
4.10pm Barton Village Hall - East Staffordshire CCG
314
EAST STAFFORDSHIRE CCG GOVERNING BODY A G E N D A OPEN SECTION Thursday 27 November 2014 1.00pm – 4.10pm Barton Village Hall, Barton under Needwood, DE13 8AF Lead Time 1. Apologies Chair 13:00 2. (a) Declarations of Interest If any member or anyone present has any pecuniary / non-pecuniary interest in any contract, proposed contract or other matter under consideration at this meeting, he/she shall disclose the fact to the Chair and shall not take part in the consideration or discussion of the matter or vote on any question with respect to it. Chair / All 13:02 3. Minutes of Meeting held on 25 September 2014 Enc. 1 Chair 13:05 4. Actions from Meeting held on 25 September 2014 Enc. 2 Chair 13:10 5. Chairman’s Report Enc. 3 Chair 13:15 6. Accountable Officer’s Report Enc. 4 Tony Bruce 13:20 7. Patient Board Update Enc. 5 Ann Tunley 13:25 8. Personal Health Budget Policy Ratification Enc. 6 Christine Brown 13:30 Strategic Items 9. Mental Health Strategy (Rita Symons/Nicky Harkness) Enc. 7 Sarah Laing 13:40 10. KPMG Recommendations – Staffordshire Strategy Frail Elderly Care (Nicky Harkness Enc. 8 Sarah Laing 13:50 11. TECS Strategy – Dave Whatton Enc. 9 Dave Whatton 14:00 12. Improving Lives Update Enc. 10 Emily Davies 14:10 Quality & Safety 13. Quality Report Enc. 11 Heather Johnstone 14:20 Performance 14. • Finance Report - Month 7 • Financial Recovery Plans 2015/16 Enc. 12 Enc. 12a Wendy Kerr 14:30 15. Performance Report – Months 6 & 7 Enc. 13 Wendy Kerr 14:40 1
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of 4.10pm Barton Village Hall - East Staffordshire CCG
EAST STAFFORDSHIRE CCG GOVERNING BODY
A G E N D A
OPEN SECTION Thursday 27 November 2014
1.00pm – 4.10pm Barton Village Hall, Barton under Needwood, DE13 8AF
Lead Time 1. Apologies Chair 13:00
2.
(a) Declarations of Interest If any member or anyone present has any pecuniary / non-pecuniary interest in any contract, proposed contract or other matter under consideration at this meeting, he/she shall disclose the fact to the Chair and shall not take part in the consideration or discussion of the matter or vote on any question with respect to it.
Chair / All 13:02
3. Minutes of Meeting held on 25 September 2014 Enc. 1 Chair 13:05
4. Actions from Meeting held on 25 September 2014 Enc. 2 Chair 13:10
5. Chairman’s Report Enc. 3 Chair 13:15
6. Accountable Officer’s Report Enc. 4 Tony Bruce 13:20
7. Patient Board Update Enc. 5 Ann Tunley 13:25
8. Personal Health Budget Policy Ratification Enc. 6 Christine Brown 13:30
Strategic Items
9. Mental Health Strategy (Rita Symons/Nicky Harkness) Enc. 7 Sarah Laing 13:40
10. KPMG Recommendations – Staffordshire Strategy Frail Elderly Care (Nicky Harkness Enc. 8 Sarah Laing 13:50
11. TECS Strategy – Dave Whatton Enc. 9 Dave Whatton 14:00
12. Improving Lives Update Enc. 10 Emily Davies 14:10
Quality & Safety
13. Quality Report Enc. 11 Heather Johnstone 14:20
Performance
14. • Finance Report - Month 7• Financial Recovery Plans 2015/16
Enc. 12 Enc. 12a Wendy Kerr 14:30
15. Performance Report – Months 6 & 7 Enc. 13 Wendy Kerr 14:40
1
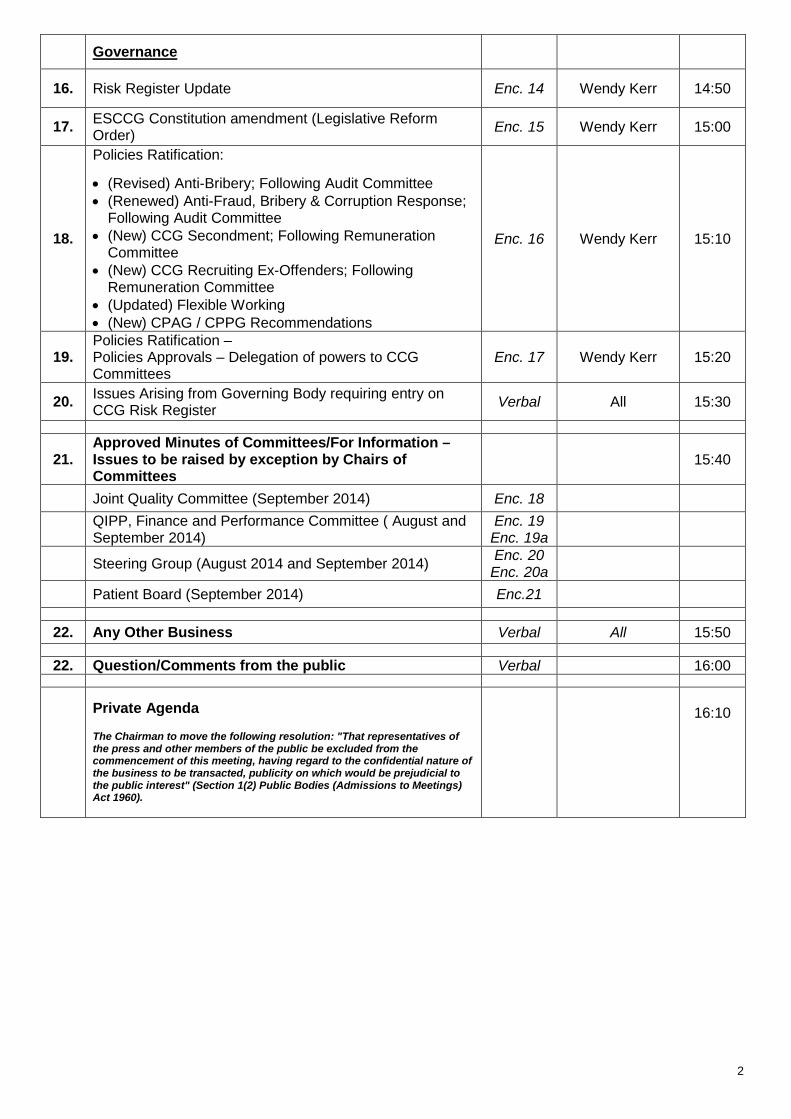
Governance
16. Risk Register Update Enc. 14 Wendy Kerr 14:50
17. ESCCG Constitution amendment (Legislative Reform Order) Enc. 15 Wendy Kerr 15:00
18.
Policies Ratification:
• (Revised) Anti-Bribery; Following Audit Committee • (Renewed) Anti-Fraud, Bribery & Corruption Response;
Following Audit Committee • (New) CCG Secondment; Following Remuneration
Committee • (New) CCG Recruiting Ex-Offenders; Following
Remuneration Committee • (Updated) Flexible Working • (New) CPAG / CPPG Recommendations
Enc. 16 Wendy Kerr 15:10
19. Policies Ratification – Policies Approvals – Delegation of powers to CCG Committees
Enc. 17 Wendy Kerr 15:20
20. Issues Arising from Governing Body requiring entry on CCG Risk Register Verbal All 15:30
21. Approved Minutes of Committees/For Information – Issues to be raised by exception by Chairs of Committees
15:40
Joint Quality Committee (September 2014) Enc. 18
QIPP, Finance and Performance Committee ( August and September 2014)
Enc. 19 Enc. 19a
Steering Group (August 2014 and September 2014) Enc. 20 Enc. 20a
Patient Board (September 2014) Enc.21
22. Any Other Business Verbal All 15:50
22. Question/Comments from the public Verbal 16:00
Private Agenda The Chairman to move the following resolution: "That representatives of the press and other members of the public be excluded from the commencement of this meeting, having regard to the confidential nature of the business to be transacted, publicity on which would be prejudicial to the public interest" (Section 1(2) Public Bodies (Admissions to Meetings) Act 1960).
16:10
2

EAST STAFFORDSHIRE CLINICAL COMMISSIONING GROUP GOVERNING BODY
Minutes of the East Staffordshire Clinical Commissioning Group Governing Body HELD IN PUBLIC
Held on Thursday 25 September 2014, at 2pm-4.20pm ABBOTS BROMLEY VILLAGE HALL
Present Dr Charles Pidsley
Tony Bruce Wendy Kerr Sarah Laing Ann Tunley Dr Wai Lim David Harding Dr John Tansey Dr Ajitha Prasad Lynne Smith Dr Catherine Faarup Paul Winter
Chair Chief Accountable Officer Chief Finance Officer Chief Operating Officer Patient and Public Involvement Lay Member GP Executive Governance Lay Member GP Executive GP Executive Co-opted Quality Lay Member GP Executive Head of Performance and Governance
In Attendance
Jeanette Cole Deborah Neal Sue Wilson Karen McGowan Members of the Public: Cyril Burton John Bridges Rupert Hill Susan Adey Steve Sambrook
PA to AO & COO (Minutes) Communication and Engagement Lead Clinical Quality Improvement Manager Head of Quality and Nursing John Hough Dr Judith Bull Leon Knowles R. Suhan
MINUTES OF THE MEETING OF THE EAST STAFFORDSHIRE CLINICAL COMMISSIONING GROUP GOVERNING BODY
ACTION
WELCOME AND INTRODUCTION Dr Charles Pidsley welcomed all present to the East Staffordshire Clinical Commissioning Group (CCG) Governing Body meeting being held in public.
GB(09)01 APOLOGIES Apologies were received from Dr Liz Gunn, Mike Chester, Heather Johnstone and Lucy Heath. Dr Wai Lim apologised for late arrival (2:45pm).
GB(09)02 DECLARATIONS OF INTEREST All GPs expressed an interest in the GP federation named Alexin. GB(09)03 MINUTES OF THE MEETING HELD ON 26 June 2014 • Page 5: bullet point 4; to read ‘Patient safety incident’ numbers are not
always reflective; a good open organisation will report high numbers; an organisation reporting low numbers could mean a culture of secrecy or bullying.
• Page 4 GB(06)08: Key Areas for Discussion; bullet point 4; to read ‘The work programme for experience lead commissioning over the next 12-18 months…….’
The minutes to reflect the above amendments were agreed as an accurate record.
Enc. 1
1
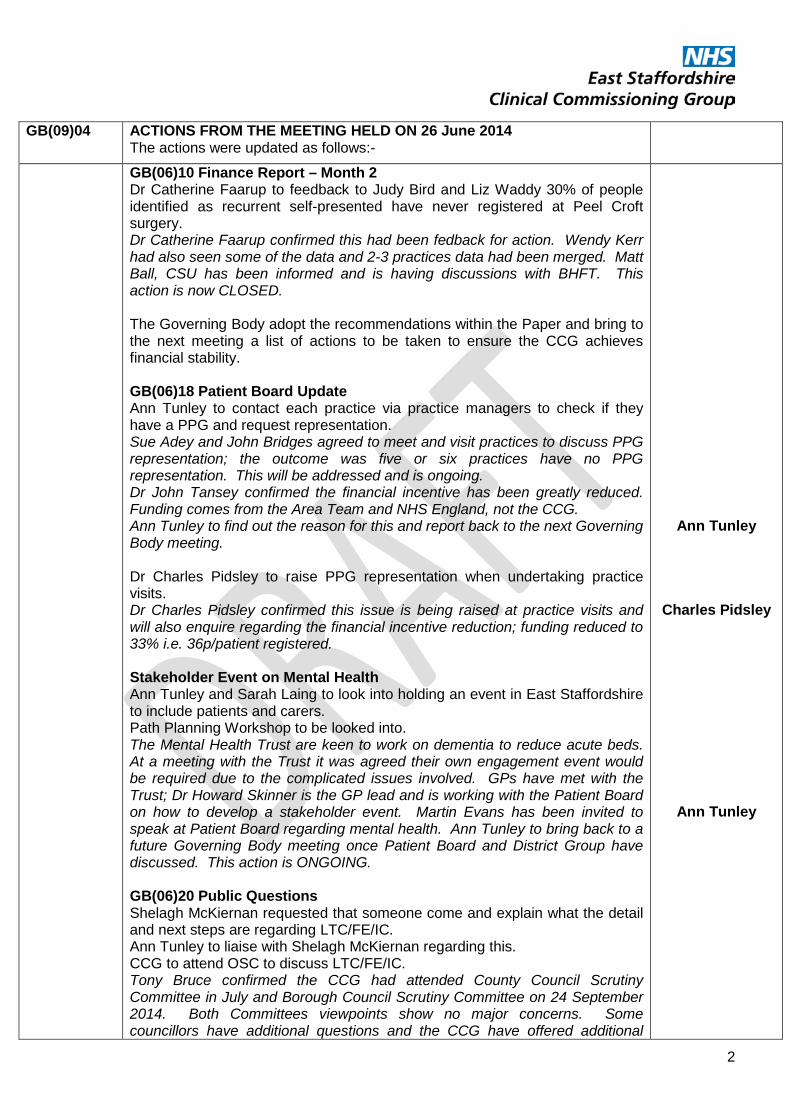
GB(09)04 ACTIONS FROM THE MEETING HELD ON 26 June 2014 The actions were updated as follows:-
GB(06)10 Finance Report – Month 2 Dr Catherine Faarup to feedback to Judy Bird and Liz Waddy 30% of people identified as recurrent self-presented have never registered at Peel Croft surgery. Dr Catherine Faarup confirmed this had been fedback for action. Wendy Kerr had also seen some of the data and 2-3 practices data had been merged. Matt Ball, CSU has been informed and is having discussions with BHFT. This action is now CLOSED. The Governing Body adopt the recommendations within the Paper and bring to the next meeting a list of actions to be taken to ensure the CCG achieves financial stability. GB(06)18 Patient Board Update Ann Tunley to contact each practice via practice managers to check if they have a PPG and request representation. Sue Adey and John Bridges agreed to meet and visit practices to discuss PPG representation; the outcome was five or six practices have no PPG representation. This will be addressed and is ongoing. Dr John Tansey confirmed the financial incentive has been greatly reduced. Funding comes from the Area Team and NHS England, not the CCG. Ann Tunley to find out the reason for this and report back to the next Governing Body meeting. Dr Charles Pidsley to raise PPG representation when undertaking practice visits. Dr Charles Pidsley confirmed this issue is being raised at practice visits and will also enquire regarding the financial incentive reduction; funding reduced to 33% i.e. 36p/patient registered. Stakeholder Event on Mental Health Ann Tunley and Sarah Laing to look into holding an event in East Staffordshire to include patients and carers. Path Planning Workshop to be looked into. The Mental Health Trust are keen to work on dementia to reduce acute beds. At a meeting with the Trust it was agreed their own engagement event would be required due to the complicated issues involved. GPs have met with the Trust; Dr Howard Skinner is the GP lead and is working with the Patient Board on how to develop a stakeholder event. Martin Evans has been invited to speak at Patient Board regarding mental health. Ann Tunley to bring back to a future Governing Body meeting once Patient Board and District Group have discussed. This action is ONGOING. GB(06)20 Public Questions Shelagh McKiernan requested that someone come and explain what the detail and next steps are regarding LTC/FE/IC. Ann Tunley to liaise with Shelagh McKiernan regarding this. CCG to attend OSC to discuss LTC/FE/IC. Tony Bruce confirmed the CCG had attended County Council Scrutiny Committee in July and Borough Council Scrutiny Committee on 24 September 2014. Both Committees viewpoints show no major concerns. Some councillors have additional questions and the CCG have offered additional
Ann Tunley
Charles Pidsley
Ann Tunley
2

meetings to discuss these. This action is CLOSED. GB(04)04 and GB(01)09 ESCCG Commissioning Intentions 2014-15 Update Tony Bruce confirmed the meeting to discuss alignment of Cancer Commissioning was to take place on Friday 25 April. An update will be provided at the next meeting. Sarah Laing provided a verbal update: A very successful meeting has taken place with the Shropshire and Staffordshire Area Team to discuss aligning commissioning of cancer services. Screening programmes to ensure people are screened and given an appropriate route into cancer services was discussed. QIPP shows some improvements are needed. If additional data is required contact Lucy Heath. This item to be retained on the action list for the next two meetings. This action is ONGOING. This item to be discussed later on the Agenda.
GB(01)11 Quality Report The Governing Body noted that further work is being done to look at the provision of the Out of Hours service. A specific report on progress as outlined and change in the structure of the service to be completed. Heather Johnstone confirmed work is ongoing regarding the wider review on Out of Hours. This will be brought back to a future meeting. This action is ONGOING. Update (25 September): Work and analysis regarding whether patients are referred and where is being completed through the operational resilience planning work. This action is ONGOING.
Tony Bruce requested the Action List is distributed and updated prior to the meeting to form part of the papers taken as read.
Dr Charles Pidsley introduced Sue Wilson and Karen McGowan from the Quality Sub Committee to present the Quality paper.
Jeanette Cole
GB(09)05 CHAIRMAN’S REPORT The paper was taken as read and accepted. Dr Charles Pidsley requested any
questions/comments. No further questions/comments were raised.
GB(09)06 ACCOUNTABLE OFFICER’S REPORT The Paper was taken as read.
Tony Bruce provided verbal key updates to the paper: • The Better Care Fund submission has been submitted and thanks to
Sarah Laing and Wendy Kerr for all their work on this. Challenges exist. Staffordshire County Council has a £30m budget problem, of which £15m has been requested from the NHS; this has been declined. The first additional £1.9m savings generated across the County through Integrated Commissioning will fund the implementation of Care Act through the County Council. Any additional savings achieved will be split 50:50 on a gain share basis between the NHS and Staffordshire County Council over and above existing organisational QIPP schemes. A risk share arrangement has not yet been agreed if savings are not made. There is huge potential for integrated commissioning and gains to the local health economy to serve people better and save money. The big schemes are: stroke prevention, public health schemes and continuing care.
3

Action: Sarah Laing to circulate a headline summary of lead areas from the Better Care Fund submission to Governing Body members.
• System Resilience Plan has been submitted. This is a detailed, joint
plan; Sarah Laing is the lead alongside South East Staffordshire and Seisdon Peninsula CCG (SESP). The Plan incorporates 18 week standard and how this is achieved; and the correct levels for non-elective care over winter and beyond. National money could be available if the right case is put forward. The Regional Team hold the decision on this.
• KPMG are helping the NHS develop a 5 year clinical and sustainable plan. Publication is awaited. A key recommendation is a single frail elderly pathway delivering consistency for Staffordshire. Dr Charles Pidsley, Tony Bruce and Nicky Harkness are working with partners to develop this pathway. The plan will be brought to a future Governing Body meeting for sign off.
• ESCCG Delivery priorities for 2014-15 to be discussed for approval. • The Quality Committee have met and confirm services are safe. BHFT
are continuing to develop collaborative relationships in a positive and sustained way with other hospitals. Sustainability of services at BHFT is included on the CCG risk register. The financial position is challenged. Urgent action is required on discussions held at the Informal Governing Body meeting in August regarding the rising elective referrals from GPs. This rise is higher than planned and budgeted for. The commercial impact will be discussed in the ‘Confidential’ section of today’s meeting.
• Feedback from the Area Team for Q4 and Q1 was good. Thanks go to all partners and CCG staff for their help in producing this result.
ESCCG Delivery Priorities 2014/15 discussion:
• Appendix 2, Item 12: ‘To develop and strengthen specifically our QIPP and Contract Management capability through effective OD and relationships with the CSU…..’ This to be broadened to read ‘relationships with the CSU or alternative arrangements’.
Sarah Laing
Tony Bruce / Wendy Kerr / Sarah Laing
In relation to the paper the Governing Body:
• APPROVE formally the CCGs Delivery Priorities for 2014/15 with the addition within Item 12 of: effective OD and relationships with the CSU ‘or alternative arrangements’; aiding the effective achievement of service and financial arrangements.
• Agree to adopt all other recommendations contained within the report.
GB(09)07 PATIENT BOARD UPDATE The paper was taken as read.
Ann Tunley provided a verbal update:
• A NHS citizens’ assembly at Westminster event took place last week. • Diabetic Support Group event takes place on 2 October between 5pm-
9pm. • Andrew Griffiths, MP will be speaking at the District Group of PPGs
October meeting. • Patient Board members will be visiting St Giles Hospice to see the
range of services available.
4

Key areas for discussion: • To help fulfil pending actions for Patient Board to mobilise engagement
with the public; contact with surgeries to gain representation will continue. Arrangements to visit the Uttoxeter group have been made.
• A meeting with Sarah Laing regarding the mental health event to be arranged.
Key actions:
• Ann Tunley to speak to the PPG regarding flu vaccination uptake within practices.
• Sarah Laing to meet with Ann Tunley regarding CCG engagement with Patient Board to ensure priorities and strategic approach are discussed. This action comes from a CPPG prioritisation meeting Sarah Laing attended where controversial decisions as a Staffordshire wide collaboration of CCGs are taken back to Patient Board for discussion and engagement. Sarah Laing to report back to the next Governing Body meeting.
Ann Tunley
Sarah Laing / Ann Tunley
GB(09)08 CONTINUOUS IMPROVEMENT TOOL Due to absence; this item to be presented to the next Governing Body meeting. STRATEGIC ITEMS GB(09)09 Commissioning Intentions 2015-16 Sarah Laing provided a verbal update:
Due to the timing of meetings a formal paper is not yet available for issue. Meetings have taken place with CSU and the Contract Management Team to discuss all contracts in detail. A meeting is arranged for 2 October with Wendy Kerr, Sarah Laing and Nicky Harkness to finalise the Commissioning Intentions and will be circulated by Friday 3 October. Key areas for discussion:
• A plan of the financial implications will be completed by December 2014 giving time to work up the contract transfer values.
• The operating framework is awaited. The Q1 review with NHS England indicated an approved deficit for CCGs next year of a smaller number than this year, in year spend deficit; the value is as yet unknown.
• The system resilience plan covers winter planning more comprehensively than previously. The plan includes elective and non-elective care for winter and beyond. Planning for surge is more difficult. Commissioning Intentions will bear in mind areas of pressure and aligned with the system resilience plan.
• The KPMG report, 5 year and 2 year plans, BCF, System Resilience Plan and Commissioning Intentions will all be aligned.
Action: Commissioning Intentions 2015-16 to be circulated to Governing Body members for comment and approval. No response will be seen as approval. Dr Charles Pidsley and Tony Bruce to be given delegated authority to sign off the documentation.
Sarah Laing
The Governing Body: • Agree to give Dr Charles Pidsley and Tony Bruce delegated
authority to sign off the Commissioning Intentions 2015-16.
GB(09)10 Better Care Fund This item was discussed as part of the Accountable Officer report previously on
the Agenda.
5

QUALITY & SAFETY GB(09)11 Quality Report
The paper was taken as read. Sue Wilson provided a verbal update:
• Page 1: NSL (none urgent ambulance service): since the Quality Committee meeting the assurance level moves from assured to limited assurance. This is due to recruitment issues reported by the provider, concerns raised due to late transfers at BHFT and renal dialysis patients. These concerns will be discussed by Quality Committee and brought back to the next meeting.
• Page 3, item (iv); Additional Issues for escalation to Governing Body. Members were asked to note this section of the report.
Key areas for discussion:
• Work is underway to improve discharge communications to GPs and forms part of the Commissioning for Quality Innovation (CQUIN) schedule. Agreement is reached with providers to meet a certain set of criteria. Dr Charles Pidsley is meeting with Colin Rogers on 26 September to discuss discharge letters and medication changes. An audit of discharge letters and information on medication on discharge will be included and whether any differences exist.
Action: GP members to email Dr Charles Pidsley by lunchtime on 26 September if they have any issues they would like to be raised at the meeting with Colin Rogers.
• Patients with heart failure discharged without their usual medication can be fedback through Dr Liz Gunn who attends Quality Committee.
• Cdiff is exceeding trajectory. Every case of Cdiff is investigated and concluded whether ‘avoidable’ or ‘unavoidable’. Notification is awaited from NHS England regarding ‘unavoidable’ cases being removed from the tally. A fine is imposed if the trajectory of 15 is exceeded.
• Page 4: Graph shows Burton trend is downward. The Quality Committee is concerned regarding the CQC report. An action plan is underway but not yet completed. The Trust is in special measures, e.g. MRSA case, Cdiff, number of falls causing harm has gone up, number of falls causing less harm are up. Wards Anna and Darwin give concern. The Committee are not as assured as previously.
• Arrangements are in place to raise the level of assurance at SSOTP. Information flow is the issue; currently information is requested but not forthcoming. A breakdown of staff sickness figures within ESCCG and specialities is required.
• More clarity is required around weekend mortality and the potential lack of specialist staff at weekends.
• Mental Health Trust figures regarding death: evidence received shows the Trust is not an outlier, although some information can be out of date. The Committee are sighted on weekend deaths as an action. Mike Chester could be requested to provide some additional work on this issue.
• Sue Wilson and Heather Johnstone to continue to monitor the quality and safety concerns raised regarding high hospital admissions; patients not discharged; quality indicators are red; conversion rates are high and wards are full.
GP members
6

Key actions: • Clarity is required around the system for approval of reports using
delegated power from the Governing Body. Paul Winter to check and report back to the next Governing Body meeting.
• Sarah Laing and Heather Johnstone to meet to discuss the resilience plan and whether mitigating actions incorporated will lessen the pressure on the hospital.
• SSOTP contract checks by CSU are required to provide assurance. A breakdown of staff sickness figures within ESCCG and specialities is also required.
• Sue Wilson to feedback to the next Governing Body meeting the ‘Stop the Clock’ rates for Serious Incidents in Burton which could cause actual delayed investigation reporting and learning from the incident. ‘Stop the Clock’ provides investigation time for Serious Incidents including police investigation where required (up to 45 days).
• Dr Charles Pidsley to speak to Craig Stenhouse regarding patients admitted at the weekend that fair less well than patients admitted during the week.
Paul Winter
Sarah Laing /
Heather Johnstone Sue Wilson
Sue Wilson
Charles Pidsley
In relation to the paper the Governing Body: • Are assured that services are safe but understand the areas
requiring further work in the respective providers to ensure consistently high quality services are provided to the local patient population.
PERFORMANCE GB(09)12 Finance Report – Month 5 The Paper was taken as read.
Wendy Kerr provided a verbal update: Page 4, Table 3 shows the CCGs summary position as at the end of month 5 and is forecast to achieve planned deficit and an unidentified QIPP of £2m. Page 7, Table 6 shows potential mitigating actions with a best, likely and worst case scenario. There are additional mitigating actions e.g. impact of the non-elective CQUIN and GP LIS implemented in August. These will be monitored over the next two months. Key areas for discussion:
• Pharmacy underpayment is not reflected within the report; possible Scriptswitch buy in may help. Drugs are made unavailable by pharmaceutical companies and when made available they are 3 or 4 times price. These are not high cost drugs but volume sales.
• Wendy Kerr is checking figures regarding 45% specialised services coming back and CCG wider risk share arrangements.
Key actions:
• Heather Johnstone to discuss the possible quality implications of drug availability through Scriptswitch with Sue Bamford.
• Dr Charles Pidsley to discuss specialised services extended risk share and clarification of community elective work at the Chairs meeting.
Heather Johnstone
Charles Pidsley
In relation to the paper the Governing Body: • Recognises the impact of month four performance, which shows
an adverse variation against planned deficit of £308k, but noting that a significant percentage of the CCGs reserves have been used (excluding NICE and CHC as these will be required).
7
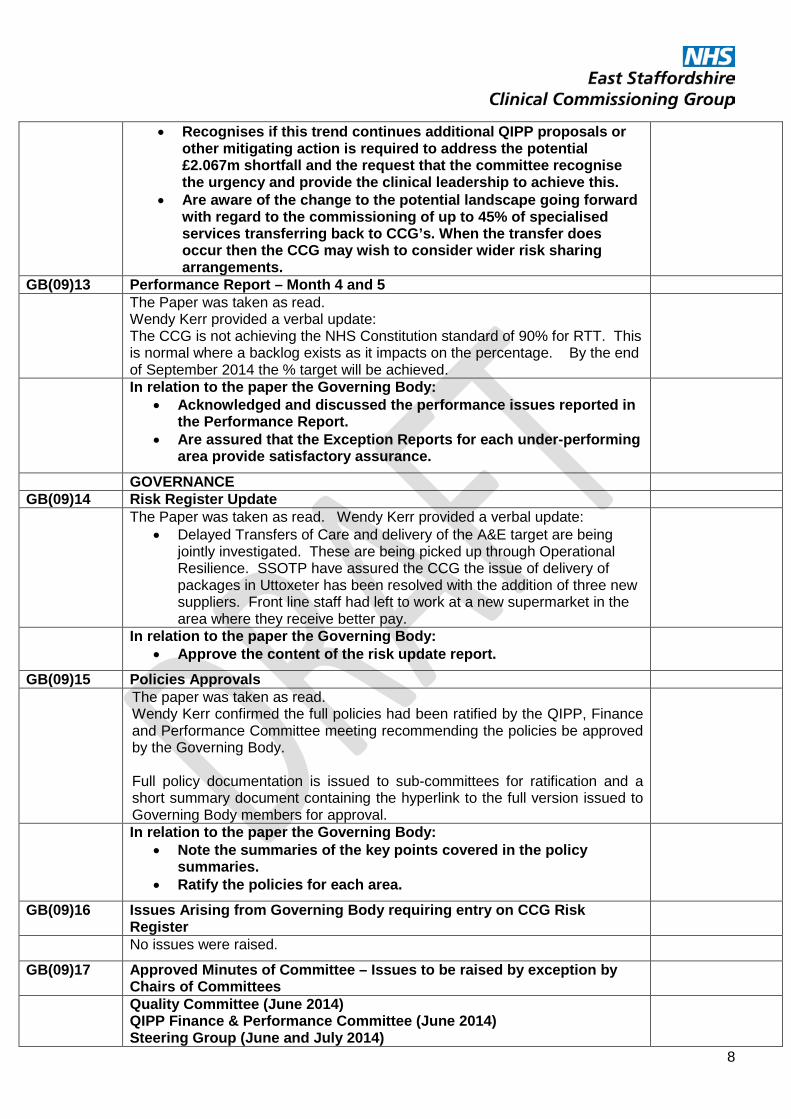
• Recognises if this trend continues additional QIPP proposals or other mitigating action is required to address the potential £2.067m shortfall and the request that the committee recognise the urgency and provide the clinical leadership to achieve this.
• Are aware of the change to the potential landscape going forward with regard to the commissioning of up to 45% of specialised services transferring back to CCG’s. When the transfer does occur then the CCG may wish to consider wider risk sharing arrangements.
GB(09)13 Performance Report – Month 4 and 5 The Paper was taken as read.
Wendy Kerr provided a verbal update: The CCG is not achieving the NHS Constitution standard of 90% for RTT. This is normal where a backlog exists as it impacts on the percentage. By the end of September 2014 the % target will be achieved.
In relation to the paper the Governing Body: • Acknowledged and discussed the performance issues reported in
the Performance Report. • Are assured that the Exception Reports for each under-performing
area provide satisfactory assurance.
GOVERNANCE GB(09)14 Risk Register Update The Paper was taken as read. Wendy Kerr provided a verbal update:
• Delayed Transfers of Care and delivery of the A&E target are being jointly investigated. These are being picked up through Operational Resilience. SSOTP have assured the CCG the issue of delivery of packages in Uttoxeter has been resolved with the addition of three new suppliers. Front line staff had left to work at a new supermarket in the area where they receive better pay.
In relation to the paper the Governing Body: • Approve the content of the risk update report.
GB(09)15 Policies Approvals The paper was taken as read.
Wendy Kerr confirmed the full policies had been ratified by the QIPP, Finance and Performance Committee meeting recommending the policies be approved by the Governing Body. Full policy documentation is issued to sub-committees for ratification and a short summary document containing the hyperlink to the full version issued to Governing Body members for approval.
In relation to the paper the Governing Body: • Note the summaries of the key points covered in the policy
summaries. • Ratify the policies for each area.
GB(09)16 Issues Arising from Governing Body requiring entry on CCG Risk Register
No issues were raised. GB(09)17 Approved Minutes of Committee – Issues to be raised by exception by
Chairs of Committees
Quality Committee (June 2014) QIPP Finance & Performance Committee (June 2014) Steering Group (June and July 2014)
8

SIRO Report No issues were raised. GB(09)18 Any Other Business Dr John Tansey raised the issue of accessibility, time, efficiency and cost of
Governing Body meetings being held in the surrounding villages of Burton upon Trent and whether more central locations i.e. Burton and Uttoxeter would be more appropriate. The members of the public present agreed that the Governing Body engage well with the public but there is apathy among patients in getting them to join PPG or attend meetings whether held in the evening or during the day; public transport links and distance are important considerations. Action: The East Staffordshire Newsletter to include the proposal to hold future meetings in Burton upon Trent; two of the six meetings to be held in Uttoxeter; comments and questions to be invited. Dr Charles Pidsley to discuss this with Deborah Neal. There were no additional items requested for discussion. Ann Tunley left the meeting at 3:10pm.
Charles Pidsley / Deborah Neal
The Governing Body: • Agreed the central location for future meetings should be Burton
upon Trent; two of the six meetings to be held in Uttoxeter. If discussions could be contentious to a particular neighbourhood then a suitable meeting room should be booked within that location to ensure inclusion of comment by local people affected.
GB(09)19 Continuous Improvement Tool Due to absence; this item to be presented to the next Governing Body meeting. Questions/Comments from the Public Susan Adey
Q1 I am concerned about patient discharges from Queen’s; can you please confirm whether this is getting better? A Sarah Laing confirmed this was due to provider packages issues and movement of staff within Uttoxeter. Staff left the health service for better pay at a new supermarket which has opened in the area. Twenty more packages were put in place last week; therefore, this issue has now been resolved. The meeting closed at 3:45pm.
GB(09)20 DATE OF NEXT MEETING The next Meeting in Public is scheduled to take place on 27 November 2014 at
1pm at Barton under Needwood Village Hall.
Private Agenda The Chairman to move the following resolution: - "That representatives of the press and other members of the public be excluded from the remainder of this meeting, having regard to the confidential nature of the business to be transacted, publicity on which would be prejudicial to the public interest" (Section 1(2) Public Bodies (Admissions to Meetings) Act 1960).
SIGNED:………………………………………………. DATE:……………….......................... (Chairman)
9
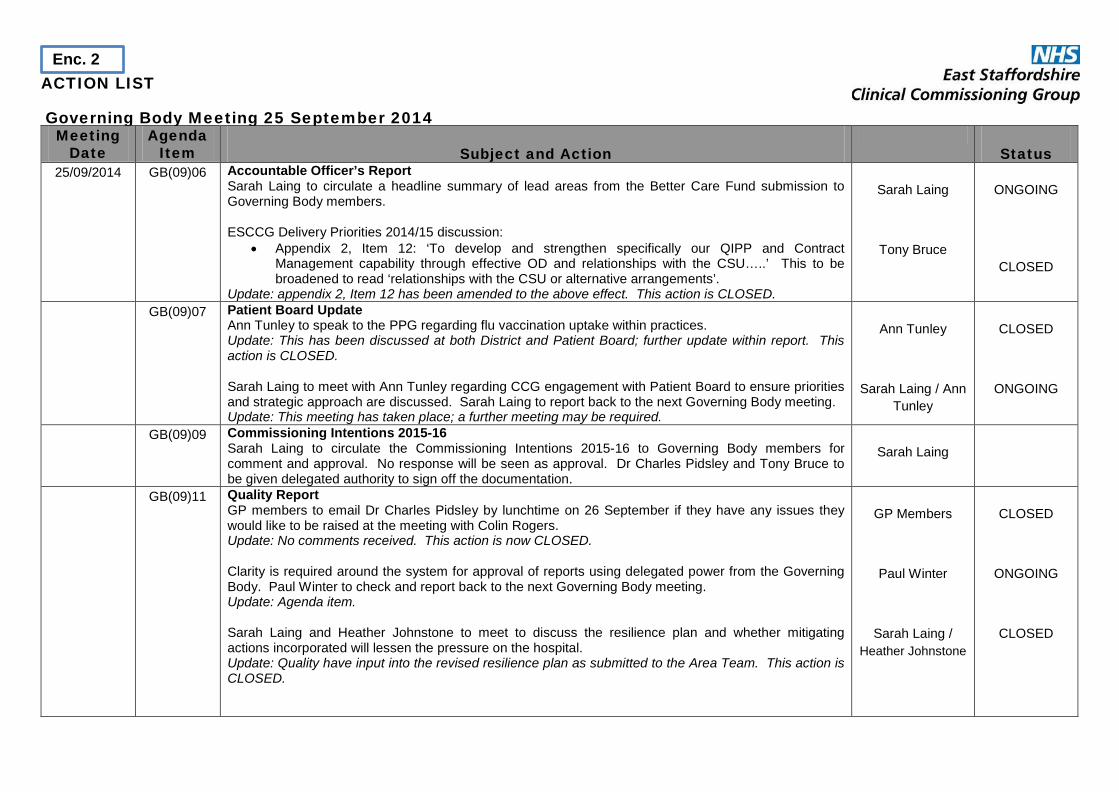
ACTION LIST Governing Body Meeting 25 September 2014
Meeting Date
Agenda Item
Subject and Action
Status
25/09/2014 GB(09)06 Accountable Officer’s Report Sarah Laing to circulate a headline summary of lead areas from the Better Care Fund submission to Governing Body members. ESCCG Delivery Priorities 2014/15 discussion:
• Appendix 2, Item 12: ‘To develop and strengthen specifically our QIPP and Contract Management capability through effective OD and relationships with the CSU…..’ This to be broadened to read ‘relationships with the CSU or alternative arrangements’.
Update: appendix 2, Item 12 has been amended to the above effect. This action is CLOSED.
Sarah Laing
Tony Bruce
ONGOING
CLOSED
GB(09)07 Patient Board Update Ann Tunley to speak to the PPG regarding flu vaccination uptake within practices. Update: This has been discussed at both District and Patient Board; further update within report. This action is CLOSED. Sarah Laing to meet with Ann Tunley regarding CCG engagement with Patient Board to ensure priorities and strategic approach are discussed. Sarah Laing to report back to the next Governing Body meeting. Update: This meeting has taken place; a further meeting may be required.
Ann Tunley
Sarah Laing / Ann
Tunley
CLOSED
ONGOING
GB(09)09 Commissioning Intentions 2015-16 Sarah Laing to circulate the Commissioning Intentions 2015-16 to Governing Body members for comment and approval. No response will be seen as approval. Dr Charles Pidsley and Tony Bruce to be given delegated authority to sign off the documentation.
Sarah Laing
GB(09)11 Quality Report GP members to email Dr Charles Pidsley by lunchtime on 26 September if they have any issues they would like to be raised at the meeting with Colin Rogers. Update: No comments received. This action is now CLOSED. Clarity is required around the system for approval of reports using delegated power from the Governing Body. Paul Winter to check and report back to the next Governing Body meeting. Update: Agenda item. Sarah Laing and Heather Johnstone to meet to discuss the resilience plan and whether mitigating actions incorporated will lessen the pressure on the hospital. Update: Quality have input into the revised resilience plan as submitted to the Area Team. This action is CLOSED.
GP Members
Paul Winter
Sarah Laing / Heather Johnstone
CLOSED
ONGOING
CLOSED
Enc. 2
Meeting Date
Agenda Item
Subject and Action
Status
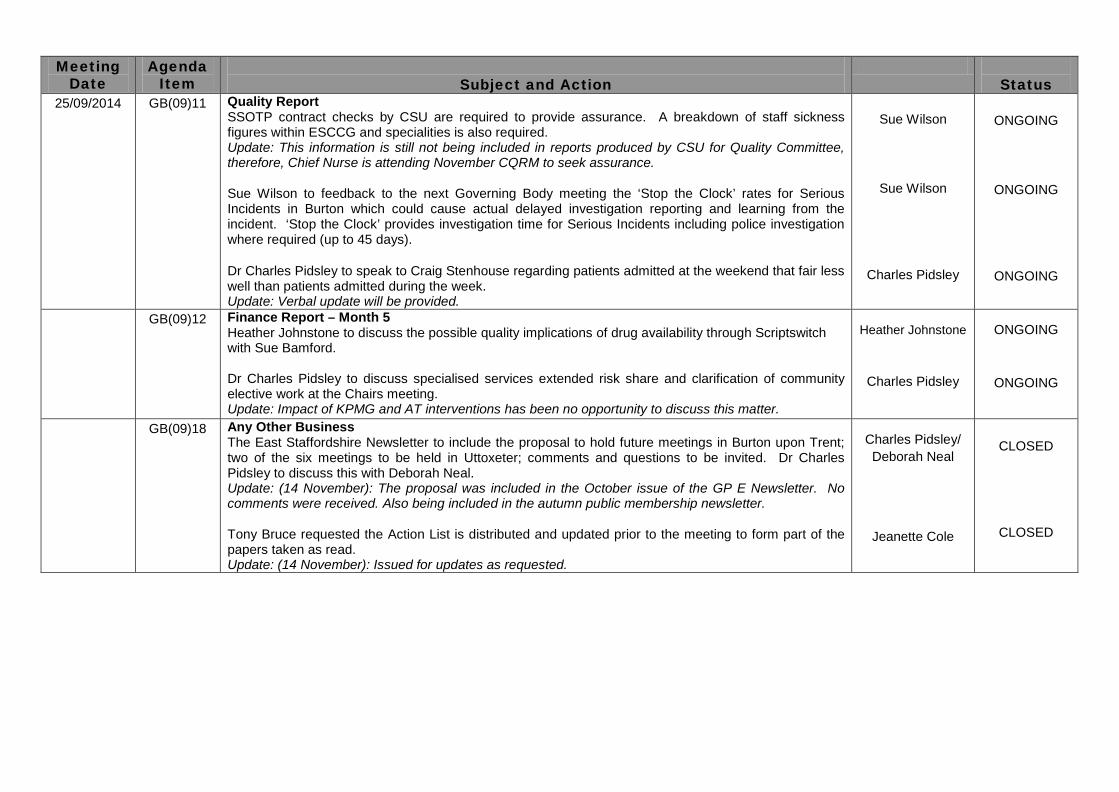
25/09/2014 GB(09)11 Quality Report SSOTP contract checks by CSU are required to provide assurance. A breakdown of staff sickness figures within ESCCG and specialities is also required. Update: This information is still not being included in reports produced by CSU for Quality Committee, therefore, Chief Nurse is attending November CQRM to seek assurance. Sue Wilson to feedback to the next Governing Body meeting the ‘Stop the Clock’ rates for Serious Incidents in Burton which could cause actual delayed investigation reporting and learning from the incident. ‘Stop the Clock’ provides investigation time for Serious Incidents including police investigation where required (up to 45 days). Dr Charles Pidsley to speak to Craig Stenhouse regarding patients admitted at the weekend that fair less well than patients admitted during the week. Update: Verbal update will be provided.
Sue Wilson
Sue Wilson
Charles Pidsley
ONGOING
ONGOING
ONGOING
GB(09)12 Finance Report – Month 5 Heather Johnstone to discuss the possible quality implications of drug availability through Scriptswitch with Sue Bamford. Dr Charles Pidsley to discuss specialised services extended risk share and clarification of community elective work at the Chairs meeting. Update: Impact of KPMG and AT interventions has been no opportunity to discuss this matter.
Heather Johnstone
Charles Pidsley
ONGOING
ONGOING
GB(09)18 Any Other Business
The East Staffordshire Newsletter to include the proposal to hold future meetings in Burton upon Trent; two of the six meetings to be held in Uttoxeter; comments and questions to be invited. Dr Charles Pidsley to discuss this with Deborah Neal. Update: (14 November): The proposal was included in the October issue of the GP E Newsletter. No comments were received. Also being included in the autumn public membership newsletter. Tony Bruce requested the Action List is distributed and updated prior to the meeting to form part of the papers taken as read. Update: (14 November): Issued for updates as requested.
Charles Pidsley/ Deborah Neal
Jeanette Cole
CLOSED
CLOSED

ACTIONS STATUS FROM PREVIOUS MEETINGS Meeting
Date Agenda
Item
Subject and Action
Status 26/06/2014 GB(06)10 Finance Report – Month 2
Dr Catherine Faarup to feedback to Judy Bird and Liz Waddy 30% of people identified as recurrent self-presented have never registered at Peelcroft surgery. The Governing Body adopt the recommendations within the Paper and bring to the next meeting a list of actions to be taken to ensure the CCG achieves financial stability. Dr Catherine Faarup confirmed this had been fedback for action. Wendy Kerr had also seen some of the data and 2-3 practices data had been merged. Matt Ball, CSU has been informed and is having discussions with BHFT. This action is now CLOSED.
Catherine Faarup
ALL
CLOSED
GB(06)18 Patient Board Update Ann Tunley to contact each practice via practice managers to check if they have a PPG and request representation. Sue Adey and John Bridges agreed to meet and visit practices to discuss PPG representation; the outcome was five or six practices have no PPG representation. This will be addressed and is ongoing. Dr John Tansey confirmed the financial incentive has been greatly reduced. Funding comes from the Area Team and NHS England, not the CCG. Ann Tunley to find out the reason for this and report back to the next Governing Body meeting. Update: Letters have been issued to practices offering support and a meeting to discuss. This action is CLOSED.
Ann Tunley
CLOSED
GB(06)18 Patient Board Update Dr Charles Pidsley to raise PPG representation when undertaking practice visits. Dr Charles Pidsley confirmed this issue is being raised at practice visits and will also enquire regarding the financial incentive reduction; funding reduced to 33% i.e. 36p/patient registered. Ann Tunley contact the Area Team regarding the DES reduction and received responses from Sian Huszak & Tracey Shewan.
Charles Pidsley
CLOSED
GB(06)18 Stakeholder event on mental health Ann Tunley and Sarah Laing to look into holding an event in East Staffordshire to include patients and carers. Path Planning Workshop to be looked into. The Mental Health Trust are keen to work on dementia to reduce acute beds. At a meeting with the Trust it was agreed their own engagement event would be required due to the complicated issues involved. GPs have met with the Trust; Dr Howard Skinner is the GP lead and is working with the Patient Board on how to develop a stakeholder event. Martin Evans has been invited to speak at Patient Board regarding mental health. Ann Tunley to bring back to a future Governing Body meeting once Patient Board and District Group have discussed. Update: Ann Tunley is meeting with Lisa Agell on Tuesday 18 November 2014. This action is ONGOING.
Ann Tunley/ Sarah Laing
ONGOING
Meeting Date
Agenda Item
Subject and Action
Status
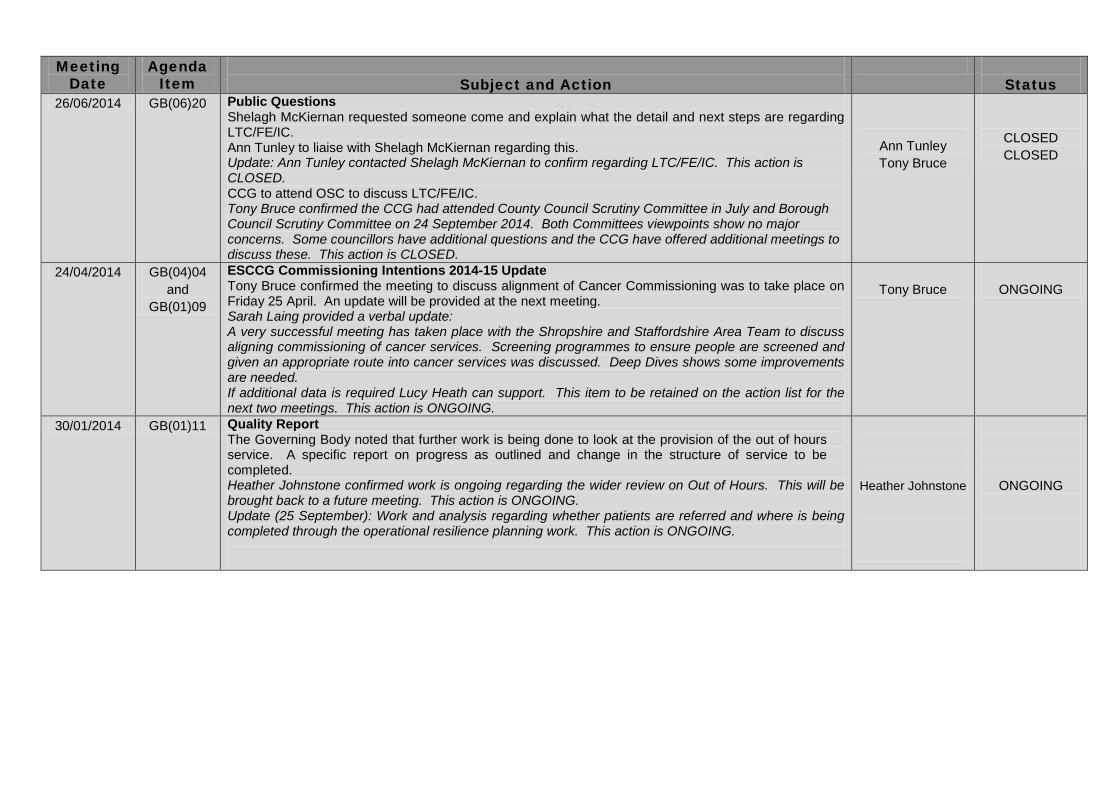
26/06/2014 GB(06)20 Public Questions Shelagh McKiernan requested someone come and explain what the detail and next steps are regarding LTC/FE/IC. Ann Tunley to liaise with Shelagh McKiernan regarding this. Update: Ann Tunley contacted Shelagh McKiernan to confirm regarding LTC/FE/IC. This action is CLOSED. CCG to attend OSC to discuss LTC/FE/IC. Tony Bruce confirmed the CCG had attended County Council Scrutiny Committee in July and Borough Council Scrutiny Committee on 24 September 2014. Both Committees viewpoints show no major concerns. Some councillors have additional questions and the CCG have offered additional meetings to discuss these. This action is CLOSED.
Ann Tunley Tony Bruce
CLOSED CLOSED
24/04/2014 GB(04)04 and
GB(01)09
ESCCG Commissioning Intentions 2014-15 Update Tony Bruce confirmed the meeting to discuss alignment of Cancer Commissioning was to take place on Friday 25 April. An update will be provided at the next meeting. Sarah Laing provided a verbal update: A very successful meeting has taken place with the Shropshire and Staffordshire Area Team to discuss aligning commissioning of cancer services. Screening programmes to ensure people are screened and given an appropriate route into cancer services was discussed. Deep Dives shows some improvements are needed. If additional data is required Lucy Heath can support. This item to be retained on the action list for the next two meetings. This action is ONGOING.
Tony Bruce
ONGOING
30/01/2014 GB(01)11 Quality Report The Governing Body noted that further work is being done to look at the provision of the out of hours service. A specific report on progress as outlined and change in the structure of service to be completed. Heather Johnstone confirmed work is ongoing regarding the wider review on Out of Hours. This will be brought back to a future meeting. This action is ONGOING. Update (25 September): Work and analysis regarding whether patients are referred and where is being completed through the operational resilience planning work. This action is ONGOING.
Heather Johnstone
ONGOING

Title Chairman’s report Reporting to Governing Body Date of Meeting 27th November 2014
Commissioning Lead(s) Author(s) Dr C Pidsley
Purpose of the Report (Please select) Approval Assurance Discussion
Key Points/Executive Summary This report contains items of information for members of the Governing Body and members of the public relating to recent events.
Recommendations (what is expected from the Board) For information and discussion.
Enclosures Report
x X
Enc. 3
1 Author: Date: East Staffs CCG
Chairman’s Report to the Governing Body (27th November 2014).
Improving Lives Procurement.
This procurement process encompasses the care of adults with Long term conditions, frail elderly, their Intermediate care needs and unplanned admissions.
The names of the shortlisted bidders have been published. They are Optum and Virgin Health Care. Initial meetings with both organisations have taken place over the past 4 weeks to progress towards establishing an outcomes based contract.
The Outcomes have been developed jointly with GP clinicians, patients and their carers. This process has involved Experience Lead Commissioning, which highlights the gap between current experiences as patient and carer and desired experience. It has proven a very powerful tool and we believe this enables us to be confident that the outcomes specified in our contract are the ones, which will ensure the best possible health for the population we serve. By the time the Governing Body convenes, a meeting between the shortlisted bidders and Stakeholders will have further tested this.
Because this is an Outcomes based contract with a fixed financial envelope the variable that we will judge bidders on will be their solution to the challenge. That challenge is; how do we shape and transform care for adults with LTC over the next 7 years in a way that will meet increasing demand, and at the same time improve peoples lives. Over the next few months there will be opportunities for Patients and Carers to help shape the solutions. Dates will be publicised once confirmed and also will be found on the CCG web site by clicking on the Improving Lives tab on the top horizontal bar.
http://www.eaststaffsccg.nhs.uk
Primary Care GP lead.
Dr Liz Waddy has now moved to Norwich and although we expect to see her in Burton from time to time in connection with her St Giles work, she has finished her work for the CCG. Most of you will have met her on the practice visits and of course she has been key to supporting practices getting the LIS (Local Improvement Scheme) up and running. The workload shared of course with Judy Bird and Julie Hughes has been considerable, and I believe the implementation of the scheme has been made largely possible by her hard work and persistence. I have had the added benefit of working for the last 26 years with Liz as a partner at Bridge surgery, and
can vouch for her reliability, hard work and exceptional capabilities as a GP. I would like to formally note my thanks personally and on Governing body member’s behalf to Liz.
Dr Ajitha Prasad has agreed to take over the role from Liz. She is eminently suitable for this task being a GP appraiser, and I wish her every success.
Clinical meetings.
As Clinical Chair, I have meetings in the last 4 weeks with Dr Aftab Gill who is now the Queen’s cardiology department lead. Amongst topics discussed were future developments in the cardiac catheter lab, and adoption of newer technologies in the diagnosis of Ischaemic heart disease. Some of the options discussed would allow patients to receive more of their care locally, and avoid some of the travelling that a number of patients have to Leicester. Further discussions are taking place with the CCG executive team.
I also attended a meeting with Dr David Watmough, the lead for gastroenterology at Queen’s and Anthony Bullock. Anthony is the lead for the joint commissioning of Drugs and Alcohol services by Staffordshire Public Health. Sarah Laing of the ESCCG is involved with this process on our behalf. Discussions revolved around the recently introduced prime contractor service across Staffordshire and as part of that service the role of the alcohol liaison service nurse. There was also debate about the adoption of pathways for a variety of conditions within this specialism.
Hospital Discharge letters.
There have recently been renewed efforts to improve the information provided by hospital discharge letters. This has been an on-going concern of GPs in the area for some time. Two main problems exist for the hospital. One is that often they are not presented with the information they require about patient medication. The second is that the patterns of working mean that letters are often completed by junior doctors who may not have been involved in the whole of the care of the patient. The former will be addressed by wider uptake of access to the summary care record and the latter by changes to the discharge letter template which requires specific responses to a number of questions regarding medication on discharge, any changes made during the admission and rationale for those changes. An audit of letters carried out in the last 2 weeks demonstrated some progress has been made.

GP Steering Group meeting 18th November.
At this meeting GPs discussed the local Dementia Strategy, services currently provided, services proposed and the recently announced payment by the government for diagnosis. A key element of the discussion was that adequate and well signposted support services were needed pre and post diagnosis.
Updates on the Improving Lives procurement were given using a novel role play of reporter interviewing lead clinician. The GP membership have expressed a desire to meet with the shortlisted bidders, to hear more about their organisations work in other areas and to understand their approach to system change.
Other updates were received on the LIS and the update to the Medicines Management Strategy.

Title Chief Accountable Officer’s Report Reporting to Governing Body Date of Meeting 27th November 2014
Commissioning Lead(s) Author(s) Tony Bruce
Purpose of the Report (Please select) Approval Assurance Discussion
Key Points/Executive Summary This paper gives an overview of the strategic and operational agenda facing the CCG. Its purpose is to give a view “in the round” to frame the more detailed business included on the agenda. It is structured in the same format as the Agenda.
Further details of the specific areas of work and issues referenced in this report are contained within the Directors’ reports. Recommendations (what is expected from the Board) The Governing Body is invited to:
• Be assured that the key strategic and operational functions of the CCG are being discharged and action plans are in place where appropriate to address any shortfalls.
Specifically and actively: • APPROVE its arrangements for contingency cost saving schemes in 2014/15 to be
developed and implemented should the need arise; either by the use of delegated powers or the use of extraordinary meetings.
• CONFIRM its commitment to its previously agreed approach to meeting the financial requirements set out by NHS England; recognizing the difficulty in developing “firm” numbers for items 2 and 4 particularly.
• EXPRESS an initial view of the Five Year Forward View. • RESERVE TIME at the informal Workshop in December to consider the implications and
shape our way forward more fully in respect of the Five Year Forward View; prior to further discussion at the Governing Body in January 2015.
• APPROVE urgent priority continue to be given to implementing the clinical, contractual and managerial actions contained within the QIPP Programme and developed at the GB workshop in August; including implementing more effective approaches to improving follow up ratios and POLCVs already contractualised; implementation of the GP LIS schemes; and agreeing a system of working with Practices to understand and address (as appropriate) rising elective referral rates.
• OFFER THE THANKS of the Governing Body to the staff of the CCG and the CSU; and to our partners for their contribution to this achievement.
• OFFER CONGRATULATIONS to the Medicines Management team and participating Practices on securing a National Award for the “What a Waste” campaign.
Enclosures Attached report and Appendices.
x x
Enc. 4
East Staffs CCG

Report to: ESCCG Governing Body (GB)
Report from: Tony Bruce – Accountable Officer
Subject: Chief Accountable Officer’s Report
Date: 27th November 2014
1. Introduction This paper gives an overview of the strategic and operational agenda facing the CCG. Its purpose is to give a view “in the round” to frame the more detailed business included on the agenda. It is structured in the same format as the Agenda.
Further details of the specific areas of work and issues referenced in this report are contained within the Directors’ reports.
The Governing Body is invited to: • Be assured that the Strategic Planning requirements are being effectively
progressed. • Specifically be assured of the positive progression of the KPMG recommendations
and the approvals being sought today and at the next meeting. • Be assured that the Staffordshire County BCF has been submitted on time and
Approved with Support. • Be cognisant of the financial requirements placed upon the CCG by NHS England. • APPROVE its arrangements for contingency cost saving schemes in 2014/15 to be
developed and implemented should the need arise; either by the use of delegated powers or the use of extraordinary meetings.
• CONFIRM its commitment to its previously agreed approach to meeting the financial requirements set out by NHS England; recognizing the difficulty in developing “firm” numbers for items 2 and 4 particularly.
• Be assured that the work to implement Integrated Commissioning with CCGs and SCC ASC continues to be progressed and that proposals will be brought for development/approval in due course.
• Be aware of changes to NHS England; details to follow. • EXPRESS an initial view of the Five Year Forward View • RESERVE TIME at the informal Workshop in December to consider the implications
and shape our way forward more fully in respect of the Five Year Forward View; prior to further discussion at the Governing Body in January 2015.
• Be assured that commissioned services are judged as safe; subject to a verbal report from the Joint Quality Committee. Furthermore be assured that BHFT is continuing to indicate its intention to develop partnerships and alliances to enhance future clinical and financial sustainability.
• Be assured by the positive overall performance against performance indicators and assured t h a t a c t i o n i s b e i n g taken in respect of the small number of under- performing areas.
• Be assured that the CCG is currently on course to achieve its deficit financial control total.
Enc. 4
East Staffs CCG
• Be cognisant of the risks in the financial projection and the need for a strong clinical and managerial focus in securing the benefits in the approved QIPP programme.
• APPROVE urgent priority c o n t i n u e to be given to implementing the clinical, contractual and managerial actions c o n t a i n e d w i t h i n t h e Q I P P P r o g r a m m e a n d developed at the GB workshop in August; including implementing more effective approaches to improving follow up ratios and POLCVs already contractualised; i m p l e m e n t a t i o n o f t h e G P L I S s c h e m e s ; and agreeing a system of working with Practices to understand and address (as appropriate) rising elective referral rates.
• Be assured that the CCGs corporate risks have been identified and t h a t mitigation plans are in place.
• Be assured by the formal letter in respect of the Quarter 1 Checkpoint review meeting.
• OFFER THE THANKS of the Governing Body to the staff of the CCG and the CSU; and to our partners for their contribution to this achievement.
• OFFER CONGRATULATIONS to the Medicines Management team and participating Practices on securing a National Award for the “What a Waste” campaign.
2. Strategic Matters Strategic Planning: “A Call to Action”/ Health and Wellbeing Strategy (HWBS) / Five Year Plans / Five Year Financial Recovery Plans/ Challenged Health Economies (KPMG)/ 2 Year Plans/ Better Care Fund(BCF)
Sarah Laing continues to lead the CCGs work in this suite of planning activities. In relation to the Call to Action, HWBS, 5 year plans, 5 year financial recovery plans, 2 year plans a n d t h e Be t t e r Ca r e Fu n d all the requirements to date have been met and there are no further significant assurances or decisions required at this stage, other than by exception below. Challenged Health Economies (KPMG) Work In relation to the “Challenged Health Economies” (KPMG) work; in my last report I referenced the work being undertaken collaboratively with partner CCGs in respect of “a single frail elderly pathway” and “greater collaborative working” to increase commissioner capacity. A single frail elderly strategy, including a single pathway is included on the agenda for approval today; together with priorities for early collaborative commissioning to drive improvement in services and outcomes. I am also pleased to report that high level meetings have taken place of clinical and professional managerial leaders across Staffordshire and that we are now actively exploring together an active collaborative approach based on that already used in Nottinghamshire. This includes a Collaborative Commissioning Congress to shape the wider strategic decisions and commissioning priorities together. Proposals will be brought for approval at the next meeting of the Governing Body. The Staffordshire BCF In my last report I referred to the challenge of agreeing the BCF given the respective Local Government and NHS national frameworks and the extent of financial challenge in Staffordshire. Following the top level negotiations referred to in my last report a BCF was agreed and submitted on 19th September in accordance with the timetable. The agreement manages the downside risks for the CCG whilst still encouraging and enabling the benefits of joint working to be shared through a “gain share” arrangement between the CCGs locally and Local Government. The Staffordshire BCF has been approved with Support and we are now moving to implement the plan.
East Staffs CCG

Five Year Plans and Five Year Financial Recovery Plan As the Governing Body will be aware the CCG has been working collaboratively with partner CCGs to develop the 5 year plan, based on the Unit of Planning of Staffordshire and Stoke on Trent. Each CCG must also show that it can live within the financial resources allocated to it. This is a legal requirement. The NHS organisations in Staffordshire are working in challenged circumstances and therefore received national support to identify solutions. This was provided in Staffordshire by KPMG. The KPMG report has provided some insight into financial solutions for part of the financial challenge. These are now being expanded on and developed further by the NHS bodies; with further support from KPMG. The financial planning requirements have recently been clarified in a letter received from NHS England, by me, as the CCGs Accountable Officer. The letter sets out a number of requirements, these have been reproduced below:
• You are required to deliver a set of planned actions that ensures in-year delivery of your control total set for 14/15. For some this will mean a set of short term financial recovery actions that deliver this.
• You are required to have in place a set of plans that show recovery to a sustainable financial position by the end of 16/17 and continuous improvement within that time frame. For clarity, sustainability is defined as meeting all NHS England financial metrics on a recurrent basis.
• You are required to plan to pay back your deficits over the following two financial years (i.e. by the end of 18/19) and be clear what action needs to be taken to achieve this.
The letter is reproduced at Appendix A to this report. In respect of the 2014/15 financial year the Governing Body will be aware that there is some risk that not all the implemented QIPP schemes will deliver the intended benefits. There is therefore an urgent need to agree a package of contingency measures (Plan B’s) which can be implemented quickly if necessary. The Governing Body is asked to approve its arrangements for such schemes to be developed; and implemented should the need arise; either by the use of delegated powers or the use of extraordinary meetings. In respect of the sustainable position by 2016/17 and repayment of deficits thereafter the Governing Body will be cognizant of the Benchmarking analysis which shows that movement to best practice performance will achieve gross savings of £4m to £6m annually; and of the distance from fair shares target. Achieving the 2016/17 requirement will require net savings of £11.3m. It is clear that there is a considerable volume of savings still to be achieved to satisfy the requirements placed on us. This will require levels of quality and performance beyond those already exhibited in the NHS; an ambitious goal which the Governing Body has already set its sights on in pursuing excellence through its Improving Lives Programme, its use of CQUINs, the BCF and its pursuit of Integrated Commissioning with Local Government. Pursuit of transformational change will bring quality, performance and financial benefits. However it is recognized that as this takes us to “beyond current best practice performance”, and that “gain share” arrangements will be used; the quantification will be challenging and will require reasonable estimates to be made. The Governing Body has previously agreed its Financial Approach at its meeting in January 2014. This has been reproduced below.
East Staffs CCG
Our approach is based on 4 streams of work and an underpinning principle: 1. Driving an ambitious and genuine QIPP Programme towards being in the best decile of comparative performance in all that we do. For example improving LTC services and reducing non elective ACS admissions. 2. Seizing innovative and creative opportunities to improve Outcomes, services and value; alone and with partners; aligned with the Vision of the Health and Wellbeing Strategy. For example the exploration of integrated commissioning, pooled budgeting, outcome based commissioning and prime contracting models. 3. Continuing to articulate the case and press for the distance from “fair shares” target to be addressed and for local people to receive their “fair share” of NHS resources. 4. Considering, as a last resort, reducing access to services for the people of East Staffordshire to reflect the lower level of funding available and the statutory financial duties of the Governing Body to live within the funding limit. This would have to be clinically led and carry the confidence of the Governing Body, Member Practices; and be subject to scrutiny and public consultation and the “Lansley tests”. Given the significant financial challenges faced by our partner CCGs in south Staffordshire; it may be appropriate to explore this jointly; if this becomes necessary. 5. The underpinning principle is to maintain a sustainable health system; whilst recognising
the need expressed in the Health and Wellbeing Strategy for a transformation in both culture and practices.
The Governing Body is asked to confirm its commitment to its previously agreed approach to meeting the financial requirements set out by NHS England; recognizing the difficulty in developing “firm” numbers for items 2 and 4 particularly. Integrated Commissioning with Staffordshire County Council – Adult Social Care The Governing Body has previously agreed to move towards Integrated Commissioning; initially with Adult Social care. Work is continuing and both the proposed benefits and governance arrangements will be brought for Governing Body approval in due course. Following the most recent OD event arrangements have now been put in place to adopt a more aligned approach to commissioning and contracting with SSOTP for the 2015/16 contract. This will involve the 2 lead collaborative CCGs (Cannock Chase for the South) working more closely together and with SCC ASC. In part this will take forward the priority development areas from the Single Frail Elderly Pathway work referred to earlier. Changes in NHS England I continue to await any firm announcements regarding changes to NHS England locally. NHS Five Year Forward View In October the national NHS leadership published the “Five Year Forward View”. I have reproduced the Foreword and the Executive Summary at Appendix B to this report. The full report has already been shared with Governing Body members. I have not attempted to summarise the report further on the basis that: - The Executive Summary is highly effective in doing this - The report is of such significance that the Governing Body will need to consider it fully and
carefully; and determine what actions to take. I also represented the CCG at a Regional Meeting at which national leaders, including Simon Stevens presented and discussed the Forward View.
East Staffs CCG
Key messages from that meeting are summarized below: - “There is a better version of the NHS out there , but a lot of work to do to get there” - Delivery in 2014/15 is key; we have significant challenges and risks and need to have a
granular focus on operational discipline - We have a good track record of delivery - 2015/16 will be a difficult year as we deliver the current and prepare for the future - The future is based on acting on Demand, Efficiency and Resourcing - Most of the efficiencies in the 5 Year View will need to be system efficiencies rather than
organizational efficiencies - The national bodies are determined to work together on a system basis and issue
guidance and system rules which are aligned - National bodies will expect local bodies to work as systems together to deliver system
performance and improvement - National bodies want us to be ambitious; but honest with them about what is really
possible. - National Bodies will be working with us over the next 6 months to inform which of the
models should be used; this will involve some pattern recognition of similar health environments/economies and discussion about which models will work best in those environments
- Clinical leadership and engagement is seen as “the active ingredient” and “a renewable energy”
- There will be consistency with current direction and priorities in the 2015/16 Planning Guidance which will be published in early December
- There will be increased scope for joint commissioning between CCGs and NHS England; both for co-commissioning Primary Care and for some Specialized Services
It is suggested that the Governing Body: - Give an initial view of the Five Year Forward View - Reserve time at the informal Workshop in December to consider the implications and
shape our way forward more fully; prior to further discussion at the Governing Body in January 2015.
3. Quality The Quality Committee of the Governing Body undertakes the detailed assurance work across the CCGs commissioned services on behalf of the Governing Body, testing through lay member challenge and appreciative inquiry, the conclusions reached by the executive quality management function. The joint Quality Committee now established between ourselves and our partners in SE&SP CCG. Its conclusions will be reported verbally at the meeting. Based on the information available at the time of writing I expect the meeting to confirm that all services commissioned by the CCG are safe. I further expect that the positive progress being made by BHFT in relation to demonstrable quality; and the CCGs increasing level of assurance; will be maintained. I have previously reported that in the context of BHFTs sustainability risks to its services and finances the Trust is supportive of using clinical and other partnerships and alliances to enhance both its clinical and financial sustainability. Specific work is currently ongoing with Derby Hospitals Foundation Trust on Stroke and TIA services and the Five Year Forward view supports such approaches to maintaining viability. The CCG also continues to support this approach.
East Staffs CCG

4. Performance and Finance
Performance
Performance across the range of indicators continues to be generally strong. The few exceptions where performance is not meeting expectations are:
- 18 week target for Admitted patients - Certain 31 day and 62 day cancer waits - Category A ambulance response times - Mixed sex accommodation breaches
Each of these has plans in place to address the shortfall in performance. Finance The CCG continues to forecast achievement of its agreed deficit control total. There is some risk to this and the next 2 months activity data at BHFT particularly will provide assurance or otherwise that the QIPP schemes relating to Non Elective Admissions (GP LIS and NEL CQUIN), POLCVs and Follow Up Outpatients are having the desired effect on the quality of patient care and on costs. Performance of the Medicines management Team continues to be strong. The CCG clinical and managerial team must maintain a strong and effective focus on the successful implementation of the agreed QIPP programme to deliver the overall financial position; together with agreed action to address some areas of rising elective referrals. Given the risks there is a need to develop proactively a set of contingency plans to reduce costs in the event of the QIPP programme not being fully successful; and to be clear on the authority to execute those contingency plans if necessary. It will not be possible to wait until the January Governing Body meeting to approve the plan or its implementation. 5. Governance and Organisational Development
Risk Management
The risk register continues to be effectively maintained. The principal risks continue to be:
• Finances related to the scale of the 14/15 and 5 year financial challenge, linked to the initial evidence of average or better than average performance across many of the CCGs commissioning domains and evidence of being significantly below the “fair shares” funding target.
• The impact on the NHS of SCC ASC funding and service changes; linked to the risks associated with implementing the agreed integrated commissioning arrangements in a challenged financial context.
• Capacity and capability of the CCG, particularly capacity to identify and deliver significant QIPP requirements in year and in the future, meet growing long term planning requirements; and to assure quality across the commissioning portfolio, with financially challenged providers.
• Clinical and financial sustainability of local services going forward, reflecting national factors locally.
East Staffs CCG
Quarter 1 2014/15 Checkpoint Review of CCG Performance and Development On 10th September the CCG had its Q1 review meeting with the Area Team of NHS England. The overall tone and messages regarding the CCGs performance and development were again very positive; consistent with the Full Year (Q4) review for 2013/14. I have now received the formal letter relating to 2014/15 Quarter 1 and this is attached as Appendix C I would like to echo again my sincere thanks to the staff of the CCG and CSU; together with our partners; for their support in delivering the results and improvements we achieved for our patients. Awards I am pleased to report that the ESCCG Medicines Management Team has been successful in winning a National Award for the “What a Waste” campaign. This is a great tribute to a hard working and highly successful team; and the work of the Practices in the CCG. AO Report November 2014.
East Staffs CCG
Shropshire & Staffordshire Area Team Anglesey House
Towers Plaza Wheelhouse Road
Rugeley WS15 1UL
14 October 2014
Dear Colleague Re: Long Term Financial Recovery for Commissioning in Staffordshire
Following the launch on Friday of the financial recovery process, I am writing to re-iterate the importance of the leadership and clinical engagement required to deliver a sustainable position in Staffordshire.
There are a clear set of requirements of your CCGs. I have set these out below;
• You are required to deliver a set of planned actions that ensures in-year delivery of your control total set for 14/15. For some this will mean a set of short term financial recovery actions that deliver this.
• You are required to have in place a set of plans that show recovery to a sustainable
financial position by the end of 16/17 and continuous improvement within that time frame. For clarity, sustainability is defined as meeting all NHS England financial metrics on a recurrent basis.
• You are required to plan to pay back your deficits over the following two financial
years (i.e. by the end of 18/19) and be clear what action needs to be taken to achieve this.
The work with KPMG and NHS England is designed to support those arrangements that you already have in place. It is not a substitute for, or separate to, the role of effective governance within your CCGs, nor the underpinning operational and commissioning arrangements that should be in place. The task to be completed by end of November is the production of a clear plan that will demonstrate how each CCG can effectively commission within the resources available. This is the task of all of those in a position of leadership in Staffordshire for the foreseeable future.
Yours sincerely
Graham Urwin Director – Shropshire & Staffordshire cc. Ros Francké – Director of Finance – Shropshire & Staffordshire Area Team
Rachel Hardy – Director of Finance – Midlands & East Region, NHS England Phil Morris – Head of Finance – Midlands & East Region Dawn Wickham – Director of Ops & Delivery, Shropshire & Staffordshire Area Team
Sent by email

FIVE YEARFORWARD VIEW
October 2014

CONTENTS
Foreword…..page 2
Executive summary…..page 3
Chapter One – Why will the NHS need to change?.....page 7
Chapter Two – What will the future look like? A new relationship with patients and communities…..page 10
- Getting serious about prevention…..page 10 - Empowering patients…..page 13 - Engaging communities…..page 14 - The NHS as a social movement…..page 15
Chapter Three – What will the future look like? New models of care…..page 17
- Emerging models…..page 17 - One size fits all?.....page 18 - New care models….page 20 - How we will support local co-design and implementation…..page 26
Chapter Four – How can we get there?.....page 29
- We will back diverse solutions and local leadership…..page 29 - We will create aligned national NHS leadership…..page 29 - We will support a modern workforce…..page 30 - We will exploit the information revolution…..page 32 - We will accelerate useful health innovation…..page 33 - We will drive efficiency and productive investment…..page 36
2
FOREWORD The NHS may be the proudest achievement of our modern society. It was founded in 1948 in place of fear - the fear that many people had of being unable to afford medical treatment for themselves and their families. And it was founded in a spirit of optimism - at a time of great uncertainty, coming shortly after the sacrifices of war. Our nation remains unwavering in that commitment to universal healthcare, irrespective of age, health, race, social status or ability to pay. To high quality care for all. Our values haven’t changed, but our world has. So the NHS needs to adapt to take advantage of the opportunities that science and technology offer patients, carers and those who serve them. But it also needs to evolve to meet new challenges: we live longer, with complex health issues, sometimes of our own making. One in five adults still smoke. A third of us drink too much alcohol. Just under two thirds of us are overweight or obese. These changes mean that we need to take a longer view - a Five-Year Forward View – to consider the possible futures on offer, and the choices that we face. So this Forward View sets out how the health service needs to change, arguing for a more engaged relationship with patients, carers and citizens so that we can promote wellbeing and prevent ill-health. It represents the shared view of the NHS’ national leadership, and reflects an emerging consensus amongst patient groups, clinicians, local communities and frontline NHS leaders. It sets out a vision of a better NHS, the steps we should now take to get us there, and the actions we need from others.

EXECUTIVE SUMMARY 1. The NHS has dramatically improved over the past fifteen years.
Cancer and cardiac outcomes are better; waits are shorter; patient satisfaction much higher. Progress has continued even during global recession and austerity thanks to protected funding and the commitment of NHS staff. But quality of care can be variable, preventable illness is widespread, health inequalities deep-rooted. Our patients’ needs are changing, new treatment options are emerging, and we face particular challenges in areas such as mental health, cancer and support for frail older patients. Service pressures are building.
2. Fortunately there is now quite broad consensus on what a better future should be. This ‘Forward View’ sets out a clear direction for the NHS – showing why change is needed and what it will look like. Some of what is needed can be brought about by the NHS itself. Other actions require new partnerships with local communities, local authorities and employers. Some critical decisions – for example on investment, on various public health measures, and on local service changes – will need explicit support from the next government.
3. The first argument we make in this Forward View is that the future health of millions of children, the sustainability of the NHS, and the economic prosperity of Britain all now depend on a radical upgrade in prevention and public health. Twelve years ago Derek Wanless’ health review warned that unless the country took prevention seriously we would be faced with a sharply rising burden of avoidable illness. That warning has not been heeded - and the NHS is on the hook for the consequences.
4. The NHS will therefore now back hard-hitting national action on obesity, smoking, alcohol and other major health risks. We will help develop and support new workplace incentives to promote employee health and cut sickness-related unemployment. And we will advocate for stronger public health-related powers for local government and elected mayors.
5. Second, when people do need health services, patients will gain far greater control of their own care – including the option of shared budgets combining health and social care. The 1.4 million full time unpaid carers in England will get new support, and the NHS will become a better partner with voluntary organisations and local communities.
6. Third, the NHS will take decisive steps to break down the barriers in how care is provided between family doctors and hospitals, between physical and mental health, between health and social care. The future will see far more care delivered locally but with some services in specialist centres, organised to support people with multiple health conditions, not just single diseases.
4
7. England is too diverse for a ‘one size fits all’ care model to apply everywhere. But nor is the answer simply to let ‘a thousand flowers bloom’. Different local health communities will instead be supported by the NHS’ national leadership to choose from amongst a small number of radical new care delivery options, and then given the resources and support to implement them where that makes sense.
8. One new option will permit groups of GPs to combine with nurses, other community health services, hospital specialists and perhaps mental health and social care to create integrated out-of-hospital care - the Multispecialty Community Provider. Early versions of these models are emerging in different parts of the country, but they generally do not yet employ hospital consultants, have admitting rights to hospital beds, run community hospitals or take delegated control of the NHS budget.
9. A further new option will be the integrated hospital and primary care provider - Primary and Acute Care Systems - combining for the first time general practice and hospital services, similar to the Accountable Care Organisations now developing in other countries too.
10. Across the NHS, urgent and emergency care services will be redesigned to integrate between A&E departments, GP out-of-hours services, urgent care centres, NHS 111, and ambulance services. Smaller hospitals will have new options to help them remain viable, including forming partnerships with other hospitals further afield, and partnering with specialist hospitals to provide more local services. Midwives will have new options to take charge of the maternity services they offer. The NHS will provide more support for frail older people living in care homes.
11. The foundation of NHS care will remain list-based primary care. Given the pressures they are under, we need a ‘new deal’ for GPs. Over the next five years the NHS will invest more in primary care, while stabilising core funding for general practice nationally over the next two years. GP-led Clinical Commissioning Groups will have the option of more control over the wider NHS budget, enabling a shift in investment from acute to primary and community services. The number of GPs in training needs to be increased as fast as possible, with new options to encourage retention.
12. In order to support these changes, the national leadership of the NHS will need to act coherently together, and provide meaningful local flexibility in the way payment rules, regulatory requirements and other mechanisms are applied. We will back diverse solutions and local leadership, in place of the distraction of further national structural reorganisation. We will invest in new options for our workforce, and raise our game on health technology - radically improving patients’ experience of interacting with the NHS. We will

5
improve the NHS’ ability to undertake research and apply innovation – including by developing new ‘test bed’ sites for worldwide innovators, and new ‘green field’ sites where completely new NHS services will be designed from scratch.
13. In order to provide the comprehensive and high quality care the people of England clearly want, Monitor, NHS England and independent analysts have previously calculated that a combination of growing demand if met by no further annual efficiencies and flat real terms funding would produce a mismatch between resources and patient needs of nearly £30 billion a year by 2020/21. So to sustain a comprehensive high-quality NHS, action will be needed on all three fronts – demand, efficiency and funding. Less impact on any one of them will require compensating action on the other two.
14. The NHS’ long run performance has been efficiency of 0.8% annually, but nearer to 1.5%-2% in recent years. For the NHS repeatedly to achieve an extra 2% net efficiency/demand saving across its whole funding base each year for the rest of the decade would represent a strong performance - compared with the NHS' own past, compared with the wider UK economy, and with other countries' health systems. We believe it is possible – perhaps rising to as high as 3% by the end of the period - provided we take action on prevention, invest in new care models, sustain social care services, and over time see a bigger share of the efficiency coming from wider system improvements.
15. On funding scenarios, flat real terms NHS spending overall would represent a continuation of current budget protection. Flat real terms NHS spending per person would take account of population growth. Flat NHS spending as a share of GDP would differ from the long term trend in which health spending in industrialised countries tends to rise as a share of national income.
16. Depending on the combined efficiency and funding option pursued, the effect is to close the £30 billion gap by one third, one half, or all the way. Delivering on the transformational changes set out in this Forward View and the resulting annual efficiencies could - if matched by staged funding increases as the economy allows - close the £30 billion gap by 2020/21. Decisions on these options will be for the next Parliament and government, and will need to be updated and adjusted over the course of the five year period. However nothing in the analysis above suggests that continuing with a comprehensive tax-funded NHS is intrinsically un-doable. Instead it suggests that there are viable options for sustaining and improving the NHS over the next five years, provided that the NHS does its part, allied with the support of government, and of our other partners, both national and local.

