
Meseret rabies final paper (1)
41
UNIVERSITY OF GONDAR COLLEGE OF MEDICINE AND HEALTH SCIENCES SCHOOL OF BIOMEDICAL AND LABORATORY SCIENCES Incidence of human rabies exposure and its associated risk factors at Gondar Health Center, Gondar, North west Ethiopia: A three years retrospective study. By: Meseret Yibrah Advisor: Debasu Damtie(BSc., MSc.) A research paper to be submitted to the School of Biomedical and Laboratory Sciences, College of Medicine and Health Sciences, University of Gondar for partial fulfilment of the requirements for the degree of Bachelor of Science in Medical Laboratory Science i
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Meseret rabies final paper (1)
UNIVERSITY OF
GONDAR
COLLEGE OF MEDICINE AND HEALTH SCIENCES
SCHOOL OF BIOMEDICAL AND LABORATORY SCIENCES
Incidence of human rabies exposure and its associated risk
factors at Gondar Health Center, Gondar, North west
Ethiopia: A three years retrospective study.
By: Meseret Yibrah
Advisor: Debasu Damtie(BSc., MSc.)
A research paper to be submitted to the School of
Biomedical and Laboratory Sciences, College of
Medicine and Health Sciences, University of Gondar
for partial fulfilment of the requirements for the
degree of Bachelor of Science in Medical Laboratory
Sciencei

June, 2014
Gondar, Ethiopia
ii
Acknowledgement
I sincerely appreciate my advisor Mr. Debasu Damtie for his
invaluable support and advice during this research work. I
also would like to acknowledge School of Biomedical and
Laboratory Sciences for selecting my topic of interest.
Lastly, my deepest gratitude goes to Gondar Health Centre for
allowing me to use the rabies post exposure data for this
study.
I
Table of contents
Contents
page
Acknowledgement..............................................I
Table of contents...........................................II
List of
tables .......................................................
..............................................................
.......IV
List of
figures.......................................................
..............................................................
.......V
Acronyms......................................................
..............................................................
.............VI
II
Abstract......................................................
..............................................................
...............VII
1. Introduction.............................................1
1.1.
Background....................................................
..............................................................
...1
1.2. Statement of the problem...............................3
2. Literature review....................................................................................................................4
3. Justification of the study................................5
4.Objectives.................................................6
4.1. General objective......................................6
4.2. Specific objectives....................................6
5. Materials and methods.....................................7
5.1. Study area.............................................7
5.2. Study design and period................................7
5.3. Population.............................................7
5.3.1. Source population..................................7
5.3.2. Study population...................................7
5.4. Inclusion and Exclusion criteria………………………………………………………...7
5.5. Variables...........................................7
III
5.5.1. Independent variables..............................7
5.5.2. Dependent variables................................7
5.6. Sample size and sampling technique.....................8
5.7. Data collection methods................................8
5.8. Quality control........................................8
5.9. Data analysis and interpretation.......................8
5.10. Result dissemination..................................8
5.11. Ethical consideration.................................8
6.
Result........................................................
..............................................................
................9
7.Discussion..................................................
..............................................................
.............14
8. Conclusion and recommendations
.........................................................
.............................16
8.1. Conclusion............................................16
8.2. Recommendations.......................................16
9.Limitation of the
study.........................................................
.................................................17
10. References..............................................18
11. Annex...................................................20
IV
Annex I....................................................20
List of tables
Table1. Socio-demographic and seasonal distribution of human
rabies exposure cases between 2011-2013 at Gondar Health
Centre ………………………………………………10
Table2. Time of arrival to health centre for post exposure
prophylaxis after human rabies exposure at Gondar Health
Centre from 2011-
2013..........................................................
......11
Table3. Incidence of human rabies exposure cases in Gondar
Health Center by sex from 2011-
2013…………………………………………………………………………………....12
V
Table4. Incidence of human rabies exposure cases in North
Gondar Administrative Zone by residence from 2011-
2013…………………………………………………………………...13
List of figures
Fig 1. Human rabies exposure cases by year between 2011–2013
at Gondar Health Center………………………………………………………………………………………….9
VI
Fig 2. Dog statuses at the time of health centre visit for
post exposure prophylaxis Gondar Health Center from 2011-
2013..........................................................
......................................11.
VII
Acronyms
CDC- Centre for Disease Control
EHNRI -Ethiopian Health and Nutrition Research Institute
OR-odds ratio
PEP-Post Exposure Prophylaxis
RIG-Rabies Immune Globulin
WHO-World Health Organization
VIII
Abstract
Back ground: Rabies is one of the oldest known and most feared
human diseases recognized since the early period of
civilization. It is one of the main zoonotic diseases caused
by a virus and death nearly always follows once an animal or
human has been clinically ill with the disease.
Epidemiological studies provide basic information about the
burden of the disease and enhance prevention and control
interventions.
Objective: To assess the incidence of human rabies exposure
and associated risk factors at Gondar Health Centre from 2011
up to 2013, Gondar, North west Ethiopia.
Methods: A retrospective cross sectional study was conducted
at Gondar Health Centre where post exposure prophylaxis for
rabies was available for the whole population in the North
Gondar Zone catchment area. Data of human rabies exposure
cases between 2011 and 2013 was collected from rabies post
exposure prophylaxis registration book using data abstraction
sheets. The data was entered and analyzed using SPSS version
16 statistical software. A descriptive analysis was performed
for categorical variables. Bivariate analysis was used to
IX
determine association of explanatory variables and outcome
variable.
Result: A total of 261 human rabies exposures were reported to
Gondar Health Centre from 2011 up to 2013 with a decreasing
trend. The sex and age specific distribution showed that the
majority of rabies exposure cases were among males (142/226,
62.8%) and children less than 14 years old (87/261, 38.5%).
Also Predominant numbers of rabies exposure cases (161/220,
73.2%) were observed from rural area and during fall and
winter with the same proportion (67/222, 30.18%). Significant
number of human rabies exposure cases (23.2%) came to health
centre beyond 2 weeks time after injury for PEP and The
incidence of human rabies exposure cases was 4.6, 2.61 and
1.27 per 100, 000 population in 2011, 2012 and 2013
respectively. Being male and living in urban setting was found
to be risk factors for human rabies exposure from bivariate
analysis.
Conclusion: Significant number of human rabies exposure was
reported at Gondar Health Centre and being male and living in
urban area was found to be associated with rabies exposure. A
community based follow up study is recommended to accurately
estimate the incidence of human rabies exposure. There is a
need for deliberate efforts to educate the public about the
risks of rabies and where to go in case of rabies exposure.
Key words: Exposure, Incidence, Rabies, Risk factors
X
1. Introduction
1.1. BackgroundRabies is one of the very dangerous viral zoonoses and all
mammals can be infected by the virus. The cause of rabies is a
neurotrop virus belonging to the class Mononegavirales, the
family Rhabdoviridae, and the genus Lyssavirus[1]. The disease
mainly is transferable through biting and sometimes through
mucous tissues, respiration, placenta, contaminated instruments
and plantation of organs. This disease is endemic in tropical
areas and more cases are observed in developing countries [2].
Almost 99.9% of mortalities caused by human rabies as well as
98.5% of animal bite cases are related to tropical areas [3].
