Diffusion-weighted lesions after carotid artery stenting are associated with cognitive impairment
Upload
independentCategory
view
0download
0
Mesoaortic compression of the left renal vein (the so-called nutcracker syndrome): Repair by a new stenting procedure Rober t W. Barnes, MD, H o m e r L. Fleisher I I I , MD, John F. Redman, MD, John Wayne Smith, MD, David L. Harshfield, ME), and Ernest J. Ferris, MD, Little Rock, Ark.
Compression of the left renal vein (LRV) between the superior mesenteric artery and the aorta has been termed the nutcracker syndrome. Although often asymptomatic, this syn- drome may result in varicocele, ovarian vein syndrome, and rarely LRV hypertension, pelviureteral varices, hematuria, and flank pain. Previous surgical approaches have in- cluded nephrectomy, variceal ligation, nephropexy, or renocaval reimplantation. We re- port a new LKV stenting procedure that provided relief for a young woman incapacitated by daily left flank pain and microscopic hematuria. Phlebography of the LKV revealed mesoaortic compression associated with a pressure gradient of 12 mm Hg and preferential outflow down large pelviureteral varices. At operation compression of the LRV was corrected with an external stent of reinforced polytetrafluoroethylene. The patient was asymptomatic and free of hematuria for 9 months after operation and follow-up phle- bography documented normal renocaval flow, elimination of the pressure gradient, and reduction of the pelviureteral varices. This represents the first description in the vascular surgical literature of this venous compression syndrome, which has been recognized in previous urologic and radiologic reports reviewed herein. Vascular surgeons should be cognizant of the nutcracker syndrome, and we recommend this new stenting procedure as a more simple and physiologic therapy than previous approaches to this problem. (J VASC SuRG 1988;8:415-21.)
Compression of the left renal vein (LRV) be- tween the superior mesenteric artery (SMA) and the aorta by a mechanism similar to that of a nutcracker has been recognized by anatomists for 50 years. 1'2 Mesoaortic compression of the LRV has been con- sidered the pathogenesis of the left-sided predomi- nance of varicoceles 3'~ and the ovarian vein syn- drome. 5,6 However, the nutcracker syndrome has been invoked only recently to explain the less common condition of left flank pain and hema- turia associated with RLV hypertension and pel- viureteral varices. 7 Such clinical problems of es-
From the Departments of Surgery (Drs. Barnes and Fleisher), Urology (Dr. Redman), and Radiology (Drs. Harshfield and Ferris), University of Arkansas for Medical Sciences, and the practice of nephrology (Dr. Smith).
Presented at the Twelfth Annual Meeting of the Southern Asso- ciation for Vascular Surgery, St. Thomas, Virgin Islands, Jan. 27-30, 1988.
Reprint requests: Robert W. Barnes, MD, Professor and Chair- man, Department of Surgery, Slot 520, University of Arkansas for Medical Sciences, 4301 West Markaham St., Little Rock, AR 72205.
sential hematuria 8-1° were previously treated by nephrectomy 11'12 or variceal ligation 13 and more re- cently by venolysis, 14 nephropexy, ~5 or renocaval reimplantation.16
Although the nutcracker syndrome represents a form of vascular compression, no previous reports have appeared in the vascular surgical literature. We recently treated a young woman incapacitated by left flank pain and hematuria with a new external stenting procedure, which relieved the nutcracker syndrome. This case is reported with a review of the literature to acquaint vascular surgeons with this syndrome and to describe a more simple and physiologic method to treat the venous compression.
CASE REPORT A 17-year-old, thin, white, nulligravida female student
first consulted her referring nephrologist (J. W. S.) for recurrent left flank and lower abdominal pain. Urinalysis revealed only microscopic hematuria. An excretory uro- gram revealed enlargement of the left renal pelvis and a convolution at the pelviureteral junction, which was doc-
415

416 Barnes et al.
Journal of VASCULAR
SURGERY
Fig. 1. Duplex scan (transverse right anterior oblique view) of left renal vein between SMA (small arrow) and aorta (large arrow).
umented by retrograde urography. Renal ultrasound re- vealed edema of the left renal pelvis. The arterial phase of a renal angiogram was normal but the venous phase sug- gested varices in the renal hilum with a tortuous collateral vessel at the site of convolution of the ureteropelvic junc- tion. Renal phlebography showed compression of the left LRV at the level of the aorta and a prominent ovarian vein. A C T scan suggested compression of the left LRV between the aorta and a large, questionably aneurysmal SMA. The patient continued to have daily episodes of left flank and abdominal pain often aggravated by meals and occasionally relieved by leaning forward. She required frequent visits to the emergency department where microscopic hematuria was documented. She became dependent on narcotics for pain relief. Because of persistence of the pain and inter- ference with her school work, she was referred to our center on March 23, 1987, for further evaluation and management.
