Meeting Agenda (Open Session) Governing Body Wednesday ...
224
Meeting Agenda (Open Session) Governing Body Wednesday 04 August 2021 (9:00 – 10:50) Virtual meeting via Zoom Time Item Presenter Reference 09.00 Introductory Items 1. Welcome, introductions and apologies Jon Towler GB/21/049 – Verbal 2. Confirmation of quoracy Jon Towler GB/21/050 – Verbal 3. Declarations of interest for any item on the agenda Jon Towler GB/21/051 4. Management of any real or perceived conflicts of interest Jon Towler GB/21/052 5. Questions from the public Jon Towler GB/21/053 – Verbal 6. Minutes from the meeting held on 2 June 2021 Jon Towler GB/21/054 7. Action log from the meeting held on 2 June 2021 Jon Towler GB/21/055 09:10 Strategy and Leadership 8. Accountable Officer Report Amanda Sullivan GB/21/056 9. Joint Clinical Leaders’ Report Stephen Shortt GB/21/057 – Verbal 09:50 Commissioning Developments 10. Primary Care Commissioning Committee Highlight Report – 16 June 2021 and 21 July 2021 Eleri de Gilbert GB/21/058 11. Patient and Public Engagement Committee Highlight Report – 29 June 2021 and 27 July 2021 Sue Clague GB/21/059 10:00 Financial Stewardship and Resources 12. Finance and Resources Committee Highlight Report – 23 June 2021 and 28 July 2021 Shaun Beebe GB/21/060 13. 2021/22 Financial Report Month Three Michael Cawley GB/21/061 10:10 Quality and Performance 14. Quality and Performance Committee Highlight Report – 24 June 2021 and 22 July 2021 Eleri de Gilbert GB/21/062 15. Quality Report Rosa Waddingham GB/21/063 16. Integrated Performance Report Michael Cawley GB/21/064 Chair: Jon Towler Enquiries to: [email protected] Agenda 1 of 224 09:00 - 10.50-04/08/21
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Meeting Agenda (Open Session) Governing Body Wednesday ...

Meeting Agenda (Open Session)
Governing Body
Wednesday 04 August 2021 (9:00 – 10:50)
Virtual meeting via Zoom
Time Item Presenter Reference
09.00 Introductory Items
1. Welcome, introductions and apologies Jon Towler GB/21/049 – Verbal
2. Confirmation of quoracy Jon Towler GB/21/050 – Verbal
3. Declarations of interest for any item on theagenda
Jon Towler GB/21/051
4. Management of any real or perceived conflictsof interest
Jon Towler GB/21/052
5. Questions from the public Jon Towler GB/21/053 – Verbal
6. Minutes from the meeting held on 2 June 2021 Jon Towler GB/21/054
7. Action log from the meeting held on 2 June 2021 Jon Towler GB/21/055
09:10 Strategy and Leadership
8. Accountable Officer Report Amanda Sullivan GB/21/056
9. Joint Clinical Leaders’ Report Stephen Shortt GB/21/057 – Verbal
09:50 Commissioning Developments
10. Primary Care Commissioning CommitteeHighlight Report – 16 June 2021 and 21 July2021
Eleri de Gilbert GB/21/058
11. Patient and Public Engagement CommitteeHighlight Report – 29 June 2021 and 27 July2021
Sue Clague GB/21/059
10:00 Financial Stewardship and Resources
12. Finance and Resources Committee HighlightReport – 23 June 2021 and 28 July 2021
Shaun Beebe GB/21/060
13. 2021/22 Financial Report Month Three Michael Cawley GB/21/061
10:10 Quality and Performance
14. Quality and Performance Committee HighlightReport – 24 June 2021 and 22 July 2021
Eleri de Gilbert GB/21/062
15. Quality Report Rosa Waddingham GB/21/063
16. Integrated Performance Report Michael Cawley GB/21/064
Chair: Jon Towler
Enquiries to: [email protected]
Agenda
1 of 22409:00 - 10.50-04/08/21

Time Item Presenter Reference
10:40 Corporate Assurance
17. Audit and Governance Committee Highlight Report – 10 June 2021
Sue Sunderland GB/21/065
18. Corporate Risk Report Lucy Branson GB/21/066
- Information Items
The following items are for information and will not be individually presented. Questions will be taken by exception.
19. Ratified minutes of CCG committee meetings: N/A GB/21/067
a) Patient and Public Engagement Committee – 25 May 2021 and 29 June 2021
b) Quality and Performance Committee
– 27 May 2021 and 24 June 2021
c) Finance and Resources Committee
– 26 May 2021 and 23 June 2021
d) Primary Care Commissioning Committee
– 19 May 2021 and 16 June 2021
e) Audit and Governance Committee
– 23 April 2021
10:50 Closing Items
21. Any other business Jon Towler GB/21/068 – Verbal
22. Date of the next meeting:
06/10/2021
To be held virtually
Jon Towler GB/21/069 – Verbal
Confidential Motion:
The Governing Body will resolve that representatives of the press and other members of the public be
excluded from the remainder of this meeting, having regard to the confidential nature of the business to be
transacted, publicity on which would be prejudicial to the public interest (Section 1[2] Public Bodies
[Admission to Meetings] Act 1960)
Agenda
2 of 224 09:00 - 10.50-04/08/21

Name Current position(s)
held in the CCG
Declared
Interest
(Name of the
organisation
and nature of
business)
Nature of Interest
Fin
an
cia
l In
tere
st
No
n-f
inan
cia
l P
rofe
ssio
nal
Inte
rests
No
n-f
inan
cia
l P
ers
on
al
Inte
rests
Ind
irect
Inte
rest
Date
Fro
m:
Date
To
:
Action taken to mitigate risk
ARORA, Dr Manik Governing Body GP
Representative
Nottingham City GP Alliance Limited
- a federation of GP practices to
work together to develop and deliver
solutions for member practices to
deliver services to the local
community
Rivergreen Medical Centre (of
which Dr Arora is a GP Partner) is a
member of the NCGPA. As a
shareholder the practice is entitled
to receive a dividend payment
(albeit no dividend is currently paid
to members).
01/04/2013 Present To be excluded from all commissioning decisions
(including procurement activities and contract
management arrangement) relating to services
that are currently, or could be, provided by the
Nottingham City GP Alliance.
ARORA, Dr Manik Governing Body GP
Representative
Rivergreen Medical Centre GP Partner 01/04/2013 Present To be excluded from all commissioning decisions
(including procurement activities and contract
management arrangements) relating to services
that are currently, or could be, provided by GP
Practices.
BALL, Alex Director of Communications
and Engagement
Keyworth Medical Practice Registered Patient 01/12/2019 Present This interest will be kept under review and
specific actions determined as required - as a
general guide, the individual should be able to
participate in discussions relating to this practice
but be excluded from decision-making.
BEEBE, Shaun Non-Executive Director University of Nottingham Senior manager with the University
of Nottingham
-
Present This interest will be kept under review and
specific actions determined as required.
BEEBE, Shaun Non-Executive Director Nottingham University Hospitals
NHS Trust
Patient in Ophthalmology -
Present This interest will be kept under review and
specific actions determined as required.
BRANSON, Lucy Associate Director of
Governance
St George’s Medical Practice Registered Patient 01/11/2005 Present This interest will be kept under review and
specific actions determined as required - as a
general guide, the individual should be able to
participate in discussions relating to this practice
but be excluded from decision-making.
Register of Declared Interests
• As required by section 14O of the NHS Act 2006 (as amended), the CCG has made arrangements to manage conflicts and potential conflicts of interest to ensure that decisions made by the CCG will be taken and seen to be taken without being unduly influenced by
external or private interests.
• This document is extracted, for the purposes of this meeting, from the CCG’s full Register of Declared Interests (which is publically available on the CCG’s website).
This document was extracted on 30 July 2021 but has been checked against the full register prior to the meeting to ensure accuracy.
• The register is reviewed in advance of the meeting to ensure the consideration of any known interests in relation to the meeting agenda. Where necessary (for example, where there is a direct financial interest), members may be fully excluded from participating in
an item and this will include them not receiving the paper(s) in advance of the meeting.
• Members and attendees are reminded that they can raise an interest at the beginning of, or during discussion of, an item if they realise that they do have a (potential) interest that hasn’t already been declared.
• Expired interests (as greyed out on the register) will remain on the register for six months following the date of expiry.
Declarations of Interest
3 of 22409:00 - 10.50-04/08/21
Name Current position(s)
held in the CCG
Declared
Interest
(Name of the
organisation
and nature of
business)
Nature of Interest
Fin
an
cia
l In
tere
st
No
n-f
inan
cia
l P
rofe
ssio
nal
Inte
rests
No
n-f
inan
cia
l P
ers
on
al
Inte
rests
Ind
irect
Inte
rest
Date
Fro
m:
Date
To
:
Action taken to mitigate risk
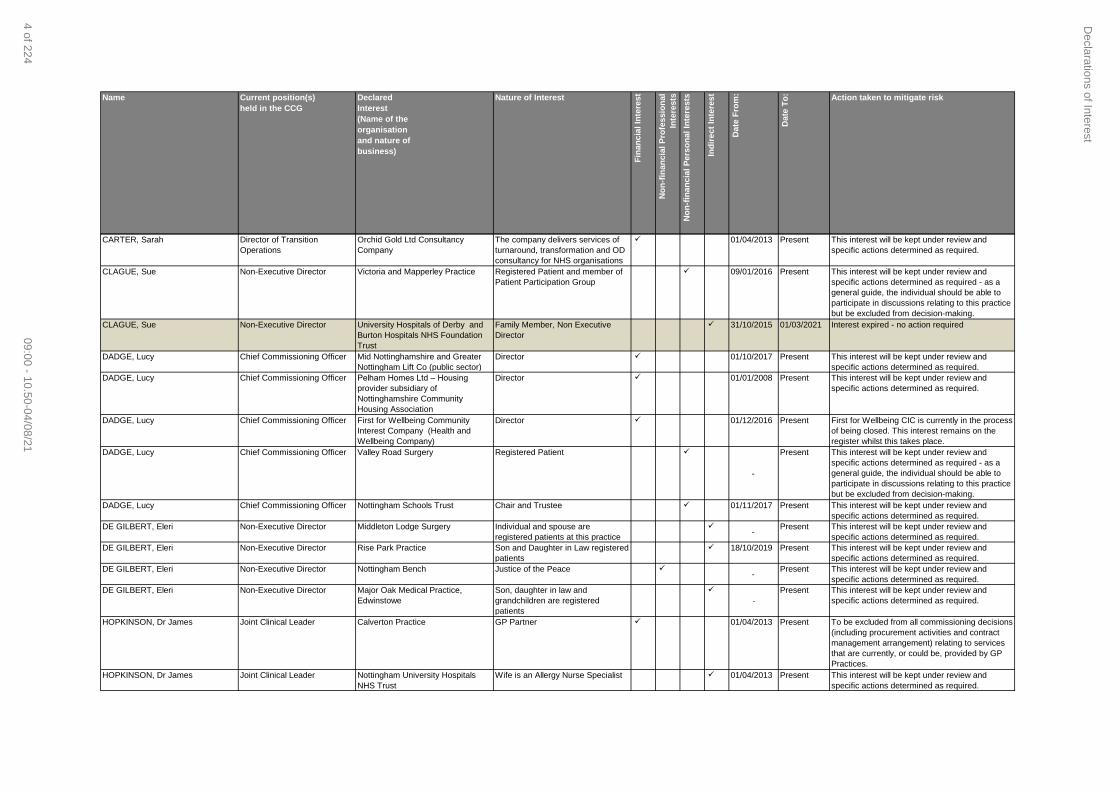
CARTER, Sarah Director of Transition
Operations
Orchid Gold Ltd Consultancy
Company
The company delivers services of
turnaround, transformation and OD
consultancy for NHS organisations
01/04/2013 Present This interest will be kept under review and
specific actions determined as required.
CLAGUE, Sue Non-Executive Director Victoria and Mapperley Practice Registered Patient and member of
Patient Participation Group
09/01/2016 Present This interest will be kept under review and
specific actions determined as required - as a
general guide, the individual should be able to
participate in discussions relating to this practice
but be excluded from decision-making.
CLAGUE, Sue Non-Executive Director University Hospitals of Derby and
Burton Hospitals NHS Foundation
Trust
Family Member, Non Executive
Director
31/10/2015 01/03/2021 Interest expired - no action required
DADGE, Lucy Chief Commissioning Officer Mid Nottinghamshire and Greater
Nottingham Lift Co (public sector)
Director 01/10/2017 Present This interest will be kept under review and
specific actions determined as required.
DADGE, Lucy Chief Commissioning Officer Pelham Homes Ltd – Housing
provider subsidiary of
Nottinghamshire Community
Housing Association
Director 01/01/2008 Present This interest will be kept under review and
specific actions determined as required.
DADGE, Lucy Chief Commissioning Officer First for Wellbeing Community
Interest Company (Health and
Wellbeing Company)
Director 01/12/2016 Present First for Wellbeing CIC is currently in the process
of being closed. This interest remains on the
register whilst this takes place.
DADGE, Lucy Chief Commissioning Officer Valley Road Surgery Registered Patient
-
Present This interest will be kept under review and
specific actions determined as required - as a
general guide, the individual should be able to
participate in discussions relating to this practice
but be excluded from decision-making.
DADGE, Lucy Chief Commissioning Officer Nottingham Schools Trust Chair and Trustee 01/11/2017 Present This interest will be kept under review and
specific actions determined as required.
DE GILBERT, Eleri Non-Executive Director Middleton Lodge Surgery Individual and spouse are
registered patients at this practice
-
Present This interest will be kept under review and
specific actions determined as required.
DE GILBERT, Eleri Non-Executive Director Rise Park Practice Son and Daughter in Law registered
patients
18/10/2019 Present This interest will be kept under review and
specific actions determined as required.
DE GILBERT, Eleri Non-Executive Director Nottingham Bench Justice of the Peace -
Present This interest will be kept under review and
specific actions determined as required.
DE GILBERT, Eleri Non-Executive Director Major Oak Medical Practice,
Edwinstowe
Son, daughter in law and
grandchildren are registered
patients
-
Present This interest will be kept under review and
specific actions determined as required.
HOPKINSON, Dr James Joint Clinical Leader Calverton Practice GP Partner 01/04/2013 Present To be excluded from all commissioning decisions
(including procurement activities and contract
management arrangement) relating to services
that are currently, or could be, provided by GP
Practices.
HOPKINSON, Dr James Joint Clinical Leader Nottingham University Hospitals
NHS Trust
Wife is an Allergy Nurse Specialist 01/04/2013 Present This interest will be kept under review and
specific actions determined as required.
Declarations of Interest
4 of 22409:00 - 10.50-04/08/21
Name Current position(s)
held in the CCG
Declared
Interest
(Name of the
organisation
and nature of
business)
Nature of Interest
Fin
an
cia
l In
tere
st
No
n-f
inan
cia
l P
rofe
ssio
nal
Inte
rests
No
n-f
inan
cia
l P
ers
on
al
Inte
rests
Ind
irect
Inte
rest
Date
Fro
m:
Date
To
:
Action taken to mitigate risk
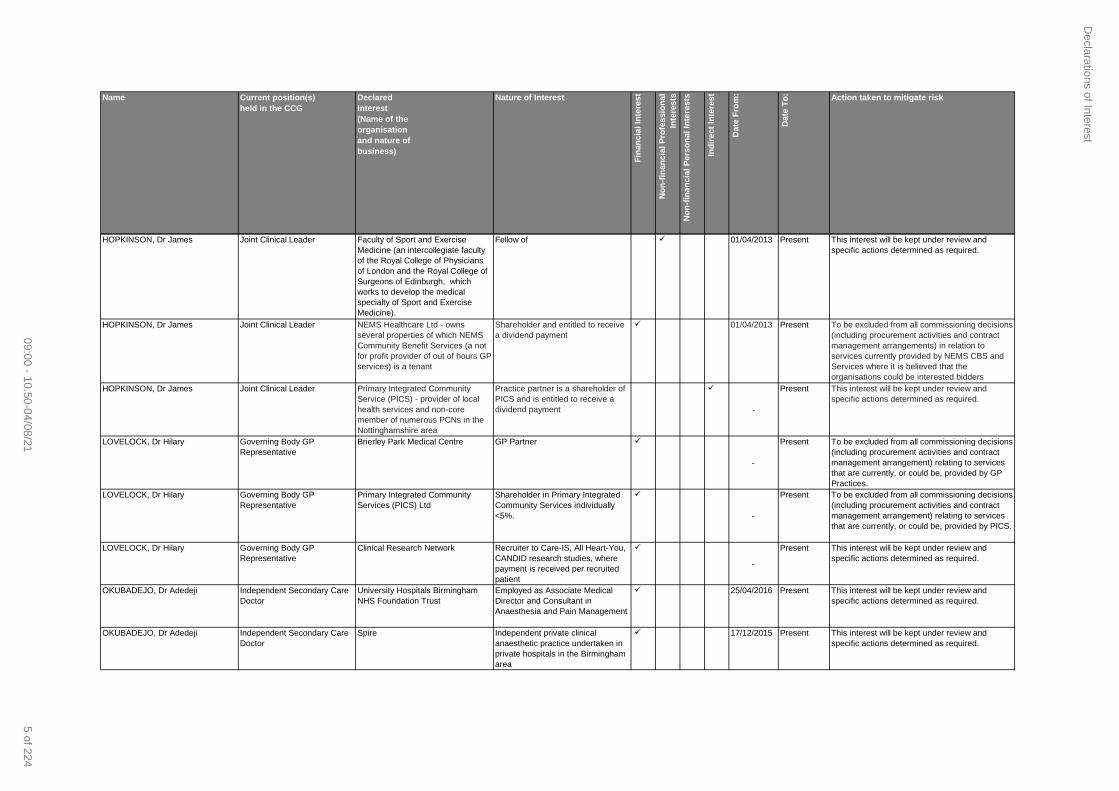
HOPKINSON, Dr James Joint Clinical Leader Faculty of Sport and Exercise
Medicine (an intercollegiate faculty
of the Royal College of Physicians
of London and the Royal College of
Surgeons of Edinburgh, which
works to develop the medical
specialty of Sport and Exercise
Medicine).
Fellow of 01/04/2013 Present This interest will be kept under review and
specific actions determined as required.
HOPKINSON, Dr James Joint Clinical Leader NEMS Healthcare Ltd - owns
several properties of which NEMS
Community Benefit Services (a not
for profit provider of out of hours GP
services) is a tenant
Shareholder and entitled to receive
a dividend payment
01/04/2013 Present To be excluded from all commissioning decisions
(including procurement activities and contract
management arrangements) in relation to
services currently provided by NEMS CBS and
Services where it is believed that the
organisations could be interested bidders
HOPKINSON, Dr James Joint Clinical Leader Primary Integrated Community
Service (PICS) - provider of local
health services and non-core
member of numerous PCNs in the
Nottinghamshire area
Practice partner is a shareholder of
PICS and is entitled to receive a
dividend payment
-
Present This interest will be kept under review and
specific actions determined as required.
LOVELOCK, Dr Hilary Governing Body GP
Representative
Brierley Park Medical Centre GP Partner
-
Present To be excluded from all commissioning decisions
(including procurement activities and contract
management arrangement) relating to services
that are currently, or could be, provided by GP
Practices.
LOVELOCK, Dr Hilary Governing Body GP
Representative
Primary Integrated Community
Services (PICS) Ltd
Shareholder in Primary Integrated
Community Services individually
<5%.
-
Present To be excluded from all commissioning decisions
(including procurement activities and contract
management arrangement) relating to services
that are currently, or could be, provided by PICS.
LOVELOCK, Dr Hilary Governing Body GP
Representative
Clinical Research Network Recruiter to Care-IS, All Heart-You,
CANDID research studies, where
payment is received per recruited
patient
-
Present This interest will be kept under review and
specific actions determined as required.
OKUBADEJO, Dr Adedeji Independent Secondary Care
Doctor
University Hospitals Birmingham
NHS Foundation Trust
Employed as Associate Medical
Director and Consultant in
Anaesthesia and Pain Management
25/04/2016 Present This interest will be kept under review and
specific actions determined as required.
OKUBADEJO, Dr Adedeji Independent Secondary Care
Doctor
Spire Independent private clinical
anaesthetic practice undertaken in
private hospitals in the Birmingham
area
17/12/2015 Present This interest will be kept under review and
specific actions determined as required.
Declarations of Interest
5 of 22409:00 - 10.50-04/08/21
Name Current position(s)
held in the CCG
Declared
Interest
(Name of the
organisation
and nature of
business)
Nature of Interest
Fin
an
cia
l In
tere
st
No
n-f
inan
cia
l P
rofe
ssio
nal
Inte
rests
No
n-f
inan
cia
l P
ers
on
al
Inte
rests
Ind
irect
Inte
rest
Date
Fro
m:
Date
To
:
Action taken to mitigate risk
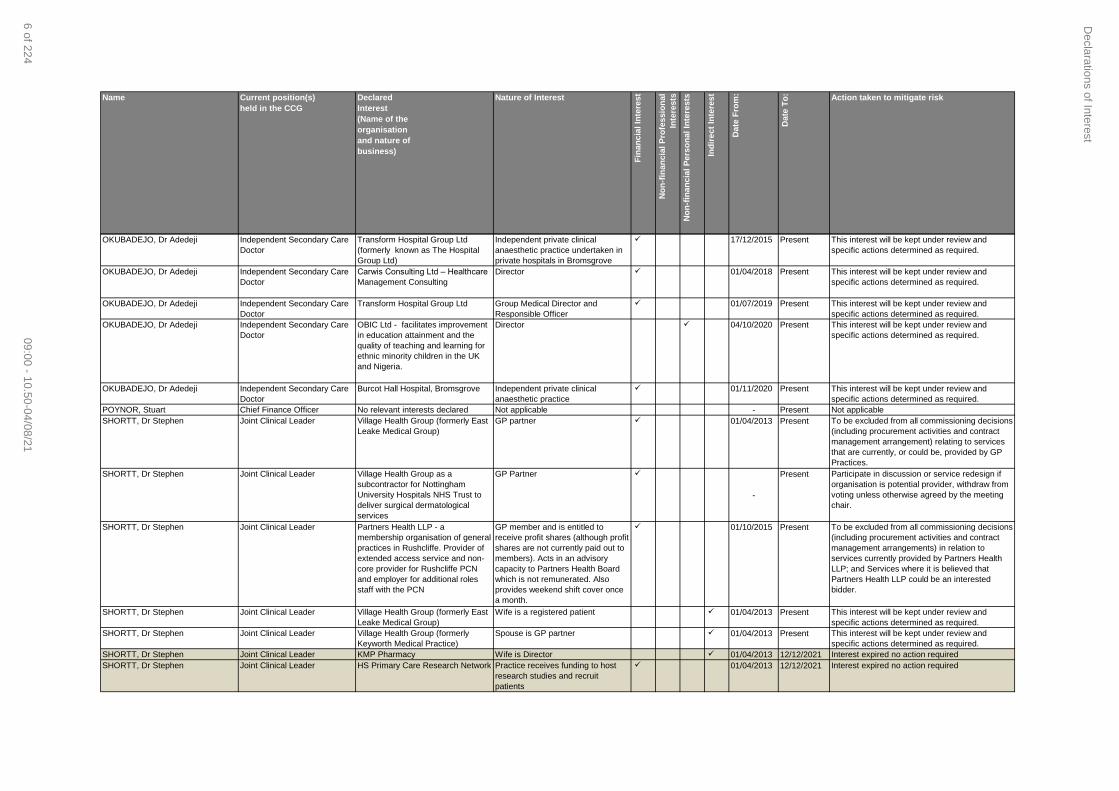
OKUBADEJO, Dr Adedeji Independent Secondary Care
Doctor
Transform Hospital Group Ltd
(formerly known as The Hospital
Group Ltd)
Independent private clinical
anaesthetic practice undertaken in
private hospitals in Bromsgrove
17/12/2015 Present This interest will be kept under review and
specific actions determined as required.
OKUBADEJO, Dr Adedeji Independent Secondary Care
Doctor
Carwis Consulting Ltd – Healthcare
Management Consulting
Director 01/04/2018 Present This interest will be kept under review and
specific actions determined as required.
OKUBADEJO, Dr Adedeji Independent Secondary Care
Doctor
Transform Hospital Group Ltd Group Medical Director and
Responsible Officer
01/07/2019 Present This interest will be kept under review and
specific actions determined as required.
OKUBADEJO, Dr Adedeji Independent Secondary Care
Doctor
OBIC Ltd - facilitates improvement
in education attainment and the
quality of teaching and learning for
ethnic minority children in the UK
and Nigeria.
Director 04/10/2020 Present This interest will be kept under review and
specific actions determined as required.
OKUBADEJO, Dr Adedeji Independent Secondary Care
Doctor
Burcot Hall Hospital, Bromsgrove Independent private clinical
anaesthetic practice
01/11/2020 Present This interest will be kept under review and
specific actions determined as required.
POYNOR, Stuart Chief Finance Officer No relevant interests declared Not applicable - Present Not applicable
SHORTT, Dr Stephen Joint Clinical Leader Village Health Group (formerly East
Leake Medical Group)
GP partner 01/04/2013 Present To be excluded from all commissioning decisions
(including procurement activities and contract
management arrangement) relating to services
that are currently, or could be, provided by GP
Practices.
SHORTT, Dr Stephen Joint Clinical Leader Village Health Group as a
subcontractor for Nottingham
University Hospitals NHS Trust to
deliver surgical dermatological
services
GP Partner
-
Present Participate in discussion or service redesign if
organisation is potential provider, withdraw from
voting unless otherwise agreed by the meeting
chair.
SHORTT, Dr Stephen Joint Clinical Leader Partners Health LLP - a
membership organisation of general
practices in Rushcliffe. Provider of
extended access service and non-
core provider for Rushcliffe PCN
and employer for additional roles
staff with the PCN
GP member and is entitled to
receive profit shares (although profit
shares are not currently paid out to
members). Acts in an advisory
capacity to Partners Health Board
which is not remunerated. Also
provides weekend shift cover once
a month.
01/10/2015 Present To be excluded from all commissioning decisions
(including procurement activities and contract
management arrangements) in relation to
services currently provided by Partners Health
LLP; and Services where it is believed that
Partners Health LLP could be an interested
bidder.
SHORTT, Dr Stephen Joint Clinical Leader Village Health Group (formerly East
Leake Medical Group)
Wife is a registered patient 01/04/2013 Present This interest will be kept under review and
specific actions determined as required.
SHORTT, Dr Stephen Joint Clinical Leader Village Health Group (formerly
Keyworth Medical Practice)
Spouse is GP partner 01/04/2013 Present This interest will be kept under review and
specific actions determined as required.
SHORTT, Dr Stephen Joint Clinical Leader KMP Pharmacy Wife is Director 01/04/2013 12/12/2021 Interest expired no action required
SHORTT, Dr Stephen Joint Clinical Leader HS Primary Care Research Network Practice receives funding to host
research studies and recruit
patients
01/04/2013 12/12/2021 Interest expired no action required
Declarations of Interest
6 of 22409:00 - 10.50-04/08/21

Name Current position(s)
held in the CCG
Declared
Interest
(Name of the
organisation
and nature of
business)
Nature of Interest
Fin
an
cia
l In
tere
st
No
n-f
inan
cia
l P
rofe
ssio
nal
Inte
rests
No
n-f
inan
cia
l P
ers
on
al
Inte
rests
Ind
irect
Inte
rest
Date
Fro
m:
Date
To
:
Action taken to mitigate risk
SHORTT, Dr Stephen Joint Clinical Leader Partners Health LLP - a
membership organisation of general
practices in Rushcliffe. Provider of
extended access service and non-
core provider for Rushcliffe PCN
and employer for additional roles
staff with the PCN
Wife is a GP member and also
provides weekend shift cover once
a month.
01/10/2015 Present To be excluded from all commissioning decisions
(including procurement activities and contract
management arrangements) in relation to
services currently provided by Partners Health
LLP; and Services where it is believed that
Partners Health LLP could be an interested
bidder.
SHORTT, Dr Stephen Joint Clinical Leader Village Health Group (formerly
Keyworth Medical Practice)
Registered Patient
-
Present This interest will be kept under review and
specific actions determined as required - as a
general guide, the individual should be able to
participate in discussions relating to this practice
but be excluded from decision-making.
SHORTT, Dr Stephen Joint Clinical Leader Rushcliffe Primary Care Network
(funded by NHS England and NHS
Improvement via the CCG and the
Integrated Care System)
Voting Member 01/10/2019 Present This interest will be kept under review and
specific actions determined as required.
SHORTT, Dr Stephen Joint Clinical Leader Rushcliffe Primary Care Network
(funded by NHS England and NHS
Improvement via the CCG and the
Integrated Care System)
Sppouse is a Voting Member 10/06/2021 Present This interest will be kept under review and
specific actions determined as required.
SHORTT, Dr Stephen Joint Clinical Leader Village Health Group as a
subcontractor for Nottingham
University Hospitals NHS Trust to
deliver surgical dermatological
services
Spouse is a GP Partner 10/06/2021 Present Participate in discussion or service redesign if
organisation is potential provider, withdraw from
voting unless otherwise agreed by the meeting
chair.
STRATTON, Dr Richard GP Representative Belvoir Health Group GP Partner 01/08/2012 Present To be excluded from all commissioning decisions
(including procurement activities and contract
management arrangements) relating to services
that are currently, or could be, provided by GP
Practices.
STRATTON, Dr Richard GP Representative Partners Health LLP - a
membership organisation of general
practices in Rushcliffe. Provider of
extended access service and non-
core provider for Rushcliffe PCN
and employer for additional roles
staff for the PCN
GP member and is entitled to
receive profit shares (although profit
shares are not currently paid out to
members). Also acts in an advisory
capacity to Partners Health Board
which is not remunerated.
01/11/2015 Present To be excluded from all commissioning decisions
(including procurement activities and contract
management arrangements) in relation to
services currently provided by Partners Health
LLP; and Services where it is believed that
Partners Health LLP could be an interested
bidder.
STRATTON, Dr Richard GP Representative Fosse Medicare Ltd: a property
company which owns the Cotgrave
Surgery which Belvoir Health Group
have a lease to occupy.
Director/Shareholder 01/11/2018 Present This interest will be kept under review and
specific actions determined as required.
Declarations of Interest
7 of 22409:00 - 10.50-04/08/21

Name Current position(s)
held in the CCG
Declared
Interest
(Name of the
organisation
and nature of
business)
Nature of Interest
Fin
an
cia
l In
tere
st
No
n-f
inan
cia
l P
rofe
ssio
nal
Inte
rests
No
n-f
inan
cia
l P
ers
on
al
Inte
rests
Ind
irect
Inte
rest
Date
Fro
m:
Date
To
:
Action taken to mitigate risk
STRATTON, Dr Richard GP Representative Nottingham University Hospitals
NHS Trust
NUH Clinical Director for Integration 01/04/2021 Present To be excluded from all commissioning decisions
(including procurement activities and contract
management arrangements) relating to services
that are currently, or could be, provided by
Nottingham University Hospitals Trust.
SULLIVAN, Amanda Accountable Officer Hillview Surgery Registered Patient 2013 Present This interest will be kept under review and
specific actions determined as required - as a
general guide, the individual should be able to
participate in discussions relating to this practice
but be excluded from decision-making.
SUNDERLAND, Sue Non-Executive Director Joint Audit Risk Assurance
Committee, Police and Crime
Commissioner (JARAC) for
Derbyshire / Derbyshire
Constabulary
Chair 01/04/2018 Present This interest will be kept under review and
specific actions determined as required.
SUNDERLAND, Sue Non-Executive Director NHS Bassetlaw CCG Governing Body Lay Member 16/12/2015 Present This interest will be kept under review and
specific actions determined as required.
SUNDERLAND, Sue Non-Executive Director Inclusion Healthcare Social
Enterprise CIC (Leicester City)
Non-Executive Director 16/12/2015 Present This interest will be kept under review and
specific actions determined as required.
TOWLER, Jon Non-Executive Director Sherwood Medical Practice. Registered Patient
-
Present This interest will be kept under review and
specific actions determined as required - as a
general guide, the individual should be able to
participate in discussions relating to this practice
but be excluded from decision-making.
TOWLER, Jon Non-Executive Director Major Oak Medical Practice,
Edwinstowe
Family members are registered
patients
-
Present This interest will be kept under review and
specific actions determined as required - as a
general guide, the individual should be able to
participate in discussions relating to this practice
but be excluded from decision-making.
TOWLER, Jon Non-Executive Director YPO - a publicly owned central
purchasing body based in
Wakefield, Yorkshire. It is owned
and governed by a consortium of
county, metropolitan and borough
councils in Yorkshire and the North
West England. It provides a wide
range of resources and services to
schools, councils, charities,
emergency services, and other
public sector organisations.
Independent Director (remunerated) 01/10/2020 Present This interest will be kept under review and
specific actions determined as required.
WADDINGHAM, Rosa Chief Nurse No relevant interests declared Not applicable - - Not applicable
Declarations of Interest
8 of 22409:00 - 10.50-04/08/21

Page 1 of 2
Managing Conflicts of Interest at Meetings
1. A “conflict of interest” is defined as a “set of circumstances by which a reasonable person
would consider that an individual’s ability to apply judgement or act, in the context of
delivering commissioning, or assuring taxpayer funded health and care services is, or could
be, impaired or influenced by another interest they hold”.
2. An individual does not need to exploit their position or obtain an actual benefit, financial or
otherwise, for a conflict of interest to occur. In fact, a perception of wrongdoing, impaired
judgement, or undue influence can be as detrimental as any of them actually occurring. It is
important to manage these perceived conflicts in order to maintain public trust.
3. Conflicts of interest include:
Financial interests: where an individual may get direct financial benefits from the
consequences of a commissioning decision.
Non-financial professional interests: where an individual may obtain a non-financial
professional benefit from the consequences of a commissioning decision, such as
increasing their reputation or status or promoting their professional career.
Non-financial personal interests: where an individual may benefit personally in ways
which are not directly linked to their professional career and do not give rise to a direct
financial benefit.
Indirect interests: where an individual has a close association with an individual who has
a financial interest, a non-financial professional interest or a non-financial personal
interest in a commissioning decision.
The above categories are not exhaustive and each situation must be considered on a case
by case basis.
4. In advance of any meeting of the Committee, consideration will be given as to whether
conflicts of interest are likely to arise in relation to any agenda item and how they should be
managed. This may include steps to be taken prior to the meeting, such as ensuring that
supporting papers for a particular agenda item are not sent to conflicted individuals.
5. At the beginning of each formal meeting, Committee members and co-opted advisors will be
required to declare any interests that relate specifically to a particular issue under
consideration. If the existence of an interest becomes apparent during a meeting, then this
must be declared at the point at which it arises. Any such declaration will be formally
recorded in the minutes for the meeting.
Management of any real or perceived conflicts of interest
9 of 22409:00 - 10.50-04/08/21

Page 2 of 2
6. The Chair of the Committee (or Deputy Chair in their absence, or where the Chair of the
Committee is conflicted) will determine how declared interests should be managed, which is
likely to involve one the following actions:
Requiring the individual to withdraw from the meeting for that part of the discussion if the
conflict could be seen as detrimental to the Committee’s decision-making arrangements.
Allowing the individual to participate in the discussion, but not the decision-making
process.
Allowing full participation in discussion and the decision-making process, as the potential
conflict is not perceived to be material or detrimental to the Committee’s decision-making
arrangements.
Management of any real or perceived conflicts of interest
10 of 224 09:00 - 10.50-04/08/21

Governing Body (Open Session)
UNRATIFIED minutes of the meeting held on
03/06/2021, 09:00-10:45
Teleconference
Members present:
Jon Towler Non-Executive Director and Chair of the meeting
Shaun Beebe Non-Executive Director
Sue Clague Non-Executive Director
Eleri de Gilbert Non-Executive Director
Dr James Hopkinson Joint Clinical Leader
Dr Hilary Lovelock GP Representative, Mid-Nottinghamshire
Dr Adedeji Okubadejo Secondary Care Specialist
Stuart Poynor Chief Finance Officer
Dr Stephen Shortt Joint Clinical Leader
Dr Richard Stratton GP Representative, South Nottinghamshire
Amanda Sullivan Accountable Officer
Sue Sunderland Non-Executive Director
Rosa Waddingham Chief Nurse
In attendance:
Alex Ball Director of Communication and Engagement
Lucy Branson Associate Director of Governance
Rachel Illingworth Head of Research and Evidence (item GB 21 044)
Sue Wass Corporate Governance Officer (minutes)
Apologies:
Dr Manik Arora GP Representative, Nottingham City
Lucy Dadge Chief Commissioning Officer
Cumulative Record of Members’ Attendance (2021/22)
Name Possible Actual Name Possible Actual
Dr Manik Arora 2 1 Stuart Poynor 2 2
Shaun Beebe 2 2 Dr Stephen Shortt 2 2
Sue Clague 2 2 Dr Richard Stratton 2 2
Lucy Dadge 2 1 Amanda Sullivan 2 2
Eleri de Gilbert 2 2 Sue Sunderland 2 2
Dr James Hopkinson 2 2 Jon Towler 2 2
Dr Hilary Lovelock 2 2 Rosa Waddingham 2 2
Dr Adedeji Okubadejo 2 2
Introductory Items GB 21 027 Welcome and Apologies Jon Towler welcomed everyone to the open session of NHS Nottingham and
Nottinghamshire CCG’s Governing Body meeting. The meeting was being held virtually due to the Covid-19 pandemic and was being live streamed to allow members of the
Minutes from the meeting held on 6 June 2021
11 of 22409:00 - 10.50-04/08/21

Page 2 of 9
public access to the discussion. Apologies were noted as above.
GB 21 028 Confirmation of Quoracy The meeting was declared quorate. GB 21 029 Declaration of interest for any item on the shared agenda No interests were noted on any item on the agenda. Jon Towler reminded members of
their responsibility to highlight any interests should they transpire as a result of discussions during the meeting.
GB 21 030 Management of any real or perceived conflicts of interest No interests had been declared; therefore this item was not required. GB 21 031 Questions from the Public There were no questions. GB 21 032 Minutes from the meeting held on 07 April 2021 The minutes were agreed as an accurate record of the discussions held. GB 21 033 Action log from the meetings held on 07 April 2021 Action GB/21/008 was noted as deferred. It was agreed that a report would be brought
to the Quality and Performance Committee, which would incorporate input from Stuart Poynor from a human resources perspective, and a summary of actions would be detailed in the Quality and Performance Highlight Report to be presented at the August meeting. All other actions were noted as completed.
Strategy and Leadership
GB 21 034 Accountable Officer Report Amanda Sullivan presented the item and highlighted the following key points:
a) Covid-19 infection rates were beginning to decline; however more recent data had noted fluctuations and an increase in admissions at Nottingham University Hospitals NHS Trust (NUH). 75% of all covid-19 cases nationally were of the Delta variant, which appeared much more transmissible and vigilance needed to be maintained as lockdown measures eased.
b) Demand for services was increasing in a number of areas, including accident and emergency, General Practice, 111, and mental health services.
c) The vaccination programme continued, with over 900,000 people in the CCG area having been vaccinated. The second dose appointments for people over the age of 50 were being brought forward, as it had been evidenced that a second dose gave a greater protection against serious illness. The programme was now open to people over the age of 30; and people over the age of 40 could receive a vaccination at drop in centres without an appointment.
d) Nottingham and Nottinghamshire had been identified as an ‘accelerator site’ for increased funding to reduce the waiting lists for planned care. The funding would be used in areas such as buying additional equipment and piloting new ways of working.
e) The report included an overview of the planned transformation of community services, which would be used to test and learn from new integrated ways of working under the Integrated Care System (ICS).
f) Following on from Dementia action week the CCG had launched a period of engagement to understand the experiences of those people living with or caring for
Minutes from the meeting held on 6 June 2021
12 of 224 09:00 - 10.50-04/08/21

Page 3 of 9
an individual with dementia, to shape future service provision. g) A review of the CCG’s emergency governance arrangements had been undertaken,
which had confirmed that the Emergency Scheme of Reservation and Delegation can now be removed, which ends the emergency decision-making powers delegated to the Service Change Cell (now the Service Change Group) and the Executive Management Team. The Emergency Delegated Financial Limits had also been reviewed to determine where it was now appropriate to revert back to the limits set out in the CCG’s Standing Financial Instructions, or where a permanent change was proposed. The proposed changes, as detailed in the report, were recommended for approval.
h) At its meeting on 1 May, the ICS Board had approved a Partnership Agreement to guide joint working over the coming period. This was appended to the report for endorsement.
The following points were raised in discussion: i) Members queried how the engagement on Dementia services would ensure
meaningful interaction with this patient cohort. It was noted that there were strong networks of dementia and care home groups to engage with and links would be made with local authorities’ carers and community groups. It was noted that the original timescale for the engagement had been extended into July to allow face to face meetings to be held.
j) As Chair of the Patient and Public Engagement Committee, Sue Clague noted an interest in the outcome of six engagement workshops, which had been held to inform the development of community services provision. It was agreed to ask Lucy Dadge to provide an update to Sue outside of the meeting.
The Governing Body:
RECEIVED the Accountable Officer Report.
APPROVED the removal of the Emergency Scheme of Reservation and Delegation and the proposed permanent amendments to the CCG’s Delegated Financial Limits.
ENDORSED the ICS Partnership Agreement.
ACTION:
Lucy Dadge to discuss with Sue Clague the outcome of the engagement workshops for community services provision.
GB 21 035 Joint Clinical Leaders’ Report Stephen Shortt and James Hopkinson presented the item and highlighted the following
key points: a) GP practices continued to see increased numbers of people, with an increased
workload from appointments traditionally undertaken in secondary care. Over 50% of appointments were face to face. There was a plea for patients to be understanding, as practices still needed to adhere to PPE and social distancing requirements.
b) A piece of work was being undertaken to audit current and future risks to the resilience of General Practice, which would build into further integrated working under the ICS. This would examine how to resolve long-term systemic issues and the targeting of resources.
The following points were raised in discussion: c) Members noted that national system recovery plans tended to focus on secondary
care; however General Practice also needed to have a plan for recovery, as the pressures of the past months had been significant and would be sustained long term. Members discussed how the stated audit related to the development of a Nottingham and Nottinghamshire ‘heat map’ that the Primary Care Commissioning
Minutes from the meeting held on 6 June 2021
13 of 22409:00 - 10.50-04/08/21

Page 4 of 9
Committee was overseeing, which assessed the pressures and risks faced by individual practices and localities. A number of points were noted, including capacity and resource within the CCG in light of the imminent devolvement of wider primary care commissioning responsibilities by NHS England; the need to restructure primary care governance arrangements; interdependencies with community services; and different demands on General Practice as a result of the pandemic. It was agreed that time would be dedicated in the July Governing Body Development Session to discuss this further; and in preparation, a set of recommendations for action, with indicative timescales would be drafted.
The Governing Body:
NOTED the verbal update.
ACTION:
Executive Team to lead on the drafting of a high level plan for support to General Practice, to be discussed at the Development Session on 7 July.
Commissioning Developments
GB 21 036 Primary Care Commissioning Committee Highlight Report – 21 April and 19 May
2021 Eleri de Gilbert presented the item and highlighted the following key points:
a) As discussed under item GB 21 035, a development session took place on 28 April 2021 around the emerging heath framework as a method of identification of pressures and risks faced by individual practices and localities. Work continued to develop the framework alongside the emerging ICS architecture and governance.
b) Hillview surgery successfully took on Farnsfield surgery as planned on 4 May. Feedback to date had been positive around the transition.
c) As discussed under item GB 21 035, practices had reported an increase in demand for face to face appointments following recent media reports as a result of a letter to GPs from NHS England, which asked practices to respect preference for face to face care unless there were good clinical reasons to the contrary and also required practice receptions to be open. The Committee noted that local practices had been offering patients a range of appointments, whilst ensuring the safety of practice staff and patents throughout the pandemic.
The Governing Body:
NOTED the Primary Care Commissioning Committee Highlight Report. GB 21 037 Patient and Public Engagement Committee (PPEC) Highlight Report – 27 April and
25 May 2021 Sue Clague presented the item and highlighted the following key points:
a) Two programmes had been reviewed using the PPEC Effectiveness Framework, which had been developed by the Committee to confirm that engagement had been properly embedded within CCG programmes of work.
b) PPEC members had provided advice regarding engagement to support the development of a Tier 3 weight management service for children and young people. Broader health prevention strategies were also discussed and it was agreed to schedule a preventative programme update on a future PPEC agenda.
c) Advice was provided by PPEC members to support the engagement that would inform the strategy and commissioning of the Dementia Well Pathway.
The following points were raised in discussion: d) Members noted the good alignment of the Committee’s work programme to the
CCG’s transformation projects and the good progress that had been made to embed
Minutes from the meeting held on 6 June 2021
14 of 224 09:00 - 10.50-04/08/21
Page 5 of 9
strategic engagement throughout commissioning processes. e) It was noted that the intention was to move towards a more rolling systematic
approach, rather than project-based engagement.
The Governing Body:
NOTED the Patient and Public Engagement Committee Highlight Report.
Financial Stewardship and Resources GB 21 038 Finance and Resources Committee Highlight Report – 28 April and 26 May 2021 Shaun Beebe presented the item and highlighted the following key points:
a) The Committee had reviewed progress against the CCG’s Organisational Development Strategy and the draft Staff Survey Action Plan. It was noted that two Non-Executive members of the Committee would be attending the June meeting of the Staff Engagement Group to gauge how the organisation was responding.
b) The CCG had met all key financial targets and indicators for 2020/21, which had been commendable during a difficult year.
c) The Committee had endorsed the draft financial plan for April to September 2021 at its May meeting.
d) Following a request by the Governing Body at its April meeting, the Committee had received a detailed update on the current activity and financial plans that were supporting the drafting of the pre-consultation business case for the Tomorrow’s NUH Programme. The Committee received assurance that a comprehensive approach to modelling had been undertaken and the plans ensured flexibility to respond to changing activity pressures.
The Governing Body:
NOTED the Finance and Resources Committee Highlight Report. GB 21 039 2021/22 Financial Report Month One Stuart Poynor presented the item and highlighted the following points:
a) The temporary financial regime implemented by NHS England and Improvement in the last financial year had been extended for the first six months of the new financial year; this period was termed ‘H1’.
b) The report covered the revised H1 draft financial plan, the ICS H1 draft financial plan, the month one financial position, an update on the 2021/22 capital plan, and an update on month one Covid-19 spend.
c) The CCG had developed a financial plan for this period and this plan was balanced overall in terms of income and expenditure. At this stage this budget had not yet been signed off formally by NHS England and Improvement.
d) Planning was underway for ‘H2’ (October 2021 to March 2022), which would be a cultural change in working, with the movement from organisational plans to an overall system financial plan.
The Governing Body:
NOTED the 2021/22 Financial Report Month One.
Quality and Performance GB 21 040 Quality and Performance Committee Highlight Report – 28 April and 27 May 2021 Eleri de Gilbert presented the item and highlighted the following key points:
a) The Committee had discussed a number of areas of concern raised by the Governing Body at its April meeting:
Concern around the increased numbers of suicide and self-harm incidents: a further deep dive report would be received at the Committee’s next meeting.
Minutes from the meeting held on 6 June 2021
15 of 22409:00 - 10.50-04/08/21

Page 6 of 9
Concern around waiting times and communication with patients on waiting lists: System wide agreement had been reached regarding the need to communicate with patients on waiting lists. There was a strong drive from the Committee to see sustained improvement in customer service.
Accident & Emergency (A&E) attendance; and the possible impact of NHS 111 dispositions: the Committee noted that in terms of NHS 111, a low proportion of calls were converting to A&E attendance.
b) The Committee had approved the CCG’s modern slavery statement for inclusion on the CCG website.
The following points were raised in discussion: c) Noting that block contract arrangements had been in place for over 12 months,
which removed the necessity for contract monitoring arrangements, members queried how provider performance continued to the routinely monitored. It was noted that partnership arrangements put in place during the pandemic had facilitated the better sharing of data. Further oversight mechanisms would be put in place as the CCG moved towards system working.
The Governing Body:
NOTED the Quality and Performance Committee Highlight Report. GB 21 041 Quality Report Rosa Waddingham presented the item and highlighted the following key points:
a) The report brought together the key quality and safety metrics for NHS commissioned services in Nottingham and Nottinghamshire.
b) A factual inaccuracy was noted in the previous reporting of the CQC status of Nurture Care Ltd. It was clarified that Nurture Care Ltd.’s CQC rating was ‘Good’ and not ‘Requires Improvement’, as had been reported.
c) Following a number of incidents at premises managed by Nottinghamshire Healthcare NHS Foundation Trust (NHT), a focused discussion on suicide prevention and trends and on wider quality concerns would be undertaken at the June meeting of the Quality and Performance Committee.
d) The CCG continued to provide enhanced support and surveillance for maternity services at NUH and an improvement plan, supported by system partners, was in place.
e) Learning Disability and Autism inpatient numbers for adults and children and young people ended quarter four was slightly over trajectory, largely due to delays to discharges affected by Covid-19 restrictions. However significant progress had been made in the completion of annual health checks for this cohort of patients.
f) The CCG Primary Care Quality and Safeguarding Teams continued to strengthen the support given; building upon the new ways of working developed throughout the pandemic response; and the CCG Safeguarding Team continued to meet the statutory and partnership duties.
The following points were raised in discussion: g) Discussing NHT, members noted their disappointment that changes in the Trust’s
leadership were not yet having a marked impact on the quality of services. It was noted that although the responsiveness of the Trust had improved, many of the concerns were similar to issues raised previously. An update would be provided to the Governing Body following the deep dive report on the Trust to be discussed at the next meeting of the Quality and Performance Committee.
The Governing Body:
NOTED the Quality Report.
Minutes from the meeting held on 6 June 2021
16 of 224 09:00 - 10.50-04/08/21

Page 7 of 9
GB 21 042 Integrated Performance Report Stuart Poynor presented the item and highlighted the following key points:
a) The report detailed the performance against key standards and targets for the CCG as of end March 2021. Areas of poor performance were in line with the national position, due to the impact of Covid-19.
b) The increase in referral to treatment performance had been discussed in detail at the last Quality and Performance Committee meeting. The CCG was in the process of submitting draft recovery plans and trajectories to NHS England and Improvement.
The following points were raised in discussion: c) Members discussed whether Nottingham and Nottinghamshire, as an accelerator
site for recovery of services, could have any significant impact on waiting lists, considering recent increases in activity. It was acknowledged that recovery would be a long term process.
d) Members discussed whether visibility in the rate of recovery of individual services was possible and whether plans were to expect existing providers of services to accelerate activity or would capacity be created elsewhere. It was noted that all providers were looking to maximise recovery actions; however the limiting factor would be workforce. It was noted that actions would include the use of best practice, different pathways and the validation of waiting lists. It was agreed that a report should be brought to the Quality and Performance Committee that gave further detail of plans and trajectories for recovery by specialty.
e) Members sought assurance that patients continued to be seen in order of clinical priority; and it was confirmed that the Quality and Performance Committee was monitoring this.
f) Members noted metrics in the report were in the main, for secondary care. It was confirmed that the scope of the performance report would be reviewed over the coming months to ensure its fitness for purpose in line with the transition to an ICS (subject to legislation).
The Governing Body:
NOTED the Integrated Performance Report.
ACTION:
Stuart Poynor to present a detailed report by specialty of plans and trajectories for recovery to the July meeting of the Quality and Performance Committee.
Corporate Assurance
GB 21 043 Audit and Governance Committee Highlight Report – 23 April 2021 Sue Sunderland presented the item and highlighted the following key points:
a) The Committee had overseen the preparation of the draft Annual Report and Accounts and would approve the final versions prior to the national deadline of 15 June. No issues had arisen to date. The hard work of the Corporate Governance and Finance Teams in the preparation of the documents was noted.
b) The Committee had received a risk management end of year report and was assured hat the CCG’s strategic and operational risk management processes continued to be robustly managed.
The Governing Body:
NOTED the Audit and Governance Committee Highlight Report. GB 21 044 Research and Evidence Annual Report 2020/21
Minutes from the meeting held on 6 June 2021
17 of 22409:00 - 10.50-04/08/21

Page 8 of 9
Rachel Illingworth was in attendance to present the item and highlighted the following key points: a) The report detailed the research, evaluation and evidence activities that had taken
place over the past year and provided assurance to the Governing Body that the CCG was meeting its statutory duties in relation to research.
b) Covid-19 had highlighted the importance and public awareness of clinical research in the NHS and the report detailed the Covid-related research activity that had taken place in Nottinghamshire. The contribution of the University of Nottingham Health Service to Covid-19 research was of particular note.
c) A significant focus of the team related to primary care research capacity building, with research activity now analysed at Primary Care Network, Place and System levels to inform strategic allocations of NIHR Research Capacity Funding. This aimed to increase research capacity and reduce inequalities in access to research by ensuring research is delivered in locations where patient need is greatest, involving patients and the public from more diverse and underserved communities.
d) An increasingly collaborative approach to research is developing across the ICS and the report provided an example of research opportunities being opened up across patient pathways between primary care and secondary care.
e) A CCG commissioned a research study had recently concluded, which related to improving the mental health outcomes of LGBT+ people in Nottingham City. This had produced important evidence with a range of recommendations and work is ongoing to ensure the evidence is mobilised throughout the ICS.
f) There had been two successful new developments in year: the in-housing of the Research Passport Service for the CCG and member GP practices since November 2020; and the development of a new Knowledge and Library Service for the CCG from February 2021.
g) The team work closely with the Knowledge and Library Service to bring together expertise in literature searching, evidence synthesis and knowledge mobilisation, and examples of this were set out within the report.
h) An Evaluation Framework had been developed for the CCG to support the commissioning process, which provides a practical tool and guide to decisions on what, when and how to evaluate commissioned services. The Prioritisation and Investment Committee had endorsed the framework and this organisational approach to evaluation at its May meeting and this will now be rolled out.
i) Next steps were noted as contributing to an ICS-wide approach to collaborative research, supporting the delivery of research in areas of high disease prevalence where currently research activity was relatively low; the further integration of evidence and evaluation support into commissioning processes; and the piloting of the evaluation framework.
The following points were raised in discussion: j) Members noted that the team undertook extensive and important work, which would
be invaluable to the ICS to drive better outcomes and support robust evidence-based strategies.
k) Reference was made to the national Research Excellence Framework (REF); a national assessment of the quality and impact of research in UK universities. Once published in about a year’s time, this would identify the key research strengths of all universities, including the University of Nottingham and Nottingham Trent University.
l) Early conversations were taking place regarding an ICS Research Group. m) It was noted that the CCG’s Patient and Public Engagement Committee would be
interested in the research relating to LGBT+ mental health outcomes. n) Following earlier discussions in the meeting about the recovery of services and
current long waiting lists for treatment, it was suggested that the team could support with an evidence review of clinical prioritisation across the system.
The Governing Body:
Minutes from the meeting held on 6 June 2021
18 of 224 09:00 - 10.50-04/08/21

Page 9 of 9
RECEIVED the Annual Report as assurance that the CCG is meeting its statutory research duties.
ENDORSED the identified key next steps. GB 21 045 2021/22 Governing Body Assurance Framework and Corporate Risk Report Lucy Branson presented the item and highlighted the following key points:
a) The report presented the CCG’s proposed strategic risks for review and approval, which would be used as the basis for the 2021/22 Governing Body Assurance Framework. It also provided an update on the current major operational risks from the CCG’s Corporate Risk Register.
b) In recognition of 2021/22 being a year of transition, 14 of the strategic risks would be jointly owned by the CCG and the ICS. These 14 strategic risks, which had been endorsed by the ICS Transition and Risk Committee, would also form the basis of an Assurance Framework for the ICS Board.
c) The fully developed Assurance Framework would be presented to the Governing Body in the form of mid-year and year-end position statements.
d) There were currently seven major operational risks on the CCG’s Risk Register. An update on each had been provided in the report and all continued to be overseen by the CCG’s respective committees.
The following points were raised in discussion: e) No new risks were raised. The Governing Body:
APPROVED the CCG’s strategic risks to enable the full development of the 2021/22 Governing Body Assurance Framework.
NOTED the next steps being taken in relation to the Assurance Framework.
NOTED the current major operational risks being managed by the CCG.
For Information GB 21 046 Ratified minutes of Governing Body committee meetings The minutes were NOTED. Annual Patient Experience Report The Annual Patient Experience Report was NOTED.
Closing Items GB 21 047 Any other business There was no other business. GB 21 048 Date of the next meeting: 04/08/21 to be held virtually.
Minutes from the meeting held on 6 June 2021
19 of 22409:00 - 10.50-04/08/21

Page 1 of 2
Governing Body
ACTION LOG for the meeting held on 02/06/21
Meeting
date
Agenda
reference
Agenda item Action Lead Date to be
completed
Comment
ACTIONS OUTSTANDING
- - - No actions outstanding - - -
ACTIONS ONGOING / NOT YET DUE
- - - No actions ongoing - - -
ACTIONS COMPLETE
07/04/2021 GB 21 008 Accountable
Officer Report
To lead on a report to the brought to the
June meeting on suicide prevention
actions.
Amanda
Sullivan
- Discussed at the Quality and
Performance Committee at its
meeting on 24 June and
presented under item QP/21/062
02/06/2021 GB 21 034 Accountable
Officer Report
To discuss with Sue Clague the outcome
of the engagement workshops for
community services provision.
Lucy Dadge - Outputs from the workshops
shared, with an offer to discuss
further if required.
02/06/2021 GB 21 035 Joint Clinical
Leaders’ Update
To lead on the drafting of a high level
plan for support to General Practice.
Executive
Team
- The Primary Care
Commissioning Committee is
oversighting work being
completed in relation to GP
Practice resilience, including
updates from the ICS Primary
Action log from
the meeting held on 6 June 2021
20 of 22409:00 - 10.50-04/08/21

Page 2 of 2
Meeting
date
Agenda
reference
Agenda item Action Lead Date to be
completed
Comment
Care Transition Workstream
(which formally reports to the ICS
Transition and Risk Committee).
02/06/2021 GB 21 042 Integrated
Performance
Report
To present a detailed report by speciality
of plans and trajectories for recovery to
the July meeting of the Quality and
Performance Committee.
Stuart
Poynor
- This information is not currently
available, but is expected as part
of the next planning round,
covering the second half of
2021/22.
Action log from
the meeting held on 6 June 2021
21 of 22409:00 - 10.50-04/08/21
Meeting Title: Governing Body (Open Session) Date: 04 August 2021
Paper Title: Accountable Officer’s Report Paper Reference:
GB 21 056
Sponsor:
Presenter:
Amanda Sullivan, Accountable Officer Attachments/ Appendices:
A: ICS Board Summary Briefing July 2021
Amanda Sullivan, Accountable Officer
Summary Purpose:
Approve ☐ Endorse ☐ Review ☐ Receive/Note for:
∑ Assurance∑ Information
☒
Executive Summary
The purpose of the Accountable Officer’s Report is to summarise recent local and national developments and areas of interest for Clinical Commissioning Groups and the wider NHS. As appropriate, the report may also include specific items requiring approval or for noting by Governing Body members.
Relevant CCG priorities/objectives:
Compliance with Statutory Duties ☒ Establishment of a Strategic Commissioner ☒
Financial Management ☐ Wider system architecture development (e.g. ICP, PCN development)
☒
Performance Management ☒ Cultural and/or Organisational Development ☐
Strategic Planning ☒ Procurement and/or Contract Management ☐
Conflicts of Interest:
☒ No conflict identified
Completion of Impact Assessments:
Equality / Quality Impact Assessment (EQIA)
Yes ☐ No ☐ N/A ☒ Not required for this item.
Data Protection Impact Assessment (DPIA)
Yes ☐ No ☐ N/A ☒ Not required for this item.
Risk(s):
No risks are identified within this report.
Confidentiality:
☒No
Accountable Officer Report
22 of 224 09:00 - 10.50-04/08/21

Recommendation(s):
The Governing Body is requested to:
1. RECEIVE the Accountable Officer’s Report for information.
Accountable Officer Report
23 of 22409:00 - 10.50-04/08/21

Page 3
Accountable Officer’s Report
COVID-19 Update
1. Local Prevalence and Response
As social distancing measures have eased, there has been an increase in the infection rate, with Nottinghamshire's ‘R’ rate remaining slightly above that of England as a whole. This has seen Bassetlaw, Broxtowe, Gedling, Newark and Sherwood, and Rushcliffe recording their highest ever infection rates.
Hospital admission rates have also been rising. As of 20 July, 107 beds in Nottinghamshire’s hospitals were occupied by patients with Covid-19; with many of these patients either unvaccinated or having had only one dose of the vaccination. This compares to mid-May, when there were 11 admissions to hospital. Information on the latest Covid-19 related data is published on a weekly basis on the CCG’s website at https://nottsccg.nhs.uk/news/.
GP practices continue to see high volumes of patients. Using the latest figures available, during May over 463,000 appointments were made, with 56% of these appointments face-to-face and 50% of patients seen on the same day or next.
2. Covid-19 Vaccination Programme
So far, in total 1,221,176 vaccinations have been administered in Nottingham and Nottinghamshire, with 527,099 of these being second doses.
Focus remains on increasing the number of people under the age of 40 taking the vaccination, with the ‘Grab a Jab’ campaign. The latest figures show that:
∑ 81.3% of people aged 35-39, 76.7% of people aged 30-34, 59.3% of people aged 25-29 and 58.7% of people aged 18-24 have received a first vaccination; and
∑ 42.3% of people aged 35-39, 30.2% of people aged 30-34, 20.9% of people aged 25-29 and 16.1% of people aged 18-24 have received a second.
Local vaccination centres in Nottingham and Nottinghamshire remain open and nine walk-in sites are open for anyone aged 18 or over. A mobile bus continues to be used across the CCG area and 11 pharmacy-led sites are open for vaccinations. Information on the latest vaccination developments can be found on the CCG’s website at https://nottsccg.nhs.uk/covid-19/. Also provided on the website is information relating to Covid-19 testing arrangements and guidance to support recovery from Covid-19.
The Nottingham and Nottinghamshire Integrated Care System (ICS) Mass Vaccination Team has been shortlisted for ‘The University of Bradford award for cross-sector working’ in the Healthcare People Management Association Excellence in People Awards. The vaccination programme in Nottingham and Nottinghamshire was a complete system response, involving the acute providers, community teams, commissioners, local authorities, volunteers and general practice. Given the pace and scale of the required roll-out, individual organisations
Accountable Officer Report
24 of 224 09:00 - 10.50-04/08/21

