
The vulnerability to alcohol and substance abuse in individuals diagnosed with schizophrenia

ARTICLE IN PRESS
1353-8292/$ - se
doi:10.1016/j.he
�Correspondfax: +1204474
E-mail addr
(G. DeVerteuil
Health & Place 13 (2007) 310–323
www.elsevier.com/locate/healthplace
Mental health and the city: Intra-urban mobility amongindividuals with schizophrenia
Geoffrey DeVerteuila,�, Aynslie Hindsb, Lisa Lixb, John Walkerc,Renee Robinsond, Leslie L. Roosb
aDepartment of Environment & Geography, University of Manitoba, Isbister 211, Winnipeg, Man., Canada R3T 2N2bDepartment of Community Health Sciences, Manitoba Centre for Health Policy, University of Manitoba, Winnipeg, MB, Canada R3E 3P5
cDepartment of Clinical Health Psychology University of Manitoba St. Boniface, General Hospital, 409 Tache Avenue, Winnipeg, MB
Canada R2H 2A6dFaculty of Health Studies, Brandon University, 270 18th Street, Brandon, MB R7A 6A9
Received 14 February 2005; received in revised form 23 January 2006; accepted 6 February 2006
Abstract
Intra-urban residential mobility of a cohort with schizophrenia was compared to a matched cohort with no mental
illness using population-based administrative data. The percentage of individuals with one or more changes in postal code
in the three-year mobility study period was examined, along with measures of the movement between different intra-urban
areas. The schizophrenia cohort was more likely to move than the matched cohort; however, this depends on their age,
income level, and area of residence at baseline. Age, gender, marital status, income quintile, and use of physicians and
hospitalizations were associated with mobility. Individuals in the schizophrenia cohort were significantly more likely to
move from the suburb to the inner city, and significantly less likely to move from the inner city to the suburb than those
with no mental illness. Implications of the findings and directions for future research are discussed, with particular
attention paid to the utility of administrative data for further mental health research.
r 2006 Elsevier Ltd. All rights reserved.
Keywords: Mental health; Schizophrenia; Residential mobility; Winnipeg; Administrative data; Neighbourhood scale
Introduction
In their landmark study on the geographicvariability of mental illness in the city, Faris andDunham (1939) observed an association betweenhigh rates of certain severe and enduring mental
e front matter r 2006 Elsevier Ltd. All rights reserved
althplace.2006.02.001
ing author. Tel.: +1204 474 8255;
7699.
ess: [email protected]
).
illness, particularly schizophrenia (less so forbipolar and affective disorders), and residence indisadvantaged and socially disorganized inner-cityneighbourhoods in Chicago. An extensive literatureon ‘‘psychiatric geographies’’ (Giggs, 1973; Lapouseet al., 1956; Dear and Wolch, 1987; Wolch andPhilo, 2000; Silver et al., 2002; Almog et al., 2004)has largely confirmed the pattern Faris and Dun-ham first identified—that individuals with schizo-phrenia continue to cluster in disadvantaged inner-city areas. There are two well-established theories
.

ARTICLE IN PRESSG. DeVerteuil et al. / Health & Place 13 (2007) 310–323 311
for the over-representation of individuals withschizophrenia in the inner city and their under-representation in suburban areas: the social selec-tion and social causation hypotheses. The socialselection hypothesis focuses on whether individualswith schizophrenia drift into deprived, service-richinner-city areas, while the social causation hypoth-esis focuses on the disproportionate development ofthe disease in socially disorganized and residualneighbourhoods (Dear et al., 1980; Dohrenwendet al., 1992; Timms, 1998; Wolch and Philo, 2000;Silver et al., 2002).
Despite the well-established findings on the geo-graphic distribution of individuals with schizophre-nia, there has been limited study about theirresidential mobility (DeVerteuil, 2003; Bhugra,2004; Lix et al., 2006). Understanding residentialmobility patterns—including the degree to whichindividuals with schizophrenia move, where theymove from and to, and whether these patterns differfrom the general population—is important forseveral reasons. First, in a post-asylum, post-mentalhealth reform era, it is more important than ever tohave an accurate ‘‘big picture’’ of the dominant flowsof individuals with schizophrenia, in order to providethe most equitable distribution of services (Wolchand Philo, 2000). From the perspective of individualswith schizophrenia, there are equity concerns invol-ving the social and built environments in which theymust live and cope with—in particular, the degree towhich mobility patterns are intersecting with stigma-tized and disadvantaged neighbourhoods. This canpossibly lead to spatial entrapment which in turn canworsen mental health problems and even facilitateadditional disorders, such as substance abuse. Fromthe perspective of neighbourhoods, there are equityconcerns over why so few are obliged to supportthe majority of individuals with schizophrenia,and why most neighbourhoods are not similarlyobliged. Second, moving can be a stressful life event,negatively affecting both physical and mentalhealth (Torrey et al., 1992; DeVerteuil, 2003; Bhugra,2004; Larson et al., 2004). High levels of mobility,particularly homelessness, can create discontinuitiesin the receipt of health care and disrupt employment,education and social support networks, as well asprecipitate a relapse (Bastide, 1972; Bachrach, 1987;Abood et al., 2002; Harkness et al., 2004). Alter-natively, moving may be positive when it involves areduction in the distance to health care and/or familysupports (Dear and Wolch, 1987; Milligan, 1996;Breslow et al., 1998).
A more systematic understanding of the varia-tions in the likelihood of mobility (i.e. the likelihoodof making at least one permanent residential movein a designated time period) as well as the overalldirection of mobility (i.e. the direction of permanentresidential moves across different environments,such as rural to urban, suburbs to inner city, etc.)among individuals with schizophrenia would help toclarify these issues. In terms of the likelihood ofmobility, previous research is inconsistent aboutwhether individuals with schizophrenia are moremobile than the general population. This incon-sistency partly stems from limited samples thatmake the detection of mobility differences betweendifferent populations difficult to detect. In addition,studies of the direction of mobility have beenlimited by coarse levels of geography, such ascounties, which may not provide a sufficientlysensitive scale to detect differences among groups.Systematic studies of mobility at an intra-urban,neighbourhood scale have rarely been undertaken.
This paper re-examines, with the advantage ofpopulation-based administrative health data, boththe likelihood and direction of intra-urban mobilityamong individuals with schizophrenia, a numeri-cally important subgroup of the severely mentallyill. Using population-based data enables us toidentify all individuals with a diagnosed mentalillness in a specified period of time, as well as anappropriate non-mentally ill comparison group, andto track the movement of both groups over time at afine level of geographic scale. The goals of this studywere to: (1) examine the geographic variability of acohort diagnosed with schizophrenia in a particularcity; (2) examine and compare the socio-demo-graphic characteristics of the schizophrenia cohortand a matched control cohort; and (3) compare thelikelihood and direction of residential mobility ofthese cohorts and examine the variables associatedwith residential mobility within a particular city. Toaddress these goals, we first review the literature,identify gaps and propose two research questions.Second, we present the methods and data, followedby the results. Finally, we discuss the results and itsimplications, suggesting future lines of research tobetter understand the complex and dynamic geo-graphies of schizophrenia in the city.