Real-time ultrasonic imaging and Doppler flow anal- ysis (duplex scanning) revealed a patent LRV, which be- came narrow between the aorta and the SMA, which was not aneurysmal (Fig. 1). Gonadal venous varices were seen. Renal phlebography suggested a cavernous hemangioma of the renal hilum and lower pole of the left lddney and flow of contrast material predominantly down variceal col- lateral vessels of the left ureteric and ovarian veins (Fig. 2). An attempt at hypertonic glucose sclerotherapy of the renal venous malformations was unsuccessful because of inability to occlude the varices with a balloon catheter. Because the patient was considered initially to have a ve- nous malformation, heminephrectomy or renal autotrans- plantation was recommended but she refused surgical in- tervention. She returned one month later with recurrent episodes of flank pain and hematuria. A repeat renal phle- bogram was performed to document the presence of me- soaortic compression of the LRV as a possible explanation
Fig. 2. Retrograde left renal phlebogram shows outflow via dilated left renal pelviureteral and ovarian venous var- ices. No contrast material enters the inferior vena cava.
for the pelviureteral varices. A constant pressure gradient of 12 mm Hg between the LRV and the inferior vena cava was present at the level between the aorta and the SMA. This gradient persisted with the patient in the supine, prone, sitting, or standing positions but decreased to 2 mm Hg with the patient leaning forward.
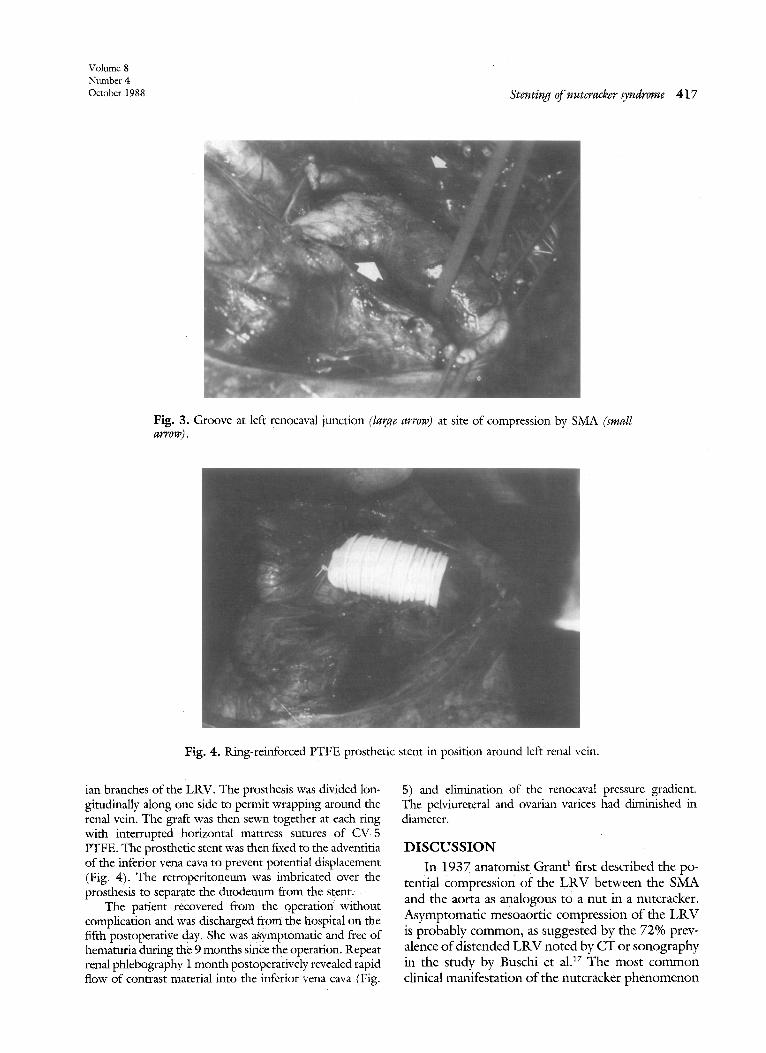
