Agenda Governing Body Board (Part 1) - NHS North East ...
132
Agenda Governing Body Board (Part 1) [28 October 2015] Agenda Governing Body Board (Part 1) Date: 28 October 2015 Time: 14.00-16.00 Venue: Boardrooms A, B and C, Kirkdale House, Leytonstone, E11 1HP Chair: Dr Anwar Khan Topic Action Required Clinical Lead/ Lead Lead Officer(s) Page No. General Business Apologies and announcements To discuss Dr Anwar Khan - Declarations of interest (register on public view) To declare All - Draft minutes from September’s Board To discuss Matters Arising To note 1 Chair’s update To note - Questions from Members and Public To note - 2 Governance No items 3 Performance and Quality 3.1 Performance and Quality Report For discussion Dr Dinesh Kapoor Les Borrett & Helen Davenport 4
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Agenda Governing Body Board (Part 1) - NHS North East ...

Agenda Governing Body Board (Part 1) [28 October 2015]
Agenda
Governing Body Board (Part 1)
Date: 28 October 2015
Time: 14.00-16.00
Venue: Boardrooms A, B and C, Kirkdale House, Leytonstone, E11 1HP
Chair: Dr Anwar Khan
Topic Action Required
Clinical Lead/
Lead
Lead Officer(s)
Page No.
General Business
Apologies and announcements To discuss Dr Anwar Khan
-
Declarations of interest (register on public view)
To declare All -
Draft minutes from September’s Board To discuss
Matters Arising To note 1
Chair’s update To note -
Questions from Members and Public To note -
2 Governance
No items
3 Performance and Quality
3.1 Performance and Quality Report For discussion Dr Dinesh Kapoor
Les Borrett & Helen Davenport
4

Topic Action Required
Clinical Lead/
Lead
Lead Officer(s)
Page No.
3.2 Children’s Services To note Dr Tonia Myers
Jane Mehta 23
3.3 Nursing and Midwifery Council Revalidation
To note Dr Anwar Khan
Helen Davenport
33
4 Finance and QIPP
4.1 Finance Report For discussion Alan Wells
Les Borrett 41
5 Strategy and Planning
5.1 Communication Strategy To approve Richard Griffin
Helen Davenport
57
5.2 Community Participation Strategy To approve Richard Griffin
Helen Davenport
67
6
For information
6.1 Minutes of Performance and Quality Committee (September 2015)
For info Dr Dinesh Kapoor
Helen Davenport
87
6.2 Minutes of Planning and Innovation Committee (September 2015)
For info Alan Wells
Jane Mehta 96
6.3 Minutes of Finance and QIPP Committee (September 2015)
For info Alan Wells
Les Borrett 102
6.4 Minutes of IT Committee (September 2015)
For info Dr Mayank Shah
Les Borrett 105
6.5 Minutes of Medicines Management Committee (September 2015)
For info Dr Mayank Shah
Helen Davenport
112

Topic Action Required
Clinical Lead/
Lead
Lead Officer(s)
Page No.
6.6 Minutes of Primary Care Commissioning Committee (July 2015)
For info Alan Wells
Jane Mehta 120
6.7 Summary of Safety Net Executive (LBWF) (September 2015)
For info - Andrew Taylor and
Alastair Macorkindale
125
6.8 Summary of Leyton/Leytonstone Locality Meeting (September 2015)
For info Dr Syed Ali
Jane Mehta 126
6.9 Summary of Walthamstow Locality Meeting (September 2015)
For info Dr Mayank Shah
Jane Mehta 127
6.10 Summary of Chingford Locality Meeting (September 2015)
For info Dr Tonia Myers
Jane Mehta 128
7 AOB
7.1 AOB -
8 Forward plan ALL
8.1 Forward plan For discussion ALL 129
9 Photographer in attendance Room D ALL
Next meeting
Date: 25 November 2015
Time: Formal Board 1400-1800
Venue: Boardrooms A, B and C, Kirkdale House, Leytonstone, E11 1HP

Page 1 Action Log Waltham Forest CCG Governing Body Part 1 on 23 September 2015 including earlier Brought Forward Items [October 2015]
Action log Waltham Forest CCG Governing Body Part 1 on 23 September 2015 including earlier Brought Forward Items Date: 23 September 2015 and earlier
Time: 2-4pm
Minute No.
Action Lead/ Owner
Due Date
Status Date Completed
146/15 NKL drew attention to Risk 7 in relation to Whipps Cross Hospital being non-compliant with eight standards of care identified in November 2014 by the Care Quality Commission (CQC). NKL suggested the CCG should write to Barts Health to raise concerns in relation to the slow progress in reducing this risk. It was agreed that HD write to Barts Health Chief Executive Officer.
Action HD to write to Barts Health Chief Executive Officer
HD
Oct Meeting
Open
147/15 MS informed the governing body that in relation to prescribing there was some good news, although cautioned this relates to the summer season. SA noted that previously leaflets informing patients about the use of antibiotics had
MS Oct Meeting
Open – Action passed to Meds Mngt. Information sign-posting to CCG website has been circulated to all practices.
1

Page 2 Action Log Waltham Forest CCG Governing Body Part 1 on 23 September 2015 including earlier Brought Forward Items [October 2015]
Minute No.
Action Lead/ Owner
Due Date
Status Date Completed
previously been sent out. SA asked if the leaflet could be re-produced. MS agreed to look into this. Action MS to explore the possibility of reproducing the antibiotics leaflet for distribution.
147/15 SA commented that some practices had been given access to the electronic Friends and Family Test, this has produced a good response rate, whereas as the paper based survey does not produce the same level of response. SA asked if the figures are based on electronic responses. HD will bring data back to the next governing body meeting. Action HD to provide data on FFT responses.
HD Oct Meeting
Open
149/15 HD outlined that it was important to have formal evidence if Diagnostic Performance Data reports do not have the necessary quality of information, examples of this should be sent to HD. Action C Edmonds to be notified to add to the locality meeting agendas and item
HD Oct Meeting
Open
2

Page 3 Action Log Waltham Forest CCG Governing Body Part 1 on 23 September 2015 including earlier Brought Forward Items [October 2015]
Minute No.
Action Lead/ Owner
Due Date
Status Date Completed
outlining that poor quality diagnostic reports should be notified to the CCG via the GP Alert System
3

Item 3.1
Title of report Performance and Quality Report (CCG Scorecard)
From Les Borrett, Director of Financial Strategy and Performance – WFCCG Helen Davenport, Director of Quality and Governance - WFCCG
Purpose of report
The purpose of this report is to inform the CCG Governing Body of the CCG’s performance against the CCG Scorecard and other national performance and quality standards at the end of August 2015 (Month 5). Where standards are not being met the report provides a narrative describing the issues and the actions being taken to ensure recovery to the planned target. At the end of August 2015 the following indicators were considered to be at a high risk of not meeting their targets: Integrated Care for Children (6) Diabetes Care Plans (11) Cardiology Referrals (12) CHC Community Assessments (14) A&E All Types Performance at Whipps Cross (17) Urgent Care Centre Utilisation at Whipps Cross (18)
Changes/additions/amendments to paper as a result of discussions held at other committees
Not applicable
Recommendations
The CCG Governing Body are asked to review the report and make any necessary recommendations for further investigation.
Impact on patients & carers
The CCG is not meeting several performance targets, including the 4hr waiting time target for A&E at Whipps Cross Hospital. The report details the actions being taken by the CCG and by providers to address these and other areas of under-performance. The Scorecard is the principle tool for the CCG to ensure it is reporting on the impact of the CCG’s work programmes for 2015/16 in terms of improved patient care and outcomes. The report supports the delivery of improved care by providing a process for recording progress each month and highlighting any risks to delivery, so that these risks can be appropriately mitigated by the CCG.
Risk implications
Failure to ensure that there are improvements to the quality and performance of services commissioned may result in a failure to manage and mitigate risks with potential harm to patients and reputational damage to the CCG.
4

Performance and Quality Report (CCG Scorecard)
Financial implications
Failure to meet NHS Constitution standards or CCG Local Priorities may affect the size of the Quality Premium, an additional incentive payment made to CCGs in 2015/16.
Equality analysis
The report has considered the CCG’s equality duty and where relevant has identified relevant actions which address any likely impact on equality and human rights.
Other committees/groups, including the CCG Reference Group and Rapid Feedback Group
An earlier version of the report was presented to the Performance and Quality Committee in September 2015.
5

Performance and Quality Report (CCG Scorecard)
October 2015
6

Performance and Quality Report (CCG Scorecard)
Page ii
Contents Scorecard Aims and Objectives 1
CCG Scorecard 2
Integrated Care 3
Mental Health 4
Children 5
Maternity 5
Learning Disability 6
Cancer 6
Long-term Conditions 7
End of Life Care 8
Integrated Commissioning 8
Community Health Services 9
Planned Care 9
Urgent Care 10
Prescribing 11
Quality and Safety 11
Primary Care 12
Exception Reporting 12
Appendices 15
Appendix A Waltham Forest CCG Business Grid 15
7

Performance and Quality Report (CCG Scorecard)
Page 1
Scorecard Aims and Objectives
NHS Waltham Forest Clinical Commissioning Group (WFCCG) has developed the Scorecard to report progress against key performance and quality targets in 2015/16.
The 2015/16 Scorecard has been designed around the CCG workstreams as identified in the CCG Business Grid (Appendix A). In order to create the Scorecard each CCG workstream lead was asked to develop a maximum of two indicators and targets that reflect the key goals for that programme. These goals have been developed in collaboration with the relevant Clinical Director and/or Clinical Leads. They have been further refined through two CCG away-days (24 and 29 April 2015). The Scorecard has also been reviewed and signed-off by the Performance and Quality Committee (13 May 2015) and approved by the Governing Body (27 May 2015).
The intention of the Scorecard is to identify specific measurable indicators that can be used to demonstrate improvements in patient care and outcomes over the course of the year. The focus of the Scorecard is on improvements to patient outcomes. Where it has not been possible to measure health outcomes, or where outcomes cannot be tracked on a monthly basis, indicators have been chosen that most closely reflect the work being undertaken by the CCG workstreams to influence improvements in outcomes.
The Scorecard reflects Waltham Forest priorities and objectives rather than replicating national performance frameworks. This makes the Scorecard more meaningful and relevant to the CCG. It enables the CCG to measure the effectiveness of its local strategic plans. Where appropriate, the Scorecard has used existing national indicators and targets. This is the case for the key national targets that CCG was not meeting at the end of 2014/15. Local CCG plans should support national performance objectives. Where relevant the Scorecard targets have been aligned with the levels of ambition set out in the CCG Operating Plan and Quality Premium submissions to simplify reporting processes.
The CCG performance reporting process will focus on the latest performance information, progress made in the past month, the identification of any risks to delivery, and actions being taken to resolve underperformance or mitigate adverse impact. Whilst the reporting process will focus on performance of the Scorecard indicators, the intention is also to capture the key elements of the wider work being undertaken within each workstream, to the extent that this supports making a difference for the residents of Waltham Forest.
The monthly reporting process will also be used to report by exception on the CCG’s performance against national performance and quality targets not covered by the Scorecard so that the CCG is aware of any risks to the local population. This exception reporting includes the NHS Constitution standards and the CCG requirements outlined in the 2015/16 Operating Plan guidance.
8

Performance and Quality Report (CCG Scorecard)
Page 2
CCG Scorecard Month 5 (August data)
Notes: Dementia and IAPT baseline figures are average values for 2014/15. IAPT performance will be assessed based on a quarterly basis in line with agreed targets with NELFT. RTT incomplete pathway shows the officially reported CCG position, but does not include Barts Health data (not reporting) - see narrative below for full update. A&E and Cancer (62 day) targets are based on CCG trajectories agreed with NHSE that assume mid-year compliance and are rated on the basis of this trajectory. RAG rating for other end-of-year targets (for example Virtual Ward and Prescribing) is also done on the basis of trajectories developed by the project leads. Methodology for Integrated Care and for District Nursing have been updated at M5 based improved information (see report for details). Both changes have been approved by the Performance and Quality Committee.
Workstream # IndicatorBasel ine 2014/15
Target 2015/16
Project lead
Exec Lead
Cl inica l Director
Apr May Jun Jul Aug YTD Trend Risk Assessment
1 Emergency admiss ions for targeted cohort patients 6840 10% reduction GF JM SA ‐6% ‐16% 10% ‐7% ‐21% ‐7% Medium ri sk
2 Emergency admiss ions from care homes (QP) 947 5% reduction GF JM SA ‐5% ‐13% 9% ‐9% 20% 1% Medium ri sk
3 Dementia diagnos is rate 57.6%* 67.0% NA JM JS ‐ ‐ ‐ 69% 70% 70% Low ‐ on track
4 IAPT access rate 3.1%* 3.75% NA LB JS 1.20% 1.18% 3.48% Medium ri sk
5 RTT performance for paediatric services at NELFT 79% 95% KH JM TM 100% 100% 100% 100% 33% 87% Medium ri sk
6 Integrated Care for Chi ldren 0 40 KH JM TM 0 0 0 0 0 0 High ri sk
Materni ty 7 Early antenata l booking at Whipps Cross (13 weeks) 84.8% (Apr 15) 85% KH JM TM 85% 92% 96% 96% 96% 91% Low ‐ on track
Learning Disabi l i ty 8 Health and socia l care community assessments New indicator 90% at M12 KH JM 1% 8% 7% 18% ‐ 18% Medium ri sk
9 Cancer GP referra l to fi rs t treatment within 62 days 74% 85% from Q2 JD/EP LB NKL 87% 76% 82% 73% 83% 80% Medium ri sk
10 Bowel cancer screening 52.7% 57.7% JD JM NKL 49% 50% 55% 49% 50% 51% Medium ri sk
11 Diabetes patients on new pathway with care plans NA 80% LS JM SA 25% 26% 26% 27% 26% High ri sk
12 Reduction in cardiology outpatient referra ls 2899 5% reduction LS JM SA 11% 45% 67% 42% 43% 73% High ri sk
End of Li fe Care 13 Patients registered as pal l iative care 434 (Apr 15) 500 at M12 JR JM NKL 434 417 423 412 420 421 Medium ri sk ‐ tra jectory from M6
Integrated Commiss ioning 14 CHC el igibi l i ty assessments within 28 days New indicator 80% KH HD 50% 64% 60% 0% 0% 35% High ri sk
Community Health Services 15 District nurs ing waiting times – GP referra ls within 48hrsNew indicator 90% KH JM AS 80% 72% 55% 69% 89% 73% Medium ri sk
Planned Care 16 RTT incomplete pathway performance 87.30% 92% LB LB DK 96.7%* 95.9%* 95.4%* 95% 93% 95% Medium ri sk
17 A&E 4hr al l types performance at Whipps Cross 89.8% 95% from Q3 EP LB NKL 87% 89% 90% 85% 89% 88% High ri sk
18 Proportion of patients us ing the WX Urgent Care Centre 32% 34% EP JM NKL 32% 31% 27% 27% 27% 30% High ri sk
Prescribing 19 Antibiotic prescribing in primary care 1.111 (13/14) <1.11 AO HD MS 1.06 1.04 1.03 1.02 ‐ 1.04 Low ‐ on track
20 Improvement in Whipps Cross FFT score 90.4% 91.4% DM HD DK 93.5% 91.1% 94.8% 92.9% ‐ 93.3% Low ‐ on track
21 Number of C.Di ff cases within planned tra jectory 43 <=45 LS HD DK 2 2 4 2 ‐ 8 Low ‐ on track
Primary Care 22 Genera l Practice FFT score (QP) 85.6% 86.6% SR JM AK 81% 89% 86% 88% ‐ 85% Medium ri sk
3.48%
Urgent Care
Qual i ty and Safety
Integrated Care
Menta l health
Chi ldren
Cancer
Long term conditions
9

Performance and Quality Report (CCG Scorecard)
Page 3
Integrated Care
1. Barts Health Integrated Care Emergency Admissions
The CCG has adjusted the measurement for this indicator so that it only counts changes in activity in the moderate to very high risk population (the top 20% of the Waltham Forest population at risk of being admitted to hospital). This is an improvement in methodology as it allows the CCG to measure impact in a more specific group of patients targeted by the integrated care programme. The change in methodology was approved by the Performance and Quality Committee on 14 October 2015.
The new indicator shows that activity has fallen by 117 in the first five months of 2015/16. This represents a 7% reduction in activity compared to 2014/15 against a 10% target. There have been significant reductions in emergency admissions for Urinary Tract Infections compared to 2014/15. However there have been some increases in high cost cardiac patients that the CCG is currently investigating to ensure there has not been any change in coding practice at Barts Health. Emergency admissions at Whipps Cross continues to fall and the hospital site has seen 14% fewer emergency admissions in 2015/16 compared to the same period in 2014/15. This indicates a large impact from Integrated Care and other out-of-hospital admission reduction initiatives. A deep dive into Integrated Care performance was conducted by the CCG on 1 October 2015 and further actions to confirm which groups of patients are no longer being admitted to Whipps Cross have been agreed. The extension of integrated care to moderate risk has been delayed by recruitment issues at NELFT. Currently there are nine posts vacant in this team. NELFT have been undertaking recruitment and have been asked to consider a wider range of clinical roles and grade bands. NELFT are using the wider workforce to support delivery of the programme.
2. Ambulance Conveyances from Waltham Forest Care Homes (CCG Quality Premium Local Measure)
August data saw a spike in ambulance attendances compared to previous months. There were 103 London Ambulance Service attendances to nursing and care homes in August compared to 83 in the previous month. The total number of patients conveyed from nursing and care home locations also increased. The increase was not confined to any particular location. Year to date conveyances from care homes has increased marginally by 1%. Falls account for 13% of attendances and this should be addressed by the new Falls Prevention Service commissioned from 1 October 2015. The Rapid Response team has been expanded in 2015/16 to include dedicated staff to work with care homes and support education and development as well as manage patients. A full schedule of education programmes for care homes is being developed with NELFT.
10

Performance and Quality Report (CCG Scorecard)
Page 4
Mental Health
3. CCG Dementia Diagnosis Rate
NHSE have updated CCGs that national data on dementia diagnosis will not be updated until September. This update has been delayed. This will change the way in which the dementia prevalence rate is calculated. The change in methodology is expected to reduce the predicted prevalence rates for most CCGs (this is therefore expected to improve the dementia diagnosis rates for most CCGs). WFCCG agreed a new set of indicators in the NELFT contract for dementia and NELFT are currently meeting these targets. Internal figures from Health Analytics show at the end of August the CCG was at 70% based on the former prevalence rate. Figures for the previous two months have been lower although above the target of 67%. This has been found to be due to some GPs not coding patients who have been diagnosed. This has been picked up by the Memory Clinic GP Link Worker and addressed in August. Monthly performance meetings continue to look at reasons for any discrepancy and to ensure the level is maintained at the March level due to the expected fall when the new prevalence figures are announced. This internal reporting is shown in the current scorecard, and this will be updated to reflect national figures as soon as these are available.
National data for dementia diagnosis rates based on the new methodology was made available to CCGs for September 2015. This shows that Waltham Forest CCG currently has performance of 75.6%. Data is yet to be published for previous months, but the scorecard will be updated as this becomes available.
4. Improving Access to Psychological Therapies (Access Rate)
Performance for Q1 was 3.39% against a target of 3.75%. This reflects a shortfall of 79 patients. NELFT have reported that this under-performance is related to seasonal patterns in the service and in part due to the number of bank holidays in Q1. Performance in July and August remains below the target to deliver 3.75%. The shortfall in August was 20 patients. NELFT have provided a monthly recovery plan to ensure they meet the target for the full year. Referrals to IAPT did improve in August and were sufficient to meet the target.
The CCG performance is significantly improved from this time last year and we continue to work with NELFT to increase the number of referrals. Increasing referrals remains a priority for the CCG in order to meet the target. The CCG is focusing on expanding the range of patients targeted for IAPT referrals, specifically to include patients being treated for Hepatitis C, FGM (Female Genital Mutilation) and patients identified as having issues with hoarding. NELFT will be establishing contacts with the relevant organisations and also working with the Local Authority to increase referrals from older adults. The CCG is working with NELFT to identify rooms in GP practices for NELFT to provide IAPT sessions closer to patient’s homes. The CCG is meeting the 50% recovery rate. 100% of patients are entering treatment within 6 weeks against the national 75% target.
11

Performance and Quality Report (CCG Scorecard)
Page 5
A risk has been identified concerning the way in which NELFT report data to the HSCIC which has resulted in variances between the locally understood performance and the nationally reported position. This is being investigated and will be picked up by the CCG Deep Dive into scorecard performance on 20 October 2015.
Children
5. Referral to Treatment (18 weeks) for Consultant Led Children’s Services at NELFT
There were 2 breaches in August, out of three referrals. One patient was delayed due to the patient and family going on holiday and a new date has been offered to the family. The other delay was due to a referral being lost, which was made to the Barts Health Central Referral System for the Epilepsy Clinic (Run at Barts but provided by NELFT Paediatricians), the patient has now been seen. Further discussions will be taking place with NELFT during performance meetings to understand the issues and action being taken. The last breach was in November 2014
6. Integrated Care for Children (NELFT)
The plan was for this service to start seeing patients in July. There has been delays in recruiting staff. This has been raised through the contracting meeting with NELFT. NELFT are in the process of recruiting candidates. The service has been commissioned to see up to 40 children in 2015/16.
CCG performance on this indicator is being followed up at a Deep Dive meeting on 20 October 2015.
Maternity
7. Early Antenatal Booking (Whipps Cross Hospital)
The indicator measures the proportion of women who have their first antenatal assessment within 13 weeks (12 weeks plus 6 days) of their pregnancy at Whipps Cross, for those women that are known to the service by ten weeks. This is a good measure of the quality and performance of this service. Early booking is associated with better outcomes for both women and their babies, and can be particularly important for women who develop complications in pregnancy. Performance has been on target for July and August.
The CCG is working with Barts Health to implement a comprehensive action plan to improve early booking for those not known to the service before 10 weeks. This programme includes: engagement with our Maternity Service Liaison Committee (MSLC) to help increase awareness about the importance of early booking, improving signposting, GP education, increasing options for self-referral, and working with Whipps Cross staff to increase access.
12

Performance and Quality Report (CCG Scorecard)
Page 6
Learning Disability
8. Health and Social Care Learning Disability Community Assessments (NELFT)
The CCG target reports on the completion of annual health and social care community assessments. The CCG expects performance to be 90%. This indicator details the support and review process for people with a Learning Disability who are supported by Waltham Forest.
Figures have been reported for the first time showing that performance is below the plan at the end of June. A meeting with NELFT and the Local Authority has been set up to review the trajectory and agree an action plan.
CCG performance on this indicator is being followed up at a Deep Dive meeting on 20 October 2015.
Cancer
9. CCG GP Referral to Treatment (62 Days) Performance
In July performance was 72.9% against a target of 85%, this was a deterioration from the previous month (81.8%). Challenges remain in Breast, Lung, and Urological pathways. In July 6 out of 10 breaches for Waltham Forest CCG were for urological cancer patients. Five Waltham Forest CCG patients had waits of over 100 days. Four of these breaches were for urological tumours (excluding testicular) and all involved patients that were first seen at Barts Health but received first treatment at UCLH. The other 100 day wait was for haematology. Provisional figures for August shows some improvement at Barts Health with Whipps Cross provisionally meeting the 85% target.
A contract performance notice was issued on 3 June 2015. A remedial action plan (RAP) has now been agreed which assumes that the Trust will be compliant with the 62 day GP referral target from October. Weekend clinics have been opened to work on the 100 day backlog and a best practice prostrate pathway (to address patients referred to UCLH) is to be agreed by all consultants and planned to be implemented from November 2015. Barts have set up a weekly tracker and telephone call with UCLH. Actions also include the redevelopment of the triple assessment clinic at Whipps Cross (by November 2015) and detailed endoscopy plan covering outsourcing and recruitment. Barts Health conducts a Root Cause Analysis for all 62 day breaches and all patients waiting over 100 days have a clinical harm review. The CCG has submitted a trajectory to NHSE that ensures compliance with the national target from Q2 2015/16. The WEL commissioners hold bi-weekly cancer speciality level deep dives with management and clinicians to challenge delivery at speciality level. Performance across London and England remains below the target.
13