Literature review
Research findings on the likelihood of residentialmobility among individuals with schizophrenia

ARTICLE IN PRESSG. DeVerteuil et al. / Health & Place 13 (2007) 310–323312
remain inconclusive. On one hand, there is evidencesuggesting that the likelihood of moving forindividuals with schizophrenia is greater than forthe general population (Lix et al., 2006). Demblinget al. (2002) found that one-third of individuals withthree or more inpatient admissions to Virginia statepsychiatric facilities had changed their county ofresidence between their first and last admission(which corresponded to a mean observation periodof 5.6 years). In comparison, Census data showedonly 15% of the general population reporting acounty change of residence in a five-year period.Small-scale research by Hopper et al. (1997)indicated that of a sample of 36 individuals withschizophrenia and other severe mental illnessesapplying for shelter in Westchester County NY in1995, 20 were suffering from excessive mobilityacross unrelated, inadvertent and inappropriateinstitutional settings.
On the other hand, not all research has supportedthe thesis of greater residential mobility amongindividuals with schizophrenia compared to thegeneral population (Lesage and Tansella, 1989;McNaught et al., 1997). Lesage and Tansella(1989) found that the likelihood of residentialmobility of individuals with schizophrenia was lessthan that of individuals with non-psychotic dis-orders. In a five-year period, they found approxi-mately 18% of a schizophrenia cohort, 30% of aneurotic cohort, and 22% of a cohort representingthe general population moved. These differenceswere not statistically significant, which the authorsattributed to small sample sizes. Chesteen et al.(1970) found that only 4% of their psychiatricpatient sample moved an average of once a year,while 8% moved on average once every two years.These rates were significantly lower than thereported national mobility rate of 20% (from the1964 US Census Bureau of Statistics).
These inconclusive results stem partly frommethodological limitations of research conductedto date. For example, Larson et al. (2004) noted thatstudies examining the relationship between healthand mobility have been hindered by the lack ofdatabases that combine person-specific informationon health status and changes in location ofresidence. This is certainly the case with studies onthe residential mobility of individuals with schizo-phrenia. Data that are primarily obtained from thecase registries of specific facilities or service provi-ders (e.g., Abood et al., 2002; Chesteen et al., 1970;Lamont et al., 2000) limit the generalizability of
study findings to the larger population of indivi-duals with schizophrenia. Moreover, population-based data have only rarely been used to selectcomparison groups representative of the generalpopulation or of populations with different types ofhealth conditions (e.g., Lesage and Tansella, 1989).Such comparative data are critical for understand-ing to what degree mobility of individuals withschizophrenia differs from other groups.
There is also some inconclusive evidence tosuggest that the direction of mobility amongindividuals with schizophrenia differs from thegeneral population, albeit at a very coarse geo-graphic scale of analysis. A number of studies havedefined residential mobility on the basis of move-ment between counties or other large geographicareas (Milligan, 1996; Breslow et al., 1998; Dem-bling et al., 2002); this may be too insensitive todetect differences among groups or within specificcities (i.e. at the intra-urban, neighbourhood scale).With these limitations in mind, Dembling et al.(2002) demonstrated that the flow of individuals inthe patient population into and out of countiesdiffered from the pattern of the general popula-tion—such that counties with the largest out-migration of the patient population experiencedthe greatest growth rates in the general population.Mental health consumers also tended to migrate tolow-income, medium-sized urban counties withlower per capita income, higher age-adjusted deathrates, higher proportion of institutionalized popula-tions, and higher proportion of non-family house-holds, and away from rural and large urbancounties. The authors further noted that countieshaving a state psychiatric facility experienced a netincrease in the patient population. Similarly, Bre-slow et al. (1998) found that patients accessingservices in a county outside of their county ofresidence were more likely to have moved (to thecounty with the psychiatric services) at follow-upthan patients who accessed services within theircounty of residence. This finding is consistent withLamont et al. (2000), who found that patients whowere hospitalized outside of their catchment areawere five times more likely to move than those whowere hospitalized inside their catchment area.
Research questions
Given these methodological and data limitationsin previous research on the mobility of individuals

ARTICLE IN PRESSG. DeVerteuil et al. / Health & Place 13 (2007) 310–323 313
with schizophrenia, it seems appropriate to examinetwo key questions within mental health geography:
1.
Is the likelihood of moving higher among acohort of individuals with schizophrenia thanamong an age–sex matched cohort?2.
Is a cohort of individuals with schizophreniamore likely to move to lower income, inner-cityneighbourhoods and less likely to move tosuburban, higher-income neighbourhoods thanan age–sex matched cohort?Data and methods
Data sources
The data are from the Winnipeg Regional HealthAuthority (WRHA), which encompasses the City ofWinnipeg (the provincial capital of Manitoba,Canada) and several exurban areas. As of June 1,2002, the population of the WRHA was approxi-mately 650,000, or 60% of the province’s entirepopulation (WRHA, 2004). A regional healthauthority in Manitoba has ‘‘the responsibility forproviding for the delivery and administration ofhealth services in specified geographic areas’’(Manitoba Health, 2004). As of 2005, there wereten rural health authorities, plus the urban WRHA,in the province. Not unlike other provinces inCanada, the Manitoba mental health system hasexperienced dramatic changes in the delivery ofhealth services in the last two decades: a model ofservice delivery centred on acute care institutionshas been replaced by one of community-basedprimary care. Most notably, mental health reformhas de-emphasized institutional residence and carein favour of integration of both individuals andtreatment options into mainstream communities.
The Manitoba Centre for Health Policy (MCHP)houses a Population Health Research Data Repo-sitory which contains anonymized administrativehealth records for all Manitoba residents eligible toreceive health services. Virtually all residents of theprovince and almost all contacts with physicians(i.e. licensed medical doctors who are salaried orworking on a fee-per-service basis) and hospitals arecaptured in the Repository. The databases in thePopulation Health Research Data Repository canbe linked to create a history of health service usefor all Manitoba residents as well as a history oflocation of residence. Moreover, diagnosis informa-tion contained in the administrative files can be used
to identify individuals receiving health services forspecific conditions or diseases. The Repository datafiles accessed for this project were the populationregistry, hospital abstracts, and medical claims.
