Metacognitive beliefs and psychological well-being in paranoia and depression
19
This article was downloaded by: [Biblioteca Universidad Complutense de Madrid] On: 27 April 2012, At: 01:38 Publisher: Psychology Press Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Cognitive Neuropsychiatry Publication details, including instructions for authors and subscription information: http://www.tandfonline.com/loi/pcnp20 Metacognitive beliefs and psychological well-being in paranoia and depression Carmen Valiente a , Jose M. Prados b , Diego Gómez a & Filiberto Fuentenebro c a Department of Clinical Psychology, Complutense University of Madrid, Madrid, Spain b Department of Cognitive Processes, Complutense University of Madrid, Madrid, Spain c Department of Psychiatry, Complutense University of Madrid, Madrid, Spain Available online: 25 Apr 2012 To cite this article: Carmen Valiente, Jose M. Prados, Diego Gómez & Filiberto Fuentenebro (2012): Metacognitive beliefs and psychological well-being in paranoia and depression, Cognitive Neuropsychiatry, DOI:10.1080/13546805.2012.670504 To link to this article: http://dx.doi.org/10.1080/13546805.2012.670504 PLEASE SCROLL DOWN FOR ARTICLE Full terms and conditions of use: http://www.tandfonline.com/page/terms-and- conditions This article may be used for research, teaching, and private study purposes. Any substantial or systematic reproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form to anyone is expressly forbidden. The publisher does not give any warranty express or implied or make any representation that the contents will be complete or accurate or up to date. The accuracy of any instructions, formulae, and drug doses should be independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings, demand, or costs or damages whatsoever or howsoever caused
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Metacognitive beliefs and psychological well-being in paranoia and depression

This article was downloaded by: [Biblioteca Universidad Complutense de Madrid]On: 27 April 2012, At: 01:38Publisher: Psychology PressInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Cognitive NeuropsychiatryPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/pcnp20
Metacognitive beliefs andpsychological well-being in paranoiaand depressionCarmen Valiente a , Jose M. Prados b , Diego Gómez a &Filiberto Fuentenebro ca Department of Clinical Psychology, Complutense University ofMadrid, Madrid, Spainb Department of Cognitive Processes, Complutense University ofMadrid, Madrid, Spainc Department of Psychiatry, Complutense University of Madrid,Madrid, Spain
Available online: 25 Apr 2012
To cite this article: Carmen Valiente, Jose M. Prados, Diego Gómez & Filiberto Fuentenebro(2012): Metacognitive beliefs and psychological well-being in paranoia and depression, CognitiveNeuropsychiatry, DOI:10.1080/13546805.2012.670504
To link to this article: http://dx.doi.org/10.1080/13546805.2012.670504
PLEASE SCROLL DOWN FOR ARTICLE
Full terms and conditions of use: http://www.tandfonline.com/page/terms-and-conditions
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make anyrepresentation that the contents will be complete or accurate or up to date. Theaccuracy of any instructions, formulae, and drug doses should be independentlyverified with primary sources. The publisher shall not be liable for any loss, actions,claims, proceedings, demand, or costs or damages whatsoever or howsoever caused

arising directly or indirectly in connection with or arising out of the use of thismaterial.
Dow
nloa
ded
by [
Bib
liote
ca U
nive
rsid
ad C
ompl
uten
se d
e M
adri
d] a
t 01:
38 2
7 A
pril
2012

Metacognitive beliefs and psychological well-being
in paranoia and depression
Carmen Valiente1, Jose M. Prados2, Diego Gomez1, andFiliberto Fuentenebro3
1Department of Clinical Psychology, Complutense University of
Madrid, Madrid, Spain2Department of Cognitive Processes, Complutense University of
Madrid, Madrid, Spain3Department of Psychiatry, Complutense University of Madrid,
Madrid, Spain
Introduction. Despite the growing interest in the effects of metacognitive beliefs andpsychological well-being on psychiatric conditions, little is known about how thesetwo variables interact in clinical samples. The central aim of this study was toinvestigate the role of some metacognitive beliefs in the relationship betweenpsychological well-being dimensions and psychopathology.Methods. Fifty-five participants with persecutory delusions diagnosed with schizo-phrenia or other psychotic disorders, 38 participants with a major depressiveepisode, and 44 healthy controls completed the 30-item short form of theMetacognitions Questionnaire (MCQ-30) and the 54-item form of the Ryff Scalesof Psychological Well-Being (PWB).Results. MANCOVA analyses revealed group differences on four subscales of PWB(self-acceptance, autonomy, personal growth, and environmental mastery), as wellas on three subscales of MCQ-30 (uncontrollability of worry, need to controlthoughts, and lack of memory confidence). Moderation analyses showed theinteraction between persecutory thinking and cognitive self-consciousness to be apredictor of psychological well-being.Conclusions. These findings suggest that psychological well-being is particularlycompromised in participants with a high level of persecutory thinking when theyhave low levels of cognitive self-consciousness.
Correspondence should be addressed to Carmen Valiente, Department of Clinical Psychology,
Complutense University of Madrid, 28223 Pozuelo de Alarcon, Madrid, Spain.
E-mail: [email protected]
This research was supported by grants from the Spanish Ministry of Science and Innovation
(PSI2009-13472). We thank Dolores Cantero for her assistance with data collection.
COGNITIVE NEUROPSYCHIATRY
2012, 1�17, iFirst
# 2012 Psychology Press, an imprint of the Taylor & Francis Group, an Informa business
http://www.psypress.com/cogneuropsychiatry http://dx.doi.org/10.1080/13546805.2012.670504
Dow
nloa
ded
by [
Bib
liote
ca U
nive
rsid
ad C
ompl
uten
se d
e M
adri
d] a
t 01:
38 2
7 A
pril
2012

Keywords: Depression; Metacognitive Beliefs; Paranoia; Psychological
well-being.
INTRODUCTION
Metacognition has recently become a research focus in the study and
treatment of most psychiatric conditions (Corcoran & Segal, 2008; Fisher &
Wells, 2009; Lysaker et al., 2011; Wells, 2000, 2009). Some authors have
claimed that psychotic symptoms are associated with deficits in metacogni-
tion that lead to unawareness of the agency of one’s own thoughts and
actions (e.g., Frith, 1992), and others have argued that metacognitive beliefs
can lead to interpretation biases that bring about psychotic experiences (e.g.,
Morrison, 2001; Morrison & Wells, 2003). Most of the research on
metacognition in patients with schizophrenia has been carried out with
individuals experiencing hallucinations (Baker & Morrison, 1998). Several
studies have also found an association between delusional ideation and
metacognition in subjects with a clinical profile similar to panic disorder,
halfway between people with hallucinations and healthy controls (Morrison
& Wells, 2003). More precisely, Freeman and Garety (1999) found that
people with persecutory delusions tend to experience ‘‘meta-worry’’, i.e.,
worry about their ability to control their delusive thinking.
Maladaptive metacognitive beliefs have been found to correlate positively
with psychopathology, not only in psychotic samples but also in nonclinical
psychotic-prone groups (Larøi & van der Linden, 2005; Morrison, French, &
Wells, 2007; Morrison & Petersen, 2003). It may be important to consider
carefully the type of metacognitive belief. For example, Reeder, Rexhepi-
Johansson, and Wykes (2010) have pointed out that only negative beliefs
about thoughts were significantly associated with psychotic-like experiences,
but not beliefs about one’s own cognitive skills.In contrast to numerous studies of metacognition in psychotic disorders,
its potential involvement in depression has received considerably less
attention. Nevertheless, evidence already suggests that it plays at least a
partial role in the disorder (Papageorgiou & Wells, 2009). Papageorgiou and
Wells (2001) have found that positive beliefs about rumination (e.g.,
‘‘Ruminating about my depression helps me to understand past mistakes
and failures’’) correlate with higher levels of depressive symptomatology. In
fact, the role of metacognitive awareness is seen as particularly relevant to
the treatment of depression. For instance, it has been argued that the ability
to shift to a decentred metacognitive perspective mediates the ability of
cognitive therapy to prevent depressive relapse (Teasdale et al., 2002).
In this way, the importance of metacognition in explanatory models has
become central in most prominent mental health disorders. Indeed, the
2 VALIENTE ET AL.
Dow
nloa
ded
by [
Bib
liote
ca U
nive
rsid
ad C
ompl
uten
se d
e M
adri
d] a
t 01:
38 2
7 A
pril
2012