Performance and Quality Report (CCG Scorecard)
Page 7
10. Bowel Cancer Screening
The CCG bowel cancer screening pilot was re-launched on 1 August and will run until 31 March 2016. The project aims to increase the uptake of screening and improve the early identification of patients with possible bowel cancer. Fifteen practices have signed up, with no change from the end of August. Another round of contact with practices is required to improve sign up to the scheme. The main reason practices have been saying to the cancer clinical leads that bowel screening is already covered by the National Screening Programme and that telephone calling is time intensive. Health Analytics analysis shows uptake of the test remaining at approximately 50%.
The CCG is working with the Bowel Cancer Screening Hub to enable GPs to access patient notification lists. Whilst these remain unavailable practices have been advised to contact patients who turn 60 years of age during the pilot. There has been some improvement in the performance figures in the last two months although the CCG is just below the target for 2015/16. The CCG has appointed a Macmillan GP who started in post at the end of July. This post will assist in promoting messages around the importance of bowel screening. Community outreach to improve understanding of bowel cancers screening started on 14 September and is being undertaken by Community Links Newham. This will be targeting a range of community organisations and will report on their activities in January 2016.
CCG performance on this indicator is being followed up at a Deep Dive meeting on 20 October 2015.
Long-term Conditions
11. High Risk Diabetes Patients with Care Plans
The pilot for the new diabetes pathway for high risk patients was originally due to commence on 1 July 2015. The project was delayed due to recruitment issues. A project manager has been recruited and started on 1 October 2015. GPs are now able to refer eligible patients (with HbA1C of nine or above) into the service. Issues with consent processes have been addressed and are being communicated to practices.
CCG performance on this indicator is being followed up at a Deep Dive meeting on 20 October 2015.
12. Cardiology Referrals (Heart Failure Service)
Data from Barts Health shows an increasing number of cardiology activity in 2015/16 compared to the same period in 2014/15. A significant proportion of cardiology outpatient referrals to secondary care are from GPs seeking advice on medications and interpretation of diagnostic results. A cardiology consultant advice and guidance email service to GPs has been piloted to support GPs manage some of these patients in primary care (without needing to make a referral). The CCG has marketed and promoted the service to GPs through our locality commissioning meetings. This will be repeated in September/October to continually keep GPs aware of the service. Work has
14

Performance and Quality Report (CCG Scorecard)
Page 8
begun with medication management and Bart’s pharmaceutical team who will be submitting a proposal to offer a similar email advice service to GPs by a pharmaceutical consultant at Barts. The CCG has identified issues with the timeliness of the response to contacts to the advice and guidance service and these have been escalated to the Clinical Director to resolve. Issues with the data from Barts showing very large increases in referrals for a specific procedure (Electrocardiogram Monitoring and Stress Testing) have been escalated to the CSU contracting team to investigate whether there has been any change in how this is recorded at Barts Health.
CCG performance on this indicator is being followed up at a Deep Dive meeting on 20 October 2015.
End of Life Care
13. Patients on the Palliative Care Register
Figures for the palliative care register have been analysed and are showing some patients have been on the register for over two years. Whilst this is possible in some cases it is feared that some patients should be removed and as such the figures are lower than the baseline taken at the end of April would suggest. In the meantime we have now liaised with UCL Partners who were the successful bidders for the HENCEL money and will be working alongside them and using their tools to plan the role out of training and education. Those GP surgeries showing the highest number of patients added over two years ago will be prioritised for the training, which will cover use of the palliative care register, difficult conversations and identifying palliative patients. There will additionally be three sessions at County Hotel and attendance at the October Locality meetings with an emphasis on increasing the number of patients being added to the register.
CCG performance on this indicator is being followed up at a Deep Dive meeting on 20 October 2015.
Integrated Commissioning
14. Continuing Healthcare Eligibility Assessments (28 days)
The indicator measures the performance of NELFT in completing eligibility assessments in the community within 28 days. This is a new measure for NELFT from April 2015. Performance data for July shows that NELFT continues to not meet this target.
In August no Decision Support Tools (DSTs) were completed within 28 days, giving a performance of 0% (no change from the previous month). NELFT have confirmed that the 10 outstanding from July have now been completed during August. Of the 10 referrals in August, 9 of these were delayed due to social care input and one due to service capacity issues. NELFT have agreed with London Borough of Waltham Forest an escalation process and protocol to resolve issues before breaches can occur. Assurance has been given that we will see an improvement in Month 6.
CCG performance on this indicator is being followed up at a Deep Dive meeting on 20 October 2015.
15

Performance and Quality Report (CCG Scorecard)
Page 9
Community Health Services
15. District Nursing Waiting Times (community referrals seen within 48hrs)
This indicator measures the waiting times for patients referred by GPs for district nursing services. Following discussions with NELFT during month one they confirmed that work has been ongoing to improve the performance of the service. August figures show performance was 65% of referrals from primary care responded to within 48 hours (against a 90% target). This is a small deterioration from the previous month. NELFT advised that the main issue has been the reporting of performance, rather than a decline in services, of which a programme of work has been put in place to improve data capture on the NELFT system. For August NELFT have undertaken analysis of the referrals received. Twelve referrals were clinically not appropriate to be seen within 48 hours, as indicated by the referral, for example patients requiring wound care in 7 days from referral. If adjusted for these patients then performance is 89%. The change in methodology was approved by the Performance and Quality Committee on 14 October 2015. This change only applies to the most recent data (August) reported in the above scorecard. Data will continue to be monitored to ensure only clinically appropriate patients are excluded.
At the CCG’s request NELFT submitted an action plan, which was signed off on 9 July 2015. In August the CCG issued a Contract Performance Notice to NELFT for the failure to meet the target. On 20 August 2015 the CCG agreed a remedial action plan. Further work is being undertaken to understand capacity issues as part of the Recovery Action Plan.
Planned Care
16. RTT incomplete pathway performance
The reported CCG performance for July does not include figures for Barts Health. Figures reported directly from the trust show that Whipps Cross underachieved against the 92% target with 78.79% in July 2015. This was a small deterioration on the previous month (79.72%) but demonstrates month on month improvement since October 2014. The Trust was below the standard in 12 out of 19 specialties. The most significant areas of under-performance are trauma and orthopaedics, urology and general surgery. A contract performance notice was issued to Barts Health on 2 June 2015 in respect to RTT, A&E, Cancer and Diagnostics. The Remedial Action Plan has been accepted apart from the trajectory for the clearance of the 52 week waiters. An independent consultancy has been hired to provide an independent opinion on the clearance trajectory for 52 week waiters. The Trust data quality plan published on 31 March 2015 included the construction of a new patient tracking list (PTL) to cover all sites. The first round of validation has been completed and
16

Performance and Quality Report (CCG Scorecard)
Page 10
excluded 194,580 pathways. The second round of validation on the remaining 120,380 is expected to last until March 2016. 2,679 patients are being directly contacted to ensure they are still active and that records are accurate (646 of these are Waltham Forest patients). The total Barts Health waiting list waiting over 18 weeks has fallen to 11,375 in July from 15,946 in November 2014. Barts is currently outsourcing approximately 300 patients a month to the independent sector. In total, there have been c2200 patients that have been treated in the independent sector and a further c400 that have been rejected due to a variety of reasons. 276 patients were treated by the independent sector in August. Internal capacity is being enhanced to reduce backlogs especially in surgical specialities.
Urgent Care
17. A&E 4hr all types performance at Whipps Cross
August performance was 88.9% against a target of 95%. This was an improvement on the previous month (84.5%). However performance has deteriorated since the end August and Whipps Cross have not met the agreed improvement trajectory since the end of June. The CCG has set a new performance meeting to manage the Whipps Cross site improvement plan and this meeting is now taking place fortnightly to manage the performance back to trajectory and review the improvement plan. Whipps Cross are focusing on embedding the new improvement plan with clinical staff. There are daily meetings to review breaches and patient flow meetings take place three times a day. Improvement actions include the expansion of ambulatory care, a focus on recruitments and the establishment of a paediatric observation unit. The Trust is working with PELC to improve the utilisation of the Urgent Care Centre. The majority of breaches are in non-admitted patients. However overall attendances remain level with 2014/15 and overall admissions are down substantially at Whipps Cross.
18. Proportion of patients using the WX Urgent Care Centre
The scorecard target is to improve the utilisation of the urgent care centre. Utilisation is measured as the proportion of all A&E attendances at Whipps Cross that are seen at the Urgent Care Centre. This proportion has fallen over the last year and was 32% in 2014/15. Utilisation has continued to fall in 2015/16 but has remained stable for the last three months at 27%. The declining utilisation has been raised at contract review meetings and PELC asked to provide a response. There are no obvious explanations for the reduction. PELC are working with Barts Health to pilot a potential increase in activity by re-triaging minor injury patients and shifting these from Barts Health to the UCC. The CCG has asked Barts Health to work with PELC to provide an improved solution for patients presenting at the hospital front-door. The CCG is also continuing to work with the LAS to reduce ambulances taken directly to Emergency Department.
17

Performance and Quality Report (CCG Scorecard)
Page 11
Prescribing
19. Antibiotic prescribing in primary care
The overall aim of indicator is to reduce the volume of antibiotic prescribing which forms part of the national Quality Premium for 2015/16. The Quality Premium also contains a target to reduce the use of broad spectrum antibiotics including co-amoxiclav, cephalosporins, and quinolones and the CCG is aiming to make improvements on both of these targets.
The July annualised antibiotic prescribing rate was 1.024, which was a further improvement on the May figure (1.031) and also below the target (1.110). For the prescribing of the broad spectrum antibiotics cephalosporins, quinolones and co-amoxiclav the result for July is 14.76% a slight improvement from last month (14.99%) but above the NHSE target of 12.9%. The CCG focus has been on reducing the use of co-amoxiclav, cephalosporins and quinolones. The CCG is currently putting together an Antimicrobial strategy to ensure practices are making full use of the resources that are available to them as highlighted by the recent PHE and NHSE Patient Safety Alert published in late August. We are also planning to have a microbiologist from Bart’s Health give a talk to GPs about antimicrobial stewardship in our next GP Prescribing Forum. The CCG will be sending monthly updates to practices and targeting practices with high usage of antibiotics.
Quality and Safety
20. Improvement in Whipps Cross FFT score
The A&E and Inpatients combined score for July was 92.6%. This is a small deterioration from the previous month but still above the target rate of 91.4%. The data by Inpatient and A&E is available for July and is as follows. 96% of inpatients at Whipps Cross would recommend the hospital to friends and family, this is slightly above the national average of 95.6%, the response rate was 21% which is below the national average of 26.7%. The A&E score was 86% of attendees would recommend the hospital to friends and family, this benchmarks slightly below the national average of 88.2%. However the response rate is very low at 2.7% (national average 15.2%) and this makes the validity of the score questionable. The total number of responses for Whipps Cross was 567 (lower than previous month of 888). The CCG Deputy Director of Integrated Governance continues to work with the Patient Experience Lead at Whipps Cross to plan consistency in performance and how the results are being used to improve the quality of patient care.
21. Number of C.Diff cases within planned trajectory
In July there were two reported cases of C.Difficile for Waltham Forest CCG against a planned threshold of four cases. The CCG remains within its planned trajectory for the year. The provisional C.Difficile data for August is 0 for Whipps Cross Hospital and 14 for Barts Health. All patients who have tested positive for C.Difficile at Barts Health are reviewed by the Consultant Microbiologist and an Infection Prevention & Control Practitioner. IPC lead working within the CSU reviews all RCA’s monthly to establish themes and trends.
18

Performance and Quality Report (CCG Scorecard)
Page 12
Primary Care
22. General Practice FFT score (CCG Quality Premium Local Measure)
Friends and Family test data has been available from January 2015. The baseline has been calculated as the average score for Waltham Forest for January -March 2015. The CCG aims to improve on this score during 2015/16. The GP bi-annual survey has shown a drop in patient experience in the last three years. The July performance was 88% which is above the target of 86.6%. The total number of responses was 1246, which although below the previous month (1750) is above the figures for April and May. Increasing response rates was noted as an action from the Performance and Quality Committee and the Primary Care Development Sub-Committee. Increasing numbers of response provides a much more robust indicator and also allows the CCG to identify areas of variation between practices. The CCG is planning on establishing a Primary Care Dashboard that is due to be agreed in October to provide assurance across a wider range of quality and performance metrics.
Performance Exception Reporting
23. Ambulance Category A Response Times (8 min)
June performance for Waltham Forest was 59% against a standard of 75%. This shows no change from the previous month and only minor improvement from April (58%). London Ambulance Service (LAS) performance across London remains below the target and has deteriorated in the last couple of months. LAS attribute underperformance to a diminished paramedic workforce. London CCGs have agreed additional investment to support performance delivery of £32m in 2015/16. LAS have met their pan-London improvement trajectory for Q1 but are not on track for Q2. Investment will be used to build capacity and develop non-emergency alternative transport for low acuity calls. From March two motorcycle response units have been based at Whipps Cross. The implementation of push bicycle response units in Walthamstow has been delayed but now is expected in October 2015. The CCG is working with the LAS to improve the utilisation of alternative care pathways and make better use of Rapid Response services, especially in relation to calls from nursing and care homes in the borough. One plan being explored is the location of a member of the rapid response service with the LAS crews.
19

Performance and Quality Report (CCG Scorecard)
Page 13
Quality Exception Reporting
24. Whipps Cross CQC Improvement/Action Plan
A review of the plan presented at the Whipps Cross Clinical Quality Review Oversight and Assurance Meeting (CQROA) held 10 September 2015 cross referencing the original plan published in “Whipps Cross Hospital – Stepping into the Future” has highlighted that progress of actions is significantly behind plan as shown below;
62.3% of actions are overdue. 16.3% of actions are marked as completed. Noting that 30% were closed out of date. 21.3% of actions remain in date. Of these 61.5% are due for completion during September 2015.
This was escalated at the Trust Oversight and Assurance Group (TOAG) and Barts Health have indicated that this position is unlikely to move forward during the next few weeks and assurance is not obtained. A formal progress report has been requested for presentation at the November CQROA meeting.
25. Serious Incident Management
Whipps Cross Hospital
Whipps Cross Hospital currently has one SI that has breached the required STEIS reporting deadline, the report being overdue by 4 months. There has been a sustained reduction in the number of overdue reports. There are however 10 reports where further information has been requested and 5 grade 2 incidents again waiting on evidence and information from Whipps Cross. This delay in providing information may impact on the Trust’s ability to share learning in a timely manner. The Deputy Director of Quality is meeting with the CSU to identify key actions to improve this position.
NELFT
NELFT have 2 SIs that have breached the STEIS reporting dates, 1 has now been submitted. The second report was sent to the CSU but is subject to a request for further information. The requirement to report all incidents within 2 days of knowledge was breached with an incident taking 31 days, NELFT have been asked to investigate and provide the reasons for the delay. There are 8 further information requests outstanding with 7 relating to pressure ulcers. The Deputy Director of Quality will address this with the CSU.
20

Performance and Quality Report (CCG Scorecard)
Page 14
26. Complaints Management
NELFT have 11 complaints that have been open longer than 90 days. This was raised for discussion at the October 2015 CQRM and an updated position that 5 had now been closed and for the remaining rationale given as to the delay. 3 are due to the complainant not being happy with the response. This will continue to be monitored via the CQRM on a monthly basis.
27. Safeguarding
NELFT Prevent training compliance in Waltham Forest is at 42% against target of 85%. The Trust has set a trajectory for compliance identifying the numbers of staff to be trained by month to achieve full compliance by March 2016. The Trust has not achieved the 85% target for staff completing DOLS and MCA training and further rationale has been requested. Both areas will be reviewed monthly at the Clinical Quality Review Meeting.
28. Appraisal Rates
NELFT appraisal compliance is at 63% below the target of 85%. There has been improvement from the previous month of 7%. The Trust have put in place a number of actions to improve this position and have given assurance that compliance will be obtained by November 2015.
29. Staffing Metrics
NELFT has not met the staffing metrics required targets year to date, showing high staff turnover at 17%, staff sickness at 17% and a 22% vacancy rate. This was raised as a concern at the September CQRM meeting and NELFT have provided the CCG with a separate report to be presented.
21

Performance and Quality Report (CCG Scorecard)
Page 15
Appendices
Appendix A Waltham Forest CCG Business Grid
22

Item 3.2
Title of report Emergency Care for Children and Young People
From Jane Mehta, Director of Strategic Commissioning - WFCCG
Purpose of report
The purpose of this report is to update the Governing Body on the challenges in services for Children and Young People and the current priorities to improve services for Waltham Forest children and young people. The report highlights the urgent access performance issues and the new services the CCG are commissioning to improve care.
Changes/additions/amendments to paper as a result of discussions held at committees
The contents of the paper have been discussed through various forums including Urgent Care Working Group, Integrated Care for Children and Young People and Joint Commissioning Board.
Recommendations
N/A
Impact on patients & carers
The expectations of this programme is to result in an improvement in the coordination and management of Children and Young People, and their families, in the health care system. This will include better integration of health and social care services.
Risk implications
N/A
Financial implications
N/A
Equality analysis
N/A
Other committees/groups, including the CCG Reference Group and Rapid Feedback Group
N/A
23

Emergency Care for Children and Young People
October 2015
24

Report Emergency Care for Children and Young People 28 October 2015
Contents
1 Purpose of report Page 1
2 Children’s Emergency Care Page 1
2.1 A&E Performance at Whipps Cross Page 1
2.2 Whipps Cross Urgent Care Centre Page 2
2.3 Audit of Paediatric Emergency Breaches Page 2
3 Out of Hospital Service Improvement Programme Page 3
3.1 Care Coordination (Virtual Ward at Home pilot) Page 3
3.2 Review of high volume pathways Page 4
3.3 Paediatric Rapid Referral Clinic Page 5
3.4 CAMHS - Crisis Page 5
3.5 Child Health and Common Illness programme Page 5
4 Partnership Working Page 5
5 High Level Model Page 7
25

Report Emergency Care for Children and Young People 28 October 2015
Page 1
1 Purpose of report
The purpose of this report is to update the Governing Body on the challenges in services for Children and Young People and the current priorities to improve services for Waltham Forest children and young people. This report is presented to the governing body to provide a more detailed understanding of the urgent care access issues relating to children which are contributing to the poor performance figures; it also outlines the mitigating actions that are being taken to improve performance.
2 Children’s Emergency Care
In 2014/15 there were 20,745 A&E attendances for Waltham Forest CCG patients aged under 18yrs old. This is an average of 58 attendances per day. Approximately 50% of these attendances were for children under 5yrs old. The large majority of attendances were at Whipps Cross hospital (71%) although 8% attended at Homerton Hospital.
Total A&E attendances for WFCCG patients under 18yrs old increased by 8% in 2014/15; this is in contrast to the significant reduction we have seen in adults and most notably over 80 year olds. Data for 2015/16 suggest that there has been further increase in the first five months of the year. This may be linked to reduced activity being seen in the Urgent Care Centre, located at the front door of the hospital. However, Waltham Forest also has a growing young population.
Whipps Cross Hospital sees 23,500 patients in Children’s Emergency Department in 2014/15. The Children’s A&E sees patients up to 17yrs old but occasionally 17-18yrs old patients.
2.1 A&E Performance at Whipps Cross
For the past few years Whipps Cross Hospital has struggled to reach the 95% target for patients to be seen and treated within 4hrs. In 2015/16 the hospital has not reached this standard for any week since the start of the year.
A high proportion of 4hr breaches are attributed to paediatrics, i.e. the Children’s Emergency Department. An average of 12 breaches per day at WX have been attributed to paediatrics in 2015/16. Paediatrics is overall responsible for approximately 23% of all breaches in 2015/16. Performance for paediatrics is extremely volatile and linked to the rate of attendances at the Emergency Department and a lack of paediatric beds, which creates a bottleneck and means that the Emergency Department cannot admit patients on to the wards.
The “One Version of the Truth” analysis completed by McKinsey in early 2015 and shared throughout the health and social care system in April 2015 identified breaches in the paediatric non admitted pathway as a key component of the overall A&E performance issues at Whipps Cross. At that time the paediatric pathway was estimated to be 13% of the problem (the discharge process was identified as the major contributing factor to poor performance, responsible for 36% of the problem). McKinsey identified the non-admitted pathway as responsible for the majority of paediatric breaches and for the volatility in performance. Breaches were attributed to flow and Emergency Department processes. Underlying factors included a lack of paediatric beds, lack of senior staff and the high utilisation of the Children’s Observation Area, which reduced capacity to assess and treat non-admitted patients. Recommendations included dedicated early senior assessment for paediatric patients, changes to the process for staffing the nursing rota, and tighter performance management of paediatrics.
The chart below shows the daily number of paediatric breaches at Whipps Cross Hospital in 2015/16, from 1 April 2015 to 12 October 2015. The horizontal line shows the average for the year of 12 breaches per day. The number of breaches shows dramatic spikes. For example, there were 38 paediatric breaches on 6 July 2015. These spikes are largely related to the same issues identified by McKinsey.
26

Report Emergency Care for Children and Young People 28 October 2015
Page 2
2.2 Whipps Cross Urgent Care Centre
The Whipps Cross Urgent Care Centre (UCC) is located within the A&E and run by the Partnership of East London Cooperatives (PELC). PELC are also responsible for the streaming function at the A&E front door, which streams patients to the most appropriate service (the Urgent Care Centre, Paediatrics, Majors or Minors). The UCC typically treats 8,000 children per year, whilst the Children’s Emergency Department sees around 23,500 (i.e. the UCC treats approximately 25% of children attending A&E). Some of the patients that are treated by the Children’s Emergency Department arrive by ambulance and are conveyed directly to the Children’s Emergency Department due to the protocols used by the ambulance service.
There have been concerns raised by the CCG that PELC’s activity has fallen over recent years and that the proportion of patients treated in the UCC relative to the Whipps Cross Emergency Department has also fallen. The overall proportion of patients attending the A&E front door that have been streamed to the Children’s Emergency Department has increased over the last two years. At the same time the proportion of patients streamed to the UCC (the PELC primary care led facility) has fallen. The total proportion of A&E attendances seen in the Urgent Care Centre fell from 35% in 2013/14 to 32% in 2014/15 and has fallen below 30% in 2015/16.
2.3 Audit of Paediatric Emergency Breaches
In order to better understand the reasons for breaches in the Children’s Emergency Department the CCG participated in a joint audit with Whipps Cross of paediatric breaches in July 2015. One of the aims of the audit was to investigate the impact of paediatric cases that cause breaches because they require ongoing treatment for more than 4 hours but do not require admission. This might include patients with asthma or moderate dehydration.
The audit showed that:
14.2% of children breached the 4hrs target 62% of all breaches were from non-admitted patients (83% of attendances were for non-admitted
patients) 32% of breaches were deemed “appropriate” and could potentially be avoided by the
implementation of a paediatric assessment unit (PAU). These children received ongoing medical care beyond 4hrs in the Emergency Department but could have been managed in a PAU or on a ward.
Other preventable breaches could have been avoided by improved hospital decision making and improved utilisation of primary care pathways. 24% could have been prevented if they had been seen in the Urgent Care Centre or dealt with in primary or community care settings.
21% were considered unavoidable, due to lack of beds or unstable children in Resus.
27