According to WHO report, worldwide human deaths from endemic
canine rabies were estimated to be 55000 per annum [4], with 56%
share from South East Asia Region [5].
An effective rabies vaccine was developed over a century ago
making rabies a preventable disease. When human diploid cell
vaccine in combination with rabies immune globulin is
administered promptly to rabies-exposed patients following
appropriate wound care, it is virtually 100% effective in
preventing human death [6]. Although rabies can infect and be
maintained by several different host species, domestic dogs are
by far the most important source of infection to humans with more
than 95% of human cases caused by bite from rabid dogs [7].
1
Rabies has the highest case fatality rate of any conventional
infectious disease, approaching 100%. The likelihood of a
productive rabies infection after exposure to a lyssa virus is
known to depend on a variety of factors, including but not
limited to dose, route of exposure, site of exposure, variant,
host genetic makeup, pre- and/or post-exposure prophylaxis
etc[8]. All mammals are susceptible to lyssa virus infection, but
species-level variation in susceptibility has long been
recognized [9].
Rabies in Africa constitutes a serious public health problem [10-
12]. In Ethiopia it is an important disease that has been
recognized for many centuries. The treatments recommended for
people bitten by rabid animals mainly dogs have been recorded in
many Ethiopian medical books since the early 17th century
(Sterleyn 1968) cited by Fekadu [13]. Rabies satisfies all the
World Health Organization (WHO) criteria for diseases that are a
priority for control [14] and, unlike many other emerging
zoonosis (such as West Nile virus), safe and effective animal and
human vaccines are widely available for its prevention and
control. Despite this, rabies remains a neglected disease that is
poorly controlled throughout much of the developing world,
particularly Africa and Asia, where most human rabies deaths
occur [14, 15]. A major factor in the failure of rabies control
is the low level of political commitment, partly arising from a
lack of quantitative data on the true public health impact of the
2
disease [14] and the cost-effectiveness and cost benefits of
controlling it [16].
Epidemiological studies provide basic information about the
burden of the disease and enhance prevention and control
interventions. To this regard, there are limited studies
conducted regarding incidence of rabies and associated factors in
Ethiopia in general and the study area in particular. Therefore,
this study was aimed to assess the incidence of human rabies
exposure cases and associated factors at Gondar Health Center.
3
1.2. Statement of the problemRabies is widely distributed across the globe. More than 55,000
people die of rabies each year [17]. About 95% of human deaths
occur in Asia and Africa. India is the most severely affected,
and China is the next [18]. Rabies is endemic in developing
countries of Africa and Asia, and most human deaths from the
disease occur in these endemic countries [19]. More than 99% of
all human deaths from rabies occur in the developing world [19].
Ethiopia being one of the developing countries is highly endemic
for rabies. Approximately 10, 000 people were estimated to die of
rabies annually in Ethiopia which makes it to be one of the worst
affected countries in the world [20]. Dogs are the principal
source of infection for humans and livestock [21]. However
incidence of human rabies exposure and its associated factors has
not been assessed at Gondar Health Center, Gondar. Hence, this
study was aimed to avail information required in combating the
disease.
4
2. Literature review
There are studies conducted about rabies anywhere else in the
globe. A retrospective study conducted in New York reported a
total of 2,216 PEP cases from 1995 to 2000, with 317–469 cases
each year. Annual PEP incidence was 23–34 cases/100,000 during
the 6-year period with 6-year average incidence of 27/100,000
reported higher mean annual incidence of PEP in rural areas and
during early spring/late summer, but no significant differences
were observed among sex or age distributions and PEP [23]. On the
other hand Chinese Centre for Disease Control and prevention5
(CDC) , reported 19,806 human rabies cases between 1996 and 2008
with an average of 1,524 cases each year, and the incidence
almost was rising rapidly, with the peak in 2007 (3,300 cases)
[24].
A community-based active surveillance for rabies in Machakos
District, Kenya showed 234 per 100 000 people annual incidence of
animal-bites of humans and the point estimate of human-rabies
incidence per year was 25 per million people. Almost all (97%)
animal-bites of humans were due to dogs [25].
Another study conducted in Zaria, Nigeria reported that males are
significantly more affected and incidence of dog bite was highest
during the hot season (April-June) and low during the wet season
(July-October) [26].
A 5-year (2002-2006) retrospective study conducted in Tanzania at
Bugando Hospital reported a total of 767 bite injuries by rabies-
suspected animals giving a mean annual incidence of ~58 cases per
100,000. A Tanzanian study revealed majority of human exposure
cases in each year were recorded during the period between June
and October and unlike the New York study children less than 18
were the most affected group [27]. A retrospective record review
study conducted in Ethiopia between 2001 and 2009 at EHNRI using
the rabies record book reported annual post exposure prophylaxis
for human rabies ranges between 1026 and 1580 every year for the
last nine years in Addis Ababa. It ranged from 300 to 1922 for
areas outside Addis Ababa. This study determined fatal human
6
rabies cases in 2001-2009 reported that children under 14 years
of age and males were highly affected segments of the community
[28]. A one year follow up of rabies incidence in humans and
domestic animals in North Gondar zone depicted an estimated human
rabies incidence of 2.33 cases per 100, 000 populations per year
[29].
3. Justification of the studyMany households own dogs usually for guarding property. Although
there are no formal studies, it is estimated that there is one
owned dog per five household nationally [20]. Dog management is
often poor and dog vaccination is limited to few dogs in urban
centres. High population of dogs with poor management contributes
for high endemicity of canine rabies in Ethiopia. In canine
rabies endemic countries like Ethiopia, rabies has also
significant economic importance by its effect on livestock [22],
so need to be investigated still. Local data are limited and old
regarding the incidence and associated factors of rabies exposure
in the study area. Hence, the findings of this study will be
useful to health service providers, planners, policy makers and
community at large for planning interventions targeting
prevention and control of rabies in the study area and beyond.
Moreover the findings of this study will serve as baseline
information for the further studies.
7
4. Objectives
4.1. General objective To assess incidence of human rabies exposure and associated
factors at Gondar Health Center.
4.2. Specific objectives To determine incidence of human rabies exposure at Gondar
Health Centre.
8
To identify associated risk factors of human rabies exposure
at Gondar Health Centre.
5. Materials and methods
5.1. Study areaThe study was conducted at Gondar Health Center, Gondar town.
Gondar town is located in the North Gondar zone of the Amhara
9
regional state, Northwest Ethiopia, at 748 km away from the
capital Addis Ababa. The town has a latitude and longitude
of 12°36′N 37°28′E with an elevation of 2133 meters above sea
level. Based on figures from the Central Statistical Agency in
2008, Gondar has an estimated total population of 231,977. Gondar
Health Center is one of the governmental health centers in
Gondar. This Health center is the only health center providing
rabies post exposure prophylaxis in the zone.
5.2. Study design and period
A retrospective cross sectional study was conducted to assess
incidence of human rabies exposure and associated risk factors
from 2011 up to 2013.
5.3. Population
5.3.1. Source populationAll population in Gondar health center who lived between 2011 and
2013 was source population of this study.
5.3.2. Study populationAll rabies exposure cases who visited Gondar Health Center for post exposure prophylaxis (PEP) between 2011 and 2013 were study population.
