
meeting of drugs technical advisory board (dtab) to be held on ...
158
78 th MEETING OF DRUGS TECHNICAL ADVISORY BOARD (DTAB) TO BE HELD ON 12 th FEBRUARY 2018 AT 11.30 A.M. IN NIRMAN BHAWAN, NEW DELHI
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of meeting of drugs technical advisory board (dtab) to be held on ...
78th
MEETING OF
DRUGS TECHNICAL
ADVISORY BOARD (DTAB)
TO BE HELD ON
12th
FEBRUARY 2018
AT 11.30 A.M.
IN NIRMAN BHAWAN,
NEW DELHI

Page 2 of 33
AGENDA INDEX
S. No. AGENDA ITEMS PAGE NO.
1. Action taken report for 77th DTAB meeting held on 16.06.2017 4
2.
Consideration of the proposal for examination of cases of banning of 344 FDCS + 05 FDCS by DTAB/ Sub-Committee and send report to the Central Government as directed by the Hon’ble Supreme Court of India within six months from the date on which this judgment is received by the DTAB
6
3. Consideration of the proposal for amendment of rule 96 under Drugs & Cosmetics rules, 1945 for disclosure of prices at first point of sale/price to trade (PTT)/ Ex-factory price or import price
10
4. Consideration of the proposal for notifying (I) Kamarajar port ltd., Chennai, Tamilnadu and (II) Mundra Port, Kutch, Gujarat; for import /export of drugs/pharmaceuticals
11
5.
Consideration of the proposal for exemption under para 15 of DMR(OA), 1954 to communicate "fever" for creating public awareness on management of fever associated with common self-limiting conditions such as fever associated with common cold and flu, dengue, chikungunya, fever associated with vaccination etc.
12
6. Consideration of the proposal regarding inclusion of separate form for issuing test reports to other than manufacturers like the procurement agencies and others
13
7. Consideration of the proposal to include Ultrasound equipments and similar imaging equipments under the purview of Section 3 (b) (iv) of the Drugs and Cosmetics Act, 1940 as Medical Devices
14
8.
Consideration of the proposal to amend Drugs & Cosmetics Rules to have Single Licensing Authority instead of multiple licensing authorities having experience in manufacture or testing of drugs or enforcement of provisions of the act for a minimum period of 10 years
15
9. Reconstitution of sub-committee of Drugs Technical Advisory Board on Homeopathy
16
10.
Consideration of the proposal to clarify whether the Centchroman (30mg) tablets to be exempted from the provisions of chapter IV of the D& C act and Rules under schedule K or to sell the remaining strengths under schedule H of D& C rules
17
11.
Consideration of the proposal for denotification of GSR 743(E) dated 10.08.1989 issued under section 26A for prohibition of all fixed dose combination injectable preparations containing synthetic Oestrogen and progesterone
18
12. Consideration of the proposal to explore the feasibility of providing a separate shelf/rack for generic medicines in pharmacy
20

Page 3 of 33
S. No. AGENDA ITEMS PAGE NO.
13.
Consideration of the proposal for amendment of Rule 127(2) of the Drugs And Cosmetics Rules, 1945, so as to remove the ambiguity and scope of different interpretations in case of use of colours in empty gelatine capsules (hard and soft)
21
14.
Consideration of the proposal to amend Schedule D of the Drugs and Cosmetics Rules, 1945 to provide exemption for radiopharmaceuticals from the provisions of the Chapter III of the Drugs and Cosmetics Act, 1940
23
15.
Consideration of the proposal for review of prophylactic doses
mentioned under Schedule ‘V’ of Drugs And Cosmetics Rules,1945
vis a vis the doses prescribed under FSS Act
24
16.
Consideration of the proposal for amendment of Para 10.9 of Schedule ‘M’ of Drugs and Cosmetics Rules, 1945 for waiver of requirement for vaccines manufactured using less than 60% residual shelf-life period in the country
25
17. Consideration of the proposal to amend the Medical Devices Rules, 2017- issue general clarification for smooth and uniform implementation
27
18. Additional agenda (if any) with the approval of the Chair 33
19. Annexure- 1 to 6 34
Page 4 of 33
AGENDA NO.1
ACTION TAKEN REPORTFOR 77thDTAB MEETING HELD ON 16.06.2017
AG.
NO. AGENDA ISSUES ACTION TAKEN
1. Action taken report for 76th DTAB meeting
held on 31.01.2017 Approved
2.
Consideration of the proposal to amend
form 12-B of the Drugs And Cosmetics
Rules for permit to import of small
quantities of drugs for personal use for
longer periods instead of six months in
case of chronic diseases
Draft notification published vide G.S.R.
No.1367 (E) dated 03.11.2017 and under
finalization.
3.
Consideration of the proposal to amend
schedule H to include certain steroid
preparations which are misused mainly as
topical steroids leading to extensive tinea
infections
Draft notification published vide G.S.R.
No.1357 (E) dated 01.11.2017 and under
finalization.
4.
Consideration of the proposal to label iron
tablets and polio drops distributed to the
children under government programmes
with name and expiry date in Hindi also
The proposal is agreeable in principle and
may be kept voluntary for multilingual
labelling where ever practical. Committee
further opined that the proposal needs to be
considered in broader prospective for making
provision under the Drugs and Cosmetics
Rules, 1945 requiring the manufacturers of
drugs to provide Patient Information with the
drugs.
5.
Consideration of the proposal to make a
provision under the Drugs And Cosmetics
Rules, 1945 for permission to sell /
distribute remaining quantities of unused
clinical trial batch of a biological drug
within its shelf life, if results of clinical trial
have been found satisfactory
Draft notification is under consideration by
Ministry.
6.
Consideration of the proposal to exempt
under Schedule-K for manufacturing of
Oxygen 93%
Draft notification published vide GSR
No.1368 (E) dated 03.11.2017.
7.
Consideration of the proposal for
inclusion of “Stem Cells and Cell Based
Products” under the definition of new
drugs and its regulation under the Drugs
And Cosmetics Rules, 1945
Draft notification is under consideration by
Ministry.
8. Consideration of report of sub-committee The DTAB noted the report of the sub-

Page 5 of 33
AG.
NO. AGENDA ISSUES ACTION TAKEN
of DTAB in respect of the directions of the
Hon’ble high court of judicature of Patna
for analyzing the components of
ingredients and their effect on human
body if consumed as food in respect of
the Neutraceutical products under
consideration in the Case of CWJC of
2425 of 2006
committee and recommended that it should
be presented to the Director General of
Health Services for further consideration.
9.
Consideration of the proposal for making
the engagement of pharmacist having
relevant qualification mandatory for blood
banks/blood storage centers
The DTAB recommended that details
giving full background objective of the
agenda should be placed before the Board
for consideration.
10.
Consideration of proposal to amend
Drugs And Cosmetics Rules, 1945,
pertaining Part XB– Requirements for
the collection, storage , processing and
distribution of whole human blood ,
human blood components by blood banks
& Part XII B- Requirements for the
functioning and operation of a blood bank
and/or for preparation of blood
components
The DTAB agreed with the proposal and
required that the Chairman may further
discuss the issue with some experts in this
field for further consideration of notification
of draft rules.
11.
Consideration of proposal to amend
Drugs And Cosmetics Rules, 1945
incorporating a provision for
Pharmacovigilance fee to be levied on the
marketing permission holder of new drugs
as well as other drugs
DTAB opined that the proposal does not
come under their purview.
S-1
Consideration of the proposal to prohibit
antibody detection Rapid Diagnostic
Tests for routine diagnosis of MALARIA to
manufacture/ import and sale of in Indian
market
The matter has been placed before
Directorate of National Vector Borne Disease
Control Programme (NVBDCP) for their
expert comments.
S-2
Amendment in notification of BA/BE
requirement from for “Oral Dosage Form”
to “Oral Solid Dosage Form”
Draft notification is under consideration by
Ministry.
S-3
Measures for uniform
implementation of provisions of Drugs &
Cosmetics Act And Rules throughout the
country
Agreed

Page 6 of 33
AGENDA NO. 2
CONSIDERATION OF THE PROPOSAL FOR EXAMINATION OF CASES OF
BANNING OF 344 FDCS + 05 FDCS BY DTAB/ SUB-COMMITTEE AND SEND
REPORT TO THE CENTRAL GOVERNMENT AS DIRECTED BY THE HON’BLE
SUPREME COURT OF INDIA WITHIN SIX MONTHS FROM THE DATE ON
WHICH THIS JUDGMENT IS RECEIVED BY THE DTAB
The Department Related Parliamentary Standing Committee (PSC) on Health
and Family Welfare had, in its 59th Report, observed that some State Licensing
Authorities had issued manufacturing licences for a very large number of FDCs
without prior clearance from CDSCO and this had resulted in the availability of many
FDCs in the market which have not been tested for efficacy and safety. The
Committee had also noted that this could put patients at risk.
The Parliamentary Standing Committee had also expressed the view that
those unauthorized FDCs that pose risk to patients and communities, such as a
combination of two antibacterials, need to be withdrawn immediately due to the
danger of developing resistance that would affect the entire population. DCG (I) had
requested all State/UT Drug Controllers to ask the concerned manufacturers in their
States to prove the safety and efficacy of such FDCs as had been licensed by SLAs
prior to 01.10.2012 without obtaining the approval of DCG (I) within a period of 18
months, failing which, such FDCs would be considered for being prohibited for
manufacture and marketing in the country.
In reply, CDSCO received approximately 6320 applications from
manufacturers for proving the safety and efficacy of these FDCs. On scrutiny, it was
observed that many FDCs are being manufactured by a number of applicants. With
the approval of the Ministry, CDSCO constituted 10 Expert Committees on
03.02.2014 for examining the safety and efficacy of these FDCs. These Committees
could, however, examine only about 295 applications. Subsequent to that the Central
Government appointed another Expert Committee to examine the matter. The
Committee was also assisted by eminent experts in different therapeutic areas from
premier Medical Institutions and hospitals.
The Expert Committee, after detailed examination and deliberations
recommended that some of these FDCs lacked therapeutic justification; were found
to be pharmacokinetically or pharmacodynamically incompatible; had abuse

Page 7 of 33
potential; or could lead to antibiotic resistance in the population. The Expert
Committee carried out a comprehensive review of the FDCs keeping in view the
contemporary scientific knowledge and expertise. On the basis of the
recommendations of the Expert Committee, the Government examined the matter
further and requested the Committee to provide specific reasons in respect of each
FDC that was found to be irrational. The Committee, accordingly reviewed the matter
further and finalized its recommendations. After careful consideration of the matter,
the Government issued show cause notices to all the manufacturers whose products
were found to be irrational and who had submitted their applications to the Central
Drugs Standard Control Organization. At the request of the manufacturers, additional
time of three months was given to them to respond to the show cause notices.
Thereafter, due consideration of the report and replies, the Government vide Gazette
Notifications S.O. Nos. 705(E) to 1048(E) dated 10.03.2016 prohibited the
manufacture for sale, sale and distribution for human use of 344 FDCs with
immediate effect in public interest as use of such FDCs was likely to involve risk to
human beings whereas safer alternatives to these drugs were available. The FDCs
that have been held irrational had been licensed by the State Licensing Authorities
without approval of the DCG(I). However, in case of a few of these FDCs, approval
had also been given by the DCGI.
Further, in pursuance of the action taken note on the 59th PSC report, based
on the examination by the Subject Expert Committee constituted by the Central
Government, the Government vide Gazette Notifications S.O. Nos.1851(E) to
1855(E) dated 08.06.2017 prohibited the manufacture for sale, sale and distribution
for human use of 5 FDCs with immediate effect in public interest
The Hon’ble Supreme Court of India in its Judgement dated 15.12.2017
pertaining to the issue of FDCs has directed DTAB and/or a Sub-Committee formed
by DTAB for the purpose, to have a relook into these cases.
The DTAB/ Sub-committee shall examine/deliberate these cases on the
parameters as laid down by Hon’ble Supreme Court of India in its Judgement as
follows:
“On the facts of these cases, a suggested course of action was stated by
learned counsel appearing on behalf of the petitioners/appellants. This course

Page 8 of 33
is that instead of now remitting the matter back to the Delhi High Court for an
adjudication on the other points raised in the writ petitions, the case of 344
FDCs that have been banned, plus another 5 FDCs that have been
banned, which comes to 349 FDCs, (barring 15 FDCs that are pre 1988
and 17 FDCs which have DCG(I) approval) pursuant to the Kokate
Committee report, by notifications of the Central Government under
Section 26A of the Drugs Act, should be sent to the DTAB, constituted
under Section 5 of the Drugs Act, so that it can examine each of these
cases and ultimately send a report to the Central Government.
In order that an analysis be made in greater depth, we, therefore, feel that
these cases should go to the DTAB and/or a Sub-Committee formed by the
DTAB for the purpose of having a relook into these cases. It is important,
however, that the DTAB/Sub-Committee appointed for this purpose will
not only hear the petitioners/ appellants before us, but that they also hear
submissions from the All India Drugs Action Network. The DTAB/Sub-
Committee set up for this purpose will deliberate on the parameters set
out in Section 26A of the Drugs Act, as follows:
First and foremost in each case, the DTAB/Sub-Committee appointed by it
must satisfy itself that the use of the Fixed Dose Combinations (FDC) in
question is likely to involve any one of the aforesaid three things:
(a) that they are likely to involve any risk to human beings or animals; or
(b) that the said FDCs do not have the therapeutic value claimed or purported
to be claimed for them; or
(c) that such FDCs contain ingredients and in such quantity for which there is
no therapeutic justification.
The DTAB/Sub-Committee must also apply its mind as to whether it is then
necessary or expedient, in the larger public interest, to regulate, restrict or
prohibit the manufacture, sale or distribution of such FDCs. In short, the
DTAB/Sub-Committee must clearly indicate in its report:
(1) as to why, according to it, any one of the three factors indicated above is
attracted;

Page 9 of 33
(2) post such satisfaction, that in the larger public interest, it is necessary or
expedient to (i) regulate, (ii) restrict, or (iii) prohibit the manufacture, sale or
distribution of such FDCs.
The DTAB/Sub-Committee must also indicate in its report as to why, in case it
prohibits a particular FDC, restriction or regulation is not sufficient to control the
manufacture and use of the FDC. We request the DTAB/Sub-Committee to be
set up for this purpose to afford the necessary hearing to all concerned, and
thereafter submit a consolidated report, insofar as these FDCs are concerned,
to the Central Government within a period of six months from the date on
which this judgment is received by the DTAB.”
The list of 344 FDCs + 05 FDCs i.e. 349 FDCs is annexed as ANNEXURE-1.
The copy of Judgment of Hon’ble Supreme Court of India dated 15.12.2017 is
enclosed as ANNEXURE-2.
As per the order of Hon’ble Supreme Court of India dated 15.12.2017, DTAB
may examine the matter and devise the mechanism/method of communication to the
Appellants/Petitioners along with schedule for undertaking such exercise including
hearing from the Appellants and All India Drug Action Network (AIDAN), so that it
could be completed in 06 months time.
Page 10 of 33
AGENDA NO. 3
CONSIDERATION OF THE PROPOSAL FOR AMENDMENT OF RULE 96 UNDER
DRUGS & COSMETICS RULES, 1945 FOR DISCLOSURE OF PRICES AT FIRST
POINT OF SALE/PRICE TO TRADE (PTT)/ EX-FACTORY PRICE OR IMPORT
PRICE
A proposal is received from Ministry to amend Rule 96 of Drugs and
Cosmetics Rules, 1945 to make it mandatory for the manufacturers/ importers to
disclose the first point sale price/ Price to Trade (PTT)/ ex-factory price or import
price of drugs on the label of packing.
A copy of the draft amendment on the said subject prepared and shown to
DGHS for his in-principle approval as the Chairman of DTAB before the draft
notification is published in the official gazette for inviting comments of
public/stakeholders. Copy of draft notification to amend rule 96 of Drugs &
Cosmetics Rules, 1945 is placed as ANNEXURE-3.
DTAB may kindly deliberate and give their views/comments/suggestions on
proposed amendment.

Page 11 of 33
AGENDA NO. 4
CONSIDERATION OF THE PROPOSAL FOR NOTIFYING (I) KAMARAJAR PORT
LTD., CHENNAI, TAMILNADU AND (II) MUNDRA PORT, KUTCH, GUJARAT;
FOR IMPORT /EXPORT OF DRUGS/PHARMACEUTICALS
I) Several proposals were received for notifying Kamarajar Port Ltd.
(formerly known as Ennore Port Ltd.) for import /export of
drugs/pharmaceuticals as it is presently having five nos. of Terminals on
Operation, out of which, two are captive users, two are BOT’s and one
own Car Import/Export Terminals. The port is equipped to handle export
and import of Drugs and Cosmetics. The port is also provided with facilities
for handling of refrigerated containers with continuous power supply
through 150 refers plug points till the goods are cleared from the port. The
container terminal was operational with effect from June, 2017. Further,
this port was declared as Customs area under section 8(b) of the Customs
Act, 1962 for the purpose of loading/unloading of import and export cargo
or any class of such goods by customs, Chennai vide public notice No.
11/2001 dated 31.01.2001.
II) Mundra Port is located in the Gulf of Kutch region and has carved niche for
itself amongst shipping lines and trade by providing world class
infrastructure. The port has handled more than 100 MMT (2.73 Million
TEUs containers) of cargo in 2015-16 & 85 MMT (3 Million TEUs
container) of cargo in 2016-17(up to January-17). Mundra Port given
significant revenue earned by Customs on cargo handled, Mundra Port is
an important set-up for the department Rs. 6232.77 Crores (2015-16) and
Rs. 6683.06 Crores ( up to January 16-17) respectively.
Accordingly, it was recommended that Kamarajar Port Ltd. and Mundra Port
Ltd. may be permitted for import/ export of Drugs, Pharmaceuticals and Cosmetics
and may also be notified under rule 43A.
Therefore, DTAB may consider and give its suggestions in the matter.
Page 12 of 33
AGENDA NO. 5
CONSIDERATION OF THE PROPOSAL FOR EXEMPTION UNDER PARA 15 OF
DMR(OA), 1954 TO COMMUNICATE "FEVER" FOR CREATING PUBLIC
AWARENESS ON MANAGEMENT OF FEVER ASSOCIATED WITH COMMON
SELF-LIMITING CONDITIONS SUCH AS FEVER ASSOCIATED WITH COMMON
COLD AND FLU, DENGUE, CHIKUNGUNYA, FEVER ASSOCIATED WITH
VACCINATION ETC.
Representations received regarding the exemption of advertisement under
Para 15 of Drugs and Magic Remedies (Objectionable Advertisements) Act, 1954, to
communicate “Fever” for creating awareness on management of Fever associated
with common Cold and Flu, Dengue, Chikungunya, Fever associated with
Vaccination etc. and role of Paracetamol in initial self-management of such
conditions.
It is stated that “Paracetamol” is already exempted under Schedule K of Drugs
& Cosmetics Rules, 1945, at Serial No. 13 vide GSR 1060 (E) dated 05.09.1986, as
household remedy from the provisions of Chapter IV of the Drugs & Cosmetics Act,
1940 and Rules thereunder which require them to be covered with a sale license
subject to certain conditions.
Representations received emphasized that the exemption of advertising will
enable the deployment of education programs designed to provide consumers with
information to foster an understanding of about “Fever”. Several references are
communicated regarding the exemptions under Para 15 of DMR (OA), 1954,
including the publication from the Ministry of Health and Family Welfare.
As it is a policy matter which is dealt by the Ministry accordingly the DTAB
may deliberate the issue regarding exemptions under Para 15 of DMR (OA), 1945.

Page 13 of 33
AGENDA NO. 6
CONSIDERATION OF THE PROPOSAL REGARDING INCLUSION OF
SEPARATE FORM FOR ISSUING TEST REPORTS TO OTHER THAN
MANUFACTURERS LIKE THE PROCUREMENT AGENCIES AND OTHERS
Providing a separate Form on lines of Form 39 of Drugs & Cosmetics, Rules,
1945 for other than manufacturers like procurement agencies and other institutions
for carrying out tests on drugs, cosmetics and raw materials was deliberated in 51st
DCC meeting held on 09.06.2017. This was also agreed in 77th DTAB meeting held
on 16.06.2017 as one of the points of Additional Agenda.
At present there is no provision in Drugs & Cosmetics Rules, 1945, for issue
of test reports for other than manufacturers like procurement agencies and others
except Form 39, which is meant for institutions carrying out tests on drugs,
cosmetics and raw materials used in their manufacture on behalf of licencees for
manufacture for sale or drugs or cosmetics.
As per Part XV (A), Rule 150E of D& C Rules, Form 39 is issued only to the
licenced manufacturers. Accordingly, a draft rule is prepared and enclosed as
ANNEXURE- 4.
DTAB may review the proposal for the suitable amendment in the D & C
Rules

Page 14 of 33
AGENDA No. 7
CONSIDERATION OF THE PROPOSAL TO INCLUDE ULTRASOUND
EQUIPMENTS AND SIMILAR IMAGING EQUIPMENTS UNDER THE PURVIEW
OF SECTION 3 (b) (iv) OF THE DRUGS AND COSMETICS ACT, 1940 AS
MEDICAL DEVICES
The Central Supervisory Board (CSB), constituted under the Pre-conception
and Pre-natal Diagnostics Techniques Act (PC & PNDT Act), 1994 in its 22nd
meeting held on 13th October, 2014 under the Chairmanship of Hon’ble HFM
recommended to include Ultrasound machines and its accessories under Section 3
of the Drugs and Cosmetic Act, 1940.
DTAB in its 70th meeting held on 18.08.2015, deliberated the agenda for
inclusion of Ultrasound equipments under the purview of Section 3 (b) (iv) of Drugs
And Cosmetics Act, 1940, so that Ultrasound equipments and similar imaging
equipments could be regulated for their manufacture and import after introducing the
Drugs and Cosmetics (Amendment Bill 2015) in the Parliament for comprehensive
provision for regulating medical devices in general.
Recently, Medical Device Rules, 2017 have been notified vide GSR 78(E)
dated 31.01.2017, coming into force with effect from 1st day of January, 2018 for the
regulation of medical devices. Therefore, proposal to include Ultrasound equipments
and similar imaging equipments under the purview of Section 3 (b) (iv) of the Drugs
and Cosmetics Act, 1940 as Medical Devices is submitted for consideration of DTAB
in the light of Pre-conception and Pre-natal Diagnostics Techniques Act (PC & PNDT
Act), 1994.
DTAB may kindly deliberate the issue and give its recommendation on the
matter.

Page 15 of 33
AGENDA NO. 8
CONSIDERATION OF THE PROPOSAL TO AMEND DRUGS & COSMETICS
RULES TO HAVE SINGLE LICENSING AUTHORITY INSTEAD OF MULTIPLE
LICENSING AUTHORITIES HAVING EXPERIENCE IN MANUFACTURE OR
TESTING OF DRUGS OR ENFORCEMENT OF PROVISIONS OF THE ACT FOR A
MINIMUM PERIOD OF 10 YEARS
DCC in its 51st meeting held on 09.06.2017 deliberated and taken a
consensus opinion that minimum experience required for Licensing Authority related
to manufacturing and sale of drugs should be raised to minimum of 10 years
regulatory experience instead of existing 5 years experience to be a Licensing
Authority.
Further this matter was placed before DTAB in its 77th meeting held on
16.06.2017 and agreed by the members.
DTAB may deliberate and give its suggestions in the matter for necessary
amendments in the rules.

Page 16 of 33
AGENDA NO. 9
RECONSTITUTION OF SUB-COMMITTEE OF DRUGS TECHNICAL ADVISORY
BOARD ON HOMEOPATHY
Ministry of AYUSH vide its F. No. K-11022/01/2014 HPC) dated 27.07.2017
informed to re-constitute the sub-committee of DTAB on Homeopathy.
The sub-committee of Drug Technical Advisory Board on Homeopathy was
constituted on 18.08.2015 and under terms of reference it was mentioned that the
tenure of the sub-committee shall be of two years. The term of the sub- committee
therefore expired on 17.08.2017.
In view of the above, DTAB may consider for reconstitution of the sub-
committee or for extension of the tenure of the existing sub-committee.
Page 17 of 33
AGENDA NO. 10
CONSIDERATION OF THE PROPOSAL TO CLARIFY WHETHER THE
CENTCHROMAN (30MG) TABLETS TO BE EXEMPTED FROM THE
PROVISIONS OF CHAPTER IV OF THE D& C ACT AND RULES UNDER
SCHEDULE K OR TO SELL THE REMAINING STRENGTHS UNDER
SCHEDULE H OF D& C RULES
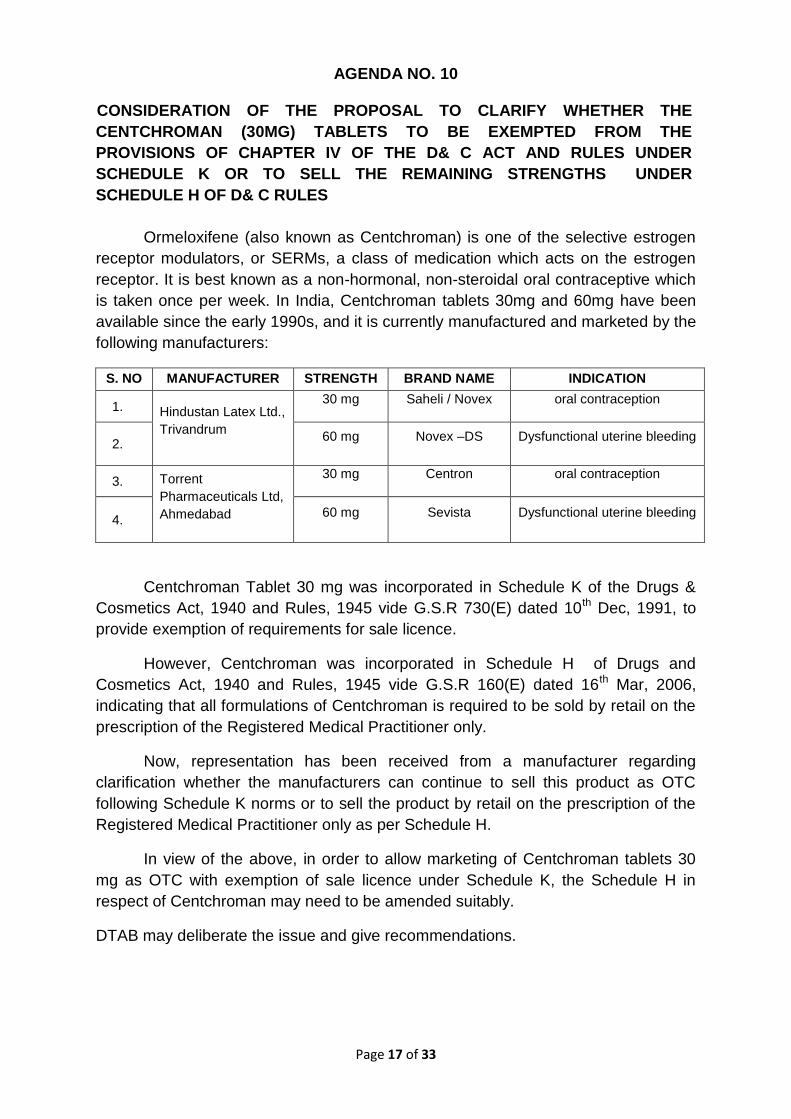
Ormeloxifene (also known as Centchroman) is one of the selective estrogen
receptor modulators, or SERMs, a class of medication which acts on the estrogen
receptor. It is best known as a non-hormonal, non-steroidal oral contraceptive which
is taken once per week. In India, Centchroman tablets 30mg and 60mg have been
available since the early 1990s, and it is currently manufactured and marketed by the
following manufacturers:
S. NO MANUFACTURER STRENGTH BRAND NAME INDICATION
1. Hindustan Latex Ltd.,
Trivandrum
30 mg Saheli / Novex oral contraception
2. 60 mg Novex –DS Dysfunctional uterine bleeding
3. Torrent
Pharmaceuticals Ltd,
Ahmedabad
30 mg Centron oral contraception
4. 60 mg Sevista Dysfunctional uterine bleeding
Centchroman Tablet 30 mg was incorporated in Schedule K of the Drugs &
Cosmetics Act, 1940 and Rules, 1945 vide G.S.R 730(E) dated 10th Dec, 1991, to
provide exemption of requirements for sale licence.
However, Centchroman was incorporated in Schedule H of Drugs and
Cosmetics Act, 1940 and Rules, 1945 vide G.S.R 160(E) dated 16th Mar, 2006,
indicating that all formulations of Centchroman is required to be sold by retail on the
prescription of the Registered Medical Practitioner only.
Now, representation has been received from a manufacturer regarding
clarification whether the manufacturers can continue to sell this product as OTC
following Schedule K norms or to sell the product by retail on the prescription of the
Registered Medical Practitioner only as per Schedule H.
In view of the above, in order to allow marketing of Centchroman tablets 30
mg as OTC with exemption of sale licence under Schedule K, the Schedule H in
respect of Centchroman may need to be amended suitably.
DTAB may deliberate the issue and give recommendations.
Page 18 of 33
AGENDA NO. 11
CONSIDERATION OF THE PROPOSAL FOR DENOTIFICATION OF G.S.R 743(E)
DATED 10.08.1989 ISSUED UNDER SECTION 26A FOR PROHIBITION OF ALL
FIXED DOSE COMBINATION INJECTABLE PREPARATIONS CONTAINING
SYNTHETIC OESTROGEN AND PROGESTERONE
Earlier all Fixed Dose Combination injectable preparations containing
synthetic Oestrogen and Progesterone were prohibited for manufacture for sale, sale
and distribution in the country vide GSR No. 743(E) dated 10.08.1989. A
representation has been received from one of the manufacturers for revocation of
the above notification for FDC of Medroxyprogesterone Acetate + Estradiol
Cypionate (cyclofem) injection from list of banned drugs.
The same was deliberated earlier by NDAC (Reproductive and Urology) on
17.09.2013 and the committee recommended that all FDC injectable preparations
containing synthetic Oestrogen and Progesterone were prohibited in the country,
most probably due to report of misuse of such preparations for pregnancy detection.
At present, chances of such misuse are insignificant as at present many pregnancy
detection kits which are very sensitive and various means for satisfactory
contraception are available. A copy of recommendations of the NDAC (Reproductive
and Urology) meeting held on 17.09.2013 is enclosed at ANNEXURE - 5.
ICMR has also conducted the clinical trial with the Cyclofem in 1275 subjects
who were followed up for 10934 women- months of use. The clinical data has been
found satisfactory. Available data shows that FDC injectable preparations containing
synthetic Oestrogen and Progesterone are not associated with change in Bone
Mineral Density. Therefore the committee recommended considering revocation of
banning of the FDC injectable preparations containing synthetic Oestrogen and
Progesterone by appropriate authority. The committee recommended the grant of
permission of clinical trial of Cyclofem and Norethisterone Enanthate (NET-EN)
subject to the following conditions:
1. The study should be titled as extended phase III clinical trial.
2. The study should be conducted at multispecialty hospitals having
emergency facilities and institutional ethics committee registered with
CDSCO.
3. Details of such sites along with undertaking by the investigators as per
appendix VII of Schedule Y should be submitted.

Page 19 of 33
4. Informed consent document as per appendix V of schedule Y should be
submitted.
5. Undertaking as per Rule 122DAB for compensation and providing medical
management as per the Rule in case of injury/death in clinical trial.
6. Denotification of the banning of Cyclofem i.e. Fixed Dose Combination
injectable preparations containing synthetic Oestrogen and Progesterone
7. The recommendation may be placed before DTAB for further
consideration. (Dr. Sunita Mittal and Dr. Lakbir Dhaliwal did not take part in
decision making process due to conflict of interest).
This proposal was earlier deliberated in 65th DTAB held on 25.11.2013 and
DTAB recommended that An Expert Committee consisting of at least three
Gynecologists, three endocrinologists, Dr. Anoop Mishra and Dr. Y. K. Gupta, HOD,
Department of Pharmacology, AIIMS, New Delhi under the Chairmanship of DGHS
may be constituted to examine the essentiality of the clinical trial as well as the
requirement, if any, of the amendment of entry number 27 in respect of the FDC of
injectable preparations containing synthetic oestrogen and progesterone, in the
context of present day knowledge. However, no further proceeding took place in the
matter. A copy of minutes of 65th DTAB is enclosed as ANNEXURE- 6.
In view of above, the DTAB may kindly give their recommendations in respect
of denotification of G.S.R 743(E) dated 10.08.1989 issued under Section 26A for
prohibition of all FDC injectable preparations containing synthetic Oestrogen and
Progesterone.
Page 20 of 33
AGENDA NO. 12
CONSIDERATION OF THE PROPOSAL TO EXPLORE THE FEASIBILITY OF
PROVIDING A SEPARATE SHELF/RACK FOR GENERIC MEDICINES IN
PHARMACY
Issue of exploring to keep a separate shelf / rack of generic medicines in
every pharmacy so as to promote the availability of “Generic Medicines” was
deliberated in 52nd DCC held on 18-09-2017 and agreed to the proposal.
Similar provisions are also exists under Rule 65, clause (12) for Schedule X
drugs and clause (20) for veterinary medicines. Accordingly, a provision under Rule
65 may need to be incorporated in Rule 65 as clause (22) in D & C Rules. A draft
prepared in this respect is given below:
In the Drugs and Cosmetics Rules, 1945, in Rule 65, after clause (21), the
following clause shall be inserted namely-
“(22) The licensee shall maintain a separate rack / shelf reserved solely
for the storage of “Generic Medicines” in a part of the premises
separated from other medicines.”.
In view of above, the DTAB may kindly deliberate and give their
recommendations to keep a separate shelf / rack of generic medicines in every
pharmacy so as to promote the availability of “Generic Medicines” in Rule 65 of
Drugs and Cosmetics Act, 1940 and Rules, 1945 made thereunder.

Page 21 of 33
AGENDA NO. 13
CONSIDERATION OF THE PROPOSAL FOR AMENDMENT OF RULE 127(2) OF
THE DRUGS AND COSMETICS RULES, 1945, SO AS TO REMOVE THE
AMBIGUITY AND SCOPE OF DIFFERENT INTERPRETATIONS IN CASE OF USE
OF COLOURS IN EMPTY GELATINE CAPSULES (HARD AND SOFT)
Representations have been received from various State Drugs Controllers
that the Government Analysts of various States declaring the samples as of
Standard Quality with a note that it does not meet the requirement of labelling (as
name of approved colour used in the empty capsule shell is not mentioned on the
label), thus contravening the provision of rule 127(2) of Drugs & Cosmetics Rules,
1945.
Drugs & Cosmetics Rules, 1945, rule 127(2) specifies that
“The label on the container of a drug containing a permitted colour shall
indicate the common name of the colour.”
However, at the same time it is also true that there is more number of repeated
manufacturers who are also not mentioning the name of the colours used in the
empty capsule shell and as a practice writing the common statement on the label as
“approved colours used in capsule shell”.
It was felt that, whether the Government Analyst(s) is/are empowered to put
such a note that sample does not meet the requirement of labelling (“as name of
approved colour used in the empty capsule shell is not mentioned on the label”
instead a statement of “approved colours used in capsule shell”.) though the sample
is of standard quality for the reasons “the sample conforms to declared formula on
the basis of tests done” if so, whether it attract the administrative action or legal
action. This matter was referred to a sub-committee and following recommendations
were suggested:
1. Rule 127(2) provides that the labelling on the container of the drug
containing permitted colours shall indicate common name of the colour.
2. Empty Gelatine Capsules were included as drug in the definition of Drugs
in 1982.
3. Thereafter the issue of declaring colour on the label of the empty gelatine
capsule was discussed in DCC meeting held at New Delhi on 22nd

Page 22 of 33
September, 1983. In the said meeting it was decided that “ In the
manufacture of gelatine capsule colours permitted for manufacture of drug
should be used and label need not indicate the name of colour added as
more than one colour are quite often used.”
4. Monograph of gelatine capsules shell is included in IP Monograph 2014,
Page 1848 and 1849. In the labelling of monograph it is provided that the
labels state that only permitted colours, if any has to be declared.
5. In labelling requirements under Food Safety and Standards Act, 2006 it is
necessary to declare that permitted colour used. It is not necessary to
declare name and specific colour.
6. It is noted that Rule 127 was inserted under S.O. 289 dtd.20/12/1972
(w.e.f. 03/02/1973). Rule 96 was substituted by GSR 19 dtd.15/12/1977
(w.e.f. 07/01/1978). However, Rule 96 does not contain provision for
declaring colours.
7. In view of the decision taken by the DCC and having regard to the fact that
empty gelatine capsules or soft gelatine capsules are not active ingredient,
but are used as vehicle for providing active ingredient (Drugs) to the
patient and labelling directions under the monograph, it is felt that insisting
declaration of colour used in capsule shell will be considered as not
consistent with spirit of law.
DTAB may please consider the proposal and give its recommendations.

Page 23 of 33
AGENDA NO. 14
CONSIDERATION OF THE PROPOSAL TO AMEND SCHEDULE D OF THE
DRUGS AND COSMETICS RULES, 1945 TO PROVIDE EXEMPTION FOR
RADIOPHARMACEUTICALS FROM THE PROVISIONS OF THE CHAPTER III OF
THE DRUGS AND COSMETICS ACT, 1940
DTAB in its 76th meeting held on 31st January 2017, deliberated the issue
regarding providing exemption for import of radiopharmaceuticals under Schedule D
of Drugs and Cosmetics Rules, 1945 and referred to Atomic Energy Regulatory
Board (AERB), Mumbai for their opinion for having holistic approach in the matter.
In response to this the AERB suggested that the decision regarding
exemption for import of radiopharmaceuticals as drug under the Drugs and
Cosmetics Act and the Rules promulgated thereunder rests with CDSCO. However,
they assured for continued coordination and support in having holistic approach in
the matter.
Under the Drugs and Cosmetics Rules, 1945, exemption has been provided
at Serial No 20, under Schedule K from the provisions of the Chapter IV of the Act
and the rules made there under. As such radiopharmaceuticals are not subjected to
regulatory controls in respect of their manufacture and sale. It is however observed
that no such exemption is provided for the radiopharmaceuticals imported into the
country.
In view of this it is proposed to provide exemption under Schedule D from the
provisions of Chapter III for radiopharmaceutical products imported into the country.
DTAB may please consider the proposal and give its recommendations.
Class of drug Extent and conditions of exemption
“10. Radiopharmaceuticals All provisions of chapter III of the Act and Rules
made there under”
Page 24 of 33
AGENDA NO. 15
CONSIDERATION OF THE PROPOSAL FOR REVIEW OF PROPHYLACTIC
DOSES MENTIONED UNDER SCHEDULE ‘V’OF DRUGS AND COSMETICS
RULES VIS A VIS THE DOSES PRESCRIBED UNDER FSS ACT
A proposal has been received from FSSAI proposing that Drugs and
Cosmetics rules may be amended to delete the preparations containing the
prophylactic doses under Schedule ‘V’ considering the provisions of doses under
Section 22 of FSS Act especially products formulated in Tablets, Capsules, Liquids,
etc. meant for oral administration.
As per Section 22 of FSS Act, 2006 it is evident that the products in drug type
matrix (i.e. Tablets, capsules, etc.) covered under FSS Act which is containing
vitamins below RDA also falls under prophylactic and some of the therapeutic doses
prescribed in schedule V of the Drugs and Cosmetics Rules.
Secondly, FSSAI has also proposed for amending the Schedule K (10) for
revising the scope of substances which are used both as articles of food as well as
drugs so that same are exempted from the provisions of Chapter IV of D&C Act and
Rules made there under.
Accordingly, DCC in its 52nd DCC meeting held on 18.09.2017 deliberated the
proposal and recommended that a provision may be incorporated in Drugs and
Cosmetics Rules, 1945 especially in Sch ‘V’ and Sch ‘K’ to exclude multivitamin
preparations containing vitamins in a strength which is lower than Recommended
Daily Allowance (RDA) for Indians as recommended by ICMR and FSSAI, from the
provisions of Drugs and Cosmetics Rules, 1945.
DTAB may discuss the issue and give further recommendations so that
necessary amendment may be made under schedule ‘V’ as well as under schedule
K (10) respectively considering the provisions under FSS Act.