On May 1, 1987, the patient had exploratory surgery through a median celiotomy. The retroperitoneum was divided over the proximal infrarenal aorta, the fourth por- tion of the duodenum was mobilized to the right, and the LRV was identified. The LRV was found to be compressed between the aorta and the 8MA, which coursed more pos- teriorly than normal in the root of the small bowel mes- entery. A groove in the anterior surface of the renal vein was evident where it passed posterior to the SMA (Fig. 3). The renal vein was soft and compliant without evidence of thrombus. To relieve the compression, a 14 mm ring-reinforced polytetrafluoroethylene (PTFE) prosthesis (Gore-Tex) was selected to create an external stent around the LRV. Tile graft was cut to an appropriate length to fit between the inferior vena cava and the adrenal and ovar-
Volume 8 Number 4 October 1988 Stenting of nutcracker syndrome 417
Fig. 3. Groove at left renocaval junction (large arrow) at site of compression by SMA (small arrow).
Fig. 4. Ring-reinforced PTFE prosthetic stent in position around left renal vein.
ian branches of the LRV. The prosthesis was divided lon- gitudinally along one side to permit wrapping around the renal vein. The graft was then sewn together at each ring with interrupted horizontal mattress sutures of CV-5 PTFE. The prosthetic stent was then fixed to the adventitia of the inferior vena cava to prevent potential displacement (Fig. 4). The retroperitoneum was imbricated over the prosthesis to separate the duodenum from the stent. ~
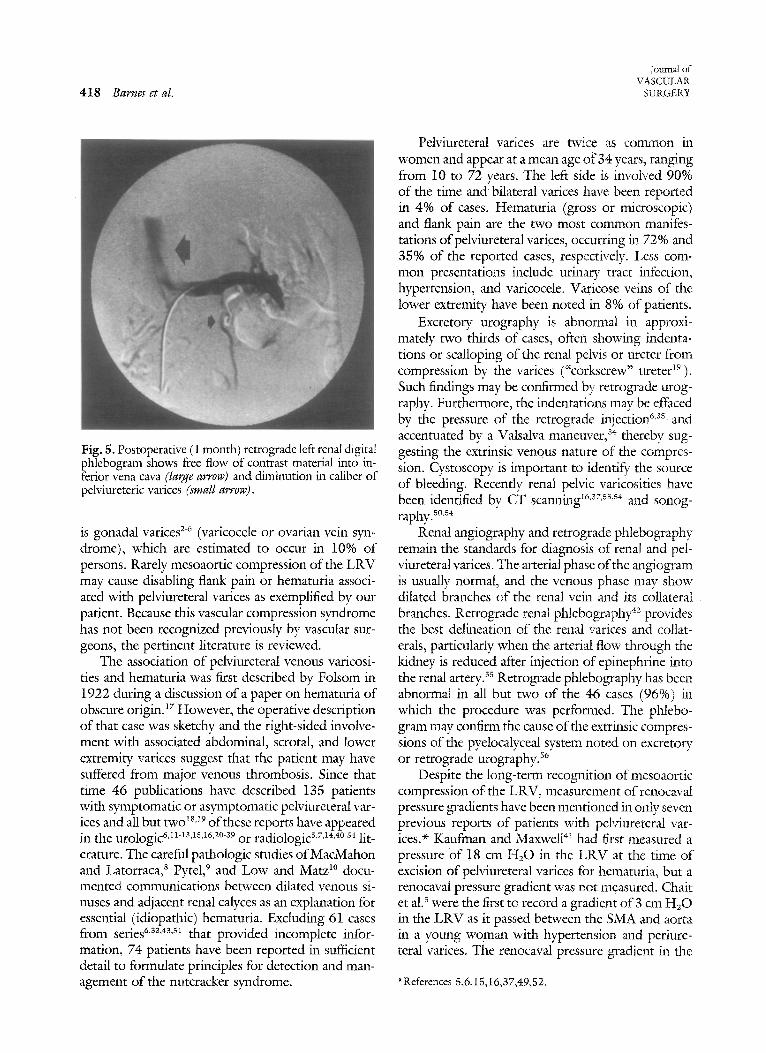
The patient recovered from the operation without complication and was discharged from the hospital on the fifth postoperative day. She was ~ymptomatic and frec of hematuria during the 9 months since the operation. Repeat renal phlebography 1 month postoperatively revealed rapid flow of contrast material into the inferior vena cava (Fig.