Page 4
needed to take the lead on different elements of the programme and work seamlessly together in delivery.
3. Restoration of Services
As reported in my last report, funding to help hospitals continue to reduce long waits for non-urgent patient care has been allocated across local health systems, including Nottingham and Nottinghamshire, as part of an elective recovery accelerator initiative. The funding will play an instrumental role in supporting hospitals to more quickly reduce waiting times that have grown due to the Covid-19 pandemic. In recent months, thanks to the hard work and dedication of our staff, we have already been able to provide far more planned care for people with non-Covid concerns.
In May and June 2021 alone the accelerator initiative enabled: 2,221 more patients to have surgery; 4,932 more patients to have a diagnostic test; and 6,376 more patients to be seen in outpatients.
£4.3 million of new capital equipment has also been ordered, which will aid future sustainability and an ability to increase productivity for elective and cancer care, once theaccelerator initiative has concluded. The capital equipment includes:
∑ £1.2 million for a mobile endoscopy unit;
∑ £300,000 for information and communications technology (ICT) equipment to improve the effectiveness of outpatient clinics; and
∑ £2.4 million for theatre equipment (e.g. operating trolleys, microscopes, new instruments for use in surgery and voice recognition software).
Over the next three months, some of the benefits to patients will include:
∑ Expansion of the Post-Anaesthetic Care Unit (PACU) at Nottingham University HospitalsNHS Trust to help reduce pressure on critical care units and increase the number of elective patients receiving treatment;
∑ Some mobile capacity for endoscopy and CT scanning will be imported to speed up diagnostics and treatment for patients; and
∑ New ophthalmology and ear, nose and throat (ENT) equipment at Sherwood Forest Hospitals NHS Foundation Trust will enable them to see and assess more patients.
We will be working closely with NHS England and NHS Improvement to monitor the impact of these interventions, so that learning can be shared with, and adopted by, our neighbours and other health systems across England, hopefully helping many more patients get the care they need quicker.
CCG Updates and Developments
4. 2020/21 Annual Report and Accounts
The CCG’s 2020/21 Annual Report and Accounts has been published on the CCG’s website in line with the Department of Health and Social Care reporting requirements. The Annual
Accountable Officer Report
25 of 22409:00 - 10.50-04/08/21

Page 5
Report provides an overview of the organisation, its purpose and a summary as to how the organisation has performed over the last year. The report also describes how governance, risk management and decision-making arrangements have operated over the last year and provides assurance on the overall stewardship of the organisation, along with information about the CCG’s workforce. The annual accounts for 2020/21 are appended to the Annual Report.
The Annual Report and Accounts can be accessed at https://nottsccg.nhs.uk/about-us/publications. Arrangements for the CCG’s 2020/21 Annual Public Meeting are currently being developed.
5. 2020/21 CCG Annual Assessment
NHS England has a legal requirement to undertake an annual assessment of CCG performance. In previous years this has been undertaken under a NHS Oversight Framework, with an overall assessment rating. However, taking into account the different circumstances and challenges that CCGs have faced in managing recovery from the pandemic, a simplified process was put in place for the assessment for 2020/21. This saw NHS England completing a review of the CCG’s performance across five key priority areas, based on the CCG’s self-assessment.
Feedback from the process has been positive, particularly noting the CCG’s rapid response and partnership arrangements to responding to the pandemic; oversight of quality and patient experience and how lessons learnt are being taken forward to benefit system working. Going forward, the assessment noted the need for the system to continue to focus on addressing health inequalities; tackle unwarranted variation; and address the underlying financial deficit.
6. CCG Governing Body Member to Step Down
Dr Richard Stratton, who has been a member of the CCG’s Governing Body since April 2020 as GP Representative for South Nottinghamshire, is stepping down from his role at the end of September 2021 to relocate out of the Nottingham and Nottinghamshire area. I would like to extend my best wishes to him and his family for the future and thank him for his valuable input and insight, not only as a member of our Governing Body, but also as a member of the Quality and Performance Committee and Primary Care Commissioning Committee.
Partner Updates
7. Bassetlaw to join the Nottingham and Nottinghamshire Integrated Care System (ICS)
As part of the Health and Care Bill proposals, it was suggested that some ICS boundaries should be changed to align with upper tier local authority boundaries. A decision has now been taken to include the district of Bassetlaw within the Nottingham and Nottinghamshire ICS. This will not affect patients within Bassetlaw, who will continue to be seen and treated by their local GP practice and they will also carry on receiving other health and care services
Accountable Officer Report
26 of 224 09:00 - 10.50-04/08/21

Page 6
in the same way. The key difference will be the development of stronger connections between Nottinghamshire County Council and the NHS in the planning of health and care services to improve the health and wellbeing of Bassetlaw people. Over the coming days and weeks, we will work in partnership with health and care organisations in Bassetlaw to ensure a smooth transition into this newly formed way of working.
8. Kathy McLean confirmed as Integrated Care Board Chair Designate
Kathy McLean has now been confirmed as Nottingham and Nottinghamshire’s Integrated Care Board Chair Designate. The recruitment process that was undertaken in relation to Kathy’s role has been confirmed as appropriate for the anticipated establishment of the statutory Integrated Care Board.
The second reading of the Health and Care Bill took place on 14 July. The Bill aims to move existing ICSs to a statutory footing to allow for further integration of the health and social care system in order to deliver better, more efficient services and ensure sustainability; as well as wider reforms, including formally merging NHS England and NHS Improvement and making changes to procurement and competition rules relating to health services. This second reading means that the intention remains to establish a statutory Integrated Care Board on 1 April 2022.
9. Nottingham University Hospitals NHS Trust Maternity Services
In December 2020 the Care Quality Commission (CQC) rated the Trust’s maternity services as ‘Inadequate’. Following another focused visit to the service in May 2021 the CQC announced that improvements had been made in some areas. The Trust has taken a number of steps to improve services and the CCG continues to work very closely and proactively with the Trust to make the required changes. There is more work to be done and the Trust has confirmed its commitment to working closely with partners, including the local Maternity Voices Partnership, to ensure further improvements to maternity services, which will include learning lessons from past failures.
The CCG is developing a system-wide action plan to address and resolve, in a collaborative manner, key concerns that not only impact on maternity services, but the Trust as a whole. These challenges relate to culture, leadership and governance and quality of care. The CCG is also working closely with NHS England and Improvement to ensure that all issues come to light, that families are listened to and that all issues are addressed.
10.Additional National Funding for Ambulance Trusts
East Midlands Ambulance Service NHS Trust will receive £3,758,000 as part of an extra £55 million funding boost from NHS England to ambulance trusts to increase staff numbers ahead of winter. The funding aims to help services to recruit more 999 call handlers, crews and clinicians to work in control rooms. Each service will decide locally how best to spend their budget to increase staffing numbers such as offering part time workers full time roles, recruiting extra call handlers or offering staff incentives to help with retention.
Accountable Officer Report
27 of 22409:00 - 10.50-04/08/21

Page 7
11. ICS Board Meeting Update
The Nottingham and Nottinghamshire Integrated Care System (ICS) Board last met virtually on 1 July. A summary of the meeting is provided for information at Appendix A.
All meeting papers are published on the ICS website at https://healthandcarenotts.co.uk/. The next ICS Board meeting is scheduled for 2 September 2021.
12.Health and Wellbeing Board Updates
Nottinghamshire County Health and Wellbeing Board
The Nottinghamshire County Health and Wellbeing Board last met virtually on 9 June. The meeting focussed on the County Council’s approach to Local Area Coordination. This is an all age support model and community based approach, which supports individuals to stay as independent as possible within their own communities and to ensure that all interventions seek to maximise their independence.
The papers and minutes from the meeting are published on Nottinghamshire County Council’s website here: https://www.nottinghamshire.gov.uk/care/health-and-wellbeing/health-and-wellbeing-board.
Nottingham City Health and Wellbeing Board
The Nottingham City Health and Wellbeing Board last met virtually on 28 July. The meeting focussed on the developing ICS in Nottingham and Nottinghamshire; Children and Adult safeguarding challenges; and a Speech, Language and Communication Strategy.
The papers and minutes from the meeting are published on Nottingham City Council’s website here:https://committee.nottinghamcity.gov.uk/ieListMeetings.aspx?CId=185&Year=0.
National Updates
13.Chief Executive of NHS England Appointed
Amanda Pritchard has been appointed as the new Chief Executive of NHS England. Amanda will be the first woman in the health service’s history to hold the post, which she will take up on 1 August 2021. As NHS Chief Executive, she will be responsible for an annual budget of more than £130 billion. Amanda takes up the role after serving as the NHS’ Chief Operating Officer (COO) for two years. Her appointment follows an open and competitive recruitment process by the Board of NHS England and NHS Improvement.
Recommendation(s)
The Governing Body is requested to:
∑ RECEIVE: the Accountable Officer’s Report for information.
Accountable Officer Report
28 of 224 09:00 - 10.50-04/08/21

Page 1 of 3
ICS Board Summary Briefing – July 2021 Please find below the Nottingham and Nottinghamshire Integrated Care System (ICS) update following the ICS Board on 1
st July. Please ensure this is cascaded to Governing Boards/Bodies, Management Teams
and other key stakeholders and teams across your respective organisations. Minutes from the ICS Board meetings held earlier in the year are always published on the system’s website – https://healthandcarenotts.co.uk/about-us/ics-board/
Introduction The Chair of the ICS, Dr Kathy McLean, welcomed the Board members to the meeting and also noted that this would be the final meeting as ICS Clinical Lead for Dr Nicole Atkinson. Kathy led the Board’s tributes to Nicole’s work and noted that she would be continuing as Clinical Lead for the South Nottinghamshire ICP. Kathy also welcomed a number of citizens and staff from across the system to the virtual Board meeting, streamed live on YouTube. Patients, citizens and staff from organisations across the system are always welcome to the Board to hear the discussions – all the papers for the meeting are available at https://healthandcarenotts.co.uk/about-us/ics-board/. Interested parties can also submit questions to be asked to the Board – details of how to do this are included with the papers on the website and promoted on social media. Citizen Story – Improving Musculoskeletal Health in Mid Nottinghamshire Dr Thilan Bartholomeuz, GP and Clinical Lead for Mid Nottinghamshire ICP presented the citizen story of the work to deliver better Musculoskeletal (MSK) outcomes in Mid Nottinghamshire including the showing of a short video from patient representative, Debs Dulake. By way of introduction, Dr Bartholomeuz noted that MSK is the third largest cause of reduction in health life expectancy in the country and that around one fifth of the population have some sort of MSK condition. The Board heard via the video of the recent improvements in MSK care in Mid Notts including a more collaborative and integrated approach. This new approach was based on the feedback from patients who had previously noted that care was disjointed and often involved periods where patients were unclear who was in charge of their condition. The new approach does not involve additional resources, just better deployment of existing staff and money to achieve improved outcomes. The Board welcomed this presentation of the improved approach and discussed how these learnings would be translated to other ICPs within the ICS. They also discussed how a Health Inequalities approach underpinned this work, seeking to ensure that those in potentially excluded groups could access this kind of elective treatment on a more equitable basis. The Board also noted that this was not about matching patients to a pathway but about creating a more personalised approach and helping patients to navigate through it. Report of the Executive Lead and Chair
Accountable Officer Report
29 of 22409:00 - 10.50-04/08/21
Page 2 of 3
In a new, regular, agenda item, Kathy and Amanda Sullivan, Interim ICS Executive Lead, shared a round-up of developments from across the system recent weeks. In particular, Amanda and Kathy heralded the pending publication of the Government’s Health and Care Bill but noted that the change to Secretary of State for Health and Social Care might impact on the timetable for this. In the period before the publication of the Bill, leaders from across the ICS were continuing to make progress on ensuring the structures, processes and arrangements were in place for an anticipated April 2022 commencement of the Government’s reforms. This progress has been boosted in recent days by the publication of NHSE/I’s ICS ‘Design Framework’ setting out the expectations for Systems, pending confirmation via the Parliamentary process. Amanda and Kathy were able to confirm to the Board that good progress was being made and the expectations set out in the Design Framework were in line with our working assumptions so far. ICS ‘Partnership Agreement’ Dr Kathy McLean confirmed to the Board that the ICS’s Partnership Agreement was nearing its completion and adoption across the system. Many organisations had already endorsed it with others just waiting on their formal meetings to complete that process. Cllr Adele Williams from Nottingham City Council confirmed that the Agreement would also be going through the formal adoption process at the Council but also proposed a number of additional elements for the Agreement which were broadly accepted for inclusion. Insights on Health and Wellbeing – Joint Strategic Needs Assessment Led by Jonathan Gribbin, Director of Public Health, Nottinghamshire County Council and Lucy Hubber, Director of Public Health, Nottingham City Council, the Board had an in-depth and wide-ranging discussion on the development and use of the system’s Joint Strategic Needs Assessments (JSNAs). JSNAs are a continuous process of strategic assessment and planning. The JSNA process ensures that a comprehensive picture of health and wellbeing needs for the local population is formed and used to shape commissioning priorities to improve health and wellbeing and reduce health inequalities in our communities. Local Authorities and CCGs have joint responsibility to ensure that JSNAs are produced and used to inform commissioning priorities and activities. Nottingham City and Nottinghamshire County have, in recent years, collaborated closely on the production of their JSNAs, ensuring a common format and approach wherever possible. Work to develop a fresh JSNA for both Local Authority areas has been impacted by the Covid-19 pandemic but as that work starts to abate, and with the publication of the Government’s White Paper and the anticipated transition to a statutory ICS, it is now timely to refresh the approach and direction of the development of the JSNAs to ensure that their work and outputs is central to the work of the ICS. Jonathan and Lucy asked ICS Board members to consider two questions – what topics and themes would be appropriate for prioritisation within the JSNA production process; and, what resources and approaches would ICS partners be able to offer to support the production of the JSNAs. Colleagues from all partners confirmed their support of this refreshed approach and offered a number of possible areas for focus including: the impact of Covid-19 (including ‘Long Covid’) on population health; the impact of neurological conditions; support to PCNs to understand their populations; longstanding factors on health including smoking, alcohol and obesity; health inequalities; and, the appropriate Restoration of NHS and Local Authority services paused during the Pandemic.
Accountable Officer Report
30 of 224 09:00 - 10.50-04/08/21

Page 3 of 3
Jonathan and Lucy welcomed the wide variety and depth of inputs in this discussion as well as offers of support and committed to return with a proposed workplan and work with partners to take forward specific topics. Priority Population Groups The ICS Board agreed in May 2021 to focus on three transformation areas to embed the Outcomes Framework within clinical transformation, with a focus on key population groups within Nottingham and Nottinghamshire as follows:
a) Community Care; b) Children and Young People; and c) Integration of Person Centred Commissioning
Amanda Sullivan, Interim Executive Lead, updated the Board on progress since the last public meeting. This included broad-based engagement with relevant parties on the Community Care work to develop the approach; a review of Commissioning arrangements and the submission of an Expression of Interest to NHSE/I to be a pilot area for Children and Young People transformation; and, the development of a high-level roadmap for Person Centred Commissioning. The Board welcomed this update and confirmed its ongoing support for the work. Other Business including Performance Report The Board received reports from the Transition and Risk Committee, the Quality Committee and the Finance Committee. This included confirming that the work to manage the transition to a statutory system by April 2022 was on track (as described above) and the endorsement of an overall ICS approach to Quality. Amanda Sullivan described some headlines from the Performance Report for the system. These included increased pressure on A&E and also 111 as well as the local impact of the nationally recognised increase in elective operation waiting lists. A new report format was welcomed by the Board and it was noted that the data clearly displayed the Health Inequalities present in access to care, including for elective operations, as discussed earlier in the MSK Citizen Story. The Board reviewed the meeting against the Partnership Agreement and confirmed that the next meeting in public would be on 2nd September 2021. Dr Kathy McLean, Independent Chair, Nottingham and Nottinghamshire ICS Amanda Sullivan, Interim Executive Lead, Nottingham and Nottinghamshire ICS
Accountable Officer Report
31 of 22409:00 - 10.50-04/08/21

Page 1 of 2
Meeting Title: Governing Body (Open Session) Date: 04 August 2021
Paper Title: Highlight report from the (virtual)
meeting of the CCG’s Primary Care
Commissioning Committee
Paper Reference: GB 21 058
Chair of the
meeting:
Eleri de Gilbert – Non - Executive
Director
Attachments/
Appendices:
Summary
Purpose:
Approve ☐ Endorse ☐ Review
☐ Receive/Note for:
Assurance
Information
☒
Summary of the Meetings
The Primary Care Commissioning Committee (PCCC) met on the 16 June 2021 and 21 July 2021. Due to
the current Coronavirus (Covid-19) situation, the meetings were held virtually.
At the June meeting, the Committee:
RECEIVED routine reports in relation to; Primary Care Contracting, additional expenses in relation
to Covid-19 and a summary of OPEL reporting. OPEL reporting had reflected the increased
pressures in Primary Care and the accuracy with which practices are recording their OPEL status.
RECEIVED the month two financial report noting that the 2020/21 Accounts had been submitted to
NHS England/Improvement (NHSE/I). A clean audit report had been received with no changes to
the previously reported spend.
SCRUTINISED the risk register and were ASSURED that all risks adequately capture primary care
pressures as discussed at the June 2021 meeting of the Governing Body and recent Primary Care
Commissioning Committee meetings.
At the July meeting, the Committee:
NOTED that demand in general practice remains high.
NOTED that two new enhanced services for Long Covid and Weight management would be
established following receipt of guidance from NHS England/Improvement (NHSE/I). Practices have
until 31 July 2021 to sign up to deliver the services. The Committee will receive an update in August
detailing practice sign up.
NOTED that 15 practices had been randomly selected to take part a programme established by
NHS England titled, ‘Access Improvement Programme Funding’. The funding will support the
selected practices over a 12 month period. The aim of the programme is to support
practices/Primary Care Networks (PCNs) to overcome challenges that are currently being faced and
implement new ways of working to optimise the workforce, efficiency and patient experience.
RECEIVED an update on work undertaken with PCNs around extended access arrangements from
April 2022. The national specification is anticipated imminently.
RECEIVED an update on GP Information Technology (IT) issues, this included: a summary of the
Primary Care Commissioning Committee Highlight Report – 16 June 2021 and 21 July 2021
32 of 224 09:00 - 10.50-04/08/21

Page 2 of 2
work of the IT Steering group and an update on the GP IT Futures programme (a national
programme to re-procure GP IT systems). In addition, the CCG continues to bid for access to NHS
England capital funding for a number of IT schemes, including the provision of up-to-date hardware
and software to practices. A programme of work whereby the CCG and Nottinghamshire Health
Informatics (NHIS) colleagues visit individual practices over the remainder of 2021/22 is underway.
The visits will provide an opportunity to discuss any IT-related area which the practice may want to
pursue or require further support; and to ensure that practices are meeting their contractual
obligations with regard to IT and access to information.
RECEIVED a report on Learning Disability Annual Health checks. The NHS Long Term Plan gave a
commitment that at least 75% of people with a Learning Disability (LD) aged 14 years and over
would receive an Annual Health Check from their GP practice by 2023/24. The target for 2021/22 is
70% by the end of March 2022 and the CCG focus for 2021/22 is to improve the quality of the
health checks.
NOTED that the Clinical Director uplift payment to support the Covid-19 vaccination programme
would continue through quarter two.
APPROVED the work programme for the open and confidential meetings of the Committee for
2021/22; noting that the CCG would need to continue to discharge its duties as per the primary care
delegation agreement with NHSE until 31 March 2022.
AGREED that in light of the Primary Care survey results it would be timely to review the scores of
risks associated with workforce and workload pressures
RECEIVED a quarterly report on PCN activity, recognising the level of activity taking place across
PCNs.
Key messages for the Governing Body
The Committee:
RECEIVED the summary findings following a survey of general practice, conducted jointly by the
CCG and LMC, to which 300 responses had been received. The aim of the survey was to listen to
the views and needs of general practice, given the current challenges being faced by general
practice as demand continues to increase. The survey was open to all primary care staff and
recipients were urged to respond to the survey on an individual basis rather on behalf of the
practice. The key findings included; increased demand on primary care services, workload
pressures causing physical and mental health issues for practice staff; many expressing a desire to
retire early or reduce their commitment. Responders supported the role of the LMC and recognised
the benefit of locality working within the CCG and the CCGs role in coordinating the Covid 19
vaccination programme. Many responders expressed that they did not understand what the ICS
does or their role within it. The committee welcomed the survey but was keen that an action plan is
developed to address the issues raised. It was confirmed that the Committee will receive regular
updates on action plans developed as part of the transition planning.
The ratified minutes of the July meeting will be received by the Governing Body on the 06 October 2021.
Primary Care Commissioning Committee Highlight Report – 16 June 2021 and 21 July 2021
33 of 22409:00 - 10.50-04/08/21

Page 1 of 2
Meeting Title: Nottingham and Nottinghamshire Patient and Public Engagement Committee
Date: 04 August 2021
Paper Title: Highlight report from meetings held on
29 June and 27 July 2021 Paper Reference: GB 21 059
Chair of the meeting:
Sue Clague, Chair of the Nottingham and Nottinghamshire Patient and Public Engagement Committee
Attachments/ Appendices:
-
Summary Purpose:
Approve ☐ Endorse ☐ Review
☐ Receive/Note for:
Assurance
Information
☒
Summary of the Meeting
The Nottingham and Nottinghamshire Patient and Public Engagement Committee (PPEC) has continued to
meet virtually on a monthly basis and most recently, meetings have taken place on 29 June and 27 July
2021. PPEC members have valued the attendance of Dr James Hopkinson and Rosa Waddingham at their
meetings representing the Executive Team.
Community and voluntary sector representatives from each ICP area are now included in the PPEC
membership, Jane Hildreth, Jules Sebelin and Carolyn Perry are fulfilling these roles.
Key agenda items considered by PPEC members during the above mentioned meetings have included;
The development of community engagement for the Integrated Care System.
Focus on the Mid Nottinghamshire ICP vision, objectives, associated breakthrough objectives and
delivery of engagement through the Voluntary Sector Alliance contract for patient and public
engagement. Key outcomes shared included recovery engagement; seeking out insight from the
most vulnerable, diabetes and learning disabilities engagement, end of life and musculo skeletal
pathway development and support for the Covid Vaccination Programme.
Update on the impact of engagement to develop the Children and Young People’s Emotional
Wellbeing Early Support, Training and Consultation Service.
Updates on Covid infection rates, details of ongoing plans to vaccinate anyone over the age of 18
years via the ‘Big Weekend’ and the opportunity to walk into any of the nine vaccination centres
currently administering the vaccination were shared with PPEC members.
Communication and engagement undertaken in relation to the Platform One Practice transition and
mobilisation was reviewed by PPEC members. Recommendations arising from the Health Scrutiny
Committee had led to the establishment of a Stakeholder Group chaired by Healthwatch, who had
supported a smoother transition for patients and delivered good communication resources.
Plans for restoration of elective activity, planned care transformation consisting of 3 core
workstreams; cancer, diagnostics and elective and out-patient transformation were shared with
PPEC members.
Patient and Public Engagement Committee Highlight Report
34 of 224 09:00 - 10.50-04/08/21

Page 2 of 2
Key Messages for the Governing Body
The key messages that PPEC members agreed to share with the Governing Body from its meetings held
on 29 June and 27 July 2021 are;
1. PPEC members welcomed the development of plans to support community engagement as part of
ICS transition and to their involvement in planned workshops to develop this further. PPEC
members suggested reference to co-production should be included in the plans.
2. The Mid Nottinghamshire Voluntary Sector Alliance update was welcomed and the need to focus on
areas of deprivation and ethnically diverse communities who may be isolated geographically due to
lower prevalence was highlighted by PPEC members.
3. The children and young people engagement provided an excellent example of co-production in
service transformation. Immediate improvements had also been achieved through provision of
better communication resources.
4. Discussion regarding Platform One Practice transition had highlighted the need for earlier and better
engagement in Primary Care Commissioning decisions working with local groups and networks who
support the most vulnerable within our communities. A stronger link between PPEC and the
Primary Care Commissioning Committee was also recommended.
The ratified minutes of Patient and Public Engagement Committee held on 29 July 2021 will be presented to the Governing Body on 06 October 2021.
Patient and Public Engagement Committee Highlight Report
35 of 22409:00 - 10.50-04/08/21

Page 1 of 2
Meeting Title: Governing Body (Open Session) Date: 04 August 2021
Paper Title: Finance and Resources Committee
Highlight report – 23 June and 28 July
2021.
Paper Reference: GB 21 060
Chair of the
meeting:
Shaun Beebe – Non-Executive Director Attachments/
Appendices:
None
Summary
Purpose:
Approve ☐ Endorse ☐ Review
☐ Receive/Note for:
Assurance
Information
☒
Summary of the Meeting
The Finance and Resources Committee (FRC) met on the 23 June and 28 July 2021. Due to the current
Coronavirus (COVID-19) situation, the meetings were held virtually. Over the course of the meetings, the
Committee:
RECIEVED an update on the development of the CCG’s agile working model. Plans to welcome staff
back to the office had been postponed to the 19th July in line with the Government announcement to
postpone easing of COVID-19 measures.
RECEIVED the finance reports for month two at the June meeting, which showed a pre Elective
Recovery Fund (ERF) deficit of £3.7m for the H1 period. At the July meeting, the month three finance
reports were received. This showed that in respect to ERF a re-submission exercise took place that
excludes elective recovery costs (for independent sector activity); elective recovery income and an
element of ICS associated activity costs. As a result, the CCG position shows a pre-ERF surplus of
£4.0m for H1; moving to a break even position, based on delivering the ERF activity target.
RECEIVED the reinstated Cross Provider Report, which gave an overview of financial and activity
performance for the Nottingham and Nottinghamshire CCG at months two and three, with a particular
focus on the major acute contracts.
RECEIVED a briefing on the financial aspects of the Nottingham and Nottinghamshire ICS’ Vaccination
Programme in order to provide context for wider discussions on other financial issues relating to the
CCG and ICS.
RECIEVED the workforce report summarising information relating to the CCG’s workforce. The key
Key Workforce Indicators currently stand at:
Target Actual (as at end May 2021)
Sickness Absence 2.5% 1.52%
Monthly Turnover 1% Exceeded 1% in 6 of the last 12 months
Completion of Appraisals 92% 76%
Finance and Resources Committee Highlight Report – 23 June 2021 and 28 July 2021
36 of 224 09:00 - 10.50-04/08/21

Page 2 of 2
CONSIDERED risks specific to the Committee’s remit.
Key Messages for the Governing Body
None.
The ratified minutes of the June 2021 meeting will be received by the Governing Body on the 4
August 2021. The ratified minutes of the July meeting will be received by the Governing Body on 6
October 2021.
Finance and Resources Committee Highlight Report – 23 June 2021 and 28 July 2021
37 of 22409:00 - 10.50-04/08/21

Page 1 of 18
Meeting Title: Governing Body (Open Session) Date: 04 August 2021
Paper Title: Finance Report Month Three
Paper Reference: GB 21 061
Sponsor:
Presenter:
Stuart Poynor, Chief Financial Officer Attachments/ Appendices:
Michael Cawley, Operational Director of Finance
Purpose: Approve ☐ Endorse ☐ Review
☐ Receive/Note for:
Assurance
Information
☒
Executive Summary
The CCG currently remains under a temporary financial regime due to the continuing COVID-19 situation; which splits the financial year into two reporting periods H1, April to September and H2, October to March.
The CCG has updated the financial plan for H1 between month two and month three reporting for aspects associated with the Elective Recovery Fund (ERF). The update involved adjusting the financial plan for independent sector (IS) provider costs associated with elective recovery. The CCG is reporting a break-even plan position (year to date (YTD) and forecast H1 out-turn position), after accounting for delivery of the ERF plan.
Key financial risks include those associated with the non-delivery of the ERF activity plan alongside recent changes that increases the threshold for attaining ERF income from Q2 onwards. The potential adverse impact on the CCG is in the range £0.5m to £0.76m.
Continuing healthcare costs continue to be a cost pressure for the CCG. Year to date there is an adverse variance of £0.65 million, and a forecast adverse variance of £1.3 million.
At the end of June, NHS organisations are presenting an ICS favourable variance of £2.1m (YTD) with a forecast to the end of H1 being break-even. (This is before accounting for any impact as a result of the change in ERF guidance).
The CCG capital plan for the full year is £2.1 million, utilising the full capital resource limit (CRL) notified by NHSEI.
The report was discussed by the Finance and Resources Committee at its July meeting and the Committee approved it for onward submission to the Governing Body.
2021/22 Financial Report Month Three
38 of 224 09:00 - 10.50-04/08/21
Page 2 of 18
Relevant CCG priorities/objectives:
Compliance with Statutory Duties ☐ Wider system architecture development (e.g. ICP, PCN development)
☐
Financial Management ☒ Cultural and/or Organisational Development
☐
Performance Management ☐ Procurement and/or Contract Management ☐
Strategic Planning ☐
Conflicts of Interest:
☒ No conflict identified
☐ Conflict noted, conflicted party can participate in discussion and decision
☐ Conflict noted, conflicted party can participate in discussion, but not decision
☐ Conflict noted, conflicted party can remain, but not participate in discussion or decision
☐ Conflict noted, conflicted party to be excluded from meeting
Completion of Impact Assessments:
Equality / Quality Impact Assessment (EQIA)
Yes ☐ No ☐ N/A ☒ Not required
Data Protection Impact Assessment (DPIA)
Yes ☐ No ☐ N/A ☒ Not required
Risk(s):
N/A
Confidentiality:
☒No
☐Yes (please indicate why it is confidential by ticking the relevant box below)
Recommendation(s):
1. To NOTE the Finance Report
2021/22 Financial Report Month Three
39 of 22409:00 - 10.50-04/08/21

Page 3 of 18
2021/22 Financial R
eport Month T
hree
40 of 22409:00 - 10.50-04/08/21
Page 4 of 18
2021/22 Financial R
eport Month T
hree
41 of 22409:00 - 10.50-04/08/21

Page 5 of 18
2021/22 Financial R
eport Month T
hree
42 of 22409:00 - 10.50-04/08/21

Page 6 of 18
2021/22 Financial R
eport Month T
hree
43 of 22409:00 - 10.50-04/08/21

Page 7 of 18
2021/22 Financial R
eport Month T
hree
44 of 22409:00 - 10.50-04/08/21

Page 8 of 18
2021/22 Financial R
eport Month T
hree
45 of 22409:00 - 10.50-04/08/21
Page 9 of 18
2021/22 Financial R
eport Month T
hree
46 of 22409:00 - 10.50-04/08/21

Page 10 of 18
2021/22 Financial R
eport Month T
hree
47 of 22409:00 - 10.50-04/08/21

Page 11 of 18
2021/22 Financial R
eport Month T
hree
48 of 22409:00 - 10.50-04/08/21
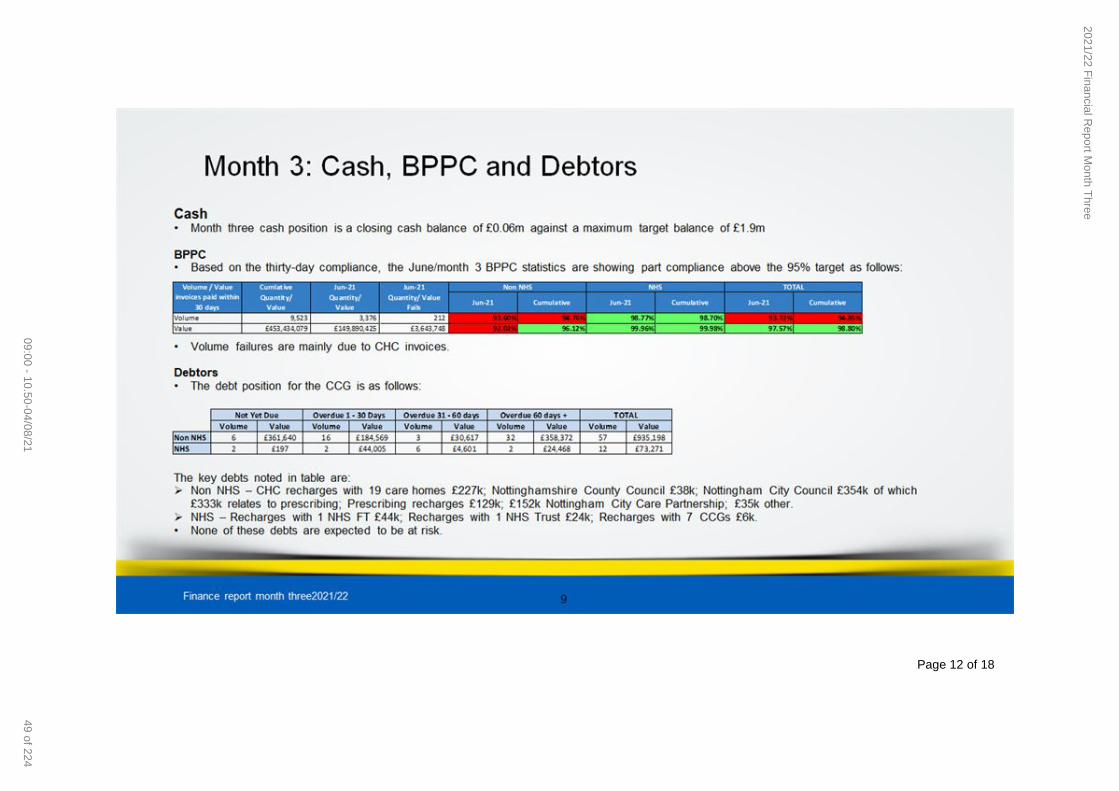
Page 12 of 18
2021/22 Financial R
eport Month T
hree
49 of 22409:00 - 10.50-04/08/21

Page 13 of 18
2021/22 Financial R
eport Month T
hree
50 of 22409:00 - 10.50-04/08/21

Page 14 of 18
2021/22 Financial R
eport Month T
hree
51 of 22409:00 - 10.50-04/08/21

Page 15 of 18
MONTHS 1-6 YEAR TO DATE MONTHS 1-6 FORECAST
Plan
£m
Actual
£m
Variance
£m
H1 Plan
£m
Forecast
Outturn
£m
Forecast
Variance
£m
Acute Services
Nottingham University Hospitals 157.20 157.20 0.00 314.40 314.40 0.00
Nottingham University Hospitals - Treatment Centre 0.00 0.00 0.00 0.00 0.00 0.00
Nottingham University Hospitals - Non Core 0.13 0.13 (0.00) 0.13 0.13 (0.00)
Sherwood Forest Hospitals 74.39 74.39 (0.00) 148.78 148.78 0.00
Sherwood Forest Hospitals - Non Core 0.03 0.03 (0.00) 0.03 0.03 0.00
East Midlands Ambulance Service 10.14 10.14 0.00 20.28 20.28 0.00
University Hospitals Of Derby And Burton 1.69 1.69 0.00 3.38 3.38 0.00
United Lincolnshire Hospitals 1.36 1.36 0.00 2.72 2.72 0.00
Doncaster & Bassetlaw 0.89 0.89 0.00 1.79 1.79 0.00
University Hospitals Leicester 0.51 0.51 0.00 1.03 1.03 0.00
Sheffield Teaching 0.33 0.33 0.00 0.65 0.65 0.00
Chesterfield Royal 0.00 0.00 0.00 0.00 0.00 0.00
Acute - NHS - Other Block Contracts 0.00 0.00 0.00 0.00 0.00 0.00
Acute - NHS 0.00 0.00 0.00 0.00 0.00 0.00
Acute Contracts - Position on Prior Year 0.00 0.00 0.00 0.00 0.00 0.00
Other NHS - NCA's 0.38 0.38 0.00 0.76 0.76 0.00
Ramsay Woodthorpe 3.68 3.16 0.52 7.46 6.81 0.65
BMI Healthcare 2.03 1.49 0.54 5.29 4.32 0.97
Barlborough 0.25 0.25 0.00 0.50 0.50 0.00
Spire 1.08 0.55 0.54 2.17 1.19 0.98
Other Non NHS - Acute 0.13 0.10 0.03 0.26 0.23 0.03
Cancer Monies 0.91 0.91 (0.00) 1.24 1.24 (0.00)
Diabetes Projects 0.00 0.00 0.00 0.00 0.00 0.00
Resilience 0.00 0.00 (0.00) 0.00 0.00 (0.00)
Urgent Care Centres 0.72 0.73 (0.02) 1.43 1.46 (0.03)
Acute Investment QIPP 0.00 0.00 0.00 0.00 0.00 0.00
Activity - Other 0.01 0.00 0.01 0.01 0.00 0.01
Acute - COVID 0.00 0.00 0.00 0.00 0.00 0.00
ERF ICS system adjustment budget (6.18) 0.00 (6.18) (12.36) 0.00 (12.36)
Acute - CCG Coding Change Adjustments 0.00 (2.33) 2.33 0.00 (2.71) 2.71
Total Acute Services 249.67 251.91 (2.23) 499.95 506.99 (7.04)
Community Services
Nottinghamshire Healthcare - General Health 24.23 24.23 (0.00) 48.46 48.46 0.00
Sherwood Forest Hospitals 2.62 2.62 (0.00) 5.24 5.24 0.00
Sherwood Forest Hospitals - Activity Reserve / QIPP / FRP 0.00 0.00 0.00 0.00 0.00 0.00
Other NHS - Community 0.83 0.83 (0.00) 1.66 1.66 0.00
Other Non NHS - Community 15.07 14.76 0.31 30.13 29.99 0.14
End of Life 0.43 0.42 0.01 0.86 0.85 0.02
Community QIPP not transacted 0.00 0.00 0.00 0.00 0.00 0.00
Community Investment QIPP 0.00 0.00 0.00 0.00 0.00 0.00
Community - Other 0.00 0.00 0.00 0.00 0.00 0.00
Community - COVID 0.27 0.27 (0.00) 0.55 0.55 0.00
Community - Balancing Adjustments to NHSE/I Model (0.29) 0.00 (0.29) (0.59) (0.43) (0.16)
Community - CCG Coding Change Adjustments 0.00 0.00 0.00 0.00 0.00 0.00
Total Community Services 43.16 43.13 0.03 86.32 86.32 (0.00)
Mental Health Services
Nottinghamshire Healthcare - Mental Health 33.09 33.09 0.00 66.62 66.62 0.00
Other NHS - Mental Health 0.21 0.21 (0.00) 0.43 0.43 0.00
Other Non NHS - Mental Health 4.80 4.90 (0.10) 9.60 9.81 (0.21)
S117 Placements 7.45 7.37 0.08 14.90 14.85 0.05
Mental Health QIPP not transacted 0.00 0.00 0.00 0.00 0.00 0.00
Mental Health Investment QIPP 0.00 0.00 0.00 0.00 0.00 0.00
Mental Health - Other 0.00 0.00 0.00 0.00 0.00 0.00
Mental Health - COVID 0.01 0.01 0.00 0.01 0.01 0.00
Mental Health - Balancing Adjustments to NHSE/I Model 4.06 4.06 0.00 8.12 8.12 0.00
Mental Health - CCG Coding Change Adjustments 0.00 0.00 0.00 0.00 0.00 0.00
Total Mental Health Services 49.62 49.65 (0.02) 99.68 99.84 (0.16)
Primary Care Services
Primary Care Contracting 39.23 39.13 0.10 81.78 81.59 0.20
Primary Care Contracting - Balancing Adjustments to NHSE/I Model 0.00 0.00 0.00 0.00 0.00 0.00
Prescribing 40.07 39.83 0.24 80.14 80.09 0.06
Prescribing - QIPP 0.00 0.00 0.00 0.00 0.00 0.00
Medicine Management - Clinical 0.81 0.71 0.09 1.61 1.43 0.18
CCG Pathways 0.00 0.00 0.00 0.00 0.00 0.00
EH - Primary Care 1.14 1.13 0.01 2.28 2.27 0.01
EH - GP Forward View 1.94 1.94 0.00 3.52 3.52 0.00
Enhanced Services 2.56 2.56 0.00 5.12 5.12 0.00
Practice Transformation fund 0.00 0.00 0.00 0.00 0.00 0.00
GPIT 0.22 0.19 0.04 0.44 0.40 0.04 Out of Hours 2.80 2.80 0.00 5.61 5.61 0.00
Primary Care - Other 0.13 0.11 0.02 0.26 0.21 0.05
Primary Care - COVID 0.04 0.04 (0.00) 0.06 0.06 0.00
Primary Care - Balancing Adjustments to NHSE/I Model 0.00 0.00 0.00 0.00 0.00 0.00
Primary Care - CCG Coding Change Adjustments 0.00 0.00 0.00 0.00 0.00 0.00
Total Primary Care Services 88.95 88.44 0.50 180.83 180.29 0.54
Other Healthcare
Continuing Care & Free Nursing Care 25.94 26.60 (0.65) 51.89 53.20 (1.31)
City Care CHC Assessment 0.67 0.65 0.02 1.34 1.31 0.03
Continuing Care - COVID 3.25 3.25 (0.00) 6.50 6.50 0.00
Continuing Care - Balancing Adjustments to NHSE/I Model 0.00 0.00 0.00 0.00 0.00 0.00
Continuing Care - CCG Coding Change Adjustments 0.00 0.00 (0.00) 0.00 0.00 (0.00)
Total Other Healthcare Costs 29.86 30.50 (0.64) 59.73 61.01 (1.28)
0.00 0.00 0.00 0.00
TOTAL PROGRAMME HEALTHCARE COSTS 461.27 463.63 (2.36) 926.51 934.44 (7.93)
NOTTINGHAM & NOTTINGHAMSHIRE CCG
Appendix 1
Operating Cost Statement: M3
2021/22 Financial Report Month Three
52 of 224 09:00 - 10.50-04/08/21

Page 16 of 18
Other Contracts
Other Non-NHS Services 0.14 0.14 (0.00) 0.28 0.29 (0.01)
Patient Transport 1.72 1.72 (0.00) 3.45 3.45 0.00
Other Non-NHS Services - 111 1.39 1.39 0.00 2.78 2.78 0.00
HDP - COVID 0.00 2.79 (2.79) 0.00 6.28 (6.28)
Social Care 9.03 9.03 0.00 18.06 18.06 0.00
Other - COVID 0.28 0.29 (0.01) 0.56 0.66 (0.10)
Other - Balancing Adjustments to NHSE/I Model 0.00 0.00 0.00 0.00 0.00 0.00
Other - CCG Coding Change Adjustments 0.00 0.00 0.00 0.00 0.00 0.00
Total Other Contracts 12.56 15.37 (2.80) 25.13 31.51 (6.38)
Corporate Non-Running Costs
Corporate - Estates 3.42 3.42 0.00 7.08 7.08 0.00
Corporate Costs - Chief Officer 0.32 0.28 0.04 0.64 0.54 0.10
Corporate Costs - Chief Commissioning Officer 0.54 0.56 (0.02) 1.07 1.09 (0.02)
Corporate Costs - Chief Finance Officer 0.00 (0.00) 0.00 0.00 (0.00) 0.00
Corporate Costs - ICS 1.11 0.53 0.57 2.59 2.59 0.00
Corporate Costs - ICS - Income (0.83) (0.26) (0.57) (1.66) (1.66) 0.00
Corporate Costs - Chief Nurse 0.99 1.04 (0.05) 1.99 2.11 (0.12)
Corporate - COVID 0.00 0.00 0.00 0.00 0.00 0.00
Corporate - Balancing Adjustments to NHSE/I Model 0.00 0.00 0.00 0.00 0.00 0.00
Corporate - CCG Coding Change Adjustments 0.00 0.00 0.00 0.00 0.00 0.00
Vaccination Costs 0.00 0.00 (0.00) 0.00 0.00 0.00
Depreciation, provisions & technical adjustments 0.00 0.00 0.00 0.00 0.00 0.00
Total Corporate Non-Running Costs 5.54 5.58 (0.04) 11.70 11.75 (0.04)
Programme Reserves
Risk Reserves (inc. running cost headroom) 0.00 0.00 0.00 0.00 0.00 0.00
PCCC 0.00 0.00 0.00 0.00 0.00 0.00
QIPP 0.00 0.00 0.00 0.00 0.00 0.00
Other Reserves 0.00 0.00 0.00 0.00 0.00 0.00
Reserves - COVID 0.00 0.00 0.00 0.00 0.00 0.00
Other Reserves - Balancing Adjustments to NHSE/I Model 0.00 0.00 0.00 0.69 0.69 0.00
Other Reserves - CCG Coding Change Adjustments 0.00 0.00 0.00 0.00 0.00 0.00
Total Programme Reserves 0.00 0.00 0.00 0.69 0.69 0.00
TOTAL PROGRAMME NON- HEALTHCARE COSTS 18.11 20.94 (2.84) 37.53 43.95 (6.42)
TOTAL NET OPERATING EXPENDITURE - PROGRAMME 479.37 484.57 (5.20) 964.03 978.39 (14.36)
Planned Surplus 2.00 0.00 2.00 4.01 0.00 4.01
TOTAL AVAILABLE RESOURCE - PROGRAMME 481.38 484.57 (3.20) 968.04 978.39 (10.35)
Running Costs
Running Costs 0.00 0.00 0.00 0.00 0.00 0.00
Running Costs - Chief Officer 0.39 0.36 0.03 0.77 0.71 0.06
Running Costs - Chief Finance Officer 1.35 1.33 0.02 2.70 2.62 0.08
Running Costs - Chief Commissioning Officer 1.37 1.43 (0.06) 2.75 2.88 (0.14)
Running Costs - Chief Nurse 0.32 0.36 (0.03) 0.65 0.72 (0.07)
Running Costs - Special Projects 0.27 0.27 0.00 0.55 0.57 (0.02)
Running Costs - Communications 0.14 0.17 (0.04) 0.28 0.32 (0.05)
Running Costs - Estates 0.68 0.68 0.00 1.37 1.38 (0.01)
Running Costs - Reserves 0.00 0.00 0.00 0.00 0.00 0.00
Running Costs - COVID 0.00 0.00 0.00 0.00 0.00 0.00
Running Costs - Balancing Adjustments to NHSE/I Model 0.00 0.00 0.00 0.00 0.00 0.00
Running Costs - CCG Coding Change Adjustments 0.00 0.00 0.00 0.00 0.00 0.00
TOTAL AVAILABLE RESOURCE - ADMIN 4.53 4.60 (0.08) 9.06 9.21 (0.15)
TOTAL 485.90 489.18 (3.27) 977.10 987.60 (10.50)
2021/22 Financial Report Month Three
53 of 22409:00 - 10.50-04/08/21

Page 17 of 18
2021/22 Financial R
eport Month T
hree
54 of 22409:00 - 10.50-04/08/21
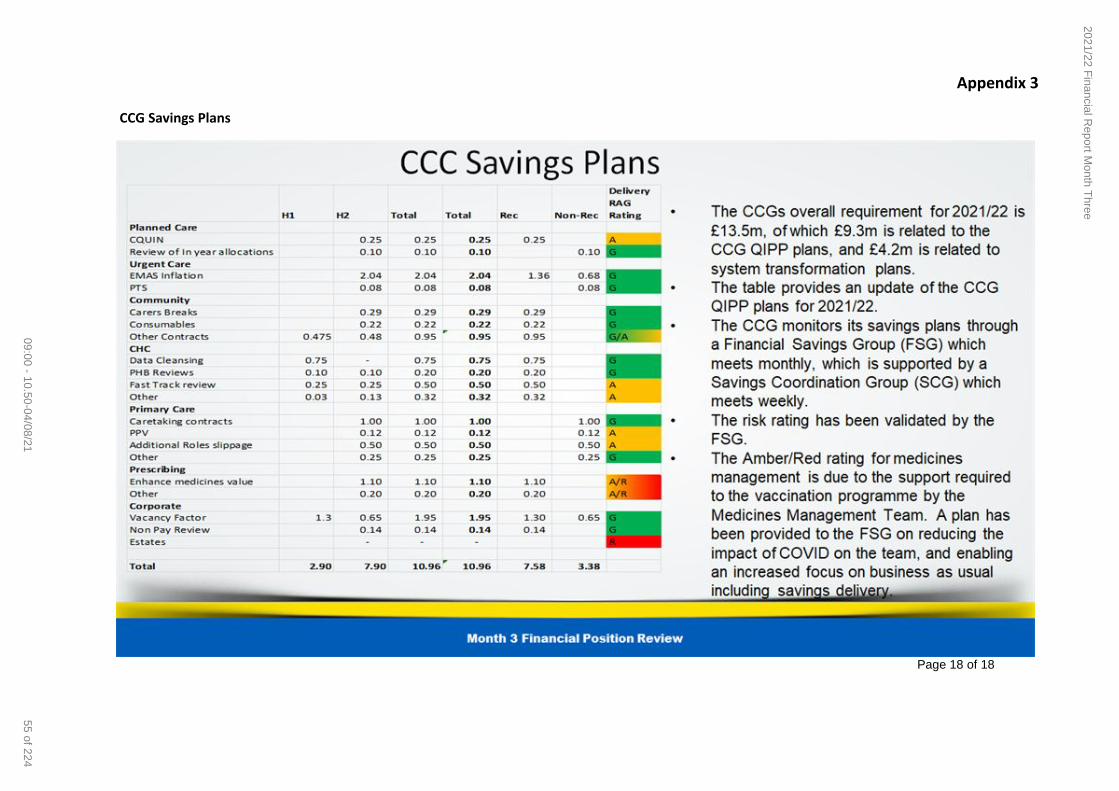
Page 18 of 18
Appendix 3
CCG Savings Plans
2021/22 Financial R
eport Month T
hree
55 of 22409:00 - 10.50-04/08/21

Page 1 of 2
Meeting Title: Governing Body (Open Session) Date: 04 August 2021
Paper Title: Highlight Report from the meeting of
the CCG’s Quality and Performance
Committee
Paper Reference: GB 21 062
Chair of the
meeting:
Eleri de Gilbert, Non-Executive Director Attachments/
Appendices:
None
Summary
Purpose:
Approve ☐ Endorse ☐ Review
☐ Receive/Note for:
Assurance
Information
☒
Summary of the Meetings
The Quality and Performance Committee met on the 24 June and 22 July 2021. Due to the current
Coronavirus (Covid-19) situation, the meetings were held virtually.
At its June meeting the Committee:
APPROVED the Committee’s work programme for 2021/22 and agreed to alternate the meeting
cycle between ‘deep dive’ meetings, focussed on particular areas of concern; and routine meetings
where the standard items would be addressed to ensure the Committee fulfils its duties under the
terms of reference.
a) Undertook a deep dive focus of Nottinghamshire Healthcare NHS Foundation Trust (NHFT) and
AGREED to maintain the associated risk score (RR 116) at 16. This reflected that NHFT is on an
improvement trajectory but recognised that concerns remain in relation to some sub-contracted
services and the sustainability of improvements being made.
RECEIVED a presentation from Public Health colleagues on the suicide and self-harm prevention
strategy and were ASSURED that a system approach to prevention is in place. ASSURANCE was
also provided regarding the CCG focus on suicide awareness training and support.
ENDORSED the Learning Disabilities Death Review (LeDeR) Annual report for publication by 30
June 2021.
At its July meeting the Committee:
a) RECEIVED the routine Integrated Performance report. The Governing Body at its June meeting had
asked the Committee to review specialty plans and trajectories for recovery for each provider. The
Committee were advised that this information is not currently available but is expected as part of the
next planning round, covering the second half of 2021/22.
APPROVED the Serious Incident and Never Event Annual Report for 2020/21. The top five
categories with the highest numbers of reported serious incidents during this reporting period were;
Pressure ulcers, Self-harm (including suicide), Sub optimal care of the deteriorating patient,
Maternity, and Slips, trips and falls. The report included actions for 2021/22.
Quality and Performance Committee Highlight Report – 24 June 2021 and 22 July 2021
56 of 224 09:00 - 10.50-04/08/21

Page 2 of 2
RECEIVED a paper on the oversight and monitoring of Preventing Future Deaths (PFD) reports
issued by the Coroner and APPROVED the approach to align an oversight process with the existing
serious incident management process.
RECEIVED two reports from the Chief Pharmacist; Nottinghamshire Area Prescribing Committee
Report and Medicine Safety Officer’s (MSO) Annual Report and recorded their APPRECIATION to
the team for their significant achievement in progressing business as usual whilst being diverted by
the requirements of the Covid-19 response.
RECEIVED an update on the implementation of Recommended Summary Plan for Emergency Care
and Treatment (ReSPECT) and were ASSURDED by the progress reported. An audit would take
place in the coming months with the outcome reported to the Committee in January 2022.
Key messages for the Governing Body:
The Committee:
Carried out a focused review of the NHT risk following a previous deep dive report and considered
reports related to suicide and self-harm. In conclusion, the Committee AGREED to maintain the
current risk, RR 116 at a score of 16 which reflects both the improvement journey and current
challenges.
RECEIVED annual reports pertaining to; Serious Incidents and Never events and Medicines safety.
AGREED to escalate concerns in relation to the performance of Nottingham University Hospitals
NHS Trust (NUH) after a number of potential and actual, complex and significant quality issues had
been identified. The risk relates to the lack of assurance regarding systematic improvements in the
quality of services provided which may present a risk of unsafe care, poor clinical outcomes and/or
patient safety issues for members of the CCG’s population. The risk score is 20 and as such is
escalated to the Governing Body.
AGREED to elevate the risk score related to NUH Maternity services from 20 to 25 due to the pace
of change. As such this risk is escalated to the Governing Body.
The ratified minutes of the July meeting will be received by the Governing Body on 06 October
2021.
Quality and Performance Committee Highlight Report – 24 June 2021 and 22 July 2021
57 of 22409:00 - 10.50-04/08/21

Page 1 of 2
Meeting Title: Governing Body (Open Session) Date: 04 August 2021
Paper Title: Nursing & Quality Report Paper Reference: GB 21 063
Sponsor:
Presenter:
Rosa Waddingham – Chief Nurse Attachments/ Appendices:
Nursing & Quality Report
Rosa Waddingham – Chief Nurse
Purpose: Approve ☐ Endorse ☐ Review ☐ Receive/Note for:
∑ Assurance∑ Information
☒
Executive Summary
The purpose of this paper is to provide a summary of local quality requirements and monitoring across the services which as commissioned by NHS Nottingham and Nottinghamshire CCG. The report also provides an update on the CCG’s statutory functions or quality improvement work which the CCG lead/are integral to.
The paper updates on the key quality and safety metrics and should be read in collaboration with the CCG Integrated Performance Report (IPR).
Key areas to note:∑ An increased number of serious incidents; however reporting guidance has changed with the inclusion of
healthcare acquired COVID infections since February 2021 and a number of deep dive and look back exercises are being undertaken.
∑ Updates on the twelve providers under enhanced surveillance for quality across the whole health and care sector.
∑ An update on the partnership focus on safe sleeping.
∑ Host commissioner arrangements and activity during the quarter, plus a progress report on inpatient performance for people with a learning disability and/or autism.
Relevant CCG priorities/objectives:
Compliance with Statutory Duties ☒ Wider system architecture development (e.g. ICP, PCN development)
☐
Financial Management ☐ Cultural and/or Organisational Development
☒
Performance Management ☒ Procurement and/or Contract Management ☐
Strategic Planning ☐
Conflicts of Interest:
☐ No conflict identified
☐ Conflict noted, conflicted party can participate in discussion and decision
☐ Conflict noted, conflicted party can participate in discussion, but not decision
Quality Report
58 of 224 09:00 - 10.50-04/08/21

Page 2 of 2
☐ Conflict noted, conflicted party can remain, but not participate in discussion or decision
☐ Conflict noted, conflicted party to be excluded from meeting
Completion of Impact Assessments:
Equality / Quality Impact Assessment (EQIA)
Yes ☐ No ☐ N/A☒ Not applicable to this item
Data Protection Impact Assessment (DPIA)
Yes ☐ No ☐ N/A☒ Not applicable to this item
Risk(s):
N/A
Confidentiality:
☒No
Recommendation(s):
1. To NOTE the Report
Quality Report
59 of 22409:00 - 10.50-04/08/21

1
QUALITY & PERFORMANCE COMMITTEE
NURSING & QUALITY REPORT
JULY 2021

2
EXECUTIVE SUMMARY We continue to review and adapt our approach to quality assurance and improvement, building upon work to date and re-evaluating previous methodologies and processes. Across the services we commission the CCG Nursing & Quality Team are working with 12 providers as part of ‘enhanced surveillance’ where additional support and oversight is in place. This includes: Working with Nottingham University Hospitals as part of the Maternity Safety and Quality
Improvement;
Working with Nottinghamshire Healthcare NHS FT as part of their organisational-wide Improvement Plans across all areas;
Working with the CCG Contracting Team due to concerns identified by CQC and actions taken in
relation to an Independent Provider for Non-Obstetric Ultrasound; Providing support to 4 General Practices following concerns identified by CQC inspection; and
Providing support to 5 Care Homes all with suspensions and support plans in place to improve
the quality of services being provided All providers within the system are working on COVID-19 restoration and recovery plans, including a review and assessment of COVID-19 related harms and focus on waiting lists. Infection control and cascading learning are areas of focus, whilst ensuring that the impact of the pandemic and the welfare of staff is understood and monitored. The CCG Nursing & Quality Team continues to maintain regular contact with providers and insight visits have recommenced. In general providers have continued to offer safe and high quality services and systems are in place to identify areas of concern. Work is progressing to refine and enhance the CCGs approach to system working in terms of Quality Planning, Quality Control, and Quality Improvement. This includes the development of a more effective ‘early warning’ system and surveillance framework. This includes longer term aims to develop a ‘one version of the truth’ quality narrative which will support and inform the commissioning cycle.

