Metabolic and Nutritional Profile of Obese Adolescents With Nonalcoholic Fatty Liver Disease
7
Copyright © 2007 by Lippincott Williams & Wilkins.Unauthorized reproduction of this article is prohibited. Metabolic and Nutritional Profile of Obese Adolescents With Nonalcoholic Fatty Liver Disease Aline de Piano, Wagner L. Prado, Danielle A. Caranti, Ka ˜li O. Siqueira, Se ´rgio G. Stella, Mara Lofrano, Lian Tock, Dejaldo M.J. Cristofalo, Henrique Lederman, Se ´rgio Tufik, Marco Tu ´lio de Mello, and Ana R. Da ˆmaso Federal University of Sa ˜o Paulo, Escola Paulista de Medicina UNIFESP-EPM, Sa ˜o Paulo, Brazil ABSTRACT Background: The incidence of nonalcoholic fatty liver disease (NAFLD) is increasing due to its prevalence in obesity, diabetes, and insulin-resistance syndrome. The best treatment protocol for NAFLD has not been determined. However, there is evidence that exercise and nutritional intervention can improve and prevent it. The aim of the present study was to evaluate the dietary and metabolic profiles of obese adolescents with NAFLD who participated in a multidisciplinary program. Patients and Methods: We studied 43 adolescents ages 15 to 19 years (17.18 1.66 years) with a body mass index (BMI) 30, consisting of 30 patients without NAFLD (BMI ¼ 35.80 3.44 kg/m 2 ) and 13 with NAFLD (BMI ¼ 33.47 2.34 kg/m 2 ). The NAFLD diagnosis was determined by ultrasonography. Blood samples were collected to analyze glycemia, hepatic aminotransferase levels, and lipid profiles. Insulin resistance was measured by homeostasis model assessment insulin-resistance index (HOMA-IR). The analyses of baseline and postintervention food intake were made by a 3-day inquiry. Results: At baseline conditions, the patients with NAFLD showed significant differences in body mass, BMI, and vis- ceral and subcutaneous fat. Glucose and visceral and subcutane- ous fat presented a significant reduction after treatment in patients with NAFLD. Analyzing the food intake, at baseline we observed a positive correlation between the visceral obesity and lipid consumption only in patients with NAFLD. We also observed significant decrease in energy and cholesterol con- sumption in patients with NAFLD after the multidisciplinary therapy. Conclusions: The intervention promoted a decrease in the prevalence of NAFLD, a significant decrease in visceral obesity, and improved HOMA-IR, glycemia, and serum lipid levels that are risk factors for NAFLD. In summary, the multidisciplinary program is essential in the treatment and prevention of NAFLD. JPGN 44:446–452, 2007. Key Words: Food intake—Nutrition—Visceral adipose tissue. # 2007 by European Society for Pediatric Gastroenterology, Hepatology, and Nutrition and North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition INTRODUCTION Obesity is increasing worldwide, especially in adoles- cents, affecting more than 15% of Brazilian children and adolescents (1–3). Studies have shown the relationship between obesity and several diseases in adult life, such as arterial hypertension, type 2 diabetes mellitus, cancer, and cardiovascular mortality (4–8). Body fat excess, mainly in the form of central obesity, is closely correlated with dyslipidemia, high blood pressure, hyperinsuline- mia, and high fasting glucose levels (7,9,10). The visceral obesity increases plasma free fatty acid (FFA) levels because these adipocytes have higher lipo- lytic activity. Consequently, the visceral obesity increases the FFA levels in the portal circulation, and insulin resistance can also be responsible for this increase (7,11). A large amount of FFA increases triglycerides serum levels, and may exceed the very low–density lipoprotein (VLDL) synthetic capacity, promoting storage in the liver, known as fatty liver (12). Nonalcoholic fatty liver disease (NAFLD) is an emer- ging clinical problem among patients of all ages. NAFLD includes a broad spectrum of liver tissue alterations, ranging from pure steatosis to cirrhosis (13,14) to nonalcoholic steatohepatitis (NASH). NASH is defined by the presence of lobular necroinflammatory activity Received May 15, 2006; accepted January 17, 2007. Address correspondence and reprint requests to Nadja Ana R. Da ˆmaso, Rua Marselhesa no. 535-Vila Clementino, Sa ˜o Paulo/SP 04020-060, Brazil (e-mail: [email protected]). Financial support was received from AFIP, CNPq, CAPES, FAPESP 2006/00684-3, CENESP, FADA, FAPESP (CEPID/Sleep #9814303-3 S.T), UNIFESP, and the CEPE Multidisciplinary Obesity Intervention Program. Journal of Pediatric Gastroenterology and Nutrition 44:446–452 # 2007 by European Society for Pediatric Gastroenterology, Hepatology, and Nutrition and North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition 446
Transcript of Metabolic and Nutritional Profile of Obese Adolescents With Nonalcoholic Fatty Liver Disease

Copy
Metabolic and Nutritional Profile of Obese Adolescents WithNonalcoholic Fatty Liver Disease
Aline de Piano, Wagner L. Prado, Danielle A. Caranti, Kali O. Siqueira, Sergio G. Stella,Mara Lofrano, Lian Tock, Dejaldo M.J. Cristofalo, Henrique Lederman, Sergio Tufik,
Journal of Pediatric Gastroenterology and Nutrition44:446–452 # 2007 by European Society for Pediatric Gastroenterology, Hepatology, and Nutrition andNorth American Society for Pediatric Gastroenterology, Hepatology, and Nutrition
right © 2007 by
Marco Tulio de Mello, and Ana R. Damaso
3-day inquiry.
arterial hypertensionand cardiovascularmainly in the form of
Received May 15, 200Address corresponden
Damaso, Rua Marselhes04020-060, Brazil (e-mai
Financial support was r2006/00684-3, CENESP,S.T), UNIFESP, and the CProgram.