Report Emergency Care for Children and Young People 28 October 2015
Page 3
The audit showed that there are measures in both primary care and hospital that could be implemented in order to reduce breaches. The results suggest that 4.5% of all paediatric attendances could be seen in a Paediatric Assessment Unit and this would potentially reduce paediatric breaches by 32%. The audit also confirmed earlier findings that improved early decision-making and improved primary care could have an important impact.
Actions being taken to improve Emergency Care for Children at Whipps Cross
Squirrel Paediatric Assessment Short Stay Unit (PASSU): The Acorn Children’s Unit at Whipps Cross has been split into two separate wards (Acorn and Squirrel) to accommodate a short stay unit that will enable patients to be assessed and rapidly discharged.
Paediatric Clinical Decision Unit (CDU): Barts Health have developed a business case for the implementation of a Clinical Decision Unit for paediatric patients in the Emergency Department. This will see patients that require more than 4hrs of treatment as identified in the audit described above. Subject to approval by the trust, capital works are scheduled to be completed by April 2016.
Urgent Care Centre: PELC have been asked to work with Barts Health to consider new ways of joint working that should increase activity in the Urgent Care Centre and reduce demand pressures on the Emergency Department. WFCCG have also commissioned Attain to review the current Urgent Care Centre model and make recommendations for improvement.
Winter Surge Plans: Plans developed by Barts Health include investments to bring forward the actions above. The trust also plans to increase paediatric doctor capacity through the winter months with staffing targeted at surges in the evening and weekend, as this was proven to be effective in the winter of 14/15.
3 Out of Hospital Service Improvement Programme
To address the issues above the commissioning team have a programme in place to improve services in the community, resulting on less reliance of acute service, the programme has been developed in line with the emerging TST strategy for Children and Young People, Below are the schemes being developed:
3.1 Care Coordination (Virtual Ward at Home pilot)
The CCG has commissioned NELFT to deliver a pilot scheme for phase one care coordination for children and young people, who will be identified in the top 2% of risk, using Health Analytics Risk Stratification Tool. This is similar to the care co-ordination service we already have in place for adults which has been so successful in reducing hospital admissions by over 20% in two years. Initially the plan had been for the service to start in September 2015, however NELFT have had issues with recruitment pushing back the start of the service.
The service will work with appropriate health and social care service across the partnership to develop integrated care plans for the highest risk children and young people of the borough.
28

Report Emergency Care for Children and Young People 28 October 2015
Page 4
3.2 Review of high volume pathways
To help realise our commissioning vision and deliver real improvements for patients and their families, a rage of pathways are currently being reviewed and redesigned during 2015/16. Two simultaneous processes are facilitating this development:
1. A range of key pathways have been identified for adoption across the WELC footprint 2. Waltham Forest has targeted a range of local pathways for redesign.
The principles that we are applying to the development of a good care pathways means having:
o The right people o In the right order o In the right place o Doing the right thing o In the right time o With the right outcomes o All with attention to the patient experience
Waltham Forest CCG is leading on the below pathways:
o Epilepsy o Sickle Cell o Asthma o Orthopaedics o Dermatology
The following pathways are being developed by WEL colleagues, which following sign off locally the CCG will consider localisation and adoption.
Vitamin D Acute Wheezy Episode Acute Asthma Attack
Obesity Lymphadenopathy Chronic Abdominal Pain
Constipation Eczema Food Allergy
Virtual Ward MDT
NELFT -Community
ServicesBarts Health
- Acute Care
Primary Care
(Virtual Input)
Schools
Social Care
Parents (Virtual Input)
Substance and Alcohol
Services
CAMHS
29

Report Emergency Care for Children and Young People 28 October 2015
Page 5
Management of Gastroesophageal Reflux (GOR) in infants up to 6 months
Headache in children Management of nocturnal enuresis
Urinary Tract Infection (UTI) in Children
3.3 Paediatric Rapid Referral Clinic
Initial planning has taken place on developing a Paediatric Rapid Referral Clinic (HOT clinic). The Rapid Referral Clinic is a rapid access general paediatric outpatient clinic for children aged 0-16 years who require an urgent paediatric specialist opinion within 4 weeks. It is for children who are not unwell enough to require same day attendance at the emergency department, but who cannot wait more than 4 weeks for a routine outpatient appointment. Criteria and funding is currently being developed with planned discussions with Barts Health in November.
3.4 CAMHS – Crisis
Waltham Forest has a CAMHS crisis service called “Interact”, initiated seven years ago, providing adolescent crisis care by North East London Foundation Trust (NELFT) across all four outer-North East London Boroughs, Waltham Forest, Barking and Dagenham, Havering, and Redbridge (BHR). In addition it has gate-keeping Tier 4 inpatient and day hospital facilities at Brookside and operates as an intensive support Tier 4 outreach service providing crisis resolution and prevention. Crisis care in this model should refer to a crisis ‘in the experience of the person’, therefore if that person or family feels they are in a crisis and need such support then the service should be responsive to that need.
Developing our support for children and families in a mental health or behavioural crisis is a key part of the CCG CAMHS transformation plan. In order to improve the system, pathways and deliver care closer to home the CCG plans to develop CAMHS management pathways at Barts Health to improve crisis care and decrease out of hours admissions. The impact of the transformation plan will be from November 2015.
3.5 Child Health and Common Illness programme
In 2015 the CCG developed and launched a new resource for parents, and parents of children aged up to 5 years. The scheme includes a self-help guide which is available as a booklet, issued with the red book, dedicated website and phone app. The CCG plan to promote the scheme in late 2015 / early 2016 across primary care and as part of a bus stop campaign.
The Integrated Care approach for Children and Young People (0-25) aims to develop a joint approach and
deliver an effective early intervention and prevention model of targeted support and care, ensuring
principles around high quality services which are available at the right time for children and young people,
and their families, from conception to 25 years of age ensuring that robust and appropriate transition
arrangements are put in place with adult services.
4 Partnership Working
To further improve services for children and families the CCG and LA are currently working together to
develop an Integrated Care Programme. The overarching outcomes of this approach are to ensure that
children and young people and their families measurably improve health and wellbeing, only access
services and interventions when required and to ensure there is a reduction in health and social care
30

Report Emergency Care for Children and Young People 28 October 2015
Page 6
inequalities. The programme will deliver this objective by developing and focussing on the below areas,
some of which are already being progressed:
Integrated health and social care pathways, including the development of care coordination and
acute avoidance schemes
Developing an end to end commissioning plan for children with Learning Disabilities and children
and young people in receipt of a Health and Social Care Plan (SEND)
Transformation plan for CAMHS
Improved maternity pathway and support to new parents
Development of Early Help and self-care offers for children and young people and their families,
including the increase in usage of Personal Budgets
The overarching objectives of the approach are to be:
Service User focused – the approach will be based on the need of individuals receiving targeted
support and care. Developments will be based on health and social care partners listening to the
voice of the child and parents on what/how/where/why.
Prevention focused – the approach will ensure services are developed and commissioned with a
focus on early intervention and prevention. Identifying and addressing the needs of children and
their families as early as possible
Consistent – the approach will focus on improving standard and quality of intervention and care
including reductions in variation of provision and access across Waltham Forest.
Integration of services – the programme will ensure that the planning, commissioning and
delivery of services will be focussed on integration across health and social care pathways. Plans
will be aligned with the wider national and local agendas for integration.
Value for Money – we will ensure services provide and are delivered within value for
money constraints which takes into account sound commissioning principles
Throughout the life of the programme we aim to learn from both national and international best practice
models, including what works well in adult services which could be considered and benefit children’s and
young people’s pathways. We aim to ensure that local innovation is supported and evaluated in a range
of ways to ensure services are appropriate and supportive to Waltham Forest residents.
31

Report Emergency Care for Children and Young People 28 October 2015
Page 7
5 High Level Model
Below are some of the services that could be in scope by applying this approach, this list is not exhaustive
and further mapping will be required:
Very High Intensity (Top 5%) – Services currently available to children and young people include
(but not exhaustive) Care Coordination Pilot, CAMHS Tier 4 and high end Tier 3, End of Life Care
Services, Complex Care for Children, Safeguarding for Children and Tripartite funding for high
needs children
High / Medium Intensity (Specialist Interventions) – Services include CAMHS Tier 3, CAMHS
Tier 2, Specialist School Nursing, high level Therapies, Specialist Community Nursing Service,
child development team and short breaks.
Low Intensity / No Needs (Universal / Early Help) – Services include Primary Care, Midwifery,
Health Visiting, School Nursing, Children Centres, Waltham Forest Early Help offer
Waltham Forest CCG and London Borough of Waltham Forest have had very initial discussions on developing a joint vision and integration approach for Children and Young People. Initial thinking has been around developing a “Better Care Fund” style arrangement, to have a roadmap for better commissioned integrated pathways across partners. Initially this arrangement will exclude plans to pool resources. A series of workshops will begin in November 2015 to further develop the plan.
Very High
Intensity (Top 5%)
High/Medium Intensity (Specilaist Interventions)
Low Intensity / No Needs (Universal / Early Help)
Saf
egu
ard
ing
Chi
ldre
n
Look
ed A
fter
Chi
ldre
n
Leve
l of N
eed
32

Item 3.3
Title of report Nursing and Midwifery Council - Revalidation for Nurses
From Helen Davenport, Director of Nursing, Quality and Governance - WFCCG
Purpose of report
NHS England requested that each Clinical Commissioning Group (CCG) submit an organisational state of readiness for Nursing Revalidation.
This report provides the Governing Body with an overview of how prepared nurses employed directly by NHS Waltham Forest Clinical Commissioning Group (WF CCG) and Practice Nurses within Waltham Forest are for the process of revalidation.
Recommendations
The Governing Body is requested to confirm whether the report provides assurance that the CCG is prepared for and ready for Nursing Revalidation.
Impact on patients & carers
It is imperative that we support our nursing colleagues in their preparation for revalidation. Nurses who are unable to fulfil the requirements for revalidation, as set out by the Nursing and Midwifery Council (NMC) will be unable to practice.
This could potentially have a significant impact on the services delivered placing delivery of high quality of care and patient experience at risk, particularly within primary care.
Risk implications
Failure of nurses to achieve the requirements necessary for revalidation may lead to a disruption of the services currently provided and therefore a reduction in the quality of care and experience for our patients.
Financial implications
Not applicable.
Equality analysis
The CCG is committed to fulfilling its obligations under the Equality Act 2010 and to ensure services commissioned by the CCG are non-discriminatory on the grounds of any protected characteristics. The CCG will work with providers, service users and communities of interest to ensure that any issues relating to equality of service within this report are identified and addressed.
Other committees/groups, including the CCG Reference Group and Rapid Feedback Group
N/A
33

Nursing and Midwifery Council - Nurse Revalidation
How prepared are nurses employed by NHS Waltham Forest Clinical Commissioning Group for Revalidation?
34

Nursing and Midwifery Council - Nurse Revalidation
ii
Contents
1 Introduction 1
2 Background 1
3 Revalidation requirements 1
4 Minimum standards which need to be achieved for revalidation 2
5 Assurance for NHSE on our state of readiness 2
35

Nursing and Midwifery Council - Nurse Revalidation
1
1 Introduction
1.1 This paper outlines how Nurses and Midwives will maintain their registration through
the revalidation at the point of renewal of registration. Revalidation is applicable to all
Nurses and Midwives irrespective of their role be that staff in frontline clinical care,
education, research, policy, advisory, management and leadership roles. It applies to
substantive, temporary and short term contract staff including bank staff.
2 Background
2.1 From 31 December 2015 The Nursing and Midwifery Council (NMC) are
changing the requirements that nurses and midwives must meet when they
renew their registration every three years. This will replace the current post registration
education and practice (PREP) standards.
Revalidation supports professionalism through a close alignment with the NMC
Code for Nurses and Midwives which has been revised in March 2015.
The four themes of the code are;
Prioritise people
Practice effectively
Preserve safety
Promote professionalism.
NHS England has established a Regional Programme Board which has good stakeholder
representation to ensure an efficient and structured implementation programme is progressed.
3 Revalidation requirements
3.1 The provisional revalidation standards are currently being piloted in a number of organisations.
The final revalidation process and standards will be confirmed in the autumn, before
implementation in December 2015.
All registrants are required to meet the following minimum standards for the three year period
preceding the date of their application for renewal. Individuals who fail to meet revalidation
standards are not legally able to work in the UK in their profession.
36

Nursing and Midwifery Council - Nurse Revalidation
2
4 Minimum standards which need to be achieved for revalidation
4.1 A minimum of 450 practice hours within their scope of practice. This scope of practice
can be direct patient care, management, education, policy or research in a wide range of
health, social care and independent care settings;
To undertake 40 hours of continuous professional development (CPD) relevant to the scope of practice
To obtain at least five pieces of practice related feedback, which can be from patients, carers, service users, students, colleagues and annual appraisals
Reflection and discussion through a minimum of 5 written reflections on the code, practice and CPD
Declaration of health and character Confirmation of personal indemnity arrangements
Confirmation from a third party, usually the manager for the purpose of verifying the
declarations
5 Assurance for NHSE on our state of readiness
5.1 NHS Waltham Forest Clinical Commissioning Group are required to submit an
organisational readiness self-assessment to NHS England in October to identify any risks
and challenges to the process. This includes a requirement for boards to be aware of their
organisational plan and any risks to delivery.
37

Nursing and Midwifery Council - Nurse Revalidation
3
Information in relation to Primary Care
NAME OF ORGANISATION
NHS Waltham Forest Clinical Commissioning Group (WF CCG)
NAME AND CONTACT DETAILS OF PERSON COMPLETING
Deirdre Malone, Deputy Director of Integrated Governance
Tel: 020 36882610
Mobile: 07908414557
Email: [email protected]
Yes No Comments
Has the CCG had assurance that all practices are aware of the dates when staff in the practice are due to revalidate?
Yes WF CCG contacted all 44 GP practices within the borough, as requested by Vanessa Lodge in May 2015.
Revalidation is discussed at monthly Practice Nurse forums across the borough.
Do the GP practices understand the requirements for revalidation?
Yes The requirements regarding revalidation have been discussed at monthly Practice Nurse forums. This has also been discussed during individual practice meetings.
Has the CCG had assurance that all the registered nurses working in GP practices in their patch have been communicated with?
Yes The Director of Nursing, Quality and Governance has communicated the requirements regarding revalidation to each of the GP practices within Waltham Forest.
The Deputy Director of Integrated Governance attends the Practice Nurse forums to support this process.
Has the CCG had assurance that a paper on revalidation and state of readiness has been discussed appropriately amongst the practice leadership teams?
Yes WF CCG have requested a position paper to be tabled at the Primary Care Committee in November 2015.
38

Nursing and Midwifery Council - Nurse Revalidation
4
Is there any good practice that you believe in terms of GP practices that could be shared across London/England?
Yes The Strategic Commissioning Directorate within WF CCG facilitate monthly educational events for GPs and Practice Nurses.
The lead Practice Nurse within the borough, leads on education through Community Education Provider Networks (CEPNs).
There is a structured education session embedded into each monthly Practice Nurse forum.
If the answer is no to any of the above questions, please would you describe the obstacles you face in relation to assurance or practices in relation to readiness and the actions to address?
Information in relation to NHS Waltham Forest Clinical Commissioning Group
NAME OF ORGANISATION
NHS Waltham Forest Clinical Commissioning Group (WF CCG)
NAME AND CONTACT DETAILS OF PERSON COMPLETING
Deirdre Malone, Deputy Director of Integrated Governance
Tel: 020 36882610
Mobile: 07908414557
Email: [email protected]
Yes No Comments
Are you aware of all the registered nurses working in your CCG?
Yes
Do you know the dates when staff in your CCG are due to revalidate?
Yes
Do you and the registered Nurses in your CCG understand the requirements for revalidation?
Yes
39

Nursing and Midwifery Council - Nurse Revalidation
5
Has a paper on revalidation and your state of readiness gone to your Governing Body meeting?
Yes Position paper presented to Governing Body 28 October 2015
Is there any good practice that you would like to share with other CCGs in London/England?
Yes Registered nurses are encouraged to have a professional portfolio. Professional practice is discussed during appraisal meetings.
If the answer is no to any of the above questions, please would you describe the obstacles you face and the actions to address?
N/A
40

Item 4.1
Title of report Finance Report
From Les Borrett, Director of Financial Strategy - WFCCG
Purpose of report
To provide an update to the Governing Body covering the financial position of the CCG as at the end of September 2015.
Changes/additions/amendments to paper as a result of discussions held at relevant Committee
Not applicable.
Recommendations
The Governing Body is asked to note this report.
Impact on patients & carers
None
Risk implications
There are some financial risks inherent within the CCG’s 2015/16 QIPP programme.
Financial implications
As a result of the information available to date the CCG is projected to achieve its planned surplus of £8.6 million for 2015/16 and to manage CCG management costs within the “capped” running cost allowance.
Equality analysis
Not relevant for this report.
Other committees/groups, including the CCG Reference Group and Rapid Feedback Group
The Finance and QIPP Committee receives a more detailed report covering financial performance.
41

Finance Report Update regarding the financial position of the CCG as at the end of
September 2015.
42

Finance Report
Page ii
Contents
1 Introduction 1
2 CCG summary income and expenditure position 1
2.1 Key headlines for M6 2
3 Commissioning expenditure 2
3.1 Barts Health contract 4
3.2 Associate acute contracts 5
3.3 Non acute 7
3.4 Prescribing 8
4 Other financial risks and mitigations 8
5 QIPP 9
6 Balance sheet, cash management, PSPP and debtors 10
7 Conclusion and recommendation 10
Appendix A Detailed income and expenditure position 11
Appendix B Detailed QIPP performance 12
Appendix C Statement of financial position (balance sheet) 13
43

Finance Report
Page 1
1 Introduction
The purpose of this report is to update the Governing Body on the financial position as at the end of September (month 6) and provide projections of income and expenditure to year end. The report goes on to describe any key variances to the commissioning budget and identifies financial risks and mitigating actions.
The Governing Body is asked to note that the CCG is forecasting that it will achieve the planned surplus of £8.6 million although there are risks to this position which will be outlined within the report.
2 CCG summary income and expenditure position
A detailed budget position is attached at Appendix A and a summary position is shown in the following table:
Annual Budget
£’000
Year to Date
(surplus)deficit
£’000
Forecast Outturn M6
£’000
Barts Health 131,208 2,348 3,357
Other Acute 51,472 1,666 3,900
Mental Health 33,380 - (311)
Other Non-Acute 57,798 (744) (1,206)
Prescribing 35,081 (398) (728)
Corporate 7,547 16 89
Delegated PC Expenditure 34,901 164 178
Sub-Total 351,387 3,053 5,279
CCG Reserves 18,084 (3,053) (5,279)
TOTAL EXPENDITURE 369,471 - -
TOTAL INCOME 378,071 - -
TOTAL CCG POSITION 8,600 0 0
44

Finance Report
Page 2
2.1 Key Headlines for M6 to note are:
The CCG is reporting breakeven against plan year to date (YTD) and is forecasting to deliver a total surplus of £8.6 million at year end after the application of reserves. The CCG’s in year planned and actual forecast position is to break even, after excluding the brought forward surplus less agreed drawdown of £0.9 million. The drawdown has been set aside to partially offset RTT backlog costs.
Barts have submitted SLAM data for M5 that if extrapolated results in a headline full year claim of £4.4 million above contract value after taking account of estimated readmissions, threshold and productivity metrics adjustments which have been calculated using precedent established during 2014/15. This represents an improvement of £0.5 million against the headline position reported last month based on M4 SLAM. We are now projecting a £3.4 million risk at year end and more detail will be provided later in this report.
Based on M5 SLAM claims received form associate providers we are now projecting a £3.9 million
risk against other acute and further details will be provided within this report.
We have reviewed our 2015/16 QIPP schemes and applied risk ratings which are detailed within Appendix B.
We have received actual prescribing data up to July 2015 and have used this to extrapolate
2015/16 costs up to M6 on the basis of the average daily prescribing costs over the last 6 months which results in a FOT surplus of £0.7 million. This projection now includes some provision for the impact of category M contractual drug price changes which will be implemented from October.
Performance against the delegated primary care budget is shown separately within Appendix A.
The delegated budget includes a £0.5 million QIPP target (1.4 percent) with limited plans provided for the delivery of these savings. The CCG has now submitted a summary primary care QIPP plan to NHSE which could result in £0.1 million of centrally held non recurrent headroom being released to help mitigate in year risks.
3 Commissioning expenditure
At month 6 the CCG is reporting a £3.1 million deficit against commissioning budgets and a projected deficit of £5.3 million at year end. This deficit is covered by uncommitted contingency and reserves as detailed later in the report. The following graphs show changes in activity over the period from April 2014 to August 2015 for accident and emergency attendances, outpatient first attendances and births broken down by activity at Barts and all other providers along with total activity.
45

Finance Report
Page 3
0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
8,000
9,000
A&E Activity ‐ Barts & AssociatesApril 2014‐ August 2015
Barts Health NHS Trust All Other Providers Total ‐ All providers
Linear ( Barts Health NHS Trust) Linear (All Other Providers) Linear (Total ‐ All providers )
0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
8,000
9,000
FA outpatient GP referral activity ‐ Barts & AssociatesApril 2014‐ August 2015
Barts Health NHS Trust All Other Providers Total ‐ All providers
Linear ( Barts Health NHS Trust) Linear (All Other Providers) Linear (Total ‐ All providers )
y = ‐0.0045x + 317.68
y = 0.0247x ‐ 794.41
y = 0.0202x ‐ 476.73
‐
50
100
150
200
250
300
350
400
450
Deliveries ‐Waltham Forest CCG
Other Providers Barts Health Grand Total
Linear (Other Providers) Linear (Other Providers) Linear (Barts Health)
Linear (Barts Health) Linear (Grand Total) Linear (Grand Total)
46

Finance Report
Page 4
This data indicates that attendances at accident and emergency departments and first outpatient appointments have been increasing over the 17 month period from April 2014 and that births have been reasonably stable over the same period.
Key commissioning variances and projected risk are as follows:
3.1 Barts Health contract
The M5 SLAM claim submitted by the Trust indicates an extrapolated full year claim totalling £4.4 million above contract value after taking account of estimated readmissions, threshold and productivity metrics adjustments which have been calculated using precedent established during 2014/15. A summary showing all of the adjustments made to the headline M5 claim extrapolated for the full year is contained within the following table:
The table details the value of the adjustments we have made reflecting a risk assessment of
challenges which have been made to the Trust. As can be seen from the table, there are both upside and downside risks associated with the above projection and the scale of the range at M6 is £1.3 million.
In addition, the M5 claim includes a number of significant variances against plan that when extrapolated forward result in the headline figure of £140 million shown in the table above. These are detailed below:
o £1.1 million relating to the maternity pathway. Initial data on births shows that we are on plan however there is a significant over-performance against ante and post natal care which is being challenged with the trust.
M6 Reporting Upside Base Downside M5 FOT
£'000 £'000 £'000 £'000
Extrapolated FOT from M5 SLAM 140,953 140,953 140,953 141,430
Readmissions penalty (2,710) (2,710) (2,710) (2,712)Emergency Threshold (1,210) (1,210) (1,210) (1,135)Impact of Productivity Metrics (1,535) (1,395) (1,256) (1,483)Claims (4,451) (4,046) (3,439) (5,188)Penalties ‐RTT, ED, Cancer (3,006) (2,405) (1,804) (2,405)Potential re‐investment of penalties 3,006 2,405 1,804 2,405Penalties Other (111) (89) (67) (89)Critical Care Work In Progress 124 124 124 593Cardiac Imaging Adjustment 69 69 69 0
Sub‐Total 131,130 131,696 132,465 131,416
CQUIN (base case assumes 90%) 2,869 2,869 2,869 2,859Sub‐Total 133,999 134,565 135,334 134,275
Contract Value 131,208 131,208 131,208 131,208Total Forecast Risk 2,791 3,357 4,126 3,067
47