3
PART ONE: PROVIDER QUALITY & SAFETY METRICS AND INTELLIGENCE 1. PATIENT SAFETY & QUALITY METRICS
There were 138 serious incidents reported in the system during 2021/22 Q1. This is an increase of 76 in comparison to 2020/21 Q1 and an increase of 38 in comparison to 2020/21 Q4. A significant contributing factor to is the number of deep dives and look back exercises, explained further below. The top three themes for reportable SIs continue to be related to Maternity, Pressure Ulcers, and Apparent/ Actual/Suspected Self-Inflicted Harm: Maternity: During Quarter 1, 22 maternity-related SIs were reported, in the main relating to services provided by NUH. There has been a retrospective review of some incidents through the Local Maternity and Neonatal System, led by the safer care and outcomes group. This has led to cases being retrospectively reported during this quarter when incidents have been identified as meeting the SI criteria. Additional surveillance of these cases is in place to respond to immediate concerns. Pressure Ulcer Incidents: 45 pressure ulcer incidents meeting the SI criteria reported during 2020/21 Q1. 37 of the 45 were reported by NUH. 30 of the 37 were reported retrospectively after being reviewed at the Trust’s internal Pressure Ulcer Incident Review Group Meeting as part of an internal review.
Apparent/Actual/Suspected Self-Inflicted Harm: 24 incidents were reported during Q1. 20 persons were in receipt of Adult Mental Health Services, 4 under the care of Children’s and Adolescent Mental Health Services (CAMHS). 15 of the 24 resulted in death, with three suspected suicides and a further two awaiting coroner’s findings. 7 of the 9 resulted in injury which required admission to an acute hospital for treatment. Nottinghamshire Healthcare NHS FT (NHT) reports increased levels in acuity of distress and presentations. NHT are actively working with Public Health Partners and continue to further implement the suicide prevention strategy.
Never Events (NE): There have been 3 Never Events reported during Quarter 1. Duty of Candour has been enacted for all 3: • Nottingham University Hospitals (NUH) reported a ‘retained foreign object post procedure’. NHS
England Specialised Commissioning is the lead commissioners for this service and is following up the learning.
• Both of the 2 Never Events reported by Sherwood Forest Hospitals (SFH) were ‘wrong site surgery’. The Trust are undertaking an in depth learning exercise around these in observational auditing,

4
ensuring positive patient identification is taking place, and that STOP moments are happening. This will be shared with the CCG and progress reviewed.
A number of providers across the system have highlighted organisational capacity challenges with respect to their serious incident (SI) management process which is impacting on their ability to submit timely SI reports. The CCG Nursing & Quality Team is actively working with provider patient safety specialists and governance leads to identify short, medium and longer term solutions. Hospital Onset COVID19: Requirements to report Hospital Onset Covid-19 is also having an impact on reporting and investigation capacity. Nottingham University Hospitals: Plans are in place for a single Trust-wide investigation/learning report around the management of hospital onset COVID-19. NUH’s Project Lead has reviewed, advised and added to any complaint letters associated with hospital onset COVID-19 narrative around the investigation / learning work. Progress in these areas will be discussed at the joint NUH and CCG patient safety touch point meetings. Sherwood Forest Hospitals: Root Cause Analysis investigations are completed for all hospital associated cases of COVID-19 and the learning is disseminated weekly across the organisation. The Trusts screening program for COVID-19 continues and 3 and 5-7 day swabbing compliance continues to improve. Learning outcomes have been developed and shared and these tally to those seen across the region such as the need to increase compliance with COVID-19 screening, support and monitoring of visitors using PPE, increasing compliance with patients wearing face masks. There have been no further reported nosocomial /hospital acquired cases since March 2021. Nottinghamshire Healthcare Trust: Root cause analysis investigations are completed on all COVID-19 outbreaks and all nosocomial infections outside of outbreaks have a concise investigation completed. Identified areas for improvement are the monitoring of lateral flow testing compliance and the recording of results on staff, cleaning, communication, ventilation and the challenges of safely isolating mental health patients. Learning and themes from hospital onset COVID cases have been shared at the Nottingham and Nottinghamshire Healthcare System Infection prevention and Control Assurance Group (HSIPCAG) and the ICS Quality Group. Oversight and monitoring will continue SafeToday Metrics The CCG Integrated Performance Report (IPR) for Quarter 1 outlines additional quality and safety metrics monitored as part of routine national quality requirements. The IPR illustrates a number of outliers and areas for focus for the quality team in terms of impact and outcomes: • VTE risk assessment completion at Nottingham University Hospitals and Sherwood Forest Hospitals
– both providers cite the launch of EPMR as the solution to compliance with this, however timelines and mitigations to be updated. No serious patient harms have been reported in relation to VTE risk assessment at either organisation
• Sherwood Forest Hospitals (HSMR) – apparent outliers for this metric however mitigations are
provided and the Trust has a plan to address data quality

5
• Sherwood Forest Hospitals (Family and Friends Test) for ED & Maternity – low recommendation rates for both areas over the last year. The Trust has identified low response rates (during COVID-19 and due to technical issues) which contribute to apparently low recommendation rates
• Nottingham University Hospitals (Ambulance Handover Times) – the Trust has identified data quality
concerns with this metric. Further work is underway to standardise, working closely with SFH 2. IPC BOARD ASSURANCE FRAMEWORK (BAF)
The CCG are working with providers to gain assurance in terms of infection, prevention and control (IPC). Information is gained from the submitted BAFs, provider quality reports and face to face visits. This is alongside monthly system wide meetings (chaired by the CCG system lead) where lessons learnt are discussed. Sherwood Forest Hospitals identified in May 2021 that the Trust was compliant with 120 of 121 key lines of enquiry in the BAF. The Trust’s IPC team have maintained a proactive approach and have on-going improvements planned including a Back to Basics campaign, additional training, new guidance posters and promotion of the link champion’s role. IPC BAFs for NUH, SFH, and NHT to be part of regular CCG Quality Reporting & Quality Insights going forward 3. NHS PROVIDER UPDATES – Key Highlights
Care Quality Commission (Status)
CQC Assessment NHS Trusts Nursing Homes Residential Homes GPs
Q4 2020/2021 Q4 2020/2021 Q4 2020/2021 Q4 2020/2021 Outstanding 0 6 16 19 Good 3 54 160 102 Requires Improvement 2 21 37 1 Inadequate 0 2 5 1 Not Rated 0 1 11 3 Across Nottingham and Nottinghamshire 9% of our CQC registered providers are rated as Outstanding, 72% Good, 14% Requires Improvement and 2% Inadequate. 2 of our largest NHS providers are subject to enhanced surveillance and system-wide oversight following CQC visit outcome and improvement work required: Nottingham University Hospital Maternity Services (Inadequate for Maternity however the Trust remains rated as Good Overall) and Nottinghamshire Healthcare Trust FT (Requires Improvement Overall). This includes working with NHT and partners on forensic inpatient / secure wards due to an inadequate rating of these specific services).
Nottingham University Hospitals NHS Trust (NUH)
Current organisational issues / areas for focus at NUH:
o Estate: impact on quality and risks due to limiting social distancing o Staff Wellbeing & Training: concern about post COVID vulnerabilities including morale and
burnout o A notable increase in the number of violence & aggression incidents o Impact of backlogs on elective care o Improvements to the response to the deteriorating patient and Recognise and Rescue
programme

6
Internal Assurance Insight Visits: NUH undertook a 3 day internal assurance inspection during June. A team (including CCG staff) visited a variety of divisions across Trust following an internal table top exercise which identified over a number of achievements and concerns which NUH wanted to gain a deeper understanding and learning around these. The findings of these visits have yet to be shared formally. Maternity Services: CQC conducted an unannounced inspection to the Maternity Service on 20 April 2021 at both City Hospital and QMC sites in order to follow up on the Section 29A Warning Notice which was issued to the Trust in October 2020. CQC reported that improvements had been made, as well as areas where further action is still required. The CQC were satisfied that progress had been made to meet the significant improvement outlined in the Section 29A Warning Notice. The Trust are developing an overarching action plan which brings together all the recommendations from serious incidents and Health Care Safety Investigation (HSIB) reports. This will be aligned to the actions to the maternity improvement plan. The CCG Quality Team continues to provide on-going support with embedding maternity SafeToday in addition to a retrospective review of maternity incidents following a look back exercise. There is also a single item quality assurance and oversight group in place to oversee maternity improvements. The CCG will continue to work with system partners and patient groups to oversee and support this work so babies, women and their families get the safe, effective and personalised care that they deserve. Sherwood Forest Hospitals FT (SFH)
Current organisational issues / areas for focus at SFH:
o Staff Wellbeing & Training particularly post COVID o Elective recovery programme o Equality, Diversity and Inclusion and the development of an action plan for the High Impact
Actions o Impact of COVID and consideration for monitoring harm and experience of care o Embedding the role of the Maternity Provider Safety Champion and Maternity Improvement /
transformation programme Hospital Standardised Mortality Ratios (HSMRs): The Trust identified that HSMR remains an outlier, and key areas of focus have been identified: Low activity; Palliative care coding; and Sub-optimal first contact / early decision making. A project improvement plan has been described and external/peer support engaged. The plan includes an emphasis on data quality to improve reporting. The ‘sub optimal first contact & decision making’ may have contributed to the outlier status for Sundays, this is included in the project plan. Harm Free Care: The Harm Free Committee has been re-established. A Falls Deep Dive has been conducted which has generated a number of actions. The rate has now fallen back below the national average as the pressures of COVID-19 have eased alongside the strengthening of the Falls Team. Nottinghamshire Healthcare NHS FT (NHT)
Priory Hospital: The CCG and NHT continue to work together with the CQC to monitor the action plans that have been developed by The Priory Arnold Hospital. Following a short cessation of admissions, the CQC have now reinstated admissions on the basis of two per week once the CQC have authorised
7
them. Monthly meetings are in place that includes mental health CCG Commissioning and CCG Quality teams, NHT and CQC. Specialised Services: NHT have proposed using a RAG rating approach to the quality management and oversight of regionally commissioned specialised services such as adult low/medium secure settings and CAMHS tier 4 wards. This enables the newly formed provider collaborative to provide a level of challenge to providers through the provider collaborative boards, peer reviews to take place to maintain impartiality as well as the ability to share good practice and innovation. Where local specialised services have been given and amber or red rating this will be notified to the CCG and discussed within the NHT Quality Assurance Group (QAG). Suicide Prevention: On-going work is taking place with NHT’s suicide prevention lead regarding specific services and specific trends in relation to serious self-harm and suicide. Following a focused discussion during June 2021 CCG Quality & Performance Committee it was agreed that further work was required to cleanse, understand and report back on the data when available NHT and the CCG are agreeing a standard definition of a serious reportable incident, definition of deliberate self-harm and definition of suicide in order to ensure that reporting is consistent and that it is comparable. Themes and trends within NHT data are informing the Nottinghamshire Suicide Prevention Real Time Surveillance Group, and are collated with the data relating to all suicides, both those known and not known to mental health services. From this information, cross partnership actions are agreed. This includes but not limited to: • Targeted bespoke training both for NHT staff and wider partners such as police, social care • Cross organisational awareness of prevalent methods e.g. social media • Changes to physical environments such as ligature risk points in wards, clinics and public places of
safety e.g. section 136 suites • Increased safety measures at public places where incidents have been noted e.g. train tracks • Identifying gaps in provision and ensuring that adequate resource is in place for mental health crisis
services including third sector, helplines etc Lings Bar: Following an internal Quality First visit across the three wards, an internal trust led improvement board has been established, with system support, meeting monthly. An update is expected at the July NHT Quality Assurance Group. Mediscan
On 23 June 2021, Mediscan a Non-Obstetric Ultrasound (NOUS) Provider received a CQC s.31 as a service provider in respect of regulated activities from 23 June - 25 August 2021. NHS England and NHS Improvement (North West) commissioned a single-item quality surveillance group (QSG) investigation to verify the scale of quality concerns that have been identified by CCGs with Mediscan contracts. We have taken appropriate local action to provide alternative NOUS services and the CCG have suspended our contract with Mediscan.

8
PART TWO: CCG STATUTORY RESPONSIBILITY/FUNCTION
4. Safeguarding, Looked After Children, and SEND The Safeguarding Team continue to work with the local safeguarding partnerships to progress statutory reviews, identifying the learning along good practice within primary care and wider the system. Liberty Protection Safeguards (LPS): The Nottingham & Nottinghamshire LPS ICS Stakeholder Forum has been developed with membership from all the responsible bodies from across our system. The Terms of Reference including the governance arrangements have been agreed and a Project Delivery Plan will be developed by this group and presented to CCG Executive group in September 2021.The CCG also has representation on the LPS National Clinical Reference Group. Sudden Infant Death – Safe Sleep local (UPDATE): Previous Nursing & Quality Reports have indicated that Safe Sleep remains a priority are for focus for the safeguarding team, below provides an update on the actions being taken: • CCG Safeguarding team continue to contribute to the Safeguarding Children’s Partnerships
responses to the National report “Out of Routine: A review of sudden unexpected death in infancy (SUDI) in families where the children are considered at risk of significant harm”(July 2020). The report has informed the four stages of a local project plan that has been based upon the responses to the national report
• CCG Safeguarding team now attends the Safe Sleep forum, contributing to a mapping exercise to help identify the work about safe sleep that is being carried out across the system. This exercise has identified further opportunities to add Safe Sleep messaging and distributing of information to other organisations that come into contact with families
• The Parent / Family Engagement Subgroup have been consulted in relation to supporting with a safe sleep survey and this work is currently being updated for the July Safe Sleep forum.
• CCG Safeguarding team are making links with the LMNS Perinatal Steering Group, substance misuse midwives and reflecting this work stream in the Safeguarding Children’s Partnership revised Neglect Strategy work
• CCG Safeguarding team are actively seeking assurance from all main providers in relation to actions being taken. Responses to date have been received from CityCare, NUH & Primary Care.
NUH Child Death Overview Panel (CDOP) & Sudden Infant Death (UPDATE): Following the CQC NUH Maternity report a CDOP audit was instigated to look at all neonatal deaths since 2018, focussing initially on NUH but it will then be broadened to include SFH & Bassetlaw. The first draft of the report is expected to be available by the end of July 2021. PART THREE: QUALITY & TRANSFORMATION 5. Learning Disability & Autism (LD/A) Inpatient Host Commissioner Throughout 2020/2021 Nottingham and Nottinghamshire CCG maintained oversight of acute and rehab LD/A inpatient settings that are located within the County, irrespective of whether we are actively commissioning beds. This includes Nottinghamshire Healthcare inpatient beds for which the CCG are lead commissioner, as well as independent beds that are spot purchased by CCGs regionally and nationally. Providers are asked to notify Nottingham and Nottinghamshire CCG when a new patient is placed and provide contact details for the placing commissioner which are held file by the CCG. Where quality issues are noted locally or by placing commissioners, these are triangulated by the LD/A Transformation Programme Team and safeguarding concerns and trends noted by the Multi-Agency

9
Safeguarding Hub (MASH) are investigated by the safeguarding team. Where concerns are raised relating to individual patients the placing commissioner is notified by Nottingham and Nottinghamshire CCG and a safe and well check is offered where it is impractical for the placing commissioner to undertake. Where concerns raised are thought to be systemic within the service, all placing commissioners are notified and an agreement is made as to how safe and well checks and quality improvement plans will be undertaken and overseen. Nottingham and Nottinghamshire CCG place very few numbers of people with LD/A into out of area acute/rehab beds (currently 3 out of 20 patients) and have robust processes of oversight for these patients, including liaising with the host commissioner of those areas where systemic issues are identified. During Q1 the CCG LDA and Quality Team have been actively involved in one ‘out of area’ placement working with the local authority to seek additional assurances. The CCG receives an average of 6 requests per month from placing commissioners regarding oversight of beds that are in our area. Using a combination of LD/A transformation, quality assurance and safeguarding intelligence, the CCG triangulates the data and concerns, informs all placing commissioners as required and undertakes safe and well checks on behalf of placing CCGs as necessary. 6. Learning Disability & Autism (LD/A) Inpatient Performance
Key Points for Consideration • 2 CCG discharge have taken place in the past month, there is good levels of confidence of achieving
the end of year CCG target which includes factoring in potential delays with accommodation and builds
• 1 NHSE Adults admission has taken place in the past month.
0
10
20
30
40
50
60
Apr May Jun July Aug Sep Oct Nov Dec Jan Feb Mar
2021/22 Inpatient performance and trajectories
Total Adult
Target Adults
Total CYP
Target CYP

Page 1 of 4
Meeting Title: Governing Body (Open Session) Date: 04 August 2021
Paper Title: Integrated Performance Report Paper Reference: GB 21 064
Sponsor:
Presenter:
Stuart Poynor, Chief Finance Officer Attachments/Appendices:
IntegratedPerformance Report
Michael Cawley, Operational Director ofFinance
Purpose: Approve ☐ Endorse ☐ Review ☐ Receive/Note for:
∑ Assurance∑ Information
☒
Executive Summary
This report sets out the performance against key standards and targets for the NHS Nottingham andNottinghamshire CCG with supplementary information showing, where appropriate, the equivalentperformance for individual provider organisations.
The report is broken down into sections for Planned Care, Urgent Care, Mental Health and Quality indicatorsoffering assurance by indicating:
∑ The root cause of performance issues being reported?∑ What mitigating actions are in place to recover performance?∑ What assurance can be given to its sustainability?∑ Are there any gaps in assurances?
Monitoring of the H1 (April to September) is included within this report by metric.
A summary of the position for the CCG against the agreed H1 plan can be seen on page 3. This alsoincludes a comparison against the equivalent period of 2019/20 and a spark line to indicate the run rate ofassociated trend data. Granular charts for each metric are shown from page 38 to 49 of this report.21/22 Priorities and operational planning guidance.
The 21/22 Planning guidance sets out a range of national priorities for the year ahead, which are summarised below:
A. Supporting the health and wellbeing of staff and taking action on recruitment and retentionB. Delivering the NHS COVID vaccination programme and continuing to meet the needs of patients with
COVID-19C. Building on what we have learned during the pandemic to transform the delivery of services,
accelerate the restoration of elective and cancer care and manage the increasing demand on mentalhealth services
D. Expanding primary care capacity to improve access, local health outcomes and address healthinequalities
E. Transforming community and urgent and emergency care to prevent inappropriate attendance atemergency departments (ED), improve timely admission to hospital for ED patients and reduce
Integrated Performance Report
69 of 22409:00 - 10.50-04/08/21

Page 2 of 4
length of stayF. Working collaboratively across systems to deliver on these priorities.
The Nottingham and Nottinghamshire Integrated Care System (ICS) submitted a set of fully triangulated plans across activity, workforce and finance on 3rd June 2021. Following a benchmarking exercise led by NHS England (NHSE), a number of small revisions were made to the plans to bring the CCG into the Inter Quartile Range of performance. Monitoring within this report is shown against the revised H1 plans.
This month’s highlightsIn this month’s report, Member’s attention is drawn to the following areas:
1. A new section has been introduced at the beginning of the report to address the enquiries made at the previous Governing Body meeting, specifically around the level of demand into Primary Care. Members are asked to note the analysis aims to estimate the number of patients who would have received a primary care service during 2020/21, but due the COVID pandemic have not accessed healthcare to a receive preventative interventions. Further metrics will be included when they become available.
2. A small improvement in the elective care Referral to Treatment (RTT) incomplete performance reported against the March position reported last time for both acute trusts and the CCG population.However, the overall number of patients waiting for their first definitive treatment continues to rise.
3. Overall the number of CCG-registered patients on the waiting list has increased to 84,213, and increase of around 2,000 patients since the March position was reported in May. Members are asked to note figure relates to all pathways (admitted and non-admitted) whereas those data quoted in respect to the Elective Recovery Fund relate only to patients on the admitted Patient Treatment List (PTL).
4. The shape of the waiting list continues to be challenging although page 12 illustrates a reduction in the number of very long-waiting patients, i.e. those over 52-weeks. This is true for the CCG population as well as those patients waiting for treatment at our local acute trusts. Members are reminded the CCG continues to monitor this and produces a suite of reports weekly so this can be managed across providers, with discussions taking place across the system on flexibilities which might exist in common specialties and within the independent sector.
5. Diagnostic services are showing an improvement in performance in with respect to the number of patients waiting against 6-week national standard.
6. Cancer services overall continue to show relatively good levels of performance compared to similar populations across the country, although a recent surge in 2 week wait referrals has deteriorated the measured performance in this area. Treatment volumes remain high and the use of the independent sector continues.
7. Performance around the 31-day and 62-day standards remains stable. The number of patients waiting more than 62-day has shown a recent reduction but the position remains challenging. Nottingham University Hospitals Trust (NUH) has negotiated a local arrangement for accessing independent sector capacity following the cessation of the national arrangements put in place last year. Bed and theatre utilisation have improved.
8. Attendance volumes to A&E departments continue to show an increase, but remain below pre-pandemic levels. Trusts continue to collaborate in terms of the availability of clinical staffing as this continues to be a challenge. A total of six 12-hour breaches have been reported in May, with a further 3 in June (page 66), at local acute trusts. Conveyance rates via East Midlands Ambulance Service (EMAS) remain low and static.
9. The number of people entering treatment for Improving Access to Psychological Therapies (IAPT)has increased since the last report but remains lower than the required standard. Waiting times and recovery rates continue to be good and better than target for both the 6-week and 18-week target.
10. The increased use of telephone consultation for perinatal mental health services continues to
Integrated Performance Report
70 of 224 09:00 - 10.50-04/08/21

Page 3 of 4
manifest itself as a reported lower performance. Local data continues to demonstrate a higher, and improved, performance. Despite some improvement in performance, the distance from target from April 2021 has shifted following a increase n the target from 7.1% to 8.6%.
11. The proportion of patients with severe mental illness who received primary care health check continues to improve slowly although remains below the national standard at 25.7% in June. Some variation is seen between the Integrated Care Partnership-defined areas. The standard for this service shifted in April from 60% to 68%.
12. The number of occupied bed days for acute mental health patients placed Out of Area shows a small reduction in Q4 with 505 reported compared to 536 in the previous quarter. However, the numbers remain above the trajectory of 180.
13. Children & Younger People continue to access Mental Health Services above the required standard.14. Access to eating disorder services for children and younger people improved for urgent patients with
72.2% of patients being seen within 1 week (Q4) compared to 63.6% the previous quarter. However, the measured performance for routine patients (defined as 4-weeks) reduced slightly to 86.6% (Q4) compared to the previously reported position of 91.0%.
15. Progress against H1 plans is shown on pages 42 – 53. Overall, demand remains static whilst activity within secondary care continues to increase, with elective care services, in most cases, above those levels planned for April – September. Non-elective care remains below the expected levels set out in the H1 plans.
16. The proportion of patients who receive “harm-free care” continues to be reported above the national standard at SFH, with NUH reporting internally only whilst the national reporting requirement has been paused due to COVID.
17. Cleaning audit scores remain high and above the national standard for all reported sites.18. Venous Thromboembolism (VTE) risk assessments for patient admissions were below the 95%
national standard at NUH, with 94.2% of patients being assessed in May.19. NUH and Nottinghamshire Healthcare Trust (NHCT) both continue to report challenges in meeting
the 80% standard for ward staffing, largely caused by staff sickness and self-isolation levels.20. The Summary Hospital Mortality Indicator rate for both acute trusts remains below or close to 100,
whilst both trusts continue to show Hospital Standardised Mortality Ratio rates above 100.21. No mixed-sex accommodation breaches were reported in the latest period.22. The proportion of positive responses to the Friends and Family tests are shown on page 63 of the
report. All responses are above the standard, with the exception of NHT and maternity at Sherwood Forest Hospitals Foundation Trust (SFH), where month-on-month improvements are being seen.
23. SFH continues to show a high level of patients admitted for 21 days or over, with NUH reporting a level lower than target. Both trusts continue to cite acuity and pressures due to COVID as the main drivers.
24. The Ambulance Handover standard continues to be unmet at NUH with a reported level of 66% of patients being handed-over in 15 minutes, compared to a national standard of 100%. SFH remain better than standard.
25. At 49.0%, the March level of eligible patients asked case finding question, or diagnosis of dementia or delirium at SFH remains significantly lower than the 90% national standard but continues to show an improvement.
Mitigating actions and assurances are provided in the relevant sections of the Integrated Performance Report.
Relevant CCG priorities/objectives:
Compliance with Statutory Duties ☒ Wider system architecture development (e.g. ICP, PCN development)
☐
Integrated Performance Report
71 of 22409:00 - 10.50-04/08/21

Page 4 of 4
Financial Management ☒ Cultural and/or Organisational Development
☐
Performance Management ☒ Procurement and/or Contract Management ☒
Strategic Planning ☐
Conflicts of Interest:
☒ No conflict identified
☐ Conflict noted, conflicted party can participate in discussion and decision
☐ Conflict noted, conflicted party can participate in discussion, but not decision
☐ Conflict noted, conflicted party can remain, but not participate in discussion or decision
☐ Conflict noted, conflicted party to be excluded from meeting
Completion of Impact Assessments:
Equality / Quality Impact Assessment (EQIA)
Yes ☐ No ☐ N/A☒ Not required for this paper.
Data Protection Impact Assessment (DPIA)
Yes ☐ No ☐ N/A☒ Not required for this paper.
Risk(s):
N/A
Confidentiality:
☒No
☐
Recommendation(s):
1. To NOTE the report and its content.
Integrated Performance Report
72 of 224 09:00 - 10.50-04/08/21
1
NHS Nottingham & Nottinghamshire CCG
Performance Report
August 2021
Table of Contents
Page 1 Introduction
Page 2-3 Indicator Summary
Page 8-22 Planned Care
Page 23-30 Urgent Care
Page 31-41 Mental Health
Page 42-53 H1 Activity Plan Monitoring
Page 54-74 Quality
Page 75 Glossary
This report sets out the performance against key standards and targets for the NHS Nottingham and Nottinghamshire CCG with supplementary information showing, where appropriate, the equivalent performance for individual provider organisations. The report is broken down in to sections for Planned Care, Urgent Care, Mental Health and Quality indicators offering assurance by indicating:
The root cause of performance issues being reported?
What mitigating actions are in place to recover performance?
What assurance can be given to its sustainability?
Are there any gaps in assurances? Monitoring of the H1 (April to September) is included within this report by metric. A summary of the position for the CCG against the agreed H1 plan can be seen on page 3. This also includes a comparison against the equivalent period of 2019/20 and a spark line to indicate the run rate of associated trend data. Granular charts for each metric are shown from page 38 to 49 of this report. 21/22 Priorities and operational planning guidance The 21/22 Planning guidance sets out a range of national priorities for the year ahead, which are summarised below: A. Supporting the health and wellbeing of staff and taking action on recruitment and retention B. Delivering the NHS COVID vaccination programme and continuing to meet the needs of patients with COVID-19 C. Building on what we have learned during the pandemic to transform the delivery of services, accelerate the
restoration of elective and cancer care and manage the increasing demand on mental health services D. Expanding primary care capacity to improve access, local health outcomes and address health inequalities E. Transforming community and urgent and emergency care to prevent inappropriate attendance at emergency
departments (ED), improve timely admission to hospital for ED patients and reduce length of stay F. Working collaboratively across systems to deliver on these priorities. The Nottingham and Nottinghamshire ICS submitted a set of fully triangulated plans across activity, workforce and finance on 3rd June 2021. Following a benchmarking exercise led by NHSE, a number of small revisions were made to the plans to bring the CCG into the Inter Quartile Range of performance. Monitoring within this report is shown against the revised H1 plans.
Integrated Performance Report
73 of 22409:00 - 10.50-04/08/21

2
NHS Nottingham & Nottinghamshire CCG Indicator Summary
Provider Indicator Summary
The table below provides a view of the performance metrics and associated standards for the key providers of healthcare for
the CCG population.
The table below provides an overview of the performance metrics within this report along with the required standard. Further
insight around these indicators can be found at the corresponding page.
Theme Indicator 1 Indicator 2 PeriodPage
Number
Percentage of Incomplete Patients Waiting Less Than 18 Weeks => 92% 8-9
Incomplete Waiting List Size 10-11
Incomplete number of 52 week waiters = 0 12-14
Diagnostics Percentage of Patients Waiting Longer Than 6 Weeks May-21 <= 1% 15-16
2 Week Wait => 93% 17
2 Week Wait - Breast Symptoms => 93% 17
28 Day Faster Diagnosis Standard => 70% 18
31 Day Decision to Treat to First Treatment => 96% 19
62 Day GP Urgent Referral to Treatment => 85% 20-22
A&E 4 Hour Standard May-21 => 95% 23-30
NHS111 NHS 111 - Percentage answered within 60 seconds Mar-21 => 95% 23-30
Category 1 – Life-threatening illnesses or injuries - Average <= 00:07:00 23-30
Category 2 – Emergency calls - Average <= 00:18:00 23-30
Category 1 – Life-threatening illnesses or injuries - 90th centile <= 00:15:00 23-30
Category 2 – Emergency calls - 90th centile <= 00:40:00 23-30
Category 3 – Urgent calls - 90th centile <= 02:00:00 23-30
Category 4 – Less urgent calls - 90th centile <= 03:00:00 23-30
Entering Treatment - Rolling Three Months => 6575 31-32
Recovery Rate - Rolling Three Months => 50% 31-32
Waiting Times - First Treatment within 6 Weeks => 75% 31-32
Waiting Times - First Treatment within 18 Weeks => 95% 31-32
Dementia Diagnosis Rate Apr-21 => 66.7% 33
Perinatal MH % of Population Birthrate May-21 => 7.1% 34
SMI Physical Health Checks for People With an SMI May-21 => 60% 35-36
OAP Inappropriate Out of Area Bed DaysQ3 2020-
21< 364 37-38
EIP Started Treatment in Two Weeks - Rolling Three Months Feb-21 => 60% 39
Routine Cases <4 Weeks - Rolling Twelve Months => 95% 41
Urgent Case <1 Week - Rolling Twelve Months => 95% 41
May-21
May-21
May-21
Mar-21
Q4 2020-
21
74.66%
92.31%
Improving
Access to
Psychological
Therapies
CYP Eating
Disorders
Planned
Care
RTT
Cancer
Ambulance -
Nottinghamshire
Division
(including
Bassetlaw)
Mental
Health
Urgent
Care
00:54:10
00:12:11
00:27:08
00:07:00
73.27%
96.68%
53.30%
6005
03:26:36
04:44:31
5.98%
24.4%
536
84.0%
N/A
Standard
84213
69.77%
72.22%
86.60%
68.52%
100.00%
92.23%
79.11%
89.67%
74.42%
32.95%
4153
Performance
NUH SFH
Percentage of Incomplete Patients Waiting Less Than 18 Weeks => 92% 68.47% 66.20% 8-9
Incomplete Waiting List Size 53,279 37,358 10-11
Incomplete number of 52 week waiters = 0 3,422 1,340 12-14
Diagnostics Percentage of Patients Waiting Longer Than 6 Weeks May-21 <= 1% 40.63% 23.05% 15-16
2 Week Wait => 93% 87.31% 95.20% 17
2 Week Wait - Breast Symptoms => 93% 68.49% 100.00% 17
28 Day FD => 70%
31 Day Decision to Treat to First Treatment => 96% 90.34% 97.73% 19
62 Day GP Urgent Referral to Treatment => 85% 71.18% 71.13% 20-22
4 Hour Standard => 95% 91.75% 23-30
12hr trolley waits = 0 5 1 23-30
Urgent
CareA&E May-21
Planned
Care
RTT May-21
Cancer May-21
Theme Indicator 1 Indicator 2 PeriodPerformance
StandardPage
Number
N/A
Integrated Performance Report
74 of 224 09:00 - 10.50-04/08/21

3
H1 Plans Monitoring
The following charts show the progress against the H1 activity plans submitted in April 2021
NHS Nottingham & Nottinghamshire CCG
H1 Plan Summary
May-21
Actual
May-21
Plan
%
Difference
to Plan
Comparison
against
2019/20
Direction of
Travel
Total outpatient attendances - Face to face (All TFC) 68,613 60,461 13.5% -36.9%
Total outpatient attendances - Telephone/virtual (All TFC) 26,018 28,804 -9.7% 638.1%
Total outpatient attendances (All TFC) 94,631 89,265 6.0% -15.7%
Consultant-led first outpatient attendances (Spec acute) 17,266 14,106 22.4% -26.1%
Consultant-led first outpatient attendances with procedures (Spec acute) 3,018 2,090 44.4% -38.2%
Consultant-led follow-up outpatient attendances (Spec acute) 43,060 37,896 13.6% -14.7%
Consultant-led follow-up outpatient attendances with procedures (Spec acute) 6,684 5,900 13.3% -28.2%
Total Advice and Guidance requests processed/answered 2,358
Number of patients moved or discharged to a PIFU pathway for the first time 774
Specific Acute elective day case spells in the period 9,736 7,977 22.1% -7.9%
Specific Acute elective ordinary spells in the period 1,319 1,450 -9.0% -18.6%
Specific Acute elective spells in the period 11,055 9,427 17.3% -9.3%
Specific Acute elective day case spells in the period under 18 years of age 258 247 4.5% -15.4%
Specific Acute elective ordinary spells in the period under 18 years of age 82 48 70.8% 3.8%
Specific Acute non-elective spells in the period with a LOS of zero days 3,643 3,926 -7.2% 16.5%
Specific Acute non-elective spells in the period with a LOS of 1 or more days (COVID) 41 275 -85.1%
Specific Acute non-elective spells in the period with a LOS of 1 or more days (Non-COVID) 6,590 6,954 -5.2% -2.2%
Specific Acute non-elective spells in the period with a LOS of 1 or more days 6,521 7,229 -9.8% -3.2%
Specific Acute non-elective spells in the period 10,164 11,155 -8.9% 3.0%
Attendances at Type 1 and Type 2 A&E departments, exc planned follow-up attendances 22,649 24,549 -7.7% -10.3%
Attendances at Type 3 and Type 4 A&E departments, exc planned follow-up attendances 7,062 7,763 -9.0% -9.9%
Attendances at all A&E departments, excluding planned follow-up attendances 29,711 32,312 -8.0% -10.2%
Diagnostic Tests - Magnetic Resonance Imaging 5,009 5,164 -3.0% -7.6%
Diagnostic Tests - Computed Tomography 9,560 7,749 23.4% 14.3%
Diagnostic Tests - Non-Obstetric Ultrasound 8,583 8,667 -1.0% -20.3%
Diagnostic Tests - Colonoscopy 935 1,048 -10.8% -16.9%
Diagnostic Tests - Flexi Sigmoidoscopy 379 427 -11.2% 6.8%
Diagnostic Tests - Gastroscopy 1,171 1,060 10.5% -7.4%
Diagnostic Tests - Cardiology - Echocardiography 2,610 2,233 16.9% -11.5%
Mental Health Indicator Summary - July 2021 UpdateNHS Nottingham & Nottinghamshire CCG
Target Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21 Jun-21
IAPT Access Rate 6.25% 3.60% 3.85% 4.46% 4.11% 3.69% 4.18% 4.82% 5.45% 5.15% 5.48%
IAPT Recovery Rate 50.0% 54.8% 55.1% 54.6% 53.9% 54.9% 55.6% 55.2% 54.7% 54.3% 53.3%
IAPT Waiting times 6 weeks 75.0% 84.9% 92.0% 94.8% 98.2% 98.7% 97.5% 97.4% 98.2% 97.1% 96.7%
IAPT waiting times 18 weeks 95.0% 99.4% 99.7% 99.1% 100.0% 100.0% 100.0% 99.6% 99.6% 99.6% 100.0%
Dementia diagnosis rate - 12mth Rolling 66.7% 71.1% 70.6% 70.5% 70.2% 70.2% 70.0% 69.8% 69.1% 68.5% 68.7% 68.5% 68.4%
Perinatal Access (Local data) - 12mth Rolling 1008 862 828 790 766 750 750 739 712 670 663 676 700
Perinatal Access Rate - 12mth Rolling 8.60% 7.36% 7.07% 6.75% 6.54% 6.40% 6.40% 6.31% 6.08% 5.72% 5.66% 5.77% 5.98%
SMI % achievement - 12mth Rolling 68.0% 30.5% 27.5% 25.9% 24.4% 24.1% 22.1% 22.1% 20.6% 19.7% 20.5% 22.5% 24.4% 25.7%
Out of Area Placement bed days (Local) - 3mth 0 680 619 468 393 318 435 536 592 469 505 516 554
Out of Area Placement bed days (MHSDS) - 3mth 0 780 690 515 430 390 465 550 590 500 510 535
EIP Waiting times - MHSDS - 3mth Rolling 60.0% 79.0% 81.0% 84.0% 80.0% 84.0% 86.0% 86.0% 86.0% 84.0% 85.0% 84.0%
CYP Access Rate - 12mth Rolling 38% tbc 29.60% 29.40% 29.90% 30.30% 29.90% 32.20% 34.30% 36.40% 38.30% 40.90% 44.30%
CYP Eating Disorder WT - Urgent (4 QTR) 95.0% 100.0% 100.0% 63.6% 72.2%
CYP Eating Disorder WR - Routine (4 QTR) 95.0% 86.7% 90.0% 91.0% 86.6%
Integrated Performance Report
75 of 22409:00 - 10.50-04/08/21

4
Impact of the COVID Pandemic on Primary Care Demand The analysis below aims to estimate the number of patients who would have received a primary care service during 2020/21, but due the COVID pandemic have not accessed healthcare to a receive preventative interventions. There are no nationally-defined measures for the number of patients waiting in primary care. However, in an attempt to begin to understand the proportion of patients who have not received their expected level of access during the COVID pandemic, and importantly to see the trend of this data, this report introduces some basic metrics. Initially the report will look at routine vaccinations, screening programmes and secondary care referrals. However, it is our ambition that more detailed information can be sourced to illustrate this better. As an example the QOF scores for each GP practice will be reportable once this is published nationally in October. In the meantime, Members of the Committee are asked to recognise this is work in progress.
1. Vaccinations The national PHE COVER (Cover of Vaccinations Evaluated Rapidly) data has been utilised to undertake the analysis by comparing the volume of patients’ vaccinated during Q1-4 2020/21 against the same period of 2019/20. The calculation focused on the volume of patients required to achieve the previous year’s performance, rather than the number required to achieve a local or national standard. The approximate number of vaccinations required across the ICS to equal the number delivered in the previous year is 1373, which can be seen by locality and vaccination type within the chart below. The requirement by locality is as follows – Mid Notts 436, City 576 and the South locality 361.
Integrated Performance Report
76 of 224 09:00 - 10.50-04/08/21

5
2. Cervical Screening All women aged 25 to 64 should be invited to receive regular cervical screening. The frequency of invitations varies depending on the age of the patient and is between 3 and 5 year intervals. The analysis undertaken has compared the GP Practice level performance during Q3 2019/20 against the same period of 2020/21. The volume of additional screening events required has been calculated based on each GP Practice equalling the level of performance that they achieved during 2019/20 Q3. This methodology focuses on returning to the historical level of GP Practice level performance, rather than achieving a national or local ambition. The analysis has identified that there were 3569 fewer screening events undertaken during the Q3 2020/21 than during the previous period. The chart below illustrates the additional screening events required by each locality within the ICS.
3. Referrals The analysis summarised below has compared the volume of referrals made via ERS against the equivalent period of the previous year. The analysis includes patients registered with GP Practices within N&N CCG and also includes referrals to all secondary care providers. A significant fall in the volume of referrals made was seen in April 2020 for 2 week wait, urgent and routine priorities. Reductions seen were between 18% and 32% of the previous levels. The number of referrals gradually increased over time and in March 2021 volumes of 2ww and Urgent referrals exceeded 100% of previous volumes. Note that the growth in demand for 2ww cancer services has previously been highlighted within the IPR. The volume of routine referrals remains significantly below historic levels.
Integrated Performance Report
77 of 22409:00 - 10.50-04/08/21

6
The chart overleaf displays the cumulative variance of referrals against the previous year. It illustrates that as the pandemic progressed, the volume of referrals that were not made increased month by month. At May 2021, the estimated cumulative volume of referrals that have not been made since the Pandemic began for registered patients of the N&N CCG is 72,877, which can be segmented by priority as follows:
Routine – 57,351
Urgent – 7,976
2 Week Wait - 7550
Integrated Performance Report
78 of 224 09:00 - 10.50-04/08/21
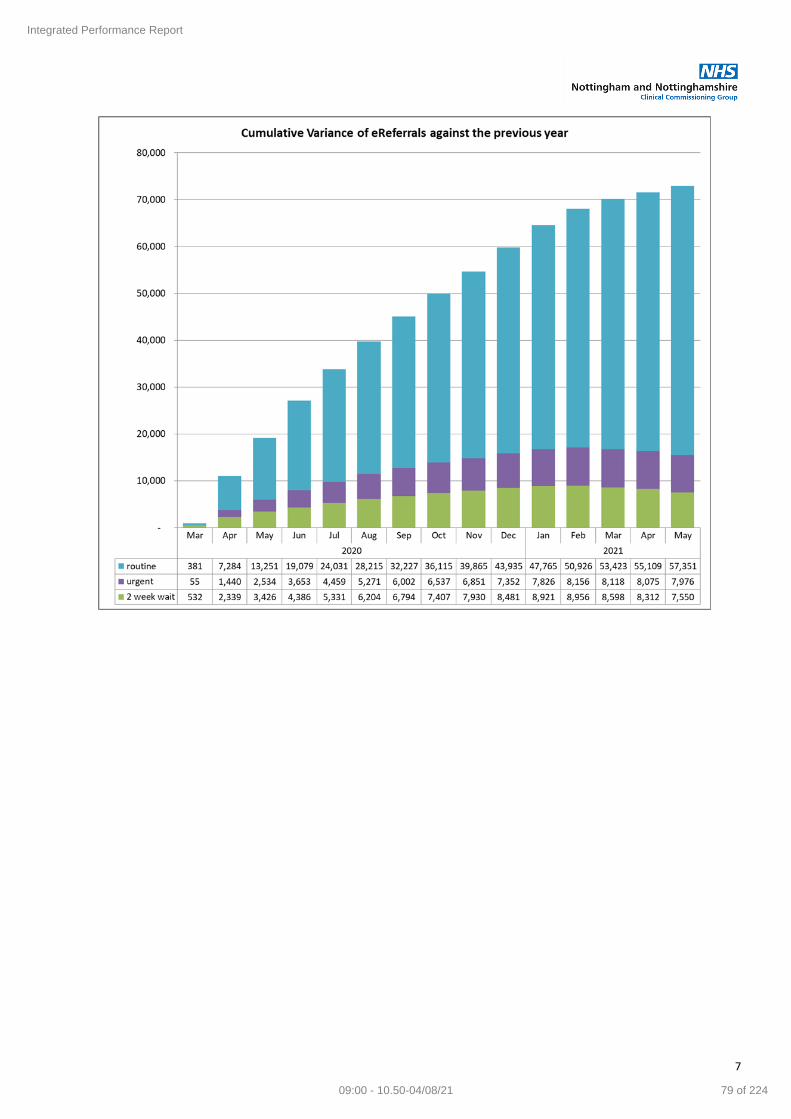
7
Integrated Performance Report
79 of 22409:00 - 10.50-04/08/21

8
Theme Indicator Indicator Overview CCG Lead Focus
Planned Care
RTT Waiting Times
The percentage of patients waiting less than 18 weeks between referral and treatment for Incomplete pathways (patients still waiting for treatment at the end of the reporting period)
Lisa Durant CCG Acute Providers
Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
N&N CCG 64.35% 57.75% 62.44% 68.04% 70.42% 71.49% 69.58% 68.08% 67.31% 67.07% 66.68% 69.77% h
NUH 58.64% 50.61% 56.75% 64.26% 67.92% 70.83% 70.21% 69.47% 68.19% 66.75% 65.39% 68.47% h
SFH 70.83% 66.03% 67.74% 70.56% 71.01% 69.78% 66.17% 62.96% 62.12% 63.58% 63.92% 66.20% h
Organsation StandardMost Recent 12 Months Performance Performance
Direction
Greater than
or equal to
92%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
Nottingham and Nottinghamshire CCG - RTT Performance - Most Recent 12 Months
N&N CCG Standard
Patients Breaches >18Wks Patients Breaches >18Wks Patients Breaches >18Wks
General Surgery 4368 1505 65.54% 897 448 50.06% 3655 1130 69.08%
Trauma & Orthopaedics 8907 4109 53.87% 6821 3269 52.07% 2712 1113 58.96%
Ear, Nose & Throat (ENT) 8210 3799 53.73% 4216 1532 63.66% 5385 2961 45.01%
Ophthalmology 13334 5297 60.27% 7065 3069 56.56% 6157 2623 57.40%
Oral Surgery 12 3 75.00% 2484 1191 52.05% 879 563 35.95%
Neurosurgery 223 65 70.85% 511 142 72.21% 0 0
Plastic Surgery 642 219 65.89% 775 275 64.52% 123 22 82.11%
General Medicine 27 4 85.19% 12 1 91.67% 0 0
Gastroenterology 6319 1605 74.60% 3799 1250 67.10% 2823 559 80.20%
Cardiology 3203 1031 67.81% 1441 248 82.79% 2180 924 57.61%
Dermatology 3503 270 92.29% 2802 78 97.22% 1337 212 84.14%
Thoracic Medicine 2608 729 72.05% 1637 396 75.81% 1531 480 68.65%
Neurology 568 24 95.77% 623 8 98.72% 0 0
Geriatric Medicine 629 49 92.21% 98 2 97.96% 577 52 90.99%
Gynaecology 5815 1721 70.40% 2376 489 79.42% 2149 488 77.29%
Cardiology 3203 1031 67.81% 1441 248 82.79% 2180 924 57.61%
Other – Medical Services 6366 670 89.48% 6366 485 92.38% 6366 274 95.70%
Other – Mental Health Services 12 3 75.00% 12 0 100.00% 12 0 100.00%
Other - Paediatric Services 3855 560 85.47% 3855 364 90.56% 3855 306 92.06%
Other – Other Services 3865 94 97.57% 3865 60 98.45% 3865 0 100.00%
Other (Total) 18746 3171 83.08%
Total 84213 25454 69.77% 53279 16800 68.47% 37358 12626 66.20%
NUH SFHRTT Specialty - May 2021
N&N CCG
Integrated Performance Report
80 of 224 09:00 - 10.50-04/08/21

9
Root Cause The specialty level breakdown of the May 2021 position details that performance for Nottingham and Nottinghamshire CCG is 69.77% against the national standard of 92%. This is an improvement from the April position of 66.68%. NUH and SFH failed to meet the national standard with performance of: NUH – 68.47% SFH – 66.20% However this is an improvement by both Trusts from their position in April. The specialties with the highest proportion of patients waiting beyond 18 weeks for the Nottingham and Nottinghamshire CCG were Ophthalmology, Trauma and Orthopaedics and ENT. Outpatient activity continues to increase, but is not yet at pre- Covid levels
Mitigating Actions
Senior oversight is in place by the ICS Clinical Executive Group
Where possible, providers have reinstated elective capacity, whilst undertaking outpatients, diagnostics and surgery in line with social distancing limitations and PPE/Testing requirements
Continued focus on non-face to face outpatient activity, with a significant shift in the proportion of outpatient activity delivered via Telephone or Video
Waiting list management continues to be based on clinical priority and taking appropriate consideration of chronological order when listing patients
The system has agreed changes to the case mix undertaken by the Independent Sector to enable cancer and urgent complex cases to be prioritised
Clinical validation of patients takes place in all specialties.
The Elective Hub undertakes collective review of waiting lists of the NHS trusts and including IS providers
Patients are regularly reviewed by specialties according to their priority level and re-prioritised if necessary. Theatre timetables have been adjusted following the second wave to accommodate specialties with higher backlogs, additional emergency theatre capacity has been identified and flexible lists created.
Assurances The capacity cell has oversight of all system wide recovery plans, to ensure a whole system approach. This is supported by good provider engagement
Established reports track the recovery of services against the agreed system plans
The CCG is working with Trusts via the capacity cell to align capacity with predicted demand. This reflects constrained capacity due to IPC requirements.
An ICS wide Planned Care Transformation Programme Board has been set up as part of the system wide transformation programme and revised system governance.
Trusts have developed plans to mitigate the risk of the impact of a 3rd wave of Covid 19 which were submitted to NHS E/I
Gaps in Assurance
Referral demand is a key variable that will impact on waiting list size. Although we have not seen total referrals return yet to pre-Covid levels we are seeing a significant rise in 2ww referrals
Patients will wait longer for elective care and may feel anxiety when attending an acute setting and adhering to social distancing requirements
It is likely to take many months to recover performance to pre COVID 19 levels
Integrated Performance Report
81 of 22409:00 - 10.50-04/08/21
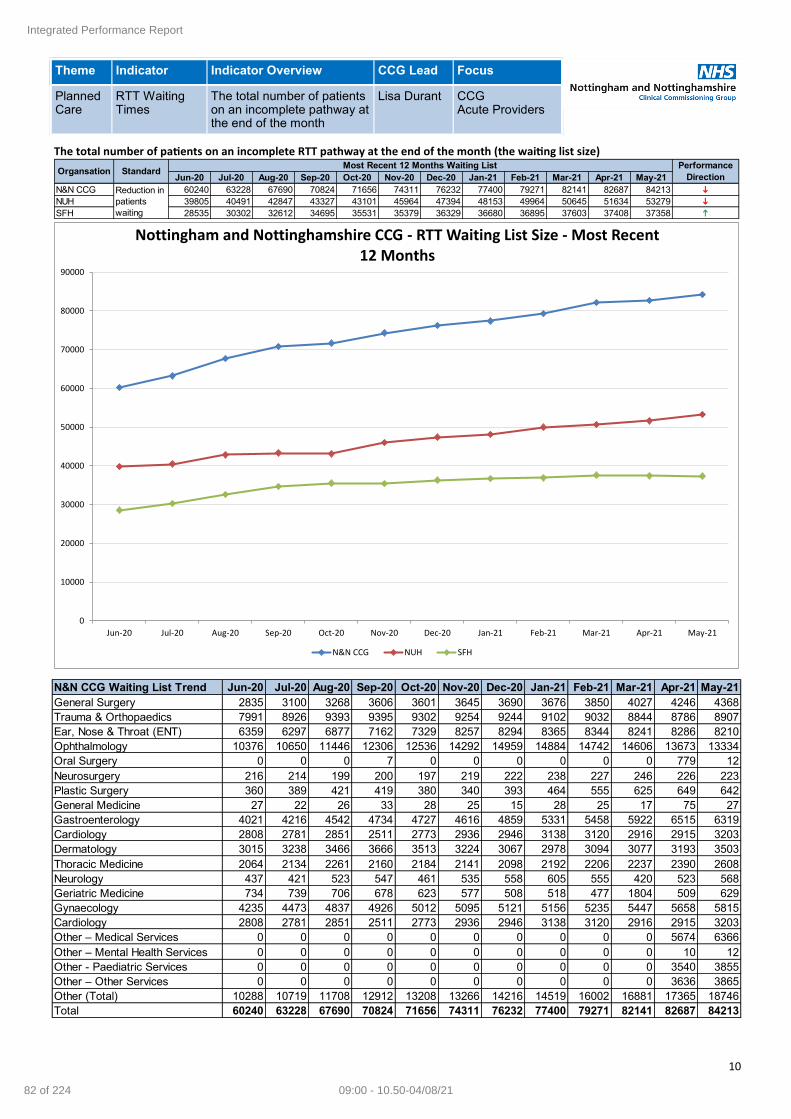
10
Theme Indicator Indicator Overview CCG Lead Focus
Planned Care
RTT Waiting Times
The total number of patients on an incomplete pathway at the end of the month
Lisa Durant CCG Acute Providers
The total number of patients on an incomplete RTT pathway at the end of the month (the waiting list size)
Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
N&N CCG 60240 63228 67690 70824 71656 74311 76232 77400 79271 82141 82687 84213 i
NUH 39805 40491 42847 43327 43101 45964 47394 48153 49964 50645 51634 53279 i
SFH 28535 30302 32612 34695 35531 35379 36329 36680 36895 37603 37408 37358 h
Reduction in
patients
waiting
Organsation StandardMost Recent 12 Months Waiting List Performance
Direction
0
10000
20000
30000
40000
50000
60000
70000
80000
90000
Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
Nottingham and Nottinghamshire CCG - RTT Waiting List Size - Most Recent 12 Months
N&N CCG NUH SFH
N&N CCG Waiting List Trend Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
General Surgery 2835 3100 3268 3606 3601 3645 3690 3676 3850 4027 4246 4368
Trauma & Orthopaedics 7991 8926 9393 9395 9302 9254 9244 9102 9032 8844 8786 8907
Ear, Nose & Throat (ENT) 6359 6297 6877 7162 7329 8257 8294 8365 8344 8241 8286 8210
Ophthalmology 10376 10650 11446 12306 12536 14292 14959 14884 14742 14606 13673 13334
Oral Surgery 0 0 0 7 0 0 0 0 0 0 779 12
Neurosurgery 216 214 199 200 197 219 222 238 227 246 226 223
Plastic Surgery 360 389 421 419 380 340 393 464 555 625 649 642
General Medicine 27 22 26 33 28 25 15 28 25 17 75 27
Gastroenterology 4021 4216 4542 4734 4727 4616 4859 5331 5458 5922 6515 6319
Cardiology 2808 2781 2851 2511 2773 2936 2946 3138 3120 2916 2915 3203
Dermatology 3015 3238 3466 3666 3513 3224 3067 2978 3094 3077 3193 3503
Thoracic Medicine 2064 2134 2261 2160 2184 2141 2098 2192 2206 2237 2390 2608
Neurology 437 421 523 547 461 535 558 605 555 420 523 568
Geriatric Medicine 734 739 706 678 623 577 508 518 477 1804 509 629
Gynaecology 4235 4473 4837 4926 5012 5095 5121 5156 5235 5447 5658 5815
Cardiology 2808 2781 2851 2511 2773 2936 2946 3138 3120 2916 2915 3203
Other – Medical Services 0 0 0 0 0 0 0 0 0 0 5674 6366
Other – Mental Health Services 0 0 0 0 0 0 0 0 0 0 10 12
Other - Paediatric Services 0 0 0 0 0 0 0 0 0 0 3540 3855
Other – Other Services 0 0 0 0 0 0 0 0 0 0 3636 3865
Other (Total) 10288 10719 11708 12912 13208 13266 14216 14519 16002 16881 17365 18746
Total 60240 63228 67690 70824 71656 74311 76232 77400 79271 82141 82687 84213
Integrated Performance Report
82 of 224 09:00 - 10.50-04/08/21
11
Root Cause
The size of the waiting list (PTL) is driven by:
Volume of clock starts (new referrals and overdue reviews)
Volume of clock stops (for treatment or no treatment required) The total number of Nottingham and Nottinghamshire CCG patients waiting for treatment at the end of May 2021 was 84,213, an increase of 1,526 patients from the April position. The majority of patients are waiting for treatment at:
NUH – 53,279 patients (includes Nottingham Treatment Centre)
SFH – 37,358 patients ‘Other’ has the largest waiting list at specialty level, although ENT, Orthopaedics, Gastroenterology and Ophthalmology also have large waiting lists. Note: ‘Other’ specialty includes a wide range of specialties including colorectal surgery, Allergy and Upper GI. At the end of May both Acute Trusts had a number of patients waiting over 52 and 75 weeks:
Over 52 weeks: NUH had 3,342 and SFH had 1,270 patients waiting
Over 75 weeks: NUH had 893 and SFH had 169 patients waiting
10.35% of the NUH waiting lists are waiting over 40 weeks, which compares to 9.35% for SFH
The 3 main Independent Sector hospitals within Nottingham & Nottinghamshire have a total of 290 patients waiting over 52 weeks covering Orthopaedics, Ophthalmology, General Surgery, Urology, Gastroenterology, and ENT.
Mitigating Actions
Executive oversight is in place by the ICS Clinical Executive Group and in addition the CCG Quality & Performance Committee
Where possible, providers have reinstated elective capacity, whilst undertaking outpatients, diagnostics and surgery in line with social distancing limitations and PPE/Testing requirements
Continued focus on non-face to face outpatient activity, with a significant shift in the proportion of outpatient activity delivered via Telephone or Video
Waiting list management continues to be based on clinical priority and taking appropriate consideration of chronological order when listing patients. The system agreed changes to the case mix undertaken by the Independent Sector to enable cancer and urgent complex cases to be prioritised
N&N ICS are an Accelerator site for elective recovery, focusing on:-
Increased capacity
Pathway innovations, including digital enablers
Pathway vetting, clinical review and validation
The Elective hub commenced in April 2021 to review surgical long waits within the system. In future, the remit will progress to outpatients and diagnostic waits.
The high volume specialties are reviewed weekly. There is also consideration of the transfer of patients between providers, which is strongly linked to clinical suitability.
The Independent Sector providers attend the elective hub to ensure capacity is maximised across system.
Assurances The capacity cell has oversight of all system wide recovery plans, to ensure a whole system approach. This is supported by good provider engagement.
Established reports track the recovery of services against system plans via the capacity cell.
The CCG is working with Trusts via the capacity cell to align capacity with predicted demand.
Elective Hub is in place.
PTLs are discussed in detail within each organisation, and reviewed and managed at the weekly system Elective Hub, chaired by the ICS lead
Performance is underpinned by whole system transformation. An ICS Planned Care, Cancer and Diagnostics Board has been established to oversee all transformation and ensure operational delivery.
Gaps in Assurance
Patients will wait longer for elective care and may feel anxiety when attending an acute setting and adhering to social distancing requirements
Integrated Performance Report
83 of 22409:00 - 10.50-04/08/21
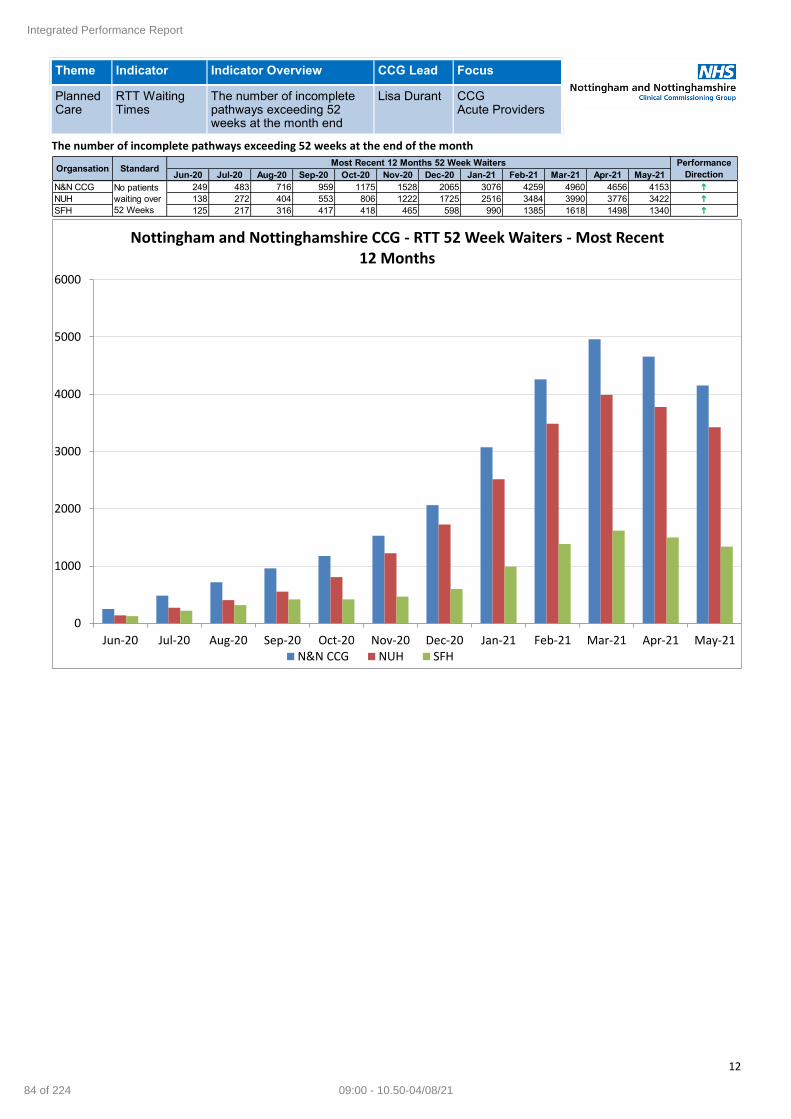
12
Theme Indicator Indicator Overview CCG Lead Focus
Planned Care
RTT Waiting Times
The number of incomplete pathways exceeding 52 weeks at the month end
Lisa Durant CCG Acute Providers
The number of incomplete pathways exceeding 52 weeks at the end of the month
Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
N&N CCG 249 483 716 959 1175 1528 2065 3076 4259 4960 4656 4153 h
NUH 138 272 404 553 806 1222 1725 2516 3484 3990 3776 3422 h
SFH 125 217 316 417 418 465 598 990 1385 1618 1498 1340 h
Organsation StandardMost Recent 12 Months 52 Week Waiters Performance
Direction
No patients
waiting over
52 Weeks
0
1000
2000
3000
4000
5000
6000
Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
Nottingham and Nottinghamshire CCG - RTT 52 Week Waiters - Most Recent 12 Months
N&N CCG NUH SFH
Integrated Performance Report
84 of 224 09:00 - 10.50-04/08/21
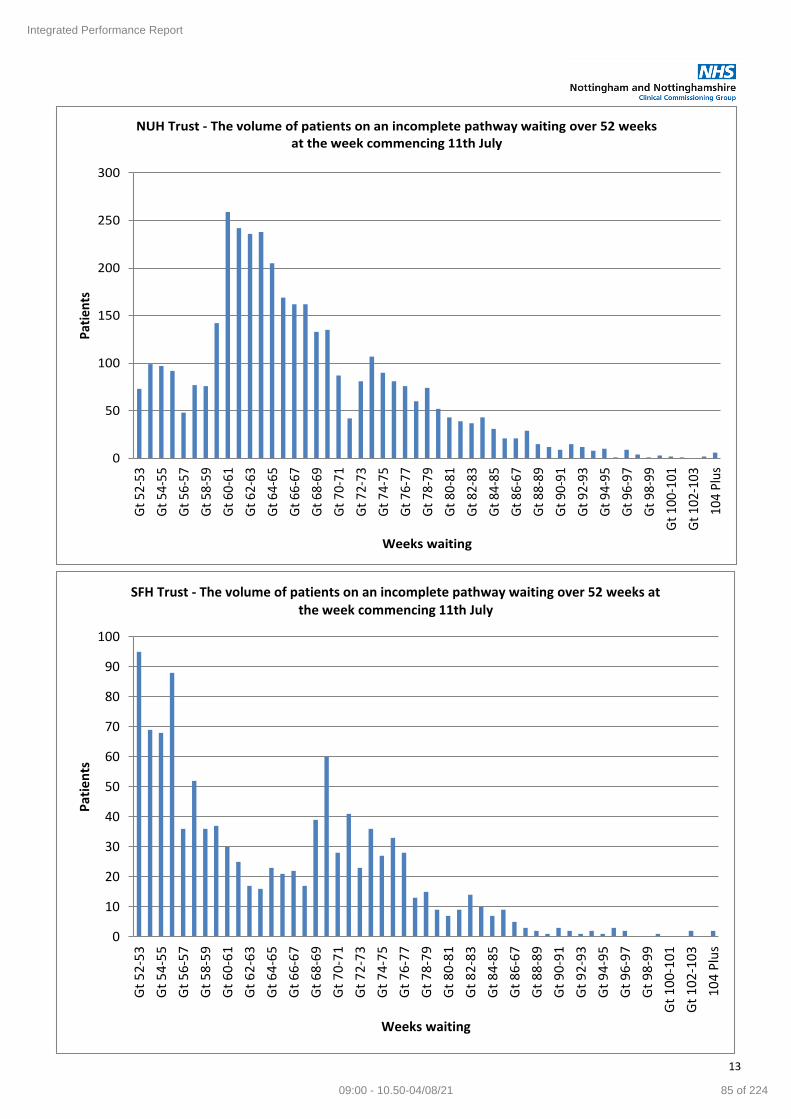
13
0
50
100
150
200
250
300
Gt
52-5
3
Gt
54-5
5
Gt
56-5
7
Gt
58-5
9
Gt
60-6
1
Gt
62-6
3
Gt
64-6
5
Gt
66-6
7
Gt
68-6
9
Gt
70-7
1
Gt
72-7
3
Gt
74-7
5
Gt
76-7
7
Gt
78-7
9
Gt
80-8
1
Gt
82-8
3
Gt
84-8
5
Gt
86-6
7
Gt
88-8
9
Gt
90-9
1
Gt
92-9
3
Gt
94-9
5
Gt
96-9
7
Gt
98-9
9
Gt
100-
101
Gt
102-
103
104
Plu
s
Pat
ien
ts
Weeks waiting
NUH Trust - The volume of patients on an incomplete pathway waiting over 52 weeks at the week commencing 11th July
0
10
20
30
40
50
60
70
80
90
100
Gt
52
-53
Gt
54
-55
Gt
56
-57
Gt
58
-59
Gt
60
-61
Gt
62
-63
Gt
64
-65
Gt
66
-67
Gt
68
-69
Gt
70
-71
Gt
72
-73
Gt
74
-75
Gt
76
-77
Gt
78
-79
Gt
80
-81
Gt
82
-83
Gt
84
-85
Gt
86
-67
Gt
88
-89
Gt
90
-91
Gt
92
-93
Gt
94
-95
Gt
96
-97
Gt
98
-99
Gt
10
0-1
01
Gt
10
2-1
03
10
4 P
lus
Pat
ien
ts
Weeks waiting
SFH Trust - The volume of patients on an incomplete pathway waiting over 52 weeks at the week commencing 11th July
Integrated Performance Report
85 of 22409:00 - 10.50-04/08/21