5) and elimination of the renocaval pressure gradient. The pelviureteral and ovarian varices had diminished in diameter.
DISCUSSION
In 1937 anatomist Grant 1 first described the po- tential compression of the L R V between the SMA and the aorta as analogous to a nut in a nutcracker. Asymptomatic mesoaortic compression o f the L R V is probably common, as suggested by the 72% prev- alence o f distended L R V noted by CT or sonography in the study by Buschi et alJ 7 The most common clinical manifestation of the nutcracker phenomenon
4 1 8 Barnes et al.
Journal of VASCULAR
SURGERY
Fig. 5. Postoperative (1 month) retrograde left renal digital phlebogram shows flee flow of contrast material into in- ferior vena cava (large arrow) and diminution in caliber of pelviureteric varices (small arrow).
is gonadal varices 2-~ (varicocele or ovarian vein syn- drome), which are estimated to occur in 10% of persons. Rarely mesoaortic compression of the LRV may cause disabling flank pain or hematuria associ- ated with pelviureteral varices as exemplified by our patient. Because this vascular compression syndrome has not been recognized previously by vascular sur- geons, the pertinent literature is reviewed.
The association of pelviureteral venous varicosi- ties and hematuria was first described by Folsom in 1922 during a discussion of a paper on hematuria of obscure origin. 17 However, the operative description of that case was sketchy and the right-sided involve- ment with associated abdominal, scrotal, and lower extremity varices suggest that the patient may have suffered from major venous thrombosis. Since that time 46 publications have described 135 patients with symptomatic or asymptomatic pelviureteral var- ices and all but two 18,~9 of these reports have appeared in the u ro log i c 6,n'ls'ls'16,2°'s9 o r r ad io log ic s,7'14,a°-s4 lit- erature. The careful pathologic studies of MacMahon and Latorraca, s Pytel, 9 and Low and Matz ~° docu- mented communications between dilated venous si- nuses and adjacent renal calyces as an explanation for essential (idiopathic) hematuria. Excluding 61 cases from series 6'3s'4s'sz that provided incomplete infor- mation, 74 patients have been reported in sufficient detail to formulate principles for detection and man- agement of the nutcracker syndrome.
Pelviureteral varices are twice as common in women and appear at a mean age of 34 years, ranging from 10 to 72 years. The left side is involved 90% of the time and bilateral varices have been reported in 4% of cases. Hematuria (gross or microscopic) and flank pain are the two most common manifes- tations of peMureteral varices, occurring in 72% and 35% of the reported cases, respectively. Less com- mon presentations include urinary tract infection, hypertension, and varicocele. Varicose veins of the lower extremity have been noted in 8% of patients.
Excretory urography is abnormal in approxi- mately two thirds of cases, often showing indenta- tions or scalloping of the renal peMs or ureter from compression by the varices ("corkscrew; ureter 19 ). Such findings may be confirmed by retrograde urog- raphy. Furthermore, the indentations may be effaced by the pressure of the retrograde injection 6,ss and accentuated by a Valsalva maneuver, s4 thereby sug- gesting the extrinsic venous nature of the compres- sion. Cystoscopy is important to identify the source of bleeding. Recently renal pelvic varicosities have been identified by CT scanning I6"37,ss's4 and sonog- raphy, s°,s4
Renal angiography and retrograde phlebography remain the standards for diagnosis of renal and pel- viureteral varices. The arterial phase of the angiogram is usually normal, and the venous phase may show dilated branches of the renal vein and its collateral branches. Retrograde renal phlebography 42 provides the best delineation of the renal varices and collat- erals, particularly when the arterial flow through the kidney is reduced after injection of epinephrine into the renal artery, ss Retrograde phlebography has been abnormal in all but two of the 46 cases (96%) in which the procedure was performed. The phtebo- gram may confirm the cause of the extrinsic compres- sions of the pyelocalyceal system noted on excretory or retrograde urography, s6
Despite the long-term recognition of mesoaortic compression of the LRV, measurement of renocaval pressure gradients have been mentioned in only seven previous reports of patients with pelviureteral vat- ices. ~ Kaufman and Maxwell 41 had first measured a pressure of 18 cm H20 in the LRV at the time of excision of pelviureteral varices for hematuria, but a renocaval pressure gradient was not measured. Chair et al. s were the first to record a gradient of 3 cm H20 in the LRV as it passed between the SMA and aorta in a young woman with hypertension and periure- teral varices. The renocaval pressure gradient in the
*References 5,6,15,16,37,49,52.