Page 25 of 33
AGENDA NO.16
CONSIDERATION OF THE PROPOSAL FOR AMENDMENT OF PARA 10.9 OF
SCHEDULE ‘M’ OF DRUGS AND COSMETICS RULES, 1945 FOR WAIVER OF
REQUIREMENT FOR VACCINES MANUFACTURED USING LESS THAN 60%
RESIDUAL SHELF-LIFE PERIOD IN THE COUNTRY
Representation has been received from Shantha Biotechnics Pvt. Ltd.
Hyderabad for waiver of Para 10.9 of Schedule M in case of manufacturing of
vaccines using import of bulk concentrated vaccine components whose residual
shelf life is less than 60% when they used in the formulation which is contravening
the existing provision in Para 10.9 of Schedule M.
The firm has submitted that for import and use of Inactivated Poliomyelitis
Vaccine (IPV) bulk (concentrated trivalent) batches with less than 60% residual shelf
life period for formulation and filling of Inactivated Poliomyelitis Vaccine IP, Trivalent
stating that as recommended by Annexure 3 of WHO TRS 962 Guidelines on
stability evaluation of Vaccines, (Para 5.3) the stability of the characteristics of a final
product should be guaranteed during the whole shelf-life, irrespective of the age of
the intermediates at the time they are used in the production process.
The firm was earlier issued NOC from DCGI Office for the import and use of
Inactivated Poliomyelitis Vaccine bulk (concentrated trivalent) (IPV) batches with less
than 60% residual shelf-life period for formulation and filling of Inactivated
Poliomyelitis Vaccine IP, Trivalent with a condition to comply the provision as laid
down in Para 10.9 of PART 1 of Good Manufacturing Practices for Premises and
Materials of Schedule M of Drugs and Cosmetics Rules 1945. Accordingly, the firm
had imported IPV bulk batches with less than 60% residual shelf life under Form-11
from M/s Sanofi Pastuer, France and manufactured 6 batches of Inactivated
Poliomyelitis Vaccine IP, Trivalent using residual shelf-life period of 6.3%, 20.5%,
21.6%, 6.3%, 20.5% and 21.6% respectively.
The firm has reported that these Inactivated Poliomyelitis Vaccine batches
were found to be stable up to 24 months shelf life period when stored at 2 to 8ºC, 6
months at 25±2ºC and 7 days at 37±2ºC. The firm has also stated that drug product
batches manufactured with less residual shelf life bulks are stable up to the shelf-life

Page 26 of 33
period i.e. 36 months and submitted the stability data up to 24 months when stored
at 2 to 8ºC against the claimed shelf life.
In view of above, DTAB may deliberate as whether such type of vaccine bulks
with less than 60% residual shelf life, imported may be permitted to be used for
manufacturing/formulation of vaccines (product licences) with the expiry of 2 years
keeping the view of above stated rule position and suggest any suitable amendment
required exclusively for vaccines.

Page 27 of 33
AGENDA NO.17
CONSIDERATION OF THE PROPOSAL TO AMEND THE MEDICAL DEVICES
RULES, 2017- ISSUE GENERAL CLARIFICATION FOR SMOOTH AND UNIFORM
IMPLEMENTATION
The Ministry of Health & Family Welfare, Government of India has notified the
Medical Devices Rules 2017 vide G.S.R. 78(E) dated 31.01.2017 under the
provisions of the Drugs and Cosmetics Act, 1940.
Said rules are effective from 01.01.2018 to regulate the Clinical Investigation,
Manufacture, Import, Sale and Distribution of the medical devices in the country.
Further, representation received from the Industry/ Stakeholders/ Associations
regarding the consideration of the proposal to amend in the Medical Device Rules,
2017.
Accordingly, following agendas are placed below for the consideration of DTAB:
1) CONSIDERATION OF THE PROPOSAL TO DEFINE PATHWAY RELATED TO
DISPOSAL OF APPLICATIONS RELATED TO CLAA RECEIVED AFTER 31ST
DECEMBER 2017
Medical Devices Rules 2017 have been implemented from 1st January 2018.
Further, this Directorate has received applications for Additional products
endorsement, Grant of manufacturing licence in form 28 and renewal applications
in Hard copy after 31st December 2017. (List attached for the reference)
It is pertinent to mention that some applications of endorsement has
forwarded by various State Licensing Authorities before 31.12.2017 but received
by this office after 31.12.2017.
It is proposed to define pathway related to disposal of applications related to
CLAA received after 31st December 2017.
In this regard, it is proposed that if application is done& joint inspection is
carried out and recommended by State Licensing Authority with effective date
earlier to 31.12.2017, it may be considered for signing by DCG (I ) effective from
that date (undertaking clause).
In case of renewal of manufacturing licenses, if firm has applied with fees it
used to be considered as deemed renewed till orders are passed as per earlier
rule of 75 and 77 of Drugs & Cosmetics Rules, 1945. If no orders are passed, such
license shall be considered valid till 31.07.2018 in the light of rule 97 of MDR-2017
& clarification in this regard may be issued to bring clarity & uniformity of
implementation.
DTAB may deliberate & give its recommendation

Page 28 of 33
2) CONSIDERATION OF THE PROPOSAL RELATED TO ENDORSEMENT OF
ADDITIONAL PRODUCTS IN OLD REGISTRATION CERTIFICATE/ IMPORT
LICENSE/ MANUFACTURING LICENCE
As per the Rule 97, the manufacturing licenses as well as import licenses
which have validity post January 2018 will remain valid till their expiry. However,
there is not adequate provision in the Rules for endorsements of additional
products in these licenses. This is an operational bottleneck for the manufacturers
and importers.
Stakeholders have requested to make provisions in the old SUGAM for
endorsement of additional product at discounted fees as compared to the fees in
New MDR as they will be getting a limited validity. Alternately, if discounted fee is
not a viable option for the CDSCO. Further, Industry suggested for a provision to
apply for endorsement under the new Rules, on the new portal, with approvals
having perpetual validity as per Medical Device Rules 2017.Plant Master File
documentation and applicable fee should not be required in this scenario as the
site is already registered in India.
It is stated that validity of manufacturing license (as per Rule 29) and import
license (as per rule 37) remain valid in perpetuity, subject to payment of licence
retention fee. Further, in this regard, it is informed that firm can get endorsement in
old Registration Certificate/ Import License/ Manufacturing licence; however there
is no provision for discounted fee. Further, it is proposed that firm may apply for
addition of products in existing Registration Certificate/ Import License/
Manufacturing licence provided that documents and fees will be submitted as per
Medical Device Rules, 2017.
DTAB may deliberate & give its recommendation.
3) CONSIDERATION OF THE PROPOSAL TO AMEND ENVIRONMENTAL
REQUIREMENTS IN RESPECT OF MANUFACTURING FACILITY AS
SPECIFIED IN THE FIFTH SCHEDULE OF MEDICAL DEVICES RULES, 2017
It has been pointed out and informed by stakeholders that the Fifth Schedule
[for rule 20 (3), 20(5), 20(8), 22 (j)] (Quality Management System for Medical
Devices and in vitro diagnostic medical devices), Annexure A – Environmental
Requirement for medical devices and in-vitro diagnostic medical devices, has
prescriptive requirements of manufacturing environmental conditions, which is not
in harmony with International (IMDRF) regulations.
This Directorate has received suggestions from Industry/ Stakeholders. They
have stated that this is leading to a situation that all indigenous manufacturers
need to make alterations to the manufacturing facilities which are not in line with
global manufacturing conditions. The manufacturing conditions have been

Page 29 of 33
prescribed based on the extrapolation of drug manufacturing condition which is not
suitable for medical devices.
Hence, the environmental conditions in Fifth Schedule of the Medical Device
Rules should be removed from the Fifth Schedule or should be redrafted as
guidance rather than as statutory requirements.
Further, Surgical Dressings Manufacturers Association has also made
representation regarding the amendment for environmental requirements in
respect of manufacturing facility for surgical dressings as specified in the
Annexure- A of the Fifth Schedule of Medical Devices Rules, 2017.
In their representation, they have stated that, presently the manufacturers of
surgical dressings complying the requirement as specified in “Schedule M” of
Drugs & Cosmetics, Act, 1940 and Rules 1945 by arranging neat, clean & dust
and free environment for the manufacturing of surgical dressings.
The “Schedule M” does not prescribe the specific environmental requirement
for the manufacturing of Surgical Dressings. However, in the Medical Devices
Rules, 2017, fifth Schedule specified the specific environmental requirement for
the type of operation as per ISO Class as under:
Name of the device Type of operation ISO Class(At rest)
Surgical Dressings Weaving 9
Assembly and Gauzing 9
Final primary packing 9
In this regard, the association members have raised concerns for their inability
to maintain environmental requirement to have an ISO Class 9 room for weaving,
assembly and gauzing and final primary packing as they are small and tiny
manufacturers.
Further, the representatives of the associations were called for personal
hearing by CDSCO in order to have detailed deliberation in the matter where the
stakeholders requested to put these conditions in abeyance.
Accordingly, following changes are proposed to be made in Annexure A of the
fifth Schedule of MDR, 2017 regarding the environmental requirement of
manufacturing of surgical dressings:
a) Annexure A of the fifth schedule of said rules shall be deleted and treated as
guidance document.
In this document
I. Instead of surgical dressing, sterile surgical dressing to be substituted.
II. Weaving and Assembly and Gauzing to be replaced by final primary
packing for sterile surgical dressings.
III. Similarly, for condoms neat & clean environment free from dust etc. shall
be replaced instead of 5 µ filter.

Page 30 of 33
DTAB may deliberate & give its recommendation.
4) CONSIDERATION OF THE PROPOSAL TO DEFINE PATHWAY TO SUBMIT
ABRIDGED APPLICATIONS (WITH TRUNCATED DOCUMENTATION) FOR
SUBSEQUENT IMPORT LICENSE APPLICATIONS
Industry/ stakeholders requested for a defined pathway to submit abridged
applications (with truncated documentation) for subsequent import license
applications for the site and products already approved under MD-15.
In this regard, it is proposed that abridges pathway may be accepted provided
that an undertaking from the manufacturer should be submitted stating that No
change have been made in the document submitted earlier while registering with
earlier agent.
DTAB may deliberate & give its recommendation.
5) CONSIDERATION OF THE PROPOSAL FOR THE DIGITAL SIGNATURE,
WHEREVER APPEARING IN THE RULES, MAY BE MADE OPTIONAL
In the Medical Devices Rules, 2017 submission of some applications required
Digital signature. Further, in case of technical error, it is proposed to use routine
signature for the submission of application form.
It is requested by stakeholders that Digital Signature, wherever appearing in
the rules, may be made optional by amending the rules.
DTAB may deliberate & give its recommendation.
6) CONSIDERATION OF THE PROPOSAL TO ADD PROVISIONS IN RESPECT
OF THE WAIVER OF CLINICAL PERFORMANCE EVALUATION FOR IVDs, IN-
LINE WITH WAIVER GIVEN FOR MEDICAL DEVICE UNDER RULE 63 OF
MEDICAL DEVICES RULES, 2017
Rules 63 of the Medical Device Rules (Chapter VIII) – Import or Manufacture
Medical Device Which Does Not Have Predicate Device - regarding Permission to
import or manufacture medical device which does not have its predicate device.
There are provisions that clinical investigation be waived off if the device has
2 years of marketing experience in UK, USA, Australia, Canada or Japan.
However, a corresponding provision is missing for Rule 64 – Permission to import
or manufacture new in-vitro diagnostic medical device.
In view of the above, it is proposed to add identical provisions in rule 64 for
IVD devices.
DTAB may deliberate & give its recommendation.
Page 31 of 33
7) CONSIDERATION OF THE PROPOSAL FOR THE SUBMISSION OF
APPLICATIONS OF MEDICAL DEVICES AND IVDS THROUGH OFFLINE
MODE
All applications for obtaining licenses will be made through online portal of the
Central Government. New Medical Device portal is functional for uploading the
applications for Import License, Registration and Manufacturing License etc.
It is proposed that, in case of failure of online portal for submission of
applications for import and manufacture, there should be a provision to accept &
process application in offline mode under MDR 2017 in order to dispose of the
applications.
8) CONSIDERATION OF THE PROPOSAL TO INCREASE THE TIMELINE OF
SUSAR REPORTING IN MDR,2017
As per the said rules, Serious Unexpected Serious Adverse
Reaction (SUSAR) need to be reported within 15 days of occurrence where as
SUSAR will be confirmed only after detailed investigation of the incident. This will
not be completed within 15 days. Industry/ Stakeholder suggested that the timeline
of SUSAR reporting need to be at-least 45 days of occurrence.
Further, it is proposed to increase the timeline of SUSAR reporting.
9) CONSIDERATION OF THE PROPOSAL TO INCREASE THE TIMELINE OF ANY
REGULATORY ACTION TAKEN ACROSS THE WORLD
As per the said rules, any regulatory action taken across the world need to be
reported within 15 days of such action and the industry feel that it is too short a
time frame for the member companies to comply with the requirement. Industry/
Stakeholder suggested that the timeline may be raised to 45 days from 15 days.
Further, it is proposed to increase the timeline for the same.
10) CONSIDERATION OF THE PROPOSAL TO INCLUDE MEDICAL DEVICE
EXPERT IN DTAB
Industry/ stakeholders requested for the seat for Medical device sector/
industry in Drug Technology Advisory Board (DTAB). It is proposed to include
medical device expert whenever medical device related proposals are being
discussed.
Page 32 of 33
11) IMPORT LICENSE REQUIREMENTS SHOULD NOT BE MANDATORY FOR
COMPONENTS THAT ARE IMPORTED FOR FURTHER PROCESSING BY
MEDICAL DEVICE /PHARMACEUTICAL MANUFACTURERS WITH VALID
MANUFACTURING LICENSE
Industry/ stakeholders requested that Import license requirements should not
be mandatory for Components i.e. manufacturing that are imported for further
processing by medical device/pharmaceutical manufacturers with valid
manufacturing license. One time NOC to be issued for such components on
submission of valid manufacturing license to the CDSCO. If any license is issued
previously for import of components for further processing of Medical devices then
it should be treated only as a trading license.
DTAB may deliberate & give its recommendation for issue of clarification.
12) WHEN MEDICAL DEVICES WHICH ALREADY EXIST IN THE INDIAN MARKET
FOR USE ARE BROUGHT IN FUTURE UNDER REGULATION, THEN SUCH
DEVICES SHALL NOT BE A NEW MEDICAL DEVICES.
It is requested by stakeholders to clarify as per the present rules, the definition
of Investigational medical devices and Predicate devices amounts to those devices
which are not approved by CDSCO. However, there are many devices in the
country which are not regulated and when they are brought under regulation will
fall under the ambit of investigational medical device as well as that we will not be
leverage it as predicate device. This anomaly need to be addressed such that
when new devices are brought under regulation, manufacturers should not be
asked to take the path of investigational medical device.
DTAB may deliberate & give its recommendation for amendment of rule.
13) CONSIDERATION OF THE PROPOSAL FOR NOTIFICATION OF ORGAN
PRESERVATIVE SOLUTION AS MEDICAL DEVICE UNDER SECTION 3(b) (iv)
OF THE DRUGS AND COSMETICS ACT, 1940
Organ preservative solution are intended to be used for flushing and cold
storage of organs like heart, lungs, kidney, liver and pancreas at the time of
removal from donor in preparation for storage, transportation and eventual
transplantation in to the recipient. The solution consists of Glutathione, Mannitol,
Lactobionic acid, glutamic acid, sodium Hydroxide, Calcium Chloride 2H2O,
Potassium Chloride, Magnesium Chloride, Histidine, Water for Injection etc. in
order to achieve a specific osmolarity required for organ preservation.
This office has received various applications on the regulatory status of Organ
Preservative solution. This office has given clarifications to the applicant that the
same is not notified under Section 3 (b) (iv) of Drugs and cosmetic Act 1940 and
therefore not regulated as Medical Devices. The clarification issued is annexed for
reference. However, the same is regulated as Drugs and permission for same has

Page 33 of 33
given by Import Division. It may however be stated that, the Organ Preservative
Solutions are regulated as medical Devices in many countries.
It is therefore proposed, that the Organ Preservative Solution may be notified
under Section 3 (b) (iv) of Drugs and Cosmetic Act 1940 so that the same may be
brought under the regulation.
In view of the above, the DTAB may kindly consider the said proposals and
recommended for amendment in the Medical Devices Rules, 2017 and inclusion of
Nebulizer, Glucometer and Organ preservative solution under Section 3 (b) (iv) of
Drugs and Cosmetics Act 1940.
AGENDA NO.18
Additional agenda (if any) with the approval of the Chair.

S. No. Name of Drug Recommendation under Second Assessment by the Kokate Committee (Dated 16.04.2015) Prohibition
Notification No.
1 Aceclofenac + Paracetamol
+ Rabeprazole
a,
1.There is pharmacokinetics incompatibility among the three drugs, as the dosing intervals are BD for
aceclofenac, OD for rabeprazole and TDS/QID for paracetamol.
2.The FDC is not approved anywhere in the world
3.The literature regarding safety and efficacy of this combination is not available in Pubmed & Google scholar
S.O. 705 (E)
2 Nimesulide + Diclofenac a,
1. Nimesulide in combination has potential of misuse and have documanted safety concern.
2. No additional advantage but hepatotoxic potential of nimesulide and adverse effects add up.
3.Pharmacodynamically irrationale FDC as both have same mechanism of action (both drugs acting on the same
enzyme). Thus, combining two NSAIDs does not and cannot improve the efficacy of treatment. It only adds to
the cost of therapy and more importantly, to the adverse effects
Chandler S. Gautam, Lekha Saha. Fixed dose drug combinations (FDCs): rational or irrational: a view point Br
J Clin Pharmacol / 65:5 / 795–796.
Kasarla Raju, A. Elumalai2, Eddla Srid. IRRATIONAL DRUG COMBINATIONS. Vol 3|Issue 2| 2013 | 52-56.
S.O. 706 (E)
3 Nimesulide + Cetirizine
+Caffeine
a,
1. Nimesulide in combination has potential of misuse in indications for allergic conditions.
2. Nimesulide has documanted safety concern.
S.O. 707 (E)
4 Nimesulide +Tizanidine a,
1. Nimesulide in combination form has potential of misuse.
2. The FDC is pharmacokinetically incompatible as both have different dosing schedule.
3. Safety concern with Nimesulide
S.O. 708 (E)
Annexure-I
List of 344 FDCs + 05 FDCs already prohibited for manufacutre and sale through gazette notifications under Section 26A of Drugs & Cosmetics Act 1940 by the Ministry
of Health and Family Welfare for further deliberation by DTAB/Sub-committee as per the Judgement given by Hon'ble Supreme Court of India on 15.12.2017
Admin
Typewriter
Annexure -1
Admin
Typewriter

5 Paracetamol + cetrizine +
caffeine
a,
1. Pharmacokinetic incompatibility, as dosing interval for paracetamol is TDS/QID and for cetrizine it is OD/BD.
2. No trial could be found in PUBMED and google scholar.
3. An important safety debate concerning multi- ingredient, multi-symptom relief products for common cold and
flu is that they commonly contain paracetamol (acetaminophen) and that users who may not be aware of this may
accidentally overdose when they take the multi- ingredient product with other medicines also containing
paracetamol.
Eccles, R., Fietze, I. and Rose, U.-B. (2014) Rationale for Treatment of Common Cold and Flu with Multi-
Ingredient Combination Products for Multi-Symptom Relief in Adults. Open Journal of Respiratory Diseases, 4,
73-82.
S.O. 709 (E)
6 Diclofenac + Tramadol +
Chlorzoxazone
a,
1. Tramadol is an opoid analgesic with abuse liability.
2. The combination will lead to additive sedation.
http://reference.medscape.com/drug-interactionchecker.
S.O. 710 (E)
7 Dicyclomine +Paracetamol
+Domperidone
a,
1.Pharmacodynamic irrelevant as each ingredient has different therapeutic use and FDC will lead to misuse and
toxicity.
2. Combining can result in dangerous elevation of the body temperature.
Chandler S. Gautam, Lekha Saha. Fixed dose drug combinations (FDCs): rational or irrational: a view point Br
J Clin Pharmacol / 65:5 / 795–796
Eccles, R., Fietze, I. and Rose, U.-B. (2014) Rationale for Treatment of Common Cold and Flu with Multi-
Ingredient Combination Products for Multi-Symptom Relief in Adults. Open Journal of Respiratory Diseases, 4,
73-82.
S.O. 711 (E)
8 Nimesulide +Paracetamol
dispesible tablets
a,
1. Nimesulide in combination as a dispersible dosage form has potential of misuse in children. There are safety
concerns with nimesuilide FDC with paracetamol.
2. Dose of paracetamol 500mg not approved in FDC with NSAIDs
Chandler S. Gautam, Lekha Saha. Fixed dose drug combinations (FDCs): rational or irrational: a view point Br
J Clin Pharmacol / 65:5 / 795–796
S.O. 712 (E)

9 Paracetamol +
Phenylephrine + Caffeine
a,
Pharmacodynamically irrelevant -
misuse and overuse of one of the ingredient of FDC in case it is not indicated.
Eccles, R., Fietze, I. and Rose, U.-B. (2014) Rationale for Treatment of Common Cold and Flu with Multi-
Ingredient Combination Products for Multi-Symptom Relief in Adults. Open Journal of Respiratory Diseases, 4,
73-82.
S.O. 713 (E)
10 Diclofenac +Tramadol
+Paracetamol
a,
1.Tramadol is itself a potent opoid analgesic. FDC is not rational as addition of Paracetamol and Diclofenac will
not provide any additional benefit.
S.O. 714 (E)
11 Diclofenac + paracetamol +
chlorzoxazone + famotidine
a,
1. Pharmacodynamic irrelevant as each ingredient has different dosing shedule/dosing requirement.
2. FDC will lead to misuse and toxicity.
S.O. 715 (E)
12 Naproxen+Paracetamol This FDC was discussed by previous Committee on 04.06.14-
There is no scientific justification, the only published literature of this combination has used Paracetamol 4g/day
which is much higher than the proposed dose in the FDC. Hence, the committee did not recommend.
S.O. 716 (E)
13 Nimesulide +
serratiopeptidase
a,
1. Safety concern with nimesulide
2.No evidence to support that Serratiopeptidase offer any particular advantage over Nimesulide.
3. On the other hand, the patient is exposed to greater risk of gastrointestinal (GI) irritation and serious bleeding
from unsuspected peptic ulceration.
Chandler S. Gautam, Lekha Saha. Fixed dose drug combinations (FDCs): rational or irrational: a view point Br
J Clin Pharmacol / 65:5 / 795–796.
S.O. 717 (E)
14 Paracetamol +Diclofenac
+Famotidine
a,
1.Pharmacodynamic irrelevant as each ingredient has different therapeutic use and FDC will lead to misuse.
2. Paracetamol dose is high
3. Both diclofenac and paracetamol hepatotoxic
4. An important safety debate concerning multi- ingredient, multi-symptom relief products for common cold and
flu is that they commonly contain paracetamol (acetaminophen) and that users who may not be aware of this may
accidentally overdose when they take the multi- ingredient product with other medicines also containing
paracetamol.
Eccles, R., Fietze, I. and Rose, U.-B. (2014) Rationale for Treatment of Common Cold and Flu with Multi-
Ingredient Combination Products for Multi-Symptom Relief in Adults. Open Journal of Respiratory Diseases, 4,
73-82.
S.O. 718 (E)

15 Nimesulide + Pitofenone +
Fenpiverinium + benzyl
alcohol
a,
1.There are no evidences on safety and efficacy of the FDC.
2. Safety concern with nimesulide
S.O. 719 (E)
16 Omeprazole + Paracetamol
+ Diclofenac
a,
1.Pharmacodynamic irrelevant as each ingredient has different therapeutic use and FDC will lead to misuse.
2. Paracetamol dose is high
3. Both diclofenac and paracetamol hepatotoxic
4. An important safety debate concerning multi- ingredient, multi-symptom relief products for common cold and
flu is that they commonly contain paracetamol (acetaminophen) and that users who may not be aware of this may
accidentally overdose when they take the multi- ingredient product with other medicines also containing
paracetamol.
Eccles, R., Fietze, I. and Rose, U.-B. (2014) Rationale for Treatment of Common Cold and Flu with Multi-
Ingredient Combination Products for Multi-Symptom Relief in Adults. Open Journal of Respiratory Diseases, 4,
73-82.
S.O. 720 (E)
17 Nimesulide + Paracetamol
injection
a,
1.There are safety concerns with nimesuilide
2. Both ingredients are hepatotoxic
S.O. 721 (E)
18 Tamsulosin + diclofenac a,
Pharmacodynamically irrelevant - misuse and overuse of one of the ingredient of FDC in case it is not indicated.
S.O. 722 (E)
19 Paracetamol
+Phenylephirine
+Chlorpheniramine
+Dextromethorphan
+Caffeine
a,
1 Dosing schedule is incompatible.
2. Ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with the
reflexes.
3.Centrally acting anti-tussive not to be combined with anti-histaminic drug.
S.O. 723 (E)
20 Diclofenac +Zinc Carnosine a,
Pharmacodynamically irrelevant - misuse and overuse of one of the ingredient of FDC in case it is not indicated.
S.O. 724 (E)

21 Diclofenac + paracetamol+
chlorpheniramine maleate +
magnesium trisillicate
a,
1.Pharmacodynamic irrelevant - each ingredient has different therapeutic use and FDC will lead to misuse and
toxicity (hepato and renal).
Eccles, R., Fietze, I. and Rose, U.-B. (2014) Rationale for Treatment of Common Cold and Flu with Multi-
Ingredient Combination Products for Multi-Symptom Relief in Adults. Open Journal of Respiratory Diseases, 4,
73-82.
S.O. 725 (E)
22 Paracetamol +
pseudoephdrine + cetrizine
a,
1. Pharmacokinetic incompatibility, as dosing interval for paracetamol is TDS/QID and for cetrizine it is OD/BD.
2. No trial could be found in PUBMED and google scholar.
3. An important safety debate concerning multi- ingredient, multi-symptom relief products for common cold and
flu is that they commonly contain paracetamol (acetaminophen) and that users who may not be aware of this may
accidentally overdose when they take the multi- ingredient product with other medicines also containing
paracetamol.
Eccles, R., Fietze, I. and Rose, U.-B. (2014) Rationale for Treatment of Common Cold and Flu with Multi-
Ingredient Combination Products for Multi-Symptom Relief in Adults. Open Journal of Respiratory Diseases, 4,
73-82.
S.O. 726 (E)
23 Phenylbutazone+Sodium
Salicylate
a,
1.Safety not established and FDC has high risk of toxicity
2. There is no synergism when two drugs acting on the same enzyme are combined. Thus combining two
NSAIDs does not and cannot improve the efficacy of treatment. It only adds to the cost of therapy and more
importantly, to the adverse effects
3. Already prohibited in the country for use in human.
Chandler S. Gautam, Lekha Saha. Fixed dose drug combinations (FDCs): rational or irrational: a view point Br
J Clin Pharmacol / 65:5 / 795–796.
S.O. 727 (E)
24 Lornoxicam+Paracetamol+T
rypsin
This FDC was discussed by previous Committee on 04.06.14-
There is no scientific evidence as well as justification for use of this combination. Hence the committee did not
recommend.
S.O. 728 (E)
25 Paracetamol +Mefenamic
Acid +Ranitidine
+Dicyclomine
This FDC was discussed by previous Committee on 04.06.14-
There is no scientific evidence as well as justification for use of this combination. Hence the committee did not
recommend.
S.O. 729 (E)

26 Nimesulide + Dicyclomine a,
1.Pharmacodynamic irrelevant as each ingredient has different therapeutic use and FDC will lead to misuse and
toxicity.
2. Combining can result in elevation of the body temperature.
Chandler S. Gautam, Lekha Saha. Fixed dose drug combinations (FDCs): rational or irrational: a view point Br
J Clin Pharmacol / 65:5 / 795–796
Eccles, R., Fietze, I. and Rose, U.-B. (2014) Rationale for Treatment of Common Cold and Flu with Multi-
Ingredient Combination Products for Multi-Symptom Relief in Adults. Open Journal of Respiratory Diseases, 4,
73-82.
S.O. 730 (E)
27 Heparin +Diclofenac a,
Pharmacodynamically irrelevant-
Topical use of heparin is irrelevant.
S.O. 731 (E)
28 Glucosamine +Methyl
Sulfonyl Methane+Vitamin
D3 + Manganese + Boron+
Copper +Zinc
a,
1. Pharmacodynamic irrelevant as each ingredient has different therapeutic use.
2. therapeutic efficacy of FDC not established and will lead to misuse.
S.O. 732 (E)
29 Paracetamol +Tapentadol This FDC was discussed by previous Committee on 04.06.14-
The firm did not turn up for the presentation. The committee noted that the proposal had already been discussed
in NDAC on 17.03.2012 and the committee agreed with the recommendations of the NDAC. Hence the
committee did not recommend.
S.O. 733 (E)
30 Tranexamic Acid +
Proanthocyanidin
a,
Safety and efficacy of Proanthocyanidin in FDC is not established
S.O. 734 (E)
31 Benzoxonium
Chloride+Lidocaine
a,
Pharmacodynamic irrelevant - each ingredient has different therapeutic use and FDC will lead to misuse.
S.O. 735 (E)
32 Lornoxicam +Paracetamol
+Tramadol
This FDC was discussed by previous Committee on 04.06.14-
There is no scientific evidence as well as justification for use of this combination. Hence the committee did not
recommend.
S.O. 736 (E)
33 Lornoxicam +Paracetamol
+Serratiopeptidase
This FDC was discussed by previous Committee on 04.06.14-
There is no scientific evidence as well as justification for use of this combination. Hence the committee did not
recommend.
S.O. 737 (E)

34 Diclofenac +Paracetamol
+Magnesium trisilicate
a,
1.Pharmacodynamic irrelevant - each ingredient has different therapeutic use and FDC will lead to misuse and
toxicity (hepato and renal).
Eccles, R., Fietze, I. and Rose, U.-B. (2014) Rationale for Treatment of Common Cold and Flu with Multi-
Ingredient Combination Products for Multi-Symptom Relief in Adults. Open Journal of Respiratory Diseases, 4,
73-82.
S.O. 738 (E)
35 Paracetamol +Domperidone
+Caffeine
a,
1.Pharmacodynamic irrelevant as each ingredient has different therapeutic use and FDC will lead to misuse and
toxicity.
Chandler S. Gautam, Lekha Saha. Fixed dose drug combinations (FDCs): rational or irrational: a view point Br
J Clin Pharmacol / 65:5 / 795–796
Eccles, R., Fietze, I. and Rose, U.-B. (2014) Rationale for Treatment of Common Cold and Flu with Multi-
Ingredient Combination Products for Multi-Symptom Relief in Adults. Open Journal of Respiratory Diseases, 4,
73-82.
S.O. 739 (E)
36 Ammonium Chloride
+Sodium Citrate
+Chlorpheniramine Maleate
+Menthol
a,
1.Potential of misuse in peadiatric population.
2.Pharmaceutical incompatibility and also the dose of each ingredient is subtherapeutic.
S.O. 740 (E)
37 Paracetamol
+Prochlorperazine Maleate
a,
1. Pharmacodynamically irrelevant and subtherapeutic dose of Paracetamol.
2. Both ingredients have different indications.
S.O. 741 (E)
38 Combikit of 3 tablets of
Serratiopeptidase (enteric
coated 20000 units) +
Diclofenac Potassium & 2
tablets of Doxycycline
a,
1.It will lead to antibiotic resistance.
2. Documented efficacy of Serratiopeptidase not available.
3. May lead to misuse
4. Do not offer any particular advantage over the individual drugs. On the other hand, the patient is exposed to
greater risk of gastrointestinal (GI) irritation and serious bleeding from unsuspected peptic ulceration.
Chandler S. Gautam, Lekha Saha. Fixed dose drug combinations (FDCs): rational or irrational: a view point Br
J Clin Pharmacol / 65:5 / 795–796
S.O. 742 (E)
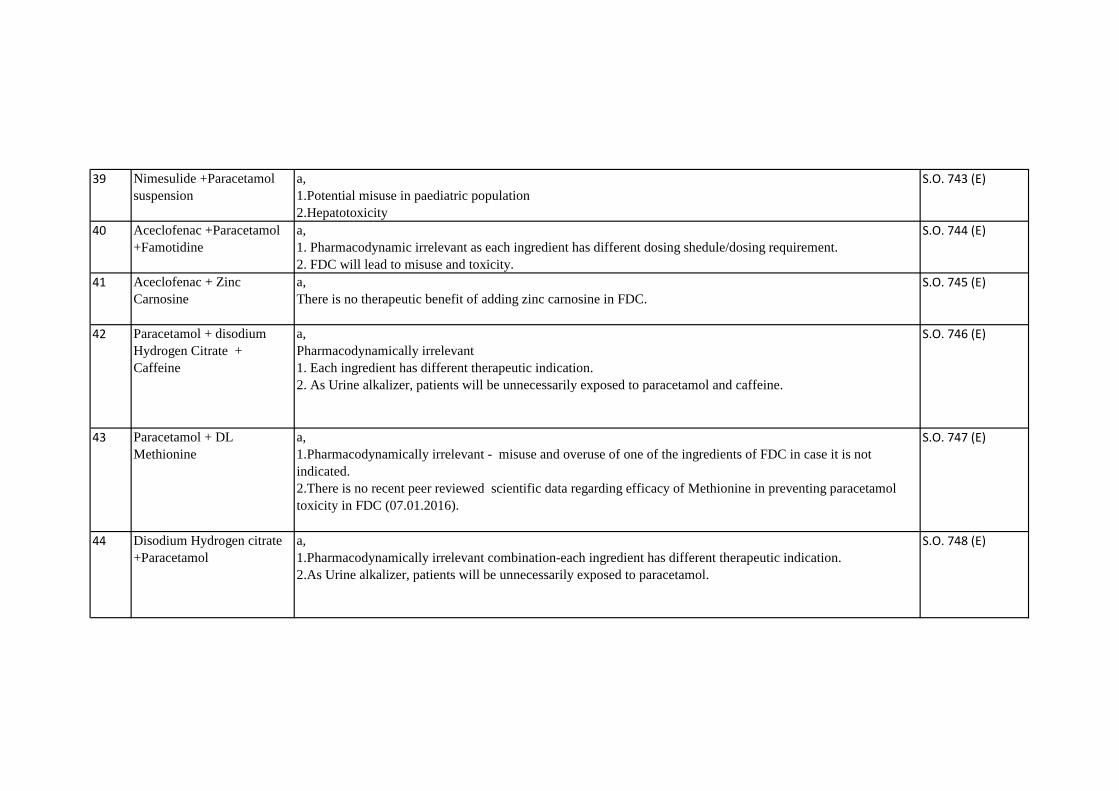
39 Nimesulide +Paracetamol
suspension
a,
1.Potential misuse in paediatric population
2.Hepatotoxicity
S.O. 743 (E)
40 Aceclofenac +Paracetamol
+Famotidine
a,
1. Pharmacodynamic irrelevant as each ingredient has different dosing shedule/dosing requirement.
2. FDC will lead to misuse and toxicity.
S.O. 744 (E)
41 Aceclofenac + Zinc
Carnosine
a,
There is no therapeutic benefit of adding zinc carnosine in FDC.
S.O. 745 (E)
42 Paracetamol + disodium
Hydrogen Citrate +
Caffeine
a,
Pharmacodynamically irrelevant
1. Each ingredient has different therapeutic indication.
2. As Urine alkalizer, patients will be unnecessarily exposed to paracetamol and caffeine.
S.O. 746 (E)
43 Paracetamol + DL
Methionine
a,
1.Pharmacodynamically irrelevant - misuse and overuse of one of the ingredients of FDC in case it is not
indicated.
2.There is no recent peer reviewed scientific data regarding efficacy of Methionine in preventing paracetamol
toxicity in FDC (07.01.2016).
S.O. 747 (E)
44 Disodium Hydrogen citrate
+Paracetamol
a,
1.Pharmacodynamically irrelevant combination-each ingredient has different therapeutic indication.
2.As Urine alkalizer, patients will be unnecessarily exposed to paracetamol.
S.O. 748 (E)

45 Paracetamol + Caffeine +
Codeine Phosphate
a,
Pharmacodynamically irrelevant.
1.Close Monitoring is required as codeine increases and caffeine decreases sedation.
2.Effect of interaction is not clear, Potential for drug-drug interaction.
3. An important safety debate concerning multi- ingredient, multi-symptom relief products for common cold and
flu is that they commonly contain paracetamol (acetaminophen) and that users who may not be aware of this may
accidentally overdose when they take the multi- ingredient product with other medicines also containing
paracetamol.
http://reference.medscape.com/drug-interactionchecker.
Eccles, R., Fietze, I. and Rose, U.-B. (2014) Rationale for Treatment of Common Cold and Flu with Multi-
Ingredient Combination Products for Multi-Symptom Relief in Adults. Open Journal of Respiratory Diseases, 4,
73-82.
S.O. 749 (E)
46 Aceclofenac (SR) +
Paracetamol
a,
1.Pharmocokinetic incompatibility-dosing shedule of aceclofenac (SR) and paracetamol are of different duration
S.O. 750 (E)
47 Diclofenac + Paracetamol
injection
a,
1.Hypersensitivity reaction with lignocaine.
2.Paracetamol dose is subtherapeutic which may increase adverse effects (07.01.2016).
S.O. 751 (E)
48 Azithromycin+Cefixime Already discussed by previous Committee on 11.06.2014 as under-
This FDC is not a standard antibiotic combination. This is not the first line combination to be used in any clinical
condition and there is no published scientific data in combining this two drugs. Also in the NDAC meeting held
on 23.08.2013, it was observed that misuse potential of this FDC is very high. Although the FDC may be useful
for certain population of patients of multi-drug resistant typhoid fever or moderate to severe lower respiratory
tract infections, the misuse potential is very high which will cause antimicrobial drug resistance. The firms did
not produce any data on pharmacokinetic and pharmacodynamic interaction as well as safety & efficacy of the
FDC. This FDC is also not approved anywhere in the world. Hence it is not recommended for approval.
S.O. 752 (E)
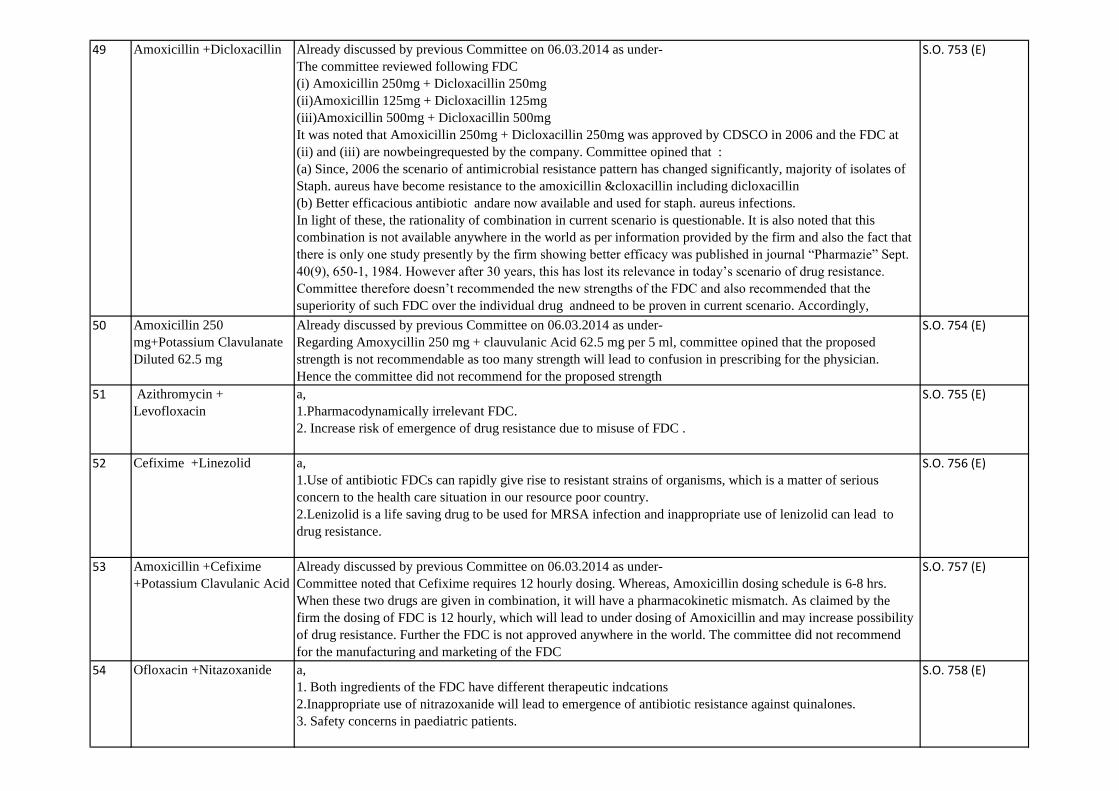
49 Amoxicillin +Dicloxacillin Already discussed by previous Committee on 06.03.2014 as under-
The committee reviewed following FDC
(i) Amoxicillin 250mg + Dicloxacillin 250mg
(ii)Amoxicillin 125mg + Dicloxacillin 125mg
(iii)Amoxicillin 500mg + Dicloxacillin 500mg
It was noted that Amoxicillin 250mg + Dicloxacillin 250mg was approved by CDSCO in 2006 and the FDC at
(ii) and (iii) are nowbeingrequested by the company. Committee opined that :
(a) Since, 2006 the scenario of antimicrobial resistance pattern has changed significantly, majority of isolates of
Staph. aureus have become resistance to the amoxicillin &cloxacillin including dicloxacillin
(b) Better efficacious antibiotic andare now available and used for staph. aureus infections.
In light of these, the rationality of combination in current scenario is questionable. It is also noted that this
combination is not available anywhere in the world as per information provided by the firm and also the fact that
there is only one study presently by the firm showing better efficacy was published in journal “Pharmazie” Sept.
40(9), 650-1, 1984. However after 30 years, this has lost its relevance in today’s scenario of drug resistance.
Committee therefore doesn’t recommended the new strengths of the FDC and also recommended that the
superiority of such FDC over the individual drug andneed to be proven in current scenario. Accordingly,
Protocol should be submitted within 3 months and data shall be generated within next one and half year. Non-
S.O. 753 (E)
50 Amoxicillin 250
mg+Potassium Clavulanate
Diluted 62.5 mg
Already discussed by previous Committee on 06.03.2014 as under-
Regarding Amoxycillin 250 mg + clauvulanic Acid 62.5 mg per 5 ml, committee opined that the proposed
strength is not recommendable as too many strength will lead to confusion in prescribing for the physician.
Hence the committee did not recommend for the proposed strength
S.O. 754 (E)
51 Azithromycin +
Levofloxacin
a,
1.Pharmacodynamically irrelevant FDC.
2. Increase risk of emergence of drug resistance due to misuse of FDC .
S.O. 755 (E)
52 Cefixime +Linezolid a,
1.Use of antibiotic FDCs can rapidly give rise to resistant strains of organisms, which is a matter of serious
concern to the health care situation in our resource poor country.
2.Lenizolid is a life saving drug to be used for MRSA infection and inappropriate use of lenizolid can lead to
drug resistance.
S.O. 756 (E)
53 Amoxicillin +Cefixime
+Potassium Clavulanic Acid
Already discussed by previous Committee on 06.03.2014 as under-
Committee noted that Cefixime requires 12 hourly dosing. Whereas, Amoxicillin dosing schedule is 6-8 hrs.
When these two drugs are given in combination, it will have a pharmacokinetic mismatch. As claimed by the
firm the dosing of FDC is 12 hourly, which will lead to under dosing of Amoxicillin and may increase possibility
of drug resistance. Further the FDC is not approved anywhere in the world. The committee did not recommend
for the manufacturing and marketing of the FDC
S.O. 757 (E)
54 Ofloxacin +Nitazoxanide a,
1. Both ingredients of the FDC have different therapeutic indcations
2.Inappropriate use of nitrazoxanide will lead to emergence of antibiotic resistance against quinalones.
3. Safety concerns in paediatric patients.
S.O. 758 (E)