Self-Regulatory Executive Function Model (S-REF; Wells & Mathews, 1994,
1996) holds that metacognition affects the development and persistence of
psychological disorders. More precisely, psychological disorders are main-
tained by maladaptive coping strategies (e.g., perseverative thinking) that
perpetuate dysfunctional self-beliefs and increase the accessibility of negativeinformation about self (Wells, 2000).
Increasing the attention paid to metacognition may make cognitive-
behavioural interventions more effective at improving psychological well-
being, which has evolved into the main outcome of psychotherapy. For
example, measuring the success of recovery from schizophrenia (Liberman &
Kopelowicz, 2005) involves assessing functional as well as subjective
dimensions, i.e., psychological well-being (Brekke, Levin, Wolkon, Sobel,
& Slade, 1993; Chino, Nemoto, Fujii, & Mizuno, 2009). In some approachesto treating psychosis, the main objective is to reduce not the symptoms but
the distress associated with them (Chadwick, Birchwood, & Trower, 1996).
Yanos and Moos (2007) have argued that a wide range of environmental and
personal factors influence well-being in schizophrenia. In particular,
cognitive appraisals are crucial to understanding well-being since they are
directly linked to patients’ efforts to manage their subjective experiences
(Brett, Johns, Peters, & McGuire, 2009). Furthermore, psychotherapeutic
strategies that enhance well-being, such as ‘‘well-being therapy’’, have provento be a valid approach for people suffering recurrent depression (Fava, 1999;
Fava et al., 2004).
Despite growing academic interest in both metacognition and psycholo-
gical well-being, little is known about the interaction between these two
variables (Harrington & Loffredo, 2001). Metacognitive beliefs may
moderate, at least in part, the relationship between well-being and paranoia
or depression. We believe that ascertaining the dynamic interaction between
well-being and metacognitive beliefs is crucial to improving our clinicalinterventions. Most cognitive-behavioural interventions aim to reduce
distress and increase well-being by increasing metacognitive introspection
and changing metacognitive evaluation (Chadwick, 2006; Sheppard &
Teasdale, 2004; Wells, 2007, 2009; Wells et al., 2009).
The regulatory role of metacognitive beliefs may depend upon the type of
psychopathology experienced. Nevertheless, evidence suggests that, as a
general rule, self-consciousness is related with the tendency to engage in
paranoid inferences (Fenigstein & Vanable, 1992). Bentall, Corcoran,Howard, Blackwood, and Kinderman (2001) have argued that assuming
that disappointments in life are caused by the intentional actions of others is
a characteristic paranoid strategy to avoid negative effects on self-esteem.
Accordingly, one could expect that individuals with paranoia use self-
consciousness (defined as the process of directing attention towards the self)
to monitor self-threats. Thus, self-consciousness could be linked to subjective
METACOGNITIVE BELIEFS AND WELL-BEING 3
Dow
nloa
ded
by [
Bib
liote
ca U
nive
rsid
ad C
ompl
uten
se d
e M
adri
d] a
t 01:
38 2
7 A
pril
2012

well-being when the level of paranoia is high. Recently, Valiente, Provencio,
Espinosa, Chaves, and Fuentenebro (2011) have suggested that a defensive-
self plays a role in persecutory delusions, but this self-pattern is absent in
depression. In fact, patients with major depression have been found to have
low scores on public self-consciousness (Ruiperez & Belloch, 2003).
AIMS AND PREDICTIONS OF THE CURRENT STUDY
The general goal of this study was to examine psychological well-being and
certain metacognitive beliefs in three groups: participants with persecution
delusions, participants with depression, and healthy participants. Seconda-
rily, we wanted to determine how the relationship between self-conscious-
ness, as a metacognitive dimension, and psychological well-being depends on
the level of paranoia and depressive symptomatology.Based on previous findings, we expected to find that (1) clinical patients,
in comparison with healthy controls, would exhibit higher levels of
dysfunctional metacognitive beliefs, in particular negative beliefs about
worry including uncontrollability and danger; and (2) clinical patients, in
comparison with healthy controls, would exhibit lower levels of psycholo-
gical well-being. In line with the self-serving model of paranoia (Bentall
et al., 2001), we expected to find (3) a moderating effect of cognitive self-
consciousness on the relationship between the level of persecutory thinkingand the level of psychological well-being. In other words, participants with
a high level of persecutory thinking would experience more subjective well-
being when cognitive self-consciousness was high, whereas participants with
a low level of persecutory thinking would experience more subjective well-
being when cognitive self-consciousness was low. However, we did not
expect to find a moderating effect of cognitive self-consciousness on the
relationship between severity of depressive symptoms and psychological
well-being.
METHODS
Participants and procedure
One hundred and thirty-seven individuals (58.4% women) aged between 16and 65 (M�37.80, SD�12.26) volunteered to collaborate in this study after
reading and signing a consent form. Three groups of participants were
formed: the current persecutory beliefs group, the depression group, and the
nonpsychiatric control group.
The current persecutory beliefs group (PG) included 55 participants
(28 men and 27 women) who were treated at a university hospital inpatient
4 VALIENTE ET AL.
Dow
nloa
ded
by [
Bib
liote
ca U
nive
rsid
ad C
ompl
uten
se d
e M
adri
d] a
t 01:
38 2
7 A
pril
2012