Volume 8 Number 4 October 1988 Stenting of nutcracker syndrome 419
10 reported patients with varices has ranged from 2 to 10 mm Hg with an average of 6 mm Hg. Beinart et al. s7 measured pullback pressures from the LRV to the inferior vena cava in 50 normal patients and found a gradient more than 1 mm Hg in only one patient. Zerhouni et al.s8 noted renocaval pressure gradients of 17, 16, and 4 mm Hg in three patients with varicoceles, whereas the gradient in five normal controls ranged from zero to 3 mm Hg.
Thirty-nine of the 74 reported patients with doc- umented pelviureteral varices did not receive specific therapy. Follow-up data were reported in only four patients, three of whom continued to manifest he- maturia. 37"38'42 Five patients had varices documented at operation without mention of specific therapy. Sporer and Pollock 11 first reported nephrectomy for bleeding renal varices in a patient who died of pul- monary hemorrhage. Maslow and Aron 12 carried out the first successful nephrectomy for this problem, which was performed in two other patients 2~'22 before recognition of the relationship between pelviure- teral varices and essential hematuria. 8'9 Berman and Copeland 13 were the first to ligate ureteric varices discovered incidentally in follow-up of a patient with bladder tumor and Woodard 23 excised pyeloureteric varices in a 20-year-old man with hematuria. Liga- tion or excision ofvarices has been performed in 21 patients and of 16 who were observed, only one had recurrent hematuria. 4~ However, Coolsaet s9 sug- gested that ligation of collateral vessels might increase the renocaval pressure gradient in patients with nut- cracker syndrome and recommended bypass of the venous compression as the procedure of choice.
Since the association of the nutcracker syndrome with pyeloureteric varices by Chair et al. 5 in 1971 and de Schepper 7 in 1972, only three reports 14-16 have described operative procedures designed to relieve the venous obstruction. Pastershank 14 reported on a 30-year-old man whose hematuria was resolved with division of a fibrous tunnel between the SMA and aorta, which had indented the LRV. Wendel et al? s excised renal varicosities in a 45-year-old woman with hematuria and relieved compression of the LRV stretched over the aorta by medial fixation of the left kidney (nephropexy). Pressure gradients and follow- up angiography were not performed. The procedure eliminated a renocaval pressure gradient of 7 cm H20. Stewart and Reiman ~6 performed direct reno- caval reimplantation tO relieve three patients of pain associated with documented renal venous hyper- tension with pressure gradients between 5.5 and 6.3 cm HzO. Two patients had hematuria and pel- viureteral varices, which were also excised. Postop-
erative pressure gradients and angiography were not performed.
