Carriageway Skidding Resistance Procedure - Leicestershire ...
Upload
khangminh22Category
view
14download
0
Leicester City Clinical Commissioning Group West Leicestershire Clinical Commissioning Group
East Leicestershire and Rutland Clinical Commissioning Group `
Meeting Title
Commissioning Collaborative Board (Joint Committee) - Meeting in Public Date Thursday 28 March 2019
Meeting no. 2 Time 11:00am – 11:50am
Chair Professor Azhar Farooqi Leicester City CCG
Venue / Location
Conference Room, 8th Floor, LC CCG, St John’s House, 30 East Street, Leicester, LE1 6NB
REF AGENDA ITEM ACTION PRESENTER PAPER TIMING
CCBP/19/10 Welcome and Introductions Professor
Farooqi 11:00am
CCBP/19/11
Apologies for Absence: Dr Ursula Montgomery Professor Mayur Lakhani Mr Clive Wood Ms Gillian Adams
To receive
Professor Farooqi verbal 11:00am
CCBP/19/12 Notification of Any Other Business
To
receive Professor Farooqi verbal 11:00am
CCBP/19/13 Declarations of Interest on Agenda Topics
To receive
Professor Farooqi verbal 11:00am
CCBP/19/14 To receive questions from the Public in relation to items on the agenda only
To receive
Professor Farooqi
verbal 11:05am
GOVERNANCE ARRANGEMENTS
CCBP/19/15 Minutes of the meeting held on 21 February 2019
To approve
Professor Farooqi A
11:10am
CCBP/19/16 Matters Arising: Update on actions from the meeting held on 21 February 2019
To receive
Professor Farooqi B
ITEMS FOR DECISION, ACTION AND ESCALATION
CCBP/19/17 LLR guidance on self-care for Minor Aliments and Self Limiting Conditions
To approve
Gillian Stead C 11:15am
CCBP/19/18 Progress update on QIPP Schemes To
receive
Spencer Gay D 11:25am
CCBP/19/19 Update on 2019/20 Contract Negotiations
To receive
Managing Directors verbal 11:35am
DATE OF NEXT MEETING The next meeting of the Commissioning Collaborative Board will take place on Thursday 18 April 2019, Conference Room, 8th Floor, Leicester City CCG, St John’s House, 30 East Street, Leicester, LE1 6NB East Leicestershire and Rutland CCG to Chair meetings from January – April 2019
Professor Farooqi verbal

A

Blank Page

Paper A LLR CCGs’ Commissioning Collaborative Board (CCB) meeting
28 March 2019
Page 1 of 4
LEICESTER, LEICESTERSHIRE AND RUTLAND CCGs COMMISSIONING COLLABORATIVE BOARD
Minutes of the Public Commissioning Collaborative Board held on Thursday 21
February 2019 at 1:00pm in the Conference Room, 8th Floor, St John’s House, 30 East Street, Leicester, LE1 6NB
PRESENT: Dr Ursula Montgomery Clinical Chair, East Leicestershire and Rutland CCG (Chair) Professor Mayur Lakhani Clinical Chair, West Leicestershire CCG Dr Andy Ker Vice Clinical Chair, East Leicestershire and Rutland CCG Mrs Caroline Trevithick Interim Managing Director, West Leicestershire CCG Ms Sue Lock Managing Director, Leicester City CCG Mrs Michelle Iliffe Director of Finance, Leicester City CCG Mrs Karen English Managing Director, East Leicestershire and Rutland CCG Mr Nick Carter Independent Lay Member, Leicester City CCG Ms Donna Enoux Chief Finance Officer, East Leicestershire and Rutland CCG Mr Spencer Gay, Chief Finance Officer, West Leicestershire CCG Ms Tamsin Hooton Director Lead for Community Services Redesign Ms Sarah Prema Director of Strategy and Implementation, Leicester City CCG Ms Gillian Adams Independent Lay Member, West Leicestershire CCG Ms Chris West Director of Nursing & Quality, Leicester City CCG
Professor Farooqi Clinical Chair, Leicester City CCG Dr Nick Pulman Deputy Clinical Chair, West Leicestershire CCG Dr Avi Prasad Co-Chair, Leicester City CCG IN ATTENDANCE Mr Tim Sacks Chief Operating Officer, East Leicestershire and Rutland CCG Mrs Jayshree Raval Commissioning Collaborative Support Officer, East
Leicestershire and Rutland CCG (minutes)
ITEM DISCUSSION LEAD RESPONSIBLE
CCB/19/01 Welcome and Introductions The Chair welcomed all to the Commissioning Collaborative Board (CCB) meeting.
CCB/19/02 Apologies received The following apologies were noted:
Mr Zuffar Haq, Independent Lay Member, Leicester City CCG
Mr Clive Wood, Independent Lay Member, East Leicestershire and Rutland CCG
Ms Tracy Burton, Interim Chief Nurse, East Leicestershire and Rutland CCG
CCB/19/03 Notification of Any Other Business The Chair had not received notification of any other business for discussion.
CCB/19/04 Declarations of Interest on Agenda Items The Chair reminded members of their obligation to declare any interest they may have on any business arising at committee meeting which might conflict with the business of NHS Leicester City CCG, East Leicestershire and Rutland CCG or West Leicestershire CCG.

Paper A LLR CCGs’ Commissioning Collaborative Board (CCB) meeting
28 March 2019
Page 2 of 4
There were no further conflicts recorded.
CCB/19/05 To receive questions from the Public in relation to the items on the agenda only There were no public present in the public gallery.
CCB/19/06 To APPROVE the minutes of the Public Commissioning Collaborative Board meeting held on 20 December 2018 (Paper A) The minutes of the Public Commissioning Collaborative Board meeting held in December 2018 were approved as an accurate record of the meeting. It was RESOLVED to:
APPROVE the minutes of the public CCB meeting.
CCB/19/07 To RECEIVE the Matters Arising: actions from Commissioning Collaborative Board held on 20 December 2018 (Paper B) There were no matters arising following the meeting held on 20 December 2018 as actions have been concluded. It was RESOLVED:
RECEIVE no matters arising.
CCB/19/08 To RECEIVE update on QIPP Schemes (Paper C)
Mr Gay presented the paper which outlined the current position at Month 10. He stated that at month 10 QIPP achievement was for £48.2m year to date with forecast of £57.8m achievement by the end of the year against the plans of £46.7m and £58.2m respectively. He stated that LLR CCGs are forecasting under delivery on the QIPP plan for 2018/19 of £0.625m, which is a favourable movement of £0.305m from last month. Mr Gay highlighted that the LLR PMO team undertakes a monthly assurance exercise on the forecasts to ensure delivery of the QIPP savings.
Furthermore Mr Gay informed that work is in progress to further develop the 2019/20 QIPP programme through the planning and contracting process. CCB noted that the PMO is engaging in networking via NHS England, with other CCG PMOs in the region in order to share best practice methodology and to benchmark both the PMO and LLRs QIPP Plans against other CCGs. In addition the PMO is drafting a Project Management Handbook, which will act as a reference manual for project management across the CCGs in LLR and will be available to project teams by the beginning of new financial year. In terms of data analysis, Dr Pulman asked how information was being shared across the three CCGs, for example he was aware of the good work by Dr Shepherd in City and would be interested how this could be applied in West and East CCGs. There was some discussion on the data mapping and how it could support with Primary Care Networks going forward.

Paper A LLR CCGs’ Commissioning Collaborative Board (CCB) meeting
28 March 2019
Page 3 of 4
Dr Montgomery informed that the purpose of this report is to receive update on the current QIPP schemes and asked in terms of the work for development of the 2019/20 QIPP schemes whether there is any clinical input that could be taken forward collaboratively. Ms Prema stated that Dr Shepherd have worked on analysing Leicester City CCG’s data and would however require other clinical input to cascade this piece of work across all the relevant areas of the three CCGs. She requested nominations for the East Leicestershire and Rutland and West Leicestershire CCGs to meet with Dr Shepherd. Dr Ker and Dr Pulman nominated themselves to work with Dr Shepherd in taking this work forward before e end of March 19. It was RESOLVED to:
NOTE and DISCUSS the content of this report CCB/19/09 To RECEIVE Update on the Work-streams arrangements for
Integrated Primary and Community Care (Paper D) Ms Hooton presented the paper which detailed the proposals in respect of organising some of the collaborative working arrangements in LLR CCGs in order to effectively deliver key elements of the Long Term Plan and Integrated Care Systems. Particularly the Primary Care Networks (PCNs) and the Integrated Community Services (ICS). Mr Sacks informed that currently within LLR CCGs there is a good progress towards developing primary care at scale, although the approach is slightly different across the three CCGs. It was noted that this work provides a platform for building PCNs as groupings of GP practices to enable them to deliver core and enhanced care and work with community services and other partners to deliver integrated care to local populations. In order to work more effectively, the recommendations were to review the current terms of reference for the GP Resilience Group to reform into the Primary Care Board with explicit responsibilities. Furthermore support revising the terms of reference for the integrated Community Boards which describes the delineation of responsibility in regards to integrated community teams and PCNs and how the interdependencies between the two groups will be managed. Lastly CCB was requested to support the plan to hold development sessions with the Governing Bodies in respect of PCNs as integrated provider models within an Integrated Care System. In addition to develop a clear strategic approach to the organisational and contractual framework in LLR. This should include consideration of the future contracting framework for community health services. Professor Lakhani welcomed the reported and added that his view on the End of Life (EoL) work-stream was that it requires dedicated leadership, similar to the Frailty work-stream. Dr Pulman added that the IM&T group do work closely with frailty and EoL work. There was some ambiguity in respect of where some of these groups were reporting and if they should be reviewed and refreshed in order to get appropriate governance arrangements in

Paper A LLR CCGs’ Commissioning Collaborative Board (CCB) meeting
28 March 2019
Page 4 of 4
place. Ms Lock added that some aspects of this work will be considered via the Commissioning Capability Programme work. Dr Montgomery summarised that:
To strengthen the governance process around some of the groups by either refreshing them or expanding them as per the report.
To understand what mechanisms will be in place for decisions
Certain aspects of this work to be taken via the Commissioning Capability Programme work.
Having clear contracting strategy in respect of the Community Services Redesign work.
To look at arranging a Joint Board Session on proposed changes.
It was RESOLVED to: SUPPORT the proposal that the GP Resilience Group’s Terms
of Reference should be reviewed. SUPPORT a revision to the Integrated Community Board’s
Terms of Reference to describe the delineation of responsibility in relation to integrated community teams and primary care networks.
SUPPORT the plan to hold development sessions with governing bodies about the role of PCNs as integrated provider models within an Integrated Care System, to develop a clear strategic approach to the organisational and contractual framework in LLR. This should include consideration of the future contracting framework for community health services.
Date of Next Meeting Thursday 28 March 2019, in the Conference Room, 8th Floor, St John’s House, 30 East Street, Leicester, LE1 6NB East Leicestershire and Rutland CCG to Chair the meeting from January – April 2019 Inclusive.

B

Blank Page

Paper B Commissioning Collaborative Board - Public
28 March 2019
1
Commissioning Collaborative Board (CCB)
Public Action Notes
Minute No Meeting Date
Item Responsible Officer
Action Required To be completed
by
Progress as at 28 March 2019
Status
There are no matters arising to follow up from the CCB held in February 2019.
No progress made
On-Track Completed
Key

C

Blank Page

COMMISSIONING COLLABORATIVE BOARD MEETING
Front Sheet
Paper C Title of the report: LLR Guideline for the treatment of minor ailments and self-
limiting conditions
Report to: Commissioning Collaborative Board
Section:
Public
Date of the meeting:
28 March 2019
Report by:
Gill Stead Head of Medicines Optimisation West Leicestershire CCG
Sponsoring Director:
Tim Sacks SRO for Medicines Optimisation, Chief Operating Officer, East Leicestershire and Rutland CCG
Presented by:
Gill Stead Head of Medicines Optimisation West Leicestershire CCG
CCG Involvement to date: City East West Insert name of
any other groups i.e. ECN
Clinician Paul Danaher
Anuj Chahal James Ogle
Manager Lesley Gant Vishal Mashru Gill Stead Received by CCG (sub-group or equivalent) prior to CCB: City East West IG sub group IG sub group Q&P subgroup SUMMARY: 1. The LLR Guidelines for the treatment of minor ailments and self-limiting conditions (Appendix A ) are based on the NHSE National Guidance for CCGs published in March 2018 following a national public consultation on “Conditions for which over the counter items should not routinely be prescribed in primary care”.1,2 2. As a result the three Leicestershire CCGs have developed this joint guideline to reduce variation and develop a system wide approach in all care settings within the context of OTC treatments for minor ailments and self-limiting conditions. 3. The views of patients through a patient engagement survey, GPs including Prescribing Lead GPs, the LPC, senior colleagues in CCG through governance committees, UHL, LPT and DHU have been sought and the guidelines were supported by LMSG in February. With full sight of the national guidance and public engagement exercises, the three CCGs have agreed to delegate final approval to the Clinical Commissioning Board and will then be hosted on the LMSG website.

4. From the public engagement exercises we learnt that the majority of people do already buy their own medicines to treat minor ailments. We also learnt that the majority of people are willing or very willing to buy medicines for minor ailments. People also told us that the information, advice and guidance that the pharmacists gave them was really helpful and that it was unnecessary to see their GP and they would rather people only used their GP for series conditions which in the long run would improve access for everyone to their GP surgery. The main concerns that emerged were:
• Would patient be affected if they had a long term condition that could be treated by an OTC medication.
• Others wanted reassurance as whether community pharmacists could give advice about drug interactions if they were also on prescription only medication
• Concerns that the quality and strength of over the counter medicines was not as good as medicines prescribed on FP10.
• Some people were also concerned about affordability of some medicines. The concerns that have arisen around long term conditions and affordability are addressed by the general exception criteria in the LLR guidance submitted for approval. A Q&A has been written to provide clarity on some of the other issues that were raised. Implementation of the guidance will be through the LLR STP Medicines Optimisation workstream. REFERENCES 1. NHS England and NHS Clinical Commissioners. Conditions for which over the counter items should not routinely be prescribed in primary care. Guidance for CCGs. March 2018. Available at: https://www.england.nhs.uk/wp-content/uploads/2018/03/otc-guidance-for-ccgs.pdf 2. NHS consultation https://www.england.nhs.uk/medicines/over-the-counter-items-which-should-not-routinely-be-prescribed/ RECOMMENDATIONS: The Commissioning Collaborative Board is requested to:
• APPROVE the LLR Guideline for the treatment of minor ailments and self-limiting condition.

LLR Guideline for the treatment of minor ailments and self-limiting conditions
1. INTRODUCTION The LLR Guidelines for the treatment of minor ailments and self-limiting conditions (Appendix A) are based on the NHSE National Guidance for CCGs published in March 2018 following a national public consultation on “Conditions for which over the counter items should not routinely be prescribed in primary care”.1 The national joint clinical working group consisted of NHS England and NHS Clinical Commissioners (NHSCC) and relevant stakeholders including the Royal College of GPs and The Royal Pharmaceutical Society. The mandate from NHSE was that the guidance issued is to be reflected in local polices, unless there is a valid reason to do otherwise, and for prescribers to reflect local policies in their prescribing practice.
2. GOVERNANCE As a result the three Leicestershire CCGs have developed this joint guideline to reduce variation and develop a system wide approach in all care settings to self-caring within the context of OTC treatments for minor ailments and self-limiting conditions. Each CCG has undertaken separate engagement processes with their respective populations to inform the guideline process ensuring they take into account their legal duties to advance equality and have regard to reduce health inequalities. In addition, the views of GPs including Prescribing Lead GPs, the LPC, senior colleagues in CCG through governance committees, UHL, LPT and DHU have been sought. The three CCGs have agreed to delegate final approval to the Clinical Commissioning Board. The scope of the NHSE guidance has been expanded so that it applies to all patients in all care settings across Leicestershire within the context of OTC treatments for minor ailments and self-limiting conditions. The reasons for this are:
• Equity for patients as they may present with the same problem. • Manage patient expectations from the outset that they will be expected to purchase
OTC. • Avoid patients seeking treatment in non-primary care settings because of the supply
of the medication. Oversight of implementation across LLR will be provided by the Medicines Value work stream (Medicines Optimisation STP) to enable the change in culture and empower patients. The guideline was supported at the February LMSG meeting and will be archived on the LMSG website following approval at CCB. References
1. NHS England and NHS Clinical Commissioners. Conditions for which over the counter items should not routinely be prescribed in primary care. Guidance for CCGs. March 2018. Available at: https://www.england.nhs.uk/wp-content/ uploads/2018/03/otc-guidance-for-ccgs.pdf. Last accessed 06/08/2018.
RECOMMENDATIONS The Commissioning Collaborative Board is requested to: APPROVE the LLR Guideline for the treatment of minor ailments and self-limiting conditio

Appendix A LLR Guidelines for the treatment of minor ailments and self limiting conditions Contents
1. Rationale 2. How the guidance has been developed 3. General principles 4. Exceptions to the guidance 5. Information and advice for patients 6. Appendix 1 OTC restrictions in pregnant and breast feeding women and
children 7. Appendix 2 Referral to local pharmacy form 8. Appendix 3 Guide for Health care professionals on treatment of minor
ailments and self limiting conditions
1. Rationale In the year prior to June 2017, the NHS spent approximately £569 million on prescriptions for medicines, which could otherwise be purchased over the counter (OTC) directly by patients from a pharmacy and/or other outlets such as petrol stations or supermarkets minor ailments, self-limiting conditions and items of limited clinical effectiveness. By reducing spend on these items resources can be used for other higher priority areas that have a greater impact for patients, support improvements in services and/or deliver transformation that will ensure the long-term sustainability of the NHS. 1 A wide range of information is available to the public on the subjects of health promotion and the management of minor self- treatable illnesses. Advice from organisations such as the Self Care Forum and NHS website is readily available on the internet. Many community pharmacies are also open extended hours including weekends and are ideally placed to offer advice on the management of minor conditions and lifestyle interventions.1 Research shows that in many cases, people can take care of their minor conditions if they are provided with the right information; thereby releasing health care professionals to focus on patients with more complex and/or serious health concerns. Past experience with self-care builds confidence in patients, with 84 per cent choosing to self-care for new episodes. More cost-effective use of stretched NHS resources allows money to be spent where it is most needed, whilst improving patient outcomes.1
2. How has this guidance been developed These guidelines are based on the NHSE national guidance for CCGs published in March 2018 following a national public consultation on “Conditions for which over the counter items should not routinely be prescribed in primary care”.3 The national joint clinical working group consisted of NHS England and NHS Clinical Commissioners (NHSCC) and relevant stakeholders including the Royal College of GPs and The Royal Pharmaceutical Society. The mandate from NHSE was that the guidance

issued is to be reflected in local polices, unless there is a valid reason to do otherwise, and for prescribers to reflect local policies in their prescribing practice. 2 Each CCG has undertaken separate engagement processes with their respective populations to inform the guideline process ensuring they take into account their legal duties to advance equality and have regard to reduce health inequalities. For the purposes of continuity, two other indications have been included in the guidance that were not part of the NHSE consultation (acute diarrhoea in children and genital thrush) as these are included in current West Leicestershire guidance and are now part of standard practice. As a result this joint LLR guideline has been developed for implementation across all care settings to reduce variation and develop a system wide approach in all care settings to self-caring within the context of OTC treatments for minor ailments and self limiting conditions. *This guidance is issued as general guidance under s14Z10 and S2 of the NHS Act 2006. The objective of this guidance is to support CCGs in their decision-making, to address unwarranted variation, and to provide clear national advice to make local prescribing practices more effective.
3. General Principles Appendix 3 of this guideline lists the conditions for which a prescription for treatment should not routinely be offered as the condition is appropriate for self-care. This is based primarily on type and severity of condition rather than the treatment itself and includes:
1. A condition that is self-limiting and does not require medical advice or treatment as it will clear up on its own.
2. A condition that is a minor illness and is suitable for self-care and treatment with items that can easily be purchased over the counter from a pharmacy.
In addition Appendix 3 also includes some treatments where there is a lack of robust evidence for clinical effectiveness unless an exception is identified under the relevant item. This guidance is intended to encourage people to self-care for minor illnesses as the first stage of treatment which may include self funding for over the counter treatments are appropriate . It is envisioned that in most cases (unless specified) these minor conditions will clear up with appropriate self-care. If symptoms are not improving or responding to treatment, then patients should be encouraged to seek further advice. It is not intended to discourage patients from going to the GP when it is appropriate to do so. This guidance applies to all patients in all care settings within the context of OTC treatments for minor ailments and self limiting conditions. It also includes those who would be exempt from paying prescription charges, unless they fall under the exceptions outlined.

4. Exceptions to the Guidance
Exceptions to the guidance are either specific to the condition, or may relate to a general scenario. In addition health care professionals are also reminded that they are responsible for prescribing, recommending or supplying an appropriate medicine taking into account that no contraindications apply and that special precautions have been considered. If in doubt the Summary of Product Characteristics (SPC) should be checked before making any recommendation.3 Specific exceptions These are specific to the condition and often relate to a “red flag symptom” indicating a more serious underlying condition. 4-5 General exceptions Several general exceptions were identified by the NHSE public consultation whereby patients should have their treatment prescribed. If a patient meets any of these criteria, they should not be expected to self-care. Note that being exempt from paying a prescription charge does not automatically warrant an exception to the guidance. For items of limited clinical effectiveness the general exceptions do not apply. There are specific exceptions listed under the items if applicable. This covers vitamins, minerals and probiotics but also includes over the counter treatments for some self-limiting conditions (e.g. acute sore throat, coughs, colds, nasal congestion, infant colic and mild cystitis) where there is limited evidence for the treatments used.
• Patients prescribed an OTC treatment for a long term condition (e.g. regular pain relief for chronic arthritis or treatments for inflammatory bowel disease).
• For the treatment of more complex forms of minor illnesses (e.g. severe migraines that are unresponsive to over the counter medicines).
• For those patients that have symptoms that suggest the condition is not minor i.e. those with red flag symptoms for example indigestion with very bad pain.
• Treatment for complex patients (e.g. immunosuppressed patients. • Patients on treatments that are only available on prescription (POMs) • Patients prescribed OTC products to treat an adverse effect or symptom of a
more complex illness and/or prescription only medications should continue to have these products prescribed on the NHS.
• Circumstances where the product licence doesn’t allow the product to be sold over the counter to certain groups of patients. This may vary by medicine, but could include babies, children and/or women who are pregnant or breastfeeding or may relate to quantities. See Appendix 1
• Patients with a minor condition suitable for self-care that has not responded sufficiently to treatment with an OTC product.
• Circumstances where the prescriber believes that, in their clinical judgement, exceptional circumstances exist that warrant deviation from the recommendation to self-care.

• Individual patients where the clinician considers that their ability to self-manage is compromised as a consequence of medical, mental health or significant social vulnerability to the extent that their health and/or wellbeing could be adversely affected, if reliant on self-care.
• Consideration should also be given to safeguarding issues.
5. Information and advice for patients
Information can be found on each of the CCG websites addressing some of the more common questions that were asked as part of the public survey they undertook in the development of this guidance.6-8 Health professionals can help to empower patients to self-care by:
• Sign posting patients to information resources for advice on symptoms, how to treat, which symptoms are likely to be of a more serious nature and when to seek advice from a GP :
NHS website Health A-Z section. 9 (link) Patient.co.uk website also has lots of useful advice for patients.10 (link)
• Educating patients at the point of care for future reference.
• Promote the “what to keep in your medicine cabinet” video on their website or in the waiting room or community pharmacies.
• Ensuring all staff are aware of the guidance.
• Liaising with local community pharmacists to ensure that patients are receiving consistent advice.
• Use the referral form (Appendix 2) if appropriate to help with communication between practices, patients and community pharmacies.
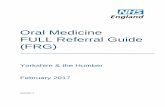
Appendix 1 OTC restrictions in pregnant and breast feeding women and children
Pregnant and breast feeding women and OTC restrictions Many OTC medicines can’t be sold by community pharmacists to pregnant or breast feeding women because they are unlicensed in these groups of patients. However, some simple analgesics which are used to treat many self-limiting illnesses can be sold OTC to pregnant or breast feeding women.
Analgesics in pregnancy
Paracetamol is the analgesic of choice during pregnancy and can be sold OTC by community pharmacists and supermarkets in small quantities. 11-12 Preparations containing codeine or ibuprofen are generally not suitable during pregnancy and should only be prescribed following a discussion with the patient’s GP. 11-12
Analgesics in breast feeding women
Paracetamol and ibuprofen are the analgesics of choice in breast feeding women and can be sold OTC by community pharmacists and supermarkets in small quantities. Preparations containing codeine should be avoided in breast feeding women. 12 Non pharmacological therapies should always be used first line wherever possible.
There is comprehensive advice on the NHS website to inform health care professionals and patients should the need arise although the information is not intended to replace the individual care and advice with a health care provider.
Age groups and OTC restrictions
The sale of some OTC preparations is restricted in infants and children and a few are restricted in older people. If unsure please check the summary of product characteristics or the pharmacist.
Analgesics in infants and children
The following analgesics cannot be sold OTC for the following age groups 3: • Paracetamol for infants < 3 months of age. • Ibuprofen for infants < 3 months of age. • Ibuprofen in infants 3-6 months <5kg body weight. • Preparations containing codeine for children< 12 years of age. • Topical NSAIDs for children <12 years of age unless advised by a doctor.
OTC medicines and restrictions in quantities that can be sold OTC
Products containing paracetamol can only be sold in quantities of 32 by the community pharmacy unless considered appropriate and approved by the pharmacist who can authorise the sale of up to 96 tablets for personal use.13a Products containing codeine and dihydrocodeine are restricted to quantities of 32 when sold over the counter.13b

Appendix 2
REFERRAL TO LOCAL PHARMACY - NO PRESCRIPTION REQUIRED You have a minor condition that can be treated with a medication that is available to buy over the counter from your local pharmacy. You do not need to make an appointment to speak to the pharmacist, just pop in anytime and they will be happy to help you.
Acne Infant colic
Burns or scald Insect bites or stings
Constipation Migraine / headache
Coughs/colds/flu / nasal congestion Mouth ulcers
Conjunctivitis bacterial /allergic Pain
Cold sores of the lip Head lice
Cystitis (women) Nappy rash
Cradle cap Oral thrush
Dandruff Piles (haemorrhoids)
Dental caries -prevention Ringworm/ athlete’s foot
Dry/ sore/tired eyes Sore throat
Diarrhoea Sunburn/ sun protection
Dry skin Teething/ mild toothache
Ear wax build up Threadworm
Excessive sweating (hyperhidrosis) Thrush genital
Hayfever / allergic rhinitis Travel/ motion sickness
Indigestion /heartburn Warts/ verrucae
Prescriber to circle the indication above that requires treatment and write any further advice or recommendations in this space:
If at any time you are concerned about your condition or if your symptoms are not improving after a few days of treatment, contact the local pharmacist or the surgery for more advice or visit NHS website Health A-Z or Patient co.uk . Link to the NHS decision on over-the-counter medicines https://www.england.nhs.uk/2018/03/nhs-england-frees-up-millions-of-pounds-which-could-be-used-for-frontline-services/

Appendix 3
Reference guide for health care professionals for the treatment of minor ailments and self limiting conditions Page Items of low clinical effectiveness Page Minor ailments & self-limiting
conditions suitable for self care 1 Probiotics 22 Headlice 2 Vitamins and minerals 23 Indigestion/ heartburn 3 Sore throat (acute) 24 Infant colic Minor ailments & self-limiting
25 Insect bites and stings
4 Acne (mild) 26 Migraine and headache (infrequent) 5 Burns and scalds (minor) 27 Mouth ulcers 6 Cold sores of the lip (infrequent) 28 Nappy rash 7 Conjunctivitis 29 Oral thrush 8 Constipation (infrequent) 30 Pain conditions (minor) 9 Cough colds, nasal congestion 31 Ringworm/ athletes foot 10 Cradle cap 32 Sun burn 11 Cystitis (mild) 33 Sun protection 12 Dandruff 34 Teething/mild toothache 13 Dental caries (prevention) 35 Threadworm 14 Dermatitis (mild irritant ) 36 Thrush in men and women 15 Diarrhoea(acute) 37 Travel/motion sickness 16 Dry skin (mild) 38 Warts and verrucae 17 Dry/ sore tired eyes 18 Ear wax build up 19 Excessive sweating 20 Haemorrhoids 21 Hayfever and allergic rhinitis
Before you use this quick reference guide It is intended that this quick reference guide is used in conjunction with the general information within the guideline. Where appropriate, links have been made to specific information within the guideline to assist your decision making. Health care professionals are also reminded that they are responsible for prescribing, recommending or supplying an appropriate medicine taking into account that no contraindications apply and that special precautions have been considered. If in doubt the Summary of Product Characteristics (SPC) should be checked before making any recommendation.

Go back to contents page
Appendix 3 Reference guide for prescribers
Probiotics There is currently insufficient clinical evidence to support prescribing of probiotics within the NHS for the treatment or prevention of diarrhoea of any cause. (Link to LLR Low Priority Prescribing Guidance) Both the Public Health England .difficile guidance14 and NICE CG 8415 recommend that probiotics cannot be recommended currently and that “Good quality randomised controlled trials should be conducted in the UK to evaluate the effectiveness and safety of a specific probiotic using clearly defined treatment regimens and outcome measures before they are routinely prescribed”.
Exceptions • ACBS approved indication or as per local policy (link to LMSG guidance). The ACBS recommends some foods and
toilet preparations that may be regarded as drugs for the treatment of specified conditions. If a doctor is satisfied that the product can be safely prescribed, that patients will be adequately monitored and have access to hospital supervision if needed, they can prescribe these products on a prescription endorsed with “ACBS”.

Go back to contents page
1. Probiotics
Vitamins and minerals There is insufficient high quality evidence to demonstrate the clinical effectiveness of vitamins and minerals.16
(Link to LLR Low Priority Prescribing Guidance)
Vitamins and minerals are essential nutrients which most people can and should get from eating a healthy, varied and balanced diet. In most cases, dietary supplementation is unnecessary. Many vitamin and mineral supplements are classified as foods and not medicines. They therefore do not have to go through the strict criteria laid down by the Medicines and Healthcare products Regulatory Agency (MHRA) to confirm their quality, safety and efficacy before reaching the market. It is therefore not deemed appropriate for such preparations to be routinely funded on the NHS. Any prescribing not in-line with listed exceptions should be discontinued.
This guidance does not apply to Healthy Start Vitamins but these are not currently prescribed on an NHS prescription but are commissioned separately.
Exceptions • Medically diagnosed deficiency or those considered to be high risk outlined in LMSG guidance including those patients
who may have a lifelong or chronic condition or have undergone surgery that results in malabsorption. Continuing need should however be reviewed on a regular basis and maintenance or preventative treatment is not an exception.
• Calcium and vitamin D for osteoporosis. • Malnutrition including alcoholism.

Go back to contents page
2. Vitamins and Minerals
Illness
Sore throat - Acute There is little evidence to suggest that treatments such as lozenges or throat sprays help to treat the cause of sore throat. (Link to LLR Low Priority Prescribing Guidance)
Advice to patients
Sore throats are very common and normally get better within a week. Patients should be advised to take simple painkillers and implement some self-care measures such as gargling with warm salty water or hot (honey and lemon) instead. Link to patient advice on the NHS website
Exceptions Red flag symptoms - https://www.gponline.com/education/medical-red-flags
Link to general exceptions Examples of medicines available to purchase OTC
• Paracetamol or ibuprofen
• Antiseptic or local anaesthetic (benzocaine) throat sprays
• Lozenges
OTC restrictions3
• See Appendix 1 for paracetamol and ibuprofen OTC restrictions. • There are restrictions on all antiseptic and local anaesthetics in children under 3 years and breast feeding/
pregnant women that can be supplied OTC. For children 3 years and over the pharmacist will be able to advise of a suitable preparation that can be supplied OTC.
3. Sore throat - Acute

Go back to contents page
Illness
Acne - Mild Acne is a common skin condition that affects most people at some point. Although acne cannot be cured, it can be controlled with treatment.
Advice to patients
Several creams, lotions and gels for treating acne are available at pharmacies. Treatments can take up to three months to work. Link to patient advice on the NHS website
Exceptions No specific exceptions have been identified.
Link to general exceptions
Examples of medicines available to
• Benzoyl peroxide-containing topical preparations 2.5%, 5% and 10%: • Nicotinamide gel 4%
OTC restrictions3
• Nicotinamide- • Nicotinamide gel 4%- avoid in the first trimester
4. Acne – Mild

Go back to contents page
Illness
Burns and scalds - Minor Burns and scalds are damage to the skin caused by heat. Both are treated in the same way. Depending on how serious a burn is, it is possible to treat minor burns at home.
Advice to patients
It is advisable to keep something ready to treat burns in a medicine cabinet or first aid box at home. Link to patient advice on the NHS website
Exceptions
Serious burns always require professional medical attention. Burns requiring hospital A and E treatment include but are not limited to:
• All chemical and electrical burns
• Large or deep burns
• Burns that cause white or charred skin
• Burns on the face, hands, arms, feet, legs or genitals that cause blisters. Link to general exceptions
Examples of medicines available to purchase OTC
• Topical antiseptics e.g. containing either povidone iodine 2.5%, chlorhexidine or zinc oxide.
OTC restrictions3 • Betadine® powder (povidone-iodine) - Pregnancy, breastfeeding, children under 2 years.
5. Burns and scalds – Minor

Go back to contents page
Illness
Cold sores of the lip - Infrequent Cold sores caused by the herpes simplex virus usually clear up without treatment within seven to ten days. (Link to LLR Low Priority Prescribing Guidance)
Advice to patients
Antiviral creams are available OTC from pharmacies without a prescription. If used correctly, they may help ease symptoms but will only reduce the healing time by a day or so. To be effective, apply as soon as the first signs of a cold sore appear. Using an antiviral cream after this initial period is unlikely to have much of an effect. Link to patient advice on the NHS website
Exceptions
Red flag symptoms-https://www.gponline.com/education/medical-red-flags#s
Immunocompromised patients
Link to general exceptions
Examples of medicines available to purchase OTC
Aciclovir cream 5% (General Sales List GSL)
OTC restrictions3 Only for face and lips
6. Cold sores of the lip - Infrequent

Go back to contents page
Illness
Conjunctivitis Treatment is not usually needed for conjunctivitis as the symptoms usually clear within a week. There are several self-care measures that may help with symptoms. If treatment is needed, then treatment is dependent on the cause: • In severe bacterial cases, antibiotic eye drops and eye ointments can be used to clear the infection.
• Irritant conjunctivitis will clear up as soon as whatever is causing it is removed.
• Allergic conjunctivitis can usually be treated with anti-allergy medications such as antihistamines. The substance that caused the allergy should be avoided.
Advice to patients
Treatments for conjunctivitis can be purchased over the counter however almost half of all simple cases of conjunctivitis clear up within ten days without any treatment. Link to patient advice on the NHS website
Exceptions
Red flag symptoms-https://www.gponline.com/education/medical-red-flags#s Link to general exceptions
Examples of medicines available to purchase OTC
Bacterial conjunctivitis
• Chloramphenicol 0.5% eye drops (pharmacy only P)
• Chloramphenicol 1% eye ointment (pharmacy only P) Allergic conjunctivitis
• Sodium cromoglycate eye drops
• Antazoline/ xylometazoline eye drops
OTC restrictions3
Children < 2 years(chloramphenicol and sodium cromoglycate)
• Children < 12 years antazoline / xylometazoline eye drops • Pregnancy and breastfeeding women
7. Conjunctivitis

Go back to contents page
Illness
Constipation - Infrequent Constipation can affect people of all ages and can be just for a short period of time.
Advice to patients
It can be effectively managed with a change in diet or lifestyle and short term use of over the counter laxatives. Link to patient advice on the NHS website
Exceptions No specific exceptions have been identified. Note the NHS website states that laxatives are not recommended for children unless prescribed by a GP. Link to general exceptions
Examples of medicines available to purchase OTC
• Lactulose liquid
• Bisacodyl suppositories • Senna tablets of liquid • Ispaghula Husk granules- oral sachets
OTC restrictions5
• Bisacodyl - pregnancy and breastfeeding and children under 10 years. • Senna - severe dehydration, children under 6 years, pregnancy and breastfeeding. • Ispaghula Husk Granules - children under 6 years. • Use for longer than 7 days duration at any one time. • Note NHS website states that laxatives are not recommended for children unless prescribed by a GP.
8. Constipation – Infrequent

Go back to contents page
Illness
Coughs and colds and nasal congestion Most colds start to improve in seven to ten days. Most coughs clear up within two to three weeks. Both conditions can cause nasal congestion. Neither condition requires any treatment. However, some over the counter medicines help to relieve short term fevers and nasal congestion. Link to LLR Low Priority Prescribing Guidance.
Advice to patients These conditions do not require any treatment. However, some over the counter medicines had relieve
short term fevers and nasal congestion. Hot honey and lemon has a similar effect to cough medicines. (Link to patient advice on the NHS website)
Exceptions Red flag symptoms- https://www.gponline.com/education/medical-red-flags Link to general exceptions
Examples of medicines available to purchase OTC
• Ibuprofen tablets/capsules and suspension • Paracetamol tablets/capsules and suspension • Aromatic inhalations
• Pseudoephedrine containing preparations • Sodium chloride 0.9% nasal drops and spray • Pholcodeine linctus
OTC restrictions3
• See Appendix 1 for paracetamol and ibuprofen OTC restrictions • Pseudoephedrine - children under 12 years, pregnancy, breastfeeding. • Pholcodine children under 6 years, pregnant and breast feeding women. • Check with the pharmacist regarding age restrictions aromatic inhalations
9. Coughs and colds and nasal congestion

Go back to contents page
10. Cradle cap (seborrhoeic dermatitis – infants)
Illness
Cradle cap (seborrhoeic dermatitis – infants) Cradle cap is harmless and does not usually itch or cause discomfort. It usually appears in babies in the first two months of their lives, and clears up without treatment within weeks to a few months.
Advice to patients
Cradle cap treatment should not routinely be offered in primary care as the condition is self-limiting and will clear up on its own without the need for treatment.
(Link to patient advice on the NHS website)
Exceptions If causing distress to the infant and not improving
Link to general exceptions
Emulsifying ointments and shampoos (General Sales List GSL).
OTC restrictions3
• If it has spread to the face • Do not use on broken skin or infected skin

Go back to contents page
Illness
Cystitis - Mild Mild cystitis is a common type of urinary tract inflammation, normally caused by an infection; however it is usually more of a nuisance than a cause for serious concern. Mild cases can be defined as those that are responsive to symptomatic treatment but will also clear up on their own. If symptoms do not improve in three days, despite self-care measures, then the patient should be advised to see their GP.
Advice to patients
Symptomatic treatment using products that reduce the acidity of the urine to reduce symptoms are available, but there is a lack of evidence to suggest they are effective. Link to patient advice on the NHS website
Exceptions Red flag symptoms including if you are a man or child with symptoms of cystitis.
https://www.gponline.com/education/medical-red-flags
Link to general exceptions Examples of medicines available to purchase OTC
• Paracetamol/ ibuprofen
• Sodium citrate 4g sachets products
• Potassium citrate preparations
OTC restrictions3
• See Appendix 1 for paracetamol OTC restrictions • Sodium citrate 4g sachet products – men, children under 16 years, pregnant and
breastfeeding women • Potassium citrate products - children under 6 years, pregnancy and breastfeeding
11. Cystitis – Mild

Go back to contents page
Illness
Dandruff Dandruff is a common skin condition. It can be defined as mild scaling of the scalp without itching. Dandruff is not contagious or harmful.
Advice to patients
Dandruff can be easily treated with over the counter antidandruff or antifungal shampoos. Link to patient advice on the NHS website
Exceptions No specific exceptions identified
Link to general exceptions Examples of medicines available to purchase OTC
• Ketoconazole
• Coal tar shampoo
• Selenium sulfide shampoo
• Salicylic acid
• Some preparations contain several ingredients at different strengths
OTC restrictions3
• The pharmacist can advise on the suitability of different preparations for each individual according to age or if pregnant or breast feeding.
• Coal tar and selenium cannot be sold OTC to pregnant and breastfeeding women.
12. Dandruff

Go back to contents page
Illness
Dental caries (dental decay) - Prevention The dentist may advise on using higher-strength fluoride toothpaste if a patient is particularly at risk of tooth decay.
Advice to patients
Higher fluoride toothpastes and mouthwashes can be purchased over the counter. Prescription only preparations such as high strength fluoride toothpastes (2,800 and 5,000 ppm) need to be re-directed to a dentist to prescribe. Link to patient advice on the NHS website (tooth decay) Link to patient advice on the NHS website (fluoride)
Exceptions No specific exceptions have been identified. Link to general exceptions
Examples of medicines available to purchase OTC
• Mouthwashes chlorhexidine digluconate.
• Fluoride up to 1500 ppm can be bought over the counter
OTC restrictions5
• POM- the dentist will advise. • GSL- For standard prevention- advise patients to look at recommendations on the side of the
toothpaste tube to determine the appropriate quantity to use
13. Dental caries – Prevention

Go back to contents page
Illness
Dermatitis - Mild irritant Irritant dermatitis is a type of eczema triggered by contact with a particular substance. Once treated most people can expect their symptoms to improve and/or clear up completely if the irritant or allergen can be identified and removed or avoided. It is most commonly caused by irritants such as soaps, washing powders, detergents, solvents or regular contact with water.
Advice to patients
Treatment normally involves avoiding the allergen or irritant and treating symptoms with over the counter emollients and topical corticosteroids. Link to patient advice on the NHS website
Exceptions No specific exceptions identified
Link to general exceptions
Examples of medicines available to
purchase OTC
• Emollients
• Crotamiton cream or lotion (with or without hydrocortisone) • Steroid creams, for example hydrocortisone 1% cream
OTC restrictions3
Crotamiton / hydrocortisone preparations
• Age restriction: crotamiton OTC restricted in children under 3 years and treatments containing hydrocortisone 1% cream are restricted in children under 10 years
• Pregnancy, breastfeeding • Broken or inflamed skin • Use on the eyes, face or ano-genital region
14. Dermatitis - Mild irritant