The population registry contains histories foreach individual registered with the Manitoba HealthServices Insurance Plan since 1970. The registryincludes a unique encrypted personal health identi-fication number, demographic characteristics (e.g.,age and sex), location of residence at the level of thesix-digit postal code, and family composition foreach registrant. The registry files are updated every6 months (i.e. June 30 and December 31); this allowschanges to these characteristics to be tracked overtime via the linked encrypted identification number.The accuracy of the registry is enhanced byinformation from other sources, such as the vitalstatistics file and hospital abstracts (Roos andNicol, 1999). Hospital abstracts and medical claimsfiles were linked to the registry via the encryptedidentification number. Hospital abstracts are com-pleted at the point of discharge for all separationsfrom hospitals in the province. Medical claims aresubmitted to the provincial health ministry byManitoba physicians who are paid on a fee-for-service basis. Almost all salaried physicians alsosubmit parallel claims for administrative purposes.Both specialists and general-practice physicianssubmit billing claims. Hospital abstracts and med-ical claims include both diagnostic and proceduralcodes. The International Classification of Diseases,9th revision (ICD-9-CM) diagnostic codes con-tained in these records were used to identifymembers of the two mutually exclusive studycohorts. Ethics approval was secured throughthe Health Research Ethics Board of the Universityof Manitoba, and access to the data was grantedby the Health Information Privacy Committee ofManitoba.
Definition of cohorts
Individuals who were continuous residents of theWRHA for the entire study period (i.e. April 1, 1996to December 31, 2002) and who were 19 years of agein 1999 (i.e. study mid-point) were eligible forinclusion. Diagnoses contained in the administrativedata for the fiscal years of April 1, 1996 to March31, 2000 were used to define the study cohort—thisrepresents the definition period. During this four-year definition period, individuals with a diagnosisof schizophrenia (ICD-9-CM 295) in either hospital

ARTICLE IN PRESSG. DeVerteuil et al. / Health & Place 13 (2007) 310–323314
abstracts or medical claims were included in theschizophrenia cohort. Those individuals whosepostal code corresponded to a public trustee’soffice (which was clearly not their residence) wereexcluded. A control group with no mental healthdiagnoses (as defined by ICD-9-CM codes in therange 290–319 inclusive in either hospital abstractsor medical claims for the period April 1, 1996 toMarch 31, 2000) was selected on the basis ofmatching age (in 1999/2000) and sex to theschizophrenia cohort. Five controls were selectedfor every case. Members from both cohorts werethen prospectively followed from June 30, 1999 toJune 30, 2002 to monitor changes in residencelocation using the six-digit postal code captured inthe population registry—this represents the actualmobility study period.
Definitions of mobility
Previous studies of residential mobility of indivi-duals with schizophrenia have examined mobilitybetween counties or other large geographic areas. Inthis study, we were interested in monitoring themovement of individuals at the intra-urban scale.To this end, the WRHA was divided into threeintra-urban areas that reflect different social andbuilt environments. Using the geographic bound-aries of 75 neighbourhoods (as defined by the areasurrounding a Winnipeg Community Centre build-ing), the WRHA was divided into inner core, outercore, and suburb areas. Given that no singlegeographical classificatory scheme can encompassall of the multifaceted complexities of the city (Ley,2001), we decided to limit our focus to a combina-tion of (1) measures of housing age and density,which were used by McLemore et al. (1975), Ramet al. (1989) and Walks (2001) to distinguish theCanadian inner city as older, denser areas vis-a-visthe rest of the metropolis, and (2) a common socio-economic measure, household income, that isessential in delineating areas of urban disadvantageand deprivation from more prosperous ones (Thor-nicroft, 1991; Silver et al., 2002). Operationally, weused 2001 Statistics Canada Census data for density(persons per hectare), housing age (proportion ofhousing stock built before 1946), and income(median household income). These variables werethe most straightforward way to measure housingage, population density and income. WRHAmedian values for each of these variables were usedto assign the neighbourhoods to areas.
As Table 1 indicates, core neighbourhoods hadpopulation density and pre-1946 housing age valuesabove the WRHA median. However, neighbour-hoods in the inner core were poorer, with householdincome values below the WRHA median, whilethose in the outer core were substantially moreaffluent. The suburb area included neighbourhoodswhose proportion of pre-1946 housing and popula-tion density were below median WRHA values.
Table 1 also profiles the three intra-urban areasaccording to four key variables that are relevant tothe everyday survival of individuals with schizo-phrenia: the availability of low-cost housing, asmeasured by average gross rent (Canadian CensusAnalyser, 2004) and rooming home units (defined aslow-end, private rental accommodation that act ashousing of last resort for many individuals withsevere mental illness, parolees, etc., and that usuallydo not offer treatment) per 1000 population; andpotential sites of mental health care, as measured bythe number of psychiatric beds and licensed mentalhealth care facility beds per 1000 population. It isimportant to note that there are no stand-alonemental health care in-patient facilities in theWRHA. The inner core has the most low-renthousing and the greatest concentration of psychia-tric services. Further, the average rent for the innercore is almost twice the amount allowed through theprovince’s income assistance housing allowance forlow-income individuals.
The six-digit postal code in the populationregistry at June 30, 1999 was used to establish thebaseline location of residence for the purposes of theensuing mobility study period. In Winnipeg, a singlepostal code tends to occupy a very small area,limited usually to one side of a residential block, ora medium-sized apartment building. As of 2001,there were approximately 19,000 postal codes in theWRHA.
Three definitions of residential mobility wereadopted. The first definition focused on the like-
lihood of a move, measured by at least one change inpostal code within the WRHA between the mobilitystudy period baseline (June 30, 1999) and endpoint(June 30, 2002) dates. This definition was usedto create a dichotomous variable with the categoriesof mover and non-mover. Two other mobilitydefinitions assessed the direction of residentialmobility and were based on a comparison ofarea of residence at the baseline and endpoint dates.The second mobility definition was a change inpostal code between baseline and endpoint that

ARTICLE IN PRESS
Table 1
Intra-urban area characteristics in the WRHA
Intra-urban
area
Median % pre-
1946 housing
(SD)a
Median
household
income in
$Cdn (SD)b
Median
population
density per
hectare
(SD)c
Total
population
Average
Gross Rent in
$Cdn
Psychiatric
beds per 1000
populationd
Licensed
mental health
care facility
beds per 1000
populatione
Rooming
home units
per 1000
populationf
Inner core 44.8 (15.1) $33,579 (7395) 31.03 (17.01) 181,090 $518.51 0.61 1.39 3.92
Outer core 40.8 (9.9) $49,152 (12,490) 26.95 (7.83) 44,393 $882.50 0 0.16 0.36
Suburb 4.6 (1.2) $59,557 (15,937) 18.87 (4.92) 408,107 $603.00 0.19 0.24 0.06
All three types of facilities were geocoded in a GIS and then aggregated by area.aMedian WRHA value for % pre-1946 housing was 19.75%.bMedian WRHA value for household income was $46,425.cMedian WRHA value for population density was 23.36 persons per hectare.dData for psychiatric beds were obtained from the Winnipeg Regional Health Authority (WRHA), December 2000.eData for licensed mental health care facilities (which provide space for 4–6 residents) was provided directly by the WRHA, December
2001.fRooming home data were obtained from a 1999 City of Winnipeg survey.