l University of Sao Paulo, Escola Paulista de Medicina UNIFESP-EPM, Sao Paulo, B
Federa razilABSTRACT
Background: The incidence of nonalcoholic fatty liver disease(NAFLD) is increasing due to its prevalence in obesity,diabetes, and insulin-resistance syndrome. The besttreatment protocol for NAFLD has not been determined.However, there is evidence that exercise and nutritionalintervention can improve and prevent it. The aim of thepresent study was to evaluate the dietary and metabolicprofiles of obese adolescents with NAFLD who participatedin a multidisciplinary program.Patients and Methods: We studied 43 adolescents ages 15 to19 years (17.18� 1.66 years) with a body mass index (BMI)�30, consisting of 30 patients without NAFLD (BMI¼35.80� 3.44 kg/m2) and 13 with NAFLD (BMI¼ 33.47�2.34 kg/m2). The NAFLD diagnosis was determined byultrasonography. Blood samples were collected to analyzeglycemia, hepatic aminotransferase levels, and lipid profiles.Insulin resistance was measured by homeostasis model
Lippincott Williams & Wilkins.Un
, type 2 diabetes mellitus, cancer,mortality (4–8). Body fat excess,central obesity, is closely correlated
6; accepted January 17, 2007.ce and reprint requests to Nadja Ana R.a no. 535-Vila Clementino, Sao Paulo/SPl: [email protected]).eceived from AFIP, CNPq, CAPES, FAPESPFADA, FAPESP (CEPID/Sleep #9814303-3EPE Multidisciplinary Obesity Intervention
446
Results: At baseline conditions, the patients with NAFLDshowed significant differences in body mass, BMI, and vis-ceral and subcutaneous fat. Glucose and visceral and subcutane-ous fat presented a significant reduction after treatment inpatients with NAFLD. Analyzing the food intake, at baselinewe observed a positive correlation between the visceral obesityand lipid consumption only in patients with NAFLD. We alsoobserved significant decrease in energy and cholesterol con-sumption in patients with NAFLD after the multidisciplinarytherapy.Conclusions: The intervention promoted a decrease in theprevalence of NAFLD, a significant decrease in visceralobesity, and improved HOMA-IR, glycemia, and serum lipidlevels that are risk factors for NAFLD. In summary, themultidisciplinary program is essential in the treatment andprevention of NAFLD. JPGN 44:446–452, 2007. Key Words:Food intake—Nutrition—Visceral adipose tissue. # 2007 by
assessment insulin-resistance index (HOMA-IR). The analyses
European Society for Pediatric Gastroen of baseline and postintervention food intake were made by aterology, Hepatology,and Nutrition and North American Society for Pediatric
Gastroenterology, Hepatology, and NutritionINTRODUCTION
Obesity is increasing worldwide, especially in adoles-cents, affecting more than 15% of Brazilian children andadolescents (1–3). Studies have shown the relationshipbetween obesity and several diseases in adult life, such as
with dyslipidemia, high blood pressure, hyperinsuline-mia, and high fasting glucose levels (7,9,10).
The visceral obesity increases plasma free fatty acid(FFA) levels because these adipocytes have higher lipo-lytic activity. Consequently, the visceral obesity increasesthe FFA levels in the portal circulation, and insulinresistance can also be responsible for this increase(7,11). A large amount of FFA increases triglyceridesserum levels, and may exceed the very low–densitylipoprotein (VLDL) synthetic capacity, promotingstorage in the liver, known as fatty liver (12).
Nonalcoholic fatty liver disease (NAFLD) is an emer-ging clinical problem among patients of all ages. NAFLDincludes a broad spectrum of liver tissue alterations,
authorized reproduction of this article is prohibited.
ranging from pure steatosis to cirrhosis (13,14) tononalcoholic steatohepatitis (NASH). NASH is definedby the presence of lobular necroinflammatory activity

Cop
OF
with or without the presence or perisinusoidal fibrosisthat can evolve to cirrhosis and can be detected on liverbiopsy (15). Differentiating between the 2 is importantbecause as many as 28% of patients with steatohepatitis,in contrast to those with simple steatosis, may progress tocirrhosis, but the only reliable method of differentiatingthem is by biopsy, which is costly and carries risks topatients (16). Therefore, ultrasonography (US), a non-invasive method to diagnose NAFLD in an ambulatorycare setting, is common (17–21).
Considering the grading for steatosis, a variation fromgrades I to III was observed (grade I, <33%; grade II,33%–66%, and grade III, >66% of hepatocytes areaffected) (20). NAFLD affects 10% to 39% of the worldpopulation, 50% of diabetic patients, 57% to 74% ofobese people, and as many as 90% of morbidly obesepeople (13,14). The prevalence in obese adolescents isbetween 22.5% and 52.8% (20,22–24).
The treatment of NAFLD is based on the associatedfactors of the disease and consists of gradual body massreduction, glycemia, and lipid control (ie, cholesteroland triglycerides). The main goal is not only to treat thefatty liver disease but also obesity, diabetes, and hyper-lipidemia (25–28). Although there is no accepted treat-ment that can reverse fatty liver disease, all patientsshould be given a low-fat diet and triglyceride-loweringagents. They should also be encouraged to exerciseregularly (6).
Because of the scarcity of studies related to theinfluence of diet on NAFLD, the purpose of this studywas to assess the short-term (12 weeks) effect of amultidisciplinary program on the dietary and metabolicprofiles of obese adolescents with NAFLD.
PATIENTS AND METHODS
Population
A total of 43 postpuberes obese adolescents (19 boys and24 girls) were recruited. Their ages ranged from 15 to 19 years,and their BMI was 34.22� 2.93 kg/m2. The inclusion criteriawere pubertal stage as assessed by means described by Tanneret al (29) and severe primary obesity (body mass index [BMI]>30), and agreement by the adolescents and their families toparticipate in a 12-week multidisciplinary weight loss program.The exclusion criteria were identified as genetic, metabolic, orendocrine disease; chronic alcohol consumption; previous druguse; and other causes of liver steatosis. The subjects volunteeredin response to statements on radio and television and in localnewspapers.