Go back to contents page
Illness
Diarrhoea (acute) Diarrhoea normally affects most people from time to time and is usually nothing to worry about. However, it can take a few days to a week to clear up.
Acute diarrhoea is usually caused by a bacterial or viral infection and other causes include drugs, anxiety or a food allergy.
Advice to patients
Over the counter treatments can help replace lost fluids or reduce bowel motions. Link to patient advice on the NHS website
Exceptions Please note: Acute diarrhoea in children was not included in the NHSE consultation Red flag symptoms in under 5s (link) Red flag symptoms https://www.gponline.com/education/medical-red-flags
No routine exceptions have been identified in adults.
Link to general exceptions Examples of medicines available to purchase OTC
• Loperamide 2mg capsule products
• Oral rehydration sachets
OTC restrictions3
• Loperamide – cannot be sold OTC children <12 years; pregnant and breastfeeding women; acute
episodes of IBS in patients <18 years old.
15. Diarrhoea (acute)

Go back to contents page
Illness
Dry skin - Mild Patients with mild dry skin can be successfully managed using over the counter products on a long term basis.
Advice to patients
Emollients are often used to help manage dry, itchy or scaly skin conditions. Link to patient advice on NHS website
Exceptions No specific exceptions have been identified. Link to general exceptions
Examples of medicines available to purchase OTC
Emollient brands should be based on personal preference
OTC restrictions3
None A pharmacist can recommend the best products to help with dry skin
16. Dry Skin – Mild

Go back to contents page
Illness
Dry eyes/sore tired eyes Dry eye syndrome, or dry eye disease, is a common condition that occurs when the eyes do not make enough tears, or the tears evaporate too quickly. Most cases of sore tired eyes resolve themselves.
Advice to patients
Patients should be encouraged to manage both dry eyes and sore eyes by implementing some self-care measures such as good eyelid hygiene and avoidance of environmental factors alongside treatment. Mild to moderate cases of dry eye syndrome or sore tired eyes can usually be treated using lubricant eye treatments that consist of a range of drops, gels and ointments that can be easily be purchased over the counter. Link to patient advice on the NHS website
Exceptions Pre-existing long–term conditions affecting the eyes.
Link to general exceptions Examples of medicines available to purchase OTC
• Lubricant eye treatments include hypromellose 0.3% and carbomer preparations.
OTC restrictions3
• Carbomer cannot be sold OTC for pregnant or breastfeeding women as safety has not been
established
17. Dry eyes/sore tired eyes

Go back to contents page
Illness
Earwax build up Earwax is produced inside ears to keep them clean and free of germs. It usually passes out of the ears harmlessly, but sometimes too much can build up and block the ears.
Advice to patients
A build-up of earwax is a common problem that can often be treated using eardrops bought over the counter. These can help soften the earwax so that it falls out naturally. Link to patient advice on the NHS website)
Exceptions • Perforated ear drum.
• Medical supervision is recommended in children <5 years
• Link to general exceptions
Examples of medicines available to purchase OTC
• Olive oil drops • Arachis oil/chlorobutanol hemihydrate drops
• Docusate sodium 0.5% drops. • Sodium bicarbonate 5% ear drops
OTC restrictions3
• Some preparations may be less suitable for children. The pharmacist will be able to advise.
18. Earwax build up

Go back to contents page
Illness
Excessive sweating (hyperhidrosis) Hyperhidrosis is a common condition in which a person sweats excessively. First line treatment involves simple lifestyle changes.
Advice to patients
An antiperspirant containing aluminium chloride is usually the first line of treatment and is sold in most pharmacies. Things you can do to help with excessive sweating are:
• Wear loose-fitting clothes to minimise signs of sweating
• Wear socks that absorb moisture and change your socks at least twice a day if possible
• Wear leather shoes and try to wear different shoes day to day
• Don’t wear tight clothes or man-made fabrics – for example, nylon
• Don’t wear enclosed boots or sports shoes that may cause your feet to sweat more • Don’t do things that might make your sweating worse e.g., drinking alcohol or eating spicy food
Link to patient advice on the NHS website
Exceptions No routine exceptions have been identified. Link to general
ti
Examples of medicines available to purchase OTC
Aluminium chloride
OTC restrictions3
None
19. Excessive sweating (hyperhidrosis)

Go back to contents page
Illness
Haemorrhoids (piles) In many cases, haemorrhoids do not cause symptoms and some people do not even realise they have them. Haemorrhoids often clear up by themselves after a few days.
Making simple dietary changes and not straining on the toilet are often recommended first.
Advice to patients
Treatments (creams, ointments and suppositories) can reduce itching and discomfort and these are available over the counter for purchase.
Link to patient advice on the NHS website
Exceptions Red flag symptoms- https://www.gponline.com/education/medical-red-flags
Link to general exceptions
Examples of medicines available to purchase OTC
• Haemorrhoidal creams and ointments usually contain multiple ingredients including astringents such as zinc oxide, lubricants, antiseptics, local anaesthetics and corticosteroids
• Paracetamol (not codeine or NSAIDs)
OTC restrictions3
• See Appendix 1 for paracetamol OTC restrictions
• Haemorrhoidal preparations
• Children under 18 years
• Pregnancy
• Breastfeeding
• Rectal bleeding or blood in the stool
• 7 day maximum duration
20. Haemorrhoids (piles)

Go back to contents page
Illness Hayfever/allergic rhinitis - Mild to moderate
Hay fever is a common allergic condition that affects up to one in five people.
Advice to patients There is currently no cure for hay fever, but most people with mild to moderate symptoms are able to relieve symptoms with OTC treatments recommended by a pharmacist.
Link to patient advice on the NHS website
Exceptions No specific exceptions have been identified. Link to general
ti Examples of medicines available to purchase OTC
• Acrivastine 8mg capsules • Cetirizine 10mg tablets and 1mg/ml oral solution • Loratadine 10mg tablets and 5mg/5ml syrup • Chlorphenamine 4mg tablets 2mg/5ml oral solution • Beclomethsone 50mcg/ml nasal spray • Fluticasone 0.05% w/w nasal spray
OTC Restrictions3
• Antihistamines cannot be sold OTC to children as follows: • Acrivastine <12 years.21 • Cetrizine children < 6 years • Loratadine children <2 years • Chlorphenamine < 1 year • Beclomethasone <18 years • Fluticasone <4 years • Pregnant and breast feeding women should be treated by their GP for hay fever as these preparations
cannot be sold OTC to this group. • Older people • Acrivastine cannot be sold OTC to adults over 65 years.
21. Hayfever/allergic rhinitis - Mild to moderate

Go back to contents page
Illness Headlice Headlice are a common problem, particularly in school children aged 4-11. They are largely harmless, but can live in the hair for a long time if not treated and can be irritating and frustrating to deal with.
Advice to patients
It is not always possible to prevent head lice infestation, as they are spread by close head to head contact, especially when children are playing. However, these self-care tips will help with detection and prevention. Frequent checking - carefully looking at your child’s scalp and hair for head lice, especially at the start of the school year. Ideally do this weekly. ‘Wet combing’- Wash hair as usual then use conditioner, do not wash this off. Use a normal comb to untangle hair, then a fine-toothed head lice detection comb to remove live head lice. Avoid sharing - Hats, combs, hairbrushes, towels, pillows.
Hair length - People with longer hair are more likely to catch head lice, simply because it is easier for the head lice to transfer to and from longer hair. Head lice eradication products containing alcohol: there is a risk of serious burns if treated hair is exposed to open flames or other sources of ignition, e.g. cigarettes. Link to patient advice on the NHS website
Exceptions
Current skin conditions of the scalp. Side effects of a severe infestation. Link to general exceptions
Examples of medicines available to purchase OTC
• Headlice comb – for wet combing hair after treatment with conditioner, lotions, solutions or sprays • Dimeticone gel, lotion or spray 4%
• Malathion aqueous lotion 0.5% (not recommended unless repeated use of dimethicone has failed.
OTC restrictions3 • Children under 6 months
22. Headlice

Go back to contents page
Illness
Indigestion and heartburn Most people have indigestion at some point. Usually, it is not a sign of anything more serious and can be treated at home without the need for medical advice, as it is often mild and infrequent and specialist treatment is not required.
Advice to patients
Most people are able to manage their indigestion by making simple diet and lifestyle changes, or taking medication such as antacids. Most people can ease symptoms by simple changes to diet and lifestyle and avoiding foods that make indigestion worse (e.g. rich spicy or fatty foods, caffeinated drinks). Link to patient advice on the NHS website - indigestion Link to patient advice on the NHS website - heartburn
Exceptions No specific exceptions have been identified. Link to general exceptions
Examples of medicines available to purchase OTC
• Co-magaldrox (aluminium and magnesium hydroxide mixture) • Sodium alginate raft forming suspension, calcium carbonate, sodium bicarbonate e.g. gaviscon® • Esomeprazole 20mg tablets
• Pantoprazole 20mg tablets • Rantidine 75mg tablets
OTC restrictions3
• Co-magaldrox- children under 14 years of age and breastfeeding women • Gaviscon® - children under 12 years • Gaviscon® Infant – premature infants and children under 1 year and over 2 years • Esomeprazole and pantoprazole - children under 18 years or adults over 55 years with new or
recently changed symptoms • Ranitidine - children under 16 years or for anyone for longer than 6 days
23. Indigestion and heartburn

Go back to contents page
Illness
Infant colic As colic eventually improves on its own, medical treatment is not usually recommended. (Link to LLR Low Priority Prescribing Guidance)
Advice to patients
There are some over the counter treatments available that could be tried. However, there is limited evidence for the effectiveness of these treatments. The most useful intervention is support for parents and reassurance that colic will resolve itself. Link to patient advice on the NHS website
Exceptions Red flag symptoms- https://www.gponline.com/education/medical-red-flags
Link to general exceptions
Examples of medicines available to purchase OTC
• Simeticone 40mg/ml
• Dimeticone 42mg/5ml (avoid in glucose-galactose or sucrose intolerant patients) OTC restrictions3
None
24. Infant colic

Go back to contents page
Illness
Insect bites and stings Most insect bites and stings are not serious and will get better within a few hours or days Advice to patients
Over-the-counter treatments can help ease symptoms, such as painkillers, creams for itching and antihistamines. Link to patient advice on the NHS website
Exceptions No specific exceptions have been identified. Link to general exceptions
Examples of medicines available to purchase OTC
• Acrivastine 8mg capsules • Cetirizine 10mg tablets and 1mg/ml oral solution • Loratadine 10mg tablets and 5mg/5ml syrup • Chlorphenamine 4mg tablets 2mg/5ml oral solution • Hydrocortisone cream 1% • Crotamiton cream or lotion 10% • Crotamiton cream 10% hydrocortisone 0.25% • Mepyramine 2% cream
OTC restrictions
3
• Oral anthistamines • Acrivastine <12 years and >65 years • Cetrizine children < 6 years • Loratadine children <2 years • Chlorphenamine < 1 year
Oral antihistamine preparations are restricted OTC in pregnant and breast feeding women Crotamiton / hydrocortisone topical preparations • Age restriction: OTC crotamiton restricted in children under 3 years and OTC preparations containing
hydrocortisone 1% are restricted in children under 10 years • Pregnancy, breastfeeding • Broken or inflamed skin • Use on the eyes, face or ano-genital region
25. Insect bites and stings

Go back to contents page
Illness
Migraine and headache - Infrequent Migraine is a common health condition, affecting around one in every five women and around one in every 15 men.
Advice to patients
Mild infrequent migraines and headaches can be adequately treated with over the counter painkillers and a number of combination medicines for migraine are available that contain both painkillers and anti-sickness medicines. Link to patient advice on the NHS website - migraine Link to patient advice on the NHS website - headaches
Exceptions No specific exceptions have been identified. Link to general exceptions
Examples of medicines available to purchase OTC
• Ibuprofen tablets, capsules and suspension • Paracetamol tablets, capsules and suspension • Co-codamol 8/500mg (paracetamol and codeine)
• Anti-sickness - prochlorperazine maleate • Sumatriptan 50mg tablets
OTC restrictions3
• See Appendix 1 for paracetamol, codeine and ibuprofen OTC restrictions (link) • Co-codamol - children under 12 years; pregnant and breastfeeding women. • Prochlorperazine maleate - children < 18 years;
• Sumatriptan – children under 18 years; adults over 65 years; pregnant and breastfeeding women.
26. Migraine and headache – Infrequent

Go back to contents page
Illness
Mouth ulcers Mouth ulcers are usually harmless and do not need to be treated because most clear up by themselves within a week or two. Mouth ulcers are common and can usually be managed at home, without seeing your dentist or GP.
Advice to patients
OTC treatment with antimicrobial mouthwashes, local anaesthetics, analgesics or hydrocortisone can help to reduce swelling and ease any discomfort. Link to patient advice on the NHS website
Exceptions No specific exceptions have been identified. Link to general exceptions
Examples of medicines available to purchase OTC
• Antimicrobial mouthwashes • Local anaesthetics are available as a mouthwash, lozenge, gel or spray e.g. Lidocaine hydrochloride
and benzocaine/chlorocresol cetylpyridinium chloride /Choline salicylate/cetalkonium chloride • Hydrocortisone oral mucosal pellets • Paracetamol or ibuprofen
OTC restrictions5
• Ask the pharmacist which antibacterial or anaesthetic preparations are suitable for children and pregnant or breast feeding women
• Hydrocortisone oral mucosal pellets cannot be sold for children< 12 years. • See Appendix 1 for paracetamol, and ibuprofen OTC restrictions
27. Mouth ulcers

Go back to contents page
Illness
Nappy rash Up to a third of babies and toddlers in nappies have nappy rash at any one time.
Advice to patients
Nappy rash can usually be treated at home using a barrier cream. Nappy rash usually clears up after about three days if recommended hygiene tips are followed. If the baby develops persistent bright red moist rash with red/ white pimples that spreads into the folds they may have an infection and an antifungal cream may be required Link to patient advice on the NHS website
Exceptions No specific exceptions have been identified. Link to general exceptions
Examples of medicines available to purchase OTC
• Titanium dioxide, titanium peroxide, titanium salicylate. Zinc oxide, benzyl alcohol, benzyl benzoate, lanolin
• Antifungal creams e.g. clotrimazole 1% or miconazole 2% cream
OTC restrictions3
No restrictions
28. Nappy rash

Go back to contents page
Illness
Oral thrush Oral thrush is a minor condition that can be treated without the need for a GP consultation or prescription in the first instance. It is common in babies and older people with dentures or those using steroid inhalers.
Advice to patients
It can easily be treated with over the counter gel for use in the mouth which usually lasts for 7 days. Link to patient advice on the NHS website (adults) Link to patient advice on the NHS website (babies)
Exceptions No specific exceptions have been identified. Link to general exceptions
Examples of medicines available to purchase OTC
Miconazole 2% oral gel (15g) , for example Daktarin® oral gel (pharmacy only P)
OTC restrictions3
• Children under 4 months • Pregnancy, breastfeeding
29. Oral thrush

Go back to contents page
Illness
Pain Conditions - Minor In most cases, headaches, period pain, mild fever and back pain can be treated at home with OTC painkillers and lifestyle changes, such as getting more rest and drinking enough fluids.
Advice to patients
Patients should be encouraged to keep a small supply of OTC analgesics in their medicines cabinets at home so they are able to manage minor ailments at home without the need for a GP appointment.
Link to patient advice on the NHS website (back) Link to patient advice on the NHS website (menstrual)
Exceptions No routine exceptions have been identified.
Link to general exceptions Examples of medicines available to purchase OTC
• Ibuprofen tablets, capsules and suspension
• Paracetamol tablets, capsules and suspension • Co-codamol 8/500mg (paracetamol and codeine)
OTC restrictions3
• See Appendix 1 for paracetamol, codeine and ibuprofen OTC restrictions
30. Pain Conditions – Minor

Go back to contents page
31. Ringworm/athletes foot
Illness
Ringworm/athletes foot Ringworm is a common fungal infection that can cause a red or silvery ring-like rash on the skin. Despite its name, ringworm doesn’t have anything to do with worms. Athlete’s foot is a rash caused by a fungus that usually appears between the toes.
Illness
These fungal infections, medically known as “tinea”, are not serious and are usually easily treated with over the counter treatments. However, they are contagious and easily spread so it is important to practice good foot hygiene. Link to patient advice on the NHS website - ringworm Link to patient advice on the NHS
Exceptions Lymphoedema or history of lower limb
cellulitis. Link to general exceptions Examples of medicines available to purchase OTC
• Terbinafine hydrochloride 1% cream, gel, powder or spray for 1-2 weeks. (first line for ringworm)
• Miconazole 2% cream0.16% powder for 10 days after the lesions have healed. • Clotrimazole 1% cream for 4 weeks
• (Miconzole and clotrimazole with hydrocortisone 1% is available OTC if there is marked inflammation).
OTC restrictions3 • All products –Most preparations can only be used in pregnancy, breastfeeding under medical supervision.
• Terbinafine hydrochloride – children under 16 years.

Go back to contents page
Illness
Sunburn due to excessive sun exposure Most people manage sun burn symptoms themselves or prevent symptoms developing by using sun protection. These products can easily be bought in a pharmacy or supermarket.
Advice to patients
Cool your skin by having a cold bath or shower, sponging it with cold water or holding a flannel to it. Use lotions containing aloe vera to soothe and moisturise the skin and drink plenty of fluids to avoid dehydration. Take painkillers such as paracetamol or ibuprofen to relieve the pain if required. (Link to patient advice on the NHS website)
Exceptions No specific exceptions have been identified. Link to general exceptions
Examples of medicines available to purchase OTC
• Calamine lotion After sun preparations
• Paracetamol/ ibuprofen
OTC restrictions3
• See Appendix 1 for paracetamol, and ibuprofen OTC restrictions (link)
32. Sunburn due to excessive sun exposure

Go back to contents page
Illness
Sun protection Most people prevent symptoms of sun damage developing using sun protection. These products can easily be bought in a pharmacy or supermarket.
Advice to patients
Sun protection products can readily be bought in a pharmacy or supermarket. Link to patient advice on the NHS website
Exceptions ACBS approved indication of photodermatoses, i.e. where skin protection should be prescribed.
Examples of medicines available to purchase OTC
• Sun protection lotion, gels and creams (General Sales List GSL)
OTC restrictions3
• No restrictions
33. Sun protection

Go back to contents page
Illness
Teething/mild toothache Teething can be distressing for some babies, but there are ways to make it easier for them.
Toothache can come and go, or be constant. Eating or drinking can make the pain worse, particularly if the food or drink is hot or cold.
Advice to patients
Teething gels often contain a mild local anaesthetic, which helps to numb any pain or discomfort caused by teething and these can be purchased from a pharmacy. If the baby is in pain or has a mild raised temperature (less than 38oC) then paracetamol or ibuprofen suspension can be given. Mild toothache in adults can also be treated with over the counter painkillers.
Link to patient advice on the NHS website
Exceptions No specific exceptions have been identified.
Link to general exceptions
Examples of medicines available to purchase OTC
• Ibuprofen tablets and suspension • Paracetamol tablets and suspension. • Teething gels containing local anaesthetics
OTC restrictions3
• See Appendix 1 for paracetamol, and ibuprofen OTC restrictions (link) • Teething gels are restricted for OTC sale in - babies under 5 months.
34. Teething/mild toothache

Go back to contents page
Illness
Threadworms Threadworms (pinworms) are tiny worms that pass in the stools. They are common in children and can be spread easily. They can be effectively treated without the need to visit the GP.
Advice to patients
Treatment for threadworms can easily be bought from pharmacies. This is usually a chewable tablet or liquid formulation. Strict hygiene measures can also help clear up a threadworm infection and reduce the likelihood of reinfection. Information is available on NHS website Everyone in the household will require treatment, even if they do not have symptoms. Link to patient advice on the NHS website
Exceptions No specific exceptions have been identified. Link to general exceptions
Examples of medicines available to purchase OTC
• Mebendazole 100mg tablets and chewable tablets are available as an individual or family pack.
OTC restrictions3
• Children under 2 years • Pregnancy • Breastfeeding
35. Threadworms

Go back to contents page
Illness
Thrush in men and women Thrush is a common yeast infection that affects men and women. It's usually harmless but it can be uncomfortable and keep coming back. It isn't classed as a sexually transmitted infection (STI).
Advice to patients
If patients have had their symptoms previously confirmed by their GP and they think have them again then it can be treated with OTC preparations bought from the local pharmacy.
However the following patients should seek advice from their GP first: <16 years of age; > 60 years of age; pregnancy or breast feeding; unusual symptoms; you're under 16 or over 60; recurrent symptoms more than twice in 6 months); treatment hasn't worked.
Link to patient advice on the NHS website
Exceptions Patients who are immunocompromised
Please note: Genital thrush was not included in the NHSE consultation
Link to general exceptions
Examples of medicines available to purchase OTC
• Clotimazole 1%, 2% creams, 500mg pessary, 10% intravaginal cream • Fluconazole 150mg capsule
OTC restrictions3 • Children < 16 years old of age • Adults >60 years • Pregnant or breast feeding women
36. Thrush in men and women

Go back to contents page
Illness
Travel (motion) sickness Mild motion sickness can be treated by various self-care measures (e.g. staring at a fixed object, getting some fresh air, listening to music etc).
Advice to patients
Severe motion sickness can be treated with over the counter medicines. It’s usually better to take the medication before the journey to prevent symptoms developing. These medicines may cause drowsiness. Link to patient advice on the NHS website
Exceptions No specific exceptions have been identified. Link to general exceptions
Examples of medicines available to purchase OTC
• Antihistamines such as cinnarizine 15mg tablets and cyclizine 50mg tablets • Hyoscine hydrobromide tablets 150mcg
OTC restrictions3
• Cinnarizine and Hyoscine hydrobromide cannot be supplied OTC in children <5 years of age.
• Cyclizine cannot be supplied OTC in children < 6 years of age
• There are no OTC preparations suitable for pregnant and breast feeding women
37. Travel (motion) sickness

Go back to contents page
Illness
Warts and verrucae Most people will have warts at some point in their life.
Advice to patients
They are generally harmless and tend to go away on their own eventually.
Several treatments can be purchased from a pharmacy to get rid of warts and verrucae more quickly if patients require treatment.
Link to patient advice on the NHS website
Exceptions No specific exceptions have been identified. Link to general
ti Examples of medicines available to purchase OTC
• A variety of topical treatments are available OTC containing salicylic acid/ lactic acid which burns the top layer of affected skin.
• Cold sprays containing dimethyl ether propane which freezes the wart is also available OTC but these are not thought to work as well as salicylic acid
OTC restrictions3
• Face, neck, ano-genital area or broken skin • Cold sprays containing dimethyl ether propane cannot be sold for: • Warts and verrucae bigger than 7.5mm • Children < 4 years old of age • Diabetics • Pregnant or breast feeding women
38. Warts and verrucae

Leicester City Clinical Commissioning Group West Leicestershire Clinical Commissioning Group
East Leicestershire and Rutland Clinical Commissioning Group
Go back to contents page
References 1. NHS England and NHS Clinical Commissioners. Conditions for
which over the counter items should not routinely be prescribed in primary care. Guidance for CCGs. March 2018. Available at: https://www.england.nhs.uk/wp-content/ uploads/2018/03/otc-guidance-for-ccgs.pdf. Last accessed 06/08/2018.
2. NHS consultation https://www.england.nhs.uk/medicines/over-the-counter-items-which-should-not-routinely-be-prescribed/
3. Electronic Medicines Compendium (eMC). Directory of prescribing and patient information for licensed medicines. Available at: https://www.medicines.org.uk/emc/ . Last accessed 05/12/2018.
4. GP online RED flags https://www.gponline.com/education/medical-red-flags
5. NICE clinical evidence https://www.evidence.nhs.uk/search?q=abdominal+red+flags
6. West Leicestershire CCG website (add page once live) 7. Leicester City CCG website (add page once live) 8. East Leicestershire and Rutland CCG website (add page once live) 9. NHS website https://www.nhs.uk/ 10. Patient https://patient.info / 11. Bumps website http://www.medicinesinpregnancy.org/Medicine--pregnancy/ 12. NHS website https://www.nhs.uk/conditions/pregnancy-and-
baby/breastfeeding-and-medicines/ 13. NHS websitehttps://www.nhs.uk/common-health-questions/medicines/what-
is-the-law-on-the-sale-of-medicines/ 14. Public Health England. Updated guidance on the management and
treatment of Clostridium difficile infection. May 2013. Available at: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/321891/Clostridium_ difficile_management_and_treatment.pdf. Last accessed 06/08/2018.
15. National Institute for Health and Care Excellence (NICE). Clinical Guideline 84. Diarrhoea and vomiting caused by gastroenteritis in under 5s: diagnosis and management. April 2009. Available at: https://www.nice.org.uk/guidance/cg84. Last accessed 06/08/2018.
16. NHS PrescQIPP. The Prescribing of Vitamins and Minerals including B Vitamin Preparations (DROP-List). August 2015. Available at: https://www.prescqipp.info/resources/send/212-vitamins-and-minerals-drop-list/2104-bulletin-107-vitamins-and- minerals-drop-list. Last accessed 06/08/2018.

Q&A regarding Self Care for Over the Counter Preparations for Minor Ailments and Self Limiting Conditions
What are over the counter (OTC) medicines?
Over the counter medicines (OTC) are those that can be purchased in a pharmacy under the supervision of a pharmacist. A limited number of medicines can also be purchased without pharmacy supervision in shops and supermarkets but are often sold in lower pack sizes or lower strengths.
Can Community Pharmacists diagnose minor ailments?
Pharmacists have to complete 4 years of undergraduate training and one year post graduate training and also pass a professional exam before they qualify and practice as a pharmacist. Part of this training includes completion of an accredited training program on minor ailments.
If you are feeling unwell, speak to your community pharmacist as the first port of call. They will be able to recognise symptoms of a minor ailment and offer you advice or treatment accordingly. They will also recognise symptoms are of a more serious or persistent nature and if it is appropriate recommend that you seek further medical advice. However if you are still worried you should make an appointment to see your GP.
You can always call NHS 111, which will help you find the right NHS service.
Can community pharmacists advise me if an OTC will interact with my prescription medicines?
If you are taking medicines prescribed by your GP and you are worried about taking an OTC treatment, a pharmacist will be able to advise you on drug interactions. The pharmacy that dispenses your repeat prescription will be able to check their records of all the medicines that they have supplied you so that they can advise you. Community pharmacists can also view your Summary Care Record which has details of any medicines supplied directly by the pharmacy and also the hospital pharmacy if you are also receiving treatment there.
So wherever you are, the local community pharmacist will be able to check what medicines you take and advise if you are suitable to take OTC remedies. If they have any queries they will speak to your GP.
You can also be prepared by asking your GP on your next routine visit whether there are any OTC preparations you should avoid.
Can my community pharmacist advise which is the most suitable OTC medicine for me if I have a long term condition?
Again speak to your pharmacist if you have any concerns. They will be able to advise patients on the safe use of OTC of medicines in the majority of cases. If they need further information that you

cannot provide, they will be able to contact your GP surgery or advise you to see your GP if appropriate.
What if I want to discuss something in private that is intimate or upsetting?
The majority of community pharmacists have a private room for consultations which you can request to use if you want to discuss an intimate or personal problem. At busy times you may have to wait a little while but the counter assistant will be able to advise you if this is the case and how long you will have to wait. However, normally it shouldn’t be a problem to see the pharmacist reasonably quickly.
Your pharmacist can also talk to you confidentially without anything being noted in your medical records, which some people may prefer.
I can’t easily get to my community pharmacy
Most people have access to a community pharmacy within a short distance of their home. However, if you genuinely struggle to get to a pharmacy, then talk to your pharmacist to see if they can help to find a solution.
It is also worth keeping a small supply of some OTC treatments at home in your medicines cabinet so that you have them at hand in the first instance if you don’t feel well. Watch our short video for advice on what to keep at home.
The quality of OTC medicines is not as good as medicines supplied on a prescription
The quality of medicinal treatments is regulated by the Medicines and Health Regulatory Authority (MHRA). This means that all licensed medicines bought over the counter must go through detailed safety and quality tests. There should be no noticeable difference in treatment of symptoms between a medicine that you can buy and those supplied on prescription.
I can only buy a small quantity of medicine over the counter
There are restrictions on the quantity of some OTC medicines that you can buy at any one time but these should be enough to manage a minor illness. Larger quantities can be sold by a pharmacy than in supermarkets. Your pharmacist can advise you on what the limits are.
Will I have to purchase OTC medicines if I have a long term condition?
If you require regular, long-term treatment with a medicine then this will be prescribed for you if your GP thinks you need it, even if it can be purchased OTC. However, unless you require a medicine on a regular basis you will be expected to purchase OTC preparations for minor illnesses like everyone else.
Your GP may also remove some OTC medicines from your repeat prescription if you are not taking them regularly and ask you to purchase it when you need it. You can help by letting your GP practice know if you have over the counter medicines on your repeat prescription and you don’t take it regularly.

Why do the prices of OTC medicines vary so much?
Prices of similar preparations vary between pharmacies and it is worth shopping around if you know what you need. Some pharmacies have websites which will tell you the products that they stock and prices.
Contact a Pharmacy near you. Link Compare supermarket prices of some OTC preparations. Link
It may be worth asking your pharmacy if they stock non-branded products which may be cheaper than their branded equivalents.
Will this affect me if I have a pre-paid certificate?
If you have a pre-paid certificate you will also be asked to purchase your OTC treatments for minor ailments. However, if you need regular treatment for a chronic condition, then this will be supplied on prescription covered by your pre-paid certificate.
What about administering OTC to small children at school or nursery?
The majority of treatments for minor ailments can be given before the school day starts and last long enough so that another dose does not have to be given until the child returns home. These should be purchased over the counter. Please don’t ask your GP to prescribe paracetamol or ibuprofen “just in case” for this purpose.
This advice does not apply to you if your child receives paracetamol or another analgesic on prescription for long term management of chronic pain. If this is the case please refer to your school’s Medicine Policy.
What if an OTC medicine has been started by the hospital?
If you are admitted to hospital, you will be given an adequate supply of medicines when you are discharged which will be free of charge. This may also include medicines for minor ailments if you have been prescribed these during your stay and it is thought that a further supply will help your recovery when you go home. However, if they are not required on a regular long term basis, then they will not be added to your repeat prescription and you will be asked to purchase them in the future.
What if I am in a residential home?
In Leicestershire, Care Homes are expected to provide a limited range of OTC medicines to adult service users who require symptom relief for treatment of headache, back ache or muscular pains, fever, constipation, cough, indigestion and coughs for up to 48hrs. The medicines can be provided without calling out the GP.
However, if there is cause for concern, the care home staff should consult with either their community pharmacist or their GP practice.

C1

Blank Page
Engagement analysis report – Conditions for which Over The Counter (OTC) items should not routinely be prescribed September 2018

2
Executive summary Introduction This engagement report details feedback and analysis obtained during a six-week period of public engagement undertaken by East Leicestershire and Rutland Clinical Commissioning Group (ELR CCG) on conditions for which over the counter (OTC) items should not routinely be prescribed in Primary Care. NHS England published guidance in March 2018, calling for restrictions to the prescribing of certain OTC items. The aim is that this will lead to a more equitable process for making decisions about the CCG’s policy on prescribing medicines. The purpose of engagement ELR CCG’s activities involved engagement rather than a public consultation because, following its own national public consultation, NHS England has already decided what changes to prescribing all Clinical Commissioning Groups (CCGs) need to implement. These changes are detailed in guidance from NHS England on its website: https://www.england.nhs.uk/medicines/conditions-for-which-over-the-counter-items-should-not-routinely-be-prescribed/ Whilst the CCG understands that it is required to support NHS England’s recommendations, it was keen to engage with its local population first. The purpose was to inform people of the CCG’s obligatory duty to apply NHS England’s guidance, but also to understand from patients what they thought, whether they had any concerns and to help identify any risks which the CCG may need to address before implementing any changes. Who responded? A total of 358 people responded during the engagement period via online and hardcopy surveys. The majority of respondents (90%) are registered with a practice in East Leicestershire and Rutland and the majority (76%) are also in receipt of a repeat prescription. What did they say? 92% of respondents agreed that they would be happy to pay for OTC items and 86% agreed that medication for self-limiting conditions should not be prescribed. Next steps for the CCG This engagement analysis report evidences strong support (substantially higher than the national average) from those ELR CCG’s patients who responded, to restrict the prescribing of certain OTC items. However, the CCG should consider the qualitative comments and concerns of patients before introducing any changes.

3
Background In the 12 months up to June 2017, the NHS spent approximately £569 million on prescriptions for medicines, which could otherwise be purchased over the counter (OTC), from a pharmacy and/or outlets such as petrol stations or supermarkets. These prescriptions include items for a condition:
• That is considered to be self-limiting and so does not need treatment as it will heal or be cured of its own accord
• Which lends itself to self-care These prescriptions can also include other common items:
• That can be purchased over the counter, sometimes at a lower cost than that which would be incurred by the NHS
• For which there is little evidence of clinical effectiveness By reducing spend on treating conditions that are self-limiting or which lend themselves to self-care, or on items for which there is little evidence of clinical effectiveness, these resources can be used for other higher priority areas that have a greater impact for patients, support improvements in services and or deliver transformation that will ensure the long-term sustainability of the NHS. NHS England’s consultation
NHS England undertook a 12-week public consultation between December 2017 and 14 March 2018. As a result of this work, NHS England and NHS Clinical Commissioners (NHSCC) developed restrictions based on type and severity of condition rather than products. Feedback from this consultation showed that there was general support (65% agreed with NHS England’s criteria to assess items for potential restrictions). ELR CCG has previously stopped prescribing paracetamol as well as gluten-free products, following engagement with patients. The move to stop paracetamol being routinely prescribed was supported by the majority of people that the CCG engaged with although there was a level of concern amongst some patients with more serious or longer-term conditions. The engagement process ELR CGG undertook engagement over six weeks between Monday 30 July 2018 and Sunday 9 September 2018, to gather public opinion on the proposals and to encourage people to self-care. The CCG sought to obtain feedback to:
• Educate people about the rationale behind why items may not routinely be prescribed
• Make people aware of the NHSE consultation and its findings

4
• Identify any other risks and themes relating to conditions or groups of people which may require further engagement or work, before any changes are implemented
• Reassure those people with long-term conditions and/or complex conditions that they will continue to receive their prescriptions
• Prepare patients for the changes so that they are aware and prepared for the changes before implementation
• Allow the CCG to determine whether people are generally in support of the proposals, so that appropriate communication and any further necessary actions can be put in place
• Achieve behavior change in patients by encouraging them to self-care Who did the CCG engage with?
• The above pie chart shows that the majority of participants responded to the survey on behalf of themselves (330 people)
• 10 people responded on behalf of an organisation
• 18 people didn’t provide these details
Participants' details
Individuals 97.06%
Organisations 2.94%

5
• The majority of respondents (298 people) were ELR patients
• 21 people were not ELR patients
• 12 people were not sure whether they are ELR patients
• 27 people did not provide these details
• The majority of respondents were female (227 people)
Participants' details
ELR patients 90.03%
Other 6.34%
Not sure 3.63%
Participants' gender
Female 67.16%
Male 31.95%
Prefer not to say 0.89%

6
• 108 of those who responded were male
• 3 people preferred not to say
• 20 people did not provide these details
• The majority of those who responded to the survey questionnaire were aged between 60 to 75 years (124 people)
• This majority group was closely followed by people aged 35 to 59 years (108 people)
• 45 people who responded were aged above 76 years
• 45 people who responded were aged between 25 to 34
• 14 people who responded were aged between 16 to 24
• 3 people preferred not to say
• 19 people did not provide these details
Participants' age
16-24 4.13%
25-34 13.27%
35-59 31.86%
60-75 36.58%
76+ 13.27%
Prefer not to say 0.88%

7
• The majority of those who responded were of White British ethnicity (296 people)
• 23 people were of Indian ethnicity (23 people)
• Participants also came from other ethnic backgrounds listed above, with 3 people being of dual-heritage
• Of those who responded more than 20% had a disability (68 people)
Participants' ethnicities Bangladeshi 0.30%
Caribbean 0.30%
Chinese 0.30%
Indian 6.80%
Irish 0.30%
Pakistani 0.30%
Somali 0.30%
White British 87.57%
Prefer not to say 2.96%
Mixed or other ethnicities0.89%
Participants' health
Disabled 20.42%
Poor health 8.11%
Neither 68.77%
Prefer not to say 2.70%

8
• More than 8% (27 people) were in poor health
• The majority were neither disabled nor in poor health (229 people)
• 9 people preferred not to say
• 25 people did not provide this information
The data pertaining to those who the CCG engaged with and who completed a survey questionnaire demonstrates a good mix of responses from ELR’s diverse communities. The CCG has engaged with patients covering each of its localities, including older people and people with disabilities. Channels and strategy
• Survey A survey was devised to gather public opinion. The survey comprised of 13 questions relating to the initiative and how it may affect patients, followed by equality questions to enable the CCG to understand the group/background that respondents belonged to. The survey was promoted on the CCG’s website, GP practice websites and through local media. Paper copies were made available at the CCG’s 31 GP practices and at six face-to-face engagement events hosted at some of ELR CCG’s largest GP practices. The survey was promoted for the duration of the engagement period on social media channels. Further information relating to social media activities is available on page 10.
• Listening Booth events The Listening Booth allows the CCG to speak to patients and carers about their experiences of healthcare. It forms an integral part of the CCG’s engagement and consultation activities and enables the CCG to collate both positive and negative feedback. By visiting an ELRCCG practice in each of its six localities, the CCG was able to ensure a good mix of responses from the geographical area that it serves. The CCG took the Listening Booth to the following practices for half-day engagement events at each:
• Glenfield Surgery, North Blaby • Northfield Medical Practice, South Blaby • Market Harborough Medical Centre, Harborough District • Oakham Medical Practice, Uppingham

9
• Latham House, Melton Mowbray • Wigston Central Surgery, Wigston
The Listening Booth enabled direct dialogue with patients about the changes and allowed the CCG to guarantee additional qualitative verbatim comments.
- Emails were sent to stakeholders and seldom heard groups, briefing them on the initiative, the rationale and requirements for all CCGs to implement the changes. The email also provided contact details, should any individuals or seldom heard groups want to request more information or a meeting.
- Emails were also sent to all practices in ELR, before and during the
engagement, explaining the aims of the engagement, the role of practices and GPs and instructions on how they could support the initiative through promotion
• Electronic toolkit
All ELR practices were emailed an electronic toolkit and instructions on how to use the toolkit. The toolkit comprised of:
- A patient-friendly one-page leaflet explaining the initiative, providing a link to the survey and CCG contact details, for use during the course of the engagement
- The survey for use during the course of the engagement - Poster promoting the initiative for immediate and longer-term use - Graphics for GP practice screens for immediate and longer-term use - Web article with a link to the survey for GP websites - Social media content for practices to use on their Facebook and Twitter
pages, covering the six-week engagement period
• Hardcopy material for GP practices In addition to the electronic toolkit, the CCG produced and delivered the following material to practices, encouraging them to promote the material around their sites:
- A patient-friendly one-page leaflet explaining the initiative, providing a link to the survey and CCG contact details, for use during the course of the engagement (Appendix X)
- Paper copies of the survey for use during the course of the engagement (Appendix X)
- Web article for use on practice websites and linking to the survey online - Poster promoting the initiative for immediate and longer-term use

10
• Website The initiative and survey was promoted on the CCG’s website as well as practice websites. The web page included links to the NHS England consultation and guidance, the survey, and e-toolkit.
• Social media The CCG used Facebook and Twitter regularly during the six-week period to encourage people to participate in the survey and to explain the changes. The below table shows the number of posts, reach and level of engagement achieved through the CCG’s social media platforms alone: Facebook Twitter Totals
Posts 6 13 19 Post reach (people/users who saw the post)
7,100 8,129 15,229
Interactions (number of times people/users engaged with the posts)
781 (389 reactions, comments, shares 392 post clicks)
96 877
*GP practices also used their social media channels to promote the initiative therefore the actual reach and engagement across ELR is likely to be much higher.
• Press release A press release was issued to local print and broadcast media to help promote the initiative and to encourage people to participate in the survey. This secured media coverage in the Leicester Mercury.
• Media opportunity with BBC East Midlands Today The CCG’s Communications team proactively pitched a news item to BBC East Midlands Today. The news item included an interview with Dr. Andy Ker and was broadcast twice on the 6 o’clock and 10’clock news programmes, during the week that the engagement was launched. The piece was very positive and included supportive vox pops from several members of the public. Survey findings A total of 358 survey responses were returned during the engagement period. The results of responses to each question are as follows:

11
Q1. Do you currently receive a repeat prescription from your doctor? 327 People answered this question. Answer choices Responses Yes 76.26% 273 No 23.74% 85 Not sure 0.00% 0 TOTAL 358 Issues for consideration The majority of those who took part in the survey receive a repeat prescription and therefore, if they have additional concerns about their current prescriptions, more educational awareness may be necessary to explain that longer-term conditions are exempt from the initiative and that they will continue to receive their prescriptions. Q2. If you answered yes to question 1, what is it for? 228 people answered this question. Repeat prescriptions listed included treatment for a range of conditions including pain, arthritis, hayfever, blood pressure, diabetes, eczema and asthma. *For a full list of responses of items prescribed and conditions see Annex A Issues for consideration Some of the conditions could be exempt from the changes, but other prescribed items prescribed such as nasal spray and shampoo may no longer be prescribed. This could affect patients who no longer receive prescriptions for items that are available over the counter (if their condition isn’t complex or long-term) and so, they may require additional information on why the changes are happening. Q3. Do you pay for your prescriptions? 356 people answered this question. Answer choices Responses Yes 35.11% 125 No 64.89% 231 Not sure 0.00% 0 TOTAL 356 Issues for consideration The majority of respondents (nearly 65%) do not pay for their prescriptions and so, unless their condition is complex and/or long-term, they may stop receiving

12
prescriptions for self-limiting or short-term conditions. Depending on their circumstances and reception, GPs may need to take a view on the items they prescribe and may also need to provide further information. Q4. Some over the counter medication (for example; vitamins and minerals, lotion for mild dry skin conditions, eye drops, painkillers and indigestion remedies) are available for you to buy at a considerably reduced cost, in comparison to what it would cost the NHS. Would you be happy paying for over the counter medication to treat short-term illnesses and conditions? 343 people answered this question. Answer choices Responses Yes 92.13% 316 No 7.87% 27 TOTAL *For detailed comments see Appendix B Issues for consideration An overwhelming majority of respondents (more than 92%) agreed that they would be happy paying for OTC medication to treat short-term conditions. This compares to a national response rate of 65%, during NHS England’s public consultation. Despite the majority of these respondents currently not paying for their prescriptions, the response is extremely positive and supportive of the proposed changes. The number of people who responded (343 people out of a total of 358) is significantly high too and therefore, can be used as a helpful indicator, when implementing the changes. Q5. Did you know a self-limiting condition is a condition which will clear up on its own without the need for medication? 349 people answered this question. Answer choices Responses Yes 69.91% 244 No 30.09% 105 TOTAL 349 Issues for consideration The majority of respondents understand what a self-limiting condition is (nearly 70%), but more awareness could be focused on those patients who are not aware of what it is. If more patients are made aware that self-limiting conditions eventually clear with time on their own, the likelihood of an increase in support for the proposed changes could also increase. Q6. Do you agree that medication for self-limiting conditions should not be prescribed?