psychiatric unit. The mean age of the PG was 34.64 years (SD�11.14). All
participants were suffering persecutory beliefs at the time of the study, as
assessed by the Present State Examination (10th ed.; PSE-10) of the
Schedules for Clinical Assessment in Neuropsychiatry (World Health
Organisation, 1992). Participants with delusions of guilt were excluded, asthese contents are usually associated with major depressive disorders with
psychotic characteristics. Participants were selected through hospital records,
and diagnoses were confirmed using the MINI International Neuropsychia-
tric Interview (MINIPLUS; Sheehan & Lecrubier, 2002), a structured
clinical interview. Participants met criteria of the Diagnostic and Statistical
Manual of Mental Disorders (4th ed.; DSM-IV; American Psychiatric
Association [APA], 1994) for the following categories: schizophrenia
paranoid type (n�28), schizophreniform disorder (n�9), schizoaffectivedisorder (n�6), delusional disorder (n�8), brief psychotic disorder (n�2),
and psychotic disorder not otherwise specified (n�2). All participants were
receiving antipsychotic medication at the time of the study. The mean age of
illness onset for this group was 25.42 (SD�7.68), and the average mean
illness duration was 8.75 years (SD�9.90).
The depression group (DG) included 38 participants (nine men and 29
women) who were recruited from an outpatient mental health service. The
mean age of the DG was 42.84 (SD�11.51). Participants in the DG metDSM-IV criteria for a current depressive disorder and had never experienced
persecutory delusions. Diagnoses were confirmed using MINIPLUS
(Sheehan & Lecrubier, 2002). Participants met criteria of the DSM-IV
(APA, 1994) for the following categories: major depressive disorder, single
episode (n�11), major depressive disorder, recurrent episode (n�22), and
bipolar depression I (n�5). All but four participants were receiving
antidepressants at the time of the study. The mean age of onset of the
disorder for this group was 34.84 years (SD�9.74).The nonpsychiatric control group (CG) comprised 44 participants
(20 men and 24 women) who were recruited via informal contacts. The
mean age of the CG was 37.41 years (SD�13.06). They were screened for
the absence of any clinical syndrome, and they had never required
psychological assistance for any mental disorder or any concurrent medical
condition.
In the clinical groups, participants had a clinical interview that included
the MINIPLUS; participants with persecutory delusions also completed thePSE-10. For the control group, the interview was designed to screen for the
absence of mental illness. After the interview, all participants were given a set
of questionnaires to fill out. After receiving a brief explanation about the
purpose of the study and after having time to ask questions, the participants
were dismissed. Data collection took place between Spring 2009 and
Winter 2010.
METACOGNITIVE BELIEFS AND WELL-BEING 5
Dow
nloa
ded
by [
Bib
liote
ca U
nive
rsid
ad C
ompl
uten
se d
e M
adri
d] a
t 01:
38 2
7 A
pril
2012
Measures
Metacognitions Questionnaire (MCQ-30; Wells & Cartwright-Hatton,
2004). The MCQ-30 is a self-report scale that assesses different beliefs
about worry and cognition. This instrument has 30 items that are rated on a
4-point scale from 1 (‘‘do not agree’’) to 4 (‘‘agree very much’’) and that
cover five different domains: (1) positive beliefs about worry, Positive beliefs
(e.g., ‘‘Worrying helps me to avoid problems in the future’’); (2) negative
beliefs about worry concerning uncontrollability and danger, Uncontroll-
ability and danger (e.g., ‘‘My worrying is dangerous for me’’); (3) beliefsabout lack of confidence in memory, Cognitive confidence (e.g., ‘‘I have a
poor memory’’); (4) beliefs concerning the need to control one’s own
thoughts, Need to control thoughts (e.g., ‘‘If I could not control my
thoughts, I would not be able to function’’); and (5) beliefs about one’s own
tendency to monitor and focus on thoughts, Cognitive self-consciousness
(e.g., ‘‘I think a lot about my thoughts’’). The MCQ-30 has demonstrated
acceptable to good internal consistency and test�retest reliability across
different samples (Cronbach’s a from .72 to .93, and r from .74 to .87; Spada,Mohiyeddini, & Wells, 2008; Wells & Cartwright-Hatton, 2004; Yilmaz,
Gencoz, & Wells, 2008). In this study the Cronbach’s a ranged from .78
to .92.
Psychological Well-Being Scales (PWB; Ryff, 1989; Ryff & Singer,2002). The PWB is a construct-oriented self-report scale that integrates
mental health and life span developmental theories about positive psycho-
logical functioning in six different domains: autonomy, positive relations
with others, self-acceptance, environmental mastery, purpose in life, and
personal growth (Ryff & Keyes, 1995). Each item of this instrument scores
on a 6-point scale from 1 (‘‘disagree very much’’) to 6 (‘‘agree very much’’).
The PWB has demonstrated good internal consistency and test�retest
reliability across different samples (Cronbach’s a from .86 to .93, and r
from .81 to .88; Ryff & Singer, 2002, 2006; van Dierendonck, 2004). In this
study we used the 54-item version, and its Cronbach’s a was .91 in the overall
sample.
Persecution and Deservedness Scale (PaDS; Melo, Corcoran, Shryane, &
Bentall, 2009). This is a brief measure to assess both the severity ofpersecutory thinking and the perceived deservedness of persecution, and it is
suitable for both clinical and nonclinical populations. In this study we used
only the 10 statements of the persecution subscale (PaDS-P), which assume
that the individual is the object of others’ malevolence (e.g., ‘‘There are times
when I worry that others might be plotting against me’’). The PaDS-P items
cover a broad conceptualisation of persecution (e.g., ‘‘I believe that some
6 VALIENTE ET AL.
Dow
nloa
ded
by [
Bib
liote
ca U
nive
rsid
ad C
ompl
uten
se d
e M
adri
d] a
t 01:
38 2
7 A
pril
2012

people want to hurt me deliberately’’), including general mistrust (e.g., ‘‘You
should only trust yourself ’’). Participants were asked to rate each statement
on a 5-point scale ranging from 0 (‘‘certainly false’’) to 4 (‘‘certainly true’’).
Melo et al. (2009) have reported good internal reliability (Cronbach’s a�.84)
and a high correlation (r�.78) with the Paranoia Scale (Fenigstein &Vanable, 1992). In this study we found a Cronbach’s a of .91.
Beck Depression Inventory�2nd edition (BDI-II; Beck, Steer, & Brown,
1996). The BDI-II is a 21-item self-report questionnaire of depression
symptom severity over the two preceding weeks. As each item of this
instrument has a 3-point score, the total score ranges between 0 and 63. The
BDI-II has demonstrated good internal consistency and acceptable test�retest reliability across different samples (Cronbach’s a�.91, r�.71; see
Dozois & Covin, 2004; Dozois, Dobson, & Ahnberg, 1998). In this study wefound a Cronbach’s a of .94.
Statistical analyses
We used one-way analyses of variance (ANOVA) to compare the threegroups with respect to age and years of education, and chi-squared tests to
compare them with respect to gender, marital status, and employment.
Multivariate analyses of covariance (MANCOVA) were used to investigate
clinical, metacognitive beliefs, and psychological well-being differences
among the three groups; a Type IV sum of squares was applied when data
were missing. Pair-wise comparisons were made using Bonferroni and
Games-Howell post hoc comparisons. Finally, hierarchical multiple regres-
sions were used to predict PWB score.
RESULTS
Demographic and clinical status
Table 1 shows sociodemographic parameters of the sample. One-way
analysis of variance revealed significant group differences for age, h2�.07.
Post hoc Bonferroni comparisons indicated that participants with persecu-
tory delusions were younger than participants with depression, t(91)�3.27,p�.004. However, there were no differences between CG and DG,
t(80)�2.06, p�.123, or between CG and PG, t(97)�1.15, p�.753.
Another one-way analysis of variance also revealed significant group
differences for years of education, h2�.16. Post hoc Bonferroni compar-
isons indicated that participants with persecutory delusions had fewer years
of education than participants with depression, t(91)�3.75, p�.001, or
METACOGNITIVE BELIEFS AND WELL-BEING 7
Dow
nloa
ded
by [
Bib
liote
ca U
nive
rsid
ad C
ompl
uten
se d
e M
adri
d] a
t 01:
38 2
7 A
pril
2012