Finance Report
Page 5
o £0.8 million relating to non-emergency patient transport which is treated on a pass-
through basis. Again, this is being challenged with the trust on the basis that new costs have been identified which were not in CCG plans.
o £1.1 million over performance projected for direct access diagnostic services which represents a 14 percent increase above 2014/15 outturn. The increased claim relates predominantly to biochemistry and haematology tests.
o £1.2 million over performance projected against the outpatient follow up plan which is a
significant increase on 2014/15 outturn. Analysis is being undertaken to clarifying any key changes driving this claim.
Commissioners are currently negotiating with the provider to close down a number of Q1 claims.
The total claim at Q1 for WFCCG is £1.9 million and to date £0.5 million has been conceded by Barts, £0.4 million has been subsequently corrected through future SLAM submissions, £0.6 million has been conceded by the CCG which leaves £0.4 million still open for settlement. Our M6 projected FOT is underpinned by an assumption of £1.0 million of successful claims.
There has been a significant level of increased claims against the Redbridge CCG contract with an apparent 12 percent price variance for non-elective activity so it does appear that there is an element of coding and counting changes at Whipps Cross which are feeding into reported activity levels and subsequent claims from the trust.
3.2 Associate acute contracts
Based on M5 SLAM data received from other providers we are projecting a full year risk of £3.9 million with material risks developing at the following Trusts:
£0.3 million risk projected against the £0.7 million Royal National Orthopaedic Hospital contract. Data shows that there have been a large number of very high cost procedures undertaken during the first 5 months and further detailed analysis will be undertaken to review whether there are any underlying issues here.
£0.3 million risk projected against the £1.7 million Guys and St Thomas contract. Much of this risk is associated with non-elective activity which accounts approximately half of this total risk. There has been a small increase in attendances at accident and emergency across the last 17 months but this would not explain the growth in non-elective claims. The contracting team have been asked to do some comparative analysis around non elective volumes and case mix. The following graph also indicates that there has been a steady growth in patients being referred to this provider.
48

Finance Report
Page 6
£0.8 million risk projected against the £11.9 million Homerton contract. Data indicates that there is a steady increase in both referrals and accident and emergency attendances at this provider as indicated within the following graphs:
£0.4 million risk projected against the £4.4 million North Middlesex contract. The majority of this risk is associated with the maternity pathway where we have seen 125 ante natal registrations recorded up to M5 against a plan of 97 (29 percent over performance). In addition, there has been a 27 percent increase in births during the first 5 months of 2015/16 compared to the same period in 2014/15 (an increase from 73 to 93). The following graph also indicates that there is a steady growth in patients being referred to this provider.
01020304050607080
First Attendances GP Referrals April 2014 ‐ Aug 2015
Series2 Linear (Series2)
0
100
200
300
400
500
600
A&E ActivityApril 2014 ‐ Aug 2015
Series2 Linear (Series2)
0
200
400
600
800
1000
1200
First Attendances GP Referrals April 2014 ‐ Aug 2015
Series2 Linear (Series2)
0
50
100
150
200
250
300
First Attendances GP Referrals April 2014 ‐ Aug 2015
49

Finance Report
Page 7
£0.2 million risk projected against the £0.6 million Whittington contract. There has been no
change in the volume of accident and emergency attendances at this provider year on year however there has been an increase in the number of outpatient first attendances which is feeding through into higher spend on elective procedures.
£0.2 million risk projected against the £0.5 million Princess Alexandra contract. Detailed analysis is being undertaken by the contracting team to understand the drivers for this claim.
In terms of inherent contract risk, agreement on 2015/16 plans have yet to be finalised with UCLH and Royal Free and our planning values are £5.0 million and £1.3 million respectively. All outstanding contracts across London were escalated for mitigation or arbitration at the beginning of September.
£1.0 million risk projected against the £5.0 million contracts covering independent sector planned care and diagnostics providers. There is some evidence that this increase is linked to those specialties where Whipps Cross have long waits so should support reduced waiting times overall.
3.3 Non Acute
We are now projecting a £0.5 million surplus against community health services reflecting recruitment delays at Q2 associated with new investments which went into the 2015/16 contract. These delays are linked to some of the CCG’s QIPP schemes such as Phase 4 integrated care and therefore present a risk which is being escalated with the trust through the contract route.
We are reporting a £0.2 million risk against the learning disabilities continuing care budget associated with the part year financial implications of 8 clients that have transitioned from the children’s service and have been assessed as eligible for full CHC funding.
Based on business cases received regarding the crisis concordat and meeting RTT targets for psychosis services we are reporting a £0.5 million surplus against the funds set aside for investment in MHS services during 2015/16. This is a non-recurrent benefit recognising the phased implementation of new services.
We are reporting a £0.2 million surplus against our out of hospital budget associated with community MSK services provided by Barts Health. The costs of this service are now being claimed for by the trust through their main contract.
We are projecting a £0.1 million surplus against our adult continuing care budgets. The following graph indicates changes in the number of placements funded by the CCG since April 2014 covering adults, older people and “fast track”. The total number of placements has been reducing slightly since April 2015 but there was an additional 12 fast track patients agreed during September which has been reflected in our financial projection.
50

Finance Report
Page 8
3.4 Prescribing
We are now projecting a £0.7 million surplus at M6 against the GP prescribing budget based on extrapolating actual prescribing data covering the 6 month period from February 2015 to July 2015 for a full year and then adjusting for the delivery of phased QIPP savings of £1.0 million. In addition, we are reflecting a further £0.2 million benefit associated with recovering costs related to an out of area GP whose prescribing costs had been charged incorrectly to Waltham Forest and a risk of £0.2 million associated with drug price increase due to be implemented in October 2015 linked to the renegotiation of Category M Medicines and Pharmacy Contract income.
4 Other financial risks and mitigations
Other financial risks faced by the CCG and mitigations are:
Work continues with Barts around understanding the volumes of additional activity required and
timelines involved with meeting RTT targets. It is possible that meeting the targets will involve increased elective costs above the levels contained within the 2015/16 contract activity plan. The 2015/16 CCG budget includes a reserve of £2.3 million to mitigate this risk. Projections from M5 SLAM claims are currently showing a £0.7 million elective risk for private providers.
Negotiations between NHSE specialised commissioning, Barts and CCGs have been undertaken to resolve some misattribution issues which came to light during 2014/15 closedown which will have a recurrent impact. The total risk to CCGs arising from this issue is £8 million of which £1.0 million would fall to Waltham Forest.
New guidance has been issued to the NHS regarding charging for treatment provided to overseas
visitors who are not entitled to free NHS care. Under the revised regime, the risk of none recovery of debt will be shared with local commissioners and current estimates from Barts suggest that this will impact the CCG by £0.4 million. At present, we have not included this risk within our Barts projection.
0
50
100
150
200
250
300
350
Adults
Older People
Fast Track
Total
Linear (Total)
51

Finance Report
Page 9
Work continues with the London Borough of Waltham Forest to understand risks around the number of young learning disability adults who will be eligible for CHC and we have currently estimated a part year risk of £0.3 million.
The 2015/16 budget assumes successful delivery of the £9.0 million QIPP programme. Non delivery of red rated schemes has been reflected in our M6 reporting and the latest risk assessment of the overall programme will be provided later in the report.
The CCG has established a contingency reserve of £1.6 million within its 2015/16 plan and this
has not been applied within our projected outturn at M6.
The CCG established non recurrent headroom of £6.4 million within the 2015/16 plan. The CCG
have subsequently made commitments totalling £6.9 million however after taking projections of actual expenditure into account there is currently a small underspend projected.
As at M6 the acute risk reserve totals £4.5 million and we have applied £3.1 million to offset risks
within our commissioning budgets. Therefore £1.4 million remains uncommitted to help mitigate any further risks that emerge during the year.
5 QIPP
Appendix B shows the latest detailed risk assessment of the CCG’s QIPP plan which now includes £0.5 million associated with primary care co-commissioning and has therefore increased to £9.5 million. The appendix also provides a projection of the level of QIPP which will be achieved at year end. The risk rating is summarised in the following table.
Current
Value
Current
Percentage
Previous
Assessment
£m
Red 0.4 4% 4%
Amber 3.7 39% 39%
Green 5.4 57% 57%
Total 9.5 100% 100%
Appendix B shows that we are now projecting delivery of £8.55 million of QIPP savings within our reporting which is 90 percent achievement against plan.
52

Finance Report
Page 10
6 Balance sheet, cash management, performance against public sector payment policy (PSPP) and debtors
Details of the CCG’s closing statement of financial performance or balance sheet along with comparable figures at M6 are shown within Appendix D.
The CCG had drawn down cash totalling £150.2 million at the end of M6 from the government banking service and had cash holdings of £0.1 million as at the end of September which is approximately 0.4 percent of the cash drawn down in the month. The level of cash holdings has reduced slightly during the month. Revised cash management rules introduced for 2015/16 requires that we minimise the level of cash held at month end to at or below 1.25 percent and the CCG has met this target each month since it was introduced.
The CCG, in common with all public sector bodies, is mandated to pay suppliers within 30 days from submission of a valid invoice. As at the end of September the CCG’s cumulative performance was measured at 86.4 percent (based on the value of invoices paid) and 85.2 percent (based on volume of invoices paid against a target of 90 percent).
The CCG currently has £102k worth of debtors within our balance sheet which have been outstanding for 90 days or more. We will monitor progress on a monthly basis in respect of reducing this figure as these could develop into bad debts and impact our income and expenditure position.
7 Conclusion and recommendation
The Governing Body is asked to note this report.
53
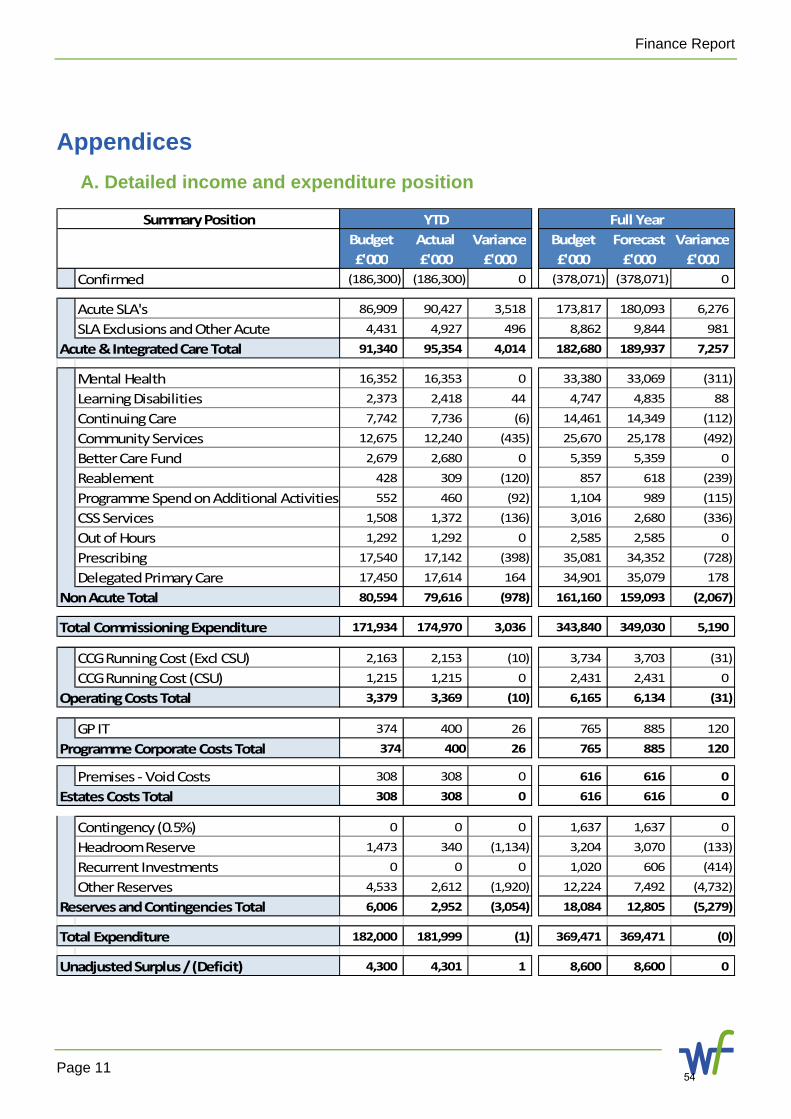
Finance Report
Page 11
Appendices
A. Detailed income and expenditure position
Budget Actual Variance Budget Forecast Variance
£'000 £'000 £'000 £'000 £'000 £'000
Confirmed (186,300) (186,300) 0 (378,071) (378,071) 0
Acute SLA's 86,909 90,427 3,518 173,817 180,093 6,276
SLA Exclusions and Other Acute 4,431 4,927 496 8,862 9,844 981
Acute & Integrated Care Total 91,340 95,354 4,014 182,680 189,937 7,257
Mental Health 16,352 16,353 0 33,380 33,069 (311)
Learning Disabilities 2,373 2,418 44 4,747 4,835 88
Continuing Care 7,742 7,736 (6) 14,461 14,349 (112)
Community Services 12,675 12,240 (435) 25,670 25,178 (492)
Better Care Fund 2,679 2,680 0 5,359 5,359 0
Reablement 428 309 (120) 857 618 (239)
Programme Spend on Additional Activities 552 460 (92) 1,104 989 (115)
CSS Services 1,508 1,372 (136) 3,016 2,680 (336)
Out of Hours 1,292 1,292 0 2,585 2,585 0
Prescribing 17,540 17,142 (398) 35,081 34,352 (728)
Delegated Primary Care 17,450 17,614 164 34,901 35,079 178
Non Acute Total 80,594 79,616 (978) 161,160 159,093 (2,067)
Total Commissioning Expenditure 171,934 174,970 3,036 343,840 349,030 5,190
CCG Running Cost (Excl CSU) 2,163 2,153 (10) 3,734 3,703 (31)
CCG Running Cost (CSU) 1,215 1,215 0 2,431 2,431 0
Operating Costs Total 3,379 3,369 (10) 6,165 6,134 (31)
GP IT 374 400 26 765 885 120
Programme Corporate Costs Total 374 400 26 765 885 120
Premises ‐ Void Costs 308 308 0 616 616 0
Estates Costs Total 308 308 0 616 616 0
Contingency (0.5%) 0 0 0 1,637 1,637 0
Headroom Reserve 1,473 340 (1,134) 3,204 3,070 (133)
Recurrent Investments 0 0 0 1,020 606 (414)
Other Reserves 4,533 2,612 (1,920) 12,224 7,492 (4,732)
Reserves and Contingencies Total 6,006 2,952 (3,054) 18,084 12,805 (5,279)
Total Expenditure 182,000 181,999 (1) 369,471 369,471 (0)
Unadjusted Surplus / (Deficit) 4,300 4,301 1 8,600 8,600 0
YTD Full YearSummary Position
54

Finance Report
Page 12
B. Detailed QIPP performance
Heading Proposed Project Planned Gross
Savings £M
Forecast Gross
Savings £M
RISK
Assessmen
t
Expansion of integrated care £1.23 £0.75Rapid Response £0.20 £0.20Falls £0.80 £0.80Respiratory £0.22 £0.22Ambulatory Care/ DVT Pathway redesign £0.20 £0.20Urgent Care Procurement £0.20 £0.00
Continuing Health Care Continuing Care Assessments £0.20 £0.13
Primary CareOut of Hours Primary Care to reduce A&E attendances (8‐8)
£0.30 £0.30
MH Wellbeing/Primary care liasion to support recovery & discharge
£0.10 £0.10
Metropolitan £0.20 £0.20Cardiac Pathway £0.05 £0.00Lower GI Pathway £0.04 £0.04Haemaglobinopathy £0.26 £0.26Diabetes £0.10 £0.10Gynaecology (Day Cases) £0.00 £0.00NELEC Procurement £0.10 £0.00
Women & Children Children's Virtual Ward £0.15 £0.15
Medicines Management Medicines Management £1.00 £1.00All Acute ProvidersProcurementNELFTAll non acute providersReduce Property Voids (Highams and others)
£0.20 £0.20
Operating cost efficiencies based on 10 percent RCA reduction
£0.70 £0.70
Primary Care Co‐
commissioning
The CCG is awaiting details from NHSE but list cleansing will be the main scheme.
£0.50 £0.16
£9.50 £8.55 90.0%
Planned Care
£2.75
Transform
ation
Integrated care
Urgent Care
Mental Health
£3.04
Transactual
Productivity & Contract
Efficiencies
Corporate
55

Finance Report
Page 13
C. Statement of financial position (balance sheet)
£000 £000Mar 2015
Sep 2015
NON-CURRENT ASSETS
Property, Plant and Equipment 3 1 Trade and Other receivables - -
TOTAL Non Current Assets 3 5
CURRENT ASSETSInventories - - Trade and Other Receivables 4,688 581 Other Financial Assets - - Cash and Cash Equivalents 6 (111)
TOTAL Current Assets 4,694 470
TOTAL ASSETS 4,697 475
CURRENT LIABILITIESTrade and Other Payables (26,365) (20,701)
Provisions - -
TOTAL Current Liabilites (26,365) (20,701)
NET CURRENT ASSETS/(LIABILITIES) (21,671) (20,230)
TOTAL ASSETS EMPLOYED (21,668) (21,678)
FINANCED BY:
General Fund (21,668) (20,230) TOTAL TAXPAYERS EQUITY (21,668) (20,230)
Waltham Forest CCGStatement of Financial PositionPosition as at 30th September 2015
56

Item 5.1
Title of report Communications Strategy
From Helen Davenport, Director of Nursing, Quality and Governance - WFCCG
Purpose of report
Communications at Waltham Forest Clinical Commissioning Group (CCG) have evolved naturally since the organisation was first formed in 2013. A communications strategy was drafted at this time, however as the CCG has matured and the needs of our key stakeholders have been better established, the communications function has responded flexibly and adapted its approach to support as effectively as possible.
The purpose of this report is to agree a refreshed communications strategy that better reflects how the communications function is currently working, and its future aspirations.
Changes/additions/amendments to paper as a result of discussions held at Planning and Innovation Committee
No amendments.
In January 2015 a proposed communications and engagement strategy was presented to the Planning and Innovation Committee. All aspects were supported and the refreshed strategy is a reflection of this.
Recommendations
Approve the refreshed communications strategy, including a review of resourcing to ensure all objectives can be met.
Impact on patients & carers
This refreshed strategy will positively impact on patients and carers, as effective communications are critical in helping people understand what the CCG is doing and how they can get involved in shaping health services.
Extensive work already being undertaken to support communication with patients and carers, and in the future this will be enhanced through additional communications channels, such as a community mailing list.
Risk implications
The CCG currently faces reputational risk, as highlighted by a poor 360° stakeholder survey earlier in the year. In particular, two-way communication with GP practices needs to be strengthened and better coordinated. There is also a need to improve relationships with the third sector and improve communication with CCG staff. The communications strategy works to address this.
57

Communications Strategy
Financial implications
Dependent on outcome of resourcing review, which will be undertaken as part of the refreshed communications strategy.
Equality analysis
We want to make sure that we are communicating with people from as many groups as possible, whether or not they have one or more of the ‘protected characteristics’ described in the Equality Act 2010. (These protected characteristics are age, disability, gender reassignment, marriage and civil partnership, pregnancy and maternity, race, religion and belief, sex and sexual orientation.) Given our commitment to this, we will consider the impact that this strategy is having on different groups and take any action that is required to ensure no group is adversely impacted.
Other committees/groups, including the CCG Reference Group and Rapid Feedback Group
The refreshed communications strategy is a reflection of the existing communications function. The function has developed naturally over time through the valued input of staff from across the CCG, patient representatives, Healthwatch and providers. It will continue to evolve to meet the changing needs of all of the CCG’s stakeholders.
58

Communications Strategy 2015 - 2018
59

Communications Strategy
Page ii
Contents
1 Foreword 1
2 Where are we now? 2
3 Our objectives 3
4 Opportunities for improvement 3
4.1 Improve current communications platforms 3
4.2 Establish new communications platforms and processes 3
4.3 Improve coordination of communication channels across the CCG 4
4.4 Embed high quality communication across the organisation 4
4.5 Review governance and resources 4
5 Evaluating the strategy 4
6 Conclusion 5
Appendices 6
Appendix A Information on Waltham Forest CCG 6
60
Communications Strategy
Page 1
1 Foreword
Good communication is at the heart of a well-functioning Clinical Commissioning Group. First and foremost, we need to listen to and engage with our local community, the residents of Waltham Forest. Many aspects of the CCG’s communication are discussed in our separate Community Participation Strategy and these two documents should be read together.
This document focuses on how we communicate within our organisation; with our partners in health and social care; and with the wider community. Our objective is to improve communications with our GP member practices and staff; and with our external stakeholders such as Waltham Forest Council, MPs and provider organisations.
Communication is a ‘two way street’: it is not just about informing people of what we are doing, but also about listening to stakeholders and collaborating closely to improve the delivery of local health care services and ensure value for money. This will help avoid duplication or gaps in service provision and make sure that we focus on the areas of greatest need.
The key to successful communication will be finding the most effective methods to keep everyone informed and to receive feedback. This strategy lays out our current plans. We would of course welcome your ideas and would be delighted to hear your suggestions.
The Communications Strategy should be read in conjunction with the Community Participation Strategy.
With best wishes,
Alan Wells OBE
Deputy Chair and Lay Member for Governance
61

Communications Strategy
Page 2
2 Where are we now?
Our previous communications strategy for 2013-2016 was developed when the CCG was first formed. It was focused on building strong relationships with our stakeholders and making sure they were always up to date, fulfilling our statutory communications responsibilities (such as responding to Freedom of Information requests), providing communications and engagement support to CCG staff, forward planning, working flexibly and ensuring the communications function is proactive.
Two years on we have had many successes, including the recent re-launch of a more patient-focused public website, and establishing a range of channels that help us communicate and engage with different stakeholder groups on a regular basis. They are:
Audience Channels of communication
Patients
CCG reference group (local residents who meet every two month to review CCG policies and strategies)
CCG rapid feedback group (local residents who provide email feedback) Focus groups and workshops Healthwatch newsletter1 Maternity Services Liaison Committee (patients who advise on maternity
services) SMS messaging through GP practices
Public
Public website Press releases Publications, such as flyers and posters Awareness outdoor advertising campaigns Public events, such as the annual general meeting
GP and practice staff
GP website Email briefings Monthly e-bulletin Monthly locality meetings Monthly training meetings Practice manager’s forum Practice nurse’s forum
CCG staff
Email briefings Monthly e-bulletin Staff meetings Centralised filing system of key communications resources and information about
CCG work
1 We would like to extend our thanks to Healthwatch for their support in disseminating key CCG information
62