5.4. Inclusion and Exclusion criteria
5. 4.1. Inclusion criteria
Human rabies exposure cases who visited Gondar health center
for post exposure proph ylaxis (PEP) from 2011 up to 2013
were included in this study.10
5. 4.1. Exclusion criteria
Human rabies exposure cases who didn’t visit Gondar health
center for post exposure prophylaxis (PEP) from 2011 up to
2013 were excluded from this study.
5.5. Variables
5.5.1. Independent variableso Ageo Sexo Seasono Residenceo Dog status
5.5.2. Dependent variableso Human rabies exposure
5.6. Sample size and sampling techniqueAll human exposure cases visiting Gondar Health Centre between2011 and 2013 was included in the study.
5.7. Data collection methodsData of human rabies exposure cases between 2011 and 2013 will becollected from rabies post exposure prophylaxis registration bookusing data abstraction sheets.
5.8. Quality controlTraining regarding data entry and analysis using SPSS version 16was given to the principal investigator of the study to make surethat the data collected from the PEP log book is properly enteredand analyzed.
11
5.9. Data analysis and interpretationThe data was entered and analysed using SPSS version 16statistical software. A descriptive analysis was performed forcategorical variables. Bivariate analysis was performed toexamine possible risk factors of human rabies exposure. Oddsratio has been used to assess the presence and strength ofassociation between the outcome variable and explanatoryvariables. To obtain adjusted estimates of the odds ratio whileaccounting for all possible risk factors, multivariate analysiswill be used. In all cases, P-value less than 0.05 wereconsidered statistically significant. The findings of the studyare presented in narratives, tables and graphs.
5.10. Result disseminationAfter the completion of this study, a copy of the document willbe given to Gondar Health Centre, North Gondar Zone Health Deskand to the School of Biomedical and Laboratory Sciences each.Moreover efforts will be made to publish on one of the peerreviewed journals.
5.11. Ethical considerationEthical approval was obtained from the School of Biomedical andLaboratory Sciences Research and Ethical Review Committee,College of Medicine and Health Sciences, University of Gondar.Moreover, the Health Centre was communicated through officialletter for smooth conduct of the study.
6. Result
1. Human rabies exposure
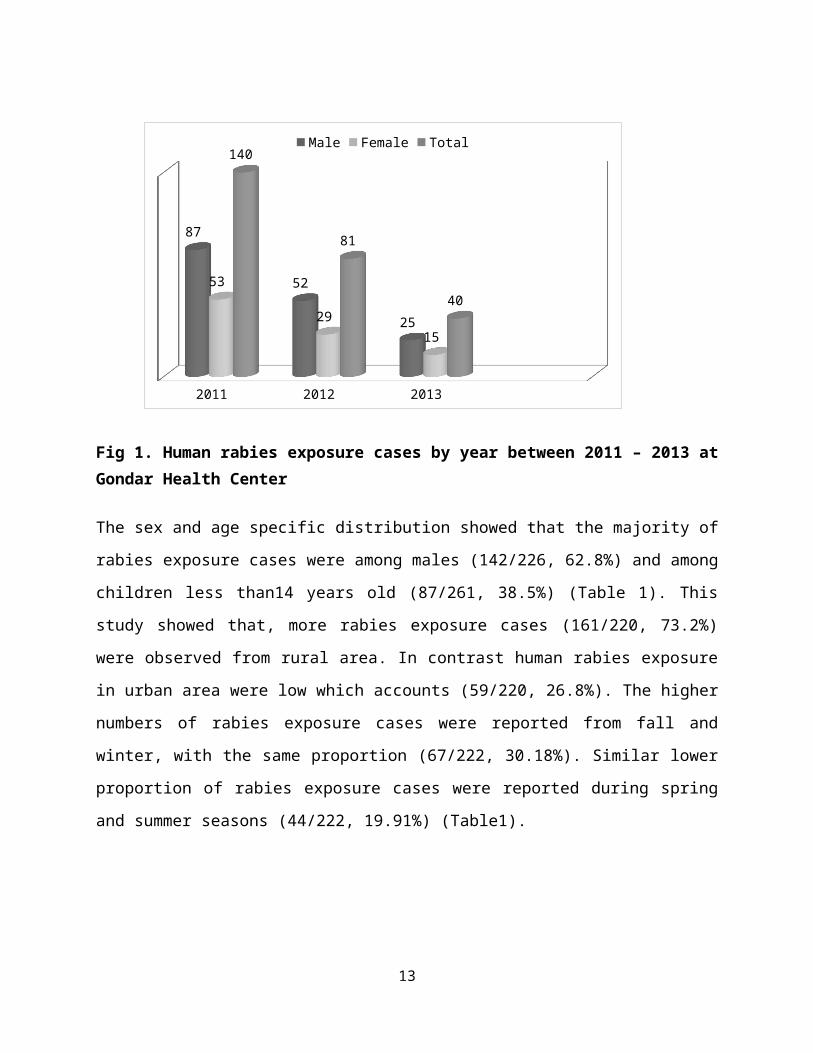
A total of 261 human rabies exposures were reported to Gondar
health centre from 2011 up to 2013. The distribution of human
rabies exposure cases from year to year was observed to decrease
(Fig 1).
12
2011 2012 2013
87
52
25
53
2915
140
81
40
Male Female Total
Fig 1. Human rabies exposure cases by year between 2011 – 2013 atGondar Health Center
The sex and age specific distribution showed that the majority of
rabies exposure cases were among males (142/226, 62.8%) and among
children less than14 years old (87/261, 38.5%) (Table 1). This
study showed that, more rabies exposure cases (161/220, 73.2%)
were observed from rural area. In contrast human rabies exposure
in urban area were low which accounts (59/220, 26.8%). The higher
numbers of rabies exposure cases were reported from fall and
winter, with the same proportion (67/222, 30.18%). Similar lower
proportion of rabies exposure cases were reported during spring
and summer seasons (44/222, 19.91%) (Table1).
13
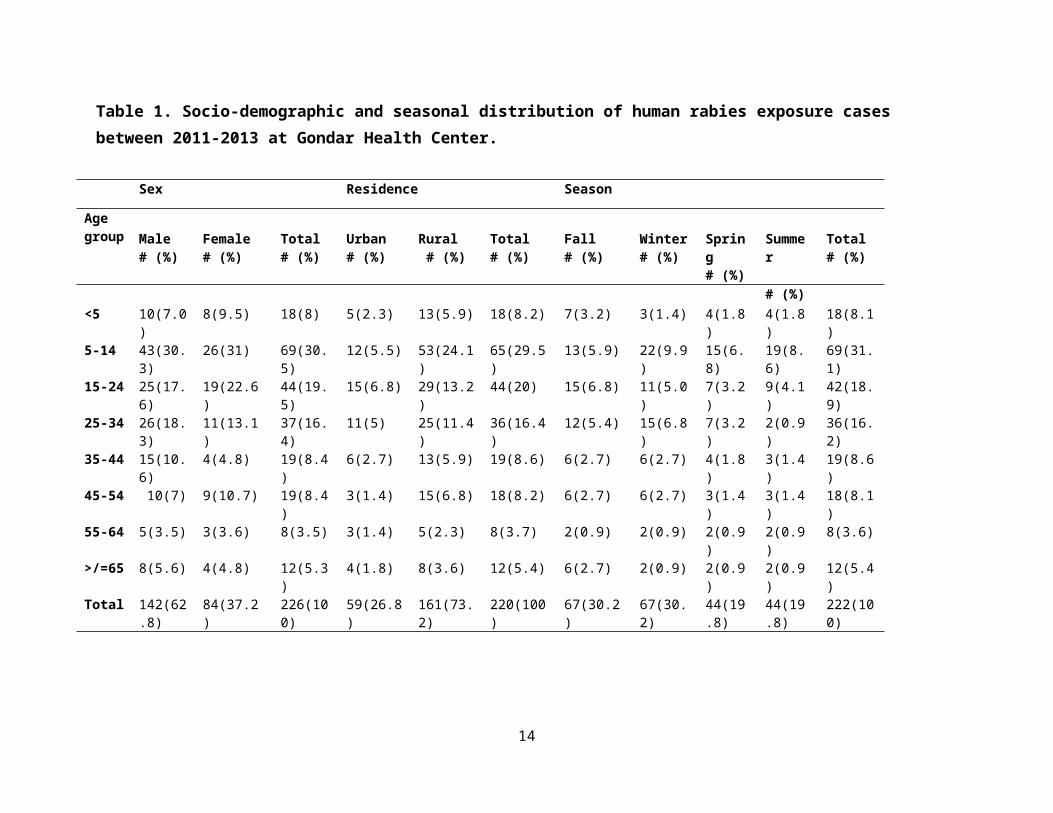
Table 1. Socio-demographic and seasonal distribution of human rabies exposure cases between 2011-2013 at Gondar Health Center.