G. DeVerteuil et al. / Health & Place 13 (2007) 310–323 315
corresponded to a move from the suburb to theinner core; this definition was used to create adichotomous variable with categories of suburb-to-inner core mover and non-mover. The thirdmobility definition was a change in postal codebetween baseline and endpoint that corresponded toa move from the inner core to the suburb. Thisdefinition was used to create a dichotomous variablewith categories of inner core-to-suburb mover andnon-mover. The number of individuals inhabitingthe outer core was too small to assess direction ofmobility (see Table 1).
Determinants of mobility
Demographic, socio-economic, and health serviceuse variables were explored as determinants ofmobility. Demographic characteristics included agegroup (19–44 years, 45–64 years, and 65+ years),sex, intra-urban area of residence at baseline (innercore, outer core, and suburb), and marital status(single, married, and widowed). These variableswere defined from baseline registry data (i.e. June1999). An area-level socio-economic measure, in-come quintile, was derived from Statistics CanadaCensus data. Each quintile (i.e. Q1–Q5) represents20% of the population (Roos and Mustard, 1997).
The health care utilization measures were countsof the number of hospitalizations and the numberof physician visits for each member of the cohortsin the fiscal year 1999/2000. Three categories ofhospital separations and physician claims wereformed based on the frequency distributions of the
data for each of the study cohorts. The categoriesfor hospital use were 0, 1–2, and 3 or more, and thecategories for physician visits were 0–3, 4–9, and 10or more.
Analyses
The data were initially described using frequencydistributions. Logistic regression analyses were usedto model mobility as a function of cohort, demo-graphic, socio-economic, and health service usevariables. All independent variables were categori-cal; the reference categories were matched controlcohort, 65 years and older, female, lowest incomequintile, and married, 0 hospitalizations and 0–3physician visits. The logistic regression modelsincluded main effects as well as two-way interac-tions between the cohort variable and some of thedeterminants of mobility. Wald w2 tests were used toassess statistical significance of the main andinteraction effects. Model fit statistics were used toassess the adequacy of each model (Fox, 1997).Odds ratios (ORs) and 95% confidence intervals arereported. The analyses were conducted using PROCGENMOD in SAS (SAS Institute, 1999).
Results
A total of 2443 individuals continuously residentin the WRHA during the entire study period wereidentified with a diagnosis of schizophrenia in thedefinition period (April 1, 1996 to March 31, 2000).There were 12,135 individuals in the matched

ARTICLE IN PRESS
Table 2
Characteristics of schizophrenia and matched cohorts
Variable Schizophrenia
cohort
Matched cohort
ðN ¼ 2443Þ ðN ¼ 12; 135Þ
n % n %
Age
19–44 years 1230 50.4 6109 50.3
45–64 years 880 36.0 4364 36.0
65+ years 333 13.6 1662 13.7
Sex
Male 1323 54.2 6557 54.0
Female 1120 45.9 5578 46.0
Marital status
Married 570 23.3 6868 56.6
Single 1780 72.9 4740 39.1
Widowed 87 3.6 500 4.1
Unknown 6 0.3 27 0.2
Area of residence at
baseline
Inner core 1333 54.6 3458 28.5
Outer core 163 6.7 858 7.1
Suburb 947 38.8 7819 64.4
Income quintile
Q1 (poorest) 1009 42.3 2221 18.4
Q2 564 23.6 2479 20.5
Q3 397 16.6 2295 19.0
Q4 240 10.1 2544 21.1
Q5 (wealthiest) 176 7.4 2549 21.1
Hospitalizations
0 1820 74.5 11,559 95.3
1–2 537 22.0 511 4.2
3 or more 86 3.5 65 0.5
Physician visits
0–3 206 8.4 4840 39.9
4–9 513 21.0 3703 30.5
10 or more 1724 70.6 3592 29.6
G. DeVerteuil et al. / Health & Place 13 (2007) 310–323316
cohort. Socio-demographically, the schizophreniacohort and matched cohort differed in severalrespects, as shown in Table 2.
The majority of the schizophrenia cohort was inthe youngest age group (50.4%) and was more likelyto be male (54.2%). Similar age and sex distribu-tions of the two cohorts attested to the success ofthe matching process. Marital status differedmarkedly between the two cohorts; individuals inthe schizophrenia cohort were predominately single(72.9%), while the majority of individuals in thematched cohort were married (56.6%). Health care
use also differed substantially between the twocohorts; members of the schizophrenia cohort weremore likely than the matched cohort to behospitalized and to visit a physician.
The geographic distribution of the schizophreniacohort at baseline (June 1999) is displayed in Fig. 1.The figure first shows a distinctly concentric patternto the three intra-urban areas. The inner corecoincided with the central neighbourhoods sur-rounding the Central Business District (CBD),including the North and West Ends, while the outercore—associated with areas of established wealththat have maintained their integrity over time, suchas River Heights—was primarily to the southwest ofthe CBD. The suburb encompassed all of theoutlying neighbourhoods. Although the patternappears quite concentric, it does obscure a some-what more complex geography of income (but nothousing age and population density), includingpockets of suburban poverty in newer, low-densityneighbourhoods such as St. Vital and Transcona,as well as more middle-class neighbourhoods inolder, denser areas such as Osborne Village and St.Boniface. Second, individuals with schizophreniawere strongly concentrated in the inner core. Atbaseline, the majority of the schizophrenia cohortlived in the inner core (54.6%), while most of thematched cohort lived in the suburb areas (64.4%).Few individuals in either cohort lived in the outercore. Two-thirds of the schizophrenia cohort,compared to fewer than 40% of the matchedcohort, resided in areas categorized as among thepoorest two income quintiles, while over 40% of thematched cohort and less than 18% of the schizo-phrenia cohort were found in the wealthiest twoincome quintiles.
1. Is the likelihood of moving higher among a
cohort of individuals with schizophrenia than among
an age– sex matched cohort?
During the three-year mobility study period (June30, 1999 to June 30, 2002), the majority ofindividuals in both cohorts did not move. However,persons in the schizophrenia cohort were moremobile than the matched cohort: approximately35% of the former cohort, compared to approxi-mately 22% of the latter cohort, moved over thethree years. Given that almost three-quarters of theschizophrenia cohort is single, we can safely assumethat they are mostly moving alone. Whether home-lessness, a common condition among individualswith severe mental illness (DeVerteuil, 2003), isdriving part of the ‘‘excess’’ residential mobility

ARTICLE IN PRESS
Fig. 1. Distribution of Schizophrenia cohort at baseline (June 1999) by neighbourhood, Winnipeg Regional Health Authority.