6
CHAPTER ONE Why does the NHS need to change?
Over the past fifteen years the NHS has dramatically improved. Cancer survival is its highest ever. Early deaths from heart disease are down by over 40%. Avoidable deaths overall are down by 20%. About 160,000 more nurses, doctors and other clinicians are treating millions more patients so that most long waits for operations have been slashed – down from 18 months to 18 weeks. Mixed sex wards and shabby hospital buildings have been tackled. Public satisfaction with the NHS has nearly doubled.
Over the past five years - despite global recession and austerity - the NHS has generally been successful in responding to a growing population, an ageing population, and a sicker population, as well as new drugs and treatments and cuts in local councils’ social care. Protected NHS funding has helped, as has the shared commitment and dedication of health service staff – on one measure the health service has become £20 billion more efficient. No health system anywhere in the world in recent times has managed five years of little or no real growth without either increasing charges, cutting services or cutting staff. The NHS has been a remarkable exception. What’s more, transparency about quality has helped care improve, and new research programmes like the 100,000 genomes initiative are putting this country at the forefront of global health research. The Commonwealth Fund has just ranked us the highest performing health system of 11 industrialised countries.
Of course the NHS is far from perfect. Some of the fundamental challenges facing us are common to all industrialised countries’ health systems:
• Changes in patients’ health needs and personal preferences. Long term health conditions - rather than illnesses susceptible to a one-off cure - now take 70% of the health service budget. At the same time many (but not all) people wish to be more informed and involved with their own care, challenging the traditional divide between patients and professionals, and offering opportunities for better health through increased prevention and supported self-care.
• Changes in treatments, technologies and care delivery. Technology is transforming our ability to predict, diagnose and treat disease. New treatments are coming on stream. And we know, both from examples within the NHS and internationally, that there are better ways of organising care, breaking out of the artificial boundaries between hospitals and primary care, between health and social care, between generalists and specialists—all of which get in the way of care that is genuinely coordinated around what people need and want.

7
• Changes in health services funding growth. Given the after-effects of
the global recession, most western countries will continue to experience budget pressures over the next few years, and it is implausible to think that over this period NHS spending growth could return to the 6%-7% real annual increases seen in the first decade of this century.
Some of the improvements we need over the next five years are more specific to England. In mental health and learning disability services. In faster diagnosis and more uniform treatment for cancer. In readily accessible GP services. In prevention and integrated health and social care. There are still unacceptable variations of care provided to patients, which can have devastating effects on individuals and their families, as the inexcusable events at Mid-Staffordshire and Winterbourne View laid bare.
One possible response to these challenges would be to attempt to muddle through the next few years, relying on short term expedients to preserve services and standards. Our view is that this is not a sustainable strategy because it would over time inevitably lead to three widening gaps:
The health and wellbeing gap: if the nation fails to get serious about prevention then recent progress in healthy life expectancies will stall, health inequalities will widen, and our ability to fund beneficial new treatments will be crowded-out by the need to spend billions of pounds on wholly avoidable illness.
The care and quality gap: unless we reshape care delivery, harness technology, and drive down variations in quality and safety of care, then patients’ changing needs will go unmet, people will be harmed who should have been cured, and unacceptable variations in outcomes will persist.
The funding and efficiency gap: if we fail to match reasonable funding levels with wide-ranging and sometimes controversial system efficiencies, the result will be some combination of worse services, fewer staff, deficits, and restrictions on new treatments.
We believe none of these three gaps is inevitable. A better future is possible – and with the right changes, right partnerships, and right investments we know how to get there.
That’s because there is broad consensus on what that future needs to be. It is a future that empowers patients to take much more control over their own care and treatment. It is a future that dissolves the classic divide, set almost in stone since 1948, between family doctors and hospitals, between physical and mental health, between health and social care, between prevention and treatment. One that no longer sees expertise locked into often out-dated buildings, with services fragmented, patients

8
having to visit multiple professionals for multiple appointments, endlessly repeating their details because they use separate paper records. One organised to support people with multiple health conditions, not just single diseases. A future that sees far more care delivered locally but with some services in specialist centres where that clearly produces better results. One that recognises that we cannot deliver the necessary change without investing in our current and future workforce.
The rest of this Forward View sets out what that future will look like, and how together we can bring it about. Chapter two – the next chapter – outlines some of the action needed to tackle the health and wellbeing gap. Chapter three sets out radical changes to tackle the care and quality gap. Chapter four focuses on options for meeting the funding and efficiency challenge.
BOX 1: FIVE YEAR AMBITIONS ON QUALITY
The definition of quality in health care, enshrined in law, includes three key aspects: patient safety, clinical effectiveness and patient experience. A high quality health service exhibits all three. However, achieving all three ultimately happens when a caring culture, professional commitment and strong leadership are combined to serve patients, which is why the Care Quality Commission is inspecting against these elements of quality too.
We do not always achieve these standards. For example, there is variation depending on when patients are treated: mortality rates are 11% higher for patients admitted on Saturdays and 16% higher on Sundays compared to a Wednesday. And there is variation in outcomes; for instance, up to 30% variation between CCGs in the health related quality of life for people with more than one long term condition.
We have a double opportunity: to narrow the gap between the best and the worst, whilst raising the bar higher for everyone. To reduce variations in where patients receive care, we will measure and publish meaningful and comparable measurements for all major pathways of care for every provider – including community, mental and primary care – by the end of the next Parliament. We will continue to redesign the payment system so that there are rewards for improvements in quality. We will invest in leadership by reviewing and refocusing the work of the NHS Leadership Academy and NHS Improving Quality. To reduce variations in when patients receive care, we will develop a framework for how seven day services can be implemented affordably and sustainably, recognising that different solutions will be needed in different localities. As national bodies we can do more by measuring what matters, requiring comprehensive transparency of performance data and ensuring this data increasingly informs payment mechanisms and commissioning decisions.

9
CHAPTER TWO What will the future look like? A new relationship with patients and communities
One of the great strengths of this country is that we have an NHS that - at its best - is ‘of the people, by the people and for the people’.
Yet sometimes the health service has been prone to operating a ‘factory’ model of care and repair, with limited engagement with the wider community, a short-sighted approach to partnerships, and under-developed advocacy and action on the broader influencers of health and wellbeing.
As a result we have not fully harnessed the renewable energy represented by patients and communities, or the potential positive health impacts of employers and national and local governments.
Getting serious about prevention
The future health of millions of children, the sustainability of the NHS, and the economic prosperity of Britain all now depend on a radical upgrade in prevention and public health. Twelve years ago, Derek Wanless’ health review warned that unless the country took prevention seriously we would be faced with a sharply rising burden of avoidable illness. That warning has not been heeded - and the NHS is on the hook for the consequences.
Rather than the ‘fully engaged scenario’ that Wanless spoke of, one in five adults still smoke. A third of people drink too much alcohol. A third of men and half of women don’t get enough exercise. Almost two thirds of adults are overweight or obese. These patterns are influenced by, and in turn reinforce, deep health inequalities which can cascade down the generations. For example, smoking rates during pregnancy range from 2% in west London to 28% in Blackpool.
Even more shockingly, the number of obese children doubles while children are at primary school. Fewer than one-in-ten children are obese when they enter reception class. By the time they’re in Year Six, nearly one-in-five are then obese.
And as the ‘stock’ of population health risk gets worse, the ‘flow’ of costly NHS treatments increases as a consequence. To take just one example – Diabetes UK estimate that the NHS is already spending about £10 billion a year on diabetes. Almost three million people in England are already living with diabetes and another seven million people are at risk of becoming diabetic. Put bluntly, as the nation’s waistline keeps piling on

10
the pounds, we’re piling on billions of pounds in future taxes just to pay for preventable illnesses.
We do not have to accept this rising burden of ill health driven by our lifestyles, patterned by deprivation and other social and economic influences. Public Health England’s new strategy sets out priorities for tackling obesity, smoking and harmful drinking; ensuring that children get the best start in life; and that we reduce the risk of dementia through tackling lifestyle risks, amongst other national health goals.
We support these priorities and will work to deliver them. While the health service certainly can’t do everything that’s needed by itself, it can and should now become a more activist agent of health-related social change. That’s why we will lead where possible, or advocate when appropriate, a range of new approaches to improving health and wellbeing.
Incentivising and supporting healthier behaviour. England has made significant strides in reducing smoking, but it still remains our number one killer. More than half of the inequality in life expectancy between social classes is now linked to higher smoking rates amongst poorer people. There are now over 3,000 alcohol-related admissions to A&E every day. Our young people have the highest consumption of sugary soft drinks in Europe. So for all of these major health risks – including tobacco, alcohol, junk food and excess sugar - we will actively support comprehensive, hard-hitting and broad-based national action to include clear information and labelling, targeted personal support and wider changes to distribution, marketing, pricing, and product formulation. We will also use the substantial combined purchasing power of the NHS to reinforce these measures.
Local democratic leadership on public health. Local authorities now have a statutory responsibility for improving the health of their people, and councils and elected mayors can make an important impact. For example, Barking and Dagenham are seeking to limit new junk food outlets near schools. Ipswich Council, working with Suffolk Constabulary, is taking action on alcohol. Other councils are now following suit. The mayors of Liverpool and London have established wide-ranging health commissions to mobilise action for their residents. Local authorities in greater Manchester are increasingly acting together to drive health and wellbeing. Through local Health and Wellbeing Boards, the NHS will play its part in these initiatives. However, we agree with the Local Government Association that English mayors and local authorities should also be granted enhanced powers to allow local democratic decisions on public health policy that go further and faster than prevailing national law – on alcohol, fast food, tobacco and other issues that affect physical and mental health.

11
Targeted prevention. While local authorities now have responsibility for many broad based public health programmes, the NHS has a distinct role in secondary prevention. Proactive primary care is central to this, as is the more systematic use of evidence-based intervention strategies. We also need to make different investment decisions - for example, it makes little sense that the NHS is now spending more on bariatric surgery for obesity than on a national roll-out of intensive lifestyle intervention programmes that were first shown to cut obesity and prevent diabetes over a decade ago. Our ambition is to change this over the next five years so that we become the first country to implement at scale a national evidence-based diabetes prevention programme modelled on proven UK and international models, and linked where appropriate to the new Health Check. NHS England and Public Health England will establish a preventative services programme that will then expand evidence-based action to other conditions.
NHS support to help people get and stay in employment. Sickness absence-related costs to employers and taxpayers have been estimated at £22 billion a year, and over 300,000 people each year take up health-related benefits. In doing so, individuals collectively miss out on £4 billion a year of lost earnings. Yet there is emerging evidence that well targeted health support can help keep people in work thus improving their wellbeing and preserving their livelihoods. Mental health problems now account for more than twice the number of Employment and Support Allowance and Incapacity Benefit claims than do musculoskeletal complaints (for example, bad backs). Furthermore, the employment rate of people with severe and enduring mental health problems is the lowest of all disability groups at just 7%. A new government-backed Fit for Work scheme starts in 2015. Over and above that, during the next Parliament we will seek to test a win-win opportunity of improving access to NHS services for at-risk individuals while saving ‘downstream’ costs at the Department for Work and Pensions, if money can be reinvested across programmes.
Workplace health. One of the advantages of a tax-funded NHS is that - unlike in a number of continental European countries - employers here do not pay directly for their employees’ health care. But British employers do pay national insurance contributions which help fund the NHS, and a healthier workforce will reduce demand and lower long term costs. The government has partially implemented the recommendations in the independent review by Dame Carol Black and David Frost, which allow employers to provide financial support for vocational rehabilitation services without employees facing a tax bill. There would be merit in extending incentives for employers in England who provide effective NICE recommended workplace health programmes for employees. We will also establish with NHS Employers new incentives to ensure the NHS as an employer sets a national example in the support it offers its own 1.3 million staff to stay healthy, and serve as “health ambassadors” in their local communities.

12
BOX 2.1: A HEALTHIER NHS WORKPLACE
While three quarters of NHS trusts say they offer staff help to quit smoking, only about a third offer them support in keeping to a healthy weight. Three quarters of hospitals do not offer healthy food to staff working night shifts. It has previously been estimated the NHS could reduce its overall sickness rate by a third – the equivalent of adding almost 15,000 staff and 3.3 million working days at a cost saving of £550m. So among other initiatives we will: ● Cut access to unhealthy products on NHS premises, implementing food standards, and providing healthy options for night staff. ● Measure staff health and wellbeing, and introduce voluntary work-based weight watching and health schemes which international studies have shown achieve sustainable weight loss in more than a third of those who take part. ● Support “active travel” schemes for staff and visitors. ● Promote the Workplace Wellbeing Charter, the Global Corporate Challenge and the TUC’s Better Health and Work initiative, and ensure NICE guidance on promoting healthy workplaces is implemented, particularly for mental health. ● Review with the Faculty of Occupational Medicine the strengthening of occupational health.
Empowering patients
Even people with long term conditions, who tend to be heavy users of the health service, are likely to spend less than 1% of their time in contact with health professionals. The rest of the time they, their carers and their families manage on their own. As the patients’ organisation National Voices puts it: personalised care will only happen when statutory services recognise that patients’ own life goals are what count; that services need to support families, carers and communities; that promoting wellbeing and independence need to be the key outcomes of care; and that patients, their families and carers are often ‘experts by experience’.
As a first step towards this ambition we will improve the information to which people have access—not only clinical advice, but also information about their condition and history. The digital and technology strategies we set out in chapter four will help, and within five years, all citizens will be able to access their medical and care records (including in social care contexts) and share them with carers or others they choose.
Second, we will do more to support people to manage their own health – staying healthy, making informed choices of treatment, managing conditions and avoiding complications. With the help of voluntary sector partners, we will invest significantly in evidence-based approaches such as group-based education for people with specific conditions and self-management educational courses, as well as encouraging independent peer-to-peer communities to emerge.
A third step is to increase the direct control patients have over the care that is provided to them. We will make good on the NHS’ longstanding

13
promise to give patients choice over where and how they receive care. Only half of patients say they were offered a choice of hospitals for their care, and only half of patients say they are as involved as they wish to be in decisions about their care and treatment. We will also introduce integrated personal commissioning (IPC), a new voluntary approach to blending health and social care funding for individuals with complex needs. As well as care plans and voluntary sector advocacy and support, IPC will provide an integrated, “year of care” budget that will be managed by people themselves or on their behalf by councils, the NHS or a voluntary organisation.
Engaging communities
More broadly, we need to engage with communities and citizens in new ways, involving them directly in decisions about the future of health and care services. Programmes like NHS Citizen point the way, but we also commit to four further actions to build on the energy and compassion that exists in communities across England. These are better support for carers; creating new options for health-related volunteering; designing easier ways for voluntary organisations to work alongside the NHS; and using the role of the NHS as an employer to achieve wider health goals.
Supporting carers. Two thirds of patients admitted to hospital are over 65, and more than a quarter of hospital inpatients have dementia. The five and a half million carers in England make a critical and underappreciated contribution not only to loved ones, neighbours and friends, but to the very sustainability of the NHS itself. We will find new ways to support carers, building on the new rights created by the Care Act, and especially helping the most vulnerable amongst them – the approximately 225,000 young carers and the 110,000 carers who are themselves aged over 85. This will include working with voluntary organisations and GP practices to identify them and provide better support. For NHS staff, we will look to introduce flexible working arrangements for those with major unpaid caring responsibilities.
Encouraging community volunteering. Volunteers are crucial in both health and social care. Three million volunteers already make a critical contribution to the provision of health and social care in England; for example, the Health Champions programme of trained volunteers that work across the NHS to improve its reach and effectiveness. The Local Government Association has made proposals that volunteers, including those who help care for the elderly, should receive a 10% reduction in their council tax bill, worth up to £200 a year. We support testing approaches like that, which could be extended to those who volunteer in hospitals and other parts of the NHS. The NHS can go further, accrediting volunteers and devising ways to help them become part of the extended NHS family – not as substitutes for but as partners with our skilled employed staff. For example, more than 1,000 “community first responders” have been recruited by Yorkshire Ambulance in more rural

14
areas and trained in basic life support. New roles which have been proposed could include family and carer liaison, educating people in the management of long-term conditions and helping with vaccination programmes. We also intend to work with carers organisations to support new volunteer programmes that could provide emergency help when carers themselves face a crisis of some kind, as well as better matching volunteers to the roles where they can add most value.
Stronger partnerships with charitable and voluntary sector organisations. When funding is tight, NHS, local authority and central government support for charities and voluntary organisations is put under pressure. However these voluntary organisations often have an impact well beyond what statutory services alone can achieve. Too often the NHS conflates the voluntary sector with the idea of volunteering, whereas these organisations provide a rich range of activities, including information, advice, advocacy and they deliver vital services with paid expert staff. Often they are better able to reach underserved groups, and are a source of advice for commissioners on particular needs. So in addition to other steps the NHS will take, we will seek to reduce the time and complexity associated with securing local NHS funding by developing a short national alternative to the standard NHS contract where grant funding may be more appropriate than burdensome contracts, and by encouraging funders to commit to multiyear funding wherever possible.
The NHS as a local employer. The NHS is committed to making substantial progress in ensuring that the boards and leadership of NHS organisations better reflect the diversity of the local communities they serve, and that the NHS provides supportive and non-discriminatory ladders of opportunity for all its staff, including those from black and minority ethnic backgrounds. NHS employers will be expected to lead the way as progressive employers, including for example by signing up to efforts such as Time to Change which challenge mental health stigma and discrimination. NHS employers also have the opportunity to be more creative in offering supported job opportunities to ‘experts by experience’ such as people with learning disabilities who can help drive the kind of change in culture and services that the Winterbourne View scandal so graphically demonstrated is needed.
The NHS as a social movement
None of these initiatives and commitments by themselves will be the difference between success and failure over the next five years. But collectively and cumulatively they and others like them will help shift power to patients and citizens, strengthen communities, improve health and wellbeing, and—as a by-product—help moderate rising demands on the NHS.
So rather than being seen as the ‘nice to haves’ and the ‘discretionary extras’, our conviction is that these sort of partnerships and initiatives are

15
in fact precisely the sort of ‘slow burn, high impact’ actions that are now essential.
They in turn need to be matched by equally radical action to transform the way NHS care is provided. That is the subject of the next chapter.
BOX 2.2: SUPPORT FOR PEOPLE WITH DEMENTIA
About 700,000 people in England are estimated to have dementia, many undiagnosed. Perhaps one in three people aged over 65 will develop dementia before they die. Almost 500,000 unpaid carers look after people living with dementia. The NHS is making a national effort to increase the proportion of people with dementia who are able to get a formal diagnosis from under half, to two thirds of people affected or more. Early diagnosis can prevent crises, while treatments are available that may slow progression of the disease.
For those that are diagnosed with dementia, the NHS’ ambition over the next five years is to offer a consistent standard of support for patients newly diagnosed with dementia, supported by named clinicians or advisors, with proper care plans developed in partnership with patients and families; and the option of personal budgets, so that resources can be used in a way that works best for individual patients. Looking further ahead, the government has committed new funding to promote dementia research and treatment.
But the dementia challenge calls for a broader coalition, drawing together statutory services, communities and businesses. For example, Dementia Friendly Communities – currently being developed by the Alzheimer’s Society – illustrate how, with support, people with dementia can continue to participate in the life of their community. These initiatives will have our full support—as will local dementia champions, participating businesses and other organisations.

16
CHAPTER THREE What will the future look like? New models of care
The traditional divide between primary care, community services, and hospitals - largely unaltered since the birth of the NHS - is increasingly a barrier to the personalised and coordinated health services patients need. And just as GPs and hospitals tend to be rigidly demarcated, so too are social care and mental health services even though people increasingly need all three.
Over the next five years and beyond the NHS will increasingly need to dissolve these traditional boundaries. Long term conditions are now a central task of the NHS; caring for these needs requires a partnership with patients over the long term rather than providing single, unconnected ‘episodes’ of care. As a result there is now quite wide consensus on the direction we will be taking.
• Increasingly we need to manage systems – networks of care – not just organisations.
• Out-of-hospital care needs to become a much larger part of what the NHS does.
• Services need to be integrated around the patient. For example a patient with cancer needs their mental health and social care coordinated around them. Patients with mental illness need their physical health addressed at the same time.
• We should learn much faster from the best examples, not just from within the UK but internationally.
• And as we introduce them, we need to evaluate new care models to establish which produce the best experience for patients and the best value for money.
Emerging models
In recent years parts of the NHS have begun doing elements of this. The strategic plans developed by local areas show that in some places the future is already emerging. For example:
In Kent, 20 GPs and almost 150 staff operate from three modern sites providing many of the tests, investigations, minor injuries and minor surgery usually provided in hospital. It shows what can be done when general practice operates at scale. Better results, better care, a better experience for patients and significant savings.
In Airedale, nursing and residential homes are linked by secure video to the hospital allowing consultations with nurses and consultants both in

17
and out of normal hours - for everything from cuts and bumps to diabetes management to the onset of confusion. Emergency admissions from these homes have been reduced by 35% and A&E attendances by 53%. Residents rate the service highly.
In Cornwall, trained volunteers and health and social care professionals work side-by-side to support patients with long term conditions to meet their own health and life goals.
In Rotherham, GPs and community matrons work with advisors who know what voluntary services are available for patients with long term conditions. This “social prescribing service” has cut the need for visits to accident and emergency, out-patient appointments and hospital admissions.
In London, integrated care pioneers that combine NHS, GP and social care services have improved services for patients, with fewer people moving permanently into nursing care homes. They have also shown early promise in reducing emergency admissions. Greenwich has saved nearly £1m for the local authority and over 5% of community health expenditure.
All of these approaches seem to improve the quality of care and patients’ experience. They also deliver better value for money; some may even cut costs. They are pieces of the jigsaw that will make up a better NHS. But there are too few of them, and they are too isolated. Nowhere do they provide the full picture of a 21st century NHS that has yet to emerge. Together they describe the way the NHS of the future will look.
One size fits all?
So to meet the changing needs of patients, to capitalise on the opportunities presented by new technologies and treatments, and to unleash system efficiencies more widely, we intend to support and stimulate the creation of a number of major new care models that can be deployed in different combinations locally across England.
However England is too diverse – both in its population and its current health services – to pretend that a single new model of care should apply everywhere. Times have changed since the last such major blueprint, the 1962 Hospital Plan for England and Wales. What’s right for Cumbria won’t be right for Coventry; what makes sense in Manchester and in Winchester will be different.
But that doesn’t mean there are an infinite number of new care models. While the answer is not one-size-fits-all, nor is it simply to let ‘a thousand flowers bloom’. Cumbria and Devon and Northumberland have quite a lot in common in designing their NHS of the future. So do the hospitals on the
18
outer ring around Manchester and the outer ring around London. So do many other parts of the country.
That’s why our approach will be to identify the characteristics of similar health communities across England, and then jointly work with them to consider which of the new options signalled by this Forward View constitute viable ways forward for their local health and care services over the next five years and beyond.
In all cases however one of the most important changes will be to expand and strengthen primary and ‘out of hospital’ care. Given the pressures that GPs are under, this is dependent on several immediate steps to stabilise general practice – see Box 3.1.
BOX 3.1: A new deal for primary care
General practice, with its registered list and everyone having access to a family doctor, is one of the great strengths of the NHS, but it is under severe strain. Even as demand is rising, the number of people choosing to become a GP is not keeping pace with the growth in funded training posts - in part because primary care services have been under-resourced compared to hospitals. So over the next five years we will invest more in primary care. Steps we will take include:
• Stabilise core funding for general practice nationally over the next two years while an independent review is undertaken of how resources are fairly made available to primary care in different areas.
• Give GP-led Clinical Commissioning Groups (CCGs) more influence over the wider NHS budget, enabling a shift in investment from acute to primary and community services.
• Provide new funding through schemes such as the Challenge Fund to support new ways of working and improved access to services.
• Expand as fast as possible the number of GPs in training while training more community nurses and other primary care staff. Increase investment in new roles, and in returner and retention schemes and ensure that current rules are not inflexibly putting off potential returners.
• Expand funding to upgrade primary care infrastructure and scope of services.
• Work with CCGs and others to design new incentives to encourage new GPs and practices to provide care in under-doctored areas to tackle health inequalities.
• Build the public’s understanding that pharmacies and on-line resources can help them deal with coughs, colds and other minor ailments without the need for a GP appointment or A&E visit.

19
Here we set out details of the principal additional care models over and above the status quo which we will be promoting in England over the next five years.
New care model – Multispecialty Community Providers (MCPs)
Smaller independent GP practices will continue in their current form where patients and GPs want that. However, as the Royal College of General Practitioners has pointed out, in many areas primary care is entering the next stage of its evolution. As GP practices are increasingly employing salaried and sessional doctors, and as women now comprise half of GPs, the traditional model has been evolving.
Primary care of the future will build on the traditional strengths of ‘expert generalists’, proactively targeting services at registered patients with complex ongoing needs such as the frail elderly or those with chronic conditions, and working much more intensively with these patients. Future models will expand the leadership of primary care to include nurses, therapists and other community based professionals. It could also offer some care in fundamentally different ways, making fuller use of digital technologies, new skills and roles, and offering greater convenience for patients.
To offer this wider scope of services, and enable new ways of delivering care, we will make it possible for extended group practices to form – either as federations, networks or single organisations.
These Multispecialty Community Providers (MCPs) would become the focal point for a far wider range of care needed by their registered patients.
• As larger group practices they could in future begin employing consultants or take them on as partners, bringing in senior nurses, consultant physicians, geriatricians, paediatricians and psychiatrists to work alongside community nurses, therapists, pharmacists, psychologists, social workers, and other staff.
• These practices would shift the majority of outpatient consultations and ambulatory care out of hospital settings.
• They could take over the running of local community hospitals which could substantially expand their diagnostic services as well as other services such as dialysis and chemotherapy.
• GPs and specialists in the group could be credentialed in some cases to directly admit their patients into acute hospitals, with out-of-hours

20
inpatient care being supervised by a new cadre of resident ‘hospitalists’ – something that already happens in other countries.
• They could in time take on delegated responsibility for managing the health service budget for their registered patients. Where funding is pooled with local authorities, a combined health and social care budget could be delegated to Multispecialty Community Providers.
• These new models would also draw on the ‘renewable energy’ of
carers, volunteers and patients themselves, accessing hard-to-reach groups and taking new approaches to changing health behaviours.
There are already a number of practices embarking on this journey, including high profile examples in the West Midlands, London and elsewhere. For example, in Birmingham, one partnership has brought together 10 practices employing 250 staff to serve about 65,000 patients on 13 sites. It will shortly have three local hubs with specialised GPs that will link in community and social care services while providing central out-of-hours services using new technology.
To help others who want to evolve in this way, and to identify the most promising models that can be spread elsewhere, we will work with emerging practice groups to address barriers to change, service models, access to funding, optimal use of technology, workforce and infrastructure. As with the other models discussed in this section, we will also test these models with patient groups and our voluntary sector partners.
New care model – Primary and Acute Care Systems (PACS)
A range of contracting and organisational forms are now being used to better integrate care, including lead/prime providers and joint ventures.
We will now permit a new variant of integrated care in some parts of England by allowing single organisations to provide NHS list-based GP and hospital services, together with mental health and community care services.
The leadership to bring about these ‘vertically’ integrated Primary and Acute Care Systems (PACS) may be generated from different places in different local health economies.
• In some circumstances – such as in deprived urban communities where local general practice is under strain and GP recruitment is proving hard – hospitals will be permitted to open their own GP surgeries with registered lists. This would allow the accumulated surpluses and investment powers of NHS Foundation Trusts to kick-start the expansion of new style primary care in areas with high health inequalities. Safeguards will be needed to ensure that they do

21
this in ways that reinforce out-of-hospital care, rather than general practice simply becoming a feeder for hospitals still providing care in the traditional ways.
• In other circumstances, the next stage in the development of a mature
Multispecialty Community Provider (see section above) could be that it takes over the running of its main district general hospital.
• At their most radical, PACS would take accountability for the whole health needs of a registered list of patients, under a delegated capitated budget - similar to the Accountable Care Organisations that are emerging in Spain, the United States, Singapore, and a number of other countries.
PACS models are complex. They take time and technical expertise to implement. As with any model there are also potential unintended side effects that need to be managed. We will work with a small number of areas to test these approaches with the aim of developing prototypes that work, before promoting the most promising models for adoption by the wider NHS.
New care model - urgent and emergency care networks
The care that people receive in England’s Emergency Departments is, and will remain, one of the yardsticks by which the NHS as a whole will be judged. Although both quality and access have improved markedly over the years, the mounting pressures on these hospital departments illustrate the need to transition to a more sustainable model of care.
More and more people are using A&E – with 22 million visits a year. Compared to five years ago, the NHS in England handles around 3,500 extra attendances every single day, and in many places, A&E is running at full stretch. However, the 185 hospital emergency departments in England are only a part of the urgent and emergency care system. The NHS responds to more than 100 million urgent calls or visits every year.
Over the next five years, the NHS will do far better at organising and simplifying the system. This will mean:
• Helping patients get the right care, at the right time, in the right place, making more appropriate use of primary care, community mental health teams, ambulance services and community pharmacies, as well as the 379 urgent care centres throughout the country. This will partly be achieved by evening and weekend access to GPs or nurses working from community bases equipped to provide a much greater range of tests and treatments; ambulance services empowered to make more decisions, treating patients and making referrals in a more flexible way; and far greater use of pharmacists.
22
• Developing networks of linked hospitals that ensure patients with the most serious needs get to specialist emergency centres - drawing on the success of major trauma centres, which have saved 30% more of the lives of the worst injured.
• Ensuring that hospital patients have access to seven day services
where this makes a clinical difference to outcomes.
• Proper funding and integration of mental health crisis services, including liaison psychiatry.
• A strengthened clinical triage and advice service that links the system together and helps patients navigate it successfully.
• New ways of measuring the quality of the urgent and emergency services; new funding arrangements; and new responses to the workforce requirements that will make these new networks possible.
New care model – viable smaller hospitals
Some commentators have argued that smaller district general hospitals should be merged and/or closed. In fact, England already has one of the more centralised hospital models amongst advanced health systems. It is right that these hospitals should not be providing complex acute services where there is evidence that high volumes are associated with high quality. And some services and buildings will inevitably and rightly need to be re-provided in other locations - just as they have done in the past and will continue to be in every other western country.
However to help sustain local hospital services where the best clinical solution is affordable, has the support of local commissioners and communities, we will now take three sets of actions.
First, NHS England and Monitor will work together to consider whether any adjustments are needed to the NHS payment regime to reflect the costs of delivering safe and efficient services for smaller providers relative to larger ones. The latest quarterly figures show that larger foundation trusts had EBITDA margins of 5% compared to -0.4% for smaller providers.
Second, building on the earlier work of Monitor looking at the costs of running smaller hospitals, and on the Royal College of Physicians Future Hospitals initiative, we will work with those hospitals to examine new models of medical staffing and other ways of achieving sustainable cost structures.
Third, we will create new organisational models for smaller acute hospitals that enable them to gain the benefits of scale without necessarily having to centralise services. Building on the recommendations of the

23
forthcoming Dalton Review, we intend to promote at least three new models:
• In one model, a local acute hospital might share management either of the whole institution or of their ‘back office’ with other similar hospitals not necessarily located in their immediate vicinity. These type of ‘hospital chains’ already operate in places such as Germany and Scandinavia.
• In another new model, a smaller local hospital might have some of its services on a site provided by another specialised provider – for example Moorfields eye hospital operates in 23 locations in London and the South East. Several cancer specialist providers are also considering providing services on satellite sites.
• And as indicated in the PACS model above, a further new option is that a local acute hospital and its local primary and community services could form an integrated provider.
New care model - specialised care
In some services there is a compelling case for greater concentration of care. In these services there is a strong relationship between the number of patients and the quality of care, derived from the greater experience these more practiced clinicians have, access to costly specialised facilities and equipment, and the greater standardisation of care that tends to occur. For example, consolidating 32 stroke units to 8 specialist ones in London achieved a 17% reduction in 30-day mortality and a 7% reduction in patient length of stay.
The evidence suggests that similar benefits could be had for most specialised surgery, and some cancer and other services. For example, in Denmark reducing by two thirds the number of hospitals that perform colorectal cancer surgery has improved post-operative mortality after 2 years by 62%. In Germany, the highest volume centres that treat prostate cancer have substantially fewer complications. The South West London Elective Orthopaedic Centre achieves lower post-operative complication rates than do many hospitals which operate on fewer patients.
In services where the relationship between quality and patient volumes is this strong, NHS England will now work with local partners to drive consolidation through a programme of three-year rolling reviews. We will also look to these specialised providers to develop networks of services over a geography, integrating different organisations and services around patients, using innovations such as prime contracting and/or delegated capitated budgets. To take one example: cancer. This would enable patients to have chemotherapy, support and follow up care in their local community hospital or primary care facility, whilst having access to world-leading facilities for their surgery and radiotherapy. In line with
24
the UK Strategy for Rare Diseases, we will also explore establishing specialist centres for rare diseases to improve the coordination of care for their patients.
New care model - modern maternity services
Having a baby is the most common reason for hospital admission in England. Births are up by almost a quarter in the last decade, and are at their highest in 40 years.
Recent research shows that for low risk pregnancies babies born at midwife-led units or at home did as well as babies born in obstetric units, with fewer interventions. Four out of five women live within a 30 minute drive of both an obstetric unit and a midwife-led unit, but research by the Women’s Institute and the National Childbirth Trust suggests that while only a quarter of women want to give birth in a hospital obstetrics unit, over 85% actually do so.
To ensure maternity services develop in a safe, responsive and efficient manner, in addition to other actions underway – including increasing midwife numbers - we will:
• Commission a review of future models for maternity units, to report by next summer, which will make recommendations on how best to sustain and develop maternity units across the NHS.
• Ensure that tariff-based NHS funding supports the choices women make, rather than constraining them.
• As a result, make it easier for groups of midwives to set up their own NHS-funded midwifery services.
New care model – enhanced health in care homes
One in six people aged 85 or over are living permanently in a care home. Yet data suggest that had more active health and rehabilitation support been available, some people discharged from hospital to care homes could have avoided permanent admission. Similarly, the Care Quality Commission and the British Geriatrics Society have shown that many people with dementia living in care homes are not getting their health needs regularly assessed and met. One consequence is avoidable admissions to hospital.
In partnership with local authority social services departments, and using the opportunity created by the establishment of the Better Care Fund, we will work with the NHS locally and the care home sector to develop new shared models of in-reach support, including medical reviews, medication reviews, and rehab services. In doing so we will build on the success of

25
models which have been shown to improve quality of life, reduce hospital bed use by a third, and save significantly more than they cost.
How will we support the co-design and implementation of these new care models?
Some parts of the country will be able to continue commissioning and providing high quality and affordable health services using their current care models, and without any adaptation along the lines described above.
However, previous versions of local ‘five year plans’ by provider trusts and CCGs suggest that many areas will need to consider new options if they are to square the circle between the desire to improve quality, respond to rising patient volumes, and live within the expected local funding.
In some places, including major conurbations, we therefore expect several of these alternative models to evolve in parallel.
In other geographies it may make sense for local communities to discuss convergence of care models for the future. This will require a new perspective where leaders look beyond their individual organisations’ interests and towards the future development of whole health care economies - and are rewarded for doing so.
It will also require a new type of partnership between national bodies and local leaders. That is because to succeed in designing and implementing these new care models, the NHS locally will need national bodies jointly to exercise discretion in the application of their payment rules, regulatory approaches, staffing models and other policies, as well as possibly providing technical and transitional support.
We will therefore now work with local communities and leaders to identify what changes are needed in how national and local organisations best work together, and will jointly develop:
• Detailed prototyping of each of the new care models described above, together with any others that may be proposed that offer the potential to deliver the necessary transformation - in each case identifying current exemplars, potential benefits, risks and transition costs.
• A shared method of assessing the characteristics of each health economy, to help inform local choice of preferred models, promote peer learning with similar areas, and allow joint intervention in health economies that are furthest from where they need to be.
• National and regional expertise and support to implement care model change rapidly and at scale. The NHS is currently spending several

26
hundred million pounds on bodies that directly or indirectly could support this work, but the way in which improvement and clinical engagement happens can be fragmented and unfocused. We will therefore create greater alignment in the work of strategic clinical networks, clinical senates, NHS IQ, the NHS Leadership Academy and the Academic Health Science Centres and Networks.
• National flexibilities in the current regulatory, funding and pricing
regimes to assist local areas to transition to better care models.
• Design of a model to help pump-prime and ‘fast track’ a cross-section of the new care models. We will back the plans likely to have the greatest impact for patients, so that by the end of the next Parliament the benefits and costs of the new approaches are clearly demonstrable, allowing informed decisions about future investment as the economy improves. This pump-priming model could also unlock assets held by NHS Property Services, surplus NHS property and support Foundation Trusts that decide to use accrued savings on their balance sheets to help local service transformation.
BOX 3.2: FIVE YEAR AMBITIONS FOR MENTAL HEALTH
Mental illness is the single largest cause of disability in the UK and each year about one in four people suffer from a mental health problem. The cost to the economy is estimated to be around £100 billion annually – roughly the cost of the entire NHS. Physical and mental health are closely linked – people with severe and prolonged mental illness die on average 15 to 20 years earlier than other people – one of the greatest health inequalities in England. However only around a quarter of those with mental health conditions are in treatment, and only 13 per cent of the NHS budget goes on such treatments when mental illness accounts for almost a quarter of the total burden of disease.
Over the next five years the NHS must drive towards an equal response to mental and physical health, and towards the two being treated together. We have already made a start, through the Improving Access to Psychological Therapies Programme – double the number of people got such treatment last year compared with four years ago. Next year, for the first time, there will be waiting standards for mental health. Investment in new beds for young people with the most intensive needs to prevent them being admitted miles away from where they live, or into adult wards, is already under way, along with more money for better case management and early intervention.
This, however, is only a start. We have a much wider ambition to achieve genuine parity of esteem between physical and mental health by 2020. Provided new funding can be made available, by then we want the new waiting time standards to have improved so that 95 rather than 75 per cent of people referred for psychological therapies start treatment within six weeks and those experiencing a first episode of psychosis do so within a

27
fortnight. We also want to expand access standards to cover a comprehensive range of mental health services, including children’s services, eating disorders, and those with bipolar conditions. We need new commissioning approaches to help ensure that happens, and extra staff to coordinate such care. Getting there will require further investment.

28
CHAPTER FOUR How will we get there?
This ‘Forward View’ sets out a clear direction for the NHS – showing why change is needed and what it will look like. Some of what is needed can be brought about by the NHS itself. Other actions require new partnerships with local communities, local authorities and employers. Some critical decisions – for example on investment, on local reconfigurations, or on various public health measures – need the explicit support of the elected government.
So in addition to the strategies we have set out earlier in this document we also believe these complementary approaches are needed, and we will play our full part in achieving them:
We will back diverse solutions and local leadership
As a nation we’ve just taken the unique step anywhere in the world of entrusting frontline clinicians with two thirds – £66 billion – of our health service funding. Many CCGs are now harnessing clinical insight and energy to drive change in their local health systems in a way that frankly has not been achievable before now. NHS England intends progressively to offer them more influence over the total NHS budget for their local populations, ranging from primary to specialised care.
We will also work with ambitious local areas to define and champion a limited number of models of joint commissioning between the NHS and local government. These will include Integrated Personal Commissioning (described in chapter two) as well as Better Care Fund-style pooling budgets for specific services where appropriate, and under specific circumstances possible full joint management of social and health care commissioning, perhaps under the leadership of Health and Wellbeing Boards. However, a proper evaluation of the results of the 2015/16 BCF is needed before any national decision is made to expand the Fund further.
Furthermore, across the NHS we detect no appetite for a wholesale structural reorganisation. In particular, the tendency over many decades for government repeatedly to tinker with the number and functions of the health authority / primary care trust / clinical commissioning group tier of the NHS needs to stop. There is no ‘right’ answer as to how these functions are arranged – but there is a wrong answer, and that is to keep changing your mind. Instead, the default assumption should be that changes in local organisational configurations should arise only from local work to develop the new care models described in chapter three, or in response to clear local failure and the resulting implementation of ‘special measures’.

29
We will provide aligned national NHS leadership
NHS England, Monitor, the NHS Trust Development Authority, the Care Quality Commission, Health Education England, NICE and Public Health England have distinctive national duties laid on them by statute, and rightly so. However in their individual work with the local NHS there are various ways in which more action in concert would improve the impact and reduce the burden on frontline services. Here are some of the ways in which we intend to develop our shared work as it affects the local NHS:
• Through a combined work programme to support the development of new local care models, as set out at the end of chapter three. In addition to national statutory bodies, we will collaborate with patient and voluntary sector organisations in developing this programme.
• Furthermore, Monitor, TDA and NHS England will work together to create greater alignment between their respective local assessment, reporting and intervention regimes for Foundation Trusts, NHS trusts, and CCGs, complementing the work of CQC and HEE. This will include more joint working at regional and local level, alongside local government, to develop a whole-system, geographically-based intervention regime where appropriate. NHS England will also develop a new risk-based CCG assurance regime that will lighten the quarterly assurance reporting burden from high performing CCGs, while setting out a new ‘special measures’ support regime for those that are struggling.
• Using existing flexibilities and discretion, we will deploy national regulatory, pricing and funding regimes to support change in specific local areas that is in the interest of patients.
• Recognising the ultimate responsibilities of individual NHS boards for the quality and safety of the care being provided by their organisation, there is however also value in a forum where the key NHS oversight organisations can come together regionally and nationally to share intelligence, agree action and monitor overall assurance on quality. The National Quality Board provides such a forum, and we intend to re-energise it under the leadership of the senior clinicians (chief medical and nursing officers / medical and nursing directors / chief inspectors / heads of profession) of each of the national NHS leadership bodies alongside CCG leaders, providers, regulators and patient and lay representatives.
We will support a modern workforce
Health care depends on people — nurses, porters consultants and receptionists, scientists and therapists and many others. We can design innovative new care models, but they simply won’t become a reality unless we have a workforce with the right numbers, skills, values and

30
behaviours to deliver it. That’s why ensuring the NHS becomes a better employer is so important: by supporting the health and wellbeing of frontline staff; providing safe, inclusive and non-discriminatory opportunities; and supporting employees to raise concerns, and ensuring managers quickly act on them.
Since 2000, the workforce has grown by 160,000 more whole-time equivalent clinicians. In the past year alone staff numbers at Foundation Trusts are up by 24,000 – a 4% increase. However, these increases have not fully reflected changing patterns of demand. Hospital consultants have increased around three times faster than GPs and there has been an increasing trend towards a more specialised workforce, even though patients with multiple conditions would benefit from a more holistic clinical approach. And we have yet to see a significant shift from acute to community sector based working – just a 0.6% increase in the numbers of nurses working in the community over the past ten years.
Employers are responsible for ensuring they have sufficient staff with the right skills to care for their patients. Supported by Health Education England, we will address immediate gaps in key areas. We will put in place new measures to support employers to retain and develop their existing staff, increase productivity and reduce the waste of skills and money. We will consider the most appropriate employment arrangements to enable our current staff to work across organisational and sector boundaries. HEE will work with employers, employees and commissioners to identify the education and training needs of our current workforce, equipping them with the skills and flexibilities to deliver the new models of care, including the development of transitional roles. This will require a greater investment in training for existing staff, and the active engagement of clinicians and managers who are best placed to know what support they need to deliver new models of care.
Since it takes time to train skilled staff (for example, up to thirteen years to train a consultant), the risk is that the NHS will lock itself into outdated models of delivery unless we radically alter the way in which we plan and train our workforce. HEE will therefore work with its statutory partners to commission and expand new health and care roles, ensuring we have a more flexible workforce that can provide high quality care wherever and whenever the patient needs it. This work will be taken forward through the HEE’s leadership of the implementation of the Shape of Training Review for the medical profession and the Shape of Care Review for the nursing profession, so that we can ‘future proof’ the NHS against the challenges to come.
More generally, over the next several years, NHS employers and staff and their representatives will need to consider how working patterns and pay and terms and conditions can best evolve to fully reward high performance, support job and service redesign, and encourage

31
recruitment and retention in parts of the country and in occupations where vacancies are high.
We will exploit the information revolution
There have been three major economic transitions in human history – the agricultural revolution, the industrial revolution, and now the information revolution. But most countries’ health care systems have been slow to recognise and capitalise on the opportunities presented by the information revolution. For example, in Britain 86% of adults use the internet but only 2% report using it to contact their GP.
While the NHS is a world-leader in primary care computing and some aspects of our national health infrastructure (such as NHS Choices which gets 40 million visits a month, and the NHS Spine which handles 200 million interactions a month), progress on hospital systems has been slow following the failures of the previous ‘connecting for health’ initiative. More generally, the NHS is not yet exploiting its comparative advantage as a population-focused national service, despite the fact that our spending on health-related IT has grown rapidly over the past decade or so and is now broadly at the levels that might be expected looking at comparable industries and countries.
Part of why progress has not been as fast as it should have been is that the NHS has oscillated between two opposite approaches to information technology adoption – neither of which now makes sense. At times we have tried highly centralised national procurements and implementations. When they have failed due to lack of local engagement and lack of sensitivity to local circumstances, we have veered to the opposite extreme of ‘letting a thousand flowers bloom’. The result has been systems that don’t talk to each other, and a failure to harness the shared benefits that come from interoperable systems.
In future we intend to take a different approach. Nationally we will focus on the key systems that provide the ‘electronic glue’ which enables different parts of the health service to work together. Other systems will be for the local NHS to decide upon and procure, provided they meet nationally specified interoperability and data standards.
To lead this sector-wide approach a National Information Board has been established which brings together organisations from across the NHS, public health, clinical science, social care, local government and public representatives. To advance the implementation of this Five Year Forward View, later this financial year the NIB will publish a set of ‘road maps’ laying out who will do what to transform digital care. Key elements will include:
• Comprehensive transparency of performance data – including the results of treatment and what patients and carers say – to help health

32
professionals see how they are performing compared to others and improve; to help patients make informed choices; and to help CCGs and NHS England commission the best quality care.
• An expanding set of NHS accredited health apps that patients will be able to use to organise and manage their own health and care; and the development of partnerships with the voluntary sector and industry to support digital inclusion.
• Fully interoperable electronic health records so that patients’ records are largely paperless. Patients will have full access to these records, and be able to write into them. They will retain the right to opt out of their record being shared electronically. The NHS number, for safety and efficiency reasons, will be used in all settings, including social care.
• Family doctor appointments and electronic and repeat prescribing available routinely on-line everywhere.
• Bringing together hospital, GP, administrative and audit data to support the quality improvement, research, and the identification of patients who most need health and social care support. Individuals will be able to opt out of their data being used in this way.
• Technology – including smartphones - can be a great leveller and,
contrary to some perceptions, many older people use the internet. However, we will take steps to ensure that we build the capacity of all citizens to access information, and train our staff so that they are able to support those who are unable or unwilling to use new technologies.
We will accelerate useful health innovation
Britain has a track record of discovery and innovation to be proud of. We’re the nation that has helped give humanity antibiotics, vaccines, modern nursing, hip replacements, IVF, CT scanners and breakthrough discoveries from the circulation of blood to the DNA double helix—to name just a few. These have benefited not only our patients, but also the British economy – helping to make us a leader in a growing part of the world economy.
Research is vital in providing the evidence we need to transform services and improve outcomes. We will continue to support the work of the National Institute for Health Research (NIHR) and the network of specialist clinical research facilities in the NHS. We will also develop the active collection and use of health outcomes data, offering patients the chance to participate in research; and, working with partners, ensuring use of NHS clinical assets to support research in medicine.

33
We should be both optimistic and ambitious for the further advances that lie within our reach. Medicine is becoming more tailored to the individual; we are moving from one-size-fits-all to personalised care offering higher cure rates and fewer side effects. That’s why, for example, the NHS and our partners have begun a ground-breaking new initiative launched by the Prime Minister which will decode 100,000 whole genomes within the NHS. Our clinical teams will support this applied research to help improve diagnosis and treatment of rare diseases and cancers.
Steps we will take to speed innovation in new treatments and diagnostics include:
• The NHS has the opportunity radically to cut the costs of conducting Randomised Controlled Trials (RCTs), not only by streamlining approval processes but also by harnessing clinical technology. We will support the rollout of the Clinical Practice Research Datalink, and efforts to enable its use to support observational studies and quicker lower cost RCTs embedded within routine general practice and clinical care.
• In some cases it will be hard to test new treatment approaches using RCTs because the populations affected are too small. NHS England already has a £15m a year programme, administered by NICE, now called “commissioning through evaluation” which examines real world clinical evidence in the absence of full trial data. At a time when NHS funding is constrained it would be difficult to justify a further major diversion of resources from proven care to treatments of unknown cost effectiveness. However, we will explore how to expand this programme and the Early Access to Medicines programme in future years. It will be easier if the costs of doing so can be supported by those manufacturers who would like their products evaluated in this way.
• A smaller proportion of new devices and equipment go through NICE’s assessment process than do pharmaceuticals. We will work with NICE to expand work on devices and equipment and to support the best approach to rolling out high value innovations—for example, operational pilots to generate evidence on the real world financial and operational impact on services—while decommissioning outmoded legacy technologies and treatments to help pay for them.
• The Department of Health-initiated Cancer Drugs Fund has expanded access to new cancer medicines. We expect over the next year to consult on a new approach to converging its assessment and prioritisation processes with a revised approach from NICE.
• The average time it takes to translate a discovery into clinical practice is however often too slow. So as well as a commitment to research, we are committed to accelerating the quicker adoption of cost-effective innovation - both medicines and medtech. We will explore with
34
partners—including patients and voluntary sector organisations—a number of new mechanisms for achieving this.
Accelerating innovation in new ways of delivering care
Many of the innovation gains we should be aiming for over the next five or so years probably won’t come from new standalone diagnostic technologies or treatments - the number of these blockbuster ‘silver bullets’ is inevitably limited.
But we do have an arguably larger unexploited opportunity to combine different technologies and changed ways of working in order to transform care delivery. For example, equipping house-bound elderly patients who suffer from congestive heart failure with new biosensor technology that can be remotely monitored can enable community nursing teams to improve outcomes and reduce hospitalisations. But any one of these components by itself produces little or no gain, and may in fact just add cost. So instead we need what is now being termed ‘combinatorial innovation’.
The NHS will become one of the best places in the world to test innovations that require staff, technology and funding all to align in a health system, with universal coverage serving a large and diverse population. In practice, our track record has been decidedly mixed. Too often single elements have been ‘piloted’ without other needed components. Even where ‘whole system’ innovations have been tested, the design has sometimes been weak, with an absence of control groups plus inadequate and rushed implementation. As a result they have produced limited empirical insight.
Over the next five years we intend to change that. Alongside the approaches we spell out in chapter three, three of the further mechanisms we will use are:
• Develop a small number of ‘test bed’ sites alongside our Academic Health Science Networks and Centres. They would serve as real world sites for ‘combinatorial’ innovations that integrate new technologies, bioinformatics, new staffing models and payment-for-outcomes. Innovators from the UK and internationally will be able to bid to have their proposed discovery or innovation deployed and tested in these sites.
• Working with NIHR and the Department of Health we will expand NHS operational research, RCT capability and other methods to promote more rigorous ways of answering high impact questions in health services redesign. An example of the sort of question that might be tested: how best to evolve GP out of hours and NHS 111 services so as to improve patient understanding of where and when to seek care, while improving clinical outcomes and ensuring the most appropriate

35
use of ambulance and A&E services. Further work will also be undertaken on behavioural ‘nudge’ type policies in health care.
• We will explore the development of health and care ‘new towns’. England’s population is projected to increase by about 3 to 4 million by 2020. New town developments and the refurbishment of some urban areas offers the opportunity to design modern services from scratch, with fewer legacy constraints - integrating not only health and social care, but also other public services such as welfare, education and affordable housing. The health campus already planned for Watford is one example of this.
We will drive efficiency and productive investment
It has previously been calculated by Monitor, separately by NHS England, and also by independent analysts, that a combination of a) growing demand, b) no further annual efficiencies, and c) flat real terms funding could, by 2020/21, produce a mismatch between resources and patient needs of nearly £30 billion a year.
So to sustain a comprehensive high-quality NHS, action will be needed on all three fronts. Less impact on any one of them will require compensating action on the other two.
Demand
On demand, this Forward View makes the case for a more activist prevention and public health agenda: greater support for patients, carers and community organisations; and new models of primary and out-of-hospital care. While the positive effects of these will take some years to show themselves in moderating the rising demands on hospitals, over the medium term the results could be substantial. Their net impact will however also partly depend on the availability of social care services over the next five years.
Efficiency
Over the long run, NHS efficiency gains have been estimated by the Office for Budget Responsibility at around 0.8% net annually. Given the pressures on the public finances and the opportunities in front of us, 0.8% a year will not be adequate, and in recent years the NHS has done more than twice as well as this.
A 1.5% net efficiency increase each year over the next Parliament should be obtainable if the NHS is able to accelerate some of its current efficiency programmes, recognising that some others that have contributed over the past five years will not be indefinitely repeatable. For example as the economy returns to growth, NHS pay will need to stay broadly in line with private sector wages in order to recruit and retain frontline staff.
36
Our ambition, however, would be for the NHS to achieve 2% net efficiency gains each year for the rest of the decade – possibly increasing to 3% over time. This would represent a strong performance - compared with the NHS' own past, compared with the wider UK economy, and with other countries' health systems. It would require investment in new care models and would be achieved by a combination of "catch up" (as less efficient providers matched the performance of the best), "frontier shift" (as new and better ways of working of the sort laid out in chapters three and four are achieved by the whole sector), and moderating demand increases which would begin to be realised towards the end of the second half of the five year period (partly as described in chapter two). It would improve the quality and responsiveness of care, meaning patients getting the 'right care, at the right time, in the right setting, from the right caregiver'. The Nuffield Trust for example calculates that doing so could avoid the need for another 17,000 hospital beds - equivalent to opening 34 extra 500-bedded hospitals over the next five years.
Funding
NHS spending has been protected over the past five years, and this has helped sustain services. However, pressures are building. In terms of future funding scenarios, flat real terms NHS spending overall would represent a continuation of current budget protection. Flat real terms NHS spending per person would take account of population growth. Flat NHS spending as a share of GDP would differ from the long term trend in which health spending in industrialised countries tends to rise a share of national income.
Depending on the combined efficiency and funding option pursued, the effect is to close the £30 billion gap by one third, one half, or all the way.
• In scenario one, the NHS budget remains flat in real terms from 2015/16 to 2020/21, and the NHS delivers its long run productivity gain of 0.8% a year. The combined effect is that the £30 billion gap in 2020/21 is cut by about a third, to £21 billion.
• In scenario two, the NHS budget still remains flat in real terms over the period, but the NHS delivers stronger efficiencies of 1.5% a year. The combined effect is that the £30 billion gap in 2020/21 is halved, to £16 billion.
• In scenario three, the NHS gets the needed infrastructure and operating investment to rapidly move to the new care models and ways of working described in this Forward View, which in turn enables demand and efficiency gains worth 2%-3% net each year. Combined with staged funding increases close to ‘flat real per person’ the £30 billion gap is closed by 2020/21.

37
Decisions on these options will inevitably need to be taken in the context of how the UK economy overall is performing, during the next Parliament. However nothing in the analysis above suggests that continuing with a comprehensive tax-funded NHS is intrinsically undoable – instead it suggests that there are viable options for sustaining and improving the NHS over the next five years, provided that the NHS does its part, together with the support of government. The result would be a far better future for the NHS, its patients, its staff and those who support them.
BOX 5: WHAT MIGHT THIS MEAN FOR PATIENTS? FIVE YEAR AMBITIONS FOR CANCER
One in three of us will be diagnosed with cancer in our lifetime. Fortunately half of those with cancer will now live for at least ten years, whereas forty years ago the average survival was only one year. But cancer survival is below the European average, especially for people aged over 75, and especially when measured at one year after diagnosis compared with five years. This suggests that late diagnosis and variation in subsequent access to some treatments are key reasons for the gap.
So improvements in outcomes will require action on three fronts: better prevention, swifter access to diagnosis, and better treatment and care for all those diagnosed with cancer. If the steps we set out in this Forward View are implemented and the NHS continues to be properly resourced, patients will reap benefits in all three areas:
Better prevention. An NHS that works proactively with other partners to maintain and improve health will help reduce the future incidence of cancer. The relationship between tobacco and cancer is well known, and we will ensure everyone who smokes has access to high quality smoking cessation services, working with local government partners to increase our focus on pregnant women and those with mental health conditions. There is also increasing evidence of a relationship between obesity and cancer. The World Health Organisation has estimated that between 7% and 41% of certain cancers are attributable to obesity and overweight, so the focus on reducing obesity outlined in Chapter two of this document could also contribute towards our wider efforts on cancer prevention.
Faster diagnosis. We need to take early action to reduce the proportion of patients currently diagnosed through A&E—currently about 25% of all diagnoses. These patients are far less likely to survive a year than those who present at their GP practice. Currently, the average GP will see fewer than eight new patients with cancer each year, and may see a rare cancer once in their career. They will therefore need support to spot suspicious combinations of symptoms. The new care models set out in this document will help ensure that there are sufficient numbers of GPs working in larger practices with greater access to diagnostic and specialist advice. We will
38
also work to expand access to screening, for example, by extending breast cancer screening to additional age groups, and spreading the use of screening for colorectal cancer. As well as supporting clinicians to spot cancers earlier, we need to support people to visit their GP at the first sign of something suspicious. If we are able to deliver the vision set out in this Forward View at sufficient pace and scale, we believe that over the next five years, the NHS can deliver a 10% increase in those patients diagnosed early, equivalent to about 8,000 more patients living longer than five years after diagnosis.
Better treatment and care for all. It is not enough to improve the rates of diagnosis unless we also tackle the current variation in treatment and outcomes. We will use our commissioning and regulatory powers to ensure that existing quality standards and NICE guidance are more uniformly implemented, across all areas and age groups, encouraging shared learning through transparency of performance data, not only by institution but also along routes from diagnosis. And for some specialised cancer services we will encourage further consolidation into specialist centres that will increasingly become responsible for developing networks of supporting services.
But combined with this consolidation of the most specialised care, we will make supporting care available much closer to people’s homes; for example, a greater role for smaller hospitals and expanded primary care will allow more chemotherapy to be provided in community. We will also work in partnership with patient organisations to promote the provision of the Cancer Recovery Package, to ensure care is coordinated between primary and acute care, so that patients are assessed and care planned appropriately. Support and aftercare and end of life care – which improves patient experience and patient reported outcomes – will all increasingly be provided in community settings.

39
ABBREVIATIONS A&E Accident & Emergency AHSCs Academic Health Science Centres AHSNs Academic Health Science Networks BCF Better Care Fund CCGs Clinical Commissioning Groups CQC Care Quality Commission CT Computerised Tomography EBITDA Earnings before interest, taxes, depreciation and
amortisation GP General Practitioner HEE Health Education England IPC Integrated Personal Commissioning IVF In Vitro Fertilisation LTCs Long term conditions NHS IQ NHS Improving Quality NHS TDA NHS Trust Development Authority NIB National Information Board NICE National Institute for Health and Care Excellence NIHR National Institute of Health Research PHE Public Health England RCTs Randomised Controlled Trials TUC Trades Union Congress WHO World Health Organisation


Dear Charles and Tony Re: CCG Quarter 1 Assurance Thank you for meeting with members of the Area Team on the 10 September 2014 to discuss delivery and improving the areas that are going less well. This letter sets out the key points arising from the discussion. NHS Constitution standards Referral to Treatment Times (RTT): Delivery of RTT has been good, but performance in the admitted standard has marginally missed the standard for Q1 as expected. This was planned due to the backlog clearance. It is acknowledged there have been issues with Derby Hospitals due to introduction of new IT and a lack of robust waiting list information, both of which are being monitored closely. A&E: The A&E 4 hour standard has continued to be achieved at Burton Hospitals. The CCG recognise the underlying pressures in the system and are working with their neighbouring South East Staffordshire and Seisdon Peninsula CCG to address areas within their control, these include the use of community matrons, healthcare at home and increased packages. The revised system resilience plan will build on stronger collaboration across the health economy to address and monitor these issues. Cancer:
Shropshire and Staffordshire Area Team Anglesey House
Wheelhouse Road Rugeley
Staffordshire WS15 1UL
Email address: [email protected] Telephone Number: 01138253713
Our Ref: DW/GU/EM 17 October 2014 Dr Charles Pidsley, Chair, Tony Bruce, Accountable Officer East Staffordshire CCG Edwin House Centrum 100 Burton on Trent DE14 2WF

Delivery of cancer waiting times still remains a challenge due to the complexity of the cancer pathways. There are a number of factors that are impacting on delivery of this standard that include: number of transfers, increased diagnostics, frequency of multi-disciplinary team meetings, and the number of providers involved. The CCG receives breakdown by case of any delays and root causes behind this and confirmation that no harm has come to patients. The CCG are exploring a tracking system on delays that is proactive and how best to simplify the patients journey Dementia: The Area Team noted that delivery of the CCGs Dementia recovery standard is off plan. The CCG reported that historic changes with provider and subsequent backlog have now been resolved. There are currently 790 dementia patients on the QoF Dementia register which requires an additional 359 dementia patients to be identified. The CCG recognises the challenge and are taking a number of actions which include: a steering group debate planned for November, clinical pathway discussions and seeking member practice assurance through CCG quality visits programme. The CCG is committed to achieving the target and are developing an action plan to deliver this. IAPT: The CCG are confident the service being delivered to patients is good, but have failed to upload data nationally during 13/14 and Q1 14/15 to comply with national reporting standards. The Area Team expressed significant disappointment that this has not yet been resolved. This is being addressed by the Provider and a remedial action plan is in place. Finance: The Area Team acknowledged the CCG was within the expected financial control total for Q1. The CSU contract management support has been strengthened and the CCG is confident of the support it receives but will monitor closely to ensure this delivers. NHS Statutory Duties Good partnership arrangements have been made with the Health and Wellbeing Board. The CCG has engaged with and involved the Overview and Scrutiny Committee with regards to public and patient engagement within the commissioning process. Key Areas of Challenge The CCG is working within a challenged health economy and would benefit from strengthening the collaborative commissioning arrangements with other CCGs. The Area Team recommended further partnership working using the KPMG challenged health economy work to assist in this area. Conclusion
The CCG has always done very well for its patients but not reducing the spend still remains an issue. A&E performance remains good and you are aware of system pressures which you are taking steps to address. It is important to work as a health economy, but also to focus on the areas you have responsibility and influence over. If performance then slips it will then be clearly identifiable what areas are not working well. It is important to drive and own the system resilience plan, as well as your own control processes. RTT performance is good and we are confident this standard will soon be fully achieved. There are good conversations around cancer and the processes you have in place, but by understanding what is going wrong in a provider you can be confident that the actions they are taking are the right ones. Further work is required on dementia so that there is a clear plan, broken down to at practice level, to deliver the standard. The CCG have given assurances on holding the financial position, but even the smallest degree of improvement will give you and us confidence. We recognise you are a small CCG with a hardworking team. It is important to continue to secure collaboration where you will be able to increase your capacity and capability. The attached enclosure 1 outlines the domain ratings, and where a domain is assured with support the agreed actions are outlined in the support/action section. Under the assurance guidance for 2014/15 finance can fall into more than one domain. Domain 3 refers to signed contracts and performance systems in place. Domain 4 is linked to governance, value for money commissioning, risk management and working with other commissioners to secure excellent affordable commissioning support services. For quarter 1, finance is shown under domain 4. Thank you for meeting with us and for the open and constructive dialogue. I trust this letter provides an accurate summary of the discussions and clearly indicates the next steps. Yours sincerely
Graham Urwin Area Team Director
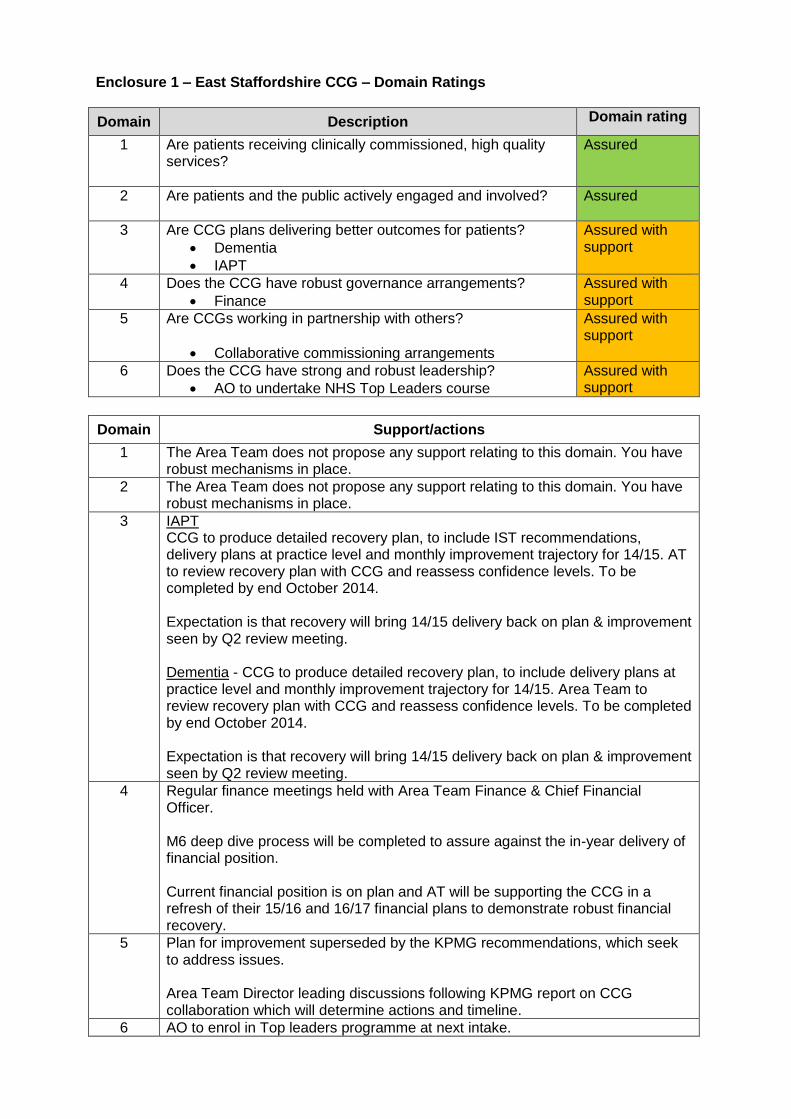
Enclosure 1 – East Staffordshire CCG – Domain Ratings
Domain Description Domain rating
1 Are patients receiving clinically commissioned, high quality services?
Assured
2 Are patients and the public actively engaged and involved?
Assured
3 Are CCG plans delivering better outcomes for patients?
Dementia
IAPT
Assured with support
4 Does the CCG have robust governance arrangements?
Finance
Assured with support
5 Are CCGs working in partnership with others?
Collaborative commissioning arrangements
Assured with support
6 Does the CCG have strong and robust leadership?
AO to undertake NHS Top Leaders course
Assured with support
Domain Support/actions
1 The Area Team does not propose any support relating to this domain. You have robust mechanisms in place.
2 The Area Team does not propose any support relating to this domain. You have robust mechanisms in place.
3 IAPT CCG to produce detailed recovery plan, to include IST recommendations, delivery plans at practice level and monthly improvement trajectory for 14/15. AT to review recovery plan with CCG and reassess confidence levels. To be completed by end October 2014. Expectation is that recovery will bring 14/15 delivery back on plan & improvement seen by Q2 review meeting. Dementia - CCG to produce detailed recovery plan, to include delivery plans at practice level and monthly improvement trajectory for 14/15. Area Team to review recovery plan with CCG and reassess confidence levels. To be completed by end October 2014. Expectation is that recovery will bring 14/15 delivery back on plan & improvement seen by Q2 review meeting.
4 Regular finance meetings held with Area Team Finance & Chief Financial Officer. M6 deep dive process will be completed to assure against the in-year delivery of financial position. Current financial position is on plan and AT will be supporting the CCG in a refresh of their 15/16 and 16/17 financial plans to demonstrate robust financial recovery.
5 Plan for improvement superseded by the KPMG recommendations, which seek to address issues. Area Team Director leading discussions following KPMG report on CCG collaboration which will determine actions and timeline.
6 AO to enrol in Top leaders programme at next intake.

Title Lay Member report on PPE Reporting to Governing Body Date of Meeting November 2014
Author(s) Ann Tunley
Purpose of the Report Information Assurance Discussion
Key Points/Executive Summary Report from Lay Member for PPE about Patient Engagement in the local area
• Information from Patient Board • Information from District Group of Patient Participation Groups • Information from Diabetes Support Group
Recommendations (what is expected from the Board) To provide assurance to the Governing Body
Enclosures Report
X x
Enc. 5
1 Author: DW Date: 20/2/14 East Staffs CCG
Report on Patient and Public Engagement for November 2014 Improving Lives developments The Chair and Vice Chair of the Patient Board were invited to a session called Learn at Lunch where they spoke to a group of people from the CSU and the CCG about their roles and what the Patient Board required of the CSU. Following this meeting, we met with the Chief Operating Officer and a member of the CSU to discuss ways forward and working more closely together especially on the Improving Lives programme. A further meeting included the same people plus the two newly appointed Patient Reps from the Improving Lives Board whom we met for the first time. Both the Chair and Vice Chair attended the Improving Lives evening event at Deferrers Academy for employers & employees. Although attendance was low, we were able to speak to several people as well as to the CSU personnel present. We were able to ask the attendees about their experiences of Burton Hospital and their own GP practices. Improving Lives is now a standard agenda item at each Patient Board meeting. We can now support the CCG with patient engagement in consultations towards the procurement process. Patient Board events Members of the Patient Board were invited to visit St Giles Hospice by Ian Leech, Community Engagement Officer. This was an idea following a discussion with Dr Liz Waddy. Ian showed us around both buildings and talked to us about the range of activities that are held there. These ranged from Computer clubs, Craft activities, Lunch clubs, Holistic therapies as well as morning drop in clubs for Patients and Carers in the community. We were really impressed by the Education activities, which ranged from visits to schools and Training at the Hospice for students and volunteers. Then he showed us around the new building, which was so unlike a
hospital with light, airy rooms and a quiet and calm atmosphere with very little equipment on view. We saw how local schools – both Primary and Secondary - were involved in bereavement activities to encourage pupils to talk about dying and raise their awareness. We also listened to Talfryn Evans talk about the Buddies scheme for Carers - a project which is just beginning and will support the Carers of patients in the community. We were very interested in the work that is done in the community – in fact 80% of their work takes place in the community, which is very impressive. We saw this in the report on a project. This recent project involved elderly people in residential homes like Chestnut Grange where they conducted before and after tests of their physical capabilities. Results showed a strong improvement in a variety of exercises including grips and walking distances. We felt that the visit had opened our eyes to what is offered to patients and carers and it enabled us to see what we can then pass on to patients in our PPGs and other organisations. Three of us on Patient Board are currently working to provide support to practices and their Patient Participation Groups. (PPGs). Letters have been sent to GP practices offering to meet to discuss ways in which we could support them, either by working alongside the PPGs or helping them to set up a PPG from the start. We are currently awaiting responses. District Group of PPGs and Patient Board events Recently we fed back to both forums a query that arose at a Governing Body meeting when one of the Doctors asked us to find out about the number of patients taking up on flu jabs. We took this to both District and Patient Board and all the reports came back to say that patients were very clearly taking up the offers of flu jabs at the GP practices. In fact several reported queues waiting for them.

Several members of Patient Board and District Group took part in the Fair Deal for Well Being training run by Lucy Heath and Jon Topham (Public Health) at Burton Library. Members will be receiving packs for their Surgery or organisation, which they can now use with the members in their own practice groups. We are very grateful to them both for setting up this training for us. Also in attendance was Dianne Wheeler, Library Manager who told the group about the range of events at the Library available to the public. Again this has made us aware of what is on offer to our patients, which we can then take back to our own organisations and PPGs to enable us to support our patients. Dianne also spoke about Bookfriends – the new Peer Support Book Club. Bookfriends The first meeting took place and three people attended. We expect this to grow as word gets around about this Peer Support Book Club. Diabetes UK events Following our very successful evening event at Deferrers with over 50 people attending, the Chair and Vice Chair of Patient Board were asked to speak to a group of 60 students at Burton College about Diabetes and their experiences. These students were on Levels 1, 2 and 3 of the Health Care and Social Studies courses. We have made links with the college now and will be returning to talk about the CCG and the way Local Health is changing in the area. We are also working with the Course tutors to set up a Youth Forum, where we can make regular contact with these young people. This will be a two way process – gaining their views as well as communicating information to them about such things as Improving Lives. The Course tutors were very interested in this idea as a way of getting their students to learn more

about Local Health. In this way we are ensuring that young people have a voice in their own healthcare. The feedback from the Deferrers event was very useful and we have made many more contacts with Diabetes patients. As a Diabetes UK Champion, I have now been asked to go to London to their conference. I have been asked to talk to other volunteers about what has happened in the area, since setting up the local support group over four years ago and how it has evolved. We will both be attending the Diabetes UK event in Nottingham in a few weeks time. This event is specifically for Voluntary Group leaders to share good practice and ideas on how to connect with patients as well as promoting the 15 Healthcare Essentials. I have also been to talk to a group of newly diagnosed Diabetes patients about the Support group to tell them about the Support Group, what we do and how we support others with Diabetes as well as carers or partners. In this way, diabetes patients gain more knowledge and support to help them to self manage their own healthcare. Both of us will also be attending the Patient Leader Network event at Rugeley run by NHS England. This will enable us to meet other Patient Leaders and learn from each other’s experiences. Networking in this way means that we stay in touch with current issues and concerns, which we can then feed back to both Patient Forums to help them in their work.