This study was carried out in accordance with the principlesof the Declaration of Helsinki and was formally approved by theethical committee of the Federal University of Sao Paulo
METABOLIC AND NUTRITIONAL PROFILE
yright © 2007 by Lippincott Williams & Wilkins.U
Paulista Medicine School (#0135/04). Informed consent wasobtained from all subjects and/or their parents. All subjectsunderwent electrocardiography.
Study Protocol
During the first visit, subjects were medically screened, hadtheir pubertal stage assessed, and had their anthropometricsprofile measured (height, weight, BMI, and body composition).During the second visit a blood sample was collected andanalyzed for various variables. At the third visit US wasperformed. The patients were divided into 2 groups: NAFLD(n¼ 13) and non-NAFLD (n¼ 30). For each subject, theprocedures were scheduled for the same time of day and atleast 15 hours after the last training session to remove anyinfluence of diurnal variations. Thereafter, obese adolescentsstarted the multidisciplinary weight loss program, as describedin the subsequent sections.
Anthropometric Measurements and BodyComposition
Subjects were weighed wearing light clothing and no shoeson a Filizola scale to the nearest 0.1 kg. Height was measured tothe nearest 0.5 cm by using a wall-mounted stadiometer(Sanny, model ES 2030). BMI was calculated as body weightdivided by height squared. Body composition was estimated byplethysmography in the BOD POD body composition system(version 1.69; Life Measurement Instruments, Concord, CA)(30).
Serum Analysis
Blood samples were collected in the outpatient clinic atapproximately 8:00 AM after an overnight fast. Insulinresistance was assessed by homeostasis model assessmentinsulin-resistance index (HOMA-IR). HOMA-IR was calcu-lated by the fasting blood glucose (FBG) and the immuno-reactive insulin (I): [FBG (mg/dL) � I (mU/L)]/405. Totalcholesterol, high-density lipoprotein (HDL), triacylglycerol,and hepatic alanine aminotransferase were analyzed using acommercial kit (CELM, Barueri, Brazil). The HOMA-IR, lipidserum level, and aminotransferase data were analyzed accord-ing to reference values described by Schwimmer et al (31).
Hepatic Steatosis and Visceral and SubcutaneousAdiposity Measurements
All abdominal US procedures and measurements of visceraland subcutaneous fat tissue and fatty liver before and afterintervention were performed in a double-blinded fashion by thesame physician specializing in image diagnostic using a3.5-MHz multifrequency transducer (broadband). This pro-cedure permits a reduction of risk margin for misclassification.The intraexamination coefficient of variation for US was 0.8%.
The US measurements of intraabdominal (ie, visceral) andsubcutaneous fat were taken. US-determined subcutaneous fatwas defined as the distance between the skin and external faceof the rectus abdominis muscle, and visceral fat was defined asthe distance between the internal face of the same muscle and
OBESE ADOLESCENTS WITH NAFLD 447
nauthorized reproduction of this article is prohibited.
the anterior wall of the aorta. Cutoff points to define visceralobesity by US parameters were based on previous methodo-logical descriptions by Ribeiro-Filho et al (32).
J Pediatr Gastroenterol Nutr, Vol. 44, No. 4, April 2007

Copy
34 subjects (24 without NAFLD and 10 with NAFLD)because 9 patients dropped out of the program. Indeed,the dietary data were available for only 23 subjects
30,23
69,77
18,6
81,4
0
20
40
60
80
100
AfterBaseline
With NAFLDWithout NAFLD
IANO
The US definition of fatty liver was based on previouslyreported diagnostic criteria and detected liver steatosis wasclassified as grade I (liver attenuation slightly less than spleen),grade II (more pronounced difference between liver and spleenand intrahepatic vessels not seen or slightly higher attenuationthan liver), or grade III (markedly reduced liver attenuation withsharp contrast between liver and intrahepatic vessels) (19,22).In the present study the group with NAFLD presented withsome liver steatosis diagnosed by US, and all of the patientspresented with normal alanine aminotransferase levels, whichwas diagnosed as simple steatosis.
Medical Program
To accomplish their health and clinical parameters, thepatients visited the endocrinologist once per month.
Dietary Program
Energy intake was set at the levels recommended by thedietary reference intake for subjects with low levels of physicalactivity of the same age and sex (33). However, no fixed level ofenergy intake was prescribed; they were encouraged only toreduce their food intake and follow a balanced diet. No drugsand antioxidants were recommended.
Once each week, adolescents attended dietetics classes thatincluded information on the food pyramid, recording energyunits intake, weight loss, dieting, diet versus ‘‘light,’’ fat andcholesterol, and nutrition facts.
At the beginning and end of the 12-week program, a 3-daydietary record was made by all of the adolescents with the helpof their parents because most obese people underreport theirfood consumption (34). The degree of underreporting may besubstantial; however, this is a valid method of evaluatingnutrition consumption (35). Portions were measured in termsof familiar volume and size and by reference to an atlas of localfood portions. The dietitian taught the parents and adolescentshow to record food consumption. These dietary data weretransferred to a computer by the same dietitian, and nutrientcomposition was analyzed by a software program developed atthe Federal University of Sao Paulo Paulista Medicine School(Nutwin software for Windows, version 1.5, 2002) basedon Western and local food tables. In addition, the parentswere encouraged by a dietitian to call if they needed extrainformation.
Exercise Program
During the 12-week multidisciplinary intervention period,adolescents followed a personalized aerobic training programincluding 60-minute sessions 3 times per week (180 minutes/week) under the supervision of a sports therapist. Each programwas developed according to the results of an initial oxygenuptake test for aerobic exercises (cycle ergometer andtreadmill). The intensity was set at a workload correspondingto ventilatory threshold 1 (50%–70% of oxygen uptake test). Atthe end of 6 weeks, aerobic tests were performed to assessphysical capacities and to adjust physical training intensity
448 DE P
right © 2007 by Lippincott Williams & Wilkins.Un
individually (data not shown). During the aerobic sessions,adolescents underwent heart rate monitoring. The exerciseprogram was based on the American College of Sports
J Pediatr Gastroenterol Nutr, Vol. 44, No. 4, April 2007
Medicine position statement of 2001 (36). Information aboutlifestyle changes related to activity was also provided andspontaneous physical activity (eg, walking, stair climbing)was encouraged but not measured.