14
Root Cause Long waiting patients and associated root causes were being actively managed by providers prior to the COVID pandemic across a range of specialties. However prior to the incident neither NUH nor SFH had any patients waiting over 52 weeks for treatment. As a result of the COVID 19 pandemic there has been a substantial increase in the number of long wait patients awaiting routine surgery locally and nationally. This is due to:
National instruction at the beginning of the Covid 19 pandemic
The level of non-elective demand acute trusts have experienced due to Covid 19
Reduced productivity due to IPC requirements and social distancing
Prioritisation of cancer and urgent categories of patients waiting before patients waiting over 52 weeks Please note: local Independent Sector providers also have patients waiting in excess of 52 week waits, currently 290, an increase of 18 since last month. This is due to prioritisation of clinically urgent patients from NHS providers.
Mitigating Actions
CCG closely monitors patients waiting at all providers by time band, with focus on patients waiting 52wks and over
Trust PTLs are discussed in detail within each organisation, and reviewed and managed at the weekly system Elective Hub, chaired by the ICS lead. Mutual aid between organisations is considered where appropriate.
Restoration of elective capacity across Notts system includes on-going use of all Independent Sector capacity. IS providers are monitored and managed against the activity plan that forms the basis of the IS contract.
Trusts have internal governance processes established including senior sign off for waiting list validation and oversight of clinical prioritisation.
Elective Hub undertakes collective review of waiting lists of the NHS trusts, including IS, which is informed by weekly performance reports distributed within the system
Letters have been sent in Q1 21/22 to all patients on a waiting list who have received no contact from their provider within the last 10 weeks to provide an update on current situation.
The Capacity Cell is reviewing all available capacity against predictions of future demand with potential mitigations and associated action
Assurances Key points:
Collaborative working is in place between CCG, IS and NHS providers to maximise all available capacity in the system and to align capacity with predicted future demand
Royal College of Surgeons guidance in relation to clinical prioritisation of patients waiting for elective care has been implemented by NHS Providers. Clinical Executive Group and the Quality & Performance Committee has oversight of this process and considers the level of risk associated with long waits.
Weekly monitoring of patients at NUH and SFH is undertaken at specialty level.
Assurances are routinely requested from IS provides as well as NHS providers with regard to long waits and appropriate clinical prioritisation
An improved position was seen in May for routine services that have been restored along with associated capacity increases.
Gaps in Assurance
Patients will wait longer for elective care and may feel anxiety when attending an acute setting and adhering to social distancing requirements
N&N CCG Patients Waiting Over 52 Wks - Top 10 Providers Patients
NOTTINGHAM UNIVERSITY HOSPITALS NHS TRUST 2342
SHERWOOD FOREST HOSPITALS NHS FOUNDATION TRUST 1070
PRIMARY INTEGRATED COMMUNITY SERVICES LTD 178
UNIVERSITY HOSPITALS OF DERBY AND BURTON NHS FOUNDATION TRUST 151
WOODTHORPE HOSPITAL 87
UNIVERSITY HOSPITALS OF LEICESTER NHS TRUST 69
SPIRE NOTTINGHAM HOSPITAL 60
BMI - THE PARK HOSPITAL 50
CHESTERFIELD ROYAL HOSPITAL NHS FOUNDATION TRUST 16
DONCASTER AND BASSETLAW TEACHING HOSPITALS NHS FOUNDATION TRUST 15
OTHER PROVIDERS 130
TOTAL 4153
Integrated Performance Report
86 of 224 09:00 - 10.50-04/08/21
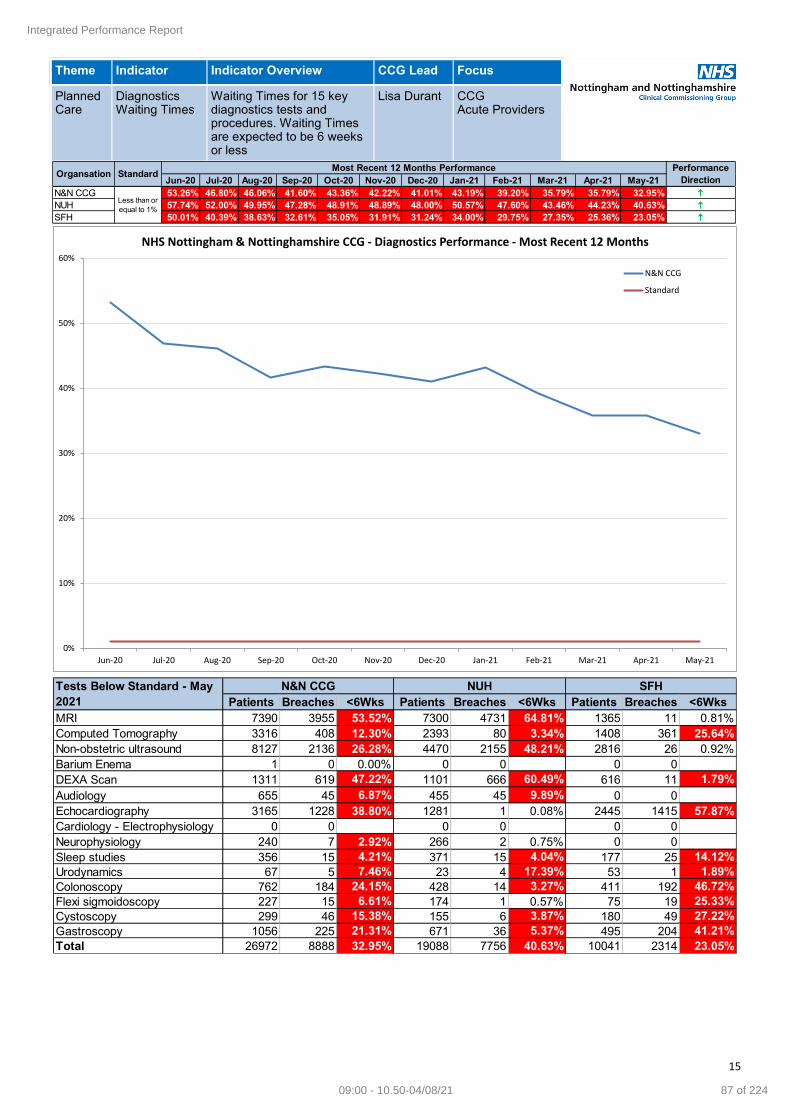
15
Theme Indicator Indicator Overview CCG Lead Focus
Planned Care
Diagnostics Waiting Times
Waiting Times for 15 key diagnostics tests and procedures. Waiting Times are expected to be 6 weeks or less
Lisa Durant CCG Acute Providers
Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
N&N CCG 53.26% 46.80% 46.06% 41.60% 43.36% 42.22% 41.01% 43.19% 39.20% 35.79% 35.79% 32.95% h
NUH 57.74% 52.00% 49.95% 47.28% 48.91% 48.89% 48.00% 50.57% 47.60% 43.46% 44.23% 40.63% h
SFH 50.01% 40.39% 38.63% 32.61% 35.05% 31.91% 31.24% 34.00% 29.75% 27.35% 25.36% 23.05% h
Organsation StandardMost Recent 12 Months Performance Performance
Direction
Less than or
equal to 1%
0%
10%
20%
30%
40%
50%
60%
Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
NHS Nottingham & Nottinghamshire CCG - Diagnostics Performance - Most Recent 12 Months
N&N CCG
Standard
Patients Breaches <6Wks Patients Breaches <6Wks Patients Breaches <6Wks
MRI 7390 3955 53.52% 7300 4731 64.81% 1365 11 0.81%
Computed Tomography 3316 408 12.30% 2393 80 3.34% 1408 361 25.64%
Non-obstetric ultrasound 8127 2136 26.28% 4470 2155 48.21% 2816 26 0.92%
Barium Enema 1 0 0.00% 0 0 0 0
DEXA Scan 1311 619 47.22% 1101 666 60.49% 616 11 1.79%
Audiology 655 45 6.87% 455 45 9.89% 0 0
Echocardiography 3165 1228 38.80% 1281 1 0.08% 2445 1415 57.87%
Cardiology - Electrophysiology 0 0 0 0 0 0
Neurophysiology 240 7 2.92% 266 2 0.75% 0 0
Sleep studies 356 15 4.21% 371 15 4.04% 177 25 14.12%
Urodynamics 67 5 7.46% 23 4 17.39% 53 1 1.89%
Colonoscopy 762 184 24.15% 428 14 3.27% 411 192 46.72%
Flexi sigmoidoscopy 227 15 6.61% 174 1 0.57% 75 19 25.33%
Cystoscopy 299 46 15.38% 155 6 3.87% 180 49 27.22%
Gastroscopy 1056 225 21.31% 671 36 5.37% 495 204 41.21%
Total 26972 8888 32.95% 19088 7756 40.63% 10041 2314 23.05%
Tests Below Standard - May
2021
N&N CCG NUH SFH
Integrated Performance Report
87 of 22409:00 - 10.50-04/08/21

16
Root Cause
Backlogs and long waits due to reduction in capacity during Covid, particularly Endoscopy where procedures were classified as Aerosol Generating Procedures (AGPs). A Significant increase in GP referrals seen in Q1 21/22, particularly urgent cancer referrals.
Mitigating Actions
Extensive use of the IS provider hospitals for endoscopy (Ramsay Woodthorpe, BMI Park, The Spire), and mobile IS Diagnostic mobile capacity located at both Trusts for CT and MRI.
Extensive use of Day Surgery facilities to increase internal Endoscopy capacity. SFH have increased the use of Newark Hospital to increase capacity levels.
Major estates work completed at City Campus Endoscopy unit to ensure compliance with latest ventilation standards, which generate improved productivity.
Evening and weekend capacity expanded at both trusts to increase capacity.
NUH utilising portable ventilation system where appropriate to enable increased productivity per session.
Assurances
Month on Month Improvement in performance against diagnostic access standards.
Activity currently at 100+% of pre-COVID levels across the main diagnostic modalities which benchmarks well against national average and peers.
DNA rates reducing as vaccination programme rolls out.
The ICS is an Accelerator system for Elective Recovery, which has enabled extension of IS Mobile diagnostic capacity.
ICS secured significant year 1 Community Diagnostic Hub funding to expand IS mobile diagnostic capacity in 21/22 – CT, MRI and Endoscopy. £5.6m revenue. Awaiting confirmation of £762k capital funding.
Gaps in Assurance
Seeking assurance from National Diagnostics Team on Year 2-5 funding for Community Diagnostic Hubs.
Integrated Performance Report
88 of 224 09:00 - 10.50-04/08/21

17
Theme Indicator Indicator Overview CCG Lead Focus
Planned Care
Cancer—2 Week Wait
Waiting Times against the 2 week wait cancer standard
Simon Castle
CCG Acute Providers
Root Cause NUH
May performance was 87.3%, an increase on previous month.
Skin and Head & Neck have both seen above 130% demand compared to pre-COVID levels.
LGI / Gynae / Urology are all above 110% demand – as sustained higher demand continues.
There has been a direct impact on outpatient capacity as in order to create enough new 2WW capacity, follow up slots have been utilised.
Performance in Breast and LGI sites are having the largest impact on the lower performance.
Breast continues to have sustained high demand. The service normally date patients at 10 days, but this has increased to 14 due to the recent surge in demand and it will be challenging to flex capacity any further.
SFH
SFH achieved the 2 week wait standard for May 2021.
Mitigating Actions NUH
Referral rates have reduced towards the pre-COVID average, following the significant rise in March and to a lesser extent in April.
Discussions continue with Primary Care regarding the importance of 2WW referrals following face to face consultation wherever possible.
Specific tumour site education sessions around referral criteria are being organised e.g. Lung and H&N are examples
Assurances NUH
62-day backlog has peaked and has started to decrease.
Treatment volumes have remained high even with surgical and HDU capacity issues.
Continued access to IS capacity with local agreement has been maintained following the end of national IS contract.
Improved access to theatres and beds across Trust from 19th April.
Gaps in Assurance NUH
Recent 2ww referral surge in March and April has impacted 2ww performance. This has started to reduced, with H&N, Skin, UGI, LGI, and Breast all seeing significant increases.
Outpatient capacity is becoming increasingly impacted by 2ww referral increases, as follow-up slots have been utilised in some areas to increase 2ww capacity, leading to longer waits for follow up appointments.
Increasing levels of COVID infection may result in a rising number of staff isolating
Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
N&N CCG 93.39% 91.78% 93.11% 94.74% 95.14% 95.53% 95.32% 88.77% 95.84% 96.44% 86.25% 89.67% h
NUH 91.87% 89.67% 91.74% 93.87% 95.39% 95.82% 95.30% 87.40% 95.38% 96.65% 82.56% 87.31% h
SFH 97.70% 96.60% 96.62% 96.46% 94.79% 95.70% 95.62% 91.43% 96.76% 96.44% 95.17% 95.20% h
Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
N&N CCG 96.97% 97.80% 98.75% 97.96% 95.79% 93.64% 93.69% 97.59% 96.94% 96.15% 63.11% 74.42% h
NUH 97.87% 98.51% 100% 96.67% 95.06% 97.98% 91.11% 97.01% 98.63% 96.81% 45.71% 68.49% h
SFH 100% 100% 100% 100% 100% 100% 100% 100% 97.50% 100% 100% 100% n
Greater than or
equal to 93%
Organsation StandardMost Recent 12 Months Performance - Two Week Wait - Breast Symptoms Performance
Direction
Organsation StandardMost Recent 12 Months Performance - Two Week Wait Performance
Direction
Greater than or
equal to 93%
Integrated Performance Report
89 of 22409:00 - 10.50-04/08/21

18
Theme Indicator Indicator Overview CCG Lead Focus
Planned Care
Cancer—28 day FDS
Waiting Times against the 28 Fast Diagnosis cancer standard
Simon Castle
CCG Acute Providers
Please note: The release of NUH & SFH data has been delayed due to the response to the COVID-19 pandemic. This table will be updated as soon as the data is available.
Root Cause The Faster Diagnosis Standard is intended to ensure that all patients who are referred for the investigation of suspected cancer find out, within 28 days, if they do or do not have a cancer diagnosis. The data is available at CCG as reported above, however data release has been delayed at provider level due to the COVID 19 pandemic. This standard is designed to:
Reduce anxiety for patients who will be diagnosed with cancer or receive an ‘all clear’ but do not currently hear this information in a timely manner;
Speed up time from referral to diagnosis, particularly where faster diagnosis is proven to improve clinical outcomes;
Reduce unwarranted variation in England by understanding how long it is taking patients to receive a diagnosis or ‘all clear’ for cancer across the country.
There are three main factors that require consideration by providers in order to deliver the Faster Diagnosis Standard. They are: 1. Time to first seen and test - This requires alignment of 2 week wait demand and diagnostic capacity 2. The volume of tests required to confirm or rule out cancer 3. Method of communication—this is often face to face, however telephone clinics are increasingly being utilised The performance level for the Nottingham and Nottinghamshire CCG was 79.11% in May 2021, which is above the national standard of 70%. Performance within the twelve months prior was above the national standard in all months. In four of those months, performance was above 80%.
Mitigating Actions The COVID 19 Pandemic has impacted capacity for diagnostic procedures, largely due to the increase in infection control requirements. SFH are reviewing all tumour sites to review methods of communication used for FDS. Moving to telephone clinics where possible to reduce the number of days patients are waiting for outcomes. SFH are reviewing the 2WW capacity as part of the work taking place around service restoration and recovery. All tumour sites are operating with a mix of face to face, non face to face appointments and triage straight to test where appropriate.
Assurances Collecting the data from April 19 has enabled a more granular understanding to be reached around the key areas for improvement at local providers which include the level of Outpatient and Diagnostic capacity as well as timely methods of communication. System wide dialogue continues to take place around the recovery and restoration of services.
Gaps in Assurance Patient choice remains a risk with some patients currently choosing to decline appointments due to COVID fears. In addition to comparison against the national standard, provider benchmarking is a useful resource against which to assess provider performance. However, this is not currently possible for 28 day FDS as a national decision has been taken to delay the publication of provider level FDS data. A publication date is not yet known.
Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
N&N CCG 79.69% 81.04% 79.37% 76.12% 87.69% 79.58% 79.87% 74.68% 83.44% 83.83% 79.25% 79.11% i
NUH n
SFH n
Organsation StandardMost Recent 12 Months Performance - Twenty Eight Day FDS Performance
Direction
Greater than or
equal to 70%
Integrated Performance Report
90 of 224 09:00 - 10.50-04/08/21

19
Theme Indicator Indicator Overview CCG Lead Focus
Planned Care
Cancer—31 Day
Waiting Times against the 31 day wait cancer standard
Simon Castle
CCG Acute Providers
Root Cause NUH
31 Day performance was 90.3%, very similar to last month’s performance. (90.1%)
The key reasons for breaches are surgical capacity for Urology (5), Gynae (7), H&N (2), and LGI (3), which continues to be linked to surgical and HDU capacity, clinical priority and Pre surgery 2 week self isolation requirements
Allocation of patients to surgical lists is more complex than pre COVID periods as specialties are unable to plan surgical capacity more than 2 weeks ahead.
SFH
SFH achieved 31 day target for May 2021.
Mitigating Actions NUH Surgical capacity
A new Skin consultant began in February 21, but theatre capacity is limited with waits of around 40 days. The Spire Hospital continues to be utilised for Skin where appropriate
Improved Capacity
From 19th April, there was improvement in access to theatres and beds. Theatre lists have returned to around 90% of pre-COVID levels.
Assurances NUH
62-day backlog has peaked and has started to decrease.
Treatment numbers have remained high even with surgical and HDU capacity issues.
Continued access to IS capacity with local agreement, following the end of the national IS contract.
Improved access to theatres and beds across Trust from 19th April.
Gaps in Assurance NUH
Recent 2ww referral surge in March and April has impacted 2ww performance. This has started to reduced slightly. H&N, Skin, UGI, LGI, and Breast all saw significant increases in demand.
Outpatient capacity is becoming increasingly impacted by 2ww referral increases, as follow-up slots have been utilised in some areas to increase 2ww capacity, leading to longer waits for follow up appointments.
Increasing levels of Covid infection are likely to result in a rising number of staff self-isolating.
Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
N&N CCG 92.01% 93.01% 89.81% 94.58% 95.06% 94.55% 91.39% 87.96% 93.01% 92.66% 91.72% 92.23% h
NUH 93.09% 93.91% 91.77% 95.17% 94.17% 91.70% 90.69% 86.58% 91.40% 91.13% 90.09% 90.34% h
SFH 92.11% 92.00% 81.93% 92.45% 94.44% 99.18% 95.79% 89.74% 99.00% 96.97% 95.88% 97.73% h
Greater than or
equal to 96%
Organsation StandardMost Recent 12 Months Performance - 31 Day Performance
Direction
Integrated Performance Report
91 of 22409:00 - 10.50-04/08/21

20
Theme Indicator Indicator Overview CCG Lead Focus
Planned Care
Cancer—62 Day
Waiting Times against the 62 day wait cancer standard
Simon Castle
CCG Acute Providers
Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
N&N CCG 74.23% 76.42% 70.26% 75.20% 76.34% 74.91% 75.73% 68.15% 71.50% 73.26% 79.10% 74.66% i
NUH 77.41% 78.35% 73.91% 78.82% 76.20% 75.00% 76.22% 71.43% 67.51% 73.83% 75.12% 71.18% i
SFH 64.71% 68.03% 60.61% 67.55% 70.91% 74.19% 69.57% 63.16% 72.79% 68.75% 73.61% 71.13% i
Greater than or
equal to 85%
Organsation StandardMost Recent 12 Months Performance - 62 Day Performance
Direction
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Jun-
20
Jul-2
0
Aug
-20
Sep
-20
Oct
-20
Nov
-20
Dec
-20
Jan-
21
Feb
-21
Mar
-21
Apr
-21
May
-21
Nottingham & Nottinghamshire CCG - Cancer 62 Day Performance - Most Recent 12 Months
0
50
100
150
200
250
300
06-O
ct-
19
20-O
ct-
19
03-N
ov-1
9
17-N
ov-1
9
01-D
ec-1
9
15-D
ec-1
9
29-D
ec-1
9
12-J
an-2
0
26-J
an-2
0
09-F
eb-2
0
23-F
eb-2
0
08-M
ar-
20
22-M
ar-
20
05-A
pr-
20
19-A
pr-
20
03-M
ay-2
0
17-M
ay-2
0
31-M
ay-2
0
14-J
un-2
0
28-J
un-2
0
12-J
ul-2
0
26-J
ul-2
0
09-A
ug-2
0
23-A
ug-2
0
06-S
ep-2
0
20-S
ep-2
0
04-O
ct-
20
18-O
ct-
20
01-N
ov-2
0
15-N
ov-2
0
29-N
ov-2
0
13-D
ec-2
0
27-D
ec-2
0
10-J
an-2
1
24-J
an-2
1
07-F
eb-2
1
21-F
eb-2
1
07-M
ar-
21
21-M
ar-
21
04-A
pr-
21
18-A
pr-
21
02-M
ay-2
1
16-M
ay-2
1
30-M
ay-2
1
13-J
un-2
1
27-J
un-2
1
To
tal
Ba
cklo
g
Week Ending
NUH - Cancer - 62 Day Backlog
Over 104 Days 63-103 Days
0
50
100
150
200
250
06-O
ct-
19
20-O
ct-
19
03-N
ov-1
9
17-N
ov-1
9
01-D
ec-1
9
15-D
ec-1
9
29-D
ec-1
9
12-J
an-2
0
26-J
an-2
0
09-F
eb-2
0
23-F
eb-2
0
08-M
ar-
20
22-M
ar-
20
05-A
pr-
20
19-A
pr-
20
03-M
ay-2
0
17-M
ay-2
0
31-M
ay-2
0
14-J
un-2
0
28-J
un-2
0
12-J
ul-2
0
26-J
ul-2
0
09-A
ug-2
0
23-A
ug-2
0
06-S
ep-2
0
20-S
ep-2
0
04-O
ct-
20
18-O
ct-
20
01-N
ov-2
0
15-N
ov-2
0
29-N
ov-2
0
13-D
ec-2
0
27-D
ec-2
0
10-J
an-2
1
24-J
an-2
1
07-F
eb-2
1
21-F
eb-2
1
07-M
ar-
21
21-M
ar-
21
04-A
pr-
21
18-A
pr-
21
02-M
ay-2
1
16-M
ay-2
1
30-M
ay-2
1
13-J
un-2
1
27-J
un-2
1
To
tal
Ba
cklo
g
Week Ending
SFH - Cancer - 62 Day Backlog
Over 104 Days 63-103 Days
Integrated Performance Report
92 of 224 09:00 - 10.50-04/08/21
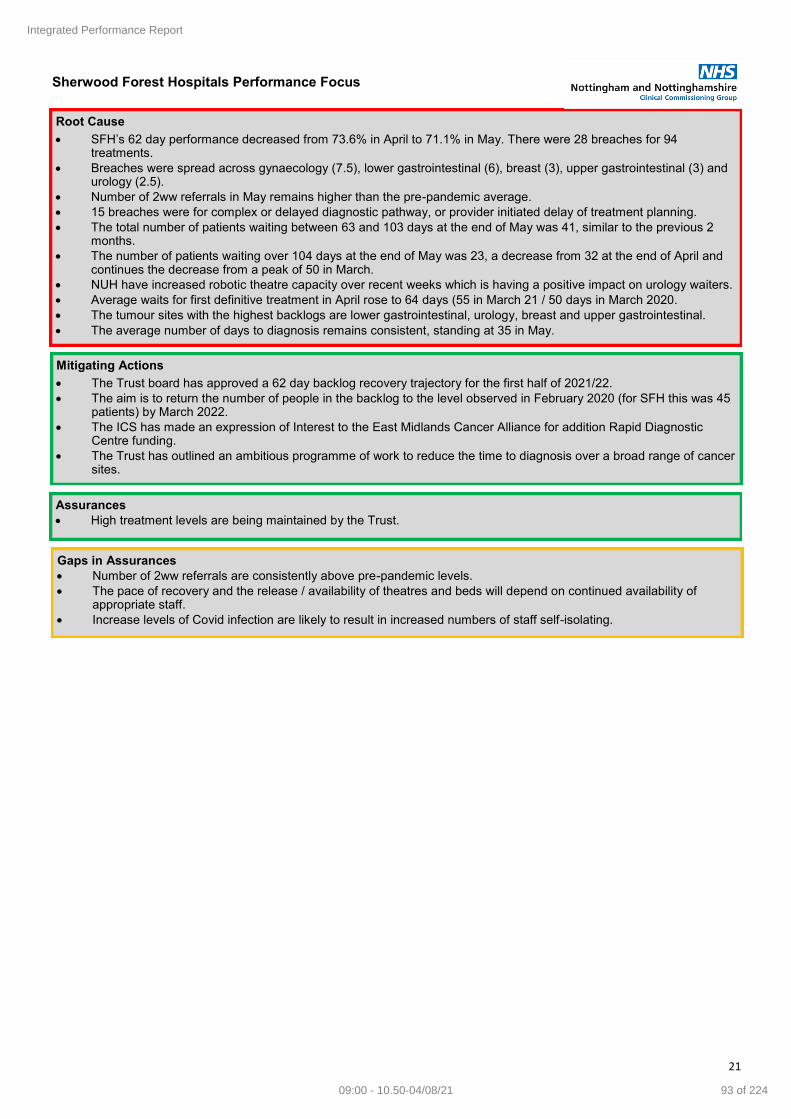
21
Root Cause
SFH’s 62 day performance decreased from 73.6% in April to 71.1% in May. There were 28 breaches for 94 treatments.
Breaches were spread across gynaecology (7.5), lower gastrointestinal (6), breast (3), upper gastrointestinal (3) and urology (2.5).
Number of 2ww referrals in May remains higher than the pre-pandemic average.
15 breaches were for complex or delayed diagnostic pathway, or provider initiated delay of treatment planning.
The total number of patients waiting between 63 and 103 days at the end of May was 41, similar to the previous 2 months.
The number of patients waiting over 104 days at the end of May was 23, a decrease from 32 at the end of April and continues the decrease from a peak of 50 in March.
NUH have increased robotic theatre capacity over recent weeks which is having a positive impact on urology waiters.
Average waits for first definitive treatment in April rose to 64 days (55 in March 21 / 50 days in March 2020.
The tumour sites with the highest backlogs are lower gastrointestinal, urology, breast and upper gastrointestinal.
The average number of days to diagnosis remains consistent, standing at 35 in May.
Mitigating Actions
The Trust board has approved a 62 day backlog recovery trajectory for the first half of 2021/22.
The aim is to return the number of people in the backlog to the level observed in February 2020 (for SFH this was 45 patients) by March 2022.
The ICS has made an expression of Interest to the East Midlands Cancer Alliance for addition Rapid Diagnostic Centre funding.
The Trust has outlined an ambitious programme of work to reduce the time to diagnosis over a broad range of cancer sites.
Sherwood Forest Hospitals Performance Focus
Assurances
High treatment levels are being maintained by the Trust.
Gaps in Assurances
Number of 2ww referrals are consistently above pre-pandemic levels.
The pace of recovery and the release / availability of theatres and beds will depend on continued availability of appropriate staff.
Increase levels of Covid infection are likely to result in increased numbers of staff self-isolating.
Integrated Performance Report
93 of 22409:00 - 10.50-04/08/21

22
Root Cause May Performance
May performance declined to 71.2% from 75.1% in April.
Treatment numbers have increased to 223.
Theatre capacity now back to approx. 90% of pre COVID levels across most specialities.
Outpatient capacity has been impacted, as follow up slots are being utilised for 2ww appointments, following surge in demand.
Post lockdown – increases in DNA / fitness for surgery issues. Patient choice issues increasing as patients unable to attend offered appoints.
62 day backlog - there has been some improvement in total backlog - is at 191 (29/6)
Total breaches are forecast to be high at 70 with highest breach numbers in:- Urology 14.5, LGI 11, Lung 10, Gynae 9.5, and UGI 7.5.
Some loss of flexibility depending on location for treatment. (ie - patients in Private Sector, or Treatment Centre, some locations don’t have HDU beds, TC don’t take high BMI patients) Allocation of patients to different lists is not as straight forward as pre covid and is causing challenges for larger / high number specialities.
Oncology and Histology performance impacted by consultant recruitment issues - Impacting on breast oncology follow up appointments and Histology impacted across the board.
Gynae front end of the pathway and performance impacted by inability to cover list allocation with consultant vacancy and allocation of 3 lists on same day.
Nottingham University Hospitals Performance Focus
Mitigating Actions
Surgical prioritisation continues to take place matching available capacity with clinical need across different specialties.
National IS agreement ended on 31st March, however, NUH have negotiated on-going agreement locally and so access to IS capacity continues.
From 19th April, there was an improvement in access to theatres and beds. Theatre lists have return to approx. 90% of pre-COVID levels.
62-day backlog peaked at 225 recently and has started to decrease. All specialties have produced an action plan and trajectory for improvement.
Assurances
See assurances for Cancer 31 day on page 15.
Gaps in Assurances
See gaps in assurances for Cancer 31 day on page 15.
Integrated Performance Report
94 of 224 09:00 - 10.50-04/08/21

23
Theme Indicator Indicator Overview CCG Lead Focus
Urgent Care
A&E—4 hour Wait
The percentage of patients waiting under 4 hours in A&E departments
Caroline Nolan
Acute Providers CCG
Theme Indicator Indicator Overview CCG Lead Focus
Urgent Care
A&E—12 Hour Trolley waits
Period from the decision to admit to formal admission to an emergency inpatient bed
Caroline Nolan
Acute Providers CCG
Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
N&N CCG 85.99% 85.06% 82.03% 80.71% 78.22% 79.85% 75.71% 73.01% 76.64% 76.04% 76.30% 73.27% i
NUH n
SFH 95.74% 96.73% 95.53% 96.45% 95.20% 93.50% 89.67% 85.41% 92.26% 94.11% 93.77% 91.75% i
Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
N&N CCG 22013 25369 26108 25324 24163 22794 22781 20438 19930 24735 26651 29282 N/A
NUH 15259 17997 18854 18565 17519 16548 15855 14526 14134 18627 19607 22179 N/A
SFH 9894 11025 11646 11338 10612 9901 10029 9279 8932 11654 12284 13930 N/A
Performance
Direction
Reporting suspended due to trial of new indicators
Organsation StandardMost Recent 12 Months Performance Performance
Direction
N/A
Greater than or
equal to 95%
Organsation StandardMost Recent 12 Months - Attendances
0
5000
10000
15000
20000
25000
30000
35000
Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
A&E Attendances - Most Recent 12 Months
N&N CCG NUH SFH
Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
N&N CCG N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A N/A n
NUH 0 0 0 0 1 0 0 8 27 8 0 5 i
SFH 0 0 0 0 0 0 7 1 2 1 0 1 i
Organsation StandardMost Recent 12 Months - 12hr Performance
Direction
N/A
0
5
10
15
20
25
30
Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
A&E 12 Hour Trolley Waits - Most Recent 12 Months
NUH SFH
Integrated Performance Report
95 of 22409:00 - 10.50-04/08/21

24
Root Cause
NHS111 saw an increase of 146 (13.9%) patients per day from May to April. Despite this increase, the number of ED dispositions referred to ED has stayed static, which shows that this increase in patient numbers are either having their consultation sessions closed at the NHS111 stage or are being referred to alternative pathways for their treatment needs.
Conveyance rates had remained relatively static to both trusts since December 2020 until May. In May, SFH saw an increase of over 14% to 60.5% when compared to April (46.1%). This increase can be attributed to an increase in higher acuity patients which has also increased bed occupancy for the same period, by 4% to just below 90%, for May. For NUH at the same time, only a 1% increase was recorded when compared to April.
Both ED departments have also continued to see an increase in attendances in May compared to April and this has been the trend since the beginning of 2021. A main contributor to this increase can be attributed to the increasing numbers of unheralded patients attending at both NUH and SFHFT. At NUH this type of patient increased from 58.9% to 60.0% and at SFHFT from 63.7% to 65.3% when comparing May to April figures.
In May, NUH saw an additional 47 patients per day compared to April, whilst at SFHFT an additional 22 patients per day were seen compared to April. At the same time, the % of attendances resulting in admission has decreased by 2.5% for NUH whilst at SFHFT it had decreased by less than 1% compared to April. However, the numbers of patients admitted to both acute trusts has remained relatively static with an increase at NUH of 11 patients per day and SFHFT 3 per day, in May.
MSFT levels in both Mid and Greater Notts remained higher that target levels in May for both NUH and SFHFT. This can be contributed to several factors including internal process issues within the acute trusts, increasing demand for Pathway 1 services, with insufficient care package provision both of which are the focus of the D2A collaborative improvement work.
In May, the daily average number of beds occupied by confirmed Covid-19 positive patients in both NUH and SFHFT was 35, as opposed to 77 in April.
Pre ED ACTIVITY Primary Care Primary care on the day demand gives an indication of the level of urgent care need in the wider system being met by Primary care. Table 1 – Primary Care activity for 6 months up to May 2021 Current data is based on appointment data extracted from GP clinical systems, not recorded consultations, and hence fails to capture the additional ‘remote’ work that primary care has been doing over this period in the form of triage calls, online consultations and clinical ‘tasks’. Discussions are underway at Primary Care Incident Management Group (PCIMG) to resolve how our systems can capture all activity from GP appointment systems in a consistent way in line with the new guidance releases 31st March 2021. NHS111 During May, DHU 111 achieved 1 of the 2 key performance standards as reported in the table below. Table 2 – DHU performance standards for March 2021 Please note the percentage of triaged calls to a clinician metric is currently unavailable due to being changed to ICS level metrics. The new reporting metric is due to be available September 2021. During May, DHU saw an increase of 146 calls per day compared to April, DHU 111 are managing this demand extremely well however; the rest of the country are seeing real impacts to performance with several providers invoking national contingency measures. The ability for 111 to directly book to GP appointments has been enabled fully as part of 111 first developments, the on-going growth of this service has continued.
Performance Indicator Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
% of Same Day Appointments 43% 46% 46% 44% 44%
Number of Same Day Appointments Booked 200,912 199,083 201,437 235,593 204,398
Total Number of Appointments Booked 465,913 436,384 436,409 534,353 461,437
Data not
released
Nottingham & Nottinghamshire Period Standard Performance
Percentage answered within 60 seconds May-21 95% 92%
Percentage abandoned after 30 seconds May-21 <5% 0.40%
Integrated Performance Report
96 of 224 09:00 - 10.50-04/08/21

25
Table 3 – Direct bookings into Primary Care over 6 months up to May 2021
In addition, the use of alternatives to ED continues to be managed well by the Clinical Advisory Service (CAS) provided by NEMS. In May the number of patient dispositions recommended for ED from 111 that were redirected away from the front door of ED by CAS was 75% an increase of 1% over April and well above the target >50%. EMAS Performance standards remained relatively stable in May in comparison to April, with the Nottinghamshire division achieving national standards against CAT 1 Mean and 90th Centile. Cat 4 performance improvements that were seen in April unfortunately weren’t continued into May. Cat 2 and Cat 3 performance standards have not been met in May. Table 4 – EMAS Performance standard monthly comparison Demand
On scene responses were above plan in April (+10.6%)
Incidents were above plan in April (+14.6%)
Duplicates as a % of calls saw a deterioration in April at 17.2% compared to 16.1% in March Resourcing to demand continues to be an issue. In April, 449 hours were lost to ‘drift’ , which is the highest numbers of hours lost across the five divisions within EMAS and is an increase on the March position. Handover Delays > than 30 minutes: The % of handover delays > than 30 minutes increased across the system by 1.6% to 5.6% in May, when compared to April (4.0%). This rise can be attributed to the increasing volumes month on month, of patients attending both EDs. Pre handover delays above 60+ minutes were less than 1 a day across both NUH and SFHFT. Conveyance Performance Conveyance rates had remained relatively static to both trusts since December 2020, until May. In May, SFH saw an increase of over 14% to 60.5% when compared to April (46.1%). This increase can be attributed to an increase in higher acuity patients which has also increased bed occupancy at the same time, by 4% to just below 90%, for May. Table 5 – EMAS Conveyance Rate to NUH and SFH - 6 monthly comparisons For NUH at the same time, only a 1% increase when compared to April has been seen. Overall, the trajectory for conveyance is still below pre-pandemic levels.
Performance Indicator Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
Total Direct Bookings into Primary Care from 111 500 668 771 1624 1785Not
Available
NHS111 dispositions recommended for ED diverted by the Clinical Advisory Service 75% 77% 75% 73% 74% 75%
Performance Indicator Performance
MetricDec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
Conveyance Rate to NUH for GN incidents Monthly % 56.50% 53.30% 55.80% 58.00% 56.60% 57.60%
Conveyance Rate to SFH for MN Incidents Monthly % 44.90% 43.70% 44.10% 46.70% 46.10% 60.50%
Integrated Performance Report
97 of 22409:00 - 10.50-04/08/21
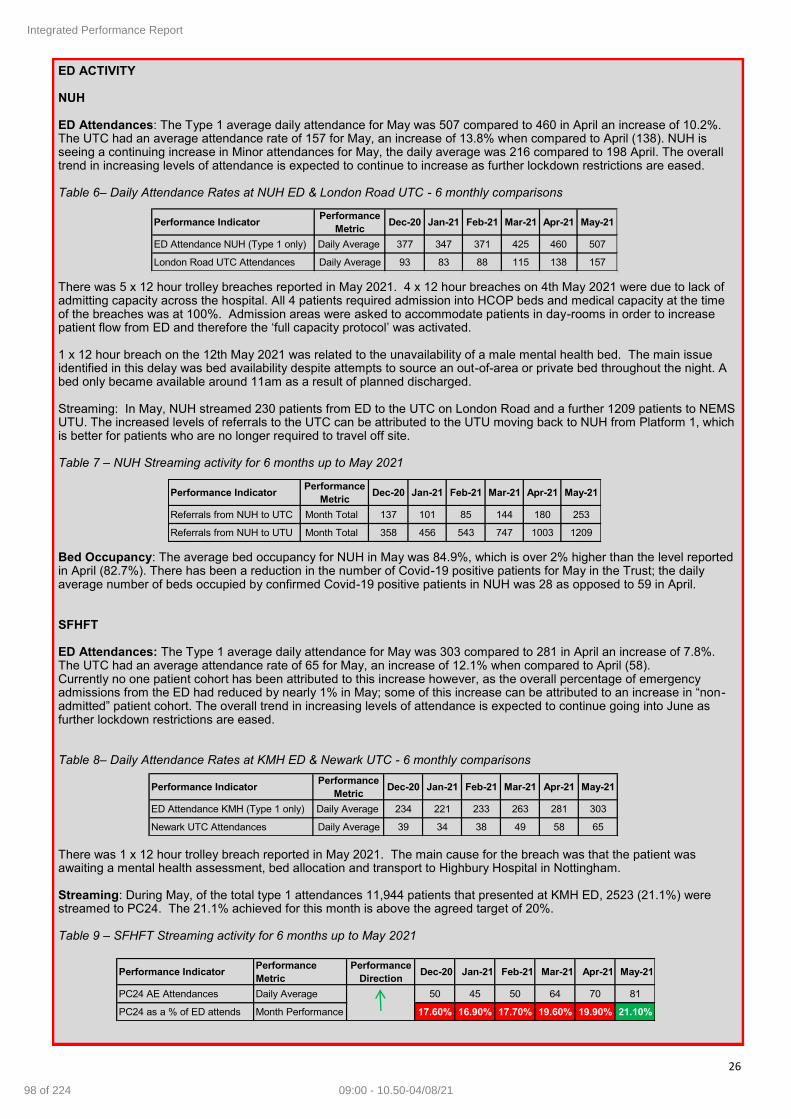
26
ED ACTIVITY NUH ED Attendances: The Type 1 average daily attendance for May was 507 compared to 460 in April an increase of 10.2%. The UTC had an average attendance rate of 157 for May, an increase of 13.8% when compared to April (138). NUH is seeing a continuing increase in Minor attendances for May, the daily average was 216 compared to 198 April. The overall trend in increasing levels of attendance is expected to continue to increase as further lockdown restrictions are eased. Table 6– Daily Attendance Rates at NUH ED & London Road UTC - 6 monthly comparisons There was 5 x 12 hour trolley breaches reported in May 2021. 4 x 12 hour breaches on 4th May 2021 were due to lack of admitting capacity across the hospital. All 4 patients required admission into HCOP beds and medical capacity at the time of the breaches was at 100%. Admission areas were asked to accommodate patients in day-rooms in order to increase patient flow from ED and therefore the ‘full capacity protocol’ was activated. 1 x 12 hour breach on the 12th May 2021 was related to the unavailability of a male mental health bed. The main issue identified in this delay was bed availability despite attempts to source an out-of-area or private bed throughout the night. A bed only became available around 11am as a result of planned discharged. Streaming: In May, NUH streamed 230 patients from ED to the UTC on London Road and a further 1209 patients to NEMS UTU. The increased levels of referrals to the UTC can be attributed to the UTU moving back to NUH from Platform 1, which is better for patients who are no longer required to travel off site. Table 7 – NUH Streaming activity for 6 months up to May 2021 Bed Occupancy: The average bed occupancy for NUH in May was 84.9%, which is over 2% higher than the level reported in April (82.7%). There has been a reduction in the number of Covid-19 positive patients for May in the Trust; the daily average number of beds occupied by confirmed Covid-19 positive patients in NUH was 28 as opposed to 59 in April. SFHFT ED Attendances: The Type 1 average daily attendance for May was 303 compared to 281 in April an increase of 7.8%. The UTC had an average attendance rate of 65 for May, an increase of 12.1% when compared to April (58). Currently no one patient cohort has been attributed to this increase however, as the overall percentage of emergency admissions from the ED had reduced by nearly 1% in May; some of this increase can be attributed to an increase in “non-admitted” patient cohort. The overall trend in increasing levels of attendance is expected to continue going into June as further lockdown restrictions are eased. Table 8– Daily Attendance Rates at KMH ED & Newark UTC - 6 monthly comparisons There was 1 x 12 hour trolley breach reported in May 2021. The main cause for the breach was that the patient was awaiting a mental health assessment, bed allocation and transport to Highbury Hospital in Nottingham. Streaming: During May, of the total type 1 attendances 11,944 patients that presented at KMH ED, 2523 (21.1%) were streamed to PC24. The 21.1% achieved for this month is above the agreed target of 20%. Table 9 – SFHFT Streaming activity for 6 months up to May 2021
Performance Indicator Performance
MetricDec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
ED Attendance NUH (Type 1 only) Daily Average 377 347 371 425 460 507
London Road UTC Attendances Daily Average 93 83 88 115 138 157
Performance Indicator Performance
Metric Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
Referrals from NUH to UTC Month Total 137 101 85 144 180 253
Referrals from NUH to UTU Month Total 358 456 543 747 1003 1209
Performance Indicator Performance
MetricDec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
ED Attendance KMH (Type 1 only) Daily Average 234 221 233 263 281 303
Newark UTC Attendances Daily Average 39 34 38 49 58 65
Performance Indicator Performance
Metric
Performance
DirectionDec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
PC24 AE Attendances Daily Average 50 45 50 64 70 81
PC24 as a % of ED attends Month Performance 17.60% 16.90% 17.70% 19.60% 19.90% 21.10%
Integrated Performance Report
98 of 224 09:00 - 10.50-04/08/21

27
Performance: The overall monthly performance was 91.6% in May, which is nearly 2% lower than the April’s performance of 93.65% and below the 95% performance target. This decrease in performance can be attributed to the both May bank holiday periods and school half term where changes in staffing levels, clinical team mix and reduced community based services would have had an impact on performance. Table 10 – SFHFT 4hr performance over 6 months up to May 2021 Bed Occupancy: The average bed occupancy for SFHFT in May was 89.6% nearly 4% higher than April’s (85.9%). Although there has been a good reduction in the number of Covid-19 positive patients in the Trust during this period, this has been offset by the increasing numbers of MSFT seen during May due to a lack of capacity in Pathway 1 provision in the Mid Notts area. In May, the daily average number of beds occupied by confirmed Covid-19 positive patients in SFHFT was 7 as opposed to 18 in April. ACUTE TRUST FLOW Same day Emergency Care (SDEC) Performance SDEC as a percentage of admissions continues to be well over target for both trusts. The specialties providing pathways for SDEC and the health care professionals that can refer to these pathways are being expanded, to further improve the SDEC offer. Table 11 – SDEC performance over 6 months up to May 2021 Admissions During May, the % of attendances resulting in admission has decreased by 2.5% for NUH whilst at SFHFT it had decreased by less than 1% when compared to April however; the numbers of patients admitted to both acute trusts has remained relatively static, with an increase at NUH of 11 patients per day and SFHFT 3 per day in May, this shows the increase are for lower acuity patients. NUH Table 12 – NUH ED Attendance to Admissions over 6 months up to May 2021 SFHFT Table 13 – SFHFT ED Attendance to Admissions over 6 months up to May 2021
Performance Indicator Performance
Metric
Performance
DirectionDec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
4hr Performance 95% 89.67% 85.11% 92.11% 94.03% 93.65% 91.60%
Performance Indicator Target Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
% of admissions classed as SDEC - NUH 30% 34.60% 34.30% 36.40% 38% 38.60% 35.00%
% of admissions classed as SDEC – SFH 30% 34.40% 35.30% 38.00% 39% 38.20% 38.20%
Performance Indicator Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
ED Attendance to Admission 38.40% 39.50% 37.60% 33.90% 33.30% 30.80%
Admissions from ED 145 137 142 152 160 164
Total Admissions 272 265 280 301 303 314
Care Homes Admissions 188 194 187 210 200 162
Performance Indicator Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
ED Attendance to Admission 38.20% 40.40% 41.00% 36.80% 34.00% 33.10%
Admissions from ED 73 72 74 74 75 77
Total Admissions 81 82 82 84 85 88
Care Homes Admissions 181 223 141 151 154 143
Integrated Performance Report
99 of 22409:00 - 10.50-04/08/21

28
Discharge NUH A daily target of 37 medically safe for transfer (MSFT) patients remains in place and a slightly improving trend is shown in the graph below for Greater Nottingham MSFT Delays over 24 hours in NUH up to 18th June: The current main delay reasons are: Table 14 – Greater-Nottingham Main Delay Reasons in NUH – Mitigating Actions
System partners continue with the 3pm team huddle Wednesdays and Thursdays to focus on those patients with a PDMS (“Predicted Date Medically Safe” for transfer) for Friday/Saturday/Sunday to ensure discharge plans are in place and reducing delay related harm. SFHFT Focus continues on the medically safe for transfer process and the actions taking place to achieve these discharges. Daily calls now include ward staff from those wards that have a higher degree of challenging discharges, participating on these calls. This measure has helped improve communication between ward staff, the IDAT team and outside providers which had on occasions slowed down the discharge process. MSFT numbers have seen an upward trend during May, which has continued into the latter part of June despite a reduction in numbers at the beginning of that month. Work is still on going on the recruitment of additional temporary LA case workers to help reduce the level of MSFTs. Other mitigating actions taken to bring the trend back to a downward trend a small POC/Bridging service operated by NCC and support from community services in the GN Notts area where their input can make a difference. See graph for Mid Notts MSFT Delays over 24 hours in SFHFT, over a 30 working day period up to 18th June 2021. Graph 3 – Mid Notts MSFT Delays over 24 hours in SFHFT up to 18th June 2021
Reason for delay Mitigating Action
Code 8: (Pathway 1)
The system has supported the funding of an additional 450 hours per week home care in the city through Covid-19
discharge funds. A further addition of 150 hours on top of the previous 450 hours per week has recently been agreed
and is planned to be on line as soon as possible.
Code 10: (Pathway 3))
Partners working through potential solutions to support the placement of these individuals that have complex needs.
The process to streamline is also being discussed however; it is recognised delays are multifactorial including
working closely to manage communication and expectations of individuals and their families and working across
many different care homes.
Integrated Performance Report
100 of 224 09:00 - 10.50-04/08/21

29
Main delay reasons for the last 7 days and mitigating actions are shown in the table below: Table 15 – Mid-Nottingham Main Delay Reasons in SFHT – Mitigating Actions Despite the efforts of system partners, MSFT delays across both trusts continue to be above target with no current evidence of continued improvement or deterioration in numbers, however there are multiple schemes in place across the county coming online during June and July that are devised to aid in reducing the numbers of delays across the ICS. Details of these D2A schemes are shown in below in the Mitigation Actions.
Reason for delay Mitigating Action
Code 8: (Pathway 1) SFHFT to fund additional case workers to reduce backlog of unallocated MSFT patients
Code 9 (Pathway 2) Support from GN in providing potential flexibility in accessing current bed stock
D2A Schemes: Pathway 1 capacity in the city will be bolstered by the additional block coming online from 12th July, providing an additional 150 hours service per week. Case manager trials and mobilisation plan for D2A initiatives to support P1 has been agreed and submitted as well. P1 capacity in Mid Notts has been improved with additional support from MHFT and the CURT team who are picking up interim packages of care to facilitate quicker discharges while the longer term D2A plans and LA recruitment com online through the summer. In the south the Pathway 3 waits that were building up are being reviewed in a different way, ensuring that all patients listed against P3 are reviewed by the bed meeting daily to ensure that any patient that has the ability to improve their outcomes from being in a P2 bed goes down that route. This has made an impact on the waits and will inform the future model.
Integrated Performance Report
101 of 22409:00 - 10.50-04/08/21
30
Gaps in Assurance Patient Transport: Patient transportation services are still being hit by social distancing rules, meaning that currently they are unable to fully utilise their fleet causing additional strain with an accelerated elective recovery programme and high levels on discharges as well. Additional capacity is currently in place to mitigate any negative impact. This issue has been escalated both locally and regionally to NHSE/I colleagues who are having national discussions on our behalf to see if these restrictions could be eased in line with national lockdown restrictions – we are not alone in this request as is affecting all areas equally. AMH community beds: AMH community beds remain an issue due to the work being done at the Priory unit with the CQC and other agencies. Alternative capacity is being identified whilst this work at the Priory continues.
Integrated Performance Report
102 of 224 09:00 - 10.50-04/08/21

31
Theme Indicator Indicator Overview CCG Lead Focus
Mental
Health
Improving
Access to
Psychological
Therapies
Performance information for
patients undergoing IAPT
treatment
Maxine
Bunn
CCG
Root Cause
ICS access performance at March has increased to 5.48% against the target of 6.25%. Referrals have increased and the percentage of people entering treatment (conversion rate) has remained at 67% as workforce capacity issues in some providers have been addressed.
The service continues to achieve and exceed waiting time and recovery standards. The average wait for an appointment in May 2021 remains at 18 days.
Benchmarking shows that the ICS is the third highest performing system in the Midlands region in March in terms of access and is above the England average. Waiting time performance has been above the England average since July 2020 and recovery rate since April 2020.
Patients Entering Treatment—2019/20 (% target)
Recovery Rate
Waiting Times—6 Week Standard
Waiting Times—18 Week Standard
Patients Entering Treatment—2020/21 (Numerical target)
Apr-20 May-20 Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21
Rolling Three
Months
Performance
4.90% 3.97% 3.60% 3.85% 4.46% 4.11% 3.69% 4.18% 4.82% 5.45% 5.15% 5.48% h
Standard 5.70% 5.70% 5.70% 5.90% 5.90% 5.90% 6.10% 6.10% 6.10% 6.25% 6.25% 6.25% N/A
Patients
Entering
Treatment
5370 4355 3950 4225 4895 4510 4050 4580 5285 5970 5645 6005 h
Additional
Patients
Required
879 1894 2299 2243 1573 1958 2637 2107 1402 882 1207 847 i
N&N CCG
Organsation StandardMost Recent 12 Months Performance - Patients Entering Treatment (Rolling Three Months) Performance
Direction
Apr-20 May-20 Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21
N&N CCGGreater than or
equal to 50%52.49% 53.11% 54.76% 55.13% 54.59% 53.86% 54.86% 55.59% 55.24% 54.66% 54.25% 53.30% i
Organsation StandardMost Recent 12 Months Performance - Recovery Rate (Rolling Three Months) Performance
Direction
Apr-20 May-20 Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21
N&N CCGGreater than or
equal to 75%82.45% 82.61% 84.88% 92.00% 94.81% 98.21% 98.69% 97.50% 97.39% 98.15% 97.05% 96.68% i
Organsation StandardMost Recent 12 Months Performance - Waiting Times - First Treatment Within 6 Weeks Performance
Direction
Apr-20 May-20 Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21
N&N CCGGreater than or
equal to 95%99.06% 99.33% 99.38% 99.67% 99.13% 100% 100% 100% 99.63% 99.63% 99.58% 100% h
Organsation StandardMost Recent 12 Months Performance - Waiting Times - First Treatment Within 18 Weeks Performance
Direction
Apr-20 May-20 Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21
Patients
Entering
Treatment
5370 4355 3950 4225 4895 4510 4050 4580 5285 5970 5645 6005 h
Additional
Patients
Required
879 1894 2299 2243 1573 1958 2637 2107 1402 882 1207 847 i
Standard 6303 6303 6303 6575 6575 6575 6848 6848 6848 7121 7121 7121 N/A
N&N CCG
Organsation StandardMost Recent 12 Months Performance - Patients Entering Treatment (Rolling Three Months) Performance
Direction
Integrated Performance Report
103 of 22409:00 - 10.50-04/08/21

32
Assurances
An established monthly steering group with IAPT providers is in place, with focussed monitoring of targeted actions to assess impact of improvement actions. Spending review investment on training, marketing and additional roles to increase community engagement will start to impact on referrals from H2.
Gaps in Assurance
None identified
Mitigating Actions Local data is utilised to identify and discuss performance issues with providers and agree actions to improve capacity and service delivery, including workforce issues. Priority actions for quarter 2
Service promotion and awareness raising through social media animations, videos and blogs, newsletters, community advertising, and attendance at community events
Roll out of direct access through Silvercloud to reduce waits further and help to better engage patients to reduce DNAs and drop outs; digital groups and online materials to enhance service offer
Expansion of the workforce through recruitment, use of agency and affiliates and trainees
Recruitment of Community Development roles and community champions to improve engagement with and access for under-represented groups
Development of links and pathways with City LTC services to increase access for patients with LTC
Commence BAME specific training and Compassionate Mind Training
Integrated Performance Report
104 of 224 09:00 - 10.50-04/08/21

33
Theme Indicator Indicator Overview CCG Lead Focus
Mental Health
Dementia Diagnosis Rate
The rate of dementia diagnosis against the estimated prevalence
Maxine Bunn
CCG
Root Cause
The ICS continues to meet the dementia diagnosis rate standard, however performance is declining and this is being reviewed.
Long waiting times and variations in localities (pre-Covid) for memory assessments have been reducing from their peak in September 2020 (19 weeks) following additional investment in the service and the reinstatement of the Memory Assessment Service (MAS) in September 2020. As at June 2021, the waiting time has reduced to 6 weeks, now lower than pre-Covid levels (10 weeks at March 2020).
Mitigating Actions
As waiting times have now reduced in these areas in areas with the longest waits (Gedling, Newark and Rushcliffe), the focus is to bring other areas in line with the lower waiting times that have been achieved, whilst maintaining the lower waits across the system.
To increase capacity the MAS has implemented remote consultations / assessments where clinically appropriate.
Assurances
The MAS has reduced waiting times since its reinstatement in September 2020.
A waiting time recovery trajectory was agreed to ensure the historical backlog will be cleared and an 8 week waiting time to diagnosis achieved by January 2022; progress is reviewed at the monthly MAS steering group.
Further modelling has been undertaken as new roles have been embedded into the service, to enable the service to achieve the Memory Services National Accreditation Programme (MSNAP) 6 week wait to diagnosis standard by April 2022.
Gaps in Assurance
The service currently captures referral to assessment and referral to treatment. The performance team are reconfiguring their data system in order to accurately record referral to diagnosis.
Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
N&N CCG
Greater than
or equal to
66.7%
71.07% 70.60% 70.52% 70.23% 70.22% 69.98% 69.75% 69.14% 68.52% 68.67% 68.52% 68.42% i
Organsation StandardMost Recent 12 Months Performance - Dementia Diagnosis Rate Performance
Direction
Integrated Performance Report
105 of 22409:00 - 10.50-04/08/21
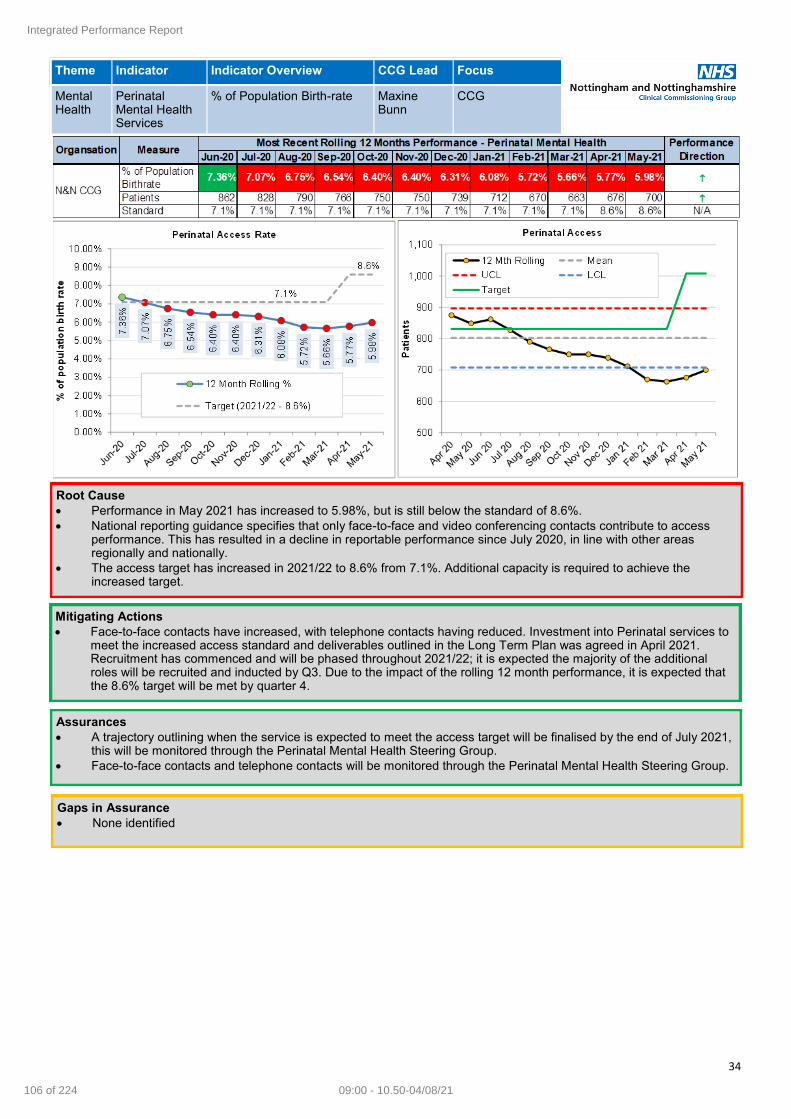
34
Theme Indicator Indicator Overview CCG Lead Focus
Mental Health
Perinatal Mental Health Services
% of Population Birth-rate Maxine Bunn
CCG
Root Cause
Performance in May 2021 has increased to 5.98%, but is still below the standard of 8.6%.
National reporting guidance specifies that only face-to-face and video conferencing contacts contribute to access performance. This has resulted in a decline in reportable performance since July 2020, in line with other areas regionally and nationally.
The access target has increased in 2021/22 to 8.6% from 7.1%. Additional capacity is required to achieve the increased target.
Mitigating Actions
Face-to-face contacts have increased, with telephone contacts having reduced. Investment into Perinatal services to meet the increased access standard and deliverables outlined in the Long Term Plan was agreed in April 2021. Recruitment has commenced and will be phased throughout 2021/22; it is expected the majority of the additional roles will be recruited and inducted by Q3. Due to the impact of the rolling 12 month performance, it is expected that the 8.6% target will be met by quarter 4.
Assurances
A trajectory outlining when the service is expected to meet the access target will be finalised by the end of July 2021, this will be monitored through the Perinatal Mental Health Steering Group.
Face-to-face contacts and telephone contacts will be monitored through the Perinatal Mental Health Steering Group.
Gaps in Assurance
None identified
Integrated Performance Report
106 of 224 09:00 - 10.50-04/08/21

35
Theme Indicator Indicator Overview CCG Lead Focus
Mental Health
PHSMI Physical health checks for people with a SMI
Maxine Bunn
CCG
UPDATE FROM MH FILE FROM TRACEY—SMI TAB
Root Cause
There has been improvement in June 2021 for a fourth consecutive month and performance is now 25.7% above the regional (22.3%) and national average (23.4%).
Performance against the national standard declined from April 2020; this level of reduction locally is in line with the regional trend during this period and is attributable to reduced face-to-face access in primary care throughout Covid-19.
Mitigating Actions Actions currently in progress to support improvements in performance include:
Monthly monitoring of practice and PCN level data continues, identifying areas requiring additional focussed support. Performance dashboards are reviewed at GP and ICP level.
The Primary Care QOF has been updated for 2021/22 and includes all 6 core components of the SMI physical health checks, rewarding those practices who achieve 50-90% of their SMI cohort having their 6 core checks recorded in the 12 month period.
The PHSMI LES went live on 1 May 2021, with 98% of practices signed up to the incentive scheme to deliver the 5 additional supporting indicators. Remaining practices are being followed up to understand reasons for their decision for not signing the LES and encouraged to sign up.
Performance against the QOF and PHSMI LES will be monitored monthly, enabling the system to respond in a timely manner and flex support accordingly. This data is shared with the PH SMI Steering Group to agree prioritisation of support from the HIWs/HINs. Additional support to City South has been identified as one of the next priority areas for the HIWs. As with other LES incentives, it is expected most of the activity undertaken by GPs will be in Q3 and Q4. Communications to practices will continue to promote the undertaking of physical health checks across the year, for example inviting patients for their health checks in their birthday month.
All Health Improvement Worker (HIW) posts continue to support the uptake of physical health checks for patients accessing secondary care mental health services. The HIWs also provide outreach support to people who have not engaged with primary care for their physical health checks. These roles will be targeted to support lower performing areas, identified through performance monitoring and data profiling.
Outreach support also is also being provided by the HIWs to people who have not responded to the COVID vaccination invites from their GP.
Recruitment to the Health Improvement Nurses continues with the outstanding 1WTE post re-advertised. As well as supporting the physical health checks, the nurses will provide clinical oversight and training across secondary and primary care.
Integrated Performance Report
107 of 22409:00 - 10.50-04/08/21

36
UPDATE FROM MH FILE FROM TRACEY—SMI TAB
Assurances
Oversight of delivery of the standard has been integrated into the Community Mental Health Transformation Programme within the Primary Care Interface Group. This will ensure coordination with all service developments, including the development and expansion of Local Mental Health Teams and introduction of Mental Health Practitioners in PCNs.
Gaps in Assurance
None identified
Integrated Performance Report
108 of 224 09:00 - 10.50-04/08/21