Vascular and general surgeons treat various vas- cular compression syndromes, including the thoracic outlet, celiac axis, and left iliac vein syndromes. How- ever, the nutcracker syndrome has not been previ- ously recognized by our discipline. The analogous syndrome-- albeit controversial-- of SMA compres- sion of the duodenum has been recognized 6° but has been associated with LRV compression only in the report by Nishimura et al. 46 We believe that our case provides several instructive principles in dealing with the nutcracker syndrome. We initially did not con- sider this diagnosis even though as a young woman she initially had the classic symptoms of recurrent left flank pain and hematuria. Her diagnostic evaluation showed characteristic deformities of the left pelvi- ureteral system on urography and venous abnor- malities on renal angiography. However, the varices noted on retrograde phlebography were initially thought to be associated with a renal venous mal- formation. Fortunately, an attempt to sclerose the varices was unsuccessful because of inability to oc- clude them with a balloon. Once the diagnosis of mesoaortic compression of the LRV was considered, physiologic documentation was carried out with re- peat phlebography and pullout pressure measure- ments. The 12 mm Hg pressure gradient was the highest yet reported for someone with this syndrome. Of interest is the fact that the gradient was nearly eliminated with the patient leaning forward--a po- sition she had previously assumed on occasion for relief of pain. Presumably the resulting anterior movement of the small bowel and SMA lessened the compression on the LRV. The fact that her symp- toms occasionally worsened after meals might be ex- plained by increased pressure within the abdomen or in the third portion of the duodenum, which in turn further compressed the LRV. Braedel et al? 1 docu- mented positional effects in one patient who had renal varices only in the prone position.
Our patient represents the first case of nutcracker syndrome relieved by external stenting of the LRV. This simple procedure avoids the complexity and thrombotic risk of renocaval reimplantation while eliminating the venous pressure gradient. Further- more, the procedure does not require the extensive dissection necessary for ligation of periureteric col- laterals, which were documented to regress once the renal venous hypertension was eliminated.
Intravascular stents have recently been employed by interventional radiologists to improve vascular pa- tency after balloon angioplasty of peripheral after-

4 2 0 Barnes et al.
~oumai of VASCULAR
SURGERY
ies? ~ Theoretically such devices might be used to treat patients with the nutcracker syndrome or go- nadal varices. However, until intraluminal stents can be shown to be without significant risk of thrombosis or migration in the venous system, we would not recommend such intervention on patients with LRV compression.
In conclusion, we believe that vascular and gen- eral surgeons shottld be aware of the nutcracker syn- drome. Patients with disabling left flank pain, he- maturia (gross or microscopic), or both should be initially evaluated with cystoscopy and urography. If these studies are normal or show left ureteral bleeding and telltale scalloping pyeloureteric deformities, then renal angiography, retrograde phlebography, and renocaval pressure measurements should be per- formed. If mesoaortic compression of the LRV is documented, external stenting with reinforced PTFE should be considered. We believe that this simple procedure may offer physiologic relief for the dis- abling but often unrecognized nutcracker syndrome.
We would agree with the prophetic statement of MacMahon and Latorraca 8 who stated in 1954:
As long as one has no idea o f the possibilities that are likely to exist in the kidney in cases o f essential hematuria, nephrectomy would seem to be the therapy of choice, but if the lesion that we have demonstrated in these three suc- cessive kidneys should prove to be a common finding in "essential hemamria" then it does not seem beyond the realm o f modern surgery to devise a method to treat the lesion and possibly save the kidney. (p. 676)
We acknowledge the assistance o f Nasrin Rahman for help with the bibliography and Bea H e n & i x for prepara- t ion o f the manuscript. The W. L. Gore Company supplied the PTFE prosthesis and suture.
REFERENCES
L Grant JCB. Method of anatomy. Baltimore: Williams & Wil- kins, 1937:158.
2. Fagarasanu I. Recherches anatomiques sur la veine renale gauche et ses collaterales; leurs rapports avec la pathogenic du varicocele essential et des varices du ligament large. (Dem- onstrations experimentales) Ann Anat Pathol 1938;15:9-52
3. EI-Sadr AR, Mina E. Anatomical and surgical aspects in the operative management of varicoceles. Urol Cutan Rev 1950;54:257-62.
4. Vassilev I. Etude radiographique de la veine spermatique gauche au cours des varicoceles idiopathiques. Presse Med 1962; 70: 704.
5. Chait A, Matasar KW, Fabian CE, Mellins HZ. Vascular impressions on the ureters. Am J Roetgen Rad Ther 1971;3:729-49.
6. Coolsaet BL. Ureteric pathology in relation to right and left gonadal veins. Urology1978;12:40-9.
7. de Schepper A. "Nutcracker" fenomeen van de vena renalis
en veneuze pathologie van de linker nier. J Beige de Radiol- ogle 1972;55:507-11.