14
Sex Residence Season
Agegroup Male
# (%)Female # (%)
Total# (%)
Urban# (%)
Rural # (%)
Total# (%)
Fall# (%)
Winter# (%)
Spring# (%)
Summer
Total# (%)
# (%)<5 10(7.0
)8(9.5) 18(8) 5(2.3) 13(5.9) 18(8.2) 7(3.2) 3(1.4) 4(1.8
)4(1.8)
18(8.1)
5-14 43(30.3)
26(31) 69(30.5)
12(5.5) 53(24.1)
65(29.5)
13(5.9) 22(9.9)
15(6.8)
19(8.6)
69(31.1)
15-24 25(17.6)
19(22.6)
44(19.5)
15(6.8) 29(13.2)
44(20) 15(6.8) 11(5.0)
7(3.2)
9(4.1)
42(18.9)
25-34 26(18.3)
11(13.1)
37(16.4)
11(5) 25(11.4)
36(16.4)
12(5.4) 15(6.8)
7(3.2)
2(0.9)
36(16.2)
35-44 15(10.6)
4(4.8) 19(8.4)
6(2.7) 13(5.9) 19(8.6) 6(2.7) 6(2.7) 4(1.8)
3(1.4)
19(8.6)
45-54 10(7) 9(10.7) 19(8.4)
3(1.4) 15(6.8) 18(8.2) 6(2.7) 6(2.7) 3(1.4)
3(1.4)
18(8.1)
55-64 5(3.5) 3(3.6) 8(3.5) 3(1.4) 5(2.3) 8(3.7) 2(0.9) 2(0.9) 2(0.9)
2(0.9)
8(3.6)
>/=65 8(5.6) 4(4.8) 12(5.3)
4(1.8) 8(3.6) 12(5.4) 6(2.7) 2(0.9) 2(0.9)
2(0.9)
12(5.4)
Total 142(62.8)
84(37.2)
226(100)
59(26.8)
161(73.2)
220(100)
67(30.2)
67(30.2)
44(19.8)
44(19.8)
222(100)
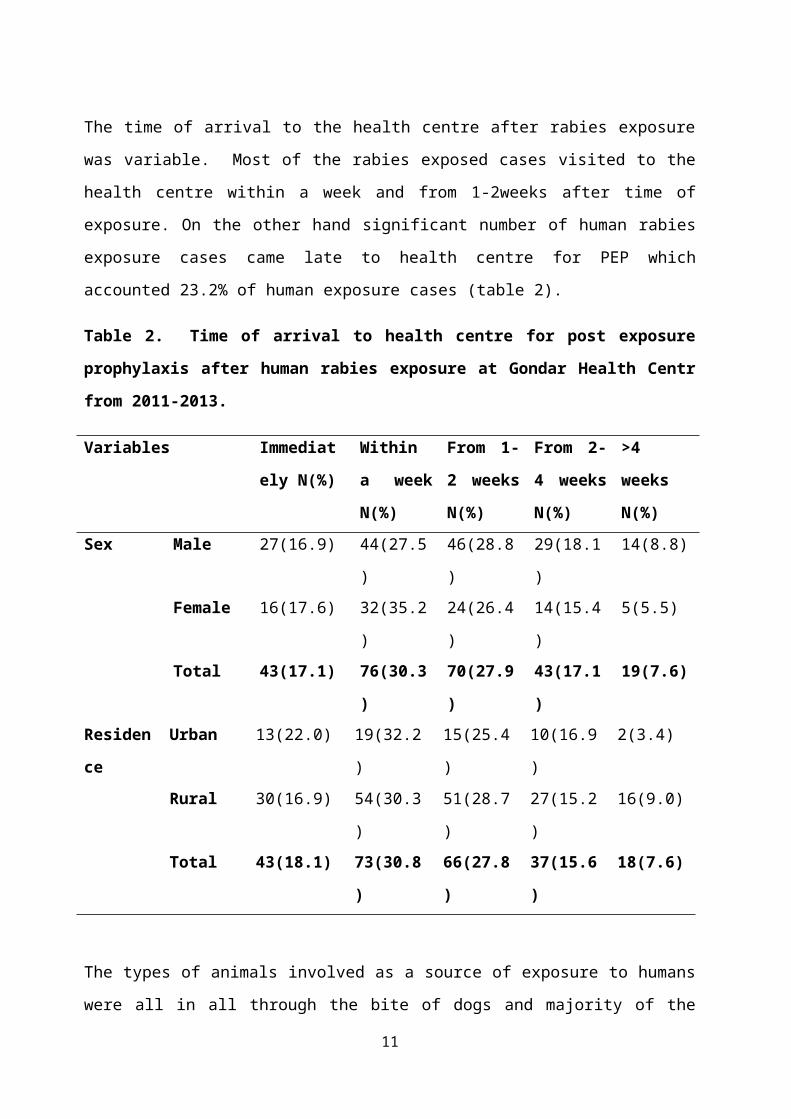
The time of arrival to the health centre after rabies exposure
was variable. Most of the rabies exposed cases visited to the
health centre within a week and from 1-2weeks after time of
exposure. On the other hand significant number of human rabies
exposure cases came late to health centre for PEP which
accounted 23.2% of human exposure cases (table 2).
Table 2. Time of arrival to health centre for post exposure
prophylaxis after human rabies exposure at Gondar Health Centr
from 2011-2013.