37
Theme Indicator Indicator Overview CCG Lead Focus
Mental Health
Out of Area Placements
Out of Area Occupied Bed Days
Maxine Bunn
Mental Health Trust
Root Cause
In quarter 4 2020/21 there were 505 OBDs, against a local trajectory of 180. The number of OBDs reported in May 2021 has decreased to 153, from 180 in April 2021. Performance continues to be impacted due to COVID-19 guidance that requires isolation beds; this has resulted in patients being admitted to out of area placements, and the temporary closure of the subcontracted beds at The Priory.
Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
NHFT Data 159 188 121 84 113 238 185 169 115 221 180 153
NHSD Data 190 170 155 110 125 230 185 170 140 200 170
Organsation Measure
NHS N&N CCG
Monthly Performance - Inappropriate Out of Area Occupied Bed Days
Q1
2019-20
Q2
2019-20
Q3
2019-20
Q4
2019-20
Q1
2020-21
Q2
2020-21
Q3
2020-21
Q4
2020-21
NHFT Actual 2555 2085 618 306 680 393 536 505
Revised Trajectory 3432 2024 1748 1440 279 364 288 180
Organsation Measure
Quarterly Performance - Inappropriate Out of Area Occupied Bed Days
Nottinghamshire
Healthcare Trust
Integrated Performance Report
109 of 22409:00 - 10.50-04/08/21
38
Mitigating Actions Actions in place include:
On-going implementation and review of the Crisis and urgent mental health pathway, including:
Crisis Resolution and Home Treatment Teams (CRHT) meeting core fidelity quality standards delivering Intensive Home Support and in-reach to wards. CRHT are providing 24/7 home treatment, with staffing commissioned to core fidelity levels.
Crisis sanctuaries commenced in Q4 2020/21
Integration of the Crisis Line and Helpline functions to deliver a single 24/7 Crisis Helpline took place in June 2021.
Multi Agency Discharge Coordinator in street triage is being recruited to (temporary staff member tested the role, job currently out to advert and interviews planned for August), which will improve patient outcomes, reduce repeat mental health related callers, and co-ordinate a response with system partners to improve joint working and ensure joint crisis plans.
Development of post crisis support is currently being scoped, with the aim to implement support in Q3.
The review of a therapeutic/MDT staffing model on inpatient wards (commenced in 2020/21 and will continue throughout 2021/22), including in-reach to wards, and work with patients with complex presentations; this includes the revised Personality Disorder pathway implementation.
Tier 3 Personality Disorder pathway has been recruited to, and commenced in Q1. Recruitment is on track for roles in the community and will be implemented from Q2 in Mid Notts.
System working with partners to utilise discharge funding, to increase ward in-reach to support more robust discharge planning and onward care in community services; this includes close working with social care, VCSE and substance misuse services.
The CCG (Commissioning and Quality) is facilitating case reviews of long stay patients during Q2 to identify reasons for discharge delays and system actions that need to be agreed and utilise discharge funding where required.
NHT is scheduled to open a new unit in November 2021, under the dormitories eradication programme. The unit will increase the number of acute beds by 14, with plans to reduce the reliance on sub-contracted beds.
EMAS and the Clinical Network are supporting the development of regional and local plans to improve ambulance response to mental health. In 2021/22, the focus will be on:
Training
Access to pathways
Staffing in contact centres
Linking 111/999 to an effective Directory of Services
Assurances
A revised trajectory has been submitted to NHSE to reach zero OBDs by end of Quarter 2 2021/22.
The Mental health Crisis and Urgent Care Steering Group reviews agreed developments and actions on a monthly basis. Partnership meetings are also in place to identify actions that can be taken to alleviate system pressures.
Gaps in Assurance
None identified
Integrated Performance Report
110 of 224 09:00 - 10.50-04/08/21

39
Theme Indicator Indicator Overview CCG Lead Focus
Mental Health
EIP Early Intervention in Psychosis Waiting Times
Maxine Bunn
CCG
Root Cause
The access standard has been consistently met at an ICS level.
Development of a number of EIP specific interventions were postponed due to COVID-19. This has impacted on the service achieving level 3 NICE compliance; originally planned for quarter 4 2020/21, revised to quarter 1 22021/22. A Quality Improvement Plan has been in place for the remaining standards (physical health checks, carer focussed education and outcome measures), two of the three, carer focussed education and physical health checks, have now been achieved and outcome measures have improved to 18%, against a required standard of 25% (this will be reported in June/ July local data). Due to a delay in achieving the outcome measures, NICE level 3 will now be achieved in quarter 2 2021/22.
There is a time lag between initial and paired outcome score, which needs to be undertaken at assessment and then at 6 month review and completion of this has been impacted by the pandemic.
Mitigating Actions
An updated service model, which includes testing of an ‘At Risk Mental State’ (ARMS) pathway, has been developed and built into Community Mental Health Transformation Plans, and includes milestones for delivery from Q2 2021/22.
A workforce model to deliver transformation has been recruited to and will enable the achievement of NICE level 3 standard by the revised date of Q2 2021/22. An action plan for improvement against each of NICE standards to achieve overall level 3 is in place. A Quality Improvement Plan (QIP) has been developed for the remaining 3 standards and is reviewed on a weekly basis.
Exception reports for breaches of the access standard are included in the EIP monthly activity reports; this enables the identification and review of any themes and actions being taken to improve performance.
Assurances
EIP Transformation meetings with NHT are in place to review progress against agreed actions.
Gaps in Assurance
None identified.
In addition to the access standard the service is required to meet NICE standards. Current performance against NICE EIP
standards based on local data in May 2021:
The ICS is currently rated as a Level 2 (Needs Improvement) overall (assessed through local audit).
May-20 Jun-20 Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21
Started treatment
in 2 weeks73.0% 79.0% 81.0% 84.0% 80.0% 84.0% 86.0% 86.0% 86.0% 84.0% 85.0% 84.0% i
Standard 60.0% 60.0% 60.0% 60.0% 60.0% 60.0% 60.0% 60.0% 60.0% 60.0% 60.0% 60.0% N/A
Organsation MeasureMost Recent 12 Months Performance - EIP Waiting Times (Rolling Three Months) Performance
Direction
N&N CCG
NICE standard Current performance Rating
Access Level 4 Top Performer
CBTp Level 2 Needs Improvement
Family Interventions Level 3 Performing Well
Supported employment and education Level 4 Top Performer
Physical Health Checks Level 2 Needs Improvement
Carer Focussed education Level 2 Needs Improvement
Outcome measures Level 1 Greatest Need for Improvement
Integrated Performance Report
111 of 22409:00 - 10.50-04/08/21

40
Theme Indicator Indicator Overview CCG Lead Focus
Mental Health
Children & Young People Increasing Access
Children & Young People Increasing Access
Maxine Bunn
CCG
Root Cause
The cumulative position for April 2021 (44.3%) is above the local and national trajectory of 38.0%.
The improved performance is from activity delivered by additional services commissioned and mobilised in Q3 20/21 and data flow to the MHSDS.
Children & Young People Increasing Access
Mitigating Actions
A data subgroup convened in June 2021 to provide ongoing support to providers, to focus on data quality and flow improvements and increase the focus on outcome data reporting. The group will meet quarterly to progress delivery on a data quality improvement plan. The system action plan will be finalised as part of the Local transformation Plan refresh (end of July 2021).
Providers continue to offer digital and face to face appointments to ensure ongoing access throughout the pandemic.
Assurances
Regular service transformation meetings are taking place with providers and commissioning leads to agree further improvement actions and to review transformation plans.
As demand increases there are pressures in some provider service waiting times and system recovery plans have been developed and are reviewed on a monthly basis.
Investment has agreed as to deliver the Long Term Plan objectives in 2021/22 which enables service expansion and transformation across a range of services; schemes will be implemented throughout the current financial year with project plans being developed by end of July 2021. In addition, in June 2021 NHS England funding has been awarded to the ICS as part of a national 4-week waiting time pilot, which will run throughout 2021/22. An implementation plan will be completed during quarter 2 in line with the terms of the funding, including completion of learning logs and case studies.
Gaps in Assurance None identified
Integrated Performance Report
112 of 224 09:00 - 10.50-04/08/21
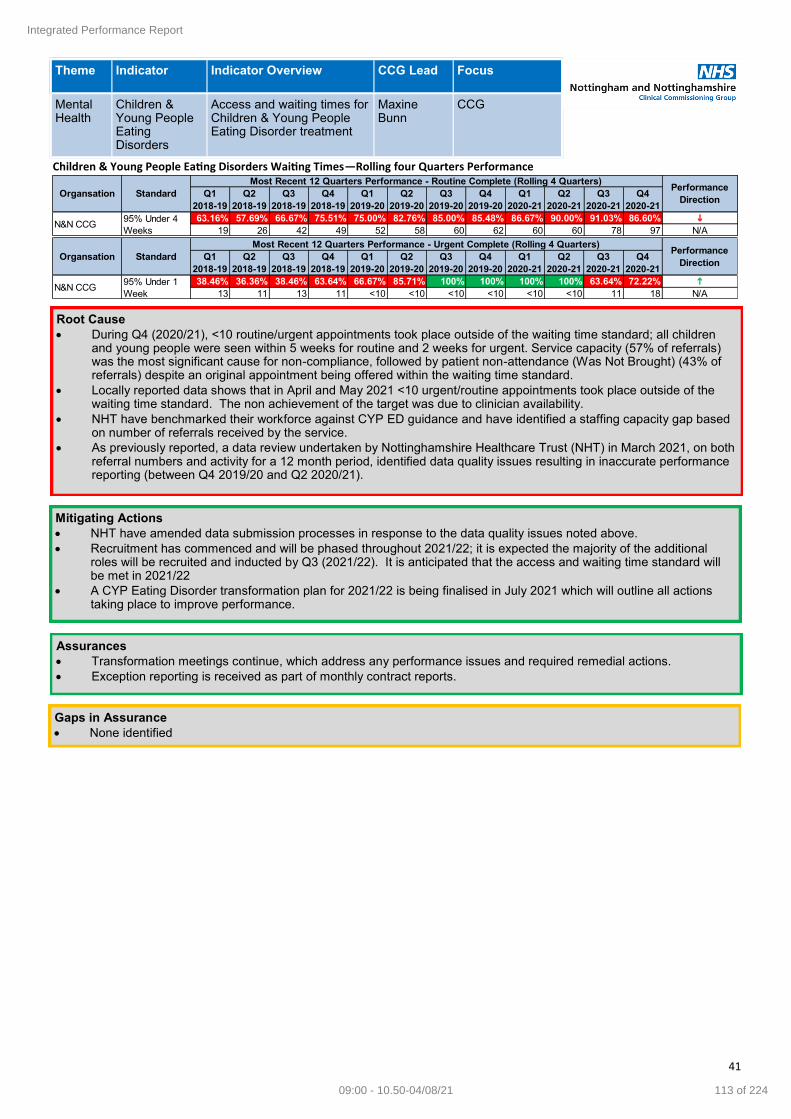
41
Theme Indicator Indicator Overview CCG Lead Focus
Mental Health
Children & Young People Eating Disorders
Access and waiting times for Children & Young People Eating Disorder treatment
Maxine Bunn
CCG
Root Cause
During Q4 (2020/21), <10 routine/urgent appointments took place outside of the waiting time standard; all children and young people were seen within 5 weeks for routine and 2 weeks for urgent. Service capacity (57% of referrals) was the most significant cause for non-compliance, followed by patient non-attendance (Was Not Brought) (43% of referrals) despite an original appointment being offered within the waiting time standard.
Locally reported data shows that in April and May 2021 <10 urgent/routine appointments took place outside of the waiting time standard. The non achievement of the target was due to clinician availability.
NHT have benchmarked their workforce against CYP ED guidance and have identified a staffing capacity gap based on number of referrals received by the service.
As previously reported, a data review undertaken by Nottinghamshire Healthcare Trust (NHT) in March 2021, on both referral numbers and activity for a 12 month period, identified data quality issues resulting in inaccurate performance reporting (between Q4 2019/20 and Q2 2020/21).
Children & Young People Eating Disorders Waiting Times—Rolling four Quarters Performance
Mitigating Actions
NHT have amended data submission processes in response to the data quality issues noted above.
Recruitment has commenced and will be phased throughout 2021/22; it is expected the majority of the additional roles will be recruited and inducted by Q3 (2021/22). It is anticipated that the access and waiting time standard will be met in 2021/22
A CYP Eating Disorder transformation plan for 2021/22 is being finalised in July 2021 which will outline all actions taking place to improve performance.
Assurances
Transformation meetings continue, which address any performance issues and required remedial actions.
Exception reporting is received as part of monthly contract reports.
Gaps in Assurance
None identified
Q1
2018-19
Q2
2018-19
Q3
2018-19
Q4
2018-19
Q1
2019-20
Q2
2019-20
Q3
2019-20
Q4
2019-20
Q1
2020-21
Q2
2020-21
Q3
2020-21
Q4
2020-21
63.16% 57.69% 66.67% 75.51% 75.00% 82.76% 85.00% 85.48% 86.67% 90.00% 91.03% 86.60% i
19 26 42 49 52 58 60 62 60 60 78 97 N/A
Organsation
Most Recent 12 Quarters Performance - Routine Complete (Rolling 4 Quarters)Performance
DirectionStandard
95% Under 4
WeeksN&N CCG
Q1
2018-19
Q2
2018-19
Q3
2018-19
Q4
2018-19
Q1
2019-20
Q2
2019-20
Q3
2019-20
Q4
2019-20
Q1
2020-21
Q2
2020-21
Q3
2020-21
Q4
2020-21
38.46% 36.36% 38.46% 63.64% 66.67% 85.71% 100% 100% 100% 100% 63.64% 72.22% h
13 11 13 11 <10 <10 <10 <10 <10 <10 11 18 N/AN&N CCG
95% Under 1
Week
Organsation Standard
Most Recent 12 Quarters Performance - Urgent Complete (Rolling 4 Quarters)Performance
Direction
Integrated Performance Report
113 of 22409:00 - 10.50-04/08/21
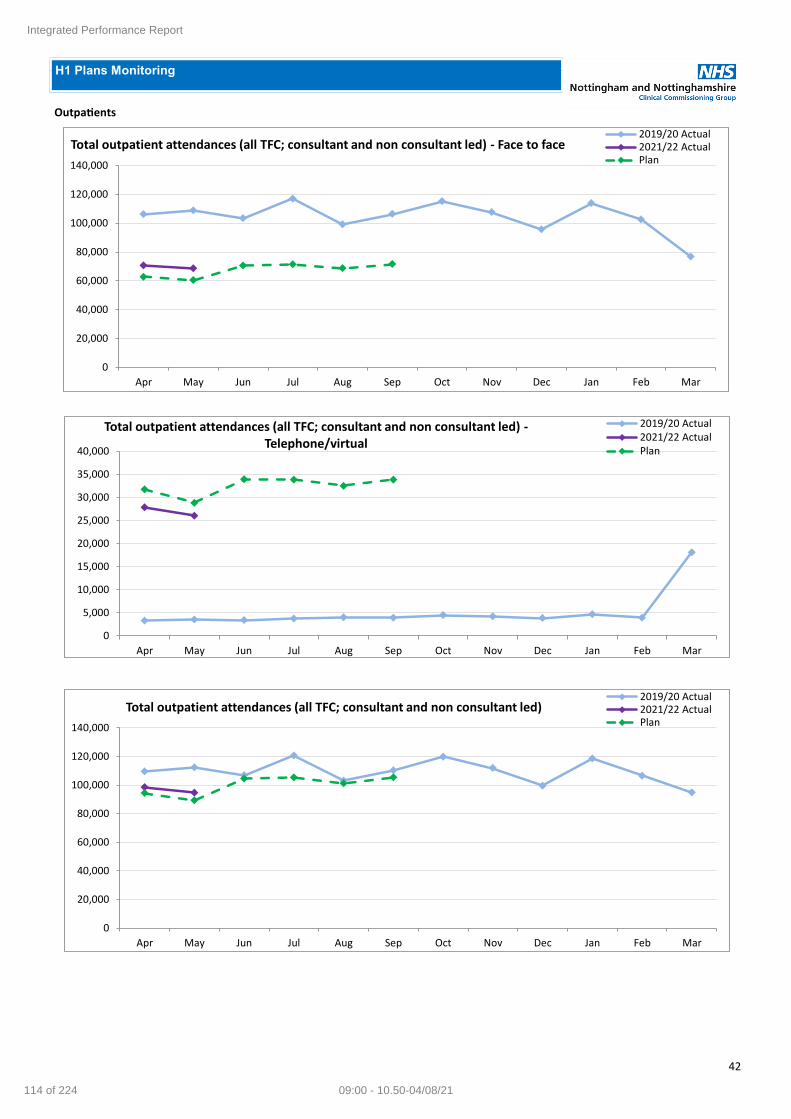
42
Outpatients
H1 Plans Monitoring
0
20,000
40,000
60,000
80,000
100,000
120,000
140,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Total outpatient attendances (all TFC; consultant and non consultant led) - Face to face2019/20 Actual2021/22 ActualPlan
0
5,000
10,000
15,000
20,000
25,000
30,000
35,000
40,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Total outpatient attendances (all TFC; consultant and non consultant led) -Telephone/virtual
2019/20 Actual2021/22 ActualPlan
0
20,000
40,000
60,000
80,000
100,000
120,000
140,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Total outpatient attendances (all TFC; consultant and non consultant led)2019/20 Actual2021/22 ActualPlan
Integrated Performance Report
114 of 224 09:00 - 10.50-04/08/21

43
H1 Plans Monitoring (continued)
Outpatients (continued)
0
5,000
10,000
15,000
20,000
25,000
30,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Consultant-led first outpatient attendances (Spec acute)2019/20 Actual2021/22 ActualPlan
0
1,000
2,000
3,000
4,000
5,000
6,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Consultant-led first outpatient attendances with procedures (Spec acute)2019/20 Actual2021/22 ActualPlan
0
10,000
20,000
30,000
40,000
50,000
60,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Consultant-led follow-up outpatient attendances (Spec acute)2019/20 Actual2021/22 ActualPlan
Integrated Performance Report
115 of 22409:00 - 10.50-04/08/21

44
H1 Plans Monitoring (continued)
Outpatients (continued)
0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
8,000
9,000
10,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Consultant-led follow-up outpatient attendances with procedures (Spec acute)2019/20 Actual2021/22 ActualPlan
0
500
1,000
1,500
2,000
2,500
3,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Total Advice and Guidance requests processed/answered2019/20 Actual2021/22 ActualPlan
0
200
400
600
800
1,000
1,200
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Number of patients moved or discharged to a PIFU pathway for the first time2019/20 Actual2021/22 ActualPlan
Integrated Performance Report
116 of 224 09:00 - 10.50-04/08/21

45
Elective
H1 Plans Monitoring (continued)
0
2,000
4,000
6,000
8,000
10,000
12,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Total number of Specific Acute elective day case spells in the period2019/20 Actual2021/22 ActualPlan
0
200
400
600
800
1,000
1,200
1,400
1,600
1,800
2,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Total number of Specific Acute elective ordinary spells in the period2019/20 ActualPlan2021/22 Actual
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Total number of Specific Acute elective spells in the period2019/20 Actual2021/22 ActualPlan
Integrated Performance Report
117 of 22409:00 - 10.50-04/08/21

46
Elective (continued)
H1 Plans Monitoring (continued)
0
50
100
150
200
250
300
350
400
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Total number of Specific Acute elective day case spells in the period of which children under 18 years of age
2019/20 Actual2021/22 ActualPlan
0
20
40
60
80
100
120
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Total number of Specific Acute elective ordinary spells in the period of which children under 18 years of age
2019/20 Actual2021/22 ActualPlan
Integrated Performance Report
118 of 224 09:00 - 10.50-04/08/21
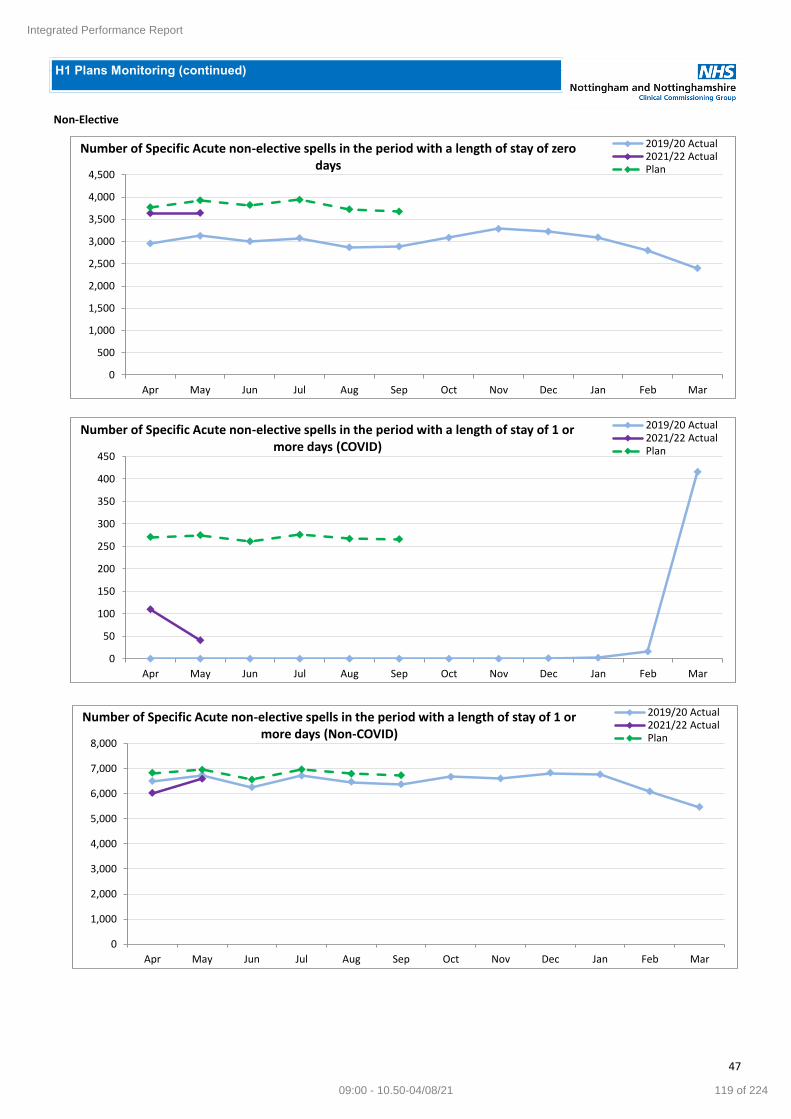
47
Non-Elective
H1 Plans Monitoring (continued)
0
500
1,000
1,500
2,000
2,500
3,000
3,500
4,000
4,500
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Number of Specific Acute non-elective spells in the period with a length of stay of zero days
2019/20 Actual2021/22 ActualPlan
0
50
100
150
200
250
300
350
400
450
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Number of Specific Acute non-elective spells in the period with a length of stay of 1 or more days (COVID)
2019/20 Actual2021/22 ActualPlan
0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
8,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Number of Specific Acute non-elective spells in the period with a length of stay of 1 or more days (Non-COVID)
2019/20 Actual2021/22 ActualPlan
Integrated Performance Report
119 of 22409:00 - 10.50-04/08/21

48
Non-Elective (continued)
H1 Plans Monitoring (continued)
0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
8,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Number of Specific Acute non-elective spells in the period with a length of stay of 1 or more days
2019/20 Actual2021/22 ActualPlan
0
2,000
4,000
6,000
8,000
10,000
12,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Number of Specific Acute non-elective spells in the period 2019/20 Actual2021/22 ActualPlan
Integrated Performance Report
120 of 224 09:00 - 10.50-04/08/21
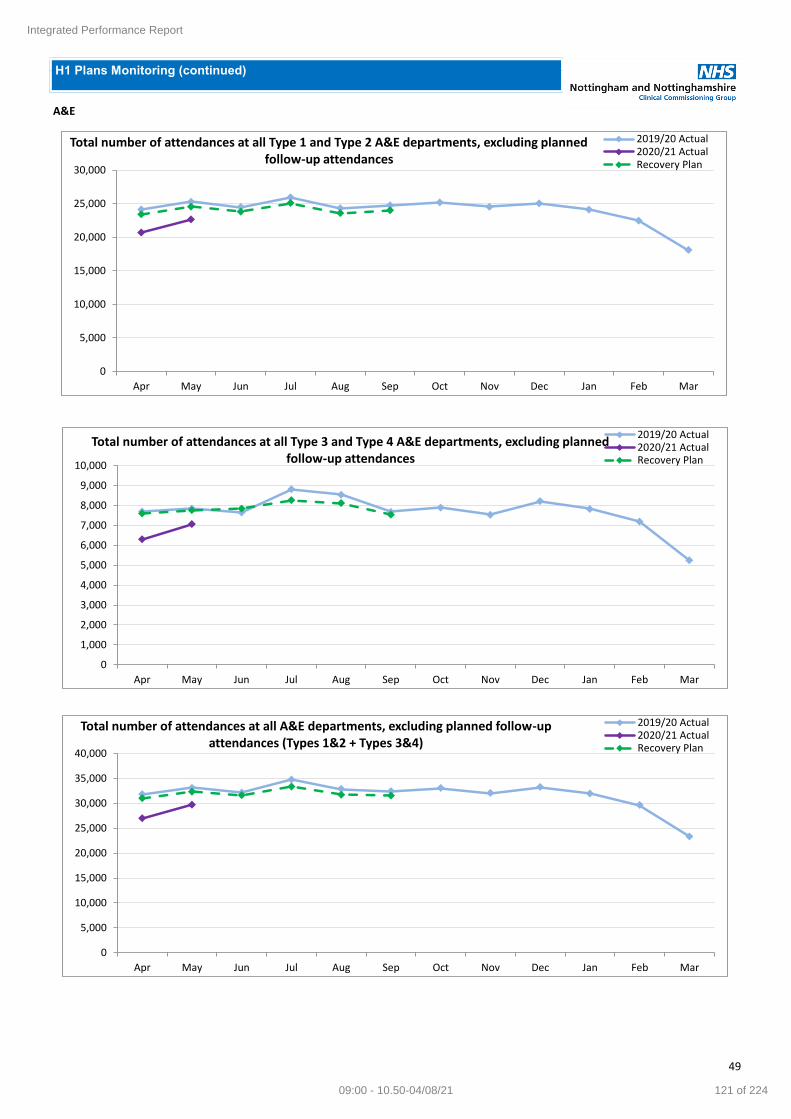
49
H1 Plans Monitoring (continued)
A&E
0
5,000
10,000
15,000
20,000
25,000
30,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Total number of attendances at all Type 1 and Type 2 A&E departments, excluding planned follow-up attendances
2019/20 Actual2020/21 ActualRecovery Plan
0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
8,000
9,000
10,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Total number of attendances at all Type 3 and Type 4 A&E departments, excluding planned follow-up attendances
2019/20 Actual2020/21 ActualRecovery Plan
0
5,000
10,000
15,000
20,000
25,000
30,000
35,000
40,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Total number of attendances at all A&E departments, excluding planned follow-up attendances (Types 1&2 + Types 3&4)
2019/20 Actual2020/21 ActualRecovery Plan
Integrated Performance Report
121 of 22409:00 - 10.50-04/08/21

50
H1 Plans Monitoring (continued)
Referrals
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
16,000
18,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
GP Referrals2019/20 Actual
2021/22 Actual
0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
8,000
9,000
10,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Other Referrals2019/20 Actual
2021/22 Actual
0
5,000
10,000
15,000
20,000
25,000
30,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Total Referrals2019/20 Actual
2021/22 Actual
Integrated Performance Report
122 of 224 09:00 - 10.50-04/08/21

51
H1 Plans Monitoring (continued)
Diagnostics
0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Diagnostic Tests - Magnetic Resonance Imaging2019/20 Actual2021/22 ActualPlan
0
2,000
4,000
6,000
8,000
10,000
12,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Diagnostic Tests - Computed Tomography2019/20 Actual2021/22 ActualPlan
0
2,000
4,000
6,000
8,000
10,000
12,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Diagnostic Tests - Non-Obstetric Ultrasound2019/20 Actual2021/22 ActualPlan
Integrated Performance Report
123 of 22409:00 - 10.50-04/08/21

52
H1 Plans Monitoring (continued)
Diagnostics (continued)
0
200
400
600
800
1,000
1,200
1,400
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Diagnostic Tests - Colonoscopy2019/20 Actual2021/22 ActualPlan
0
100
200
300
400
500
600
700
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Diagnostic Tests - Flexi Sigmoidoscopy2019/20 Actual2021/22 ActualPlan
0
200
400
600
800
1,000
1,200
1,400
1,600
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Diagnostic Tests - Gastroscopy2019/20 Actual2021/22 ActualPlan
Integrated Performance Report
124 of 224 09:00 - 10.50-04/08/21

53
H1 Plans Monitoring (continued)
Diagnostics (continued)
0
500
1,000
1,500
2,000
2,500
3,000
3,500
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Diagnostic Tests - Cardiology - Echocardiography2019/20 Actual2021/22 ActualPlan
0
5,000
10,000
15,000
20,000
25,000
30,000
35,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
All Diagnostic Tests2019/20 Actual2021/22 ActualPlan
Integrated Performance Report
125 of 22409:00 - 10.50-04/08/21

54
Theme Indicator Indicator Overview CCG Lead Focus
Safe Harm Free Care Standard
The proportion of patients who received ‘harm free’ care.
Sandy Smith CCG Acute Providers
Current Issue/Risk NUH This indicator refers to the safety thermometer and this was stopped nationally by NHSE. NUH collected it internally for a while but with COVID this has been paused (and the value is limited now with no national data collection system). SFH Indicator appears to remains consistently above the standard of 95% so no exception reporting by the Trust, however method of collection is unclear since national tool was suspended.
Mitigating Actions (Provider) NUH The Trust has set up monthly Pressure Ulcer Learning Group and Falls Learning Group meetings which are specialist forums to promote best practice and support the patient safety agenda. These meetings are chaired by the Deputy Chief Nurse (Strategy) and are attended by all Divisional Leads from the Trust. SFH There are a number of internal groups including Deteriorating Patient Group; Mobility and Falls Group and the overarching Harms Free Care Group which are attended by a member of the CCG QA team. Regular data and exception reporting identifies any areas of concern/good practice
Assurances (CCG) NUH The Quality Assurance Team continues to monitor and gain further assurance by reviewing Trust Board papers and discussing cases directly with NUH’s Harm Free Care Team. A member of the Quality Assurance Team attends the Trust’s monthly Pressure Ulcer Learning Group, Falls Learning Group meetings and Falls Incident Review meetings to gain further assurance around the actions being taken by the Trust in providing Harm Free Care. SFH The Quality Assurance Team continue to gain further assurance by attending the monthly group meetings for Mobility and falls and Harm Free Care to monitor and review actions and learning, alongside reviewing monthly Trust Board papers. They have had no serious incidents that were attributed to their staffing levels. Falls reduction work remains high on the agenda with a continued focus on reducing deconditioning through mobility awareness to promote patient independence. May has again seen a decrease in the number of fall per 1000 bed days. Hospital acquired pressure ulcers remain consistently low, there have been no category 3 PUs since Nov 18 and no category 4s since August 2017 and just four category 2s reported during May
Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
NUH 99.00% 96.80% 95.50% - - - - - -YTD Actual
98.5%
SFH 97.30% 98.50% 97.60% 98.40% 98.30% 97.50% 98.00% N/A N/AYTD Actual
97.4%
Organisation StandardPerformance
Direction
Greater than
or equal to
95%
Next Steps for QA Team
Continue to work with providers to strengthen and maintain relationships
Develop a team approach to information sharing/collaboration which will support system wide learning (eg pressure ulcer prevention)
Gain further information from SFH about the data which informs their harms free care metrics now that national tool suspended.
Integrated Performance Report
126 of 224 09:00 - 10.50-04/08/21

55
Theme Indicator Indicator Overview CCG Lead Focus
Safe Cleaning Audit Score
Outcome of audits reviewing the cleanliness of provider environments
Sandy Smith CCG Acute Providers
Current Issue/Risk NUH NUH’s Cleaning Audit Score has been consistently above the national target. SFH Cleaning/environment audit data has routinely been collected using the Perfect Ward metrics. This data is shared via the Trust’s IPC committee and latest figures for May 21 demonstrate performance against cleanliness for commodes; hand hygiene; PPE; patient environment; waste; catheters and lines
Mitigating Actions (Provider) NHT Cleaning and deep cleaning is in place as part of the management of outbreaks on ward areas & communal areas. Updates on the correct use of PPE are continually shared with all staff along with regular training sessions. Regular audits are undertaken of all areas. Increased touch point cleaning remains in place. There are multiple locations across all sites where staff/patients can access PPE.
Assurances (CCG) The Quality Assurance Team continues to monitor and gain further assurance reviewing Trust Board papers and IPC BAFs with providers. Insight visits to NUH and SFH were undertaken in May 2021 in partnership with Trust IPC colleagues. The team were assured that both NUH and SFH were sighted to the relevant issues as a result of routine audits. SFH have articulated an action plan to address areas of improvement The SFH BAF reported in July 2021 demonstrates compliance with 120 of 121 key lines of enquiry.
Next Steps for QA Team Conduct further insight visit at SFH with support from the CCG IPC team.
Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
NUH 97.60% 97.20% 98.10% 98.90% 98.60% 98.40% 98.00% 98.60% 98.00%YTD Actual
98.3%
SFH - - - - - - - - - -
NHT Millbrook 53.00% 93.00% 93.00% 67.80% 94.40% 94.40% 94.00% 93.00% - h
NHT Lings Bar 92.00% 94.00% 95.00% 94.60% 94.00% 95.30% 93.60% 94.00% - h
NHT Highbury 97.69% 96.88% 97.02% 97.53% 100.00% 100.00% 96.75% 99.00% - h
CityCare 93.80% 93.00% 93.60% 93.30% 93.60% 93.00% 93.50% 94.50% - h
Organisation StandardPerformance
Direction
Greater than
or equal to
92.3%
Integrated Performance Report
127 of 22409:00 - 10.50-04/08/21

56
Theme Indicator Indicator Overview CCG Lead Focus
Safe Venous Thromboembolism (VTE) risk assessment
Assessment of risk of VTE for all patients admitted to hospital
Sandy Smith CCG Acute Providers
Current Issue/Risk NUH VTE risk assessment performance for May was below target at 94.2%. However, from August 2020 performance has improved and the target was met once in 2021. Electronic VTE risk assessment compliance has fallen since the introduction of the new VTE RA platform on Nervecentre. SFH National reporting of VTE risk assessment screening was stopped in March 2020 in response to the Covid pandemic. SFH continued with data collection for our own internal monitoring process. The data collection process for VTE risk assessment is a manual data process which takes a significant investment of time to complete. Covid infection control requirements changed the manual collection processes which have had a detrimental impact on compliance figures.
Mitigating Actions (Provider) NUH
The following actions to recover performance are in place:
Previous local audit has shown overall prescription of prophylaxis exceeds 95% in the areas investigated
The recent GIRFT thrombosis audit confirmed 100% prescription of enoxaparin in surgery and critical care
Local Hospital Associated Thrombosis (HAT) data has consistently shown a low rate of preventable HAT
GIRFT HAT data indicated no preventable HAT in the audit cohort during the 6 month audit period (October 2019 – March 2020)
VTE risk assessment has been introduced as a mandatory field in the maternity medway electronic records system (February 2021)
Correspondence has gone out to medical teams within NUH regarding VTE and the need to ensure VTE RA is completed and Divisional teams have been requested to report on plans to improve the overall position via the QSC
When E prescribing (EPMA) is introduced, VTE risk assessment will be linked as a mandatory field (December 2021)
SFH
The GSU team resumed the pre-COVID method of form collection; this was commenced on the 1st April 2021.
EPMA will resolve the data collection issues as the VTE assessment will be included as part of the package and will be mandatory. The EPMA VTE screening tool will be based on the NG89 standards
A one off audit undertaken by pharmacy in November 2020 demonstrated :
• 97% of patients have the correct decision made in relation to their VTE prophylaxis requirements.
• The majority of patients have a dose prescribed, if pharmacological prophylaxis is required, that is appropriate
for their current renal function.
Assurances (CCG)
Exceptional patient safety incidents related to VTE risk assessment are picked up via the SI route, however the data and mitigations shared above are outdated. Further work is needed to understand how VTE risk assessment continues to be prioritised at both Trusts.
Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
NUH 91.50% 92.70% 92.90% 93.00% 93.80% 94.30% 96.20% 94.50% 94.20%YTD Actual
94.3%
SFH 95.10% 95.10% 95.00% 90.90% 93.20% N/A N/A N/A N/AYTD Actual
94.1%
Greater than
or equal to
95%
Organisation StandardPerformance
Direction
Next Steps for QA Team
Confirm timeframes for the recommencement or launch of VTE risk assessments via EPMA
Seek clarity on SFH data post April 21
Integrated Performance Report
128 of 224 09:00 - 10.50-04/08/21

57
Theme Indicator Indicator Overview CCG Lead Focus
Safe Falls Falls (resulting in harm per 1,000 bed days or total number)
Sandy Smith CCG Acute Providers
There is not a nationally set target in regards to falls hence why the providers listed have different internal targets set by their respective Boards. Current issue/risk NUH The Trust’s Integrated Performance Report for June 2021 did not report on Falls. SFH The rate of falls per 1000 occupied bed days nationally has increased during the pandemic and the SFH figures are comparable but above the RCP indicative figure of 6.63. SFH have been tracking actions as appropriate since the initial pandemic peak and subsequent surge. The number of repeat falls remains high and of concern. SFH are learning from others to address this. NHT Figures for May were 94 which has seen an decrease compared to 130 falls in April. There is no set target. The Falls strategy has been started to align with the frailty work. Good work has been completed with MHSOP on falls prevention and other initiatives. There was nothing to escalate CityCare There was 1 recorded for May at CityCare. There is no set target.
Mitigating Actions (Provider) NUH
A revised investigation process has been implemented
Continue IRM and QRC processes
Education around falls is enhanced through a Trust podcast
Divisional Falls related performance data and themes from investigations are shared at the Falls Learning Group to support trust wide improvements
SFH The falls team has expanded with physiotherapy involvement from May 21 and a Chief Nurse Fellow in April 21. They are collectively working on reducing deconditioning through mobility awareness to promote patient independence. NHT Mitigations previously detailed remain in place, we have asked for additional assurances due to the increase in falls numbers between February, March and April.
Assurances (CCG) NUH A member of the Quality Assurance team attends the monthly Falls Learning Group and Incident Review meetings set up at NUH to gain assurance around the Trust’s actions around falls, processes of reporting falls, etc. The Falls Incident Review meetings have been set up to review retrospective and current falls and ensure appropriate escalation. SFH A CCG representative attends the Mobility and Falls Meeting and the Harm Free Care group going for further assurance Appointment of Chief Nurse Clinical Fellow to investigate and implement accurate monitoring to reduce functional decline EPO and Dementia specialist nurse linked to the falls team. Regular reviews under the heading ‘Connected Care’ Improve operational oversight of mo9bility and falls with 2 days of rehabilitation therapy lead (band 8a) The falls team are working to be more proactive with on-going monitoring of in month falls and using this to target actions. Datix to be investigated to create daily dashboard for review Strengthen the falls team with appointment of FT band 6 to support the part-time band 6 giving WTE of 1.3 (1.5 with 8a) NHT The CCG Quality Assurance team meet weekly with the Head of Safety at NHT to discuss any serious incidents or emerging themes from incidents. CityCare The CCG Quality Assurance team meet fortnightly with the Quality Lead at CityCare to discuss serious incidents, emerging themes and actions being taken.
Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
NUH <= 0.98 - 1.24 - 0.94 - - - 1.28 - i
SFH 100 105 120 132 138 106 105 114 100 i
NHT 93 100 91 115 100 101 156 130 94 i
CityCare 1 0 1 1 0 1 0 2 1 i
Organisation StandardPerformance
Direction
Total Falls
Integrated Performance Report
129 of 22409:00 - 10.50-04/08/21

58
Theme Indicator Indicator Overview CCG Lead Focus
Safe Number of wards below 80% fill rate / safe staffing
Actual v. planned staffing Sandy Smith CCG Acute Providers
The current pandemic has impacted on providers’ ability to safely staff wards. Increased staff sickness, self-isolation and shielding have all contributed to increase staff absence. There has been some mutual aid at times however each provider is risk assessing each ward when declared unsafe and managing appropriately in house. Current issue/risk NUH Five wards in May 2021 reported fill rates <80% - the reasons are varied, associated with environmental closures ( in the case of Jenner and relocation to a smaller base; a reduction in required capacity for E12 in line with the surge management of intensive care and staffing challenges through the same period). With respect to Winifred 2, the bed demand decreased due to reduced demand as high acuity elective patient’s pathway was altered. With regards to Children’s hospital areas, short term sickness and staff relocated to non-clinical roles due to the 28 week pregnancy rule. Shifts were covered relocating appropriate nursing resource, additional hours and off framework agencies and where appropriate. External patient referrals were reviewed in line with associated acuity and occupancy and discussed with the network where required. SFH The Trust report by exception with this target met however the Trust did state that they had experienced unprecedented workforce loss and had been heavily reliant on agency staffing particularly in nursing. They have had no serious incidents declared that were attributed to staffing levels. NHT There has been a decrease in May.
Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
NUH 0 1 7 2 2 7 9 6 2 5 YTD = 7 h
SFH
Safe staffing
care hours
per patient
day >8
10.7 10.3 10.1 9.8 9.1 9.5 9.5 9.5 9.3 YTD = 9.1
NHT 0 5 4 8 4 7 7 9 5 4YTD Actual =
49 h
Organisation StandardPerformance
Direction
Integrated Performance Report
130 of 224 09:00 - 10.50-04/08/21
59
Assurances (CCG) In the absence of routine quality review meetings, the CCG has sought to monitor this standard through Trust Board reports and with discussions with the patient safety team of individual cases. Maternity staffing levels are also detailed in the Safe Today submission to the CCG (at NUH) and tracked via Datix reporting and use of a bespoke acuity tool (at SFH).
Mitigating Actions (Provider) NUH
Both SafeCare and the staffing app records when wards declare unsafe. This is reported per shift through the staffing report and safety wheel. SafeCare is currently in phase 7 of 8, Trust wide roll out. When rolled out, this will change the reporting to include staffing versus acuity.
Divisions manage patient safety and staffing on a daily basis, through movement of staff and increasing staffing through use of temporary staff – where a ward was declared as unsafe, staff were relocated to that ward to support. An establishment review is carried out annually to review safe staffing requirements. The senior leadership establishment on one of the low fill wards has now been increased.
Maternity overfill rate is 95.6%
Additional mitigating actions to support safe staffing include:
Temporary staff altered cascade and added additional agencies
Supervision from senior nursing leads divisionally in hours and bronze flow teams out of hours
Healthcare assistant recruitment- aiming to keep vacancies at near zero. The majority of international recruitment currently paused due to travel restrictions from India.
SFH
Sickness absence has returned to their expected seasonal norm post the pandemic; they are still seeing low levels of COVID related absence however these additional losses are recorded as 0.5% additional to the sickness absence rate of 3.8%.
Overall resourcing indicators for M2 are positive with levels of vacancy’s (7.3%) and turnover (0.4%) remaining low.
There has been a focus on increasing access for colleagues’ staff COVID-19 vaccine. This has resulted in 4,923 (91%) of substantive staff vaccinated, with 4,461 (83%) receiving their second dose. This is above the regional benchmark (87%). They have vaccinated 87% of BAME staff (regional benchmark 77%) and 97% of their over 60 and 91% of CEV staff.
Integrated Performance Report
131 of 22409:00 - 10.50-04/08/21
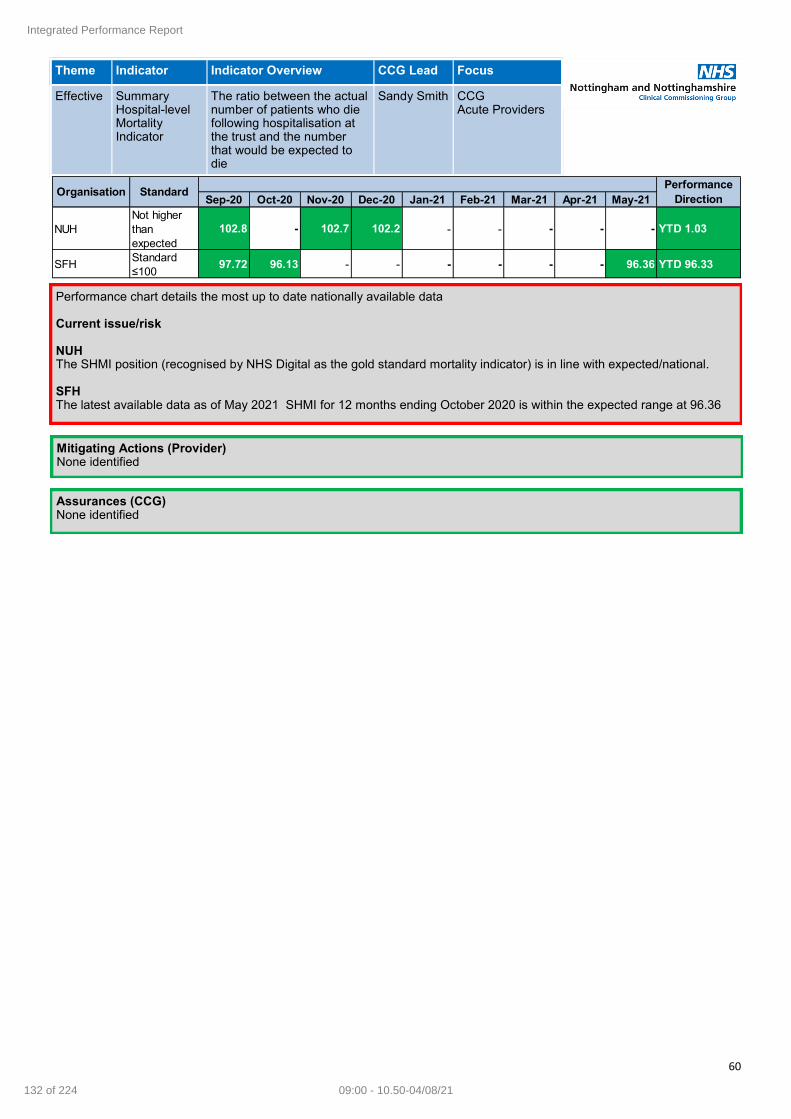
60
Theme Indicator Indicator Overview CCG Lead Focus
Effective Summary Hospital-level Mortality Indicator
The ratio between the actual number of patients who die following hospitalisation at the trust and the number that would be expected to die
Sandy Smith CCG Acute Providers
Performance chart details the most up to date nationally available data Current issue/risk NUH The SHMI position (recognised by NHS Digital as the gold standard mortality indicator) is in line with expected/national. SFH The latest available data as of May 2021 SHMI for 12 months ending October 2020 is within the expected range at 96.36
Mitigating Actions (Provider) None identified
Assurances (CCG) None identified
Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
NUH
Not higher
than
expected
102.8 - 102.7 102.2 - - - - - YTD 1.03
SFHStandard
≤10097.72 96.13 - - - - - - 96.36 YTD 96.33
Organisation StandardPerformance
Direction
Integrated Performance Report
132 of 224 09:00 - 10.50-04/08/21

61
Theme Indicator Indicator Overview CCG Lead Focus
Safe HSMR (basket of 56 diagnosis groups)
Adjust mortality data to take account of some of the factors known to affect the underlying risk of death
Sandy Smith CCG Acute Providers
Current issue/risk NUH
HSMR for 12-months ending March 2021 (latest data) is outside the expected range at 112.8. Crude HSMR position (3.2%) is below the national rate (3.6%) for 12 months to March 2021 (latest data).
SFH
HSMR; performance 117.1 against a target of 100. The trust consistently has higher than the national average but continues to track the peer groups. Issues identified with data submission have been identified which as a trusts they
Mitigating Actions (Provider) NUH
Extensive analysis (both via internal and external stakeholders) has been undertaken to understand NUH’s elevated HSMR position.
Specific diagnostic groups have been reviewed in detail (such as pneumonia) which alone do not account for the above expected position.
Other sources of intelligence such as NUH’s national audit outcomes and care quality reviews through the Structured Judgement Case Review process do not suggest systemic issues with outcomes/care quality (SJCR provides significant assurance of care in general being rated as good or excellent).
SFH
HSMR has increased at 117.1 to March 2021 (November 20 data). The effects of the COVID pandemic are clear within this data and they outline their proposals for meeting the requirements of investigation of Hospital acquired COVID and learning from other COVID related mortality data. They continue to review their HSMR and SHMI data and work closely with Dr Foster to understand what drives the changes in their data Preliminary discussions with an alternative mortality intelligence provider CHKS have raised some interesting areas for further exploration
Interim findings of their review of Trust Mortality Review Process and proposals for further actions. The COVID pandemic has significantly affected their ability to achieve the target of 90% reviews using the mortality tool. They have noted that the quality assurance of their Learning from Death processes requires strengthening and they propose to address this with SIR training delivered and review of their governance processes
Expansion of their Medical Examiner Service has allowed independent scrutiny of 97% of hospital deaths which partially mitigates this underachievement of the MRT target and a powerful example of learning from the process is provided
Assurances (CCG)
The CCG continues to monitor this standard through attendance at provider Mortality and End of Life and Learning from Deaths groups. SFH meet monthly and NUH meet bi-monthly. Any issues are raised with appropriate teams across the CCG e.g. commissioning and contracting. Mortality outlier alert notifications from the Dr Foster Unit are shared with the CCG by the providers as received with responses shared to the Chief Nurse at the CCG.
Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
NUHStandard ≤
100122.6 127.1 - 103.4 116 112.6 109.8 - - 112.8
SFHStandard ≤
100111.9 108.6 113.1 110.6 - 110.5 117.1 - -
106.2
(Exc COVID)
Organisation Standard12 Month
Position
Integrated Performance Report
133 of 22409:00 - 10.50-04/08/21
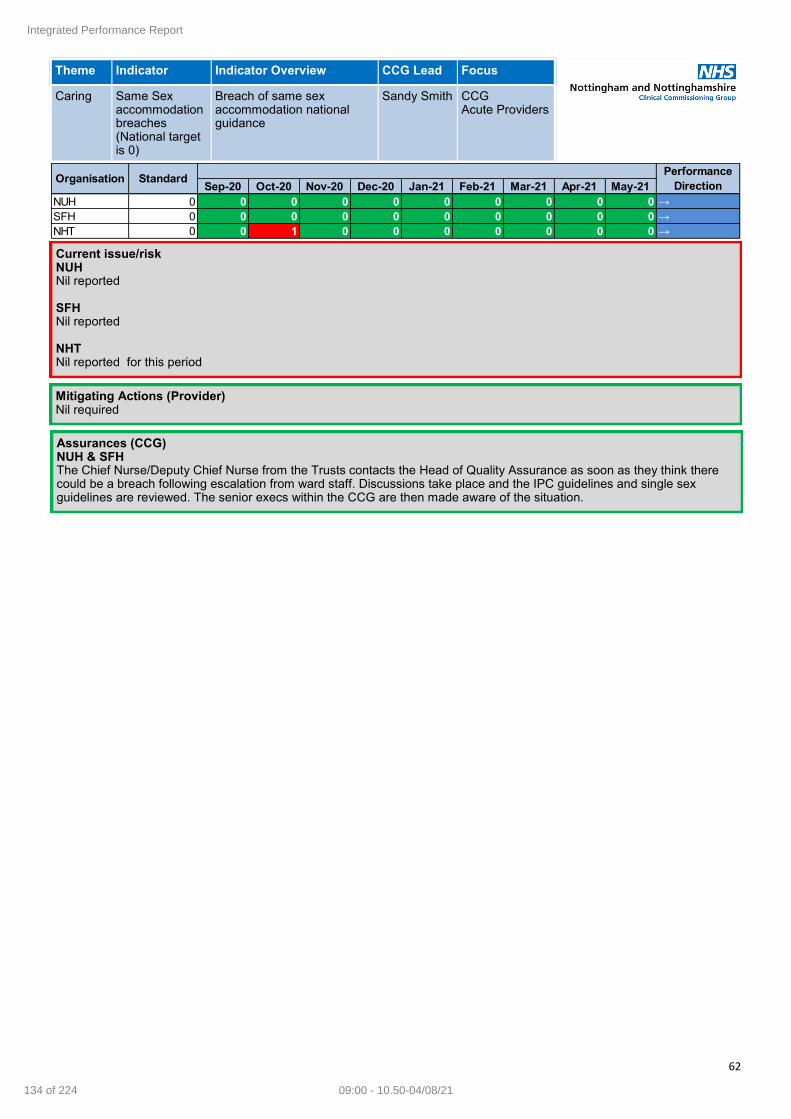
62
Theme Indicator Indicator Overview CCG Lead Focus
Caring Same Sex accommodation breaches (National target is 0)
Breach of same sex accommodation national guidance
Sandy Smith CCG Acute Providers
Current issue/risk NUH Nil reported SFH Nil reported NHT Nil reported for this period
Mitigating Actions (Provider) Nil required
Assurances (CCG) NUH & SFH The Chief Nurse/Deputy Chief Nurse from the Trusts contacts the Head of Quality Assurance as soon as they think there could be a breach following escalation from ward staff. Discussions take place and the IPC guidelines and single sex guidelines are reviewed. The senior execs within the CCG are then made aware of the situation.
Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
NUH 0 0 0 0 0 0 0 0 0 0 →
SFH 0 0 0 0 0 0 0 0 0 0 →
NHT 0 0 1 0 0 0 0 0 0 0 →
Organisation StandardPerformance
Direction
Integrated Performance Report
134 of 224 09:00 - 10.50-04/08/21
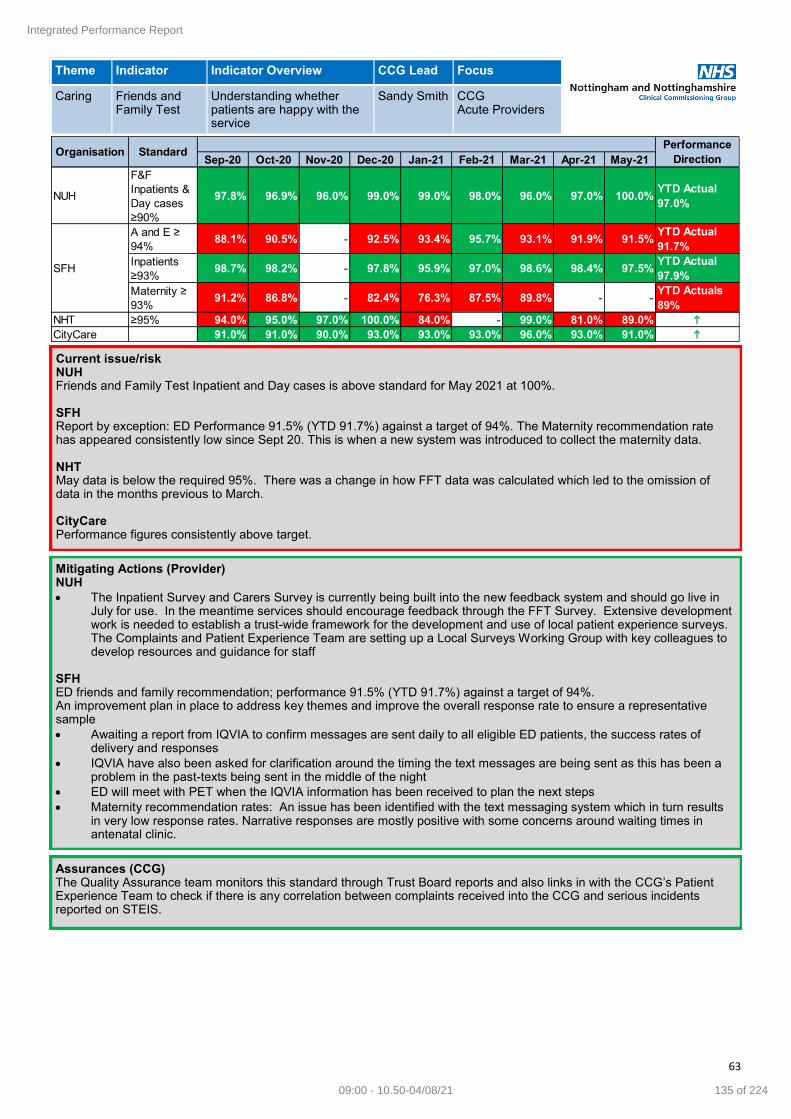
63
Theme Indicator Indicator Overview CCG Lead Focus
Caring Friends and Family Test
Understanding whether patients are happy with the service
Sandy Smith CCG Acute Providers
Current issue/risk NUH Friends and Family Test Inpatient and Day cases is above standard for May 2021 at 100%. SFH Report by exception: ED Performance 91.5% (YTD 91.7%) against a target of 94%. The Maternity recommendation rate has appeared consistently low since Sept 20. This is when a new system was introduced to collect the maternity data. NHT May data is below the required 95%. There was a change in how FFT data was calculated which led to the omission of data in the months previous to March. CityCare Performance figures consistently above target.
Mitigating Actions (Provider) NUH
The Inpatient Survey and Carers Survey is currently being built into the new feedback system and should go live in July for use. In the meantime services should encourage feedback through the FFT Survey. Extensive development work is needed to establish a trust-wide framework for the development and use of local patient experience surveys. The Complaints and Patient Experience Team are setting up a Local Surveys Working Group with key colleagues to develop resources and guidance for staff
SFH ED friends and family recommendation; performance 91.5% (YTD 91.7%) against a target of 94%. An improvement plan in place to address key themes and improve the overall response rate to ensure a representative sample
Awaiting a report from IQVIA to confirm messages are sent daily to all eligible ED patients, the success rates of delivery and responses
IQVIA have also been asked for clarification around the timing the text messages are being sent as this has been a problem in the past-texts being sent in the middle of the night
ED will meet with PET when the IQVIA information has been received to plan the next steps
Maternity recommendation rates: An issue has been identified with the text messaging system which in turn results in very low response rates. Narrative responses are mostly positive with some concerns around waiting times in antenatal clinic.
Assurances (CCG) The Quality Assurance team monitors this standard through Trust Board reports and also links in with the CCG’s Patient Experience Team to check if there is any correlation between complaints received into the CCG and serious incidents reported on STEIS.
Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
NUH
F&F
Inpatients &
Day cases
≥90%
97.8% 96.9% 96.0% 99.0% 99.0% 98.0% 96.0% 97.0% 100.0%YTD Actual
97.0%
A and E ≥
94%88.1% 90.5% - 92.5% 93.4% 95.7% 93.1% 91.9% 91.5%
YTD Actual
91.7%
Inpatients
≥93%98.7% 98.2% - 97.8% 95.9% 97.0% 98.6% 98.4% 97.5%
YTD Actual
97.9%
Maternity ≥
93%91.2% 86.8% - 82.4% 76.3% 87.5% 89.8% - -
YTD Actuals
89%
NHT ≥95% 94.0% 95.0% 97.0% 100.0% 84.0% - 99.0% 81.0% 89.0% h
CityCare 91.0% 91.0% 90.0% 93.0% 93.0% 93.0% 96.0% 93.0% 91.0% h
Organisation Standard
SFH
Performance
Direction
Integrated Performance Report
135 of 22409:00 - 10.50-04/08/21
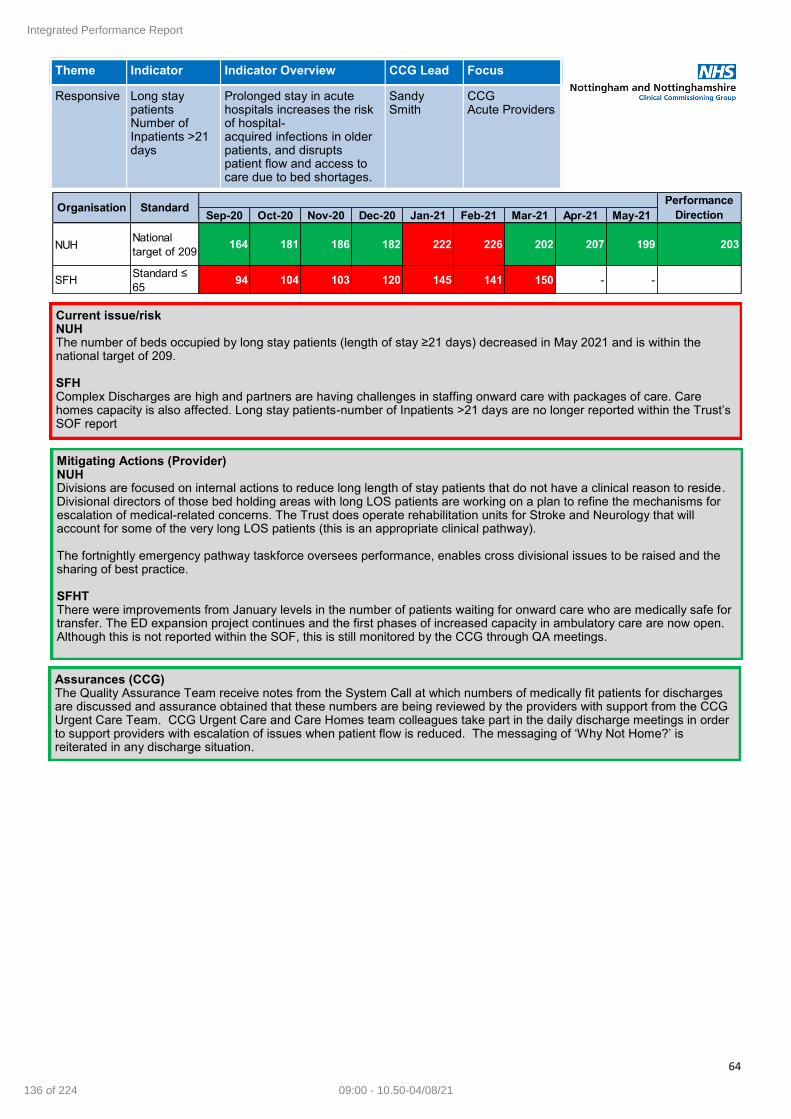
64
Theme Indicator Indicator Overview CCG Lead Focus
Responsive Long stay patients Number of Inpatients >21 days
Prolonged stay in acute hospitals increases the risk of hospital-acquired infections in older patients, and disrupts patient flow and access to care due to bed shortages.
Sandy Smith
CCG Acute Providers
Current issue/risk NUH The number of beds occupied by long stay patients (length of stay ≥21 days) decreased in May 2021 and is within the national target of 209. SFH Complex Discharges are high and partners are having challenges in staffing onward care with packages of care. Care homes capacity is also affected. Long stay patients-number of Inpatients >21 days are no longer reported within the Trust’s SOF report
Mitigating Actions (Provider) NUH Divisions are focused on internal actions to reduce long length of stay patients that do not have a clinical reason to reside. Divisional directors of those bed holding areas with long LOS patients are working on a plan to refine the mechanisms for escalation of medical-related concerns. The Trust does operate rehabilitation units for Stroke and Neurology that will account for some of the very long LOS patients (this is an appropriate clinical pathway). The fortnightly emergency pathway taskforce oversees performance, enables cross divisional issues to be raised and the sharing of best practice. SFHT There were improvements from January levels in the number of patients waiting for onward care who are medically safe for transfer. The ED expansion project continues and the first phases of increased capacity in ambulatory care are now open. Although this is not reported within the SOF, this is still monitored by the CCG through QA meetings.
Assurances (CCG) The Quality Assurance Team receive notes from the System Call at which numbers of medically fit patients for discharges are discussed and assurance obtained that these numbers are being reviewed by the providers with support from the CCG Urgent Care Team. CCG Urgent Care and Care Homes team colleagues take part in the daily discharge meetings in order to support providers with escalation of issues when patient flow is reduced. The messaging of ‘Why Not Home?’ is reiterated in any discharge situation.
Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
NUHNational
target of 209 164 181 186 182 222 226 202 207 199 203
SFHStandard ≤
6594 104 103 120 145 141 150 - -
Organisation StandardPerformance
Direction
Integrated Performance Report
136 of 224 09:00 - 10.50-04/08/21