nonpsychiatric control participants, t(97)�4.71, pB.001. However, no
differences were found between DG and CG, tB1.
Finally, chi-square tests showed the three groups differed significantly in
gender, with a smaller number of men in DG than in PG or CG. However,
the groups showed no differences in employment or marital status.
Gender, years of education, and gender differences between groups were
statistically controlled in the following analyses.
Table 2 shows means and standard deviations of scores on BDI-II and
PaDS-P scales for the three groups. In the MANCOVA, BDI-II, and PaDS-P
scores were introduced as dependent variables, and age, years of education,
and gender were introduced as covariates. The analysis revealed a significant
main effect for group, Wilks’s lambda�0.47, F(4, 216)�23.98, pB.001,
h2�.31. There were significant group differences for the BDI-II, h2�.44,
and for the PaDS-P, h2�.20. As Levene’s tests indicated heteroscedasticity
for BDI-II, F(2, 112)�5.37, p�.006, and PaDS-P, F(2, 112)�13.17,
pB.001, group differences for these variables were corroborated using the
Kruskall-Wallis test, x2(2, N�117)�51.33, pB.001; and x2(2, N�119)�24.69, pB.001.
As expected, post hoc Games-Howell comparisons showed that scores on
BDI-II were higher for the DG than for the PG, t(86)�7.61, pB.001, or
CG, t(63)�9.47, pB.001. Moreover, BDI-II scores were higher for the PG
than for CG, t(79)�3.09, p�.002. Compared to controls, PaDS-P scores
were higher for the PG, t(81)�5.55, pB.001, and for DG, t(64)�4.38,
pB.001. However, there were no significant differences between the two
clinical groups, t B1.
TABLE 1Participant characteristics
Nonclinical
(n�44)
Depression
(n�38)
Paranoia
(n�55) F x2 p
Mean age (SD) 37.41 (13.06) 42.84 (11.51) 34.64 (11.14) 5.39 .006
Years of education
(SD)
14.75 (3.69) 14.15 (4.07) 11.23 (3.38) 12.98 B.001
Gender
Men 20 9 28 7.25 .027
Women 24 29 27
Marital status 5.59 �.05
Never married 22 18 38
Ever married 22 20 17
Employment 5.56 �.05
Not employed 19 15 34
Employed 25 23 21
8 VALIENTE ET AL.
Dow
nloa
ded
by [
Bib
liote
ca U
nive
rsid
ad C
ompl
uten
se d
e M
adri
d] a
t 01:
38 2
7 A
pril
2012

Group differences on MCQ-30
Table 2 shows means and standard deviations of the MCQ-30 subscales for
the three groups. Another MANCOVA was used to assess group differences
in MCQ-30 subscales; here, again, the covariates were age, years of
education, and gender. After determining that Box’s test was nonsignificant
(M�37.02), F(30, 45008)�1.16, p�.247, we found a significant main effect
for group, Wilks’s lambda�0.58, F(10, 240)�7.38, pB.001, h2�.23, and
gender, Wilks’s lambda�0.85, F(5, 120)�4.12, p�.002, h2�.14. There
were significant differences in three MCQ-30 subscales: uncontrollability and
danger, h2�.32; need to control thoughts, h2�.18; and cognitive con-
fidence, h2�.10.
Post hoc Bonferroni analysis revealed that participants in the DG scored
higher on the uncontrollability and danger subscale than those in the PG,
t(86)�2.96, p�.011, or CG, t(77)�7.58, pB.001. In addition, the PG
scored higher than nonclinical participants, t(91)�4.48, pB.001. A
significant gender effect was found for the uncontrollability and danger
TABLE 2Means and standard deviations (in parenthesis) on BDI-II, PaDS-P, MCQ-30, and
PWQ scales
Scale
Nonclinical
(n�44)
Depression
(n�38)
Paranoia
(n�55) F p
BDI-II 6.31 (6.68) 31.05 (9.82) 13.96 (12.65) 43.98 B.001
PaDS-P 4.86 (5.01) 15.80 (10.20) 16.54 (10.90) 13.67 B.001
MCQ-30
Cognitive confidence 12.02 (4.35) 15.83 (4.37) 12.64 (4.59) 7.01 .001
Positive beliefs 12.50 (4.78) 12.16 (4.43) 14.45 (5.65) 1.07 .346
Cognitive self-
consciousness
15.92 (4.02) 16.51 (3.20) 16.84 (4.44) 0.99 .374
Uncontrollability and
danger
10.88 (3.57) 18.89 (4.64) 15.39 (4.69) 29.39 B.001
Need to control
thoughts
11.78 (3.41) 16.21 (3.65) 15.05 (4.32) 13.72 B.001
PWQ
Autonomy 33.55 (5.42) 30.22 (5.34) 33.32 (7.22) 4.47 .013
Relations with others 34.44 (5.77) 31.30 (6.43) 33.59 (7.85) 2.52 .084
Self-acceptance 33.83 (6.30) 27.33 (5.14) 32.46 (6.46) 10.36 B.001
Environmental mastery 33.02 (6.20) 29.02 (5.52) 31.19 (6.92) 4.83 .009
Purpose in life 30.00 (5.15) 27.55 (5.72) 30.90 (7.83) 2.60 .078
Personal growth 31.48 (5.60) 28.41 (6.12) 31.61 (7.57) 3.24 .042
BDI-II, Beck Depression Inventory (2nd edition); PaDS-P, Persecution and Deservedness
Scale�Persecutory thinking dimension; MCQ-30, Metacognitions Questionnaire; PWB, Scales of
Psychological Well-Being.
METACOGNITIVE BELIEFS AND WELL-BEING 9
Dow
nloa
ded
by [
Bib
liote
ca U
nive
rsid
ad C
ompl
uten
se d
e M
adri
d] a
t 01:
38 2
7 A
pril
2012

