AGENDA NHS Leeds CCG Governing Body Meeting
185
AGENDA NHS Leeds CCG Governing Body Meeting Date: Wednesday 25 November 2020 Time: 14:00 – 17:00 Venue: Microsoft Teams Please note: agenda timings are approximate Item Description Lead Paper Time GB 20/82 Welcome and Apologies Purpose: To record apologies for absence and confirm the meeting is quorate. Chair N 14:00 GB 20/83 Declarations of Interest Purpose: To record any Declarations of Interest relating to items on the agenda: a) Financial Interest Where an individual may get direct financial benefit from the consequences of a decision they are involved in making; b) Non-Financial professional interest Where an individual may obtain a non-financial professional benefit from the consequences of a decision they are involved in making; c) Non-financial personal interest Where an individual may benefit personally in ways that are not directly linked to their professional career and do not give rise to a direct financial benefit, because of the decisions they are involved in making; and d) Indirect Interests Where an individual has a close association with another individual who has a financial interest, a non-financial professional interest or a non-financial personal interest who would stand to benefit from a decision they are involved in making. Chair Y GB 20/84 Questions from Members of the Public Purpose: To receive questions from members of the public Chair N 14:05 GB 20/85 Minutes of the Governing Body Meeting and the Annual General Meeting held on 23 September 2020 Purpose: To receive the minutes for approval Chair Y 14:10 GB 20/86 Matters Arising Chair N
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of AGENDA NHS Leeds CCG Governing Body Meeting

AGENDA NHS Leeds CCG
Governing Body Meeting
Date: Wednesday 25 November 2020
Time: 14:00 – 17:00
Venue: Microsoft Teams
Please note: agenda timings are approximate
Item Description Lead Paper Time
GB 20/82
Welcome and Apologies Purpose: To record apologies for absence and confirm the meeting is quorate.
Chair N
14:00
GB 20/83
Declarations of Interest Purpose: To record any Declarations of Interest relating to items on the agenda: a) Financial Interest
Where an individual may get direct financial benefit from the consequences of a decision they are involved in making;
b) Non-Financial professional interest Where an individual may obtain a non-financial professional benefit from the consequences of a decision they are involved in making;
c) Non-financial personal interest Where an individual may benefit personally in ways that are not directly linked to their professional career and do not give rise to a direct financial benefit, because of the decisions they are involved in making; and
d) Indirect Interests Where an individual has a close association with another individual who has a financial interest, a non-financial professional interest or a non-financial personal interest who would stand to benefit from a decision they are involved in making.
Chair Y
GB 20/84
Questions from Members of the Public Purpose: To receive questions from members of the public
Chair N 14:05
GB 20/85
Minutes of the Governing Body Meeting and the Annual General Meeting held on 23 September 2020 Purpose: To receive the minutes for approval
Chair Y 14:10
GB 20/86
Matters Arising
Chair N

Item Description Lead Paper Time
Purpose: To consider any matters arising that are not considered elsewhere on the agenda
GB 20/87
Action Log Purpose: To review the outstanding actions
Chair Y
CHIEF EXECUTIVE’S REPORT GB 20/88
Chief Executive’s Report Purpose: To receive a report from the Chief Executive, including an update on the current position relating to COVID-19
Tim Ryley Y 14:20
GB 20/89
Winter Planning & Impact of Covid-19 Purpose: To receive an update on the current position
Helen Lewis Y 14:40
GB 20/90
Financial Update
a) Financial Plan for 20-21
Purpose: To receive an update on the current financial plan
b) Financial Position – Month 7
Purpose: To receive the finance report for information
Visseh Pejhan-Sykes
Y 15:00
RISK
GB 20/91
Corporate Risk Register Purpose: To receive the corporate risks for review
Sabrina Armstrong
Y 15:20
GB 20/92
Governing Body Assurance Framework Purpose: To receive the Governing Body Assurance Framework for review
Sabrina Armstrong
Y
BREAK FOR 5 MINUTES
STRATEGY GB 20/93
People & OD Strategy Refresh Purpose: To receive an update and approve the updated version
Sabrina Armstrong
Y 15:40
COMMITTEE CHAIRS SUMMARIES GB 20/94
Primary Care Commissioning Committee – 7 October 2020 Purpose: To receive the summary for information and assurance
Sam Senior Y 15:55
GB 20/95
Remuneration & Nomination Committee – 14 October 2020
Sam Senior Y

Item Description Lead Paper Time
Purpose: To receive the summary for information and assurance
GB 20/96
Audit Committee – 18 November 2020 a) Purpose: To receive the summary for information and assurance and approve the recommendations
Auditor Panel – 18 November 2020 b)
Purpose: To receive the summary for information and assurance and approve the recommendations
Cheryl Hobson Y
GB 20/97
Quality & Performance Committee – 11 November 2020 Purpose: To receive the summary for information and assurance
Phil Ayres Y
COMMISSIONING & FINANCE GB 20/98
Integrated Quality & Performance Report Purpose: To receive the IQPR and consider any issues escalated by the Quality & Performance Committee
Helen Lewis Y 16:10
GOVERNANCE GB 20/99
Policy Approval a) Conflicts of Interest and Standards of Business
Conduct Policies
Purpose: To receive the policies for approval b) Pharmaceutical and Related Industries Joint Working
Policy Purpose: To receive the policies for approval
Sabrina Armstrong Simon Stockill Presented by Sally Bower
Y
16:20
GB 20/100
Forward Work Programme 2020/21 Purpose: To receive the forward work programme for 2020/21
Chair Y
16:30
GB 20/101
Any Other Business Chair N
Exclusion of the public - it is recommended that the following resolution be passed: "That representatives of the press and other members of the public be excluded from the remainder of the meeting, having regard to the confidential nature of the business to be transacted, publicity on which would be prejudicial to the public interest"
Confidential Section - Held in private GB 20/102
Confidential Minutes of the Governing Body held on 23 September 2020 Purpose: To receive the minutes for approval
Chair Y 16:35
GB 20/103
Ratification of Lay Member Appointment
Chair N 16:40

Item Description Lead Paper Time
Purpose: To ratify the lay member appointment
GB 20/104
Recommendations from Remuneration & Nomination Committee
a) Recommendation from Remuneration & Nomination Committee – Non-Executive
b) Recommendation from Remuneration & Nomination Committee – Executive
Purpose: To approve the recommendation from the Remuneration & Nomination Committee
Chair Sam Senior
Y 16:50
Dates of Future Meetings:
27 January 2021
24 March 2021
ITEMS FOR INFORMATION IFI1. Minutes of the West Yorkshire & Harrogate Joint
Committee – 20 July 2020 Purpose: To receive the minutes for information
Chair Y N/A
IFI2. Summary of Key Decisions – West Yorkshire & Harrogate Joint Committee – 6 October 2020 Purpose: To receive the key decisions for information
Chair Y N/A

Title Name Job Title
(where applicable)
Role Practice B
Code
(Practice
Only)
Declared Interest- (Name of the organisation and
nature of business)
Type of Interest Is the interest
direct or
indirect?
Interest From Interest Until Action Taken to Mitigate Risk
Angela Collins Lay Member for Patient and
Public Participation
Governing Body Member N/A Nil Declaration
Dr Ben Browning Member Representative Governing Body Member B86020 GP Partner at Lofthouse Surgery Financial Interests Direct 01/02/2019 01/04/2020 Declare any potential or perceived conflict of
interest at relevant meetings/workshops
Dr Ben Browning Member Representative Governing Body Member B86020 Shareholder in Leodis Care Ltd (now dormant) Financial Interests Direct 01/01/2011 Ongoing Declare any potential or perceived conflict of
interest at relevant meetings/workshops
Dr Ben Browning Member Representative Governing Body Member B86020 Member of Leodis Care LLP (Shell Company) Financial Interests Direct 01/01/2011 Ongoing Declare any potential or perceived conflict of
interest at relevant meetings/workshops
Dr Ben Browning Member Representative Governing Body Member B86020 Spouse is a Salaried GP Indirect Interests Indirect 01/01/2019 Ongoing Declare any potential or perceived conflict of
interest at relevant meetings/workshops
Dr Ben Browning Member Representative Governing Body Member B86020 Spouse is city-wide lead for Disability Services (NHS
Leeds CCG)
Indirect Interests Indirect 01/01/2015 Ongoing Declare any potential or perceived conflict of
interest at relevant meetings/workshops
Cheryl Hobson Lay member, Audit &
Conflicts of Interest
Governing Body Member N/A Member of South Yorkshire Joint Independent Audit
Committee for the Office of the Police and Crime
Commissioner
Financial Interests Direct 01/12/2019 Ongoing Declare interest in any relevant agenda items
and absent as appropriate
Cheryl Hobson Lay member, Audit &
Conflicts of Interest
Governing Body Member N/A Contracted to provide online tutoring for HFMA on
Post Graduate Leadership and Financial Management
qualifications
Financial Interests Direct 01/02/2019 Ongoing Declare interest in any relevant agenda items
and absent as appropriate
Cheryl Hobson Lay member, Audit &
Conflicts of Interest
Governing Body Member N/A Deputy Chair and Board Member, Chair of Finance and
Resources Committee and Member of Audit
Committee for Wellspring Academy Trust which has
academies across Yorkshire and the Humber including
in Leeds. Voluntary, unremunerated role.
Non-Financial Personal Interests Direct 01/12/2018 Ongoing Declare interest in any relevant agenda items
and absent as appropriate
Cheryl Hobson Lay member, Audit &
Conflicts of Interest
Governing Body Member N/A Sibling is a Non-Executive Director at Barnsley Hospital
NHS FT and also contracted to provide interim
financial support to Connect Healthcare Rotherham
CIC
Indirect Interests Indirect 04/11/2020 Ongoing Declare interest in any relevant agenda items
and absent as appropriate
Helen Lewis Interim Director of Acute
and Specialised
Commissioning.
Governing Body Member N/A Trustee, Leeds Jewish Welfare Board Non-Financial Personal Interests Direct 01/12/2017 Up to 9 year
term
Declare any potential or perceived conflict of
interest at relevant meetings/workshops
Dr Jason Broch Clinical Chair Governing Body Member B86022 Partner at Oakwood Lane Medical Practice Financial Interests Direct 01/01/2006 Ongoing Declare any potential conflict/interest at
relevant Governing Body/Committee
meetings
Dr Jason Broch Clinical Chair Governing Body Member B86022 Director Jemjo Healthcare Ltd Financial Interests Direct 01/05/2007 Ongoing Declare any potential conflict/interest at
relevant Governing Body/Committee
meetings
Dr Jason Broch Clinical Chair Governing Body Member B86022 Spouse business Airtight International Ltd Indirect Interests Indirect 10/05/2012 Ongoing Declare any potential conflict/interest at
relevant Governing Body/Committee
meetings
Dr Jason Broch Clinical Chair Governing Body Member B86022 Spouse business Nails 17 Ltd Indirect Interests Indirect 10/05/2012 Ongoing Declare any potential conflict/interest at
relevant Governing Body/Committee
meetings
Dr Jason Broch Clinical Chair Governing Body Member B86022 Director Leeds Jewish free school Non-Financial Personal Interests Direct 16/01/2014 Ongoing Declare any potential conflict/interest at
relevant Governing Body/Committee
meetings
Dr Jason Broch Clinical Chair Governing Body Member B86022 Director/trustee Brodetsky Primary School Foundation Non-Financial Personal Interests Direct 17/06/2014 Ongoing Declare any potential conflict/interest at
relevant Governing Body/Committee
meetings
Dr Jason Broch Clinical Chair Governing Body Member B86022 Chair of Governor's Brodetsky Primary School Non-Financial Personal Interests Direct 01/09/2012 Ongoing Declare any potential conflict/interest at
relevant Governing Body/Committee
meetings
Dr Jason Broch Clinical Chair Governing Body Member B86022 Founding Fellow of the Faculty of Clinical Informatics Non-Financial Professional Interests Direct 01/05/2018 Ongoing Declare any potential conflict/interest at
relevant Governing Body/Committee
meetings
Dr Jason Broch Clinical Chair Governing Body Member B86022 Gartner UK - Clinical Advisor Financial Interests Direct 01/06/2018 01/05/2020 Declare any potential conflict/interest at
relevant Governing Body/Committee
meetings
NHS Leeds CCG Governing Body Meeting - 25 November 2020
Declarations of Interest

Dr Jason Broch Clinical Chair Governing Body Member B86022 Calibre Care Partners Ltd OLMP is a member of this GP
federation, which is part of Leeds GP Confederation
Financial Interests Direct 01/06/2018 Ongoing Declare any potential conflict/interest at
relevant Governing Body/Committee
meetings
Dr Jason Broch Clinical Chair Governing Body Member B86022 Shareholder / Director Chapeloak Services Ltd Financial Interests Direct 01/01/2019 Ongoing Declare any potential conflict/interest at
relevant Governing Body/Committee
meetings
Dr Jason Broch Clinical Chair Governing Body Member B86022 Leeds Acupuncture Clinic - father's and brother's
business
Indirect Interests Indirect 10/05/2012 Ongoing Declare any potential conflict/interest at
relevant Governing Body/Committee
meetings
Dr Jason Broch Clinical Chair Governing Body Member B86022 Clinical Lead - Yorkshire & Humber Local Health & Care
record Exemplar, inc membership of NHSE Clinical
Advisory Group
Financial Interests Direct 01/11/2018 Ongoing Declare any potential conflict/interest at
relevant Governing Body/Committee
meetings
Dr Jason Broch Clinical Chair Governing Body Member B86022 Clinical Chair role, NHS Leeds CCG Financial Interests Direct 01/07/2020 Ongoing Was Assistant Clinical Chair between
1/4/2018-1/7/2020
Joanne Harding Executive Director of
Quality and
Safety/Governing Body
Nurse
Governing Body Member N/A Joint Chair of the NHSCC National Nurses Forum Non-Financial Professional Interests Direct 01/07/2019 Ongoing Declare any conflict of interest at relevant
meetings/workshops.
Dr Julianne Lyons GP Member Representative Governing Body Member B86110 GP Partner at Leeds Student Medical Practice Financial Interests Direct 01/01/2016 Ongoing Declare any potential conflict of interest at
Governing Body/Board, sub committees and
relevant meetings
Dr Julianne Lyons GP Member Representative Governing Body Member B86110 Leeds Local Medical Committee Member Financial Interests Direct 01/09/2013 31/03/2020 Declare any potential conflict of interest at
Governing Body/Board, sub committees and
relevant meetings
Dr Julianne Lyons GP Member Representative Governing Body Member B86110 Spouse is a Director of Leeds Haematology Ltd Indirect Interests Indirect 01/05/2013 Ongoing Declare any potential conflict of interest at
Governing Body/Board, sub committees and
relevant meetings
Dr Julianne Lyons GP Member Representative Governing Body Member B86110 Spouse is a trustee of UK Myeloma Forum Indirect Interests Indirect 01/01/2013 Ongoing Declare any potential conflict of interest at
Governing Body/Board, sub committees and
relevant meetings
Dr Julianne Lyons GP Member Representative Governing Body Member B86110 Spouse is an employee of the University of Leeds Indirect Interests Indirect 01/01/2015 Ongoing Declare any potential conflict of interest at
Governing Body/Board, sub committees and
relevant meetings
Dr Julianne Lyons GP Member Representative Governing Body Member B86110 GP lead for Leeds Primary Care Workforce and Training
Hub
Financial Interests Direct 01/05/2018 Ongoing Declare any potential conflict of interest at
Governing Body/Board, sub committees and
relevant meetings
Dr Julianne Lyons GP Member Representative Governing Body Member B86110 Spouse has an honorary contract with Leeds Teaching
Hospitals NHS Trust
Indirect Interests Indirect 01/01/2015 Ongoing Declare any potential conflict of interest at
Governing Body/Board, sub committees and
relevant meetings
Dr Julianne Lyons GP Member Representative Governing Body Member B86110 Shareholder of Leeds West Primary Care Limited Financial Interests Direct 01/10/2015 Ongoing Declare any potential conflict of interest at
Governing Body/Board, sub committees and
relevant meetings
Dr Julianne Lyons GP Member Representative Governing Body Member B86110 I am a member of LSMP and The Light PCN Financial Interests Direct 01/07/2019 Ongoing Declare any potential or perceived conflict of
interest at relevant meetings/workshops
Dr Julianne Lyons GP Member Representative Governing Body Member B86110 Daughter employee of Leeds Primary Care Workforce
and Training Hub
Indirect Interests Indirect 01/07/2019 Ongoing Declare any potential or perceived conflict of
interest at relevant meetings/workshops.
Dr Keith Miller GP Member Representative Governing Body Member B86109 Spouse - Advanced Nurse Practitioner, LTHT Financial Interests Indirect 01/01/2008 Ongoing Declare any potential conflict of interest at
Governing Body/Board, sub committees and
relevant meetings
Dr Keith Miller GP Member Representative Governing Body Member B86109 *Expired*
GP Partner at Kirkstall Lane Medical Centre
Financial Interests Direct 01/01/2010 31/08/2020 Declare any potential conflict of interest at
Governing Body/Board, sub committees and
relevant meetings
Dr Keith Miller GP Member Representative Governing Body Member B86033 GP Partner at Crossley Street Surgery Financial Interests Direct 01/09/2020 Ongoing Declare any potential conflict of interest at
Governing Body/Board, sub committees and
relevant meetings
Dr Keith Miller GP Member Representative Governing Body Member B86109 *Expired*
Temporary ad hoc role as Project Lead for Care Homes
for Woodsley and Holt Park PCNs
Financial Interests Direct 20/05/2020 31/08/2020 Declare any potential conflict of interest at
Governing Body/Board, sub committees and
relevant meetings
Dr Keith Miller GP Member Representative Governing Body Member B86109 NHS Leeds Clinical Commissioning Group – Member
Representative
Financial Interests Direct 01/01/2018 Ongoing Declare any potential conflict of interest at
Governing Body/Board, sub committees and
relevant meetings
Dr Keith Miller GP Member Representative Governing Body Member B86109 Member of GP Confederation Non-Financial Professional Interests Direct 01/01/2018 Ongoing Declare any potential conflict of interest at
Governing Body/Board, sub committees and
relevant meetings

Phil Ayres Secondary Care Consultant
and Chair of the Quality and
Pewrformance Committee
Governing Body Member N/A Personal friendship with the Chief Executive of Leeds
Community Healthcare
Indirect Interests Indirect 27/11/2019 Ongoing The action required to manage any conflicts
of interest will be agreed with the Chair of
the relevant meeting. In relation to the
Quality and Performance Committee which I
chair, the Deputy chair will be asked to agree
any required actions.
No confidential/sensitive information to be
shared or discussed with the LCH Chief
Executive.
Phil Ayres Governing Body Member Governing Body Member N/A I have personal friendships with GP of the Rawdon
Surgery
Indirect Interests Indirect 01/01/2017 Ongoing Maintain awareness of potential influence
over decisions I may take as independent
practitioner. Abide by GMC code of conduct.
Declare this interest at relevantmeetings.
Sabrina Armstrong Director of Organisational
Effectiveness
Governing Body Member N/A Personal friendship with a non-executive director of
Leeds Community Healthcare NHS Trust.
Non-Financial Personal Interests Direct 01/05/2019 Ongoing Declare any potential or perceived conflict of
interest at relevant meetings/workshops.
Sabrina Armstrong Director of Organisational
Effectiveness
Governing Body Member N/A Close friend works as Director of System Capability and
Operations at NHS England.
Indirect Interests Indirect 01/01/2014 Ongoing Declare any potential or perceived conflict of
interest at relevant meetings/workshops.
Sabrina Armstrong Director of Organisational
Effectiveness
Governing Body Member N/A Pool member with NHS Interim Management and
Support (NHS IMAS).
Non-Financial Professional Interests Direct 01/01/2014 Ongoing Declare any potential or perceived conflict of
interest at relevant meetings/workshops.
Samantha Ramsey Corporate Governance
Manager
Band 8d and above or
Employee Decision Maker
N/A Close friend works as an Advanced Health
Improvement Specialist (Public Health)
Indirect Interests Indirect 01/01/2014 Ongoing Declare any potential or perceived conflict of
interest at relevant meetings/workshops
Sam Senior Lay Member for Primary
Care Co-Commissioning
Governing Body Member N/A Lay Member for Primary Care Bassetlaw CCG Financial Interests Direct 01/09/2013 Ongoing Declare any potential or perceived conflict of
interest at relevant meetings/ workshops
Sam Senior Lay Member for Primary
Care Co-Commissioning
Governing Body Member N/A Lay Representative National School of Healthcare
Science
Financial Interests Direct 01/05/2016 Ongoing Declare any potential or perceived conflict of
interest at relevant meetings/ workshops
Sam Senior Lay Member for Primary
Care Co-Commissioning
Governing Body Member N/A Lay Advisor Health Education England (West Midlands) Financial Interests Direct 01/05/2016 Ongoing Declare any potential or perceived conflict of
interest at relevant meetings/ workshops
Sam Senior Lay Member for Primary
Care Co-Commissioning
Governing Body Member N/A Patient and Public Panel Member - National Institute
Health Research
Financial Interests Direct 01/04/2017 Ongoing Declare any potential or perceived conflict of
interest at relevant meetings/ workshops
Sam Senior Lay Member for Primary
Care Co-Commissioning
Governing Body Member N/A *Expired*
Chairperson - Brampton United Junior Football Club
(S63 6BB)
Non-Financial Personal Interests Direct 01/05/2013 18/05/2020 Declare any potential or perceived conflict of
interest at relevant meetings/ workshops
Sam Senior Lay Member for Primary
Care Co-Commissioning
Governing Body Member N/A *Expired*
Independent Lay Member to Rotherham Federation
Connect Healthcare
Non-Financial Professional Interests Direct 29/05/2019 10/08/2020 Declare any potential or perceived conflict of
interest at relevant meetings/ workshops
Sam Senior Lay Member for Primary
Care Co-Commissioning
Governing Body Member N/A Volunteer for CortonWood Miners Welfare Scheme
(registered charity)
Non-Financial Personal Interests Direct 15/10/2019 Ongoing Declare any potential or perceived conflict of
interest at relevant meetings/ workshops
Dr Simon Stockill Medical Director Governing Body Member N/A Partner at Sleights and Sandsend Medical Practice,
Whitby (Hambleton, Richmondshire & Whitby CCG)
Financial Interests Direct 01/04/2016 Ongoing Declare any conflict or perceived conflict
within context of any relevant meeting or
project work
Dr Simon Stockill Medical Director Governing Body Member N/A GP Appraiser, NHS England (Yorkshire & Humber) Financial Interests Direct 01/12/2013 Ongoing Declare any conflict or perceived conflict
within context of any relevant meeting or
project work
Dr Simon Stockill Medical Director Governing Body Member N/A Clinical Lead for Quality Improvement, Royal College of
GPs
Financial Interests Direct 01/09/2016 Ongoing Declare any conflict or perceived conflict
within context of any relevant meeting or
project work
Dr Simon Stockill Medical Director Governing Body Member N/A Clinical Director, Whitby Coast & Moors Primary Care
Network
Financial Interests Direct 01/07/2019 Ongoing Declare any conflict or perceived conflict
within context of any relevant meeting or
project work
Tim Ryley Chief Executive Officer Governing Body Member N/A Spouse to carry out LeDeR reviews for the CCG which
is a financial benefit to her.
Indirect Interests Indirect 31/07/2020 Ongoing Exclude self from all conversations to do with
LeDeR except pure performance in terms of
numbers. Declare at any relevant meetings
Visseh Pejhan-Sykes Chief Finance Officer Governing Body Member N/A Niece works for CCG as Digital Communications Officer Indirect Interests Indirect 11/12/2017 Ongoing Declare any potential or perceived conflict of
interest at relevant meetings/workshops

1
Draft Minutes NHS Leeds CCG – Governing Body Meeting
Wednesday 23 September 2020 1.00pm – 4.00pm
Microsoft Teams Virtual Meeting
Members Initials Role Present Apologies
Dr Jason Broch (Chair) JB Clinical Chair
Dr Phil Ayres PA Secondary Care Specialist Doctor
Dr Ben Browning BB Member Representative
Angela Collins AC Lay Member – Patient & Public Involvement
Jo Harding JH Executive Director of Quality and Nursing
Dr Julianne Lyons JL Member Representative
Dr Keith Miller KM Member Representative
Visseh Pejhan-Sykes VPS Executive Director of Finance
Tim Ryley TR Chief Executive
Samantha Senior (Deputy Chair)
SS Lay Member – Primary Care Co-Commissioning
Dr Simon Stockill SSt Medical Director
Additional Attendees
Sabrina Armstrong SA Director of Organisational Effectiveness
Victoria Eaton VE Director of Public Health
Helen Lewis HL Interim Director of Acute & Specialist
Commissioning
Laura Parsons LP Head of Corporate Governance & Risk
Sam Ramsey SR Corporate Governance Manager
Rachel Howitt RH
Head of Clinical Governance
(item GB 20/61)
Dr Bryan Power BP
Clinical Lead
(item GB 20/65)
John Tatton JT Associate Director of Planning
(item GB 20/66)
Members of public/staff observing - 0
No. Agenda Item Action
GB 20/55
Welcome and Apologies JB welcomed everyone to the virtual Governing Body meeting.

2
No. Agenda Item Action
Apologies had been received from Phil Ayres and Sabrina Armstrong. The Chair confirmed the meeting was quorate.
GB 20/56
Declarations of interest Members were asked to raise any declarations of interest in relation to agenda items. No declarations were raised.
GB 20/57
Questions from Members of the Public No questions had been received.
GB 20/58
Minutes from Previous Meetings JB presented the minutes from the NHS Leeds Governing Body 22 July 2020 for approval. The Governing Body:
(a) approved the minutes of the NHS Leeds Governing Body held on 22 July 2020.
GB 20/59
Matters Arising There were no matters arising.
GB 20/60
Action Log The Governing Body reviewed the action log and noted that all actions were complete. The Council of Members meeting, in relation to action 20/40 was due to take place on 30 September 2020.
GB 20/61
Patient Voice The Governing Body received a presentation which provided detail of patient experience by those who use the Special Allocation Service (SAS) in Leeds. Members were informed that the service was a GP practice for registered patients in Leeds who have been asked to leave their own (usual) GP practice due to unsafe or inappropriate behaviour. It was acknowledged that this was not something that was used frequently and there were strict criteria and thresholds that must be reached in order for it to happen. Two patient stories were presented, which outlined the difficult and complex reasons for removal, and highlighted the importance of safety, but that it was a difficult balance to meet. The importance of patient experience was recognised and the impact on patients. The stories provided important feedback that they had not understood what was happening at the time and explanations hadn’t been provided. Feedback had also been provided that once removed, patients had difficulties accessing and registering with the SAS.

3
No. Agenda Item Action
Further engagement work had also been undertaken with other groups and services that supported patients who used the service. The overall responses had been positive and were satisfied with the care and support received. Following the engagement and feedback received, a patient information leaflet had been developed for practices to use to ensure there was not a gap between the removal and registration with the new service. In addition to this, a summary flow chart was being developed to support staff in understanding the policy. Further improvements were being considered and what could be learnt from the feedback provided. It was acknowledged that the changes may be small, but were significant. Members recognised the importance of the service and that it provided continued service for those patients identified. It was also highlighted that it was important to consider the staff members affected within practices. A suggestion was made to link to the zero tolerance policy to indicate concerns about safety. Members recognised the actions that had been taken as a result of the patient experience and highlighted the importance of using engagement to inform the decision making process. Patient Experience & Complaints Annual Report The Patient Experience and Complaints Annual Report was presented for information. Members noted that the report had been discussed in detail at the Quality & Performance Committee and they had agreed full assurance that there were robust processes in place for the patient experience function in the CCG.
GB 20/62
Chief Executive Report An overview of the current Covid-19 situation was provided and it was acknowledged that it was a fast paced situation and that winter and reset was extremely challenging. As a city, Leeds had 88.3 per 100k people identified with Covid-19 and there had been a notable increase in hospital admissions. It was acknowledged that there would be a knock on consequence to the stabilisation and reset and as an organisation there was a need to consider how to manage the challenging targets and continue to support the health of the population. The Director of Public Health provided a detailed overview of the situation in Leeds in relation to Covid-19. It was acknowledged that it was challenging to have a high rate of infection; however this reflected the national position. The highest proportion of cases was in the younger adults’ age group; however Leeds was seeing a rise across all ages.
Members were informed that the Health Inequalities framework would be launched and recognised the importance of the piece of work, but also the challenges in relation to investment discussions as a result of the knock on consequences of the wider challenges faced. The impact of Covid had been

4
No. Agenda Item Action
considered alongside the launch of the framework and the subsequent impact on inequalities in relation to the restrictions made in light of Covid.
The Communications & Engagement report had been included and members were asked to receive the information as assurance that the CCG was delivering its statutory duties to ensure public involvement and consultation.
A query was raised in relation to the expectations from NHS England, where we currently are and where we predict to be in terms of the response to the pandemic as well as resuming elective activity. It was acknowledged that the impact of Covid-19 had affected the services undertaking elective surgery and if the situation deteriorated further, it would not be possible to deliver the targets set. It was noted that the situation was different for the second wave as the first wave resulted in the cancellation of all elective activity and services. Members recognised the hard work that was ongoing and the virtual work taking place. The system was prioritising clinically and maximising elective activity and would continue to do so whilst possible.
The Medical Director provided an overview of the current position within general practice and it was highlighted that there was increased demand with 11 practices reporting level 2, however it was manageable. There was a proactive system in place in terms of managing demand, as it was highlighted that contact levels in primary care were as high and now exceeding the levels pre Covid-19. The Primary Care Silver group were considering the BAME population and workforce to understand which practices had higher numbers and prioritising the business continuity plans within those practices. The response and support from the GP Confederation and Primary Care Commissioning teams to general practice was commended. In relation to staff testing, members were informed that this had been extended to include symptomatic children of staff. Although there was further work to be done in terms of testing, it was acknowledged that the demand was being managed well.
Members were informed that in relation to care homes, the Silver and Bronze care home groups were actively meeting and considered intelligence form all care homes via the capacity tracker. There were good relationships with care homes and care home managers sat on the Silver and Bronze groups. It was recognised that test and trace continued to be a challenge; however the position in care homes was stable due to the hard work and systems that had been put into place. Members were informed that the care home Silver group had agreed to consider support to the wider social care sector and the home care sector. It was noted that in relation to the national guidance on care home visiting, a local approach was being considered in order for the decision to be taken on an individual basis to have a more ethical approach. The Governing Body:

5
No. Agenda Item Action
a) noted the contents of the CEO Report; and; b) received the communications and engagement update as assurance that the CCG is delivering its statutory duties to ensure public involvement and consultation.
GB 20/63
Corporate Risk Register The Corporate Risk Register was presented. Members were informed that there were two corporate (red) risks on the operational risk register. This was an increase from 1 to 2 red risks. Risk 548, Statutory Financial Duties had increased due to national planning principles not being received and the uncertainty in relation to current projections. It was noted that the risk would be reviewed and updated once the guidance had been received. Members were informed that the risk relating to Information Security following the penetration testing would be lowered by March 2021 once the action plan had been implemented. The high amber risk in relation to Shaping our Future was discussed and the potential impact on staff given the current circumstances and remote working. The Governing Body: a) reviewed the corporate risks; b) reviewed the high scoring amber risk aligned to the Governing Body; and c) agreed that the controls and actions were effective and assurances were sufficiently robust.
GB 20/64
Governing Body Assurance Framework The Governing Body Assurance Framework (GBAF) was presented and it was noted that this had been reviewed and risk descriptions had been updated following feedback from the previous meeting.
It was noted that no scores had been changed, and additional controls had been added where required. Members were informed that a deep dive of Risk 4 (failure to overcome local and national workforce shortages) had been presented to the Audit Committee on 16 September 2020 and the Committee had been assured regarding the governance arrangements. The Chief Executive highlighted the impact of Covid on service delivery and that this could increase the risk level to the organisation. It was noted that the position was changing rapidly in Leeds and there was a timing issue with the paperwork but it was important to note the increasing risk. The Governing Body: a) reviewed the Governing Body Assurance Framework; b) considered the controls and assurances; and c) noted the review and assurance processes.

6
No. Agenda Item Action
GB 20/65
Covid-19 impact on provision of health services for non Covid conditions BP presented with the key findings from the work stream ‘Covid 19 – Impact on the Provision of Healthcare services on non-covid conditions’. The work was undertaken to understand the healthcare of those whose care had been negatively impacted by the arrangements made to meet Covid-19 demands. Members were informed that a multi-agency steering group had been set up to shape and lead the work, including a strong clinical representation and representation from Healthwatch to ensure the patients were at the forefront. A hypothesis led approach was taken in developing the recommendations. There were 74 recommendations made through the hypothesis with 5 cross cutting themes. It was noted that the report had been divided into themes, quick wins and successes and the work would be taken forward through existing forums and partnerships. Members found the report useful and comprehensive. A query was raised in relation to a focus on the increase in domestic violence and it was acknowledged that further work could be undertaken through the recommendations to ensure this was included. The challenge of the timing of data was recognised within the timescales that the report had been produced. A further query was raised in relation to more detail of the inclusion of care homes within the report and recommendations. Members were assured that there was detailed work ongoing within the care home scheme in practices and the report considered the frail population as a whole. It was agreed that the report would link directly with the health inequalities framework to identify the needs of those in care homes as a population cohort. In relation to the cross cutting themes, a question was asked as to whether there were any implications for the CCG’s strategic commitments and whether these would require adapting. Members were assured that the work supported the development of the left shift blue print and Shaping our Future. A query was raised in relation to whether the lessons learnt were being used in the current second wave and it was confirmed that the report had been discussed at the Stabilisation and Reset group and would be taken through individual forums and proactive work was already being undertaken in both primary care and through the Silver Care Home group. The Governing Body expressed thanks to all those involved and highlighted the quality of the report and the effort that had been put into developing this piece of work. Members agreed that the report should be shared widely to promote the work that had been undertaken and that it was reflective of a good position in Leeds.
JH

7
No. Agenda Item Action
The Governing Body:
a) approved the Covid19 – impact on provision of health services for non-COVID Conditions report; and
b) noted the recommendations within the report.
GB 20/66
NHS Leeds CCG Green Plan JT presented the NHS Leeds CCG Green Plan. The Governing Body was informed that NHS Organisations were required to publish a Green Plan that articulated their commitment to achieving national climate change/carbon reduction priorities along with the key actions that would be taken to ensure delivery. Members were informed of three areas that would be measured - reducing the CCG’s direct impact on carbon, pollution and waste; commissioned services and a role in supporting sustainability; and partnership working. It was noted that the carbon reduction had been significant over the last 6 months due to Covid-19 and the number of staff working from home. It was acknowledged that work was ongoing with partners in relation to the estates across the city and the wider role that the CCG had. Conversations were ongoing in relation to a system headquarters and how partners plan to work in the future. The need to invest in technology to maximise use when working from home was highlighted. NHS Leeds CCG was described as small as an organisation in terms of carbon footprint, however there was a role in terms of commissioning services that could be utilised.
The role of digital and technology was discussed and the importance of the Leeds Informatics Board to consider the priorities across the city in terms of technology. The Governing Body: a) agreed the focus of the NHS Leeds CCG Green Plan; and b) approved the publication of the plan.
GB 20/67
Committee Chair’s Summary – Primary Care Commissioning Committee – 5 August 2020 Members were informed that the Committee had approved the branch closure at Adel following a robust discussion. Members had been assured that proper engagement had been completed and this had been reviewed and analysed. The Governing Body:
a) received the report.

8
No. Agenda Item Action
GB 20/68
Committee Chair’s Summary – Remuneration & Nomination Committee – 29 July 2020 The report was presented and members were asked to note the further work that would be undertaken on the Workforce Race Equality Standard (WRES) and would be presented to a future Remuneration and Nomination Committee meeting. The Governing Body:
a) received the report.
GB 20/69
Committee Chair’s Summary – Audit Committee – 16 September 2020 Members were informed that the Committee had received a deep dive of Risk 4 of the Governing Body Assurance Framework (relating to local and national workforce shortages) and were assured by the work that was being undertaken. The Committee had noted the limited assurance in relation to penetration testing and an update would be provided with a more detailed discussion at the November Audit Committee. An update had been received from internal audit and it was noted that further resource would be allocated to considering personal health budgets. The Governing Body:
a) received the report.
GB 20/70
Committee Chair’s Summary – Quality & Performance Committee – 09 September 2020 The Governing Body received the report for information and the focus on annual reports at the Committee was highlighted. The Governing Body:
a) received the report.
GB 20/71
Integrated Quality & Performance Committee The Governing Body received an overview of current performance levels and noted the sustained activity in primary care in relation to learning disability assessments. Members were informed that cancer performance measures were back up to 95% for 2 week waits and it was acknowledged that the IQPR does not always reflect the targets that are being worked on. A query was raised in relation to the Continuing Healthcare assessment backlog and the actions taken to address this. Members were assured that work was ongoing and as of 1 September, new patients had to be assessed within 6 weeks. It was noted that the performance target would be included in the next version of the IQPR in order to inform Governing Body members of the position.
9
No. Agenda Item Action
The Governing Body: a) received and reviewed the IQPR dashboards; discussed the
information, and noted the current areas of underperformance and mitigating action.
GB 20/72
Finance Update The finance update was presented to members and it was noted that in line with the previous regime, retrospective top ups would be provided to bring organisations to breakeven where appropriate. Members were informed that there had been no increase to service changes as part of developments of commissioning and the commissioning budgets were currently unclear. It was acknowledged that there was no financial issue for the first half of the financial year.
The Governing Body: a) considered the Month 5 financial position.
GB 20/73
2020-21 Operational Financial Planning and Annual Budgets Update The Governing Body was informed of the basis of the budget setting, and once further detail was known, it would return to the Governing Body. It was recognised that the position had changed since the report had been submitted as allocations had been received. Members were informed that growth money planned in terms of new investments would be given to the ICS to oversee as a lump sum. Ordinarily the CCG would receive growth monies to spend on activity increase and investments; however the total figure would now be given to the ICS. Conversations were ongoing with partners across the system and there was an assumption that any activity taken with independent providers would be paid centrally through a national contract. VPS highlighted ambiguity in terms of winter for hospices and the third sector. It was recognised that there were still large details to clarify. Members discussed the affordability of activity within the acute sector and the risks associated with not doing so. It was highlighted that Leeds were considering the impacts and costs and consequences across the system. The increase in mental health demand was also recognised. It was acknowledged that the risks were smaller than £30million and EMT would consider and present a sensible proposal to a future meeting once further work had been undertaken on the allocations. Members recognised the challenges, noted the position and welcomed the opportunity to inform thinking.
It was highlighted that discussion and decisions should take place in the public domain where possible but the Governing Body was mindful of

10
No. Agenda Item Action
restrictions in terms of time and national direction. The Executive Management Team would focus on the needs of the population of Leeds and negotiate the best position for Leeds as a whole. The Governing Body expressed thanks to the Chief Finance Officer for the ongoing hard work in relation to the financial position. The Governing Body: a) noted the current position with the CCG financial plan for 2020-21; b) noted potential exposure to an anticipated financial risk (deficit) of c£30m for September to March 2021; and c) discussed and agreed that EMT would consider and present a sensible proposal to a future Governing Body meeting.
GB 20/74
Any Qualified Provider Update Report Members were informed that following the decision made in May 2020 at the Governing Body to offer direct financial support to AQP providers considered to be of local strategic importance for the recovery of services across the city, further guidance had been released. The Finance team had reviewed the position, considered the PPN 04/20 (Procurement Policy Note – Recovery and Transition from COVID-19) and proposed to continue the arrangement to the end of the financial year.
The Governing Body reaffirmed the decision taken to continue the revised contracting arrangements with providers beyond 31st October 2020, as per PPN 04/20 based on the current financial regime and pending the issue of updated financial planning guidance. The Governing Body:
a) noted the contents of this update report; and b) reaffirmed the decision taken in May 2020 to continue the revised
contracting arrangements with providers beyond 31st October 2020, as per PPN 04/20 based on the current financial regime and pending the issue of updated financial planning guidance.
GB 20/75
Governing Body Effectiveness JB presented the report and it was highlighted that work had begun in terms of the recommendations from the survey and actions from the independent review of the Audit Committee. It was acknowledged that there was a recommendation that the Audit Committee receives information in relation to all procurement waivers, rather than just those above the procurement thresholds. This would require an amendment to the Committee’s terms of reference, Procurement Policy and Operational Scheme of Delegation. The Governing approved these amendments in line with the Constitution.
The Chair highlighted the importance of ensuring that the Governing Body

11
No. Agenda Item Action
has leadership that was representative of the people of Leeds and that this was high on the agenda of the CCG. The PWC report and actions, and the feedback from the internal effectiveness review would be considered with the new Audit Committee Chair once in post. The Governing Body:
a) received the report; b) considered the issues raised; and c) approved the minor amendments to the Audit Committee Terms of
Reference, Procurement Policy and Operational Scheme of Delegation to confirm that all procurement waivers will be presented to the Audit Committee.
GB 20/76
Forward Work Programme 2020/21 The Governing Body’s work programme was presented for information. The Governing Body:
a) received the forward work programme.
GB 20/77
Any Other Business No other business was raised.
The Governing Body resolved that representatives of the press and other members of the public be excluded from the remainder of the meeting, having regard to the confidential nature of the business to be transacted, publicity on which would be prejudicial to the public interest.
Date of next meeting: 25 November 2020
Approved and signed by: Dr Jason Broch, Clinical Chair, NHS Leeds CCG Date:

1
Minutes NHS Leeds CCG – Annual General Meeting (AGM)
Wednesday 23 September 2020 16:15 – 17:30
Live Event, MS Teams (Virtual)
Attendees Initials Role Present Apologies
Dr Jason Broch JB Clinical Chair
Tim Ryley TR Chief Executive Officer
Dr Ben Browning BB Member Representative
Angela Collins AC Lay Member – Patient & Public Involvement
Jo Harding JH Director of Nursing & Quality
Dr Julianne Lyons JL Member Representative
Dr Keith Miller KM Member Representative
Visseh Pejhan-Sykes VPS Chief Finance Officer
Samantha Senior SS Lay Member – Primary Care Co-Commissioning
Dr Simon Stockill SSt Medical Director
Helen Lewis HL Interim Director of Acute & Specialist
Commissioning
Dr Sarah Forbes SF Associate Medical Director
Victoria Eaton VE Director of Public Health
Sabrina Armstrong SA Director of Organisational Effectiveness
Dr Bryan Power BP Clinical Lead for Long Term Conditions
Becky Barwick RB Head of System Integration
Laura Parsons LP Head of Corporate Governance & Risk
Sam Ramsey SR Corporate Governance Manager
Cheryl Lee (minutes) CL Corporate Governance Officer
Members of the public/staff members observing – 21
Item. Notes Action
1 Welcome & Introductions

2
Item. Notes Action
Jason Broch (JB), Chair welcomed everyone to the meeting. JB thanked his predecessor, Gordon Sinclair for his time in the role of Clinical Chair. JB reflected on the previous year and sent thanks and well wishes to members of staff and lay members who had moved on to new roles or retired. Ian Cameron, previous Director of Public Health was thanked for his time and commitment and Victoria Eaton was welcomed to the role.
2 Review of Achievements 2019-2020 Tim Ryley (TR) provided an overview of NHS Leeds CCG for the previous year and highlighted key achievements for the year. These included:
Leeds mental wellbeing service launched in November 2019
5 year contract, worth up to £76m including new investment of up to £20m
Follows significant review of primary care mental health services for common mental ill health conditions
Gives people access to services depending on their needs such as Improving access to psychological therapies (IAPT), primary care mental health liaison and perinatal mental health support Over £4.5 million investment to support GP practices with link workers
Investment in social prescribing makes a positive difference
Single citywide service run by community and voluntary organisations led by Community Links
Example: Foundry Lane Surgery in Seacroft: refers patients to 8 week art therapy course to help those experiencing a range of emotions including anger, low mood, depression or anxiety. Leeds Cancer Programme
City-wide partnership strategy; core team embedded in the CCG
Leeds Teledermatology service for suspected skin cancer patients
Last year, 8,927 two week-wait skin referrals received by LTHT; 5,798 patients (65%) appointed to a Teledermatology Triage Clinic; all patients appointed to triage assessed within48 working hours
Key challenges were identified as:
Coronavirus • Struck in the last quarter of 2019-2020 • Rapidly developed new ways of working to provide safe care • Changes to how the CCG works
System / winter pressures
• NHS experiences pressures every year; winter less challenging but pressure remains constant throughout the year

3
Item. Notes Action
• System-wide initiatives to reduce delayed transfers of care taking effect; more to do to improve patient experience and outcomes
• Good progress made on system flow System integration (both challenge and success)
• Leeds ‘Place’ • West Yorkshire and Harrogate Integrated Care Partnership
TR detailed the positive responses to the challenges faced including the adoption of new ways of working, improved technology, virtual meetings, system wide initiatives and the ever developing integrated and collaborative working across organisations.
3 Financial Review 2019-20 Visseh Pejhan-Sykes (VPS) presented a review of the finances of NHS Leeds CCG. VPS stated that the Leeds economy is worth £69 billion and 4 out of 5 NHS national offices are based here in Leeds including NHS England and NHS Digital. 196,000 people were employed within health and science in the public sector. VPS reported on how the CCG had spent the allocated funds:
£1.316 billion received
Half of this is spent on hospital care
Quarter is spent in primary care including prescribing
15% spent on Community Care and Care Homes
12% spent on Mental Health services
2% other areas
VPS presented the running costs of the CCG:
CCG – £17million allocation, of which £13 billion spent with the balance transferred to patient care.
From 2021, CCG running costs allocation will be reduced to £15 million, all underspend will be transferred to health services.
Key Financial Achievements:
• Financial Balance – despite emerging pressures from COVID in March
• High audit assurance – financial systems
• Leeds Mental Health and Well Being Service
• Keeping the NHS Operating during COVID
4 Adoption of Annual Report and Accounts 2019-20 JB presented the Annual Report and Accounts 2019-20 for adoption.
5 Covid-19
Impact on the city

4
Item. Notes Action
Victoria Eaton (VE) provided an overview of the current cases of Covid-19 in Leeds. VE explained there had been steep rises during late summer and September which is earlier than had been anticipated. The highest rates of infection were in 18-34 year olds but VE acknowledged that all age groups are seeing rising numbers of infection. VE discussed the impact being felt now along with the ongoing impact across the city including mental health, economic impacts and the interrupted care of chronic conditions.
Impact on health services Bryan Power (BP) presented on a study carried out around Covid19 – impact on provision of health services for non-COVID Conditions, which had been commissioned by Health and Social Care Gold Command. BP shared that people had rapidly adapted to new ways of accessing healthcare. By focussing on inequalities, specific areas were identified with a focus on deprived areas. 75 hypotheses and recommendations along with cross cutting themes were identified and being taken forward. Clear consistent communications was identified as being a key factor.
Stabilisation and Reset (StAR) Sarah Forbes (SF), Associate Medical Director presented an overview of the stabilisation and reset plan. SF explained the benefit and strength in partnership working and the group members included those from community healthcare, hospitals, mental health trusts, Social Care, Public Health along with the third sector and peoples’ voices represented. SF stated that capturing peoples’ voices had been invaluable and that one focus had been on ensuring service delivery along with improving the lives of the poorest the fastest.
6 Look Forward – Health Inequalities Framework Becky Barwick (BB) shared a video around improving the health of the poorest the fastest. This included the 5 intended outcomes; 1 – People will live longer and have healthier lives; 2 – People will live full, active and independent lives; 3 - People’s quality of life will be improved by access to quality services; 4 - People will be actively involved in their health and their care; 5 – People will live in healthy, safe and sustainable communities. BB introduced the Health Inequalities Framework which was signed off in May.

5
Item. Notes Action
BB shared the ‘strategy to action’ for 2020-21.
7 Questions & Answers Attendees were invited to pose questions to the CCG’s Governing Body:
1. “Do you know where the transmission of Covid-19 is occurring for it to be rising amongst all age groups?”
Information is gathered both from NHS Test and Trace and local contact tracing activities. This enables trends to be identified along with specific places. The main trend for transmission in Leeds has been found to be socialising, both in private households and hospitality venues. This particularly escalated in mid-August. The levels of transmission have been shown to be much lower in organised settings such as schools and workplaces. 2. “Are funding cuts to the CCG for administration fuelling CCG
mergers in West Yorkshire and Harrogate?”
The position in West Yorkshire is for CCGs to be closely aligned to our local communities at city level. Although financial challenges with administration costs in some areas may have led to mergers, this is not the case for Leeds CCG or Bradford. The ambition and intent remains to have close links with the Local Authority. 3. “Do you have an action plan to address a 3rd and 4th wave?”
The work carried out by the group Bryan Power led is driving some of the thinking around the third wave, particularly around the management of chronic conditions. Work is already underway to ensure a more integrated, holistic approach is adopted. The 4th wave will be around the economic impact as well as the mental health and well-being. The biggest challenge for mental well-being is where the NHS will distribute the money, either for targeting elective mental health and the backlog that has been created or to target the increase that is anticipated in the coming months and years. The CCG is committed to not only meet the mental health investment standard but to go faster where we are able to. A mental health plan is developing city-wide with a strategy board meeting and including all partners in the city. In terms of the economic impact, the CCG will be an active player in the commissioning of services to support the health inequalities agenda and to mitigate wherever possible the economic wave. We will also be driving

6
Item. Notes Action
innovation working with the universities and the business sector to boost that part of the economy. An example of this in new Leeds hospital buildings. 4. “As you will be aware, the CCG’s combined prescribing costs for
stoma and continence appliances is one of the highest nationally. Many CCGs are advancing plans to centralise services with the aims of improving patient experience, ensuring patients have an annual review with a nurse specialist and containing costs. Do you have any plans to look into this area? And if so, who will be leading on this?”
NHS Leeds CCG have invested in the past two years in clinical nurse specialists, who working as integral members of the Community Continence and Colorectal service, undertake reviews and clinical assessment of patients who are catheterised and who require stoma review. This has significantly increased the numbers of people who are now living without catheters as a result of successful trials without catheter. Stoma care patients are being reviewed and the appropriate products prescribed reducing accessories and product use in addition to promoting clinically effective stoma care. These reviews take place as clinically indicated and at a minimum annually following recent investment in nursing staff (Nurses are CCG funded rather than sponsored by one of the stoma companies.)
5. “Given the emerging evidence around Childhood Adverse
Experiences (ACEs) and the cross-cutting health impacts generating from them – many of which will have been compounded by Covid19. Combined with the increasingly robustly evidenced needs of sexual violence victims across the lifespan - evidenced by the Independent Inquiry Child Sexual Abuse (IICSA) and the recent Police & Crime Commissioners review of 3rd sector specialist sexual violence services in West Yorkshire. What plans do the Board have for supporting the gaps in Leeds 3rd sector specialist sexual violence services funding for children, young people and adults, female and male - as we emerge into a post Covid19 environment?”
The NHS Leeds health and the care system recognise the profound and lifelong impact that Adverse Childhood Experiences (ACEs) can have. We share a commitment to identify and support children who are experiencing, or adults who have experienced these. Earlier this year, the Leeds Health & Well-being Board signed off the new all age Mental Health Strategy and one of the key priorities within this strategy is to ensure existing and new services provide trauma informed care. In taking this forward we recognise the importance of working with those who are experiencing, or who are survivors of ACEs, in developing our support and services. We ensure that children are at the centre of any development of support and services; for example Leeds CCG funds the MindMate Ambassadors (who are young people with lived experience and often have had experience of ACEs), as well as working closely with the children in care council in the city. Leeds

7
Item. Notes Action
CCG also funds the Visible Project, which is survivor led group, who campaign for better outcomes for adult survivors of child sexual abuse. In addition, NHS Leeds CCG have worked with NHS providers in terms of developing quality standards relating to developing trauma informed care services and we plan expand this work to other providers and sectors. There is also a dedicated work-stream in the city where health, social care and education partners are working together to join up the support and service offer, as well as developing a programme to encourage a trauma informed approach in school settings. As a system, we recognise there is more to do but are well placed to make good progress in this area over the next few years. In response to your specific query about supporting the gaps in Leeds 3rd sector funding for specialist sexual violence services, we are not currently in a position to make any firm commitments around any funding in any areas. The CCG has no clarity yet at all about its allocations from NHS England for next year, or the national mandated expectations that will come with them. We fully recognise the pressures this sector is under and are in ongoing dialogue with Forum Central and other 3rd sector partners and with LCC colleagues. We recognise that the pressures in the Council budgets will bring additional pressures to the City’s resources. Within the available resources Leeds CCG is committed to addressing gaps within the 3rd sector, which will be informed by our recently developed health inequalities framework and CCG strategic plan. We recognise that as a system, we need to shift resources to preventative and early intervention services and 3rd sector have a crucial role in this. Survivors of sexual abuse are a priority group and as commissioners, we will ensure that future investments consider carefully the needs of this group and other vulnerable groups. Currently, commissioners are reviewing current 3rd sector provision relating to mental health support and city wide engagement is planned for November 2020. The findings from their engagement will also help to inform future investments and new models of care support. More details will shared on the CCG website.
6. “Can you tell us about prescribing physical activity in different
localities in Leeds?”
The new Primary Care Healthy Living template for monitoring levels of physical activity and enabling quick electronic referral to Healthy Living services is planned to go live on 21st September 2020. This is the first time that Leeds Primary Care staff including GP’s will be able to refer patients directly to One You Leeds and Active Leeds for Physical Activity Opportunities. Active Leeds offer a range of physical activity behaviour change programmes, initiatives and interventions – including, for example, long term conditions, Leeds Girls Can, couch to 5km, bike rides and group walks. Active Leeds are accepting referrals from Healthcare Professionals, Healthy Living Services, Social Prescribing Teams, community groups and self-referrals via the online enquiry form, email or by phone. PH fund work

8
Item. Notes Action
around Falls Prevention and a Strength and Balance Programme for Frailer Older People. Active Leeds Team have also supported the place based approach outlined in the Director of Communities and Environments report of November 2017 and have Localities Officers working with the 6 x 1% priority communities identified in the report (the 4 areas outlined below plus Lincoln Green, Burmantofts and Richmond Hill and Clifton and Nowells, in Seacroft). Sport England funding has enabled a Get Set Leeds Local approach to PA in our 1% neighbourhoods, where a community chest pot is available to support local innovative projects. 55 staff across primary and secondary care have attended followed by HCAs, GPs and physiotherapists. The training supports professionals to look at the benefits of signposting and referring patients to physical activity opportunities as well as promoting opportunities in Leeds. We have recently developed, in response to Covid and more people wanting to be active at home, a set of webinars focused on increasing knowledge and awareness of the benefits of physical activities and signposting opportunities in the Leeds area. A number of Leeds GP practices refer patients to Parkrun (opportunity to walk, run or volunteer). A survey of GP practices we did in 2018 looked at GP referrals into OYL/Active Leeds and Parkrun, which suggests 16% current signpost into parkrun. Leeds is also one of the areas in the UK with a 5K Your Way programme which links Cancer pathways into parkrun via primary and secondary care signposting. Walking Groups have also started from GP surgeries supported by Walk Leader training from Active Leeds. The Public Health contract reported 42 referrals from Health Services (GPs, Social Prescribing, Midwives, other Health professionals) in 19/20. All partners deliver a range of physical activity options. In WNW, Barca delivers yoga and walking groups. In ENE, Orion and Touchstone deliver a walking group, Zumba, gardening groups, swimming, pilates, yoga, Ramgarhia fitness. In the SE, Health For All and Hamara are able to offer a community gym, but also offer activities such as walking groups, exercise classes, gardening groups, swimming group, pilates, and Zumba. Physical Activity Clinical champions training, run by Public Health England. The majority are nurses or trainee nurses,
7. “I am very disturbed to hear that NHSE have noted their intention to
“streamline commissioning through a single ICS/STP approach” which will “typically lead to a single CCG across the system” and are requiring formal written applications to merge CCGs on 1 April 2021 to be submitted by 30 September 2020. When the CCGs were set up following the Health and Social Care Act 2012 a key argument for the change was that planning and commissioning health care would be put in the hands of local GPs who were said to be best placed to understand the needs of their
9
Item. Notes Action
patients and neighbourhoods. We have already seen the 3 CCGs reduce to one with an inevitable loss of accountability. Now that Covid 19 is shedding a harsh light on gross inequalities between diverse populations, income groups and geographical areas, surely it is even more important that vital decisions regarding commissioning health and social care are taken at ground level by people who know Leeds well and are familiar not just with the challenges but with a string of good intentions and past local initiatives which have barely scratched through the rust on the issue. It also seems more important than ever to insist on championing and building local decision making and accountability as early Government decisions to bypass local public health and other bodies well placed to manage test and trace systems, PPE provision etc. in favour of putting resources into privatised, remote, often unaccountable and sadly inadequate providers has been fairly disastrous. Some time ago the West Yorkshire and Harrogate joint CCGs reassured us that they were not in favour of amalgamating CCGs across the ICS. I hope that this is still the case and would be grateful if you could clarify the position of Leeds CCG. Should there be any plans for further mergers I would like reassurance such plans would be widely publicised and subject to rigorous public consultation as required by the Health and Social Care Act and NHS (Clinical Commissioning Groups) Regulations 2012.”
The WYH joint CCGs are not in favour of amalgamating and that remains our position. Where there are areas we can work on together we will through the Joint Committee and this will be an open meeting at which the public can attend. Leeds CCG is committed to remaining as an independent CCG. Any mergers can only happen in two-ways. One as CCGs we decide to consider that, in which case I can give assurance that if we change our position then we will include public consultation. However, the second means is through changes in legislation or direction from NHS England. In those circumstances decisions on consultation will be outside the CCG’s control.
8. “While Public Health England has effectively been abolished and moved into a new organisation with a central role in dealing with pandemics, it is unclear who will pick up other important aspects of PHE including screening, vaccination, intelligence and health improvement. The whole thrust of NHS reorganisation is based on shift of services from hospital to community coupled with effective public health interventions that will lead to a reduction in demand for health care and reduce costs. What assessment has the CCG made of the implications of the abolition of PHE (in the current pandemic, likened to removing the wings from a malfunctioning aircraft in flight

10
Item. Notes Action
in order to achieve a safe landing) in terms of achieving its strategic objectives?”
The CCG has limited engagement with Public Health England currently as most of our Public Health relationship is with those aspects commissioned or delivered with the Public Health Department in Leeds City Council. We continue to strengthen these relationships with an Integrated Commissioning framework and further joint posts. PHE is continuing to operate across its remit currently and once more detail of the future is understood we will review the position.
9. “The number of positive tests for coronavirus in Leeds is rising
alarmingly. There has been an outbreak at Gregg’s distribution centre in Leeds, and recently the Food Standards Authority was investigating approximately 40 outbreaks in food factories around the country. In meat packing plants, infection has been attributed to cramped working conditions, background noise (which leads to shouting), and poor ventilation. Worryingly, similar compound risk situations might occur in other crowded, noisy, indoor environments, such as pubs, live music venues, gyms and schools. The German meat processing plant outbreak in which 1500 workers were infected was investigated very thoroughly, including with genetic finger printing of the virus isolated. This showed the outbreak was a super-spreader event in the plant and not related to spread in the community (as commonly assumed). Transmission of the virus occurred indoors over distances of 8 metres and more. Such outbreaks have demonstrated that current precautions for controlling spread of infection in workplaces are inadequate, and airborne transmission a much more significant problem than previously thought. UK experts have been calling for urgent recognition of the key role of ventilation in work places in preventing COVID-19. This issue is not yet reflected in government advice regarding reduction in risk of viral spread. How is the Governing body raising the importance of airborne viral transmission with its various partners, with a focus on effective ventilation to reduce risk of further outbreaks in schools and workplaces?”
From a national government perspective there are guidelines and restrictions in place that seek to reduce the potential of infection of airborne transmission. Social distancing and the rule of 6 is now a legal requirement in the hospitality sector along with a restriction on levels of music to prevent shouting and the need for excessively close talking. In addition new legislation announced on the 22nd September 2020 requires all staff working in the retail sector to wear face coverings. Government guidance targeted at businesses does make reference to the importance of providing as much ventilation in workplaces as is practically possible although it does not make this a legal requirement at present. From a Leeds perspective following outbreaks in food processing

11
Item. Notes Action
plants across Europe and closer to home in Kirklees the Leeds Environmental Health Team contacted all food processors and manufacturers in Leeds to provide advice and support to ensure they were clear taking all necessary safeguards. This included the offer of visits and inspections by EHO’s and Infection Control Specialists. The offer was well received and taken up by many businesses. This has now been rolled out to other workplace settings including the hospitality sector and our universities and FE colleges. To date Leeds has seen approximately 15 outbreaks linked to workplace transmission and a rapid response allied to good relationships with businesses has meant that outbreaks have been quickly brought under control and further transmission prevented.
10. “Last year the CCG adopted commissioning guidance from NHS
England based on recommendations to restrict access to 17 Evidence Based Interventions (17 EBI). A further consultation over an additional 31 procedures has now been completed and CCGs will at some point once again be asked to endorse recommendations made. I would therefore like to draw attention to a response to this consultation by the Patients Association (PA) which stated that the claim it was extensively consulted is false, that it was commissioned to undertake patient focus groups with a timetable that then made it impossible for findings to be fed back before the close of the consultation, and that the risk that these proposals may cause harm could have been reduced by engaging with patients and listening to their views. In addition the PA questioned why the whole consultation was focused on reducing NHS activity rather than how to benefit patients. In the light of this, when recommendations are made to the CCG over commissioning these 31 procedures, will the CCG look critically at these and endorse the concerns of patients with NHSE, as articulated by the PA? Furthermore, has the Governing body published data on changes in numbers of procedures and any adverse clinical consequences for patients following implementation of guidance on commissioning the 17 EBI?”
Thank you for drawing our attention to the Patients’ Association concern that patients were not fully consulted. The process that the Integrated Care System of West Yorkshire and Harrogate took with the first 17 was to review the extent to which they were a significant change from any existing local policies, and then to adopt these as an ICS in line with our approach to commissioning policies. We did ask about patient engagement for the first set as we felt it was sensible to rely on national engagement rather than incurring additional costs repeating such engagement locally. Given your feedback, it would be helpful to know whether the PA feedback could be made available to the ICS to consider before we discuss our local adoption of the further EBI list. It would be really helpful if you could arrange to share this or give us a contact.
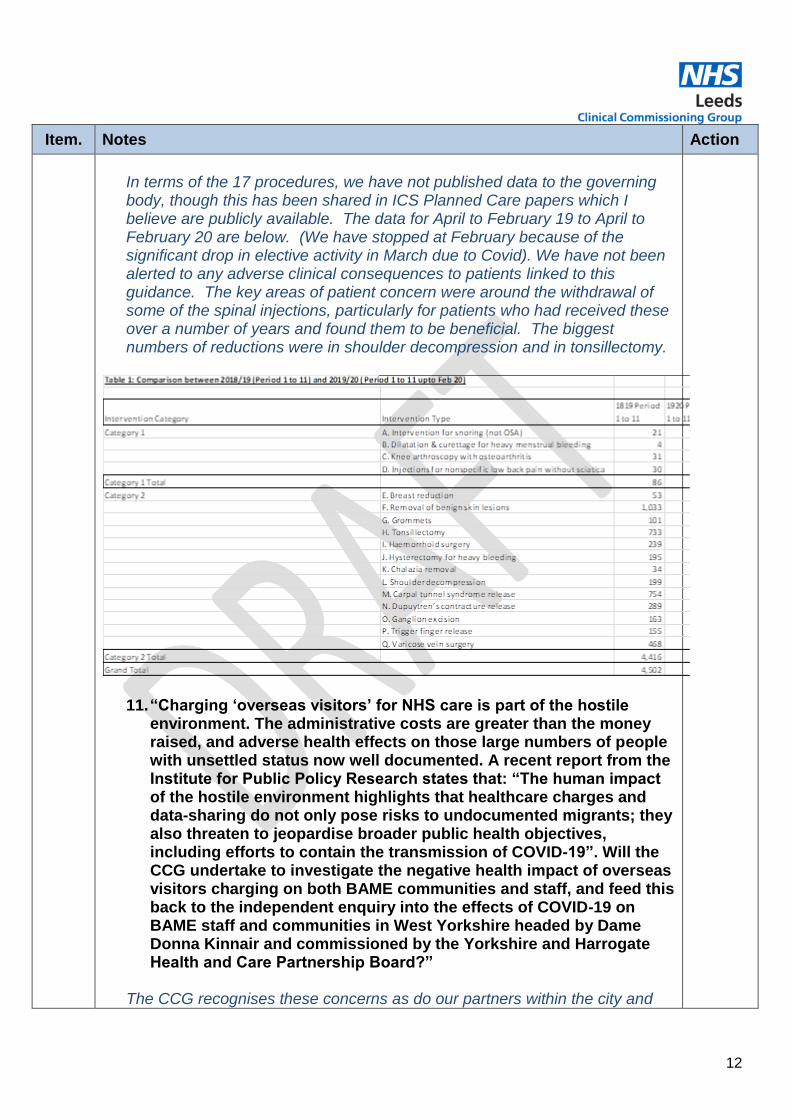
12
Item. Notes Action
In terms of the 17 procedures, we have not published data to the governing body, though this has been shared in ICS Planned Care papers which I believe are publicly available. The data for April to February 19 to April to February 20 are below. (We have stopped at February because of the significant drop in elective activity in March due to Covid). We have not been alerted to any adverse clinical consequences to patients linked to this guidance. The key areas of patient concern were around the withdrawal of some of the spinal injections, particularly for patients who had received these over a number of years and found them to be beneficial. The biggest numbers of reductions were in shoulder decompression and in tonsillectomy.
11. “Charging ‘overseas visitors’ for NHS care is part of the hostile environment. The administrative costs are greater than the money raised, and adverse health effects on those large numbers of people with unsettled status now well documented. A recent report from the Institute for Public Policy Research states that: “The human impact of the hostile environment highlights that healthcare charges and data-sharing do not only pose risks to undocumented migrants; they also threaten to jeopardise broader public health objectives, including efforts to contain the transmission of COVID-19”. Will the CCG undertake to investigate the negative health impact of overseas visitors charging on both BAME communities and staff, and feed this back to the independent enquiry into the effects of COVID-19 on BAME staff and communities in West Yorkshire headed by Dame Donna Kinnair and commissioned by the Yorkshire and Harrogate Health and Care Partnership Board?”
The CCG recognises these concerns as do our partners within the city and

13
Item. Notes Action
recognise that they are likely to further drive health inequalities. We are currently waiting for the publication of the report of Dame Donna Kinnair report and will take forward any findings arising from that.
12. “It has been a very disappointing year for the residents who live in
Adel who after an extensive campaign lost their one and only surgery. How many more small surgeries going to be closed?”
Applications for branch surgery closures can be made by the practice who holds the contract at any time (as opposed to a CCG led process). There is a clear process which should be followed in considering any application as part of NHS England’s Policy and Guidance Manual (PGM) (Part B, Section 7.15.10). Specifically, the guidance sets out what commissioners should consider when deciding on branch closures. This includes:
financial viability
registered list size and patient demographics
condition, accessibility and compliance to required standards of the premises;
accessibility of the main surgery premises including transport implications;
the Commissioner’s strategic plans for the area;
other primary health care provision within the locality (including other providers and their current list provision, accessibility, dispensaries and rural issues);
dispensing implications (if a dispensing practice);
whether the contractor is currently in receipt of premises costs for the relevant premises;
other payment amendments;
possible co-location of services;
patient feedback;
any impact on groups protected by the Equality Act 2010 (for further detail see chapter 4 (General duties of NHS England);
the impact on health and health inequalities; Both sites at Adel and Alwoodley are operated by the same practice and therefore the level of service should be consistent however recognising that the premises at Alwoodley are modern which meet current healthcare guidance relating to estate.
JB thanked attendees for their contributions to the meeting. The AGM closed at 17:35

MINUTES ACTION LOG – GOVERNING BODY
1
ITEM NO:
ACTION NO:
ACTION: ACTION BY: COMPLETED/UPDATE
22 July 2020
20/40 1 Shaping our Future Operating Model Recommendation that the CCG Membership (at the next opportunity) approves the changes in the voting members’ job titles in the CCG Constitution.
LP/JB Complete. Council of Members meeting to take place on 30 September. Changes will be presented for approval.
23 September 2020
20/65 1 Covid-19 impact on provision of health services for non Covid conditions Members were assured that there was detailed work ongoing within the care home scheme in practices and the report considered the frail population as a whole. It was agreed that the report would link directly with the health inequalities framework to identify the needs of those in care homes as a population cohort.
JH Complete. Primary Care Colleagues are working to establish the enhanced health in care homes scheme as per the national requirements. The scope to apply a health inequalities lens in terms of is probably reasonably limited during this set up phase but we certainly have a long term ambition to implement proactive care based on need to all people living with frailty – focusing on maximising independence – wherever the person lives.