Title Personal Health Budgets
Reporting to East Staffordshire Clinical Commissioning Group Governing Body
Date of Meeting 27 November 2014
Commissioning Lead(s) Author(s) Christine Brown/ Matt Oakley
Purpose of the Report (Please select) Approval Assurance Discussion
Key Points/Executive Summary Personal Health Budgets (PHBs) are part of a model of person-centred care that also includes support for self-management, shared decision making, improving information and understanding, and promoting prevention All 211 Clinical Commissioning Groups across England have signed up to the NHS England personal health budget support programme From April 2014 people eligible for NHS Continuing Health Care have had the “right to ask” for a personal health budget. From October 2014 this will be strengthened and this group will have the “right to have” a personal health budget. From April 2015 people with long term conditions must have a personalised care plan (which could include a PHB if the CCG think they would benefit). The National Health Service Commissioning Board and Clinical Commissioning Groups (Responsibilities and Standing Rules) Regulations 2012, the National Health Service Commissioning Board and Clinical Commissioning Groups (Responsibilities and Standing Rules) (Amendment) Regulations 2013 and the National Health Service Commissioning Board and Clinical Commissioning Groups (Responsibilities and Standing Rules) (Amendment) (No. 3) Regulations 2014 along with the National Health Service (Direct Payments) Regulations 2013 and the National Health Service (Direct Payments) (Amendment) Regulations 201317 set out CCGs’ legal duties relating to NHS Continuing Health Care and Continuing Care rights and personal health budgets. These include duties to publicise and promote their availability, to provide information, advice and support, to consider requests for personal health budgets and to ensure they have the systems and processes in place to be able to make this provision. Staffordshire CCGs had set up a Personal Health Budgets (PHBs) Steering Group in 2013, and have engaged the services of a project manager from within Staffordshire County Council to roll out PHBs out locally across Staffordshire
A part-time interim PHB Lead was also appointed to progress the work in February 2014 to support the PHB Project Manager in the production of the attached PHB Policy for the Staffordshire CCGs in line with the National guidance and in the development of patient information, and guidance for practitioners. Further partnership work is on-going with Shropshire CCG in the recruitment of PHB
x
Enc. 6
1 Author: DW Date: 20/2/14 East Staffs CCG

Implementation Manager and Care Manager to take PHBs forward with the CHC team and to work with the CCG Commissioners to support the roll out of personal health budgets to people with long term conditions in April 2015. Recommendations (what is expected from the Board)
• To approve the attached Personal Health Budgets Policy for the future management
of care provision to patients eligible for Continuing Health Care Funding and future patients with long term conditions across East Staffordshire.
Enclosures
PHB policy exec summary.docx
PHB Policy v3 280714.docx
Appendix 1 Delegation of Level 3
Appendix 2 Practical guide for Personal He
Appendix 4 Staffordshire CCGs PH
2 Author: DW Date: 20/2/14 East Staffs CCG

Personal Health Budgets Operational Policy: Executive Summary From April 2014 everyone eligible for Continuing Health Care had the right to ask for their care to be delivered as a Personal Health Budget (PHB) and CCGs needed to be in the position to respond to any requests. From October 1st 2014 those eligible for Continuing Health care NHS funding will have the right to have a PHB. The right has also included children with special educational needs and disabilities who are in receipt of an integrated budget. As of April 2015, CCG Commissioners should be ready to offer a PHB to anyone with a long term condition who could benefit from one.
This summary explains the purpose and contents of each document contained within the Personal Health Budget Operational Policy. The key documents that the CCG need to note, are the Financial Framework and the Delegation of Level 3 tasks policy. Other documents have been produced and will be made available to support the practical implementation of PHBs for service users, carers and practitioners
Risk Management CCGs are required to commit to the promotion of Personal Health Budgets to service users, as well as supporting them to manage risks positively, proportionately and realistically. Supporting people to make informed decisions with an awareness of risks in their daily lives enables them to achieve their full potential and to do the things that most people take for granted. Enabling people to exercise choice and control over their lives, and therefore their own management of risk, is central to achieving better outcomes for individuals. A degree of risk can be accommodated within the aim of enhancing the quality of people’s lives. CCGs are required to acknowledge that service users who have the mental capacity to make a decision, and choose to live with a level of risk, are entitled to do so. CCGs are required to assure that Care Providers document clearly any evidence of decision making and rationale in relation to the management and reduction of risk where appropriate or necessary. This will be considered as part of the PHB approval process that has been put in place clinically and financially for the CCGs across Staffordshire. Health Professionals will be required to ensure that any clinical and financial risks identified are fully understood and managed in the context of ensuring that the individual’s needs and their best interests are safeguarded and that appropriate governance arrangements are in place. The CCG needs to acknowledge that this is a very different way of working, and it may be a challenge for professionals to balance the need to work alongside a service user to deliver their choices, and a concern over whether a proposed activity or service provision will meet the need and deliver the outcomes. The Staffordshire CCGs PHB Steering Group will be required to support the development of a shared forum of clinical and finance staff to discuss complex, unusual or higher risk PHB requests which will include representation from the appropriate CCG. This will support shared learning, and the development of a shared approach to improving quality of care to the service user and identifying possible financial risks.
1. PHB Operational Policy
The Operational Policy outlines the principles for achieving the implementation of personal health budgets by balancing choice, risk, rights and responsibilities. It recognises that, in the right circumstances, a positive approach to risk can promote a culture of choice and independence that encourages responsible support and shared decision making. The Government's aim is that in future, everyone in England who could benefit
Item 08 Enc 06 PHB policy exec summary, Created September 14
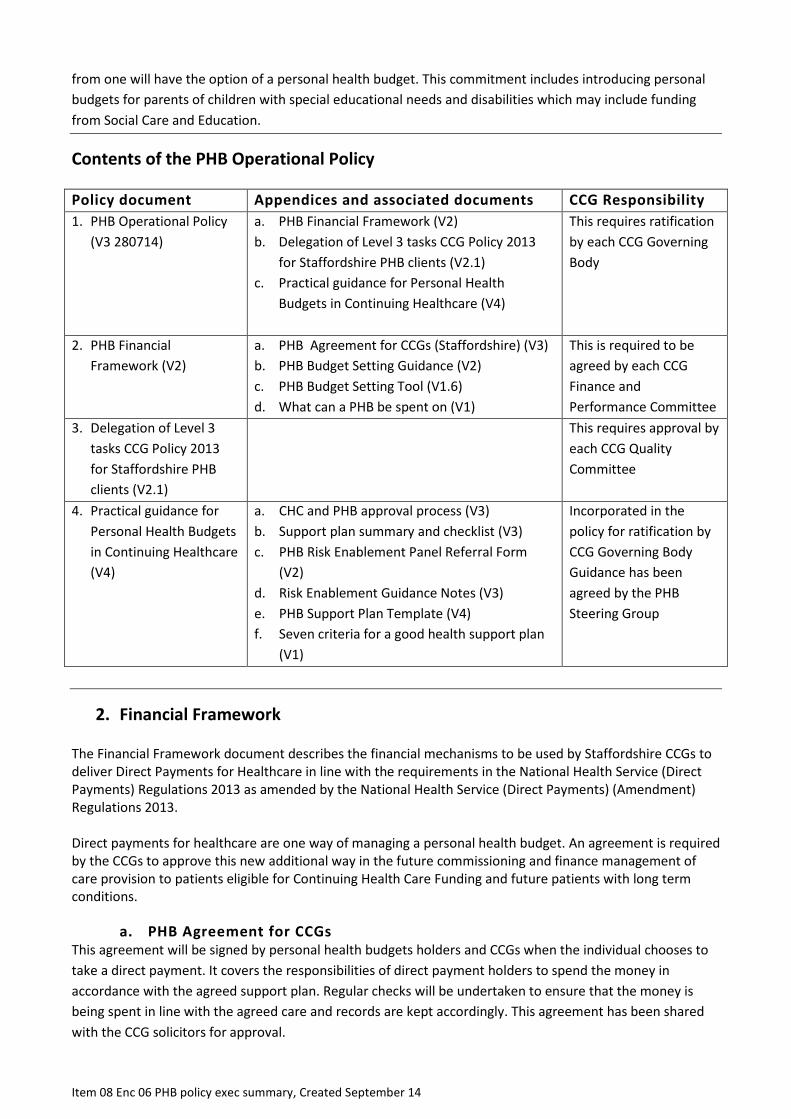
from one will have the option of a personal health budget. This commitment includes introducing personal budgets for parents of children with special educational needs and disabilities which may include funding from Social Care and Education.
Contents of the PHB Operational Policy
Policy document
Appendices and associated documents CCG Responsibility 1. PHB Operational Policy
(V3 280714) a. PHB Financial Framework (V2) b. Delegation of Level 3 tasks CCG Policy 2013
for Staffordshire PHB clients (V2.1) c. Practical guidance for Personal Health
Budgets in Continuing Healthcare (V4)
This requires ratification by each CCG Governing Body
2. PHB Financial Framework (V2)
a. PHB Agreement for CCGs (Staffordshire) (V3) b. PHB Budget Setting Guidance (V2) c. PHB Budget Setting Tool (V1.6) d. What can a PHB be spent on (V1)
This is required to be agreed by each CCG Finance and Performance Committee
3. Delegation of Level 3 tasks CCG Policy 2013 for Staffordshire PHB clients (V2.1)
This requires approval by each CCG Quality Committee
4. Practical guidance for Personal Health Budgets in Continuing Healthcare (V4)
a. CHC and PHB approval process (V3) b. Support plan summary and checklist (V3) c. PHB Risk Enablement Panel Referral Form
(V2) d. Risk Enablement Guidance Notes (V3) e. PHB Support Plan Template (V4) f. Seven criteria for a good health support plan
(V1)
Incorporated in the policy for ratification by CCG Governing Body Guidance has been agreed by the PHB Steering Group
2. Financial Framework
The Financial Framework document describes the financial mechanisms to be used by Staffordshire CCGs to deliver Direct Payments for Healthcare in line with the requirements in the National Health Service (Direct Payments) Regulations 2013 as amended by the National Health Service (Direct Payments) (Amendment) Regulations 2013. Direct payments for healthcare are one way of managing a personal health budget. An agreement is required by the CCGs to approve this new additional way in the future commissioning and finance management of care provision to patients eligible for Continuing Health Care Funding and future patients with long term conditions.
a. PHB Agreement for CCGs This agreement will be signed by personal health budgets holders and CCGs when the individual chooses to take a direct payment. It covers the responsibilities of direct payment holders to spend the money in accordance with the agreed support plan. Regular checks will be undertaken to ensure that the money is being spent in line with the agreed care and records are kept accordingly. This agreement has been shared with the CCG solicitors for approval.
Item 08 Enc 06 PHB policy exec summary, Created September 14

b. Budget Setting Guidance This document explains the process for setting provisional (indicative) budgets for prospective personal health budget holders. When possible, the approach will use existing cost of an individual’s care package. Other methods to support the calculation of the provisional budget are the use of a care specification that is completed by a CHC Nurse and a budget setting tool.
c. PHB Budget Setting Tool The tool will be used for the calculation of provisional (indicative) budgets. This is required to provide an estimate of the budget that will be made available to people and families before they begin support planning. It is based on the scores in the categories covered by the Decision Support Tool. (for CHC patients only)The tool has been adapted from one that was developed during the Manchester PHB pilot programme. A key principle of personal health budgets is to provide people with an estimate of the funding that will be made available. Best practice in support planning states that providing an early upfront amount can help people to better plan their care and support. The tool will be used when an existing cost is unavailable; instances when this may occur are detailed in the Budget Setting Guidance.
d. What a PHB can be spent on This summarises the principles of how personal health budgets should be used; with a focus on outcomes and what can be achieved rather than what it is being spent on.
There is also a list of what a personal health budget cannot be spent on which is based on national guidance.
3. Delegation of Level 3 tasks CCG Policy 2013 for Staffordshire PHB clients
This guidance provides clarity on the key issues relating to delegation of care from employed registered professionals to third party individuals who are not employed by Staffordshire and Stoke on Trent Clinical Commissioning Groups (CCGs). This will provide assurance that delegation is always undertaken within the clear parameters of safe delegation as stated by the Nursing and Midwifery Council (NMC).
This document needs to be ratified by each Clinical Commissioning Group in order for people that are receiving a personal health budget who wish to employ their own personal assistants to meet their care needs can, if they choose to, delegate clinical care tasks to them.
4. Practical guidance for Personal Health Budgets in Continuing Healthcare
The practical guidance is a resource for staff involved in the delivery of personal health budgets for Continuing Healthcare patients. It breaks down the seven step process that has been adopted in Staffordshire; explains what tasks should be undertaken as part of each step, who will be responsible for ensuring that these tasks are completed and also the likely individuals that will, or could, carry out each tasks.
At present the guidance is a proposed approach for how personal health budgets will operate when a dedicated PHB team is established and the following has been developed to assist practitioners with the process
.
Item 08 Enc 06 PHB policy exec summary, Created September 14

a. CHC and PHB approval process This process flow describes the stages of the approval process and specifically the involvement of Continuing Healthcare with the personal health budget process, highlighting additional tasks that need to be carried out when a personal health budget is being set up.
b. Support plan summary and checklist This document will be used as part of the approval process of support plans. It is made up of three parts. The Support Plan summary should be signed by the service user or their representative, the appropriate clinician overseeing the support plan, the PHB Lead and the CHC Lead.
c. PHB Risk Enablement Panel Referral Form Where there is a complex or challenging risk issues in relation to provision of a PHB a clear process has been identified to assist in resolving the issues. The referral form is also included as part of the support plan summary and checklist.
d. Risk Enablement Guidance Notes These notes support the Risk Enablement Panel.
e. PHB Support Plan Template This template is to form part of the information pack that will be given to people who express an interest in having a personal health budget.
Best practice in support planning is to promote self-directed development of support plans and that it can be presented in a way that best suits them. In combination with the Support plan summary and use of the seven criteria for a good health support plan this should allow people
f. Seven criteria for a good health support plan This document explains the criteria that must be covered by a support plan. This is to be used as reference as part of the approval process for evaluation of the quality of support plans to ensure that what is included is lawful, likely to be effective, affordable and appropriate.
Item 08 Enc 06 PHB policy exec summary, Created September 14

PHB Policy Version 3 July 28th 2014
Personal Health Budgets Operational Policy Date Approved
Date Ratified
Signature Reference Number Version 03 Lead Officer Christine Brown Review Date

Table of Contents
1. INTRODUCTION ............................................................................................................ 3
2. THE SCOPE OF THE POLICY ....................................................................................... 3
3. UNDERPINNING PRINCIPLES ...................................................................................... 3
4. IMPLEMENTATION OF THE POLICY ............................................................................ 4
5. PURPOSES AND PRINCIPLES OF PERSONAL HEALTH BUDGETS ......................... 4
6. COMMUNICATION WITH PATIENTS ............................................................................ 5
7. THE STAFFORDSHIRE APPROACH ............................................................................ 5
8. PATIENT CHOICE .......................................................................................................... 6
9. RESPONSIBLITIES OF KEY STAFF .............................................................................. 7
10. THE PROCESS .............................................................................................................. 7
11. TRAINING ...................................................................................................................... 8
12. FINANCE ........................................................................................................................ 8
13. REVIEWS AND MONITORING ...................................................................................... 8
14. DISPUTES/DISAGREEMENTS ...................................................................................... 9
REFERENCES .......................................................................................................................... 9
APPENDICES ......................................................................................................................... 10
2
1. INTRODUCTION
1.1 Background
Following the evaluation of the national pilot programme for personal health budgets in November 2012 the government announced that anyone eligible for NHS Continuing healthcare will have “the right to ask” for a personal health budget. From October 2014 for people not in residential or nursing homes placements this will become a “right to have”.
The government also re-confirmed a commitment in the NHS mandate that anyone with a long term condition, who can benefit from a personal health budget will have the “right to ask” by April 2015.
Staffordshire Clinical Commissioning Groups (CCGs) which includes Stoke-on-Trent are to introduce personal health budgets (PHBs) to those eligible for NHS Continuing Healthcare.
This policy outlines the principles for achieving the implementation of personal health budgets by balancing choice, risk, rights and responsibilities. It recognises that, in the right circumstances, a positive approach to risk can promote a culture of choice and independence that encourages responsible support and shared decision making. The Government's aim is that in future, everyone in England who could benefit from one will have the option of a personal health budget. This commitment includes introducing personal budgets for parents of children with special educational needs and disabilities which may include funding from Social Care and Education.
1.2. What is a Personal Health Budget?
A personal health budget is an amount of money to support a person's identified health and wellbeing needs, planned and agreed between the person and their local NHS team.
By April 2014, people eligible for fully funded NHS continuing healthcare will have the right to ask for a personal health budget, including a direct payment for healthcare. This becomes a right to have a personal health budget in October 2014. The NHS will also be able to offer personal health budgets more widely - for example to people with long term health conditions or people with mental health problems that could benefit.
2. THE SCOPE OF THE POLICY
The policy applies to all patients who are eligible for continuing health care funding living in the community (not in nursing or residential care homes) that are or were registered with Staffordshire General Practitioners at the time of decision. This policy builds on the existing collaborations and joint protocols between Multi Agencies and local social care. Personal Health Budget will be discussed with the patient following their first three month review or following their Continuing Care review.
3. UNDERPINNING PRINCIPLES
Notional Budgets and third party budgets could be carried out under existing NHS legislation prior to the pilot programme. Direct payments required new legislation. The 2010 Health Act allowed Primary Care Trusts (as they were then) to legally make direct payments using NHS
3
money. The Act stated that personal health budgets pilot sites with specific permission from the Secretary of State for Health can make direct payments for the pilot period. Following the pilot period, the Act allowed the Secretary of State to extend direct payments to other commissioning organisations. Direct payments powers have been extended to all Clinical Commissioning Groups in England. The principles in this policy are underpinned by the National Health Service (Direct Payments) Regulations 2013 as amended by the National Health Service (Direct Payments) (Amendment) Regulations 2013 and the National Framework for NHS Continuing Healthcare and NHS funded care (DoH 2012) Procedures relating to the protection of vulnerable adults, use of the Mental Capacity Act (2005) will be followed and wherever appropriate interpreting or advocacy services will be provided. Local Multi-Disciplinary guidelines will be adhered to in conjunction with Staffordshire Continuing Healthcare Policy.
4. IMPLEMENTATION OF THE POLICY
The successful implementation of this policy is based upon a robust system of Multi- Disciplinary and inter-agency working with in local communit ies. The Clinical Commissioning Groups will work collaboratively with external organizations to ensure that t the policy is a working document, which takes into account current legislation and local policies and procedures.
5. PURPOSES AND PRINCIPLES OF PERSONAL HEALTH BUDGETS
The person with the personal health budget (or their representative) will:
• be able to choose the health and wellbeing outcomes they want to achieve, in agreement with a healthcare professional
• know how much money they have for their health care and support • be enabled to create their own care plan, with support if they want it • be able to choose how their budget is held and managed, including the right to ask for
a direct payment • be able to spend the money in ways and at times that make sense to them, as agreed
in their plan.
The approach to personalisation and personal health budgets in the NHS: • The NHS stands by its promise that it is there for everyone, based on need not ability
to pay. • The NHS care and support you get should be safe and effective. It should be a
positive experience. • Personal health budgets should help people to get a better service not make things
worse. • You will not have to get healthcare in this way if you do not want to. • You should have as much control over decisions as you want
4
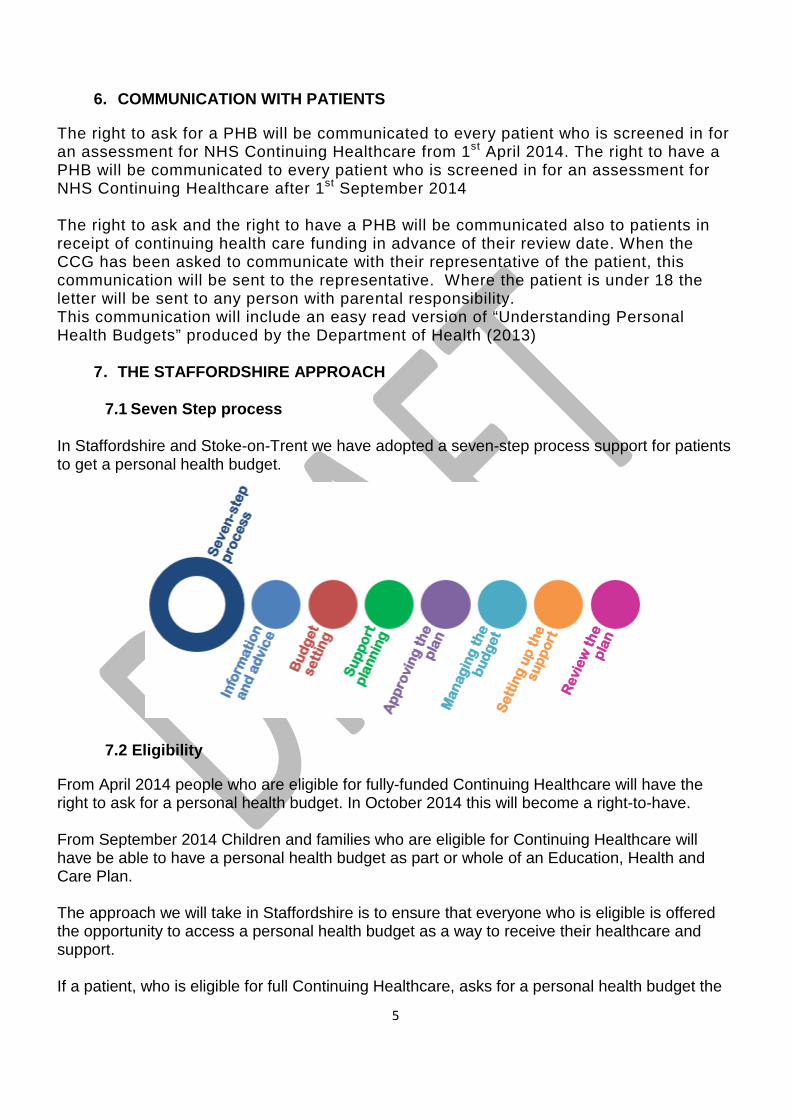
6. COMMUNICATION WITH PATIENTS
The right to ask for a PHB will be communicated to every patient who is screened in for an assessment for NHS Continuing Healthcare from 1st April 2014. The right to have a PHB will be communicated to every patient who is screened in for an assessment for NHS Continuing Healthcare after 1st September 2014 The right to ask and the right to have a PHB will be communicated also to patients in receipt of continuing health care funding in advance of their review date. When the CCG has been asked to communicate with their representative of the patient, this communication will be sent to the representative. Where the patient is under 18 the letter will be sent to any person with parental responsibility. This communication will include an easy read version of “Understanding Personal Health Budgets” produced by the Department of Health (2013)
7. THE STAFFORDSHIRE APPROACH
7.1 Seven Step process
In Staffordshire and Stoke-on-Trent we have adopted a seven-step process support for patients to get a personal health budget.
7.2 Eligibility
From April 2014 people who are eligible for fully-funded Continuing Healthcare will have the right to ask for a personal health budget. In October 2014 this will become a right-to-have. From September 2014 Children and families who are eligible for Continuing Healthcare will have be able to have a personal health budget as part or whole of an Education, Health and Care Plan. The approach we will take in Staffordshire is to ensure that everyone who is eligible is offered the opportunity to access a personal health budget as a way to receive their healthcare and support. If a patient, who is eligible for full Continuing Healthcare, asks for a personal health budget the
5

seven step process will commence at the three month review following eligibility. In deciding whether to offer a direct payment for healthcare, the CCG must consider:
• The indicative budget that the CCG is willing to offer(likely to be based on the cost of a traditional care package)
• The CCG’s alternative offer of care • Whether a direct payment is appropriate given the patient’s condition • The impact of that condition on the patient’s life
The CCG will also consider both the complexity and any changing nature of the patients health needs Where a patient (or their representative indicates to the CCG their wish to exercise their right to ask for/have a PHB, arrangements will be made to discuss this with them, including the form of PHB may be most appropriate to them A patient who becomes eligible for continuing healthcare on a “fast track” will also be entitled to be considered for a PHB. However, as such the patient will have a terminal condition that will rapidly deteriorate; therefore the CCG will prioritise arranging a suitable care package for them.
7.3 How Personal Health Budgets are used:
Personal health budgets are intended to give people a high level of choice and control in how their care and support is provided and the flexibility to try creative and innovative solutions. During the national pilot programme people used their personal health budget in a variety of ways; employing their own care staff (personal assistants) to support them in their home, physiotherapy, equipment and training to improve managing their own care more effectively and respite care in alternative settings.. What the patients choose to purchase through their personal health budget will be linked to their health needs and personal outcomes that are described in their support plan
8. PATIENT CHOICE
Patients and their carers are to be actively involved in all decisions regarding their care. In the majority of cases patient choice will be to return to their own home if at all possible. When this cannot be achieved safely a patient may need to transfer to a care home of their choice. Patients and Carers are to be provided with as much information and support as possible to allow for informed decision making. Where the CCG has been made aware that the individual may not have capacity to consent to the making of a PHB for them, the CCG will arrange for their capacity to be tested, in line with the Mental Capacity Act (2005). Where that person does not have capacity to consent for a PHB a best interest decision will be taken as to whether they should have a personal health budget.
6
9. RESPONSIBLITIES OF KEY STAFF
Responsibilities of key staff are laid out in detail in the National Framework for Continuing Healthcare (2012) Medical staff, Ward Nurses, Therapists, Community Nurses, Social Services and Care Co-ordinators. As a general principle, health and social staff will be responsible for the continuing healthcare assessments of patients, which do require the involvement of multi-agency services and identification of a named Care Co-ordinator. A Delegation of Level Three tasks to Personal Assistants employed through Personal Health Budgets for Staffordshire CCGs patients Guidance has been developed for health professionals regarding their responsibilities in identifying the key clinical skills and training is required and identifying what of these skills can be delegated to Personal Assistants (PAs) employed by patients(or their representatives) (see Appendix 1) Clinicians involved with the patient will have an important role to play helping to determine and agree the clinical competences that PAs need but decisions about how training to reach these competences needs to be identified with the patient during the support planning stage and agreed and signed up to by the patient.
10. THE PROCESS
Practice Guidance has been developed to allow health and social care professionals to understand the process and where their responsibilities lie in terms of the development of the patients personal support plan. (See appendix 2) The Support Plan will be completed by their Support Planner with the appropriate health care professional. This will include what is important to the person, what they want to see changed, how they want to be supported, how support will be managed, how the person will stay in control of their life, how the person will make the plan happen. From this will emerge a clear set of health and personal outcomes from which to commission the services required as well as a framework in which to review the patient’s care. To enable the Personal Support Plans to be approved by the CCG the proposals for meeting the patients assessed health needs will be:
• Lawful - the proposals will be legitimately within the scope of the funds and resources that will be used. The proposals will be lawful and regulatory requirements relating to specific measures proposed will be addressed
• Effective - the proposals must meet the patient’s assessed eligibility needs and support the patient’s independence, health and well-being. A risk assessment will be carried out and any risks identified that might jeopardise the effectiveness of the plan or threaten the safety or wellbeing of the patient or others must be addressed. The proposals will make effective use of the funds and resources available in accordance with the principle of best value.
• Affordable - All costs will be identifies and can realistically be met within the budget. • Appropriate - the patients support plan will have clear and strong links to the patients’
health and social care outcomes.
A strategic overview flowchart can be seen in appendix 3
7

11. TRAINING
A joint health and social care training programme on PHBs will be arranged across Staffordshire for health and social care professionals
12. FINANCE
The support planning process helps the patient decide how they would like the PHB fund to be managed. Some people will simply not want employer’s responsibilities, and in these cases a third party arrangement may be preferred, where all money, purchases and employment contracts are handled on the patient’s behalf. Though legal responsibilities lie with the third party organisation the patient retains choice and control. It is vital that the Continuing Healthcare budget setting methods is fully transparent t to the patients (or their representative) from the outset. No Personal Health Budget will be allocated unless the potential Personal Health Budget Holder demonstrates to the Support Planner full appreciation of the implications of PHB uptake. If a direct payment is chosen, the patient is required to sign a service agreement with the CCG, committing them to spend the budget as agreed in their support plan. They take on full employer’s responsibilities, including advertising for staff, decisions on rates of pay and employee requirements The Support Planner may help with some of these tasks. The PHB may also fund extra staff training on certain clinical tasks which has been identified within the Support Plan and also consider a contingency fund to factor in long term sickness and redundancy costs to the patient, this mechanism would allow the CCG to monitor PHB efficiency more closely Where the PHBs are underspent, the balance will be returned to the CCG. The patient will not be permitted to spend funds on anything not identified in their personal support plan. Guidance of the process is found in Appendix 4 (Personalising Healthcare - Framework for Direct Payments of Personal Health Budgets Guidance)
National guidance provides a list of inappropriate spend: • Alcohol • Tobacco • Gambling • Debt repayment • The purchase of primary care services provided by GPs • Urgent or emergency treatment services • To pay a close family carer living in the same household except in circumstances when
“it is necessary to meet satisfactorily the patient’s need for that service; or to promote the welfare the welfare of a patient who is a child”
• The employment of people in ways which breach national employment regulations
13. REVIEWS AND MONITORING
The National Framework for Continuing Healthcare and Funded Nursing Care ( Nov. 2012) recommends that patients who have been deemed eligible for continuing healthcare funding should be reviewed initially at 3 months and then annually unless there are any changes in the patients’ needs. There is no national guidance regarding PHB reviews however the frequency of the reviews and monitoring should be guided by the needs of each individual and their circumstances. Some people may have relatively straightforward care arrangements others
8

may have more complex arrangements and particularly vulnerable. At the minimum, new PHB holders will have a review at three months and twelve months and yearly thereafter as the CHC Framework states. Individuals will have access to the Support Planner contact details if at any point healthcare needs change.
14. DISPUTES/DISAGREEMENTS
The Staffordshire and Stoke on Trent CCGs and the Local Authorities have the right to insist on a different support package, or end a Personal health budget if there is serious concern that the care being funded via the personal health budget is not achieving the agreed outcomes identified in the patient’s support plan, involves an inappropriate level of risk, or is proving harmful to the patient. Complains by patients, families, professionals will be addressed in the first instance through the appropriate organisations Complaint teams
REFERENCES
Department of Health (2012) Personal health budgets guide: implementing effective care planning London Department of Health (2012) Budget setting for NHS Continuing healthcare London. Department of Health (2012) National Framework for NHS Continuing Healthcare and NHS funded care. London Department of Health (2014) Guidance on Direct Payments for Healthcare Understanding the Regulations. London NHS England (2013) The CCG Assurance Guide 2013/4: Operational Guidance London
9

APPENDICES
10

Appendix 3
11

Title Staffordshire Mental Health is Everyone’s Business Strategy 2014
Reporting to Governing Body Date of Meeting 27th November 2014
Commissioning Lead(s) Author(s)
Nicola Harkness Dawn Jennens
Mental Health Lead Staffordshire Joint Commissioning Unit
Purpose of the Report (Please select) Approval Assurance Discussion
Key Points/Executive Summary The South Staffordshire Mental Health Commissioning Board led by SES&SP CCG and supported by the Staffordshire Joint Commissioning Unit has developed the Mental Health Is Everyone’s Business Strategy.
Our ESCCG GP colleague Dr John Cleary has been involved in reviewing the development of the strategy through his role on the South Staffordshire Mental Health Commissioning Board.
Key Points:
• It is a well-known fact that 1 in 4 of us will suffer from mental health problems in our lives. We know that individuals with mental health problems often manage their conditions well and lead full and productive lives. We also know, however, that people with mental health issues are much less likely to have a job, stable housing and their life expectancy is lower. This is unacceptable and we strongly support the concept of ‘parity of esteem’ and ‘closing the gap’ for individuals and will work to ensure that for our citizens, mental ill health is not a barrier to achieving good life outcomes.
• It is recognised that we need to focus more generally on the population and what
we need to do to promote good mental wellbeing. We know what makes people happy is not just material goods, but a sense of community and giving. As partners, we have developed this strategy to clearly mark our intentions to improve outcomes for service users across Staffordshire and Stoke on Trent.
• The strategy focuses on adults; however, we recognise the key need to link to
children’s mental health services to ensure smooth transition. This document outlines the proposals, both in terms of priority outcomes and actions to deliver. If agreed, we will move forward to develop implementation plans for the north and south of the areas.
x
Enc. 7

Recommendations (what is expected from the Board) The Governing Body is asked to:-
1. Approve the Staffordshire Mental Health is Everyone’s Business Strategy 2014 including the outcomes and actions to be taken both as a CCG and in collaboration with all Mental Health Commissioning Board Partners
Enclosures
1. Staffordshire Mental Health is Everyone’s Business Strategy 2014.
We will support people to be healthier and more independent, feel safer, happier and more supported in and by their community
Mental Health is Everybody’s Business
Contents Foreword – Mental Health Strategy 5
01 Our Vision 7
02 Introduction 12
03 Why do we need change 15
04 Prevention 18
05 We will improve access to and the delivery of mental health services with better outcomes for 22
individuals with mental illness
06 People will be able to access the right level of assessment, advice, support and intervention at the earliest opportunity 25
07 Early intervention and care as close to home as possible 28
08 People will have good healthcare 30 and enjoy healthy lifestyles
09 People Can and Will Recover 33
10 People will feel safer, happier and more supported in and by their communities
36
11 Fewer people will experience stigma and discrimination 37
12 People with a mental illness will gain and retain paid work 39
13 How will you know we have delivered our vision 41
3

Foreword –Mental Health Strategy
It is a well-known fact that 1 in 4 of us will suffer from mental health problems in our lives. Suffering from mental ill health can feel just as bad if not worse than being in physical pain due to illness, however, there is still a lack of understanding and a stigma associated with it.
We know that individuals with mental health problems often manage their conditions well and lead full and productive lives. We also know, however, that people with mental health issues are much less likely to have a job, stable housing and their life expectancy is lower. This is unacceptable and we strongly support the concept of ‘parity of esteem’ and ‘closing the gap’ for individuals and will work to ensure that for our citizens, mental ill health is not a barrier to achieving good life outcomes.
We also need to focus more generally on the population and what we need to do to promote good mental wellbeing.
We know what makes people happy is not just material goods, but a sense of community and giving.
As partners, we have developed this strategy to clearly mark our intentions to improve outcomes for service users across Staffordshire and Stoke on Trent. The strategy focusses on adults; however, we recognise the key need to link to children’s mental health services to ensure smooth transition.
This document outlines our proposals, both in terms of priority outcomes and actions to deliver. If agreed, we will move forward to develop implementation plans for the north and south of the areas.
Ultimately, we want to get on with making things better for our citizens and for
people with mental health problems.
Signaturies
5

Our Vision
We have 3 clear Outcomes:
People will be Healthier and More Independent
They will feel Safer, Happier and more Supported in and by their communities
They will be able to access more, and appropriate, employment
We will inspire, influence and empower people to be more independent, to achieve this:-
We will tackle the stigma and discrimination associated with mental illness
We will build on the strengths that exist in our communities so that they can make a difference to the wellbeing of the people around them
We will make sure that those people at the greatest risk of developing a mental illness understand when and how to find the right support
We will intervene early when there is a problem
We will ensure people get the right and response to their mental health need 24 hours a day, 7 days a week.
No one with a mental illness will be detained in a police cell unless there are exceptional circumstances
01
7

We will increase the number of people with lived experience of mental illness across our workforce and build networks of peer support to help people of all ages understand how to manage their problems
We will increase the number of people with a mental illness in paid work or volunteering
We will ensure that people are supported to access accommodation options appropriate to their needs.
We will ensure that the emotional wellbeing of people is managed alongside their physical health problems to improve their recovery.
We will also ensure that people with severe mental illness live longer because their physical health needs are met effectively.
We will drive innovation and maximize the use of new technology and social media
We want to reduce suicide
8
We know that to deliver our vision we must fundamentally change the way we commission and deliver services for people with mental illness.
We will use our infl uence across the economy to embed mental health into everything that we do across public services:
We are changing the way that we work, with a new focus on working together in partnership, to ensure that mental illness is considered with equal parity to physical illness across all aspects of our services:
We will commission services based on the principle that only the person using services or experiencing illness can attach value to the outcome of the care they receive … placing them truly at the centre of what we deliver ..
We see this as the start of new relationships, more choice and control for people using our services and greater innovation and new ways of delivering our outcomes through collaboration, engagement and co-production with the people who understand what good looks like.
9
Everybody’s BusinessMental illness is common and expensive and where stigma and discrimination continue to be an issue, people would simply rather not talk about it.
Because we don’t talk about it, it is easy to underestimate the impact that these conditions can have on individuals, their families, our communities and the local economy
But poor mental health is both a cause and a consequence of family breakdown, debt and unemployment, homelessness and isolation; it is consistently linked with lower levels of educational achievement as well as poor physical health and it is no coincidence that the most deprived communities have the poorest health and well-being and the highest levels of mental illness.
This has to change … We have to talk about it!
Mental ill health accounts for over a third of all illness in Britain and 40% of all disability.
At any one time one in six working age adults (16 % of the population) will experience depression and/or anxiety
Children from the poorest households are 3 times more likely to have mental health problems than children from more affl uent households
The most recent fi gures available show that only around 27% of working age adults in England with a mental illness are in employment.
About 50% of lifetime cases of diagnosable mental illnesses begin by age 14 and It is estimated that a quarter of all older people suffer from depression
Mental illness accounts for over 20% of the total burden of disease in the UK, more than cardiovascular disease or cancer.
Mental disorder accounts for around 5% of A&E attendances, 25% of primary care attendances, 30% of acute inpatient bed occupancy and 30% of acute readmissions
People with severe mental illness are less likely to have their physical health problems diagnosed and treated and as a result die on average 15 - 20 years sooner than the general population.
People with physical health problems often have undiagnosed mental health problems. Depression is two to three times more common in people with chronic physical health problems.
People who have been abused or been victims of domestic violence have higher rates of mental health problems
10
People with mental health problems are much more likely to smoke and to drink more alcohol than is healthy.
Mental illness carries a stigma, and people with a mental illness are more likely to be living in poverty and be unemployed - unemployed people are twice as likely to have depression as people in work
Suicide accounts for 8 deaths per 100,000 population every year
Tackling these issues is complex and measuring the true cost is almost impossible.
11

We will achieve New Ways of thinking about Health
Mental health is as important as physical health.
everyone has mental health needs;
mental well-being underpins all aspects of health and well-being; and
mental health, like physical health, is a resource that we all need to promote and protect
Everyone has a role in creating an environment that promotes mental well-being to improve the lives of individuals, families and communities.
To achieve this:
We will Increase collaborative working among and across key agencies to embed a clear understanding that poor life chances such as unemployment, poor housing and education poor parenting and family breakdown, and unhealthy lifestyle including excessive use of alcohol, substance misuse, smoking, and obesity are inextricably linked to physical and mental illness in our communities and that together we can make a difference.
Integrated care will be seen as a ‘must do’ priority – the argument is not just about providing better care and support to people often with complex needs, but also about making the best use of public services and reducing the use of expensive specialist services – this can only be achieved on an economy wide basis, integration will break down the barriers of separate funding streams and improve outcomes.
The local Suicide Prevention plan operates within the context of this strategy reflecting the key outcomes of the National Strategy, Preventing Suicide in England (DoH 2011).
We recognise that suicide devastates families and communities and its impact can be felt for many years.
Last year, local suicide prevention plans were developed and we are committed to making sure that theses plans are driven forward.
This joint strategy endorses a key principle that mental health is everybody’s business and we will use our influence across the economy to embed mental health into everything that we do.
13
Introduction
We have set out a clear vision to ensure that everything we do supports and empowers people to be healthier and more independent and to feel safer, happier and more supported in and by their communities: This includes people with a mental illness.
Growing evidence supports the principle that good mental health underpins everything we do and its absence is reflected in costs to individuals, to our communities and to the local economy and is strongly associated with inequalities in both health and wellbeing.
The strategy draws on the national direction set out in ‘No Health without Mental Health’ (DoH 2011) and the associated guidance, and has 2 distinct themes:-
To improve the mental health and wellbeing of the population, including those recovering from a mental illness;
To improve access to and the delivery of mental health services with better outcomes for individuals with mental illness and their carers:
We have set out our commitment to ensure that through greater integration we will enable positive behaviour and support for those who need it most, whilst helping people to take control of their own lives.
We want our communities to be able to:-
stay in control of their lives
access high quality services when they need them
receive care which is focused on recovery and independence
We are committed to leading an integrated agenda that ensures local people with a mental illness have the opportunity to prosper, be healthy and happy.
02
12
14
Why do we need to change? The causes of mental illness are complex, some of which we cant easily infl uence, however what we do know is that everyone has periods in their life when they feel sad, lonely or stressed – sometimes there is no explanation – we also know that there are some factors that can cause prolonged periods of poor mental health, such as isolation and loneliness, unemployment, debt, family breakdown, abuse or trauma, physical health problems and poor housing or homelessness. These are factors where we believe we can make a difference.
Poor mental health can in turn lead to a more defi ned mental illness and we want to prevent this wherever we can.
We know
Mental Wellbeing is essential for each of us to reach our full potential.
Mental illness often starts early in life interrupting education and limiting life chances
If we can make a difference at an early stage then we can begin to impact on the future.
Where mental illness does occur, if we take a positive approach to recovery then people with a mental illness can retain or gain control of their lives
Mental wellbeing is more than the absence of mental illness it is about people being able to realise his or her own abilities to cope with the normal stresses of life, to be able to work productively, and to be able to engage with and make a contribution to his or her community: This includes people who have a mental illness.
03
15
The detail of how our aims and priorities will be delivered will be set out in clear locally developed implementation plans refl ecting local strategies that will be co-produced with partners, with local people and with people who have lived experience of mental illness.
These plans will refl ect much of the action required to deliver the suicide prevention plans, however we will set up focused action groups, with clear leadership, to review the suicide plans and set clear priorities for action.. We specifi cally want to see action to increase suicide awareness training for frontline staff,particularly GPs, and targeted work to encourage responsible reporting of suicide in the local media.
The scope of this strategy is focused on adults of all ages; however there is a strong link with those set out for children and young people to ensure continuity across a life time approach with a seamless transition taking place as young people become adults.
We will champion our agenda across all aspects of the Public Sector in order to reduce the impact of mental illness on people, families, communities, services and our economy, working closely with our district councils and locality teams.
Action
We will identify mental health champions who can infl uence change in all aspects of public services including: Council Cabinet members: Senior Police Offi cers: GP Champions and Experts through lived experience.
We will ensure that ‘good mental health’ is a service specifi c goal and outcome of all public provided and commissioned services.
There are incalculable costs associated with mental illness to the individual, their family and their community it is diffi cult to quantify lost potential and unrealised hopes and goals - but there is also a cost to economy:
We spend more than £120 million on treatment care and support to adults with a mental illness, in the current climate this is not likely to increase but demand is growing:
Locally around 45% of the people are claiming incapacity benefi ts have a mental or behavioral disorder, this is at a cost of over £60 million
Where people with long term physical health conditions also have mental health problems, evidence suggests that £1 in every £8 spent is linked to depression and anxiety.
A detailed report published by the Offi ce of the Police and Crime commissioner in May 2013 set out the cost associated with police time spent dealing with issues relating to mental illness at around £600,000 for the period January – December 2012
And we can keep adding to that, the cost of absence from work with stress related illness, the cost associated with caring for a person with mental illness, the cost of family breakdown … it is diffi cult to place a fi nancial value on everything but there is non the less a cost to the economy - if we are going to make a difference we need to use our infl uence to harness this resource locally to prevent mental health problems escalating to mental illness and to support people with a mental illness to recover and reduce dependency on services
Under the umbrella of our Health and Well-Being strategies for both the County and the City we are clear that tackling the wider determinants of health and well-being and investing in early help and prevention underpins our agenda for mental illness and improving mental wellbeing underpins the successful achievement of our outcomes across public services.
We will work with our public health leads and local councils to promote mental wellbeing and prevent mental illness and where mental illness occurs to maximise the opportunities for recovery.
We will support people and communities to use their knowledge and strength to build the foundation, with more access to support locally, when it is needed, to make sure that intervention is early when there is a problem with the aim of reducing long term dependence on services:
This agenda is not just about what happens in health or social care settings, it is about infl uencing change so that everybody understands their responsibility for mental health and wellbeing - this will only be delivered by partnerships between and across public services, voluntary organisations and service providers and between local communities and the people who use services.
Mental health and wellbeing is everybody’s business and through the collective leadership of our Health and Wellbeing Boards we will make the best use of our combined resources to improve our identifi ed outcomes.
We know we can’t solve everyone’s problems but we can start the conversations, change minds, infl uence new ways of thinking and working and show people that it is time to change our ways of thinking about mental wellbeing and mental illness.
16 17
Prevention We will do everything we can to influence change so that more people will have good mental health including those recovering from a mental illness.
Improved mental well-being is associated with a range of better outcomes including improved physical health, better educational achievement, improved employment rates and reduced anti-social behaviour – all contributing to a healthier and more productive future.
Effective prevention and early intervention are essential if we are to reduce the impact of mental illness on our communities and our economy.
The key areas to achieve this objective are the same as those set out in the Public Health White Paper ‘Healthy lives Healthy people’ :-
Starting Well
People’s earliest years and all that they experience has a profound impact upon the rest of their life.
Maternal mental health, postnatal care, and effective parenting are key to promoting the positive development of children and lay the foundations for their future particularly because half of life time mental health problems have already developed by the age of 14 years.
04
18
Developing Well
Developing independence and individual resilience continues as a child becomes a young adult – however it is also important to target young people who are at particular risk of developing mental health problems, this would include
Victims of abuse or neglect
Those in contact with the criminal justice system
Underachievers in school
Children in the looked after system
Children of a parent with a mental illness
Children living in poverty
Adolescence in itself is a time of major developmental change at all levels, the major influences on their lifestyle shift from their parents to their peers.
There are clear local strategies that reflect the specific complexities in addressing the mental health needs of children and young people but the interface with the adult strategy is key to a seamless approach where young people will transition to adult services: The interface is also key to the long term objectives as the foundations preventing mental illness are laid in the early years.
Living Well
We all need to take responsibility for our own health and well being – however our communities and environment can influence behaviours – Housing, families, social networks and community safety and community involvement are all key factors:
Physical activity, social interaction, leisure, involvement and awareness all contribute to a wider sense of wellbeing and belonging.
The ‘5 ways to mental wellbeing’ which were developed from evidence gathered in the government’s Foresight Project on Mental Capital and Wellbeing published in 2008, provide a framework not only for developing our agenda, but for the wellbeing agenda as it applies to the wider population and specific vulnerable groups within our communities.
Connect
Be active
Take notice
Keep learning
Give
19

Working Well
Employment not only has economic benefits but there are significant psychological benefits – not least a sense of self-worth: the longer someone is out of work the harder it is to re-join the job market
Support with job seeking can prevent the deterioration that can lead to long term unemployment and potential for mental illness, just as targeted support for people recovering from mental illness assists recovery and reduces the demand for care services.
For those with mental illness, being employed can be an important step to recovery, improving self-esteem and confidence and reducing psychological distress. Conversely, unemployment increases the risk of developing mental illness, and is associated with increased rates of depression and suicide as well as higher use of health services and hospital admission. Employment is therefore vital for maintaining good mental health and promoting recovery from mental illness.
However employment and employers can also be the cause of stress and mental ill health – healthy workplace initiatives need to extend beyond the environment to take account of psychological well-being – and raising awareness of mental health issues has benefits not only for the individuals but also can reduce the costs associated with sickness absence due to mental illness.
Ageing Well
As people live longer, problems associated with ageing – social isolation, physical health problems, grief and loss and increasingly the need for care and support lead to the increasing likelihood of mental health problems, depression being the most common mental disorder in older people particularly linked to bereavement and social isolation, and leads to poor diet, confusion, falls, which in return leads to increasing dependence on care services: Bereavement counselling for older people is not considered and yet they are the one part of our population most likely to experience loss.
Social networks, support for carers and safer communities all increase the opportunities for older people to continue to be involved members of their families and communities.
20
How will we tackle this?
We will influence a broad span of activities to reduce risk and prevent mental illness, this will include:
Driving the delivery of effective Parenting programmes targeting those areas where children are most likely to be at risk including teenage parents, and parents with a mental illness or problems with substance misuse
Working with Children’s Services and Education to develop effective programmes to raise emotional awareness both amongst teachers and carers and through school based education programmes for children and young people
Ensuring that mental illness and mental wellbeing is integral to the management of the ‘ whole family’ particularly where there is evidence of violence or abuse, mental illness or substance misuse
Drive continued improvement in access to age appropriate Talking Therapies increasing the scope of options available in line with best practice and guidance, particularly for children and older people, and maximising the potential of modern technology to support this agenda.
Working with Health Promotion colleagues to develop effective campaigns which include programmes specifically focusing on access for people with Mental Illness
Influence the development of new business locally to include opportunities for people with mental illness such as apprentice schemes and supported employment opportunities
Working with employers to understand Stress in the workplace through effective information, education and achievement of the Healthy Workplace Awards
Work alongside our district and local councils and housing providers to improve housing opportunities
Develop the opportunities for volunteering, especially in local communities
Influence contracting and procurement opportunities to ensure that wellbeing is embedded in all of our contracted services
Work with local police to maximise the opportunities to improve wellbeing and provide targeted support for individuals and families who are known to the criminal justice system.
21

We will improve access to and the delivery of mental health services with better outcomes for individuals with mental illness. What people have told us
We have heard what people who use mental health services locally have said - whether this has been through engagement with people who use services or their carers or through feedback from surveys – the messages have been clear.
People want:-
Services closer to home and family
Access to services when they need them in a crisis, especially where this will avoid admission to hospital
Information on the options available to them
Services that are appropriate to them
Choice
Greater support in the community
More active support and help with day to day living so that they can live more independently
To be treated as a whole person not a diagnosis
05
22
They have asked that:-
There are clear pathways through services so that they get the intervention they need quickly without being referred over and over again
If they are unwell that treatment at home is considered before admission to hospital
If they are admitted to hospital there is a discharge plan agreed with them and they know who to contact if they are in crisis so that they don’t have to go back into hospital
If they are admitted it is for as short a time as possible and it is clear to them why where ever possible
They are involved in planning their care – wherever that is delivered
They are part of setting their own outcomes and that these outcomes matter
They suggested that:
Information on the side-effects of medication is provided by a range of health professionals at different times, so that they have a chance to absorb the information at the right time for them. - Pharmacists were considered effective and under-used.
Information about their condition and treatment is shared between their GP and specialist services to reduce repeating details about themselves to numerous different professionals
Social care, peer-support and the voluntary sector to be part of the same pathway
They have one care-plan that includes their mental and physical health needs and well-being.
Everyone involved in their care understand all of their medication
We have heard but now we need to listen and respond:
We know that we need to extend our methods of engagement to become more innovative asking the right questions of the right people.
Moving forward:
We will develop a robust communications plan that extends our methods of engagement to become more innovative across all of our partners – asking the right questions of the right people.
We will work with service users and professionals to co-produce the plans that will deliver the expectations of this strategy
23

Where people are accessing services we also need to be confi dent that they are of the highest quality, therefore services will be monitored against the principles set out below:
Decisions about care will be made with the person
Care will delivered as close to home as possible
Interventions will be planned around the outcomes agreed by the person
Services will be appropriate to the age and development of the person referred
Services will meet the cultural needs of the individual
Early intervention will be provided when someone needs support
Families and carers will be involved as appropriate
The right Information will be available to support choice and decision making
Patient Reported Outcome Measures will be recorded and demonstrate how they support continuous improvement
Services will be able to demonstrate innovation and new ways of working
We will target areas where we know there is dissatisfaction and address the problems
We will work with care providers to ensure that we can demonstrate that these principles are embedded in the delivery of care
24 25
People will be able to access the right level of assessment, advice, support and intervention at the earliest opportunity: Mental illness will occur, it is common and varies in its nature and severity, for some the disorders are long term and disabling for others it is less severe and many recover fully
We need to ensure that people can access services when they need them:
We need professionals to work more closely with people to understand how a crisis referral can be avoided, but when a crisis does occur that a swift and appropriate response can be initiated.
People who use mental health services and their families or carers often know when they are approaching crisis and many know what they need to avoid it – we need to listen and be able respond effectively.
For many people the fi rst point of contact is their GP, whether this is the fi rst time they experience a problem or when they are approaching a crisis – GPs are central to achieving effective early intervention. We need our GPs to work differently – to share care with but be better supported by specialist services.
We will work with the Local Area team of NHS England to infl uence primary care commissioning.
We actively support the recently published priorities for change in mental health and aim to ensure that ‘No one experiencing a mental health crisis should ever be turned away from services’ early recognition of, and response to, mental illness at the fi rst point of contact is key to the achievement of this and whilst it is often through the GP the fi rst point of contact may also be through other services including the Police, Emergency Departments, an Acute
06
Hospital or Community Health Service, local pharmacy services or even housing providers and advice services.
Too many people wait for too long to get the services they need and too often people are turned away because services don’t have capacity or are not open outside of offi ce hours or care is just delayed because information is not shared between services and professionals.
We will change this.
Signifi cantly, in 2012/13, 25% of people in Staffordshire, detained under the Mental Health Act by the police, were held in police cells because care services were not able to respond quickly, this has a profound impact on the mental health of the person already in crisis or distress and takes up an unacceptable amount of police time, who are not equipped with the skills to support someone with a mental illness: Our aspiration is that no individual, detained under section 136, will be held in police custody unless there are exceptional circumstances, but equally that people are not detained under Section 136 unless it is appropriate, and that requires a new level of understanding and intervention at the frontline of policing.
Delays in care often lead to a crisis for that person as their needs have increased as a result of delays:
We also recognise that there are local people, with a mental illness whose needs are often poorly met because they fall between services when it comes to getting the right intervention, especially when they have complex needs that require more than one service or intervention; collectively we commission a range of services from both health and social care, voluntary organisations and independent providers which have been developed in isolation with a range of criteria and outcomes or success measures:
It is the gaps that exist between services that increase the cost both to the individual and to the wider economy
We are clear that we need to understand the impact that gaps in service pathways have on individuals and the cost of these gaps to the economy and then close them.
We are focused on ensuring that we have a clear model of care, that sits across the whole system, that is able to deliver a more effi cient and effective experience for people who have mental health needs and that proactive work will be undertaken to improve pathways and deliver clear outcomes making our services more responsive, fl exible, and tailored to individual need – Mental health care will be solution focused rather than criteria driven
26
We will strengthen connectivity between services and professionals to both improve the outcomes for the individual and to drive greater effi ciency and effectiveness across services, through clear and integrated pathways of care.
Priorities for Development
24 Hour Response to People in Crisis
Single Point of Access
Extended Services in the Community to bridge the gaps between Primary and Secondary care
Police community triage linked to liaison and diversion
Suffi cient Place of Safety provision for people detained under the Mental Health Act:
- People who are intoxicated as a result of Alcohol or Substance abuse
- People who have Physical Health Problems
We will work with our children’s commissioners to identify a Place of Safety for people under the age of 18.
Clear transition policy for children with a mental illness moving from CAMHS to Adult services
27

Early intervention and care as close to home as possible. We have seen an increasing demand for talking therapies in recent years but coverage is still not in place for all adults, for children and young people, people with physical health problems and for frail older people, nor is it in place for many people with complex mental health needs and personality disorders:
Talking therapies help people to manage their mental health problems or support them to recover. They are an effective means of early intervention where there are mild to moderate levels of depression and anxiety, simple short term interventions can prevent the need for longer term care and treatment options and for many these can be very practical self-help approaches that support recovery and prevent longer term mental illness:
Identifying problems early and supporting people to access advice, information and simple self-help options can be achieved through raising awareness within the existing workforce across organisations and professionals this could include staff within Job Centres, Community Police Offi cers or Pharmacists it should not be restricted to just health and social care but wherever someone comes into contact with public services or community groups
Talking therapies can also support people with more complex needs to cope with or manage their mental illness allowing them to live their lives, people with psychotic illness, personality disorders and those who self- harm can all achieve greater and more sustained recovery through access to appropriate talking therapies.
We will be creative in our thinking working closely with providers and service users to understand what makes a difference:
There are times when someone has a level of need such that 24 hour care is required but we don’t want hospital to be the fi rst option considered. Where someone could be supported at home and this would give them a better outcome, then that approach should be taken. Every decision must be based on the need of the individual and the views of the professionals involved at the time.
07
28
This is not a new idea and it is not always the easiest option – but where people have experienced effective treatment at home they have been very positive about the experience and felt that being with their family helped them to recover sooner:
We want care to be delivered as close to home as possible in a setting that will deliver the best outcome for the individual:
We will deliver the right care option in the right setting supporting independence, choice and control
Priorities for Development
Increased access to talking Therapies and Psychological Interventions for all people with mental health needs
Shared Care options between GPs and Specialist services
Work with libraries to extend the reading well project to include self-help reading groups
Provide alternative care and support wherever possible to avoid hospital admission
29

People will have good healthcare and enjoy healthy lifestyles. Many people with long-term physical health conditions also have some degree of mental illness – usually depression or anxiety. These can lead to significantly poorer health outcomes, reduced quality of life and longer term dependence on health or social care services. The cost to the care system is significant.
Primary care services are central to effective integration of care across physical and mental health services but wider collaborative approaches can improve the management and outcomes of both conditions – we need to behave differently to achieve different outcomes.
We will influence our partners, both providers and commissioners of care, support and treatment services in acute and community settings, to embed mental wellbeing in the care they provide: We are confident that not only will this improve the outcomes for people and give them greater independence but we will reduce the demand for a range of services including the number of people attending emergency departments, admissions to hospital, community services and social care packages including residential care.
The evidence is overwhelming that poor mental wellbeing delays recovery from physical illness – we have to view mental and physical health with equal importance.
Mental wellbeing will be an integral aspect of pathways for people with long term conditions including for those with physical and sensory impairment - assessment and appropriate interventions will be embedded in all aspects of care reducing the likelihood of people requiring specialist interventions in the future, but where need is identified there will be clear pathways into psychological therapies with the overall aim to improve their health outcomes and recovery.
08
30 31
We will support partners to:
Develop integrated care pathways managing the mental health needs of people with physical health problems both in primary and secondary care ensuring screening, psychological support and access to talking therapies across care pathways.
Develop the skills of professionals working with people with physical health needs in assessing emotional and mental health needs and providing low level interventions to support their overall recovery
Implement a single care co-ordination approach reducing the need for cross referral between parts of the health and care system
We know that having a mental illness increases the risk of physical ill health – having both a physical and mental illness delays recovery from both,
We don’t have local data on the physical health of people with mental health problems
However, national data/research shows:
69% of people with a psychotic illness and 55% of people with depression are smokers
16% of people with schizophrenia drink above the recommended levels for adults – this is higher in people with Bi Polar disorder and extends to other substance misuse.
42% of people with schizophrenia are obese
19% of people with schizophrenia will suffer from hypertension (compared to 15% of the general population)
People taking some anti-psychotic medications are more likely to develop diabetes than the general population.

All of these contributors and the other identified causes of mental illness basically mean that people with schizophrenia and bi-polar disorder die on average 15 - 20 years sooner than the general population because of higher rates of respiratory and cardiovascular disorders.
We want people to live long and healthy lives – that includes people with a mental illness: We will drive a programme of awareness and support to help people with a mental illness to take care of their own health but we also expect GPs and mental health professionals to understand and take responsibility for ensuring that the physical health needs of people with a mental illness are met.
We know we can’t make a difference overnight but we can make a difference and reduce the number of people dying too soon. We will adapt services such as smoking cessation or weight management to ensure they are relevant for people recovering from a mental illness.
But most importantly we will do more to enable people to take care of their own physical health – encouragement, information, advice and support so that they do access health screening and health checks, visit the dentist or optician, feel confident in attending their GP for regular health checks and understand the side effects of the medication they may be taking so that they can take action early.
People with mental health problems will be supported to access physical health care and lifestyle services as an integral aspect of care planning
People with a mental illness, will be supported to access an NHS Health Check from their GP
We will ensure that lifestyle services are designed to support people with complex mental health needs
Explore opportunities for providing effective medicines management through local pharmacies
People Can and Will Recover We will support and encourage people with a mental illness to move forward, set new goals and develop relationships that give their lives meaning:
Recovery is a personal journey of discovery: It involves making sense of, and finding meaning in, what has happened; it is about people becoming experts in their own self-care; and building a new sense of self and purpose in life; discovering their own resourcefulness and possibilities and using these, and the support available to them, to pursue their aspirations and goals.
Recovery is about people staying in control of their life; the guiding principle being is that it is possible for someone to regain a meaningful life, despite mental illness.
Mental illness and social attitudes to mental illness often impose limits on people experiencing ill health, professionals, friends and families can be overly protective or pessimistic about what someone with a mental illness problem will be able to achieve.
Taking a recovery approach across services we will support people to achieve their own goals and aspirations.
The challenge then is for us to help people on this journey, to look beyond symptoms and to help people build satisfying and meaningful lives.
The key factors important to recovery include:
good relationships
financial security
satisfying work
personal growth
the right living environment
developing one’s own cultural or spiritual perspectives
developing resilience to possible adversity or stress in the future
being believed in listened to and understood
getting explanations for problems or experiences
having the opportunity to temporarily resign responsibility during periods of crisis.
09
32 33
We will work together to reduce the number of people in contact with specialist mental health services by remodelling the system to support people in the community to recover, and we want to take this forward the through a proactive education and learning approach
We will support people to live their lives as they want and to take the risks that we all take – but with the knowledge that they can regain access to services quickly if they need additional support.
We will empower people to take personal responsibility for their own recovery.
We will support and encourage people with a mental health problem to move forward, set new goals and develop relationships that give their lives meaning
Recovery needs to start at the first intervention and we need new and innovative ways of working because we believe that recovery is not only possible but is the right of everyone
People will have a positive experience of care and support
As far as possible people should be able to control and manage their own care and support so that it matches a recovery plan that has been developed with them; Placing the individual at the centre of their own care is key to improving the experience of and key to ensuring that our services take a problem solving approach.
We not only want to know that the quality of the service they received was good but that it made a difference, and this can only be achieved if the care plan reflects what the person needs to support that recovery process – this will require everyone to think differently about what is offered.
We will introduce a Patient Reported Outcomes tool – a way of working or a tool for measuring outcomes from the patient’s perspective, across all services to ensure that people are supported and empowered to create their own recovery action plan to achieve their own aspirations, setting out their goals, what help they need to get there, what helps keep them well and what puts their recovery at risk giving individuals: a sense of control over their life despite having a mental illness.
We will evidence that we are making a difference to people’s lives by working with all of our providers to ensure that an individual outcome tool is integral to the delivery of services and monitored through the contracting process
We will reward innovation for services that are supporting people in their recovery and achieving outcomes
We will
Develop a Recovery college approach to supporting independence
Develop peer support approaches to support self-management and recovery including peer recovery workers in services
We will maximise the use of technology and social media
We know that measuring outcomes with people works – because we already use a recovery star across some of our services and the feedback from people is positive: We want to embed this approach across all of our services.
When people have identified their needs we want to make it easier for everyone to get the care that best suits them, therefore we will drive the development of integrated personal health budgets ensuring that everyone is fully involved in discussions and decisions about their health and wellbeing enabling the individual to work in equal partnership with professionals about how their needs can best be met.
We will test the introduction of personal health budgets with a small group of people initially building on experience from elsewhere and then extend the programme over the next 2-3 years
34 35

People will feel safer, happier and more supported in and by their communitiesA person’s home environment can either promote or hinder good mental health: when people live in a place that helps them feel safe and secure it will support recovery.
Currently we don’t have a clearly defined model or strategic plan to ensure that the needs of people with mental health problems are effectively addressed:
We will work with our local and district councils and local housing associations to ensure that good quality housing advice and information is available at the appropriate time to support people with a mental illness and to enable them to make informed choices as to their future housing options, and that strategic plans specifically address the needs of people with mental illness in the future.
People with a mental illness will be supported to live in settled and appropriate accommodation
We will work with each district or locality to understand the blocks to achieving our outcomes and agree how we can move forward
We will undertake a housing needs analysis for people with a mental illness and identify the gaps we need to address.
10
36 37
Stigma and discrimination is essentially driven by ignorance and fear Stigma can stop people from seeking help, sadly even within support services professionals hold attitudes and beliefs that negatively stereotype people with mental illness and they can have low expectations therefore people become isolated and unable to engage in ordinary life or activities that could improve their mental wellbeing.
Discrimination is costly to the individual their families and to communities – not least discrimination is illegal. The Equality Act 2010 makes it illegal to discriminate directly or indirectly against people with mental illness in public services and functions, access to premises, work, education and transport.
Stigma and discrimination can also worsen someone’s mental illness and delay or impede their getting help, treatment and their recovery. Social isolation, poor housing, unemployment and poverty are all linked to mental ill health so stigma can trap people in a cycle of illness.
The situation is made worse by the media where reports often link mental illness with violence, or portray people with mental illness as dangerous, criminal or very disabled and unable to live normal fulfilled lives.
We will make a concerted effort to actively tackle discrimination through innovative approaches in order to begin to shift attitudes and institutionalised discrimination in many organisations.
11

We will raise the profi le of mental health and challenge discrimination wherever we see it
We Will
Undertake effective campaigns, programmes and projects to raise awareness and understanding built around ‘Time to Change’ principles
Build capacity within advocacy and engagement services to support people and families with mental illness to have more say about local services
Delivering equity of access to comprehensive, appropriate high quality services where mental illness is not an exclusion criterion and all services are responsive to the needs of people with mental illness
We will undertake a Survey of service users and their experience of stigma and discrimination- using the outcomes of this to target campaigns
We will use our infl uence to change the attitudes of the local media to improve reporting where mental illness is a factor.
People with a mental illness will gain and retain paid work We know that Work is good for mental wellbeing , and that mental illness can be the reason for people becoming unemployed:
However people with a mental illness fi nd it hard to access the workplace.
Mental illness makes up the single greatest number of incapacity benefi ts claimants.
It is a complex and challenging agenda requiring a joined up approach to resolution:
Targeted support for people recovering from mental illness assists recovery and reduces the demand for care services.
For those with a mental illness, being employed is important step to recovery, whether that is paid employment, volunteering or just having something meaningful to contribute to the local community. Employment improves self-esteem and confi dence.
12
38 39
Employment is therefore vital for promoting recovery from mental illness.
We will be proactive in building the links between employment and mental health services to increase the opportunities for people with a mental illness to access employment:
Priorities for Development
To proactively identify work opportunities for people in contact with mental health services
To ensure employment is a priority as part of all assessment and care planning.
Increase the range and level of support available to support people with a mental illness into employment and to retain employment building on the success of our current services operating an Individual Placement Support model
Support employers to create a healthier workplace and raise awareness of mental health issues
Focus on employers to tackle discrimination in the workplace
Increase opportunities for volunteering
Work with our business development leads in the council to develop apprenticeships and supported work opportunities particularly for young people.
How will you know we have delivered our vision Some of the developments we have identifi ed are clearly service changes or new ways of working – these developments are building blocks to help us to achieve the outcomes we have identifi ed and of paramount importance is to be able to demonstrate that not only are our services high quality and evidence based, but that they make a difference to the people that access them.
Commissioning for outcomes means that, in many cases we don’t have a baseline position from which to measure success and how we measure success requires a new way of capturing data – and this will take time to develop.
The strategy is an overarching commitment to people in Staffordshire and Stoke on Trent, there will be localised delivery plans to refl ect the north and south footprint of commissioning and provider economy, this is to ensure that local people and local partners are able to refl ect local need; one size will not fi t all.
A key outcomes framework is being developed to refl ect each of the strategic aims and this will continue to be developed and adapted to refl ect local priorities for action.
We will produce this in year one.
Much of the information that will demonstrate delivery is new therefore for the fi rst year it will be about setting baselines but there is a view to the outcomes frameworks for the NHS, Adult Social Care and Public Health to ensure we harness those indicators which will demonstrate out achievement..
Our challenge to ourselves, to all of our providers and our partners is to demonstrate that we are making a difference to people, particularly to those with a mental illness:
Good is only good if it makes a difference, and this is a new way of thinking and working.
13
40 41

How will you will be able to hold us to account?
We will ensure that our governance structure is adjusted to refl ect the complexity of delivering such a wide ranging strategy – and we will set out our plans and the measures that we will use to demonstrate progress against the outcomes we want to achieve at a local level.
Our key aims are to:
Strengthen early recognition and intervention
Reduce long term disability
Increase recovery rates
Improve access to services including shorter waiting times
Maximise choice and control,
Reduce inequality through targeting those at risk,
Listen to what people say
Build capacity through innovative approaches
Focus on effective and effi cient models of commissioning and provision
Reduce demand for and time spent within specialist mental health services where appropriate
42

Stafford & Surrounds Clinical Commissioning Group
North Staffordshire Clinical Commissioning Group
East Staffordshire Clinical Commissioning Group
Cannock Chase Clinical Commissioning Group
Stoke-on-Trent Clinical Commissioning Group
Print and design by Staffordshire County Council, Print Commissioning Services. Telephone: 01785 276051 74500/5/14

Mental Health Strategy Everyone’s Business Staffordshire Health and Wellbeing Board July 2014
AIMS To improve the mental health and wellbeing of the population, including those recovering from a mental illness; To improve access to and the delivery of mental health services with better outcomes for individuals with mental illness and their carers

Some Facts
• Mental ill health accounts for over a third of all illness in Britain and 40% of all disability.
• At any one time one in six working age adults (16 % of the population) will experience depression and/or anxiety
• Children from the poorest households are 3 times more likely to have mental health problems than children from more affluent households
• About 50% of lifetime cases of diagnosable mental illnesses begin by age 14 and It is estimated that a quarter of all older people suffer from depression
• Mental illness accounts for over 20% of the total burden of disease in the UK, more than cardiovascular disease or cancer.
Priority Outcomes
• Physical Health • Work • A safe place to live • Part of the community and reduced social
stigma • No S136 detentions in police custody • Reduced Demand • Support for Carers

The Person aged 16+,
with a non dementia mental
health difficulty
SPA/CMHT 0300 5555001 CRHT
01283 505166
PWBT 0300 790 7000
EIT 01785 257888
Brendon House 01543 899465
CHANGES 01543 679000
Work4You 01785 887813 07843268042
QUEST
Provide: the first point of contact for advice & assessment, intervention & care coordination, in hours gate-keep Crisis Referrals. Work with people who have moderate to severe difficulties requiring Multi Disciplinary Team involvement.
IAPT service, people with mild to moderate anxiety & depression up to & including step 3 NICE Guidance.
Recovery focussed interventions, group & 1-1 promote social inclusion & meaningful activity.
24 hr crisis response up to 72 hrs, home treatment up to 6-8 wks for people at risk of requiring hospital admission. Gate keep admissions to hospital
3 night stay in supported house to prevent relapse, deterioration.
Assessment & intervention up to 3yrs for people aged 14 – 37 experiencing 1st episode of psychosis.
Mental health helpline
0808 800 2234
Carers Association 01785 606675
People Need Support Navigating!!!

Mental Wellbeing
Good mental wellbeing is about being confident, happy and being able to cope with the stresses of everyday life. We know some factors can increase the risk of poor mental wellbeing. They include: • social isolation, loneliness or discrimination • homelessness or poor housing • a long-term physical health condition • social disadvantage, poverty or debt • unemployment • caring for a family member or friend
To do something about these issues; we need a partnership approach

Recovery Based Approaches Make a Difference
• Meet Danni…….

Title Frail Elderly Care – A Staffordshire Strategy Reporting to ESCCG Governing Body Date of Meeting 27th November 2014
Commissioning Lead(s) Author(s) Nicola Harkness/Emily Davies Nicola Harkness/Emily Davies
Purpose of the Report (Please select) Approval Assurance Discussion
Key Points/Executive Summary Purpose The Governing Body are asked to approve and adopt the Frail Elderly Strategy for Staffordshire. Context
Staffordshire has been identified as one of 11 ‘Distressed Health Economies’ across England. KMPG were commissioned by NHS England, the TDA and monitor to undertake a rapid assessment of the issues (both clinical and financial) and to proffer solutions that will improve quality and the long term affordability of the Local Health Economy.
A key recommendation of the KMPG report issued on the 11th August 2014, was for the development of ‘a single frail elderly pathway across the Local Health Economy to replace the two pathways that currently exist. This will remove duplication of resources and improve the quality for patients.’ The benefits of a single integrated pathway outlined in the report include reduced admissions to hospital, reduced delayed discharges and an increase in the number of patients returning to their usual place of residence. Consistent with the recommendation within the KMPG report of ‘do it once where possible, and six times where necessary’ Stoke on Trent Clinical Commissioning Group has taken a leadership role in development of a Frail Elderly strategy on behalf of all Staffordshire CCGs and the County Council. Dr Charles Pidsley, Tony Bruce and Nicola Harkness from East Staffordshire CCG have been actively involved in the co-production of the strategy and helped to inform and shape its content, to ensure it is consistent with the CCG’s organisational priorities and objectives, 5 year plan, and policy decisions agreed at the Health and Wellbeing Board.
x
Enc. 8
1 Author: Date: East Staffs CCG

Key Points The Frail Elderly strategy for Staffordshire outlines a shared vision for the Local Health Economy: ‘That people of Staffordshire have a coherent integrated model of care that is consistently available across the County while being locally responsive to the needs of communities and individuals.’ A key message of the strategy is that commissioners will ‘centralise where possible and localise where necessary.’ This will enable the co-design of the pathway, achieving economies of scale and reduction in duplication where possible but also allow for services to continue to be commissioned on a locality basis to ensure that they reflect the needs of local populations and communities. This is consistent with the agreement at the Health and Wellbeing Board in January 2014, where it was agreed that integrated commissioning for older people would be undertaken at a local level. In order to achieve consistency of provision across Staffordshire, the strategy highlights a number of critical service components, identified by KMPG and local commissioners, for an integrated frail elderly pathway based on evidence and best practice. These include:
• Achieving Personal Responsibility • Single Assessment • Intermediate Care • Step up and step down practice • Frail Elderly Assessment activity • Parity for mental health and approach to dementia • Access to diagnostics including access to specialist interpretation and advice • Care facilitation, coordination and navigation • Making effective use of Technology enabled care • Information management
These critical service components are entirely consistent with the vision set out by East Staffordshire CCG for the Improving Lives Programme, which aims to support people with long term conditions, and/or are frail and older to remain as independent as possible for as long as possible. The shortlisted bidders for the Improving Lives Programme will be asked to demonstrate how their solutions for future service delivery meet the above components and this will be evaluated as part of the final tender process. Recommendations (what is expected from the Board) The Governing Body are asked to approve and adopt the Frail Elderly Strategy for Staffordshire.
Enclosures
1. Draft Frail Elderly Strategy for Staffordshire
2 Author: Date: East Staffs CCG

Staffordshire Frail Elderly Strategy
Prepared by Stoke on Trent CCG, North Staffordshire CCG & Cross Economy Transformation Team for Staffordshire’s Health and Social Care Commissioners
The contributions to this strategy by Health and Social Care Commissioners are acknowledged
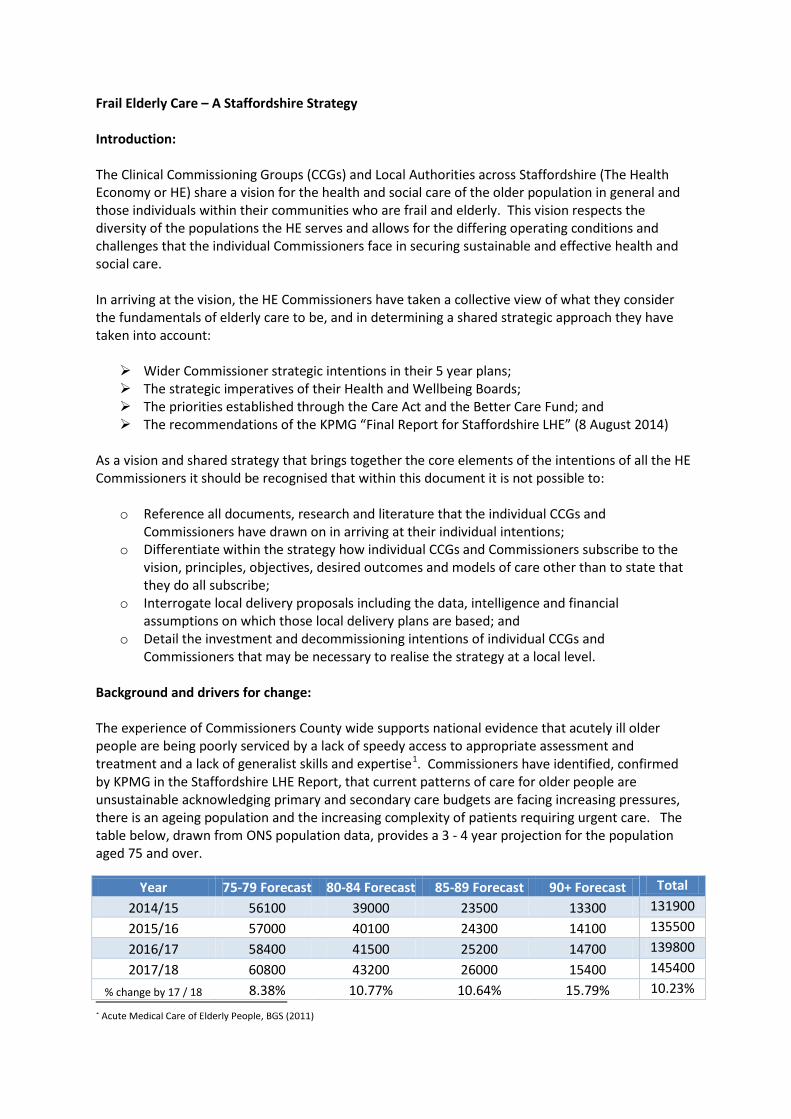
Frail Elderly Care – A Staffordshire Strategy Introduction: The Clinical Commissioning Groups (CCGs) and Local Authorities across Staffordshire (The Health Economy or HE) share a vision for the health and social care of the older population in general and those individuals within their communities who are frail and elderly. This vision respects the diversity of the populations the HE serves and allows for the differing operating conditions and challenges that the individual Commissioners face in securing sustainable and effective health and social care. In arriving at the vision, the HE Commissioners have taken a collective view of what they consider the fundamentals of elderly care to be, and in determining a shared strategic approach they have taken into account: Wider Commissioner strategic intentions in their 5 year plans; The strategic imperatives of their Health and Wellbeing Boards; The priorities established through the Care Act and the Better Care Fund; and The recommendations of the KPMG “Final Report for Staffordshire LHE” (8 August 2014)
As a vision and shared strategy that brings together the core elements of the intentions of all the HE Commissioners it should be recognised that within this document it is not possible to:
o Reference all documents, research and literature that the individual CCGs and Commissioners have drawn on in arriving at their individual intentions;
o Differentiate within the strategy how individual CCGs and Commissioners subscribe to the vision, principles, objectives, desired outcomes and models of care other than to state that they do all subscribe;
o Interrogate local delivery proposals including the data, intelligence and financial assumptions on which those local delivery plans are based; and
o Detail the investment and decommissioning intentions of individual CCGs and Commissioners that may be necessary to realise the strategy at a local level.
Background and drivers for change: The experience of Commissioners County wide supports national evidence that acutely ill older people are being poorly serviced by a lack of speedy access to appropriate assessment and treatment and a lack of generalist skills and expertise1. Commissioners have identified, confirmed by KPMG in the Staffordshire LHE Report, that current patterns of care for older people are unsustainable acknowledging primary and secondary care budgets are facing increasing pressures, there is an ageing population and the increasing complexity of patients requiring urgent care. The table below, drawn from ONS population data, provides a 3 - 4 year projection for the population aged 75 and over.
1 Acute Medical Care of Elderly People, BGS (2011)
Year 75-79 Forecast 80-84 Forecast 85-89 Forecast 90+ Forecast Total 2014/15 56100 39000 23500 13300 131900 2015/16 57000 40100 24300 14100 135500 2016/17 58400 41500 25200 14700 139800 2017/18 60800 43200 26000 15400 145400
% change by 17 / 18 8.38% 10.77% 10.64% 15.79% 10.23%

Consistently across Staffordshire, (in line with national benchmarks) older people, > 65, account for the majority of general hospital users (65%); frail older people in the acute care setting represent a low volume, high impact group; they have the longest length of stay, the highest rate of inpatient complications and subsequent re-admissions2. At any one time, patients in this group account for 70% of bed days. Commissioners are responding to the concept of frailty as a determinant in the management of older people and in particular, for many older people, a stay in hospital is disempowering: the environment itself, the noise, and the routines on the wards overwhelm and undermine them in ways that affect their ability to recover who they were and how they were living before they were admitted3.
The table below illustrates A&E Attendance projections by age band (based on ONS population projections and modelled A&E attendance patterns).
Year 75-79
Forecast 80-84 Forecast 85-89 Forecast 90+ Forecast Total
2014/15 25,453 24,096 19,598 13,383 82,530 2015/16 25,862 24,776 20,265 14,188 85,091 2016/17 26,497 25,640 21,016 14,792 87,945 2017/18 27,586 26,691 21,683 15,496 91,456
% change by 17 / 18 8.38% 10.77% 10.64% 15.79% 10.82% The table below illustrates A&E Admission projections by age band (based on ONS population projections and modelled A&E admission patterns). Frailty: While commissioners agree that frailty is a state of vulnerability resulting from the cumulative decline in physiological systems which occurs progressively over a lifetime there is currently no County wide shared definition of frailty and no single frailty index is applied. However, in the work to date the following characteristics are referenced by Commissioners as factors:
i. Usually, but not exclusively, Commissioners reference frailty linked to older age; ii. Commissioners generally agree the person will have two or more long term conditions;
iii. It is consistent that Commissioners mean the person has no functional reserve (ie: no physical capacity to endure a further incidence of ill health);
iv. Polypharmacy is commonly associated with frailty by Commissioners;
2 Age and Ageing, BGS (2011) 3 Kings Fund – Continuity of Care for Older Hospital Patients March 2012
Year 75-79
Forecast 80-84 Forecast 85-89 Forecast 90+ Forecast Total
2014/15 15,162 16,151 14,349 10,317 55,979 2015/16 15,405 16,607 14,838 10,938 57,788 2016/17 15,783 17,187 15,387 11,403 59,760 2017/18 16,432 17,891 15,876 11,946 62,145
% change by 17 / 18 8.38% 10.77% 10.64% 15.79% 11.01%

v. Commissioners expect frail persons will either have higher levels of social care input to support them in their own home or be resident in a Care Home (Residential or Nursing);
vi. It is anticipated by Commissioners that frail persons are likely to have or be at great risk of developing dementia; and
vii. All Commissioners assume that once frail patients decompensate if they develop a further complication/illness they decompensate further very quickly.
National evidence suggests that up to one quarter of hospital beds are occupied by people with dementia4. Across the County, those patients with dementia, or who display symptoms or behaviours associated with dementia, stay in hospital longer (often with multiple transfers of their care) than other people for the same procedures. In recent years practice across the County, by all Commissioners, has been reactive to system pressures which has led to “silo” interventions and fragmented pathways from crisis responses to need through to meeting long term health and social care needs in primary care and eventually end of life and palliative care needs. All Commissioners identify, at a local level, the vital importance of commissioning integrated services that allows for the management of people before their needs escalate, to respond to their needs in an anticipated and planned way, reducing the need for expensive crisis responses and unscheduled care. In addition, Commissioners recognise there is a disconnect between the delivery of health and social care services and wider well-being support with inconsistent and sometimes limited community and volunteer involvement and the use of community social capital or community assets with varied and inconsistent approaches to the involvement of carers. Custom and practice has become to respond to the needs of frail older people and patients in a reactive way through structured services and programmes where these exist with an emphasis on managing people through the system rather than being person centred wrapping responsive services around individuals in anticipation of their needs. Consistently in their local plans and statements of intent, Commissioners focus on areas where they identify the need for change: improvement in the model of care and the management of patients; improving the patient / user experience; reducing transfers of care within and between organisations and where possible eliminating the
need for transfers of care completely; more and better joint and integrated working between health, social care and mental health
services; better and timely information sharing between those involved in a person’s care including the
sharing of information with people themselves and importantly their carers; planned and “in time” care co-ordination with simplification of what are often complex and
involved patient management processes; establish the utilisation of Technology Enhanced Care Services (TECS) to support people in their
self-management and to support clinicians / professionals in securing health and social care outcomes; and
access to intermediate community-based services as an alternative to acute hospital attendances and acute hospital admission.
4 Commission on Improving Dignity in Care for Older People (2011)

Vision:
That the people of Staffordshire have access to and benefit from a coherent integrated model of care that is consistently available across the County while being locally responsive to the needs of communities and individuals.
The HE are determined that in pursuit of the vision and the coherent model of care there will be latitude for innovation at a local level where this builds the local capacity to deliver services effectively within financial and other resource constraints. The vision reinforces the HE common goals of securing true integration in the delivery of all care including social care and mental health, promoting independence, preventing avoidable admissions, supporting individuals to manage crises in their health and wellbeing, securing the right care in the right place for the individual at the appropriate level of care while enabling people to live well, live independently and live confidently. HE Commissioners are determined to realise a vibrant participation of the third sector and community and voluntary organisations and importantly to recognise and nurture the valuable contribution made by family and carers. The Fundamentals of Elderly Care: Before stating the Commissioner shared fundamentals of elderly care, this strategy builds on an underpinning set of principles integral to all HE Commissioners – the HE are committed to the NHS England mission of high quality care for all; that Commissioners are striving for parity for mental health; and that the Commissioners respond to and seek to promulgate the best practice guidance from the Royal College of Physicians, the British Geriatrics Society and Kings Fund. Fundamental 1: Elderly Care should be a whole system approach where all elements of the
system link by design and work together to proactively support the patient anticipating, planning and delivering for their needs;
Fundamental 2: There should be timely, proportionate and appropriate communication
between all those involved in a person’s care and support that always engages the person and their carer(s) where the ability to provide for excellence in a person’s care is enabled by access to information;
Fundamental 3: That irrespective of where people present in the system, they have access to
an appropriate and rigorous assessment of their needs, that this assessment is trusted and informs the diagnosis of their health, social care and wider well-being needs and that they are able to access treatment and care services in the setting appropriate to their assessed needs promptly without unnecessary transfers of their care and without unnecessary admission to hospital;
Fundamental 4: That the quality of care received and the experience of individuals should
not be adversely affected by where they normally reside, the time their care is needed, the place where their care is delivered, or by the person or organisation delivering their care;
Fundamental 5; There is a requirement for case finding and case management that navigates
people through to the services they need that leads to achievement of

outcomes, these outcomes being determined by screening and assessment processes that inform the care plan and the actions taken to deliver care;
Fundamental 6: An emphasis on prevention and support for living well, including after
episodes of illness or where an individual’s well-being has been compromised, is essential and at all times individuals should be supported to achieve optimal recovery, their best level of reablement, rehabilitation, and confidence; and
Fundamental 7: Preserving dignity, respect and privacy for all must be at the heart of our
model of care and by design we should eliminate health inequalities.
While not a fundamental, the HE believe that under this strategy they should centralise where possible and localise where necessary – this reflects wider ambitions to commission care and other services that reflect the specific needs of local populations and that routine health and social care should take place in the home or as close to home as possible recognising that where necessary care will be delivered in acute and community hospitals and other centres.
Our objectives:
Through consistent commissioning across the County, and where appropriate the wider operating footprints of the individual CCGs, the CCGs and their associate commissioners will:
Focus on prevention and have as a priority supporting older people to live well where there are accessible opportunities for the health and wellbeing of older people to be sustained;
Drive a culture change that delivers individual independence where people (and the important people in their lives and their living arrangements) are able, confident and empowered to participate in their self-care, where they are able to make informed decisions on their care and the first response to their needs;
Focus on design and delivery of services that support and add value to patient care from General Practice and Primary Care that utilises community and acute provision effectively under an integrated continuum of care;
Secure better anticipatory and preventative care that focusses on the needs of the individual where the person is involved in the assessment of their need and the putting in place of a care plan;
Develop innovative and robust approaches to risk stratification and case finding that leads to the effective objective based case management of people and health and social care case management with purpose;
Build the capacity of local practitioners at all levels so that they respond confidently and appropriately to the needs of local people on a day to day basis and at times of crisis or uncertainty;
Ensure that information, necessary so that practitioners can deliver integrated services to people and patients, is available and accessible at any and all times that interventions or actions with individuals are being planned, reviewed or delivered;
Drive for single trusted assessments of an individual’s needs that inform a single care plan which patients and their carers have ownership of and to which the individual can allow access to practitioners involved in their care and wellbeing;