G. DeVerteuil et al. / Health & Place 13 (2007) 310–323 317
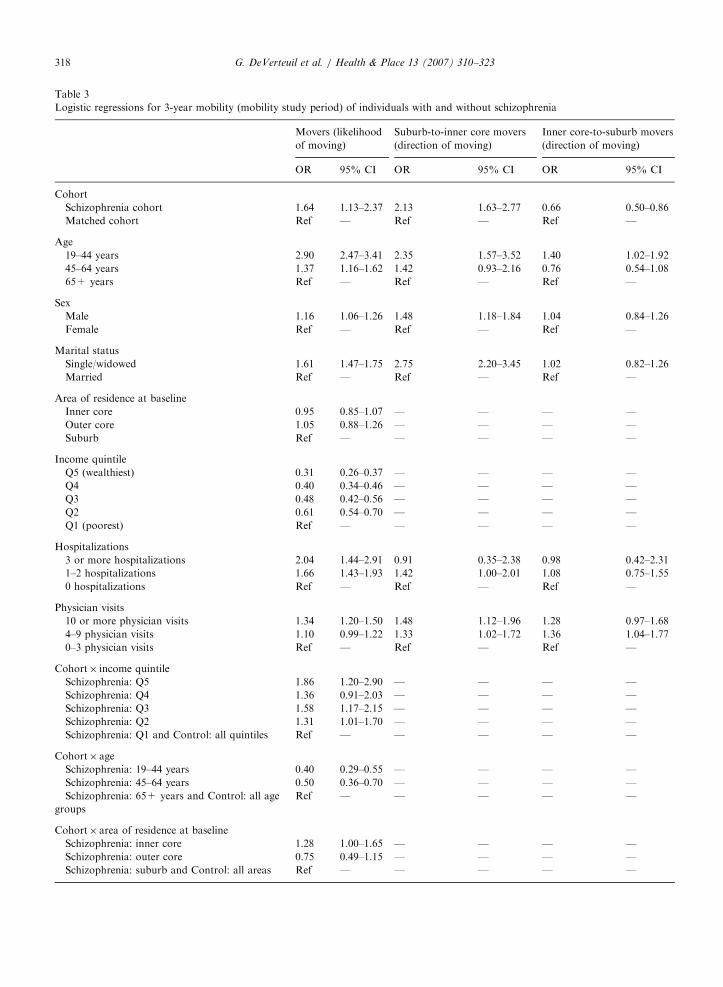
among the schizophrenia cohort is impossible todeduce from the administrative data.1 Tests ofsignificance of these differences are reported inTable 3.
The first logistic regression analysis focused onthe likelihood of residential movement. The ratio ofthe model deviance to its degrees of freedom (df)for this model was 1.02. Values close to oneindicate good model fit (Littell et al., 2002). Themain effects, with the exception of region ofresidence at baseline, were statistically significant,as well as the following two-way interactions:cohort� age group ðpo0:0001Þ, cohort� incomequintile ðp ¼ 0:0123Þ, and cohort� region of resi-dence at baseline ðp ¼ 0:0207Þ. The ORs for thismodel are reported in Table 3.
1More generally, studies and counts of homeless individuals in
urban Canada have suggested that individuals with severe mental
illness are over-represented (Peressini and McDonald, 2001).
The odds of moving were higher for the schizo-phrenia cohort than the matched cohort althoughthis depended on their age, income level and regionof residence at baseline. The odds of moving werehigher for males, for individuals who were single orwidowed, and for those with greater numbers ofhospitalizations and physician visits.
The cohort� age group interaction revealed low-er ORs for the schizophrenia cohort in the 19–44years and 45–64 years age groups. Table 4 containsthe age distribution of movers and non-movers forboth cohorts which illustrates the nature of thisparticular interaction.
Despite the higher overall percentage of moversin the schizophrenia cohort, younger individuals inthe matched cohort were more likely to move thanin the schizophrenia cohort.
The cohort� income quintile interaction revealedhigher ORs for the schizophrenia cohort in thesecond (Q2), third (Q3), and fifth (Q5) income
ARTICLE IN PRESS
Table 3
Logistic regressions for 3-year mobility (mobility study period) of individuals with and without schizophrenia
Movers (likelihood
of moving)
Suburb-to-inner core movers
(direction of moving)
Inner core-to-suburb movers
(direction of moving)
OR 95% CI OR 95% CI OR 95% CI
Cohort
Schizophrenia cohort 1.64 1.13–2.37 2.13 1.63–2.77 0.66 0.50–0.86
Matched cohort Ref — Ref — Ref —
Age
19–44 years 2.90 2.47–3.41 2.35 1.57–3.52 1.40 1.02–1.92
45–64 years 1.37 1.16–1.62 1.42 0.93–2.16 0.76 0.54–1.08
65+ years Ref — Ref — Ref —
Sex
Male 1.16 1.06–1.26 1.48 1.18–1.84 1.04 0.84–1.26
Female Ref — Ref — Ref —
Marital status
Single/widowed 1.61 1.47–1.75 2.75 2.20–3.45 1.02 0.82–1.26
Married Ref — Ref — Ref —
Area of residence at baseline
Inner core 0.95 0.85–1.07 — — — —
Outer core 1.05 0.88–1.26 — — — —
Suburb Ref — — — — —
Income quintile
Q5 (wealthiest) 0.31 0.26–0.37 — — — —
Q4 0.40 0.34–0.46 — — — —
Q3 0.48 0.42–0.56 — — — —
Q2 0.61 0.54–0.70 — — — —
Q1 (poorest) Ref — — — — —
Hospitalizations
3 or more hospitalizations 2.04 1.44–2.91 0.91 0.35–2.38 0.98 0.42–2.31
1–2 hospitalizations 1.66 1.43–1.93 1.42 1.00–2.01 1.08 0.75–1.55
0 hospitalizations Ref — Ref — Ref —
Physician visits
10 or more physician visits 1.34 1.20–1.50 1.48 1.12–1.96 1.28 0.97–1.68
4–9 physician visits 1.10 0.99–1.22 1.33 1.02–1.72 1.36 1.04–1.77
0–3 physician visits Ref — Ref — Ref —
Cohort� income quintile
Schizophrenia: Q5 1.86 1.20–2.90 — — — —
Schizophrenia: Q4 1.36 0.91–2.03 — — — —
Schizophrenia: Q3 1.58 1.17–2.15 — — — —
Schizophrenia: Q2 1.31 1.01–1.70 — — — —
Schizophrenia: Q1 and Control: all quintiles Ref — — — — —
Cohort� age
Schizophrenia: 19–44 years 0.40 0.29–0.55 — — — —
Schizophrenia: 45–64 years 0.50 0.36–0.70 — — — —
Schizophrenia: 65+ years and Control: all age
groups
Ref — — — — —
Cohort� area of residence at baseline
Schizophrenia: inner core 1.28 1.00–1.65 — — — —
Schizophrenia: outer core 0.75 0.49–1.15 — — — —
Schizophrenia: suburb and Control: all areas Ref — — — — —
G. DeVerteuil et al. / Health & Place 13 (2007) 310–323318

ARTICLE IN PRESS
Table 4
Age distribution of movers and non-movers by cohort
Movers Schizophrenia
cohort
Matched cohort
ðN ¼ 2443Þ ðN ¼ 12; 135Þ
n % n %
19–44 years 516 59.79 1813 67.15
45–64 years 240 27.81 648 24.00
65+ years 107 12.40 239 8.85
Total 863 2700
Non-movers
19–44 years 714 45.19 4296 45.53
45–64 years 640 40.51 3716 39.39
65+ years 226 14.30 1423 15.08
Total 1580 9435
Table 5
Income quintile distribution of movers and non-movers by cohort
Movers Schizophrenia
cohort
Matched cohort
ðN ¼ 2386Þ ðN ¼ 12; 088Þ
n % n %
Q1 (poorest) 422 49.47 800 29.74
Q2 197 23.09 628 23.35
Q3 132 15.47 472 17.55
Q4 58 6.80 442 16.43
Q5 (wealthiest) 44 5.16 348 12.94
Total 853 2690
Non-movers
Q1 (poorest) 587 38.29 1421 15.12
Q2 367 23.94 1851 19.70
Q3 265 17.29 1823 19.40
Q4 182 11.87 2102 23.37
Q5 (wealthiest) 132 8.61 2201 23.42
Total 1533 9398
G. DeVerteuil et al. / Health & Place 13 (2007) 310–323 319
quintiles. Table 5 contains the income quintiledistribution of movers and non-movers for theschizophrenia cohort and the matched cohort.
