
Tayside NHS Board
137
1 Please note any items relating to Committee business are embargoed and should not be made public until after the meeting Tayside NHS Board A meeting of Tayside NHS Board Performance and Resources Committee will be held at 9:45am on Thursday 10 February 2022 via Microsoft Teams Apologies/enquiries to: Ms Pauline Ireland, 01382 660111 extension 55761 or email [email protected] AGENDA LEAD OFFICER REPORT NUMBER 1. WELCOME AND APOLOGIES 2. DECLARATION OF INTERESTS 3. MINUTE AND CHAIR’S ASSURANCE REPORT 3.1 Minute of the Performance and Resources Committee meeting of 19 December 2021 – for approval Chair Attached 3.2 Chair’s Assurance Report to the Board following the Performance and Resources Committee of 9 December 2021 – for noting Chair Attached 4. ACTION POINTS UPDATE AND MATTERS ARISING 4.1 Action Points Update S Lyall Attached 4.2 Matters Arising 5. COMMITTEE ASSURANCE AND WORKPLAN 2021/2022 5.1 Performance and Resources Committee Assurance and Workplan 2021/22 Chair Attached 5.2 Record of Attendance 2021/2022 Attached 6. ITEMS FOR ASSURANCE Financial Planning and Monitoring 6.1 Revenue Financial Report for Period Ended 31 December 2021 / Long Term Financial Sustainability Risk Assurance Report (risk ref 724) / Financial Annual Plan Risk Assurance Report (risk ref 849) S Lyall PRC01/2022 6.2 Capital Financial Report and Programme Update Period Ended 31 December 2021 / Prioritisation & Management of Capital Funding Risk Assurance Report (risk ref 636) L Lyall PRC02/2022 6.3 Best Value Review S Lyall Verbal Update Performance Monitoring 6.4 a) Performance Report H Barnett PRC03/2022
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Tayside NHS Board
1
Please note any items relating to Committee business are embargoed and should not be made public until after the meeting Tayside NHS Board A meeting of Tayside NHS Board Performance and Resources Committee will be held at 9:45am on Thursday 10 February 2022 via Microsoft Teams Apologies/enquiries to: Ms Pauline Ireland, 01382 660111 extension 55761 or email [email protected]
AGENDA LEAD OFFICER
REPORT NUMBER
1. WELCOME AND APOLOGIES 2. DECLARATION OF INTERESTS 3. MINUTE AND CHAIR’S ASSURANCE REPORT 3.1 Minute of the Performance and Resources Committee meeting of
19 December 2021 – for approval Chair Attached
3.2 Chair’s Assurance Report to the Board following the
Performance and Resources Committee of 9 December 2021 – for noting
Chair Attached
4. ACTION POINTS UPDATE AND MATTERS ARISING 4.1 Action Points Update S Lyall Attached 4.2 Matters Arising 5. COMMITTEE ASSURANCE AND WORKPLAN 2021/2022 5.1 Performance and Resources Committee Assurance and
Workplan 2021/22 Chair
Attached
5.2 Record of Attendance 2021/2022 Attached 6. ITEMS FOR ASSURANCE Financial Planning and Monitoring
6.1
Revenue Financial Report for Period Ended 31 December 2021 / Long Term Financial Sustainability Risk Assurance Report (risk ref 724) / Financial Annual Plan Risk Assurance Report (risk ref 849)
S Lyall
PRC01/2022
6.2
Capital Financial Report and Programme Update Period Ended 31 December 2021 / Prioritisation & Management of Capital Funding Risk Assurance Report (risk ref 636)
L Lyall
PRC02/2022
6.3 Best Value Review S Lyall Verbal
Update Performance Monitoring 6.4 a) Performance Report H Barnett PRC03/2022
2
b) Remobilisation Plan (RMP3) 2021/22 Action Tracker
Verbal update
10 minute comfort break
Digital Strategy 6.5 Unapproved Minute from Digital Transformation Partnership
Meeting of held on 5 November 2021 L Khalique Attached
Items for assurance
6.6 Climate Emergency and Sustainable Development
P Wilde
PRC04/2022
RESERVED BUSINESS OF THE COMMITTEE IN ACCORDANCE WITH THE GUIDE TO THE EXEMPTION UNDER THE FREEDOM OF INFORMATION (SCOTLAND) ACT 2002
7. MINUTES 7.1 Reserved Minute of the Performance and Resources Committee
Meeting held on 9 December 2021 – for approval Chair Attached
7.2 Minutes of Asset Management Group Meetings held on
13 December 2021 and 20 January 2022 – for noting L Lyall Attached
8. ACTION POINTS UPDATE AND MATTERS ARISING 8.1 Reserved Action Points Update S Lyall Attached 8.2 Matters Arising 9. ITEMS FOR ASSURANCE 9.1 Update on Development of Draft Strategic Financial Plan
2022/23 S Lyall PRC05/2022
9.2 Draft Five Year Capital Plan 2022/23 to 2026/27 L Lyall PRC06/2022 9.3
Property Disposal Update
J Henderson
PRC07/2022
10. MEETING REFLECTIONS AND CONSIDERATION OF MATTERS FOR CHAIR’S ASSURANCE
REPORT FOR TAYSIDE NHS BOARD MEETING ON 24 FEBRUARY 2022 11. The next meeting of the Performance and Resources Committee is at 9.45am on Thursday 14
April 2022 Ms Pat Kilpatrick Chair Performance and Resources Committee February 2022 Level of Assurance System Adequacy Controls
3
Comprehensive Assurance
Robust framework of key controls ensures objectives are likely to be achieved.
Controls are applied continuously or with only minor lapses.
Moderate Assurance
Adequate framework of key controls with minor weaknesses present.
Controls are applied frequently but with evidence of non-compliance.
Limited Assurance
Satisfactory framework of key controls but with significant weaknesses evident which are likely to undermine the achievement of objectives.
Controls are applied but with some significant lapses.
No Assurance
High risk of objectives not being achieved due to the absence of key internal controls.
Significant breakdown in the application of controls.
DISTRIBUTION MEMBERS
REGULAR ATTENDEES
FOR INFORMATION
Mrs Jenny Alexander Ms Anne Buchanan Mr Peter Drury (Vice Chair) Cllr Eric Drysdale Ms Pat Kilpatrick (Chair) Mr Donald McPherson Cllr Bob Myles
Mr Grant Archibald Mr Mark Anderson Mrs Hazel Barnett Mrs Lorna Birse-Stewart Mr George Doherty Mr James Henderson Mr Laic Khalique Ms Karen Kidd Mrs Louise Lyall Mr Stuart Lyall (Lead Officer) Mr Raymond Marshall (APF) Mr John Paterson Ms Lorna Wiggin
Mr Bob Benson Mr Niall Deuchar Mrs Claire Pearce Ms Margaret Dunning Cllr Ken Lynn Mrs Trudy McLeay Dr Norman Pratt Prof Peter Stonebridge Audit Scotland FTF Internal Audit
48
Minute NHS Tayside TAYSIDE NHS BOARD PERFORMANCE AND RESOURCES COMMITTEE - OPEN BUSINESS
Minute of the meeting of Tayside NHS Board Performance and Resources Committee held at 9:45am on Thursday 9 December 2021 via Microsoft Teams. Present: Mrs Jenny Alexander, Non Executive Member & Employee Director, Tayside NHS Board Mr Peter Drury, Non Executive Member, Tayside NHS Board (Vice Chair) Cllr Eric Drysdale, Non Executive Member, Tayside NHS Board Ms Pat Kilpatrick, Non Executive Member, Tayside NHS Board (Chair) Mr Donald McPherson, Non Executive Member, Tayside NHS Board Attendees Mr Grant Archibald, Chief Executive, Tayside NHS Board Mrs Hazel Barnett, Director of Performance and Activity, NHS Tayside Mr Adrian Caddick, ACT Officer, NHS Tayside (item 6.13) Mr David Coulson, Director of Pharmacy, NHS Tayside Mr John Davidson, Consultant Physician, NHS Tayside (item 6.13) Ms Beth Hamilton, Non Executive Member, Tayside NHS Board Mr James Henderson, Property Asset Manager, NHS Tayside Ms Pauline Ireland, Committee Support Officer, NHS Tayside Ms Karen Kidd, Senior Finance Manager, NHS Tayside Mrs Louise Lyall, Head of Finance – Capital & Resources, NHS Tayside (deputising for Mr Stuart Lyall) Mr Raymond Marshall, Representative Area Partnership Ms Louise McTaggart, Head of Strategic Delivery, NHS Tayside (deputising for Mr Laic Khalique and Mr Ally Gentles) Mr John Paterson, Director of Facilities, NHS Tayside Mr Christopher Smith, Deputy Director of Workforce, NHS Tayside (deputising for Mr George Doherty) Ms Audrey Warden, Associate Director Clinical Services, NHS Tayside (deputising for Ms Lorna Wiggin) Apologies Mr Mark Anderson, Head of Property, NHS Tayside Mr George Doherty, Director of Workforce, NHS Tayside Ms Margaret Dunning, Board Secretary, NHS Tayside Mr Ally Gentles, Head of Operations, Digital Directorate, NHS Tayside Mr Laic Khalique, Director of Digital Technology, NHS Tayside Mr Stuart Lyall, Director of Finance, NHS Tayside Cllr Bob Myles, Non Executive Member, Tayside NHS Board Ms Lorna Wiggin, Chief Officer Acute Services, NHS Tayside Mr Drury and Ms Kilpatrick in the Chair
Item Number 3.1
49
1. WELCOME AND APOLOGIES
ACTION
Mr Drury welcomed all to the meeting.
Apologies were noted as above.
2. DECLARATION OF INTERESTS There were no declaration of interests.
3. MINUTE AND CHAIR’S ASSURANCE REPORT 3.1
Minute of the Performance and Resources Committee Meeting of 14 October 2021
The open Minute of the Performance and Resources Committee meeting of 14 October 2021 was approved on the motion of Mr McPherson and seconded by Cllr Drysdale.
3.2
Chair’s Assurance Report to the Board following the Performance and Resources Committee meeting of 14 October 2021 The Committee noted the Chair’s Assurance report to Tayside NHS Board meeting of 28 October 2021.
4.
ACTION POINTS UPDATE AND MATTERS ARISING
4.1
Action Points Update Members were asked to note the Action Points Update and noted the status of each action point. • Action point 6.1 from 12 August 2021 – complete. • Action point 6.1 from 14 October 2021 – complete. • Action point 6.5 from 14 October 2021 – Mrs Barnett noted Appendix B of
the Action Points update and reported that an executive slide set was being produced and would be submitted to Performance and Resources Committee in February 2022. Mr Archibald highlighted the challenges being faced due to Omicron, and that timeframes may need to be subsequently adapted.
The Committee noted the Action Points Update
4.2 Matters arising
No other matters were discussed.
5. COMMITTEE ASSURANCE AND WORKPLAN 2021/2022
50
5.1 5.2 6. 6.1
Performance and Resources Committee Assurance and Workplan 2020/21 The Committee were asked to note the Committee Assurance and Workplan 2021/22. The Committee:
• Noted the Performance and Resources Committee Assurance Workplan 2021
Record of Attendance 2021/22 The Committee noted the Record of Attendance 2021/22. ITEMS FOR ASSURANCE Revenue Financial Report for period ended 31 October 2021 / Long Term Financial Sustainability Risk Assurance Report / Financial Annual Plan Risk Assurance Report (PRC51/2021) Ms Kidd spoke to the report and provided members with a brief summary of the key points. Members heard that the report provided moderate assurance which was an improvement on the limited assurance previously provided. Ms Kidd advised that the reason for the improvement was that a second tranche of Covid-19 funding had been received in October, with a commitment from Scottish Government of further funding following Quarter 3 where necessary and applicable. Ms Kidd reported a reduced level of 16 for the current risk exposure rating for the Finance Annual Plan 2021/22 Strategic Risk. This was a reduction from level 20 which reflected further clarity around the funding allocations for 2021/22 and current position against financial plan trajectory. Ms Kidd reported an overspend of £1.7m for the year to date against a financial plan trajectory of £2.5m. The Financial Plan submitted in March projected a breakeven position, with financial savings of £27.0m required; of which £8.0m were high risk. Mr Drury asked what, if any, were the major concerns for the finance team. Ms Kidd advised the uncertainty of the financial impact of Covid-19 remained a concern for the next financial year. Cllr Drysdale noted the overspend within Mental Health Services and queried if there was more NHS Tayside could be doing in association with Local Authorities to reduce the overspend. Mr Archibald advised that NHS Tayside were trying to recruit Psychiatrists with a view to reducing locum costs within Mental Health Services, as well as working alongside Scottish Government reviewing the current Mental Health Services model in NHS Tayside. He added that the plan was to improve the current service issue which should then have a positive impact on the financial position. Mr Archibald advised that although he was unable to provide an immediate timescale of said plan,
51
6.2
he assured members that a regular update would be provided in due course. Following a query from Mr McPherson on the Integrated Joint Boards (IJBs) overspend, Ms Kidd noted that 2021/22 was the first year that all 3 IJBS had break-even financial plans, and all had a level of reserves that supported the break-even projection. Following brief discussion, members agreed moderate assurance was provided from the report The Committee:
• Noted the content of the Revenue Financial Report for period ended 31 October 2021
• Noted a reduction in the current risk exposure rating to level 16 for the Finance Annual Plan 2021/22 Risk
• Agreed moderate assurance was provided from the Revenue Financial Report for period ended 31 October 2021
Capital Financial Report and Programme Update for Period Ended 31 October 2021 / Prioritisation & Management of Capital Funding Risk Assurance Report (PRC52/2021) Mrs Lyall spoke to the report and noted that the purpose of the report was to advise the Committee of NHS Tayside’s financial performance against the Five Year Capital Plan 2021/22 to 2025/26 for the seven months to 31 October 2021. The key points highlighted were as follows:
• The total capital programme forecast outturn at 31 October 2021 was £31.540m, with a breakeven position forecast, including Covid-19 expenditure.
• The total capital programme expenditure to 31 October 2021 was £10.754m, which was 34% of the total forecast outturn and included Covid-19 expenditure of £0.960m.
• Confirmation has now been received from Scottish Government Health Finance Corporate Governance and Value Directorate (SGHFCGVD) that additional capital funding of £2.776m will be provided for Covid-19 capital costs in 2021/22.
• There had been no change to the current risk exposure rating of 20, and planned risk exposure rating of 12, for the Prioritisation and Management of Capital Funding Strategic Risk since the last report in October 2021. The risk scores reflects the financial position as at month 7 and the continued risk of further slippage in planned expenditure, but mainly because of capacity issues within the Property Team to support the delivery of the capital programme.
Following a query from Mr Drury regarding the 34% spend of the total forecast outturn, Mrs Lyall advised that this level spend after a 7 month period was normal as, due to the nature of the capital programme, the majority of spend usually falls in the last quarter of the year. The Committee agreed a moderate level assurance was received from the
52
6.3 6.4 6.5
report. The Committee:
• Noted the content of the Capital Financial Report and Programme Update for Period Ended 31 October 2021
• Noted no change was reported to the current risk exposure rating for Prioritisation and Management of Capital Funding Strategic Risk 636
• Agreed moderate assurance was provided from the Capital Financial Report for the period ended 31 October 2021.
Draft Financial Plan Ms Kidd provided members with a verbal update, and noted that the Scottish Government was publishing the Draft Budget on 9 December 2021, which would inform assumptions made in the development of the Draft Financial Plan. Members heard that the process for Financial Planning was reverting back to a 3 year cycle, with a view to submit the final 3 year Financial Plan 2022/23 to 2024/25 to Scottish Government at the end of July 2022. In the interim a one year plan was required to be approved by the end of financial year 2021/22 and a draft will be presented to members at the next Performance and Resources Committee meeting in February 2022, ahead of submission to Tayside NHS Board for approval. The Committee noted the Draft Financial Plan update Draft Five Year Capital Plan Mrs Lyall advised the development of the next iteration of the NHS Tayside Five Year Infrastructure Investment Plan was discussed at the Asset Management Group (AMG) meeting held on 13 December 2021. The intention is to roll over the current approved plan, and undertake a reassessment of the key strategies priorities to be taken forward in the Five Year Capital Plan. Further information on funding planning assumptions was expected to be announced in the Draft Scottish Budget later that afternoon, and a detailed report would be considered at the January 2022 AMG meeting. She added that once the draft Five Year Capital Plan was finalised, it would be submitted to the Performance and Resources Committee for consideration, before submission to Tayside NHS Board for approval. The Committee noted the Draft Five Year Capital Plan update a) Performance Report (PRC53/2021) Mrs Barnett spoke to the report and members were asked to consider a moderate level of assurance in respect of NHS Tayside’s current performance. Mrs Barnett highlighted the following key points: Mrs Barnett advised that Remobilisation Plan 4 (RMP4) would be tabled at Tayside NHS Board on 16 December 2021, and thereafter will be made
53
available in the NHS Tayside website. Members heard that following some fault diagnostics within TrakCare, the Business Unit and Digital colleagues were working with InterSystems to provide a solution. A timeline was not determinable at present, however Mrs Barnett advised that we remain able to report on out patients, diagnostics and in-patient/day case waiting times which contribute to the 18 Week pathway. The number of patients waiting greater than 12 weeks for an elective Inpatient / Daycase procedures continued to increase. However, NHS Tayside’s routine elective activity has been progressing across all sites with activity remaining above remobilisation planned levels over April-October 2021. Theatre 3 in Stracathro Regional Treatment Centre remobilised in November. New outpatient clinics continued in line with the Remobilisation Plan. The volume of new outpatients waiting beyond 12 weeks was reducing up until June following which a month on month increase had been recorded. The new outpatient Did Not Attend (DNA) rate had plateaued over the previous 2 reported months at 8.9% which brings it into line with the Scotland average which also increased to 8.9% in September 2021. The volume of patients waiting beyond 6 weeks for a key diagnostic test rose at the end of August but was reducing over the past 2 months. The overall volume of patients waiting beyond 6 weeks for a key diagnostic test as at end October 2021 reduced by just under 500. Both Endoscopy and Radiology activity remained above Remobilisation planned levels. Over 5,500 Endoscopy tests had been undertaken in the Vanguard mobile unit since April 2021 and Scottish Government recently confirmed funding for this mobile unit would continue would continue throughout the next financial year 2022/23. NHS Tayside continued to deliver the 31 day national standard for cancer services. (98.7% in October). The 62 day performance remained below target (95%) at 90.6% in October 2021. Performance had been fluctuating since January; however NHS Tayside remained in the top percentile Scottish Boards in cancer waiting times performance. Both CAMHS and Psychological Therapies performance are above the 90% target. CAMHS 18 week referral to treatment performance had dipped in November but remained at 90.4% in October 2021. Psychological Therapies 18 week referral to treatment performance had improved to 93.6% in October 2021. Unscheduled care performance remained the highest performance in mainland boards in Scotland and had increased throughout the previous 2 months to 91.7% in October 2021. Mental Health presentations to the Emergency Department being seen within 4 hours showed a fractional dip to 89.3% in October from 90.5% reported in September. It was noted that the volume of attendances to the Emergency Department had increased overall.
54
The volume of Delayed Discharges had continued to rise since June 2021, with the number of bed days lost also increasing significantly. Stage 1 (5 working days) complaint response performance showed a slight improvement from September to October 2021 with current performance at 71.4%. The National average is 80%. Stage 2 (20 working days) responses times have deteriorated and performance is still low. It was noted that a Complaints Manager had been recruited with the main focus on the longest outstanding complaints. Alcohol Brief Interventions (ABI) was still well below target due to reduced face to face contact. An ABI co-ordinator had now been appointed, due to start mid-January, and will focus on training and delivery of ABI’s in key settings. Ms Kilpatrick welcomed the report and in particular the cancer performance data. Mr McPherson noted the ongoing TrakCare Update issues and queried what prompted the change to this system. Mrs Barnett advised that it was an update to the current TrakCare system and that the ongoing issues were in connection with InterSystems. Ms McTaggart provided assurance that the digital team were working very closely with InterSystems with a view to resolving the ongoing issues with TrakCare and advised members that an update would be provided at the next Performance and Resources Committee meeting in February 2022. Mr McPherson noted the ABI data and queried if other Boards were having similar issues. Mrs Barnett advised that she was aware of NHS Grampian having the similar issues, and suggested that benchmarking for ABIs would be included in the next Performance Report submitted to the Committee in February 2022. Cllr Drysdale raised a concern regarding the rapid increase in Delayed Discharges and noted that this figure had doubled in the 6 months to October 2021. Mrs Barnett advised that delays regarding Guardianship applications attributed to a number of the Delayed Discharges, as well as Covid-19 restrictions in Care Homes. The Committee agreed a moderate level of assurance was provided from the report. The Committee:
• Noted the content of the Performance Report • Noted benchmarking for ABIs to be included in future Performance
Reports • Agreed moderate assurance was provided from the Performance
Report b) Remobilisation Plan (RMP3) 2021/22 Action Tracker (PRC53/2021) Mrs Barnett spoke to the report and members were asked to acknowledge and take moderate assurance in respect of progress with delivery of the
HB
55
6.6 6.7
Remobilisation Plan 2021/22. Mrs Barnett advised that RMP4 would be reported in the next quarter. Mr McPherson noted the age range for CAMHS referrals had been increased to 25 years of age. Mrs Barnett advised the service were involved in discussions at a national level as widening the age range would impact on capacity at a local level. It is anticipated the change would help children transition between children’s and adolescent services, if needed, rather than impose an arbitrary end point. Mr Archibald advised the National Chief Executives Group are sighted on this and were considering the implications. Mrs Barnett agreed to include an update in the next performance report The Committee agreed moderate assurance was provided from the report Workforce Information Report (PRC54/2021) Mr Smith presented the report and advised members that the purpose of it was to outline NHS Tayside’s workforce metrics and trends ensuring that governance was embedded into the workforce strategies and processes. He added that a similar report had been submitted to the Staff Governance Committee as a single suite of workforce data to provide assurance. Mr Smith highlighted 4 issues to the Committee, namely: Absence Age profile Workforce profile Corporate Workforce Plan Members were asked to consider the Workforce Information report both in terms of presentation as well as its content. They were asked to consider and examine the wide range of metrics and determine the level of assurance and governance the report provided, along with the appropriate associated narrative. Ms Kilpatrick noted the age profile data within the report and in particular the high level of staff who were over 50 years of age. She queried if there were opportunities for staff to work flexible hours and Mr Smith confirmed that there were a number of different options for staff to work flexibly. Mrs Alexander noted that she was not confident that all areas within NHS Tayside implemented flexible working for staff in a consistent way. Following discussion, members agreed moderate assurance was provided from the Workforce Information Report. The Committee:
• Noted the Workforce Information Report • Agreed moderate assurance was provided from the report •
Waiting Times and RTT Targets Risk Assurance Report (PRC55/2021)
HB
56
6.8 6.9
Mr Archibald spoke to the report in Ms Wiggin’s absence. He advised that due to the prevailing Covid-19 restrictions, capacity had been reduced since the commencement of the pandemic and activity had been materially lower than pre-Covid levels. This had resulted in the number patients waiting for TTG and diagnostic procedures continuing to increase month on month. Members heard that during June and July 2021, the increasing community prevalence of Covid-19 translated into a third wave of presentations with an increase in hospital admissions. This required reconfiguration of hospital wards to create the necessary inpatient and critical care capacity which impacted on NHS Tayside’s ability to maintain its entire planned care programme. Mr Archibald noted that despite all of this, NHS Tayside had managed services appropriately and continued to do so. Ms Kilpatrick noted the additional funding secured from Scottish Government to support 10 additional theatre sessions per week and queried if this was required due to physical capacity and Mr Archibald advised this was due to workforce capacity. Ms Kilpatrick queried if the MRI and CT mobile units were still currently on-site and Ms Warden advised that she would follow this query up out-with the meeting and feedback to members in due course. The Committee agreed moderate assurance was provided from the report Effective Prescribing Risk Assurance Report (PRC56/2021) Mr Coulson presented the report and noted that the proposed current risk rating of 12 reflected the dynamic nature of the medicines supply chain and the influence of prescribing behaviour, the current and proposed controls continued to improve the clinical and financial governance related to medicines in primary and secondary care across NHS Tayside. Members heard that members of the Prescribing Management Group (PMG) previously debated and agreed the reduction of the planned risk exposure rating. The reduction from 12 to 9 recognised the progress to date and the expected outcomes from the planned / proposed controls were detailed in the report. The Committee agreed moderate assurance was received from the report. Mrs Alexander left the meeting at 11.50am Estates Infrastructure Risk Assurance Report (PRC57/2021) Mr Paterson spoke to the report and members were asked to note the level of assurance was currently moderate, with no change until the relevant programmes of activity were adequately planned and resourced to meet the
AW
57
6.10 6.11
requirements set out in the risk overview. He added that the current controls to manage the risk reflected the necessary prioritisation of available financial funding. Members heard that the Estates Department had been experience ongoing workforce issues and were currently trying to recruit a number of posts to join the management team. Cllr Drysdale noted the Fire Safety Risk (ref 866) and queried if NHS Tayside held a contingency plan in the event of a major fire. Mr Paterson confirmed that NHS Tayside had a Fire Safety Policy and also a Fire Safety Team had been established. He added that a Fire Safety Report was submitted to the Health and Safety Committee 6 times per year. The Committee agreed moderate assurance was provided from the report. Mr Archibald left the meeting at 12.00pm Digital Strategy and Annual Operation Plan Update (PRC58/2021) Ms McTaggart spoke to the report and members were asked to note the progress made in several areas across the Digital Directorate and consider a moderate level of assurance. Cllr Drysdale noted the work progressing in connection with the Electronic Patient Record (EPR) system and questioned when the EPR system is complete, will systems across the Health and Social Care Partnerships (HSCP), hospitals and GP’s be compatible. Ms McTaggart advised that GP reports were currently shared on the clinical portals which were accessible across the organisation. She was unaware whether reports from HSCPs were shared with NHS Tayside and GPs, and would discuss this with her colleagues and feedback to members in due course. Following discussion, members agreed moderate assurance was provided from the report. The Committee:
• Noted the Digital Strategy and Annual Operation Plan Update • Agreed moderate assurance was provided from the report
Cyber Attack Risk Assurance Report (PRC59/2021) Ms McTaggart presented the report and members were asked to consider a moderate level of assurance. It was noted that this was an improvement from limited assurance in the last report to the Committee in October. Members heard that the current risk exposure rating was now assessed as level 9 which was noted as a significant development. Mr McPherson noted the desktop based simulation of a malware attack for Senior Managers and Executives which was held on 16 November 2021 and queried what the key points from this exercise were. Ms McTaggart advised she would feedback the outcome of the exercise to the Committee in due
LM
LM
58
6.12 6.13
course. The Committee:
• Noted the improvement in the current risk exposure rating to 9 • Agreed a moderate level of assurance was provided from the
report eHealth Technical Infrastructure and Modernisation Programme Risk Assurance Report (PRC60/2021) Ms McTaggart presented the report and members were asked to note a limited level of assurance, due to the reasons outlined in the report. The Committee:
• Noted the eHealth Technical Infrastructure and Modernisation Programme Risk Assurance Report
• Agreed limited assurance was provided from the report Additional Cost of Teaching (ACT) Annual Update Report 2020/21 (PRC61/2021) Mr Caddick spoke to the report and highlighted the following key points: In 2021/22 the overall allocation of funding was £14.0m which reflected an increase of 3%. During 2021/22 there had been an increase in funding nationally due to increased student numbers. NHS Tayside received a further £752,891 of funding to be spent by 31 March 2022. It was noted that the funds were unable to be carried forward to 2022/23. Scottish Graduate Entry Medical Programme (ScotGEM) funding from NES was ring-fenced and based on a different funding allocation model to core ACT funding. For 2021/22, NHS Tayside’s allocation had increased to £641,210, funding 13 year three students in Tayside and year four hospital placements for 53 students. Following a query from Mr McPherson regarding the process of funding for students joining NHS Tayside versus students joining another Health Board, Mr Caddick advised that Dundee students would often have placements in other Board areas to study specialties that were not delivered in Tayside, or for GP placements which were across Scotland. Students from other Medical Schools would come to Tayside to study specialties not delivered in their Board areas. Mr McPherson noted the low level of student feedback noted in the report from students and Mr Caddick advised that the level of feedback was currently being reviewed by University of Dundee Medical School. He also added that the Quality Review Panel questions had been revised by NHS Education for Scotland (NES) for 2021/22. Mr McPherson queried why the ‘Treated with respect’ option was ‘greyed out’ within the Undergraduate Survey and Mr Caddick noted this comment and advised that he would investigate this further and feedback to members in due course.
AC
59
7. 7.1
Discussion took place regarding the possibility of not being able to spend all of the current year new monies funding unless it could be carried forward to 2021/22 and Cllr Drysdale offered his support with a view to lobbying Scottish Government regarding carrying the funding forward to the next financial year. Ms Kidd noted Cllr Drysdale comments and advised that she was not aware of discussions but would raise these points through the National Corporate Finance Network. Members agreed a moderate level of assurance was provided from the report. The Committee:
• Noted the possibility of not being able to spend all of the current year new monies funding unless it could be carried forward to the 2022/2023. This concern to be highlighted at the next National Corporate Finance Network meeting
• Agreed moderate assurance was provided from the report ITEMS FOR AWARENESS Children’s Theatre Suite (CTS) – Projected Overspend (PRC62/2021) Ms Fowlie spoke to the report and the key points highlighted were as follows: The original CTS project plan anticipated the project being completed in October 2020, however due to the impact of Covid-19 and several other unpredictable major issues affecting the timescale, the current projected completion date was mid February 2022. The impact on the projected financial outturn of the delay was considerable. Members noted the Approved Compensation Events and also the Compensation Events Pending Approval. The total forecast expenditure for the CTS project as at 31 October 2021 was £11.072m which represented an increase of £1.402m against the Full Business Case (FBC) budget of £9.671m. The £1.402m forecast additional expenditure excluded costs in relation to Covid-19 and remedial works as a result of a major ingress of water, as these costs were being separately funded by Scottish Government.
Ms Fowlie confirmed that there was an external Cost Advisor (Gardiner & Theobald) and external Contracts Manager (Currie & Brown) appointed by NHS Tayside whose responsibility it was to support NHS Tayside in scrutinising and challenging the compensation events.
Ms Fowlie highlighted the impact that capacity issues had on the development of the business cases and delivery of the project. She added that the challenges in relation to the preferred site were much greater than envisaged at the start of the project, and that learning from the CTS project should be considered for future projects. Mr Paterson advised that the Post Project Evaluation would pick up on these points.
KK
60
Mrs Lyall advised that, following completion, the next stage for the project was a Post Project Evaluation which would be brought to the required governance committees. The Committee noted the report for awareness
8. 8.1 8.2 9. 9.1 9.2
For Governance reasons the following items were taken in reserved business MINUTES Reserved Minute of the Performance and Resources Committee Meeting held on 14 October 2021 The Reserved Minute of the Performance and Resources Committee meeting of 14 October 2021 was approved on the motion of Mr Drury and seconded by Mr McPherson. Unapproved Minute of the Asset Management Group meeting held on 9 September 2021 The Committee noted the Unapproved Minute of the Asset Management Group meeting of 4 November 2021. ACTION POINTS UPDATE AND MATTERS ARISING Reserved Action Points Update There were no outstanding reserved action points. Matters arising There were no matters arising.
10. 10.1 11. 12.
ITEMS FOR ASSURANCE Property Disposal Update (PRC63/2021) The Committee noted the Property Disposal Update. MEETING REFLECTIONS AND CONSIDERATION OF MATTERS FOR CHAIR’S ASSURANCE REPORT FOR TAYSIDE NHS BOARD MEETING 16 DECEMBER 2021 Mr McPherson highlighted the reasons behind the additional costs for the CTS project and suggested these should be highlighted at the next Board meeting. DATE OF NEXT MEETING The Committee noted the date of the next Performance and Resources Committee meeting would be held on Thursday 10 February 2022 at 9.45am via Microsoft Teams.
61
The meeting concluded at 13.15pm
Subject to any amendments recorded in the Minute of the subsequent meeting of the Committee, the foregoing Minute is a correct record of the business proceedings of the meeting of Tayside NHS Board Performance and Resources Committee held on 9 December 2021, and approved by the Performance and Resources Committee at its meeting held on 10 February 2022. .............................................……..….... ................................................. CHAIR DATE
1
Item Number 3.2
Performance and Resources Committee 10 February 2022
CHAIR’S ASSURANCE REPORT PERFORMANCE AND RESOURCES COMMITTEE 9 December 2021 1
Performance against work plan
REVENUE FINANCIAL REPORT FOR PERIOD ENDED 31 OCTOBER 2021 / LONG TERM FINANCIAL SUSTAINABILITY RISK ASSURANCE REPORT / FINANCIAL ANNUAL PLAN RISK ASSURANCE REPORT Members heard that the report provided moderate assurance which was an improvement on the limited assurance previously provided. The reason for the improvement was that a second tranche of Covid-19 funding had been received in October, with a commitment from Scottish Government of further funding following Quarter 3 where necessary and applicable. The ongoing overspend within Mental Health Services was raised. The Chief Executive provided assurance to the committee that NHS Tayside were trying to recruit Psychiatrists with a view to reducing locum costs within Mental Health Services, as well as working alongside Scottish Government reviewing the current Mental Health Services model in NHS Tayside. The committee noted that all 3 IJBS had break-even financial plans, and all had a level of reserves that supported the break-even projection. CAPITAL FINANCIAL REPORT AND PROGRAMME UPDATE FOR PERIOD ENDED 31 OCTOBER 2021 / PRIORITISATION & MANAGEMENT OF CAPITAL FUNDING RISK ASSURANCE REPORT (PRC52/2021) The purpose of the report was to advise the Committee of NHS Tayside’s financial performance against the Five Year Capital Plan 2021/22 to 2025/26 for the seven months to 31 October 2021. The total capital programme forecast outturn at 31 October 2021 was £31.540m, with a breakeven position forecast, including Covid-19 expenditure. The total capital programme expenditure to 31 October 2021 was £10.754m, which was 34% of the total forecast outturn and included Covid-19 expenditure of £0.960m. Confirmation has now been received from Scottish Government Health Finance Corporate Governance and Value Directorate (SGHFCGVD) that additional capital funding of £2.776m will be provided for Covid-19 capital costs in 2021/22. There had been no change to the current risk exposure rating of 20, and planned risk exposure rating of 12, for the Prioritisation and Management of Capital Funding Strategic Risk since the last report in October 2021. The risk scores
2
reflects the financial position as at month 7 and the continued risk of further slippage in planned expenditure, but mainly because of capacity issues within the Property Team to support the delivery of the capital programme. DRAFT FINANCIAL PLAN It was noted that the Scottish Government was publishing the Draft Budget on 9 December 2021, which would inform assumptions made in the development of the Draft Financial Plan. Members heard that the process for Financial Planning was reverting back to a 3-year cycle, with a view to submit the final 3-year Financial Plan 2022/23 to 2024/25 to Scottish Government at the end of July 2022. In the interim a one-year plan was required to be approved by the end of financial year 2021/22 and a draft will be presented to members at the next Performance and Resources Committee meeting in February 2022, ahead of submission to Tayside NHS Board for approval. DRAFT FIVE YEAR CAPITAL PLAN It was reported that the next iteration of the NHS Tayside Five Year Infrastructure Investment Plan was discussed at the Asset Management Group (AMG) meeting held on 13 December 2021. The intention is to roll over the current approved plan and undertake a reassessment of the key strategies priorities to be taken forward in the Five-Year Capital Plan. Once the draft Five Year Capital Plan has been finalised, it would be submitted to the Performance and Resources Committee for consideration, before submission to Tayside NHS Board for approval. PERFORMANCE REPORT The committee agreed a moderate level of assurance in respect of NHS Tayside’s current performance. DRAFT FINANCIAL PLAN Ms Kidd provided members with a verbal update, and noted that the Scottish Government was publishing the Draft Budget on 9 December 2021, which would inform assumptions made in the development of the Draft Financial Plan. Members heard that the process for Financial Planning was reverting back to a 3 year cycle, with a view to submit the final 3 year Financial Plan 2022/23 to 2024/25 to Scottish Government at the end of July 2022. In the interim a one year plan was required to be approved by the end of financial year 2021/22 and a draft will be presented to members at the next Performance and Resources Committee meeting in February 2022, ahead of submission to Tayside NHS Board for approval. The Committee noted the Draft Financial Plan update DRAFT FI VE YEAR CAPITAL PLAN Mrs Lyall advised the development of the next iteration of the NHS Tayside Five Year Infrastructure Investment Plan was discussed at the Asset Management Group (AMG) meeting held on 13 December 2021. The intention is to roll over the current approved plan, and undertake a reassessment of the key strategies
3
priorities to be taken forward in the Five Year Capital Plan. Further information on funding planning assumptions was expected to be announced in the Draft Scottish Budget later that afternoon, and a detailed report would be considered at the January 2022 AMG meeting. She added that once the draft Five Year Capital Plan was finalised, it would be submitted to the Performance and Resources Committee for consideration, before submission to Tayside NHS Board for approval. The Committee noted the Draft Five Year Capital Plan update. PERFORMANCE REPORT The number of patients waiting greater than 12 weeks for an elective Inpatient / Day case procedures continued to increase. However, NHS Tayside’s routine elective activity has remained above remobilisation planned levels over April-October 2021. The volume of patients waiting beyond 6 weeks for a key diagnostic test rose at the end of August but was reducing over the past 2 months. Both Endoscopy and Radiology activity remained above Remobilisation planned levels. Over 5,500 Endoscopy tests had been undertaken in the Vanguard mobile unit since April 2021 and Scottish Government recently confirmed funding for this mobile unit would continue throughout the next financial year 2022/23. NHS Tayside continued to deliver the 31-day national standard for cancer services. (98.7% in October). The 62-day performance remained below target (95%) at 90.6% in October 2021. Performance had been fluctuating NHS Tayside remained in the top percentile Scottish Boards in cancer waiting times performance. Both CAMHS and Psychological Therapies performance are above the 90% target. Unscheduled care performance remained the highest performance in mainland boards in Scotland and had increased throughout the previous 2 months to 91.7% in October 2021. Mental Health presentations to the Emergency Department being seen within 4 hours achieved a 89.3% performance level, it was noted that the volume of attendances to the Emergency Department had increased overall. The volume of Delayed Discharges had continued to rise, with the number of bed days lost also increasing significantly. It was noted that a Complaints Manager had been recruited to improve responses performance. WORKFORCE INFORMATION REPORT In the presentation of the report the age profile of staff and in particular the high numbers over 50 years of age was noted. The issue of flexible working for staff was noted. The Employee Director expressed concern that flexible working for staff was not available consistently for all staff throughout NHS Tayside.
4
2.
WAITING TIMES AND RTT TARGETS RISK ASSURANCE REPORT The Chief Executive spoke to the report and advised that due to the prevailing Covid-19 restrictions, capacity had been reduced since the commencement of the pandemic and activity had been materially lower than pre-Covid levels. This had resulted in the number patients waiting for TTG and diagnostic procedures continuing to increase month on month. Members heard that during June and July 2021, the increasing community prevalence of Covid-19 translated into a third wave of presentations with an increase in hospital admissions. This required reconfiguration of hospital wards to create the necessary inpatient and critical care capacity which impacted on NHS Tayside’s ability to maintain its entire planned care programme. It was noted that despite all of this, NHS Tayside had managed services appropriately and continued to do so. EFFECTIVE PRESCRIBING RISK ASSURANCE REPORT Mr Coulson presented the report and noted that the proposed current risk rating of 12 reflected the dynamic nature of the medicines supply chain and the influence of prescribing behaviour, the current and proposed controls continued to improve the clinical and financial governance related to medicines in primary and secondary care across NHS Tayside. ESTATES INFRASTRUCTURE RISK ASSURANCE REPORT Mr Paterson spoke to the report and members were asked to note the level of assurance was currently moderate, with no change until the relevant programmes of activity were planned and resourced to meet the requirements set out in the risk overview. DIGITAL STRATEGY AND ANNUAL OPERATION PLAN UPDATE ( Members were asked to note the progress made in several areas across the Digital Directorate and consider a moderate level of assurance. CYBER ATTACK RISK ASSURANCE REPORT Ms McTaggart presented the report and members were asked to consider a moderate level of assurance. Members heard that the current risk exposure rating was now assessed as level 9 which was noted as a significant improvement ADDITIONAL COST OF TEACHING (ACT) ANNUAL UPDATE REPORT In 2021/22 the overall allocation of funding was £14.0m which reflected an increase of 3%. During 2021/22 there had been an increase in funding nationally due to increased student numbers. NHS Tayside received a further £752,891 of funding to be spent by 31 March 2022. It was noted that the funds were unable to be carried forward to 2022/23. Members agreed a moderate level of assurance was provided from the report. Children’s Theatre Suite (CTS) – Projected Overspend
5
Due to the impact of Covid-19 and several other unpredictable serious issues affecting the timescale, the projected completion date was revised to mid-February 2022. The impact on the projected financial outturn of the delay was considerable. Members noted the Approved Compensation Events and the Compensation Events Pending Approval. The total forecast expenditure for the CTS project as at 31 October 2021 was £11.072m which represented an increase of £1.402m against the Full Business Case (FBC) budget of £9.671m. The £1.402m forecast additional expenditure excluded costs in relation to Covid-19 and remedial works because of a major ingress of water, as Scottish Government were separately funding these costs. Capital Planning advised that, following completion, the next stage for the project was a Post Project Evaluation which would be brought to the required governance committees. Horizon Scanning -
Pat Kilpatrick Chair Performance and Resources Committee 9 December 2021
ACTION POINTS UPDATE Item Number 4.1
Performance and Resources Committee – Open Business – 10 February 2022 MEETING MINUTE
REF HEADING ACTION POINT RESPONSIBILITY STATUS
9 December 2021
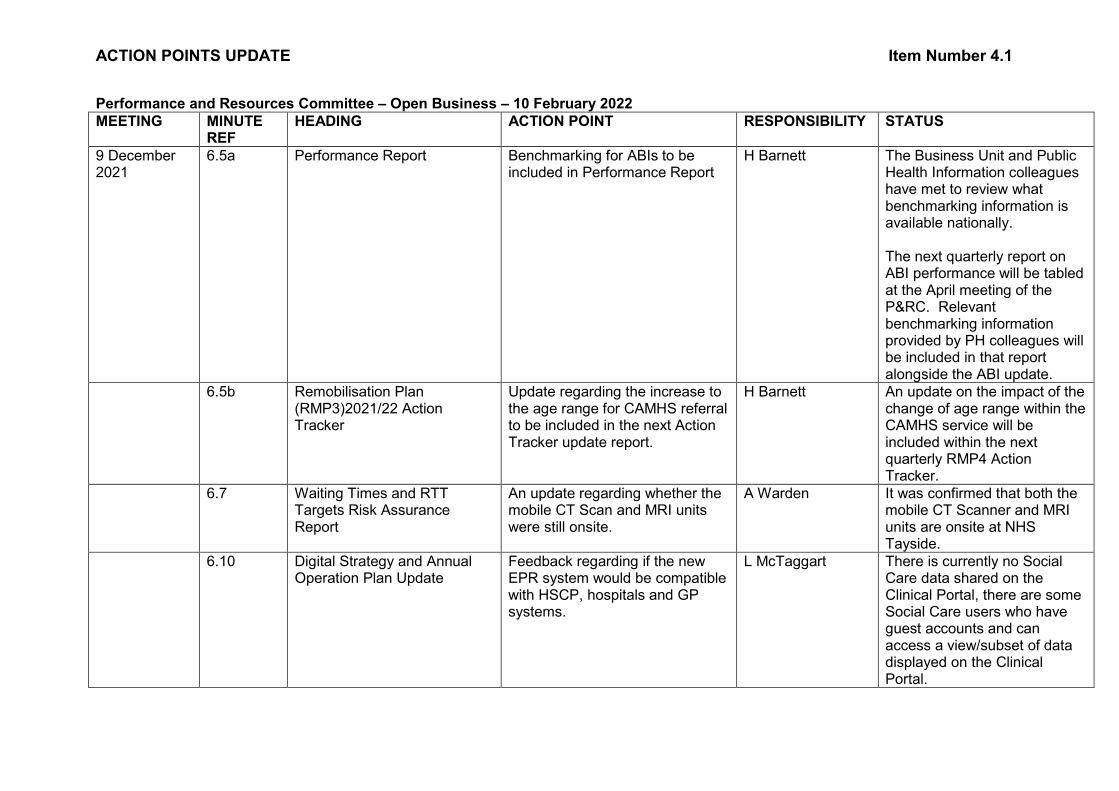
6.5a Performance Report Benchmarking for ABIs to be included in Performance Report
H Barnett The Business Unit and Public Health Information colleagues have met to review what benchmarking information is available nationally. The next quarterly report on ABI performance will be tabled at the April meeting of the P&RC. Relevant benchmarking information provided by PH colleagues will be included in that report alongside the ABI update.
6.5b Remobilisation Plan (RMP3)2021/22 Action Tracker
Update regarding the increase to the age range for CAMHS referral to be included in the next Action Tracker update report.
H Barnett An update on the impact of the change of age range within the CAMHS service will be included within the next quarterly RMP4 Action Tracker.
6.7 Waiting Times and RTT Targets Risk Assurance Report
An update regarding whether the mobile CT Scan and MRI units were still onsite.
A Warden It was confirmed that both the mobile CT Scanner and MRI units are onsite at NHS Tayside.
6.10 Digital Strategy and Annual Operation Plan Update
Feedback regarding if the new EPR system would be compatible with HSCP, hospitals and GP systems.
L McTaggart There is currently no Social Care data shared on the Clinical Portal, there are some Social Care users who have guest accounts and can access a view/subset of data displayed on the Clinical Portal.
ACTION POINTS UPDATE Item Number 4.1
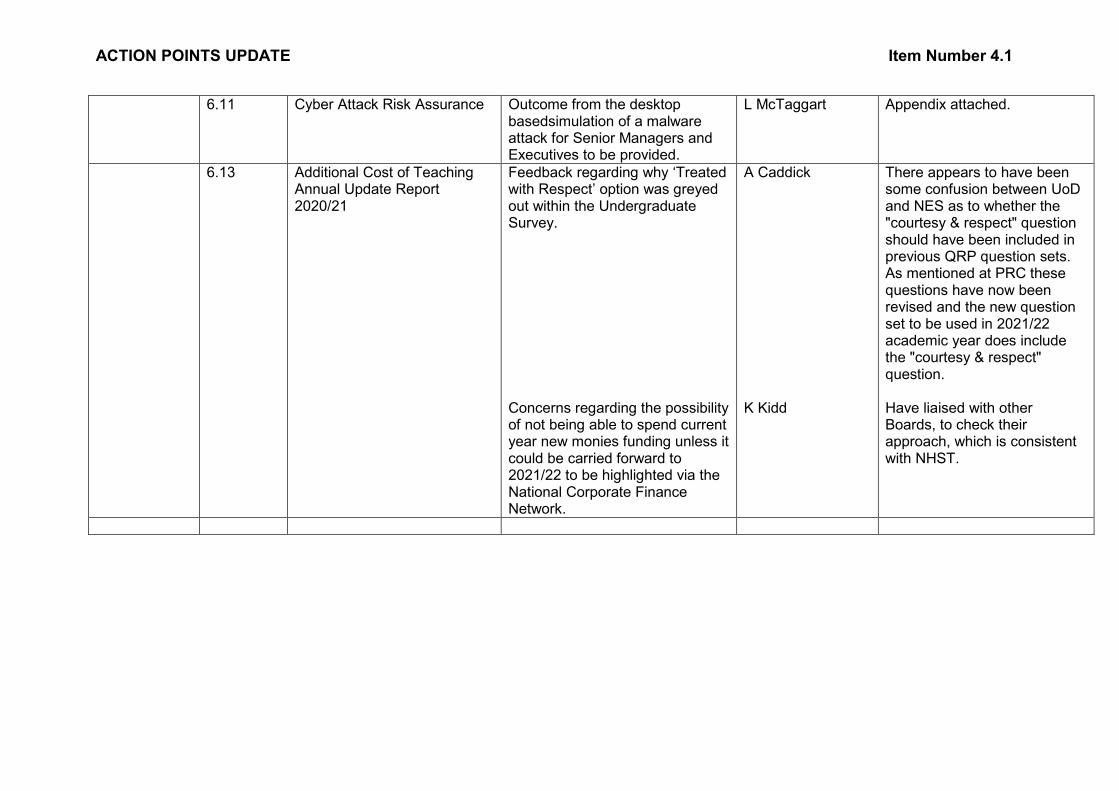
6.11 Cyber Attack Risk Assurance Outcome from the desktop basedsimulation of a malware attack for Senior Managers and Executives to be provided.
L McTaggart Appendix attached.
6.13 Additional Cost of Teaching Annual Update Report 2020/21
Feedback regarding why ‘Treated with Respect’ option was greyed out within the Undergraduate Survey. Concerns regarding the possibility of not being able to spend current year new monies funding unless it could be carried forward to 2021/22 to be highlighted via the National Corporate Finance Network.
A Caddick K Kidd
There appears to have been some confusion between UoD and NES as to whether the "courtesy & respect" question should have been included in previous QRP question sets. As mentioned at PRC these questions have now been revised and the new question set to be used in 2021/22 academic year does include the "courtesy & respect" question. Have liaised with other Boards, to check their approach, which is consistent with NHST.
ACTION POINTS UPDATE Item Number 4.1
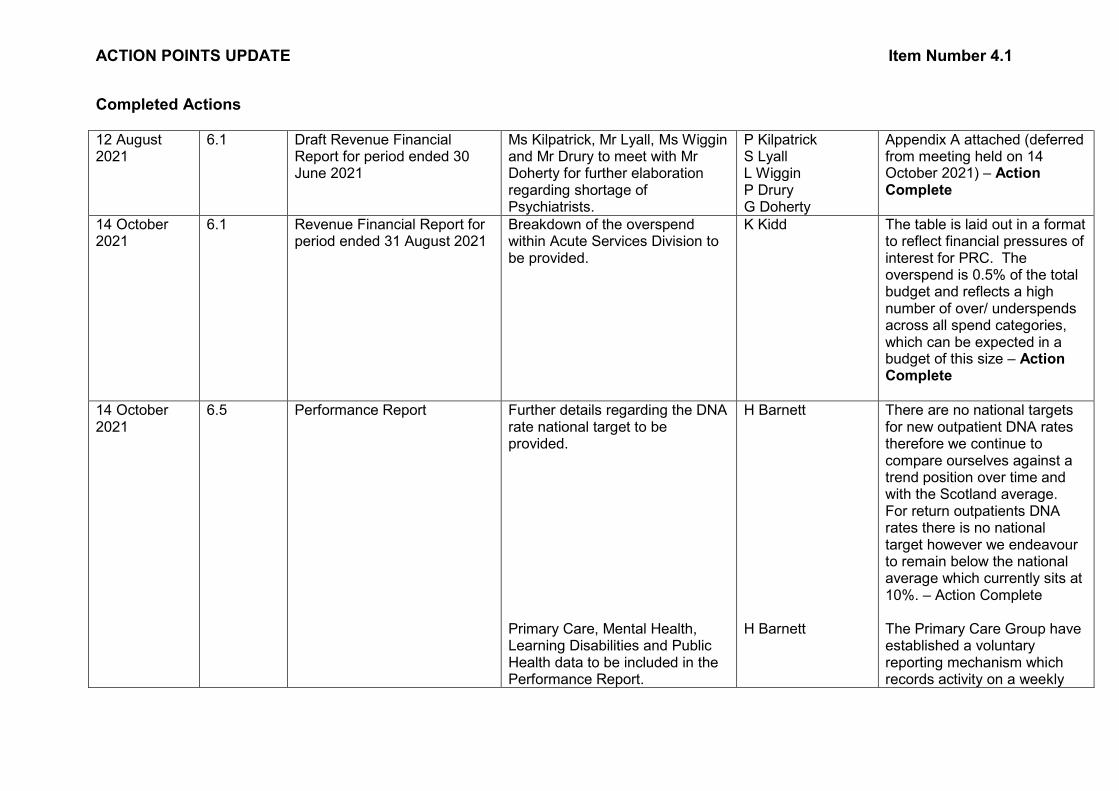
Completed Actions
12 August 2021
6.1 Draft Revenue Financial Report for period ended 30 June 2021
Ms Kilpatrick, Mr Lyall, Ms Wiggin and Mr Drury to meet with Mr Doherty for further elaboration regarding shortage of Psychiatrists.
P Kilpatrick S Lyall L Wiggin P Drury G Doherty
Appendix A attached (deferred from meeting held on 14 October 2021) – Action Complete
14 October 2021
6.1 Revenue Financial Report for period ended 31 August 2021
Breakdown of the overspend within Acute Services Division to be provided.
K Kidd The table is laid out in a format to reflect financial pressures of interest for PRC. The overspend is 0.5% of the total budget and reflects a high number of over/ underspends across all spend categories, which can be expected in a budget of this size – Action Complete
14 October 2021
6.5 Performance Report Further details regarding the DNA rate national target to be provided. Primary Care, Mental Health, Learning Disabilities and Public Health data to be included in the Performance Report.