subscale, F(1, 124)�8.48, p�.004, h2�.06, reflecting higher scores for
women (M�16.22, SD�5.34) than men (M�12.77, SD�4.70). Follow-up
ANOVA using group and gender as factors and the uncontrollability and
danger subscale as the dependent variable corroborated the main group and
gender effects, but showed no interaction effect, FB1.Finally, post hoc comparisons showed that scores on the need to control
thoughts subscale were lower for the CG than for the DG, t(77)�5.10,
pB.001, or the PG, t(91)�3.39, p�.003. However, there were no differences
between participants in clinical groups, t(86)�1.64, p�.309.
Regarding the cognitive confidence subscale, participants in the DG had
higher scores than participants in the PG, t(86)�3.03, p�.009, and CG,
t(77)�3.45, p�.002. But no differences were found between participants in
the PG and CG, tB1.
Group differences on PWB
Table 2 shows means and standard deviations of the PWB subscales for thethree groups. MANCOVA was used to assess group differences in the six
PWB subscales while controlling age, years of education, and gender as
covariates. This analysis revealed only a significant group effect, Wilks’s
lambda�0.81, F(12, 240)�2.21, pB.012, h2�.10. In particular, there were
significant group differences on four PWB dimensions: self-acceptance,
h2�.14; environmental mastery, h2�.07; autonomy, h2�.06; and personal
growth, h2�.04.
Post hoc Bonferroni comparison revealed that participants in the DGscored lower than participants in the CG on the subscales for self-
acceptance, t(77)�4.45, pB.001, environmental mastery, t(77)�3.10,
p�.007, autonomy, t(77)�2.57, p�.033, and personal growth,
t(77)�2.42, p�.050. In addition, participants in the DG scored lower
than participants in the PG on the self-acceptance subscale, t(86)�3.21,
p�.005, and autonomy subscale, t(86)�2.67, p�.026. But no differences
were found between the PG and CG on any PWB subscale (p�.05).
Predicting PWB: A moderation analysis
After preliminary analyses conducted to ensure that assumptions ofregression were not violated, hierarchical multiple regression analyses were
used to examine whether cognitive self-consciousness (MCQ-30-CSC)
moderated the relationship between severity of persecutory thinking
(PaDS-P) and psychological well-being (PWB). Standardised scores for
PaDS-P and MCQ-30-CSC were introduced at Step 1 and their interaction
(PaDS-P�MCQ-CSC) was introduced at Step 2.
10 VALIENTE ET AL.
Dow
nloa
ded
by [
Bib
liote
ca U
nive
rsid
ad C
ompl
uten
se d
e M
adri
d] a
t 01:
38 2
7 A
pril
2012
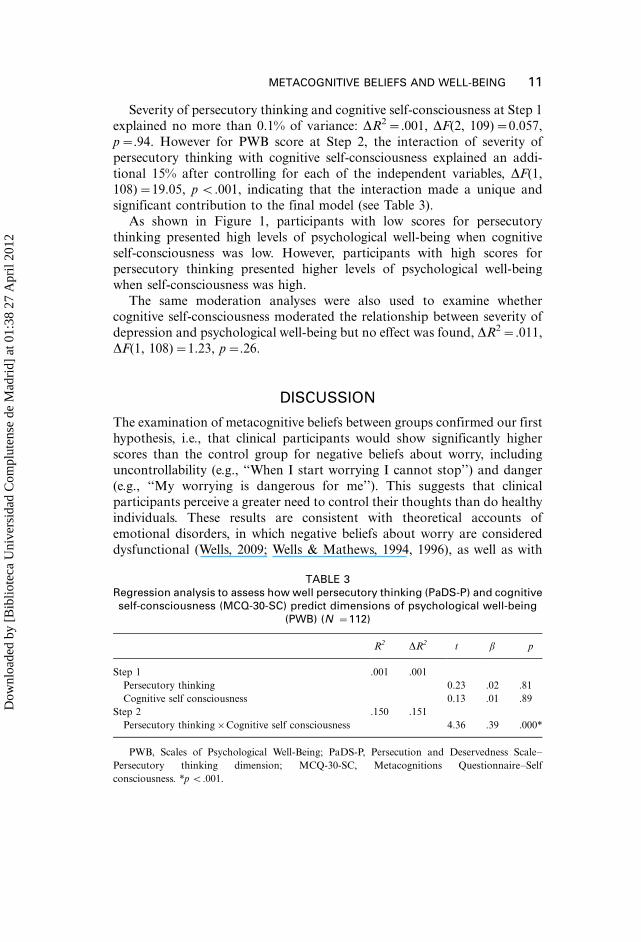
Severity of persecutory thinking and cognitive self-consciousness at Step 1
explained no more than 0.1% of variance: DR2�.001, DF(2, 109)�0.057,
p�.94. However for PWB score at Step 2, the interaction of severity of
persecutory thinking with cognitive self-consciousness explained an addi-
tional 15% after controlling for each of the independent variables, DF(1,108)�19.05, p B.001, indicating that the interaction made a unique and
significant contribution to the final model (see Table 3).
As shown in Figure 1, participants with low scores for persecutory
thinking presented high levels of psychological well-being when cognitive
self-consciousness was low. However, participants with high scores for
persecutory thinking presented higher levels of psychological well-being
when self-consciousness was high.
The same moderation analyses were also used to examine whethercognitive self-consciousness moderated the relationship between severity of
depression and psychological well-being but no effect was found, DR2�.011,
DF(1, 108)�1.23, p�.26.
DISCUSSION
The examination of metacognitive beliefs between groups confirmed our first
hypothesis, i.e., that clinical participants would show significantly higher
scores than the control group for negative beliefs about worry, includinguncontrollability (e.g., ‘‘When I start worrying I cannot stop’’) and danger
(e.g., ‘‘My worrying is dangerous for me’’). This suggests that clinical
participants perceive a greater need to control their thoughts than do healthy
individuals. These results are consistent with theoretical accounts of
emotional disorders, in which negative beliefs about worry are considered
dysfunctional (Wells, 2009; Wells & Mathews, 1994, 1996), as well as with
TABLE 3Regression analysis to assess how well persecutory thinking (PaDS-P) and cognitiveself-consciousness (MCQ-30-SC) predict dimensions of psychological well-being
(PWB) (N �112)
R2 DR2 t b p
Step 1 .001 .001
Persecutory thinking 0.23 .02 .81
Cognitive self consciousness 0.13 .01 .89
Step 2 .150 .151
Persecutory thinking�Cognitive self consciousness 4.36 .39 .000*
PWB, Scales of Psychological Well-Being; PaDS-P, Persecution and Deservedness Scale�Persecutory thinking dimension; MCQ-30-SC, Metacognitions Questionnaire�Self
consciousness. *p B.001.
METACOGNITIVE BELIEFS AND WELL-BEING 11
Dow
nloa
ded
by [
Bib
liote
ca U
nive
rsid
ad C
ompl
uten
se d
e M
adri
d] a
t 01:
38 2
7 A
pril
2012