8. MacMahon HE, Latorraca R. Essential renal hematuria. 3" Urol 1954;71:667-76.
9. Pytel A. Renal fornical hemorrhages: their pathogenesis and treatment. J Urol 1960;83:783-9.
10. Low AI, Matz LR. Haematuria and renal fornical lesions. Br J Urol 1972;44:681-91.
11. Sporer A, Pollock R. Renal varix. J Urol 1947;48:424-7. 12. Maslow LA, Aron E. Varicosities of the kidney peMs. Case
report. J Urol 1949;61:719-24. 13. Berman MH, Copdand H. Filling defects of ureterogram
caused by a varicose ureteral vein. J Urol 1953;70:168-70. 14. Pastershank SP. Left renal vein obstruction by a superior
mesenteric artery. J Can Assoc Radiol 1974;25:52-4. 15. Wendel RG, Crawford ED, Hehman RaN. The "nutcracker"
phenomenon: an unusual cause for renal varicosities with hematuria. }" Urol 1980;123:761-3.
16. Stewart BH, Reiman G. Left renal venous hypertension "nutcracker" syndrome. Managed by direct renocaval reim- plantation. Urology 1982;20:365-9.
17. Buschi AJ, Harrison R_B, Brenbridge ANAG, Williamson BRJ, Gentry R R , Cole R. Distended left renal vein: CT/sonographic normal variant. AIR 1980;135:339-42.
18. Folsom AI. Discussion following Stevens AR. Hematuria of obscure origin, lAMA 1922;79:1302-5.
19. Heal MR. Ureteral varicosities--a cause of the corkscrew ureter. Br J Surg 1970;57:274-6.
20. Gruber GB, Frank P. Klinisch-pathologische Beitr~ige zum Gebiet der Urologie. Uber ein sogenarmtes intrarenales Aneu- rysma der Nierenarterie und tiber intrarenale Varixbildtmg der Nicrenvenen. Z Urol Chir 1923;13:107-15.
21. Brin AR, Mellinger GT, Sharp RE. Varix of the renal vein: report of a case. J Urol 1949;62:18-21.
22. Keshin JG, Joffe A. Varices of the Upper urinaDr tract and their relationship to portal hypertension. J Urol 1956; 76:350-6.
23. Woodard JR. Vascular imprints on the upper ureter. J Urol 1962;87:666-8.
24. Gillenwater JY, Burros HM, Nackphairajj S. Varicosities of the renal pelvis and ureter. J Urol !963;90:37-9.
25. LorenzT, DobrzeckiW. Ureteralvaricosis as a probable cause of urolithiasis. Polski Tygodnik Lekarski 1964; 19:1863-4.
26. Samellas W. Varices of the ureter: a rare cause of hemamria. J UroI 1965;94:55.
27. Karanjavala DK. Varicose ureteral veins as a cause of symptom-free haemamria. Br J Urol 1966;38:16-7.
28. Martelli A, Vitullo F. Microscopic hemamria due to peri- ureteral varices. Urol Int 1970;25:457-65.
29. Goswami AP. Anatomical variation of the renal veins with varicosity presenting as pseudommor of the kidney. J Urol 1976;116:648-9.
30. Blaivas JG, Previte SR, Pais VM. Idiopathic pelviureteric var- ices. Urology 1977;9:207-11.
31. Braedel H-U, Schindler E, Polsky MS. Selective renal phle- bography in the diagnosis of renal peNic and ureteric varices. Br J Urol 1977;49:365-70.
32. Taylor WN, Schillinger IF, Gaum L. Renal vein compression. I Urol 1977;118:1061-3.
33. Lopatkin NA, Morozov AV, Lopatkina LN. Essential renal haemorrhages. Eur Urol 1978;4:115-9.
34. Rosenthal JT, Costello P, Roth RA. Varicosities of renal venous system. Urology. 1980;15:427-9.
Voltmae 8 Number 4 October 1988 Stenting of nutcracker syndrome 421
35. Camuzzi FA, Kleinman SZ, Pohtano VA. Ureteral varices. Urology 1980;15:588-9.
36. Hayashi M, Kume T, Nihira H. Abnormalities of renal venous system and unexplained renal hematuria. J Urol 1980; 124:12-6.
37. Weiner SN, Bemstein RG, Morehouse H, Golden RA. He- maturia secondary to left peripelvic and gonadal vein varices. Urology 1983;22:81-4.