1
Leeds Health & Wellbeing Strategy Outcomes – that this report relates to:
1. People will live longer and have healthier lives
2. People will live full, active and independent lives
3. People’s quality of life will be improved by access to quality services
4. People will be actively involved in their health and their care
5. People will live in healthy, safe and sustainable communities
NHS Leeds CCG Strategic Commitments We will focus resources to:
1. Deliver better outcomes for people’s health and wellbeing
2. Reduce health inequalities across our city
We will work with our partners and the people of Leeds to:
3. Support a greater focus on the wider determinants of health
4. Increase their confidence to manage their own health and wellbeing
5. Achieve better integrated care for the population of Leeds
6. Create the conditions for health and care needs to be addressed around local neighbourhoods
Assurance Framework – which risks on the GBAF does this report relate to: 1. Failure to deliver the CCG commitment to reduce health inequalities across our city.
2. Quality of commissioned care is compromised and does not reflect best practice.
3. Failure to achieve financial stability and sustainability.
4. Failure to overcome local and national workforce shortages.
5. Business continuity of health and care services disrupted as a result of a significant event.
6. Ineffective patient and public engagement and lack of transparency in translation of engagement into decisions.
7. Partners and Professionals do not support the CCG strategy.
8. Constraints on CCG organisational effectiveness impact the delivery of the CCG’s plans.
9. Inadequate system infrastructure to support the CCG’s plans.
Agenda Item: GB 20/88 FOI Exempt: N
NHS Leeds CCG Governing Body Meeting
Date of meeting: 25th November 2020
Title: Chief Executives Report
Lead Governing Body Member: Tim Ryley, Chief Executive
Category of Paper Tick as
appropriate
()
Report Author: Tim Ryley, Chief Executive
Decision
Reviewed by EMT/Date: N/A
Discussion
Reviewed by Committee/Date: N/A
Information
Checked by Finance (Y/N/N/A - Date): N/A
Approved by Lead Governing Body member (Y/N): Y

2
EXECUTIVE SUMMARY: The report provides an overview of the key areas of focus and provides updates on work to implement a number of key areas discussed by the Governing Body. In particular, it sets out:
- The medium term implications of the Covid Pandemic and the likely medium-term financial pressures with an eye to implications on the level of risk and future planning priorities
- The changing NHS landscape and implications for Leeds going forwards - The plans for management of EU Exit impact as the transition period ends - Development of the local Integrated Care Partnership - Implementation of Shaping Our Future - Addressing BAME inequalities and diversity within the CCG - First steps on implementing the CCG Health Inequalities Framework
RECOMMENDATION: The Governing Body is asked to:
a) DISCUSS and NOTE the Chief Executive report; b) DISCUSS and NOTE the attached BAME Health Inequalities Report; and c) RECEIVE the communications and engagement update as assurance that the CCG
is delivering its statutory duties to ensure public involvement and consultation.

3
Chief Executives Report:
1. INTRODUCTION 1.1 This report provides an overall context to the current work of the CCG including an element
of Horizon Scanning. In doing so it is intended to give some context for further detailed reports and discussions. It also updates on key areas of work that have been set in motion by the Governing Body in recent months.
2. HORIZON SCANNING 2.1 Covid Implications
2.1.1 Governing Body members will note that the GBAF and the Risk Report indicate an
increasing level of risk across all areas of the CCG business. Given the unprecedented scale of the pandemic it would be a surprise otherwise. It will also be clear in the IQPR that the system is not operating at a normal level of service.
2.1.2 There is the immediate pressure that presents considerable risks to access, clinical quality, finance and staffing. The demand on colleagues and resource constraints within the CCG and across our partners also limits our capacity to push forward other agendas at the pace we might have normally expected to.
2.1.3 Members of the Governing Body will also recall the report from Dr. Bryan Power on the medium and long-term implications of Wave 1 which will clearly now be exacerbated. These include: the implications on planned activity which is now scaled back increasing waiting lists; access to long-term condition management; the implications on mental health; and the impact of economic hardship in health especially health inequalities.
2.1.4 The CCG believes that the best way to minimise these impacts is to continue to share
the risks across the city with our partners and to continue to engage with the public in Leeds. The shorter the time period that Wave 2 lasts the less the impact and equally the more service we can retain during this period the greater the mitigation. There are no intentions to stop services but reductions in the scale of the offer and delays in access are inevitable.
2.1.5 In the medium term the back-log of elective activity is likely to become the dominant
feature of NHS planning for at least the next three years, potentially something akin to the focus in the early years of the 2000’s. This will have an impact on other areas of development.
2.1.6 The paper on the Covid response later on the agenda will detail more on the work being
undertaken to manage the situation.

4
2.2 Finances
2.2.1 The financial challenges of this current period and how these are being managed will be detailed in the financial report later in the papers.
2.2.2 However, the Governing Body needs to be sighted on the potential implications of a number of changes in the financial position going forward and the implications on the CCG Strategy and previous commitments.
2.2.3 It is likely that the changes to the funding regime set out for the last six months of 20-21 will continue into the next financial year. This, with the planned care recovery noted above, will put considerable pressure on the CCG’s budget and thus our commissioning intentions. The attention given to cost reductions and efficiency across the city will be much higher than in previous years. The implications of reductions in Adult and Children’s Social care will also need to be played-in.
2.2.4 Work is underway on developing revised plans and budgets. The Governing Body will
be discussing these in more detail over the next three months.
2.3 NHS Landscape
2.3.1 As Governing Body members will be aware there are on-going conversations at a national level between the NHS and DHSC on the future of the NHS and in particular commissioning and the strong possibility of legislation in the spring.
2.3.2 The clear picture emerging is that there will be a very strong emphasis on Integrated Care Partnerships at place, in line with our strategy. These will have a number of commissioning responsibilities. At the same time there will be a single strategic commissioner or similar at an ICS level.
2.3.3 Clearly the balance of decision making and the nature of this relationship will need
working through.
2.3.4 The other strong message is that there is a desire that legislation removes barriers to evolving the right solutions for each area rather than prescribes the exact nature of all arrangements.
2.3.5 It is expected that guidance on the transitional nature of ICS will be published shortly
and probably at some point in December there will be a consultation published on future legislative changes.
2.3.6 The CCG will continue to work closely with the ICS and fellow CCGs to set out our
preferred options on how we evolve towards this new thinking, whilst at the same time strengthening the place based approach adopted through Shaping Our Future. These are set out in the work being done under Commissioning Futures. I intend to bring a report to the next CCG Governing Body on this and the revised Operating Model of the ICS in which the CCG is also involved.
5
2.3.7 It will be important too to develop a strong narrative for all CCG colleagues and as a Leeds partnership describing our approach. The CCG will continue to work across our partnerships and take forward the principles agreed in the last board development workshop.
2.4 EU Exit
2.4.1 The Emergency Preparedness leads in the City have updated their EU Exit planning
assumptions and risks, as we get closer to December we may again face the end of the transition period without a trade agreement. The main risk areas identified locally remain medicines and equipment supply, and the risk to fuel supplies. Local organisation have confirmed that they are in a much stronger position now due to actions taken in Covid in respect of PPE supply, and recent centralised distribution models adopted for medicines in Covid-19 may mitigate some of the previously assessed supply risks.
2.4.2 A national NHSE/I Webinar hosted on 4th November 2020 gave detailed information on the ongoing national work and associated developments on a wide spectrum of areas including medicine supplies, clinical consumables, workforce, data, information governance, reciprocal healthcare, adult social care and primary care. There is now a much clearer picture on the mechanisms in place to mitigate identified risk, as well as clarity on channels to communicate up and down the structures. There continues to be strong messages not to stockpile, and to escalate through established routes.
2.4.3 The Leeds Health and Social Care Resilience Group is now meeting and the first half of
it focusses on Leeds Health and Social Care EU Exit Planning and will comprise organisational updates and a review of key risks and an update from the Leeds City Council Executive Office. This format replaces the previous Leeds Health and Social Care EU Exit Task and Finish group that was led by Dr Ian Cameron as Director of Public Health; members welcome the supportive approach which enables a shared understanding of issues and risk. The CCG is committed to supporting delivery across the system, including obtaining assurance from Primary Care and contracted providers.
3. INTEGRATED CARE PARTNERSHIP (ICP) DEVELOPMENT
3.1 Progress and Next Steps
3.1.1 In the past two months further conversations have taken place across Leeds building on
the already strong relationships to agree the next steps on developing an Integrated Care Partnership across the city. This has included a number of meetings of NHS Chief Executives with the Director of Adult Social Care and the Confederation Chief Executive; the wider city Partnership Executive Group and at the Health & Wellbeing Board. These have been supported and facilitated by CCG members of staff with advice from strategic partners.

6
3.1.2 The Chief Executive group has been formed to meet at least monthly to drive the agenda forward and agreed that in building a truly Integrated Care System we need to strengthen and accelerate four areas:
- Strengthen our shared vision and ambition by more sharply defining measurable goals. This will be supported by the work underway in the Left Shift Blue-Print. - Create a single source of truth that drives decision making across the system, accelerating the creation of joined-up information systems and analysis - Develop governance to hold the partnership together in development and in time as things move forward to create the underpinning governance for an integrated networked partnership - Ensure that there is an engine room to drive the change building around the CCG plans for a Director of Business Integration with support from a remodeled Health Partnership Team
Each of these four has named city chief executives leading on it and reporting back accordingly. I have been asked by provider colleagues to chair the ICP development board.
3.2 Workforce
3.2.1 In September 2020, a permanent Director of Strategic Workforce and the Health and
Care Academy (Kate O’Connell) was appointed on behalf of the city, to advance the full programme of work underpinning the Strategic Workforce Priorities, including effective alignment and integration with the city’s wider enabling strategies, and developing the Academy to realise its full potential.
3.2.2 The Strategic Workforce Priorities continue to provide a cohesive focus for Health and Care organisations across the city, but there is recognition of different challenges within different parts of the system, dissonance between governance requirements, and unique organisational pressures all of which can make alignment with system level priorities a challenge.
3.2.3 Workforce pressures in health and care are even greater than before, with the
resourcing, safety and wellbeing of our current and future workforce under substantial strain.
3.2.4 The collective response to these disruptions has however stimulated innovation and an
increase in pace of the Leeds Left Shift and person-centred care, prioritising digital transformation, workforce redesign, and cross-organisational working and learning.
3.2.5 This provides an impetus to progress key programmes of work advancing the
introduction of new roles into the health and care system; rebalancing and enhancing our educational pathways; working with local communities to learn together and improve

7
opportunities; develop city-wide leadership and expertise; realise the value of digital, technical and data advances; and improve workforce mobility.
3.2.6 Progress on the shared workforce strategy has been challenging over the last year, with
immediate staffing pressures often taking precedence over some of the longer term ambitions. Despite this, there have been some important system level achievements:
- The successful expansion and diversity of nursing placement opportunities
- The growth of System Leadership development across the city, stimulating cross-
boundary working and innovation
- Development of a Mental Health First Aid infrastructure to better support
workforce wellbeing
- The increasing impact of Springboard in career progression for women in health
and care, specifically from minority communities
- Launch of the first city cohort of Data Analyst Apprentices building workforce
capacity and connectivity
- The culture change programme Better Conversations has now reached over 100
organisations helping to unify a city-wide approach to working ‘with’ our citizens
and patients
- Completion of a successful pilot for new roles in GP practice providing essential
learning for future workforce planning
3.2.7 As part of Shaping Our Future the CCG is looking to appoint a workforce planning individual to work closely with the Pathway Integration Teams and Primary Care to ensure that there is an end to end understanding of workforce changes and needs to support the city approach to workforce planning.
4. CCG DEVELOPMENT
4.1 Shaping Our Future - Staffing
4.1.1 We have now begun the post-filling activity in line with our Organisational Change policy
and follow ACAS and CIPD best practice. At present, that is limited to Band 8C, 8D and VSM. We have appointed one of the three vacant Director posts, the Director of Pathway Integration, and a second is currently advertised on NHS Jobs, the Director of Population Health Planning. We are still in consultation with partners on the potential joint post of Director of Business System Integration, and anticipate this being agreed for advert by the end of November. In the meantime we have secured some interim support to cover aspects of the two current vacancies given the Covid challenges.
4.1.2 At the Governing Body level we have recruited to the vacant Lay Post for Audit and Conflicts of Interest and welcome Cheryl Hobson.
4.1.3 Directors have now had initial discussions with colleagues in the first tranche (VSM, Bands 8C and 8D) and will issue individual letters outlining next steps. We are including those senior staff embedded within the GP Confederation. In line with our policies, we

8
have reviewed current roles against those identified in the new structure and either ‘slotting in’ clear matches; assessing in ring-fenced ‘pools’; or identifying other options. We expect most of our people will transition into the new structure and are committed to avoiding compulsory redundancies.
4.1.4 We also plan to move quickly to resolve the position for Bands 2-4 where their roles are far less likely to change significantly in the new model other than a greater likelihood of matrix working, as will apply to all staff.
4.1.5 We are finalising our development offer to support colleagues which will begin with a programme from December commencing with Population Health Management; and Matrix-working. We will also launch a series of co-development design workshops in January.
4.2 Shaping Our Future – Organisational Development
4.2.1 Our Organisational Design plans include: - Finalising our new behaviours, ways of working (matrix and extreme teaming) and
cultural change requirements - Designing the skeletal architecture (Directorates, Portfolio Holders and Business Units)
required to enable the delivery of the new operating model - Agreeing resourcing envelopes for the Business Units - Agreeing an approach to resource management to ensure expertise from within BUs
are deployed swiftly and effectively into virtual teams; and - Supporting briefing, consultation and activity to populate the teams and directorates.
5. BLACK LIVES MATTER AND BAME NETWORK
5.1 West Yorkshire Review on BAME Health Inequalities
5.1.1 The West Yorkshire Partnership (ICS) commissioned Dame Donna Kinnair to undertake a rapid review over the summer of the public sector approach to the commissioning and provision of services across West Yorkshire. The report was published in October and is attached for note, “Tackling health inequalities for Black, Asian and minority ethnic communities and colleagues - understanding impact, reducing inequalities, supporting recovery”
5.1.2 The Governing Body are asked to discuss and note the report and the implications for the CCG as commissioners. There is a close fit to the work we have already undertaken within the Health Inequalities Framework but with an additional lens.
5.1.3 In particular the key recommendations for commissioners are set out below:
Ethnicity recording is 100% in all settings and that this data, coupled with local insight, is used across the Partnership to inform the design and delivery of care.

9
Community representation, that reflects local population ethnicity, is visible throughout the planning process, including procurement of services.
Service access, uptake and outcomes by ethnicity are monitored to identify inequalities.
Ethnicity recording is 100% in all settings and that this data, coupled with local insight, is used across the Partnership to inform the design and delivery of care.
Clear local and Partnership arrangements for commissioning with the voluntary, community and social enterprise (VCSE) sector are in place.
Demonstrate that services are culturally competent and are contributing towards reducing inequalities identified.
5.2 CCG Response to West Yorkshire BAME Staff Action Plan
5.2.1 The Governing Body will recall that at the September meeting we signed-up to the West
Yorkshire BAME Staff Action Plan following a presentation by Shak Rafiq and Kaysha Maynard. Our BAME network was already established but is now increasingly involved in key decision making. They are receiving training to enable them to be actively and meaningfully involved in all senior appointments, and members of the Network have been involved in all recent senior appointments.
5.2.2 In tandem with two other CCGs, we have commissioned Unconscious Bias training for
all staff. It is and is due for delivery in December and will include a targeted offer for Governing Body members.
5.2.3 Some actions are still in progress including offering active representation at the WY&H
BAME Review action planning group. All of our planned future actions are in line with those recommended by the review, but we are now looking at how we can spread these across the system to increase impact.
5.2.4 As the Chief Executive Officer, I met with the CCG BAME Network last month and we
agreed a set of areas to focus on which are being built into our organisational development plan. These included:
- Further strengthening of the arrangements for BAME colleagues in the
appointment processes - Building into my one-to-ones with directors a focus on their active support to
Black, Asian and other heritage staff in their directorate - Ensure our processes for secondments and acting-up roles are as inclusive as
our permanent recruitment process to create developmental opportunities - We will ensure that colleagues with Black, Asian and other heritages receive
recognition as authors of work etc. - We will ensure colleagues from a variety of backgrounds are actively invited to
influence our planning and design of services.

10
6. HEALTH INEQUALITIES UPDATE
6.1 The CCG launched its Health Inequalities Framework in September at the CCG Annual General Meeting, the Health & Wellbeing Board and through a week long set of articles in the Yorkshire Evening Post. We also announced a series of investments in this financial year that are aligned to the framework with a focus on the Voluntary Sector, Local Care Partnerships and Digital Inclusion. The challenging financial position has meant some minor scaling back on the scale of these.
6.2 We are now working to ensure that in setting our plans for the next financial year the principles set out in the Health Inequalities Framework are applied across all areas of our business and in line with the Commissioning elements of the West Yorkshire Black Lives Review described above. This includes further work to look at data in amore granular way.
7. SUMMARY
7.1 The NHS is in unchartered territory and the pressures on all aspects are significant. As a
CCG it is important that we both support our colleagues to manage the very intense challenges of the pandemic in the current time-zone, whilst at the same-time maintain that strategic population and medium to long-term focus set out in our Strategic Plan. The report summarises the likely pressures on the system arising from the current challenges and indicates progress that we have made in key areas of our strategy in the past few months.
7.2 As ever Governing Body members are asked to note the Engagement Report which is attached. Maintaining a strong communications and engagement presence at times like this remains critical.
8. RECOMMENDATION
The Governing Body is asked to:
a) DISCUSS and NOTE the Chief Executive report; b) DISCUSS and NOTE the attached BAME Health Inequalities Report; and c) RECEIVE the communications and engagement update as assurance that the CCG is
delivering its statutory duties to ensure public involvement and consultation.

West Yorkshire and Harrogate Health and Care Partnership Review Report
Understanding impact, reducing inequalities, supporting recovery
October 2020
Tackling health inequalities for Black, Asian and minority ethnic communities and colleagues

Contents01Foreword
Introduction
Purpose of the review
The Review Panel
Building on existing work
Supporting Black, Asian and minority ethnic (BAME) communities
Supporting BAME colleagues
Review themes
Improving access to safe work for BAME people in West Yorkshire and Harrogate
Ensuring the Partnership’s leadership is reflective of communities
Population planning – using information to make sure services meet different groups of people’s needs
Reducing inequalities in mental health outcomes by ethnicity
Summary of recommendations
Action plan
Closing comments
Supporting information
Contributors
References
03
05
09
11
13
14
15
19
20
24
28
33
38
42
43
45
45
48
Despite historic events and the stark reality of the compelling evidence before us, I like many others want to know why people from BAME communities have been disproportionately affected by COVID-19 and continue, yet again, to be impacted by health inequalities and an unjust society. Furthermore, I want to know what is happening to address this symbol of social injustice.
Being involved in this important review has given me both the opportunity to learn more about West Yorkshire and Harrogate’s cultural vibrancy, strong diverse communities and identities, and to facilitate a much needed conversation which builds on the work already well underway by the Partnership. There is much to be proud of and it gives me genuine hope for current and future BAME generations.
I am especially keen to ensure that the review work carried out doesn’t sit as a report on a shelf, collecting dust. I know this is absolutely not the intention. There is a genuine commitment for real change and you only need to look at the themes covered on page 19 to know this is the case. You can be reassured that an action plan for implementation, monitoring and evaluation is firmly underway.
>>
Everyone deserves the same opportunities to lead a healthy life, no matter where they live or who they are – their background, whether they are wealthy or not. Difference should not lead to disadvantage.
Yet, evidence shows that people from Black, Asian and minority ethnic (BAME) communities continue to face health inequalities, discrimination in the workplace and are more likely to develop and die as a result of a plethora of diseases, most recently COVID-19.
Health inequalities we know exist have been further exacerbated by recent events, namely the pandemic and economic recession. Whilst it may be uncomfortable for some, now, once again, we have the opportunity to act with passion and conviction like never before.
Closing these gaps which exist in all BAME communities remains the biggest challenge we face, and essentially one of the biggest of our life time. This is one of the many reasons I was delighted to hear that West Yorkshire and Harrogate Health and Care Partnership (WY&H HCP) were commissioning an independent review. Knowing that more must be done was an important step.
Foreword from the chair of the review sessions
/ 3West Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and Wakefield

Photo credit: Leeds Gypsy and Traveller Exchange (also known as Leeds GATE)
BAME communities and colleagues, like everyone else, deserve to have the best start in life - to live a long and happy one in good health with fair access to education opportunities, a warm and loving home and an income sufficient to meet their needs. And because we understand that reducing health inequalities is about jobs that local people can get, decent housing and preventing people becoming isolated, it follows that we should recognise that local places and communities have the most critical role to play in West Yorkshire and Harrogate.
The collective strength behind this report will give it the determined force and the resources it needs around key areas of work, such as addressing the wider determinants of mental health for BAME communities, fairer career opportunities for colleagues, addressing racism and indirect discrimination.
I’m heartened by the work of the review panel. It has been built and informed by an extensive amount of insight, hard work, dedication and commitment from all involved. This includes the Partnership’s leadership, the West Yorkshire and Harrogate BAME Network, and the strength of voluntary and community sector partners – to name a few. I look forward to following the outcomes from the recommendations made here and most importantly hearing about the positive difference it has made to people’s live.
Professor Dame Donna Kinnair
(Professor Dame Donna Kinnair is the Chief Executive and General Secretary of the Royal College of Nursing, a leading figure in national health and care policy.)
The 2011 census data shows Black Asian and minority ethnic (BAME) communities make up 20% of the population of West Yorkshire and Harrogate, around 490,000 people. Bradford has the highest proportion of BAME groups of people (31.2%) and Craven has the lowest (3.6%). In 2019/20 the percentage of BAME children in school across West Yorkshire ranged from around 6 in pupils in Bradford to around 2 in 10 pupils in Wakefield. There are approximately 7,000 people from Gypsy, Roma and Traveller communities living across West Yorkshire.
Our Partnership and population
West Yorkshire and Harrogate Health and Care Partnership (WY&H HCP), is the fourth largest Integrated Care System in the country, covering a population of 2.7 million people. It covers six local places, Bradford district and Craven; Calderdale, Harrogate, Kirklees, Leeds and Wakefield. It is made up of NHS organisations, councils, Healthwatch, social enterprises, charities, community and voluntary organisations, which collectively employ over 100,000 colleagues.
The majority of work takes place locally in the six places where people live. The Partnership only works across West Yorkshire and Harrogate where it can add value, share good practice or tackle difficult issues together.
Introduction
Watch Professor Dame Donna Kinnair’s film here where she explains more about her involvement.
Percentage of Black, Asian and minority ethnic population groups by local authority area and overall across West Yorkshire and Harrogate
Calder
dale
Bradfo
rd
Harro
gate
25
20
15
10
5
0
Crave
n
Tota
l
Leeds
Kirkle
es
Wak
efie
ld
All other White
Mixed / multiple ethnic groups
Asian / Asian British
Black / African / Caribbean / Black British
Other ethnic group
/ 54 / West Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and WakefieldWest Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and Wakefield

Percentage of ethnic groups by local authority area and overall in West Yorkshire and Harrogate
100
90
80
70
60
50
40
30
20
10
0
White British
All other White
Mixed / multiple ethnic groups
Asian / Asian British
Black / African / Caribbean / Black British
Other ethnic group
Calder
dale
Bradfo
rd
Harro
gate
Crave
n
Leeds
Kirkle
es
Wak
efie
ld
Photo credit: Feel Good Factor, Leeds
West Yorkshire and Harrogate has a long history of welcoming refugees and asylum seekers. Obtaining current numbers for these communities can be difficult and complex to understand with no overall figure at any one time. For more information visit Migration Yorkshire.
The COVID-19 pandemic has highlighted the impact of deep-seated and long-standing health inequalities faced by BAME communities. What causes these inequalities is the subject of much debate but much can be linked to the deeper impact of wider societal inequalities beyond the operation of health and social care services. These include broader environmental, social and economic factors that exert a profound ability to shape health outcomes for communities.
You can read more about this in ‘Delivering better health and wellbeing for everyone: Our five year plan’.
1
Better health and
wellbeing for everyone:
Our five year plan
EasyRead
The Partnership has big ambitions to tackle health inequalities and support BAME communities and colleagues.
“Our ambition is to have a more diverse leadership that better reflects the broad range of talent in West Yorkshire and Harrogate, helping to ensure that the poor experiences in the workplace that are particularly high for Black, Asian and minority ethnic (BAME) staff will become a thing of the past.”
(West Yorkshire and Harrogate Health and Care Partnership, March 2020)
As our awareness of the emergent health inequalities that have been brought into sharp focus by the COVID-19 pandemic both broadens and deepens, we believe it is vital to seize this moment and build our knowledge in this space. We will focus on taking decisive and clear action to make a powerful and sustained impact on the lives of the communities that we are privileged to serve.
Photo credit: Harrogate and District NHS Foundation Trust
Differences in the impact of the pandemic by ethnicity
The direct impacts of the pandemic can be seen by the number of people diagnosed with the virus and the number of deaths from COVID-19. Analysis by Public Health England (PHE, June 2020) showed that the proportion of cases testing positive for COVID-19 varied by ethnicity.
Tota
l
/ 76 / West Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and WakefieldWest Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and Wakefield

Photo credit: Keighley Healthy Living
You can read more examples of the impact of COVID-19 on communities here.
In England the highest diagnosis rates of COVID-19 per 100,000 population were in Black ethnic groups of people (486 per 100,000 in females and 649 per 100,000 in males) and the lowest were in people of White ethnic groups (220 per 100,000 in females and 224 per 100,000 in males). It is important to state that the differential impact of COVID-19 on BAME communities is not specifically as a result of genetic vulnerability to the disease but largely as a result of forces that shape and structure labour markets, housing and workplace cultures which culminate in an elevated risk profile for some BAME communities.
Indirect impacts from COVID-19 arise from the effects of various factors, such as whether healthcare services are appropriate to the needs of different groups, food or job insecurity, education, communities being together in harmony, safety and access to safe spaces to be physically active.
We have also observed inequalities in the indirect impacts of COVID-19 by ethnicity from communities in West Yorkshire and Harrogate, for example, ‘39% of parents of children from BAME backgrounds said they worried about taking their children into healthcare settings, compared to 31% of parents of White British children’ (Healthwatch Leeds, June 2020). In Halifax, ‘people are just not going out, there’s fear that if they go into hospital they won’t come home again’ (Voluntary Community Organisation Manager, June 2020).
Higher rates of mortality were also seen for some ethnic groups compared to others. In comparison to previous years, all-cause death was almost four times higher than expected amongst Black people in March-May 2020, almost three times higher in Asian males and almost twice as high in White males. Among females, deaths were almost three times higher in this period in Black, mixed and other females, and 2.4 times higher in Asian females compared with 1.6 times higher in White females.
The causes of these inequalities are often structurally located, multi-faceted and intersecting in nature, for example gender. These might take the form of differences by ethnicity, for example overcrowded living conditions (English Housing Survey, July 2020), high risk occupations, existing health conditions and differences in the provision of appropriate health services that meet people’s needs. Working with communities allows us to influence wider factors such as housing, employment, education, social networks and the environment, which make a big difference to people’s health.
We recognise that the term BAME has limitations. While this report uses the acronym BAME to describe people from Black, Asian and minority ethnic backgrounds, we recognise that this grouping will include a number of groups with different experiences, cultural backgrounds and health needs.
The COVID-19 pandemic has affected every child, adult, family and community in West Yorkshire and Harrogate, with some of the biggest impacts experienced by the most economically disadvantaged and those from BAME communities.
This review specifically aimed to understand this impact on BAME communities and staff. The aim was to review existing work, to explore if this work was sufficient to address this impact and to identify recommendations for action to reduce this impact.
This review builds on the Partnership’s work so far and includes new themed areas of work (see page 19). This review did not aim to address all issues related to COVID-19 such as the restoration of health and care services or increases in waiting times.
Purpose of the review
You can read the Terms of Reference for the Review here.
Photo credit: Born in Bradford
Some issues are likely to affect everyone living in an area and some only specific groups of people. Other issues are likely to be compounding and intersectional – such as people experiencing oppression due to concurrent racism, sexism and other forms of prejudice or systemic deprivation. For example, a Black lesbian woman will have different needs and experiences to a Black heterosexual woman. These factors further amplify the disadvantages experienced by some groups.
Also, not everyone from one of these groups will identify with the term BAME. We are mindful of the current work taking place called #BAMEover and will be keeping this in view as we move forward. For the purpose of this review we have used the term BAME and will explore the needs of some ethnic groups disproportionately affected.
/ 98 / West Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and WakefieldWest Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and Wakefield

West Yorkshire and Harrogate has a diverse population which has a complex profile across the region as a whole and within the six local places. Therefore activity in this arena should be locally-led and driven in order to address the nuances and differences of each area and to have the greatest impact.
Integral to this review is the impact of interpersonal, institutional and structural racism on inequalities in health outcomes for the BAME population. These refer to the range of different issues people might experience. For example, direct experiences of racism from other people, ways in which organisations might act to exclude certain groups of people, and fundamental differences in life opportunities for different groups of people.
Racism is experienced differently and to different degrees by different groups of people. The experiences of BAME communities and colleagues, in and out of the workplace, differ considerably. These factors were considered throughout the review and tackling these head on, however uncomfortable, is instrumental to the success of this report’s recommendations (see page 38).
Watch this film narrated by West Yorkshire and Harrogate young people about their ambitions for a fairer society for everyone.
Current events, such as COVID-19 and the Black Lives Matter Movement, have brought into focus inequalities in health outcomes that disproportionately affect people from BAME communities. This makes the review carried out and the subsequent findings (see page 21) extremely important if the Partnership is to improve BAME people’s health and ensure a fairer society for all living across the area.
Photo credit: Mid Yorkshire Hospitals NHS Trust
Five initial independent review sessions were chaired by Professor Dame Donna Kinnair, Chief Executive and General Secretary of the Royal College of Nursing, a leading figure in national health and care policy. The review panel included the Chair of West Yorkshire and Harrogate Health and Care Partnership Board, Cllr Tim Swift; leaders of the executive team; public health specialists, doctors, members of the West Yorkshire and Harrogate BAME Network and colleagues from the voluntary, community and social enterprise (VCSE) sector. An advisory group of VCSE representatives was established to support the inclusivity of the panel. You can listen to their podcast here which describes their journey through the process. Both the review panel and the VCSE group had a wide diversity of voices including people from different ethnicities, sectoral backgrounds and ages. The sessions took place between July and October 2020.
The Review Panel first considered the demographics of West Yorkshire and Harrogate in relation to ethnicity. The panel also received intelligence and insight related to inequalities in health observed for specific ethnic groups and underlying factors that may contribute towards these. The panel coupled this information on population need with information on Partnership work to date to formulate the four key themes (see page 19).
Subsequently the panel received intelligence and insight related to these themes to inform the review recommendations.
The Review PanelThe recommendations were required to be ambitious and action focused so they could contribute towards a reduction in health inequalities by ethnicity for people living in West Yorkshire and Harrogate.
Launching the review, Councillor Tim Swift, Chair of the West Yorkshire and Harrogate Health and Care Partnership Board, said:
“We are in full agreement that rapid action is needed to understand and tackle deep-seated and longstanding health inequalities facing people. Although tackling wider inequalities cannot fall to us alone, we are in an ideal position to both listen and lead, and have a responsibility to demonstrate by our actions that we can be part of the solution. The excellent relationships we have with other key players, including the West Yorkshire Combined Authority and our local universities, mean we can ensure that action on reducing these inequalities becomes a major part of our recovery plans.”
(July, 2020)
Photo: Cllr Tim Swift (MBE), Chair of the West Yorkshire and Harrogate Health and Care Partnership Board.
/ 1110 / West Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and WakefieldWest Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and Wakefield

Accountability
This reports sets out a series of recommendations to the leadership of the West Yorkshire and Harrogate Health and Care Partnership. The Partnership will develop an action plan in response to the recommendations. The action plan will capture all the information about the changes we are going to make as a system – it will detail what we will do and why, who will be responsible for the changes, and the timescales for delivery.
This action plan will be considered and approved by the Partnership Board in December 2020. The Partnership board will periodically review progress against these recommendations and this information will be made available to the public on our website and wider through our community networks. The action plan will be accompanied by a set of indicators to measure progress over time.
Alongside the above, we aim to strengthen the role of the VCSE panel, which was set up to inform the review. This panel will ensure progress is made on the recommendations and will support the Partnership to engage with communities who might not otherwise be aware of this work. This will be achieved through community assets and influencers. We will also aim to strengthen the role of the West Yorkshire and Harrogate BAME network in delivering change.
The aim is to complement and support system-wide working at both a local and West Yorkshire and Harrogate level. This review does not replace local place based work in Bradford district and Craven; Calderdale, Harrogate, Kirklees, Leeds and Wakefield.
The intention is to share this report and action plan with the Government’s Commission on ‘Race and Ethnic Disparities’ to influence nationally what can be done to eradicate racial and social inequality. It will also be used to support national reviews, including the independent review into the Government’s coronavirus response and the NHS People Plan, which published its latest edition in July 2020.
Photo: Members of West Yorkshire and Harrogate Health and Care Partnership BAME Network.
Photo credit: St Augustine’s Centre, Halifax
This review is built on local knowledge, insight and intelligence as well as existing work carried out by the Partnership.
Building on existing work
“With much to do we are hopeful that we will achieve better wellbeing for everyone by working with community partnerships. This involves recognising that the relationship between healthiness and ethnicity is complex and ultimately a life and death situation for many who are at an increased risk of contracting coronavirus and sadly dying.”
West Yorkshire and Harrogate Health and Care Partnership Board, June 2020
• COVID-19 feedback received from partners including West Yorkshire Healthwatch organisations, Yorkshire Cancer Community, Sikh Alliance Yorkshire, Carers UK and Bradford Talking Media (August 2020). This was specifically regarding the impact of coronavirus on individual people and communities.
• A rapid insight report developed with the support of the Yorkshire & Humber Academic Health Science Network (June 2020). Recommendations included undertaking further investigations into the experiences of BAME communities and colleagues working across the Partnership.
Recent Partnership insight includes:
• A report produced in July 2020 titled ‘Third Sector Resilience: Before and during COVID-19’. This highlights the impact of COVID-19 across the voluntary and community sector enterprise (VCSE), and makes various recommendations including long term investment in the VCSE and in volunteering; investment in training and developing people and organisations, and better connecting commissioning of health and care service delivery across West Yorkshire and Harrogate.
• A diversity of programmes across the Partnership which can link with the health of our BAME populations, including our carers programme, maternity programme, children and young people programme and many more.
/ 1312 / West Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and WakefieldWest Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and Wakefield
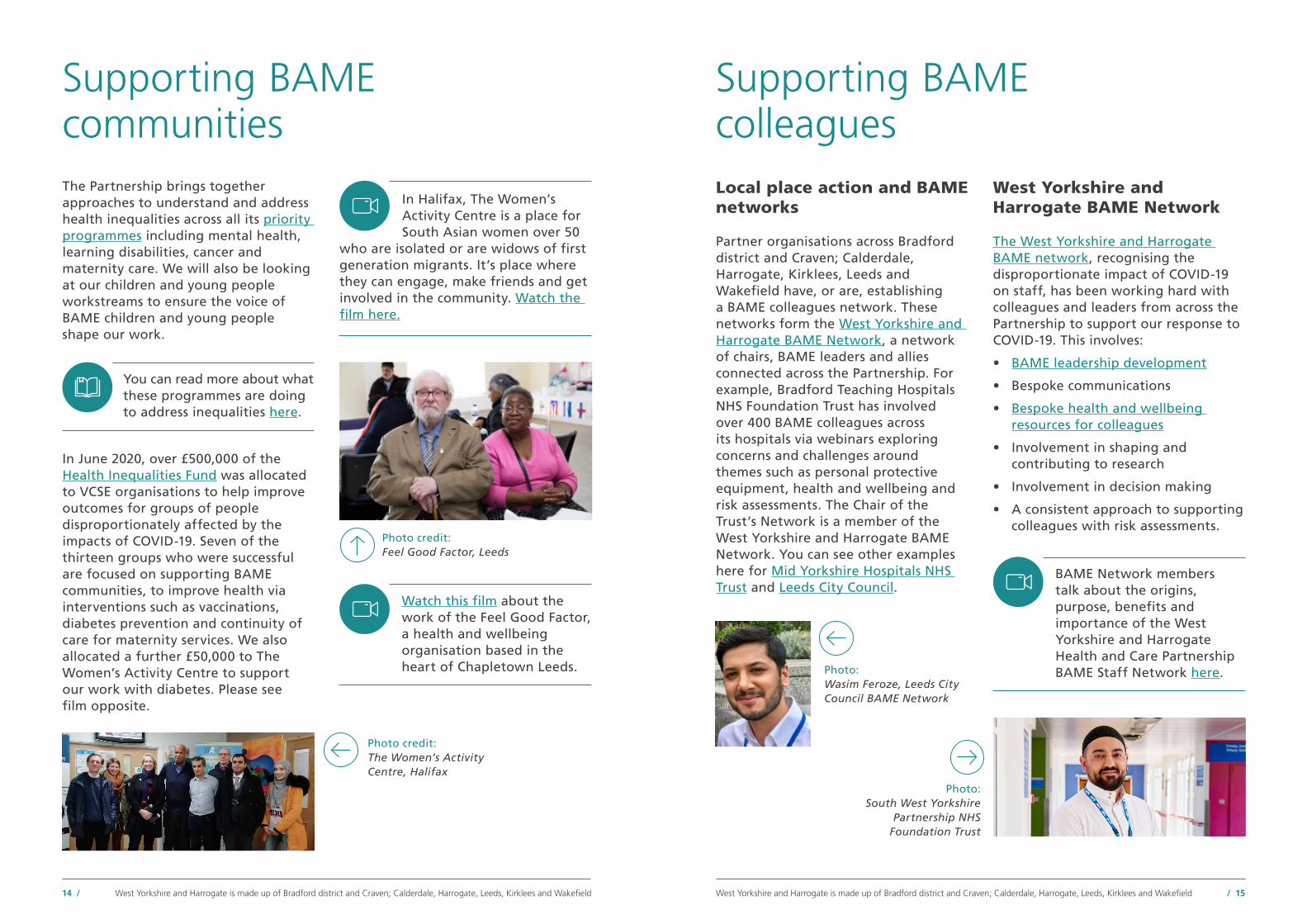
The Partnership brings together approaches to understand and address health inequalities across all its priority programmes including mental health, learning disabilities, cancer and maternity care. We will also be looking at our children and young people workstreams to ensure the voice of BAME children and young people shape our work.
Supporting BAME communities
You can read more about what these programmes are doing to address inequalities here.
In June 2020, over £500,000 of the Health Inequalities Fund was allocated to VCSE organisations to help improve outcomes for groups of people disproportionately affected by the impacts of COVID-19. Seven of the thirteen groups who were successful are focused on supporting BAME communities, to improve health via interventions such as vaccinations, diabetes prevention and continuity of care for maternity services. We also allocated a further £50,000 to The Women’s Activity Centre to support our work with diabetes. Please see film opposite.
Watch this film about the work of the Feel Good Factor, a health and wellbeing organisation based in the heart of Chapletown Leeds.
In Halifax, The Women’s Activity Centre is a place for South Asian women over 50
who are isolated or are widows of first generation migrants. It’s place where they can engage, make friends and get involved in the community. Watch the film here.
Photo credit: Feel Good Factor, Leeds
Photo credit: The Women’s Activity Centre, Halifax
Photo: Wasim Feroze, Leeds City Council BAME Network
Photo: South West Yorkshire
Partnership NHS Foundation Trust
Supporting BAME colleagues Local place action and BAME networks
Partner organisations across Bradford district and Craven; Calderdale, Harrogate, Kirklees, Leeds and Wakefield have, or are, establishing a BAME colleagues network. These networks form the West Yorkshire and Harrogate BAME Network, a network of chairs, BAME leaders and allies connected across the Partnership. For example, Bradford Teaching Hospitals NHS Foundation Trust has involved over 400 BAME colleagues across its hospitals via webinars exploring concerns and challenges around themes such as personal protective equipment, health and wellbeing and risk assessments. The Chair of the Trust’s Network is a member of the West Yorkshire and Harrogate BAME Network. You can see other examples here for Mid Yorkshire Hospitals NHS Trust and Leeds City Council.
West Yorkshire and Harrogate BAME Network
The West Yorkshire and Harrogate BAME network, recognising the disproportionate impact of COVID-19 on staff, has been working hard with colleagues and leaders from across the Partnership to support our response to COVID-19. This involves:
• BAME leadership development
• Bespoke communications
• Bespoke health and wellbeing resources for colleagues
• Involvement in shaping and contributing to research
• Involvement in decision making
• A consistent approach to supporting colleagues with risk assessments.
BAME Network members talk about the origins, purpose, benefits and importance of the West Yorkshire and Harrogate Health and Care Partnership BAME Staff Network here.
/ 1514 / West Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and WakefieldWest Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and Wakefield

A series of West Yorkshire and Harrogate Health and Care Partnership Podcasts called ‘Can you hear me?’ was launched early 2020, giving a voice to the diverse talent working to improve health and care for people in West Yorkshire and Harrogate. The first episode (launched on 14 May 2020) focused on the impact of COVID-19 on our BAME population – this approach has been seen as national good practice.
‘Can You Hear Me?’ Episode 1: Everything you wanted to know about coronavirus but were afraid to ask. ‘This is about how we change the way people view other people, view other people’s lives. It is about empathy… we want people to understand and then to empathise, and that’s what senior leaders need to actually start doing and thinking about now’ said Yvonne Coghill, Former Director for Workforce Race Equality Standard Implementation, NHS England.
This group has focused on using their collective lived experience and knowledge to support action on:
• Recruitment, selection and succession planning
• Talent, culture and organisational development
• Reporting on measurement and impact
• Influencing decision-making
• Health inequalities.
“Building on the support of the executive leadership session, colleagues explained the importance of visible role models, peer support, a safe space to share experiences, and a forum to shape and influence change across the Partnership, as well as what already exists within their organisations.”
(Fatima Khan-Shah, West Yorkshire and Harrogate Health and Care Partnership, Director for Unpaid Carers and Personalised Care)
Photo: Fatima Khan-Shah, member of West Yorkshire and Harrogate Health and Care Partnership BAME Network
Listen to the Podcast here.
‘Can You Hear Me?’ Episode 2: Carers ‘I think there’s a recognition now that the kind of ‘one size fits all’ (approach) that typically institutions like ours have, is just not sufficient. We have to find a way of getting into a conversation with communities that says ‘what would good look like?’ said Dr Owen Williams (OBE), Chief Executive, Calderdale and Huddersfield NHS Foundation Trust.
‘Can You Hear Me?’ Episode 4: Workforce ‘My father’s work ethics were to respect people – and some may feel they have to work twice as hard’ said Kez Hayat, Bradford Teaching Hospitals NHS Foundation Trust.
Listen to the Podcast here.
Listen to the Podcast here. ‘Can You Hear Me?’ Episode 3: White Privilege ‘It’s not just about what we do in our own organisations. We have to carry it over into society every single day’ said Wallace Sampson (OBE), Chief Executive, Harrogate Borough Council.
Listen to the Podcast here.
Photo: Wallace Sampson (OBE), CEO for Harrogate Borough Council
Photo: Kez Hayat, Bradford Teaching Hospitals NHS Foundation Trust.
Photo: Dr Owen Williams (OBE)
/ 1716 / West Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and WakefieldWest Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and Wakefield

Through the review’s work original themes, such as population health inequalities and workforce, the areas of work were refined into four distinct themes, through panel member contributions, initial review of the evidence and further discussion by the panel:
• Improving access to safe work for BAME colleagues in West Yorkshire and Harrogate
• Ensuring the Partnership’s leadership is reflective of communities
• Population planning (using information to make sure that services meet different groups’ needs)
• Reducing inequalities in mental health outcomes by ethnicity.
Review themes
07The Partnership’s System Leadership Development Programme
The Partnership’s System Leadership Development Programme recognisingthe importance of building inclusiveleadership, has put in place varioussupport packages with a focus onunderstanding BAME issues and aroundhow white leaders will be required to demonstrably use that insight to create better outcomes and experiences for BAME staff and communities. This includes the BAME Fellowship Programme which is all about developing future senior system leaders that reflect the local populations. Development of competencies to form a pivotal element of judgement on performance is underway for those working through the programme and for those leaders supporting the stretch opportunities.
It is anticipated this will promote and embed systemic change leading to increased accountability. Developed and designed by BAME colleagues, it aims to recognise the talent of colleagues and give them the missing leadership skills and opportunities required to progress their career. The unique element of the fellowship programme is that as well as offering traditional taught sessions on system leadership, it also guarantees a career coach and works in partnership with organisations to identify stretch opportunities and associated competencies. Recognising the responsibility organisations have in increasing the diversity of senior leadership, this programme works collaboratively to achieve different outcomes.
The programme supports the Partnership’s ambition to increase the number of BAME colleagues in senior leadership and board level positions.
Photo credit: Leeds and York Partnership NHS Foundation Trust
/ 1918 / West Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and WakefieldWest Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and Wakefield

The Partnership aims to reduce any disproportionate health or economic impact resulting from COVID-19 for people working in West Yorkshire and Harrogate. You can read the insight which was gathered for this section here.
Key lines of inquiry for review
• Are occupations at highest risk of exposure to COVID-19 infection over-represented by BAME population groups? This element of the report includes both the impact on health and also the economic impact on people due to the lock down.
• What have West Yorkshire and Harrogate organisations and local places done to mitigate and communicate risk?
Improving access to safe work for BAME people in West Yorkshire and Harrogate
What does the evidence tell us?
The Office of National Statistics (ONS) data (May 2020), tells us that some jobs have a higher risk of exposure to the virus because of the need to work closely with others. This is especially true in health and social care environments where there is a likelihood of direct exposure because of the need for direct physical contact with others. Wide ranging analysis highlighted in the Health Service Journal (May 2020), shows the significantly higher risk to BAME health and care workers of catching COVID-19. 60% of healthcare colleagues who have died of COVID-19 are from a BAME background whereas they make up around 20% of the overall NHS workforce.
The West Yorkshire Association of Acute Trusts (WYAAT) and the Mental Health, Learning Disability and Autism Collaborative have worked with HR colleagues and the BAME Networks to develop a consistent approach to risk assessment in the workplace. This covers all areas of risk including age, weight, pregnancy and underlying health conditions - as well as ethnicity. In response to the risk assessments a number of actions have been put in place for people.
This includes homeworking or temporarily working in non-patient facing roles. It also aims to ensure colleagues feel confident requesting access to personal protective equipment. Managers are trying to ensure that any extended change to normal working arrangements does not disadvantage BAME colleagues in the longer term that could be a consequence of the resulting limiting range of duties, visibility, exposure and access to career development opportunities.
The increased risk to health is also true for any occupation where there is close contact with other people every day; for example bus and taxi drivers, hairdressers and cleaners, and for people working in factories, such as food production and manufacturing. The ONS data (May 2020) highlights a higher proportion of Black, Asian and ethnic minority people are working in these types of jobs. For example, Health Foundation analysis of the ONS labour force survey (June 2019) shows in West Yorkshire and Harrogate, 23% of food production, processing and food sales involves BAME colleagues. For some of these roles the underlying risk cannot be fully mitigated by social distancing measures or more general advice and guidance. As well as increasing awareness for some roles it may be necessary to increase physical protection to mitigate the increased health risk of the workers.
The risk to our workforce is not only about catching COVID-19. The lockdown has resulted in large numbers of people with reduced employment and earning potential, totalling around 24% of the workforce. Analysis by McKinsey (May 2020), shows that people with the lowest incomes are most at risk of this at around 44% for roles such as cleaners, kitchen assistants and waiting staff. People working in part time roles, via an agency or on zero hours contracts, are especially vulnerable to changes in their job situation. For example, the NHS Workforce Race Equality Standard and local council information shows that BAME colleagues don’t always receive the same opportunities as their White colleagues with equivalent qualifications.
What further action to do we need to take?
It is clear from the review findings that the Partnership must make concerted efforts to reach, inform and support colleagues most at risk in our communities. It is also imperative that safety and wellbeing messages are understood by the high proportion of BAME people working in high risk roles. It is important for their health, and that of their families and communities.
/ 2120 / West Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and WakefieldWest Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and Wakefield

Communication with colleagues and communities recognises
the impact of racism on people’s lives. It is important that particular attention is given to the fact that BAME communities are not of one homogenous ethnicity.
The review recommends amplifying communications messages at a local level whilst not making assumptions about language or method. It is also important to consider the impact of racism and digital exclusion.
This should take place through local communication channels and VCSE networks. Consideration should also be given to the co-production of a West Yorkshire and Harrogate anti-racism and a myth busting campaign to combat COVID-19 racism.
Watch this film about the South West Yorkshire Partnership NHS Foundation Trust’s Black, Asian and minority ethnic staff network, which is one of many local organisation networks.
Channel support to the most vulnerable colleagues as the job
retention and self-employed support schemes end. The aim is to provide support for people in sectors most impacted by lockdown. This includes the provision of retraining and reskilling schemes for potential new roles in the future and the introduction of new short term working and training schemes for disproportionately affected BAME young people and women. This will include supporting people returning to work on reduced hours, helping them to maintain working knowledge in their job while the economy recovers. Initiatives are needed to narrow the educational attainment gap and raise aspirations, supporting people from BAME communities into employment.
The review recommends strategic partners, such as West Yorkshire Combined Authority ensures equality of opportunities for BAME groups are explicit in all economic development and recovery plans, and that positive action such as the inclusion of specific plans to improve opportunities for BAME communities, and the promotion of schemes such as the government KickStart Scheme to young BAME people, are prioritised.
This should also include wider work on apprenticeships, post-university employment, job creation and start up grants. The review also recommends that strategic partners ensure that COVID-19 related safe working practices are incorporated in any and all work done to ensure quality employment for the population of West Yorkshire and Harrogate.
The risk assessment process is only the first step. The Partnership
should aim to ensure that appropriate actions are taken in each place to mitigate risk for all colleagues, where they don’t already exist. We recognise that individual organisations hold accountability for doing risk assessments and protecting those most vulnerable to harm, and that work is ongoing across the Partnership to do this.
The review therefore recommends that all organisations engage with their BAME networks (setting one up if it doesn’t already exist) to seek assurance regarding the impact and effectiveness of risk assessments, and ensure that the emotional load related to racism is considered in the risk assessments and resulting mitigating actions. Good practice found in organisations and networks will also be shared through the BAME network of networks.
The Partnership will ensure that this recommendation is reflected in the Partnership’s People Plan (expected January 2021) and progress is monitored through the West Yorkshire and Harrogate People Board and the Partnership Board.
Recommendations
Immediate action is needed to share information and reach those
hardest hit by COVID-19. It is important to shine a light on the people who are working in high risk roles which haven’t been given a high profile in the media in the same way that some areas of the NHS have been. This includes colleagues working in social care settings, in transport and food service roles, and people working in factory environments. We will work with organisations, such as The West Yorkshire Combined Authority to deliver co-designed ethnically appropriate advice and support for people who are working in high risk roles to mitigate risk to their health, their families and communities. In addition to this where advice will not be sufficient; action to mitigate the risk should be taken, such as the provision of personal protective equipment for people working in public-facing roles.
/ 2322 / West Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and WakefieldWest Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and Wakefield

The Partnership aims to ensure their leadership is reflective of communities, within partner organisations, and at a system and board level. You can read the insight gathered to support this work here.
Key lines of inquiry for review
• Are boards within the Partnership ethnically representative of the communities they serve?
• What are the barriers for colleagues in applying and being successful at reaching this level?
• What representation do BAME colleagues have on key decision making forums?
What does the evidence tell us?
Based on census data from 2011 for West Yorkshire and Harrogate residents, overall 19.6% are from a BAME background. Bradford has the highest proportion of BAME groups at 31.2% and Craven has the lowest at 3.6%.
Ensuring the Partnership’s leadership is reflective of communities
We know from analysis by McKinseyand Company (February 2020) thathaving diverse representation insenior decision making is critical totruly understand and represent theviews and needs of the communitiesserved. Evidence from a McKinseyand Company report (January, 2020)highlighted that diverse boardscan also lead to improving theexperiences of BAME workforces. A diverse Board offers a breadth of perspective and leadership styles that improve collective decision-making. Our Partnership must strive to betruly representative of the communities we serve.
Photo credit: Airedale NHS Foundation Trust
The panel acknowledged the data reviewed relates to the previous year and some progress has been made since the publication of the local NHS Workforce Race Equality Standard data (2019).
However organisation boards on the whole are not representative of the communities they serve and the process of change is glacial and uneven across the NHS. Based on available data (local NHS Workforce Race Equality Standard data 2019) Board representation varies from 0% to 28.6% across NHS organisations in West Yorkshire and Harrogate.
The panel recognised the important role inclusive cultures and processes play in the experience and progression of BAME people. Similarly, the McGregor-Smith Review (2017) recommendations are wide-ranging in nature and ask that organisations focus on improving workplace cultures, improve processes and systematically support progression.
This review identified a number of barriers for the progression of BAME colleagues in our organisations, and found that structural racism and white privilege play a part. Experiencing structural racism and micro aggressions can have an extremely negative impact on people and can falter their progression, for example everyday verbal and nonverbal slights or snubs, which are frequently not intended to cause harm or hurt feelings, yet their impact often does just that.
The review also found the likelihood of being appointed from shortlisting for roles is over double for White people than for BAME colleagues in some of our organisations. The relative likelihood of entering formal disciplinary action is also greater for BAME colleagues and they are less likely to access nonmandatory training and continuous professional development. All of these are indicators of career success and role progression. More detailed information on these findings can be found in the insight report here.
Insight from the experiences of the West Yorkshire and Harrogate BAME network and review of Roger Kline’s (2020) work highlights that recruitment and selection processes are unfair, there is increased scrutiny of performance rather than potential, and that social exclusion impacts on opportunities to network.
“White privilege doesn’t mean or suggest that you have had an easy life. Nor does it suggest you haven’t earned your successes but it does mean that your life hasn’t been harder because of the colour of your skin”
/ 2524 / West Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and WakefieldWest Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and Wakefield
https://www.wyhpartnership.co.uk/application/files/2115/9724/8015/Paper_C_-_Leadership_Deep_Dive.pdf
https://www.wyhpartnership.co.uk/application/files/2115/9724/8015/Paper_C_-_Leadership_Deep_Dive.pdf
https://www.wyhpartnership.co.uk/application/files/2115/9724/8015/Paper_C_-_Leadership_Deep_Dive.pdf
https://www.wyhpartnership.co.uk/application/files/2115/9724/8015/Paper_C_-_Leadership_Deep_Dive.pdf
https://www.wyhpartnership.co.uk/application/files/2115/9724/8015/Paper_C_-_Leadership_Deep_Dive.pdf

This offers the opportunity for a career coach to tailor the development needs of BAME colleagues for career progression and offers a variety of stretch and secondment opportunities across the Partnership. The review acknowledged that whilst there are pockets of good practice being delivered against the system ambition, such as the increased representation in some decision making forums and the BAME focused development programme and work on bias and privilege training, there was some concern about the lack of progress in other areas and this inquiry could serve as a reminder of the previously agreed actions.
What further action do we need to take?
There is still much work to do to implement the Partnership’s commitment to deliver the system ambition of a more diverse leadership that better reflects the broad range of talent in West Yorkshire and Harrogate. This includes helping to ensure that the poor experiences in the workplace that are particularly high for BAME staff will become a thing of the past.
Recommendations
To increase the fairness and equity of access to roles, the review
recommends that all organisational leaders develop and embed clear leadership standards that ensure we have inclusive workplaces. That leaders pledge to personally uphold these standards within their own organisations, starting with a review of recruitment and selection processes; where process is not followed ensure immediate action is taken to support learning, reward success and sanction poor performance.
This builds on the commitment made in March 2020 to deliver the recruitment and retention recommendations made in the ‘Achieving our ambition to increase the diversity of our leadership’ paper written by the West Yorkshire and Harrogate BAME network. It is also a fundamental area of focus for the NHS People Plan 2020, which highlights the importance of compassionate and inclusive cultures that value our people and create a sense of belonging with a particular focus on tackling the discrimination that some staff face.
The evidence found that the Partnership needs to provide
more development opportunities for all BAME staff working at every level across organisations.
The review recommends that a new BAME mentorship framework is developed. This will provide additional, flexible development opportunities for people across the Partnership and further enhance opportunities provided by the West Yorkshire and Harrogate BAME Fellowship Programme (see page 7) in the West Yorkshire and Harrogate System Leadership Programme.
It is helpful to note that work is already underway across the Partnership. A recent call to action asked all the Partnership’s Chief Executives to ensure representatives from the BAME network are involved in the recruitment and selection of senior leadership level appointments. This was part of delivering the West Yorkshire and Harrogate BAME Network recommendations in March 2020 where recommendations include making equality and diversity and unconscious bias training mandatory across all partnership organisations. There are examples of good practice where structural privilege and White privilege discussions are now being built into unconscious bias training packages. Whilst evidence informs us that training alone does not make a huge difference to reducing disparity in experience, undertaking it alongside all the other system ambitions will be more impactful. Systemic reviews of our recruitment and wider employment processes and policies are integral to shaping lasting change and delivering on our commitments by ensuring that inclusion and equality are built into the fabric of our day-to-day operations.
A fellowship programme has also been developed for BAME colleagues as recommended by the BAME network (please see page 7).
Photo: Sal Uka, Clinical Lead for West Yorkshire Association of Acute Trusts
Photo credit: Yorkshire Ambulance Service NHS Trust
To reduce the disparity in disciplinary and complaints
processes, the review recommends all organisations across West Yorkshire and Harrogate develop independent panels with BAME representation to review cases of racial discrimination on people who access care and services as well as staff.
The panels should also be responsible for assuring all grievance and disciplinary cases are reviewed to ensure racism has not been a contributing factor prior to cases progressing through to formal disciplinary stages.
In addition, to eliminate discrimination, identify ways of providing independent support for BAME people going through processes and promote inclusion; panels should support organisations to undertake root cause analysis of existing systems and processes when managing disciplinary and complaint cases. Care should be taken to ensure the process for making complaints does not penalise people and complaints are handled seriously.
To ensure leadership is representative of communities,
the review recommends that all Partnership organisations should actively seek out local, ethnically representative talent through positive action and embed accountability by setting targets for recruitment and retention, particularly at senior levels. This should include talent within partnership organisations and proactive engagement with schools, colleges, universities and local communities for recruitment drives with planned engagement events.
/ 2726 / West Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and WakefieldWest Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and Wakefield

Key lines of inquiry for review
To identify and embed approaches to reduce health inequalities for specific ethnic groups throughout population planning processes. Pressures on funding may exacerbate inequalities where limited resource is not aligned to local need. You can read the insight gathered to support this work here.
Population planning moves us on from the term commissioning to a whole system approach to; understanding needs, designing pathways, procuring services and evaluating impact to ensure local need is met. It involves a partnership approach for a population across a defined geography whether this is a local neighbourhood, a local authority area or an integrated care system, such as ours.
Population planning - using information to make sure services meet different groups of people’s needs
What does the evidence tell us?
Effective planning of services starts with understanding groups of people’s ‘needs’. This requires access to data and insight. Intelligence related to ethnicity is often not included in local, regional and national data sets. Improvements have been made locally in the recoding of ethnicity in primary care. For example, in Leeds gaps in ‘unknown or not recorded’ data has reduced from 22% in 2013 to 6% in 2020. Recording of ethnicity data varies across the NHS Trusts in the Partnership, with completeness ranging from 86.4% to 99.3%.
The Partnership has developed a combined impact assessment for large scale service change. Equality impact assessments (EQIAs) are completed locally for service changes or revised policies. It was felt that EQIAs were often undertaken without assurance that positive action would follow where disadvantage was identified.
Review members highlighted the importance of co-producing services with communities and of sustainable funding models for the VCSE and a clear commitment to a commissioning intention that is co-designed with local VCSE partners. Work is ongoing within the Partnership regarding ‘Commissioning Futures’. The review advised further opportunities must be sought to connect this work with the needs of BAME communities across the Partnership and that high-level buy-in should be secured.
What further action do we need to take?
Intelligence informed action
The Partnership should foster a culture of recording and understanding of ethnicity data in all sectors. This requires improvements in the quality of coding of ethnicity across all of our health and care settings. This data should feed into population health management models to support decision making in relation to local need and prioritisation of care.
Data should be coupled with relevant local insight to complete the picture. This includes meaningful engagement with communities to understand people’s needs, strengths and experiences.
We should use intelligence to inform thinking as to where we have the greatest opportunity to take preventative action to improve health outcomes for people - this includes refugees, asylum seekers, and Gypsy, Traveller and Roma groups of people.
Photo credit: Feel Good Factor, Leeds
Photo credit: Keighley Healthy Living
Photo credit: Yorkshire Cancer Community
Photo credit: Leeds Irish Health and Homes
/ 2928 / West Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and WakefieldWest Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and Wakefield

This should include specific action, such as easy to understand language, procurement mechanisms and contract security.
Approaches to micro-commissioning (the process of identifying and addressing needs at an individual level through creating additional activities in local communities) of services should be supported, underpinned by knowledge of need at a neighbourhood level.
Approaches for consultation, engagement and coproduction should be adapted as relevant to meet preferred methods and styles of specific groups of people, where they don’t exist already.
Photo credit: Wakefield NHS Clinical Commissioning Group
Photo credit: Touchstone, Leeds
The engagement we undertake needs to be fit for purpose for what we need to deliver to improve people’s health. Being clear on the purpose of the engagement, where the findings will be shared and to what extent it can influence change is essential.
Photo credit: Keighley Healthy Living
To receive the best experience from the process we should go to places where people are, in settings that are accessible and, importantly, where people are most comfortable. We also need to consider the impact of participation in public involvement, including the support which may be needed for the psychological impact of those sharing their experiences.
Accelerated improvements
Partnerships should come together to understand inequalities in relation to access and use of health and care services by ethnicity.
Positive action should be taken to mitigate the widening of inequalities. Options for delivering models for care, such as digital access or social prescribing offers, should consider the needs for specific ethnic groups of people. Equality impact assessment processes need to reform to become a catalyst for change. Effective alternatives should be developed that have more direct accountability aligned to improved health outcomes for people.
You can see an example of this from two experiences of care for one person who spoke only Farsi. They were referred
to a doctor following a night in A&E due to an attempted suicide. Her number was passed to the Integrated Access to Psychological Therapies Service with no access to an interpreter or explanation to what was happening.
In the same period of hospital care, mental health liaison team colleagues used Language Line to support them and stayed in contact to ensure they received the care needed. We need to learn from examples such as these to improve the way we work.
It is also essential that we keep in view overseas visitor charging which is a national government policy in terms of health inequalities.
A key part of the pathway of care is personalised care planning. When working with BAME communities, colleagues should consider the cultural, religious and communication needs of specific ethnic groups of people. Digital inclusion should also be considered, including reducing barriers to access related to language, connectivity and access to technology. Public facing roles, including receptionists, mental health workers etc. should be reflective of the ethnic diversity of communities, with culturally competent services being provided.
The intelligence we use should be captured and considered at relevant population geographies within the system, including in neighbourhoods working with the data Primary Care Networks hold, in local places bringing intelligence together in partnership, and at a system level to inform the work we do across the Partnership.
We need to do more to triangulate the data from relevant sources with system-wide approach to intelligence to underpin this. We also need to do more to resource and embed Population Health Management models across the Partnership to support the effective use of data and insight in understanding need. Equal partners in population planning
We should seek to shift the balance of power towards those with the greatest knowledge of the needs of specific ethnic groups, i.e. the people in our communities. This involves taking positive action to seek the views of under-represented groups to ensure the views sought for engagement reflect the ethnic diversity of our populations. This engagement should happen throughout the population planning process, including the development of co-design principles with the Voluntary Community and Social Enterprise (VCSE) and the community they serve.
The VCSE play a key role in this, as they are agile and responsive to local community needs. An approach to service planning should be adopted, one that creates an equal playing field for all providers, including the VCSE, in the design and delivery of services.
/ 3130 / West Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and WakefieldWest Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and Wakefield