Variables Immediat
ely N(%)
Within
a week
N(%)
From 1-
2 weeks
N(%)
From 2-
4 weeks
N(%)
>4
weeks
N(%)Sex Male 27(16.9) 44(27.5
)
46(28.8
)
29(18.1
)
14(8.8)
Female 16(17.6) 32(35.2
)
24(26.4
)
14(15.4
)
5(5.5)
Total 43(17.1) 76(30.3
)
70(27.9
)
43(17.1
)
19(7.6)
Residen
ce
Urban 13(22.0) 19(32.2
)
15(25.4
)
10(16.9
)
2(3.4)
Rural 30(16.9) 54(30.3
)
51(28.7
)
27(15.2
)
16(9.0)
Total 43(18.1) 73(30.8
)
66(27.8
)
37(15.6
)
18(7.6)
The types of animals involved as a source of exposure to humans
were all in all through the bite of dogs and majority of the
11
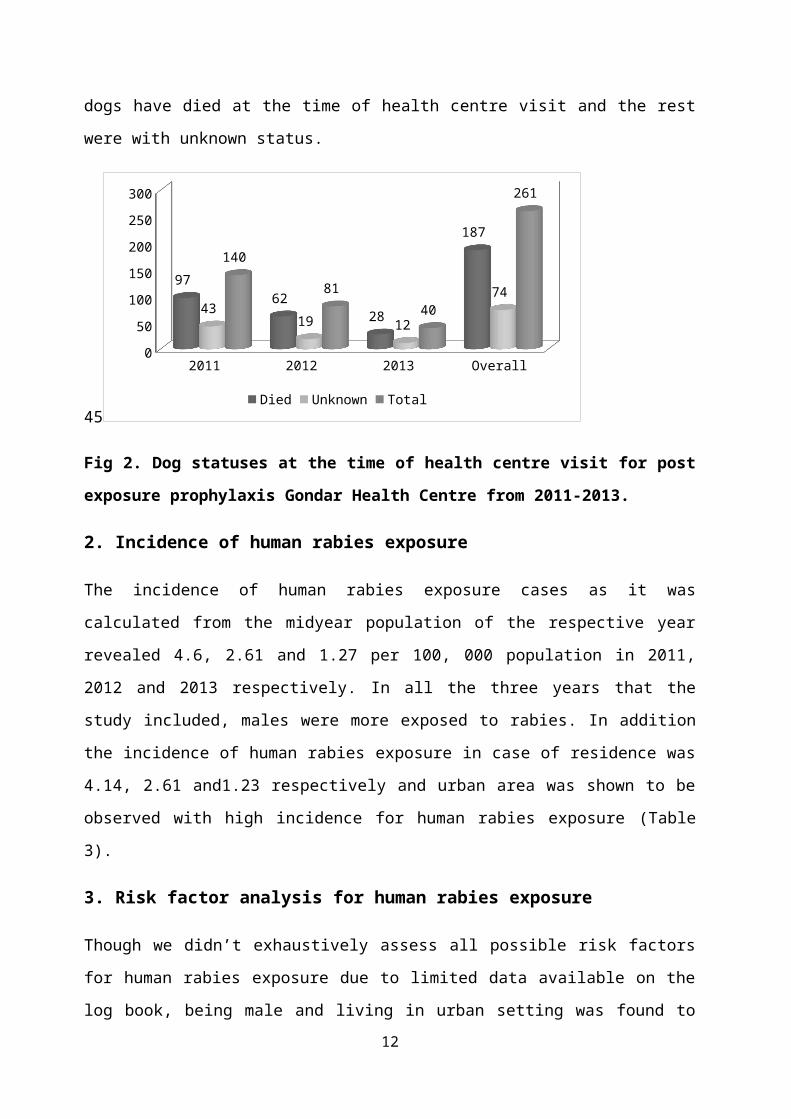
dogs have died at the time of health centre visit and the rest
were with unknown status.
45
2011 2012 2013 Overall050100150200250300
9762
28
187
4319 12
74
140
8140
261
Died Unknown Total
Fig 2. Dog statuses at the time of health centre visit for post
exposure prophylaxis Gondar Health Centre from 2011-2013.
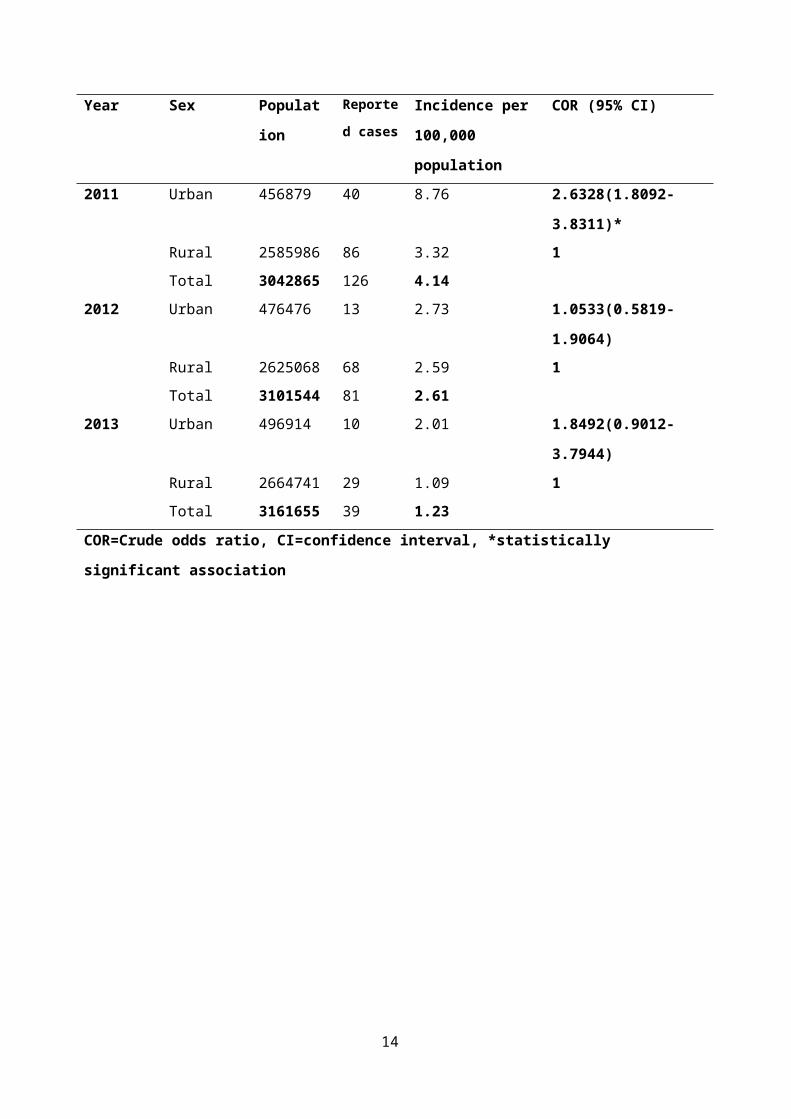
2. Incidence of human rabies exposure
The incidence of human rabies exposure cases as it was
calculated from the midyear population of the respective year
revealed 4.6, 2.61 and 1.27 per 100, 000 population in 2011,
2012 and 2013 respectively. In all the three years that the
study included, males were more exposed to rabies. In addition
the incidence of human rabies exposure in case of residence was
4.14, 2.61 and1.23 respectively and urban area was shown to be
observed with high incidence for human rabies exposure (Table
3).