Provide for co-ordination of services and support patient and person navigation through to services that meet their needs so that care is delivered in the right place, at the right time, by the person best able to meet their needs;
Ensure that older people who present to services (in primary care, community or acute settings) have speedy access to comprehensive geriatric assessment as an integral part of a whole assessment of their needs;
Provide for the prompt assessment of the needs of frail older people who present in acute settings so that patients can step down or step across to appropriate services as an alternative to admission or, if admission is necessary, patients are managed effectively under an informed care plan, improving health outcomes, supporting independence and minimising length of stay;
Improve medicines management for older people at home, in homes, in community services, under intermediate care or in acute settings so that unnecessary or inappropriate prescribing is avoided;
By design, integrate mental health care into all services and facilities so that the needs of individuals, and in particular frail older people, with dementia and other age related conditions are accounted for and met;
Provide pathways of care that are simple and unambiguous and provide clarity that individuals will receive appropriate, proportionate and responsive services that ensure safe care in the most appropriate setting without unnecessary delays, transfers of care or unnecessary admission to hospital;
Ensure that older people and in particular frail older people stay in an acute hospital only when they are acutely ill and require treatment or interventions or a level of specialist care or rehabilitation that can only be provided in the acute setting;
Ensure that older people and in particular frail older people stay in a rehabilitation, recovery or reablement setting only when they continue to benefit and require treatment or interventions or a level of specialist care or therapy that can only be provided in these settings;
Ensure that older people who reside in homes benefit from health and social care equality and incentivise homes to follow pathways of care and to participate in meeting the needs of individuals at home, or in the most appropriate setting without unnecessary delays, transfers of care or unnecessary admission to hospital; and
Encourage and enable use of Technology Enhanced Care Services through wider adoption of assistive technology, telecare and telehealth.
The Continuum of Care:
The HE are committed to ensuring a continuum of care that focusses on the needs of individuals and takes account of the circumstances of the individual and their degree of vulnerability so that the best care is provided at the right time, in the right place by those best equipped to meet the person’s needs where the intent is to respond to the acuity of the person supporting their independence and optimal recovery.
Under the prevention and self-care elements of this strategy there will be specific cross over to the local Long Term Conditions work stream, the staying healthy and active work stream and the urgent care work stream of the HE. There will be a local emphasis on engaging, mobilising and working in partnership with the 3rd Sector and Local Authorities (including but not limited to the Better Care Fund) to develop local models of support that allow older people, particularly those with high

support needs, live well and to live confidently in later life. Evidence shows these models are greatly valued by communities and achieve significant outcomes for individuals particularly when they link to other services.
The continuum of care assumes a vital role for carers so there will be a cross over with local carer strategies where the emphasis will be on supporting carers to keep well themselves.
The HE will promote interactions between clinicians and practitioners along the continuum of care as a vehicle for continuous improvement, personal and organisational development and to encourage better networking, care planning and exchange of information leading to an improved patient experience and better patient outcomes. The important place of information across the continuum is recognised and the HE will continue to search for the effective sharing of records, real time communication between primary, secondary, community and mental health including with equal standing local authority services (particularly social care) and the 3rd Sector.
As individuals move through the continuum of care access to specialist and consultant medical input, senior clinical input, and specialist service practitioners needs to be assured.
The Continuum of Care
Prevention
Empowering Self-Care
and Education
Support at
Home
Enhanced Services at Home
Managed crisis and planned
responses to need
Step Up
Acute services including admission
where necessary
Manage Discharge effectively avoiding
readmissions
Step Down
Enhanced Services at Home
Support at
Home
Empowering Self-Care
and Education
Community and
Voluntary Sector
support
An integrated delivery system involving public health, community and voluntary sector, primary care, community service, acute and secondary care services and the patient .
The outcomes under this strategy:
The outcomes are based on securing improvements in the commissioning of health care of elderly people generally and specifically for those with complex requirements. In delivering these outcomes the CCGs will: Establish and embed relationships between the CCGs and their associated commissioners in
health, social care and third sector services for frail older populations; Ensure consistency of services across the County, demand equality of access for all communities,
and coherent local delivery of the continuum of care; and Ensure joint working including shared commissioning. The CCGs agree that effective care for frail people with complex needs demands integrated and coordinated patient-centred journeys which; building on the core care provided by General Practice and Primary Care; recognise and respond to the scope and complexity of need, are proactive whenever possible, are promptly reactive whenever necessary, maximise continuity of care and minimise sudden or unplanned transitions of care, particularly towards the end of life. Strategy into deliverables / what success will look like: Non-elective admissions of people identified as frail older people not to exceed XXXX in a stated
year; or Non-elective admissions of people identified as frail older people to be in line with Better Care
Fund plans;

Number of GP led intermediate care based episodes of care for frail older people not to be less than XXXXX; or
Number of GP led intermediate care based episodes of care for frail older people to increase by Y%;
100% of frail older people under an integrated single care plan will benefit from care navigation and care co-ordination;
Number of integrated single care plans that have an active and sustained contribution from a community and voluntary sector organisation not be less than XXXX or Y% of all plans;
Number of referrals to acute settings of frail older people from homes not to exceed XXXXX; or Number of referrals to acute settings of frail older people from homes to reduce by Y%; XX% of Older people and / or their carers are able to discuss how their care is organised and the
actions they are taking or their contribution under the integrated single care plan; XX% of older people and / or their carers are able to name the key clinician involved in their care
and where applicable how to contact their care co-ordinator or navigator; XX% of GPs confirm there is an accessible comprehensive geriatric assessment process which
informs health and social care planning and supports excellence in the delivery of care; 100% of all single integrated care plans include an assessment of the mental health needs of
patients and state the actions under the care plan and anticipate the outcomes to be delivered by the care provided;
Care is co-ordinated through a single care plan that anticipates patient need and eliminates the necessity for patient transfers throughout the episode of care;
There are no incidents of breakdowns in communication between clinicians and practitioners involved in care such that patients and / or carers report that on all occasions care has been discussed or required there has been access to the current and up to date version of their single integrated care plan;
100% of patient or service user and their families and carers report they have been engaged (appropriately and consistently) in the setting and agreement of their care plan, this will include offering patients the opportunity to be involved in advance care planning supported by skilled practitioners;
XX% of patients or users under the service confirm that, where they can make a judgement, they received care that met their needs, delivered at their home when it was appropriate to do so and that patients stepped up into other services as their needs required it;
XX% of patients beginning inpatient stays, in any setting, have their discharge organised within YY hours of admission (engaging General Practice and the wider Primary Care team) so that patients can step down at the first opportunity delivering the shortest length of stay needed by the individual patient and in line with their individual needs;
Discharge planning and the continuation of care post discharge will ensure that patients achieve their expected health outcomes such that any re-admission to a bed based service is a cause for concern and a driver for continuous improvement so all re-admissions within 14 days will be subject to a root cause analysis (RCA);
Timely and informed diagnosis and assessment (starting within 1 hour of attendance) allows and enables utilisation of local services directly from emergency portals;
Following any episode of care, through any combination of services, XX% of beneficiaries and / or their carers report they have achieved an acceptable return to wellbeing;
Following any episode of care, through any combination of services, XX% of care practitioners suggest that beneficiaries have achieved an acceptable return to their normal state or have secured optimal recovery;
End of Life care will be anticipated and planned for, such that 100% of patients receive high quality co-ordinated end of life care;
XX% of patients will be supported to die in their place of choice; and
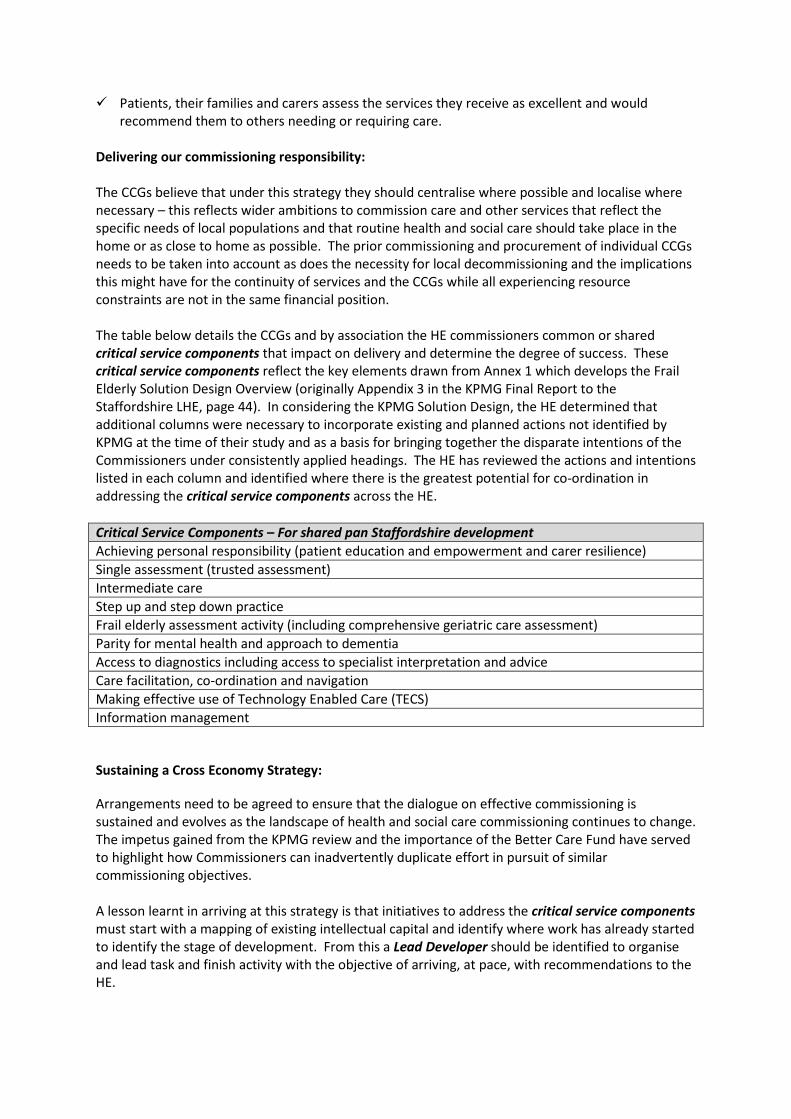
Patients, their families and carers assess the services they receive as excellent and would recommend them to others needing or requiring care.
Delivering our commissioning responsibility: The CCGs believe that under this strategy they should centralise where possible and localise where necessary – this reflects wider ambitions to commission care and other services that reflect the specific needs of local populations and that routine health and social care should take place in the home or as close to home as possible. The prior commissioning and procurement of individual CCGs needs to be taken into account as does the necessity for local decommissioning and the implications this might have for the continuity of services and the CCGs while all experiencing resource constraints are not in the same financial position. The table below details the CCGs and by association the HE commissioners common or shared critical service components that impact on delivery and determine the degree of success. These critical service components reflect the key elements drawn from Annex 1 which develops the Frail Elderly Solution Design Overview (originally Appendix 3 in the KPMG Final Report to the Staffordshire LHE, page 44). In considering the KPMG Solution Design, the HE determined that additional columns were necessary to incorporate existing and planned actions not identified by KPMG at the time of their study and as a basis for bringing together the disparate intentions of the Commissioners under consistently applied headings. The HE has reviewed the actions and intentions listed in each column and identified where there is the greatest potential for co-ordination in addressing the critical service components across the HE. Critical Service Components – For shared pan Staffordshire development Achieving personal responsibility (patient education and empowerment and carer resilience) Single assessment (trusted assessment) Intermediate care Step up and step down practice Frail elderly assessment activity (including comprehensive geriatric care assessment) Parity for mental health and approach to dementia Access to diagnostics including access to specialist interpretation and advice Care facilitation, co-ordination and navigation Making effective use of Technology Enabled Care (TECS) Information management
Sustaining a Cross Economy Strategy:
Arrangements need to be agreed to ensure that the dialogue on effective commissioning is sustained and evolves as the landscape of health and social care commissioning continues to change. The impetus gained from the KPMG review and the importance of the Better Care Fund have served to highlight how Commissioners can inadvertently duplicate effort in pursuit of similar commissioning objectives. A lesson learnt in arriving at this strategy is that initiatives to address the critical service components must start with a mapping of existing intellectual capital and identify where work has already started to identify the stage of development. From this a Lead Developer should be identified to organise and lead task and finish activity with the objective of arriving, at pace, with recommendations to the HE.

All recommendations should be underpinned with an appropriate level of service design and indicative specifications from which pan Staffordshire and where appropriate localised commissioning decisions can made. Lead Commissioner and other arrangements should respond to the recommendations. Throughout, there should be proportionate commissioner participation in support of the Lead Developer where the HE commits its intellectual property and knowledge to ensure that the best solutions possible are proposed. This should ensure first a robust and inclusive development process and second deliver ownership of the outcome at an individual commissioner level. Oversight arrangements will be necessary, these should however be aligned with or take account of: • Priorities established by Health and Wellbeing Boards; • The integrated work stream arrangements of the HE Commissioners (driven by Better Care
Fund); • Existing Cross Economy Strategic Leadership arrangements - such as Accountable Officer and
COO forums and CELG (it is recognised these arrangements are being reviewed); • Clinical Senate, Clinical Forums and Clinical Network arrangements (eg Star Chamber established
in Northern Staffordshire) as proportionate clinical representation in the oversight arrangements will be required; and
• Economic imperatives driving the necessity for system wide QIPP and efficiency gains. Lead Developers should carry responsibility for reporting to all HE Commissioners (through the COO forums and cross economy arrangements) and should expect to support individual Commissioners through their individual decision making and governance processes.
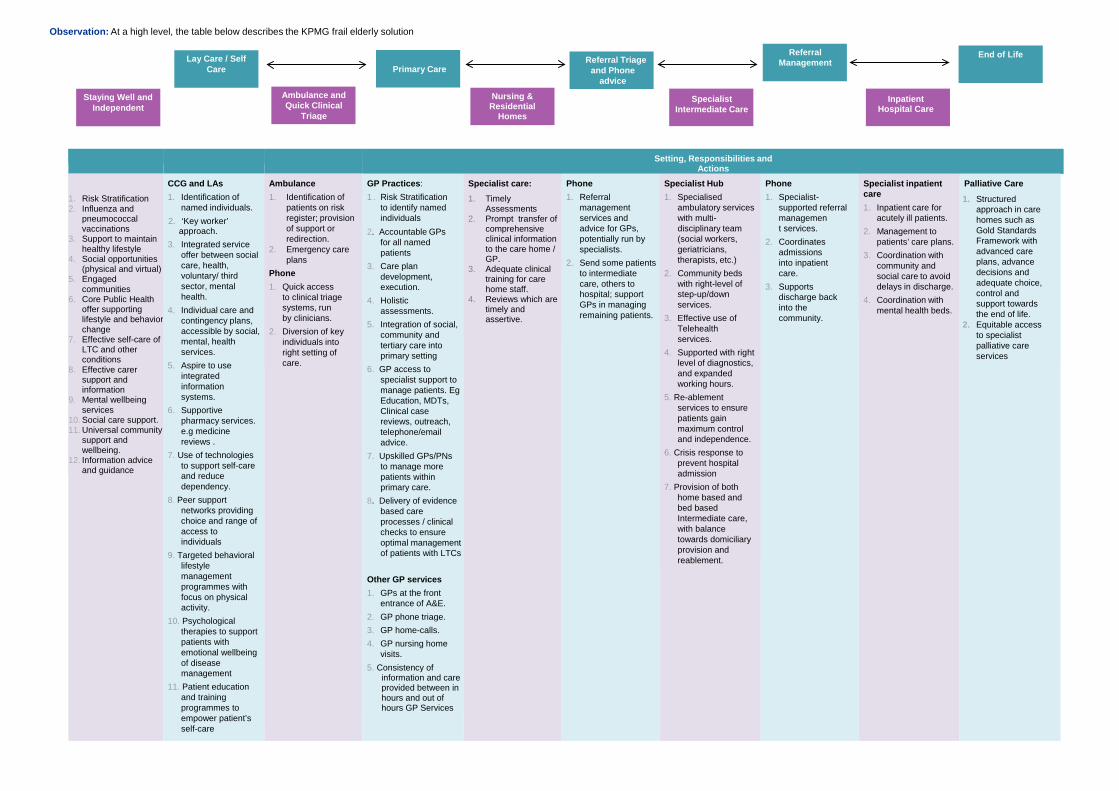
Lay Care / Self Care Primary Care
Specialist Intermediate Care
Inpatient Hospital Care
Ambulance and Quick Clinical
Triage
Nursing & Residential
Homes
Referral Management
End of Life Referral Triage and Phone
advice
Observation: At a high level, the table below describes the KPMG frail elderly solution
Setting, Responsibilities and Actions
1. Risk Stratification 2. Influenza and
pneumococcal vaccinations
3. Support to maintain healthy lifestyle
4. Social opportunities (physical and virtual)
5. Engaged communities
6. Core Public Health offer supporting lifestyle and behavior change
7. Effective self-care of LTC and other conditions
8. Effective carer support and information
9. Mental wellbeing services
10. Social care support. 11. Universal community
support and wellbeing.
12. Information advice and guidance
CCG and LAs 1. Identification of
named individuals. 2. ‘Key worker’
approach. 3. Integrated service
offer between social care, health, voluntary/ third sector, mental health.
4. Individual care and contingency plans, accessible by social, mental, health services.
5. Aspire to use integrated information systems.
6. Supportive pharmacy services. e.g medicine reviews .
7. Use of technologies to support self-care and reduce dependency.
8. Peer support networks providing choice and range of access to individuals
9. Targeted behavioral lifestyle management programmes with focus on physical activity.
10. Psychological therapies to support patients with emotional wellbeing of disease management
11. Patient education and training programmes to empower patient’s self-care
Ambulance 1. Identification of
patients on risk register; provision of support or redirection.
2. Emergency care plans
Phone 1. Quick access
to clinical triage systems, run by clinicians.
2. Diversion of key individuals into right setting of care.
GP Practices: 1 . Risk Stratification
to identify named individuals
2. Accountable GPs for all named patients
3. Care plan development, execution.
4. Holistic assessments.
5. Integration of social, community and tertiary care into primary setting
6. GP access to specialist support to manage patients. Eg Education, MDTs, Clinical case reviews, outreach, telephone/email advice.
7. Upskilled GPs/PNs to manage more patients within primary care.
8. Delivery of evidence based care processes / clinical checks to ensure optimal management of patients with LTCs
Other GP services 1. GPs at the front
entrance of A&E. 2. GP phone triage. 3. GP home-calls. 4. GP nursing home
visits. 5. Consistency of
information and care provided between in hours and out of hours GP Services
Specialist care: 1. Timely
Assessments 2. Prompt transfer of
comprehensive clinical information to the care home / GP.
3. Adequate clinical training for care home staff.
4. Reviews which are timely and assertive.
Phone 1. Referral
management services and advice for GPs, potentially run by specialists.
2. Send some patients to intermediate care, others to hospital; support GPs in managing remaining patients.
Specialist Hub 1. Specialised
ambulatory services with multi- disciplinary team (social workers, geriatricians, therapists, etc.)
2. Community beds with right-level of step-up/down services.
3. Effective use of Telehealth services.
4. Supported with right level of diagnostics, and expanded working hours.
5. Re-ablement services to ensure patients gain maximum control and independence.
6. Crisis response to prevent hospital admission
7. Provision of both home based and bed based Intermediate care, with balance towards domiciliary provision and reablement.
Phone 1. Specialist-
supported referral management services.
2. Coordinates admissions into inpatient care.
3. Supports discharge back into the community.
Specialist inpatient care 1. Inpatient care for
acutely ill patients. 2. Management to
patients’ care plans. 3. Coordination with
community and social care to avoid delays in discharge.
4. Coordination with mental health beds.
Palliative Care
1. Structured approach in care homes such as Gold Standards Framework with advanced care plans, advance decisions and adequate choice, control and support towards the end of life.
2. Equitable access to specialist palliative care services
Staying Well and Independent

. 12. Supporting
anticipatory planning to scenario plan events and responses
13. Ongoing support and liaison services and crisis support
14. Default choice of control, offering DPs, PBs and PHBs.
15. Commission in partnership for shared outcomes.

Lay Care / Self Care Primary Care
Specialist Intermediate Care
Inpatient Hospital Care
Ambulance and Quick Clinical
Triage
Nursing & Residential
Homes
Referral Management
End of Life Referral Triage and Phone
advice
Observation: At a high level, the table below describes the KPMG frail elderly solution
Setting, Responsibilities and Actions
1. Risk Stratification 2. Influenza and
pneumococcal vaccinations
3. Support to maintain healthy lifestyle
4. Social opportunities (physical and virtual)
5. Engaged communities
6. Core Public Health offer supporting lifestyle and behavior change
7. Effective self-care of LTC and other conditions
8. Effective carer support and information
9. Mental wellbeing services
10. Social care support. 11. Universal community
support and wellbeing.
12. Information advice and guidance
CCG and LAs 1. Identification of
named individuals. 2. ‘Key worker’
approach. 3. Integrated service
offer between social care, health, voluntary/ third sector, mental health.
4. Individual care and contingency plans, accessible by social, mental, health services.
5. Aspire to use integrated information systems.
6. Supportive pharmacy services. e.g. medicine reviews.
7. Use of technologies to support self-care and reduce dependency.
8. Peer support networks providing choice and range of access to individuals
9. Targeted behavioral lifestyle management programmes with focus on physical activity.
10. Psychological therapies to support patients with emotional wellbeing of disease management
11. Patient education and training programmes to empower patient’s self-care
Ambulance 1. Identification of
patients on risk register; provision of support or redirection.
2. Emergency care plans
Phone 1. Quick access
to clinical triage systems, run by clinicians.
2. Diversion of key individuals into right setting of care.
CCG and LAs (cont.) 12. Supporting
anticipatory planning to scenario plan events and responses
13. Ongoing support and liaison services and crisis support
14. Default choice of control, offering DPs, PBs and PHBs.
15. Commission in partnership for shared outcomes.
GP Practices: 1 . Risk Stratification
to identify named individuals
2. Accountable GPs for all named patients
3. Care plan development, execution.
4. Holistic assessments.
5. Integration of social, community and tertiary care into primary setting
6. GP access to specialist support to manage patients. E.g. Education, MDTs, Clinical case reviews, outreach, telephone/email advice.
7. Upskilled GPs/PNs to manage more patients within primary care.
8. Delivery of evidence based care processes / clinical checks to ensure optimal management of patients with LTCs
Other GP services 1. GPs at the front
entrance of A&E. 2. GP phone triage. 3. GP home-calls. 4. GP nursing home
visits. 5. Consistency of
information and care provided between in hours and out of hours GP Services
Specialist care: 1. Timely
Assessments 2. Prompt transfer of
comprehensive clinical information to the care home / GP.
3. Adequate clinical training for care home staff.
4. Reviews which are timely and assertive.
Phone 1. Referral
management services and advice for GPs potentially run by specialists.
2. Send some patients to intermediate care, others to hospital; support GPs in managing remaining patients.
Specialist Hub 1. Specialised
ambulatory services with multi- disciplinary team (social workers, geriatricians, therapists, etc.)
2. Community beds with right-level of step-up/down services.
3. Effective use of Telehealth services.
4. Supported with right level of diagnostics, and expanded working hours.
5. Re-ablement services to ensure patients gain maximum control and independence.
6. Crisis response to prevent hospital admission
7. Provision of both home based and bed based Intermediate care, with balance towards domiciliary provision and reablement.
Phone 1. Specialist-supported
referral Management services.
2. Coordinates admissions into inpatient care.
3. Supports discharge back into the community.
Specialist inpatient care 1. Inpatient care for
acutely ill patients.
2. Management to patients’ care plans.
3. Coordination with community and social care to avoid delays in discharge.
4. Coordination with mental health beds.
Palliative Care
1. Structured approach in care homes such as Gold Standards Framework with advanced care plans, advance decisions and adequate choice, control and support towards the end of life.
2. Equitable access to specialist palliative care services
Staying Well and Independent

Title The Technology Enabled Care Services (TECS) Strategy for Staffordshire and Stoke-on-Trent
Reporting to Governing Body Date of Meeting 27th November 2014
Commissioning Lead(s) Author(s) Nicola Harkness/Dave Whatton Dave Whatton
Purpose of the Report (Please select) Approval Assurance Discussion
Key Points/Executive Summary The Governing Body are requested to agree the goals and approach to delivery of those goals detailed in the summary document accompanying this paper and reproduced below.
The Technology Enabled Care Services (TECS) Board for Staffordshire and Stoke-on-Trent is a partnership between Providers, NHS CCG commissioners and Social Care representatives. The TECS strategy is a collaborative approach designed to make the best use of TECS to support people and their carers by giving patients and families the confidence and support to maximise their control of their health conditions. It outlines the strategic direction for Staffordshire and Stoke-on-Trent and recognizes the benefits of an integrated approach to implementation at scale and pace.
TECS support our CCG goals and in particular, aligns with the Improving Lives programme aimed to support people at the lowest point of dependency. We can build TECS into the increased adoption of personal health and care budgets to improve person centred outcomes and support self-care.
The attached summary document provides a high level description of a strategy to deliver, promote and expand Technology Enabled Care Services in Staffordshire & Stoke-on-Trent. It provides a mechanism for TECS Board member organisations to commit to a set of TECS related goals and an approach to their delivery. It should be noted that the role of the TECS Board in the delivery of the TECS Strategy is one not of governance but of guidance, co-ordination, awareness raising and support.
The summary document calls for formal adoption by each member organisation of both the proposed goals and approach to achieving them;
The key goals that the TECS Strategy aims to achieve are:
1. Optimise the appropriate use of technology to support self-management by patients, service users and the general public in order both to improve outcomes and prevent or
X
Enc. 9
Author: Dave Whatton Date: 17/11/2014 East Staffs CCG

delay deterioration in condition, and to reduce service delivery costs across the economy.
2. Support the delivery of efficient, effective and productive remote care, and facilitate integrated care delivery.
3. Minimise cost and complexity for users and service providers across the economy by establishing a strategic direction for and, where possible implementing, common or interoperable technology for specific relevant functions.
In order to support delivery of the agreed goals, TECS Board member organisations will:
1. Ensure that they and their staff understand the benefits and implications of the technologies in scope that are relevant to them and the services that they provide
2. Take these technologies into account when reviewing/designing services and integrate/implement them wherever feasible
3. Share best practice across member organisations
4. Share the TECS related elements of their organisation strategy with other members
5. Adopt an approach to branding TECS within their organisation and target population that is consistent across member organisations and avoids confusing people with different names / labels for the same thing.
6. Ensure that all relevant parts of their organisation are aware of the TECS Strategy and the role of the TECS Board in helping to deliver it
7. Raise awareness of appropriate technology in their target populations
8. Encourage a culture of appropriate technology exploitation within their staff and include an appropriate focus on TECS in workforce development and training
9. Agree, across the economy, target technologies that would benefit from strategic direction, agree that strategic direction and, wherever feasible, take decisions aligned with that direction
10. Where appropriate and relevant, collaborate on and provide resource to joint projects with other member organisations
11. Provide information to support effective measurement of the benefits of the strategy and evaluation of TECS delivery
Recommendations (what is expected from the Board) The Governing Body are requested to agree the goals and approach to delivery of those goals detailed above.
Enclosures 1. A Strategy to support TECS in Staffordshire & Stoke-on-Trent - Summary
2. A Strategy to support TECS in Staffordshire & Stoke-on-Trent - Context, Background and Vision
Author: Dave Whatton Date: 17/11/2014 East Staffs CCG
A Strategy to support
Technology Enabled Care Services
in
Staffordshire & Stoke-on-Trent
Context, Background and Vision Version 1.0
01.10.14
Page 1 of 38

Effective Date: 01.10.14
Version No. Effective Date Summary of Significant Changes Previous
Version no.
1.0 01.10.14 Initial draft for development and feedback n/a
Page 2 of 38

CONTENTS
1 FOREWORD 5
2 INTRODUCTION & BACKGROUND 6
3 DEFINITION OF WHAT WE MEAN BY TECHNOLOGY ENABLED CARE SERVICES 6
4 WHY HAVE A TECS STRATEGY FOR STAFFORDSHIRE? 8
5 NATIONAL VISION FOR TECHNOLOGY ENABLED CARE SERVICES INTEGRATED CARE 8
6 VISION STATEMENT FOR TECHNOLOGY ENABLED CARE SERVICES IN STAFFORDSHIRE 9
7 WHAT OUTCOMES IS THE STRATEGY AIMING TO ACHIEVE 9
7.1 To improve access to TECS across Staffordshire & Stoke-0n-Trent for staff and service users 9
7.2 TO DEMONSTRATE a focus on prevention and early intervention 9
7.3 To establish clear process pathways 9
7.4 To facilitate partnerships for effective commissioning 9
7.5 To demonstrate value for money, quality and efficiency 10
8 IDENTIFYING BENEFITS? 11
9 RECOGNISING THE CHALLENGES TO DELIVERY OF A TECS STRATEGY FOR STAFFORDSHIRE & STOKE ON TRENT 13
9.1 Identifying where to start 13
9.2 Identifying Service Users to target using an agreed method of risk stratification and associated assessment 13
9.3 Agreeing technology that’s on offer within Staffordshire and ensure people know where and how to get it 14
9.4 Establish a process to introduce new technologies that are either for testing or deployment. 14
9.5 Measurement of quality & productivity outcomes. 14
10 MAKING IT HAPPEN 15
Page 3 of 38

11 APPENDIXES 16
11.1 Appendix 1 – Summary of National Drivers and key documents supporting TECS 17
11.2 Appendix 2 - Digital health modalities Current Situation in Staffordshire 21
11.3 Appendix 3 – A closer look at the evidence base 31
Page 4 of 38

1 FOREWORD
By Joanne Harding - Associate Director of Transformation & Innovation, Staffordshire & Stoke on Trent Partnership Trust & Jim Ellam - Commissioning Manager & Assistive Technology Project Lead, Staffordshire County Council On behalf of Staffordshire TECS Programme Board
The Technology Enabled Care Services (TECS) Strategy for Staffordshire and Stoke-on-Trent is a collaborative partnership approach to making the best use of TECS to support people and their carers. It outlines the strategic direction for Staffordshire and Stoke-on-Trent and recognizes the benefits of an integrated approach to implementation at scale and pace. The benefits will be for our people, their carers and the partner agencies who will transform services and through integrated investment deliver better outcomes for all. It is applicable to people of all ages and across the spectrum of health and social care needs.
TECS support our goals to reduce admissions and readmissions to hospital and long term care among older people as well as support people of all ages to take greater responsibility for their own health and wellbeing and that of their families. We can build TECS into the increased adoption of personal health and care budgets to improve person centered outcomes and support self-care.
The population we serve is increasingly looking to TECS to support them to better co-ordinate their health, care and wellbeing as part of their everyday lives. TECS will range from simple items that help in everyday tasks to well established TECS such as community alarms and linked tele-care sensors, and will embrace the emerging TECS which are now readily available through mobile phones and the internet.
The adoption of TECS is happening all around us. We know that we are increasingly using technology throughout our lives, whether that be online shopping, internet banking, Skype or FaceTime calls with relatives and friends or using mobile apps to search for information or services. These technologies will support self-care, support carers and help people better manage long term conditions.
As commissioners and providers of services across Staffordshire and Stoke-on-Trent it is paramount that we have an agreed strategic direction and communicate our intentions to support the future of Staffordshire’s health and well-being through a personalised approach
We recognize that as TECS are becoming inexpensive and easily accessible for everyone we must take advantage of that to improve quality and productivity of the services we commission and transform the way we provide advice, care and support to our population.
The Staffordshire and Stoke-on-Trent TECS Board is the structure we have put in place collectively to share developments and agree on strategic intentions regarding recognition of need, commissioning and provision.
This has the advantage of integrated procurement at scale where applicable and will coordinate and register interest for new developments and funding opportunities that support innovation as they
Page 5 of 38

arise. These will harness and utilize the collective skills and expertise within our local health economy.
2 INTRODUCTION & BACKGROUND Technology can play a much bigger part in enabling more convenient, accessible, and better care for individuals, just as it has transformed banking, booking holidays and communicating with smartphones. However, in a fragmented and complex health and social care landscape, we should be mindful of the immense transformational cultural shift this will require. TECS should be seen as an enabler for improvement of health and social care services and within Staffordshire and Stoke on Trent we have the chance to develop an integrated approach to commissioning the right TECS to support the right care in the right place at the right time. Through aligning commissioning intentions, smarter procurement and transforming provider services we can harness TECS to deliver personalized care and support. Through public and community engagement we can understand and support the development of the prevention and self-funded markets for TECS. Staffordshire and Stoke-on-Trent is committed to moving the TECS agenda forward both in terms of infrastructure and interfaces with patients, service users and the public. We are a diverse group of stakeholders including CCG’s, Acute Trusts, Community & Mental Health Providers, Housing, Voluntary Sector Organisations, Local Authorities and patient and carer groups. We are all agreed that TECS is increasingly available; the conundrum we have is understanding the evidence to support particular TECS for specific groups whether they are staff or service users. We need to understand and utilise resources that people already have and consider the best products when supporting self-purchase.
3 DEFINITION OF WHAT WE MEAN BY TECHNOLOGY ENABLED CARE
SERVICES TECS means something different to virtually everyone we speak to and a single clear definition is not easily found. For the purposes of this document we have defined TECS into the five modalities described below:-
TECHNOLOGY ENABLED CARE SERVICE Modality Descriptions
Assistive Technology
Devices designed to support or enable independence for disabled and older people. It acknowledges the cross over between inclusively designed, mainstream products and the technology specifically made available to assist disabled and older people and reflects the wide range of equipment and services that assists older and disabled people to maximise their independence.
Page 6 of 38

TECHNOLOGY ENABLED CARE SERVICE Modality Descriptions
Tele-care
Devices in or away from the home that support independence, and can be used as stand-alone or linked to a support service such as a call centre. Many of these devices relate to social needs in relation to activities of daily living and increasingly can be purchased on the high street and through the internet
Tele-health
Devices used in or away from the home that enable health parameter measurements such as blood pressure, glucose, weight, wound management that supports decision making around personalised care planning and appropriate interventions. Tele-health can be used as stand-alone or linked to a response service. Many devices are now available and can purchased on-line and in the high street
Mobile Apps & online self-management
A growing area of support where people use a mobile device, smartphone or desktop PC to manage their own health and well-being. This area is mainly aimed at self-management and so is most appropriate for the lower levels of need, however increasing use of mobile apps is having an impact in supporting staff and carers in monitoring and care co-ordination
Video Consultations & Tele-Diagnostics
Growing in popularity and relies on infrastructure being available to support, this includes WebEx, FaceTime and Skype. This can be between people patients and staff, groups of people and staff and between staff & staff. All allow a non-face to face consultation that enables decisions to be made without the need for anyone to leave their desk or home. Tele-diagnostics include near patient testing and this needs to be used in selected environments / cohorts. This could be people / carers testing themselves or could be community staff doing testing in the person’s home. These will support working age carers contributing to MDT and linking to those they care for remotely and support peer – peer communication to help reduce isolation and loneliness.
Note: the modalities above overlap. The is especially relevant with regard to ‘Apps and Self-Management’ as other modalities, such as ‘Telecare’ and ‘Telehealth’ may actually be delivered via ‘Apps’, and self-management is also enabled by the other categories above
Page 7 of 38

4 WHY HAVE A TECS STRATEGY FOR STAFFORDSHIRE? Everything we do to support TECS must have a measurable outcome to deliver improved quality and efficiency for the services we collectively commission and provide for the population of Staffordshire & Stoke-on-Trent.
1. To coordinate and communicate the effective and proportional adoption and use of TECS across the local health economy and to encourage and stimulate the self-care market
2. Alignment with the national vision and delivery plan for TECS 3. Agree a broad strategic direction that every organisation can sign up to and use as a
basis for their individual organisation's plans. 4. To encourage joint working and partnerships wherever possible. 5. To build on the existing infrastructure and previous commissioning intentions. 6. To identify economies of scale that all organisations can support in terms of
procurement and interoperability. 7. To support the personalization and transformation of health and social care 8. To provide a consistent approach to raising awareness amongst staff, service users
and the public. 9. To identify workforce requirements and to jointly offer skills and competencies
across all organisations that meet the needs of Staffordshire. 10. To ensure that the strategy is informed by experts by having a clear programme
structure and process by which advisory groups shape strategic direction and local choice.
11. To have a clear process by which all partners can consider the latest evidence and make recommendations for future inclusion in the Staffordshire TECS Programme and to develop and harness the potential of the self-funded market
12. To understand benefits realisation with regard to TECS for Staffordshire and be clear what the benefits are and to who they are applicable in order to inform commissioning plans through shared investment
13. To support a delivery plan that has a regional perspective but that considers local needs
5 NATIONAL VISION FOR TECHNOLOGY ENABLED CARE SERVICES
INTEGRATED CARE The National Vision for TECS
Technology Enabled Care Services are underpinned by the idea of service integration to improve patient care and outcomes. When different services and sectors work together, towards shared goals, patients get far more flexible, better, and more appropriate care. To achieve true service integration, we recognise that this needs to be delivered through a genuine partnership across partner agencies – facilitating collaboration between agencies and professions and empowering people and their carers to better self-manage health and wellbeing with the use of technology.”
Page 8 of 38
The Vision of “Technology Enabled Care Services” being supported by technology is what sits at the core of the Staffordshire TECS Strategy. We recognise the potential of technology to transform tradition al models of care and support and to enable greater self-management of care and to support people and their carers to be as independent as possible.
6 VISION STATEMENT FOR TECHNOLOGY ENABLED CARE SERVICES IN
STAFFORDSHIRE
“People living in Staffordshire and Stoke on Trent will be supported to
manage and improve their health and well-being through Technology Enabled Care Services”
7 WHAT OUTCOMES IS THE STRATEGY AIMING TO ACHIEVE
7.1 TO IMPROVE ACCESS TO TECS ACROSS STAFFORDSHIRE & STOKE-0N-TRENT FOR STAFF AND
SERVICE USERS • So people know where to find out more about TECS and how and where it can be
accessed or purchased To support the self-care agenda – empowering people to exercise choice and control
• So people are able to research and find their own solutions without the need for “specialist” assessment or support.
• Increase in direct purchase/ self-funding of TECS to support independence.
7.2 TO DEMONSTRATE A FOCUS ON PREVENTION AND EARLY INTERVENTION • To reduce the proportion of people who reach a point of crisis that requires emergency
admission to hospital, admission to a care home, or GP call out. • To increase the ability to respond quickly to an emergency or react to deterioration in
health at home. • To open up opportunities for self-purchase by people who have concerns and want to
take early action to monitor changes or protect their independence. • To suport people live as independently as possible and for carers to feel reassured.
7.3 TO ESTABLISH CLEAR PROCESS PATHWAYS • To encourage the health & social care workforce to consider TECS as an integral part of
support planning, not an add-on. • To enable work across traditional agency boundaries, encouraging people to understand
the outcomes required and then consider the most effective way of supporting these.
7.4 TO FACILITATE PARTNERSHIPS FOR EFFECTIVE COMMISSIONING • To create a seamless process for the end user
Page 9 of 38

• To balance the use of TECS resources both to deal appropriately with severe and complex needs, whilst building up the use of resources for preventative purposes in the longer term.
• To support clinicians to proactively manage their caseloads by appropriate introduction of TECS earlier in the care pathway as part of the risk stratification process
• To support use of tele-care and tele-health to more people who are recovering in hospital and can be helped to return home safely, as part of the re-ablement and intermediate care processes.
7.5 TO DEMONSTRATE VALUE FOR MONEY, QUALITY AND EFFICIENCY • To help people maximise their personal budgets and help self-funders get best value. • To better target resources where needed. • To enable the use of tele-care more widely as part of a support package, including those
arranged through a personal care and / or health budget.
Changes to the way TECS are commissioned can release significant efficiencies and improved outcomes from the following sources: 1. Improved use of resources and a more effective service provision, through:
• More people using TECS - Investment will be re-directed towards growing the market, through a try-before-you-buy model, and helping people to find the right digital health solutions for them.
• Increased prevention and early interventions, reducing unplanned hospital admissions and dependency on acute care services.
• Speedier hospital discharges, with TECS aligned to re-ablement through free installation and free service provision for the first 12 weeks.
2. Economies of scale – Overcoming existing problems of a fragmented local market for TECS services.
3. Economies of scope – Pulling together a continuum of TECS into a seamless service offer, irrespective of whether funded by the individual or the public purse.
4. Disinvesting provision where needs are not identified – Thousands of community alarm systems are currently delivered to people who don’t need or want them, with pull-cords are tied up to the ceiling and hard-wired into properties where the tenant is not vulnerable.
5. Technological advances drive productivity – TECS continues to develop at pace, with thousands of new devices coming onto the market every year and, over time, production costs falling. From an organisational perspective, investing in TECS increases speed, frees up valuable time and helps people to have information at their fingertips.
6. Competitive procurement – The majority of contracts have not faced competitive tendering, or been subject to efficiency targets.
7. Opportunities from integration and pooled funding – A joined-up approach which builds on shared processes, avoids duplication and allows commissioners to work towards shared outcomes.
8. Maximise personal contributions – Recognising (i) the efficiencies that arise from consumer driven market forces, where the end users of TECS are best placed to judge what works for them and what offers them best value, and (ii) aside from a statutory duty for care, many people recognise the value of TECS and are willing to self-fun
Page 10 of 38

8 IDENTIFYING BENEFITS? High Level Benefits Matrix
Modality
Stakeholder Group
Patients CCGs
Acute Trusts
Mental Health Trusts
Community Provider
Voluntary Sector
Local Authority GPs
Assistive Technology
Promotes self care, choice and control. Less stigma than state provision. Can offer VFM compared to receiving care and support
Supports self care and support for carers . Earlier awareness of TECS as part of care journey..
Promote self care through A&E ie falls, dementia and carer breakdown
Range of practical, options to support self care and management.
Opportunity to support enablement and rebuild or maintain individuals skills and abilities reducing dependency
Peer endorsement and promotion of self care and management. Carers support.
Information, advice and guidance, promotion of self care and welbeingCan improve levels of self care,
Can help people reduce likelihood of falls, self medicate and maintain food and fluid intake
Tele-care
Greater independence Increased Self-management Supported decision making
Increased self-management and thus reducing demand on services due to earlier intervention
Not usually directly impacting on an acute Trust
Increased ability for patients to stay at home remaining independent Medication reminders are effective in supporting compliance
increased early intervention and support of independence with minimal costs avoiding crisis intervention
Can provide means for engagement and interaction with voluntary sector
Directly reduces need for home visits and can trigger earlier interventions thus avoiding crisis
Reduced interaction with GPs, particularly phone calls or unnecessary GP Visits
Tele-health
Improved experience Early decision making Improved communication Reduced travel Improved access
Reduced utilisation costs in terms GP visits and community care costs Improved medication compliance & associated costs
Reduced admission and length of stay costs
Reduced admissions and length of stay. Reassurance re quality & safety allowing pts to stay at home
Reduced costs in terms of home visits Can aid patient monitoring and increase self-management
Not usually directly impacting engagement with Voluntary sector but can support earlier referral to a voluntary service if required
May result in reduced social care need if health managed holistically
Reduced face to face interaction with GP Increased self management
Mobile apps & Self Management
Education, support & self-management Supported decision making Improved access
increased access to credible advice and so aid decision making Impacts on preventive agenda and long term cost savings Reduces demand
Can reduce follow-ups and support improved interaction Gives greater control and understanding to patients and their families
increased access to support and decision aids Can capture patient data and assure compliance
Aids communication & co-ordination Improves access to community team Can capture patient data
Can provide a “touch” point for the voluntary sector Can provide access to high quality validated information and support when required
Can support navigation of services and signpost to most relevant information
Can give access to credible advice and so aid decision making Can allow capture of patient data
Page 11 of 38

across all sectors
Video consultations & tele-diagnostics
Reduced travel Improved access Improved experience
Reduced costs across all sectors Reduced travel
Reduced admission and length of stay costs Reduced travel
Reduced admissions and length of stay Improved satisfaction & experience
Aids communication & co-ordination Improves access to community team Improved experience Reduced travel requirements
Able to use infrastructure to support patients through support groups Reduced travel
Reduced travel Improved access Improved experience
Improved access Greater no. of consultations Avoid lengthy appointments Reduced travel
Page 12 of 38

9 RECOGNISING THE CHALLENGES TO DELIVERY OF A TECS STRATEGY FOR
STAFFORDSHIRE & STOKE ON TRENT
9.1 IDENTIFYING WHERE TO START Establish what we already have available within each modality across all partner organisations and ensure we are making the most of opportunities already available at minimal costs. Increase awareness of what’s already there and encourage people to use it, across all modalities such as:-
• Staff training and development across public, private and third sector. • Assessment for Technology Enabled Care Services integrated into all care pathways and
commissioning intentions. • Increased use of Tele-care through increased awareness and availability via e-
marketplace and supported by workforce development across the LHE • Embed the proportional use of TECS in all Institutional care setting • Increased use of Simple Tele-health for approved cohorts where we know there are
measureable benefits, publicise the benefits calculator • Expansion of Patient Portal to support self-management and care planning for people
with long Term Conditions, share outcomes of deployments to date • Work with clinicians and people to Idenify and establish Apps that we wish to promote
to population of Staffordshire • Look at other forms of Tele-health that may enable easier monitoring and care co-
ordination for service users, for example WoundSense for patients requiring regular dressings in hospital or the community.
• Identify infrastructure in place for video-consultations and establish clinic operating models across all partner organisations.
• Identify which Tele-diagnostics could and should be used in primary, community and community hospital settings to allow faster decision making and prevent travel costs whilst ensuring increased quality and user experience.
• Continually keeping abreast of emerging technologies and evidence where this is being used and making a difference
9.2 IDENTIFYING SERVICE USERS TO TARGET USING AN AGREED METHOD OF RISK STRATIFICATION AND
ASSOCIATED ASSESSMENT • Identify what method of risk stratification we are going to use and be consistent across
all of Staffordshire. We need to understand need and target initially those service users who are in greatest need; we need an agreed process to do this.
• Understand what are the local trends and opportunities for influencing people who choose to make their own arrangements e.g. through self-funding apps and equipment
Page 13 of 38
9.3 AGREEING TECHNOLOGY THAT’S ON OFFER WITHIN STAFFORDSHIRE AND ENSURE PEOPLE KNOW
WHERE AND HOW TO GET IT • Publish and maintain a menu of what’s available online and ensure it is maintained and
up to date, offering choice to consumers who wish to self-fund and to those that can be offered digital health following referral and assessment
• We need to understand the impact of the care bill and the challenges and opportunities around earlier assessment, improved advice information and guidance to share understanding and access to TECS.
• Establish a marketing campaign for staff, partners and service users – be consistent • Agreeing on an assessment process prior to deployment across all partner organisations • Support people to optimize technology through personal health and social care budgets. • Examine current assessment process, ensure routine consideration for digital
technologies • Agreeing routes to procurement – Identify benefits to each stakeholder and agree
individual costs based on benefits. • Ensuring service users and staff have sufficient skills to utilise technology effectively,
work with partners like libraries to build digital literacy where required • identify skills and competencies required for each modality through a training needs
analysis for service users and carers and staff • Commission the required training • Ensure training is consistent, recurrent and regularly refreshed across all organisations
in a variety of formats
9.4 ESTABLISH A PROCESS TO INTRODUCE NEW TECHNOLOGIES THAT ARE EITHER FOR TESTING OR
DEPLOYMENT. • First - process system that takes best evidence base and looks at potential to adopt and
spread • Second – process system by which new technologies / innovations can be tested within
Staffordshire and look at “fit”with use of existing technologies • Third - consider the use of technology in all settings: community, extra care housing,
hospital and care homes • Ensure we have clear guidance in relation to Information Governance so users and staff
are not confused
9.5 MEASUREMENT OF QUALITY & PRODUCTIVITY OUTCOMES. • Agree a set of quality & productivity measures that can align with the national
requirements but also show value to Staffordshire’s commissioners & providers. • The outcomes we might want to see are:-
Page 14 of 38

o Increase in service user confidence and perception of ability to self-manage
o Increase in contact via digital means with associated less face to face contact
o Increase in improved experience of care o Increase in carers’ perception of support o Decrease in GP Visits o Decrease in out-patient visits o Decrease in emergency calls and associated A&E attendances o Decrease in travel and associated costs
10 MAKING IT HAPPEN In order to deliver the strategy and achieve the vision, we need to:-
1. Define a clear set of outcomes with associated measures 2. Agree an approach to workforce requirements for awareness, education and training 3. Agree clear guidance based on national advice for Information Governance in relation to
TECS
In addition, there are a number of considerations that need to be addressed within the strategy, these include:-
1. Identifying the types of TECS that work and that people want to use. • Initial focus needs to be on the things that can be adopted / expanded at scale at
low costs and utilization of existing services through an integrated approach 2. Identifying the right TECS for the right people at the right time and in the right place
• Using risk stratification and integrating early consideration of the range of technologies within all care pathways
• Working with Hospitals and care homes to manage risks and personalise care delivery
3. Increasing awareness and public understanding and access to TECS • Engagement, marketing and communication. • Demonstration facilities and online resources
4. Increasing staff awareness, understanding and application of TECS • Engagement, marketing and communication. • Performance management to support and manage the consistent adoption of
technology across services. 5. Increasing the knowledge, skills and competencies for staff, service users and the public
to be equipped to use digital health
Page 15 of 38

• Training needs analysis and delivery of training programmes at a number of levels
i. Basis awareness and understanding at induction ii. Generic knowledge, skills and competencies to include digital health
assessment iii. Specific skills and expertise for particular types of digital health
modalities. 6. Changing the perception of the existing and emerging evidence base
• Highlighting innovation, new ways of working and captured benefits realisation. • Gaining recognition for achievements through awards and external funding • Public endorsement from people carers and staff • Performance management to monitor investment in technology against
efficiencies achieved to support service transformation and 7. Service Transformation through use of TECS and supporting a cultural shift within our
services and within our communities.
11 APPENDIXES
Appendix 1 – A summary of National Drivers and key documents supporting TECS
Appendix 2 - Digital health modalities Current Situation in Staffordshire
Appendix 3 – A closer look at the evidence base
Page 16 of 38

11.1 APPENDIX 1 – SUMMARY OF NATIONAL DRIVERS AND KEY DOCUMENTS SUPPORTING TECS In considering national strategic context and strategy, the following national drivers and work programmes have been referenced as they support the digital strategy and partnership working in Staffordshire. Further background and information can be found on the associated url links.
11.1.1 The National Digital Strategy http://digitalhealth.dh.gov.uk/digital-strategy/
Technology and the internet are transforming society. They are changing the way we talk to each other, work with one another and organise our lives. The impact technology can have in healthcare is profound and transformative. More open access to quality data increases our understanding of how diseases develop and spread. Linking data – to industry and research as well as to patients, service users and the public – gives us insight into the whole patient journey, not just isolated episodes of care. Sharing experiences through social channels equips people with information to help them to get the right support or care. Remote diagnosis and surgery are no longer the stuff of science fiction.
11.1.2 Paperless NHS by 2018
http://www.youtube.com/watch?v=p2eiiBujIv4 On the way towards the 2018 goal, the Health Secretary wants to see:
• By March 2015 – everyone who wishes will be able to get online access to their own health records held by their GP.
• Adoption of paperless referrals – instead of sending a letter to the hospital when referring a patient to hospital, the GP can send an email instead.
• Clear plans in place to enable secure linking of these electronic health and care records wherever they are held, so there is as complete a record as possible of the care someone receives.
• Clear plans in place for those records to be able to follow individuals, with their consent, to any part of the NHS or social care system.
• By April 2018 – digital information to be fully available across NHS and social care services, barring any individual opt outs.
Page 17 of 38

11.1.3 Pioneering Integrated Care & Support http://www.nhsiq.nhs.uk/resource-search/publications/integrated-care-leaflet.aspx
https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/198748/DEFINITIVE_FINAL_VERSION_Integrated_Care_and_Support_-_Our_Shared_Commitment_2013-05-13.pdf
Person-centered coordinated care and support is key to improving outcomes for individuals who use health and social care services. Too often, we don’t communicate properly with each other, don’t work together as a team or don’t treat people as whole individuals. As a result, care and support is often fragmented, delayed or duplicated, which can result in missed opportunities to prevent needs from escalating and intervening early. This leads to poorer outcomes and experiences for the people who use our services. Our growing older population, and children and young people with long term and complex conditions, are particularly vulnerable; outside these groups, many more people have physical and mental health needs which mean they need support from their community, be it for housing, help with personal care such as washing and dressing, or companionship. Every time someone has an unplanned trip to hospital, it can reduce his or her capacity to cope independently. People deserve better than this and we all need to play our part in delivering services that are better coordinated around preventing and meeting their needs. Alongside the toughening financial climate, we have no option but to work together, think creatively, and identify new ways of doing more for patients and people who use services, so that every pound spent on care and support counts while we strive to improve outcomes for individuals and local communities.
11.1.4 Digital First http://digital.innovation.nhs.uk/pg/dashboard
Digital first (formerly Digital by default) is a Department of Health initiative which aims to reduce unnecessary face-to-face contact between patients and healthcare professionals by incorporating technology into these interactions. By ‘unnecessary’ we mean, for example, attending a hospital or GP appointment to receive a test result that says everything is OK; or a visit to an outpatient clinic or GP surgery for something that could be discussed on the phone or via email or SKYPE. Digital first is not about replacing doctors or nurses with technology. Patients will still be able to get an appointment with a doctor or a healthcare professional if they choose to. Instead, it is about using technology in healthcare where it can deliver the same high standards in a way that is more flexible and convenient for patients, and at a lower cost.
11.1.5 Technology Enabled Care Services (previously known as 3MillionLives) http://3millionlives.co.uk/
http://www.england.nhs.uk/2013/11/15/new-tech-imprv-hlt-serv/
Page 18 of 38
http://3millionlives.co.uk/about-3ml#3millionlives_-_nhs_england_vision_statement
3millionlives is underpinned by the idea of service integration to improve patient care and outcomes. When different services and sectors work together, towards shared goals, patients get far more flexible, better, and more appropriate care. To achieve true service integration, we recognise that 3millionlives needs to be delivered through a genuine partnership across NHS England – facilitating collaboration between clinicians, and empowering patients to better self-manage their conditions, with the use of technology. We also recognise that this cannot be achieved through technology alone – the key will be to deliver service transformation through realising the potential of that technology to support clinicians, patients and carers. Under the overall leadership of NHS England Medical Directorate, 3millionlives will be delivered going forward by combining clinical advocacy, service improvement and technology strategy – making it a true partnership and synergy within NHS England. We are committed to the delivery and success of 3millionlives, and we are confident that this approach will put 3millionlives right at the heart of our ambition to deliver High Quality Care for All.
11.1.6 The NHS Mandate https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/256497/13-15_mandate.pdf
The NHSE Mandate Section 2.6 (November 2013) states that:
In a digital age, it is crucial that the NHS not only operates at the limits of medical science, but also increasingly at the forefront of new technologies. The Board’s objective is to achieve a significant increase in the use a wide range of technology to help people manage their health and care. In particular, the Government expects that by March 2015:
o everyone who wishes will be able to get online access to their own health records held by their GP. The Board should promote the implementation of electronic records in all health and care settings and should work with relevant organisations to set national information standards to support integration;
o clear plans will be in place to enable secure linking of these electronic health and care records wherever they are held, so there is as complete a record as possible of the care someone receives;
o clear plans will be in place for those records to be able to follow individuals, with their consent, to any part of the NHS or social care system;
o everyone will be able to book GP appointments and order repeat prescriptions online;
o everyone will be able to have secure electronic communication with their GP practice, with the option of e-consultations becoming much more widely available;
o Significant progress will be made towards three million people with long-term conditions being able to benefit from tele-health and tele-care by 2017; supporting them to manage and monitor their condition at home, and reducing
Page 19 of 38

the need for avoidable visits to their GP practice and hospital.
11.1.7 The NHS Outcomes Framework 2013/2014 https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/213055/121109-NHS-Outcomes-Framework-2013-14.pdf
The Digital Health Strategy for Staffordshire will clearly define how it supports the NHS Outcomes Framework within the benefits realisation section.
Page 20 of 38

11.2 APPENDIX 2 - DIGITAL HEALTH MODALITIES CURRENT SITUATION IN STAFFORDSHIRE
11.2.1 Tele-care A range of tele-care support is already widely available and greater emphasis will be placed on what this is, how to purchase it and in what circumstances it is best used. There are plans to open an e-marketplace shop and high street store in order to increase accessibility to tele-care. Assessment tools like Just Checking support the assessment process and evidence how the adoption of technology can support independence and reduce admissions to hospital and long term care. Staffordshire currently commissions community alarm and tele-care services through a complex set of 150 contracts with 22 provider organisations. The combined annual contract value is over £1.7 million. The majority are community alarms provided by housing organisations. Around 10,000 alarms are delivered in community settings, mostly in socially rented properties, with a further 4,500 in sheltered or extra care housing. There is a slow-growing number of alarms with peripheral tele-care devices, such as fall detectors, gas sensors, activity monitors, flood detectors, etc. The table below shows spread and trend of tele-care devices being used. (Data from Joining the Dots)
Websites such as http://www.livingmadeeasy.org.uk/, http://www.atdementia.org.uk/ and http://asksara.dlf.org.uk/ are to support people to find the right gadgets and equipment to help them remain independent. These will be enhanced by the development of the Staffordshire e-market place as part of the Staffordshire cares suite.
Page 21 of 38
http://www.youtube.com/watch?v=joMWzGq9Oak&list=PLRjtunFnmEOfSruqSU7AEcg7dPwG_V70n
Telecare has potential to support more personalised care, manage and mitigate risks in acute and care home settings freeing up staff resources to deliver better care and helping to manage care costs. Intelligent Tele-care systems like Myamego are being introduced within inpatient beds for the first time nationally within Staffordshire, for people with the most complex needs supporting a transformation of traditional care.
Page 22 of 38
There is substantial scope for the further expansion of tele-care, especially where it is jointly commissioned with health partners as part of the wider commissioning of services. There are potential benefits for both the quality and costs of support.
11.2.2 Evaluation - Tele-care - Care Services Efficiency Delivery Model (2010) Updated by Care performance partners 2013
Tele-care is a well-established technology within social care and housing and it has seen numerous evaluations. It is still largely funded by Social Care and self-funders but the outcomes it supports benefit the whole local health economy and so it makes a natural place to develop shares investment
The CSED model analysed tele-care services in nine English councils, covering 858 service users, and compared the cost of supporting people with tele-care to the cost of supporting them without tele-care.
Page 23 of 38
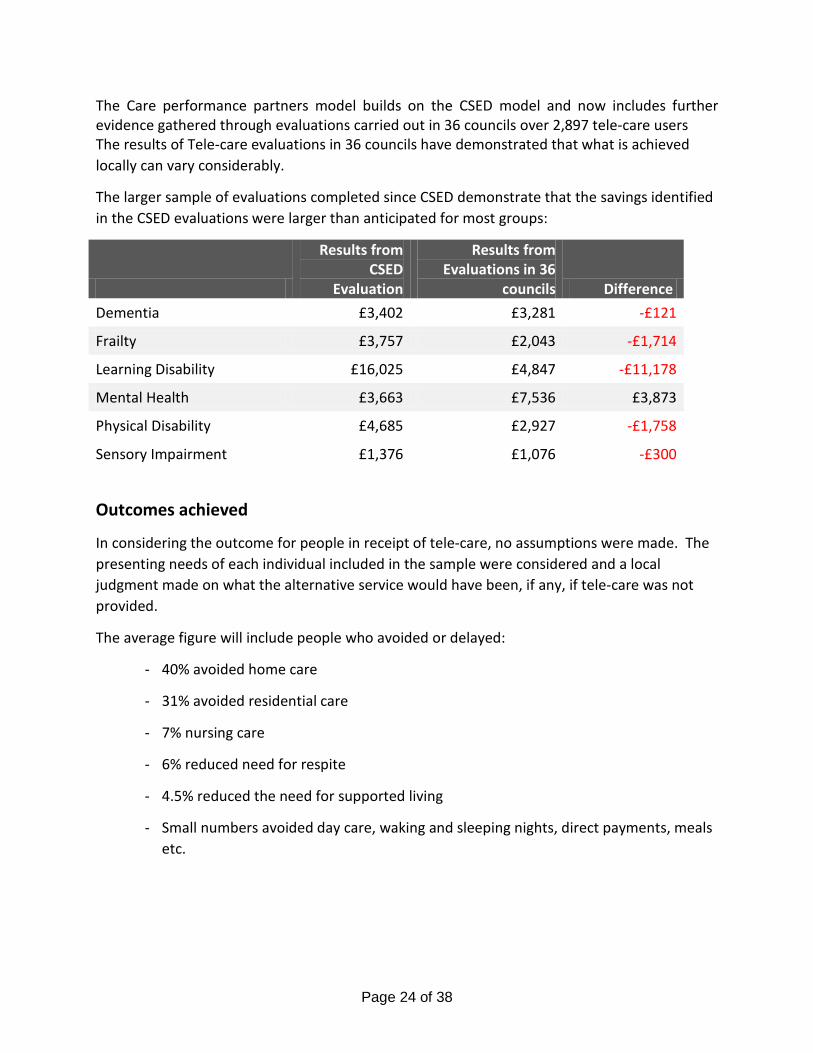
The Care performance partners model builds on the CSED model and now includes further evidence gathered through evaluations carried out in 36 councils over 2,897 tele-care users The results of Tele-care evaluations in 36 councils have demonstrated that what is achieved locally can vary considerably.
The larger sample of evaluations completed since CSED demonstrate that the savings identified in the CSED evaluations were larger than anticipated for most groups:
Results from CSED
Evaluation
Results from Evaluations in 36
councils Difference Dementia £3,402 £3,281 -£121
Frailty £3,757 £2,043 -£1,714
Learning Disability £16,025 £4,847 -£11,178
Mental Health £3,663 £7,536 £3,873
Physical Disability £4,685 £2,927 -£1,758
Sensory Impairment £1,376 £1,076 -£300
Outcomes achieved
In considering the outcome for people in receipt of tele-care, no assumptions were made. The presenting needs of each individual included in the sample were considered and a local judgment made on what the alternative service would have been, if any, if tele-care was not provided.
The average figure will include people who avoided or delayed:
- 40% avoided home care
- 31% avoided residential care
- 7% nursing care
- 6% reduced need for respite
- 4.5% reduced the need for supported living
- Small numbers avoided day care, waking and sleeping nights, direct payments, meals etc.
Page 24 of 38

The extent of the outcomes achieved for people using the service is directly influenced by how well the tele-care service is integrated with the community care assessment and the confidence social workers have in tele-care managing the identified risk.
Consideration needs to be given to the proportion of tele-care that will be provided for reassurance or preventative purposes and that supporting an individual in place of an alternative social care service.
Tele-care, if used to support an identified assessed need, can deliver the following benefits:
- Individual: reassurance that support is available when needed, reducing anxiety and improving well-being, maintaining independence and improved dignity.
- Carers: reassurance that risks are being managed and support will be available when needed. The reassurance should reduce the pressure from carers to increase the level of support package including pressure for residential placements.
- Adult Social Care: more effective and appropriate use of resources
- Care Commissioning Group: more effective and appropriate use of resources e.g. someone who is elderly frail and a known faller and unable to get up on their own, could have ended up in hospital if a fall happened during the night where there was no-one to assist them to get up. With the support of tele-care this scenario could be responded to within a short time and reassurance provided to the individual, resulting in removing or reducing the risk of hospital admission.
The links between tele-care and tele-health should be explored with clear step up / step down pathways. The use of tele-health on its own cannot deliver benefits for the individual or health and social care organisations and must be embedded within clear care pathways and support mechanisms. If used effectively and integrated into the healthcare pathway, tele-health can provide early warning of an exacerbation, enabling local health teams to provide a quick and targeted intervention reducing the likelihood of escalation into more acute or unplanned care.
The Benefits Model is intended to be baseline to aid discussion within Staffordshire to inform the following:
• Targeting of tele-care service
• Scale of change
• Pace of change
• Infrastructure changes needed to support the change
• Project costs to make the changes
Page 25 of 38
11.2.3 Tele-health A recent scoping document shows Staffordshire currently has small numbers of service users supported by Tele-health equipment. Historically equipment in this category has included such devices like Tunstall’s MyMedic http://www.tunstall.co.uk/solutions/mymedic and Docobo’s Healthhub. http://www.docobo.co.uk/ArticlePage.aspx?articleId=7&topParentId=7 All are relatively expensive per patient and attract on-going costs in terms of software and hardware updates, they require peripherals to support continued use and also require a high level of motivation from staff and users to interact with the equipment regularly. There is a requirement to ensure the right patients are selected and they are usually deployed at small scale and thus will have difficulty in achieving the kind of benefits we would expect. Thinking has moved towards buying or leasing low cost peripherals just as:-
• Blood pressure machines • Pulse oximetry • Weighing scales • Digital thermometers • Peak flow readers • Glucose monitoring
When done well Tele-health can deliver benefits for the individual as well as efficiencies for the health and social care services. Evidence suggests the following key factors in implementing Tele-health service:
• careful planning of the care pathway that will support Tele-health monitoring • integration of Tele-health into existing teams and support provided to patients • careful identification of suitable patients • focus on benefits realization
Emphasis is now pointing towards supporting patients and their families to better look after themselves and to remotely monitor at home or work where possible and be supported by a personalised care plan so that service users and carers know what to do should a circumstance arise. This has implications for high cost suppliers, call centres and support staff in that requirements are reduced. The growth of over the counter peripheral availability has meant that people are already doing home health checks for weight, blood pressure and so on, however the missing link is the support to make sense of the information. The challenge is to understand when, where and to whom the benefits accrue. This will support the business case for investment and support the case for decommissioning and realignment of services where effective use of Tele-health has created additional capacity.
Page 26 of 38
11.2.4 NHS Simple Tele-health “FLO” http://www.networks.nhs.uk/nhs-networks/simple-telehealth/about
The STH programme aims to provide information and tools to help clinicians develop innovative and practical ways to help patients to help themselves. What does Flo do?
• Improve adherence with treatment regimes through encouragement, reminders and interactive contact
• Regularly collect any self-reported information and give instant automated feedback. • Enable improvements in clinical team productivity and outcome quality • Engage patients in their health and social care pathways and services • Enables multiple healthcare teams to work together to assist patients in the
management of their own care. • Due to the low cost of STH, its ease of use and universal acceptability of the methods,
STH is affordable and deployable on an unequalled scale across an unrivalled range of conditions and pathways.
Simple Tele-health encompasses Florence (Flo) the friendly interface & persona, technical assets, methodologies, patents, business cases and an open and honest approach to sharing best practice across health and social care.
11.2.5 Mobile Apps & Online self-management http://apps.nhs.uk/
Mobile Apps and online self-management support is the direction every healthcare provider in the UK and worldwide is heading. With the huge growth in mobile devices and smartphones and the ever increasing availability of broadband in our homes and Wi-Fi in public spaces it has become easier for people to use digital technologies in their everyday lives and to look to the internet to support decision making.
Page 27 of 38

This has resulted in a vast number of health related apps being developed and to date there are 250 Apps accredited for use on the NHS Apps Library. NHS England Apps library was launched in March 2013 and hosts information regarding a growing number of apps that have been accredited and approved as recommended for use within the NHS. All the apps in the Health Apps Library have been reviewed to ensure that they are:
• Relevant to people living in England • Use information from a verifiable or a trusted source • Comply with the Data Protection Act, to make sure that they hold and use your
information appropriately • Most importantly, we work with the Developers of apps listed in the Library to ensure
they are clinically safe. We do this by understanding what the app does and then consider the potential clinical safety implications before deciding whether to include the app in the Library.
What the NHS Apps library does not do is to make any requirements to prove effectiveness in terms of quality and value to the consumer. When you search the Apple App store for “NHS”, you find the following:-
• 26 iPad only Apps across all categories that have NHS in the title • 144 iPhone only Apps across categories
Most are to support navigation and location of services as well as access to information. Some apps support healthy lifestyle such as losing weight, reducing alcohol consumption, stopping smoking, increasing and tracking exercise. There are a broad range of Apps to support shared decision making. Most Apps are aimed at service users, informal carers and the public. There is a rapidly growing number of free and commercial apps on all digital platforms which the public can and do access. We are aware there is a tension between the view of clinicians and the public right to choose what suits them. This market grows weekly and we are recognise that the public will choose what works for them and public pressure will be a major driver in transforming the medical model of care and support a new model which embraces and harness potential for self-care. With regard to using Mobile Apps and online self-management support, Staffordshire County Council has developed http://apps.nhs.uk/app/me-myself-i/
Page 28 of 38

A user-led support planning tool, using game play, which puts the individual in control of identifying their social care and health needs. This is integrated within the Staffordshire cares website and its associated web support tools, It supports personalisation agenda and helps [people identify a wide range of ways in which that can achieve their outcomes Staffordshire and Stoke have recently commenced a pilot using the Mobile App Health Fabric. This is an App (developed in Staffordshire in conjunction with Gnosall medical practice) that is used on a tablet device, smart phone or desktop computer that allows users to create a profile and start to understand and take control of their own health and well-being. The Health Fabric App is fully integrated with the GP Clinical system EMIS and extracts relevant data from EMIS to pre-populate the patient’s own profile. This enables sharing of the GP clinical record and promotes a greater understanding and interaction for the patient and those supporting their health and social care needs. The innovative aspect of the Health Fabric App is that the patient chooses who to share their profile with thus putting them firmly in control and shifting the emphasis towards them taking more responsibility for their own health and decision making. The pilot has just commenced and the team plans to capture benefits from working & interacting with patients, their friends and families in this way. By using risk stratification patients are invited to create a profile for themselves. Currently the App is funded through a licencing model, however early 2014, it becomes free to the public and available for download from the App store.
Page 29 of 38

Evidence to date shows that where used appropriately, we can better co-ordinate care, improve communication, reduce unnecessary utilisation of services whilst improving clinical and quality outcomes as well as user experience. APP’S are now being used widely, supporting most aspects of daily living so their use within health and social care is a natural extension of this.
11.2.6 Video-conferencing and Tele-diagnostics Video consultations are reliant on the necessary infrastructure being in place in terms of hardware (video cameras, microphones, speakers etc.). The IM&T roadmap across Staffordshire will see all relevant staff having access to video-consultations via their work computers (with built in cameras). Video consultations are not yet embedded in everyday practice, however enthusiasm is high to start working in this way, particularly between acute trusts and community hospitals / nursing homes. Work is on-going nationally via NHS England to determine information governance and security requirements which will allow use through everyday software such as Skype and Facetime and how this is incorporated to work flow assignment as well as payment mechanisms for working in this way.
Page 30 of 38
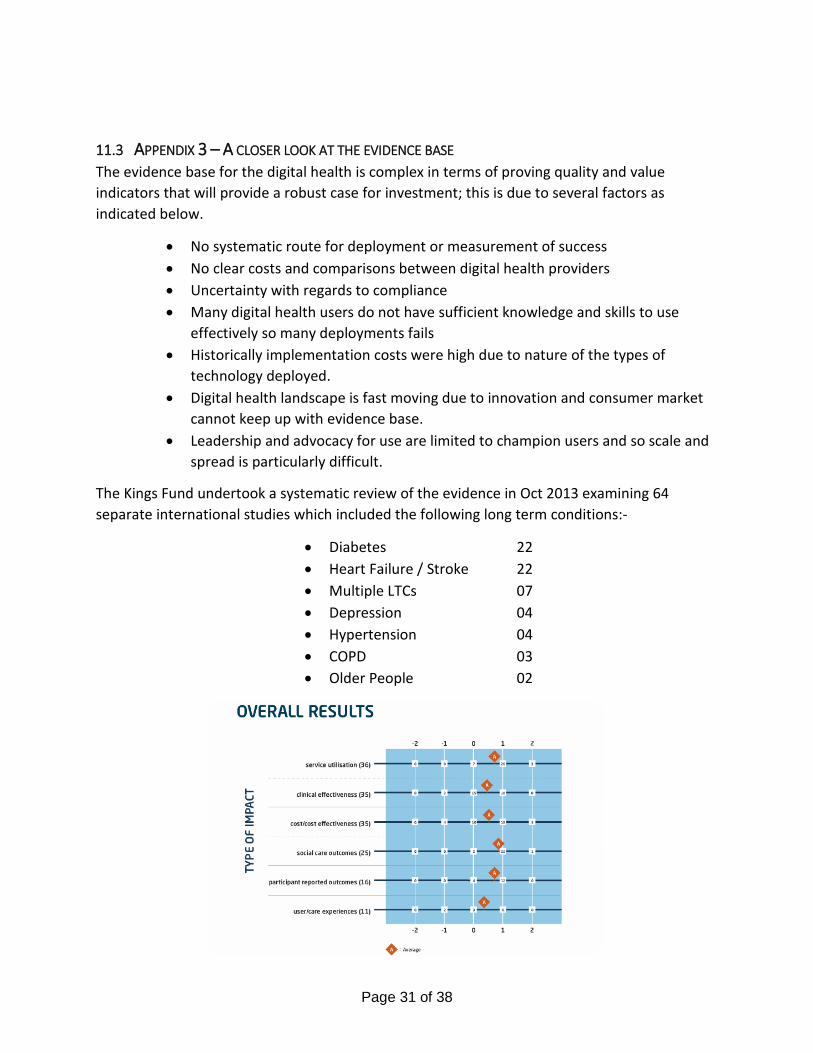
11.3 APPENDIX 3 – A CLOSER LOOK AT THE EVIDENCE BASE The evidence base for the digital health is complex in terms of proving quality and value indicators that will provide a robust case for investment; this is due to several factors as indicated below.
• No systematic route for deployment or measurement of success • No clear costs and comparisons between digital health providers • Uncertainty with regards to compliance • Many digital health users do not have sufficient knowledge and skills to use
effectively so many deployments fails • Historically implementation costs were high due to nature of the types of
technology deployed. • Digital health landscape is fast moving due to innovation and consumer market
cannot keep up with evidence base. • Leadership and advocacy for use are limited to champion users and so scale and
spread is particularly difficult.
The Kings Fund undertook a systematic review of the evidence in Oct 2013 examining 64 separate international studies which included the following long term conditions:-
• Diabetes 22 • Heart Failure / Stroke 22 • Multiple LTCs 07 • Depression 04 • Hypertension 04 • COPD 03 • Older People 02
Page 31 of 38
11.3.1 Tele-health - Whole System Demonstrator Evidence (June 2012) http://www.bmj.com/content/344/bmj.e3874
The Department of Health Whole System Demonstrator model (2008) involved 6,191 patients and 179 GP practices in the UK.
The results showed that when using tele-health correctly, patients and healthcare professionals would benefit. These results included:
• 45% reduction in mortality rates • 14% reduction in the number of patient bed days • 20% reduction in emergency admissions • 14% reduction in elective admissions • 15% reduction in emergency department visits • 8% reduction in tariff costs
Not surprisingly, the costs savings were not shown to be overall significant, as the trial was started in 2009 and based on low scale payment models used ageing technology and did not link with a transformation service change. . Despite this, there was an overall reduction of £188 per head. The trial did not look at impact on community care quality or costs.
The outcomes from the Whole system demonstrators raise questions we need to consider to progress the proportional and effective use of Tele-health devices:
• Change management: particularly how to secure GP’s commissioners and finance managers’ commitment with adequate evidence of effectiveness – increasingly, this is seen as essential ground work. There are a few commissioning champions who are maintaining the impetus and interest, but there is a substantial task ahead to inform and persuade GPs and the new Commissioning Consortia that tele-health is, or should be, an adequately-evidenced development priority.
• High start-up costs quoted by suppliers: especially where there is supplier pressure to purchase a large number of units: and their lack of interest in quoting for smaller scale schemes or for stand-alone equipment
• Some scepticism about the predicted pace of impact on productivity: efficiency gains may be slower to realise than anticipated, due to slower recruitment of suitable patients, and technical issues with the connection of equipment
• Lack of access to independent reviews of equipment, and impartial horizon scanning, to inform choices about equipment – for example to help avoid the risks of purchasing equipment that is likely to become rapidly obsolescent.
11.3.2 The Evidence for Simple Tele-Health “Florence Simple Tele-health has been deployed for the last 3 years or so across a wide range of providers with differing levels of success, which has been due to effective leadership, clinical engagement and effective deployment for the right patients.
Page 32 of 38