Psychological Intervention
A diagnosis was established by validated questionnairesconsidering some psychological problems caused by obesitythat have been described in the literature, such as depression,disturbances of body image, anxiety, and decrease ofself-esteem. During the multidisciplinary intervention, theadolescents attended weekly psychological orientation groupsessions in which they discussed body image and alimentarydisorders such as bulimia and anorexia nervosa; binge eating;their signals, symptoms, and consequences for health; relationbetween feelings and food; familiar problems such asalcoholism; and other topics. An individual psychologicaltherapy was recommended when we found nutritional andbehavioral problems.
Statistical Analysis
All data were analyzed by means of Statistica version 6 forWindows with significance set at P< 0.05. All of the data areexpressed as mean� SD unless otherwise stated.
Comparisons between measures at baseline and after theweight loss program were made using paired t tests, betweengroups by independent t tests, and Pearson correlation.
RESULTS
The present study comprised 43 obese adolescentsdivided into 30 patients without NAFLD and 13 withNAFLD. The prevalence of NAFLD was 30.23% in thispopulation, but only 18.6% at the end of the multidisci-plinary program (Fig. 1).
Complete data after the intervention were available for
ET AL.
authorized reproduction of this article is prohibited.
intervention
FIG. 1. Prevalence of NAFLD (%) in obese adolescents at base-line and after multidisciplinary weight loss program.
Cop
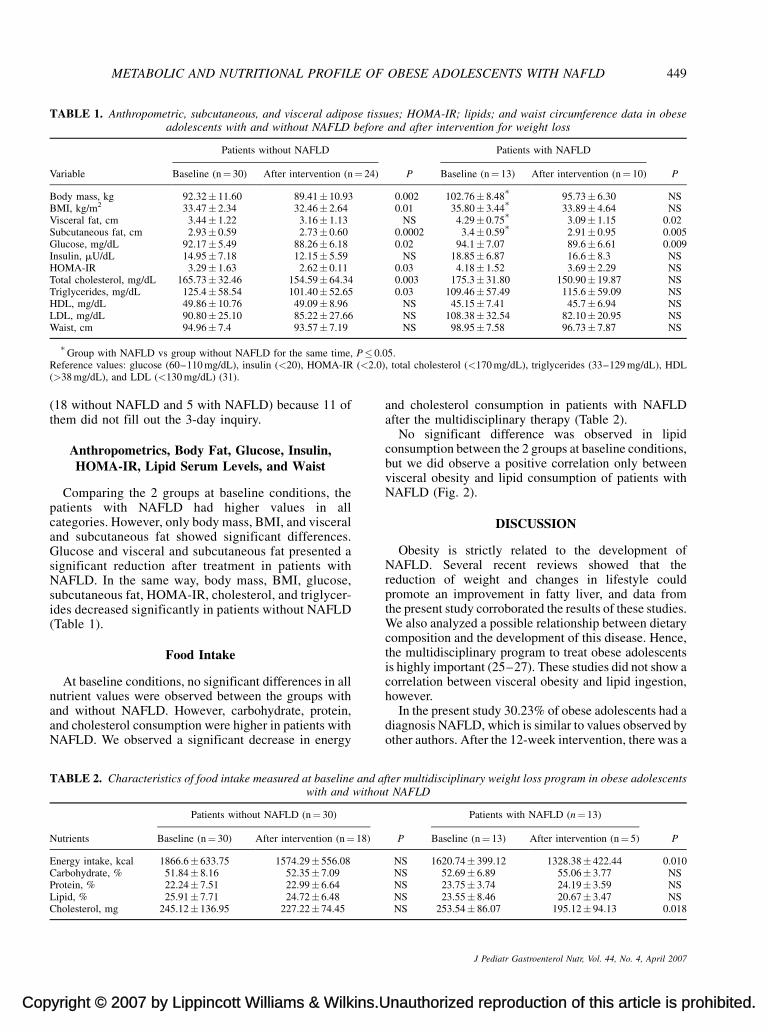
TABLE 1. Anthropometric, subcutaneous, and visceral adipose tissues; HOMA-IR; lipids; and waist circumference data in obeseadolescents with and without NAFLD before and after intervention for weight loss
Variable
Patients without NAFLD
P
Patients with NAFLD
PBaseline (n¼ 30) After intervention (n¼ 24) Baseline (n¼ 13) After intervention (n¼ 10)
Body mass, kg 92.32� 11.60 89.41� 10.93 0.002 102.76� 8.48�
95.73� 6.30 NSBMI, kg/m2 33.47� 2.34 32.46� 2.64 0.01 35.80� 3.44
�33.89� 4.64 NS
Visceral fat, cm 3.44� 1.22 3.16� 1.13 NS 4.29� 0.75�
3.09� 1.15 0.02Subcutaneous fat, cm 2.93� 0.59 2.73� 0.60 0.0002 3.4� 0.59
�2.91� 0.95 0.005
Glucose, mg/dL 92.17� 5.49 88.26� 6.18 0.02 94.1� 7.07 89.6� 6.61 0.009Insulin, mU/dL 14.95� 7.18 12.15� 5.59 NS 18.85� 6.87 16.6� 8.3 NSHOMA-IR 3.29� 1.63 2.62� 0.11 0.03 4.18� 1.52 3.69� 2.29 NSTotal cholesterol, mg/dL 165.73� 32.46 154.59� 64.34 0.003 175.3� 31.80 150.90� 19.87 NSTriglycerides, mg/dL 125.4� 58.54 101.40� 52.65 0.03 109.46� 57.49 115.6� 59.09 NSHDL, mg/dL 49.86� 10.76 49.09� 8.96 NS 45.15� 7.41 45.7� 6.94 NSLDL, mg/dL 90.80� 25.10 85.22� 27.66 NS 108.38� 32.54 82.10� 20.95 NSWaist, cm 94.96� 7.4 93.57� 7.19 NS 98.95� 7.58 96.73� 7.87 NS
P� 0.(<2.0)
METABOLIC AND NUTRITIONAL PROFILE OF OBESE ADOLESCENTS WITH NAFLD 449
(18 without NAFLD and 5 with NAFLD) because 11 ofthem did not fill out the 3-day inquiry.