Find out more about involving people in service delivery by watching
this film about the Sikh Alliance Yorkshire and Sikh Elders Service.
Photo credit: Sikh Elders Service, Touchstone
Reducing inequalities in mental health outcomes by ethnicity
Accelerated improvements include continuous cycles of intelligence-
based service developments to make sure services are culturally able and meet local need. We will work across the Partnership to demonstrate the actions we have taken to reduce inequalities for specific ethnic groups. The review recommends monitoring service access, uptake and outcomes by ethnicity. Services should demonstrate how they are contributing towards reducing inequalities. This would involve working with West Yorkshire Association of Acute Trusts, mental health providers, Primary Care Networks and other partner organisations to identify opportunities to reduce inequalities through service improvements.
To explore inequalities in mental health for BAME communities, in order to develop targeted approaches for improving mental health. You can read the insight gathered to support this work here.
Key lines of inquiry for review
This review focused on the mental health needs of people from different BAME communities, including the following groups of people who experience particularly high levels of inequality:
• Men from Black or Black British backgrounds
• Women from South Asian backgrounds
• People from Gypsy, Roma and Traveller communities
• People who are asylum seekers or refugees.
*It is important to note that within each of these groups, there are diverse communities with different experiences, needs and strengths.
The Health Inequalities Prevention Pathway (HIPP) approach was used to understand the causes of inequality in mental health. This included three key issues:
1. Are there inequalities in living conditions and risk factors that affect mental ill health? What can be done to reduce this?
2. Are communities able to see a health professional and get a diagnosis? What can be done to improve access to health care?
3. Is treatment and support for mental illness high quality and appropriate? How can this be improved?
>>
Photo credit: Yorkshire Ambulance Service NHS Trust
Recommendations
Insight and Intelligence: Understanding the needs of
different population groups and improved recording of ethnicity is shared to improve racial inequalities for the decision makers across the Partnership.
This review recommends that ethnicity recording is 100% in all settings and that data is visible in integrated intelligence models.
The review also recommends that the Partnership take system action for specific groups requiring more focus, for example refugees, asylum seekers, Roma, Gypsy and Traveller groups of people and to better understand the links between ethnicity and poverty.
Equal partners: Redressing the balance of power towards those
with the best knowledge of why inequalities exist and the solutions of how they can be addressed.
The review recommends community representation that reflects the diverse ethnicity of local areas, is embedded throughout the population planning process; including in the design, mobilisation, delivery and evaluation of services. The review also recommends the VCSE are treated as equal partners with clear mechanisms in place to enable this.
/ 3332 / West Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and WakefieldWest Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and Wakefield

Evidence on rates of mental illness by ethnicity is complex and mixed. Black men are three times more likely to be diagnosed as having a psychotic condition than any other group and there is evidence that Black women are more likely to have depression or anxiety (McManus et al 2016).
Refugees and asylum seekers have much higher rates of mental ill health than the general population, and it has been estimated that over 30% experience depression, and over 30% experience post-traumatic stress disorder (Blackmore et al 2020).
It can also be difficult to understand differences locally, due to issues with data collection. For example, Gypsy, Roma and Traveller background information is rarely recorded, so inequalities in mental health for people from these communities are ‘invisible’.
People who are suffering from mental ill health do not always get a diagnosis and the care that they need. Research has shown that depression and anxiety in pregnancy was more likely to be missed for women from Pakistani backgrounds in some areas (Prady et al 2016). People from Gypsy, Roma and Traveller communities, and asylum seekers and refugees, often find it very difficult to get the health care they need. For people with English as an additional language, making an appointment in the first instance can be difficult. Other barriers include stigma, trust and concerns about discrimination, and lack of understanding of how the health care system works.
The Voluntary Community and Social Enterprise (VCSE) sector and individual people, such as teachers or youth workers, provide considerable support, for example to people who have mild to moderate illness, or people who are waiting to receive appropriate health care. This puts pressure on these organisations and individual people. The emotional toll of providing support is high, with impacts on their wellbeing. This was illustrated to the Review Panel (September, 2020) with examples put forward from VCSE organisations supporting refugees and asylum seekers who help people with complex trauma to navigate the health and care system.
High quality of treatment and support is essential to help people to manage their conditions and recover. There is some evidence of differences by ethnicity.
After starting psychological therapies for anxiety disorders and depression, completion rates are lower for people from Black, Asian or minority ethnic backgrounds. For example, in West Yorkshire and Harrogate 46% of White men complete treatment, compared with 39% of Black/Black British men and 38% of men from mixed backgrounds (IAPT 2019/20 figures). Issues raised include a lack of culturally appropriate services, including support in different languages.
In West Yorkshire and Harrogate there are many examples of innovative approaches and good practice to support the mental health of BAME communities. This ranges from individual people and community organisations, through to health care providers, commissioners and mental health hospitals. Sharing learning from these across the area could help to reduce inequalities in mental health.
Photo credit: South West Yorkshire Partnership NHS Foundation Trust
What does the evidence tell us?
The conditions of everyday life, such as income, employment, housing and the local environment, have an impact on mental health. Experiences of discrimination and racism are also likely to impact on people’s mental health. In West Yorkshire, people from BAME backgrounds are more likely to live in the most deprived 10% of areas (West Yorkshire Combined Authority, 2020).
The Office of National Statistics (ONS) has shown that income levels vary by ethnicity, with people from Bangladeshi backgrounds having the lowest median hourly pay. People from non-White backgrounds are more likely to be unemployed than people from a White background (ONS, 2019).
There is some evidence that air pollution is linked to depression, anxiety and suicide, and we know that air quality is worse in areas with high BAME populations. There are also differences in the use of greenspace by ethnicity, which is linked to both physical and mental health.
COVID-19 has had an unequal impact on BAME populations, including loss of employment and income, increased caring responsibilities and loss of support networks. There are likely to be ongoing mental health support needs, including for people who have lost friends and family or been unwell with the virus.
>>
/ 3534 / West Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and WakefieldWest Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and Wakefield
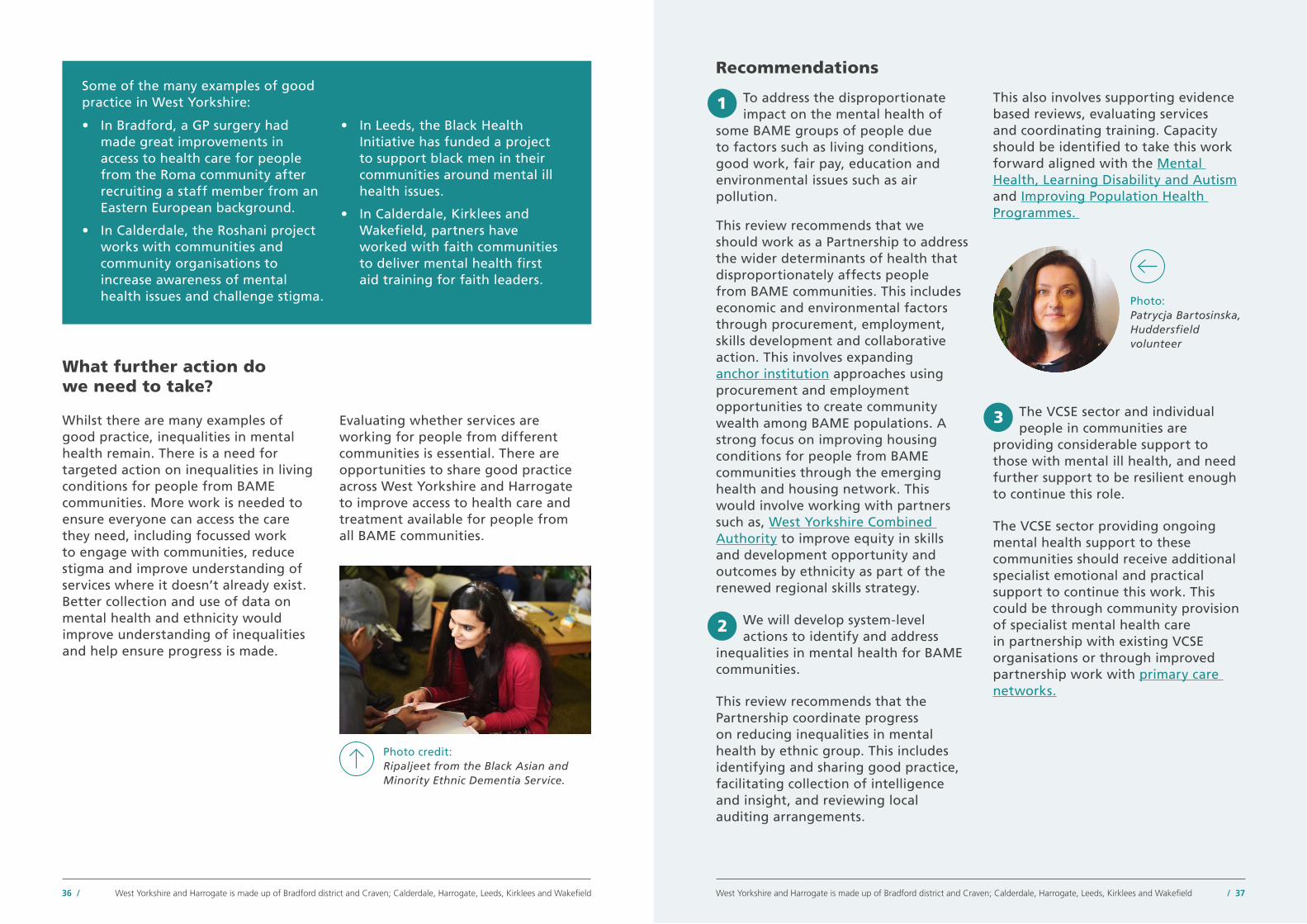
What further action do we need to take?
Whilst there are many examples of good practice, inequalities in mental health remain. There is a need for targeted action on inequalities in living conditions for people from BAME communities. More work is needed to ensure everyone can access the care they need, including focussed work to engage with communities, reduce stigma and improve understanding of services where it doesn’t already exist. Better collection and use of data on mental health and ethnicity would improve understanding of inequalities and help ensure progress is made.
Recommendations
To address the disproportionate impact on the mental health of
some BAME groups of people due to factors such as living conditions, good work, fair pay, education and environmental issues such as air pollution.
This review recommends that we should work as a Partnership to address the wider determinants of health that disproportionately affects people from BAME communities. This includes economic and environmental factors through procurement, employment, skills development and collaborative action. This involves expanding anchor institution approaches using procurement and employment opportunities to create community wealth among BAME populations. A strong focus on improving housing conditions for people from BAME communities through the emerging health and housing network. This would involve working with partners such as, West Yorkshire Combined Authority to improve equity in skills and development opportunity and outcomes by ethnicity as part of the renewed regional skills strategy.
We will develop system-level actions to identify and address
inequalities in mental health for BAME communities.
This review recommends that the Partnership coordinate progress on reducing inequalities in mental health by ethnic group. This includes identifying and sharing good practice, facilitating collection of intelligence and insight, and reviewing local auditing arrangements.
This also involves supporting evidence based reviews, evaluating services and coordinating training. Capacity should be identified to take this work forward aligned with the Mental Health, Learning Disability and Autism and Improving Population Health Programmes.
Some of the many examples of good practice in West Yorkshire:
• In Bradford, a GP surgery had made great improvements in access to health care for people from the Roma community after recruiting a staff member from an Eastern European background.
• In Calderdale, the Roshani project works with communities and community organisations to increase awareness of mental health issues and challenge stigma.
• In Leeds, the Black Health Initiative has funded a project to support black men in their communities around mental ill health issues.
• In Calderdale, Kirklees and Wakefield, partners have worked with faith communities to deliver mental health first aid training for faith leaders.
Photo credit: Ripaljeet from the Black Asian and Minority Ethnic Dementia Service.
Photo: Patrycja Bartosinska, Huddersfield volunteer
Evaluating whether services are working for people from different communities is essential. There are opportunities to share good practice across West Yorkshire and Harrogate to improve access to health care and treatment available for people from all BAME communities.
The VCSE sector and individual people in communities are
providing considerable support to those with mental ill health, and need further support to be resilient enough to continue this role.
The VCSE sector providing ongoing mental health support to these communities should receive additional specialist emotional and practical support to continue this work. This could be through community provision of specialist mental health care in partnership with existing VCSE organisations or through improved partnership work with primary care networks.
/ 3736 / West Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and WakefieldWest Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and Wakefield

Summary of recommendations
Work with partners, such as The West Yorkshire Combined Authority to deliver co-designed, ethically appropriate advice and support for people who are in high risk roles. This will help to mitigate risk to their health, their families and communities.
1
All organisations in West Yorkshire and Harrogate should engage in positive action to actively seek out local, ethnically representative talent with local recruitment targets for senior level roles.
4
The Partnership should develop and embed inclusive leadership standards which leaders pledge to personally uphold within their organisations, starting with recruitment and selection processes.
1
Work with strategic partners, such as West Yorkshire Combined Authority, to ensure equality of opportunities for BAME groups in all economic development and recovery plans, including work on apprenticeships, job creation and start up grants.
2
All West Yorkshire and Harrogate partner organisations should engage with their BAME networks (setting one up if it doesn’t already exist) to seek assurance regarding the impact and effectiveness of risk assessments and the resulting actions - ensuring the impact of racism is fully considered and mitigated.
3
The Partnership should support the co-production of an anti-racism campaign. Recognising and appreciating that BAME people are not one homogenous population. Communications messages should be amplified at a local level to consider the impact of racism and digital exclusion.
4
A West Yorkshire and Harrogate System Leadership Programme is commissioned to develop a BAME mentorship framework.
2
To ensure the Partnership’s leadership is reflective of communities, the review recommends that...
To improve access to safe work for Black, Asian and minority ethnic (BAME) people in West Yorkshire and Harrogate, the review recommends that...
It is helpful to note that these recommendations build on knowledge, insight and intelligence as well as existing work carried out by the Partnership. You can read more in the main report.
All health and care organisationsin West Yorkshire and Harrogateshould develop independentdiscrimination panels with BAMErepresentation to review allcases of racial discrimination indisciplinary and complaints casesprior to progressing through toformal stages.
3
/ 3938 / West Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and WakefieldWest Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and Wakefield

Summary of recommendations continued...
To reduce inequalities in mental health outcomes by ethnicity, the review recommends all West Yorkshire and Harrogate Partnership organisations...
Ethnicity recording is 100% in all settings and that this data, coupled with local insight, is used across the Partnership to inform the design and delivery of care.
1
Service access, uptake and outcomes by ethnicity are monitored to identify inequalities.
4
Demonstrate that services are culturally competent and are contributing towards reducing inequalities identified.
5
Work together to co-ordinate, lead and measure progress on reducing inequalities in mental health by ethnicity. This includes sharing good practice, improving use of evidence and coordinating training.
2
Support the voluntary, community and social enterprise sector to provide ongoing mental health support to Black, Asian and minority ethnicity communities. Colleagues from this sector should receive additional specialist emotional and practical support to continue this work.
3
Work to address the determinants that lead to ethnic inequalities in mental health. This includes using procurement and employment opportunities to create community wealth among BAME populations, improving housing conditions for people and equity in skills opportunities.
1
Community representation that reflects local population ethnicity, is visible throughout the planning process, including procurement of services.
2
Clear local and Partnership arrangements for commissioning with the voluntary, community and social enterprise (VCSE) sector are in place.
3 Watch the Partnership’s film to see why all the review recommendations are so important.
Please see full report for more information on recommendations.
To use information to plan services to meet different groups of people’s needs through population planning. The review recommends that services are culturally competent and are contributing towards reducing inequalities identified...
/ 4140 / West Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and WakefieldWest Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and Wakefield

Action plan Closing comments from Rob Webster
This reports sets out a series of recommendations to the leadership of the West Yorkshire and Harrogate Health and Care Partnership. The Partnership will develop an action plan in response to the recommendations, outlining roles and responsibilities and aligning it to our People Plan.
This action plan will be considered and approved by the Partnership Board in December 2020, before being published here.
During this time we will engage meaningfully with stakeholders in developing the plan.
The Partnership Board will periodically review progress against the report recommendations. This information will be made available to the public. The action plan will be accompanied by a set of indicators to measure progress over time.
Along with the above, we also aim to strengthen the role for the VCSE panel, which was set up to inform the review. This will help ensure progress is made on the recommendations. Their role will be important in supporting the Partnership to engage with communities who might not otherwise be aware of this work. This will be achieved through community assets and influencers. We will also aim to strengthen the role of the regional BAME network in implementing and delivering change.
West Yorkshire and Harrogate’s cultural vibrancy is borne from cities, towns, villages with strong diverse communities and even stronger identities. As a Partnership we are extremely proud to work alongside and represent the 2.7million people living across the area.
The healthy life expectancy of people living in some areas is below the national average, and the inequalities between communities are significant. Working together with communities is what motivates local health and care partners to work as one partnership together, putting the needs of people first.
As set out in this review report (summary) West Yorkshire and Harrogate Health and Care Partnership has big ambitions to tackle health inequalities and support Black, Asian and minority ethnic (BAME) communities and staff. The COVID-19 pandemic has brought these issues into even sharper focus, with inequalities seen in deaths for specific ethnic groups.
We will now act on the findings from this review, built on the dual foundations of good evidence and the testimony of people with lived experience.
Our independent review has again repeated the facts about the inequalities by ethnicity and has shown that BAME communities can be vulnerable to poorer health outcomes for far too many reasons. There are key factors that can increase inequalities further such as intersectionality with deprivation. In West Yorkshire and Harrogate around half a million people are living in the 10% most deprived communities nationally; a clear picture is that of a social gradient - the more deprived the place where you live, the higher the mortality rate and the shorter your life expectancy.
People from BAME backgrounds, like all people, experience a range of risks to their health throughout their lives. These risks vary significantly depending on their ethnicity. For example, people from BAME backgrounds are overrepresented in the most deprived 10% of our population across West Yorkshire and Harrogate, and income varies by ethnic group.
The economic impact of COVID-19 has led to a recession which brings additional risks to the mental and physical health of our population – all themes covered in this report.
The report also shines a light on the economic benefits of the health and care system. We are creators of good jobs, have large capital schemes underway, lead innovation in med tech and digital work. These potential benefits for both the economy and for local people must be secured as we invest in health and care.
/ 4342 / West Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and WakefieldWest Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and Wakefield

Thank you to contributors Review Panel Membership
• Professor Dame Donna Kinnair, Chief Executive and General Secretary, Royal College of Nursing (Independent Chair)
• Dr Sohail Abbas, GP and Deputy Clinical Chair at NHS Bradford District and Craven Clinical Commissioning Group (CCG) and Chair of the West Yorkshire and Harrogate Health and Care Partnership (WY&H HCP) Health Inequalities Network
• Brendan Brown, Chief Executive, Airedale NHS Foundation Trust and Senior Responsible Officer (SRO) for the WY&H HCP Workforce Programme
• Marie Burnham, Independent Lay Chair of the WY&H HCP Joint Committee of CCGs
>>
Rob Webster (CBE)
CEO Lead for West Yorkshire and Harrogate Health and Care Partnership (also known as an integrated care system (ICS) and CEO for South West Yorkshire Partnership NHS Trust
It is our time to step up, to better support staff, and to build a new resilient workforce for the future which is truly reflective of the communities we serve with a leadership that has the talent, which has often gone unrecognised, and the commitment from us all.
As we continue through the COVID-19 pandemic, it will be important to rebuild and shape our local economy to meet the needs of all people – irrespective of social class, ethnicity or other factors. The Partnership sees that we have a role in tackling economic, social and health inequalities barriers to achieving long-term prosperity and considerably reducing the impact on BAME communities and colleagues.
Not all experiences are equal and our current language does not account for the different ways in which different ethnic minorities experience racism. Racism is experienced differently and to different degrees by different groups of people. It is unhelpful to suggest that BAME groups are in perfect racial solidarity - that all racism is the same and that all ‘BAME’ people have the same life experiences and values. The experiences of BAME communities and staff, in and out of the workplace, differ considerably and it is our role as a large health and care partnership to take this into account and make a positive difference to people’s lives with them.
I would personally like to thank everyone for their hard work and involvement in this report. This includes the Partnership’s leadership executive group, our People Board and of course the West Yorkshire and Harrogate BAME network. I would like to also take the
opportunity to thank all colleagues involved in the Review Panel, including voluntary and community partners who have given their time freely without hesitation to do what is right for all communities across West Yorkshire and Harrogate. My thanks also to Professor Dame Donna Kinnair for her inspirational leadership in challenging us all to think differently, to make change happen and giving us the confidence we need to get on and move forward at pace without hesitation.
We have the potential to make the work of this review something unique and special. I’m reassured that this is a significant step forward that will be closely monitored as progress is made through our action plan with clear timescales for delivery. This will amplify and extend the work already underway. Above all, we now have an opportunity to improve and to save lives – it’s imperative we seize the moment to make something of value we can be proud of together.
Watch this film here about why the review is important, and for more information on
the recommendations and what is next.
A report summary is available in British Sign Language, Easy Read and audio version. It is also available in community languages.
There is also a range of information on our website to support this important report. This includes personal reflections from the review panel members, voluntary and community sector partner case studies and a series of short films. You can also listen to a podcast from review panel members talking about their personal experience as part of the review process here. The voluntary and community sector enterprise sub-group (VCSE) review sub group also recorded a podcast which is here.
All information was accurate at September 2020. Please note some of the photos and film footage may have been produced pre-COVID-19.
Supporting information
/ 4544 / West Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and WakefieldWest Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and Wakefield

• Yvonne Coghill, Former Director of Workforce Race Equality Standard at NHS England
• Hannah Davies, Chief Executive, Healthwatch Leeds
• Stephen Featherstone, Co-opted Member, WY&H HCP Health and Care Partnership Board
• Fatima Khan-Shah, Programme Director, WY&H HCP Unpaid Carers and Personalised Care programme and member of the WY&H BAME Network
• Alison Lowe, Chief Executive, Touchstone (voluntary and community sector representative)
• Dr Habib Naqvi, Interim Director for the NHS Workforce Race Equality Standard at NHS England / NHS Improvement
• Sara Robinson, Centre Lead, St Augustine’s (voluntary and community sector representative)
• Wallace Sampson, Chief Executive, Harrogate Borough Council
• Kim Shutler, Chief Executive, The Cellar Trust (voluntary and community sector representative)
• Sarah Smith, Consultant in Public Health and Programme Director, WY&H HCP Improving Population Health programme
• Rachel Spencer-Henshall, Strategic Director Corporate Strategy, Commissioning and Public Health , Kirklees Council
• Richard Stubbs, Chief Executive, Yorkshire & Humber Academic Health Science Network
• Cllr Tim Swift, Leader, Calderdale Council and Chair of the WY&H HCP Health and Care Partnership Board
• Dr James Thomas, Clinical Chair, NHS Bradford Districts and Craven CCG, Co-Chair of the WY&H HCP Clinical Forum and Joint SRO for the WY&H Improving Population Health Programme
• Robin Tuddenham, Chief Executive, Calderdale Council and Joint SRO for the WY&H HCP Improving Population Health Programme
• Rob Webster, Chief Executive, South West Yorkshire Partnership NHS Foundation Trust and CEO Lead for the WY&H HCP
• Dr Owen Williams, Chief Executive, Calderdale and Huddersfield NHS Foundation Trust and Chair of the NHS England / NHS Improvement Health Inequalities Expert Advisory Group
• Professor John Wright, Director, Bradford Institute of Health Research.
Review Panel Membership continued... Voluntary and Community Sector Enterprise Sub-group Membership
• Jo Baker, Programme Director, WY&H HCP Harnessing the Power of Communities Programme
• Humayun Islam, Chief Executive, BEAP Community Partnership
• Dipika Kaushal, Chief Executive Officer, Voluntary Action Calderdale
• Javed Khan, Chief Executive Officer, CNet Bradford
• Kaneez Khan, Local Coordinator (West Yorkshire), Near Neighbours
• Corrina Lawrence, Chief Executive Officer, Feel Good Factor
• Alison Lowe, Chief Executive, Touchstone
• Heather Nelson, Chief Executive, Black Health Initiative
• Portia Roberts-Popham, Chief Executive Officer, Locorum Care Services Ltd
• Santokh Sidhu, (Harrogate voluntary community sector representative)
• Sayed Ahmed from Pakistan and Kashmir Welfare Association
• Hilary Thompson, Chair, Third Sector Leaders Kirklees and SRO for the WY&H HCP Harnessing the Power of Communities Programme.
West Yorkshire and Harrogate Health and Care Partnership (WY&H HCP) Project Support Team
• Heather McKnight, WY&H HCP Programme Support
• Ian Holmes, Director, WY&H HCP
• Jonathan Booker, WY&H HCP Senior Analyst
• Karen Coleman, WY&H HCP Communications and Engagement Lead
• Lauren Phillips, Head of Programmes for WY&H HCP.
• Pam Bhupal, Calderdale Council, Regional Health Partnership Support.
Report Contributors
• Pippa Bird, WY&H HCP, Specialist Registrar in Public Health
• Madi Hoskin, Programme Manager, West Yorkshire Association of Acute Trusts
• Sayma Mirza, Senior Head of Collaboration, Act as One -System Transformation. Programme for Bradford District and Craven
• Yannish Naik, WY&H HCP Climate Change Lead / Acting Consultant in Public Health
/ 4746 / West Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and WakefieldWest Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and Wakefield

ReferencesTitle Date Geography Subject Population
groupAuthor
Mental health and wellbeing in the NHS
2014 National Mental health All S. McManus, P. Bebbington, R. Jenkins, T Brugha
Diversity matters Feb 2015
National Workforce All Vivian Hunt, Dennis Layton and Sara Prince
Evaluation of ethnic disparities in detection of depression and anxiety in primary care during the maternal period: combined analysis of routine and cohort data
May 2016
National Mental health, access of health services
Black, Asian and minority ethnic communities (BAME)
S. Prady, K Pickett, E. Petherick, S. Gilbody, T. Croudace, D. Mason, T, Sheldon, J. Wright
Race in the workplace: The McGregor-Smith Review
Feb 2017
National Workforce All Dept. of Business, Energy and Industrial strategy
Access and experiences of mental health crisis care services in Leeds by black and minority ethnic communities
2018 Leeds Mental health BAME John Halsall
Delivering through diversity
Jan 2018
National Workforce All Vivian Hunt, Sara Prince, Sundiatu Dixon-Fyle and Lareina Yee
Social, Emotional and Mental Health Needs Assessment: children and young people from Black, Asian and ethnic minority communities in Leeds
Oct 2019
Leeds Mental health All Children and young people
Charlotte Hanson Parminder Grewal
UK labour market June 2019
National Employment,Workforce
All Office of National Statistics
Air Pollution (Particulate Matter) Exposure and Associations with Depression, Anxiety, Bipolar, Psychosis and Suicide Risk: A Systematic Review and Meta-Analysis
Dec 2019
National Environmental, Mental health
All Isobel Braithwaite, Shuo Zhang, James Kirkbride, David Osborn, Joseph Hayes
Health needs data update 2019:End of life care services for adults in Leeds
Dec 2019
Leeds Palliative Care All Leeds Palliative Network
Deaths of NHS staff from Covid-19 analysed
April 2020
National Mortality All Tim Cook, Emira Kursumovic, Simon Lennane
Gig workers among the hardest hit by coronavirus pandemic
April 2020
International Covid-19, Employment
All Josephine Moulds
Are some ethnic groups more vulnerable to Covid-19 than others?
May 2020
National Covid-19, Employment
BAME Lucinda Platt Ross Warwick
Assessing jobs at risk and the impact on people and places
May 2020
National Employment,Workforce
All Tera Allas, Marc Canal and Vivian Hunt
Covid-19 in-patient hospital mortality by ethnicity
May 2020
Bradford Covid-19, Ethnicity, Mortality, Gender
BAME John Wright,Gillian Santorelli, Trevor Sheldon, Jane West, Chris Cartwright
Homelessness and Rough Sleeping Strategy 2019- 2022
May 2020
Leeds Homelessness,Rough Sleepers
All Leeds City Council: Housing Options
The effects of the coronavirus crisis on workers
May 2020
National Covid-19 Employment
All Laura Gardiner Hannah Slaughter
Which occupations have the highest potential exposure to the coronavirus (COVID-19)?
May 2020
National Employment, Workforce,Economy
All Office of National Statistics
Covid-19 transport survey
June2020
West Yorkshire
Covid-19, Employment,Travel
All West Yorkshire Combined Authority
/ 4948 / West Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and WakefieldWest Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and Wakefield

How Covid-19 is affecting the mental health of young people in the BAME community
June2020
National Mental health Children andYoung people
Kooth
Sikhs Covid-19 report June 2020
Yorkshire Covid-19 Sikhs Sikh Alliance Yorkshire
Stabilisation and Reset Programme: Rapid Insight Report
June 2020
West Yorkshire and Harrogate
Covid-19
Workforce West Yorkshire and Harrogate Health and Care PartnershipYorkshire & Humber Academic Health Science Network
A review on how the health of babies and young children from disadvantaged backgrounds can be improved
July 2020
National Health inequalities
All Children Dept. of Health and Social Care Jo Churchill MP Andrea Leadsom MP Matt Hancock MP
Commission on Race and Ethnic Disparities
July 2020
National Employment Health, Criminal Justice
BAME Dr Tony Sewell (Chair)
Covid-19 and Brexit: Real-time updates on business performance in the United Kingdom
July 2020
National Covid-19, Brexit
All Josh De Lyon Swati Dhingra
English Housing Survey July 2020
National Housing All Ministry of Housing, Communities and Local Government
Race disparities in innovation
July 2020
International Innovation BAME Eszter Czibor
Third sector resilience in West Yorkshire and Harrogate: Before and during Covid-19
July 2020
West Yorkshire and Harrogate
Covid-19 All Voluntary Action Leeds
Action required to tackle health inequalities in latest phase of COVID-19 response and recovery
Aug 2020
National Covid-19, Ethnicity
BAME Dr Owen Williams OBE (Chair) NHS England and NHS Improvement
Coronavirus engagement report for stabilisation and reset
Aug2020
West Yorkshire and Harrogate
Covid-19,Voluntary, Community Sector
All West Yorkshire and Harrogate Health and Care Partnership
Disparities in the risk and outcomes of Covid-19
Aug 2020
National Covid-19 BAME Prof. Kevin Fenton
NHS England / Improvement Planning Guidance – Implementing Phase 3 of the NHS response to the COVID-19 pandemic
Aug 2020
National Covid-19,Mental health, Health services
All NHS England/ NHS Improvement
Over-Exposed and Under-Protected: The devastating impact of Covid-19 on black and minority ethnic communities in Great Britain
Aug 2020
National Economy, Ethnicity Inequalities
BAME adult and children
Zubaida Haque Laia Becares Nick Treloar
We are the NHS: the NHS People Plan 2020/21
Aug 2020
National Covid-19,Workforce, Employment,Leadership
BAME NHS England/ NHS Improvement
Kickstart scheme Sept 2020
National Employment All Department for Work and Pensions
The prevalence of mental illness in refugees and asylum seekers: A systematic review and meta-analysis
Sept 2020
National Mental health Refugees and asylum seekers
Rebecca Blackmore, Jaqueline Boyle, Mina Fazel, Sanjeeva Ranasinha, Kyle Gray, Grace Fitzgerald, Marie Misso, Melanie Gibson-Helm
/ 5150 / West Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and WakefieldWest Yorkshire and Harrogate is made up of Bradford district and Craven; Calderdale, Harrogate, Leeds, Kirklees and Wakefield

A Partnership made up of the NHS, local councils, care providers, Healthwatch, voluntary and community organisations and charities.
Publication date: October 2020
For more information contact:
01924 317659
NHS Wakefield CCG White Rose House West Parade Wakefield WF1 1LT
www.wyhpartnership.co.uk
@WYHpartnership

Communications and engagement report
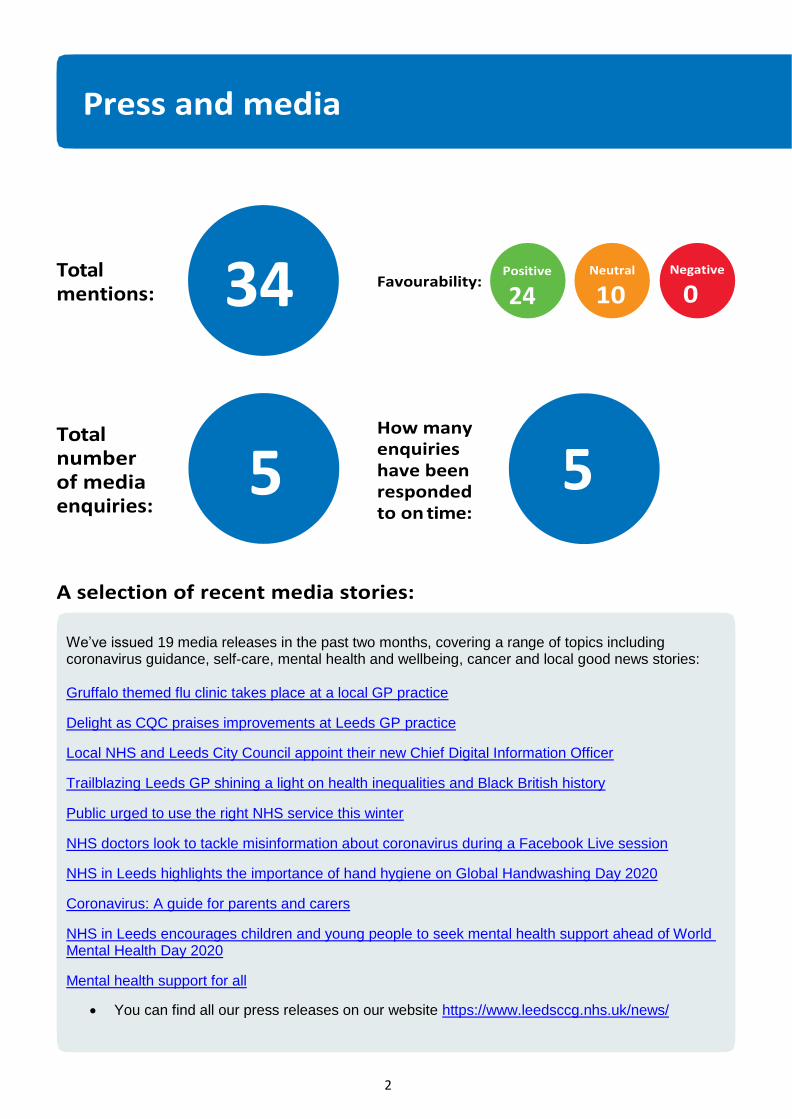
2
We’ve issued 19 media releases in the past two months, covering a range of topics including coronavirus guidance, self-care, mental health and wellbeing, cancer and local good news stories: Gruffalo themed flu clinic takes place at a local GP practice
Delight as CQC praises improvements at Leeds GP practice
Local NHS and Leeds City Council appoint their new Chief Digital Information Officer
Trailblazing Leeds GP shining a light on health inequalities and Black British history
Public urged to use the right NHS service this winter
NHS doctors look to tackle misinformation about coronavirus during a Facebook Live session
NHS in Leeds highlights the importance of hand hygiene on Global Handwashing Day 2020
Coronavirus: A guide for parents and carers
NHS in Leeds encourages children and young people to seek mental health support ahead of World Mental Health Day 2020
Mental health support for all
You can find all our press releases on our website https://www.leedsccg.nhs.uk/news/
Total mentions:
Total number of media enquiries:
Favourability:
How many enquiries have been responded to on time:
A selection of recent media stories:
34
5 5
24

3
Most popular content
September
This video describing the symptoms of Covid-19 and the importance of booking a test if you display any of these symptoms was September’s most popular content. The post reached an audience of 236,145, pulling in 7,696 engagements, 532 reactions as well as 42 shares. To view the post please click on the image on the left

4
Most popular content
This post describing the importance of washing your hands to help stop the spread of Covid 19 (click on image to view the Facebook post). The post received 268 reactions, reaching an audience of 74,929 and with 715 engagements. To view the post please click on the image on the left

5
Covid-19 – during the last two months, our campaigns and communications activity has still largely focused on issues surrounding the pandemic and the city’s stabilisation and reset work, which is a partnership approach involving colleagues across the local healthcare system. We continue to support messages that promote appropriate use of healthcare services and actions people can take to reduce the rate of infections.
In September, we ran our first Facebook Live event with local doctors and public health experts to address coronavirus questions and misinformation. The video from the session has had just under 4,000 views.
AGM – we supported governance colleagues with this year’s virtual annual general meeting, including writing and publishing the CCG’s annual report and annual review.
City/regional meetings and representation – we continue to hold key roles as part of the West Yorkshire and Harrogate communications network and the Leeds citywide communications network.
Citywide work – we are continuing to provide communications support for the city digital team. We are also supporting communications around mental health, an area of significant concern because of the impact of Covid-19. In addition, we are working with colleagues across the city on the 2020-21 flu vaccination campaign.
Health inequalities – we worked with the Yorkshire Evening Post to launch our health inequality framework leading to a series of features highlighting the work of partner organisations in tackling health inequalities.
Internal communications – we have continued our regular (three times a week) briefings for primary care and CCG staff and support our chief executive with a monthly team briefs via Teams Live. For World Mental Health Day, we organised a virtual staff wellbeing event with a local mental health specialist.
Local campaigns – we continue to work with commissioners, clinical colleagues and our partners to develop campaigns in response to current issues, including Feel Better, our student health and wellbeing campaign, and continuing our work to highlight NHS services (#NHSHereForYou and #ReopeningSafely).
National campaigns – we continue to support national information and awareness campaigns, including Black History Month, World Mental Health Day and Global Handwashing Day.
Primary care communications – we have supported practices by providing patient-facing materials, social media advice and media relations guidance, including press releases to highlight good news stories. We continue to support the new primary care BAME network.
Website accessibility – we ensured out website met new public sector accessibility standards, ahead of the 23 September deadline. Winter preparedness – with flu season and coronavirus likely to significantly affect health and care service capacity, we continue to work with colleagues across the city to ensure clear, consistent and effective communications help people access he right services at the right time as well as taking preventative action to keep themselves and others stay well.

6
Number of e-bulletins (staff and primary care)
Number of extranet users
Number of people registered on Workplace by Facebook
Average open rate * *We have temporarily changed the way we send out daily staff and primary care briefings and are currently unable to access open rates
Average number of users per week
144
725
429
N/A
267

7
Number of live consultations/engagements
Number of people involved in our events / activities
Number of parliamentary enquiries
Number of engagement events / activities
Number of people signed up to patient & public network
Number of PQs responded to on time
122
0
7
N/A

8
As a result of the ongoing Covid-19 pandemic, no new engagements were started during September and October; however, members of our team are involved in several work groups. In addition, we continue to consider alternative approaches to patient and public involvement.
Mental health community commissioning review – the CCG commissioning team and Leeds City Council are reviewing third sector and community-based mental health services in Leeds. Our team, alongside two CCG volunteers, is supporting this work.
Children’s constipation – we had our first steering group meeting in October. We now are contacting families who may want to be involved and gathering insight.
Community neuro service review – the insight report has been completed, and a survey is now live, asking patients for thoughts on the current service. This will conclude in December when commissioners and providers will agree on options for the new service. Engagement will start February 2021.
Insight reviews – we completed an insight review for the Primary Care Pro-active Team into what people in the Lincoln Green area think about accessing health and care services, and are working on a similar review for the Belle Isle area.
Insight repository – we are supporting work in the CCG to explore the development of an Insight repository and grey literature library. These resources will enable us to collate and code patient insight so that we can use existing patient experience data to inform commissioning decisions in the city.
Primary care networks engagement – we are working with Leeds Voices and Cross Gates Primary Care Network to develop a pilot to strengthen patient participation groups (PPGs) to facilitate stronger links between practices and the local patient population.
Digitising engagement – the working group, of patient and public volunteers from the CCG Network, met in October to look at priorities and focus. This will enable us to develop an aim, objectives and outcomes for this project.
CCG volunteers – We held one virtual group catch-up sessions during this time, and are developing more opportunities for our volunteers to get involved online. We continue to provide mentoring to our volunteers via phone and video calls.
Patient Assurance Group (PAG) – no PAG meetings were held in September or October.
Patient participation groups (PPGs) – we have continued to support PPGs during this time, attending meetings and planning a virtual PPG event.
Winter preparation engagement – Leeds Voices are leading an engagement to understand the communication needs of key seldom-heard communities and coproduce essential winter/Covid-19 messages for those communities.
People’s Voices Group (PVG) – we continue to support the PVG and associated sub-groups. These include the Digital Inclusion, Big Leeds Chat, and Citywide Network subgroups.
Networked Data Lab – we are continuing to provide support and guidance to the Business Intelligence Team with the engagement aspects of their Networked Data Lab.
Co-Production Training – we ran a virtual session of our co-production training through Zoom in October. We hope to create a video resource of the session to share online.

9
Covid-19 – we will continue to support the Leeds system with clear and consistent communications. Campaigns – we will be working with colleagues to develop new campaigns and communications plans around antimicrobial resistance, advance care planning, Brexit and mental health. We are also developing a harms minimization programme for people aged 60 and above to encourage people to stay active and socially, but not physically, connected. We will be supporting the West Yorkshire and Harrogate Health and Care Partnership with several regional campaigns, including Positive Vibes (mental wellbeing), Islamophobia awareness, Healthy Hearts (cardiovascular disease awareness) and Looking out for our Neighbours (social isolation). We will also be supporting national initiatives, including the new Help Us Help You campaign. Internal communications – we will continue to look at new ways to engage staff working remotely via our internal communications channels The mental health community service engagement plan is being developed. Proactive engagement – the Cross Gates PCN engagement will begin in November. Stabilisation and reset – we will continue to lead on communications around the Leeds healthcare system’s reset to the new ‘normal.’ Volunteers - we are holding a CCG volunteer refresher session in November, and hosting two safeguarding training sessions for the volunteers which have been developed by the CCG safeguarding team Winter / Covid-19 pressures – the health and care system in Leeds is currently under significant pressure. We will be working with colleagues across the city to ensure clear, consistent and effective communications so that people understand how services may be affected and how they can help. As part of this work we will be developing an information booklet that will be posted to every home in Leeds.

If you wish to contact us, please use the details below:
NHS Leeds Clinical Commissioning Group Suites 2- 4, WIRA House, West Park Ring Road, Leeds LS16 6EB
Tel: 0113 843 5470 Email: [email protected] Website: www.leedsccg.nhs.uk Facebook: facebook.com/nhsleeds Twitter: @nhsleeds
If you have special communication needs or would like this information in another format or in a different language, please contact us or ask a carer or friend to contact us on 0113 8435457.

1
Leeds Health & Wellbeing Strategy Outcomes – that this report relates to:
1. People will live longer and have healthier lives
2. People will live full, active and independent lives
3. People’s quality of life will be improved by access to quality services
4. People will be actively involved in their health and their care
5. People will live in healthy, safe and sustainable communities
NHS Leeds CCG Strategic Commitments We will focus resources to:
1. Deliver better outcomes for people’s health and wellbeing
2. Reduce health inequalities across our city
We will work with our partners and the people of Leeds to:
3. Support a greater focus on the wider determinants of health
4. Increase their confidence to manage their own health and wellbeing
5. Achieve better integrated care for the population of Leeds
6. Create the conditions for health and care needs to be addressed around local neighbourhoods
Assurance Framework – which risks on the GBAF does this report relate to: 1. Failure to deliver the CCG commitment to reduce health inequalities across our city.
2. Quality of commissioned care is compromised and does not reflect best practice.
3. Failure to achieve financial stability and sustainability.
4. Failure to overcome local and national workforce shortages.
5. Business continuity of health and care services disrupted as a result of a significant event.
6. Ineffective patient and public engagement and lack of transparency in translation of engagement into decisions.
7. Partners and Professionals do not support the CCG strategy.
8. Constraints on CCG organisational effectiveness impact the delivery of the CCG’s plans.
9. Inadequate system infrastructure to support the CCG’s plans.
Agenda Item: GB 20/89 FOI Exempt: N
NHS Leeds CCG Governing Body Meeting
Date of meeting: 25 November 2020
Title: Update on Winter Planning and the Impacts of COVID-19
Lead Governing Body Member: Helen Lewis, Director of Pathway Integration
Category of Paper Tick as
appropriate
()
Report Author: Helen Lewis, Director of Pathway Integration
Decision
Reviewed by EMT/Date: N/A
Discussion
Reviewed by Committee/Date: N/A
Information
Checked by Finance (Y/N/N/A - Date): N/A
Approved by Lead Governing Body member (Y/N): Y

2
EXECUTIVE SUMMARY: This paper outlines the preparations for winter and surge planning in light of the significant constraints on the system caused by COVID-19. It describes the way in which system partners are working together and the impact of the increase in COVID-19 patients during the second wave on further recovery of planned care.
NEXT STEPS: Governing Body is asked to note the continued oversight of System Resilience through the city-wide Health and Care Silver and Gold command arrangements, and the ongoing reporting of risks and mitigation through Governing Body subcommittee structures.
RECOMMENDATION: The Governing Body is asked to:
(a) NOTE the actions and processes within the system and the significant risks to
‘business as usual’ caused by the need to respond to the surge of patients with COVID-19.

3
1. SUMMARY 1.1 The purpose of this paper is to update on planning for Winter and surge in relation to
COVID-19, usual winter demand, and flu. It also describes the key impacts of the second wave of COVID-19 on other parts of the NHS system.
2. BACKGROUND 2.1 In line with the NHSE approach, the CCG is taking an integrated approach to overseeing
winter, Covid and EU Exit planning over the coming weeks and months. System partners have all identified their own key actions which include both phased additional capacity and actions to respond to expected seasonal demands, and triggered actions to be taken as demand increases through Covid or other demand factors such as a flu outbreak, or other winter related disease peaks. Clearly because of the very early and unexpectedly large surge in Covid cases, we have already gone beyond some of the expected surge plans, and are developing new plans on a weekly basis to cope with the unprecedented volume of cases and the complexity of the infection control implications of these patients.
2.2 Each provider in the City has their own comprehensive set of actions internally, and the
system also has a number of cross-cutting task groups to ensure key areas of focus are addressed. The difference between this winter and others is that we have had a chance to test out some very extreme versions of stopping services and deploying staff, earlier in the year. This means that providers have refined their thinking, but also that their staff are in the main are trained and ready to redeploy when essential so the lead times to do this will be less, and the potential for doing so greater. All our providers are committed to trying to not cease the provision of whole services, but will adjust their service offers in line with available staffing and clinical need.
2.3 At the time of writing, it seems extremely likely that we face a prolonged period in which we will only be able to deliver scaled back versions of many services. However, many services have been able to alter the way in which they are provided, which means that they will be more able to continue in some form than they were in May. Some services were ceased altogether while risk assessment and new ways of working were introduced, and so can still continue safely this time.
2.4 The risks to the waiting times in both outpatient and elective services at LTHT, but more widely across all our providers are noted in the IQPR and the report from the Quality and Performance Committee. Depending on how long the current surge in cases continues, the numbers of people waiting for treatment and the length of that wait will both increase. However, the situation is better than in the first wave, in that most diagnostic services are continuing to operate, and we are back up to around 80% or more of the usual ‘pre pandemic’ operating levels. Cancer pathways and cancer diagnostics continue to be in place despite the major constraints, and the backlog of people waiting more than 62 and more than 104 days for Cancer Treatment is falling. Cancer referral rates are back up to and higher than pre-pandemic rates. All elective capacity is used for those most clinically urgent, but depending on the impact of the COVID admissions on critical care facilities, there may continue to be some delays even for this group.

4
2.5 Partners meet regularly to review operational situation and consider further mutual aid. The Health and Care Silver Group (also operating as System Reset Group) which consists of Chief Operating Officers and key partners oversees the System Operational Group, serves as the A&E Delivery Board and is also overseeing reset plans and the attempts by partners to maintain as much of the recovery as possible during the second wave. This group also oversees Communications to public and staff around system and service delivery during this period.
2.6 At time of writing there were 11 wards at LTHT occupied by patients with COVID-19. This is close to the maximum numbers of wards that can be used in this way, and has been created by swapping the use of existing wards rather than opening new ones. Space and staffing remain constraints to further expansion. While the Nightingale hospital remains a potential venue for further patients, there is no pool of additional staffing to open these beds. The system continues to try to maximise outflow from LTHT and prevention of admission for any patients who can be cared for safely in their own homes or in a community bed.
2.7 Primary Care is currently also facing increased demand with more practices reporting increasing levels of Opel 2 and 3. Very strong mutual aid arrangements have been put in place, to try to maximise continuity of service for patients with support from neighbouring practices. Additional funding has been identified to increase same day demand response over the winter period which includes a combination of PCN and practice based plans. New national funding and national guidance on how primary care should prioritise its workforce was received in mid-November, but this continues to be a moving position. The requirement to also create sufficient staffing to deliver the COVID-19 vaccine during the coming months will provide an extra set of challenges. Recruitment of suitable staff to be able to deliver these expanded requirements will be a key challenge.
3. PROPOSAL 3.1 The Governing Body is asked to note the wide range of actions under way within the City
coordinated by the CCG in ensuring we maximise capacity to maintain both our acute/emergency responses to patients and as far as possible slow any deterioration in waiting times for planned care. We note the risks that proactive and elective care may suffer during the coming weeks, which may then further impact upon outcomes for patients and may further reinforce inequalities.
3.2 In light of all the work done earlier in the year on the impact of COVID on non-COVID conditions, the Governing Body is asked to be assured that all partners remain extremely mindful of this in their planning and delivery during this second wave. This has added to system pressures.
4. NEXT STEPS 4.1 The Governing Body is asked to note the content of this report.

5
5. STATUTORY/LEGAL/REGULATORY/CONTRACTUAL
5.1 This section sets out in any statutory/legal/regulatory or contractual issues. 6. FINANCIAL IMPLICATIONS AND RISK 6.1 The financial position around meeting the costs of surge capacity is described elsewhere in
the Board papers but remains a moving position as additional funds become identified (e.g. for primary care capacity, Winter funding for Mental health services etc.)
7. COMMUNICATIONS AND INVOLVEMENT 7.1 Public communications and stakeholder engagement remain critical at this period, because
of the very fast moving nature of the local situation and frequent updates on national guidance. Balancing the messages between encouraging patients to seek help for their healthcare against the need to remind people the NHS is significantly under pressure remains a challenging tightrope.
8. WORKFORCE
8.1 Workforce is significantly constrained across the system due to the levels of COVID and the levels of self-isolation required after contacts. The implementation of staff testing in the next weeks may impact on this somewhat, though there are concerns that proactive staff testing may add to pressures if they identify high levels of asymptomatic staff who then cannot work. Registered staffing remains a major pressure area- recruitment of non-registered staff has been more encouraging.
9. EQUALITY IMPACT ASSESSMENT 9.1 No new EIA has been completed 10. ENVIRONMENTAL
10.1 No new environmental issues have been identified.
11. RECOMMENDATION
The Governing Body is asked to:
(a) NOTE the actions and processes within the system and the significant risks to ‘business
as usual’ caused by the need to respond to the surge of patients with COVID-19.
1
Leeds Health & Wellbeing Strategy Outcomes – that this report relates to:
1. People will live longer and have healthier lives
2. People will live full, active and independent lives
3. People’s quality of life will be improved by access to quality services
4. People will be actively involved in their health and their care
5. People will live in healthy, safe and sustainable communities
NHS Leeds CCG Strategic Commitments We will focus resources to:
1. Deliver better outcomes for people’s health and wellbeing
2. Reduce health inequalities across our city
We will work with our partners and the people of Leeds to:
3. Support a greater focus on the wider determinants of health
4. Increase their confidence to manage their own health and wellbeing
5. Achieve better integrated care for the population of Leeds
6. Create the conditions for health and care needs to be addressed around local neighbourhoods
Assurance Framework – which risks on the GBAF does this report relate to: 1. Inadequate patient and public engagement results in ineffective decisions and challenge
2. Failure to assure the delivery of high quality services, leading to commissioned services not reflecting best practice and improving care
3. Failure to achieve financial stability and sustainability
4. Lack of provider and clinical support for change will impact on the development and implementation of the CCG strategy
5. Resources are not targeted effectively to areas of most need, leading to failure to improve health in the poorest areas
6. Insufficient workforce capacity, capability and adaptability to deliver the ambitions
7. Failure to enable partners to work together to deliver the CCG commitments
8. Failure of system to be adaptable and resilient in the event of a significant event
9. Inadequate system infrastructure to support the CCG’s plans.
Agenda Item: GB 20/90a FOI Exempt: N
NHS Leeds CCG Governing Body Meeting
Date of meeting: 25th November 2020
Title: 2020-21 Operational Financial Planning and Annual Budgets Update
Lead Governing Body Member: Visseh Pejhan-Sykes, Chief Finance Officer
Category of Paper Tick as
appropriate
()
Report Author: Judith Williams, Head of Corporate Reporting & Strategic Financial Planning
Decision
Reviewed by EMT/Date: N/A Discussion
Reviewed by Committee/Date: N/A Information
Checked by Finance (Y/N/N/A - Date): Y
Approved by Lead Governing Body member (Y/N): Y

2
EXECUTIVE SUMMARY: This paper provides an overview of the latest financial planning position for NHS Leeds Clinical Commissioning Group (CCG), and the context of the system within which it operates, both at a place based level, and the wider Integrated Care System (ICS). The latest planning submission to NHSEI reflects a deficit position for the CCG of £14.8m for the six months October 2020 to March 2021. The forecast deficit position is net of a number of material risks and assumptions around the current position, including the anticipated receipt of additional allocations of c£20m (£11m retrospective COVID reimbursement allocation requested by the CCG for Aug/Sept still awaited, and £9m of retrospective drawdowns of resources from NHSE/I in M7-12 to cover spend for which resources are deemed to be held centrally to cover the costs of out of hospital capacity and place based initiatives that ensure we have sufficient bed base available to deal with COVID and non- COVID activity. Examples include the Hospital Discharge Programme and support for strategic Any Qualified Provider/local Independent Sector capacity to maximise patient activity throughput. The forecast position also assumes the delivery of £2.4m of QIPP savings which we are in the process of identifying. Leeds needs to ensure that across the NHS Organisations we are financially balanced in aggregate. There are risks across all NHS organisations within Leeds as well as significant pressures on social care at Leeds City Council, all of which will have service and financial implications. Although the NHS financial regime for 2021-22 is yet to be published, the expectation is that it will follow the principles of the M7-12 2020-21 regime. This is expected to result in a reduction in allocations of c£50m for Leeds CCG. Both the Leeds Healthcare system and Leeds City Council are forecasting significant financial shortfalls going forwards, together with the uncertainty of increased ongoing costs associated with the pandemic. This emphasises the need for all organisations, at both place level and the wider regional level to work together to transform services to ensure financial sustainability across the system.
NEXT STEPS: Work will continue to identify efficiencies. And to develop a shared financial understanding across place and at system level We will continue to bring updates to Governing Body on planning
RECOMMENDATION: The Governing Body is asked to:
(a) NOTE the current position with the CCG financial plan for 2020-21, which is a deficit of £14.8m with further risk on top of. The plan was approved by the Accountable Officer and Chief Finance Officer as per the authority previously delegated by Governing Body. EMT, the CCG Chair and Lay Members have been kept abreast of the reported position as it evolved, during the Integrated Care System submission process;
(b) APPROVE the high level budgets for 2020-21, recognising the savings still to be found;

3
(c) DISCUSS and RECOMMEND how the CCG should proceed in the remainder of 2020-21 with balancing its statutory duties to provide care for the population of Leeds, progress with our health inequalities agenda and continue with service developments that have already commenced prior to Covid in the light of the changing financial position and the need to find significant efficiencies; and
(d) DISCUSS and RECOMMEND the approach to be adopted to develop a cohesive plan for 2021-22 within the anticipated financial constraints, to ensure financial sustainability, and limit risk to services. With due consideration to the context of the Place and the wider Integrated Care System (ICS) and the associated requirements to work closely with other organisations both at a Leeds place based level and at the wider ICS level.
4
1. SUMMARY 1.1 This paper provides an overview of the latest financial planning position for NHS Leeds
Clinical Commissioning Group, and the system context.
1.2 The Leeds health and social care system has been operating on revised national funding arrangements as a result of Covid and is subject to ongoing significant associated cost pressures.
1.3 The latest planning submission, for M7-12 reflects a forecast outturn deficit position of £14.8m. Leeds as a place has the opportunity to deliver a balanced position if support towards lost commercial income is received by local trusts.
1.4 The forecast deficit position is net of a number of material risks and assumptions around the current position, including the anticipated receipt of additional allocations of c£20m (£11m retrospective COVID reimbursement allocation requested by the CCG for Aug/Sept still awaited, and £9m of retrospective drawdowns of resources from NHSE/I in M7-12 to cover spend for which resources are deemed to be held centrally to cover the costs of out of hospital capacity and place based initiatives that ensure we have sufficient bed base available to deal with COVID and non- COVID activity. Examples include the Hospital Discharge Programme and support for strategic Any Qualified Provider/local Independent Sector capacity to maximise patient activity throughput.
1.5 The forecast position also assumes the delivery of £2.4m of QIPP savings which we are in the process of identifying. Budgets have been set on a full forecast spend basis, and work has started to identify the efficiencies required to reduce our deficit gap.
1.6 Leeds needs to ensure that across the NHS Organisations we are financially balanced in aggregate. There are risks across all NHS organisations within Leeds as well as significant pressures on social care at Leeds City Council, all of which will have service and financial implications.
1.7 A high level reconciliation of the flow of funds in and out of Leeds as a result of the COVID finance regime suggest that Leeds has ended up with a reduced level of resources as a Place. Therefore based on this assessment (and our deficit position which has emerged as a result of our allocation changes) our planned investments will now have to be stopped and in some areas, we will need to start to decommission services in order to remain within the revised and reduced allocation envelopes post these regime changes.
1.8 Although the NHS financial regime for 2021-22 is yet to be published, the expectation is that it will follow the principles of the M7-12 2020-21 regime. This is expected to result in a reduction in allocations of c£50m for Leeds CCG. Both the Leeds Healthcare system and Leeds City Council are forecasting significant financial shortfalls going forwards, together with the uncertainty of increased ongoing costs associated with the pandemic.
1.9 The Governing Body is asked to note the current position with the financial plan, which is a deficit of £14.8m, and the further risks inherent in that forecast position. The Governing Body is asked to approve the high level budgets for 2020-21, recognising the savings still to be found.
1.10 Specifically, the Governing Body is asked to recommend how the CCG should proceed with in the remainder of 2020-21with balancing its statutory duties to provide care for the

5
population of Leeds, progress with our health inequalities agenda and continue with service developments that have already commenced prior to Covid in the light of the changing financial position and the need to find significant efficiencies.
1.11 The Governing Body is also asked to discuss and recommend the approach to be adopted to develop a cohesive plan for 2021-22 within the anticipated financial constraints, to ensure financial sustainability, limit risk to services and progress the system Sustainability and Transformation Plan
2. BACKGROUND
2.1 The Leeds health and social care system has been operating on revised national funding arrangements as a result of Covid and is subject to ongoing significant associated costs pressures. For NHS organisations the revised funding arrangements have been broken down into two phases.
2.2 Phase 1 of the NHS revised financial regime applied from April to September 2020, and the aim was to ensure that NHS organisations retained a balanced position during this period operated through a ‘top up’ regime. Leeds Clinical Commissioning Group (CCG) are still awaiting confirmation of associated August and September retrospective allocation to the value of £11m and this remains a significant risk.
2.3 Phase 2 applies from October 2020 until the end of March 2021. The CCG has submitted an operational plan for these six months to the West Yorkshire and Harrogate Integrated Care System (ICS) on 16th October for a consolidated submission to NHSEI, and a more detailed organisational plan on the same basis to NHSEI on 22nd October 2020 (Appendix A).
2.4 The plan assumes that the retrospective allocation for August/September of £11.3m is received in full and so the position at the end of September 2020 is breakeven. Based on the reduced allocations for the CCG for October to March, plus a share of the ICS covid allocation for these months, the CCG plan reflects a deficit position of £14.8m for these six months. Included within this is an unidentified QIPP figure of £2.4m.
2.5 The financial plan meets the requirements of the Mental Health Investment Standard (MHIS) and the Better Care Fund. However note that within the calculation of the MHIS assumptions have had to be made around block contract values which have been nationally mandated and which do not match the original planned contract values, and have had to be pro-ratad back to previous year splits.
2.6 The CCG holds no reserves or contingency.
2.7 The retained historic cumulative surplus for the CCG continues to equate to £35.6m (3% of original allocation as opposed to national requirement of 1%).
2.8 The plan does not include planned spend on the Hospital Discharge Programme (HDP) (£3m for M7-12) or spend on strategic Any qualified Providers (AQP)/local Independent Sector (IS) above a baseline (£3.6m for M7-12) as per the guidance from NHSEI. And so in that sense the expenditure in the plan is understated. The intent is that the spend on these areas will show in month as an overspend and be matched by a retrospective allocation. The process around HDP is ongoing and clear, that for AQP/IS and the elective incentive scheme less so.
2.9 Block payments to NHS providers, based on nationally mandated figures, with minor changes in the second half of the year, are continuing. So of the £1.3bn allocation for the

6
CCG £828m is committed for NHS providers. Budgets within the ledger are currently based on a mismatch of M1-6 budgets per the national model (with a shortfall of £11.3m based on the M05/M06 retro allocation not received) and planned spend for M7-12. Assuming that the M05/M06 retro allocation is received, budgets would be adjusted and the full year budgets are shown in Appendix B.
2.10 A process of close working between commissioners, finance and planners has been followed to produce the M7-12 budgets. Note that the first six months element of the full year budgets is based on actual spend and an assumption that the M05/M06 retrospective allocation will be received. And that the NHS element is nationally mandated for the full year. Note that unidentified QIPP of £2.4m is within “other” and the deficit is out with this. The budgets include the full retrospective allocation for M1-6 which is £22.5m. Work is ongoing to identify potential efficiencies to contribute to the gap.
2.11 The CCG’s Executive Team and Governing Body are reviewing their investment plans for 20-21 (and beyond) that were designed to tackle our Health Inequalities agenda and for which significant headroom had been created in 19-20 in preparation for these investments
2.12 A high level reconciliation of the flow of funds in and out of Leeds as a result of the COVID finance regime suggest that Leeds has ended up with a reduced level of resources as a Place. Therefore based on this assessment (and our deficit position which has emerged as a result of our allocation changes) our planned investments will now have to be stopped and in some areas, we will need to start to decommission services in order to remain within the revised and reduced allocation envelopes post these regime changes.
2.13 The NHS financial regime for 2021-22 is yet to be published but funding is expected to follow the principles in the 2020-21 M7-12 regime. This is expected to result in a significant reduction in available funds and there will be a need for urgent work to be undertaken across the system to balance the desired investments and real efficiency savings required to put the Leeds healthcare system in a strong position if the CCG budget is reduced by the c£50m anticipated.
2.14 The Left Shift Blueprint programme should give a sense of potential efficiencies for 2021-22, based on the current work to provide the top 3 priorities for each area.
3. PROPOSAL
3.1 The Governing Body is advised of the current position with the financial plan as per the plan submitted in late October to NHSE/I, which is a deficit of £14.8m, with further inherent risks (see risks section)
3.2 This plan will form the basis of high level and detailed budgets for the 2020- 2021 financial year. The budget levels will include inherent risks and rely on additional central resources whilst also recognizing the savings still to be found within the reported forecast position.
3.3 The Governing Body inevitably needs to balance its statutory duties to remain in financial balance while providing care for the population of Leeds, progressing with our health inequalities agenda and continuing with service developments that have already commenced prior to Covid. In the light of the changing financial position and the need to find significant efficiencies, some of our original planned initiatives will be delayed.
3.4 In order for the CCG to start to develop a cohesive plan for 2021-22 within the anticipated financial constraints, the Governing Body is asked to provide a steer around this balance in order to ensure financial sustainability, and limit risk to services, with due consideration to

7
the context of the wider system and the associated requirements to work closely with other organisations both at a Leeds place based level and at the wider ICS level
4. NEXT STEPS
4.1 Work will continue internally to identify potential efficiencies and any associated impact on services. There will also be ongoing work on both a place based and system basis to ensure that the there is a shared and cohesive financial understanding, and that the implications of decisions in one organization are understood and recognized across the system.
4.2 We will continue to bring updates to Governing Body on planning and budgets.
5. STATUTORY/LEGAL/REGULATORY/CONTRACTUAL
5.1 Not achieving balance is a breach of a statutory duty
6. FINANCIAL IMPLICATIONS AND RISK
6.1 Deficit of £14.8m, after assumptions of further resource allocations in 6.2 and 6.3, and assuming unidentified QIPP of £2.4m is found. Risk around the receipt of the anticipated retrospective allocation for Aug/Sept of £11.3m.
6.2 Anticipated further resource allocation of £8.8m in relation to national primary care allocations, Hospital Discharge Programme and national funding for strategically important local AQP/IS spend.
6.3 Unidentified QIPP of £2.4m to find as minimum, plus further requirement to contribute towards deficit
6.4 Leeds has the opportunity to deliver financial balance as a system if non recurrent support towards lost commercial income is received by local trusts.
6.5 Risks across Leeds as a place:
6.5.1 LTHT’s break even position relies not just on significant national support towards lost commercial income during the Pandemic but also on the continuation of their ambitious waste reduction programme which is progressing despite the challenges of COVID but is clearly also carrying more risk.
6.5.2 The Leeds and York Partnership FT position carries significant risks around the costs of out of area placements which is particularly challenging during the COVID Pandemic.
6.5.3 LCH are also facing fluctuating pressures to ensure out of hospital capacity and support is maintained during the current COVID waves with associated financial and service risks.
6.5.4 Whilst the Council has been significantly impacted by COVID its core funding has not been amended by government. However, in recognition of the pressures incurred by local authorities, in-year one-off grant funding has been received. Decisions being made now by the local authority will have implications for the health and care system going forward.
6.6 Further risks that are not quantifiable at this point include:
6.6.1 Any potential impact of Elective Incentive System, currently the status of this scheme and its impact is unclear, and relates to the whole system activity levels within the ICS, the NHS and non NHS sectors.