The Simple Tele-Health in Stoke have been gathering evidence to support implementation of “Flo” for quality & productivity benefits.
Below is an example of some of the more popular protocols and associated use with aims and benefits clearly identified.
Type of Protocol Aim of protocol Benefits Medication reminder for adults and teenagers, tablets, injections , inhalers or nebulisers
Medication compliance Avoidance of crisis Improve long term outcomes
Reduced waste of medications
Hypertension poor control or newly diagnosed
To monitor and maintain blood pressure
Reduced travel costs Reduced home visits to monitor BP early recognition of trends
Hypertension medication titration
To monitor and maintain blood pressure
Reduced travel and home visits to monitor BP, early recognition of trends Faster titration of medication
COPD, Oxygen saturation, Sputum & temperature monitoring
To avoid exacerbation and unplanned admission To support self-management
Reduced home visits Reduced travel Costs Reduced exacerbation due to earlier intervention
Blood Glucose Monitoring To monitor and maintain diabetes control To prompt to take action when required
To support self-management Reduce home visits to monitor blood glucose Reduced Travel Costs
Woundsense - dressing monitoring
To dress wounds when clinically indicated
Reduced unnecessary dressing changes Reduced Travel Costs Reduced home visits by approximately 33%
Appointment Reminder To reduce DNA’s Offer alternative appointment
Reduced costs due to under utilisation of clinics Increased productivity
Heart Failure – weight monitoring
To control symptoms and spot early exacerbation of heart failure
Reduction in home visits by up to 50% Reduced Travel Costs
Heart Failure Question Set To control symptoms and spot early exacerbation of heart failure
Reduction in home visits by up to 50% Reduced Travel Costs
Weight Tracking for obesity Reduced long term costs Urine Testing Reduced ? UTI visits for patients with
catheters Nebuliser reminders Reduced exacerbations Reduced Home Visits by Respiratory
Nurses Reduced Travel Costs
Page 33 of 38
Each team wishing to use “Flo” needs to work up benefits on a team by team basis, recommended starting points are to look at Community Matron / Case Management for patients with COPD, Heart Failure, Diabetes & Hypertension and determine which patients may benefit from the Simple Tele-health “Flo” service. The Staffordshire digital programme board provides the resources to evaluate the cost benefits of these applications to support where it is best used at scale and pace.
11.3.3 Mobile apps & Online self management Mobile health apps have the potential to contribute to the improvement of health, both from the perspective of staff, service users and the public. However, there are usually defined specific aspects that reveal whether an app is safe or not. There seems to be no real criteria needs or usefulness in the development of the vast majority of apps. In addition, many organisations and individuals have the capacity to develop apps for their own needs, all of which is related to an even greater diversity in design and use of apps. The existence of several guidelines and the considerable number of publications, related to the quality and impact of health apps in healthcare, implies that there is a growing interest. In a survey conducted by PwC mHealth, one third of patients surveyed were convinced that mHealth would improve the convenience, cost and quality of health care received in the next three years. 59% of respondents indicated that mobile health applications would change the way health information is sought and 50% felt that these apps will radically change the way they manage their chronic disease.
http://www.pwc.com/en_GX/gx/healthcare/mhealth/assets/pwc-emerging-mhealth-exec-summary.pdf
The most recent trends suggest that mobile health applications as a set of tools and technologies show great potential in health promotion and education in both lifestyle and clinical care settings. The phenomenal growth mainly in individual downloads of health apps however has not been accompanied by clear frameworks of regulation and control to ensure quality design, appropriate recommendations on the use and application as well as a legal vacuum on such essential issues as privacy and confidentiality or safety data.
11.3.4 Understanding Apps There are thousands of downloadable apps that people can use that interface with health with over 40,000 mobile health apps currently available in iTunes. The public are indentifying their preferred apps and rating them: http://myhealthapps.net/ The IMS Institute for Healthcare Informatics in the USA analyzed 43,689 health, fitness and medical apps in the Apple iTunes store as of June 2013. These split into what IMS categorized as 23,682 “genuine” health care apps, and 20,007 falling into miscellaneous categories such as product-specific apps, fashion and beauty, fertility, veterinary, and apps with “gimmicks” (IMS’s word) with no obvious health benefit.
Page 34 of 38
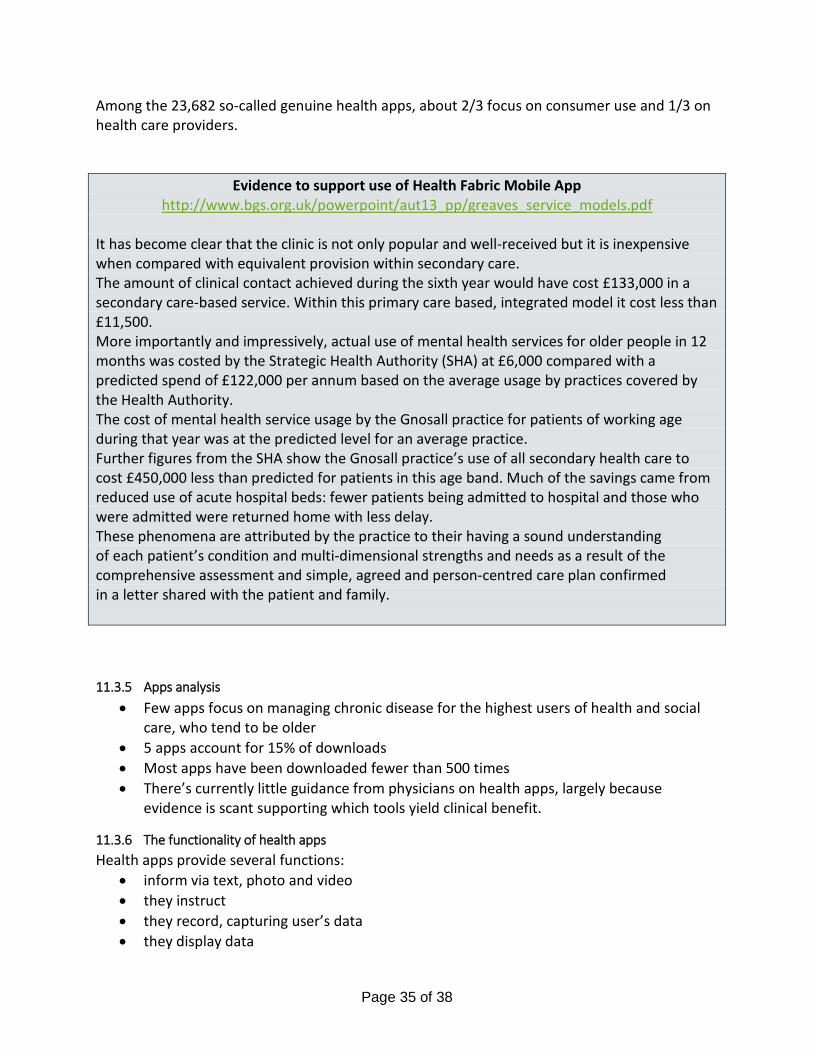
Among the 23,682 so-called genuine health apps, about 2/3 focus on consumer use and 1/3 on health care providers.
Evidence to support use of Health Fabric Mobile App http://www.bgs.org.uk/powerpoint/aut13_pp/greaves_service_models.pdf
It has become clear that the clinic is not only popular and well-received but it is inexpensive when compared with equivalent provision within secondary care. The amount of clinical contact achieved during the sixth year would have cost £133,000 in a secondary care-based service. Within this primary care based, integrated model it cost less than £11,500. More importantly and impressively, actual use of mental health services for older people in 12 months was costed by the Strategic Health Authority (SHA) at £6,000 compared with a predicted spend of £122,000 per annum based on the average usage by practices covered by the Health Authority. The cost of mental health service usage by the Gnosall practice for patients of working age during that year was at the predicted level for an average practice. Further figures from the SHA show the Gnosall practice’s use of all secondary health care to cost £450,000 less than predicted for patients in this age band. Much of the savings came from reduced use of acute hospital beds: fewer patients being admitted to hospital and those who were admitted were returned home with less delay. These phenomena are attributed by the practice to their having a sound understanding of each patient’s condition and multi-dimensional strengths and needs as a result of the comprehensive assessment and simple, agreed and person-centred care plan confirmed in a letter shared with the patient and family.
11.3.5 Apps analysis • Few apps focus on managing chronic disease for the highest users of health and social
care, who tend to be older • 5 apps account for 15% of downloads • Most apps have been downloaded fewer than 500 times • There’s currently little guidance from physicians on health apps, largely because
evidence is scant supporting which tools yield clinical benefit.
11.3.6 The functionality of health apps Health apps provide several functions:
• inform via text, photo and video • they instruct • they record, capturing user’s data • they display data
Page 35 of 38

• they guide or diagnose • they remind and alert the user (say, to take a medication or test blood) • they communicate to social networks or health providers. Providing information is the
most common function across the health apps: while two-thirds can display information, one-half provide instructions, and only one-fifth track or capture user’s data.
11.3.7 App categories include: • Healthy living, promoting modifiable health risk factors such as healthy weight, smoking
cessation, and exercise. The most popular apps in this category are the Calorie Counter and Diet Tracker from MyFitnessPal, the Calorie Counter PRO by MyNetDiary, the Chest Trainer from Fitness Buddy, Cycle Tracker Pro, Quit It 3.0 to stop smoking, and Quit Smoking Now HD hypnotherapy with Max Kirsten.
• Self-diagnosis, which the FDA intends to regulate per its September 25, 2013, guidance. The top apps in this category were HealthTap, iTriage, and WebMD.
• Filling prescriptions, via pharmacy apps. Top apps were GoodRx, MyRefill Rx, and Walgreens.
• Medication compliance, helping patients stick to prescribed dosing regimens. Top apps were Dosecast, Pill Monitor, and RemindMe Prescription.
• By therapy area, IMS found mental health and behavioral disorders, eyes and hearing, endocrine and nutrition, heart/circulatory, musculoskeletal, and cancer to be the most prevalent areas apps cover. Within mental and behavioral health, autism, anxiety, depression, and ADHD were covered by a total of 558 apps.
• Health apps specifically for seniors are addressed by only 27 apps.
11.3.8 Video-conferencing & Tele-diagnostics think we should consider peer to peer and person to carer benefits too
11.3.8.1 Video Conferencing Use Case Scenarios Video conferencing has the following use case scenarios.
1. For education and training purposes to train across multiple sites and reach more people therefore reducing training time required by multiple sessions and reducing travelling time for staff
2. For case conferences and collaboration between teams either routine or urgent 3. For direct patient / carer remote consultation, to avoid an appointment or home visits, this
could be routine or urgent 4. Between patients, carers and independent / voluntary sector to support information, education
and sign posting 5. For follow up support and education, either 1:1 or in a group as part of rehabilitation or
counselling.
11.3.8.2 Background and latest developments in video-conferencing in health • Cloud-based services and Web browsers can now offer video conferencing access to
anyone with a mobile device.
Page 36 of 38

• Video conferencing is becoming less expensive and more easily available. • Cloud services and browser-based video conferencing allow inexpensive face-to-face
interoperability, regardless of the system being used. • Video conferencing offers a rich collaboration for a wide span of providers across all
sectors of health and social care. • In terms of patient care, video provides access to consultations to avoid a travel to a
clinic or hospital. • Community staff and GPs especially, are at the centre of coordinating care related to the
patients’ health and well-being. Pathology results, prescribing, patient referrals and GP interactions all rely on effective contact.
• Cloud services and Web access enable smaller community clinics and GP Surgeries, to offer video conferencing instead of a GP, community visit or Hospital appointment.
• Home visits are no longer necessary as staff can now monitor and communicate with patients at home who have a smartphone, tablet or a PC with Internet access.
The challenge rests in enabling those involved in patient care to have increased capabilities and convenience through sharing information, while also protecting privacy rights of patients whilst maintaining information integrity. As these issues recede, increased numbers of providers and patients will use video to help them achieve their health goals through a personalised care plan.
11.3.8.3 Recognised benefits of video-conferencing
1. Reduced Travel Costs The ability to be in several places at once without leaving the office base can increase productivity whilst reducing travel costs. Though face-to-face interactions with your other members of staff, service users and the public, will never be replaced, the huge leaps in quality, availability, and ease-of-use make videoconferencing the closest thing to being there. When you calculate the number of trips taken annually and determine the associated travel costs it is clear why videoconferencing is such an attractive alternative.
2. Decreased Hospital Appointments 3. Decreased GP Visits 4. Decreased unnecessary emergency admissions 5. Increased Productivity Among Teams
In Health & Social Care we have numerous offices and organisations across all of Staffordshire, most of which will communicate with phone calls, email, or instant messages. The lack of face-to-face communication can cause misunderstandings within teams, and worse, can result in lost or nonexistent communication. When video is implemented, participants are more likely to stay alert and focused on what is being discussed. As a result, projects and tasks are completed faster, productivity increases, and staff feel part of a team.
6. Improves Communication & Reinforces Relationships
Page 37 of 38

During a videoconference you can see the facial expressions and body language of conference participants, leading to faster and more effective collaboration. These are both important aspects of communication that are lost with a basic telephone call. Allowing organisational or multi-organisational meetings in real time with offices across geographical boundaries often supports partnership working and collaboration.
Page 38 of 38

A Strategy to support
Technology Enabled Care Services
in
Staffordshire & Stoke-on-Trent
Summary Document
Version 1.1
23.10.14

Version Control Effective Date: 23/10/14
Version No. Effective Date Summary of Significant Changes Previous
Version no.
1.0 1/10/14 Initial version for TECS Board Member review and feedback n/a
1.1 23/10/14
Includes • Additional ‘Goal’ around support for
remote care and facilitation of integrated care delivery
• A section describing requirements defined by the Patient Advisory Group for delivery of the strategy
• Additional accountabilities/activities for the TECS Board o summary of TECS implementations o identification of benefits
1.0
Contents Introduction ............................................................................................................... 1
Context ...................................................................................................................... 1
Goals .......................................................................................................................... 1
Scope ......................................................................................................................... 2
Approach to Delivering the Goals ............................................................................... 2
The Role of Member Organisations in delivering the Goals ..................................... 2
The Role of TECS Board in delivering the Goals ....................................................... 3
TECS Benefits Summary ............................................................................................. 4
Measurement and Evaluation .................................................................................... 5
Appendix 1 – Organisations and Groups Supporting the Strategy .............................. 6
Introduction This document provides a high level description of a strategy to deliver, promote and expand Technology Enabled Care Services in Staffordshire & Stoke-on-Trent. It provides a mechanism for TECS Board member organisations to commit to a set of TECS related goals and an approach to their delivery.
It is based on the extensive work already done by the TECS Board in creating a detailed draft strategy, plus subsequent detailed consultation with TECS Board members and input from the TECS Board Patient Advisory Group.
In this version, it comprises:
• A summary of the context and background for the Strategy • The proposed goals for TECS within Staffordshire and Stoke-on-Trent (to be formally agreed with TECS
Board member organisations and the Patient Advisory Group) • A proposed approach to achievement of those goals, including the role of the TECS Board and of member
organisations (to be formally agreed with TECS Board member organisations and the Patient Advisory Group)
• A summary of the benefits of TECS for all stakeholders • A proposed approach to measurement and evaluation
It should be read in conjunction with ‘A Strategy to support Technology Enabled Care Services in Staffordshire & Stoke-on-Trent – Context, Background and Vision’ which provides extensive information on the need for, benefits of, and vision for TECS in the area, and the challenges that need to be overcome to enable successful delivery.
Context The National Vision for TECS:-
Technology Enabled Care Services are underpinned by the idea of service integration to improve patient care and outcomes. When different services and sectors work together, towards shared goals, patients get far more flexible, better, and more appropriate care. To achieve true service integration, we recognise that this needs to be delivered through a genuine partnership across partner agencies – facilitating collaboration between agencies and professions and empowering people and their carers to better self-manage health and wellbeing with the use of technology.”
This vision of “Technology Enabled Care Services” being supported by technology is what sits at the core of this Staffordshire TECS Strategy. We recognise the potential of technology to transform traditional models of care and support and to enable greater self-management of care and to support people and their carers to be as independent as possible. This will help people of all ages to take greater responsibility for their own health and wellbeing and that of their families, as well as reducing admissions and readmissions to hospital and enhancing long term care among older people
Goals The key goals that the TECS Strategy aims to achieve are:
Page 1 of 6

1. Optimise the appropriate use of technology to support self-management by patients, service users and the general public in order both to improve outcomes and prevent or delay deterioration in condition, and to reduce service delivery costs across the economy.
2. Support the delivery of efficient, effective and productive remote care, and facilitate integrated care delivery.
3. Minimise cost and complexity for users and service providers across the economy by establishing a strategic direction for and, where possible implementing, common or interoperable technology for specific relevant functions.
Scope In the context of the TECS Strategy, ‘technology’ includes the following overlapping categories:
• Assistive Technology. In broad terms, this covers any product designed to support or enable independence. It acknowledges the cross-over between inclusively designed, mainstream products and the technology specifically made available to provide assistance to people with specific needs, and reflects the wide range of equipment and services that help people to maximise their independence.
• Telecare. This category includes devices in or away from the home that support independence, that can be used as stand-alone or linked to a support service such as a call centre. Many of these devices relate to social needs in relation to activities of daily living and increasingly can be purchased on the high street and through the internet
• Telehealth. This category includes devices used in or away from the home that enable health parameter measurements such as blood pressure, glucose, weight, and wound management, and support decision making around personalised care planning and appropriate interventions. Tele-health can be used as stand-alone or linked to a response service. Many devices are now available and can purchased on-line and on the high street
• Apps and self-management. This category, which covers a growing area of support where people use a mobile device, smartphone or desktop PC to manage their own health and well-being, is sometimes seen as a separate category or ‘modality’. It is mainly aimed at self-management and so is most appropriate for the lower levels of need, although increasing use of mobile apps is having an impact in supporting staff and carers in monitoring and care co-ordination. However, it should be noted that other categories, such as ‘Telecare’ and ‘Telehealth’ may actually be delivered via ‘Apps’, and that self-management is also specifically enabled by the other categories above.
• Video consultations and tele-diagnostics. This category enables electronic ‘face to face’ consultation between service users or patients and staff, and between staff & staff. It enables decisions to be made without the need for anyone to leave their desk or home. Tele-diagnostics could involve people / carers testing themselves or could be community staff doing testing in the person’s home. This category includes tools such as WebEx, FaceTime and Skype and relies on availability of appropriate infrastructure.
Approach to Delivering the Goals
The Role of Member Organisations in delivering the Goals In order to support delivery of the agreed goals, TECS Board member organisations will:
1. Ensure that they and their staff understand the benefits and implications of the technologies in scope that are relevant to them and the services that they provide
2. Take these technologies into account when reviewing/designing services and integrate/implement them wherever feasible
3. Share best practice across member organisations 4. Share the TECS related elements of their organisation strategy with other members
Page 2 of 6

5. Adopt an approach to branding TECS within their organisation and target population that is consistent across member organisations and avoids confusing people with different names / labels for the same thing.
6. Ensure that all relevant parts of their organisation are aware of the TECS Strategy and the role of the TECS Board in helping to deliver it
7. Raise awareness of appropriate technology in their target populations 8. Encourage a culture of appropriate technology exploitation within their staff and include an appropriate
focus on TECS in workforce development and training 9. Agree, across the economy, target technologies that would benefit from strategic direction, agree that
strategic direction and, wherever feasible, take decisions aligned with that direction 10. Where appropriate and relevant, collaborate on and provide resource to joint projects with other member
organisations 11. Provide information to support effective measurement of the benefits of the strategy and evaluation of
TECS delivery
The Role of TECS Board in delivering the Goals The role of the TECS Board in the delivery of the TECS Strategy is one not of governance but of guidance, co-ordination, awareness raising and support. This role will include the following activities and accountabilities:
1. Sharing information, ideas, benefits and best practice related to TECS across member organisations and the wider economy and population of Staffordshire and Stoke-on-Trent
2. Horizon scanning to support future proofing of solutions implemented by member organisations and to identify innovative uses of TECS
3. Identifying technologies where benefits might accrue from common platforms and an agreed strategic direction and make proposals for agreement
4. Working with member organisations and solution providers to support market development of new products and services
5. Highlighting priority areas for action (both by member organisations and by the Board itself) 6. Interfacing with, and co-ordinating direction and action with, other relevant initiatives (e.g. ICR) 7. Agreeing a consistent approach to branding TECS across member organisations 8. Understanding and promoting the art of the possible with regard to the appropriate application of
available technology 9. Measuring the impact of the Strategy and its delivery 10. Where appropriate, in line with input and proposals from member organisations:
a. facilitating joint procurement across member organisations in order to achieve economies of scale b. facilitating establishment of joint projects c. collaborating on joint funding bids for specific projects d. initiating and running projects
11. Maintaining a summary of TECS implementations across Staffordshire & Stoke-on-Trent 12. Producing an annual plan for TECS summarising member organisation and joint initiatives
The Board will set up sub-groups as needed to fulfil the role described above.
Patient Advisory Group Requirements The agreed goals of the TECS strategy should be delivered with a focus on • equal choice and access;
Page 3 of 6

• ensuring that: o TECS are implemented in a way that is tailored to individual needs (not ‘one size fits all’); o the introduction of technical solutions does not cause or exacerbate social isolation.
TECS Benefits Summary The table below includes examples of benefits accruing to, and generated by, various stakeholder groups as a result of TECS implementations. It is not intended to be an exhaustive list.
Stakeholder Group
TECS Category/Modality
Assistive Technology
Tele-care
Tele-health
Mobile apps & Self Management
Video consultations & tele-diagnostics
People
Promotes self-care, choice and control. Less stigma than state provision. Can offer value for money compared to receiving care and support
Greater independence Increased Self-management Supported decision making
Improved experience Early decision making Improved communication Reduced travel Improved access
Education, support & self-management Supported decision making Improved access Increased opportunities to access resources via e-marketplace
Reduced travel Improved access Improved experience Transferable skills for social interaction e.g. FaceTime to reduce loneliness
CCGs Supports self-care and support for carers . Earlier awareness of TECS as part of care journey..
Increased independence and self-management and thus reducing demand on services due to earlier intervention
More effective utilisation of GP and community care resource. Improved medication compliance & associated costs
increased access to credible advice and so aid decision making Impacts on, for instance, preventive agenda and long term cost savings Reduces demand across all sectors
Reduced costs across all sectors Reduced travel
Acute Trusts Promote self-care through A&E falls, dementia and carer breakdown
Not usually directly impacting on an acute Trust.
Reduced admission and length of stay costs
Can reduce follow-ups and support improved interaction Gives greater control and understanding to patients and their families
Reduced admission and length of stay costs Reduced travel
Mental Health Trusts
Range of practical, options to support self care and management.
Increased ability for patients to stay at home remaining independent Medication reminders are effective in supporting compliance
Reduced admissions and length of stay Reassurance re quality & safety allowing pts to stay at home
increased access to support and decision aids Can capture patient data and assure compliance
Reduced admissions and length of stay Improved satisfaction & experience
Community Provider
Opportunity to support enablement and rebuild or maintain individuals skills and abilities reducing dependency
increased early intervention and support of independence with minimal costs avoiding crisis intervention
Reduced costs in terms of home visits Can aid patient monitoring and increase self-management
Aids communication & co-ordination Improves access to community team Can capture patient data
Aids communication & co-ordination Improves access to community team Improved experience Reduced travel requirements
Voluntary Sector
Peer endorsement and promotion of self-care and management. Carers support.
Can provide means for engagement and interaction with voluntary sector
Not usually directly impacting engagement with Voluntary sector but can support earlier referral to a voluntary service if required
Can provide a “touch” point for the voluntary sector Can provide access to high quality validated information and support when required
Able to use infrastructure to support patients through support groups Reduced travel
Page 4 of 6

Stakeholder Group
TECS Category/Modality
Assistive Technology
Tele-care
Tele-health
Mobile apps & Self Management
Video consultations & tele-diagnostics
Local Authority
Information, advice and guidance, promotion of self-care and wellbeing. Can improve levels of self-care,
Directly reduces need for home visits and can trigger earlier interventions thus avoiding crisis
May result in reduced social care need if health managed holistically
Can support navigation of services and signpost to most relevant information
Reduced travel Improved access Improved experience
General Practice teams
Can help people reduce likelihood of falls, self-medicate and maintain food and fluid intake
Reduced interaction with GPs, particularly phone calls or unnecessary GP Visits
Reduced face to face interaction with GP Increased self-management
Can give access to credible advice and so aid decision making Can allow capture of patient data
Improved access Greater no. of consultations Avoid lengthy appointments Reduced travel
Note: the benefits listed against CCGs are those that could result from effective TECS related commissioning rather than necessarily accruing directly to the CCGS
Measurement and Evaluation The approach to measurement of the success of the strategy will be in line with proposals for core measures and metrics within the national TECS Improvement Plan generated by the TECS Stakeholder Forum, namely:
1. Generalised “Goal Attainment Score” (GAS). This measures how technology enabled care services can support individuals’ goal attainment (within the context of their long term condition). Goals are set by the individual patient or informal carer in consultation with their healthcare professional or social worker. Specific goals could include lowering blood pressure, being able to walk in the park, or return to work, for example. The Goal Attainment Score will test the premise that the appropriate use of technology enabled care services will empower patients and improve lives. The National Voices’ narrative for patient-centred, integrated care could be adapted at a local level to set out what good looks like from the user perspective.
2. Key risk indicator. This could measure the effectiveness of technology enabled care services in slowing the progression of illness, frailty, the loss of independence or accelerating rehabilitation, self-management or re-ablement. This measure will test the premise that appropriate use of technology enabled care services could help reduce dependence on and use of primary and secondary services by people with long term conditions or frailty.
3. Service utilisation metric. This could measure the effectiveness of technology enabled care services to reduce avoidable or unplanned service activity by evaluating the cost avoided and capacity released as a result of these technologies. This would demonstrate the increase in efficiency of service delivery and the net-positive cost impact on a local health economy.
4. Patient experience metric. This could measure the impact that technology enabled care services have on patient experience and satisfaction levels.
5. Social impact metric. This could demonstrate the wider societal impact of technology enabled care services, for example by measuring level of social contact or the increased participation in employment by patients and informal carers using these technologies.
6. Economic impact metric. This could demonstrate the contribution to the UK economy made by technology enabled care services by measuring the commercial value of the sector within commissioned services in England, including benchmarking against other countries.
************************************
Page 5 of 6
Appendix 1 – Organisations and Groups Supporting the Strategy This Strategy is supported by the following partner organisations and Advisory Groups across Staffordshire
(to be completed)
Organisation Name Type of Organisation
Key Contact Role Date agreed
Page 6 of 6

Title Improving Lives Reporting to Governing Body Date of Meeting 27th November 2014
Commissioning Lead(s) Author(s) Emily Davies/Nicola Harkness Emily Davies
Purpose of the Report (Please select) Approval Assurance Discussion
Key Points/Executive Summary
Purpose of Paper
The Governing Body are asked to be assured that the Improving Lives Programme is progressing in accordance with the agreed framework and timetable set by the Governing Body.
Context
The attached briefing outlines the background to the Improving Lives Programme and how the CCG aims to improve health and life experience outcomes for people living in East Staffordshire with long term conditions, and/or are frail and older. This includes:
• The rationale for change
• The vision for the future
• The method/vehicle of delivery to realise improvements to patient care
• Current status of the work programme and next steps
Key Points
• On the 29th October 2014, East Staffordshire Clinical Commissioning Group announced the shortlisted bidders for the competitive dialogue stage of the process. This includes Optum (part of UnitedHealth Group) and Virgin Care.
• Both bidders have had to submit responses to a range of questions which tested and clarified their approach towards key issues including quality, safety, patient and public involvement and finances as part of a pre-qualification stage. These will continue to be tested through the process.
• Both bidders have been invited to participate in competitive dialogue, which is now underway, to work with the CCG collaboratively to develop the solutions to improve patient and carer outcomes and life experiences.
X
Enc. 10
1 Author: DW Date: 20/2/14 East Staffs CCG

• The current programme of work is currently on track to deliver as agreed. Contract award is scheduled for 2015, with go live in early 2016.
• A supply chain network event and community leaders event has been scheduled for the 20th November 2014. The first of these events is for the shortlisted bidders to meet with new and existing providers who can help realise the future vision as part of the Prime Contractor’s supply chain. The Community Leaders event will provide people who represent patients and their carers locally, with the opportunity to meet with the bidders, share the views of the local population and open up lines of communication for the coming months.
• In addition, a public ‘Call to Action’ event is planned for the evening of the 15th January 2015. This is a follow up to the event held in June 2014, where the Improving Lives programme was launched. The CCG will be providing an update on Improving Lives at this event. Anyone interested in registering for this event should contact the Improving Lives Team at [email protected]
Recommendations (what is expected from the Board) The Governing Body are asked to be assured that the Improving Lives Programme is progressing in accordance with the agreed framework and timetable set by the Governing Body.
Enclosures
1. Improving Lives Briefing Paper – October 2014
2 Author: DW Date: 20/2/14 East Staffs CCG

3 Author: DW Date: 20/2/14 East Staffs CCG

Improving Lives Briefing – 29 October 2014 Improving Lives - Background East Staffordshire Clinical Commissioning Group (CCG) is the organisation, led by GPs, which buys many of the health services for local people.
• As a CCG, we have a duty to patients and the public to improve health outcomes and reduce health inequalities.
• Improving outcomes for patients with long term conditions and /or are frail elderly is East Staffordshire CCG’s number one improvement priority as determined by our key stakeholders.
• Amongst the challenges we face are that
o there are approximately 38,000 people in East Staffordshire with long term health
issues such as breathing problems, diabetes and heart disease
o as we live longer, the number of older people is growing year on year and most people aged over 60 have one long term health issue, and those over 65 have an average of three ongoing health issues. East Staffordshire’s ageing population is increasing above national rate, with an additional 10,000 people predicated by 2023.
o the money we are allocated will not be sufficient to provide care for everyone in the future unless we re-think our approach.
• We know, from listening to patients over the past 18 months, that they want to be more in control of their health. Local people have told us that the essence of great healthcare is to feel ‘confident, supported, informed and safe.’ Patients have told us they often feel anxious or scared, particularly when they are first diagnosed with a long term condition or on discharge from hospital following an inpatient stay.
Helping local people to live more independent, healthier lives
1

• At the moment, the quality of health care that these people get in East Staffordshire isn’t as good as that in many other parts of the country. Some of the facts we have to face include:
o There are inequalities across the CCG area. The gap between life expectancy for men and women living in the least deprived and most deprived areas is nine and six years respectively.
o Long term conditions are health conditions that could be better managed in the community. However, in East Staffordshire, the hospital admission rate for long term conditions is higher than the national average. (2013/14)
o Hospital readmission rates are high, particularly for respiratory diseases such as Chronic Obstructive Pulmonary Disease. In the adult population, readmission rates are highest amongst those aged 80 and over.
o There are poor outcomes for some disease areas e.g. The CCG is in the
bottom 25% of CCGs nationally for its attainment of optimal treatment targets for diabetes including blood glucose, blood pressure and cholesterol collectively. (2012/13)
o The minor (below the ankle) amputation rate in diabetics is 2.9 per 1000 in
East Staffordshire. This is almost double the national rate of 1.7 per 1000. (2010-2013)
o Falls admissions into hospital of people aged over 65 are higher than the
national average. (2012/13)
o Care is not joined up between the GP, community and hospital. We know this from the evidence we have from independent reviews e.g. The West Midlands Quality Review for Long Term conditions.
o Audit and modelling work undertaken across South East Staffordshire and
East Staffordshire health economies indicates that fewer intermediate care beds are required, there is a need to rebalance the number of step up to step down beds (25%:75%) and increase the amount of home based care.
• That is why our Governing Body, led by GPs - and backed by all 19 GP practices in East Staffordshire - took the decision early in 2014 to focus on helping people to be healthier for longer and helping those people with long term health issues to take more control over their own care.
• The CCG aim to improve health outcomes and life experiences of patients and their families who live in East Staffordshire through
o providing more support earlier to people with long term conditions
Helping local people to live more independent, healthier lives
2

o ensuring people have the right information, knowledge and skills to make
informed decisions about their care and how they live their lives
o offering a wider choice of and more accessible services and
o joining up care across the healthcare system.
• Some of our current ideas for services include:
o offering people access to local support networks where they can meet and socialise, either face to face or online, with others who have similar conditions
o targeted education programmes which provide information and support to enable people to make better lifestyle choices eg. Exercise groups, Cook and Eat sessions
o tailored telephone helplines led by clinically trained professionals which will
offer information and support to people during difficult times.
• The CCG has decided to use a competitive procurement process to achieve this end. This is the ‘Improving Lives’ procurement, which was launched to the public at the CCG’s ‘Call to Action Event’ in June 2014.
• In procurement processes such as this one, all ‘qualified providers’, including NHS organisations and private companies, are invited to participate. The reason for competition is that it can drive real improvements in care.
• This process will mean that we will appoint a ‘Prime Contractor’ of services who will then sub contract services to other organisations to deliver a set of outcomes. It is likely that, as is the present case, there will be a mixture of NHS, private organisations and voluntary sector involved in providing services. The Prime Contractor will be responsible for improving outcomes through organising these services operationally.
• The contract is for a set amount, and it is for the bidders to develop their solutions for achieving what needs to be achieved, within the budget available.
• The Improving Lives procurement process started this summer 2014. The contract is likely to commence in early 2016.
• At this point in time, patients will continue to receive services as usual.
Helping local people to live more independent, healthier lives
3

Improving Lives Update – 29 October 2014
• The CCG has now shortlisted two bidders from those organisations who submitted
responses to a whole range of questions which tested and clarified their approach towards key issues including quality, safety, patient and public involvement and finances.
• The shortlisted organisations are Optum (part of UnitedHealth Group) and Virgin Care.
• Over the coming months, the shortlisted organisations bidding for the contract will
work with us to develop what we call ‘outcomes’ – that is what the end results for patients and their families should be – for example
o reducing the number of people dying prematurely from heart and respiratory diseases
o reducing the numbers of patients with these conditions having to be admitted into hospital
o improved quality of life for the carers and families, and many more.
The CCG will use the insights collected from patients and their carers over the last 18 months to ensure the outcomes include those things that really matter to East Staffordshire patients when living with a long term condition and/or are frail and older.
• Once the outcomes are finalised, then the bidding organisations will work on ‘solutions’ – what services they will offer to achieve the agreed outcomes, and how they would propose to be able to deliver all the outcomes within the budget available
• The winning bidder will not be decided until 2015. This organisation will become our Prime Contractor and may not itself be a provider of services. It will be the one which demonstrates that it has the capability to deliver change and has organisations around it which can work together successfully so that patients receive the right care at the right time.
• Before there are any major changes to services there will be further engagement with patients and with Overview and Scrutiny Committees.
• The Prime Contractor will use the same criteria as we do for making sure that the quality and safety of care is of the right standard and we will be holding them directly to account to ensure that this happens.
• Services will continue to be NHS funded and free at the point of access for patients.
Helping local people to live more independent, healthier lives
4
Title Quality Report Reporting to Governing Body Date of Meeting 27th November 2014
Lead Director Author(s)
Heather Johnstone Sue Wilson/Heather Johnstone/Karen McGowan
Purpose of the Report (Please select) Approval Assurance Discussion
Key Points/Executive Summary
The Quality Committee meets on a monthly basis to review information and data relating to all commissioned services. The October meeting was the first meeting of the East Staffs and South East Staffs and Seisdon Peninsula Joint Quality Committee. The revised approach was considered by all present to be a success. The Joint Chairs report is attached at Appendix A. Recommendations (what is expected from the Board) The Governing Body is asked to read and understand the detail in this report and take assurance from the contents and the continuing work to improve quality and patient safety monitoring in the CCG. Furthermore, members of the governing body are asked to take assurance in respect of the Committees conclusion that all services are safe but members must understand that there are areas requiring further work in the respective providers to ensure consistently high quality services are provided to the local patient population. In addition and if considered necessary, members of the Governing Body are invited to suggest any further actions they would like to see in respect of any of the issues raised. Enclosures (1). Quality Report
X
Enc. 11
2 Author: Sue Wilson/Heather Johnstone Date: 18/11/2014 East Staffs CCG

Quality Report – November 2014
Update and exception report from Quality Committee The Quality Committee met on the 15th October and 12th November 2014 to review formally the submitted data and associated reports in respect of key providers and also to review additional items in line with the Committee business cycle. The October meeting was the first meeting of the East Staffs CCG (ESCCG) and South East Staffs and Seisdon Peninsula CCG (SES&SP CCG) Joint Quality Committee. Key information from the meeting is summarised below:
i) Provider Assurance The Committee received reports in respect of all key providers and decisions were made regarding the level of assurance regarding the safety and quality of each provider as follows: BHFT –for the first time since the trust went into special measures, members of the Quality Committee agreed they were assured regarding the quality and safety of the care that is provided. SSOTP – East Staffs and South East & Seisdon Peninsula Quality Committee members in October agreed that they had Limited Assurance in respect of quality and care at SSOTP. At the November meeting members stated they were Not Assured.
The October Committee highlighted the lack of workforce data, lack of confirmation from the Trust of their plans to replace the Medical and Nursing Directors, concerns about District Nursing in the south and particularly in East Staffs. Members agreed that work should be carried out to:
• Improve the quality of the reports to the committee, in line with other providers • Escalate to Governing Body and suggest a board to board meeting • Raise concerns with the Lead Commissioner about the continued lack of assurance • Consider raising a contract query as Associate Commissioners • Ask the Lay representatives to raise with members of the Patient Groups
SSSFT - members of the Quality Committee agreed they were assured by the data and information that was provided. Derby Hospitals FT – although far more information had been made available, members of the Quality Committee concluded they were not assured, based on the areas of concern detailed in the report. NSL – at the October Quality Committee members agreed they were assured based upon the data and information provided. SDUC – at the October Quality Committee members agreed they were partially assured in respect of quality of care at SDUC.
1

ii) Reports and updates received by the Committee Alex Fox, Lay Member for Quality at SES&SP CCG, was proposed as Chair of the Joint Quality Committee and Lynne Smith Associate Lay Representative for East Staffs, as Deputy Chair. This was agreed by all present. The approach for the new Joint Quality Committee is as follows:
- Core Members – responsible for reviewing quality and attending the entire meeting - Advisors – Quality Improvement Leads (QiLs) from both CCGs, responsible for advising
core members on the issues that require scrutiny and will also attend the entire meeting.
- Experts – attend to present reports they are responsible for and may attend for their report only or for the entire meeting.
Subject to a small number of amendments, the Joint Quality Committee Terms of Reference were approved. The Joint Quality Committee has a business cycle which lists when the key reports are to be presented to the committee. This was agreed at the October meeting. In addition, reports may be received on an ad hoc basis in line with publications, reports and relevant submissions, normally from the CCG Chief Nurse. At the Joint Quality Committee in October, the following reports and updates were received and discussed:
- regular update and feedback report from the ES Patient Board - Participation Toolkit produced for SES&SP CCG - CCGs’ clinical risks were reviewed and items to be added to the risk register, identified - Quarterly Complaints Report. A number of suggestions for improvement to the report
were made - update on the work of the Quality Surveillance Group - Infection Control Quarterly Report - Medicines Management regular report - Serious Incident Monthly Report from the CSU - Update on primary care quality was provided along with an update on GP avoidable
incidents in SES&SP CCG. It was suggested that the scheme is discussed at the ES Steering Group with a view to adoption by ESCCG.
At the Quality committee in November, the following reports were received and discussed:
- CCG Quality Escalation Process - Regular Medicines Management Update - Serious Incident Monthly Report from the CSU - Revised update report around local engagement and involvement activity - An update on the work of the Area Team Quality Surveillance Group
2
- The Quarterly Research Report was received for information. The low numbers of
practices actively involved in research was highlighted and proposals were suggested to improve this position.
- The Quarterly Winterbourne View Action Plan for Learning Disabilities Services was received. The Committee noted the content of the plan and the progress made to date. In future the report will be known as ‘Transforming Care’
- Quarterly updates for Safeguarding children and adults were received and improvements in both reports were recognised.
- Quarterly Soft Intelligence Report was received. This is to be shared with ESCCG Steering Group.
- Six monthly report on Individual Funding Requests was received and the content noted.
iii) Decisions made by the Joint Committee In October, the following decisions were made:
- Subject to a small number of amendments, the Terms of Reference were approved - Members approved the amended cover sheet and reminded all members that the
cover sheet for reports must be completed in full - At the first joint committee meeting, members agreed that in the absence of the East
Staffs secondary care consultant (who facilitates a different system of rating) assurance for providers would be agreed as assured, partial assurance, limited assurance or not assured. Further information in respect of this is provided below.
In November, the following decisions were made:
- The CCG Quality Escalation Process was approved for use by the Joint Quality Committee and the CCGs more broadly
- The Care Home Strategy for SES&SP CCG was not approved as the lead officer was not available to answer queries and provide additional assurance in relation to links with quality.
- Revised versions of the Standard Operating Procedures for the Medicines Optimisation clinics and the associated Quality Impact Assessment forms were approved.
iv) Additional Issues for escalation to Governing Body
Members are asked to note the concerns in respect of staffing at SSOTP, including the departure of the Medical Director and the Director of Nursing. In addition, the lack of assurance and concerns around workforce highlighted in the body of this report and above are brought to the attention of the Governing Body.
v) Assurance
Previously, ESCCG Quality Committee rated providers using the Modified Nominal Group Technique, introduced by ESCCG Secondary Care Clinician. Unfortunately, he has been unable to attend the Joint Quality Meetings so far and so, in order to provide consistency, members
3

used the criteria common to both CCGs to assess levels of assurance in respect of quality and safety. This is as follows:
1. Assured – certain, complete assurance 2. Partially Assured – only part, not generally, or incomplete information or data 3. Limited Assurance – restricted through lack of data, poor patient experience or
refusal to respond to challenges 4. Not Assured – complete lack of confidence or absence of significant
information/action following requests from previous quality committees
Members were in agreement that all provider services are considered to be safe. However, members are asked to note the specific concern in relation to falls at Burton Hospital which is being closely monitored with patient safety in mind.
vi) Provider Reports
The Committee received and reviewed reports in respect of quality for all key providers on the key quality indicators. A summary of each of these is provided below, highlighting areas by exception only.
4

BURTON HOSPITALS NHS FOUNDATION TRUST (Lead Commissioner - East Staffordshire CCG) SUMMARY ASSURANCE LEVEL Current RAG Rating based on information received and external reviews
Assured
Exceptions and Actions Patient Experience: There have been sustained improvements in helping patients with eating and drinking and staying clean. A consistent green score has been achieved for staff treating patients with kindness and compassion. The Trust overall patient experience score dropped down one point to amber in August and maintained the same score in September. Despite this, during August and September the Trust had the highest number of green domains since the start of the financial year. The question ‘Being involved in decisions about treatment and care’; ‘being able to get attention from staff’, and ‘getting help in time to get to the toilet’, continue to be the key areas for improvement. Discharge Question: The trust has continued to offer the discharge survey to patients, along with the Friends and Family Survey, at the point of discharge. The scores have remained reasonably consistent with previous months with “patients receiving answers that they understood about discharge” scoring highest. Ward Assurance: The Trust has sustained green rating for the 6th consecutive month. All areas that failed to achieve 95% or above (green) will continue to submit action plans to the Director of Nursing. In addition, the senior nursing team responsible for these areas now meet with the Director of Nursing to discuss action plans and confirm reasons for either deterioration or persistent low score. Performance management measures are considered within these meetings. Mixed Sex Accommodation Breaches: 7 breaches were reported in August. 4 were reported in ITU due to the lack of ward capacity to move the patient out to a medical ward. 3 breaches occurred in HDU due to the lack of ward capacity when a patient was ready to be transferred out of HDU. No breaches were reported in September. Falls: The number of falls is now increasing despite the significant amount of work being undertaken within the Trust. 5 falls resulting in harm (fractures) were reported as serious incidents in August and 4 falls resulting in fractures were reported in September. The NRLS data shows BHFT reports more Patient Accidents (Includes Slip Trips and Falls) than many other organisations (BHFT 23% of reported incidents against 20.6 % for all Small Acute Trusts). The Trust is undertaking extensive work to reduce the number of falls, yet the number of falls resulting in fractures is not reducing. The CQRM will be seeking assurance from the Trust on actions they are taking in relation to the NRLS publication, and a potential CQUIN for 2015-2016 is a CQUIN aimed at reducing the number of falls resulting in harm. Blood transfusion related incidents: This issue relates to the completion of the transfusion issue cards that have to be returned to the Blood Bank within 3 days of administering the blood product. The information required from the card is entered onto the blood history of the patient,
5

and then reported to external organisations as required. The Trust reports that no apparent harm came to the patients as a result of this. It is being addressed at ward and departmental meetings, senior staff team meetings and used during training sessions. The reduction in the number of incidents is a reflection of this work. Delayed reporting onto STEIS: In meetings between the Commissioners and the Trust, the Trust acknowledged that there has been a problem with the timely reporting of Serious Incidents onto STEIS. This is due to an internal process set up by the previous interim Director of Governance which required SIs to be signed off by a Senior Manager before being entered on to STEIS. The Trust has now revised this approach and has implemented a new process to ensure SIs are reported within 2 working days, in line with reporting requirements. The new process has resulted in improved performance which the Trust expects to be fully implemented by 1st November. The subject of delayed reporting is mirrored in their NRLS reporting times which are significantly higher than the reporting times of many other Providers. Following the commencement in employment of the new Head of Governance, reporting times have been seen to improve, and it is anticipated this will be sustained going forward. This will continue to be monitored on an on-going basis by commissioners. Medication Incidents: The reporting of medication incidents has shown an improvement in reporting, which is encouraging as the NRLS has identified BHFT as being in the lowest 25% of reporters of small acute Trusts between October 2013 and March 2014. The more reporting improves, the more likely that themes and areas of concern will be identified and actions taken to address issues allowing wider learning to take place across the organisation. Mortality Update: The Trust’s mortality measures are all as expected. The HSMR for the year to date is 102, and the SHMI is 98. Following the actions that have already taken place as a result of the previous high mortality rates which led to the Keogh Review, the present mortality data demonstrates the positive influence this has had on reducing the mortality rates at the Trust.
MRSA: No cases reported since July. C. Difficile: The Trust are current at risk of breaching their annual maximum of 15 cases as the present figure shows 15 cases have already occurred. However, in a new system introduced this year Cdiff figures are subject to review for avoidability and to date only one of the 15 cases has been found to be avoidable, thus 14 unavoidable. Complaints: The Trust has internal KPIs for dealing with complaints which are measured over a 12 month period. The Trust wants to ensure their complaints process is robust and so has invited Healthwatch to come into the trust to review their complaints process and to make recommendation for improvements where appropriate. The CQRM raised concerns about the recurrent themes within complaints and questioned what the Trust is doing to address these. The Trust assured the CQRM that specific work is underway with staff in response to the following complaints:
- Communication: where communication is identified as an issue the Trust addresses the
6

issue with individuals and teams
- Attitude: this is managed by the Senior Nurses who speak to the individuals / teams and explain the expectations of employees
Ownership of complaints is with the wards, and addressed through shared learning at ward and team meetings. Cancer 62 Day Wait: Performance was achieved in July, August and September. Safer Staffing: The Trust published their compliance with the safer staffing requirements via their website, in line with national requirements. No issues were identified at the last CQRM although the on-going issue of recruitment difficulties continues and has resulted in several trips overseas to successfully recruit additional nurses. The Trust has given assurance that all wards are adequately staffed and that staff are moved to other wards when patient needs dictate. The Trust stated that national reporting requirements do not reflect bed occupancy and that they strive to staff wards correctly at all times.
7

SOUTH STAFFORDSHIRE AND SHROPSHIRE HEALTHCARE FOUNDATION TRUST
(Lead Commissioner - South East Staffs and Seisdon Peninsula CCG)
SUMMARY ASSURANCE LEVEL
Current RAG Rating based on information received and external reviews
Assured
Exceptions and Actions
7 day follow up: There were 3 breaches during September 2014. These were as follows: • East Staffs CCG – there was a miscommunication between the ward, the care co-ordinator and
the patient. The patient was seen, but outside of the 7 days target • Cannock Chase CCG – the patient was seen but not showing on RiO at the time of reporting • South East Staffs and Seisdon Peninsula CCG – the patient DNA, the CRHT were informed and
were asked to visit the patient at the weekend Crisis Resolution/Home Treatment: 100% admissions via CRHT CRHT Four Hourly Responses: There were 7 breaches, 2 of which involved patients from Stafford & Surround CCG and 5 from East Staffordshire CCG. Of the 5, 3 were due to staff being unable to locate the service user within the 4hr response time, 1 was not medically fit at the time of referral, and 1 was a genuine staff breach due to staff attending another assessment IAPT: There has been a significant reduction in referrals in East Staffordshire which is reflected in the dip in activity. A meeting to discuss the Activity Notice from East Staffs CCG was held on the 12th Sept. An Action plan is being developed to encourage GPs to refer into the service. Under 18 Admissions: There was 1 under age admission in September. Another patient was admitted and discharged on the same day so did not count as an actual Occupied Bed Day (OCBD). 18 weeks Community Paediatrics: This breach involved audiology. The Trust advised commissioners that the delays were due to difficulties obtaining suitable audiology suites. The delays also had a detrimental impact on the recruitment and retention of audiologists. The Trust is now at full establishment, both audiology suites are complete and equipment has been ordered for installation into the new suite. 18 weeks Adult Mental Health: The 18 week dip is being investigated. Assurance will be sought at the next CQRM. 18 weeks older Adult Mental Health: As predicted, the service is now hitting the target as all MAC UK patients have been seen. Patient safety Incidents: The total number of incidents reported for the month of September 2014 is 77 and is split as follows:
• Older Adult Inpatient Services – 19, of which 30% were falls • Adult Mental Health Inpatient Services - 50, a 40% decrease from last month.
8
The highest reported types of incidents are self-harm (30%), assault (10%), absconding (30%) and medication incidents (12%). No trends are identified. Community Mental Health Reporting of Patient Safety Incidents remains within control limits for the combined Community Mental Health Teams. There was one unexpected death in the community which is currently subject to investigation. Infection Control: No MRSA or C.Difficile cases were reported in August or September
Adult and Children Safeguarding Update: There have been 20 referrals relating to safeguarding adults, compared to 28 in the previous quarter. There have been no allegations against members of staff related to safeguarding children and there are no current large scale investigations underway within the service. Workforce: The annual turnover rate for the Trust was 13.58% as at 31 August 2014. The areas that are over the upper control limit of 15% are the Forensic and Criminal Justice Directorate (16.2%) and HR/OD (29.4%). Whilst the Medical Directorate is showing a high turnover rate, this can be explained by rotations of junior medical staff which occurs four times per year. The Trust-wide appraisal rate remains at 87% as at 31 August 2014. Whilst the Trust is not reporting any further increases, this does represent an increase of 7% over the last 12 months. The largest improvements have been in the Finance Directorate where rates have improved from 79% to 94% over the last 12 months and Mental Health Staffordshire where rates have improved from 74% to 95%. The Trust-wide vacancy rate as at 31 August 2014 was 11.6%. The highest Divisional vacancy rates are Forensic and Criminal Justice Directorate (17%), Specialist Learning Disabilities Directorate (17.6%) and Facilities and Estates (26%). The Chief Operating Officer Directorate has the lowest vacancy rate (-9% - this is an over-establishment). The highest vacancy rate by professional group is Estates and Ancillary (24.9%) and the lowest is Nursing and Midwifery Registered (8.2%). Hotspot areas (at ward/team level) with high vacancy rates are reported to Trust Management Team and Divisional Management Teams. Complaints and PALs: The top themes for complaints are staff attitude, clinical treatment, and communication/attitude. 28 complaints were received in Q1 and lessons learned shared across the Trust. The Complaints and PALS report includes a Qualitative Summary of Upheld and Partially Upheld Complaints. The total number of PALS concerns received in Q1 was 133. Patient experience: During Q1, the Board continued to hear patient stories at Board meetings. The stories were conveyed in different formats, ensuring that there were a number of ways in which service users, with the necessary support, were able to bring their voice to the Board. CQUIN Q1 Update: All Q1 milestones were achieved.
9

STAFFORDSHIRE AND STOKE ON TRENT PARTNERSHIP TRUST (Lead Commissioner Cannock Chase CCG)
SUMMARY ASSURANCE LEVEL
Current RAG Rating based on information received and external reviews
Not Assured
Exceptions and Actions In October, members of the Joint Quality Committee agreed that they had Limited Assurance in respect of quality and care at SSOTP. This deteriorated to Not Assured at the November meeting. At the October meeting, committee members highlighted the lack of workforce data, the lack of assurance from the Trust with regard to their plans to replace the Medical and Nursing Directors, and concerns about District Nursing in the south particularly in East Staffs. Members agreed that work should be carried out to:
• Improve the quality of the reports to the committee, in line with other providers • Escalate to Governing Body and suggest a board to board meeting • Raise concerns about the continued lack of assurance to the Lead Commissioner • Consider raising a contract query as Associate Commissioner • Ask the Lay representatives to raise with members of the Patient Groups
In November, the committee highlighted the inaccuracy of the data in the reports, e.g. YTD columns incorrectly tallied and targets missing. The overall toolkit information was poor with data missing for September. It is unclear if members of the SSOTP Board had viewed the reports. Members of the committee queried whether this should be escalated to CQC and agreed that initially the issue should be raised by the Chair of the Lead Commissioners, emphasising the level of concern expressed by the CCGs.
Serious Incidents: There were 16 new Serious Incidents in September with a total of 13 ‘Stop the Clocks’. A breakdown for the South division was not provided. No further information for the South was submitted by SSOTP for September. Pressure Ulcers: A total of 6 Grade 3 pressure ulcers were reported for August, with 41 year to date. 1 Grade 4 pressure ulcer was reported, 2 year to date. All pressure ulcers will go through the Trust internal pressure ulcer validation panel, following which re-categorisation may occur. Pressure ulcers reported as Serious Incidents are reviewed and validated by the trust’s Tissue Viability Panel. Pressure Ulcers reported in August and reviewed by the panel in September, resulted in the following classifications; 2 were de-escalated, 1 was avoidable, 6 were non avoidable, and 1 was avoidable but not attributable. There was no information submitted on Pressure Ulcers for September.
Tissue Viability: The Trust has not tabled a Pressure Ulcer Q2 Update Report.
Sickness Absence: The sickness rate for the trust at the end of August was 4.56% which shows a small increase from July, against a stretch target of 3.39%. The report for September was 4.62%.
10

Long Term Sickness this accounts for 3.19% with Short Term Sickness at 1.37%. There has been an increase of 6 cases since last month where staff absence has hit the trigger of 28 days or more and therefore registered as Long Term Sickness. An analysis of the longer term cases has identified that managers are not closing down sickness episodes in a timely manner and therefore all managers of cases over 100 days (42 cases) will be required to audit whether the individuals are still off sick. Long Term Sickness for September was 3.22%, with Short Term Sickness at 1.40%. There had been a decrease of 11 cases since the previous month where staff absence has hit the trigger of 28 days for Long Term Sickness. The feedback from the audit by managers had resulted in 6 cases removed from the data as the individual had left or returned to work.
The increase in August was across all divisions except specialist services which had seen a small decrease. In September, there was a steady increase in Long Term Sickness cases in the Children’s Directorate, which is to be investigated.
Turnover Levels: In August and September, the Trust’s turnover level was well below its target of 10%. The highest recorded reason for staff leaving the Trust is reported to be retirement.
The Workforce Matters Committee Task to Finish group met to consider the reason for the low uptake of Exit interviews. It appeared to be related to the high number of staff taking retirement. Further work is planned to look at ways to retain an aging workforce. No update was provided for September.
Statutory and Mandatory Training: The Trust reported an increase in compliance levels for Statutory and Mandatory training courses except for Manual Handling and Basic Life Support, which is down by 0.5% in August, and Fire Safety down by 2.05% in September.
Appraisal Completion: Appraisal compliance figures remain below target for both August and September. The Trust reported that the Workforce Matters Committee is keeping a close eye on progress for each directorate but no improvement is reported to date.
11

DERBY HOSPITALS FOUNDATION TRUST (Lead Commissioner - Southern Derbyshire CCG)
SUMMARY ASSURANCE LEVEL
Current RAG Rating based on information received and external reviews
Not Assured
Exceptions and Actions In view of the concerns reported below for stroke performance, the Joint Quality Committee concluded they were not assured around the quality of services at the trust. The Lead Commissioner has changed the meeting schedule for the Quality Committee with Derby Hospitals. It is anticipated that from December, the timings of the Quality Assurrance Group and the Trust Board meetings will support the sharing of information in a more timely manner. The QAG in October reported an expected improvement in the available data at the December 2014 meeting. Stroke Services: An announced visit took place on the 21st October in response to poor performance against the national Stroke targets. The report is currently being compiled by SDCCG. Underperformance is shown for the target of ‘90% of Time spent on a Stroke Unit’. Data sources are being investigated to ensure that these figures are accurate. The number of Transient Ischaemic Attacks (TIAs) treated within 24 hours decreased following achievement the previous month. There is still a delay in coding, which has resulted in the August figures being amended on the Contract Management Delivery Group dashboard. As a consequence of non-achievement of the Stroke KPIs, the CCG has issued the Trust with a Contract Query Notice. An action plan has been developed to support the improvement of performance against targets as follows:
• TIA - breach information has been shared with the CCG. As the majority of the TIA breaches arrived at Hospital more than 24 hours after being seen by the first Health Professional, the CCG are working on education for GPs to ensure the importance of a speedy referral and ensure patients are aware of the consequences of not attending the TIA clinic on the same day
• 90% Time spent on a Stroke Unit – comparisons to the same time period on Sentinel Stroke National Audit Programme data is showing different compliance to the data reported from the corporate Information team. The two datasets are to be reconciled to identify the differences in reporting. At present there is a backlog of coding which is delaying the production of performance data. The Business Unit will be undertaking root cause analysis to understand the reasons for non-compliance.
A Business case for Stroke Hyper Acute, Acute and High Risk TIA has been developed and presented to Management Executive and the Trust Board. A proposal to provide the service to the Burton population from April 2015 has been shared with Commissioners. Workforce Update based on July Data: The Trust covered all shifts to ensure patient safety was
12

not compromised, although having more temporary staff on the wards did place pressure on the system. Particular workforce issues included:
• There were a high number of patients requiring increased nursing support. This lead to a need for additional staff on some wards. The demand was met by adjusting rotas and booking temporary staff
• Staffing matched patient dependency. Recruitment is on-going • Vacancies were covered by temporary staff or nurses being moved from other areas • There are no specific issues but a current workforce review is in process • Despite staffing levels falling below agreed levels, moving staff around the division has
enabled safer staffing to be adhered to The Trust overall shows an overfill rate of unregistered staff which is often an indication of providing additional support to patients who need increased supervision, e.g. those who are confused, wander, and are liable to increased risks of falling. A significant amount of recruitment activity has already been undertaken with bespoke and generic adverts. The fourth pooled recruitment event for unregistered staff took place during the weekend of the 16th August. The current vacancy position of registered and unregistered staff in the ward areas is 148.8wte of which 52.21wte have been appointed but are not yet in post. Friends and Family Test: In September, the results for the in-patient areas was 95 with a response rate of 38%. Complaint themes for August: Limited information was provided in September. It is anticipated that the Trust will be sharing more indepth information at future meetings MRSA: The MRSA case which occurred in August has been investigated. The route cause appears to be a lack of screening on admission. C.Diff: Year to date there have been 32 cases of C. diff reported. Investigations have been undertaken for all cases. The results are as follows: • 5 cases reported due to lapse in care • 21 cases reported which were not due to lapse in care • 6 cases are still under review
VTE: The list of exemptions has been reviewed against other local Trusts and, following agreement from the Medical Director and Lead for Thrombosis, additional exemptions have been included. The exemptions had not been reviewed since monitoring of the VTE risk assessments began.This mirrors the local agreement with Nottingham University Hospital and Leicester. Following achievement of the 95% target in August, it is anticipated that the performance will continue to improve with the other actions which are taking place throughout the Trust
Termination of Pregnancy services: There is a locally required standard of 95% of women, where clinically appropriate, to receive Termination of Pregnancy within 21 days of referral. An action plan was put in place to support the recovery and sustainability of this target, which is now being achieved.
13
OTHER PROVIDERS Staffordshire Doctors Urgent Care (SDUC) – Partial Assurance (October) It was noted that SDUC need to strengthen their written reporting of assurances in order to validate their current processes around complaints, incidents and patient experience and evidence outcomes and lessons learnt. Concerns were voiced around staffing between the North and South of the county. The next CQRM will seek assurances that the South has appropriate cover. An update is required from the Provider around the National Patient Survey, following recognition that there are areas for improvement. The provider has carried out an Infection Prevention and Control clinical audit and rated services as GREEN, compliant. Six doctors are reported to be non-compliant and resistant to attending Safeguarding Training. The matter is to be escalated to the Area Team. In addition, the Registrar Induction is to be escalated to Health Education England to allow for timely inductions as there are delays in the current system. NSL Non Urgent Patient Transport – Assured (October) Complaints in relation to NSL, continue to be low in relation to the number of journeys undertaken. The two complaints for September both relate to staff attitude. A central complaints telephone number has been introduced and a Complaints Manager is in post. One incident was reported. This was a patient who trapped their finger in the door of an ambulance. The patient was taken to Minor Injuries for treatment. Commissioners undertook a quality visit to the Hixon Depot in September. The visit provided a good opportunity to discuss issues and queries directly with staff. The outcome was very positive. It was noted that quarterly patient experience reports are produced and NSL is working on increasing the number of returns they receive. The return rate is low but very positive. The options for increasing uptake were discussed and included working with the local hospital trusts to include a question in their patient experience surveys as a means of improving response rates. The provider has been struggling to recruit appropriate staff, especially in the Burton area. They are now advertising in the local newspapers and were interviewing at the time of the visit.
Conclusion The Joint Quality Committee discusses and agrees the level of assurance for each provider at each committee meeting. This includes a discussion about the quality and safety of all commissioned services. As previously highlighted, the Committee concluded that all provider services are safe and therefore no additional immediate action was required in respect of safety. Where it was agreed that the quality issues highlighted above require further action these are raised with lead commissioners as part of the routine quality monitoring activity.
The work of the virtually integrated quality team through the CQRMs and Quality Committee alongside on-going work with all providers and/or lead commissioners continues to enable the CCG Governing Body to remain informed of key developments and areas of concern with all providers. Recent developments to further enhance this work have been highlighted within this report.
14

FEEDBACK SHEET SOUTH EAST STAFFORDSHIRE AND SEISDON PENINSULA AND EAST
STAFFORDSHIRE CLINICAL COMMISSIONING GROUP Joint Quality Committee
Wednesday 12th November 2014
1 Members present: Alex Fox, Chair, Dr Liz Gunn, Heather Johnstone, Sue Wilson, Debbie Vucetic, Rob
Boland, Nigel Williams, Angie Nisbett (Part meeting) Sue Bamford (Part meeting) Judy Bird, Heather Widdowson, Ann Tunley, Rosemary Crawley, Mark Seaton, Karen McGowan, Paul Winter
Administrator – Tracey Finney Quorate: Yes
2 Declarations of Interest: None
3 Key Points discussed:
• This was the second meeting of the newly formed Joint Quality Committee which was very well attended.
• A revised escalation process was presented and members of the Committee approved this. It is important to note that the CCGs must act in a timely and disciplined manner over issues that have been escalated to the relevant section or body for action. Future action lists are being amended to incorporate specific reference to escalated items.
• The Quality reports for key providers were discussed. Of these, the main concerns of the Committee related to HEFT, Derby and SSOTP. The issues for escalation are detailed in the relevant section below.
• The latest data for Derby suggests that the apparent improvement in cancer two week wait times has been achieved to the detriment of the 62 day target.
• Reports in respect of safeguarding adults and children were received. • A summary report in respect of Spotter Practices was received. Members of
the Committee were concerned at possible suggestions that this work does not continue and have made a strong recommendation that not only is this continued, but also that the pilot is widened to include practices in the East Staffs area.
• A helpful summary of local research activity was received. This identified that very low numbers of practices currently participate in research activity. Keele University are working on a scheme to encourage more research activity amongst GPs and the numbers in SES & SP and ES are particularly low compared to the rest of Staffordshire.
• A concern was raised in respect of GP Out of Hours, specifically anecdotal evidence that a number of GPs were resigning from their roles with Staffordshire Doctors Urgent Care (SDUC). An urgent action in respect of this
1

was identified to ensure continuity of service. • The Committee was pleased to agree that they were assured in respect of
Burton Hospitals Foundation Trust. 4 Next steps:
1. The Committee will have a considered debate at the next meeting in respect of
the use of patient experience to better triangulate quality issues. 2. It is important to note that the new committee structure is intended to bring
together experts (the core committee) and specialists (officer leads) to scrutinise and challenge health. Attendance by those nominated to fill specific roles is vital to continue improving quality surveillance.
5 Issues for escalation: 1. Heart of England – the reported action by Monitor and the CQC should be shared
urgently with GP practices. 2. Derby – assurance to be requested from Southern Derbyshire CCG in respect of
Derby Hospital’s failure to achieve the stroke indicators. It was agreed that due to the patient safety aspect of this matter, the Chief Nurse and the GP Lead for Quality, Dr Gunn, would take urgent action.
3. SSOTP – continued poor quality reports received in respect of this provider. The Chief Nurse undertook to discuss with the Accountable Officer and Chairman to discuss what further action can be taken.
4. Safeguarding – following a helpful update the Committee request that the Governing Bodies reinforce the need to ensure that safeguarding training for both adults and children is prioritised at both a practice but also a CCG level.
5. Spotter Practices – the committee asked the Governing Bodies to consider the future of Spotter Practices with the recommendation that the pilot is widened to take in more practices in the East.
6. Research – the Governing Bodies are asked to consider current involvement in research activity by local GPs and to decide whether or not a stronger commitment should be encouraged.
7. Attendance – the Governing Body is asked to consider the continuing role of the CCG secondary care representatives to ensure acute provider issues are appropriately and independently challenged. Similarly, concern in respect of a lack of response from Public Health is considered to leave a significant gap in the new Committee’s function.
2

Title Finance Report Month Seven 2014/15 (Period 1st April 2014 – 31st October 2014)
Reporting to Governing Body Date of Meeting 27th November 2014
Commissioning Lead(s) Author(s) W Kerr W Kerr / M Richards / L Squire
Purpose of the Report (Please select) Approval Assurance Discussion
Key Points/Executive Summary The Burton contract forecast outturn reflected at month seven is £4.5m and is materially
unchanged from month six. The year-to-date financial position shows an over spend of £3.946m which is an adverse
variation against planned deficit of £454k. In order to offset the over performance at Burton and hence maintain the agreed forecast deficit
of £5.882m, all uncommitted reserves have been released totalling £2.290m. This includes the release of £350k decommissioning reserve. In addition, £250k LIS savings have been released.
In order to achieve the agreed forecast deficit of £5.882m, a gap of £1.278m remains. This has been reduced from £1.515m at month six.
A number of transactional proposals have been included in the report to support mitigation of the remaining £1.278m gap, although additional areas need to be identified to provide headroom for slippage.
There are financial risks currently not reflected in the position and if these were to materialise, additional cost pressures would occur. The position will be closely monitored in case there is any deterioration. “Plan B” should therefore be to make savings in excess of £1.278m.
Recommendations (what is expected from the Board) Recommendations:-
The Governing Body are asked to: Recognise the impact of month seven performance, which shows an adverse year-to-date
variation against planned deficit of £454k. The target is to deliver the agreed £5.882m deficit and all appropriate mitigating action must
be undertaken to achieve this. Recognise the potential risks that currently exist and therefore must be appropriately
managed to ensure delivery of the planned deficit. Additional QIPP proposals/other mitigating actions have been identified to support
achievement of the £1.278m shortfall. It is requested that the committee recognise the urgency and provide the clinical leadership to achieve the savings required.
Understand the impact of achieving QIPP savings non recurrently on the underlying recurrent position going forward into 2015/16.
Enclosures Attached report.
X
Enc. 12
East Staffs CCG
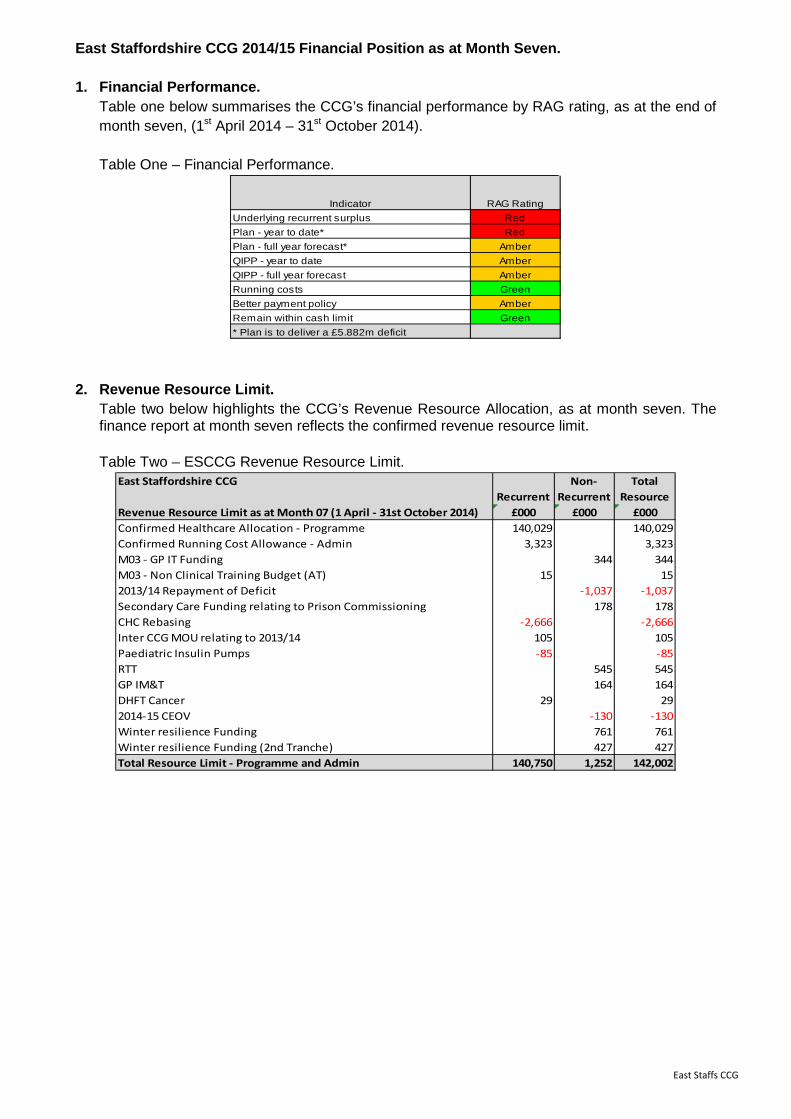
East Staffordshire CCG 2014/15 Financial Position as at Month Seven.
1. Financial Performance. Table one below summarises the CCG’s financial performance by RAG rating, as at the end of month seven, (1st April 2014 – 31st October 2014). Table One – Financial Performance.
Indicator RAG RatingUnderlying recurrent surplus RedPlan - year to date* RedPlan - full year forecast* AmberQIPP - year to date AmberQIPP - full year forecast AmberRunning costs GreenBetter payment policy AmberRemain within cash limit Green* Plan is to deliver a £5.882m deficit
2. Revenue Resource Limit. Table two below highlights the CCG’s Revenue Resource Allocation, as at month seven. The finance report at month seven reflects the confirmed revenue resource limit.
Table Two – ESCCG Revenue Resource Limit. East Staffordshire CCG
RecurrentNon-
RecurrentTotal
ResourceRevenue Resource Limit as at Month 07 (1 April - 31st October 2014) £000 £000 £000Confirmed Healthcare Allocation - Programme 140,029 140,029Confirmed Running Cost Allowance - Admin 3,323 3,323M03 - GP IT Funding 344 344M03 - Non Clinical Training Budget (AT) 15 152013/14 Repayment of Deficit -1,037 -1,037Secondary Care Funding relating to Prison Commissioning 178 178CHC Rebasing -2,666 -2,666Inter CCG MOU relating to 2013/14 105 105Paediatric Insulin Pumps -85 -85RTT 545 545GP IM&T 164 164DHFT Cancer 29 292014-15 CEOV -130 -130Winter resilience Funding 761 761Winter resilience Funding (2nd Tranche) 427 427Total Resource Limit - Programme and Admin 140,750 1,252 142,002
East Staffs CCG

3. Financial Summary.
Table three shows the CCG’s summary position as at the end of month seven (1st April to 31st October 2014). Table Three – Financial Overview.
East Staffordshire CCG - Finance Report Annual Budget
YTD Budget
YTD Expenditure
YTD Variance
Forecast Expenditure
Forecast Variance
Month 07 (1 April - 31st October 2014)£,000 £,000 £,000 £,000 £,000 £,000
Revenue Resource Allocation -142,002 -82,009 -82,009 0 -142,002 0
ExpenditureMental Health 11,884 6,865 6,843 -22 11,848 -37Acute 85,232 49,050 51,480 2,431 89,477 4,245Primary Care 22,663 13,233 13,017 -217 22,375 -288Cont Care & FNC 9,708 5,890 5,752 -138 9,579 -129Community 10,698 6,241 6,239 -2 10,695 -3Other 1,891 956 913 -43 1,817 -75Total HCHS 142,077 82,235 84,244 2,009 145,791 3,714
General Reserves 2,485 1,449 0 -1,449 195 -2,290Total Reserves / Contingencies / QIPP 2,485 1,449 0 -1,449 195 -2,290
Total Healthcare 144,562 83,684 84,244 560 145,986 1,424
Corporate/Running Costs 3,322 1,817 1,712 -105 3,176 -146
Total Expenditure 147,884 85,501 85,955 454 149,162 1,278
Total Deficit Reported 5,882 3,492 3,946 454 7,160 1,278
Further Savings Required to Address Deficit -1,278 -1,278
Potential Financial Risks Excluded From Position Full Risk Probability Potential Narrative £'000 % £'000
Acute Contracts 1,000 40% 400 Possible further movement Qtr 4QIPP Under Delivery 1,278 50% 639 Part of overall requirementCat M Drugs 160 50% 80 Total 2,438 1,119
Breakdown of General Reserves Total Released
£'000 £'000National Contingency 0.5% 700 700Local Contingency 328 328Nice / Lucentis Reserves 465 270Investment Reserves 290 290Decommissioning Budget 350 350Acute Contract Fines 151 151QIPP Line By Line Review 107 107Child Health Information System 94 94Total 2,485 2,290£2.290m has been released to support the financial position
As at month seven, acute contract monitoring has been received from most providers up to month six, although the report contains the assumption that current trends continue into month seven. Burton Hospitals is showing a forecast outturn of £4.5m over performance (£5.4m less £0.9m emergency funding outside of the contract). The Burton forecast excludes any assumption regarding delivery of QIPP for periods eight to twelve (achievement of QIPP in the year to date position is included in the forecast; future delivery is incorporated within the mitigating actions). The other acute providers are currently showing relatively small variances. In order to mitigate the over performance at Burton and achieve the planned deficit outturn of £5.882m, all uncommitted reserves totalling £2.290m have been incorporated into the forecast
East Staffs CCG
outturn position. These include the £700k national contingency, £328k local contingency, £290k investment reserve, £350k decommissioning budget, 7/12ths of the £465k NICE reserve, £257k relating to fines and budget reductions following a line-by-line review, and £94k funding contribution from the Area Team relating to Child Health Information System representing a reimbursement of payments made by the CCG. Additional savings to the value of £1.278m needs to be achieved in the remaining five months. The current forecast outturn position for contracts cannot deteriorate further otherwise the CCG’s ability to achieve the planned deficit could be jeopardised. There are other key financial risks that could materialise, which have not been reflected in the current forecast outturn position:
• Acute contracts non elective activity/elective could continue to over perform, with increased activity in quarter 4 resulting from unprecedented winter pressures. Current forecast represents some seasonal variation, however if the trend is significantly different to previous years then it will impact on the forecast position. Where possible the CCG will aim to reduce this risk by working with our two major providers, Burton and Derby, in obtaining the Trust’s view of the forecast outturn position each month, to validate how aligned we are. In addition the CCG will also attempt to enter into discussion with providers to agree year end agreements to close contracts down prior to the end of the financial year. The CCG has been successful in agreeing a year end settlement with Burton in prior years; however given the financial deficits both the CCG and Trust are facing this may be challenging to achieving.
• A number of challenges remain open with Burton Trust which is yet to be finalised and hence if not agreed could impact on the forecast position.
• Continuing Healthcare/complex cases risk has reduced due to renegotiation of the risk share. Current forecast assumptions are that activity will grow by 1% for each remaining month of the financial year, and that the QIPP of £1.67m will be delivered (ES CCG share for the remaining financial year is £246k). The forecast is currently shown £129k under spent, which is the value achieved to month 7. If the QIPP delivers and the 1% growth is not exceeded, then a further surplus would be achieved. However, at the present time the prudent position is being reflected. The key cost pressures arising from Continuing Health Care are the complex cases, which tend to be low volume in terms of numbers of patients but high cost.
• The CCG has been informed of a price increase in Generic M drugs, which based on script
switch data is likely to give an in year additional cost pressure of £160k. The BSA prescribing data which provides an indicative forecast outturn value currently excludes this impact. Overall the current trend in spending levels within Prescribing indicates that this can be accommodated within the overall prescribing resources. GP prescribing overspends are currently being offset by under spends from other prescribing budgets such as Home Oxygen. Forecast outturn position does not currently reflect the under spend from the other prescribing budgets, since these are currently being held in reserve until the BDA month 9 forecast has been released. The BDA prescribing data is not reliable until at least month 9. Further mitigation has also been undertaken by the Medicines Management team, in identifying and promoting further QIPP savings initiatives which have been communicated to all GP practices for implementation.
East Staffs CCG
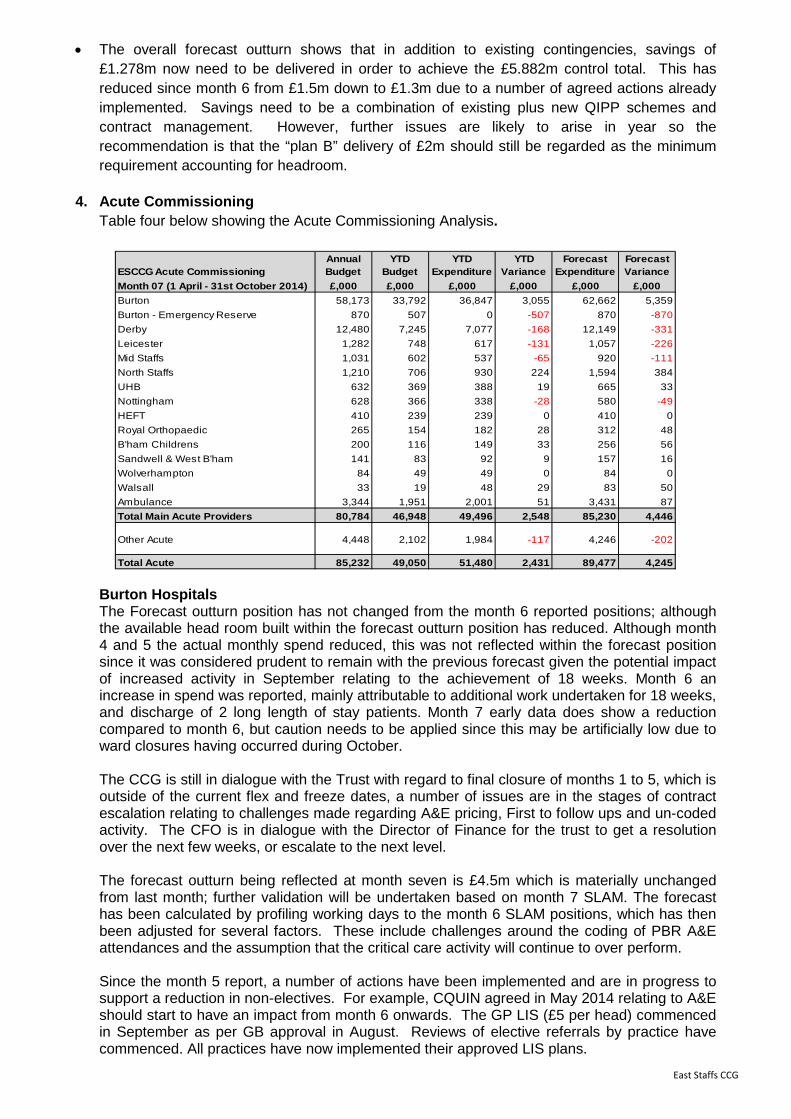
• The overall forecast outturn shows that in addition to existing contingencies, savings of £1.278m now need to be delivered in order to achieve the £5.882m control total. This has reduced since month 6 from £1.5m down to £1.3m due to a number of agreed actions already implemented. Savings need to be a combination of existing plus new QIPP schemes and contract management. However, further issues are likely to arise in year so the recommendation is that the “plan B” delivery of £2m should still be regarded as the minimum requirement accounting for headroom.
4. Acute Commissioning Table four below showing the Acute Commissioning Analysis.
ESCCG Acute CommissioningAnnual Budget
YTD Budget
YTD Expenditure
YTD Variance
Forecast Expenditure
Forecast Variance
Month 07 (1 April - 31st October 2014) £,000 £,000 £,000 £,000 £,000 £,000Burton 58,173 33,792 36,847 3,055 62,662 5,359Burton - Emergency Reserve 870 507 0 -507 870 -870Derby 12,480 7,245 7,077 -168 12,149 -331Leicester 1,282 748 617 -131 1,057 -226Mid Staffs 1,031 602 537 -65 920 -111North Staffs 1,210 706 930 224 1,594 384UHB 632 369 388 19 665 33Nottingham 628 366 338 -28 580 -49HEFT 410 239 239 0 410 0Royal Orthopaedic 265 154 182 28 312 48B'ham Childrens 200 116 149 33 256 56Sandwell & West B'ham 141 83 92 9 157 16Wolverhampton 84 49 49 0 84 0Walsall 33 19 48 29 83 50Ambulance 3,344 1,951 2,001 51 3,431 87Total Main Acute Providers 80,784 46,948 49,496 2,548 85,230 4,446
Other Acute 4,448 2,102 1,984 -117 4,246 -202
Total Acute 85,232 49,050 51,480 2,431 89,477 4,245
Burton Hospitals The Forecast outturn position has not changed from the month 6 reported positions; although the available head room built within the forecast outturn position has reduced. Although month 4 and 5 the actual monthly spend reduced, this was not reflected within the forecast position since it was considered prudent to remain with the previous forecast given the potential impact of increased activity in September relating to the achievement of 18 weeks. Month 6 an increase in spend was reported, mainly attributable to additional work undertaken for 18 weeks, and discharge of 2 long length of stay patients. Month 7 early data does show a reduction compared to month 6, but caution needs to be applied since this may be artificially low due to ward closures having occurred during October. The CCG is still in dialogue with the Trust with regard to final closure of months 1 to 5, which is outside of the current flex and freeze dates, a number of issues are in the stages of contract escalation relating to challenges made regarding A&E pricing, First to follow ups and un-coded activity. The CFO is in dialogue with the Director of Finance for the trust to get a resolution over the next few weeks, or escalate to the next level. The forecast outturn being reflected at month seven is £4.5m which is materially unchanged from last month; further validation will be undertaken based on month 7 SLAM. The forecast has been calculated by profiling working days to the month 6 SLAM positions, which has then been adjusted for several factors. These include challenges around the coding of PBR A&E attendances and the assumption that the critical care activity will continue to over perform. Since the month 5 report, a number of actions have been implemented and are in progress to support a reduction in non-electives. For example, CQUIN agreed in May 2014 relating to A&E should start to have an impact from month 6 onwards. The GP LIS (£5 per head) commenced in September as per GB approval in August. Reviews of elective referrals by practice have commenced. All practices have now implemented their approved LIS plans.
East Staffs CCG
Close monitoring will need to be undertaken over the next few months to see if an impact is demonstrated. If the required outcomes are not achieved, then other mitigating action will be required.
North Staffordshire The forecast outturn reflected for University Hospitals North Staffordshire is £384k, reflecting a small adverse movement compared to month 6, due to an increase in non elective activity. It should be recognised that activity from Mid Staffordshire has now transferred to North Staffordshire and a contract variation has been undertaken to reflect this change. A challenge has been made to the trust regarding the mechanism for funding of ventilators. The CCG is still awaiting a response. Derby Hospitals The CCG has a reserve to cover the potential impact of RTT issues above the funding allocated by the Area Team of £129k. As at month seven the contract is under performing, but the cautious approach is to hold the RTT reserve until the CCG is confident it is not required. Review of the CCG 18 weeks profile for Derby shows that the RTT position has not improved and therefore the RTT funding is likely to be required prior to the yearend if performance is to be achieved.
5. Extract from Month 7 QF&P Contract Management Report East Staffordshire CCG Forecast at all Acute Providers using M6 SLAM YTD
• Base forecasts provided by Contract Management Team (CMT)/ CCG Contract leads across region. Reviewed by local CMT and adjusted for known local issues where required.
• Key Assumptions – Heart of England - Joint Managed Risk Agreement so Contract performance capped.
• Key Assumptions – Burton Foundation Trust - Successful outcome from A&E Coding Challenge of £286k in Best/Likely - Successful Critical care unit challenge of £56k re coding to Specialised Commissioning. - Reducing Critical care unit forecast by £123k now long stay patients discharged. - Reducing Day case/Elective forecast to remove non recurrent expenditure on 18 week delivery in months 1 to 6. - Forecast assumes QIPP delivery per current performance levels in months 1 to 6 in underlying activity position.
• Key Assumptions – Derby / Leicester - Increase forecast to remove under-performance in Day case/Elective that will be delivered in months 7 to 9 via 18 weeks initiatives and to adjust for Contract variation order to transfer funding from University Hospital Leicester to University Hospital North Staffs for vascular service changes.
Burton NHS Foundation Trust i) Summary
• Overall contract performing at +£3.8m v plan (all Commissioners) • East Staffordshire CCG +£2.7m v contract plan (for analysis of split see section below) • A number of contract levers have been enacted to challenge activity and service
performance • 18 weeks initiatives complete at Burton Foundation Trust within July-Sept time frame set
out by NHS England, with no Variations for October and November required. 18 weeks penalties will apply in full.
East Staffs CCG