H Barnett H Barnett
There are no national targets for new outpatient DNA rates therefore we continue to compare ourselves against a trend position over time and with the Scotland average. For return outpatients DNA rates there is no national target however we endeavour to remain below the national average which currently sits at 10%. – Action Complete The Primary Care Group have established a voluntary reporting mechanism which records activity on a weekly
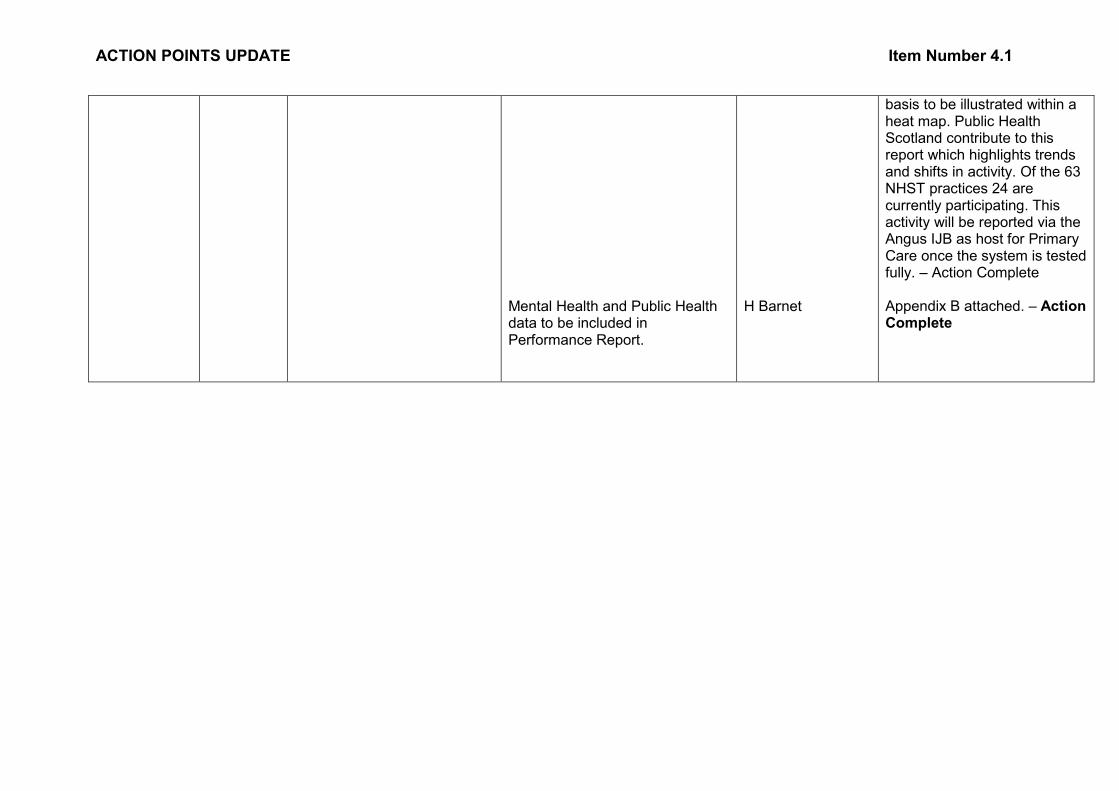
ACTION POINTS UPDATE Item Number 4.1
Mental Health and Public Health data to be included in Performance Report.
H Barnet
basis to be illustrated within a heat map. Public Health Scotland contribute to this report which highlights trends and shifts in activity. Of the 63 NHST practices 24 are currently participating. This activity will be reported via the Angus IJB as host for Primary Care once the system is tested fully. – Action Complete Appendix B attached. – Action Complete
APPENDIX
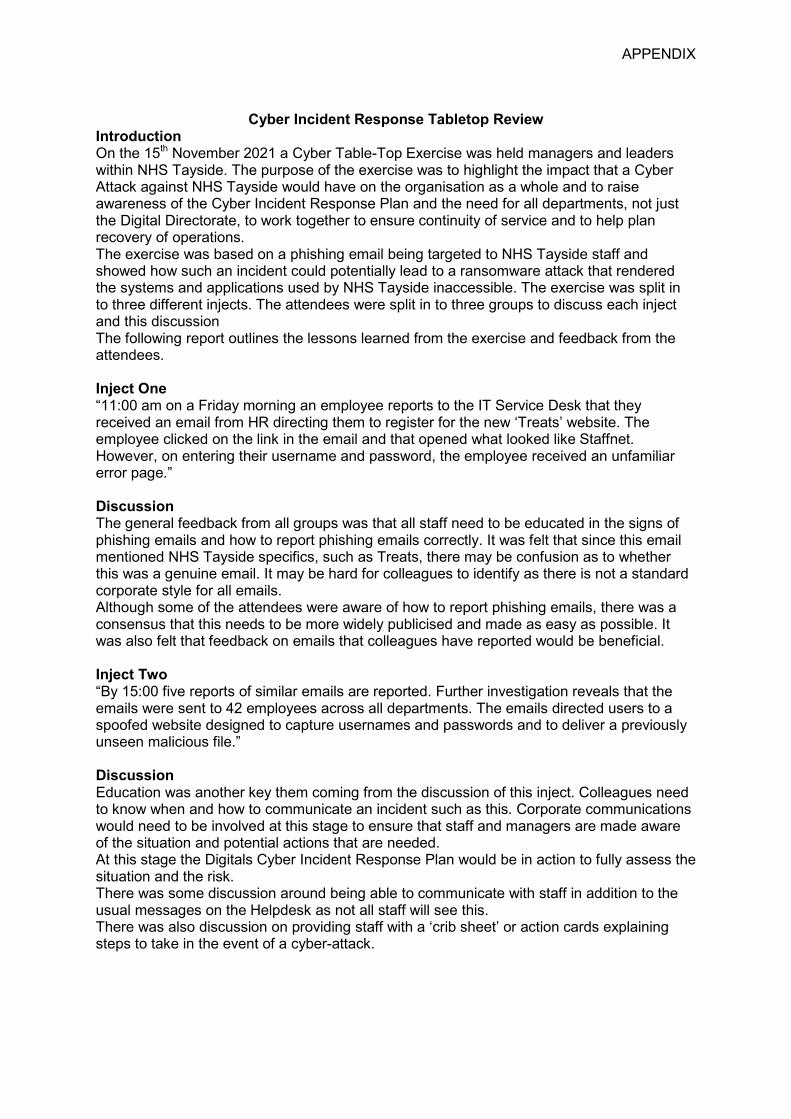
Cyber Incident Response Tabletop Review
Introduction On the 15th November 2021 a Cyber Table-Top Exercise was held managers and leaders within NHS Tayside. The purpose of the exercise was to highlight the impact that a Cyber Attack against NHS Tayside would have on the organisation as a whole and to raise awareness of the Cyber Incident Response Plan and the need for all departments, not just the Digital Directorate, to work together to ensure continuity of service and to help plan recovery of operations. The exercise was based on a phishing email being targeted to NHS Tayside staff and showed how such an incident could potentially lead to a ransomware attack that rendered the systems and applications used by NHS Tayside inaccessible. The exercise was split in to three different injects. The attendees were split in to three groups to discuss each inject and this discussion The following report outlines the lessons learned from the exercise and feedback from the attendees. Inject One “11:00 am on a Friday morning an employee reports to the IT Service Desk that they received an email from HR directing them to register for the new ‘Treats’ website. The employee clicked on the link in the email and that opened what looked like Staffnet. However, on entering their username and password, the employee received an unfamiliar error page.” Discussion The general feedback from all groups was that all staff need to be educated in the signs of phishing emails and how to report phishing emails correctly. It was felt that since this email mentioned NHS Tayside specifics, such as Treats, there may be confusion as to whether this was a genuine email. It may be hard for colleagues to identify as there is not a standard corporate style for all emails. Although some of the attendees were aware of how to report phishing emails, there was a consensus that this needs to be more widely publicised and made as easy as possible. It was also felt that feedback on emails that colleagues have reported would be beneficial. Inject Two “By 15:00 five reports of similar emails are reported. Further investigation reveals that the emails were sent to 42 employees across all departments. The emails directed users to a spoofed website designed to capture usernames and passwords and to deliver a previously unseen malicious file.” Discussion Education was another key them coming from the discussion of this inject. Colleagues need to know when and how to communicate an incident such as this. Corporate communications would need to be involved at this stage to ensure that staff and managers are made aware of the situation and potential actions that are needed. At this stage the Digitals Cyber Incident Response Plan would be in action to fully assess the situation and the risk. There was some discussion around being able to communicate with staff in addition to the usual messages on the Helpdesk as not all staff will see this. There was also discussion on providing staff with a ‘crib sheet’ or action cards explaining steps to take in the event of a cyber-attack.
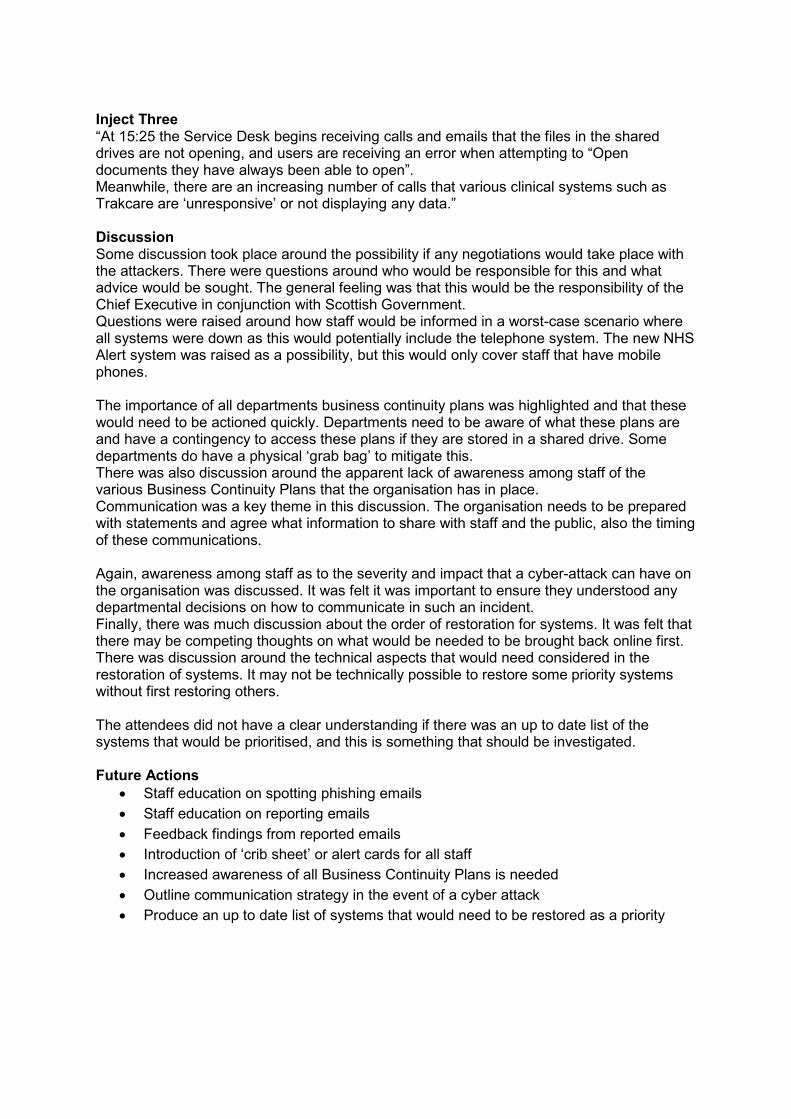
Inject Three “At 15:25 the Service Desk begins receiving calls and emails that the files in the shared drives are not opening, and users are receiving an error when attempting to “Open documents they have always been able to open”. Meanwhile, there are an increasing number of calls that various clinical systems such as Trakcare are ‘unresponsive’ or not displaying any data.” Discussion Some discussion took place around the possibility if any negotiations would take place with the attackers. There were questions around who would be responsible for this and what advice would be sought. The general feeling was that this would be the responsibility of the Chief Executive in conjunction with Scottish Government. Questions were raised around how staff would be informed in a worst-case scenario where all systems were down as this would potentially include the telephone system. The new NHS Alert system was raised as a possibility, but this would only cover staff that have mobile phones. The importance of all departments business continuity plans was highlighted and that these would need to be actioned quickly. Departments need to be aware of what these plans are and have a contingency to access these plans if they are stored in a shared drive. Some departments do have a physical ‘grab bag’ to mitigate this. There was also discussion around the apparent lack of awareness among staff of the various Business Continuity Plans that the organisation has in place. Communication was a key theme in this discussion. The organisation needs to be prepared with statements and agree what information to share with staff and the public, also the timing of these communications. Again, awareness among staff as to the severity and impact that a cyber-attack can have on the organisation was discussed. It was felt it was important to ensure they understood any departmental decisions on how to communicate in such an incident. Finally, there was much discussion about the order of restoration for systems. It was felt that there may be competing thoughts on what would be needed to be brought back online first. There was discussion around the technical aspects that would need considered in the restoration of systems. It may not be technically possible to restore some priority systems without first restoring others. The attendees did not have a clear understanding if there was an up to date list of the systems that would be prioritised, and this is something that should be investigated. Future Actions
• Staff education on spotting phishing emails • Staff education on reporting emails • Feedback findings from reported emails • Introduction of ‘crib sheet’ or alert cards for all staff • Increased awareness of all Business Continuity Plans is needed • Outline communication strategy in the event of a cyber attack • Produce an up to date list of systems that would need to be restored as a priority
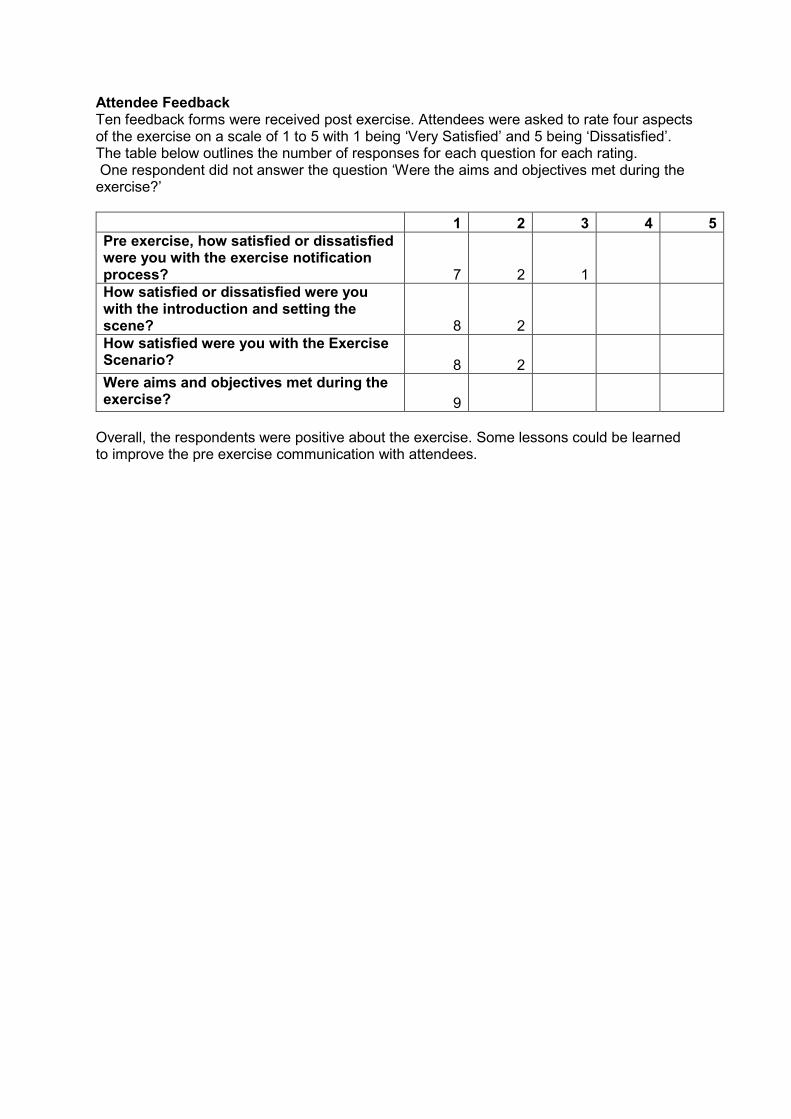
Attendee Feedback Ten feedback forms were received post exercise. Attendees were asked to rate four aspects of the exercise on a scale of 1 to 5 with 1 being ‘Very Satisfied’ and 5 being ‘Dissatisfied’. The table below outlines the number of responses for each question for each rating. One respondent did not answer the question ‘Were the aims and objectives met during the exercise?’ 1 2 3 4 5 Pre exercise, how satisfied or dissatisfied were you with the exercise notification process? 7 2 1 How satisfied or dissatisfied were you with the introduction and setting the scene? 8 2 How satisfied were you with the Exercise Scenario? 8 2 Were aims and objectives met during the exercise? 9
Overall, the respondents were positive about the exercise. Some lessons could be learned to improve the pre exercise communication with attendees.
2
Item Number 5.1
PERFORMANCE AND RESOURCES COMMITTEE Committee Assurance Plan and Workplan 2021/2022
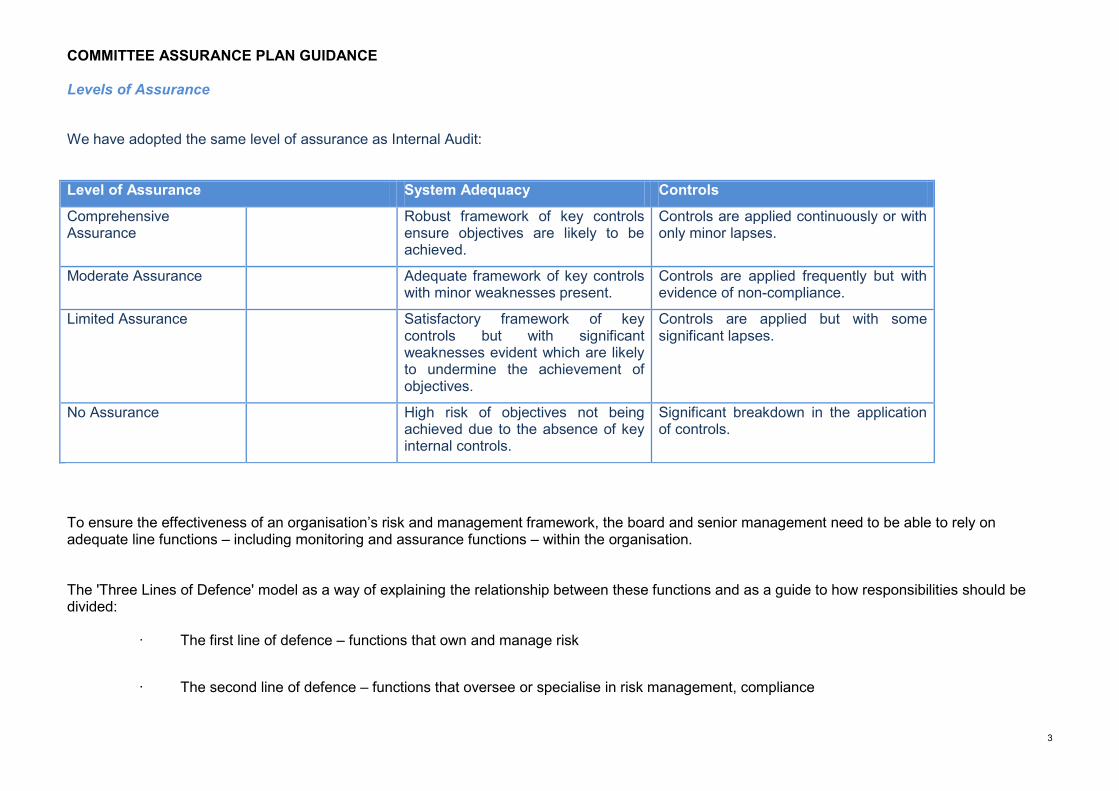
COMMITTEE ASSURANCE PLAN GUIDANCE
3
Levels of Assurance We have adopted the same level of assurance as Internal Audit:
Level of Assurance System Adequacy Controls
Comprehensive Assurance
Robust framework of key controls ensure objectives are likely to be achieved.
Controls are applied continuously or with only minor lapses.
Moderate Assurance Adequate framework of key controls with minor weaknesses present.
Controls are applied frequently but with evidence of non-compliance.
Limited Assurance Satisfactory framework of key controls but with significant weaknesses evident which are likely to undermine the achievement of objectives.
Controls are applied but with some significant lapses.
No Assurance High risk of objectives not being achieved due to the absence of key internal controls.
Significant breakdown in the application of controls.
To ensure the effectiveness of an organisation’s risk and management framework, the board and senior management need to be able to rely on adequate line functions – including monitoring and assurance functions – within the organisation. The 'Three Lines of Defence' model as a way of explaining the relationship between these functions and as a guide to how responsibilities should be divided:
· The first line of defence – functions that own and manage risk
· The second line of defence – functions that oversee or specialise in risk management, compliance
COMMITTEE ASSURANCE PLAN GUIDANCE
4
· The third line of defence – functions that provide independent assurance, above all internal audit.
The group looking at a topic is 1st line, telling the committee about having done this and what the outcome was (through a report, not just minutes) is 2nd line First line of defence Under the first line of defence, operational management has ownership, responsibility and accountability for directly assessing, controlling and mitigating risks. Second line of defence The second line of defence consists of activities covered by several components of internal governance (compliance, risk management, quality, IT and other control departments). This line of defence monitors and facilitates the implementation of effective risk management practices by operational management and assists the risk owners in reporting adequate risk related information up and down the organisation. Third line of defence Internal audit forms the organisation’s third line of defence. An independent internal audit function will, through a risk-based approach to its work, provide assurance to the organisation’s board of directors and senior management. This assurance will cover how effectively the organisation assesses and manages its risks and will include assurance on the effectiveness of the first and second lines of defence. It encompasses all elements of an institution’s risk management framework (from risk identification, risk assessment and response, to communication of risk related information) and all categories of organisational objectives: strategic, ethical, operational, reporting and compliance.
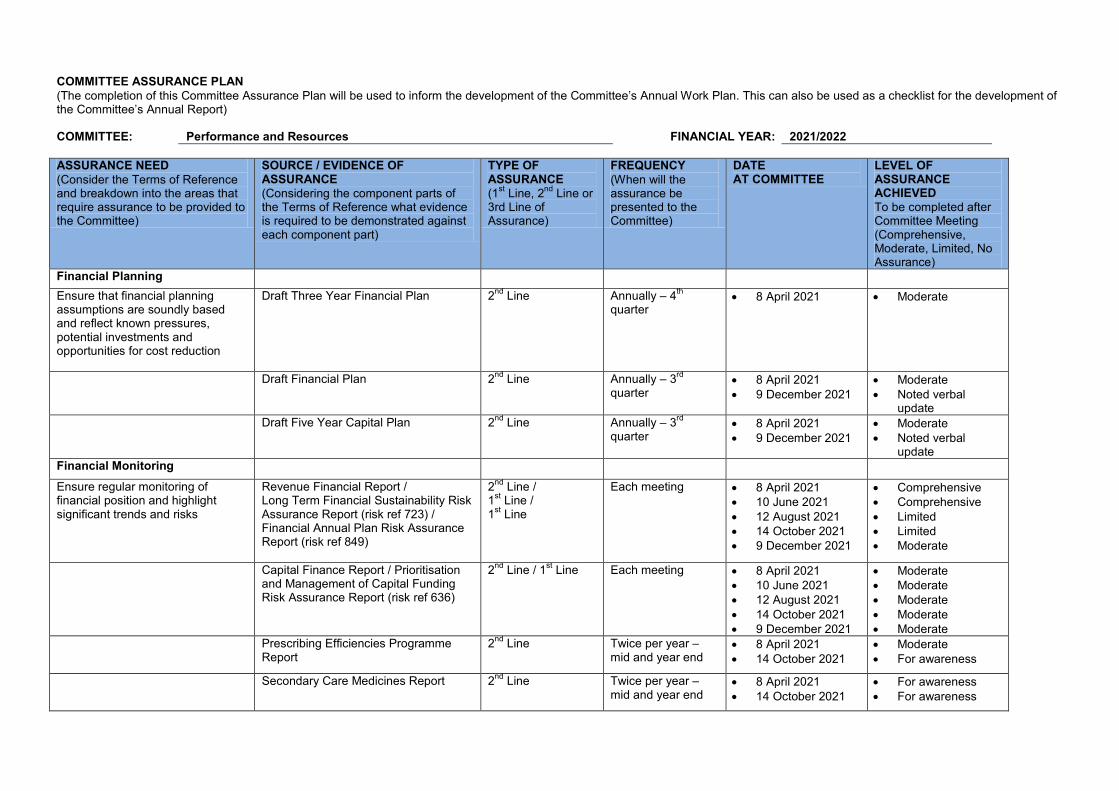
COMMITTEE ASSURANCE PLAN (The completion of this Committee Assurance Plan will be used to inform the development of the Committee’s Annual Work Plan. This can also be used as a checklist for the development of the Committee’s Annual Report) COMMITTEE: Performance and Resources FINANCIAL YEAR: 2021/2022 ASSURANCE NEED (Consider the Terms of Reference and breakdown into the areas that require assurance to be provided to the Committee)
SOURCE / EVIDENCE OF ASSURANCE (Considering the component parts of the Terms of Reference what evidence is required to be demonstrated against each component part)
TYPE OF ASSURANCE (1st Line, 2nd Line or 3rd Line of Assurance)
FREQUENCY (When will the assurance be presented to the Committee)
DATE AT COMMITTEE
LEVEL OF ASSURANCE ACHIEVED To be completed after Committee Meeting (Comprehensive, Moderate, Limited, No Assurance)
Financial Planning Ensure that financial planning assumptions are soundly based and reflect known pressures, potential investments and opportunities for cost reduction
Draft Three Year Financial Plan 2nd Line Annually – 4th quarter
• 8 April 2021 • Moderate
Draft Financial Plan 2nd Line Annually – 3rd quarter
• 8 April 2021 • 9 December 2021
• Moderate • Noted verbal
update Draft Five Year Capital Plan 2nd Line Annually – 3rd
quarter • 8 April 2021 • 9 December 2021
• Moderate • Noted verbal
update Financial Monitoring
Ensure regular monitoring of financial position and highlight significant trends and risks
Revenue Financial Report / Long Term Financial Sustainability Risk Assurance Report (risk ref 723) / Financial Annual Plan Risk Assurance Report (risk ref 849)
2nd Line / 1st Line / 1st Line
Each meeting • 8 April 2021 • 10 June 2021 • 12 August 2021 • 14 October 2021 • 9 December 2021
• Comprehensive • Comprehensive • Limited • Limited • Moderate
Capital Finance Report / Prioritisation and Management of Capital Funding Risk Assurance Report (risk ref 636)
2nd Line / 1st Line Each meeting • 8 April 2021 • 10 June 2021 • 12 August 2021 • 14 October 2021 • 9 December 2021
• Moderate • Moderate • Moderate • Moderate • Moderate
Prescribing Efficiencies Programme Report
2nd Line Twice per year – mid and year end
• 8 April 2021 • 14 October 2021
• Moderate • For awareness
Secondary Care Medicines Report
2nd Line Twice per year – mid and year end
• 8 April 2021 • 14 October 2021
• For awareness • For awareness
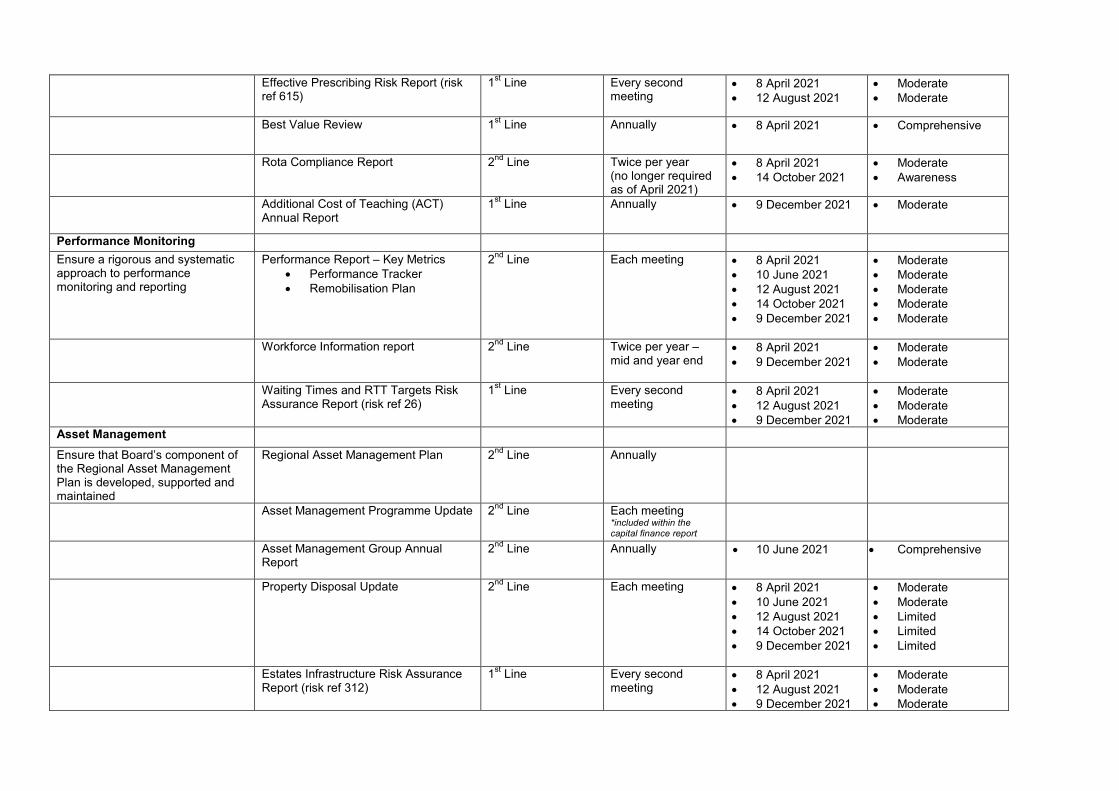
Effective Prescribing Risk Report (risk ref 615)
1st Line Every second meeting
• 8 April 2021 • 12 August 2021
• Moderate • Moderate
Best Value Review 1st Line Annually • 8 April 2021 • Comprehensive
Rota Compliance Report 2nd Line Twice per year (no longer required as of April 2021)
• 8 April 2021 • 14 October 2021
• Moderate • Awareness
Additional Cost of Teaching (ACT) Annual Report
1st Line Annually • 9 December 2021 • Moderate
Performance Monitoring Ensure a rigorous and systematic approach to performance monitoring and reporting
Performance Report – Key Metrics • Performance Tracker • Remobilisation Plan
2nd Line Each meeting • 8 April 2021 • 10 June 2021 • 12 August 2021 • 14 October 2021 • 9 December 2021
• Moderate • Moderate • Moderate • Moderate • Moderate
Workforce Information report 2nd Line Twice per year – mid and year end
• 8 April 2021 • 9 December 2021
• Moderate • Moderate
Waiting Times and RTT Targets Risk Assurance Report (risk ref 26)
1st Line Every second meeting
• 8 April 2021 • 12 August 2021 • 9 December 2021
• Moderate • Moderate • Moderate
Asset Management
Ensure that Board’s component of the Regional Asset Management Plan is developed, supported and maintained
Regional Asset Management Plan 2nd Line Annually
Asset Management Programme Update 2nd Line Each meeting *included within the capital finance report
Asset Management Group Annual Report
2nd Line Annually • 10 June 2021 • Comprehensive
Property Disposal Update 2nd Line Each meeting • 8 April 2021 • 10 June 2021 • 12 August 2021 • 14 October 2021 • 9 December 2021
• Moderate • Moderate • Limited • Limited • Limited
Estates Infrastructure Risk Assurance Report (risk ref 312)
1st Line Every second meeting
• 8 April 2021 • 12 August 2021 • 9 December 2021
• Moderate • Moderate • Moderate
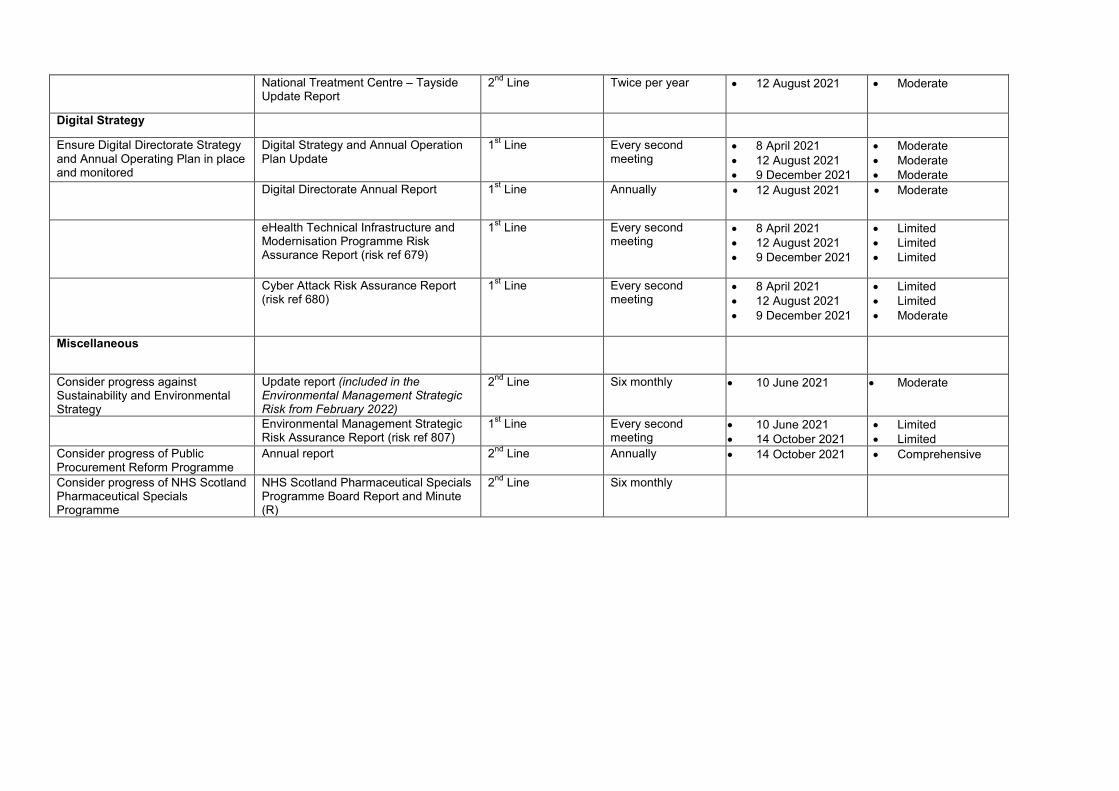
National Treatment Centre – Tayside Update Report
2nd Line Twice per year • 12 August 2021 • Moderate
Digital Strategy
Ensure Digital Directorate Strategy and Annual Operating Plan in place and monitored
Digital Strategy and Annual Operation Plan Update
1st Line Every second meeting
• 8 April 2021 • 12 August 2021 • 9 December 2021
• Moderate • Moderate • Moderate
Digital Directorate Annual Report 1st Line Annually • 12 August 2021 • Moderate
eHealth Technical Infrastructure and Modernisation Programme Risk Assurance Report (risk ref 679)
1st Line Every second meeting
• 8 April 2021 • 12 August 2021 • 9 December 2021
• Limited • Limited • Limited
Cyber Attack Risk Assurance Report (risk ref 680)
1st Line Every second meeting
• 8 April 2021 • 12 August 2021 • 9 December 2021
• Limited • Limited • Moderate
Miscellaneous
Consider progress against Sustainability and Environmental Strategy
Update report (included in the Environmental Management Strategic Risk from February 2022)
2nd Line Six monthly • 10 June 2021
• Moderate
Environmental Management Strategic Risk Assurance Report (risk ref 807)
1st Line Every second meeting
• 10 June 2021 • 14 October 2021
• Limited • Limited
Consider progress of Public Procurement Reform Programme
Annual report 2nd Line Annually • 14 October 2021 • Comprehensive
Consider progress of NHS Scotland Pharmaceutical Specials Programme
NHS Scotland Pharmaceutical Specials Programme Board Report and Minute (R)
2nd Line Six monthly
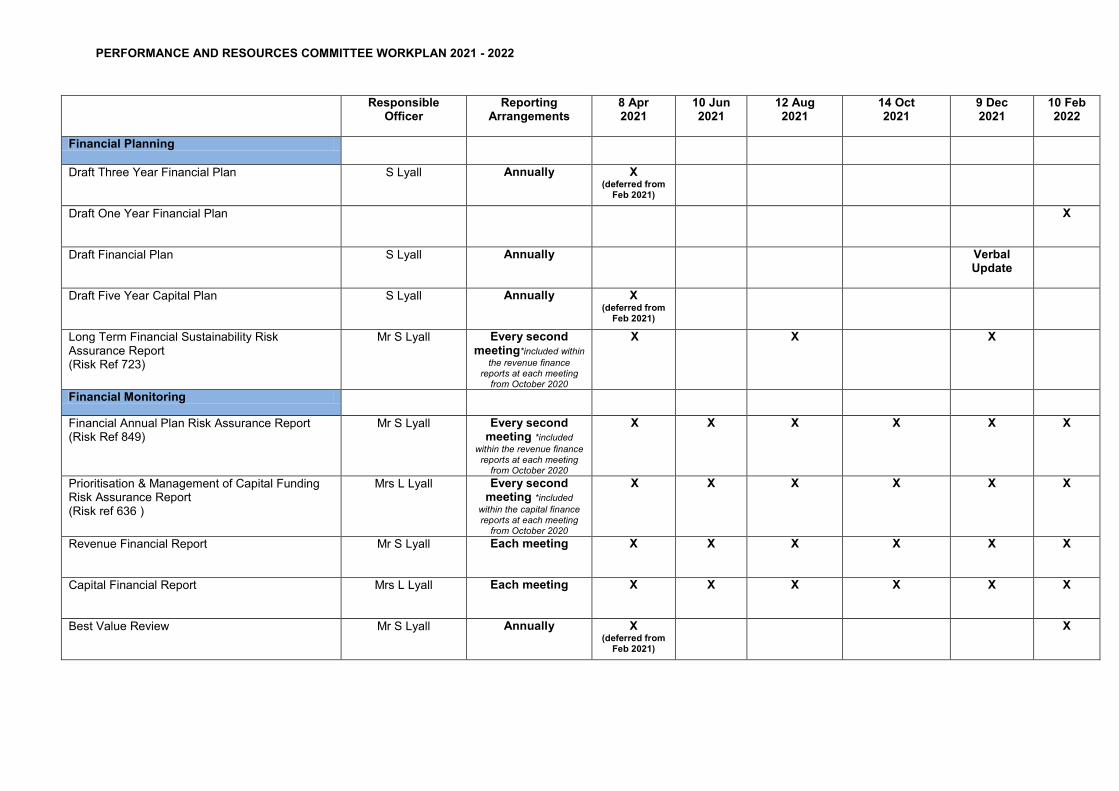
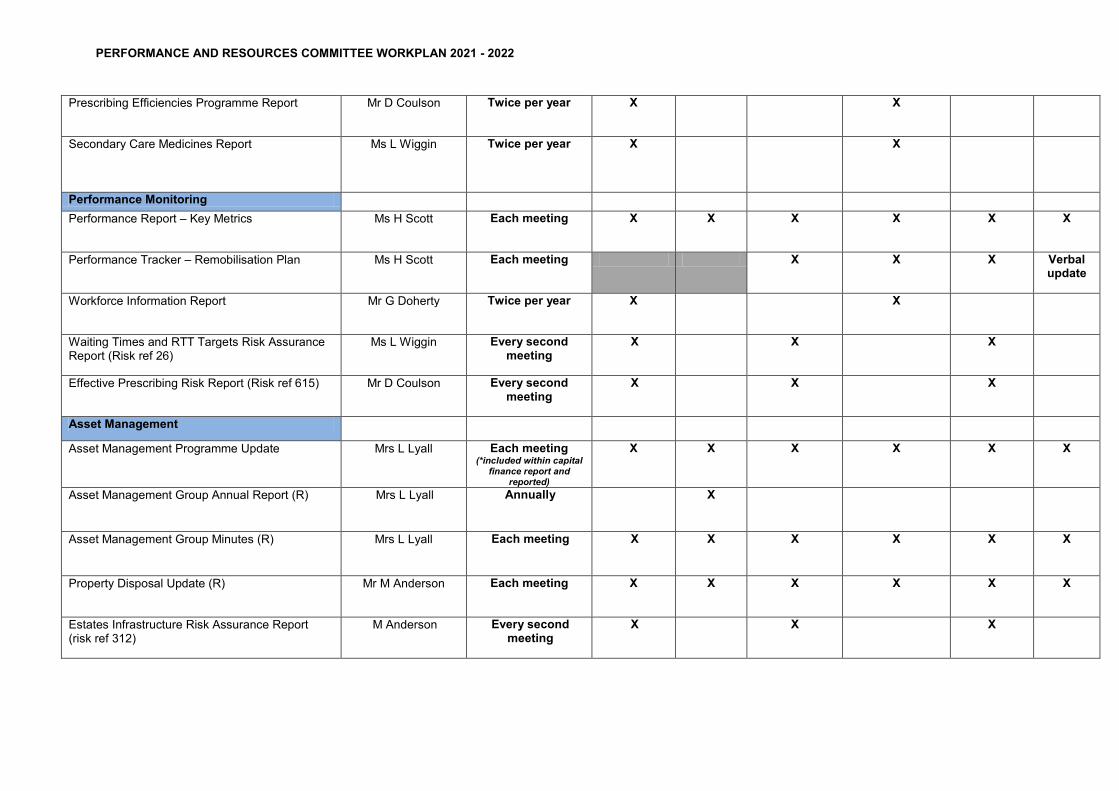
PERFORMANCE AND RESOURCES COMMITTEE WORKPLAN 2021 - 2022
Responsible Officer
Reporting Arrangements
8 Apr 2021
10 Jun 2021
12 Aug 2021
14 Oct 2021
9 Dec 2021
10 Feb 2022
Financial Planning
Draft Three Year Financial Plan S Lyall Annually X (deferred from
Feb 2021)
Draft One Year Financial Plan X
Draft Financial Plan S Lyall Annually Verbal Update
Draft Five Year Capital Plan S Lyall Annually X (deferred from
Feb 2021)
Long Term Financial Sustainability Risk Assurance Report (Risk Ref 723)
Mr S Lyall Every second meeting*included within
the revenue finance reports at each meeting
from October 2020
X X X
Financial Monitoring
Financial Annual Plan Risk Assurance Report (Risk Ref 849)
Mr S Lyall Every second meeting *included
within the revenue finance reports at each meeting
from October 2020
X X X X X X
Prioritisation & Management of Capital Funding Risk Assurance Report (Risk ref 636 )
Mrs L Lyall Every second meeting *included
within the capital finance reports at each meeting
from October 2020
X X X X X X
Revenue Financial Report Mr S Lyall Each meeting X X X X X X
Capital Financial Report Mrs L Lyall Each meeting X X X X X X
Best Value Review Mr S Lyall Annually X (deferred from
Feb 2021)
X
PERFORMANCE AND RESOURCES COMMITTEE WORKPLAN 2021 - 2022
Prescribing Efficiencies Programme Report Mr D Coulson Twice per year X X
Secondary Care Medicines Report
Ms L Wiggin Twice per year X X
Performance Monitoring Performance Report – Key Metrics Ms H Scott Each meeting X X X X X X
Performance Tracker – Remobilisation Plan Ms H Scott Each meeting X X X Verbal update
Workforce Information Report Mr G Doherty
Twice per year X X
Waiting Times and RTT Targets Risk Assurance Report (Risk ref 26)
Ms L Wiggin Every second meeting
X X X
Effective Prescribing Risk Report (Risk ref 615) Mr D Coulson Every second meeting
X X X
Asset Management
Asset Management Programme Update Mrs L Lyall Each meeting (*included within capital
finance report and reported)
X X X X X X
Asset Management Group Annual Report (R) Mrs L Lyall Annually
X
Asset Management Group Minutes (R) Mrs L Lyall Each meeting X X X X X X
Property Disposal Update (R) Mr M Anderson Each meeting X X X X X X
Estates Infrastructure Risk Assurance Report (risk ref 312)
M Anderson Every second meeting
X X X
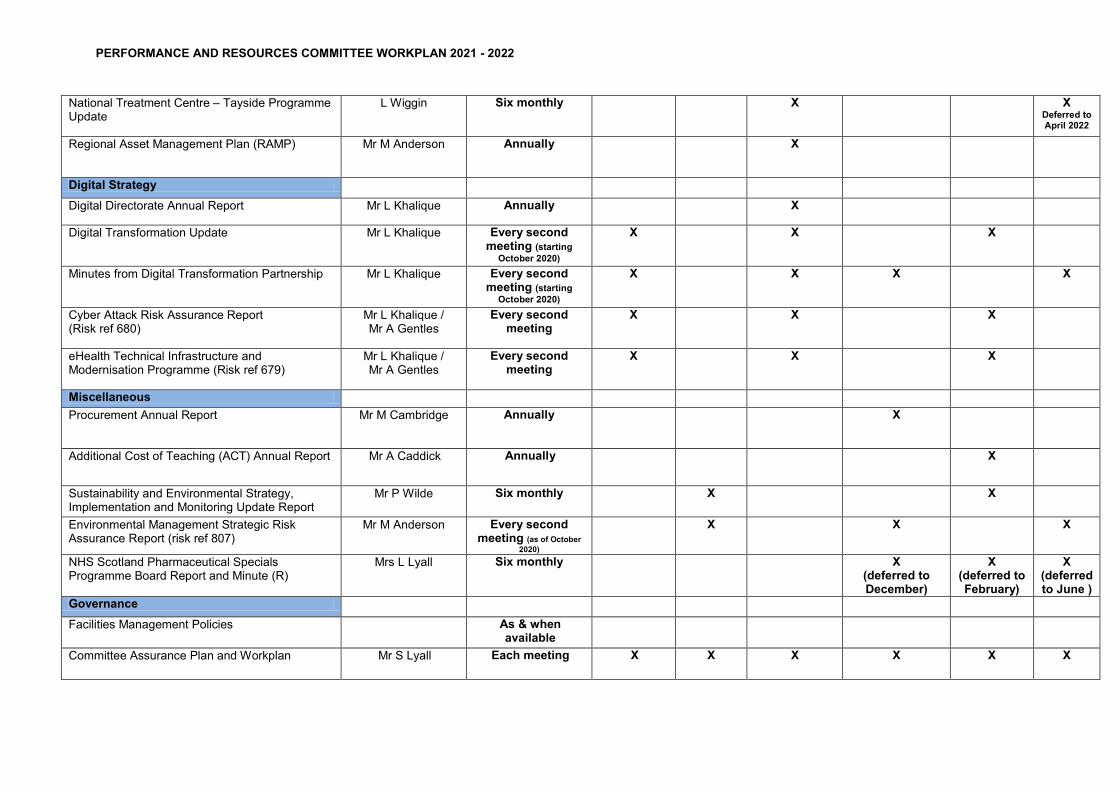
PERFORMANCE AND RESOURCES COMMITTEE WORKPLAN 2021 - 2022
National Treatment Centre – Tayside Programme Update
L Wiggin Six monthly
X X Deferred to April 2022
Regional Asset Management Plan (RAMP) Mr M Anderson Annually X
Digital Strategy Digital Directorate Annual Report Mr L Khalique Annually X
Digital Transformation Update Mr L Khalique Every second meeting (starting
October 2020)
X X X
Minutes from Digital Transformation Partnership Mr L Khalique Every second meeting (starting
October 2020)
X X X X
Cyber Attack Risk Assurance Report (Risk ref 680)
Mr L Khalique / Mr A Gentles
Every second meeting
X X X
eHealth Technical Infrastructure and Modernisation Programme (Risk ref 679)
Mr L Khalique / Mr A Gentles
Every second meeting
X X X
Miscellaneous Procurement Annual Report Mr M Cambridge Annually
X
Additional Cost of Teaching (ACT) Annual Report Mr A Caddick Annually X
Sustainability and Environmental Strategy, Implementation and Monitoring Update Report
Mr P Wilde Six monthly X X
Environmental Management Strategic Risk Assurance Report (risk ref 807)
Mr M Anderson Every second meeting (as of October
2020)
X X X
NHS Scotland Pharmaceutical Specials Programme Board Report and Minute (R)
Mrs L Lyall Six monthly X (deferred to December)
X (deferred to February)
X (deferred to June )
Governance
Facilities Management Policies As & when available
Committee Assurance Plan and Workplan Mr S Lyall Each meeting X X X X X X
PERFORMANCE AND RESOURCES COMMITTEE WORKPLAN 2021 - 2022
Committee Annual Report Mr S Lyall Annually
X
Committee Terms of Reference Mr S Lyall Annually
X
Chair: Pat Kilpatrick Vice Chair: Peter Drury Lead Officer: Stuart Lyall
NAME Meeting Date
Meeting Date
Meeting Date
Meeting Date
Meeting Date
Meeting Date
8 April 2021
10 June 2021
12 August 2021
14 October 2021
10 December 2021
11 February 2022
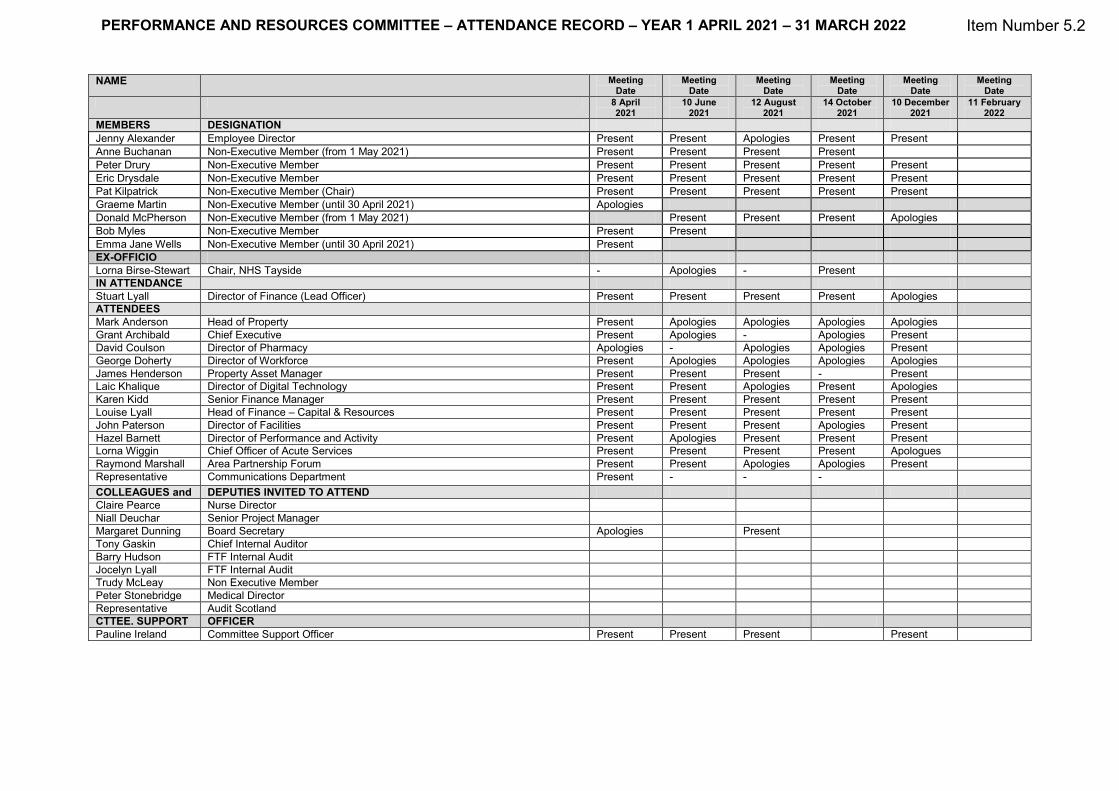
MEMBERS DESIGNATION Jenny Alexander Employee Director Present Present Apologies Present Present Anne Buchanan Non-Executive Member (from 1 May 2021) Present Present Present Present Peter Drury Non-Executive Member Present Present Present Present Present Eric Drysdale Non-Executive Member Present Present Present Present Present Pat Kilpatrick Non-Executive Member (Chair) Present Present Present Present Present Graeme Martin Non-Executive Member (until 30 April 2021) Apologies Donald McPherson Non-Executive Member (from 1 May 2021) Present Present Present Apologies Bob Myles Non-Executive Member Present Present Emma Jane Wells Non-Executive Member (until 30 April 2021) Present EX-OFFICIO Lorna Birse-Stewart Chair, NHS Tayside - Apologies - Present IN ATTENDANCE Stuart Lyall Director of Finance (Lead Officer) Present Present Present Present Apologies ATTENDEES Mark Anderson Head of Property Present Apologies Apologies Apologies Apologies Grant Archibald Chief Executive Present Apologies - Apologies Present David Coulson Director of Pharmacy Apologies - Apologies Apologies Present George Doherty Director of Workforce Present Apologies Apologies Apologies Apologies James Henderson Property Asset Manager Present Present Present - Present Laic Khalique Director of Digital Technology Present Present Apologies Present Apologies Karen Kidd Senior Finance Manager Present Present Present Present Present Louise Lyall Head of Finance – Capital & Resources Present Present Present Present Present John Paterson Director of Facilities Present Present Present Apologies Present Hazel Barnett Director of Performance and Activity Present Apologies Present Present Present Lorna Wiggin Chief Officer of Acute Services Present Present Present Present Apologues Raymond Marshall Area Partnership Forum Present Present Apologies Apologies Present Representative Communications Department Present - - - COLLEAGUES and DEPUTIES INVITED TO ATTEND Claire Pearce Nurse Director Niall Deuchar Senior Project Manager Margaret Dunning Board Secretary Apologies Present Tony Gaskin Chief Internal Auditor Barry Hudson FTF Internal Audit Jocelyn Lyall FTF Internal Audit Trudy McLeay Non Executive Member Peter Stonebridge Medical Director Representative Audit Scotland CTTEE. SUPPORT OFFICER Pauline Ireland Committee Support Officer Present Present Present Present
PERFORMANCE AND RESOURCES COMMITTEE – ATTENDANCE RECORD – YEAR 1 APRIL 2021 – 31 MARCH 2022 Item Number 5.2
1
Item Number 6.1 PRC01/2022
Performance and Resources Committee 10 February 2022 REVENUE FINANCIAL REPORT FOR THE PERIOD ENDED 31 DECEMBER 2021 Responsible Executive: Stuart Lyall, Director of Finance Report Author Karen Kidd, Senior Finance Manager Jaime Lyon, Senior Finance Manager 1. PURPOSE This is presented to the Committee for:-
• Assurance The report relates to:- • Annual Operating Plan
This aligns to the following NHS Scotland quality ambition(s):- • Effective
2. REPORT SUMMARY 2.1 Situation The purpose of this report is to set out in summary:-
i. Tayside NHS Board’s financial performance for the nine months to 31 December, 2021;
ii. the risks to delivery of the Board’s Financial Plan 2021/22, and iii. an assessment of the impact on Strategic Risk 723: Long Term Financial
Sustainability and Risk 1033: Finance Annual Plan 2021/22. The report provides moderate assurance based on the current forecast outturn and the
outstanding confirmation from Scottish Government (SG) Health Finance Corporate Governance and Value Directorate (SGHFCGVD) on outstanding funding allocation adjustments anticipated in the final quarter of the financial year.