8
6.6.2 The impact of major Independent Sector contracts returning from national to local control.
6.6.3 The impact of Brexit on areas such as CCG prescribing. Prescribing spend has been very volatile to date, and the first four months spend from the NHS Business Services Authority this year is £3.5m higher than in 2019-20. This is due to drug switches and changes to recommended practice (NICE guidance), as well as price increases experienced over the past 7 months across a range of drugs.
6.7 The risk of increasing levels of Covid activity across the system could also impact on the position currently reported.
6.8 Implications for 2021-22 if the funding follows the principles in the 2020-21 M7-12 regime.
7. RECOMMENDATION
The Governing Body is asked to:
(a) NOTE the current position with the CCG financial plan for 2020-21, which is a deficit of £14.8m with further risk on top of. The plan was approved by the Accountable Officer and Chief Finance Officer as per the authority previously delegated by Governing Body. EMT, the CCG Chair and Lay Members have been kept abreast of the reported position as it evolved, during the Integrated Care System submission process;
(b) APPROVE the high level budgets for 2020-21, recognising the savings still to be found;
(c) DISCUSS and RECOMMEND how the CCG should proceed in the remainder of 2020-21 with balancing its statutory duties to provide care for the population of Leeds, progress with our health inequalities agenda and continue with service developments that have already commenced prior to Covid in the light of the changing financial position and the need to find significant efficiencies; and
(d) DISCUSS and RECOMMEND the approach to be adopted to develop a cohesive plan for 2021-22 within the anticipated financial constraints, to ensure financial sustainability, and limit risk to services. With due consideration to the context of the Place and the wider Integrated Care System (ICS) and the associated requirements to work closely with other organisations both at a Leeds place based level and at the wider ICS level.

9
Appendix A
Plan submission for October 2020 to March 2021(six months)
Revenue Resource Limit Total
Plan
31/03/2021
Year Ending
£'000
Total In-Year allocation 645,742
Expenditure
Acute 314,802
Mental Health 86,527
Community 75,911
Continuing Care 28,177
Primary Care 81,569
Other Programme 2,913
Primary Care Co-Commiss ioning 63,393
Total Programme Costs 653,292
Running Costs 7,280
Contingency 0
Total Costs 660,572
Underspend/(Defici t) In-Year Movement (14,830)
In-Year (RAG) 3
Net Risk/Headroom 2,176
Risk Adjusted Underspend/(Defici t) (12,654)
Risk Adjusted Underspend/(Defici t) (RAG) 3
Underlying pos i tion - Underspend/ (Defici t) (14,830)
Contingency 0
Noti fied Running Cost Al location 7,690
Running Cost 7,280
Under / (Overspend) 410
Population Size (000) 889
Spend per head (£) 8
Efficiencies 2,400
% of Recurrent Noti fied Resource 0.4%
BALANCE SHEET memorandum - Movement on historic underspend/(deficit)
Brought forward underspend/(defici t) 35,568
Underspend/(Defici t) M1 - M6 0
Underspend/(Defici t) M6 - M12 (14,830)
Balance carried forward 20,738
Risk Adjusted Underspend/(Defici t) Cumulative 22,914

10
Appendix B
2020-21 Budgets based on plan submissions
2020-21 2020-21 2020-21
NHS Leeds CCG
2020-21 High Level Budgets NHS NON NHS
Total
Budget
£'000 £'000 £'000
Programme ServicesAcute Services 596,696 29,481 626,177
Mental Health Services 116,651 52,687 169,338
Community Health Services 114,490 38,317 152,807
Continuing Care Services 63,826 63,826
Prescribing 134,378 134,378
Primary Care Services 33,028 33,028
Primary Care Co-Commissioning 125,854 125,854
Other 9,088 9,088
Total Programme Services 827,838 486,658 1,314,496
RUNNING COSTS 13,446 13,446
RESERVES 0
CONTINGENCY 0
CCG Net Expenditure 827,838 500,104 1,327,942
Allocations M1-6 M7-12 Total
Programme 578,145 571,207 1,149,352
Primary care co commissioning 61,244 60,951 122,195
Running Costs 5,446 7,690 13,136
Base allocations 644,835 639,848 1,284,683Retrospective allocation M1-4 11,203 11,203
Retrospective allocation M5/6 (currently under review at centre) 11,332 11,332
Share of ICS growth/covid pot 5,474 5,474
System Development Funding allocations 420 420
Non recurrent allocations 22,535 5,894 28,429Total allocations at time of plan 667,370 645,742 1,313,112
Surplus/(deficit) -14,830

1
Leeds Health & Wellbeing Strategy Outcomes – that this report relates to:
1. People will live longer and have healthier lives
2. People will live full, active and independent lives
3. People’s quality of life will be improved by access to quality services
4. People will be actively involved in their health and their care
5. People will live in healthy, safe and sustainable communities
NHS Leeds CCG Strategic Commitments We will focus resources to:
1. Deliver better outcomes for people’s health and wellbeing
2. Reduce health inequalities across our city
We will work with our partners and the people of Leeds to:
3. Support a greater focus on the wider determinants of health
4. Increase their confidence to manage their own health and wellbeing
5. Achieve better integrated care for the population of Leeds
6. Create the conditions for health and care needs to be addressed around local neighbourhoods
Assurance Framework – which risks on the GBAF does this report relate to: 1. Inadequate patient and public engagement results in ineffective decisions and challenge
2. Failure to assure the delivery of high quality services, leading to commissioned services not reflecting best practice and improving care
3. Failure to achieve financial stability and sustainability
4. Lack of provider and clinical support for change will impact on the development and implementation of the CCG strategy
5. Resources are not targeted effectively to areas of most need, leading to failure to improve health in the poorest areas
6. Insufficient workforce capacity, capability and adaptability to deliver the ambitions
7. Failure to enable partners to work together to deliver the CCG commitments
8. Failure of system to be adaptable and resilient in the event of a significant event
9. Inadequate system infrastructure to support the CCG’s plans.
Agenda Item: GB 20/90b FOI Exempt: N
NHS Leeds CCG Governing Body Meeting
Date of meeting: 25th November 2020
Title: Finance Report for the seven months ended 31st October 2020
Lead Governing Body Member: Visseh Pejhan-Sykes, Chief Finance Officer
Category of Paper Tick as
appropriate
()
Report Author: Judith Williams, Head of Corporate Reporting & Strategic Financial Planning
Decision
Reviewed by EMT/Date: N/A
Discussion
Reviewed by Committee/Date: N/A Information
Checked by Finance (Y/N/N/A - Date):
Approved by Lead Governing Body member (Y/N): Y

2
EXECUTIVE SUMMARY: This report provides an update on the financial performance of NHS Leeds Clinical Commissioning Group for the seven months to 31st October 2020, compared to the amended allocations for this period. Full year allocations have now been received. Baseline funding for the year, excluding retrospective allocation and other non-recurrent funding is £1,285m. This will have implications for planning for 2021-22 if the funding is on the same basis going forwards. The latest planning submission, for the six months October 2020 to March 2021 reflects a deficit position of £14.8m for the CCG. Leeds has the opportunity to deliver financial balance as a system if non recurrent support towards lost commercial income is received by local trusts. There are also a number of further material risks and assumptions around the current position, including receipt of additional allocations of c£20m. Of this £11.3m relates to retrospective allocation for August/September, still under review by NHSEI. £2m relates to anticipated primary care allocations. And £6.5m relates to funding for the Hospital Discharge Programme and support for strategic Any Qualified Provider/local Independent Sector activity. These latter costs are not currently within the forecast as per NHSEI guidance. The plan also includes unidentified QIPP of £2.4m, currently within other. Work is ongoing to identify efficiencies to cover this and potentially contribute towards improving the deficit position. The year to date position includes HDP spend of £0.8m, and spend on AQP/local IS of £0.5m, these will show as an overspend as budget for these was taken out of the plan (full year effect of both £6.5m). The anticipation is that these will be funded as a retrospective allocation. The process around HDP is clear and ongoing, that around AQP/local IS less so. As a result, to comply with current guidance, the October HDP spend is included in the forecast £0.8m, however the AQP/local IS spend is not. There is a small benefit relating to conditional system development funding for mental health, where spend was already in plan so receipt of allocations covers this (£155k). But this is offset by a retrospective element payable to Yorkshire Ambulance Service in relation to April 2020(£137k). Net impact is an improvement of £18k in the deficit position from £14,830k to £14,812k. Overspends by area mainly relate to variance as at end of September, which would be cleared if retrospective allocation for August/September was given.
NEXT STEPS: Updates on the 2020-21financial position will continue to be presented to the Governing Body and/or Executive Management Team (EMT) on alternate months to ensure that the CCGs’ financial position is formally reported and reviewed each month under the CCGs’ governance arrangements.
RECOMMENDATION: The Governing Body is asked to:

3
(a) CONSIDER the Month 7 financial position; and (b) DISCUSS, COMMENT and HIGHLIGHT ACTIONS required to progress and report to the next meeting of the Executive Management Team.

NHS Leeds Clinical Commissioning Group
Finance Report for the Seven Months ended 31st October 2020
Page 1

Financial Performance Report 31st October 2020
NHS Leeds Clinical Commissioning Group
At 31st October
2020 At Year End
2020-21 RAG RAG
CCG Expenditure does not exceed planned level
Programme spend less than allocation
Running costs spend less than allocation
Delegated Co-commissioning less than allocation
Planned Surplus in year
QIPP
Clear identification of risks against financial delivery & mitigations
Delivery of Mental Health Investment Standard (MHIS)Better Payment Practice Code - to pay 95% of valid invoices by due date or
within 30 days of receipt of a valid invoice, whichever is later
Cash at bank balance within 1.25% of the monthly amount requested or £250k,
whichever is greater
The current temporary financial regime means that most of the usual metrics are not achievable under these conditions, and so have not been RAG rated
Page 2

Overview 31st October 2020
This report provides an update on the financial performance of NHS Leeds Clinical Commissioning Group for the seven months to 31st October 2020, compared to the amended allocations for this period.
Full year allocations have now been received. Baseline funding for the year, excluding retrospective allocation and other non recurrent funding is £1,285m. This will have implications for planning for 2021-22 if the funding
is on the same basis going forwards.
The latest planning submission, for the six months October 2020 to March 2021 reflects a deficit position of £14.8m for the CCG. Leeds has the opportunity to deliver financial balance as a system if non recurrent support
towards lost commercial income is received by local trusts.
There are also a number of further material risks and assumptions around the current position, including receipt of additional allocations of c£20m. Of this £11.3m relates to retrospective allocation for August/September,
still under review by NHSEI. £2m relates to anticipated primary care allocations. And £6.5m relates to funding for the Hospital Discharge Programme and support for strategic Any Qualified Provider/local Independent
Sector activity. These latter costs are not currently within the forecast as per NHSEI guidance. The plan also includes unidentifed QIPP of £2.4m, currently within other. Work is ongoing to identify efficiencies to cover this
and potentially contribute towards improving the deficit position.
The year to date position includes HDP spend of £0.8m, and spend on AQP/local IS of £0.5m, these will show as an overspend as budget for these was taken out of the plan (full year effect of both £6.5m). The anticipation is
that these will be funded as a retrospective allocation. The process around HDP is clear and ongoing, that around AQP/local IS less so. As a result, to comply with current guidance, the October HDP spend is included in the
forecast £0.8m, however the AQP/local IS spend is not.
There is a small benefit relating to conditional system development funding for mental health, where spend was already in plan so receipt of allocations covers this (£155k). But this is offset by a retrospective element
payable to Yorkshire Ambulance Service in relation to April 2020(£137k). Net impact is an improvement of £18k in the deficit position from £14,830k to £14,812k. Overspends by area mainly relate to variance as at end of
September, which would be cleared if retrospective allocation for August/September was given.
Page 3
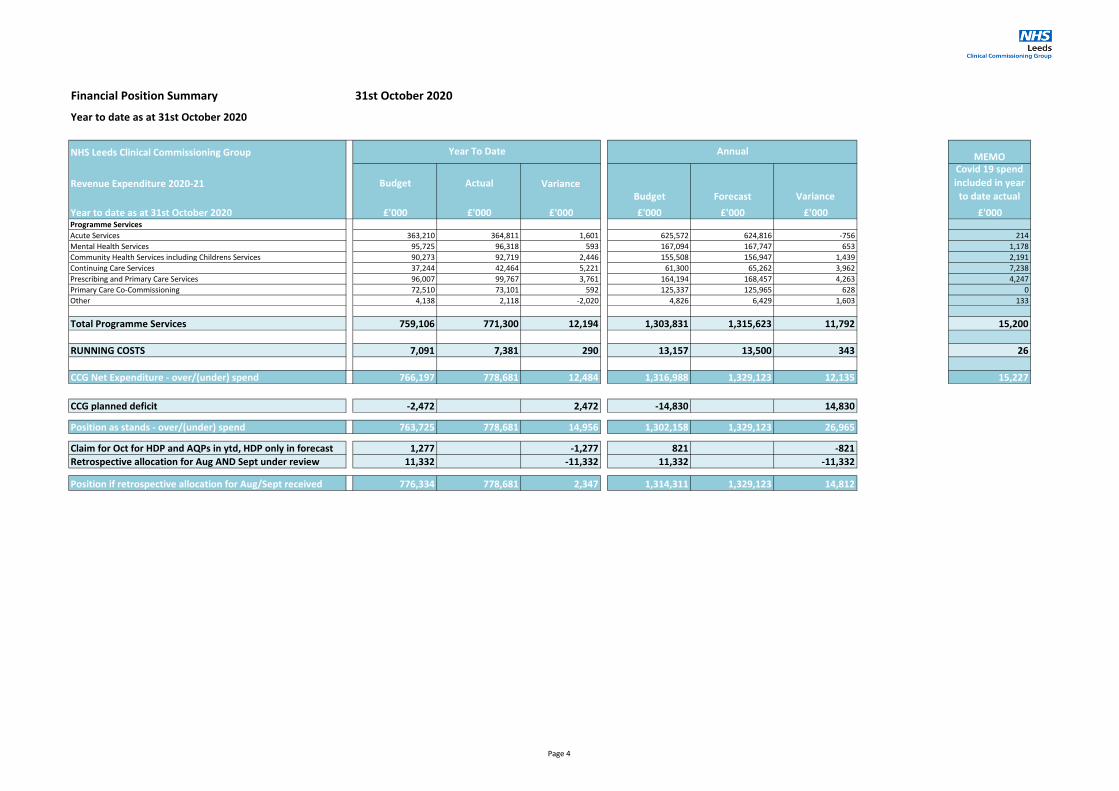
Financial Position Summary 31st October 2020
Year to date as at 31st October 2020
NHS Leeds Clinical Commissioning Group MEMO
Revenue Expenditure 2020-21 Budget Actual VarianceBudget Forecast Variance
Covid 19 spend
included in year
to date actual
Year to date as at 31st October 2020 £'000 £'000 £'000 £'000 £'000 £'000 £'000Programme Services
Acute Services 363,210 364,811 1,601 625,572 624,816 -756 214
Mental Health Services 95,725 96,318 593 167,094 167,747 653 1,178
Community Health Services including Childrens Services 90,273 92,719 2,446 155,508 156,947 1,439 2,191
Continuing Care Services 37,244 42,464 5,221 61,300 65,262 3,962 7,238
Prescribing and Primary Care Services 96,007 99,767 3,761 164,194 168,457 4,263 4,247
Primary Care Co-Commissioning 72,510 73,101 592 125,337 125,965 628 0
Other 4,138 2,118 -2,020 4,826 6,429 1,603 133
Total Programme Services 759,106 771,300 12,194 1,303,831 1,315,623 11,792 15,200
RUNNING COSTS 7,091 7,381 290 13,157 13,500 343 26
CCG Net Expenditure - over/(under) spend 766,197 778,681 12,484 1,316,988 1,329,123 12,135 15,227
CCG planned deficit -2,472 2,472 -14,830 14,830
Position as stands - over/(under) spend 763,725 778,681 14,956 1,302,158 1,329,123 26,965
Claim for Oct for HDP and AQPs in ytd, HDP only in forecast 1,277 -1,277 821 -821
Retrospective allocation for Aug AND Sept under review 11,332 -11,332 11,332 -11,332
Position if retrospective allocation for Aug/Sept received 776,334 778,681 2,347 1,314,311 1,329,123 14,812
Year To Date Annual
Page 4

Allocations 31st October 2020
NHS Leeds Clinical Commissioning Group
Allocations 2020-21
£'000 £'000 £'000 £'000
Opening Baseline Allocation Apr to July 2020 385,430 3,631 40,829 429,890
Subtotal Month 3 Adjustments 2,596 267 0 2,863
Subtotal Month 4 Adjustments 1,637 76 0 1,713
Baseline Allocation Aug to Sep 2020 192,715 1,815 20,415 214,945
Retrospective allocation 5,839 88 700 6,627
Subtotal Month 5 Adjustments (incl baseline Aug/Sept) 198,554 1,903 21,115 221,572
Subtotal Month 6 Adjustments 0 0 0 0
Baseline for October 2020 to March 2021 571,207 7,690 60,951 639,848
STP Plan Transfer - System Covid distribution to other CCGs 5,474 5,474
CYPMH Green Paper 400 400
Tobacco Early Implementer Sites 20 20
Adult MH - Individual Placement Support (IPS) -(Conditional SDF) 142 142
Learning Disabilities Mortality Review Programme (LeDeR) (Conditional SDF) 13 13
Community/CETR - (Conditional SDF) 223 223
Subtotal Month 7 Adjustments (baseline Oct to March) 577,479 7,690 60,951 646,120
Closing Allocation 1,165,696 13,567 122,895 1,302,158
MEMO: Full Year Baseline Allocation 1,149,352 13,136 122,195 1,284,683
Month 07 allocations
Running CostsCo-
commissioning
IN YEAR
ALLOCATIONProgramme
Note that no retrospective allocation has been received at this point in respect of top up or covid reimbursement for M05 or M06. This is still under review by NHSE and an update is expected in late November. This is
£11.3m for Leeds CCG
Allocations received in M07 are the baseline allocations for M7-12 (£639,848k), plus a share of the ICS covid allocation (£5.5k), and non recurrent amounts for specific areas under the umbrella of System Development
Funding (SDF) (£798k)
Page 5
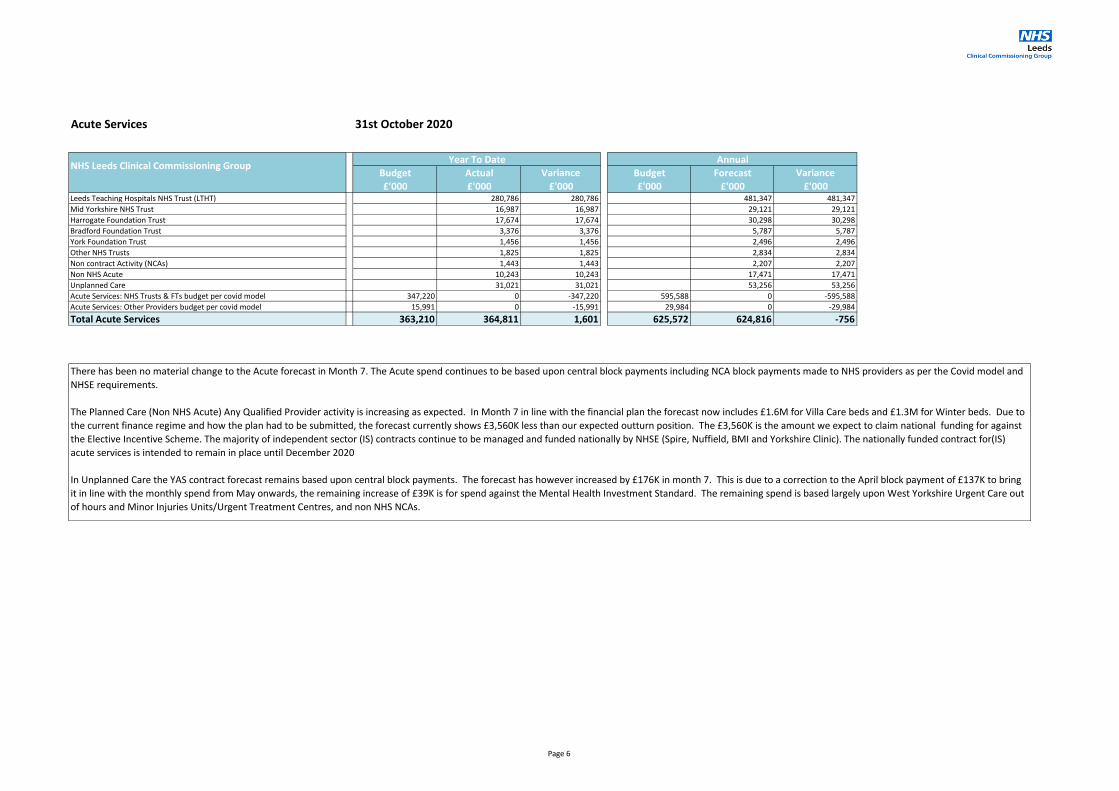
Acute Services 31st October 2020
Budget Actual Variance Budget Forecast Variance
£'000 £'000 £'000 £'000 £'000 £'000Leeds Teaching Hospitals NHS Trust (LTHT) 280,786 280,786 481,347 481,347
Mid Yorkshire NHS Trust 16,987 16,987 29,121 29,121
Harrogate Foundation Trust 17,674 17,674 30,298 30,298
Bradford Foundation Trust 3,376 3,376 5,787 5,787
York Foundation Trust 1,456 1,456 2,496 2,496
Other NHS Trusts 1,825 1,825 2,834 2,834
Non contract Activity (NCAs) 1,443 1,443 2,207 2,207
Non NHS Acute 10,243 10,243 17,471 17,471
Unplanned Care 31,021 31,021 53,256 53,256
Acute Services: NHS Trusts & FTs budget per covid model 347,220 0 -347,220 595,588 0 -595,588
Acute Services: Other Providers budget per covid model 15,991 0 -15,991 29,984 0 -29,984
Total Acute Services 363,210 364,811 1,601 625,572 624,816 -756
Year To DateNHS Leeds Clinical Commissioning Group
Annual
There has been no material change to the Acute forecast in Month 7. The Acute spend continues to be based upon central block payments including NCA block payments made to NHS providers as per the Covid model and
NHSE requirements.
The Planned Care (Non NHS Acute) Any Qualified Provider activity is increasing as expected. In Month 7 in line with the financial plan the forecast now includes £1.6M for Villa Care beds and £1.3M for Winter beds. Due to
the current finance regime and how the plan had to be submitted, the forecast currently shows £3,560K less than our expected outturn position. The £3,560K is the amount we expect to claim national funding for against
the Elective Incentive Scheme. The majority of independent sector (IS) contracts continue to be managed and funded nationally by NHSE (Spire, Nuffield, BMI and Yorkshire Clinic). The nationally funded contract for(IS)
acute services is intended to remain in place until December 2020
In Unplanned Care the YAS contract forecast remains based upon central block payments. The forecast has however increased by £176K in month 7. This is due to a correction to the April block payment of £137K to bring
it in line with the monthly spend from May onwards, the remaining increase of £39K is for spend against the Mental Health Investment Standard. The remaining spend is based largely upon West Yorkshire Urgent Care out
of hours and Minor Injuries Units/Urgent Treatment Centres, and non NHS NCAs.
Page 6

Mental Health Services 31st October 2020
Budget Actual Variance Budget Forecast Variance
£'000 £'000 £'000 £'000 £'000 £'000Leeds and York Partnership Foundation Trust (LYPFT) 65,123 65,123 113,696 113,696
Tees Esk and Wear Valley NHS Foundation Trust (TEWV) 783 783 1,342 1,342
South West Yorkshire Partnership Foundation Trust 759 759 1,301 1,301
Bradford District Care NHS Foundation Trust 100 100 100 100
Mental Health NHS budget 0 0 0 0
Independent/Voluntary Sector/LCC/Other NHS 3,891 3,891 6,768 6,768
Learning Disabilities 19,219 19,219 32,977 32,977
Improving Access to Psychological Therapies (IAPT) 335 335 1,339 1,339
Mental Health Specialist Services 5,749 5,749 9,781 9,781
Mental Health Non Contract Activity (NCA) 213 213 220 220
Mental Health Other 147 147 223 223
Mental Health Services: NHS Trusts & FTs budget per covid model 67,773 0 -67,773 117,448 0 -117,448
Mental Health Services: Other Providers budget per covid model 27,951 0 -27,951 49,646 0 -49,646
Total Mental Health Services 95,725 96,318 593 167,094 167,747 653
NHS Leeds Clinical Commissioning Group Year To Date Annual
The block payments to Leeds and York Partnership Foundation Trust have increased for months 7-12 increasing the 12 month forecast by £2.8m all reflected in months 7-12, increasing expenditure in the second half of the
year.
The other significant increase to forecast is the inclusion of the commissioning intention to clear the IAPT backlog of £1.07m again reflected in the second half of the year.
There is a small reduction of £198k in the 12 month forecast for Rotherham Doncaster and South Humber NHS Foundation Trust (MH NCAS) and a reduction of £100k for Bradford District Care Trust, as the block payments
to these providers have stopped from October as they are below the de-minimum payment limit.
Page 7

Community Health Services 31st October 2020
Budget Actual Variance Budget Forecast Variance
£'000 £'000 £'000 £'000 £'000 £'000Leeds Community Healthcare NHS Trust (LCH) 67,373 67,373 114,490 114,490
Community Reserves 0 0 0 0
Voluntary Sector/Local Authority (LA) 11,966 11,966 20,783 20,783
Community Beds 4,747 4,747 8,024 8,024
Hospices 3,435 3,435 5,881 5,881
Reablement 3,492 3,492 4,662 4,662
Safeguarding 441 441 761 761
Community Health Services: NHS Trusts & FTs budget per covid model 62,722 0 -62,722 110,007 0 -110,007
Community Health Services: Other Providers budget per covid model 27,551 0 -27,551 45,501 0 -45,501
Sub Total Community Health Services 90,273 91,454 1,182 155,508 154,602 -907Children's Services excluding Continuing Care 1,265 1,265 2,346 2,346
Total Community Health Services including Childrens 90,273 92,719 2,446 155,508 156,947 1,439
Year To Date AnnualNHS Leeds Clinical Commissioning Group
Community Services
The main change in the 12 month forecast is a reduction in the Leeds Community Healthcare NHS Trus block payment which reduces the 12 month forecast by £1,007k.
In Voluntary Sector the 12 month forecast has increased with the inclusion in months 7-12 of £242k for the East Recovery Hub (part of the £3.5m Winter Beds), however there will be less expenditure in the second half of
the year due to non-continuation of Covid expenditure of £334k at the Leeds Equipment Store which is in months 1-6 only.
In Reablement there is no change to the 12 month total forecast however there is Covid expenditure in the first 6 months only of £1,855k which significantly reduces the amount to be paid in the second half of the year.
No material change to any other area
Children's Services
The 12 month forecast has not changed materially from month 6. There will be slightly more expenditure in the second half of the year as the commissioning intention for the Family Drugs and Alcohol team at LCC will be
paid
Page 8

Continuing Care Services 31st October 2020
Budget Actual Variance Budget Forecast Variance
£'000 £'000 £'000 £'000 £'000 £'000Continuing Healthcare (CHC) 25,300 25,300 36,882 36,882
Continuing Healthcare Personal Health Budgets (PHBs) 8,507 8,507 14,597 14,597
Funded Nursing Care (FNC) 4,474 4,474 7,127 7,127
Children Continuing Care including PHBs 729 729 1,252 1,252
Continuing Healthcare - operational 1,457 1,669 212 2,222 2,723 501
Neuro-rehab 1,785 1,785 2,681 2,681
Continuing Care Services: NHS Trusts & FTs budget per covid model 113 0 -113 113 0 -113
Continuing Care Services: Other Providers budget per covid model 35,674 0 -35,674 58,966 0 -58,966
Total Continuing Care Services 37,244 42,464 5,221 61,300 65,262 3,962
AnnualNHS Leeds Clinical Commissioning Group
Year To Date
Continuing Care Services:
The CHC year to date has increased by £800k for Hospital Discharge Programme (HDP) Covid related costs as of month 7. As per NHSE guidance, any further spend for HDP from Nov to Mar has not been included in the
forecast outturn.
Page 9

Prescribing and Primary Care Services 31st October 2020
Budget Actual Variance Budget Forecast Variance
£'000 £'000 £'000 £'000 £'000 £'000Prescribing (budget as per covid model) 75,783 76,703 920 130,047 131,491 1,444
Ex centrally funded drugs 2,173 2,173 3,773 3,773
Oxygen contract 565 565 1,040 1,040
Primary Care Schemes 16,429 16,429 25,538 25,538
Clinical Leads 310 310 543 543
Primary Care - GP Information Technology (GP IT) 1,555 1,555 2,565 2,565
Out Of Hours 35 35 65 65
Medicines Optimisation NHSE Non Recurring Funded Projects 196 160 -36 196 196 0
Primary Care Services: NHS Trusts & FTs budget per covid model 374 0 -374 374 0 -374
Primary Care Services: Other Providers budget per covid model 18,057 0 -18,057 30,839 0 -30,839
Sub Total Prescribing and Primary Care Services 94,410 97,930 3,520 161,456 165,212 3,756Prescribing Staff 1,009 920 -90 1,730 1,688 -43
Primary Care Staff 464 498 34 795 837 41
Confederation Staff and Delivery Costs 124 420 296 212 721 509
Sub Total GP Confederation 1,597 1,837 240 2,738 3,246 508
Total Prescribing & Primary Care Services 96,007 99,767 3,761 164,194 168,457 4,263
Primary Care: Forecast spend is anticipated to be in line with original plans, and includes additional expenditure relating to Covid 19. The position for the year shows the impact of schemes from the original plan, with a
slight decrease for the year due to anticipated expenditure no longer materialising.
AnnualNHS Leeds Clinical Commissioning Group
Year To Date
GP Confederation: Budget set for embedded staff costs only. Forecast includes delivery costs which were planned to be funded from transformation.
GP IT: Overall spend for the remainder of the year is expected to continue at a similar level as Apr to October, with a reduction in Covid related spend.
Staffing: Prescribing staffing underspends relates to vacancies. Primary Care Staff overspend relates to additional Covid 19 Costs
Prescribing (inc centrally funded drugs and out of hours): August 2020 data has now been received and the data shows a decrease compared to previous months . Year to date costs remain £4.1M more compared to
previous year’s costs at the end of August 2019. The Prescribing forecast for the year is an estimated £7.4m overtrade against planned budgets and includes adverse impacts in relation to final 19/20 expenditure. The
forecast assumes there will be increases in the next few months due to seasonal demand and continued effects due to Covid 19, the expected costs are estimated to be more in line with the higher April-July 2020 costs.
Home Oxygen includes a year-end benefit and expenditure in relation to Covid 19.
Page 10

Primary Care Co-Commissioning 31st October 2020
Budget Actual Variance Budget Forecast Variance£'000 £'000 £'000 £'000 £'000 £'000
GMS 18,155 19,227 1,071 31,124 32,960 1,836
PMS 29,478 29,946 468 50,535 51,337 802
APMS 6,017 6,262 246 10,146 10,735 590
Premises cost reimbursements 8,882 8,975 93 15,226 15,385 159
Other premises costs 587 498 -90 1,006 853 -153
Enhanced Services 1,589 1,888 299 2,664 3,236 572
QOF 5,741 6,100 359 9,841 10,457 616
Other GP Services(inc PCO) 2,060 85 -1,976 4,795 793 -4,002
Reserves 0 121 121 0 208 208
Total Primary Care Co-Commissioning 72,510 73,101 592 125,337 125,965 628
Year To DateNHS Leeds Clinical Commissioning Group
Annual
Co-Commissioning expenditure is expected to remain in-line with the original pre Covid planned expenditure. This would have included transferring £1.8m budget from primary care budgets to cover the equitable funding
scheme as in previous years.
Page 11

Other Services 31st October 2020
Budget Actual Variance Budget Forecast Variance
£'000 £'000 £'000 £'000 £'000 £'000
Total Other Services 4,138 2,118 -2,020 4,826 6,429 1,603
Year to date underspend relates to the fact that M1-6 budget includes a significant amount set per the national model to cover PTS/111, but the costs are wrapped up in acute spend. This has been adjusted for in M7-12
and would be corrected for M1-6 if retrospective allocation is given and CCG is able to amend budgets for that period.
Forecast overspend reflects that a negative budget for unidentifed QIPP of £2.4m in M7-12 has been set here. Schemes are currently being worked up across different areas to provide efficiences in future months.
NHS Leeds Clinical Commissioning Group Year To Date Annual
Page 12

Running Costs 31st October 2020
Budget Actual Variance Budget Forecast Variance£'000 £'000 £'000 £'000 £'000 £'000
Pay, set on establishment, as per original allocation 5,850 5,559 -291 10,029 9,651 -377
Non Pay/Income, set as per original allocation 2,538 1,822 -715 5,351 3,849 -1,502
Defund/negative budget to match covid model -1,297 0 1,297 -2,223 0 2,223
Total Running Costs (incl retrospective allocation) 7,091 7,381 290 13,157 13,500 343
NHS Leeds Clinical Commissioning Group Year To Date Annual
Additional allocation has been provided for the remander of the financial year in line with anticipated spend. However, the £290k overspend for Aug and Sep is still under review by NHSEI as part of retrospective allocation,
and forecast outturn including this is now £343k overspent. Current vacancies and an underspend on non pay would have shown an underspend against pre Covid 19 original NHS England notified budget allocation of
£15.380m.
Page 13

Consolidated Statement of Financial Position
31st October 202031st October
2020
31st March
2020
£'000 £'000
Current AssetsTrade & Other Receivables 78,198 7,882
Cash & Cash Equivalents 464 315
Total Current Assets 78,662 8,197
Total Assets 78,662 8,197
Current LiabilitiesTrade & Other Payables: (56,946) (58,903)
Borrowings 0 0
Provisions (392) (538)
Total Current Liabilities (57,338) (59,441)
Total Assets less Current Liabilities 21,324 (51,244)
Non-current LiabilitiesProvisions (6,530) (5,650)
Total Non-current Liabilities (6,530) (5,650)
Total Assets Employed 14,794 (56,894)
Financed by Taxpayers’ EquityGeneral Fund 14,794 (56,894)
Total Taxpayers’ Equity 14,794 (56,894)
The significant movement of total assets employed is mainly due to measures taken to support the temporary financial regime to ensure NHS Providers have certainty regarding cash inflows in response to Covid-19;
notably the nationally mandated NHS block monthly payments in advance from April onwards (£68.9m per month).
Page 14

1
Leeds Health & Wellbeing Strategy Outcomes – that this report relates to:
1. People will live longer and have healthier lives
2. People will live full, active and independent lives
3. People’s quality of life will be improved by access to quality services
4. People will be actively involved in their health and their care
5. People will live in healthy, safe and sustainable communities
NHS Leeds CCG Strategic Commitments We will focus resources to:
1. Deliver better outcomes for people’s health and wellbeing
2. Reduce health inequalities across our city
We will work with our partners and the people of Leeds to:
3. Support a greater focus on the wider determinants of health
4. Increase their confidence to manage their own health and wellbeing
5. Achieve better integrated care for the population of Leeds
6. Create the conditions for health and care needs to be addressed around local neighbourhoods
Assurance Framework – which risks on the GBAF does this report relate to: 1. Failure to deliver the CCG commitment to reduce health inequalities across our city.
2. Quality of commissioned care is compromised and does not reflect best practice.
3. Failure to achieve financial stability and sustainability.
4. Failure to overcome local and national workforce shortages.
5. Business continuity of health and care services disrupted as a result of a significant event.
6. Ineffective patient and public engagement and lack of transparency in translation of engagement into decisions.
7. Partners and Professionals do not support the CCG strategy.
8. Constraints on CCG organisational effectiveness impact the delivery of the CCG’s plans.
9. Inadequate system infrastructure to support the CCG’s plans.
Agenda Item: GB 20/91 FOI Exempt: N
NHS Leeds CCG Governing Body Meeting
Date of meeting: 25 November 2020
Title: Corporate Risk Register (Operational Risks)
Lead Governing Body Member: Sabrina Armstrong, Director of Organisational Effectiveness
Category of Paper Tick as
appropriate
()
Report Author: Anne Ellis, Risk Manager
Decision
Reviewed by EMT/Date: 28 October 2020 Discussion
Reviewed by Committee/Date: Quality and Performance Committee 11 November 2020
Information
Checked by Finance (Y/N/N/A - Date): N/A
Approved by Lead Governing Body member (Y/N): Y

2
EXECUTIVE SUMMARY:
1. The CCG uses Datix as an internal risk management system which enables operational
risks to be recorded and managed by all members of staff. Risks are aligned to the
appropriate CCG committee for overview and scrutiny.
2. The risks are included on the CCG operational risk register and reviewed within
individual directorates on a regular basis. In line with the Risk Management Strategy,
the Executive Management Team (EMT) and relevant CCG Committees receive and
review the operational risks rated as high amber (12) and above. The CCG Governing
Body receives the corporate risk register (all red operational risks scored at 15 and
above) for review at each meeting, supported by the CCG committee chair updates.
Summary Table
Current Previous (Sept 20)
Total Risks 68 66
Red Risks 15+ 5 2
Amber 12+ 10 9
Accepted Risks 25 26
New Risks 2 7
Closed Risks 0 1
Accepted Risks
3. There are currently 68 active risks on the CCG risk register, 25 of these risks are
categorised as ‘Accepted’ risks. This means that the current level of risk is deemed
acceptable. Accepted risks are risks that are at, or below, the target risk score
(approved by the responsible Director) or are green on the risk matrix (score <6). These
risks are reviewed by management at least on an annual basis or when the CCG
becomes aware of a change to the risk. High amber (12) or red risks are unlikely to be
accepted and will continue to be reported to the relevant Committee and Governing
Body.
Corporate Risks
4. There has been an increase from 2 to 5 red risks, the following changes have taken place:
a. R732 – Risk of Harm post Covid-19 (Planned Care and Mental Health): the risk has increased from 12 to 20. The likelihood of harm is now certain for some patients waiting for treatment, with an impact of a significant reduction in health outcomes and / or life expectancy.
b. R729 – Risk of Harm post Covid-19 (Primary Care): the risk has increased from 12 to 16. The impact of the mitigating actions in relation to capacity and workforce on the changing situation is unknown and therefore the current score has been aligned with the unmitigated score.
c. R707 – System Flow: the risk has increased from 12 to 16. The risk is more challenging to manage due to the more complex Infection Prevention Control (IPC) requirements needed to manage Covid-19 related demand.

3
A summary of the corporate risks is provided in the table below but further detail,
including controls, actions and assurances, can be seen in Appendix 1.
Ris
k I
D
Ris
k T
itle
Current Position
Risk Rating
Cu
rren
t
Previous
Ta
rge
t S
co
re
Ta
rge
t D
ate
Ch
an
ges t
o
Ta
rge
t D
ate
Sep
t 20
Ju
ly 2
0
732
Ris
k o
f h
arm
durin
g a
nd p
ost
Co
vid
-19 (
Pla
nn
ed
Ca
re a
nd
Me
nta
l H
ealth
)
Risk score increased from 12 to 20. The
likelihood of harm is now certain for
patients waiting for treatment, with risk of a
significant reduction in health outcomes
and / or life expectancy.
Recovery has been progressing well over
the summer, however, given the surge in
Covid-19 cases, the recovery will be
impacted and it is expected that backlogs
will increase further. Detail of the impact of
Covid-19 has been included in appendix 1.
Phase 3 action plans in place; these will
be reviewed at each monthly planned care
meeting. Due date set to 31/3/21 as
review is ongoing.
20 12 9
31/0
3/2
02
1
0
548
Sta
tuto
ry F
inan
cia
l D
uties
Work is ongoing to understand and
challenge national assumptions in relation
to the Phase 3 Covid-19 financial regime
and associated allocations; challenge
regarding flaws in way the allocations
have been derived nationally. Work is
ongoing with WY&H ICS to balance the
ICS position. Work is ongoing across
Leeds place to mitigate Leeds system
shortfall. Work is ongoing in Leeds CCG
to reduce non-committed commissioning
intentions, investments and other spend.
All non-committed expenditure suspended
until further notice.
16 16 4 4
31/1
0/2
02
1
0

4
Risks Aligned to the Governing Body
5. There are 14 risks aligned to the Governing Body. These relate to Finance,
Procurement and the Shaping Our Future programme. Six of these 14 risks are
categorised as ‘Accepted’ risks.
707
Syste
m F
low
Risk score increased from 12 to 16. The
risk is more challenging to manage due to
the more complex IPC requirements
needed to manage Covid-19 related
demand.
The Winter Resilience Plan refresh is
ongoing, and includes planned Covid-19
specific winter responses and trigger
actions to enact as a result of surges in
demand.
StaR Group formalised as Silver response
and providing escalation forum from
pressures identified at Bronze.
16 12 12 8
2/8
/202
1
0
729
Ris
k o
f h
arm
durin
g a
nd p
ost
Co
vid
-19
(Prim
ary
Care
)
The risk has been reviewed and the score
increased to 16. The impact score has
been increased due to the increasing rate
of Covid-19 cases, patients waiting for
elective surgery needing to manage their
symptoms for longer and the impact of this
on the quality of life. The impact of the
mitigating actions in relation to capacity
and workforce on the changing situation is
unknown and therefore the current score
has been aligned with the unmitigated
score.
There is limited funding available to
support practices with staff absences and
therefore impacting further on the backlog.
16 12 9
31/0
3/2
02
1
0
721
Info
rmatio
n S
ecurity
Ma
turity
The risk score remains red, mitigating
actions are recorded in the Penetration
Test action plan. The action plan is risk
rated and implementation is overseen by
the Business Intelligence, Information
Governance and Information Technology
Assurance Committee.
15 15 15 9
01/0
3/2
02
1
0

5
Current Previous (Sept 20)
Total Risks 14 14
Red Risks 15+ 1 1
Amber 12+ 1 1
Accepted Risks 6 6
New Risks 0 1
Closed Risks 0 0
6. Of the remaining eight risks aligned to the Governing Body, there is currently one red
corporate risk and one high amber risk. The red corporate risk is summarised above at
paragraph 4 (R548: Statutory Financial Duties) ; the high amber risk is summarised
below, but further detail of the risks, including controls and assurances, can be seen in
Appendix 1.
Covid-19 Risks
7. Risks and issues specifically relating to COVID-19 continue to be logged within task
groups, and are escalated by exception through the command structure via SitReps.
Strategic risks and red risks are reported to Gold Command by exception.
8. All operational risks continue to be monitored where they are impacted by the outbreak.
Ris
k I
D
Ris
k T
itle
Current Position
Risk Rating C
urr
en
t
Previous
Ta
rge
t S
co
re
Ta
rge
t D
ate
Ch
an
ges t
o
Ta
rge
t D
ate
Sep
t 20
Ju
ly 2
0
719
Sh
ap
ing O
ur
Futu
re –
Imp
act
on S
taff
Risk score remains at 12 due to:
The impact on current remote
working arrangements and general
levels of staff anxiety during Covid-
19. This is key to considerations in
the way in which the SOF programme
has been re-started and delivered
remotely.
The publication of the operating
model makes the programme real to
staff and could increase the likelihood
of some staff leaving.
Additional controls and actions have
been identified and added to Datix.
12 12 12 6
31/1
2/2
02
0
0

6
NEXT STEPS:
All operational risks will be reviewed as per the bi-monthly cycle in accordance with the CCG risk management strategy and presented to the assigned committee for review. The Corporate Risk Register and high amber risks aligned to the Governing Body will be presented to the CCG Governing Body at each meeting.
Risks arising from the COVID-19 outbreak will continue to be monitored and escalated by exception via the command structure.
RECOMMENDATION: The Governing Body is asked to:
(a) REVIEW the five corporate risks; (b) REVIEW the high scoring amber risk aligned to the Governing Body; and, for each
risk; (c) CONSIDER whether the controls, actions are effective and whether assurances are
sufficiently robust; and (d) AGREE any further actions required to manage the risks to the target level set.

ID
Titl
e
Op
ened
Description
Rev
iew
dat
e
Acc
ou
nta
ble
Dir
ecto
r
Man
age
r
Co
mm
itte
e
Res
po
nsi
ble
Co
nse
qu
ence
Like
liho
od
Rat
ing
Controls Assurance
Co
nse
qu
ence
Like
liho
od
Rat
ing
Gaps in controls Gaps in assurance
Is t
he
risk
aff
ecte
d
or
as a
res
ult
of
Co
vid
-19
?
Please provide details Actions
Co
nse
qu
ence
Like
liho
od
Rat
ing
Exp
ecte
d d
ate
to
reac
h t
arge
t gr
adin
g
732
Ris
k o
f h
arm
du
rin
g an
d p
ost
-Co
vid
-19
19
(P
lan
ne
d C
are
and
Men
tal H
ealt
h)
07
/08
/20
20
There is a risk of harm due to 1) Patients not
presenting with symptoms due to Covid-19
fears/concerns, including some urgent
presentations/referrals 2) Routine referral routes
into hospital settings being stopped from approx.
26th March through to June 2020, and 3) The
backlog generated in terms of patients waiting for a
diagnostic, first outpatient appointment, follow-up
or surgery - all resulting in potentially increased
morbidity, mortality and widening of health
inequalities. While Mental Health services in the
main remained open, some of our more specialist
services were closed while staff were redeployed,
and some of our services have been delivered in
non face to face ways that may have been less
accessible. There is therefore some evidence of
increased demand both linked to reduced services
but also due to increased pressure on mental
health conditions during lockdown.
15
/10
/20
20
Hel
en L
ewis
Lew
is,
Hel
en
Qu
alit
y an
d P
erfo
rman
ce C
om
mit
tee
Maj
or
Exp
ecte
d t
o o
ccu
r in
mo
st c
ircu
mst
ance
s.
20
Stabilisation and reset group formed.
Work has also been undertaken to identify and prioritise the highest risk
patients.
Planned Care team have worked to coordinate recovery plans with our
local AQP providers; i.e. backlog at LTHT worked through tackling longest
waiters/urgent cases first for ophthalmology, ENT and gastro/endoscopy.
Working with LTHT to track/manage backlog utilising NHSE Sourced IS
contracts.
Close working with Cancer Alliance to manage cancer backlog and PTL.
Currently working with LTHT to write to all patients waiting longer than 18
weeks with advise re pain management and how they might manage
symptoms whilst waiting for an appointment.
Focused work across pathways undertaken for LTCs via Diabetes,
Respiratory and CVD Steering Groups, with recommendations reviewed by
our Leeds LTCs programme board.
Mental health partners working together to see how they can further
expand capacity using 3rd sector partners and new ways of working, and a
focus on primary care MH offers to help preventative approaches as far as
possible.
Reviewing Mental Health Issues at System Rest Group, involving all
partners
Waiting times/progress monitored via Planned Care
programme board with LTHT and IS/LTHT weekly meetings.
The Commissioning team is working closely with quality
colleagues to identify and address themes arising from
incidents reported on Datix and from soft intelligence.
Close monitoring of mental health demand through
fortnightly system calls
Maj
or
Exp
ecte
d t
o o
ccu
r in
mo
st c
ircu
mst
ance
s.
20
Implementation of actions identified from
Phase 3 letter Yes
Number of patients waiting over 18 weeks for First Outpatient Appointment totalled
18,440 in September (down on previous months), but higher than pre-Covid-19 levels
(8,800 in March). Outpatient activity during September was 90% (with majority of
contacts non-face-to-face). There is a risk that recovery will now be impacted due to
growing Covid-19 cases within LTHT and staff absence due to illness/isolation and
caring requirements; i.e. children. The number of patients waiting over 18 weeks is
likely to increase during November, as first week in November will mark 18 weeks
since services were reinstated in June.
35,700 patients are waiting long than 3 months for an appointment, which is a
significant risk particularly in the area of ophthalmology, where there is a risk of
harm relating to sight loss. In the specialty of ophthalmology, 7964 patients are
currently waiting longer than 3 months for a follow-up appointment with 915
ophthalmology patients also waiting over 18 weeks for a first outpatient
appointment. Meetings are taking place with LTHT to agree a joint approach to
recovery with AQP/CLODN members.
13,700 patients are currently awaiting a diagnostic at LTHT; diagnostic capacity at
LTHT is currently at 82% of pre-Covid-19 levels due to social distancing; which is a
great achievement. Patients waiting longer than 52 weeks totalled 1606 at the end of
September, in the specialities of urology, colorectal, adult spines, paediatric urology
and dentistry. Urgent referral rates have returned to pre-Covid-19 levels; with the
cancer 2ww referral rate exceeding pre-Covid-19 levels at 104%. The rate of other
'urgent' referrals is at 77%; this requires attention.
Referrals into mental health services are also increasing.
Phase 3 Action Plan
Mo
der
ate
Mig
ht
occ
ur
at s
om
e ti
me.
9
31
/03
/20
21
548
Stat
uto
ry F
inan
cial
Du
ties
27/1
1/20
15
There is a risk of overspend; due to unforeseen
financial pressures; resulting in failing to achieve
statutory financial duties e.g. Planned Surplus,
Running Cost/Programme Expenditure limits, Cash
Limit (MCD)
08/1
0/20
20
Vis
seh
Pej
han
-Syk
es -
Ch
ief
Fin
anci
al O
ffic
er
R R
eyn
old
s
Go
vern
ing
Bo
dy
Maj
or
Exp
ecte
d t
o o
ccu
r in
mo
st c
ircu
mst
ance
s.
20
Budget Control & Reporting
Contingency / Reserves
Audited accounts
Policies and Procedures
Maj
or
Will
pro
bab
ly o
ccu
r in
mo
st c
ircu
mst
ance
s.
16
National planning principles still to be
received.
COVID phase 3 financial regime and financial
allocations to be notified beyond month 4,
also some funding being directed to ICS as
opposed to direct to CCG.
Yes
Work is ongoing to understand and challenge national assumptions in relation to the
Phase 3 Covid-19 financial regime and associated allocations; challenge regarding
flaws in way the allocations have been derived nationally. Work is ongoing with
WY&H ICS to balance the ICS position. Work is ongoing across Leeds place to
mitigate Leeds system shortfall. Work is ongoing in Leeds CCG to reduce non-
committed commissioning intentions, investments and other spend. All non-
committed expenditure suspended until further notice.
Work is ongoing to understand and challenge
national assumptions in relation to the Phase 3
Covid-19 financial regime and associated
allocations
Maj
or
Do
no
t ex
pec
t to
hap
pe
n. C
an o
nly
imag
ine
hap
pe
nin
g
in e
xcep
tio
nal
cir
cum
stan
ces
4
31/1
0/20
21
707
Syst
em F
low
01/0
8/20
19
There is a risk that the Leeds system will deliver
sub-optimal care and patient experience due to an
inability to respond / coordinate response to a
surge in demand, resulting in poor patient quality
and experience, failed constitutional targets and
reputational risk.
This encompasses patients presenting urgently,
admission avoidance activity, treatment in the
hospital and smooth discharge arrangements and
capacity for those admitted.
13/1
0/20
20
Hel
en L
ewis
Tayl
or-
Tate
, D
ebra
Qu
alit
y an
d P
erfo
rman
ce C
om
mit
tee
Maj
or
Exp
ecte
d t
o o
ccu
r in
mo
st c
ircu
mst
ance
s.
20
Leeds System Resilience Plan - Associated Delivery Action Plans
Leeds System Dashboard
Predictive System Capacity & Demand Modelling
System Agreed Escalation Processes and Mutual Aid
5 Year Commissioning Plans
West Yorkshire Integrated Care System Development
System Pressures & OPEL reporting
Winter Review and Evaluation Programme
System Resilience Operational Group
Integrated Commissioning Executive
Partnership Executive Group
Governing Body
IQPR to Q&P Committee
Covid-19 Gold Command
Covid-19 Silver / Stabilisation And Reset
Covid-19 Bronze Commands
Maj
or
Will
pro
bab
ly o
ccu
r in
mo
st c
ircu
mst
ance
s.
16
Winter review programme will identify
learning from existing surge/escalation
plans - including the positives from
interventions as a result from Covid-19 that
would be beneficial to continue.
Winter review programme ongoing;
completed initial phases of reviewing winter
19/20, evaluated learning from Covid-19
response, and currently triangulating system
winter plans.
Learning from the Covid-19 response to
system pressures is also being captured by
EPRR review.
Yes
Covid-19 has added another dimension to winter planning; some services are
adapting their capacity and service models according to national guidance.
Positives from the initial response such as greater use of technical solutions such as
online consultations are being introduced where possible.
The risk more challenging to manage due to the more complex IPC requirements
needed to manage Covid-19 related demand.
StaR Group formalised as Silver Response and
providing escalation forum for pressures
identified at Bronze.
Winter Resilience Plan refresh ongoing to
include planned Covid-19 specific winter
responses an trigger actions to enact as a result
of surges in demand.
Min
or
No
t ex
pec
ted
bu
t co
nce
ivab
le.
Co
uld
occ
ur
som
etim
e
4
02/0
8/20
21
729
Ris
k o
f H
arm
du
rin
g an
d p
ost
Co
vid
-19
(Pri
mar
y C
are)
16/0
7/20
20
There is a risk of harm to patients given the backlog
of work post COVID-19 due to pauses on QOF, QIS,
screening, referrals, patients not presenting with
symptoms and challenges faced with “reset”
resulting in increase morbidity and mortality and
widen health inequalities.
13/1
0/20
20
Dr
Sim
on
Sto
ckill
- M
edic
al D
irec
tor
Turn
er, M
rs K
irst
y
Pri
mar
y C
are
Co
mm
issi
on
ing
Co
mm
itte
e
Maj
or
Will
pro
bab
ly o
ccu
r in
mo
st
circ
um
stan
ces.
16
Amendments to national GP contract to re-prioritise work including a re-
focus of the Quality and Outcomes Framework
National commitment to reduce unnecessary bureaucracy to focus on
clinical care
Local amendments proposed to re-focus QIS to support clinical capacity
utilisation of EA activity to support capacity
Continue to use PQI to monitor progress
Alignment of some contract measures to support a focus in
key areas i.e. QoF / flu
Continued engagement of CDs, PMs and LMC to respond to
feedback and address any concerns
Maj
or
Will
pro
bab
ly o
ccu
r in
mo
st
circ
um
stan
ces.
16
Lack of certainty on flu cohort / vaccine
availability
Impact of a potential 2nd peak
Limited funding available to support
practices with staff absences and therefore
creating further backlog
Assurance in the provision of
vaccine to 50-64 cohort given
national message regarding
vaccine availability
Yes
At the height of the pandemic / lockdown, routine work in primary was paused in line
with the national direction to cope with Covid-19 activity. As services begin to open
up and services are re-started, there is understandably a backlog of work such as LTC
reviews, cervical screening which needs to be covered.
The impact score has been increased due to the increasing rate of Covid-19 cases,
patients waiting for elective surgery needing to manage their symptoms for longer
and the impact of this on the quality of life. The impact of the mitigating actions in
relation to capacity and workforce on the changing situation is unknown and
therefore the current score has been aligned with the unmitigated score.
Ongoing review of flu plans and performance.
Ongoing review of key indicators including
cytology, LD and SMI. Mo
der
ate
Mig
ht
occ
ur
at s
om
e ti
me.
9
31/0
3/20
21
721
Info
rmat
ion
Sec
uri
ty M
atu
rity
30/0
1/20
20
There is a risk of malicious file types gaining entry
into the enterprise and taking hold as a result of:
- Outdated software
- SMBv1 Enabled
- Poor Password Culture
- System misconfigurations
- Authentication Mechanisms
Resulting in:
- Loss of data
- Access to data
- Integrity of data
- Access to network.
In addition could result in failure of the DSPT,
resulting in Data flows from NHSD and other
organisations being restricted.
09/1
0/20
20
Vis
seh
Pej
han
-Syk
es -
Ch
ief
Fin
anci
al O
ffic
er
Step
hen
s, N
ich
ola
Au
dit
Co
mm
itte
e
Maj
or
Exp
ecte
d t
o o
ccu
r in
mo
st c
ircu
mst
ance
s.
20
Microsoft patching on Desktop and Servers is provided by LCC
Anti-virus is installed on all desktop and server estate
NHSMail is a centrally controlled ingress
Redcentric firewall has been installed on the internet boundary; not yet
fully configured
Windows ATP(Advanced Threat Prevention) is installed on all Windows 10
devices
Symantec Endpoint Protection (SEPP) in installed on all Windows 7 devices
System Event Management installed for Solarwinds to improve monitoring
position
Mo
der
ate
Exp
ecte
d t
o o
ccu
r in
mo
st c
ircu
mst
ance
s.
15
Engagement with LCC on Full patching
Engagement with LCC on Third party
patching (Ivanti)
Upgrade affected server estate to eradicate
SMBv1 & .Net
Network (RAS) hardening activities
Assessment of Protective monitoring and
implementation of controls
Updated password protocol -
communications and testing of passwords
Windows 10 roll out and standardisation
Applocker installation to reduce unmanaged
applications on desktop and address out of
support desktop applications
Update configuration of desktop and server
estate, including, but not limited to: SMB
signing, denied anonymous logons and
unique community strings
Segregate Active Directory from LCH
Move from HTTP to HTTPs to secure
internet facing services
Yes
As a result of Covid-19 there have been delays in creating and implementing an
action plan to resolve critical and high risk vulnerabilities. In addition as a result of
an increase in scam emails, text messaging, there is a higher likelihood of a cyber
breach.
Penetration Test action plan in place, risk rated
and overseen by the BIGIT Committee.
LCC are arranging for licences that the CCG will
require for Ivanti to allow us to keep third party
applications patched.
Applocker installation to reduce unmanaged
applications on desktop and address out of
support desktop applications.
Network (RAS) hardening activities.
Update configuration of desktop and server
estate, including, but not limited to: SMB signing,
denied anonymous logons and unique
community strings.
Disabling of the SMBv1 - The total removal of
this issue is reliant on the migration away from
the aging hardware in Yeadon. There is a plan in
place for migrating our file structure from this
platform and onto the Microsoft Azure tenancy
during Dec 2020/Jan 2021
Segregate Active Directory from LCH.
Mo
der
ate
No
t ex
pec
ted
bu
t co
nce
ivab
le.
Co
uld
occ
ur
som
etim
e
6
31/0
5/20
21
Unmitigated Risk Score Current Risk Score Target Risk Score
Corporate Risks
Governing Body High Amber Risk

719
Shap
ing
Ou
r Fu
ture
- Im
pac
t o
n S
taff
22/0
1/2
02
0 There is a risk of key CCG staff leaving the
organisation due to the uncertainty created by the
Shaping Our Future Programme; resulting in
inability to deliver core services and to support
transformation.
12/1
0/2
02
0
Sab
rin
a A
rmst
ron
g, D
irec
tor
of
Org
anis
atio
nal
Eff
ecti
ven
ess
Sco
tt,
Joh
n
Go
vern
ing
Bo
dy
Maj
or
Will
pro
bab
ly o
ccu
r in
mo
st c
ircu
mst
ance
s.
16
Targeted conversations with key staff, individually and as part of wider SLT
development
Honest conversations regarding opportunities and implications of new
staffing structures and requirements
Communication Plan - Communication and engagement with all staff so
that they are clear on the rationale for change and the potential
implications.
OD planning and support key part of the programme - resource allocated
from within partners and CCG lead.
Reports to EMT
Staff survey results
Staff absence reports
Mo
der
ate
Will
pro
bab
ly o
ccu
r in
mo
st c
ircu
mst
ance
s.
12Capacity to fill roles / loss of knowledge
Staff may not disclose their
concerns or intentions to leave
until they secure roles outside
the CCG
Yes Programme was paused in April, now restarted.
Weekly updates about the programme in the
CCG staff bulletin
All staff invited to participate in staff information
sessions before Christmas
Questions and Answers section produced for the
extranet. Clear message re no planned
compulsory redundancies
Names of members of the Shaping Our Future
Delivery Group circulated to enable people to
have conversations with members of this group
as required
Implementation approach to be shared with SOF
delivery group to understand impact on staff and
how we can respond to this.
Regular meetings with Staff Side and
commitment to work transparently with them as
the programme progresses.
Confirmation provided by TR that bands 2-4
would be mapped into role, and that band 5 is
being reviewed at present
Process to allow targeted unfreezing of
recruitment of key roles has begun.
Min
or
Mig
ht
occ
ur
at s
om
e ti
me.
6
31/1
2/2
02
0

1
Leeds Health & Wellbeing Strategy Outcomes – that this report relates to:
1. People will live longer and have healthier lives
2. People will live full, active and independent lives
3. People’s quality of life will be improved by access to quality services
4. People will be actively involved in their health and their care
5. People will live in healthy, safe and sustainable communities
NHS Leeds CCG Strategic Commitments We will focus resources to:
1. Deliver better outcomes for people’s health and wellbeing
2. Reduce health inequalities across our city
We will work with our partners and the people of Leeds to:
3. Support a greater focus on the wider determinants of health
4. Increase their confidence to manage their own health and wellbeing
5. Achieve better integrated care for the population of Leeds
6. Create the conditions for health and care needs to be addressed around local neighbourhoods
Assurance Framework – which risks on the GBAF does this report relate to: 1. Failure to deliver the CCG commitment to reduce health inequalities across our city.
2. Quality of commissioned care is compromised and does not reflect best practice.
3. Failure to achieve financial stability and sustainability.
4. Failure to overcome local and national workforce shortages.
5. Business continuity of health and care services disrupted as a result of a significant event.
6. Ineffective patient and public engagement and lack of transparency in translation of engagement into decisions.
7. Partners and Professionals do not support the CCG strategy.
8. Constraints on CCG organisational effectiveness impact the delivery of the CCG’s plans.
9. Inadequate system infrastructure to support the CCG’s plans.
Agenda Item: GB 20/92 FOI Exempt: N
NHS Leeds CCG Governing Body Meeting
Date of meeting: 25 November 2020
Title: Governing Body Assurance Framework (Risks to the Strategic Commitments)
Lead Governing Body Member: Sabrina Armstrong, Director of Organisational Effectiveness
Category of Paper Tick as
appropriate
()
Report Author: Anne Ellis, Risk Manager
Decision
Reviewed by EMT/ Date: 04 November 2020 Discussion
Reviewed by Committee/Date: N/A
Information
Checked by Finance (Y/N/N/A - Date): N/A
Approved by Lead Governing Body member (Y/N): Y

2
EXECUTIVE SUMMARY:
1. The Governing Body Assurance Framework (GBAF) provides a structure and process that enables the CCG to focus on the principal (strategic) risks to achieving its strategic commitments and be assured that adequate controls are operating to reduce these risks to acceptable levels (the risk appetite).
2. The GBAF format enables the Governing Body to review each of the risks, analyse the
controls and assurances, clearly identify any gaps and the actions needed to address them. The graph illustrates the movement of the risk score throughout the year in relation to the target risk score. The target risk score is the total impact of risk the CCG is prepared to accept in pursuit of its strategic commitments and has been agreed for each risk, based on the risk appetite.
3. As part of the review cycle, each of the principal risks has been reviewed and updated
by the director leads. Updates made since the previous version are highlighted in bold italics.
4. All risks are currently operating above the agreed risk appetite. Mitigating actions have
been identified and once implemented; the risk level should reduce to the level of risk appetite the CCG has agreed to tolerate.
5. The Executive Management Team and Governing Body receive the GBAF bi-monthly. The risks aligned to the Governing Body Committees are also reported to the relevant Committee bi-monthly in the risk report.
6. The Risk Management Strategy includes a review of the assurances provided by the
GBAF. The review is designed to provide assurance to the Audit Committee that the CCG can place reliance on the assurances provided by the GBAF. The strategy states that principal risks outside risk appetite will be reviewed in detail at least once a year to assess the adequacy and completeness of the assurances. The Audit Committee will receive Risk 8: Constraints on CCG organisational effectiveness impacts the delivery of the CCG’s plans at the next Audit Committee meeting (18 November 2020). The Governing Body will receive assurance from the Audit Committee Chair in relation to the GBAF assurance paper as part of the Audit Committee Chairs summary.
7. As stated in the paragraph above, the strategy states that principal risks outside risk appetite will be reviewed in detail (deep dive) at least once a year to assess the adequacy and completeness of the assurances. As a result of the impact of the Covid-19 pandemic on the principal risks, and all principal risks currently being outside risk appetite, the number of principal risks having a deep dive review at each Audit Committee would need to be increased to enable all risks to be reviewed during the year. The Governing Body is requested to consider operating outside the strategy during 2020/21 by postponing some deep dive reviews outside risk appetite and to continue to present one risk at each Audit Committee meeting. This is due to the current demands on the executive team in responding to the pandemic leading to reduced capacity of Directors to undertake a deep dive of all risks outside appetite by the end of 2020/21.