13
333 people answered this question. Answer choices Responses Yes 85.59% 285 No 14.41% 48 TOTAL 333 *For additional comments relating to this question, see Appendix C. Issues for consideration The majority of patients agree that medication for self-limiting conditions should not be prescribed (nearly 86%). However the responses show that a small percentage of people still believe that medication for self-limiting conditions should be prescribed. More work can be undertaken with these patients to establish what their reasoning may be. Q7. If you were suffering from a self-limiting condition or minor illness, where would you go for more information in the first instance? 347 people answered this question. Answer choices Responses Pharmacy 67.72% 235 NHS website 11.53% 40 Dial NHS 111 2.31% 8 GP surgery 11.82% 41 Other (please specify) 6.63% 23 TOTAL 347 The following list shows the other places that patients go to for this information:
1. Walk-in facility or chemist 2. No one 3. We do try to solve it with home remedies before going to the GP surgery 4. Internet 5. Call 111, NHS Website 6. NHS Website, G.P Surgery 7. NHS Website 8. Ask my mum 9. Online 10. Google 11. Google 12. Relative 13. Google 14. N/A

14
15. Google, friends and family 16. Pharmacy and NHS Website 17. Pharmacy & NHS website 18. Allow it to take its course 19. Internet 20. Internet via search engine 21. Internet 22. Pharmacy, unless related to my allergies / rhinitis when i would go straight to
my GP as nothing the pharmacy can offer is strong enough 23. Generally internet and pharmacy unless tonsillitis
Issues for consideration The responses show that the majority of patients visit their pharmacy in the first instance for information and advice on self-limiting conditions. The results, including the list (although this does duplicate many of the categories offered in the specific question), are a helpful indicator in highlighting the most popular platforms. The CCG could target these, should it want to promote more information on self-limiting conditions. Q8. Do you currently purchase over the counter medication? 349 people answered this question. Answer choices Responses Yes 70.20% 245 No 29.80% 104 TOTAL 349 Issues for consideration Although the majority (70%) of respondents purchase OTC medication nearly 30% indicated that they do not. This means that either all of their medication is prescribed or they do not take any OTC medication. The results could indicate that if some patients have to pay for OTC items, they would choose not to take these items. For self-limiting conditions however, their condition would eventually clear without OTC treatments and so, the items are not absolutely necessary. Q9. If you answered yes to question 8, please tell us what condition the item is for, where you purchase it from, and any further comments. 234 people answered this question and provided a list of conditions. Here is a random selection of some of the conditions:
1. Paracetamol. migraine tablets, calpol and hayfever syrup 2. Painkillers- anti-inflammatories for general aches and pains. Tendonopathy
Hydrocortisone and cream for dry skin 3. Paracetamol- tesco 4. Ibuprofen/ paracetamol- tesco

15
5. Pain, flu/cold symptoms, cold sores, dry skin conditions 9/17/2018 1:45 PM 6. Paracetamol- back pain - supermarkets Nurofen- back pain - supermarkets
vitamins supermarket 7. Arthritis 8. Cod liver oil, glucosomine 9. Cetirizine recommended by GP and purchased 10. Aspirin 9/17/2018 1:27 PM 11. Cold remedies, sore throat remedies, glucosamine- from supermarkets 12. Paracetamol for various aches and pains from supermarkets 13. Back pain 14. Hayfever 15. Turmeric (arthritis) 16. Vitamin D 17. Diarrhoea from chemist 18. Pain killers, Olbas oil for sinuses 19. Cocodamol 20. Eyedrops – pharmacy
* The full list of conditions (234) can be viewed in Appendix D. Issues for consideration The majority of respondents purchase OTC items. They provided a list of these conditions and OTC items. The results indicate that respondents use OTC items for self-limiting conditions and short-term pain relief. The cost of the items described is not excessive and this information could be provided to patients with self-limiting conditions. They would then have an option to purchase the items for relief or wait for their condition to clear on its own. Q10. If there are any medicines that you have any particular concerns about please tell us which one and why. 98 people answered this question and provided a list of medicines. Here is a random selection of some of the conditions:
1. Emollient creams 2. Lanzoprazole (should be for limited time?) 3. Atorvastatin- side effects 4. penicillin 5. No 6. Blood pressure medication- strong painkillers should be regularly reviewed. 7. Some medications react with each other and should only be taken under
suspension 8. The medications mentioned above plus the skin medications/creams which
help me manage my long term condition/illness 9. Insulin, and eye drops 10. Ibuprofin as I am buying it from the supermarket, I am not monitored on this
medication, I have had a dystonia for over 20 years and this, along with botox injections is the only medication for pain relief
11. Paracetamol, rheumatoid arthritis which is very painful

16
12. Co-codemol I take this prescribed for pain x4 tablets a day 13. All my meds 14. Statins. Concern about efficacy if no previous incidents 15. A lot of codeine products are so easily available 16. All of the medicines I am prescribed- they all carry potential side effects 17. Branded medication which advertises widely, is more costly than non-branded
and costs much more 18. Why are paracetamol etc. still widely available over the counter. It's asking for
trouble 19. I have to buy Neil’s Sinus Rinse for my daughters long term condition the
sachets cost £20 per month because they are not prescribed 20. Mild lotion cream as I can only use a few due to allergies and my condition
goes from mild to severe which requires much use *The full list of medicines can be viewed in Appendix E. Issues for consideration The list of items and conditions provided indicates that some of these items would still be available on prescription as they are for longer-term conditions. Others items may no longer be prescribed, if required for short-term conditions. GPs would have to apply their judgement when consulting with patients and decide based on the patient’s condition, whether OTC medicines should be prescribed. The information also suggests that more promotion on conditions that are exempt from the changes may be helpful to reduce patients’ concerns. Q11. If you are aware of any groups of people who may be affected by this change more than others, please tell us which groups below. 150 people answered this question. Here is a random selection of some of the responses:
1. Low income families 2. People with life time chronic conditions 3. Children (dosages) 4. My 20 year old special needs grandson 5. Low income 6. Low income, pensioners 7. Renal patients 8. Elderly with long-term condition with no access to local pharmacy 9. Low income families and long term illnesses 10. Disadvantaged with small resources 11. The poorest people in our society, that's why I think it's a very serious concern 12. Elderly people 13. People who can't afford 14. Elderly/ pensioners/ low income families/ single parents/ unemployed/
students 15. Diabetics and high risk patients 16. Poor families 17. Low income

17
18. Those who find it difficult to get to a pharmacy / we live in a village with limited bus service
19. The very elderly or people that are unable to get out. People that have their prescription delivered
20. Possible people with limited or low income
Issues for consideration The responses indicate that the following groups may be more affected by the changes: • People with complex and/or long-term conditions • People on low incomes including the unemployed • Older people • People who are less mobile or housebound • People who require longer-term use of pain killers People with complex and/or long-term conditions however, would be exempt from the changes. They could be reassured to avoid concerns. Many of the most popular OTC items are no longer prescribed across Leicester, Leicestershire and Rutland (for example, paracetamol, cough syrups, medicated shampoo, antihistamines for hayfever), unless these are required for complex or longer-term conditions, so there would be little change for patients, regardless of their income or age. Patients who require longer-term pain relief would also be exempt from the changes so again, there would be little impact on them. Consideration should be given however, to vulnerable individuals with short-term conditions who are housebound or less mobile, particularly if they are likely to have to purchase OTC items more than once for the same condition (for example, paracetamol). GPs would need to apply their judgement to reduce potential adverse impact on vulnerable patients. Q12. If you are aware of any situations or groups of people where you think some or all of the medicines should still be prescribed, please tell us. 140 responded to this question. Here is a random selection of some of the responses:
1. Treatment for chronic conditions 2. People who are prescribed multiple medicines 3. Those with chronic conditions 4. Low income state assisted people and their children 5. Elderly, babies and children 6. Children (antibiotics) 7. Grandson as above

18
8. Low income, pensioners 9. Low income 10. Elderly people on few incomes 11. Those with chronic conditions where over the counter medications are
restricted in quantity 12. The poorest people are generally the most vulnerable group of people. Highly
paid. GPs should not ration prescriptions. 13. For all over 60s 14. OAPs 15. Pensioners 16. All high risk patients as mentioned above as they are more prone to infection 17. Income support 18. Low income families 19. People over 75 may find it more difficult to get out to shops to collect larger
quantities of painkillers 20. Those who have difficulty getting to outlets supplying the subject medication
or cannot afford to buy same A full list of responses to this question can be viewed in Appendix F. Issues for consideration The groups identified from the responses is the same as the groups identified from question 11: • People with complex and/or long-term conditions • People on low incomes including the unemployed • Older people • People who are less mobile or housebound • People who require longer-term use of pain killers The issues for consideration deriving from the previous responses can also be applied to mitigate adverse impact on the identified groups. GPs would need to apply their judgement to reduce potential adverse impact on these groups. It is important to acknowledge however, that self-limiting conditions would eventually clear without any OTC items, whether prescribed or purchased by the patient. 13. Please use this space to provide additional comments, to tell us how the changes may affect you or to request any additional information. 70 people responded to this question. The following is a snapshot of some of the comments:

19
*All comments relating to this question can be viewed in Appendix G. Issues for consideration The comments demonstrate that although there is strong support for the proposed changes to prescribing, some people do have some concerns. Whilst the proposed changes would not affect patients with complex and/or long-term conditions, consideration should be given to the impact on the vulnerable groups identified. Responses show that there is a lack of understanding relating to the groups of people or conditions that would be exempt from the proposed changes. For example, some respondents were very concerned for patients with life threatening or serious conditions who may not be able to afford medication. Under the new changes, such patients would continue to receive their prescriptions and so, there would be no additional adverse effect on them when the NHS England guidance is applied. The price of over the counter items was also a factor, with some respondents willing to purchase low cost over the counter medication. However, the results do not indicate how these same respondents would feel about purchasing more expensive items. Other respondents were fully supportive of the proposed changes regardless of the cost of OTC items. Some patients requiring paracetamol indicated their concern relating to limitations on the amount of pain killers they would be able to purchase over the counter. However, the CCG stopped prescribing paracetamol in October 2016. Patients who require Paracetamol/Ibuprofen/Aspirin for long-term conditions are likely to be exempt from the proposed changes and GPs would be expected to make a clinical judgement to prescribe in certain cases. Listening Booth analysis The table below shows the number of people who the CCG spoke to at each practice. These patients also completed a survey during the face-to-face engagement: Practice Number of patients engaged with Glenfield Surgery 37 Northfield Medical Practice 39 Market Harborough Medical Centre 34 Oakham Medical Practice 23 Latham House 32 Wigston Central Surgery 29 TOTAL 194

20
Other feedback from the Listening Booth events
• 194 surveys completed in total • 30 people out of 194 felt that people with low incomes would be affected more
than others from the proposed changes • 54 people out of 194 felt the elderly would be affected more than others from
the proposed changes • 3 people out of 194 felt people with diabetics would be affected more than
others from the proposed changes • 3 people out of 194 were concerned that higher strength co-codamol available
on prescription only, may no longer be available The responses obtained from the completed questionnaires at the engagement events were analysed with all other questionnaires. A summary of analyses from all feedback is below: Summary of engagement analysis
• The majority of respondents (more than 92%) agree that they would be happy paying for OTC medication to treat short-term conditions. The national average is 65%, therefore support in ELR is much higher than the national average.
• There is concern from some groups (people with low incomes, older people and people who are housebound) that they will be adversely affected by the changes.
• Some patients are not aware that the proposed changes will apply to short-term and self-limiting conditions only.
• Not all patients are aware of what a self-limiting condition actually is.
• There is concern amongst some respondents that patients with long-term or more serious conditions would be affected by the proposed changes.
• A small percentage of respondents feel that OTC items should continue to be prescribed.
• Some respondents are unaware that certain OTC items ceased being prescribed two years ago.
• Pharmacies are the first point of contact for the majority of patients, when they have questions relating to short-term or self-limiting conditions. This is followed by the NHS website and GP practices.

21
Recommendations/key considerations for the CCG
• Further publicity and promotion of the initiative should be considered to reach as many patients as possible and on a long-term basis.
• Emphasis should be placed on what short-term conditions are in order to reduce unnecessary concerns relating to more serious and longer-term conditions that will not be affected by the changes.
• The above can be demonstrated by promoting more widely, the full list of conditions that the NHS England guidance would apply to.
• GPs will have a role in deciding when certain OTC items may still be prescribed. A patient’s circumstances may need to be taken into account to reduce any potential inequalities in health provision.
• The CCG can support GPs to implement the changes by providing supporting material and/or contact details for patients who wish to ask questions or find out more.
• The CCG can ensure that GPs are fully aware of their roles in implementing the changes by writing to them and offering support.
• It should be highlighted at every opportunity that those with complex and/or longer-term and more serious conditions will be exempt from the changes. GPs will have a pivotal role in explaining this during patient consultations.
Next steps The recommendations and key considerations should be considered by the CCG in implementing the changes. After a set time period following implementation, the CCG may choose to revisit the initiative to ascertain from GPs what the response has been from their patients. This may help identify any further areas of work or engagement.

22
Appendix A
A

23
If you answered yes to question 1, what is it for? (Please skip this question if you answered no) RESPONSES WITH DATE AND TIME OF RESPONSE 1 Paracetamol, movicol haeworrloids, macrogal 9/17/2018 1:55 PM 2 Fedofenadine and skin creams and inhailers 9/17/2018 1:54 PM 3 Hypromellose and dexamethasom 9/17/2018 1:49 PM 4 Fluxetine 9/17/2018 1:46 PM 5 Chronic pain, thyroin replacement, heart problem, BP 9/17/2018 1:45 PM 6 Blood pressure, polymyalgia rheumatica 9/17/2018 1:44 PM 7 Ibandronic acid- osteoarthritis, statins- high cholestrol and angina, fluoxetine- depression 9/17/2018 1:42 PM 8 Losartan and atorvastatin 9/17/2018 1:37 PM 9 Paracetamol, citalopram, amitriptyline 9/17/2018 1:37 PM 10 Statins 9/17/2018 1:29 PM 11 Risk of stroke 9/17/2018 1:27 PM 12 Phenelzine, levothyroxine and naratriptan 9/17/2018 1:23 PM 13 Diclofenac sodium fluoxetine, lansoprazok, latanoprost eye drops 9/17/2018 1:16 PM 14 Blood pressure 9/17/2018 1:16 PM 15 Hayfever 9/17/2018 1:14 PM 16 ramipril, tamsulosin, co-codamol 9/17/2018 1:13 PM 17 Hypertension 9/17/2018 1:12 PM 18 Insulin, statin and levothryroxine 9/17/2018 1:10 PM 19 Heart faliure 9/17/2018 12:57 PM 20 Asthma, enlarged prostate, nose blockage and heart condition 9/17/2018 12:55 PM 21 Various aliments atm 9/17/2018 12:44 PM 22 Several things 9/12/2018 4:27 PM 23 Heart/ stomach and arthritis 9/12/2018 4:19 PM 24 Mononitane 9/12/2018 4:19 PM 25 All my regular prescription 9/12/2018 4:15 PM 26 Condesartan 9/12/2018 4:03 PM 27 metaformin tablets, latanprost eye drops and azopt eye drops 9/12/2018 4:02 PM 28 Venofaxin lamsoprol 9/12/2018 3:54 PM 29 Bendiofluazido, amlodipine, adcol, disoprolol, lansoprazole 9/12/2018 3:52 PM 30 various 9/12/2018 3:49 PM 31 Amlodidine, aspirin, atorvastatin, bisoprolol 9/12/2018 3:48 PM 32 Asthma and hayfever 9/12/2018 3:39 PM 33 Latanaprost eye drops 9/12/2018 3:37 PM 34 Heart, pain relief, blood pressure 9/12/2018 3:33 PM 35 For eczema berodouble gel, atorvastin, mouthwash, toothpaste, biotene saliver gel, alfobosin, for side effects of head/neck cancer treatment for prostate condition 9/12/2018 3:30 PM 36 Zolmitripton 9/12/2018 3:26 PM 37 Eliquis, axtal, various stofia supplies 9/12/2018 3:23 PM 38 Type 2 diabetes 9/12/2018 3:19 PM 39 Thyroid 9/12/2018 3:13 PM 40 Blood pressure and vertigo shingles in head, numb scalp 9/12/2018 3:12 PM

24
41 Diabetic 9/12/2018 3:10 PM 42 HRT 9/12/2018 3:09 PM 43 Several 9/12/2018 3:08 PM 44 Statins, Hipitor 9/12/2018 3:07 PM 45 My meds 9/12/2018 2:59 PM 46 Quite a few medications for COPd and Rhumatoid arthritus 9/12/2018 2:52 PM 47 Diabetes Glaucoma 9/12/2018 2:42 PM 48 Asthma, raised BP and bone density pills 9/12/2018 2:41 PM 49 Metformin and spironolactone 9/12/2018 2:40 PM 50 Regular diabetic medicine 9/12/2018 2:36 PM 51 Thyroxin, Amlopodin, lanzaroprol, Bisopirol, Losantin, Clopidegrel 9/12/2018 2:31 PM 52 Amlodogine 5Mlg 9/12/2018 2:26 PM 53 Inhaler 9/12/2018 2:23 PM 54 Levothyroxine 9/12/2018 2:11 PM 55 Lansoprole Fursuide 9/12/2018 2:08 PM 56 Angina, utiania, blood pressure 9/12/2018 2:06 PM 57 Multiple issues 9/12/2018 2:03 PM 58 Type 2 diabetes, statins, blood pressure 9/12/2018 2:00 PM 59 Evorel patches, Omeprazole and bisopropolol 9/12/2018 1:47 PM 60 Statins 9/12/2018 1:33 PM 61 Thyroid function, osteo arthritis, osteo malacia, oesophagul problems and heart flutters due to thyroxine 62 Glacoma, Hypertension 9/12/2018 1:31 PM 63 Thyroxide, Fexafenadine 9/12/2018 1:23 PM 64 High Blood pressure, Cholesterol, Blood thinning 9/12/2018 1:21 PM 65 Digoxin, Bisoprol and rivaroxaban 9/12/2018 1:18 PM 66 Contraceptve pill 9/12/2018 1:16 PM 67 Fibromyaligia and chronic back pain 9/12/2018 1:14 PM 68 Romipril Levothyroxine 9/12/2018 1:12 PM 69 Blood pressure Control 9/12/2018 1:09 PM 70 Psorasis 9/12/2018 1:06 PM 71 Citalopram, fexafendadine 9/12/2018 1:05 PM 72 Amitriptyline for muscle spasm, Tolterodine for bladder control both connected to MS 9/12/2018 1:01 PM 73 Shampoo 9/12/2018 12:53 PM 74 High blood pressure 9/12/2018 12:49 PM 75 Prosifired 9/12/2018 12:49 PM 76 Nasal spray 9/12/2018 12:46 PM 77 Sertraline, Sumatriptan, Neditol 9/12/2018 12:46 PM 78 High chloresterol 9/12/2018 12:43 PM 79 Inhailer and co-codamol 9/12/2018 12:37 PM 80 Diabetes Hyperterusion 9/12/2018 12:35 PM 81 Thyiziod 9/12/2018 12:30 PM 82 Blood pressure 9/12/2018 11:58 AM 83 Thyroid and Anytriplene 9/12/2018 11:54 AM 84 Sertraline 9/12/2018 11:42 AM 85 Too many to list 9/12/2018 11:38 AM 86 Tramadol and anti-depressants 9/12/2018 11:36 AM 87 Blood pressure 9/12/2018 11:15 AM

25
88 Epilepsy 9/12/2018 11:14 AM 89 Heart failiure 9/12/2018 11:13 AM 90 Various 9/12/2018 10:52 AM 91 LVD AF 9/12/2018 10:46 AM 92 Blood pressure and cholestrol 9/12/2018 10:41 AM 93 A.F 9/12/2018 10:39 AM 94 Lavzaprazole 9/12/2018 10:33 AM 95 HRT Migrane prevent 9/12/2018 10:21 AM 96 Reeumatid arthritis 9/12/2018 10:16 AM 97 Various 9/12/2018 9:57 AM 98 Seroxat and femoston 9/12/2018 9:56 AM 99 Diabetes 9/12/2018 9:54 AM 100 High blood pressure and high cholestrol 9/12/2018 9:44 AM 101 Arthritus 9/12/2018 9:40 AM 102 Alendronic acid, amlodipine and lansoprazole 9/12/2018 9:37 AM 103 Rivaroxaban 9/12/2018 9:33 AM 104 Paracetamol 9/12/2018 9:31 AM 105 POM 9/12/2018 9:29 AM 106 Co-codomol and Celuizine hydrochloride 9/12/2018 9:27 AM 107 High Cholestrol 9/12/2018 9:23 AM 108 Seretide inhailer, Betnovate, nasal spray and hydrocorstitode cream 9/11/2018 4:25 PM 109 Various- blood thinning and heart 9/11/2018 4:18 PM 110 Epilepsy 9/11/2018 4:15 PM 111 Bratius, Ventolin, Atimos, Eyedrops 9/11/2018 4:12 PM 112 Contraceptive pill and anxiety tablets 9/11/2018 4:10 PM 113 Contraceptive pill 9/11/2018 4:08 PM 114 Ganfort, Eye drops, Lisinopril, Rheumatoid arthens 9/11/2018 4:01 PM 115 High Blood pressure 9/11/2018 3:58 PM 116 Prefer not to state 9/11/2018 3:55 PM 117 Blood pressure 9/11/2018 3:51 PM 118 Anti-depressant, my children have have movacol, senna, gluten free bread, sertlaline, microgejnon for mood fluctuation (not contraception) 119 Ramapril- eye drops 9/11/2018 3:34 PM 120 Paracetamol and Codene 9/11/2018 3:14 PM 121 Crohns Disease 9/11/2018 3:12 PM 122 Propranolol 9/11/2018 3:01 PM 123 Various POM's 9/11/2018 2:57 PM 124 Fexofenadine 9/11/2018 2:51 PM 125 Asprin, Atov astatin, Brattus, Salbutamol 9/11/2018 2:42 PM 126 Blood pressure, thyroid-hypo 9/11/2018 2:31 PM 127 Bisopodol and apixaban 9/11/2018 2:29 PM 128 Contraception 9/11/2018 2:24 PM 129 Heart Problems 9/11/2018 2:22 PM 130 Itylo tear drops, hay fever tablets and nasal spray sestraline 9/11/2018 1:59 PM 131 BP Tablets, thyroxine, fluoxetine, pain relief meds 9/11/2018 1:54 PM 132 Blood pressure / chlorestrol 9/11/2018 1:52 PM 133 Levothyroxine and pregabalin 9/11/2018 1:38 PM 134 Asthma 9/11/2018 1:34 PM 135 Ramipril 9/11/2018 1:16 PM

26
136 Furosemide 9/11/2018 1:13 PM 137 Various conditions 9/11/2018 1:05 PM 138 Salbutamol 9/11/2018 1:01 PM 139 Lansoprozole, naproxen, paracetamol, pregablin, tramodol, antidepressants 9/11/2018 12:59 PM 140 Sertraline and the contraceptive pill 9/11/2018 12:56 PM 141 Acid reflux 9/11/2018 12:47 PM 142 AF 9/11/2018 12:37 PM 143 artorvastatin and amlopodine 9/11/2018 12:05 PM 144 Too many 9/11/2018 11:58 AM 145 Depession 9/11/2018 11:54 AM 146 Inhailers for asthma 9/11/2018 11:51 AM 147 Tamoxifen 9/11/2018 11:41 AM 148 Fibromyalgia Asthma 9/11/2018 11:29 AM 149 Heart attack 9/11/2018 10:50 AM 150 Blood pressure 9/11/2018 10:47 AM 151 Inhailer 9/11/2018 10:41 AM 152 BP and DVT 9/11/2018 10:39 AM 153 Diabetic 9/11/2018 10:37 AM 154 Skin conditions 9/11/2018 10:16 AM 155 Gasapentin, fostair, ventolin, flu 9/11/2018 10:05 AM 156 Several 9/11/2018 10:02 AM 157 IBS, BP 9/11/2018 9:58 AM 158 Ursodeoxychloc acid, Citalaplam, Ferrus sulphate, Alovasliatin, Eye drops (Glaucoma) 9/11/2018 9:54 AM 159 Loratadine and flixonaise 9/11/2018 9:51 AM 160 Cancer/ BP 9/11/2018 9:46 AM 161 Inhailers 9/11/2018 9:18 AM 162 Pain Relief- store products, Anti-depressant 9/11/2018 8:57 AM 163 Blood pressure 9/11/2018 8:40 AM 164 Sertraline 9/10/2018 12:29 PM 165 polichistic ovarian 9/10/2018 12:24 PM 166 BP, Cholesterol R, Prostate fentanyl, cramorph, paracetamol 9/10/2018 12:19 PM 167 Anxiety & Depression 9/10/2018 12:14 PM 168 Asthma 9/10/2018 11:36 AM 169 All my needs 9/10/2018 11:34 AM 170 Chlestrol 9/10/2018 11:25 AM 171 Boots blood pressure tablets & Anti Depressants 9/10/2018 11:18 AM 172 Heart Valve Leak Blood pressure AF 9/10/2018 10:58 AM 173 Depression 9/10/2018 10:54 AM 174 Statins 9/10/2018 10:51 AM 175 Sertraline, Atenolol, Doxasosin, Amitriptyline, Symbicort 9/10/2018 10:43 AM 176 Desloratadyne Hayfever tablets 9/10/2018 10:31 AM 177 Escitalopram 9/10/2018 10:25 AM 178 Lanotrogine 9/10/2018 10:22 AM 179 Anti-deppressants statins & Pain relief for MS 9/10/2018 9:50 AM 180 Asthma medications 9/10/2018 9:41 AM 181 Allopurinol 9/10/2018 7:28 AM 182 Citalepram 9/9/2018 1:48 PM

27
183 Long term illness 9/7/2018 4:07 PM 184 Diabetes 2, High BP, Chronic Back Pain (Stenosis), Asthma 9/7/2018 3:44 PM 185 T.I.A 9/6/2018 11:50 AM 186 Blood pressure, Cholesterol 9/5/2018 8:30 PM 187 diabetes,cholesteral 9/5/2018 10:33 AM 188 Various 9/4/2018 11:53 AM 189 Lanzoprazole 9/3/2018 6:39 PM 190 Asthma meds, meberverine and ppis 9/3/2018 5:57 PM 191 Ulcerative colitis asacol 9/3/2018 3:56 PM 192 Degenerative spinal problem 9/3/2018 2:32 PM 193 Multiple medications 9/3/2018 2:16 PM 194 Asthma and hayfever 8/30/2018 4:36 PM 195 High blood pressure 8/30/2018 4:00 PM 196 asthma cholesterol high blood pressure 8/30/2018 10:36 AM 197 many conditions long term 8/29/2018 2:13 PM 198 multiple 8/29/2018 1:40 PM 199 Reflux Esophagitis, Hypertension, Arthritis, Ischaemia of the heart 8/28/2018 11:16 AM 200 Metformin500mg Clopidogrel.75mg Levothyroxine.75mgAmlodipine5mg.Bezafibrat200mge Isossorbide mononitmgrate 30mg Pavastatin40mg Aspirin 75mg Glyceryl trinitrate spray 201 Lamotrigine 8/21/2018 6:16 PM 202 COPD/Heart Failure/Diabetes/High Cholesterol/Anxiety/Blefharitis/Disseminated superficial porokeratosis 8/21/2018 5:08 PM 203 Anal fissure 8/20/2018 6:28 PM 204 Allergies 8/20/2018 3:10 PM 205 Hay fever medicine, diabetic medicine, cramp, cholesterol 8/20/2018 3:08 PM 206 Paroxetine and Amitriptyline 8/17/2018 5:35 PM 207 Cocodamol30/500 Sulfasalazine, nasonex spray, ceterizine , Ramipril, Amlodipine 8/16/2018 1:10 PM 208 High blood pressure 8/16/2018 9:51 AM 209 Hay fever allergy 8/14/2018 8:50 PM 210 Depression 8/14/2018 2:27 PM 211 Menopausal night sweats 8/14/2018 9:01 AM 212 Roaccutane and amitriptyline 8/13/2018 9:53 PM 213 Lamotrigine 8/13/2018 11:10 AM 214 Hypertension 8/10/2018 7:43 PM 215 Simvastatin; Hylo-forte; Xailin 8/10/2018 2:39 PM 216 Back,leg,arm and shoulder pain 8/10/2018 2:17 PM 217 Son's serious hayfever 8/9/2018 6:07 PM 218 Mental health, fibromyalgia, chronic migraine, to combat side effects from other medications. 8/4/2018 11:38 AM 219 statin 8/3/2018 3:10 PM 220 Asthma, constipation, patch for menopause and reflux (duodenal ulcer) 8/3/2018 10:30 AM 221 Diclafenac ointment 8/2/2018 11:57 PM 222 osteoporosis 8/2/2018 4:20 PM 223 Roscea 8/1/2018 2:00 PM

28
224 methotrexate, folic acid, tramadol, amitriptyline, lansaprazole, Lisinopril levothyroxine,simvastatin. I am also vitamin D deficient, and agreed with the doctor that I will buy my own tablets for that. 8/1/2018 8:30 AM 225 Thyroxine 7/31/2018 8:42 PM 226 Inhaler 7/31/2018 7:43 PM 227 Underactive Thyroid 7/31/2018 7:30 PM 228 None 7/31/2018 6:56 PM

29
Appendix B
B

30
FURTHER COMMENTS AND DATE AND TIME OF COMMENT 1 The hypromellose eye drops 9/17/2018 1:49 PM 2 But I can afford it. It might be different for someone who cannot afford it. 9/17/2018 1:37 PM 3 Already do 9/17/2018 1:23 PM 4 Do so already 9/17/2018 1:13 PM 5 Advised to take colecalciferol due to renal disease 9/17/2018 1:06 PM 6 However, it is worrying that this is happening. Surely there should be a middle ground. NHS should only pay what it costs the pharmacy not prescription charge. Further, the responsibility is put on the pharmacist to give the correct medication- this should be responsibility of the GP as he has the records.9/17/2018 12:55 PM 7 Medication for headaches as such. I don't mind paying over the counter 9/12/2018 4:27 PM 8 If medicines cost cheaper, I would be happy to pay for them. However it would be discriminatory towards the elderly/ disabled/ single parents/ low paid and unemployed 9/12/2018 4:15 PM 9 We already pay enough national insurance contributions, just because we work we are being punished, yet people on benefits get everything free. Unfair to the working class 9/12/2018 4:02 PM 10 Definitely for short term, would the medication be better from the NHS if needed for long term 9/12/2018 3:52 PM 11 Pharmacy and GSL medicines should be for purchase from the appropriate outlet from medicines should be the principal ones on prescription 9/12/2018 3:46 PM 12 Gaviscon 9/12/2018 3:33 PM 13 as long as sufficient notice is given to the patient of any withdrawal of prescribed items. As long as the items withdrawn from prescription are available locally (it is important that older people who cannot drive or have no means of travelling a mile or two are not made to suffer 9/12/2018 3:30 PM 14 Because I have several long term conditions EDS/ME/CFS/ The NHS needs to negotiate and get their medications as cheaply as Boots and, therefore they will not cost me 9/12/2018 3:18 PM 15 Totally agree with purchasing over the counter medication 9/12/2018 3:08 PM 16 I have paid it to the service all my life so I am entitled 9/12/2018 2:59 PM 17 I need antiacid tablets on a regular basis 9/12/2018 2:31 PM 18 N/A the issues are not short term 9/12/2018 2:03 PM 19 Always do now, consult local pharmacist at chemist 9/12/2018 2:00 PM 20 Unless the symptoms get worse 9/12/2018 1:50 PM 21 I already do this- laxatives, gaviscon and eye drops etc 9/12/2018 1:31 PM 22 The NHS as a major buyer should negotiate equal or lower purchase prices 9/12/2018 1:21 PM 23 I do require 200 co-codamol every month for pain so would this be affected by this change? 9/12/2018 1:14 PM 24 I already purchased asprin rather than getting on prescription 9/12/2018 1:09 PM 25 I could not afford over the counter medicines that I would need on benefits 9/12/2018 1:06 PM 26 absolutely no problems with this paracetamol is only zap 101 9/12/2018 12:57 PM 27 Always have done this 9/12/2018 12:32 PM 28 Don't know 9/12/2018 11:14 AM

31
29 If it helps the NHS then yes I would pay for these things. I am only on sick pay at the moment so I do find this hard but if I was working yes I would be willing 9/12/2018 11:13 AM 30 I already do! 9/12/2018 10:58 AM 31 Why does it cost the NHS more? 9/12/2018 10:37 AM 32 It will help 9/12/2018 10:18 AM 33 Rarely pay for these so happy to pay 9/11/2018 4:15 PM 34 Usually a similar price if not cheaper over the counter 9/11/2018 4:13 PM 35 For myself not a problem, however having a son with excema and hay fever I would prefer for him to still receive these on prescription 36 I do anyway- However as someone who has had no choice but to claim benefits due to being a carer, I now have to pay for GF bread and pasta and so on. This can cost me £20 or more a mouth. For people on benefits this will affect them. 9/11/2018 3:50 PM 37 There is too much waste in the NHS it works to be sorted out and run properly 9/11/2018 3:34 PM 38 Only up to a certain amount e.g. £10 and for a limited period. 9/11/2018 2:57 PM 39 Vitamins, moisturisers- aveeno 9/11/2018 2:51 PM 40 Short term I do, but e.g. hay fever etc ongoing 9/11/2018 1:59 PM 41 As long as vulnerable people still have access via NHS 9/11/2018 1:45 PM 42 I am 60 years old and always paid for my tablets e.t. Why should I have to pay now? 9/11/2018 12:59 PM 43 Happy to continue to purchase anything that doesn't need a prescription 9/11/2018 12:42 PM 44 Regular use of all 9/11/2018 11:58 AM 45 If the prescription can be bought e.g. paracetamo. It shouldn't be prescribed at such a cost to patient and the NHS 9/11/2018 11:24 AM 46 Find it easier to have on prescription 9/11/2018 10:50 AM 47 It depends on what the illness is and the cost of the medication 9/11/2018 9:43 AM 48 Pain relief medication is only available in boxes of 16, this is not enough for me as I use more and 500G 9/11/2018 8:57 AM 49 I do this anyway 9/10/2018 11:40 AM 50 These should be paid for by the user and not the NHS 9/7/2018 4:07 PM 51 So long as not a slippery slope to all prescriptions. 9/6/2018 11:50 AM 52 If I can still get out to do this 9/5/2018 8:30 PM 53 feel this is reasonable 9/4/2018 2:55 PM 54 I didn't even realise I could go to my gp for a prescription for these things. 9/3/2018 7:03 PM 55 I don’t think my GARD medication is available over the counter so I am concerned where this will leave me. I am happy to pay for my medication. 9/3/2018 6:39 PM 56 Being on a fixed income with ever rising living costs, I feel that this is the thin end of a very big wedge. 9/3/2018 2:32 PM 57 I have said "no" - in general I don't have an issue with this for short-term conditions (even though if it was prescribed I wouldn't need to pay for it) but my father-in-law, who is end of life, is still being told to take paracetamol but that it can't be prescribed, so we have to buy it. I don't think that is right at all. 9/1/2018 6:42 PM 58 It makes sense, most of them are not the £8 of the prescription cost and it would clearly benefit the NHS 8/30/2018 4:00 PM

32
59 Yes only if short term 8/29/2018 2:13 PM 60 Not always about cost, something mild ie. infant colic may be an opportunity for the GP to check mums well-being. If mums are stopped visiting for something that keeps them awake all night this could have a detrimental impact on a person the 8/28/2018 11:09 PM 61 personally it makes sense to buy otc as it's cheaper for me, but also where medications are available otc they shouldn't need patients to see a Dr in the first place. Patients should be educated to seek help from a pharmacist or 111 initially and treat themselves so that resources can focus on patients who do need Dr intervention 8/21/2018 6:16 PM 62 Why can't the nhs give them at this cost? 8/20/2018 6:28 PM 63 Yes, but my medication is fexofenadine for allergies, particularly hayfever between April - September when it is very bad. No other anti-histamines work to reduce my symptoms and without fexofen I am sneezing constantly and this then turns in to a sinus infection. 8/20/2018 3:10 PM 64 Yes as this helps the NHS. 8/20/2018 3:08 PM 65 No - because due to my progressive illness (MS) I am unable to work and I have an exemption certificate for prescriptions as I am on a low income. Making certain exemptions for the prescribing of medication that is available over the counter will be detrimental to my health as I will not be able to afford it. 8/17/2018 5:35 PM 66 This depends very much on what it is for. There is one probiotic, VSL#3 which is prescribable for the maintenance of pouchitis. This is a serious condition and affects a very small number of patients so the economic burden to the CCG is insignificant. However you can save money by prescribing Vivomixx as this s not only less expensive than VSL#3 but also contains the original De Simone formulation, or DSF which VSL#3 does not as they changed the formulation 2 years ago. The CCG can therefore reduce costs and ensure that patients who really need this product to treat their condition receives a genuine product at a low price 8/16/2018 6:39 PM 67 Please ask yourself this very simple question - WHY CAN THIS MEDICATION BE BOUGHT OVER THE COUNTER MUCH MORE CHEAPLY THAN IT CAN BE OBTAINED BY THE NHS??? ..... my suggested answer is that you (the NHS) have done a very bad job over the years at negotiating competitive costs and now you are reaping the rewards of your previous incompetence in that the drugs concerned are being blocked. What else would anyone do???? 8/14/2018 10:17 PM 68 I believe everyday items should be bought over the counter by everyone ie even those with hypothesis problems and diabetes etc. Patients just order prescriptions each month without considering the cost. Oh yes I will have another inhaler at £62 (or more) I think I lost the other one! 8/14/2018 9:01 AM 69 Most people would, I believe buy such items from pharmacies. 8/10/2018 7:43 PM 70 I buy that type of item already over the counter, but it is expensive if you are on a tight budget. 8/10/2018 2:39 PM 71 I do now anyway always have even for things for the chikdren . My gp has always told me what to get 8/10/2018 2:17 PM 72 Concerned that Son, Daughter and Husbands serious / severe hay fever and allergies will still be available on prescription as they need max dose fexofenadine 8/9/2018 6:07 PM 73 I already get a lot of medications on prescription that I cannot get OTC that help keep me stable and in regards to me mental health, keep me safe and alive, so I do

33
not have a problem with paying for OTC treatments for short term or mild illness. 8/4/2018 11:38 AM 74 Already do so 8/2/2018 11:57 PM 75 This is a silly question, it is not as clear as yes or know. A real example is vitamin D. When first diagnosed with deficiency I was put on a very high dose for a while (I think a couple of months but certainly several weeks), which was then reduced to a lower dose for maintenance. The GP asked if I would be prepared to buy them myself and I 'negotiated' that the practice would give me prescriptions for the high doses, as the amount I was prescribed initially would have cost me in excess of about £30 per week, as the doses sold in pharmacies and other legitimate shops are low dose, so would have needed more than 10 pills a day. Not only that but getting enough dosage would require either a good stock of money lying around to afford all the pills needed, or necessitate very frequent trips to buy them, which is not compatible with full time working. It is interesting you use the term 'short term illnesses and conditions' because Vit D deficiency is treated for life. Does that mean it will remain as a prescription available item? This would need to be clarified before implementation. That said, there are some treatments which I feel can be bought rather than prescribed which are low cost. Has consideration been given to none financial implications? Again a real life example is that paracetamol is cheap and readily available but I am prescribed up to 8 a day as needed. That means a minimum of 2 trips to buy enough for a week, when my conditions flare up. When they flare up is the time I am least able to get out of the house. Could there be a generic letter that comes from GP practices that explains the need for the patient to buy more than 32 pills, which can be shown to pharmacists (not other shops)? Getting enough supplies is very aggravating, paying for them is not. 8/1/2018 8:30 AM 76 I already spend a fair amount on vitamins and minerals and have never expected the NHS to fund these. However I find the current restrictions on the purchase of paracetamol inconvenient, especially when, if I also buy Calpol for my Grandson I’m precluded from buying two packets of 16 paracetamol!!! 7/31/2018 8:42 PM