3. Risk factor analysis for human rabies exposure
Though we didn’t exhaustively assess all possible risk factors
for human rabies exposure due to limited data available on the
log book, being male and living in urban setting was found to12
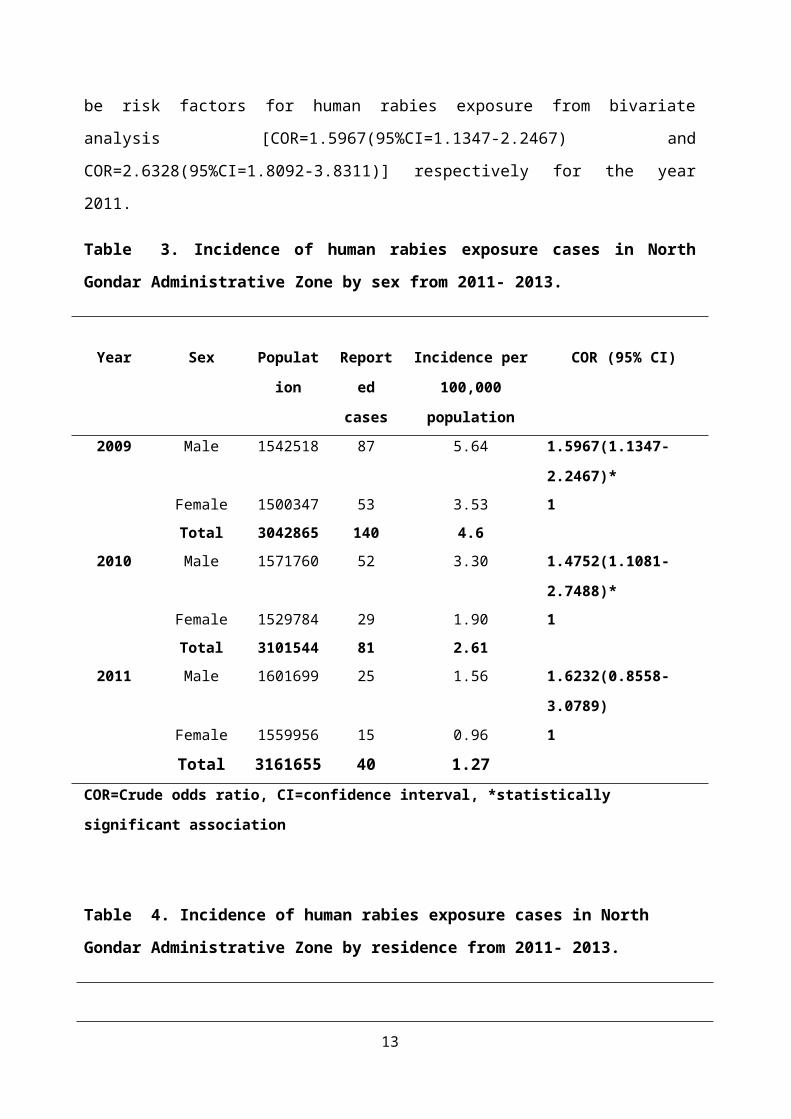
be risk factors for human rabies exposure from bivariate
analysis [COR=1.5967(95%CI=1.1347-2.2467) and
COR=2.6328(95%CI=1.8092-3.8311)] respectively for the year
2011.
Table 3. Incidence of human rabies exposure cases in North
Gondar Administrative Zone by sex from 2011- 2013.
Year Sex Populat
ion
Report
ed
cases
Incidence per
100,000
population
COR (95% CI)
2009 Male 1542518 87 5.64 1.5967(1.1347-
2.2467)*Female 1500347 53 3.53 1Total 3042865 140 4.6
2010 Male 1571760 52 3.30 1.4752(1.1081-
2.7488)*Female 1529784 29 1.90 1Total 3101544 81 2.61
2011 Male 1601699 25 1.56 1.6232(0.8558-
3.0789)Female 1559956 15 0.96 1
Total 3161655 40 1.27COR=Crude odds ratio, CI=confidence interval, *statistically
significant association
Table 4. Incidence of human rabies exposure cases in North
Gondar Administrative Zone by residence from 2011- 2013.
13
Year Sex Populat
ion
Reporte
d casesIncidence per
100,000
population
COR (95% CI)
2011 Urban 456879 40 8.76 2.6328(1.8092-
3.8311)*Rural 2585986 86 3.32 1Total 3042865 126 4.14
2012 Urban 476476 13 2.73 1.0533(0.5819-
1.9064)Rural 2625068 68 2.59 1Total 3101544 81 2.61
2013 Urban 496914 10 2.01 1.8492(0.9012-
3.7944)Rural 2664741 29 1.09 1Total 3161655 39 1.23
COR=Crude odds ratio, CI=confidence interval, *statistically
significant association
14
7. Discussion
In the present study, animal bite cases during 2011-2013 were
140, 81 and 40 respectively. Also, the Incidence cases per
100,000 were respectively 4.6, 2.61 and 1.27.This finding is by
far lower than a report from New York (23-34/100,000), Kenyan
active surveillance report (234/100,000) and Tanzanian study
which reported 58/100,000 population [23, 25, 27]. These
discrepancies might be explained by multiple socio-cultural
factors and methodological differences. In Ethiopia many people
prefer to go to traditional and faith healers than getting
modern medical care after exposure. Hence vast majority of
human exposure cases might not be reported to the health
facilities as a result it falsely reduces the incidence of
human rabies exposure.
The distribution of human rabies exposure cases from year to
year was observed to decrease. This might be explained by the
fact that dog vaccination services are being common practices
from time to time particularity in urban settings thereby
reducing possibility of dog bite.
The sex specific distribution showed that the majority (62.8%)
of rabies exposure cases were among males. This finding was
supported by a previous Ethiopian study conducted at the former
15
EHNRI and a Nigerian study which showed higher proportion of
males being exposed to rabies [26, 28]. This might be explained
by the day and night outdoor activities males are frequently
involved in and females are more likely to remain in-doors for
cultural and religious reasons. On the other hand majority of
human rabies exposure cases were reported among children less
than 14 years old (38.5%). This finding is in line with the
study done in Tanzania and Ethiopian study which reported
higher incidence of human rabies exposure among under 18 and
under 14 years old children respectively [27, 28]. This could
be probably due to children are more likely to have the dogs
provoked and are also less likely to defend themselves thereby
sustaining dog bite injuries. Unlike the present study a study
in New York reported no significant differences among sex or
age distributions and rabies exposure [23].
This study showed that, more rabies exposure cases (161/220,
73.2%) were observed from rural area. This finding is
concurrent with the study done in New York [23]. This might
possibly be explained by the large population being residing in
rural areas compared to urban settings.
The majority of rabies exposure cases were reported from fall
and winter, with the same proportion (67/222, 30.18%). In
contrary to this finding, studies from New York, Tanzania and
Nigeria reported high incidence of rabies exposure during
spring and summer seasons [23, 27, and 26]. This seasonal
16
variation could be due to variation in geographical locations
which determine the weather condition of each season.
Significant number of human rabies exposure cases came late to
health centre for PEP which accounted 23.2% of human exposure
cases while only 17.1% of victims have visited the health
centre immediately after bite. Unlike our finding, a Nigerian
retrospective study revealed that most (87.7%) of the victims
afflicted with dog bite injuries presented within 24 hours of
the bite which is quite commendable [26]. This might be due to
inaccessibility of the health centre in terms of distance for
majority of the rural catchment area since Gondar Health Centre
is the only facility providing PEP service. Therefore, the
efficacy of the PEP would be hampered by late arrival of the
victims at health facility.