3
NEXT STEPS: The Governing Body will continue to review the GBAF at each meeting and directors will continually monitor and update their risks accordingly. Deep dive reviews of principal risks outside risk appetite will continue to be presented to the Audit Committee.
RECOMMENDATION: The Governing Body is asked to:
(a) REVIEW the Governing Body Assurance Framework; (b) CONSIDER whether the controls and assurances are sufficiently robust; (c) AGREE any further actions required to manage the risks to the target set; (d) NOTE the review and assurance processes; and (e) APPROVE the postponement of some deep dive reviews of risks outside risk
appetite and to continue to present one risk at each Audit Committee meeting.

1
Governing Body Assurance Framework (GBAF) 2020/2021
Introduction
The Governing Body Assurance Framework (GBAF) sets out how the CCG will manage the principal risks to delivering the strategic commitments. The GBAF enables the Governing Body to corporately assure itself (gain confidence, based on evidence). The framework aligns principal risks with the commitments, and highlights key controls and assurances.
Where gaps are identified, or key controls and assurances are insufficient to reduce the risk of non-delivery to acceptable levels (within the CCG risk appetite), action needs to be taken. Planned actions will enable the Governing Body to monitor progress in addressing gaps or weaknesses and to ensure that resources are allocated appropriately. Governing Body responsibility for the GBAF
It is for the Governing Body to:
Establish strategic commitments.
Identify the principal risks that threaten the achievement of these aims.
Identify and evaluate the design of key controls intended to manage these principal risks.
Set out the arrangements for obtaining assurance on the effectiveness of key controls across all areas of principal risk.
Evaluate the assurance across all areas of principal risk.
Identify positive assurances and areas where there are gaps in controls and / or assurances
Put in place plans to take corrective action where gaps have been identified in relation to principal risks.
Maintain dynamic risk management arrangements including a well-founded risk register.
Assurance
The Executive Management Team and Governing Body receive the GBAF bi-monthly. The risks aligned to the Governing Body Committees are also reported to the relevant Committee bi-monthly in the risk report. The Audit Committee annual work plan will ensure that principal risks outside risk appetite are reviewed in detail at least once a year, to assess the adequacy and completeness of the assurances, the Governing Body will receive a copy of the assurance provided to the Audit Committee. The GBAF provides the basis for the preparation of a fair and representative Annual Governance Statement. It is the subject of annual review by both Internal and External Audit. CCG Commitments: We will focus our resources to:
Deliver better outcomes for people’s health and well-being
Reduce health inequalities across our city
We will work with our partners and the people of Leeds to:
Support a greater focus on the wider determinants of health
Increase their confidence to manage their own health and well-being
Achieve better integrated care for the population of Leeds
Create the conditions for health and care needs to be addressed around local neighbourhoods
CCG Risk Appetite Statement NHS Leeds CCG recognises that the long-term health of its population depends upon the delivery of its strategic ambitions and its relationships with its service providers, staff, public and partners. As such, NHS Leeds CCG will not accept risks that have a material adverse impact on quality of healthcare, health inequalities or life expectancy. NHS Leeds CCG has a greater appetite to take considered risks in relation to opportunities where positive gains can be anticipated such as clinical and contractual innovation, where necessary, testing the constraints of the regulatory environment.
Appendix 1

2
Summary of Principal Risks
Ref Risk Title Risk
Appetite Current Score
Target Score
Key changes since last review
1 Failure to deliver the CCG commitment to reduce health inequalities across our city.
Averse 20 12 No change to the current score, however investment plans are on hold pending review of CCG financial position. Depending on the outcome of the review of finances the risk score may be increased.
2 Quality of commissioned care is compromised and does not reflect best practice
Averse 16 6 The risk score has increased from 8 to 16 due to the risk that the demands of Covid-19 on our providers and primary care will put the quality of care of non Covid-19 patients at risk due to reduced access to services. There is also a risk that some reporting and responding of quality measures will be paused again due to a second wave of Covid-19. i.e. complaints , CQUINS and other quality indicators. As such the consequence score has increased to 4 (major).
3 Failure to achieve financial stability and sustainability.
Cautious 16 8 By month 6 the CCG would normally expect this risk to start to reduce, however risk levels for 2020-21 are very high following the publication of revised allocations in September that have significantly reduced the Leeds CCG’s resources in 2020-21. In particular in relation to our Commissioning intentions and progress towards our health Inequalities agenda. For months 1-4 the finance regime nationally was to ensure all organisations remained in financial balance. The CCG has yet to receive assurances that it will also be in balance from months 5 and 6 before entering the months 7-12 planning process with all the risks described above. Following the allocations changes the Leeds system financial performance for 2021-22 in particular is predicated on the delivery of a significant QIPP/CIP programme; that needs to be initiated quickly in 2020-21.
4 Failure to overcome local and national workforce shortages
Averse 9 6 No change to the current score. This risk was subject of a Deep Dive Assurance at the Audit Committee on 16 September 2020.
5 Business continuity of health and care services disrupted as a result of a significant event
Averse 20 15 No change to the current score. The CCG is embedding learning identified by both the Covid-19 Incident Coordination Centre evaluation, and the Winter 19/20 review.
6 Ineffective patient and public engagement and lack of transparency in translation of engagement into decisions.
Averse 8 4 The risk score has been reduced from 12 to 8. Commissioning projects were paused during the pandemic therefore there was a lack of engagement. The risk score was increased to recognise that some changes were made in response to the pandemic. Temporary changes are permitted under regulation 23(2) of the s.244 Regulations in the interests of protecting the health of patients and staff. If it is proposed that a temporary change is to be made permanent as business as usual, the expectation is that engagement or consultation should occur. As services are restarting, where appropriate, there are a number of projects in the planning stages that have already factored in a requirement for patient and public insight and involvement therefore the risk score can be reduced.
7 Partners and Professionals do not support the CCG strategy
Open 12 8 No change to the current score. New action added relating to a review of Membership Engagement and Clinical Leadership in the CCG.
8 Constraints on CCG organisational effectiveness impacts the delivery of the CCG’s plans.
Medium 12 6 No change to current score. New action added in relation to the development of internal assurance process around delivery of outcomes identified under the Left Shift Blueprint work and through commissioning intentions. Internal assurance through the Executive Management Team meetings.
9 Inadequate system infrastructure to support the CCG’s plans.
Medium 16 8 No change since the last review. Actions are ongoing.
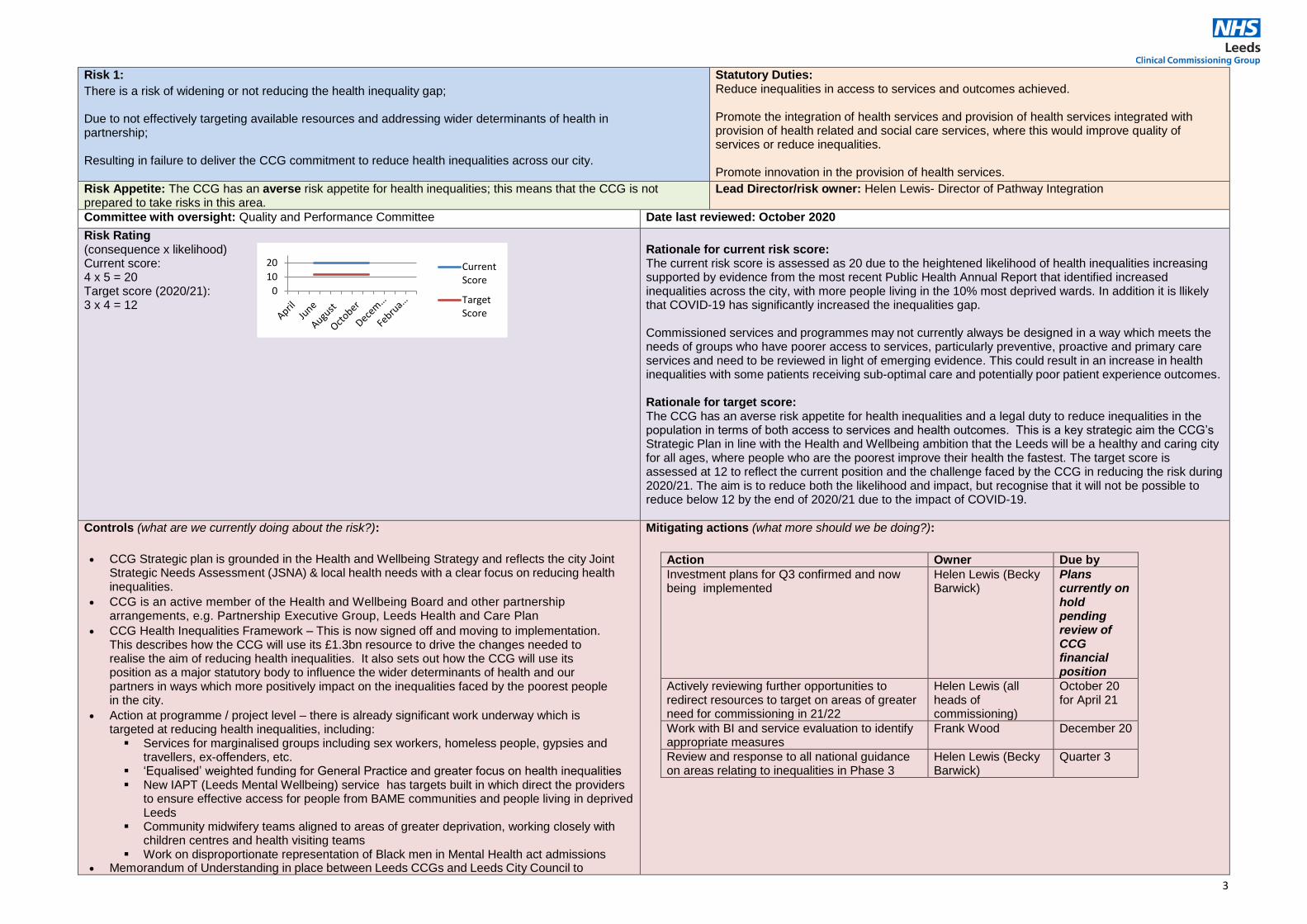
3
Risk 1:
There is a risk of widening or not reducing the health inequality gap; Due to not effectively targeting available resources and addressing wider determinants of health in partnership; Resulting in failure to deliver the CCG commitment to reduce health inequalities across our city.
Statutory Duties: Reduce inequalities in access to services and outcomes achieved. Promote the integration of health services and provision of health services integrated with provision of health related and social care services, where this would improve quality of services or reduce inequalities. Promote innovation in the provision of health services.
Risk Appetite: The CCG has an averse risk appetite for health inequalities; this means that the CCG is not prepared to take risks in this area.
Lead Director/risk owner: Helen Lewis- Director of Pathway Integration
Committee with oversight: Quality and Performance Committee Date last reviewed: October 2020
Risk Rating (consequence x likelihood) Current score: 4 x 5 = 20 Target score (2020/21): 3 x 4 = 12
Rationale for current risk score: The current risk score is assessed as 20 due to the heightened likelihood of health inequalities increasing supported by evidence from the most recent Public Health Annual Report that identified increased inequalities across the city, with more people living in the 10% most deprived wards. In addition it is llikely that COVID-19 has significantly increased the inequalities gap. Commissioned services and programmes may not currently always be designed in a way which meets the needs of groups who have poorer access to services, particularly preventive, proactive and primary care services and need to be reviewed in light of emerging evidence. This could result in an increase in health inequalities with some patients receiving sub-optimal care and potentially poor patient experience outcomes. Rationale for target score: The CCG has an averse risk appetite for health inequalities and a legal duty to reduce inequalities in the population in terms of both access to services and health outcomes. This is a key strategic aim the CCG’s Strategic Plan in line with the Health and Wellbeing ambition that the Leeds will be a healthy and caring city for all ages, where people who are the poorest improve their health the fastest. The target score is assessed at 12 to reflect the current position and the challenge faced by the CCG in reducing the risk during 2020/21. The aim is to reduce both the likelihood and impact, but recognise that it will not be possible to reduce below 12 by the end of 2020/21 due to the impact of COVID-19.
Controls (what are we currently doing about the risk?):
CCG Strategic plan is grounded in the Health and Wellbeing Strategy and reflects the city Joint Strategic Needs Assessment (JSNA) & local health needs with a clear focus on reducing health inequalities.
CCG is an active member of the Health and Wellbeing Board and other partnership arrangements, e.g. Partnership Executive Group, Leeds Health and Care Plan
CCG Health Inequalities Framework – This is now signed off and moving to implementation. This describes how the CCG will use its £1.3bn resource to drive the changes needed to realise the aim of reducing health inequalities. It also sets out how the CCG will use its position as a major statutory body to influence the wider determinants of health and our partners in ways which more positively impact on the inequalities faced by the poorest people in the city.
Action at programme / project level – there is already significant work underway which is targeted at reducing health inequalities, including:
Services for marginalised groups including sex workers, homeless people, gypsies and travellers, ex-offenders, etc.
‘Equalised’ weighted funding for General Practice and greater focus on health inequalities New IAPT (Leeds Mental Wellbeing) service has targets built in which direct the providers
to ensure effective access for people from BAME communities and people living in deprived Leeds
Community midwifery teams aligned to areas of greater deprivation, working closely with children centres and health visiting teams
Work on disproportionate representation of Black men in Mental Health act admissions Memorandum of Understanding in place between Leeds CCGs and Leeds City Council to
Mitigating actions (what more should we be doing?):
Action Owner Due by
Investment plans for Q3 confirmed and now being implemented
Helen Lewis (Becky Barwick)
Plans currently on hold pending review of CCG financial position
Actively reviewing further opportunities to redirect resources to target on areas of greater need for commissioning in 21/22
Helen Lewis (all heads of commissioning)
October 20 for April 21
Work with BI and service evaluation to identify appropriate measures
Frank Wood December 20
Review and response to all national guidance on areas relating to inequalities in Phase 3
Helen Lewis (Becky Barwick)
Quarter 3
0
10
20 CurrentScore
TargetScore

4
deliver Public Health Healthcare Advisory Service (PHHCAS) with action plan. CCG commitment to Population Health Management approach will enable providers to work
together at very local levels (through LCPs) to shape services around needs.
Commissioning for value programme now established to understand how commissioning investments impact on finance, quality and health outcomes.).
Joint data analysis team in place across Local Authority and CCG.
Each Commissioning lead reviewing actions to reduce health inequalities within their own areas as part of the work on the Left Shift Blueprint
Data consistently broken down into ‘deprived Leeds’, all Leeds to help identify areas with biggest gaps
Starting work to look at the underrepresentation of some communities in proactive mental health services
Assurances (how do we know if the things we are doing are having an impact?): Internal Assurance
Process measures being developed which clearly identify data on a Leeds/deprived Leeds/PCN basis to identify variation to drive actions to address these
All commissioning intention/business cases and Blueprint plans reviewed to ensure sufficiently focused on the needs of most deprived/BAME communities/vulnerable groups as relevant to specific areas of work
Independent Assurance There are a number of external reporting mechanisms which will be used to build the CCG’s reporting framework, including:- Public Health England Local Authority Health Profiles Public Health Annual Report Local Authority Quarterly Report
Gaps in assurances (what additional assurances should we seek):
Further work needed to be able to provide more timely data because of very significant lags in national datasets
Further work needed to evaluate within marginal groups where data is not available at granular enough levels to evidence impact through routine data sets and will require proxy measures
Link to Risk Register (operational risks): 305: Compliance with the Equality Act 2010 Public Sector Equality Duty (6) 688: Utilising patient experience data to inform commissioning decisions (6) 695: Learning Disabilities Mortality Review Programme (LeDeR) (12)

5
Risk 2:
There is a risk that the quality of commissioned care is compromised, and does not reflect best practice;
Due to inadequate quality assurance and improvement processes, in both commissioning and delivery of care;
Resulting in failure to deliver the CCG’s strategic commitment to focus resources to deliver better outcomes for
people’s health and well-being.
Statutory Duties: Secure improvement in the quality of services and outcomes for patients, with particular regard to clinical effectiveness, safety and patient experience. Promote the integration of health services and provision of health services integrated with provision of health related and social care services, where this would improve quality of services or reduce inequalities.
Risk Appetite: The CCG has an averse risk appetite for service quality; this means that the CCG is not prepared to take risks in this area.
Lead Director/risk owner: Jo Harding – Executive Director of Quality and Nursing
Committee with oversight: Quality and Performance Committee Date last reviewed: October 2020
Risk Rating (consequence x likelihood) Current score: 24 x 4 = 816 Target score: 2 x 3 = 6
Rationale for current risk score: Whilst the CCG has in place quality standards, and measures quality outcomes via a range of methods and processes to assure the quality of care we commission for our patients. The risk score has increased from 8 to 16 due to the risk that the demands of Covid-19 on our providers and primary care will put the quality of care of non Covid-19 patients at risk due to reduced access to services. There is also a risk that some reporting and responding of quality measures will be paused again due to a second wave of Covid-19. i.e. complaints , CQUINS and other quality indicators. As such the consequence score has increased to 4 (major). Rationale for target score: A target score of six has been applied to this risk as the CCG aims to minimise the likelihood and consequence of the risk occurring. However it is recognised that it is not possible to eradicate risk to quality and safety completely and as such the target likelihood due to error is 3 (possible) and the target consequence remains 2 (minor).
Controls (what are we currently doing about the risk?):
The CCG has multiple team and work streams that encompass all the elements of monitoring and assurance of quality including patient safety, patient experience, effectiveness (clinical outcomes) and safeguarding.
Various assurance methods and improvement strategies are used in collaboration with all providers. This includes intelligence from our IQPR, quality visits, regulatory feedback and compliance with national standards and contractual requirements. This also includes integrated processes with local authority in relation to the monitoring and improvement quality in care homes. Unable to conduct quality visits at this time due to Covid-19
The WY&H QEIA tool, used across the ICS and adopted by the CCG, is utilised to ensure all quality and equality impacts are considered in all service changes and commissioning/decommissioning decisions.
The CCG is leading the local implementation of the NHS England Early Adopter Programme with LTHT for new Patient Safety Incident Response Framework and planning ongoing for rollout to all providers. Progress with implementation delayed in LTHT currently due to Covid-19
The CCG leads a Patient Experience Collaborative to ensure robust mechanisms for utilising all Patient Experience in commissioning decisions. This involves wider system partners and will feed into the city wide PE strategy.
The CCG has developed population health management work programmes to ensure quality lens is applied to the commissioning and delivery of care with specific reference to vulnerable groups and health inequalities. Quality outcomes as part of the left shift blueprint work are currently being worked up and will link in with the SOF work around outcomes for populations
CCG is working towards embedding the new liberty protection safeguards (MCA/DoLS). The judicial process needed for implementation of LPS is delayed needing to an increased risk as the current DOLs process has significant backlogs.
The CCG is currently working towards the implementation of the host commissioner assurance arrangements for people in LD and autism who reside in locked rehabilitation to ensure in particular patients who are placed out of area receive a safe and quality service
Mitigating actions (what more should we be doing?):
Action Owner Due by
Review of AQP quality assurance process to completed and presented to the Quality and Performance Committee in September 2020.
Deputy Director of Nursing and Quality
Complete
Embed Patient Experience further in the initial stages of the commissioning cycle to strengthen and inform developments focused on patients’ experience of care.
Head of Patient Safety and Experience
January 2021
Lead colleagues across the city to consider a new vision and approach to QA and QI with a strong emphasis on mutual accountability
Director of Nursing and Quality
March 2021
Host commissioner assurance arrangements for people with LD and autism to be presented at Q&P once agreed with LYPFT
Head of Quality December 2020
0
10
20 CurrentScore
TargetScore

6
Assurances (how do we know if the things we are doing are having an impact?): Internal Assurance
Joint Clinical Quality Review Groups (CQRG) and Primary Care Quality Surveillance
Review and monitor key quality, clinical governance and safeguarding (adults and children) requirements and standards, performance information, expectations and performance requesting and monitoring remedial action plans where required. The approach of CQRG has changed to encompass assurance against increased risk of Covid-19
West Yorkshire Quality Surveillance Group (QSG) and Quality Leads Meeting (QLM)
oversight of quality / sharing of intelligence and actions
Contract Management Board
update briefings from Providers identifying key areas of concern/under performance and actions
Quality and Performance Committee review of quality:
Integrated Quality and Performance Report, providers under enhanced surveillance, patient experience, incident management, updates around Covid-19 and impact on non Covid-19 services discussed at the committee
Robust governance structure in place within the CCG provides assurance on the quality of services to Governing Body
Safeguarding annual declaration for care homes and private hospitals
Qualitative and quantitative monitoring of LeDeR reviews
GP Safeguarding Standards Framework to monitor SG performance of primary care SG
CCG is implementing the host commissioner framework for learning disabilities/autism in in patient settings
Independent Assurance
CQC inspection programme – reports/action plans monitored via provider quality meetings
New emergency inspection framework for CQC inspections implemented due to Covid-19.
New IPC targeted inspection framework launched and has included care homes and health
care settings across Leeds.
Internal audits – 2018/19 High assurance of Individual Funding Requests and Patient Experience, Significant assurance of Personal Health Budgets, Safeguarding, Continuing Healthcare and Performance Reporting. 2019/20 High assurance of Incident Management, Significant assurance of Contract Management and the Mental Capacity Act
Gaps in assurances (what additional assurances should we seek):
Lack of joined up city wide approach to patient experience
Lack of city wide approach to quality assurance and improvement across the city
Link to Risk Register (operational risks): 732: Risk of Harm During and Post Covid-19 (Planned Care and Mental Health) (20) 729: Risk of Harm During and Post Covid-19 (Primary Care) (16) 723: Deprivation of Liberty (12) 726: Post Covid-19 backlog of Local Resolution and assessments (12) 695: Learning Disabilities Mortality Review Programme LeDeR (12) 697: Care Home Medicine Management (9) 664: Community Care Beds – Medicine Review (9) 660: Delivery of high quality primary care services (9) 28: Learning from medication related incidents (9)

7
Risk 3:
There is a risk of failure to achieve financial stability and sustainability for the Leeds health and care system; Due to increasing demands on the system, and / or failure of financial controls; Resulting in a breach of financial duties and an adverse impact on delivery of the CCG commitments.
Statutory Duties: Fulfil the financial duties.
Risk Appetite: Given the statutory nature of financial duties of the CCG, the CCG has a cautious risk appetite for financial efficiency; this means the CCG will accept a low level of risk in this area.
Lead Director/risk owner: Visseh Pejhan-Sykes – Chief Finance Officer
Committee with oversight: Governing Body Date last reviewed: October 2020
Risk Rating (consequence x likelihood) Current score: 4 x 4 = 16 Target score: 4 x 2 = 8
Rationale for current risk score: Risk levels for 2020-21 are very high following the publication of revised allocations in September that have
significantly reduced the Leeds CCG’s resources in 20-21- in particular in relation to our Commissioning intentions and progress towards our health Inequalities agenda
Failure to achieve financial stability could normally lead to a breach in our statutory duties and have an adverse effect on our local population. This risk relates to both 20-21 and 21-22 financial years – although some mitigations have been identified non-recurrently for 20-21.
Following the allocations changes the Leeds system financial performance for 21-22 in particular is predicated on the delivery of a significant QIPP/CIP programme, that needs to be initiated quickly in 20-21
The system is heavily reliant on financial delivery at Place level and the CCG will be relying on LTHT to achieve a surplus to cover some elements of the CCG’s deficit in 20-21. The CCG will need to address its potential shortfall in 20-21 via QIPP schemes to be identified and put in train to start 21-22 with a break even plan.
For months 1-4 the finance regime nationally was to ensure all organisations remained in financial balance. The CCG has yet to receive assurances that it will also be in balance from months 5 and 6 before entering the
months 7-12 planning process with all the risks described above.
Rationale for target score: The consequences of failing our financial duties will always be high from a patient care perspective so our ideal target score would be to retain the likelihood levels at 2 and below to manage the risks.
Controls (what are we currently doing about the risk?):
Revised financial policies and budgetary control framework produced in May 2020 to reflect new finance regime introduced in March 2020 to combat the COVID 19 Pandemic – shared with Audit Committee and Governing Body. Internal Audit has reviewed and compared with peers.
Revised allocations received for 20-21 in September 2020 and led to a deficit position for
the CCG
Regular CFO meetings across Leeds & West Yorkshire and the CCG have led to the potential for Leeds as a system balancing its finances but with some significant risks and caveats. The CCG has also developed a RAG rated list of QIPP opportunities for 20-21 and in preparation for 21-22 financial planning.
Monthly budget reports will be issued from November once the CCG plans have been accepted by NHSE/I in November and positions will be discussed at budget holder meetings.
Mitigating actions (what more should we be doing?):
Action Owner Due by Financial plans submission to NHSE/I at the end of October 2020 with major caveats including the assumption of significant revenue national resources drawdowns leading to adjustments between the CCG and LTHT to achieve financial balance across Leeds.
Governing Body
NSHE/I response expected in early November
Continuing to work closely across Leeds NHS and Leeds City Council, West Yorkshire and the Reginal NHSE/I Team to clarify rules around finances and centrally held funds during the COVID financial regime.
Governing Body
Attend daily / weekly informal and formal forums and keep abreast of all deadlines for financial reporting, resource allocations and informing the centre throughout the next 6 months.
Assurances (how do we know if the things we are doing are having an impact?): Internal Assurance
Monthly finance reports to EMT, Audit Committee and Governing Body identifying any current financial risks.
Escalation of exception reports to EMT and to Governing Body, and in the current year to the WY system and the regional NHSE/I team.
Procurement Programme monitoring and delivery reporting.
Lead commissioner monthly forecasts.
Financial impacts of primary care commissioning appear to be less significant at current stage of planning.
Independent Assurance Budgetary and governance control systems for identifying and controlling financial risks –
ranked high assurance by the Internal Auditors again as we enter 2020-21.
NHSE assurance meetings have resulted in the Leadership of the CCG across all areas being rated Green.
Gaps in assurances (what additional assurances should we seek): Health and social care economy nationally (including in Leeds) is severely financially challenged as a result of the
COVID-19 Pandemic. Over the course of the year, some resources have been allocated to cover major gaps but
the position for the second half of the year looks very precarious.
Within the context of the West Yorkshire Integrated Care System (ICS), we are able to aim for a balance plan for 20-
21 at each Place level but only after some major assumptions around national financial support for a number of
technical and successful applications by CCGs and Trusts against centrally held pots for specific areas of
spend.
Post COVID there will be significant pressures on the systems to ‘catch up’ on backlog elective activity and maximise capacity and at the same time as having significantly restricted resources . The need to find innovative ways to delivery care therefore is fundamental and urgent
Link to Risk Register (operational risks): 548: Statutory Financial Duties (16) 551: Fraud and
Corruption (9) 708: National Shortage of Capital (8)
0
10
20 CurrentScore
TargetScore

8
Risk 4:
There is a risk of an inability to attract, develop and retain people to work in the Leeds health and care system;
Due to our failure to overcome local and national workforce shortages;
Resulting in failure to deliver the CCG commitment to deliver better outcomes for people’s health and well-being.
Statutory Duties: Secure improvement in the quality of services and outcomes for patients, with particular regard to clinical effectiveness, safety and patient experience. Have regard to the need to promote education and training of current or future health service staff.
Risk Appetite: The CCG has an averse risk appetite for service quality; this means that the CCG is not prepared to take risks in this area.
Lead Director/risk owner: Jo Harding – Executive Director of Quality and Nursing
Committee with oversight: Quality and Performance Committee Date last reviewed: October 2020
Risk Rating (consequence x likelihood) Current score: 3 x 3 = 9 Target score: 3 x 2 = 6
Rationale for current risk score: Ensuring we have the workforce to deliver a sustainable health and care today and a workforce to deliver a transformed health and care for tomorrow is hugely complex. Leeds needs to ensure that this is being addressed at city-wide levels within the context of workforce challenges across the system. We know there are gaps in required workforce now and the potential for more due to the halt in international recruitment as a result of the pandemic. The National People Plan has just been published. The Leeds system will need to take account of its requirements locally. As a result the likelihood score is assessed as 3 (possible). Rationale for target score: The changing nature of healthcare delivery and the introduction of new models of care require an adaptive, agile and integrated system. Keeping abreast of workforce requirements and planning for future skills and competencies will be challenging. There are likely to be workforce shortages as a consequence. As a result the actions detailed below are designed to reduce the likelihood from 3 (possible) to 2 (unlikely).
Controls (what are we currently doing about the risk?):
Leaders of main health and care organisations have come together with commissioning and care leaders across the city as the Partnership Executive Group (PEG). This group aims to ensure coherence of strategy and approach across the city, and delivery of the goals set out in the Health and Wellbeing Strategy. This includes our approach to Workforce in the City.
Governance for Leeds Workforce programme has been reviewed and the new Leeds One
Workforce Strategic Board (LOWSB) was established to replace the former arrangements and
their first quarterly meeting was held in November 2019. The purpose of the LOWSB is: to
ensure that the Leeds based health and care workforce is fit for now and the future.
7 Shared Workforce Priorities have been developed and agreed by the LOWSB.
The Leeds Health and Care Academy (LHCA) is funded by and works with all partners in the
city. LOWSB works with the LHCA to bring together planning, coordination, resource and
delivery of learning and development for staff working in health and care in the city, to meet the
citywide workforce challenge. LHCA work programme directly links to the strategic workforce
priorities.
Primary Care Workforce sub-group and action plan is in place – TOR and membership has
been reviewed to ensure alignment with Strategic workforce priorities and PCN workforce
challenges and links to the wider system. Workforce action plans being developed at PCN level
which supports the new GP contract setting out the new roles developing within general
practice and the funding to support these roles e.g. care navigation; Rotational Paramedic; role
of occupational therapists in primary care pilot; shared roles across a number of practices and
many more.
Leeds actively participates in the national and regional West Yorkshire and Harrogate ICS
Workforce Groups and workforce activity is linked/mapped against regional workforce plan.
Mitigating actions (what more should we be doing?):
Action Owner Due by
The LOWSB to review the Leeds ‘One Workforce’ vision statement and the 7 shared priorities in light of the pandemic and agree a clear strategy for successful delivery.
Jo Harding as the CCG representative on the LOWSB
Complete
Seek to better understand the role and vision of the Academy in delivering the ‘Leeds One Workforce’ ambition statement Due date extended as the LOWSB does not meet until middle of November
Jo Harding as the CCG representative on the LOWSB
October 2020 December 2020
The LOWSB to consider the requirement for a workforce needs analysis to better understand the systems priorities in light of the pandemic. Due date extended as the LOWSB does not meet until middle of November
Jo Harding as the CCG representative on the LOWSB
October 2020 December 2020
0
10
20 CurrentScore
TargetScore

9
Assurances (how do we know if the things we are doing are having an impact?):
The LOWSB provides assurance to the Health and Wellbeing Board and reporting to PEG on the delivery and impact of the workforce priorities in respect of its own plan, leading on the workforce requirements outlined in the strategic drivers of the city through including the Leeds Health and Wellbeing Strategy, Leeds Health and Care Plan, Children & Young People’s Plan, Inclusive Growth Strategy and tackling Climate Change.
Additional Comments: Leeds Health and Care System risk owner: Dr Sara Munro – Chief Executive of LYPFT She is the Senior Responsible Officer for Leeds Health and Care Academy and Workforce – Chair of Leeds One Workforce Strategic Board (LOWSB) and a Member of Partnership Executive Group (PEG).
Gaps in assurances (what additional assurances should we seek):
There is a lack of understanding to develop, agree and establish a baseline of accurate workforce data across the whole Leeds Health and Care System to identify workforce gaps in existing and new roles in order to model the future workforce requirements short/medium/long term.
Workforce Programme of work and action plans to feed into a Leeds One Workforce Strategy has been delayed due to the impact of COVID-19. Next business as usual meeting due 14 July 2020.
Leeds accepts the associated workforce risks and that workload and capacity has been negatively impacted by COVID-19 and the new challenges that changed the focus of our system led work.
Former Director left the post in September 2019 LHCA and Workforce have appointed a Director and they join the team September 2020.
The establishment of the Leeds GP Confederation brings new opportunity to engage with primary care ‘at scale’ and develop workforce initiatives for general practice across the city. This is yet to be realised.
Link to Risk Register (operational risks): 651: General Practice Workforce (12)
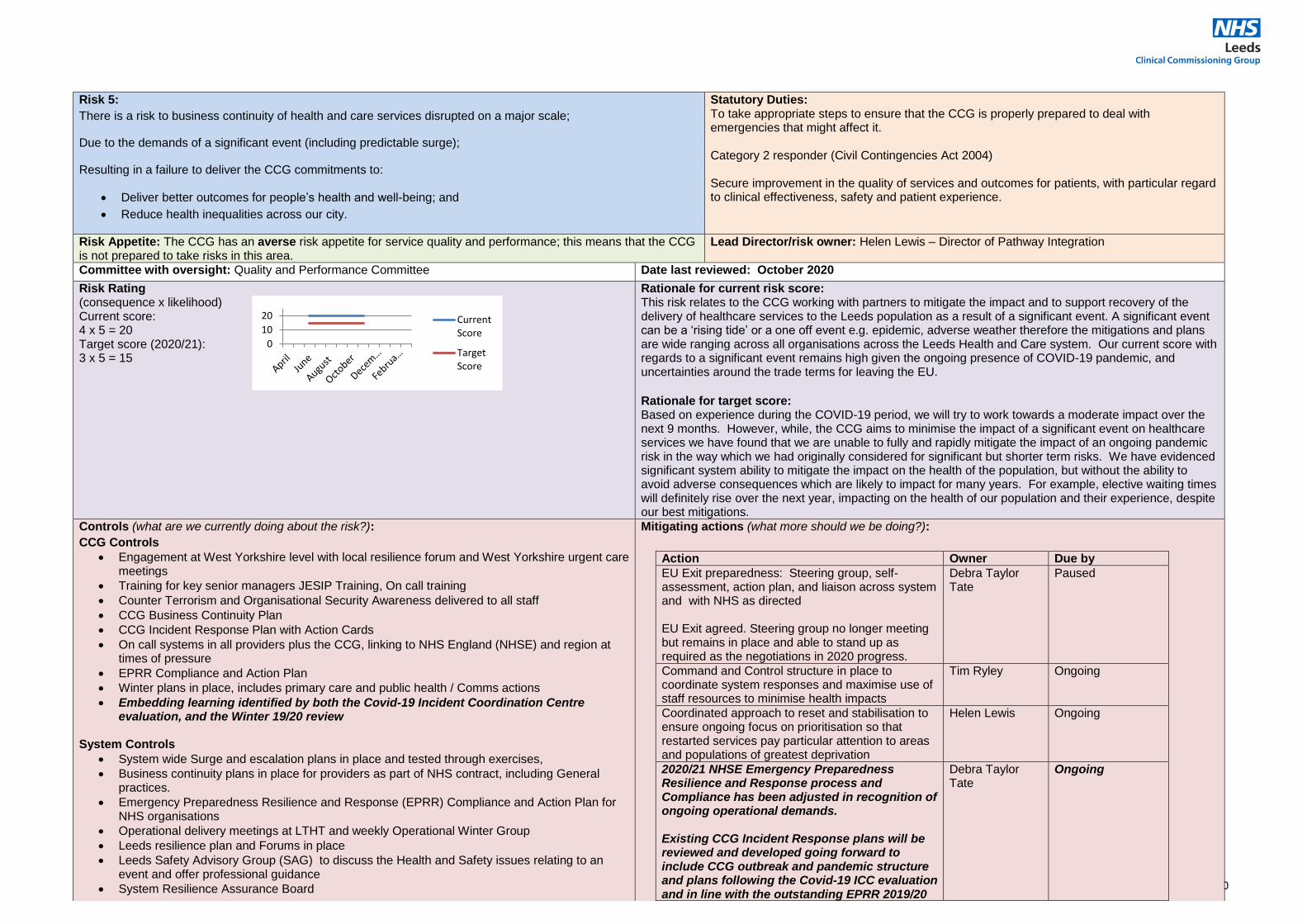
10
Risk 5:
There is a risk to business continuity of health and care services disrupted on a major scale;
Due to the demands of a significant event (including predictable surge);
Resulting in a failure to deliver the CCG commitments to:
Deliver better outcomes for people’s health and well-being; and
Reduce health inequalities across our city.
Statutory Duties: To take appropriate steps to ensure that the CCG is properly prepared to deal with emergencies that might affect it. Category 2 responder (Civil Contingencies Act 2004) Secure improvement in the quality of services and outcomes for patients, with particular regard to clinical effectiveness, safety and patient experience.
Risk Appetite: The CCG has an averse risk appetite for service quality and performance; this means that the CCG is not prepared to take risks in this area.
Lead Director/risk owner: Helen Lewis – Director of Pathway Integration
Committee with oversight: Quality and Performance Committee Date last reviewed: October 2020
Risk Rating (consequence x likelihood) Current score: 4 x 5 = 20 Target score (2020/21): 3 x 5 = 15
Rationale for current risk score: This risk relates to the CCG working with partners to mitigate the impact and to support recovery of the delivery of healthcare services to the Leeds population as a result of a significant event. A significant event can be a ‘rising tide’ or a one off event e.g. epidemic, adverse weather therefore the mitigations and plans are wide ranging across all organisations across the Leeds Health and Care system. Our current score with regards to a significant event remains high given the ongoing presence of COVID-19 pandemic, and uncertainties around the trade terms for leaving the EU.
Rationale for target score: Based on experience during the COVID-19 period, we will try to work towards a moderate impact over the next 9 months. However, while, the CCG aims to minimise the impact of a significant event on healthcare services we have found that we are unable to fully and rapidly mitigate the impact of an ongoing pandemic risk in the way which we had originally considered for significant but shorter term risks. We have evidenced significant system ability to mitigate the impact on the health of the population, but without the ability to avoid adverse consequences which are likely to impact for many years. For example, elective waiting times will definitely rise over the next year, impacting on the health of our population and their experience, despite our best mitigations.
Controls (what are we currently doing about the risk?):
CCG Controls
Engagement at West Yorkshire level with local resilience forum and West Yorkshire urgent care meetings
Training for key senior managers JESIP Training, On call training
Counter Terrorism and Organisational Security Awareness delivered to all staff
CCG Business Continuity Plan
CCG Incident Response Plan with Action Cards
On call systems in all providers plus the CCG, linking to NHS England (NHSE) and region at times of pressure
EPRR Compliance and Action Plan
Winter plans in place, includes primary care and public health / Comms actions
Embedding learning identified by both the Covid-19 Incident Coordination Centre evaluation, and the Winter 19/20 review
System Controls
System wide Surge and escalation plans in place and tested through exercises,
Business continuity plans in place for providers as part of NHS contract, including General practices.
Emergency Preparedness Resilience and Response (EPRR) Compliance and Action Plan for NHS organisations
Operational delivery meetings at LTHT and weekly Operational Winter Group
Leeds resilience plan and Forums in place
Leeds Safety Advisory Group (SAG) to discuss the Health and Safety issues relating to an event and offer professional guidance
System Resilience Assurance Board
Mitigating actions (what more should we be doing?):
Action Owner Due by
EU Exit preparedness: Steering group, self-assessment, action plan, and liaison across system and with NHS as directed EU Exit agreed. Steering group no longer meeting but remains in place and able to stand up as required as the negotiations in 2020 progress.
Debra Taylor Tate
Paused
Command and Control structure in place to coordinate system responses and maximise use of staff resources to minimise health impacts
Tim Ryley Ongoing
Coordinated approach to reset and stabilisation to ensure ongoing focus on prioritisation so that restarted services pay particular attention to areas and populations of greatest deprivation
Helen Lewis Ongoing
2020/21 NHSE Emergency Preparedness Resilience and Response process and Compliance has been adjusted in recognition of ongoing operational demands. Existing CCG Incident Response plans will be reviewed and developed going forward to include CCG outbreak and pandemic structure and plans following the Covid-19 ICC evaluation and in line with the outstanding EPRR 2019/20
Debra Taylor Tate
Ongoing
0
10
20 CurrentScore
TargetScore

11
System and regional meetings. Local Health Resilience Partnership (LHRP). Health and Social Care Resilience Group.
Health Protection Board
EPRR framework for NHS organisations includes clear roles and responsibilities for system wide response
Clear roles and responsibilities for outbreak planning (NHSE, CCG, LA)
Leeds Outbreak Plan and Outbreak Roles and Responsibilities.
Command and control structure in place to coordinate the city’s response to Covid-19
action
Update training needs analysis and create a testing and evaluation schedule in response to the three yearly External Audit review of CCG BC arrangements
Debra Taylor-Tate
March 2021 (to be informed by the new CCG Operating Model)
Recommendations from the Internal Audit of the CCGs response to Wave One of Covid-19 to be reviewed and reflected upon.
Debra Taylor-Tate
Ongoing. Recommendations still in draft form.
Assurances (how do we know if the things we are doing are having an impact?): Internal Assurance
Assurance from providers on EPRR compliance, and business continuity plans..
Regular testing of the CCG Business Continuity Plan
Annual self-assessment against EPRR – goes to Governing Body
Outputs from real or tested scenarios and learning – reports and action plans produced e.g. winter reviews.
Oversight Group in place to ensure mutual aid to areas of greatest clinical needs
Coordinated ICS response to ensure prioritisation of staff and capacity for most urgent cases
Planned care boards and other boards overseeing impacts on routine care to ensure shared understanding of ongoing risks
Ongoing feedback from Healthwatch to help identify areas requiring greatest mitigation Independent Assurance NHSE complete an annual CCG assurance assessment through quarterly reviews.
Internal Audit review undertaken on EPRR and Business Continuity
NHSE Review of EPRR response during COVID-19
Gaps in assurances (what additional assurances should we seek):
None identified
Link to Risk Register (operational risks): 650: CCG Business Continuity (6) 706: Emergency Preparedness Resilience and Response (8) 729: Risk of Harm During and Post Covid-19 (Primary Care) (16) 732: Risk of Harm During and Post Covid-19 (Planned Care and Mental Health) (20) 721: Information Security Maturity (15) 707: System Flow (16) 690: EU Exit (12)

12
Risk 6:
There is a risk of commissioning services that do not meet population needs;
Due to ineffective engagement with patients and public and lack of transparency in translation of engagement
outcomes into decisions;
Resulting in failure to deliver the CCG’s strategic commitment to work with our partners and the people of Leeds to:
Support a greater focus on the wider determinants of health
Increase their confidence to manage their own health and well-being
Achieve better integrated care for the population of Leeds
Create the conditions for health and care needs to be addressed around local neighbourhoods
Statutory Duties: Involve the public in the planning of, and proposed changes to, commissioning arrangements. Promote the integration of health services and provision of health services integrated with provision of health related and social care services, where this would improve quality of services or reduce inequalities. Provide patient choice. Promote innovation in the provision of health services.
Risk Appetite: The CCG has an averse risk appetite for public engagement; this means that the CCG is not prepared to take risks in this area.
Lead Director/risk owner: Sabrina Armstrong – Director of Organisational Effectiveness
Committee with oversight: Governing Body Date last reviewed: October 2020
Risk Rating (consequence x likelihood) Current score: 4 x 2 = 8 Target score: 4 x 1 = 4
Rationale for current risk score: All appropriate controls are in place to plan and deliver effective patient and public involvement (PPI). However the consequence of these controls failing has the potential to result in challenge and ultimate referral by Scrutiny board to judicial review. This would impact on the CCG’s reputation as well as delaying
any proposed changes. Commissioning projects were paused during the pandemic therefore there was a lack of engagement. The risk score was increased to recognise that some changes were made in response to the pandemic. Temporary changes are permitted under regulation 23(2) of the s.244 Regulations in the interests of protecting the health of patients and staff. If it is proposed that a temporary change is to be made permanent as business as usual, the expectation is that engagement or consultation should occur. As services are restarting, where appropriate, there are a number of projects in the planning stages that have already factored in a requirement for patient and public insight and involvement therefore the risk score can be reduced. In March 2020 the CCG published an extensive insight report and engagement about changing the way people accessed hospital outpatient services, which includes support for greater use of technology, and therefore supports some of the changes already made. The CCG is now about to undertake a similar review and engagement into changes to primary care services. The CCG has contingency to move to facilitated online engagement and work with Leeds Voices to engage with people through their volunteer programme. Feedback from an in-depth deliberative event which took place in March 2020 now ensures that the commissioning, contracting and procurement teams act in accordance with the expressed priorities that patients have on patient choice, which is reflected in our procurement policies and service specifications. Rationale for target score: A target score of 4 reflects an averse risk appetite. It would not be possible to reduce the risk to a score lower than 4. This is due to the potential consequence of a control failure supplemented by circumstances outside our control.
Controls (what are we currently doing about the risk?):
Volunteer panel in place (PAG): Remit to provide assurance around engagement and/or
consultation plans.
Significant and major engagement/consultation plans taken to Scrutiny Board for discussion
and approval to proceed.
CCG has a full complement of staff in place to support engagement activity.
Communications and engagement incorporated into Left Shift Blueprint /Commissioning for
Value (CfV) process.
Mitigating actions (what more should we be doing?):
Action Owner Due by
Ensure communications or engagement team reps co-opted onto appropriate commissioning steering groups to ensure the patient voice is heard.
Strategy and Commissioning teams Communications and Engagement Team
Ongoing
0
10
20 CurrentScore
TargetScore

13
The engagement plan template includes the Equality and Quality Impact Assessment to identify
impact on protected characteristics and discrete communities.
Contract with Voluntary Action Leeds (VAL) to support CCG engagement work across as wide
a reach as possible, and also to undertake broad asset-based engagement in harder to
reach/engage communities. VAL is continuing to recruit to their volunteer Health Champions.
CCG has a lead role in continuing to develop the citywide engagement hub which includes
engagement colleagues from provider teams.
CCG works closely with Healthwatch as part of the People’s Voice network.
CCG community network continues to grow.
Bi-monthly communications and engagement reports published and shared
CCG undertakes regular engagement with GP patient and public groups.
Deliberative events are independently facilitated, analysed and reported on.
Formal consultation and engagement processes are independently analysed and reported on.
Equality and Diversity lead works with engagement team to ensure all aspects of protected characteristics are covered in line with the Equality Act 2010.
There is a greater focus on collecting, analysing and using existing insight from patients and the public in planning
Further enhance our approach to engagement and involvement activity beyond our statutory duties. Our focus will be on proactive, ongoing conversations with communities and individuals to build a foundation of evidence that supports commissioning plans for health outcomes.
Communications and Engagement Team
Ongoing
The website is currently being audited to ensure it meets national mandated accessibility standards
Communications team
Complete
Engagement team working more closely with patient experience and complaints team to triangulate feedback and ensure robust processes in place.
Communications and Engagement Team
Ongoing
Assurances (how do we know if the things we are doing are having an impact?): Internal Assurance
Evaluation reports written and provided to commissioning teams to incorporate in their plans and influence service change.
Reports published on the CCG website and shared with members of the public who expressed an interest for further detail: ‘You said, we did’.
Regular liaison with, and attendance as appropriate at, Scrutiny Board to support commissioning colleagues.
Annual PPI review published in July 2019
Monthly VAL contract meetings and VAL KPIs reviewed quarterly. Independent Assurance
‘Amber’ assessment rating for PPI from NHS England in 2018/19 (latest rating).
Internal stakeholder engagement audit October / November 2018; this has been rated High Assurance (highest rating).
NHS Leeds CCG invited by NHS England to present examples of good practice to Amber rated CCGs at a North of England workshop on Improvement and Assessment Framework (IAF) for engagement and community involvement.
Gaps in assurances (what additional assurances should we seek):
Need to ensure feedback from engagement is joined up with insight and intelligence from patient experience reports and monitoring of contract delivery.
Link to Risk Register (operational risks): 305: Compliance with the Equality Act Public Sector Duty (6)

14
Risk 7:
There is a risk to the development and implementation of the CCG strategy;
Due to failure to enable partners and professionals to work with and support the CCG
Resulting in failure to deliver the CCG’s strategic commitment to work with our partners and the people of Leeds to:
Support a greater focus on the wider determinants of health
Increase their confidence to manage their own health and well-being
Achieve better integrated care for the population of Leeds
Create the conditions for health and care needs to be addressed around local neighbourhoods
Statutory Duties: Co-operate with relevant local authorities. Co-operate with other NHS bodies. Promote the integration of health services and provision of health services integrated with provision of health related and social care services, where this would improve quality of services or reduce inequalities. Promote innovation in the provision of health services.
Risk Appetite: The CCG has an open risk appetite for partnership working; this means the CCG is willing to consider a higher level of risk in this area.
Lead Director/risk owner: Simon Stockill – Medical Director (Professionals) Tim Ryley – Chief Executive (Partners)
Committee with oversight: Governing Body/Primary Care Commissioning Committee Date last reviewed: October 2020
Risk Rating (consequence x likelihood) Current score: 3 x 4 = 12 Target score: 2 x 4 = 8
Rationale for current risk score: There has been a long period of partnership development and through the COVID-19 response this has deepened further. There are a wide range of controls in place to maintain this level of commitment. Rationale for target score: The CCG is open to taking a managed risk that, partners and professionals do not support the development and implementation of the CCG strategy, to take the opportunity to further integrate care. The CCG recognises that to proceed in delivering greater integration, there is a fine balance in ensuring partners and professionals are on board and will need to take a more significant level of risk in order to do this. The higher level of risk will be mitigated through the targeted engagement and work with partners and professionals and the risk that partners and professionals do not work with the CCG will continue to be monitored on the integration journey.
Controls (what are we currently doing about the risk?):
A wide range of partnership multi-agency, multi-professional boards and task groups are in
place at all levels across the city where issues can be addressed (PEG, ICE, SRAB,
Programme Boards, Clinical senate, HWB, HWB Board-to-Board,
The Chief Executive meets at least monthly with each of his equivalent and there are regular
Exec-to-Exec meetings
A range of joint city-wide capabilities in digital, workforce and estates
New contracting approaches are in place to encourage greater partnership working
Commissioning teams develop new models of care with partners and always with clinical
leadership
All levels of staff heavily involved in West Yorkshire & Harrogate Partnership
Wide range of clinical leadership in all areas of change
Mitigating actions (what more should we be doing?):
Action Owner Due by
Refresh of the city-wide governance with partners
Tim Ryley March 2021
Further develop the coordination depth and range of joint core city functions
Tim Ryley Review March 2021
Develop a CCG and city-wide approach to working with West Yorkshire ICS
Tim Ryley Dec 2020
Review of Membership Engagement and Clinical Leadership in the CCG
Simon Stockill Dec 2020
Assurances (how do we know if the things we are doing are having an impact?): Internal Assurance
Commissioning for Value monthly EMT meetings to review progress on key plans
Progress in key areas of improvement where partnership necessary for example TCP, IAPT, Waiting Lists
Independent Assurance
Internal Audit Partnership Review
CCG Annual Leadership Rating which includes reflection on partnerships
Gaps in assurances (what additional assurances should we seek):
Develop a local replacement for the 360 review to gain feedback from partners.
Outcomes to monitor progress on Leeds level integration
Link to Risk Register (operational risks): 655: Member engagement (12) 718: Shaping Our Future Stakeholder Engagement (9)
0
10
20 CurrentScore
TargetScore

15
Risk 8:
There is a risk of the effectiveness of the CCG being constrained;
Due to internal weaknesses and external threats, for example, capacity, structure, business intelligence and
cybercrime;
Resulting in failure to deliver the CCG’s strategic commitments, which are:
We will focus our resources to:
Deliver better outcomes for people’s health and well-being
Reduce health inequalities across our city
We will work with our partners and the people of Leeds to:
Support a greater focus on the wider determinants of health
Increase their confidence to manage their own health and well-being
Achieve better integrated care for the population of Leeds
Create the conditions for health and care needs to be addressed around local neighbourhoods.
Statutory Duties: To carry out functions effectively, efficiently and economically.
Risk Appetite: The CCG has a medium risk appetite for the transformation of the CCG function and purpose; this means the CCG will accept a medium level of risk In this area.
Lead Director/risk owner: Sabrina Armstrong – Director of Organisational Effectiveness Visseh Pejhan-Sykes – Chief Finance Officer
Committee with oversight: Governing Body Date last reviewed: October 2020
Risk Rating (consequence x likelihood) Current score: 4 x 3 = 12 Target score: 3 x 2 = 6
Rationale for current risk score: The current risk score of 12 reflects that the CCG is testing new ways of operating that are not yet proven; at this point in time there is a risk that the consequence of doing this could impede or significantly delay the CCGs transformation. The likelihood has been scored as possible during the period of uncertainty; however the CCG has well established governance arrangements to manage the risk. Rationale for target score: A target score of 6 represents a medium risk appetite for transformation of the CCG function and purpose towards strategic commissioner of population outcomes. The CCG is taking a risk in reshaping its structure and function in order to better deliver against its strategic commitments. The risk score of 6 represents a moderate consequence that a decision affecting contract, collaborations, or governance delays the CCGs transformation, the target likelihood would be that this would be unlikely following implementation of the actions identified.
Controls (what are we currently doing about the risk?):
‘Shaping Our Future’ established to transform the way the CCG operates to better enable the achievement of the CCG’s strategic commitments to deliver improved population outcomes, reduce inequalities and greater provider integration.
NHS England has introduced the People Plan for which we have a programme of activity to implement to meet our local needs.
Returning Stronger programme of work to identify better ways of working to improve outcomes.
Annual reviews of Governing Body and Committee effectiveness as well as ongoing review to ensure continuing effectiveness (e.g. Quality & Performance Committee, Audit Committee).
Comprehensive Risk Management Strategy approved by Governing Body and implementation
is overseen by Risk Manager.
Cyber Essentials Assurance roadmap supported by a detailed IT, IG and BI delivery plan for
the CCG and areas in Primary Care the CCG supports.
BI, IG and IT Committee providing assurance on all aspects of IT, IG and BI to the Audit
Committee.
Increasing leadership capability re analytics infrastructure support to Commissioning and all
other functions of the CCG.
Development of a Leadership Behaviour Framework for, initially, our senior staff to support our new ways of working as part of the Shaping our Future programme of work.
Mitigating actions (what more should we be doing?):
Action Owner Due by
Green Plan in terms of climate change and carbon reduction, planned to go to Governing Body in September 2020.
Sabrina Armstrong September 2020 Complete. Due to be published shortly and implementation to begin.
Development of internal assurance process around delivery of outcomes identified under the Left Shift Blueprint work and through commissioning intentions. Internal assurance through the Executive Management Team meetings.
Sabrina Armstrong January 2021
Stage One Shaping Our Future – redesigning the CCG
Sabrina Armstrong March 2021
Establish Outcomes based contract the Covid-19 finance regime is expected to continue until April 2022.
Visseh Pejhan-Sykes
April 2021 April 2022
0
10
20 CurrentScore
TargetScore

16
Introduction of a range of development opportunities to enhance and develop new capabilities.
Enhancement of our Health and Wellbeing support for staff to support new ways of working.
Supporting the development of a BAME Network and engaging members in key decisions across the CCG, including senior appointments, to ensure the CCG is an inclusive employer.
Reducing reliance on physical premises to develop more agile working capability for the CCG
in preparation for its System Integrator function in particular.
NHS Digital has stepped up nationally to reduce cyber risk for all NHS organisations by
providing a single NHS Cloud tenancy nationally and contracts with Microsoft for all O365
products including security related options.
Risk assessments carried out on all staff during pandemic phase to ensure that health and
wellbeing is being supported effectively and changes to working patterns and locations are
being assessed and supported as appropriate. Where a risk is identified, action (including
redeployment) will be considered to ensure staff can continue to work in a safe environment.
Regular formal reporting of the CCG’s delivery plan progress (BI, IT, IG) to the Audit Committee/ EMT / GB
Visseh Pejhan-Sykes
Ongoing
Reducing further our operational reliance on premises as a CCG
Governing Body Mid 2022
Assurances (how do we know if the things we are doing are having an impact?): Internal Assurance
Staff survey results.
Cohesive commissioning decisions with high assurance and regular review and affirmation of progress against strategic objectives supported and informed by robust support systems.
Remuneration and Nominations Committee receives assurance on workforce issues through quarterly reports and regular updates on such as the Gender Pay Gap and Workforce Race Equality Action Plan.
Independent Assurance
All internal audits undertaken during 2019/20 were rated as ‘significant’ or ‘high’ assurance. Head of Internal Audit Opinion provided significant assurance that there is a generally sound system of internal control.
CCG rated as ‘outstanding’ under the NHS Oversight Framework.
NHS Digital Audit, Self-Assessed annual Toolkit review of CCG’s BI, IT and IG processes and controls plus annual Internal Audit review of toolkit
Key outcome metrics and national / local tracking of delivery trajectory confirming positive impact on reducing health inequalities in line with CCG aspirations.
Quarterly Place assurance meeting with NHS E/I.
Gaps in assurances (what additional assurances should we seek):
Impact of climate change on CCG effectiveness
Assurance to the Governing Body on CCG workforce issues
Organisation structured around Strategic Commissioning and System Integration capabilities.
New, long term population-level outcomes based contracts established.
CCG’s Business Intelligence reporting and Analytics has been identified as a key areas for development on both the CCG ad the city wide footprint
Link to Risk Register (operational risks): 650: CCG Business Continuity (6) 305: Compliance with the Equality Act 2010 Public Sector Equality Duty (6) 578: Cyber Security (12) 721: Information Security Maturity (15) 718: Shaping Our Future Stakeholder Engagement (9) 719: Shaping Our Future Impact on Staff (12) 731: Legal claims/challenges to decisions (8) 730: Authentication Vulnerability with MS Teams (12) 733: Home Working – Staff Physical Health (9) 734: Home Working – Managing Remotely (9)

17
Risk 9:
There is a risk to delivery of the CCG strategy;
Due to inadequate system infrastructure to support plans, such as, estates and or digital provision;
Resulting in failure to deliver the CCG’s strategic commitments, which are:
We will focus our resources to:
Deliver better outcomes for people’s health and well-being
Reduce health inequalities across our city
We will work with our partners and the people of Leeds to:
Support a greater focus on the wider determinants of health
Increase their confidence to manage their own health and well-being
Achieve better integrated care for the population of Leeds
Create the conditions for health and care needs to be addressed around local neighbourhoods.
Statutory Duties: Promote innovation in the provision of health services. Secure improvement in the quality of services and outcomes for patients, with particular regard to clinical effectiveness, safety and patient experience.
Risk Appetite: The CCG has a medium risk appetite towards enablers (digital and estates); this means the CCG will accept a medium level of risk In this area.
Lead Director/risk owner: Visseh Pejhan-Sykes – Chief Finance Officer
Committee with oversight: Governing Body/Primary Care Commissioning Committee Date last reviewed: October 2020
Risk Rating (consequence x likelihood) Current score: 4 x 4 = 16 Target score: 4 x 2 = 8
Rationale for current risk score: Three critical non-workforce related support areas have been identified as Estates, Technology and Intelligence. Post COVID, the weightings assigned to Estates and Technology respectively may alter depending on the nature of service delivery, but the data intelligence on which the system should rely on when making decisions remains of the highest importance. Without access to all three in the right measure, service delivery across the system will be highly challenging or potentially less than optimally relevant. As Estates costs tend to be high with associated flexibilities being lower, the COVID era has highlighted the benefits of transferring reliance on premises to technology where practical in terms of mode of delivery of care – as new developments emerge this will increasingly become the case and Leeds is well equipped to be at the forefront of new ways of working. Our ability to deliver high quality intelligence is currently in the development stages. We currently have a significant backlog maintenance challenge for NHS premises – mainly in the Acute sector – and in some pockets in Primary Care. Rationale for target score: Ideally, our commissioning functions would have access to and rely more heavily on infrastructure and support functions such as IT, Cyber and Analytics to more effectively commission using sophisticated actuarial analytics to inform decisions. If this were the case the consequences of unavailability would be higher as would the benefits of access to this capability when available and working well. Our ideal score would be high reliance but low likelihood of failure due to well maintained and supported infrastructure. Treasury funding made available to LTHT to replace the Leeds General Infirmary will significantly eradicate the City’s NHS backlog maintenance and quality of care delivery issues in Secondary care. We are expecting an accelerated trajectory to the rebuilding of the LGI over the next 5 years. Critical next steps are the approval of the Outline Business Case and proceeding to Full Business Case and procurement processes. Ensuring that the new buildings are affordable to the Leeds System is also an important aspect of the planning process next steps. Business Intelligence development roadmap and leadership are in the process of being put in place.
Controls (what are we currently doing about the risk?):
System review of COVID learning to reduce reliance on estates and to increase our full potential in terms
of use of Technology.
NHS Digital developments around N365 and a common single cloud tenancy for the NHS has significantly
improved cyber security for the NHS to build its technological service delivery platforms on.
New Director Portfolios to increase leadership focus on business intelligence and separation of Digital
leadership from Analytics to give the space and time to both agendas
CCG’s roadmap to cyber assurance compliance and Business Intelligence capability developed and
phased for Audit review and feedback / assurances.
Mitigating actions (what more should we be doing?):
Action Owner Due by Leadership role in reviewing, seizing and embedding change post COVID to ensure that transformation of service delivery resulting from the COVID era is retained and adopted sustainably by the Leeds system.
Governing Body Late 2020
Set up Programme of delivery for Analytics support to the CCG which is co-designed and owned by SLT, Commissioners and the Wider System
New Director for Business Intelligence
December 2021
System wide Estates and Digital Strategy resets for the City post COVID
Strategic Estates Group (SEG) and Leeds Informatics Board (LIB)
March 2021
0
10
20 CurrentScore
TargetScore

18
Assurances (how do we know if the things we are doing are having an impact?): Internal Assurance
BI – availability of and feedback from leadership and system leaders and stakeholders on impact and relevance of business intelligence as a timely and relevant tool for decision making.
System wide Estates (SEG) and Digital (LIB) strategic developments continue to address barriers to optimal delivery of care.
Independent Assurance Internal Audit Reviews of progress against plans for delivery
Annual reports of progress from LIB and SEG to City wide forums such as PEG and the HWB Board
Gaps in assurances (what additional assurances should we seek):
IT infrastructure adequately developed across the Leeds and wider NHS system to provide a robust and relevant platform for analytics development and support infrastructure – needs more committed partnership working across both Health and Council.
Information Governance and other related governance and statutory arrangements support the development of the ideal infrastructure and support systems.
Link to Risk Register (operational risks): 707: System Flow (16) 653: Primary Care Infrastructure (12) 708: National Shortage of Capital (8)

1
Leeds Health & Wellbeing Strategy Outcomes – that this report relates to:
1. People will live longer and have healthier lives
2. People will live full, active and independent lives
3. People’s quality of life will be improved by access to quality services
4. People will be actively involved in their health and their care
5. People will live in healthy, safe and sustainable communities
NHS Leeds CCG Strategic Commitments We will focus resources to:
1. Deliver better outcomes for people’s health and wellbeing
2. Reduce health inequalities across our city
We will work with our partners and the people of Leeds to:
3. Support a greater focus on the wider determinants of health
4. Increase their confidence to manage their own health and wellbeing
5. Achieve better integrated care for the population of Leeds
6. Create the conditions for health and care needs to be addressed around local neighbourhoods
Assurance Framework – which risks on the GBAF does this report relate to: 1. Failure to deliver the CCG commitment to reduce health inequalities across our city.
2. Quality of commissioned care is compromised and does not reflect best practice.
3. Failure to achieve financial stability and sustainability.
4. Failure to overcome local and national workforce shortages.
5. Business continuity of health and care services disrupted as a result of a significant event.
6. Ineffective patient and public engagement and lack of transparency in translation of engagement into decisions.
7. Partners and Professionals do not support the CCG strategy.
8. Constraints on CCG organisational effectiveness impact the delivery of the CCG’s plans.
9. Inadequate system infrastructure to support the CCG’s plans.
Agenda Item: GB 20/93 FOI Exempt: No
NHS Leeds CCG Governing Body Meeting
Date of meeting: 25 November 2020
Title: Position Statement: People and Organisational Development Strategy
Lead Governing Body Member: Sabrina Armstrong, Director of Organisational Effectiveness
Category of Paper Tick as
appropriate
()
Report Authors: John Scott and Lara Parkinson, former and current Head of People & OD
Decision
Reviewed by EMT/Date: 11 November 2020 Discussion
Reviewed by Committee/Date: Workforce & Diversity Group on 10 November 2020; EMT on 11 November 2020.
Information
Checked by Finance (Y/N/N/A - Date): N/A
Approved by Lead Governing Body member (Y/N): Y

2
EXECUTIVE SUMMARY: Leeds CCG’s People and Organisational Development (P&OD) Strategy 2018-21 was endorsed by the Governing Body in October 2018 and reviewed in January 2020. Despite a radically changing environment, the Strategy remains broadly fit for purpose. The Remuneration and Nominations Committee now has a programme to regularly review workforce data and specific diversity reports. The impact of COVID-19 and lockdown has both challenged our capacity to maintain our support to people management but also shown our Strategy to be robust, flexible and adaptable. The P&OD Strategy, through its six Ambitions and eight Themes, set out how the organisation should focus its People and OD activities in anticipation of changes in the wider system. As in the previous update, this report seeks to:
Identify which key developments since the Strategy’s publication have been the most significant for the P&OD function
Describe the function’s response, and plans, around the impact of these developments
Provide an opportunity for the Governing Body to note these developments and consider ways in which the CCG can further capitalise on the opportunities they present
Provide assurance to the Governing Body that the steps being taken now and over the next 12 months will increase the organisation’s resilience and capacity for delivery and, where appropriate, development and transformation. In that respect, our response to the NHS People Plan and Promise will be pivotal.
NEXT STEPS: Publication of the update and associated communication and engagement with our people and partners.
RECOMMENDATION: The Governing Body is asked to:
(a) NOTE the continuing progress made during 2020; (b) COMMENT on the content of this report; and (c) ENDORSE and SUPPORT the plans described for 2021.