55 Cefpodoxime Proxetil
+Levofloxacin
Already discussed by previous Committee on 11.06.2014 as under-
Infectious Disease Society of America (IDSA)/ American Thoracic Society (ATS) recommends the combination
of B-lactam + Macrolide for the treatment of community acquired pneumonia and cefpodoxime has been
mentioned as one of the B-lactams. However, the dosage of Azithromycin is 500 mg on day one followed by 250
mg once daily for 4 days while cefpodoxime has to be given 200 mg twice daily for 7 days. Therefore, there is a
mismatch in the dosage schedule of Cefpodoxime + Azithromycin. Although concomitant therapy of two drugs
may be required in some patients of CAP however there is no dose compatibility. It was observed that misuse
potential of this FDC is very high which will cause antimicrobial drug resistance. Hence, the FDC for CAP is not
recommended for approval.
In gonorrhea, the recommended dose is either azithromycin 1g as single dose or cefpodoxime 400 mg single
dose. Therefore the proposed FDC is not recommended for approval.
S.O. 759 (E)
56 Combikit of Azithromycin
dihydrate, secnidazole and
fluconazole
a,
1. Pharmacodynamically irrelevant due to different therapeutic indications of ingredients. FDC may Increase risk
of emergence of drug resistance.
2. Patient may require only one ingredient
3. Azithromycin and fluconazole both increase QTc interval, Potential cardiac toxicity.
http://reference.medscape.com/drug-interactionchecker.
4.The Committee reexamined the combikit of this formulation and it was opined that all the three drugs are not
used for same duration in treatment of PID, Vaginal infection.The use of azithromycin is not as per the CDC
guidelines (07.01.2016).
S.O. 760 (E)
57 Levofloxacin +Ornidazole
+Alpha Tocopherol Acetate
a,
1. Patient may need only one ingredient and the use of FDC may lead to misuse.
2. Increased risk of emergence of drug resistance due to misuse of FDC .
S.O. 761 (E)
58 Nimorazole+Ofloxacin a,
1. Patient may need only one ingredient and the use of FDC may lead to misuse.
2. Increased risk of emergence of drug resistance due to misuse of FDC .
S.O. 762 (E)
59 Azithromycin + ofloxacin a,
1.Pharmacodynamically irrelevant FDC.
2. Increased risk of emergence of drug resistance due to misuse of FDC .
S.O. 763 (E)
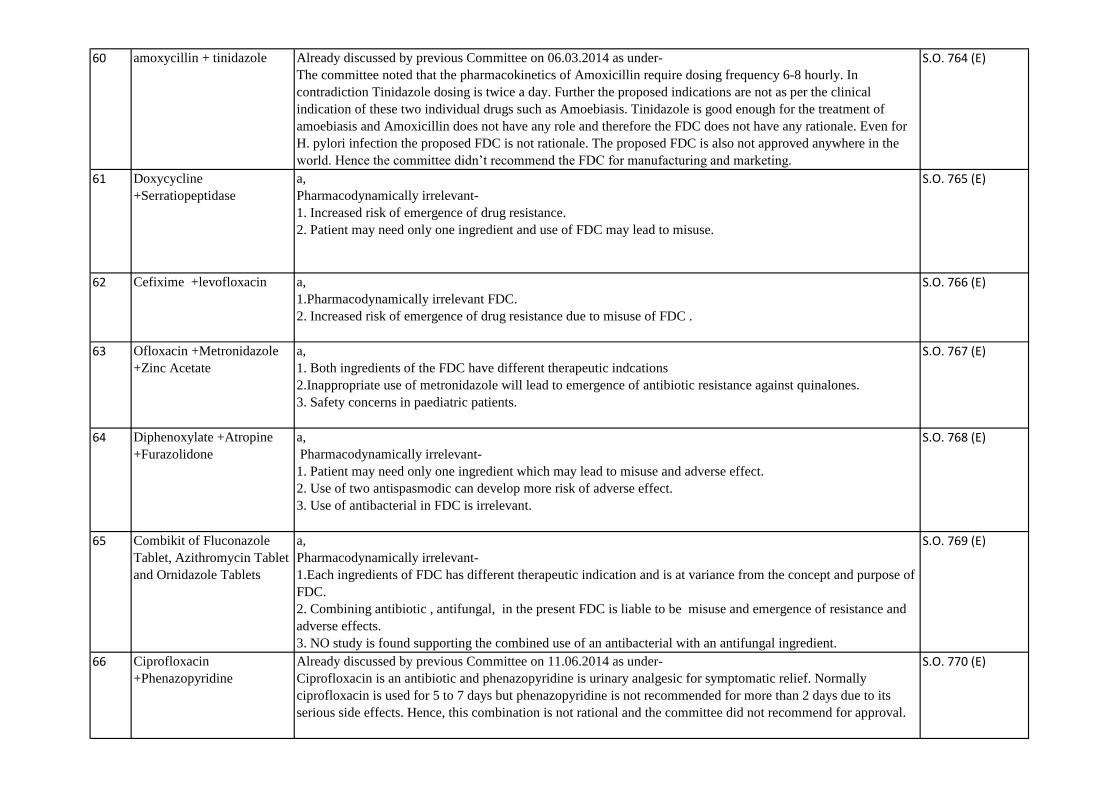
60 amoxycillin + tinidazole Already discussed by previous Committee on 06.03.2014 as under-
The committee noted that the pharmacokinetics of Amoxicillin require dosing frequency 6-8 hourly. In
contradiction Tinidazole dosing is twice a day. Further the proposed indications are not as per the clinical
indication of these two individual drugs such as Amoebiasis. Tinidazole is good enough for the treatment of
amoebiasis and Amoxicillin does not have any role and therefore the FDC does not have any rationale. Even for
H. pylori infection the proposed FDC is not rationale. The proposed FDC is also not approved anywhere in the
world. Hence the committee didn’t recommend the FDC for manufacturing and marketing.
S.O. 764 (E)
61 Doxycycline
+Serratiopeptidase
a,
Pharmacodynamically irrelevant-
1. Increased risk of emergence of drug resistance.
2. Patient may need only one ingredient and use of FDC may lead to misuse.
S.O. 765 (E)
62 Cefixime +levofloxacin a,
1.Pharmacodynamically irrelevant FDC.
2. Increased risk of emergence of drug resistance due to misuse of FDC .
S.O. 766 (E)
63 Ofloxacin +Metronidazole
+Zinc Acetate
a,
1. Both ingredients of the FDC have different therapeutic indcations
2.Inappropriate use of metronidazole will lead to emergence of antibiotic resistance against quinalones.
3. Safety concerns in paediatric patients.
S.O. 767 (E)
64 Diphenoxylate +Atropine
+Furazolidone
a,
Pharmacodynamically irrelevant-
1. Patient may need only one ingredient which may lead to misuse and adverse effect.
2. Use of two antispasmodic can develop more risk of adverse effect.
3. Use of antibacterial in FDC is irrelevant.
S.O. 768 (E)
65 Combikit of Fluconazole
Tablet, Azithromycin Tablet
and Ornidazole Tablets
a,
Pharmacodynamically irrelevant-
1.Each ingredients of FDC has different therapeutic indication and is at variance from the concept and purpose of
FDC.
2. Combining antibiotic , antifungal, in the present FDC is liable to be misuse and emergence of resistance and
adverse effects.
3. NO study is found supporting the combined use of an antibacterial with an antifungal ingredient.
S.O. 769 (E)
66 Ciprofloxacin
+Phenazopyridine
Already discussed by previous Committee on 11.06.2014 as under-
Ciprofloxacin is an antibiotic and phenazopyridine is urinary analgesic for symptomatic relief. Normally
ciprofloxacin is used for 5 to 7 days but phenazopyridine is not recommended for more than 2 days due to its
serious side effects. Hence, this combination is not rational and the committee did not recommend for approval.
S.O. 770 (E)
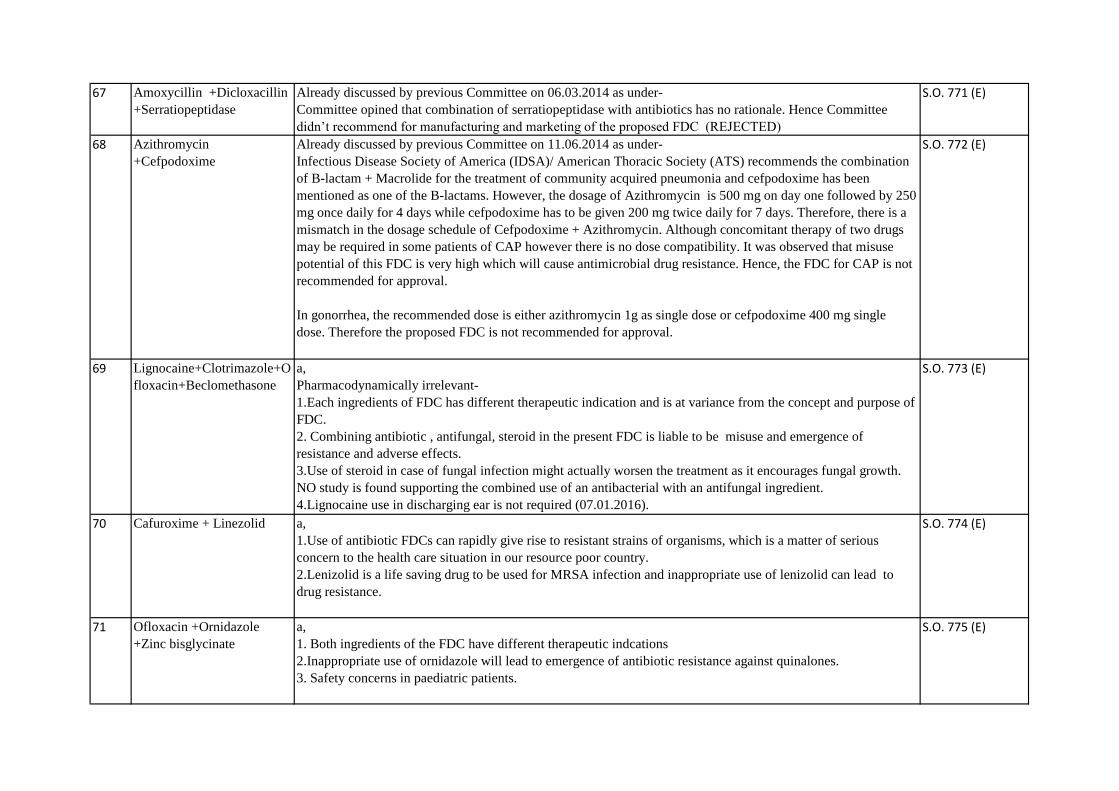
67 Amoxycillin +Dicloxacillin
+Serratiopeptidase
Already discussed by previous Committee on 06.03.2014 as under-
Committee opined that combination of serratiopeptidase with antibiotics has no rationale. Hence Committee
didn’t recommend for manufacturing and marketing of the proposed FDC (REJECTED)
S.O. 771 (E)
68 Azithromycin
+Cefpodoxime
Already discussed by previous Committee on 11.06.2014 as under-
Infectious Disease Society of America (IDSA)/ American Thoracic Society (ATS) recommends the combination
of B-lactam + Macrolide for the treatment of community acquired pneumonia and cefpodoxime has been
mentioned as one of the B-lactams. However, the dosage of Azithromycin is 500 mg on day one followed by 250
mg once daily for 4 days while cefpodoxime has to be given 200 mg twice daily for 7 days. Therefore, there is a
mismatch in the dosage schedule of Cefpodoxime + Azithromycin. Although concomitant therapy of two drugs
may be required in some patients of CAP however there is no dose compatibility. It was observed that misuse
potential of this FDC is very high which will cause antimicrobial drug resistance. Hence, the FDC for CAP is not
recommended for approval.
In gonorrhea, the recommended dose is either azithromycin 1g as single dose or cefpodoxime 400 mg single
dose. Therefore the proposed FDC is not recommended for approval.
S.O. 772 (E)
69 Lignocaine+Clotrimazole+O
floxacin+Beclomethasone
a,
Pharmacodynamically irrelevant-
1.Each ingredients of FDC has different therapeutic indication and is at variance from the concept and purpose of
FDC.
2. Combining antibiotic , antifungal, steroid in the present FDC is liable to be misuse and emergence of
resistance and adverse effects.
3.Use of steroid in case of fungal infection might actually worsen the treatment as it encourages fungal growth.
NO study is found supporting the combined use of an antibacterial with an antifungal ingredient.
4.Lignocaine use in discharging ear is not required (07.01.2016).
S.O. 773 (E)
70 Cafuroxime + Linezolid a,
1.Use of antibiotic FDCs can rapidly give rise to resistant strains of organisms, which is a matter of serious
concern to the health care situation in our resource poor country.
2.Lenizolid is a life saving drug to be used for MRSA infection and inappropriate use of lenizolid can lead to
drug resistance.
S.O. 774 (E)
71 Ofloxacin +Ornidazole
+Zinc bisglycinate
a,
1. Both ingredients of the FDC have different therapeutic indcations
2.Inappropriate use of ornidazole will lead to emergence of antibiotic resistance against quinalones.
3. Safety concerns in paediatric patients.
S.O. 775 (E)
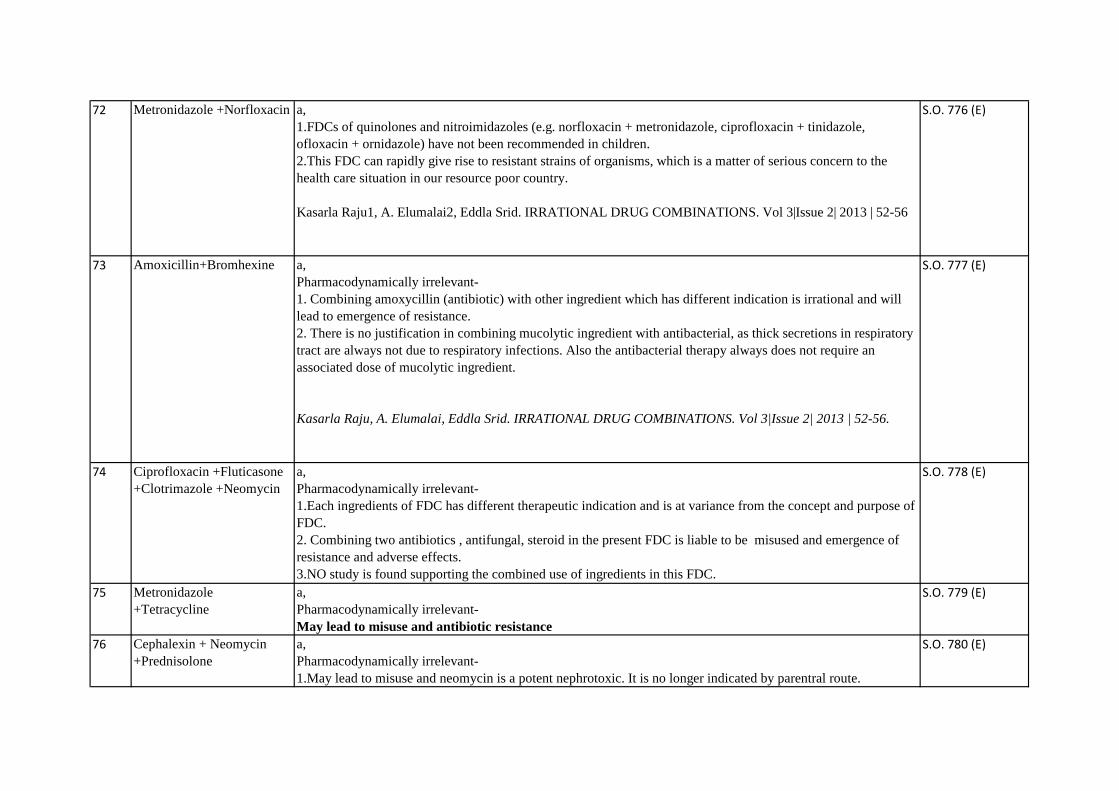
72 Metronidazole +Norfloxacin a,
1.FDCs of quinolones and nitroimidazoles (e.g. norfloxacin + metronidazole, ciprofloxacin + tinidazole,
ofloxacin + ornidazole) have not been recommended in children.
2.This FDC can rapidly give rise to resistant strains of organisms, which is a matter of serious concern to the
health care situation in our resource poor country.
Kasarla Raju1, A. Elumalai2, Eddla Srid. IRRATIONAL DRUG COMBINATIONS. Vol 3|Issue 2| 2013 | 52-56
S.O. 776 (E)
73 Amoxicillin+Bromhexine a,
Pharmacodynamically irrelevant-
1. Combining amoxycillin (antibiotic) with other ingredient which has different indication is irrational and will
lead to emergence of resistance.
2. There is no justification in combining mucolytic ingredient with antibacterial, as thick secretions in respiratory
tract are always not due to respiratory infections. Also the antibacterial therapy always does not require an
associated dose of mucolytic ingredient.
Kasarla Raju, A. Elumalai, Eddla Srid. IRRATIONAL DRUG COMBINATIONS. Vol 3|Issue 2| 2013 | 52-56.
S.O. 777 (E)
74 Ciprofloxacin +Fluticasone
+Clotrimazole +Neomycin
a,
Pharmacodynamically irrelevant-
1.Each ingredients of FDC has different therapeutic indication and is at variance from the concept and purpose of
FDC.
2. Combining two antibiotics , antifungal, steroid in the present FDC is liable to be misused and emergence of
resistance and adverse effects.
3.NO study is found supporting the combined use of ingredients in this FDC.
S.O. 778 (E)
75 Metronidazole
+Tetracycline
a,
Pharmacodynamically irrelevant-
May lead to misuse and antibiotic resistance
S.O. 779 (E)
76 Cephalexin + Neomycin
+Prednisolone
a,
Pharmacodynamically irrelevant-
1.May lead to misuse and neomycin is a potent nephrotoxic. It is no longer indicated by parentral route.
S.O. 780 (E)
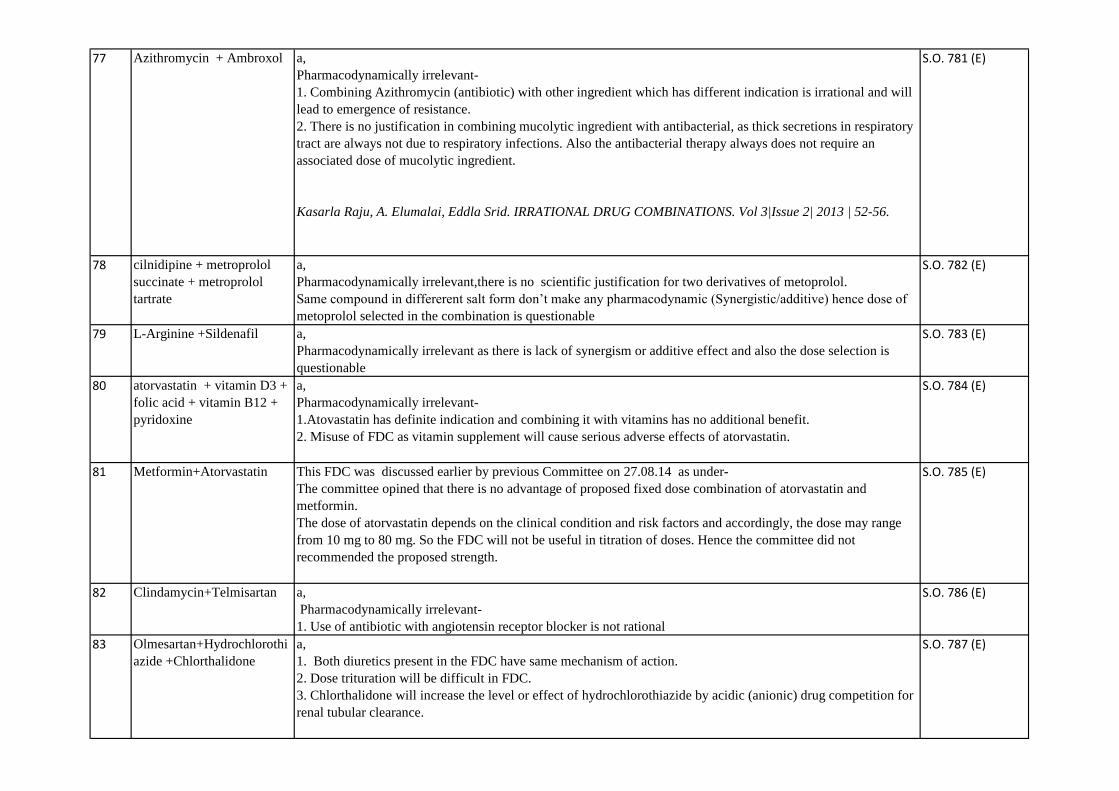
77 Azithromycin + Ambroxol a,
Pharmacodynamically irrelevant-
1. Combining Azithromycin (antibiotic) with other ingredient which has different indication is irrational and will
lead to emergence of resistance.
2. There is no justification in combining mucolytic ingredient with antibacterial, as thick secretions in respiratory
tract are always not due to respiratory infections. Also the antibacterial therapy always does not require an
associated dose of mucolytic ingredient.
Kasarla Raju, A. Elumalai, Eddla Srid. IRRATIONAL DRUG COMBINATIONS. Vol 3|Issue 2| 2013 | 52-56.
S.O. 781 (E)
78 cilnidipine + metroprolol
succinate + metroprolol
tartrate
a,
Pharmacodynamically irrelevant,there is no scientific justification for two derivatives of metoprolol.
Same compound in differerent salt form don’t make any pharmacodynamic (Synergistic/additive) hence dose of
metoprolol selected in the combination is questionable
S.O. 782 (E)
79 L-Arginine +Sildenafil a,
Pharmacodynamically irrelevant as there is lack of synergism or additive effect and also the dose selection is
questionable
S.O. 783 (E)
80 atorvastatin + vitamin D3 +
folic acid + vitamin B12 +
pyridoxine
a,
Pharmacodynamically irrelevant-
1.Atovastatin has definite indication and combining it with vitamins has no additional benefit.
2. Misuse of FDC as vitamin supplement will cause serious adverse effects of atorvastatin.
S.O. 784 (E)
81 Metformin+Atorvastatin This FDC was discussed earlier by previous Committee on 27.08.14 as under-
The committee opined that there is no advantage of proposed fixed dose combination of atorvastatin and
metformin.
The dose of atorvastatin depends on the clinical condition and risk factors and accordingly, the dose may range
from 10 mg to 80 mg. So the FDC will not be useful in titration of doses. Hence the committee did not
recommended the proposed strength.
S.O. 785 (E)
82 Clindamycin+Telmisartan a,
Pharmacodynamically irrelevant-
1. Use of antibiotic with angiotensin receptor blocker is not rational
S.O. 786 (E)
83 Olmesartan+Hydrochlorothi
azide +Chlorthalidone
a,
1. Both diuretics present in the FDC have same mechanism of action.
2. Dose trituration will be difficult in FDC.
3. Chlorthalidone will increase the level or effect of hydrochlorothiazide by acidic (anionic) drug competition for
renal tubular clearance.
S.O. 787 (E)

84 L-5-Methylterahydrofolate
calcium + Escitalopram
a,
Pharmacodynamically irrelevant-
1. No supporting published literature available on the combination.
2. Both ingredients have different indications.
S.O. 788 (E)
85 pholcodine +Promethazine a,
1 Dosing schedule is incompatible.
2. Ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with the
reflexes.
3.Centrally acting anti-tussive not to be combined with anti-histaminic drug.
S.O. 789 (E)
86 Paracetamol +Promethazine a,
1. Pharmacodynamically irrelevant.
2. Both ingredients have different indications.
S.O. 790 (E)
87 Betahistine +Ginkgo Biloba
Extract+Vinpocetine+Pirace
tam
a,
Pharmacodynamic irrelevant - each ingredient has different therapeutic use and FDC will lead to misuse.
S.O. 791 (E)
88 Cetirizine Dihydrochloride
+Diethyl Carbamazine
a,
1. Patient may need only one ingredient and use of FDC may lead to misuse.
S.O. 792 (E)
89 Doxylamine +Pyridoxine
+Mefenamic
Acid+Paracetamol
a,
Pharmacodynamically irrelevant-
1. No published literature supporting the FDC.
2. Users who may not be aware of this mefanamic acid content and may accidentally overdose when they take the
multi- ingredient product with other medicines also containing paracetamol.
3. If misused for morning sickness, it is teratogenic.
Eccles, R., Fietze, I. and Rose, U.-B. (2014) Rationale for Treatment of Common Cold and Flu with Multi-
Ingredient Combination Products for Multi-Symptom Relief in Adults. Open Journal of Respiratory Diseases, 4,
73-82.
S.O. 793 (E)
90 Drotaverine + Clidinium
+ Chlordiazepoxide
This FDC was earlier discussed by previous Committee on 05.09.2014 as under-
There is no scientific evidence as well as justification for use of this combination. Hence the committee did not
recommend.
S.O. 794 (E)

91 Imipramine + Diazepam a,
Pharmacodynamically irrelevant-
1. Diazepam and imipramine both increase sedation.
2. Potential for interaction.
http://reference.medscape.com/drug-interactionchecker.
S.O. 795 (E)
92 Flupentixol +Escitalopram a,
Pharmacodynamically irrelevant-
1. No supporting published literature for this FDC.
2. The combination will aggravate the adverse effects.
S.O. 796 (E)
93 Paracetamol +
Prochloperazine
a,
1. Pharmacodynamically irrelevant.
2. Both ingredients have different indications.
S.O. 797 (E)
94 Gabapentin +Mecobalamin
+Pyridoxine +Thiamine
a,
Pharmacodynamically irrelevant-
gabapentin decreases levels of cyanocobalamin by inhibition of GI absorption.
http://reference.medscape.com/drug-interactionchecker.
S.O. 798 (E)
95 Imipramine
+Chlordiazepoxide
+Trifluoperazine
+Trihexyphenidyl
a,
Pharmacodynamically irrelevant-
1.Trifluoperazine and imipramine both increase QTc interval.
2. High likelihood serious or life-threatening interaction.
3.Trihexyphenidyl and imipramine both decrease cholinergic effects/transmission.
4.chlordiazepoxide and trifluoperazine both increase sedation.
5.Trihexyphenidyl decreases levels of trifluoperazine by pharmacodynamic antagonism.
http://reference.medscape.com/drug-interactionchecker.
S.O. 799 (E)
96 Chlorpromazine
+Trihexyphenidyl
a, Pharmacodynamically irrelevant-
1.In current scenerio chlorpromazine is not a drug of choice for the treatment of depression.
2. dose adjustment of Trihexyphenidyl to counteract the adverse effect of chlorpromazine is not possible in FDC
formulation
3.There is a risk of potential abuse
S.O. 800 (E)
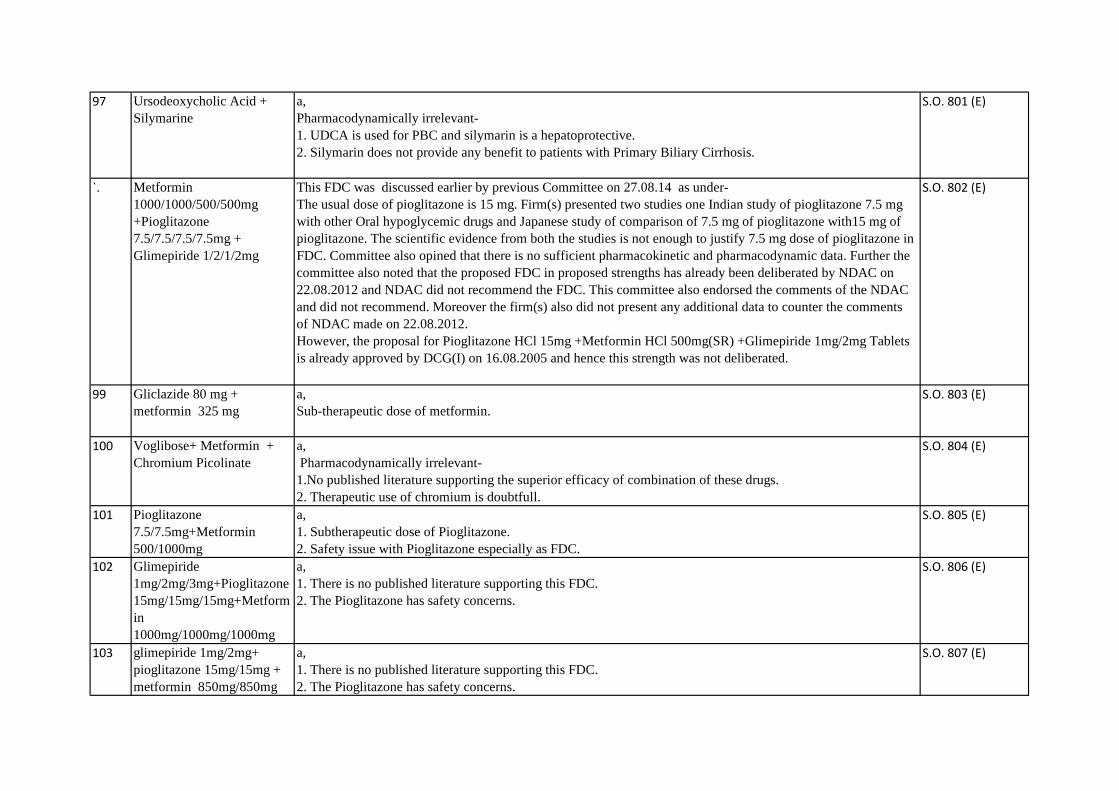
97 Ursodeoxycholic Acid +
Silymarine
a,
Pharmacodynamically irrelevant-
1. UDCA is used for PBC and silymarin is a hepatoprotective.
2. Silymarin does not provide any benefit to patients with Primary Biliary Cirrhosis.
S.O. 801 (E)
`. Metformin
1000/1000/500/500mg
+Pioglitazone
7.5/7.5/7.5/7.5mg +
Glimepiride 1/2/1/2mg
This FDC was discussed earlier by previous Committee on 27.08.14 as under-
The usual dose of pioglitazone is 15 mg. Firm(s) presented two studies one Indian study of pioglitazone 7.5 mg
with other Oral hypoglycemic drugs and Japanese study of comparison of 7.5 mg of pioglitazone with15 mg of
pioglitazone. The scientific evidence from both the studies is not enough to justify 7.5 mg dose of pioglitazone in
FDC. Committee also opined that there is no sufficient pharmacokinetic and pharmacodynamic data. Further the
committee also noted that the proposed FDC in proposed strengths has already been deliberated by NDAC on
22.08.2012 and NDAC did not recommend the FDC. This committee also endorsed the comments of the NDAC
and did not recommend. Moreover the firm(s) also did not present any additional data to counter the comments
of NDAC made on 22.08.2012.
However, the proposal for Pioglitazone HCl 15mg +Metformin HCl 500mg(SR) +Glimepiride 1mg/2mg Tablets
is already approved by DCG(I) on 16.08.2005 and hence this strength was not deliberated.
S.O. 802 (E)
99 Gliclazide 80 mg +
metformin 325 mg
a,
Sub-therapeutic dose of metformin.
S.O. 803 (E)
100 Voglibose+ Metformin +
Chromium Picolinate
a,
Pharmacodynamically irrelevant-
1.No published literature supporting the superior efficacy of combination of these drugs.
2. Therapeutic use of chromium is doubtfull.
S.O. 804 (E)
101 Pioglitazone
7.5/7.5mg+Metformin
500/1000mg
a,
1. Subtherapeutic dose of Pioglitazone.
2. Safety issue with Pioglitazone especially as FDC.
S.O. 805 (E)
102 Glimepiride
1mg/2mg/3mg+Pioglitazone
15mg/15mg/15mg+Metform
in
1000mg/1000mg/1000mg
a,
1. There is no published literature supporting this FDC.
2. The Pioglitazone has safety concerns.
S.O. 806 (E)
103 glimepiride 1mg/2mg+
pioglitazone 15mg/15mg +
metformin 850mg/850mg
a,
1. There is no published literature supporting this FDC.
2. The Pioglitazone has safety concerns.
S.O. 807 (E)