Communications Strategy
Page 3
Audience Channels of communication
Other stakeholders
Briefing papers for and attendance at Health Scrutiny Committee meetings Briefing papers for attendance at Health and Wellbeing Board meetings Email correspondence and meetings with local MPs and councillors Email correspondence and meetings with Waltham Forest Council Email correspondence and meetings with healthcare provider organisations Email correspondence and meetings with neighbouring CCGs Email correspondence with NHS England and Department of Health
There are also areas where our communications need to improve. A recent evaluation highlighted that communication to GPs in Waltham Forest could be much better, and more support needs to be given to CCG staff to ensure messaging about the CCG’s work is clear and consistent.
This revised strategy has considered the changing needs of the CCG and our stakeholders, and builds on those areas where there are opportunities to make improvements.
3 Our objectives
Key stakeholders will know what we’re doing, and the CCG will be seen as the local healthcare leader
Staff and GPs will have access to the information and communications and engagement support they need to do their jobs well
Patient and public engagement will be innovative and delivered in line with the NHS Constitution The CCG will have communications and engagement support to improve the health outcomes of
our local population Communication and engagement projects will be delivered in line with our statutory
responsibilities Work will be managed proactively and urgent issues will be dealt with effectively
4 Opportunities for improvement
4.1 Improve current communications platforms
We will improve current platforms, including the GP website, to ensure they are all clear, engaging and accessible.
4.2 Establish new communications platforms and processes
We believe that the following additional platforms and processes are required to communicate more effectively with our stakeholders. These are:
Mailing list and newsletter for patients and key stakeholders A platform for communicating regularly with voluntary and community organisations Staff intranet
63

Communications Strategy
Page 4
Formalised processes for communicating regularly with the Overview and Scrutiny Committee, Local Medical Committee and Adult and Child Safeguarding Boards
The use of social media will be reviewed and introduced if we believe it will provide tangible benefits to the community
4.3 Improve coordination of communication channels across the CCG
In the past, some communication platforms have been managed by the communications team, with others (such as GP locality meetings) managed elsewhere in the organisation. We will improve governance structures to ensure the communications team is involved with all key communications platforms and there is consistent messaging across them.
4.4 Embed high quality communication across the organisation
We have developed a central communications resource to ensure that CCG communications on key work streams are consistent. We will do further work to embed the use of this resource throughout the organisation, and ensure the materials are updated regularly. This will help ensure that messaging is aligned across all our channels.
We will also provide more guidance to staff on how the communications and community participation function can support them.
4.5 Review governance and resources
We will review the resourcing and governance arrangements within the communications and community participation functions to ensure they are robust, that new channels are of a high quality and that the team is working as effectively as possible.
We will ensure the communications and community participation functions are aligned and work together to develop plans that support staff within the CCG, and the local community, and is able to address the following challenges:
the CCG’s new responsibility for commissioning GP services delivering the Transforming Services Together transformational change programme addressing pressure on A&E services increasing demand for communications and engagement support as our newly formed organisation
develops and undertakes larger and more complex pieces of commissioning work
introduction of the NHS England accessible information standard
5 Evaluating the strategy
Once the strategy has been approved, an action plan for 2015-2016 will be devised to help deliver it. At the end of every year progress will be reviewed, and the strategy itself will be refreshed if required.
We also want to make sure that we are communicating with people from as many groups as possible, whether or not they have one or more of the ‘protected characteristics’ described in the Equality Act 2010. (These protected characteristics are age, disability, gender reassignment, marriage and civil partnership, pregnancy and maternity, race, religion and belief, sex and sexual orientation.) Given our commitment to this, we will consider the impact that this strategy is having on different groups and take any action that is required to ensure no group is adversely impacted.
64

Communications Strategy
Page 5
6 Conclusion
Good communication is at the heart of any well-functioning Clinical Commissioning Group. Through this strategy we hope to improve all forms of communications at Waltham Forest CCG so that we can support the CCG in delivering its vision, its objectives, and the tenets that lie at the heart of the NHS.
We want this strategy to be successful and positive for everyone it impacts and will follow the principles we have outlined in order to achieve this. We will monitor our progress carefully to ensure that we are achieving our objectives.
Most of all, we hope to hear your feedback and suggestions. With your help we know we can improve our standards of communication to the level that the organisation and our stakeholders deserve, and maintain those high standards on an ongoing basis.
To request a copy of this document in another format or language, please contact: [email protected]
65

Communications Strategy
Page 6
Appendices
Appendix A Information on Waltham Forest CCG
NHS Waltham Forest Clinical Commissioning Group became the new statutory leader for commissioning local NHS services from 1 April 2013. CCGs are different from previous health organisations in that they are led by GPs and other clinicians to help ensure that services reflect local patients’ needs. Having leaders who have clinical expertise and maintain close contact with patients offers great potential to make improvements in health and social care for local people. The CCG’s commitment to community participation will also help improve health and social care for the residents of Waltham Forest.
It is essential that the CCG communicates well with its residents and its stakeholders in order to achieve our vision. This vision is: ‘we will put patients at the heart of everything we do and use our joint experience to improve the delivery of local health care and ensure value for money.’ Through effective communication we also want to support our organisation in achieving its objective.
Our objective is to improve the health outcomes of our local population through the effective commissioning of high quality services by:
meeting our statutory requirements; being clinically led; strengthening collaboration with WEL/WELC (our partners in East London and the City) and local
providers; and establishing commissioning arrangements; improving the patient experience across all services; and involving patients, communities and hard to reach groups.
This strategy sets out how we will establish formal communications pathways that will support the CCG to achieve these aims.
It provides a guide for staff, GP member practices and everyone with an interest in working with us. It is part of our approach to working in partnership and our aim to bring the best of modern healthcare to local people.
66
Item 5.2
Title of report Community Participation Strategy
From Helen Davenport, Director of Nursing, Quality and Governance - WFCCG
Purpose of report
The purpose of this report is to inform the Governing Body that the community participation strategy has been revised and updated. The revised strategy sets out how NHS Waltham Forest Clinical Commissioning Group (WF CCG) intend to engage with and involve the public in our work. The strategy reflects on achievements to date and sets out our priorities for 2015/16.
Recommendations
The Governing Body are requested to review and approve the contents of the Community Participation Strategy.
Impact on patients & carers
It is essential that patients and the public are involved in the services which we commission from providers. It is important to capture and act on patient experience, as this will assist us to evaluate the quality and clinical effectiveness.
Listening to patient experience, will assist WF CCG to ensure that it commissions services which meet the needs of our residents.
Risk implications
Failure to implement and monitoring the effectiveness of the Community Participation Strategy, may result in the objectives of the strategy not being met.
Financial implications
Failure to include the views and opinions of our local population, could potentially result in WF CCG commissioning services which do not offer value for money for our residents.
Equality analysis
The CCG is committed to fulfilling its obligations under the Equality Act 2010 and to ensure services commissioned by the CCG are non-discriminatory on the grounds of any protected characteristics. The CCG will work with providers, service users and communities of interest to ensure that any issues relating to equality of service within this report are identified and addressed.
67

Community Participation Strategy
Other committees/groups, including the CCG Reference Group and Rapid Feedback Group
WF CCG Reference Group were involved with developing the original Community Participation Strategy.
68

Community Participation Strategy 2015 - 2018
1
Waltham Forest Clinical Commissioning Group
Community Participation Strategy 2015- 2018
69

Community Participation Strategy 2015 - 2018
2
Contents Foreword 3
Community participation: the statutory basis 4
Community participation: our approach 4
Our structure 8
Further information on our structure 10
Priority areas for 2015/16 14
Evaluating our strategy 15
Conclusion 15
Appendix: Information on Waltham Forest CCG 16
70

Community Participation Strategy 2015 - 2018
3
Foreword NHS Waltham Forest Clinical Commissioning Group (WF CCG) are committed to involving our local community, including patients and the public, in the commissioning decisions we take. WF CCG have pledged to involve our community not just because the Health and Social Care Act 2012 places considerable importance on people in the community participating in decisions taken by Clinical Commissioning Groups; but because we believe involving people is essential if we are to spend the money available to us as effectively as possible to improve local healthcare. For us, involving people in our community means more than just consulting; it means listening to the views of the people of Waltham Forest. These views are taken into account, for all significant decisions we take. We hope we have already shown our keenness to listen in the engagement work we have undertaken since our initial strategy was approved in September 2013. This work has included:
Establishing our face-to-face Reference Group and virtual Rapid Feedback Group. These were established in the winter of 2013-14, following an extensive marketing campaign.
Consulting and engaging on a host of local healthcare issues, including formal consultations (Naseberry Court and the CCG / local authority mental health strategy for adults) and engagement on key workstreams (such as Transforming Services Together and the CCG’s primary care and urgent care strategies).
Revitalising our Maternity Services Liaison Committee. This is now managed by a local community organisation, Social Action for Health.
Extensive work with the local authority on ensuring the voices of children and young people (including looked after children) are heard in commissioning.
These are just a few highlights. Full reports on our participation activities are available online in our Governing Body papers: www.walthamforestccg.nhs.uk/about/previous-governing-body-meeting-papers.htm (The report on our 2013-14 activities is available in the October 2014 minutes, and the report on our 2014-15 activities will be available in the October 2015 minutes.) Our Community Participation Strategy 2015-18 builds on our 2013-16 strategy. It sets out how we intend to develop our community participation function over the next three years, and should be read in conjunction with our Communications Strategy 2015-18. We want to ask people regularly how well our strategy is working. We hope that your feedback will tell us that you understand what the CCG is, what we are trying to do and how well we are doing. Of course, we hope that you will say: “I understand what the CCG is trying to do.” “I feel that the CCG listens to what I have to say.” “Even if I disagree with a decision the CCG took, I know that they thought about what I said.” If we do not get comments like these, we will know we have further work to do. Richard Griffin Lay Member for Community Participation
71

Community Participation Strategy 2015 - 2018
4
Community participation: the statutory basis The Health and Social Care Act 2012 includes a clear commitment to involving patients and the public in decisions taken. The NHS Constitution includes the right of the public: ‘to be involved, directly or through representatives, in the planning of healthcare services, the development and consideration of proposals for changes in the way services are provided, and in decisions to be made affecting the operation of those services’. The Health and Social Care Act 2012 places a responsibility on Clinical Commissioning Groups (CCGs) to involve patients and the public in the area that they serve in decisions the CCG takes. We intend to do this through our Community Participation Strategy. The NHS Outcomes Framework 2014/15 clearly sets out within Domain 4 – Ensuring that people have a positive experience of care, how organisations including CCGs measure and evaluate patient experience. Community participation: our approach Introduction NHS Waltham Forest CCG is committed to commissioning high-quality health services for people living in Waltham Forest. We believe that the only way we can achieve this is by making sure that we involve people in our community in the decisions we take and the services we develop. Historically, the NHS has not always been very good at involving patients and the public in decisions about their healthcare taken with public money. This has been particularly true of groups and people in the community who are seldom heard, but it is also true for involvement in general. We intend to change this. Above all, our Community Participation Strategy will ensure that people in our community:
feel that they have been listened to; are able to put their views to us; know how to get involved in decisions we make; and understand how their views were taken into account in decisions we have made.
How we involve people We want to involve people in our community at every stage of our commissioning. This includes helping to:
assess needs in our population to determine what and where services need to be provided;
review existing services to identify gaps and potential improvements; decide priorities and identify what we give priority to; design services through involvement at the beginning of the development of a service;
and monitor performance against our plans.
We also want to hear your views on your experiences of our local health services, and so we want you to be able to contribute views. These will not be one-off activities, but a continuous process. This is demonstrated in the diagram overleaf.
72

Community Participation Strategy 2015 - 2018
5
Community participation in the commissioning cycle
PLANNING
Helping to assess needs in our population to determine what and where services need to be provided.
Helping to review existing services to identify gaps and potential improvements.
Helping to decide priorities and identify what we give
priority to.
DESIGNING
Helping to design services through involvement at the
beginning of the development of a service.
MONITORING
Helping to monitorperformance against our
plans. Contribute views on your experiences of local health
services.
EVALUATING
Helping to evaluate our community participation strategy and activities
73

Community Participation Strategy 2015 - 2018
6
Working with our partners A key characteristic of our approach is working with partners on our participation activities. The section below lists our key partners, and describes some of our current and future work with them. Waltham Forest Local Authority We work closely with the local authority on many initiatives, in particular integrating health and social care through our ‘Better Care Together’ programme. Better Care Together is our local workstream to deliver the national Better Care Fund programme. This scheme seeks to promote integration of health and social care services via a pooled budget, which for Waltham Forest is £18.6 million. During 2014/15 we successfully agreed a plan to deliver this work, laying the foundations for mobilisation during 2015/16. Another area where we work closely with the local authority is in ensuring that the voice of children and young people is heard in health and social care. All health organisations must demonstrate how they have listened to the voice of children and young people, and how this will improve their health outcomes. Patient and family experiences should not only include the experience of the patient and carer going through the service but also demonstrate how they are involved in assessments, and running and developing future services. (London Children’s Strategic Clinical Network, NHS England 2014). Under the Healthy Child Programme (Department of Health, 2008), the personal child health record, commonly referred to as ‘the red book’, has been made available to all children in England under the age of five. However numerous placement changes experienced by looked after children (LAC) result in the misplacement of this health record. Furthermore, there is a requirement that all LAC have a documentary record of their health history for their period of time in care. This contributes to their life story work and provides a snapshot of the individual child’s health journey while in care. A significant piece of work was undertaken by the CCG designated nurse for LAC to develop a health passport which incorporates all health records for LAC, which can be easily shared with other health care professionals. We have also developed an app to support this project. In addition, some of the main messages from serious case reviews nationally with regard to the voice of the child are that:
• In too many cases, the child was not seen frequently enough by the professionals involved, or was not asked about their views and feelings.
• Often agencies do not listen to adults who try to speak on behalf of the child, and who have important information to contribute.
• Parents and carers prevent professionals from seeing and listening to the child. • Practitioners focus too much on the needs of parents, especially vulnerable parents, and
overlook the implications for the child.
In response, Waltham Forest CCG commissioned Social Action for Health to undertake a project across provider services in Waltham Forest, to capture the voice of the child. The purpose of this project is to:
• Ensure that the CCG are putting children, young people and their families at the heart of our work.
• Enable children and young people’s opinions and experiences of health services within Waltham Forest to be included in the commissioning and development of future services.
In particular, as part of this project, Social Action for Health will scope and set up focus groups with health service users in Waltham Forest. The aim of the focus groups is to ensure that we
74
Community Participation Strategy 2015 - 2018
7
are capturing the voice of the child to obtain services that are shaped around the needs, aspirations and preferences of children, young people and those around them. Healthwatch Waltham Forest Healthwatch Waltham Forest is the independent ‘consumer champion’ for health and social care. They were created by the Health and Social Act 2012 to represent the views of patients and the public in our local area. Whether it's improving them today or helping to shape them for tomorrow, Healthwatch Waltham Forest is all about local voices being able to influence the delivery and design of local services. Not just people who use them, but anyone who might need to in future. We will continue working closely with our local Healthwatch, for instance by meeting regularly to share patient engagement and experience information, and by working together to deliver focus groups and other participation activities. Voluntary and Community Organisations Waltham Forest has a considerable number of voluntary and community organisations representing our community, including black and ethnic minority organisations, disability organisations and also organisations that represent the lesbian, gay, bisexual and transgendered (LGBT) population. Many of these have a very wide area of interest, while others focus on a particular issue. We plan to strengthen our relationship with these organisations, either individually or through an umbrella network. We will also meet voluntary and community organisations when decisions we may take would have an impact on the people they represent. WF CCG have commissioned Age UK to assist in our work to engaging with the vulnerable and socially isolated people in our neighbourhood. Community of Interest Groups In addition to more established voluntary organisations, there are a number of usually smaller and less formal, groups that focus on a particular interest or group. Sometimes these groups are concerned with a specific clinical issue (e.g. diabetes or sickle cell disease); sometimes they are concerned with a particular area or locality (e.g. a housing estate); sometimes they are focused on a particular community (e.g. Polish people). We want to encourage these community of interest groups to become involved in helping us commission the right services for Waltham Forest. We intend to convene meetings with specific community of interest groups when action we plan to take is likely to have a particular impact of the people they represent. Other organisations We will work closely with the Care Quality Commission (CQC) and other NHS organisations, including NHS England, Monitor, the Trust Development Authority and provider organisations. One of the major pieces of work we will be undertaking with our local healthcare partners is the ‘Transforming Services Together’ programme, which looks at how to provide safer, more effective and sustainable healthcare services in east London. We will also build on the work we have done with Leyton College, and partner with local organisations where possible.
75

Community Participation Strategy 2015 - 2018
8
Principles We have established a number of principles that inform our strategy. We will be:
Inclusive: allowing everyone who has an interest in or is affected by decisions we take to be involved.
Honest: being honest and open about the reasons we have taken every decision. Clear: explaining what we do and issues we are addressing in clear and simple
language. Flexible: making sure that there are different ways to be involved to reflect the diversity
of our community and ensuring no one is excluded. Accountable: responding in the shortest possible time about decisions taken and why
contributions from people in the community have or have not influenced the decisions taken.
Responsive: open to ideas about changing ways we encourage our community to participate.
Willing to Learn: making sure that we learn from experience. Working in Partnership: working with, and avoiding duplicating other statutory partners,
particularly Waltham Forest Council and local voluntary and community organisations (as outlined in the Waltham Forest Compact).
Our structure Although we use a number of informal approaches to involving people in the decisions we plan to take, we recognise that we need a structured approach as well. This structure is outlined on the following page. The blue boxes represent community participation structures and activities, while the pink boxes represent written reports relating to community participation. Green marking indicates where patients, public and their representatives link into the structure.
76

Community Participation Strategy 2015 - 2018
9
CCG Governing Body
Community Participation pooling mechanism (TBC)
Community Participation
report (report on activities conducted
outside the main platforms)
Ad hoc Community Participation activities
(including focus groups and participation conferences)
Patients, public and their
representatives
Communications report (including digital and social
media)
Patient experience report
Complaints from patients/public
Patients and public
Experience info received directly
from patients/public
Patients and public
NHS patient experience metrics
Patients and public
Primary care team report
(kiosk intelligence etc)
Patients and public
Healthwatch intelligence
Patients and public
Rapid Feedback Group report
Rapid Feedback Group
CCG Reference Group
Expert patient representatives
TBC
Expert patients for each CCG
Committee and TST
Healthwatch representative x1
Patients and public
Voluntary / community organisation
representatives x TBC
Voluntary and community organisations
Patients and public
PPG representatives
x3
PPGs in Chingford,
Walthamstow and Leyton / Leytonstone
Maternity representative x1
Whipps MSLC
Patients and public
Held in public: patients, public and their representatives attend
77

Community Participation Strategy 2015 - 2018
10
Further information on our structure CCG Reference Group The CCG Reference Group was set up in the lifetime of the last Community Participation Strategy. It was formed as representative of the diverse nature of Waltham Forest; and so that the members have the skills needed to advise us. We consulted on the timing of the group, and ensured that the venue is accessible to people from all groups (irrespective of whether they have one or more ‘protected characteristics’). We are also committed to paying out-of-pocket travel expenses for members; and confirmed in the group’s Terms of Reference that people attend as individuals, not representatives of particular organisations. The group has been operational since January 2014, and meets every two months to provide input on CCG strategies and plans. Over time the group will be developed so that it is involved in all stages of the commissioning cycle, with a focus on assessing the needs of the people of Waltham Forest, providing advice on our overall commissioning strategy, and overseeing the progress of our Community Participation Strategy. The subjects they have addressed are varied, and have included: the CCG primary care strategy; plans for an enhanced GP service (i.e. evening and weekend appointments); integrated discharge planning; and the CCG urgent care strategy. Rapid Feedback Group The Rapid Feedback Group was also set up in the lifetime of the last Community Participation Strategy, and has been operational since December 2013. Some decisions we have to take need to be taken very quickly; within a couple of days. So sometimes there is not the time to convene a meeting or get our Reference Group together. That’s where the Rapid Feedback Group comes in: they are an email group who can provide us with immediate feedback when time is short. The group is larger than the Reference Group, and some members are members of the Reference Group. We do not intend for the Rapid Feedback Group to be used instead of the Reference Group but only when circumstances mean that the Reference Group has not time to meet. We will regularly review the group, to ensure it remains representative of the diversity of Waltham Forest. In particular we are keen to ensure that members of the Armed Forces are given the same opportunity to participate in the CCG, and we will work to ensure this is the case. Topics of engagement have included the CCG’s IT and digital strategies, looked after children strategy, and proposed changes to ophthalmology services. GP Patient Participation Groups (PPGs) Some GP practices in Waltham Forest have Patient Participation Groups (sometimes called Patient Engagement Groups). We want to change this, so that all of the GP practices in Waltham Forest have a group. Some PPGs meet fairly regularly; others meet more sporadically. Some PPGs usually meet in face-to-face meetings; others are virtual groups, contacted and consulted by email. The focus of all PPGs is on ways to improve how their GP practice works. We believe that Patient Participation Groups can provide a useful forum for testing out CCG plans and proposals. So we plan to work with GP PPGs to identify how they can include discussion of wider commissioning plans in their meetings. We also want to help PPGs make sure that they reflect the make-up of the population served by the GP practice.
78

Community Participation Strategy 2015 - 2018
11
Although it is for individual GP practices to decide how their Patient Participation Group operates, we will help and support PPGs to become as effective as possible. We also want to ensure that the views of patients in PPGs about services are considered by the CCG and/or referred on to NHSE or any other appropriate organisation. In order to achieve this, we intend to:
establish a key patient contact for each PPG; regularly suggest areas of health provision that PPGs might wish to discuss and
comment on; provide briefings on each topic we propose; ask our PPG patient contact to provide feedback on the views expressed at PPG
meetings; and pass on, as appropriate, to the CCG Governing Body or NHSE, the views of PPGs about
services they receive. As a first step towards this, we will be running a PPG development programme with the Patients Association (‘Patients in Participation’) from September 2015 to August 2016. The aims and objectives of this project are as follows. Project Aim To provide a development programme for Patient Participation Groups across Waltham Forest in order to increase their effectiveness and commissioning influence at practice, local, regional and national level and increase the level of patient and public patent participation. Project Objectives
To provide a communication and co-ordination channel for PPGs across Waltham Forest;
To develop a structure and model for a Patient Participation Group Networks working with Clinical Commissioning Groups to avoid repetition/duplication;
To provide a source of information to improve the level of patient and public awareness of and involvement in Patient Participation Groups;
To share knowledge and best practice between Groups; To provide roll out and facilitation for the Patients Association Patient Participation
Group Information and Support pack; To provide training and support for Patient Participation Group members to develop as
a positive resource and critical friend to the practices face to face, on-line and including webinars;
To assist with the development of future work plans for Patient Participation Groups with clear roles and responsibilities for monitoring and improving services;
To provide development opportunities for young people and other minority groups to be involved in Patient Participation Group and have greater influence over commissioning;
To develop a resource for revalidation of GPs; To raise public awareness about the need for appropriate use of primary care services
such as reducing “did not attends” and unnecessary contacts with GPs by including patients views and suggestions about this;
To develop Patient Participation Group as a resource for health promotion/education, encouraging self-care and smarter preventative services for the benefits of patients and the practices;
79

Community Participation Strategy 2015 - 2018
12
To contribute to CQC inspections and compliance and other national requirements such as the Friends and Family Test;
To assist with funding bids and submissions for improvement grants; To build in evaluation and action learning throughout the project including the
production of a final report, film and other methods to capture stories of the learning in progress;
To develop ‘PPG friendly practice’ criteria and an award process that is linked to the above objectives designed by patients and carers.
Maternity Services Liaison Committee One of the areas we are keen to develop is our collaboration with local voluntary and community organisations. One area we have delivered on this has been in running the Maternity Services Liaison Committee for Whipps Cross Hospital, which we now commission from a local organisation, Social Action for Health. Much of our recent activity has been in setting up this new group, and we are pleased to say 19 members of the local community have now been recruited. These people have also completed a comprehensive training programme, to enable them to undertake inspections and review of maternity units. This committee convened its first meeting in June 2015, and reports to the Performance and Quality Committee, which reports directly to the Governing Body. Patient Experience Reports All information the CCG receives on patient choice and feedback will be kept track of in a patient experience report that will go to the Performance and Quality Committee every month. This committee will then make decisions on any action that needs to be taken:
to convert insights about patient choice into plans and decision-making; and to respond to any quality issues that have been identified, including safety issues.
This report will include intelligence from sources like the patient experience kiosks we have established in some GP practices in Waltham Forest, and also intelligence from complaints. Because complaints are so important, they will also be reviewed by our Governing Body. A list of all complaints we receive and how we have dealt with them will be considered by our Governing Body every month at our meeting which is open to the public to attend. In addition, our Deputy Chair will regularly review all complaints to identify points made that could influence our commissioning plans. The Deputy Chair will raise these issues with our Governing Body to ensure that complaints are taken into account when commissioning services. Focus Groups and Participation Conferences Sometimes we will set up small focus groups around a particular topic or issue. Focus groups will allow us to get feedback and advice on a specific issue (mental health, for example) from people who have lots of knowledge and experience of the issue. We also plan to hold Participation Conferences. These conferences will report on what we have been doing and plan to do, as well as feature some sessions on specific clinical issues, such as managing diabetes and living with dementia.
80