34
Appendix C
C

35
Do you agree that medication for self-limiting conditions should not be prescribed? FURTHER COMMENTS WITH DATE AND TIME OF COMMENT 1 They should never have been prescribed, I have bought my own for years 9/17/2018 1:42 PM 2 Depends on the person e.g age and their condition 9/17/2018 1:16 PM 3 Dependent on illness or condition for example, cold sores, sinuses. 9/17/2018 1:08 PM 4 Self limiting conditions can be uncomfortable and painful. The correct medicine needs to be prescribed by a doctor. Again, the doctors knows the medical history. 9/17/2018 12:55 PM 5 Allow the body to heal it self 9/17/2018 12:44 PM 6 There are many medications which are available upon prescription only 9/12/2018 4:15 PM 7 For certain patients who have certain illnesses should be granted every medication that they need 9/12/2018 4:02 PM 8 The major saving is not in the cost of otc medicines but the cost of consultation with a GP so a system e.g. triage needs to be delivered to avoid unnecessary GP consultation 9/12/2018 3:46 PM 9 Depends what other conditions the patient has 9/12/2018 3:37 PM 10 But not for me because of my long term illnesses 9/12/2018 3:18 PM 11 So why prescribe if this is the case, penny pinching NHS 9/12/2018 2:59 PM 12 In general yes, but there could be exceptions for people with weak immune system which does not clear up quickly 9/12/2018 2:57 PM 13 That depends E.G; if painfully ill or long term it ought to be on prescription 9/12/2018 2:49 PM 14 Need to have a uniform policy for this, it varies so much between each surgery and the CCG's 9/12/2018 2:36 PM 15 This question should be answered by professionals 9/12/2018 2:03 PM 16 Unless you have a low immune system like myself 9/12/2018 1:50 PM 17 Unless the patient is at risk from some other condition 9/12/2018 1:47 PM 18 Although I worry that by the time some people may not realise a condition is not self limiting it may be too late to treat the same serious condition e.g brain tumor. The least time to get to G.P appointment make this extremely dangerous 9/12/2018 1:31 PM 19 Depends on the condition and the short term impact on the patient 9/12/2018 1:21 PM 20 Fexafindine only works for my hayfever and I cannot buy over the counter 9/12/2018 1:05 PM 21 Yes makes perfect sense 9/12/2018 12:57 PM 22 I don't like to go to the doctors, it is easier to go for example to Tesco and buy it straight away 9/12/2018 11:18 AM 23 Unless it comes back 9/12/2018 11:14 AM 24 Special needs people don't have capacity to buy or know if what is needed so to stop them or anyone trying to cure patients is ridiculous 9/12/2018 10:52 AM 25 Life- changes should be followed 9/12/2018 10:33 AM 26 There is no need 9/12/2018 10:18 AM 27 Depends how bad it is 9/12/2018 9:31 AM 28 As long as the individual can afford to purchase it themselves- otherwise then I agree 9/11/2018 4:08 PM

36
29 providing it is not causing pain/ anxiety 9/11/2018 3:58 PM 30 I agree that the NHS needs to save money. For above/ many people this will not be a problem, but this will hit the poor and the vulnerable. 9/11/2018 3:50 PM 31 People on a low income / benefits would struggle to pay especially If they had to have time off work for appointment / illness and cannot afford to pay 9/11/2018 3:20 PM 32 Depends what the condition is 9/11/2018 2:27 PM 33 Need is to allow virus etc to have time to go through system 9/11/2018 1:59 PM 34 Depends on level of pain having 9/11/2018 1:54 PM 35 Depends on the type of pain you (the person) are going through 9/11/2018 1:50 PM 36 If it clears up quicker and there's a patient need it should be available 9/11/2018 1:45 PM 37 As long as the higher strength pain killer is available on prescription only and I would be able to get more from a doctor, letter or pharmacy 9/11/2018 1:28 PM 38 Depends on if deliberating for the time period 9/11/2018 12:50 PM 39 May cause a reaction with other meds being prescribed 9/11/2018 12:47 PM 40 Some people can't always afford these medications 9/11/2018 11:43 AM 41 Depends on the condition 9/11/2018 11:41 AM 42 Depends on the patients circumstances 9/11/2018 11:37 AM 43 Depends if you get free prescriptions- i.e elderly/ children 9/11/2018 11:22 AM 44 Depending on time it takes to clear up, if short-term then ok. 9/10/2018 12:29 PM 45 Don't know 9/10/2018 11:59 AM 46 Depends on the severity of the condition 9/10/2018 11:40 AM 47 Depends on patient 9/10/2018 11:34 AM 48 Personally if I get a cold I often succumb to a chest infection due to my asthma. 9/10/2018 10:43 AM 49 Unless causing discomfort/embarassement 9/10/2018 10:22 AM 50 In principle yes but some conditions, depending on patient age, severity etc, can take a long time to clear up. So maybe exceptions to a blanket policy. 9/6/2018 11:50 AM 51 Unless there are overriding reasons why this should happen in the opinion of a doctor 9/5/2018 8:30 PM 52 use funds for more appropriate treatments 9/5/2018 10:33 AM 53 But not all patients have the knowledge or understanding about this and what alternatives are available, especially vulnerable people. 9/4/2018 11:53 AM 54 Will guidance be issued for if it does not clear up ie bacterial infection instead of a virus. 9/3/2018 6:39 PM 55 As long as there are alternative, funded methods available to help cope with the condition until it heals. 9/3/2018 2:32 PM 56 People should not be going to the doctors for coughs/colds etc unless they have had symptoms for 3+ weeks. 8/30/2018 4:00 PM 57 The fact they are no longer prescribed may confuse patients when to visit the GP, so are more likely to not to visit anyway as they don’t want to bother the doctor. The medicine actually states not to use more than 3 days in a row... 8/28/2018 11:09 PM 58 We shouldn't provide anything on the NHS that isn't necessary. 8/21/2018 6:16 PM 59 Although things may clear up they may be very painful before they do, or take longer to clear up without medication 8/20/2018 6:28 PM

37
60 Surely medication speeds up the process of recovery? If you have to go to work a self-limiting condition can cause you to feel awful and risk having sick days. 8/20/2018 3:10 PM 61 Yes because it’s a short term use and you can save the NHS money. 8/20/2018 3:08 PM 62 Except as above 8/16/2018 6:39 PM 63 Tell the patient what's required and leave them to get it themselves - it will probably be cheaper than the Prescription Charge anyway. 8/14/2018 10:17 PM 64 Sometimes seems unfair though, as some patients with out long term conditions still get these medications - it really all depends on which doctor you see 8/14/2018 2:27 PM 65 So many minor illnesses get better on their own. 8/14/2018 9:01 AM 66 I had not heard that phrase before. It is a complex idea to put forward. The condition might well go on its own but could be very painful in the process (eg cold sore) 8/10/2018 2:39 PM 67 OTC medicine should be sought of needed. 8/4/2018 11:38 AM 68 Generally yes, however I get strep throat and I get very ill temperatures of 39.8, throat swelling with strep and without antibiotics I’m really really scared what will happen. It started after a serious bout of glandular fever in my teens and comes once or twice a year. I’m a carer for a disabled child and it’s usually at times when she’s got ill with something different I get so run down that I get ill with tonsillitis. 8/3/2018 10:30 AM 69 However those in poverty who cannot buy over the counter need support especially if children vulnerable adults involved 8/2/2018 11:57 PM 70 Depends on the timescale and the person's other medical needs and conditions. 8/1/2018 2:00 PM 71 I think this is travelling into a shady area. A torn muscle could be described as self-limiting but is exceptionally painful. Everyone I know who has had this (I am linked to a mens hockey team) has required pain relief stronger than can be bought over the counter. Therefore, it may be self-limiting but a GP could (and many would) decline a request for painkillers as it is a self-limiting condition. This is just one example off the top of my head, there will be many more, but there is a very fine line when it comes to the difference between 'want' and 'need' and I don't think this has been sufficiently ironed out yet. 8/1/2018 8:30 AM 72 Prescribing a medicine for a condition that will clear up on its own is quite clearly a waste of money.

38
Appendix D
D

39
Q9. RESPONSE AND RESPONSE DATE AND TIME 1 Paracetamol. migrane tablets, calpol and hayfever syrup 9/17/2018 1:54 PM 2 Painkillers- anti inflammatories for general aches and pains. Tendonopathy. Hydrocortisone and cream for dry skin 9/17/2018 1:52 PM 3 Paracetamol- tesco 9/17/2018 1:49 PM 4 Ibuprofen/ paracetamol- tesco 9/17/2018 1:46 PM 5 Pain, flu/cold symptoms, cold sores, dry skin conditions 9/17/2018 1:45 PM 6 Paracetamol- back pain - supermarkets Neurofen- back pain - supermarkets vitaminssupermarket 9/17/2018 1:42 PM 7 Arthritis 9/17/2018 1:37 PM 8 Cod liver oil, glucosomine 9/17/2018 1:37 PM 9 Cetrizine recommended by GP and purchased 9/17/2018 1:34 PM 10 Asprin 9/17/2018 1:27 PM 11 Cold remedies, sore throat remedies, glucosamine- from supermarkets 9/17/2018 1:23 PM 12 Paracetamol for various aches and pains from supermarkets 9/17/2018 1:16 PM 13 Back pain 9/17/2018 1:16 PM 14 Hayfever 9/17/2018 1:14 PM 15 Turmeric (arthiritis) 9/17/2018 1:13 PM 16 Vitamin D 9/17/2018 1:12 PM 17 Diarrhoea from chemist 9/17/2018 1:10 PM 18 Pain killers Olbas oil for sinuses 9/17/2018 1:08 PM 19 Cocodamol 9/17/2018 1:06 PM 20 Eyedrops- pharmacy 9/17/2018 1:02 PM 21 Paracetamol for occasional aches and pains Chemist and supermarket Anusol - piles Glycerine and honey - irritable coughs 9/17/2018 1:01 PM 22 Cough and cold- chemist 9/17/2018 12:59 PM 23 Headache/joint pain 9/17/2018 12:55 PM 24 Ibuprofen, paracetamol, cold and flu syrups. 9/17/2018 12:44 PM 25 Any medicine you don't need a prescription for 9/12/2018 4:27 PM 26 Hayfever, vitamins, iron supplement 9/12/2018 4:15 PM 27 Skin, mouth ulcers 9/12/2018 4:06 PM 28 Bad knee and ankle etc 9/12/2018 4:03 PM 29 paracetamol, ibuprofen, cough remedies 9/12/2018 4:02 PM 30 ibuprofen and paracetamol 9/12/2018 3:54 PM 31 Paracetamol from local shops 9/12/2018 3:52 PM 32 paracetamol 9/12/2018 3:49 PM 33 Pain relief, antihistamines for stings etc OTC hand cream all from pharmacy 9/12/2018 3:46 PM 34 Colds or headaches 9/12/2018 3:39 PM 35 General aspirin 9/12/2018 3:37 PM 36 Retimax Max for mocular degeneration 9/12/2018 3:30 PM 37 Vicks sinex, ibuprofen and paracetamol 9/12/2018 3:26 PM 38 Paracetamol from supermarkets 9/12/2018 3:23 PM 39 Dry Skin Condition 9/12/2018 3:20 PM 40 paracetamol and ibuprofen 9/12/2018 3:19 PM 41 NeilMed Sinus rinse for rhinitis, cost £20. Some items magnesium, vitamins B1 and 12, Rennie for indigestion. Pharmacy or grocery wherever the cheaper 9/12/2018 3:18 PM 42 Vitamins, Painkillers, Cold and flu remedies 9/12/2018 3:13 PM

40
43 Cough, initial pain relief and thrush 9/12/2018 3:08 PM 44 Iboprofin for neck and joint pain. Along with the statins it is the only thing I take it is the only medication that helps with my pain 9/12/2018 3:07 PM 45 Dry skin 9/12/2018 2:59 PM 46 Skin Conditions, athletes foot 9/12/2018 2:57 PM 47 Vitamin D, Vitamin C, Pain Killers, Votorol from the chemist 9/12/2018 2:52 PM 48 Vitamins Glucosamine 9/12/2018 2:49 PM 49 Just general pain killers etc as and when needed 9/12/2018 2:46 PM 50 Paracetamol 9/12/2018 2:41 PM 51 Hayfever, insect Bites, headaches 9/12/2018 2:40 PM 52 General painkillers, indigestion remedies and creams for insect bites 9/12/2018 2:36 PM 53 Paracetamol occasional headache 9/12/2018 2:35 PM 54 Paracetamol for pain relief 9/12/2018 2:31 PM 55 Vitamin D- Pharmacy. Cod liver oil- pharmacy or Holland Barrett 9/12/2018 2:26 PM 56 Paracetamol Headaches, Iboprofin, Stiff joints 9/12/2018 2:23 PM 57 Ibuprofen for arthritic pain from supermarket. Paracetamol for arthritic pain from supermarket. Calcium carbonate for acid reflux from supermarket. 9/12/2018 2:11 PM 58 Ibuprofen and paracetamol bought from the supermarket 9/12/2018 2:06 PM 59 Visionaid- Boots/ chemist/ H & Barrat 9/12/2018 2:03 PM 60 Golden eye cream, Dry eye mist spray, Paracetamol, Voctarol, travel pills and pile treatment 9/12/2018 2:00 PM 61 Paracetamol- painkillers. Indigestion tablets- heart burn and indigestion 9/12/2018 1:50 PM 62 Vocal cones from the pharmacy 9/12/2018 1:47 PM 63 Asprin 9/12/2018 1:33 PM 64 I purchase gaviscon from the supermarket when I have forgotten to buy any from the Eppingham dispensary 9/12/2018 1:31 PM 65 Insect bites rashes headaches, supermarket or pharmacy (least Likely) 9/12/2018 1:31 PM 66 Headaches/Migrain, Pharmacy 9/12/2018 1:23 PM 67 Ibuprofen from the pharmacy 9/12/2018 1:22 PM 68 Pain relief iboprofin, vitamins, pharmacy or supermarket where they are cheaper 9/12/2018 1:21 PM 69 Dry eyes 9/12/2018 1:18 PM 70 Cold remedies and voltorol 9/12/2018 1:14 PM 71 Paracetamol, headache, Lloyds chemist 9/12/2018 1:12 PM 72 Asprin to work in conjunction with B.P medication purchased at pharmacy 9/12/2018 1:09 PM 73 Painkillers with codeine from boots for bad bones and pain from psoriasis 9/12/2018 1:06 PM 74 Paracetamol general pain, local chemist/supermarket 9/12/2018 1:05 PM 75 Vitamin D 3 Boots recommended by hospital many years ago for potential oesteoporosis 9/12/2018 1:01 PM 76 Headaches 9/12/2018 12:58 PM 77 Paracetamol, Ibuprofin, Vitamins, cough/flu medication 9/12/2018 12:57 PM 78 Paracetamol for headaches and otex ear drops 9/12/2018 12:53 PM 79 Dry skin and pain killers 9/12/2018 12:49 PM

41
80 Hayfever 9/12/2018 12:46 PM 81 Pharmacy or supermarket 9/12/2018 12:43 PM 82 Paracetamol- to have at home if needed Antihistamines- for allergies 9/12/2018 12:37 PM 83 Dry skin cream- Tesco's Hay fever tablets- supermarket/ local shop 9/12/2018 12:32 PM 84 Pain killers, cold and flu tablets 9/12/2018 12:30 PM 85 Painkillers 9/12/2018 11:58 AM 86 Co-codomol 9/12/2018 11:51 AM 87 Paracetamol and anti-diarrhoea from boots or wilko's 9/12/2018 11:42 AM 88 Painkillers- cream etc All from various supermarkets 9/12/2018 11:36 AM 89 Tesco- pregnancy vitamins 9/12/2018 11:18 AM 90 Vitamin D 9/12/2018 11:13 AM 91 Paracetamol and ibuprofen 9/12/2018 10:58 AM 92 Ibuprofen and hay fever tablets 9/12/2018 10:52 AM 93 Paracetamol from Sainsbury's 9/12/2018 10:44 AM 94 Day eye drops, anti-histamine tablets and vitamin tablets 9/12/2018 10:43 AM 95 Headaches and general aches and pains 9/12/2018 10:41 AM 96 Headaches and hay fever 9/12/2018 10:37 AM 97 If needed, co-codamol 9/12/2018 10:34 AM 98 Paracetamol 9/12/2018 10:30 AM 99 Gum disease, fungal nail infections- purchased from any chemist 9/12/2018 10:24 AM 100 Allergy tablets 9/12/2018 10:21 AM 101 Pain killers- local chemist and asthma tablets 9/12/2018 10:16 AM 102 Probiotics, paracetamol, ibuprofen and vitamins 9/12/2018 9:56 AM 103 Pain relief from supermarkets 9/12/2018 9:54 AM 104 Paracetamol tablets and liquid, ibuprofen 9/12/2018 9:53 AM 105 Sciatica, menstrual problems, headaches, aches and pains, anti-histamines, athletes foot, fungal nail infection, toothaches etc 9/12/2018 9:51 AM 106 Paracetamol 9/12/2018 9:40 AM 107 Gaviscon, anti-histamines, pain relief 9/12/2018 9:37 AM 108 Zantac- pain relief 9/12/2018 9:29 AM 109 Gaviscon and ibuprofen 9/12/2018 9:21 AM 110 Cough medicine, painkillers and baby ointment 9/12/2018 9:20 AM 111 Paracetamol and hay fever relief 9/11/2018 4:25 PM 112 Co-codamol 9/11/2018 4:22 PM 113 Paracetamol 9/11/2018 4:18 PM 114 Ad hoc for coughs 9/11/2018 4:15 PM 115 Gaviscon and paracetamol 9/11/2018 4:13 PM 116 paracetamol, cough relief, hayever relief, all from supermarkets 9/11/2018 4:08 PM 117 Germaline 9/11/2018 4:01 PM 118 Blocked sinus 9/11/2018 3:58 PM 119 Pain Relief- supermarkets 9/11/2018 3:55 PM 120 Cold and flu 9/11/2018 3:51 PM 121 Painkillers and cold remedies. My daughter has a long term pain condition which won't go away and I have arthritis which won't go away. 9/11/2018 3:50 PM 122 Vitamins, child pain relief, headaches 9/11/2018 3:26 PM
42
123 Paracetamol/ ibuprofen general aches/ pains e.g. headaches 9/11/2018 3:20 PM 124 Oral thrush, hay fever 9/11/2018 3:12 PM 125 Paracetamols, calpol 9/11/2018 3:02 PM 126 Paracetamol/ ibuprofen for aches and pains, cold medications 9/11/2018 3:01 PM 127 Eczema, hayfever 9/11/2018 2:51 PM 128 Vitamins, Digestive things, Skin dryness, Hayfever and pain relief 9/11/2018 2:46 PM 129 Various 9/11/2018 2:42 PM 130 Anti acid medication, steroid cream for skin, boots pharmacy 9/11/2018 2:40 PM 131 Mild pain- paracetamol 9/11/2018 2:31 PM 132 Antihistamine and paracetamol 9/11/2018 2:27 PM 133 Coughs, cold and thrush 9/11/2018 2:24 PM 134 Aches and pains 9/11/2018 2:22 PM 135 Hayfever tablets 9/11/2018 2:02 PM 136 Paracetamol, ibuprofen for headaches and back pain 9/11/2018 1:59 PM 137 Antihistamine for hay fever. Sudafed for sinus congestion etc. Purchased in pharmacy 9/11/2018 1:38 PM 138 Ibuprofen and paracetamol 9/11/2018 1:34 PM 139 Cold, cough 9/11/2018 1:28 PM 140 Vitamin D 9/11/2018 12:59 PM 141 Ibuprofen 9/11/2018 12:48 PM 142 Vitamin supplement and ibuprofen from chemist 9/11/2018 12:39 PM 143 Cough and cold/ flu medication. Cold sores, insect bites. Mainly bought from boots or supermarkets. Whichever is cheapest! 9/11/2018 12:35 PM 144 Paracetamol 9/11/2018 12:05 PM 145 Painkillers and vitamins for zinc deficiency 9/11/2018 11:51 AM 146 Aspirin and antihistamines 9/11/2018 11:44 AM 147 Hayfever, ibuprofen, paracetamol 9/11/2018 11:43 AM 148 Sometimes 9/11/2018 11:41 AM 149 Paracetamol- pain Loratadine- allergy 9/11/2018 11:37 AM 150 Pain killers and vitamins 9/11/2018 11:32 AM 151 Pain relief (arthritic) 9/11/2018 11:29 AM 152 Ibuprofen for pain relief 9/11/2018 11:01 AM 153 Cough and cold medications purchased from pharmacy 9/11/2018 10:58 AM 154 Tension Headphones- supermarket 9/11/2018 10:55 AM 155 N/a 9/11/2018 10:50 AM 156 Paracetamol for headaches, cough syrups for cough/ cold 9/11/2018 10:41 AM 157 Paracetamol 9/11/2018 10:39 AM 158 Paracetamol- migrane/ headaches 9/11/2018 10:35 AM 159 Headaches/ period pain- paracetamol/ ibuprofen - any shops that sell them 9/11/2018 10:12 AM 160 Painkillers- local shops 9/11/2018 10:07 AM 161 Nurofen Plus 9/11/2018 10:04 AM 162 Imodium 9/11/2018 10:02 AM 163 Paracetamol 9/11/2018 9:58 AM 164 Paracetamol, ibroprofen, athletes foot treatment 9/11/2018 9:51 AM 165 Cough mixture 9/11/2018 9:46 AM 166 paracetamol 9/11/2018 9:42 AM

43
167 Anadin, gaviscon 9/11/2018 9:28 AM 168 Paracetamol, calpol, vitamin C 9/11/2018 9:24 AM 169 Eye drops for dry eyes, Antihistamines- hayfever, painkillers- occasional headkillers 9/11/2018 9:20 AM 170 Creams 9/11/2018 8:57 AM 171 Calpol/ beconase 9/11/2018 8:43 AM 172 Nasal spray/ anti-histamine/ painkiller - supermarkets 9/11/2018 8:40 AM 173 Hospital prescribed and I purchased from pharmacy buy my GP prescribed. 9/10/2018 12:24 PM 174 Dermatitus - I buy steroid cream over the counter. Also painkillers 9/10/2018 12:14 PM 175 Cough medicine & Paracetamol. chemist 9/10/2018 12:07 PM 176 Pain relief 9/10/2018 11:40 AM 177 My business 9/10/2018 11:34 AM 178 Purchase from the pharmacy for coughs/colds 9/10/2018 11:31 AM 179 Ear wax, Boots 9/10/2018 11:21 AM 180 Anti histamines at market Harborough pharmacy 9/10/2018 11:18 AM 181 Paracetamol - Back & Leg pain 9/10/2018 10:58 AM 182 Boots skin cream 9/10/2018 10:51 AM 183 Gaviscon for occasional heartburn 9/10/2018 10:43 AM 184 cracked heals 9/10/2018 10:31 AM 185 Pain & pharmacy 9/10/2018 10:25 AM 186 Aches & pains paracetamol, cold relief medication. insect bite cream pharmacy 9/10/2018 10:22 AM 187 Eye drops/Hay Fever tablets 9/10/2018 10:12 AM 188 Paracetamol - Pain relief 9/10/2018 9:57 AM 189 Paracetamol Ibuprophen from Wilinsons 9/10/2018 9:50 AM 190 Paracetamol - For headaches and minor aches and pains 9/10/2018 9:41 AM 191 Dry skin 9/9/2018 1:48 PM 192 Regurgitation, acid reflux Gaviscon Double Action 9/7/2018 3:44 PM 193 Mild painkillers for occasional headaches. 9/6/2018 11:50 AM 194 Hayfever/allergy- Supermarket 9/5/2018 8:30 PM 195 colds and flu like symptoms 9/4/2018 2:55 PM 196 Migraine tablets, migraine balm, antihistamines, pain relief creams and gels and patches, eye drops. Purchase from a pharmacy. 9/4/2018 11:53 AM 197 I go to the pharmacy or supermarket for: Calpol for kids temperature Cough medicine in winter. Thrush treatment from time to time Travel sickness tablets Antihistamines for occasional hives. Treatment for boils Sudocreme for nappy rash/ sunburn/ grazes 9/3/2018 7:03 PM 198 Cystitis 9/3/2018 6:39 PM 199 Painkillers 9/3/2018 5:57 PM 200 Painkillers from supermarket for joint pains; allergy relief. 9/3/2018 2:16 PM 201 I buy standard painkillers such as Paracetamol and anti-inflammatories such as Ibuprofen 9/1/2018 6:42 PM 202 Hayfever - anti hystamines from various supermarkets and chemists 8/30/2018 4:36 PM 203 cough medicine, eye drops, paracetemol 8/30/2018 10:36 AM 204 cold remedies dioreha 8/29/2018 1:40 PM 205 Liquid piriton for my daughters allergy, but didn’t realise as this was drowsy this was more problematic than her over the prescription 8/28/2018 11:09 PM

44
206 Analgesics. Cold and cough remedies.Indigestion.eye drops etc. 8/26/2018 3:57 PM 207 Hayfever tablets Painkillers Eyedrops Purchased from chemist 8/24/2018 3:26 PM 208 Paracetamol Ibuprofen Gastro medication for dietary intolerance symptoms (if accidentally eaten) Vitamin D Hydrocortisone cream for eczema All purchased from pharmacies 8/22/2018 10:18 AM 209 Ibuprofen etc for occasional pain relief 8/21/2018 6:16 PM 210 Dry Itchy Scalp. Purchased from a Chemist. Recommended by the GP. 8/21/2018 5:08 PM 211 Painkillers, antihistamines and teething medication 8/20/2018 6:28 PM 212 Eye drops - hayfever 8/20/2018 3:10 PM 213 Cough and cold, fever, thrush, pain relief for carpal tunnel. 8/20/2018 3:08 PM 214 The items I currently buy over the counter are paracetamol and ibuprofen for pain relief. I can purchase these cheaply at supermarkets and high street stores. 8/17/2018 5:35 PM 215 NSAIDs, cold remedy 8/16/2018 6:39 PM 216 Germolene / plasters / eyewash / cold and flu remedies / painkillers / moisturising cream /cough medicine etc 8/14/2018 10:17 PM 217 Headaches, medication bought from pharmacies/supermarkets 8/14/2018 8:50 PM 218 Vitamin D - purchased from superdrug Hypromellose eye drops for dry eye - Lloyds Pharmacy Loratadine - hayfever tablets – Aldi 8/14/2018 2:27 PM 219 Coughs and colds, painkillers 8/13/2018 6:27 PM 220 eczema - hydrocortisone cream 8/13/2018 9:37 AM 221 Antihistamine cream for stings 8/10/2018 7:43 PM 222 Hay Fever 8/10/2018 2:53 PM 223 Vitamins, Gaviscon 8/10/2018 2:39 PM 224 Paracetamol, idpudeanin, capol, cough meds, exma cream. Bum cream all for different things 8/10/2018 2:17 PM 225 purchase OTC from Boots or other pharmacy for most self limiting and minor conditions where OTC available 8/9/2018 6:07 PM 226 Vitamin D - I buy it from somewhere such as Wilkinson or a store that sells OTC medicine cheaply. 8/4/2018 11:38 AM 227 warts, insect bites, sinusitis, athletes goit, headaches etc 8/3/2018 3:10 PM 228 Paracetamol taken once daily before bed re back pain as otherwise can’t sleep with pain. Vitamins to support menopause Canestan for infection 8/3/2018 10:30 AM 229 Emollient bath oil and creams vitamins / supplements seasonal items eg for colds hay fever- supermarkets and pharmacies 8/2/2018 11:57 PM 230 Indigestion remedy 8/2/2018 4:20 PM 231 Paracetamol for headaches Ibuprofen for strains Anti-histamine for bites and stings All from Boots 8/1/2018 2:00 PM 232 Most of the items below are from Superdrug I buy Vitamin D tablets for diagnosed deficiency. I buy paracetamol to be taken alongside tramadol for psoriatic arthritis and fibromyalgia. I take anti-histamine occasionally for hay fever. I have just started taking cannabis oil (no THC, 5%) and bought it from Holland and Barratt - incidentally for future consultations it is improving my health considerably - 8/1/2018 8:30 AM

45
233 Paracetamol. I buy from local supermarket and only being able to buy 32 tabets at one time is frankly inconvenient as 32 tablets only last me 8 days!! 7/31/2018 8:42 PM 234 Hay fever and allergies 7/31/2018 7:43 PM

46
Appendix E
E

47
If there are any medicines that you have any particular concerns about please tell us which one and why. RESPONSE AND RESPONSE DATE AND TIME 1 Emoliant creams 9/17/2018 1:54 PM 2 Lanzoprazole (should be for limited time?) 9/17/2018 1:45 PM 3 Atorvastatin- side effects 9/17/2018 1:37 PM 4 penicillin 9/17/2018 1:37 PM 5 No 9/17/2018 1:08 PM 6 Blood pressure medication- strong painkillers should be regularly reviewed. 9/12/2018 4:15 PM 7 Some medications react with each other and should only be taken under supension 9/12/2018 3:37 PM 8 The medications mentioned above plus the skin medications/creams which help me manage my long term condition/illness 9/12/2018 3:18 PM 9 Insulin, and eye drops 9/12/2018 3:10 PM 10 Ibuprofin as I am buying it from the supermarket, I am not monitored on this medication, I have had a dystonia for over 20 years and this, along with botox injections is the only medication for pain relief 9/12/2018 3:07 PM 11 Paracetamol, rheumatoid arthritis which is very painful 9/12/2018 3:04 PM 12 Co Codemol I take this prescribed for pain x4 tablets a day 9/12/2018 3:00 PM 13 All my meds 9/12/2018 2:59 PM 14 Statins. Concern about efficacy if no previous incidents 9/12/2018 2:49 PM 15 A lot of codeine products are so easily available 9/12/2018 2:36 PM 16 All of the medicines I am prescribed- they all carry potential side effects 9/12/2018 2:35 PM 17 Branded medication which advertises widely, is more costly than non-branded and costs much more 9/12/2018 2:11 PM 18 Why are paracetamol etc. still widely available over the counter. It's asking for trouble 9/12/2018 1:31 PM 19 Nil 9/12/2018 1:31 PM 20 I have to buy Nlls Sinks Rinse for my daughters long term condition the sachets cost £20 per month because they are not prescribed 9/12/2018 1:21 PM 21 No Follow up advice of pharmacist 9/12/2018 1:09 PM 22 Mild lotion cream as I can only use a few due to allergies and my condition goes from mild to severe which requires much use 9/12/2018 1:06 PM 23 Why are capsules so much more expensive? 9/12/2018 12:57 PM 24 Co-codomol short term use 9/12/2018 12:30 PM 25 Anti-depressants - cost if it was private Tramadol - most needed 9/12/2018 11:36 AM 26 Amitriptyline- too many side effects. Me and my daughter have both come off it and noticed a positive difference 9/12/2018 11:13 AM 27 All of them can help suicidal patients to end their lives 9/12/2018 10:52 AM 28 No 9/12/2018 10:46 AM 29 You are not saying which medications are included in this- so I am concerned that aloracol and GF products come under this. 9/11/2018 3:50 PM 30 Co-codamol can be abused. Patients can buy from multiple pharmacies which the use cannot be monitored. 9/11/2018 3:26 PM 31 N/A 9/11/2018 3:20 PM 32 Sedative 9/11/2018 3:14 PM 33 Paracetamol- buying every few days 9/11/2018 3:12 PM

48
34 No 9/11/2018 3:01 PM 35 No 9/11/2018 1:34 PM 36 Painkillers for long term pain. 9/11/2018 1:28 PM 37 No 9/11/2018 1:05 PM 38 Reason for attending surgery 9/11/2018 12:37 PM 39 Recurring conditions can build up cost of over counter medication over time. Any medicines that cost more than prescription cost. 9/11/2018 12:35 PM 40 No 9/11/2018 11:51 AM 41 No 9/11/2018 11:46 AM 42 Nasal decongesralts- often used inappropriately 9/11/2018 11:37 AM 43 No 9/11/2018 11:32 AM 44 N/a 9/11/2018 11:15 AM 45 Co-codomol, many people misusing codeine based products on regular basis 9/11/2018 11:10 AM 46 N/a 9/11/2018 10:50 AM 47 None 9/11/2018 10:41 AM 48 N/a 9/11/2018 10:12 AM 49 N/a 9/11/2018 10:04 AM 50 Predaxa 9/11/2018 10:02 AM 51 No 9/11/2018 9:58 AM 52 None 9/11/2018 9:48 AM 53 No 9/11/2018 9:46 AM 54 none 9/11/2018 9:28 AM 55 N/A 9/11/2018 9:24 AM 56 N/A 9/11/2018 9:18 AM 57 n/a 9/11/2018 8:43 AM 58 No 9/11/2018 8:40 AM 59 No 9/10/2018 12:29 PM 60 No 9/10/2018 12:19 PM 61 Diazapam & Anti depressents 9/10/2018 12:14 PM 62 No 9/10/2018 12:02 PM 63 Life threatening medicines 9/10/2018 11:44 AM 64 No 9/10/2018 11:34 AM 65 All medicines, I have worked all my life and paid national insurance and tax. 9/10/2018 11:21 AM 66 Am prescribed coated aspirin as part of diabetes meds, re preventing BP and heart disease complications 9/7/2018 3:44 PM 67 Statins - a lot of contra-indications. 9/6/2018 11:50 AM 68 over use of indigestion/reflux relief that may be disguising a more serious condition 9/5/2018 8:30 PM 69 you mention dental cries in consultation . I have a family memner who is under the care of Dental hospitals as paed and adult and has Duraphat toothpaste prescribed and is not available over the counter 9/4/2018 2:55 PM 70 Migraine tablets as they are not always available and there is no alternative when there is non around as I'm currently experiencing. 9/4/2018 11:53 AM 71 Lanzoprazole- I have GARD but it is commonly for heartburn. I have a hernia . 9/3/2018 6:39 PM 72 N/a 9/3/2018 5:57 PM

49
73 Paracetamol. I would have difficulty obtaining the amount I receive on prescription without making several journeys (by car as no bus service) each month. 9/3/2018 2:32 PM 74 None 9/3/2018 2:16 PM 75 None 8/30/2018 4:36 PM 76 painkillers possible interactions with current meds and health issues 8/29/2018 1:40 PM 77 Allergy products are more expensive and could stop people accessing the right products 8/28/2018 11:09 PM 78 n/a 8/21/2018 6:16 PM 79 My concern is waste on packaging:- Candesartan 2mg 1 a day.1 mth supply=4 cartons. Braltus capsules (plus new applicator which is not required each month) 8/21/2018 5:08 PM 80 Fexofenadine (180mg) and Avamays - I am concerned as there is nothing over the counter in this strength that prevents me from feeling awful for half the year. 8/20/2018 3:10 PM 81 N/A 8/20/2018 3:08 PM 82 I would be concerned if the eye drops and cream for a skin condition were no longer available on prescription as they are relatively expensive. 8/17/2018 5:35 PM 83 Vivomixx should be your treatment of choice for your pouchitis patients and will save you money 8/16/2018 6:39 PM 84 None 8/16/2018 9:51 AM 85 I don't understand this question! 8/14/2018 10:17 PM 86 n/a 8/14/2018 2:27 PM 87 Why should hyperthyroid patients have to pay and not hypothyroid patients not? With prepayment certificates available should they not be treated the same? 8/14/2018 9:01 AM 88 None 8/10/2018 7:43 PM 89 None 8/10/2018 2:39 PM 90 5% versatis medicated plaster (lidocaine) i heard you maybe stopping these. I use two nightly they help me so much with sleep and being able to get up in morning. I could not afford to buy these myself my day to day life would be affected 8/10/2018 2:17 PM 91 Hayfever / Severe Allergies - concerned that my family will not be able to access these on prescription - they cannot function without them 8/9/2018 6:07 PM 92 OTC opiate based pain killers such a co-codamol, even at the lower dose can lead to addiction and pain killers in general due to the risk of too much is taken.8/4/2018 11:38 AM 93 none 8/3/2018 3:10 PM 94 I take movicol for continued constipation. The consultant said it was highly likely from symptoms I had IBS and a disorder of defaccation. I refused further test and said I would try and carry on with movicol and diet to manage. I worry that I will no longer be prescribed the movicol. I also worry about my strep throat wIth which I get so very ill. I get very ill temperatures of 39.8, throat swelling with strep and without antibiotics I’m really really scared what will happen. It started after a serious bout of glandular fever and comes once or twice a year. I’m a carer for a disabled child and it’s usually at times when she’s got ill with something different I get so run down that I get ill with tonsillitis. 8/3/2018 10:30 AM

50
95 Diclafenac/Volterol 12 hour cream to treat athritic pain topically as NSAID oral meds cause gastric problems - as oap prohibitively expensive if had to self fund. 8/2/2018 11:57 PM 96 None 8/1/2018 2:00 PM 97 I am concerned that Tramadol seems to be going down the same root as co-proxamol did. All of a sudden GP's couldn't prescribe it and so they put me on Tramadol which is effective at reducing pain. I do not find paracetamol on it's own does anything to reduce pain levels. I can't take ibuprofen. It is hard living with pain, after 26 years you get worn down, and there seems to be a culture of blaming the patient some of whom may become addicted to medication, for most patients it is not a choice to take medication, even addictive ones. I can categorically state that for me, a life without pain relief would be a life that is not worth living and there would only be one way out of that life. 8/1/2018 8:30 AM 98 All of them. Because we want to cure everything and take no responsibility for prevention. 7/31/2018 10:15 PM

51
Appendix F
F
52
RESPONSES AND DATE AND TIME OF RESPONSE 1 Treatment for chronic conditions 9/17/2018 1:45 PM 2 People who are prescribed multiple medicines 9/17/2018 1:44 PM 3 Those with chronic conditions 9/17/2018 1:37 PM 4 Low income state assisted people and their children 9/17/2018 1:23 PM 5 Elderly, babies and children 9/17/2018 1:16 PM 6 Children (antibiotics) 9/17/2018 1:14 PM 7 Grandson as above 9/17/2018 1:13 PM 8 Low income, pensioners 9/17/2018 1:08 PM 9 As above 9/17/2018 1:06 PM 10 Elderly people on few incomes 9/17/2018 1:02 PM 11 Those with chronic conditions where over the counter medications are restricted in quantity 9/17/2018 1:01 PM 12 As above, the poorest people are generally the most vulnerable group of people. Highly paid GPs should not ration prescriptions. 9/17/2018 12:51 PM 13 For all over 60's 9/17/2018 12:44 PM 14 OAPs 9/12/2018 4:27 PM 15 As above 9/12/2018 4:15 PM 16 All high risk patients as mentioned above as they are more prone to infection 9/12/2018 4:02 PM 17 Income support 9/12/2018 3:54 PM 18 As above 9/12/2018 3:37 PM 19 People over 75 may find it more difficult to get out to shops to collect larger quantities of painkillers 9/12/2018 3:31 PM 20 Those who have difficulty getting to outlets supplying the subject medication or cannot afford to buy same 9/12/2018 3:30 PM 21 People who are entitled to free prescriptions should still have that option 9/12/2018 3:26 PM 22 As above 9/12/2018 3:19 PM 23 As above in 11 9/12/2018 3:18 PM 24 Over 75 years 9/12/2018 3:12 PM 25 Diabetic People 9/12/2018 3:10 PM 26 Yes, long term usage of painkillers so the patient is monitored on use. If this is not possible it should be noted on their records as regular users and checks made 9/12/2018 3:07 PM 27 Financial problems and chronically ill 9/12/2018 3:04 PM 28 Painkillers for chronic pain, so they can be monitored on use 9/12/2018 3:00 PM 29 All people over the age of 60 9/12/2018 2:59 PM 30 Long Term Conditions/palliative 9/12/2018 2:46 PM 31 Low income families, people handicapped by mental issues 9/12/2018 2:41 PM 32 Elderly/Disabled 9/12/2018 2:40 PM 33 People who need antacid to prevent stomach damage from other drugs 9/12/2018 2:00 PM 34 As above 9/12/2018 1:47 PM 35 Those who are unable to pay who would otherwise get free prescriptions 9/12/2018 1:31 PM 36 Sufferers of long term conditions, hayfever, eczma, asthma 9/12/2018 1:21 PM 37 Limited income, elderly and people with long term conditions that will not improve 9/12/2018 1:14 PM 38 N/A 9/12/2018 1:09 PM

53
39 Lansoprosal as medicine can cause stomach issues 9/12/2018 1:06 PM 40 As above 9/12/2018 1:05 PM 41 My husband has paracetamol capsules prescribed for arthiritis. he cannot tolerate other forms of paracetamol due to Crohns disease. This should be available on prescription 9/12/2018 1:01 PM 42 Chronic suffers 9/12/2018 1:01 PM 43 Apprentices- I don't earn minimum wage yet. I spend half my wage on prescriptions. I probably earn less than those on benefits and they get it for free 9/12/2018 12:57 PM 44 Low income, physical disability, mentally challenged 9/12/2018 12:49 PM 45 As above 9/12/2018 12:43 PM 46 Elderly 9/12/2018 12:32 PM 47 Mental institute 9/12/2018 11:58 AM 48 Chronic conditions and life threatening conditions 9/12/2018 11:36 AM 49 Children and pregnant women 9/12/2018 11:16 AM 50 Long term illnesses 9/12/2018 11:13 AM 51 Everyone 9/12/2018 10:52 AM 52 If medication not received regularly by GP 9/12/2018 10:46 AM 53 Chronic conditions where medication is needed for life 9/12/2018 10:43 AM 54 Benefits recipients 9/12/2018 10:30 AM 55 Diabetic and asthmatic 9/12/2018 10:21 AM 56 Elderly and maternity leave 9/12/2018 9:43 AM 57 Disabled 9/12/2018 9:31 AM 58 O.A.Ps and people on fixed/ reduced income 9/12/2018 9:27 AM 59 If it's cheaper 9/11/2018 4:22 PM 60 As above 9/11/2018 4:10 PM 61 Low income groups 9/11/2018 3:58 PM 62 For people on low incomes, OTC medications on a long term basis, struggle financially. 9/11/2018 3:50 PM 63 As above 9/11/2018 3:20 PM 64 Mental health 9/11/2018 3:12 PM 65 As above 9/11/2018 3:01 PM 66 As above 9/11/2018 2:57 PM 67 People with serious illnesses and elderly 9/11/2018 2:46 PM 68 People with long term conditions 9/11/2018 2:40 PM 69 People on very low incomes Carers 9/11/2018 2:31 PM 70 People without financial means to pay themselves 9/11/2018 2:02 PM 71 Cancer patients 9/11/2018 1:54 PM 72 Low income, elderly, students 9/11/2018 1:45 PM 73 Pregnant mums, low income, elderly 9/11/2018 1:34 PM 74 N/A 9/11/2018 1:05 PM 75 Lower income, vulnerable 9/11/2018 12:50 PM 76 The very elderly, with limited movement to go shopping. Cheap prescribed medication to be delivered 77 Old age 9/11/2018 12:37 PM 78 Need to be mindful of people taking medication they shouldn't- probably need more info available to help people 9/11/2018 12:35 PM 79 Perhaps people with a history of substance abuse and who could be vulnerable to having easier access 9/11/2018 11:51 AM 80 No 9/11/2018 11:46 AM