104 Metformin
850mg+Pioglitazone 7.5
mg+Glimepiride 2mg
This FDC was discussed earlier by previous Committee on 27.08.14 as under-
The usual dose of pioglitazone is 15 mg. Firm(s) presented two studies one Indian study of pioglitazone 7.5 mg
with other Oral hypoglycemic drugs and Japanese study of comparison of 7.5 mg of pioglitazone with15 mg of
pioglitazone. The scientific evidence from both the studies is not enough to justify 7.5 mg dose of pioglitazone in
FDC. Committee also opined that there is no sufficient pharmacokinetic and pharmacodynamic data. Further the
committee also noted that the proposed FDC in proposed strengths has already been deliberated by NDAC on
22.08.2012 and NDAC did not recommend the FDC. This committee also endorsed the comments of the NDAC
and did not recommend. Moreover the firm(s) also did not present any additional data to counter the comments
of NDAC made on 22.08.2012.
However, the proposal for Pioglitazone HCl 15mg +Metformin HCl 500mg(SR) +Glimepiride 1mg/2mg Tablets
is already approved by DCG(I) on 16.08.2005 and hence this strength was not deliberated.
S.O. 808 (E)
105 Metformin
850mg+Pioglitazone 7.5
mg+Glimepiride 1mg
This FDC was discussed earlier by previous Committee on 27.08.14 as under-
The usual dose of pioglitazone is 15 mg. Firm(s) presented two studies one Indian study of pioglitazone 7.5 mg
with other Oral hypoglycemic drugs and Japanese study of comparison of 7.5 mg of pioglitazone with15 mg of
pioglitazone. The scientific evidence from both the studies is not enough to justify 7.5 mg dose of pioglitazone in
FDC. Committee also opined that there is no sufficient pharmacokinetic and pharmacodynamic data. Further the
committee also noted that the proposed FDC in proposed strengths has already been deliberated by NDAC on
22.08.2012 and NDAC did not recommend the FDC. This committee also endorsed the comments of the NDAC
and did not recommend. Moreover the firm(s) also did not present any additional data to counter the comments
of NDAC made on 22.08.2012.
However, the proposal for Pioglitazone HCl 15mg +Metformin HCl 500mg(SR) +Glimepiride 1mg/2mg Tablets
is already approved by DCG(I) on 16.08.2005 and hence this strength was not deliberated.
S.O. 809 (E)
106 Metformin
500mg/500mg+Gliclazide
SR
30mg/60mg+Pioglitazone
7.5mg/7.5mg
a,
Pharmacodynamically irrelevant-
1. Subtherapeutic dose of Pioglitazone.
2. Pioglitazone has safety concerns.
S.O. 810 (E)
107 Voglibose+Pioglitazone+Me
tformin
a,
Pharmacodynamically irrelevant-
1. Subtherapeutic dose of pioglitazone.
2. Safety concerns of pioglitazone.
3. No published literature supporting this FDC.
S.O. 811 (E)
108 Metformin +bromocriptine a,
Pharmacodynamically irrelevant-
1. No published literature supporting the use of combination.
2. Both ingredients have different indication.
S.O. 812 (E)
109 Metformin +Glimepiride
+Methylcobalamin
a,
Pharmacodynamically irrelevant-
1. No published literature supporting the superior efficacy of combination of three drugs.
2. Use of methylcobalamine as prophylaxis in FDC is not documented.
S.O. 813 (E)
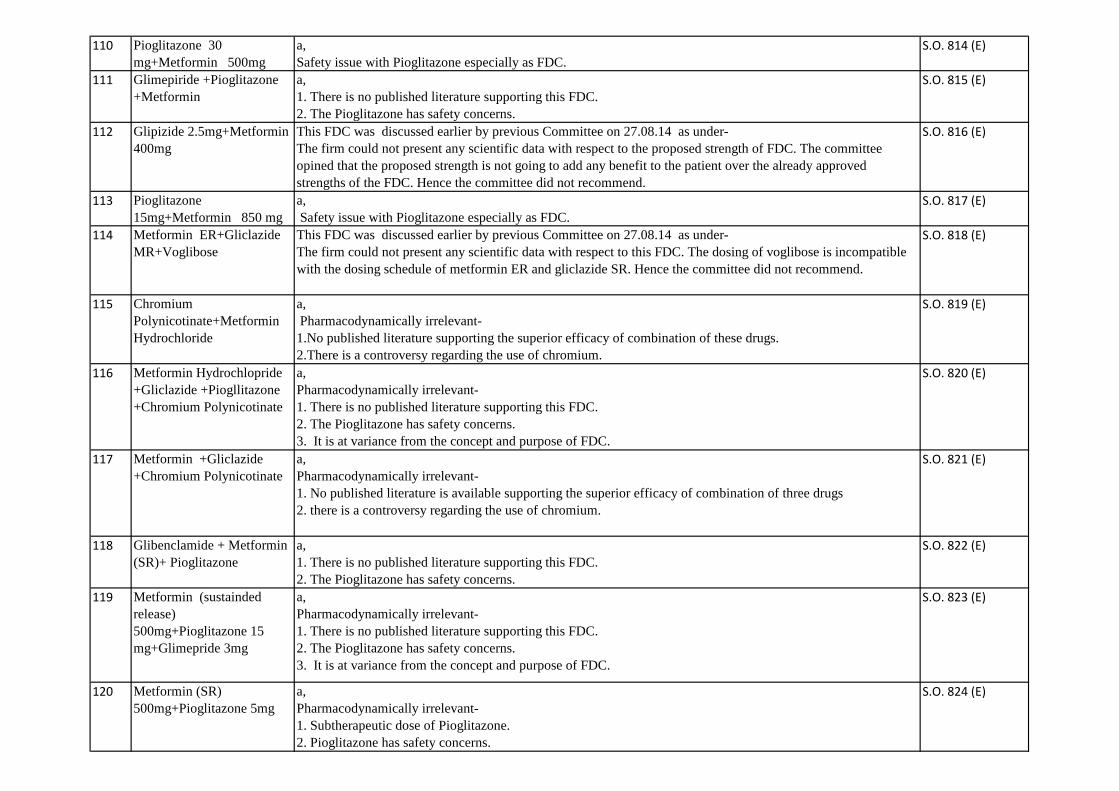
110 Pioglitazone 30
mg+Metformin 500mg
a,
Safety issue with Pioglitazone especially as FDC.
S.O. 814 (E)
111 Glimepiride +Pioglitazone
+Metformin
a,
1. There is no published literature supporting this FDC.
2. The Pioglitazone has safety concerns.
S.O. 815 (E)
112 Glipizide 2.5mg+Metformin
400mg
This FDC was discussed earlier by previous Committee on 27.08.14 as under-
The firm could not present any scientific data with respect to the proposed strength of FDC. The committee
opined that the proposed strength is not going to add any benefit to the patient over the already approved
strengths of the FDC. Hence the committee did not recommend.
S.O. 816 (E)
113 Pioglitazone
15mg+Metformin 850 mg
a,
Safety issue with Pioglitazone especially as FDC.
S.O. 817 (E)
114 Metformin ER+Gliclazide
MR+Voglibose
This FDC was discussed earlier by previous Committee on 27.08.14 as under-
The firm could not present any scientific data with respect to this FDC. The dosing of voglibose is incompatible
with the dosing schedule of metformin ER and gliclazide SR. Hence the committee did not recommend.
S.O. 818 (E)
115 Chromium
Polynicotinate+Metformin
Hydrochloride
a,
Pharmacodynamically irrelevant-
1.No published literature supporting the superior efficacy of combination of these drugs.
2.There is a controversy regarding the use of chromium.
S.O. 819 (E)
116 Metformin Hydrochlopride
+Gliclazide +Piogllitazone
+Chromium Polynicotinate
a,
Pharmacodynamically irrelevant-
1. There is no published literature supporting this FDC.
2. The Pioglitazone has safety concerns.
3. It is at variance from the concept and purpose of FDC.
S.O. 820 (E)
117 Metformin +Gliclazide
+Chromium Polynicotinate
a,
Pharmacodynamically irrelevant-
1. No published literature is available supporting the superior efficacy of combination of three drugs
2. there is a controversy regarding the use of chromium.
S.O. 821 (E)
118 Glibenclamide + Metformin
(SR)+ Pioglitazone
a,
1. There is no published literature supporting this FDC.
2. The Pioglitazone has safety concerns.
S.O. 822 (E)
119 Metformin (sustainded
release)
500mg+Pioglitazone 15
mg+Glimepride 3mg
a,
Pharmacodynamically irrelevant-
1. There is no published literature supporting this FDC.
2. The Pioglitazone has safety concerns.
3. It is at variance from the concept and purpose of FDC.
S.O. 823 (E)
120 Metformin (SR)
500mg+Pioglitazone 5mg
a,
Pharmacodynamically irrelevant-
1. Subtherapeutic dose of Pioglitazone.
2. Pioglitazone has safety concerns.
S.O. 824 (E)
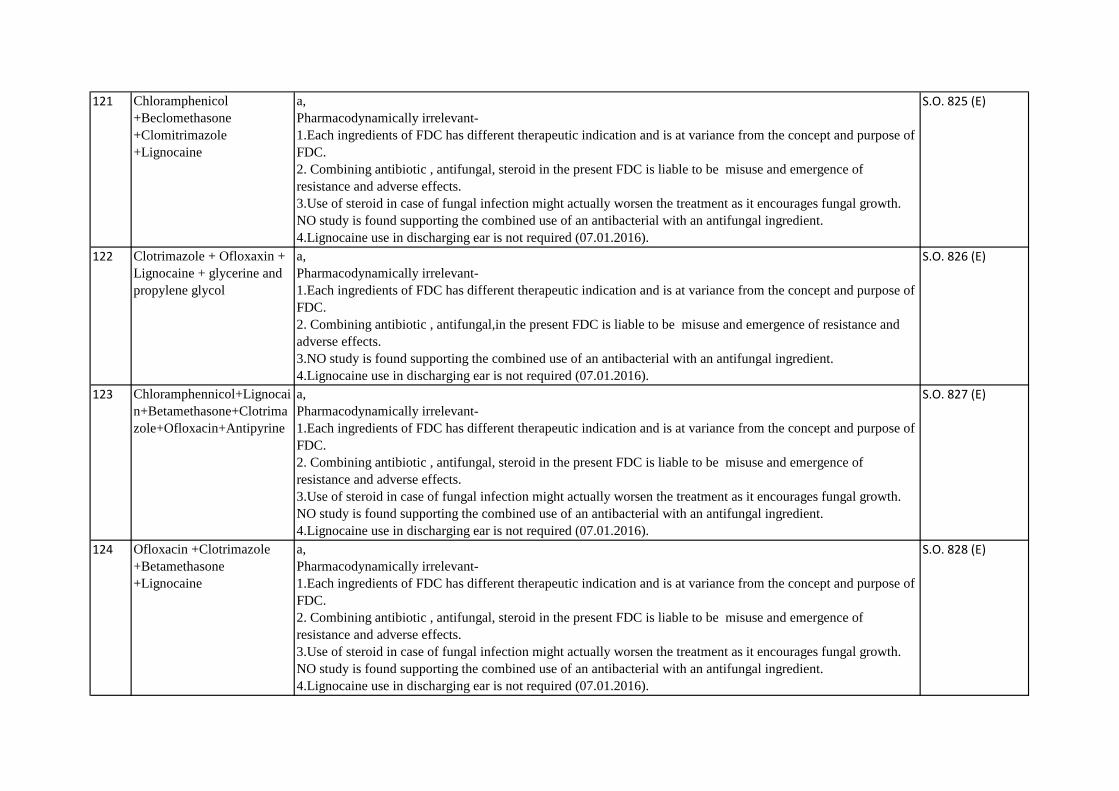
121 Chloramphenicol
+Beclomethasone
+Clomitrimazole
+Lignocaine
a,
Pharmacodynamically irrelevant-
1.Each ingredients of FDC has different therapeutic indication and is at variance from the concept and purpose of
FDC.
2. Combining antibiotic , antifungal, steroid in the present FDC is liable to be misuse and emergence of
resistance and adverse effects.
3.Use of steroid in case of fungal infection might actually worsen the treatment as it encourages fungal growth.
NO study is found supporting the combined use of an antibacterial with an antifungal ingredient.
4.Lignocaine use in discharging ear is not required (07.01.2016).
S.O. 825 (E)
122 Clotrimazole + Ofloxaxin +
Lignocaine + glycerine and
propylene glycol
a,
Pharmacodynamically irrelevant-
1.Each ingredients of FDC has different therapeutic indication and is at variance from the concept and purpose of
FDC.
2. Combining antibiotic , antifungal,in the present FDC is liable to be misuse and emergence of resistance and
adverse effects.
3.NO study is found supporting the combined use of an antibacterial with an antifungal ingredient.
4.Lignocaine use in discharging ear is not required (07.01.2016).
S.O. 826 (E)
123 Chloramphennicol+Lignocai
n+Betamethasone+Clotrima
zole+Ofloxacin+Antipyrine
a,
Pharmacodynamically irrelevant-
1.Each ingredients of FDC has different therapeutic indication and is at variance from the concept and purpose of
FDC.
2. Combining antibiotic , antifungal, steroid in the present FDC is liable to be misuse and emergence of
resistance and adverse effects.
3.Use of steroid in case of fungal infection might actually worsen the treatment as it encourages fungal growth.
NO study is found supporting the combined use of an antibacterial with an antifungal ingredient.
4.Lignocaine use in discharging ear is not required (07.01.2016).
S.O. 827 (E)
124 Ofloxacin +Clotrimazole
+Betamethasone
+Lignocaine
a,
Pharmacodynamically irrelevant-
1.Each ingredients of FDC has different therapeutic indication and is at variance from the concept and purpose of
FDC.
2. Combining antibiotic , antifungal, steroid in the present FDC is liable to be misuse and emergence of
resistance and adverse effects.
3.Use of steroid in case of fungal infection might actually worsen the treatment as it encourages fungal growth.
NO study is found supporting the combined use of an antibacterial with an antifungal ingredient.
4.Lignocaine use in discharging ear is not required (07.01.2016).
S.O. 828 (E)

125 Gentamicin Sulphate
+Clotrimazole
+Betamethasone
+Lignocaine
a,
Pharmacodynamically irrelevant-
1.Each ingredients of FDC has different therapeutic indication and is at variance from the concept and purpose of
FDC.
2. Combining antibiotic , antifungal, steroid in the present FDC is liable to be misuse and emergence of
resistance and adverse effects.
3.Use of steroid in case of fungal infection might actually worsen the treatment as it encourages fungal growth.
NO study is found supporting the combined use of an antibacterial with an antifungal ingredient.
4.Lignocaine use in discharging ear is not required (07.01.2016).
S.O. 829 (E)
126 Clotrimazole
+Beclomethasone
+Ofloxacin +Lignocaine
a,
Pharmacodynamically irrelevant-
1.Each ingredients of FDC has different therapeutic indication and is at variance from the concept and purpose of
FDC.
2. Combining antibiotic , antifungal, steroid in the present FDC is liable to be misuse and emergence of
resistance and adverse effects.
3.Use of steroid in case of fungal infection might actually worsen the treatment as it encourages fungal growth.
NO study is found supporting the combined use of an antibacterial with an antifungal ingredient.
4.Lignocaine use in discharging ear is not required (07.01.2016).
S.O. 830 (E)
127 Becloemthasone
+Clotrimazole+Chloramphe
nicol+Gentamycin
+Lignocaine Ear drops
a,
Pharmacodynamically irrelevant-
1.Each ingredients of FDC has different therapeutic indication and is at variance from the concept and purpose of
FDC.
2. Combining antibiotic , antifungal, steroid in the present FDC is liable to be misuse and emergence of
resistance and adverse effects.
3.Use of steroid in case of fungal infection might actually worsen the treatment as it encourages fungal growth.
NO study is found supporting the combined use of an antibacterial with an antifungal ingredient.
4.Lignocaine use in discharging ear is not required (07.01.2016).
S.O. 831 (E)
128 Flunarizine +
Paracetamole+
Domperidone
a,
Pharmacodynamically irrelevant-
1. Indication for each drug is different.
2. There is no common condition in which all three drugs are useful.
3. In case of migraine, flunarizine is used for prophylaxis, whereas paracetamol and domperidone are used for
acute attack treatment.
S.O. 832 (E)
129 Rabeprazole +Zinc
carnosine
a,
Pharmacodynamically irrelevant-
1.No published literature supporting the FDC.
2.Potential for adverse effects.
S.O. 833 (E)
130 magaldrate + famotidine +
simethicone
a,
Pharmacodynamically irrelevant-
1. Subtherapeutic dose of Famotidine.
2. No evidence of efficacy exists supporting the use of triple drug combination.
S.O. 834 (E)
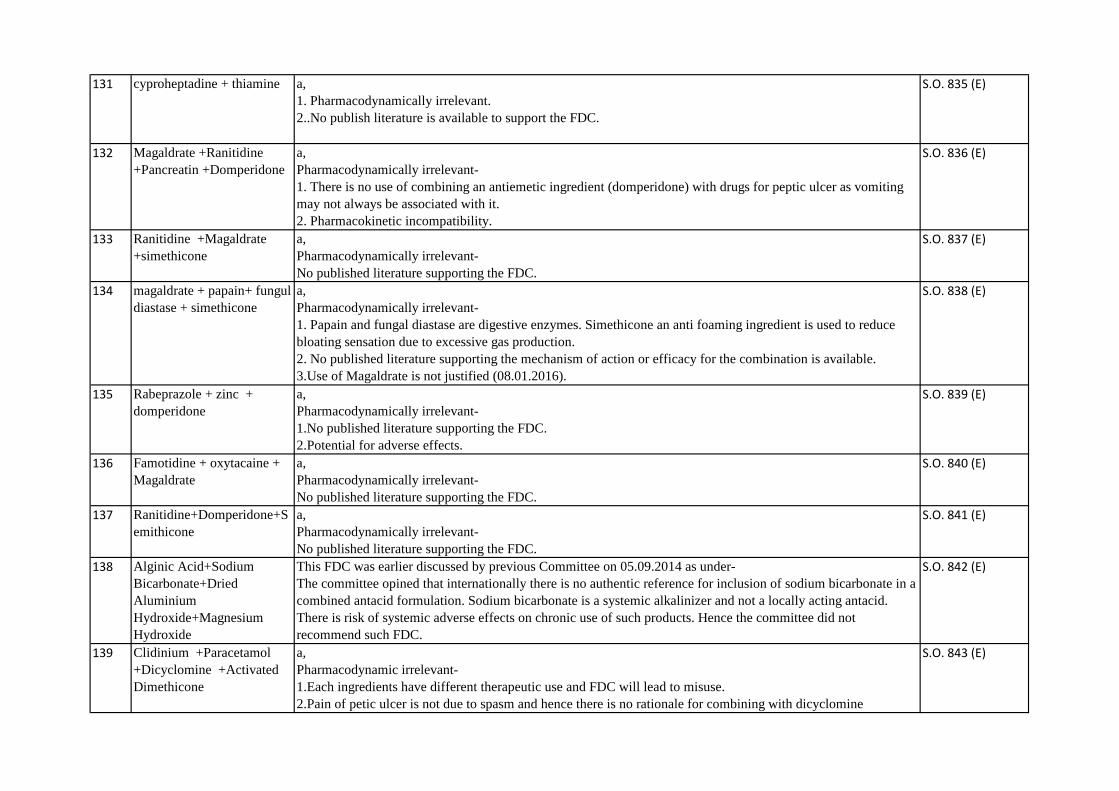
131 cyproheptadine + thiamine a,
1. Pharmacodynamically irrelevant.
2..No publish literature is available to support the FDC.
S.O. 835 (E)
132 Magaldrate +Ranitidine
+Pancreatin +Domperidone
a,
Pharmacodynamically irrelevant-
1. There is no use of combining an antiemetic ingredient (domperidone) with drugs for peptic ulcer as vomiting
may not always be associated with it.
2. Pharmacokinetic incompatibility.
S.O. 836 (E)
133 Ranitidine +Magaldrate
+simethicone
a,
Pharmacodynamically irrelevant-
No published literature supporting the FDC.
S.O. 837 (E)
134 magaldrate + papain+ fungul
diastase + simethicone
a,
Pharmacodynamically irrelevant-
1. Papain and fungal diastase are digestive enzymes. Simethicone an anti foaming ingredient is used to reduce
bloating sensation due to excessive gas production.
2. No published literature supporting the mechanism of action or efficacy for the combination is available.
3.Use of Magaldrate is not justified (08.01.2016).
S.O. 838 (E)
135 Rabeprazole + zinc +
domperidone
a,
Pharmacodynamically irrelevant-
1.No published literature supporting the FDC.
2.Potential for adverse effects.
S.O. 839 (E)
136 Famotidine + oxytacaine +
Magaldrate
a,
Pharmacodynamically irrelevant-
No published literature supporting the FDC.
S.O. 840 (E)
137 Ranitidine+Domperidone+S
emithicone
a,
Pharmacodynamically irrelevant-
No published literature supporting the FDC.
S.O. 841 (E)
138 Alginic Acid+Sodium
Bicarbonate+Dried
Aluminium
Hydroxide+Magnesium
Hydroxide
This FDC was earlier discussed by previous Committee on 05.09.2014 as under-
The committee opined that internationally there is no authentic reference for inclusion of sodium bicarbonate in a
combined antacid formulation. Sodium bicarbonate is a systemic alkalinizer and not a locally acting antacid.
There is risk of systemic adverse effects on chronic use of such products. Hence the committee did not
recommend such FDC.
S.O. 842 (E)
139 Clidinium +Paracetamol
+Dicyclomine +Activated
Dimethicone
a,
Pharmacodynamic irrelevant-
1.Each ingredients have different therapeutic use and FDC will lead to misuse.
2.Pain of petic ulcer is not due to spasm and hence there is no rationale for combining with dicyclomine
S.O. 843 (E)

140 Furazolidone
+Metronidazole
+Loperamide
a,
Pharmacodynamically irrelevant-
1.antimotility drug will cause toxic megacolon in infective diarrhoea.
2. Loperamide is contra-indicated in infective diarrhea and in patients with bacterial enterocolitis caused by
invasive organisms including Salmonella, Shigella, and Campylobacter as it reduces the clearance of pathogens.
Hence there is no rationale for combining with antibiotic in an FDC.
3. In bacterial diarrhoea only anti-bacterial drug is effective and antiamoebic drug is useless. Similarly, in
intestinal amoebiasis only antiamoebic drug is effective while antibacterial drug is useless.
4.Amoebiasis and bacterial diarrhoea rarely coexist.
5. Only one drug of the combination would be effective and the other one would be useless.
S.O. 844 (E)
141 Rabeprazole +Diclofenac
+Paracetamol
a,
1.Pharmacokinetic/Pharmacodynamic incompatibility.
2.Subtherapeutic dose of rabeprazole.
3.No published literature support combination of rabeprazole with diclofenac and paracetamol.
S.O. 845 (E)
142 Ranitidine +Magaldrate a,
Pharmacodynamically irrelevant-
No published literature supporting the FDC.
S.O. 846 (E)
143 Norfloxacin+ Metronidazole
+ zinc Acetate
a,
1.FDCs of quinolones and nitroimidazoles (e.g. norfloxacin + metronidazole, ciprofloxacin + tinidazole,
ofloxacin + ornidazole) have not been recommended in children.
2.This FDC can rapidly give rise to resistant strains of organisms, which is a matter of serious concern to the
health care situation in our resource poor country.
Kasarla Raju, A. Elumalai, Eddla Srid. IRRATIONAL DRUG COMBINATIONS. 2013;3(2):52-56.
S.O. 847 (E)
144 Zinc Carnosine+Oxetacaine a,
Pharmacodynamically irrelevant-
1. No published literature supporting this FDC.
S.O. 848 (E)
145 Oxetacaine +Magaldrate
+Famotidine
a,
Pharmacodynamically irrelevant-
No published literature supporting the FDC.
S.O. 849 (E)
146 Pantoprazole (as Enteric
Coated Tablet)+Zinc
Carnosine (as Film Coated
Tablets)
a,
Pharmacodynamically irrelevant-
No published literature supporting the FDC.
S.O. 850 (E)
147 Zinc
Carnosine+MagnesiumHydr
oxide +Dried Aluminium
Hydroxide +Simethicone
a,
Pharmacodynamically irrelevant-
1. No published literature supporting this FDC.
S.O. 851 (E)
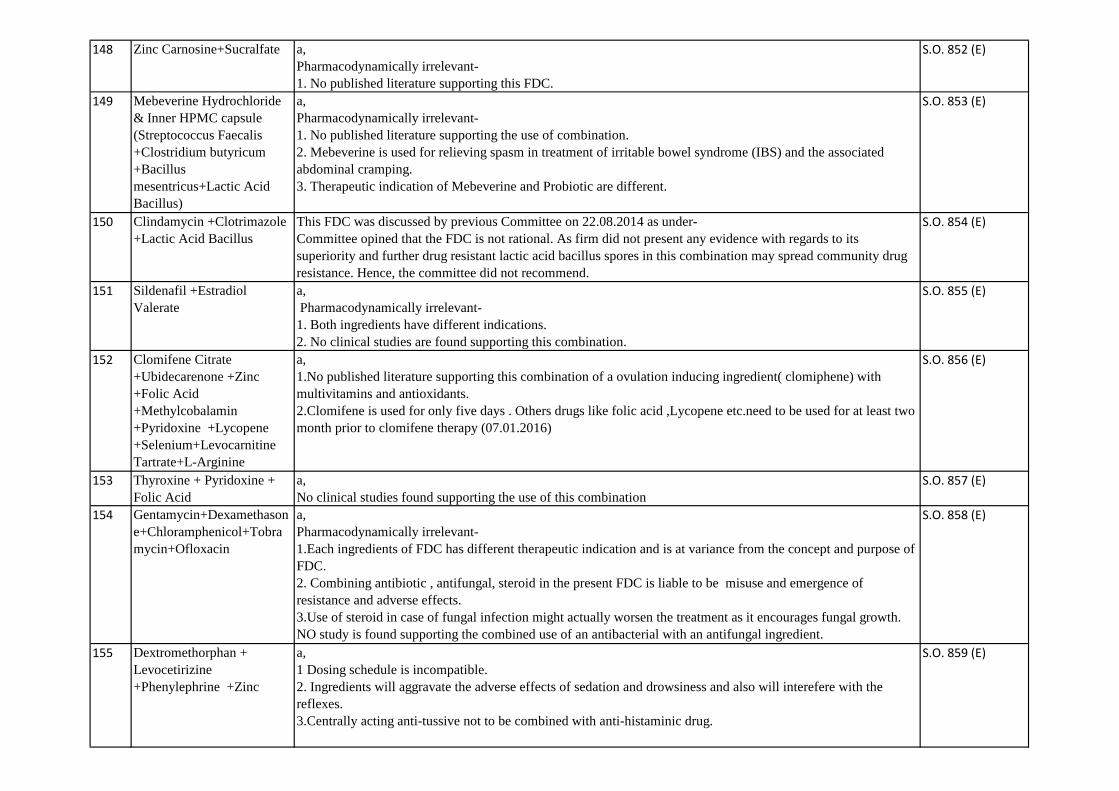
148 Zinc Carnosine+Sucralfate a,
Pharmacodynamically irrelevant-
1. No published literature supporting this FDC.
S.O. 852 (E)
149 Mebeverine Hydrochloride
& Inner HPMC capsule
(Streptococcus Faecalis
+Clostridium butyricum
+Bacillus
mesentricus+Lactic Acid
Bacillus)
a,
Pharmacodynamically irrelevant-
1. No published literature supporting the use of combination.
2. Mebeverine is used for relieving spasm in treatment of irritable bowel syndrome (IBS) and the associated
abdominal cramping.
3. Therapeutic indication of Mebeverine and Probiotic are different.
S.O. 853 (E)
150 Clindamycin +Clotrimazole
+Lactic Acid Bacillus
This FDC was discussed by previous Committee on 22.08.2014 as under-
Committee opined that the FDC is not rational. As firm did not present any evidence with regards to its
superiority and further drug resistant lactic acid bacillus spores in this combination may spread community drug
resistance. Hence, the committee did not recommend.
S.O. 854 (E)
151 Sildenafil +Estradiol
Valerate
a,
Pharmacodynamically irrelevant-
1. Both ingredients have different indications.
2. No clinical studies are found supporting this combination.
S.O. 855 (E)
152 Clomifene Citrate
+Ubidecarenone +Zinc
+Folic Acid
+Methylcobalamin
+Pyridoxine +Lycopene
+Selenium+Levocarnitine
Tartrate+L-Arginine
a,
1.No published literature supporting this combination of a ovulation inducing ingredient( clomiphene) with
multivitamins and antioxidants.
2.Clomifene is used for only five days . Others drugs like folic acid ,Lycopene etc.need to be used for at least two
month prior to clomifene therapy (07.01.2016)
S.O. 856 (E)
153 Thyroxine + Pyridoxine +
Folic Acid
a,
No clinical studies found supporting the use of this combination
S.O. 857 (E)
154 Gentamycin+Dexamethason
e+Chloramphenicol+Tobra
mycin+Ofloxacin
a,
Pharmacodynamically irrelevant-
1.Each ingredients of FDC has different therapeutic indication and is at variance from the concept and purpose of
FDC.
2. Combining antibiotic , antifungal, steroid in the present FDC is liable to be misuse and emergence of
resistance and adverse effects.
3.Use of steroid in case of fungal infection might actually worsen the treatment as it encourages fungal growth.
NO study is found supporting the combined use of an antibacterial with an antifungal ingredient.
S.O. 858 (E)
155 Dextromethorphan +
Levocetirizine
+Phenylephrine +Zinc
a,
1 Dosing schedule is incompatible.
2. Ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with the
reflexes.
3.Centrally acting anti-tussive not to be combined with anti-histaminic drug.
S.O. 859 (E)

156 Nimesulide +Loratadine
+Phenylephrine +Ambroxol
a,
Pharmacodynamic irrelevant-
1.Each ingredient has different therapeutic use and FDC will lead to misuse and toxicity.
2. Pharmacokinetic mismatch.
Chandler S. Gautam, Lekha Saha. Fixed dose drug combinations (FDCs): rational or irrational: a view point Br
J Clin Pharmacol / 65:5 / 795–796
Eccles, R., Fietze, I. and Rose, U.-B. (2014) Rationale for Treatment of Common Cold and Flu with Multi-
Ingredient Combination Products for Multi-Symptom Relief in Adults. Open Journal of Respiratory Diseases, 4,
73-82.
S.O. 860 (E)
157 Bromhexine
+Phenylephrine
+Chlorepheniramine
Maleate
a,
Pharmacodynamically irrelevant-
1.chlorpheniramine + phenylephrine
chlorpheniramine increases and phenylephrine decreases sedation. Effect of interaction is not clear, use caution.
2.Dosing shedule of the ingredients are not compatible
S.O. 861 (E)
158 Dextromethorphan +
bromhexine +Guaiphenesin
a,
Pharmacodynamically irrelevant-
1. Guiaphenesin: a mucolytic which increases mucus secretion should not given in combination with
antihistaminic with anti cholinergic properties, because due to anti cholinergic properties mucus secretions is
dried up.
2. Dextromethorphan: it decreases the cough impulse so expulsion of secretion would be hampered
3.Patients may need only one ingredient and use of FDC may lead to misuse.
4.Dosing shedule of the ingredients is incompatible.
S.O. 862 (E)
159 Paracetamol + Loratadine +
phenylephrine +
Dextromethorphan +
caffeine
a,
1.Pharmacodynamically and phamacokinetically irrational FDC.
2.Patients may need only one ingredient and use of FDC may lead to misuse.
S.O. 863 (E)
160 Nimesulide + Phenylephrine
+ Ceffeine+ levocetirizine
a,
1. Pharmacodynamically irrelevant-Patients may not need all the ingredients and use of FDC may lead to misuse
and adverse effects.
2.Pharmacokinetically irrelevant-different dosing shedule.
3. Nimesuilide- Safety concern
S.O. 864 (E)
161 Azithromycin +
acebrophyline
a,
1. Pharmacodynamically irrelevant-combining anti-bacterial with bronchodialator is not indicated.
2. Potential misuse as bronchodialator with anti-bacterial will increase the emergence of drug resistance to
azithromycin and its adverse effects .
S.O. 865 (E)

162 Diphenhydramine +Terpine
+Ammonium Chloride
+Sodium Chloride
+Menthol
a,
Pharmacodynamically irrelevant.
No published literature supporting the combination
S.O. 866 (E)
163 Nimesulide+Paracetamol+C
etrizine +Phenylephrine
a,
1. Nimesulide in combination has potential of misuse in indications for allergic conditions. Users who may not
be aware of this paracetamol content and may accidentally overdose when they take the multi- ingredient product
with other medicines also containing paracetamol.
2. There is pharmacokinetic incompatibility among the drugs.
3.Nimesuilide has documanted safety concern.
4. Hepatotoxic potential of both the drugs
Eccles, R., Fietze, I. and Rose, U.-B. (2014) Rationale for Treatment of Common Cold and Flu with Multi-
Ingredient Combination Products for Multi-Symptom Relief in Adults. Open Journal of Respiratory Diseases, 4,
73-82.
S.O. 867 (E)
164 paracetamol+ loratadine +
dextromethophan +
pseudoepheridine + caffeine
a,
1.Pharmacodynamically and phamacokinetically irrational FDC.
2.Patients may need only one ingredient and use of FDC may lead to misuse.
3.Dosing shedule of the ingredients is incompatible.
S.O. 868 (E)
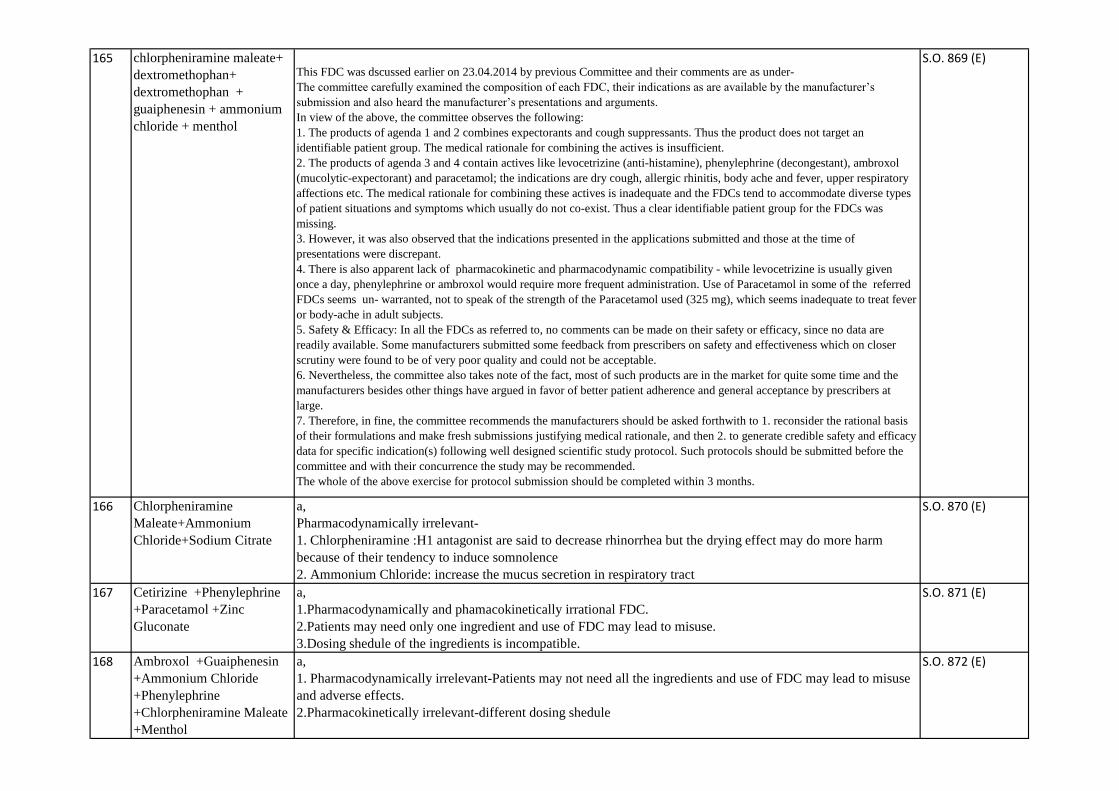
165 chlorpheniramine maleate+
dextromethophan+
dextromethophan +
guaiphenesin + ammonium
chloride + menthol
This FDC was dscussed earlier on 23.04.2014 by previous Committee and their comments are as under-
The committee carefully examined the composition of each FDC, their indications as are available by the manufacturer’s
submission and also heard the manufacturer’s presentations and arguments.
In view of the above, the committee observes the following:
1. The products of agenda 1 and 2 combines expectorants and cough suppressants. Thus the product does not target an
identifiable patient group. The medical rationale for combining the actives is insufficient.
2. The products of agenda 3 and 4 contain actives like levocetrizine (anti-histamine), phenylephrine (decongestant), ambroxol
(mucolytic-expectorant) and paracetamol; the indications are dry cough, allergic rhinitis, body ache and fever, upper respiratory
affections etc. The medical rationale for combining these actives is inadequate and the FDCs tend to accommodate diverse types
of patient situations and symptoms which usually do not co-exist. Thus a clear identifiable patient group for the FDCs was
missing.
3. However, it was also observed that the indications presented in the applications submitted and those at the time of
presentations were discrepant.
4. There is also apparent lack of pharmacokinetic and pharmacodynamic compatibility - while levocetrizine is usually given
once a day, phenylephrine or ambroxol would require more frequent administration. Use of Paracetamol in some of the referred
FDCs seems un- warranted, not to speak of the strength of the Paracetamol used (325 mg), which seems inadequate to treat fever
or body-ache in adult subjects.
5. Safety & Efficacy: In all the FDCs as referred to, no comments can be made on their safety or efficacy, since no data are
readily available. Some manufacturers submitted some feedback from prescribers on safety and effectiveness which on closer
scrutiny were found to be of very poor quality and could not be acceptable.
6. Nevertheless, the committee also takes note of the fact, most of such products are in the market for quite some time and the
manufacturers besides other things have argued in favor of better patient adherence and general acceptance by prescribers at
large.
7. Therefore, in fine, the committee recommends the manufacturers should be asked forthwith to 1. reconsider the rational basis
of their formulations and make fresh submissions justifying medical rationale, and then 2. to generate credible safety and efficacy
data for specific indication(s) following well designed scientific study protocol. Such protocols should be submitted before the
committee and with their concurrence the study may be recommended.
The whole of the above exercise for protocol submission should be completed within 3 months.
S.O. 869 (E)
166 Chlorpheniramine
Maleate+Ammonium
Chloride+Sodium Citrate
a,
Pharmacodynamically irrelevant-
1. Chlorpheniramine :H1 antagonist are said to decrease rhinorrhea but the drying effect may do more harm
because of their tendency to induce somnolence
2. Ammonium Chloride: increase the mucus secretion in respiratory tract
S.O. 870 (E)
167 Cetirizine +Phenylephrine
+Paracetamol +Zinc
Gluconate
a,
1.Pharmacodynamically and phamacokinetically irrational FDC.
2.Patients may need only one ingredient and use of FDC may lead to misuse.
3.Dosing shedule of the ingredients is incompatible.
S.O. 871 (E)
168 Ambroxol +Guaiphenesin
+Ammonium Chloride
+Phenylephrine
+Chlorpheniramine Maleate
+Menthol
a,
1. Pharmacodynamically irrelevant-Patients may not need all the ingredients and use of FDC may lead to misuse
and adverse effects.
2.Pharmacokinetically irrelevant-different dosing shedule
S.O. 872 (E)

169 dextromethophen +
bromhexine +
chlorpheniramine maleate +
guaiphenesin
a,
1 Dosing schedule is incompatible.
2. Ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with the
reflexes.
3.Centrally acting anti-tussive not to be combined with anti-histaminic drug.
S.O. 873 (E)
170 levocetirizine + ambroxol +
phenylephrine
+guaiphenesin
a,
1. Pharmacodynamically irrelevant-Patients may not need all the ingredients and use of FDC may lead to misuse
and adverse effects.
2.Pharmacokinetically irrelevant-different dosing shedule
S.O. 874 (E)
171 dextromethorphan +
chlorpheniramine +
chlorpheniramine maleate
a,
1 Dosing schedule is incompatible.
2. Ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with the
reflexes.
3.Centrally acting anti-tussive not to be combined with anti-histaminic drug.
S.O. 875 (E)
172 cetirizine + ambroxol +
Guaiphenesin + ammonium
chloride+ phenylephrine+
menthol
a,
1.Pharmacodynamically and phamacokinetically irrational FDC.
2.Patients may need only one ingredient and use of FDC may lead to misuse.
S.O. 876 (E)
173 chlorpheniramine +
phenylephrine + caffiene
a,
1.Pharmacodynamically irrationale FDC.
2.Patients may need only one ingredient and use of FDC may lead to misuse.
S.O. 877 (E)
174 dextromethorphan +
triprolidine + phenylephrine
a,
1 Dosing schedule is incompatible.
2. Ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with the
reflexes.
3.Centrally acting anti-tussive not to be combined with anti-histaminic drug.
S.O. 878 (E)
175 Terpinhydrate+
dextromethorphan +
menthol
a,
Pharmacodynamically irrelevant.
No published literature supporting the combination.
S.O. 879 (E)
176 dextromethorphan +
phenylephrine + zinc
gluconate+ menthol
a,
Pharmacodynamically irrelevant-
1 Dosing schedule is incompatible.
2. Ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with the
reflexes.
S.O. 880 (E)

177 chlorpheniramine + codeine
+ sodium citarte + menthol
syrup
1 Dosing schedule is incompatible.
2. Both the ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with
the reflexes.
3.Centrally acting anti-tussive not to be combined with anti-histaminic drug.
4.There is also a risk of abuse potential.
S.O. 881 (E)
178 Enrofloxacin + bromhexin a,
Pharmacodynamically irrelevant-
1. Enrofloxacin is not approved for human use.
S.O. 882 (E)
179 Bromhexine
+Dextromethorphan
+Phenylephrine +Menthol
a,
Pharmacodynamically irrelevant-
1. Dextromethorphan: it decreases the cough impulse so expulsion of secretion would be hampered
2. Bromhexine:a mucolytic which increases mucus secretion should not given in combination with antihistaminic
with anti cholinergic properties, because due to anti cholinergic properties mucus secretions is dried up.
S.O. 883 (E)
180 Levofloxacin +Bromhexine a,
Pharmacodynamically irrelevant-
1. Patient may need only one ingredient and the use of FDC may lead to misuse.
2. Increased risk of emergence of drug resistance due to misuse of FDC .
S.O. 884 (E)
181 Levocetirizine +Ranitidine a,
Pharmacodynamically irrelevant as both ingredients are indicated for different indications.
S.O. 885 (E)
182 Levocetirizine
+Phenylephrine +Ambroxol
+Guaiphenesin
+Paracetamol
a,
Pharmacodynamically irrelevant-
1. Patients may not need all the ingredients and use of FDC may lead to misuse and adverse effects.
2.Pharmacokinetically irrelevant-different dosing shedule.
3.Potential drug interactions.
S.O. 886 (E)
183 cetirizine +
dextromethorphan +
phenylephrine + zinc
gluconate + paracetamol+
menthol
a,
1.Pharmacodynamically and phamacokinetically irrational FDC.
2.Patients may need only one ingredient and use of FDC may lead to misuse.
3.Centrally acting anti-tussive not to be combined with anti-histaminic drug.
S.O. 887 (E)
184 paracetamol+
pseudoephedrine +
dextromethorphan +
cetirizine
a,
1 Dosing schedule is incompatible.
2. Ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with the
reflexes.
3.Centrally acting anti-tussive not to be combined with anti-histaminic drug.
S.O. 888 (E)
185 diphenhydamine +
guaiphenesin + ammonium
chloride + bromhexine
a, Pharmacodynamically irrelevant.
• Anticholinergic property of diphenhydramine will lead to drying up of secretions while mucolytics increase.
S.O. 889 (E)
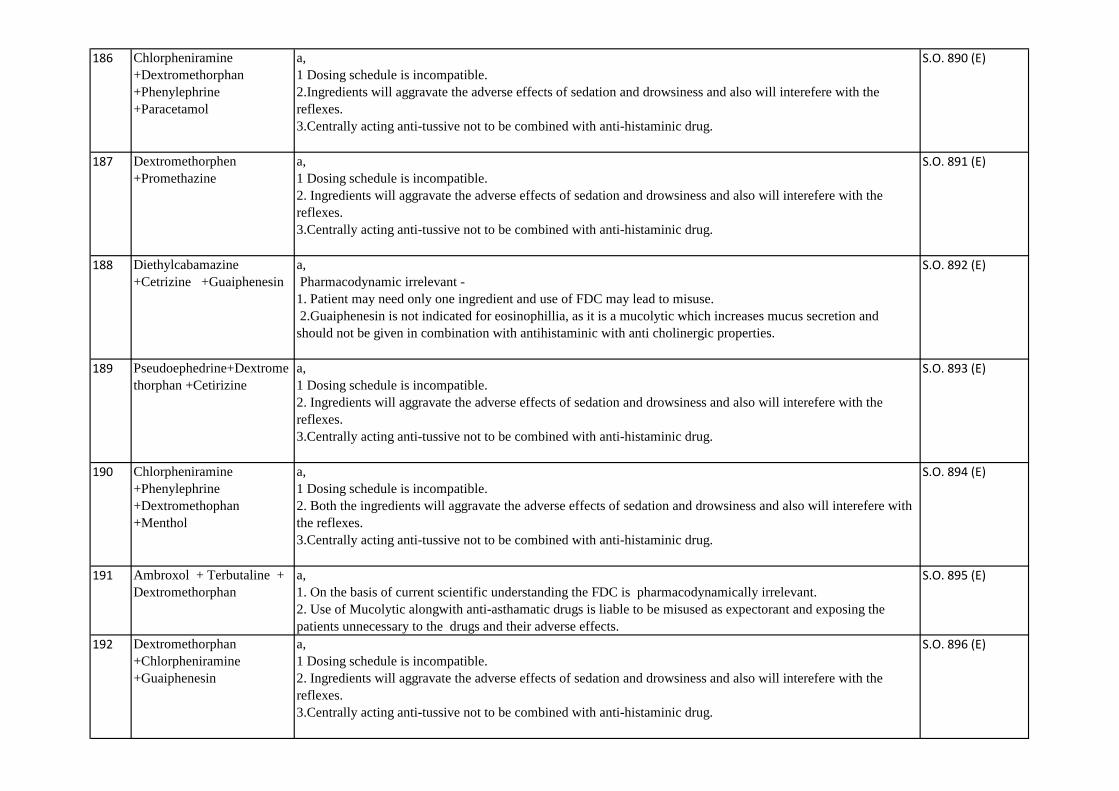
186 Chlorpheniramine
+Dextromethorphan
+Phenylephrine
+Paracetamol
a,
1 Dosing schedule is incompatible.
2.Ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with the
reflexes.
3.Centrally acting anti-tussive not to be combined with anti-histaminic drug.
S.O. 890 (E)
187 Dextromethorphen
+Promethazine
a,
1 Dosing schedule is incompatible.
2. Ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with the
reflexes.
3.Centrally acting anti-tussive not to be combined with anti-histaminic drug.
S.O. 891 (E)
188 Diethylcabamazine
+Cetrizine +Guaiphenesin
a,
Pharmacodynamic irrelevant -
1. Patient may need only one ingredient and use of FDC may lead to misuse.
2.Guaiphenesin is not indicated for eosinophillia, as it is a mucolytic which increases mucus secretion and
should not be given in combination with antihistaminic with anti cholinergic properties.
S.O. 892 (E)
189 Pseudoephedrine+Dextrome
thorphan +Cetirizine
a,
1 Dosing schedule is incompatible.
2. Ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with the
reflexes.
3.Centrally acting anti-tussive not to be combined with anti-histaminic drug.
S.O. 893 (E)
190 Chlorpheniramine
+Phenylephrine
+Dextromethophan
+Menthol
a,
1 Dosing schedule is incompatible.
2. Both the ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with
the reflexes.
3.Centrally acting anti-tussive not to be combined with anti-histaminic drug.
S.O. 894 (E)
191 Ambroxol + Terbutaline +
Dextromethorphan
a,
1. On the basis of current scientific understanding the FDC is pharmacodynamically irrelevant.
2. Use of Mucolytic alongwith anti-asthamatic drugs is liable to be misused as expectorant and exposing the
patients unnecessary to the drugs and their adverse effects.
S.O. 895 (E)
192 Dextromethorphan
+Chlorpheniramine
+Guaiphenesin
a,
1 Dosing schedule is incompatible.
2. Ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with the
reflexes.
3.Centrally acting anti-tussive not to be combined with anti-histaminic drug.
S.O. 896 (E)
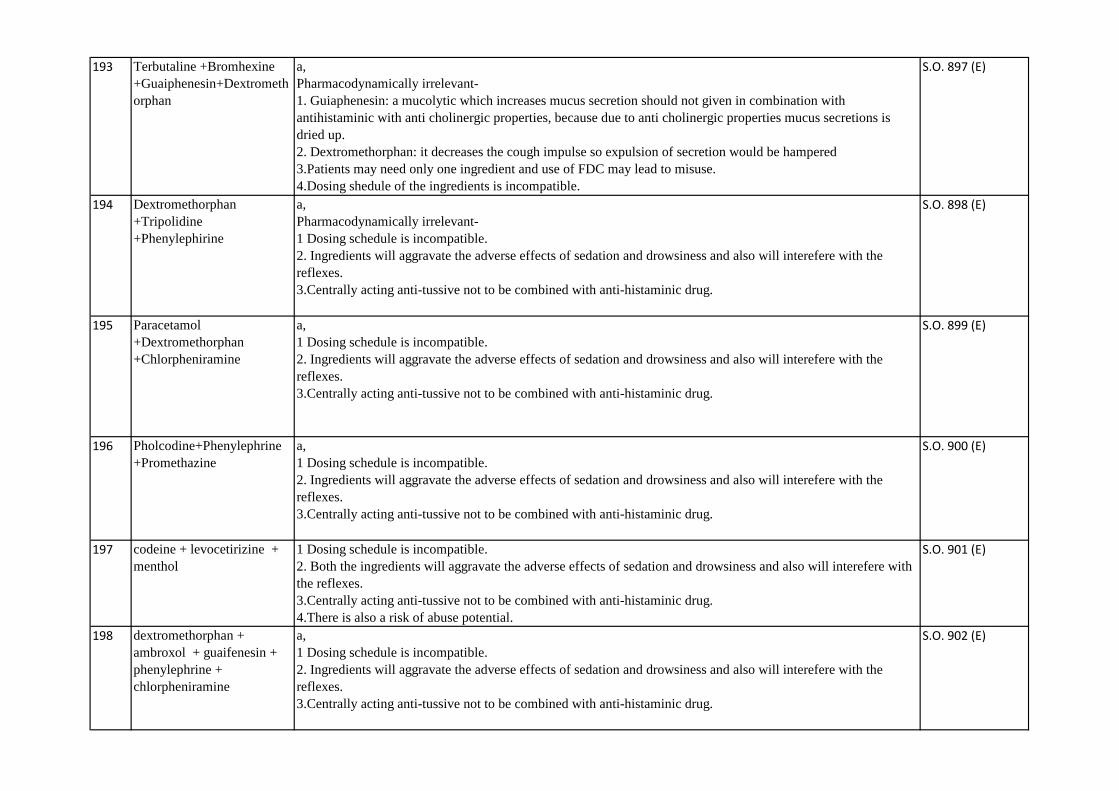
193 Terbutaline +Bromhexine
+Guaiphenesin+Dextrometh
orphan
a,
Pharmacodynamically irrelevant-
1. Guiaphenesin: a mucolytic which increases mucus secretion should not given in combination with
antihistaminic with anti cholinergic properties, because due to anti cholinergic properties mucus secretions is
dried up.
2. Dextromethorphan: it decreases the cough impulse so expulsion of secretion would be hampered
3.Patients may need only one ingredient and use of FDC may lead to misuse.
4.Dosing shedule of the ingredients is incompatible.
S.O. 897 (E)
194 Dextromethorphan
+Tripolidine
+Phenylephirine
a,
Pharmacodynamically irrelevant-
1 Dosing schedule is incompatible.
2. Ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with the
reflexes.
3.Centrally acting anti-tussive not to be combined with anti-histaminic drug.
S.O. 898 (E)
195 Paracetamol
+Dextromethorphan
+Chlorpheniramine
a,
1 Dosing schedule is incompatible.
2. Ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with the
reflexes.
3.Centrally acting anti-tussive not to be combined with anti-histaminic drug.
S.O. 899 (E)
196 Pholcodine+Phenylephrine
+Promethazine
a,
1 Dosing schedule is incompatible.
2. Ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with the
reflexes.
3.Centrally acting anti-tussive not to be combined with anti-histaminic drug.
S.O. 900 (E)
197 codeine + levocetirizine +
menthol
1 Dosing schedule is incompatible.
2. Both the ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with
the reflexes.
3.Centrally acting anti-tussive not to be combined with anti-histaminic drug.
4.There is also a risk of abuse potential.
S.O. 901 (E)
198 dextromethorphan +
ambroxol + guaifenesin +
phenylephrine +
chlorpheniramine
a,
1 Dosing schedule is incompatible.
2. Ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with the
reflexes.
3.Centrally acting anti-tussive not to be combined with anti-histaminic drug.
S.O. 902 (E)