3
1. SUMMARY
1.1 This paper summarises progress during 2020 on the key elements of the P&OD Strategy and planned activity to ensure we embrace and embed the content and ambitions of the NHS People Plan and Promise.
2. BACKGROUND
2.1 The P&OD Strategy was written as a companion piece to the Leeds CCG Strategic Plan and so adopted the ambition of the Strategic Plan and echoed a Workforce Ambition to: ‘…attract and develop a flexible, dynamic and responsive group who can lead and support the health and care system to achieve this ambition.’
2.2 An Action Plan listed tasks and initiatives that would support the eight themes. These have been reviewed regularly and are summarised at Annex A. The RAG rating in January suggested that we had established a strong basis but needed to place greater emphasis on wider leadership development and the broader talent agenda.
2.3 Developments that have impacted on the Strategy during 2020
2.3.1 2020 has been a year like no other most of us have experienced. It has presented many challenges and potential barriers and severely tested the different elements of emotional intelligence of all our people. But equally it has resulted in an explosion of new ways of working and an increase in innovation. Some of the issues, benefits and implications to be drawn from the experience include:
Agile working and redeployment. In the early stages of the pandemic, we swiftly gathered information about our people’s skills, personal circumstances and availability so that people might be deployed to priority areas within the CCG and the wider system. This activity has highlighted the flexibility and commitment across the organisation and sets a template for the second wave and subsequent remote management and matrix-working in the future. It also flagged a need for up-to-date information on our people and their skills.
Homeworking. Since March 2020 the CCG has effectively operated as a predominantly home-based organisation. This has tested, and largely found effective, our ability to adapt to online operation, in terms of keeping in touch, management meetings, decision making and recruitment and selection. This was facilitated by the immediate issue of laptops and, where requested, mobile phones to all staff and the introduction of MS Teams to enable online conversations. Although we have re-opened WIRA House on a limited basis, it seems unlikely that we will return fully to our previous office-based operations as they were. We have conducted a Returning Stronger survey that seeks to identify some of the positive outcomes driven by the pandemic. The impact of COVID-19 and the changed working environment will also be addressed in this year’s Staff Survey, currently underway.

4
Health and Wellbeing. A direct impact of remote working was an increased call for practical and emotional support. Our established Occupational Health, counselling and wellbeing offer was enhanced by an online 24/7 Employee Assistance Programme, renewed publicity for our Health and Wellbeing Group (HWG), our Mental Health First Aiders and the Freedom to Speak Up Guardians. We also established, initially, daily written updates to all staff including supportive messages from the Chief Executive and Directors; ‘Kitchen Chat’ e-drop in sessions. A DSE (Display Screen Equipment) Assessment also gauged colleagues’ comfort and safety in working from home and, as a result, additional equipment issued for home use.
Black Lives Matter and disproportionate impact of COVID-19. Like the rest of the NHS and the Integrated Care System (ICS), we have begun to systematically review all our people processes and are proactively involving colleagues from the BAME (Black, Asian and Minority Ethnic) network in key decision-making including senior level appointments. A comprehensive COVID-19 risk assessment was completed for all CCG staff and actions taken to limit risk. This and the DSE review will be repeated periodically and when circumstances change.
Further development of our diversity and inclusion offer. The BAME network has proved very successful and perhaps offers a template for developing further support to staff facing particular challenges (for example: staff with disabilities, premature birth, caring responsibilities and historical abuse). We continue to source support and adapt our policies and working practices. We have recently, for example, carried out a staff survey in relation to disabilities with the aim of understanding some of the challenges colleagues across the CCG experience and to explore the interest in developing a Disability and Wellbeing Network. Analysis of the responses to the survey is currently underway.
The NHS People Plan. The NHS People plan has provided all NHS organisations with a clear set of actions that we must undertake to embody the behaviours set out in the People Promise. Many of the actions were already underway by means of our HWG, our Workforce Race Equality Standard (WRES) action plan and the P&OD Strategy action plan. This includes making our recruitment processes more inclusive, increased promotion of the physical and mental health and wellbeing of our staff and continuing to offer learning and development opportunities to increase the capability of our staff. These action plans are being brought together to provide clear oversight of the further interventions needed to be developed by the team.
Shaping Our Future. We paused briefly on this programme trailed in January, during the first wave of the pandemic, but have now entered the post-filling phase to support the new operating model and organisational structure. This has included development work on capability requirements and a Leadership Behaviour Framework which we have begun to socialise with our senior managers.
Social Partnership Forum. We now have effective engagement and consultation arrangements in place with our Staff Side colleagues including a regular Forum.

5
3. PROPOSAL 3.1 What is planned to prepare the CCG for future developments?
3.1.1 Our future plans will be largely dictated by the fulfilment of Shaping Our Future. Delayed by COVID-19, we remain committed to introducing the new working arrangements required to deliver the new operating model from the start of 2021-22. The people ambitions include:
a. Greater partnership working and integration with our partners with wider use of shared posts and management, and more extensive matrix working along extreme teaming principles.
b. A clear deployment model within the CCG to enable agile resourcing and working.
c. Building on the Leadership Behaviour Framework and rolling these values out through the organisation.
d. A greater understanding of the capabilities of our people and what gaps exist to fulfil current and emerging organisational and system needs.
e. Further development of coaching, mentoring and learning including workshops, secondment and shadowing opportunities and the offer of Executive Coaching;
f. Continued engagement with Culture Change initiatives at national, place and local levels. Ensuring we remain fully informed and involved in developments around Inclusive and Compassionate Leadership and embedding those principles into all our activities, processes and practices.
g. An unremitting commitment to addressing inequality across the organisation and, in particular, representation at senior levels in the CCG.
4. NEXT STEPS 4.1 The Strategy continues to reflect our broad direction of travel characterised by ever greater
collaboration and partnership working across the system. We would normally see no reason for any significant reorientation of the Strategy – it has served us well.
4.2 However, the NHS People Plan and Promise offers an alternative framework to describe our intentions for how we engage and manage our people. We will want to track developments in its use by NHS England, NHS Improvement and our partners and may return to Governing Body with a further proposal during 2021.In the interim; we will continue to monitor progress and report via the Remuneration and Nominations Committee.
5. STATUTORY/LEGAL/REGULATORY/CONTRACTUAL
5.1 The CCG has existing contractual relationships with providers of professional People and
OD services that are necessary for the realisation of its strategic plans.

6
5.2 This report does not seek to change these so there are no additional statutory, legal, regulatory or contractual implications.
6. FINANCIAL IMPLICATIONS AND RISK 6.1 The contract for developing the new operating model for Shaping Our Future had a limited
timescale and the costs were agreed as part of a rigorous tender process that met all necessary procurement and governance requirements. The additional in-house OD capacity set out in this report is provided through either secondment or temporary arrangements within existing budgets. Service arrangements, such as those via LTHT, give improved value for money through partnership working that enables the CCGs to shape those services within existing budgets.
6.2 The CCG has to be both resilient and agile in order to respond to the dynamic environment in which it operates, which in turn, requires responsivity and agility from our P&OD function. If that cannot deliver effective support, the risk is that it will fail to create the right conditions to enable the CCG to achieve its ambitions.
7. COMMUNICATIONS AND INVOLVEMENT 7.1 The original P&OD Strategy covered the period 2018 – 21. The communication and
involvement activities around its review will include:
7.1.1 Assuming Governing Body agreement that it remains broadly fit for purpose, it will remain publicly available on the CCG’s website
7.1.2 A communications plan will be needed for the People Plan and, should this supersede the Strategy, that proposal will be presented to Governing Body.
7.1.3 Continued monitoring of Workforce and Diversity reports by the CCG’s Workforce and Diversity Group; Executive Management Team and the Remuneration and Nominations Committee.
7.1.4 Publication of this report and other supporting material on the CCG website and Extranet.
8. WORKFORCE
8.1 The plans set out in this report are designed to build the CCG’s capacity through, amongst other things, employee and leadership development. This will increase awareness of, and competence in ‘soft skills’ such as Coaching, which will support people to operate more confidently and effectively across a broader range of scenarios.
8.2 Better engagement through the staff survey, involvement, inclusion and development through appraisal, health and wellbeing through staff-led groups and collaborative working through active pursuit of partnership, will all work together to further attract, develop and retain a workforce that is more motivated, capable and engaged.

7
8.3 No negative workforce implications are anticipated, though the change to working arrangements will require sensitive handling.
9. EQUALITY IMPACT ASSESSMENT 9.1 The staff survey response rate of 80% for 2019 was encouraging, and in line with the
national average completion rate for CCGs. This gives confidence that the results will provide a reliable baseline in terms of representation of staff opinions. We will need to do all we can to replicate that engagement for the 2020 survey.
9.2 Similarly the introduction of an improved and consistent appraisal system, and the encouragement for staff-led communications and groups, deliver tangible benefits for involvement, equality and staff voice.
10. ENVIRONMENTAL
10.1 There are no anticipated environmental issues, though the increased use of homeworking
and other remote working will contribute to a reduction in the CCG’s carbon footprint.
11. RECOMMENDATION
The Governing Body is asked to:
(a) NOTE the continuing progress made during 2020; (b) COMMENT on the content of this report; and (c) ENDORSE and SUPPORT the plans described for 2021.

ANNEX A: PEOPLE & OD STRATEGY. ACTION PLAN SUMMARY STOCKTAKE
The diagram below describes the actions completed in the first two years of the strategy (in green) and indicates key activity for the coming 12 months (in
red). The table that follows lists the activities as described in the Action Plan and uses a RAG rating to assess progress in each workstrand against the
original plan.
People & OD Strategy
Leadership Framework
Appraisal process
Recruitment, Selection and Onboarding
Inclusion
Learning opportunities
Senior Leadership Tier development
Shaping Our Future -
impact on OD
Health & Wellbeing
Coaching offer

THEME
ACTION
Resourcing 1 Apprenticeship Guidance, including a city-wide approach Complete
Resourcing 2
Review the promotion of alternative channels of recruitment i.e. LinkedIn,
local communities, primary care, Leeds employers city-wide
Complete
Resourcing 3
Alternative method of recruitment i.e. alternative to NHS Jobs and internal
administration (E-track)
Superseded by link to
LTHT. Will explore
alternatives
Resourcing 4 Offer broader induction including an understanding of commissioning
process, teams and impacts on each other. Including Biographies, structure
charts and extranet information
Complete
Resourcing 5 Standardised approach to recruitment Complete
Resourcing 6 Recruitment toolkit for managers, including a suite of values based interview
questions for recruitment
Some work, but still a
need
Resourcing 7 Understanding and collating internal pools of resources, skills and
capabilities internally
SoF leading to better
understanding
Resourcing 8 Review recruitment and promotion practices to make sure
that staffing reflects the diversity of the community, and regional and national labour markets
New
Resourcing 9 Explore greater use of jointly-funded posts New
Resourcing 10 Explore organisations commitment to flexible working for all including roll
out of carers passport
New

Talent 1 Review appraisal process, including a talent matrix approach, train people appropriately in the appraisal process
Complete
Talent 2 Scope the meaning of the skills gap analysis and agree approach/timeframe Work begun as part of SoF post-filling activity
Talent 3 Formalising the CCG's approach for access to mentoring, Planned as part of coaching offer
Talent 4 Consider adopting the Citywide network approach, that is used for coaching to support mentoring
Complete
Talent 5 Using data from workforce planning, identify 'at risk' roles and agree a succession planning approach to address the gap (including Clinical Leadership)
Emerging issue from SoF, but needs more targeted work
Talent 6 Review previous approaches to Governing Body development and work with Corporate Governance team to identify future approach
New Chair has embarked on review
Engagement 1 Revisit previous communications survey outcomes, temperature check,
engagement thermometer and take appropriate action (eg refresh team
brief, workplace launch etc)
Complete
Engagement 2 Development a schedule of Staff Away Days inform content and implement Complete
Engagement 3 Evaluation and Review the Building Champions network Complete
Engagement 4 Increase the Champions cohort Complete – two tranches
Engagement 5 Suggestions Box and Bright Ideas, you said we did model Complete
Engagement 6 Conduct Staff Survey Complete – 2019 done,
2020 in train
Health & WB
1
Clarify the accountability of the H&WB Group and publicise the role of the
group and it's outcomes
Complete

H&WB 2 Director level responsibility for H&WB and H&WB Champions Complete
H&WB 3 Learning from other organisations where we can share good practice and
shared arrangements i.e. WIRA Business Park, city-wide organisations, LCC,
LTHT, etc.
Ad hoc learning so far
H&WB 4 Extranet page specific to H&WB Complete
H&WB 5 Re-procurement of OH and counselling services (widening the offer/scope
of services i.e. MSK)
Complete. EAP added in
2020
H&WB 6 Promotion of H&WB at induction, manager training and as part of
organisational value
Complete
H&WB 7 Link flexible work arrangements (and it's support) to induction and appraisal
conversations. Explore extension to current flexible work patterns and
examples of best practice.
Partially addressed, though
still more to do in terms
of publicity, further
development
H&WB 8 Revise Special Leave Policy to include provision for voluntary work/time out
to improve H&WB and support corporate social responsibility
Complete
Inclusion 1 WRES action plan actions published and reviewed annually Complete for 2019 and
2020
Inclusion 2 Review membership of all CCG formal meetings, to ensure protective characteristics are considered (board diversity)
Complete
Inclusion 3 Update self-assessment for disability confident standard for the single CCG Complete
Inclusion 4 Research development opportunities which target under- represented groups and share
Under review, but no formal output, as yet
Inclusion 5 Review protected characteristic data that is available as a check and balance for all people related processes
Ongoing activity

Inclusion 6 Developing Managers awareness of their responsibility to support any reasonable adjustments for new starters and current employees
Ongoing. Unconscious Bias training due in 2020
Inclusion 7 Review Gender Pay Gap analysis and action plan New – Paused in 2020
Learning &
Development
Review appraisal process, train people appropriately in the appraisal process Complete
L&D 2 Capture individual development needs from appraisal discussions and inform
learning & development needs for the organisation
Complete
L&D 3 Capture organisational wide development need from directorates and
inform the learning & development needs
Complete for 2019
L&D 4 Statutory/Mandatory compliance, ongoing monitoring and maintenance of
the provision, transition from current arrangements i.e. impact of eMBED
contract end
Complete. Compliance at
90%+
L&D 5 Link into wider Leeds resources i.e. training programmes, coaching etc.…,
Influencing and developing a portfolio
Ad hoc. Link to LTHT not
fully actioned
L&D 6 Support for existing coaches Complete
L&D 7 Address the need for clear management of Learning and Development
applications - consider broader approaches for CPD across the city
Discussions began with
Health & Care Academy
but paused. Some alliance.
L&D 8 Develop and implement a Management skills programme Manager as Coach
delivered. Will pick up as
part of SoF.
Workforce Planning & Transition 1
Consider the validity of the development of a long term workforce plan that includes information about future alignment of work streams to other organisations
Greater focus on workforce planning, but more to do.

W P & T 2 Audit of current New Ways of Working arrangements, following its implementation in April 2018
Overtaken by impact of COVID-19. Still requires documentation
W P & T 3 Agree an approach of aligning resources to support the work of the Academy
Paused whilst Academy agrees approach
W P & T 4 Scoping the approach to matrix management for discussion with EMT Key element of SoF,
W P & T 5 Flexible deployment toolkit for managers including an examplar way of working document
Due to be includedin development under SoF
Leadership 1 Agree the approach on adopting the Healthcare Leadership Framework, including use of 360 feedback
Paused pending outcomes of SoF
Leadership 2 Develop the Management Development Programme Paused pending outcomes of SoF
Leadership 3 Contribution to the Citywide development of system induction and leadership approach
Attending meetings. System Leadership programme agreed and resource allocated
Leadership 4 Review Temperature Check and Staff Survey results to understand current culture around trust and support. Dependant on outcomes agree an appropriate plan
Partly completed. Awaiting 2020 results to compare trend analysis.

1
Agenda Item: GB 20/94 FOI Exempt: N
NHS Leeds CCG Governing Body Meeting
Date of meeting: 25 November 2020
Title: Chair’s Summary – Primary Care Commissioning Committee held on 7 October 2020
Lead Governing Body Member: Sam Senior, Lay Member & Chair – Primary Care Commissioning Committee
Category of paper
Tick as appropriate
()
Report Author: Cheryl Lee, Corporate Governance Officer
Decision
Discussion
Information
Approved by Lead Governing Body Member (Y/N) Y
EXECUTIVE SUMMARY: This report provides the NHS Leeds CCG Governing Body with a summary of items discussed and outcomes and risks identified at the Primary Care Commissioning Committee (PCCC) meeting held on 7 October 2020.
RECOMMENDATION: The Governing Body is asked to: (a) RECEIVE the report.
Description of key items of business discussed and key outcomes
1. Please note that this is a brief summary of the items considered and decisions taken at the meeting of the PCCC meeting held on 7 October 2020. Further information can be obtained by reference to the minutes of that meeting.
Chief Executive’s Update 2. Members were informed of the current Covid-19 position in Leeds which has seen numbers
in the mid to high 200’s per 100,000 people. The highest levels of infection are strongly amongst the lower age groups but all age groups are affected across all parts of Leeds. It was recognised that the implications would be more severe if a growth was seen in the older population. Members were informed that hospital admissions had increased and a third ward had already been opened and amid the increasing pressure, it is likely that some aspects of elective surgery may have to be cancelled. It was highlighted that workforce and testing remained high in terms of potential additional pressure. The need to be aware of recognising the impact on mental health and well-being should further restrictions come into place was stressed, along with the importance of the flu vaccine.
3. A significant challenge was noted in terms of finances for both the CCG and the NHS as a whole. The budget allocation leaves NHS Leeds CCG with financial challenges for the latter half of this year and a lack of clarity on the primary care funding position.

2
4. Multiple challenges were noted –the rising cases of Covid-19, pressures on elective
procedures, flu vaccinations and the significant financial challenges and uncertainty faced.
5. It was shared that the ‘shaping our future’ programme was not believed to have a significant impact on primary care resources or support. There have been changes in relation to GP contracts across Leeds whereby they are more widely integrated and aligned to broader outcomes.
6. A good example of the work and initiative being undertaken across Leeds was shared with the Committee; Wetherby surgery were arranging a mass flu vaccination drive-through event where 7000 patients would be vaccinated at one time.
Closure of Branch Surgery at Adel – Update 7. Members received an update on the branch closure at Adel. The landlord may decide to
give notice to the pharmacy therefore options available to the pharmacy were shared. There may be implications for the pharmacy needs assessment (PNA) and include the need to work within existing pharmacy regulations. It was noted that positive steps had been taken in mobilising patient transportation solutions and that formal arrangements would be confirmed at the next Committee meeting.
Primary Care Networks 8. The Committee was informed that revised national guidance had been circulated on PCN
and DES implementation.
9. The key focus would now be in relation to the investment and impact fund which is a points-based system in place to reward quality service and the additional role reimbursement scheme.
10. Challenges were noted with an identified forecast of workforce underspend of £680,000.
Some of the PCN’s with the biggest underspends were from the most deprived areas which could then have a negative impact on health inequalities. It was acknowledged that there was also the possibility that the anticipated underspend may be even greater. It was confirmed that 60% of the funding was within the financial baseline and confirmation was awaited for the remaining 40%.
11. Further challenges were noted regarding the progress of estates and utilising space for
newly recruited posts. Although clarity was needed about where the responsibility for that sits, a senior level estates member would be recruited within shaping our future.
Summary from the Primary Care Operational Group meetings in August and September 2020 12. The Committee was informed that Oakwood Surgery had now re-opened their list, meaning
all lists across Leeds were open.
13. There had been a notable increase in the number of asylum seekers across Leeds with additional support being provided by York Street Practice.

3
14. Target training had taken place in September and had received positive feedback.
15. An action was agreed for a shared risk approach to be revisited as part of the wider system integration work.
Impact of Covid on Quality in Primary Care 16. Members received an update on the impact of Covid-19 in primary care, highlighting the
findings of the work carried out by Dr Bryan Power. During the initial findings looking at March, April and May there was a significant decrease in access to appointments along with a change in how they are being accessed. There had been a marked decrease in LD health checks along with a decrease in cervical smears. Vaccination levels had continued without a significant drop. 100% of practices have provided assurance they are now offering face-face appointments and the number of appointments was now increasing to pre-Covid levels.
17. The Committee received assurance that all patient feedback received was followed up and
shared.
18. Members recognised that the biggest challenge facing primary care was the ongoing pandemic and the knock-on impact on health and well-being but the overview of quality highlighted that support was in place.
19. Positive news was relayed to members that 100% of practices in Leeds are now rated as
good or outstanding by the CQC.
CCG Enhanced care home scheme 2021/22 update 20. Members were updated on the 1-year agreement in place to support care homes whilst
awaiting the national guidance update which has been delayed due to Covid-19. The enhanced health and care home scheme would move towards less duplication.
21. Data regarding frailty was shared and a stepped approach to this was discussed. The importance of member feedback was acknowledged in developing the scheme and the primary care team will be running a care home session to ensure the ongoing dialogue and meaningful engagement.
22. The Committee approved the direction of travel, but recognized that this was a complex
area with significant work to be undertaken.
Primary Care Risk Report 23. Members noted there were eleven active risks aligned to the Committee rated at 12 and
above. A new addition reported was the alignment to the Governing Body Assurance Framework.
24. Two high amber (12) risks were reported: R651: General Practice Workforce, and high amber risk; R729: Risk of Harm post Covid-19 (Primary Care). An action was agreed for discussions to take place in relation to the levels of risk due to the pandemic and imminent Brexit along with the financial challenges faced.

4
Primary Care Finance and Estates Update 25. Members were presented with the position reported at month 5. The time-lag in reporting
was also noted. The Committee was informed of a budget overspend at month 5 – a continuation of the trend for months 1-4 with the gap relating mainly to Covid-19 costs having been refunded by NHSE to break even retrospectively in months 1-4 . We are still awaiting our refund for month 5.
26. Reports throughout 20-21 to PCC have highlighted consistently a forecast over spend for
Primary Care Co-Commissioning Budgets due to the CCG’s inability to move £1.8M of budget from the core allocation to cover the equitable funding scheme in Primary Care under the emergency finance rules introduced by NHSE/I for the pandemic period. Based on our indicative allocation now received for the remainder of the financial, it is clear that we will not be able to close this gap over the remainder of the year and that this deficit will continue. The NHS Leeds CCG has also not received a further allocation for the Impact and Investment Fund currently being paid to PCNs each month but it is likely that a separate allocation will ensue over the next 6 months.
27. The prescribing budget is also subject to overspending, in part due to changes in drug
prescribing recommendations resulting in more expensive regimes along with an increase in the prescription of Sertraline. The second factor in the budget overspend is the inability to pursue more cost-effective drugs due to the Covid-19 pandemic and restrictions.
28. Members were informed that an indicative budget allocation had now been provided for the remainder of 20-21. Our financial planning assumptions have led to a starting position of estimated overspend by the end of the year to be £25m. Assuming the reimbursement of costs from NHSE for Covid-19 in months 5 and 6 and also for related additional activity spend with independent sector providers for months 7-12, this deficit would be reduced to £15m. It was noted the CCG has been defunded £53min total against its original allocation for 20-21 with circa only half of planned spend (circa £25) with the Independent Sector having been taken on centrally as an offset. This is then main reason for the initial deficit position as highlighted above.
29. Leeds CCG is not alone in this position as many CCGs across Yorkshire, and the Country,
are also finding themselves with deficits.
Strategies/Policies approved N/A
Items of positive assurance or issues to be raised with the NHS Leeds Governing Body
N/A
Any additional comments
N/A
1
Agenda Item: GB 20/95 FOI Exempt: N
NHS Leeds CCG Governing Body
Date of meeting: 25 November 2020
Title: Chair’s Summary of Remuneration & Nomination Committee Meeting held on 14 October 2020
Lead Governing Body Member: Sam Senior, Lay Member – Primary Care Co-Commissioning / Deputy Chair
Category of Paper Tick as
appropriate
()
Report Author: Laura Parsons, Head of Corporate Governance & Risk
Decision
Discussion
Information
Approved by Lead Governing Body member (Y/N): Y
EXECUTIVE SUMMARY: 1. This report provides the NHS Leeds CCG Governing Body with a summary of items
discussed, outcomes and risks identified at the Remuneration & Nomination Committee meeting held on 14 October 2020.
RECOMMENDATION: The Governing Body is asked to: (a) RECEIVE the report.
Description of key items of business discussed
1. Please note that this is a brief summary of the items considered and decisions taken at the meeting of the Remuneration & Nomination Committee on 14 October 2020. Further information can be obtained by reference to the minutes of that meeting (subject to exemptions under the Freedom of Information Act).
Non Executive Posts – Succession Planning
2. The Committee noted that the terms of office for the three Member Representatives were due to end on 31 March 2021, therefore an election process would be undertaken in line with the Constitution. The Secondary Care Consultant had indicated that he would be retiring from 31 March 2021, therefore a recruitment process would be undertaken. Job descriptions were agreed for both roles.
VSM Pay
3. The Committee agreed to make recommendations to the Governing Body in relation to pay for some VSM staff, this is included in a separate item on today’s agenda (GB 20/104).
Quarterly Workforce Report 4. The Committee’s responsibilities now include oversight of workforce within the CCG. The
quarterly report was presented which provided detail on the current workforce profile and benchmarked performance in key HR areas such as sickness and recruitment. The Committee was pleased to note that statutory and mandatory training levels have reached

2
90% in all areas. A query was raised in relation to staff turnover which was 12.32% on average over the last 12 months. This was in line with other CCGs and was not of concern. Turnover rates had reduced recently due to Covid-19. Assurance was provided that turnover levels would be assessed at directorate level to ensure there were no areas with unusually high rates, and any concerns would be reported to the Committee by exception.
Staff Survey – Update on Harassment Figures 5. The Committee received an update on the results reported as part of the Workforce Race
Equality Standard (WRES) report. This identified harassment and bullying from colleagues as a significant issue. This will continue to be monitored and any further action will be informed by the 2020 staff survey results. There may be a decrease compared to last year as the majority of staff are now working from home.
Gender Pay Gap – Further Analysis 6. An update was provided further to the Committee’s request for a further comparison of the
Gender Pay Gap, following the report which showed results of a mean difference of 29.4% and median difference of 15.7%. Due to COVID-19 priorities, NHS organisations were not required to report for 2019 and, as a consequence, few comparators were available.
7. The next report was due in the next few months and would therefore be presented to the next Remuneration & Nomination Committee meeting, in February 2021. It was agreed that this should include a review of each pay band.
Lay Member Reappointments
8. The Clinical Chair presented a proposal in relation to Lay Member reappointments. Further detail is included in a separate item on today’s agenda (GB 20/104).
Strategies/Policies approved
Five policies have recently been agreed by Staff Side, and will be circulated to the Committee for approval by e-mail rather than delay approval until the next meeting in February.
Items of positive assurance or issues to be raised with the NHS Leeds CCG Governing Body
In particular, the Committee wished to highlight the Gender Pay Gap and inform the Governing Body that further analysis would be presented to the next Remuneration & Nomination Committee (including an analysis by pay band), to inform any action required.
Items of discussion regarding Strategic Risks to the CCG
This summary provides assurance in relation to strategic risk 8 (Constraints on CCG organisational effectiveness impact the delivery of the CCG’s plans). In particular, no concerns were reported as part of the quarterly workforce update, however the Committee will be considering more detailed analysis in relation to the Gender Pay Gap, and will continue to monitor harassment figures reported through the staff survey and agree actions as required.
Any other Comments
N/A

1
Agenda Item: GB 20/96a FOI Exempt: No
NHS Leeds CCG Governing Body Meeting
Date of meeting: 25 November 2020
Title: Chair’s Summary – Audit Committee meeting held on 18 November 2020
Lead Governing Body Member: Cheryl Hobson, Lay Member – Audit & Conflicts of Interest
Category of Paper Tick as
appropriate
()
Report Author: Anne Ellis, Risk Manager Decision
Discussion
Information
Approved by Lead Governing Body member (Y/N): Y
EXECUTIVE SUMMARY: This report provides the NHS Leeds CCG Governing Body with a summary of items discussed and outcomes and risks identified at the Audit Committee meeting held on 18 November 2020.
RECOMMENDATION: The Governing Body is asked to:
(a) RECEIVE the report; (b) APPROVE the minor changes to the Detailed Financial Policies; and (c) APPROVE the minor change to the Operational Scheme of Delegation;
Description of key items of business discussed and key outcomes
1. Please note that this is a brief summary of the items considered and decisions taken at the meeting of the Audit Committee held on 18 November 2020. Further information can be obtained by reference to the minutes of that meeting.
Finance
2. The Committee was provided with an update on the impact of the finance regime for 2020/21 on the ICS and the CCG financial position. The consolidated system financial plan was submitted to NHS England on 5 October 2020 with an accompanying letter setting out the planning assumptions and risks associated with the plan. The shortfall from the ICS system envelope considered at the last meeting of the System Oversight and Assurance Group was £72m. This included a Leeds CCG deficit of £13m; however this position was predicated on the system receiving significant further national funding which is so far indicated but not confirmed. The CCG has limited control over payments under the financial regime, the areas the CCG has control over include prescribing, Continuing Healthcare and investments relating to tackling health inequalities.

2
3. The Audit Committee noted that the Governing Body will receive an updated paper outlining the risks and proposed actions to manage the financial position in the ICS and in the CCG.
4. The members received an update on progress relating to VAT provisions and noted that
the final outcomes were awaited.
Risk Management 5. The Committee received an update on the operation of the risk management
arrangements and the current risk profile. There are 68 active risks on the CCG register, of which 25 are accepted risks. There are five corporate (red) risks reported, this is an increase from two. The increase is as a result of the impact of covid-19 increasing risks relating to the risk of harm to non-covid-19 patients and pressure on the system. The increased risk profile was also reflected in the Governing Body Assurance Framework (GBAF), in particular for the principal risks around health inequalities, quality of care and financial stability. The Committee was assured that risk management arrangements were operating in line with the CCG’s risk management strategy.
6. Members were presented with the report for the deep dive of GBAF risk 8: Constraints on
CCG Organisational Effectiveness Impacts the Delivery of the CCG’s plans. The Committee received an update on the current position in relation to the risk and the impact of covid-19 on the CCG and the unknowns going forward. The Committee noted that there were additional pressures on all teams and the CCG was working towards reaching the target score but that this was unlikely to be met by the end of March 2021. The Committee was assured on the position and was clear on the challenges being faced.
7. The Committee received a further paper on the progress towards managing the cyber
security risk, which is part of GBAF risk 8. The CCG has an action plan and governance in place to become compliant with Cyber Essentials Plus by 31 July 2021. The Committee was assured on the progress being made and the contribution that the actions will have on managing the overall organisational effectiveness risk.
Information Governance 8. The Committee was updated by the Data Protection Officer. Specific areas to highlight
included the change in reporting format, which is now based on the Accountability Framework recently introduced by the Information Commissioner’s Office which is divided into 10 categories to aid demonstration of compliance with relevant legislation. The Committee was assured that overall the CCG is fulfilling a good level of compliance with legislation despite the current conditions. There had been some slippage in processing activities. Information asset registers and data flows are reviewed on a six monthly basis, however this year, due to Covid-19, this was relaxed to be completed annually. Reviews had started and aim to be completed by the end of November 2020.
Internal Audit 9. The Committee was presented with the Internal Audit Progress Report which detailed the

3
audits undertaken in 2020/21. Two final reports have been issued for: Covid-19 Business Continuity, Significant assurance was provided and Full assurance was provided for the Primary Care Commissioning and Contracting audit. Work was ongoing on six audits. Progress against the plan had been delayed due to Covid-19 and audit staff being redeployed in the first wave, Internal Audit assured the Committee that the audits required to inform the Head of Audit Opinion would be completed as planned but could not assure that the full plan would be delivered by the end of March 2021. The Committee agreed to include an item on the agenda for the January 2021meeting to review any impact on delivery of the audit plan.
10. The Committee was presented with an update on open internal audit recommendations. The Committee noted that the number of open recommendations was reducing and there was good engagement with Internal Audit in implementing recommendations.
Counter Fraud 11. The Committee received and considered the Counter Fraud Progress Report. External Audit 12. The Committee received an update on planning for the External Audit of the 2020/21
accounts. A full plan would be brought to the Committee meeting in January 2021. External Audit was in the process of identifying the value for money (VFM) risks.
Governance 13. The Committee received assurance on the governance arrangements within the city for
managing the pandemic. 14. The Committee was assured that all tender waivers have been approved in line with the
CCG’s Procurement Policy. 15. The Committee received an update on progress against the PWC Audit Committee
Effectiveness action plan. Losses and Special Payments 16. There were no losses and special payments to report in the period since the last Audit
Committee meeting in September 2020.
Strategies/Policies approved
The Committee approved the following Information Governance policies: o Information Governance and Framework policy o Data Security and Information Governance Training Strategy o Data Subject Information Rights Including Subject Access Requests Policy

4
The Committee recommended minor changes to the following policies for approval by the Governing Body:
o Managing Conflicts of Interest Policy o Standards of Business Conduct Policy o Detailed Financial Policies o Minor change to the Operational Scheme of Delegation in relation to the approval
of tender waivers.
Items of positive assurance or issues to be raised with the NHS Leeds Governing Body
The Audit Committee highlighted the following:
The impact of the finance regime for 2020/21 on the ICS and the CCG financial position;
Good assurance on the governance arrangements across the city to manage the pandemic;
The impact of Covid-19 on the CCG is a recurring theme across the Audit Committee agenda.
Any additional comments
N/A

1
Agenda Item: GB 20/96b FOI Exempt: No
NHS Leeds CCG Governing Body
Date of meeting: 25 November 2020
Title: Chair’s Summary – Auditor Panel meeting held on 18 November 2020
Lead Governing Body Member: Cheryl Hobson, Lay Member – Audit & Conflicts of Interest
Category of Paper Tick as
appropriate
()
Report Author: Anne Ellis, Risk Manager Decision
Discussion
Information
Approved by Lead Governing Body member (Y/N): Y
EXECUTIVE SUMMARY: This report provides the NHS Leeds CCG Governing Body with a summary of items discussed and outcomes and risks identified at the Auditor Panel meeting held on 18 November 2020.
RECOMMENDATION: The Governing Body is asked to:
(a) RECEIVE the report; (b) APPROVE the Auditor Panel Terms of Reference.
Description of key items of business discussed and key outcomes
1. Please note that this is a brief summary of the items considered and decisions taken at the meeting of the Auditor Panel meeting held on 18 November 2020. Further information can be obtained by reference to the minutes of that meeting.
2. The Auditor Panel received an update on the joint external audit procurement exercise being undertaken with West Yorkshire CCGs. A procurement timetable is in place to award a contract to commence from 1 April 2021. The procurement is being led by Huddersfield CCG. Leeds CCG will be represented by Sam Jones, Senior Finance Manager.
3. The Panel received the Auditor Panel Terms of Reference and noted that there were no
proposed amendments. The Panel recommended the terms of reference for approval by the Governing Body.

1
Agenda Item: GB 20/97 FOI Exempt: No
NHS Leeds CCG Governing Body
Date of meeting: 25 November 2020
Title: Chair’s Summary of Quality & Performance Committee Meeting held on 11 November 2020
Lead Board Member: Dr Phil Ayres, Chair – Quality & Performance Committee & Secondary Care Specialist Doctor
Category of Paper Tick as
appropriate
()
Report Author: Sam Ramsey, Interim Head of Corporate Governance & Risk
Decision
Discussion
Information
Approved by Lead Governing Body member (Y/N): Y
EXECUTIVE SUMMARY: 1. This report provides the NHS Leeds CCG Governing Body with a summary of items
discussed at the Quality & Performance Committee meeting held on 11 November 2020.
RECOMMENDATION: The Governing Body is asked to: (a) RECEIVE the report.
Description of key items of business discussed
1. Please note that this is a brief summary of the items considered and decisions taken at themeeting of the Quality & Performance Committee on 11 November 2020. Furtherinformation can be obtained by reference to the minutes of that meeting.
Integrated Quality & Performance Report (IQPR) 2. The Committee received the Integrated Quality & Performance Report. Members noted
that many areas covered by the report; particularly in secondary care, were affected by thesecond wave of Covid infections in the City. Therefore, the report offered no assurance tothe Committee due to key performance indicators not being in line with nationally settargets/trajectories and no reasonable mitigation for this with no identifiable action thatcould be taken to rectify issues.
3. It was acknowledged that in terms of numbers, particularly delays to treatment, there willbe a degree of harm because of the second wave. Whilst the timescales for a recovery tonormal activity levels remained uncertain, the residual risk of significant harm would remainuntil the waiting times had reduced to a more acceptable level. The committee acceptedand agreed that there was little else that could have been foreseen or done to avoid thissituation.
4. The Chair highlighted that the Governing Body should note that in relation to the level of noassurance, there were no additional actions that could have been taken to provide a higherlevel of assurance; the Committee recognised that the timeline to recovery was unknown.

2
5. It was acknowledged that the entire IQPR had been rated at a level of no assurance due to
the level of unmet need but that there were areas of service that were still performing well. The Committee was informed that there was confidence in relation to cancer response times and diagnostics along with many elements of primary and community care (see below).
6. The Committee was informed that during phase 3, stabilisation and reset, national
performance expectations were set and as a city LTHT had ben commended for their ambitious targets and had over performed. This had been highlighted by the Integrated Care System (ICS) who had provided positive feedback to Leeds.
7. The Committee was assured that across providers, a commitment had been made to
continue services where possible, therefore it was noted that a better service had been maintained, however, not sufficient to prevent delayed waiting times.
8. In relation to Primary Care, the view was supported that during the second wave, routine
services had been maintained. Locally, practices had been invested in to increase capacity and manage winter and the backlog. Positive news was detailed in terms of the ambitious targets that had been set for flu vaccinations and at the current position; 30 practices had met over 75% for the over 65 year old cohort.
9. The need to understand and find ways to support GPs, their teams and the wider PCNs in
the delivery of a Covid 19 vaccination programme was expressed. Further pressures were expected on an already stretched workforce when the vaccine was rolled out. The Committee agreed to reflect to the Governing Body that there were concerns about levels of fatigue and that the expected vaccine programme would place the system under further stress.
10. The Committee acknowledged the rising demand within mental health and although there
had been sustained activity levels based on last years’ prevalence; unmet need was almost certainly rising because of system pressures.
11. An update was provided to the Committee on the current situation of care homes in Leeds.
It was noted that although there were a significant number of care homes with infections, procedures were well established with a number of support offers, including daily calls, regular bulletins and data from capacity trackers. PPE availability was noted to be good and staff absences were deemed manageable.
12. The Committee agreed the level of no assurance, recognised that the recovery path was
currently unknown and accepted that all staff in the system were making every feasible effort in the face of mounting pressure.
Providers Under Enhanced Monitoring 13. The Committee received a summary of the providers that were currently under Routine+
Monitoring, Enhanced Monitoring and Formal Action and the actions being taken as a result.
3
14. Members were assured that surveillance had continued during Covid-19 and six homes
had now been removed from the surveillance process due to the assurance gained. Relationships were ongoing between the CCG and Leeds City Council and meetings were taking place on a monthly basis to share intelligence.
15. Members agreed that they were fully assured of the process in place. CCG Risk Register 16. The risk register was presented. It was noted that there had been a change to the risk
profile and there had been an increase to two red risks, ‘Risk of Harm during and post Covid-19’ and ‘System Flow’. A further high amber risk has increased from 12 to 16 (red risk), relating to the risk of harm during and post Covid-19 in primary care (R729); this risk was aligned to the Primary Care Commissioning Committee.
17. Members acknowledged the risks linked to Covid-19 and the EU Exit. This was reflected in the risk profile in the Governing Body Assurance Framework risks aligned to the Committee.
CCG Emergency Planning Statement of Compliance 18. The CCG Emergency Planning Statement of Compliance report was presented. Members
were informed that a different assurance process had taken place this year in which the Accountable Officer signed off the statement.
19. Members noted good practice and were assured that the correct process had been followed and returned to NHS England.
Individual Funding Request Annual Report 20. The Committee received the Individual Funding Request Annual Report. Differences were
noted in approval rates between different areas of deprivation (fewer approvals in higher deprived areas). The Committee requested that further interrogation of the data be undertaken to explore possible explanations for this the variation. The ability of this report to describe such variation was noted as good practice.
21. Members were fully assured of the Individual Funding Request process in place. Forward Work Programme 2020-21 22. The Committee agreed to receive an update on the backlog of Continuing Healthcare
(CHC) assessments and reviews at the January 2021 Committee meeting.
Strategies/Policies approved
N/A
Items of positive assurance or items for escalation to the NHS Leeds CCG Governing Body and/or Audit Committee.
N/A

4
Items of discussion regarding Strategic Risks to the CCG
This summary provides details of discussion in relation to the strategic risks aligned to the Quality & Performance Committee.
Any other Comments
N/A

1
Leeds Health & Wellbeing Strategy Outcomes – that this report relates to:
1. People will live longer and have healthier lives
2. People will live full, active and independent lives
3. People’s quality of life will be improved by access to quality services
4. People will be actively involved in their health and their care
5. People will live in healthy, safe and sustainable communities
NHS Leeds CCG Strategic Commitments We will focus resources to:
1. Deliver better outcomes for people’s health and wellbeing
2. Reduce health inequalities across our city
We will work with our partners and the people of Leeds to:
3. Support a greater focus on the wider determinants of health
4. Increase their confidence to manage their own health and wellbeing
5. Achieve better integrated care for the population of Leeds
6. Create the conditions for health and care needs to be addressed around local neighbourhoods
Assurance Framework – which risks on the GBAF does this report relate to: 1. Failure to deliver the CCG commitment to reduce health inequalities across our city.
2. Quality of commissioned care is compromised and does not reflect best practice.
3. Failure to achieve financial stability and sustainability.
4. Failure to overcome local and national workforce shortages.
5. Business continuity of health and care services disrupted as a result of a significant event.
6. Ineffective patient and public engagement and lack of transparency in translation of engagement into decisions.
7. Partners and Professionals do not support the CCG strategy.
8. Constraints on CCG organisational effectiveness impact the delivery of the CCG’s plans.
9. Inadequate system infrastructure to support the CCG’s plans.
Agenda Item: GB 20/98 FOI Exempt: N
NHS Leeds CCG Governing Body Meeting
Date of meeting: 25th November 2020
Title: Integrated Quality and Performance Report
Lead Governing Body Member: Helen Lewis, Director of Pathway Integration
Category of Paper Tick as
appropriate
()
Report Author: Tamara McCabe – Planning and Performance
Decision
Reviewed by EMT/Date: N/A
Discussion
Reviewed by Committee/Date: Quality and Performance Committee Wednesday 11
th
November 2020 Information
Checked by Finance: N
Approved by Lead Governing Body member: Y

2
EXECUTIVE SUMMARY: This report provides an overview of current performance levels against the measures set out in the NHS Mandate and Constitution.
Following the NHS declaration of a Level 4 National Incident on 30 January due to Covid-19, and subsequently those levels falling and rising since then, many of these performance measures have been adversely affected to the requirement to follow national instruction.
The dashboards included with this report are:
NHS Constitution and Operational Planning
The indicators and metrics in each dashboard have been chosen to provide a balanced view for each sector. Please note that the metrics are flexible and may change depending on sustained performance.
No assurance is being recommended to the Governing Body due to performance not being in line with nationally set targets/trajectories and there is no reasonable mitigation for this and/or there is no identifiable action that can be taken to rectify issues.
NEXT STEPS: The key actions which will be undertaken in relation to performance are as follows:
To continue to closely monitor the commissioner and provider-led actions as part of phase 3 stabilisation and reset towards national performance expectations and system recovery towards at least national performance expectations as part of the phase 3 stabilisation and reset NHS Planning.
To continue to maximise all possible out of hospital capacity to free up beds for elective activity; however redeployment and sickness are still likely to impact very substantially.
RECOMMENDATION: The level of assurance being recommended to the Governing Body is:
No assurance – performance/quality is not in line with agreed targets/trajectories and there is no reasonable mitigation for this and/or there is no identifiable action that can be taken to rectify issues
The Governing Body is asked to:
a) CONSIDER the recommended level of assurance; b) RECEIVE and REVIEW the IQPR dashboards; discuss the information, note the current
areas of underperformance and mitigating action, and the major risks to improvement faced by the level of Covid infection as of October 2020.
3
1. Background 1.1 This report provides an overview of current performance levels against the measures set
out in the NHS Mandate and Constitution.
1.2 Following the NHS declaration of a Level 4 National Incident on 30 January due to Covid-19, and subsequently those levels falling and rising since then, many of these performance measures have been adversely affected by the requirement to follow national instruction.
2. Summary
2.1 Primary and Proactive Care
Access to primary and proactive care services continue to perform well with the proportion of the population with access to online consultations in Quarter 4 above the target of 75%. Many routine services were suspended for the latter part of 2019/20 and Quarter 1 of 2020/21 to focus clinical resources in managing patients with Covid or to support patient/staff safety. There are five areas of impact for primary care and these include reducing the numbers of health checks undertaken for SMI and LD, reducing the numbers of cervical screening, reducing the number of incidents being reported through Datix maintaining childhood vaccinations and increasing the number of patients eligible to use a registered NHS app. NHS England have outlined some key areas of focus, either through the use of restart letters or through the amendments to the QOF arrangements. The Primary Care team has refreshed the PQI so that it reflects a more population based approach in line with the strategic direction for the organisation with a focus on the key priority areas. In order to align these arrangements, NHS England has amended elements of the contract through the QOF arrangements for additional incentives to support the delivery of these priority areas. The overall quality position is now that 100% of practices are rated good or outstanding with the CQC.
2.2 Planned Care and Long Term Conditions 18 week performance increased to 60.5% in August 2020, an increase of 8.2% from June 2020. Outpatient capacity during August was approximately 77% pre-Covid levels during August due to social distancing and staff annual leave absence over the summer months to ensure that staff are not too fatigued as winter approaches. There are continued challenges within the specialties of ophthalmology, spines, colorectal, ENT, plastic surgery and oral surgery even though all specialties were face to face where required. As with 18 weeks and electives, all routine diagnostics were paused from 23rd March although urgent diagnostics (excluding endoscopy) continued. During April and May, a number of cancer diagnostics/treatments were placed on hold as services paused in line with national Covid-19 guidance. This therefore has continued long-terms impacts on 2 Week Waits, 31 day and 62 day performance during August.

4
The number of patients waiting over 18 weeks for a First Outpatient Appointment totalled 18,440 in September (down on previous months), but higher than pre-Covid levels (8,800 in March). Outpatient activity during September was 90% (with majority of contacts non-face to face). There is a risk that recovery will now be impacted due to growing Covid-19 cases within LTHT and staff absence due to illness/isolation and caring requirements i.e. children who are required to isolate. The number of patients waiting over 18 weeks is likely to increase during November regardless of activity levels, as the first week in November will mark 18 weeks since services were reinstated in June. At the end of September, 35,700 patients are waiting longer than 3 months for an appointment, which is a significant risk particularly in the area of ophthalmology, where there is a risk of harm relating to sight loss. In the specialty of ophthalmology, 7964 patients are currently waiting longer than 3 months for a follow-up appointment with 915 ophthalmology patients also waiting over 18 weeks for a first outpatient appointment. 13,700 patients are currently awaiting a diagnostic at LTHT; diagnostic capacity at LTHT is currently at 82% of pre-Covid levels due to social distancing; which is a great achievement, up from 55% in August. There were 1606 patients waiting longer than 52 weeks at the end of September, in the specialties of urology, colorectal, adult spines, paediatric urology and dentistry. This is a very steep rise from 346 at the end of June. This growth reflects the reality that very little routine surgery has been carried out, while the focus is on the most urgent clinical priorities, which are often also larger cases. Outpatient waits continue to increase too, then tipping onto surgical pathways later in a patient’s journey. Urgent referral rates have returned to pre-Covid levels; with cancer 2 Week Waits referral rate exceeding pre-Covid levels at 104%. The rate of other 'urgent' referrals is at 77% and this therefore merits investigation and potentially attention as to why this has not returned to normal in the same way. . Whilst services continue to do all they can to continue to deliver electives and outpatients, our planning assumptions will be at risk, depending on Covid-19 infection rates and the conversion to inpatient stays. The opening of additional Covid-19 wards, and the staffing required to support these, has substantially impacted on inpatient capacity and is likely to begin to impact outpatient and diagnostic services as staff and resources are redeployed to staff the many additional rotas required in the service configurations to create ‘hot wards’. LTHT continues to work closely with Spire and Nuffield to maximize the use of independent sector theatres and beds, but these are limited compared to the volumes of patients usually treated across the City.
2.3 Unplanned Care The Emergency Care Standard (ECS) in September was below target at 82.8%. There has been a continued reduction in the ECS since May, when 95% was achieved for the first time in five years. Since the peak of the first wave of Covid, month on month increases in attendances have been recorded. By August attendances had returned to 85% of the figure in August 2019, with the reduction in attendances predominately within the lower acuity

5
patient cohorts. A&E department footprints and processes have been reconfigured in line with, and to meet national Covid-19 response guidance, as have admission processes, leading to some inefficiencies in patient flow. This has therefore impacted delivery against the ECS. Lower bed occupancy levels earlier in the year also contributed to improved performance in previous months. Recent increases in demand across ED that includes a high prevalence of symptomatic Covid-19 and related presentations are likely to continue to impact on performance. Local Covid-19 infection rates suggest that growing demand and the requirement to meet national IPC guidance and reduce the transmission of infection will result in some delays to allocating beds for admissions. In August, the Yorkshire Ambulance Service (YAS) showed a decrease in performance compared to previous months, with YAS achieving 4 out of 6 response targets. August performance indicates that 90% of patients requiring an urgent response within 7 minutes waited no longer than 12 minutes and 44 seconds. Activity in August was 4.3% over plan in Leeds. This was the highest variance in activity plans year to date. High activity levels of contract plans were mainly within the Hear, Treat and Convey division of the shadow Payment by Results (PBR) tariff (40% over plan). This indicates that YAS are experiencing higher call volumes; however calls are being managed within the Emergency Operations Centre (EOC) as opposed to requiring an ambulance dispatch and conveyance. Conveyance remained below normal rates in August.
2.4 Mental Health and Learning Disabilities IAPT rates have been affected by reduced referrals/assessments due to Covid. Therefore the access rate is still below target at 12.4% against a target of 22%. Teams are working on a number of communication campaigns for November 2020 to market and promote the service which should result in increased access to the service during Q3 and Q4. Commissioners are also in the process of developing an access recovery plan with the service. With regard to IAPT waiting times for 6 and 18 weeks, there are some discrepancies currently in the reporting of these metrics and so those quoted within the IQPR dashboard are not a true reflection of the figures being reported by the Leeds Mental Health and Wellbeing Service. These discrepancies are being invested. The dementia diagnosis rate has declined since March 2020 because the usual, expected mortality of people with a dementia diagnosis, plus the excess deaths during the Covid period, have not been offset by people newly-diagnosed with dementia. The memory assessment services were paused, but have now restarted. The initial estimate is that the backlog of referrals from January to March will be seen during October to December. The service is operating with a mix of remote and face to face assessment and will be testing out how to triage people between these methods. The LYPFT older people’s service leads have been in touch with LTHT radiology colleagues to factor in the capacity for brain imaging. Therefore, it is anticipated that there may be a decline in diagnosis rates as these level off during October and we stay just above national target or, we might fall below target and then stabilise around 65%, before recovering above it.

6
2.5 Children’s and Maternity During 2019/20 a huge amount of work has been undertaken to enable all providers to be able to submit to the Mental Health Services dataset. From November 2019 all providers have been able to submit and therefore going forward the figures published will demonstrate a true reflection of activity. In addition, an exercise was undertaken during April and May 2020 to allow providers to submit data for the whole year had they not been able to do so. We are therefore awaiting this updated position for 2019/20. The latest data run has shown what seem to be some inaccuracies in the MHSDS figures in comparison to what providers have submitted, and this is currently being investigated between commissioners and providers with the support of BI. During the Covid period, services have altered their provision. The majority of CAMHS services were classified as critical services and therefore continued to support young people. Other third sector services were impacted initially and provision has been altered to ensure safe delivery however this will have an impact of future access rate figures. It should be noted though that services have contacted and risk assessed all service users to ensure they continue to receive the appropriate level of support. Demand continues to rise in all children’s mental health services as an impact of Covid-19. Additional waiting list initiative funding has been provided to the MindMate Wellbeing Service – this was mobilised for a 1st September start date using a new contracting mechanism which will enable data not previously flowed to the MHSDS to be captured. Waiting times for routine referrals to CYP Eating Disorder Service are currently at 93.3%. This is impacted by patient choice where first appointment time was rejected, and second appointment offer was cancelled. It is anticipated that demand will continue to rise within the Eating Disorder Service as an impact of Covid.
2.6 Continuing Health Care The Leeds position on the 28 day and 15% targets continues to be reported to NHSE on a quarterly basis. This reporting has remained in place throughout the Covid-19 pandemic. From 1st September 2020 until 31st March 2021 there is additional reporting on deferred assessment activity occurring on a fortnightly basis. There has been a notable improvement in both Quality Premiums in Quarter 2 where NHS CHC eligibility decision made within 28 days was above target at 86.3%. This has improved due to reduced number of CHC referrals and staffing shielding at home having the capacity to undertake the assessments. Although increased to 1.3% in Quarter 2 of 2020/21, the full NHS CHC assessments taking place in an acute hospital setting still remains above the target of less than 15%. This is due to an increase in Discharge to Assess beds enabling staff to undertake assessments outside of acute settings. Staff continue to complete most assessments as virtual assessments and this has been readily accepted by most patients and their families.
Throughout the pandemic there has been a notable increase in the proportion Fast Track referrals to other referral types compared to last year and this continues to be monitored.

7
The service anticipates a significant increase in complaints and challenges to the outcome of assessment as patients and their families have acclimatised to having fully funded care for many months. To try and reduce this, the team has RAG rated all patients.
3. NEXT STEPS
3.1 The key actions which will be undertaken in relation to performance are as follows:
To continue to closely monitor the commissioner and provider-led actions as part of phase 3 stabilisation and reset towards national performance expectations and system recovery towards at least national performance expectations as part of the phase 3 stabilisation and reset NHSE Planning.
To continue to maximise all possible out of hospital capacity to free up beds for elective activity; however redeployment and sickness are still likely to impact very substantially.
4. STATUTORY/LEGAL/REGULATORY/CONTRACTUAL
4.1 Not applicable. 5. FINANCIAL IMPLICATIONS AND RISK
5.1 Not applicable. 6. COMMUNICATIONS AND INVOLVEMENT
6.1 Not applicable. 7. WORKFORCE
7.1 Not applicable.
8. EQUALITY IMPACT ASSESSMENT
8.1 Not applicable.
9. ENVIRONMENTAL
9.1 Not applicable. 10. RECOMMENDATION The level of assurance being recommended to the Governing Body is:
Overall: No assurance – performance/quality is not in line with agreed targets/trajectories and there is no reasonable mitigation for this and/or there is no identifiable action that can be taken to rectify issues

8
The Governing Body is asked to:
a) CONSIDER the recommended level of assurance; b) RECEIVE and REVIEW the IQPR dashboards; discuss the information, note the current
areas of underperformance and mitigating action, and the major risks to improvement faced by the level of Covid infection as of October 2020.
Indicator Tables
NHS Constitution and Operational Planning Measures Page 2-3
RAG Rating
92.5%
88.0%
85.0%
Interpreting Trends
Sparklines
The most recent period of data is shown furthest to the right in each sparkline.
The Integrated Quality and Performance Report
Report Period: August 2020
Contents
Report Key
Note: The RAG rating applied within this report is based upon calculating a limit of
5% higher/lower relative to the expected standard/target.
For example, if the expected Standard is a minimum of 92%...
'Green' performance would be ≥ 92%
'Amber' performance would be 87.4% ≤ x < 92%
'Red' performance would be < 87.4%
Performance measures shown to be 'Amber' should still be interpreted as
underperforming - a RAG rating has only been applied to serve as a visual guide to
understand how close performance is to the expected standard.
They should not be interpreted as being currently within a tolerance level.
Trend analysis is currently based upon comparing the latest performance with the
performance in the previous period.
A green arrow represents an improvement in performance
An amber arrow represents no change in performance
A red arrow represents a deterioration in performance
Sparklines have been produced to demonstrate the distance
away from the expected target level, with green representing a
positive position and red representing underperformance.

NHS Constitution and Operational Planning Measures
Measure Target Data Period Current
NHS Constitution - RTT
RTT - Incomplete Pathway (18 week wait compliance) 92% Aug-20 60.5%
RTT - Incomplete Pathway (number of patients waiting) 47,411 Aug-20 41,014
RTT - 52 Week Waits 0 Aug-20 825
A&E
A&E Waiting Times: % 4 hours or less (LTHT - All Types of A&E)95% National
(93.3% Local)Sep-20 82.8%
NHS Constitution
Diagnostic Waiting Times99% National
(99.5% Local)Aug-20 73.3%
Cancer - 2 Week Wait 93% Aug-20 65.7%
Cancer - 2 Week Wait (Breast) 93% Aug-20 29.1%
Cancer - 31 Day First Treatment 96% Aug-20 96.8%
Cancer - 31 Day Surgery94% National
(94.3% Local)Aug-20 92.3%
Cancer - 31 Day Drugs 98% National
(98.2% Local)Aug-20 99.5%
Cancer - 31 Day Radiotherapy 94% Aug-20 100.0%
Cancer - 62 Day GP Referral 85% National
(85.3% Local)Aug-20 76.8%
Cancer - 62 Day Screening 90% National
(94.4% Local)Aug-20 0.0%
Cancer - 62 Day Upgrade 90% National
(68.6% Local)Aug-20 81.1%
Mental Health
Dementia - Estimated Diagnosis Rate 67% Aug-20 67.5%
IAPT Access (12 month equivalent based on rolling 3 months)22% National
(19.0% Local)Jul-20 12.4%
IAPT Recovery Rate 50% Jul-20 54.4%
IAPT Waiting Times - 6 Weeks 75% Jul-20 15.5%
IAPT Waiting Times - 18 Weeks 95% Jul-20 89.9%
EIP - Psychosis treated within two weeks of referral60% National
(57.1% Local)Jul-20 60.0%
People with a severe mental illness receiving a full annual physical health check
and follow-up interventions (Rolling 12 Months)60% 2020/21 Q1 55.1%
Improve access rate to CYPMH (YTD) 32% 2019/20 23.1%
Improve access to CYPMH (Rolling 12 Months) 34% Jul-20 25.2%
Waiting Times for Routine Referrals to CYP Eating Disorder Services - Within 4
Weeks (Rolling 12 Months)95% 2020/21 Q1 74.3%
Waiting Times for Urgent Referrals to CYP Eating Disorder Services - Within 1 Week
(Rolling 12 Months)95% 2020/21 Q1 100.0%
IAPT Trainees 8 2019/20 Q4 5
Therapists co-located in primary Care 14 2019/20 Q4 47
Performance Measures (1 of 2)
Trend

NHS Constitution and Operational Planning Measures
Measure Target Period Current
Primary Care Target Period Current
Proportion of the population with access to online consultations 75% 2019/20 Q4 90.6%
Extended Access Appointment Utilisation 75% Aug-20 86.6%
Learning Disability Target Period Current
Reliance on Inpatient Care for People with LD or Autism - CCGs (All Length of Stays) 13 2020/21 Q2 14
Reliance on Inpatient Care for People with LD or Autism - NHSE (All Length of
Stays)11 2020/21 Q2 6
Other Commitments
Number of personal health budgets that have been in place, at any point during
the financial year300 2020/21 Q1 503
Children Waiting no more than 18 Weeks for a Wheelchair 92% 2020/21 Q2 97.6%
Annual Health Checks (AHCs) delivered by GPs for patients on the Learning
Disability Register (YTD)186 2020/21 Q1 177
Performance Measures (2 of 2)
Trend

1
Agenda Item: GB 20/99a FOI Exempt: N
NHS Leeds CCG Governing Body Meeting
Date of meeting: 25 November 2020
Title: Managing Conflicts of Interest and Standards of Business Conduct Policies
Lead Governing Body Member: Sabrina Armstrong, Director of Organisational Effectiveness
Category of Paper Tick as
appropriate
()
Report Author: Sam Ramsey, Interim Head of Corporate Governance and Risk
Decision
Reviewed by EMT/Date: N/A Discussion
Reviewed by Committee/Date: N/A Information
Checked by Finance (Y/N/N/A - Date): N/A
Approved by Lead Governing Body member (Y/N): Y
Leeds Health & Wellbeing Strategy Outcomes – that this report relates to
1. People will live longer and have healthier lives
2. People will live full, active and independent lives
3. People’s quality of life will be improved by access to quality services
4. People will be actively involved in their health and their care
5. People will live in healthy, safe and sustainable communities
NHS Leeds CCG Strategic Commitments We will focus resources to:
1. Deliver better outcomes for people’s health and wellbeing
2. Reduce health inequalities across our city
We will work with our partners and the people of Leeds to:
3. Support a greater focus on the wider determinants of health
4. Increase their confidence to manage their own health and wellbeing
5. Achieve better integrated care for the population of Leeds
6. Create the conditions for health and care needs to be addressed around local neighbourhoods
Assurance Framework – which risks on the GBAF does this report relate to: 1. Failure to deliver the CCG commitment to reduce health inequalities across our city.
2. Quality of commissioned care is compromised and does not reflect best practice.
3. Failure to achieve financial stability and sustainability.
4. Failure to overcome local and national workforce shortages.
5. Business continuity of health and care services disrupted as a result of a significant event.
6. Ineffective patient and public engagement and lack of transparency in translation of engagement into decisions.
7. Partners and Professionals do not support the CCG strategy.
8. Constraints on CCG organisational effectiveness impact the delivery of the CCG’s plans.
9. Inadequate system infrastructure to support the CCG’s plans.

2
EXECUTIVE SUMMARY: In line with Statutory Guidance on Managing Conflicts of Interest, the Conflicts of Interest and Standards of Business Conduct policies must be reviewed on an annual basis. The policies have been reviewed and there are no amendments proposed. The policies are included within the supporting information documents. The policies were presented to the Audit Committee on 18 November 2020 and were recommended for approval.
NEXT STEPS: The policies will be published on the website with the review date amended.
RECOMMENDATION: The Governing Body is asked to:
a) REVIEW the Managing Conflicts of Interest and Standards of Business Conduct
Policies, NOTE that there are no proposed amendments, and APPROVE for publication.
1
Leeds Health & Wellbeing Strategy Outcomes – that this report relates to:
1. People will live longer and have healthier lives
2. People will live full, active and independent lives
3. People’s quality of life will be improved by access to quality services
4. People will be actively involved in their health and their care
5. People will live in healthy, safe and sustainable communities
NHS Leeds CCG Strategic Commitments We will focus resources to:
1. Deliver better outcomes for people’s health and wellbeing
2. Reduce health inequalities across our city
We will work with our partners and the people of Leeds to:
3. Support a greater focus on the wider determinants of health
4. Increase their confidence to manage their own health and wellbeing
5. Achieve better integrated care for the population of Leeds
6. Create the conditions for health and care needs to be addressed around local neighbourhoods
Assurance Framework – which risks on the GBAF does this report relate to: 1. Failure to deliver the CCG commitment to reduce health inequalities across our city.
2. Quality of commissioned care is compromised and does not reflect best practice.
3. Failure to achieve financial stability and sustainability.
4. Failure to overcome local and national workforce shortages.
5. Business continuity of health and care services disrupted as a result of a significant event.
6. Ineffective patient and public engagement and lack of transparency in translation of engagement into decisions.
7. Partners and Professionals do not support the CCG strategy.
8. Constraints on CCG organisational effectiveness impact the delivery of the CCG’s plans.
9. Inadequate system infrastructure to support the CCG’s plans.
Agenda Item: GB 20/99b FOI Exempt: No
NHS Leeds CCG Governing Body Meeting
Date of meeting: 25 November 2020
Title: Pharmaceutical and Related Industries Joint Working Policy
Lead Governing Body Member: Simon Stockill, Medical Director
Category of Paper Tick as
appropriate
()
Report Author: Sally Bower, Head of Medicines Optimisation
Decision
Reviewed by EMT/Date: NA
Discussion
Reviewed by Committee/Date: N/A Information
Checked by Finance (Y/N/N/A - Date): NA
Approved by Lead Governing Body member (Y/N): Y

2
EXECUTIVE SUMMARY: Department of Health Guidance encourages NHS organisations and their staff to consider opportunities for joint working with the pharmaceutical industry, where there are clear advantages to patient care and improvements to patients’ health and well-being. The NHS does not always have the expertise or necessary tools to aid implementation of innovation or best practice at the pace or scale that it desires. Pharmaceutical and other health care companies may wish to partner with the CCG to support this adoption of innovation. It is essential that all projects or dealings with the Industry are open and transparent and are subject to the widest scrutiny to enable likely pitfalls to be highlighted at an early stage. This policy aims to:
Provide all staff working for or on behalf of NHS Leeds CCG with a framework and
guidance for appropriate joint working
Ensure at all times that the interests of patients, public and NHS Leeds CCG are upheld
and maintained
Assist NHS Leeds CCG to achieve its objectives and delivery of national and local
priorities by building effective and appropriate working relationships with the
pharmaceutical and related industries
Inform and advise staff of their responsibilities when entering into joint working arrangements with the pharmaceutical and related industries.
NEXT STEPS: Receive and explore opportunities for joint working.
RECOMMENDATION: The Governing Body is asked to:
(a) APPROVE the policy.