Anthropometrics, Body Fat, Glucose, Insulin,HOMA-IR, Lipid Serum Levels, and Waist
Comparing the 2 groups at baseline conditions, thepatients with NAFLD had higher values in allcategories. However, only body mass, BMI, and visceraland subcutaneous fat showed significant differences.Glucose and visceral and subcutaneous fat presented asignificant reduction after treatment in patients withNAFLD. In the same way, body mass, BMI, glucose,subcutaneous fat, HOMA-IR, cholesterol, and triglycer-ides decreased significantly in patients without NAFLD(Table 1).
Food Intake
At baseline conditions, no significant differences in allnutrient values were observed between the groups with
�Group with NAFLD vs group without NAFLD for the same time,
Reference values: glucose (60–110 mg/dL), insulin (<20), HOMA-IR(>38 mg/dL), and LDL (<130 mg/dL) (31).
yright © 2007 by Lippincott Williams & Wilkins.U
and without NAFLD. However, carbohydrate, protein,and cholesterol consumption were higher in patients withNAFLD. We observed a significant decrease in energy
TABLE 2. Characteristics of food intake measured at baseline and awith and withou
Nutrients
Patients without NAFLD (n¼ 30)
Baseline (n¼ 30) After intervention (n¼ 18)
Energy intake, kcal 1866.6� 633.75 1574.29� 556.08Carbohydrate, % 51.84� 8.16 52.35� 7.09Protein, % 22.24� 7.51 22.99� 6.64Lipid, % 25.91� 7.71 24.72� 6.48Cholesterol, mg 245.12� 136.95 227.22� 74.45
and cholesterol consumption in patients with NAFLDafter the multidisciplinary therapy (Table 2).
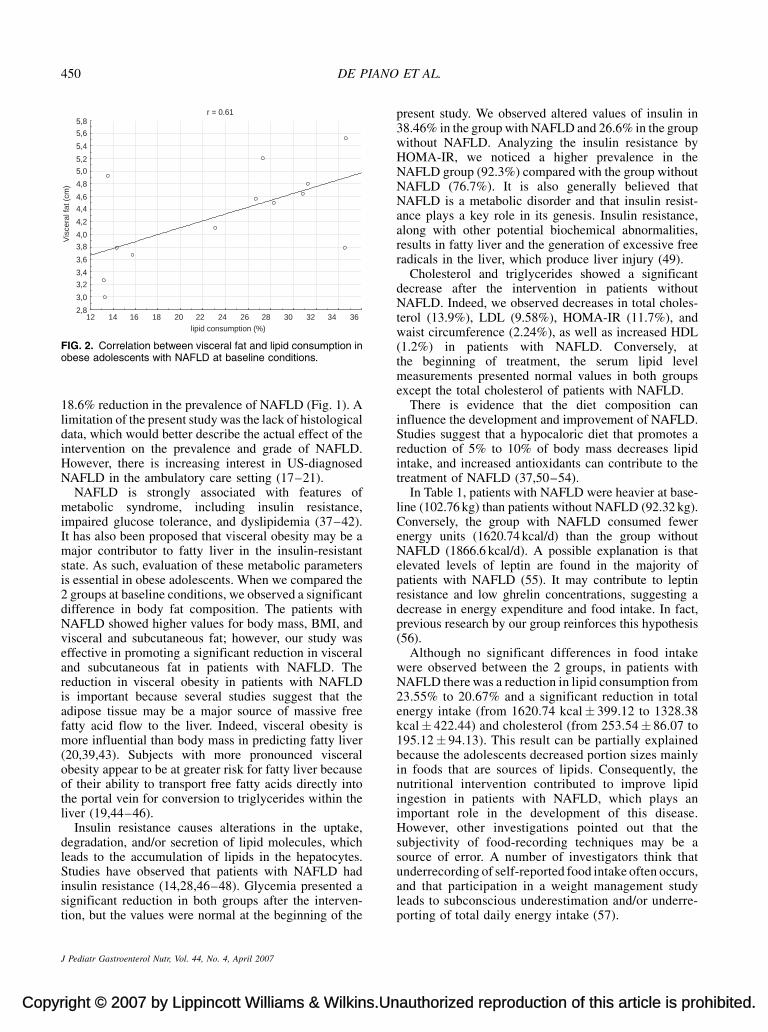
No significant difference was observed in lipidconsumption between the 2 groups at baseline conditions,but we did observe a positive correlation only betweenvisceral obesity and lipid consumption of patients withNAFLD (Fig. 2).
DISCUSSION
Obesity is strictly related to the development ofNAFLD. Several recent reviews showed that thereduction of weight and changes in lifestyle couldpromote an improvement in fatty liver, and data fromthe present study corroborated the results of these studies.We also analyzed a possible relationship between dietarycomposition and the development of this disease. Hence,the multidisciplinary program to treat obese adolescentsis highly important (25–27). These studies did not show acorrelation between visceral obesity and lipid ingestion,however.
05., total cholesterol (<170 mg/dL), triglycerides (33–129 mg/dL), HDL
nauthorized reproduction of this article is prohibited.
In the present study 30.23% of obese adolescents had adiagnosis NAFLD, which is similar to values observed byother authors. After the 12-week intervention, there was a
fter multidisciplinary weight loss program in obese adolescentst NAFLD
P
Patients with NAFLD (n¼ 13)
PBaseline (n¼ 13) After intervention (n¼ 5)
NS 1620.74� 399.12 1328.38� 422.44 0.010NS 52.69� 6.89 55.06� 3.77 NSNS 23.75� 3.74 24.19� 3.59 NSNS 23.55� 8.46 20.67� 3.47 NSNS 253.54� 86.07 195.12� 94.13 0.018
J Pediatr Gastroenterol Nutr, Vol. 44, No. 4, April 2007
Copy
r = 0.61
36343230282624222018161412lipid consumption (%)
2,8
3,0
3,2
3,4
3,6
3,8
4,0
4,2
4,4
4,6
4,8
5,0
5,2
5,4
5,6
5,8
Vis
cera
l fat
(cm
)450 DE PIANO
18.6% reduction in the prevalence of NAFLD (Fig. 1). Alimitation of the present study was the lack of histologicaldata, which would better describe the actual effect of theintervention on the prevalence and grade of NAFLD.However, there is increasing interest in US-diagnosedNAFLD in the ambulatory care setting (17–21).