previous research that has reported a high level of these beliefs in paranoia
and depression (Foster, Startup, Potts, & Freeman, 2010; Moritz, Peters,
Larøi, & Lincoln, 2010; Morrison & Wells, 2007; Startup, Freeman, &
Garety, 2007). These findings support new clinical interventions to treat
psychosis that encourage acceptance of internal experience (e.g., Chadwick,
2006) and unavoidable private events (Bach & Hayes, 2002).
In line with prior studies that indicate memory deficits in depression (e.g.,
Hermens, Naismith, Redoblado-Hodge, Scott, & Hickie, 2010), our study
shows a significant lack of memory confidence in the depression group. This
may be linked to their high level of worry (Starcevic, 1995), because some
evidence suggests that worry restricts working memory capacity (Hayes,
Hirsch, & Mathews, 2008; Rapee, 1993). Interestingly, our participants with
persecutory delusions had similar memory confidence as healthy controls,
which is consistent with previous research (Moritz et al., 2010). The possible
link between worry and memory in deluded patients should be explored in
further research.
Similar to other clinical comparisons (Wells & Carter, 2001), our study
did not find differences among groups in positive beliefs about worry.
Although self-consciousness has been linked to paranoid thinking
(Fenigstein & Vanable, 1992), our groups did not show differences in
cognitive self-consciousness scores. Other research has also suggested that
cognitive self-consciousness, as assessed with the MCQ-30, is not linked to
depression severity (Yilmaz et al., 2008). Future research should address
these apparent discrepancies about the effect of self-consciousness.
155
160
165
170
175
180
185
190
195
200
Low Persecutory Thinking(PaDS)
High Persecutory Thinking(PaDS)
Psy
cho
log
ical
Wel
l-b
ein
g (
PW
B)
Low Self-Consciousness(MCQ-30)
High Self-Consciousness(MCQ-30)
Figure 1. Moderating effect of cognitive self-consciousness and persecution thinking on psycholo-
gical well-being. PWB, Scales of Psychological Well-Being; PaDS, Persecution and Deservedness
Scale; MCQ-30, Metacognitions Questionnaire.
12 VALIENTE ET AL.
Dow
nloa
ded
by [
Bib
liote
ca U
nive
rsid
ad C
ompl
uten
se d
e M
adri
d] a
t 01:
38 2
7 A
pril
2012

The findings of our study partially support our second hypothesis.
Participants with depression rated their psychological well-being lower
than did participants with persecution delusions and healthy controls,
especially in the self-acceptance and autonomy domains. However, partici-
pants with persecutory delusions and healthy controls did not differ insubjective psychological well-being. An inflated sense of well-being could
reflect a motivational bias in paranoia that seeks to preserve a positive sense
of self (Bentall et al., 2001; McKay, Langdon, & Coltheart, 2007; Valiente
et al., 2011). It would be interesting to try to replicate this finding using
objective measures of well-being.
Our third hypothesis predicted that the level of cognitive self-
consciousness would moderate the effects of persecutory thinking on well-
being. Our results showed that neither the level of persecutory thinkingnor the level of cognitive self-consciousness on their own was able to explain
the observed variance in well-being. Nevertheless, we did find that the level
of cognitive self-consciousness moderated the relationship between well-
being and persecutory thinking, though not the relationship between well-
being and depression severity. Participants with higher persecutory thinking
reported better well-being when they had higher cognitive self-consciousness
than when they had lower cognitive self-consciousness. And participants
with lower persecutory thinking reported worse well-being when they hadhigher cognitive self-consciousness than when they had lower cognitive self-
consciousness. These results suggest that the participants with higher
persecution thinking use cognitive self-consciousness as a strategy to
maintain a sense of wellness. The cross-sectional nature of our study
prevents us from reaching any definitive conclusions about causality, but
we speculate that the use of cognitive self-consciousness, as a way to regulate
well-being, may have positive effects in the short term, while perpetuating a
defensive self in the long term.This last finding has important clinical implications. For instance,
psychotherapy should build on people’s personal resources and mechanisms
(Tarrier et al., 1993), while redirecting self-effort towards more coherence
and authenticity (Kernis, 2003). This suggestion is also in line with recent
metacognitively oriented therapy for schizophrenia (Aghotor, Pfueller,
Moritz, Weisbrod, & Roesch-Ely, 2010; Buck & Lysaker, 2009; Lysaker,
Buck, & Ringer, 2007).
As a first attempt to study the relationship between metacognitive beliefsand psychological well-being, this study has several limitations that must be
addressed in future research. For example, external validity could be
enhanced by the inclusion of multiple measures of main variables; these
measures could be subjective, objective, and implicit. Future studies
could also address whether experimental manipulation of cognitive self-
consciousness affects the level of psychological well-being in clinical and
METACOGNITIVE BELIEFS AND WELL-BEING 13
Dow
nloa
ded
by [
Bib
liote
ca U
nive
rsid
ad C
ompl
uten
se d
e M
adri
d] a
t 01:
38 2
7 A
pril
2012

control samples. Further studies could explore how changes in cognitive self-
consciousness in context*over time and with different daily stresses*are
associated with changes in clinical and psychological adjustment.
Manuscript received 13 April 2011
Revised manuscript received 9 February 2012
First published online 24 April 2012
REFERENCES
Aghotor, J., Pfueller, U., Moritz, S., Weisbrod, M., & Roesch-Ely, D. (2010). Metacognitive training
for patients with schizophrenia (MCT): Feasibility and preliminary evidence for its efficacy.
Journal of Behavior Therapy and Experimental Psychiatry, 41, 207�211. doi:10.1016/
j.jbtep.2010.01.004
American Psychiatric Association (APA). (1994). Diagnostic and statistical manual of mental
disorders (4th ed.). Washington, DC: Author.
Bach, P., & Hayes, S. C. (2002). The use of acceptance and commitment therapy to prevent the
rehospitalization of psychotic patients: A randomized controlled trial. Journal of Consulting
and Clinical Psychology, 70, 1129�1139. doi:10.1037//0022-006X.70.5.1129
Baker, C. A., & Morrison, A. P. (1998). Cognitive processes in auditory hallucinations:
Attributional biases and metacognition. Psychological Medicine, 28, 1199�1208. doi:10.1017/
S0033291798007314
Beck, A. T., Steer, R. A., & Brown, G. K. (1996). Beck Depression Inventory�second edition manual.
San Antonio, TX: Psychological Corporation.
Bentall, R. P., Corcoran, R., Howard, R., Blackwood, N., & Kinderman, P. (2001). Persecutory
delusions: A review and theoretical integration. Clinical Psychology Review, 21, 1143�1192.
doi:10.1016/S0272-7358(01)00106-4
Brekke, J. S., Levin, S., Wolkon, G. H., Sobel, E., & Slade, E. (1993). Psychosocial functioning and
subjective experience in schizophrenia. Schizophrenia Bulletin, 19, 559�608. doi:10.1093/schbul/
19.3.599
Brett, C. M. C., Johns, L. C., Peters, E. P., & McGuire, P. K. (2009). The role of metacognitive
beliefs in determining the impact of anomalous experiences: A comparison of help-seeking and
non-help-seeking groups of people experiencing psychotic-like anomalies. Psychological
Medicine, 39, 939�950. doi:10.1017/S0033291708004650
Buck, K. D., & Lysaker, P. H. (2009). Addressing metacognitive capacity in the psychotherapy for
schizophrenia: A case study. Clinical Case Studies, 8, 463�472. doi:10.1177/1534650109352005.
Chadwick, P. (2006). Person based cognitive therapy for distressing psychosis. Chichester, UK: Wiley.
Chadwick, P., Birchwood, M. J., & Trower, P. (1996). Cognitive therapy for delusions, voices and
paranoia. Chichester, UK: Wiley.
Chino, B., Nemoto, T., Fujii, C., & Mizuno, M. (2009). Subjective assessments of the quality of life,
well-being and self-efficacy in patients with schizophrenia. Psychiatry and Clinical Neuros-
ciences, 63, 521�528. doi:10.1111/j.1440-1819.2009.01995.x
Corcoran, K. M., & Segal, Z. V. (2008). Metacognition in depressive and anxiety disorders:
Current directions. International Journal of Cognitive Therapy, 1, 33�44. doi:10.1680/
ijct.2008.1.1.33
Dozois, D. J. A., & Covin, R. (2004). The Beck Depression Inventory�II, Beck Hopelessness Scale
(BHS), and Beck Scale for Suicide Ideation (BSS). In M. Hersen, M. J. Hilsenroth, & D. L.
Segal (Eds.), Comprehensive handbook of psychological assessment: Personality assessment
(pp. 50�69). New York, NY: Wiley.
14 VALIENTE ET AL.
Dow
nloa
ded
by [
Bib
liote
ca U
nive
rsid
ad C
ompl
uten
se d
e M
adri
d] a
t 01:
38 2
7 A
pril
2012