1
GB 20/100 GOVERNING BODY FORWARD WORK PLAN 2020/21
ITEM MAY JUN JULY SEPT
NOV JAN MAR Lead
Officer
STANDING ITEMS
Welcome & apologies X X X X X X X Chair
Declarations of interest X X X X X X X Chair
Minutes of previous meeting X X X X X X Chair
Matters arising X X X X X X Chair
Action log X X X X X X Chair
Questions from members of the public X X X X X X X Chair
Patient Voice X JH
PERFORMANCE
Chief Officer’s Report X X X X X X TR
Integrated Quality & Performance Report
X X
X X X
HL/SA
FINANCE
Finance Report X X X X X VPS
AQP Update Paper X VPS
Approval of Annual Report & Accounts X VPS
Approval of Annual Budget X VPS
STRATEGY
CCG Operating Plan (incl. high level budgets)
X SA/VPS
People & OD Strategy/Refresh X SA
Shaping Our Future – New Operating Model
X
TR
Left Shift Blue Print X VPS
Climate Change X SA
RISK
Governing Body Assurance Framework
X X X
X X X SA
Corporate Risk Register X X X X X X SA
GOVERNANCE
Approval of Procurement Plan 2020/21 X VPS
Approval of Business Cases/Investments over £1.5m (as required)
Various
Chair’s Summary of Committee Meetings
X X X X X X Committee Chairs
Committee Terms of Reference X
Committee Chairs

2
ITEM MAY JUN JULY SEPT
NOV JAN MAR Lead
Officer
Update to Committee Terms of Reference & Scheme of Reservation & Delegation
Chair
Committee Annual Reports X
Committee Chairs
Governing Body Effectiveness X GS
Maternity and Neonatal Services Consultation
X
TR
Approval of Governing Body Appointments / Reappointments (as required)
Chair
Approval of amendments to Constitution (as required)
Chair
Forward Work Plan X X X X X X Chair
Policy Approval (as required) Various
Review of Operational Scheme of Delegation
X VPS
Patient Experience & Complaints Annual Report
X
JH
System Resilience Plan (included in Q&P Summary)
PA/HL
EPRR Compliance (included in Q&P Summary)
PA/HL

1
Joint Working Criteria (adapted from the Association of British Pharmaceutical Industry Joint Working Guide) All potential parties should review this checklist and satisfy themselves that each criterion would be met under the project. If the answer to any of the questions below is no, the project is not a true joint working arrangement and should not be viewed as such. Appropriate steps to address the outstanding areas should be taken before proceeding further.
YES NO
1 The main benefit of the project is focused on the patient
2 All parties acknowledge the arrangements may also benefit the NHS and pharmaceutical partners involved
3 Any subsequent benefits are at an organisational level and not specific to any individual
4 There is a significant contribution of pooled resources (taking into account people, finance, equipment, & time) from each of the parties involved
5 There is a shared commitment to joint development, implementation, and successful delivery of a patient‐centred project by all parties involved
6 Patient outcomes of the project will be measured and documented
7 All partners are committed to publishing an executive summary of the Joint Working Agreement
8 All proposed treatments involved are in line national guidance where it exists and based on evidence‐based clinical practice
9 All activities are to be conducted in an open and transparent manner
10 Exit strategy and any contingency arrangements have been agreed
11 Are you satisfied with your knowledge of the collaborating organisation i.e. is there evidence of audited accounts, is the organisation and ownership known?
12 Is the proposal on offer consistent with NHS Leeds West CCG priorities?

West Yorkshire & Harrogate Joint Committee of Clinical Commissioning Groups
Minutes of the meeting held in public on Tuesday 7th July 2020 Held virtually by Microsoft Teams
Members Initials Role and organisation Marie Burnham MB Independent Lay Chair
Richard Wilkinson RW Lay member
Stephen Hardy SH Lay member
Dr James Thomas JT Chair, NHS Bradford District and Craven CCG
Michelle Turner MT Strategic Director of Quality and Nursing, Bradford District and Craven CCG
Dr Steven Cleasby SC Chair, NHS Calderdale CCG
Neil Smurthwaite NS Deputy Chief Officer, NHS Calderdale CCG
Dr Steve Ollerton SO Chair, NHS Greater Huddersfield CCG
Carol McKenna CMc Chief Officer, NHS Greater Huddersfield CCG and NHS North Kirklees CCG
Dr Jason Broch JB Chair, NHS Leeds CCG
Tim Ryley TR Chief Officer, NHS Leeds CCG
Dr Adam Sheppard AS Chair, NHS Wakefield CCG
Jo Webster JW Chief Officer, NHS Wakefield CCG
Apologies
Helen Hirst HH Chief Officer, NHS Bradford District and Craven CCG
Dr Khalid Naeem KN Chair, NHS North Kirklees CCG
Dr Charles Parker CP Chair, NHS North Yorkshire CCG
Amanda Bloor AB Chief Executive, NHS North Yorkshire CCG
In attendance Esther Ashman EA Programme Director, Commissioning Futures
Stephen Gregg SG Governance Lead, Joint Committee of CCGs (minutes)
Ian Holmes IH Director, WY&H HCP
Anthony Kealy AKe Locality Director WY&H, NHS England & NHS Improvement
Catherine Thompson CT Improving Planned Care
Jonathan Webb JWb Director of Finance Lead, WY&H Health and Care Partnership
Item No. Action
76/20 Welcome, introductions and apologies
The Chair welcomed everyone to the meeting, and apologies were noted. As a result of the COVID-19 restrictions, this was the first in public since January 2020 and was being held via Microsoft Teams. Members of the public were able to watch the livestream of the meeting.

WY&H Joint Committee of CCGs – 07/07/2020
Page 2 of 5
Item No. Action
77/20 Chair’s update
The Chair noted that since the last meeting, partners had been dealing with the impact of the COVID-19 pandemic. Staff in all organisations had played a huge part in responding to the pandemic, and the Chair thanked them for their hard work and commitment. COVID-19 had also meant that we had refocused and reprioritised our work as a Partnership. In such challenging times, collaborative working was more important than ever. The Chair noted changes in the commissioning landscape. The Bradford and Craven CCGs had merged to form a single CCG. Harrogate CCG had merged to form North Yorkshire CCG, which was now an associate member of this Committee. The Chair proposed a vote of thanks to members who had left the Committee – Andy Withers, Gordon Sinclair, David Kelly and Sohail Abbas. She also thanked Richard Wilkinson who was attending his last meeting.
78/20 Questions and deputations
The Chair advised that because the meeting was being held virtually, questions would be handled differently today. Members of the public had been invited to send questions to the Partnership Team so that a member of our team could read them out on their behalf. One question had been received: Question: What, in the view of the JCCC, have been the effects on WYH ICS’s ability to respond to the Covid-19 Pandemic, of:
a) decade-long cuts to NHS funding, hospital beds and clinical staff - including ICU beds and staff?
b) the government’s failure to promptly authorise and direct widespread testing and tracing, from the start of the pandemic?
c) the government’s failure to source and provide adequate PPE? These questions were followed by a number of more detailed questions. As the questions largely related to the wider Partnership rather than the Joint Committee specifically, it was agreed that a written response would be prepared, drawing on the comments of partners.
79/20 Declarations of Interest
MB asked Committee members to declare any interests that might conflict with the business on today’s agenda. There were none.
80/20 Minutes of the meeting in public – 14 January 2020
The Committee reviewed the minutes of the last meeting.
The Joint Committee: Approved the minutes of the meeting on 14 January 2020, subject to the correction of a minor typographical error.
81/20 Actions and matters arising – 14 January 2020
The Joint Committee reviewed the action log.
The Joint Committee: Noted the action log.
82/20 Joint Committee governance
SG presented an update on key governance issues.

WY&H Joint Committee of CCGs – 07/07/2020
Page 3 of 5
Item No. Action COVID had significantly disrupted governance arrangements and some ‘business as usual’, including approval of the Committee’s annual report, had been carried out ‘virtually’. Programmes had been refocussed and the existing Joint Committee work plan had largely run its course, which had meant that there has been no requirement for the Joint Committee to take any formal commissioning decisions during the lockdown. In March, members had agreed that a revised MoU and work plan be presented to the individual CCGs for approval. The main changes were the delegation of new commissioning decisions and changes in Committee membership, with North Yorkshire CCG becoming an associate member, able to contribute to the discussion but not to vote. The new MoU and work plan would come into effect once it had been approved by all of the West Yorkshire CCGs. The risk framework would be refreshed to reflect the Committee’s new work plan. CCG mergers had meant that the PPI Assurance Group now had a core membership of only 5. SH said that further work was being done on the membership and role of the PPI Assurance Group to enable it to continue its core role of providing assurance to the Joint Committee. JW noted the importance of the Group drawing on the wide range of engagement activity that was taking place across all Partnership programmes.
The Joint Committee: a) Noted the 2019/20 annual report. b) Noted the progress in agreeing the new MOU and work plan and that the
MoU would be presented to the Accountable Officers once it had been agreed by all of the CCGs.
c) Requested that an agenda planner, based on the revised work plan, be presented to the meeting in public in October, together with the refreshed risk framework.
d) Requested that further work be done to explore the future membership and role of the PPI Assurance Group.
SG
83/20 Our response on COVID-19: Implications for the Joint Committee
IH report on the response of the health and care system to the initial surge in the COVID-19 pandemic. As we moved to a more stable situation our focus was turning towards how we continue to meet the needs of people with COVID and other conditions. The paper set out the approach and how we had refocused our programmes to support the response. In this uniquely fast moving environment, priorities and pressure points would change frequently and an agile response was essential. While the specific focus of our work had changed, our Five year plan continued to set the high level objectives. The report included revised summary plans for each of the work programmes where decisions had been delegated to the Joint Committee. Alongside stabilisation and reset, the main development which would influence the Joint Committee’s future priorities and approach was the commissioning futures work. Moving forward, the Committee’s work plan and role would evolve to reflect these new priorities. JT noted the need for the Committee to be involved in the further development of the commissioning futures work. JW confirmed that an update on the work would be brought to a future meeting.
JW/EA

WY&H Joint Committee of CCGs – 07/07/2020
Page 4 of 5
Item No. Action
The Joint Committee: a) Noted the approach set out in response to the pandemic, and the programme
priorities for the next phase of the response. b) Noted the next steps to develop a revised forward plan for the Joint
Committee based on these new priorities.
84/20 Improving Planned Care: Programme Refresh
CT presented a summary of the changes to the Improving Planned Care programme as a result of the response to COVID-19. The proposed new priorities supported the stabilisation and reset of health and care services and included: • A single programme of work bringing together the Elective Care programme
and the WYAAT Elective Surgery programme, under new leadership and overseen by a new Alliance Board.
• Supporting places with restarting planned care and limiting the growth of waiting lists. This included a bid for a proposed elective care ‘hub’.
• Optimising the use of diagnostic capacity. • Supporting a different approach to pathways, focusing on prevention, shared
decision-making between primary and secondary care and personalisation. Elements of the pre-existing work programme had been re-started where they supported the re-start of planned care, for example time-critical eye services. SO highlighted the need to manage carefully the transfer of work between primary and secondary care. JW acknowledged that the impact of changing pathways would be felt across the system and that effective partnership would be needed. TR noted the need to be clear that the work at WY&H level and in particular the elective care ‘hub’ would support work at place level. He also noted the need to join up work with places and other Partnership programmes around prevention. CT noted the importance of putting the health of the population at the centre of the Programme’s work. She added that the Programme was working closely with other programmes on shared care, personalisation and prevention. JT noted the need to embed personalised care within all Programmes. The Clinical Forum supported the need to focus on population health and to ensure that learning was shared effectively across the Partnership. IH welcomed the establishment of a system-wide Programme designed to support place. SC highlighted the critical importance of the Programme, which would involve fundamental transformation across the system. Strong relationships and clinical leadership would be needed to ensure that shared responsibility was embedded across the whole system. JW added that system transformation was needed to ensure that capacity was used effectively to improve outcomes and reduce inequalities. Winning ‘hearts and minds’ would be key.
The Joint Committee: a) Noted the integration of the two programmes to form the Improving Planned
Care programme b) Supported the proposals to address access to diagnostic testing and elective
surgery c) Supported the proposals to address referrals and support proactive
approaches to managing planned care. d) Recommended that CCGs take the proposals back into their individual
CCGs for further consideration.

WY&H Joint Committee of CCGs – 07/07/2020
Page 5 of 5
Item No. Action
85/20 Any other business
RW thanked the Chair and members for their support and for their contribution to the work of the Joint Committee over the past 3 years.
Next Joint Committee in public – Tuesday 6 October 2020, 11am – 1pm.

1
Pharmaceutical and Related Industries Joint Working Policy

2
Review and Amendment Log / Version Control Sheet
Responsible Officer: Dr Simon Stockill, Medical Director
Clinical Lead: Dr Simon Stockill, Medical Director
Author: Sally Bower, Head of Medicines Optimisation, Commissioning team
Date Approved: November 2020
Committee: Governing Body
Version: 4.0
Review Date: November 2023
Version History
Version no. Date Author Description Circulation
1.0 February
2016 Sally Bower
Initial draft approved by Senior Management team, NHS Leeds West CCG
Senior Management Team Patient leaders
2.0 March 2018 Sally Bower Amended NHS Leeds West CCG to Leeds CCG Partnership
Senior Management Team Patient leaders
3.0 April 2019 Kim Mooring Annual update completed
Senior Management Team Patient leaders
4.0 October
2020 Sally Bower
Revision of previous versions following updated ABPI Code 2019,(particularly clause 20) and associated guidance
Clinical Directors Head of Corporate Governance and Risk Patient leaders

3
Contents
Page
1. Introduction 4
2. Purpose 4
3 Definition of Joint Working 5
4 Values 5
5 Principles of Assessing Joint Working Approval 6
6 Minimum Dataset for Project Approval 7
7 Confidential and Patient Identifiable Information 7
8 Freedom of Information 8
9 Duties / Accountabilities / Responsibilities 8
10 Responsibilities for Approval 9
11 Public Sector Equality Duty 9
12 Scope of the Policy 9
13 Monitoring Compliance with the Document 9
14 Arrangements for Review 9
15 Dissemination 9
16 References 10
17 Appendices 10
Appendices
Appendix 1 Equality Impact Assessment
Appendix 2 Joint Working Criteria

4
1 Introduction
Department of Health Guidance encourages NHS organisations and their staff
to consider opportunities for joint working with the pharmaceutical industry,
where there are clear advantages to patient care and improvements to
patients’ health and well-being.
In the past, contact between the Pharmaceutical Industry and primary health
care professionals has revolved around the purchase or promotion of specific
products and the provision of sponsorship e.g. to support educational events
or training. More recently, the Industry has begun to focus on enhancing its
links with the NHS. Many companies have developed internal structures to
encourage closer liaison with GP practices, CCGs and health care
professionals working for CCGs.
The NHS does not always have the expertise or necessary tools to aid
implementation of innovation or best practice at the pace or scale that it
desires. Pharmaceutical and other health care companies may wish to
partner with the CCG to support this adoption of innovation. The ‘Innovation
Health and Wealth, Accelerating Adoption and Diffusion in the NHS’ report
sets out a strategy for collaboration between the NHS and industry to improve
health outcomes for patients.
It is essential that all projects or dealings with the Industry are open and
transparent and are subject to the widest scrutiny to enable likely pitfalls to be
highlighted at an early stage.
2 Purpose
The aim of this policy is to:
Provide all staff working for or on behalf of NHS Leeds CCG with a
framework and guidance for appropriate joint working
Ensure at all times that the interests of patients, public and NHS Leeds
CCG are upheld and maintained
Assist NHS Leeds CCG to achieve its objectives and delivery of national
and local priorities by building effective and appropriate working
relationships with the pharmaceutical and related industries
Inform and advise staff of their responsibilities when entering into joint
working arrangements with the pharmaceutical and related industries.
Specifically, it aims to:

5
Assist NHS Leeds CCG and its staff in maintaining appropriate
ethical standards in the conduct of NHS business.
Highlight that NHS staff are accountable for achieving the best
possible health care within the resources available.
Staff are reminded that at all times they have a responsibility to comply with their own professional codes of conduct and CCG’s standards of business conduct policy. In the interests of transparency staff must comply with CCG’s Hospitality, gifts and sponsorship policy and Declarations of interest’s policy.
Representatives of the pharmaceutical industry must comply with the ABPI
Code of Practice for the Pharmaceutical Industry as a condition of their
membership. Pharmaceutical companies must publicly disclose all ‘Transfers
of Value’ to health care professionals and health care organisations on an
annual basis for the preceding year. Non-member pharmaceutical industries
who promote prescription medicines are also encouraged by the ABPI and
MHRA. If staff believe that a pharmaceutical industry representative has
broken the Code, they can report their complaint to the Director of the
Prescription Medicines Code of Practice Authority (PMCPA) at
Further details on the ABPI Code including a guide for health professionals, is
available at https://www.pmcpa.org.uk/the-code
3 Definition of Joint Working
For the purpose of this policy, joint working is defined as situations where, for
the benefit of patients, the NHS and commercial organisations pool skills,
experience and/or resources for the joint development and implementation of
patient centred projects and share a commitment to successful delivery. Joint
working differs from sponsorship, where pharmaceutical companies simply
provide funds for a specific event or work programme.
4. Values
In line with the NHS Code of Conduct three public service values underpin the
work of the NHS:

6
Accountability – everything done by those who work in the NHS must be
able to stand the test of parliamentary scrutiny, public judgements of propriety
and professional codes of conduct;
Probity – there should be an absolute standard of honesty in dealing with the
assets of the NHS. Integrity should be the hallmark of all personal conduct in
decisions affecting patients, staff and suppliers, and in the use of information
acquired in the course of NHS duties. This includes ensuring that integrity is
not only ensured in all decision making processes, but that it is also clearly
perceivable from the point of view of a stakeholder or third party, and
Openness – there should be sufficient transparency about NHS activities to
promote confidence between the organisation and its staff, patients and the
public
5 Principles for Joint Working Arrangements
Joint working arrangements should be of mutual benefit, with the principal
beneficiary being the patient. The length of the arrangement, the potential
implications for patients and the NHS, together with the perceived benefits for
all parties, should be clearly outlined before entering into any joint working
arrangement.
The following principles also apply:
Staff must be aware of NHS guidance, the legal position and
appropriate and relevant professional codes of conduct in relation to
joint working initiatives.
Contracts will be negotiated in line with NHS values.
Confidentiality of information received in the course of duty must be
respected and never used outside the scope of the specific project.
Whilst joint working arrangements should take place at a corporate,
rather than an individual level the role (or lack thereof) of sales
representatives must be agreed during scoping and them and
appropriate NHS staff made aware.
Clinical and financial outcomes will be assessed through a process of
risk assessment.

7
Each company that enters into a joint venture with NHS Leeds CCG
will be acknowledged for resources provided. NHS Leeds CCG will
only endorse a particular medicine as a result of the joint venture in line
with national or local guidance provided that all parties are agreed that
the activity is ethical and in patients’ best interest and the marketing
authorisation of the medicine involved.
NHS Leeds CCG or its staff will not agree to practice under any
condition that compromises professional independence or judgement,
or imposes such conditions on other health care professionals.
A mutually agreed and effective exit strategy will be in place at the
outset of any joint working arrangement detailing the responsibilities of
each party and capable of dealing with a situation where premature
termination may become necessary.
Where such collaborations are being considered then the proposal
must be presented at a Governing Body meeting for approval before
any formal agreement is made. Legal advice may also be necessary.
NHS Leeds CCG will retain control of all projects whilst
accommodating joint working partners’ involvement and their regulatory
obligations.
6 Minimum Data Set Required for Project Approval
Each joint working arrangement will be supported by a project initiation
document setting out the following:
The vision, objectives and outcomes of the project
The benefits to the patient of the proposed joint working initiative
The benefits to NHS Leeds CCG
The benefits for the pharmaceutical company
Deliverables and key success factors
The resources the pharmaceutical company will provide

8
The resources that NHS Leeds CCG will provide
Timelines and milestones
Accountabilities, roles and responsibilities
Governance and Project Management arrangements
Any issues identified in relation to information governance and/or
information sharing including the need for transparency, (executive
summary published before implementation, disclosure of
pharmaceutical company involvement in all documentation and
communication, public disclosure of the pharmaceutical company
resource as a Transfer of Value to NHS Leeds CCG.
Any issues identified in relation to public sector procurement duties
Arrangements for monitoring and evaluation
An exit strategy
7 Confidential and Patient Identifiable Data
The project should be assessed at an early stage to determine if access to
sensitive data such as confidential or patient identifiable information is
proposed as part of the project.
The Senior Information Risk Owner should be approached for advice where
the project may require access to confidential or sensitive CCG information.
The CCG Caldicott Guardian should be approached for advice where the
proposal may require access to patient identifiable information.
8 Freedom of Information
NHS Leeds CCG supports the principles of transparency enshrined in the
Freedom of Information Act. Arrangements made between the CCG and the
Pharmaceutical and related industries will be made available in line with
Freedom of Information legislation.

9
9 Duties / Accountabilities and Responsibilities
Duties within organisation
The CCG’s lead project manager will be responsible for developing the project
proposal and getting advice from the CCG’s Head of Medicines Optimisation,
Commissioning team, Senior Information Risk Owner, Caldicott Guardian,
Head of Contracting and Communication and Engagement team on the
appropriateness of the proposed project.
The CCG’s Head of Medicines Optimisation, Commissioning team will be
responsible for providing advice on whether the joint working initiative meets
best practice guidelines. A check of all joint working proposals will also be
made to ensure that the proposed initiatives do not conflict with existing CCG
prescribing policies and guidelines.
The Senior Information Risk Owner will be responsible for ensuring that any
proposed information sharing as part of a joint working agreements is in line
with the CCG’s legal duties.
The CCG Caldicott Guardian is responsible for assessing if any proposed
access to patient identifiable data meets the Caldicott principles.
The CCG’s Head of Contracting is responsible for advising if there are any
implications from the CCG’s public sector procurement duties.
The CCG’s Head of Communication and Engagement is responsible for
including in the engagement plan outlining information in section 6 and
ensuring that risks identified are managed.
10 Responsibilities for approval
Proposals for joint working will be reviewed by the CCG Quality team to
consider the quality aspects of the proposal and Finance team to consider
financial, procurement and links to CCG priorities.
Recommendations from the Quality and Finance teams will be taken to a
public Governing Body Meeting for formal approval of the joint working
proposal.

10
The pharmaceutical company is required to review and formally approve the
final version of the project initiation document and executive summary of the
joint working agreement before implementation.
11 Public Sector Equality Duty NHS Leeds CCG aims to design and implement services, policies and measures that meet the diverse needs of our service, population and workforce, ensuring that none are placed at a disadvantage over others.
12 Scope of the Policy
This policy applies to NHS Leeds CCG including all employees, co-opted
members and members of the Governing Body and its committees, who must
comply with the arrangements outlined in this policy.
13 Monitoring Compliance with the Document
The NHS Leeds CCG Audit Committee will monitor compliance with the
policy.
14 Arrangements for Review
This policy will be reviewed three years after the date of authorisation. The
policy may be reviewed sooner if there is a change in legislation or new
national guidance.
15 Dissemination
This policy will be shared with all members of the Executive Management
Team, Clinical Directors and Governing Body. It will be published on both the
CCG intranet and internet sites.

11
16 References
The following policies were used as the basis of this policy
1. Department of Health, February 2008. Best practice guidance for joint
working between the NHS and the pharmaceutical industry.
2. Standards of business conduct for NHS Staff HSG (93).
3. ABPI, 2006. Best practice guidance for joint working between the NHS and
the pharmaceutical industry. Department of Health, 2004. Code of Practice
for the Pharmaceutical Industry. ABPI, 2019. Code of Conduct: Code of
Accountability in the NHS. 2019 ABPI, 2009. Guidance Notes on Joint
Working between pharmaceutical companies and the NHS and others for
the benefit of patients.
4. Leeds CCG Standards of business conduct policy, Hospitality, gifts and
sponsorship policy and Declaration of interest’s policy.
5. Innovation Health and Wealth, Accelerating Adoption and Diffusion in the
NHS. Department of Health. 2011.
17. Appendices
1 – EQIA
2 – Criteria for joint working

12
Appendix 1: Equality Impact Assessment
Title of policy
Names and roles of people completing the
assessment
Date assessment started/completed
1. Outline
Give a brief summary
of the policy
What outcomes do you
want to achieve
2. Evidence, data or research
Give details of
evidence, data or
research used to
inform the analysis of
impact
3. Consultation, engagement
Give details of all
consultation and
engagement activities
used to inform the
analysis of impact

13
4. Analysis of impact
This is the core of the assessment, using the information above detail the actual or
likely impact on protected groups, with consideration of the general duty to; eliminate
unlawful discrimination; advance equality of opportunity; foster good relations
Are there any likely
impacts?
Are any groups going to
be affected differently?
Please describe.
Are these
negative
or
positive?
What action will be
taken to address any
negative impacts or
enhance positive
ones?
Age
Carers
Disability
Sex
Race
Religion or
belief
Sexual
orientation
Gender
reassignment
Pregnancy and
maternity
Marriage and
civil
partnership
Other relevant
group
If any negative/positive impacts were
identified are they valid, legal and/or
justifiable?

14
Please detail.
5. Monitoring, Review and Publication
How will you review/monitor
the impact and effectiveness of
your actions
Lead Officer Review date:
6.Sign off
Lead Officer
Director Date approved:

1
Managing conflicts of interest policy
Version 2.2
Ratified by Governing Body
Date ratified
Name and title of originator/Authors Head of Corporate Governance & Risk
Name of responsible Committee/Individual
Audit Committee
Date issued
Review date December 2021
Target audience See section 1.6

2
CONTENTS
Page
1. Introduction
3
2. Definition of an interest
4
3. Equality statement
7
4. Principles
7
5. Roles and responsibilities
8
6. Declaring interests
9
7. Register of interests
10
8. Publication of registers
11
9. Appointing Governing Body or committee members and senior staff
12
10. Conflicts of interest at meetings
13
11. Managing conflicts of interest throughout the commissioning cycle
16
12. Raising concerns and breaches
21
13. Conflicts of interest training
23
APPENDIX 1- Declaration of interests form
24
APPENDIX 2 – Register of interests template
29
APPENDIX 3 – Declarations of interest checklist for chairs
30
APPENDIX 4 – Minutes template for recording declarations of interest
33
APPENDIX 5 – Procurement checklist
34
APPENDIX 6 – Register of procurement decisions template
36
APPENDIX 7 – Declaration of interests for bidders/contractors template
37
APPENDIX 8 – Confidentiality and Conflicts of Interest Form for Procurements
39
APPENDIX 9 - Summary of key aspects of the NHS England statutory guidance on managing conflicts of interest relating to commissioning of new care models
43

3
1. Introduction
1.1 Managing conflicts of interest appropriately is essential for protecting the integrity of the NHS commissioning system and to protect Leeds CCG and GP practices from any perceptions of wrongdoing. Commissioners need the highest level of transparency so they can demonstrate that conflicts of interest are managed in a way that cannot undermine the probity and accountability of the organisation.
1.2 It will not be possible to avoid conflicts of interest. They are inevitable in many
aspects of public life, including the NHS. Healthcare professionals have always had to manage competing interests. However, by recognising where and how they arise and dealing with them appropriately, commissioners will be able to ensure proper governance, robust decision-making and appropriate decisions about the use of public money.
1.3 A conflict of interest is defined as:
“a set of circumstances by which a reasonable person would consider that an individual’s ability to apply judgement or act, in the context of delivering, commissioning, or assuring taxpayer funded health and care services is, or could be, impaired or influenced by another interest they hold”
1.4 This policy seeks to ensure that conflicts are identified, declared and recorded,
and that clear mechanisms exist to manage or diffuse conflicts of interest when they arise. It is also important to acknowledge that conflicts may not always be obvious to, or recognised by, the individuals concerned. Therefore, a policy based on full disclosure regarding competing interests will best safeguard healthcare professionals as they exercise their new commissioning responsibilities. NHS Leeds CCG’s Managing Conflicts of Interest Policy is based on the principle of: “If in doubt, disclose”.
1.5 The Health and Social Care Act 2012 places a duty on the NHS Commissioning Board to publish guidance for CCGs on managing conflicts and a duty on CCGs to have regard to such guidance. It also requires that CCGs set out in their constitution their proposed arrangements for managing conflicts of interest. This policy provides more specific, additional safeguards that the CCG has put in place. It reflects the revised statutory guidance for CCGs on Managing Conflicts of Interest, issued by NHS England in June 2017, and the Best Practice Update on Conflicts of Interest Management: Call to Action for CCGs, issued by NHS England in February 2019.
1.6 This policy applies to:
All CCG employees, including all full and part-time staff, staff on sessional or short term contracts, students and trainees (including apprentices), agency staff, seconded staff.
Members of the CCG’s Governing Body, Committees, Sub Committees and Sub Groups, including co-opted members, appointed

4
deputies and members of committees/groups from other organisations (where the CCG is participating in a joint committee alongside other CCGs, any interests which are declared by the committee members should be recorded on the register(s) of interest of each participating CCG).
Members of the CCG – defined as GP partners (or where the practice is a company, each director) and any individual directly involved with the business or decision making of the CCG.
Who are referred to collectively in this policy as ‘individuals within the CCG’.
2. Definition of an interest 2.1 For the purposes of this policy a conflict of interest is defined as “a set of
circumstances by which a reasonable person would consider that an individual’s ability to apply judgement or act, in the context of delivering, commissioning, or assuring taxpayer funded health and care services is, or could be, impaired or influenced by another interest they hold” 1.
2.2 A conflict of interest may be:
Actual Potential
There is a material conflict between one or more interests.
There is the possibility of a material conflict between one or more interests in the future.
2.3 Individuals within the CCG may hold interests for which they cannot see
potential conflict. However, caution is always advisable because others may see it differently. It will be important to exercise judgement and to declare such interests where there is otherwise a risk of imputation of improper conduct. The perception of an interest can be as damaging as an actual conflict of interest.
2.4 Conflicts of interest can arise in many situations, environments and forms of
commissioning, with an increased risk in primary care commissioning, out-of- hours commissioning and involvement with integrated care organisations and new care models, as individuals within the CCG may here find themselves in a position of being both commissioner and provider of services. Conflicts of interest can arise throughout the whole commissioning cycle from needs assessment, to procurement exercises, to contract monitoring. References in this policy to ‘new care models’ refer to Multi-speciality Community Providers (MCP), Primary and Acute Care Systems (PACS) or other arrangements of a similar scale or scope.
1 Managing conflicts of interests in the NHS: Guidance for staff and organisations
https://www.england.nhs.uk/wp-content/uploads/2017/02/guidance-managing-conflicts-of-interest-nhs.pdf

5
2.5 Interests fall into the four categories outlined below. A benefit may arise from the making of a gain or the avoidance of a loss:
2.6 Financial interests
This is where an individual may get direct financial benefits from the consequences of a commissioning decision. This could, for example, include an individual being:
A director, including a non-executive director, or senior employee in a private company or public limited company or other organisation which is doing, or which is likely, or possibly seeking to do, business with health or social care organisations. This includes involvement with a potential provider of a new care model;
A shareholder (or similar ownership interests), a partner or owner of a private or not-for-profit company, business, partnership or consultancy which is doing, or which is likely, or possibly seeking to do, business with health or social care organisations;
A management consultant for a provider;
A provider of clinical private practice;
In employment outside of the CCG;
In receipt of secondary income;
In receipt of a grant from a provider;
In receipt of any payments (for example honoraria, one-off payments, day allowances or travel or subsistence) from a provider;
In receipt of research funding, including grants that may be received by the individual or any organisation in which they have an interest or role;
Having a pension that is funded by a provider (where the value of this might be affected by the success or failure of the provider); or
Substantively employed by another organisation, i.e. when on secondment.
2.7 Non-financial professional interests
This is where an individual may obtain a non-financial professional benefit from the consequences of a commissioning decision, such as increasing their professional reputation or status or promoting their professional career. This may, for example, include situations where the individual is:
An advocate for a particular group of patients;
A GP with special interests e.g. in dermatology, acupuncture, etc.;
An active member of a particular specialist professional body (although routine GP membership of the Royal College of General Practitioners (RCGP), British Medical Association (BMA) or a medical defence organisation would not usually by itself amount to an interest which needed to be declared);
An advisor for the Care Quality Commission (CQC) or the National Institute for Health and Care Excellence (NICE);
Engaged in a research role;

6
Involved in the development and holding of patents and other intellectual property rights which allow staff to protect something that they create, preventing unauthorised use of products or the copying of protected ideas;
GPs and practice managers, who are members of the Governing Body or committees of the CCG, should declare details of their roles and responsibilities held within their GP practices.
2.8 Non-financial personal interests
This is where an individual may benefit personally in ways which are not directly linked to their professional career and do not give rise to a direct financial benefit. This could include, for example, where the individual is:
A voluntary sector champion for a provider;
A volunteer for a provider;
A member of a voluntary sector board or has any other position of authority in or connection with a voluntary sector organisation;
Suffering from a particular condition requiring individually funded treatment;
A member of a lobby or pressure group with an interest in health. 2.9 Indirect interests
This is where an individual has a close association with an individual who has a financial interest, a non-financial professional interest or a non-financial personal interest in a commissioning decision (as described above) for example, a:
Spouse / partner
Close relative e.g., parent, grandparent, child, grandchild or sibling;
Close friend or associate;
Business partner.
A declaration of interest for a “business partner” in a GP partnership should include all relevant collective interests of the partnership, and all interests of their fellow GP partners (which could be done by cross referring to the separate declarations made by those GP partners, rather than by repeating the same information verbatim).
Whether an interest held by another person gives rise to a conflict of interests will depend upon the nature of the relationship between that person and the individual, and the role of the individual within the CCG.
2.10 NHS England has published conflicts of interests case studies which are available on its website here.
2.11 The above categories and examples are not exhaustive and a common sense approach should be adopted. Individuals within the CCG should exercise discretion on a case by case basis, including in relation to new care model arrangements, having regard to the principles set out in section 4 of this policy, in deciding whether any other role, relationship or interest may impair

7
or otherwise influence the individual’s judgement or actions in their role within the CCG. If so, this should be declared and appropriately managed.
3. Equality statement 3.1 This policy applies to all employees, Governing Body and Committee
members and members of the NHS Leeds CCGs Partnership irrespective of age, race, colour, religion, disability, nationality, ethnic origin, gender, sexual orientation or marital status, domestic circumstances, social and employment status, HIV status, gender reassignment, political affiliation or trade union membership.
3.2 A full Equality Impact Assessment is not considered to be necessary as this
policy will not have a detrimental impact on a particular group.
4. Principles 4.1 The CCG observes the following principles of good governance:
The Nolan Principles of selflessness, integrity, objectivity, accountability, openness, honesty and leadership2
The Good Governance Standards for Public Services (2004), Office for Public Management (OPM) and Chartered Institute of Public Finance and Accountancy (CIPFA)3
The seven key principles of the NHS Constitution4
The Equality Act 20105
The UK Corporate Governance Code6
Standards for members of NHS boards and CCG governing bodies in England7
4.2 The CCG endorses other principles that can safeguard against conflicts of
interest:
Doing business appropriately;
Being proactive about identifying and minimising the risks of conflicts;
Being balanced and proportionate in managing conflicts;
Being transparent and documenting every stage in the commissioning cycle; and
2 The 7 principles of public life https://www.gov.uk/government/publications/the-7-principles-of-public-
life 3 The Good Governance Standards for Public Services, 2004, OPM and CIPFA
https://www.jrf.org.uk/sites/default/files/jrf/migrated/files/1898531862.pdf 4 The seven key principles of the NHS Constitution
http://www.nhs.uk/NHSEngland/thenhs/about/Pages/nhscoreprinciples.aspx 5 The Equality Act 2010 http://www.legislation.gov.uk/ukpga/2010/15/contents
6 UK Corporate Governance Code https://www.frc.org.uk/Our-Work/Codes-Standards/Corporate-
governance/UK-Corporate-Governance-Code.aspx 7 Standards for members of NHS boards and CCG governing bodies in England
https://www.professionalstandards.org.uk/docs/default-source/publications/standards/standards-for-members-of-nhs-boards-and-ccgs-2013.pdf?sfvrsn=d5f77f20_2

8
Creating an environment and culture where individuals feel supported and confident in declaring relevant information and raising any concerns.
4.3 The CCG also recognises that:
A perception of wrongdoing, impaired judgement or undue influence can be as detrimental as any of them actually occurring.
If in doubt, it is better to assume the existence of a conflict of interest and manage it appropriately rather than ignore it.
For a conflict of interest to exist, financial gain is not necessary. 4.4 This policy reflects ‘Managing Conflicts of Interests: Revised Statutory
Guidance for CCGs 2017’ (Issued by NHS England, June 2017). It should be read alongside the following Leeds CCG documents:
Anti-Fraud, Bribery and Corruption Policy;
Code of Conduct for NHS Managers, also contained within individual contracts of employment;
Whistleblowing Policy;
Working Time Regulations Policy (including Secondary Employment);
Disciplinary Policy;
Procurement Policy; and
Standards of Business Conduct Policy.
5. Roles and responsibilities 5.1 The Accountable Officer has overall accountability for the CCG’s
management of conflicts of interest. 5.2 The Conflicts of Interest Guardian, who will be the Chair of the Audit
Committee, will:
Act as a conduit for GP practice staff, members of the public and healthcare professionals who have any concerns with regards to conflicts of interest;
Be a safe point of contact for employees or workers of the CCG to raise any concerns in relation to this policy;
Support the rigorous application of conflict of interest principles and policies;
Provide independent advice and judgment where there is any doubt about how to apply conflicts of interest policies and principles in an individual situation;
Provide advice on minimising the risks of conflicts of interest; and
If an individual requests that information is not included in the public register(s), decide whether the information should be published or not.
5.3 The Head of Corporate Governance & Risk has day to day responsibility for
managing conflict of interests, including:

9
Maintaining the CCG’s register(s) of interest and the other registers referred to in this policy;
Supporting the Conflicts of Interest Guardian to enable them to carry out the role effectively;
Providing advice, support, and guidance on how conflicts of interest should be managed; and
Ensuring that appropriate administrative processes are put in place. 5.4 All members of the Governing Body must act in accordance with this policy
and lead by example in acting with the utmost integrity and ensuring adherence to all relevant regulations, policies and procedures.
5.5 Line Managers are responsible for assisting employees in complying with this
policy by ensuring that this policy and its requirements are brought to the attention of employees for whom they are responsible, and that those employees are aware of its implications for their work.
5.5 All individuals within the CCG are required to be aware of and comply with
the policy.
5.6 If any individual within the CCG has any doubt about the relevance of an interest, this should be discussed with the Conflicts of Interest Guardian or the Head of Corporate Governance.
6. Declaring interests 6.1 All individuals within the CCG must declare any interests that might have any
bearing on the work of the CCG:
a) on appointment - applicants for any appointment to the CCG or its Governing Body or any committees should be asked to declare any relevant interests. When an appointment is made, a formal declaration of interests should again be made and recorded.
b) annually - declarations will be sought from all relevant individuals on an annual basis and where there are no interests or changes to declare, a “nil return” will be recorded.
c) at meetings - all attendees are required to declare their interests as a standing agenda item for every Governing Body, committee, sub-committee or working group meeting, before the item is discussed. Even if an interest has been recorded in the register of interests, it should still be declared in meetings where matters relating to that interest are discussed. Declarations of interest must be recorded in minutes of meetings.
d) on changing role, responsibility or circumstances - whenever an individual’s role, responsibility or circumstances change in a way that affects the individual’s interests (e.g. where an individual takes on a new role outside the CCG, enters into a new business or relationship, starts a new project/piece of work or may be affected by a procurement decision e.g. if their role may transfer to a proposed new provider), a further declaration should be made to reflect the change in circumstances as soon as possible, and in any event within 28 days. This could involve a

10
conflict of interest ceasing to exist or a new one materialising. It is the individual’s responsibility to make a further declaration as soon as possible, rather than waiting to be asked.
e) if they come to know that the CCG has entered into (or proposes to enter into) a financial arrangement in which they or any person connected with them has any interest, direct or indirect.
6.2 CCG staff should declare any interests by completing the declaration of
interests form at Appendix 1 and submitting this to their Line Manager, within 28 days. Line Managers will record the interests and make a decision on whether the declaration is deemed to require any action to ensure transparency and avoid a conflict of interest. If required, Line Managers should seek advice on appropriate action from the Head of Corporate Governance & Risk and/or Conflicts of Interest Guardian.
6.3 Line Managers should hold any interests declared on the individual’s personal
file. All interests should be declared as and when they arise. Individuals are responsible for ensuring that their registered interests are kept up to date at all times.
6.4 Once any arrangements for mitigating the risk have been agreed by the
individual’s Line Manager, these should be documented on the approved form and submitted to the Head of Corporate Governance & Risk. Such arrangements will specify:
• whether and when an individual should withdraw from a specified activity, on a temporary or permanent basis; and
• monitoring of the specified activity undertaken by the individual, either by a line manager, colleague or other designated individual.
6.5 Where an individual is unclear about the arrangements for managing the
interest, they should seek advice from their Line Manager. 6.6 All other individuals should submit declarations directly to the Head of
Corporate Governance & Risk using the form at Appendix 1, who will decide, in conjunction with the Conflicts of Interest Guardian, whether any specific arrangements are required to manage the conflicts or potential conflicts declared.
6.7 Although the interest may be declared, this does not remove the individual’s
personal responsibilities of removing themselves from a position or situation which may result in a potential breach of this policy.
7. Register of Interests 7.1 Registers will be maintained of the interests of individuals within the CCG,
specified in paragraph 1.6.

11
7.2 The registers for all the above will be published on the CCG’s website and maintained by the Head of Corporate Governance & Risk. The register(s) will be reviewed annually, and updated as necessary. For a new declaration, the relevant register will be updated inside 28 days. All individuals within the CCG must submit a nil declaration where they have no interests or changes to declare. All interests will remain on the register for a minimum of 6 months after the interest has expired. The CCG will retain a private record of historic interests for a minimum of 6 years after the date on which it expired.
7.3 Where an individual is unable to provide a declaration in writing, e.g. if a
conflict becomes apparent in the course of a meeting, they will make an oral declaration before witnesses, and provide a written declaration as soon as possible thereafter.
7.4 Registers will include:
Name of the person declaring the interest;
Position within, or relationship with, the CCG (or NHS England in the event of joint committees);
Type of interest e.g., financial interests, non-financial professional interests;
Description of interest, including for indirect interests details of the relationship with the person who has the interest;
The dates from which the interest relates; and
The actions to be taken to mitigate risk - these should be agreed with the individual’s line manager or a senior manager within the CCG.
7.5 A template is attached at Appendix 2. 7.6 The register of interests will be reviewed at every Audit Committee meeting.
The Governing Body will review the register of interests on an annual basis.
8. Publication of registers 8.1 The CCG will publish the register of interests and gifts and hospitality and the
register of procurement decisions described below, in a prominent place on the CCG’s website.
8.2 Although all individuals must declare interests, the CCG will only publish the interests of decision makers. Decision makers are defined as follows:
All governing body members;
Members of advisory groups which contribute to direct or delegated decision making on the commissioning or provision of taxpayer funded services such as working groups involved in service redesign or stakeholder engagement that will affect future provision of services;
Members of the Primary Care Commissioning Committee (PCCC);
Members of other committees of the CCG e.g., audit committee, remuneration committee etc.;

12
Members of new care models joint provider / commissioner groups / committees;
Members of procurement (sub-)committees;
Individuals on Agenda for Change band 8d and above;
Management, administrative and clinical staff who have the power to enter into contracts on behalf of the CCG;
Management, administrative and clinical staff involved in decision making concerning the commissioning of services, purchasing of goods, medicines, medical devices or equipment, and formulary decisions; and
Management, administrative and clinical staff responsible for processing payments on behalf of the CCG.
8.2 In exceptional circumstances, where the public disclosure of information could give rise to a real risk of harm or is prohibited by law, an individual’s name and/or other information may be redacted from the publicly available register(s). Where an individual believes that substantial damage or distress may be caused, to him/herself or somebody else by the publication of information about them, they are entitled to request that the information is not published. Such requests must be made in writing. Decisions not to publish information will be made by the Conflicts of Interest Guardian for the CCG, who will seek appropriate legal advice where required, and a confidential un-redacted version of the register(s) will be retained.
8.3 All decision making staff will be made aware, in advance of publication, that the register(s) will be kept, how the information on the register(s) may be used or shared and that the register(s) will be published. This will be done by the provision of a fair processing notice that details the identity of the data controller, the purposes for which the registers are held and published, how the information on the register(s) may be used or shared and contact details for the data protection officer. This information will also be provided to individuals identified in the register(s) because they are in a relationship with the person making the declaration.
8.4 All individuals who are not decision makers but who are still required to make a declaration of interest(s) will be made aware that the register(s) will be kept and how the information on the register(s) may be used or shared. This will be done by the provision of a separate fair processing notice that details the identity of the data controller, the purposes for which the register(s) are held, how the information on the register(s) may be used or shared and contact details for the data protection officer. This information will also be provided to individuals identified in the register(s) because they are in a relationship with the person making the declaration.
9. Appointing Governing Body or committee members and senior staff
9.1 On appointing Governing Body, committee or sub-committee members and
senior staff, the CCG will consider whether conflicts of interest should exclude individuals from being appointed to the relevant role. The CCG will assess the

13
materiality of the interest, in particular whether the individual (or any person with whom they have a close association could benefit (whether financially or otherwise) from any decision the CCG might make. This will be particularly relevant for Governing Body, committee and sub-committee appointments, but should also be considered for all employees and especially those operating at senior level.
9.2 The CCG will also determine the extent of the interest and the nature of the
appointee’s proposed role within the CCG. If the interest is related to an area of business significant enough that the individual would be unable to operate effectively and make a full and proper contribution in the proposed role, then that individual should not be appointed to the role.
9.3 Any individual who has a material interest in an organisation which provides,
or is likely to provide, substantial services to the CCG (whether as a provider of healthcare or commissioning support services, or otherwise) should recognise the inherent conflict of interest risk that may arise and should not be a member of the Governing Body or a committee or sub-committee of the CCG, in particular if the nature and extent of their interest and the nature of their proposed role is such that they are likely to need to exclude themselves from decision-making on so regular a basis that it significantly limits their ability to effectively perform that role.
10. Managing conflicts of interest at meetings 10.1 Declarations of interests will be a standing item on all meeting agendas. The
chair of a meeting of the CCG’s Governing Body or any of its committees, sub-committees or groups has ultimate responsibility for deciding whether there is a conflict of interest and for taking the appropriate course of action in order to manage the conflict of interest. In reaching this decision the chair will seek advice from the Head of Corporate Governance & Risk or their representative, or where there is not one, another senior manager.
10.2 In the event that the chair of a meeting has a conflict of interest, the vice chair
is responsible for deciding the appropriate course of action in order to manage the conflict of interest. If the vice chair is also conflicted then the remaining non-conflicted voting members of the meeting should agree between themselves how to manage the conflict(s).
10.3 In making such decisions, the chair (or vice chair or remaining non-conflicted
members as above) may wish to consult with the Conflicts of Interest Guardian or another member of the Governing Body.
10.4 It is good practice for the chair, with support of the CCG’s Head of Corporate
Governance & Risk and, if required, the Conflicts of Interest Guardian, to proactively consider ahead of meetings what conflicts are likely to arise and how they should be managed, including taking steps to ensure that supporting papers for particular agenda items of private sessions/meetings are not sent to conflicted individuals in advance of the meeting where relevant.

14
10.5 Chairs will be provided with a declaration of interests checklist (attached at
Appendix 3) with the meeting papers, which will include details of any declarations of interest which have already been made by members of the Governing Body / committee / sub-group.
10.6 The chair should ask at the beginning of each meeting if anyone has any
conflicts of interest to declare in relation to the business to be transacted at the meeting. Each member of the group should declare any interests which are relevant to the business of the meeting whether or not those interests have previously been declared. Any new interests which are declared at a meeting must be included on the CCG’s relevant register of interests to ensure it is up-to-date. Similarly, any new offers of gifts or hospitality which are declared at a meeting must be added to the register of gifts and hospitality.
10.7 It is the responsibility of each individual member of the meeting to declare any
relevant interests which they may have. However, should the chair or any other member of the meeting be aware of facts or circumstances which may give rise to a conflict of interests but which have not been declared then they should bring this to the attention of the chair who will decide whether there is a conflict of interest and the appropriate course of action to take in order to manage the conflict of interest.
10.8 If, after a meeting, the chair or any other member becomes aware that a
conflict of interest has not been declared, they should raise this with the Head of Corporate Governance & Risk or Conflicts of Interest Guardian who will consider the appropriate course of action.
10.9 When a member of the meeting (including the chair or vice chair) has a
conflict of interest in relation to one or more items of business, the chair (or vice chair or remaining non-conflicted members where relevant as described above) must decide how to manage the conflict. The appropriate course of action will depend on the particular circumstances, but could include one or more of the following:
Where the chair has a conflict of interest, deciding that the vice chair (or another non-conflicted member of the meeting if the vice chair is also conflicted) should chair all or part of the meeting;
Requiring the individual who has a conflict of interest (including the chair or vice chair if necessary) not to attend the meeting;
Ensuring that the individual does not receive the supporting papers or minutes of the meeting which relate to the matter(s) which give rise to the conflict;
Requiring the individual to leave the discussion when the relevant matter(s) are being discussed and when any decisions are being taken in relation to those matter(s). In private meetings, this could include requiring the individual to leave the room and in public meetings to either leave the room or join the audience in the public gallery;
Allowing the individual to participate in some or all of the discussion when the relevant matter(s) are being discussed but requiring them to leave the

15
meeting when any decisions are being taken in relation to those matter(s). This may be appropriate where, for example, the conflicted individual has important relevant knowledge and experience of the matter(s) under discussion, which it would be of benefit for the meeting to hear, but this will depend on the nature and extent of the interest which has been declared;
Noting the interest and ensuring that all attendees are aware of the nature and extent of the interest, but allowing the individual to remain and participate in both the discussion and in any decisions. This is only likely to be the appropriate course of action where it is decided that the interest which has been declared is either immaterial or not relevant to the matter(s) under discussion.
10.10 Where the conflict of interest relates to outside employment and an individual
continues to participate in meetings pursuant to the preceding two bullet points, he or she should ensure that the capacity in which they continue to participate in the discussions is made clear and correctly recorded in the meeting minutes. Where it is appropriate for them to participate in decisions they must only do so if they are acting in their CCG role.
10.11 Where over half of members withdraw from a part of a meeting – due to the
arrangements agreed for the management of conflicts of interests - the chair (or deputy) will determine whether or not the discussion can proceed. In making this decision the chair will consider whether the meeting is quorate in accordance with the required number /balance of membership.
10.12 Where the meeting is not quorate the discussion will be deferred until such
time as a quorum can be convened. Where a quorum cannot be convened from the membership of the meeting, owing to the arrangements for managing conflicts of interest or potential conflicts of interests, the chair of the meeting shall consult with the Conflicts of Interest Guardian on the action to be taken. This may include:
requiring another committee or sub-committee which can be quorate to progress the item of business; or if this is not possible,
inviting on a temporary basis one or more of the following to make up the quorum (where these are permitted members of the Governing Body or committee / sub-committee in question) so that the group can progress the item of business:
a member of the CCG who is interest free; an individual nominated by a member to act on their behalf in the
dealings between it and the CCG; a member of a relevant Health and Wellbeing Board; a member of a board/Governing Body for another CCG.
10.13 The minutes will record all declarations of interest and actions taken in
mitigation. A minutes template for recording declarations is attached at Appendix 4.

16
11. Managing conflicts of interest throughout the commissioning cycle
11.1 Conflicts of interest need to be managed appropriately throughout the whole
commissioning cycle. Discussions around conflicts will take place when procurement specifications are produced, bids are scored, and in meetings where final procurement decisions are made. At the outset of a commissioning process, the relevant interests of all individuals involved should be identified and clear arrangements put in place to manage any conflicts of interest. This includes consideration as to which stages of the process an individual should not participate in, and, in some circumstances, whether they should be involved in the process at all. The CCG will identify and appropriately manage any conflicts of interest that may arise where staff are involved in both the management of existing contracts and the procurement of related / replacement contracts. The CCG will also identify as soon as possible where staff might transfer to a provider (or their role may materially change) following the award of a contract. This will be treated as a relevant interest, and the CCG will manage the potential conflict.
Designing service requirements
11.2 The way in which services are designed can either increase or decrease perceived or actual conflicts of interest. Public involvement supports transparent and credible commissioning decisions. It should happen at every stage of the commissioning cycle from needs assessment, planning and prioritisation to service design, procurement and monitoring. The CCG has a legal duty under the Act to involve patients and the public in their respective commissioning processes and decisions.
Provider engagement
11.3 It is good practice to engage relevant providers, especially clinicians, in confirming that the design of service specifications will meet patient needs. This may include providers from the acute, primary, community, and mental health sectors, and may include NHS, third sector and private sector providers. Such engagement, done transparently and fairly, is entirely legal. However, conflicts of interest, as well as challenges to the fairness of the procurement process, can arise if a commissioner engages selectively with only certain providers (be they incumbent or potential new providers) in developing a service specification for a contract for which they may later bid. Individuals should be particularly mindful of these issues when engaging with existing / potential providers in relation to the development of new care models.
11.4 Provider engagement should follow the three main principles of procurement law, namely equal treatment, non-discrimination and transparency. This includes ensuring that the same information is given to all at the same time and procedures are transparent. This mitigates the risk of potential legal challenge.

17
11.5 As the service design develops, it is good practice to engage with a range of providers on an on-going basis to seek comments on the proposed design e.g., via the commissioners website and/or via workshops with interested parties (ensuring a record is kept of all interaction). NHS Improvement has issued guidance on the use of provider boards in service design.8
11.6 Engagement should help to shape the requirement to meet patient need, but it is important not to gear the requirement in favour of any particular provider(s). If appropriate, the advice of an independent clinical adviser on the design of the service should be secured.
11.7 Individuals should ensure that decisions are documented to ensure that the CCG meets its obligations under, but not limited to, the National Health Service (Procurement, Patient Choice and Competition) (No 2) Regulations 2013 and the Public Contracts Regulations 2015.
Specifications
11.8 The CCG will seek, as far as possible, to specify the outcomes that it wishes to see delivered through a new service, rather than the process by which these outcomes are to be achieved. As well as supporting innovation, this helps prevent bias towards particular providers in the specification of services. The CCG will also ensure that careful consideration is given to the appropriate degree of financial risk transfer in any new contractual model.
11.9 Specifications should be clear and transparent, reflecting the depth of engagement, and set out the basis on which any contract will be awarded.
Procurement and awarding grants
11.10 The CCG will seek to recognise and manage any conflicts or potential conflicts of interest that may arise in relation to the procurement of any services or the administration of grants. Anyone taking part in a procurement panel will be required to complete a Confidentiality and Conflicts of Interest form (Appendix 8). “Procurement” relates to any purchase of goods, services or works and the term “procurement decision” should be understood in a wide sense to ensure transparency of decision making on spending public funds. The decision to use a single tender action, for instance, is a procurement decision and if it results in the CCG entering into a new contract, extending an existing contract, or materially altering the terms of an existing contract, then it is a decision that should be recorded.
11.11 NHS England and CCGs must comply with two different regimes of procurement law and regulation when commissioning healthcare services: the NHS procurement regime, and the European procurement regime:
The NHS procurement regime – the NHS (Procurement, Patient Choice and Competition (No.2)) Regulations 2013: made under S75 of the 2012
8 Monitor, Case closure decision on Greater Manchester and Cheshire cancer surgery services,
January 2014 https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/284832/ManchesterCaseClosure.pdf

18
Act; apply only to NHS England and CCGs; enforced by NHS Improvement; and
The European procurement regime – Public Contracts Regulations 2015 (PCR 2015): incorporate the European Public Contracts Directive into national law; apply to all public contracts over the threshold value; enforced through the Courts. The general principles arising under the Treaty on the Functioning of the European Union of equal treatment, transparency, mutual recognition, non-discrimination and proportionality may apply even to public contracts for healthcare services falling below the threshold value if there is likely to be interest from providers in other member states.
11.12 Whilst the two regimes overlap in terms of some of their requirements, they are not the same – so compliance with one regime does not automatically mean compliance with the other. The National Health Service (Procurement, Patient Choice and Competition) (No.2) Regulations 2013 state:
CCGs must not award a contract for the provision of NHS health care services where conflicts, or potential conflicts, between the interests involved in commissioning such services and the interests involved in providing them affect, or appear to affect, the integrity of the award of that contract; and
CCGs must keep a record of how it managed any such conflict in relation to NHS commissioning contracts it has entered into.
11.13 Paragraph 24 of PCR 2015 states: “Contracting authorities shall take appropriate measures to effectively prevent, identify and remedy conflicts of interest arising in the conduct of procurement procedures so as to avoid any distortion of competition and to ensure equal treatment of all economic operators”. Conflicts of interest are described as “any situation where relevant staff members have, directly or indirectly, a financial, economic or other personal interest which might be perceived to compromise their impartiality and independence in the context of the procurement procedure”.
11.14 The Procurement, Patient Choice and Competition Regulations (PPCCR) place requirements on commissioners to ensure that they adhere to good practice in relation to procurement, run a fair, transparent process that does not discriminate against any provider, do not engage in anti-competitive behaviour that is against the interest of patients, and protect the right of patients to make choices about their healthcare. Furthermore the PPCCR places requirements on commissioners to secure high quality, efficient NHS healthcare services that meet the needs of the people who use those services. The PCR 2015 are focussed on ensuring a fair and open selection process for providers.
11.15 The CCG will use a procurement checklist (see Appendix 5) to record the factors that should be addressed when drawing up its plans to commission services. This will help to evidence the CCG’s deliberations on conflicts of interest. The CCG will make the evidence of its management of conflicts publicly available, and the relevant information from the procurement template

19
will be used to complete the register of procurement decisions. Complete transparency around procurement will provide:
Evidence that the CCG is seeking and encouraging scrutiny of its decision-making process;
A record of the public involvement throughout the commissioning of the service;
A record of how the proposed service meets local needs and priorities for partners such as the Health and Wellbeing Boards, local Healthwatch and local communities;
Evidence to the audit committee and internal and external auditors that a robust process has been followed in deciding to commission the service, in selecting the appropriate procurement route, and in addressing potential conflicts.
11.16 External services such as commissioning support services (CSSs) can play an important role in helping CCGs decide the most appropriate procurement route, undertake procurements and manage contracts in ways that manage conflicts of interest and preserve the integrity of decision-making. The CCG will assure itself that a CSS’ business processes are robust and enable the CCG to meet its duties in relation to procurement (including those relating to the management of conflicts of interest). This will require the CSS to declare any conflicts of interest it may have in relation to the work commissioned by the CCG.
11.17 A CCG cannot, however, lawfully delegate commissioning decisions to an external provider of commissioning support. Although CSSs are likely to play a key role in helping to develop specifications, preparing tender documentation, inviting expressions of interest and inviting tenders, the CCG itself will need to:
Determine and sign off the specification and evaluation criteria;
Decide and sign off decisions on which providers to invite to tender; and
Make final decisions on the selection of the provider.
Register of procurement decisions
11.18 The CCG will maintain a register of procurement decisions taken with a value in excess of £100,000, either for the procurement of a new service or any extension or material variation of a current contract. This will include:
The details of the decision;
Who was involved in making the decision (including the name of the CCG clinical lead, the CCG contract manager, the name of the decision making committee and the name of any other individuals with decision-making responsibility);
A summary of any conflicts of interest in relation to the decision and how this was managed by the CCG; and
The award decision taken.
11.19 The register of procurement decisions will be updated whenever a procurement decision is taken, using the register at Appendix 6. The Procurement, Patient Choice and Competition Regulations 9(1) place a

20
requirement on commissioners to maintain and publish on their website a record of each contract it awards. The register of procurement decisions will be made publicly available and easily accessible to patients and the public by:
Ensuring that the register is available in a prominent place on the CCG’s website; and
Making the register available upon request for inspection at the CCG’s headquarters.
Declarations of interests for bidders / contractors
11.20 As part of the CCG’s procurement processes, bidders will be asked to declare any conflicts of interest. This allows the CCG to ensure that it complies with the principles of equal treatment and transparency. When a bidder declares a conflict, the CCG will decide how best to deal with it to ensure that no bidder is treated differently to any other. A declaration of interests for bidders/ contractors template is attached at Appendix 7.
11.21 It will not usually be appropriate to declare such a conflict on the register of procurement decisions, as it may compromise the anonymity of bidders during the procurement process. However, the CCG will retain an internal audit trail of how the conflict or perceived conflict was dealt with to allow it to provide information at a later date if required. The CCG is required under regulation 84 of the Public Contract Regulations 2015 to make and retain records of contract award decisions and key decisions that are made during the procurement process (there is no obligation to publish them). Such records must include “communications with economic operators and internal deliberations” which should include decisions made in relation to actual or perceived conflicts of interest declared by bidders. These records must be retained for a period of at least three years from the date of award of the contract.
Contract Monitoring
11.22 The management of conflicts of interest applies to all aspects of the commissioning cycle, including contract management. Any contract monitoring will consider conflicts of interest as part of the process i.e., the chair of a contract management meeting will invite declarations of interests; record any declared interests in the minutes of the meeting; and manage any conflicts appropriately and in line with this guidance. This equally applies where a contract is held jointly with another organisation such as the Local Authority or with other CCGs under lead commissioner arrangements.
11.23 The individuals involved in the monitoring of a contract should not have any direct or indirect financial, professional or personal interest in the incumbent provider or in any other provider that could prevent them, or be perceived to prevent them, from carrying out their role in an impartial, fair and transparent manner. The CCG will be mindful of any potential conflicts of interest when it disseminates any contract or performance information/reports on providers, and manage the risks appropriately.

21
12. Raising concerns and breaches
12.1 There will be situations when interests will not be identified, declared or managed appropriately and effectively. This may happen innocently, accidentally, or because of the deliberate actions of staff or organisations. For the purposes of this policy these situations are referred to as ‘breaches’.
12.2 It is the duty of every individual within the CCG to speak up about genuine
concerns in relation to the management of conflicts of interests, and to report any concerns in accordance with the terms of this policy and the CCG’s Whistleblowing Policy or with the whistleblowing policy of the relevant employer organisation (where the breach is being reported by an employee or worker of another organisation). Individuals should not ignore their suspicions or seek to investigate them, but speak to the CCG’s Conflict of Interest Guardian or the Head of Corporate Governance.
12.3 Where a breach is suspected or has occurred, this will be investigated by the
Head of Corporate Governance & Risk who will draw on other expertise available to the organisation such as internal audit. The findings will be shared with the Conflicts of Interest Guardian and the breach formally reported to the Audit Committee.
12.4 A review of lessons learned will be conducted by the Head of Corporate
Governance & Risk following any incident of non-compliance with this policy and the report reviewed by the CCG’s Audit Committee. Anonymised details of breaches will be published on the CCG’s website for the purpose of learning and development.
12.5 Anyone who wishes to report a suspected or known breach of the policy, who
is not an employee or worker of the CCG, should ensure that they comply with their own organisation’s whistleblowing policy, since most such policies should provide protection against detriment or dismissal.
12.6 All notifications will be treated with appropriate confidentiality at all times, in
accordance with the CCG’s policies and applicable laws, and the person making such disclosures can expect an appropriate explanation of any decisions taken as a result of any investigation.
12.7 Providers, patients and other third parties can make a complaint to NHS
Improvement in relation to a commissioner’s conduct under the Procurement Patient Choice and Competition Regulations. The regulations are designed as an accessible and effective alternative to challenging decisions in the courts.
Fraud or Bribery
12.8 Any suspicions or concerns of acts of fraud or bribery can be reported online via https://www.reportnhsfraud.nhs.uk/ or via the NHS Fraud and Corruption Reporting Line on 0800 0284060. This provides an easily accessible and confidential route for the reporting of genuine suspicions of fraud within or

22
affecting the NHS. All calls are dealt with by experienced trained staff and any caller who wishes to remain anonymous may do so. Please refer to the CCG’s Anti-Fraud, Bribery and Corruption Policy for further details.
Impact of non-compliance
12.9 Failure to comply with the CCG’s policy on conflicts of interest management can have serious implications for the CCG and any individuals concerned.
Civil implications
12.10 If conflicts of interest are not effectively managed, CCGs could face civil challenges to decisions they make. For instance, if breaches occur during a service re-design or procurement exercise, the CCG risks a legal challenge from providers that could potentially overturn the award of a contract, lead to damages claims against the CCG, and necessitate a repeat of the procurement process. This could delay the development of better services and care for patients, waste public money and damage the CCG’s reputation. In extreme cases, staff and other individuals could face personal civil liability, for example a claim for misfeasance in public office.
Criminal implications
12.10 Failure to manage conflicts of interest could lead to criminal proceedings including for offences such as fraud, bribery and corruption. This could have implications for CCGs and linked organisations, and the individuals who are engaged by them. The Fraud Act 2006 created a criminal offence of fraud and defines three ways of committing it:
Fraud by false representation;
Fraud by failing to disclose information; and,
Fraud by abuse of position.
12.11 In these cases, the offender’s conduct must be dishonest and their intention must be to make a gain, or cause a loss (or the risk of a loss) to another. Fraud carries a maximum sentence of 10 years imprisonment and /or a fine if convicted in the Crown Court or 6 months imprisonment and/or a fine in the Magistrates’ Court. The offences can be committed by a body corporate.
12.12 Bribery is generally defined as giving or offering someone a financial or other
advantage to encourage that person to perform certain functions or activities. The Bribery Act 2010 reformed the criminal law of bribery, making it easier to tackle this offence proactively in both the public and private sectors. It introduced a corporate offence which means that commercial organisations, including NHS bodies, will be exposed to criminal liability, punishable by an unlimited fine, for failing to prevent bribery.
12.13 The offences of bribing another person, being bribed or bribery of foreign
public officials in relation to an individual carries a maximum sentence of 10 years imprisonment and/or a fine if convicted in the Crown Court and 6

23
months imprisonment and/or a fine in the Magistrates’ Court. In relation to a body corporate the penalty for these offences is a fine.
Disciplinary implications
12.14 Individuals who fail to disclose any relevant interests or who otherwise breach this policy will be subject to investigation and, where appropriate, to disciplinary action in accordance with the CCG’s Disciplinary Policy. Individuals should be aware that the outcomes of such action may, if appropriate, result in the termination of their employment or position with the CCG.
Professional regulatory implications
12.15 Statutorily regulated healthcare professionals who work for, or are engaged by, CCGs are under professional duties imposed by their relevant regulator to act appropriately with regard to conflicts of interest. The CCG will report statutorily regulated healthcare professionals to their regulator if they believe that they have acted improperly, so that these concerns can be investigated. Statutorily regulated healthcare professionals should be made aware that the consequences for inappropriate action could include fitness to practise proceedings being brought against them, and that they could, if appropriate, be struck off by their professional regulator as a result.
13. Conflicts of interest training
13.1 The CCG will ensure that training is offered to all individuals within the CCG
on the management of conflicts of interest. This is to ensure staff and others within the CCG understand what conflicts are and how to manage them effectively. All individuals within the CCG are required to complete this mandatory training on an annual basis.