199 Cetirizine +Phenylephrine
+ Dextromethorphan +
Menthol
a,
1.Pharmacodynamically and phamacokinetically irrational FDC.
2.Patients may need only one ingredient and use of FDC may lead to misuse.
3.Centrally acting anti-tussive not to be combined with anti-histaminic drug.
S.O. 903 (E)
200 Roxithromycin +
Serratiopeptidase
a,
Pharmacodynamically irrelevant-
May lead to misuse and drug resistance
S.O. 904 (E)
201 Paracetamol +Phenylephrine
+Triprolidine
a,
1.Pharmacodynamically and phamacokinetically irrational FDC.
2.Patients may need only one ingredient and use of FDC may lead to misuse.
3.Dosing shedule of the ingredients is incompatible.
S.O. 905 (E)
202 Acetaminophen+Loratadine
+ambroxol +Phenylephrine
a,
1.Pharmacodynamically and phamacokinetically irrational FDC.
2.Patients may need only one ingredient and use of FDC may lead to misuse.
S.O. 906 (E)
203 Cetirizine
+Acetaminophen+Dextrome
thorphan +Phenyephrine
+Zinc gluconate
a,
1.Pharmacodynamically and phamacokinetically irrational FDC.
2.Patients may need only one ingredient and use of FDC may lead to misuse.
3.Centrally acting anti-tussive not to be combined with anti-histaminic drug.
S.O. 907 (E)
204 Diphenhydramine
+Guaifenesin +Bromhexine
+Ammonium Chloride
+Menthol
a, Pharmacodynamically irrelevant.
• Anticholinergic property of diphenhydramine will lead to drying up of secretions while mucolytics increase.
S.O. 908 (E)
205 Chlopheniramine Maleate
+Codeine syrup
1 Dosing schedule is incompatible.
2. Both the ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with
the reflexes.
3. Centrally acting anti-tussive not to be combined with anti-histaminic drug.
4.There is also a risk of abuse potential.
S.O. 909 (E)
206 Cetirizine
+Dextromethorphan +Zinc
Gluconate +Menthol
a, Pharmacodynamically irrelevant.
1.Patients may need only one ingredient and use of FDC may lead to misuse.
2..Pharmacokinetic incompatibility amongst ingredients.
3..Use of anti-histamine with centrally acting anti- tussive ingredient is not rationale
S.O. 910 (E)
207 Paracetamol +Phenylephrine
+Desloratadine+Zinc
Gluconate +Ambroxol
a,
1.Pharmacodynamically and phamacokinetically irrational FDC.
2.Patients may need only one ingredient and use of FDC may lead to misuse.
3.Dosing shedule of the ingredients is incompatible.
S.O. 911 (E)
208 levocetirizine + montelukast
+ acebrophylline
a,
Pharmacodynamically irrelevant-
1. There is no published literature supporting FDC of three drugs.
2. Pharmacokinetic imcompatibilty.
S.O. 912 (E)
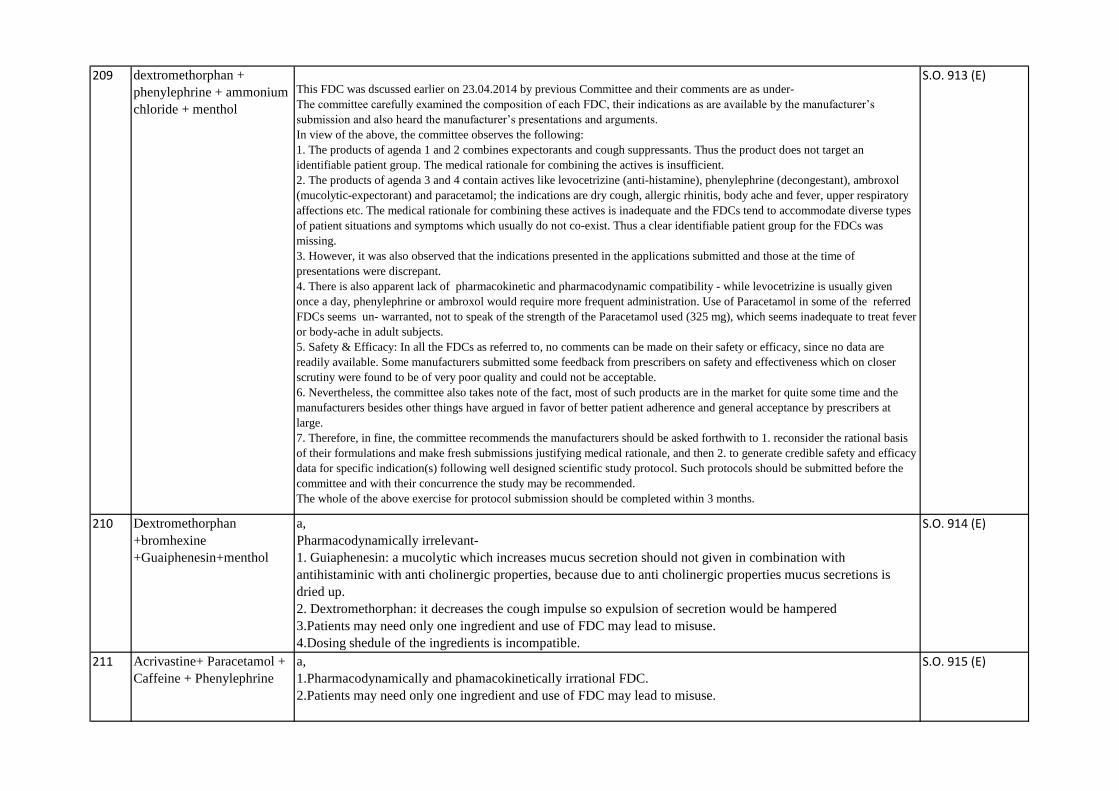
209 dextromethorphan +
phenylephrine + ammonium
chloride + menthol
This FDC was dscussed earlier on 23.04.2014 by previous Committee and their comments are as under-
The committee carefully examined the composition of each FDC, their indications as are available by the manufacturer’s
submission and also heard the manufacturer’s presentations and arguments.
In view of the above, the committee observes the following:
1. The products of agenda 1 and 2 combines expectorants and cough suppressants. Thus the product does not target an
identifiable patient group. The medical rationale for combining the actives is insufficient.
2. The products of agenda 3 and 4 contain actives like levocetrizine (anti-histamine), phenylephrine (decongestant), ambroxol
(mucolytic-expectorant) and paracetamol; the indications are dry cough, allergic rhinitis, body ache and fever, upper respiratory
affections etc. The medical rationale for combining these actives is inadequate and the FDCs tend to accommodate diverse types
of patient situations and symptoms which usually do not co-exist. Thus a clear identifiable patient group for the FDCs was
missing.
3. However, it was also observed that the indications presented in the applications submitted and those at the time of
presentations were discrepant.
4. There is also apparent lack of pharmacokinetic and pharmacodynamic compatibility - while levocetrizine is usually given
once a day, phenylephrine or ambroxol would require more frequent administration. Use of Paracetamol in some of the referred
FDCs seems un- warranted, not to speak of the strength of the Paracetamol used (325 mg), which seems inadequate to treat fever
or body-ache in adult subjects.
5. Safety & Efficacy: In all the FDCs as referred to, no comments can be made on their safety or efficacy, since no data are
readily available. Some manufacturers submitted some feedback from prescribers on safety and effectiveness which on closer
scrutiny were found to be of very poor quality and could not be acceptable.
6. Nevertheless, the committee also takes note of the fact, most of such products are in the market for quite some time and the
manufacturers besides other things have argued in favor of better patient adherence and general acceptance by prescribers at
large.
7. Therefore, in fine, the committee recommends the manufacturers should be asked forthwith to 1. reconsider the rational basis
of their formulations and make fresh submissions justifying medical rationale, and then 2. to generate credible safety and efficacy
data for specific indication(s) following well designed scientific study protocol. Such protocols should be submitted before the
committee and with their concurrence the study may be recommended.
The whole of the above exercise for protocol submission should be completed within 3 months.
S.O. 913 (E)
210 Dextromethorphan
+bromhexine
+Guaiphenesin+menthol
a,
Pharmacodynamically irrelevant-
1. Guiaphenesin: a mucolytic which increases mucus secretion should not given in combination with
antihistaminic with anti cholinergic properties, because due to anti cholinergic properties mucus secretions is
dried up.
2. Dextromethorphan: it decreases the cough impulse so expulsion of secretion would be hampered
3.Patients may need only one ingredient and use of FDC may lead to misuse.
4.Dosing shedule of the ingredients is incompatible.
S.O. 914 (E)
211 Acrivastine+ Paracetamol +
Caffeine + Phenylephrine
a,
1.Pharmacodynamically and phamacokinetically irrational FDC.
2.Patients may need only one ingredient and use of FDC may lead to misuse.
S.O. 915 (E)

212 Naphazoline +carboxy
Methyl cellulose +Menthol
+Camphor +Phenylephrine
a,
Pharmacodynamically irrelevant-
1. Therapeutic area not clear
2. Multiple ingredients with diverse pharmacological profile susceptible to pharmaceutically incompatibility
S.O. 916 (E)
213 Dextromethorphan
+Cetirizine
a,
1 Dosing schedule is incompatible.
2. Ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with the
reflexes.
3.Centrally acting anti-tussive not to be combined with anti-histaminic drug.
S.O. 917 (E)
214 nimesulide + paracetamol +
levocetirizine +
phenylephrine + caffeine
a,
1. Pharmacodynamically irrelevant-Patients may not need all the ingredients and use of FDC may lead to misuse
and adverse effects.
2.Pharmacokinetically irrelevant-different dosing shedule.
3. Nimesuilide- Safety concern
S.O. 918 (E)
215 Terbutaline +Ambroxol
+Guaiphenesin+Zinc+Ment
hol
a,
1. On the basis of current scientific understanding the FDC is pharmacodynamically irrelevant.
2. Use of Mucolytic alongwith anti-asthamatic drugs is liable to be misused as expectorant and exposing the
patients unnecessary to the drugs and their adverse effects.
S.O. 919 (E)
216 Codeine +Chlorpheniramine
+Alcohol syrup
1 Dosing schedule is incompatible.
2. Both the ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with
the reflexes.
3. Centrally acting anti-tussive not to be combined with anti-histaminic drug.
4.There is also a risk of abuse potential.
S.O. 920 (E)
217 Dextromethorphan
+Phenylephrine
+Guaifenesin+Triprolidine
a,
Pharmacodynamically irrelevant-
1. Guiaphenesin: a mucolytic which increases mucus secretion should not given in combination with
antihistaminic with anti cholinergic properties, because due to anti cholinergic properties mucus secretions is
dried up.
2. Dextromethorphan: it decreases the cough impulse so expulsion of secretion would be hampered
3.Patients may need only one ingredient and use of FDC may lead to misuse.
4.Dosing shedule of the ingredients is incompatible.
S.O. 921 (E)
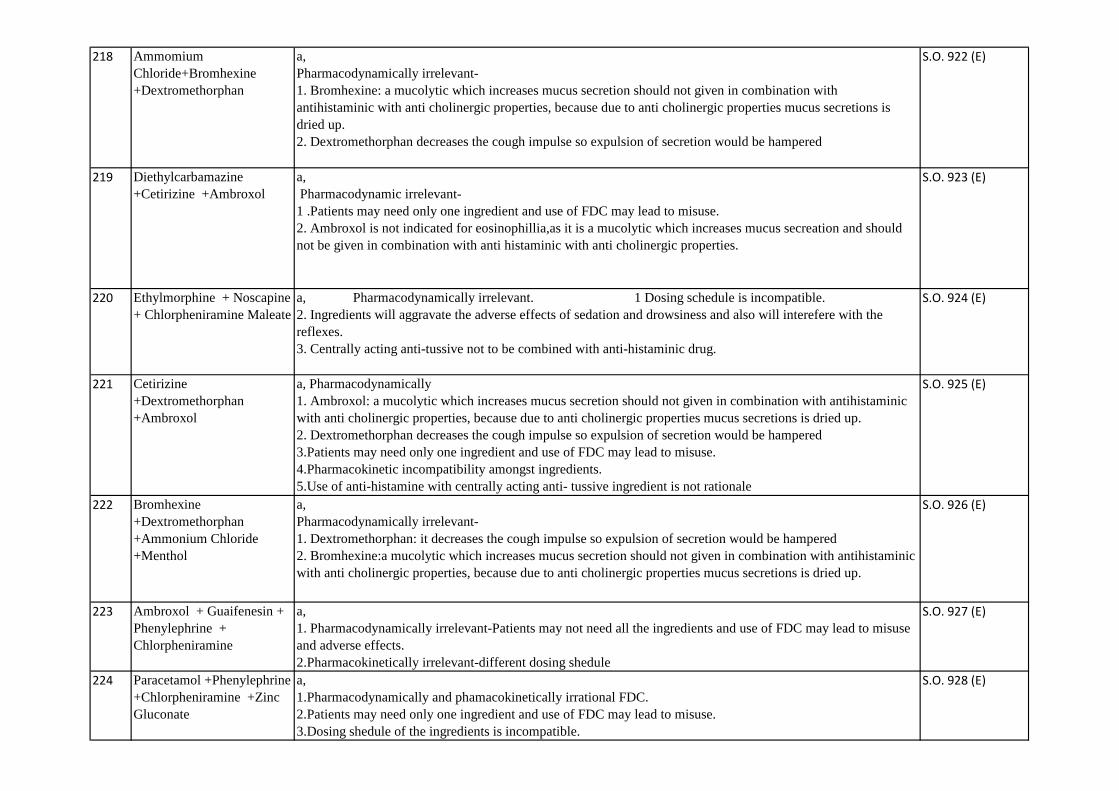
218 Ammomium
Chloride+Bromhexine
+Dextromethorphan
a,
Pharmacodynamically irrelevant-
1. Bromhexine: a mucolytic which increases mucus secretion should not given in combination with
antihistaminic with anti cholinergic properties, because due to anti cholinergic properties mucus secretions is
dried up.
2. Dextromethorphan decreases the cough impulse so expulsion of secretion would be hampered
S.O. 922 (E)
219 Diethylcarbamazine
+Cetirizine +Ambroxol
a,
Pharmacodynamic irrelevant-
1 .Patients may need only one ingredient and use of FDC may lead to misuse.
2. Ambroxol is not indicated for eosinophillia,as it is a mucolytic which increases mucus secreation and should
not be given in combination with anti histaminic with anti cholinergic properties.
S.O. 923 (E)
220 Ethylmorphine + Noscapine
+ Chlorpheniramine Maleate
a, Pharmacodynamically irrelevant. 1 Dosing schedule is incompatible.
2. Ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with the
reflexes.
3. Centrally acting anti-tussive not to be combined with anti-histaminic drug.
S.O. 924 (E)
221 Cetirizine
+Dextromethorphan
+Ambroxol
a, Pharmacodynamically
1. Ambroxol: a mucolytic which increases mucus secretion should not given in combination with antihistaminic
with anti cholinergic properties, because due to anti cholinergic properties mucus secretions is dried up.
2. Dextromethorphan decreases the cough impulse so expulsion of secretion would be hampered
3.Patients may need only one ingredient and use of FDC may lead to misuse.
4.Pharmacokinetic incompatibility amongst ingredients.
5.Use of anti-histamine with centrally acting anti- tussive ingredient is not rationale
S.O. 925 (E)
222 Bromhexine
+Dextromethorphan
+Ammonium Chloride
+Menthol
a,
Pharmacodynamically irrelevant-
1. Dextromethorphan: it decreases the cough impulse so expulsion of secretion would be hampered
2. Bromhexine:a mucolytic which increases mucus secretion should not given in combination with antihistaminic
with anti cholinergic properties, because due to anti cholinergic properties mucus secretions is dried up.
S.O. 926 (E)
223 Ambroxol + Guaifenesin +
Phenylephrine +
Chlorpheniramine
a,
1. Pharmacodynamically irrelevant-Patients may not need all the ingredients and use of FDC may lead to misuse
and adverse effects.
2.Pharmacokinetically irrelevant-different dosing shedule
S.O. 927 (E)
224 Paracetamol +Phenylephrine
+Chlorpheniramine +Zinc
Gluconate
a,
1.Pharmacodynamically and phamacokinetically irrational FDC.
2.Patients may need only one ingredient and use of FDC may lead to misuse.
3.Dosing shedule of the ingredients is incompatible.
S.O. 928 (E)

225 Dextromethorphan
+Phenylephrine +Cetirizine
+Paracetamol +Caffeine
a,
1 Dosing schedule is incompatible.
2. Ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with the
reflexes.
3.Centrally acting anti-tussive not to be combined with anti-histaminic drug.
S.O. 929 (E)
226 Dextromethophan
+Chlorpheniramine
+Guaifenesin +Ammonium
Chloride
a,
1 Dosing schedule is incompatible.
2. Ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with the
reflexes.
3.Centrally acting anti-tussive not to be combined with anti-histaminic drug.
S.O. 930 (E)
227 Levocetirizine
+Dextromethorphan +Zinc
a,
1 Dosing schedule is incompatible.
2. Ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with the
reflexes.
3.Centrally acting anti-tussive not to be combined with anti-histaminic drug.
S.O. 931 (E)
228 Paracetamol +Phenylephrine
+Levocetirizine +Caffeine
a,
1.Pharmacodynamically and phamacokinetically irrational FDC.
2.Patients may need only one ingredient and use of FDC may lead to misuse.
3.Dosing shedule of the ingredients is incompatible.
S.O. 932 (E)
229 Chlorpheniramine
+Ammonium Chloride
+Sodium Chloride
a,
Pharmacodynamically irrelevant-
1. Chlorpheniramine :H1 antagonist are said to decrease rhinorrhea but the drying effect may do more harm
because of their tendency to induce somnolence
2. Ammonium Chloride: increase the mucus secretion in respiratory tract
S.O. 933 (E)
230 Paracetamol
+Dextromethorphan
+Bromhexine
+Phenylephrine
+Diphenhydramine
a,
1 Dosing schedule is incompatible.
2. Ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with the
reflexes.
3.Centrally acting anti-tussive not to be combined with anti-histaminic drug.
4.Paracetamol dose is subtherapeutic.
S.O. 934 (E)
231 Salbutamol +Bromhexine
+Guaiphenesin +Menthol
a,
1. On the basis of current scientific understanding the FDC is pharmacodynamically irrelevant.
2. Use of Mucolytic alongwith anti-asthamatic drugs is liable to be misused as expectorant and exposing the
patients unnecessary to the drugs and their adverse effects.
S.O. 935 (E)
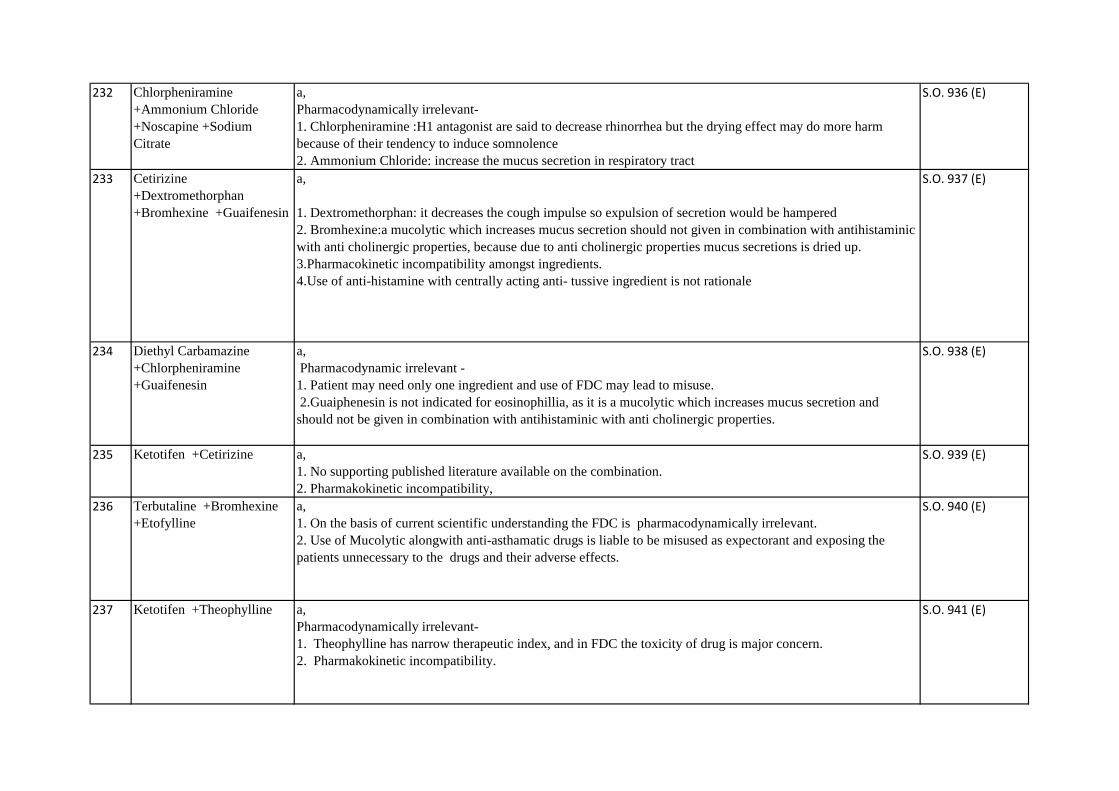
232 Chlorpheniramine
+Ammonium Chloride
+Noscapine +Sodium
Citrate
a,
Pharmacodynamically irrelevant-
1. Chlorpheniramine :H1 antagonist are said to decrease rhinorrhea but the drying effect may do more harm
because of their tendency to induce somnolence
2. Ammonium Chloride: increase the mucus secretion in respiratory tract
S.O. 936 (E)
233 Cetirizine
+Dextromethorphan
+Bromhexine +Guaifenesin
a,
1. Dextromethorphan: it decreases the cough impulse so expulsion of secretion would be hampered
2. Bromhexine:a mucolytic which increases mucus secretion should not given in combination with antihistaminic
with anti cholinergic properties, because due to anti cholinergic properties mucus secretions is dried up.
3.Pharmacokinetic incompatibility amongst ingredients.
4.Use of anti-histamine with centrally acting anti- tussive ingredient is not rationale
S.O. 937 (E)
234 Diethyl Carbamazine
+Chlorpheniramine
+Guaifenesin
a,
Pharmacodynamic irrelevant -
1. Patient may need only one ingredient and use of FDC may lead to misuse.
2.Guaiphenesin is not indicated for eosinophillia, as it is a mucolytic which increases mucus secretion and
should not be given in combination with antihistaminic with anti cholinergic properties.
S.O. 938 (E)
235 Ketotifen +Cetirizine a,
1. No supporting published literature available on the combination.
2. Pharmakokinetic incompatibility,
S.O. 939 (E)
236 Terbutaline +Bromhexine
+Etofylline
a,
1. On the basis of current scientific understanding the FDC is pharmacodynamically irrelevant.
2. Use of Mucolytic alongwith anti-asthamatic drugs is liable to be misused as expectorant and exposing the
patients unnecessary to the drugs and their adverse effects.
S.O. 940 (E)
237 Ketotifen +Theophylline a,
Pharmacodynamically irrelevant-
1. Theophylline has narrow therapeutic index, and in FDC the toxicity of drug is major concern.
2. Pharmakokinetic incompatibility.
S.O. 941 (E)

238 Ambroxol +Salbutamol
+Theophylline
a,
1. On the basis of current scientific understanding the FDC is pharmacodynamically irrelevant.
2. Use of Mucolytic alongwith anti-asthamatic drugs is liable to be misused as expectorant and exposing the
patients unnecessary to the drugs and their adverse effects.
S.O. 942 (E)
239 Cetirizine +Nimesulide
+Phenylephrine
a,
1.Pharmacodynamically irrelevant as different ingredients have different therapeutic indication
2. Nimesulide: safety concern
S.O. 943 (E)
240 Chloropheniramine
+Phenylephrine+Paracetamo
l+Zinc Gluconate
a,
1.Pharmacodynamically and phamacokinetically irrational FDC.
2.Patients may need only one ingredient and use of FDC may lead to misuse.
3.Dosing shedule of the ingredients is incompatible.
S.O. 944 (E)
241 Acetaminophen+Guaifenesi
n+Dextromethorphan
+Chlorpheniramine
a,
1. Use of anti-histamine with centrally acting anti- tussive ingredient is not rationale
2. Patients may need only one ingredient and use of FDC may lead to misuse.
3.Different mechanism of action without synergistic action.
4.Also the Acetaminophen, an antipyretic, is not indicated in the cough syrup. (04.01.2016)
S.O. 945 (E)
242 Cetirizine
+Dextromethorphan
+Phenylephrine +Tulsi
a,
1.Pharmacodynamically and phamacokinetically irrational FDC.
2.Patients may need only one ingredient and use of FDC may lead to misuse.
3.Use of anti-histamine with centrally acting anti- tussive ingredient is not rationale
S.O. 946 (E)
243 Cetirizine +Phenylephrine
+Paracetamol+Ambroxol
+Caffeine
a,
1.Pharmacodynamically and phamacokinetically irrational FDC.
2.Patients may need only one ingredient and use of FDC may lead to misuse.
S.O. 947 (E)
244 Guaifenesin+Dextromethorp
han
a,
Pharmacodynamically irrelevant-
1. Guaiphenesin :a mucolytic which increases mucus secretion.
2. Dextromethorphan: it decreases the cough impulse so expulsion of secretion would be hampered (04.01.2016)
S.O. 948 (E)
245 Levocetirizine +Paracetamol
+Phenylephirine +Caffeine
a,
1. Pharmacodynamically irrelevant-Patients may not need all the ingredients and use of FDC may lead to misuse
and adverse effects.
2.Pharmacokinetically irrelevant-different dosing shedule.
S.O. 949 (E)
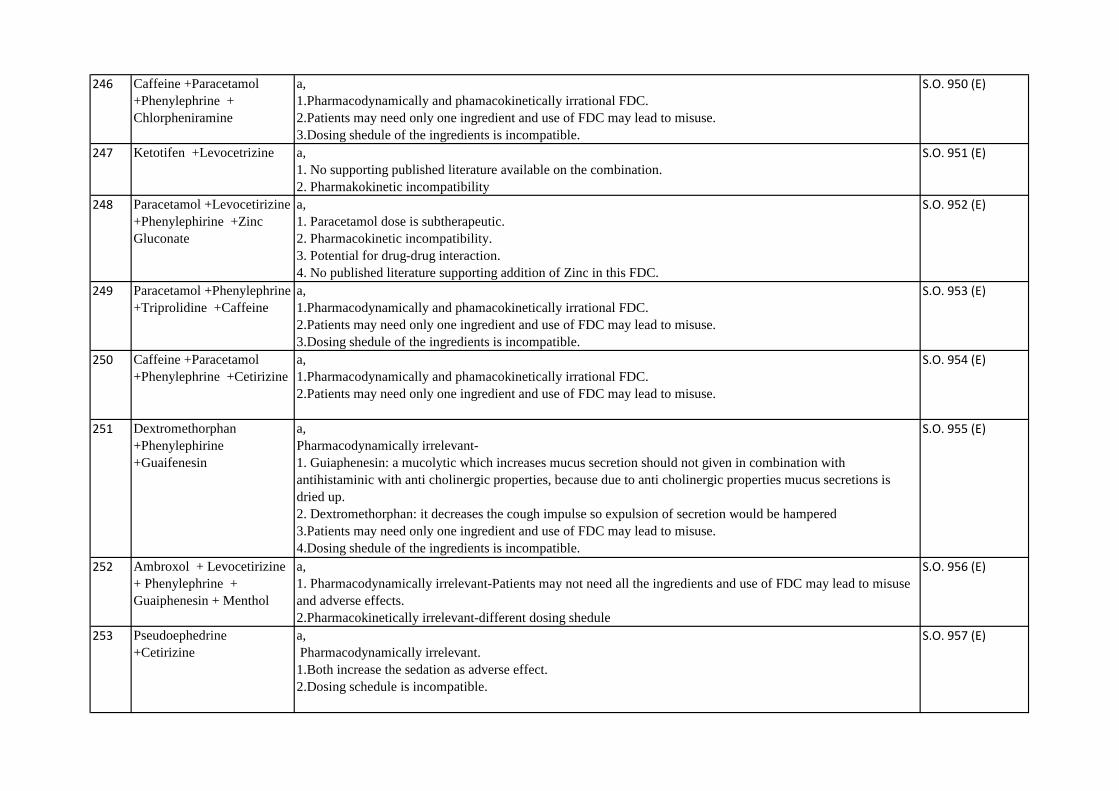
246 Caffeine +Paracetamol
+Phenylephrine +
Chlorpheniramine
a,
1.Pharmacodynamically and phamacokinetically irrational FDC.
2.Patients may need only one ingredient and use of FDC may lead to misuse.
3.Dosing shedule of the ingredients is incompatible.
S.O. 950 (E)
247 Ketotifen +Levocetrizine a,
1. No supporting published literature available on the combination.
2. Pharmakokinetic incompatibility
S.O. 951 (E)
248 Paracetamol +Levocetirizine
+Phenylephirine +Zinc
Gluconate
a,
1. Paracetamol dose is subtherapeutic.
2. Pharmacokinetic incompatibility.
3. Potential for drug-drug interaction.
4. No published literature supporting addition of Zinc in this FDC.
S.O. 952 (E)
249 Paracetamol +Phenylephrine
+Triprolidine +Caffeine
a,
1.Pharmacodynamically and phamacokinetically irrational FDC.
2.Patients may need only one ingredient and use of FDC may lead to misuse.
3.Dosing shedule of the ingredients is incompatible.
S.O. 953 (E)
250 Caffeine +Paracetamol
+Phenylephrine +Cetirizine
a,
1.Pharmacodynamically and phamacokinetically irrational FDC.
2.Patients may need only one ingredient and use of FDC may lead to misuse.
S.O. 954 (E)
251 Dextromethorphan
+Phenylephirine
+Guaifenesin
a,
Pharmacodynamically irrelevant-
1. Guiaphenesin: a mucolytic which increases mucus secretion should not given in combination with
antihistaminic with anti cholinergic properties, because due to anti cholinergic properties mucus secretions is
dried up.
2. Dextromethorphan: it decreases the cough impulse so expulsion of secretion would be hampered
3.Patients may need only one ingredient and use of FDC may lead to misuse.
4.Dosing shedule of the ingredients is incompatible.
S.O. 955 (E)
252 Ambroxol + Levocetirizine
+ Phenylephrine +
Guaiphenesin + Menthol
a,
1. Pharmacodynamically irrelevant-Patients may not need all the ingredients and use of FDC may lead to misuse
and adverse effects.
2.Pharmacokinetically irrelevant-different dosing shedule
S.O. 956 (E)
253 Pseudoephedrine
+Cetirizine
a,
Pharmacodynamically irrelevant.
1.Both increase the sedation as adverse effect.
2.Dosing schedule is incompatible.
S.O. 957 (E)
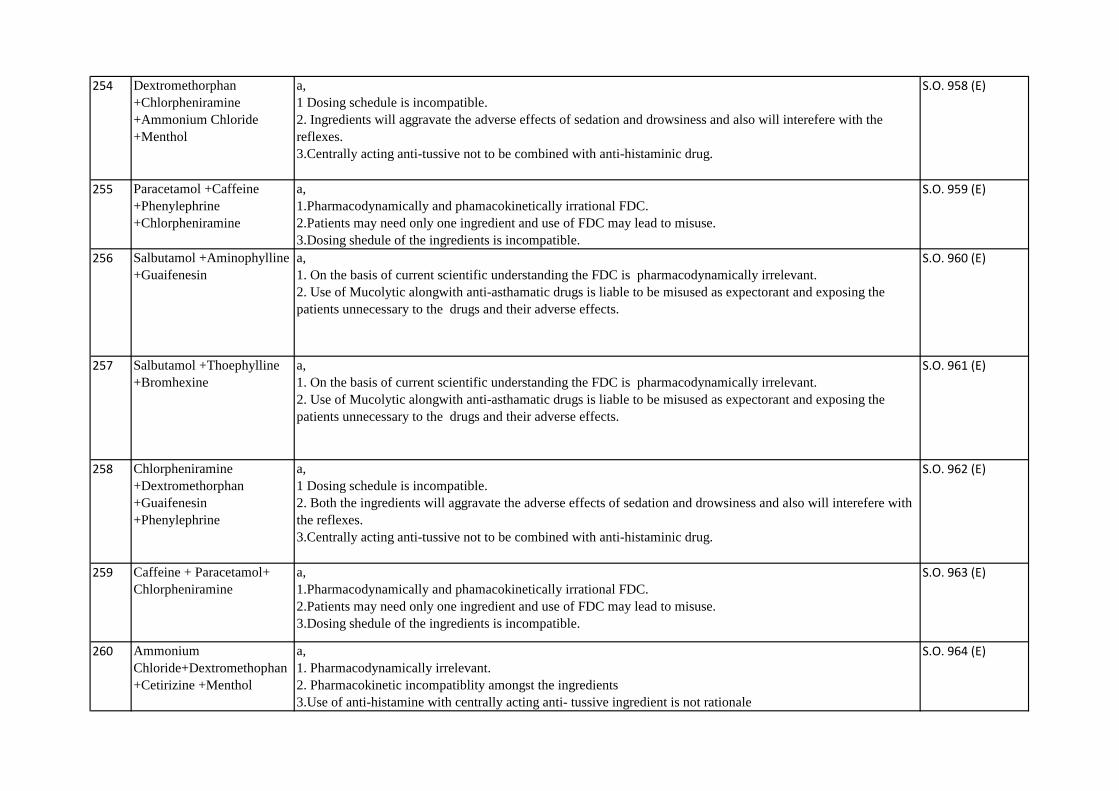
254 Dextromethorphan
+Chlorpheniramine
+Ammonium Chloride
+Menthol
a,
1 Dosing schedule is incompatible.
2. Ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with the
reflexes.
3.Centrally acting anti-tussive not to be combined with anti-histaminic drug.
S.O. 958 (E)
255 Paracetamol +Caffeine
+Phenylephrine
+Chlorpheniramine
a,
1.Pharmacodynamically and phamacokinetically irrational FDC.
2.Patients may need only one ingredient and use of FDC may lead to misuse.
3.Dosing shedule of the ingredients is incompatible.
S.O. 959 (E)
256 Salbutamol +Aminophylline
+Guaifenesin
a,
1. On the basis of current scientific understanding the FDC is pharmacodynamically irrelevant.
2. Use of Mucolytic alongwith anti-asthamatic drugs is liable to be misused as expectorant and exposing the
patients unnecessary to the drugs and their adverse effects.
S.O. 960 (E)
257 Salbutamol +Thoephylline
+Bromhexine
a,
1. On the basis of current scientific understanding the FDC is pharmacodynamically irrelevant.
2. Use of Mucolytic alongwith anti-asthamatic drugs is liable to be misused as expectorant and exposing the
patients unnecessary to the drugs and their adverse effects.
S.O. 961 (E)
258 Chlorpheniramine
+Dextromethorphan
+Guaifenesin
+Phenylephrine
a,
1 Dosing schedule is incompatible.
2. Both the ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with
the reflexes.
3.Centrally acting anti-tussive not to be combined with anti-histaminic drug.
S.O. 962 (E)
259 Caffeine + Paracetamol+
Chlorpheniramine
a,
1.Pharmacodynamically and phamacokinetically irrational FDC.
2.Patients may need only one ingredient and use of FDC may lead to misuse.
3.Dosing shedule of the ingredients is incompatible.
S.O. 963 (E)
260 Ammonium
Chloride+Dextromethophan
+Cetirizine +Menthol
a,
1. Pharmacodynamically irrelevant.
2. Pharmacokinetic incompatiblity amongst the ingredients
3.Use of anti-histamine with centrally acting anti- tussive ingredient is not rationale
S.O. 964 (E)