54
81 Elderly- low income Parents and children 9/11/2018 11:37 AM 82 No 9/11/2018 11:32 AM 83 Paracetamol should not be prescribed but instead be bought from a pharmacy. Encourage patients to buy from pharmacy instead of doctor prescribing 9/11/2018 11:10 AM 84 Elderly 9/11/2018 10:50 AM 85 No pensioners 9/11/2018 10:47 AM 86 As above 9/11/2018 10:39 AM 87 Unemployed 9/11/2018 10:37 AM 88 Perhaps some genetic conditions 9/11/2018 10:16 AM 89 As above 9/11/2018 10:12 AM 90 No 9/11/2018 10:02 AM 91 No 9/11/2018 9:58 AM 92 As above 9/11/2018 9:24 AM 93 The poor/ those claiming benefits 9/11/2018 9:20 AM 94 N/A 9/11/2018 9:18 AM 95 O.A.P 9/11/2018 8:43 AM 96 As above 9/11/2018 8:40 AM 97 No 9/10/2018 12:29 PM 98 Older people 9/10/2018 12:19 PM 99 PKU and & Diabetes and mental health groups. 9/10/2018 12:14 PM 100 One parent family 9/10/2018 12:07 PM 101 N/A 9/10/2018 12:02 PM 102 Elderly, those with transplant problems 9/10/2018 11:44 AM 103 Low income patients 9/10/2018 11:40 AM 104 No 9/10/2018 11:21 AM 105 lower income families 9/10/2018 10:51 AM 106 Those with Asthma, COPD, HIV/Aids 9/10/2018 10:43 AM 107 Under 16s because parents may not know what to give 9/10/2018 9:50 AM 108 as above 9/5/2018 8:30 PM 109 Perhaps those on low incomes and for children and the elderly and other vulnerable groups. 9/4/2018 11:53 AM 110 Low income groups 9/3/2018 7:03 PM 111 Repeat illnesses- I had tonsillitis 5 times a year and eventually they were constantly infected and were removed. If someone is just going to a pharmacy how will repeat illnesses be progressed. 9/3/2018 6:39 PM 112 N/a 9/3/2018 5:57 PM 113 Pensioners. Those with a terminal illness. Members of the Armed Forces who have served overseas. 9/3/2018 2:32 PM 114 No 9/3/2018 2:16 PM 115 End of life 9/1/2018 6:42 PM 116 Eczema sufferers 8/30/2018 4:36 PM 117 People on PIP and disability benefit 8/29/2018 2:13 PM 118 perhaps some flexibility for a bit of common sense 8/29/2018 1:40 PM 119 Those who are unable to afford them. Refugees.and homeless. Chronic disabled. 8/26/2018 3:57 PM 120 None. They are cheap enough to fund through pharamacy. NHS is struggling and funds are needed for Mental health services and others. 8/22/2018 10:18 AM 121 See answer to 11 8/20/2018 6:28 PM 122 Summer time - allergies 8/20/2018 3:10 PM

55
123 Those with long-term health conditions that are also on a low income and those who have an exemption certificate for items on prescription. 8/17/2018 5:35 PM 124 Pouchitis patients should be prescribed Vivomixx for reasons above 8/16/2018 6:39 PM 125 None 8/16/2018 9:51 AM 126 In my opinion this is a meaningless question - where would I go to get sufficient information to make an informed choice? 8/14/2018 10:17 PM 127 The elderly or those with long term health conditions 8/14/2018 2:27 PM 128 Unfortunately I believe that some of the patients who do really require these medications will not now attend the surgery and may suffer more as a result of leaving a serious condition until too late. 8/14/2018 9:01 AM 129 Vulnerable adults Patients with learning difficulties Elderly which are house bound 8/13/2018 9:53 PM 130 Old/vulnerable people - better to monitor medication and side effects. Vey low income- may struggle to with cost. 8/13/2018 11:10 AM 131 Those in SEVERE financial difficulties who cannot afford to smoke or drink alcohol. 8/10/2018 7:43 PM 132 severe allergies / hay fever - still needing strong antihistamines that are not available OTC 8/9/2018 6:07 PM 133 It should be assessed on a case by case basis 8/4/2018 11:38 AM 134 patients with physical disability 8/3/2018 3:10 PM 135 -Patients with a history of annual or more tonsilitus or indeed those who are carers. –Children with Down’s syndrome to be treated with antibiotics at a lower threshold for coughs /chest infection or more careful consideration/follow up. 8/3/2018 10:30 AM 136 As at 11 those in poverty those who are vulnerable whether though age mental health or disability who cannot make choices judgements without carer / adult support 8/2/2018 11:57 PM 137 people with long term health conditions 8/2/2018 4:20 PM 138 Those with dementia. 8/1/2018 2:00 PM 139 I have addressed this question earlier I the document 8/1/2018 8:30 AM 140 None at all. I believe that medications for short term self limiting conditions should definitely not be prescribed 7/31/2018 8:42 PM

56
Appendix G
G

57
13. FURTHER COMMENTS AND DATE AND TIME OF COMMENT 1 Pain relief for chronic conditions is needed immediately if pain severe 9/17/2018 1:45 PM 2 Specially prescribed drugs by the NHS for treatment only, all other medicines should be purchased and paid for by the patient 9/17/2018 1:44 PM 3 I think all medications I am supplied are essential 9/17/2018 1:42 PM 4 Originally the GP set me to a trainer at Enderby Gym. I have belonged to this gym over 10 years. Important for my for my arthiritis and limits medication that I need. It used to include a free cup of coffee for 10 weeks - the trainer introduced us to others in the café and we remained a supportive and encouraging group. Included 'Heart Smart'. This investment into prevention in the long run saved the NHS money.9/17/2018 1:37 PM 5 Leave time to see GP 9/17/2018 1:14 PM 6 Long term medication 9/17/2018 1:08 PM 7 Limited budget- cost more 9/17/2018 12:55 PM 8 I am struggling financially and buy a pre-payment certificate, otherwise I could not have all the prescriptions I need to stay well. When people are sitting in an office highly paid by the NHS they have no idea how the poorer people in society struggle. 9/17/2018 12:51 PM 9 Cuts not needed 9/17/2018 12:44 PM 10 It Wouldn't as I pay anyway 9/12/2018 4:27 PM 11 Lot of wastage in the NHS, especially at hospitals. Too top heavy in management and admin staff. 9/12/2018 4:15 PM 12 We are too dependant on prescribed medication, home remedies have worked for generations 9/12/2018 4:06 PM 13 Patients need to be assessed on a one to one basis due to their illnesses 9/12/2018 4:02 PM 14 I take paracetamol as one of my main painkillers for arthritis and wonder If I would be able to buy more than the very limited numbers at present 9/12/2018 3:31 PM 15 Sine I have EDS,CFS, ME and POTS I need the medication/skincare creams to manage my conditions which are long term 9/12/2018 3:18 PM 16 As this stage it will not effect me as I buy Ibuprofin over the counter 9/12/2018 3:07 PM 17 Savings from not prescribing these items is fair. a small charge e.g. 20p per each item ordered on any prescriptions by anyone. 9/12/2018 2:36 PM 18 They won't effect me 9/12/2018 2:35 PM 19 I don't think it will affect me 9/12/2018 1:50 PM 20 If the cost of the pharmacy drugs. Escalate because of the new policies there should be a limit to how much individuals should be expected to spend at a time or over the course of an illness 9/12/2018 1:47 PM 21 A saving of £4 I may be dwarfed by the cost of any measures designed to reduce cost of the items 9/12/2018 1:31 PM 22 My daughter who has been home bound for almost 10 years nees to manage her condition and many of the products affected help her to do this 9/12/2018 1:21 PM 23 It's broadly a good thing 9/12/2018 12:58 PM 24 Changes will not affect me greatly as I would always try to self medicate a self limiting condition before coming to see a GP 9/12/2018 12:43 PM 25 I agree that certain medications should not be available on prescription why it can be brought from a shop for £0.16 9/12/2018 11:42 AM 26 Would have to be flexible 9/12/2018 11:36 AM

58
27 I have fibromyalgia and spondylitis so to stop prescribed painkillers is ludicrous 9/12/2018 10:52 AM 28 No 9/12/2018 10:46 AM 29 I am retired but as yet do not receive state pension so paying for medication would affect me and others in the same situation. 9/12/2018 9:37 AM 30 Do not foresee any changes that will impact me 9/11/2018 4:22 PM 31 I think this is a blanket approach without care or consideration for those who are likely to be affected 9/11/2018 3:50 PM 32 I will not be affected personally but my mother will struggle with change 9/11/2018 3:20 PM 33 People could self medicate when not realising they could have other medical problems 9/11/2018 2:40 PM 34 Hardly at all at present 9/11/2018 2:31 PM 35 None 9/11/2018 1:05 PM 36 It would be a lot more convenient for me to be able to purchase my repeat prescriptions over the counter 9/11/2018 12:56 PM 37 No change 9/11/2018 12:44 PM 38 N/a 9/11/2018 12:37 PM 39 I pay for my Rx. I would rather buy directly from the pharmacy if I could, instead of paying £8.80 prescription charge. OTC would in most cases be cheaper. 9/11/2018 11:10 AM 40 N/a 9/11/2018 10:12 AM 41 No 9/11/2018 9:58 AM 42 Unsure 9/11/2018 8:57 AM 43 Good thing, enhance the NHS service 9/11/2018 8:43 AM 44 No 9/10/2018 11:34 AM 45 I worry that I might not be prescribed antibiotics should a cough lead to a chest infection. 9/10/2018 10:43 AM 46 I am just becoming stable and my meds and if changes are made I will become ill. I also have MS so need what I have to have com fort. 9/10/2018 9:50 AM 47 It is long overdue, the NHS has too long been a cash cow! 9/10/2018 9:41 AM 48 I hope this is a UK wide policy. If this only affects LEICESTERSHIRE then I’d be against it, as this would be unfair. If this is UK wide then I approve of the policy. 9/9/2018 2:49 PM 49 See reply to Qn 10. Will I have to buy these in future? 9/7/2018 3:44 PM 50 I have first hand knowledge of people receiving off the shelve items such as cosmetic style creams and give them to members of their family which is blatent abuse of the NHS and all it stands for and questions should be asked of the GP's perscribing these types of items 9/5/2018 10:33 AM 51 I do not understand why our gps point blank refuse to accept or acknowledge complimentary treatments. In this day and age in the U.K. This I find unacceptable. People should be empowered to take more responsibility for their own health and wellbeing by raising awareness. There is so much out there but no partnership working. Personally, I have seen and experienced a huge lack of partnership working from my own gp with not only the pharmacy where I get my repeat prescriptions from but also but hospital gp just doesn't want to know and work in silo at the detriment of my health. 9/4/2018 11:53 AM 52 I am happy to pay as long as I can get my medication. 9/3/2018 6:39 PM 53 The main thing is consistency - my experience is that, depending on which doctor or nurse you speak to, you get different answers, and then you don;t know what is

59
actually a policy decision and what is just the view of that individual 9/1/2018 6:42 PM 54 won't affect me 8/30/2018 4:36 PM 55 The fact that if you are not able to work due to ill health and that every penny counts. It is not great to hear that such measures are being put in place when even with exemptions these changes will still be put through. Its the same as always marginalise the poorest of society. If the changes go ahead and I am not able to afford medications that I need to take on a regular basis it will leave me questioning where I will get the money from next to pay for these extra costs that have are now coming my way. 8/29/2018 2:13 PM 56 Vivomixx is approved under the ACBS regulations for use in pouchitis patients 8/16/2018 6:39 PM 57 All my prescriptions are for longstanding conditions, I wouldn’t expect any of them to become non prescribed. 8/16/2018 1:10 PM 58 They won't affect me and they shouldn't affect most other people - I don't think the NHS was established to provide free cough medicine or painkillers. 8/14/2018 10:17 PM 59 It is an excellent idea to make some medication only available over the counter. Too much appears to be “given away” and this may make people think twice before seeking GP advice for unnecessary complaints. 8/14/2018 8:50 PM 60 n/a 8/14/2018 2:27 PM 61 This scheme is a win win for gp dispensing practises , it will free up time to dispense necessary medication. My answer to question 7 is the fact that I work at a gp practice and would speak to one of my colleagues. 8/14/2018 9:01 AM 62 I have a medical exemption but I'm happy to buy medication available over the counter from my pharmacy. 8/13/2018 11:10 AM 63 It might cost me a little more, but save the NHS time and money to spend on people who have life-threatening illnesses or who require expensive investigations such as MRI scans. 8/10/2018 7:43 PM 64 I hope very much the eye drops and ointment will not be taken off of my prescription as they are expensive items every month now I am retired. 8/10/2018 2:39 PM 65 N/A 8/4/2018 11:38 AM 66 sensible move 8/3/2018 3:10 PM 67 I think there are a lot of positive changes, but I do have concerns. 8/3/2018 10:30 AM 68 I care for someone with dementia. He could not manage his own over the counter medicines if I was not here. 8/1/2018 2:00 PM 69 please don't rush this through, this will be life changing for some patients so all the medications, conditions they are prescribed for as well as illnesses that hunt in packs (often go together) should be considered before introducing a blanket ban on the prescription of medications. 8/1/2018 8:30 AM 70 As mentioned before the only problem I have is being prevented from purchasing two packets of 16 paracetamol in the same transaction as buying Calpol for a child. It’s ridiculous and very inconvenient 7/31/2018 8:42 PM

C2

Blank Page

Report S. Venables 1
Over the counter medicines including Vitamin D and infant formula
Survey Report
1. INTRODUCTION
1.1 This report outlines the findings of research undertaken between the Monday 17 July and
Wednesday 9 August 2017 to understand the impact of any changes on people in relation to:
• The prescribing of medications available to buy over the counter for minor ailments • The prescribing of Vitamin D and Vitamin D3 • The prescribing of Infant Formula excluding specialised products
1.2 Detailed analysis and evaluation of the data of the quantitative and qualitative insights has
been undertaken and this report outlines insights and emerging themes highlighted by people who completed the survey.
2. BACKGROUND 2.1 West Leicestershire Clinical Commissioning Group (CCG) wants to understand how people
would be affected if they had to buy certain over the counter medicines, instead of requesting a prescription for some minor conditions. These include minor conditions like headaches, indigestion, head lice, travel sickness, athlete’s foot, diarrhoea, insect bites and stings and hay fever, which many people already do purchase without prescription. It also includes Vitamin D supplements. The CCG also wants to understand the impact on relevant people if they were asked to buy specialised infant formula which can be prescribed for babies with reflux or lactose intolerance instead of it being supplied on prescription. This does not apply to specialised products for infants with cows’ milk protein allergy which is very expensive and not readily available in supermarkets.
2.2 Using an online survey promoted across West Leicestershire the CCG asked a number of
questions to gain quantitative and qualitative insights. 2.3 We captured data and insights from:
• 269 people with regard to medications available to buy over the counter and Vitamin D supplements
• 23 people with regard to Infant Formula

Report S. Venables 2
3. ANALYSIS: WORK UNDERTAKEN 3.1 A detailed analysis and evaluation of the quantitative and qualitative data has been
undertaken. This work will enable the CCG to make an evidenced based decision on prescribing over the counter medicines, vitamin D and infant formula, which were the subject of this research.
3.2 This report outlines the key quantitative data and outlines the key themes from the
qualitative insights. 3.3 The quantitative and qualitative data is anonymised so that individuals and organisations
cannot be identified. Appendix 1 is an analysis of profile information including equality and diversity insights.
4. QUANTATIVE DATA ON THE PRESCRIBING OF MEDICATION AVAILABLE TO BUY OVER THE
COUNTER 4.1 269 people responded to the survey
4.2 197 people stated that they were eligible for a free prescription, 71 stated they were not eligible and 1 person was unsure
4.3 We asked if people had dependents and 80 said yes and 189 said no they had no dependents.

Report S. Venables 3
4.4 We asked if one or more dependents had been prescribed the following medicines by their GP:

Report S. Venables 4
4.5 We asked how willing on a scale of 1-5 they would be to purchases medicines over the counter rather than request them on prescription for the treatment of minor ailments. 153 said they were very willing and 27 not willing at all. However, the analysis of the qualitative insights does highlight some provisos that some people make when stating they are very willing to buy over the counter medicines for minor ailments, which are discussed in section 5.
5. KEY EMERGING THEMES – OVER THE COUNTY MEDICINES (QUALITATIVE DATA) 5.1 A number of themes emerge from the detailed insights gathered through the survey. Our
analysis and evaluation has grouped the insights into emerging themes and sub themes which are outlined below, with some examples of the verbatim comments which illustrate the theme:
GP appointments
1. Some people find it hard to get an appointment with their GP and therefore use their pharmacists to avoid waiting for an appointment and because they find it quicker and easier.
“Firstly it’s too difficult to even get an appointment with my GP, so I just go to
the pharmacy. Makes more sense, but also this is bad because if I actually need to see the GP for something and need prescribed medication, I can’t even do
that.”
Routinely buy over the counter medicines
2. Buying over the counter medicines is an automatic thing for many people and they have never gone to their GP for minor ailments.

Report S. Venables 5
“I already do this. I only request medication on prescription that I cannot get without a prescription.”
GP provides reassurance service
3. For some people buying over the counter medicines might be automatic but
they do feel that it is important to see your GP for ongoing or long term issues.
“If it is something minor, that will go away quickly, then I don’t see the point in bothering a doctor for these things in the first place, let along the cost of getting
tablets on prescription that are easy to obtain from a chemist (and can be cheaper from a chemist if you only need a small quantity.) If something is an ongoing/long-term issue then I think it should be looked at by a doctor and
covered by prescriptions.”
4. Many people are worried about the effect of mixing over counter medicines
without GP advice, with long-term medicines they are taking.
“Some ‘minor’ ailments can be side-effects of my long-term medications required for a serious chronic illness. It is important that my GP is aware of these issues
and can advise on possible help in view of all my health problems.”
5. Many people feel that they want a diagnosis and explanation prior to taking any medicines.
“Because I want diagnosis and explanation first so that I know what is happening
to my body. Not just the special ailment. There is no pattern to follow back if I go directly to the pharmacy.”
6. People say they value reassurance from their GP about their medicine and
would want that reassurance from their pharmacist
“Sometimes all you need is advice from the doctor about what treatment would be best, paying over the counter is fine, as long as you are reassured it’s the
best course of treatment.” Quantity and quality
7. Some people perceive that the strength of the medicines they require mean that
over the counter medicines are not an option, or perceive they are not as effective as those prescribed. Some need to buy in larger quantities.
“If I am not sure what would be appropriate e.g. I had an eye infection and
accepted a prescription from the doctor for this as I felt it would be preferable rather than purchase something over the counter from a pharmacy because it
was more likely to be stronger.”
Report S. Venables 6
“I would want to know that the medicines available over the counter are as effective as those that are prescribed.”
“I do buy paracetamol and ibuprofen over the counter, but would prefer to buy in
larger quantities.”
Using NHS resources appropriately
8. Many people feel that it is important that NHS resources are used to treat more serious conditions rather than on over the counter medicines. Many also state that they have a good understanding of the constraints of the NHS and wish to see them appropriately used.
“It makes sense, takes away a drain on the NHS – prescriptions are not free, they
are costly and paid for from another source. The funds could be used for innovative projects or just plain health care.”
Route to privatisation 9. Some people feel that this survey and likely outcome is a move to privatise the
NHS by the back door.
“I do not agree in any way to pay at supermarkets or anywhere else you are trying to privatise by the back door.”
Finance and affordability
10. Some people have prepayment certificates and feel unwilling to pay for over the
counter medicines. Others use prepayment certificates to manage household expenditure including medicines.
“I pay for a prepayment certificate so I would be unwilling to have to pay
again. I can afford to buy many things from the pharmacy such as ibuprofen and vitamin D but that doesn’t make it right for everyone. If someone is entitled to free prescriptions it is because they can’t afford to pay so don’t make them pay at the chemist. I know that the CCG is trying to cut spending. You’ve already taken away my transport to hospital appointments. Don’t make other people suffer because of
your penny pinching.”
“Currently I have a prepayment certificate so all my medicines costs are fixed. My dependants are all eligible for free prescriptions o having to pay for
medicines would come out of our household budget.”
11. People feel that if you require the medicines for a longer period of time it makes it difficult financially to purchase over the counter.

Report S. Venables 7
“Managing on a state pension is difficult enough without having to pay for over the counter medicines which are needed for 6 months of every year.”
12. Some people feel that if you are eligible for a free prescription it is your
entitlement and others ways to save money should be found.
“We are eligible for free NHS prescription and we should be entitled to this locally. It is extremely unfair of the local CCG to make patients buy such items when the national NHS has no such restrictions or guidelines. Surely there are other ways of saving the NHS money by reducing unnecessary managers in the local CCG or perhaps capping manager pay at less than £35k. It is unnecessary
to have healthcare professionals such as doctors, pharmacists and nurses undertaking management roles. Healthcare professionals should be employed
within their professions helping people and management professionals should be employed in management roles. That would result in a more efficient local NHS
service and patients would receive a better service.”
13. Some people who are on a low income feel they would not be able to afford it.
“I do have to take a large amount of drugs for various illnesses so have to purchase some of these over the counter may make considerable impact on my
income (Pensions).
14. Some people feel that over the counter medicines are cheap.
“I do already, I feel my diabetic medication is free, and you can get paracetamol etc. so cheaply at certain supermarkets.”
Information, advice and guidance from community pharmacies 15. Some people recognise that it is beneficial to talk to your pharmacist to get
information, advice and guidance.
“If it is over the counter, maybe the pharmacist could be the person I talk to about it and not the GP. It’s easier to talk to a pharmacist than get a GP
appointment.”
“Pharmacists are highly qualified professionals and the range of ailments that they can treat is growing especially in the pharmacy only market. I would prefer
a pharmacy to a supermarket.”
Medicines waste 16. Some people feel that if you have purchased medicines you are less likely to
waste them.
“I think if you have to purchase your own medicines you are more likely not to waste them.”

Report S. Venables 8
17. Only one person mentioned a postcode lottery in prescribing.
Medicines that some surgeries prescribe through NHS are not prescribed by other surgeries. Why this ‘bar’ from one surgery to the other?”
My willingness to buy over the counter medicines is dependent on other factors
18. Some people state that their answer really depends on other factors e.g. cost,
affordability for themselves and for more vulnerable, the ailment and the time they have suffered from the condition, strength of medicines needed. “Depends on what the medical problem is. You can't always be certain that
your symptoms are from a "minor" ailment and sometimes need more advice/help.”
“Depends if the medicine is cheaper to get it over the counter or if the
amount can be doubled up to get it on prescription.”
“Willing if it was cheaper than the cost of a prescription and it was the correct strength.”
“I don’t mind the principle of doing it, but feel that, taken to extremes this could
represent quite a hefty extra financial commitment for some people who may already be vulnerable.”
“Unless a patient has an ongoing need for a regular prescription it is no
unreasonable to pay for cheap and simple remedies, many of which are a matter of personal choice rather than a medical necessity.”
“I generally buy generic over the counter medicines and multi-vitamin
supplements also paracetamol or ibuprofen as required. These are easily affordable on my state pension. The only medicines I require are a cough which becomes persistent over a 2 to 3 week period (usually antibiotics) otherwise over
the counter medicines suffice.”
“I am willing to do so where the treatment is appropriate for me the time to organise a prescription is easily off-set by the medication costs. Specifically for
me, a visit to the GP for a prescription has only been where OTC treatments failed to resolve the issues. I also appreciate that my level of education and also financial situation is somewhat different to many others and they would not be able to pay for OTC treatment for many minor ailments even if they do pay for
their prescriptions.”
6. QUANTATIVE DATA ON THE PRESCRIBING OF VITAMIN D 6.1 In addition to the list of minor ailments, the CCG wanted to understand the views of people
who get vitamin D (also known as colecalciferol or Cholecalceferol or Vitamin D3) on

Report S. Venables 9
prescription. We asked who was in receipt of prescription for Vitamin D or Calcium and Vitamin D. We also asked them if they had not been prescribed Vitamin D in any form. 33 people confirmed that they or their dependents had been prescribed Vitamin D; 19 confirmed that they or their dependents had been prescribed Calcium and Vitamin D and 220 had not been prescribed Vitamin D in any form. Therefore 220 had not been prescribed Vitamin D in any form. The answers given are therefore based on their opinions rather than their experiences.
6.2 We then asked who had been prescribed calcium with Vitamin D. 28 people answered yes.
6.3 We then asked the reason that Vitamin D had been prescribed. 6 people said it was to prevent Vitamin D deficiency reoccuring following treatment of severe deficiency. 6 said that it was to treat aches and pains, but not diagnosed as Vitamin D deficient. 16 said they were in a high risk group and 27 said it was to treat Vitamin D deficiency.

Report S. Venables 10
6.4 The high risk groups that people and their dependents fall into are:
• 1 – infants and young children under 5 years of age • 11 – people aged 65 years and over • 2 – people with darker skin • 5 – other broken to Osteoporosis and prevention of Osteoporosis, auto
immune disease, was on high dose of steriods and Lupus SLE
6.5 We asked if the following applied to people:
• Diagnosed with Osteoporosis – 17 people said yes • Diagnosed with malabsorption – 1 person said yes • Poor mobility – 12 people said yes • Taking oral steroids or anti-epileptics medication – 6 people said yes

Report S. Venables 11
• 17 people confirmed they were affect by any other the above
6.6 We asked how willing on a scale of 1-5 they would be to purchase low dose Vitamin D over the counter rather than request them on prescription. 162 said they were very willing and 33 not willing at all.
6.7 We then asked people to tell us if they had ever been given any diet or lifestyle advice by a health professional to help them to increase Vitamin D intake. 45 people said they had and 220 people said they hadn’t.

Report S. Venables 12
7. KEY EMERGING THEMES - VITAMIN D (QUALITATIVE DATA) 7.1 A number of themes emerge from the detailed insights gathered through the survey. Our
analysis and evaluation has grouped the insights into emerging theme which are outlined below, with some examples of the verbatim comments which illustrate the theme:
1. Many people were happy to purchase Vitamin D highlighting a number of different
reasons including getting the best use of NHS resources, it is cheaper, affordability and it cuts down on unnecessary GP appointments. They also felt it was quicker and easier to do so.
“Because I believe we should contribute more to the health service for treatments non-
serious or urgent conditions.”
“NHS should deal with matters that are urgent or with acute, long term illnesses. Vitamins, cough medicines, weak pain relief should not be funded by NHS.”
“Because I can afford this and I think that most people could. It would also cut down on
people making unnecessary appointments with their GP for repeat prescriptions etc., thereby freeing up GP time.”
“Cheaper than prescription charge – I pay for prescriptions.”
“Easy to do and cheap.”
2. Many people sight affordability as the reason why Vitamin D should be available on
prescription. Other people said they couldn’t afford to purchase. Others discussed variable cost in the market place.
“I can afford to, but a lot of people eligible for free prescriptions could not afford to buy
these over the counter.”
“Should take already and don’t bother, because I need it in such high does I couldn’t afford to.”
“I have been taking the prescription Vitamin D at 3000 units. When the three month
course finishes, I need to buy my own Vitamin D at 1000 units. Have looked around and a popular health food shop costs £13.99 for 30 days, which I certainly can’t afford, but

Report S. Venables 13
after ages looking for an affordable supply, I have found a small chemist that sells the equivalent strength at £1.50 for two months supply, which I can afford. So I would say it would depend on where you were, if there was an affordable supplier. Many cheap ones are available, but they appear to be extremely small dose ones, so in my case would not
be sufficient.” 3. Many people want to have reassurance from their GP prior to buying Vitamin D and
value medical supervision, if they are on other medicines.
“I have had Vitamin D in the past as the result of a blood test. I think it is important to find out properly if you are deficient, and I understand that there are different types of
Vitamin D and it would be correct to have the right one for you.”
“I try to eat a well-balanced diet and have never been advised to take Vitamin D supplements. However, if this were the case I would rather that it was under medical
supervision.” 4. Some people believe that diet and lifestyle changes negate the need for
supplements.
“No need for Vitamins to be prescribed as many deficiencies can be reduced by lifestyle and diet changes.”
“A well balanced diet and good lifestyle choices (plenty of fresh air, exercise, spending
time in day light) I would hope not to find myself in a position where I need to take Vitamin D supplement.”
5. Some people think that to have these medicines on prescription would save money
in the long term or prove more expensive not to provide them and lead to increases in A&E attendances. Others feel we should consider the link between Vitamin D and prevention of conditions. Others call for consideration of those with particular conditions e.g. MS and osteoporosis.
“Vitamin D deficiency is linked to a number of chronic diseases. I believe it is important for the NHS to treat vitamin D deficiency and insufficiency or symptoms linked to this
with appropriate vitamin D supplements. Prevention is always better than cure and by supplying vitamin D supplements funded by the NHS is likely to reduce the future health
care burden on the NHS through prevention of chronic conditions.”
“It depends so much on the individual circumstances, but if you withdrew these medications from very low paid patients they probably couldn’t afford them and then
you’ve got an A&E attendance on your hands and that’s far more costly.”
“Vitamin d deficiency is linked to a number of chronic diseases. I believe it is important for the NHS to treat vitamin d deficiency and insufficiency or symptoms linked to this
with appropriate vitamin d supplements. Prevention is always better than cure and by supplying vitamin d supplements funded by the NHS is likely to reduce the future health care burden on the NHS through prevention of chronic conditions. As per my previous

Report S. Venables 14
response it is better to spend NHS money on prevention of disease through vitamin D supplements than to pay high manager salaries in local NHS structures such as CCGs.
“I have the financial means to do so, and it saves me having to have a GP appointment.
Though please consider that Vitamin D is closely linked to conditions such as MS, and any barriers to individuals being able to access Vitamin D may lead to an increase in
symptoms.”
“I do currently buy my vitamin D over the counter but that's because I didn't realise I could get it on prescription. Having MS it is medically recommended that I take a sizable dose every day. Athough I am not completely housebound yet, (it is predicted that it will happen in less than a year) due to my condition I am forced to spend most of my time at home. So perhaps you need to rethink who gets a prescription. Needing regular intake of
a drug that you describe as for "minor ailments" may seem frivolous to you but is actually a medical necessity to some, especially those of us with chronic conditions.”
“I have osteoporosis as a consequence of long-term drug therapy. My bone density must
not deteriorate further.”
“I get free prescriptions and I require it for the long term - was prescribed by my haematologist and by staying on my repeat prescription, my GP can see what I'm taking
whereas it would be overlooked if I was buying it and wasn't listed as an active prescription on my medical notes.”
6. Many people automatically buy Vitamins over the counter. Many people didn’t
realise they could get them on prescription; others said that they were told by their practice they weren’t available on prescription.
“I already buy Vitamin D as an OTC medicine.”
“My surgery does not prescribe Vitamin D, told to get it over the counter”
“I do currently buy my Vitamin D over the counter but that's because I didn't realise I
could get it on prescription.”
7. Some people feel they pay their taxes to get this service.
“We pay taxes to get this service. NHS needs to find more efficient ways of operating or reduce NI. My outgoings are more than income, even at earning £20k. So I am unable
then to pay for medicines.”
8. People have differing views as to whether they perceive Vitamin D as a medical necessity or a supplement.
“Personally I am happy, but if considered a medical necessity then it is appropriate
that the NHS provide such medication. They should also be a low cost to the NHS under these circumstance, and be provided free might well increase compliance in taking them.

Report S. Venables 15
Patients paying for prescriptions will already be discouraged from using the NHS route if informed by the pharmacist or their doctor that they can be bought at a lower price.”
“This is a supplement and doesn't need monitoring by a GP.”
“Because it is a dietary supplement not a condition that has occurred.”
“Although diagnosed by GP as having a vitamin level of 17, I had to purchase my
own Vitamin D and was given a leaflet by GP to choose which brand I decided to buy. I think vitamin D should be available on prescription for those who have been diagnosed as needing
a supplement.”
9. Some people would benefit from advice and guidance on supplements.
“How do you know what strength the item would be that people buy? Also if that person was then receiving the set amounts. I suppose if a GP told you which brand, or if
obtaining it from a pharmacy, set items of drugs could be bought . But most may pick items that are most likely to be multi vitamins and think they are ok doing this. Some may not even bother with additives like this? I believe some sort of brand, would have to be specified, if it
was important to certain people.”
8. QUANTATIVE DATA ON THE PRESCRIBING OF INFANT FORMULA 8.1 The CCG wanted to understand, in situations where it is necessary to use specialised infant
formulas, how any change to prescribing would impact on them. We clarified that any change was not applicable to specialised products for infants with cows’ milk protein allergy.
8.2 As the target audience for this survey was ‘niche’ we created a separate survey that was
marketed to appropriate target audiences through partner organisations. 8.3 Response rates to the survey are low with only 24 people completing it and only 3 people
stating they are drawing from personal experience. Therefore the CCG does need to consider if the engagement does give use sufficient insights into the impact on people, that allows us to make a decision or if further work needs to be undertaken to reach out to this very niche group.
8.4 Only 1 person out of 24 completing the survey was a parent or guardian of a child who has
been prescribed a specialised infant formula for lactose intollerance.

Report S. Venables 16
8.5 We asked how old the child was. 1 was less than 3 month, 1 was 3 – 6 months and the other was 1 – 2 year. In addition we asked how old the child was when they stopped. 1 was 6 – 12 months, 1 was 1 – 2 year and the third was 2 – 3 years.
8.6 We asked for the name of the formula:
8.7 We asked how on a scale of 1-5 it would affect people if they were asked to purchase specialised infant formula. 2 people said they would be affected a lot, 3 mid-range and 17 would be affected a little
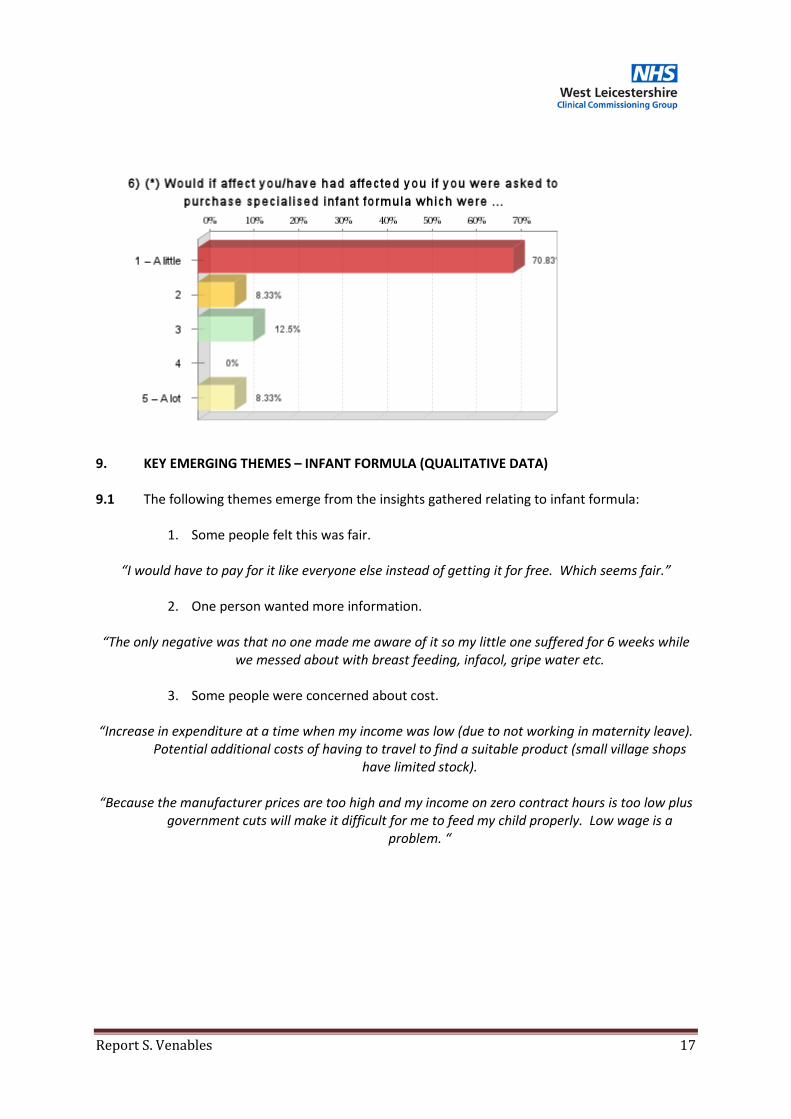
Report S. Venables 17
9. KEY EMERGING THEMES – INFANT FORMULA (QUALITATIVE DATA) 9.1 The following themes emerge from the insights gathered relating to infant formula:
1. Some people felt this was fair.
“I would have to pay for it like everyone else instead of getting it for free. Which seems fair.”
2. One person wanted more information. “The only negative was that no one made me aware of it so my little one suffered for 6 weeks while
we messed about with breast feeding, infacol, gripe water etc.
3. Some people were concerned about cost. “Increase in expenditure at a time when my income was low (due to not working in maternity leave).
Potential additional costs of having to travel to find a suitable product (small village shops have limited stock).
“Because the manufacturer prices are too high and my income on zero contract hours is too low plus
government cuts will make it difficult for me to feed my child properly. Low wage is a problem. “

Report S. Venables 18
Appendix 1 Profiles – Over the counter medicines and Vitamin D Postcodes LE2 X 3 LE3 X 10 LE4 X 3 LE5 X 2 LE6 X 9 LE7 X 11 LE8 X- 1 LE9 X 30 LE10 X 22 LE11 X 61 LE12 X 52 LE18 X 1 LE19 X 1 LE65 X 13 LE67 X 47 CV13 X 5 DE74 X 7 NG13 X 1 DE12 X 2

Report S. Venables 19

Report S. Venables 20

Report S. Venables 21

Report S. Venables 22

Report S. Venables 23

Report S. Venables 24
Profiles – Infant formula Postcodes LE3 X 1 LE4 X 1 LE6 X 2 LE7 X 3 LE9 X 1 LE10 X 3 LE11 X 5 LE12 X 1 LE67 X 2 DE12 X 1 De74 X 2

Report S. Venables 25

Report S. Venables 26

Report S. Venables 27

Report S. Venables 28

Report S. Venables 29

Report S. Venables 30

Your NHS partner for improving health and integrating care
West Leicestershire CCG –
Phase 2 - Prescribing of
OTC medicines for minor
ailments Survey
Patient Survey September 2018

NHS Midlands & Lancashire Commissioning Support Unit 2
Introduction West Leicestershire Clinical Commissioning Group (CCG) engaged with patients to understand the impact it would have, if they were asked to buy certain medicines for some minor ailments instead of requesting a prescription from their GP. An online survey was created which ran from Monday 30th July 2018 and closed on Sunday 9th September 2018 and was disseminated via the online survey platform Elesurvey. Overall 26 responses were received to this survey. The main findings and themes have been summarised in this report. A full analysis of all results is available in the raw data report, which accompanies this highlight report.
Background In the 12 months up to June 2017, the NHS spent approximately £569 million on prescriptions for medicines, which could otherwise be purchased over the counter (OTC), from a pharmacy and/or outlets such supermarkets. These prescriptions include items for:
• self-limiting conditions (i.e. those that do not need treatment) • conditions that will heal or be cured of their own accord • conditions which lend themselves to self-care
These prescriptions can also include other common items including:
• medicines that can be purchased over the counter, sometimes at a lower cost than that which would be incurred by the NHS
• medicines for which there is little evidence of clinical effectiveness By reducing spend on treating conditions that are self-limiting or which lend themselves to self-care, or on items for which there is little evidence of clinical effectiveness, these resources can be used for other higher priority areas that have a greater impact for patients, support improvements in services and or deliver transformation that will ensure the long-term sustainability of the NHS. NHS England’s consultation NHS England undertook a 12-week public consultation between December 2017 and 14 March 2018. As a result of this work, NHS England and NHS Clinical Commissioners (NHSCC) developed restrictions based on type and severity of condition rather than products. Feedback from this consultation showed that there was general support (65% agreed with NHS England’s criteria to assess items for potential restrictions). CCGs were asked to carry out local engagement in taking forward the implementation of the recommendations of the NHSE report. In West Leicestershire this engagement was limited to those ailments not covered by previous engagements carried out last year. In Leicester City and East Leicestershire and Rutland CCGs engagement covered all ailments covered in the NHSE review.