Dozois, D. J. A., Dobson, K. S., & Ahnberg, J. L. (1998). A psychometric evaluation of the Beck
Depression Inventory�II. Psychological Assessment, 10, 83�89.
Fava, G. A. (1999). Well-being therapy: Conceptual and technical issues. Psychotherapy and
Psychosomatics, 68, 171�179. doi:10.1159/000012329
Fava, G. A., Ruini, C., Rafanelli, C., Finos, L., Conti, S., & Grandi, S. (2004). Six-year outcome of
cognitive behavior therapy for prevention of recurrent depression. American Journal of
Psychiatry, 161, 1872�1876. doi:10.1176/appi.ajp.161.10.1872
Fenigstein, A., & Vanable, P. A. (1992). Paranoia and self-consciousness. Journal of Personality and
Social Psychology, 62, 129�134. doi:10.1037/0022-3514.62.1.129
Fisher, P., & Wells, A. (2009). Metacognitive therapy. Hove, UK: Routledge.
Foster, C., Startup, H., Potts, L., & Freeman, D. (2010). A randomised controlled trial of a worry
intervention for individuals with persistent persecutory delusions. Journal of Behavior Therapy
and Experimental Psychiatry, 41, 45�51. doi:10.1016/j.jbtep.2009.09.001
Freeman, D., & Garety, P. A. (1999). Worry, worry processes and dimensions of delusions: An
exploratory investigation of a role for anxiety processes in the maintenance of delusional
distress. Behavioural and Cognitive Psychotherapy, 27, 47�62.
Frith, C. D. (1992). The cognitive neuropsychology of schizophrenia. Hove, UK: Lawrence Erlbaum
Associates Ltd.
Harrington, R., & Loffredo, D. A. (2001). The relationship between life satisfaction, self-
consciousness and the Myers-Briggs Type Inventory dimensions. Journal of Psychology, 135,
439�450. doi:10.1080/00223980109603710
Hayes, S., Hirsch, C. R., & Mathews, A. (2008). Restriction of working memory capacity during
worry. Journal of Abnormal Psychology, 117, 712�717. doi:10.1037/a0012908
Hermens, D. F., Naismith, S. L., Redoblado-Hodge, M. A., Scott, E. M., & Hickie, I. B. (2010).
Impaired verbal memory in young adults with unipolar and bipolar depression. Early
Intervention in Psychiatry, 4, 227�233. doi:10.1111/j.1751-7893.2010.00194.x
Kernis, M. H. (2003). Toward a conceptualization of optimal self-esteem. Psychological Inquiry, 14,
1�26. doi:10.1207/S15327965PLI1401_01
Larøi, F., & van der Linden, M. (2005). Metacognition in proneness towards hallucinations and
delusions. Behaviour Research and Therapy, 43, 1425�1441. doi:10.1016/j.brat.2004.10.008
Liberman, R. P., & Kopelowicz, A. (2005). Recovery from schizophrenia: A concept in search of
research. Psychiatric Services, 56, 735�742. doi:10.1176/appi.ps.56.6.735
Lysaker, P. H., Buck, K. D., & Ringer, J. (2007). The recovery of metacognitive capacity in
schizophrenia across 32 months of individual psychotherapy: A case study. Psychotherapy
Research, 17, 713�720. doi:10.1080/10503300701255932]
Lysaker, P. H., Dimaggio, G., Buck, K. D., Callaway, S. S., Salvatore, G., Carcione, A., et al.
(2011). Poor insight in schizophrenia: Links between different forms of metacognition with
awareness of symptoms, treatment need, and consequences of illness. Comprehensive Psychiatry,
52, 253�260. doi:10.1016/j.comppsych.2010.07.007
McKay, R., Langdon, R., & Coltheart, M. (2007). The defensive function of persecutory delusions:
An investigation using the implicit association test. Cognitive Neuropsychiatry, 12, 1�24.
doi:10.1080/13546800500363996
Melo, S., Corcoran, R., Shryane, N., & Bentall, R. P. (2009). The persecution and deservedness
scale. Psychology and Psychotherapy: Theory, Research and Practice, 82, 247�260. doi:10.1348/
147608308X398337
Moritz, S., Peters, M. J. V., Larøi, F., & Lincoln, T. M. (2010). Metacognitive beliefs in obsessive-
compulsive patients: A comparison with healthy and schizophrenia participants. Cognitive
Neuropsychiatry, 15, 531�548. doi:10.1080/13546801003783508
Morrison, A. P. (2001). The interpretation of intrusions in psychosis: An integrative cognitive
approach to hallucinations and delusions. Behavioural and Cognitive Psychotherapy, 29,
257�276. doi:10.1017/S1352465801003010
METACOGNITIVE BELIEFS AND WELL-BEING 15
Dow
nloa
ded
by [
Bib
liote
ca U
nive
rsid
ad C
ompl
uten
se d
e M
adri
d] a
t 01:
38 2
7 A
pril
2012