261 Dextromethorphan
+Paracetamol+Cetirizine
+Phenylephrine
a,
1 Dosing schedule is incompatible.
2. Ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with the
reflexes.
3.Centrally acting anti-tussive not to be combined with anti-histaminic drug.
S.O. 965 (E)
262 Chlorpheniramine +Terpin
+Antimony Potassium
Tartrate+Ammonium
chloride+Sodium
Citrate+Menthol
a,
Pharmacodynamically irrelevant-
1. Chlorpheniramine :H1 antagonist are said to decrease rhinorrhea but the drying effect may do more harm
because of their tendency to induce somnolence
2. Ammonium Chloride: increase the mucus secretion in respiratory tract
S.O. 966 (E)
263 Terbutaline
Sulphate+Etofylline+Ambro
xol
a,
1. On the basis of current scientific understanding the FDC is pharmacodynamically irrelevant.
2. Use of Mucolytic alongwith anti-asthamatic drugs is liable to be misused as expectorant and exposing the
patients unnecessary to the drugs and their adverse effects.
S.O. 967 (E)
264 Paracetamol +Codeine
+Chlorpheniramine
a,
1 Dosing schedule is incompatible.
2. Both the ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with
the reflexes.
3.Paracetamol dose is subtherapeutic.
4.There is also a risk of abuse potential.
S.O. 968 (E)
265 Paracetamol
+Pseudoephedrine
+Cetirizine +Caffeine
a,
1.Pharmacodynamically and phamacokinetically irrational FDC.
2.Patients may need only one ingredient and use of FDC may lead to misuse.
3.Caffeine is CNS stimulant where as Pseudoephedrine leads to sedation.
4.Dosing shedule of the ingredients is incompatible.
S.O. 969 (E)
266 Chlorpheniramine
+Ammonium Chloride
+Menthol
a,
Pharmacodynamically irrelevant-
1. Chlorpheniramine :H1 antagonist are said to decrease rhinorrhea but the drying effect may do more harm
because of their tendency to induce somnolence
2. Ammonium Chloride: increase the mucus secretion in respiratory tract
S.O. 970 (E)
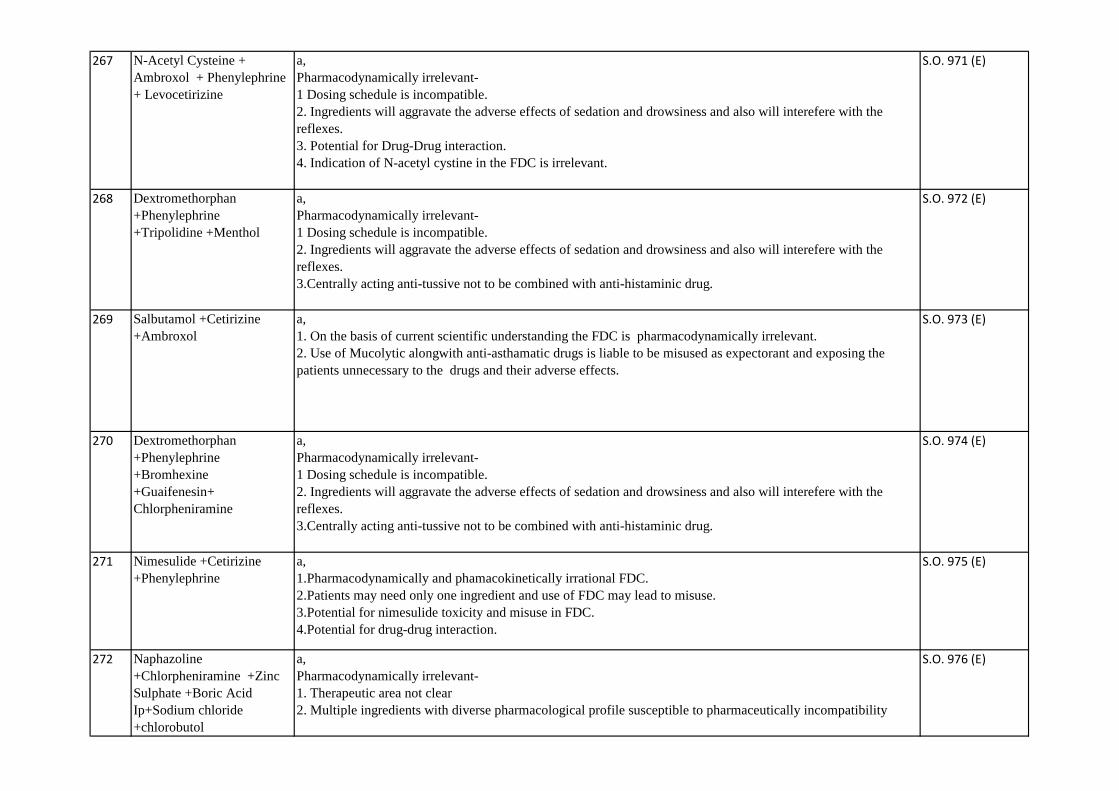
267 N-Acetyl Cysteine +
Ambroxol + Phenylephrine
+ Levocetirizine
a,
Pharmacodynamically irrelevant-
1 Dosing schedule is incompatible.
2. Ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with the
reflexes.
3. Potential for Drug-Drug interaction.
4. Indication of N-acetyl cystine in the FDC is irrelevant.
S.O. 971 (E)
268 Dextromethorphan
+Phenylephrine
+Tripolidine +Menthol
a,
Pharmacodynamically irrelevant-
1 Dosing schedule is incompatible.
2. Ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with the
reflexes.
3.Centrally acting anti-tussive not to be combined with anti-histaminic drug.
S.O. 972 (E)
269 Salbutamol +Cetirizine
+Ambroxol
a,
1. On the basis of current scientific understanding the FDC is pharmacodynamically irrelevant.
2. Use of Mucolytic alongwith anti-asthamatic drugs is liable to be misused as expectorant and exposing the
patients unnecessary to the drugs and their adverse effects.
S.O. 973 (E)
270 Dextromethorphan
+Phenylephrine
+Bromhexine
+Guaifenesin+
Chlorpheniramine
a,
Pharmacodynamically irrelevant-
1 Dosing schedule is incompatible.
2. Ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with the
reflexes.
3.Centrally acting anti-tussive not to be combined with anti-histaminic drug.
S.O. 974 (E)
271 Nimesulide +Cetirizine
+Phenylephrine
a,
1.Pharmacodynamically and phamacokinetically irrational FDC.
2.Patients may need only one ingredient and use of FDC may lead to misuse.
3.Potential for nimesulide toxicity and misuse in FDC.
4.Potential for drug-drug interaction.
S.O. 975 (E)
272 Naphazoline
+Chlorpheniramine +Zinc
Sulphate +Boric Acid
Ip+Sodium chloride
+chlorobutol
a,
Pharmacodynamically irrelevant-
1. Therapeutic area not clear
2. Multiple ingredients with diverse pharmacological profile susceptible to pharmaceutically incompatibility
S.O. 976 (E)

273 Paracetamol+Bromhexine
+Phenylephrine
+Chlorpheniramine
+Guaifenesin
a,
Pharmacodynamically irrelevant.
1.Mucolytic increases mucus secretion and antihistaminic with anti cholinergic properties dry up secretions.
2.Dosing schedule is incompatible.
3. Paracetamol dose is subtherapeutic.
S.O. 977 (E)
274 Salbutamoll+Bromhexine a,
1. On the basis of current scientific understanding the FDC is pharmacodynamically irrelevant.
2. Use of Mucolytic alongwith anti-asthamatic drugs is liable to be misused as expectorant and exposing the
patients unnecessary to the drugs and their adverse effects.
S.O. 978 (E)
275 Dextromethorphan
+Phenylephrine
+Guaifenesin +Cetirizine
+Acetaminophen
a,
1 Dosing schedule is incompatible.
2. Ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with the
reflexes.
3.Centrally acting anti-tussive not to be combined with anti-histaminic drug.
S.O. 979 (E)
276 Guaifenesin+ Bromhexine +
Chlorpheniramine +
Paracetamol
a,
Pharmacodynamically irrelevant-
1. Guaiphenesin:a mucolytic which increases mucus secretion should not given in combination with
antihistaminic with anti cholinergic properties, because due to anti cholinergic properties mucus secretions is
dried up.
2. paracetamol : addition of paracetamol express the consumers to the hepatotoxic effect of antipyretic
unnecessarily
3. Chlorpheniramine :H1 antagonist are said to decrease rhinorrhea but the drying effect may do more harm
because of their tendency to induce somnolence
4.All ingredients present in the FDC have different indications.
S.O. 980 (E)
277 Chlorpheniramine
+Ammonium Chloride
+Chloroform +Menthol
a,
Pharmacodynamically irrelevant-
1. Chlorpheniramine :H1 antagonist are said to decrease rhinorrhea but the drying effect may do more harm
because of their tendency to induce somnolence
2. Ammonium Chloride: increase the mucus secretion in respiratory tract
S.O. 981 (E)
278 Salbutamol +Choline
Theophylinate +Ambroxol
a,
1. On the basis of current scientific understanding the FDC is pharmacodynamically irrelevant.
2. Use of Mucolytic alongwith anti-asthamatic drugs is liable to be misused as expectorant and exposing the
patients unnecessary to the drugs and their adverse effects.
S.O. 982 (E)
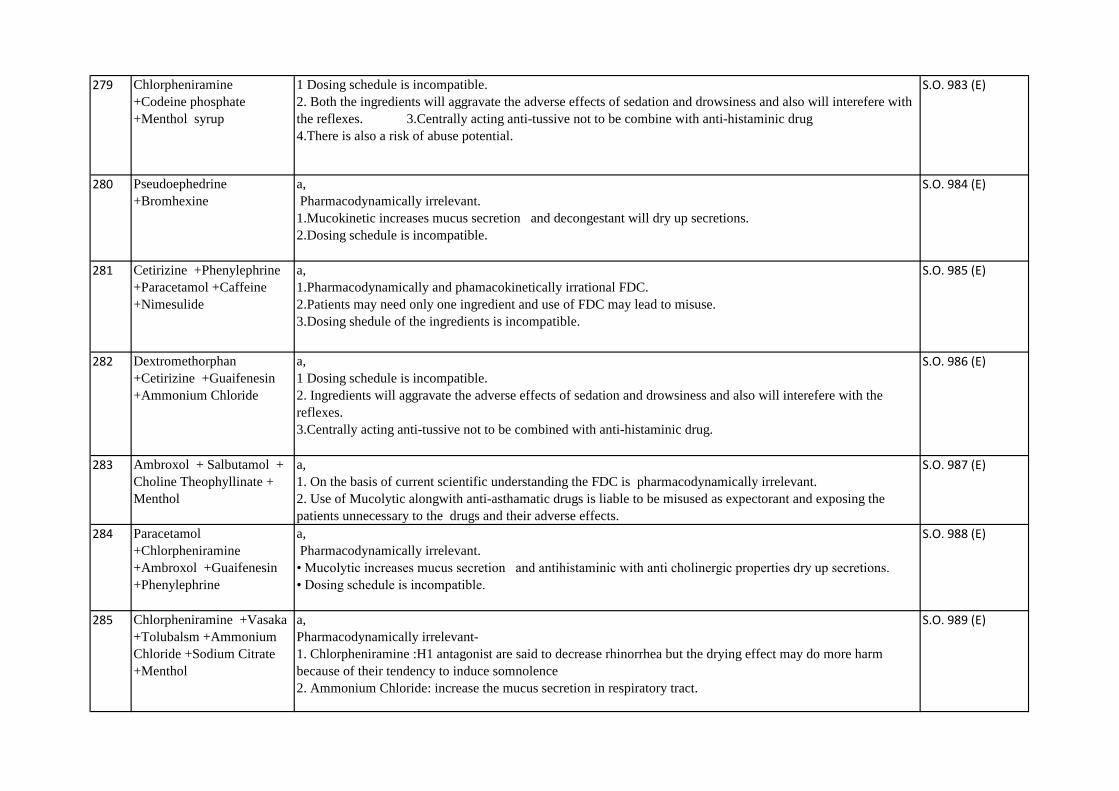
279 Chlorpheniramine
+Codeine phosphate
+Menthol syrup
1 Dosing schedule is incompatible.
2. Both the ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with
the reflexes. 3.Centrally acting anti-tussive not to be combine with anti-histaminic drug
4.There is also a risk of abuse potential.
S.O. 983 (E)
280 Pseudoephedrine
+Bromhexine
a,
Pharmacodynamically irrelevant.
1.Mucokinetic increases mucus secretion and decongestant will dry up secretions.
2.Dosing schedule is incompatible.
S.O. 984 (E)
281 Cetirizine +Phenylephrine
+Paracetamol +Caffeine
+Nimesulide
a,
1.Pharmacodynamically and phamacokinetically irrational FDC.
2.Patients may need only one ingredient and use of FDC may lead to misuse.
3.Dosing shedule of the ingredients is incompatible.
S.O. 985 (E)
282 Dextromethorphan
+Cetirizine +Guaifenesin
+Ammonium Chloride
a,
1 Dosing schedule is incompatible.
2. Ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with the
reflexes.
3.Centrally acting anti-tussive not to be combined with anti-histaminic drug.
S.O. 986 (E)
283 Ambroxol + Salbutamol +
Choline Theophyllinate +
Menthol
a,
1. On the basis of current scientific understanding the FDC is pharmacodynamically irrelevant.
2. Use of Mucolytic alongwith anti-asthamatic drugs is liable to be misused as expectorant and exposing the
patients unnecessary to the drugs and their adverse effects.
S.O. 987 (E)
284 Paracetamol
+Chlorpheniramine
+Ambroxol +Guaifenesin
+Phenylephrine
a,
Pharmacodynamically irrelevant.
• Mucolytic increases mucus secretion and antihistaminic with anti cholinergic properties dry up secretions.
• Dosing schedule is incompatible.
S.O. 988 (E)
285 Chlorpheniramine +Vasaka
+Tolubalsm +Ammonium
Chloride +Sodium Citrate
+Menthol
a,
Pharmacodynamically irrelevant-
1. Chlorpheniramine :H1 antagonist are said to decrease rhinorrhea but the drying effect may do more harm
because of their tendency to induce somnolence
2. Ammonium Chloride: increase the mucus secretion in respiratory tract.
S.O. 989 (E)

286 Bromhexine +Cetrizine
+Phenylephrine
+Guaifenesin +Menthol
a,
1.Pharmacologically no synergistic effect
2. Multiple ingredients with diverse pharmacological profile susceptible to pharmaceutically incompatibility.
3. Pharmacokinetically incompatibiliy.
S.O. 990 (E)
287 Dextromethorphan
+Ambroxol +Ammonium
Chloride +Chlorpheniramine
+Menthol
a,
1 Dosing schedule is incompatible.
2. Ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with the
reflexes.
3.Centrally acting anti-tussive not to be combined with anti-histaminic drug.
S.O. 991 (E)
288 Dextromethorphan
+Phenylephrine +Cetirizine
+Zinc +Menthol
a,
Pharmacodynamically irrelevant-
1 Dosing schedule is incompatible.
2. Ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with the
reflexes.
3.Centrally acting anti-tussive not to be combined with anti-histaminic drug.
S.O. 992 (E)
289 Terbutaline + N-Acetyl L-
Cysteine + Guaifenesin
a,
1. On the basis of current scientific understanding the FDC is pharmacodynamically irrelevant.
2. Use of Mucolytic alongwith anti-asthamatic drugs is liable to be misused as expectorant and exposing the
patients unnecessary to the drugs and their adverse effects.
S.O. 993 (E)
290 Calcium Gluconate
+Levocetirizine
a,
Pharmacodynamically irrelevant-
1.Each ingredients have different indication.
2.This combination does not follow the concept and purpose of FDC
S.O. 994 (E)
291 Paracetamol
+Levocetirizine+Pseudoeph
edrine
a,
1. Paracetamol dose high
2. Pharmacokinetic incompatibility.
3. Potential for drug-drug interaction.
S.O. 995 (E)
292 Salbutamol +Choline
Theophylinate
+Carbocisteine
a,
1. On the basis of current scientific understanding the FDC is pharmacodynamically irrelevant.
2. Use of Mucolytic alongwith anti-asthamatic drugs is liable to be misused as expectorant and exposing the
patients unnecessary to the drugs and their adverse effects.
S.O. 996 (E)

293 Chlorpheniramine +Vitamin
C
a,
Pharmacodynamically irrelevant FDC
S.O. 997 (E)
294 Calcium Gluconate
+Chlorpheniramine
+Vitamin C
a,
Pharmacodynamically irrelevant-
1.Each ingredients have different indication.
2.This combination does not follow the concept and purpose of FDC
S.O. 998 (E)
295 Chlorpheniramine+Paraceta
mol +Pseudoephedrine
+Caffeine
a,
1.Pharmacodynamically irrationale FDC.
2.Patients may need only one ingredient and use of FDC may lead to misuse.
3.Caffeine is CNS stimulant where as Pseudoephedrine leads to sedation.
S.O. 999 (E)
296 Guaifenesin +Bromhexine
+Chlorpheniramine
+Phenylephrine
+Paracetamol
+Serratiopeptidase (as
enteric coated
granules)10000 SP Units
a,
Pharmacodynamically irrelevant-
1. Guaiphenesin :a mucolytic which increases mucus secretion should not given in combination with
antihistaminic with anti cholinergic properties, because due to anti cholinergic properties mucus secretions is
dried up.
2. Chlorpheniramine :H1 antagonist are said to decrease rhinorrhea but the drying effect may do more harm
because of their tendency to induce somnolence
3. paracetamol : as cough and cold not allows accompanied by fever, addition of paracetamol express the
consumers to the hepatotoxic effect of antipyretic unnecessarily
4. All ingredients have different therapeutic indications.
S.O. 1000 (E)
297 Paracetamol +Pheniramine a,
Pharmacodynamically irrelevant-
1. Both ingredients have different indications.
2. Misuse and toxicity of paracetamol.
S.O. 1001 (E)
298 Betamethasone +Fusidic
Acid+Gentamycin
+Tolnaftate+Iodochlorhydro
xyquinoline(ICHQ)
a,
Pharmacodynamically irrelevant-
1.Each ingredients of FDC has different therapeutic indication and is at variance from the concept and purpose of
FDC.
2. Combining antibiotics , antifungal, steroid in the present FDC is liable to be misused and emergence of
resistance and adverse effects 3.use of steroid in case of fungal infection might actually worsen the treatment as it
encourages fungal growth.No study is found supporting the combined use of an anti bacterial with an anti fungal
ingredient.
S.O. 1002 (E)

299 Clobetasol
+Ofloxacin+Miconazole
+Zinc Sulphate
a,
Pharmacodynamically irrelevant-
1.Each ingredients of FDC has different therapeutic indication and is at variance from the concept and purpose of
FDC.
2. Combining antibiotics , antifungal, steroid in the present FDC is liable to be misused and emergence of
resistance and adverse effects 3.use of steroid in case of fungal infection might actually worsen the treatment as it
encourages fungal growth.No study is found supporting the combined use of an anti bacterial with an anti fungal
ingredient.
S.O. 1003 (E)
300 Clobetasole +Gentamicin
+Miconazole +Zinc
Sulphate
a,
Pharmacodynamically irrelevant-
1.Each ingredients of FDC has different therapeutic indication and is at variance from the concept and purpose of
FDC.
2. Combining antibiotics , antifungal, steroid in the present FDC is liable to be misused and emergence of
resistance and adverse effects 3.use of steroid in case of fungal infection might actually worsen the treatment as it
encourages fungal growth.No study is found supporting the combined use of an anti bacterial with an anti fungal
ingredient.
S.O. 1004 (E)
301 levocetirizine + ambroxol +
phenylephrine +
paracetamol
a,
1 Dosing schedule is incompatible.
2. Patients may need only one or two ingredients and use of FDC may lead to misuse.
S.O. 1005 (E)
302 Permethrin + Cetrimide +
Menthol
a,
1.This FDC has no therapeutic value.
S.O. 1006 (E)
303 beclomethasone +
clotimazole + neomycin +
iodochlorohydroxyquinone
a,
Pharmacodynamically irrelevant-
1.Each ingredients of FDC has different therapeutic indication and is at variance from the concept and purpose of
FDC.
2. Combining antibiotics , antifungal, steroid ,iodochlorohydroxyquinone in the present FDC is liable to be
misused and emergence of resistance and adverse effects 3.use of steroid in case of fungal infection might
actually worsen the treatment as it encourages fungal growth.No study is found supporting the combined use of
an anti bacterial with an anti fungal ingredient.
S.O. 1007 (E)
304 Neomycin + Doxycycline a,
Pharmacodynamically irrelevant-
1. Patient may need only one ingredient
2. Drug misuse should not be there for diagnostic uncertainty
3. Inadvertent use of antimicrobials may lead to emergence of resistence
4. No published literature supporting this combination of products found
S.O. 1008 (E)

305 Ciprofloxacin +
Fluocinolone +
Clotrimazole + Neomycin +
Chlorocresol
a,
Pharmacodynamically irrelevant-
1.Each ingredients of FDC has different therapeutic indication and is at variance from the concept and purpose of
FDC.
2. Combining two antibiotics , antifungal, steroid in the present FDC is liable to be misused and emergence of
resistance and adverse effects.
3.NO study is found supporting the combined use of ingredients in this FDC.
S.O. 1009 (E)
306 Clobetasol + Ofloxacin +
Ketoconazole + Zinc
Sulphate
a,
Pharmacodynamically irrelevant-
1.Each ingredients of FDC has different therapeutic indication and is at variance from the concept and purpose of
FDC.
2. Combining antibiotics , antifungal, steroid in the present FDC is liable to be misused and emergence of
resistance and adverse effects 3.use of steroid in case of fungal infection might actually worsen the treatment as it
encourages fungal growth.No study is found supporting the combined use of an anti bacterial with an anti fungal
ingredient.
S.O. 1010 (E)
307 Betamethasone
+Gentamicin +Tolnaftate
+Iodochlorhydroxyquinoline
a,
Pharmacodynamically irrelevant-
1.Each ingredients of FDC has different therapeutic indication and is at variance from the concept and purpose of
FDC.
2. Combining antibiotics , antifungal, steroid ,iodochlorohydroxyquinone in the present FDC is liable to be
misuse and emergence of resistance and adverse effects 3.Use of steroid in case of fungal infection might actually
worsen the treatment as it encourages fungal growth.No study is found supporting the combined use of an anti
bacterial with an anti fungal ingredient.
S.O. 1011 (E)
308 Clobetasol +Gentamicin
+Tolnaftate
+Idochlorhydroxyquinone
+Ketoconazole
a,
Pharmacodynamically irrelevant-
1.Each ingredients of FDC has different therapeutic indication and is at variance from the concept and purpose of
FDC.
2. Combining antibiotics , antifungal, steroid in the present FDC is liable to be misuse and emergence of
resistance and adverse effects 3.Use of steroid in case of fungal infection might actually worsen the treatment as
it encourages fungal growth.No study is found supporting the combined use of an anti bacterial with an anti
fungal ingredient.
S.O. 1012 (E)
309 Allantoin+Dimethieone+Ure
a+Propylene+Glycerin+Liqu
id paraffin
This FDC was earlier discussed by previous Committee on 22.8.2014 as under:
Firm did not turn up for presentation. The FDC is not rational as ingredients present in the FDC have antagonistic
functions. Further, there are no supporting documents to prove that the FDC is rational for the proposed
indication. Hence, the committee did not recommend.
S.O. 1013 (E)
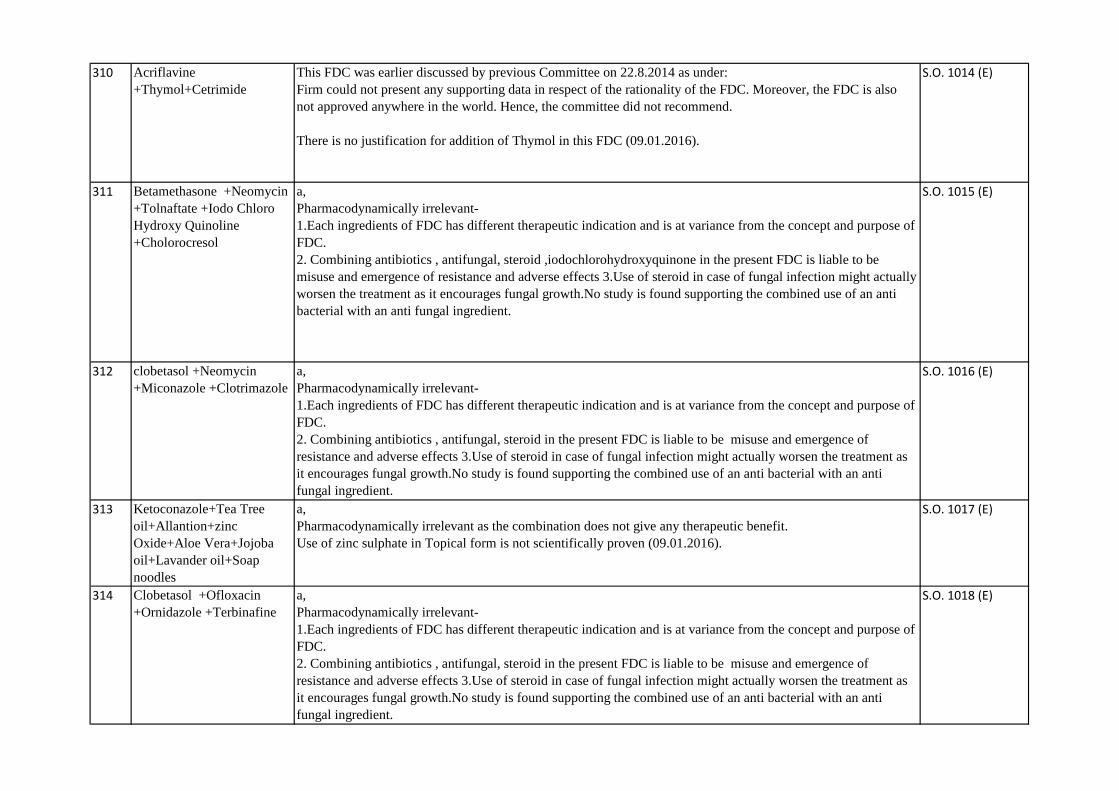
310 Acriflavine
+Thymol+Cetrimide
This FDC was earlier discussed by previous Committee on 22.8.2014 as under:
Firm could not present any supporting data in respect of the rationality of the FDC. Moreover, the FDC is also
not approved anywhere in the world. Hence, the committee did not recommend.
There is no justification for addition of Thymol in this FDC (09.01.2016).
S.O. 1014 (E)
311 Betamethasone +Neomycin
+Tolnaftate +Iodo Chloro
Hydroxy Quinoline
+Cholorocresol
a,
Pharmacodynamically irrelevant-
1.Each ingredients of FDC has different therapeutic indication and is at variance from the concept and purpose of
FDC.
2. Combining antibiotics , antifungal, steroid ,iodochlorohydroxyquinone in the present FDC is liable to be
misuse and emergence of resistance and adverse effects 3.Use of steroid in case of fungal infection might actually
worsen the treatment as it encourages fungal growth.No study is found supporting the combined use of an anti
bacterial with an anti fungal ingredient.
S.O. 1015 (E)
312 clobetasol +Neomycin
+Miconazole +Clotrimazole
a,
Pharmacodynamically irrelevant-
1.Each ingredients of FDC has different therapeutic indication and is at variance from the concept and purpose of
FDC.
2. Combining antibiotics , antifungal, steroid in the present FDC is liable to be misuse and emergence of
resistance and adverse effects 3.Use of steroid in case of fungal infection might actually worsen the treatment as
it encourages fungal growth.No study is found supporting the combined use of an anti bacterial with an anti
fungal ingredient.
S.O. 1016 (E)
313 Ketoconazole+Tea Tree
oil+Allantion+zinc
Oxide+Aloe Vera+Jojoba
oil+Lavander oil+Soap
noodles
a,
Pharmacodynamically irrelevant as the combination does not give any therapeutic benefit.
Use of zinc sulphate in Topical form is not scientifically proven (09.01.2016).
S.O. 1017 (E)
314 Clobetasol +Ofloxacin
+Ornidazole +Terbinafine
a,
Pharmacodynamically irrelevant-
1.Each ingredients of FDC has different therapeutic indication and is at variance from the concept and purpose of
FDC.
2. Combining antibiotics , antifungal, steroid in the present FDC is liable to be misuse and emergence of
resistance and adverse effects 3.Use of steroid in case of fungal infection might actually worsen the treatment as
it encourages fungal growth.No study is found supporting the combined use of an anti bacterial with an anti
fungal ingredient.
S.O. 1018 (E)
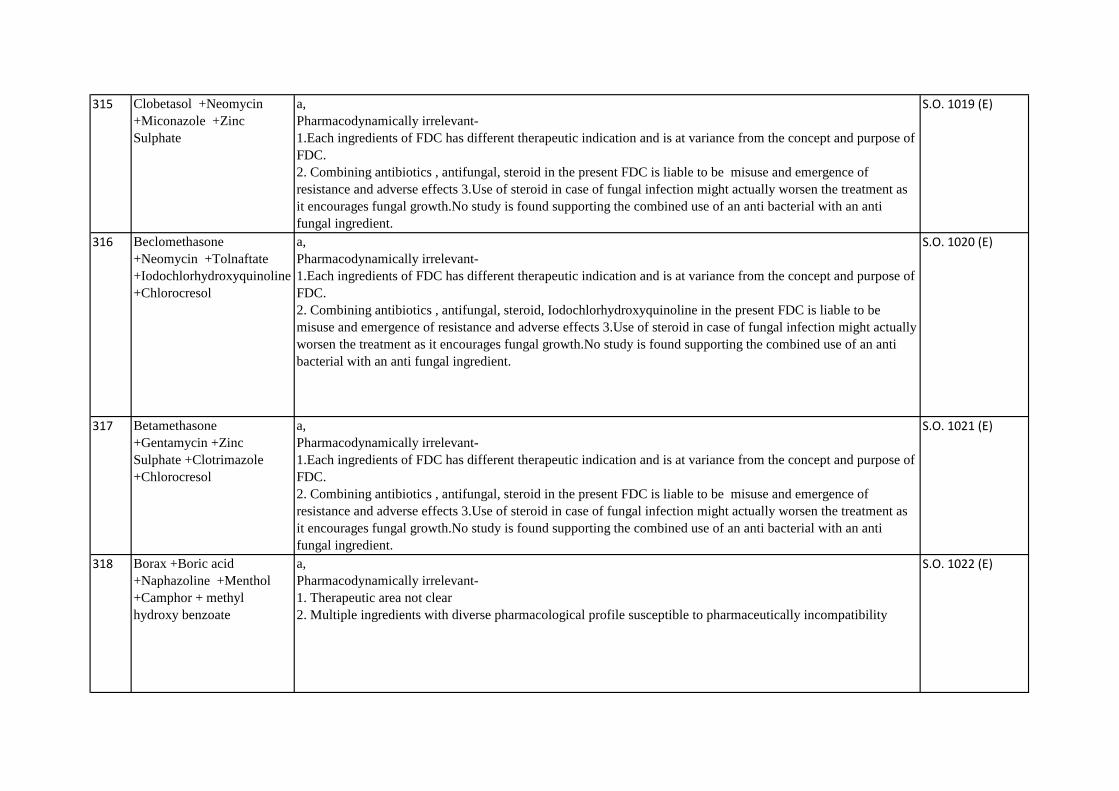
315 Clobetasol +Neomycin
+Miconazole +Zinc
Sulphate
a,
Pharmacodynamically irrelevant-
1.Each ingredients of FDC has different therapeutic indication and is at variance from the concept and purpose of
FDC.
2. Combining antibiotics , antifungal, steroid in the present FDC is liable to be misuse and emergence of
resistance and adverse effects 3.Use of steroid in case of fungal infection might actually worsen the treatment as
it encourages fungal growth.No study is found supporting the combined use of an anti bacterial with an anti
fungal ingredient.
S.O. 1019 (E)
316 Beclomethasone
+Neomycin +Tolnaftate
+Iodochlorhydroxyquinoline
+Chlorocresol
a,
Pharmacodynamically irrelevant-
1.Each ingredients of FDC has different therapeutic indication and is at variance from the concept and purpose of
FDC.
2. Combining antibiotics , antifungal, steroid, Iodochlorhydroxyquinoline in the present FDC is liable to be
misuse and emergence of resistance and adverse effects 3.Use of steroid in case of fungal infection might actually
worsen the treatment as it encourages fungal growth.No study is found supporting the combined use of an anti
bacterial with an anti fungal ingredient.
S.O. 1020 (E)
317 Betamethasone
+Gentamycin +Zinc
Sulphate +Clotrimazole
+Chlorocresol
a,
Pharmacodynamically irrelevant-
1.Each ingredients of FDC has different therapeutic indication and is at variance from the concept and purpose of
FDC.
2. Combining antibiotics , antifungal, steroid in the present FDC is liable to be misuse and emergence of
resistance and adverse effects 3.Use of steroid in case of fungal infection might actually worsen the treatment as
it encourages fungal growth.No study is found supporting the combined use of an anti bacterial with an anti
fungal ingredient.
S.O. 1021 (E)
318 Borax +Boric acid
+Naphazoline +Menthol
+Camphor + methyl
hydroxy benzoate
a,
Pharmacodynamically irrelevant-
1. Therapeutic area not clear
2. Multiple ingredients with diverse pharmacological profile susceptible to pharmaceutically incompatibility
S.O. 1022 (E)
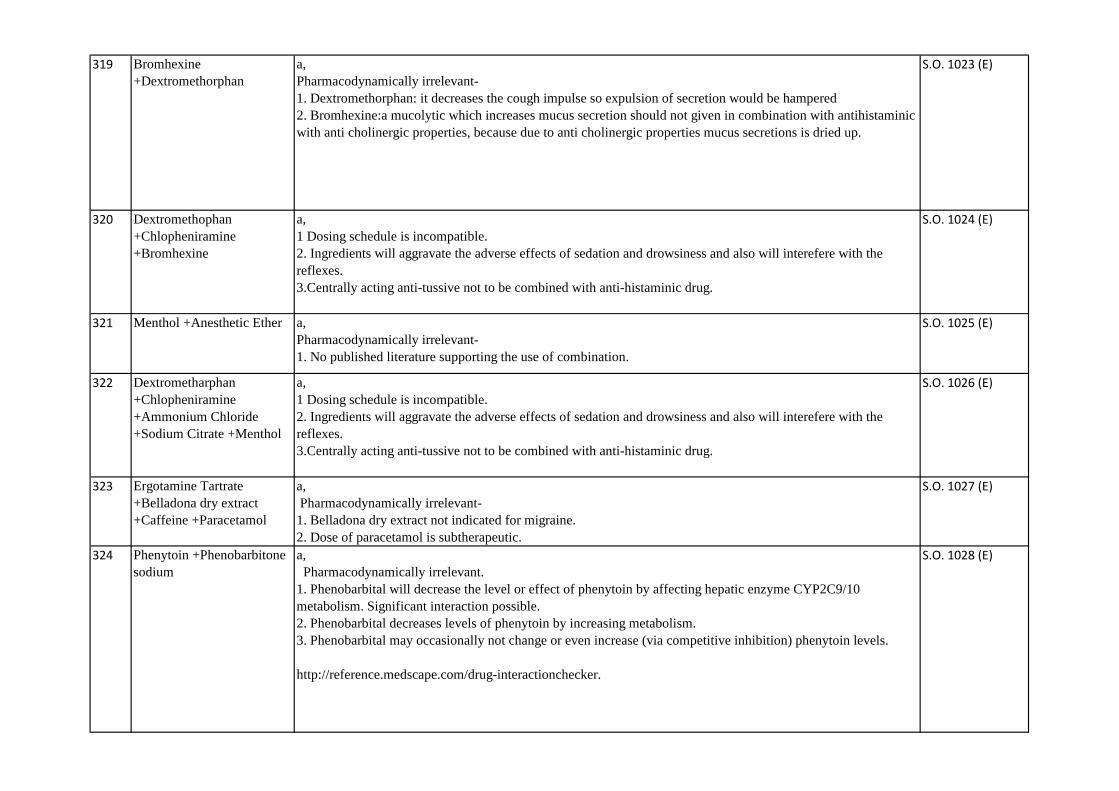
319 Bromhexine
+Dextromethorphan
a,
Pharmacodynamically irrelevant-
1. Dextromethorphan: it decreases the cough impulse so expulsion of secretion would be hampered
2. Bromhexine:a mucolytic which increases mucus secretion should not given in combination with antihistaminic
with anti cholinergic properties, because due to anti cholinergic properties mucus secretions is dried up.
S.O. 1023 (E)
320 Dextromethophan
+Chlopheniramine
+Bromhexine
a,
1 Dosing schedule is incompatible.
2. Ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with the
reflexes.
3.Centrally acting anti-tussive not to be combined with anti-histaminic drug.
S.O. 1024 (E)
321 Menthol +Anesthetic Ether a,
Pharmacodynamically irrelevant-
1. No published literature supporting the use of combination.
S.O. 1025 (E)
322 Dextrometharphan
+Chlopheniramine
+Ammonium Chloride
+Sodium Citrate +Menthol
a,
1 Dosing schedule is incompatible.
2. Ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with the
reflexes.
3.Centrally acting anti-tussive not to be combined with anti-histaminic drug.
S.O. 1026 (E)
323 Ergotamine Tartrate
+Belladona dry extract
+Caffeine +Paracetamol
a,
Pharmacodynamically irrelevant-
1. Belladona dry extract not indicated for migraine.
2. Dose of paracetamol is subtherapeutic.
S.O. 1027 (E)
324 Phenytoin +Phenobarbitone
sodium
a,
Pharmacodynamically irrelevant.
1. Phenobarbital will decrease the level or effect of phenytoin by affecting hepatic enzyme CYP2C9/10
metabolism. Significant interaction possible.
2. Phenobarbital decreases levels of phenytoin by increasing metabolism.
3. Phenobarbital may occasionally not change or even increase (via competitive inhibition) phenytoin levels.
http://reference.medscape.com/drug-interactionchecker.
S.O. 1028 (E)

325 Gliclazide 40mg+Metformin
400mg
a,
Sub-therapeutic dose of metformin.
S.O. 1029 (E)
326 Paracetamol + Ambroxol +
Phenylephrine
+Chlorpheniramine
a,
Pharmacodynamically irrelevant
1. Dosing schedule is incompatible.
2. Ingredients will aggravate the adverse effects of sedation and drowsiness and also will interefere with the
reflexes.
3.Potential for drug-drug interaction.
S.O. 1030 (E)
327 Oflaxacin + Ornidazole
suspension
a,
1. Both ingredients of the FDC have different therapeutic indcations
2.Inappropriate use of ornidazole will lead to emergence of antibiotic resistance against quinalones.
3. Safety concerns in paediatric patients.
S.O. 1031 (E)
328 Albuterol + Etofylline +
Bromhexine + Menthol
a,
1. Etofylline is a narrow therapeutic indexed drug and requires close monitoring.
2.Patients may need only one ingredient and use of FDC may lead to misuse.
S.O. 1032 (E)
329 Albuterol + Bromhexine +
Theophylline
a,
1. Theophylline is a narrow therapeutic indexed drug and requires close monitoring.
2.Patients may need only one ingredient and use of FDC may lead to misuse.
S.O. 1033 (E)
330 Salbutamol +
Hydroxyethyltheophylline
(Etofylline)+ Bromhexine
a,
1. On the basis of current scientific understanding the FDC is pharmacodynamically irrelevant.
2. Use of Mucolytic alongwith anti-asthamatic drugs is liable to be misused as expectorant and exposing the
patients unnecessary to the drugs and their adverse effects.
S.O. 1034 (E)
331 Paracetamol +Phenylephrine
+Levocetirizine +Sodium
Citrate
a,
1.Pharmacodynamically and phamacokinetically irrational FDC.
2.Patients may need only one ingredient and use of FDC may lead to misuse.
3.Dosing shedule of the ingredients is incompatible.
4. Potential for drug-drug interaction.
S.O. 1035 (E)
332 Paracetamol
+Propyphenazone +Caffeine
a,
Pharmacodynamically irrelevant-
1. Paracetamol dose is subtherapeutic.
2. Suceptibility of adverse drug reaction is very high.
3. Misuse potential.
S.O. 1036 (E)