NHS Tayside has submitted the Board’s Quarter 3 financial position to Scottish
Government Health Finance Corporate Governance and Value Directorate (SGHFCGVD) at the end of January 2022. Quarter 1 and Quarter 2 returns having been submitted in July and October 2021 respectively.
2.1 Background Tayside NHS Board approved the Board’s one year Strategic Financial Plan 2021/22 at its
meeting of 29 April, 2021.
The Plan presented a forecast breakeven position for 2021/22 based on a set of key assumptions relating to funding allocations, growth in costs, and related recovery plans.
2
The Plan was dependent on delivery of efficiency savings to close a net financial gap of £27.0 million. SGHFCGVD provided an initial allocation for 2021/22 Covid-19 related expenditure in June, and a subsequent allocation in October following the Quarter 1 financial review. Any balance of funding that is required is anticipated to be received after a review of the Quarter 3 financial position. The issue of anticipated funding allocations from SGHFCGVD continues to be addressed at national level through a SG led review of all Boards’ financial results and performance. This report provides moderate assurance, based on the results to date and the additional Covid-19 funding received in October.
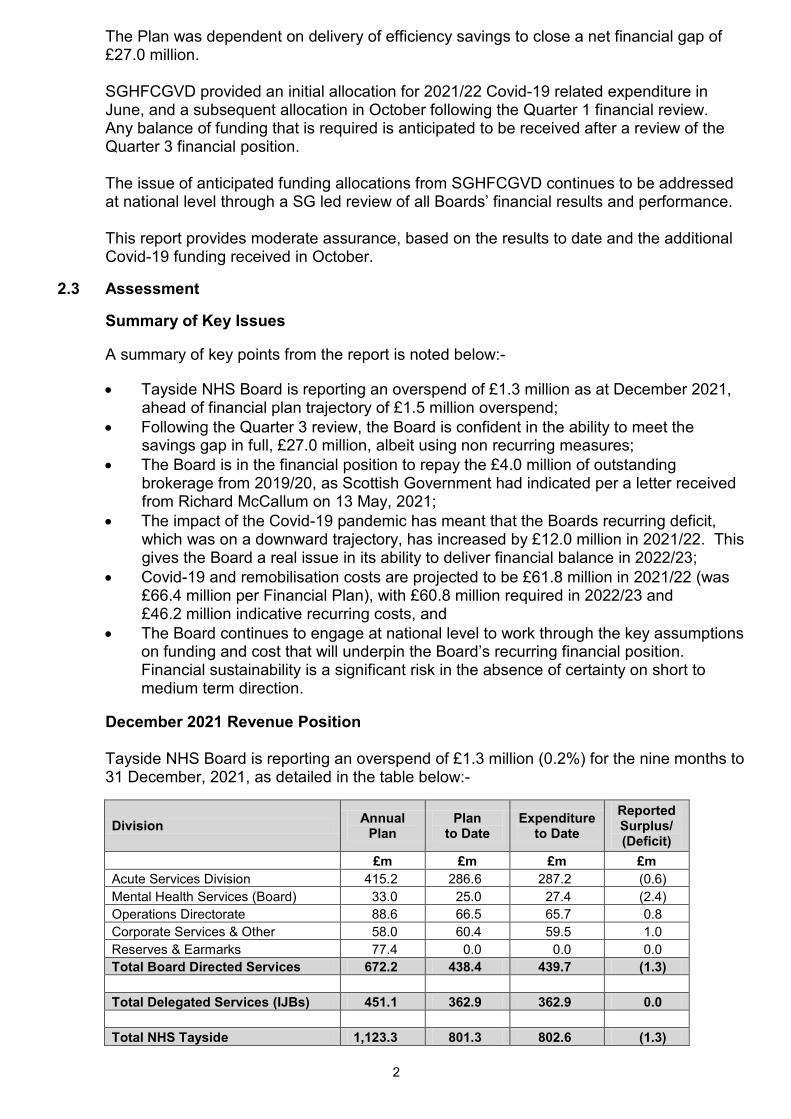
2.3 Assessment Summary of Key Issues A summary of key points from the report is noted below:-
• Tayside NHS Board is reporting an overspend of £1.3 million as at December 2021, ahead of financial plan trajectory of £1.5 million overspend;
• Following the Quarter 3 review, the Board is confident in the ability to meet the savings gap in full, £27.0 million, albeit using non recurring measures;
• The Board is in the financial position to repay the £4.0 million of outstanding brokerage from 2019/20, as Scottish Government had indicated per a letter received from Richard McCallum on 13 May, 2021;
• The impact of the Covid-19 pandemic has meant that the Boards recurring deficit, which was on a downward trajectory, has increased by £12.0 million in 2021/22. This gives the Board a real issue in its ability to deliver financial balance in 2022/23;
• Covid-19 and remobilisation costs are projected to be £61.8 million in 2021/22 (was £66.4 million per Financial Plan), with £60.8 million required in 2022/23 and £46.2 million indicative recurring costs, and
• The Board continues to engage at national level to work through the key assumptions on funding and cost that will underpin the Board’s recurring financial position. Financial sustainability is a significant risk in the absence of certainty on short to medium term direction.
December 2021 Revenue Position Tayside NHS Board is reporting an overspend of £1.3 million (0.2%) for the nine months to
31 December, 2021, as detailed in the table below:-
Division Annual Plan
Plan to Date
Expenditure to Date
Reported Surplus/ (Deficit)
£m £m £m £m Acute Services Division 415.2 286.6 287.2 (0.6) Mental Health Services (Board) 33.0 25.0 27.4 (2.4) Operations Directorate 88.6 66.5 65.7 0.8 Corporate Services & Other 58.0 60.4 59.5 1.0 Reserves & Earmarks 77.4 0.0 0.0 0.0 Total Board Directed Services 672.2 438.4 439.7 (1.3) Total Delegated Services (IJBs) 451.1 362.9 362.9 0.0 Total NHS Tayside 1,123.3 801.3 802.6 (1.3)
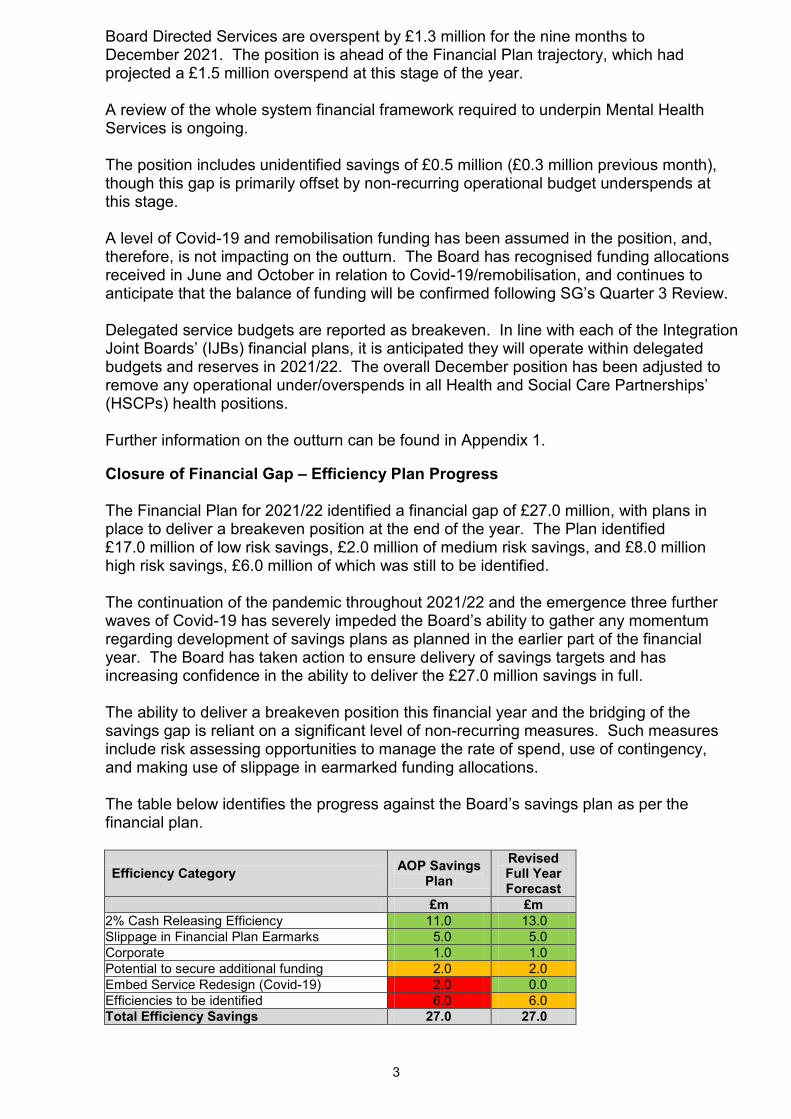
3
Board Directed Services are overspent by £1.3 million for the nine months to December 2021. The position is ahead of the Financial Plan trajectory, which had projected a £1.5 million overspend at this stage of the year. A review of the whole system financial framework required to underpin Mental Health Services is ongoing. The position includes unidentified savings of £0.5 million (£0.3 million previous month), though this gap is primarily offset by non-recurring operational budget underspends at this stage. A level of Covid-19 and remobilisation funding has been assumed in the position, and, therefore, is not impacting on the outturn. The Board has recognised funding allocations received in June and October in relation to Covid-19/remobilisation, and continues to anticipate that the balance of funding will be confirmed following SG’s Quarter 3 Review.
Delegated service budgets are reported as breakeven. In line with each of the Integration Joint Boards’ (IJBs) financial plans, it is anticipated they will operate within delegated budgets and reserves in 2021/22. The overall December position has been adjusted to remove any operational under/overspends in all Health and Social Care Partnerships’ (HSCPs) health positions.
Further information on the outturn can be found in Appendix 1. Closure of Financial Gap – Efficiency Plan Progress
The Financial Plan for 2021/22 identified a financial gap of £27.0 million, with plans in place to deliver a breakeven position at the end of the year. The Plan identified £17.0 million of low risk savings, £2.0 million of medium risk savings, and £8.0 million high risk savings, £6.0 million of which was still to be identified. The continuation of the pandemic throughout 2021/22 and the emergence three further waves of Covid-19 has severely impeded the Board’s ability to gather any momentum regarding development of savings plans as planned in the earlier part of the financial year. The Board has taken action to ensure delivery of savings targets and has increasing confidence in the ability to deliver the £27.0 million savings in full. The ability to deliver a breakeven position this financial year and the bridging of the savings gap is reliant on a significant level of non-recurring measures. Such measures include risk assessing opportunities to manage the rate of spend, use of contingency, and making use of slippage in earmarked funding allocations. The table below identifies the progress against the Board’s savings plan as per the financial plan.
Efficiency Category AOP Savings Plan
Revised Full Year Forecast
£m £m 2% Cash Releasing Efficiency 11.0 13.0 Slippage in Financial Plan Earmarks 5.0 5.0 Corporate 1.0 1.0 Potential to secure additional funding 2.0 2.0 Embed Service Redesign (Covid-19) 2.0 0.0 Efficiencies to be identified 6.0 6.0 Total Efficiency Savings 27.0 27.0
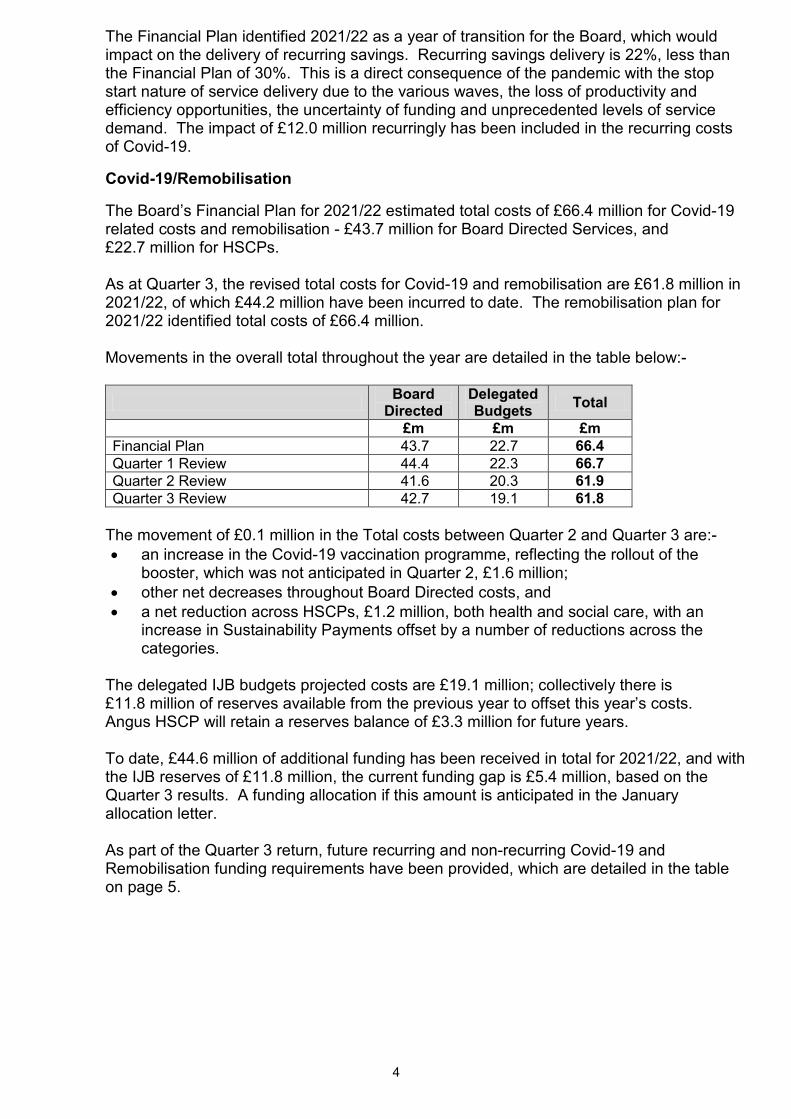
4
The Financial Plan identified 2021/22 as a year of transition for the Board, which would impact on the delivery of recurring savings. Recurring savings delivery is 22%, less than the Financial Plan of 30%. This is a direct consequence of the pandemic with the stop start nature of service delivery due to the various waves, the loss of productivity and efficiency opportunities, the uncertainty of funding and unprecedented levels of service demand. The impact of £12.0 million recurringly has been included in the recurring costs of Covid-19.
Covid-19/Remobilisation The Board’s Financial Plan for 2021/22 estimated total costs of £66.4 million for Covid-19
related costs and remobilisation - £43.7 million for Board Directed Services, and £22.7 million for HSCPs.
As at Quarter 3, the revised total costs for Covid-19 and remobilisation are £61.8 million in
2021/22, of which £44.2 million have been incurred to date. The remobilisation plan for 2021/22 identified total costs of £66.4 million.
Movements in the overall total throughout the year are detailed in the table below:-
Board Directed
Delegated Budgets Total
£m £m £m Financial Plan 43.7 22.7 66.4 Quarter 1 Review 44.4 22.3 66.7 Quarter 2 Review 41.6 20.3 61.9 Quarter 3 Review 42.7 19.1 61.8
The movement of £0.1 million in the Total costs between Quarter 2 and Quarter 3 are:-
• an increase in the Covid-19 vaccination programme, reflecting the rollout of the booster, which was not anticipated in Quarter 2, £1.6 million;
• other net decreases throughout Board Directed costs, and • a net reduction across HSCPs, £1.2 million, both health and social care, with an
increase in Sustainability Payments offset by a number of reductions across the categories.
The delegated IJB budgets projected costs are £19.1 million; collectively there is
£11.8 million of reserves available from the previous year to offset this year’s costs. Angus HSCP will retain a reserves balance of £3.3 million for future years.
To date, £44.6 million of additional funding has been received in total for 2021/22, and with
the IJB reserves of £11.8 million, the current funding gap is £5.4 million, based on the Quarter 3 results. A funding allocation if this amount is anticipated in the January allocation letter.
As part of the Quarter 3 return, future recurring and non-recurring Covid-19 and
Remobilisation funding requirements have been provided, which are detailed in the table on page 5.
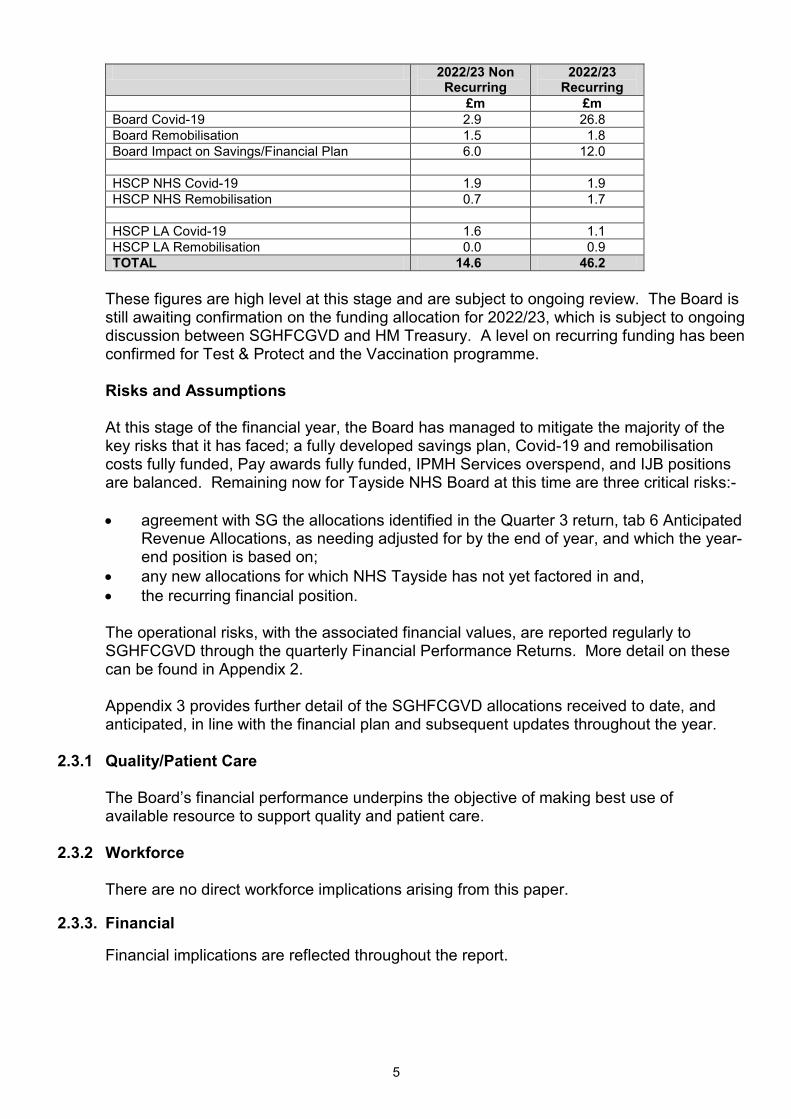
5
2022/23 Non Recurring
2022/23 Recurring
£m £m Board Covid-19 2.9 26.8 Board Remobilisation 1.5 1.8 Board Impact on Savings/Financial Plan 6.0 12.0 HSCP NHS Covid-19 1.9 1.9 HSCP NHS Remobilisation 0.7 1.7 HSCP LA Covid-19 1.6 1.1 HSCP LA Remobilisation 0.0 0.9 TOTAL 14.6 46.2
These figures are high level at this stage and are subject to ongoing review. The Board is
still awaiting confirmation on the funding allocation for 2022/23, which is subject to ongoing discussion between SGHFCGVD and HM Treasury. A level on recurring funding has been confirmed for Test & Protect and the Vaccination programme.
Risks and Assumptions At this stage of the financial year, the Board has managed to mitigate the majority of the
key risks that it has faced; a fully developed savings plan, Covid-19 and remobilisation costs fully funded, Pay awards fully funded, IPMH Services overspend, and IJB positions are balanced. Remaining now for Tayside NHS Board at this time are three critical risks:-
• agreement with SG the allocations identified in the Quarter 3 return, tab 6 Anticipated
Revenue Allocations, as needing adjusted for by the end of year, and which the year-end position is based on;
• any new allocations for which NHS Tayside has not yet factored in and, • the recurring financial position.
The operational risks, with the associated financial values, are reported regularly to
SGHFCGVD through the quarterly Financial Performance Returns. More detail on these can be found in Appendix 2.
Appendix 3 provides further detail of the SGHFCGVD allocations received to date, and
anticipated, in line with the financial plan and subsequent updates throughout the year. 2.3.1 Quality/Patient Care The Board’s financial performance underpins the objective of making best use of
available resource to support quality and patient care. 2.3.2 Workforce There are no direct workforce implications arising from this paper. 2.3.3. Financial Financial implications are reflected throughout the report.
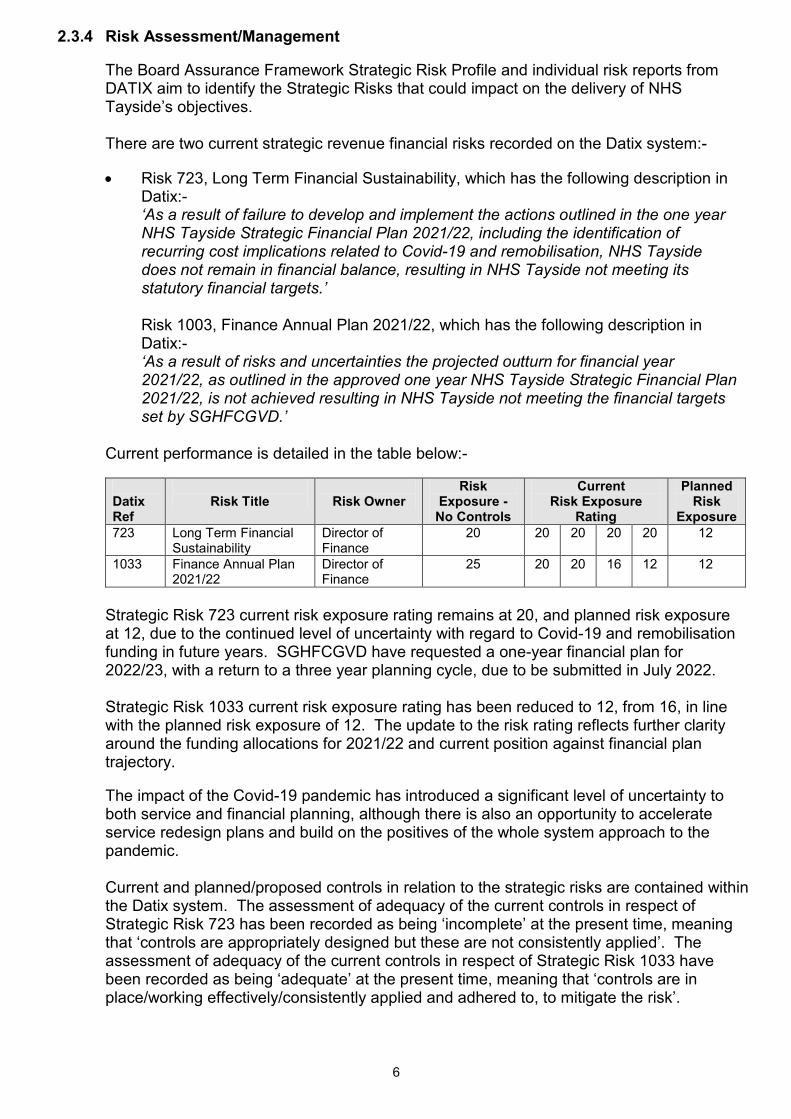
6
2.3.4 Risk Assessment/Management The Board Assurance Framework Strategic Risk Profile and individual risk reports from
DATIX aim to identify the Strategic Risks that could impact on the delivery of NHS Tayside’s objectives.
There are two current strategic revenue financial risks recorded on the Datix system:-
• Risk 723, Long Term Financial Sustainability, which has the following description in Datix:- ‘As a result of failure to develop and implement the actions outlined in the one year NHS Tayside Strategic Financial Plan 2021/22, including the identification of recurring cost implications related to Covid-19 and remobilisation, NHS Tayside does not remain in financial balance, resulting in NHS Tayside not meeting its statutory financial targets.’ Risk 1003, Finance Annual Plan 2021/22, which has the following description in Datix:-
‘As a result of risks and uncertainties the projected outturn for financial year 2021/22, as outlined in the approved one year NHS Tayside Strategic Financial Plan 2021/22, is not achieved resulting in NHS Tayside not meeting the financial targets set by SGHFCGVD.’
Current performance is detailed in the table below:-
Datix Ref
Risk Title
Risk Owner
Risk Exposure - No Controls
Current Risk Exposure
Rating
Planned Risk
Exposure 723 Long Term Financial
Sustainability Director of Finance
20 20 20 20 20 12
1033 Finance Annual Plan 2021/22
Director of Finance
25 20 20 16 12 12
Strategic Risk 723 current risk exposure rating remains at 20, and planned risk exposure at 12, due to the continued level of uncertainty with regard to Covid-19 and remobilisation funding in future years. SGHFCGVD have requested a one-year financial plan for 2022/23, with a return to a three year planning cycle, due to be submitted in July 2022. Strategic Risk 1033 current risk exposure rating has been reduced to 12, from 16, in line with the planned risk exposure of 12. The update to the risk rating reflects further clarity around the funding allocations for 2021/22 and current position against financial plan trajectory. The impact of the Covid-19 pandemic has introduced a significant level of uncertainty to both service and financial planning, although there is also an opportunity to accelerate service redesign plans and build on the positives of the whole system approach to the pandemic.
Current and planned/proposed controls in relation to the strategic risks are contained within the Datix system. The assessment of adequacy of the current controls in respect of Strategic Risk 723 has been recorded as being ‘incomplete’ at the present time, meaning that ‘controls are appropriately designed but these are not consistently applied’. The assessment of adequacy of the current controls in respect of Strategic Risk 1033 have been recorded as being ‘adequate’ at the present time, meaning that ‘controls are in place/working effectively/consistently applied and adhered to, to mitigate the risk’.
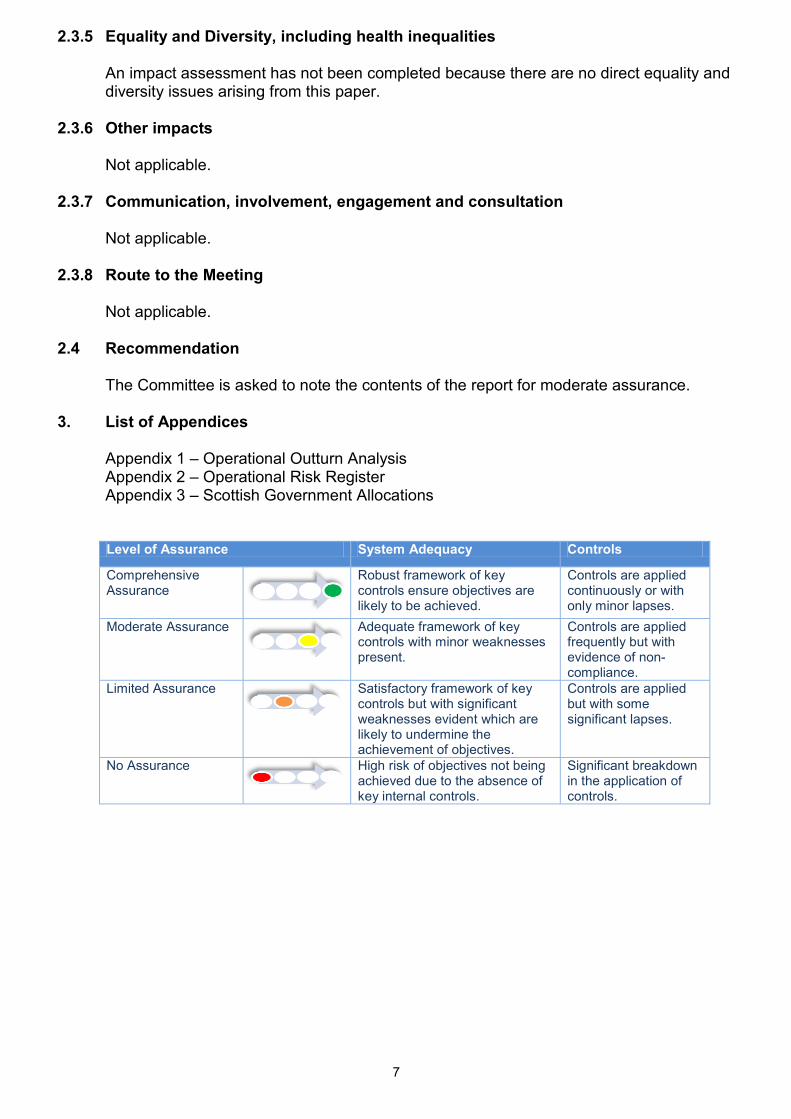
7
2.3.5 Equality and Diversity, including health inequalities An impact assessment has not been completed because there are no direct equality and
diversity issues arising from this paper. 2.3.6 Other impacts Not applicable. 2.3.7 Communication, involvement, engagement and consultation Not applicable. 2.3.8 Route to the Meeting Not applicable. 2.4 Recommendation The Committee is asked to note the contents of the report for moderate assurance. 3. List of Appendices Appendix 1 – Operational Outturn Analysis Appendix 2 – Operational Risk Register
Appendix 3 – Scottish Government Allocations
Level of Assurance System Adequacy Controls
Comprehensive Assurance
Robust framework of key controls ensure objectives are likely to be achieved.
Controls are applied continuously or with only minor lapses.
Moderate Assurance
Adequate framework of key controls with minor weaknesses present.
Controls are applied frequently but with evidence of non-compliance.
Limited Assurance
Satisfactory framework of key controls but with significant weaknesses evident which are likely to undermine the achievement of objectives.
Controls are applied but with some significant lapses.
No Assurance
High risk of objectives not being achieved due to the absence of key internal controls.
Significant breakdown in the application of controls.
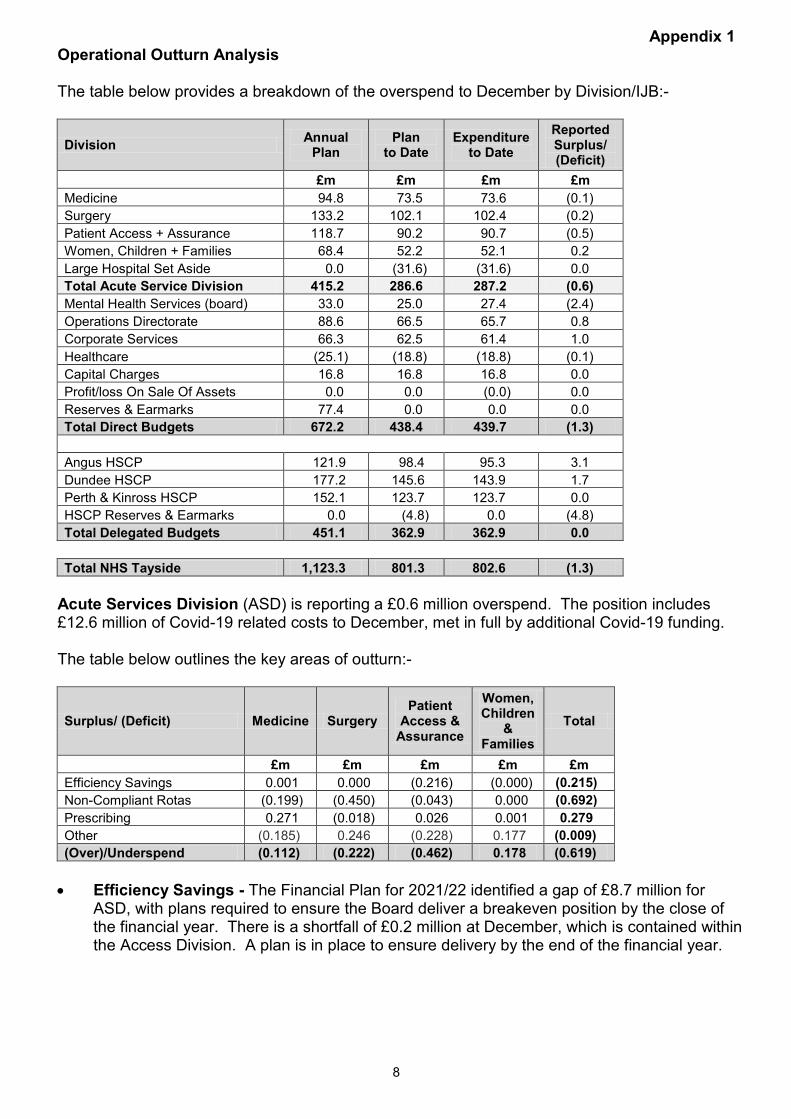
8
Appendix 1 Operational Outturn Analysis The table below provides a breakdown of the overspend to December by Division/IJB:-
Division Annual Plan
Plan to Date
Expenditure to Date
Reported Surplus/ (Deficit)
£m £m £m £m Medicine 94.8 73.5 73.6 (0.1) Surgery 133.2 102.1 102.4 (0.2) Patient Access + Assurance 118.7 90.2 90.7 (0.5) Women, Children + Families 68.4 52.2 52.1 0.2 Large Hospital Set Aside 0.0 (31.6) (31.6) 0.0 Total Acute Service Division 415.2 286.6 287.2 (0.6) Mental Health Services (board) 33.0 25.0 27.4 (2.4) Operations Directorate 88.6 66.5 65.7 0.8 Corporate Services 66.3 62.5 61.4 1.0 Healthcare (25.1) (18.8) (18.8) (0.1) Capital Charges 16.8 16.8 16.8 0.0 Profit/loss On Sale Of Assets 0.0 0.0 (0.0) 0.0 Reserves & Earmarks 77.4 0.0 0.0 0.0 Total Direct Budgets 672.2 438.4 439.7 (1.3) Angus HSCP 121.9 98.4 95.3 3.1 Dundee HSCP 177.2 145.6 143.9 1.7 Perth & Kinross HSCP 152.1 123.7 123.7 0.0 HSCP Reserves & Earmarks 0.0 (4.8) 0.0 (4.8) Total Delegated Budgets 451.1 362.9 362.9 0.0
Total NHS Tayside 1,123.3 801.3 802.6 (1.3) Acute Services Division (ASD) is reporting a £0.6 million overspend. The position includes £12.6 million of Covid-19 related costs to December, met in full by additional Covid-19 funding. The table below outlines the key areas of outturn:-
Surplus/ (Deficit) Medicine Surgery Patient
Access & Assurance
Women, Children
& Families
Total
£m £m £m £m £m Efficiency Savings 0.001 0.000 (0.216) (0.000) (0.215) Non-Compliant Rotas (0.199) (0.450) (0.043) 0.000 (0.692) Prescribing 0.271 (0.018) 0.026 0.001 0.279 Other (0.185) 0.246 (0.228) 0.177 (0.009) (Over)/Underspend (0.112) (0.222) (0.462) 0.178 (0.619)
• Efficiency Savings - The Financial Plan for 2021/22 identified a gap of £8.7 million for
ASD, with plans required to ensure the Board deliver a breakeven position by the close of the financial year. There is a shortfall of £0.2 million at December, which is contained within the Access Division. A plan is in place to ensure delivery by the end of the financial year.
9
• Non-Compliant Rotas - £0.7 million of unfunded costs as a result of non compliant rotas, mainly across the Surgical Division, which is the result of recent monitoring. Actionable steps are being taken to review and remedy to avoid a significant cost pressure moving into 2022/23. Whilst monitoring was paused for the second time recently with the emergence of the Omicron wave, notification has been received from the central office around recommencement once again. This will allow Acute Services to address all non-compliance from previous monitoring.
• Other – Across the Division cost pressures continue with high cost locums in the Breast Service to ensure cancer services can be maintained. There is a national shortage of breast consultants across the country and recruitment has been challenging. The service continues to review options for a sustainable service model which removes the premium cost of off-contract agency locums as the Board move into 2022/23.
Within PRI, the opening of additional beds to increase capacity has put pressure on Nursing budgets. This is multi-factorial and linked to higher admissions, longer length of stay for frail and older patients as well as increases within delayed discharges as a consequence of the workforce shortages being experienced in social care. These two main pressures continue to be offset in the main by benefits in relation to Hepatitis C medication, and other operational workforce underspends across the Division.
Board Mental Health Services include both In-patient Mental Health Services, £2.9 million overspent, and other Mental Health Services, £0.5 million underspent (Forensic Services, junior doctors). In-patient Mental Health budgets transferred from a hosting arrangement with Perth & Kinross HSCP, following operational responsibility being aligned to the Board in June 2020. The service transferred with significant financial pressures, which were previously offset by operational underspends on Community Mental Health budgets within the three IJBs. The split between IJBs and Board has de-stabilised the financial model underpinning Mental Health Services, with the Board picking up a significant overspend on in-patient services, forecast at £3.5 million for 2021/22 (the other side being a financial benefit to IJBs of the same amount).
• In-patient Mental Health Medical Pay is £1.4 million overspent. Expenditure to December
2021 on medical locums is £3.3 million, which is offset in part by a number of wte consultant vacancies; £1.9 million.
• In-patient Mental Health Nursing pay is £1.0 million overspent. Supplementary costs have increased this financial year due to increased activity, a number of delayed discharges and high sickness absence rates (8.46% as at December).
• Historical unidentified savings continues to have a bearing on the financial performance of In-patient Mental Health.
Operations Directorate is reporting a £0.8 million underspend. The main driver of the underspend is a high level of vacancies across both soft facilities management and estates with challenges with both recruitment and retaining of staff in both areas. Work is ongoing to progress the Estates review, which will significantly increase the number of staff in post and reduce the requirement for external contractors. The operational non-recurring pay underspend position is partially offset by pressures with shortfalls in catering income, waste contingency measures as well as a return to pre Covid-19 levels for fees relating to the Central Legal Office. Corporate Services are collectively £1.0 million underspent. There are pressures within the Digital Directorate and Corporate Affairs, offset by services with underspends due to vacancies, e.g. Pharmacy and Medical Records.
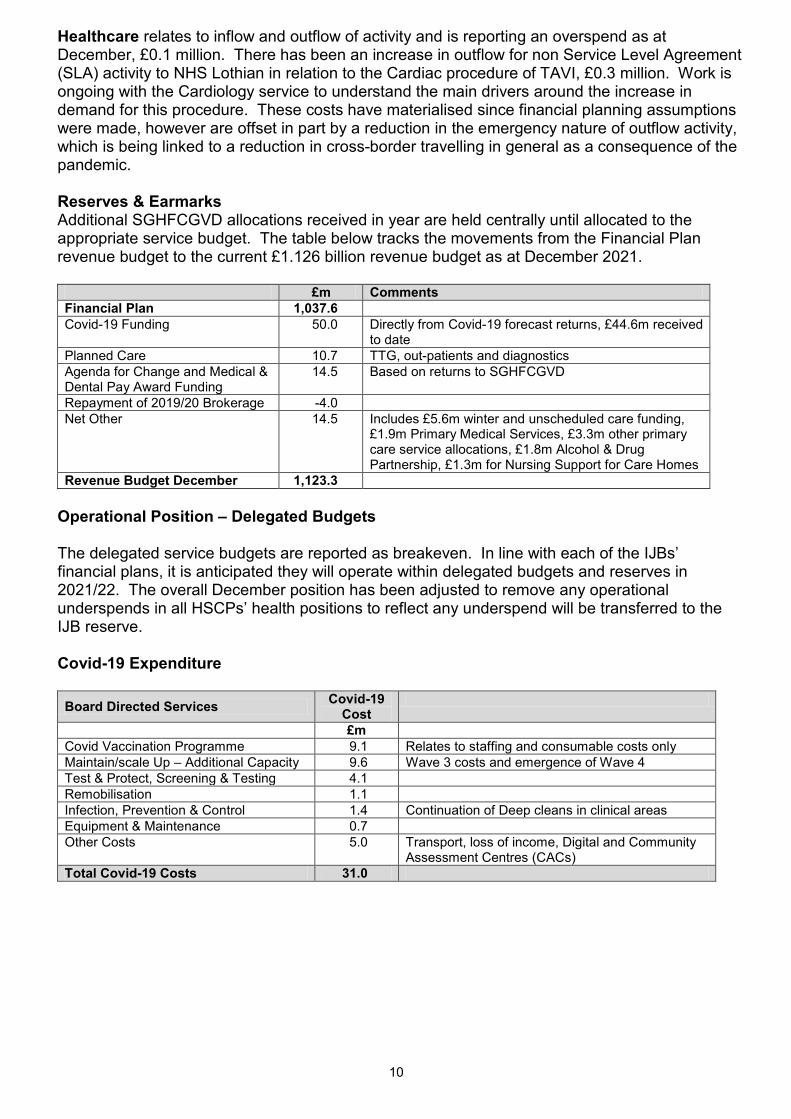
10
Healthcare relates to inflow and outflow of activity and is reporting an overspend as at December, £0.1 million. There has been an increase in outflow for non Service Level Agreement (SLA) activity to NHS Lothian in relation to the Cardiac procedure of TAVI, £0.3 million. Work is ongoing with the Cardiology service to understand the main drivers around the increase in demand for this procedure. These costs have materialised since financial planning assumptions were made, however are offset in part by a reduction in the emergency nature of outflow activity, which is being linked to a reduction in cross-border travelling in general as a consequence of the pandemic. Reserves & Earmarks
Additional SGHFCGVD allocations received in year are held centrally until allocated to the appropriate service budget. The table below tracks the movements from the Financial Plan revenue budget to the current £1.126 billion revenue budget as at December 2021. £m Comments Financial Plan 1,037.6 Covid-19 Funding 50.0 Directly from Covid-19 forecast returns, £44.6m received
to date Planned Care 10.7 TTG, out-patients and diagnostics Agenda for Change and Medical & Dental Pay Award Funding
14.5 Based on returns to SGHFCGVD
Repayment of 2019/20 Brokerage -4.0 Net Other 14.5 Includes £5.6m winter and unscheduled care funding,
£1.9m Primary Medical Services, £3.3m other primary care service allocations, £1.8m Alcohol & Drug Partnership, £1.3m for Nursing Support for Care Homes
Revenue Budget December 1,123.3 Operational Position – Delegated Budgets The delegated service budgets are reported as breakeven. In line with each of the IJBs’ financial plans, it is anticipated they will operate within delegated budgets and reserves in 2021/22. The overall December position has been adjusted to remove any operational underspends in all HSCPs’ health positions to reflect any underspend will be transferred to the IJB reserve. Covid-19 Expenditure Board Directed Services Covid-19
Cost
£m Covid Vaccination Programme 9.1 Relates to staffing and consumable costs only Maintain/scale Up – Additional Capacity 9.6 Wave 3 costs and emergence of Wave 4 Test & Protect, Screening & Testing 4.1 Remobilisation 1.1 Infection, Prevention & Control 1.4 Continuation of Deep cleans in clinical areas Equipment & Maintenance 0.7 Other Costs 5.0 Transport, loss of income, Digital and Community
Assessment Centres (CACs) Total Covid-19 Costs 31.0
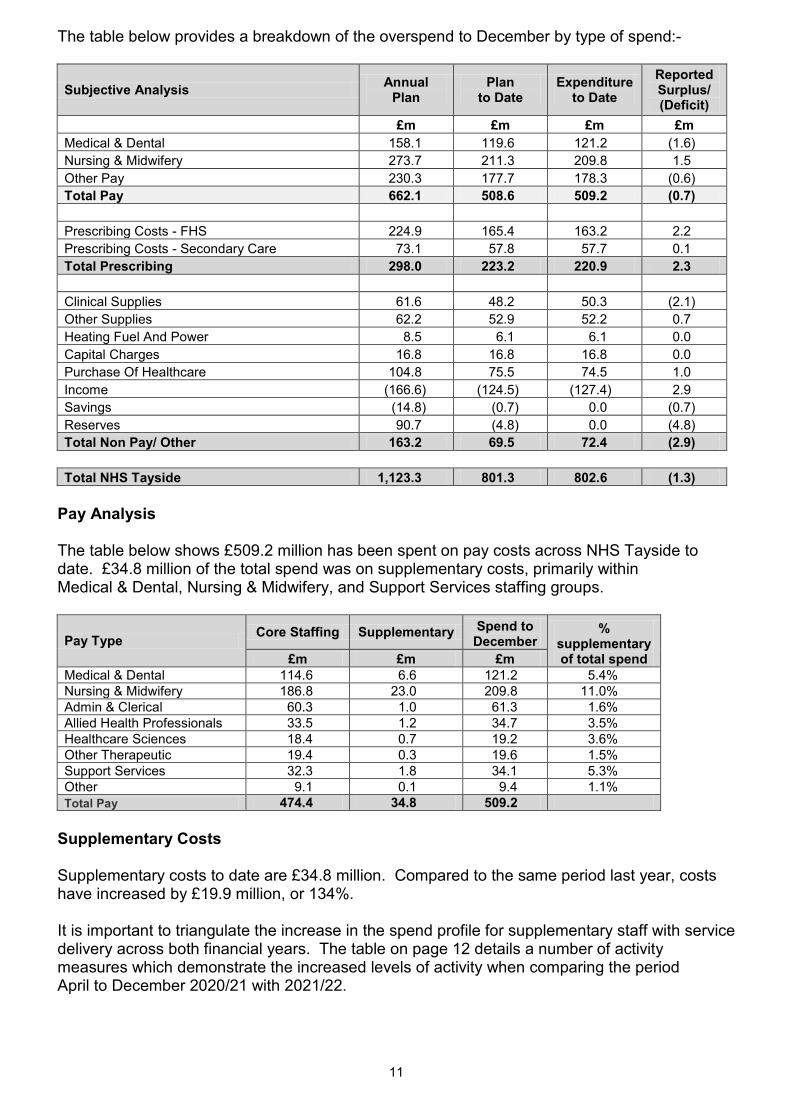
11
The table below provides a breakdown of the overspend to December by type of spend:-
Subjective Analysis Annual Plan
Plan to Date
Expenditure to Date
Reported Surplus/ (Deficit)
£m £m £m £m Medical & Dental 158.1 119.6 121.2 (1.6) Nursing & Midwifery 273.7 211.3 209.8 1.5 Other Pay 230.3 177.7 178.3 (0.6) Total Pay 662.1 508.6 509.2 (0.7) Prescribing Costs - FHS 224.9 165.4 163.2 2.2 Prescribing Costs - Secondary Care 73.1 57.8 57.7 0.1 Total Prescribing 298.0 223.2 220.9 2.3 Clinical Supplies 61.6 48.2 50.3 (2.1) Other Supplies 62.2 52.9 52.2 0.7 Heating Fuel And Power 8.5 6.1 6.1 0.0 Capital Charges 16.8 16.8 16.8 0.0 Purchase Of Healthcare 104.8 75.5 74.5 1.0 Income (166.6) (124.5) (127.4) 2.9 Savings (14.8) (0.7) 0.0 (0.7) Reserves 90.7 (4.8) 0.0 (4.8) Total Non Pay/ Other 163.2 69.5 72.4 (2.9)
Total NHS Tayside 1,123.3 801.3 802.6 (1.3) Pay Analysis The table below shows £509.2 million has been spent on pay costs across NHS Tayside to date. £34.8 million of the total spend was on supplementary costs, primarily within Medical & Dental, Nursing & Midwifery, and Support Services staffing groups.
Pay Type Core Staffing Supplementary Spend to December
% supplementary of total spend £m £m £m
Medical & Dental 114.6 6.6 121.2 5.4% Nursing & Midwifery 186.8 23.0 209.8 11.0% Admin & Clerical 60.3 1.0 61.3 1.6% Allied Health Professionals 33.5 1.2 34.7 3.5% Healthcare Sciences 18.4 0.7 19.2 3.6% Other Therapeutic 19.4 0.3 19.6 1.5% Support Services 32.3 1.8 34.1 5.3% Other 9.1 0.1 9.4 1.1% Total Pay 474.4 34.8 509.2
Supplementary Costs Supplementary costs to date are £34.8 million. Compared to the same period last year, costs have increased by £19.9 million, or 134%. It is important to triangulate the increase in the spend profile for supplementary staff with service delivery across both financial years. The table on page 12 details a number of activity measures which demonstrate the increased levels of activity when comparing the period April to December 2020/21 with 2021/22.
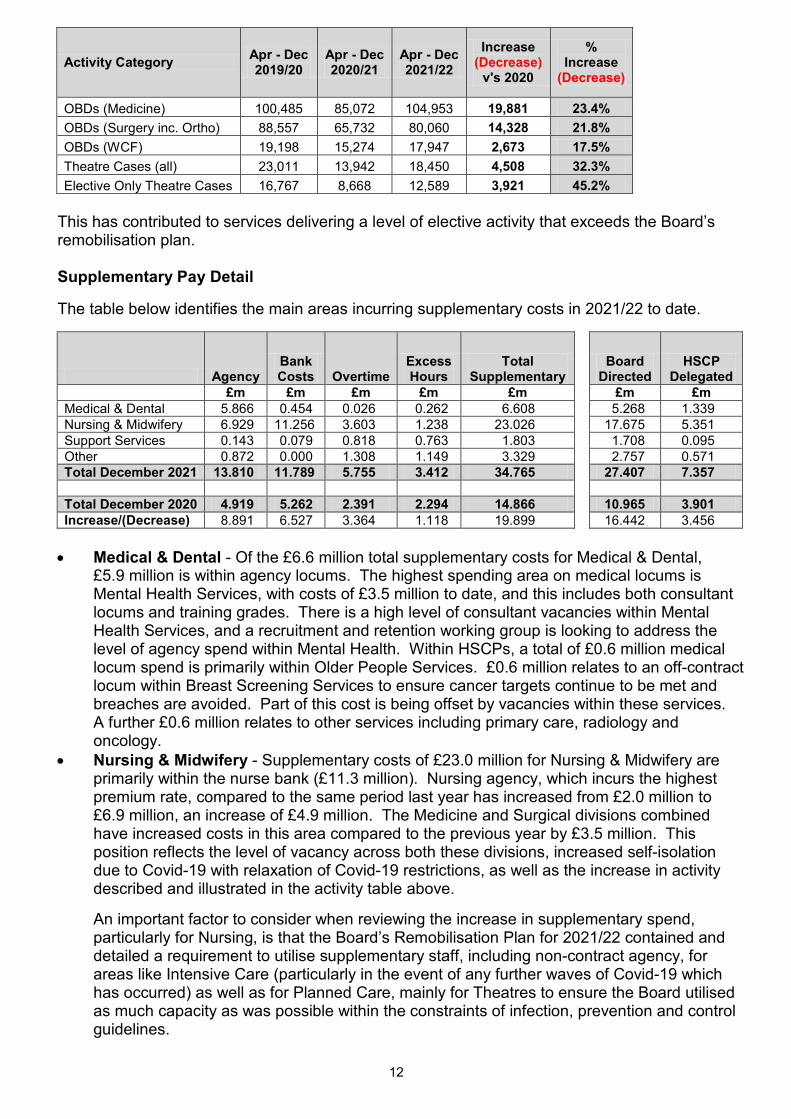
12
Activity Category Apr - Dec 2019/20
Apr - Dec 2020/21
Apr - Dec 2021/22
Increase (Decrease)
v's 2020
% Increase
(Decrease)
OBDs (Medicine) 100,485 85,072 104,953 19,881 23.4% OBDs (Surgery inc. Ortho) 88,557 65,732 80,060 14,328 21.8% OBDs (WCF) 19,198 15,274 17,947 2,673 17.5% Theatre Cases (all) 23,011 13,942 18,450 4,508 32.3% Elective Only Theatre Cases 16,767 8,668 12,589 3,921 45.2%
This has contributed to services delivering a level of elective activity that exceeds the Board’s remobilisation plan. Supplementary Pay Detail The table below identifies the main areas incurring supplementary costs in 2021/22 to date.
Agency Bank Costs Overtime
Excess Hours
Total Supplementary
Board Directed
HSCP Delegated
£m £m £m £m £m
£m £m Medical & Dental 5.866 0.454 0.026 0.262 6.608
5.268 1.339
Nursing & Midwifery 6.929 11.256 3.603 1.238 23.026
17.675 5.351 Support Services 0.143 0.079 0.818 0.763 1.803
1.708 0.095
Other 0.872 0.000 1.308 1.149 3.329
2.757 0.571 Total December 2021 13.810 11.789 5.755 3.412 34.765
27.407 7.357
Total December 2020 4.919 5.262 2.391 2.294 14.866
10.965 3.901
Increase/(Decrease) 8.891 6.527 3.364 1.118 19.899
16.442 3.456 • Medical & Dental - Of the £6.6 million total supplementary costs for Medical & Dental,
£5.9 million is within agency locums. The highest spending area on medical locums is Mental Health Services, with costs of £3.5 million to date, and this includes both consultant locums and training grades. There is a high level of consultant vacancies within Mental Health Services, and a recruitment and retention working group is looking to address the level of agency spend within Mental Health. Within HSCPs, a total of £0.6 million medical locum spend is primarily within Older People Services. £0.6 million relates to an off-contract locum within Breast Screening Services to ensure cancer targets continue to be met and breaches are avoided. Part of this cost is being offset by vacancies within these services. A further £0.6 million relates to other services including primary care, radiology and oncology.
• Nursing & Midwifery - Supplementary costs of £23.0 million for Nursing & Midwifery are primarily within the nurse bank (£11.3 million). Nursing agency, which incurs the highest premium rate, compared to the same period last year has increased from £2.0 million to £6.9 million, an increase of £4.9 million. The Medicine and Surgical divisions combined have increased costs in this area compared to the previous year by £3.5 million. This position reflects the level of vacancy across both these divisions, increased self-isolation due to Covid-19 with relaxation of Covid-19 restrictions, as well as the increase in activity described and illustrated in the activity table above.