NHS Midlands & Lancashire Commissioning Support Unit 3
Main findings and themes 1. Most people are willing to pay for OTC medications for minor ailments
1.1 A majority of respondents to this survey (<62%) said that they would be ‘very willing’ or ‘willing’ to pay for OTC medication for minor ailments. This compares to a national response rate of 65%, during NHS England’s public consultation and suggests the majority of people support the policy of paying for OTC medications for minor ailments.
1.2 Although 19 respondents (73%) to this survey are eligible for free prescriptions, only 5 (20%) said that they would be unwilling to pay for prescriptions for minor ailments. As above, this is extremely positive and suggests that the respondents to this survey were generally very supportive of the proposed changes.
1.3 5 respondents (19%) appeared undecided as to whether they would be either ‘willing’ or ‘unwilling’ to pay for medications for minor ailments OTC.
Point to note: Further awareness raising among this ‘undecided’ group may be needed to explain why these changes are happening (in other words, further promotion and awareness raising may migrate this ‘undecided’ group of people into the ‘willing’ or ‘very willing’ categories).
2. Some remain unsure as to what a ‘minor ailment’ is, and what is exempt 2.1 One comment in particular highlights that some people may not understand what conditions will
be affected by the proposed changes, or what the definition of a minor ailment is:
“My IBS condition is life limiting. If I did not have the medications prescribed to me it would be even
worse - I would be unable to leave the house…I do not feel my condition is "minor."
Point to note: Further education / awareness raising may be needed in order to clarify exactly which conditions will be affected by the change (i.e. what is classed as a ‘minor ailment’). The above quote reveals some confusion as to whether potentially long-term conditions such as IBS will be affected.
Further education/awareness raising to reassure patients who will not be affected by the proposed changes (i.e. those with LTCs) may be needed, as well as helping people with ‘minor ailments’ to understand the reasons for the proposed change.
3. Majority of people agree with/support the reasons behind the proposed change
3.1 Over half (55%) of those who said they are willing to purchase OTC medicines for minor ailments cited expense to the NHS as a chief reason. This is a positive response and suggests a significant number of respondents understand – and agree with – why the current changes are necessary.
Point to note: Further education and awareness raising around the reasons behind the proposed changes (cost to the NHS, importance of self-care etc.) may persuade more people to be supportive. This is especially so given that one in five appeared undecided as to whether they would be willing to pay for OTC medications for minor ailments (see 1.3 above).
3.2 One comment revealed that there are fears that the proposed changes could adversely affect low income families, which is something that further messaging could potentially address:

NHS Midlands & Lancashire Commissioning Support Unit 4
“I am concerned about the impact on low income families and individuals. Surely a lot of the prescribed list is a side effect of poverty in the first place?”
3.3 Another comment revealed that, for people who perceive themselves as ‘hard working, tax-
paying families’ who use NHS resources relatively infrequently, there may be an expectation that, when they do require NHS expertise or resource, that it is free at the point of need, in every case:
“My family & I have rarely used the NHS…however when…we…rely on the NHS due to unforeseen circumstances…I feel we should not have to pay for prescriptions…My spouse & I both
work full time & have done so since graduating (as well as pay taxes) - we both feel that we don't abuse a system like the NHS, but when we require its use, it should be free as that is what is was built for”
4. Other trends to note
4.1 The vast majority of respondents to this survey were white British (96%) and over 55 (73%). This should be borne in mind when considering the effect of the proposed changes on more diverse populations.
4.3 6 respondents (23%) have a long-term illness. Further analysis could usefully look at how this group answered Q7 (…how willing would you be to purchase medicines over the counter from
a pharmacy or supermarket rather than request a prescription for the treatment or a minor
ailment?)
4.2 Other comments to note centred on the issue of NHS expertise and ‘getting the right advice’. Even for those prepared to pay for OTC medicines, many still want access to GP/Pharmacy reassurance to ensure they are buying the most effective option:
“Aware of costs to surgery. Willing to buy but just need advice to ensure making informed choice”.

Get to know us or get in touch
mlcsu
Midlands and Lancashire Commissioning Support Unit
midlandsandlancashirecsu.nhs.uk

C3

Blank Page

Prescribing Medicine for Minor Illnesses and Ailments and the Pharmacy First Minor Ailments Scheme Patient and public engagement report 30th July – 9th September 2018

Background In the year prior to June 2017, the NHS spent approximately £569million on prescriptions for medicines, which could otherwise be purchased over the counter (OTC), from a pharmacy and/or outlets such as petrol stations or supermarkets. These prescriptions include items for a condition:
• That is considered to be self-limiting and so does not need treatment as it will heal or be cured of its own accord;
• Which lends itself to self-care
These prescriptions can also include other common items:
• That can be purchased over the counter, sometimes at a lower cost than that which would be incurred by the NHS
• For which there is little evidence of clinical effectiveness By reducing spend on treating conditions that are self-limiting or which lend themselves to self-care, or on items for which there is little evidence of clinical effectiveness, these resources can be used for other higher priority areas that have a greater impact for patients, support improvements in services and or deliver transformation that will ensure the long-term sustainability of the NHS. NHS England undertook a 12-week public consultation between December 2017 and 14 March 2018. As a result of this work, NHSE and NHSCC (NHS Clinical Commissioners) developed restrictions based on type and severity of condition rather than products. Feedback from this consultation showed that there was general support (65% agreed with NHSE’s criteria to assess items for potential restriction). Leicester City CCG no longer routinely prescribes paracetamol as well as some gluten-free products, following engagement with patients. The move for paracetamol to stop being routinely prescribed was supported by the majority of people that the CCG engaged with although there was a level of concern amongst some patients with more serious or longer-term conditions. Methodology Leicester City CGG undertook a six-week engagement exercise to gather public opinion on the two proposals. The feedback would help to:
• Educate people about the rationale behind why items will not routinely be prescribed/ summarise the findings of the NHSE consultation
• Listen to any concerns and prepare our patients for the changes so that they’re not impacted when they visit their practice/pharmacy
• Allow the CCG to determine whether people are generally in support of the proposals, so that appropriate communication and mitigation can be put in place before rolling out the initiative

• Achieve behavior change in patients by encouraging them to self-care • Understand the impact on patients, pharmacies and GP practice staff if we
took the decision to stop the Pharmacy First Minor Ailments Scheme The engagement focused on an online survey which was available on the CCG’s website. It was promoted via GP practice websites, at GP practices, pharmacies and in the local media. Printed hard copies were available on request. Additionally, the CCG engaged face-to-face with patients at local GP practices and Pharmacies across Leicester City. This was initially focused on areas where there is high demand for the Pharmacy First Minor Ailments Scheme, before being rolled across the city. This enabled staff to encourage responses and talk to patients directly about the changes. Pharmacies with high usage of the Minor Ailments Scheme 1. 7-11 Pharmacy, Berners St 2. Health Serve Pharmacy,4 Egginton St 3. Health Serve Pharmacy, St Peters Shopping Centre, Melbourne Rd 4. Medicare Pharmacy Ltd, 140 St Saviours Rd 5. Parkview Leicester Ltd, 276 East Park Road 6. Pearl Chemists,185-187 Evington Rd 7. Yakub Chemist Ltd, 67 Hartington Rd 8. Parkem Chemists Ltd, 102 Dominion Rd 9. Moin's Chemist (M.N. Kolia Ltd T/A) , 137a East Park Rd Neighbouring GP Practices
• Community Health Centre (Melbourne Rd) • Spinney Hill Medical Centre • Melbourne St Surgery • East Park Medical Centre • Sayeed Medical Centre • Shefa Medical Practice • Evington Medical Centre • Al-Waqas Medical Centre • Oakmeadow Surgery
The following communication vehicles were employed to promote the engagement:
• Press release for media • Proactive and reactive media interviews • A simple, 1-sided informative sheet with relevant info and box to be completed
by the GP and handed to the patient • Email to stakeholders • Email to seldom heard groups with e-toolkit and hard copy survey • Graphics for GP practice screens • Web story • Leaflets • Posters • Social media content covering the 6 weeks

• Face-to-face briefings with identified vulnerable groups on request Dependent on reception of the initiative, a flexible approach would enable the CCG to react accordingly, in addition to the above proactive communications. Summary of survey responses During the six week engagement period we visited 9 GP practices and 24 pharmacies across the city. We received 185 completed surveys. 17 were completed online, 4 through the post and 164 during visits to GP practices. Below is a summary of the findings (if you would like to see a copy of the full responses please email [email protected] or telephone 0116 295 1116). Q1. In the last 12 months, have you received medication prescribed by your GP practice for any of the following conditions (please tick all that apply): 11 Conjunctivitis 1 Mild Cystitis 2 Cradle Cap – infants 10 Mild Dry Skin/Sunburn 4 Dandruff 10 Mild to Moderate Hay fever/Allergic Rhinitis 8 Diarrhoea (Adults) 0 Minor burns and scalds 18 Dry Eyes/Sore tired Eyes 8 Mouth ulcers 7 Earwax 5 Nappy Rash 0 Excessive sweating 3 Oral Thrush 4 Haemorrhoids 1 Prevention of dental caries 2 Head Lice 3 Ringworm/Athletes foot 15 Indigestion and Heartburn 15 Sleep problems 9 Infrequent Constipation 2 Sun Protection 8 Infrequent Migraine 3 Teething/Mild toothache 6 Insect bites and stings 2 Threadworms 7 Irritable bowel syndrome 6 Travel Sickness 2 Mild Acne 3 Warts and Verrucae 4 Mild contact dermatitis The three highlighted conditions were the most popular choices selected by participants. Q2. Did you know that you can buy medication for the above conditions without a prescription? The majority of participants were aware that the medication for the aforementioned conditions could be purchased without a prescription with 143 answering “yes” and 36 answering “no”. Q3. Do you pay for your prescriptions?

81 participants stated that they pay for their prescriptions per item or with a pre-payment certificate. This is 45% of the total number who completed the survey. 100 participants advised that they received free prescriptions. Q4. Some over the counter medication (for example; lotion for mild dry skin conditions, eye drops, painkillers and indigestion remedies) are available for you to buy at a considerably reduced cost, in comparison to what it would cost the NHS. Would you be happy paying for over the counter medication to treat short-term illnesses and conditions? 130 out of 182 (71%) participants stated that they would be happy paying for over the counter medication to treat short-term illnesses and conditions. Please provide any further comments: The following comments and themes were identified:
• Participants often already have these self-care medications at home • It is not always necessary to visit a GP for these conditions • Some medications are cheap to buy over the counter • Asking patients to pay for over the counter medication to treat short term
illnesses encourages self-care awareness A number of areas of caution were identified, some of which include:
• Families on low income may not be able to afford over the counter medication • Unable to get appropriate dosage without a prescription (i.e. buying multiple
boxes or higher strengths) • Some of the medications listed are quite expensive • Dry eyes are not always self-limiting • Correct diagnosis is important • Some ailments are caused by other conditions that patients may have
“People need advice and a diagnosis as many do not recognise or misdiagnose their conditions. Advice needs to be provided. As long as medication is cheap then most people will be able to afford it. Some, however, will not. This is a concern. What provision is being made for those who really cannot afford it?” (Female, aged 60 – 75)
Q5. Did you know a self-limiting condition is a condition which will clear up on its own without the need for medication?
130 out of 181 participants (72%) stated that they knew what a self-limiting condition is.
Q6. Do you agree that medication for self-limiting conditions should not be prescribed by your GP practice? 120 out of 178 participants (67%) agreed that medication for self-limiting conditions should not be prescribed by your GP practice.

Please provide any further comments: The following comments and themes were identified:
• Caution should be taken when patients are diagnosing and selecting medication without the direction of a GP
• Batteries for hearing aids should be included • It is easier to visit the chemist than get an appointment with a GP • Patients should take ownership on self-care
A number of areas of caution were identified, some of which included:
• Caution should be taken when considering patients with long term health issues
• Participants questioned what if the condition in question is not self-limiting or serious
• The conditions listed are not all self-limiting • Children should be considered with more caution • Dry eye syndrome could be serious • Symptoms of these conditions can be distressing • Some self-limiting conditions can repeatedly occur • The effectiveness of over the counter medicines compared to prescription
medicines should be considered • Patients are open to misdiagnosis without prescription
“I agree with this in principle, however I have suffered from a dreadful throat infection in the past as a result of the GP waiting another week to 'see if it clears up on its own', even though I was already off work because of it. It could have been caught early but I ended up suffering for a month in total (including a week with no voice) waiting for the antibiotics to kick in. However, common sense has to work both ways; patients taking responsibility for their own health and GPs realising when someone who never comes to the GP has already waited long enough before booking an appointment to see if it will 'self-limit'. Currently I don't trust them to make this distinction.” (Male, aged 25 – 34) Q7. If you were suffering from a self-limiting condition or minor illness, where would you go for more information in the first instance? 91 Pharmacy 55 GP Surgery 28 NHS Website 5 Dial NHS 111 17 Other: Google, NHS 111, Optician A total of 91 participants (51%) stated that they would visit a pharmacy for more information on a self-limiting condition or minor illnesses. The second most popular choice was GP surgery (31%).

Q8. If you are aware of any groups of people who may be affected by this change more than others, please tell us which groups below: A number of groups were identified, some of which include:
• People whose first language isn’t English • People on benefits / unemployed • Elderly / Pensioners • Refugees / Asylum seekers • People with learning disabilities and limited communication skills • People with long term conditions • Children • People on low incomes / can’t afford medication • Homeless • Single parents • Students • Black and Asian minority • Dementia patients • Vulnerable people
“Those people who are not able to understand what is self limiting or those who are confused and vulnerable” (Female, aged 60 -75) “Disabled people (all categories), especially those receiving DLA/PIP or other benefits. The Elderly, especially people over 65 with long-term chronic conditions and disabilities due to conditions like rheumatoid arthritis, osteoarthritis etc. Children of low-income families.” (Male, aged 60 – 75) “None English speaking/limited English who may not understand what is available and when or where you should go depending on what the ailment is.” (Male, aged 35 – 59) “- Children under the age of 16 -Elderly over 65 -People who get their malediction free (Exemption certificate) -People on benefits” (Female, aged 16 – 24) Q9. If you are aware of any situations or groups of people where you think some or all of the medicines for the above listed conditions should still be prescribed, please tell us below: A number of groups were identified, some of which include:
• People on benefits / low income • Cancer patients • People with severe mental health problems • People with disabilities which restrict income • Elderly people over 65 • Children • People with long term conditions

• People with dry eyes • People with head lice • People with severe hay fever who need lots of types of medication • People with dementia • People with IBS • Vulnerable people, homeless and asylum seekers
“Hayfever medicines should be prescribed, so should Diarrhoea. So should infants' medicines. It would be easier for new mothers to go to the Pharmacy and obtain their medicine rather than going to the GP first, requesting an appointment and then going to the Pharmacy with the prescription.” (Female, aged 16 – 24) “elderly, people who don't pay for their prescriptions” (Female, aged 60 – 75) “people at the lower end of the financial scale might no see paying for lice control as a priority. The end result is a whole school with the problem and then you need more nit nurses and how much does that cost. Of course, you then have the scenario of the parents saying the child has a condition and its really them, you would have to have a system that prevents such abuse.” (Male, aged 60 – 75) “There should always be room for discretion - my son needed Benadryl, nasal spray & eye drops for severe hay fever - cheaper alternatives were not effective. The cost was extortionate without prescription” (Female, aged 35 – 59) Q10. If you have any particular concerns about any of the conditions listed please tell us which one and why: A number of concerns were raised, some of which include:
• Self-diagnosis and usage of medication instructions • IBS • Sleep problems • Haemorrhoids which may need surgery • Diarrhoea may need to be admitted because of dehydration • Conjunctivitis • Fibromyalgia • Migraines • Chronic dry eyes • Minor ailments of the fungal cause can cause further complications e.g.
athletes foot could spread to several people if not treated • Ringworms / threadworms could spread to different people • Hay fever • Indigestion and heart burn • Elderly and those with dementia • Children’s conditions; cradle cap / nappy rash • Head lice • Worms • Cystitis • These conditions could become major if left untreated

• Conditions which could be caused by something underlying and undiagnosed “Left untreated, Minor ailments of the fungal cause can cause further complications. E.g Athletes foot could spread to several people if not treated. Nappy rash can become aggressively infected. Ringworms, threadworms could also spread to different people” (Male, aged 60 – 75) “Sleep problems as these are not minor. Sleep is as vital to our health as food, water and oxygen. You wouldn't sanction long term deprivation of any of these as a minor ailment yet you class sleep in that way. Bad sport old chap” (Female, aged 35 – 59) “children's conditions conjunctivitis, cradle cap, moderate + nappy rash, headline, thread worms, cystitis (kidney reflux in under 5s and women's. health) (was this proposal written by a man? Sleep problems might be a really good prescription to outlaw! huge pressure on GPs to prescribe.” (Male, aged 60 – 75) Q11. Please use this space to provide additional comments, to tell us how the changes may affect you or to request any additional information. A number of comments were made as follows:
• People could suffer in silence • Could have a serious underlying issue causing symptoms • Cost could deter patients from buying medication and therefore worsen
conditions • GP demand would increase especially for families wanting Calpol for children • Conditions could be left untreated • Deciding whether symptoms are self-limiting or part of a more serious chronic
condition should require individual and holistic medical input • Proposals may turn out to be false economy • A patient formulary should be produced • Scheme has been very helpful and a good cost and time saver for patients
“I would not be too sereiously effected as I already buy many items for some of my minor conditions. I have prescription eye drops for the side effect of some of my other prescribed medication and at present these eye drops are relatively inexspensive but that may not always be the case.” (Male, aged 65 – 70) “As a single parent with young children in school who are forever picking up head lice and illness its too expensive to keep treatment going that the scheme is very hellful” (Female, aged 25 – 34) “It is not for an administrative system or alogrithm to determine whether my symptoms are self-limiting or part of a more serious chronic condition. I need individual and holistic medical input to make such decsions with myself. Some of the proposals may turn out to be false economies.” (Female, aged 60 – 75)

“Won't affect me as i pay for prescriptions and tend to buy them over the counter” (Female, aged 16 – 24) Q12. The Pharmacy First Minor Ailments Scheme is where a patient in Leicester City can have an appointment in selected pharmacies to get advice about a minor illness or ailment, and can receive medicine free of charge without visiting a GP. Have you ever used the Pharmacy First Minor Ailments Scheme? 48 out of 180 participants (27%) advised that they had used the Pharmacy First Minor Ailments Scheme. Q13. We are reviewing whether to continue to provide the Minor Ailments Scheme because:
- After October 2018, medicines may no longer be routinely prescribed for minor ailments and illnesses.
- The demand for this service is low across the city
If we stop this scheme, you would still be able to speak to any pharmacy for advice about health problems, and they will still be able to offer you medicines to buy over the counter, if appropriate. What do you think about this proposal? I support the stopping of the Minor Ailments Scheme: 60 I do not support the stopping of the Minor Ailments Scheme: 68 I am not sure: 53 68 of 181 participants (38%) did not support stopping the scheme; however, 33% did support the proposal. Please tell us reasons for your answer: Those that supported stopping the Minor Ailments Scheme gave the following reasons:
• You can get advice from Pharmacists already for free • Support this as long as pharmacists continue to offer impartial advice • Messages to patients need to be consistent • Chemists can abuse system/misuse the facility • Support this as pharmacists are not knowledgeable enough – need GP
appointments for diagnosis • Support this as pharmacists do not have access to patient medical records to
give specific advice “There is a lot of information on NHS Choice website about minor conditions and pharmacy's are able to provide advice and guidance on products to use.” (Female, aged 60 – 75)

“If medications for minor ailments are going to be charged I can’t see the need for this scheme as long as pharmacists can still give impartial advice to patients/customers about suitable treatments My only concern would be that patients would go to their gp instead and thus use appointment times that would be more valuable to someone else.” (Respondent aged 60 – 75) Those that did not support stopping the Minor Ailments Scheme gave the following reasons:
• More awareness of the scheme is needed • Will not pay for medication • Scheme means that patients do not need to wait for unnecessary GP
appointments • Useful for families on low income or in an emergency
• Difficult financially especially for large families • Some of these conditions are not self-limiting • The low uptake may have been due to the failure to offer the system across
the city • Goes against advice to visit Pharmacist instead of GP for minor ailments
Having the scheme has been essential to obtain medication for my 3 year old granddaughter over her short life, as she has suffered many different minor ailments. The availability and efficiently to be able to get medication at short notice has been beneficial not only to treat her quickly, but also, as we are pensioners being free has been a godsend. We have had to rely on it on her behalf on lots of occasions. PLEASE don't stop it. (Male, aged 60 – 75) “Its a matter of cost and many young mother and the elderly may have limited means making the purchasing of these medicines beyond their budget.” (Female, aged 76+) Q14. Are you are aware of any way in which people may be affected if we stop the Pharmacy First Minor Ailments Scheme? If so, please tell us how below: Participants provided the following suggestions:
• Low income families • Elderly • More GPs and emergency calls • People having to wait to get seen by health professionals • Children • Young families • People on benefits • Telephone calls to health professionals will increase • Those who suffer pain and discomfort • Sick people will suffer more and longer. It may give rise to more instances of
working people ringing in sick for minor ailments. Many children may miss

school and their parents would also need to take time off from work to look after them.
• People who cannot get to GP's/appointments at set times can instead access a local pharmacy
• A&E attendance may rise “More pressure of GP Practices. Extend it back into the county and make it really work. It was a great scheme and saved patient time too.” (Male aged 35 – 59) “Vulnerable groups, young children, the elderly, people who cannot get to GP's/appointments at set times can instead access a local pharmacy and am sure this would be more helpful.” (Transgender, aged 25 – 34) “Yes, sick people will suffer more and longer. It may give rise to more instances of working people ringing in sick for minor ailments. Many children may miss school and their parents would also need to take time off from work to look after them. The elderly, especially those without the support of friends, relatives or helpful neighbours would suffer more.” (Male, aged 60 – 75) The majority of participants were registered with Leicester City Central GP surgeries (50%), residing in the LE2 and LE5 areas (totally 66%). Of this, 67% of participants were women, with 72% of patients being aged between 35 and 75, of Indian (55%) ethnic origin. Summary of findings Of the participants who completed the survey, the majority were aware that medication for the minor ailments named could be purchased over the counter and declared that they were happy to do so. Although most participants were aware what the term “self-limiting” meant, many disputed whether some of the conditions listed were more than self-limiting. Most felt that medications for self-limiting conditions should not be prescribed however raised a number of concerns. The most predominant of which were around misdiagnosis in self-care and the ability of patients being able to afford medication. A number of groups of people were highlighted, most commonly being those on low-income and the elderly. It was also identified that most people used the pharmacy as their first port of call when suffering from a minor ailment. When looking at groups of people for which the changes may affect more than others, there were a number of areas identified. These were predominantly around children, the elderly and those on low-income. Patients with learning disabilities or those whose first language isn’t English were also referenced where understanding of the changes could be missed. The major concerns raised regarding the changes were around costs to those on low incomes, misdiagnosis and prolonged suffering if symptoms are left untreated. Only a small proportion of those that responded to the survey had used the Pharmacy First Minor Ailment Scheme. However, the majority of respondents felt that they were unsure or did not support stopping the minor ailment scheme. The main concerns raised were that of cost to the patient and the consequences to those

who cannot afford it. It was further noted that many respondents were unaware of the scheme, and should awareness and coverage across the city be raised, the scheme would be better utilized. It was felt that removal of the scheme would result in increased pressure on GP surgeries and other parts of the health system such as A&E. Next steps Please complete – paper going to IGC and when decisions will be made.

D

Blank Page

Leicester City Clinical Commissioning Group
East Leicestershire & Rutland Clinical Commissioning Group West Leicestershire Clinical Commissioning Group
Commissioning Collaborative Board
Paper D Title of the report: LLR Programme Management Office (PMO) and Finance QIPP
Report
Report to: Commissioning Collaborative Board
Section: Public
Date of the meeting: 28 March 2019
Report by:
Sarah Ferrin, Head of Financial Planning & Project Delivery Nigel Brady, PMO Manager
Sponsoring Director: Spencer Gay, CFO West Leicestershire CCG
Presented by:
Spencer Gay, CFO West Leicestershire CCG
Report supports the following LLR CCG’s goal(s): Improve health outcomes
Improve the quality of health-care services
Use our resources wisely CCG Involvement to date: City East West Insert name
of any other groups ie ECN
Clinician N/A N/A N/A Manager PMO – C Nixon PMO – C Richardson PMO – N Brady QAG, CFO’s
SUMMARY: LLR CCGs are forecasting an under delivery of the QIPP plan for 2018/19 of £0.866m, an adverse movement of £0.241m from last month. LC CCG is reporting an over delivery against plan of £1.012m, ELR CCG is reporting an under delivery of £0.413m and WL CCG an under delivery of £1.465m. SROs are forecasting QIPP delivery of £57.334m which is reported formally on a monthly basis. The LLR PMO undertakes a monthly assurance exercise on the forecasts provided to provide an ‘assured value’ which represents the amount of QIPP savings that the PMO is confident will be delivered. During the month, the PMO assurance process resulted in an assured value of £55.923m. Further work is required to further develop the 19/20 QIPP programme through the planning and contracting process.
RECOMMENDATIONS: The Commissioning Collaborative Board is asked to:
• NOTE and DISCUSS the content of this report

2
CONTENTS
Page
1. QIPP Delivery 3
1.1: Introduction 3
1.2: Month 11 Position 3 1.3 Overall scheme risks 4
2. PMO Progress 5
2.1: QIPP Assurance Group (QAG) 5
2.2: Risks by Programme Area 6 2.3: Additional PMO Team Activities 7 2.4: PMO Next Steps 7
3. QIPP Schemes 2019/20 7
4. CONCLUSION & RECOMMENDATIONS 7 Appendices
Appendix 1: Finance Red Rated QIPP Schemes Appendix 2: Full LLR QIPP Dashboard Appendix 3: Full LC CCG QIPP Dashboard Appendix 4: Full WL CCG QIPP Dashboard Appendix 5: Full ELR CCG QIPP Dashboard Appendix 6: 2019/20 QIPP Schedule

3
1. QIPP Delivery 1.1 Introduction: SRO’s have submitted workbooks for QIPP schemes, including risk adjusted forecasts of the likely financial delivery for the year. These workbooks have been reviewed and their contents analysed by the LLR PMO. This report highlights key points and items of interest from these workbooks.
1.2 Month 11 Position Month 11 position as reported by SRO’s at the start of March indicated QIPP achievement of £52.081m year to date and forecast £57.334m achievement by the end of the year against plans of £52.455m and £58.200m respectively. This is shown at summary level in tables 1 and 2 below. TABLE 1 - Summary Performance by Programme Area
Programme Area YTD Plan
(£'000) YTD Actuals
(£'000) YTD Variance
(£'000) Annual Plan
(£'000)
Forecast Outturn (£'000)
Annual Variance (£'000)
Annual variance %
CHC (6,204) (7,491) (1,287) (6,769) (8,224) (1,455) 21%Community (3,494) (1,398) 2,096 (3,993) (1,598) 2,395 -60%CommunityServices Redesign (1,091) (58) 1,033 (1,334) (112) 1,222 -92%Contracting (4,609) (3,101) 1,508 (5,072) (3,178) 1,894 -37%Corporate (2,183) (1,211) 973 (2,415) (1,399) 1,016 -42%Finance (4,789) (12,726) (7,937) (5,235) (13,117) (7,882) 151%Integrated Teams workstream (1,805) 369 2,175 (1,973) 368 2,341 -119%Medicine Management (11,678) (12,249) (571) (12,841) (13,411) (571) 4%Mental Health/LD (3,636) (4,457) (821) (4,074) (5,105) (1,031) 25%Planned Care Workstream (5,109) (2,184) 2,925 (5,874) (2,495) 3,379 -58%Primary Care (4,836) (4,952) (116) (5,321) (6,183) (862) 16%Urgent Care Workstream (3,020) (2,623) 397 (3,301) (2,881) 420 -13%Grand Total (52,455) (52,081) 374 (58,200) (57,334) 866 -1% This can be broken down by CCG as follows: TABLE 2 - Summary Performance by CCG
CCG YTD Plan
(£'000) YTD Actuals
(£'000) YTD Variance
(£'000) Annual Plan
(£'000)
Forecast Outturn (£'000)
Annual Variance (£'000)
Annual variance %
PMO Confidence/
Assured ELR (17,609) (16,759) 850 (19,647) (19,234) 413 -2% (18,849)LC (16,335) (17,732) (1,397) (18,055) (19,067) (1,012) 6% (18,693)WL (18,511) (17,590) 921 (20,498) (19,033) 1,465 -7% (18,380)Grand Total (52,455) (52,081) 374 (58,200) (57,334) 866 -1% (55,923) The forecast out-turn of £57.334m across LLR has moved adversely from month 10 by £0.241m. Table 3 below outlines the main movements in month by CCG:

4
TABLE 3 - Movement in Month LLR (£'000) ELR (£000) WL (£'000) LC (£'000)
Favourable Movements:Pathway 3/Risk Share (107) (34) (33) (39)LD Pooled (186) (91) (95)Section 117 and AHP (101) (6) (30) (65)
Adverse Movements:HCD - biosimilars 141 50 46 45MH OOA Placements - additional provision in LPT 191 41 54 96Planned Care 165 21 88 56Fed QIPP 63 63LPT CQUIN 100 27 33 41
Other (26) (36) 54 (44)
Total Movement 241 (29) 179 90 Main Favourable Movements: An improvement for the Pathway 3 scheme has been observed. This is based on modelled expenditure within the supporting Business Case, which showed a potential QIPP opportunity of c£1.6m, with a view taken of 50% delivery in 2018/19, which was deemed a conservative estimate. Given the magnitude of the opportunity, this over-delivery seems plausible. LD Pool reviews with the Local Authority have resulted in a higher level of savings in January than previously forecast. This has then been replicated in the forecasts for February and March. Main Adverse Movements: The High Cost Drugs position has deteriorated due to a reduction in Biosimilar savings which were forecast in December and did not materialise. The adverse movement in relation to MH OOA placements is due to a reduction in actual QIPP delivered in January from that originally forecast and a subsequent halving of forecast delivery for the months of February and March. The adverse movement in Planned Care is due to an increase in activity during January at UHL for new and follow up outpatients. The WL CCG Federation QIPP scheme has deteriorated further this month due to further payments to Federations. LC CCG is reporting an over delivery against plan of £0.914m, ELR CCG is reporting an under delivery of £0.472m and WL CCG an under delivery of £1.433m. 1.3 Overall Scheme Risks:
All schemes have been allocated an overall PMO RAG rating by the LLR PMO in relation to the completeness of documentation and the level of assurance that this gives regarding delivery. This review is focussed on documentation and rating the schemes across a number of categories (E.g. Milestones, deliverables, risks, issues) – it does not include a review of the likelihood of financial delivery. This is shown in the table below:

5
TABLE 4 - Forecast Out-turn by PMO overall RAG rating & PMO confidence/Assured Value
Programme Area Green Amber Red Blue
(Completed) Purple
(Deferred) Grey (Closed) Grand Total
PMO Confidence/Assured Value
CHC (8,224) 0 0 0 0 0 (8,224) (8,224)Community (317) (84) 0 (1,197) 0 0 (1,598) (1,598)CommunityServices Redesign 0 0 0 (112) 0 0 (112) (112)Contracting (1,537) 0 0 (1,641) 0 0 (3,178) (3,088)Corporate (1,399) 0 0 0 0 0 (1,399) (1,399)Finance (5,387) 0 0 (7,730) 0 0 (13,117) (13,117)Integrated Teams workstream 0 0 368 0 0 0 368 549Medicine Management (11,311) 0 0 (2,100) 0 0 (13,411) (13,411)Mental Health/LD (4,975) (130) 0 0 0 0 (5,105) (5,105)Planned Care Workstream (2,379) (116) 0 0 0 0 (2,495) (2,096)Primary Care (4,686) (300) (777) (420) 0 0 (6,183) (5,883)Urgent Care Workstream (2,365) 0 (329) (187) 0 0 (2,881) (2,439)Grand Total (42,580) (630) (738) (13,387) 0 0 (57,334) (55,923)
High Financial Confidence (41,842) (611) (82) (13,387) 0 0 (55,923)Medium Financial Confidence (738) (19) 0 0 0 0 (756)Low Financial Confidence 0 0 (655) 0 0 0 (655)Total (42,580) (630) (738) (13,387) 0 0 0 (57,334) There is also a separate financial review undertaken by the LLR PMO which provides a level of confidence in the financial delivery of QIPP for each scheme: Red - Low confidence in delivery of the financial element of QIPP Amber - Medium confidence in the delivery of the financial element of QIPP Green - High confidence in the delivery of the financial element of QIPP (‘Assured Value’ in Table 4 above) These financial RAG ratings are shown on Appendices 1 to 5. The PMO assured value of £55.923m has improved by £0.282m from last month’s assured value of £55.641m. There have been movements in relation to changes in FOTs provided by SROs which are fully assured as outlined in Table 3. There have also been favourable movements due to increased levels of assurance around schemes such as BCF contingency (£0.701m) and LPT contract review (£0.130m). Appendix 1 shows the schemes for which the financial RAG rating is red (i.e. low confidence). All of these schemes also have an overall PMO Red Rated RAG status, reflecting that the scheme is still in the scoping phase, is behind in relation to its deliverables and milestones or has a number of high risks associated with it. A full list of LLR QIPP schemes, their current levels of delivery and RAG ratings is attached in Appendix 2, along with supporting PMO commentary. Appendices 3 to 5 show the overall QIPP performance per CCG. 2 PMO Progress.
2.1 QAG: The QIPP Assurance group meet twice a month, once to review the overall QIPP position and once to receive updates and further clarity from specific schemes which are causing concern. During the month, an escalation report in relation to the Falls scheme was provided due to concerns in relation to 18/19 delivery. It was determined that further discussions were to be undertaken by the planning team and the project lead to ensure the situation is fully

6
understood before committing further investment next year. A verbal update was also provided in relation to High Cost Drugs to reassure the committee that appropriate completion of the monthly workbook was being undertaken and support provided to the project lead who is relatively new in post. An initial review of 19/20 QIPP schemes was undertaken to determine the project documentation required to enable appropriate monitoring. During the month, 1 scheme was recommended to JMT (by QAG), for closure (scheme no longer viable), and 3 schemes for deferral into the 2019/20 QIPP plan. These were approved by JMT on 25th February 2019. The table below identifies the schemes involved and the agreed action. Table 5 - Closed, Completed & Deferred Schemes
Scheme Number
Scheme Name Exec lead Value in Plan Current FOT Rationale Proposed Action
26 LLR MPC controls Spencer Gay£51k (£17k per
CCG)£43k (£14k per
CCG)The process has been revised and completed, however no QIPP saving materialised. To be reviewed as part of the MH element of 19/20 plan.
Closed
NEW I LLR Telehealth - Dedicated line for Care/Nursing/Residential Homes
Mike Ryan £0k £0k Identified mitigating scheme which has not progressed or resulted in savings Defer
NEW K LLRReduction of EMAS conveyancing activity/Transfer of activity to UCCs
Mike Ryan £0k £0k Identified mitigating scheme which has not progressed or resulted in savings Defer
47 LC & WL Joint Funding University of Leicester Ian Potter£48k (£24k LC;
£24k WL)£0k Scheme deferred into 19/20 QIPP plan Defer
2.2 Risks by Programme Area 2.2.1 Primary Care: West Leicestershire CCG Federation QIPP This QIPP scheme had a delivery plan of £1.3m, with high confidence in delivering £0.9m against this plan. However, a number of payments to Federations pertaining to adherence to the pre-agreed KPIs have resulted in a drop in FOT. A further recent payment to the Federations has been made resulting in a FOT of £0.777m. Furthermore, a new agreement has been made with the Federations in that £0.3m of the £0.450m allocated to the NE element has been reallocated to support a two stage approach in to ensure a specific checklist of actions is completed. There is high confidence in the completion of these actions and thus payment of the £0.3m, which will result in the incommodious further drop in PMO Assured value to £0.477m. 2.2.2 Urgent Care: A&E Since this scheme is inextricably linked to A&E activity, it is naturally subject to month-on-month and seasonal variance. Against a plan of £0.860m, the FOT is now depicted as £0.274m, which represents deterioration in FOT of £0.063m from last month. The PMO has assured delivered to £0.150m. 2.2.3 Integrated Teams: Falls The Falls programme has experienced a number of delays, resulting in only three of the five key programme areas being mobilised. Consequently, the service is not delivering the expected savings. Some of this variance can be attributed to a seasonally-induced activity increase, colloquially known as Winter Pressures. Currently, the programme is delivering a cost, which is partly mitigated by an under-delivery. The combination of activity stabilisation and implementation of the other two programmes is expected to result in an improvement in financial delivery 2.2.4 Planned Care Adverse movement for this month can be attributed to an increase in activity at UHL around New and Follow-Up Outpatients. There is a distinct possibility of further deterioration on FOT due to the difficulty in managing how the provider manages their demand. 2.2.5 Continuing Healthcare (CHC) Month-on-month variance in delivery for CHC has been observed, with large inter-CCG variances being recorded. Although it has been suggested that this was due to adjustments being made for initial over reporting earlier in the year, assurance around the calculation and

7
assumptions has been requested to provide further clarity and justification for the approach. High confidence around delivery exists. 2.2.6 LD Pool: Joint Panel Reviews An update is now to be received every Friday on the outcome of scheduled panels. A number of panels were cancelled due to the lack of appropriate personnel to attend from the Local Authority. Discussions are currently underway to ensure appropriate representation is in place henceforth to ensure that no further delay is experienced to the panels and the outcomes are supported by all attendees. 2.3 Additional PMO team activities: The PMO successfully completed an LLR 2019-20QIPP Plan submission to NHS England on 21st February 2019. This consisted of completing NHS England templates, which prompted the PMO to evaluate the deliverability of the schemes in the QIPP Plan, but also to illustrate the Governance structure across LLR, and the roles that the PMO plays across the organisations. To underpin and support the responses, an array of business cases and PIDs were submitted to NHS England, with explanatory narrative to compliment. The PMO is drafting a Project Management Handbook, which is expected to be disseminated amongst project teams in April. Significant time has been invested by the PMO into working with Project Leads to aid them in project planning, business case and PID writing and providing face-to-face ad hoc training. 2.4 PMO Next Steps A series of workshops will be run by the PMO between April and July to cover a range of topics. The workshops will be delivered by the PMO and/or guest presenters and will be held either at County Hall or Woodgate. The timetable is being finalised and will be distributed in the next week or two. A timetable of 2019-20 workbook submissions is being finalised by the PMO. Once the CSU have committed to the timetable, it will be distributed to project teams. 3 QIPP Schemes 2019/20 The latest financial plan submission on 12th February 2019, identified £48.630m QIPP against a target of £56.250m, resulting in a gap of £7.620m. PIDs and business cases were completed as part of the planning round and initial PMO workbooks requested for submitted by 15th February outlining the key deliverables and detailed financial breakdown. A small number of workbooks were submitted at this time, a number of which omitted the detailed financial workings required. A second PMO workbook submission was set for 8th March 2019, to enable project leads to further progress their schemes and complete the appropriate documentation. Appendix 6 outlines the progress made to date in terms of workbooks and documentation submitted, issues arising from some submissions and refinements to QIPP figures reported. As can be seen, a large number of schemes have failed to submit completed workbooks by the deadline and some which have contain quality issues. Figures highlighted in yellow show where the original planned figures have been refined; where figures have increased, these have been captured, where they have reduced, stretch schemes have been added. These amendments have resulted in the QIPP gap reducing from £7.620m (LLR) to £5.809m (LLR), although it should be noted that LC CCG is over performing against its QIPP target by £0.653m.