The types of animals involved as a source of exposure to humans
were all in all through the bite of dogs. The present study
finding is consistent with another community based active
surveillance study conducted in Kenya which revealed 97% of
animal bites of humans were attributed to dogs [25]. Among dogs
responsible for human rabies exposure, majority (72.8%) have
died at the time of health centre visit by the victim and the
rest was with unknown status. This implies that dogs were
potential sources of rabies infection to humans.
Though we didn’t exhaustively assess all possible risk factors
for human rabies exposure due to limited data available on the
log book, being male was found to be risk factors for human
rabies exposure from bivariate analysis respectively for the
17
year 2011. This was supported by studies from Nigeria, Tanzania
and Ethiopia [26, 27, 28]. The present study also found out
that and living in urban setting is also a risk factor unlike
the report from New York which reported living in rural setting
as a risk factor. This might be due to the fact that in
Ethiopia people in rural settings settle very far apart in
contrary to urban area where people live in crowded conditions
which may favour dog bite exposure. On other hand in urban
settings stray dogs are abundant which may contribute for human
rabies exposure.
8. Conclusion and recommendations
8.1. Conclusion Significant number of human rabies exposure was reported at
Gondar Health Centre despite the fact that majority of victims
would prefer traditional healers for post exposure management
of rabies which probably may reduce the actual figure. Majority
of human rabies exposure cases were reported among children and
males. Human rabies exposure was common during fall and winter
seasons. Dog bite was the only source of exposure reported.
Significant number of rabies exposed cases came late to the
Health Centre to seek medical attention. Being male and living
in urban seating was found to be risk factors for rabies
exposure in humans.
18
8.2. RecommendationsBased on this study the following recommendations are made:
A community based follow up study is recommended to
accurately estimate the incidence of human rabies
exposure.
There is a need for deliberate efforts to educate the
public about the risks of rabies and where to go in case
of rabies exposure.
It is vital to vaccinate dogs for rabies in North Gondar
Zone.
Human diploid cell vaccine together with human rabies immune
globulin should be made available in every health care
facility.
19
9. Limitation of the study
Since the data for this study was from secondary sources
(document review), it was not complete and difficult to get
important variables. All the rabies cases reported to Gondar
health centre was considered treated with anti rabies vaccine
but the number of cases completed PEP regime and the status of
exposed cases after PEP was not documented. Moreover, this
study compiled data of exposure cases who did report to the
health centre. Hence those victims who didn’t come to the
health centre were not considered in the study which may
underestimate the true incidence of rabies exposure.
20
10. References
1. Azizi F, Janghorbani M, Hatami H. Epidemiology and Control of
Common Diseases in Iran. 2nd Ed. Tehran: Khosravi Pub; 2011,
p.542-557.
2. Riahi M, Latifi M, Bakhttyari M, Yavari P, Khezeli M, Hatami
H,et al. Epidemiologic survey of animal bites and causes of
delay ingetting preventive treatment in tabbas during 2005-
2010. Toloee Behdasht 2012; 11(1): 20-31.
3. Simani S. Rabies Disease. 1st Ed. Tehran: Pasteur Institute
of Iran pub; 2004.
4. World Health Organization. WHO technical report series 931:
WHO expert consultation on rabies; first report. Geneva
Switzerland: WHO; 2005. p13
5. World Health Organization, Regional Office for South East
Asia. Prevention and control of rabies in South-East Asia
Region 2004, New Delhi. SEA-Rabies; 2004.
6. Quiambao BP, Dimaano EM, Ambas C, Davis R, Banzhoff A,
Malerczyk C. Reducing the cost of post-exposure rabies
prophylaxis: Efficacy of 0.1ml PCEC rabies vaccine
administered intradermally using the Thai Red Cross post-
exposure regimen in patients severely exposed to laboratory
confirmed rabid animal. Vaccine 2005; 23:1709-14.
21
7. World health Organization. World survey of rabies No 34 for
the year 1998 WHO/CDS/CSR/APH/99.6 World Health Organization,
Geneva, Switzerland, 1999.
8. Centre for Disease Prevention and Control. Human rabies
prevention—United States, 2008: recommendations of the
Advisory Committee on Immunization Practices. MMWR Recomm Rep
57: 1–28.
9. Rupprecht CE, Hanlon CA, Hemachudha T. Rabies re-examined.
Lancet Infect Dis 2002; 2:327–343.
10. Owolodun BY. Rabies in cattle in Northern States/Nigeria.
Bull. Epizoot Dis Afri 1968; 16:425-427.
11. Rweyemamu MM, Loretu K, Jackob H, Gorton E. Observation on
rabies in Tanzania Bull Epizoot Dis Afri 1973;21:19-27.
12. Kitala P, Perry B, Barrat J, King A. Proceedings of the
Southern and Eastern African Rabies Group (SEARG) Meeting, 4
_ 6 March 1997, Nairobi, Kenya, 1997.
13. Fekadu M. Rabies in Ethiopia. Am J Epidemiol 1982; 115:266-
73.
14. World Health Organization. Strategies for the control and
elimination of rabies in Asia. Report of a WHO interregional
consultation. Geneva: The Organization; 2002.
15. Rutebarika C, Winyi-Kaboyo R, Barrat J, King A.
Proceedings of the Southern and Eastern African Rabies Group
meeting. Entebbe, Uganda: Foundation Marcel Merieux; 2000.
16. Bögel K, Meslin F-X. Economics of human and canine rabies
elimination: guidelines for programme orientation. Bull World
Health Organ 1990; 68:281–91.
22
17. Knobel DL, Cleave land S, Coleman PG: Re-evaluating the
burden of rabies in Africa and Asia. Bull World Health Organ 2005,
83:3.
18. Tang Q, Zhao XQ, Tao XX: Analysis on the present situation
of human rabies epidemic in China. Chinese Journal of Epidemiology
2001, 22:8-10. 60-8.
19. World Health Organization (1998) World rabies survey No.
32 for the year 1996. Geneva: WHO document WHO/EMC/ZDI/98.4.
20. Fekadu M. Human rabies surveillance and control in
Ethiopia. In: proceeding of the southern and eastern African
rabies group meeting 1997 March 4–6; Nairobi, Kenya.
21. Deressa A, Ali A, Beyene M, Newaye Selassie B, Yimer E.
The status of rabies in Ethiopia: A retrospective record
review. Ethiopian Journal of Health Development 2010; 24:127–132.
22. Knobel DL, Cleaveland S, Coleman PG, Fevre EM, Meltzer MI.
Re-evaluating the burden of rabies in Africa and Asia.
Bulletin of the World Health Organization 2005; 83: 360–368.
23. Jesse DB, Nadine YB et’al. Rabies Post-exposure Prophylaxis,
New York, 1995–2000.
24. Miao S., Qing T. Epidemiological investigations of human
rabies in China1996 to 2008.
25. Kitalaa P.M., McDermotta J.J., Kyulea M.N., Gathuma J.M.
Community-based active surveillance for rabies in Machakos
District, Kenya. Preventive Veterinary Medicine 1999; 44 (2000): 73-
85.