An important factor to consider when reviewing the increase in supplementary spend,
particularly for Nursing, is that the Board’s Remobilisation Plan for 2021/22 contained and detailed a requirement to utilise supplementary staff, including non-contract agency, for areas like Intensive Care (particularly in the event of any further waves of Covid-19 which has occurred) as well as for Planned Care, mainly for Theatres to ensure the Board utilised as much capacity as was possible within the constraints of infection, prevention and control guidelines.
13
In-patient Mental Health Services have incurred £4.2 million of nursing supplementary costs to date, primarily nurse bank costs, and largely related to a high number of vacancies. Public Health are the next highest users of nursing supplementary with costs of £2.0 million in relation to Covid-19 Vaccination and Test and Protect, followed by Dundee HSCP (£2.0 million), primarily in Older People Services.
• Support Services - The use of supplementary staffing for support services is £1.8 million for 2021/22. The Operations Directorate incurs the majority of the supplementary spend associated with Support Services. The costs relate to supporting extended rotas in relation to enhanced cleaning within clinical and non clinical areas, as well as additional drivers to ensure PPE stock levels are maintained across all healthcare facilities within Tayside, including care homes and GP practices. A further increase in February 2021 in this area relates to the rollout of Lateral Flow Testing across NHS Tayside sites and the increased transport costs associated with delivery of these kits.
Prescribing • FHS Prescribing
FHS prescribing outturn to December 2021 is a cumulative underspend of £1.8 million to date, and a forecast underspend of £2.5 million for the year. This is based on actual prescribing data for April to October, and estimates for November and December. Actual prescribing volumes to October are higher compared to previous year, but slightly lower than 2021/22 Financial Plan. Average pricing per prescription to October remains close to financial planning expectations. The position with GP practice prescribing patterns was fluid and dynamic throughout 2020/21, given the impact of Covid-19. 2021/22 information available for April to September has shown less volatility than previous months, although prescribing volumes were lower in October, and this situation continues to be monitored. There is a further improvement in the reported position due to actual rebate information received showing higher rebates than in previous months.
The table below outlines the FHS prescribing position against each of the three HSCPs:-
Annual
Plan Plan
to Date Expenditure
to Date Surplus/ (Deficit)
£m £m £m £m FHS - Angus IJB 22.095 16.525 16.293 0.232 FHS - Dundee IJB 33.051 24.741 23.511 1.229 FHS - Perth & Kinross IJB 27.444 20.501 20.149 0.352 Total 82.590 61.767 59.954 1.813
• Secondary Care Prescribing
Expenditure for the nine months to 31 December, 2021, is £57.7 million on secondary care medicines, with a £0.09 million underspend position reported. Spend has increased by £7.2 million (14%) compared with the same period in 2020/21. Given the increase in urgent and unscheduled activity as well as the increase within cancer and elective services, the Board would anticipate a level of increase when compared to previous year. Growth is in line with projections on both activity and new medicines and the projected outturn for the year is breakeven. The chart on page 14 outlines the monthly spend on secondary care medicines, comparable to last financial year:-
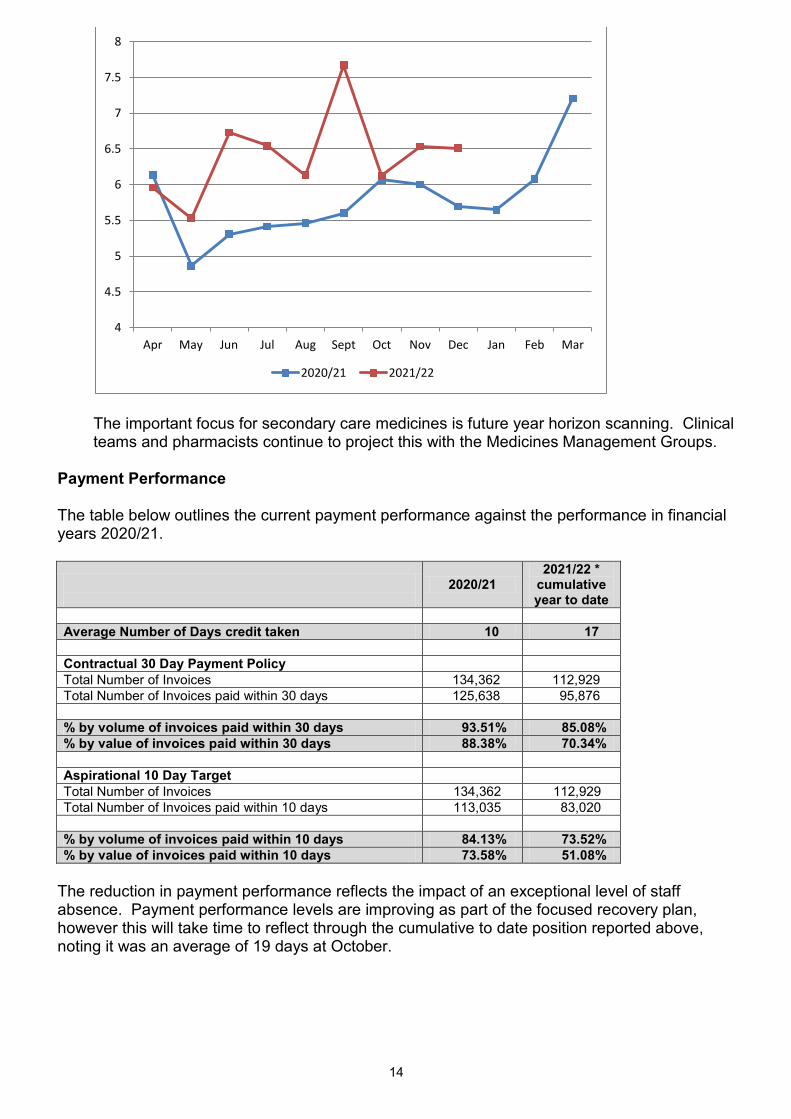
14
The important focus for secondary care medicines is future year horizon scanning. Clinical teams and pharmacists continue to project this with the Medicines Management Groups.
Payment Performance The table below outlines the current payment performance against the performance in financial years 2020/21.
2020/21 2021/22 *
cumulative year to date
Average Number of Days credit taken 10 17
Contractual 30 Day Payment Policy Total Number of Invoices 134,362 112,929
Total Number of Invoices paid within 30 days 125,638 95,876
% by volume of invoices paid within 30 days 93.51% 85.08% % by value of invoices paid within 30 days 88.38% 70.34%
Aspirational 10 Day Target Total Number of Invoices 134,362 112,929
Total Number of Invoices paid within 10 days 113,035 83,020
% by volume of invoices paid within 10 days 84.13% 73.52% % by value of invoices paid within 10 days 73.58% 51.08%
The reduction in payment performance reflects the impact of an exceptional level of staff absence. Payment performance levels are improving as part of the focused recovery plan, however this will take time to reflect through the cumulative to date position reported above, noting it was an average of 19 days at October.
4
4.5
5
5.5
6
6.5
7
7.5
8
Apr May Jun Jul Aug Sept Oct Nov Dec Jan Feb Mar
2020/21 2021/22
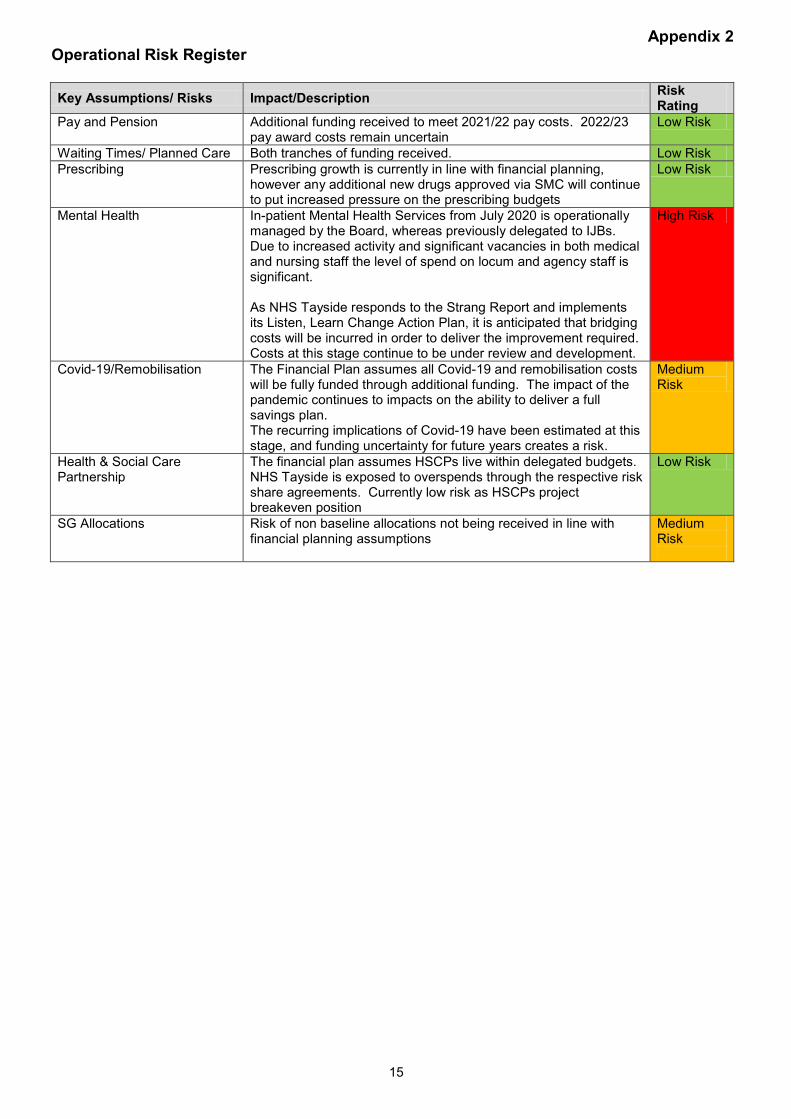
15
Appendix 2 Operational Risk Register Key Assumptions/ Risks Impact/Description Risk
Rating Pay and Pension Additional funding received to meet 2021/22 pay costs. 2022/23
pay award costs remain uncertain Low Risk
Waiting Times/ Planned Care Both tranches of funding received. Low Risk Prescribing Prescribing growth is currently in line with financial planning,
however any additional new drugs approved via SMC will continue to put increased pressure on the prescribing budgets
Low Risk
Mental Health In-patient Mental Health Services from July 2020 is operationally managed by the Board, whereas previously delegated to IJBs. Due to increased activity and significant vacancies in both medical and nursing staff the level of spend on locum and agency staff is significant. As NHS Tayside responds to the Strang Report and implements its Listen, Learn Change Action Plan, it is anticipated that bridging costs will be incurred in order to deliver the improvement required. Costs at this stage continue to be under review and development.
High Risk
Covid-19/Remobilisation The Financial Plan assumes all Covid-19 and remobilisation costs will be fully funded through additional funding. The impact of the pandemic continues to impacts on the ability to deliver a full savings plan. The recurring implications of Covid-19 have been estimated at this stage, and funding uncertainty for future years creates a risk.
Medium Risk
Health & Social Care Partnership
The financial plan assumes HSCPs live within delegated budgets. NHS Tayside is exposed to overspends through the respective risk share agreements. Currently low risk as HSCPs project breakeven position
Low Risk
SG Allocations Risk of non baseline allocations not being received in line with financial planning assumptions
Medium Risk
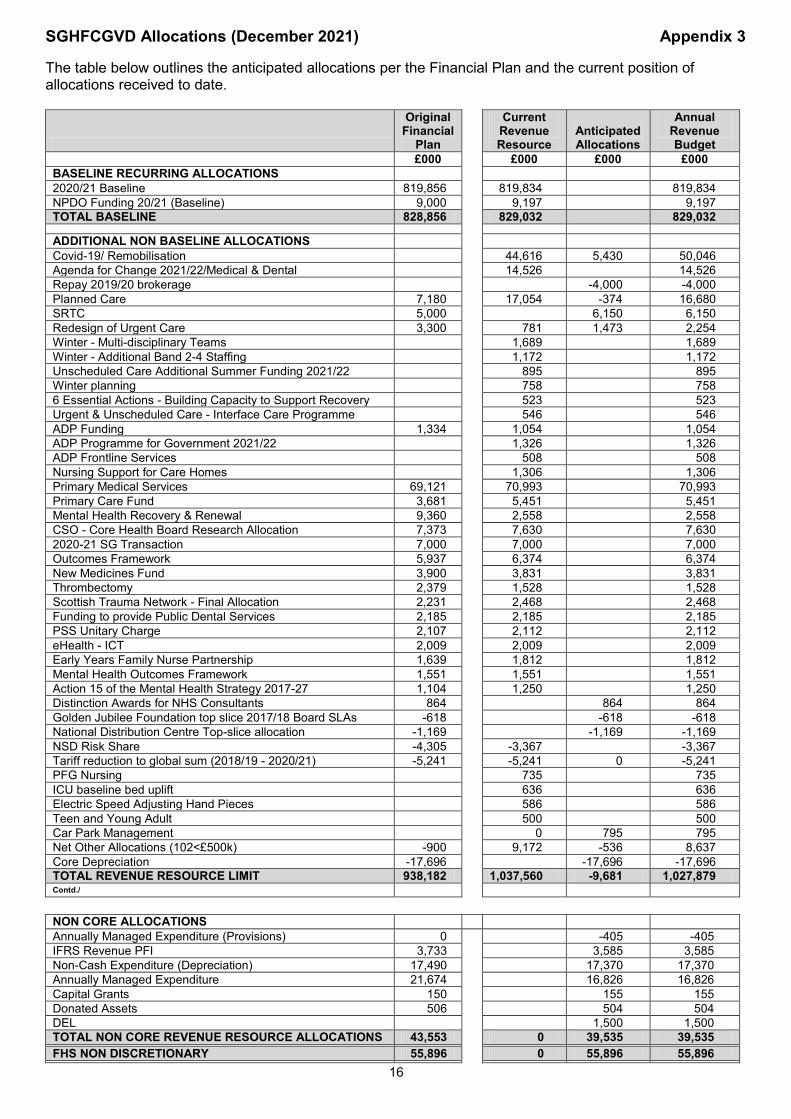
16
SGHFCGVD Allocations (December 2021) Appendix 3 The table below outlines the anticipated allocations per the Financial Plan and the current position of allocations received to date.
Original Financial
Plan
Current Revenue Resource
Anticipated Allocations
Annual Revenue Budget
£000 £000 £000 £000 BASELINE RECURRING ALLOCATIONS 2020/21 Baseline 819,856 819,834 819,834 NPDO Funding 20/21 (Baseline) 9,000 9,197 9,197 TOTAL BASELINE 828,856 829,032 829,032 ADDITIONAL NON BASELINE ALLOCATIONS Covid-19/ Remobilisation 44,616 5,430 50,046 Agenda for Change 2021/22/Medical & Dental 14,526 14,526 Repay 2019/20 brokerage -4,000 -4,000 Planned Care 7,180 17,054 -374 16,680 SRTC 5,000 6,150 6,150 Redesign of Urgent Care 3,300 781 1,473 2,254 Winter - Multi-disciplinary Teams 1,689 1,689 Winter - Additional Band 2-4 Staffing 1,172 1,172 Unscheduled Care Additional Summer Funding 2021/22 895 895 Winter planning 758 758 6 Essential Actions - Building Capacity to Support Recovery 523 523 Urgent & Unscheduled Care - Interface Care Programme 546 546 ADP Funding 1,334 1,054 1,054 ADP Programme for Government 2021/22 1,326 1,326 ADP Frontline Services 508 508 Nursing Support for Care Homes 1,306 1,306 Primary Medical Services 69,121 70,993 70,993 Primary Care Fund 3,681 5,451 5,451 Mental Health Recovery & Renewal 9,360 2,558 2,558 CSO - Core Health Board Research Allocation 7,373 7,630 7,630 2020-21 SG Transaction 7,000 7,000 7,000 Outcomes Framework 5,937 6,374 6,374 New Medicines Fund 3,900 3,831 3,831 Thrombectomy 2,379 1,528 1,528 Scottish Trauma Network - Final Allocation 2,231 2,468 2,468 Funding to provide Public Dental Services 2,185 2,185 2,185 PSS Unitary Charge 2,107 2,112 2,112 eHealth - ICT 2,009 2,009 2,009 Early Years Family Nurse Partnership 1,639 1,812 1,812 Mental Health Outcomes Framework 1,551 1,551 1,551 Action 15 of the Mental Health Strategy 2017-27 1,104 1,250 1,250 Distinction Awards for NHS Consultants 864 864 864 Golden Jubilee Foundation top slice 2017/18 Board SLAs -618 -618 -618 National Distribution Centre Top-slice allocation -1,169 -1,169 -1,169 NSD Risk Share -4,305 -3,367 -3,367 Tariff reduction to global sum (2018/19 - 2020/21) -5,241 -5,241 0 -5,241 PFG Nursing 735 735 ICU baseline bed uplift 636 636 Electric Speed Adjusting Hand Pieces 586 586 Teen and Young Adult 500 500 Car Park Management 0 795 795 Net Other Allocations (102<£500k) -900 9,172 -536 8,637 Core Depreciation -17,696 -17,696 -17,696 TOTAL REVENUE RESOURCE LIMIT 938,182 1,037,560 -9,681 1,027,879 Contd./
NON CORE ALLOCATIONS Annually Managed Expenditure (Provisions) 0 -405 -405 IFRS Revenue PFI 3,733 3,585 3,585 Non-Cash Expenditure (Depreciation) 17,490 17,370 17,370 Annually Managed Expenditure 21,674 16,826 16,826 Capital Grants 150 155 155 Donated Assets 506 504 504 DEL 1,500 1,500 TOTAL NON CORE REVENUE RESOURCE ALLOCATIONS 43,553 0 39,535 39,535 FHS NON DISCRETIONARY 55,896 0 55,896 55,896

17
TOTAL OPERATING COSTS 1,037,631 1,037,560 86,124 1,123,310
Page 1 of 21
Item Number 6.2 PRC02/2022
Performance and Resources Committee 10 February 2022 CAPITAL FINANCIAL REPORT AND PROGRAMME UPDATE FOR THE PERIOD ENDED 31 DECEMBER, 2021 Responsible Officer: Stuart Lyall, Director of Finance Report Authors: Louise Lyall, Head of Finance - Capital and Resources Wilma Mason, Senior Capital Accountant 1. Purpose
This is presented to the Performance and Resources Committee for:- • Assurance This report relates to the:- • Annual Operation Plan (AOP) This aligns to the following NHS Scotland quality ambitions:- • Effective
2. Report summary 2.1 Situation The purpose of this report is to advise the Committee on the following:-
i. NHS Tayside’s financial performance against the Five Year Capital Plan 2021/22 to 2025/26 for the nine months to 31 December, 2021, and forecast outturn;
ii. the impact of the Covid-19 pandemic on the capital position to date and forecast outturn;
iii. implications of budget movements in the 2021/22 Capital Plan on future years; iv. the risks to delivery of NHS Tayside’s Capital Plan 2021/22 and provide a level of
assurance around the management of risk; v. emerging issues and impact on future years, and vi. the programme of works being progressed by the Asset Management Group
(AMG). Scottish Government Health Finance, Corporate Governance and Value Directorate
(SGHFCGVD) set three financial targets at Health Board level each year - Revenue Resource Limit (RRL), Capital Resource Limit (CRL) and Cash Requirement. Health Boards are required to contain their net expenditure within these limits.
This paper monitors progress against the CRL, which is a resource budget for net
capital investment. As at 31 December, 2021, the 2021/22 core CRL is £18.717 million, with further allocations anticipated.
Page 2 of 21
A moderate level of assurance has been reported, on the basis that planned expenditure continues to be impacted by delays in major capital projects under construction and the availability of staff resource to support further initiatives.
2.2 Background
The Five Year Capital Plan sets out Tayside NHS Board’s priorities for managing the infrastructure that will support the delivery of patient care and associated services across NHS Tayside. The Plan is focused on actions across four main areas:- • investment in infrastructure consistent with NHS Tayside’s strategic health
priorities; • reduction in high and significant risk backlog maintenance and compliance
with statutory requirements; • replacement of essential equipment, and • disposal of assets declared surplus to requirements.
In terms of allocation of resources, the Plan recognises the complexity of decisions and choices regarding the prioritisation of available funding, and the requirement to keep this under review on at least an annual basis.
By taking a balanced approach the Five Year Plan will ensure that NHS Tayside is able to:-
• improve estate and asset performance on all key indicators, including a targeted
reduction in significant and high risk backlog maintenance, and a continued programme of essential equipment replacement, and
• disinvest from buildings with high operating costs, backlog maintenance requirements, or short remaining life where these do not meet future service requirements.
2.3 Assessment
The total capital programme forecast outturn at 31 December, 2021 is £32.649 million, with a breakeven position forecast. The Five Year Capital Plan is attached at Appendix 1, reflecting the December 2021 position in the Quarter 3 Financial Performance Return (FPR) submitted to SGHFCGVD on 31 January, 2022. A detailed financial assessment is shown in section 2.3.3. The Capital Plan has a number of funding sources including core formula allocation, project specific funding, net book value (NBV) on disposal of assets retained to support the Capital Plan, donated funding, capital grants and revenue to capital transfer to support the non added value (NAV) elements of the Capital Plan. The Plan includes project specific capital funding in addition to the core formula allocation to support key infrastructure projects, including Neonatal Intensive Care Unit (NICU), Multi-storey Plant Room (MSPR), Ninewells Electrical Infrastructure (NEI), National Treatment Centre - Tayside (NTC-T), Cancer Centre (CC), Shaping Critical Care (SCC), Endoscopy Decontamination Replacement (EDR) and Tayside Thrombectomy Imaging Facilities (TTIF).
Page 3 of 21
It should be noted that the phasing and indicative costs in future years for the NEI projects has been updated in the plan following a review carried out by NHS Tayside’s external cost advisors. Indicative costs and timings were originally based on the NEI Outline Business Case (OBC), however due to the time lapse since approval of the OBC in 2018, and also the knowledge gained during the construction of NEI Zones 1 and 2, more realistic costs and phasing of the projects have been developed. Major Projects Update:
The current status of major projects within the capital programme is as follows:- • Children’s Theatre Suite (CTS) - currently in construction with planned
completion in February 2022. An overspend of circa £1.276 million is forecast, which equates to 13.2% over the approved Full Business Case (FBC) budget of £9.671 million. As CTS is funded through NHS Tayside’s core formula allocation, any overspend will impact on NHS Tayside’s forecast position. The forecast excludes costs associated with flood remedial works, as a separate funding stream for the loss incurred has been identified. The forecast also excludes Covid-19 costs associated with the project, which are funded through the Covid-19 capital allocation received from SGHFCGVD in 2020/21 and the confirmed funding for 2021/22.
• NICU - the project is now complete and the final account received which includes a gain share for NHS Tayside of £0.159 million. An underspend of circa £0.015 million is forecast, which equates to 0.2% under the approved FBC budget of £7.204 million. The forecast includes estimated costs for minor works outwith the main contract plus re-charges due in respect of shared costs with the CTS project. The financial status of the project will continue to be reported until these costs are confirmed and the final financial position is known. This forecast excludes Covid-19 costs associated with the project, which have been funded through the Covid-19 capital allocation received from SGHFCGVD in 2020/21.
• MSPR - construction is now complete and awaiting Final Account. The project is forecasting an underspend of circa £0.159 million, which equates to 8.7% under the approved FBC budget of £1.841 million. As MSPR is funded by SGHFCGVD, any underspend will not impact on NHS Tayside’s forecast position. Cost advisors are currently forecasting a gain share of circa £0. 271 million for NHS Tayside on the combined MSPR and CTS projects (single contract). Should this materialise, any benefit to this project would not be realised until the CTS project is complete and the financial status of the project will continue to be reported until this time. This forecast excludes Covid-19 costs associated with the project, which have been funded through the Covid-19 capital allocation received from SGHFCGVD in 2020/21.
• NEI Zone 2 - currently in construction. The project is currently reporting a 13 week delay with a planned construction completion now in Quarter 2 of 2022/23. The approved FBC budget is £7.922 million, however the Lead Advisor has advised the project team of potential additional expenditure requirements which have been accepted by the Project Board and AMG. The project is, therefore, currently projecting an overspend of circa £0.950 million, which equates to 11.99% of the approved FBC budget. Additional funding has been sought from SGHFCGVD. A detailed report on the overspend will be submitted to a future meeting of the Performance and Resources Committee.
• NEI Zone 3 - early preparatory work has commenced to inform development of the FBC, which is now expected to be completed in 2022/23.
Page 4 of 21
• TTIF – The OBC is now complete and was considered at AMG in November, 2021 and Tayside NHS Board in December, 2021. Submission to SGHFCGVD Capital Investment Group (CIG) is planned for mid-year 2022, following completion of the National Services Scotland (NSS) Assure process and approval of the National Initial Agreement (IA).
• NTC-T - The OBC has been completed but is currently caveated with the requirement that it will need to be updated to reflect the impact of the new Scottish Government policy re Sustainability/Net Zero Carbon on the proposed design once this is fully quantified. The project plan will need to be updated to reflect the impact this will have on timelines.
• CC - The IA is now complete and is progressing through NHS Tayside’s internal governance approvals process prior to being submitted to CIG. It was considered by AMG in January 2022 and Executive Leadership Team (ELT) on 24 January, 2022, and is expected to be presented to Tayside NHS Board for approval in due course. The impact of new policy including “Sustainable Design and Construction (SDaC) Guide (SHTN 02-01)”, published October 2021 by Health Facilities Scotland (HFS) and DL (2021) 38 - “A Policy for NHS Scotland on the Climate Emergency and Sustainable Development”, published November 2021 and the fit with the wider infrastructure and development plan for Ninewells Hospital requires further consideration.
• SCC - The IA is now complete and is progressing through NHS Tayside’s internal governance approvals process prior to being submitted to CIG. It has been considered by the Project Board and AMG in July 2021, and ELT on 24 January, 2022, and is expected to be presented to Tayside NHS Board for approval in due course. The impact of new policy including “Sustainable Design and Construction (SDaC) Guide (SHTN 02-01)”, published October 2021 by HFS and DL (2021) 38 - “A Policy for NHS Scotland on the Climate Emergency and Sustainable Development”, published November 2021 and the fit with the wider infrastructure and development plan for Ninewells Hospital requires further consideration.
• EDR - The IA is now complete and was considered at AMG in November 2021 and Tayside NHS Board in December 2021, and has now been submitted to CIG for consideration.
Major projects currently in construction were procured under a Frameworks New Engineering Contract (NEC3) Option C, which is a Target Cost contract, with activity schedule where the outturn financial risks are shared between the client and the contractor in an agreed proportion. The aim of the contract is to motivate the contractor to deliver the works in the most cost efficient way. NHS Tayside’s NEC3 cost advisors are currently forecasting a gain share for NHS Tayside on completion of CTS/MSPR and NEI Zone 1 projects (NICU gain share is confirmed), which could result in a reduction in total project cost at final account stage.
Decisions Update The meeting of AMG held on 13 December, 2021, was a single item agenda to consider the prioritisation of funding for NHS Tayside Five Year Infrastructure Investment Plan 2022/23 to 2026/27, ahead of submission to Performance and Resources Committee and Tayside NHS Board for final approval. At the most recent AMG meeting held on 20 January, 2022, four items for decision were considered as noted on page 5.
Page 5 of 21
1. AMG02/2022 CC IA - Members approved the CC IA to continue with the required governance process of presenting the IA to ELT on Monday 24 January, 2022.
2. AMG03/2022 , Post Occupancy Evaluation and Post Project Evaluation Updates -Members were asked to approve placing mandatory post project evaluation and project monitoring activities on hold to focus on legally committed projects due to capacity constraints within the Property Department. The Senior Project Manager has been asked to seek a view from the chair of CIG and National Infrastructure Board (NIB) before reaching a decision.
3. AMG04/2022 Draft Five Year Capital Plan 2022/23 to 2026/27 - Members agreed to approve the submission of the draft Five Year Capital Plan 2022/23 to 2026/27 to ELT and PRC.
4. Verbal Update Primary Care Premises Strategy Update - Members noted the Primary Care Premises Strategy verbal update, and noted a further written update would be provided in due course following discussions with the Interim Medical Director, Primary Care Services.
At the Senior Capital Review Group (SCRG) meetings held on 1 December, 2021, and 10 January, 2021, no items for decision were considered. One item for decision in respect of Additional Cost of Teaching (ACT) funding bids of £74,902 was considered and approved electronically by SCRG Members on 18 January, 2022. Two items for decision in respect of a new plotter at £9,600 and upgrade to wet rooms at Stracathro Hospital at £29,070 were considered and approved electronically by the Director of Finance and Chief Officer - Acute Services on 13 January, 2022, and 24 January, 2022, respectively. The delegated authority control sheet can be found at Appendix 2.
In addition to the above, AMG noted reports on the following:-
Major Project Updates • Children’s Theatre Suite; • Thrombectomy Imaging Facilities; • National Treatment Centre – Tayside, and • Infrastructure Programme Board.
Information • Assurance Report – Prioritisation and Management of Capital Funding
Strategic Risk 636; • Assurance Report – Estate Infrastructure Condition Strategic Risk 312; • A Policy for NHS Scotland on the Climate Emergency and Sustainable
Development – DL (2021) 38; • Hub Initiative Key Performance Indicators (KPIs) Report 2020-21; • Regional Asset Management Plan/CEL 35(2010) Meetings Progress Update,
and • Asset Management Group Work Plan 2021/22.
2.3.1 Quality/Patient Care
The Five Year Capital Plan supports the delivery of patient care and associated services across a range of environments in NHS Tayside.
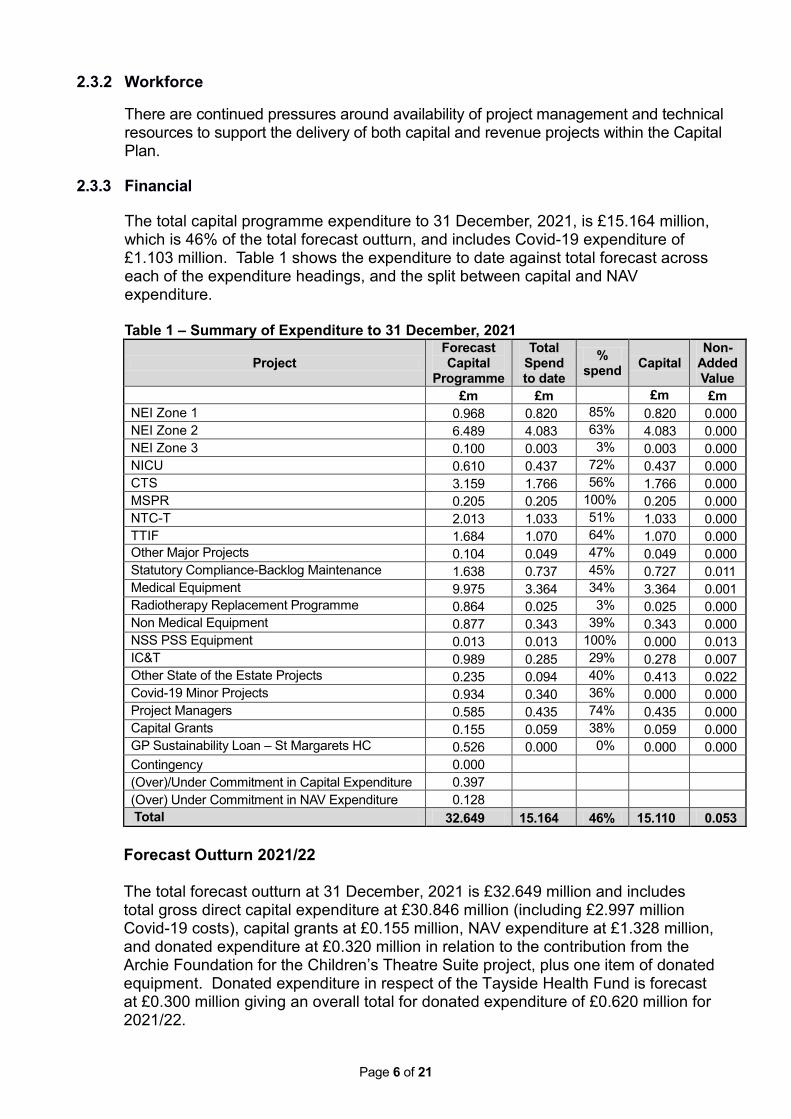
Page 6 of 21
2.3.2 Workforce
There are continued pressures around availability of project management and technical resources to support the delivery of both capital and revenue projects within the Capital Plan.
2.3.3 Financial
The total capital programme expenditure to 31 December, 2021, is £15.164 million, which is 46% of the total forecast outturn, and includes Covid-19 expenditure of £1.103 million. Table 1 shows the expenditure to date against total forecast across each of the expenditure headings, and the split between capital and NAV expenditure. Table 1 – Summary of Expenditure to 31 December, 2021
Project Forecast Capital
Programme
Total Spend to date
% spend Capital
Non-Added Value
£m £m £m £m NEI Zone 1 0.968 0.820 85% 0.820 0.000 NEI Zone 2 6.489 4.083 63% 4.083 0.000 NEI Zone 3 0.100 0.003 3% 0.003 0.000 NICU 0.610 0.437 72% 0.437 0.000 CTS 3.159 1.766 56% 1.766 0.000 MSPR 0.205 0.205 100% 0.205 0.000 NTC-T 2.013 1.033 51% 1.033 0.000 TTIF 1.684 1.070 64% 1.070 0.000 Other Major Projects 0.104 0.049 47% 0.049 0.000 Statutory Compliance-Backlog Maintenance 1.638 0.737 45% 0.727 0.011 Medical Equipment 9.975 3.364 34% 3.364 0.001 Radiotherapy Replacement Programme 0.864 0.025 3% 0.025 0.000 Non Medical Equipment 0.877 0.343 39% 0.343 0.000 NSS PSS Equipment 0.013 0.013 100% 0.000 0.013 IC&T 0.989 0.285 29% 0.278 0.007 Other State of the Estate Projects 0.235 0.094 40% 0.413 0.022 Covid-19 Minor Projects 0.934 0.340 36% 0.000 0.000 Project Managers 0.585 0.435 74% 0.435 0.000 Capital Grants 0.155 0.059 38% 0.059 0.000 GP Sustainability Loan – St Margarets HC 0.526 0.000 0% 0.000 0.000 Contingency 0.000 (Over)/Under Commitment in Capital Expenditure 0.397 (Over) Under Commitment in NAV Expenditure 0.128 Total 32.649 15.164 46% 15.110 0.053
Forecast Outturn 2021/22
The total forecast outturn at 31 December, 2021 is £32.649 million and includes total gross direct capital expenditure at £30.846 million (including £2.997 million Covid-19 costs), capital grants at £0.155 million, NAV expenditure at £1.328 million, and donated expenditure at £0.320 million in relation to the contribution from the Archie Foundation for the Children’s Theatre Suite project, plus one item of donated equipment. Donated expenditure in respect of the Tayside Health Fund is forecast at £0.300 million giving an overall total for donated expenditure of £0.620 million for 2021/22.
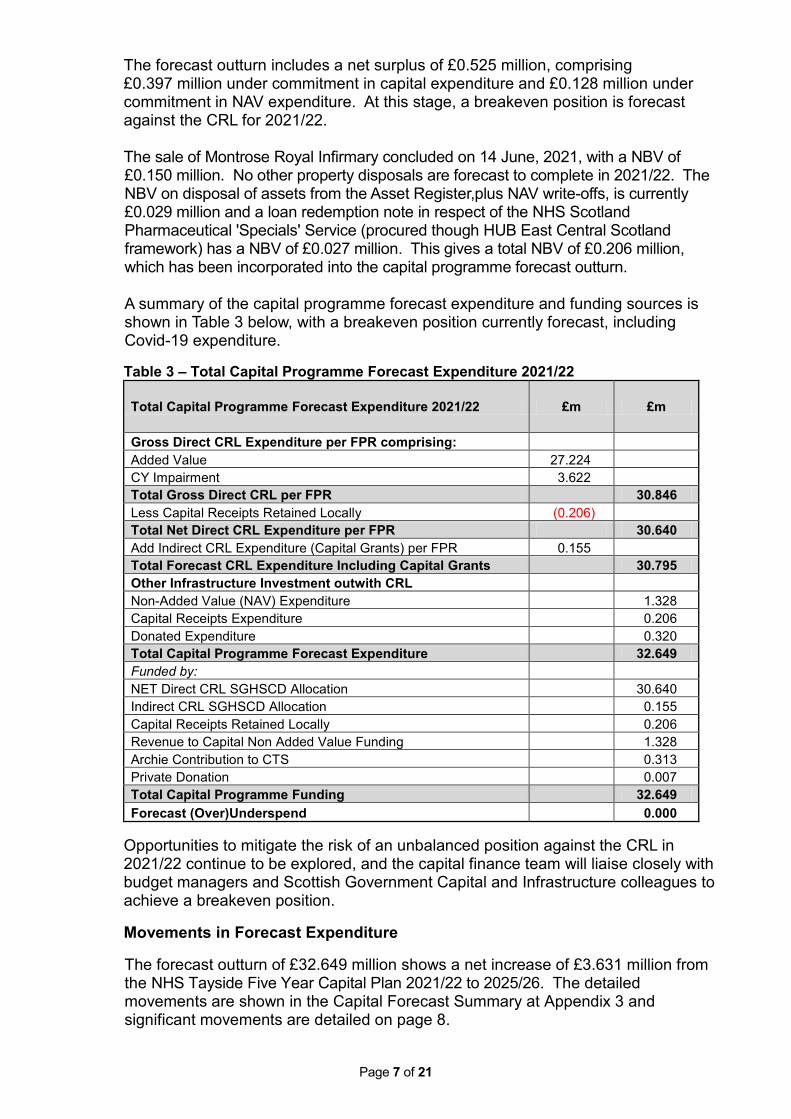
Page 7 of 21
The forecast outturn includes a net surplus of £0.525 million, comprising £0.397 million under commitment in capital expenditure and £0.128 million under commitment in NAV expenditure. At this stage, a breakeven position is forecast against the CRL for 2021/22. The sale of Montrose Royal Infirmary concluded on 14 June, 2021, with a NBV of £0.150 million. No other property disposals are forecast to complete in 2021/22. The NBV on disposal of assets from the Asset Register,plus NAV write-offs, is currently £0.029 million and a loan redemption note in respect of the NHS Scotland Pharmaceutical 'Specials' Service (procured though HUB East Central Scotland framework) has a NBV of £0.027 million. This gives a total NBV of £0.206 million, which has been incorporated into the capital programme forecast outturn. A summary of the capital programme forecast expenditure and funding sources is shown in Table 3 below, with a breakeven position currently forecast, including Covid-19 expenditure. Table 3 – Total Capital Programme Forecast Expenditure 2021/22
Total Capital Programme Forecast Expenditure 2021/22 £m £m
Gross Direct CRL Expenditure per FPR comprising: Added Value 27.224
CY Impairment 3.622 Total Gross Direct CRL per FPR
30.846
Less Capital Receipts Retained Locally (0.206) Total Net Direct CRL Expenditure per FPR 30.640
Add Indirect CRL Expenditure (Capital Grants) per FPR 0.155 Total Forecast CRL Expenditure Including Capital Grants
30.795
Other Infrastructure Investment outwith CRL Non-Added Value (NAV) Expenditure
1.328 Capital Receipts Expenditure
0.206
Donated Expenditure
0.320 Total Capital Programme Forecast Expenditure
32.649
Funded by: NET Direct CRL SGHSCD Allocation
30.640 Indirect CRL SGHSCD Allocation
0.155
Capital Receipts Retained Locally
0.206 Revenue to Capital Non Added Value Funding
1.328
Archie Contribution to CTS
0.313 Private Donation
0.007
Total Capital Programme Funding
32.649 Forecast (Over)Underspend
0.000
Opportunities to mitigate the risk of an unbalanced position against the CRL in 2021/22 continue to be explored, and the capital finance team will liaise closely with budget managers and Scottish Government Capital and Infrastructure colleagues to achieve a breakeven position.
Movements in Forecast Expenditure
The forecast outturn of £32.649 million shows a net increase of £3.631 million from the NHS Tayside Five Year Capital Plan 2021/22 to 2025/26. The detailed movements are shown in the Capital Forecast Summary at Appendix 3 and significant movements are detailed on page 8.
Page 8 of 21
Increase in Annual Forecast Expenditure 2021/22 • NEI Zone1 - £0.968 million net increase in forecast expenditure for 2021/22,
of which £0.916 million relates to slippage in expenditure from 2020/21 to 2021/22 not captured in the AOP, due to timing of the submission. The remaining £0.052 million relates to an increase in the Target Cost not factored into the 2021/22 forecast.
• CTS - £1.756 million net increase in forecast expenditure for 2021/22, of which £0.384 million relates to slippage in expenditure from 2020/21 to 2021/22 not captured in the AOP, due to timing of the submission. An additional £0.105 million relates to the inclusion of the NICU Uninterruptable Power Supply (UPS) works, £0.510 million for additional costs associated with flood works, £0.106 million for projected Covid-19 costs in 2021/22, £0.336 million for pipe work modifications in Pipe Street, and £0.315 million for other increases within the Target Cost.
• TTIF - £1.684 million net increase in forecast expenditure, which relates to additional funding approved by SGHFCGVD in respect of Sections 1 and 2 - construction work and Section 3 - development of the FBC, professional fees to progress the design to Royal Institute of British Architecture (RIBA) Stage 3, and appointment of a Principal Supply Chain Partner (PSCP).
• Medical Equipment - £6.039 million net increase in forecast expenditure for 2021/22, of which £0.178 million relates to slippage in expenditure from 2020/21 to 2021/22 not captured in the AOP, due to timing of the submission. An additional £1.241 million, relates to funding provided by SGHFCGVD in respect of the Robotic Assisted Surgery (RAS) project, dental pods, spectrophotometer, dose calibrator, imaging and ultrasound equipment, scope, dental scanner and genetics analyser. Additional funding of £3.018 million has also been allocated through the NIB Equipping Group for the replacement of prioritised medical equipment. Core capital funding of £0.915 million has been approved in relation to the Radiology Angiography project, and priority medical equipment to be funded from anticipated slippage in the capital programme, with the balance of £0.687 million relating to approved emergency bids and net budget variances.
• IC&T - £0.953 million net increase in forecast expenditure for 2021/22, of which £0.253 million relates to slippage in expenditure from 2020/21 to 2021/22 not captured in the AOP, due to timing of the submission. An additional £0.033 million, relates to funding provided by SGHFCGVD in respect of the Audio Visual Immersion Room (ACT) project. Core capital funding of £0.638 million, has been approved in relation to a Digital Pathology System and £0.015 million, for uninterruptable power supplies (2). The balance of £0.014 million relates to minor budget variances.
Reduction in Annual Forecast Expenditure 2021/22 • NEI Zone 3 - £1.4 million net reduction in forecast expenditure for 2021/22, of
which £0.060 million relates to slippage in expenditure from 2020/21 to 2021/22 not captured in the AOP due to timing of the submission. A reduction of £1.460 million relates to slippage in the 2021/22 expenditure projection due to a delay in development of the FBC.
• NTC-T - £3.411 million net reduction in forecast expenditure for 2021/22, of which £0.049 million relates to slippage in expenditure from 2020/21 to 2021/22 not captured in the AOP, due to timing of the submission. A reduction of £3.460 million relates to slippage in the 2021/22 expenditure projection as advised by NHS Tayside’s cost advisors.

Page 9 of 21
• Statutory Compliance and Backlog Maintenance - £1.362 million net reduction in forecast expenditure due to slippage in the planned programme of works for 2021/22.
• Radiotherapy Replacement Programme - £3.196 million net reduction in forecast expenditure for 2021/22, of which £0.511 relates to slippage in the Record and Verify System due to an unforeseen requirement to upgrade the windows operating system for associated Linear accelerators. Slippage of £2.940 million has been incurred on the MRI Simulator not deliverable until April 2022, due to a delay in approval of final costs by the Technical Specification and Evaluation Sub-Group (TSE). Additional funding of £0.098 million has been provided by SGHFCGVD in respect of the Brachytherapy Unit in 2021/22. Core capital funding of £0.141 million has been approved in relation to the Treatment Planning System, with the balance of £0.016 million being net budget increases.
Capital Allocations The CRL allocation from SGHFCGVD is confirmed in the December capital allocation letter at £18.717 million. This includes the initial core formula allocation of £9.473 million, and further allocations totalling £9.244 million in respect of the following:- • The return of £0.854 million funding to NHS Tayside with regard to CRL slippage
returned to SGHFCGVD in 2020/21; • Additional funding over and above the core formula allocation for:-
o Covid-19 costs - £2.997 million; o NICU/CC/SCC and EDR major projects - £0.667 million; o Brachytherapy project/MRI Simulator/Dose Calibrator - £0.174 million; o RAS project - £0.540 million; o Dental Education Infrastructure - £0.159 million; o Medical and non-Medical equipment (NIB bids) - £3.485 million; o Fluorescence Spectrophotometer and PCR System (National Services
Division bids) - £0.075 million; o Ultrasound Machine, Diagnostic Laboratory Equipment and Imaging System
- £0.168 million, and o Allocations received in error to be transferred to revenue - £0.125 million.
Specific ring-fenced allocations and adjustments of £11.923 million are currently anticipated in 2021/22 and shown in Table 4 on page 10.
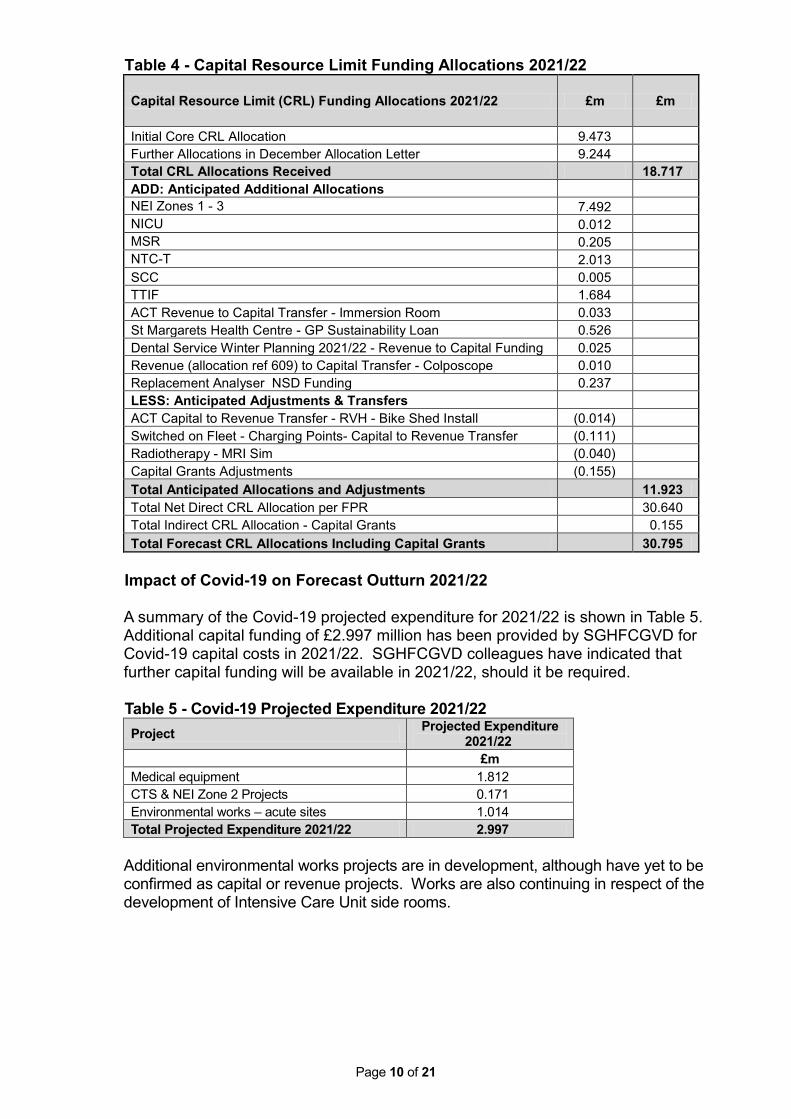
Page 10 of 21
Table 4 - Capital Resource Limit Funding Allocations 2021/22
Capital Resource Limit (CRL) Funding Allocations 2021/22 £m £m
Initial Core CRL Allocation 9.473 Further Allocations in December Allocation Letter 9.244 Total CRL Allocations Received 18.717
ADD: Anticipated Additional Allocations NEI Zones 1 - 3 7.492
NICU 0.012 MSR 0.205 NTC-T 2.013 SCC 0.005 TTIF 1.684 ACT Revenue to Capital Transfer - Immersion Room 0.033 St Margarets Health Centre - GP Sustainability Loan 0.526 Dental Service Winter Planning 2021/22 - Revenue to Capital Funding 0.025 Revenue (allocation ref 609) to Capital Transfer - Colposcope 0.010 Replacement Analyser NSD Funding 0.237 LESS: Anticipated Adjustments & Transfers
ACT Capital to Revenue Transfer - RVH - Bike Shed Install (0.014) Switched on Fleet - Charging Points- Capital to Revenue Transfer (0.111) Radiotherapy - MRI Sim (0.040) Capital Grants Adjustments (0.155) Total Anticipated Allocations and Adjustments
11.923
Total Net Direct CRL Allocation per FPR
30.640 Total Indirect CRL Allocation - Capital Grants
0.155
Total Forecast CRL Allocations Including Capital Grants
30.795
Impact of Covid-19 on Forecast Outturn 2021/22
A summary of the Covid-19 projected expenditure for 2021/22 is shown in Table 5. Additional capital funding of £2.997 million has been provided by SGHFCGVD for Covid-19 capital costs in 2021/22. SGHFCGVD colleagues have indicated that further capital funding will be available in 2021/22, should it be required.
Table 5 - Covid-19 Projected Expenditure 2021/22 Project Projected Expenditure
2021/22 £m Medical equipment 1.812 CTS & NEI Zone 2 Projects 0.171 Environmental works – acute sites 1.014 Total Projected Expenditure 2021/22 2.997
Additional environmental works projects are in development, although have yet to be confirmed as capital or revenue projects. Works are also continuing in respect of the development of Intensive Care Unit side rooms.
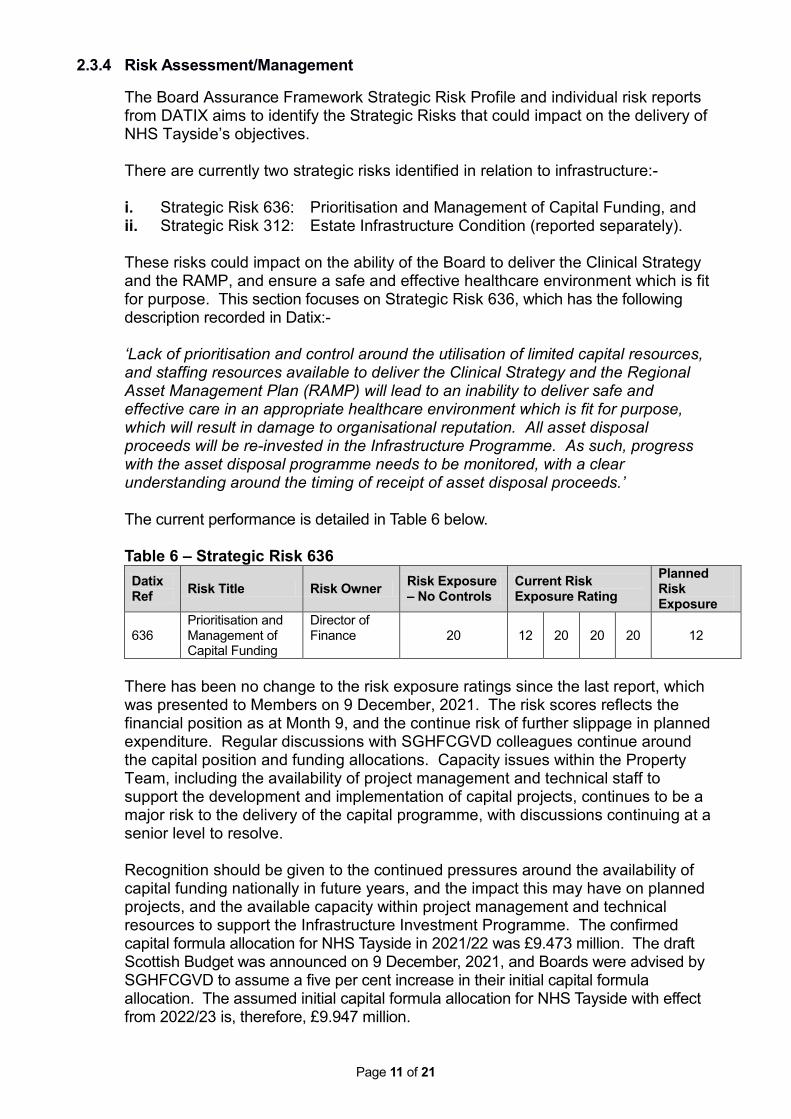
Page 11 of 21
2.3.4 Risk Assessment/Management
The Board Assurance Framework Strategic Risk Profile and individual risk reports from DATIX aims to identify the Strategic Risks that could impact on the delivery of NHS Tayside’s objectives. There are currently two strategic risks identified in relation to infrastructure:- i. Strategic Risk 636: Prioritisation and Management of Capital Funding, and ii. Strategic Risk 312: Estate Infrastructure Condition (reported separately). These risks could impact on the ability of the Board to deliver the Clinical Strategy and the RAMP, and ensure a safe and effective healthcare environment which is fit for purpose. This section focuses on Strategic Risk 636, which has the following description recorded in Datix:- ‘Lack of prioritisation and control around the utilisation of limited capital resources, and staffing resources available to deliver the Clinical Strategy and the Regional Asset Management Plan (RAMP) will lead to an inability to deliver safe and effective care in an appropriate healthcare environment which is fit for purpose, which will result in damage to organisational reputation. All asset disposal proceeds will be re-invested in the Infrastructure Programme. As such, progress with the asset disposal programme needs to be monitored, with a clear understanding around the timing of receipt of asset disposal proceeds.’