65
Theme Indicator Indicator Overview CCG Lead Focus
Responsive Ambulance handover
Ambulance handover delays can be a symptom of system-wide issues, a mismatch of capacity and demand and inadequacy of patient flow
Sandy Smith
CCG Acute Providers
Current issue/risk NUH The national standard has not been met at NUH with improved performance being maintained since first contact process changes were enacted in April 2019 There are two main issues:
Hospital flow challenges can result in NUH’s Emergency Department not being able to deliver timely handover due to the department being full (or over-capacity) as a result of limited flow into assessment areas. The challenge in the assessment areas relates to timely flow out into the base wards due to lack of timely base ward bed availability. The maximum ED occupancy is also constrained by infection prevention and control measures as we operate in the ‘living with COVID’ era.
Data quality/validation component. The data is provided to NUH by EMAS and does not always enable the Trust to understand the driving factors.
SFH Ambulance handovers remained within target
Mitigating Actions (Provider) NUH NUH is generally a strong performing Trust in the region for this metric in comparison to other Trusts. Key actions that align to the issues described are:
System effort together with the Trust’s own improving patient stays work programme to support with effective flow through and out of hospital. This is to release hospital capacity to prevent patients waiting in ED for a bed and providing ED with space to be able to receive new patients in a timely manner.
A data quality / validation proposal has been drafted by NUH and shared with colleagues at EMAS to seek commitment to review in order to identify the next steps to improve performance.
NUH is also working to improve communication channels for EMAS and Trust command centre. Ambulance handover performance oversight takes place within ED and the site operations team on a daily basis with oversight at the fortnightly ED Pathway Taskforce.
Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21
NUH
(completed
within 15
minutes)
National
target of
100%
68.5% 68.5% 71.0% 66.0% 68.0% 66.0% 67.0% 68.0% 66.0%YTD Actuals
67%
SFH
(Percentage
of Ambulance
Arrivals > 30
minutes)
<10% 4.4% 3.5% 2.9% 2.9% 3.1% 3.1% 2.9% 2.1% 3.3%YTD Actuals
2.8%
Performance
DirectionOrganisation Standard
Next steps (QA team) Confirm data source for SFH data in view of NUH data quality concerns -action as appropriate.
Integrated Performance Report
137 of 22409:00 - 10.50-04/08/21

66
Theme Indicator Indicator Overview CCG Lead Focus
Safe 12 hour trolley breaches
Sandy Smith
CCG Acute Providers
Current issue/risk NUH
There were no 12 hour trolley breached reported in June 2021. SFH
There were 3 x 12 hour trolley breaches reported in June 2021. Factors influencing the delays include: Covid-19 swab result process delay and psychiatric bed unable to be allocated to patient until existing patient’s COVID-19 result was processed which in turn allowed transfer to another ward therefore allowing allocation of said bed for patient; allocation of a mental health bed and there was no evidence of any Registered Nurse chasing for a bed or escalation to DMN/NIC; requirement for a male psychiatric bed in Derbyshire mental health services.
Mitigating Actions (Provider) NUH
To support better flow through ED, NUH’s transformation and improvement teams are working closely with operational teams to deliver an ‘improving inpatient stays’ work programme. Also, a mental health task and finish group are now receiving and acting upon information pertaining to patients presenting to ED with mental health issues with specific actions being developed to improve patient pathways and experience.
SFH
All medical Consultants are asked to attend wards and undertake senior medical reviews of all patients and escalate any delays to discharge to the Divisional General Manager
Senior nursing representatives attend the Board rounds to take escalations and where appropriate, challenge decisions to encourage safe, earlier discharge
Assurances (CCG) NUH & SFH
The Quality Assurance team receives the notes from the daily System Call where any 12 hour trolley breaches are declared. The QA team follows up with the CCG’s Urgent Care Team and Head of Operational Planning and Assurance at NUH and SFH to obtain details of the breach and review the Breach Incident Response Template. The QA Team and the Urgent Care Team also have monthly meetings to discuss any breaches that happened during the month. RCAs once completed are reviewed by the QA team who request for further assurance as needed.
Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21 Jun-21
NUH 1 0 0 8 27 8 0 5 0 i
SFH 0 0 7 1 2 1 0 1 3 h
Performance
DirectionOrganisation Standard
National
target of 0
Integrated Performance Report
138 of 224 09:00 - 10.50-04/08/21
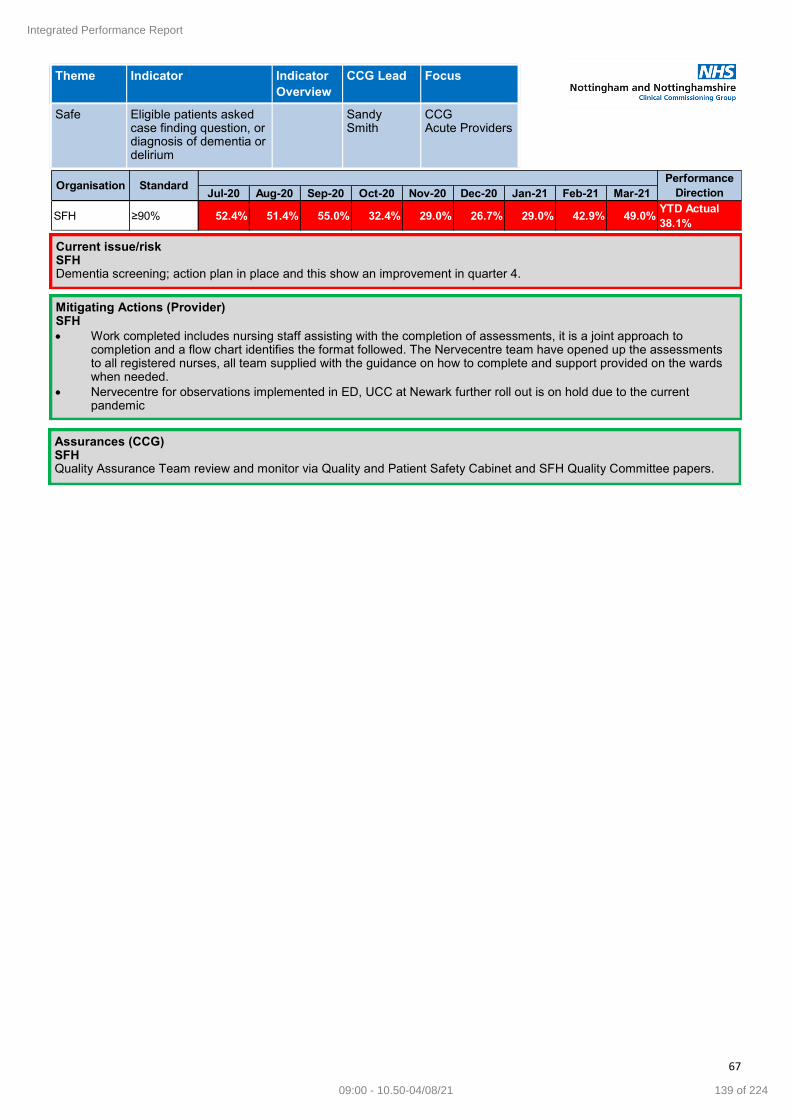
67
Theme Indicator Indicator
Overview
CCG Lead Focus
Safe Eligible patients asked case finding question, or diagnosis of dementia or delirium
Sandy Smith
CCG Acute Providers
Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21
SFH ≥90% 52.4% 51.4% 55.0% 32.4% 29.0% 26.7% 29.0% 42.9% 49.0%YTD Actual
38.1%
Performance
DirectionOrganisation Standard
Current issue/risk SFH Dementia screening; action plan in place and this show an improvement in quarter 4.
Mitigating Actions (Provider) SFH
Work completed includes nursing staff assisting with the completion of assessments, it is a joint approach to completion and a flow chart identifies the format followed. The Nervecentre team have opened up the assessments to all registered nurses, all team supplied with the guidance on how to complete and support provided on the wards when needed.
Nervecentre for observations implemented in ED, UCC at Newark further roll out is on hold due to the current pandemic
Assurances (CCG) SFH Quality Assurance Team review and monitor via Quality and Patient Safety Cabinet and SFH Quality Committee papers.
Integrated Performance Report
139 of 22409:00 - 10.50-04/08/21

68
Theme Indicator Indicator
Overview
CCG Lead Focus
Safe
OrganisationIndicator
Overview
CCG
Quality
Lead
Focus
NNCCGContinuing
CareSally Dore
Percentage of
CHC decisions
made within 28
days
>80%
Percentage of
CHC
assessments
completed in
hospital
<15% 1%
Indicator TargetPerformance for
2020/21 Quarter 4
93%
The CCG has continued to meet both quality performance targets in June 2021 with both being well within
tolerance levels.
Integrated Performance Report
140 of 224 09:00 - 10.50-04/08/21

69
Theme Indicator Indicator
Overview
CCG Lead Focus
Safe C-Diff
Current issue/risk There are no formal reduction targets in place. Plans are based on previous objectives. Revised reduction targets are expected to be issued in Q2.
Mitigating Actions (Provider) None identified
Assurances (CCG) None identified
YTD TOTAL
2021-22 2021-22
Plan 20 20 23 23 22 22 24 23 24 24 21 20 63 266
COCA 6 3 6 15 15
COIA 1 5 1 7 7
COHA 8 4 6 18 18
HOHA 5 6 6 17 17
Total acquired 20 18 19 0 0 0 0 0 0 0 0 0 57 57
Cumulative
Variance0 -2 -6 -29 -51 -73 -97 -120 -144 -168 -189 -209 -6 -209
Plan 6 6 6 6 7 7 7 7 7 7 7 6 18 79
COHA 5 4 4 13 15
HOHA 4 2 2 8 13
Total acquired 9 6 6 0 0 0 0 0 0 0 0 0 21 21
Cumulative
Variance3 3 3 -3 -10 -17 -24 -31 -38 -45 -52 -58 3 -58
Plan 9 9 12 10 10 10 10 10 10 10 10 10 30 120
COHA 4 0 3 7 18
HOHA 3 4 7 14 30
Total acquired 7 4 10 0 0 0 0 0 0 0 0 0 21 21
Cumulative
Variance-2 -7 -9 -19 -29 -39 -49 -59 -69 -79 -89 -99 -9 -99
Sherwood Forest
Hospital NHS
Trust
Nottingham
University
Hospitals NHS
Trust
Dec-21 Jan-22 Feb-22 Mar-22
NHS Nottingham
and
Nottinghamshire
CCG
Jul-21 Aug-21 Sep-21 Oct-21 Nov-21C-Diff Total 2021-
22Apr-21 May-21 Jun-21
Integrated Performance Report
141 of 22409:00 - 10.50-04/08/21

70
Theme Indicator Indicator
Overview
CCG Lead Focus
Safe MRSA
Current issue/risk
There is a zero target for MRSA BSI
Citycare reported 1 community MRSA BSI June
Mitigating Actions (Provider)
Citycare are in the process of completing an RCA
Assurances (CCG)
CCG RCA provider review process in place
Themes and learning are shared as a system monthly at IPC RCA meeting
YTD TOTAL
2021-22 2021-22
Plan 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Community-
onset1 1 1 3 3
Hospital-onset 0 0 0 0 0
Total 1 1 1 0 0 0 0 0 0 0 0 0 3 3
Cumulative
Variance1 2 3 3 3 3 3 3 3 3 3 3 3 3
Plan 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Hospital-onset 0 0 0 0 0
Total 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Cumulative
Variance0 0 0 0 0 0 0 0 0 0 0 0 0 0
Plan 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Hospital-onset 0 0 0 0 0
Total 0 0 0 0 0 0 0 0 0 0 0 0 0 0
Cumulative
Variance0 0 0 0 0 0 0 0 0 0 0 0 0 0
Mar-22
NHS Nottingham
and
Nottinghamshire
CCG
Sherwood Forest
Hospital NHS
Trust
Nottingham
University
Hospitals NHS
Trust
Oct-21 Nov-21 Dec-21 Jan-22 Feb-22May-21 Jun-21 Jul-21 Aug-21 Sep-21MRSA Total 2021-
22Apr-21
Integrated Performance Report
142 of 224 09:00 - 10.50-04/08/21

71
Theme Indicator Indicator
Overview
CCG Lead Focus
Safe E-Coli
Current issue/risk
A revised national ambition is in place to reduce all healthcare associated cases by 25% by 2021/22. The 50% reduction is now required by 2023/24, this reflects the complexity of these infections.
There are no formal Gram negative reduction targets in place these are expected to be introduced in Q2. This plan is based on the 10% reduction from 2016 baseline.
Mitigating Actions (Provider)
All cases are reviewed and related data is inputted onto the national data capture system for wider scrutiny and collation of themes
Assurances (CCG)
All cases are reviewed at an individual level to extract themes and shared learning for improvement, themes and learning are shared as a system at monthly IPC RCA meetings
YTD
2021-22
20% reduction 67 67 66 65 68 65 64 63 65 65 68 69 200
15% reduction 71 71 69 69 71 69 68 68 69 70 71 71 211
Plan 10%
reduction74 74 74 75 77 74 70 71 74 74 74 75 222
COCA 55 38 39 132
COHA 14 17 14 45
HOHA 16 11 13 40
Total acquired 85 66 66 0 0 0 0 0 0 0 0 0 217
Cumulative
Variance11 3 0 -146 -223 -297 -367 -438 -512 -586 -660 -735 -5
Plan 3 3 3 4 4 4 4 4 4 3 3 3 9
HOHA 6 4 0 10
Cumulative
Variance3 4 1 1
Plan 17 17 17 17 17 17 17 17 17 17 17 17 51
HOHA 14 7 16 37
Cumulative
Variance-3 -13 -14 -14
Sherwood Forest
Hospital NHS
Trust
42
10
-32
Nottingham
University
Hospitals NHS
Trust
204
37
-167
NHS Nottingham
and
Nottinghamshire
CCG
792
837
886
484
119
134
217
-669
Dec-21 Jan-22 Feb-22 Mar-22TOTAL
2021-22Jul-21 Aug-21 Sep-21 Oct-21 Nov-21
E-Coli Total 2021-
22Apr-21 May-21 Jun-21
Integrated Performance Report
143 of 22409:00 - 10.50-04/08/21

72
Theme Indicator Indicator
Overview
CCG Lead Focus
Safe COVID-19
YTD
2021-22
Sherwood Forest
Hospital NHS
Trust
Total 2 0 0 2
Nottingham
University
Hospitals NHS
Trust
Total 5 0 0 5
YTD
2021-22
Sherwood Forest
Hospital NHS
Trust
Total 0 0 1 1
Nottingham
University
Hospitals NHS
Trust
Total 15 1 0 16
YTD
2021-22
Sherwood Forest
Hospital NHS
Trust
Total 3 1 4
Nottingham
University
Hospitals NHS
Trust
Total 7 6 13
Mar-22
Feb-22 Mar-22
Number of
COVID-19 deathsApr-21 May-21 Jun-21 Jul-21 Aug-21 Sep-21 Oct-21 Nov-21 Dec-21 Jan-22 Feb-22
Dec-21 Jan-22 Feb-22 Mar-22
Number of
confirmed
COVID-19
swabbed within
15+ days of
Apr-21 May-21 Jun-21 Jul-21 Aug-21 Sep-21 Oct-21 Nov-21 Dec-21 Jan-22
Jul-21 Aug-21 Sep-21 Oct-21 Nov-21
Number of
confirmed
COVID-19
swabbed within
8-14 days of
Apr-21 May-21 Jun-21
Integrated Performance Report
144 of 224 09:00 - 10.50-04/08/21

73
Current issue/risk
There is an increasing number of COVID-19 related outbreaks across the system. This is against a backdrop of increasing levels of COVID-19 infection in circulation locally. The predominant strain remains the highly transmissible Delta variant (B.1.617.2) first detected in India.
Mitigating Actions (Provider)
Implementation of IPC advice, guidance and training support. Increased testing,
Cohorting/zoning positive cases, contact cases from those currently negative.
Enhanced cleaning schedules.; Monitoring PPE use with audits and ‘spot checks’ of compliance;
Monitoring of safe staffing levels ; Adherence to guidance re reduced visitor access.
Reduced staff movement across different sites and services; Promoting staff vaccination.
Action plans developed following CIPCT audit. Review of outbreaks and nosocomial infections for shared learning and improvement
Assurances (CCG)
Monthly IPC system assurance meetings with escalation to ICS Quality Group
Public Health COVID-19 outbreak meetings 3 x week
Integrated Performance Report
145 of 22409:00 - 10.50-04/08/21

74
Theme Indicator Indicator
Overview
CCG Lead Focus
Safe Individual Funding Requests & Service Restricted Procedures 01/06 – 30/06 2021
Fertility Requests
NHS Nottingham & Nottinghamshire CCG updated the Gamete and Embryo storage eligibility criteria in July 2020. It was
amended to include reference to the prior approval form development which includes eligibility criteria which will be used un-
til EMACC policy for gamete and embryo storage has been adopted. Of the 15 requests for storage, 13 patients were ap-
proved for storing products prior to commencing treatment where they are at risk of permanent infertility, including those re-
ceiving cancer treatments. 1 request is still outstanding and being looked into and 1 was declined due to it not being submit-
ted by an appropriate Consultant led service. 1 request was for IVF.
Online Prior Approval Requests
The IFR Team are responsible for the triaging and monitoring of online prior approvals from secondary care providers. We
received a total of 1293 online prior approval requests. Out of the 1293, 1269 were approved and 24 were not approved. The
100% indicator refers to the turnaround time as stated in the Service Restriction Policy. Indicator remains consistent meeting
the 100% target so no exception reported is required.
Prior Approval Requests
The CCG IFR Team have a 10 working day turnaround from date of receipt for all Primary Care requests.
The IFR Team are responsible for the triaging and monitoring of prior approval request from GP’s. We received a total of 822
prior approval requests. Out of the 822, 704 were approved and 118 were not approved. The 100% indicator refers to the
turnaround time as stated in the Service Restriction Policy. Indicator remains consistent meeting the 100% target so no ex-
ception reported is required.
Out of Area Treatment
The IFR Team are responsible for the triaging and monitoring of Out of Area Requests from both GP’s and secondary care
Consultants. We received a total of 3 requests. All 3 requests were approved. The 100% indicator refers to the turnaround
time as stated in the Service Restriction Policy. Indicator remains consistent meeting the 100% target so no exception report-
ed is required.
Treatment Abroad
No Treatment abroad requests received this month.
There are strict criteria under which they have to assess each application. See attached link
https://www.england.nhs.uk/wp-content/uploads/2016/03/s2-directv-guid-comms-mar16.pdf.
IFR Requests
In line with the CCGs IFR Policy all requests must be acknowledged, screened and considered by the Panel (if exceptionality
is demonstrated within 40 days of the receipt of the application. 5 requests have been received this month, all 5 which were
declined at the screening stage. Indicator remains consisted meeting the 100% target from last month and so no exception
reporting is required.
Fertility Requests 100% 14 2
Online Prior Approval Requests 100% 1269 24
Prior Approval Requests 100% 705 118
Out of Area Requests 100% 3 0
Treatment Abroad Requests100% NHS E Target of
7 day turnaround0 0
IFR Requests 100% 0 5
Type of Request
Percentage of SRP
assessments
completed within 10
days (target 100%)
Approved Not Approved
Percentage of IFR
decision made within
40 days (target
>100%)
Integrated Performance Report
146 of 224 09:00 - 10.50-04/08/21

75
Glossary
Acronym Meaning Acronym Meaning
A&E Accident and Emergency LD Learning Disabilities
A&E DB Accident and Emergency Delivery Board LoS Length of Stay
ACS Accountable Care System LTWB Let's Talk Well Being
ADD Attention Deficit Disorder MHST Mental Health Support Team
ADHD Attention Deficit and Hyperactivity Disorder MN Mid Nottinghamshire
ANP Advanced Nurse Practitioner MOU Memorandum of Understanding
ASD Autism Spectrum Disorder NEL Non-Elective
BAU Business As Usual NEMS Nottinghamshire Emergency Medical Services
CBT Cognitive Behavioural Therapy NHCT Nottinghamshire Healthcare NHS Trust
CCG Clinical Commissioning Group NHSE NHS England
CETR Care Education and Treatment Review NHSI NHS Improvement
CFIDD Community Forensic Intellectual and Development Disability ServiceNNICS Nottingham & Nottinghamshire ICS
CHC Continuing Healthcare NICE National Institute for Health and Care Excellence
CoP Court of Protection NUH Nottingham University Hospitals NHS Trust
CQUIN Commissioning for Quality and Innovation OAPs Out of Area Placements
CT Computed Tomography OBD Occupied Bed Days
CV Contract Variation OP Outpatient
CP Children and Younger People PCN Primary Care Network
DCO Director of Commissioning Operations PHE Public Health England
DST Decision Supporting Tool PHSMI Physical Health for SMI patients
DToC Delayed Transfer of Care PICU Psychiatric Intensive Care Unit
DTT Diagnosis to Treatment Times PID Project Initiation Document
EBUS Endobronchial Ultrasound POD Point of Delivery
ED Emergency Department - often referred to as A&E PTL Patient Targeted List
EIP Early Intervention in Psychosis QIPP Quality Innovation Productivity and Prevention
EMAS East Midlands Ambulance Service NHS Trust QMC Queens Medical Centre
EMCA East Midlands Cancer Alliance RAP Remedial Action Plan
EOL End of Life RTT Referral to Treatment Times
G&A General & Acute SFHFT Sherwood Forest Hospitals NHS Foundation Trust
GI Gastro-Intestinal - often referred to as Upper GI or Lower GI SLA Service Level Agreement
GN Greater Nottingham SLAM Service Level Agreement Monitoring
HEE Health Education England SMI Severe Mental Illness
HFID Home First Integrated Discharge SOP Standard Operating Procedure
IAPT Improving Access to Psychological Therapies SRO Senior Responsible Officer
IBN Information Breach Notice STP Sustainability and Transformation Plan
ICATT Intensive Community Assessment and Treatment Team TCP Transforming Care Partnership
ICP Integrated Care Partnership UEC Urgent & Emergency Care
ICS Integrated Care System UTC Urgent Treatment Centre
IR Identification Rules YOC Year of Care
KMH Kings Mill Hospital YTD Year to Date
Integrated Performance Report
147 of 22409:00 - 10.50-04/08/21

Page 1 of 2
Meeting Title: Governing Body (Open Session) Date: 04 August 2021
Paper Title: Highlight report from the (virtual)
meeting of the CCG’s Audit and
Governance Committee
Paper Reference: GB 21 165
Chair of the
meeting
Sue Sunderland, Non-Executive
Director
Attachments/
Appendices:
-
Summary
Purpose:
Approve ☐ Endorse ☐ Review
☐ Receive/Note for:
Assurance
Information
☒
Summary of the Meeting
The Audit and Governance Committee met on the 10 June 2021. Due to the current Coronavirus (Covid-
19) restrictions, the meeting was held virtually.
At the meeting, the Committee:
APPROVED the CCG’s final Annual Report and audited accounts for submission to NHS England
ahead of the deadline of 15 June 2021. The Committee also endorsed the signing of the letter of
representation, which stated compliance with accounting and auditing standards. This approval had
followed scrutiny of the External Audit report of the accounts; third party assurance reports; and the
Head of Internal Audit Opinion report, which had provided an overall rating of ‘significant assurance’.
The External Audit opinion was ‘unqualified’.
APPROVED the Counter Fraud, Bribery and Corruption Annual Report; and noted that baseline
measurements had been taken for the CCG for the NHS Counter Fraud Authority’s new counter fraud
standards, which had been introduced in April 2021. The Committee noted that many of the standards
were new, which effectively meant that the CCG was not yet complaint with all standards. However, the
CCG’s annual counter-fraud work plan for 2021/22 had been based around actions to meet all
standards.
APPROVED the CCG’s 2020/21 Health and Safety, Security and Fire Compliance Annual Report; and
supported the next steps for action.
ENDORSED the sign off of the 2020/21 Data Security and Protection Toolkit submission by the Senior Information risk Owner by 30 June, subject to the outstanding evidence items being satisfactorily addressed.
RETROSPECTIVELY APPROVED invoice payments and credit notes transacted outside of delegated
limits. The Committee had received a report that noted that 1.95% of all transactions during the
previous financial year had been approved outside of limits set in the CCG’s Standing Financial Orders.
All had been investigated and errors were found to be as a result of the limitations of the financial
reporting systems rather than intentional breaches and mitigating actions had been put in place. The
Committee will continue to monitor compliance.
Audit and Governance Committee Highlight Report – 10 June 2021
148 of 224 09:00 - 10.50-04/08/21

Page 2 of 2
Key Messages for the Governing Body
Strong assurance received from the Information Governance and Health and Safety Reports.
The Committee thanked the Corporate Governance and Finance Teams for the huge amount of work that had been undertaken to produce the Annual Report and Accounts by the stated deadline. The Committee also thanked both external and internal audit for their positive reports.
The ratified minutes of the meeting will be received by the Governing Body on the 6 October 2020.
Audit and Governance Committee Highlight Report – 10 June 2021
149 of 22409:00 - 10.50-04/08/21
1
Meeting Title: Governing Body (Open Session) Date: 04 August 2021
Paper Title: Corporate Risk Report Paper Reference: GB 21 066
Sponsor: Rosa Waddingham, Chief Nurse Attachments/ Appendices:
Appendix A -Extract from CCG’sCorporate Risk Register
Presenter: Lucy Branson, Associate Director of Governance
Purpose: Approve ☐ Endorse ☐ Review ☐ Receive/Note for:
∑ Assurance∑ Information
☒
Executive Summary
The purpose of this paper is to present the Governing Body with the major (red) operational risks from the CCG’s Corporate Risk Register. This paper is a standing agenda item, presented to each meeting to ensure that the Governing Body is kept informed of the key risks facing the CCG and assured that robust management actions are in place to manage and mitigate them.
Relevant CCG priorities/objectives:
Compliance with Statutory Duties ☒ Wider system architecture development (e.g. ICP, PCN development)
☐
Financial Management ☒ Cultural and/or Organisational Development
☒
Performance Management ☐ Procurement and/or Contract Management ☐
Strategic Planning ☐
Conflicts of Interest:
☒ No conflict identified
Completion of Impact Assessments:
Equality / Quality Impact Assessment (EQIA)
Yes ☐ No ☐ N/A☒ Not applicable to this report
Data Protection Impact Assessment (DPIA)
Yes ☐ No ☐ N/A☒ Not applicable to this report
Risk(s):
The paper details the current major (red) risks in the Corporate Risk Register.
Corporate Risk Report
150 of 224 09:00 - 10.50-04/08/21

2
Confidentiality:
☒No
Recommendation(s):
1. NOTE the major risks shown at Section 2.1 and comment on whether sufficient controls and actions are in place.
2. HIGHLIGHT any risks identified during the course of the meeting for inclusion within the Corporate Risk Register.
Corporate Risk Report
151 of 22409:00 - 10.50-04/08/21
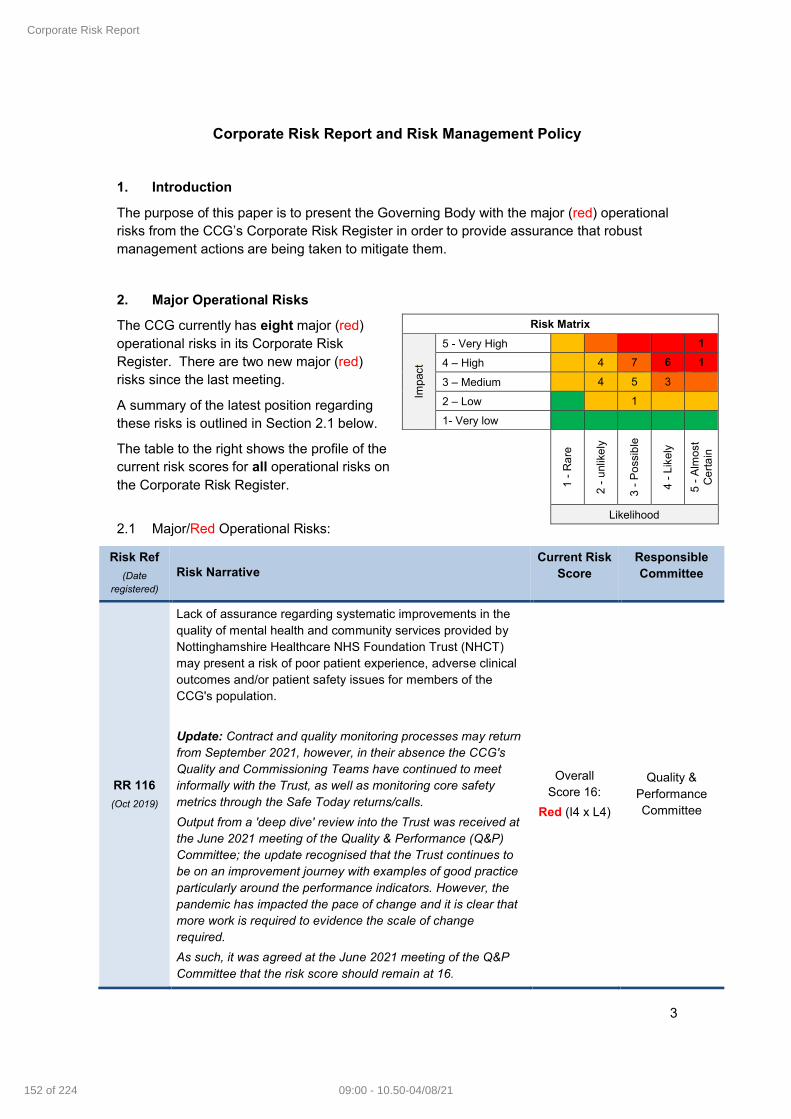
3
Corporate Risk Report and Risk Management Policy
1. Introduction
The purpose of this paper is to present the Governing Body with the major (red) operational risks from the CCG’s Corporate Risk Register in order to provide assurance that robust management actions are being taken to mitigate them.
2. Major Operational Risks
The CCG currently has eight major (red) operational risks in its Corporate Risk Register. There are two new major (red) risks since the last meeting.
A summary of the latest position regarding these risks is outlined in Section 2.1 below.
The table to the right shows the profile of the current risk scores for all operational risks on the Corporate Risk Register.
2.1 Major/Red Operational Risks:
Risk Ref
(Date registered)
Risk Narrative Current Risk
ScoreResponsible Committee
RR 116
(Oct 2019)
Lack of assurance regarding systematic improvements in the quality of mental health and community services provided by Nottinghamshire Healthcare NHS Foundation Trust (NHCT)may present a risk of poor patient experience, adverse clinical outcomes and/or patient safety issues for members of the CCG's population.
Update: Contract and quality monitoring processes may return from September 2021, however, in their absence the CCG's Quality and Commissioning Teams have continued to meet informally with the Trust, as well as monitoring core safety metrics through the Safe Today returns/calls.
Output from a 'deep dive' review into the Trust was received at the June 2021 meeting of the Quality & Performance (Q&P)Committee; the update recognised that the Trust continues to be on an improvement journey with examples of good practice particularly around the performance indicators. However, the pandemic has impacted the pace of change and it is clear that more work is required to evidence the scale of change required.
As such, it was agreed at the June 2021 meeting of the Q&P Committee that the risk score should remain at 16.
Overall Score 16:
Red (I4 x L4)
Quality & Performance Committee
Risk Matrix
Impa
ct
5 - Very High 1
4 – High 4 7 6 1
3 – Medium 4 5 3
2 – Low 1
1- Very low
1 -
Ra
re
2 -
unl
ike
ly
3 -
Po
ssib
le
4 -
Lik
ely
5 -
Alm
ost
Ce
rta
in
Likelihood
Corporate Risk Report
152 of 224 09:00 - 10.50-04/08/21
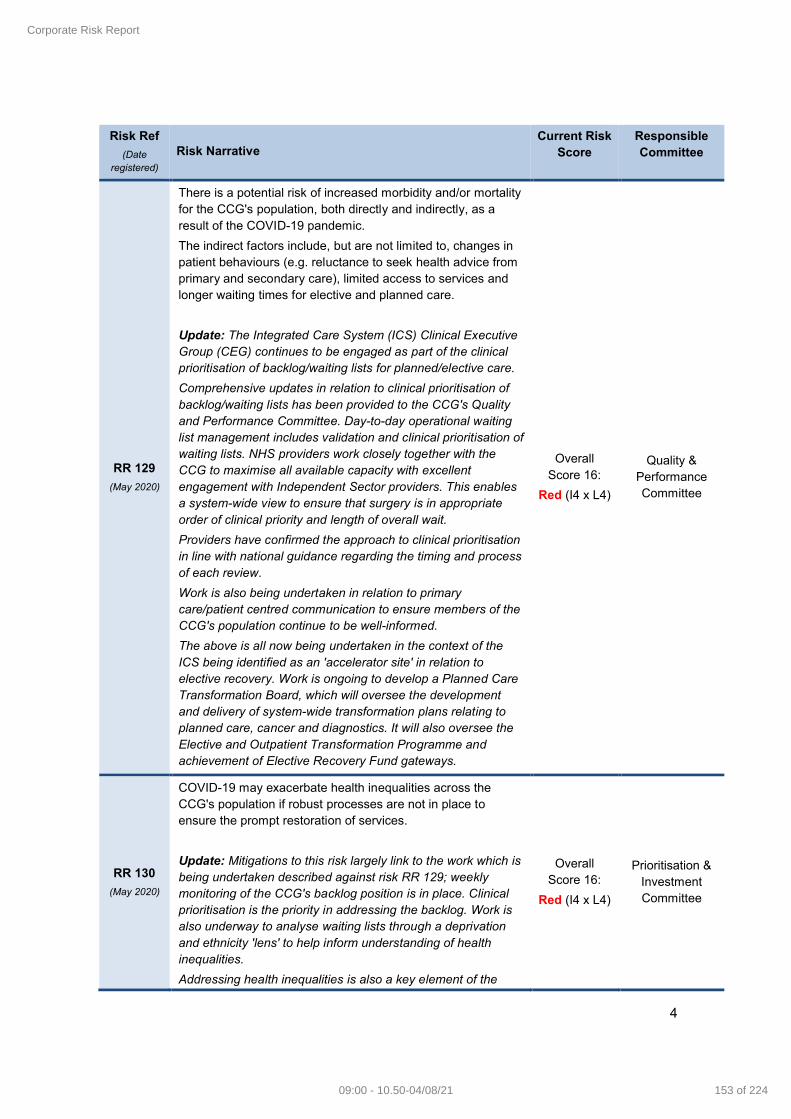
4
Risk Ref
(Date registered)
Risk Narrative Current Risk
ScoreResponsible Committee
RR 129
(May 2020)
There is a potential risk of increased morbidity and/or mortality for the CCG's population, both directly and indirectly, as a result of the COVID-19 pandemic.
The indirect factors include, but are not limited to, changes in patient behaviours (e.g. reluctance to seek health advice from primary and secondary care), limited access to services and longer waiting times for elective and planned care.
Update: The Integrated Care System (ICS) Clinical Executive Group (CEG) continues to be engaged as part of the clinical prioritisation of backlog/waiting lists for planned/elective care.
Comprehensive updates in relation to clinical prioritisation of backlog/waiting lists has been provided to the CCG's Quality and Performance Committee. Day-to-day operational waiting list management includes validation and clinical prioritisation of waiting lists. NHS providers work closely together with the CCG to maximise all available capacity with excellent engagement with Independent Sector providers. This enables a system-wide view to ensure that surgery is in appropriate order of clinical priority and length of overall wait.
Providers have confirmed the approach to clinical prioritisation in line with national guidance regarding the timing and process of each review.
Work is also being undertaken in relation to primary care/patient centred communication to ensure members of the CCG's population continue to be well-informed.
The above is all now being undertaken in the context of the ICS being identified as an 'accelerator site' in relation to elective recovery. Work is ongoing to develop a Planned Care Transformation Board, which will oversee the development and delivery of system-wide transformation plans relating to planned care, cancer and diagnostics. It will also oversee the Elective and Outpatient Transformation Programme and achievement of Elective Recovery Fund gateways.
Overall Score 16:
Red (I4 x L4)
Quality & Performance Committee
RR 130
(May 2020)
COVID-19 may exacerbate health inequalities across the CCG's population if robust processes are not in place to ensure the prompt restoration of services.
Update: Mitigations to this risk largely link to the work which is being undertaken described against risk RR 129; weekly monitoring of the CCG's backlog position is in place. Clinical prioritisation is the priority in addressing the backlog. Work is also underway to analyse waiting lists through a deprivation and ethnicity 'lens' to help inform understanding of health inequalities.
Addressing health inequalities is also a key element of the
Overall Score 16:
Red (I4 x L4)
Prioritisation & Investment Committee
Corporate Risk Report
153 of 22409:00 - 10.50-04/08/21

5
Risk Ref
(Date registered)
Risk Narrative Current Risk
ScoreResponsible Committee
2021/22 Planning Submission (April – September); five priority areas in relation to health inequalities are outlined:
∑ Restore NHS services inclusively;
∑ Mitigate against digital exclusion;
∑ Ensure datasets are complete and timely;
∑ Accelerate preventative programmes that proactively engage those at greatest risk of poor health outcomes; and
∑ Strengthen leadership and accountability.
The planning submission also outlines work being undertaken to expand primary care capacity to improve access, local health outcomes and health inequalities. Health inequalities is included in the System Performance Dashboard to the ICS Board.
The implementation of population health management and personalised care approaches are also key mitigations to this risk.
RR 151
(Sept 2020)
There is a risk that the CCG may incur increased costs of service provision due to COVID related requirements and the resulting reduction in productivity. This may manifest in increased prices for services that the CCG seeks to procure in the future, as well as increased costs to the NHS provider cost base. This, in turn, would have a cost pressure on the system.
Update: The 2021/22 planning submissions for the first half of the financial year have been co-produced by system partners and submitted to regulators. Contracts have been put in place with Independent Sector providers for 2021/22, however, the financial regime put in place in response to the pandemiccontinues for NHS providers.
The CCG, and ICS, have submitted a balanced financial plan for the first half of 2021/22. As such, the score in relation to this risk will be reviewed at an upcoming Committee meeting.
Overall Score 16:
Red (I4 x L4)
Prioritisation & Investment Committee
RR 156
(Nov 2020)
Lack of assurance regarding systematic improvements required in the quality of maternity services provided by Nottingham University Hospitals (NUH), may present a risk of unsafe care, poor clinical outcomes and/or patient safety issues for members of the CCG's population.
Update: Terms of Reference for a proposed thematic review of NUH Maternity Services are being drafted. This review is due to be co-commissioned by the CCG and NHS England and Improvement.
The latest NUH Maternity Safety Oversight and Quality
Overall Score 25:
Red (I5 x L5)
Quality & Performance Committee
Corporate Risk Report
154 of 224 09:00 - 10.50-04/08/21
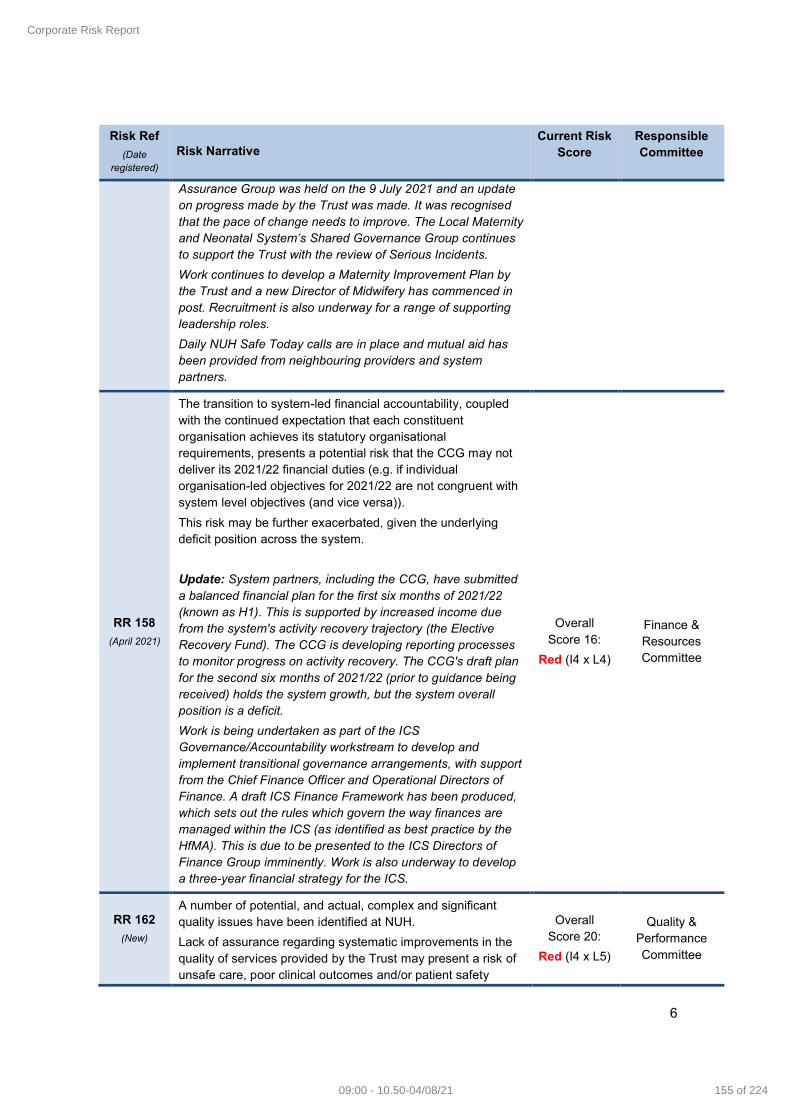
6
Risk Ref
(Date registered)
Risk Narrative Current Risk
ScoreResponsible Committee
Assurance Group was held on the 9 July 2021 and an update on progress made by the Trust was made. It was recognised that the pace of change needs to improve. The Local Maternity and Neonatal System’s Shared Governance Group continues to support the Trust with the review of Serious Incidents.
Work continues to develop a Maternity Improvement Plan by the Trust and a new Director of Midwifery has commenced in post. Recruitment is also underway for a range of supporting leadership roles.
Daily NUH Safe Today calls are in place and mutual aid has been provided from neighbouring providers and system partners.
RR 158
(April 2021)
The transition to system-led financial accountability, coupled with the continued expectation that each constituent organisation achieves its statutory organisational requirements, presents a potential risk that the CCG may not deliver its 2021/22 financial duties (e.g. if individual organisation-led objectives for 2021/22 are not congruent with system level objectives (and vice versa)).
This risk may be further exacerbated, given the underlyingdeficit position across the system.
Update: System partners, including the CCG, have submitted a balanced financial plan for the first six months of 2021/22 (known as H1). This is supported by increased income due from the system's activity recovery trajectory (the Elective Recovery Fund). The CCG is developing reporting processes to monitor progress on activity recovery. The CCG's draft plan for the second six months of 2021/22 (prior to guidance being received) holds the system growth, but the system overall position is a deficit.
Work is being undertaken as part of the ICS Governance/Accountability workstream to develop and implement transitional governance arrangements, with support from the Chief Finance Officer and Operational Directors of Finance. A draft ICS Finance Framework has been produced, which sets out the rules which govern the way finances are managed within the ICS (as identified as best practice by the HfMA). This is due to be presented to the ICS Directors of Finance Group imminently. Work is also underway to develop a three-year financial strategy for the ICS.
Overall Score 16:
Red (I4 x L4)
Finance & Resources Committee
RR 162
(New)
A number of potential, and actual, complex and significant quality issues have been identified at NUH.
Lack of assurance regarding systematic improvements in the quality of services provided by the Trust may present a risk of unsafe care, poor clinical outcomes and/or patient safety
Overall Score 20:
Red (I4 x L5)
Quality & Performance Committee
Corporate Risk Report
155 of 22409:00 - 10.50-04/08/21

7
Risk Ref
(Date registered)
Risk Narrative Current Risk
ScoreResponsible Committee
issues for members of the CCG's population.
Update: Further work has been undertaken to understand current challenges around culture and leadership, governance, quality of care, and performance recovery and restoration.
Actions are being taken through Executive and ICS forums, 'mock' internal CQC inspections and quality improvement programmes, Safe Today progress and the development of a local Quality Schedule (to include dashboard metrics).
A focused discussion for NUH is scheduled for the August 2021 meeting of the CCG’s Quality and Performance Committee. An update on the activities undertaken will be presented, including the system-wide support action plan. An assessment of the current risk score will be undertaken at this meeting.
RR 165
(New)
There is a potential risk that H1 funding received by the system (for the first six months of 2021/22) may not be sufficient to address recovery of services for the CCG's population (e.g. meeting planning/performance trajectories and addressing backlog).
Update: The CCG, and the system, have submitted a balanced financial plan for the first six months of 2021/22 (known as H1). This is supported by increased income due from the system's activity recovery trajectory (the Elective Recovery Fund). The CCG is developing reporting processes to monitor progress on activity recovery. Financial management and reporting processes are in place at system, and CCG, level to ensure delivery against the H1 plan continues to be monitored.
In July 2021, it was announced that the Q2 thresholds for elective recovery will be increased from 85% to 95%, which would result in a reduction in expected allocation (which was planned to fund recovery). The impact of this change is being worked through with ICS system partners, however, would result in reduced income. As such, the likelihood of this risk has been increased from a 3 to 4, resulting in an overall score of 16.
Overall Score 16:
Red (I4 x L4)
Finance & Resources Committee
2.2 Since the last meeting, the Finance and Resources Committee has agreed a reduction in the likelihood score for risk RR 135 (the CCG may not be spending its allocation in line with commissioning intentions/priorities) from 4 to 2, resulting in an overall score of 8 (I4 x L2). As such, this risk no longer requires escalation to the Governing Body.
2.3 The overall risk score for risk RR 156 (quality of maternity services provided by Nottingham University Hospitals (NUH)) has been increased from 20 to 25 following
Corporate Risk Report
156 of 224 09:00 - 10.50-04/08/21
8
assurances received, and subsequent discussions, at the July 2021 Quality and Performance Committee meeting.
2.4 Relevant senior CCG colleagues are considering an increase to the score for risk RR 160 (primary care staff exhaustion and 'burn out'), with a proposal on this due to be presented to the August meeting of the Primary Care Commissioning Committee.
3. Recommendations
3.1 The Governing Body is requested to:
a) NOTE the major risks shown at Section 2.1 and comment on whether sufficient controls and actions are in place; and
b) HIGHLIGHT any risks identified during the course of the meeting for inclusion within the Corporate Risk Register.
Siân Gascoigne
Head of Corporate Assurance
August 2021
Corporate Risk Report
157 of 22409:00 - 10.50-04/08/21

Risk Ref Oversight Committee Directorate Date Risk
Identified Risk Description Risk Category Existing Controls Mitigating Actions Mitigating Actions Progress Update:
Last Review
DateTrend
(Relevant committee in
the CCG's governance
structure responsible for
monitoring risks relating
to their delegated duties)
(Date risk
originally
identified)
(These are operational risks, which are by-products of day-to-day business delivery. They
arise from definite events or circumstances and have the potential to impact negatively on
the organisation and its objectives.) Imp
act
Like
liho
od
Sco
re
(The measures in place to control risks and reduce the likelihood of them occurring).
(Actions required to manage / mitigate the identified risk. Actions
should support achievement of target risk score and be SMART (e.g.
Specific, Measurable, Assignable, Realistic and Time-bound). Imp
act
Like
liho
od
Sco
re (To provide detailed updates on progress being made against any mitigating actions identified. Actions taken should bring risk to level which can be
tolerated by the organisation).
(Movement
in risk score
since
previous
month)
RR116 Quality and Performance
Committee
Quality and
Governance
Oct-19 Lack of assurance regarding systematic improvements in the quality of mental health and
community services provided by NHCT, may present a risk of poor patient experience,
adverse clinical outcomes and/or patient safety issues for members of the CCG's
population.
Quality
Ro
sa W
add
ingh
am
Dan
ni B
urn
ett
4 4 16 • Delegated role and responsibilities of the Quality & Performance Committee (and
membership);
• Quality Assurance Group;
• Integrated Performance reporting / Nursing and Quality reporting (including NHCT
focussed reporting) to Quality & Performance Committee;
• Safe Today quality assurance programme;
• Provider oversight and monitoring of provider Board Assurance Framework action plans.
Action: To embed the Quality Assurance Group (QAG) to be chaired
by the CCG as lead commissioner. The QAG to have oversight of
the quality improvement plans across the Trust
Action: CCG to liaise with NHSE Spec Comms regarding local
agreement for SI reporting
Action: CCG to discuss with partners to review support offers to the
Trust
Action: CCG to support internal discussions to address SI backlog
Action: Safe Today Quality & Safety metrics to be reviewed as part
of Recovery & Restoration of the Quality Assurance function
Action: Safe Today dashboard to be expanded to include other
elements e.g. safeguarding, medicines safety, and comparative
data.
4 4 16 August 2021: The usual contract and quality monitoring processes will return from September 2021 (H2), however, in their absence the CCG's Quality and
Commissioning Teams have continued to meet informally with the Trust, as well as monitoring core safety metrics through the Safe Today returns/calls.
Output from a 'deep dive' review into the Trust was received at the June 2021 meeting of the Q&P Committee; the update recognised that the Trust
continues to be on an ‘improvement journey’ with examples of good practice particularly around the performance indicators. However, the pandemic has
impacted the pace of change and it is clear that more work is required to evidence the scale of change required.
As such, it was agreed at the June 2021 meeting of the Q&P Committee that the risk score should remain at 16.
01/08/2021 ↔
RR129 Quality and Performance
Committee
Commissioning May-20 There is a potential risk of increased morbidity and/or mortality for Nottingham and
Nottinghamshire system's population, both directly and indirectly, as a result of the COVID-
19 pandemic.
The indirect factors which may contribute to this include, but are not limited to:
• Increasing elective/planned care waiting times (e.g. increasing waiting lists and backlog);
• Non-achievement of elective recovery targets;
• Limited access to services;
• Public behaviours in not raising concerns/accessing primary care (e.g. reluctance to seek
health advice from primary and secondary care).
This risk may be exacerbated by poor, or delayed, communication with the public and/or
patients in relation to access and/or position on waiting lists.
Commissioning
Lucy
Dad
ge /
Ro
sa W
add
ingh
am
Lisa
Du
ran
t /
Dan
ni B
urn
ett
5 4 20 • Establishment of Capacity Cell and Data Cell within the CCG's Incident Response
infrastructure;
• Restoration of planned/elective activity (via the Recovery Cell);
• Recovery Cell (system engagement);
• Elective Hub (being established);
• ICS Clinical Reference Group (chaired by ICS Medical Lead);
• Weekly reporting of waiting list/backlog figures.
Action: To continue with the restoration of services through the
Recovery Cell and ICS Clinical Executive Group
Action: To establish the Elective Hub
Action: To ensure weekly reporting of backlog/waiting list figures is
in place, published to all key stakeholders (Complete)
Action: To establish the ICS-wide Elective Hub (that will sit alongside
the Capacity Cell) to monitor delivery of waiting lists (to ensure
equitable across the patch).
4 4 16 August 2021: The ICS Clinical Executive Group (CEG) continues to be engaged as part of the clinical prioritisation of backlog/waiting lists for
planned/elective care.
Comprehensive updates in relation to clinical prioritisation of backlog/waiting lists was provided to the March and April 2021 meetings of the CCG's Quality
and Performance Committee. Day-to-day operational waiting list management includes validation and clinical prioritisation of waiting lists. Both providers
(NUH and SFH) work closely together with the CCG to maximise all available capacity with excellent engagement with the Independent Sector (IS)
providers. This enables a system-wide view to ensure that surgery is in appropriate order of clinical priority and length of overall wait.
Both providers have confirmed the approach to clinical prioritisation in line with national guidance regarding the timing and process of each review.
Work is also being undertaken in relation to primary care/patient centred communication to ensure members of the CCG's population continue to be well-
informed. Further assurance has been requested in relation to this.
The above is all now being undertaken in the context of the ICS being identified as an 'accelerator site' in relation to elective recovery. Work is ongoing to
develop a Planned Care Transformation Board, which will oversee the development and delivery of system-wide transformation plans relating to planned
care, cancer and diagnostics. It will also oversee the Elective and Outpatient Transformation Programme and achievement of Elective Recovery Fund (ERF)
gateways.
01/08/2021 ↔
RR130 Prioritisation and
Investment Committee
Commissioning May-20 COVID-19 may exacerbate health inequalities across the CCG's population if robust
processes are not in place to ensure the prompt restoration of services.
Commissioning
Ro
sa W
add
ingh
am
Lisa
Du
ran
t /
Haz
el B
uch
anan
4 4 16 • Restoration of services (led by the Capacity Cell); establishment of the Planned Care
Transformation governance;
• CCG's commissioning intentions/system planning priorities (System and Co-production
Framework);
• Prioritisation and Investment Committee (duties regarding health inequalities);
• Quality and Performance Committee (duties regarding equality of access);
• Various commissioning policies (e.g. Service Benefit Review, CHC, Service Restriction);
• ICS Outcomes Framework/performance metrics (work in progress).
Action(s):
• To work with system partners to strengthen the work around
health inequalities, learning from COVID-19, aligning to the
Outcomes Framework and future recovery and restoration plans;
capture data to inform future planning and service provision
• To continue the EQIA process during COVID-19 with continued
oversight of the impacts of service change to those people within
protected characteristic groups, particularly disability, those within
inclusion health, and other disadvantaged groups such as new
emerging and travelling communities, the homeless, and people
experiencing economic or social deprivation
• To ensure the oversight of health inequalities is integral to
routine quality assurance processes and business continuity
planning
Action: Development of PPEC effectiveness frameworks; greater
integration of public involvement and equalities, diversity and
inclusion (EDI) through the work of the EDI Steering Group and
delivery of a number of programmes of engagement that evidence
involvement across different stages of the commissioning cycle.
4 4 16 August 2021: Mitigations to this risk largely link to the work which is being undertaken described against risk RR 129 (refer to Quality and Performance
Committee risk); weekly monitoring of the CCG's backlog position is in place, which includes reporting to Quality and Performance Committee members.
Clinical prioritisation is the priority in addressing backlog. Work is also underway to analyse waiting lists through a deprivation and ethnicity 'lens' to help
inform understanding of health inequalities.
Addressing health inequalities is also a key element of the H1 2021/22 Planning Submission; five priority areas in relation to HI are outlined:
• Restore NHS services inclusively;
• Mitigate against digital exclusion;
• Ensure datasets are complete and timely;
• Accelerate preventative programmes which proactively engage those at greatest risk of poor health outcomes; and
• Strengthen leadership and accountability.
The H1 planning submission also outlines work being undertaken to expand primary care capacity to improve access, local health outcomes and health
inequalities. HI is included in the System Performance Dashboard to the ICS Board.
Work is ongoing to develop a Planned Care Transformation Board, which will oversee the development and delivery of system-wide transformation plans
relating to planned care, cancer and diagnostics. It will also oversee the Elective and Outpatient Transformation Programme and achievement of Elective
Recovery Fund (ERF) gateways.
The implementation of population health management and personalised care approaches are also key mitigations to this risk.
01/08/2021 ↔
RR151 Prioritisation and
Investment Committee
Commissioning Sep-20 There is a risk that the CCG may incur increased costs of service provision due to COVID
related requirements and the resulting reduction in productivity. This may manifest in
increased prices for services that the CCG seeks to procure in the future, as well as
increased costs to the NHS provider cost base.
This in turn would have a cost pressure on the system.
Commissioning
Lucy
Dad
ge /
Stu
art
Po
yno
r
Mar
k Sh
epp
ard
/ A
nd
rew
Mo
rto
n
4 4 16 • 2021/22 H1 Finance Plan; associated governance and reporting processes to monitor its'
delivery.
• Block payment arrangements in place for early 2021/22 with larger providers (short term
mitigation).
Action: Development of 2021/22 H2 financial plan based on
guidance (when received).
4 4 16 August 2021: 2021/22 planning submissions for H1 have been co-produced by system partners and submitted to Regulators. Contracts have been put in
place with the Independent Sector (IS) providers for 2021/22, however, the financial regime put in place during COVID continues for NHS providers. The
CCG and ICS have submitted a balanced financial plan for H1 2021/22; guidance is awaited in relation to H2.
H1 guidance focused on uplifts to historical costs and, due to a separate allocation being made for COVID costs, means that any change in costs of services
is either linked to inflationary costs, or for a specifically identified non-recurrent purpose, allowing it to be revised when COVID (e.g. IPC) mitigations are
reduced.
01/08/2021 ↔
RR156 Quality and Performance
Committee
Quality and
Governance
Nov-20 Lack of assurance regarding systematic improvements required in the quality of maternity
services provided by NUH, may present a risk of unsafe care, poor clinical outcomes
and/or patient safety issues for members of the CCG's population.
Quality
Ro
sa W
add
ingh
am
Dan
ni B
urn
ett
4 5 20 • Role and remit of the CCG's Quality and Performance Committee;
• Governance and oversight of NUH improvement programme: Maternity Oversight
Group; Committee reporting into Quality Assurance Committee and ultimately into NUH
Trust Board. CCG has strong links with all of these controlled meetings to minimise risk;
• Safe Today Programme;
• NUH Maternity Quality Assurance Group, co-chaired by NHS England and NHS
Improvement Regional Chief Nurse & the CCG Accountable Officer. Focus will be on the
progress of the Quality Improvement and the necessary actions in response to an
Inadequate CQC rating. An update will be provided at the next Quality & Performance
Committee;
• Daily NUH Maternity Safe Today Returns are completed with a Daily CCG/NUH Safe Today
call.
Action: To continue to work with NUH to seek assurance in relation
to the Assurance Assessment Tool; required as part of the
Ockenden Review (due to be submitted 15 February 2021)
Action: Safe Today Quality & Safety metrics to be reviewed as part
of Recovery & Restoration of the Quality Assurance function
Action: Safe Today dashboard to be expanded to include other
elements e.g. safeguarding, medicines safety, and comparative data
Action: NUH Next Steps 2020/21 Priorities for Maternity Quality
Improvement Projects.
5 5 25 August 2021: Terms of Reference for a proposed thematic review of NUH Maternity Services are being drafted. This review is due to be co-commissioned
by CCG and NHSEI.
The latest NUH Maternity Safety Oversight and Quality Assurance Group was held on the 9 July 2021 and an update on progress made by the Trust was
made. It was recognised that the pace of change needs to improve. The LMNS Shared Governance Group continues to support the Trust with the review of
Serious Incidents (SIs).
Work continues to develop a Maternity Improvement Plan by the Trust and a new Director of Midwifery has commenced in post. Recruitment is also
underway for a range of supporting leadership roles.
Daily NUH Safe Today calls are in place and mutual aid has been provided from neighbouring providers and system partners
01/08/2021
Current Risk
RatingInitial Risk Rating
NHS Nottingham and Nottinghamshire CCG Corporate Risk Register (August 2021)
Exec
uti
ve L
ead
Ris
k O
wn
er
Corporate R
isk Report
158 of 22409:00 - 10.50-04/08/21