Community Participation Strategy 2015 - 2018
13
Every conference will include a report on the information on the patient choice and feedback the CCG has received in the past six months, as well as a summary of how the CCG has responded to this. Digital and Social Media Our website will contain as much information as possible about what we are doing and what we plan to do. It will be updated regularly. There will also be a section that will allow anyone to give their views or make suggestions, and a section on what people have said to us about what we plan to do or have done. We will also assess the value that social media can bring to our function.
81

Community Participation Strategy 2015 - 2018
14
Priority areas for 2015/16 Over time we will develop the community participation function so that it resembles the function described above. As our next step towards this, and during 2015/16, we will deliver the following key improvements.
1. Although there has been community participation activity on the participation duties, we have not always governed this activity consistently and demonstrated its impact, so this will be a real focus for us going forward. This will be delivered by implementing a governance structure as outlined on page 9. In the short term we will draw the structures and reports we have in place into this arrangement; and in the long term we will develop the remaining structures and reports.
2. We will ensure better alignment between the CCG’s objectives and resources, so that:
There is sufficient resource allocated to deliver participation duties; The Reference Group’s work programme is linked to the Governing Body’s
agenda; and We review the issue of remuneration for patient participation.
3. During 2015/16 we will review the membership of our community participation groups,
to confirm whether groups identified in the Equality Act as having protected characteristics are adequately represented. We will begin with our Reference Group, Rapid Feedback Group and Maternity Services Liaison Committee.
4. We will establish ‘you said, we did’ feedback loops for all community participation
activities.
5. We will deliver the ‘Patients in Participation’ project.
82

Community Participation Strategy 2015 - 2018
15
Evaluating our strategy We want to make sure that our Community Participation Strategy is working and that people in Waltham Forest feel able to be involved in the decisions we plan to take. From September 2015 onwards we will undertake annual surveys of patients and public involved in the CCG’s community participation structure, to find out whether they feel that our strategy helps them get involved. We will ask questions around the four key indicators outlined at the start of the strategy (i.e. do they feel that they have been listened to; have been able to put their views to us; do they know how to get involved in decisions we make; and do they know how their views were taken into account in decisions we have made). We will also ask questions to help us monitor the impact this strategy is having on groups with protected characteristics. After each annual survey we will consider whether the feedback supports a revision of the Community Participation Strategy, and if so then we will undertake a revision. Conclusion We are committed to involving people of Waltham Forest in the commissioning decisions we take because we believe that this is crucial if we are to make the right decisions. We know we are responsible for spending your money (the money you pay in taxes to pay for healthcare) and so we need to spend it wisely. This is necessary for us to be able to develop and sustain first class healthcare for you, the people of Waltham Forest. We want to thank the people who have participated so far, and invite all local residents to get in touch and find out how to get involved. To request a copy of this document in another format or language, please contact: the communications team at [email protected]
83
Community Participation Strategy 2015 - 2018
16
Appendix 1 Information on Waltham Forest CCG Our Vision, Values and Objectives Our Vision, Values, Objectives and Priorities will drive all that we do. Our Vision is: ‘we will put patients at the heart of everything we do and use our joint experience to improve the delivery of local health care and ensure value for money.’ Our Values are:
we will act with integrity, treating everyone with respect and equity; we will actively listen to enable everyone to maximise their potential and fully contribute
to the organisation; and we will work in close collaboration with our partners across health and social care.
Our objective is to improve the health outcomes of our local population through the effective commissioning of high quality services by:
meeting our statutory requirements; being clinically led; strengthening collaboration with our partners in East London and the City and local
providers and establishing commissioning arrangements; improving the patient experience across all services; and involving patients, communities and hard to reach groups.
Our Priorities It would be all too easy to say that everything is a priority. In some senses everything is. However, we need to decide where we focus most of our effort in the next few years so that we use the money we have as wisely as possible. Everything NHS organisations do is guided by:
patient safety; patient experience; and effectiveness of care.
What this means is that Waltham Forest CCG, just like every other NHS organisation, is trying to:
prevent people from dying prematurely; enhance the quality of life for people with long-term conditions; help people to recover from episodes of ill health or following injury; ensure people have a positive experience of care; and treat and care for people in a safe environment, and protect them from avoidable harm.
We have agreed 11 commissioning priorities for 2015-16. These are:
care for older people; mental health; diabetes; children and maternity; cancer; integrated commissioning; community health services; quality; urgent care and planned care;
84

Community Participation Strategy 2015 - 2018
17
prescribing; and primary care.
At this point, you might be asking “what exactly is a Clinical Commissioning Group (CCG)”? The Role of CCGs Clinical Commissioning Groups are GP-led organisations which were set up in April 2013 to be responsible for planning and designing local health services in England. There are just over 200 CCGs in England. In Waltham Forest, our CCG covers exactly the same area as Waltham Forest Council (that is, Chingford, Leyton, Leytonstone and Walthamstow). The CCG commissions (or in simple terms, ‘buys’) many health services for the people of Waltham Forest. We commission:
maternity services; most community health services; health services for people with learning disabilities; most mental health services; A&E services; urgent care services; out-of-hours services; elective hospital care (care that is provided at a planned or prearranged time rather than
in response to an emergency); infertility services; rehabilitation services; NHS Continuing Care (care for people who need long-term support as a result of a
disability, accident or illness); some services for children and young people; and end of life care.
In April 2015 we received delegated responsibility for commissioning services. We are not responsible for commissioning most specialist healthcare or work carried out by dentists, pharmacists (chemists) and opticians; this is currently the responsibility of NHS England. We also do not manage public health, as this is managed by Waltham Forest Council. Our Clinical Commissioning Group is a membership organisation and all of the GP practices in Waltham Forest are members of the CCG. We have a Governing Body, responsible for running the CCG and a small staff team. Our Governing Body includes GPs, a hospital doctor, a nurse, lay members, senior members from Public Health and Waltham Forest Council, and our senior staff. All Clinical Commissioning Groups are overseen by NHS England. You can find out more about NHS England at: www.england.nhs.uk Boards have been set up to make sure that CCGs meet the needs of local people. Health and Wellbeing Boards bring together Clinical Commissioning Groups and the local Council to understand the health, social and wellbeing needs of its community. You can find out more about the Waltham Forest Health and Wellbeing Board at: www.walthamforest.gov.uk. Our Community Waltham Forest is a diverse place, with people from all parts of the world, many of whom have rich cultural heritage. We have just fewer than 260,000 people, and a relatively young population (almost 1 in 5 of the people who live here are under 20 years of age) compared with other areas. Our population is also growing and the number of children and older people is expected to increase significantly in the next few years. Our population is also fairly mobile, with people moving in and out of the area. We are quite a deprived area (the 15th most deprived Local Authority in England) although deprivation varies from area to area.
85

Community Participation Strategy 2015 - 2018
18
Our Health Needs We have a lot of challenges to improve the health of people living in Waltham Forest. We know that we have higher than average death rates for cancer, cardiovascular disease (heart attack and stroke) and asthma. Also more people in the area we serve have diabetes and mental health disorders than in many other areas of England. All too many people end up in hospital in an emergency because they have a chronic condition or mental health issues or problems with alcohol. We also know that a significant number of patients are dissatisfied with aspects of hospital care and access to GP services. All of this presents us with a very real challenge. We know that we need to improve the coordination of care for the elderly and people with long term conditions. We also need to prevent people being admitted to hospital when they could be cared for more effectively in their own home. We need to improve the care of people with cancer and get survival rates up to the national level. The care people receive when they are in the community needs to be better than it is at present and we need to get to a position where most patients are very positive about the health care they receive in Waltham Forest. None of this will be easy, particularly as we have limited funds and we will need to make some savings in the next few years in order to balance our budget. We want you to help us make the decisions that are right for our community. If you want to find out more about the health needs of the local community in Waltham Forest, you can find information about the most recent Joint Strategic Needs Assessment (JSNA) here: www.walthamforest.gov.uk/documents/wf-jsna2013.doc
86

Highlights [Performance and Quality Committee] [September 2015]
Item 6.1
Committee Minutes
Performance and Quality Committee September 2015
From Dr Dinesh Kapoor, Clinical Director Quality and Performance -WFCCG
Key highlights
Chair’s Report
The Pathology Task and Finish group established July 2015 following concerns raised to remain in place till key metric of 80% of practices are using Tquest is achieved.
Work is ongoing relating to the glaucoma report recommendations to have a triage
for ophthalmic services and feedback of the eye treatment centre. These workstreams will be combined and is recognised these will reduce A&E admissions.
Cancer Services
Macmillan nurse in post since July 2015 The CCG have written to Barts Health Trust about endoscopy and 2 week waits. 15 practices signed up to the bowel screening pilot. The CCG requested full
patient prior notification lists, response inconclusive so to be added to the risk register.
There is a risk that the bowel screening target would not be met, mitigation in place and for review.
2 week wait times being met, challenges relate to 62 day waits and remedial action plan produced by Barts Health for sign off at the Contract Review Group.
Performance and Quality scorecard
Only 1 practice provided feedback of the pilot dashboard. Medium and high risk areas were highlighted to the committee. 62 day cancer target is high risk. Cardiology shows large increase in patient referrals. Performance notice sent to NELFT relating to District Nursing waiting times and
remedial action plan in place. 52 week wait RTT issues. FFT score improved since April and doubled since July 15.
87

Highlights [Performance and Quality Committee] [September 2015]
Patient Experience 3 quality visits undertaken at Whipps Cross and feedback provided to the CQR OA
meeting; Bracken Ward No significant concerns, good leadership and patients complimentary of the care received. Blackthorn Ward A number of quality concerns noted. Lack of a ward manager and leadership, 5 patients acquired MRSA, one patient unhappy with care. The issues were escalated on the day. B3 Ward Well managed ward with no significant issues noted.
The Gold Standard Charter was launched 7 July 2015 Quality
The findings of the CQC visit to Homerton Maternity unit showed it to be inadequate and 3 warning notices issued. An action plan is in place and a risk summit will be held with City and Hackney CCG and NHSE at the end of September. It was suggested this would be a good time for alignment with the TST strategy.
The Reaching out East and CCG joint project ran from November 2014 to March
2015 and focused on diabetes. Concerns noted; access of GP surgeries for disabled patients; short appointment times and lack of information about their medication. Key recommendations re communications; literature needs to be widely available in a variety of languages, education and training.
Safeguarding
The deep dive requirements have been established. The designated nurse safeguarding children is a member of the LBWF Strategic
Think Families Group. The launch of the Think Family Safeguarding project is on 30 November.
MCA and DOLs training bid has been secured and training was held for 290 staff. Mandatory Prevent training has been attended so far by 40 staff.
Social Action for Health has been commissioned to do lead on a specific Voice of the Child project. An event will be held at the Town Hall on 3 November to launch the project.
There are 3 ongoing serious case reviews. Work from the lessons learnt from the cases will be taken to a conference to be held in January.
The Clinical Lead for Safeguarding Children has been appointed and will start in November.
88

Performance and Quality Committee Meeting
Date: Wednesday 9 September 2015
Time: 10.00am – 12.00pm
Venue: Boardroom, Kirkdale House, Leytonstone
Chair: Dinesh Kapoor (DK)
Attendees: Les Borrett (LB)
Kate Brintworth (KB)
James Driver (JD)
Carl Edmonds (CE)
Emily Grundy (EG)
Kelvin Hankins (KH)
Anna Jones (AJ)
Naheed Khan-Lodhi (NKL)
Tony Lawlor (TL)
Deirdre Malone (DM)
Tonia Myers (TM)
Enrico Panizzo (EP)
Helen Davenport (HD)
Apologies:
Agenda items
1. Welcome and apologies DK
Apologies were noted as above.
2. Declaration of interest register DK
There was no conflict of interests declared.
3. Minutes of last meeting
The minutes were agreed as an accurate record of the meeting held 8 July 2015
Actions outstanding from previous meeting / Matters Arising Deadline Action
1. HD confirmed that there will be a national NHS staff survey but a date has not been confirmed, an internal survey has been sent out to all staff. Item closed.
2. It was confirmed that the CCG had written to Barts Health, who had apologised for the issues around phlebotomy and not implementing the CCG’s plans. A meeting with BH next week is organised to look at the business case and plan for implementation. If the outcome of the meeting does not offer assurance then re- procurement will take place. CE met with Healthwatch who are reviewing patient experiences with phlebotomy, and DM will report
14 Oct
DM
89

Meeting minutes Performance and Quality Committee 9 September 2015
Page 2 of 7
findings of the review carried out by Healthwatch at the next P&Q meeting on 7 October.
3. Cerner issues and pathology issues have been taken up and progressed well at the Pathology Task and Finish group. Item closed
4. The Primary Care Commissioning Committee agreed to stay with the metric for the Friends and Family test, but with work currently ongoing will continue to increase the number of responses. There were increases in responses in month 3, and month 4 data is being collected and will discuss the possibility of taking FFT to locality meetings. Item closed
4. Chair’s Report Chair
The Chair informed the Committee that the Pathology Task and Finish Group have been established since 15 July. The main discussion on the 28 August meeting focused mainly on Cerner and Tquest issues. It seems that only 10% of practices are using Tquest and it was agreed that communications would be sent to increase take up, Pathology T&F group meetings would continue until take up is 80%. Red top bottles are not to be used for specimens, this was confirmed.
Papers are awaited from Pathology advising about the usefulness and appropriateness of various tests. These will be communicated to GPs.
Eye treatment centre feedback on the bulletin for GPs has been forwarded to Anwar Khan for comment, and will be rolled out to GPs before the next Clinical Forum meeting on 16 September. CE is also working on the recommendations from a report looking at glaucoma services, and on having a triage for eye services. There is a need to ensure both pieces of work are connected. It was recognised the treatment centre will reduce admissions in A&E for eye problems.
4.1 ACTION:
DM to liaise with Zoe Hooper, to understand what the communications have been with GPs relating to the changes to the eye services.
It was discussed that there are issues with radiology results as GPs are not clear about what they mean. A direct email advice line would be helpful and this was requested at the last Clinical Forum meeting. A formal request should be submitted to the Clinical Forum and added to the next agenda on 16 September. If there is no satisfactory response then the P&Q Committee will need to be informed.
4.2 ACTION:
DK/TM to take Radiology advice line request to Clinical Forum meeting on 16 September.
DM
DK/TM
90

Meeting minutes Performance and Quality Committee 9 September 2015
Page 3 of 7
5. Cancer Services Update JD/TL
5.1
Cancer Services Update The Committee heard that the Macmillan GP has been in post since July. The CCG has written to BH Trust about endoscopy capacity and 2 week waits but a response has not been received. Issues with lung pathway are more around referral processes rather than with screening. Public Health have been invited to provide an update. 15 practices have signed up to the bowel screening pilot which was launched at the start of August. Work will be done to increase up take. The CCG have written to the head of the bowel cancer screening programme asking for full patient prior notifications lists, however the response received was inconclusive. HD requested this be added to the risk register as a governance issue. NKL confirmed the biggest risk was that the bowel screening target would not be met. Mitigation steps taken were outlined; mailshots were sent to practices setting out the advantages of bowel screening, and the alternatives. A meeting was held with clinical leads that will target practices to get a good uptake in September. The Macmillan GP was to have made a presentation at the locality meetings but the item was stood down. A presentation will be made to GPs and other attendees of the AGM on 10 September by a facilitator from Cancer UK, and at next month’s locality meetings. He will also visit practices to offer support. It was confirmed that more administrative resource would be required. 5.1 ACTION:
JD to ensure that the risk relating to the two week wait referral for lung pathway is added to the risk register.
JD
5.2
Cancer Review of Acute Services A presentation of cancer services at BH and its key messages was presented. The first section of the report outlines performance information, policy information around common cancers commissioned by the CCG, and work being done to improve quality and performance across WEL. The 2 cancer waiting measures, the 2 week cancer wait, and the 62 days GP pathway were discussed. The 2 week wait times are being met. The challenge relates to the 62 days waits both regionally and nationally. Remedial action plans are drawn up, and this will be signed off at a meeting of the Contract Review Group later in the week. A national cancer peer review programme flagged up a number of issues but there has not been a forum where these can be taken up. There are locality based Clinical Quality Review Meetings (CQRMs) where they are being addressed. TL went through the issue with common cancers such as lung and informed the Committee that cancer will be discussed at the next Medical Senate meeting. It was confirmed that everything possible has been done to meet the 62 day target which hasn’t been met for 16 months. NKL confirmed however that patients are having follow up treatment but the difficulty is of transferring patient information to different hospitals. It is therefore necessary to recognise that the issue is not with WX hospital.
91

Meeting minutes Performance and Quality Committee 9 September 2015
Page 4 of 7
5.2 ACTION: HD requested that JD and TL chronologically record all actions taken by CCG. HD emphasised the importance of the CCG having an accurate audit trail of actions and mitigation. HD to liaise with JD and TL about the detail of this work.
HD/JD/TL
6. Public Health – Scorecard Update EG
The committee was updated on the key changes with the scorecard. Only 1 practice responded to the email to clinical directors’ practices about dashboard testing.
Still awaiting data from NELFT and from NHSE which will be reported to P&Q meeting next month. CE confirmed that the dashboard will be taken to locality meetings every 3 months.
7. Patient Experience Update DM
It was confirmed that the Gold Standard Charter was launched on 7 July at the Waltham Forest Nursing Conference, and has been rolled out across the borough.
A joint nursing and pharmacy review of Healthlands in the Chingford locality was undertaken to ascertain whether the recommendations made at the previous visit in May were followed through. There is a strong process in place with regards to pharmacy prescriptions, however there was no system of monitoring stock and there were discrepancies. The medicines management policy needs to be updated to reflect changes. A large number of nutritional supplements are stored and distributed unnecessarily, this needs to be monitored as they should only be given by prescription. Training has been offered but declined due to lack of time.
3 quality assurance visits have been made at WX and comments noted below;
Bracken Ward
Had strong leadership and was fully staffed. Skin assessments and nutritional charts were updated. Patients were complimentary of the care they were receiving; they did
however say that the menu was repetitive. Staff were complimentary about senior staff visits and it was noted
that since the special measures were put in place there have been significant improvements.
Blackthorn Ward
The ward does not have a ward manager and lacked leadership. 5 patients acquired MRSA. One patient was extremely unhappy, his daughter was bringing in
food, and he was dehydrated. Staff were unaware of this issue amongst others. DM escalated this issue, and the ward will be revisited.
B3 Ward
Was visited in May and was noted to be well managed. Measures at this visit were found to be maintained.
92

Meeting minutes Performance and Quality Committee 9 September 2015
Page 5 of 7
Highlights of the above 3 visits will be taken to the CQRM and Oversight and Assurance meetings.
7.1 ACTION:
To feedback to the CQRM and Oversight and Assurance meetings the findings of Quality Assurance visits completed.
A report by Healthwatch highlighted failings on hospital discharge, which the internal discharge team is looking into.
The vacant post for Patient Experience and GP Alerts is expected to be appointed to shortly.
HD
8. Performance EP
The medium and high risk areas of the performance report were highlighted to the Committee, including:-
IAPT – Referral issues with this indicator. NELFT have a new trajectory which will help to meet the target. There is a data quality risk on this target.
The 62 day cancer target is high risk, this has been discussed above. Cardiology, there are large increases in patients referred for
appointments. CE has met with Dr Syed Ali regarding the diabetes pilot launched this
month. There is concern that it is the responsibility of the GPs to refer patients. It seems that GPs were not aware of any issues with diabetes pilot, although it was questioned why a consent form needs to be completed.
Dr Ali has not received a response from Dr Raj Amersey about cardiology and this has been added to the risk register. Assistance offered by HD if further assistance is required.
8.1 ACTION:
Failure of BH to respond to emails requesting advice not being responded to by BH to be raised at the Clinical Forum.
A performance notice has been sent to NELFT about district nursing waiting times, and a remedial action plan is in place.
RTT issue remains with more than 52 week waits. There has been some improvement with A&E target; however there
are ongoing issues with PELC. It was reported that the FFT Score has improved since April and has
more than doubled since June.
8.2 ACTION:
EP was requested to produce a report highlighting what is being done to mitigate risks, detailing the person responsible for actions and a timeframe.
DK/TM
EP
93

Meeting minutes Performance and Quality Committee 9 September 2015
Page 6 of 7
9. Quality NA/AJ/KB/DM/
9.1
NELFT Crisis Care
This item has been deferred to the next meeting in October. Action NA
9.2
Clinical Governance Final Report The report was circulated for information.
9.3
Think Family Safeguarding The Committee received a progress report for Think Family Safeguarding. The Designated Nurse Safeguarding Children informed the members that she is a member of the LBWF Strategic Think Families Group. The launch of this project is on 30 November. Local Safeguarding Children’s and Adults wards in Waltham Forest are both chaired by the same person.
MCA and DOLs training bid has been secured and training was held by 290 staff. Mandatory Prevent training has been attended so far by 40 staff, and a final session is planned shortly.
Capturing the Voice of Children and Young People is imperative to informing commissioning intentions. Social Action for Health have been commissioned to do lead on a specific Voice of the Child project. An event will be held at the Town Hall on 3 November to launch the project.
Serious case reviews, there are 3 ongoing cases, 1 case will be published. Work from the lessons learnt from the cases will be taken to a conference to be held in January.
The report was noted.
9.4
CQC Homerton Maternity Unit The Head of Maternity Commissioning across the 7 CCGs presented a report outlining the outcome of the CQC visit to the Homerton Maternity unit. This was triggered as a result of 5 maternal deaths from July 2013 to January 2015. The findings were inadequate, and 3 warning notices issued. An action plan is in place. A risk summit will be held with City and Hackney CCG and NHSE at the end of September involving NHSE. It was suggested this would be a good time for alignment with the TST strategy. KB requested some input around the Homerton being aligned with TST. KH will attend the alliance meeting. 9.4 ACTION: The committee requested that KB provides an update report relating to the Homerton Maternity Unit CQC Report in December 2015. KH informed the Committee that he has asked for regular updates from C&H CCG on action plans and progress.
KB
9.5
Reaching Out East The Committee were informed that the Reaching out East and CCG joint project ran from November 2014 to March 2015, and focused on diabetes. Access of GP surgeries was a concern for disabled patients. Other concerns were the amount of time GPs gave them, and lack of information
94

Meeting minutes Performance and Quality Committee 9 September 2015
Page 7 of 7
about their medication. Black and ethnic minority focus groups were held; Google translate link provides issues with language problems. Experiences of LGBT people were looked at and it was recognised these need to be addressed. Key recommendations listed included communications, literature needs to be widely available in a variety of languages, education and training. The report will be taken to the Primary Care Development Committee on 16 September. TM stressed that the language should be kept simple as some patients have literacy issues. 9.5 ACTION: The integrated governance framework requires updating to reflect reporting lines.
DM
9.6 Deep Dive Review for Safeguarding HD informed the meeting that the deep dive requirements have been established. It was confirmed that the family with 3 children from Waltham Forest who were going to Syria are safe and being looked after 9.6 ACTION: HD recommended that a representative from Medicines Management be invited to future meetings. Proposal agreed.
HD
10. A.O.B All
HD recommended that a representative from Medicines Management be invited to future meetings. Proposal agreed.
All
Details of next meeting: Date: 14 October 2015
Time: 10.00am – 12.00 noon
Venue: Boardroom Kirkdale House
95