333 Guaifenesin
+Diphenhydramine
+Bromhexine
+Phenylephrine
a,
Pharmacodynamically irrelevant-
• Anticholinergic property of diphenhydramine will lead to drying up of secretions while mucolytics increase.
S.O. 1037 (E)
334 Dried Alumnium Hydroxide
Gel +Propantheline Bromide
+Diazepam
a,
Pharmacodynamically irrelevant-
1. No published literature supporting the FDC.
2. In present scenario Propanthaline has safety concerns.
3. Use of diazepam is irrational.
S.O. 1038 (E)
335 Bromhexine
+Phenylephrine
+Chlorpheniramine
+Paracetamol
a,
Pharmacodynamically irrelevant-
1. Bromhexine :a mucolytic which increases mucus secretion should not given in combination with
antihistaminic with anti cholinergic properties, because due to anti cholinergic properties mucus secretions is
dried up.
2. Chlorpheniramine :H1 antagonist are said to decrease rhinorrhea but the drying effect may do more harm
because of their tendency to induce somnolence
3. Potential misuse in FDC formualtion is likely to be hepatotoxic .
S.O. 1039 (E)
336 Beclomethasone
+Clotrimazole+Gentamicin+
IodoChlorhydroxyquinoline
a,
Pharmacodynamically irrelevant-
1.Each ingredients of FDC has different therapeutic indication and is at variance from the concept and purpose of
FDC.
2. Combining antibiotics , antifungal, steroid, Iodochlorhydroxyquinoline in the present FDC is liable to be
misuse and emergence of resistance and adverse effects 3.Use of steroid in case of fungal infection might actually
worsen the treatment as it encourages fungal growth.No study is found supporting the combined use of an anti
bacterial with an anti fungal ingredient.
S.O. 1040 (E)
337 Telmisartan + Metformin a,
Pharmacodynamically irrelevant as no study supports this combination.
S.O. 1041 (E)
338 Ammonium
Citrate+Vitamin B 12+Folic
Acid+Zinc Sulphate
a,
Pharmacodynamically irrelevant-
1. Therapeutic area not clear
2. ingredients susceptible to pharmaceutically incompatibility
S.O. 1042 (E)

339 levothyroxine pyridoxine+
nicotinamide
a,
Pharmacodynamically irrelevant-
1.Each ingredients of FDC has different therapeutic indication and is at variance from the concept and purpose of
FDC.
S.O. 1043 (E)
340 benfotiamine+ metformin This was discussed by previous Committee on 27.08.14 as under-
The committee noted that the proposed FDC was also discussed earlier by NDAC on 06.10.2012.
There is not enough published data particularly in the human subjects regarding the efficacy. The data
presented by the firm(s) has been examined scientifically and firm has presented only animal study
data. The firm fails to present clinical data about synergistic effect of this FDC over other drugs present
in FDC. Moreover no scientific publication recommends this combination. This combination is also not
approved anywhere in the world. Hence the committee did not recommend for the manufacturing and
marketing of this FDC.
S.O. 1044 (E)
341 Thyroid +Thiamine +
Riboflavin + Pyridoxine +
Calcium Pantothenate +
Tocopheryl Acetate
+Nicotinamide
a,
No clinical studies found supporting the use of this combination
S.O. 1045 (E)
342 Ascorbic Acid + Manadione
Sodium Bisulphate+ Rutin +
Dibasic Calcium Phosphate
+ Adrenochrome Mono
Semicarbazone
a, Pharmacodynamically irrelevant-
1. Therapeutic area not clear
2. Multiple ingredients with diverse pharmacological profile.
S.O. 1046 (E)
343 Phenylephrine
+Chlorpheniramine
+Paracetamol +Bromhexine
+Caffeine
a,
1.Pharmacodynamically and phamacokinetically irrational FDC.
2.Patients may need only one ingredient and use of FDC may lead to misuse.
3.Dosing shedule of the ingredients is incompatible.
4.Mucolytic increases mucus secretion and antihistaminic with anti cholinergic properties dry up secretions.
S.O. 1047 (E)
344 Clotrimazole
+Beclomethasone
+Lignocaine +Ofloxacin
+Acetic Acid + Sodium
Methyl Paraben +Propyl
Paraben
a,
Pharmacodynamically irrelevant-
1.Each ingredients of FDC has different therapeutic indication and is at variance from the concept and purpose of
FDC.
2. Combining antibiotic , antifungal, steroid in the present FDC is liable to be misuse and emergence of
resistance and adverse effects.
3.Use of steroid in case of fungal infection might actually worsen the treatment as it encourages fungal growth.
NO study is found supporting the combined use of an antibacterial with an antifungal ingredient.
4.Lignocaine use in discharging ear is not required (07.01.2016).
S.O. 1048 (E)

345 Nimesulide + Levocetirizine
The FDC of Nimesulide + Levocetirizine was deliberated by SEC (Pulmonary) in its meeting held on
24.09.2014.
The committee examined and opined that the FDC is not rational as levocetirizine is anti-histaminic whereas
Nimesulide is an antipyretic analgesic and the combination is likely to be misused/overused in situations where
single drug is required. Further this FDC is not approved anywhere in the world. Hence the committee did not
recommended for its continued marketing in the country.
S.O.1851 (E)
DATED
08.06.2017
346 Ofloxacin + Ornidazole
injection
The FDC of Ofloxacin + Ornidazole injection was deliberated by NDAC (Antimicrobial, Antiparasitic,
Antifungal & Antiviral) in its meeting held on 28.02.2014 . The Committee noted the recommendation of the
Parliament Standing Committee (PSC) and evaluated this drug in present scenario. The firm presented the data of
phase III trial data. The committee noted that parenteral use of antibacterial in acute diarrhoea is not
recommended routinely. There is no specific advantage of giving Fluroquinolone and imidazole in parental form
as both can be given individually, if indicated. The FDC will not be rationale. Hence, the committee did not
recommend the FDC for continued marketing in India for the present approved indication of diarrhoea.
S.O.1852 (E)
DATED
08.06.2017
347 Gemifloxacin + Ambroxol The FDC of Gemifloxacin with Ambroxol was deliberated by SEC (Pulmonary) in its meeting held on 23-12-
2015. The proposal of continued marketing of Gemifloxacin + Ambroxol was deliberated in current scenario.
The Committee opined that Ambroxol being a mucolytic agent does not have any added advantage in the
antimicrobial activity. Therefore the Committee considered the FDC as irrational in current scenario and did not
recommend for its continued marketing.
S.O.1853 (E)
DATED
08.06.2017
348 Glucosamine + Ibuprofen The FDC of Glucosamine with Ibuprofen was deliberated by SEC (Analgesic & Rheumatology) in its meeting
held on 15.01.2016.
The Committee reviewed the FDC for its continued marketing in the Country. Committee opined that
glucosamine is required for long term use whereas Ibuprofen being NSAID is not recommended for long term.
Thus the FDC would lead to unnecessary overuse of NSAID leading to toxicity. Further the FDC is also not
approved Internationally. Hence the Committee did not recommend for its continued marketing.
S.O.1854 (E)
DATED
08.06.2017
349 Etodolac + Paracetamol The FDC of Etodolac + Paracetamol was deliberated by NDAC (Analgesics, Anesthetics & Rheumatology) in its
meeting held on 19.02.2014. The committee noted the recommendations of the PSC. The committee evaluated
the safety and efficacy reports presented by the firm. The committee observed that the product shall not be
prescribed more than 10 days as claimed by the firm. The committee opined that FDC is not required for short
term use as Paracetamol can be prescribed separately when required and can be tapered off early if need arises.
The committee recommended that the FDC is not rationale as present scenario.
S.O.1855 (E)
DATED
08.06.2017
Details of 05 FDCs are as under:

REPORTABLE
IN THE SUPREME COURT OF INDIA
CIVIL APPELLATE JURISDICTION
CIVIL APPEAL NO. 22972 OF 2017(ARISING OUT OF SLP (C) NO.7061 OF 2017
UNION OF INDIA AND ANR. …APPELLANTS
VERSUS
PFIZER LIMITED AND ORS. ...RESPONDENTS
WITH
CIVIL APPEAL NOS. 22973-22981 OF 2017(ARISING OUT OF SLP (C) NO.10170-10178 OF 2017)
CIVIL APPEAL NOS. 22982-23404 OF 2017(ARISING OUT OF SLP (C) NO.28960-29382 OF 2017)
TRANSFERRED CASE (C) NO.29 OF 2017
TRANSFERRED CASE (C) NO.30 OF 2017
TRANSFERRED CASE (C) NO.31 OF 2017
TRANSFERRED CASE (C) NO.32 OF 2017
TRANSFERRED CASE (C) NO.33 OF 2017
TRANSFERRED CASE (C) NO.34 OF 2017
TRANSFERRED CASE (C) NO.35 OF 2017
TRANSFERRED CASE (C) NO.36 OF 2017
1
Admin
Typewriter
Annexure -2
Admin
Typewriter
TRANSFERRED CASE (C) NO.38 OF 2017
TRANSFERRED CASE (C) NO.39 OF 2017
TRANSFERRED CASE (C) NO.40 OF 2017
TRANSFERRED CASE (C) NO.41 OF 2017
TRANSFERRED CASE (C) NO.42 OF 2017
TRANSFERRED CASE (C) NO.43 OF 2017
TRANSFERRED CASE (C) NO.44 OF 2017
TRANSFERRED CASE (C) NO.45 OF 2017
TRANSFER PETITION (C) NOS.1176-1182 OF 2017
TRANSFERRED CASE (C) NO.258 OF 2017
TRANSFERRED CASE (C) NO.259 OF 2017
TRANSFERRED CASE (C) NO.260 OF 2017
TRANSFERRED CASE (C) NO.261 OF 2017
TRANSFERRED CASE (C) NO.262 OF 2017
TRANSFERRED CASE (C) NO.263 OF 2017
TRANSFERRED CASE (C) NO.264 OF 2017
TRANSFERRED CASE (C) NO.265 OF 2017
TRANSFERRED CASE (C) NO.266 OF 2017
CIVIL APPEAL NOS. 23405-23472 OF 2017(ARISING OUT OF SLP (C) NOS. 36044-36111 OF 2017
Diary No.28274 of 20172
TRANSFERRED CASE (C) NOS. 308-317 OF 2017(ARISING OUT OF T.P. (C) NOS.2108-2117 OF 2017)
J U D G M E N T
R.F. Nariman, J.
1. Leave granted.
2. The present appeals and transfer petitions relate to the
interpretation of Section 26A of the Drugs and Cosmetics Act,
1940 (hereinafter referred to as “the Drugs Act”). By the
impugned judgment of the learned single Judge of the Delhi
High Court dated 1.12.2016, the learned single Judge has held
that the mandatory condition precedent for the exercise of the
power by the Central Government under Section 26A of the
Drugs Act is the prior consultation of the Drugs Technical
Advisory Board (DTAB) set up under Section 5 of the said Act.
It must be stated that the learned single Judge differed from
judgments of the Karnataka and Madras High Courts in this
regard, wherein two other learned single Judges of two other
3
High Courts have held that such consultation with the DTAB is
not mandatory before exercise of such power under Section
26A. Since we are concerned only with this narrow question
that has been decided by the learned single Judge of the Delhi
High Court, we are not going into any other contentions that
have been raised by learned counsel for the parties.
3. The issue regarding the prevalence of many Fixed Dose
Combinations (hereinafter referred to “FDCs”) that were
flooding the Indian market and had not been tested for efficacy
or safety was considered by the Parliamentary Standing
Committee on Health and Family Welfare in its 59th Report in
May, 2012. The Standing Committee observed that some of
the State Licensing Authorities have issued manufacturing
licenses for a very large number of FDCs without prior
clearance from the Central Drugs Standard Control
Organization (CDSCO). Such FDCs can pose significant risks
to persons and need to be withdrawn immediately in that
human lives can be at risk. The Committee recommended that
a clear and transparent policy may be framed for approving
FDCs based on scientific principles, and that, at present,
4

Section 26A of the Drugs Act is adequate to deal with the
problem of FDCs not cleared by the CDSCO. Pursuant to the
aforesaid report, the Ministry of Health in October, 2012 issued
directions to States and Union Territories under Section 33P of
the Drugs Act not to grant licenses to FDCs falling under the
definition of “new drugs” and not approved by the Drug
Controller General of India (DCG(I)). The DCG(I), in turn, had
requested all States/Union Territories Drug Controllers to ask
concerned manufacturers in their respective States/Union
Territories to prove the safety and efficacy of such FDC licenses
issued prior to 1.10.2012, without due approval of the DCG(I),
within a period of 18 months, failing which such FDCs would be
considered for being prohibited, both qua manufacture and
marketing in the country. On 5.7.2013, the DCG(I) vide its
communication to the State Drug Controllers asked
manufacturers to make applications as per the procedure
prescribed within this 18 month period. We have been informed
that a large number of applications were received from the
manufacturers within the 18 month period for 2911 products,
which had to be subjected to examination.
5

4. With the approval of the Ministry of Health and Family
Welfare, the CDSCO constituted 10 different Committees for
examination of the said applications which were received on
3.2.2014. As the said Committees could examine only about
295 applications, on 16.9.2014, the Ministry of Health and
Family Welfare constituted a Committee under the
Chairmanship of Professor C.K. Kokate, Vice Chancellor of KLE
University, Belgaum, Karnataka for examining the safety and
efficacy as per the following terms of reference:
a. Those FDCs which are considered grosslyirrational/unsafe based on pharmacokinetic andpharmacodynamic interaction, dosagecompatibilities of FDCs vis-a-vis that of singleingredients present in the FDC and availableliterature/evidence.b. Those FDCs which the Committee mayconsider necessary for further deliberation with anyof the 10 Expert Committees already constituted.
c. Those FDCs which are considered as safeand effective based on pharmacokinetic andpharmacodynamic interaction, dosagecompatibilities of FDCS vis-a-vis that of singleingredients present in the FDC, availableliterature/evidence, clinical experience and otherdata available.
d. Those FDCs which may be considered asrational, based on present data and knowledgeavailable. However, data in post market scenario is
6
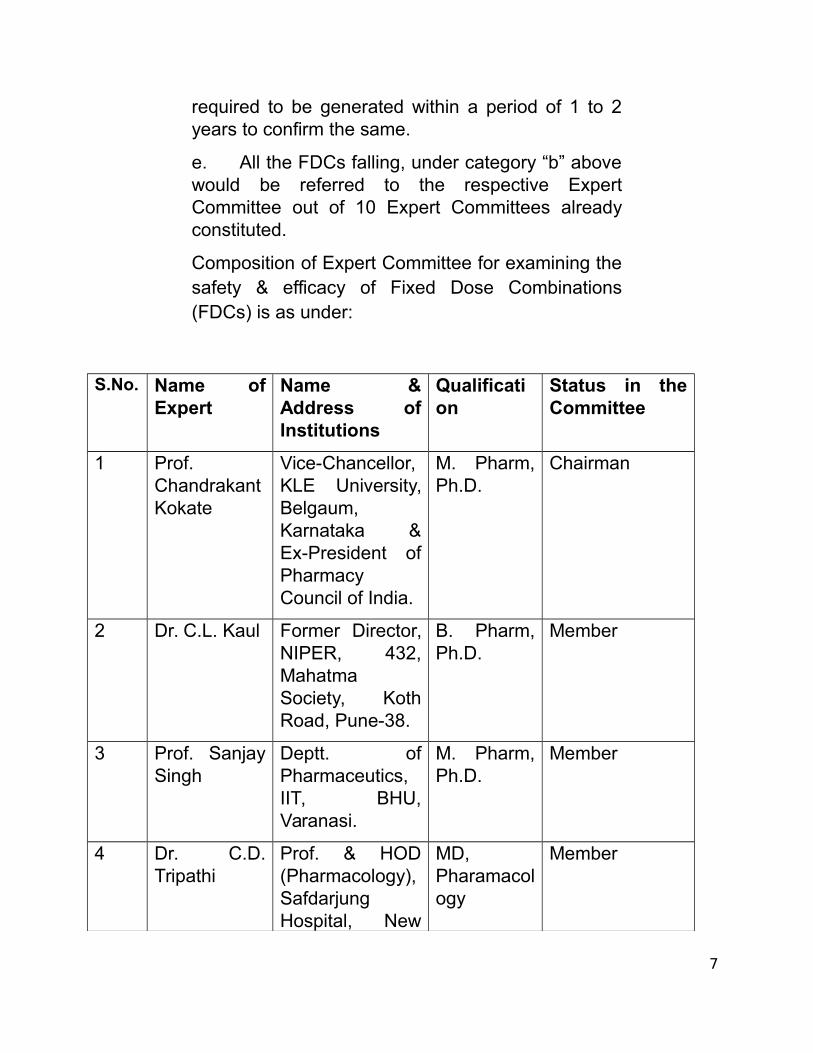
required to be generated within a period of 1 to 2years to confirm the same.
e. All the FDCs falling, under category “b” abovewould be referred to the respective ExpertCommittee out of 10 Expert Committees alreadyconstituted.
Composition of Expert Committee for examining thesafety & efficacy of Fixed Dose Combinations(FDCs) is as under:
S.No. Name ofExpert
Name &Address ofInstitutions
Qualification
Status in theCommittee
1 Prof.ChandrakantKokate
Vice-Chancellor,KLE University,Belgaum,Karnataka &Ex-President ofPharmacyCouncil of India.
M. Pharm,Ph.D.
Chairman
2 Dr. C.L. Kaul Former Director,NIPER, 432,MahatmaSociety, KothRoad, Pune-38.
B. Pharm,Ph.D.
Member
3 Prof. SanjaySingh
Deptt. ofPharmaceutics,IIT, BHU,Varanasi.
M. Pharm,Ph.D.
Member
4 Dr. C.D.Tripathi
Prof. & HOD(Pharmacology),SafdarjungHospital, New
MD,Pharamacology
Member
7
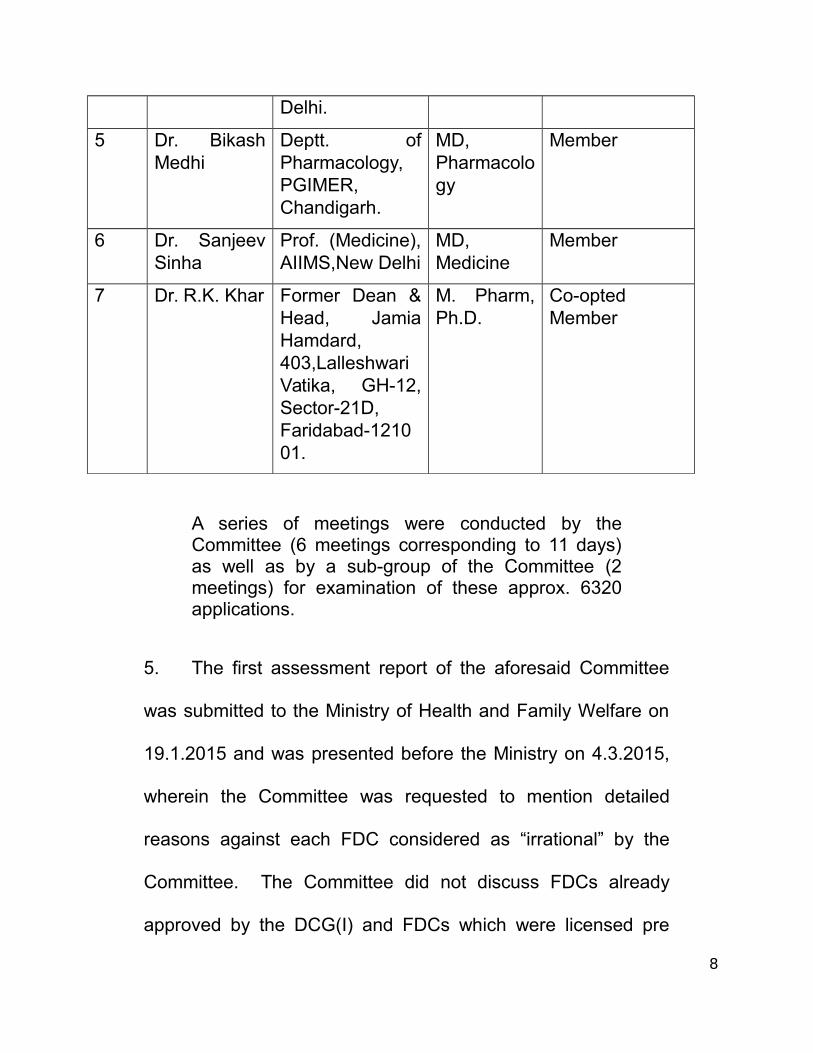
Delhi.
5 Dr. BikashMedhi
Deptt. ofPharmacology,PGIMER,Chandigarh.
MD,Pharmacology
Member
6 Dr. SanjeevSinha
Prof. (Medicine),AIIMS,New Delhi
MD,Medicine
Member
7 Dr. R.K. Khar Former Dean &Head, JamiaHamdard,403,LalleshwariVatika, GH-12,Sector-21D,Faridabad-121001.
M. Pharm,Ph.D.
Co-optedMember
A series of meetings were conducted by theCommittee (6 meetings corresponding to 11 days)as well as by a sub-group of the Committee (2meetings) for examination of these approx. 6320applications.
5. The first assessment report of the aforesaid Committee
was submitted to the Ministry of Health and Family Welfare on
19.1.2015 and was presented before the Ministry on 4.3.2015,
wherein the Committee was requested to mention detailed
reasons against each FDC considered as “irrational” by the
Committee. The Committee did not discuss FDCs already
approved by the DCG(I) and FDCs which were licensed pre
8

21.9.1988 i.e. before the introduction of Schedule Y to the
Drugs Act. The Committee stated, “in case the Committee
made any comment with respect to the above inadvertently, it
shall be treated as not discussed.”
6. On 16.4.2015, a detailed report in this regard was
submitted by the Kokate Committee to the Ministry stating the
reasons for declaring FDCs as irrational. We have been
informed that for the FDCs which were considered as irrational
by the Committee, the Committee wrote to various
manufacturers/associations calling upon them to submit
material to establish the therapeutic justification/rationality of
the FDCs. Replies received from such associations were
examined by the Expert Committee and final recommendations
therein were given only on 10.2.2016. In category A, following
the final recommendations of the Expert Committee, the Central
Government has banned 344 FDCs. In category B, 944 FDCs
needed to be considered/deliberated upon further, which meant
that they would be referred to the respective Expert
Committees out of the 10 Expert Committees already
constituted for further examination. In category C, 1493 FDCs
9

have been declared “rational” and we are informed that
approvals have since been issued by the DCG(I) in respect of
these FDCs. In category D, 126 FDCs have to be considered
for further generation of data by the prospective applicants. It is
only after carrying out of this exercise, that by notifications
dated 10.3.2016 issued under Section 26A, the Central
Government banned manufacture and sale of 344 FDCs.
7. In March 2016, a large number of writ petitions were filed
in the Delhi High Court against the aforesaid notifications. The
impugned judgment then followed on 1.12.2016 disposing of
454 petitions, followed by an order dated 21.12.2016, in which
the Delhi High Court disposed of 51 further writ petitions in
terms of the judgment dated 1.12.2016.
8. Letters Patent Appeals were filed before the Delhi High
Court. Meanwhile, the Union of India filed transfer petitions in
this Court. This is how these matters have been heard by us in
civil appeals arising out of SLPs against the judgment of the
single Judge dated 1.12.2016 and in transfer cases in which the
10

LPAs pending before the Delhi High Court have been
transferred to us.
9. Ms. Pinky Anand, learned Additional Solicitor General,
took us through various provisions of the Drugs Act, and
emphasized that Section 26A does not expressly refer to the
DTAB. According to her, a large number of provisions of the
Drugs Act expressly refer to the DTAB in various contexts and,
therefore, it is not permissible for the Court to read a mandatory
requirement of consultation with the DTAB into Section 26A,
when such mandatory consultation is present in other
provisions, but is conspicuous by its absence in Section 26A.
She further went on to state that the provisions of Section 26A
are legislative in nature, and ultimately, once the Central
Government arrives at a satisfaction based on relevant
materials, judicial review of the Central Government decision
taken on the basis of Expert Committee reports is extremely
limited. She launched an all out attack against the single
Judge’s judgment and stated that the Madras and Karnataka
view, with which the Delhi High Court differed, is the correct
view in law. Shri Colin Gonsalves, learned senior counsel,
11

supported her arguments, and appeared in civil appeal arising
out of SLP(C) Nos.10170-10178 of 2017.
10. By way of reply, Shri C.S. Vaidyanathan, learned senior
counsel, argued that the impugned single Judge judgment was
based on an earlier Division Bench judgment in E. Merck
(India) Ltd. and another v. Union of India and another,
(2001) 90 DLT 60, which upheld the constitutional validity of
Section 26A on the ground that since the DTAB had to be
consulted before passing an order under Section 26A, the said
Section would pass constitutional muster. He also referred us
to this Court’s judgment in Systopic Laboratories (Pvt) Ltd. v.
Dr. Prem Gupta & Ors., 1994 Supp (1) SCC 160 in furtherance
of the same proposition. According to learned counsel, it is
clear on a reading of Section 5 of the Drugs Act, that it will
apply to both the Central Government and the State
Governments on all technical matters that arise out of the
administration of the Drugs Act. Since Section 26A deals only
with such technical matters, it is obvious that the DTAB’s advice
has to be taken in every such case as otherwise, if it were open
to the Central Government to pick and choose in which case
12
they would take such advice and which case they would not
take such advice, the provision itself would become arbitrary
and unreasonable. According to the learned senior counsel,
Section 5(5) of the Drugs Act is very important in that it is the
DTAB alone who may constitute sub-committees consisting of
persons who are not members of the DTAB, who may consider
particular matters, thereby making it clear that the DTAB alone
can induct experts who are outside Section 5 and not the
Central Government. He further referred to the Drugs and
Cosmetics Rules, 1945 (hereinafter referred to as the “Drugs
Rules”), in particular Rules 21, 68A, 122A, 122D and 122DA, to
buttress his submission that a detailed filtration process has to
be gone through before a drug can be manufactured and put on
the market and that the Central Government cannot ban such
drug without consulting the technical expert under the Drugs
Act namely, the DTAB, that is set up under Section 5. He also
argued that Sections 10A and 26A were introduced by way of
an amendment in 1982 and this being so, it is clear that it is
assumed by Parliament that Section 5 of the Drugs Act will be
13
read along with both of them so as to make the DTAB a
mandatory consultee before action is taken under Section 26A.
11. Shri Vashisht, learned senior counsel appearing for some
of the respondents, adverted to Section 5 and stated that it was
in two parts, the first being advice to the Central Government
on all technical matters arising out of the administration of the
Drugs Act and the second (and distinct part) being to carry out
other functions assigned to it by the Drugs Act. It is clear,
therefore, that in all matters which fall within the first part, the
advice of the Board would be mandatory before the Central
Government were to take action under Section 26A. He also
referred us to Section 7A of the Drugs Act and argued that
when the said Drugs Act expressly states that nothing in
Section 5 is to apply, it is expressly so stated and that,
therefore, the necessary inference would be that Section 5
would apply in all situations other than those covered by
Section 7A. He further argued that Section 26A does not have a
non obstante clause which puts out of harm’s way Section 5,
but only a “without prejudice” clause and that too restricted only
to Chapter IV, making it clear that Section 26A would have to be
14

read along with Section 5. According to him, therefore, there is
no reason to interfere with the judgment of the Delhi High
Court.
12. Dr. A.M. Singhvi, learned senior counsel, argued that on a
cursory look at the persons who constitute the DTAB under
Section 5, it is an extremely high ranking body which is the
technical expert set up by the statute and, therefore, the High
Court judgment is right in stating that in all cases arising under
Section 26A prior consultation with the DTAB is a must. He
argued, in the alternative, that on a purposive and harmonious
construction of the Drugs Act as a whole, a middle approach
could be that the Central Government may, in emergent
situations, not consult the DTAB, but in all other situations
should give reasons why the DTAB was not consulted,
otherwise the exercise under Section 26A would be found to be
constitutionally infirm. According to the learned senior counsel,
hearing is mandatory under the said Section and the High
Court’s reading in the requirement of hearing into the said
Section was absolutely correct. He also referred us to
judgments dealing with not only how hearing must be added
15

when it is absent, but to a judgment of this Court which stated
that conditional legislation, of which Section 26A is a clear
instance, would also require hearing the affected parties.
13. In answer to these submissions, the learned Additional
Solicitor General, in rejoinder, went through the 1982
amendment, which introduced Section 26A, and stated that
Sections 29 and 35 thereof make it clear that amendments
were made in certain Sections with reference to the DTAB
under Section 5 and that, therefore, the omission of any
reference to the DTAB in Section 26A is deliberate. She also
went on to state that Rule 66 of the Drugs Rules, which deals
with cancellation of individual licenses and which requires
compliance with natural justice, should be contrasted with
Section 26A of the Drugs Act which, according to her, is a
legislative power as opposed to an administrative power.
14. Having heard learned counsel for the parties, it is first
important to set out some of the provisions of the Drugs Act.
“5. The Drugs Technical Advisory Board.—
(1) The Central Government shall, as soon as maybe, constitute a Board (to be called the DrugsTechnical Advisory Board) to advise the Central
16

Government and the State Governments ontechnical matters arising out of the administration ofthis Act and to carry out the other functionsassigned to it by this Act.
(2) The Board shall consist of the followingmembers, namely:—
(i) the Director General of Health Services, exofficio, who shall be Chairman;
(ii) the Drugs Controller, India, ex officio;
(iii) the Director of the Central Drugs Laboratory,Calcutta, ex officio;
(iv) the Director of the Central Research Institute,Kasauli, ex officio;
(v) the Director of the Indian Veterinary ResearchInstitute, Izatnagar, ex officio;
(vi) the President of the Medical Council of India, exofficio;
(vii) the President of the Pharmacy Council of India,ex officio;
(viii) the Director of the Central Drug ResearchInstitute, Lucknow, ex officio;
(ix) two persons to be nominated by the CentralGovernment from among persons who are incharge of drugs control in the States;
(x) one person, to be elected by the ExecutiveCommittee of the Pharmacy Council of India, fromamong teachers in pharmacy or pharmaceuticalchemistry or pharmacology on the staff of an Indianuniversity or a college affiliated thereto;
(xi) one person, to be elected by the ExecutiveCommittee of the Medical Council of India, fromamong teachers in medicine or therapeutics on the
17

staff of an Indian university or a college affiliatedthereto;
(xii) one person to be nominated by the CentralGovernment from the pharmaceutical industry;
(xiii) one pharmacologist to be elected by theGoverning Body of the Indian Council of MedicalResearch;
(xiv) one person to be elected by the CentralCouncil of the Indian Medical Association;
(xv) one person to be elected by the Council of theIndian Pharmaceutical Association;
(xvi) two persons holding the appointment ofGovernment Analyst under this Act, to be nominatedby the Central Government.
(3) The nominated and elected members of theBoard shall hold office for three years, but shall beeligible for re-nomination and re-election:
Provided that the person nominated or elected, asthe case may be, under clause (ix) or clause (x) orclause (xi) or clause (xvi) of sub-section (2) shallhold office for so long as he holds the appointmentof the office by virtue of which he was nominated orelected to the Board.
(4) The Board may, subject to the previous approvalof the Central Government, make bye-laws fixing aquorum and regulating its own procedure and theconduct of all business to be transacted by it.
(5) The Board may constitute sub-committees andmay appoint to such sub-committees for suchperiods, not exceeding three years, as it maydecide, or temporarily for the consideration ofparticular matters, persons who are not members ofthe Board.
18

(6) The functions of the Board may be exercisednotwithstanding any vacancy therein.
(7) The Central Government shall appoint a personto be Secretary of the Board and shall provide theBoard with such clerical and other staff as theCentral Government considers necessary.
6. The Central Drugs Laboratory.—
(1) The Central Government shall, as soon as maybe, establish a Central Drugs Laboratory under thecontrol of a Director to be appointed by the CentralGovernment, to carry out the functions entrusted toit by this Act or any rules made under this Chapter:
Provided that, if the Central Government soprescribes, the functions of the Central DrugsLaboratory in respect of any drug or class of drugsor cosmetic or class of cosmetics shall be carriedout at the Central Research Institute, Kasauli, or atany other prescribed Laboratory and the functionsof the Director of the Central Drugs Laboratory inrespect of such drug or class of drugs or suchcosmetic or class of cosmetics shall be exercised bythe Director of that Institute or of that otherLaboratory, as the case may be.
(2) the Central Government may, after consultationwith the Board, make rules prescribing—
(a) the functions of the Central Drugs Laboratory;
********
(d) the procedure for the submission of the saidLaboratory under Chapter IV or Chapter IVA ofsamples of drugs or cosmetics for analysis or test,the forms of Laboratory’s reports thereon and thefees payable in respect of such reports;
19

(e) such other matters as may be necessary orexpedient to enable the said Laboratory to carry outits functions;
(f) the matters necessary to be prescribed for thepurposes of the proviso to sub-section (1).
7. The Drugs Consultative Committee.—
(1) The Central Government may constitute anadvisory committee to be called “the DrugsConsultative Committee” to advise the CentralGovernment, the State Governments and the DrugsTechnical Advisory Board on any matter tending tosecure uniformity throughout India in theadministration of this Act.
(2) The Drugs Consultative Committee shall consistof two representatives of the Central Government tobe nominated by that Government and onerepresentative of each State Government to benominated by the State Government concerned.
(3) The Drugs Consultative Committee shall meetwhen required to do so by the Central Governmentand shall have power to regulate its own procedure.
7A. Sections 5 and 7 not to apply to Ayurvedic,Siddha or Unani drugs.—
Nothing contained in sections 5 and 7 shall apply toAyurvedic, Siddha or Unani drugs.
8. Standards of quality.—
(1) For the purposes of this Chapter, the expression“standard quality” means—
(a) in relation to a drug, that the drug complies withthe standard set out in the Second Schedule, and
(b) in relation to a cosmetic, that the cosmeticcompiles with such standard as may be prescribed.
20
(2) The Central Government, after consultation withthe Board and after giving by notification in theOfficial Gazette not less than three months’ notice ofits intention so to do, may by a like notification addto or otherwise amend the Second Schedule, for thepurposes of this Chapter, and thereupon theSecond Schedule shall be deemed to be amendedaccordingly.
10. Prohibition of import of certain drugs orcosmetics.—
From such date as may be fixed by the CentralGovernment by notification in the Official Gazette inthis behalf, no person shall import—
(a) any drug or cosmetic which is not of standardquality;
(b) any misbranded drug or misbranded or spuriouscosmetic;
(bb) any adulterated or spurious drug;
(c) any drug or cosmetic for the import of which alicence is prescribed, otherwise than under, and inaccordance with, such licence;
(d) any patent or proprietary medicine, unless thereis displayed in the prescribed manner on the labelor container thereof the true formula or list of activeingredients contained in it together with thequantities thereof;
(e) any drug which by means of any statement,design or device accompanying it or by any othermeans, purports or claims to cure or mitigate anysuch disease or ailment, or to have any such othereffect, as may be prescribed;
(ee) any cosmetic containing any ingredient whichmay render it unsafe or harmful for use under thedirections indicated or recommended;
21
(f) any drug or cosmetic the import of which isprohibited by rule made under this Chapter:
Provided that nothing in this section shall apply tothe import, subject to prescribed conditions, of smallquantities of any drug for the purpose ofexamination, test or analysis or for personal use:
Provided further that the Central Government may,after consultation with the Board, by notification inthe Official Gazette, permit, subject to anyconditions specified in the notification, the import ofany drug or class of drugs not being of standardquality.
12. Power of Central Government to make rules.—
(1) The Central Government may, after consultationwith or on the recommendation of the Board andafter previous publication by notification in theOfficial Gazette, make rules for the purpose ofgiving effect to the provisions of this Chapter:
Provided that consultation with the Board may bedispensed with if the Central Government is ofopinion that circumstances have arisen whichrender it necessary to make rules without suchconsultation, but in such a case the Board shall beconsulted within six months of the making of therules and the Central Government shall take intoconsideration any suggestions which the Board maymake in relation to the amendment of the said rules.
(2) xxx xxx xxx
16. Standards of quality.—
(1) For the purposes of this Chapter, the expression“standard quality” means—
(a) in relation to a drug, that the drug complies withthe standard set out in the Second Schedule, and
22

(b) in relation to a cosmetic, that the cosmeticcomplies with such standard as may be prescribed.
(2) The Central Government, after consultation withthe Board and after giving by notification in theOfficial Gazette not less than three months’ notice ofits intention so to do, may by a like notification addto or otherwise amend the Second Schedule for thepurposes of this Chapter, and thereupon theSecond Schedule shall be deemed to be amendedaccordingly.
18. Prohibition of manufacture and sale ofcertain drugs and cosmetics.—
From such date as may be fixed by the StateGovernment by notification in the Official Gazette inthis behalf, no person shall himself or by any otherperson on his behalf—
(a) manufacture for sale or for distribution, or sell, orstock or exhibit or offer for sale, or distribute—
(i) any drug which is not of a standard quality, or ismisbranded, adulterated or spurious;
(ii) any cosmetic which is not of a standard qualityor is misbranded, adulterated or spurious;
(iii) any patent or proprietary medicine, unless thereis displayed in the prescribed manner on the labelor container thereof the true formula or list of activeingredients contained in it together with thequantities thereof;
(iv) any drug which by means of any statement,design or device accompanying it or by any othermeans, purports or claims to prevent, cure ormitigate any such disease or ailment, or to have anysuch other effect as may be prescribed;
23
(v) any cosmetic containing any ingredient whichmay render it unsafe or harmful for use under thedirections indicated or recommended; and
(vi) any drug or cosmetic in contravention of any ofthe provisions of this Chapter or any rule madethereunder;
(b) sell, or stock or exhibit or offer for sale, ordistribute any drug or cosmetic which has beenimported or manufactured in contravention of any ofthe provisions of this Act or any rule madethereunder;
(c) manufacture for sale or for distribution, or sell, orstock or exhibit or offer for sale, or distribute anydrug or cosmetic, except under, and in accordancewith the conditions of, a licence issued for suchpurpose under this Chapter:
Provided that nothing in this section shall apply tothe manufacture, subject to prescribed conditions,of small quantities of any drug for the purpose ofexamination, test or analysis:
Provided further that the Central Government may,after consultation with the Board, by notification inthe Official Gazette, permit, subject to anyconditions specified in the notification, themanufacture for sale, or for distribution, sale,stocking or exhibiting or offering for sale ordistribution of any drug or class of drugs not beingof standard quality.
26A. Powers of Central Government to prohibitmanufacture, etc., of drug and cosmetic inpublic interest.—
Without prejudice to any other provision containedin this Chapter, if the Central Government issatisfied, that the use of any drug or cosmetic islikely to involve any risk to human beings or animals
24

or that any drug does not have the therapeutic valueclaimed or purported to be claimed for it or containsingredients and in such quantity for which there isno therapeutic justification and that in the publicinterest it is necessary or expedient so to do, then,that Government may, by notification in the OfficialGazette, regulate, restrict or prohibit themanufacture, sale or distribution of such drug orcosmetic.
33. Power of Central Government to make rules.—
(1) The Central Government may after consultationwith, or on the recommendation of, the Board andafter previous publication by notification in theOfficial Gazette, make rules for the purpose ofgiving effect to the provisions of this Chapter:
Provided that consultation with the Board may bedispensed with if the Central Government is ofopinion that circumstances have arisen whichrender it necessary to make rules without suchconsultation, but in such a case the Board shall beconsulted within six months of the making of therules and the Central Government shall take intoconsideration any suggestions which the Board maymake in relation to the amendment of the said rules.
(2) Without prejudice to the generality of theforegoing power, such rules may—
(a) provide for the establishment of laboratories fortesting and analysing drugs or cosmetics;
(b) prescribe the qualifications and duties ofGovernment Analysts and the qualifications ofInspectors;
(c) prescribe the methods of test or analysis to beemployed in determining whether a drug orcosmetic is of standard quality;
25