The current performance is detailed in Table 6 below.
Table 6 – Strategic Risk 636 Datix Ref Risk Title Risk Owner Risk Exposure
– No Controls Current Risk Exposure Rating
Planned Risk Exposure
636
Prioritisation and Management of Capital Funding
Director of Finance
20
12
20
20
20
12
There has been no change to the risk exposure ratings since the last report, which was presented to Members on 9 December, 2021. The risk scores reflects the financial position as at Month 9, and the continue risk of further slippage in planned expenditure. Regular discussions with SGHFCGVD colleagues continue around the capital position and funding allocations. Capacity issues within the Property Team, including the availability of project management and technical staff to support the development and implementation of capital projects, continues to be a major risk to the delivery of the capital programme, with discussions continuing at a senior level to resolve. Recognition should be given to the continued pressures around the availability of capital funding nationally in future years, and the impact this may have on planned projects, and the available capacity within project management and technical resources to support the Infrastructure Investment Programme. The confirmed capital formula allocation for NHS Tayside in 2021/22 was £9.473 million. The draft Scottish Budget was announced on 9 December, 2021, and Boards were advised by SGHFCGVD to assume a five per cent increase in their initial capital formula allocation. The assumed initial capital formula allocation for NHS Tayside with effect from 2022/23 is, therefore, £9.947 million.
Page 12 of 21
AMG will consider updates around the Strategic Infrastructure Risks and Digital Directorate risk assessments in line with their Annual Work Plan, and will identify the level of risk across all assets and prioritise accordingly all available resources to reduce risk and support service transformational work. Key operational risks in relation to the management of the Capital Plan are reported to each AMG meeting and to SGHFCGVD through the quarterly FPR. Appendix 4 summarises the ongoing operational risks including, but not exclusively, the impact of Covid-19. The Statutory Compliance and Backlog Maintenance Plan continues to be reviewed in conjunction with the Director of Facilities and Head of Property. Current and planned/proposed controls in relation to Strategic Risk 636 are contained within the Datix system. The assessment of adequacy of the current controls has been recorded as being ‘incomplete’ at the present time, meaning that ‘controls are appropriately designed but these are not consistently applied’.
2.3.5 Equality and Diversity, including health inequalities
An impact assessment has not been completed as it is not applicable to the reporting of the capital month end position. Where applicable, impact assessments will be carried out for individual projects listed within the Capital Plan.
2.3.6 Other impacts The amounts and scheduling of projects beyond 2021/22 are subject to change.
Future projects cannot be robustly costed until design work has been completed. Furthermore, priorities and resources are subject to change and should align with the Board’s Clinical Strategy and RAMP. The forecast for 2022/23 onwards should, therefore, be treated as indicative at this stage.
There are a number of emerging issues with significant financial implications that will impact on the Capital Plan and capital funding requirements in future years. These issues are reported routinely to AMG, and have been included in the AOP and the RAMP.
2.3.7 Communication, involvement, engagement and consultation
The Board has carried out its duties to involve and engage external stakeholders where appropriate:-
• Major iinfrastructure projects have project teams and project/programme
boards established, with representation from key stakeholders and communication and engagement strategies developed;
• University of Dundee is represented on the membership of AMG; • Regular dialogue with SGHFCGVD Health Finance and Infrastructure Team,
and • Regular dialogue with external property valuers in respect of the NHS Tayside
estate.
2.3.8 Route to the Meeting This paper has not been circulated to any meetings prior to submission to the Committee.
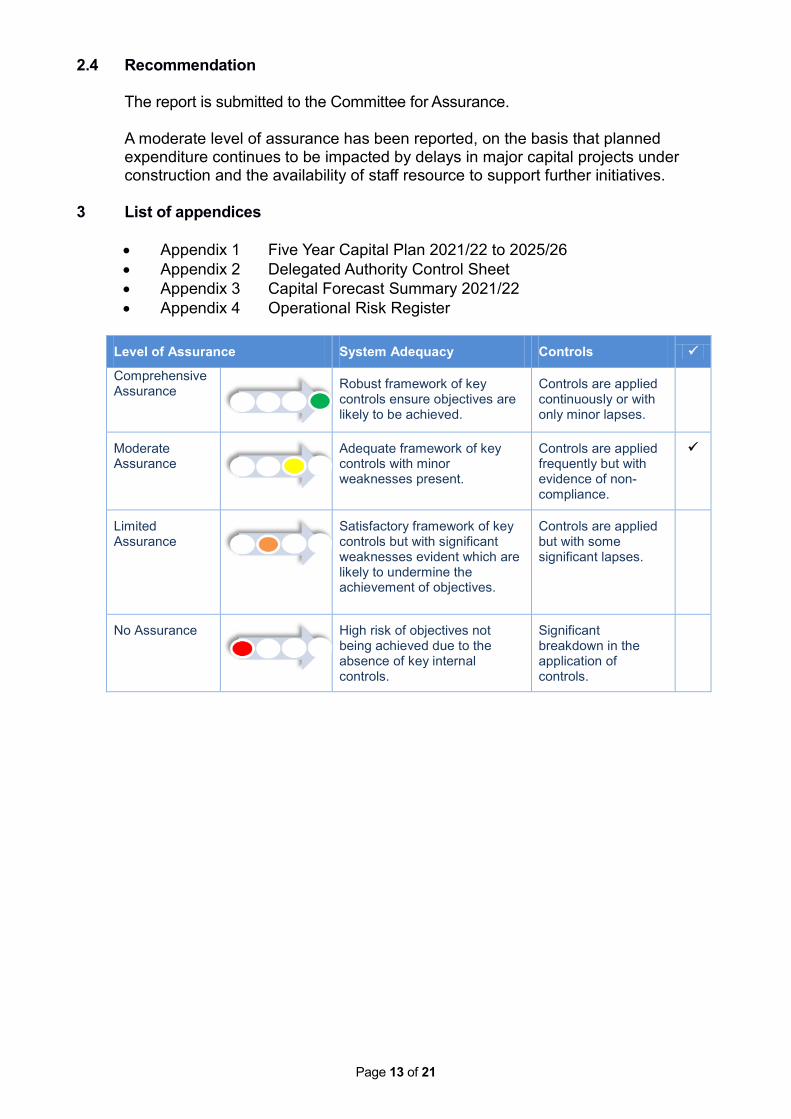
Page 13 of 21
2.4 Recommendation The report is submitted to the Committee for Assurance. A moderate level of assurance has been reported, on the basis that planned expenditure continues to be impacted by delays in major capital projects under construction and the availability of staff resource to support further initiatives.
3 List of appendices
• Appendix 1 Five Year Capital Plan 2021/22 to 2025/26 • Appendix 2 Delegated Authority Control Sheet • Appendix 3 Capital Forecast Summary 2021/22 • Appendix 4 Operational Risk Register
Level of Assurance System Adequacy Controls
Comprehensive Assurance
Robust framework of key controls ensure objectives are likely to be achieved.
Controls are applied continuously or with only minor lapses.
Moderate Assurance
Adequate framework of key controls with minor weaknesses present.
Controls are applied frequently but with evidence of non-compliance.
Limited Assurance
Satisfactory framework of key controls but with significant weaknesses evident which are likely to undermine the achievement of objectives.
Controls are applied but with some significant lapses.
No Assurance
High risk of objectives not being achieved due to the absence of key internal controls.
Significant breakdown in the application of controls.
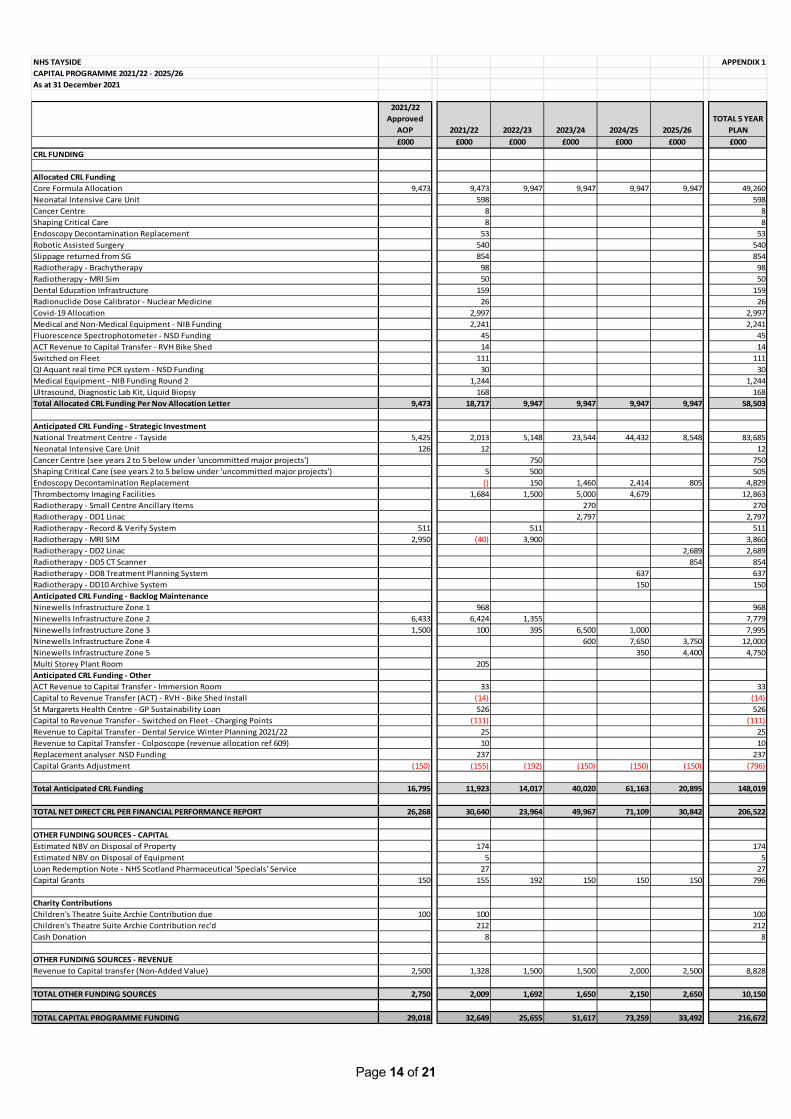
Page 14 of 21
NHS TAYSIDE APPENDIX 1CAPITAL PROGRAMME 2021/22 - 2025/26 As at 31 December 2021
2021/22 Approved
AOP 2021/22 2022/23 2023/24 2024/25 2025/26TOTAL 5 YEAR
PLAN£000 £000 £000 £000 £000 £000 £000
CRL FUNDING
Allocated CRL Funding Core Formula Allocation 9,473 9,473 9,947 9,947 9,947 9,947 49,260Neonatal Intensive Care Unit 598 598Cancer Centre 8 8Shaping Critical Care 8 8Endoscopy Decontamination Replacement 53 53Robotic Assisted Surgery 540 540Slippage returned from SG 854 854Radiotherapy - Brachytherapy 98 98Radiotherapy - MRI Sim 50 50Dental Education Infrastructure 159 159Radionuclide Dose Calibrator - Nuclear Medicine 26 26Covid-19 Allocation 2,997 2,997Medical and Non-Medical Equipment - NIB Funding 2,241 2,241Fluorescence Spectrophotometer - NSD Funding 45 45ACT Revenue to Capital Transfer - RVH Bike Shed 14 14Switched on Fleet 111 111QI Aquant real time PCR system - NSD Funding 30 30Medical Equipment - NIB Funding Round 2 1,244 1,244Ultrasound, Diagnostic Lab Kit, Liquid Biopsy 168 168Total Allocated CRL Funding Per Nov Allocation Letter 9,473 18,717 9,947 9,947 9,947 9,947 58,503
Anticipated CRL Funding - Strategic InvestmentNational Treatment Centre - Tayside 5,425 2,013 5,148 23,544 44,432 8,548 83,685Neonatal Intensive Care Unit 126 12 12Cancer Centre (see years 2 to 5 below under 'uncommitted major projects') 750 750Shaping Critical Care (see years 2 to 5 below under 'uncommitted major projects') 5 500 505Endoscopy Decontamination Replacement () 150 1,460 2,414 805 4,829Thrombectomy Imaging Facilities 1,684 1,500 5,000 4,679 12,863Radiotherapy - Small Centre Ancillary Items 270 270Radiotherapy - DD1 Linac 2,797 2,797Radiotherapy - Record & Verify System 511 511 511Radiotherapy - MRI SIM 2,950 (40) 3,900 3,860Radiotherapy - DD2 Linac 2,689 2,689Radiotherapy - DD5 CT Scanner 854 854Radiotherapy - DD8 Treatment Planning System 637 637Radiotherapy - DD10 Archive System 150 150Anticipated CRL Funding - Backlog MaintenanceNinewells Infrastructure Zone 1 968 968Ninewells Infrastructure Zone 2 6,433 6,424 1,355 7,779Ninewells Infrastructure Zone 3 1,500 100 395 6,500 1,000 7,995Ninewells Infrastructure Zone 4 600 7,650 3,750 12,000Ninewells Infrastructure Zone 5 350 4,400 4,750Multi Storey Plant Room 205Anticipated CRL Funding - OtherACT Revenue to Capital Transfer - Immersion Room 33 33Capital to Revenue Transfer (ACT) - RVH - Bike Shed Install (14) (14)St Margarets Health Centre - GP Sustainability Loan 526 526Capital to Revenue Transfer - Switched on Fleet - Charging Points (111) (111)Revenue to Capital Transfer - Dental Service Winter Planning 2021/22 25 25Revenue to Capital Transfer - Colposcope (revenue allocation ref 609) 10 10Replacement analyser NSD Funding 237 237Capital Grants Adjustment (150) (155) (192) (150) (150) (150) (796)
Total Anticipated CRL Funding 16,795 11,923 14,017 40,020 61,163 20,895 148,019
TOTAL NET DIRECT CRL PER FINANCIAL PERFORMANCE REPORT 26,268 30,640 23,964 49,967 71,109 30,842 206,522
OTHER FUNDING SOURCES - CAPITALEstimated NBV on Disposal of Property 174 174Estimated NBV on Disposal of Equipment 5 5Loan Redemption Note - NHS Scotland Pharmaceutical 'Specials' Service 27 27Capital Grants 150 155 192 150 150 150 796
Charity ContributionsChildren's Theatre Suite Archie Contribution due 100 100 100Children's Theatre Suite Archie Contribution rec'd 212 212Cash Donation 8 8
OTHER FUNDING SOURCES - REVENUERevenue to Capital transfer (Non-Added Value) 2,500 1,328 1,500 1,500 2,000 2,500 8,828
TOTAL OTHER FUNDING SOURCES 2,750 2,009 1,692 1,650 2,150 2,650 10,150
TOTAL CAPITAL PROGRAMME FUNDING 29,018 32,649 25,655 51,617 73,259 33,492 216,672
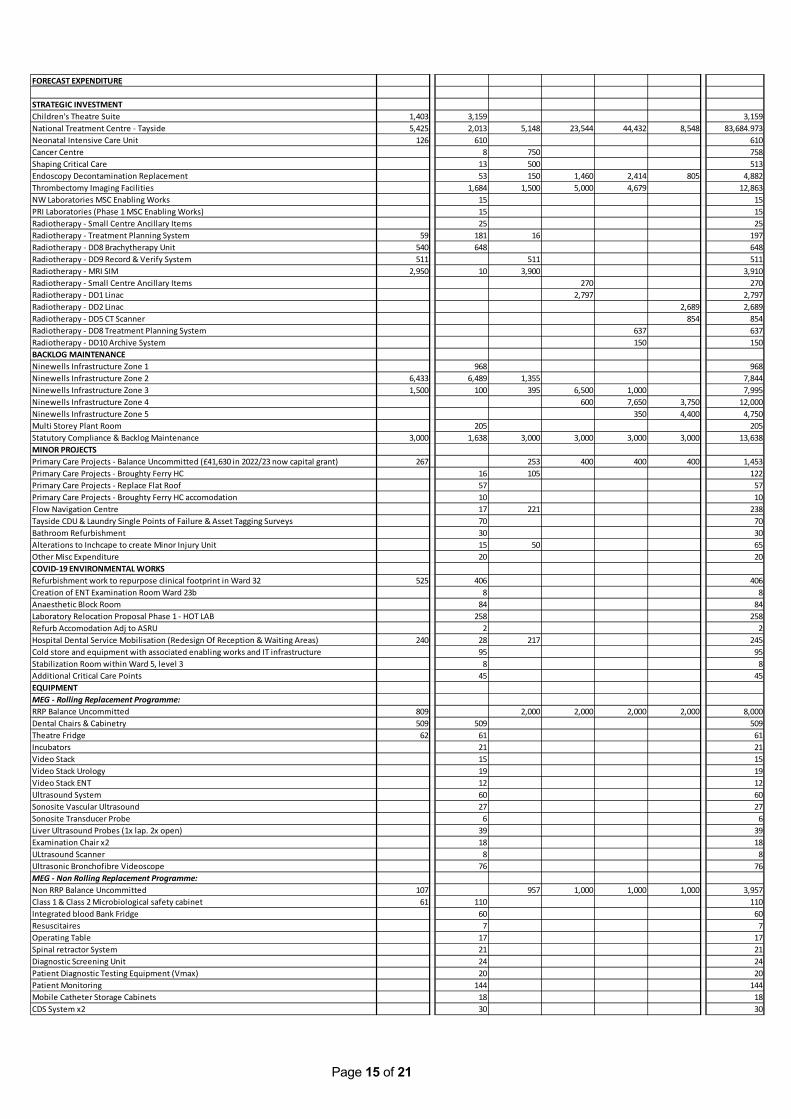
Page 15 of 21
FORECAST EXPENDITURE
STRATEGIC INVESTMENTChildren's Theatre Suite 1,403 3,159 3,159National Treatment Centre - Tayside 5,425 2,013 5,148 23,544 44,432 8,548 83,684.973Neonatal Intensive Care Unit 126 610 610Cancer Centre 8 750 758Shaping Critical Care 13 500 513Endoscopy Decontamination Replacement 53 150 1,460 2,414 805 4,882Thrombectomy Imaging Facilities 1,684 1,500 5,000 4,679 12,863NW Laboratories MSC Enabling Works 15 15PRI Laboratories (Phase 1 MSC Enabling Works) 15 15Radiotherapy - Small Centre Ancillary Items 25 25Radiotherapy - Treatment Planning System 59 181 16 197Radiotherapy - DD8 Brachytherapy Unit 540 648 648Radiotherapy - DD9 Record & Verify System 511 511 511Radiotherapy - MRI SIM 2,950 10 3,900 3,910Radiotherapy - Small Centre Ancillary Items 270 270Radiotherapy - DD1 Linac 2,797 2,797Radiotherapy - DD2 Linac 2,689 2,689Radiotherapy - DD5 CT Scanner 854 854Radiotherapy - DD8 Treatment Planning System 637 637Radiotherapy - DD10 Archive System 150 150BACKLOG MAINTENANCENinewells Infrastructure Zone 1 968 968Ninewells Infrastructure Zone 2 6,433 6,489 1,355 7,844Ninewells Infrastructure Zone 3 1,500 100 395 6,500 1,000 7,995Ninewells Infrastructure Zone 4 600 7,650 3,750 12,000Ninewells Infrastructure Zone 5 350 4,400 4,750Multi Storey Plant Room 205 205Statutory Compliance & Backlog Maintenance 3,000 1,638 3,000 3,000 3,000 3,000 13,638MINOR PROJECTSPrimary Care Projects - Balance Uncommitted (£41,630 in 2022/23 now capital grant) 267 253 400 400 400 1,453Primary Care Projects - Broughty Ferry HC 16 105 122Primary Care Projects - Replace Flat Roof 57 57Primary Care Projects - Broughty Ferry HC accomodation 10 10Flow Navigation Centre 17 221 238Tayside CDU & Laundry Single Points of Failure & Asset Tagging Surveys 70 70Bathroom Refurbishment 30 30Alterations to Inchcape to create Minor Injury Unit 15 50 65Other Misc Expenditure 20 20COVID-19 ENVIRONMENTAL WORKSRefurbishment work to repurpose clinical footprint in Ward 32 525 406 406Creation of ENT Examination Room Ward 23b 8 8Anaesthetic Block Room 84 84Laboratory Relocation Proposal Phase 1 - HOT LAB 258 258Refurb Accomodation Adj to ASRU 2 2Hospital Dental Service Mobilisation (Redesign Of Reception & Waiting Areas) 240 28 217 245Cold store and equipment with associated enabling works and IT infrastructure 95 95Stabilization Room within Ward 5, level 3 8 8Additional Critical Care Points 45 45EQUIPMENTMEG - Rolling Replacement Programme:RRP Balance Uncommitted 809 2,000 2,000 2,000 2,000 8,000Dental Chairs & Cabinetry 509 509 509Theatre Fridge 62 61 61Incubators 21 21Video Stack 15 15Video Stack Urology 19 19Video Stack ENT 12 12Ultrasound System 60 60Sonosite Vascular Ultrasound 27 27Sonosite Transducer Probe 6 6Liver Ultrasound Probes (1x lap. 2x open) 39 39Examination Chair x2 18 18ULtrasound Scanner 8 8Ultrasonic Bronchofibre Videoscope 76 76MEG - Non Rolling Replacement Programme:Non RRP Balance Uncommitted 107 957 1,000 1,000 1,000 3,957Class 1 & Class 2 Microbiological safety cabinet 61 110 110Integrated blood Bank Fridge 60 60Resuscitaires 7 7Operating Table 17 17Spinal retractor System 21 21Diagnostic Screening Unit 24 24Patient Diagnostic Testing Equipment (Vmax) 20 20Patient Monitoring 144 144Mobile Catheter Storage Cabinets 18 18CDS System x2 30 30
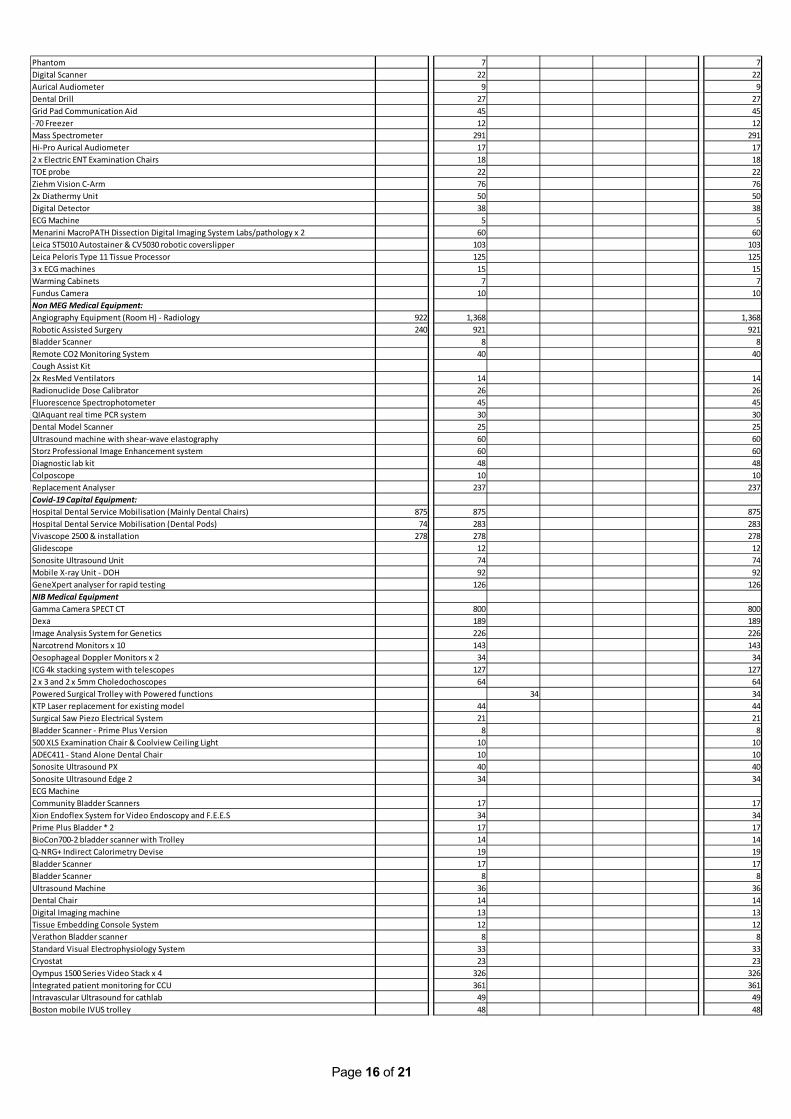
Page 16 of 21
Phantom 7 7Digital Scanner 22 22Aurical Audiometer 9 9Dental Drill 27 27Grid Pad Communication Aid 45 45-70 Freezer 12 12Mass Spectrometer 291 291Hi-Pro Aurical Audiometer 17 172 x Electric ENT Examination Chairs 18 18TOE probe 22 22Ziehm Vision C-Arm 76 762x Diathermy Unit 50 50Digital Detector 38 38ECG Machine 5 5Menarini MacroPATH Dissection Digital Imaging System Labs/pathology x 2 60 60Leica ST5010 Autostainer & CV5030 robotic coverslipper 103 103Leica Peloris Type 11 Tissue Processor 125 1253 x ECG machines 15 15Warming Cabinets 7 7Fundus Camera 10 10Non MEG Medical Equipment:Angiography Equipment (Room H) - Radiology 922 1,368 1,368Robotic Assisted Surgery 240 921 921Bladder Scanner 8 8Remote CO2 Monitoring System 40 40Cough Assist Kit2x ResMed Ventilators 14 14Radionuclide Dose Calibrator 26 26Fluorescence Spectrophotometer 45 45QIAquant real time PCR system 30 30Dental Model Scanner 25 25Ultrasound machine with shear-wave elastography 60 60Storz Professional Image Enhancement system 60 60Diagnostic lab kit 48 48Colposcope 10 10Replacement Analyser 237 237Covid-19 Capital Equipment:Hospital Dental Service Mobilisation (Mainly Dental Chairs) 875 875 875Hospital Dental Service Mobilisation (Dental Pods) 74 283 283Vivascope 2500 & installation 278 278 278Glidescope 12 12Sonosite Ultrasound Unit 74 74Mobile X-ray Unit - DOH 92 92GeneXpert analyser for rapid testing 126 126NIB Medical EquipmentGamma Camera SPECT CT 800 800Dexa 189 189Image Analysis System for Genetics 226 226Narcotrend Monitors x 10 143 143Oesophageal Doppler Monitors x 2 34 34ICG 4k stacking system with telescopes 127 1272 x 3 and 2 x 5mm Choledochoscopes 64 64Powered Surgical Trolley with Powered functions 34 34KTP Laser replacement for existing model 44 44Surgical Saw Piezo Electrical System 21 21Bladder Scanner - Prime Plus Version 8 8500 XLS Examination Chair & Coolview Ceiling Light 10 10ADEC411 - Stand Alone Dental Chair 10 10Sonosite Ultrasound PX 40 40Sonosite Ultrasound Edge 2 34 34ECG MachineCommunity Bladder Scanners 17 17Xion Endoflex System for Video Endoscopy and F.E.E.S 34 34Prime Plus Bladder * 2 17 17BioCon700-2 bladder scanner with Trolley 14 14Q-NRG+ Indirect Calorimetry Devise 19 19Bladder Scanner 17 17Bladder Scanner 8 8Ultrasound Machine 36 36Dental Chair 14 14Digital Imaging machine 13 13Tissue Embedding Console System 12 12Verathon Bladder scanner 8 8Standard Visual Electrophysiology System 33 33Cryostat 23 23Oympus 1500 Series Video Stack x 4 326 326Integrated patient monitoring for CCU 361 361Intravascular Ultrasound for cathlab 49 49Boston mobile IVUS trolley 48 48
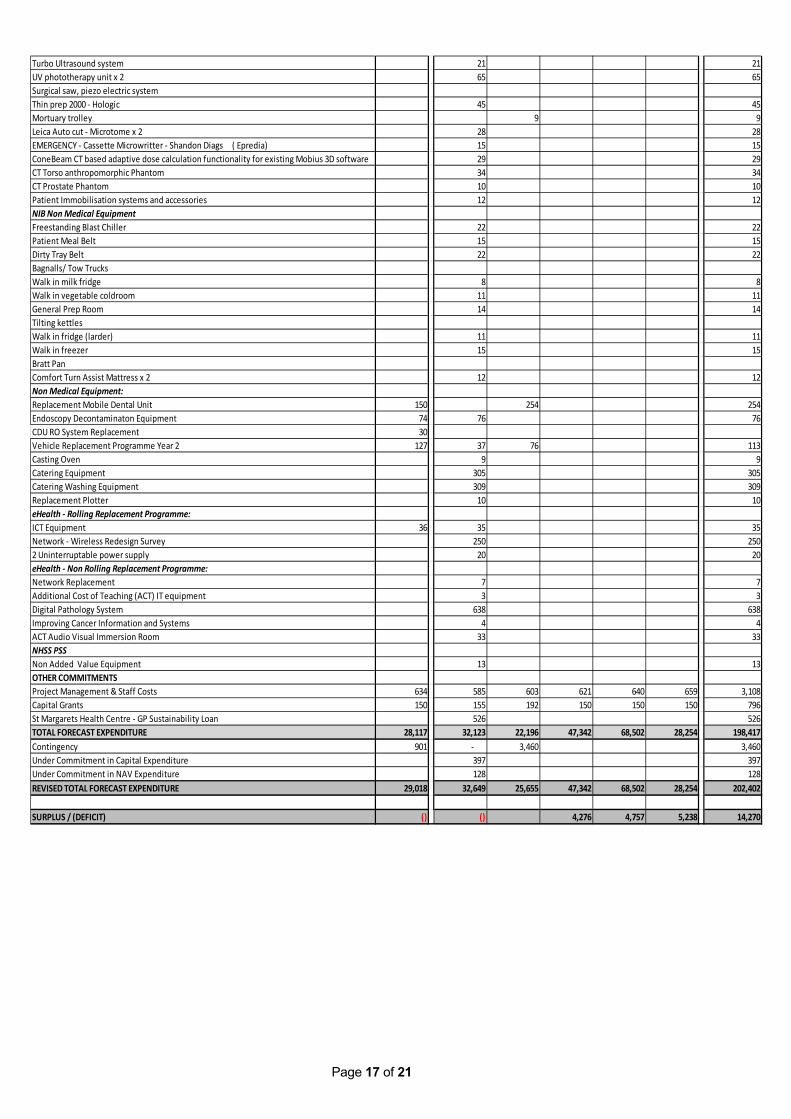
Page 17 of 21
Turbo Ultrasound system 21 21UV phototherapy unit x 2 65 65Surgical saw, piezo electric systemThin prep 2000 - Hologic 45 45Mortuary trolley 9 9Leica Auto cut - Microtome x 2 28 28EMERGENCY - Cassette Microwritter - Shandon Diags ( Epredia) 15 15ConeBeam CT based adaptive dose calculation functionality for existing Mobius 3D software 29 29CT Torso anthropomorphic Phantom 34 34CT Prostate Phantom 10 10Patient Immobilisation systems and accessories 12 12NIB Non Medical EquipmentFreestanding Blast Chiller 22 22Patient Meal Belt 15 15Dirty Tray Belt 22 22Bagnalls/ Tow TrucksWalk in milk fridge 8 8Walk in vegetable coldroom 11 11General Prep Room 14 14Tilting kettlesWalk in fridge (larder) 11 11Walk in freezer 15 15Bratt PanComfort Turn Assist Mattress x 2 12 12Non Medical Equipment:Replacement Mobile Dental Unit 150 254 254Endoscopy Decontaminaton Equipment 74 76 76CDU RO System Replacement 30Vehicle Replacement Programme Year 2 127 37 76 113Casting Oven 9 9Catering Equipment 305 305Catering Washing Equipment 309 309Replacement Plotter 10 10eHealth - Rolling Replacement Programme:ICT Equipment 36 35 35Network - Wireless Redesign Survey 250 2502 Uninterruptable power supply 20 20eHealth - Non Rolling Replacement Programme:Network Replacement 7 7Additional Cost of Teaching (ACT) IT equipment 3 3Digital Pathology System 638 638Improving Cancer Information and Systems 4 4ACT Audio Visual Immersion Room 33 33NHSS PSS Non Added Value Equipment 13 13OTHER COMMITMENTSProject Management & Staff Costs 634 585 603 621 640 659 3,108Capital Grants 150 155 192 150 150 150 796St Margarets Health Centre - GP Sustainability Loan 526 526TOTAL FORECAST EXPENDITURE 28,117 32,123 22,196 47,342 68,502 28,254 198,417Contingency 901 - 3,460 3,460Under Commitment in Capital Expenditure 397 397Under Commitment in NAV Expenditure 128 128REVISED TOTAL FORECAST EXPENDITURE 29,018 32,649 25,655 47,342 68,502 28,254 202,402
SURPLUS / (DEFICIT) () () 4,276 4,757 5,238 14,270
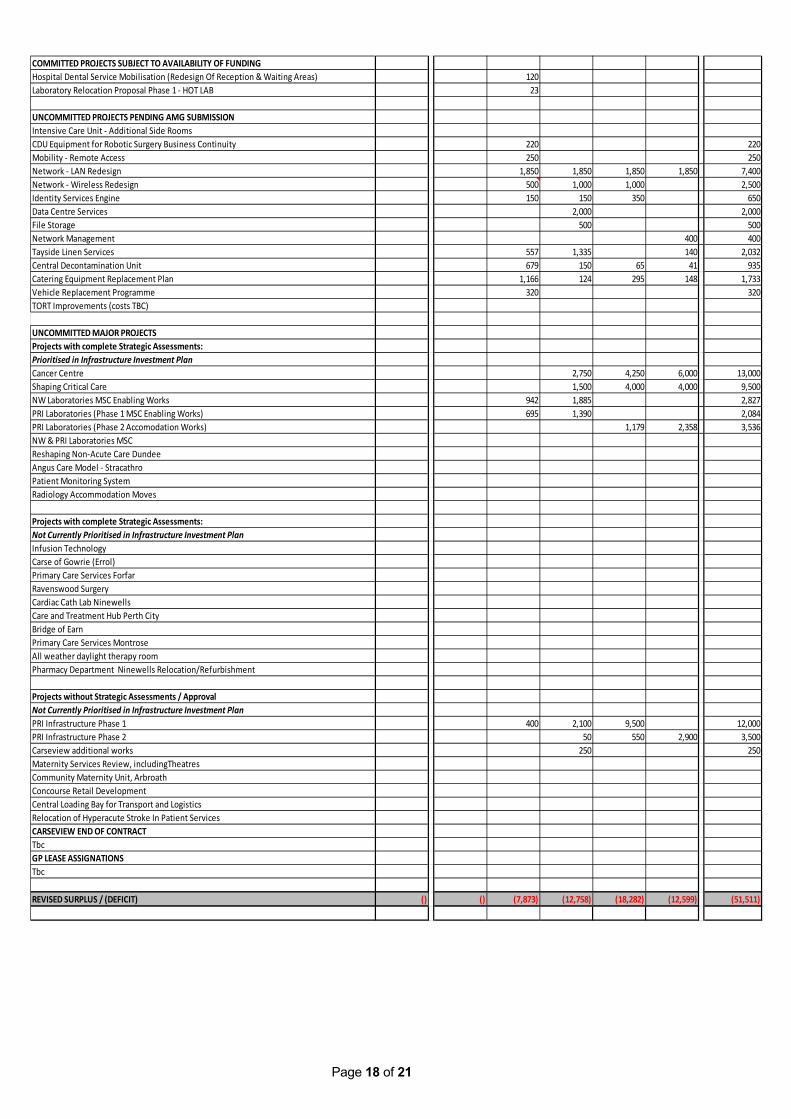
Page 18 of 21
COMMITTED PROJECTS SUBJECT TO AVAILABILITY OF FUNDINGHospital Dental Service Mobilisation (Redesign Of Reception & Waiting Areas) 120Laboratory Relocation Proposal Phase 1 - HOT LAB 23
UNCOMMITTED PROJECTS PENDING AMG SUBMISSIONIntensive Care Unit - Additional Side Rooms CDU Equipment for Robotic Surgery Business Continuity 220 220Mobility - Remote Access 250 250Network - LAN Redesign 1,850 1,850 1,850 1,850 7,400Network - Wireless Redesign 500 1,000 1,000 2,500Identity Services Engine 150 150 350 650Data Centre Services 2,000 2,000File Storage 500 500Network Management 400 400Tayside Linen Services 557 1,335 140 2,032Central Decontamination Unit 679 150 65 41 935Catering Equipment Replacement Plan 1,166 124 295 148 1,733Vehicle Replacement Programme 320 320TORT Improvements (costs TBC)
UNCOMMITTED MAJOR PROJECTSProjects with complete Strategic Assessments:Prioritised in Infrastructure Investment PlanCancer Centre 2,750 4,250 6,000 13,000Shaping Critical Care 1,500 4,000 4,000 9,500NW Laboratories MSC Enabling Works 942 1,885 2,827PRI Laboratories (Phase 1 MSC Enabling Works) 695 1,390 2,084PRI Laboratories (Phase 2 Accomodation Works) 1,179 2,358 3,536NW & PRI Laboratories MSCReshaping Non-Acute Care DundeeAngus Care Model - StracathroPatient Monitoring SystemRadiology Accommodation Moves
Projects with complete Strategic Assessments:Not Currently Prioritised in Infrastructure Investment PlanInfusion Technology Carse of Gowrie (Errol)Primary Care Services ForfarRavenswood Surgery Cardiac Cath Lab NinewellsCare and Treatment Hub Perth City Bridge of EarnPrimary Care Services MontroseAll weather daylight therapy room Pharmacy Department Ninewells Relocation/Refurbishment
Projects without Strategic Assessments / ApprovalNot Currently Prioritised in Infrastructure Investment PlanPRI Infrastructure Phase 1 400 2,100 9,500 12,000PRI Infrastructure Phase 2 50 550 2,900 3,500Carseview additional works 250 250Maternity Services Review, includingTheatresCommunity Maternity Unit, ArbroathConcourse Retail DevelopmentCentral Loading Bay for Transport and LogisticsRelocation of Hyperacute Stroke In Patient ServicesCARSEVIEW END OF CONTRACTTbcGP LEASE ASSIGNATIONSTbc
REVISED SURPLUS / (DEFICIT) () () (7,873) (12,758) (18,282) (12,599) (51,511)
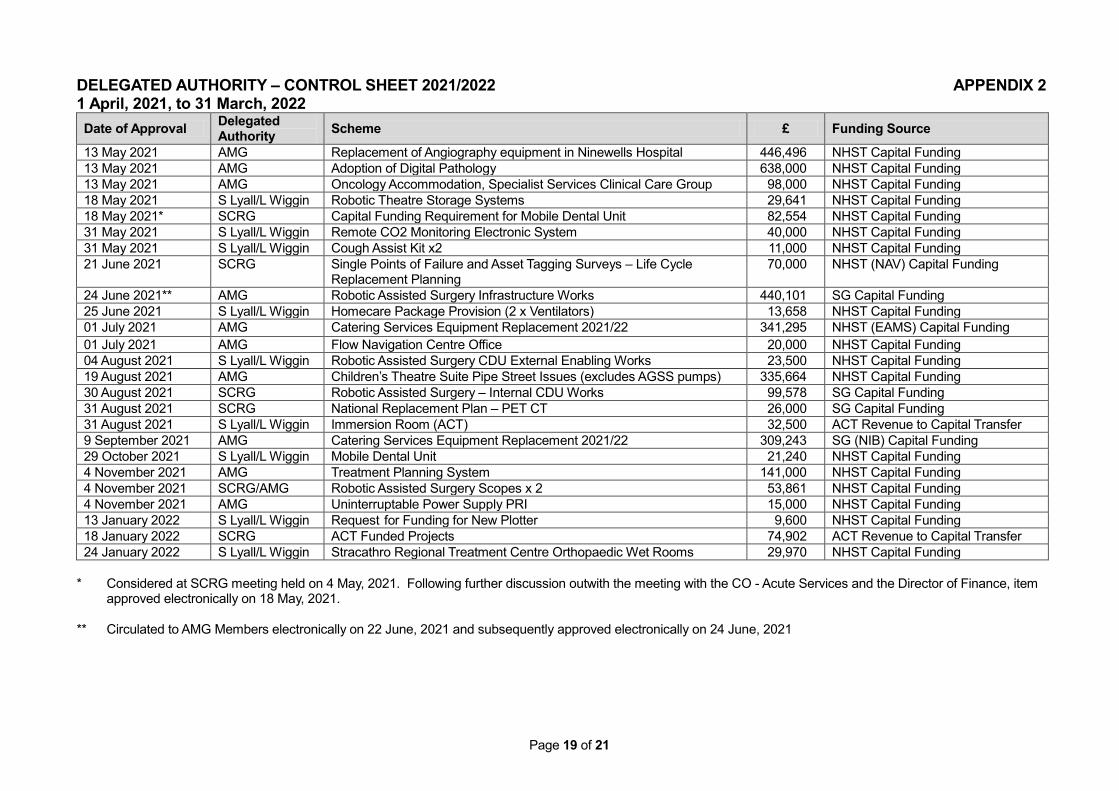
Page 19 of 21
DELEGATED AUTHORITY – CONTROL SHEET 2021/2022 APPENDIX 2 1 April, 2021, to 31 March, 2022 Date of Approval Delegated
Authority Scheme £ Funding Source
13 May 2021 AMG Replacement of Angiography equipment in Ninewells Hospital 446,496 NHST Capital Funding 13 May 2021 AMG Adoption of Digital Pathology 638,000 NHST Capital Funding 13 May 2021 AMG Oncology Accommodation, Specialist Services Clinical Care Group 98,000 NHST Capital Funding 18 May 2021 S Lyall/L Wiggin Robotic Theatre Storage Systems 29,641 NHST Capital Funding 18 May 2021* SCRG Capital Funding Requirement for Mobile Dental Unit 82,554 NHST Capital Funding 31 May 2021 S Lyall/L Wiggin Remote CO2 Monitoring Electronic System 40,000 NHST Capital Funding 31 May 2021 S Lyall/L Wiggin Cough Assist Kit x2 11,000 NHST Capital Funding 21 June 2021 SCRG Single Points of Failure and Asset Tagging Surveys – Life Cycle
Replacement Planning 70,000 NHST (NAV) Capital Funding
24 June 2021** AMG Robotic Assisted Surgery Infrastructure Works 440,101 SG Capital Funding 25 June 2021 S Lyall/L Wiggin Homecare Package Provision (2 x Ventilators) 13,658 NHST Capital Funding 01 July 2021 AMG Catering Services Equipment Replacement 2021/22 341,295 NHST (EAMS) Capital Funding 01 July 2021 AMG Flow Navigation Centre Office 20,000 NHST Capital Funding 04 August 2021 S Lyall/L Wiggin Robotic Assisted Surgery CDU External Enabling Works 23,500 NHST Capital Funding 19 August 2021 AMG Children’s Theatre Suite Pipe Street Issues (excludes AGSS pumps) 335,664 NHST Capital Funding 30 August 2021 SCRG Robotic Assisted Surgery – Internal CDU Works 99,578 SG Capital Funding 31 August 2021 SCRG National Replacement Plan – PET CT 26,000 SG Capital Funding 31 August 2021 S Lyall/L Wiggin Immersion Room (ACT) 32,500 ACT Revenue to Capital Transfer 9 September 2021 AMG Catering Services Equipment Replacement 2021/22 309,243 SG (NIB) Capital Funding 29 October 2021 S Lyall/L Wiggin Mobile Dental Unit 21,240 NHST Capital Funding 4 November 2021 AMG Treatment Planning System 141,000 NHST Capital Funding 4 November 2021 SCRG/AMG Robotic Assisted Surgery Scopes x 2 53,861 NHST Capital Funding 4 November 2021 AMG Uninterruptable Power Supply PRI 15,000 NHST Capital Funding 13 January 2022 S Lyall/L Wiggin Request for Funding for New Plotter 9,600 NHST Capital Funding 18 January 2022 SCRG ACT Funded Projects 74,902 ACT Revenue to Capital Transfer 24 January 2022 S Lyall/L Wiggin Stracathro Regional Treatment Centre Orthopaedic Wet Rooms 29,970 NHST Capital Funding
* Considered at SCRG meeting held on 4 May, 2021. Following further discussion outwith the meeting with the CO - Acute Services and the Director of Finance, item
approved electronically on 18 May, 2021. ** Circulated to AMG Members electronically on 22 June, 2021 and subsequently approved electronically on 24 June, 2021
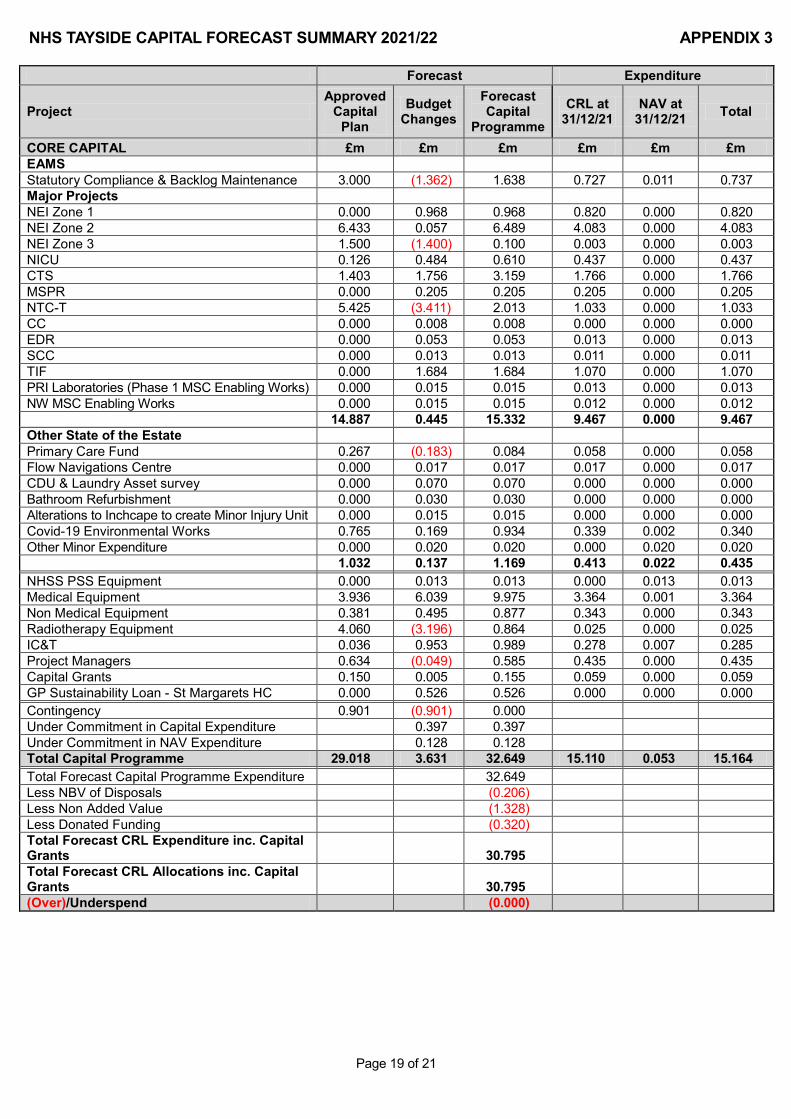
Page 19 of 21
NHS TAYSIDE CAPITAL FORECAST SUMMARY 2021/22 APPENDIX 3
Forecast Expenditure
Project Approved
Capital Plan
Budget Changes
Forecast Capital
Programme CRL at
31/12/21 NAV at
31/12/21 Total
CORE CAPITAL £m £m £m £m £m £m EAMS
Statutory Compliance & Backlog Maintenance 3.000 (1.362) 1.638 0.727 0.011 0.737 Major Projects
NEI Zone 1 0.000 0.968 0.968 0.820 0.000 0.820 NEI Zone 2 6.433 0.057 6.489 4.083 0.000 4.083 NEI Zone 3 1.500 (1.400) 0.100 0.003 0.000 0.003 NICU 0.126 0.484 0.610 0.437 0.000 0.437 CTS 1.403 1.756 3.159 1.766 0.000 1.766 MSPR 0.000 0.205 0.205 0.205 0.000 0.205 NTC-T 5.425 (3.411) 2.013 1.033 0.000 1.033 CC 0.000 0.008 0.008 0.000 0.000 0.000 EDR 0.000 0.053 0.053 0.013 0.000 0.013 SCC 0.000 0.013 0.013 0.011 0.000 0.011 TIF 0.000 1.684 1.684 1.070 0.000 1.070 PRI Laboratories (Phase 1 MSC Enabling Works) 0.000 0.015 0.015 0.013 0.000 0.013 NW MSC Enabling Works 0.000 0.015 0.015 0.012 0.000 0.012
14.887 0.445 15.332 9.467 0.000 9.467
Other State of the Estate Primary Care Fund 0.267 (0.183) 0.084 0.058 0.000 0.058
Flow Navigations Centre 0.000 0.017 0.017 0.017 0.000 0.017 CDU & Laundry Asset survey 0.000 0.070 0.070 0.000 0.000 0.000 Bathroom Refurbishment 0.000 0.030 0.030 0.000 0.000 0.000 Alterations to Inchcape to create Minor Injury Unit 0.000 0.015 0.015 0.000 0.000 0.000 Covid-19 Environmental Works 0.765 0.169 0.934 0.339 0.002 0.340 Other Minor Expenditure 0.000 0.020 0.020 0.000 0.020 0.020
1.032 0.137 1.169 0.413 0.022 0.435
NHSS PSS Equipment 0.000 0.013 0.013 0.000 0.013 0.013 Medical Equipment 3.936 6.039 9.975 3.364 0.001 3.364 Non Medical Equipment 0.381 0.495 0.877 0.343 0.000 0.343 Radiotherapy Equipment 4.060 (3.196) 0.864 0.025 0.000 0.025 IC&T 0.036 0.953 0.989 0.278 0.007 0.285 Project Managers 0.634 (0.049) 0.585 0.435 0.000 0.435 Capital Grants 0.150 0.005 0.155 0.059 0.000 0.059 GP Sustainability Loan - St Margarets HC 0.000 0.526 0.526 0.000 0.000 0.000 Contingency 0.901 (0.901) 0.000
Under Commitment in Capital Expenditure
0.397 0.397 Under Commitment in NAV Expenditure
0.128 0.128
Total Capital Programme 29.018 3.631 32.649 15.110 0.053 15.164 Total Forecast Capital Programme Expenditure
32.649
Less NBV of Disposals
(0.206) Less Non Added Value
(1.328)
Less Donated Funding
(0.320) Total Forecast CRL Expenditure inc. Capital
Grants
30.795 Total Forecast CRL Allocations inc. Capital
Grants
30.795 (Over)/Underspend
(0.000)
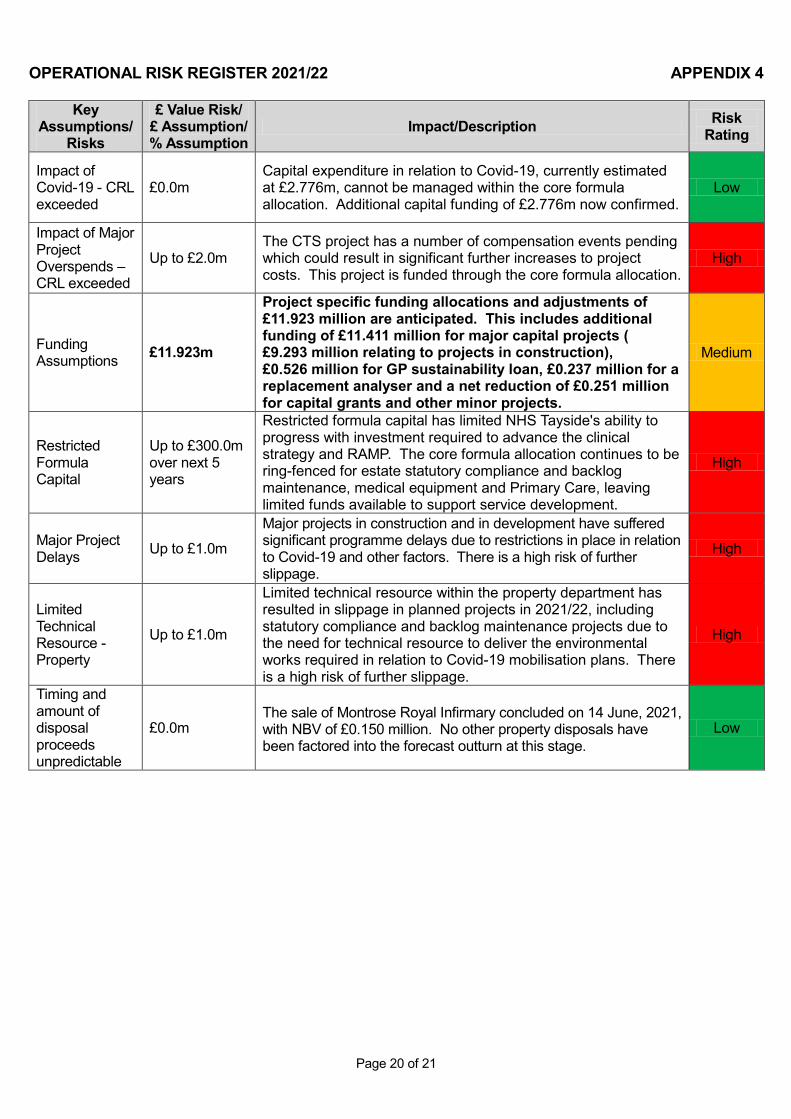
Page 20 of 21
OPERATIONAL RISK REGISTER 2021/22 APPENDIX 4
Key Assumptions/
Risks
£ Value Risk/ £ Assumption/ % Assumption
Impact/Description Risk Rating
Impact of Covid-19 - CRL exceeded
£0.0m Capital expenditure in relation to Covid-19, currently estimated at £2.776m, cannot be managed within the core formula allocation. Additional capital funding of £2.776m now confirmed.
Low
Impact of Major Project Overspends – CRL exceeded
Up to £2.0m The CTS project has a number of compensation events pending which could result in significant further increases to project costs. This project is funded through the core formula allocation.