26. Abubakar SA, Bakari AG. Incidence of dog bite injuries
and clinical rabies in a tertiary health care institution: A
23
10-year retrospective study. Annals of African Medicine 2012;
11(2):108-111
27. Humphrey D Mazigo, Fredros O Okumu, Eliningaya J Kweka.
Retrospective analysis of suspected rabies cases reported at
Bugando Referral Hospital, Mwanza, Tanzania. Journal of Global
Infectious Diseases 2010; 2(3):216-220.
28. Asefa D., Abraham A., Mekoro B., Bethelehem NS, Eshetu Y.,
Kedir H. The status of rabies in Ethiopia: A retrospective
record review. Ethiopian Journal of Health Development 2010;
24(2):127-132.
29.Wudu T., Wassie M., Gizat A., Sefinew A. Incidence of Rabies
in Humans and Domestic Animals and People's Awareness in North
Gondar Zone, Ethiopia. PLOS Neglected Tropical Diseases 2013; 7(5):
e2216.
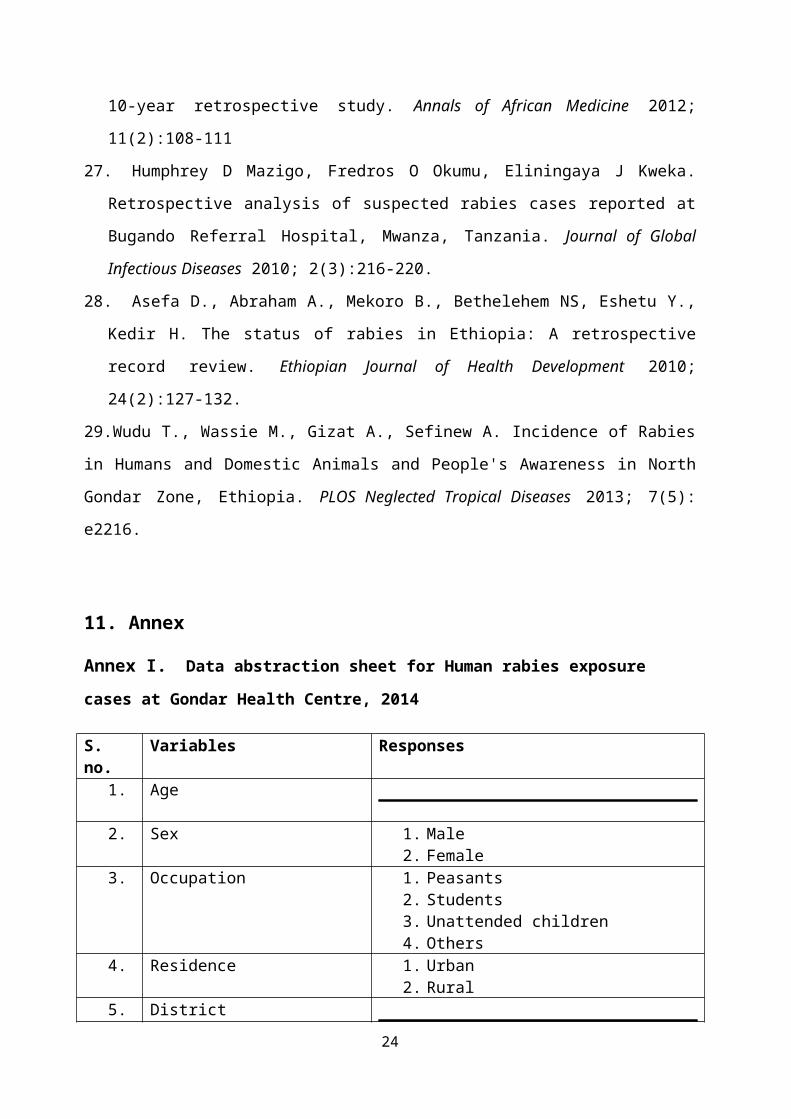
11. Annex
Annex I. Data abstraction sheet for Human rabies exposure cases at Gondar Health Centre, 2014
S. no.
Variables Responses
1. Age
2. Sex 1. Male 2. Female
3. Occupation 1. Peasants 2. Students 3. Unattended children 4. Others
4. Residence 1. Urban 2. Rural
5. District 24
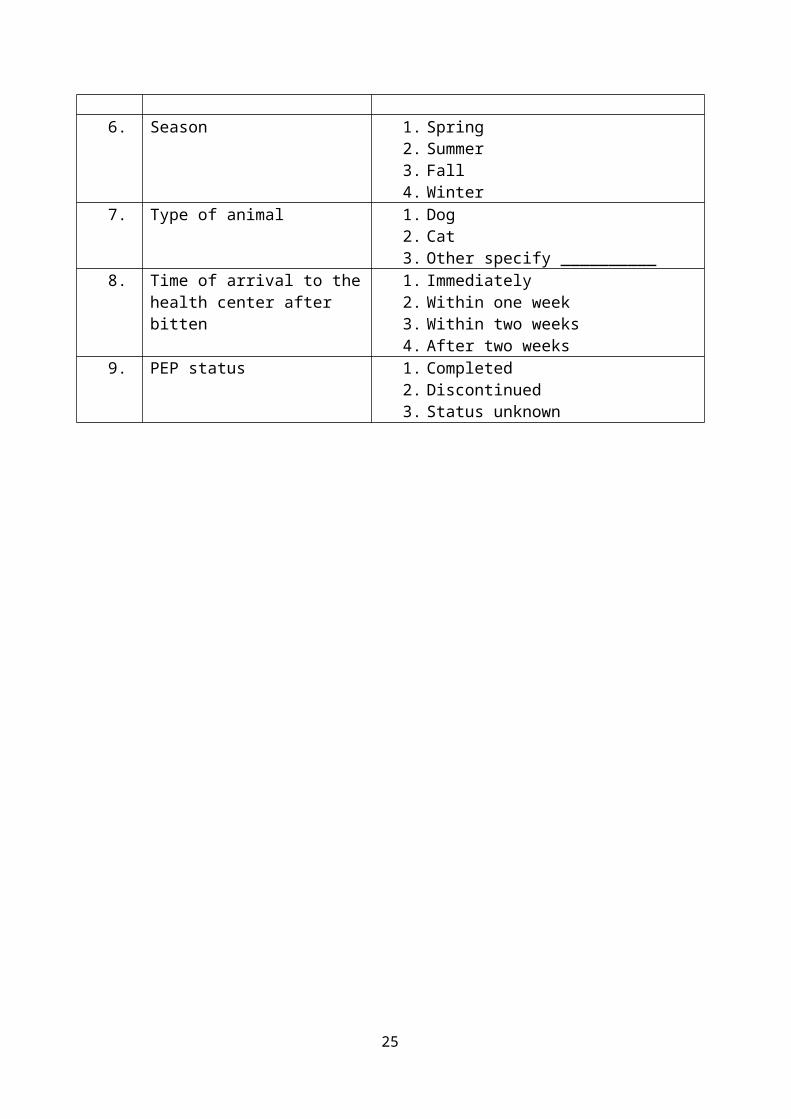
6. Season 1. Spring 2. Summer 3. Fall 4. Winter
7. Type of animal 1. Dog 2. Cat 3. Other specify __________
8. Time of arrival to thehealth center after bitten
1. Immediately 2. Within one week3. Within two weeks 4. After two weeks
9. PEP status 1. Completed 2. Discontinued 3. Status unknown
25




