24
Appendix 1: Declaration of interests form Practice Code (if applicable)
Name:
Position within, or relationship with, the CCG (or NHS England in the event of joint committees)
Details of interest held (complete all that are applicable)
Type of interest (see reverse of form)
Description of interest (including for indirect interests, details of the relationship with the person who has the interest)
Date of interest From & To
Actions to be taken to mitigate risk (if required) To be agreed with line manager (CCG employees only)
I am / am not a decision maker [delete as applicable].
Decision makers are defined as follows:
All governing body members;
Members of advisory groups which contribute to direct or delegated decision making on the commissioning or provision of

25
taxpayer funded services such as working groups involved in service redesign or stakeholder engagement that will affect future provision of services;
Members of the Primary Care Commissioning Committee (PCCC);
Members of other committees of the CCG e.g., audit committee, remuneration committee etc.;
Members of new care models joint provider / commissioner groups / committees;
Members of procurement (sub-)committees;
Individuals on Agenda for Change band 8d and above;
Management, administrative and clinical staff who have the power to enter into contracts on behalf of the CCG;
Management, administrative and clinical staff involved in decision making concerning the commissioning of services, purchasing of goods, medicines, medical devices or equipment, and formulary decisions; and Management, administrative and clinical staff responsible for processing payments on behalf of the CCG
I do / do not [delete as applicable] give my consent for this information to published on registers that the CCG holds. If consent is NOT given
please give reasons:
The information submitted will be held by the CCG for personnel or other reasons specified on this form and to comply with the organisation’s policies, notably the statutory guidance published by NHS England relating to Conflicts of Interest. This information may be held in both manual and electronic form in accordance with the General Data Protection Regulations (GDPR). Information may be disclosed to third parties in accordance with the Freedom of Information Act 2000 and published in registers that the CCG holds. The data controller is your employing CCG who can be contacted by emailing the SIRO at [email protected] If you are declaring an indirect interest, please state your relationship with the third party but do not include their name in line with GDPR. Please advise the third party that this information will be held on the register, which will be published on the CCG website if you are a decision maker (as outlined above).

26
I confirm that the information provided above is complete and correct. I acknowledge that any changes in these declarations must be notified to the Corporate Governance Office at [email protected] as soon as practicable, and no later than 28 days after the interest arises. I am aware that if I do not make full, accurate and timely declarations then civil, criminal, or internal disciplinary action may result.
Declarer’s signature: …………………………………………. Date: ………………..
For CCG employees only:
Signature of line manager: …………………………………. Name: ……………………………
Position: ………………………………………. Date: ………………..

27
Types of interest
Type of interest
Description
Financial Interests
This is where an individual may get direct financial benefits from the consequences of a commissioning decision. This could, for example, include being:
A director, including a non-executive director, or senior employee in a private company or public limited company or other organisation which is doing, or which is likely, or possibly seeking to do, business with health or social care organisations. This includes involvement with a potential provider of a new care model;
A shareholder (or similar owner interests), a partner or owner of a private or not-for-profit company, business, partnership or consultancy which is doing, or which is likely, or possibly seeking to do, business with health or social care organisations.
A management consultant for a provider;
A provider of clinical private practice;
In employment outside of the CCG;
In receipt of secondary income;
In receipt of a grant from a provider;
In receipt of any payments (for example honoraria, one off payments, day allowances or travel or subsistence) from a provider
In receipt of research funding, including grants that may be received by the individual or any organisation in which they have an interest or role; and
Having a pension that is funded by a provider (where the value of this might be affected by the success or failure of the provider.
Non-Financial Professional Interests
This is where an individual may obtain a non-financial professional benefit from the consequences of a commissioning decision, such as increasing their professional reputation or status or promoting their professional career. This may, for example, include situations where the individual is:
An advocate for a particular group of patients;
A GP with special interests e.g., in dermatology, acupuncture etc.
An active member of a particular specialist professional body (although routine GP membership of the RCGP, BMA or a medical defence organisation would not usually by itself amount to an interest which needed to be declared);
An advisor for Care Quality Commission (CQC) or National Institute for Health and Care Excellence (NICE);
Engaged in a research role;
The development and holding of patents and other intellectual property rights which allow staff to protect something that they create, preventing unauthorised use of products or the copying of protected ideas; or
GPs and practice managers, who are members of the governing body or committees of the CCG, should declare details of their roles and responsibilities held within their GP practices
Non-Financial Personal Interests
This is where an individual may benefit personally in ways which are not directly linked to their professional career and do not give rise to a direct financial benefit. This could include, for example, where the individual is:
A voluntary sector champion for a provider;
A volunteer for a provider;
A member of a voluntary sector board or has any other position of authority in or connection with a voluntary sector organisation;
Suffering from a particular condition requiring individually funded treatment;
A member of a lobby or pressure group with an interest in health and care.

28
Indirect Interests
This is where an individual has a close association with an individual who has a financial interest, a non-financial professional interest or a non-financial personal interest in a commissioning decision (as those categories are described above). For example, this should include:
Spouse / partner;
Close relative e.g., parent, grandparent, child, grandchild or sibling;
Close friend or associate; or
Business partner Decision Maker Decision makers are defined as follows:
All governing body members;
Members of advisory groups which contribute to direct or delegated decision making on the commissioning or provision of taxpayer funded services such as working groups involved in service redesign or stakeholder engagement that will affect future provision of services;
Members of the Primary Care Commissioning Committee (PCCC);
Members of other committees of the CCG e.g., audit committee, remuneration committee etc.;
Members of new care models joint provider / commissioner groups / committees;
Members of procurement (sub-)committees;
Individuals on Agenda for Change band 8d and above;
Management, administrative and clinical staff who have the power to enter into contracts on behalf of the CCG;
Management, administrative and clinical staff involved in decision making concerning the commissioning of services, purchasing of goods, medicines, medical devices or equipment, and formulary decisions; and Management, administrative and clinical staff responsible for processing payments on behalf of the CCG.

29
Appendix 2: Register of Interests template
Name Title Role Practice B Code
Declared Interest- (Name of the organisation and nature of business)
Type of Interest
Is the interest direct or indirect?
Interest From
Interest Until Action Taken to Mitigate Risk

30
Appendix 3: Declarations of interest checklist for chairs
Under the Health and Social Care Act 2012, there is a legal obligation to manage conflicts of
interest appropriately. It is essential that declarations of interest and actions arising from the
declarations are recorded formally and consistently across all CCG governing body,
committee and sub-committee meetings. This checklist has been developed with the
intention of providing support in conflicts of interest management to the Chair of the meeting-
prior to, during and following the meeting. It does not cover the requirements for declaring
interests outside of the committee process
Timing
Checklist for Chairs
Responsibility
In advance of the meeting
1. The agenda to include a standing item on declaration of interests to enable individuals to raise any issues and/or make a declaration at the meeting. 2. A definition of conflicts of interest should also be accompanied with each agenda to provide clarity for all recipients. 3. Agenda to be circulated to enable attendees (including visitors) to identify any interests relating specifically to the agenda items being considered. A form (see below) will also be circulated on which attendees can record any interests relating to the agenda items. 4. Members should return the form to the Chair or Head of Corporate Governance as soon as an actual or potential conflict is identified. 5. Chair to review a summary report from preceding meetings i.e. sub-committee, working group, etc., detailing any conflicts of interest declared and how this was managed. 6. A copy of the members’ declared interests is checked to establish any actual or potential conflicts of interest that may occur during the meeting.
Meeting Chair and secretariat Meeting Chair and secretariat Meeting Chair and secretariat Meeting members Meeting Chair Meeting Chair
During the meeting 7. Chair requests members to Meeting Chair

31
declare any interests in agenda items, including the nature of the conflict. 8. Chair makes a decision as to how to manage each interest which has been declared, including whether / to what extent the individual member should continue to participate in the meeting, on a case by case basis, and this decision is recorded. 9. As minimum requirement, the following should be recorded in the minutes of the meeting:
Individual declaring the interest;
At what point the interest was declared;
The nature of the interest;
The Chair’s decision and resulting action taken;
The point during the meeting at which any individuals retired from and returned to the meeting - even if an interest has not been declared
Visitors in attendance who participate in the meeting must also follow the meeting protocol and declare any interests in a timely manner
Meeting Chair Secretariat
Following the meeting
10. All new interests declared at the meeting should be promptly updated onto the declaration of interest form. 11. All new completed declarations of interest should be transferred onto the register of interests. 12. If, following the meeting, the chair or any other member becomes aware that a conflict of interest has not been declared, they should raise this with the Head of Corporate Governance or Conflicts of Interest Guardian who will consider the appropriate course of action.
Individual(s) declaring interest(s) Designated person responsible for registers of interest Person who becomes aware of the conflict

32
DECLARATION OF INTERESTS FORM – MEETINGS
Please complete and return this form to the Head of Corporate Governance & Risk prior to the start of the meeting, or at any point at which you
become aware of an interest during the meeting.
Name:
Meeting:
Date:
Agenda item in which you have an interest
Type of Interest:
Financial
Non Financial Professional
Non Financial Personal
Indirect
Brief Description of your interest
Arrangement for managing the conflict of interest (to be agreed with the Chair of the meeting)
Signed:

33
Appendix 4: Template for recording minutes
Item no Agenda item
Actions
Declarations of interest SK reminded committee members of their obligation to declare any interest they may have on any issues arising at committee meetings which might conflict with the business of the CCG. Declarations are listed in the CCG’s Register of Interests. The Register is available via the CCG website at the following link: [link to be inserted] Declarations of interest from sub committees None declared Declarations of interest from today’s meeting The following update was received at the meeting: With reference to business to be discussed at this meeting, MS declared that he is a shareholder in XXX Care Ltd. SK declared that the meeting is quorate and that MS would not be included in any discussions on agenda item X due to a direct conflict of interest which could potentially lead to financial gain for MS. SK and MS discussed the conflict of interest, which is recorded on the register of interest, before the meeting and MS agreed to remove himself from the table and not be involved in the discussion around agenda item X.
Agenda Item <Note the agenda item> MS left the meeting, excluding himself from the discussion regarding xx. <conclude decision has been made> MS was brought back into the meeting.

34
Appendix 5: Procurement checklist
Service:
Question
Comment/Evidence
1. How does the proposal deliver good or improved outcomes and value for money-what are the estimated benefits? How does it reflect the CCG’s proposed commissioning priorities? How does it comply with the CCG’s commissioning obligations?
2. How have you involved the public in the decision to commission this service?
3. What range of health professionals have been involved in considering the proposals?
4. What range of potential providers have been involved in considering the proposals?
5. How have you involved the Health and Wellbeing Board? How does the proposal support the priorities in the joint health and wellbeing strategy?
6. What are the proposals for monitoring the quality of the service?
7. What systems will there be to monitor and publish data on referral patterns?
8. Have all conflicts and potential conflicts of interests been appropriately declared and entered on registers?
9. In respect of every conflict or potential conflict, you must record how you have managed that conflict or potential conflict. Has the management of all conflicts been recorded with a brief explanation of how they have been managed?
10. Why have you chosen this procurement route e.g. single action tender*?
11. What additional external involvement will there be in scrutinising the proposed decisions?
12. How will the CCG make its final commissioning decision in ways that preserve the integrity of the decision making process and award of any contract?

35
Additional question when qualifying a provider on a list or framework or pre selection for tender (including but not limited to any qualified provider) or direct award (for services where national tariffs do not apply)
13. How have you determined a fair price for the service?
Additional question when qualifying a provider on a list or framework or pre selection for tender (including but not limited to any qualified provider) where GP practices are likely to be qualified providers
14. How will you ensure that patients are aware of the full range of qualified providers from whom they can choose?
Additional questions for proposed direct awards to GP providers
15. What steps have been taken to demonstrate that the services to which the contract relates are capable of being provided by only one provider?
16. In what ways does the proposed service go beyond what GP practices should expect to provide under the GP contract?
17. What assurances will there be that a GP practice is providing high quality services under the GP contract before it has the opportunity to provide any new services?
*Taking into account all relevant regulations (e.g. the NHS (Procurement, patient choice and
competition) (No.2 Regulations 2013 and guidance (e.g. that of Monitor))

36
Appendix 6: Register of Procurement Decisions Template
Ref No
Date of Decision
Providers Name
Procurement description
Existing contract or new procurement (if existing include details)
Procurement type – CCG procurement, collaborative procurement with partners
CCG clinical / Commissioning Lead
CCG contract manager
Decision making process and name of decision making committee
Summary of conflicts of interest declared and how these were managed
Estimated Contract value (£) (Total)

37
Appendix 7 - Template of conflict of interests for bidders /contractors This page requires completion of details of organisations Page 2 overleaf requires completion of details of individuals
Name of organisation:
Details of interest held
Type of interest
Details
Provision of services or other work for the CCG or NHS England
Provision of services or other work for any other potential bidder in respect of this project or procurement process
Any other connection with the CCG or NHS England or professional, which the public could perceive may impair or otherwise influence the CCG’s or nay of its members or employees’ judgments, decisions or actions

38
Name of relevant person
(complete for all relevant persons)
Details of interest held:
Type of interest
Details
Personal interest or that of a family member, close friend or other acquaintance?
Provision of services or other work for the CCG or NHS England
Provision of services or other work for any other potential bidder in respect of this project or procurement process
Any other connection with the CCG or NHS England or professional, which the public could perceive may impair or otherwise influence the CCG’s or any of its members or employees’ judgments, decisions or actions
To the best of my knowledge and belief, the above information is complete and correct. I undertake to update the information as necessary. Signed: On behalf of: Date:

39
APPENDIX 8 Confidentiality and Conflicts of Interest during Public Procurement
PROCUREMENT FOR THE PROVISION OF XXXXXXXX
All persons involved in supporting this procurement are legally required to ensure the procurement process is reasonable and transparent, and that all potential bidders are treated fairly. To ensure that this is a fair and competitive procurement process, confidentiality must be maintained, and all actual or potential conflicts of interest identified, recorded and managed. As part of this process, we need you to confirm that you agree to keep all the information in relation to this process confidential, and that there are no actual or potential conflicts of interest that may prevent your participation. For these purposes, a conflict of interest means a set of circumstances by which a reasonable person would consider that your ability to apply judgement or act, in the context of delivering, commissioning, or assuring taxpayer funded health and care services is, or could be, impaired or influenced by another interest you hold. Examples of conflicts of interest include:
Having a financial interest (e.g. holding shares or options) in a Potential Bidder or any entity involved in any bidding consortium (Bidder Party);
Having a financial or any other personal interest in the outcome of the Evaluation Process;
Being employed by or providing services to any Bidder Party;
Being employed by or providing services to any Commissioning/Contracting Party currently or prospectively engaged in a procurement exercise for the same or similar services;
Receiving any kind of monetary or non-monetary payment or incentive (including hospitality) from any Bidder Party or its representatives;
Canvassing, or negotiating with, any person with a view to entering into any of the arrangements outlined above;
Having a close association with anyone (including spouse/partner; close relative e.g. parent, grandparent, child, grandchild or sibling; close friend or associate; or business partner) who falls into any of the categories outlined above; and
Having any other close relationship (current or historical) with any Bidder Party. The above is a non-exhaustive list of examples, and it is your responsibility to ensure that any and all potential conflicts – whether or not of the type listed above – are disclosed in writing prior to you joining the process.

40
Any disclosure by you will be assessed by the CCG on a case-by-case basis. Individuals will only be excluded from the Evaluation Process where the identified conflict is, in the CCG’s opinion, material and cannot be mitigated or be reasonably dealt with in another way. Please confirm that you will maintain confidentiality in relation to the process and declare any actual or perceived conflicts of interest by completing and returning Annex 1. The form should be signed in hard copy, scanned and returned by e-mail.

41
ANNEX 1 - PROCUREMENT FOR THE PROVISION OF XXXXXX
Name:
Job title/Role:
Organisation represented:
Telephone:
Email:
FORM OF CONFIDENTIALITY UNDERTAKING Please state
“yes” or “no”
I acknowledge that as a result of my participation in the Process, I will be receiving confidential information, which is not in the public domain, including a list of the relevant organisations involved with the short-listed bidders (the Information).
In consideration of my participation in the Process, I agree, at all times, to keep the Information, and all other information I receive as part of the Process, confidential and agree not to disclose, make any copies of, retain, or discuss it with any person who is not directly involved in the Process.
CONFLICTS OF INTEREST DECLARATION Please state
“yes” or “no”
In relation to the above Procurement, I am aware that there is a requirement that all actual or potential conflicts of interest, which may arise as a result of my involvement in the procurement process, are identified, disclosed and resolved (where applicable) before I can take part in the process.
The issues regarding conflicts of interest have been explained to me. I fully understand the nature and scope of such conflicts and accept the related obligations.
I confirm that I will notify the Procurement Manager immediately if any potential or actual conflicts of interest come to light following my completion and return of this form so that they may be addressed by the CCG as appropriate.
Are there any potential Conflicts of Interest?
If you have stated yes as to whether there are any potential conflicts of interest, please provide details and any reasons where appropriate, why you may believe these to be non-material and/or any proposed mitigating controls or state ‘Not Applicable’:

42
The information submitted will be held by the CCG for personnel or other reasons specified on this form and to comply with the organisation’s policies. This information may be held in both manual and electronic form in accordance with the General Data Protection Regulations (GDPR). Information may be disclosed to third parties in accordance with the Freedom of Information Act 2000 and published in registers that the CCG holds. The data controller is the CCG who can be contacted by emailing the Data Protection Officer at [email protected]
If you have named a relative or close associate on this form, please advise them that their details may be published on the CCG’s register of procurement decisions. I confirm that the information provided above is complete and correct. I acknowledge that any changes in these declarations must be notified to the Procurement Manager immediately. I am aware that if I do not make full, accurate and timely declarations then civil, criminal, or internal disciplinary action may result.
I do / do not [delete as applicable] give my consent for this information to published on registers that the CCG holds. If consent is NOT given please give reasons:
Declarer’s signature: Date:

43
Appendix 9 - Summary of key aspects of the NHS England statutory guidance on managing conflicts of interest relating to commissioning of new care models Introduction 1. Conflicts of interest can arise throughout the whole commissioning cycle from
needs assessment, to procurement exercises, to contract monitoring. They arise in many situations, environments and forms of commissioning.
2. Where CCGs are commissioning new care models9, particularly those that include primary medical services, it is likely that there will be some individuals with roles in the CCG (whether clinical or non-clinical), that also have roles within a potential provider, or may be affected by decisions relating to new care models. Any conflicts of interest must be identified and appropriately managed, in accordance with this statutory guidance.
3. This annex is intended to provide further advice and support to help CCGs to
manage conflicts of interest in the commissioning of new care models. It summarises key aspects of the statutory guidance which are of particular relevance to commissioning new care models rather than setting out new requirements. Whilst this annex highlights some of the key aspects of the statutory guidance, CCGs should always refer to, and comply with, the full statutory guidance.
Identifying and managing conflicts of interest 4. The statutory guidance for CCGs is clear that any individual who has a material
interest in an organisation which provides, or is likely to provide, substantial services to a CCG (whether as a provider of healthcare or provider of commissioning support services, or otherwise) should recognise the inherent conflict of interest risk that may arise and should not be a member of the governing body or of a committee or sub-committee of the CCG.
5. In the case of new care models, it is perhaps likely that there will be individuals
with roles in both the CCG and new care model provider/potential provider. These conflicts of interest should be identified as soon as possible, and appropriately managed locally. The position should also be reviewed whenever an individual’s role, responsibility or circumstances change in a way that affects the individual’s interests. For example where an individual takes on a new role outside the CCG, or enters into a new business or relationship, these new interests should be promptly declared and appropriately managed in accordance with the statutory guidance.
9 Where we refer to ‘new care models’ in this note, we are referring to any Multi-speciality Community
Provider (MCP), Primary and Acute Care Systems (PACS) or other arrangements of a similar scale or scope that (directly or indirectly) includes primary medical services.

44
6. There will be occasions where the conflict of interest is profound and acute. In
such scenarios (such as where an individual has a direct financial interest which gives rise to a conflict, e.g., secondary employment or involvement with an organisation which benefits financially from contracts for the supply of goods and services to a CCG or aspires to be a new care model provider), it is likely that CCGs will want to consider whether, practically, such an interest is manageable at all. CCGs should note that this can arise in relation to both clinical and non-clinical members/roles. If an interest is not manageable, the appropriate course of action may be to refuse to allow the circumstances which gave rise to the conflict to persist. This may require an individual to step down from a particular role and/or move to another role within the CCG and may require the CCG to take action to terminate an appointment if the individual refuses to step down. CCGs should ensure that their contracts of employment and letters of appointment, HR policies, governing body and committee terms of reference and standing orders are reviewed to ensure that they enable the CCG to take appropriate action to manage conflicts of interest robustly and effectively in such circumstances.
7. Where a member of CCG staff participating in a meeting has dual roles, for
example a role with the CCG and a role with a new care model provider organisation, but it is not considered necessary to exclude them from the whole or any part of a CCG meeting, he or she should ensure that the capacity in which they continue to participate in the discussions is made clear and correctly recorded in the meeting minutes, but where it is appropriate for them to participate in decisions they must only do so if they are acting in their CCG role.
8. CCGs should take all reasonable steps to ensure that employees, committee
members, contractors and others engaged under contract with them are aware of the requirement to inform the CCG if they are employed or engaged in, or wish to be employed or engaged in, any employment or consultancy work in addition to their work with the CCG (for example, in relation to new care model arrangements).
9. CCGs should identify as soon as possible where staff might be affected by the
outcome of a procurement exercise, e.g., they may transfer to a provider (or their role may materially change) following the award of a contract. This should be treated as a relevant interest, and CCGs should ensure they manage the potential conflict. This conflict of interest arises as soon as individuals are able to identify that their role may be personally affected.
10. Similarly, CCGs should identify and manage potential conflicts of interest where
staff are involved in both the contract management of existing contracts, and involved in procurement of related new contracts.
Governance arrangements 11. Appropriate governance arrangements must be put in place that ensure that
conflicts of interest are identified and managed appropriately, in accordance

45
with this statutory guidance, without compromising the CCG’s ability to make robust commissioning decisions.
12. We know that some CCGs are adapting existing governance arrangements and
others developing new ones to manage the risks that can arise when commissioning new care models. We are therefore, not recommending a “one size fits” all governance approach, but have included some examples of governance models which CCGs may want to consider.
13. The principles set out in the general statutory guidance on managing conflicts
of interest (paragraph 19-23), including the Nolan Principles and the Good Governance Standards for Public Services (2004), should underpin all governance arrangements.
14. CCGs should consider whether it is appropriate for the Governing Body to take
decisions on new care models or (if there are too many conflicted members to make this possible) whether it would be appropriate to refer decisions to a CCG committee.
Primary Care Commissioning Committee 15. Where a CCG has full delegation for primary medical services, CCGs could
consider delegating the commissioning and contract management of the entire new care model to its Primary Care Commissioning Committee. This Committee is constituted with a lay and executive majority, and includes a requirement to invite a Local Authority and Healthwatch representative to attend (see paragraph 97 onwards of the CCG guidance).
16. Should this approach be adopted, the CCG may also want to increase the
representation of other relevant clinicians on the Primary Care Commissioning Committee when new care models are being considered, as mentioned in Paragraph 98 of this guidance. The use of the Primary Care Commissioning Committee may assist with the management of conflicts/quorum issues at governing body level without the creation of a new forum/committee within the CCG.
17. If the CCG does not have a Primary Care Commissioning Committee, the CCG
might want to consider whether it would be appropriate/advantageous to establish either:
a) A new care model commissioning committee (with membership
including relevant non-conflicted clinicians, and formal decision making powers similar to a Primary Care Commissioning Committee (“NCM Commissioning Committee”); or
b) A separate clinical advisory committee, to act as an advisory body to
provide clinical input to the Governing Body in connection with a new care model project, with representation from all providers involved or potentially involved in the new care model but with formal decision making powers

46
remaining reserved to the governing body (“NCM Clinical Advisory Committee”).
NCM Commissioning Committee 18. The establishment of a NCM Commissioning Committee could help to provide
an alternative forum for decisions where it is not possible/appropriate for decisions to be made by the Governing Body due to the existence of multiple conflicts of interest amongst members of the Governing Body. The NCM Commissioning Committee should be established as a sub-committee of the Governing Body.
19. The CCG could make the NCM Commissioning Committee responsible for
oversight of the procurement process and provide assurance that appropriate governance is in place, managing conflicts of interest and making decisions in relation to new care models on behalf of the CCG. CCGs may need to amend their constitution if it does not currently contain a power to set up such a committee either with formal delegated decision making powers or containing the proposed categories of individuals (see below).
20. The NCM Commissioning Committee should be chaired by a lay member and
include non-conflicted GPs and CCG members, and relevant non-conflicted secondary care clinicians.
NCM Clinical Advisory Committee 21. This advisory committee would need to include appropriate clinical
representation from all potential providers, but have no decision making powers. With conflicts of interest declared and managed appropriately, the NCM Clinical Advisory Committee could formally advise the CCG Governing Body on clinical matters relating to the new care model, in accordance with a scope and remit specified by the Governing Body.
22. This would provide assurance that there is appropriate clinical input into
Governing Body decisions, whilst creating a clear distinction between the clinical/provider side input and the commissioner decision-making powers (retained by the Governing Body, with any conflicts on the Governing Body managed in accordance with this statutory guidance and constitution of the CCG).
23. From a procurement perspective the Public Contracts Regulations 2015
encourage early market engagement and input into procurement processes. However, this must be managed very carefully and done in an open, transparent and fair way. Advice should therefore be taken as to how best to constitute the NCM Clinical Advisory Committee to ensure all potential participants have the same opportunity. Furthermore it would also be important to ensure that the advice provided to the CCG by this committee is considered proportionately alongside all other relevant information. Ultimately it will be the responsibility of the CCG to run an award process in accordance with the

47
relevant procurement rules and this should be a process which does not unfairly favour any one particular provider or group of providers.
24. When considering what approach to adopt (whether adopting an NCM
Commissioning Committee, NCM Clinical Advisory committee or otherwise) each CCG will need to consider the best approach for their particular circumstances whilst ensuring robust governance arrangements are put in place. Depending on the circumstances, either of the approaches in paragraph 17 above may help to give the CCG assurance that there was appropriate clinical input into decisions, whilst supporting the management of conflicts. When considering its options the CCG will, in particular, need to bear in mind any joint / delegated commissioning arrangements that it already has in place either with NHS England, other CCGs or local authorities and how those arrangements impact on its options.
Provider engagement 25. It is good practice to engage relevant providers, especially clinicians, in
confirming that the design of service specifications will meet patient needs. This may include providers from the acute, primary, community, and mental health sectors, and may include NHS, third sector and private sector providers. Such engagement, done transparently and fairly, is entirely legal. However, conflicts of interest, as well as challenges to the fairness of the procurement process, can arise if a commissioner engages selectively with only certain providers (be they incumbent or potential new providers) in developing a service specification for a contract for which they may later bid. CCGs should be particularly mindful of these issues when engaging with existing / potential providers in relation to the development of new care models and CCGs must ensure they comply with their statutory obligations including, but not limited to, their obligations under the National Health Service (Procurement, Patient Choice and Competition) (No 2) Regulations 2013 and the Public Contracts Regulations 2015.

The Joint Committee has delegated powers from the WY CCGs to make collective decisions on specific, agreed WY&H work programmes. It can also make recommendations. The Committee supports the Partnership, but does not represent all partners. Further information is available here: https://www.wyhpartnership.co.uk/meetings/west-yorkshire-harrogate-joint-committee-ccgs or from Stephen Gregg, [email protected].
West Yorkshire & Harrogate (WY&H) Joint Committee of Clinical Commissioning Groups Summary of key decisions - Meeting in public, Tuesday 6th October 2020
Joint Committee governance
The Committee welcomed 2 new CCG Lay Members to their first meeting – Ruby Bhatti from Bradford District and Craven CCG and John Mallalieu from Calderdale CCG. The delegation of new commissioning decisions to the Joint Committee was noted.
The Committee: Noted that the new Joint Committee work plan had been agreed by all the West Yorkshire CCGs and reviewed the risks to the delivery of the work plan.
Commissioning Futures
The Commissioning Futures programme is being developed in collaboration with partners across the health and care system, including providers and local authorities and is based on our successful model of place-based working. There are three levels of commissioning, each tailored to local need and focused on improving population health. With an emphasis on place, work will only be carried out at WY&H level if it adds value to our places. A proposed operating model would come to a future meeting for approval.
The Committee: Agreed the next steps in developing the Commissioning Futures operating model.
Mental health learning disabilities & autism - Assessment and Treatment Units (ATUs)
The Committee considered proposals for ATUs, which involved collaborative commissioning between commissioners and providers. The proposal considered the whole pathway for people with learning disabilities. The Committee noted plans for engaging with people who had accessed care in ATUs, their carers and staff. Formal approval for commissioning ATUs would be sought at a future meeting of the Joint Committee, once the engagement had been completed.
The Committee: a) Endorsed the proposal to commission a new care model for people with a learning disability. b) Supported the proposed approach of provider-managed risk, subject to the further work of provider
Directors of Finance and CCG Chief Finance Officers.
Urgent and emergency care – NHS 111 First
The NHS 111 First national programme builds on learning from COVID-19 about the high use of 111 by the public for advice and signposting. It encourages people to phone 111 as an alternative to ‘walking’ unheralded into Emergency Departments (EDs). The integrated offer includes alternative pathways, for example GPs, pharmacists and mental health advice. The aim was not to stop people attending ED, but to make it easier for them to access quickly the right support.
The Committee: Noted the national specification for NHS 111 First and the process for local implementation through a Yorkshire and Humber Programme Oversight Group.
Yorkshire and Humber commissioning framework for Yorkshire Ambulance Service (YAS)
YAS provides integrated urgent and emergency services across Yorkshire and the Humber (Y&H), which covers 3 Integrated Care Systems. A framework has been developed to strengthen the coordination of the commissioning of YAS services. It aims to balance the advantages of operating at scale with the need to be responsive to the needs of local places.
The Committee: Noted the development of the Yorkshire and Humber framework for integrated commissioning of Integrated Urgent and Emergency Care Services provided by Yorkshire Ambulance Service and supported the proposed next steps.

1
Standards of Business Conduct Policy
Version: 2.2
Ratified by: Governing Body
Date ratified:
Name & Title of originator/author: Head of Corporate Governance and Risk
Name of responsible committee/individual: Audit Committee
Date issued:
Review date:
Target audience: See section 3

2
Contents
Page
1. Introduction
3
2. Purpose
3
3. Scope
3
4. Duties
4
5. Receipt of Hospitality, Gifts and Commercial Sponsorship
5
6. Outside Employment
10
7. Gifts Hospitality and Sponsorship Register
10
8. Publication of registers
11
9. Contracts for Goods and Services
12
10. Intellectual Property
13
11. Confidentiality
13
12. The Bribery Act 2010
14
13. Equality Impact Assessment
14
14. Monitoring Compliance and Effectiveness
15
15. Associated Documentation
15
16. References
15
APPENDIX 1 - The Seven Principles of Public Life
16
APPENDIX 2 - Standards of Business Conduct - Quick Guide
17
APPENDIX 3 - Declaration of Gift/Hospitality/Sponsorship Form
18
APPENDIX 4 – Declaration of Gift/Hospitality/Sponsorship Register Template
22
APPENDIX 5 - Non Disclosure Agreement
23
APPENDIX 6 - Policy Consultation Process
24

3
1 Introduction 1.1 The Code of Conduct and Code of Accountability in the NHS (second revision
July 2004) sets out the following three public service values which are central to the work of the NHS:
Accountability - everything done by those who work in the NHS must be able to stand the test of parliamentary scrutiny, public judgements on propriety and professional codes of conduct.
Probity - there should be an absolute standard of honesty in dealing with the assets of the NHS: integrity should be the hallmark of all personal conduct in decisions affecting patients, officers and members and suppliers, and in the use of information acquired in the course of NHS duties.
Openness - there should be sufficient transparency about NHS activities to promote confidence between the NHS and its staff, patients and the public.
1.2 In addition to the public service values described above, all individuals within
the CCG should follow the Seven Principles of Public Life (the Nolan Principles) - see Appendix 1.
1.3 All individuals within the CCG are responsible for ensuring that they are not
placed in a position which risks conflict between their private interests and their NHS duties. Every individual is responsible for ensuring that they comply with this policy. Some individuals may additionally be required to adhere to a code of conduct of their own professional body.
2 Purpose 2.1 This policy provides guidance on what is deemed to be acceptable in terms of
receipt of gifts, hospitality and sponsorship and provides a code of conduct that individuals within the CCG are expected to follow.
2.2 This policy reflects and builds on the following national guidance:
HSG(93)5 Standards of Business Conduct for NHS Staff
Seven Principles of Public Life
The Codes of Conduct and Accountability in the NHS 2004
The Code of Conduct for NHS Managers 2002
Professional Standards Authority ‘Standards for Members of NHS Boards and Clinical Commissioning Group Governing Bodies in England’ 2012
2.3 This policy should be read in partnership with the CCG’s Conflicts of Interest
Policy, the Anti‐Fraud and Bribery Policy, the Working Time Regulations Policy (in relation to secondary employment) and the Procurement Policy.
3 Scope 3.1 This policy applies to:

4
All CCG employees, including: o All full and part time staff; o Any staff on sessional or short term contracts; o Any students and trainees; o Agency staff; and o Seconded staff.
In addition, any self-employed consultants or other individuals working for the CCG under a contract for services should declare gifts, hospitality and sponsorship in accordance with this policy, as if they were CCG employees.
Members of the governing body: All members of the CCG’s committees, sub-committees/sub-groups, including:
o Co-opted members; o Appointed deputies; and o Any members of committees/groups from other organisations.
All members of the CCG (i.e. each practice) This includes each provider of primary medical services which is a member of the CCG under Section 140 (1) of the 2006 Act. Declarations should be made by the following groups:
o GP partners o Any individual directly involved with the business or decision-
making of the CCG. Who are referred to collectively in this policy as ‘individuals within the CCG’.
4 Duties 4.1 The Chief Executive is the organisation’s designated ‘Accountable Officer’
and has overall responsibility for ensuring that the CCG operates efficiently, economically and with probity. The Chief Executive (alongside other members of the Governing Body) has a duty to ensure that the CCG provides a secure environment in which to work, and one in which people are confident to raise concerns which will be listened to and addressed.
4.2 The Chief Finance Officer is responsible for ensuring this policy is in place.
The Chief Finance Officer, in conjunction with the Chief Executive, monitors and ensures compliance with NHS Counter Fraud Authority Standards for Commissioners regarding fraud, bribery and corruption. In addition and in consultation with the Local Counter Fraud Specialist (LCFS), the Chief Finance Officer will decide whether there is sufficient cause to conduct an investigation in relation to bribery, and whether the Police and external audit need to be informed.
4.3 The Head of Corporate Governance and Risk is responsible for
administering this policy and ensuring reporting to the Audit Committee. 4.4 All members of the Governing Body must act in accordance with this policy
and lead by example in acting with the utmost integrity and ensuring adherence to all relevant regulations, policies and procedures. Governing Body members must abide by the Professional Standards Authority Standards

5
for Members of NHS Boards and Clinical Commissioning Group Governing Bodies in England.
4.5 Line Managers are responsible for assisting employees in complying with this
policy by ensuring that this policy and its requirements are brought to the attention of employees for whom they are responsible, and that those employees are aware of its implications for their work.
4.6 All individuals within the CCG are required to:
Act honestly and with integrity at all times and to safeguard the organisation’s resources for which they are responsible.
Ensure that they read, understand and comply with this policy.
Adhere to all relevant regulations, policies and procedures.
Raise concerns as soon as possible if they believe or suspect that a conflict with this policy has occurred, or may occur in the future.
Ensure that the interests of patients remain paramount at all times.
Be impartial and honest in the conduct of their official business.
Use the public funds entrusted to them to the best advantage of the service, always ensuring value for money.
Not abuse their official position for personal gain or to benefit their family or friends.
Not seek to gain advantage or further private business or other interests, in the course of their official duties.
Be aware that it is both a serious criminal offence (under the Bribery Act 2010, the Theft Act 1968 and the Fraud Act 2006) and disciplinary matter to corruptly receive or give any fee, loan, gift, reward or other advantage in return for doing (or not doing) anything or showing favour (or disfavour) to any person or organisation.
Understand that failure to follow this policy may damage the CCG and its work and so may be viewed as a disciplinary matter. The organisation’s Disciplinary Policy makes it clear that bringing the organisation into disrepute is potentially gross misconduct. As well as the possibility of civil and criminal prosecution, individuals that breach this policy will face disciplinary action, which could result in dismissal for gross misconduct.
5 Receipt of Hospitality, Gifts and Commercial Sponsorship
Hospitality
5.1 Delivery of services across the NHS relies on working with a wide range of partners (including industry and academia) in different places and, sometimes, outside of ‘traditional’ working hours. As a result, individuals within the CCG will sometimes appropriately receive hospitality. Individuals receiving hospitality should always be prepared to justify why it has been accepted, and be mindful that even hospitality of a small value may give rise to perceptions of impropriety and might influence behaviour.
5.2 For the purpose of this policy, hospitality is defined as offers of meals, refreshments, travel, accommodation, and other expenses in relation to attendance at meetings, conferences, education and training events, etc.
5.3 Overarching principles:

6
Individuals within the CCG should not ask for or accept hospitality that may affect, or be seen to affect, their professional judgement;
Hospitality must only be accepted when there is a legitimate business reason and it is proportionate to the nature and purpose of the event;
Particular caution should be exercised when hospitality is offered by actual or potential suppliers or contractors, these can be accepted if modest and reasonable, but individuals should always obtain senior approval and declare these.
5.4 Meals and refreshments:
Under a value of £25.00 – may be accepted and need not be declared;
Of a value between £25.00 - £75.00 – may be accepted and must be declared;
Over a value of £75.00 – should be refused unless (in exceptional circumstances) senior approval is given. A clear reason must be recorded in the register of gifts and hospitality as to why it was permissible to accept.
A common sense approach should be applied to the valuing of meals and refreshments (using an actual amount, if known, or an estimate that a reasonable person would make as to its value).
5.5 Travel and accommodation:
Modest offers to pay some or all of the travel and accommodation costs related to attendance at events may be accepted and must be declared.
Offers which go beyond modest or are of a type that the CCG itself might not usually offer, need senior approval, should only be accepted in exceptional circumstances, and must be declared. A clear reason must be recorded in the register of gifts and hospitality as to why it was permissible to accept travel and accommodation of this type.
A non-exhaustive list of examples includes: o Offers of business class or first class travel and accommodation
(including domestic travel); and o Offers of foreign travel and accommodation.
5.5 In cases of doubt, advice should be sought from the Head of Corporate
Governance and Risk or the hospitality should be politely declined.
Gifts 5.6 Staff in the NHS offer support during significant events in people’s lives. For
this work they may sometimes receive gifts as a legitimate expression of gratitude. We should be proud that our services are so valued. But situations where the acceptance of gifts could give rise to conflicts of interest should be avoided. Individuals within the CCG should be mindful that even gifts of a small value may give rise to perceptions of impropriety and might influence behaviour if not handled in an appropriate way.

7
5.7 A ‘gift’ is defined as any item of cash or goods, or any service, which is provided for personal benefit, free of change or at less than its commercial value.
5.8 Overarching principles:
Individuals within the CCG must not accept gifts that may affect, or be seen to affect, their professional judgement. This overarching principle should apply in all circumstances;
Any personal gift of cash or cash equivalents (e.g. vouchers, tokens, offers of remuneration to attend meetings whilst in a capacity working for or representing the CCG) must always be declined, whatever their value and whatever their source, and the offer which has been declined must be declared and recorded in the register of gifts and hospitality.
5.9 Gifts from suppliers or contractors:
Gifts from suppliers or contractors doing business (or likely to do business) with the CCG must be declined, whatever their value (subject to this, low cost branded promotional aids may be accepted and not declared where they are under the value of a common industry standard of £6.00). The person to whom the gifts were offered must also declare the offer so that it can be recorded on the register of gifts and hospitality.
5.10 Gifts from other sources (e.g. patients, families, service users):
Individuals must not ask for any gifts;
Modest gifts of less than £50.00 can be accepted and do not need to be declared;
Gifts valued at over £50.00 should be treated with caution and only be accepted, with senior approval, on behalf of an organisation (i.e. to an organisation’s charitable funds), not in a personal capacity. These must be declared;
Multiple gifts from the same source over a 12 month period must be treated in the same way as a single gift in respect of the £50.00 threshold.
5.11 In cases of doubt, advice should be sought from the Head of Corporate
Governance and Risk or the gift should be politely declined.
5.12 If an individual becomes aware that they are a named beneficiary in the will of a patient they have provided care to, they must contact the Chief Executive or Chief Finance Officer to discuss the ethics of remaining a beneficiary. Senior approval
5.13 If you wish to accept gifts worth more than £50.00, hospitality worth over £75.00, or offers of travel/accommodation which go beyond modest (see above), this must be approved by the following, who must sign Section 9 of the Gifts and Hospitality declaration form:

8
Requesting Individual Approving Manager
Chief Executive Non-Executive Members of Governing Body
CCG Chair
Directors CCG Chair
Chief Executive
Other Individuals Relevant Director or Deputy/Associate Director
Sponsored events
5.14 Sponsorship of NHS events by external providers is valued. Offers to meet some or part of the costs of running an event secures their ability to take place, benefiting NHS staff and patients. Without this funding there may be fewer opportunities for learning, development and partnership working. However, there is potential for conflicts of interest between the organiser and the sponsor, particularly regarding the ability to market commercial products or services. As a result there should be proper safeguards in place to prevent conflicts occurring.
5.15 For the purpose of this policy, sponsorship is defined as including:
NHS funding from an external source, including funding of all or part of the costs of a member of staff; and
NHS research, staff training, pharmaceuticals, equipment, meeting rooms, costs associated with meetings, meals, hotel and transport costs (including trips abroad), provision of free services (speakers), buildings or premises.
5.16 When sponsorships are offered, the following principles must be adhered to:
Sponsorship of CCG events by appropriate external bodies should only be approved if a reasonable person would conclude that the event will result in clear benefit for the CCG and the NHS.
Acceptance of commercial sponsorship must not in any way compromise the commissioning decisions of the CCG or be dependent on the purchase or supply of goods or services.
At the CCG’s discretion, sponsors or their representatives may attend of take part in the event but they should not have a dominant influence over the content or main purpose of an event, meeting, seminar, publication or training event.
The involvement of a sponsor in an event should always be clearly identified in the interests of transparency.
The sponsorship agreement must be in writing and must include the following statement: ‘The fact of sponsorship does not mean that the CCG endorses [company name]’s products or services.’ This should also be made visibly clear on any promotional or other materials relating to the event.
No information should be supplied to the sponsor from which they could gain a commercial advantage, and information which is not in the public domain should not normally be supplied.

9
Ensure there are no potential irregularities that may affect a company’s ability to satisfy the conditions of the agreement or impact upon it in any way. This would include checking the company’s financial standing and referring to the company’s accounts.
Consider the costs and benefits in relation to alternative options where appropriate. The decision making process must be transparent and defensible.
During dealings with sponsors there must be no breach of patient or individual confidentiality or data protection rules and legislation. Any disclosure of confidential information must be legally and ethically appropriate. In research purposes, disclosure should not take place without approval of the Local Research Ethics Committee.
Monitor clinical and financial outcomes and ensure break clauses are built in to enable the CCG to terminate the agreement if it becomes apparent that it is not providing expected value for money / clinical outcomes.
5.17 Any sponsorship that is offered and/or accepted must be declared and approval must be sought from the Chief Executive and Chair prior to accepting sponsorship using the form attached at Appendix 3. Other forms of sponsorship:
5.18 Organisations external to the CCG or NHS may also sponsor posts or research. However, there is potential for conflicts of interest to occur, particularly when research funding by external bodies does or could lead to a real or perceived commercial advantage, or if sponsored posts cause a conflict of interest between the aims of the sponsor and the aims of the organisation, particularly in relation to procurement and competition. There needs to be transparency and any conflicts of interest should be well managed. For further information, please refer to Managing Conflicts of Interest in the NHS: Guidance for staff and organisations. Speaking at a Meeting / Conference
5.19 Should an individual be asked to speak at an event and there is an offer of payment and delivering it during contracted hours, then there are two choices open to the individual in conjunction with agreement with the line manager:
The payment should be credited to the CCG and the relevant department within which the individual works, including the Governing Body as a “department” for GP members / Lay Members to be assigned to. Any such payments must also be declared using the form at Appendix 3. If there is no payment but other benefits are offered, such as accommodation, travel expenses, etc. then this must be declared using the form at Appendix 3.
The individual takes annual leave and the payment is made to them as a private matter between the organisation making the payment and the individual involved with the CCG. However, GPs in particular need to be mindful of the potential conflicts of interest that may still arise between their role within CCG and as a private contractor of services to the NHS. For further information please see the Conflicts of Interest Policy.

10
Inappropriate Offers of Hospitality/Gifts/Sponsorship
5.20 All staff and members must notify the Head of Corporate Governance and Risk of any inappropriate/overly generous offers of hospitality/gifts/sponsorship within 2 weeks of the offer being made. This includes any offers that would constitute a bribe, i.e. offers of a financial or other advantage as an incentive or reward to improperly perform your function or activities. For further information, please see the Anti-Fraud and Bribery Policy. The Head of Corporate Governance and Risk will ensure the Audit Committee is made aware of the inappropriate offer at the next meeting.
6. Outside Employment In accordance with the CCG’s Working Time Regulations Policy, individuals who are directly employed by the CCG must notify their line manager of their intention to undertake secondary employment by completing the Declaration of Secondary Employment form. Any existing outside employment must be declared on appointment, and any new outside employment must be declared when it arises. Amongst other things, the purpose of this is to ensure that the CCG is aware of any potential conflict with their CCG employment. For further information, please see the Conflicts of Interest Policy.
6.1 Examples of work which might conflict with the business of the CCG include:
Employment with another NHS body;
Employment with another organisation which might be in a position to supply goods/services to the CCG including paid advisory positions and paid honorariums which relate to bodies likely to do business with the CCG;
Directorships e.g. of a GP federation or non-executive roles;
Self employment, including private practice, charitable trustee roles, political roles and consultancy work, in a capacity which might conflict with the work of the CCG or which might be in a position to supply goods/services to the CCG.
6.2 Permission to engage in secondary employment will be required and the CCG
reserves the right to refuse permission where it believes a conflict will arise.
7. Gifts, Hospitality and Sponsorship Register
7.1 The following must be declared as soon as reasonably practicable using the form at Appendix 3:
All offers of gifts from suppliers and contractors, other than low cost branded promotional items under the value of £6.00;
All offers of gifts from other sources (e.g. patients, families, service users) with a value of more than £50.00;
Hospitality with a value of more than £25.00; and
All offers and/or acceptances of sponsorship.
7.2 Where gifts and hospitality have been offered and declined, they must be declared and recorded if the amount would have been subject to such a declaration.

11
7.3 All completed hospitality/gift/sponsorship forms must be submitted to the
Head of Corporate Governance and Risk for incorporating into the central register.
7.4 The Gifts and Hospitality Register will be published on the CCG website on a
quarterly basis.
7.5 A record of all gifts and hospitality will remain on the register for a minimum of
6 months after the date of offer. The CCG will retain a private record of
historic interests for a minimum of 6 years after the date on which it was
offered.
8. Publication of registers
8.1 In order to demonstrate openness the Gift and Hospitality register will be made available on the CCG’s website. Also, the register is reviewed by the Audit Committee on a quarterly basis.
8.2 Although all individuals must declare gifts, hospitality and sponsorship, the CCG will only publish those declared by decision makers. Decision makers are defined as follows:
All governing body members;
Members of advisory groups which contribute to direct or delegated decision making on the commissioning or provision of taxpayer funded services such as working groups involved in service redesign or stakeholder engagement that will affect future provision of services;
Members of the Primary Care Commissioning Committee (PCCC);
Members of other committees of the CCG e.g., audit committee, remuneration committee etc.;
Members of new care models joint provider / commissioner groups / committees;
Members of procurement (sub-)committees;
Individuals on Agenda for Change band 8d and above;
Management, administrative and clinical staff who have the power to enter into contracts on behalf of the CCG;
Management, administrative and clinical staff involved in decision making concerning the commissioning of services, purchasing of good, medicines, medical devices or equipment, and formulary decisions; and
Management, administrative and clinical staff responsible for processing payments in behalf of the CCG.
8.3 In exceptional circumstances, where the public disclosure of information could
give rise to a real risk of harm or is prohibited by law, an individual’s name and/or other information may be redacted from the publicly available register. Where an individual believes that substantial damage or distress may be caused, to him/herself or somebody else by the publication of information about them, they are entitled to request that the information is not published. Such requests must be made in writing. Decisions not to publish information

12
must be made by the Conflicts of Interest Guardian for the CCG, who should seek appropriate legal advice where required, and the CCG will retain a confidential un-redacted version of the register.
8.4 All decision making staff will be made aware, in advance of publication, that the register(s) will be kept, how the information on the register(s) may be used or shared and that the register(s) will be published. This will be done by the provision of a fair processing notice that details the identity of the data controller, the purposes for which the registers are held and published, how the information on the register(s) may be used or shared and contact details for the data protection officer. This information will also be provided to individuals identified in the register(s) because they are in a relationship with the person making the declaration.
8.5 All individuals who are not decision makers but who are still required to make a declaration of interest(s) or a declaration of gifts or hospitality will be made aware that the register(s) will be kept and how the information on the register(s) may be used or shared. This will be done by the provision of a separate fair processing notice that details the identity of the data controller, the purposes for which the register(s) are held, how the information on the register(s) may be used or shared and contact details for the data protection officer. This information will also be provided to individuals identified in the register(s) because they are in a relationship with the person making the declaration.
9. Contracts for Goods and Services
9.1 All staff who are in contact with suppliers and contractors (including external
consultants), and in particular those who are authorised to sign Purchase Orders or place contracts for goods, materials or services, are expected to adhere to professional standards of the kind set out in the Code of Conduct of the Chartered Institute of Purchasing and Supply (CIPS).
9.2 Fair and open competition between prospective contractors or suppliers for
NHS contracts is a requirement of NHS Standing Orders and of EU Directives on Public Purchasing for Works and Supplies. This means that:
No private, public or voluntary organisation which may bid for NHS business should be given any advantage over its competitors, such as advance notice of NHS requirements. This applies to all potential contractors, whether or not there is a relationship between them and the
CCG, such as a long‐running series of previous contracts.
Each new contract should be awarded solely on merit, taking into account the requirements of the NHS and the ability of the contractors to fulfil them.
9.3 Individuals should ensure that no special favour is shown to current or former
employees or their close relatives or associates in awarding contracts to private or other businesses run by them or employing them in a senior or relevant managerial capacity. Contracts may be awarded to such businesses where they are won in fair competition against other tenders, but scrupulous care must be taken to ensure that the selection process is conducted

13
impartially, and that individuals who are known to have a relevant interest play no part in the selection. Such interests must also be declared in accordance with the Conflicts of Interest Policy.
9.4 Individuals must not seek, or accept, preferential rates or benefits in kind for
private transactions carried out with companies with which they have had, or may have, official dealings on behalf of the CCG. This does not apply to officers’ and members’ benefit schemes offered by the NHS or trade unions.
9.5 Every invitation to tender to a prospective bidder for CCG business must
require each bidder to give a written undertaking not to engage in collusive tendering or other restrictive practice, and not to engage in canvassing the CCG, its employees or officers concerning the contract opportunity tendered.
10. Intellectual Property 10.1 Any patents, designs, trademarks or copyright resulting from the work (e.g.
research) of an individual, carried out as part of their work with the CCG, shall be the Intellectual Property of the CCG.
10.2 Approval should be sought from the appropriate line manager prior to entering
into an obligation to undertake external work connected with the business of the CCG, e.g. writing articles for publication, speaking at conferences.
10.3 Where the undertaking of external work, gaining patent or copyright or the
involvement in innovative work, benefits or enhances the CCG’s reputation or results in financial gain for the CCG, consideration will be given to rewarding employees subject to any relevant guidance for the management of Intellectual Property in the NHS issued by the Department of Health.
11. Confidentiality 11.1 Information concerning the CCG which is not in the public domain must not at
any time be divulged to any unauthorised person. Similarly, patient data or personal data concerning staff must not be divulged, in line with the General Data Protection Regulation (GDPR) 2018. This duty of confidence remains after termination of employment and applies to all individuals within the CCG.
11.2 Care should be taken that confidentiality is not breached inadvertently by, for
instance discussing confidential matters in public places, such as whilst travelling by train, or by leaving portable IT equipment containing confidential information where it might easily be stolen, such as on full view in a parked car. Data should only be distributed using mechanisms with an appropriate level of security.
11.3 Individuals must maintain confidentiality of information at all times, both
commercial data and personal data, as defined by the GDPR. 11.4 Individuals should guard against providing information on the operations of
the CCG which might provide a commercial advantage to any organisation (private or NHS) in a position to supply goods or services to the CCG. For particularly sensitive procurements/contracts, individuals may be asked to

14
sign a non-disclosure agreement, a copy of which can be found at Appendix 4.
11.5 Please note that nothing in this policy prevents an individual from raising a
concern in line with the CCG’s Whistleblowing Policy.
12. The Bribery Act 2010
12.1 The Bribery Act 2010 defines bribery as:
“Inducement for an action which is illegal, unethical or a breach of trust. Inducements can take the form of gifts, loans, fees, rewards or other privileges".
12.2 This can be broadly defined as the offering or acceptance of inducements,
gifts, favours, payment or benefit-in-kind which may influence the action of any person. Bribery does not always result in a loss. The corrupt person may not benefit directly from their deeds; however, they may be unreasonably using their position to give some advantage to another.
12.3 The Act also introduces a corporate offence of failing to prevent bribery
where the organisation (which includes all NHS bodies) does not have adequate preventative procedures in place.
12.4 Should members or staff wish to report any concerns or allegations they have
a number of options available to them:
Report all suspected irregularities to the Chief Finance Officer who is also the contact point for NHS Counter Fraud Authority, the Police and External Audit.
Contact the Local Counter Fraud Specialist on 01904 725145 / 01423 554548 for any potential fraud related queries.
Contact the NHS Counter Fraud Authority Fraud and Corruption Reporting Line o 0800 028 4060 o www.reportnhsfraud.nhs.uk
Contact the Public Concern at Work line on 0207 404 6609
Follow the CCG’s own Whistleblowing Policy guidelines
12.5 Failure to disclose or providing falsified information is considered as gross misconduct and may lead to internal disciplinary action and/or include the involvement of the CCG’s Local Counter Fraud Specialist in line with the CCG’s Anti-Fraud and Bribery Policy.
13. Equality Impact Assessment (EIA)
13.1 A full Equality Impact Assessment is not considered to be necessary as this policy will not have a detrimental impact on a particular group.
14. Monitoring Compliance and Effectiveness

15
14.1 Effectiveness is monitored by the Audit Committee through regular reports on declarations made in line with the policy.
14.2 Individuals should be aware that a breach of this policy could render them
liable to prosecution as well as leading to the termination of their employment or position with the CCG.
15. Associated Documentation
Managing Conflicts of Interest Policy
Anti‐Fraud and Bribery Policy
Working Time Regulations Policy
Procurement Policy
Whistleblowing Policy
16. References
HSG(93)5 Standards of Business Conduct for NHS Staff
Nolan Principles of Public Life
The Codes of Conduct and Accountability in the NHS 2004
The Code of Conduct for NHS Managers 2002
Professional Standards Authority ‘Standards for Members of NHS Boards and Clinical Commissioning Group Governing Bodies in England’ 2012
Bribery Act 2010
Chartered Institute of Purchasing and Supply (CIPS) Code of Conduct

16
Appendix 1 – The Seven Principles of Public Life (Nolan Principles)
Selflessness - Holders of public office should act solely in terms of the public
interest.
Integrity - Holders of public office must avoid placing themselves under any obligation to people or organisations that might try inappropriately to influence them in their work. They should not act or take decisions in order to gain financial or other material benefits for themselves, their family, or their friends. They must declare and resolve any interests and relationships.
Objectivity - Holders of public office must act and take decisions impartially, fairly and on merit, using the best evidence and without discrimination or bias.
Accountability - Holders of public office are accountable to the public for their decisions and actions and must submit themselves to the scrutiny necessary to ensure this.
Openness - Holders of public office should act and take decisions in an open and transparent manner. Information should not be withheld from the public unless there are clear and lawful reasons for so doing.
Honesty - Holders of public office should be truthful.
Leadership - Holders of public office should exhibit these principles in their own behaviour. They should actively promote and robustly support the principles and be willing to challenge poor behaviour wherever it occurs.

17
Appendix 2 - Standards of Business Conduct – Quick Guide
Make sure you understand the guidelines on standards of business conduct, and consult your line manager if you are not sure.
Make sure you are not in a position where your private interests and NHS duties may conflict.
Declare to any relevant interests in line with the Managing Conflicts of Interest Policy. If in doubt, ask yourself: i. Am I, or might I be, in a position where I (or my family/friends) could gain from the connection between my private interests and my employment? ii. Do I have access to information which could influence purchasing decisions? iii. Could my outside interest be in any way detrimental to the NHS or to patients' interests? iv. Do I have any other reason to think I may be risking a conflict of interest?
If still unsure - Declare it!
Declare the offer and receipt of gifts and hospitality as soon as possible.
Report any inappropriate offers of gifts/hospitality/sponsorship to the Head of Corporate Governance within 2 weeks of the offer being made.
Obtain permission from the Chief Executive and Chair (using the form at Appendix 3) before accepting any sponsorship agreement.
Adhere to the code of conduct of the Institute of Purchasing and Supply if you are involved in any way with the acquisition of goods and services.
Inform your line manager if you are intending to take on outside work, including any potential conflicts of interest this may cause.
Do not abuse your past or present official position to obtain preferential rates for private deals.
Do not unfairly advantage one competitor over another or show favouritism in awarding contracts.
Do not misuse or make available official "commercial in confidence" information.

18
Appendix 3
RECORD OF HOSPITALITY/GIFTS/SPONSORSHIP – DECLARATION FORM This form should be used to record any offers and/or acceptance of hospitality/gifts, and sponsorship agreements. Both declined and accepted offers should be declared in line with the following rules: Gifts
Gifts from suppliers or contractors: Gifts offered from other sources:
All gifts of any nature offered by suppliers or contractors linked (currently or prospectively) to the CCG’s business should be declined, whatever their value.
Gifts of cash and vouchers to individuals should always be declined.
Subject to this, low cost branded promotional aids may be accepted where they are under the value of £6.00 in total, and need not be declared.
Modest gifts of less than £50.00 can be accepted and do not need to be declared.
Gifts valued at over £50.00 should be treated with caution and only be accepted, with senior approval, on behalf of an organisation, not in a personal capacity. These must be declared.
Multiple gifts from the same source over a 12 month period should be treated in the same way as a single gift in respect of the £50.00 threshold.
Hospitality
Hospitality - meals and refreshments:
Hospitality - travel and accommodation:
Under a value of £25.00 – may be accepted and need not be declared.
Modest offers to pay some or all of the travel and accommodation costs related to attendance at events may be accepted and must be declared.
Of a value between £25.00 - £75.00 – may be accepted and must be declared.
Offers which go beyond modest (i.e. first class travel and accommodation and foreign travel and accommodation),or are of a type that the organisation itself might not usually offer, need senior approval, should only be accepted in exceptional circumstances, and must be declared.
Over a value of £75.00 – should be refused unless (in exceptional circumstances) senior approval is given. These must be declared.

19
Senior approval
If you wish to accept gifts worth more than £50.00, hospitality worth over £75.00, or offers of travel/accommodation which go beyond modest (see above), this must be approved by the following, who must sign Section 9:
Requesting Individual Approving Manager
Chief Executive Non-Executive Members of Governing Body
CCG Chair
Directors CCG Chair
Chief Executive
Other Individuals Relevant Director or Deputy/Associate Director
If you have declined gifts worth more than £50 or Hospitality worth over £25.00 respectively, this must be declared.
If you wish to enter into a sponsorship agreement, this must be approved by the Chief Executive and Chair, and they must complete section 9 below.

20
Name:
Position within the CCG:
Are you responsible for contract monitoring, ordering or approval powers? Yes / No (please delete as appropriate) If yes, please specify:
Details of Hospitality/Gifts/Sponsorship Offered and/or Accepted
1.Details of the hospitality/gift/sponsorship:
2. Approximate value:
3. Reason why the hospitality/gift/sponsorship is being offered:
4a. Name of organisation/individual offering hospitality or gift/sponsorship:
4b. Name of the organisation representative:
4c. Date of event/gift being offered:
5. Products/services provided by the organisation/individual to NHS Leeds CCG, where applicable:
6. Are the products or services being offered either used or ordered by the individual in the course of their duties?
Yes / No (please delete as appropriate)
7. Decision: Declined / Accepted (please delete as appropriate)

21
8. Declaration: I confirm that the information provided is complete and correct. I acknowledge that any changes in these declarations must be notified to the CCG as soon as practicable and no later than 28 days after the interest arises. I am aware that if I do not make full, accurate and timely declarations then civil, criminal, professional regulatory or internal disciplinary action may result.
Signed: Name: Designation: Date:
9. Approved: Yes / No (please delete as appropriate)
If yes, reason for approval / If no, reason offer declined (Continue overleaf if necessary):
Signed: Name: Designation: Date:
Please return completed forms to the Corporate Governance Team
[email protected] for inclusion on the register.
The information submitted will be held by the CCG for personnel or other reasons specified on this
form and to comply with the organisation’s policies. This information may be held in both manual and
electronic form in accordance with the Data Protection Act 2018. Information may be disclosed to third
parties in accordance with the Freedom of Information Act 2000 and in the case of ‘decision making
staff’ (as defined in the statutory guidance on managing conflicts of interest for CCGs), may be
published in registers that the CCG holds.
Decision making staff should be aware that the information provided in this form will be added to the
CCG’s registers which are held in hardcopy for inspection by the public and published on the CCG’s
website. Decision making staff must make any third party whose personal data they are providing in
this form aware that the personal data will held in hardcopy for inspection by the public and published
on the CCG’s website and must inform the third party that the CCG’s privacy policy is available on the
CCG’s website. If you are not sure whether you are a ‘decision making’ member of staff, please speak
to your line manager before completing this form.

22
Appendix 4 - Declaration of Gift/Hospitality/Sponsorship Register Template
Ref.
Name Position Details of Gift/ Hospitality Offered
From whom it was offered
Details of previous gifts and hospitality offered or accepted by this offeror/supplier
Date of Event/ Gift Offered
Estimated Value
Reason for Offer (if known)
Decision (Accepted/ Declined) and reason for acceptance/ declining
Any action taken to mitigate against a conflict
Name of Approver
Date Approved / Declined
Reasons why approved / declined

23
Appendix 5 – Non Disclosure Agreement Template
NHS Leeds CCG - express requirement for confidentiality You have been requested to be involved in [INSERT DETAILS] (the “Project”). NHS Leeds CCG or other parties participating in the Project may provide you with, as part of your role in respect of the Project, access to certain confidential information relating the Project (whether before or after the date of this letter), in writing, by email, orally or by other means (including from or pursuant to discussions with any other party or which is obtained through attendance at meetings related to the Project) and trade secrets including, without limitation, technical data and know-how relating to the Project, including in particular (by way of illustration only and without limitation) [EXAMPLES] and including (but not limited to) information that you may create, develop, receive or obtain in connection with your engagement on the Project, whether or not such information (if in anything other than oral form) is marked confidential (the "Confidential Information"). Accordingly we draw to your attention that as part of your role for NHS Leeds CCG you are required to: 1.1. maintain the Confidential Information in the strictest confidence and not divulge
any of the Confidential Information to any third party without the prior written permission of NHS Leeds CCG; and
1.2. not make use of, reproduce, copy, discuss, disclose or distribute the
Confidential Information other than for use as part of your role in the Project. The above obligations in respect of this Confidential Information are supplemental to any prior representation, understanding and commitment (whether oral or written) between us. The terms of this Letter can only be changed by a written document, agreed upon by both of us and signed by duly authorised persons. These provisions shall be governed and construed by English law. Yours faithfully
For and on behalf of NHS Leeds CCG By signing this letter you agree to comply with these terms.
Signed:
Date:
Print Name:

24
Appendix 6 - Policy Consultation Process
Title of document Standards of Business Conduct Policy
Author Corporate Governance & Risk Team
Revised document Revised October 2019
Lists of persons involved in the revision of the policy
Laura Parsons - Head of Corporate Governance and Risk Sam Ramsey – Corporate Governance Manager
List of persons involved in the consultation process:
As Above Audit Committee