High
Funding Assumptions £11.923m
Project specific funding allocations and adjustments of £11.923 million are anticipated. This includes additional funding of £11.411 million for major capital projects ( £9.293 million relating to projects in construction), £0.526 million for GP sustainability loan, £0.237 million for a replacement analyser and a net reduction of £0.251 million for capital grants and other minor projects.
Medium
Restricted Formula Capital
Up to £300.0m over next 5 years
Restricted formula capital has limited NHS Tayside's ability to progress with investment required to advance the clinical strategy and RAMP. The core formula allocation continues to be ring-fenced for estate statutory compliance and backlog maintenance, medical equipment and Primary Care, leaving limited funds available to support service development.
High
Major Project Delays Up to £1.0m
Major projects in construction and in development have suffered significant programme delays due to restrictions in place in relation to Covid-19 and other factors. There is a high risk of further slippage.
High
Limited Technical Resource - Property
Up to £1.0m
Limited technical resource within the property department has resulted in slippage in planned projects in 2021/22, including statutory compliance and backlog maintenance projects due to the need for technical resource to deliver the environmental works required in relation to Covid-19 mobilisation plans. There is a high risk of further slippage.
High
Timing and amount of disposal proceeds unpredictable
£0.0m The sale of Montrose Royal Infirmary concluded on 14 June, 2021, with NBV of £0.150 million. No other property disposals have been factored into the forecast outturn at this stage.
Low
Item Number 6.4a PRC03/2022
Page 1 of 5
Meeting: Performance and Resources Committee Meeting date: 10 February 2022 Title: NHS Tayside Performance Report Responsible Executive/ Hazel A Barnett, Director of Performance & Activity Non-Executive: Report Author: Jenni Woods, Health & Business Intelligence Lead 1 Purpose
This is presented to the Performance and Resources Committee for: • Assurance This report relates to a: • Annual Operation Plan This aligns to the following NHSScotland quality ambition(s): • Effective
2 Report summary 2.1 Situation
NHS Tayside routinely reports on our performance against a range of non-financial performance metrics. This report provides an update to the Performance and Resources Committee in respect of NHS Tayside’s performance against a range of national and local measures.
This report provides moderate assurance in respect of NHS Tayside’s current performance. 2.2 Background
NHS Tayside has developed and evolved our performance reporting over the past 3 years, where possible ensuring a focus on national measures and standards, as well as incorporating local measures that align with our strategic direction. This has largely led to a focus on the aims outlined within our Annual Operational Plan, however during 2020-21 the focus shifted towards understanding the impact of the pandemic on our performance against national measures, as well as the incorporation and development of measures aligned with our remobilisation plan. The report has evolved to align with the key objectives outlined with the remobilisation plan 2021-22, alongside the ongoing national indicators which remain in place.
2.3 Assessment Since we last reported to the Performance and Resources Committee the following progress has been made:
• NHS Tayside’s Remobilisation Plan (RMP3) 2021/22 was commissioned as a one year Annual Operational Plan, covering the period 1 April 2021 to 31 March 2022, and provided an update and further iteration of existing Remobilisation Plans which had already received Scottish Government and Board approval. The Remobilisation Plan 2021/22: Mid-Year Update (RMP4) was submitted to the Scottish Government on 30 September 2021 and acknowledged by NHST Board on 16 December 2021.
Page 2 of 5
• A mid-year update approach was adopted by SG this year due to the level of uncertainty around the trajectory of the Covid-19 pandemic and the need to take stock mid-year to determine whether Remobilisation Plans continued to reflect the current situation.
• A Remobilisation Plan (RMP3) 2021/22 Action Tracker was developed, as a tool to monitor progress of the plan’s implementation, and has been presented to the Performance and Resource Committee providing an update on Q1 (April-June) and Q2 (July-September ) performance against actions and predicted trajectories. The Action Tracker covering Q2 which was submitted to the December meeting of the Performance and Resource Committee will supply the detail to populate the first draft of the SG Q3 (October-December) update.
• Following an upgrade to TrakCare in May 2021, reporting functionality for 18 Week RTT has been affected, preventing production of the data. Work undertaken identified the reporting issue is due to a change in data structure and the existing report queries will no longer complete. The Business Unit documented reporting requirements and Intersystems are currently working through the request in order to re-produce the relevant data files from TrakCare. The timeline for completion is dependent on how this work progresses, acknowledging the complexities involved. Whilst 18 Weeks performance cannot currently be reported NHS Tayside remains able to report on out patients, diagnostics and in-patient/day case waiting times which contribute to the 18 Week pathway.
• The following measures are scheduled to have updated information available
throughout February 2022 therefore any updates will be reflected in the next report due to the Performance & Resources Committee: Drug & Alcohol treatments, Infection Control measures, and Smoking Cessation rate.
• Development to include Mental Health activity and performance measures within the
report. Work is progressing to include local and national benchmarking information available on Mental Health activity within the next report due to the Performance & Resources Committee. This work is being progressed in line with the Listen Learn Change Action Plan to ensure measures align with the programme.
This month’s performance report is available at Appendix 1 and shows the following:
• NHS Tayside has seen a continued increase in the number of patients waiting greater than 12 weeks for an elective Inpatient / Daycase procedure (TTG) reaching 6,524 at end November 2021, and 6,959 in December 2021. Routine elective activity is progressing across Ninewells, PRI and Stracathro as per the agreed phased remobilisation planning and TTG activity over April-December 2021 remained above planned levels with 12,135 patients treated against a plan of 10,942 patients.
• The volume of new outpatients waiting beyond 12 weeks fell to 9,881 at end of
November 2021, and increased further to 10,588 at the end of December 2021 following a reduction in activity over the festive period. Clinics continue to remobilise, with the number of patients waiting over 52 weeks also reducing as the Waiting List Validation exercise progresses. Outpatient delivery over April-December 2021 remained above planned levels with 73,884 patients seen against a plan of 59,256 patients.
• The volume of patients waiting beyond 6 weeks for a key diagnostic test has increased
to 6,115 at end December 2021 from 5,181 at end November 2021, compared with a position of 5,534 at end August 2021. The increase is within MRI, CT and ultrasound scans, with a reduction seen in Endoscopy waits.
Page 3 of 5
• NHS Tayside have continued to successfully deliver the national standard for 31 day cancer waiting times and reached 99.3% in December 2021. However the 62 day performance remains below target at 89.7% in December 2021. Despite being below the target, NHS Tayside ranks 2nd highest performance of the mainland Boards against the 62 days standard.
• CAMHS 18 week referral to treatment performance remains above target at 92.3% in December, which is a slight decrease from 95.9% in November 2021.
• Psychological Therapies 18 week referral to treatment performance continues to
improve above target reaching 96.1% in December 2021 compared with 91.8% in November 2021.
• Unscheduled care (A&E waits) performance remains the highest performance in
mainland boards in Scotland and achieved 93.4% in December 2021. Mental Health presentations to A&E being seen within 4 hours has been above 90% over the previous 2 months, with 91% performance in December 2021.
• NHS Tayside continues to achieve 100% for IVF waiting times. • Healthcare Associated Clostridioides difficile Infection (CDI) rate in NHS Tayside has
increased from 9.5 per 100,000 bed days in Quarter 2 2021 (Apr-Jun) to 9.8 per 100,000 Total Occupied Bed Days (TOBDs) in Quarter 3 2021 and remains below the national average.
• Healthcare Associated Staphylococcus aureus bacteraemia infection rate for has
increased from 22.8 per 100,000 Total Occupied Bed Days in Quarter 2 2021 (Apr-Jun) to 23.2 per 100,000 Total Occupied Bed Days in Quarter 3 2021 and is above the national average.
• Healthcare Associated E. coli bacteraemia infection rate has significantly increased
from 40.8 per 100,000 bed days in Quarter 2 (Apr-Jun) to 54.4 per 100,000 Total Occupied Bed Days (TOBDs) in Quarter 3 2021 and is above the national average.
• The volume of Delayed Discharges has decreased from 127 at the end of November
2021, to 121 at the end of December 2021. From June 2021, there was a significant increase in days delayed reaching 1,906 in October 2021. The number of days delayed has been reducing since then reaching 1,649 in December 2021.
• The new outpatient DNA rate rose to 9.2% in December 2021 in line with the Scottish
average, with Tayside’s New DNA rate reducing to 8.7% in November 2021 compared with the Scottish average of 8.8%.
• Stage 1 complaint response performance shows a slight improvement from November
to December with current performance at 67.6%. Whilst Stage 2 responses times have deteriorated and performance is still very low beneath our local target. Two key programmes of work have now been commenced to address performance in this area, however whilst the current caseload is addressed, performance is likely to remain low before we see improvement.
Page 4 of 5
2.3.1 Quality/Patient Care The provision and analysis of performance data will inform clinical decision making around productivity and efficiency.
2.3.2 Workforce Workforce key performance measures are included within the exception report for monitoring when appropriate.
2.3.3 Financial Significant resource implications are associated with Covid recovery, and these are being incorporated within NHS Tayside’s remobilisation plans.
2.3.4 Risk Assessment/Management Performance reporting is linked to corporate risk IDs 26 (Wafting times and RTT targets), 313/494 (Capacity and Flow) and 637 (Child and Adolescent Mental Health Service). These risks are updated accordingly by responsible risk owners.
2.3.5 Equality and Diversity, including health inequalities Capacity restrictions and waiting list delays may impact differentially on patient groups. New ways of working could result in the growth of the ‘digital care divide’ as the move to virtual healthcare may impact vulnerable groups with limited access to technology.
2.3.6 Other impacts N/A
2.3.7 Communication, involvement, engagement and consultation A summary report / infographic titled ‘How we Did’ is published on NHS Tayside Health Board web site and Facebook page illustrating outlining key measurements such as the number of outpatients seen weekly, number of Emergency Room attendances, etc. A number of Board Non-Executives have been engaged in the development of the routine performance report style.
2.3.8 Route to the Meeting Waiting times (TTG, OP, Diagnostics, A&E, CAMHs and Psychological Therapies) performance and remobilisation activity is routinely reported through the Board Business Critical Report to the Executive Leadership Team. Infection Control measures are reported through the Infection Prevention and Control Committee.
2.4 Recommendation Performance and Resources Committee are asked to: • Acknowledge the actions taken since the report in August 2021; and • Acknowledge and take moderate assurance in respect of NHS Tayside’s current
performance against non-financial measures.
3 List of appendices The following appendices are included with this report: • Appendix 1 – Performance Report – Period ending August 2021 • Appendix 2 – Performance Report Reporting Schedule
Level of Assurance System Adequacy Controls
Moderate Assurance
Adequate framework of key controls with minor weaknesses present.
Controls are applied frequently but with evidence of non-compliance.

Page 5 of 5
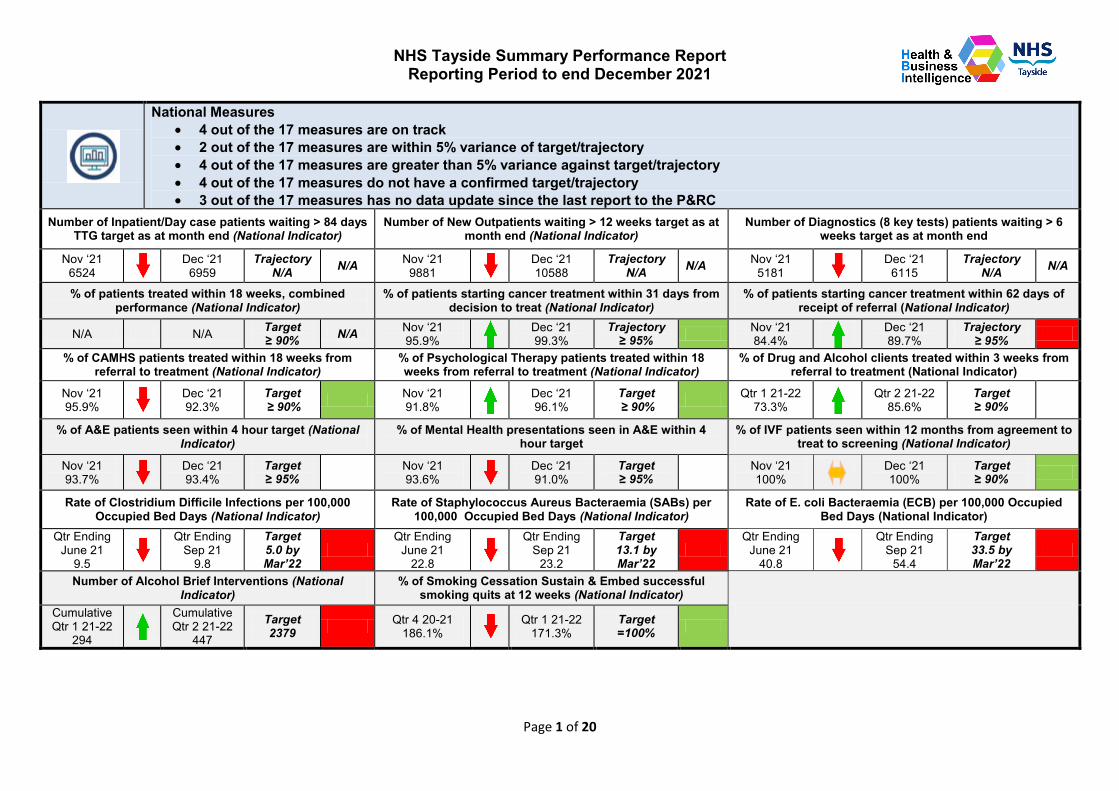
NHS Tayside Summary Performance Report Reporting Period to end December 2021
Page 1 of 20
National Measures • 4 out of the 17 measures are on track • 2 out of the 17 measures are within 5% variance of target/trajectory • 4 out of the 17 measures are greater than 5% variance against target/trajectory • 4 out of the 17 measures do not have a confirmed target/trajectory • 3 out of the 17 measures has no data update since the last report to the P&RC
Number of Inpatient/Day case patients waiting > 84 days TTG target as at month end (National Indicator)
Number of New Outpatients waiting > 12 weeks target as at month end (National Indicator)
Number of Diagnostics (8 key tests) patients waiting > 6 weeks target as at month end
Nov ‘21 6524
Dec ‘21 6959
Trajectory N/A N/A Nov ‘21
9881 Dec ‘21 10588
Trajectory N/A N/A Nov ‘21
5181 Dec ‘21
6115 Trajectory
N/A N/A
% of patients treated within 18 weeks, combined performance (National Indicator)
% of patients starting cancer treatment within 31 days from decision to treat (National Indicator)
% of patients starting cancer treatment within 62 days of receipt of referral (National Indicator)
N/A N/A Target ≥ 90% N/A Nov ‘21
95.9% Dec ‘21 99.3%
Trajectory ≥ 95% Nov ‘21
84.4% Dec ‘21 89.7%
Trajectory ≥ 95%
% of CAMHS patients treated within 18 weeks from referral to treatment (National Indicator)
% of Psychological Therapy patients treated within 18 weeks from referral to treatment (National Indicator)
% of Drug and Alcohol clients treated within 3 weeks from referral to treatment (National Indicator)
Nov ‘21 95.9%
Dec ‘21 92.3%
Target ≥ 90% Nov ‘21
91.8% Dec ‘21 96.1%
Target ≥ 90% Qtr 1 21-22
73.3% Qtr 2 21-22
85.6% Target ≥ 90%
% of A&E patients seen within 4 hour target (National Indicator)
% of Mental Health presentations seen in A&E within 4 hour target
% of IVF patients seen within 12 months from agreement to treat to screening (National Indicator)
Nov ‘21 93.7%
Dec ‘21 93.4%
Target ≥ 95% Nov ‘21
93.6% Dec ‘21 91.0%
Target ≥ 95% Nov ‘21
100% Dec ‘21
100% Target ≥ 90%
Rate of Clostridium Difficile Infections per 100,000 Occupied Bed Days (National Indicator)
Rate of Staphylococcus Aureus Bacteraemia (SABs) per 100,000 Occupied Bed Days (National Indicator)
Rate of E. coli Bacteraemia (ECB) per 100,000 Occupied Bed Days (National Indicator)
Qtr Ending June 21
9.5
Qtr Ending Sep 21
9.8
Target 5.0 by Mar’22
Qtr Ending
June 21 22.8
Qtr Ending Sep 21
23.2
Target 13.1 by Mar’22
Qtr Ending
June 21 40.8
Qtr Ending Sep 21
54.4
Target 33.5 by Mar’22
Number of Alcohol Brief Interventions (National Indicator)
% of Smoking Cessation Sustain & Embed successful smoking quits at 12 weeks (National Indicator)
Cumulative Qtr 1 21-22
294
Cumulative Qtr 2 21-22
447
Target 2379 Qtr 4 20-21
186.1% Qtr 1 21-22
171.3% Target =100%
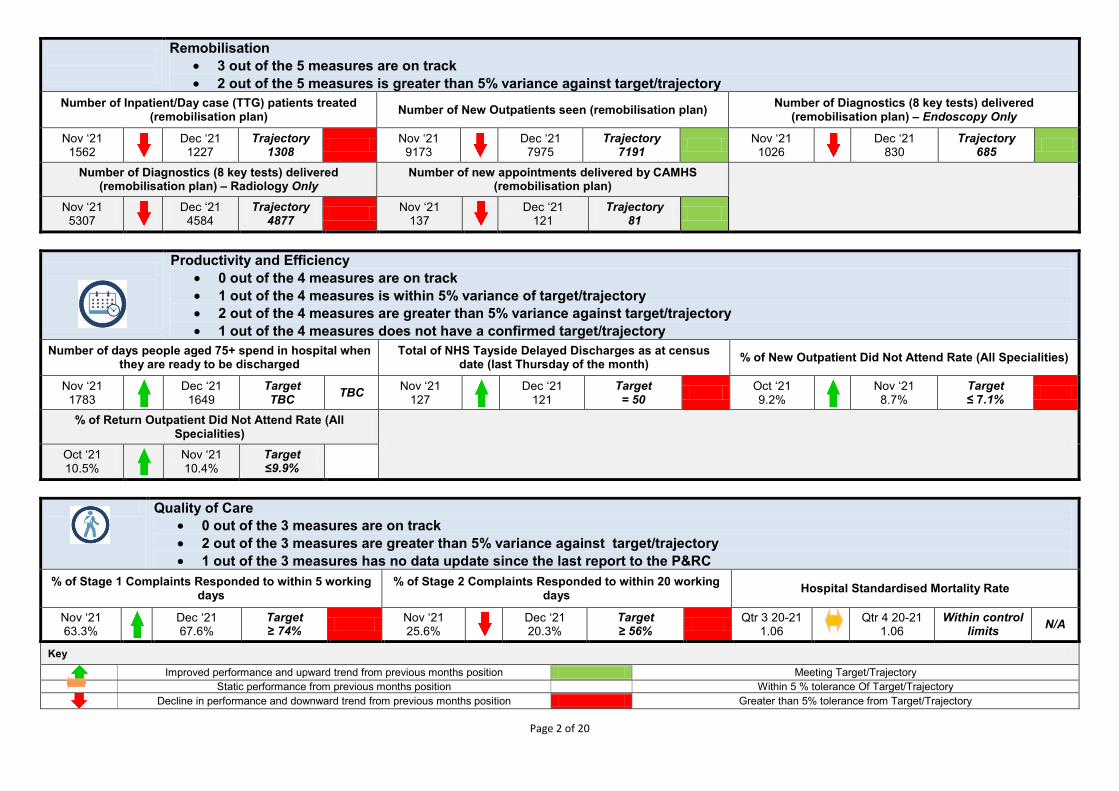
Page 2 of 20
Remobilisation • 3 out of the 5 measures are on track • 2 out of the 5 measures is greater than 5% variance against target/trajectory
Number of Inpatient/Day case (TTG) patients treated (remobilisation plan) Number of New Outpatients seen (remobilisation plan) Number of Diagnostics (8 key tests) delivered
(remobilisation plan) – Endoscopy Only
Nov ‘21 1562
Dec ‘21 1227
Trajectory 1308 Nov ‘21
9173 Dec ‘21
7975 Trajectory
7191 Nov ‘21 1026
Dec ‘21 830
Trajectory 685
Number of Diagnostics (8 key tests) delivered (remobilisation plan) – Radiology Only
Number of new appointments delivered by CAMHS (remobilisation plan)
Nov ‘21
5307 Dec ‘21
4584 Trajectory
4877 Nov ‘21 137
Dec ‘21 121
Trajectory 81
Productivity and Efficiency • 0 out of the 4 measures are on track • 1 out of the 4 measures is within 5% variance of target/trajectory • 2 out of the 4 measures are greater than 5% variance against target/trajectory • 1 out of the 4 measures does not have a confirmed target/trajectory
Number of days people aged 75+ spend in hospital when they are ready to be discharged
Total of NHS Tayside Delayed Discharges as at census date (last Thursday of the month) % of New Outpatient Did Not Attend Rate (All Specialities)
Nov ‘21 1783
Dec ‘21 1649
Target TBC TBC Nov ‘21
127 Dec ‘21
121 Target = 50 Oct ‘21
9.2% Nov ‘21 8.7%
Target ≤ 7.1%
% of Return Outpatient Did Not Attend Rate (All Specialities)
Oct ‘21 10.5%
Nov ‘21 10.4%
Target ≤9.9%
Quality of Care • 0 out of the 3 measures are on track • 2 out of the 3 measures are greater than 5% variance against target/trajectory • 1 out of the 3 measures has no data update since the last report to the P&RC
% of Stage 1 Complaints Responded to within 5 working days
% of Stage 2 Complaints Responded to within 20 working days Hospital Standardised Mortality Rate
Nov ‘21 63.3%
Dec ‘21 67.6%
Target ≥ 74% Nov ‘21
25.6% Dec ‘21 20.3%
Target ≥ 56% Qtr 3 20-21
1.06 Qtr 4 20-21
1.06 Within control
limits N/A
Key
Improved performance and upward trend from previous months position Meeting Target/Trajectory Static performance from previous months position Within 5 % tolerance Of Target/Trajectory
Decline in performance and downward trend from previous months position Greater than 5% tolerance from Target/Trajectory
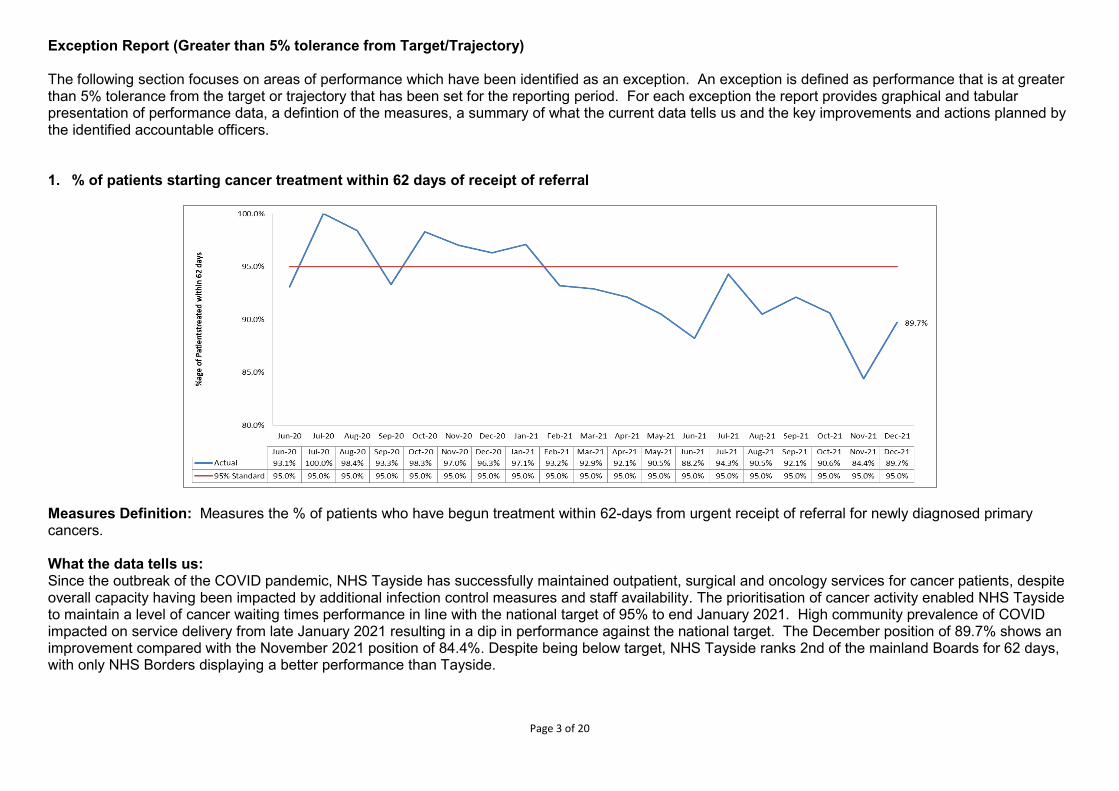
Page 3 of 20
Exception Report (Greater than 5% tolerance from Target/Trajectory) The following section focuses on areas of performance which have been identified as an exception. An exception is defined as performance that is at greater than 5% tolerance from the target or trajectory that has been set for the reporting period. For each exception the report provides graphical and tabular presentation of performance data, a defintion of the measures, a summary of what the current data tells us and the key improvements and actions planned by the identified accountable officers. 1. % of patients starting cancer treatment within 62 days of receipt of referral
Measures Definition: Measures the % of patients who have begun treatment within 62-days from urgent receipt of referral for newly diagnosed primary cancers. What the data tells us: Since the outbreak of the COVID pandemic, NHS Tayside has successfully maintained outpatient, surgical and oncology services for cancer patients, despite overall capacity having been impacted by additional infection control measures and staff availability. The prioritisation of cancer activity enabled NHS Tayside to maintain a level of cancer waiting times performance in line with the national target of 95% to end January 2021. High community prevalence of COVID impacted on service delivery from late January 2021 resulting in a dip in performance against the national target. The December position of 89.7% shows an improvement compared with the November 2021 position of 84.4%. Despite being below target, NHS Tayside ranks 2nd of the mainland Boards for 62 days, with only NHS Borders displaying a better performance than Tayside.
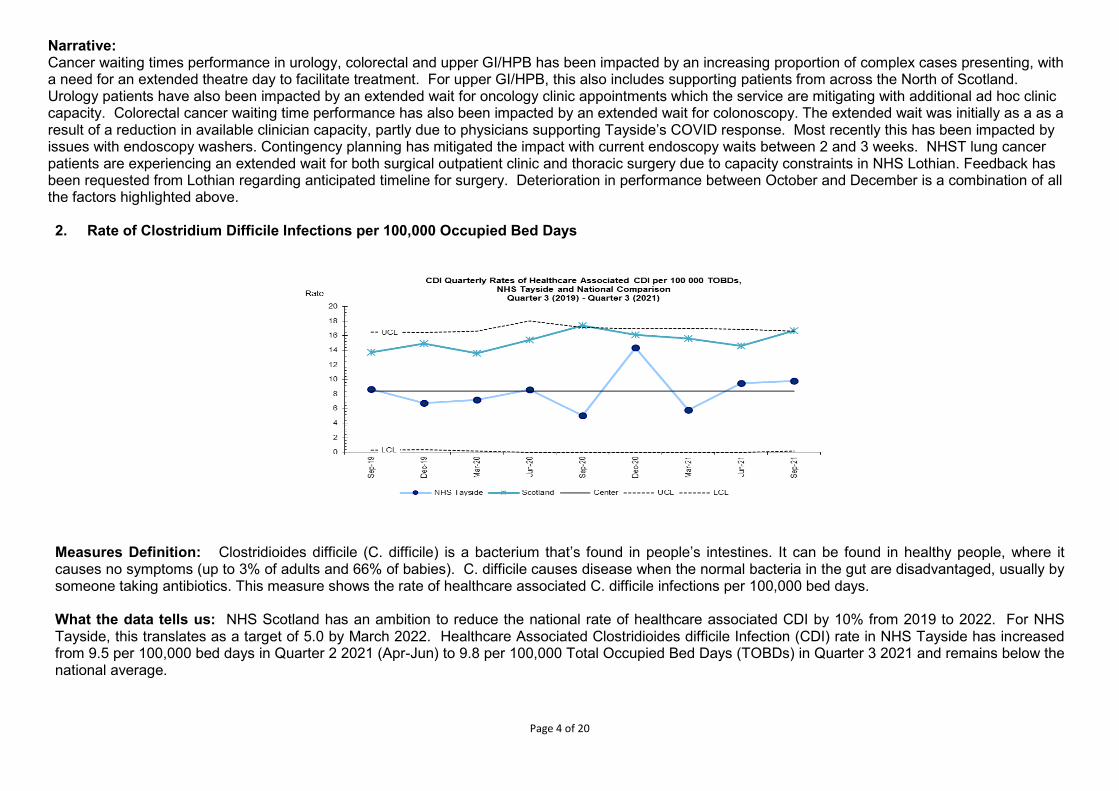
Page 4 of 20
Narrative: Cancer waiting times performance in urology, colorectal and upper GI/HPB has been impacted by an increasing proportion of complex cases presenting, with a need for an extended theatre day to facilitate treatment. For upper GI/HPB, this also includes supporting patients from across the North of Scotland. Urology patients have also been impacted by an extended wait for oncology clinic appointments which the service are mitigating with additional ad hoc clinic capacity. Colorectal cancer waiting time performance has also been impacted by an extended wait for colonoscopy. The extended wait was initially as a as a result of a reduction in available clinician capacity, partly due to physicians supporting Tayside’s COVID response. Most recently this has been impacted by issues with endoscopy washers. Contingency planning has mitigated the impact with current endoscopy waits between 2 and 3 weeks. NHST lung cancer patients are experiencing an extended wait for both surgical outpatient clinic and thoracic surgery due to capacity constraints in NHS Lothian. Feedback has been requested from Lothian regarding anticipated timeline for surgery. Deterioration in performance between October and December is a combination of all the factors highlighted above. 2. Rate of Clostridium Difficile Infections per 100,000 Occupied Bed Days
Measures Definition: Clostridioides difficile (C. difficile) is a bacterium that’s found in people’s intestines. It can be found in healthy people, where it causes no symptoms (up to 3% of adults and 66% of babies). C. difficile causes disease when the normal bacteria in the gut are disadvantaged, usually by someone taking antibiotics. This measure shows the rate of healthcare associated C. difficile infections per 100,000 bed days. What the data tells us: NHS Scotland has an ambition to reduce the national rate of healthcare associated CDI by 10% from 2019 to 2022. For NHS Tayside, this translates as a target of 5.0 by March 2022. Healthcare Associated Clostridioides difficile Infection (CDI) rate in NHS Tayside has increased from 9.5 per 100,000 bed days in Quarter 2 2021 (Apr-Jun) to 9.8 per 100,000 Total Occupied Bed Days (TOBDs) in Quarter 3 2021 and remains below the national average.
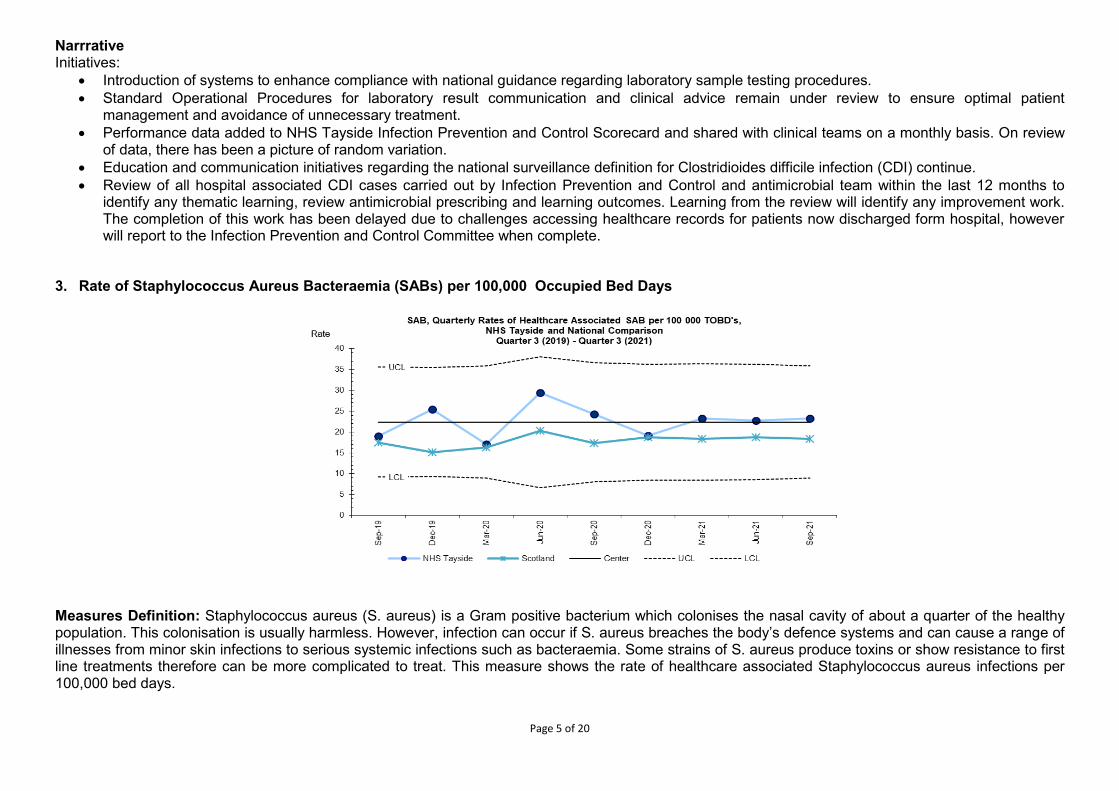
Page 5 of 20
Narrrative Initiatives:
• Introduction of systems to enhance compliance with national guidance regarding laboratory sample testing procedures. • Standard Operational Procedures for laboratory result communication and clinical advice remain under review to ensure optimal patient
management and avoidance of unnecessary treatment. • Performance data added to NHS Tayside Infection Prevention and Control Scorecard and shared with clinical teams on a monthly basis. On review
of data, there has been a picture of random variation. • Education and communication initiatives regarding the national surveillance definition for Clostridioides difficile infection (CDI) continue. • Review of all hospital associated CDI cases carried out by Infection Prevention and Control and antimicrobial team within the last 12 months to
identify any thematic learning, review antimicrobial prescribing and learning outcomes. Learning from the review will identify any improvement work. The completion of this work has been delayed due to challenges accessing healthcare records for patients now discharged form hospital, however will report to the Infection Prevention and Control Committee when complete.
3. Rate of Staphylococcus Aureus Bacteraemia (SABs) per 100,000 Occupied Bed Days
Measures Definition: Staphylococcus aureus (S. aureus) is a Gram positive bacterium which colonises the nasal cavity of about a quarter of the healthy population. This colonisation is usually harmless. However, infection can occur if S. aureus breaches the body’s defence systems and can cause a range of illnesses from minor skin infections to serious systemic infections such as bacteraemia. Some strains of S. aureus produce toxins or show resistance to first line treatments therefore can be more complicated to treat. This measure shows the rate of healthcare associated Staphylococcus aureus infections per 100,000 bed days.
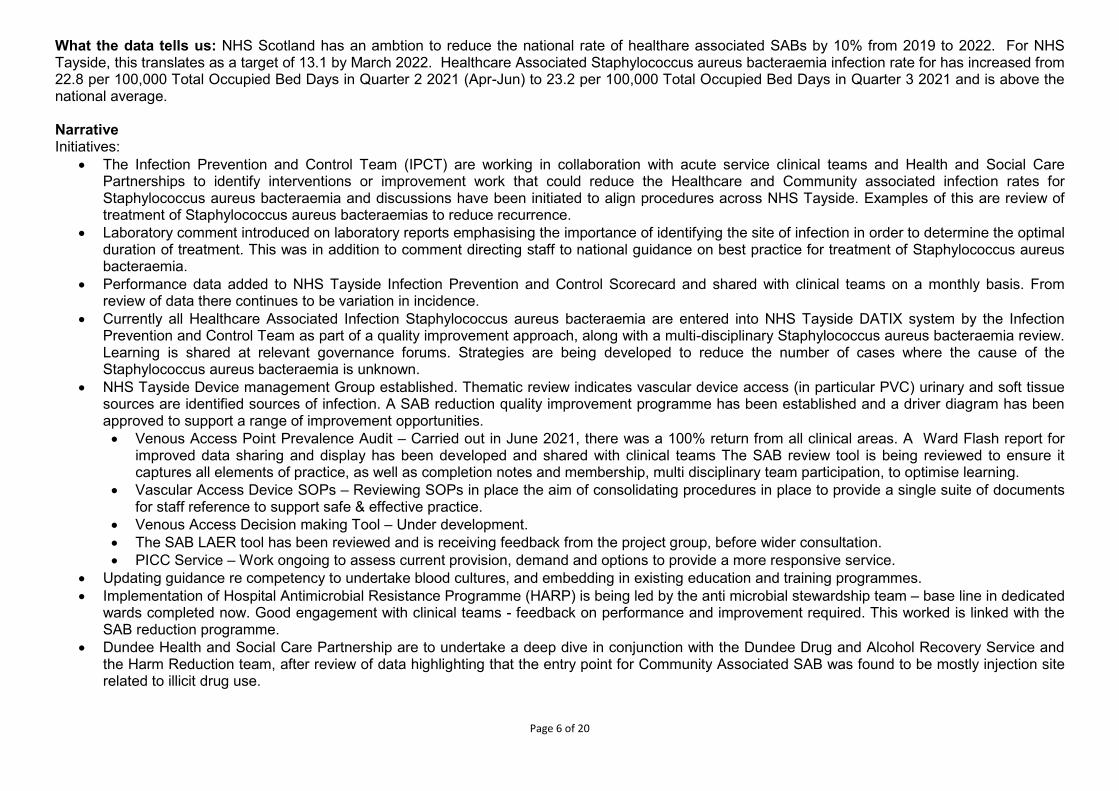
Page 6 of 20
What the data tells us: NHS Scotland has an ambtion to reduce the national rate of healthare associated SABs by 10% from 2019 to 2022. For NHS Tayside, this translates as a target of 13.1 by March 2022. Healthcare Associated Staphylococcus aureus bacteraemia infection rate for has increased from 22.8 per 100,000 Total Occupied Bed Days in Quarter 2 2021 (Apr-Jun) to 23.2 per 100,000 Total Occupied Bed Days in Quarter 3 2021 and is above the national average. Narrative Initiatives:
• The Infection Prevention and Control Team (IPCT) are working in collaboration with acute service clinical teams and Health and Social Care Partnerships to identify interventions or improvement work that could reduce the Healthcare and Community associated infection rates for Staphylococcus aureus bacteraemia and discussions have been initiated to align procedures across NHS Tayside. Examples of this are review of treatment of Staphylococcus aureus bacteraemias to reduce recurrence.
• Laboratory comment introduced on laboratory reports emphasising the importance of identifying the site of infection in order to determine the optimal duration of treatment. This was in addition to comment directing staff to national guidance on best practice for treatment of Staphylococcus aureus bacteraemia.
• Performance data added to NHS Tayside Infection Prevention and Control Scorecard and shared with clinical teams on a monthly basis. From review of data there continues to be variation in incidence.
• Currently all Healthcare Associated Infection Staphylococcus aureus bacteraemia are entered into NHS Tayside DATIX system by the Infection Prevention and Control Team as part of a quality improvement approach, along with a multi-disciplinary Staphylococcus aureus bacteraemia review. Learning is shared at relevant governance forums. Strategies are being developed to reduce the number of cases where the cause of the Staphylococcus aureus bacteraemia is unknown.
• NHS Tayside Device management Group established. Thematic review indicates vascular device access (in particular PVC) urinary and soft tissue sources are identified sources of infection. A SAB reduction quality improvement programme has been established and a driver diagram has been approved to support a range of improvement opportunities. • Venous Access Point Prevalence Audit – Carried out in June 2021, there was a 100% return from all clinical areas. A Ward Flash report for
improved data sharing and display has been developed and shared with clinical teams The SAB review tool is being reviewed to ensure it captures all elements of practice, as well as completion notes and membership, multi disciplinary team participation, to optimise learning.
• Vascular Access Device SOPs – Reviewing SOPs in place the aim of consolidating procedures in place to provide a single suite of documents for staff reference to support safe & effective practice.
• Venous Access Decision making Tool – Under development. • The SAB LAER tool has been reviewed and is receiving feedback from the project group, before wider consultation. • PICC Service – Work ongoing to assess current provision, demand and options to provide a more responsive service.
• Updating guidance re competency to undertake blood cultures, and embedding in existing education and training programmes. • Implementation of Hospital Antimicrobial Resistance Programme (HARP) is being led by the anti microbial stewardship team – base line in dedicated
wards completed now. Good engagement with clinical teams - feedback on performance and improvement required. This worked is linked with the SAB reduction programme.
• Dundee Health and Social Care Partnership are to undertake a deep dive in conjunction with the Dundee Drug and Alcohol Recovery Service and the Harm Reduction team, after review of data highlighting that the entry point for Community Associated SAB was found to be mostly injection site related to illicit drug use.
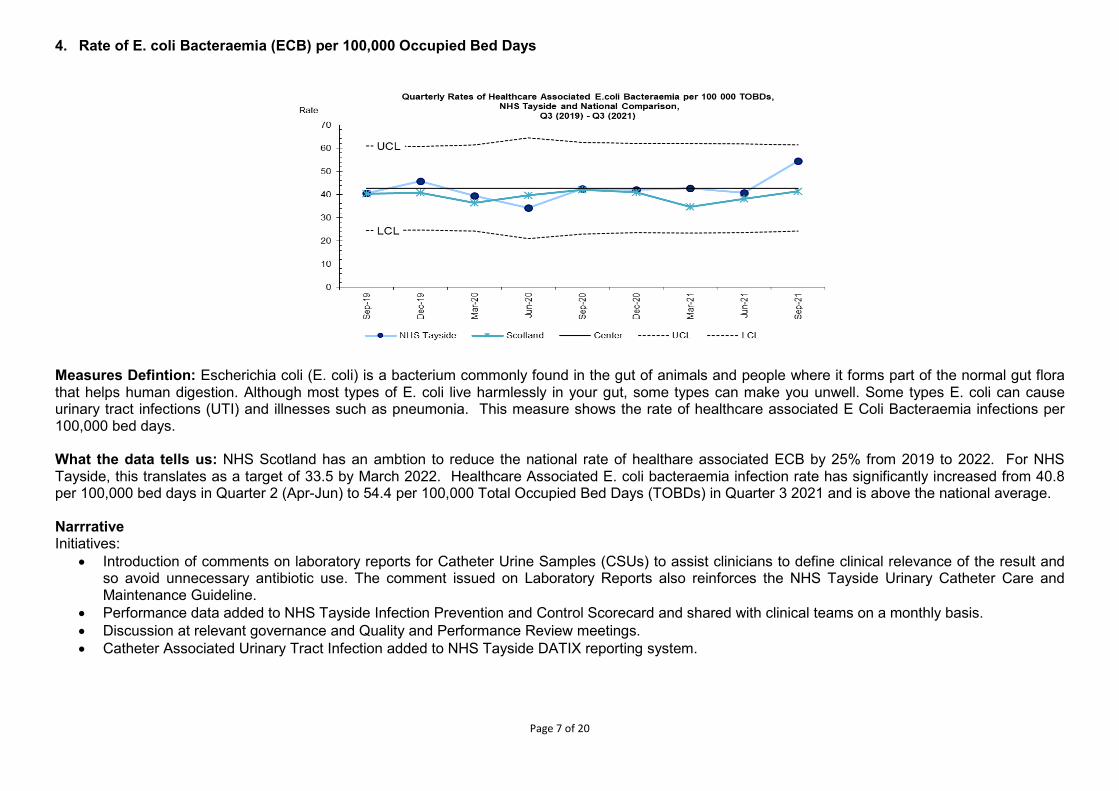
Page 7 of 20
4. Rate of E. coli Bacteraemia (ECB) per 100,000 Occupied Bed Days
Measures Defintion: Escherichia coli (E. coli) is a bacterium commonly found in the gut of animals and people where it forms part of the normal gut flora that helps human digestion. Although most types of E. coli live harmlessly in your gut, some types can make you unwell. Some types E. coli can cause urinary tract infections (UTI) and illnesses such as pneumonia. This measure shows the rate of healthcare associated E Coli Bacteraemia infections per 100,000 bed days. What the data tells us: NHS Scotland has an ambtion to reduce the national rate of healthare associated ECB by 25% from 2019 to 2022. For NHS Tayside, this translates as a target of 33.5 by March 2022. Healthcare Associated E. coli bacteraemia infection rate has significantly increased from 40.8 per 100,000 bed days in Quarter 2 (Apr-Jun) to 54.4 per 100,000 Total Occupied Bed Days (TOBDs) in Quarter 3 2021 and is above the national average. Narrrative Initiatives:
• Introduction of comments on laboratory reports for Catheter Urine Samples (CSUs) to assist clinicians to define clinical relevance of the result and so avoid unnecessary antibiotic use. The comment issued on Laboratory Reports also reinforces the NHS Tayside Urinary Catheter Care and Maintenance Guideline.
• Performance data added to NHS Tayside Infection Prevention and Control Scorecard and shared with clinical teams on a monthly basis. • Discussion at relevant governance and Quality and Performance Review meetings. • Catheter Associated Urinary Tract Infection added to NHS Tayside DATIX reporting system.
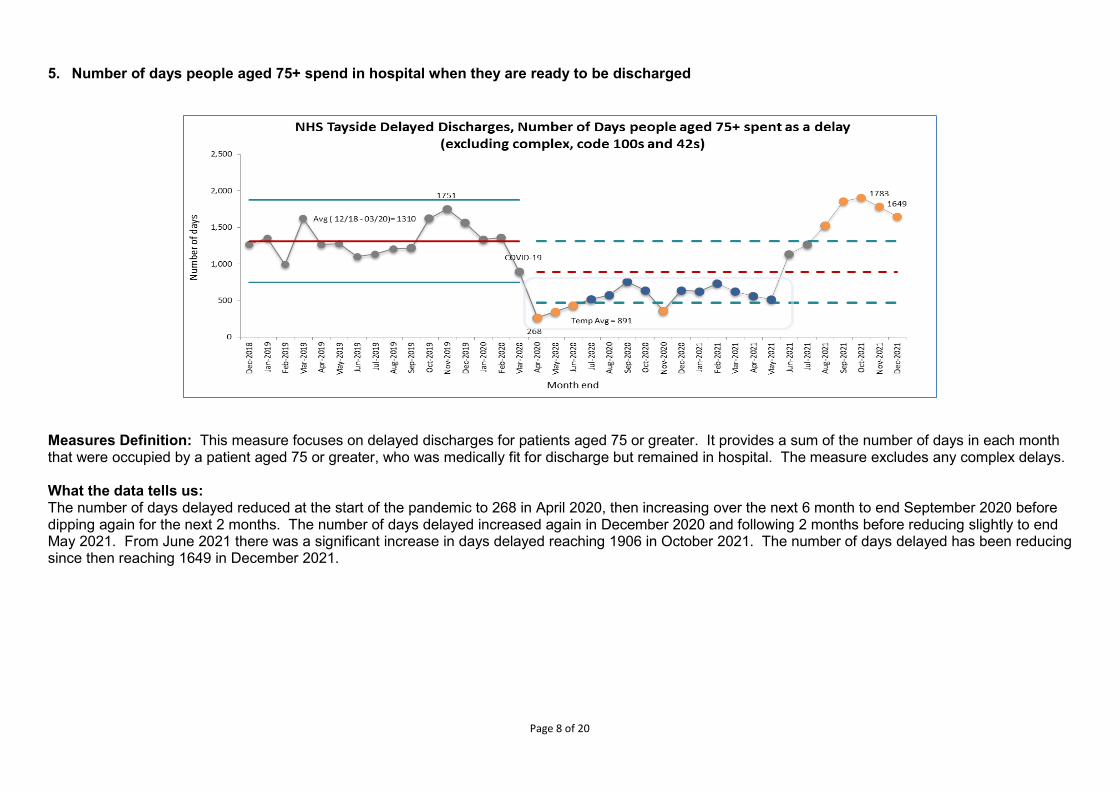
Page 8 of 20
5. Number of days people aged 75+ spend in hospital when they are ready to be discharged
Measures Definition: This measure focuses on delayed discharges for patients aged 75 or greater. It provides a sum of the number of days in each month that were occupied by a patient aged 75 or greater, who was medically fit for discharge but remained in hospital. The measure excludes any complex delays. What the data tells us: The number of days delayed reduced at the start of the pandemic to 268 in April 2020, then increasing over the next 6 month to end September 2020 before dipping again for the next 2 months. The number of days delayed increased again in December 2020 and following 2 months before reducing slightly to end May 2021. From June 2021 there was a significant increase in days delayed reaching 1906 in October 2021. The number of days delayed has been reducing since then reaching 1649 in December 2021.
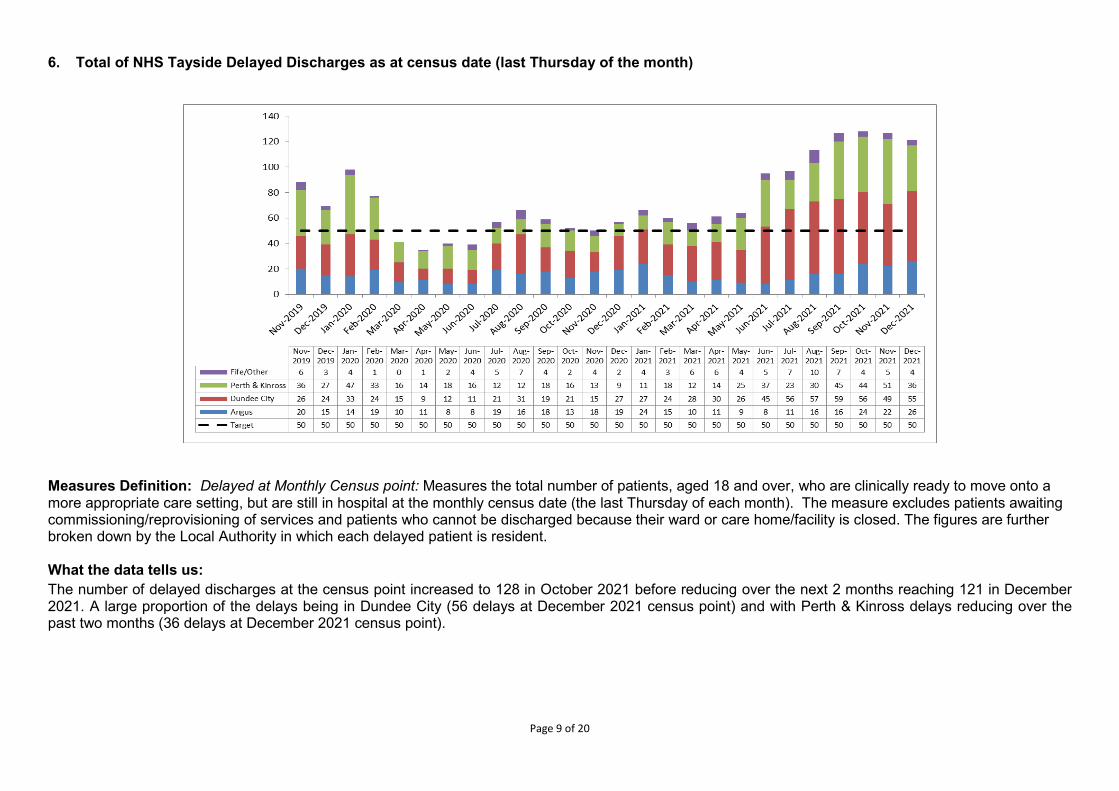
Page 9 of 20
6. Total of NHS Tayside Delayed Discharges as at census date (last Thursday of the month)
Measures Definition: Delayed at Monthly Census point: Measures the total number of patients, aged 18 and over, who are clinically ready to move onto a more appropriate care setting, but are still in hospital at the monthly census date (the last Thursday of each month). The measure excludes patients awaiting commissioning/reprovisioning of services and patients who cannot be discharged because their ward or care home/facility is closed. The figures are further broken down by the Local Authority in which each delayed patient is resident. What the data tells us: The number of delayed discharges at the census point increased to 128 in October 2021 before reducing over the next 2 months reaching 121 in December 2021. A large proportion of the delays being in Dundee City (56 delays at December 2021 census point) and with Perth & Kinross delays reducing over the past two months (36 delays at December 2021 census point).
Page 10 of 20
Narrative: Angus: Within Angus, delayed discharge rates (in over 75-year olds) were previously reduced due to ongoing good multi-disciplinary communication in the community and in hospitals and planned date of discharge process. Angus continues to perform in the top quartile in Scotland. However, there has been a small increase in delays in Angus in Autumn 2021 due to a combination of the large volume of Adults with Incapacity (AWI) work, Care at Home providers struggling with capacity issues and recruitment, and a number of complex care cases for whom accommodation solutions are not straightforward. We are working with Care at Home providers on their recruitment drives. The bed days lost to complex delays have doubled between 2019/20 and 2020/21 Q2. This means that 1154 bed days between the beginning of October 2019 and the end of September 2020 relate to complex delays. This accounts for only 1.8% of all bed days used following an admission in an emergency. This growth is largely due to the closure of Courts on 27th March 2020 due to the COVID 19 pandemic. Local Courts opened from 22nd June 2020 and have started to deal with the backlog of Guardianship applications. The situation continues to be challenging with a significant backlog of Court reports; in addition, Courts have shown a tendency to require more reviews, thereby resulting in increased report requests. Additional resources are being identified to support Mental Health Officer (MHO) activity. There is a group of Psychiatry of Old Age patients whose discharge is delayed to due to the lack of availability of appropriate community accommodation and support solutions. We continue to work with Angus Council Procurement Team with a view to commissioning an appropriate Care Home within Angus. While recognising current challenges in available social care workforce, we also recognise the strong performance of the Angus Care Model over many years focussed on enhanced community support. We continue to progress the roll out of integrated teams in the community with care managers working alongside our community nursing service. Areas of Angus who have made the greatest progress with integrated teams are experiencing less problems with access to social care at this time. Angus HSCP is also working to improve the process for patients with Incapacity, including the Guardianship process and the use of 13ZA of the Social Work (Scotland) Act 1968. A small number of complex patients who have forensic or complex needs require specific types of accommodation that are not readily available locally or across Scotland, and which may need to be commissioned elsewhere in the UK, or require special builds. Planning continues in relation to allocating the utilising the Winter Planning, MDT and Care at Home funding to support and increase provision in the community. A number of workstreams will address the need for improved capacity in care at home, Enablement, Mental Health Officer activity, care management, Occupational Therapy including equipment and adaptations, and intermediate care, community nursing and OOHs.