Risk Ref Oversight Committee Directorate Date Risk
Identified Risk Description Risk Category Existing Controls Mitigating Actions Mitigating Actions Progress Update:
Last Review
DateTrend
(Relevant committee in
the CCG's governance
structure responsible for
monitoring risks relating
to their delegated duties)
(Date risk
originally
identified)
(These are operational risks, which are by-products of day-to-day business delivery. They
arise from definite events or circumstances and have the potential to impact negatively on
the organisation and its objectives.) Imp
act
Like
liho
od
Sco
re
(The measures in place to control risks and reduce the likelihood of them occurring).
(Actions required to manage / mitigate the identified risk. Actions
should support achievement of target risk score and be SMART (e.g.
Specific, Measurable, Assignable, Realistic and Time-bound). Imp
act
Like
liho
od
Sco
re (To provide detailed updates on progress being made against any mitigating actions identified. Actions taken should bring risk to level which can be
tolerated by the organisation).
(Movement
in risk score
since
previous
month)
Current Risk
RatingInitial Risk Rating
Exec
uti
ve L
ead
Ris
k O
wn
er
RR158 Finance and Resources
Committee
Finance and
Resources
Apr-21 The transition to system-led financial accountability, coupled with the continued
expectation that each constituent organisation achieves its statutory organisational
requirements, presents a potential risk that the CCG may not deliver its 2021/22 financial
duties (e.g. if individual organisation-led objectives for 2021/22 are not congruent with
system level objectives (and vice versa)).
This risk may be further exacerbated given the underlying, deficit position across the
system.
Finance
Stu
art
Po
yno
r
Mic
k C
awle
y /
An
dre
w M
ort
on
4 4 16 • Role and remit of the CCG Finance and Resources Committee; receipt and scrutiny of
monthly finance reports;
• Role and remit of the ICS Finance Committee (in development);
• H1 2021/22 Planning Submission;
• Transformation and Efficiency Plan.
Action: To deliver the Transformation and Efficiency Plan target of
£48 million (1.6% of system cost base)
Action: To agree system 'framework' for financial decision-making
Action: To develop and implement ICS governance arrangements
(e.g. the establishment of a robust ICS Finance Committee).
4 4 16 August 2021: The CCG, and the system, have submitted a balanced financial plan for the first six months of 2021/22 (known as H1). This is supported by
increased income due from the system's activity recovery trajectory (the elective recovery fund). The CCG is developing reporting processes to monitor
progress on activity recovery. The CCG's draft plan for H2 (prior to guidance being received) holds the system growth, but the system overall position is a
deficit.
An initial meeting of the ICS Finance Committee has taken place; further work is being undertaken as part of the Governance/Accountability workstream to
develop and implement transition governance arrangements, with support from the Chief Finance Officer and Operational Directors of Finance.
A draft ICS Finance Framework has been produced, which sets out the rules which govern the way finances are managed within the ICS (as identified as
best practice by the HfMA). This is due to be presented to the ICS Director of Finance Group imminently.
More specifically, the framework:
• describes the collaborative behaviours expected of the parties;
• describes processes for reaching consensus and resolving disputes about how best to use financial and other resources available to the ICS; and
• sets out a mechanism for management of the aggregate financial position of the parties to achieve and maintain the system financial improvement
trajectory for the ICS.
Work is also underway to develop a three-year financial strategy for the ICS.
01/08/2021 ↔
RR162 Quality and Performance
Committee
Quality and
Governance
May-21 A number of potential, and actual, complex and significant quality issues have been
identified at NUH.
Lack of assurance regarding systematic improvements in the quality of services provided
by the Trust may present a risk of unsafe care, poor clinical outcomes and/or patient
safety issues for members of the CCG's population.
Quality
Ro
sa W
add
ingh
am
Dan
ni B
urn
ett
4 4 16 • CCG led confidential NUH Internal Risk Register (April 2021);
• Role and remit of the CCG's Quality and Performance Committee;
• Safe Today Programme.
Action: To take appropriate action based upon the output of the
confidential NUH internal risk review.
4 5 20 August 2021: Further work has been undertaken to understand current challenges around culture and leadership, governance, quality of care, and
performance recovery and restoration.
Actions are being taken through Executive and ICS Forums, 'mock' internal CQC inspections and quality improvement programmes, Safe Today progress
and the development of a local Quality Schedule (to include dashboard metrics).
A focused discussion for NUH is scheduled for August 2021 CCG Quality and Performance Committee. An update on the activities undertaken will be
presented, including the system-wide support action plan. An assessment of the current risk score will be undertaken at this meeting.
01/08/2021 ↔
RR165 Finance and Resources
Committee
Finance and
Resources
Apr-21 There is a potential risk that H1 funding received by the system (for 2021/22) may not be
sufficient to address recovery of services for the CCG's population (e.g. meeting
planning/performance trajectories and addressing backlog).
Finance
Stu
art
Po
yno
r
Mic
k C
awle
y /
An
dre
w
Mo
rto
n
4 4 16 • Role and remit of the CCG Finance and Resources Committee; receipt and scrutiny of
monthly finance reports;
• Role and remit of the ICS Finance Committee (in development);
• H1 2021/22 Planning Submission.
Action: To submit a financial balanced plan for the ICS and CCG; and
then to manage delivery against the plan
Action: To ensure a robust oversight framework is in place for the
delivery of the activity required to meet the elective recovery fund
(ERF).
4 4 16 August 2021: The CCG, and the system, have submitted a balanced financial plan for the first six months of 2021/22 (known as H1). This is supported by
increased income due from the system's activity recovery trajectory (the elective recovery fund). The CCG is developing reporting processes to monitor
progress on activity recovery. Financial management and reporting processes are in place at system, and CCG, level to ensure delivery against the H1 plan
continues to be monitored.
In July 2021, it was announced that the Q2 thresholds for elective recovery will be increased from 85% to 95%, which would result in a reduction in
expected allocation (which was planned to fund recovery). The impact of this change is being worked through with ICS system partners, however, would
result in reduced income from the accelerator site (£13m for the system, c£700k for the CCG). As such, the likelihood of this risk has been increased from a
3 to 4, resulting in an overall score of 16.
01/08/2021
Corporate R
isk Report
159 of 22409:00 - 10.50-04/08/21

1
Minutes of the Nottingham and Nottinghamshire Patient and Public Engagement Committee
held virtually on Tuesday 25 May 2021 2 pm to 4 pm
Attendees; Sue Clague, Chair Chitra Acharya, Patient Leader/Carer Teresa Burgoyne, Nottingham West Michael Conroy, My Sight Nottinghamshire Kerry Devine, Improving Lives Gilly Hagen, Patient Leader/Sherwood Patient Participation Groups (from 3 pm) Amdani Juma, African Institute for Social Development Roland Malkin, Nottinghamshire Cardiac Support Group Paul Midgley, Rushcliffe (from 2.30 pm) Helen Miller, Healthwatch Nottingham and Nottinghamshire Daniel Robertson, Nottingham and Nottinghamshire Refugee Forum In attendance (NHS Nottingham & Nottinghamshire Clinical Commissioning Group’s Staff): Julie Andrews, Engagement Manager Alex Ball, Executive Team Representative Sasha Bipin, Engagement Officer Lucy Dadge, Executive Team Representative Lewis Etoria, Head of Insights and Engagement Karon Foulkes, Deputy Head of Children’s Commissioning Alex Julian, Mental Health Commissioning Manager Jane Hufton, Engagement Assistant (minute taker) Charlotte Reading, Deputy Head of Commissioning, Mental Health & Learning Disabilities Katie Swinburn, Engagement Officer Apologies for absence were received from; Jasmin Howell, Vice Chair Colin Barnard, Patient Leader/Diabetes Mike Deakin, Nottinghamshire County Council
NN/138/05/21 Welcome and introductions
Sue Clague welcomed everyone to the Nottingham and Nottinghamshire Patient and Public Engagement Committee (PPEC) meeting and extended a warm welcome to Lucy Dadge, Chief Commissioning Officer, representing the Executive team, Karon Foulkes, Deputy Head of Children’s Commissioning, Alex Julian, Mental Health Commissioning Manager and Charlotte Reading, Deputy Head of Commissioning, Mental Health & Learning Disabilities.
NN/139/05/21 Declarations of interest
Sue Clague reminded PPEC members of their obligation to declare any interest they might have on any issues arising at the meeting which might conflict with the business of the CCG and any items on this agenda. No declarations were made.
NN/140/05/21 Minutes of the last meeting
The minutes of the last PPEC meeting held on 27 April 2021 were agreed as an accurate record of the discussion that took place at that meeting.
Ratified Minutes of CCG Committee meetings
160 of 224 09:00 - 10.50-04/08/21
2
NN/141/05/21 Matters arising including Action Log
An updated copy of the Action Log had been circulated to PPEC members prior to the meeting and was noted. PPEC members confirmed that the actions marked as completed accurately reflected their status. A number of updates were provided as follows; NN/134/04/21 An issue was raised around barriers to accessing services due to financial poverty and a request made for this to be raised with the Equality, Diversity and Inclusion Steering Group (EDI) with a view to being included in the Equality Inclusion and Assessment Impact (EQUIA) template. Julie Andrews confirmed that this was already included within the EQUIA which considers the impact on people experiencing economic or social deprivation. NN/132/04/21 Julie Andrews confirmed that some of the dates for conversations on community services had been changed to take place outside of Purdah. Two sessions had taken place attended by almost 50 people and further sessions are scheduled for 3, 9 and 14 June 2021. Work is ongoing to plan citizen engagement and a further update will be provided to PPEC. NN/130/04/21 Spare capacity amongst St Johns Ambulance vaccinators had been highlighted to the workforce lead for the vaccination programme who had confirmed that the programme currently had sufficient volunteers. There is a challenge of securing sufficient registered clinical professionals, but unfortunately these are not available through St John’s Ambulance. NN/115/03/21 Concerns remain around the approach to FGM support to women attending appointments. An interim response to this issue had been provided by the CCGs Chief Nurse and further information would be shared in due course. Julie Andrews provided an update on the outstanding actions as detailed below: NN/132/04/21 Community Services Transformation Programme -Community care
is one of the three specific programmes of work that will be the focus of the ICS Outcomes Framework and measure the system’s efforts to transform and make a difference to healthy life expectancy and other health and care outcomes over the next year. Detailed engagement plans will be developed to support the three projects and will be shared with PPEC. A further update will be provided in June 2021. NN/82/11/20 Platform One Practice – A PPEC Effectiveness template had been
completed for this programme of work and would be presented to PPEC in July 2021 following the transfer of patients from Platform One Practice. MNGN/32/20 Patient Experience Team (PET) - PPEC members were reminded that
any individual instances of vulnerable people being unable to access health and care services could be raised with the PET. Julie Andrews would be pleased to provide any assistance required to access the PET.
NN/142/05/21 Children and Young People’s Weight Management Service
Copies of a paper entitled Listening to and Engaging Children, Young People and Families on Weight Management Services together with a copy of the Children’s
Ratified Minutes of CCG Committee meetings
161 of 22409:00 - 10.50-04/08/21

3
Weight Management Engagement Plan had been circulated to PPEC members prior to the meeting. Karon Foulkes, Deputy Head of Children’s Commissioning, informed members that a gap in services had been identified by the Integrated Care System for those Children and Young People (CYP) with severe obesity. Severe obesity has been increasing in CYP by 1.3% a year. Local data shows Nottingham City is significantly higher than the national average at age 5-6 (reception) and 10-11 (year 6). Nottinghamshire is average or significantly lower. There is a correlation between deprivation and severe obesity but in the city there is also a significantly higher ratio of severe obesity for those from Mixed, Black and Asian ethnicity compared to the national ethnicity ratio. There is also a significant growing gap in rates of severe obesity for boys compared to girls. Currently children and young people (CYP) who are overweight or obese are funded through each Local Authorities (LA’s) public health services (Tier 1 and Tier 2 services). Children with severe obesity and comorbidities are seen by the relevant service in the acute in the department relating to their comorbidity e.g. endocrinology (Tier 3/4 services). There is a gap in service provision for CYP who are severely obese without comorbidities (Tier 3). Nottingham and Nottinghamshire CCG therefore need to scope the level of need, align pathways and engage the key stakeholders including CYP and their families in ensuring the CCG’s Tier 3 responsibilities are fulfilled. The information collated will also be used by the Nottingham University Hospitals (NUH) service as they prepare to become a regional hub for children for the treatment of complications related to excess weight (CREW). Sasha Bipin, Engagement Officer presented the Children’s Weight Management Engagement Plan that promoted engagement via existing weight management services for children up to the age of 18, parents and carers and professionals. The engagement approach includes use of surveys and virtual focus groups to capture opinions and views of these groups. The engagement would commence on 1 July and conclude on 30 July 2021 with a report to be available to commissioners in September 2021. PPEC members were invited to review and provide comment on the engagement plan by 28 May 2021 to inform delivery of this work programme. PPEC members welcomed the Engagement Plan. PPEC members participated in an engaging discussion and provided advice regarding engagement to support development of a Tier 3 weight management services for children and young people who are severely obese emphasising the need for an integrated approach. The Association for Young People’s Health have already completed a piece of work identifying barriers, links and solutions and it was suggested this be reviewed to inform this programme of work. The link to this work is [email protected]. PPEC members noted that this is a very sensitive and difficult issue to discuss with children and young people that should be approached with empathy. Sasha Bipin confirmed that resources to be used would be piloted with children and young people prior to the launch of the engagement. Discussion took place about broader public health interventions to begin to address the root cause of obesity. It was agreed that a preventative programme update should be included on a future PPEC agenda.
Ratified Minutes of CCG Committee meetings
162 of 224 09:00 - 10.50-04/08/21

4
Action: Sasha Bipin and Karon Foulkes to review work carried out by the Association for Young People’s Health. Action: PPEC members to provide comments on the Children’s Weight Management Engagement Plan to Sasha Bipin by 28 May 2021. Action: Julie Andrews to include a preventative programme update on PPEC forward programme.
NN/143/05/21 Patient and Public Engagement Annual Report
The PPEC Engagement Annual Report had been circulated to PPEC members prior to the meeting. Lewis Etoria, Head of insights and Engagement thanked PPEC members for their input and feedback that had been used to strengthen the commentary particularly around the impact of engagement. The report would be published online in June 2021. Sue Clague confirmed that the report presented was a much better iteration and something PPEC were proud of. Action: Engagement Team to circulate the link to access the Annual Report following its publication online.
NN/144/05/21 Platform One Practice Mobilisation/Transitional Arrangements
Copies of resources developed to support patients facing severe multiple disadvantage (SMD) and asylum seekers and refugees patients who would transfer from Platform One Practice had been circulated to PPEC members prior to the meeting. Lewis Etoria, Head of Insights and Engagement gave an update on the progress of the transition and confirmed that the resources had been developed with stakeholders. A credit card sized concertina leaflet would be available in the four most commonly spoken languages; Farsi, Tigrinya, Kurdish Sorani and Polish. Lucy Dadge, Chief Commissioning Officer confirmed that the Health Scrutiny Committee had a continued interest in this transition and had requested assurances regarding how the SMD enhanced service was benefitting patients and systems used to highlight patients with specific needs. Lewis Etoria agreed to present the PPEC Effectiveness Framework at the meeting in July following the transfer of patients from Platform One Practice. Action: Julie Andrews to add the Platform One Practice PPEC Effectiveness Framework to PPEC forward programme for July 2021.
NN/145/05/21 Covid Update
Alex Ball, Director of Communications and Engagement for the CCG and ICS gave an update on the Covid 19 vaccination programme and provided an overview of case rates. Increasing levels of social contact would lead to an increase in case rates and this would be monitored closely. Presently, rates in Nottingham and Nottinghamshire
Ratified Minutes of CCG Committee meetings
163 of 22409:00 - 10.50-04/08/21
5
are in line with the England average. There is a low level of bed occupancy for Covid patients in our hospitals. Further information regarding the vaccination programme was shared as follows:-
Eligibility for vaccination is moving down through the age groups with appointments opened up to anyone over 32 years of. Appointments can be booked by calling 119 or booking online through the National Booking Service
860,443 vaccinations had been administered between 8 December 2020 and 16 May 2021 and 320,789 second doses of the vaccine had been administered.
Incredibly good coverage of locations where people can have their vaccine including main sites, pharmacies, pop-up clinics mobile bus and hospital hubs.
Anyone over the age of 40 years can walk into any of the centres below to receive their first vaccination without booking an appointment. - Forest Recreation Ground - Kings Meadow Campus - Gamston Community Centre - Ashfield Health Village - Newark Showground - Richard Herrod Centre - Mansfield Vaccination Centre (former Wickes site)
Over the next week there will be a focus on Nottingham City to increase uptake.
Information was shared about the process for anyone over the age of 50 to have an 8 week gap between first and second dose of the vaccine. Patients would be contacted regarding this.
PPEC members referred to the opportunity to promote the functionality and benefits of the NHS App alongside using it as a record of Covid vaccination status. Alex Ball advised that it was difficult to promote due to it not being available across all practices. Concerns were raised about people with older operating systems on mobile devices having to contact their GP practice in relation to the technical aspects of the NHS App and this was impacting heavily on GP practices. With regard to accessing vaccination status PPEC members were reminded of the option to request this via 119. Sue Clague requested an update from Connected Notts on digital solutions and the NHS App be provided at a future PPEC meeting. There was some positive feedback regarding the vaccination bus in that it had been really helpful to clients of Nottingham and Nottinghamshire Refugee Forum many of whom had received their vaccination on the bus. There is no online booking system and this is so helpful to people who may be struggling with language barriers. Action: Julie Andrews to add to PPEC Forward Programme an update of the NHS App and digital solutions from Connected Notts.
NN/146/05/21 Dementia Well Pathway
Information regarding the Nottingham and Nottinghamshire Dementia Well Pathway had been circulated to PPEC members prior to the meeting.
Ratified Minutes of CCG Committee meetings
164 of 224 09:00 - 10.50-04/08/21

6
Alex Julian, Mental Health Commissioning Manager explained the aim of the review is to ensure future provision of services for patients with Dementia and their families is personalised, integrated, equitable, timely and meets the needs of those living with Dementia throughout their journey. There are two key objectives:
Co-create a Dementia Strategy
Develop recommendations for future commissioning of dementia care services for consideration by the CCGs Prioritisation and Investment Committee.
In order to fully understand patient, carers and health and care professionals experience of the pathway, a variety of engagement activities would commence from 17 May (Dementia Awareness Week) to the 16 July 2021. These are listed below.
A Dementia survey tailored to patient, carer and health and care professionals
Workshops
1:1 interviews
Attendance at local Dementia friendly café’s and activities.
A particular focus of the engagement will be on understanding experience of; - The post-diagnosis pathway - The impact of the pandemic - People from ethnically diverse communities
A pathway review group has been operating since January 2021 and has advised on the engagement plan. The group comprises of key stakeholders including two carer’s with lived experience of caring for someone living with Dementia. Alex Julian welcomed PPEC member’s support, feedback, comments and challenges on how improvements could be made. Katie Swinburn reported that over 120 surveys had already been completed. It was agreed that the Communications and Engagement Plan would be shared with members after the meeting and comments requested. PPEC members welcomed the programme and shared their thoughts and comments regarding the Dementia well pathway and suggested adding in a process of screening patients before they show signs of dementia. Alex Julian responded that there would need to be a really strong evidence base for screening and this would be determined nationally. There was a query about using the NHS app as a patient facing tool for screening and Alex Julian confirmed he would raise this at the next meeting of the Dementia Steering Group. Clarification was requested regarding the current waiting times for a dementia diagnosis. Alex Julian confirmed this currently was 7.2 weeks. Last year the waiting times had been significantly higher at 40+ weeks in some areas. As part of the engagement commissioners would like to understand if citizens would like to be offered support pre-diagnosis. Nottinghamshire Healthcare Trust would also begin to report on the referral to diagnosis rates. With regard to engagement, a query was raised regarding the steps and monitoring that would take place to ensure responses are received from ethnically diverse communities. Katie Swinburn, Engagement Officer, confirmed that there would be a
Ratified Minutes of CCG Committee meetings
165 of 22409:00 - 10.50-04/08/21

7
concerted effort to engage as widely as possible and data gathered would include a mix of both quantitative and qualitative data. A query was raised around extending the timescale of the engagement programme in order to be able to include face to face meetings with groups. It was confirmed that the timescale was aligned to the reporting to the Prioritisation and Investment Committee at the end of August. PPEC members suggested engagement with a range of groups that would be followed up. Action: Schedule an update on the Dementia Well Pathway on the PPEC Forward Programme for September 2021. Action: Katie Swinburn to share the Communication and Engagement Plan with PPEC members after the meeting. Action: PPEC members to support the cascade of information on the Dementia Well Pathway amongst their groups and networks.
NN/147/05/21 Equality, Diversity & Inclusion Steering Group Feedback
Lewis Etoria, Head of Insights and Engagement, advised that the Equality, Diversity & Inclusion (EDI) Steering Group had not met recently and therefore no further update was available. Sue Clague requested assurance that the group was not losing momentum. Lewis Etoria confirmed that there is an absolute commitment to progressing Equality, Diversity and Inclusion within the organisation. It was confirmed that the frequency of the meetings had changed from monthly to quarterly. PPEC members were reminded that Lucy Branson and Rosa Waddingham would be attending the next meeting to give an update on equality, diversity and inclusion. Lucy Dadge referenced how the vaccination programme had provided insight about how to access the population more equitably and had provided much learning to build upon in the future. PPEC members considered the concept of the bus to be a good one in that it provided targeted access to services and suggested that this could provide a model for the future as a way of delivering targeted programmes of work.
NN/148/05/21 Governing Body Feedback & Key Messages from PPEC
Sue Clague reported that a Governing Body development session had taken place on 7 April 2021. The development session had focused on ICS transition and overall system design that would incorporate an ICS NHS Board and ICS Health & Care Partnership. Sue Clague summarised the key messages arising from the PPEC meeting to highlight at the next Governing Body Meeting in June 2021 as;
1. PPEC members had participated in an engaging discussion and provided advice regarding engagement to support development of a Tier 3 weight management services for children and young people who are severely obese emphasising the need for an integrated approach. Broader health prevention strategies were also discussed and it was agreed to schedule a preventative
Ratified Minutes of CCG Committee meetings
166 of 224 09:00 - 10.50-04/08/21

8
programme update on a future PPEC agenda.
2. Advice was provided by PPEC members to support the engagement that would inform the strategy and commissioning of the Dementia Well Pathway. The importance of listening to the voices of both patients and carers with lived experience and future service users was emphasised. It was suggested that consideration be given to extending the timeline for engagement to provide opportunity to undertake more engagement in person post 21 June 2021 that should see the possible easing of Covid restrictions.
NN/149/05/21 Any Other Business
There were no items for discussion.
NN/150/05/21 Date of Next Virtual Meeting
The next PPEC meeting will be held virtually on Tuesday 29 June 2021 from 2 pm to 4 pm.
Ratified Minutes of CCG Committee meetings
167 of 22409:00 - 10.50-04/08/21

1
Minutes of the Nottingham and Nottinghamshire Patient and Public Engagement Committee
held virtually on Tuesday 29 June 2021 2 pm to 4 pm
Attendees; Sue Clague, Chair Chitra Acharya, Patient Leader/Carer Teresa Burgoyne, Nottingham West Michael Conroy, My Sight Nottinghamshire Kerry Devine, Improving Lives Gilly Hagen, Patient Leader/Sherwood Patient Participation Groups arrived at 3 pm Amdani Juma, African Institute for Social Development Roland Malkin, Nottinghamshire Cardiac Support Group Paul Midgley, Rushcliffe - until 2.30 pm Helen Miller, Healthwatch Nottingham and Nottinghamshire In attendance (NHS Nottingham & Nottinghamshire Clinical Commissioning Group’s Staff): Julie Andrews, Engagement Manager Alex Ball, Director of Communications and Engagement Diane Carter, Clinical Integrator Mid-Nottinghamshire Integrated Care Partnership Dr. James Hopkinson, Executive Representative Jane Hufton, Engagement Assistant (minute taker) Nichola Reed, Public Health and Commissioning Manager Children’s Integrated Commissioning Hub and Public Health Nottinghamshire Jane Hildreth, Community Voluntary Sector representing Mid Nottinghamshire ICP area Jules Seblin, Community Voluntary Sector representing City ICP area Carolyn Perry, Community Voluntary Sector representing South Nottinghamshire ICP area Apologies for absence were received from; Jasmin Howell, Vice Chair Daniel Robertson, Nottingham and Nottinghamshire Refugee Forum Lewis Etoria, Head of insights and Engagement Colin Barnard, Patient Leader/Diabetes Mike Deakin, Nottinghamshire County Council
NN/151/06/21 Welcome and introductions
Sue Clague welcomed everyone to the Nottingham and Nottinghamshire Patient and Public Engagement Committee (PPEC) meeting and extended a warm welcome to Dr. James Hopkinson, Joint Chair of the CCG and Executive Team representative. Sue Clague also welcomed new members of PPEC representing the Community and Voluntary Sector, Jane Hildreth, Jules Seblin, Carolyn Perry. Sue Clague informed PPEC member that the next meeting would be Lewis Etoria’s last as he is due to join the Yorkshire Ambulance Service as the Engagement Lead. Lewis Etoria would be missed by PPEC members.
NN/152/06/21 Declarations of interest
Sue Clague reminded PPEC members of their obligation to declare any interest they might have on any issues arising at the meeting which might conflict with
Ratified Minutes of CCG Committee meetings
168 of 224 09:00 - 10.50-04/08/21

2
the business of the CCG and any items on this agenda. No declarations were made.
NN/153/06/21 Minutes of the last meeting
The minutes of the last PPEC meeting held on 25 May 2021 were agreed as an accurate record of the discussion that took place at that meeting.
NN/154/06/21 Matters arising including Action Log
An updated copy of the Action Log had been circulated to PPEC members prior to the meeting and was noted. PPEC members confirmed that the actions marked as completed accurately reflected their status. Julie Andrews provided an update on key outstanding actions as detailed below: NN/133/04/21 Identification of a PPEC member to join a Community Diagnostic Hub Working Group had been paused whilst clarification of funding was secured. NN/133/04/21 The development of an engagement plan in relation to Community Diagnostic Hubs had also been paused whilst clarification of funding was secured. NN/130/04/21 With regard to the action regarding long waiting lists that had arisen as a consequence of the pandemic, Lisa Durant and Andrea Collis from Nottingham and Nottinghamshire Clinical Commissioning Group (CCG) hoped to attend the next meeting to provide an update.
NN/155/06/21 Developing Community Engagement for the ICS
Copies of a paper entitled Developing Community Engagement for the Integrated Care System (ICS) had been circulated to PPEC members prior to the meeting. Alex Ball explained the Government’s White Paper: Integration and innovation; working together to improve health and social care sets out legislative intentions for the future of Health and Care Systems for England. It was noted that changes within the Department of Health and Social Care had led to a slight adjustment to the timetable for the Bill to be presented to Parliament. Overall the timeframe remained the same for implementation from April 2022. The key ambition is to establish in law Integrated Care Systems (ICSs) bringing together partners to improve health and care for citizens. The recently published design framework sets out 7 key principles for citizen engagement moving forward;
1. Use of public engagement and insight to inform decision making 2. Redesign models of care and tackle system priorities in partnership with staff,
people who use care and support and unpaid carers 3. Work with Healthwatch and the voluntary, community and social enterprise
sector as key transformation partners 4. Understand your community’s experience and aspirations for health and care 5. Reach out to excluded groups, especially those affected by inequalities 6. Provide clear and accessible public information about vision, plans and
progress to build understanding and trust 7. Use community development approaches that empower people and
communities, making connections by social action.
Ratified Minutes of CCG Committee meetings
169 of 22409:00 - 10.50-04/08/21

3
The local approach to deliver the above key principles will focus on: 1. Governance 2. Embedding community engagement 3. Generating and using intelligence from communities 4. Integrating community involvement work and resources across the ICS 5. Developing a culture that enables good quality community involvement to be
embedded Alex Ball invited PPEC members to comment on the local plans. PPEC members suggested the inclusion of co-production in pathway development involving citizens and professionals. Alex Ball advised that Rosa Waddingham, Chief Nurse for the CCG was leading on co-production within the CCG. Co-production through involvement in design work and community development are separate activities but they do interrelate. Citizen intelligence will enable the ICS to learn what is important to citizens – a co-creation approach will inform the approach to this and co-production will support development of solutions together with citizens and professionals. Three important elements that should be referenced in the development of plans for engagement. The Engagement Team are undertaking some preparatory work including mapping of citizen engagement across the health and care system and planning a series of workshops to take place over the summer to refine plans for engagement. Further information and an invitation will be provided to PPEC members in due course. Action: Engagement Team to invite PPEC members to workshops. It was noted that August should be avoided for workshops due to holiday commitments. Action: Schedule regular updates on engagement and transition to ICS in PPEC’s forward programme.
NN/156/06/21 Covid Update
Alex Ball, Director of Communications and Engagement shared the latest information on the Covid Vaccination Programme. Alex Ball reported that case rates are rising rapidly across Nottingham and Nottinghamshire. This is a real concern and translating into admissions to hospitals, 17 over the past week and patients are remaining in hospital longer for longer. Overall the vaccination programme is weakening the link between hospitalisation and death. This reinforces the need to vaccinate as many people as possible before 19 July, the proposed date for easing of all restrictions. The Nottingham and Nottinghamshire CCG are promoting the ‘Big Weekend’ of walk-in vaccinations. Anyone over the age of 18 who has not received their 1st vaccination or 2nd dose of the vaccination (after 56 days of receiving their 1st dose) can walk into any of the 9 centres currently administering the vaccination. Patients may book a vaccination appointment via NHS Booking Link or by calling 119. The message is to have your vaccination. Further clarification regarding Phase 3 of the vaccination programme is awaited in relation to booster doses in the Autumn along with vaccinating the12–17 year age group. PPEC members discussed a saliva Covid test that is being piloted. Michael Conroy confirmed that MySight Nottinghamshire is part of this pilot and the University of Nottingham would be interested in involving other groups who wish to take part. Gilly
Ratified Minutes of CCG Committee meetings
170 of 224 09:00 - 10.50-04/08/21

4
Hagen agreed to contact Michael Conroy outside of the meeting regarding this. Alex Ball concluded by informing PPEC members that community briefings had been scheduled to take place through to the Autumn.
NN/157/06/21 VSA Contract Mid Nottinghamshire Focus
Copies of a presentation entitled Voluntary Sector Alliance (VSA) Contract Update Mid Nottinghamshire ICP Focus had been circulated to PPEC members prior to the meeting. Diane Carter, Clinical Integrator Mid-Nottinghamshire Integrated Care Partnership (ICP) shared information about the Mid Nottinghamshire ICP vision, objectives and associated breakthrough objectives. In relation to the VSA contract delivery related to objectives that would;
1.1 Build on the integration across the Primary Care Networks (PCNs) building on community asset based services that include the voluntary sector, care homes and care in the community settings.
2.1 Improve the connection and integration of the voluntary sector and current health and social services available to build effective services that support alcohol, diabetes, cancer, EOL and joint and bone pain (MSK). Diane Carter informed PPEC members that monthly meetings were taking place with Mid Nottinghamshire Community Voluntary Sector colleagues to support prioritisation of work aligned to ICP objectives. Key programmes of work delivered to date include;
Recovery Engagement seeking out insight from the most vulnerable
Diabetes and Learning Disabilities engagement
End of life and musculo skeletal pathway development
Support for the Covid Vaccination Programme
Membership of the Integrated Care Partnership (ICS) Board.
Diane Carter reported on close working with the Primary Care Networks looking at inequalities within the most deprived areas of Mid Nottinghamshire to ensure that citizens are at the heart of service design and development, and to identify opportunities to support communities to stay well and healthy. Sue Clague referred to the high levels of deprivation and impact on health and asked how this was being addressed. Diane Carter advised that detailed population health management data is being used to identify priority communities and engagement would take place with those communities to understand their issues and how they could be addressed. PPEC members challenged Mid Nottinghamshire ICP to accelerate this area of work. PPEC members highlighted the need to also focus on early intervention and mental health services as they were not explicit within the ICP objectives. Amdani Juma advised isolation may be experienced by ethnically diverse communities due to lower numbers across Mid Nottinghamshire and asked what steps are being taken to engage with these communities and support access to services that may previously have been accessed in Nottingham City. Diane Carter confirmed that there is a need to understand via community engagement access issues relevant to
Ratified Minutes of CCG Committee meetings
171 of 22409:00 - 10.50-04/08/21
5
ethnically diverse communities to develop solutions and agreed to progress this through the Mid Nottinghamshire Health Inequalities Group. PPEC members and CVS organisations across Nottingham and Nottinghamshire offered support to progress engagement. Julie Andrews confirmed that a recent workshop had taken place with all Voluntary Sector Alliance (VSA) partners which includes Ashfield Voluntary Action, Mansfield CVS, Newark and Sherwood CVS, Nottingham CVS and Rushcliffe CVS and the programme Directors for all ICPs to look at priority objectives for 2021/22. The outcome of the session was for VSA partners to use the information provided to confirm their priorities and develop a work plan for year 2021/22. The VSA partners also agreed to review reporting arrangements and to present a plan to the CCG by 19 July 2021. Action: Diane Carter to follow up engaging with ethnically diverse communities through the Mid Nottinghamshire Health Inequalities Group.
NN/158/06/21 Platform One Practice Transitional Update
Julie Andrews reminded PPEC members that a Stakeholder Group had been meeting regularly to support the Platform One Practice mobilisation and transitional arrangements. As part of its work, the group has advised on the development of appropriate resources and the content to support communities facing severe multiple disadvantage and asylum seekers and refugees. This information had been shared at the last meeting. Julie Andrews confirmed that Lewis Etoria would share the PPEC Effectiveness Framework at the next PPEC meeting following the transfer of patients from Platform One Practice. Action: Include Platform One PPEC Effectiveness Framework on the agenda for the next PPEC meeting on 27 July 2021.
NN/159/06/21 Children and Young People’s Mental Health Pathway
Copies of the Children and Young People’s Emotional Wellbeing Early Support, Training and Consultation Service Update Report had been circulated to PPEC members prior to the meeting. Nichola Reed advised that a full report would be shared with PPEC members following sign off and in the interim provided highlights as follows;
Following engagement events, commissioners have used feedback, along with review of the evidence base and national best practice and clinical involvement to develop the model.
It has been determined that a lead provider model utilising VCSE is the preferred model to address current challenges and improve outcomes and experience
A service specification, key performance indicators and outcomes have been developed
Tender is currently live – closing date 16th July 2021
Procurement timeframe has been extended – new service will go live 1st April 2022
Current services will continue to ensure support is available
Ratified Minutes of CCG Committee meetings
172 of 224 09:00 - 10.50-04/08/21

6
The service specification has been informed by engagement findings and MH:2K Citizen Researchers. A response to key themes arising from engagement are detailed below:
1. Raising awareness of services available including advertising on Notts Help Yourself and Ask Lion
2. Offering flexible support and delivering this from community locations across Nottingham City and Nottinghamshire County with face to face, online and digital options. Easy access to advice and guidance, self-help and self-guided help, drop in sessions, online support, face to face therapeutic support, group work and peer support groups
3. Offering more immediate support including instant access, eg. online counselling and resources, self-help/self-guided help and advice and guidance
4. Considering varying needs between people in the City and County including ease of access
5. Enabling children and young people to assist in the delivery of training to professionals where appropriate
6. Providing greater support for parent and carers including easy access to advice and guidance, self-help, online resources, self-referral, development of support networks, holistic assessment of need including emotional wellbeing and signposting on onward referral to alternative support where required
7. Providing greater communication to and involvement of parent and carers Implementing a clear and simple referral pathway
8. Providing greater training and support for staff including GPs, Schools/further education, 0-19 services and social care.
9. Promoting and encouraging greater partnership working between services which will form part of the CYP mental health system.
Nichola Reed concluded with a reminder of the next steps of the tender process. Ongoing engagement with children and young people, parents and carers will continue through the service mobilisation phase and beyond in relation to ongoing service developments. In response to a question, Nichola Reed confirmed that Equality Impact Assessments (EQIAs) had been undertaken and would continue to be undertaken at various checkpoints throughout this programme of work. Nichola Reed reported that a communication group had been established to refresh information developed by children and young people themselves and additional information would be produced regarding waiting times. Sue Clague welcomed the assurances provided regarding managing the transition and ensuring immediate actions were being taken forward in relation to communication. Action: Nichola Reed to share full report with PPEC members.
NN/160/06/21 Equality, Diversity & Inclusion Steering Group Feedback
Julie Andrews reported that the last Equality, Diversity and Inclusion (EDI) Steering Group had taken place on 17 June 2021. Key agenda items related to;
Draft Equality Improvement Plan (including equality objectives)
Ratified Minutes of CCG Committee meetings
173 of 22409:00 - 10.50-04/08/21

7
Cultural Competence Programme – Update
Staff networks and training
The next meeting would take place on 16 September 2021. PPEC members were reminded that Rosa Waddingham and Lucy Branson would be attending the next PPEC meeting to provide an update on equality, diversity and inclusion.
NN/161/06/21 Governing Body Feedback & Key Messages from PPEC
Sue Clague provided feedback from the last Governing Body meeting held on 2 June 2021 as follows;
Discussion had taken place regarding outcomes of CQC inspections at Nottingham University Hospitals Trust and Nottinghamshire Healthcare Trust. Improvement plans are in place for both providers.
For the period April-September 2021 ‘H1’, financial balance had been reported upon.
A deterioration in waiting times for elective procedures was reported. PPEC had requested an update on objective management plans to address this.
Pre-engagement for Reshaping Health Services Across Nottinghamshire was expected to recommence towards the end July.
Sue Clague summarised the key messages from PPEC to highlight at the next Governing Body Meeting as follows;
1. PPEC members welcomed the development of plans to support community
engagement as part of ICS transition. Links to co-production should be referenced in the plans.
2. The Mid Nottinghamshire Voluntary Sector update was welcomed and the need to focus on deprivation and ethnically diverse communities who may be isolated geographically was highlighted by PPEC members.
3. The children and young people engagement provided an excellent example of co-production in service transformation. Immediate improvements had also been achieved through provision of better communication resources.
NN/162/06/21 Any Other Business
There were no items for discussion.
NN/163/06/21 Date of Next Virtual Meeting
The next PPEC meeting will be held virtually on Tuesday 27 July 2021 from 2 pm to 4 pm.
Ratified Minutes of CCG Committee meetings
174 of 224 09:00 - 10.50-04/08/21
Page 1 of 9
NHS Nottingham and Nottinghamshire Clinical Commissioning GroupQuality and Performance Committee
Ratified minutes of the meeting held on27/05/2021 9:00-12:00
MS Teams Meeting
Members present:
Eleri de Gilbert Non-Executive Director (Chair)Sue Clague Non-Executive Director Jon Towler Non-Executive DirectorStuart Poynor Chief Finance OfficerAndy HallRosa Waddingham
Associate Director of Performance and InformationChief Nurse
Hazel Buchanan Associate Director of Strategic Programmes & EPRRCommissioningDanni Burnett Deputy Chief Nurse
Lisa Durant Director of Commissioning - Mid NottinghamshireCaroline Nolan System Delivery Director- Urgent CareDr Manik Arora GP RepresentativeDr Hilary Lovelock GP RepresentativeDr Richard Stratton GP Representative
In attendance:
Lucy Anderson (Deputising for Maxine Bunn)Rhonda Christian Assistant Director of Nursing & Safeguarding (Item QP 21 034)Lewis Etoria Head of Insights and Engagement (Item QP 21 035)Louise Espley Corporate Governance Officer (minutes)Jo Simmonds Head of Corporate Governance
Apologies:
Mindy Bassi Chief PharmacistSian Gascoigne Head of Corporate AssuranceMaxine Bunn Associate Director of Commissioning, Contracting and Performance
– Mental Health and Community
Ratified Minutes of CCG Committee meetings
175 of 22409:00 - 10.50-04/08/21

Page 2 of 9
Cumulative Record of Members’ Attendance (2021/22)
Name Possible Actual Name Possible Actual
Dr Manik Arora 02 02 Eleri de Gilbert 02 02
Mindy Bassi 02 0 Andy Hall 02 02
Hazel Buchanan 02 02 Dr Hilary Lovelock 02 02
Maxine Bunn 02 0 Caroline Nolan 02 02
Danni Burnett 02 02 Stuart Poynor 02 02
Lisa Durant 02 02 Dr Richard Stratton 02 02
Sue Clague 02 02 Jon Towler 02 02
Rosa Waddingham 02 02
Introductory Items
QP 21 021 Welcome and Apologies
Eleri de Gilbert welcomed members to the Quality and Performance Committee meeting which was held on MS Teams due to the current Covid-19 situation.
Apologies were noted as above.
QP 21 022 Confirmation of Quoracy
The meeting was confirmed as quorate.
QP 21 023 Declaration of interest for any item on the shared agenda
Dr Richard Stratton has an interest relating to NUH as he is an employee. This is on the Committee’s Register. The conflict is noted in relation to items:-
∑ QP/21/027 – Nottingham University Hospitals NHS Trust (NUH) Deep Dive
∑ QP/21/028 – NUH Maternity Confidential Update
∑ QP/21/030 – Integrated Performance Report
∑ QP/21/036 – Risk Report
The Chair reminded members of their responsibility to highlight any interests should they transpire as a result of discussions during the meeting.
QP 21 024 Management of any real or perceived conflicts of interest
For item QP/21/027 the agreed management action is that Dr Richard Stratton is excluded from the meeting and has not received the paper.
For items QP/21/028 and QP/20/030, the agreed management action is for Dr Stratton to remain in the meeting and participate on matters of fact. However it does need stressing that item QP/21/028 is confidential and not to be shared outside of the meeting.
Ratified Minutes of CCG Committee meetings
176 of 224 09:00 - 10.50-04/08/21

Page 3 of 9
For item QP/21/036 the proposed management action is that Dr Richard Stratton is excluded from the meeting for the discussion of the NUH risk. He had received a redacted version of the paper.
QP 21 025 Minutes from the meeting held on 22 April 2021
The minutes were agreed as an accurate record.
QP 21 026 Action log and matters arising from the meeting held on 22 April 2021
All actions were noted as complete, on the agenda for the meeting or planned for a future meeting and there were no matters arising.
Nottingham University Hospitals NHS Trust (NUH)
QP 21 027 NUH Deep Dive Review
Dr Richard Stratton left the meeting for this item.
Item redacted
QP 21 028 NUH Maternity Confidential Update
Item redacted.
Quality and Performance
QP/21/029 Nursing and Quality Quarterly Report
Danni Burnett presented the item and highlighted the following points:
a) The report for quarter four draws together key quality and safety metrics for NHS commissioned services across Nottingham and Nottinghamshire. The report also included a revised CCG Safeguarding Strategy for endorsement.
b) There is a transition from ‘safe today’ to a systems approach in terms of quality planning, quality control and quality improvement. During this year of transition, the importance of keeping a focus on the CCG’s statutory duties remains paramount.
c) The highest reporting incidents across the patch relate to: pressure ulcers, maternity and self-harm incidents.
d) Outbreak information was included in the report, particularly the learning from Covid-19. There are currently zero outbreaks.
e) Sherwood Forest Hospitals NHS Foundation Trust (SFT) was commended for their success at the recent Health Service Journal (HSJ) awards.
f) Nottinghamshire Healthcare NHS Foundation Trust (NHT) had received a number of CQC inspection reports. The Wells Road Centre report concluded that services ‘require improvement’. In addition, the Priory Arnold Hospital received an ‘inadequate’ rating. The CCG Quality and Commissioning teams are working closely with the Trust to monitor and support improvements across both services.
g) Attention was drawn to a matter of factual accuracy in relation to the CQC status
Ratified Minutes of CCG Committee meetings
177 of 22409:00 - 10.50-04/08/21

Page 4 of 9
of NurtureCare. The July 2020 report had stated Nurture Care had a CQC rating of requires improvement, this was an administrative error and the actual rating was ‘Good’.
The following points were made in discussion:
h) The Committee members raised concerns regarding performance at NHT and noted that the June 2021 meeting would focus on a report following a deep dive at this Trust.
The Quality and Performance Committee:
∑ RECEIVED and NOTED the report, APPROVED the ACTIONS andENDORSED the Safeguarding Strategy.
QP/21/030 Integrated Performance Report
Andy Hall presented the item and highlighted the following points:
a) Overall deterioration in elective referral to treatment (RTT) performance had been reported, including a further increase in the waiting list. There are an increased number of patients waiting 12 months; this trend is likely to continue, particularly as the number of referrals from primary care increases.
b) Continued improvement is reported in respect of cancer two week waits.
c) Accident and Emergency activity is increasing, with a number of 12 hour breaches reported.
d) Improving Access to Psychological Therapies (IAPT) is reporting good recovery.
e) Physical Health Checks for patients with severe mental illness remains below the national standard at 22.5%.
f) The number of occupied bed days for acute mental health patients placed out of area shows a small reduction however, the numbers remain above the trajectory of 180.
g) Children and younger people accessing mental health services continue to do so at a level above the national standard. The February 2021 position shows a continuation of the improvements in performance with a level of 38.3% compared to the 35% standard.
h) Ward staffing remains below the 80% target at both acute provider Trusts.
i) The Summary Hospital level Mortality Indicator (SHMI) rate for both acute trusts remains below or close to 100, whilst both trusts continue to show Hospital Standardised Mortality Ratio (HSMR) rates above 100.
j) SFT continues to report a high level of patients admitted for 21 days or more.k) The ambulance handover standard continues to be unmet at NUH, with 67% of
patients being handed over in 15 minutes compared to the national standard of 100%.
l) At 49.0%, the March level of eligible patients asked case finding questions, or diagnosis of dementia or delirium at SFH remains significantly lower than the 90% national standard but continues to show improvement.
The following points were made in discussion:
Ratified Minutes of CCG Committee meetings
178 of 224 09:00 - 10.50-04/08/21

Page 5 of 9
m) The Committee raised concern at the continuing position with regard to elective waiting lists. The matter had also been discussed at the May 2021 Primary Care Commissioning Committee, particularly in respect of the impact on general practice. The Committee sought assurance regarding the position and the recovery trajectory. In response, Lisa Durant outlined the systems and contractual arrangements in place to improve the position. Trusts are in the early stages of looking at how they can maximise productivity.
n) Further information was sought about the elective position as of May 2021 (figures in the report relate to March 2021 data). Andy Hall was able to provide updated data as follows: as of 23 May 2021 NUH has 53,236 patients on their waiting list, of which 17,249 are waiting over 18 weeks, within that 3,478 are 12 month waits. SFH is reporting 36,931 patients on their waiting list, 12,708 are waiting over 18 weeks, within that 1,368 are 12 month waits. Both trusts report a slight reduction in 12 month waits
o) The Committee requested clarity regarding the performance trajectory in order to be in a position to manage performance against it. In response, reference was made to detail in the report in relation to the recovery plan.
The Quality and Performance Committee:
p) RECEIVED and NOTED the Integrated Performance Report.
Sue Clague left the meeting
Quality Improvement and Assurance
Ratified Minutes of CCG Committee meetings
179 of 22409:00 - 10.50-04/08/21

Page 6 of 9
QP 21 031 ICS Quality and Outcomes Discussion Paper
Rosa Waddingham presented the item and highlighted the following points:
a) The paper provided the Committee with the detail of how the overarching ‘quality principles’ would be delivered during the move into a system space where both the ICS and constituent partnerships and organisations have shared accountability for quality assurance and improvement.
b) The paper also included an update on how the ICS outcomes framework is being translated into delivery.
c) The Chief Nurse invited members to consider the paper further and share their thoughts by Friday 04 June 2021, in order that they can be incorporated into the next iteration of the paper.
d) The Chief Nurse suggested a number of areas for consideration, including: frequency of meetings, how best to navigate the year of transition, the importance of links between this Committee and the ICS Committee, Committee Chair arrangements, how we ensure the flow of business and decision making to the Governing Body and ICS Board.
The following points were made in discussion:
e) Committee members welcomed the discussion paper and would provide feedback to the Chief Nurse within the timeframe identified. Members felt they would benefit from some time to explore the issues in more detail ahead of a more detailed proposal to the Committee in June 2021.
ACTION:
∑ Rosa Waddingham to present an update to the Committee in June 2021.
The Quality and Performance Committee:
∑ NOTED the quality principles outlined and agreed to provide feedback to the Chief Nurse ahead of a more detailed discussion and update to the Committee in June 2021.
∑ SUPPORTED the system work to develop a robust quality oversight and improvement process.
Ratified Minutes of CCG Committee meetings
180 of 224 09:00 - 10.50-04/08/21

Page 7 of 9
QP 21 032 ICS Health Inequalities
Hazel Buchanan was in attendance to present the item and highlighted the following points:
a) The ICS Health Inequalities Strategy is designed to help establish a shared commitment and vision for addressing health inequalities across the health and care system.
b) The strategy recognises the impact of Covid-19 and supports the ICS Clinical and Community Services Strategy and the five year strategic plan.
c) The strategy and ICS planning includes actions against the five national priorities for health inequalities including 1) restore NHS services inclusively 2) mitigate against digital exclusion 3) ensure datasets are complete and timely 4) accelerate preventative programmes that proactively engage those at greatest risk of poor health outcomes 5) strengthen leadership and accountability.
d) An ICS Health Inequalities, Prevention and Wider Determinants Committee had been implemented to provide cohesion and accountability and make progress alongside Health and Wellbeing Boards.
The following points were made in discussion:
e) The Committee noted that the challenge is to understand the impact of access and quality of services on health outcomes.
The Quality and Performance Committee:
∑ NOTED the ICS Health Inequalities Strategy and progress against the five national priorities.
QP 21 033 Health Inequalities Data Presentation
This item was deferred to a future meeting.
Patient and Public Engagement
QP 21 034 Engagement Development Plan
Lewis Etoria joined the meeting.
Lewis Etoria was in attendance to present the item and highlighted the following points:
a) The paper described the transition from the existing engagement approach to a system-wide ICS engagement function aligned to the ambitions in the Integration and Innovation white paper.
b) Nottingham and Nottinghamshire aim to confirm governance arrangements by September 2021 and to be operating under these arrangements in shadow form from December 2021.
c) To support the ambitions of the ICS there would be more focus on going beyond asking communities what they think of existing services and proposed changes to generating insights from local people that shape lasting changes.
Ratified Minutes of CCG Committee meetings
181 of 22409:00 - 10.50-04/08/21

Page 8 of 9
d) The paper identified five priority areas of focus for embedding community engagement in the ICS.
The following points were made in discussion:
e) The Committee noted that there are many examples of existing good practice and there is further learning to be harnessed from the engagement experience through Covid-19.
f) The paper will be presented to the Patient and Public Experience Committee(PPEC) in June 2021.
g) The link to co-production was made and would be included in the next iteration of the plan.
The Quality and Performance Committee:
∑ RECEIVED the report and ENDORSED the direction of travel described.
Lewis Etoria left the meeting.
QP 21 035 Patient Experience Annual Report
Andy Hall left the meeting.
Amanda Wright joined the meeting.
Amanda Wright presented the item and highlighted the following points:
a) During 2020/21 the patient experience team received 1,456 contacts, comprising of 185 complaints, 1,257 enquiries and 14 compliments.
b) The team received a significant number of contacts in relation to Covid-19 (increase of 33%) and experienced reduced staffing levels at times due to the pandemic.
c) The statutory function of the patient experience team had been maintainedthroughout the year. The impact of the pandemic had seen stakeholder relationships strengthen both internally and externally.
d) During 2021/22 the team would focus on: developing the patient experience in the ICS, reviewing reporting categories, strengthening links with quality leads and reinstate the Complaints Managers forum for all providers.
The following points were made in discussion:
e) The Committee expressed their thanks to Amanda and the team for their work, particularly during such a challenging year
The Quality and Performance Committee:
∑ RECEIVED and NOTED the report.
Ratified Minutes of CCG Committee meetings
182 of 224 09:00 - 10.50-04/08/21

Page 9 of 9
Amanda Wright left the meeting.
Corporate Assurance
QP 21 036 Risk Report
Rosa Waddingham presented the item and highlighted the following points:
a) The report was presented for information. The Committee noted that four risks are rated red.
b) Discussion in relation to RR162 had taken place at item 7, QP 21 027.
No further points were raised in discussion.
The Quality and Performance Committee:
∑ RECEIVED the risk report and confirmed that no additional risks had been highlighted during the course of the meeting for inclusion within the Corporate Risk Register.
Closing Items
QP 21 037 Any other business
The Committee agreed to receive and approve the Quality Accounts from provider organisations virtually.
No further business was raised.
QP 21 038 Key messages to escalate to the Governing Body
The Committee:
∑ Item redacted.
QP 21 039 Date of next meeting:
24/06/2021 via MS Teams meeting
Ratified Minutes of CCG Committee meetings
183 of 22409:00 - 10.50-04/08/21

Page 1 of 9
NHS Nottingham and Nottinghamshire Clinical Commissioning GroupQuality and Performance Committee
Ratified minutes of the meeting held on24/06/2021 9:00-12:00
MS Teams Meeting
Members present:
Eleri de Gilbert Non-Executive Director (Chair)
Sue Clague Non-Executive Director
Andy Hall
Rosa Waddingham
Associate Director of Performance and Information
Chief Nurse
Jon Towler Non-Executive Director
Hazel Buchanan Associate Director of Strategic Programmes & EPRRDanni Burnett Deputy Chief Nurse
Lisa Durant Director of Commissioning - Mid Nottinghamshire
Caroline Nolan System Delivery Director- Urgent Care
Dr Hilary Lovelock GP Representative
Dr Richard Stratton GP Representative
Maxine Bunn Associate Director of Commissioning
In attendance:
Lucy Anderson Deputy Director-Contracting
Louise Espley Corporate Governance Officer (minutes)
Jo Simmonds Head of Corporate Governance
Sian Gascoigne Head of Corporate Assurance
Theodore Philips
Cath Pritchard
Lucy Jones
Sue Barnitt
Head of Transforming Care for Learning Disabilities and Autism(item
QP/21/050 & QP/21/053)
Consultant in Public Health Nottinghamshire County Council (item
QP/21/049)
Senior Public Health Commissioning Manager Nottinghamshire County
Council (item QP/21/049)
Head of Quality – Community and Mental Health
Apologies:
Mindy Bassi Chief Pharmacist
Stuart Poyner Chief Finance Officer
Ratified Minutes of CCG Committee meetings
184 of 224 09:00 - 10.50-04/08/21

Page 2 of 9
Dr Manik Arora GP Representative
Sally Bird Head of Service Infection Prevention and Control
Cumulative Record of Members’ Attendance (2021/22)
Name Possible Actual Name Possible Actual
Dr Manik Arora 03 02 Eleri de Gilbert 03 03
Mindy Bassi 03 00 Andy Hall 03 03
Hazel Buchanan 03 03 Dr Hilary Lovelock 03 03
Maxine Bunn 03 01 Caroline Nolan 03 03
Danni Burnett 03 03 Stuart Poynor 03 02
Lisa Durant 03 03 Dr Richard Stratton 03 03
Sue Clague 03 03 Jon Towler 03 03
Rosa Waddingham 03 03
Introductory Items
QP 21 041 Welcome and Apologies
Eleri de Gilbert welcomed members to the Quality and Performance Committeemeeting which was held on MS Teams due to the current Covid-19 situation.
Apologies were noted as above.
QP 21 042 Confirmation of Quoracy
The meeting was confirmed as quorate.
QP 21 043 Declaration of interest for any item on the shared agenda
Dr Richard Stratton has an interest relating to Nottingham University Hospitals NHS Trust (NUH) as he is an employee. This is on the Committee’s Register. The conflict is noted in relation to items:-
∑ QP/21/045 – Minutes of the previous meeting
∑ QP/21/046 – Action log from previous meeting
∑ QP/21/047 – NUH Deep Dive update
∑ QP/21/047 – NUH Maternity Confidential Update
∑ QP/21/054 – Risk Register
The Chair reminded members of their responsibility to highlight any interests should they transpire as a result of discussions during the meeting.
Ratified Minutes of CCG Committee meetings
185 of 22409:00 - 10.50-04/08/21
Page 3 of 9
QP 21 044 Management of any real or perceived conflicts of interest
The Chair highlighted conflicts of interest noted and how they would be handled at this meeting:-
For item QP/21/045 the proposed management action is that Dr Richard Stratton is excluded from any discussion relating to the NUH agenda items. He has received a redaction version of the minutes.
For item QP/21/046 the proposed management action is that Dr Richard Stratton is excluded from any discussion relating to the NUH agenda items. He has received a redaction version of the action log.
For item QP/21/047, NUH Deep Dive update, the proposed management action is that Dr Richard Stratton is excluded from the meeting for this discussion. He has not received the update paper.
For item QP/21/047, NUH Maternity update, the proposed management action is that Dr Richard Stratton may remain in the meeting and may participate in the discussion.However, it was agreed that Dr Stratton would remain absent for this item due to its position on the agenda.
For item QP/21/054 the proposed management action is that Dr Richard Stratton is excluded from the meeting when the NUH risk is discussed. He has received a redacted version of the paper.
Dr Stratton joined the meeting at 09.45 when the main committee business commenced and left the meeting at 11:15 ahead of the Risk Register discussion.
QP 21 045 Minutes from the meeting held on 27 May 2021
Dr Richard Stratton was not present for this item.
The minutes were agreed as an accurate record of proceedings.
QP 21 046 Action log and matters arising from the meeting held on 27 May 2021
Dr Richard Stratton was not present for this item.
All actions were noted as complete, on the agenda for the meeting or planned for a future meeting and there were no matters arising.
QP 21 047 Actions arising from the Governing Body meeting held on 02 June 2021
∑ NUH confidential performance update
∑ NUH maternity confidential update
Dr Richard Stratton was not present for this item.
Item redacted.
NUH maternity confidential update
Dr Richard Stratton was not present for this item.
Item redacted.
Ratified Minutes of CCG Committee meetings
186 of 224 09:00 - 10.50-04/08/21

Page 4 of 9
Committee Business
QP 21 048 Revised Committee arrangements including draft committee work programme
Eleri de Gilbert introduced the item. The paper provided an update on the change ofapproach for the Committee’s meeting cycle during the transition year and the proposed Annual Work Programme for the remainder of 2021/22.
It was explained that governance arrangements are emerging in shadow form and willcontinue to evolve and adapt as ICS statutory requirements are confirmed and newways of working are embedded. It is proposed that the Committee’s meeting cycle beamended to alternate between ‘deep dive’ meetings and routine meetings which willinclude the Committee’s standard items and ensure it discharges its full range ofduties over the year. Due diligence would take place ahead of a more detaileddiscussion of quality in the ICS in the system space in October 2021.
The following points were raised in discussion:
a) Members sought any pointers to guidance (for example, from the King’s fund)that may support the transition of quality into the ICS space. It was noted that the landscape is constantly changing, hence the need for the Committeediscussion in October 2021 to review quality arrangements in the ICS system space.
b) Reference was made to a recent discussion at the Finance and Resources Committee focused on activity data and its relationship to quality. There was concern that each Committee looks at data in isolation, potentially missingconnections. The Clinical Executive Group would consider the issue and identify the important factors for patient outcomes. The Chief Nurse referred to work taking place to support the quality assurance and improvement work.
The Quality and Performance Committee:
∑ ENDORSED the proposed approach to the meeting cycle.
∑ NOTED that the deep dive programme would be developed
∑ APPROVED the Committee annual work programme for 2021/22.
Quality and Performance
Dr Richard Stratton, Lucy Jones and Cath Pritchard joined the meeting.
QP 21 049 System suicide prevention strategy
Eleri de Gilbert introduced the core business topic of the meeting; a focus on suicide prevention; self-harm and suicide within Nottinghamshire Healthcare Foundation Trustservices and a discussion on what support and suicide awareness training is in place
ACTION:∑ Committee to receive a report in October 2021 describing quality in the ICS
system space.
Ratified Minutes of CCG Committee meetings
187 of 22409:00 - 10.50-04/08/21
Page 5 of 9
for CCG staff. These issues had been raised by the Governing Body and previously by this committee as areas of concern
Colleagues from Public Health joined the meeting to inform the discussion.
Cath Pritchard (Consultant in Public Health), supported by Lucy Jones (Senior Public Health Commissioning Manager) delivered a presentation which included the national evidence in relation to suicide alongside the local picture, system overview and the role of the Suicide Prevention Strategy Group, key development areas (2019 to date) and priorities going forward.
The following points were raised in discussion:
a) Members welcomed the opportunity to have time to discuss this importantissue and thanked Public Health colleagues for joining the meeting. It was noted that there are a number of causes of suicide falling into three categories; those experiencing acute distress as a result of a change in circumstances, those who choose suicide to escape the suffering of their illness and suicides due to misadventure. The question was raised as to whether data collection defined the causes of suicide. Lucy Jones described how data is analysed to understand the circumstances leading up to suicides.
b) Discussion turned to staff suicide awareness training for those working in the NHS and Local Authorities. The Chief Nurse reported that NHS responses have been coordinated via the People and Culture Boards. There is a programme for staff in relation to their own mental health and wellbeing alongside an education programme for staff.
c) Reference was made to a 30-minute training programme provided by zero suicide alliance which is benchmarked well. The Committee suggested that system wide commitment would raise the profile of this issue and could have a significant impact. The Chief Nurse suggested the conversation be taken to the ICS Board to consider the best approach to ensure inclusion in the development of the system wide strategy.
d) The importance of training for GPs and other front line staff, including reception staff, was recognised as they are often in a position to identify a vulnerable person.
The Quality and Performance Committee:
∑ NOTED the presentation
∑ RECEIVED ASSURANCE that a system approach to prevention was in place.
Cath Pritchard and Lucy Jones left the meeting.
QP/21/050 Nottinghamshire Healthcare Foundation Trust (NHT):
Self-harm and suicide serious incidents
Theodore Philips delivered the presentation and highlighted the following points:
Ratified Minutes of CCG Committee meetings
188 of 224 09:00 - 10.50-04/08/21