(ii) Contract Actions against activity/service performance issues
• 1 Contract Query in progress – A&E at Joint Investigation stage • Activity Query Notice for First to Follow Up Ratios on going to support Month 1 and 2.
(iv) East Staffordshire CCG Performance At Month 6 (August 2014)
Burton/East Staffordshire CCG Month 6 YTDPOD Activity PlanActivity Actual Activity Diff Price Plan Price Actual Price DiffDaycases 4,329 4,822 493 £3,008,914 £3,421,416 £412,501Elective Inpatients 1,010 1,031 21 £2,214,588 £2,575,955 £361,367Non Elective Emergency Threshold 0 0 0 £0 -£371,840 -£371,840Non Elective Inpatients 7,383 8,970 1,587 £8,851,629 £10,096,700 £1,245,070Other Below line Activity 301,326 317,060 15,734 £4,192,744 £4,713,063 £520,318Outpatient First Attendances 15,330 14,956 -374 £1,936,721 £1,999,274 £62,553Outpatient Follow-Up Attendances 30,094 32,420 2,326 £2,205,936 £2,426,747 £220,811Outpatient Procedures 8,856 8,842 -14 £1,590,060 £1,571,610 -£18,450Passthrough payments 0 1,238 1,238 £1,078,989 £1,279,071 £200,082Pathway Payments 1,648 1,620 -28 £1,472,044 £1,446,002 -£26,042Queries and Adjustments 0 -195 -195 -£211,307 -£235,601 -£24,293Unbundled Diagnostics 7,641 8,954 1,313 £488,976 £563,580 £74,604Ward Attenders 2,140 2,176 36 £94,032 £93,031 -£1,001Grand Total 379,756 401,894 22,138 £26,923,326 £29,579,008 £2,655,681
(v) Contract / Activity Pressures
The table blow summarises the financial pressures that are contributing to the Month 6 YTD over performance
Service Line Value £ Value £Month 6 YTD Over Performance £2,655,681QiPP by PODDaycases -£94,857Elective -£76,744Non Elective -£260,500Fup Outpatients -£283,123A&E -£28,002QIPP Delivered £206,767QiPP Sub Total -£536,459
Critical Care Episodes incorrectly charged to ESCCG
-£27,924
A&E Counting & Coding Challenge -£134,049
Increase in elective/daycase activity in specialties due to RTT performance
-£406,000
Emergency: shortfall in plan -£435,000Remaining Financial Variance Driven by Activity Demand
£1,116,249
(vi) Headline analysis and Reasons for Over-Performance After reviewing the Burton information available for the month 6 position, an analysis of the reasons for the over performance and headline findings are summarised below:
• Over Performance: the year to date variance at month 6 is £2.655m, which means that the variance has moved by £683k from month 5 which was £1.972m.
East Staffs CCG

• Critical Care: As at month six the critical care bed days are 89 above plan with a cost variance of £172k. Within the costs to date of £619k (which is generating the £172k variance) there are £28k of charges that relate to Specialised Services. Burton have reallocated the majority of the previously identified activity, but there are some recent charges that need to be reallocated. The correct identification is based upon activity in SUS being flagged by the DMIC and is part of the reconciliation process. Included in the year to date costs are 2 patients with long stays of £84k and £39k.
• A&E change in coding: it appears that Burton Foundation Trust have changed their A&E coding which has resulted in activity being charged at higher tariffs than was planned for. Providers are required to give advance notice to commissioners if they intend to change their coding. The month two coding position has already been raised as a challenge with Burton Foundation Trust and at month six the cumulative financial impact of the coding is valued at £139k; which is included in the year to date over performance of £241k.
• A&E increased activity: Aside from the coding issue there is a cost pressure being driven by the increase in attendances above the anticipated planned levels. At present there have been 1,078 additional A&E attendances (7% above plan). The increase is coming from patients self-presenting and this emerging picture has previously being shared with the CCG Steering Group. The increase in A&E activity means that there will be pressure on Non Electives as patients convert from A&E.
• Non-elective activity increased in month six. The simple line graph below shows the comparison between plan and actual activity levels.
• Non-elective plan shortfall: It appears that the plan for 2014-15 is light on activity
compared to last year’s actuals (adjusted for part year effect of the AAC opening). The annual shortfall based on an average unit price of £1,800 is £870k, a contingency has been identified to support mitigation of this, which is shown as a separate line within the finance report for Burton.
Activity increase due to 18 weeks performance issues: As part of the 18 weeks work undertaken it was identified that Burton Foundation Trust had activity issues in three main specialties. At the end of September it appears that the originally identified backlog has been cleared. The original exercise identified circa 190 outpatient and spells at a cost of just over £400k for ESCCG. This cost is currently shown as a direct hit to the current over performance.
(vii) Steps taken to Validate Costs
• Best Practice Tariffs (BPT) we have asked the Trust to provide patient level to demonstrate compliance with parts of the BPT criteria which cannot be verified through the SUS or SLAM provided. This will be conducted as part of Q1 process.
• CCG Medicines Management colleagues are undertaking reviews of the high cost drugs data to ensure compliance and raise queries where appropriate regarding charging and dispensing.
East Staffs CCG

• The CMT are working with the Data Management Integration centre (DMIC) to set up and establish a process for validating maternity payments for the antenatal and postnatal elements of the pathway to ensure there is no double charging by individual Providers to CCGs where a mother choses to change her Provider part way through the antenatal pathway. Burton and other Providers have been requested to supply maternity pathway data.
• The monthly performance of follow-up ratios is being monitored compared to the contract
ratios. As at month five, there is a cost pressure of £85k as a result of Burton not achieving the ratios in the contract.
(viii) Detailed Contract Actions against activity/service performance issues
• Activity Query Notice raised in support of First – Follow Up Outpatient Ratio’s • Month 1 to 4 remain outstanding with issues relating to First – Follow up ratios, A&E Coding
and U Codes in SUS as substantial differences in position. In process of entering formal dispute procedure to progress.
• New monthly of internal reviews of Planned and Unscheduled Care issues to agree priorities and key actions
• Q1 reconciliation of Best Practice Tariff eligibility (ix) Supporting Information To assist the CCG in working with GP’s and demonstrating activity pressures and demand trends we have produced monthly activity trackers for Inpatient, Outpatient and A&E for East Staffordshire CCG at the two main Providers Burton and Derby Hospitals highlighting;
1) A&E referral sources by GP Practice and time of arrival 2) A&E reasons for presentation 3) Total Demand on Emergency Portal including AAC 4) Non Elective referral sources 5) Case-mix pressures in Elective care 6) Outpatient Referral Sources to key specialties
6. Mitigating Actions
Table five below shows potential mitigating actions, with a best, likely and worst case scenario.
A number of work streams are aligned to supporting reductions in non elective activity/finances, GP local improvement scheme and CQUINS. Non-elective activity plans have been developed and work is underway on elective activity management, recognising the timescale to have an impact this financial year is the end of October. Elective data has been shared with practices and discussions with practices where benchmarking shows significant movement between 13/14 and 14/15 are being undertaken.
East Staffs CCG

7. QIPP update The year to date position on planned QIPP is showing an under achievement of £330k, and a forecast outturn under achievement of £720k, against the original plan of £2.068m. The main areas under achieving are reductions in first to follow up ratios and non-elective admissions. Whilst the recurrent QIPP plans have not fully delivered the planned savings required a number of non recurrent transactional savings have been achieved to support mitigation. However this does have a detrimental impact on the CCG underlying recurrent financial position going forward into 2015/16.
8. Primary Care Table six shows Primary Care expenditure as at the end of month seven.
Primary Care Summary Annual Budget
YTD Budget
YTD Expenditure
YTD Variance
Forecast Expenditure
Forecast Variance
Month 07 (1 April - 31st October 2014) £,000 £,000 £,000 £,000 £,000 £,000CENTRAL DRUGS 535 312 249 -64 535 0COMMISSIONING SCHEMES 165 96 96 0 165 0LOCAL ENHANCED SERVICES 1,411 823 690 -133 1,161 -250MEDICINES MANAGEMENT - CLINICAL 332 156 128 -28 294 -38OUT OF HOURS 364 244 244 0 364 0PRIMARY CARE IT 356 166 150 -16 356 0OXYGEN 197 115 93 -22 197 0PRESCRIBING 19,303 11,321 11,367 46 19,303 0
Total 22,663 13,233 13,017 -217 22,375 -288 The CCG has received prescribing data for April to August. Currently the BSA is forecasting an over spend of £146k which currently can be contained within the overall prescribing budgets. Prescribing will be monitored closely particularly given the magnitude of variation in the BSA forecasting data during 2013/14 – the forecast is not regarded as reliable until at least December. CCGs have also recently been advised of increases in Generic M drugs prices which are forecast to cause an additional cost pressure of £160k. As a result the Medicines Management team have been proactive and rolled out additional QIPP schemes to offset this pressure. The forecast underspend on local enhanced services is due to slippage on the implementation date of the LIS, which commenced in September. The schemes are scheduled to run for 12 months, but only 6 months finances will accrue in 2014/15 financial year.
East Staffs CCG

9. CCG Running Costs.
The CCG running cost envelope for 2014/15 is based on the same financial value as allocated for 2013/14 at £3,322k. No uplift in recognition of increases to population has been funded, although likewise no cuts to the current allowance have been made.
Table seven - Running Costs.
Corporate Running Costs Annual Budget
YTD Budget
YTD Expenditure
YTD Variance
Forecast Expenditure
Forecast Variance
Month 07 (1 April - 31st October 2014) £,000 £,000 £,000 £,000 £,000 £,000
Pay 1,290 749 647 -102 1,153 -138
Non-Pay 2,102 1,138 1,148 10 2,100 -2
Income -70 -70 -82 -13 -76 -6
Total Corporate Running Costs 3,322 1,817 1,713 -105 3,176 -146
10. Better Payment Policy
The CCG has a business target to achieve the Government’s Prompt Payment Target of 95% of invoices being paid within 30 days both in terms of value and volume. As at month seven, the CCG was not achieving the Better Payment Policy (BPP) target in relation to the number of invoices paid within 30 days, but was achieving the % for value of invoices passed for payment within 30 days. Table eight below shows the currently reported position.
05D EAST STAFFORDSHIRE CCG Prepared by: Rebecca CrawfordDate completed: 05/11/2014
NHS Period: OCT 2014
NHS Invoices Paid Percentage ComplianceWithin Limit Outside Limit Total Paid This Month Year to Date
Number Value Number Value Number Value Number Value Number ValueAPR 126 14,372,543 59 495,325 185 14,867,868 68.1 96.7 68.1 96.7MAY 177 8,604,151 23 226,071 200 8,830,222 88.5 97.4 78.7 97.0JUN 120 8,275,676 11 5,864 131 8,281,540 91.6 99.9 82.0 97.7JUL 149 9,599,820 14 57,665 163 9,657,484 91.4 99.4 84.2 98.1AUG 152 8,726,352 28 271,105 180 8,997,457 84.4 97.0 87.7 97.8SEP 210 9,788,071 11 206,916 221 9,994,986 95.0 97.9 86.4 96.3OCT 200 9,437,295 13 263,325 213 9,700,619 93.9 97.3 87.6 96.4TOTAL 1,134 68,803,906 159 1,526,270 1,293 70,330,177 Failed Achieved Failed Achieved
NON NHS Invoices Paid Percentage ComplianceWithin Limit Outside Limit Total Paid This Month Year to Date
Number Value Number Value Number Value Number Value Number ValueAPR 116 434,793 11 94,848 127 529,641 91.3 82.1 91.3 82.1MAY 113 625,691 19 62,093 132 687,784 85.6 91.0 88.4 87.1JUN 172 1,065,754 24 83,431 196 1,149,185 87.8 92.7 88.1 89.8JUL 113 569,528 23 121,698 136 691,225 83.1 82.4 87.0 88.2AUG 154 934,814 45 283,822 199 1,218,636 77.4 76.7 84.6 84.9SEP 142 746,734 19 122,503 161 869,237 88.2 85.9 85.2 85.1OCT 150 670,923 9 36,832 159 707,754 94.3 94.8 86.5 86.2TOTAL 960 5,048,235 150 805,227 1,110 5,853,462 Failed Failed Failed Failed
Combined NHS/NON -NHS2,094 73,852,142 309 2,331,497 2,403 76,183,639 87.1 96.9
Failed Achieved 11. Cash Resource Limit.
The CCG has been advised of the Cash Resource Limit (CRL) by NHS England, confirming that the planned deficit will be funded in cash terms. Continuing careful management of cash should now ensure sufficient funds are available throughout the financial year.
East Staffs CCG

Table nine below shows the Cash Drawdown position. East Staffordshire CCG Financial Year 2014/15
Cash Book Ba lance
£000 £000 £000 £000 £000 £000 £000 % £000 % %
Apri l 15,000 1,305 16,305 1,291 15,000 16,291 16,291 10.99% -14 -0.08% 667 4.45%
May 10,500 1,431 28,236 1,391 9,000 10,391 26,682 18.00% -1,554 -5.50% 444 4.93%
June 9,000 1,399 38,635 1,408 9,000 10,408 37,090 25.02% -1,545 -4.00% 99 1.10%
July 9,000 1,433 49,068 1,403 10,500 11,903 48,993 33.05% -75 -0.15% 132 1.26%
August 10,000 1,339 60,407 1,384 10,000 11,384 60,377 41.07% -30 -0.05% 140 1.40%
September 11,000 1,467 72,874 1,464 11,000 12,464 72,841 49.55% -33 -0.04% 343 3.12%
October 10,500 1,394 84,768 1,383 10,500 11,883 84,724 57.63% -44 -0.05% 297 2.83%
November 11,000 1,377 97,145
December 10,500 1,512 109,158
January 10,500 1,418 121,075
February 11,000 1,387 133,463
March* 12,125 1,416 147,004
CRL 130,125 16,879 147,004 9,724 75,000 60,377
CASH DRAWINGS
MonthMonthly
Plan
Actual Tota l
Monthly Drawdown
% Drawings
to Date
Cumulative Variance
from Plan
% Variance from Plan
(cumulative)
BSA Prescribing Drawdown
Actual Cash Drawdown
Planned BSA Prescribing Drawdown
Actual Cumulative Drawdown
Cumulative Plan
% Variance
(target 5%)
The cash profile above recognises the planned cash advance of £5m made to Burton against the 2014/15 Service Level Agreement (SLA) in April 2014; this will be clawed back in March 2015, so that cash and the SLA are aligned.
12. Statement of Financial Position Table ten shows the Statement of Financial Position as at month 7.
Month 07 (1 April - 31st October 2014)ASSETS £'sTotal Other Non-Current Assets 0Non-Current Assets 0
£'sInventories 0Trade and other receivables 300,032- NHS receivables 223,143- NHS - Prepayments 2,321- Non- NHS Prepayments (13,074)- Other - Prepayments 0- NHS - Accrued Income 0- Non-NHS Accrued Income 58,894- Non-NHS receivables 0- Non-NHS prepayments and accrued income 0- VAT Receivable 42,414- Other Receivables 9,714- Payments received on account (23,380)Other financial assets 0Other current assets 0Cash and cash equivalents 297,749- Cash 297,749Current Assets 597,781
TOTAL ASSETS 597,781
LIABILITIES £'s- Interest payable 0- Social Security Costs 46,030- NHS payables - revenue 3,982,602- Non-NHS payables - revenue 688,787- Non-NHS accruals and deferred income 2,190,489- NHS accruals and deferred income (155,928)- Other Payables - revenue 74,065- Other liabilities 0Current Liabilities 6,826,045
EQUITY £'sShare Capital 0Revaluation Reserve 0Donated Assets Reserve 0Government Grants Reserve 0Other Reserves 0Retained Earnings (6,228,264)Total Taxpayers Equity (6,228,264)TOTAL EQUITY + LIABILITIES 597,781
East Staffs CCG
Recommendations:-
The Governing Body are asked to: Recognise the impact of month seven performance, which shows an adverse year-to-date
variation against planned deficit of £454k. The target is to deliver the agreed £5.882m deficit and all appropriate mitigating action
must be undertaken to achieve this. Recognise the potential risks that currently exist and therefore must be appropriately
managed to ensure delivery of the planned deficit. Additional QIPP proposals/other mitigating actions have been identified to support
achievement of the £1.278m shortfall. It is requested that the committee recognise the urgency and provide the clinical leadership to achieve the savings required.
Whilst mitigating actions have been identified within the report, actual implementation is key to ensure delivery of the control total. Close monitoring of schemes identified must be undertaken.
Understand the impact of achieving QIPP savings non- recurrently on the underlying recurrent position going forward into 2015/16.
East Staffs CCG
Title Medium Term Financial Recovery Plans- Financial Years 2015/16 - 2016/17.
Reporting to Governing Body Date of Meeting 27th November 2014
Commissioning Lead(s) Author(s) W Kerr W Kerr
Purpose of the Report (Please select) Approval Assurance Discussion
Key Points/Executive Summary • As part of the Distressed Health Economy review Staffordshire CCG’s have been
requested to prepare revised financial recovery plans.
• Updated plans are required to demonstrate financial balance as at the end of the financial year 2016/17, following which the ability to repay past deficits will then be required to be factored into plans for 2017/18 onwards.
• The CCG is required to identify the size of the financial gap required to be addressed by 2016/17 including achievement of a 1% surplus.
• The Gap requiring to be addressed is £9.8m.If the CCG is required to have a 1.5% National contingency in 2016/17 then this would increase by a further £1.5m, current plans include a 0.5% National contingency.
• The following areas have been identified as a priority across the Staffordshire CCG’s;
First Priority Areas Second Priority Areas
Non Elective Admissions Pricing Disinvestments Mental Health Planned Care Specialised commissioning Continuing Health Care Prevention and Public Health
X
Enc. 12a
1 Author: Date: East Staffs CCG
Recommendations (what is expected from the Board) Recommendation:-
The Governing Body are asked to: • Recognise and understand the implications of the requirements set out by NHS
England relating to the refresh of 2015/16 and 2016/17 Financial Plans.
• Understand the size of QIPP programme required to be achieved over the next 2 years, acknowledging that the phasing between the 2 financial years has yet to be confirmed.
• Approve in principle the priority areas currently identified for project initiation and evaluation, supporting delivery of the CCG’s financial gap.
Enclosures None.
2 Author: Date: East Staffs CCG
1. Overview
• As part of the Distressed Health Economy review Staffordshire CCG’s have been requested to prepare revised financial recovery plans. Updated plans are required to demonstrate financial balance as at the end of the financial year 2016/17, following which the ability to repay past deficits will then be required to be factored into plans for 2017/18 onwards.
• The 2 year plans for submission by the 28th November are required to demonstrate the following; That the CCG has capability to successfully implement recovery plans,
demonstrating appropriate internal governance and financial grip. That plans have appropriate programme leads, responsibilities, key
assumptions and milestones. Are credible Reflect the principle of “do it once not six times”, collaborating with CCG’s
and other stakeholders in developing plans together. Incorporate the KPMG Local Health Economy 23 recommendations,
where relevant. Demonstrate improvement on the CCG’s “run rate” when compared to
2014/15. Basically this requires the CCG to request approval of a planned deficit that is lower than 2014/15 deficit after excluding payback of prior year’s deficit. So for ESCCG that would mean a deficit that would be lower than £4.8m, (2014/15 planned deficit is £5.8m of which £1m relates to payback of 2013/14 £1m deficit).
The CCG is required to demonstrate achievement of the National Performance Metrics in 2016/17, which therefore requires achieving a 1% surplus, representing £1.5m.
• Financial Planning support to commissioners is being provided by KPMG and NHS England, against which progress is being monitored by a Programme Management office on a weekly basis. The end product is one which the CCG must own and be accountable for, so engagement by the Governing Body in owning the delivery of the Medium term financial plans is critical.
• The CCG received approval for a planned deficit for 2014/15 of £5.8m (£4.8m in
year deficit, combined with £1m payback of prior year’s deficit).Currently ESCCG is forecasting an outturn deficit of £5.8m which is line with the CCG’s approved plan for 2014/15. Any deterioration of outturn prior to the closure of 2014/15 would require the CCG to produce an in year financial recovery plan, against which weekly monitoring by NHS England would be undertaken. In addition any variation to 2014/15 outturn could potentially have a recurrent impact on 2015/16 plans, which would then give rise to additional savings being required. It is therefore important that all the appropriate contract levers and challenges are undertaken. Delivery of the CCG’s Local Improvement Scheme is enacted to support the achievement of the CCG’s 2014/15 forecast outturn.
3 Author: Date: East Staffs CCG

2. Refresh of Medium Term Financial plans. • East Staffordshire CCG in May 2014 submitted its 5 year financial plans, covering
the period April 2014 to March 2019. The current refresh focuses on the financial years 2015/16 and 2016/17. The CCG is required to identify the size of the financial gap required to be addressed if at the end of 2016/17 it is to achieve a 1% surplus. The Gap identified to be addressed is £9.8m. If the CCG is required to have a 1.5% National contingency in 2016/17 then this would increase by a further £1.5m, current plans include a 0.5% National contingency.
The table below highlights the movement between May’s original submission and November’s refresh.
• The key differences are:-
Achievement of 2014/15 QIPP has not been fully delivered on a recurrent
basis and hence achievement of the forecast outturn position has relied on non-recurrent benefits and savings. Therefore the underlying recurrent position being carried forward into 2015/16 is of a greater financial value than that which was anticipated in June’s version.
The requirement to demonstrate delivery of a 1% Surplus has been
incorporated within the refreshed version. However the impact of this has been partly mitigated by the assumption that 2016/17 resource allocation will increase greater than previous allocations growth for 2014/15 and 2015/16. This is due to the CCG’s distance from target (fair shares) moving from being under target by c£6m to c£9m as a result of the Continuing Health Care adjustment undertaken during 2014/15.
4 Author: Date: East Staffs CCG
3. QIPP Schemes • The overall gap identified for 2015/16 is £8.2m, given the requirement by NHS
England to ensure that any planned deficit required for 2015/16 shows an improvement against 2014/15 planned deficit position of £4.8m (excluding prior year’s deficit), then the CCG would need to deliver minimum savings in 2015/16 of £4m.
• Savings at this level would result in a planned deficit of £4.2m which fulfils NHS requirements. No predetermined level has been requested currently by NHS England for 2015/16 planned deficit level, although they will be looking for improvement against 2014/15, credible plans being submitted, and that the CCG has challenged itself with the level of QIPP aiming to be achieve in year 1, and ensuring that the CCG has not heavily back ended QIPP schemes into 2016/17. If 2015/16 delivered savings of £4m then 2016/17 would require saving of £5.8m for 2016/17.
• Until the full programme of QIPP schemes has been fully populated it is too early to confirm the profiling of the QIPP savings over the 2 years. An update will be provided to the QIPP, Finance and Performance committee and Governing Body in December.
• The key areas highlighted below are currently in the process of having detailed
Project initiation Documents produced either by the CCG or in collaboration with other CCG’s for inclusion in the November 28th Submission. Once financial values have been validated then these will be incorporated within the financial plans refresh.
• The following areas have been identified as a priority across the Staffordshire
CCG’s; First Priority Areas Second Priority Areas Non Elective Admissions Pricing Disinvestments Mental Health Planned Care Specialised commissioning Continuing Health Care Prevention and Public Health
Opportunity CCG Lead
QIPP 14/15 Areas to strengthen recovery
CHC including Complex cases ESCCG Nicky Harkness to work with Rob Lusuardi Cannock/Stafford CCG
GP Local Improvement Scheme to support reductions in Non -Elective Admissions
Julie Hughes
SSSFT Mental Health Re: Out of Area Placements
Tim Tebbs SES and Wendy Kerr
SSOTP: Quality issue
Nicky Harkness to work with Victoria Hilpert/Yohan Bhatti in CMT.
5 Author: Date: East Staffs CCG

Contract Issue & 7 day therapies NELS Immediate actions: Flu Vac uptake Palliative care Nursing Burton Trust
Julie Hughes to work with Rebecca Woods Review Specification
Priorities as per Staffordshire wide Workshop
Opportunity CCG Lead NELS
NHS 111
Paul Winter and Sharon Finney to work with Chris Oliver
Out of Hours Sharon Finney to work with Hayley Bishop from SES
Pathway for AAC Geriatrician Service spec
Sharon Finney/Lee Squire
Challenge Fund Julie Hughes Disinvestment Clinical prioritisation ( Oregon) CPAG/POLCV
Dave Whatton for POLCV Lead TBC for Oregon and clinical prioritisation
SSOTP Validation of services commissioned against services received to include a one month turn around
Nicky Harkness with Lee Squire
MSK services Dave Whatton Planned Care Referral management system Julie Hughes in partnership with Mel
Savage Transformational Change looking at national policy best practice and contractual incentives
TBC to link with CPAG possibly an accountable Board across Staffordshire
GP Education
Julie Hughes/ Dr Catherine Farrup
Cal protectin pathway Julie Hughes Telehealth Dave Whatton Data Sharing IM&T Julie Hughes/ Wendy Kerr CHC Complex conditions
Rob Luisardi/ Nicky Harkness
Frail Elderly Pathway will sit in the NEL PID.
Across CCGs Dave Sanzari leading for all CCGs. Sarah Evans pulling together response via email. Nicola Harkness ESCCG lead
Personal Healthcare Budget Wendy Kerr Medicines Management Sue Bamford
6 Author: Date: East Staffs CCG
Mental Health Nicky Harkness to liaise with R Symonds
SES. Recommendation:-
The Governing Body are asked to: • Recognise and understand the implications of the requirements set out by
NHS England relating to the refresh of 2015/16 and 2016/17 Financial Plans. • Understand the size of QIPP programme required to be achieved over the
next 2 years, acknowledging that the phasing between the 2 financial years has yet to be confirmed.
• Approve in principle the priority areas currently identified for project initiation and evaluation, supporting delivery of the CCG’s financial gap.
7 Author: Date: East Staffs CCG

Title ESCCG Performance Report 2014 – Months 6 & 7 (Sept / Oct) Reporting to Governing Body Date of Meeting 27th November 2014
Commissioning Lead(s) Author(s) Wendy Kerr Paul Winter
Purpose of the Report (Please select) Approval Assurance Discussion Key Points/Executive Summary
This report outlines the latest-available performance data against the national outcome measures (depending on national / local data availability). All measures are updated for M6, and some for M7, including provisional data that will be subject to change by the time of the meeting or after it. Exception Reports provide an overview of the actions being taken in areas of under-performance in the “Quality & Safety” and “NHS Constitution” Dashboards. A summary of current performance against these principal outcome measures in 2014-15 indicates the following non-achieving areas. All other targets are by definition currently on track.
18 Weeks Referral to Treatment – admitted patients: ESCCG, BHFT & DHFT 31-Day Cancer Waits – to second / subsequent treatments (surgery / radiotherapy): ESCCG & UHB Delayed Transfers of Care, GP Clinic Letters, Mixed Sex Accommodation & Never Events: BHFT The additional allocation for achievement of 18 Weeks RTT is currently seeing Burton and Derby on track with their plans (according to local weekly data). Performance for ESCCG and principal Acute Providers has improved in September and provisional data for October suggests achievement overall. The QF&P Committee needs to be aware that this is a result of the inclusion of already-breached patients within the denominators used to calculate monthly percentage scores. National rules mean such patients have to be included and Providers are unable to separately report these. This will skew the position of RTT achievement until such time as breached patients are fully cleared. Burton have significantly reduced their over 18 and over 40-week waiters this month over previous months, so this does provide assurance that the RTT improvement plans are working.
Recommendations (what is expected from the Committee)
The Governing Body is provided with the report to enable it to retain an active grip on performance in the areas that the CCG is held to account for delivery by the Area Team. The Committee is asked to: - Acknowledge and discuss the issues covered in the Performance Report
- Be assured that the Exception Reports for each under-performing area provide satisfactory assurance Enclosures Month 6 & 7 Performance Report 2014-15
Enc. 13
1 Author: Paul Winter Date: 19th November 2014 East Staffs CCG

Summary
"Balanced Scorecard" Summary (Areas 1 to 5 are from the CCG Assurance Framework)
Amber Green Amber Green
Amber Red Red
3.11 - B 3.1.1 - C Systems QIPP
6.3 - A 6.4 - E
"Quality Premium"Analysis
£0 QP paymentCCG achieves all Constitution targets (RTT incompletes, A&E 95%,62-d cancer waits, Cat As < 75 mins) - lose 25% of earned QP for each failure
CCG achieves it's Local Priority #3 target (Dementia prescribing: anti-psych)[this qualifies for 12.5% of the total QP]
CCG achieves it's Local Priority #2 target (DTOCs reduction)[this qualifies for 12.5% of the total QP]
CCG achieves it's Local Priority #1 target (LTCs prevalence reporting)[this qualifies for 12.5% of the total QP]
£0 QP payment
£83,166 £0 QP payment
£83,166 £0 QP paymentStep Seven
Step Seven
YES
£83,166
£166,331
£83,166
£665,325 - X%
CCG has 0 MRSA cases; achieves C.Diff target (COF Domain 5)[this qualifies for 12.5% of the total QP]
CCG rolls out F&FT; improves patient experience (COF Domain 4)[this qualifies for 12.5% of the total QP]
CCG reduces Avoidable Emergency Admissions (COF Domains 2&3)[this qualifies for 25% of the total QP]
CCG reduces Potential Years of Life Lost (COF Domain 1)[this qualifies for 12.5% of the total QP]
CCG manages within its Total Resources for 2014-15?[this is a de minima pre-qualifying criterion]
Step Four
Step Five
Step Six
Step Seven
Step One
Step Two
Step Three
NO
£0 QP payment
£0 QP payment
£83,166 £0 QP payment
£83,166 £0 QP payment
NB: NHS England reserves the right not to pay regardless of performance if there's been a serious quality failure in 14-15
ESCCG Population = 133,065; QP payment = £5 per head of population: maximum possible QP payment = £665,325
2Are local people getting good quality care?
1Are patient rights under the NHS Constitution being promoted?
ESCCG Performance Report 2014-15
CCG Report work-sheets
3Are health outcomes improving for local people?
4
5Are CCG authorisation conditions being addressed / removed?
6Delivery of CCG Strategy: clinical priorities & QIPP
Are CCGs commissioning services within their financial allocations?
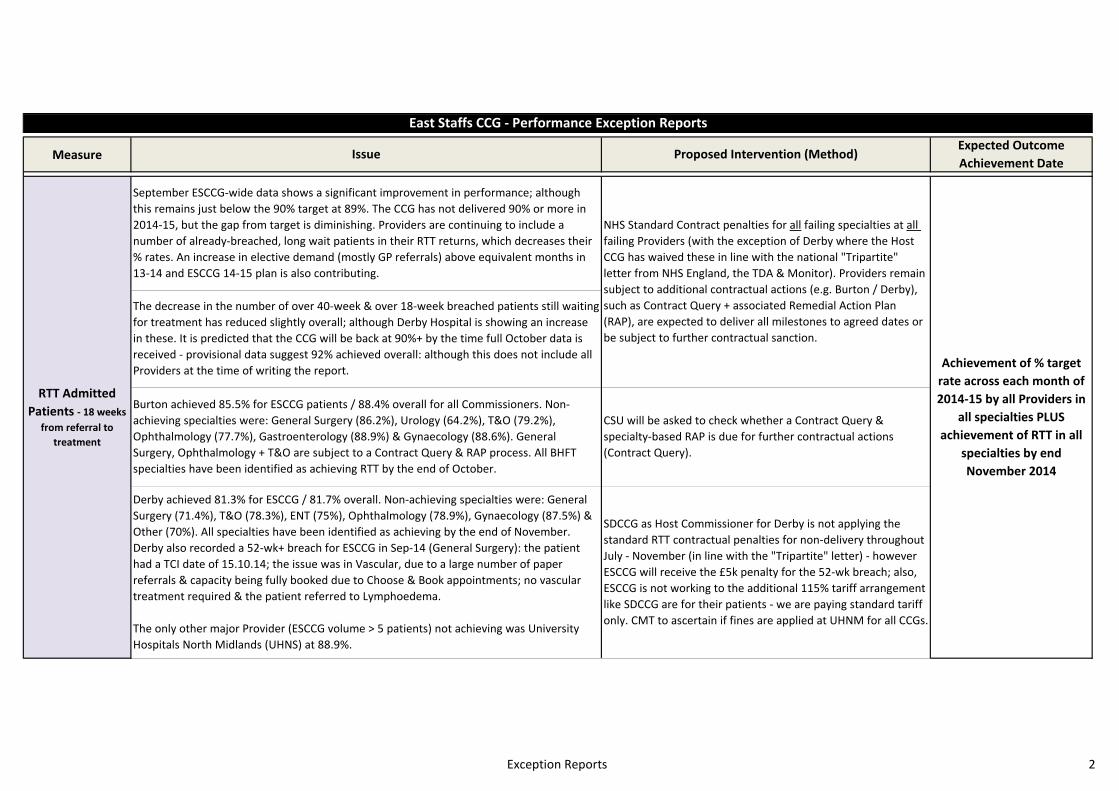
Exception Reports 2
Measure
East Staffs CCG - Performance Exception Reports
Issue Proposed Intervention (Method)Expected OutcomeAchievement Date
RTT Admitted Patients - 18 weeks
from referral to treatment
The decrease in the number of over 40-week & over 18-week breached patients still waiting for treatment has reduced slightly overall; although Derby Hospital is showing an increase in these. It is predicted that the CCG will be back at 90%+ by the time full October data is received - provisional data suggest 92% achieved overall: although this does not include all Providers at the time of writing the report. Achievement of % target
rate across each month of 2014-15 by all Providers in
all specialties PLUS achievement of RTT in all
specialties by end November 2014
September ESCCG-wide data shows a significant improvement in performance; although this remains just below the 90% target at 89%. The CCG has not delivered 90% or more in 2014-15, but the gap from target is diminishing. Providers are continuing to include a number of already-breached, long wait patients in their RTT returns, which decreases their % rates. An increase in elective demand (mostly GP referrals) above equivalent months in 13-14 and ESCCG 14-15 plan is also contributing.
Burton achieved 85.5% for ESCCG patients / 88.4% overall for all Commissioners. Non-achieving specialties were: General Surgery (86.2%), Urology (64.2%), T&O (79.2%), Ophthalmology (77.7%), Gastroenterology (88.9%) & Gynaecology (88.6%). General Surgery, Ophthalmology + T&O are subject to a Contract Query & RAP process. All BHFT specialties have been identified as achieving RTT by the end of October.
Derby achieved 81.3% for ESCCG / 81.7% overall. Non-achieving specialties were: General Surgery (71.4%), T&O (78.3%), ENT (75%), Ophthalmology (78.9%), Gynaecology (87.5%) & Other (70%). All specialties have been identified as achieving by the end of November. Derby also recorded a 52-wk+ breach for ESCCG in Sep-14 (General Surgery): the patient had a TCI date of 15.10.14; the issue was in Vascular, due to a large number of paper referrals & capacity being fully booked due to Choose & Book appointments; no vascular treatment required & the patient referred to Lymphoedema.
The only other major Provider (ESCCG volume > 5 patients) not achieving was University Hospitals North Midlands (UHNS) at 88.9%.
SDCCG as Host Commissioner for Derby is not applying the standard RTT contractual penalties for non-delivery throughout July - November (in line with the "Tripartite" letter) - however ESCCG will receive the £5k penalty for the 52-wk breach; also, ESCCG is not working to the additional 115% tariff arrangement like SDCCG are for their patients - we are paying standard tariff only. CMT to ascertain if fines are applied at UHNM for all CCGs.
CSU will be asked to check whether a Contract Query & specialty-based RAP is due for further contractual actions (Contract Query).
NHS Standard Contract penalties for all failing specialties at all failing Providers (with the exception of Derby where the Host CCG has waived these in line with the national "Tripartite" letter from NHS England, the TDA & Monitor). Providers remain subject to additional contractual actions (e.g. Burton / Derby), such as Contract Query + associated Remedial Action Plan (RAP), are expected to deliver all milestones to agreed dates or be subject to further contractual sanction.
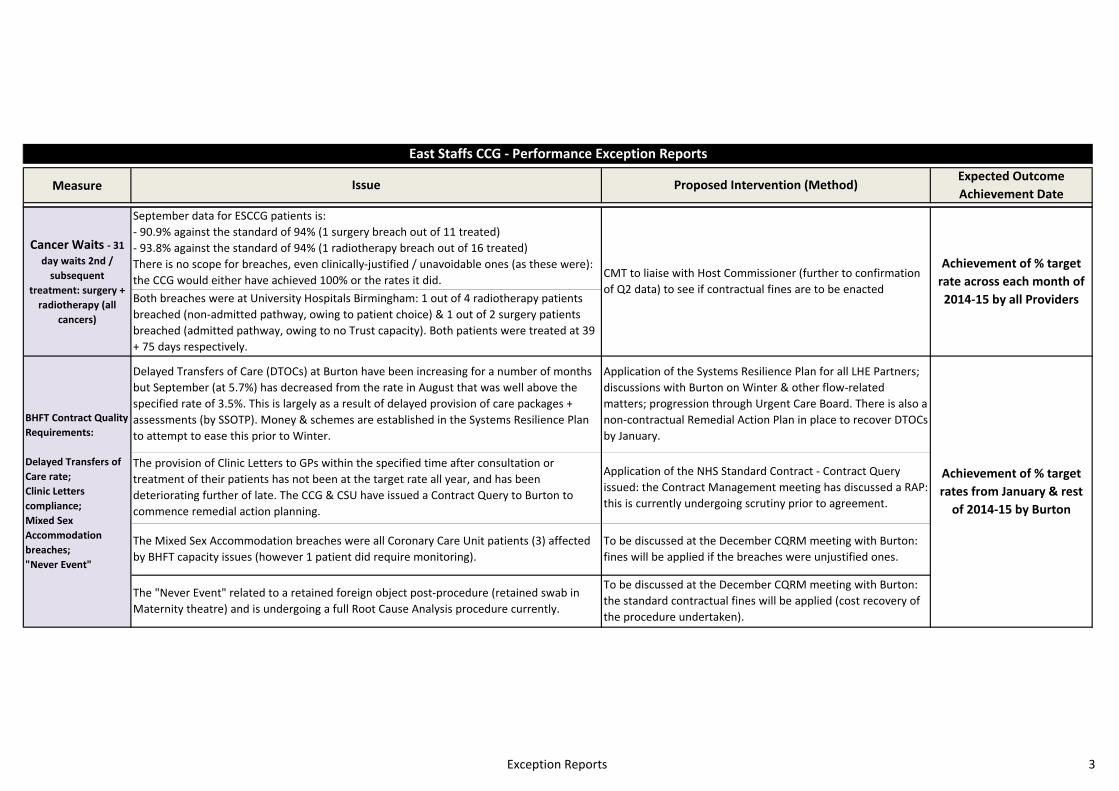
Exception Reports 3
Measure
East Staffs CCG - Performance Exception Reports
Issue Proposed Intervention (Method)Expected OutcomeAchievement Date
Both breaches were at University Hospitals Birmingham: 1 out of 4 radiotherapy patients breached (non-admitted pathway, owing to patient choice) & 1 out of 2 surgery patients breached (admitted pathway, owing to no Trust capacity). Both patients were treated at 39 + 75 days respectively.
September data for ESCCG patients is:- 90.9% against the standard of 94% (1 surgery breach out of 11 treated)- 93.8% against the standard of 94% (1 radiotherapy breach out of 16 treated)There is no scope for breaches, even clinically-justified / unavoidable ones (as these were): the CCG would either have achieved 100% or the rates it did.
Achievement of % target rate across each month of 2014-15 by all Providers
Cancer Waits - 31 day waits 2nd /
subsequent treatment: surgery +
radiotherapy (all cancers)
CMT to liaise with Host Commissioner (further to confirmation of Q2 data) to see if contractual fines are to be enacted
The "Never Event" related to a retained foreign object post-procedure (retained swab in Maternity theatre) and is undergoing a full Root Cause Analysis procedure currently.
To be discussed at the December CQRM meeting with Burton: the standard contractual fines will be applied (cost recovery of the procedure undertaken).
Achievement of % target rates from January & rest
of 2014-15 by Burton
BHFT Contract Quality Requirements:
Delayed Transfers of Care rate;Clinic Letters compliance;Mixed Sex Accommodation breaches;"Never Event"
Delayed Transfers of Care (DTOCs) at Burton have been increasing for a number of months but September (at 5.7%) has decreased from the rate in August that was well above the specified rate of 3.5%. This is largely as a result of delayed provision of care packages + assessments (by SSOTP). Money & schemes are established in the Systems Resilience Plan to attempt to ease this prior to Winter.
The Mixed Sex Accommodation breaches were all Coronary Care Unit patients (3) affected by BHFT capacity issues (however 1 patient did require monitoring).
Application of the Systems Resilience Plan for all LHE Partners; discussions with Burton on Winter & other flow-related matters; progression through Urgent Care Board. There is also a non-contractual Remedial Action Plan in place to recover DTOCs by January.
To be discussed at the December CQRM meeting with Burton: fines will be applied if the breaches were unjustified ones.
Application of the NHS Standard Contract - Contract Query issued: the Contract Management meeting has discussed a RAP: this is currently undergoing scrutiny prior to agreement.
The provision of Clinic Letters to GPs within the specified time after consultation or treatment of their patients has not been at the target rate all year, and has been deteriorating further of late. The CCG & CSU have issued a Contract Query to Burton to commence remedial action planning.

Quality & Safety 4
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
1 0 0 0 0 0 0 1
97.1% 97.6% 98.6% 98.6% 98.9% 98.3% 98.3% 98.6%
= 1 1 0 0 1 1 0 0
28 1 3 8 7 1 2 1
= 2 1 0 0 0 0 0 0
16 2 1 6 4 0 0 1
475 28 26 27 16 21 17 *
3821 367 325 332 315 212 264 *
5135 311 435 374 440 366 432 *
113 6 4 3 5 12 8 11
92 14 0 0 0 7 0 4
= 111 98 98 * * * * *
= 1.01 1.01 1.01 98 (Dec13) 98 (Mar14)
88 85 85 85 85 * 96 *
94.4% 95% 95.3% 96.7% 96.4% 97.3% 97.1%
- 185/77 - - 29 / 16 - - 20 / 19
79 1 0 0 1 2 0 2
= 31 / 0 1 / 0 1 / 0 2 / 0 1 / 0 1 / 0 1 / 0 1 / 0
= 100% 100% 100% 100% 100% 100% 100% 100%
77 / 71 72 / 70 75 / 67 79 / 63 77 / 55 73 / 62 76 / 61 *
= 88 92 93 94 95 94 94 *
= 3 0 0 0 0 0 0 0
= 1 0 0 0 0 0 0 0
= 0 0 0 0 0 0 0 0
71% 73.7% 73.0% 72.5% 68.8% 73.9% 69.5% 71.9%
84.9% 81.4% 81.3% 84.4% 80.8% 93.3% 89.7% 74.4%
52 week waits Zero 52wk+
"Friends & Family Test" (IP,A&E)
Reduction
Quality assurance: ward metrics > 95%
Pressure Ulcers (No. Level 3 / 4) Reduction
Improvement
Realtime Experience (overall) Improvement
Clinical Quality & Patient Safety
ESCCG Quality Dashboard (data presented for Burton Hospitals FT unless otherwise stated) * = awaiting data / ‽ = provisional data
Trend
Total 'EMSA' breaches (No.) Zero
Total MRSA cases (ESCCG No.) 0
Total C.Diff cases (ESCCG No.)
Total Serious Incidents (No.) Reduction
32
Quality Requirement Threshold Latest Monthly or Quarterly Performance
Total 'Never Events' (No.) Zero
Trolley Waits in A&E Zero 12hr+
Urgent ops cancelled (2nd time) Zero
Breastfeeding on discharge 68.5 - 70%
13-14
Total MRSA cases (BHFT No.) 0
Total C.Diff cases (BHFT No.)
95-97.75% (Q4)
22
Total Incidents (No.) Reduction
VTEs prophylaxis (%)
Total Complaints (No.)
Time on stroke unit 80%
Reduction
Total PALs Contacts (No.) -
"Duty of Candour" audits
Mortality: HSMR (ratio) 100
100% complete
Mortality: SHMI (ratio) 100
Mortality: RAMI (CHKS) 100
Pressure Ulcers (No. Level 2) Reduction
Safeguarding referrals (Ch / Ad)

Quality & Safety 5
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
71.8% 75.0% 62.5% 61.5% 90.9% 60.0% 65.2% 70.0%
5.7% 5.9% 5.4% 5.9% 6.5% 6.4% 5.7% 5.0%
1.9% 2.6% 2.9% 2.5% 3.2% 2.1% 2.0% 1.9%
95.0% 19 15 11 13 11 12 11
51 60 65 62 59 46 45 60
3.2% 2.5% 3.4% 3.1% 3.3% 4.4% 7.1% 5.7%
96.3% 98.2% 95.6% 96.7% 97.7% 97.5% 96.1% 96.2%
91.6% 93.0% 92.1% 97.7% 96.9% 96.2% 96.4% 96.3%
92.0% 95.2% 95.3% 93.9% 94.5% 95.8% 93.2% 87.0%
= 99.2% 100% 100% 100% 100% 100% 100% 100%
= (95.8%) 0 0 0 0 0 0 0
92.8% 93.1% 93.7% 92.0% 91.2% 93.6% 91.9% 91.8%
= (new) 100% 100% 100% 100% 100% 100% 100%
= (new) 0 0 0 0 0 0 0
= (new) 0 0 0 0 0 0 0
= (new) 0 0 0 0 0 0 0
Local Avoidable: trolley falls 0
Local Avoidable: device malfunction 0
Local Avoidable: retained cannula 0
Time to A&E treatment Ave < 60 mins
Clinic Letters sent < 5 days 100%
Diabetics: 9 care processes Improvement
Catheter care improvement 0
Time to antenatal assessment >= 90%
Minimise Delayed Discharge < = 3.5%
MRSA screening: electives 100%
MRSA screening: non-electives 100%
Time to surgery #FNOF 100% < 48hrs
TIAs scanned / treated 60% <24 hrs
A&E unplanned reattendances < = 5%
A&E left w/out being seen rate < = 5%
Time to A&E assessment 95% <15mins
13-14Quality Requirement Threshold TrendLatest Monthly or Quarterly Performance

NHS Constitution 6
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Admitted patients treated < max 18 weeks from referral 89.8% 89.9% 88.7% 83.1% 77.9% 88.8% 92.3% * 86.2%
Non-Admitted patients treated < max 18 wks from referral 99.4% 98.5% 98.4% 98.1% 98.0% 96.4% 97.9% * 98.2%
Incompletes (yet to start treatment) do not wait > 18 wks 95.3% 91.6% 93.9% 94.5% 95.7% 95.8% 97.3% * 94.6%
Number of patients waiting more than 52 weeks 0 0 0 0 0 1 0 * 1
Patients should not wait > 6 weeks from referral 98.7% 98.9% 99.5% 99.7% 99.9% 99.4% 99.4% * 99.3% =
94.6% 95.3% 97.2% 96.3% 95.9% 95.7% 95.1% 95.7%
94.5% 95.3% 97.6% 96.5% 96.0% 95.9% 95.1% 95.8%
96.7% 98.8% 95.4% 96.4% 93.6% 95.1% 96.0%10/300 3/253 14/301 12/331 17 / 266 14 / 283 70/1734
100.0% 100.0% 100.0% 95.8% 94.4% 98.1% 98.0%0/78 0/44 0/46 3/71 3 / 54 1 / 53 7/346
97.1% 94.4% 92.6% 96.3% 94.9% 96.4% 95.4%2/69 3/54 4/54 2/54 3 / 59 2 / 55 16/345
100.0% 100.0% 100.0% 92.3% 83.3% 90.9% 94.7%0/14 0/5 0/8 1/13 1 / 6 1 / 11 3/57
100.0% 100.0% 100.0% 100.0% 92.9% 100.0% 98.7%0/8 0/13 0/12 0/12 1 / 14 0 / 18 1/77
85.0% 87.5% 95.0% 95.0% 100.0% 93.8% 91.7%3/20 2/16 1/20 1/19 0 / 5 1 / 16 8/96
95.9%
97.4%88%93%
96.3%
100%
93.8%
98.0%
89%94%
93%98%
89%
Y
Subsequent treatments: radiotherapy
Subsequent treatments: anti-cancer drugs
Subsequent treatments: surgery
From diagnosis to first definitive treatment, all cancers
Breast symptom patients (cancer not initially suspected)
Patients referred by a GP with suspected cancer
94%
91%96%
88%93%
Y
Y
N
Y
Delivery of the NHS Constitution
CCG Assessment = is the NHS Constitution being delivered?
A&E Waiting Times within 4 hours of arrival - 1st figure = Burton; 2nd figure = Derby
Diagnostic Test Waiting Times - ESCCG
99.7%
95.4%
96.9%
Y
N
94%99% Y
Patients admitted, transferred or discharged < 4 hrs
Trend
Referral to Treatment / RTT Waiting Times for non-urgent, Consultant-led treatment - ESCCG
Below LT or Amber x2 consecutive months
Between Standard (Std) &Lower Threshold (LT)
At or aboveStandard (Std)Amber / Green = no indicator rated Red but future concerns
YTD Met?YTDIndicator Std 13-14LT
Y
95% Y
0 Y
90%
88.3%
98.8%
94.8%
0
87%
10
92%
85%
RAGGreen = no indicators rated Red
Red = 2 or more indicators rated Red
Amber / Red = one indicator rated Red
90%
90%95%
Cancer Waits - maximum 1 month (31 days) waits from diagnosis to 1st or subsequent treatment - ESCCG (No. breaches / treated)
Cancer Waits - maximum 2 week (14 days) waits for 1st outpatient appointment, for all patients referred urgently - ESCCG (No. breaches / treated)
N
Latest Monthly Performance (* DENOTES PROVISIONAL DATA - subject to change)
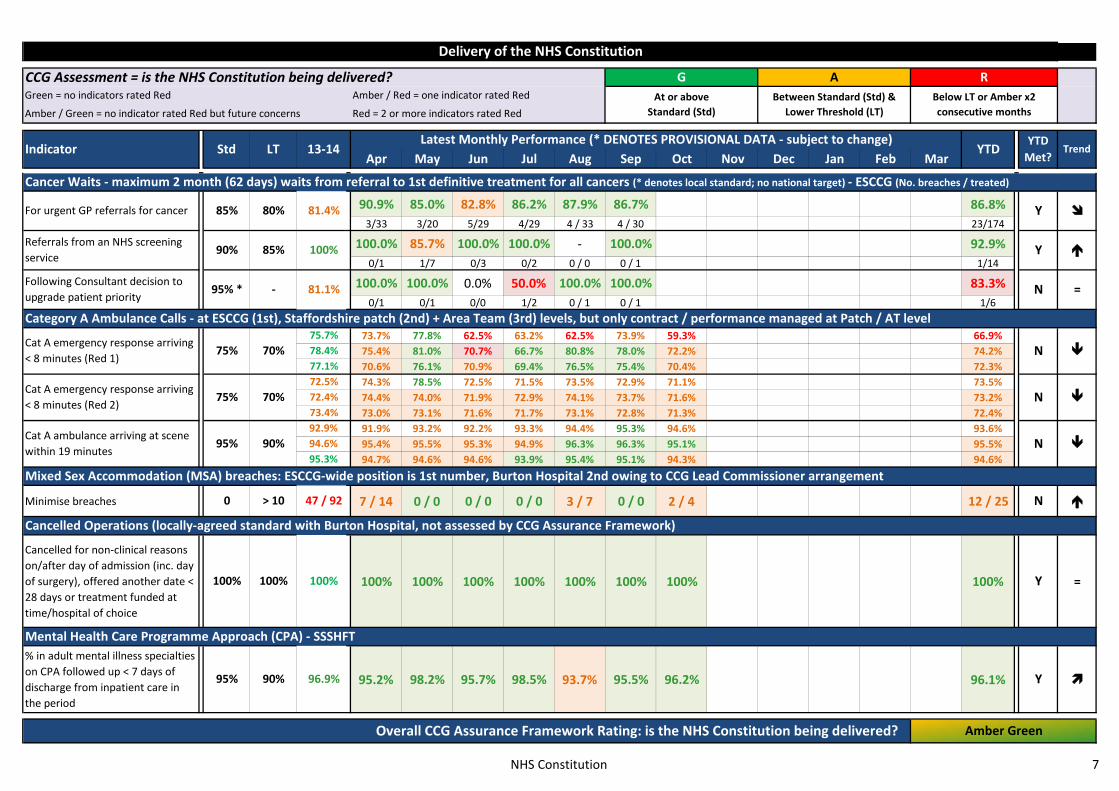
NHS Constitution 7
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Delivery of the NHS Constitution
CCG Assessment = is the NHS Constitution being delivered?
Trend
Below LT or Amber x2 consecutive months
Between Standard (Std) &Lower Threshold (LT)
At or aboveStandard (Std)Amber / Green = no indicator rated Red but future concerns
YTD Met?YTDIndicator Std 13-14LT
RAGGreen = no indicators rated Red
Red = 2 or more indicators rated Red
Amber / Red = one indicator rated Red
Latest Monthly Performance (* DENOTES PROVISIONAL DATA - subject to change)
90.9% 85.0% 82.8% 86.2% 87.9% 86.7% 86.8%3/33 3/20 5/29 4/29 4 / 33 4 / 30 23/174
100.0% 85.7% 100.0% 100.0% - 100.0% 92.9%0/1 1/7 0/3 0/2 0 / 0 0 / 1 1/14
100.0% 100.0% 0.0% 50.0% 100.0% 100.0% 83.3%0/1 0/1 0/0 1/2 0 / 1 0 / 1 1/6
73.7% 77.8% 62.5% 63.2% 62.5% 73.9% 59.3% 66.9%75.4% 81.0% 70.7% 66.7% 80.8% 78.0% 72.2% 74.2%70.6% 76.1% 70.9% 69.4% 76.5% 75.4% 70.4% 72.3%74.3% 78.5% 72.5% 71.5% 73.5% 72.9% 71.1% 73.5%74.4% 74.0% 71.9% 72.9% 74.1% 73.7% 71.6% 73.2%73.0% 73.1% 71.6% 71.7% 73.1% 72.8% 71.3% 72.4%91.9% 93.2% 92.2% 93.3% 94.4% 95.3% 94.6% 93.6%95.4% 95.5% 95.3% 94.9% 96.3% 96.3% 95.1% 95.5%94.7% 94.6% 94.6% 93.9% 95.4% 95.1% 94.3% 94.6%
Minimise breaches 7 / 14 0 / 0 0 / 0 0 / 0 3 / 7 0 / 0 2 / 4 12 / 25
Cancelled for non-clinical reasons on/after day of admission (inc. day of surgery), offered another date < 28 days or treatment funded at time/hospital of choice
100% 100% 100% 100% 100% 100% 100% 100% =
% in adult mental illness specialties on CPA followed up < 7 days of discharge from inpatient care in the period
95.2% 98.2% 95.7% 98.5% 93.7% 95.5% 96.2% 96.1%
80%85%
73.4%92.9%94.6%95.3%
81.1%
100%
81.4%
-95% *Following Consultant decision to upgrade patient priority
Referrals from an NHS screening service
For urgent GP referrals for cancer
Mixed Sex Accommodation (MSA) breaches: ESCCG-wide position is 1st number, Burton Hospital 2nd owing to CCG Lead Commissioner arrangement
Category A Ambulance Calls - at ESCCG (1st), Staffordshire patch (2nd) + Area Team (3rd) levels, but only contract / performance managed at Patch / AT level
Cancer Waits - maximum 2 month (62 days) waits from referral to 1st definitive treatment for all cancers (* denotes local standard; no national target) - ESCCG (No. breaches / treated)
77.1%78.4%75.7%
N70%75%Cat A emergency response arriving < 8 minutes (Red 1)
90%
72.5%72.4%
=N
Y
Y
85%90%
95% Y
Amber Green
Mental Health Care Programme Approach (CPA) - SSSHFT
Cancelled Operations (locally-agreed standard with Burton Hospital, not assessed by CCG Assurance Framework)
47 / 92
100%
96.9%
Overall CCG Assurance Framework Rating: is the NHS Constitution being delivered?
0 N
100% Y
90%
> 10
100%
N95%Cat A ambulance arriving at scene within 19 minutes
Cat A emergency response arriving < 8 minutes (Red 2)
70%75% N

RTT & Cancer Detail
40 week+ waits 18 week+ waits
Cancer Standard Breach ReasonsKEY: A B C D E Total
A = Patient Choice Feb-14 9 5 2 0 0 16B = Late Referral (inter-Provider) Mar-14 13 0 3 2 0 18C = No (Trust) Capacity Apr-14 10 1 4 1 1 17D = Clinical Complexity May-14 4 1 2 4 1 12E = Other Reason (e.g. admin error) Jun-14 13 2 2 5 2 24
Jul-14 15 1 1 7 0 24Aug-14 18 1 8 1 1 29Sep-14 15 0 4 3 1 23Oct-14
Nov-14
Dec-14
Jan-15
Feb-15
Mar-15
SUM 97 11 26 23 6 16362-d: all = 108, BHFT (complex diagnosis, repeat biopsy required)
31-d 2nd: radiotherapy = 75d, UHB (Trust capacity issue)
Delivery of the NHS Constitution - RTT Long Wait Analysis (Incomplete Pathways) + Cancer Breach Reasons Analysis
14-d: all = 42d, BHFT (1st date patient made themselves available)
Longest Wait: breach to eventual treatment (current month)
31-d 1st: all = 57d, UHB (Trust capacity issue)
22
24
14
13
18
28
12
7
14
0
5
10
15
20
25
30BHFT DHFT
Other ESCCG447
395 417
293
534
440 388
303 300
0
100
200
300
400
500
600BHFT DHFT
Other ESCCG
97
11
26
23
6
Cancer Standard Breach Reasons
A
B
C
D
E

Plans & Outcomes 9
(1) CCG Operational Plans 2014-15
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Plan
Actual
Plan
Actual
Plan
Actual
Plan
Actual
Plan
Actual
Plan
Actual
Plan
Actual
Plan
Actual
Plan
Actual
Plan 1 3 2 2 4 2 3 3 4 2 2 2Actual 1 3 8 7 1 2 1Plan 255 288 298 292 256 310 301 319 256 249 283 283
Actual 232 276 287 256 243 238 *
Plan 1020 1116 1099 1192 1003 1062 1137 1167 1059 1157 1100 1100
Actual 1221 1279 1221 1401 1121 1265 *
Plan 1275 1404 1397 1484 1259 1372 1438 1486 1315 1406 1383 1383
Actual 1453 1555 1508 1657 1364 1503 *
Plan 1034 1057 1043 1026 1032 1131 1158 1112 1318 1197 1110 1110
Actual 1201 1266 1226 1334 1150 1212 *
Plan 2729 2934 2945 3290 2632 3100 3272 2976 2856 3168 2989 2989
Actual 2979 2964 3163 3263 2583 3120 *
Plan 2182 2233 2106 2315 1952 1938 2347 2031 1847 2319 2128 2128
Actual 2021 2006 2224 2373 2006 2336 *
Plan 1573 1692 1645 1619 1406 1476 1590 1457 1425 1499 1538 1538
Actual 1775 1588 1575 1644 1435 1597 *
Plan 3755 3925 3751 3934 3358 3414 3937 3488 3272 3818 3666 3666
Actual 3796 3594 3799 4017 3441 3933 *
Y
EC5: all first outpatient activity (MAR view) 34871 (13-14) N
Y
EC10: other written referrals (MAR view) 18361 (13-14) Y
EC9: GP written referrals (MAR view) 24843 (13-14)
EC11: total referrals (MAR view) 43204 (13-14)
N
EC3: total elective activity (MAR view) 17318 (13-14) N
EC4: non-elective activity (MAR view) 13655 (13-14) N
-
NEAS5: number of C.Difficile infections 28 (13-14)
EAS1: dementia diagnosis rate (No. diagnosed from expected prevalence)
58% (12-13)67% or 1149 / 1714 (14-15 annual target)
Y
EAS2: IAPT recovery rate (% completing treatment with expected outcome)
[New KPI] Y50% or 772 / 1544 (14-15 annual target)
58% or 31 / 53 118% or 13 / 11 data quality alert
2004.9
3.9% or 404 / 10286
-
123.0 (14-15 annual target)
552.0 551.0 550.0 548.0
On target?Q1 Q2 Q3 Q4
ESCCG Latest Performance [ * = awaiting data ]
-
-
Y
74.0 (14-15 annual target)
Assessed Jul-15 (annual data for 14-15)
Assessed Jul-15 (annual data for 14-15)
Baseline(ESCCG 2012
unless stated)
Indicator( = also in CCG Assurance or Outcomes Framework)
6.2
ESCCG Local Priority: recorded vs. expected prevalence of Hypertension + CHD (QOF)
67% (12-13)
1991.9 (14-15 annual target)
EA2: health-related quality of life for people with long-term conditions (average EQ-5D score)
73.8
EA3: 'Improving Access to Psychological Therapies': IAPT roll-out (% entering treatment)
8.7% (13-14)3.75% or 386 / 10286 3.75% or 386 / 10286 3.75% or 386 / 10286 3.75% or 386 / 10286
Assessed Jul-15 (annual data) ; 13/14 = 58%, > CCG plan of 52.6%
EA1: potential years of life lost, causes considered amenable to healthcare (rate per 100k)
EC2: elective daycase activity (MAR view) 14126 (13-14)
3.6% or 370 / 10286
6.1 (14-15 annual target)
70% or 25400 / 36300 (14-15 annual target)
EC1: elective inpatient activity (MAR view) 3192 (13-14)
Assessed Jul-15 (annual data for 14-15)
Assessed Jul-15 (annual data for 14-15)
Assessed Jul-15 (annual data for 14-15)
Assessed Jul-15 (annual data for 14-15)EA7: composite indicator of i) GP Services ii) GP Out of Hours experience
EA4: composite measure, emergency admissions (ACS+Acute+LRTIs+Under 19s, rate per 100k)
2260.2
EA5: patient experience of hospital care 123.6 -
-
Y
Delivery of ESCCG 14/15 Operational Plans and the CCG (NHS) Outcomes Framework

Plans & Outcomes 10
(2) CCG Assurance Framework - CCG Outcomes Indicator Set based metrics [assessment based on number of outcomes not met by the CCG]
C1.1 - potential yrs of life lost (amenable to healthcare): adults + children/young people
C2.6 - unplanned hospitalisation chronic ACS conditions in adults
C2.7 - unplanned hospitalisation: asthma, diabetes & epilepsy in the under 19s
C3.1 - emergency admissions acute conditions not usually requiring hospital admission
C3.4 - emergency admissions: for children with lower respiratory tract infections
C4.3 - Friends & Family Test: Inpatients / A&E (BHFT)
C5.3 - incidence of healthcare associated infection: MRSA (CCG)
C5.3 - incidence of healthcare associated infection: MRSA (BHFT)
C5.4 - incidence of healthcare associated infection: C.Diff (BHFT)
Domain 2: enhancing quality of life for people with Long Term Conditions
Q1 14-15due Dec-14
918.7(13-14)
525.5(13-14)
N(13-14 > 12-13)
Y(13-14 < 12-13)
Q1 14-15due Dec-14
Q1 14-15due Dec-14
n/a
(1) n/a ; (2) 643.9 ;(3) 1164.7
(12-13, per 100k) 1349.7
Domain 1: preventing people from dying prematurely
N(13-14 > 12-13)
Amber / Green = not all indicators on track for achievement of the QP
Green = all relevant indicators on track for achievement of Quality Premium (QP)
Indicator Baseline (ESCCG 2012 unless stated)
(1) CCG target(2) Upper decile
(3) Nat. ave.
Threshold (inc. Quality Premium)
CCG AF Assessment = are health outcomes improving for local people?
Q1
2014 due Sep-151917.4(2013)
(12-13, per 100k) 391.2
(12-13 outturn)22 9 4 N
Overall CCG Assurance Framework Rating: are health outcomes improving? To be assessed formally at year end: total standards met, out of X
(CDI target 14-15)15
Amber-Red
(internal target)0
(BHFT target)0 1
Domain 5: treating and caring for people in a safe environment and protecting them from avoidable harm
Domain 4: ensuring that people have a positive experience of care
Domain 3: helping people to recover from episodes of ill health or following injury
Y(13-14 < 12-13)
N
N
N(12-13 outturn)1
1159.9(13-14)
339.1(13-14)
1
Q1 14-15due Dec-14
2
74 / 69 75 / 59
1
(pop rate per 100k) 1992.9
Reduce byat least -3.2%
(1) 1991.9;(2) 1534.3; (3) 2027.4
Below 95% variance or Amber for 2
consecutive quarters
R
(12-13, per 100k) 877.6
(1) n/a ; (2) 391.6 ;(3) 780.9
Q2
Between standard / threshold & 95%
variance
Latest Quarterly PerformanceQ4Q3
At or above target / threshold
AG
Red = all indicators statistically / significantly off track for achievement of the QP
Amber / Red = at least 1 indicator statistically / significantly off track for achievement of the QP
Reduce or 0% growth
Reduce or 0% growth(1) n/a ; (2) 186.5 ;
(3) 368.6
(1) n/a ; (2) 148.8 ;(3) 307.4
0 cases
n/a
(12-13 outturn)4
Rolled out + Q1 14-15 > Q1 13-14
(ave 13-14)80 / 71
awaiting data
(12-13, per 100k) 378.8
Reduce or 0% growth
Reduce or 0% growth
On target?
Y(2013 < 2012)

Plans & Outcomes 11
(3) CCG Outcomes Indicator Set [other outcomes not routinely assessed by the CCG Assurance Framework]
C1.2 - under 75s mortality from cardiovascular disease
C1.3 - cardiac rehabilitation completion
C1.4 - myocardial infarction / stroke / stage 5 kidney disease in people with diabetes
C1.5 - mortality within 30 days of hospital admission for stroke
C1.6 - under 75s mortality from respiratory disease
C1.7 - under 75s mortality from liver disease
C1.8 - emergency admissions for alcohol related liver disease
C1.9 - under 75s mortality from cancer
C1.10 - 1 year cancer survival rates: all cancers
C1.11 - 1 year cancer survival rates: breast, lung & colorectal
C1.12 - people with severe mental illness who have received a list of physical checks
C1.13 - antenatal assessment < 13 weeks
C1.14 - maternal smoking at delivery rate
C1.15 - breastfeeding prevalence at 6 to 8 weeks
C1.16 - cancer: diagnosis via emergency routes
C1.17 - cancer: record of stage at diagnosis
C1.18 - cancer: early detection (% at stage 1 / 2)(% rate)42.8%
(1) n/a; (2) 54.2%;(3) 41.6%
n/a - 2013due Sep-15
Y(> national ave)
-
(% rate)59.9%
(1) n/a; (2) 79.4%;(3) 59.4%
n/a - 2013due Sep-15
Y(> national ave)
In development Awaiting data n/a no national data
65%(Dec-11:Dec-12)
2013 due Jun-15
11.7%(Q4 13-14)
67.7%(Dec-11:Dec-12)
Due Jun-15
Awaiting data
Domain 1: preventing people from dying prematurely
no national data
1.51
IndicatorLatest Quarterly Performance
(11-12, per 100k)1.51
Q1 Q2
(1) n/a; (2) 1.41;(3) 1.98
n/a
no national data
(per 100k rate) 26.4(1) n/a; (2) 16.7;
(3) 28.1n/a
On target?
(per 100k rate) 56.3
Baseline (ESCCG 2012 unless stated)
-
N(2013 > 2012)
18.7(2013)
2014 due Sep-15
Awaiting data n/a
(1) n/a; (2) 97.6;(3) 122.1
n/a
n/a
N(13-14 > 12-13)
Awaiting data
(12-13, per 100k) 26.6(1) n/a; (2) 8.4;
(3) 24.1n/a
N(2013 > 2012)
118.9(2013)
2014 due Sep-15
Q1 14-15due Dec-14
(per 100k rate) 131.4
(1) n/a; (2) 8.4;(3) 15.5
n/a
35.6(13-14)
15.2(2013)
2014 due Sep-15
Y(2012 > 2011)
(1) CCG target(2) Upper decile
(3) Nat. ave.
Threshold (inc. Quality Premium)
(1) n/a; (2) 45.6;(3) 64.9
n/a
Awaiting data -
Q3 Q4
n/a
2013 due Mar-15 Y(> national ave)
65.9(2013)
2014 due Sep-15
no national data
No data - data quality issue
Q1 14-15due Dec-14
Q1 14-15due Dec-14
Y(2012 > 2011)
Q3 13-14due Dec-14
87.9%(Q2 13-14)
-
Y(Q2 > Q1)
N(Q4 < Q1)
2013 due Jun-15
-
Y(2013 < 2012)
No data - data quality issue
(1) n/a; (2) 76.2%;(3) 44.1%
n/a
(Q1 13-14)14.2%
(1) n/a; (2) 23.2%;(3) 12.8%
n/a
(Dec-10:Dec-11)66.8%
(1) n/a; (2) 72.5%;(3) 69.3%
n/a
(1) n/a; (2) 124.9%;(3) 95.7%
n/a
Awaiting data n/a
(Q1 13-14)84.4%
(Dec-10:Dec-11)64.8%
(1) n/a; (2) 71.2%;(3) 67.8%
Awaiting data
(per 100k rate) 14.9
Y(2013 < 2012)
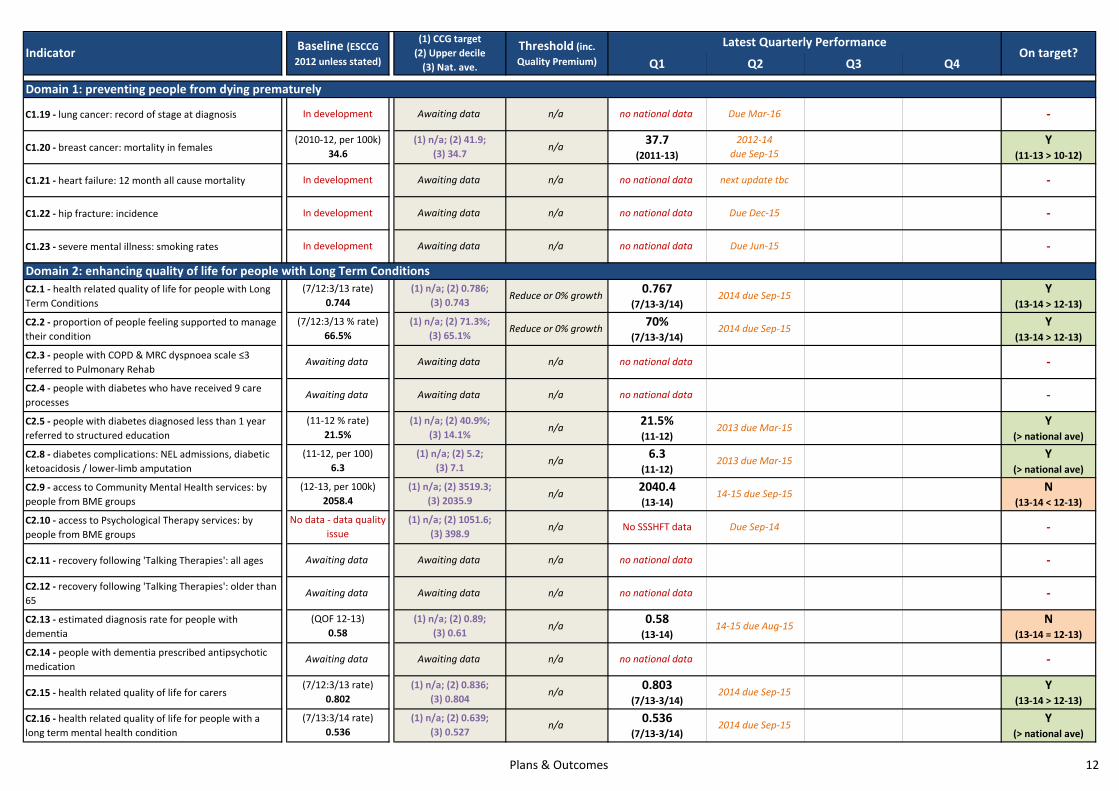
Plans & Outcomes 12
C1.19 - lung cancer: record of stage at diagnosis
C1.20 - breast cancer: mortality in females
C1.21 - heart failure: 12 month all cause mortality
C1.22 - hip fracture: incidence
C1.23 - severe mental illness: smoking rates
C2.1 - health related quality of life for people with Long Term Conditions
C2.2 - proportion of people feeling supported to manage their condition
C2.3 - people with COPD & MRC dyspnoea scale ≤3 referred to Pulmonary Rehab
C2.4 - people with diabetes who have received 9 care processes
C2.5 - people with diabetes diagnosed less than 1 year referred to structured education
C2.8 - diabetes complications: NEL admissions, diabetic ketoacidosis / lower-limb amputation
C2.9 - access to Community Mental Health services: by people from BME groups
C2.10 - access to Psychological Therapy services: by people from BME groups
C2.11 - recovery following 'Talking Therapies': all ages
C2.12 - recovery following 'Talking Therapies': older than 65
C2.13 - estimated diagnosis rate for people with dementia
C2.14 - people with dementia prescribed antipsychotic medication
C2.15 - health related quality of life for carers
C2.16 - health related quality of life for people with a long term mental health condition
-
(1) n/a; (2) 0.836;(3) 0.804
n/a 0.803(7/13-3/14)
2014 due Sep-15 Y(13-14 > 12-13)
Awaiting data Awaiting data
no national data
N(13-14 = 12-13)
n/a
In development Awaiting data n/a no national data Due Dec-15 -
In development Awaiting data n/a no national data Due Jun-15 -
(2010-12, per 100k) 34.6
(1) n/a; (2) 41.9;(3) 34.7
n/a 37.7(2011-13)
2012-14due Sep-15
Y(11-13 > 10-12)
In development Awaiting data n/a no national data next update tbc -
In development Awaiting data n/a no national data Due Mar-16 -
On target?Q1
0.58(13-14)
(1) n/a; (2) 0.89;(3) 0.61
n/a
Due Sep-14No SSSHFT data
no national data
no national data
Awaiting data Awaiting data
-
-
Y(13-14 > 12-13)
Y(13-14 > 12-13)
-
Y(> national ave)
Y(> national ave)
N(13-14 < 12-13)
-
6.3(11-12)
2040.4(13-14)
21.5%(11-12)
Domain 2: enhancing quality of life for people with Long Term Conditions
Q2 Q3 Q4
Domain 1: preventing people from dying prematurely
Indicator Baseline (ESCCG 2012 unless stated)
(1) CCG target(2) Upper decile
(3) Nat. ave.
Threshold (inc. Quality Premium)
Latest Quarterly Performance
Reduce or 0% growth
70%(7/13-3/14)
2014 due Sep-15
Awaiting data Awaiting data
0.767(7/13-3/14)
n/a
Reduce or 0% growth
2014 due Sep-15
no national data
(1) n/a; (2) 0.786;(3) 0.743
14-15 due Sep-15
(1) n/a; (2) 5.2;(3) 7.1
no national dataAwaiting data Awaiting data n/a
n/a 2013 due Mar-15
2013 due Mar-15n/a(11-12 % rate)
21.5%
-
(7/13:3/14 rate)0.536
(1) n/a; (2) 0.639;(3) 0.527
n/a 0.536(7/13-3/14)
2014 due Sep-15 Y(> national ave)
(7/12:3/13 rate)0.802
(12-13, per 100k)2058.4
(1) n/a; (2) 3519.3;(3) 2035.9
n/a
No data - data quality issue
(1) n/a; (2) 1051.6;(3) 398.9
n/a
(QOF 12-13)0.58
(11-12, per 100)6.3
(7/12:3/13 % rate)66.5%
(1) n/a; (2) 71.3%;(3) 65.1%
n/a
(1) n/a; (2) 40.9%;(3) 14.1%
Awaiting data Awaiting data n/a
14-15 due Aug-15
(7/12:3/13 rate)0.744

Plans & Outcomes 13
C3.2 - emergency readmissions within 30 days of discharge from hospital
C3.3a - average health gain assessed by patients (PROMs): hip replacement
C3.3b - average health gain assessed by patients (PROMs): knee replacement
C3.3c - average health gain assessed by patients (PROMs): groin hernia
C3.3d - average health gain assessed by patients (PROMs): varicose veins
C3.5 - people who have had a stroke: admitted to a hospital acute stroke unit < 4 hours of arrival
C3.6 - people who have had a stroke who: receive thrombolysis following an acute stroke
C3.7 - stroke: people discharged from hospital with joint health & social care plan
C3.8 - stroke: people with follow-up assessment 4-8 months after initial admission
C3.9 - patients who have had an acute stroke who spend 90% or more of their stay on a stroke unit
C3.10 - proportion of patients recovering to their previous levels of mobility or walking ability
C3.11 - hip fracture: formal hip fracture programme
C3.12 - hip fracture: timely surgery
C3.13 - hip fracture: multifactorial risk assessment
C3.14 - alcohol: admissions
C3.15 - alcohol: readmissions
C3.16 - readmissions to mental health within 30 days of discharge
C3.17 - % adults in contact with secondary mental health services in paid employment
In development Awaiting data n/a no national data Due Dec-14
In development Awaiting data n/a no national data Due Dec-14 -
In development Awaiting data n/a no national data Due Dec-14 -
In development Awaiting data n/a no national data Due Dec-15 -
In development Awaiting data n/a no national data Due Dec-14 -
In development Awaiting data n/a no national data Due Dec-15 -
In development Awaiting data n/a no national data Due Dec-15 -
In development Awaiting data n/a no national data Due Dec-15 -
In development Awaiting data n/a no national data Due Dec-15
Indicator Baseline (ESCCG 2012 unless stated)
(1) CCG target(2) Upper decile
(3) Nat. ave.
Threshold (inc. Quality Premium)
Latest Quarterly PerformanceOn target?
Q1 Q2 Q3 Q4
0.079(12-13)
13-14 due Sep-15 N(12-13 < 11-12)
n/a
no national data
n/a
0.361(12-13)
13-14 due Sep-15
Awaiting data Awaiting data n/a
Awaiting data Awaiting data n/a
Awaiting data Awaiting data n/a
no national data
(10-11, per 100k)12.5
(1) n/a; (2) 13.5;(3) 11.8
Reduce or 0% growth 12.2(11-12)
next update tbc
no national data
no national data
-
-
-
-
-
0.416(12-13)
13-14 due Sep-15
Awaiting data Awaiting data
(11-12 HES)0.433
(1) n/a; (2) 0.464;(3) 0.423
n/a
(11-12 HES)0.311
(1) n/a; (2) 0.359;(3) 0.313
Y(12-13 > 11-12)
(11-12 HES)0.112
(1) n/a; (2) 0.116;(3) 0.084
n/a
-
n/a
No data - insufficient ESCCG procedures
(1) n/a; (2) 0.145;(3) 0.095
Domain 3: helping people to recover from episodes of ill health or following injuryY
(11-12 < 10-11)
N(12-13 < 11-12)
No data - insufficient procs
13-14 due Sep-15 -