Page 11 of 20
Dundee: Increased demand for social care continues to be the key issue impacting on delayed discharge performance. Although the numbers of delayed patients remain high, there has been a levelling off with the figures stabilising this month. Social care availability has begun to improve slightly with our Home First assessment provider now reporting positive recruitment activity which is generating increased capacity. Although a significant number of local care homes have been affected by Covid in recent weeks, the policy of offering interim respite placements has continued with a total of 39 admissions to date. The revised eligibility criteria for access to social care is now fully implemented, with review processes in place to ensure existing service users have their care packages assessed against these criteria. Work is ongoing to further embed the AHP service into this process to ensure a continued focus on independent living and the maximisation of functional ability. As access to social care begins to improve, our strategic plan to focus on admission avoidance through the development of urgent care and the Home First model can be refreshed once again. This further complements the work to implement eligibility criteria based on functional ability, with needs related to social isolation becoming more aligned with our 3rd sector partnerships. In addition, a suite has been opened in Menzieshill House (Local Authority Residential Home) which will provide 6 interim beds specifically to accommodate patients whose discharge has been delayed. Admissions to this unit are ongoing this week (24th January). There are now also an additional 20 beds available on the RVH site to support patient flow from the acute hospital, and 8 beds within Turriff House Residential Unit to support step up/down care for older people with mental health needs, both in a community setting and on the Kingsway site. Our key piece of work to support capacity and flow as well as optimising the patient’s journey is the continued roll out of Planned Date of Discharge across all hospitals in Tayside. This is supported by the Tayside Unscheduled Care Board, and is a partnership between all 3 of the Tayside HSCPs. A senior coordinator has been identified within the Dundee service who has had her full time role protected to lead on this roll out, which has now been successfully implemented in Orthopaedics in Ninewells and is being rolled out in Surgical, MFE, Covid, and across the RVH site. Since the last report, we have seen the stabilising of the standard delay numbers, although they remain much higher than we would wish. In terms of the complex delays, there has been a reduction as several of the longer term plans for discharge have been activated. This has a particular impact on bed days lost to the system as the patients with complex codes tend to be delayed for significantly longer periods of time.
Page 12 of 20
Perth & Kinross: In December 2021 Perth & Kinross Health & Social Care Partnership (HSCP) in collaboration with acute colleagues and others commenced the completion of the Discharge without Delay self assessment in order to gain a better understanding of current good practice and what can be further improved to optimise the patient journey on admission to hospital through to discharge back into the community. A Discharge without Delay Steering Group has been established with representation from senior managers from PKHSCP, Acute and other sectors to provide leadership, oversight and monitoring. Two workstreams have been established to take forward the identified improvements, reporting into the Steering Group:
• Interim Care Beds • Inpatient and Community
Perth & Kinross Health & Social Care Partnership has approved additional funding to enhance our existing Locality Integrated Care Services. Posts are now being recruited to with an anticipated commencement date of early April 2022. Capacity will include clinical co-ordinators, assistant practitioners, community care assistants and overnight social care support. This additional workforce capacity will allow care to be provided over a 24/7 period, with initial test to commence in Perth City Locality. The development of our ‘Hospital at Home’ service has been slightly delayed due to recruitment challenges. However, again we are anticipating that the required nursing and clinical workforce will be in place by early April 2022. A co-located and integrated Urgent Care model is being explored, which will bring together he key elements of urgent care in hours with a single point of contact to better co-ordinate primary and community care, aligned to secondary care and urgent care out of hours. We continue to develop our Advance Nurse Practitioner service to support our urgent care approach across Perth & Kinross. We have appointed to a Nurse Consultant for Urgent Care whose role will be to support with the further development of the Urgent Care Pathway linking into community services. Two tests of change are currently being taken forward, learning from which will help to inform the development of the pathway. To support timely discharges we have invested in Care at Home services, in testing Hospital at Home and in staff to support our Discharge to Assess approach. Care at Home/HART Much progress has been made with the redesign of Care at Home and significant actions completed but given the complexities and interdependencies, work continues to develop and design a flexible, responsive, outcome-based approach to supporting a sustainable model to enable people to remain at home. Work is focused on strengthening Care at Home foundations, supporting the workforce to thrive and preparing Care at Home to be fit for the future. We are developing pathways into care with a variety of stakeholders including employability networks, Perth College UHI, Developing the Young Workforce Co-ordinators and Skills and Employment Initiative reps. These will form part of a toolkit of resources to promote careers in social care. We have employed a Digital Marketing Graduate whose sole focus is to positively present care at home on a variety of digital platforms. A Wellbeing team approach is being developed for unmet need in rural locations. This approach will bring, more flexibility of service provision and the team will provide a culture of team responsibility, shift the decision making closer to the front line. A team that is committed to wellbeing, both of the people they support and its team members. In addition to a traditional personal-care delivery CAH model, this team would also look at technology, aids and adaptations, support from family, friends, the wider community, as well as other services and paid support.
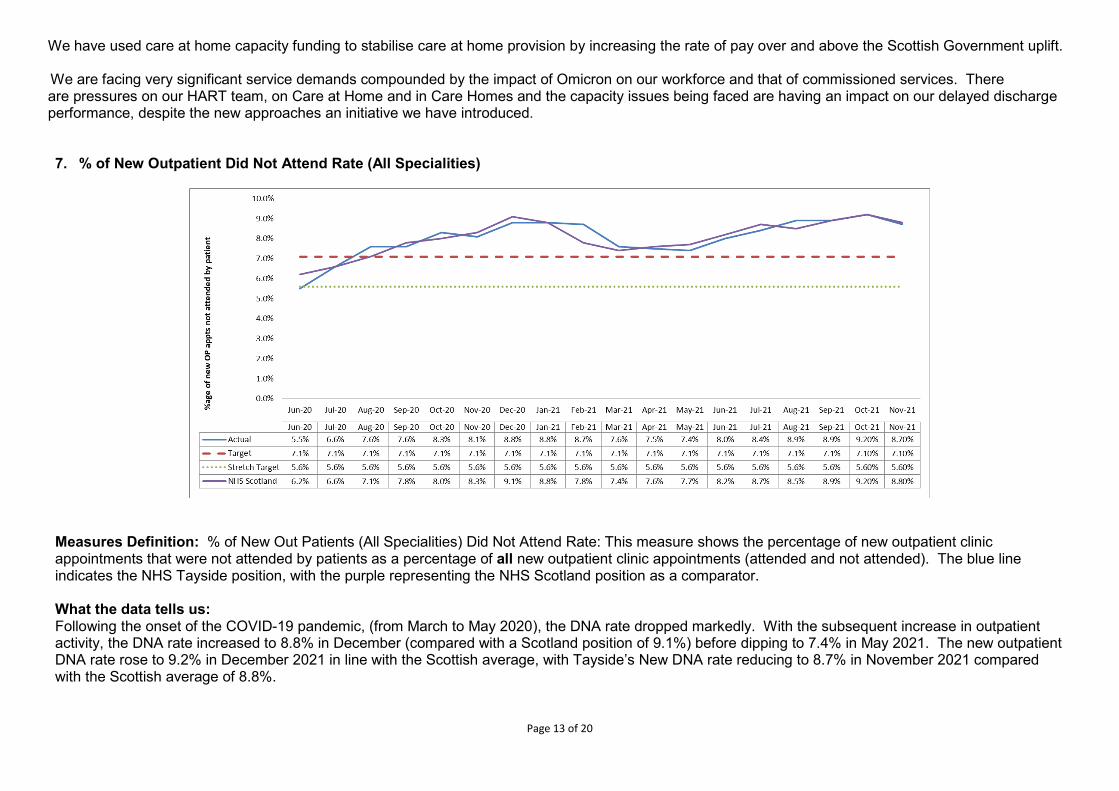
Page 13 of 20
We have used care at home capacity funding to stabilise care at home provision by increasing the rate of pay over and above the Scottish Government uplift. We are facing very significant service demands compounded by the impact of Omicron on our workforce and that of commissioned services. There are pressures on our HART team, on Care at Home and in Care Homes and the capacity issues being faced are having an impact on our delayed discharge performance, despite the new approaches an initiative we have introduced.
7. % of New Outpatient Did Not Attend Rate (All Specialities)
Measures Definition: % of New Out Patients (All Specialities) Did Not Attend Rate: This measure shows the percentage of new outpatient clinic appointments that were not attended by patients as a percentage of all new outpatient clinic appointments (attended and not attended). The blue line indicates the NHS Tayside position, with the purple representing the NHS Scotland position as a comparator. What the data tells us: Following the onset of the COVID-19 pandemic, (from March to May 2020), the DNA rate dropped markedly. With the subsequent increase in outpatient activity, the DNA rate increased to 8.8% in December (compared with a Scotland position of 9.1%) before dipping to 7.4% in May 2021. The new outpatient DNA rate rose to 9.2% in December 2021 in line with the Scottish average, with Tayside’s New DNA rate reducing to 8.7% in November 2021 compared with the Scottish average of 8.8%.
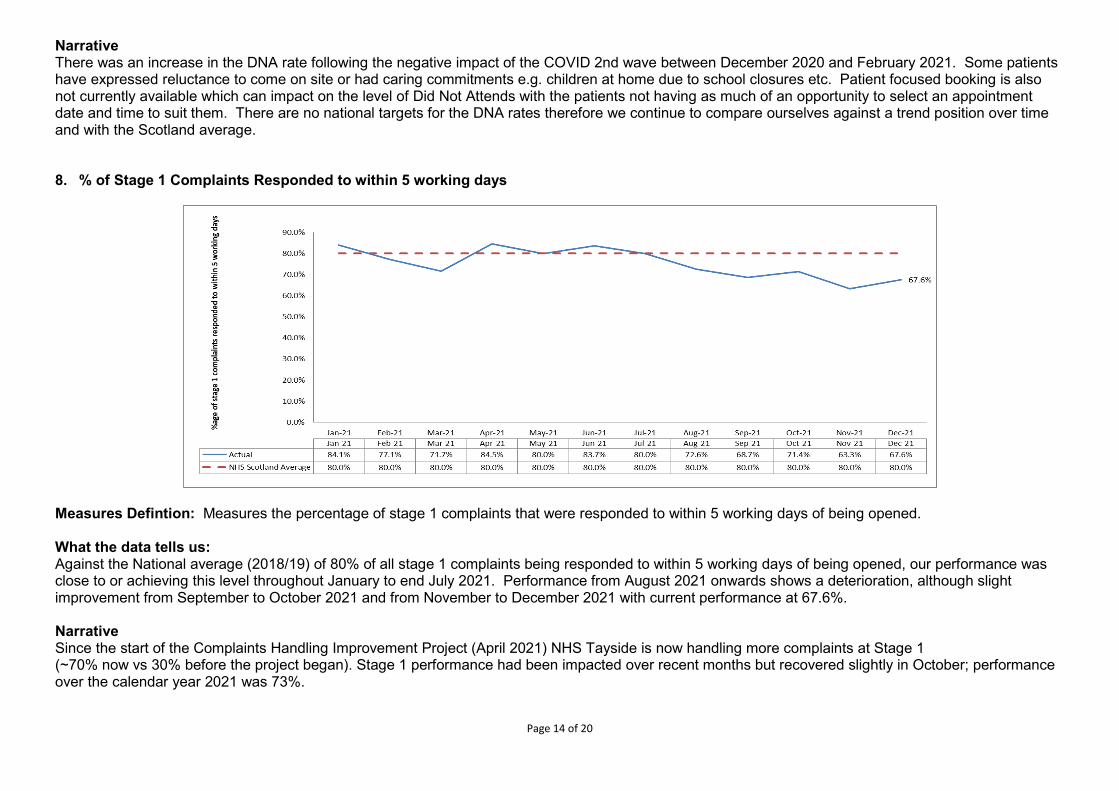
Page 14 of 20
Narrative There was an increase in the DNA rate following the negative impact of the COVID 2nd wave between December 2020 and February 2021. Some patients have expressed reluctance to come on site or had caring commitments e.g. children at home due to school closures etc. Patient focused booking is also not currently available which can impact on the level of Did Not Attends with the patients not having as much of an opportunity to select an appointment date and time to suit them. There are no national targets for the DNA rates therefore we continue to compare ourselves against a trend position over time and with the Scotland average. 8. % of Stage 1 Complaints Responded to within 5 working days
Measures Defintion: Measures the percentage of stage 1 complaints that were responded to within 5 working days of being opened. What the data tells us: Against the National average (2018/19) of 80% of all stage 1 complaints being responded to within 5 working days of being opened, our performance was close to or achieving this level throughout January to end July 2021. Performance from August 2021 onwards shows a deterioration, although slight improvement from September to October 2021 and from November to December 2021 with current performance at 67.6%. Narrative Since the start of the Complaints Handling Improvement Project (April 2021) NHS Tayside is now handling more complaints at Stage 1 (~70% now vs 30% before the project began). Stage 1 performance had been impacted over recent months but recovered slightly in October; performance over the calendar year 2021 was 73%.
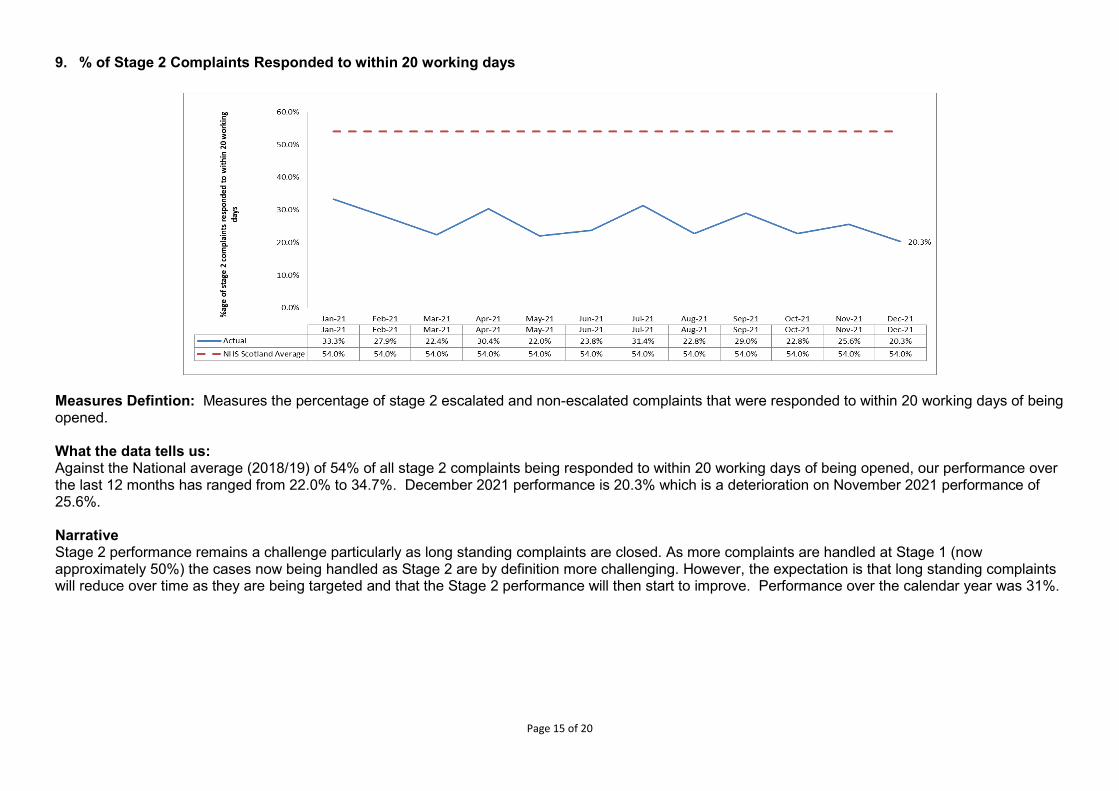
Page 15 of 20
9. % of Stage 2 Complaints Responded to within 20 working days
Measures Defintion: Measures the percentage of stage 2 escalated and non-escalated complaints that were responded to within 20 working days of being opened. What the data tells us: Against the National average (2018/19) of 54% of all stage 2 complaints being responded to within 20 working days of being opened, our performance over the last 12 months has ranged from 22.0% to 34.7%. December 2021 performance is 20.3% which is a deterioration on November 2021 performance of 25.6%. Narrative Stage 2 performance remains a challenge particularly as long standing complaints are closed. As more complaints are handled at Stage 1 (now approximately 50%) the cases now being handled as Stage 2 are by definition more challenging. However, the expectation is that long standing complaints will reduce over time as they are being targeted and that the Stage 2 performance will then start to improve. Performance over the calendar year was 31%.
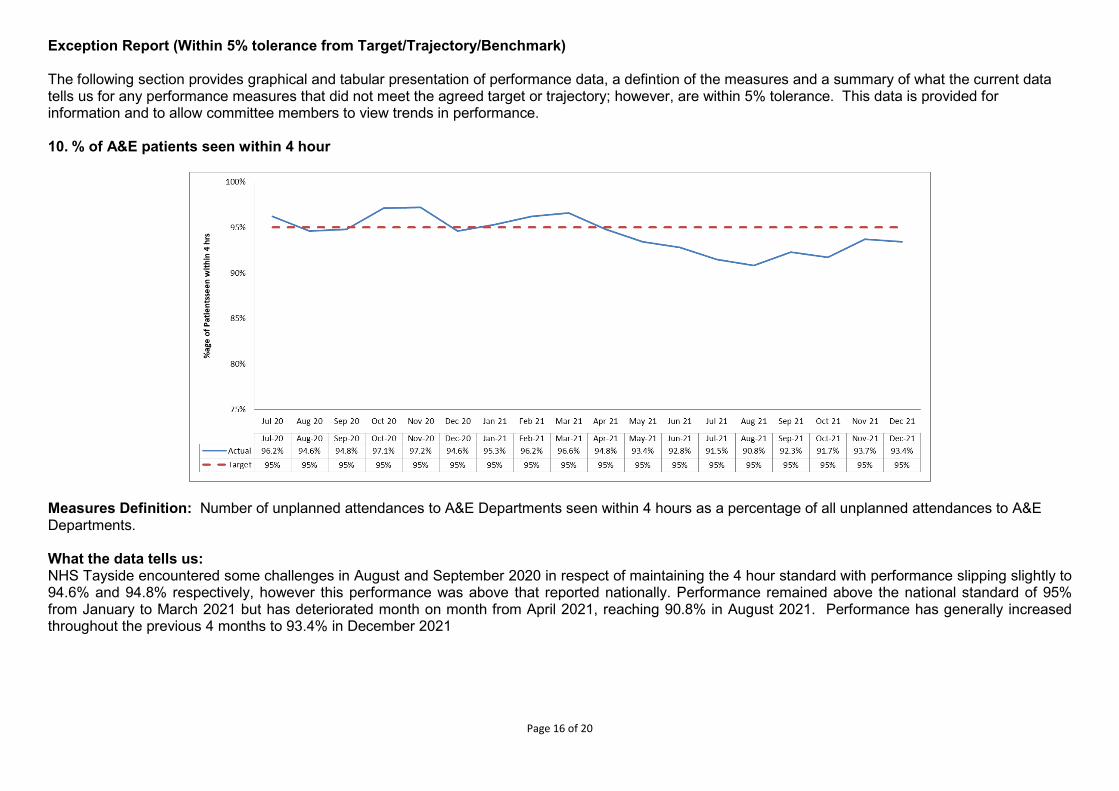
Page 16 of 20
Exception Report (Within 5% tolerance from Target/Trajectory/Benchmark) The following section provides graphical and tabular presentation of performance data, a defintion of the measures and a summary of what the current data tells us for any performance measures that did not meet the agreed target or trajectory; however, are within 5% tolerance. This data is provided for information and to allow committee members to view trends in performance. 10. % of A&E patients seen within 4 hour
Measures Definition: Number of unplanned attendances to A&E Departments seen within 4 hours as a percentage of all unplanned attendances to A&E Departments. What the data tells us: NHS Tayside encountered some challenges in August and September 2020 in respect of maintaining the 4 hour standard with performance slipping slightly to 94.6% and 94.8% respectively, however this performance was above that reported nationally. Performance remained above the national standard of 95% from January to March 2021 but has deteriorated month on month from April 2021, reaching 90.8% in August 2021. Performance has generally increased throughout the previous 4 months to 93.4% in December 2021
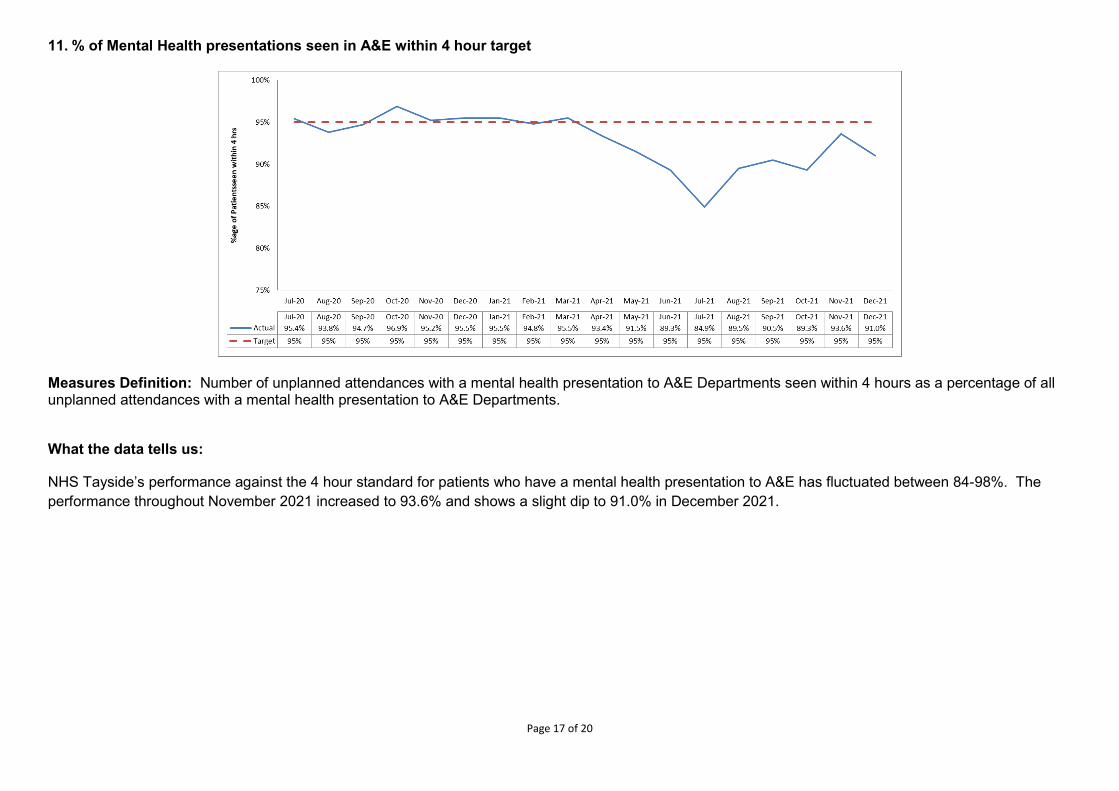
Page 17 of 20
11. % of Mental Health presentations seen in A&E within 4 hour target
Measures Definition: Number of unplanned attendances with a mental health presentation to A&E Departments seen within 4 hours as a percentage of all unplanned attendances with a mental health presentation to A&E Departments.
What the data tells us:
NHS Tayside’s performance against the 4 hour standard for patients who have a mental health presentation to A&E has fluctuated between 84-98%. The performance throughout November 2021 increased to 93.6% and shows a slight dip to 91.0% in December 2021.
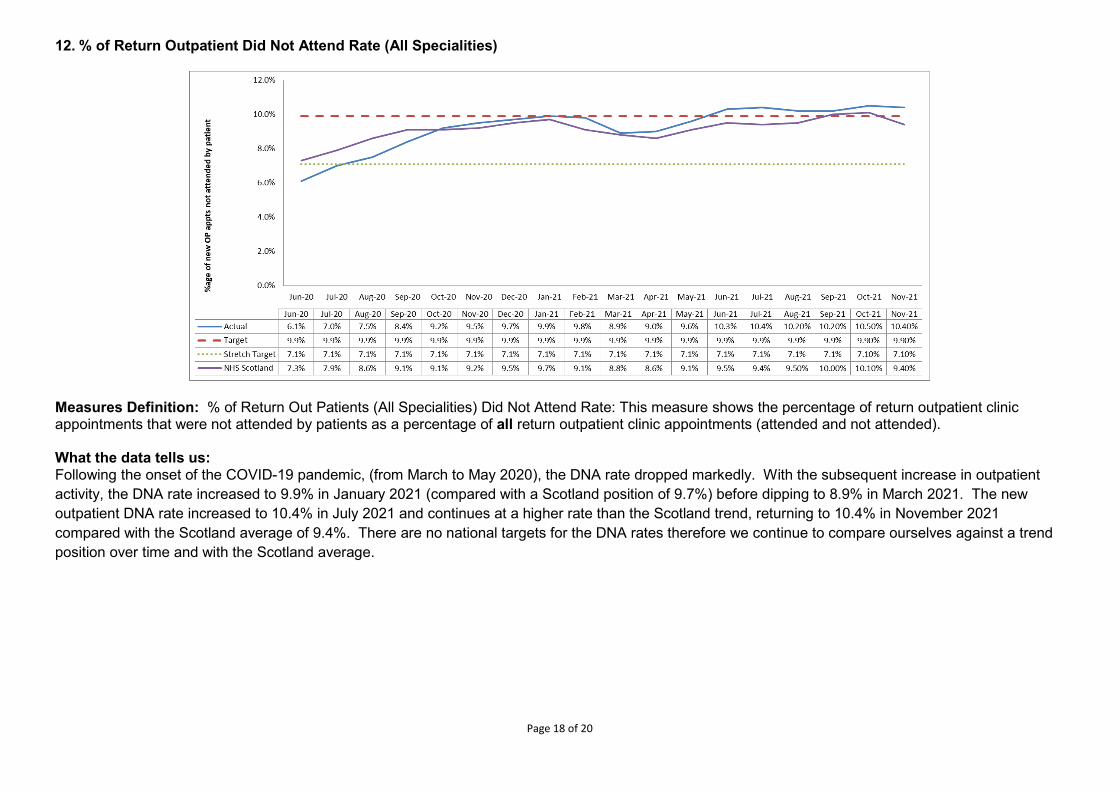
Page 18 of 20
12. % of Return Outpatient Did Not Attend Rate (All Specialities)
Measures Definition: % of Return Out Patients (All Specialities) Did Not Attend Rate: This measure shows the percentage of return outpatient clinic appointments that were not attended by patients as a percentage of all return outpatient clinic appointments (attended and not attended). What the data tells us: Following the onset of the COVID-19 pandemic, (from March to May 2020), the DNA rate dropped markedly. With the subsequent increase in outpatient activity, the DNA rate increased to 9.9% in January 2021 (compared with a Scotland position of 9.7%) before dipping to 8.9% in March 2021. The new outpatient DNA rate increased to 10.4% in July 2021 and continues at a higher rate than the Scotland trend, returning to 10.4% in November 2021 compared with the Scotland average of 9.4%. There are no national targets for the DNA rates therefore we continue to compare ourselves against a trend position over time and with the Scotland average.
Page 19 of 20
Remobilisation Plan – Waiting Times and Activity Update 13. Number of Inpatient/Daycase (IP/DC) patients waiting > 84 days TTG target as at month end
• All patients who are due to receive planned treatment on an inpatient or day case basis, which are subject to the Scottish Government standards, should wait no longer than 84 days for treatment. This measure shows all patients on the waiting list at each month’s end who have waited longer than 84 days and are, thus, breaching the Treatment Time Guarantee (TTG) maximum wait.
• Due to the Covid pandemic and the impact on elective capacity, the number of patients waiting greater than 12 weeks for an elective Inpatient / Daycase procedure (TTG) has increased over the last 9 months with the exception of a slight dip in May 2021, reaching 6,959 at end December 2021.
• Routine elective activity is progressing across Ninewells, PRI and Stracathro as per the agreed phased remobilisation planning and TTG activity over April-December 2021 remained above planned levels outlined in our Remobilisation Plan 2021-22 with 12,135 patients treated against a plan of 10,942 patients.
14. Number of New Outpatients waiting > 12 weeks target as at month end
• All new outpatient (OP) referrals, which are subject to the Scottish Government standards, should wait no longer than 12 weeks for a new OP appointment. This measure shows the number of eligible patients waiting greater than 12 weeks to be seen in an OP clinic at the end of each calendar month.
• Following the ceasing of routine elective activity in response to the COVID19 pandemic, the number of patients waiting beyond 12 weeks rose to its highest point of 13,662 patients at the end of June 2020. The volume of patients waiting beyond 12 weeks fell to 8,328 by end June 2021, and has increased over the previous 6 month period reaching 10,558 at end December 2021.
• Clinics continue to remobilise, with the number of patients waiting over 52 weeks also reducing as the Waiting List Validation exercise progresses. Outpatient delivery over April-December 2021 remained above planned levels outlined in our Remobilisation Plan 2021-22 with 73,884 patients seen against a plan of 59,256 patients.
15. Number of Diagnostics (8 key tests) patients waiting > 6 weeks target as at month end – Radiology 4 key tests only • The measure shows the number of patients at the end of each month who have been waiting for more than 6 weeks for a Radiology examination.
The 4 key Radiology tests which are reported within this measure are; MRI, CT Scan, non-obstetric ultrasound and Barium Studies. • Following the ceasing of routine elective activity in response to the COVID19 pandemic, the number of patients waiting beyond 6 weeks rose to
4,712 patients at the end of June 2020. This was the highest number of patients waiting more than 6 weeks, up until end December 2021 with 4,997 patients waiting more than 6 weeks. The greatest increase in waits is for CT Scans with staffing deficit impacting activity levels due to maternity leave, staff vacancies as well as staff isolating/covid and staff sickness. Staff are currently in training to address this deficit and Stracathro has been fully staffed since mid-January. We have also recruited a locum radiographer to increase MRI scan activity.
• The planned activity levels throughout Quarter 3 and 4 of 2021/22 have been reviewed and adjusted in line with the Remobilisation Plan bi-annual review. Radiology activity delivered October to December 2021 exceeded planned levels with 14,850 tests undertaken compared with a plan of 14,631 tests.
Page 20 of 20
16. Number of Diagnostics (8 key tests) patients waiting > 6 weeks target as at month end – Endoscopy 4 key tests only • The measure shows the number of patients at the end of each month who have been waiting for more than 6 weeks for an Endoscopic diagnostic
test. The 4 key Endoscopic diagnostic tests which are reported within this measure are; upper endoscopy, lower endoscopy, cystoscopy, and colonoscopy.
• Following the ceasing of routine elective activity in response to the COVID19 pandemic, the number of patients waiting beyond 6 weeks rose to its highest point of 2,557 patients at the end of August 2020. The volume of patients waiting beyond 6 weeks at end December 2021 is 1,118 compared with an end March 2021 position of 2,066.
• Endoscopy activity delivery over April-December 2021 remained above planned levels outlined in our Remobilisation Plan 2021-22 with 7,508 Endoscopic tests undertaken against a plan of 6,092.
Grant Archibald Chief Executive
NHS Tayside
Hazel Scott Director of Performance & Activity
NHS Tayside
Jenni Woods Health & Business Intelligence Lead
NHS Tayside
January 2022
1
Item Number 6.5
Minute NHS Tayside DIGITAL TRANSFORMATION PARTNERSHIP (DTP) Minute of the meeting of the Digital Transformation Partnership, held on Friday 5 November 2021, at 2.00pm, via TEAMS. Present: Ruth Anderson Head of Health Records, NHS Tayside Paul Arbuckle Service Improvement Lead, NHS Tayside Caroline Cooper Head of IT, Angus Council Margaret Dunning Board Secretary, NHS Tayside Dougie Elder Consultant Cardiologist & Digital AMD, NHS Tayside Garry Fraser Assoc Director for PRI and Medicine, NHS Tayside Ally Gentles Head of Digital Operations, NHS Tayside Lynne Harris IT Service Manager, Perth & Kinross Council Morag Macrae Patient Safety Development Manager, NHS Tayside Sean McArtney Deputy Assoc Nurse Director for Acute Services, NHS Tayside
(Representing Nursing) Bill McLeary IT Service Manager, Dundee City Council Angela Murphy Angus AHP Lead, NHS Tayside Brodie Paterson Consultant Emergency Medicine & Digital AMD, NHS Tayside Rachel Simpson Senior Commercialisation Manager, University of Dundee Sandy Strathearn Service Manager for Business Improvement, Perth & Kinross Council Lynn Smith Associate Director Access & Assurance, NHS Tayside Dawn Sturrock Business Change Lead, NHS Tayside (Representing Audrey Warden) Shobhan Thakore Consultant A&E, NHS Tayside Apologies: David Baty Consultant Clinical Scientist, NHS Tayside Dave Berry Chief Finance Officer, Dundee Health & Social Care Partnership,
Dundee City Council Janice Caithness Head of Service, NHS Tayside Alison Clement General Medical Practitioner James Cotton Consultant Gastroenterologist, NHS Tayside Alison Dailly Head of Information Governance & Cyber Assurance/Data Protection
Officer, NHS Tayside Hamish Dougall Cardiologist/General Practice Ellie Dow Consultant Biochemical Medicine, NHS Tayside Colin Fleming Consultant Dermatologist, NHS Tayside Paul Freeman Head of Service, NHS Tayside Jillian Galloway Head of Health & Care Services, Angus Health and Social Care
Partnership Karen Kidd Senior Finance Manager, NHS Tayside Ellie Hothersall Consultant Public Health, NHS Tayside Emily Jefferson Professor of Health Data Science & Director of Health Informatics,
Dundee University Nikki McColgan Head of Service, NHS Tayside Kate McDermott Staffside Lead - Transforming Tayside, NHS Tayside Louise McTaggart Head of Strategic Delivery, NHS Tayside Gordon Paterson Chief Officer/Director P&K HSCP, NHS Tayside Sarah Peterson General Practitioner, P&K HSCP Charlie Quipp Head of Service, NHS Tayside Beena Raschkes Portfolio GP, OOH GP and Joint Clinical IT Lead, NHS Tayside David Shaw GP and interim Associate Med Dir for Primary Care and Assoc Med Dir for
Dundee Health and Social Care Partnership Duncan Simpson Innovation Development Manager, NHS Tayside Gail Smith Interim Chief Officer Angus HSCP, NHS Tayside Lorna Wiggin Chief Officer Acute Services, NHS Tayside Kerry Wilson Associate Director Hospital Services PRI, NHS Tayside In Attendance:
2
Allison Beattie Business Development Manager, University of Dundee Susan Birse Personal Assistant, Digital Directorate, NHS Tayside Jonathan Waldheim-Ross Head of Service, Product and Delivery (Health), NHS Education for
Scotland (NES) In the Chair: Laic Khalique Director of Digital Technology, NHS Tayside in the Chair 1. WELCOME & APOLOGIES
Laic welcomed everyone to the meeting of the DTP. Introductions were made around the table. Apologies were noted as above.
2. MINUTE OF PREVIOUS MEETING – 20 JULY 2021
The Minute of the previous meeting held on 20 July 2021 was accepted as an accurate record.
3. ACTION POINT UPDATE
As per Action Point Update.
4. ReSPECT3 SBAR
Morag introduced Jonathan Waldheim-Ross, Head of Product and Delivery (Health) at NES, to the group. Jonathan and his team have been supportive of the ongoing work to test and implement the ReSPECT3 process and from within NHS Tayside. Morag provided an update on the project:-
• Paper was submitted to OLT. Endorsement and support were received. • In January received funding from the Scottish Partnership for Palliative Care to
undertake a small quality improvement project to test the ReSPECT3 process and form.
• As part of the project, working closely and collaboratively with colleagues across specialities, including Acute Care, Palliative Care and Primary Care.
• With a Steering Group and a Project Group, which oversees and supports the work, the testing has been small and focused on several wards at Ninewells and RVH, with further work commencing in a GP Practice, a Care Home and in Ward 4 at Ninewells.
• Progress has been interrupted by the pandemic. • Key drivers for the project are:-
1. Ensuring staff are confident and skilled to have meaningful
conversations with patients/families about future care and treatment. Currently in the process of developing an education/training package.
2. Developing a public awareness campaign and promoting the
importance of planning for the future and having conversations about future care. Two designs students from Duncan of Jordanstone College designed the prototype campaign which has been shared with the National ReSPECT3 Collaborative and other health boards.
3. Having the IT Infrastructure to support transitions of ReSPECT3
across the interfaces of care. The ReSPECT3 project is now at the stage to be considered by the Board for full implementation. Forth Valley has been the pilot site for ReSPECT3 and for the digital platform. As a result of the work done to date, and the support of the NES team, Tayside could be the second adopter site in Scotland. A number of steps remain to be completed before Tayside can become an adopter site (detailed in the report). These discussions have been held between NES and our local team.
3
The DTP was asked to support and endorse the roll out of the ReSPECT3 process and the digital format. Jonathan provided a high level view of the Digital ReSPECT3:-
• Cloud hosted; • National product to allow the sharing of information from emergency care and
treatment plans across Scotland; • Tayside would be the second adopter in Scotland; • The on-line form would be accessed through Clinical Portal; • Looking to start the process in Tayside in early 2022, initially with the launch in
patient context. Then look at additional features afterwards. • The concept being: information sharing across Primary Care, Secondary Care,
Unscheduled Care and in the future Social Care. It would be shared incrementally and in partnership.
How does this fit in with the National Digital Platform due to materialise in 5-10 years - The 5-10 years timescale is to have the full Digital Platform for everyone. The platform already exists and ReSPECT is the first product to sit on it. This form uses the national services that are being developed and by using ReSPECT you are contributing to that development process.
A question and answer session followed:-
1. How will the information be made accessible to the public? There is a parallel project about giving the public, their families and powers of attorney direct access to the information that is captured. Not only is it shared by clinicians when you have the conversation it is visible to people once they get home or if they want to share it with their friends and family. This is a parallel piece of work and it is in an earlier phase, but is ongoing.
2. Will sites stop using paper and go digital, and when more sites are brought on will they go straight to digital? The amount of paper form being used has been controlled. Testing release has been kept small and focused on development/training/education and on the foundations of getting the digital element. Don’t want large areas using paper then we have to pull that back.
3. How does this appear at the Primary Care end? We would want GPs to be able to view the ReSPECT data, whether that is via a
clinical portal or directly into the system. Currently in Forth Valley there is straight forward ‘copy’ button that allows you to copy it into the care information summary. This is only for the short term as we are in discussions to allow us to integrate it with the unscheduled care services. When it is released in Tayside there will be a better solution in place to make sure the information is shared with all of our colleagues in unscheduled care.
Laic asked if we could be kept up to date on the progress in this area. 4. In regard to Office 365 single sign on – will this be delivered nationally? A local AD is required to be set up to feed into the national. Ally highlighted if browser based then the national infrastructure standards are
to be moving forward, and Edge is to be the preferred default browser. Ally further highlighted that if you want to implement a project and there is not a Once for Scotland DPIA then you would need to link in with our Information Governance colleagues.
Jonathan advised a DPIA has been drafted to be Once for Scotland. Once
Tayside is on board he would contact our IG team. 5. Who is leading on the parallel project around public access and is their local
government representation on that? In regard to the public view and how will that work – research shows that read
only view does not offer much – being able to contribute is what the NES design team are looking into. In regard to identity – there is a Scottish Digital Identity
4
programme that is looking at the long term vision. We are looking at building a process for a patient ie do patients know what ReSPECT is and how they would initiate a ReSPECT conversation – these pieces will sit in the public domain ie on NHS Inform – and then there is the bit where you start to interact. The next component is your identity and that’s the Once for Scotland which has to be single sign across the entire piece. We will use what the Scottish Government suggest is the right approach and we will feed into that digital identity programme. We can however use something that already exists ie My Account or the product used to access Vaccine certification, to allow us to push through ReSPECT access quickly.
Brodie advised Tayside would look to put a link on Portal when we go to the online read version, other people will have access to a write version, and it will gently roll out as the gold standard of the life plan.
Laic thanked Alison and Jonathan for joining the meeting. The group were supportive of the project and looked forward to updates.
5. 5G OPPORTUNITIES AND HEALTHCARE IN TAYSIDE
Laic welcomed Allison Beattie, Business Development Manager, University of Dundee, to the meeting. Allison advised the University has been approached by Scotland 5G to advise us of their partnership, and what the opportunities might be in working with their businesses and their role and remit. The project has been set-up and sponsored by the Scottish Government to try and promote the adoption of 5G technology across Scottish businesses. 5G is a secure network that is provided by the larger network providers ie BT. Through the Tay Cities Deal, funding has been awarded to set-up a Hub within Tayside which is to be run from the V&A in January 2022. They are asking for partners to come forward with ideas etc or how 5G technology might support businesses and the healthcare sector. Allison understood that the more Scotland engages in 5G opportunities then we can have more pulling power with the operators to increase the infrastructure across Scotland. Ally highlighted 5G would be helpful if it was able to be used in rural areas. It would not be something that would be a replacement for our local network. Laic advised, in regard to augmented and virtual reality, that from a clinical perspective we can use those technologies in conjunction with 5G to deliver remote healthcare and the opportunities within that. Important to have that medium to long term view on how technology will impact on our working lives and patient care. Something for us to think about both from a clinical and social care perspective. Up to us to start campaigning for a real reason for 5G to be put into rural areas. Paul Arbuckle requested an update on what projects are taken forward to allow an insight into how 5G is being enacted locally and we can do a sense check on how that fits in with the plans we are making digitally in health and social care. Allison suggested this proposal could be put forward to the Hub once it was up and running. Laic gave thanks to Allison for the presentation and advised anyone interested in engaging to contact Allison.
6. DIGITAL STRATEGY
Laic advised the Digital Strategy has been out for wider consultation for the second time. We have had both patient and citizen engagement. That consultation is now complete. We have had further input from an equality and diversity perspective to ensure the EQIA for the strategy is complete. The Strategy is now with the Chief Executive for final sign off. Currently planning a launch of the Digital Strategy and hopefully engaging with Comms
5
to put together a couple of videos to be launched out in the Community and internally. It is hoped the process will be complete towards the end of this year. The Strategy has been renamed 2022-2027 as a 5-year digital strategy.
7. INHEALTHCARE PRESENTATION & PROTOCOLS
Dougie provided an update on the feedback from the presentation. Dougie, Louise, and digital colleagues, met with Inhealthcare and the Scottish Government Team who have been tasked with progressing remote health monitoring for patients via the Inhealthcare App. The Scottish Government completed the procurement exercise for remote health monitoring and awarded the contract to Inhealthcare for the next 5 years. The Scottish Government vision being that all remote health monitoring, or collection of data for patients, is conducted through the Inhealthcare App. In Tayside we have successfully used the text or SMS service called Florence and we have extended our agreement with Florence for one more year to facilitate the transition. There are currently twelve protocols being established, developed and validated by the national team, ranging from COPD to Weight Management etc. and being taken forward on a national model with national governance around the decision making aspect that these Apps handle. Tayside is being considered by the Program for some of these Apps. We currently have the Covid App running and it is working very well. Looking to bring on more Apps over the coming months. Currently in early stages of engagement with the team. Dougie referred to a Scottish Government program called Digital Scot which appears to be funding the roll out of an App, based on the Storm ID programme for managing COPD. The program is funded by the Scottish Government. Laic advised it was important that these protocols are clinically approved in Tayside and a forum established for this purpose. Action: Dougie would find out more about the Digital Scot program and provide
an update at the next meeting.
DE
8. SLWG OUTPUT ON EPR
Dougie provided an updated on the EPR SLWG. A number of sessions have been held to discuss our options in terms of moving forward with our EPR. It is hoped to submit a paper to OLT which describes the challenges and benefits of what we currently have and where we want to go. It was felt the way forward was with TrakCare for Secondary Care, this being the clinical system of choice within the active clinical notes module to record care delivered. There are a number of challenges and we hope to lay out in the paper a method by which we control them. The plan is to adopt active clinical notes in the Emergency Department, followed by a control roll out to the ED wards. Consideration would then be given to how we would move the rest of the organisation across. It was noted that the EMIS contract expires in 12 months. A group is being established to take this forward. The group noted the update.
9. eOBSERVATIONS
Dougie provided an update. Meetings have taken place between Digital and Nursing. Hoping to progress at pace
6
with acquiring and deploying a solution to manage eObservations in the hospital. The benefit of the system is early detection of a patient who is deteriorating, allowing us to provide early intervention. It becomes a key part not to leave behind on paper as you move towards an EPR. It is important that we have one system that records the observations wherever they are taken in NHS Tayside. Sean highlighted the patient safety features. A paper and Business Case have been put together and currently engaging with Finance. Laic advised this was a key piece of work and an area of focus for us to have implemented. In regard to funding, continue to engage with Finance and ensure the Business Case highlights the wireless peripherals ie a patient’s readings are automatically transmitted to the system, therefore, cutting out as many manual processes as possible. The group noted the update.
10. KEY PROJECTS UPDATE
Laic provided an update on the following programs of work:-
• GP IT Re-Provisioning:- Supplier expected to be accredited January 2022 (this is an 8 week delay); All Vision practices have agreed in principle to a Direct Award
procurement.
• Community Nursing System Replacement (EMIS Web):- We are actively engaging with our EMIS practices, with the hope of having
all practices using a single system; A Project Plan is in draft; The EMIS Web Contract is due to expire shortly; Procurement considerations are underway; Stakeholder engagements have commenced.
• CHI – National Program:-
• Successfully implemented; • Dual running of systems from February 2022; • Go Live in November 2022.
• EPR Projects:-
Update as at Agenda Item 8
• Other National Projects:-
eRostering expansion LIMS Prisons Healthcare
eROSTERING Dougie highlighted that in regard to eRostering, Tayside is quite far down the line in terms of our expected implementation of Health Roster for Medical Staff and asked if anyone knew who the medical person engaged in that piece of work was, could they advise Pamela Johnston. Sean advised in regard to eRostering, that in Tayside we are using a system called SafeCare. It has been recognised nationally, and the Scottish Government have requested a demonstration. It is a useful reporting mechanism that is part of eRostering where you can see the gaps to be plugged and share the staffing resource.
7
A great example of what we are doing in NHS Tayside. The group noted the update.
11. AOCB
11.1 DIGITAL CITIZEN DELIVERY PLAN Laic advised this was a community plan which focused on 3 priorities:-
• Digital approaches within Care Homes, in Social Care and supporting the prevention of drug related deaths through technology and digital inclusion;
• Citizen Engagement – digital knowledge of skills within the community; • Delivering remote healthcare ie NearMe, Remote Healthcare Pathways, Digital
Mental Health, Digital Telecare and Digital Front Door.
Laic organised a meeting recently with the three Chief Operating Officers in regard to taking these big pieces of work forward and establishing a new governance structure. They agreed that Laic would write to the Chief Executives of the three local authorities with a view to establishing key contacts in order to take these pieces of work forward jointly. Action: Laic would share the Digital Citizen Delivery Plan with the group.
11.2 WiFi Dougie highlighted that Patient WiFi can now be accessed by anyone at work and
advised they were seeking to have a publicity campaign to highlight the various ways you can connect to WiFi whilst at work.
LK
12. DATE OF NEXT MEETING
Date to be arranged.
Item Number 6.6 PRC04/2022
Page 1 of 5
Meeting: Performance & Resources Committee Meeting date: 10 February 2022 Title: Climate Emergency and Sustainable
Development Responsible Executive: John Paterson, Director of Facilities Stuart Lyall, Sustainability Champion Report Author: John Paterson, Director of Facilities
Philip Wilde, Property Environmental & Quality Manager 1 Purpose
This is presented to the Committee for:
• Assurance
This report relates to a: • Government policy/directive
This aligns to the following NHSScotland quality ambition(s):
• Safe 2 Report summary 2.1 Situation
The Scottish Government Health Finance, Corporate Governance & Value Directorate emailed all Chief Executives the new Policy for NHS Scotland on the Climate Emergency and Sustainable Development – DL(2021) 38 dated 10 November 2021. This policy statement supersedes CEL 2 (2012) ‘A Policy on Sustainable Development for NHSScotland 2012’. A copy of the policy is included as an appendix below. 2.2 Background
The new policy has been prepared in consultation with Health Boards and relevant Scottish Government and public sector stakeholders. It takes account of relevant wider Scottish Government policies and existing statutory duties on Health Boards. The policy sets out aims and associated targets for NHS Scotland to work towards. The forthcoming NHS Scotland Climate Emergency and Sustainability Strategy will provide proposals for action to assist in meeting those aims and targets. The Policy for NHS Scotland on the Global Climate Emergency and Sustainable Development takes immediate effect. Responding to the climate emergency is one of the Scottish Government’s highest priorities.
Page 2 of 5
2.3 Assessment Policy Aims
• Ensure that NHS Scotland bodies, as an integral part of their commitment to the health and wellbeing of the community, contribute to the achievement of the United Nation’s Sustainable Development Goals.
• Ensure that NHS Scotland becomes a net-zero greenhouse gas emissions health service by 2040 or earlier where possible.
• Ensure that NHS Scotland’s assets and activities are resilient to the impacts of a changing climate, particularly extreme weather events.
• Establish a culture of stewardship within NHS Scotland, where natural resources are safeguarded and responsibly used to provide environmentally sustainable healthcare.
• Establish NHS Scotland as part of the circular economy through designing out waste and pollution, keeping products and materials in use and contributing to the regeneration of natural systems.
• Increase NHS Scotland’s contribution to tackling the ecological emergency and restoring biodiversity.
Timescales and actions required by the policy include:
2020 New Buildings to be Carbon Net Zero 2021/22 Adopt ISO 9001/14001 Environmental Management System (EMS) 2022 Resource Board’s Climate Emergency Team 2025 Reduce Domestic Waste; 5% to landfill, 70% recycled 2025 Promote Greenspace & Biodiversity 2025 Remove Petrol/diesel cars from fleet 2030 Remove Petrol/diesel vehicles from fleet 2038 Heat buildings by renewable energy only 2040 Emissions to be “Net Zero”; waste, travel, water, leased assets
2.3.1 Quality/ Patient Care
The purpose of this policy is to provide a framework for NHS Scotland to maximise its contribution to mitigating and limiting the effects of the global climate emergency and for the development of an environmentally and socially sustainable health service that is resilient to the locked-in impacts of climate change. As such, the policy is mandatory for all NHS Scotland bodies and its scope extends to all of their activities. The aims of this policy must be fully integrated into all planning, management decisions and operational practices across NHS Scotland in order to respond fully to the global climate emergency and achieve an environmentally and socially sustainable health service. 2.3.2 Workforce Each NHS Scotland body must ensure their workforce consider the environmental impacts of treatments when making decisions about the care they provide. An assessment of the shortfall in resource required to support this agenda will be undertaken with a corresponding business case to be developed.