Page 6 of 9
a) There has been a notable increase in the reporting of serious and untoward incidents (SUIs) across Adult Mental Health Services in NHT since December 2020.
b) Additional concerns had been raised as death occurred in 72% of the incidents reported during quarter four and there was an increase in those requiring treatment.
c) The presentation provided the data and trends in more detail, particularly in respect of links with the impact of Covid-19.
d) Since January 2021, Child and Adolescent Mental Health Services (CAMHS)had seen a significant increase in crisis referrals, which reflects the national position.
e) Work is ongoing to further interrogate the data and themes and a number of next steps were included in the presentation.
The following points were made in discussion:
f) The Committee raised concern at the upward trend in reporting and sought clarification regarding the root causes to the issues reported. The Chief Nurse reported that some of these are related to known issues and other issues are still being explored to determine the root cause.
g) The Committee noted that this data only refers to patients under the care of mental health services and not those, for example, who had been accessing drug and alcohol services. It was also highlighted that the suspension of face to face consultations during the Covid-19 pandemic may have been significant.
h) The on-going work to understand the data further was welcomed., with the work to date being a good starter for 10. Further work was now required to be clear around lessons learnt and a SMART Action plan developed.
The Quality and Performance Committee:
∑ NOTED the presentation on initial findings and next steps.
QP/21/051 Risk Review update
The Chair introduced the item. A deep dive was undertaken some time ago resulting in risk RR 116 (NHCT) with a risk score of 16. The Committee has received updates since the deep dive on improvements in leadership, culture, governance, transparency and openess but has not seen sustained improvement. This meeting was now the opportunity to review progress and review the risk score.
Rosa Waddingahm presented the item and highlighted the following points:
a) The review had been delayed due to the pandemic but the current position is well understood, therefore it is timely to bring it to the Committee for review.
b) The Deputy Chief Nurse delivered a detailed presentation to summarise the position. The presentation included; a recap of CQC findings, risk scoping summary, areas of improvement/good practice, areas for focus and associated oversight, leadership and governance, risk description and update.
Ratified Minutes of CCG Committee meetings
189 of 22409:00 - 10.50-04/08/21
Page 7 of 9
c) NHT is on an improvement trajectory although there are some concerns in relation to sub-contracted services.
d) NHT is open and transparent and there is no evidence that further intervention or action is required at this time.
The following points were made in discussion:
e) Members were encouraged by the improvement trajectory that was evident from the presentation and improvements in leadership and governance. Concern was raised in respect of deterioration in some areas, with new risks also having been identified
f) It was observed that patient engagement appears to be insufficient and requires attention. It was also noted that the main focus of the presentation was on the mental health services rather than a focus on the wider community service provision. Some context was provided in respect of this.
g) Assurance was provided in terms of the management of serious incidents and leadership changes.
h) NHT is open in its approach and fully aware of the improvement journey it is on, this provides a level of assurance in terms of culture, governance and embedded change.
i) Following discussion it was agreed that the risk score should remain at 16 at this time until systematic improvement was evident
The Quality and Performance Committee:
∑ RECEIVED and REVIEWED the documents in order to assess the NHT risk.
∑ AGREED that the risk score of RR 116 should remain at 16.
QP 21 052 CCG Staff suicide awareness/support programme
Rosa Waddingham presented the item and highlighted the following points:
a) Suicide awareness is included as part of the CCG mental health awareness work. The CCG is focused on creating a culture where people feel able and empowered to talk about mental health issues and know where to go for support.
b) A recent story from a staff member about his mental health had been powerful in starting a conversation about building suicide awareness into the CCG competency programme, cultural awareness programme and disability and well-being network.
c) A mental health first aiders programme is in the initial stages of development.
d) There has been a focus on restorative supervision. The CCG has the only CCG Nurse in the country to be on this training programme. Support will be available to all staff members.
The following points were made in discussion:
e) Sian Gascoinge as Chair of the Disability and well-being network reported on
Ratified Minutes of CCG Committee meetings
190 of 224 09:00 - 10.50-04/08/21

Page 8 of 9
the progress of the network since it was established four months ago. The response to the well-being agenda and mental health awareness has been significant. A procurement exercise is underway to identify the training provider for mental health first aiders. It was accepted that it is often difficult to quantify the impact of intervention, particularly in relation to suicide prevention.
f) The impact of isolation on staff continually working at home was also noted. In response it was reported that a number of options will be available to staff to ensure it is responsive to individual needs.
The Quality and Performance Committee:
∑ NOTED the update.
QP 21 053 Learning Disabilty Mortality Review (LeDeR) annual report 2020/21
Theodore Philips presented the LeDeR annual report and highlighted the following points:
a) The LeDeR programme is commissioned by NHSE/I and managed locally by Nottingham and Nottinghamshire CCG.
b) A national initiative, LeDeR was introduced as a service improvement programme to identify the causes of early morbidity within the Learning disability (LD) population compared to the general population.
c) The age range of LeDeR deaths for Nottingham and Nottinghamshire reflects the national trend for learning disability deaths with the average age of death in 2020/21 being 59 years.
d) The annual report was signed off by the Learning Disabilities/Autism Spectrum Disorder Executive Board on 15 June 2021.
e) The biggest change during 2019/20 was the impact of Covid-19. There has been a spike in the number of deaths related to respiratory illness in the learning disability population. Further work is needed to understand this in more detail as Nottinghamshire is seen as an outlier.
f) The report included recommendations and priorities for 2021/22 and beyond.
g) The report would be published by 30 June 2021 in this format alongside an easy read version.
The following points were made in discussion:
h) It was suggested that some of the objectives in the report could be more specific and measurable.
i) The journey of improvement was noted, although concern raised regarding the high deaths due to respiratory illness. It was suggested that a review of ‘do notresuscitate’ (DNRs) in relation to the 21 cases would be appropriate.
j) The Chief Nurse suggested and action plan would be produced to sit alongside the report and clarify next steps.
ACTION:∑ LeDeR annual report to be published by 30 June 2021 with an easy read
version available too.∑ Action plan to be produced to sit alongside the report.
Ratified Minutes of CCG Committee meetings
191 of 22409:00 - 10.50-04/08/21

Page 9 of 9
The Quality and Performance Committee:
∑ ENDORSED the report for publication by 30 June 2021 alongside an easy read version and NOTED that an action plan would be developed.
Corporate Assurance
QP 21 054 Risk Report
Dr Richard Stratton was not present for this item.
Item redacted.
Information only items
QP 21 055 ICS Quality report
The report was shared for information only.
Closing Items
QP 21 056 Any other business
No further business was raised.
QP 21 057 Key messages to escalate to the Governing Body
Dr Richard Stratton was not present for this item.
The Committee:
a) Item redacted.
b) The Committee AGREED the revised Committee meeting arrangements for the transition period and agreed the work programme for 2021/22.
c) The Committee carried out a focused review of the NHT risk following a previous deep dive report and considered reports related to suicide and self-harm. In conclusion, the Committee AGREED to maintain the current risk, RR 116 at a score of 16 which reflects both the improvement journey and current challenges.
d) ENDORSED publication of the LeDeR annual report.
QP 21 058 Date of next meeting:
22/07/2021 via MS Teams meeting
Ratified Minutes of CCG Committee meetings
192 of 224 09:00 - 10.50-04/08/21
Page 1 of 6
NHS Nottingham and Nottinghamshire Clinical Commissioning Group
Finance and Resources CommitteeRatified minutes of the meeting held on
26/05/2021 09:00-12.00MS Teams Meting
Members present:
Shaun Beebe (Chair) Non-Executive Director Maxine Bunn Associate Director of Commissioning, Contracting and Performance -
Mental Health and CommunityLucy Branson Associate Director of GovernanceMichael Cawley Operational Director of FinanceLisa Durant Commissioning Director (Mid Nottinghamshire)Andy Hall Associate Director of Performance and InformationDr James Hopkinson Joint Clinical LeaderAndrew Morton Operational Director of FinanceCaroline Nolan System Delivery Director (Greater Nottingham)Stuart Poynor Chief Finance OfficerJonathon Rycroft Associate Director of Financial Recovery (Operations)Dr Stephen Shortt Joint Clinical LeaderSue Sunderland Non-Executive DirectorJon Towler Non-Executive Director
In attendance:Paul Antunes-GonclavesSian GascgoineJames GlossopJack RodberIsobel ScoffieldGemma Waring
JT TBC (Item FR 21 031)Head of Corporate AssuranceJT TBC (Item FR 21 031)JT TBC (Item FR 21 031) JT TBC (Item FR 21 031)Head of Human Resources and Organisational Development (FR 21 023)
Shannon Wilkie Corporate Governance Officer (Minutes)Sue Wass Corporate Governance Officer
Apologies:Amanda Sullivan Accountable Officer
Cumulative Record of Members’ Attendance (2021/22)Name Possible Actual Name Possible ActualShaun Beebe 02 02 Caroline Nolan 02 02
Lucy Branson 02 02 Stuart Poynor 02 02
Maxine Bunn 02 02 Jonathan Rycroft 02 02
Michael Cawley 02 02 Stephen Shortt 02 02
Lisa Durant 02 02 Amanda Sullivan 02 01
Andy Hall 02 02 Sue Sunderland 02 02
James Hopkinson 02 02 Jon Towler 02 02
Ratified Minutes of CCG Committee meetings
193 of 22409:00 - 10.50-04/08/21

Page 2 of 6
Andrew Morton 02 02
Introductory Items
FR 21 017 Welcome and Apologies
Shaun Beebe welcomed members to the Finance and Resources Committee meetingwhich was held on MS Teams due to the current Covid-19 situation.
There were apologies from Amanda Sullivan – Accountable Officer.
FR 21 018 Confirmation of Quoracy
The meeting was confirmed as quorate.
FR 21 019 Declaration of interest for any item on the shared agenda
No interests were declared in relation to any item on the agenda. The Chair reminded members of their responsibility to highlight any interests should they transpire as a result of discussions during the meeting.
FR 21 020 Management of any real or perceived conflicts of interest
As no conflicts of interest had been identified, this item was not necessary for the meeting.
FR 21 021 Minutes from the meeting held on 28 April 2021
The minutes were agreed as an accurate record.
FR 21 022 Action log and matters arising from the meeting held on 28 April 2021
Members highlighted the narrative included within the log to satisfy action FR 20 140 relating to the number of vacancies in commissioning teams. It was noted that a reporting mistake had made the number of vacancies seem higher and this had been corrected. Shaun Beebe felt that the actual number of vacancies still seemed high. Stuart Poynor explained that there is not a great concern surrounding the vacanciesheld by the commissioning team; as this is in line with managing the CCG’s vacancy factor.
All actions were noted as complete.
Workforce Management and Organisational Development
FR 21 023 Staff Survey Action Plan
Gemma Waring presented the item and highlighted the following points:
a) The first draft of the staff survey action plan had been shared at the following forums; Staff Engagement Group (SEG), Black, Asian and Minority Ethnic (BAME) Steering Group, Lesbian, Gay, Bi-sexual, Transgender, Queer/Questioning (LGBTQ+) Steering Group and the Equality, Diversity and Inclusion (EDI) Steering Group.
b) The staff survey report had been published in March 2021 and the areas with the least improvement since the previous survey had been used as the main focus for the action plan. These areas were; morale, team working, equality, diversity and inclusion, safety culture and health and wellbeing.
Ratified Minutes of CCG Committee meetings
194 of 224 09:00 - 10.50-04/08/21

Page 3 of 6
c) Staff health and wellbeing had been a particular area of focus throughout the Covid-19 pandemic.
d) Discussions had been held at SEG to consider the impact of the proposed Agile Working Model on staff health and wellbeing.
The following points were made in discussion:
e) Members queried the process and timelines to progress the staff survey action plan. It was noted that the plan will be submitted to the June 2021 Committee meeting for final approval and this iteration of the plan will include proposed timescales and action leads.
f) Members acknowledged that the staff survey report captures staff thoughts and feelings at a point in time.
The Committee:
∑ REVIEWED the staff survey action plan.
Financial Position and Contract Management
FR 21 024 Finance Report Month 1 (M1), 2021/22 plan submission and Covid-19 Related Expenditure Update
Michael Cawley presented the item and highlighted the following points:
a) The report was presented in a new format, intended to be more reader friendly. The content and level of detail remained in line with previous reports.
b) The plan for period M1 to M6 ‘H1’ of 2021/22, which had been presented to the April 2021 Committee had been revisited following publication of further guidance from NHS England/Improvement (NHSE/I). The updated plan detaileda break even position.
c) As there was limited information at M1 to comment on the financial position, the report focused on the potential variations that could be a risk to the H1 plan.
d) There had been a request from the regulators for the CCG to engage with all other organisations in the ICS to agree a joint commitment to provide detailed plans regarding delivery of transformation savings that will deliver full year effect, by the end of June 2021.
e) There had been challenge from regulators regarding the implementation of a robust governance process, financial framework and system wide approval process for investment within the ICS.
The following points were made in discussion:
f) Members discussed the risks around delivering elective activity levels in order to recover the position and the financial risks that come with not achieving targets. It was noted that activity performance is being monitored by the Elective Recovery Fund (ERF) Tracking and Co-ordination group which meets weekly.
g) Members noted that delivery of financial targets is expected to be a greater
Ratified Minutes of CCG Committee meetings
195 of 22409:00 - 10.50-04/08/21

Page 4 of 6
challenge for the second half of the financial year, the ‘H2’ period than the H1 period.
h) Members discussed the risks to delivery of the system financial position for H1 and the risk appetite of Directors of Finance (DoFs) within the ICS.
i) Members discussed a lack of oversight for Primary Care Capital Expenditure both at a Governing Body level and across the various sub Committees.
j) Members noted that there is insufficient resource to deliver the scale of change needed to deliver transformation savings. Members agreed to raise this risk in the confidential session of the Governing Body Meeting. Members noted that the ICS Finance Committee would take ownership of this risk under normal circumstances however this forum is not fully established therefore this is inappropriate.
ACTION:
∑ Michael Cawley to discuss improving Committee oversight of Primary Care Capital Expenditure with Eleri de Gilbert
∑ Stuart Poyner to brief the Governing Body on the risks surrounding delivery of transformation savings in the confidential session
The Committee:
∑ APPROVED the Finance Report
∑ APPROVED the 2021/22 plan submission update
∑ APPROVED the COVID-19 related expenditure report
FR 21 025 COVID- 19 Vaccination Programme Briefing Paper
Michael Cawley presented the item and highlighted the following points:
a) The report described a provisional position for M12 of the COVID-19 vaccination programme as work was still outstanding to finalise the position.
b) There were a number of claims yet to be substantiated and work was on-going to gather data to support claims to NHS E/I for reimbursement of funds relating to the programme.
The following points were made in discussion:
c) Members queried the figures in the report relating to the cost of delivering a vaccination, which were higher than the flat rate. The actual cost of delivering a vaccine is higher than the flat rate contribution made per vaccine, which has resulted in a financial shortfall.
d) Members acknowledged the need for balance between ensuring the vaccination programme is cost efficient versus focusing more on the patient experience and accessibility aspect of the programme.
The Committee:
Ratified Minutes of CCG Committee meetings
196 of 224 09:00 - 10.50-04/08/21

Page 5 of 6
∑ NOTED the briefing paper.
FR 21 026 Update on the reinstatement of the Cross Provider Report
Andy Hall presented the item and highlighted the following points:
a) The update described the request to reinstate the cross provider report, which was in place prior to the COVID-19 pandemic.
b) Discussions are on-going to improve the way the future report will be formatted and to ensure the most relevant data is included.
The following points were made in discussion:
c) Members debated whether the report should focus on activity rather than tariff calculations, which have been rendered redundant due to the pandemic.
d) Members considered shaping the report to describe performance against Elective Recovery Fund (ERF) targets.
e) Members noted that activity reports are received at Quality and Performance Committee and therefore changing the narrative of the Cross Provider Report could result in the report falling outside the remit of the Committee.
ACTION:
∑ Stuart Poynor and Andy Hall to refresh the content of the cross provider report.
The Committee:
∑ NOTED the verbal update.
Risk Management
FR 21 027 Risk Report
Siân Gascoigne presented the item and highlighted the following points:
a) There were seven risks pertaining to the Committee’s responsibilities on the Committee’s risk register, a reduction in five since the last report.
b) Risk 158 relating to the impact of the transfer to the ICS on delivery of the CCG’s financial duties, was rated red and would be presented to the Governing Body.
c) It was proposed that the likelihood rating for RR 165 be reduced from a four to a three resulting in an overall risk score of twelve.
The following points were made in discussion:
d) Members agreed with the reasoning behind the reduction to risk RR 165 as it relates to the H1 period and members noted that in the coming months a risk relating to the H2 period will be added to the register.
Ratified Minutes of CCG Committee meetings
197 of 22409:00 - 10.50-04/08/21

Page 6 of 6
e) No new risks were highlighted.
The Committee:
∑ APPROVED the reduction of the likelihood risk score for RR 165 from a four to a three.
Closing Items
FR 21 028 Any other business
No further business was raised.
FR 21 029 Key messages to escalate to the Governing Body
The Committee:
∑ Agreed to brief the Governing body following discussion at item FR 21 024, as per the agreed action.
FR 21 030 Date of next meeting:
23/06/2021
MS Teams meeting
Actions arising from the Governing Body
FR 21 031 Tomorrow’s NUH
Item redacted: The discussion relates to policy development not yet formalised by the organisation
The Committee:
∑ Was ASSURED by the presentation
Ratified Minutes of CCG Committee meetings
198 of 224 09:00 - 10.50-04/08/21

Page 1 of 6
NHS Nottingham and Nottinghamshire Clinical Commissioning Group
Finance and Resources Committee
Ratified minutes of the meeting held on23/06/2021 09:00-11:00
MS Teams Meting
Members present:
Jon Towler Maxine Bunn
Non-Executive Director (Chair)Associate Director of Commissioning, Contracting and Performance -Mental Health and Community
Lucy Branson Associate Director of GovernanceMichael Cawley Operational Director of FinanceLisa Durant Commissioning Director (Mid Nottinghamshire)Andy Hall Associate Director of Performance and InformationDr James Hopkinson Joint Clinical LeaderAndrew Morton Operational Director of FinanceCaroline Nolan System Delivery Director (Greater Nottingham)Jonathon Rycroft Associate Director of Financial Recovery (Operations)Dr Stephen Shortt Joint Clinical LeaderAmanda Sullivan Accountable OfficerSue Sunderland Non-Executive Director
In attendance:Siân Gascoigne Head of Corporate AssuranceShannon Wilkie Corporate Governance Officer (Minutes)
Apologies:Shaun Beebe Non-Executive Director (Chair)
Stuart Poynor Chief Finance Officer
Cumulative Record of Members’ Attendance (2021/22)Name Possible Actual Name Possible ActualShaun Beebe 03 02 Caroline Nolan 03 03
Lucy Branson 03 03 Stuart Poynor 03 02
Maxine Bunn 03 03 Jonathan Rycroft 03 03
Michael Cawley 03 03 Stephen Shortt 03 03
Lisa Durant 03 03 Amanda Sullivan 03 02
Andy Hall 03 03 Sue Sunderland 03 03
James Hopkinson 03 03 Jon Towler 03 03
Andrew Morton 03 03
Ratified Minutes of CCG Committee meetings
199 of 22409:00 - 10.50-04/08/21

Page 2 of 6
Introductory Items
FR 21 032 Welcome and Apologies
Jon Towler welcomed members to the Finance and Resources Committee meeting which was held on MS Teams due to the current Covid-19 situation. Jon assumed the position of Chair in Shaun Beebe’s absence.
There were apologies from Shaun Beebe – Non Executive Director and Committee Chair and Stuart Poynor – Chief Finance Officer.
FR 21 033 Confirmation of Quoracy
The meeting was confirmed as quorate.
FR 21 034 Declaration of interest for any item on the shared agenda
No interests were declared in relation to any item on the agenda. The Chair reminded members of their responsibility to highlight any interests should they transpire as a result of discussions during the meeting.
FR 21 035 Management of any real or perceived conflicts of interest
As no conflicts of interest had been identified, this item was not necessary for the meeting.
FR 21 036 Minutes from the meeting held on 26 May 2021
The minutes were agreed as an accurate record.
FR 21 037 Action log and matters arising from the meeting held on 26 May 2021
All actions were noted as complete.
Workforce Management and Organisational Development
FR 21 038 Agile Working Update
Jonathan Rycroft presented the item and highlighted the following points:
a) The Government had announced that the easing of COVID-19 restrictions had been postponed until 19th July 2021. This had resulted in the CCG postponing plans to welcome more staff back to office working. This was communicated at the most recent staff briefing.
b) Once restrictions are eased, office working will be an option for staff and those who are not comfortable returning to the office will be able to continue to work from home. Once COVID-19 subsides, there will be an expectation that all staff have some degree of office presence, as agreed in the agile working model.
c) Preparation work had taken place at Sir John Robinson House to make the base ready for staff to return to the office.
d) Soft phones will be rolled out to improve communications amongst staff regardless of where they are working. This functionality will in many cases replace mobile phones.
The following points were made in discussion:
e) Members discussed ways to ensure staff comply with COVID-19 office guidance; specifically around ventilation. Signs have been placed in all CCG occupied
Ratified Minutes of CCG Committee meetings
200 of 224 09:00 - 10.50-04/08/21

Page 3 of 6
office buildings to remind staff to open windows, especially in communal areas and to close these when vacating premises. Members agreed that the guidance must be reiterated to staff in preparation for return to the office. The CCG’s Health and Safety Team and Infection, Prevention and Control Team will work together to ensure the guidance is up-to-date and aligns with latest Governance guidance.
The Committee:
∑ NOTED the verbal update.
Financial Position and Contract Management
FR 21 039 Finance Report Month Two (M2), 2021/22 plan submission and Covid-19 Related Expenditure Update
Andrew Morton and Michael Cawley presented the item and highlighted the following points:
a) The CCG remained under a temporary financial regime due to the COVID-19 pandemic. Plans for the H2 period (Months 6 to 12 of the 2021/22 financial year) had not yet been published.
b) The CCG position showed a pre Elective Recovery Fund (ERF) deficit of £3.7m for H1. It was assumed that the 120% activity target linked to the ERF would be achieved at an ICS level and this would result in a breakeven position.
c) The M2 position was breakeven after accounting for assumed allocations for ERF and also for the Hospital Discharge Programme (HDP) allocation. The CCG is not able to account for anticipated allocations in the financial ledger. So instead the “off ledger” adjustments reflect the overall anticipated financial position of the CCG.
d) The most significant areas of variance to plan were Continuing Healthcare (CHC) costs and the Hospital Discharge Programme (HDP). These packages were forecasted to amount to net £400k overspend at the end of the H1 period.
e) Draft 2021/22 QIPP plans were also included for the first time.
f) The Committee were apprised of the current financial position for the COVID-19 vaccination programme (CVP) whilst noting that that CVP does not form part of the reported financial results of the CCG. The CVP had an accumulated loss of£0.5m and based on current run rate levels was incurring a deficit of £270k per month. The loss attributed to providers is mainly pay expense related. An analysis of pay per site had been provided to programme officers (based on information provided by Sherwood Forest Hospitals NHS Foundations Trust (SFHFT) as the main employing organisation for the vaccination programme). An analysis had also been provided to programme officers that sets out activity currently required to be delivered at each Local Vaccination Site (LVS) that would achieve a financial breakeven position.
The following points were made in discussion:
Ratified Minutes of CCG Committee meetings
201 of 22409:00 - 10.50-04/08/21

Page 4 of 6
g) Members requested further detail regarding performance against ERF as this is a crucial part of the overall financial plan. It was noted that in order to draw down ERF funds the entire system must deliver against targets. The CCG has requested performance information from relevant providers.
h) Members discussed staff being deployed to the COVID-19 vaccinationprogramme and the impact of this on other areas of performance and whether there are plans to repatriate these staff to their original areas of work. It was noted that this work is on-going and a milestone for repatriating staff will be shared with the Committee once agreed.
i) Members noted that the costs of the Nottinghamshire Vaccination Programme cannot be directly compared with other areas due to the approach taken across Nottingham and Nottinghamshire. This included, for example, the vaccination sites being bigger and, therefore, there are additional overhead costs to consider that other systems will not have. Nottinghamshire has the 4th highest cost per COVID-19 vaccine in the region and the cost of delivering this exceeds the income received.
Action;
∑ Andrew Morton to share further detail with the Committee surrounding the performance of providers against ERF targets.
∑ Andrew Morton to share a plan for staff deployed to the vaccination programme to be repatriated to their original work area, once agreed.
The Committee:
∑ APPROVED the Finance Report
∑ NOTED the 2021/22 plan submission update
∑ APPROVED the COVID-19 related expenditure report
FR 21 040 Cross Provider Report
Andrew Hall presented the item and highlighted the following points:
a) The report was presented in a new format highlighting activity plans for the H1 period. The report included a greater focus on performance and compared performance to 2019/20 baseline activity figures. The report also included the analysis of finance performance members were used to.
b) The impact of the Early Warning and Response System (EWRS) had not been included in the report but this will be would be included in future reports once the system wide EWRS Group provides input.
The following points were made in discussion:
c) Members discussed the level of system performance management that exists surrounding the key areas of performance described in the report and agreed this was sufficient. It was noted that the ICS Performance Oversight Group will
Ratified Minutes of CCG Committee meetings
202 of 224 09:00 - 10.50-04/08/21

Page 5 of 6
re-convene in the near future and the next step will be to include more clinical involvement to ensure performance management is clinically driven.
d) Members noted that the non-elective activity levels appeared to be higher than the 2019/20 baseline in the report and this was unlikely. The Committee requested that this be checked and clarified outside of the meeting.
e) Members discussed the interdependencies between performance and the important dimensions of quality that are not regularly discussed or reported. Members agreed the most appropriate forum to consider this matter would be the newly formed ICS Clinical Executive Group.
f) It was noted that absent members should be given the opportunity to comment on the reformatted Cross Provider Report.
Action;-
∑ Andy Hall to check the non-elective performance figures in the cross provider report for accuracy.
∑ Andy Hall to share the Cross Provider Report with Shaun Beebe for comment.
Risk Management
FR 21 041 Risk Report
Siân Gascoigne presented the item and highlighted the following points:
a) There were eight risks pertaining to the Committee’s responsibilities on the Committee’s risk register, an increase in one since the previous meeting.
b) Risk RR 158 relating to the impact of the transfer to the ICS on delivery of the CCG’s financial duties, was rated red.
c) Risk RR 98 surrounding reliance upon non-recurrent funds and mitigations is being closely monitored and may increase in the near future.
The following points were made in discussion:
d) Members agreed that the rating for the new risk RR 166 relating to delivery of ERF should be increased.
The Committee:
∑ APPROVED an increase to the score for risk RR 166 to Impact three, likelihood four.
Closing Items
FR 21 042 Any other business
No further business was raised.
FR 21 043 Key messages to escalate to the Governing Body
Ratified Minutes of CCG Committee meetings
203 of 22409:00 - 10.50-04/08/21
Page 6 of 6
The Committee:
∑ Agreed to brief the Governing body on the M2 financial position and the financial performance of the COVID-19 vaccination programme.
FR 21 044 Date of next meeting:
21/07/2021
Ratified Minutes of CCG Committee meetings
204 of 224 09:00 - 10.50-04/08/21
Page 1 of 9
NHS Nottingham and Nottinghamshire Clinical Commissioning GroupPrimary Care Commissioning Committee (Public Session)
Ratified minutes of the meeting held on19/05/2021 09:00 – 10.30
Zoom Meeting
Members present:
Eleri De Gilbert Non-Executive Director (Chair)Shaun Beebe Non-Executive DirectorDanielle Burnett Deputy Chief NurseMichael Cawley Operational Director of FinanceLucy Dadge Chief Commissioning OfficerJoe Lunn Associate Director of Primary CareHelen Griffiths Associate Director of Primary Care NetworksDr Richard Stratton GP RepresentativeSue Sunderland Non-Executive DirectorDr Ian Trimble Independent GP Advisor
In attendance:Louise Espley Corporate Governance Officer (minute taker)Lynette Daws Head of Primary CareSiân Gascoigne Head of Corporate Assurance Jo Simmonds Head of Corporate GovernanceEsther Gaskill Head of Quality – Primary CareMichael Wright Nottinghamshire Local Medical Committee
Apologies: None
Cumulative Record of Members’ Attendance (2020/21)
Name Possible Actual Name Possible Actual
Shaun Beebe 02 02 Joe Lunn 02 02
Michael Cawley 02 02 Dr Richard Stratton 02 02
Lucy Dadge 02 02 Sue Sunderland 02 02
Eleri de Gilbert 02 02 Dr Ian Trimble 02 02
Helen Griffiths 02 02 Danielle Burnett 02 02
Ratified Minutes of CCG Committee meetings
205 of 22409:00 - 10.50-04/08/21

Page 2 of 9
Introductory Items
PCC 21 026 Welcome, Introductions and Apologies
Eleri de Gilbert welcomed everyone to the public session of the Primary Care Commissioning Committee meeting, which was being held virtually due to the COVID-19 pandemic.
PCC 21 027 Confirmation of Quoracy
The meeting was confirmed as quorate.
PCC 21 028 Declaration of interest for any item on the shared agenda
No conflicts of interest were identified for this meeting.
Members were reminded that they can raise an interest at the beginning of, or during discussion of an item if they realise that they do have an interest.
PCC 21 029 Management of any real or perceived conflicts of interest
No conflicts of interest were identified.
PCC 21 030 Questions from the public
No questions had been received from the public.
PCC 21 031 Minutes from the meeting held on 21 April 2021.
The minutes of the meeting were approved as a true and accurate record of proceedings.
PCC 21 032 Action log and matters arising from the meeting held on 21 April 2021
All actions on the log are complete.
Eleri de Gilbert provided an update on the development of the primary care heat map, as follows:
a) Committee members attended a development session in April 2021 to explore the components and framework of the heat map. The session had provided the opportunity for discussion and the sharing of ideas. A number of issues influencing the heat map were explored, primarily, links with the Integrated Care System (ICS) transition programme and the sensitivity of the data held within the heat map.
b) The Committee agreed to receive an update on the Integrated Care System (ICS) framework in June 2021, with a particular focus on the implications for Primary Care and the role of the Committee.
ACTION:∑ ICS framework update to be provided the PCCC in June 2021, with
considerations for Primary Care highlighted.
Ratified Minutes of CCG Committee meetings
206 of 224 09:00 - 10.50-04/08/21

Page 3 of 9
Commissioning, Procurement and Contract Management
PCC 21 033 Covid-19 Capacity expansion fund – How the allocation was used to meet the priority goals.
Joe Lunn presented the item and highlighted the following points:a) The paper detailed the utilisation of the Covid-19 expansion fund to date
(£2.73m). b) The seven priority goals for utilisation of the fund were shared in the paper. c) Funding was distributed across all Clinical Commissioning Group (CCG) member
GP practices. The process of collecting the evidence of meeting the priority goalswas almost complete.
d) The Covid-19 expansion fund has been extended from April 2021 to September 2021 with an anticipated CCG allocation of £2.13m.
The following points were raised in discussion:e) It was confirmed that in addition to providing evidence of meeting the
requirements of the seven priority goals, practices were also submitting the necessary workforce data.
f) Clarification was provided regarding the Learning Disabilities data reported; the figure of 85% related to one practice rather than system performance.
g) All returns had been positive. Quantifiable data had not been a pre-requisite for reporting.
The Committee:∑ RECEIVED and NOTED the report.
PCC 21 034 Monthly contract update
Lynette Daws presented the report and highlighted the following key points:a) The contract log provided detail from the last 12 months of contractual action in
respect of GP providers’ contracts across Nottingham and Nottinghamshire.b) All contractual changes follow the process outlined in the NHS England
Improvement Primary Care Policy and Guidance Manual (PGM).c) Hill View surgery had completed their transition to Farnsfield Surgery. The
process had been relatively smooth with positive feedback received by the Parish Council and social media.
d) Bilborough Surgery had closed on 05 May 2021 as planned.
No further points were raised in discussion.
The Committee:
∑ RECEIVED and NOTED the contract update.
Ratified Minutes of CCG Committee meetings
207 of 22409:00 - 10.50-04/08/21

Page 4 of 9
PCC 21 035 Local Enhanced Services 2021/22: General Practice sign up
Joe Lunn presented the item and highlighted the following key points:a) The paper provided an overview of the uptake of Local Enhanced Services
(LES) for 2021/22 and alternative commissioning arrangements where practices had not signed up to the LES.
b) Sign up from practices had been similar to previous years and all 126 practices had confirmed their intention to deliver some services.
No further points were raised in discussion.
The Committee:∑ RECEIVED and NOTED the report.
PCC 21 036 General Practice Referral to Community Pharmacist Funding
Helen Griffiths presented the item and highlighted the following key points:a) The paper provided a summary of how the £4k funding would be utilised in
accordance with the NHS England Improvement (NHSEI) Memorandum of Understanding (MOU).
b) The scheme had been piloted across the country since 2019 therefore established pathways to support triage and extended consultation by Community Pharmacists are available.
c) This scheme supports the improved access agenda.d) PCN Clinical Directors had been involved in discussions and an implementation
plan will follow.
No points were raised in discussion.
The Committee:∑ RECEIVED and NOTED the report.
Quality Improvement and Assurance
PCC 21 037 Integrated Care Systems – PCN support funding
Helen Griffiths presented the item and highlighted the following key points:a) NHS England had issued a Memorandum of Understanding (MOU) to
Nottingham and Nottinghamshire CCG to support Integrated Care Systems (ICS) and their constituent Primary Care Networks (PCNs).
b) The funding (310k) would provide backfill costs for preparatory work and meetings between CCG(s) and PCN Clinical Directors as well as PCN to PCN meetings to explore how PCNs will be represented in the ICS governance structure.
c) The CCG and the ICS would work together to ensure PCNs are engaged and represented in the ICS governance structure with the CCG reporting activity and progress to NHSEI as per the requirements of the MOU.
Ratified Minutes of CCG Committee meetings
208 of 224 09:00 - 10.50-04/08/21

Page 5 of 9
No further points were raised in discussion:
The Committee:
∑ RECEIVED and NOTED the paper and MOU for information.
PCC 21 038 Primary Care Quality report
Esther Gaskill presented the item and highlighted the following key points:a) The paper provided a summary of the quarter four quality dashboard ratings and
actions alongside an update on the activity of the Primary Care Quality Groups and Primary Care Quality team.
b) Current Care Quality Commission (CQC) ratings were included in the paper along with actions being taken to support practices with ratings of ‘Inadequate’ or ‘Requires Improvement’.
c) Information was provided in respect of practices currently receiving an enhanced level of support from the Primary Care Quality Team.
The following points were raised in discussion:d) The Committee welcomed the comprehensive report which described a positive
picture and continuing improvements across practices. e) It was noted that performance differs across practices and that in some cases
good performance by one practice may disguise poorer performance elsewhere. The example of the Learning Disabilities target mentioned earlier in the meeting was used as an example. It was confirmed that practices who struggle to achieve the target receive input and support.
f) Specifically in relation to Learning Disabilities annual health checks, the Deputy Chief Nurse cited this as an area of focus in terms of the quality of checks going forward. An update would be provided to the Committee in July. 2021.
The Committee:∑ RECEIVED and NOTED the Primary Care Quality report.
Covid-19 Recovery and Planning
PCC 21 039 Overview of GP Practice additional expenses in relation to Covid-19
Joe Lunn presented the item and highlighted the following key points:a) The paper provided an update on guidance and restrictions set out by NHS
England Improvement in the letter published 4th August 2020. The claiming period covered in the report is to 31 March 2021.
b) During March 2021 £547 had been claimed for exceptional Covid-19 support. c) In the same period 16 claims had been received via the Covid-19 expansion
fund. The claims pertain to seven practices; all were approved for payment (circa
ACTION:∑ Learning Disabilities paper to be presented to the Committee in July
2021.
Ratified Minutes of CCG Committee meetings
209 of 22409:00 - 10.50-04/08/21

Page 6 of 9
£12k). d) The Covid-19 expansion fund would continue to September 2021.
No further points were raised in discussion.
The Committee:∑ RECEIVED and NOTED the paper for assurance purposes.
PCC 21 040 Covid-19 Practice Level Update: Operational Pressures Escalation Levels (OPEL)
Joe Lunn presented the item and highlighted the following points:a) The paper covered the four week period to 30 April 2021 and detailed OPEL
levels alongside the number of days spent at that level.b) A shift in reporting had been observed, 75 practices across the CCG reported
increased pressures, which impacted their ability to support other practices in the system.
c) One clinical management centre remains in place.
The following points were raised in discussion:d) Pressure in primary care had been the subject of media attention in recent days
therefore the Committee sought an update on the May position to date. The current position was outlined as follows; South Nottinghamshire is reporting greater demand with 50% of practices consistently reporting OPEL level 2 (previously level 1), mid Nottinghamshire is reporting a similar position to April, although one practice has moved to OPEL 3 during the last week. A number of Nottingham City practices had reported OPEL 3 in the last couple of weeks. The trend in May (to date) is an increasing demand in primary care.
e) Reference was made to the letter from NHSEI to General Practice regarding face to face patient consultations. The letter had not been received well in Primary Care who had felt that the considerable efforts made by practices during the pandemic had not been recognised. The letter had prompted a significant amount of national and local publicity, which had led to additional demand pressures in practices, particularly in relation to reception staff.
f) Both the Local Medical Committee (LMC) and the CCG had provided positive reassurance to the CCG’ member practices, which had been helpful.
g) Joe Lunn confirmed that March 2021 data confirms that 55% of general practice appointments were face to face appointments, with 51% of those being offered on the same or next day.
The Committee:∑ RECEIVED and NOTED the report.
ACTION:∑ Joe Lunn to share the updated Standard Operating Procedure to support the
restoration of General Practice (dated 13 May 2021) with Non-Executive Directors.
∑ Committee to receive an update on the position in June 2021.
Ratified Minutes of CCG Committee meetings
210 of 224 09:00 - 10.50-04/08/21

Page 7 of 9
Financial Management
PCC 21 041 Finance report – month one
Michael Cawley presented the item and highlighted the following points:a) The paper addressed two aspects; Primary Care Commissioning Committee
expenditure for the year ending 2020/21 (subject to external audit scrutiny) and the financial plan for the first six months of 2021/22, set alongside the month one out-turn position.
b) The CCG achieved its key financial targets for the year ended 31 March 2021, including delivery against the agreed year end position.
c) Within that position Primary Care Commissioning related spend accounted for a £1.36 million overspend when compared to delegated budgets. The position reflected the main drivers that have previously been reported; namely additional slippage on PCN Additional Roles offset by overspends in APMS, Prescribing/ Dispensing as well as Premises Costs spend lines.
d) The CCG set aside additional year end accrual adjustments based on additional information received. The CCG has been able to accommodate those accruals into its overall financial position.
e) The CCG has received confirmation on its allocations for the first six months of 2021/22, referred to as H1.
f) The report set out how those allocations are expected to be allocated across each of the areas within Primary Care Delegated budgets.
g) A Financial Plan for H1 (and therefore the delegated budget) has been submitted to NHSEI Improvement and remains subject to their approval.
The following points were raised in discussion:h) In response to a question regarding the APMS budget plan for H1 it was
confirmed that the movement in budget plans reflect current contract arrangements.
The Committee:∑ RECEIVED and NOTED the contents of the Primary Care Commissioning
Finance report. ∑ APPROVED the Primary Care Commissioning Finance report for the period
ending April 2021 (on the understanding that the overall CCG financial plan submission to NHSEI remains subject to their approval).
Risk Management
PCC 21 042 Risk Report
Siân Gascoigne presented the item and highlighted the following points:a) There are currently seven risks relating to the Committee’s responsibilities. This
is the same number of risks as presented to the Committee in April 2021.b) As agreed by the Committee in April 2021, the risk in relation to RR 126 (overall
Ratified Minutes of CCG Committee meetings
211 of 22409:00 - 10.50-04/08/21

Page 8 of 9
impact of Covid-19 on the safe and effective delivery of primary care services) had been reduced from 16 (red) to 12 (amber/red).
c) Risk RR 157 score (Farnsfield Surgery) would be reduced as a result of the report and discussion at item PCC 21 034.
No further points were made in discussion.
The Committee:∑ COMMENTED on the risks shown within the paper (including the high/red risk)
and those at Appendix A
∑ CONFIRMED that no new risks had been identified during the course of the meeting for inclusion in the corporate risk register.
Other: Covid-19 Vaccination Programme related
PCC 21 043 CVP: Q1 2021/22 Primary Care Network (PCN) ‘Clinical Director Uplift’ payments
Helen Griffiths presented the item and highlighted the following points:a) The Committee received a paper regarding this payment in March 2021. Further
notification had been received from NHSEI that the payment would be extended to quarter one of 2021/22.
b) NHSEI require the CCG sign off the proposed payments to be made directly toPrimary Care Networks.
c) The paper confirmed that all PCNs are eligible to receive payment.
The Committee∑ NOTED the revised guidance.∑ CONSIDERED the CCG’s proposal regarding the approach to manage the
transaction.∑ SUPPORTED the authorisation of payments by NHSEI to PCNs.
Closing Items
PCC 21 044 Any other business
Joe Lunn and Lynette Daws attended the Nottingham City Council Health Scrutiny Committee on 13 May 2021 to discuss the Platform One Practice. Three recommendations and one action had been received as a result of the meeting. A written response would be provided and shared with the Primary Care Commissioning Committee.
No other business was raised.
PCC 21 045 Key messages to escalate to the Governing Body
The Committee:∑ NOTED an increase in demand on General Practice as a result of NHSEI
guidance and would monitor the position. ∑ APPROVED the Primary Care Commissioning Finance report for the period
ending April 2021 (on the understanding that the overall CCG financial plan
Ratified Minutes of CCG Committee meetings
212 of 224 09:00 - 10.50-04/08/21

Page 9 of 9
submission to NHSEI remains subject to their approval). ∑ WELCOMED an update on the successful transition at Farnsfield surgery by
Hillview surgery.
PCC 21 046 Date of next meeting:16/06/2021Zoom Meeting
Confidential Motion:
The Primary Care Commissioning Committee will resolve that representatives of the press and other members of the public be excluded from the remainder of this meeting, having regard to the confidential nature of the business to be transacted, publicity on which would be prejudicial to the public interest (Section 1[2] Public Bodies [Admission to Meetings] Act 1960)
Ratified Minutes of CCG Committee meetings
213 of 22409:00 - 10.50-04/08/21

Page 1 of 5
NHS Nottingham and Nottinghamshire Clinical Commissioning GroupPrimary Care Commissioning Committee (Public Session)
Unratified minutes of the meeting held on16/06/2021 09:00 – 09.30
Zoom Meeting
Members present:
Eleri De Gilbert Non-Executive Director (Chair)Shaun Beebe Non-Executive DirectorDanielle Burnett Deputy Chief NurseMichael Cawley Operational Director of FinanceLucy Dadge Chief Commissioning OfficerJoe Lunn Associate Director of Primary CareHelen Griffiths Associate Director of Primary Care NetworksSue Sunderland Non-Executive DirectorDr Ian Trimble Independent GP Advisor
In attendance:Louise Espley Corporate Governance Officer (minute taker)Lynette Daws Head of Primary CareSiân Gascoigne Head of Corporate Assurance Jo Simmonds Head of Corporate GovernanceEsther Gaskill Head of Quality – Primary CareMichael Wright Nottinghamshire Local Medical Committee
Apologies:Dr Richard Stratton GP Representative
Cumulative Record of Members’ Attendance (2020/21)
Name Possible Actual Name Possible Actual
Shaun Beebe 03 03 Joe Lunn 03 03
Michael Cawley 03 03 Dr Richard Stratton 03 02
Lucy Dadge 03 03 Sue Sunderland 03 03
Eleri de Gilbert 03 03 Dr Ian Trimble 03 03
Helen Griffiths 03 03 Danielle Burnett 03 03
Ratified Minutes of CCG Committee meetings
214 of 224 09:00 - 10.50-04/08/21

Page 2 of 5
Introductory Items
PCC 21 048 Welcome, Introductions and Apologies
Eleri de Gilbert welcomed everyone to the public session of the Primary Care Commissioning Committee meeting, which was being held virtually due to the COVID-19 pandemic.
PCC 21 049 Confirmation of Quoracy
The meeting was confirmed as quorate.
PCC 21 050 Declaration of interest for any item on the shared agenda
No conflicts of interest were identified for this meeting.
Members were reminded that they can raise an interest at the beginning of, or during discussion of an item if they realise that they do have an interest.
PCC 21 051 Management of any real or perceived conflicts of interest
No conflicts of interest were identified.
PCC 21 052 Questions from the public
No questions had been received from the public.
PCC 21 053 Minutes from the meeting held on 19 May 2021.
The minutes of the meeting were approved as a true and accurate record of proceedings subject to two amendments:
- Page 3, PCC 21 033, £213million to be replaced with £2.13million.
- Page 4, PCC 21 035, insert the word ‘some’ before services in the last line of point b).
PCC 21 054 Action log and matters arising from the meeting held on 19 May 2021
All actions on the log are complete or to be reported to a future Committee.
PCC 21 055 Actions arising from the Governing Body meeting held on 02 June 2021
The Governing Body asked the Committee to review the risks on its risk register in light of the workload pressures being experienced in General Practice.
Commissioning, Procurement and Contract Management
PCC 21 056 Monthly contract update
Lynette Daws presented the report and highlighted the following key points:a) The contract log provided detail from the last 12 months of contractual action in
respect of GP providers’ contracts across Nottingham and Nottinghamshire.
Ratified Minutes of CCG Committee meetings
215 of 22409:00 - 10.50-04/08/21

Page 3 of 5
b) All contractual changes follow the process outlined in the NHS England Improvement Primary Care Policy and Guidance Manual (PGM).
c) The Committee’s attention was drawn to a number of entries on the contract log that would be removed following the meeting as the contractual issues areresolved. They related to Sherwood Medical Partnership (Farnsfield Surgery), Bilborough Surgery, Giltbrook Surgery and Leen View Surgery.
No further points were raised in discussion.
The Committee:
∑ RECEIVED and NOTED the contract update.
Covid-19 Recovery and Planning
PCC 21 057 Overview of GP Practice additional expenses in relation to Covid-19
Joe Lunn presented the item and highlighted the following key points:a) The paper provided an update on guidance and restrictions set out by NHS
England/Improvement in the letter published 4th August 2020. The claiming period covered in the report is to 28 May 2021.
b) The CCG received nine claims on behalf of three practices. All nine claims were approved for payment totaling £11,294.
No further points were raised in discussion.
The Committee:∑ RECEIVED and NOTED the paper for assurance purposes.
PCC 21 058 Covid-19 Practice Level Update: Operational Pressures Escalation Levels (OPEL)
Joe Lunn presented the item and highlighted the following points:a) The paper covered the four week period to 28 May 2021 and detailed OPEL
levels alongside the number of days spent at that level.b) One clinical management centre remains in place. The number of appointments
has been reduced from 22 to 11 per day since 05 May 2021. Of the 220 available appointments during this reporting period, 188 were utilised.
c) The period reported covered 19 working days. Three practices reported days at OPEL level three for a total of 16 days across all practices.
d) 92 practices reported OPEL 2, with 62 practices reporting this level for 10 days or more and 30 reporting this level for less than 10 days.
e) 34 practices reported OPEL 1 consistently. 27% of practices were OPEL 1 for the full 19 days.
The following points were raised in discussion:f) In response to a question regarding the OPEL report it was confirmed that the
current OPEL position reflects the increased demand in Primary Care and the fact that practices are becoming better at accurately reporting their OPEL status.
The Committee:
Ratified Minutes of CCG Committee meetings
216 of 224 09:00 - 10.50-04/08/21
Page 4 of 5
∑ RECEIVED and NOTED the report.
Financial Management
PCC 21 059 Finance report – month two
Michael Cawley presented the item and highlighted the following points:a) Since the May meeting, the CCG’s 2020/21 Accounts had been submitted to
NHSE/I. A clean audit report had been received with no changes to the previously reported spend.
b) The paper detailed the financial position for Primary Care Commissioning Committee (PCCC) spend for month two 2021/22. The report had been prepared in the context of the revised financial regime implemented by NHSE/I in response to the current COVID-19 pandemic for M1-6 (H1).
c) Both the year to date and forecast position show a financial position at or around budget.
d) The CCG is expecting to remain within the delegated budgets that have been set for the rest of the year.
e) Reference was made to the primary care capital budget, of which 48% is primary care related. The Committee would be kept appraised of commitments against the capital plan in terms of spend via this report.
f) It was suggested that reports on capital schemes from the Associate Director of Estates and Associate Director of Performance and Information would be beneficial to the Committee.
The following points were raised in discussion:g) It was noted that the GP IT Strategy had been deferred from this agenda to a
future agenda. However, the Committee would request an update report on GP IT at the July meeting.
h) In response to a query on available GP IT capital monies it was agreed that it would be further explored and reported to the Committee in July 2021.
The Committee:∑ RECEIVED and NOTED the contents of the Primary Care Commissioning
Finance report.
Risk Management
PCC 21 060 Risk Report
Siân Gascoigne presented the item and highlighted the following points:a) There are currently seven risks relating to the Committee’s responsibilities. This
is the same number of risks as presented to the Committee in May 2021.b) Following discussions at the May meeting, action had been taken to fully review
risks RR 023 and RR 157. In light of this, the overall risk scores for both have
ACTION:∑ Andy Hall to provide an update to the PCCC in July on GP IT issues∑ Michael Cawley and Andy Hall to discuss the availability of additional funding
for GP IT.
Ratified Minutes of CCG Committee meetings
217 of 22409:00 - 10.50-04/08/21

Page 5 of 5
been reduced to 6, which is below the threshold for inclusion on the Corporate Risk Register.
c) The narrative in relation to RR 126 and RR 160 had been reviewed following discussion at the Committee.
d) At its meeting held on 02 June 2021, the Governing Body had asked the Committee to review the content and scores of all risks within its remit to ensure that concerns around the workload pressures in Primary Care are reflected. As such, the Committee was asked to offer views on the narrative of all risks in Appendix A of the report.
The following points were raised in discussion:e) It was agreed that RR 023 would be reviewed again for the purposes of clarity,
ahead of archiving. f) The Committee confirmed they were comfortable with the risk scores as
presented in Appendix A.g) It was suggested that a consolidated, overarching strategic risk may be required
to reflect the new primary care landscape and its impact on business as usual.
The Committee:∑ APPROVED the archiving of risks RR 023 and RR 157, subject to amending RR
023.∑ COMMENTED on the risks shown within the paper (including the high/red risk)
and those at Appendix A. ∑ ENSURED that the risks currently within the Committee’s remit adequately
capture primary care related discussions at the June 2021 meeting of the Governing Body.
∑ CONFIRMED that no new risks had been identified during the course of the meeting for inclusion in the corporate risk register.
Closing Items
PCC 21 061 Any other businessNo other business was raised.
PCC 21 062 Key messages to escalate to the Governing Body
The Committee agreed that there were no specific items to be escalated to the Governing Body.
PCC 21 063 Date of next meeting:21/07/2021
Confidential Motion:
The Primary Care Commissioning Committee will resolve that representatives of the press and other members of the public be excluded from the remainder of this meeting, having regard to the confidential nature of the business to be transacted, publicity on which would be prejudicial to the public interest (Section 1[2] Public Bodies [Admission to Meetings] Act 1960)
Ratified Minutes of CCG Committee meetings
218 of 224 09:00 - 10.50-04/08/21

Page 1 of 6
Audit and Governance CommitteeRATIFIED minutes of the meeting held on
23/04/2021, 9.00-10.00Via MS Teams
Members present:Sue Sunderland Non-Executive Director (Chair)Jon Towler Non-Executive Director
In attendance:Hazel Buchanan Associate Director of Strategic Programmes and EPRR (item AG
21 007)Craig Bevan Davies Counter Fraud Specialist, 360 AssuranceLucy Branson Associate Director of GovernanceMichael Cawley Operational Director of FinanceIan Livsey Deputy Director of FinanceAudrey McDonald Assistant Director of FinanceAndrew Morton Operational Director of FinanceStuart Poynor Chief Finance OfficerTimothy Thomas Head of Internal Audit, 360 Assurance Richard Walton Senior Manager, KPMGSue Wass Corporate Governance Officer (minutes)Kevin Watkins Client Manager, 360 Assurance
Apologies: Eleri de Gilbert Non-Executive Director
Cumulative Record of Members’ Attendance (2021-22)Name Possible Actual Name Possible ActualEleri de Gilbert 1 0 Jon Towler 1 1Sue Sunderland 1 1
Introductory Items
AG 21 001 Welcome and apologies Sue Sunderland welcomed everyone to the meeting of the Audit and Governance Committee, which was held on MS Teams due to the current Covid-19 situation.
Apologies were noted a above.
AG 21 002 Confirmation of quoracy The meeting was declared quorate.
AG 21 003 Declaration of interest for any item on the agendaNo interests were noted on any item on the agenda.
Sue Sunderland reminded members of their responsibility to highlight any interests
Ratified Minutes of CCG Committee meetings
219 of 22409:00 - 10.50-04/08/21

Page 2 of 6
should they transpire as a result of discussions during the meeting.
AG 21 004 Management of any real or perceived conflicts of interestThis item was not required as no interests were declared.
AG 21 005 Minutes from the meeting held on 30 March 2021The minutes of the meeting held on 30 March were agreed as an accurate record of the discussions held.
AG 21 006 Action log and matters arising from meeting held on 30 March 2021Actions AG 20 127 and 128 were noted as not yet due and would report to the June meeting.
All other actions were noted as complete and there were no matters arising.
Emergency Preparedness, Resilience and Response (EPRR) and Business Continuity
AG 21 007 Emergency, Preparedness, Resilience and Response (EPRR) PolicyHazel Buchanan was in attendance to present this item and highlighted the following key points:a) The Policy had been brought to the Committee for approval following a scheduled
review to ensure that it remained current. At this point in time no fundamental changes had been made. Of note was the change to the role of Accountable Emergency Officer, which had been assigned to the CCG’s Chief Commissioning Officer.
b) From April 2022 there would potentially be significant changes to the role and responsibility of the statutory ICS in relation to the management of EPRR (subject to legislation), which would need to be reflected in a revised policy. This was being discussed with NHS England and NHS Improvement.
c) Any revised policy would also need to take into account changed business continuity arrangements, due to the evolving agile working arrangements.
d) As the CCG moved out of incident mode, training and EPRR business as usual arrangements would be resumed.
The following points were raised in discussion:e) Members noted that any legislative change regarding EPRR responsibilities would
be incorporated into the Bill to establish ICSs as statutory bodies.f) In her role to support the Accountable Emergency Officer for the implementation of
EPRR arrangements, Sue Sunderland noted that she would meet with Hazel Buchannan later in the year once firmer plans were in place.
The Committee:∑ APPROVED the Emergency, Preparedness, Resilience and Response (EPRR)
Policy.
At this point, Hazel Buchanan left the meeting
Annual Reporting
AG 21 008 Annual Report 2020/21: DraftLucy Branson presented this item and highlighted the following key points:a) The report presented the draft annual report for review and comment prior to its
submission to NHS England on 27 April.b) The core requirements of the document were prescribed by HM Treasury and
translated by NHS England into a template for completion. As 2020/21 had been
Ratified Minutes of CCG Committee meetings
220 of 224 09:00 - 10.50-04/08/21
Page 3 of 6
an exceptional year, NHS England had given CCGs the option to omit two sections. It was proposed to omit the detailed performance analysis section in recognition of the impact of Covid-19 on performance targets; an overview would still be incorporated into the report to explain the work being completed to restore and recover services. An option was given to omit staff sickness and turnover metrics. However, it was proposed to include these in the report, as the CCG had not been particularly impacted.
c) Further work was still required in three areas: the finalising of the Accountable Officer’s Statement; the summary of performance; and the completion of a recently received checklist from NHS England that had included a number of additional requirements.
d) Following the circulation of the report to members, the pay multiples section had been amended and a revised section had been circulated. Following re-examination of the technical advice, an error had been made in the original calculation.
e) It was noted that potential anomalies in the pension benefits section had been raised with the NHS Pensions Agency.
The following points were raised in discussion:f) Members were supportive of the proposals if there was a sufficient level of detail in
the performance overview of the actions taken by the CCG to mitigate the on-going impact of Covid-19 on service delivery targets.
g) Members queried the section on sustainable development, noting it to be a requirement; however the CCG had been unable to provide data. It was noted that data was usually drawn from the performance of CCG office bases. Due to the working from home arrangements that had been put in place during the year, CCG offices had not been used. Enquiries into whether working from home arrangements could be quantified had been undertaken, but data could not be calculated in a meaningful way. It was proposed that this explanation should be included in the narrative, which was agreed.
h) Members took assurance that the CCG was on track to submit the report by thedeadline of 27 April and congratulated the Governance Team for the hard work that had been undertaken to produce a substantially complete draft annual report.
The Committee:∑ NOTED the further work required for annual report 2020/21 prior to submitting the
final draft version;∑ REVIEWED the CCG’s draft annual report 2020/21; ∑ NOTED that the Committee will be responsible for approving the final annual report
2020/21 at the next Committee meeting on 10 June 2021.
AG 21 009 Annual Accounts 2020/21: UnauditedMichael Cawley presented this item and highlighted the following key points:a) The report provided a briefing to accompany the unaudited accounts. As the paper
had only recently been circulated it was proposed that members fed back any queries outside of the meeting upon further scrutiny of the report. A response to any queries would be presented alongside the final audited accounts at the June meeting.
b) Audrey McDonald detailed the content of the briefing paper. Of note was the need for clarity of the definition for ‘very senior manager’ posts for the purposes of the remuneration report.
c) Ian Livsey detailed the contents of the appendix to the briefing note, which gave an overview of the provisional financial performance of the CCG. All targets had been met.
Ratified Minutes of CCG Committee meetings
221 of 22409:00 - 10.50-04/08/21
Page 4 of 6
The following points were raised in discussion:d) Members took assurance that the CCG was on track to submit the unaudited
accounts by the deadline and congratulated the Finance Team for the hard work that had been undertaken ahead of the deadline for submission.
e) Members noted that the financial performance report was commensurate with the in-year reports that had been brought to the Finance and Resources Committee. Although the CCG had delivered an in-year surplus, the underlying deficit had not been addressed, which posed on-going financial challenges for the 2021/22financial year.
The Committee:∑ NOTED the report and unaudited accounts.
At this point, Ian Livsey and Audrey McDonald left the meeting
Financial Stewardship
AG 21 010 Tender Waiver RegisterLucy Branson presented this item and highlighted the following key points:a) The Committee was responsible for reviewing all instances where the CCG waived
the requirement for competitive tendering. The report presented the decisions that had been made since the last update in September 2020.
b) Since this time there had been 23 new entries, which reflected the number of contracts that had needed to be rolled forward due to the need to prioritise the CCG’s response to the pandemic. All had been through the CCG’s governance processes and had been agreed by the relevant Governing Body committees.
The following points were raised in discussion: c) A minor error on the dates in the reporting column was noted, which would be
amended.d) It was noted that each entry was well explained and assurance was taken that all
entries had been considered by other committees.
The Committee:∑ REVIEWED the Tender Waiver Register.
Internal Audit
AG 21 011 Internal Audit PlanKevin Watkins provided a verbal update in relation to this item and highlighted the following key points:a) The two outstanding audits from the 2020/21 plan were on track to be completed by
agreed deadlines and would be reported to the June Committee meeting.b) Following discussions at the previous meeting regarding the 2021/22 plan,
discussions with the Chief Nurse regarding the possible scope and timing of an audit on safeguarding had taken place; the plan had been shared with committee chairs and plans to meet with CCG executive officers had been put in place.
c) The timing of the audits would be a key issue for the final plan, as there would be no carry forward of work into 2022/23. A full update would be provided at the next meeting.
The Committee:∑ NOTED the verbal update.
Ratified Minutes of CCG Committee meetings
222 of 224 09:00 - 10.50-04/08/21
Page 5 of 6
External Audit
AG 21 012 External Audit UpdateRichard Walton was in attendance to present this verbal item and highlighted the following key points:a) The audit team had a daily work programme in place to undertake their audit during
April, May and June and would commence work following the submission of the accounts on 27 April.
The Committee:∑ NOTED the verbal update.
Policies
AG 21 013 Counter Fraud Policy Craig Bevan Davies was in attendance to present this item and highlighted the following key points:a) The Policy had been brought to the Committee for approval following a review to
ensure it incorporated changes to the new Counter Fraud Standard. b) The NHS Counter Fraud Authority had released the Government Functional
Standard 013 Counter Fraud as a suite of requirements to countering fraud across the NHS. This replaced the previous standards and became effective on 1 April 2021. The Policy also included a Fraud Response Plan, which was a requirement under the new Standard.
The Committee:∑ APPROVED the Fraud, Bribery and Corruption Policy, subject to a minor change to
Jon Towler’s email address.
Risk Management
AG 21 014 Risk Management Year End UpdateLucy Branson was in attendance to present this item and highlighted the following key points:a) The Committee was responsible for reviewing the strategic and operational risk
management processes across the CCG and satisfying themselves that the overall system in place was effective. The report provided the Committee with a year-end update on work undertaken to embed the CCG’s strategic and operational risk management arrangements during 2020/21.
b) As the CCG’s Assurance Framework had been presented to the previous meeting, it was suggested that members focus on the section on the CCG’s operational risk management arrangements and attention was drawn to the current risk profile. The turnover of risks was an indicator of how effectively the CCG was managing the risks. During the course of the year 32 risks had been identified and 19 archived. Only two risks had remained on the register for any length of time. The risks were regularly overseen by the appropriate CCG committee.
c) Separate Covid-19 incident response risk management arrangements had been put in place in April 2020 and continued to be overseen by the CCG’s Incident Management Team. A full review of these risks would be undertaken when the Incident Management Team was stepped down to determine if any risks remained live. A full programme of risk management training would also be re-started at this time.
d) Looking ahead there was a need to develop risk management arrangements for the ICS and provide risk management oversight for the transition of the CCG to the ICS
Ratified Minutes of CCG Committee meetings
223 of 22409:00 - 10.50-04/08/21

Page 6 of 6
(subject to legislation), which would be overseen by the ICS Transition and Risk Committee.
e) There were currently seven risks on the Corporate Risk Register that fell within the Audit and Governance Committee’s responsibilities, the same number of risks that had been presented previously.
The following points were raised in discussion:f) Members agreed that an assurance report should be brought to the August meeting
on the scope of the transition risks and the development of risk management arrangements for the ICS.
The Committee:∑ NOTED the progress of embedding the CCG’s strategic and operational risk
management arrangements;∑ NOTED the full Corporate Risk Register; ∑ NOTED the risk management processes that have been followed during the Covid-
19 emergency response period.
ACTION: ∑ Lucy Branson to bring to the August Committee meeting an assurance report
on the scope of the transition risks and the development of risk management arrangements for the ICS.
Closing Items
AG 21 015 Any other businessStuart Poynor gave his thanks to the hard work of the Governance and Finance Teamsfor the production of the draft annual report and accounts under challenging circumstances.
AG 21 016 Key messages to escalate to the Governing Body∑ Assurance that work was progressing to produce the CCG’s annual report and
accounts.∑ Assurance that the CCG had robust risk management arrangements in place.
AG 21 017 Date of the next meeting:10/06/2021Via MS Teams
Ratified Minutes of CCG Committee meetings
224 of 224 09:00 - 10.50-04/08/21














![10 11 Session HR Session Seri Management[1]](https://static.fdokumen.com/doc/165x107/6314ba61fc260b71020fb0ee/10-11-session-hr-session-seri-management1.jpg)