Plans & Outcomes 14
C4.1 - patient experience of Primary Care: Out Of Hours Services
C4.2 - patient experience of hospital care
C4.4 - patient experience of outpatient services
C4.5 - responsiveness to Inpatients’ personal needs
C4.6 - patient experience of A&E services
C4.7 - women’s experience of Maternity services
C4.8 - patient experience of Community Mental Health services
C4.9 - bereaved carers’ views on quality of care in last 3 months of life
C5.1 - patient safety incidents reported: rate per 1000 total provider bed days (top 5 providers)
no national data
66.9(13-14)
Awaiting data Awaiting data n/a
Awaiting data Awaiting data n/a
(13-14 out of 100)66.9
(1) n/a; (2) 74.9;(3) 68.4
n/a
Awaiting data Awaiting data n/a
(1) n/a; (2) 80.8;(3) 76.5
n/a 76.9(13-14)
2014 due Sep-15
Indicator Baseline (ESCCG 2012 unless stated)
(1) CCG target(2) Upper decile
(3) Nat. ave.
Threshold (inc. Quality Premium)
Latest Quarterly Performance
Q1 Q2 Q3 Q4
(13-14 out of 100)76.9
no national data
next update tbc
next update tbc
57.6%(7/13-3/14)
Y(> national ave)
On target?
Domain 4: ensuring that people have a positive experience of care
no national data
(7/12:3/13 % rate)76.6%
(1) n/a; (2) 77.9%;(3) 66.2%
n/a
-
-
-
N(13-14 < 12-13)
N(< national ave)
-
Awaiting data Awaiting data n/a
(Q1,2 13-14)165
(1) n/a; (2) n/a;(3) 37
n/a
Domain 5: treating and caring for people in a safe environment and protecting them from avoidable harm165
(Q1,2 13-14)N
(< national ave)Q3,4 13-14 due Mar-
15
In development Awaiting data n/a no national data next update tbc -
no national data
Title ESCCG Risk Register Update – November 2014 Reporting to Governing Body Date of Meeting 27th November 2014
Commissioning Lead(s) Author(s) Wendy Kerr Paul Winter
Purpose of the Report (Please select) Approval Assurance Discussion Key Points/Executive Summary In line with the CCG’s approach to Integrated Governance, it is a requirement for the Governing Body to receive and undertake a detailed review of all risks scoring over 12, in order to gain assurance as to the actions being undertaken to mitigate the CCG’s risks. The attached Risk Register has been renewed and updated as at November 2014; with the majority of risks updated by the Owner. The Audit Committee, Joint Quality Committee and QF&P Committee have discussed the Risk Registers in detail at their November meetings. Overview
One Clinical Risk has been rescored higher (A35: Infection Prevention – C.Diff);
One Non-Clinical Risk has been rescored higher (2.32: SSOTP Community Staffing);
No risks have been rescored lower;
Assurance Framework Risks not already reflected on the Risk Register have been updated; One newly-added Non-Clinical Risk (2.37: Impact of CSU Restructuring / Re-pricing).
Recommendations (what is expected from the Governing Body)
The Governing Body is provided with this report to enable it to be assured that risk management is being implemented effectively. The Governing Body is requested to consider the contents, and to raise any areas of new risk for logging onto the Risk Register. Recommendations:
(1) To discuss if the Governing Body is assured on risk management and associated mitigating actions for the CCG’s more-highly scoring risks;
(2) To advise of any necessary rescoring of risks logged; (3) To add or request the removal of any areas of risk to or from the register; (4) To approve the content of the accompanying risk update report.
Enclosures 12+ Scores Risk Register
Enc. 14
1 Author: Paul Winter Date: 19th November 2014 East Staffs CCG

ESCCG Comprehensive Risk Register (Clinical + Non-Clinical Risks)
A4 =
A34 =
A35
A37 =
A38 =
A39 =
SAFEGUARDING - MCA / DOLs: (added after CCG Risk Network Sep-14) Mental Capacity Act & Deprivation of Liberty risk re. Adult Safeguarding capacity c/o No. DOLs assessments needing to be undertaken likely to increase following Supreme Court decision (case of Cheshire West & Chester Council) + potential for increased costs / Individuals may be deprived of Liberty whilst in hospital / NHS funded placements without any formal and legal arrangements.[Added 12.9.14]
Operational, Clinical, Financial & Reputational Risk - this could lead to legal challenge and or increased applications to Court of Protection with significant financial impact and risk to CCG.
12(3x4)
Action plan agreed in conjunction with Staffs County Council as supervisory body to include circulation of updates to all providers; continued monitoring + reporting through Adult S/G Boards + QC. UPDATE: Oct-14= proposal to S/G Adult Board 9.10.14 re. subgroup established responsible for quality assurance of this risk; CCG to assist LA in managing this risk have agreed; Adult S/G Lead to complete BIA; LA implementing the MCA/DOLs action plan. Score unchanged. UPDATE:Nov-14= AT have released funding for Lead MCA project manager + support manager for Staffs/Stoke; SES&SP leading for all CCGs: have appointed to both posts - lead commences 3.11.14 + support manager starts 10.11.14; it is expected that these posts will assist managing the risk + identifying an action plan across the CCGs to improve understanding / implementation of the Capacity Act. Score unchanged.
9(3x3)
HJ / SF
INFECTION PREVENTION & CONTROL (IPC) - C.DIFF: (added after Apr-14 Qual Comm) Adverse effect to patient experience & health in the event of contracting avoidable C Diff infection; inherent to this is that the CCG may breach its annual CDI objective set by NHS England (30 in total 14/15)[Added 25.4.14]
Clinical & Reputational Risk due to patient exposure / health & non-delivery
12(4x3)
(original 8)
Head of IPC to: monitor Provider performance re H&S Act compliance; attend IPC Comms; monitor IPC provision (Care Homes/°1 Care); monthly QC report; CCG engagement: Shrops & Staffs IPC + Antimicrobial Prescribing forums; local RCAs scrutiny to determine avoidability of each infection re national guidance.UPDATE: Jun-14 = 12 YTD (ESCCG), most BHFT but 1 each DHFT/UHNS: no RCAs yet to est whether avoidable. Score unchanged. UPDATE: Aug-14 = 19 YTD at Jul (ES), 15 at BHFT: target at risk. Score increased. UPDATE: Sep-14 = NO UPDATE. UPDATE: Oct-14= 20 YTD at Sep (most BHFT, 2 each DHFT, UHNS); 15 agreed with HIPC as unavoidable; 5 avoidable: 2 community, 1 BHFT, 1 UHNS + 1 DHFT; Acutes have action plans to prevent recurrence; comm cases to be addressed within antimicrobial prescribing workstream (prescribers made aware of adverse effects of their prescribing). Rescored highly as a result. UPDATE:Nov-14= NO UPDATE RECEIVED
8(4x2)
JD / HJ
62-DAY CANCER STANDARD - DERBY FT: (added after May-14 Qual Comm) DHFT failed to achieve >= 85% each month from May 2013-March 2014; further to the Trust's Remedial Action Plan (RAP), improvements are expected from May & full recovery from July 2014 once all actions have been fully implemented.[Added 9.6.14]
Clinical & Operational Risk: although a date for recovery in performance is identified, until it is sustained it is a risk to patients
12(3x4)
(original 9)
RAPs in situ c/o Trust & Host CCG (S Derbys): detailed milestones + actions; signed off by Host; ATs + Monitor sighted on content.UPDATE: Aug-14 = Transformation Plan agreed + milestones being delivered, regular briefings; not expecting Q1 delivery so penalties to be applied; Host expecting Jul/Q2 delivery. UPDATE: Sep-14 =73% as at end Q1; mgt & contract actions assured (c. £40k fines for Q1) but emerging clinical concerns: SD quality summit suggested. Score increased after Aug QC. UPDATE: Oct-14= July 83.3%: SDCCG enacting financial penalties; contract meeting 13.10 to brief on further actions. ESCCG expect SD to enact all sanctions re. missed milestones in RAP. Score unchanged. UPDATE Nov-14= Aug 82.1% + deteriorating; Q2 not expected to deliver (need c. 90%+ Sep to deliver across Q2 - unlikely); repeat failure sites Urology, Gynae, Upper + Lower GI & Lung each have their own improvement trajectories; DHFT view = "work to reduce the backlog + deliver 2ww target in Q2 does increase likelihood of 62d compliance in Q3"
9(3x3)
PW /DV (CSU)
[A] CCG RISKS: CLINICAL = processed via Quality Committee (QC) + Audit Committee (AC)
DERBY HOSPITAL: (added after Feb-14 Qual Comm) Minimal data received resulting in minimal or no assurance in respect of quality; QC raised concerns about continuing lack of data & at the March meeting members NOT ASSURED in respect of quality[Added 11.4.14 - carried over to 14-15 by Qual Comm]
Clinical, Operational & Reputational Risk due to insufficient data to build assurances picture
12(4x3)
Good relationship with Host; Quality reps attend quality meetings + accompany SDCCG on visits; min core dataset c/o SDCCG + Chief Nurse (CN) invited to QC to provide overview; SDCCG GB report shared with QC; monthly report to QC by CSU Quality Improvement Lead (QIL).UPDATE: May/Jun-14 = CSU rep attends Quality Evidence Group & Assurance Comm; SD work with ES to ensure data needs met; ES CN invite to meet DHFT Dir of Nursing + SD CN; SD CN unable to attend ES QC. Score remains til data & assurances received. UPDATE: Aug-14 = SDCCG CN to attend Aug QC to provide assurances; ongoing work to access increased data/info; QIL regular attendee at meetings. Score unchanged. UPDATE: Sep-14 = SDCCG Chief Nurse attended ES QC (Aug) to provide assurances + further info; risk to remain until areas of concern resolved. Score unchanged. UPDATE: Oct-14= risk remains until issues of concern are resolved. Score unchanged. UPDATE:Nov-14= NO UPDATE RECEIVED
HJ / SW12
(4x3)
HJ / SW
TrendRisk Description Impact (Consequence of Risk) Risk Owner(s)Actions to Manage / Mitigate RiskInherent
Score(L x C)
Residual Score(L x C)
Risk
12(4x3)
(original 16 to 20 to 9 to 12)
BURTON HOSPITAL QUALITY CONCERNS: triangulation of several quality metrics (internal + external sources / agencies) covering a range of targets, quality visits & experience data indicates significant concerns about quality at BHFT [Added 1.4.13 - carried over to 14-15 by Qual Comm]
Clinical Risk - failure to protect patients; clinical quality standards compromised; investigation pressures; loss of CQC compliance
QC to AO escalation, BHFT CEO letters; QSG role; CQRM assurance; Quality Visits; Keogh outcomes & Action Plan; Monitor + "buddy" Trust support; score reduced following Feb-14 QC: increased assurances.UPDATE: May/Jun-14 = ongoing CQRM/QC process; CQC Chief Inspector of Hospitals visit: outcome awaited (end Jun), no major concerns. Score unchanged. UPDATE: Aug-14 = CQC visit rated as "requires improvement" overall; No. positive practices identified, but remain in Special Measures (SM) until further notice; additional action re ongoing quality issues. Score increased. UPDATE: Sep-14 = remains in SM; ongoing work on all recs inc inviting WMQRS to undertake a review of paediatrics (at BHFT request); all monitoring remains in place. Score unchanged. UPDATE: Oct-14= continued levels of monitoring & scrutiny. Score unchanged. UPDATE: Nov-14= no change reported by Risk Owner; score unchanged.
9(3x3)
POST-EVENT MESSAGE SERVICE (PEMS) - SDUC: (added after Apr-14 Qual Comm) the CCG's Out of Hours Provider, Staffs Drs Urgent Care, have highlighted that unregistered / untraceable NHS Spine patients seen by the service will not have their record transferred for onward care as no forwarding GP is identified[Added 6.5.14]
Clinical & Operational Risk12
(4x3)
SDUC & emergency services continue to see patients in acute relapse of illness/symptoms; CCG commissions services to meet UC needs of non-reg patients; SDUC SOP + internal processes to match how A&E handles similar events; Steering Group to consider rotational GP service; Chief Nurse chairs CQRM.UPDATE: Jun-14 = no change notified by Owner: scores t.b.c. c/o SES register. UPDATE: Aug-14 = monitoring at 1/4ly CQRM: met 11.08; once update received, necessary actions can be agreed. Score unchanged. UPDATE: Sep-14 = reports received at regular CQRMs; date / details of specific incidents are reviews. Score decreased to match SES score. UPDATE: Oct-14= SDUC CQRM (6.10) requested to undertake further work re. mitigations etc. Score unchanged.UPDATE: Nov-14 = NO UPDATE RECEIVED
6(2x3)
HJ

ESCCG Comprehensive Risk Register (Clinical + Non-Clinical Risks)
TrendRisk Description Impact (Consequence of Risk) Risk Owner(s)Actions to Manage / Mitigate RiskInherent
Score(L x C)
Residual Score(L x C)
Risk
1.2 =
1.3 =
2.1 =
2.2 =
2.5 =
2.10 =
2.15 =
16(4x4)
(12 to 16 to 12 to 16)
12(3x4)
QIPP: impact of non-implementation / delivery of agreed QIPP schemes - reduced mitigation & availability of "Plan Bs" exacerbates FOT deficit; 14/15 Provider CIPs, SLAs & knock-on to QIPP[Added 1.4.13 - carried over to 14-15 by QF&P Comm]
Operational, Reputational & Financial Risk
QF&P + QIPP Prog Board; prospective Opportunity searches + planning for further schemes; 2 & 5 yr plans to ensure schemes identified (align to BCF etc); activity shifts factored into SLAs. Rescored lower for start of new financial year.UPDATE: May/Jun-14 = score reduced to reflect new contract / fin yr; however concern that in 14/15 still finalising GP LIS re. impact on NELs reductions in BHFT contract. UPDATE: Aug-14 = contract over-perf requires further schemes to be identified + existing schemes 100% delivered to mitigate pressures. Score increased. UPDATE: Sep-14 = contract letter to BHFT re. OP ratios + actions; main concern = reductions in NELs - LIS implemented from Sep + CQUIN supports AAC so should support delivery; monitoring over next 2-3m to see impact is key. Score unchanged. UPDATE: Oct-14= no change reported. Score unchanged. UPDATE: Nov-14= driven through non-recurrent savings currently (e.g. contract penalties, CQUINs, slippage - LIS etc) so will have an impact on 15/16 financial position; therefore QIPPs going forward all need to be delivered on a recurrent basis. Score unchanged.
SL / WK
CSU DELIVERY: lack of info / performance products + outputs (regular monitoring data that's credible & reliable)[Added 1.4.13 - carried over to 14-15 by QF&P Comm]
Operational Risk - unable to operate as a viable CCG; not managing enhanced AT focus & not rescinding Conditions; potential pressure re. key vacancies unfilled
16(4x4)
(original 9)
SLA; Customer Forum; monthly review + informal op leads meetings; BI Action Plan; OD events; in-house vs. CSU provision reviews. Score remains til Plan fully delivered + high feedback scores across all functions.UPDATE: May/Jun-14 = clarity needed on CSU merger, vacancies; ongoing dialogue; May workshops (CMT + Finance) to work through issues & recommend action plans (monitored via CFO forum). Score unchanged. UPDATE: Aug-14 = interims filling permanent posts (appointed but notice periods not elapsed). Score increased as unable to manage risk. UPDATE: Sep-14 = weekly meetings scheduled, substantive posts start end Sep, phased intro Sep. Score unchanged. UPDATE: Oct-14= CSU restructure announced: revised CMT/Finance structure not yet published; meeting to discuss impact + risk; seeking satisfactory outcome with potential for CCG to be giving notice on both in collaboration with other CCGs; position to be updated post-meeting. Score increased as a result. UPDATE: Nov-14= escalated issue to CSU Director of Finance for formal resolution. Score unchanged.
12(3x4)
WK / PW
CONTINUING & FREE NURSING CARE: increased financial pressure re projected activity & new guidance for retrospective funding; Quality Assurance meeting highlighted 1705 outstanding initial assessments backlog + reassessment standard not met. ESCCG = CHC - 36 / FNC - 154 outstanding[Added 1.4.13 - carried over to 14-15 by QF&P Comm]
Financial, Operational & Clinical Risk - due to increased volume of cases, especially if higher-than-expected No. retrospective claims & backlog continues; more CHC Clinical Leads needed to undertake reviews (also reported as risk by Lead CCG Stafford)
12(4x3)
CCG + CHC-quantified impact of retro funding in baseline; Nursing Homes standard contract; collaborative commissioning; potential QIPP; +£6m in closure of 12/13 Final Accounts; CSU admin increase; prog to manage backlog; KPMG review. Score remains until mitigated.UPDATE: May/Jun-14 = Proposal to rectify backlog by end 14 to NH Quality Assurance Group; options discussed by Host; no 14/15 risk-share: CFO meeting re. future expectations; CSU process review: changes in gov structures (COO ES rep on Prog Board); CSU to est true cost of shares to clarify risk-share + drivers. No change to score. UPDATE: Aug-14 = no further update at NHQAG: requested for next meeting (Sep). Score unchanged. UPDATE: Sep-14 = Prog Board in place + QIPP plan produced; COO attended. Score unchanged. UPDATE: Oct-14= no change reported. Score unchanged. UPDATE: Nov-14= identified by all Staffs CCGs as a KPMG priority area (i.e. for Financial Recovery Plans target areas + delivery). Score unchanged.
9(3x3)
WK / SL / SW (+ CHC Team CSU)
9(3x3)
SL / WK
AUTHORISATION OUTCOME #2: Condition 3.1.1 - C (planned 1% headroom c/o NHS Commissioning Board requirement)[Added 1.4.13 - carried over to 14-15 by QF&P Comm]
Reputational Risk - formal CCG condition that needs clearing 12
(3x4)(original 9)
Rectification + Financial Recovery Plans & ongoing CCG-AT discussions on surplus control level totals; 14/15 planning work; QIPP Prog Board; AT recommend condition remains; AT supportive of CCG-raised issues. Score remains due to ongoing financial position.UPDATE: May/Jun-14 = Q4 review: remains owing to deficit plan: managed through KPMG Review, Checkpoint & AT support. Score unchanged. UPDATE: Aug-14 = Q1 review: remains (same mitigations). Score unchanged. UPDATE: Sep/Oct/Nov-14 = no change. Score unchanged.
12(3x4)
TB / WK
CONTRACTING: management of Provider contracts[Added 1.5.13 - carried over to 14-15 by QF&P Comm]
Financial Risk - financial balance re. over-performance against Activity Plans; commissioned outcomes not secured
16(4x4)
(12 to 16 to 12 to 16)
CMT operational support; Contract Exec + sub-groups focus on SUS/SLAM; alignment to QIPP; RAPs + forecasting re overspends not decreasing; GB paper re. cost reduction planning.UPDATE: May/Jun-14 = CMT vacancies/interims; 0 Derby data: Host sorting; QIPP in place but NEL not signed off by Practices, may impact outturn; MSFT disaggregation: non-ES flows to BHFT + increased £ potential (before 1 Provider so PBR) - Host to est group; national PDC guidance re. Comm Trusts (assets transferred funded or not): awaiting feedback. Score reduced (12): new contract yr. UPDATE: Aug-14 = contract challenges + over-perf experienced. Score increased. UPDATE: Sep-14 = LIS signed off (Aug GB): targets re. NELs; anticipating impact on activity; GB workshop: proposals re. Elective demand - outcome to be completed. Score unchanged. UPDATE: Oct-14=GP Refs Task & Finish (GP Execs led) re. exploring Alexin triage model using CSU-based refs analysis by Practice for debate/ownership. Score unchanged: level of risk remains. UPDATE: Nov-14= CCG Chair proposal being explored with BHFT Consultants re. referral triage process (inc retrospective analysis); LIS schemes progressing + all on track: all Practices actioning their plans. Score unchanged.
12(3x4)
WK / SL
[B] CCG RISKS: NON-CLINICAL = processed via QIPP, Finance & Performance Committee (QF&PC) + Audit Committee (AC)
AUTHORISATION OUTCOME #1: Condition 3.1.1 - B (QIPP + planned stakeholder engagement re. plans, beyond LHE Forum; showing how feedback influences CCG plans; QIPP impact on activity & workforce)[Added 1.4.13 - carried over to 14-15 by QF&P Comm]
Reputational Risk - formal CCG condition that needs clearing 12
(3x4)(original 9)
Standing QF&P item + QIPP Board; 14/15 trajectories with headroom; Rectification + Financial Recovery Plans; AT recommend condition remains until QIPP audit outcomes delivered (suggests could be removed at Q4). Rescored lower as a result.UPDATE: May/Jun-14 = Q4 review: remains owing to deficit plan: managed through KPMG Review, Checkpoint & AT support. Score unchanged. UPDATE: Aug-14 = Q1 review: remains (same mitigations). Score unchanged. UPDATE: Sep/Oct/Nov-14 = no change. Score unchanged.
9(3x3)
TB / WK
PROVIDER SUSTAINABILITY #1: general increasing pressures on LHE + non-LHE Providers (CIPs, QIPP, Winter, CCG allocations etc); impact of Monitor reviews + sustainability[Added 1.4.13 - carried over to 14-15 by QF&P Comm: now includes closed risk #2.3]
Financial & Organisational Risks - financial balance due to LHE viability + over-perf vs. Activity Plans; BHFT in Special Measures; unsecured CCG Commissioning Intentions owing to Provider fragility
12(3x4)
LHE Forum: QIPP, CIPs + resilience models / future strategy + working opps; CMT + CCG QIPP mgt; risk shares; Activity Planning Assumptions; Winter Pressures Plan; Chair, AO & CFO meetings; Urgent Care Board + LHE discussions (post-Keogh); Checkpoint Reviews. Score 9 as a result of SLA over-perf.UPDATE: May/Jun-14 = KPMG review: awaiting recs; some BHFT collaborative work with UHNS (vasc surgery); new BHFT DoF to share plans - Service Line Reporting etc for next 12m to understand £s; quality + service issues on Clinical Risk Reg. Score unchanged. UPDATE: Aug-14 = no update. Score unchanged. UPDATE: Sep-14 = KPMG not overall solution to £ gaps; further alliances by BHFT / others to support sustainability. Score unchanged. UPDATE: Oct-14= no change. Score unchanged. UPDATE: Nov-14= new LHE escalation process for closer working (SSoTP + BHFT); winter schemes all started: monitored by new gov structure - System Resilience Group (SRG) + System Resilience Operational Group (SROG), to track schemes + identify solutions for system flow. Score unchanged.

ESCCG Comprehensive Risk Register (Clinical + Non-Clinical Risks)
TrendRisk Description Impact (Consequence of Risk) Risk Owner(s)Actions to Manage / Mitigate RiskInherent
Score(L x C)
Residual Score(L x C)
Risk
2.23 =
2.25 =
2.28 =
2.29 =
2.32
2.33 =
2.36 =
2.37 New
C10 =
C11 =
PW
DERBY HOSPITAL FT: (added after Apr-14 QF&P) Migration to new PAS caused all related systems to cease provision of robust, quality data needed for national returns - e.g. RTT data not available in Feb & Mar-14; DHFT unable to separate correct RTT pathway details from deleted/amended PAS records so can’t report RTT clock stops accurately or highlight errors[Added 28.4.14]
Operational & Financial Risk - insufficient waiting list or PBR data to monitor 18 wks for CCG patients or build assurances picture re backlogs / non-RTT delivery (also on Clinical Risk Reg as #A34 re. lack of quality data)
12(4x3)
15(5x3)
WK
INTEGRATED COMMISSIONING - BETTER CARE FUND: (added after Feb Gov Body) Acknowledgement of the implications of new ways of working as posed by the Integration agenda (systems, processes, budgets, accountability + governance arrangements etc)[Added 17.3.14 - carried over to 14-15 by QF&P Comm]
Financial & Reputational Risk - not meeting the CCG's Statutory Duties; significant financial pressures to be addressed by ESCCG + re. CCG assurance frameworks
16(4x4)
Financial & Reputational Risks - not meeting the CCG's Statutory Duty of break-even = significant financial pressures to be addressed by ESCCG + potential intervention re. CCG Assurance Framework
15(5x3)
(original 20)
Full mitigations to be worked through to manage likely system / process issues.UPDATE: May/Jun-14 = emerging Integrated Commg model (OD, system planning) + ongoing revisions then approvals to 5-yr strategy. Risk score unchanged. UPDATE: Aug-14 = changing BCF guidelines expected to have (as yet unknown) impact on risk, actions, score as issues remain unclear. Score increased slightly. UPDATE: Sep-14 = revised draft due on 19 Sep; key issues to be resolved in readiness for Apr-15; delivery of QIPP with SCC share of £16.9 = major risk. Score unchanged. UPDATE: Oct-14= no change reported. Score unchanged. UPDATE: Nov-14= BCF approved with support c/o NHS England: refresh of BCF plan is due re. resolving certain ongoing challenges. Score unchanged.
16(4x4)
SL / WK
CHALLENGED ECONOMIES REVIEW: (added after Apr-14 Aud Comm) Unknown + potentially far-reaching strategic, financial, operational, systemic & structural outcomes of the proposed KPMG review, which are unclear until review's findings released: may have significant ramifications on CCG internal / external processes[Added 1.5.14]
Operational, Reputational & Financial Risk12
(3x4)
CCG input into Review scope/structure (+ AT/CSU) = some control re. known parameters & supporting analytics etc; Gov Body papers to brief on impact when known (Jun).UPDATE: Jun-14 = awaiting output (initial key issues discussed by CCGs); links to other LHE + sustainability risks. Score unchanged. UPDATE: Aug-14 = review not yet fully completed: gaps still to be addressed (while recs notified, solutions not currently resolving gaps). Score unchanged. UPDATE: Sep-14 = awaiting confirmation of delivery / Governance mechanism by Sponsors re implementation of report; gap not fully addressed + excluded the impact of report. Score unchanged. UPDATE: Oct-14= no change reported. Score unchanged. UPDATE: Nov-14= still awaiting outcome + triangulation vs. Provider assumptions; now part of wider KPMG Financial Recovery PLan process. Score unchanged.
9(3x3)
WK / TB
Activity + access plans link to correct pathways; DHFT to submit Feb & Mar RTT at Unify yr-end refresh (Jul) if granted; Lorenzo Prog Board (LPB) appraises CCGs of remedial process + recovery, inc assurances no PBR gaming nor backlogs as a result; SDCCG GB paper to brief ES for Jun QF&P.UPDATE: Jun-14 = Recovery plan approved by LPB/CCGs: aim for RTT Jun (+ retrospective); data quality risk: unvalidated RTT; potential risk re. SUS/SLAM + reporting accuracy. Score unchanged. UPDATE: Aug-14 = RTT submitted, more stable; SLAM/SUS problems: Host informed DHFT delays unacceptable (LPB had briefed no issue). Score remains but 3x4 not 4x3. UPDATE: Sep-14 = 52-wk breaches (0 ES): LPB briefed re. ongoing issues; Steering Group comms = to watch patients ref'd to DHFT. Score remains. UPDATE: Oct-14= RTT + other Unify routinely submitted & data quality stable; LPB work progressing; IMAS involved & assured worst is over (detailed report with recs received). Score reduced as a result (risk re. RTT & now far more assured). UPDATE: Nov-14= LPB still meeting: most waiting list issues (RTT + Cancer etc) now resolved. Score unchanged - stays until IMAS / Host CCG fully assured + all data flowing effectively.
4(2x2)
CCG DELIVERY OF STATUTORY BREAKEVEN DUTY: deficit plan submitted for 14/15 (to be reviewed at M6 post-Strategic Review) underlying finances represent a major pressure causing deficit to be declared - flagged to AT as a risk they need to assist / lead mitigation of not ESCCG alone[Added 7.11.13 - carried over to 14-15 by QF&P Comm]
Declared 14/15 deficit plan at M1 (£4.8m) re underlying financial position + QIPP challenge; Financial Recovery Plans (inc QIPP + SLA mgt to minimise further pressures); AT input + mitigating actions owing to causal factor (allocation). 13/14 risk score remains.UPDATE: May/Jun-14 = agreed Deficit Plan with NHSE (£5.8m); but QF&P Chair only signed off 6m awaiting response re. Distressed Economy; QIPP Working Group with BI + Public Health scoping further schemes. Score unchanged. UPDATE: Aug-14 = Deficit Plan approved: consequence reduced (residual remains). UPDATE: Sep-14 = forecast remains on plan, however risk c.£2m on QIPP or reduction in contract perf key to holding position. Score unchanged. UPDATE: Oct-14= no change reported. Score unchanged. UPDATE: Nov-14= still forecasting a planned deficit as FOT for 14/15 + likelihood to continue into 15/16 although at a lower Run Rate. Score unchanged.
Specific ESCCG Operational Plans focusing on Elective Acute Care (NHS Providers)[Added 12.9.14]
Financial, Operational & Reputational Risk due to insufficient outcomes achieved
12(3x4)
Contract Quality Requirements + KPIs; Contract Exec & Review Board reporting; BHFT position at Q1 start saw trend pressures vs. Q1 13-14 position: performance on 18 Weeks improving.UPDATE: Oct/Nov-14= Systems Resilience Plan agreed & additional NHSE monies allocated to RTT backlog clearance: delivered by BHFT by end Sept (sustainability going forward assured); Gov Body work on managing demand ongoing, inc CSU-based analysis
6(3x2)
Sl / NH
SSOTP PROVISION - COMMUNITY SERVICES: (added after CFO/COO & GB discussion Sep/Oct-14) Issues flagged by Commissioning Team & Quality Committee re. increasing community staff (District Nursing) sickness-absence rates, decreasing service capacity (notably GP Practices), increasing complaints + potential impact upon services during Improving Lives procurement [Added 10.10.14]
Operational, Financial & Reputational Risk16
(4x4)
Awaiting agreement with COO as to draft mitigating actions: inc SSOTP contractual mechanisms to apply; impact / role of Operational + Strategic Resilience Group; Operational Resilience Plan. UPDATE: Nov-14= Contract Query Notice issued - Resdiual Score to increase until RAP fully mitigates + makes improvements, as major impact on Member Practices as a consequence of reduced SSOTP staff.
12(3x4)
SL / NH
IMPACT OF LOCAL AUTHORITY CUTS: (added after QF&P Sep-14) Impact upon CCG & commissioned services / activity levels (e.g. A&E attendances etc) uncertain owing to continued, deep cuts into Staffs County Council funding - as flagged by CCG's AO [Added 10.10.14]
Operational & Financial Risk12
(3x4)
CCG response to BCF & 5-Year Strategy; Integrated Commissioning policy & approach; KPMG review & outputs (system & LHE changes); Systems Resilience Plan (e.g. activity issues: NELs + attendances). UPDATE: Nov-14= no update as situation remains as noted, however see also Risks # 2.31 & 2.32 for further info.
9(3x3)
WK / TB
IMPACT OF CSU RESTRUCTURE - PROCUREMENT SERVICES: (added after CFO request Oct-14) CSU restructuring and potential impact on the procurement staff supporting the CCG during the Improving Lives procurement.[Added 15.10.14]
Operational, Financial & Reputational Risk16
(4x4)
CCG input to ongoing 45-day CSU consultation; embedded CSU staff ensures some onsite presence; further dialogue between CCG-CSU: via customer forum, weekly meetings + AO-CSU MD / CFO-CSU DOF discussions. UPDATE: Nov-14= no change reported. Score unchanged.
6(3x2)
WK
Specific ESCCG Operational Plans for Member Practices performance (quality improvements)[Added 12.9.14]
Clinical, Operational & Reputational Risk due to insufficient processes & actions to sustain good quality
12(3x4)
Local Improvement Schemes (LIS) agreed by ES Gov Body for Member Practices, commences Sep-14 onwards; aligns to CCG QIPPs & financial position; support via PC Strategy + work of PC Change Manager; 1/4ly Practice Visits + Clinical Chair engagement; see also risks #A17 & #A18.UPDATE: Oct/Nov-14= as per risks #A17 & #A18 on Clinical Risk Reg: x2 outstanding signatures required before finance can be released but all Practices underway with plans.
9(3x3)
HJ / JH + Quality Team
IMPACT OF CSU RESTRUCTURE + REPRICING: (added after CFO request Nov-14) CSU restructuring and potential impact on staff supporting the CCG; exacerbated by ognoing debate about 15/16 finances re. CSU costs (unquantified) + impact of -10% Management Costs on both CCG + CSU. This risk merges former risks # 2.34 & 2.35, now closed.[Added 18.11.14]
Operational, Financial & Reputational Risk16
(4x4)
CCG input to ongoing 45-day CSU consultation; embedded CSU staff ensures some onsite presence; further dialogue between CCG-CSU: via customer forum, weekly meetings + AO-CSU MD / CFO-CSU DOF discussions (since escalated as unknown costs for 15/16)
9(3x3)
WK
[C] 2014-15 CCG ASSURANCE FRAMEWORK RISKS (where not already on Clinical or Non-Clinical Risk Registers - processed via QF&P, Quality & Audit Committees depending on nature of risk)

Title ESCCG Constitution Amendments Reporting to Governing Body Date of Meeting 27th November 2014
Commissioning Lead(s) Author(s) Wendy Kerr Paul Winter
Purpose of the Report (Please select) Approval Assurance Discussion Key Points / Executive Summary
CCGs are mandated to follow a specific NHS England procedure when submitting an application for variation of their Constitutions (for any change, regardless of scope). There are a number of factors that NHS England will take into account based on their guidance: “Procedures for clinical commissioning group constitution change, merger and dissolution”. Any proposed changes to CCG’s Constitution must be submitted to NHS England by 6th January 2015. As there is no public meeting in December, and the next available NHS England window for formal CCG applications is June 2015, the November meeting is requested to receive the changes outlined below.
Recommendations (what is expected from the Governing Body)
The Governing Body is asked to receive, discuss and approve the changes outlined in the sections below (the actual proposed changes to the Constitution are denoted by shading). Enclosures None
Enc. 15
1 Author: Paul Winter Date: 17th November 2014 East Staffs CCG
Proposed Amendments to the ESCCG Constitution (1) The National Legislative Reform Order (“Gateway” Reference 02281, October 2014)
This relates to changes that came into effect from 1st October 2014 as a result of the passing of a Legislative Reform Order (LRO) through Parliament, affecting all CCGs and NHS England, to enable:
(a) Two or more CCGs to form joint committees to exercise their functions jointly; and (b) One or more CCGs and NHS England to form joint committees so that the CCG(s) and NHS England
can exercise functions jointly. The LRO does not allow CCGs to form joint committees with Local Authorities. The changes amended key sections of the Health & Social Care Act 2012, meaning that CCGs no longer had to operate local work-around arrangements such as “committees in common” when wishing to make joint and binding decisions. While the 2012 Act allowed two or more CCGs to exercise their commissioning functions jointly, it made no provision for them to do so via a joint committee. Furthermore, there was no provision in the Act to allow CCGs to exercise their commissioning functions jointly with NHS England and to form a joint committee when doing so. Forming joint committees is one of a range of potential governance models for collaborative commissioning that CCGs can adopt. However the formation of a joint committee requires CCGs to amend their Constitutions. The changes to the ESCCG Constitution below use the suggested “Model Wording” for supplementing extant clauses in our Constitution, as released by NHS England in early November. These have been inserted into Chapter 6 (“Decision Making: the governing structure”): [6.8] Joint Commissioning Arrangements with other CCGs [6.8.1] - the CCG may wish to work together with other CCGs in the exercise of its commissioning functions. [6.8.2] - the CCG may make arrangements with one or more CCG in respect of: (a) delegating any of the CCG’s commissioning functions to another CCG; (b) exercising any of the commissioning functions of another CCG; or (c) exercising jointly the commissioning functions of the CCG and another CCG [6.8.3] - for the purposes of the arrangements described at paragraph 6.8.2, the CCG may: (a) make payments to another CCG; (b) receive payments from another CCG; (c) make the services of its employees or any other resources available to another CCG; or (d) receive the services of the employees or the resources available to another CCG [6.8.4] - where the CCG makes arrangements which involve all the CCGs exercising any of their commissioning functions jointly, a joint committee may be established to exercise those functions. [6.8.5] - for the purposes of the arrangements described at paragraph 6.8.2, the CCG may establish and maintain a pooled fund made up of contributions by any of the CCGs working together pursuant to paragraph 6.8.2 (c). Any such pooled fund may be used to make payments towards expenditure incurred in the discharge of any of the commissioning functions in respect of which the arrangements are made. [6.8.6] - where the CCG makes arrangements with another CCG as described at paragraph 6.8.2, the CCG shall develop and agree with that CCG an agreement setting out the arrangements for joint working, including details of: • how the parties will work together to carry out their commissioning functions;
2 Author: Paul Winter Date: 17th November 2014 East Staffs CCG

• the duties and responsibilities of the parties; • how risk will be managed and apportioned between the parties; • financial arrangements, including, if applicable, payments towards a pooled fund and management of that; • contributions from the parties, including details around assets, employees and equipment to be used under
the joint working arrangements [6.8.7] - the liability of the CCG to carry out its functions will not be affected where the CCG enters into arrangements pursuant to paragraph 6.8.2. [6.8.8] - the CCG will act in accordance with any further guidance issued by NHS England on co-commissioning. [6.8.9] - only arrangements that are safe and in the interests of patients registered with member practices will be approved by the Governing Body. [6.8.10] - the Governing Body shall require in all joint commissioning arrangements that the lead clinician and lead manager of the lead CCG make a quarterly written report to the Governing Body and hold at least annual engagement events to review aims, objectives, strategy and progress and publish an annual report on progress made against objectives. [6.8.11] - should a joint commissioning arrangement prove to be unsatisfactory, the Governing Body can decide to withdraw from the arrangement, but has to give six months’ notice to partners, with new arrangements starting from the beginning of the next new financial year. [6.9] Joint Commissioning Arrangements with NHS England for the exercise of CCG functions [6.9.1] - the CCG may wish to work together with NHS England in the exercise of its commissioning functions. [6.9.2] - the CCG and NHS England may make arrangements to exercise any of the CCG’s commissioning functions jointly. [6.9.3] - the arrangements referred to in paragraph 6.9.2 above may include other CCGs. [6.9.4] - where joint commissioning arrangements pursuant to 6.9.2 above are entered into, the parties may establish a joint committee to exercise the commissioning functions in question. [6.9.5] - arrangements made pursuant to 6.9.2 may be on such terms and conditions (including terms as to payment) as may be agreed between NHS England and the CCG. [6.9.6] - where the CCG makes arrangements with NHS England (and another CCG if relevant) as described at paragraph 6.9.2, the CCG shall develop and agree with NHS England a framework setting out the arrangements for joint working, including details of: • how the parties will work together to carry out their commissioning functions; • the duties and responsibilities of the parties; • how risk will be managed and apportioned between the parties; • financial arrangements, including, if applicable, payments towards a pooled fund and management of that; • contributions from the parties, including details around assets, employees and equipment to be used under
the joint working arrangements; and [6.9.7] - the liability of the CCG to carry out its functions will not be affected where the CCG enters into arrangements pursuant to paragraph 6.9.2. [6.9.8] - the CCG will act in accordance with any further guidance issued by NHS England on co-commissioning. [6.9.9] - only arrangements that are safe and in the interests of patients registered with Member Practices will be approved by the Governing Body. [6.9.10] - the Governing Body shall require in all joint commissioning arrangements that the Accountable Officer make a quarterly written report to the Governing Body and hold at least annual
3 Author: Paul Winter Date: 17th November 2014 East Staffs CCG
engagement events to review aims, objectives, strategy and progress and publish an annual report on progress made against objectives. [6.9.11] - should a joint commissioning arrangement prove to be unsatisfactory, the Governing Body can decide to withdraw from the arrangement, but has to give six months’ notice to partners, with new arrangements starting from the beginning of the next new financial year after the expiration of the six months’ notice period. [6.10] Joint Commissioning Arrangements with NHS England for the exercise of NHS England’s functions [6.10.1] - the CCG may wish to work with NHS England and, where applicable, other CCGs, to exercise specified NHS England functions. [6.10.2] - the CCG may enter into arrangements with NHS England and, where applicable, other CCGs to: • exercise such functions as specified by NHS England under delegated arrangements; • jointly exercise such functions as specified with NHS England [6.10.3] - where arrangements are made for the CCG and, where applicable, other CCGs to exercise functions jointly with NHS England a joint committee may be established to exercise the functions in question. [6.10.4] - arrangements made between NHS England and the CCG may be on such terms and conditions (including terms as to payment) as may be agreed between the parties. [6.10.5] - for the purposes of the arrangements described at paragraph 6.10.2, NHS England and the CCG may establish and maintain a pooled fund made up of contributions by the parties working together. Any such pooled fund may be used to make payments towards expenditure incurred in the discharge of any of the commissioning functions in respect of which the arrangements are made. [6.10.6] - where the CCG enters into arrangements with NHS England as described at paragraph 6.10.2, the parties will develop and agree a framework setting out the arrangements for joint working, including details of: • how the parties will work together to carry out their commissioning functions; • the duties and responsibilities of the parties; • how risk will be managed and apportioned between the parties; • financial arrangements, including payments towards a pooled fund and management of that; • contributions from the parties, including details around assets, employees and equipment to be used under
the joint working arrangements [6.10.7] - the liability of NHS England to carry out its functions will not be affected where it and the CCG enter into arrangements pursuant to paragraph 6.10.2. [6.10.8] - the CCG will act in accordance with any further guidance issued by NHS England on co-commissioning. [6.10.9] - only arrangements that are safe and in the interests of patients registered with Member Practices will be approved by the Governing Body. [6.10.10] - the Governing Body shall require in all joint commissioning arrangements that the Accountable Officer make a quarterly written report to the Governing Body and hold at least annual engagement events to review aims, objectives, strategy and progress and publish an annual report on progress made against objectives. [6.10.11] - should a joint commissioning arrangement prove to be unsatisfactory the Governing Body can decide to withdraw from the arrangement, but has to give six months’ notice to partners, with new arrangements starting from the beginning of the next new financial year after the expiration of the six months’ notice period.
4 Author: Paul Winter Date: 17th November 2014 East Staffs CCG
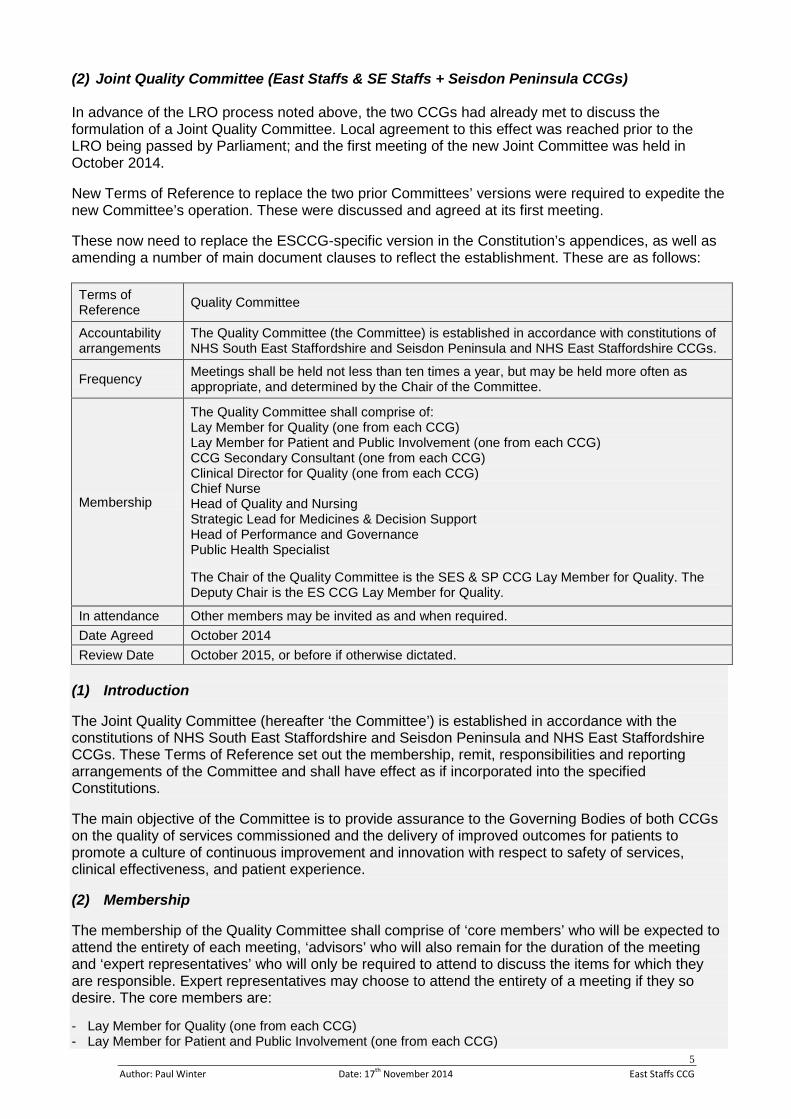
(2) Joint Quality Committee (East Staffs & SE Staffs + Seisdon Peninsula CCGs) In advance of the LRO process noted above, the two CCGs had already met to discuss the formulation of a Joint Quality Committee. Local agreement to this effect was reached prior to the LRO being passed by Parliament; and the first meeting of the new Joint Committee was held in October 2014. New Terms of Reference to replace the two prior Committees’ versions were required to expedite the new Committee’s operation. These were discussed and agreed at its first meeting. These now need to replace the ESCCG-specific version in the Constitution’s appendices, as well as amending a number of main document clauses to reflect the establishment. These are as follows:
Terms of Reference Quality Committee
Accountability arrangements
The Quality Committee (the Committee) is established in accordance with constitutions of NHS South East Staffordshire and Seisdon Peninsula and NHS East Staffordshire CCGs.
Frequency Meetings shall be held not less than ten times a year, but may be held more often as appropriate, and determined by the Chair of the Committee.
Membership
The Quality Committee shall comprise of: Lay Member for Quality (one from each CCG) Lay Member for Patient and Public Involvement (one from each CCG) CCG Secondary Consultant (one from each CCG) Clinical Director for Quality (one from each CCG) Chief Nurse Head of Quality and Nursing Strategic Lead for Medicines & Decision Support Head of Performance and Governance Public Health Specialist The Chair of the Quality Committee is the SES & SP CCG Lay Member for Quality. The Deputy Chair is the ES CCG Lay Member for Quality.
In attendance Other members may be invited as and when required. Date Agreed October 2014 Review Date October 2015, or before if otherwise dictated.
(1) Introduction The Joint Quality Committee (hereafter ‘the Committee’) is established in accordance with the constitutions of NHS South East Staffordshire and Seisdon Peninsula and NHS East Staffordshire CCGs. These Terms of Reference set out the membership, remit, responsibilities and reporting arrangements of the Committee and shall have effect as if incorporated into the specified Constitutions. The main objective of the Committee is to provide assurance to the Governing Bodies of both CCGs on the quality of services commissioned and the delivery of improved outcomes for patients to promote a culture of continuous improvement and innovation with respect to safety of services, clinical effectiveness, and patient experience. (2) Membership The membership of the Quality Committee shall comprise of ‘core members’ who will be expected to attend the entirety of each meeting, ‘advisors’ who will also remain for the duration of the meeting and ‘expert representatives’ who will only be required to attend to discuss the items for which they are responsible. Expert representatives may choose to attend the entirety of a meeting if they so desire. The core members are: - Lay Member for Quality (one from each CCG) - Lay Member for Patient and Public Involvement (one from each CCG)
5 Author: Paul Winter Date: 17th November 2014 East Staffs CCG

- CCG Secondary Consultant (one from each CCG) - Clinical Director for Quality (one from each CCG) - Chief Nurse (representing both CCGs) - Head of Quality and Nursing (representing both CCGs) - Strategic Lead for Medicines & Decision Support - Head of Performance and Governance (ESCCG) - Public Health Specialist The advisors are: - Clinical Quality Improvement Managers / Leads – two from each CCG The expert representatives are: - Quality Improvement Experts - Adult Safeguarding Lead - Child Safeguarding Lead - Head of Infection Prevention and Control - Heads of Medicines Management (from both CCGs) - Commissioning Support Unit Complaints Manager - Patient Public Engagement Representative (SES & SPCCG) - Primary Care Representative (from either CCG) - Governance Manager (SES & SPCCG) The Chair of the Quality Committee is the SES & SP CCG Lay Member for Quality. The Deputy Chair is the ES CCG Lay Member for Quality. If both the Chair and Deputy Chair are not able to attend a meeting an alternative Chair may be nominated from within the membership. (3) Attendance Other representatives may attend on an ad-hoc basis as requested or authorised by the Chair. (4) Secretary Secretarial support will be provided by the SES & SP and ES CCGs administration teams. (5) Quorum Quorum shall be no less than five core members, to include one Lay Member or Secondary Care Consultant plus one CCG representative from each CCG. If quorum is not achieved the meeting may take place, however no decisions will be able to be taken other than a decision to reconvene at a new time and place. (6) Voting The voting system will be one vote for each core member of the Quality Committee. The Chair of the Quality Committee will have the casting vote. (7) Dissenting Views Members taking a dissenting view but losing a vote can have their dissent recorded in the minutes, if so desired. (8) Frequency of Meetings Meetings shall be held not less than ten times a year. (9) Remit and Responsibilities of the Committee The main objective of the Committee is to provide assurance to the Governing Bodies of both CCGs on the quality of services commissioned. The areas in which assurance will be sought are as follows:
6 Author: Paul Winter Date: 17th November 2014 East Staffs CCG
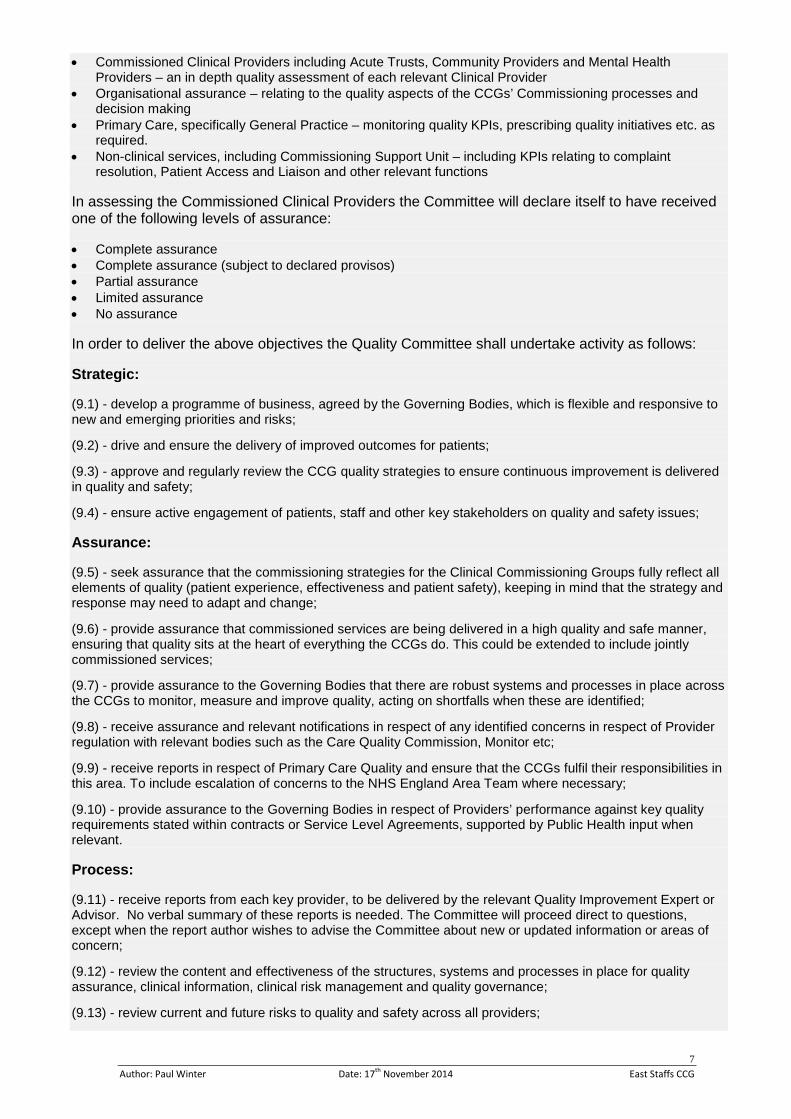
• Commissioned Clinical Providers including Acute Trusts, Community Providers and Mental Health Providers – an in depth quality assessment of each relevant Clinical Provider
• Organisational assurance – relating to the quality aspects of the CCGs’ Commissioning processes and decision making
• Primary Care, specifically General Practice – monitoring quality KPIs, prescribing quality initiatives etc. as required.
• Non-clinical services, including Commissioning Support Unit – including KPIs relating to complaint resolution, Patient Access and Liaison and other relevant functions
In assessing the Commissioned Clinical Providers the Committee will declare itself to have received one of the following levels of assurance: • Complete assurance • Complete assurance (subject to declared provisos) • Partial assurance • Limited assurance • No assurance In order to deliver the above objectives the Quality Committee shall undertake activity as follows: Strategic: (9.1) - develop a programme of business, agreed by the Governing Bodies, which is flexible and responsive to new and emerging priorities and risks; (9.2) - drive and ensure the delivery of improved outcomes for patients; (9.3) - approve and regularly review the CCG quality strategies to ensure continuous improvement is delivered in quality and safety; (9.4) - ensure active engagement of patients, staff and other key stakeholders on quality and safety issues; Assurance: (9.5) - seek assurance that the commissioning strategies for the Clinical Commissioning Groups fully reflect all elements of quality (patient experience, effectiveness and patient safety), keeping in mind that the strategy and response may need to adapt and change; (9.6) - provide assurance that commissioned services are being delivered in a high quality and safe manner, ensuring that quality sits at the heart of everything the CCGs do. This could be extended to include jointly commissioned services; (9.7) - provide assurance to the Governing Bodies that there are robust systems and processes in place across the CCGs to monitor, measure and improve quality, acting on shortfalls when these are identified; (9.8) - receive assurance and relevant notifications in respect of any identified concerns in respect of Provider regulation with relevant bodies such as the Care Quality Commission, Monitor etc; (9.9) - receive reports in respect of Primary Care Quality and ensure that the CCGs fulfil their responsibilities in this area. To include escalation of concerns to the NHS England Area Team where necessary; (9.10) - provide assurance to the Governing Bodies in respect of Providers’ performance against key quality requirements stated within contracts or Service Level Agreements, supported by Public Health input when relevant. Process: (9.11) - receive reports from each key provider, to be delivered by the relevant Quality Improvement Expert or Advisor. No verbal summary of these reports is needed. The Committee will proceed direct to questions, except when the report author wishes to advise the Committee about new or updated information or areas of concern; (9.12) - review the content and effectiveness of the structures, systems and processes in place for quality assurance, clinical information, clinical risk management and quality governance; (9.13) - review current and future risks to quality and safety across all providers;
7 Author: Paul Winter Date: 17th November 2014 East Staffs CCG
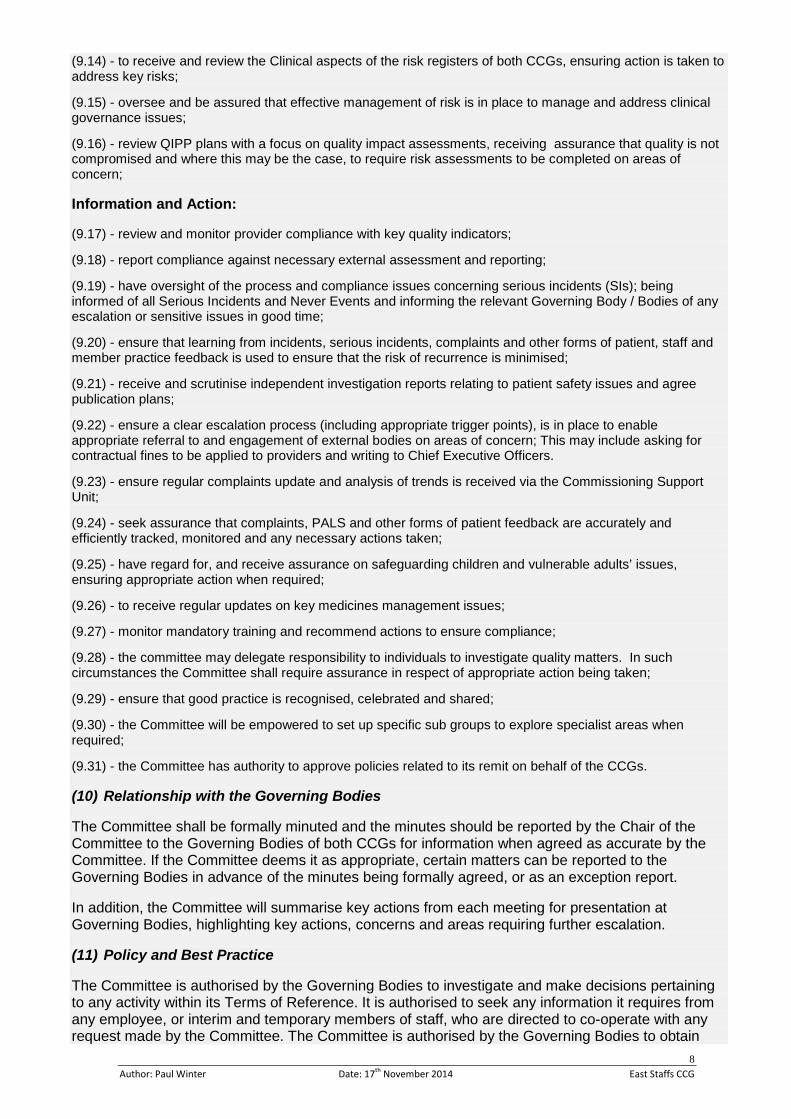
(9.14) - to receive and review the Clinical aspects of the risk registers of both CCGs, ensuring action is taken to address key risks; (9.15) - oversee and be assured that effective management of risk is in place to manage and address clinical governance issues; (9.16) - review QIPP plans with a focus on quality impact assessments, receiving assurance that quality is not compromised and where this may be the case, to require risk assessments to be completed on areas of concern; Information and Action: (9.17) - review and monitor provider compliance with key quality indicators; (9.18) - report compliance against necessary external assessment and reporting; (9.19) - have oversight of the process and compliance issues concerning serious incidents (SIs); being informed of all Serious Incidents and Never Events and informing the relevant Governing Body / Bodies of any escalation or sensitive issues in good time; (9.20) - ensure that learning from incidents, serious incidents, complaints and other forms of patient, staff and member practice feedback is used to ensure that the risk of recurrence is minimised; (9.21) - receive and scrutinise independent investigation reports relating to patient safety issues and agree publication plans; (9.22) - ensure a clear escalation process (including appropriate trigger points), is in place to enable appropriate referral to and engagement of external bodies on areas of concern; This may include asking for contractual fines to be applied to providers and writing to Chief Executive Officers. (9.23) - ensure regular complaints update and analysis of trends is received via the Commissioning Support Unit; (9.24) - seek assurance that complaints, PALS and other forms of patient feedback are accurately and efficiently tracked, monitored and any necessary actions taken; (9.25) - have regard for, and receive assurance on safeguarding children and vulnerable adults’ issues, ensuring appropriate action when required; (9.26) - to receive regular updates on key medicines management issues; (9.27) - monitor mandatory training and recommend actions to ensure compliance; (9.28) - the committee may delegate responsibility to individuals to investigate quality matters. In such circumstances the Committee shall require assurance in respect of appropriate action being taken; (9.29) - ensure that good practice is recognised, celebrated and shared; (9.30) - the Committee will be empowered to set up specific sub groups to explore specialist areas when required; (9.31) - the Committee has authority to approve policies related to its remit on behalf of the CCGs. (10) Relationship with the Governing Bodies The Committee shall be formally minuted and the minutes should be reported by the Chair of the Committee to the Governing Bodies of both CCGs for information when agreed as accurate by the Committee. If the Committee deems it as appropriate, certain matters can be reported to the Governing Bodies in advance of the minutes being formally agreed, or as an exception report. In addition, the Committee will summarise key actions from each meeting for presentation at Governing Bodies, highlighting key actions, concerns and areas requiring further escalation. (11) Policy and Best Practice The Committee is authorised by the Governing Bodies to investigate and make decisions pertaining to any activity within its Terms of Reference. It is authorised to seek any information it requires from any employee, or interim and temporary members of staff, who are directed to co-operate with any request made by the Committee. The Committee is authorised by the Governing Bodies to obtain
8 Author: Paul Winter Date: 17th November 2014 East Staffs CCG

outside legal or other independent professional advice and to secure the attendance of outsiders with relevant experience and expertise if it considers this necessary. (12) Administration Items of business to be transacted for inclusion on the agenda of a meeting need to be notified to the Chair at least 10 working days before the meeting takes place. Supporting papers for such items need to be submitted at least 10 working days before the meeting takes place. The agenda and supporting papers will be circulated to all members of a meeting at least 5 working days before the meeting will take place. As the lead for Quality across both CCGs, the Chief Nurse will be responsible for supporting the Chair in the organisation and management of the committee, its business and for drawing the committee’s attention to Quality Management best practice, national guidance and other relevant documents as appropriate. Participants will be expected to have read all the circulated information prior to attending the meeting to ensure that any necessary decision can be made at the meeting. All reports submitted to the Committee must be accompanied by a completed cover sheet this cover sheet must effectively summarise the report, explain all acronyms used and clearly specify if the report is for approval, assurance or discussion. Quality Improvement staff, as advisors, can assume that their reports have been read and that no verbal summary of these reports are needed. The Committee will proceed direct to questions, except when the report author wishes to advise the Committee about new or updated information or areas of concern. Each of the Core Members of the Committee will have lead responsibility to provide scrutiny and challenge for a specified key provider. A record of attendance will be kept from each meeting. (13) Conduct of Committee The Committee will conduct its business in accordance with Nolan’s seven principles of public life. The agenda of each Committee will be informed by a defined cycle of business. The cycle of business will be produced in conjunction with Committee members and agreed by the Chair of the Committee. This will be flexible and may be adapted to address new and emerging priorities and risks. In addition Members have agreed the following principles which will be adhered to: • We will seek assurance from other lead commissioners, on the principle that it is their responsibility to
provide assurance on the services they commission • Notwithstanding that assurance, we will challenge those lead commissioners where we think it appropriate,
based on information and intelligence • In relation to the services we commission directly, we will look at the assurances given by those providers,
but will challenge and maintain an objective and independent view • We will distinguish between quality and safety in our assessments and recognise the possibility that one or
some elements of a service may not be safe, even if the service is safe overall • We will promote patient experience as a major factor in our discussions as to quality and safety • Recognising that there is much external information about providers already available, we will make best
use of any such relevant external information to inform our opinions on the services we commission
• We will promote the use of soft intelligence as a major factor in our discussions as to quality and safety and in addition we will clarify what soft intelligence is for and what it is not for (e.g. helping with procedural issues)
9 Author: Paul Winter Date: 17th November 2014 East Staffs CCG
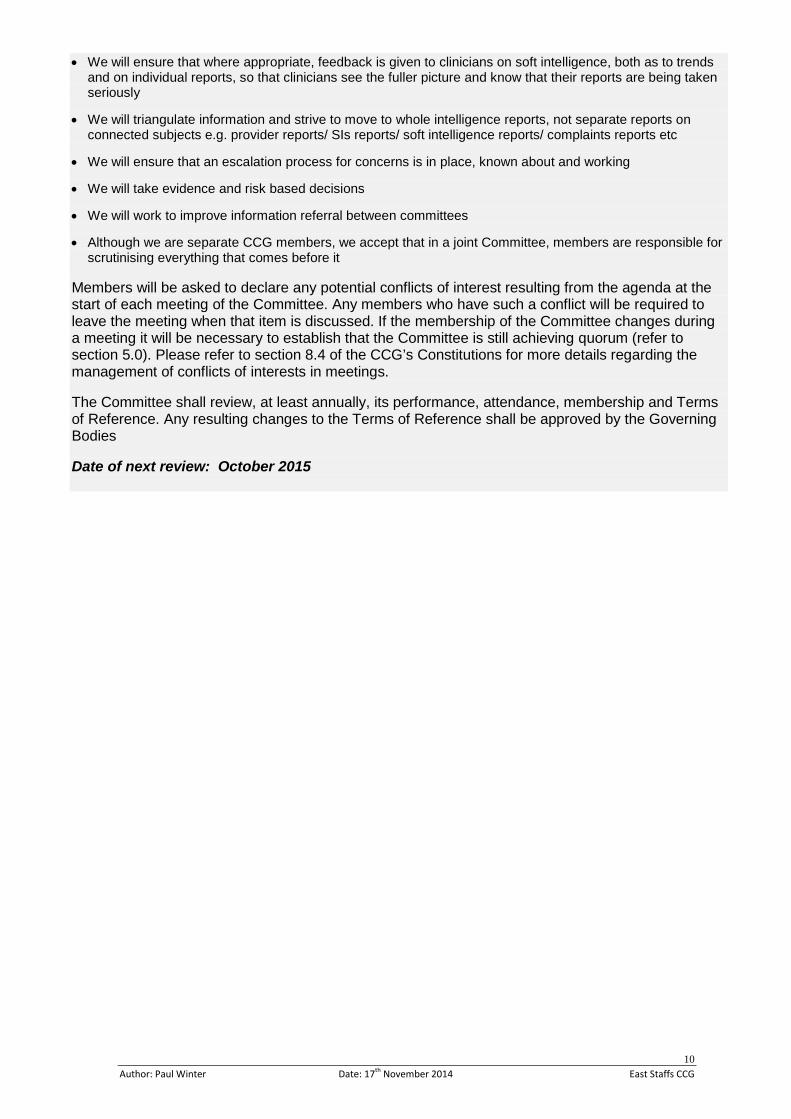
• We will ensure that where appropriate, feedback is given to clinicians on soft intelligence, both as to trends and on individual reports, so that clinicians see the fuller picture and know that their reports are being taken seriously
• We will triangulate information and strive to move to whole intelligence reports, not separate reports on
connected subjects e.g. provider reports/ SIs reports/ soft intelligence reports/ complaints reports etc • We will ensure that an escalation process for concerns is in place, known about and working • We will take evidence and risk based decisions • We will work to improve information referral between committees • Although we are separate CCG members, we accept that in a joint Committee, members are responsible for
scrutinising everything that comes before it Members will be asked to declare any potential conflicts of interest resulting from the agenda at the start of each meeting of the Committee. Any members who have such a conflict will be required to leave the meeting when that item is discussed. If the membership of the Committee changes during a meeting it will be necessary to establish that the Committee is still achieving quorum (refer to section 5.0). Please refer to section 8.4 of the CCG’s Constitutions for more details regarding the management of conflicts of interests in meetings. The Committee shall review, at least annually, its performance, attendance, membership and Terms of Reference. Any resulting changes to the Terms of Reference shall be approved by the Governing Bodies Date of next review: October 2015
10 Author: Paul Winter Date: 17th November 2014 East Staffs CCG

Title CCG Policies Update and Ratification Reporting to Governing Body Date of Meeting 27th November 2014
Commissioning Lead(s) Author(s) Wendy Kerr Paul Winter
Purpose of the Report (Please select) Approval Assurance Discussion Key Points / Executive Summary
CCG Committees and/or approved external decision-making bodies acting under delegated authority have approved the following policy summaries for the Governing Body to formally ratify. This is in accordance with the current policy approvals procedure (i.e. in advance of the proposed revision to the policy approvals / ratification procedure that is to be discussed after this agenda item). Should full versions of the policies be required, these will be made available to Governing Body members upon request prior to the meeting. These are all non-contentious in nature; and indeed some have been approved already by other CCGs (e.g. in the case of the pan-CCG HR policies, as approved through the Staff Partnership Forum or the Clinical Prioritisation Advisory Group’s processes). All policy documents will be made fully available via the CCG’s website after the Governing Body meeting.
Recommendations (what is expected from the Governing Body)
The Governing Body is asked to receive, discuss and approve the policies as outlined on the next page. Enclosures None
Enc. 16
1 Author: Paul Winter Date: 19th November 2014 East Staffs CCG

Policy Summaries for the Governing Body to Ratify
(1) Updated Anti-Bribery / Renewed Anti-Fraud, Bribery & Corruption Response Policies [Both refreshes approved by Audit Committee, Sept-14] The original policies were approved by Audit Committee in early 2013; however after discussion with the CCG’s Local Counter Fraud Specialist (CW Audit), it transpired that these required update to better reflect the 2010 Bribery Act and other key legislative matters. These policies were also updated in light of the removal of the Secretary of State Directions for Counter Fraud and new Counter Fraud arrangements imposed by the Standard NHS Contract. Furthermore the original version of the Anti-Bribery Policy was reviewed post-approval by Internal Audit, and some changes were made as part of their Audit Report’s recommendations. The changes are minimal in terms of the fundamental gist of the original policies that the Audit Committee approved. A summary is as follows:
• Anti-Bribery Policy ˗ Removal of Appendix Three (Guidelines on Secondary Employment) and short sections in the
Conflicts of Interest policy section about outside employment / private practice – both being removed from the CW Audit generic policy template provided as part of the review;
˗ Clarification in the policy about gifts not being made illegal by the 2010 Act, only inappropriate gifts, as genuine hospitality / gifts are acceptable; this now reflects the registering and consideration of the gift / hospitality as the important thing;
˗ Correction of the earlier policy quoting £20 as the threshold for gifts of low intrinsic value (£25
is the confirmed amount in the separate Gifts & Hospitality Policy);
˗ Updated cross-references to CCG Gifts & Hospitality and Commercial Sponsorship policies;
˗ Minor changes to roles set out in the Monitoring & Review section (CFO as lead, not the Accountable Officer);
˗ Addition of a ‘Conclusion’ section (re-stating the points about roles).
• Anti-Fraud, Bribery & Corruption Response Policy
˗ Section 5 (NHS Standard Contract) this section has been updated to reflect the provisions of both the 2013/14 and 2014/15 Standard NHS Contract. References to the sections only applicable to the 2013/14 have been removed;
˗ Contact details for the Nominated Local Counter Fraud Specialist (LCFS) have been updated.
˗ Anti-Fraud Manual: reference to the former NHS Counter Fraud and Corruption Manual have been removed and replaced with reference to the new manual (the Audit Committee were advised that the NHS Protect Anti-Fraud Manual are what LCFS’ are required to work to);
(2) New CCG Secondment and Recruiting Ex-Offenders Policies
[Approved by other Staffordshire CCGs & Staff Partnership Forum, Sept-14]
• Secondment Policy This policy facilitates the secondment of the CCGs’ staff (both internally within CCGs and externally within the wider NHS, and exceptionally with other non-NHS Bodies). It is also designed to encourage staff from external organisations to take up a secondment where available within the CCG, for the mutual benefit of both. This Policy will apply to all employees within the CCG.
2 Author: Paul Winter Date: 19th November 2014 East Staffs CCG
˗ Secondment requests will be considered in line with business needs and may be refused on that basis;
˗ Staff entering into secondments will be asked to sign a secondment agreement outlining the terms and parameters;
˗ Any individual who agrees to undertake a secondment will be expected to keep any information confidential that may be made available to them as a direct result of the secondment (e.g. personnel, salary, business-sensitive information);
˗ Employees on secondment with an external organisation will retain all of their continuity of service rights with the CCG;
˗ Staff undertaking a secondment will be entitled to return to their substantive post on completion: should the substantive post be subject to organisational change this will be dealt with in line with the relevant CCG procedure;
˗ The duration of a secondment will vary depending on the circumstances; however the minimum is 3 months / maximum 24 months (with exceptions to be arranged with the relevant line manager and support from Human Resources);
˗ Training and support will be provided to all Line Managers. The policy outlines a detailed procedure covering the fundamental CCG processes relating to internal and external secondments of CCG staff; as well as covering generic principles regarding funding and working arrangements, communication, manager responsibilities and extension / termination arrangements.
• Recruiting Ex-Offenders Policy This policy covers the arrangements for CCGs as recruiters / employers when using the disclosure service provided by the Disclosure Barring Service (DBS) to assess applicants’ suitability for positions of trust. It will ensure that CCGs comply fully with the DBS Code of Practice and undertake to treat all applicants fairly; and not to discriminate unfairly against any subject of a disclosure on the basis of conviction or other information received. The policy will be made available to all applicants who are required to provide a Disclosure, at the beginning of the recruitment process. The policy outlines detailed procedures covering the security, storage, handling use, retention and disposal of Disclosures / Disclosure information. It also covers a checklist of key guidelines for recruiting managers to consider about basic, standard or enhanced disclosure. (3) Updated CCG Flexible Working Policy
[Revision approved by Staffordshire CCGs & Staff Partnership Forum, Sept-14; sent to ESCCG Remuneration Committee in October 2014] This policy (as drafted by the CSU for all CCGs to adopt) was originally approved in November 2013 by the Remuneration Committee. Since then, national legislation has required that an appendix needs to be amended to reflect updated HR guidance – this is the Flexible Working Request form. This was amended to take out a list of eligibility criteria (confirmation of marital status and other child carer responsibilities that the applicant had to validate as part of the request). These are no longer mandated items since the update to employment legislation. The revised Flexible Working Request appended to the policy will be revised accordingly.
3 Author: Paul Winter Date: 19th November 2014 East Staffs CCG

(4) CPAG / CPPG Recommendations [Summary of recommendations as discussed by Quality Committee, May-14] The pan-Staffordshire Clinical Prioritisation Advisory Group (CPAG) and the Clinical Policies and Priorities Group (CPPG) have requested that Governing Bodies sign off the following list of interventions discussed by the Groups, supporting their recommendation that they should not routinely be commissioned. Feedback is required for CPPG from CCG decision bodies to understand where CCGs are in terms of adopting or still needing to adopt those recommendations: ˗ Hyaluronic acid (cystistat) for the treatment of interstitial cystitis / painful bladder syndrome ˗ Surgery for simple snoring (adult) ˗ Glucosamine prescribing in Osteoarthritis* ˗ Vitamin supplements for age related macular degeneration (AMD)* ˗ Transcranial Magnetic Stimulation (TMS) for Migraine ˗ Sodium Oxybate for the treatment of cataplexy in patients with narcolepsy ˗ Labiaplasty for cosmetic appearance ˗ Bone stimulators for non-union (PEMF- pulsed electromagnetic field) ˗ Pentosan polysulfate sodium for treatment of interstitial cystitis ˗ Endoscopic radiofrequency ablation for gastro-oesophageal reflux disease (GORD) ˗ Lucentis( Ranibizumab) for the treatment of neovascular glaucoma ˗ Silicone gel sheeting for preventing or treating hypertrophic scarring* ˗ Eflornithine cream for facial hirsutism in women* ˗ Intramedullary(ISKD) nail in lower limb length discrepancy ˗ Linx®system for management of GORD ˗ Infliximab in the treatment of sight threatening chronic non-infectious uveitis ˗ Grazax as a disease modifying treatment for grass pollen induced rhinitis and conjunctivitis in
adults and children over 5 years, with a positive skin-prick or specific IgE test to grass pollen ˗ Anti VEGF ( Ranibizumab)for macular oedema post uveitis ˗ Hyaluronic acid( & derivatives) for intra-articular injection in osteoarthritis ˗ Teriparatide for severe osteoporosis in men. ˗ Hip Arthroscopy ˗ Improving the uptake of chlamydia screening in primary care - Dash programme ˗ Modular Rotating hinge knee system ˗ Benzodiazepine Withdrawal Programme ˗ Cough Assist Device This intervention scored 160 at CPAG, well above the threshold of 100, and went to CCG decision bodies with the recommendation that this service is suitable for commissioning. CCGs should ensure the out of date SSPCT policy number 51 (Commissioning Policy on the use of Cough Assist therapy for Neuromuscular disorders and cervical spinal cord injury patients) is no longer accessible from their websites.
4 Author: Paul Winter Date: 19th November 2014 East Staffs CCG

Title CCG Policies & Procedures Approvals and Ratification Process Reporting to Governing Body Date of Meeting 27th November 2014
Commissioning Lead(s) Author(s) Wendy Kerr Paul Winter
Purpose of the Report (Please select) Approval Assurance Discussion Key Points / Executive Summary
The CCG agreed a policy for the development and management of policies in September 2013. This confirmed that all policies would be initially approved and recommended for ratification by the relevant CCG Committee (Quality, QIPP Finance & Performance, Audit and Steering Group). The agreed procedure was that a summary version of the initially-approved policy would then come to Governing Body for formal ratification – the full version being made available on request or on the CCG website for Governing Body members to apprise themselves of the full document, and should they so wish to do so. In order to retain a more strategic oversight role of the Governing Body, a proposal to amend the Policy for the Development and Management of Policies to a new approvals pathway has been formulated. This would look to confer, via the CCG’s Scheme of Delegation, full policy approvals and ratification powers to the assigned Committee (assigned depending on the nature of the actual policy itself). The vast majority of the stated policy development process would then be owned and managed by these Committees. Governing Body members would still be able to request sight of the draft policy at any stage of this process. Thereafter, only the most contentious policies would come to Governing Body for final ratification. The Policy would be amended to reflect this change in the process and made available to staff and on the CCG’s website.
Recommendations (what is expected from the Governing Body)
The Governing Body is asked to receive, discuss and approve the changes to the CCG Policy for the Development and Management of Policies as outlined on the next page. Enclosures None
Enc. 17
1 Author: Paul Winter Date: 17th November 2014 East Staffs CCG

Proposed Amendments to the Policy for the Development and Management of Policies Note: current wording is un-shaded; the proposed amendments are denoted by shading
(1.3) Responsibilities
• The Governing Body
Has overall responsibility for the policy making process. Delegated authority will be given to both the Quality and QIPP, Finance & Performance Committees to approve and to initially ratify polices. The Governing Body will then formally ratify all Policies and Procedures. (1.3) Responsibilities • The Governing Body Full delegated authority will be given to the Joint Quality Committee, QIPP Finance & Performance Committee, Audit Committee and Remuneration Committee to approve and ratify the specified polices outlined in Appendix One on the Governing Body’s behalf. The Governing Body will only formally ratify the most contentious Policies and Procedures. For the avoidance of doubt, contentious implies likely to cause significant argument among the CCG’s stakeholders about principles contained; or to be highly controversial (e.g. requiring liaison with Overview & Scrutiny Committee, other public engagement methods). Note: Other minor changes to the current wording / flowcharts of the CCG Policy will also be necessary based on this key change in the policy approvals process. Committee Terms of Reference will also be amended to confirm the new arrangement. These will be made outside of the Governing Body meeting by the Head of Performance & Governance, and in summary will amend:
• Clinical Commissioning Policies and Procedures: these may be required to be discussed by
the Steering Group first. Drafts will be shared with the Chief Nurse and Steering Group Chair (as necessary), who will consult with appropriate specialists, then to the Joint Quality Committee for formal approval and ratification.
• Human Resources / OD Policies and Procedures: these may need to be formally consulted on first at the Staffordshire & Stoke on Trent Staff Partnership Forum (and sense-checked by the CSU Human Resources Team), then to the Remuneration Committee for formal approval and ratification.
• Health & Safety Policies and Procedures: these may need to be formally consulted on first
at the Staffordshire & Stoke on Trent Staff Partnership Forum (and sense-checked by the CSU Human Resources Team), then to the QIPP Finance & Performance Committee for formal approval and ratification.
• Any Other Corporate Policies and Procedures: (e.g. communication, finance and risk
management) will be put to either the QIPP Finance & Performance or Audit Committee for formal approval and ratification.
2 Author: Paul Winter Date: 17th November 2014 East Staffs CCG