8
It is essential that SROs and project leads continue to work to fully complete PMO workbooks and submit for review as soon as possible to ensure the final plan can be finalised. 4 Conclusion and Recommendations LLR CCGs are forecasting an under delivery of the QIPP plan for 2018/19 of £0.866m, an adverse movement of £0.241m from last month. LC CCG is reporting an over delivery against plan of £1.012m, ELR CCG is reporting an under delivery of £0.413m and WL CCG an under delivery of £1.465m. SROs are forecasting QIPP delivery of £57.334m which is reported formally on a monthly basis. The LLR PMO undertakes a monthly assurance exercise on the forecasts provided to provide an ‘assured value’ which represents the amount of QIPP savings that the PMO is confident will be delivered. During the month, the PMO assurance process resulted in an assured value of £55.923. Further work is required to further develop the 19/20 QIPP programme through the planning and contracting process.
RECOMMENDATIONS: The Commissioning Collaborative Board is asked to:
• NOTE and DISCUSS the content of this report

Appendix 1: Finance Red Rag Rated Schemes
Scheme no.
for LLR
Summary
Report
Scheme Name Deliverables Milestones Total Risks IssuesOverall PMO
RAG ratingsGrouping / Function Annual Plan
Sum of
Revised FOT
Sum of Low
Finance
Confidence
Sum of
Medium
Finance
Confidence
Sum of High
Finance
Confidence
18 WL PRIMARY CARE - Federation QIPP scheme impact on acute demand Red Red Red Red Red Primary Care (1,300) (777) (300) 0 (477)
A15 ED Front Door Model 1 Green Green Red Red Red Urgent Care Workstream (167) (51) (27) 0 (24)
A16 ED Front Door Model 2 Green Green Red Red Red Urgent Care Workstream (76) (20) (10) 0 (9)
A17 Increase & Improve Ambulatory Pathways 1 Green Green Red Red Red Urgent Care Workstream (202) (63) (33) 0 (29)
A2 Respiratory Red Red Red Red Red Integrated Teams workstream (113) 22 (49) 0 71
A20 Improved Clinical Triage Green Green Red Red Red Urgent Care Workstream (25) (8) (4) 0 (4)
A21 Expansion of Clinical Navigation Hub Green Green Red Red Red Urgent Care Workstream (169) (54) (29) 0 (25)
A23 Urgent Diagnostic Pathways Red Red Red Red Red Urgent Care Workstream (24) (9) (5) 0 (4)
A24 Increase Support for EMAS to reduce conveyances Green Green Red Red Red Urgent Care Workstream (198) (48) (26) 0 (23)
A26 Frailty Red Red Red Red Red Urgent Care Workstream (177) (59) (31) 0 (28)
A27 Passporting Red Red Red Red Red Urgent Care Workstream (49) (17) (9) 0 (8)
A3 Falls Red Red Red Red Red Integrated Teams workstream (76) 197 (85) 0 281
A4 EoL - CHC Deflected Patients Red Red Red Red Red Integrated Teams workstream (1,455) 149 (48) 0 197
Grand Total (2,731) (738) (655) 0 (82)
Page 8

Appendix 2 Full LLR QIPP Dashboard
Scheme no.
for LLR
Summary
Report
Scheme Name Deliverables Milestones Total Risks IssuesOverall PMO
RAG ratingsAnnual Plan
Sum of
Revised FOT
Sum of Low
Finance
Confidence
Sum of
Medium
Finance
Confidence
Sum of High
Finance
Confidence
1 Ambulatory Care Purple Purple Purple Purple Purple 0 0 0 0 0
2 Demand Management HUB: MSK, Dermatology (RSS) Amber Green Amber Green Amber 0 (14) 0 (2) (12)
4 Orthotics Procurement(Blatchfords) Blue Blue Blue Blue Blue (215) (249) 0 0 (249)
5 Pathway 3 Control/Risk Share Green Green Green Green Green (800) (818) 0 0 (818)
6 Coding and Counting Grey Grey Grey Grey Grey 0 0 0 0 0
12 Removal of double payment to LPT for UHL discharge co-ordinators (Primary Care Co-ordinators) Purple Purple Purple Purple Purple (393) 0 0 0 0
13 Block Contracts at UHL Blue Blue Blue Blue Blue (348) (848) 0 0 (848)
14 UHL Contract Price negotiation - Follow Up Ratios Grey Grey Grey Grey Grey (891) 0 0 0 0
15 UHL Contract Price negotiation - CAU Blue Blue Blue Blue Blue (300) (469) 0 0 (469)
16 UHL Contract Price Negotiation - CDU Purple Purple Purple Purple Purple (1,000) 0 0 0 0
17 UHL Contract Price Negotiation - RDA's Purple Purple Purple Purple Purple (500) 0 0 0 0
20 All historic AQP contracts to be reviewed Grey Grey Grey Grey Grey (2,061) 0 0 0 0
22 Independent Sector Contract Control Grey Grey Grey Grey Grey 0 0 0 0 0
23 Independent Sector - manage IPT transfers from UHL Grey Grey Grey Grey Grey 0 0 0 0 0
24 NCA's tighter controls Amber Green Green Green Green 0 0 0 0 0
27 Night Nursing contract negotiation - DHU Blue Blue Blue Blue Blue (416) (103) 0 0 (103)
29 DHU - all services/contracting redesign Blue Blue Blue Blue Blue 0 (84) 0 0 (84)
31 LD Pool -improved case management Green Green Green Green Green (1,321) (1,236) 0 0 (1,236)
32 Reduce corporate clinical input Green Green Green Green Green (200) (148) 0 0 (148)
34 Review and redesign in ICS/IP Beds/District Nursing Purple Purple Purple Purple Purple (1,000) 0 0 0 0
35 EMAS - Negotiation of 18/19 contract Blue Blue Blue Blue Blue (801) (324) 0 0 (324)
36 LD Short breaks consolidation Purple Purple Purple Purple Purple (255) 0 0 0 0
37 LPT CQUIN expectation Green Green Green Green Green (576) (891) 0 0 (891)
38 Stroke Rehab Bed Numbers Reduction Following redesign and investment Blue Blue Blue Blue Blue (318) (318) 0 0 (318)
39 Agnes unit - options for use Grey Grey Grey Grey Grey 0 0 0 0 0
40 Potential realignment of Community Hospital Beds across sites Purple Purple Purple Purple Purple (209) 0 0 0 0
41 AHP/117 repatriation Grey Grey Grey Grey Grey 0 0 0 0 0
43 Vol Sector - Review VFM and service need Green Green Green Amber Green (972) (12) 0 0 (12)
44 Derbyshire Healthcare non acute SLA negotiation Grey Grey Grey Grey Grey (156) 0 0 0 0
47 Joint Funding University of Leicester Purple Purple Purple Purple Purple (48) 0 0 0 0
49 Office Accommodation savings Purple Purple Purple Purple Purple 0 0 0 0 0
50 In House Legal expertise Purple Purple Purple Purple Purple (105) 0 0 0 0
57 Readmissions reduction Purple Purple Purple Purple Purple 0 0 0 0 0
58 BCT Partnership office maintain spend in line with 17/18 outturn Green Green Green Green Green (236) (236) 0 0 (236)
59 Anticoag at UHL - moved into community Blue Blue Blue Blue Blue (630) (630) 0 0 (630)
61 Consider Staff Car Parking Charges Grey Grey Grey Grey Grey 0 0 0 0 0
63 Prior approvals (IFR's) tighter controls Purple Purple Purple Purple Purple (500) 0 0 0 0
64 Primary care transformation fund Grey Grey Grey Grey Grey 0 0 0 0 0
Page 9
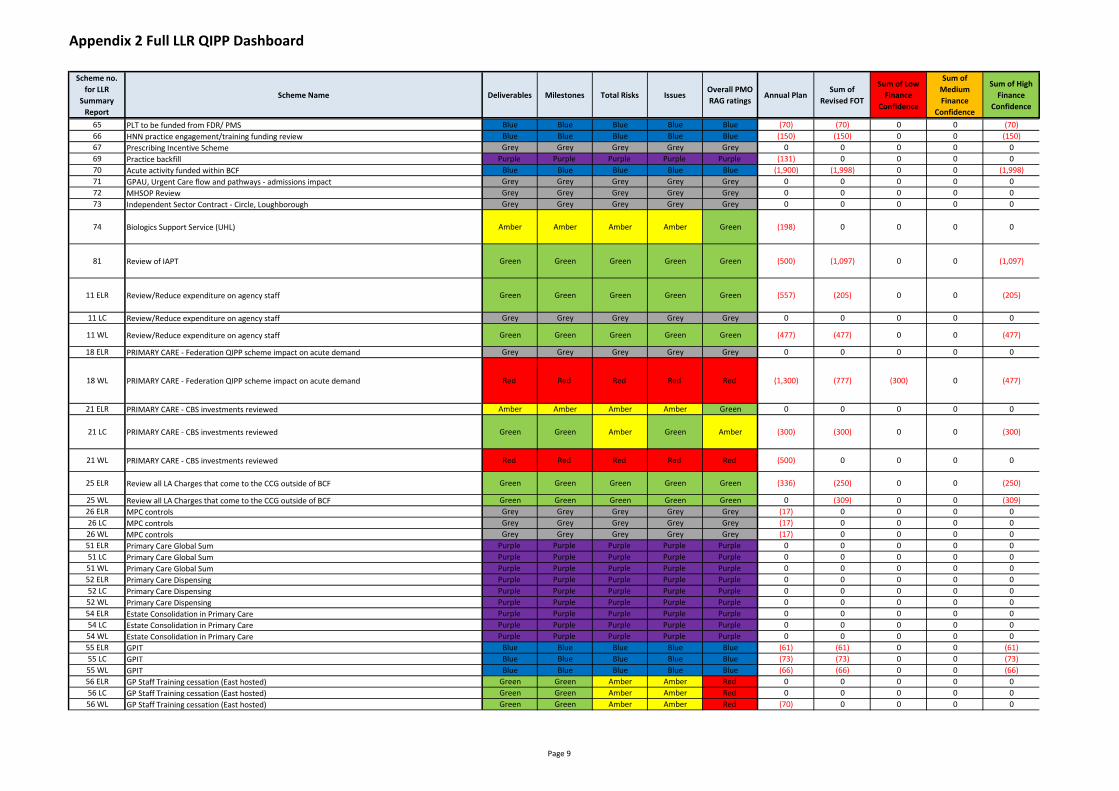
Appendix 2 Full LLR QIPP Dashboard
Scheme no.
for LLR
Summary
Report
Scheme Name Deliverables Milestones Total Risks IssuesOverall PMO
RAG ratingsAnnual Plan
Sum of
Revised FOT
Sum of Low
Finance
Confidence
Sum of
Medium
Finance
Confidence
Sum of High
Finance
Confidence
65 PLT to be funded from FDR/ PMS Blue Blue Blue Blue Blue (70) (70) 0 0 (70)
66 HNN practice engagement/training funding review Blue Blue Blue Blue Blue (150) (150) 0 0 (150)
67 Prescribing Incentive Scheme Grey Grey Grey Grey Grey 0 0 0 0 0
69 Practice backfill Purple Purple Purple Purple Purple (131) 0 0 0 0
70 Acute activity funded within BCF Blue Blue Blue Blue Blue (1,900) (1,998) 0 0 (1,998)
71 GPAU, Urgent Care flow and pathways - admissions impact Grey Grey Grey Grey Grey 0 0 0 0 0
72 MHSOP Review Grey Grey Grey Grey Grey 0 0 0 0 0
73 Independent Sector Contract - Circle, Loughborough Grey Grey Grey Grey Grey 0 0 0 0 0
74 Biologics Support Service (UHL) Amber Amber Amber Amber Green (198) 0 0 0 0
81 Review of IAPT Green Green Green Green Green (500) (1,097) 0 0 (1,097)
11 ELR Review/Reduce expenditure on agency staff Green Green Green Green Green (557) (205) 0 0 (205)
11 LC Review/Reduce expenditure on agency staff Grey Grey Grey Grey Grey 0 0 0 0 0
11 WL Review/Reduce expenditure on agency staff Green Green Green Green Green (477) (477) 0 0 (477)
18 ELR PRIMARY CARE - Federation QIPP scheme impact on acute demand Grey Grey Grey Grey Grey 0 0 0 0 0
18 WL PRIMARY CARE - Federation QIPP scheme impact on acute demand Red Red Red Red Red (1,300) (777) (300) 0 (477)
21 ELR PRIMARY CARE - CBS investments reviewed Amber Amber Amber Amber Green 0 0 0 0 0
21 LC PRIMARY CARE - CBS investments reviewed Green Green Amber Green Amber (300) (300) 0 0 (300)
21 WL PRIMARY CARE - CBS investments reviewed Red Red Red Red Red (500) 0 0 0 0
25 ELR Review all LA Charges that come to the CCG outside of BCF Green Green Green Green Green (336) (250) 0 0 (250)
25 WL Review all LA Charges that come to the CCG outside of BCF Green Green Green Green Green 0 (309) 0 0 (309)
26 ELR MPC controls Grey Grey Grey Grey Grey (17) 0 0 0 0
26 LC MPC controls Grey Grey Grey Grey Grey (17) 0 0 0 0
26 WL MPC controls Grey Grey Grey Grey Grey (17) 0 0 0 0
51 ELR Primary Care Global Sum Purple Purple Purple Purple Purple 0 0 0 0 0
51 LC Primary Care Global Sum Purple Purple Purple Purple Purple 0 0 0 0 0
51 WL Primary Care Global Sum Purple Purple Purple Purple Purple 0 0 0 0 0
52 ELR Primary Care Dispensing Purple Purple Purple Purple Purple 0 0 0 0 0
52 LC Primary Care Dispensing Purple Purple Purple Purple Purple 0 0 0 0 0
52 WL Primary Care Dispensing Purple Purple Purple Purple Purple 0 0 0 0 0
54 ELR Estate Consolidation in Primary Care Purple Purple Purple Purple Purple 0 0 0 0 0
54 LC Estate Consolidation in Primary Care Purple Purple Purple Purple Purple 0 0 0 0 0
54 WL Estate Consolidation in Primary Care Purple Purple Purple Purple Purple 0 0 0 0 0
55 ELR GPIT Blue Blue Blue Blue Blue (61) (61) 0 0 (61)
55 LC GPIT Blue Blue Blue Blue Blue (73) (73) 0 0 (73)
55 WL GPIT Blue Blue Blue Blue Blue (66) (66) 0 0 (66)
56 ELR GP Staff Training cessation (East hosted) Green Green Amber Amber Red 0 0 0 0 0
56 LC GP Staff Training cessation (East hosted) Green Green Amber Amber Red 0 0 0 0 0
56 WL GP Staff Training cessation (East hosted) Green Green Amber Amber Red (70) 0 0 0 0
Page 9

Appendix 2 Full LLR QIPP Dashboard
Scheme no.
for LLR
Summary
Report
Scheme Name Deliverables Milestones Total Risks IssuesOverall PMO
RAG ratingsAnnual Plan
Sum of
Revised FOT
Sum of Low
Finance
Confidence
Sum of
Medium
Finance
Confidence
Sum of High
Finance
Confidence
62 ELR Prescribing Stretch to £1m Green Green Green Amber Green (1,000) (1,509) 0 0 (1,509)
62 WL Prescribing Stretch to £1m Green Green Green Green Green (1,000) (587) 0 0 (587)
68 ELR Nursing Homes Grey Grey Grey Grey Grey 0 0 0 0 0
68 LC Nursing Homes Grey Grey Grey Grey Grey 0 0 0 0 0
68 WL Nursing Homes Grey Grey Grey Grey Grey 0 0 0 0 0
7 ELR Primary Care - Federation QIPP, Quality SIP etc. Green Green Green Green Green (2,000) (2,000) 0 0 (2,000)
7 WL Primary Care - Federation QIPP, Quality SIP etc. Grey Grey Grey Grey Grey 0 0 0 0 0
8 ELR Plan assumptions/Budget Reviews Blue Blue Blue Blue Blue 0 (1,015) 0 0 (1,015)
8 LC Plan assumptions/Budget Reviews Green Green Green Green Green 0 (431) 0 0 (431)
8 WL Plan assumptions/Budget Reviews Blue Blue Blue Blue Blue 0 (1,372) 0 0 (1,372)
82 ELR Stop Risk Stratification related investments Grey Grey Grey Grey Grey 0 0 0 0 0
82 LC Stop Risk Stratification related investments Grey Grey Grey Grey Grey 0 0 0 0 0
82 WL Stop Risk Stratification related investments Grey Grey Grey Grey Grey 0 0 0 0 0
9 ELR Public Health Funding Flu Vaccines Blue Blue Blue Blue Blue (300) (125) 0 0 (125)
9 LC Public Health Funding Flu Vaccines Grey Grey Grey Grey Grey (200) 0 0 0 0
9 WL Public Health Funding Flu Vaccines Blue Blue Blue Blue Blue (300) (69) 0 0 (69)
A1 Cardiology Grey Grey Grey Grey Grey (231) 0 0 0 0
A10 Audiology Purple Purple Purple Purple Purple (96) 0 0 0 0
A11 MSK Physiotherapy Green Green Amber Green Green (690) (526) 0 (84) (442)
A12 Physio Amber Amber Red Green Amber (64) 0 0 0 0
A13 Diagnostics - Imaging Amber Amber Red Amber Green (472) (393) 0 (63) (330)
A14 Diagnostics - Non Imaging Amber Amber Red Amber Amber (8) (11) 0 (2) (9)
A15 ED Front Door Model 1 Green Green Red Red Red (167) (51) (27) 0 (24)
A16 ED Front Door Model 2 Green Green Red Red Red (76) (20) (10) 0 (9)
A17 Increase & Improve Ambulatory Pathways 1 Green Green Red Red Red (202) (63) (33) 0 (29)
A18 Increase & Improve Ambulatory Pathways 2 Green Green Green Green Green (372) (885) 0 (150) (735)
A19 Increase & Improve Ambulatory Pathways 3 Green Green Green Green Green (72) (99) 0 (17) (82)
A2 Respiratory Red Red Red Red Red (113) 22 (49) 0 71
A20 Improved Clinical Triage Green Green Red Red Red (25) (8) (4) 0 (4)
A21 Expansion of Clinical Navigation Hub Green Green Red Red Red (169) (54) (29) 0 (25)
A22 Tighten Eligibility for NEPTS Green Green Green Green Green (344) (445) 0 (100) (345)
A23 Urgent Diagnostic Pathways Red Red Red Red Red (24) (9) (5) 0 (4)
A24 Increase Support for EMAS to reduce conveyances Green Green Red Red Red (198) (48) (26) 0 (23)
A25 Discharge Pathways Green Green Green Green Green (209) (119) 0 0 (119)
A26 Frailty Red Red Red Red Red (177) (59) (31) 0 (28)
A27 Passporting Red Red Red Red Red (49) (17) (9) 0 (8)
A28 ELR Medicines Optimisation (CCG) Green Green Green Green Green (2,000) (2,000) 0 0 (2,000)
A28 LC Medicines Optimisation (CCG) Green Green Green Green Green (2,700) (2,696) 0 0 (2,696)
A28 WL Medicines Optimisation (CCG) Green Green Green Green Green (2,000) (2,000) 0 0 (2,000)
A29 ELR Cat M Grey Grey Grey Grey Grey 0 0 0 0 0
A29 LC Cat M Blue Blue Blue Blue Blue (500) (500) 0 0 (500)
A29 WL Cat M Grey Grey Grey Grey Grey 0 0 0 0 0
Page 9

Appendix 2 Full LLR QIPP Dashboard
Scheme no.
for LLR
Summary
Report
Scheme Name Deliverables Milestones Total Risks IssuesOverall PMO
RAG ratingsAnnual Plan
Sum of
Revised FOT
Sum of Low
Finance
Confidence
Sum of
Medium
Finance
Confidence
Sum of High
Finance
Confidence
A3 Falls Red Red Red Red Red (76) 197 (85) 0 281
A30 ELR NSCO Grey Grey Grey Grey Grey 0 0 0 0 0
A30 LC NSCO Blue Blue Blue Blue Blue (1,600) (1,600) 0 0 (1,600)
A30WL NSCO Grey Grey Grey Grey Grey 0 0 0 0 0
A31 Biosimilar Switches Green Green Amber Amber Green (1,212) (1,251) 0 0 (1,251)
A32 Patent Expiry Humira® Green Green Amber Amber Green (570) (1,068) 0 0 (1,068)
A33 ELR Move to VAT Free Route (TMP)- Tolvaptan Green Green Amber Amber Green (20) (2) 0 0 (2)
A33 LC Move to VAT Free Route (TMP)- Tolvaptan Green Green Amber Amber Green (20) (2) 0 0 (2)
A33 WL Move to VAT Free Route (TMP)- Tolvaptan Green Green Amber Amber Green (20) (2) 0 0 (2)
A34 Adult Mental Health Grey Grey Grey Grey Grey (1,139) 0 0 0 0
A35 Section 117 and AHP Green Green Green Green Green (540) (1,723) 0 0 (1,723)
A36 MH OOA Placements - additional provision in LPT Green Green Amber Amber Green (237) (919) 0 0 (919)
A37 LD short breaks - other reviews Grey Grey Grey Grey Grey (82) 0 0 0 0
A38 Community Health Services Various schemes Purple Purple Purple Purple Purple (975) 0 0 0 0
A39 Community Equipment Scheme (returned equipment) Green Green Green Green Green (150) (305) 0 0 (305)
A4 EoL - CHC Deflected Patients Red Red Red Red Red (1,455) 149 (48) 0 197
A40 ELR CCG Efficiencies (incl Execs) Green Green Green Green Green (166) (166) 0 0 (166)
A40 LC CCG Efficiencies (incl Execs) Green Green Green Green Green (167) (167) 0 0 (167)
A40 WL CCG Efficiencies (incl Execs) Red Red Red Red Red (507) 0 0 0 0
A41 CHC Green Green Green Green Green (4,819) (7,747) 0 0 (7,747)
A42 CHC Stretch Green Green Green Green Green (1,950) (477) 0 0 (477)
A43 ELR BCF Slippage/contingency/savings plan Green Green Green Green Green (1,100) (1,169) 0 0 (1,169)
A43 WL BCF Slippage/contingency/savings plan Green Green Amber Amber Green (1,000) (967) 0 0 (967)
A44 Integrated urgent care - Primary care Green Green Green Green Green (600) (600) 0 0 (600)
A46 2. Repeat Ordering - FYE 3. Pregabalin - FYE 4. Technician Care Home Project - Reducing Waste Grey Grey Grey Grey Grey 0 0 0 0 0
A47 Ambulatory Care -look at closer to home services Grey Grey Grey Grey Grey (300) 0 0 0 0
A48 Recharge for UCC outside LLR Amber Amber Amber Amber Amber (40) (84) 0 0 (84)
A49 Primary Care Stretch Target - as part of contractual review Green Green Green Green Green 0 (2,086) 0 0 (2,086)
A5 E0L Reduction in Emergency Admissions Red Red Red Red Red (99) 0 0 0 0
A50 ELR Paediatric Pathways Grey Grey Grey Grey Grey 0 0 0 0 0
A50 LC Paediatric Pathways Grey Grey Grey Grey Grey 0 0 0 0 0
A50 WL Paediatric Pathways Grey Grey Grey Grey Grey 0 0 0 0 0
A51 ELR ICS notice (ELR - Consider alongside 34, A51, 40.) Blue Blue Blue Blue Blue (125) (112) 0 0 (112)
A51 LC ICS notice (ELR - Consider alongside 34, A51, 40.) Grey Grey Grey Grey Grey 0 0 0 0 0
A51 WL ICS notice (ELR - Consider alongside 34, A51, 40.) Grey Grey Grey Grey Grey 0 0 0 0 0
A6 Demand Savings: New Appointments Green Green Green Green Green (672) (589) 0 (94) (495)
Page 9

Appendix 2 Full LLR QIPP Dashboard
Scheme no.
for LLR
Summary
Report
Scheme Name Deliverables Milestones Total Risks IssuesOverall PMO
RAG ratingsAnnual Plan
Sum of
Revised FOT
Sum of Low
Finance
Confidence
Sum of
Medium
Finance
Confidence
Sum of High
Finance
Confidence
A7 Demand Savings: Follow Up Appointments Green Green Green Green Green (369) (291) 0 (47) (245)
A8 Demand Savings: Low Value Treatments Green Green Green Green Green (137) (115) 0 (18) (97)
A9 Pathway Redesign Green Green Green Green Green (1,305) (350) 0 (56) (294)
New 1 ELR Procurement price reduction Inflectra Green Green Green Red Green 0 (67) 0 0 (67)
New 1 LC Procurement price reduction Inflectra Green Green Green Red Green 0 (63) 0 0 (63)
New 1 WL Procurement price reduction Inflectra Green Green Green Red Green 0 (63) 0 0 (63)
NEW A PCL Utilisation Green Green Amber Green Amber 0 (33) 0 (5) (28)
NEW B Pathology - Target Tests Green Green Green Green Green 0 (114) 0 (18) (96)
NEW C Alliance at Reduced Tariff Green Green Amber Green Amber 0 (58) 0 (9) (49)
NEW D Avastin Green Green Amber Green Red 0 0 0 0 0
NEW E UHL CQUIN Delivery Green Green Amber Green Green 0 (600) 0 (90) (510)
NEW F LPT Contract review including MH parity over investment Red Red Red Red Amber 0 (130) 0 0 (130)
NEW G ELR Budget Review Blue Blue Blue Blue Blue 0 (771) 0 0 (771)
NEW G LC Budget Review Green Green Green Green Green 0 (2,261) 0 0 (2,261)
NEW G WL Budget Review Blue Blue Blue Blue Blue 0 (2,380) 0 0 (2,380)
NEW H High Volume Service Users (EMAS/A&E) Grey Grey Grey Grey Grey 0 0 0 0 0
NEW I Telehealth - Dedicated line for Care/Nursing/Residential Homes Purple Purple Purple Purple Purple 0 0 0 0 0
NEW J Audit of Readmission Rates Grey Grey Grey Grey Grey 0 0 0 0 0
NEW K Reduction of EMAS conveyancing activity/Transfer o activity to UCCs Purple Purple Purple Purple Purple 0 0 0 0 0
NEW L Reduction of isolation and unnecessary hospital activity. Frailty & Isolation - BCF and community
design; social inclusionGrey Grey Grey Grey Grey 0 0 0 0 0
NEW N ELR GPIT review: utilisation of contract efficiencies Red Red Red Red Red 0 0 0 0 0
NEW N WL GPIT review: utilisation of contract efficiencies Red Red Red Red Red 0 0 0 0 0
NEW O Assista Green Green Green Green Green 0 (46) 0 0 (46)
Grand Total (58,200) (57,334) (655) (756) (55,923)
RAG Status Key:
Scheme
StatusPriority
Financial
Confidence
Red Open High Risk Low
Amber Open Medium Risk Medium
Green Open Low Risk High
Grey Closed N/A N/A
Blue Completed N/A N/A
Purple Deferred to
19/20N/A N/A
Page 9

Appendix 3 Full LC CCG QIPP Dashboard
Scheme no.
for LLR
Summary
Report
Scheme Name Deliverables Milestones Total Risks IssuesOverall PMO
RAG ratingsGrouping / Function Annual Plan
Sum of Revised
FOT
Sum of Low
Finance
Confidence
Sum of Medium
Finance
Confidence
Sum of High
Finance
Confidence
1 Ambulatory Care Purple Purple Purple Purple Purple Integrated Teams workstream 0 0 0 0 0
2 Demand Management HUB: MSK, Dermatology (RSS) Amber Green Amber Green Amber Planned Care Workstream 0 (4) 0 (1) (4)
4 Orthotics Procurement(Blatchfords) Blue Blue Blue Blue Blue Community (75) (29) 0 0 (29)
5 Pathway 3 Control/Risk Share Green Green Green Green Green Urgent Care Workstream (300) (304) 0 0 (304)
6 Coding and Counting Grey Grey Grey Grey Grey Contracting 0 0 0 0 0
12 Removal of double payment to LPT for UHL discharge co-ordinators (Primary Care Co-ordinators) Purple Purple Purple Purple Purple Community (134) 0 0 0 0
13 Block Contracts at UHL Blue Blue Blue Blue Blue Contracting (146) (470) 0 0 (470)
15 UHL Contract Price negotiation - CAU Blue Blue Blue Blue Blue Contracting (123) (156) 0 0 (156)
16 UHL Contract Price Negotiation - CDU Purple Purple Purple Purple Purple Contracting (408) 0 0 0 0
17 UHL Contract Price Negotiation - RDA's Purple Purple Purple Purple Purple Contracting (204) 0 0 0 0
20 All historic AQP contracts to be reviewed Grey Grey Grey Grey Grey Planned Care Workstream (70) 0 0 0 0
22 Independent Sector Contract Control Grey Grey Grey Grey Grey Contracting 0 0 0 0 0
23 Independent Sector - manage IPT transfers from UHL Grey Grey Grey Grey Grey Contracting 0 0 0 0 0
24 NCA's tighter controls Amber Green Green Green Green Contracting 0 0 0 0 0
27 Night Nursing contract negotiation - DHU Blue Blue Blue Blue Blue Urgent Care Workstream (83) (41) 0 0 (41)
29 DHU - all services/contracting redesign Blue Blue Blue Blue Blue Urgent Care Workstream 0 (28) 0 0 (28)
34 Review and redesign in ICS/IP Beds/District Nursing Purple Purple Purple Purple Purple CommunityServices Redesign (345) 0 0 0 0
35 EMAS - Negotiation of 18/19 contract Blue Blue Blue Blue Blue Contracting (312) (127) 0 0 (127)
36 LD Short breaks consolidation Purple Purple Purple Purple Purple Mental Health/LD (81) 0 0 0 0
37 LPT CQUIN expectation Green Green Green Green Green Contracting (233) (360) 0 0 (360)
38 Stroke Rehab Bed Numbers Reduction Following redesign and investment Blue Blue Blue Blue Blue Community (124) (124) 0 0 (124)
39 Agnes unit - options for use Grey Grey Grey Grey Grey Mental Health/LD 0 0 0 0 0
40 Potential realignment of Community Hospital Beds across sites Purple Purple Purple Purple Purple CommunityServices Redesign (104) 0 0 0 0
41 AHP/117 repatriation Grey Grey Grey Grey Grey Mental Health/LD 0 0 0 0 0
43 Vol Sector - Review VFM and service need Green Green Green Amber Green Community (174) 0 0 0 0
47 Joint Funding University of Leicester Purple Purple Purple Purple Purple Finance (24) 0 0 0 0
49 Office Accommodation savings Purple Purple Purple Purple Purple Corporate 0 0 0 0 0
50 In House Legal expertise Purple Purple Purple Purple Purple Corporate 0 0 0 0 0
57 Readmissions reduction Purple Purple Purple Purple Purple Urgent Care Workstream 0 0 0 0 0
58 BCT Partnership office maintain spend in line with 17/18 outturn Green Green Green Green Green Corporate (90) (90) 0 0 (90)
59 Anticoag at UHL - moved into community Blue Blue Blue Blue Blue Community (257) (239) 0 0 (239)
61 Consider Staff Car Parking Charges Grey Grey Grey Grey Grey Corporate 0 0 0 0 0
63 Prior approvals (IFR's) tighter controls Purple Purple Purple Purple Purple Contracting (204) 0 0 0 0
64 Primary care transformation fund Grey Grey Grey Grey Grey Primary Care 0 0 0 0 0
65 PLT to be funded from FDR/ PMS Blue Blue Blue Blue Blue Primary Care (70) (70) 0 0 (70)
66 HNN practice engagement/training funding review Blue Blue Blue Blue Blue Primary Care (150) (150) 0 0 (150)
69 Practice backfill Purple Purple Purple Purple Purple Primary Care (131) 0 0 0 0
70 Acute activity funded within BCF Blue Blue Blue Blue Blue Finance (1,900) (1,998) 0 0 (1,998)
71 GPAU, Urgent Care flow and pathways - admissions impact Grey Grey Grey Grey Grey Urgent Care Workstream 0 0 0 0 0
72 MHSOP Review Grey Grey Grey Grey Grey Mental Health/LD 0 0 0 0 0
73 Independent Sector Contract - Circle, Loughborough Grey Grey Grey Grey Grey Contracting 0 0 0 0 0
74 Biologics Support Service (UHL) Amber Amber Amber Amber Green Medicine Management (198) 0 0 0 0
81 Review of IAPT Green Green Green Green Green Mental Health/LD 0 0 0 0 0
11 LC Review/Reduce expenditure on agency staff Grey Grey Grey Grey Grey Corporate 0 0 0 0 0
21 LC PRIMARY CARE - CBS investments reviewed Green Green Amber Green Amber Primary Care (300) (300) 0 0 (300)
26 LC MPC controls Grey Grey Grey Grey Grey Finance (17) 0 0 0 0
51 LC Primary Care Global Sum Purple Purple Purple Purple Purple Primary Care 0 0 0 0 0
52 LC Primary Care Dispensing Purple Purple Purple Purple Purple Primary Care 0 0 0 0 0
54 LC Estate Consolidation in Primary Care Purple Purple Purple Purple Purple Primary Care 0 0 0 0 0
55 LC GPIT Blue Blue Blue Blue Blue Primary Care (73) (73) 0 0 (73)
56 LC GP Staff Training cessation (East hosted) Green Green Amber Amber Red Primary Care 0 0 0 0 0
68 LC Nursing Homes Grey Grey Grey Grey Grey Medicine Management 0 0 0 0 0
8 LC Plan assumptions/Budget Reviews Green Green Green Green Green Finance 0 (431) 0 0 (431)
82 LC Stop Risk Stratification related investments Grey Grey Grey Grey Grey Primary Care 0 0 0 0 0
9 LC Public Health Funding Flu Vaccines Grey Grey Grey Grey Grey Finance (200) 0 0 0 0
A1 Cardiology Grey Grey Grey Grey Grey Integrated Teams workstream (154) 0 0 0 0
A10 Audiology Purple Purple Purple Purple Purple Planned Care Workstream (48) 0 0 0 0
A11 MSK Physiotherapy Green Green Amber Green Green Planned Care Workstream (292) (194) 0 (31) (163)
A12 Physio Amber Amber Red Green Amber Planned Care Workstream (32) 0 0 0 0
A13 Diagnostics - Imaging Amber Amber Red Amber Green Planned Care Workstream (236) (121) 0 (19) (102)
A14 Diagnostics - Non Imaging Amber Amber Red Amber Amber Planned Care Workstream (4) (4) 0 (1) (3)
A15 ED Front Door Model 1 Green Green Red Red Red Urgent Care Workstream (97) (23) (12) 0 (11)
A16 ED Front Door Model 2 Green Green Red Red Red Urgent Care Workstream (64) (15) (8) 0 (7)
A17 Increase & Improve Ambulatory Pathways 1 Green Green Red Red Red Urgent Care Workstream (113) (26) (14) 0 (12)

Appendix 3 Full LC CCG QIPP Dashboard
Scheme no.
for LLR
Summary
Report
Scheme Name Deliverables Milestones Total Risks IssuesOverall PMO
RAG ratingsGrouping / Function Annual Plan
Sum of Revised
FOT
Sum of Low
Finance
Confidence
Sum of Medium
Finance
Confidence
Sum of High
Finance
Confidence
A18 Increase & Improve Ambulatory Pathways 2 Green Green Green Green Green Urgent Care Workstream (174) (439) 0 (75) (365)
A19 Increase & Improve Ambulatory Pathways 3 Green Green Green Green Green Urgent Care Workstream (32) (44) 0 (8) (37)
A2 Respiratory Red Red Red Red Red Integrated Teams workstream (59) 9 (18) 0 27
A20 Improved Clinical Triage Green Green Red Red Red Urgent Care Workstream (16) (4) (2) 0 (2)
A21 Expansion of Clinical Navigation Hub Green Green Red Red Red Urgent Care Workstream (85) (20) (11) 0 (9)
A22 Tighten Eligibility for NEPTS Green Green Green Green Green Urgent Care Workstream (136) 0 0 0 0
A23 Urgent Diagnostic Pathways Red Red Red Red Red Urgent Care Workstream (1) (0) (0) 0 (0)
A24 Increase Support for EMAS to reduce conveyances Green Green Red Red Red Urgent Care Workstream (184) (43) (23) 0 (20)
A25 Discharge Pathways Green Green Green Green Green Urgent Care Workstream (84) (40) 0 0 (40)
A26 Frailty Red Red Red Red Red Urgent Care Workstream (79) (18) (10) 0 (9)
A27 Passporting Red Red Red Red Red Urgent Care Workstream (17) (4) (2) 0 (2)
A28 LC Medicines Optimisation (CCG) Green Green Green Green Green Medicine Management (2,700) (2,696) 0 0 (2,696)
A29 LC Cat M Blue Blue Blue Blue Blue Medicine Management (500) (500) 0 0 (500)
A3 Falls Red Red Red Red Red Integrated Teams workstream (0) 0 0 0 0
A30 LC NSCO Blue Blue Blue Blue Blue Medicine Management (1,600) (1,600) 0 0 (1,600)
A31 Biosimilar Switches Green Green Amber Amber Green Medicine Management (394) (407) 0 0 (407)
A32 Patent Expiry Humira® Green Green Amber Amber Green Medicine Management (185) (347) 0 0 (347)
A33 LC Move to VAT Free Route (TMP)- Tolvaptan Green Green Amber Amber Green Medicine Management (20) (2) 0 0 (2)
A34 Adult Mental Health Grey Grey Grey Grey Grey Mental Health/LD 0 0 0 0 0
A35 Section 117 and AHP Green Green Green Green Green Mental Health/LD (180) (915) 0 0 (915)
A36 MH OOA Placements - additional provision in LPT Green Green Amber Amber Green Mental Health/LD 0 (542) 0 0 (542)
A37 LD short breaks - other reviews Grey Grey Grey Grey Grey Mental Health/LD 0 0 0 0 0
A38 Community Health Services Various schemes Purple Purple Purple Purple Purple Community 0 0 0 0 0
A39 Community Equipment Scheme (returned equipment) Green Green Green Green Green Community (75) (113) 0 0 (113)
A4 EoL - CHC Deflected Patients Red Red Red Red Red Integrated Teams workstream (456) 49 (15) 0 64
A40 LC CCG Efficiencies (incl Execs) Green Green Green Green Green Corporate (167) (167) 0 0 (167)
A41 CHC Green Green Green Green Green CHC (1,782) (2,499) 0 0 (2,499)
A42 CHC Stretch Green Green Green Green Green CHC (650) (168) 0 0 (168)
A46 2. Repeat Ordering - FYE 3. Pregabalin - FYE 4. Technician Care Home Project - Reducing Waste Grey Grey Grey Grey Grey Medicine Management 0 0 0 0 0
A5 E0L Reduction in Emergency Admissions Red Red Red Red Red Integrated Teams workstream 0 0 0 0 0
A50 LC Paediatric Pathways Grey Grey Grey Grey Grey Elective Care 0 0 0 0 0
A51 LC ICS notice (ELR - Consider alongside 34, A51, 40.) Grey Grey Grey Grey Grey CommunityServices Redesign 0 0 0 0 0
A6 Demand Savings: New Appointments Green Green Green Green Green Planned Care Workstream (144) (189) 0 (30) (158)
A7 Demand Savings: Follow Up Appointments Green Green Green Green Green Planned Care Workstream (87) (97) 0 (16) (81)
A8 Demand Savings: Low Value Treatments Green Green Green Green Green Planned Care Workstream (40) (28) 0 (5) (24)
A9 Pathway Redesign Green Green Green Green Green Planned Care Workstream (638) (167) 0 (27) (141)
New 1 LC Procurement price reduction Inflectra Green Green Green Red Green Medicine Management 0 (63) 0 0 (63)
NEW A PCL Utilisation Green Green Amber Green Amber Planned Care Workstream 0 (11) 0 (2) (9)
NEW B Pathology - Target Tests Green Green Green Green Green Planned Care Workstream 0 (45) 0 (7) (38)
NEW C Alliance at Reduced Tariff Green Green Amber Green Amber Planned Care Workstream 0 (19) 0 (3) (16)
NEW D Avastin Green Green Amber Green Red Planned Care Workstream 0 0 0 0 0
NEW E UHL CQUIN Delivery Green Green Amber Green Green Contracting 0 (240) 0 (36) (204)
NEW F LPT Contract review including MH parity over investment Red Red Red Red Amber Mental Health/LD 0 (43) 0 0 (43)
NEW G LC Budget Review Green Green Green Green Green Finance 0 (2,261) 0 0 (2,261)
NEW H High Volume Service Users (EMAS/A&E) Grey Grey Grey Grey Grey Urgent Care Workstream 0 0 0 0 0
NEW I Telehealth - Dedicated line for Care/Nursing/Residential Homes Purple Purple Purple Purple Purple Urgent Care Workstream 0 0 0 0 0
NEW J Audit of Readmission Rates Grey Grey Grey Grey Grey Urgent Care Workstream 0 0 0 0 0
NEW K Reduction of EMAS conveyancing activity/Transfer o activity to UCCs Purple Purple Purple Purple Purple Urgent Care Workstream 0 0 0 0 0
NEW L Reduction of isolation and unnecessary hospital activity. Frailty & Isolation - BCF and community design; social inclusionGrey Grey Grey Grey Grey Urgent Care Workstream 0 0 0 0 0
NEW O Assista Green Green Green Green Green Contracting 0 (15) 0 0 (15)
Grand Total (18,055) (19,067) (115) (259) (18,693)
RAG Status Key:
Scheme
StatusPriority
Financial
Confidence
Red Open High Risk Low
Amber Open Medium Risk Medium
Green Open Low Risk High
Grey Closed N/A N/A
Blue Completed N/A N/A
Purple Deferred to
19/20 N/A N/A