Highlights [Planning and Innovation Committee] [September 2015]
Item 6.2
Committee Minutes
Planning and Innovation Committee – September 2015
From Alan Wells, Chair of the Committee - WFCCG
Key highlights
Highlights of the September 2015 meeting are summarised below: 1. Health and Well Being Strategy
The Committee was presented with a first draft of the HWB Strategy which is being co-authored by the CCG and LA.
2. Weight Management Tender
The commissioning of the tier 2 weight management service had been stopped and other options are being looked at. LA are interested in procuring tier 2 service but there is no tier 3 service. It is to be noted that with the lack of tier 3, patients cannot be referred to tier 4.
3. 111 Service
111 and OOH service has been paused nationally. Discussions have taken place locally on re-procurement. It has been proposed that the 7 CCGs would commence procurement for a 111 service as NHSE would not allow a single CCG to do this. The final proposal will be signed off by the Governing Body.
4. Utilisation Management The utilisation management project plan was presented. Further work would be carried out, 3 key work streams are: a discharge to assess programme, developing a process to get to a trusted assessor role, and the third is where acute acerbations are able to be responded to. A business case will be brought to the committee in December/January.
5. Anticoagulation Planned changes to the provision of anticoagulation services in WF and the benefits of the pilot were discussed. There are 2 phases to the pilot. The business case was approved and will be taken to other relevant committees for approval.
6. Early Intervention in psychosis / Crisis Service The members were advised that there are new national requirements for the CCG to meet the standards for EIP Services and Crisis care. Both of the business cases were approved.
7. TB DOT Service The case to gain support for the DOT service for patients with TB in the community was presented. There is a proposal for level 3 for patients to be observed by a pharmacist under the care of Barts Health. Public health data shows that 10 patients would fit this criteria.
96

Highlights [Planning and Innovation Committee] [September 2015]
8. Homeless Focus Group Report
The Homeless report by Healthwatch and its recommendations was discussed. A response to the recommendations in the report from Healthwatch has been drafted and will be taken to the Primary Care Commissioning Committee.
9. MSK Pathway Re-Design 30% of GP consultations are for MSK, and services are fragmented. Engagement with patients raised single point of access to cut down confusion for patients.
97

PLANNING AND INNOVATION COMMITTEE Notes of Meeting held on 9 September 2015
Chair: Alan Wells (AW)
Attendees:
Ian Clay (IC) Mayank Shah (MS) Dinesh Kapoor (DK) Deirdre Malone (DM) John Samuel (JS) Abdul Sheikh (AS)
Caroline Gilmartin (CG) Sharon Yepes-Mora (SYM)
Anwar Khan (AK) Nuzhat Anjum (NA) Carl Edmonds (CE) In Attendance: Aysha Patel (AP)
James Driver (JD)
Apologies: Jane Mehta (JM) Tonia Myers (TM)
Syed Ali (SA) Naheed Khan-Lodhi (NKL)
Item Summary / Actions Action 1 Apologies The apologies were noted as above.
2 Declarations of Interest MS declared an interest in the MSK Review item as he is the Chair of East 17,
and would be leaving the meeting for this item.
3 Minutes of the last meeting / Matters Arising Corrections to the minutes of the last meeting: DM was present at the meeting
and AS had sent apologies. The minutes of the last meeting were agreed with the above corrections. There were no matters arising.
4 Health and Well Being Strategy SYM informed the meeting that the LA is refreshing the HWB Strategy and this is
being co-authored by the CCG. SYM presented a summary to the Committee and the first draft is due to be available to share in the next couple of days. The three big ambitions in the strategy are the Best start in life, Healthy longer happy lives and Thriving Maturity. There are three cross cutting themes, Service development, Community development and Resilience in equalities and equity. Comments on the draft will be requested by 23 September, and a soft launch will take place when Duncan Selby, CE of Public Health England, visits Waltham Forest. The final document will be signed off by the HWBB in December. AK informed the meeting that he had met with Andrew Taylor and had been informed that the relevant clinical directors were involved with the 3 ambitions and asked for clarification. It was confirmed however that the clinical leads would be contacted for their involvement. The HWB Summary was noted.
98

5 Weight Management Tender JD informed the Committee on the progress of the weight management tender
and informed the Committee that the Local Authority Strategic Procurement Board had stopped the commissioning of the tier 2 service and are looking at other options. LA are interested in procuring tier 2 service but there is no tier 3 service. It is to be noted that with the lack of tier 3, patients cannot be referred to tier 4. The Committee noted the progress report.
6 111 Service CG presented the report to the committee and informed them that the 111 and
OOH service has been paused nationally. Discussions have taken place locally on re-procurement. The North East London Advisory Group proposed that the 7 CCGs would commence procurement for a 111 service as NHSE would not allow a single CCG to do this. The final proposal will be signed off by the Governing Body. The Committee were happy to support the proposal.
7 Utilisation Management CG updated the committee on work done around utilisation management. A
project plan was included in the report. Further work would be carried out, 3 key work streams are: a discharge to assess programme, developing a process to get to a trusted assessor role, and the third is where acute acerbations are able to be responded to. A business case will be brought to the committee in December/January. The report was noted.
8 Business Cases 8i Anticoagulation
AP reported on the planned changes to the provision of anticoagulation services in WF. Patients on Warfarin are in need of regular monitoring and this is currently provided by nine community providers. AP took members through the pathway. Current provision dates back from an SLA has been in place since 2008. There are issues with external quality assurance, lack of information sharing across pathways etc. There have been changes to NICE guidance, including the introduction of NOACs, an alternative to warfarin which has impacted on activity levels. Activity at Whipps Cross decreased as it has in the community. AP went through the benefits of the pilot. There are 2 phases to the pilot and the business case will be taken to other relevant committees for approval. AS raised concerns regarding the plans for the pilot and suggested there had been a deviation from the concept of allowing practices to provide the service. Discussions took place which highlighted that GP practices could bid should they wish to do so when the pilot is procured, but the CCG would only be commissioning one prime provider to deliver the service. AS agreed with the clinical model but had reservations about the business case. These were noted. The Committee agreed to approve the Business case.
99

8ii / 8iii
Early Intervention in psychosis / Crisis Service NA presented 2 business cases for the Committee to note and agree. NA advised the members that there are new national requirements for the CCG to meet the standards for EIP Services and Crisis care. There will be new waiting time standards from Referral to Treatment (RTT) which will be implemented in April 2016. However, CCG has received a notification that these standards will be monitored from November 2015 in shadow form. CCG commissioner has been working closely with NELFT to draw up a Business case and lots of discussion has taken up involving the finance team to come up with the model. A comprehensive monitoring template will be drawn to check the progress of the project and improvements in the service. Crisis care concordat plan was signed off by all partner agencies including WF CCG. There are clear areas identified for improvement. The services are provided jointly with BHR boroughs and they are taking a CQUIN approach and considering the business case as well. The recommended option is Option 2 in the Business case The members agreed both the Business cases.
8iv
TB DOT Service AO presented the case to gain support for the DOT service for patients with TB in the community. AO informed the Committee that problems arise with patients with poor adherence with medication for 6 months. There is a proposal for level 3 for patients to be observed by a pharmacist under the care of Barts Health. Public health data shows that 10 patients would fit this criteria. Pharmacists currently providing substance misuse service would be providing the DOT service. Follow up appointments will remain. After a discussion the Committee were happy to approve the proposal.
9 Homeless Focus Group Report CG presented the Homeless report by Healthwatch and its recommendations to
the meeting. A response to the recommendations in the report from Healthwatch has been drafted. It was suggested that it would be helpful if practices were allocated for the homeless rather that for them to be able to go to any practice. The report will be taken to the Primary Care Commissioning Committee for further discussion. The report was noted.
10 MSK Pathway Re-Design MS left the meeting for this item as he had declared an interest as he is the Chair
of East 17, a provider of MSK services. CE presented the report to the Committee and informed the meeting that 30% of GP consultations are for MSK, and services are fragmented. Engagement with patients raised single point of access to cut down confusion for patients. It was confirmed that Kam Seera is the clinical director for MSK. JS requested the addition of mental health into the project/ business case. A discussion followed on what ought to be included in the business case.
100

AS asked CE to ask Kam to get in touch with AS re adding mental health and with SA re rheumatology. The report was noted.
CE
11 AOB CG informed the meeting that this would be her last meeting as she would be
leaving the organisation shortly. The Chair and members of the Committee thanked CG for all her work and wished her well for the future.
12 Date of next meeting Date of the next meeting: - 14 October 4pm – 6pm
101

Highlight [Finance & QIPP Committee] [September 2015]
Item 6.3
Committee Minutes
Finance and QIPP Committee – September 2015
From Alan Wells, Chair of the Committee - WFCCG
Key highlights
The Committee received the month 5 (August) Finance report forecasting achievement of the planned surplus of £8.6 million. Risks to delivery and mitigation was discussed.
The Committee reviewed the month 5 QIPP performance report.
The Committee approved the proposals for 2015/16 non-recurrent funding schemes to pump prime projects that supported the delivery of CCG targets and key programme objectives.
The Committee received an update on the prescribing budget which showed that QIPP is delivering according to plan. There is currently a forecast underspend on the prescribing budget and cost pressures expected later in 2015/16 were noted. The mental health investment proposals for crisis support and early intervention in psychosis were approved.
102

1
Meeting Finance and QIPP Committee
Date and time 16 September 2015
Board Room , Kirkdale House
12.30-2.00pm
Chair Alan Wells
Attendees: Apologies: In attendance:
Les Borrett (LB), Sharon Yepes-Mora (SYM), Kelvin Hankins (KS), Ian Clay (IC), Enrico Panizzo, Dr. Abdul Sheikh, Dr. Syed Ali, Dr. Dinesh Kapoor, Jane Mehta Nuzhat Anjum, Ada Onyeagwara
Action Points
Agenda item Summary and Action Who
1. Notes of last meeting
The minutes of the last meeting were agreed as accurate.
2. Matters Arising There were no matters arising.
3. Finance Report The committee was asked to note the financial position at the end of August and to note that the CCG is forecasting that it will achieve the planned surplus of £8.6 million however there are risks to this position.
LB ran through key risks and mitigations as at M5. The M4 SLAM claim from Barts has been risk assessed and we are projecting a full year risk of £3.1 million. Based on M4 SLAM claims received from associate providers we are now projecting a £3.2 million risk. WF CCG have reviewed our 2015/16 QIPP schemes and applied risk ratings. The CCG will be submitting a summary primary care QIPP plan to NHSE at the end of September which could result in accessing additional £0.1 million of non-recurrent resource.
4. QIPP report EP took the committee through the main points.
Overall forecast remains at 90% achievement NELEC procurement has been delayed due to
investigation by Monitor. No savings expected in 2015/16. Delays and/or underperformance reported for: Continuing
Healthcare, Integrated Care for Children, Sickle Cell, Diabetes, Metropolitan and the Cardiac Pathway
103

Page 2 of 2
Medicines Management savings on track. Respiratory medication reviews commenced
Slightly improved projections for primary care received from NHSE reflecting list maintenance and clinical waste contract.
GP Extended Access pilot in operation across three hubs. Falls contract awarded to NELFT and new service
expected for 1 October 2015.
5. Prescribing Update
AO presented a prescribing update to inform the committee on the recommendations from previous report and update the committee on the prescribing budget. Key messages: QIPP is delivering according to plan. There is still further work required on the respiratory indicator to release further savings. Significant costs have been avoided by the CCG due to the successful challenge by the Medicines Management team of some charges by acute providers as reported via SLAM. Practice support pharmacists are working with the overspending practices, to help reduce their forecast overspend. There is currently a forecast underspend on the prescribing budget, however there are cost pressures expected in the latter part of the year.
6. Mental Health Business Cases
NA ran through the investment proposals for crisis support and early intervention in psychosis indicating that both models had been approved by the Planning and Innovation Committee. Both cases for investment were approved.
7. Date of next meeting
21st October 2015
104

Highlights [IT Committee minutes] [September 2015]
Item 6.4
Committee Minutes
IT Committee - September 2015
From Dr Mayank Shah, Chair of the IT Committee - WFCCG
Key highlights
Monthly Review of Connectedness Criteria
The Committee agreed that a paper putting forward a recommendation should go to the Governing Body.
Progress that TPP are making with the 4 connectedness criteria were discussed. As of today it was noted that there is no production tested solution available to meet any of the 4 criteria.
The SystmOne user group have written to the IT committee requesting an extension for the connectedness criteria decision. It was agreed that there would have to be commitment from the user group that if after the agreed period the tests had not been met that the deal is that they agree to move.
Paperless Update
A spreadsheet detailing how discharge summaries are received by all practices from each of the departments with each of the Barts and Homerton hospital – as well as PELC at FedNet was shared with the IT Committee. A Red amber green status was applied to each where green is received via DTS so it is received straight into the clinical system’s workflow for processing - Red were fax, post and duplicates.
Discharge summaries must not be sent via fax from 1st Oct 2015
IT Digital Comms & Engagement Plan
Zoe Hooper attended to present the IT Digital Comms & Engagement Plan. It was agreed that there is a need to talk to patients and public and that the CCG
need a strategic approach to do this. IT and digital teams will engage with practices and draft material for the comms
team to finalise. This will be reviewed quarterly Other Updates on Projects & Roll-outs
Emis Web rollout - Now have 34/45 practices on Emis by end of Sept another 3 to
migrate will then have 37/45 leaving 8 SystmOne. Rollout of lab tests – All practices now have access to Tquest, There are issues
with access to Cyberlabs from some practices, feedback from IT audit visits was that some practices are not confident with the training they have received to train the other staff – This is being followed up.
105

Highlights [IT Committee minutes] [September 2015]
SMS IPlato - NHS Mail Service ends 30th September. Signed a contract with iPlato, all practices to sign up and attend training sessions 21/45 signed up, 12/45 installed
MIG / HIE Update – Risk to be raised – Stakeholder engagement significant - 45 GPs Barts Cerner Newham TPP NELFT ELFT. Recommendation that any new contracts for OOH includes the stipulation that the provider must use MIG/HIE
Skype Pilot - 7 practices interested in piloting – Criteria will be applied to select 4.
106

Page 1
IT Committee
Date and time 02.09.2015 14:00-16:00
Venue Board Room, Kirkdale House
Chair Mayank Shah (MS) Clinical Director for IT
Attendees Les Borrett (LB) Director of Financial Strategy, WFCCG Carl Edmonds (CE) Deputy Director of Delivery, WFCCG Luke Readman (LR) Philip Woolley (PW) GP IT Manager Phil Koczan (PK) GP Advisor Clinical Lead for IT (Via Conference call) Nina Worley (NW) Prederi Dinesh Kapoor (DK) Deputy Chair, WFCCG Damien Pearce (DmP) Francis Mulhern (FM) Thaven Chetty (TC) Gary McGuinness (GM) David Pearce (DvP)
Apologies Bhagiyash Shah (BS) Prederi Joan Fratter (JF) Patient representative Richard Griffin (RG) Lay Member
107

Agenda items
1 Welcome and apologies
1.1 Apologies noted as above.
2 Minutes of the Last Meeting and Matters Arising
2.1 Notes agreed to be accurate.
Declarations
None
3 Connectedness Criteria
3.1 The Committee agreed that a paper putting forward a recommendation should go to the Governing Body. Progress that TPP are making with the 4 connectedness criteria were discussed. As of today it was noted that there is no production tested solution available to meet any of the 4 criteria. LB and MS attended a SystmOne user group and received a letter from 7 SystmOne practices. The letter stated that 21% of the WF patient list is looked after by the 7 SystmOne practices. There are 4 criteria remaining which have not been delivered by TPP to date. DK on behalf of the SystmOne user group commented that the connectedness criteria is important but given the speed of development the user group believe it will happen soon regardless of moving to Emis.TPP and the SystmOne user group have requested that the CCG write to Emis and Barts requesting what is a reasonable timescale to delay. It was agreed that there would have to be commitment from the user group that if after the agreed period the tests had not been met that the deal is that they agree to move. The committee requested that a closer eye be kept on progress via a monthly report. PK thinks that there may be an issue with Emis not engaging after speaking to NHS England. PK proposed we work with the NHS England team to have a co-ordinated approach as opposed to a single CCG. PK happy to broker and have a chat with Tracey Granger. LR informed the committee that informatics is going through a rapid development stage and therefore overheads over time are likely to be more than the £200k to move the 7 SystmOne practices. LR also stated that Barts have been pretty clear that they have put in significant effort and are now going to stop. The committee agreed that the best outcome for patients was to share health and care data across providers MS – summarised the options:
108
Option 1 – apply the criteria to finalise the IT strategy. Review the latest TPP progress at the September 2015 IT Committee meeting and make a recommendation based on the 4 criteria above. Based on progress to date, it is unlikely that TPP will have a fully proven IT integration solution available, which is also fully supported, by September 2015. The implication of this is that commercial technology has not developed very far in 18 months and is unlikely to progress significantly in the immediate future. Therefore, to secure the benefits of information sharing for WF patients, WF CCG should progress with the strategy to migrate the remaining SystmOne practices to EMIS Web. The evidence is that even with CCG intervention and support, TPP have not successfully developed integration technology that emulates the quality and functionality of the existing EMIS capability. It is also recommended CCG support to developing SystmOne interoperability – e.g. via current IT consultancy support – ceases so that focus can be given to implementing upgrades to EMIS Web going forward, and that eligibility for pilots for new IT projects etc. will be based on use of Emis Web in future. During discussions an alternative approach was developed whereby: WF CCG defer the decision for a specified period of time, until the November IT Committee
meeting
Gain agreement from the SystmOne user group that if TPP have not fully met all 4 criteria with a commercial quality solution (irrespective of where the fault lies) by the extended timescale that all practices will agree to migrate to Emis Web to go live from the beginning of next financial year
Regular progress reports are provided to the IT Committee members outside of the IT Committee meetings
Extra costs incurred by WF CCG and Barts (in continuing to work with TPP) are funded by WF CCG
TPP are required to provide a project manager to coordinate their work with us and Barts
The Governing Body is made aware of this proposed way forward and asked to delegate the decision to the IT committee to make in the November IT committee (as there is no Governing Body meeting in December)
It should also be noted that the benefits of connectedness, in the long run, could be eroded by the cost and complexities of maintaining multiple solutions for integrating Primary Care with systems of other providers.
Action: MS & LB to reply to the SystmOne user group letter. Requesting agreement to the revised timetable and recommendations by 18th September. Action: response from SystmOne user group to be received by 18/09 in order to feed into GB. Action: BS / NW Update paper for Governing Body devolving decision to IT committee.
4 Paperless Update
4.1 The Committee agree to share data with NELFT It was also agreed to share data with practices prior to locality meetings The committee had a discussion around how can we go about encouraging private hospitals to change the referral process away from Fax
109

Action: DP to check what governance issues around fax are, check what is in GP contract & liaise with LMC to get their view Action: NW to send spreadsheet to all Action: NW to ask LR to raise with Barts issue of duplicates
5 IT Digital Comms & Engagement Plan
5.1 Zoe Hooper attended to present the IT Digital Comms & Engagement Plan.
It was agreed that there is a need to talk to patients and public and that the CCG need a strategic approach to do this.
IT and digital teams will engage with practices and draft material for the comms team to finalise. This will be reviewed quarterly.
Action: ZH to meet with JF in next couple of weeks (and NW) to go through the plan and get JF’s comments
Action: ZH to update regarding decision from the IT committee on SystmOne
Action: ZH to consider how to include feedback loop into plan
Approved to start using
6 IT Strategy Implementation Update
6.1 Emis Web Rollout Now have 34/45 practices on Emis by end of Sept another 3 to migrate will then have 37/45 leaving 8 SystmOne. Rollout of lab tests – pathology
o All practices now have access to Tquest o There are issues with access to Cyberlabs from some practices as the IP addresses
have not been correctly set up in 5 places within Barts o Report from Rachel’s visits that some practices are not confident with the training they
have received to train the other staff o Some initial feedback on usage from Barts but not demonstrating significant usages o Action agreed at IT Implementation group for James Driver to get involved and
coordinate regular meetings (initially weekly) with Ed Keating and Barts – to micro manage with deadlines
o DK chairs Barts Pathology meeting and can feedback there if appropriate
iPlato / SMS
o NHS Mail Service ends 30th September o Signed a contract with iPlato and raised PO o Invited all practices to sign up and attend training sessions (emails to PM and
info in GP newsletter) o 21/45 signed up, 12/45 installed
110

o Training 3rd Sept Leyton / Leytonstone and Walthamstow and 10th Sept Chingford – Follow up training at PM forum 24th Sept
o Deadline for sign up was 31st Aug – still have 24 practices to sign up so re-emailing today to extend sign up to end next week 11/9 and will try to have in place before current service ceases – Also reminder in Sept locality meetings
o Great dashboard for CCG to monitor usage o App is coming Jan o Action: CE to ask Mable to include in GP Newsletter again – add to this month’s
newsletter – Mable to ZH o Action: LB will raise at Chingford locality meeting
MIG / HIE Update o LMC sign off of data sharing expected Dec 14 took till March 2015 o Recommend future data sharing agreements need to engage with LMC earlier and
be firmer with deadlines and escalate further o Risk to be raised – Stakeholder engagement significant - 45 GPs Barts Cerner
Newham TPP NELFT ELFT o Issue Cerner & issue with Emis o Action: JM raise risk that as connectivity expands there will need to be adequate
support at the CCG to manage this. o Action: JM to work with GM and LR to consider how to mitigate risk o 29 practices switched on MIG 2 practices have postponed visits several times o Agreed that if we don’t get anything in the diary for the next week to escalate to MS
to write to 2 practices o Action: JM to query with Cerner why there are only 22 practices linked to HIE when
there are 29 linked to MIG. o Recommend that any new contracts for OOH includes the stipulation that the
provider must use MIG/HIE. Action:JM to speak to Caroline Gilmartin/Enrico Panizzo
o If community CSS services are on RiO then we should consider when this could be included in MIG /HIE – Agreed all future contracts should include a clause that their IT solution works with MIG / HIE at no additional cost to CCG Action CE to raise with Kelvin
7. User Lock
Suggest run a pilot at Crawley Road medical centre and get feedback. The committee agreed to do a pilot.
IT Audit Visits – Initial View
Deferred to October meeting
Next meeting: 21st October 2015 15.00-17.00
111

Highlights [Medicines Management Committee minutes] [September 2015]
Item 6.5
Committee Minutes
Medicines Management Committee Minutes - September 2015
From Dr Mayank Shah, Clinical Director and GP Prescribing Lead - WFCCG
Key highlights
Attached are the minutes of the Medicines Management Committee (MMC) held on 9 September 2015 Key Points for the governing body:
An investment proposal to improve access to end of life medication in Waltham Forest has been approved by the MMC.
The Waltham Forest Antimicrobial Stewardship plan was discussed and agreed by the MMC with a proposal for all clinicians, including the governing body, to become antibiotic guardians.
Issues relating to a local nursing home were again discussed by the MMC and the
RAG rating for this item on the risk register was reviewed.
Controlled drug issues have been raised with NHS England but a response has not been received by the MMC.
112