The income quintile distribution for both themovers and non-movers from the schizophreniacohort show a higher proportion in the lower-income quintiles. There was also a moderategradient effect for the matched cohort. For thematched cohort, the gradient for the movers wasopposite to the non-movers, in that there was ahigher percentage of individuals in the lower-income
quintiles for the movers and a higher percentage ofindividuals in the higher-income quintiles amongthe non-movers. Finally, the cohort� region ofresidence interaction revealed a higher OR for theschizophrenia cohort residing in the inner core atbaseline.
2. Is a cohort of individuals with schizophrenia
more likely to move to lower income, inner-city
neighbourhoods and less likely to move to suburban,
higher-income neighbourhoods than an age– sex
matched cohort?
The majority of movers stayed within theirbaseline area of residence—that is, they movedwithin their incumbent intra-urban area. For thosemoving between areas, the schizophrenia cohortand the matched cohort tended to move in opposite
directions. When persons in the schizophreniacohort moved, they were more likely to move fromsuburb to inner core (12.4%) than from inner coreto suburb (7.1%), whereas the matched controlswere more likely to move from the inner core to thesuburb (9.8%) than from the suburb to the innercore (4%).
The logistic regression analysis for suburb-to-inner core movers (Table 3) displayed substantialunder dispersion ðdeviance=df ¼ 0:36Þ, which indi-cates less variation in the data than would beexpected under the binomial distribution (Littellet al., 2002). Therefore, the standard errors of theORs were adjusted (i.e. scaled) using the modelvariance as the scaling factor. Scaling ensuresthe confidence intervals for the OR are asymptoti-cally correct (Fox, 1997). None of the two-way interactions were statistically significant, andtherefore were not included in the final model.Significant main effects were observed for cohortðpo0:001Þ, age group ðpo0:001Þ, sex ðp ¼ 0:0005Þ,marital status ðpo0:0001Þ, and physician visitsðp ¼ 0:0158Þ. The odds of moving from suburb toinner core were higher for the schizophrenia cohort,for males, for individuals in the 19–44 years agegroup, for those who were single or widowed, forthose with a high number of physician visits, andthose who were hospitalized one or two times.
The logistic regression analysis for inner core-to-suburb movers (Table 3) also revealed underdisper-sion ðdeviance=df ¼ 0:60Þ. Therefore, the standarderrors of the ORs were again scaled using the modelvariance as the scaling factor. None of the two-wayinteractions were statistically significant, and there-fore were dropped from the model. There was astatistically significant main effect for cohort

ARTICLE IN PRESSG. DeVerteuil et al. / Health & Place 13 (2007) 310–323320
ðp ¼ 0:0024Þ, age group ðpo0:0001Þ, and physicianvisits ðpo0:05Þ. The odds of moving from the innercore to the suburb was lower for the schizophreniacohort, and higher for 19–44 year age group andthose who visited a physician between 4 and 9 times.
To further illustrate these results in a non-inferential manner, we extended the geographicstudy area to examine residential mobility from the10 rural Manitoba RHAs into the WRHA, based onbaseline and endpoint postal codes. Among those inthe schizophrenia cohort2 who moved to theWRHA, 80.7% had a final postal code in aninner-core area, and 14.8% had a postal codeindicating a suburban neighbourhood. In contrast,65.6% of the matched cohort who were classified asnon-WRHA-to-WRHA movers went directly to thesuburb area, while only 30.1% moved to the innercore area.
Discussion
The comparative residential mobility resultsclarified several key issues within the field of mentalhealth geography, as well as confirmed previousfindings in a more systematic way. Consistent withthe larger literature, the schizophrenia cohort isspatially concentrated in the inner-core area sur-rounding the Central Business District. As pre-viously noted, the inner core is defined by its lowersocio-economic status (lower-income quintiles),while the suburbs are generally associated withhigher socio-economic status (higher-income quin-tiles), so it was not surprising that the schizophreniacohort differed in terms of income quintile ofresidence. Second, the schizophrenia cohort wasmore likely to make at least one residential movethan the matched cohort although this depended ontheir age, income level, and region of residence atbaseline. Third, when they did move, the schizo-phrenia cohort was more likely to move from thesuburb to the inner core, opposite to the generalflow within the WRHA—inner core to suburb,symptomatic of a demographically stagnant yetgeographically sprawling city (Leo and Brown,2000). Confirming our earlier concern, the schizo-phrenia cohort does appear to be spatially en-trapped in economically disadvantaged parts of the
2Same criteria were employed to define this cohort as for the
intra-urban cohort, with the exception that they lived in a rural
RHA at baseline and moved to the WRHA at endpoint.
city, albeit ones with high levels of services andmore affordable housing.