EAST STAFFORDSHIRE CCG AND
SOUTH EAST STAFFORDSHIRE AND SEISDON PENINSULA CCG JOINT QUALITY COMMITTEE
Wednesday 15th October 2014, 1.00pm, Holiday Inn, Burton on Trent
Present: In attendance:
Alex Fox (AF) Lynne Smith (LS) Heather Johnstone (HJ) Rosemary Crawley (RC) Ann Tunley (AT) Dr Liz Gunn (LG) Dr Adrian Parkes (AP) Karen McGowan (KM) Sue Wilson (SW) Fleur Fernando (FF) Paul Winter (PW) Rob Boland (RB) Judy Bird (JB) Angie Nisbet (AN) Debbie Vucetic (DV) Jackie Derby (JD) Tracey Finney (TF)
Lay Member for Quality Assurance (SES&SP CCG) (Chair) Associate Lay Representative for Quality (ES CCG) (Deputy Chair) Chief Nurse (ES CCG/SES&SP CCG) Lay Member Patient & Public Involvement (SES&SP CCG) Lay Member Patient & Public Involvement (ES CCG) Clinical Lead (ES CCG) Clinical Director Quality (SES&SP CCG) Head of Quality & Governance (SES&SP CCG) Clinical Quality Improvement Manager (ES CCG) Engagement & Partnership Manager (SES&SP CCG) Head of Performance & Governance (ES CCG) Governance Manager (SES&SP CCG) Interim Primary Care Change Manager (ES CCG) Quality Improvement Lead (CSU) Quality Improvement Lead (CSU) Head of Infection Prevention & Control (Staffordshire Health Economy) Administrator
AGENDA ITEM NO
MINUTES ACTION
To be noted: RC arrived at 1.15 pm AN arrived at 1.50 pm and left the meeting during the Comfort Break prior to Agenda Item 9 – HEFT FF left the meeting at 2.10 pm JB arrived at 4.40 pm
Appointment of Chair/Vice Chair The first item of business discussed was the appointment of the Joint Quality Committee Chair and Vice Chair. HJ proposed AF as Chair and LS as Deputy Chair. LG seconded this. The proposal was accepted.
1. Welcome and Apologies AF welcomed members to the first meeting of the ES CCG and SES&SP CCG Joint Quality Committee. Thanks were given to both ES CCG and SES&SP CCG Governing Bodies for providing an opportunity for cooperation between both CCGs to provide more effective
1
assurance on the quality agenda. Apologies were received from: Sue Bamford (SB), Claire Dearden (CD), Julie Hughes (JH), Mark Seaton (MS), Mike Chester (MC), Katie Montgomery (KLM), Mahesh Mistry (MM), Colette Marshall (CM)
2. Declaration of Conflicts of Interest None were declared. PW requested that the wording be changed from ‘if a member’ to ‘if anyone present’. Quoracy The meeting was agreed as being quorate.
TF
3. Minutes of the ES CCG Quality Committee held on 17th September 2014 The Minutes of the meeting held on 17th September 2014 were agreed as a true and accurate record subject to LS revisions. Minutes of the SES&SP CCG Quality Committee held on 16th September 2014 The Minutes of the meeting held on 16th September 2014 were agreed as a true and accurate record.
LS/ID
4. Actions from the ES CCG Quality Committee held on 17th September 2014 Actions from the SES&SP CCG Quality Committee held on 16th September 2014 Due to the number of actions on both ES CCG and SES&SP Action Sheets, members agreed that these would be updated outside of the meeting and a closed list brought to the 12th November 2014 meeting. LS suggested a task and finish group be set up to review the outstanding actions for SSOTP which members agreed to. HJ and KM to discuss this further outside of the meeting. A new integrated action sheet for the Joint Quality Committee will be produced and circulated by TF.
HJ/KM
5. Discussion on the approach for the new Joint Committee AF set out the membership of the Joint Quality Committee as follows:
• Core members – responsible to review quality and attend the entire meeting.
• Advisors – Quality Improvement Leads from both CCGs, responsible for advising core members on the issues that require scrutiny and attend the entire meeting
• Experts – attend to present reports they are responsible for, may attend for their report only or the entire meeting as they wish.
Members were advised that a verbal summary of each report would no longer be necessary. The Committee will instead proceed directly to relevant questions from all members. Patient information will also be utilised more widely and effectively throughout the committee. Terms of Reference (TOR) AF thanked MS for his helpful comments on the TOR. Subject to the following amendments members Approved the Terms of Reference:
PW/RB
2

• Describe in more detail the purpose of the committee. • Point 9.10 – amend reference to CSU. • Governing Body to be changed to Governing Bodies throughout the
document. • Point 9.11 to be amended to state that a verbal summary of reports is no
needed longer and the committee will proceed direct to questions. • Point 9.31 delegated authority for approved Policies on the CCG to be
revisited.
6. Business Cycle HJ and KM agreed to review and amend the Business Cycle for circulation by TF. Amendments to include reviewing frequency of SDUC and NSL provider reports and Staffing Levels – Hard Truths, inclusion of Primecare and Commissioning Intentions.
HJ/KM
7. Patient Engagement ES CCG Patient Board update Members noted the report on Patient Engagement in ES CCG produced by AT. SES&SP CCG Participation Toolkit FF presented the Participation Toolkit produced for SES&SP CCG which is a practical guide to assist staff, partners, patient groups and members in implementing community engagement processes. AT asked FF for additional copies of the document. Members agreed that patient engagement organisations such as Healthwatch and Staffordshire Cares should be notified of the formation of the Joint Quality Committee and that correspondence from them on the patient engagement agenda would be welcomed. AP highlighted to members that technology that allows patients to choose the way in which clinicians can contact them will be available in the near future. This would transform patient engagement with clinicians in the future. FF agreed and stated that the use of technology is a huge area at the moment. Healthwatch have signed up to Digimind, which is an online social media monitoring software. SES&SP CCG have also taken out a three month free subscription to Patient Opinion. Members were informed by FF of two consultations that are currently being undertaken; Day Case Theatre Consultation at Sir Robert Peel Hospital and Surgery Reconfiguration at HEFT. Members agreed that RC should produce a monthly report from the Patient Council for the Joint Quality Committee. RC drew members’ attention to an issue raised at the Patient Council held on the 7th of October 2014 which she was requested to bring to the Quality Committee’s attention. Changes to surgical arrangements at Cannock Chase Hospital are impacting on patients living in the Seisdon area, when attending for surgery patients are now required to present to the hospital at 7.00 am. This was highlighted as an area of concern during the consultation; however patients felt
FF
FF
RC
3

that their concerns were not listened to. Members agreed that this was not acceptable, especially for patients who may have limited access to transport. It was agreed that KLM would raise this with the Lead Commissioner.
KLM
8. Complaints, PALS and Soft Intelligence Members were informed by HJ that discussions are currently being held with the complaints team to look at the possibility of providing an integrated report for both CCG’s in the future. Members also welcomed the suggestion of a representative from the complaints team attending the committee on a quarterly basis. The following queries were raised: • Negative patient feedback on the Cardiology service at BHFT – DV agreed to
raise this with the Trust.
• Soft Intelligence – are clinicians receiving feedback that any concerns they raise are being acted on. HJ explained that ES CCG and SES&SP CCG operate two different soft intelligence systems. The system in SES&SP CCG is more advanced with a Single Point of Contact inbox and part-time administrator time to log on Datix and work with the Quality Team to follow up and feedback on concerns. KLM is currently working on replicating this system in ES CCG. SW raised the point that as CCG’s are not allowed to receive patient identifiable data the Quality Team are unable to investigate individual concerns with providers and GP practices are still required to raise incidents directly with providers. HJ asked members to note that soft intelligence is about gathering themes and learning and using that to effect change in the future and not to manage incidents on behalf of practices. However it is recognised that feedback to GPs needs to be improved, an alert system is being set up to highlight any emerging themes and ask practices to report back their experiences. HJ agreed to circulate the Complaints Report to practices.
DV
HJ
9. Quality Reports from Key Providers All members were reminded of the following guidelines when producing reports:
• Cover sheet be completed in full including all acronyms used in the full report. Any incomplete sheets will be sent back to members by TF in future.
• A summary of the key messages only and not a summary of the whole report should be provided on the cover sheet.
• Only one recommendation should be ticked ie all provider reports are ‘for assurance’ only.
Members agreed that at the committee held today assurance for providers would be agreed as follows:
1. Assured 2. Partial Assurance 3. Limited Assurance 4. Not Assured
4

Adoption of the assurance process used by the former ES CCG Quality Committee will be discussed at the 12th of November 2014 meeting. HJ informed members that the intention going forward is for Quality Leads to produce one integrated quality report to include complaints and serious incidents. DV has agreed to pilot this for BHFT at the 12th November 2014 committee. SSOTP Members noted the Quality Report produced by Di Rochelle (DR), Interim Quality Improvement Lead KM queried whether, as part of the programme of visits, any unannounced visits are planned. AN advised that these will be agreed once the schedule of announced visits has been confirmed. The lack of workforce data provided by the Trust was raised by LS. AN reported that DR is working with the Trust to improve and refine the data produced in order to provide assurance to commissioners. The joint CQRM to be held on the 30th of October 2014 will focus on workforce and North and South directors will be in attendance. Confirmation has still not been received from the Trust however as to their plans to replace the Director of Nursing and Medical Director. Members again raised significant concerns about the Trust and District Nursing Services in the South in particular. AP reported that this had been discussed at the SES&SP CCG Clinical Delivery Group and an action plan had been formulated. AN stated that the South CQRM agenda planned for November will focus on District Nursing and meetings have taken place with Jonathan Bletcher at Cannock Chase/Stafford & Surrounds CCGs. Members agreed that the following actions needed to be carried out before the November 2014 Quality Committee:
• Work to be carried out to improve the report provided to the committee in line with reports produced for other providers.
• Escalate to both ES CCG and SES&SP CCG Governing Bodies and suggest possibility of a board to board.
• Raise concerns about continued lack of assurance with the Lead Commissioner.
• Look into possibility of raising a contract query as Associate Commissioners. • AT and RC to raise with members of the Patient Groups.
Members agreed that they had Limited Assurance in respect of quality and safety of care at SSOTP. Burton Hospital (BHFT) Members noted the Quality Report produced by DV. Members highlighted the following points:
• The number of falls occurring at the Trust and the degree of harm, in particular those being reported as SI’s. HJ reported that a presentation on falls will take place at the 7th November 2014 CQRM and agreed that she would raise this with the Trust’s Director of Nursing prior to the meeting.
AN
HJ
HJ
PW AT/RC
HJ
5
LS and AP were invited by DV to attend the CQRM for this presentation. Members agreed to discuss proposing an independent review if a satisfactory response is not received from the Trust. DV agreed to look at the possibility of a Falls CQUIN for next year.
• Misinterpretation of CT scan results. LG stated that she was concerned by
the response given by the Trust when this issue was raised at the CQRM. HJ stated that there have also been concerns raised via soft intelligence in regard to ultrasound reporting. The Trust has been asked to provide assurance on CT and Ultrasound reporting. Members agreed to wait for this response before making a decision on whether to escalate further.
• Quality of care on Anna and Darwin Wards. HJ agreed to raise this with the
Trust’s Director of Nursing. • Significant concern was raised at the QSG regarding the number of stop the
clock SI’s and HJ has been asked to give an update at the 28th October 2014 QSG.
• Car parking system. Although this has slightly improved members were still
concerned that the system is confusing and a cause of anxiety for patients. It was agreed that a letter would be sent on behalf of the Joint Quality Committee to the Trust highlighting the committee’s concerns. ES CCG and SES&SP Governing Bodies to be informed of this decision.
Members agreed that they had Partial Assurance in respect of the quality and safety of care at BHFT SSSFT Members noted the Quality Report produced by DV. Members highlighted the following points:
• SPC Charts – the Trust were challenged at the October 2014 CQRM as the upper control limit on the SPC charts appear to be flexed, this was subsequently confirmed by the Trust who have agreed to review this and report back to the November 2014 CQRM.
• Increase in the number of SI’s over 45 days. To be raised at the November 2014 CQRM.
• IAPT compliance. PW informed members that the Trust have not been reporting against the national minimum data set. However this has now been resolved contractually and no further action is required.
• Increase in the number of patients absconding. KM confirmed this had been raised at the October 2014 CQRM and the Trust had given assurance that no patients had come to any harm.
• Increase in the number of suicides. LS queried whether a further benchmarking exercise should be undertaken to ensure the Trust is still not an outlier. DV to investigate this.
DV
HJ
AF
DV
DV
6

Members went on to discuss on-going concerns about the lack of a suicide prevention strategy for Staffordshire, despite repeated assurances from Public Health that one would be produced. This issue has been raised previously with the Area Team. RC reported that at the Quality Forum held in September Dr Saher Zakai (SZ), Clinical Director for Mental Health (SES&SP CCG) had stated that she was going to take this issue forward. HJ agreed to discuss this further with SZ. LS suggested a letter be sent to the cabinet member for Health & Wellbeing in Staffordshire and members agreed. Members agreed that they were Assured in respect of quality and safety of care at SSSFT. SDUC Members noted the Quality Report produced by KLM. Members highlighted the following points:
• Safeguarding Training Level 3. Six doctors are currently overdue this training which members agreed was not acceptable. It was agreed to escalate this to the Area Team.
• Members were concerned at reports that a number of GPs are leaving SDUC and the implications this would have on staffing levels and the ability to cover shifts especially at weekends and bank holidays. HJ confirmed that concerns had been raised at the October 2014 CQRM and SDUC were asked to provide evidence that there would be no impact on patients if for example GP’s from the South were being asked to provide cover in the North. A response is expected at the December 2014 CQRM.
Members agreed that they were Partially Assured in respect of quality and safety of care at SDUC. NSL Care Services Members noted the Quality Report produced by AN. LS queried whether workforce and vacancy rates were raised at the CQRM and AN confirmed that they were discussed. AN brought to members attention that in the North the Joint Quality Review meeting has now been integrated into the Contract Review Board. A decision is required on how to take forward the Quality Review Meeting in the South. HJ stated that she would support a separate CQRM for the South and members agreed with this. Members agreed that they were Assured in respect of quality and safety of care at NSL Care Services. Heart of England Foundation Trust (HEFT) including Good Hope Hospital (GHH) Members noted the Quality Report produced by KM. Members highlighted the following points:
HJ AF
7

• MRSA screening - KM confirmed that the Trust are now reporting this data. • Falls – the Lead Commissioner are to conduct an internal review of audits
and carry out a deep dive in relation to Falls. • EMSA breaches – more detail is required on these breaches. • Quality Forum – this has still not been established. A meeting between HJ,
KM and the lead commissioners is scheduled to take place on the 28th of October 2014 to discuss this further. The lead commissioners have also been invited to attend a BHFT CQRM.
• Reporting of Serious Incidents – a contract query notice has now been issued by the Lead Commissioner.
Members raised concerns about the mortality data at HEFT. KM confirmed that following the issue of a contract variation, mortality data will now be reported by the Trust. AF asked members to consider whether the lack of data should be escalated to the CQC. HJ reminded members of the role of Monitor and CQC and assured members that CQC do review mortality data and publish this as part of Hospital Intelligent Monitoring. KM confirmed that as the Trust have been identified as outliers for mortality in certain specialities they are being monitored by CQC and action plans are in place for those areas. Members agreed that HJ/KM to review national data before a decision is taken to escalate to the CQC. Members agreed that they were Not Assured in respect of quality and safety of care at HEFT. The Dudley Group Of Hospitals Foundation Trust (DGH) Members noted the Quality Report produced by KLM. Members highlighted the following points:
• Keogh Review Follow up visit – the final report following the Quality Summit held on the 27th of June 2014 is still not available. HJ reported that she would investigate when this would be published. PW suggested that the Committee consider the possibility of sending a Freedom of Information Request to CQC.
• Reducing Ventilation Associate Pneumonia – Saving Lives. Members were concerned about poor compliance. KLM to raise with the Trust.
HJ confirmed that concerns raised at the SES&SP CCG Quality Committee held on the 16th of September had been escalated to the SES&SP CCG Governing Body held on the 1st of October 2014. A number of actions were agreed as follows:
• HJ to contact Brigid Stacey, Director of Nursing for the Area Team, to highlight the CCGs on-going Quality Committees lack of assurance for patient quality and safety at Dudley Hospital, and a request that this is shared with Brigid Stacey’s counterpart in the Birmingham and Black County Area Team.
• A letter will be written to the lead commissioner, Dudley CCG, to make clear that the CCG is not satisfied with the standards of reports being received from Dudley Hospital.
• AF/RS to attend Kinver Patient Group to determine if there is any Soft Intelligence reports around Dudley Hospital.
KM
HJ/KM
HJ
KLM
8
Members agreed that if a satisfactory response is not received the Quality Committee concerns would be escalated directly to CQC. Members agreed that they were Not Assured in respect of quality and safety of care at DGH. Derby (DHFT) Members noted the Quality Report produced by DV. Members were asked to note that the level of data contained within the Quality Report reflects the fact that the majority of reporting requirements for DHFT are quarterly and August data was not received in time for the last Quality Assurance Group. This group is now meeting on a monthly basis. Data will be available for the 12th November 2014 Quality Committee. Members highlighted the following points:
• Never Event – retained guide wire following insertion of a chest drain. DV to ask the Trust for a copy of the RCA when completed.
• Abortion Waiting Times (see dashboard circulated with ES CCG Action Sheet). DV to ask the Trust how many patients this affected in terms of terminations taking place within the correct time frame.
• Cancer 62 day standard – PW asked members to note that the Trust will fail Quarter 2. ES CCG is liaising with the Lead Commissioner and members were assured this is being dealt with via the contracting and performance route.
• A&E Current Performance on the dashboard should be rated Green not Red.
An announced visit to DHFT Stroke Services will take place on the 21st of October 2014 which DV will attend. PW highlighted that performance related to Stroke Services is falling and concerns were raised at the last Contract meeting. Members were concerned how this would affect DHFT’s business case to provide a Hyper-acute Stroke Unit. HJ assured members that both Nicky Harkness, Head of Transformation & Commissioning (ES CCG) and Frances Sutherland, Head of Transformation (SES&SP CCG) are closely involved with this project and are linking in with DV and the Quality Team regarding any quality concerns. DV agreed to share the findings of the announced visit to members via email and will raise any issues under DHFT at the 12th November 2014 Quality Committee. Members agreed that they had Limited Assurance in respect of quality and safety of care at DHFT. The Royal Wolverhampton Trust (RWT) Members noted the Quality Report produced by KLM. Members highlighted the following points:
• Never Event – Wrong Site Surgery/WHO Surgical Checklist. HJ queried whether, taking into the account the number of never events at the Trust and their reported 100% compliance with the WHO Surgical Checklist, the
DV
DV
DV
DV
9

Lead Commissioner needed to request an independent review into never events at RWT.
• Doctors Appraisal Rates – members were concerned with the number of Doctors who are overdue their annual appraisal. KLM to raise with the Lead Commissioner.
• Soft Intelligence – delay in x-ray reporting of patient’s pelvis and both knees. KLM to ask the Trust whether the patient had come to any harm due to this delay.
• Cancer 31 Day Diagnosis/Cancer 62 Day – concerns raised regarding falling targets. KLM to gain assurance from the Lead Commissioner.
Members agreed that they had Limited Assurance in respect of quality and safety of care at RWT. Primecare Members noted the Quality Report produced by KM. KM advised members that she was very assured by Primecare following her attendance at the CQRM. Members highlighted the following points:
• August Bank Holiday staffing cover - KM assured members that no problems had been experienced over the bank holiday and Primecare were now planning rotas to cover the Christmas holiday period.
• Repeat Prescribing – Primecare are currently undertaking an analysis of requests for repeat prescribing, especially within nursing homes. This will be shared at the next CQRM.
Members agreed that they were Assured in respect of quality and safety of care at Primecare.
KLM
KLM
KLM
10. Quality Surveillance Group (QSG) HJ gave a verbal update from the QSG. One area of particular concern to the Area Team was the number of serious incident stop the clocks reported for Burton. HJ was requested to given an update at the 28th October 2014 QSG and DV is working with BHFT to reduce this number.
11. Medicines Management ES CCG Medicines Optimisation Report Members expressed concerns that, although containing a substantial amount of data, no conclusions could be drawn from the report. HJ informed members that discussions have been held with the Medicines Management teams at both ES CCG and SES&SP CCG with regard to the Committee’s expectations of future Medicines Management reports. HJ to discuss this further with both teams.
HJ
10

12. Infection Prevention and Control Report LS queried if the issue of whether non-avoidable health care associated infections (HCAI) count towards the trajectory had been resolved. JD replied that the general consensus for acute providers is that the whole C-Diff objective counts, although Commissioners can then decide at the end of the year which C-Diff infections are added to the aggregate total. NHS England is advising that only avoidable infections are counted. However, CCGs are currently being challenged by the Area Team on their number of infections and are being asked to manage the unavoidable infections. Analysis will take place of the avoidable infections to look at themes and unavoidable infections to look at breaches along the care pathway. SW queried whether BHFT are aware that Commissioners make the final decision on which infections are counted at the end of the year, as they currently look as though they may fail their target. JD assured members that the Trust would be fully aware of this. HJ confirmed that ES CCG have been asked to put in place a recovery plan by the Area Team. JD reported that in order to pre-empt a HCAI summit, discussions have taken place with BHFT regarding the possibility of inviting the Area Team to a meeting to discuss any issues. HJ confirmed that this had been agreed at the CQRM and arrangements will follow shortly.
13. Serious Incidents (SI) Combined Report Members noted the report produced by Janinne Lake (JL), Head of Governance & Compliance (CSU). HJ informed members that the integrated Quality Reports, discussed earlier in the meeting under Agenda Item 9, may super-cede the need for a separate SI report. However in the interim discussions are taking place with JL regarding the possibility of attending the Quality Committee on a quarterly basis and members agreed that they would welcome JL’s attendance.
14. Clinical Risk Register ES CCG Members noted the report produced by PW. Additional items for the Risk Register were discussed - see Agenda Item 18 - Items for the Risk Register and Leads Identified. SES&SP CCG Members noted the report produced by RB. Additional items for the Risk Register were discussed - see Agenda Item 18 - Items for the Risk Register and Leads Identified.
15. Primary Care Quality ES CCG JB provided a verbal update on Primary Care Quality within ES CCG.
• On-going programme of quality visits to GP practices by Dr C Pidsley (ES CCG Chair).
• Local Incentive Visits (LIS) to GP practices. Work is being undertaken with
11
practices to reduce NELS, improve patient education and access to practices. Each practice receives two visits per year led by Dr Pidsley with input from Dr Waddy. A report is then produced which is filed in the practice. Members agreed that it would be useful for these reports to come to the Quality Committee. HJ/JB to discuss further outside of the meeting.
GP Avoidable Incidents AP gave members an update on GP Avoidable Incidents which had come out of the SES&SP CCG LIS looking at improving quality in General Practice. A workshop was held on the 6th of August 2014, facilitated by the Quality Team and the Medical Protection Society, followed by further discussion amongst GP members at the Joint Locality Board on the 9th of September 2014. Six subjects were identified for practices to report. A RCA will be completed to demonstrate learning within the practice. This will also be shared anonymously for the learning of other practices. Members agreed that this was a very welcome initiative. HJ suggested that once ratified within SES&SP CCG, the scheme be adopted by ES CCG. JB and LG agreed and suggested it be discussed at the ES CCG Steering Group, although LG felt it would need to be incorporated into the ES CCG LIS.
HJ/JB
16. Discussion on escalation process KM agreed to send the Escalation Process paper to members electronically for further discussion at the 12th November 2014 committee. Items To Report To Governing Body(s)
• Concerns regarding SSOTP, especially lack of data and possibility of holding a Board to Board to discuss concerns at SSOTP – ES CCG and SES&SP CCG
• Car parking system at BHFT, letter from Joint Quality Committee to be sent to BHFT – ES CCG and SES&SP CCG
• Lack of Staffordshire Suicide Strategy – ES CCG and SES&SP CCG • Lack of mortality data for DGH and HEFT – SES&SP CCG
17. Items To Report To Other CCG Committees
• Emerging theme of Ultrasound and CT scan reports – ES CCG Steering Group and SES&SP CCG Clinical Delivery Group
• Reports of GPs leaving SDUC - ES CCG Steering Group and SES&SP CCG Clinical Delivery Group
• District Nursing Service at SSOTP – ES CCG Patient Board and SES&SP CCG Patient Council
• GP Avoidable Incidents – ES CCG Steering Group HJ reported that a template is being designed in order to facilitate communication and feedback of concerns from the Quality Committee to other CCG committees.
18. Items for the Risk Register and Leads Identified
• District Nursing issues at SSOTP – ES CCG • Stroke Performance levels at DHFT – ES CCG and SES&SP CCG • Increase in number of suicides at SSSFT – ES CCG and SES&SP CCG • Lack of mortality data at DGH and HEFT – SES&SP CCG
12
• Loss of GPs at SDUC – ES CCG and SES&SP CCG
HJ asked members to acknowledge the work of both PW and RB and also members’ commitment in ensuring that all risks are actively updated.
19. Items for escalation to the Area Team
• Outstanding Level 3 safeguarding training at SDUC • Lack of mortality data at HEFT and DGH and assurance levels with a request
that this is shared with Brigid Stacey’s counterpart in the Birmingham and Black Country Area Team.
20. Any Other Business Members were invited to comment on how they felt the first Joint Quality Committee had run and whether any improvements could be made. All members agreed that the committee had been a success. Members comments included:
• Concern about the time spent discussing provider reports, more time to be allocated at future meetings.
• Streamline items for escalation at end of meeting. • Ensure members are aware of their role within the committee. • All members agreed they had the opportunity to contribute to discussions. • All members agreed that all out of area provider reports were useful eg
DGH, RWT and HEFT for ES CCG members. HJ reported that an integrated dashboard is being developed by the CSU Business Intelligence Team.
Date time of next meeting Wednesday 12th of November 2014, 1.00 pm, Intercontinental Hotel Group (IHG), First Avenue, Centrum 100, Burton-on-Trent DE14 2WB
13
EAST STAFFORDSHIRE CCG QIPP, Finance and Performance Committee
DRAFT Minutes of the Meeting held on Wednesday 24 September 2014, at 1.00 p.m.,
in Meeting Room 1, Edwin House, Burton-on-Trent
Present: (DH) David Harding, Governance Lay Member (Chair of the Committee) (WK) Wendy Kerr, Chief Finance Officer, ESCCG (TB) Tony Bruce, Chief Accountable Officer, ESCCG
(CP) Dr Charles Pidsley, ESCCG Clinical Chair (LG) Dr Liz Gunn, ESCCG Clinical Lead (PW) Paul Winter, Head of Performance and Governance, ESCCG
In attendance: (ID)
(NH)
Ilona Davies, Secretary, ESCCG (Minutes) part meeting
Nicola Harkness, Head of Transformation and Commissioning, ESCCG part meeting
(YB) Yohan Bhatti, Contract Manager, Midlands and Lancashire CSU part meeting
Apologies: (SL) Sarah Laing, Chief Operating Officer, ESCCG
ITEM ACTION 1. Apologies for Absence As recorded above. It was noted WK would join the meeting a little later.
DH welcomed Yohan Bhatti, Contract Manager, CSU and a brief round of introductions took place.
2. Quoracy and Declarations of Interest The meeting was quorate. There were no declarations of interest.
3. Minutes of the Previous Meeting held 27 August 2014 The open and confidential minutes were accepted as an accurate record.
4. Actions from the Previous Meeting held 27 August 2014 The actions have been updated as follows:
26.2.2014#3 – Cardiology Pathways – Carried forward. 25.6.2014#6 – POLCV – Hip and Knee – Carried forward pending confirmation if resolved. 27.8.2014#1 – The Committee agreed to request the Governing Body for exemption from the rule of having 10 meetings per annum however, a meeting will be tentatively scheduled for 17 December pending confirmation of its requirement. Post meeting note: Meeting set up. CLOSED
Enc. 1
Page 1 of 5

27.8.2014#2 – On Agenda. CLOSED
NB. All reports are taken as read.
5. Contract Management Update
YB informed the Committee that at month 4 the overperformance on BHFT contract was £1.8m. The contributing factors were:
- Critical care beds activity; - A&E change in coding resulting in activity being charged at higher tariffs –
this is being challenged with the Trust; - A&E increased activity; - Non-elective plan shortfall; - Activity increase due to RTT performance issues.
It was noted BHFT had undertaken work around patient flows, which should impact on A&E and RTT performance. WK joined the meeting at this point. DH queried the probability of reducing the overall overperformance figure. WK said ESCCG were aiming to hold the position at £5.3m gross value. However, a number of mitigating actions were in place and if these actions work, projections should be coming down each month. It was noted there were still challenges in respect of assumptions having been made on successful outcomes of some actions and non-payment for First-to-Follow Ups ratios as discussed last month. A discussion took place about financial commitments CCG has made and issues relating to overperformance on provider contracts. WK clarified that the assumptions made in the Finance Report did not include the big CQUIN, due to start in September, however, the LIS benefit had been included in the mitigating actions. Some of the reserves had not been played in the position as at month 5 since need to monitor month 6 and 7 to see if reduced. Actuals include the RTT. The Committee discussed issues around electives and GP referral levels and mitigating actions being taken to address these issues. There were no further questions on the report. DH thanked YB.
6. Finance Report – Month 5 2014/15
WK said that if the current contract overperformance with BHFT continues there would be a further gap of over £2m above the agreed deficit. This will need to found through existing, additional savings plans and contract management. WK added that a significant percentage of reserves had been used, excluding NICE and CHC, and that the Area Team were aware of the risks. WK said that Ken Deacon had been asked by the Area Team to do a deep dive into ESCCG mitigating actions being taken. The Committee recognised that despite mitigating actions, ESCCG is still projecting a deficit for 2014/15. CP confirmed that the financial issues would be raised with the Governing Body with a view of discussing options for resolution. CP noted the change needs to be
Page 2 of 5

in elective management and referral patterns. WK made the Committee aware of the potential change with regards to the commissioning of up to 45% of specialised services transferring back to CCGs. When the transfer occurs, the CCG may wish to consider wider risk sharing arrangements. The Committee noted the impact of month 4 performance on ESCCG financial position showing currently an adverse variation against planned deficit. Further discussion is to be held in the Governing Body meeting on 25 September. DH thanked WK.
7. Performance Report – Month 5 2014/15
PW highlighted the currently non-achieving areas. • 18 Weeks Referral to Treatment – admitted patients: ESCCG, BHFT & DHFT • 31-Day Cancer Waits – to second / subsequent treatments (surgery): ESCCG
& BHFT • 62-Day Cancer Waits (consultant upgrades): ESCCG & BHFT • Ambulance Response – Cat A Calls within 8 minutes: Area Team / WMAS • Healthcare Associated Infections – C. Difficile + MRSA: ESCCG, BHFT &
DHFT
It was noted that the additional allocation for achievement of 18 weeks RTT was currently seeing BHFT and DHFT on track with their plans. Further assurance is provided by the fact that BHFT had significantly reduced their over 18 and over 40-week waiters this month over previous months. DH queried if penalties were being imposed for failed target in hospital related infections. PW explained that contractually penalties could be applied and the issue had been discussed by the Quality Committee but no contractual action was taken. The Committee felt the matter needs to be pursued further. WK will e-mail Heather Johnstone to discuss and take appropriate action via the contract route. ACTION: WK CP asked about IAPT PW explained the target rate was not met but ESCCG were not far off it. WK requested PW to check if the upload had been done and evidenced. ACTION: PW The Committee noted the report and the exception reports for underperforming areas. DH thanked PW.
WK
PW
8. QIPP 2014/15 – Month 4 2014/15 NH joined the meeting.
NH informed the Committee that the overall position for QIPP delivery remained the same. NH proceeded to draw out the key points: • First to Follow Ups and Non-electives are overperforming; • POLCV – first audits have taken place and the Trust supported the process.
DH queried if the financial position reflected a reduction in First to Follow Ups.
Page 3 of 5
WK confirmed that the position assumed payment of £200k, although this was subject to the outcome of negotiations. DH asked whether the work being undertaken on non-electives would improve the financial position. NH confirmed the improvement would be due to the impact of LIS and CQUIN. WK asked about audit visits to BHFT. LG responded that the first visit took place but the outcomes were still being reviewed. WK stressed the feedback to the CMT had to be provided as soon as possible should there be any financial implications. NH assured the Committee it would be done within 10 working days. A discussion took place about hip and knee referrals and the referral forms not being filled correctly causing delays in the system. It was agreed that NH, WK and YB would have a further discussion outside of this meeting to take it forward. ACTION Outside of Meeting The Committee approved the report. DH thanked NH. NH left the meeting.
9. Local Improvement Scheme (LIS) WK cover the item for JB. It was noted the Tutbury practice had made another
submission and was now in green. There were no questions on the report. The Committee noted the review process for amber rated practices and the updated RAG rating. The Gain Strategy Incentive Proposal was approved by the Committee and its approval recommended to the Governing Body.
Escalation to GB
10. Risk Register (Non-clinical Risks) The Committee discussed the Risk Register. The following additions were
requested: • Impact of Local Authority cuts on CCG; • Impact of CSU restructure during consultation period; • CSU pricing. The Risk Register was approved subject to the above amendments. ACTION: PW Post meeting note: Risk Register had been updated in accordance with above. Action completed. CLOSED TB left the meeting.
11. Standing Item: Matters Arising from GP IM&T Steering Group The meeting took place on 22 September. Feedback will be provided at the next
meeting.
12. For Approval
No items 13. For Information
No items
Page 4 of 5

14. Items for Escalation to Governing Body
It was confirmed the items were already on the agenda for the Governing Body meeting in September.
14. Any Other Business
YB and ID left the meeting. A brief discussion took place about recent changes in CSU and their impact on CCG. There was no other business. DH closed the meeting.
15. Date and Time of the Next Meeting
Wednesday 22 October 2014, 1pm to 3pm, Meeting Room 1, Edwin House, Burton on Trent Papers due by close of business 13 October.
Page 5 of 5
EAST STAFFORDSHIRE CCG QIPP, Finance and Performance Committee
Minutes of the Meeting held on Wednesday 27 August 2014, at 1.00 p.m.,
in Meeting Room 1, Edwin House, Burton-on-Trent
Present: (DH) David Harding, Governance Lay Member (Chair of the Committee) (WK) Wendy Kerr, Chief Finance Officer, ESCCG (TB) Tony Bruce, Chief Accountable Officer, ESCCG
(LG) Dr Liz Gunn, ESCCG Clinical Lead (PW) Paul Winter, Head of Performance and Governance, ESCCG (AH) Alyas Hussain, Interim Head of Contracts, Midlands and Lancashire CSU
part meeting In attendance: (ID)
(NH)
Ilona Davies, Secretary, ESCCG (Minutes)
Nicola Harkness, Head of Transformation and Commissioning, ESCCG part meeting
(LW) Dr Liz Waddy, ESCCG Primary Care Clinical Lead, part meeting
(JB) Judy Bird, Interim Primary Care Change Manager, ESCCG part meeting Apologies: (SL) Sarah Laing, Chief Operating Officer, ESCCG
ITEM ACTION 1. Apologies for Absence As recorded above. It was noted CB would join the meeting late due to prior
commitments. Dr Waddy and Judy Bird will join the meeting for agenda item 9.
2. Quoracy and Declarations of Interest The meeting was quorate. LG made a declaration of interest with regards to item
9. There were no other declarations of interest. At this point the Committee briefly discussed the business cycle in view of July’s meeting being cancelled due to the meeting not being quorate. Terms of Reference require a minimum of 10 meetings per annum. Currently there are 9 meetings scheduled therefore it was agreed that additional meeting will be convened in November or December. (Action: ID)
ID 3. Minutes of the Previous Meeting held 25 June 2014 The open and confidential minutes were accepted as an accurate record.
4. Actions from the Previous Meeting held 25 June 2014 The actions have been updated as follows:
26.2.2014#3 – Cardiology Pathways – Not actioned – Urgent update will be requested for September’s meeting. Additional new action: WK to investigate an increase in invoices for High Dependency ambulance transfers onto Glenfield Hospital – CMT have
Enc. 1
Page 1 of 5

investigated the cause for this increase and have ensured that only South Staffordshire patients are charged as previous data included Derby patients. CLOSED 25.6.2014#1 – On agenda/CLOSED 25.6.2014#2 – Completed/CLOSED 25.6.2014#3 – On agenda/CLOSED 25.6.2014#4 – First to Follow Ups – CMT were asked to send a letter to BHFT that as of month 6, 9 and 12, if outpatient ratios for 13/14 are greater in 14/15 they would be asked for an activity and management plan. Following a discussion the Committee concluded to send a letter to BHFT emphasising that CCG will only pay for Follow Up referrals based on the activity ratios agreed in the contract schedules. Post meeting note: Letter was sent 5 September 2014. CLOSED 25.6.2014#5 – Completed/CLOSED 25.6.2014#6 – POLCV – Hip and Knee – Not resolved as yet. Update required for September’s meeting. 25.6.2014#7 – On agenda/CLOSED 25.6.2014#8 – Escalated 24 July 2014/CLOSED
NB. All reports are taken as read.
5. Contract Management Update AH joined the meeting.
AH informed the Committee that the BHFT were currently forecasting overperformance on contract of over £4.4m (£5.3m gross less £0.9m flexibility). A number of areas has been identified and CMT were working with CCG colleagues to manage the demand in those areas. CMT are also challenging the Trust on s number of areas. AH said that the referrals had increased again in July and were much higher than in previous months. AH added that if the July’s increase is validated it would have an impact on contract. DH queried if the referrals were going to Derby. WK said that Derby were underperforming for the first two months however, there was no assurance that it would continue for the rest of the year. AH added that appropriate adjustments had been made based on data due to conversion rates. AH said that he compared in his report data for activities at main providers. It was noted that the significant increase was in Urgent Care, Emergency and A&E at BHFT. LG queried if there was a possibility of double counting with AAC. AH said the increase was mainly due to self-referrals. AH added that the attendance at A&E was being challenged with the Trust. DH asked how CCG were planning to address the gap of circa £2m to ensure the planned deficit of £5m. TB answered that there were initiatives in place such as LIS to drive a reduction in non-electives. TB added that CQUIN was agreed to ensure implemented clinical pathways were adhered to at BHFT. Both schemes will commence in September. DH concluded that CCG needed to improve the figure of £5.3m and ensure
Page 2 of 5
appropriate sanctions were applied in accordance with the contract. There were no further questions. The Committee noted the report. DH thanked AH. AH left the meeting.
6. Finance Report – Month 4 2014/15
The report was taken as read. DH queried a highlighted over spend of £2.195m, which was an adverse variation against planned deficit of £221k. WK explained this was inclusive of the release of over 50% of available reserves and without the reserves, the adverse variation from plan would be £1.132m year-to-date. WK added that the assumed delivery of QIPP within contracts had been taken out and therefore the position reported is a prudent view.
WK clarified that although bottom line was at the moment £8m, CCG were taking mitigating actions as listed in table 6 which would help reduce the gap. There was a suggestion to suspend some activities to next year in addition to addressing demand. Informal workshop on 25 August will look at potential actions. WK said that if this trend continued additional QIPP proposals or other mitigating actions were required to address the potential £2.160m shortfall. The Area Team were aware of the pressures ESCCG were currently facing.
The Committee noted the comments and accepted the report with the variation against planned deficit and recognising the inclusion of reserves.
DH thanked WK.
7. Performance Report – Month 4 2014/15
The report was taken as read. PW highlighted the currently non-achieving areas. • 18 Weeks Referral to Treatment – admitted patients: ESCCG • 31-Day Cancer Waits (all cancers): ESCCG & DHFT • 31-Day Cancer Waits – to second / subsequent treatments (radiotherapy):
ESCCG & DHFT • 62-Day Cancer Waits (all cancers): ESCCG, BHFT & DHFT • Ambulance Response – Cat A Calls within 8 & 19 minutes: Area Team /
WMAS • Healthcare Associated Infections – C. Difficile + MRSA: ESCCG & BHFT PW said that other key targets were being achieved. Ambulance performance against response time targets has improved albeit there has been an increase in demand. The Committee discussed the report and noted the exception reports and contractual actions being undertaken to address non-performance. DH thanked PW.
8. QIPP 2014/15 – Month 3 2014/15
Page 3 of 5

NH joined the meeting. DH queried if the QIPP figures, the £2m plan for the year and the forecasted shortfall against the target by £173k, correlated to the assumption in the Financial Report. WK clarified that although QIPP was being delivered in some areas there were issues with contract overperformance that hence mitigated the position. Therefore, the figures had been aligned but could not be matched exactly. DH said the report format was helpful and thanked NH. NH gave a brief overview of QIPP schemes. The main concern up to the month 3 was First To Follow Ups, which £41k over. WK informed NH that a discussion took place earlier in the meeting and CCG would be writing to BHFT to reiterate enforcement of contract agreed ratios. NH added that CCG asked BHFT to separate the additional RTT money given by ESCCG. WK said that she had requested a block contract and this will be discussed with the Trust next week. Month 4 onwards QIPP for non-electives commences. The Committee approved the report. DH thanked NH. NH left the meeting.
9. Local Improvement Scheme (LIS) – Feedback from the meeting held 14 August 2014
JB and LW joined the meeting. LG declared her interest for this item. JB requested the Committee to consider and agree target for NELs reductions. JB tabled proposed targets per practice and additional information on A&E admissions. JB explained the total QIPP target for 14/15 was £582,700 (£522,996k initial QIPP target made up of NELs and £56,700 attendances). The LIS scheme proposed cost £511k therefore overall needed to achieve circa £1.2m savings on non-electives to demonstrate value for money return on investment. A discussion took place about the proposed savings target, which varied between 5% and 10%. In conclusion the Committee agreed the QIPP target of circa 6%, which would achieve the required return, and recommended its approval by the Governing Body. (Escalation to GB) The Committee agreed the proposed LIS plans and approved • the process, including the RAG rating; • the payment mechanism; and • the monitoring and evidence gathering process. The Committee also suggested a Gain Strategy if overall target of £1.5m on 13/14 outturn was achieved. JB/WK to work out proposal for September’s meeting subject to the Governing Body’s agreement to the principle. (Action: JB/WK) DH thanked JB and LW. JB and LW left the meeting.
Escalation to GB
JB/WK
Page 4 of 5
10. Risk Register (Non-clinical Risks) The Committee discussed the Risk Register. The following addition was
requested: • Impact of Local Authority cuts on hospital flows and discharges. The Risk Register was approved subject to the above amendment. TB left the meeting.
11. Standing Item: Matters Arising from GP IM&T Steering Group The action list was presented for Committee’s assurance on actions being taken.
12. For Approval
The Committee considered and approved the following: • GP IM&T Strategy • Revised Information Governance Policy • Information Governance Handbook • Display Screen Equipment Policy and Procedure The Committee recommended the adoption of the above policies by the Governing Body. (Escalation to GB, September)
Escalation
to GB (September)
13. Items for Escalation to Governing Body
Confirmed items already on the agenda for Governing Body in August. 14. Any Other Business
SIRO Report – The Committee noted the report for information and to be shared with the Governing Body in September. (GB, September) There was no other business. DH closed the meeting.
GB (September)
15. Date and Time of the Next Meeting
Wednesday 24 September 2014, 1pm to 3pm, Meeting Room 1, Edwin House, Burton on Trent Papers due by close of business 15 September.
Page 5 of 5
EAST STAFFORDSHIRE CLINICAL COMMISSIONING GROUP
Minutes of the East Staffordshire Clinical Commissioning Steering Group Meeting held on 19 August 2014 at 12.45pm
at the Holiday Inn Express, Second Avenue, Burton-on-Trent
Present: Dr Chris Gunstone ESCCG Steering Group Chair Dr Charles Pidsley ESCCG Chairman / Bridge Surgery Tony Bruce ESCCG Accountable Officer Sarah Laing ESCCG Chief Operating Officer Dr R Adams Abbots Bromley Surgery Dr K Aziz All Saints Surgery David Rose Barton Family Practice Dr Afzal Mohammed Carlton Street Practice Dr Richard Fulford Dove River Practice Dr B T O’Reilly Gordon Street Surgery Dr Sheraz Hassan King Street Surgery Dr S Poonian Millview Surgery Pauline Boden Northgate Surgery Dr K Pai Peel Croft Surgery Dr David Dickson South Staffs LMC Secretary Dr V Bammidi Stapenhill Medical Practice Dr Peter Jones Trent Meadows Practice Dr Liz Gunn Tutbury Practice Dr Ajitha K Prasad Wetmore Road Surgery Lesley Needham Winshill Surgery John Evans Yoxall Surgery Julie Hughes ESCCG Primary Care Change Manager Judy Bird
Dr Liz Waddy ESCCG Interim Primary Care Change Manager ESCCG Clinical Support
Nicky Harkness ESCCG Head of Transformation and Commissioning Dave Whatton
Annette Alexander ESCCG Change Manager ESCCG Project Manager
In Attendance
Jeanette Cole
Personal Assistant, ESCCG (minutes)
MINUTES ACTION SG(08)01 APOLOGIES No apologies were received. SG(08)02 DECLARATIONS OF INTEREST All members declare an interest in the GP Federation (Alexin). SG(08)03 Chairman’s Opening Remarks
Dr Chris Gunstone welcomed everyone to the meeting.
SG(08)04 MINUTES OF PREVIOUS MEETING HELD ON 15 July 2014 Amendment to the Attendance Sheet; Page 1 – Remove ‘Dr’ from Rob
Paton’s name.
The minutes were agreed as a true and accurate record.
SG(08)05 ACTIONS FROM MEETING HELD ON 15 July 2014 SG(07)04: Minutes of Previous Meeting held on 17 June 2014
Chairman’s Report SG(06)06, Page 2; b) CCGs to be moved nearer to the fair share allocation – this would
Enc. 1
1

move the CCG further underneath the target e.g. £6m this year to £6.8m next year. The local MP will be writing to NHS England regarding this. There may be some non-recurrent money available but this is not yet known. Tony Bruce to check the wording of this paragraph. Update: The wording should read ‘……this would move the CCG further away from the fair share allocation’. Update: Wendy Kerr, Chief Finance Officer, has re-negotiated CHC risk sharing arrangements. The CCG has previously recorded a £6.8m shortfall in funding as a result of distance from target. However, a rebasing of Continuing Healthcare has been undertaken for 2014/15 recognising that the previous risk sharing arrangements were not aligned to individual CCGs usage. As per the Memorandum of Understanding the 2013/14 resource baseline has been corrected to reflect the revised split and as a result £2.6m of funding has transferred. ESCCG risk share for CHC reduces to 14.74% and the distance from target also formally increases to £9.4m. SG(07)06: Chairman’s Report Included within the report are current media links for GPs. All members to let Dr Charles Pidsley know if they do not feel these links are helpful and require removal from future reports. Update: All members agreed the links should remain within the report. This action is now CLOSED. Members of the Steering Group commented when Dr Willis is on leave, there appears to be no urgency and the process becomes very slow. Dr Charles Pidsley to discuss this matter with Dr Willis. Update: Dr Charles Pidsley confirmed he had not received any response to his emails. Dr Chris Gunstone and Dr Charles Pidsley are meeting with Dr Crampton to discuss a joint GP-consultants meeting. This action is ONGOING. SG(07)07: Local Incentive Scheme Judy Bird to add two additional columns to the Spreadsheet: 1) Current position; 2) 3/6 months’ position.
Judy Bird to revamp the template and include level of evidence for plans. This action is now CLOSED. Dr Liz Waddy to check whether Drugs/DNRs/Palliative drop-down boxes for completion within special notes can be added for all conditions; the response to be cascaded to all practices. Action to be discussed later on the agenda. Dr Liz Waddy and Judy Bird to check the live state of the Urgent Care Dashboard and bring back to the next Steering Group meeting. Action to be discussed later on the agenda. Dr Liz Waddy and Judy Bird to discuss the design of a standard form for completion by practices to provide an audit trail of evidence without being too onerous. This action is now CLOSED. SG(07)08: Heart Failure and Diabetes Dr Charles Pidsley to take ideas back to Dr Willis and Dr Carey who will
2
be asked if the suggestions are feasible. Update: Prior to arranging a meeting a contractual request will be implemented. This action is ONGOING. Annette Alexander to correlate all feedback from the Lead of each group and send to Dr Charles Pidsley for the meeting with Dr Willis and Dr Carey. Update: Feedback has been sent to Dr Charles Pidsley. This action is now CLOSED. SG(07)10: Derby Tony Bruce to ask Heather Johnstone which specialities are behind on follow-ups and request assurance from Derby the follow-up system is secure and report back to the next Steering Group meeting. Tony Bruce to speak to Sue James, CEO and notify her of this issue and request follow up of any breaches. Tony Bruce to feedback to Steering Group members. GPs to explain what the situation is for new referrals and work on:
1. How they identify patients already within the system? 2. Are patients within the system receiving follow ups?
John Tansey to request an EMIS share search to provide information and feedback to Steering Group members. Update: Wendy Kerr will discuss EMIS at the next IM&T Group meeting. This action is ONGOING. Sarah Laing to speak to the host commissioners and request the Access Policy for Derby. This will highlight if any gaps exist. Update: The Access policy has been received and will be added to the website for information purposes. This action is now CLOSED. Dr Charles Pidsley requested this issue is discussed within practices pending the issue of further information from the CCG from a corporate perspective. Update: Heather Johnstone has sent feedback regarding Lorenzo and been advised the patient system is working. Steering Group members confirmed there had been no issues in the past month. Tony Bruce confirmed he had spoken to Sue James (CEO) regarding the concerns; Heather Johnstone would be taking these concerns to the Quality Committee; due to meet 20 August 2014. Heather Johnstone will also be asking South Derbyshire CCG how they are assuring themselves that patients referred for first referral are receiving a follow up appointment if determined required by a clinician. Dr Pai advised that renal patient follow ups in February and March had been missed; Derby Hospital is checking a different database in order to ensure patients receive follow ups. GPs are advised to be aware of this issue when referring patients to Derby. SG(06)07: Local Incentive Scheme The CCG to arrange a dialogue with Carers organisations to ensure a consistent message is delivered on behalf of the Steering Group regarding care within homes where patients are being sent straight to
Wendy Kerr
ALL
3

A&E – improved access to the practice. Update: Tony Bruce confirmed this item would be actioned and an update brought to the next meeting. Update: (19 August 2014) – This action is ONGOING. Sarah Laing to speak to Wendy Kerr to request EMIS web is raised at the next IT Sub Group meeting in order to progress the need for 100% uptake and Smartcard access. Update: Sarah Laing confirmed Smartcard access has been raised with the Area Team; some practices are not using Smartcards. With regard to EMIS Web; some practices are not utilising the system as they should. A new SLA has been written and will be presented at the QFP meeting for initial sign off. Once signed off, the SLA will be brought to the next meeting of the Steering Group. Update: (19 August 2014) The IT Sub Group is functioning as it should. This action is now CLOSED. SG(06)09: Any Other Business Tony Bruce to raise Ambulance Response Times with the Contract Management Group to clarify the service offered and whether appropriate. Update: Tony Bruce confirmed this matter had been raised and a response is awaited. Update: (19 August 2014) Tony Bruce confirmed this matter is still being pursued. This action is ONGOING. SG(06)10: Soft Intelligence Sarah Laing to request a list of cancelled or re-scheduled appointments from Burton Hospital over the last few months regarding growing waits within Cardiology. Update: Sarah Laing confirmed this matter would be progressed through the contract management route. A response is awaited but will be delayed as the process is new. Update: (19 August 2014) Sarah Laing confirmed this information had been requested and will be discussed at the Contract Management Team meeting on 20 August 2014. This action is ONGOING. SG(03)09: Any Other Business Emily Davies confirmed that an indication of what is provided as part of the ‘As Is’ specification should be received by the end of June. A breakdown of patients referred and how many had received psychological therapy would be added to this request. Update: Nicky Harkness confirmed the majority of the breakdown had been received from SSOTP and covers Community Matrons and Community Nursing. There are differences of service between practices. Speed of recruitment to vacancies is an issue. No money has been taken out of the system for District and Community Nursing; the allocation is the same as 12 months ago with spend above the national average. Action: Nicky Harkness to circulate the ‘Audit with GPs’, ‘National Specification’ and the ‘As Is’ specification; to show where any differences or gaps exist. This item to be added to the next Steering Group Meeting agenda. Action: Nicky Harkness to request a copy of the plan and raise this matter through the contract route to mitigate these issues.
Nicky Harkness
Nicky Harkness
4
Soft Intelligence has been received regarding discharge letters which are typed and ready to be sent but the practice has not received. Action: Liz Waddy to send to Nicky Harkness.
Liz Waddy SG(08)06 Chairman’s Report The report was taken as read.
Dr Charles Pidsley provided a brief overview of the Improving Lives Procurement. Second paragraph ‘issued on the 17th of July preceded by a bidder event’ should read ‘followed by’.
• The Procurement is an outcomes based contract rather than the traditional commissioning approach based on activity.
• Details regarding Competitive Dialogue can be found at the link contained within the report.
• The scope of the procurement process was outlined in the paper approved by the Steering Group in May.
Key Areas of Discussion: • David Dickson queried whether this could mean privatisation of
District Nursing and the issues arising from this regarding Union involvement and SSOTP.
• Dr Charles Pidsley confirmed it is important to emphasise services are free at point of contact; there may be no choice over privatisation, it is the current nature of the health economy. The prime contractor bids are due by close of play on Friday 22 August and these could be both public sector and private.
• Tony Bruce confirmed 3 monthly open dialogue events will be held for frontline staff to attend. HR Directors of Providers Trusts and Unions will be invited to attend. Any staff queries should be directed to Tony Bruce or Emily Davies.
• Dr Charles Pidsley confirmed the future provision of health care will be community based and inconceivable that community setting staff will be at risk. There is a recognition that workloads will increase but operated in a more efficient manner.
SECTION TWO SG(08)07 A&E Referral Data Alyas Hussain, Head of Contract Management, CSU; and Matt Ball,
Informatics and Performance Lead, CSU; presented detailed analysis of the A&E Referral Data.
• A&E Attendances dropped off when the AAC opened but have now returned to pre-AAC levels.
• Self-Referrals appear to be increasing, whereas GP Referrals dropped off when the AAC opened in Sept 2013. Between 9:00am to before 5:00pm has increased since each Quarter from Q3 2013-14. 5:00pm to before Midnight has increased by 12% since Q4 2013-14.
• The comparison between Q3, Q4 and Q1 Self-Presenters during the period after 9:00am and before 5:00pm show from Q3 the numbers have been increasing each Quarter. The main increases appear to be in the 3:00pm and 4:00pm time band.
• Between Q4 and Q1 Self Presenters during the period after 5:00pm to before 1:00am, the increases appear to be between 6:00pm and before 11:00pm.
5

Key Areas for Discussion: • The number of A&E referrals stands out against other healthcare
benchmarks. • Repeat visits may take account of some of the figures. • OOH and 111 figures are not available separately. • Hospital coding is reliable; therefore, other issues are causing
the rise; these need to be identified. • Practices are providing education and signposting patients to
alternative services e.g. minor injuries units. • Geography for some practices is still an issue e.g. closeness to
the hospital site. Key Actions Arising from the Discussion:
• The data to include 111 referrals; repeat and follow up attendances.
• There is a requirement to understand the figures at practice level for Self Presenters.
• List size comparisons need to be made. Action: Alyas Hussain to send Dr Charles Pidsley the data to include; referrals via 111, repeat visits, per 1,000 population, by age for all providers, follow-up ratios Monday to Friday and weekends including time of day. Action: Matt Ball to send Jeanette Cole the presentation for circulation to Steering Group members. Dr Chris Gunstone thanked Alyas Hussain and Matt Ball for attending.
Alyas Hussain
Matt Ball
SECTION THREE SG(08)08 LIS Liz Waddy and Judy Bird provided a verbal update:
Liz Waddy thanked all practices for receipt of their plans. The plans have been scrutinised by Tony Bruce, Wendy Kerr and Internal Audit. The comments have been added; plans amended and rag rated. The plans will be presented at Quality Committee for assurance and then Governing Body for sign off. Those rag rated: Green – are given the go ahead to start making plans but no money should be spent. Amber – a response will be issued by close of play on 20 August.
• Evidence and outcomes based on action plans will be required via completion of a CCG monitoring template. The monitoring summary will be presented at QFP Committee.
• Practices will need to show additionality within their evidence. • Payments will be made quarterly up front and providing evidence
is received Q2 and Q3 payments will be made. • Baselines to be agreed to provide parameters to measure
against. Baseline information is required to show the current level of clinical service to demonstrate additionality quarter on quarter.
• A letter of intent from the CCG will be issued to practices by close of play on 21 August.
• Submission date to be included within the template.
6

Actions Arising from 15 July 2014 meeting: Dr Liz Waddy to check whether Drugs/DNRs/Palliative drop-down boxes for completion within special notes can be added for all conditions; the response to be cascaded to all practices. Dr Peter Jones confirmed there is no minimum for special notes and can be added for all conditions. This information aids the OOH doctor, who does not know the patient, to decide whether an admission is necessary. SATs for a COPD patient are required, would save admissions and enable the most recent admission added to be reviewed. Action: Dr Peter Jones to issue a list of pointers to send out to Steering Group members. Dr Peter Jones offered support to practices and practice managers using the Adastra system. Anyone requiring support to ring: 0300 123 0812 or 0814. Dr Liz Waddy and Judy Bird to check the live state of the Urgent Care Dashboard and bring back to the next Steering Group meeting. Dr Liz Waddy confirmed this has been escalated to Sarah Laing and Wendy Kerr; this was promised by July and is now promised by the end of August. Wendy Kerr is meeting with CSU Director if this deadline is not met. This action is ONGOING. The key indicator for Burton performance for 4 hour waits from April to date is poor, the winter months, therefore, will worsen. Sarah Laing confirmed, for assurance purposes, the CCG are working closely with the hospital on CQUINs, the tariff they are entitled to and the throughput in A&E. The ambulance service are working on the contract through WMAS and providing ideas for reduction in admissions and improve responses e.g. placing a senior nurse in the ambulance along with paramedics. The LIS and WMAS together should show improvements. The population flux in Burton has been taken into consideration and an increase in demographic is included, e.g. this year’s contract is bigger than last and exceeding in contract.
Peter Jones
SG(08)09 Soft Intelligence No Soft Intelligence was reported. SG(08)10 Any other Business
(by prior agreement with the Chair of the Steering Group)
• District Nurses Dr Sheraz Hassan: King Street Practice: • Request for a patient visit at the weekend – this was not
picked up. • Service declined to do a dressing. • Blood tests declined. Yoxall: • OT referral delayed by teams not accepting referral – this
led to a 2 week delay for patient discharged from Walsall. Action: Nicky Harkness to send to soft intelligence team for
Nicky Harkness
7
SIGNED: .............................................................. DATE: ..................................................... (Chairman)
process. Action: Nicky Harkness to highlight this issue through the Contract Management Group.
• Letters to GPs
Dr Chris Gunstone referred to the Burton Fertility Clinic. There is a new provider for the service. A clinic audit highlighted referrals previously made contained incomplete information and necessitated repeat visits from the patient. Each practice should be aware of the new system; the secretaries are tasked with holding on to this paperwork and posting the forms to patients prior to their clinic visit making the patient pathway easier. David Dickson requested removal of the statement within the referral process ‘the referral will be rejected’. The service has to accept a referral and cannot bounce it back. Action: Dr Liz Gunn to request removal of the statement ‘the referral will be rejected’.
Meeting ended at 2:25pm.
Nicky Harkness
Liz Gunn
DATE AND TIME OF NEXT MEETING Tuesday 23 September 2014 at 12:45pm
Robert Peel Suite, Holiday Inn, Burton Upon Trent
8
EAST STAFFORDSHIRE CLINICAL COMMISSIONING GROUP
Minutes of the East Staffordshire Clinical Commissioning Steering Group Meeting held on 23 September 2014 at 12.45pm
at the Holiday Inn Express, Second Avenue, Burton-on-Trent
Present: Dr Charles Pidsley ESCCG Chairman / Bridge Surgery Tony Bruce ESCCG Accountable Officer – left at 1:30pm Dr J Bull Abbots Bromley Surgery Dr K Aziz All Saints Surgery Suzanne Wem Alrewas Surgery Dr D Atherton Balance Street Dr Jon White Barton Family Practice Dr Wai Lim Carlton Street Practice Dr Richard Fulford Dove River Practice Dr Phil Robinson Gordon Street Surgery Dr Sheraz Hassan King Street Surgery Dr S Poonian Millview Surgery Dr Simon Jones Northgate Surgery Dr K Pai Peel Croft Surgery Dr P Needham Stapenhill Medical Practice Dr John Tansey Trent Meadows Practice Dr Mike Salwey Tutbury Practice Dr Ajitha K Prasad Wetmore Road Surgery Amy Carter Winshill Surgery John Evans Yoxall Surgery Julie Hughes ESCCG Primary Care Change Manager Judy Bird
Dr Liz Waddy ESCCG Interim Primary Care Change Manager ESCCG
Nicky Harkness ESCCG Head of Transformation and Commissioning Dave Whatton ESCCG Change Manager In Attendance
Jeanette Cole
Personal Assistant, ESCCG (minutes)
MINUTES ACTION SG(09)01 APOLOGIES Apologies were received from Dr Chris Gunstone, David Dickson, Sarah
Laing, Sharon Finney and Emily Davies.
SG(09)02 DECLARATIONS OF INTEREST All members declare an interest in the GP Federation (Alexin). SG(09)03 Chairman’s Opening Remarks
Dr Charles Pidsley welcomed everyone to the meeting.
SG(09)04 MINUTES OF PREVIOUS MEETING HELD ON 19 August 2014 The minutes were agreed as a true and accurate record. SG(09)05 ACTIONS FROM MEETING HELD ON 19 August 2014 SG(08)07: A&E Referral Data
Alyas Hussain to send Dr Charles Pidsley the data to include; referrals via 111, repeat visits, per 1,000 population, by age for all providers, follow-up ratios Monday to Friday and weekends including time of day. Update: Dr Charles Pidsley confirmed this action is now CLOSED.
Enc. 1
1

SG(08)10: Any Other Business District Nursing Nicky Harkness to highlight the issues raised through the Contract Management Group. Update: Dr Charles Pidsley requested this be discussed later on the agenda as part of Item 8. Letters to GPs – Burton Fertility Clinic Dr Liz Gunn to request removal of the statement ‘the referral will be rejected’. Update: Dr Liz Gunn is arranging to meet with Dr Hopkinson to discuss this issue and report back to the next Steering Group meeting. Dr Charles Pidsley requested any feedback regarding referrals to be brought to the next Steering Group meeting. Minutes of previous meetings SG(07)06: Chairman’s Report Members of the Steering Group commented when Dr Willis is on leave, there appears to be no urgency and the process becomes very slow. Dr Charles Pidsley to discuss this matter with Dr Willis. Update: Dr Charles Pidsley confirmed he had not received any response to his emails. Dr Chris Gunstone and Dr Charles Pidsley are meeting with Dr Crampton to discuss a joint GP-consultants meeting. Update: (23 September 2014): Dr Charles Pidsley confirmed his difficulty in setting up this meeting; reminder emails have been sent. Nicky Harkness is setting up a meeting with Dr Carey. Separate meetings have been arranged for 24 September with Dr Crampton and David Watmough. Dr Charles Pidsley will update the next Steering Group meeting on outcomes from these meetings. Tony Bruce attended a consultant leads workshop where consultants requested discussions with GPs. Tony Bruce suggested the CCG could sponsor an event similar to the Pirelli event if sufficient interest was identified. A response is awaited. A draft Agenda to be prepared highlighting purpose and focus of the event to be brought to a future Steering Group meeting for approval. SG(07)07: Local Incentive Scheme Dr Peter Jones to issue a list of pointers to send out to Steering Group members when completing special notes. Update: This action is now CLOSED. Dr Liz Waddy and Judy Bird to check the live state of the Urgent Care Dashboard and bring back to the next Steering Group meeting. Update: (23 September 2014) The dashboard is now live. Data retrieval is not ideal but provides the information required. IT at Queens is not aligned to make it work 100%. This action is now CLOSED. SG(07)08: Heart Failure and Diabetes Dr Charles Pidsley to take ideas back to Dr Willis and Dr Carey who will be asked if the suggestions are feasible. Update: Prior to arranging a meeting a contractual request will be implemented. Update: (23 September 2014) This action now forms part of item SG(07)06: Chairman’s Report and is CLOSED.
Liz Gunn
ALL
Charles Pidsley
Tony Bruce/ Charles Pidsley
2
SG(07)10: Derby Tony Bruce to ask Heather Johnstone which specialities are behind on follow-ups and request assurance from Derby the follow-up system is secure and report back to the next Steering Group meeting. GPs to explain what the situation is for new referrals and work on:
1. How they identify patients already within the system? 2. Are patients within the system receiving follow ups?
Update: Tony Bruce confirmed this issue is proving to be challenging and has been escalated to the CEO. Information is slow coming back and the CCG are progressing this matter. Tony Bruce requested individual GPs continue to work on the assumption; if sending patients to Derby GPs are aware of the risks and are doing all they can to mitigate the risk. The Governing Body will also be discussing this issue. John Tansey to request an EMIS share search to provide information and feedback to Steering Group members. Update: Wendy Kerr will discuss EMIS at the next IM&T Group meeting. Update: (23 September 2014): The IM&T sub group have requested EMIS attend and present all processes and options available through this system. The system is currently not being used to its full potential. The outcome will be brought to a future Steering Group meeting. Dr Charles Pidsley requested this issue is discussed within practices pending the issue of further information from the CCG from a corporate perspective. Update: Heather Johnstone has sent feedback regarding Lorenzo and been advised the patient system is working. Steering Group members confirmed there had been no issues in the past month. Tony Bruce confirmed he had spoken to Sue James (CEO) regarding the concerns; Heather Johnstone would be taking these concerns to the Quality Committee; due to meet 20 August 2014. Heather Johnstone will also be asking South Derbyshire CCG how they are assuring themselves that patients referred for first referral are receiving a follow up appointment if determined required by a clinician. Dr Pai advised that renal patient follow ups in February and March had been missed; Derby Hospital is checking a different database in order to ensure patients receive follow ups. GPs are advised to be aware of this issue when referring patients to Derby. Update: (23 September 2014) Lorenzo is now up and running. This action is now CLOSED. SG(06)07: Local Incentive Scheme The CCG to arrange a dialogue with Carers organisations to ensure a consistent message is delivered on behalf of the Steering Group regarding care within homes where patients are being sent straight to A&E – improved access to the practice. Update: Tony Bruce confirmed this item would be actioned and an update brought to the next meeting. Update: (23 September 2014): This will be discussed at the Operational Resilience Group meeting. A structured dialogue and meetings with Nursing Homes and Care Homes will be instigated. This action is now
ALL
Julie Hughes / Mike Jones
3

CLOSED as work in progress. SG(06)09: Any Other Business Tony Bruce to raise Ambulance Response Times with the Contract Management Group to clarify the service offered and whether appropriate. Update: Tony Bruce confirmed this matter had been raised and a response is awaited. Update: (19 August 2014) Tony Bruce confirmed this matter is still being pursued. This action is ONGOING. Update: (23 September 2014) Tony Bruce confirmed this issue has now been escalated through the contract management route, a response is awaited. This action is ONGOING. SG(06)10: Soft Intelligence Sarah Laing to request a list of cancelled or re-scheduled appointments from Burton Hospital over the last few months regarding growing waits within Cardiology. Update: Sarah Laing confirmed this matter would be progressed through the contract management route. A response is awaited but will be delayed as the process is new. Update: (19 August 2014) Sarah Laing confirmed this information had been requested and will be discussed at the Contract Management Team meeting 20 August 2014. This action is ONGOING. Update: (23 September 2014) Sarah Laing is currently off sick. This action is ONGOING. SG(03)09: Any Other Business Emily Davies confirmed that an indication of what is provided as part of the ‘As Is’ specification should be received by the end of June. A breakdown of patients referred and how many had received psychological therapy would be added to this request. Update: Agenda item for discussion. This action is now CLOSED.
SG(09)06 Chairman’s Report The report was taken as read.
Dr Charles Pidsley provided a verbal update: • AGM takes place on Thursday 25 September at Abbots Bromley. • Tutbury patient forum fair event on 13 September. A number of
voluntary sector organisations attended; contact details providing additional help for patients are included within the report e.g. Diabetes event taking place on 2 October between 5:30pm and 8:30pm.
• Summary of the LIS. • Better Care Fund. • KPMG report. • Quality Committees for East Staffs and SESP are now combined;
a lot of work had previously been duplicated for each committee. East Staffs GP representative, Liz Gunn and lay members attend.
Key discussion areas were:
• The decision to hold the AGM at 1pm was due to a clash with Burton Hospital’s AGM at 4pm. Meetings and stakeholder events take place both during the day and evening to ensure the
4
widest spectrum of public opinion, comment and questions are taken into consideration as possible.
• Tony Bruce confirmed the Better Care Fund submission was signed off last week. The first £1.9m savings generated across the County will fund the implementation of Care Act through the County Council. Any other savings achieved will be split 50:50 between the NHS and Council. Thanks go to Wendy Kerr, Chief Finance Officer; who noticed a line within the document stating ‘if savings are not made NHS allocates £15m to help towards £30m Council deficit’. This section has since been re-written removing this statement; there is, therefore, no commitment to hand over any cash apart from through the savings plans.
SG(09)07 Improving Lives Nicky Harkness provided a verbal update. The procurement has
commenced, is live and ongoing. All work is overseen by the Programme Board, sub-committee of the Governing Body. The Programme Board meet every 6 weeks. Dr Chris Gunstone has been recruited to the clinical role and 2 lay members; Rachel Proudlove and John Bentley. The Board now has full representation. Nicky Harkness provided assurance to the Steering Group that the Board are following the planned timetable and report to the Governing Body.
SECTION TWO SG(09)08 ‘As Is’ Specification The paper was taken as read. Nicky Harkness provided a verbal
update: Action arising from SG(03)09 Any Other Business: This issue was raised with the Trust through the quality and contracting route. Vacancies within teams was raised and the ‘As Is’ specification circulated to Steering Group members.
• It is still the case the CCG fund a higher proportion of community matrons and nurses.
• Some caseloads are under against the national average. • Variance exists across practices. • The Trust is pushing for an agreement regarding a standardised
specification for district nurses and community matrons. Factual accuracy is required in order to sign off the specification. Steering Group members are asked to split into 3 groups to discuss the ‘As Is’ specification taking into consideration the following questions:
• Whether the specification is realistic? • Is this specification a true reflection of what is received; what is
missing or additional? • How shall we manage this issue regarding differing levels of
equity across practices?
Key Actions: Nicky Harkness, Julie Hughes and Dave Whatton were assigned as lead for each group. Each lead to submit their notes to Nicky Harkness.
• Nicky Harkness to highlight the difference between the National and ‘As Is’ specifications and circulate consensus view to all representatives and practices.
Nicky Harkness clarified the obstacles faced for retrieval of monies from SSOTP for nurses not provided as follows:
Julie Hughes / Dave Whatton
Nicky Harkness
5
• Length of time to query contract and withhold money. • Ensure correct questions are asked and correct contract lever
used to withhold money. • Some information queries are received through soft intelligence
and if not turned around 1% is withheld within timescale. • Monies will not be received for the whole gap but the Trust are
then aware there is going to be a challenge. • There is a threat of arbitration and risk of paying Trust costs if not
clear on challenge. Nicky Harkness acknowledged the CSU contract management role on behalf of the CCG. A number of changes have taken place with a number of vacancies whereby CCG then drive actions. The CCG will continue to discuss the pros and cons of continuing this.
SECTION THREE SG(09)09 Controlled Drugs Information Dr Charles Pidsley introduced Claire Dearden, Clinical Audit Facilitator
(Medicines Management), to the meeting and requested Steering Group members be aware the less time Medicines Management spends monitoring Controlled Drugs (CDs), the more time would be available to help practices in prescribing. The paper was taken as read. Claire Dearden provided some background information:
• A robust system and policy for monitoring CDs, schedules 2 and 3 is required.
• Brigid Stacey, Director of Nursing at the Area Team has been appointed as CDAO and is responsible for ensuring the CCG establish and operate a monitoring and audit process for the management of CDs.
• CDs are monitored on a monthly basis; patient information and doses are not received.
• If anomalies exist, a letter is sent to practice managers requesting additional information. A response to the letter is required within 10 working days; a reminder is sent if no response is received. A third letter is issued and, if no response, taken to Quality Committee. This process takes 1 month.
• Prescriptions can be recalled from the Area Team but the process is lengthy.
Key areas for discussion:
• Limiting CDs to 30 days would potentially solve this issue. • Letters could be issued to someone else within the practice to
ensure responses are received. • Possibility of 3 letters being sent over a 2 month period to cover
absence of staff at practices. • The Medicines Management Team can be called to help with any
queries practices may have. • Without dosage the system fails at the first hurdle.
Key actions:
• Governance around taking CDs out of the country. Claire Dearden to send to Jeanette Cole for circulation with the minutes.
Claire Dearden / Jeanette Cole
6

• Claire Dearden to recall prescriptions where a query exists and then judge whether issuing a letter to practices is required. If the Area Team have more prescription recall requests, dosages may become a future requirement.
• Claire Dearden to call the practice prior to issuing a letter where an anomaly exists.
• Steering Group members to be as responsive to letters as possible.
• Claire Dearden to issue a progress report in 2 months’ time.
Claire Dearden
Claire Dearden
ALL
Claire Dearden SG(09)10 Soft Intelligence Report The paper was taken as read. Steering Group members were asked if
they were happy with the format of the quarterly report. There was recognition of the gap between practices submitting soft intelligence and no direct feedback but agreed to the continued quarterly reporting. Soft Intelligence to be reported:
• Leg Ulcer Clinic; referral rejected twice and informed no staff are available.
• Rapid Chest Pain Clinic; two appointments cancelled. • Specsavers, Uttoxeter; 3 tiers of treatment. Dr Poonian spoke
directly to the branch on speaker phone whilst with a patient for referral. The member of staff accused Dr Poonian of swearing and put the phone down on him; the patient witnessed this. This issue to be reported to the Area Team.
• Cardiology; discrepancy over none receipt of letters regarding outcome for patient. Dr Charles Pidsley will also raise this issue with Dr Carey.
Jeanette Cole / Nicky Harkness
Charles Pidsley
SG(09)11 Any other Business (by prior agreement with the Chair of the Steering Group)
• Referrals to Primary Care Mental Health Dr Charles Pidsley requested Steering Group members be made aware MIND are currently oversubscribed and the Mental Health Trust are under subscribed; therefore, patients should be made aware of the current 14 week wait if referred to MIND. Steering Group members agreed no changes should be made to the current system of self-referring. If GPs are concerned about a patient they should be referred into single point of access.
• Patient Identifiable Correspondence to CCG; any received has to be logged as a risk. Dr Charles Pidsley reminded all Steering Group members the CCG are not allowed to receive any patient identifiable information; any received has to be reported through soft intelligence. Documentation needs to be anonymised prior to sending.
• Safeguarding – Children – Named GP required. Nicky Harkness to speak to Heather Johnstone or Sue Wilson regarding a joint named GP with SESP; Dr Kaur.
• LPC News: Community pharmacy management of patients with hypertension: PSNC Main site. Blood pressure checks on patients. Steering Group members agreed checks should not take place within pharmacy.
• Data referral numbers All members agreed they are happy for the data to be shared.
7

SIGNED: .............................................................. DATE: ..................................................... (Chairman)
• Pancreatic Cancer Awareness Involvement from GPs was requested regarding an awareness day taking place in November. Patient information will be circulated with local relevance.
• Dementia Diagnosis Rates Julie Hughes to circulate figures for GP % identified proportionate to estimated numbers and will form part of the discussion section of the November Steering Group meeting.
The meeting ended at 2:40pm. DATE AND TIME OF NEXT MEETING Tuesday 18 November 2014 at 12:45pm
Robert Peel Suite, Holiday Inn, Burton Upon Trent
8
Enc. 1
Minutes of the Patient Board Wednesday 10 September 2014
The Foster Suite, Citizens Advice Bureau, Units 5d/5e Anson Court, Burton Upon Trent, DE14 1NG
Present: Ann Tunley PPI Lay Member and Chair (AT) Lynne Barrell Burton Mind (LB) John Bridges Patient Participation Groups (JB)
Ian North Harvey Girls and Dads for Dads (IN) Sue Adey Patient Participation Group (SA) Keddie Bailey Homestart (KB) Lisa Beard Age UK (LB)
In Attendance: Emma Keeling ESCCG (EK) Agenda No
Actions
1. Welcome, Introduction and Apologies: AT opened the meeting and apologies noted. Apologies: Dawn Green, Paul Laffey, Deborah Neal, Mandy Rollins
2. Declarations of Interest: Standing item, no new declarations to note
3. Minutes from 7 July 2014 meeting: The minutes were agreed as a true and accurate record.
4. Action Log for update: The actions were updated on the action log.
5. Call to Action event and Questionnaire: AT to ask Emily Davies at ESCCG the following questions: Is Call to Action linked to improving lives or are they separate projects? Could the new date for the next Call to Action event be given as soon as possible? JB updated the group following Dr Charles Pidsley request at the event for Patient Board to follow up on DNA appointments in surgeries. He is currently looking into the figures and attempting to gain figures from individual surgeries but this is proving difficult. Reports will be presented to the group and ESCCG when the findings are available. SA reported that Healthwatch are currently undertaking the same piece of work and the group therefore feel this is something that Patient Board could use. The group further discussed the subject with JB to re send the link to The GP Patient Survey to group members for them to read and feedback at a future meeting. AT to ask Dr Pidsley to attend a future meeting.
AT JB AT
1

Enc. 1
6. DNA appointments: Discussed during agenda item 5
7. Car Park Letter – BHFT: JB updated the group that charges for parking have changed and they are currently looking at exemptions to be put into place. This is an on-going issue in relation to the cost of parking and the fines given out, this will continue to be followed up by The Patient Board. Andrew Griffiths MP is attending The District Group and will be asked his opinion and thoughts on this issue, feedback will be available to the group.
8. Path Planning: AT updated that the comments highlighted by MR at a previous meeting in regards to omitted information has now been updated. AT asked members what next in regards to where this piece of work will go and how will The Patient Board be involved in the future? This is an agenda item that will be on a future meeting for discussion when all Patient Board members are present.
9. Dates and Venues TBC: Daytime dates (Formal); 09:30-12:30 Wednesday 22 October – visit to St Giles 10.00 Wednesday 5 November – CAB; Dr Pidsley to be invited to this meeting Wednesday 3 December – CAB; Martin Evans, Mental Health Lead to attend, Mental Health Planning event; Kerry Lawrence South Staffordshire Mental Health Network to be invited Wednesday 4 February 2015 Wednesday 4th March 2015 Wednesday 6 May 2015 Wednesday 3 June 2015 Wednesday 8 July 2015 Wednesday 9 September 2015 Wednesday 7 October 2015 Wednesday 2 December 2015 AT to check with the Citizens Advice Bureau on dates for the formal meetings Evening dates (Informal); Wednesday 14 January 2015, 7:00 p.m at The Winery to be booked by AT Wednesday 8 April 2015, Wednesday 12 August 2015 Wednesday 11 November 2015
AT AT
10. Better Care Funding/Supporting People: Paul Laffey had in advance emailed a short commentary on the funding cuts and the impact this is having to the YMCA. The group discussed their major concerns on this topic and the pressures and impact this will have on other organisations in the area when these cuts fully happen. Especially in relation to the impact on 16/17 year olds.
2

Enc. 1
IN suggested that The Patient Board ask ESCCG re the shortfall in funding and how they intend to manage this. SA is to raise this question at the next Governing Body meeting. This question will be emailed to ESCCG in advance of the meeting. AT to also raise and include the concerns on the pro forma for Governing Body also. AT suggested that the issue be raised at The District Group on 2 October with Andrew Griffiths MP. SA commented and raised her concerns on the new Dementia Centre of Excellence being built alongside the new houses and developments in Burton and how this will impact the wider community services and the pressures this will have on the healthcare system within the area. The group discussed this issue and agreed.
SA AT
11. Mental Health Event – SES: AT suggested that in December when Martin Evans and Kerry Lawrence attend that ideas are discussed around running an event in 2015 along with SES CCG. The group agreed this would be a good event to run and further discussions will take place to organise this.
12. District Group Letters and GP’s: JB updated the group on a meeting that was held for GP’s on the friends and family test which will be implemented in surgeries from 1 December. The meeting was not well attended . This is within the NHS contract and is therefore having to be financed by GP’s and uses a scoring system on how likely you are to recommend the surgery following the appointment. No minimum number of submissions has been requested with GP’s being able to design their own questionnaire and therefore the efficacy and consistency reporting of the system is questioned.
13. Insite Report: AT will request that Andy Ruston distribute the report in the future to all members. Feedback requested by AT from members on the report with the possibility of inviting him to a future meeting.
14. Improving Lives: The group agreed that the event that took place at Barton Under Needwood was successful. AT noted that during the meeting she commented and asked if there were plans for future events and if at all possible this could be held at a central area with plenty of notice being given. AT to circulate feedback from the event to the group via email. IN is to meet with Nicola Harkness, ESCCG in October to discuss The Improving Lives project and will feedback to the group.
AT IN
15. Burton Library Pilot Reading group: AT distributed a report to members which included the Burton Library Reading group. She reported on the success and benefits of the group for those that attend. AT has also been working with Lucy Heath discussing the organising of future monthly reading groups and inviting in particular patients with Long term Conditions to encourage them to attend and socialise.
3
Enc. 1
16. Medicines Management Update: The attachment was circulated with the agenda. AT to ask The Medicines Management Team what savings have been made since the campaign begun and will feedback to members.
AT
17. AOB: Note of thanks given to Dawn Green for the use of the room at The Citizens Advice Bureau. LB asked about the tendering of a 10 year contract for cancer services and asked if any other members had heard. This question is to be asked of Dr Charles Pidsley in the future. AT and JB have organised a Diabetic event in conjunction with Diabetes UK on Thursday 2 October at De Ferrers School at the Trent Campus from 17:00 onwards. JB will email the flyer to all members for distribution and circulation to raise awareness of the event. SA asked if it is possible for funding or paper to be provided for printing. EK to check with Sarah Laing ESCCG and will email the group with a response.
JB EK
Date and time of next meeting: Wednesday 5 November, 9:30-12:30, The Foster Suite, Citizens Advice Bureau, Units 5d/5e, Anson Court, Burton Upon Trent, DE14 1NG
Future Events: September 13 2014; Tutbury PPG Health Event October 2 2014 – District Group; Andrew Griffiths is attending October 2 2014 – Diabetes Event at De Ferrers School 17:00 onwards
4