NAFLD is strongly associated with features ofmetabolic syndrome, including insulin resistance,impaired glucose tolerance, and dyslipidemia (37–42).It has also been proposed that visceral obesity may be amajor contributor to fatty liver in the insulin-resistantstate. As such, evaluation of these metabolic parametersis essential in obese adolescents. When we compared the2 groups at baseline conditions, we observed a significantdifference in body fat composition. The patients withNAFLD showed higher values for body mass, BMI, andvisceral and subcutaneous fat; however, our study waseffective in promoting a significant reduction in visceraland subcutaneous fat in patients with NAFLD. Thereduction in visceral obesity in patients with NAFLDis important because several studies suggest that theadipose tissue may be a major source of massive freefatty acid flow to the liver. Indeed, visceral obesity ismore influential than body mass in predicting fatty liver(20,39,43). Subjects with more pronounced visceralobesity appear to be at greater risk for fatty liver becauseof their ability to transport free fatty acids directly intothe portal vein for conversion to triglycerides within theliver (19,44–46).
Insulin resistance causes alterations in the uptake,degradation, and/or secretion of lipid molecules, whichleads to the accumulation of lipids in the hepatocytes.Studies have observed that patients with NAFLD had
FIG. 2. Correlation between visceral fat and lipid consumption inobese adolescents with NAFLD at baseline conditions.
right © 2007 by Lippincott Williams & Wilkins.Un
insulin resistance (14,28,46–48). Glycemia presented asignificant reduction in both groups after the interven-tion, but the values were normal at the beginning of the
J Pediatr Gastroenterol Nutr, Vol. 44, No. 4, April 2007
present study. We observed altered values of insulin in38.46% in the group with NAFLD and 26.6% in the groupwithout NAFLD. Analyzing the insulin resistance byHOMA-IR, we noticed a higher prevalence in theNAFLD group (92.3%) compared with the group withoutNAFLD (76.7%). It is also generally believed thatNAFLD is a metabolic disorder and that insulin resist-ance plays a key role in its genesis. Insulin resistance,along with other potential biochemical abnormalities,results in fatty liver and the generation of excessive freeradicals in the liver, which produce liver injury (49).
Cholesterol and triglycerides showed a significantdecrease after the intervention in patients withoutNAFLD. Indeed, we observed decreases in total choles-terol (13.9%), LDL (9.58%), HOMA-IR (11.7%), andwaist circumference (2.24%), as well as increased HDL(1.2%) in patients with NAFLD. Conversely, atthe beginning of treatment, the serum lipid levelmeasurements presented normal values in both groupsexcept the total cholesterol of patients with NAFLD.
There is evidence that the diet composition caninfluence the development and improvement of NAFLD.Studies suggest that a hypocaloric diet that promotes areduction of 5% to 10% of body mass decreases lipidintake, and increased antioxidants can contribute to thetreatment of NAFLD (37,50–54).
In Table 1, patients with NAFLD were heavier at base-line (102.76 kg) than patients without NAFLD (92.32 kg).Conversely, the group with NAFLD consumed fewerenergy units (1620.74 kcal/d) than the group withoutNAFLD (1866.6 kcal/d). A possible explanation is thatelevated levels of leptin are found in the majority ofpatients with NAFLD (55). It may contribute to leptinresistance and low ghrelin concentrations, suggesting adecrease in energy expenditure and food intake. In fact,previous research by our group reinforces this hypothesis(56).
Although no significant differences in food intakewere observed between the 2 groups, in patients withNAFLD there was a reduction in lipid consumption from23.55% to 20.67% and a significant reduction in totalenergy intake (from 1620.74 kcal� 399.12 to 1328.38kcal� 422.44) and cholesterol (from 253.54� 86.07 to195.12� 94.13). This result can be partially explainedbecause the adolescents decreased portion sizes mainlyin foods that are sources of lipids. Consequently, thenutritional intervention contributed to improve lipidingestion in patients with NAFLD, which plays animportant role in the development of this disease.However, other investigations pointed out that thesubjectivity of food-recording techniques may be asource of error. A number of investigators think thatunderrecording of self-reported food intake often occurs,
ET AL.
authorized reproduction of this article is prohibited.
and that participation in a weight management studyleads to subconscious underestimation and/or underre-porting of total daily energy intake (57).

Cop
OF
One of the most important findings of our study is thatdespite the lipid consumption at baseline conditions,there was no significant difference between the patientswith and without NAFLD, and a positive correlation(0.61) between lipid consumption and visceral obesitywas observed only in patients with NAFLD (Fig. 2).Although the r value was not extremely strong, itrepresents an important positive correlation that hasnot been discussed in the literature to our knowledgeand requires further investigation with better patientsamples.
The key observation in this clinical study is that thepatients with NAFLD accumulated more visceral fatand presented more altered insulinemia and higherHOMA-IR values than patients without NAFLD(Table 1). Under these conditions there is a disproportio-nately greater flow of free fatty acids from visceraladipose stores, which are transported to the liver byportal blood and affect hepatic lipid and glucose metab-olism and insulin sensitivity, causing insulin resistance(9,10,25,58,59). These mechanisms contribute to thedevelopment of NAFLD. It provides a unifying mech-anism that links the coordinated regulation of glucose andlipid metabolism in the liver by hormonal regulation oflipolysis in visceral adipose stores (49). This way,reduction in the HOMA-IR, visceral obesity, and lipidingestion is essential to prevent and treat fatty liverdisease.