Because we did not explicitly test for the socialselection/causation hypotheses, we cannot rule outthe effects of either (or both) in the pooling ofindividuals with schizophrenia in the inner core.However, our analysis indicated that individualswith schizophrenia do migrate into inner-city areas,offering support to the social selection theory—thatindividuals with schizophrenia are downwardlymobile and drift into service-rich, disadvantagedareas. Part of the drift may be explained by the pushfactors of unemployment, dependence on incomeassistance and poverty, all of which are higher forindividuals with schizophrenia and other severemental illnesses than for the general population(Mustard et al., 1996; Silver et al., 2002; Wilton,2004). These push factors interact with the pullfactors of low-cost housing and mental healthservices, both of which clearly cluster in the innercore and develop to create a ‘‘coping matrix’’ forindividuals with schizophrenia (see Table 1), creat-ing a co-location dynamic that approaches a service-dependent ghetto (Dear and Wolch, 1987; but seeMilligan, 1996 for a critical view on how suchghettos may not emerge in non-North Americansettings).
The advantages of using population-based ad-ministrative data to study geographic mobility ofindividuals with schizophrenia included (1) residentsof the entire health region can be followed overvarying periods of time and (2) appropriatecomparison cohorts can be selected from thepopulation registry. However, there are somelimitations to the use of these data to investigatemobility. First, the data source only allows us tocapture those individuals with a diagnosis ofschizophrenia. Nevertheless, we believe that theschizophrenia cohort is fairly representative of theactual population with schizophrenia, given thatsuch a severe mental illness usually requires contactwith a physician at some point or use of hospitalservices. Second, postal code changes of healthinsurance registrants are only captured if reportedto the provincial ministry of health. Thus, our datamay provide a conservative estimate of the numbersof individuals who actually change their location ofresidence over time. The probability of reportingaddress changes may differ between the twocohorts. Other analyses, based on comparing surveyand administrative data, suggest that such problemstend to be small (Roos and Nicol, 1999). Finally,

ARTICLE IN PRESSG. DeVerteuil et al. / Health & Place 13 (2007) 310–323 321
understanding the motivations behind the moveswould require a more qualitative approach. Indivi-duals with schizophrenia may be moving to theinner core for a variety of complex and tangledreasons, including not only affordable housing andproximity to services, but also for reasons asso-ciated with family, friends, employment, and stigma(Milligan, 1996).
Conclusions: schizophrenia and the city
This paper has contributed to a more systematicunderstanding of the dynamic and complex move-
ments of individuals with schizophrenia and, criti-cally, how they compared to the general population.By using (1) a systematic, large-scale and long-itudinal administrative database, (2) a more sensi-tive geographical scale, in the form of three intra-urban neighbourhood areas, and (3) a matchedcontrol cohort, we were able to overcome certainkey methodological and data limitations inherent inprevious studies, particularly the lack of databasesthat combine person-specific information on healthstatus and changes in location of residence. Ourfindings further contribute to what Wolch and Philo(2000) call the ‘‘third wave’’ of mental healthgeography research—the use of large-scale, repre-sentative and longitudinal databases to engage withthe implications of the current context for indivi-duals with schizophrenia, a troubling context inwhich they continue to live in, if not migrate to, theinner core.
This suggests that the promise of deinstitutiona-lization (and recent mental health care reforms tomake services closer to clients’ place of residence sothey do not have to move) remains unfulfilled, andthat the challenges of supporting individuals withschizophrenia continue to fall inequitably on just afew (inner-city) neighbourhoods. A further conclu-sion is that individuals with schizophrenia are morelikely to move, which can negatively affect mentalhealth (Abood et al., 2002). Thus, health policymakers and services providers should be cognizantof the degree, pattern, reasons for and causes ofresidential mobility among the mentally ill, andwhether there have been changes over time. This isparticularly true within a context in which far toomany individuals with schizophrenia or other severemental illnesses find themselves moving involunta-rily among inadvertent, informal and inappropriatesettings, including prison, jail, homeless shelters, the
street, and licensed care facilities (Wolch and Philo,2000; DeVerteuil, 2003).
Future research should focus on at least twoareas. First, the case study in this paper hasdemonstrated the utility of using administrativedata for clarifying critical issues in mental healthgeography. To build on this momentum, futureresearch on other unresolved topics in mental healthgeography—including the question of whether long-term residents of deprived, disorganized inner-cityneighbourhoods experience a greater likelihood ofdeveloping severe mental illness than those long-term residents of more affluent suburban neigh-bourhoods—could benefit from using administra-tive data. Second, we need to go beyond thedichotomous measure used here to see how indivi-duals with schizophrenia differ according to thenumber of moves within a specified time period. Areindividuals with schizophrenia who moved fivetimes within a year different—in terms of hospita-lizations, direction of mobility, socio-economicstatus, etc.—than those who only moved twice inthe same time period? For direction, we need toadvance qualitative research that will uncover themotivations for moving to particular neighbour-hoods in the city and not others, and how move-ment intersects with key resources (housing,employment, services) that may improve (or wor-sen) an individual’s quality of life (Milligan, 1996;DeVerteuil, 2003; Rog, 2004).
Acknowledgements
This research was supported by Canadian In-stitutes of Health Research (CIHR) Grant (#HSM-62336) and a Social Sciences and HumanitiesResearch Council of Canada (SSHRC) CanadaGraduate Scholarship to the second author. Com-ments by Jennifer Wolch were much appreciated.Thanks to Okechukwu Ekuma for assistance withdata extraction and cohort selection. The authorsare indebted to Health Information Management ofManitoba Health for providing the data used in thisstudy. The results and conclusions are those of theauthors, and no official endorsement by ManitobaHealth is intended or should be inferred.
References
Abood, Z., Sharkey, A., Webb, M., Kelly, A., Gill, M., 2002.
Are patients with bipolar affective disorder socially

ARTICLE IN PRESSG. DeVerteuil et al. / Health & Place 13 (2007) 310–323322
disadvantaged? A comparison with a control group. Bipolar
Disorders 4, 243–248.
Almog, M., Curtis, S., Copeland, A., Congdon, P., 2004.
Geographical variation in acute psychiatric admissions within
New York City 1990–2000: growing inequalities in service
use? Social Science and Medicine 59, 361–376.
Bachrach, L., 1987. Geographic mobility and the homeless
mentally ill. Hospital and City Psychiatry 38, 27–28.
Bastide, R., 1972. From ecology to the study of communities. In:
Bastide, R. (Ed.), The Sociology of Mental Disorder.
Routledge and Paul, London.
Bhugra, D., 2004. Migration and mental health. Acta Psychia-
tratrica Scandinavica 109, 243–258.
Breslow, R.E., Klinger, B.I., Erickson, B.J., 1998. County drift: a
type of geographic mobility of chronic psychiatric patients.
General Hospital Psychiatry 20, 44–47.
Canadian Census Analyser, 2004. Census of Canada 2001.
Computing in the Humanities and Social Sciences, University
of Toronto. http://datacentre.chass.utoronto.ca/census/ (accessed
December 1, 2004).
Chesteen, H.E., Bergeron, V., Addison, W.P., 1970. Geographic
mobility and mental disorder. Hospital and Community
Psychiatry 21, 31–32.