Morrison, A. P., French, P., & Wells, A. (2007). Metacognitive beliefs across the continuum of
psychosis: Comparisons between patients with psychotic disorders, patients at ultra risk and
non-patients. Behaviour Research and Therapy, 45, 2241�2246. doi:10.1016/j.brat.2007.01.002
Morrison, A. P., & Petersen, T. (2003). Trauma, metacognition and predisposition to hallucinations
in non-patients. Behavioural and Cognitive Psychotherapy, 31, 235�246. doi:10.1017/
S1352465803003011
Morrison, A. P., & Wells, A. (2003). A comparison of metacognitions in patients with
hallucinations, delusions, panic disorder, and non-patient controls. Behaviour Research and
Therapy, 41, 251�256. doi:10.1016/S0005-7967(02)00095-5
Morrison, A. P., & Wells, A. (2007). Relationships between worry, psychotic experiences and
emotional distress in patients with schizophrenia spectrum diagnoses and comparisons with
anxious and non-patient groups. Behaviour Research and Therapy, 45, 1593�1600. doi:10.1016/
j.brat.2006.11.010
Papageorgiou, C., & Wells, A. (2001). Positive beliefs about depressive rumination: Development
and preliminary validation of a self-report scale. Behavior Therapy, 32, 13�26. doi:10.1016/
S0005-7894(01)80041-1
Papageorgiou, C., & Wells, A. (2009). A prospective test of the clinical metacognitive model of
rumination and depression. International Journal of Cognitive Therapy, 2, 123�131. doi:10.1521/
ijct.2009.2.2.123
Rapee, R. M. (1993). The utilisation of working memory by worry. Behaviour Research and
Therapy, 31, 617�620. doi:10.1016/0005-7967(93)90114-A
Reeder, C., Rexhepi-Johansson, T., & Wykes, T. (2010). Different components of metacognition
and their relationship to psychotic-like experiences. Behavioural and Cognitive Psychotherapy,
38, 49�57. doi:10.1017/S1352465809990403
Ruiperez, M. A., & Belloch, A. (2003). Dimensions of the self-consciousness scale and their
relationship with psychopathological indicators. Personality and Individual Differences, 35,
829�841. doi:10.1016/S0191-8869(02)00286-6
Ryff, C. D. (1989). Happiness is everything, or is it? Explorations on the meaning of psychological
well-being. Journal of Personality and Social Psychology, 57, 1069�1081. doi:10.1037/0022-
3514.57.6.1069
Ryff, C. D., & Keyes, C. L. (1995). The structure of psychological well-being revisited. Journal of
Personality and Social Psychology, 69, 719�727. doi:10.1037/0022-3514.69.4.719
Ryff, C., & Singer, B. (2002). From social structure to biology. In C. Zinder & A. Lopez (Eds.),
Handbook of positive psychology (pp. 63�73). London, UK: Oxford University Press.
Ryff, C. D., & Singer, B. H. (2006). Best news yet on the six-factor model of well-being. Social
Science Research, 35, 1103�1119. doi:10.1016/j.ssresearch.2006.01.002
Sheehan, D. V., & Lecrubier, Y. (2002). MINI International Neuropsychiatric Interview for DSM-IV
(English version 5.0.0). Tampa, FL: University of South Florida.
Sheppard, L., & Teasdale, J. D. (2004). How does dysfunctional thinking decrease during recovery
from major depression? Journal of Abnormal Psychology, 113, 64�71. doi:10.1037/0021-
843X.113.1.64
Spada, M. M., Mohiyeddini, C., & Wells, A. (2008). Measuring metacognitions associated with
emotional distress: Factor structure and predictive validity of the Metacognitions Question-
naire 30. Personality and Individual Differences, 45, 238�242. doi:10.1016/j.paid.2008.04.005
Starcevic, V. (1995). Pathological worry in major depression: Preliminary report. Behaviour
Research and Therapy, 33, 55�57. doi:10.1016/0005-7967(93)E0028-4
Startup, H., Freeman, D., & Garety, P. A. (2007). Persecutory delusions and catastrophic worry in
psychosis: Developing the understanding of delusion distress and persistence. Behaviour
Research and Therapy, 45, 523�537. doi:10.1016/j.brat.2006.04.006
Tarrier, N., Sharpe, L., Beckett, R., Harwood, S., Baker, A., & Yusopoff, L. (1993). A trial of two
cognitive behavioural methods of treating drug-resistant residual psychotic symptoms in
16 VALIENTE ET AL.
Dow
nloa
ded
by [
Bib
liote
ca U
nive
rsid
ad C
ompl
uten
se d
e M
adri
d] a
t 01:
38 2
7 A
pril
2012

schizophrenic patients: II. Treatment-specific changes in coping and problem-solving skills.
Social Psychiatry and Psychiatric Epidemiology, 28, 5�10. doi:10.1007/BF00797826
Teasdale, J. D., Moore, R. G., Hayhurst, H., Pope, M., Williams, S., & Segal, Z. V. (2002).
Metacognitive awareness and prevention of relapse in depression: Empirical evidence. Journal
of Consulting and Clinical Psychology, 70, 275�287. doi:10.1037//0022-006X.70.2.275
Valiente, C., Provencio, M., Espinosa, R., Chaves, C., & Fuentenebro, F. (2011). Predictors of
subjective well-being in patients with paranoid symptoms: Is insight necessarily advantageous?
Psychiatry Research, 189, 190�194. doi:10.1016/j.psychres.2011.02.018
van Dierendonck, D. (2004). The construct validity of Ryff ’s scales of psychological well-being and
its extension with spiritual well-being. Personality and Individual Differences, 36, 629�643.
doi:10.1016/S0191-8869(03)00122-3
Wells, A. (2000). Emotional disorders and metacognition: Innovative cognitive therapy. Chichester,
UK: Wiley.
Wells, A. (2007). The attention training technique: Theory, effects, and a metacognitive hypothesis
on auditory hallucinations. Cognitive and Behavioral Practice, 14(2), 134�138. doi:10.1016/
j.cbpra.2006.01.010
Wells, A. (2009). Metacognitive therapy for anxiety and depression. New York, NY: Guilford Press.
Wells, A., & Carter, K. (2001). Further tests of a cognitive model of generalized anxiety disorder:
Metacognitions and worry in GAD, panic disorder, social phobia, depression and nonpatients.
Behavior Therapy, 32, 85�102. doi:10.1016/S0005-7894(01)80045-9
Wells, A., & Cartwright-Hatton, S. (2004). A short form of the metacognitions questionnaire:
Properties of the MCQ-30. Behaviour Research and Therapy, 42, 385�396. doi:10.1016/S0005-
7967(03)00147-5
Wells, A., Fisher, P., Myers, S., Wheatley, J., Patel, T., & Brewin, C. R. (2009). Metacognitive
therapy in recurrent and persistent depression: A multiple-baseline study of a new treatment.
Cognitive Therapy and Research, 33, 291�300. doi:10.1007/s10608-007-9178-2
Wells, A., & Mathews, G. (1994). Attention and emotion: A clinical perspective. Hove, UK:
Lawrence Erlbaum Associates Ltd.
Wells, A., & Mathews, G. (1996). Modelling cognition in emotional disorder: The S-REF Model.
Behaviour Research and Therapy, 34, 881�888. doi:10.1016/S0005-7967(96)00050-2
World Health Organisation. (1992). The ICD-10 classification of mental and behavioural disorders:
Clinical descriptions and diagnostic guidelines. Geneva, Switzerland: Author.
Yanos, P. T., & Moos, R. H. (2007). Determinants of functioning and well-being among individuals
with schizophrenia: An integrated model. Clinical Psychology Review, 27, 58�77. doi:10.1016/
j.cpr.2005.12.008
Yilmaz, A. E., Gencoz, T., & Wells, A. (2008). Psychometric characteristics of the Penn State
Worry Questionnaire and Metacognitions Questionnaire-30 and metacognitive predictors of
worry and obsessive-compulsive symptoms in a Turkish sample. Clinical Psychology and
Psychotherapy, 15, 424�439. doi:10.1002/cpp.589
METACOGNITIVE BELIEFS AND WELL-BEING 17
Dow
nloa
ded
by [
Bib
liote
ca U
nive
rsid
ad C
ompl
uten
se d
e M
adri
d] a
t 01:
38 2
7 A
pril
2012