CONCLUSIONS
The multidisciplinary intervention promoted a decreasein the prevalence of NAFLD, a significant decrease in thevisceral obesity, and improved HOMA-IR, glycemia, andlipid serum levels that are risk factors for NAFLD. Thepatients with NAFLD presented higher anthropometrics,visceral and subcutaneous fat, HOMA-IR, total choles-terol, LDL and waist values at baseline conditions. Afterthe intervention all of the values, except HOMA-IR,were normalized in both groups. No significant differenceswere observed in the food intake between the 2 groups,however the lipid consumption of patients with NAFLDwas correlated with visceral obesity. In summary, themultidisciplinary program, including the nutritionalintervention, is essential in the treatment and preventionof NAFLD.
Acknowledgment: The authors thank the patients and theirparents for their participation in this study.
REFERENCES
1. Balaban G, Silva GAP. Prevalencia de sobrepeso em criancas
METABOLIC AND NUTRITIONAL PROFILE
yright © 2007 by Lippincott Williams & Wilkins.U
e adolescentes de uma escola da rede privada de Recife. J Pediatr2001;77:96–100.
2. James PT, Leach R, Kalamara E, et al. The worldwide obesityepidemic. Obesity Res 2001;9:228S–33S.
3. World Health Organization, Obesity: Preventing and Managing theGlobal Epidemic. WHO Obesity Technical Report Series 894;Geneva; World Health Organization 2000.
4. Csabi G, Torok K, Jeges S, et al. Presence of metabolic cardiovascularsyndrome in obese children. Eur J Pediatr 2000;159:91–4.
5. Ezzati M, Lopez AD, Rodgers A, et al. Select major risk factors andglobal and regional burden of disease. Lancet 2002;360:1347–60.
6. Freedman DS. Clustering of coronary heart disease risk factorsamong obese children. J Pediatr Endocrinol Metab 2002;15:1099–108.
7. Oliveira CL, Mello MT, Cintra IP, et al. Obesidade e sındromemetabolica na infancia e adolescencia. Rev Nutr 2004;17:237–45.
8. Zimmermann MB, Gubeli C, Puntener C, et al. Overweight andobesity in 6–12 year old children in Switzerland. Swiss Med Weekly2004;134:523–8.
9. Marchesini G, Bugianesi E, Forlani G, et al. Nonalcoholic fattyliver, steatohepatitis, and metabolic syndrome. Hepatology2003;37:917–23.
10. Poordad FF. The role of leptin in NAFLD: contender or pretender?J Clin Gastroenterol 2004;38:841–3.
11. Shigematsu R, Okura T, Kumagai S, et al. Cutoff and target valuesfor intra-abdominal fat area for prevention of metabolic disorders inpre-and post-menopausal obese women before and after weightreduction. Circ J 2006;70:110–4.
12. Xiong MA, Zhiping LI. Pathogenesis of nonalcoholic steatohepatitis(NASH). Chin J Dig Dis 2006;7:7–11.
13. Alba LM, Lindor K. Review article: non-alcoholic fatty liverdisease. Aliment Pharmacol Ther 2003;17:977–86.
14. Angulo P. Nonalcoholic fatty liver disease. N Engl J Med 2002;346:1221–31.
15. Palekar NA, Naus R, Larson SP, et al. Clinical model for distin-guishing nonalcoholic steatohepatitis from simple steatosis inpatients with nonalcoholic fatty liver disease. Liver Int 2006;26:151–6.
16. Harrison SA, Neushwnder-Tetri BA. Nonalcoholic fatty liver disease.Gastroenterology 2002;122:1649–57.
17. Riley TR III, Kahn A. Risk factors and ultrasound can predictchronic hepatitis caused by nonalcoholic fatty liver disease. Dig DisSci 2006;51:41–4.
18. Lee S, Kim YJ, Jeon TY, et al. Obesity is the only independentfactor associated with ultrasound-diagnosed non-alcoholicfatty liver disease: a cross-sectional case-control study. Scand JGastroenterol 2006;41:566–7.
19. Sabir N, Sermez Y, Kazil S, et al. Correlation of abdominal fataccumulation and liver steatosis: importance of ultrasonographicand anthropometric measurements. Eur J Ultrasound 2001;14:121–8.
20. Nakao K, Nakata K, Otsubo N, et al. Association betweennonalcoholic fatty liver markers of obesity, and serum leptin levelin young adults. Am J Gastroenterol 2002;97:1796–801.
21. Tock L, Prado WL, Caranti DA, et al. Non-alcoholic fatty liver diseasedecrease in obese adolescents after multidisciplinary therapy. Eur JGastroenterol Hepatol 2006;18:1241–5.
22. Saadeh S, Younossi ZM, Remer EM, et al. The utility of radiologicalimaging in nonalcoholic fatty liver disease. Gastroenterology2002;123:745–50.
23. Machado M, Cortez-Pinto H. Non-alcoholic fatty liver disease andinsulin resistance. Eur J Gatroenterol Hepatol 2005;17:823–6.
24. Ten S, Maclaren N. Insulin resistance syndrome in children. J ClinEndocrinol Metabol 2004;89:2596–639.
25. Festi DA, Sacco T, Bondi M, et al. Hepatic steatosis in obesepatients: clinical aspects and prognostic significance. Obesity Rev2004;5:27–42.
26. Angulo P, Lindor K. Treatment of non-alcoholic steatohepatitis.
OBESE ADOLESCENTS WITH NAFLD 451
nauthorized reproduction of this article is prohibited.
Best Pract Res Clin Gastroenterol 2002;16:797–810.27. Bugianesi E, Marzocchi R, Villanova N, et al. Non-alcoholic
fatty liver disease/non-alcoholic steatohepatitis (NAFLD/NASH):treatment. Best Pract Res Clin Gastroenterol 2004;18:1105–16.
J Pediatr Gastroenterol Nutr, Vol. 44, No. 4, April 2007

Copy
IANO
28. Patrick L. Nonalcoholic fatty liver disease: relationship to insulinsensitivity and oxidative stress. Treatment approaches using vita-min E, magnesium and betaine. Altern Med Rev 2002;7:276–91.