Appendix 4 Full WL CCG QIPP Dashboard
Scheme no. for
LLR Summary
Report
Scheme Name Deliverables Milestones Total Risks IssuesOverall PMO
RAG ratingsGrouping / Function Annual Plan
Sum of Revised
FOT
Sum of Low
Finance
Confidence
Sum of Medium
Finance
Confidence
Sum of High
Finance
Confidence
1 Ambulatory Care Purple Purple Purple Purple Purple Integrated Teams workstream 0 0 0 0 0
2 Demand Management HUB: MSK, Dermatology (RSS) Amber Green Amber Green Amber Planned Care Workstream 0 (4) 0 (1) (3)
4 Orthotics Procurement(Blatchfords) Blue Blue Blue Blue Blue Community (75) (154) 0 0 (154)
5 Pathway 3 Control/Risk Share Green Green Green Green Green Urgent Care Workstream (300) (350) 0 0 (350)
6 Coding and Counting Grey Grey Grey Grey Grey Contracting 0 0 0 0 0
12 Removal of double payment to LPT for UHL discharge co-ordinators (Primary Care Co-ordinators) Purple Purple Purple Purple Purple Community (140) 0 0 0 0
13 Block Contracts at UHL Blue Blue Blue Blue Blue Contracting (98) (173) 0 0 (173)
15 UHL Contract Price negotiation - CAU Blue Blue Blue Blue Blue Contracting (88) (156) 0 0 (156)
16 UHL Contract Price Negotiation - CDU Purple Purple Purple Purple Purple Contracting (295) 0 0 0 0
17 UHL Contract Price Negotiation - RDA's Purple Purple Purple Purple Purple Contracting (147) 0 0 0 0
20 All historic AQP contracts to be reviewed Grey Grey Grey Grey Grey Planned Care Workstream (686) 0 0 0 0
22 Independent Sector Contract Control Grey Grey Grey Grey Grey Contracting 0 0 0 0 0
23 Independent Sector - manage IPT transfers from UHL Grey Grey Grey Grey Grey Contracting 0 0 0 0 0
24 NCA's tighter controls Amber Green Green Green Green Contracting 0 0 0 0 0
27 Night Nursing contract negotiation - DHU Blue Blue Blue Blue Blue Urgent Care Workstream (83) (34) 0 0 (34)
29 DHU - all services/contracting redesign Blue Blue Blue Blue Blue Urgent Care Workstream 0 (28) 0 0 (28)
31 LD Pool -improved case management Green Green Green Green Green Mental Health/LD (718) (666) 0 0 (666)
32 Reduce corporate clinical input Green Green Green Green Green Corporate (200) (148) 0 0 (148)
34 Review and redesign in ICS/IP Beds/District Nursing Purple Purple Purple Purple Purple CommunityServices Redesign (349) 0 0 0 0
35 EMAS - Negotiation of 18/19 contract Blue Blue Blue Blue Blue Contracting (269) (108) 0 0 (108)
36 LD Short breaks consolidation Purple Purple Purple Purple Purple Mental Health/LD (87) 0 0 0 0
37 LPT CQUIN expectation Green Green Green Green Green Contracting (189) (292) 0 0 (292)
38 Stroke Rehab Bed Numbers Reduction Following redesign and investment Blue Blue Blue Blue Blue Community (108) (108) 0 0 (108)
39 Agnes unit - options for use Grey Grey Grey Grey Grey Mental Health/LD 0 0 0 0 0
40 Potential realignment of Community Hospital Beds across sites Purple Purple Purple Purple Purple CommunityServices Redesign (105) 0 0 0 0
41 AHP/117 repatriation Grey Grey Grey Grey Grey Mental Health/LD 0 0 0 0 0
43 Vol Sector - Review VFM and service need Green Green Green Amber Green Community (580) (12) 0 0 (12)
44 Derbyshire Healthcare non acute SLA negotiation Grey Grey Grey Grey Grey Contracting (156) 0 0 0 0
47 Joint Funding University of Leicester Purple Purple Purple Purple Purple Finance (24) 0 0 0 0
49 Office Accommodation savings Purple Purple Purple Purple Purple Corporate 0 0 0 0 0
50 In House Legal expertise Purple Purple Purple Purple Purple Corporate (60) 0 0 0 0
57 Readmissions reduction Purple Purple Purple Purple Purple Urgent Care Workstream 0 0 0 0 0
58 BCT Partnership office maintain spend in line with 17/18 outturn Green Green Green Green Green Corporate (146) (146) 0 0 (146)
59 Anticoag at UHL - moved into community Blue Blue Blue Blue Blue Community (206) (189) 0 0 (189)
61 Consider Staff Car Parking Charges Grey Grey Grey Grey Grey Corporate 0 0 0 0 0
63 Prior approvals (IFR's) tighter controls Purple Purple Purple Purple Purple Contracting (147) 0 0 0 0
71 GPAU, Urgent Care flow and pathways - admissions impact Grey Grey Grey Grey Grey Urgent Care Workstream 0 0 0 0 0
72 MHSOP Review Grey Grey Grey Grey Grey Mental Health/LD 0 0 0 0 0
73 Independent Sector Contract - Circle, Loughborough Grey Grey Grey Grey Grey Contracting 0 0 0 0 0
74 Biologics Support Service (UHL) Amber Amber Amber Amber Green Medicine Management 0 0 0 0 0
81 Review of IAPT Green Green Green Green Green Mental Health/LD 0 (597) 0 0 (597)
11 WL Review/Reduce expenditure on agency staff Green Green Green Green Green Corporate (477) (477) 0 0 (477)
18 WL PRIMARY CARE - Federation QIPP scheme impact on acute demand Red Red Red Red Red Primary Care (1,300) (777) (300) 0 (477)
21 WL PRIMARY CARE - CBS investments reviewed Red Red Red Red Red Primary Care (500) 0 0 0 0
25 WL Review all LA Charges that come to the CCG outside of BCF Green Green Green Green Green Finance 0 (309) 0 0 (309)
26 WL MPC controls Grey Grey Grey Grey Grey Finance (17) 0 0 0 0
51 WL Primary Care Global Sum Purple Purple Purple Purple Purple Primary Care 0 0 0 0 0
52 WL Primary Care Dispensing Purple Purple Purple Purple Purple Primary Care 0 0 0 0 0
54 WL Estate Consolidation in Primary Care Purple Purple Purple Purple Purple Primary Care 0 0 0 0 0
55 WL GPIT Blue Blue Blue Blue Blue Primary Care (66) (66) 0 0 (66)
56 WL GP Staff Training cessation (East hosted) Green Green Amber Amber Red Primary Care (70) 0 0 0 0
62 WL Prescribing Stretch to £1m Green Green Green Green Green Medicine Management (1,000) (587) 0 0 (587)
68 WL Nursing Homes Grey Grey Grey Grey Grey Medicine Management 0 0 0 0 0
7 WL Primary Care - Federation QIPP, Quality SIP etc. Grey Grey Grey Grey Grey Primary Care 0 0 0 0 0
8 WL Plan assumptions/Budget Reviews Blue Blue Blue Blue Blue Finance 0 (1,372) 0 0 (1,372)
82 WL Stop Risk Stratification related investments Grey Grey Grey Grey Grey Primary Care 0 0 0 0 0
9 WL Public Health Funding Flu Vaccines Blue Blue Blue Blue Blue Finance (300) (69) 0 0 (69)
A1 Cardiology Grey Grey Grey Grey Grey Integrated Teams workstream (77) 0 0 0 0
A10 Audiology Purple Purple Purple Purple Purple Planned Care Workstream (48) 0 0 0 0
A11 MSK Physiotherapy Green Green Amber Green Green Planned Care Workstream (292) (245) 0 (39) (206)
A12 Physio Amber Amber Red Green Amber Planned Care Workstream (32) 0 0 0 0
A13 Diagnostics - Imaging Amber Amber Red Amber Green Planned Care Workstream (236) (93) 0 (15) (78)
A14 Diagnostics - Non Imaging Amber Amber Red Amber Amber Planned Care Workstream (4) (4) 0 (1) (3)
A15 ED Front Door Model 1 Green Green Red Red Red Urgent Care Workstream (46) (18) (9) 0 (8)
A16 ED Front Door Model 2 Green Green Red Red Red Urgent Care Workstream (10) (4) (2) 0 (2)
A17 Increase & Improve Ambulatory Pathways 1 Green Green Red Red Red Urgent Care Workstream (59) (23) (12) 0 (11)
A18 Increase & Improve Ambulatory Pathways 2 Green Green Green Green Green Urgent Care Workstream (141) (253) 0 (43) (210)
A19 Increase & Improve Ambulatory Pathways 3 Green Green Green Green Green Urgent Care Workstream (27) (29) 0 (5) (24)
A2 Respiratory Red Red Red Red Red Integrated Teams workstream (53) 7 (17) 0 24

Appendix 4 Full WL CCG QIPP Dashboard
Scheme no. for
LLR Summary
Report
Scheme Name Deliverables Milestones Total Risks IssuesOverall PMO
RAG ratingsGrouping / Function Annual Plan
Sum of Revised
FOT
Sum of Low
Finance
Confidence
Sum of Medium
Finance
Confidence
Sum of High
Finance
Confidence
A20 Improved Clinical Triage Green Green Red Red Red Urgent Care Workstream (5) (2) (1) 0 (1)
A21 Expansion of Clinical Navigation Hub Green Green Red Red Red Urgent Care Workstream (60) (23) (12) 0 (11)
A22 Tighten Eligibility for NEPTS Green Green Green Green Green Urgent Care Workstream (152) 0 0 0 0
A23 Urgent Diagnostic Pathways Red Red Red Red Red Urgent Care Workstream (21) (8) (4) 0 (4)
A24 Increase Support for EMAS to reduce conveyances Green Green Red Red Red Urgent Care Workstream (14) (5) (3) 0 (3)
A25 Discharge Pathways Green Green Green Green Green Urgent Care Workstream (83) (40) 0 0 (40)
A26 Frailty Red Red Red Red Red Urgent Care Workstream (64) (24) (13) 0 (11)
A27 Passporting Red Red Red Red Red Urgent Care Workstream (21) (8) (4) 0 (4)
A28 WL Medicines Optimisation (CCG) Green Green Green Green Green Medicine Management (2,000) (2,000) 0 0 (2,000)
A29 WL Cat M Grey Grey Grey Grey Grey Medicine Management 0 0 0 0 0
A3 Falls Red Red Red Red Red Integrated Teams workstream (76) 85 (55) 0 139
A30WL NSCO Grey Grey Grey Grey Grey Medicine Management 0 0 0 0 0
A31 Biosimilar Switches Green Green Amber Amber Green Medicine Management (394) (406) 0 0 (406)
A32 Patent Expiry Humira® Green Green Amber Amber Green Medicine Management (185) (347) 0 0 (347)
A33 WL Move to VAT Free Route (TMP)- Tolvaptan Green Green Amber Amber Green Medicine Management (20) (2) 0 0 (2)
A34 Adult Mental Health Grey Grey Grey Grey Grey Mental Health/LD (547) 0 0 0 0
A35 Section 117 and AHP Green Green Green Green Green Mental Health/LD (111) (601) 0 0 (601)
A36 MH OOA Placements - additional provision in LPT Green Green Amber Amber Green Mental Health/LD (131) (202) 0 0 (202)
A37 LD short breaks - other reviews Grey Grey Grey Grey Grey Mental Health/LD 0 0 0 0 0
A38 Community Health Services Various schemes Purple Purple Purple Purple Purple Community (383) 0 0 0 0
A39 Community Equipment Scheme (returned equipment) Green Green Green Green Green Community (75) (96) 0 0 (96)
A4 EoL - CHC Deflected Patients Red Red Red Red Red Integrated Teams workstream (460) 47 (15) 0 62
A40 WL CCG Efficiencies (incl Execs) Red Red Red Red Red Corporate (507) 0 0 0 0
A41 CHC Green Green Green Green Green CHC (1,826) (3,030) 0 0 (3,030)
A42 CHC Stretch Green Green Green Green Green CHC (650) (170) 0 0 (170)
A43 WL BCF Slippage/contingency/savings plan Green Green Amber Amber Green Finance (1,000) (967) 0 0 (967)
A44 Integrated urgent care - Primary care Green Green Green Green Green Primary Care (600) (600) 0 0 (600)
A46 2. Repeat Ordering - FYE 3. Pregabalin - FYE 4. Technician Care Home Project - Reducing Waste Grey Grey Grey Grey Grey Medicine Management 0 0 0 0 0
A5 E0L Reduction in Emergency Admissions Red Red Red Red Red Integrated Teams workstream (59) 0 0 0 0
A50 WL Paediatric Pathways Grey Grey Grey Grey Grey Elective Care 0 0 0 0 0
A51 WL ICS notice (ELR - Consider alongside 34, A51, 40.) Grey Grey Grey Grey Grey CommunityServices Redesign 0 0 0 0 0
A6 Demand Savings: New Appointments Green Green Green Green Green Planned Care Workstream (293) (151) 0 (24) (127)
A7 Demand Savings: Follow Up Appointments Green Green Green Green Green Planned Care Workstream (150) (58) 0 (9) (49)
A8 Demand Savings: Low Value Treatments Green Green Green Green Green Planned Care Workstream (65) (56) 0 (9) (47)
A9 Pathway Redesign Green Green Green Green Green Planned Care Workstream (535) (138) 0 (22) (116)
New 1 WL Procurement price reduction Inflectra Green Green Green Red Green Medicine Management 0 (63) 0 0 (63)
NEW A PCL Utilisation Green Green Amber Green Amber Planned Care Workstream 0 (11) 0 (2) (9)
NEW B Pathology - Target Tests Green Green Green Green Green Planned Care Workstream 0 (33) 0 (5) (28)
NEW C Alliance at Reduced Tariff Green Green Amber Green Amber Planned Care Workstream 0 (19) 0 (3) (16)
NEW D Avastin Green Green Amber Green Red Planned Care Workstream 0 0 0 0 0
NEW E UHL CQUIN Delivery Green Green Amber Green Green Contracting 0 (180) 0 (27) (153)
NEW F LPT Contract review including MH parity over investment Red Red Red Red Amber Mental Health/LD 0 (43) 0 0 (43)
NEW G WL Budget Review Blue Blue Blue Blue Blue Finance 0 (2,380) 0 0 (2,380)
NEW H High Volume Service Users (EMAS/A&E) Grey Grey Grey Grey Grey Urgent Care Workstream 0 0 0 0 0
NEW I Telehealth - Dedicated line for Care/Nursing/Residential Homes Purple Purple Purple Purple Purple Urgent Care Workstream 0 0 0 0 0
NEW J Audit of Readmission Rates Grey Grey Grey Grey Grey Urgent Care Workstream 0 0 0 0 0
NEW K Reduction of EMAS conveyancing activity/Transfer o activity to UCCs Purple Purple Purple Purple Purple Urgent Care Workstream 0 0 0 0 0
NEW L Reduction of isolation and unnecessary hospital activity. Frailty & Isolation - BCF and community design; social inclusionGrey Grey Grey Grey Grey Urgent Care Workstream 0 0 0 0 0
NEW M WL CFO Prescribing Stretch Red Red Red Red Red Medicine Management 0 0 0 0 0
NEW N WL GPIT review: utilisation of contract efficiencies Red Red Red Red Red Finance 0 0 0 0 0
NEW O Assista Green Green Green Green Green Contracting 0 (15) 0 0 (15)
Grand Total (20,498) (19,033) (448) (205) (18,380)
RAG Status Key:
Scheme
StatusPriority
Financial
Confidence
Red Open High Risk Low
Amber Open Medium Risk Medium
Green Open Low Risk High
Grey Closed N/A N/A
Blue Completed N/A N/A
Purple Deferred to
19/20 N/A N/A

Appendix 5 Full ELR CCG QIPP Dashboard
Scheme no.
for LLR
Summary
Report
Scheme Name Deliverables Milestones Total Risks IssuesOverall PMO
RAG ratingsGrouping / Function Annual Plan
Sum of Revised
FOT
Sum of Low
Finance
Confidence
Sum of Medium
Finance
Confidence
Sum of High
Finance
Confidence
1 Ambulatory Care Purple Purple Purple Purple Purple Integrated Teams workstream 0 0 0 0 0
2 Demand Management HUB: MSK, Dermatology (RSS) Amber Green Amber Green Amber Planned Care Workstream 0 (6) 0 (1) (5)
4 Orthotics Procurement(Blatchfords) Blue Blue Blue Blue Blue Community (65) (66) 0 0 (66)
5 Pathway 3 Control/Risk Share Green Green Green Green Green Urgent Care Workstream (200) (164) 0 0 (164)
6 Coding and Counting Grey Grey Grey Grey Grey Contracting 0 0 0 0 0
12 Removal of double payment to LPT for UHL discharge co-ordinators (Primary Care Co-ordinators) Purple Purple Purple Purple Purple Community (119) 0 0 0 0
13 Block Contracts at UHL Blue Blue Blue Blue Blue Contracting (104) (205) 0 0 (205)
14 UHL Contract Price negotiation - Follow Up Ratios Grey Grey Grey Grey Grey Contracting (891) 0 0 0 0
15 UHL Contract Price negotiation - CAU Blue Blue Blue Blue Blue Contracting (89) (156) 0 0 (156)
16 UHL Contract Price Negotiation - CDU Purple Purple Purple Purple Purple Contracting (297) 0 0 0 0
17 UHL Contract Price Negotiation - RDA's Purple Purple Purple Purple Purple Contracting (149) 0 0 0 0
20 All historic AQP contracts to be reviewed Grey Grey Grey Grey Grey Planned Care Workstream (1,305) 0 0 0 0
22 Independent Sector Contract Control Grey Grey Grey Grey Grey Contracting 0 0 0 0 0
23 Independent Sector - manage IPT transfers from UHL Grey Grey Grey Grey Grey Contracting 0 0 0 0 0
24 NCA's tighter controls Amber Green Green Green Green Contracting 0 0 0 0 0
27 Night Nursing contract negotiation - DHU Blue Blue Blue Blue Blue Urgent Care Workstream (250) (28) 0 0 (28)
29 DHU - all services/contracting redesign Blue Blue Blue Blue Blue Urgent Care Workstream 0 (28) 0 0 (28)
31 LD Pool -improved case management Green Green Green Green Green Mental Health/LD (603) (570) 0 0 (570)
34 Review and redesign in ICS/IP Beds/District Nursing Purple Purple Purple Purple Purple CommunityServices Redesign (306) 0 0 0 0
35 EMAS - Negotiation of 18/19 contract Blue Blue Blue Blue Blue Contracting (220) (89) 0 0 (89)
36 LD Short breaks consolidation Purple Purple Purple Purple Purple Mental Health/LD (87) 0 0 0 0
37 LPT CQUIN expectation Green Green Green Green Green Contracting (154) (238) 0 0 (238)
38 Stroke Rehab Bed Numbers Reduction Following redesign and investment Blue Blue Blue Blue Blue Community (86) (86) 0 0 (86)
39 Agnes unit - options for use Grey Grey Grey Grey Grey Mental Health/LD 0 0 0 0 0
40 Potential realignment of Community Hospital Beds across sites Purple Purple Purple Purple Purple CommunityServices Redesign 0 0 0 0 0
41 AHP/117 repatriation Grey Grey Grey Grey Grey Mental Health/LD 0 0 0 0 0
43 Vol Sector - Review VFM and service need Green Green Green Amber Green Community (218) 0 0 0 0
47 Joint Funding University of Leicester Purple Purple Purple Purple Purple Finance 0 0 0 0 0
49 Office Accommodation savings Purple Purple Purple Purple Purple Corporate 0 0 0 0 0
50 In House Legal expertise Purple Purple Purple Purple Purple Corporate (45) 0 0 0 0
57 Readmissions reduction Purple Purple Purple Purple Purple Urgent Care Workstream 0 0 0 0 0
58 BCT Partnership office maintain spend in line with 17/18 outturn Green Green Green Green Green Corporate 0 0 0 0 0
59 Anticoag at UHL - moved into community Blue Blue Blue Blue Blue Community (167) (202) 0 0 (202)
61 Consider Staff Car Parking Charges Grey Grey Grey Grey Grey Corporate 0 0 0 0 0
63 Prior approvals (IFR's) tighter controls Purple Purple Purple Purple Purple Contracting (149) 0 0 0 0
67 Prescribing Incentive Scheme Grey Grey Grey Grey Grey Medicine Management 0 0 0 0 0
71 GPAU, Urgent Care flow and pathways - admissions impact Grey Grey Grey Grey Grey Urgent Care Workstream 0 0 0 0 0
72 MHSOP Review Grey Grey Grey Grey Grey Mental Health/LD 0 0 0 0 0
73 Independent Sector Contract - Circle, Loughborough Grey Grey Grey Grey Grey Contracting 0 0 0 0 0
74 Biologics Support Service (UHL) Amber Amber Amber Amber Green Medicine Management 0 0 0 0 0
81 Review of IAPT Green Green Green Green Green Mental Health/LD (500) (500) 0 0 (500)
11 ELR Review/Reduce expenditure on agency staff Green Green Green Green Green Corporate (557) (205) 0 0 (205)
18 ELR PRIMARY CARE - Federation QIPP scheme impact on acute demand Grey Grey Grey Grey Grey Primary Care 0 0 0 0 0
21 ELR PRIMARY CARE - CBS investments reviewed Amber Amber Amber Amber Green Primary Care 0 0 0 0 0
25 ELR Review all LA Charges that come to the CCG outside of BCF Green Green Green Green Green Finance (336) (250) 0 0 (250)
26 ELR MPC controls Grey Grey Grey Grey Grey Finance (17) 0 0 0 0
51 ELR Primary Care Global Sum Purple Purple Purple Purple Purple Primary Care 0 0 0 0 0
52 ELR Primary Care Dispensing Purple Purple Purple Purple Purple Primary Care 0 0 0 0 0
54 ELR Estate Consolidation in Primary Care Purple Purple Purple Purple Purple Primary Care 0 0 0 0 0
55 ELR GPIT Blue Blue Blue Blue Blue Primary Care (61) (61) 0 0 (61)
56 ELR GP Staff Training cessation (East hosted) Green Green Amber Amber Red Primary Care 0 0 0 0 0
62 ELR Prescribing Stretch to £1m Green Green Green Amber Green Medicine Management (1,000) (1,509) 0 0 (1,509)
68 ELR Nursing Homes Grey Grey Grey Grey Grey Medicine Management 0 0 0 0 0
7 ELR Primary Care - Federation QIPP, Quality SIP etc. Green Green Green Green Green Primary Care (2,000) (2,000) 0 0 (2,000)
8 ELR Plan assumptions/Budget Reviews Blue Blue Blue Blue Blue Finance 0 (1,015) 0 0 (1,015)
82 ELR Stop Risk Stratification related investments Grey Grey Grey Grey Grey Primary Care 0 0 0 0 0
9 ELR Public Health Funding Flu Vaccines Blue Blue Blue Blue Blue Finance (300) (125) 0 0 (125)
A1 Cardiology Grey Grey Grey Grey Grey Integrated Teams workstream 0 0 0 0 0
A10 Audiology Purple Purple Purple Purple Purple Planned Care Workstream 0 0 0 0 0
A11 MSK Physiotherapy Green Green Amber Green Green Planned Care Workstream (106) (87) 0 (14) (73)
A12 Physio Amber Amber Red Green Amber Planned Care Workstream 0 0 0 0 0
A13 Diagnostics - Imaging Amber Amber Red Amber Green Planned Care Workstream 0 (179) 0 (29) (150)
A14 Diagnostics - Non Imaging Amber Amber Red Amber Amber Planned Care Workstream 0 (4) 0 (1) (3)
A15 ED Front Door Model 1 Green Green Red Red Red Urgent Care Workstream (24) (11) (6) 0 (5)
A16 ED Front Door Model 2 Green Green Red Red Red Urgent Care Workstream (2) (1) (0) 0 (0)
A17 Increase & Improve Ambulatory Pathways 1 Green Green Red Red Red Urgent Care Workstream (30) (14) (7) 0 (7)
A18 Increase & Improve Ambulatory Pathways 2 Green Green Green Green Green Urgent Care Workstream (57) (193) 0 (33) (160)
A19 Increase & Improve Ambulatory Pathways 3 Green Green Green Green Green Urgent Care Workstream (13) (25) 0 (4) (21)
A2 Respiratory Red Red Red Red Red Integrated Teams workstream 0 6 (13) 0 19

Appendix 5 Full ELR CCG QIPP Dashboard
Scheme no.
for LLR
Summary
Report
Scheme Name Deliverables Milestones Total Risks IssuesOverall PMO
RAG ratingsGrouping / Function Annual Plan
Sum of Revised
FOT
Sum of Low
Finance
Confidence
Sum of Medium
Finance
Confidence
Sum of High
Finance
Confidence
A20 Improved Clinical Triage Green Green Red Red Red Urgent Care Workstream (4) (2) (1) 0 (1)
A21 Expansion of Clinical Navigation Hub Green Green Red Red Red Urgent Care Workstream (24) (11) (6) 0 (5)
A22 Tighten Eligibility for NEPTS Green Green Green Green Green Urgent Care Workstream (56) (445) 0 (100) (345)
A23 Urgent Diagnostic Pathways Red Red Red Red Red Urgent Care Workstream (2) (1) (0) 0 (0)
A24 Increase Support for EMAS to reduce conveyances Green Green Red Red Red Urgent Care Workstream 0 0 0 0 0
A25 Discharge Pathways Green Green Green Green Green Urgent Care Workstream (42) (40) 0 0 (40)
A26 Frailty Red Red Red Red Red Urgent Care Workstream (34) (16) (8) 0 (7)
A27 Passporting Red Red Red Red Red Urgent Care Workstream (11) (5) (3) 0 (2)
A28 ELR Medicines Optimisation (CCG) Green Green Green Green Green Medicine Management (2,000) (2,000) 0 0 (2,000)
A29 ELR Cat M Grey Grey Grey Grey Grey Medicine Management 0 0 0 0 0
A3 Falls Red Red Red Red Red Integrated Teams workstream 0 112 (30) 0 142
A30 ELR NSCO Grey Grey Grey Grey Grey Medicine Management 0 0 0 0 0
A31 Biosimilar Switches Green Green Amber Amber Green Medicine Management (424) (438) 0 0 (438)
A32 Patent Expiry Humira® Green Green Amber Amber Green Medicine Management (200) (374) 0 0 (374)
A33 ELR Move to VAT Free Route (TMP)- Tolvaptan Green Green Amber Amber Green Medicine Management (20) (2) 0 0 (2)
A34 Adult Mental Health Grey Grey Grey Grey Grey Mental Health/LD (592) 0 0 0 0
A35 Section 117 and AHP Green Green Green Green Green Mental Health/LD (249) (206) 0 0 (206)
A36 MH OOA Placements - additional provision in LPT Green Green Amber Amber Green Mental Health/LD (106) (175) 0 0 (175)
A37 LD short breaks - other reviews Grey Grey Grey Grey Grey Mental Health/LD (82) 0 0 0 0
A38 Community Health Services Various schemes Purple Purple Purple Purple Purple Community (592) 0 0 0 0
A39 Community Equipment Scheme (returned equipment) Green Green Green Green Green Community 0 (96) 0 0 (96)
A4 EoL - CHC Deflected Patients Red Red Red Red Red Integrated Teams workstream (539) 53 (17) 0 71
A40 ELR CCG Efficiencies (incl Execs) Green Green Green Green Green Corporate (166) (166) 0 0 (166)
A41 CHC Green Green Green Green Green CHC (1,211) (2,217) 0 0 (2,217)
A42 CHC Stretch Green Green Green Green Green CHC (650) (139) 0 0 (139)
A43 ELR BCF Slippage/contingency/savings plan Green Green Green Green Green Finance (1,100) (1,169) 0 0 (1,169)
A46 2. Repeat Ordering - FYE 3. Pregabalin - FYE 4. Technician Care Home Project - Reducing Waste Grey Grey Grey Grey Grey Medicine Management 0 0 0 0 0
A47 Ambulatory Care -look at closer to home services Grey Grey Grey Grey Grey Community (300) 0 0 0 0
A48 Recharge for UCC outside LLR Amber Amber Amber Amber Amber Community (40) (84) 0 0 (84)
A49 Primary Care Stretch Target - as part of contractual review Green Green Green Green Green Primary Care 0 (2,086) 0 0 (2,086)
A5 E0L Reduction in Emergency Admissions Red Red Red Red Red Integrated Teams workstream (40) 0 0 0 0
A50 ELR Paediatric Pathways Grey Grey Grey Grey Grey Elective Care 0 0 0 0 0
A51 ELR ICS notice (ELR - Consider alongside 34, A51, 40.) Blue Blue Blue Blue Blue CommunityServices Redesign (125) (112) 0 0 (112)
A6 Demand Savings: New Appointments Green Green Green Green Green Planned Care Workstream (235) (249) 0 (40) (209)
A7 Demand Savings: Follow Up Appointments Green Green Green Green Green Planned Care Workstream (132) (136) 0 (22) (115)
A8 Demand Savings: Low Value Treatments Green Green Green Green Green Planned Care Workstream (32) (31) 0 (5) (26)
A9 Pathway Redesign Green Green Green Green Green Planned Care Workstream (132) (44) 0 (7) (37)
New 1 ELR Procurement price reduction Inflectra Green Green Green Red Green Medicine Management 0 (67) 0 0 (67)
NEW A PCL Utilisation Green Green Amber Green Amber Planned Care Workstream 0 (11) 0 (2) (9)
NEW B Pathology - Target Tests Green Green Green Green Green Planned Care Workstream 0 (35) 0 (6) (30)
NEW C Alliance at Reduced Tariff Green Green Amber Green Amber Planned Care Workstream 0 (19) 0 (3) (16)
NEW D Avastin Green Green Amber Green Red Planned Care Workstream 0 0 0 0 0
NEW E UHL CQUIN Delivery Green Green Amber Green Green Contracting 0 (180) 0 (27) (153)
NEW F LPT Contract review including MH parity over investment Red Red Red Red Amber Mental Health/LD 0 (43) 0 0 (43)
NEW G ELR Budget Review Blue Blue Blue Blue Blue Finance 0 (771) 0 0 (771)
NEW H High Volume Service Users (EMAS/A&E) Grey Grey Grey Grey Grey Urgent Care Workstream 0 0 0 0 0
NEW I Telehealth - Dedicated line for Care/Nursing/Residential Homes Purple Purple Purple Purple Purple Urgent Care Workstream 0 0 0 0 0
NEW J Audit of Readmission Rates Grey Grey Grey Grey Grey Urgent Care Workstream 0 0 0 0 0
NEW K Reduction of EMAS conveyancing activity/Transfer o activity to UCCs Purple Purple Purple Purple Purple Urgent Care Workstream 0 0 0 0 0
NEW L Reduction of isolation and unnecessary hospital activity. Frailty & Isolation - BCF and community design; social inclusionGrey Grey Grey Grey Grey Urgent Care Workstream 0 0 0 0 0
NEW M ELR ELR Unidentified QIPP Red Red Red Red Red Community 0 0 0 0 0
NEW N ELR GPIT review: utilisation of contract efficiencies Red Red Red Red Red Finance 0 0 0 0 0
NEW O Assista Green Green Green Green Green Contracting 0 (15) 0 0 (15)
Grand Total (19,647) (19,234) (93) (292) (18,849)
RAG Status Key:
Scheme
StatusPriority
Financial
Confidence
Red Open High Risk Low
Amber Open Medium Risk Medium
Green Open Low Risk High
Grey Closed N/A N/A
Blue Completed N/A N/A
Purple Deferred to
19/20 N/A N/A

APPENDIX 6
19/20 QIPP SCHEMES AS AT 11TH MARCH 2019 high
medium
WAVE 1 SCHEMES: low
Scheme Ref Scheme Name SRO Gross Savings Investment Net Savings PID Required Business Case
Required Pid Completed
Business Case
Completed
Approved by
CCB?
Workbook
Received Workbook Name Gross Savings Investment Net Savings
Confidence in
DeliveryRish Adjusted Comments
1.1 Same Day Emergency Care Tamsin Hooton £2,920,375 -£14,890 £2,905,485 Yes Yes Yes Yes Yes Yes Same Day Emergency Care PMO Workbook £2,920,375 -£14,890 £2,905,485 low £726,371 No activity or finance contained within the workbook £865,283 -£4,412 £860,872 £998,057 -£5,089 £992,968 £1,057,035 -£5,389 £1,051,645
1.2 Community Services Redesign Tamsin Hooton £1,259,000 £1,259,000 Yes Yes Yes Yes Yes PMO Workbook - CSR 2019-20 £4,799,223 -£4,026,785 £772,439 low £193,110 As per workbook £1,367,436 -£1,170,469 £196,968 £1,899,805 -£1,540,575 £359,230 £1,531,982 -£1,315,741 £216,241
1.2 a Community Services Redesign Stretch £486,913 £0 £486,913 low £121,728 Shortfall on previous plan added as stretch £162,304 £162,304 £162,304 £162,304 £162,304 £162,304
1.3 Long Term Conditions Tamsin Hooton £629,596 £629,596 Yes Yes Yes Yes Yes YesPMO Workbook LTC -
Respiratory/Cardiology/Diabetes/Hypertenstion£1,309,071 -£541,500 £767,571 low £191,893 £472,866 -£181,656 £291,210 £361,050 -£166,428 £194,622 £475,155 -£193,416 £281,739
1.4 Integrated Urgent Care Mike Ryan £1,273,182 -£430,819 £842,363 Yes Yes Yes Yes Yes Yes IUC PMO Workbook £1,273,182 -£430,819 £842,363 low £210,591 Finances need clarifying with project lead as not clear in workbook £347,253 -£112,876 £234,377 £424,629 -£138,341 £286,288 £501,300 -£179,602 £321,698
1.5 Falls (County Only) Tamsin Hooton £1,008,946 -£421,750 £587,196 Yes Yes Yes Yes Yes No £1,008,946 -£421,750 £587,196 medium £366,998 £511,375 -£213,760 £297,615 £497,571 -£207,990 £289,581 £0
2.1 Audiology Ket Chudasama £410,690 £410,690 Yes Yes Yes Yes Yes No £410,690 £410,690 medium £256,681 £140,320 £140,320 £148,860 £148,860 £121,510 £121,510
2.2 Referral Support Services Ket Chudasama £9,446,913 -£6,859,416 £2,587,497 Yes Yes Yes Yes Yes Yes Planned Care Workbook £9,456,913 -£6,859,416 £2,597,497 medium £1,623,436 Needs Grossing up in the workbook. £10k change in figures £3,179,989 -£2,313,878 £866,111 £2,804,394 -£2,010,341 £794,053 £3,472,530 -£2,535,197 £937,333
2.3 Dermatology Pathway Redesign Ket Chudasama £745,998 -£405,217 £340,781 Yes Yes Yes Yes Yes Yes Planned Care Workbook £745,998 -£405,217 £340,781 medium £212,988 Needs Grossing up in the workbook £254,823 -£134,350 £120,473 £313,492 -£186,769 £126,722 £177,684 -£84,098 £93,586
2.4 Ophthalmology Pathway Redesign Ket Chudasama £646,100 -£452,293 £193,807 Yes Yes Yes Yes Yes Planned Care Workbook £646,100 -£452,293 £193,807 medium £121,130 Needs Grossing up in the workbook £217,800 -£152,480 £65,320 £240,500 -£168,323 £72,177 £187,800 -£131,490 £56,310
2.5 Pathology Ket Chudasama £1,185,500 £1,185,500 Yes Yes Yes Yes Yes Yes Planned Care Workbook £1,185,500 £1,185,500 high £1,037,313 £374,500 £374,500 £349,500 £349,500 £461,500 £461,500
3.1 Medicines Optimisation Tim Sacks £6,669,312 -£659,312 £6,010,000 Yes Yes Yes Yes N/A? Yes Medicines Optimisation £7,434,997 -£674,996 £6,760,001 high £5,915,001
LLR Workbook presented - to be verified by ELR and LC due to annual leave.
£750k of £1m stretch included. Remaining £250k stretch to be included
within HCD figures
£2,414,620 -£174,620 £2,240,000 £2,585,757 -£325,757 £2,260,000 £2,434,620 -£174,620 £2,260,000
3.2 High Cost Drugs Tim Sacks £6,000,000 £6,000,000 Yes Yes Yes Yes N/A Yes £7,817,980 £7,817,980 medium £4,886,238 Includes £1.1m self determined stretch £2,715,860 £2,715,860 £2,551,060 £2,551,060 £2,551,060 £2,551,060
3.3 LC CCG CBS Review Richard Morris £240,000 £240,000 Yes Yes Yes Yes N/A No £240,000 £240,000 medium £150,000 £0 £0 £240,000 £0 £240,000
3.4 University of Leicester Post Ian Potter £48,000 £48,000 No No N/A N/A N/A No £48,000 £48,000 high £42,000 £0 £24,000 £24,000 £24,000 £24,000
3.5 GP Backfill Scheme Richard Morris £131,149 £131,149 No No N/A N/A N/A N/A £131,149 £131,149 high £131,149 Informed is already delivered - budget reduction in plan £0 £0 £131,149 £131,149
4.1 Continuing Healthcare Paul Gibarra £6,700,000 £6,700,000 Yes Yes Yes Yes Yes Yes 2019-20 CHC workbook £5,523,569 £5,523,569 medium £3,452,230 Amount identified in workbook - with stretch below £1,521,552 £1,521,552 £1,470,347 £1,470,347 £2,531,670 £2,531,670
5.1 Contracting Efficiencies Sarah Shuttlewood £525,000 £525,000 No No N/A N/A N/A No £525,000 £525,000 low £131,250 £155,553 £155,553 £179,422 £179,422 £190,025 £190,025
5.2 Orthotics Contract Sarah Shuttlewood £177,857 £177,857 No No N/A N/A N/A N/A £177,857 £177,857 high £177,857 £47,143 £47,143 £110,000 £110,000 £20,714 £20,714
5.3Northants Mental Health Contract Block to cost per case
(ELR Only)Sarah Shuttlewood £150,000 £150,000 No No
N/A N/AN/A No £150,000 £150,000 high £150,000 £150,000 £150,000 £0 £0
6.1 Primary Care Co-ordinators Sarah Shuttlewood £392,500 £392,500 No No N/A N/A N/A No £785,000 £785,000 medium £490,625 Updated figures provided by Colin Groom £238,000 £238,000 £280,000 £280,000 £267,000 £267,000
6.2 Reduction in Stroke Beds Sarah Shuttlewood £445,200 £445,200 No No N/A N/A N/A N/A £445,200 £445,200 high £445,200 £120,203 £120,203 £151,369 £151,369 £173,628 £173,628
6.3 ICS notice (ELR Only) Sarah Shuttlewood £600,000 £600,000 No No N/A N/A N/A N/A £600,000 £600,000 high £600,000 £600,000 £600,000 £0 £0
7.1 Children's Blood Borne Viruses Chris West £37,200 -£12,700 £24,500 Yes Yes Yes Yes Yes Yes Children's workbok £30,200 -£5,700 £24,500 medium £15,313Finances need splitting into investment and savings. Profile between CCGs
changed from assumed 1/3rds in plan.£7,800 -£1,500 £6,300 £10,700 -£2,000 £8,700 £11,700 -£2,200 £9,500
7.2 CAMHS efficiencies Chris West £231,120 £231,120 Yes Yes No No No £231,120 £231,120 low £57,780 £59,693 £59,693 £81,887 £81,887 £89,540 £89,540
8.1 Reduced Clinical Input (WL CCG Only) Ket Chudasama £74,196 £74,196 No No N/A N/A N/A No £74,196 £74,196 high £74,196 £0 £74,196 £74,196 £0
8.2 Running Costs (ELR CCG Only) Donna Enoux £746,000 £746,000 No No N/A N/A N/A Yes £746,000 £746,000 medium £466,250 £746,000 £746,000 £0 £0
Total QIPP (Wave 1 Schemes) £42,693,834 -£9,256,397 £33,437,437 £49,203,179 -£13,833,365 £35,369,814 £22,247,326 £16,670,374 -£4,459,999 £12,210,375 £15,718,899 -£4,751,613 £10,967,286 £16,813,906 -£4,621,753 £12,192,154
WAVE 2 SCHEMES (STRETCH):
Scheme Ref Scheme Name SRO Gross Savings Investment Net Savings PID Required Business Case
Required Pid Completed
Business Case
Completed
Approved by
CCB?
Workbook
ReceivedWorkbook Name Gross Savings Investment Net Savings
Confidence in
DeliveryRish Adjusted Comments
1.6 End of Life Tamsin Hooton £500,000 £500,000 Yes Yes Yes Yes No End of Life £500,000 £500,000 medium £312,500 Initial workbook received stating £300k, however work has been undertaken
to refresh the scheme and updated figures due imminently.
£166,667 £166,667 £166,667 £166,667 £166,667 £166,667
2.6 Follow Up Outpatients Ket Chudasama £1,200,000 £1,200,000 Yes Yes No No Yes Planned Care £1,200,000 £1,200,000 low £300,000 £400,000 £400,000 £400,000 £400,000 £400,000 £400,000
2.7 Diagnostics Ket Chudasama £1,000,000 £1,000,000 Yes Yes No No Yes Planned Care £1,000,000 £1,000,000 low £250,000 £333,333 £333,333 £333,333 £333,333 £333,333 £333,333
2.8 System Pathway Opportunities (Cardiology) Ket Chudasama £500,000 £500,000 Yes Yes No No Yes Planned Care - cardiology only £500,000 £500,000 low £125,000 £166,667 £166,667 £166,667 £166,667 £166,667 £166,667
2.8 a System Pathway Opportunities (Gastro) Ket Chudasama £500,000 £500,000 Yes Yes No No No £500,000 £500,000 low £125,000 £166,667 £166,667 £166,667 £166,667 £166,667 £166,667
3.1a Medicines Management - Stretch Tim Sacks £1,000,000 £1,000,000 Yes Yes Yes Yes N/A Yes Medicines Optimisation £0 high £0removed as £750k included within CCG prescribing - more than remaining
£250k included within revised HCD £0 £0 £0
3.5 City GP Office (LC CCG Only) Richard Morris £79,851 £79,851 No No N/A N/A N/A No £79,851 £79,851 high £69,870 £0 £0 £79,851 £79,851
3.6 PCCC Budget Alignment QIPP (county Only) Tim Sacks £1,463,000 £1,463,000 No No N/A N/A N/A No £1,463,000 £1,463,000 low £365,750 £809,000 £809,000 £654,000 £654,000 £0
3.7 Primary Care (ELR Only) Tim Sacks £1,500,000 £1,500,000 No No N/A N/A N/A No £1,500,000 £1,500,000 low £375,000 £1,500,000 £1,500,000 £0 £0
4.1a Adult CHC - Stretch Paul Gibarra £1,300,000 £1,300,000 Yes Yes Yes Yes Yes Yes 2019-20 CHC workbook £2,476,431 £2,476,431 low £619,108 Stretch to £8m overall LLR target £825,477 £825,477 £825,477 £825,477 £825,477 £825,477
6.4 Vol Sector Sarah Shuttlewood £577,092 £577,092 Yes Yes No No Yes Voluntary Sector £577,092 £577,092 low £144,273 No finances included £139,560 £139,560 £202,784 £202,784 £234,748 £234,748
7.3 Children’s CHC Chris West £500,000 £500,000 Yes Yes No No No £500,000 £500,000 low £125,000 £166,667 £166,667 £166,667 £166,667 £166,667 £166,667
10.1 Budget review (LC CCG Only) Michelle Iliffe £457,979 £457,979 No No N/A N/A N/A N/A Should disappear as a balancing figure £0 £0 high £0 £0 £0 £0
9.2 LD Short Breaks Sarah Warmington £0 £0 Yes Yes No NO No £160,000 £160,000 medium £100,000 New scheme identified since submission £53,333 £53,333 £53,333 £53,333 £53,333 £53,333
£0 £0 £0
WAVE 3 SCHEMES CFO ADJUSTMENTS IN FINANCIAL PLAN 12.02.19): £0 £0 £0
8.3 Clinical Director QIPP (ELR CCG Only) Donna Enoux £170,000 £170,000 No No N/A N/A N/A Yes £170,000 £170,000 medium £106,250 £170,000 £170,000 £0 £0
6.5 LPT Growth QIPP Sarah Shuttlewood £4,228,365 £4,228,365 No No N/A N/A N/A N/A £4,228,365 £4,228,365 low £1,057,091 £1,135,005 £1,135,005 £1,367,643 £1,367,643 £1,725,717 £1,725,717
9.1 MH Investment QIPP Spencer Gay £216,752 £216,752 No No N/A N/A N/A No £216,752 £216,752 low £54,188 £0 £216,752 £216,752 £0
£0 £0 £0
Total Potential QIPP (Wave 2 & 3 Schemes) £15,193,039 £0 £15,193,039 £15,071,491 £0 £15,071,491 £4,129,030 £6,032,375 £0 £6,032,375 £4,719,989 £0 £4,719,989 £4,319,126 £0 £4,319,126
Total Identified QIPP £57,886,873 -£9,256,397 £48,630,476 £64,274,670 -£13,833,365 £50,441,305 £26,376,355 £22,702,749 -£4,459,999 £18,242,750 £20,438,889 -£4,751,613 £15,687,275 £21,133,033 -£4,621,753 £16,511,280
Unidentified £7,619,796 £0 £7,619,796 £1,231,999 £4,576,968 £5,808,967 £2,068,733 £1,231,163 £3,299,896 £1,314,392 £1,847,294 £3,161,686 -£2,151,126 £1,498,511 -£652,615
Total QIPP (Including Unidentified) £65,506,669 -£9,256,397 £56,250,272 £65,506,669 -£9,256,397 £56,250,272 £24,771,482 -£3,228,836 £21,542,646 £21,753,281 -£2,904,319 £18,848,962 £18,981,906 -£3,123,241 £15,858,665
check £0 £0 £0 Target QIPP £24,771,482 -£3,228,836 £21,542,646 £21,753,281 -£2,904,319 £18,848,962 £18,981,906 -£3,123,241 £15,858,665
LC CCG
LLR WIDE FIGURES LLR WIDE FIGURES
ELR CCG WL CCG LC CCG
WL CCG
As per Financial Plan Submission on 12.02.19 Updated for Workbooks ReceivedLLR WIDE FIGURES LLR WIDE FIGURES
ELR CCG
Copyright © 2022 FDOKUMEN