38. Nielsen IT, Nielsen SM. Idiopathic renal vein varicosities. Scand J Urol Nephrol 1984;18:91-5.
39. Ali Kahn S, Jayachandran S, Desai PG, Bonheim P. Renal colic, a presenting symptom of pelviureteric varices. Int Urol Nephrol 1985; 17:11-4.
40. Halpern M, Evans JA. Coarctation of the renal artery with "notching" of the ureter. A roentgenologic sign O f unilateral renal disease as a cause of hypertension. Am J Roentgenol 1962;88:159-64.
41. Kaufman JJ, Maxwell MH. Ureteral varices. AmJ Roentgenol 1964;92: 346- 50.
42. Abrams HL. Renal venography. In: Abrams HL, ed. Angi- ography. Boston: Little, Brown, 1971:915-25.
43. Jonsson K. Renal angiography in patients with hematutia. Am J Roentgenol 1972;116:758-65.
44. Mitty HA, Goldman H. Angiography in unilateral renal bleeding with a negative urogram. Am J Roentgenol 1974; 121:508-17.
45. Braedel H-U, Haage H, Moeller J-F, Schindler E. Differential diagnostic importance of retrograde phlebography in cases of unusual ectasia and renal pelvic deformity. Radiology 1976; 119:65-8.
46. Nishimura Y, Inoue Y, Huzime M, Tor/finaga T. Angiogra- phisch gesicherte Vafizen im Bereich des Nierenbeckens und des oberen Hamleiters. Fortschr Rontgenstr 1978;128: 595-9.
47. Schreyer VH, Justich E, Gypser G. Varikose der Nierenvenen, der Nierenbecken- und Uretervenen. Fortschr Rontgenstr 1978;129:192-8.
48. Peterson RA, Peterson LR. Renal varices. J Can Assoc Radiol 1980;3!:54-6.
49. Sacks BA, Gomori J, Lerner M, Masters R, DeWolfW. Left renal venous hypertension in association with the nutcracker phenomenon. Cardiovasc Intervent Radiol 1981;4:253-5.
50. Spira R, Kwan E, Gerzof SG. Left renal vein varix simulating a pancreatic pseudocyst by sonography. AJR 1982;138:149- 50.
51. Beckmann CF, Abrams HL. Idiopathic renal vein varices: incidence and significance. Radiology 1982;143:649-52.
52. Beinart C, Sniderman KW, Saddekni S, Weiner M, Vaughan ED Jr, Sos TA. Left renal vein hypertension: a cause of occult hematuria. Radiology 1982;145:647-50.
53. Yashiro N, Yoshida H, Okumura K. Renal sinus varix: an additional differential diagnosis of a renal hilar mass. Radiat Med 1964;2:194-6.
54. Kauzlaric D, Barmeir E. Ukrasonic detection of renal pelvic and ureteric varices. J Clin Ultrasound 1984;12:569-71.
55. Olin TB, Reuter SR. A pharmacoangiographic method for improving nephrophlebography. Radiology1965;85:1036- 42.
56. Pearson JC, Tanagho EA, Palubinskas AJ. Nonoperative di- agnosis of pyelocalyceal deformity due to venous impressions. Urology 1979;13:207-10.
57. Beinart C, Sniderman KW, Tamura S, Vaughan ED Jr, Sos TA. Left renal vein to inferior vena cava pressure relationship in humans. J Urol 1982;127:1070-71.
58. Zerhouni EA, Siegelman SS, Walsh PC, White RI. Elevated pressure in the left renal vein in patients with varicocele: preliminary observations. J Urol 1980;123:512-3.
59. Coolsaet BL. RE: "Nutcracker" phenomenon: an unusual cause for renal varicosities with hematuria. (Letter) I Urol 1981;125:134.
60. Strong EK~ Mechanics of arteriomesenteric duodenal obstruc- tion and direct surgical attack upon etiology. Ann Surg 1958; 148:725-30.
61. Sigwart U, Puel J, Mirkovitch V, Joffre F, Kappenberger L. Intravascular stents to prevent occlusion and restenosis after transluminal angioplasty. N Engl J Med 1987;316:701-6.
Copyright © 2022 FDOKUMEN