Dear, M.J., Wolch, J.R., 1987. Landscapes of Despair: From
Deinstitutionalization to Homelessness. Princeton University
Press, Princeton.
Dear, M.J., et al., 1980. Coping in the Community: the Needs of
Ex-Psychiatric Patients. Canadian Mental Health Associa-
tion, Hamilton, Ont.
Dembling, B.P., Rovnyak, V., Mackey, S., Blank, M., 2002.
Effects of geographic migration on SMI prevalence estimates.
Mental Health Services Research 4, 7–12.
DeVerteuil, G., 2003. Homeless mobility, institutional settings,
and the new poverty management. Environment and Planning
A 35, 361–379.
Dohrenwend, B.P., Levav, I., Shrout, P.E., Schwartz, S., Naveh,
G., Link, B.G., Skodol, A.E., Stueve, A., 1992. Socio-
economic status and psychiatric disorders: the causation-
selection issue. Science 255, 946–952.
Faris, R.E., Dunham, W., 1939 (Reprint 1965). Mental
Disorders in Urban Areas: An Ecological Study of Schizo-
phrenia and Other Psychoses. University of Chicago Press,
Chicago, IL.
Fox, J., 1997. Applied Regression Analysis, Linear Models, and
Related Methods. Sage Publications, Thousand Oaks.
Giggs, J.A., 1973. The distribution of schizophrenics in Notting-
ham. Transactions of the Institute of British Geographers 59,
55–76.
Harkness, J., Newman, S., Salkever, D., 2004. The cost-
effectiveness of independent housing for the chronically
mentally ill: do housing and neighborhood features matter?
Health Services Research 39, 1341–1360.
Hopper, K., Jost, J., Hay, T., Welber, S., Haughland, G., 1997.
Homelessness, severe mental illness, and the institutional
circuit. Psychiatric Services 48, 659–665.
Lamont, A., Ukoumunne, O.C., Tyrer, P., Thornicroft, G., Patel,
R., Slaughter, J., 2000. The geographical mobility of severely
mentally ill residents in London. Social Psychiatry and
Psychiatric Epidemiology 35, 164–169.
Lapouse, R., Monk, M.A., Terris, M., 1956. The drift hypothesis
and socioeconomic differentials in schizophrenia. American
Journal of Public Health 46, 978–986.
Larson, A., Bell, M., Young, A.F., 2004. Clarifying the relation-
ships between health and residential mobility. Social Science
and Medicine 59, 2149–2160.
Leo, C., Brown, W., 2000. Slow growth and urban development
policy. Journal of Urban Affairs 22, 193–213.
Lesage, A.D., Tansella, M., 1989. Mobility of schizophrenic
patients, non-psychotic patients and the general population in
a case register area. Social Psychiatry and Psychiatric
Epidemiology 24, 271–274.
Ley, D., 2001. The inner city. In: Bunting, T., Filion, P. (Eds.),
Canadian Cities in Transition. Oxford University Press,
Toronto.
Littell, R.C., Stroup, W.W., Freund, R.J., 2002. SAS for Linear
Models, fourth ed. SAS Institute Inc., Cary, NC.
Lix, L., Hinds, A., DeVerteuil, G., Robinson, R., Roos, L., 2006.
Residential Mobility and Severe Mental Illness: A Popula-
tion-Based Analysis. Administration and Policy in Mental
Health and Mental Health Services Research, available
online.
Manitoba Health, 2004. Annual Report. Manitoba Health,
Winnipeg, MB.
McLemore, R., Aass, C., Keilhofer, P., 1975. The Changing
Canadian Inner-city. Ministry of State for Urban Affairs,
Ottawa, Ont.
McNaught, A.S., Jeffreys, S.E., Harvey, C.A., Quayle, A.S.,
King, M.B., Bird, A.S., 1997. The Hampstead Schizophrenia
Survey 1991. II: incidence and migration in inner London.
British Journal of Psychiatry 170, 307–311.
Milligan, C., 1996. Service dependent ghetto formation—a
transferable concept? Health and Place 2, 199–211.
Mustard, C., Derksen, S., Tataryn, D., 1996. Intensive use of
mental health care. Canadian Journal of Psychiatry 41,
93–101.
Peressini, T., McDonald, L., 2001. Urban homelessness in
Canada. In: Bunting, T., Filion, P. (Eds.), Canadian Cities
in Transition. Oxford University Press, Toronto.
Ram, B., Norris, M., Skof, K., 1989. The Inner-city in Transition.
Minister of Supply Services Canada, Ottawa, Ont.
Rog, D., 2004. The evidence on supported housing. Psychiatric
Rehabilitation Journal 27, 334–344.
Roos, L., Nicol, P., 1999. A research registry: uses, development,
and accuracy. Journal of Clinical Epidemiology 52, 39–47.
Roos, N.P., Mustard, C.A., 1997. Variation in health and health
care use by socioeconomic status in Winnipeg, Canada: does
the system work well? Yes and no. Milbank Quarterly 75,
89–111.
SAS Institute, Inc. (1999). SAS/STAT user’s guide, version 8.
Author, Cary, NC.
Silver, E., Mulvey, E.P., Swanson, J.W., 2002. Neighbourhood
structural characteristics and mental disorder: Faris and
Dunham revisited. Social Science and Medicine 55,
1457–1470.
Thornicroft, G., 1991. Social deprivation and rates of treated
mental disorder: developing statistical models to predict
psychiatric service utilization. British Journal of Psychiatry
158, 475–484.
Timms, D., 1998. Gender, social mobility, and psychiatric
diagnoses. Social Science and Medicine 46, 1235–1247.
Torrey, E., Stieber, J., Ezekiel, J., Wolfe, S., Sharfstein, J., Noble,
J., Flynn, L., 1992. Criminalizing the Seriously Mentally Ill:
The Abuse of Jails as Mental Hospitals. National Alliance for
the Mentally Ill, Arlington VA.

ARTICLE IN PRESSG. DeVerteuil et al. / Health & Place 13 (2007) 310–323 323
Walks, R.A., 2001. The social ecology of the post-Fordist/
global city? Economic restructuring and socio-spatial
polarization in the Toronto urban region. Urban Studies 38,
407–447.
Wilton, R., 2004. Putting policy into practice? Poverty and people
with serious mental illness. Social Science and Medicine 58,
25–39.
Winnipeg Regional Health Authority (WRHA), 2004. 2001
Census Profile. http://www.wrha.mb.ca/howcare/decsup/
files/population/Census_2001.pdf (accessed November 10,
2004).
Wolch, J., Philo, C., 2000. From distributions of deviance to
definitions of difference: past and future mental health
geographies. Health and Place 6, 137–157.
Copyright © 2022 FDOKUMEN



