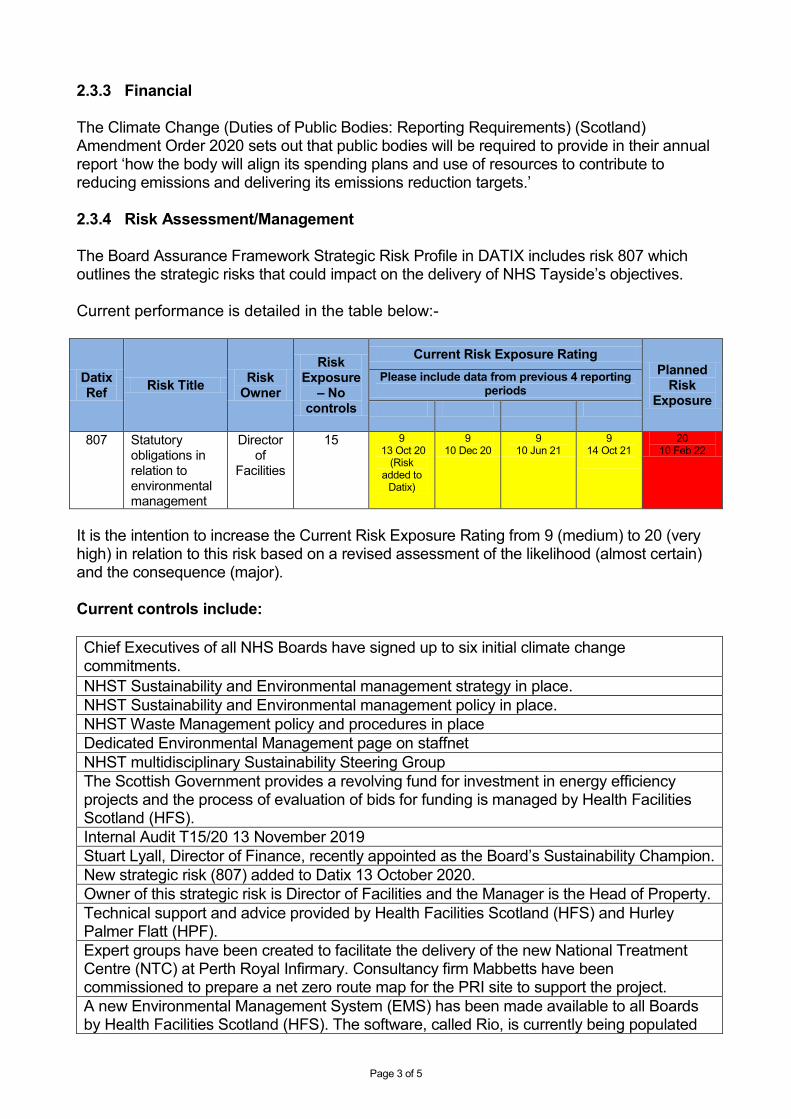
Page 3 of 5
2.3.3 Financial
The Climate Change (Duties of Public Bodies: Reporting Requirements) (Scotland) Amendment Order 2020 sets out that public bodies will be required to provide in their annual report ‘how the body will align its spending plans and use of resources to contribute to reducing emissions and delivering its emissions reduction targets.’ 2.3.4 Risk Assessment/Management The Board Assurance Framework Strategic Risk Profile in DATIX includes risk 807 which outlines the strategic risks that could impact on the delivery of NHS Tayside’s objectives. Current performance is detailed in the table below:-
Datix Ref Risk Title Risk
Owner
Risk Exposure
– No controls
Current Risk Exposure Rating Planned
Risk Exposure
Please include data from previous 4 reporting periods
807 Statutory obligations in relation to environmental management
Director of
Facilities
15 9 13 Oct 20
(Risk added to
Datix)
9 10 Dec 20
9 10 Jun 21
9 14 Oct 21
20 10 Feb 22
It is the intention to increase the Current Risk Exposure Rating from 9 (medium) to 20 (very high) in relation to this risk based on a revised assessment of the likelihood (almost certain) and the consequence (major). Current controls include: Chief Executives of all NHS Boards have signed up to six initial climate change commitments. NHST Sustainability and Environmental management strategy in place. NHST Sustainability and Environmental management policy in place. NHST Waste Management policy and procedures in place Dedicated Environmental Management page on staffnet NHST multidisciplinary Sustainability Steering Group The Scottish Government provides a revolving fund for investment in energy efficiency projects and the process of evaluation of bids for funding is managed by Health Facilities Scotland (HFS). Internal Audit T15/20 13 November 2019 Stuart Lyall, Director of Finance, recently appointed as the Board’s Sustainability Champion. New strategic risk (807) added to Datix 13 October 2020. Owner of this strategic risk is Director of Facilities and the Manager is the Head of Property. Technical support and advice provided by Health Facilities Scotland (HFS) and Hurley Palmer Flatt (HPF). Expert groups have been created to facilitate the delivery of the new National Treatment Centre (NTC) at Perth Royal Infirmary. Consultancy firm Mabbetts have been commissioned to prepare a net zero route map for the PRI site to support the project. A new Environmental Management System (EMS) has been made available to all Boards by Health Facilities Scotland (HFS). The software, called Rio, is currently being populated
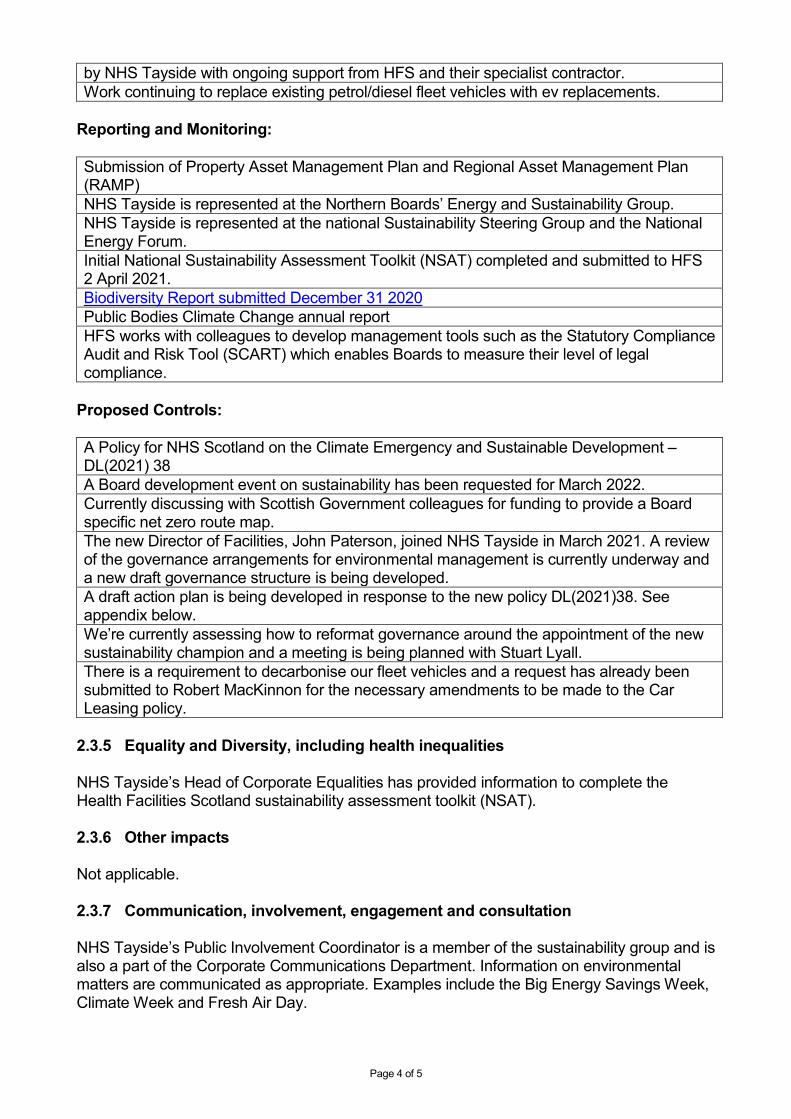
Page 4 of 5
by NHS Tayside with ongoing support from HFS and their specialist contractor. Work continuing to replace existing petrol/diesel fleet vehicles with ev replacements.
Reporting and Monitoring: Submission of Property Asset Management Plan and Regional Asset Management Plan (RAMP) NHS Tayside is represented at the Northern Boards’ Energy and Sustainability Group. NHS Tayside is represented at the national Sustainability Steering Group and the National Energy Forum. Initial National Sustainability Assessment Toolkit (NSAT) completed and submitted to HFS 2 April 2021. Biodiversity Report submitted December 31 2020 Public Bodies Climate Change annual report HFS works with colleagues to develop management tools such as the Statutory Compliance Audit and Risk Tool (SCART) which enables Boards to measure their level of legal compliance.
Proposed Controls: A Policy for NHS Scotland on the Climate Emergency and Sustainable Development – DL(2021) 38 A Board development event on sustainability has been requested for March 2022. Currently discussing with Scottish Government colleagues for funding to provide a Board specific net zero route map. The new Director of Facilities, John Paterson, joined NHS Tayside in March 2021. A review of the governance arrangements for environmental management is currently underway and a new draft governance structure is being developed. A draft action plan is being developed in response to the new policy DL(2021)38. See appendix below. We’re currently assessing how to reformat governance around the appointment of the new sustainability champion and a meeting is being planned with Stuart Lyall. There is a requirement to decarbonise our fleet vehicles and a request has already been submitted to Robert MacKinnon for the necessary amendments to be made to the Car Leasing policy.
2.3.5 Equality and Diversity, including health inequalities
NHS Tayside’s Head of Corporate Equalities has provided information to complete the Health Facilities Scotland sustainability assessment toolkit (NSAT). 2.3.6 Other impacts
Not applicable. 2.3.7 Communication, involvement, engagement and consultation
NHS Tayside’s Public Involvement Coordinator is a member of the sustainability group and is also a part of the Corporate Communications Department. Information on environmental matters are communicated as appropriate. Examples include the Big Energy Savings Week, Climate Week and Fresh Air Day.
Page 5 of 5
2.3.8 Route to the Meeting
Not applicable but noted that NHS Tayside’s sustainability group are aware of the requirement for regular updates to the P&R committee.
2.4 Recommendation
This paper is presented for assurance and the committee is asked to note the following:
• The increasing and significant workload associated with the new policy. • The Committee is asked to support the intention to increase the Current Risk
Exposure Rating from 9 (medium) to 20 (very high) in relation to this risk based on a revised assessment of the likelihood (almost certain) and the consequence (major).
• Acknowledge the requirement to allocate appropriate resources to maintain and improve the performance of environmental management within NHS Tayside as required by the policy.
• Historically the main focus for progressing this agenda has rested with the Facilities Directorate and in particular the Property Department. This will need to broaden across all sectors of NHS Tayside.
• The level of assurance is considered to be Limited. Level of Assurance System Adequacy Controls
Comprehensive Assurance
Robust framework of key controls ensures objectives are likely to be achieved.
Controls are applied continuously or with only minor lapses.
Moderate Assurance
Adequate framework of key controls with minor weaknesses present.
Controls are applied frequently but with evidence of non-compliance.
Limited Assurance
Satisfactory framework of key controls but with significant weaknesses evident which are likely to undermine the achievement of objectives.
Controls are applied but with some significant lapses.
No Assurance
High risk of objectives not being achieved due to the absence of key internal controls.
Significant breakdown in the application of controls.
3 List of appendices
• Policy for NHS Scotland on the Climate Emergency and Sustainable Development
• Draft Climate Emergency and Sustainable Development Action Plan
St Andrew’s House, Regent Road, Edinburgh EH1 3DG
www.gov.scot
Health Finance, Corporate Governance & Value Directorate Richard McCallum, Director
T: 0131-244 3475 E: [email protected]
NHS Chairs NHS Chief Executives via email
___ 10th November, 2021 Dear Colleagues A POLICY FOR NHS SCOTLAND ON THE CLIMATE EMERGENCY AND SUSTAINABLE DEVELOPMENT - DL (2021) 38
I am writing to share with you the attached policy statement, a ‘Policy for NHS Scotland on the Global Climate Emergency and Sustainable Development’.
This policy statement supersedes CEL 2 (2012) ‘A Policy on Sustainable Development for NHSScotland 2012’.
Addressees should ensure that this letter is cascaded to all appropriate staff within their area of responsibility.
The attached document has been prepared in consultation with Health Boards and relevant Scottish Government and public sector stakeholders. It takes account of relevant wider Scottish Government policies and existing statutory duties on Health Boards.
The policy sets out aims and associated targets for NHS Scotland to work towards. The forthcoming NHS Scotland Climate Emergency and Sustainability Strategy will provide proposals for action to assist in meeting those aims and targets.
The Policy for NHS Scotland on the Global Climate Emergency and Sustainable Development takes immediate effect.
Responding to the climate emergency is one of the Scottish Government’s highest priorities and I look forward to working with you on this crucial matter.
Yours sincerely
Richard McCallum Director of Health Finance and Governance
St Andrew’s House, Regent Road, Edinburgh EH1 3DG
www.gov.scot
A Policy for NHS Scotland on the Global Climate Emergency and Sustainable Development Introduction Responding to the global climate emergency is one of the Scottish Government’s highest priorities. Sustainable development, the concept that the needs of the present must be met “without compromising the ability of future generations to meet their own needs”1 is integral to the Scottish Government’s overall purpose. The Scottish Government’s National Performance Framework shares the same aims as the United Nations’ Sustainable Development Goals. The purpose of this policy is to provide a framework for NHS Scotland to maximise its contribution to mitigating and limiting the effects of the global climate emergency and for the development of an environmentally and socially sustainable health service that is resilient to the locked-in impacts of climate change. As such, the policy is mandatory for all NHS Scotland bodies and its scope extends to all of their activities. The aims of this policy must be fully integrated into all planning, management decisions and operational practices across NHS Scotland in order to respond fully to the global climate emergency and achieve an environmentally and socially sustainable health service. Background The planet is in the midst of a climate emergency as a result of human activity and urgent action is required to reduce greenhouse gas emissions, adapt to the changes caused by climate change and achieve an environmentally and socially sustainable society. Climate change presents a serious risk to the health of people around the world and has been described by the Lancet Commission on Managing the Health Effects of Climate Change as “the biggest global health threat of the 21 century”2. At the same time, many of the actions to mitigate and adapt to climate change and improve environmental sustainability also have positive health benefits to such an extent that the Lancet Commission has described tackling climate change as “the greatest global health opportunity of the 21st century”.3 It is therefore incumbent on NHS Scotland to be an exemplar in responding to the climate emergency and achieving environmental sustainability. Meeting the needs of the present requires action to address the inequalities in our society, inequalities which manifest themselves in significantly poorer health outcomes for the most deprived. Many of the health benefits of action to address the climate emergency and ecological crisis will have the greatest benefits for those with the worst health outcomes.
1 Report of the World Commission on Environment and Development: Our Common Future (1987) (“the Brundtland Report”) Para. 27. 2 Reference 3 The Lancet Commission on Managing the Health Effects of Climate Change (2015) – complete reference
St Andrew’s House, Regent Road, Edinburgh EH1 3DG
www.gov.scot
Policy Aims
Ensure that NHS Scotland bodies, as an integral part of their commitment to the health and wellbeing of the community, contribute to the achievement of the United Nation’s Sustainable Development Goals.
Ensure that NHS Scotland becomes a net-zero greenhouse gas emissions health service by 2040 or earlier where possible.
Ensure that NHS Scotland’s assets and activities are resilient to the impacts of a changing climate, particularly extreme weather events.
Establish a culture of stewardship within NHS Scotland, where natural resources are safeguarded and responsibly used to provide environmentally sustainable healthcare.
Establish NHS Scotland as part of the circular economy through designing out waste and pollution, keeping products and materials in use and contributing to the regeneration of natural systems.
Increase NHS Scotland’s contribution to tackling the ecological emergency and restoring biodiversity.
Governance
1. Each NHS Scotland body must implement a strong management structure as a means of ensuring the delivery of this policy’s aims. Each NHS Scotland body must either establish a Climate Emergency and Sustainability Group or designate an existing committee as the lead group for climate emergency and sustainability. In either case, the group must be chaired by a member of its senior / executive management team and its membership must be of sufficient authority to ensure that the aims of this policy are fully integrated into all planning, management decisions and operational practices across the NHS Scotland body.
2. The Scottish Government Health and Social Care Directorates (SGHSC) have established an NHS Scotland Climate Emergency and Sustainability Board to provide leadership and governance to NHS Scotland’s overall efforts in responding to the global climate emergency and achieving an environmentally and socially sustainable health service.
3. Each NHS Scotland body must appoint an executive lead for its climate emergency response and sustainability.
4. Each NHS Scotland body must appoint a member of its board to act as champion for its climate emergency response and sustainability at a strategic level to assist in articulating and promoting its sustainability priorities.
5. Each NHS Scotland body Chief Executive is accountable to the SGHSC for their organisation’s implementation of this policy.
6. NHS Scotland bodies which encounter issues with or barriers to the implementation of this policy or its aims which cannot be resolved at NHS Scotland body level must escalate those issues to the NHS Scotland Climate Emergency and Sustainability Board.
7. As assessment of its progress against the aims of this policy will form part of each NHS Scotland body’s annual ministerial review.
St Andrew’s House, Regent Road, Edinburgh EH1 3DG
www.gov.scot
Integrated approach and co-operation
8. NHS Scotland bodies must take an integrated approach to the achievement of the aims of this policy. In developing plans or taking action, NHS Scotland bodies must consider the full range of this policies’ aims.
9. NHS Scotland bodies must co-operate with each other with a view to achieving the aims of this policy.
10. The achievement of this policy’s aims will require NHS Scotland bodies to work with their local communities and patients and with organisations outside of the NHS who have similar aims or who can assist NHS Scotland to achieve its aims. In particular, territorial Health Boards are required to use all reasonable efforts to work with the local authorities for their areas to achieve this policy’s aims.
A Just Transition
11. In implementing this policy, NHS Scotland bodies must:
a) plan, invest and implement a transition to an environmentally and socially sustainable, climate resilient, health service in a way which builds on Scotland’s economic and workforce strengths and potential;
b) create opportunities to develop resource efficient and sustainable approaches which help address inequality and poverty; and
c) design and deliver low carbon and climate resilient investment and infrastructure, making all possible efforts to create decent, fair and high value work.
Net-zero Scope 1 and 2 emissions
12. Having regard to national plans to decarbonise the UK’s electricity supply by 2035, each NHS Scotland body must reduce the greenhouse gas emissions from its activities, the activities under its control and from the electricity, steam and heat purchased by it to net-zero by 2040 or earlier where possible. The UK’s independent, statutory Climate Change Committee advises that most sectors will need to reduce emissions close to zero without offsetting.
13. All NHS owned buildings must be heated from renewable sources by 2038 or earlier where possible. Scope 3 greenhouse gas emissions
14. NHS Scotland bodies must, as a minimum, reduce their associated greenhouse gas emissions from the following sources to net-zero by 2040 or earlier where possible:
energy transmission and distribution, having regard to national plans to decarbonise the UK’s electricity supply by 2035
waste disposal
business travel, including grey fleet
St Andrew’s House, Regent Road, Edinburgh EH1 3DG
www.gov.scot
water consumption
waste water treatment
leased assets
15. Each NHS Scotland body must take sufficient action to influence a reduction in those greenhouse gas emissions which are linked to its activities but are from sources which it does not own or control (and are not included in paragraph 14) to maximise its contribution to reducing emissions to net-zero by 2045 or earlier where possible.
Interim targets
16. Where the 1990 baseline is known for an emissions source, the NHS Scotland body
must reduce the emissions from that source by at least 75% by 2030.
17. Where the 1990 baseline is not known for an emissions source, the NHS Scotland body must set interim targets for reducing emissions from that source which are consistent with achieving the net-zero target for the emissions type.
Greenhouse gas emissions reporting
18. Each NHS Scotland body must assess their progress towards net-zero emissions via their annual Public Bodies’ Climate Change Duties Report which is to be submitted to the Scottish Government by 30 November each year. NHS Scotland bodies should, as a minimum, report on their annual emissions associated with their:
building fossil-fuel energy use
owned and leased fleet fuel use
fluorinated gases and anaesthetic gases (where relevant)
purchased energy use (electricity, heat, steam)
energy transmission and distribution
waste
water consumption
waste water treatment
business travel, including the use of grey fleet
leased assets Climate change adaptation
19. Each NHS Scotland body must undertake a Climate Change Risk Assessment covering all operational areas and produce and implement a Climate Change Adaptation Plan to ensure resilience of service under changing climate conditions and these should be reviewed and updated at least every 5 years.
20. In relation to existing facilities, these assessments and plans should cover a period at least 20 years into the future from the time of assessment.
21. In relation to planned facilities, these assessments and plans should cover a period at least 50 years into the future from the time of assessment.
22. The key risks from the Climate Change Risk Assessment must be incorporated into each NHS Scotland body’s corporate risk register.
St Andrew’s House, Regent Road, Edinburgh EH1 3DG
www.gov.scot
23. Progress on undertaking Risk Assessments and implementing Adaptation Plans, including in terms of how these are supporting national Scottish Climate Change Adaptation Programmes, is to be set out in each bodies’ annual Public Bodies’ Climate Change Duties Report.
Sustainable care
24. Each NHS Scotland body will foster and promote a culture of stewardship, where staff are mindful of the resources they use and share a vision of green and sustainable healthcare.
25. Each NHS Scotland body must ensure their workforce consider the environmental impacts of treatments when making decisions about the care they provide.
26. Each NHS Scotland body will ensure all employees are educated and trained on the principles of practising sustainably.
Procurement
27. Each NHS Scotland body must consider social and environmental sustainability when it is procuring goods and services. The procurement of goods and services by NHS Scotland bodies must further the aims of this policy.
28. NHS Scotland bodies are reminded of the sustainable procurement duty established by section 9 of the Procurement (Scotland) Act 2014, which can be viewed here: Procurement Reform (Scotland) Act 2014 (legislation.gov.uk). NHS Scotland bodies are required to follow the guidance and use the tools issued by the Scottish Government to assist in optimising the economic, social and environmental outcomes of their procurement activity.
29. It is the responsibility of each NHS Scotland body to review the supply chain of the goods and services that it procures to determine the extent of the associated greenhouse gas emissions and social and environmental impacts. Where an NHS Scotland body procures goods and services on behalf of another organisation, it is the responsibility of the procuring body to review the supply chain.
Circular economy
30. Each NHS Scotland body must contribute to the creation of a circular economy,
working with National Procurement and with suppliers to design out waste and consider the entire life cycle of products and services, reducing the environmental impact, keeping products and materials in use and contributing to the regeneration of natural systems.
31. In particular, NHS Scotland bodies must:
promote the use of items and assets which have been designed for durability and upgradability;
prolong the use of items and assets through proper maintenance and promoting their reuse; and
promote the use of items and assets which can be recycled at the end of their useful life.
St Andrew’s House, Regent Road, Edinburgh EH1 3DG
www.gov.scot
32. NHS Scotland bodies, with support from National Procurement, must identify and assess the life cycle of products and services and take action to reduce their environmental impact through the avoidance of pollution (including toxic chemicals, micro-plastics and pharmaceutical residues) and waste throughout their life cycle.
Water
33. Each NHS Scotland body must monitor its water usage and take action to reduce
unnecessary water consumption. Resource and Waste Management
34. Each NHS Scotland body must put in place a system for recording and reporting the
volume and type of waste which it generates and the destination of that waste.
Targets
35. By 2025, each NHS Scotland body must:
a) reduce its domestic waste arising by a minimum of 15%, and greater where possible, compared to a financial year 2012/13 baseline;
b) ensure that no more than 5%, and less where possible, of all its domestic waste goes to landfill;
c) reduce the food waste it produces by 33% against a financial year 2015/16 baseline; and
d) ensure that 70% of all its domestic waste is recycled or composted.
36. Each NHS Scotland body must set appropriate targets for reducing the volume of healthcare waste it produces through measures including greater use of reusable items, improvements to waste segregation and increased recycling of recyclable materials.
Biodiversity and Greenspace
37. Under section 1 of the Nature Conservation (Scotland) Act 2004, it is the duty of each NHS Scotland body in exercising its functions to further the conservation of biodiversity so far as is consistent with the proper exercise of those functions. In addition to that duty, each NHS Scotland body must promote improvements to biodiversity in so far as is consistent with the proper exercise of its functions.
38. All NHS Scotland bodies must assess, and then take action to improve:
a) the extent and quality of the greenspace they have; b) the contribution its estate makes to biodiversity; and c) the value of the ecosystem services its greenspaces provide.
39. Greenspace can have benefits for the health and wellbeing of staff, patients and
communities. NHS Scotland bodies must manage their greenspace to increase its provision and improve access, quality and regular use by staff, patients and the local community.
40. Greenspace can have benefits in relation to climate change mitigation and adaptation through, for example, reducing flooding and absorbing heat. NHS Scotland bodies
St Andrew’s House, Regent Road, Edinburgh EH1 3DG
www.gov.scot
must manage their greenspace to assist with climate change mitigation and adaptation.
41. All NHS Scotland bodies must collaborate with local partners to improve the natural links between NHS greenspace and other local areas of greenspace.
42. Where an NHS Scotland body proposes an action which would result in the loss in quantity or quality of greenspace to the NHS or its contribution to biodiversity, it must refer the proposal to the SGHSC.
43. It is the duty, under section 2A of the Nature Conservation (Scotland) Act 2004, of each NHS Scotland body to publish a report every three years on the actions taken by it in pursuance of its duty under section 1 of that Act during the period to which the report relates. These reports must be forwarded to SGHSC when they are published.
Travel and transport
44. All NHS Scotland bodies must take action to reduce the carbon emissions resulting from travel associated with their activities, including those associated with staff and patient travel. Those actions must include:
Actions to reduce the need for travel;
Actions to increase active travel;
Actions to increase the use of public or community transport to access services and sites;
Actions to reduce car use in support of the Scottish Government’s aim to reduce the number of kilometres driven in Scotland by 20% by 2030 compared to a 2019 baseline; and
Actions to support the use of vehicles powered by renewable energy in preference to vehicles powered by fossil fuels.
45. The actions set out in the paragraph above must be taken in a way which supports
access to services with a particular focus on addressing inequality of access.
46. Each NHS Scotland body must remove all petrol and diesel fuelled cars from their owned and leased fleets by 2025 or earlier where possible.
47. Each NHS Scotland body must phase out the need for it to purchase or lease any petrol or diesel light commercial vehicles by 2025 or earlier where possible.
48. Each NHS Scotland body must phase out the need for it to purchase or lease any petrol and diesel vehicles by 2030 or earlier where possible.
49. Each NHS Scotland body must decarbonise its owned and leased fleet by 2032 or earlier if possible.
50. Each NHS Scotland body will develop a sustainable transport and travel policy.
Facilities
51. All NHS Scotland bodies must take sufficient action to ensure that the buildings they own or occupy achieve net-zero greenhouse gas emissions by 2040 or earlier if possible. The UK’s independent, statutory Climate Change Committee advises that
St Andrew’s House, Regent Road, Edinburgh EH1 3DG
www.gov.scot
most sectors will need to reduce emissions close to zero without offsetting. Therefore, the public sector’s owned estate needs to achieve as close as possible to absolute zero direct emissions.
52. All NHS Scotland new buildings and major refurbishments must be designed to have net-zero greenhouse emissions. Where a net-zero design is not currently practicable, the project must only be approved where a credible route map showing how net-zero emissions will be achieved before 2040 is produced.
53. In addition, all NHS Scotland owned buildings must be heated from renewable sources by 2038. All NHS Scotland new buildings must be designed to achieve that target. Where a renewable heat source is not currently practicable, the project must only be approved where a credible route map showing how renewable heating will be achieved before 2038 is produced.
54. All NHS Scotland buildings should be assessed for resilience to the locked in impacts of climate change over the expected lifespan of that building. Where resilience is not considered sufficient, an action plan must be set out to improve this.
55. Each NHS Scotland body’s Property and Asset Management Strategy must support the achievement of this policy’s aims and in particular the requirements to reduce carbon emissions, adapt to the changing climate and promote greenspace and biodiversity.
Environmental Management Systems
56. Each NHS Scotland body must implement the following management standards to further the aims of this policy: ISO 9001 and 14001 or equivalent. NHS Scotland bodies are not required to seek external confirmation or certification of its conformance with these standards.
57. Each NHS Scotland body must have an effective Environmental Management System in place which has been approved by the SGHSC.
Resourcing
58. Each NHS Scotland body must have a Climate Emergency and Sustainability Team which is sufficiently resourced in light of the scale and complexity of the challenge of decarbonisation, sustainability and climate resilience faced by that NHS Scotland body.
59. Each NHS Scotland body must appoint an Environmental Management Representative (EMR) with the responsibility, resources and authority to implement this policy in respect of environmental management.
60. Each NHS Scotland body must appoint a Waste Management Officer with the responsibility, resources and authority to implement this policy in respect of waste. The Waste Management Officer must have responsibility for all aspects of waste management within the organisation consistent with the Scottish Government’s commitments towards zero-waste and a circular economy.
61. Each NHS Scotland body must appoint an officer with the responsibility, resources and authority to implement this policy in respect of greenspace and biodiversity.
St Andrew’s House, Regent Road, Edinburgh EH1 3DG
www.gov.scot
62. Each NHS Scotland body must appoint an officer with the responsibility, resources
and authority to implement this policy in respect of travel.
63. Each NHS Scotland body which provides clinical services must include a sustainable care medical planning team as part of its Climate Emergency and Sustainability Team.
Assessment of Sustainability
64. Each NHS Scotland body must assess its contribution to the achievement of the United Nation’s Sustainable Development Goals on an annual basis using the National Sustainability Assessment Tool provided by NHS National Services Scotland.
Awareness and Reporting
65. Each NHS Scotland body must publish a report on its public website by November
each year summarising its progress against the aims of this policy using a template approved by the SGHSC for that purpose. The progress report must be approved by the NHS Scotland body’s Chief Executive and be provided to:
The NHS Scotland body’s staff
The NHS Scotland body’s board members; and
SGHSC.
66. The annual progress report will form part of each NHS Scotland’s body annual ministerial review.
67. Each NHS Scotland body must have a clear communications plan to ensure that staff, patients and the local community are aware of that NHS Scotland body’s climate emergency and sustainability plans, policies and processes, and to support them to make sustainable choices. The communications plan must include measures to publicise the annual progress report.
Review
68. This policy and its implementation will be reviewed annually by the NHS Scotland Climate Emergency and Sustainability Board.
APPENDIX 2
A POLICY FOR NHS SCOTLAND ON THE CLIMATE EMERGENCY AND SUSTAINABLE DEVELOPMENT - DL (2021) 38
• Ensure that NHS Scotland bodies, as an integral part of their commitment to the health and wellbeing of the community, contribute to the achievement of the United Nation’s Sustainable Development Goals.
• Ensure that NHS Scotland becomes a net-zero greenhouse gas emissions health service by 2040 or earlier where possible. • Ensure that NHS Scotland’s assets and activities are resilient to the impacts of a changing climate, particularly extreme weather
events. • Establish a culture of stewardship within NHS Scotland, where natural resources are safeguarded and responsibly used to provide
environmentally sustainable healthcare. • Establish NHS Scotland as part of the circular economy through designing out waste and pollution, keeping products and
materials in use and contributing to the regeneration of natural systems. • Increase NHS Scotland’s contribution to tackling the ecological emergency and restoring biodiversity.
Action Responsibility Timescale Comments/Evidence Each NHS Scotland body must implement a strong management structure as a means of ensuring the delivery of this policy’s aims. Each NHS Scotland body must either establish a Climate Emergency and Sustainability Group or designate an existing committee as the lead group for climate emergency and sustainability. In either case, the group must be chaired by a member of its senior / executive management team and its membership must be of sufficient authority to ensure that the aims of this policy are fully integrated into all planning, management decisions and operational practices across the NHS Scotland body.
Director of Facilities Regular updates on climate emergency and sustainability provided to NHS Tayside’s Performance & Resource Committee. New governance structure being reviewed by Director of Facilities
Each NHS Scotland body must appoint an executive lead for its climate emergency response and sustainability.
Director of Facilities? Complete To be confirmed.
Each NHS Scotland body must appoint a member of its board to act as champion for its climate emergency response and sustainability at a strategic level to assist in articulating and promoting its sustainability priorities.
NHS Tayside Board Complete Peter Drury already in post.
NHS Scotland bodies must take an integrated approach to the achievement of the aims of this policy. In developing
NHS Tayside Board
APPENDIX 2
plans or taking action, NHS Scotland bodies must consider the full range of this policies’ aims. NHS Scotland bodies must co-operate with each other with a view to achieving the aims of this policy.
• NHS Tayside represented at National Environmental & Sustainability Group
• NHS Tayside is a member of the northern boards’ sustainability group. Chair is Philip Wilde.
• Other board wide projects include NTC programme for example.
The achievement of this policy’s aims will require NHS Scotland bodies to work with their local communities and patients and with organisations outside of the NHS who have similar aims or who can assist NHS Scotland to achieve its aims. In particular, territorial Health Boards are required to use all reasonable efforts to work with the local authorities for their areas to achieve this policy’s aims.
Plan, invest and implement a transition to an environmentally and socially sustainable, climate resilient, health service in a way which builds on Scotland’s economic and workforce strengths and potential.
Create opportunities to develop resource efficient and sustainable approaches which help address inequality and poverty.
Design and deliver low carbon and climate resilient investment and infrastructure, making all possible efforts to create decent, fair and high value work.
Having regard to national plans to decarbonise the UK’s electricity supply by 2035, each NHS Scotland body must reduce the greenhouse gas emissions from its activities, the activities under its control and from the electricity, steam and heat purchased by it to net-zero by 2040 or
2040
APPENDIX 2
earlier where possible. The UK’s independent, statutory Climate Change Committee advises that most sectors will need to reduce emissions close to zero without offsetting. All NHS owned buildings must be heated from renewable sources by 2038 or earlier where possible.
2038
NHS Scotland bodies must, as a minimum, reduce their associated greenhouse gas emissions from the following sources to net-zero by 2040 or earlier where possible:
2040
• Energy transmission and distribution, having regard to national plans to decarbonise the UK’s electricity supply by 2035
2040
• Waste Disposal 2040 • Business travel, including grey fleet 2040 • Water consumption 2040 • Waste water treatment 2040 • Leased assets 2040
Each NHS Scotland body must take sufficient action to influence a reduction in those greenhouse gas emissions which are linked to its activities but are from sources which it does not own or control to maximise its contribution to reducing emissions to net-zero by 2045 or earlier where possible. (Either) Where the 1990 baseline is known for an emissions source, the NHS Scotland body must reduce the emissions from that source by at least 75% by 2030.
2030
(Or) Where the 1990 baseline is not known for an emissions source, the NHS Scotland body must set interim targets for reducing emissions from that source which are consistent with achieving the net-zero target for the emissions type.
Greenhouse gas emissions reporting Each NHS Scotland body must assess their progress towards net-zero emissions via their annual Public Bodies’ Climate Change Duties Report which is to be submitted to the Scottish Government by 30 November each year. NHS Scotland bodies should, as a minimum, report on their annual emissions associated with their:
APPENDIX 2
• building fossil-fuel energy use • owned and leased fleet fuel use • fluorinated gases and anaesthetic gases (where
relevant)
• purchased energy use (electricity, heat, steam) • energy transmission and distribution • waste • water consumption • waste water treatment • business travel, including the use of grey fleet • leased assets
Climate change adaptation Each NHS Scotland body must undertake a Climate Change Risk Assessment covering all operational areas and produce and implement a Climate Change Adaptation Plan to ensure resilience of service under changing climate conditions and these should be reviewed and updated at least every 5 years.
In relation to existing facilities, these assessments and plans should cover a period at least 20 years into the future from the time of assessment.
In relation to planned facilities, these assessments and plans should cover a period at least 50 years into the future from the time of assessment.
The key risks from the Climate Change Risk Assessment must be incorporated into each NHS Scotland body’s corporate risk register.
Progress on undertaking Risk Assessments and implementing Adaptation Plans, including in terms of how these are supporting national Scottish Climate Change Adaptation Programmes, is to be set out in each bodies’
APPENDIX 2
annual Public Bodies’ Climate Change Duties Report. Sustainable care Each NHS Scotland body will foster and promote a culture of stewardship, where staff are mindful of the resources they use and share a vision of green and sustainable healthcare.
Each NHS Scotland body must ensure their workforce consider the environmental impacts of treatments when making decisions about the care they provide.
Each NHS Scotland body will ensure all employees are educated and trained on the principles of practising sustainably.
Procurement
Each NHS Scotland body must consider social and environmental sustainability when it is procuring goods and services. The procurement of goods and services by NHS Scotland bodies must further the aims of this policy.
NHS Scotland bodies are reminded of the sustainable procurement duty established by section 9 of the Procurement (Scotland) Act 2014 https://www.legislation.gov.uk/asp/2014/12/section/9 NHS Scotland bodies are required to follow the guidance and use the tools issued by the Scottish Government to assist in optimising the economic, social and environmental outcomes of their procurement activity.
It is the responsibility of each NHS Scotland body to review the supply chain of the goods and services that it procures to determine the extent of the associated greenhouse gas emissions and social and environmental impacts. Where
APPENDIX 2
an NHS Scotland body procures goods and services on behalf of another organisation, it is the responsibility of the procuring body to review the supply chain. Circular economy
Each NHS Scotland body must contribute to the creation of a circular economy, working with National Procurement and with suppliers to design out waste and consider the entire life cycle of products and services, reducing the environmental impact, keeping products and materials in use and contributing to the regeneration of natural systems.
In particular, NHS Scotland bodies must: • promote the use of items and assets which have
been designed for durability and upgradability;
• prolong the use of items and assets through proper maintenance and promoting their reuse; and
• promote the use of items and assets which can be recycled at the end of their useful life.
NHS Scotland bodies, with support from National Procurement, must identify and assess the life cycle of products and services and take action to reduce their environmental impact through the avoidance of pollution (including toxic chemicals, micro-plastics and pharmaceutical residues) and waste throughout their life cycle.
Water
Each NHS Scotland body must monitor its water usage and take action to reduce unnecessary water consumption.
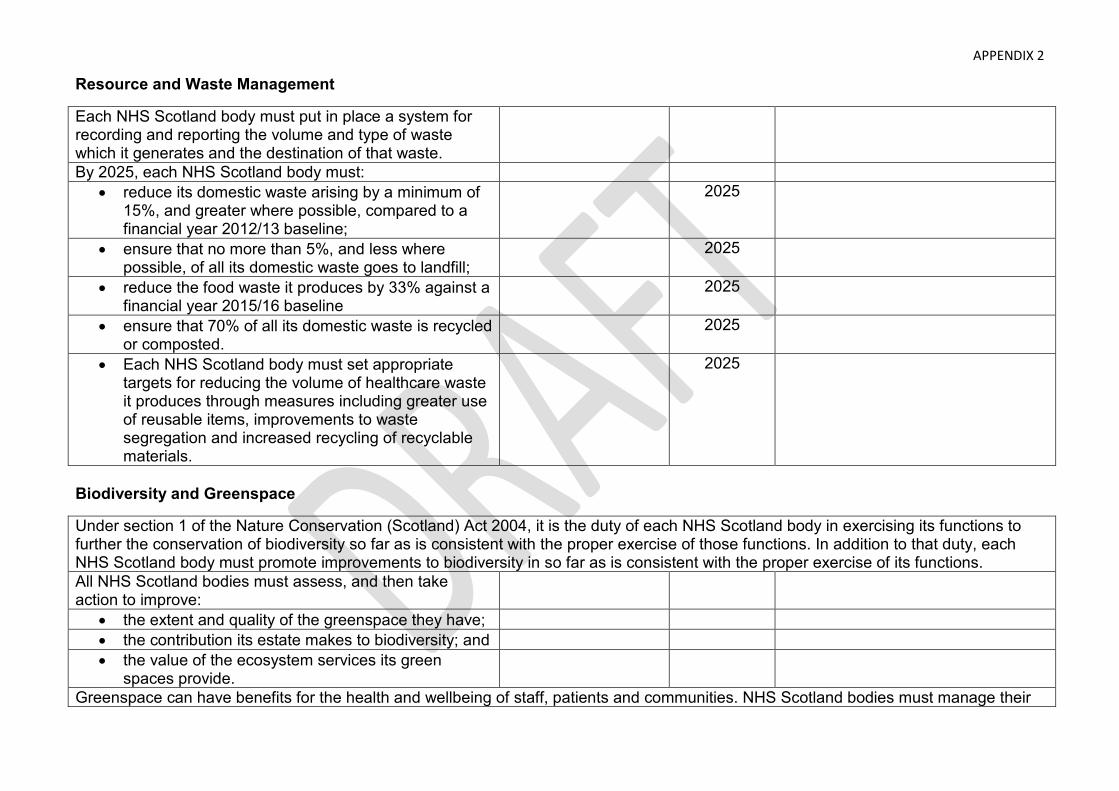
APPENDIX 2
Resource and Waste Management
Each NHS Scotland body must put in place a system for recording and reporting the volume and type of waste which it generates and the destination of that waste.
By 2025, each NHS Scotland body must: • reduce its domestic waste arising by a minimum of
15%, and greater where possible, compared to a financial year 2012/13 baseline;
2025
• ensure that no more than 5%, and less where possible, of all its domestic waste goes to landfill;
2025
• reduce the food waste it produces by 33% against a financial year 2015/16 baseline
2025
• ensure that 70% of all its domestic waste is recycled or composted.
2025
• Each NHS Scotland body must set appropriate targets for reducing the volume of healthcare waste it produces through measures including greater use of reusable items, improvements to waste segregation and increased recycling of recyclable materials.
2025
Biodiversity and Greenspace
Under section 1 of the Nature Conservation (Scotland) Act 2004, it is the duty of each NHS Scotland body in exercising its functions to further the conservation of biodiversity so far as is consistent with the proper exercise of those functions. In addition to that duty, each NHS Scotland body must promote improvements to biodiversity in so far as is consistent with the proper exercise of its functions. All NHS Scotland bodies must assess, and then take action to improve:
• the extent and quality of the greenspace they have; • the contribution its estate makes to biodiversity; and • the value of the ecosystem services its green
spaces provide.
Greenspace can have benefits for the health and wellbeing of staff, patients and communities. NHS Scotland bodies must manage their
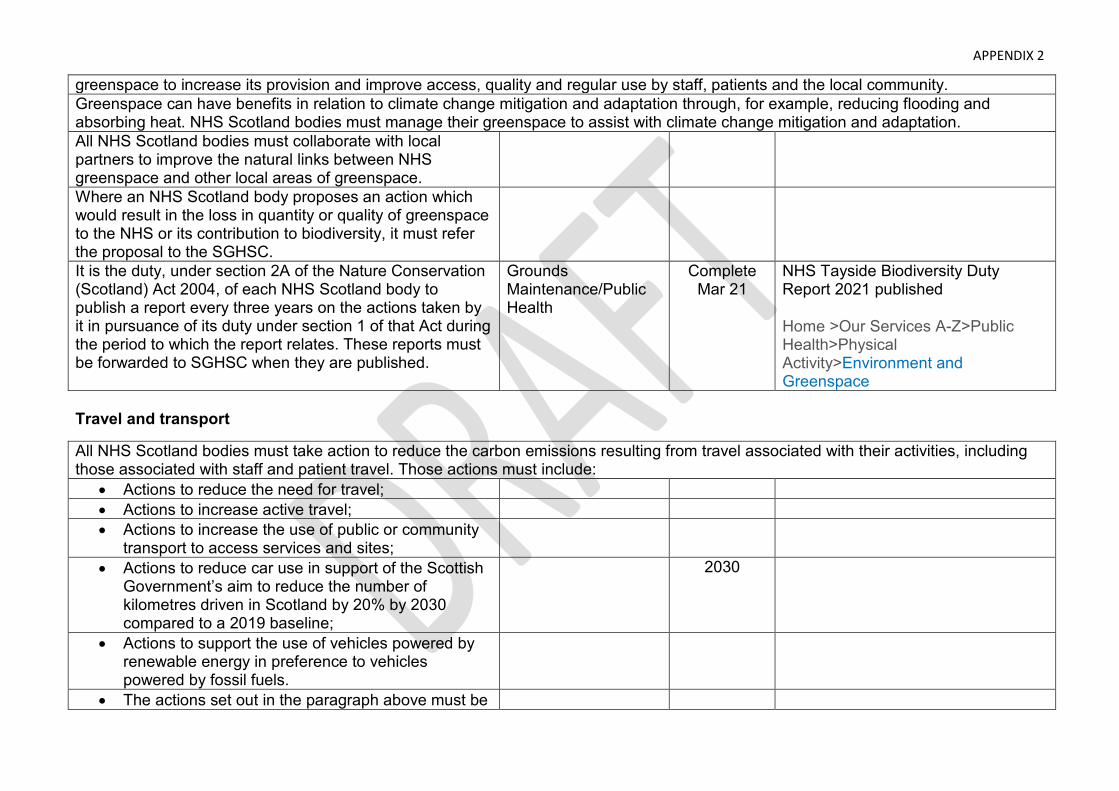
APPENDIX 2
greenspace to increase its provision and improve access, quality and regular use by staff, patients and the local community. Greenspace can have benefits in relation to climate change mitigation and adaptation through, for example, reducing flooding and absorbing heat. NHS Scotland bodies must manage their greenspace to assist with climate change mitigation and adaptation. All NHS Scotland bodies must collaborate with local partners to improve the natural links between NHS greenspace and other local areas of greenspace.
Where an NHS Scotland body proposes an action which would result in the loss in quantity or quality of greenspace to the NHS or its contribution to biodiversity, it must refer the proposal to the SGHSC.
It is the duty, under section 2A of the Nature Conservation (Scotland) Act 2004, of each NHS Scotland body to publish a report every three years on the actions taken by it in pursuance of its duty under section 1 of that Act during the period to which the report relates. These reports must be forwarded to SGHSC when they are published.
Grounds Maintenance/Public Health
Complete Mar 21
NHS Tayside Biodiversity Duty Report 2021 published
Home >Our Services A-Z>Public Health>Physical Activity>Environment and Greenspace
Travel and transport
All NHS Scotland bodies must take action to reduce the carbon emissions resulting from travel associated with their activities, including those associated with staff and patient travel. Those actions must include:
• Actions to reduce the need for travel; • Actions to increase active travel; • Actions to increase the use of public or community
transport to access services and sites;
• Actions to reduce car use in support of the Scottish Government’s aim to reduce the number of kilometres driven in Scotland by 20% by 2030 compared to a 2019 baseline;
2030
• Actions to support the use of vehicles powered by renewable energy in preference to vehicles powered by fossil fuels.
• The actions set out in the paragraph above must be
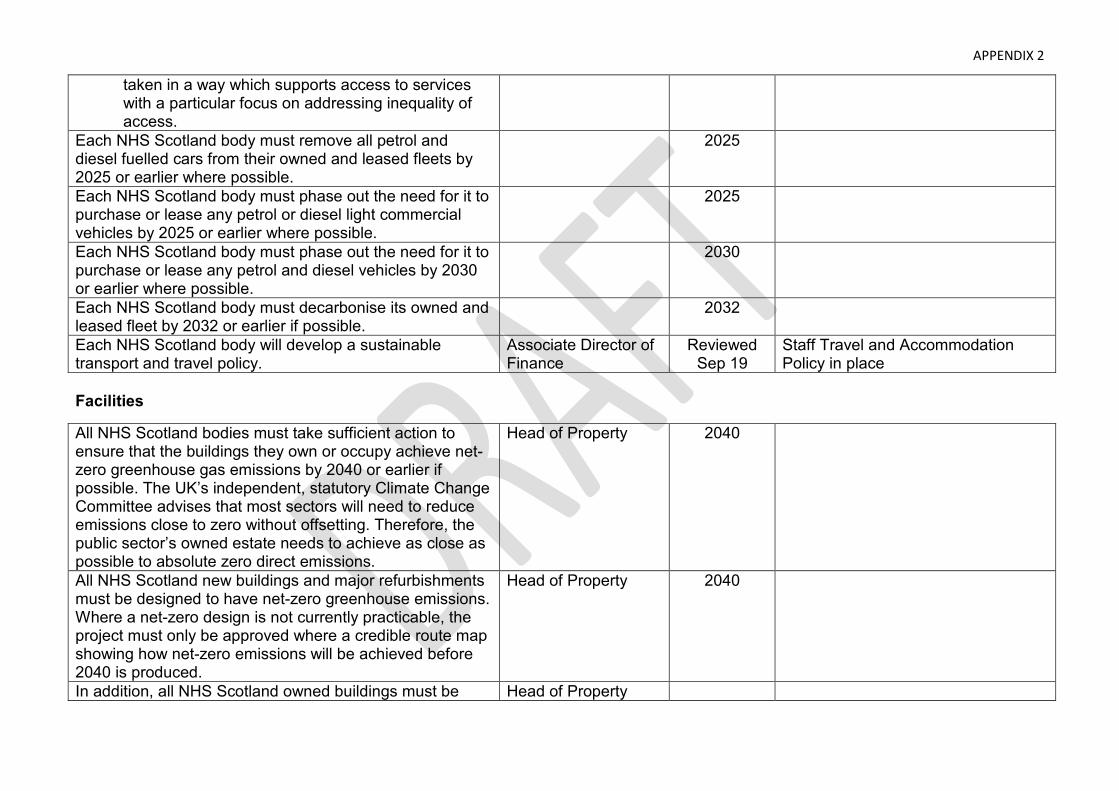
APPENDIX 2
taken in a way which supports access to services with a particular focus on addressing inequality of access.
Each NHS Scotland body must remove all petrol and diesel fuelled cars from their owned and leased fleets by 2025 or earlier where possible.
2025
Each NHS Scotland body must phase out the need for it to purchase or lease any petrol or diesel light commercial vehicles by 2025 or earlier where possible.
2025
Each NHS Scotland body must phase out the need for it to purchase or lease any petrol and diesel vehicles by 2030 or earlier where possible.
2030
Each NHS Scotland body must decarbonise its owned and leased fleet by 2032 or earlier if possible.
2032
Each NHS Scotland body will develop a sustainable transport and travel policy.
Associate Director of Finance
Reviewed Sep 19
Staff Travel and Accommodation Policy in place
Facilities
All NHS Scotland bodies must take sufficient action to ensure that the buildings they own or occupy achieve net-zero greenhouse gas emissions by 2040 or earlier if possible. The UK’s independent, statutory Climate Change Committee advises that most sectors will need to reduce emissions close to zero without offsetting. Therefore, the public sector’s owned estate needs to achieve as close as possible to absolute zero direct emissions.
Head of Property 2040
All NHS Scotland new buildings and major refurbishments must be designed to have net-zero greenhouse emissions. Where a net-zero design is not currently practicable, the project must only be approved where a credible route map showing how net-zero emissions will be achieved before 2040 is produced.
Head of Property 2040
In addition, all NHS Scotland owned buildings must be Head of Property
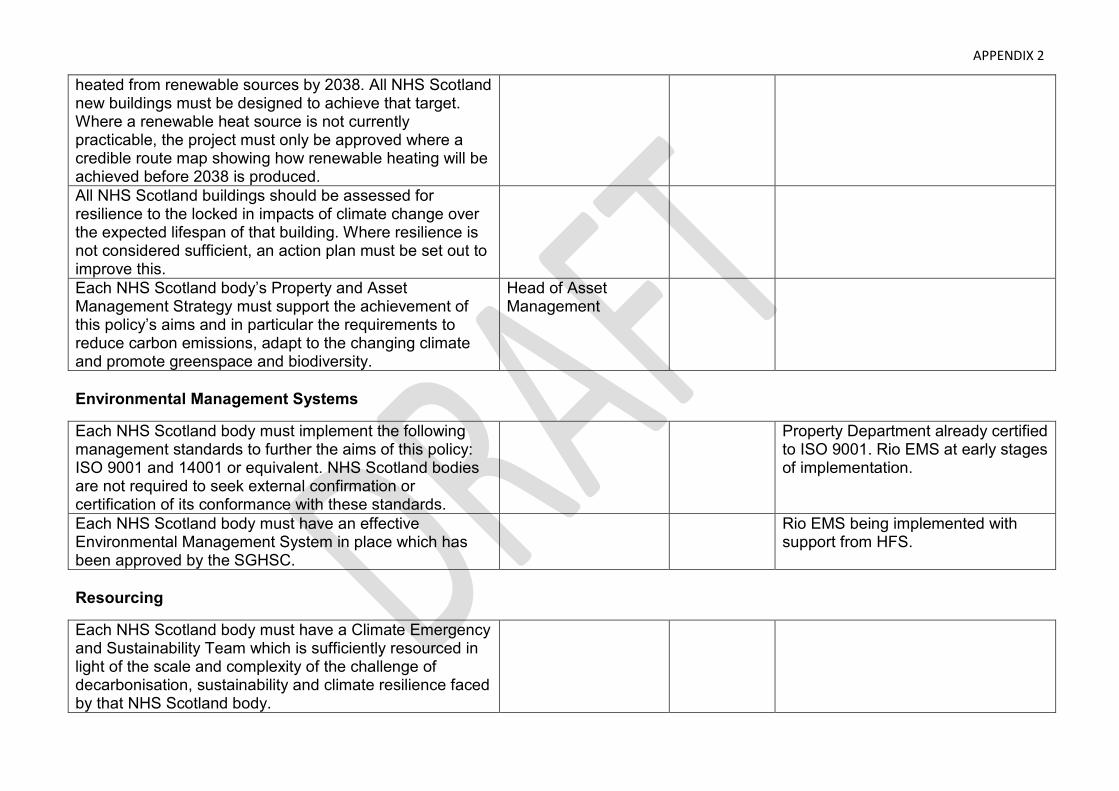
APPENDIX 2
heated from renewable sources by 2038. All NHS Scotland new buildings must be designed to achieve that target. Where a renewable heat source is not currently practicable, the project must only be approved where a credible route map showing how renewable heating will be achieved before 2038 is produced. All NHS Scotland buildings should be assessed for resilience to the locked in impacts of climate change over the expected lifespan of that building. Where resilience is not considered sufficient, an action plan must be set out to improve this.
Each NHS Scotland body’s Property and Asset Management Strategy must support the achievement of this policy’s aims and in particular the requirements to reduce carbon emissions, adapt to the changing climate and promote greenspace and biodiversity.
Head of Asset Management
Environmental Management Systems
Each NHS Scotland body must implement the following management standards to further the aims of this policy: ISO 9001 and 14001 or equivalent. NHS Scotland bodies are not required to seek external confirmation or certification of its conformance with these standards.
Property Department already certified to ISO 9001. Rio EMS at early stages of implementation.
Each NHS Scotland body must have an effective Environmental Management System in place which has been approved by the SGHSC.
Rio EMS being implemented with support from HFS.
Resourcing
Each NHS Scotland body must have a Climate Emergency and Sustainability Team which is sufficiently resourced in light of the scale and complexity of the challenge of decarbonisation, sustainability and climate resilience faced by that NHS Scotland body.
APPENDIX 2
Each NHS Scotland body must appoint an Environmental Management Representative (EMR) with the responsibility, resources and authority to implement this policy in respect of environmental management.
Director of Facilities Complete
Each NHS Scotland body must appoint a Waste Management Officer with the responsibility, resources and authority to implement this policy in respect of waste. The Waste Management Officer must have responsibility for all aspects of waste management within the organisation consistent with the Scottish Government’s commitments towards zero-waste and a circular economy.
Operational Waste Manager in post
Each NHS Scotland body must appoint an officer with the responsibility, resources and authority to implement this policy in respect of greenspace and biodiversity.
Senior Estates Manager?
Each NHS Scotland body must appoint an officer with the responsibility, resources and authority to implement this policy in respect of travel.
Each NHS Scotland body which provides clinical services must include a sustainable care medical planning team as part of its Climate Emergency and Sustainability Team.
Assessment of Sustainability
Each NHS Scotland body must assess its contribution to the achievement of the United Nation’s Sustainable Development Goals on an annual basis using the National Sustainability Assessment Tool provided by NHS National Services Scotland.
Property Environmental & Quality Manager
Progress monitored via NHS Tayside existing sustainability group.
Awareness and Reporting
Each NHS Scotland body must publish a report on its public website by November each year summarising its progress against the aims of this policy using a template approved by the SGHSC for that purpose. The progress
APPENDIX 2
report must be approved by the NHS Scotland body’s Chief Executive and be provided to:
• The NHS Scotland body’s staff • The NHS Scotland body’s board members; • SGHSC
The annual progress report will form part of each NHS Scotland’s body annual ministerial review.
Each NHS Scotland body must have a clear communications plan to ensure that staff, patients and the local community are aware of that NHS Scotland body’s climate emergency and sustainability plans, policies and processes, and to support them to make sustainable choices. The communications plan must include measures to publicise the annual progress report.
Review
This policy and its implementation will be reviewed annually by the NHS Scotland Climate Emergency and Sustainability Board.




