29. Tanner JM, Whitehouse RH, Marubini E, et al. Clinical longitudinalstandards for height, weight velocity an stages of puberty. Arch DisChild 1976;51:170–9.
30. Fields DA, Goran MI. Body composition techniques and the four-compartment model in children. J Appl Physiol 2000;89:613–20.
31. Schwimmer JB, Deutsch R, Rauch JB, et al. Obesity, insulinresistance, and other clinicopathological correlates of pediatricnonalcoholic fatty liver disease. J Pediatr 2003;143:500–5.
32. Ribeiro-Filho FF, Faria NA, Ajzen S, et al. Methods of estimation ofvisceral fat: advantages of ultrasonography. Obesity Res2003;11:1488–94.
33. Dietary Reference Intake: Applications in Dietary AssessmentWashington, DC: National Academic Press; 2001.
34. Hill RJ, Davies PS. The validity of self-reported energy intake asdetermined using the doubly labeled water technique. Br J Nutr2001;85:415–30.
35. Stanton RA. Nutrition problems in an obesogenic environment.Med J Aust 2006;184:76–9.
36. ACSM Position Stand on the Appropriate Intervention Strategiesfor Weight Loss and Prevention of Weight Regain for Adults. MedSci Sports Exercise 2001;33:2145–56.
37. Suzuki A, Lindor K, Save JS, et al. Effect of changes on bodyweight and lifestyle in nonalcoholic fatty liver disease. J Hepatol2005;43:1060–6.
38. Clark JM. The epidemiology of nonalcoholic fatty liver disease inadults. J Clin Gastroenterol 2006;40 (Suppl 1):S5–10.
39. Kaushal M, Batra Y, Gupta DS, et al. Vitamin E-based therapy iseffective in ameliorating transaminasemia in nonalcoholic fattyliver disease. Indian J Gastroenterol 2005;24:251–5.
40. Kluwe J, Lohse AW. Therapeutic options for nonalcoholic fattyliver disease and steatohepatitis. Internist (Berl) 2005;46:1324–30.
41. Loguercio C, De Girolamo V, de Sio I, et al. Non-alcoholic fattyliver disease in an area of southern Italy: main clinical, histological,and pathophysiological aspects. J Hepatol 2001;35:568–74.
42. Papadopoulou-Alataki E, Papadopoulou-Legbelou K, Doukas L,et al. Clinical and biochemical manifestations of syndrome X inobese children. Eur J Pediatr 2004;163:573–9.
43. Fishbein MH, Mogren C, Gleason T, et al. Relationship of hepaticsteatosis to adipose tissue distribution in pediatric nonalcoholic
452 DE P
right © 2007 by Lippincott Williams & Wilkins.Un
44. Stranges S, Dorn JM, Muti P, et al. Body fat distribution, relativeweight, and liver enzyme levels: a population-based study. Hepa-tology 2004;39:754–63.
J Pediatr Gastroenterol Nutr, Vol. 44, No. 4, April 2007
45. Wajchenberg LB. Subcutaneous and visceral adipose tissue: theirrelation to the metabolic syndrome. Endocr Rev 2000;21:697–738.
46. Bugianesi E, Gastaldelli A, Vanni E, et al. Insulin resistance innon-diabetic patients with non-alcoholic fatty liver disease:sites and mechanisms. Diabetologia 2005;48:634–42.
47. Mohsin R, Roberts EA. Nonalcoholic steatohepatitis in children.J Pediatr Gastroenterol Nutr 2000;30:48–53.
48. Louthan MV, Theriot JA, Zimmerman E, et al. Decreased prevalenceof nonalcoholic fatty liver disease in black obese children. J PediatrGastroenterol Nutr 2005;41:426–9.
49. Haque M, Sanyal A. The metabolic abnormalities associated withnon-alcoholic fatty liver disease. Best Pract Res Clin Gastroenterol2002;16:709–31.
50. Chang CY, Argo CK, Al-Osaimi AMS, et al. Therapy of NAFLD:antioxidants and cytoprotective agents. J Clin Gastroenterol 2006;40:S51–60.
51. Harrison AS, Torgenson S, Hayashi P, et al. Vitamin E andvitamin C treatment improves fibrosis in patients with nonalcoholicsteatohepatitis. Am J Gastroenterol 2003;98:2348–50.
52. Hasegawa T, Yoneda M, Nakamura K, et al. Plasma transforminggrowth factor-b 1 level and efficacy of a-tocopherol in patients withnonalcoholic steatohepatitis: a pilot study. Aliment Pharmacol Ther2001;15:1667–72.
53. Pessayre D, Mansouri A, Fromenty B. Nonalcoholic steatosis andsteatohepatitis. V: mitochondrial dysfunction in steatohepatitis. AmJ Physiol 2002;282:G193–9.
54. Tsukamoto H. Fat paradox in liver disease. Keio J Med 2005;54:190–2.
55. Bruun JM, Lihn AS, Verdich C, et al. Regulation of adiponectin byadipose tissue-derived cytokines: in vivo and in vitro investigationsin humans. Am J Physiol Endorinol Metab 2003;285:E527–33.
56. Damaso AR, Tock L, Tufik S, et al. Tratamento multidisciplinarreduz o tecido adiposo visceral, leptina, grelina e a prevalencia deesteatose hepatica nao alcoolica (NAFLD) em adolescentes obesos.Rev Bras Med Esporte 2006;12:263–7.
57. Wing RR, Venditi JM, Kakicic BA, et al. Lifestyle intervention inoverweight individuals with a family history of diabetes. DiabetesCare 1998;21:350–9.
58. Angelico F, Del Ben M, Conti R, et al. Insulin resistance, themetabolic syndrome, and nonalcoholic fatty liver disease. J Clin
ET AL.
Endocrinol Metabol 2005;90:1578–82.
fatty liver disease. J Pediatr Gastroenterol Nutr 2006;42:83–8.authorized reproduction of this article is prohibited.
59. Lewis GF, Carpentier A, Adeli K, et al. Disordered fat storage andmobilization in the pathogenesis of insulin resistance and type 2diabetes. Endocr Rev 2002;23:201–29.