1
Minutes
Meeting Medicines Management Committee
Date and Time: 9th September 2015, 2pm – 4pm
Venue: Boardrooms B&C, Kirkdale House, 7 Kirkdale Road, E11 1HP
Chair: Dr Mayank Shah
Attendees:
Name Title
Dr. Mayank Shah MS Waltham Forest CCG GP Clinical Director Ada Onyeagwara AO Associate Director, Head of Medicines Management Team for Waltham
Forest Dr. Imran Kazi IK GP Prescribing Lead for Chingford Consortium Dr. Rishav Dhital RD GP Prescribing Lead for Walthamstow Consortium Dr.Thaven Chetty TC GP Prescribing Lead for Leyton/Leytonstone Consortium Dr.Prakash Kawar
PK Local Medical Committees Representative for Waltham Forest
Kay Saini KS Senior Prescribing Advisor, Waltham Forest Medicines Management Team Isaac Otomewo IO Senior Prescribing Advisor, Waltham Forest Medicines Management Team Anisha Sharma AS Prescribing Advisor, Waltham Forest Medicines Management Team Hassan Serghini HS Senior Prescribing Advisor, Waltham Forest Medicines Management Team Natalie McCallam Thomas
NMT Team Administrator, Waltham Forest Medicines Management Team
Deirdre Malone DM Deputy Director of Integrated Governance, Waltham Forest CCG Lynn Snowden LS Senior Commissioning Manager, Waltham Forest CCG Mayur Patel MP Local Pharmaceutical Committee Representative for Waltham Forest
Apologies
Name Title
Helen Davenport HD Director of Nursing, Quality and Governance Carol Greening CG Assistant Director of Clinical Pharmacy Barts Health NHS Trust Carolyn Goss CGo Prescribing Support Dietitian, Waltham Forest Medicines Management
Team Kamaljit Takhar KT Deputy Chief Pharmacist, NELFT CSS Services
113

2
15/09/01 Welcome and apologies
The chair welcomed members to the meeting. Apologies received as above.
15/09/02 Declarations of Interest and Register of committee interest
There were no declarations of interest since the last meeting. Action: MMT to send a reminder email for the outstanding declarations of interest to be returned by the end of Friday 11 September.
15/09/03 Review of previous minutes, action tracker and matters arising
The minutes of the August MMC meeting were approved by the committee as accurate pending minor amendments – ‘Care home’ to be replaced with ‘nursing home’.
Review of Action Tracker MMC142 – CSS service overspend issue is still ongoing. Action: MMC recommend that a formal letter be sent to the CSS service requesting clarification on the reason for the overspend, and what processes have put in place to ensure it doesn’t reoccur. MMC141- Inclusion of an annual audit on all CSS contracts will be considered in the 16/17 contracting rounds, which will begin shortly. Item to remain on the action tracker. MMC138- To be discussed at the meeting under agenda item ‘End of Life business case’. MMC136- NELFT are currently reviewing their direction to administer policy, and are seeking advice from their nursing leads. An update will be given to MMC once the draft has been taken to the NELFT DTG meeting. Action: To request a copy of the draft policy for MMC to review when available. MMC133- Outstanding declarations of Interest to be submitted by the end of Friday 11 September. MMC132- Information regarding emergency supplies of salbutamol inhalers has not been sent out to community pharmacies. LPC to contact the Department of Health for information material. MMC121- LPC to be contacted regarding a meeting with MMT to discuss branded generics. MMC118- Awaiting a response from Barts Health Trust for representation at MMC meetings. Action: MMT to formally write to the Chief Pharmacist at Barts Health to address Trust attendance issues and governance.
15/09/04 NELMMN Update
A meeting was not held in August.
114

3
The next meeting is being held on 10th September and will focus on the future of NELMMN options paper.
15/09/05 JPG Update
The JPG meeting was held on 19th August, and the following key points were highlighted:
Dulaglutide submission – Further discussion was needed, so this was not approved.
Desmopressin and cinacalcet Shared Care Guidelines – Further information has been requested.
Omalizumab for previously treated chronic spontaneous urticaria approved. Asthma Guidelines – This still needs approval, and will be on the JPG agenda in
October. The next meeting is being held on Wednesday 16th September. ACTION: All comments on the JPG agenda/papers to be forwarded to MMC member attending JPG by the end of Friday 11 September.
15/09/06 NELFT Update
A summary of the NELFT Mental Health DTG agenda was given to MMC. MMT to provide an update to MMC at the next meeting. ACTION: All comments on the DTG agenda/papers to be forwarded by the end of Friday 11 September.
15/09/07 Information Governance issues
Risk register The format of the register was reviewed and amended since the last meeting. Monthly trends and how the risks are being managed has now been incorporated. All risks discussed will be rag rated by MMC. MMT will meet with CCG Head of Governance on a monthly basis to ensure the risks on the MMT register are aligned with the CCG’s quality and safety register. Nursing Home An overview of the nursing home was presented to MMC. There are a number of quality and governance issues that need to be addressed, as the recommendations from the last visit have not been implemented. These include ‘PRN’ medication and repeat prescribing, record keeping, prescribing of oral nutritional supplements, staff support and training. MMC agreed that the risk should be rag rated red (likelihood 4 x impact 4 = 16). This will now go to the board assurance framework. Prescribing budget This relates to the overall prescribing budget and cost pressure. Mitigations have been put in place to better control the budget, therefore reducing the likelihood of risk. MMC agreed that the risk should be rag rated amber (likelihood 3 x impact 4 = 12).
115

4
Controlled drugs The current risk should be split into two, one relating to the specific incidents raised at a practice, and the other relating the lack of clarity on role of the CCG in the management of CDs, which is a pan London issue. MMC agreed:
Risk 1: Specific incidents at a practice – RAG rating should remain the same until we have further information from the prescribing lead and practice support pharmacist who raised the issue.
Risk 2: CCG’s responsibilities with CDs - Should be rag rated amber (likelihood 3 x impact 4 = 12). This will now go to the board assurance framework.
Action: MMT to escalade issue regarding the lack of response from NHS England in relation to controlled drugs. Action: Controlled drugs to be raised at the GP prescribing forums in October.
15/09/08 End of life business case
Two documents were submitted to MMC for approval. Investment proposal for improving access to end of life medication in Waltham Forest - This will be added to the CCG’s end of life strategy in order for it to be commissioned. The LPC has suggested additional annual retention fee funding for pharmacists who stock the extra medication, as they need to be stored in a secure unit. Action: LPC to respond to MMT regarding the additional funding for CD storage units and training for community pharmacists. Good practice guidance for CD disposal and destruction for the community teams The guidance has also been sighted by NELFT and the palliative care team at Barts Health, and can also be used by healthcare professionals. A process is needed for safely disposing of CDs by community teams in exceptional circumstances. Relatives/carers need to be made aware that CDs remain the property of the patient after death, and that retaining the drugs has legal implications. Any issues arising with disposal of CDs from patient homes returned should be escalated to NHS England. MMC agreed both proposals.
15/09/09 Repeat Prescribing Policy
MMT are holding two workshops on 16th and 23rd September to provide training to GP practice staff on repeat prescribing. The structure and content of the workshops were discussed, and some of the hand-outs were reviewed. As part of the prescribing incentive scheme, GPs will be provided with a repeat prescribing policy template to adapt for their practices, which will need to be submitted to the MMT by 31st March 2016. Action:
1. Repeat prescribing checklist - Change quantity of drugs to issue from 28 days to 56 days
2. Repeat prescribing request slip - Change the drug name listed Action: To circulate the updated Repeat Prescribing Policy to MMC when complete for comments prior to the workshop.
116

5
15/09/10 Antimicrobial Stewardship plan
An update was given to MMC on the work being carried out on antimicrobial stewardship. NHS England, Public Health England and Health Education England have issued a Patient Safety Alert that encourages the use of the RCGP TARGET Toolkit, which Waltham Forest MMT have been promoting of the course of the last year. The MMT will continue to raise awareness of the RCGP TARGET Toolkit to encourage wider use by practices. MMT will be reviewing the recently issued NICE guideline on antimicrobial stewardship, with the aim of producing an antimicrobial stewardship plan that will also support achievement of the quality premium for NHS England. Additionally, the MMT will be encouraging clinicians, clinical Governing Body members and prescribing leads to become Antibiotic Guardians. The MMC were informed that locums and out of hours providers are high prescribers of antibiotics within the borough. People from overseas need to be made aware that antibiotics will not be prescribed on demand. Another suggestion was to make better use of media outlets to highlight the issue and education could be provided to children in schools. Action: MMC members to sign up to become antibiotic guardians.
15/09/11 Alogliptin submission
Three CCGs (Waltham Forest, Newham and Tower Hamlets) will be submitting a request to include alogliptin in the formulary for primary care. It is cost effective and licensed for dual and triple therapy. This was discussed by MMC. Action: Committee agreed with the recommendation to add alogliptin to the formulary, but with no specific recommendation. To be monitored over the next 3-6 months, due to the limited data and safety evidence available.
15/09/12 Insulin pen needle switch SOP
It was proposed that a switch to more cost effective pen needles will be carried out by GPs in individual practices with the support of Practice Support Pharmacists (PSPs) where possible. A standard operating procedure has been produced to assist with the switch and a letter informing patients of the change will also be made available. PSPs will identify the practices with the highest spend for support. It was suggested that rather than GPs carrying these switches, local community pharmacists could support with the switch. ACTION: To discuss further with the LPC and establish what assistance can be provided. The LPC and MMT will need to agree a process.
15/09/13 Finance Report
ScriptSwitch update The report was summarised and discussed by the Committee. Some of the key points in the summary were that uptake and acceptance of ScriptSwitch messages had reduced in the month of August. Drugs used in Overactive Bladder have the highest missed cost saving. MMC discussed prednisolone soluble tablets that have been flagged as a large potential cost saving. It was highlighting that a licensed liquid preparation is available Net savings will be monitored, as they are significantly lower this month than in previous months.
117

6
CSS prescribing data Highlights: The Adult Sickle Cell service did not prescribe any items this month. The Community Specialist Cardiology Service have been prescribing but it is still not clear who the provider of this service. The Dermatology CSS service has been prescribing homeopathic preparations, but Waltham Forest’s policy on this needs clarification. Action: MMT to provide a position statement on homeopathic preparations at the next MMC meeting.
QIPP 15/16 MMT issued the dashboard to all practices last month, and provided guidance on accessing data on NELIE. A reminder will also be circulated.
GP forum feedback No update
Practice Support No update
QIPP 16/17 – Ideas MMT will seek wider comment on the Medicines Optimisation Scheme from GP practices at the October locality meetings
Acute prescribing The minutes of the Barts Health Drug Commissioning meeting were available to MMC for information. The key highlight was that it has been agreed that a biosimilar of Infliximab is to be used for gastrointestinal patients.
15/09/14 Queries
The Prescription Pricing Division (PPD) advised that on a monthly basis of any drugs over £75 that have been prescribed. These are NP8 drugs, which are not listed on the Drug Tariff and therefore are not subject to the normal pricing structure. MMC discussed the list of drugs WF practices had been charged for. ACTION: LPC to provide MMT with a copy of the NP8 drug tariff list. Action: To add a ScriptSwitch message noting that any drug highlighted should prescribed by brand
15/09/15 NICE Update
The Committee reviewed the update
The antimicrobial stewardship is to be reviewed, as agreed by MMC.
118

7
Vedolizumab and Bevacizumab to be provided by the acute trust. Edoxaban is a newly approved oral anticoagulant. To be reviewed by JPG. NICE guidance for diabetes is to be published in October.
15/09/16 LPC Update
No update
15/09/17 LMC Update
No update
15/09/18 AOB
Barts Health Parkinson's Disease Guideline: Clinician input is required before September JPG.
The Annual General Meeting for Waltham Forest CCG is being held on Thursday 10th September at Kirkdale House.
MMT to enquire what involvement the flu committee requires from the GP lead (TH).
Next meeting: Wednesday 14th October 2015
Boardrooms B&C, Kirkdale House, 7 Kirkdale Road, Leytonstone, E11 1HP 2:00 - 4:00pm
119

Highlights [Primary Care Commissioning Committee] [July 2015]
Item 6.6
Committee Minutes
Primary Care Commissioning Committee – July 2015
From Alan Wells, Chair of the Committee - WFCCG
Key highlights
Highlights of the July 2015 meeting are summarised below: 1. MOU Sign-off and Reports
Feedback on the document has been sent and also requested that where NHSE team will provide support, that they also provide recommendations. It was agreed to review the MOU in 6 months.
2. Decision Making 2 types of urgent decisions might need to be made in between main meetings; those that need to be made before the next committee meeting and those within 24 hours. NHSE and CCG officers will make the decision how urgent the issues are. An urgent decision making group will be set up to meet to discuss decisions that cannot wait until the next meeting.
3. NHSE Primary Care Update Report PMS contract review - Waltham Forest has 23 practices with a PMS contract, a review needs to be carried out by the end of March 2016. A meeting will be held on 20 July to go through the PMS review process with WEL CCGs and NHSE.
Primary Care Enhanced Service uptake by practice and coverage - an analysis will be carried out on Enhanced Services.
4. Issues raised by the Primary Care Development sub-Committee NHS Choices was discussed. A link has been sent amendments or additions, as there were concerns about not being able to make amendments to practice details on the website. Patient experience kiosks, careers projects in 15 practices, and digital health strategy to help GPs manage demand were discussed. Also, data procurement looking at extracting primary care data to use it to drive up quality. Video conferencing, NHS mail was discussed. An estates working group in the organisation will be looking at section 106 bids, the HWBB will continue to make approvals. The primary care strategy will be completed in a couple of months.
120

Highlights [Primary Care Commissioning Committee] [July 2015]
5. Risk Register (Primary Care) Primary care risks from the risk register were presented. This item will be added to the agenda as a standing item.
6. AOB Primary Care QIPP Members were informed that it is unclear what the QIPP requirements are for the year, this was noted. Frequency of Meetings Members were informed that meetings will take place bi-monthly in future with urgent meetings arranged if necessary. The next meeting will therefore take place in October.
121

PRIMARY CARE COMMISSIONING COMMITTEE
Notes of Meeting held on 10 July 2015 Board Room
Kirkdale House
Chair: Alan Wells (AW) (Dept) Cllr Ahsan Khan (CAK)
Attendees:
Attracta Asika (AA)
Andrew Taylor (AT)
Bansilai Gurtu (BG)
Les Borrett (LB)
Dinesh Kapoor (DK)
Abdul Sheikh (AS)
In Attendance Jane Mehta (JM)
Apologies Terry Huff (TH)
Anwar Khan (AK)
Jaime Walsh (JW)
Item Summary / Actions
Action
1 Welcome and Apologies The Chair welcomed the members to the meeting of the PCCC.
2 Minutes of the last meeting/Actions
Minutes of the last meeting were agreed. Actions outstanding from the last meeting:
Are refusals by GPs to provide a home visit a breach of contract – AA to update at the next meeting. AA would provide an update at the next meeting.
It was suggested that a confidentiality clause would be signed by all members. David Pearce would consider how this would be managed. This is still outstanding and an update will be provided at the next meeting.
AA
JM/
David Pearce
3 MOU Sign-off and Reports
CE updated the Committee on the MOU which is a guidance document on making primary care decisions. Feedback on the document has been sent and also requested that where NHSE team will provide support, that they also provide recommendations. Steve Gilvin will be writing to NHSE and a copy will be sent to the LMC as requested by BG. AA made a recommendation that the communications team from the CCG and NHSE work together on communications, however it was suggested that one communications team should take responsibility. It was agreed to discuss this and clarify at the next meeting.
AA
122

It was agreed to review the MOU in 6 months.
4 Decision Making Paper
CE presented the paper to the Committee informing them of the 2 types of urgent decisions that might need to be made. Those that need to be made before the next committee meeting and those within 24 hours. NHSE and CCG officers will make the decision how urgent the issues are. An urgent decision making group will be set up to meet to discuss decisions that cannot wait until the next meetings. Meetings will be diarised and stood down if not required. Members will be able to be represented by their deputies if they are unable to attend. It was agreed to add ‘Urgent Decisions’ as a standard item to the agenda. Any issues regarding urgent decisions would also be emailed to the members of the Committee in between meetings. The process would be reviewed in 6 months.
CE
5 NHSE Primary Care Update Report
PMS contract review AA informed the Committee that as Waltham Forest has 23 practices with a PMS contract, a review needs to be carried out by the end of March 2016. NHSE has set up a PMO to lead on the review and an offer will be made to the CCG to accept the offer for the PMO office to lead on the review or to conduct it themselves. It was noted that the review will be negotiated and not imposed. A meeting will be held on 20 July to go through the PMS review process with WEL CCGs and NHSE. It was noted that at this point the CCG had not taken any decision about accepting the proposals. Recommendation was received from the Primary Care Development Committee stating that the Primary Care Commissioning Committee, when undertaking a PMS review, is to consult and negotiate with Waltham Forest PMS GP Group, as was the case with the PCT in the past and NHSE recently. This was discussed and agreed that the WFPMS Group would be consulted and negotiations would take place during the entire process of the review. NHSE will be informed of this decision. Primary Care Enhanced Service uptake by practice and coverage AA went through the paper and informed the members that an analysis will be carried out on Enhanced Services.
CE
6 Issues raised by the Primary Care Development sub-Committee CE explained that there are 2 sets of minutes of the Primary Care Sub Committee
for information. At the 20 May meeting, NHS Choices was discussed. A link has been sent to DK to make amendments or additions, as he had raised concerns about not being able to make amendments to practice details on the website. Patient experience kiosks, careers projects in 15 practices, and digital health strategy to help GPs manage demand were discussed. Also, data procurement looking at extracting primary care data to use it to drive up quality. At the 16 June meeting, a plan to pilot video conferencing was discussed. The end of NHS mail was discussed and alternatives for this. An estates working group in the organisation will be looking at section 106 bids, the HWBB will continue to make approvals. The primary care strategy will be completed in a couple of months. My
123

Self Care Plan was presented by the pharmacist in the Committee. AS acknowledged the hard work done by CE and his team. DK raised homelessness at the last meeting and felt that there ought to be an APMS to take on homeless patients as care is patchy as it stands.
7 Risk Register (Primary Care) CE presented the extracted primary care risks from the risk register. AW
suggested adding this item to the agenda as a standing item, and having the risk register showing trends in risks going up or down.
CE
8 AOB Primary Care QIPP
CE informed the meeting that it is unclear what the QIPP requirements are for the year, this was noted.
Frequency of Meetings
CE informed the members that meetings will take place bi-monthly in future. The next meeting will therefore take place in October. As meetings have been diarised on a monthly basis, meetings now not required for PCCC will be used for Decision making Group meetings (see item 4). Any decisions will be fed back to the PCCC.
Date of the next meeting:
Wednesday 7 October 2015, 3pm-5pm Board Room, Kirkdale House 7 Kirkdale Road, London E11 1HP
124

Summary [SafetyNet Exec (LBWF)] [September 15]
Item 6.7
Committee Minutes
SafetyNet Executive Board (LBWF) – September 2015
From Andrew Taylor & Alastair Macorkindale – London Borough of Waltham Forest
Key highlights
Business Management Report – update on off target violence with injury, higher than desired reoffending rate of young offenders, proposal to tackle open drug market emerging on Hoe Street, and review of KPIs. Stock Take on Gang Programme – progress report updating the Executive on regional and local developments, regional and local (e)-commissioning plans, and community engagement. Think Family – update on forthcoming WFSCB/SAB workshop and system of champions to spread the word and help develop “professional curiosity” across disciplines. Integrated Offender Management – Update on IOM implementation and new sub-regional project to enhance IOM in North/East London, worth £1.4M across 8 boroughs, with Waltham Forest leading for the East. Civil Protection Service: Adoption of the Mass Shelter Plan and agreement of Borough Risk Register. VAWG Update: procurement exercise had covered 4 lots of service provision; DV Refuge, IDVAs, Perpetrators and Community Based Support. A report is being submitted to Deputy Chief Exec for Families for approval of panel’s recommendations. Shortfall in funding for therapeutic interventions for children and young people. Prevent – discussion about plans to engage with partners and communities about the local approach to Prevent in order to improve levels of understanding and buy-in. Safer Neighbourhood Board – update on progress with the successful bids to MOPAC’s Safer Neighbourhood fund and future plans. Forward Plan: Items for discussion at the next meeting include: the Annual Strategic Assessment AOB: The Board noted the on-going reorganisation of the London Community Rehabilitation Company and the impact on engagement at a borough level.
125

Summary [Leyton/Leytonstone Locality minutes] [September 2015]
Item 6.8
Committee Minutes
September – Leyton/Leytonstone Locality Minutes
From Dr Syed Ali, Clinical Director - WFCCG
Key highlights
IT issues Transforming Services Together – Primary Care Strategy MSK engagement CCG Performance reports • QIPP and Borough reports Clinical Director and Board Update:
o Diabetes pilot o New SMS service
126
Summary [Walthamstow Locality minutes] [September 2015]
Item 6.9
Committee Minutes
Walthamstow Locality Minutes – September 2015
From Dr Mayank Shah, Clinical Director - WFCCG
Key highlights
IT issues Transforming Services Together – Primary Care Strategy MSK engagement CCG Performance reports • QIPP and Borough reports Clinical Director and Board Update:
o Diabetes pilot o New SMS service
127

Summary [Leyton/Leytonstone Locality minutes] [September 2015]
Item 6.10
Committee Minutes
Chingford Locality Minutes – September 2015
From Dr Tonia Myers, Clinical Director - WFCCG
Key highlights
• Transforming Services Together – Primary Care Strategy • MSK engagement • CCG Performance reports • QIPP and Borough reports • Clinical Director and Board Update:
o Diabetes pilot o New SMS service
• IT issues
128

Item 8.1
28/10/2015 25/11/2015 27/01/2016 24/02/2016 23/03/2016 25/05/2016 22/06/2016 27/07/2016PART 1GENERAL BUSINESS GENERAL BUSINESS GENERAL BUSINESS GENERAL BUSINESS GENERAL BUSINESS GENERAL BUSINESS GENERAL BUSINESS GENERAL BUSINESS
Chair's update Chair's update Chair's update Chair's update Chair's update Chair's update Chair's update Chair's update
Questions from Members and Public
Questions from Members and Public
Questions from Members and Public
Questions from Members and Public
Questions from Members and Public
Questions from Members and Public
Questions from Members and Public
Questions from Members and Public
GOVERNANCE GOVERNANCE GOVERNANCE GOVERNANCE GOVERNANCE GOVERNANCE GOVERNANCE GOVERNANCEBAF BAF BAF BAF BAF
Co‐Commissioning
Governance Review
PERFORMANCE AND QUALITY
PERFORMANCE AND QUALITY
PERFORMANCE AND QUALITY
PERFORMANCE AND QUALITY
PERFORMANCE AND QUALITY
PERFORMANCE AND QUALITY
PERFORMANCE AND QUALITY
PERFORMANCE AND QUALITY
P&Q Report P&Q Report P&Q Report P&Q Report P&Q Report P&Q Report P&Q Report P&Q ReportChildren's Services RTT
Urgent CareNursing and Midwifery Council Revalidation Primary Care Performance
FINANCE AND QIPP FINANCE AND QIPP FINANCE AND QIPP FINANCE AND QIPP FINANCE AND QIPP FINANCE AND QIPP FINANCE AND QIPP FINANCE AND QIPPFinance Report Finance Report Finance Report Finance Report Finance Report Finance Report Finance Report Finance Report
STRATEGY AND PLANNING
STRATEGY AND PLANNING
STRATEGY AND PLANNING
STRATEGY AND PLANNING
STRATEGY AND PLANNING
STRATEGY AND PLANNING
STRATEGY AND PLANNING
STRATEGY AND PLANNING
WX Estates Strategy Estates Strategy
Communication Strategy
Community Participation Strategy
PART 2
Procurement update Procurement updatePMS Review
129