(d) prescribe, in respect of biological andorganometallic compounds, the units or methods ofstandardisation;
(dd) prescribe under clause (d) of section 17A thecolour or colours which a drug may bear or containfor purposes of colouring;
(dda) prescribe under clause (d) of section 17E thecolour or colours which a cosmetic may bear orcontain for the purpose of colouring;
(e) prescribe the forms of licences for themanufacture for sale or for distribution, for the saleand for the distribution of drugs or any specifieddrug or class of drugs or of cosmetics or anyspecified cosmetic or class of cosmetics, the form ofapplication for such licences, the conditions subjectto which such licences may be issued, the authorityempowered to issue the same, the qualifications ofsuch authority and the fees payable therefor; andprovide for the cancellation or suspension of suchlicences in any case where any provision of thisChapter or the rules made thereunder iscontravened or any of the conditions subject towhich they are issued is not complied with;
(ee) prescribe the records, registers or otherdocuments to be kept and maintained under section18B;
(eea) prescribe the fees for the inspection (for thepurposes of grant or renewal of licences) ofpremises, wherein any drug or cosmetic is being oris proposed to be manufactured;
(eeb) prescribe the manner in which copies are tobe certified under sub-section (2A) of section 22;
(f) specify the diseases or ailments which a drugmay not purport or claim to prevent, cure or mitigate
26

and such other effects which a drug may not purportor claim to have;
(g) prescribe the conditions subject to which smallquantities of drugs may be manufactured for thepurpose of examination, test or analysis;
(h) require the date of manufacture and the date ofexpiry of potency to be clearly or truly stated on thelabel or container of any specified drug or class ofdrugs, and prohibit the sale, stocking or exhibitionfor sale, or distribution of the said drug or class ofdrugs after the expiry of a specified period from thedate of manufacture or after the expiry of the date ofpotency;
(i) prescribe the conditions to be observed in thepacking in bottles, packages, and other containersof drugs or cosmetics, including the use of packingmaterial which comes into direct contact with thedrugs and prohibit the sale, stocking or exhibition forsale, or distribution of drugs or cosmetics packed incontravention of such conditions;
(j) regulate the mode of labelling packed drugs orcosmetics, and prescribe the matters which shall orshall not be included in such labels;
(k) prescribe the maximum proportion of anypoisonous substance which may be added orcontained in any drug, prohibit the manufacture,sale or stocking or exhibition for sale, or distributionof any drug in which that proportion is exceeded,and specify substances which shall be deemed tobe poisonous for the purposes of this Chapter andthe rules made thereunder;
(l) require that the accepted scientific name of anyspecified drug shall be displayed in the prescribedmanner on the label or wrapper of any patent orproprietary medicine containing such drug;
27

[****]
(n) prescribe the powers and duties of Inspectorsand the qualifications of the authority to which suchInspectors shall be subordinate and specify thedrugs or classes of drugs or cosmetics or classes ofcosmetics in relation to which and the conditions,limitations or restrictions subject to which, suchpowers and duties may be exercised or performed;
(o) prescribe the forms of report to be given byGovernment Analysts, and the manner ofapplication for test or analysis under section 26 andthe fees payable therefor;
(p) specify the offences against this Chapter or anyrule made thereunder in relation to which an orderof confiscation may be made under section 31;
(q) provide for the exemption, conditionally orotherwise, from all or any of the provisions of thisChapter or the rules made thereunder, of anyspecified drug or class of drugs or cosmetic or classof cosmetics; and
(r) sum which may be specified by the CentralGovernment under section 32-B.
33EED. Power of Central Government to prohibitmanufacture, etc., of Ayurvedic, Siddha or Unanidrugs in public interest.—
Without prejudice to any other provision containedin this Chapter, if the Central Government issatisfied on the basis of any evidence or othermaterial available before it that the use of anyAyurvedic, Siddha or Unani drug is likely to involveany risk to human beings or animals or that anysuch drug does not have the therapeutic valueclaimed or purported to be claimed for it and that inthe public interest it is necessary or expedient so todo then, that Government may, by notification in the
28

Official Gazette, prohibit the manufacture, sale ordistribution of such drug.
33N. Power of Central Government to makerules.—
(1) The Central Government may, after consultationwith, or on the recommendation of, the Board andafter previous publication by notification in theOfficial Gazette, make rules for the purpose ofgiving effect to the provisions of this Chapter:
Provided that consultation with the Board may bedispensed with if the Central Government is ofopinion that circumstances have arisen whichrender it necessary to make rules without suchconsultation, but in such a case, the Board shall beconsulted within six months of the making of therules and the Central Government shall take intoconsideration any suggestions which the Board maymake in relation to the amendment of the said rules.
(2) Without prejudice to the generality of theforegoing power, such rules may—
(a) provide for the establishment of laboratories fortesting and analysing Ayurvedic, Siddha or Unanidrugs;
(b) prescribe the qualification and duties ofGovernment Analysts and the qualifications ofInspectors;
(c) prescribe the methods of test or analysis to beemployed in determining whether any Ayurvedic,Siddha or Unani drug is labelled with the true list ofthe ingredients which it is purported to contain;
(d) specify any substance as a poisonoussubstance;
(e) prescribe the forms of licences for themanufacture for sale of Ayurvedic, Siddha or Unani
29
drugs, and for sale of processed Ayurvedic, Siddhaor Unani drugs, the form of application for suchlicences, the conditions subject to which suchlicences may be issued, the authority empowered toissue the same and the fees payable therefor; andprovide for the cancellation or suspension of suchlicences in any case where any provision of thisChapter or rules made thereunder is contravened orany of the conditions subject to which they areissued is not complied with;
(f) prescribe the conditions to be observed in thepacking of Ayurvedic, Siddha and Unani drugsincluding the use of packing material which comesinto direct contact with the drugs, regulate the modeof labelling packed drugs and prescribe the matterswhich shall or shall not be included in such labels;
(g) prescribe the conditions subject to which smallquantities of Ayurvedic, Siddha or Unani drugs maybe manufactured for the purpose of examination,test or analysis;
(gg) prescribe under clause (d) of section 33EE thecolour or colours which an Ayurvedic, Siddha orUnani drug may bear or contain for purposes ofcolouring;
(gga) prescribe the standards for Ayurvedic, Siddhaor Unani drugs under section 33EEB;
(ggb) prescribe the records, registers or otherdocuments to be kept and maintained under section33 KB; and
(h) any other matter which is to be or may beprescribed under this Chapter.”
15. Having heard learned counsel for the parties, it is clear
that Section 26A has been introduced by an amendment in
30

1982. A bare reading of this provision would show, firstly, that it
is without prejudice to any other provision contained in this
Chapter (meaning thereby Chapter IV). This expression only
means that apart from the Central Government’s other powers
contained in Chapter IV, Section 26A is an additional power
which must be governed by its own terms. Under Section 26A,
the Central Government must be “satisfied” that any drug or
cosmetic is likely to involve (i) any risk to human beings or
families; or (ii) that any drug does not have the therapeutic
value claimed or purported to be claimed for it; or (iii) contains
ingredients in such quantity for which there is no therapeutic
justification. Obviously, the Central Government has to apply its
mind to any or all of these three factors which has to be based
upon its “satisfaction” as to the existence of any or all of these
factors. The power exercised under Section 26A must further be
exercised only if it is found necessary or expedient to do so in
public interest. When the power is so exercised, it may
regulate, restrict or prohibit manufacture, sale or distribution of
any drug or cosmetic.
31
16. Undoubtedly, Section 26A has to be read with the rest of
the Drugs Act. So read, it is clear that unlike Section 6(2),
Section 8(2), second proviso to Section 10, proviso to Section
12(1), Section 16(2), proviso to Section 18(2), Section 33 and
Section 33N, there is no explicit requirement to consult the
DTAB set up under Section 5 of the Drugs Act. The question is
did the Parliament do so deliberately or is it something that the
Court should read into the provision?
17. As has been stated hereinabove, Section 26A was
brought in by an amendment in 1982. The amendment
specifically made changes in Sections 33 and 33N in which it
added the words “on the recommendation of the Board”. From
this, it is clear that Parliament in the very Amendment Act which
introduced Section 26A made certain changes which involved
the DTAB under Section 5 of the said Act. It is clear that the
additional power that is given to the Central Government under
Section 26A does not refer to and, therefore, mandate any
previous consultation with the DTAB. On the contrary, the
Central Government may be “satisfied” on any relevant material
that a drug is likely to involve any risk to human beings etc. as a
32
result of which it is necessary in public interest to regulate,
restrict or prohibit manufacture, sale or distribution thereof. So
long as the Central Government’s satisfaction can be said to be
based on relevant material, it is not possible to say that not
having consulted the DTAB, the power exercised under the said
Section would be non est. Take the case of an FDC that is
banned in 50 countries of the world owing to the fact that the
said FDC involved significant risk to human beings. Assuming
that the Central Government is satisfied based on this fact
alone, which in turn is based on expert committee reports in
various nations which pointed out the deleterious effects of the
said drug, can it be said that without consulting the DTAB set up
under Section 5, the exercise of the power under Section 26A
to prohibit the manufacture or sale or distribution of a drug that
is banned in 50 countries would be bad only because the DTAB
has not been consulted? The obvious answer is no inasmuch
as the Central Government’s satisfaction is based upon
relevant material, namely, the fact that 50 nations have banned
the aforesaid drug, which in turn is based on expert committee
reports taken in each of those nations. Take another example.
33
Suppose the Central Government were to ban an FDC on the
ground that, in the recent past, it has been apprised of the fact
that the FDCs taken over a short period of time would lead to
loss of life, which has come to the notice of the Central
Government through reports from various district authorities, in
let us say, a majority of districts in which the said FDC has been
consumed. Could not the Central Government then base its
ban order on material collected from district authorities which
state that this particular drug leads to human mortality and
ought, therefore, to be prohibited? The obvious answer again is
yes for the reason that the Central Government has been
satisfied on relevant material that it is necessary in public
interest to ban such drug. Examples of this nature can be
multiplied to show that the width of the power granted under
Section 26A cannot be cut down by artificially cutting down the
language of Section 26A.
18. We were referred to a judgment of this Court in Systopic
Laboratories (supra) at 169. Paragraph 19 of the said
judgment reads as follows:-
34
“19. Having considered the submissions made bythe learned counsel for the petitioners and thelearned Additional Solicitor General in this regard,we must express our inability to make anassessment about the relative merits of the variousstudies and reports which have been placed beforeus. Such an evaluation is required to be done by theCentral Government while exercising its powersunder Section 26-A of the Act on the basis of expertadvice and the Act makes provision for obtainingsuch advice through the Board and the DCC.”
19. It is clear that a stray sentence in a judgment without a
focused argument cannot be considered as the ratio of such a
judgment. Also, on a careful reading of the second sentence in
paragraph 19, it is clear that all that is stated by this Court is
that, while exercising its power under Section 26A of the Drugs
Act, the basis of the Central Government’s decision must be
“expert advice”. The sentence then goes on to add that the
Drugs Act makes provision for obtaining such advice through
the Board and the DCC. According to us, there was no focused
argument on whether such advice is or is not mandatory before
powers under Section 26A of the Drugs Act can be exercised,
and merely reading a stray sentence in this judgment does not
lead to such a conclusion. Equally, the single Judge’s reliance
upon a Division Bench judgment contained in E. Merck (supra),
35
where, in holding Section 26A to be constitutional, the Court
stated:
“Before the Government records its satisfaction toprohibit the manufacture, sale, distribution etc. of aparticular drug, opinion of the DTAB and/or DrugsConsultative Committee is obtained.”
This is an equally stray sentence and what has been
stated with respect to Systopic Laboratories (supra), applies
equally to this sentence.
20. We have now to consider certain other arguments made
on behalf of the respondents. One argument was that Section
5 is in two parts and that the first part necessarily applies to all
technical matters that arise out of the administration of the
Drugs Act, and that, therefore, the Central Government is
bound to take the advice of the DTAB in all such matters. We
must first advert to the fact that the DTAB is only an advisory
body. No doubt, it would be desirable for the Central
Government to take its advice on technical matters arising out
of the administration of the Drugs Act, but this does not lead to
the conclusion that if such advice is not taken power under
Section 26A cannot be exercised. Indeed, the Central
36

Government’s satisfaction may be based on a number of
factors, one of which may be advice tendered to it by the DTAB
under Section 5. There is no warrant to read Section 26A to
constrict the wide powers granted to the Central Government
by a so-called harmonious construction of the statute. Another
argument made is that Section 5 makes it clear that the DTAB
alone can constitute sub-committees which may have persons
who are not members of the Board on them. We are afraid that
this again does not lead us very far. It is clear that the reason
for Section 5(5) is completely different. Sub-committees may
be appointed for such periods not exceeding three years or
temporarily for the consideration of particular matters. Such
sub-committees may be set up in the wisdom of the DTAB for
short periods of time or temporarily to consider certain matters
and make reports which the DTAB may then utilize. This is a
power of the DTAB which can be exercised when the DTAB
deems it desirable. From this power, it cannot be inferred, as a
matter of logic, that since Section 5(5) permits persons who are
not members of the board to sit on sub-committees, the Central
Government may not, under Section 26A, refer to any persons
37

other than those who are board members. This argument,
therefore, is also rejected.
21. Yet another argument has been made that since Section
10A and 26A were brought in together by an Amendment Act in
1982, it must, therefore, somehow be assumed that the
Amendment Act necessarily included a mandatory consultation
with the DTAB set up under Section 5. We have already
pointed out how the very amendment Act of 1982 also
amended Sections 33 and 33N by referring to the DTAB and
that, therefore, it is obvious that the omission of any reference
to the DTAB under Sections 10A and 26A cannot but be said to
be deliberate. This argument also need not detain us further.
22. A negative argument was made stating that Section 7A of
the Drugs Act makes it clear that Section 5 will not apply to
Ayurvedic, Siddha or Unani drugs and that, therefore, it will
apply to all other drugs. The reason for Section 7A is again
something very different from what has been argued. It must
first be pointed out that under Chapter IVA, which is a separate
Chapter introduced by Act 13 of 1964, Ayurvedic, Siddha and
38
Unani drugs are completely separately dealt with. Indeed,
Section 33A, which must be read with Section 7A, expressly
provides that save as provided in this Drugs Act, nothing
contained in this Chapter, i.e. Chapter IV, shall apply to
Ayurvedic, Siddha or Unani drugs. Chapter IVA consists of a
separate and distinct drill to be followed in the case of
Ayurvedic, Siddha and Unani drugs. Under Section 33C, there
is a separate technical advisory board for Ayurvedic and Unani
drugs and a separate consultative committee for Ayurvedic,
Siddha and Unani drugs (see Section 33D). When Section 7A
says that nothing in section 5 shall apply to Ayurvedic, Siddha
or Unani drugs, all that it affirms is that the DTAB set up under
Section 5 will apply to all drugs except Ayurvedic, Siddha or
Unani medicines. The Latin maxim “expressio unius est
exclusio alterius” cannot apply, as has been held in State of
Karnataka v Union of India & Ors., (1977) 4 SCC 608 at 662,
making it clear that the said maxim should be very carefully
applied and when misapplied would turn out to be a “dangerous
master” as opposed to a “useful servant”. This has also been
held in Assistant Collector of Central Excise, Calcutta
39

Division v. National Tobacco Co. of India Ltd., (1972) 2 SCC
560 at 575 as follows:
“The High Court's view was based on an applicationof the rule of construction that where a mode ofperforming a duty is laid down by law it must beperformed in that mode or not at all. This rule flowsfrom the maxim: “Expressio unius ast exclusioalterius”. But, as was pointed out by Wills, J.,in Colguoboun v. Brooks [(1888) 21 QBD 52, 62]this maxim “is often a valuable servant, but adangerous master….”. The rule is subservient to thebasic principle that Courts must endeavour toascertain the legislative intent and purpose, andthen adopt a rule of construction which effectuatesrather than one that may defeat these. “
This argument, therefore, also need not detain us.
23. It was also argued that Section 26A had no non obstante
clause to keep Section 5 out of harm’s way. On our
construction of Section 26A, it is clear that no such non
obstante clause was necessary in that the width of the
expression “is satisfied” contained in Section 26A cannot be cut
down by reference to Section 5. As has been stated by us
hereinabove, the expression “without prejudice” makes it clear
that Section 26A is an additional power given to the Central
Government which must be exercised on its own terms.
40
24. An argument was made that unless the provisions of
Section 5 requiring consultation with the DTAB are read into
Section 26A, the said Section would be arbitrary. In our
opinion, there are sufficient indicators in the Section to eschew
any ground of arbitrariness. The power can only be exercised
based on satisfaction of material that is relevant to form an
opinion that the drug in question falls within any of the three
categories outlined by the Section and that, further, it is
necessary or expedient to either regulate, restrict or prohibit
manufacture, sale or distribution of the said drug in public
interest. Indeed, this is made explicit in Section 33 EED of the
Drugs Act, wherein a similar power is given to the Central
Government qua Ayurvedic, Siddha or Unani drugs, where the
Section states:
“… the Central Government is satisfied on the basisof any evidence or other material available before itthat …”
25. If the power under Section 26A is exercised on the basis
of irrelevant material or on the basis of no material, the
satisfaction itself that is contemplated by Section 26A would not
41

be there and the exercise of the power would be struck down
on this ground. Further, it is argued that the provision may be
read down to make it constitutionally valid, but in so doing,
words cannot be added as a matter of constitutional doctrine.
26. In Cellular Operators Association of India and others
v. Telecom Regulatory Authority of India and others, (2016)
7 SCC 703 at 740-741, this Court held as under:
“50. But it was said that the aforesaid Regulationshould be read down to mean that it would applyonly when the fault is that of the service provider.We are afraid that such a course is not open to us inlaw, for it is well settled that the doctrine of readingdown would apply only when general words used ina statute or regulation can be confined in aparticular manner so as not to infringe aconstitutional right. This was best exemplified in oneof the earliest judgments dealing with the doctrine ofreading down, namely, the judgment of the FederalCourt in Hindu Women’s Rights to Property Act,1937, In re [Hindu Women’s Rights to Property Act,1937, In re, AIR 1941 FC 72]. In that judgment, theword “property” in Section 3 of the Hindu Women’sRights to Property Act was read down so as not toinclude agricultural land, which would be outside theCentral Legislature’s powers under the Governmentof India Act, 1935. This is done because it ispresumed that the legislature did not intend totransgress constitutional limitations. While soreading down the word “property”, the Federal Courtheld:
42

“… If the restriction of the general wordsto purposes within the power of thelegislature would be to leave an Act withnothing or next to nothing in it, or an Actdifferent in kind, and not merely indegree, from an Act in which the generalwords were given the wider meaning,then it is plain that the Act as a wholemust be held invalid, because in suchcircumstances it is impossible to assertwith any confidence that the legislatureintended the general words which it hasused to be construed only in thenarrower sense: Owners of SS Kalibia v.Wilson [(1910) 11 CLR 689 (Aust)],Vacuum Oil Co. Pty. Ltd. v. Queensland[(1934) 51 CLR 677 (Aust)], R. v.Commonwealth Court of Conciliationand Arbitration, ex p Whybrow & Co.[(1910) 11 CLR 1 (Aust)] and BritishImperial Oil Co. Ltd. v. Federal Commr.of Taxation [(1925) 35 CLR 422 (Aust)].”
51. This judgment was followed by a ConstitutionBench of this Court in DTC v. Mazdoor Congress[1991 Supp (1) SCC 600 : 1991 SCC (L&S) 1213].In that case, a question arose as to whether aparticular regulation which conferred power on anauthority to terminate the services of a permanentand confirmed employee by issuing a noticeterminating his services, or by making payment inlieu of such notice without assigning any reasonsand without any opportunity of hearing to theemployee, could be said to be violative of theappellants’ fundamental rights. Four of the learnedJudges who heard the case, the Chief Justice alonedissenting on this aspect, decided that theregulation cannot be read down, and must,therefore, be held to be unconstitutional. In the lead
43

judgment on this aspect by Sawant, J., this Courtstated: (SCC pp. 728-29, para 255)
“255. It is thus clear that the doctrine ofreading down or of recasting the statutecan be applied in limited situations. It isessentially used, firstly, for saving astatute from being struck down onaccount of its unconstitutionality. It is anextension of the principle that when twointerpretations are possible — onerendering it constitutional and the othermaking it unconstitutional, the formershould be preferred. Theunconstitutionality may spring fromeither the incompetence of thelegislature to enact the statute or fromits violation of any of the provisions ofthe Constitution. The second situationwhich summons its aid is where theprovisions of the statute are vague andambiguous and it is possible to gatherthe intentions of the legislature from theobject of the statute, the context inwhich the provision occurs and thepurpose for which it is made. However,when the provision is cast in a definiteand unambiguous language and itsintention is clear, it is not permissibleeither to mend or bend it even if suchrecasting is in accord with good reasonand conscience. In such circumstances,it is not possible for the court to remakethe statute. Its only duty is to strike itdown and leave it to the legislature if itso desires, to amend it. What is further,if the remaking of the statute by thecourts is to lead to its distortion thatcourse is to be scrupulously avoided.One of the situations further where the
44

doctrine can never be called into play iswhere the statute requires extensiveadditions and deletions. Not only it is nopart of the court’s duty to undertakesuch exercise, but it is beyond itsjurisdiction to do so.”
(emphasis supplied)
52. Applying the aforesaid test to the impugnedRegulation, it is clear that the language of theRegulation is definite and unambiguous — everyservice provider has to credit the account of thecalling consumer by one rupee for every single calldrop which occurs within its network. TheExplanatory Memorandum to the aforesaidRegulation further makes it clear, in Para 19 thereof,that the Authority has come to the conclusion thatcall drops are instances of deficiency in servicedelivery on the part of the service provider. It is thusunambiguously clear that the impugned Regulationis based on the fact that the service provider isalone at fault and must pay for that fault. In thesecircumstances, to read a proviso into the Regulationthat it will not apply to consumers who are at faultthemselves is not to restrict general words to aparticular meaning, but to add something to theprovision which does not exist, which would benothing short of the court itself legislating. For thisreason, it is not possible to accept the learnedAttorney General’s contention that the impugnedRegulation be read down in the manner suggestedby him.”
27. Also, as a matter of statutory interpretation, words can
only be added if the literal interpretation of the Section leads to
an absurd result. As has been stated by us, the construction of
45

Section 26A on a literal reading thereof does not lead to any
such result. Dr. Singhvi’s argument to read in words to save
Section 26A must, therefore, be rejected.
28. We may also mention that the Madras High Court in its
judgment in Macleods Pharmaceuticals Limited v. Union of
India & Ors., Writ Petition Nos.21933 and 25442 of 2011,
specifically held as under:
“38. Thus, the Act gives in every Chapter, anindication of the functions to be exercised by theDTAB. In other words, the territory within which theDTAB is to operate and exercise its functions, isclearly demarcated in various provisions of the Actsuch as 5(1), 6(2), 7(1), 8(2), second proviso toSection 10, 12(1) and 33(1). But Section 26-A iscompletely silent about any consultation with DTAB.It is so even with Section 26-B.
39. While the advisory role of DTAB is indicated inbroad and general terms in Section 5(1), it isindicated in specific terms in Sections 6(2), 7(1),8(2), second proviso to Section 10, 12(1) and 33(1).Therefore, the absence of any reference to suchrequirement of consultation in Section 26-Aassumes great significance. It is a well settledprinciple of interpretation of statutes that the Courtsare not expected to supply the omission. TheParliament had consciously incorporated theexpressions “after consultation with the Board” or“on the recommendation of the Board”, in certainprovisions of the Act such as Sections 5(1), 6(2),7(1), 8(2), second proviso to Section 10, 12(1) and33(1). But it has deliberately omitted to include any
46
of those expressions while inserting Sections 26-Aand 26-B. It is a case of casus omisus. Therefore,the argument that the Central Government ought tohave taken the consultation of the DTAB beforeissuing the ban order, can hold good only if I cansupply into Section 26-A, what was deliberately leftout by the Parliament. This cannot be done by meand hence the first contention has to be rejected.”
29. To similar effect is the judgment of a single Judge of the
Karnataka High Court in Lundbeck India Pvt. Ltd. v Union of
India, (2014) 5 Kant LJ 440.
30. We approve of these two judgments as having laid down
the correct law on the construction of Section 26A of the Drugs
Act.
31. Though arguments have been made as to whether
Section 26A is legislative in nature and therefore excludes
natural justice, we do not propose to go into the same
inasmuch as since the learned single Judge’s judgment is being
set aside on one point and one point alone. In this view of the
matter, we are of the opinion that the impugned judgment dated
1.12.2016 deserves to be set aside.
47
32. On the facts of these cases, a suggested course of action
was stated by learned counsel appearing on behalf of the
petitioners/appellants. This course is that instead of now
remitting the matter back to the Delhi High Court for an
adjudication on the other points raised in the writ petitions, the
case of 344 FDCs that have been banned, plus another 5 FDCs
that have been banned, which comes to 349 FDCs, (barring 15
FDCs that are pre 1988 and 17 FDCs which have DCG(I)
approval) pursuant to the Kokate Committee report, by
notifications of the Central Government under Section 26A of
the Drugs Act, should be sent to the DTAB, constituted under
Section 5 of the Drugs Act, so that it can examine each of these
cases and ultimately send a report to the Central Government.
We reiterate that only on the peculiar facts of these cases, we
think that such a course commends itself to us, which would
obviate further litigation and finally set at rest all other
contentions raised by the petitioners. We say so because we
find that the Kokate Committee did deliberate on the 344 FDCs
plus 5 FDCs and did come to a conclusion that the aforesaid
FDCs be banned, but we are not clear as to what exactly the
48

reasons for such conclusions are, and whether it was
necessary in the public interest to take the extreme step of
prohibiting such FDCs, instead of restricting or regulating their
manufacture and supply. In order that an analysis be made in
greater depth, we, therefore, feel that these cases should go to
the DTAB and/or a Sub-Committee formed by the DTAB for the
purpose of having a relook into these cases. It is important,
however, that the DTAB/Sub-Committee appointed for this
purpose will not only hear the petitioners/appellants before us,
but that they also hear submissions from the All India Drugs
Action Network. The DTAB/Sub-Committee set up for this
purpose will deliberate on the parameters set out in Section
26A of the Drugs Act, as follows.
33. First and foremost in each case, the
DTAB/Sub-Committee appointed by it must satisfy itself that the
use of the Fixed Dose Combinations (FDC) in question is likely
to involve any one of the aforesaid three things:
(a) that they are likely to involve any risk to human beings or
animals; or
49
(b) that the said FDCs do not have the therapeutic value
claimed or purported to be claimed for them; or
(c) that such FDCs contain ingredients and in such quantity for
which there is no therapeutic justification.
34. The DTAB/Sub-Committee must also apply its mind as to
whether it is then necessary or expedient, in the larger public
interest, to regulate, restrict or prohibit the manufacture, sale or
distribution of such FDCs. In short, the DTAB/Sub-Committee
must clearly indicate in its report:
(1) as to why, according to it, any one of the three factors
indicated above is attracted;
(2) post such satisfaction, that in the larger public interest, it is
necessary or expedient to (i) regulate, (ii) restrict, or (iii) prohibit
the manufacture, sale or distribution of such FDCs.
35. The DTAB/Sub-Committee must also indicate in its report
as to why, in case it prohibits a particular FDC, restriction or
regulation is not sufficient to control the manufacture and use of
the FDC. We request the DTAB/Sub-Committee to be set up
for this purpose to afford the necessary hearing to all50

concerned, and thereafter submit a consolidated report, insofar
as these FDCs are concerned, to the Central Government
within a period of six months from the date on which this
judgment is received by the DTAB. We may also indicate that
the Central Government, thereafter, must have due regard to
the report of the DTAB and to any other relevant information,
and ultimately apply its mind to the parameters contained in
Section 26A of the Drugs Act and, accordingly, either maintain
the notifications already issued, or modify/substitute them or
withdraw them.
36. With these directions given on the peculiar facts and
circumstances of these cases, the appeals are disposed of.
37. Insofar as the drugs that have been banned and which
were manufactured pre 21st September, 1988, a list of 15 such
drugs has been given to us by Mr. Kapil Sibal, learned senior
counsel for the respondents. We set aside the Central
Government notifications banning them as these cases were
never meant to be referred to the Kokate Committee. It will be
open, however, for the Central Government, if it so chooses, de
51
novo, to carry out an inquiry as to whether such drugs should
be the subject matter of a notification under Section 26A of the
Drugs Act.
38. Insofar as the list of 17 cases handed over by Shri Sibal,
in which DCG(I) approvals have allegedly been granted, we are
of the view that since the Parliamentary Standing Committee
itself refers to DCG(I) approvals and the manner in which they
were granted, we do not accede to Mr. Sibal's request that
these 17 cases be kept outside the purview of the fresh look
that has to be given by the DTAB/Sub-Committee in these
cases.
39. Insofar as the status quo, obtaining as on today, is
concerned, that will continue in all cases (including the 5 FDCs
which are not the subject matter of stay orders already made)
until the Central Government issues fresh notifications in this
behalf.
MADRAS CASES (TRANSFERRED CASES)
T.C.(C)Nos. 308-317_of 2017 @ T.P.(C)Nos.2108-2117 of 2017
52

40. Mr. Gopal Subramanium, learned senior counsel
appearing on behalf of the original petitioners in these cases,
stated that these cases have been transferred to this Court
from the Madras High Court. A Section 33 ban, which was
imposed on 294 FDCs in these cases, has been stayed by the
Madras High Court, and the very exercise that we have
proposed in the Delhi cases has apparently been carried out in
this group of cases. A report of the expert committee of the
DTAB to review the rationality and safety of 294 FDCs is taken
on record. The report indicates that 42 FDCs reportedly were
repeated or duplicate; 44 were already prohibited for
manufacture in the country; 83 were considered rational; 56
were considered not rational; 49 required further generation of
data; 17 were considered inadequate so far as rationality, safety
and efficacy is concerned; and 3 other cases were sent for
further examination by an expert committee constituted by the
Ministry of Health and Family Welfare. The DTAB after review
of the report and deliberations recommended that the FDC
Ofloxacin and Prednisolone at serial number 75 under the
category of GI in Annexure C does not appear to be rational
53

and should be re-examined. The list of the drugs mentioned in
Annexure D are required to be prohibited/withdrawn from the
market as these are not rational. Considering that an expert
body has already deliberated upon and decided these cases,
we accept the report, and accordingly dispose of these petitions
in accordance therewith.
……………………….J.(R.F. Nariman)
……………………….J.(Sanjay Kishan Kaul)
New Delhi;December 15, 2017.
54

ANNEXURE 3
(To be published in part II, Section 3, Sub-section (i) of the Gazette of India, Extraordinary, dated the…..)
Government of India Ministry of Health and Family Welfare
(Department of Health and Family Welfare)
New Delhi, the , 2017
Notification
G.S.R._______ (E).-The following draft of certain rules which the Central
Government proposes to make in exercise of the power conferred by sections 12
and 33 of the Drugs and Cosmetic Act, 1940 (23 of 1940) and in consultation after
publication with the Drugs Technical Advisory Board is hereby published for
information of all persons likely to be affected thereby and notice is hereby given that
the said draft rules shall be taken into consideration or after the expiry of a period of
thirty days from the date on which the copies of the Gazette of India these draft rules
are made available to public.
Objections and suggestions which may be received from any person within
the period specified above will be considered by the Central Government.
Objections and suggestions, if any, may be addressed to the Under Secretary
(Drugs), Ministry of Health and Family Welfare, Government of India, Room No. 414
A, D Wing, Nirman Bhawan, New Delhi – 110011 or sent on email drugsdiv-
Draft Rules
1. (1) These rules may be called Drugs and Cosmetics (________Amendment)
Rules, 2017.
(2) They shall come into force after their final publication in the Official
Gazette.
2. In the Drugs and Cosmetics Rules, 1945, in rule 96 sub-rule (1),-
(a) in clause (ii) at the end for the words “Metric system” the words “Metric
system; and Ex-factory price or import price as the case may be, in figures.”
shall be substituted;
(b) at the end of clause (ii) so amended the following Explanation shall be
inserted, namely,-
“Explanation.- For the purpose of these rules,-
(i) “Ex-factory price” means price on which the goods and service tax is payable
under the Central Goods and Service Tax Act, 2017 (12 of 2017) by the first
buyer.
(ii) “Import price” means the price on which custom duty is to be payable by the
importer or by agent under the Custom Act, 1962(52 of 1962) and the Customs
Tariff Act, 1975 (51 of 1975) on clearance from the port.
[F. No. X.11014/20/2017-DRS]
(Sudhir Kumar) Joint Secretary to the Government of India
Note.- The principal rules were published in the Gazette of India vide notification No.F.28-10/45-H (1) dated 21stDecember, 1945 and last amended vide ---------.
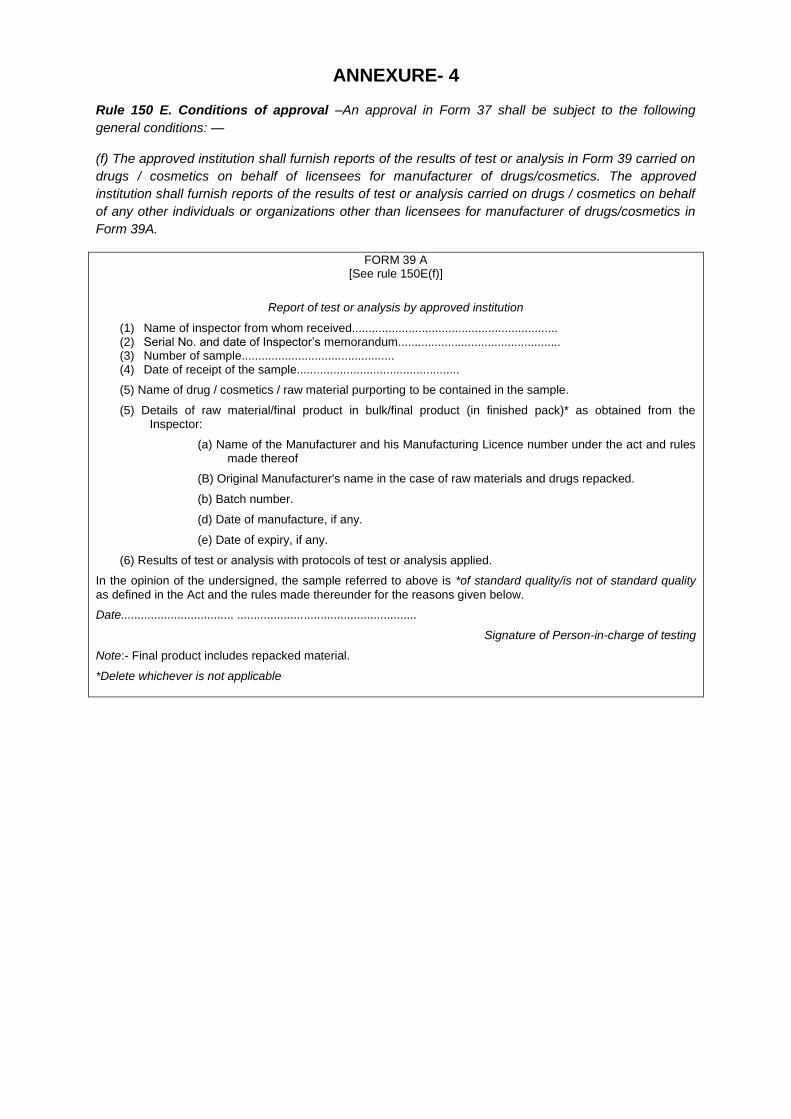
ANNEXURE- 4
Rule 150 E. Conditions of approval –An approval in Form 37 shall be subject to the following
general conditions: —
(f) The approved institution shall furnish reports of the results of test or analysis in Form 39 carried on
drugs / cosmetics on behalf of licensees for manufacturer of drugs/cosmetics. The approved
institution shall furnish reports of the results of test or analysis carried on drugs / cosmetics on behalf
of any other individuals or organizations other than licensees for manufacturer of drugs/cosmetics in
Form 39A.
FORM 39 A [See rule 150E(f)]
Report of test or analysis by approved institution
(1) Name of inspector from whom received.............................................................. (2) Serial No. and date of Inspector’s memorandum................................................. (3) Number of sample.............................................. (4) Date of receipt of the sample.................................................
(5) Name of drug / cosmetics / raw material purporting to be contained in the sample.
(5) Details of raw material/final product in bulk/final product (in finished pack)* as obtained from the Inspector:
(a) Name of the Manufacturer and his Manufacturing Licence number under the act and rules made thereof
(B) Original Manufacturer's name in the case of raw materials and drugs repacked.
(b) Batch number.
(d) Date of manufacture, if any.
(e) Date of expiry, if any.
(6) Results of test or analysis with protocols of test or analysis applied.
In the opinion of the undersigned, the sample referred to above is *of standard quality/is not of standard quality
as defined in the Act and the rules made thereunder for the reasons given below.
Date.................................. ......................................................
Signature of Person-in-charge of testing
Note:- Final product includes repacked material.
*Delete whichever is not applicable

RECOMMENDATIONS OF THE (REPRODUCTIVE AND UROLOGY) HELD ON 17.09.2013:-
The NDAC (Reproductive and Urology) deliberated the proposals on 17.09.2013 and recommended the following:-
Agendano. Drug Name Recommendations
1 /
V . - ' '
Cyclofem
Committee opined that all Fixed Dose Combination injectable preparations containing synthetic Oestrogen and Progesterone were prohibited in the country vide GSR No. 743(E) dated 10.08.1989 most probably due to report of misuse of such preparations for pregnancy detection. In present scenario the chances of such misuse is not there as at present many pregnancy detection kits which are very sensitive and various means for satisfactory contraception are available. ICMR has already conducted the clinical trial with the cyclofem in 1275 subjects who were followed up for 10934 women- months of use. The clinical data has been found satisfactory. Available data shows that Fixed Dose Combination injectable preparations containing synthetic Oestrogen and Progesterone (cyclofem) are not associated with change in Bone Mineral Density. Therefore the committee recommended to consider de-notification of banning of the Fixed Dose Combination injectable preparations containing synthetic Oestrogen and Progesterone by appropriate authority. The committee recommended the grant of permission of clinical trial of Cyclofem and NET-EN subject to the following conditions:
1. The study should be titled as extended phase III clinical trial.
2. The study should be conducted at multispecialty hospitals having emergency facilities and institutional ethics committee registered with CDSCO.
3. Details of such sites along with undertaking by the investigators as per appendix VII of schedule Y should be submitted.
4. Informed consent document as per appendix V of schedule Y should be submitted.
5. Undertaking as per Rule 122DAB
Admin
Typewriter
Annexure -5
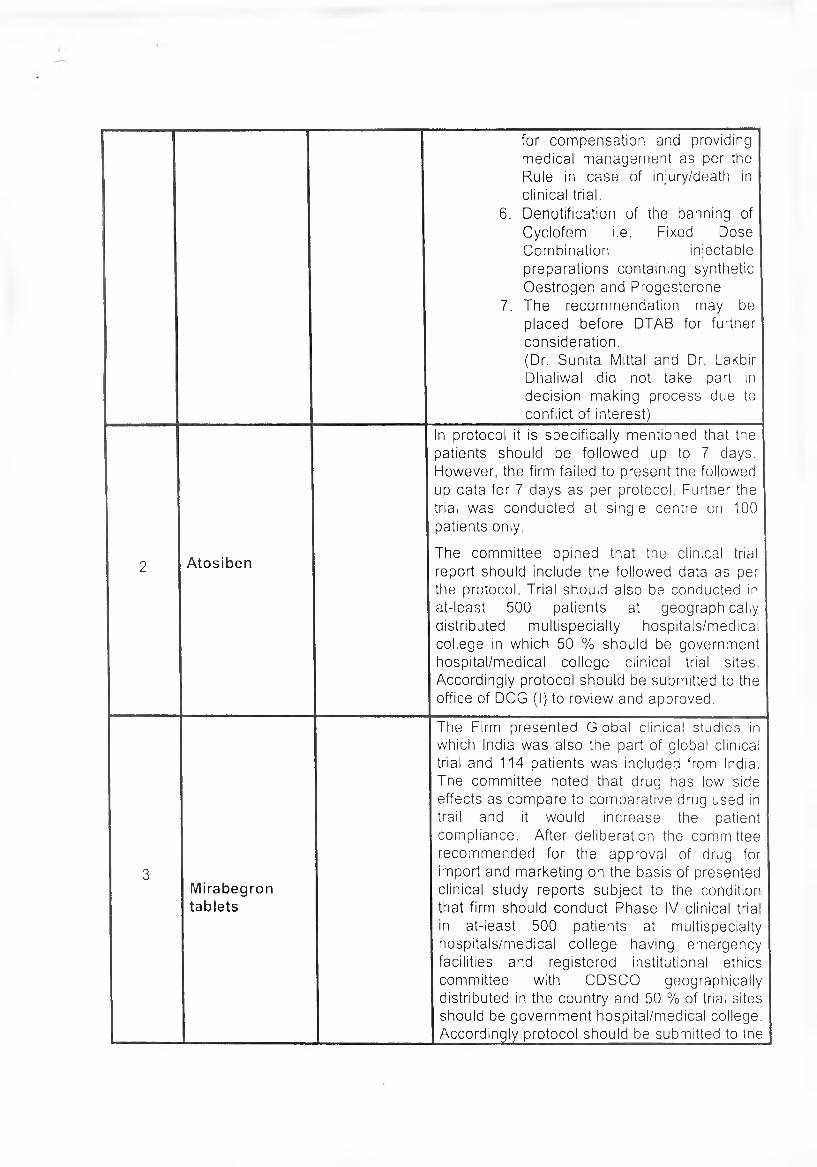
for compensation and providing medical management as per the Rule in case of injury/death in clinical trial.
6. Denotification of the banning of Cyclofem i.e. Fixed Dose Combination injectable preparations containing synthetic Oestrogen and Progesterone
7. The recommendation may be placed before DTAB for further consideration.(Dr. Sunita Mittal and Dr. Lakbir Dhaliwal did not take part in decision making process due to conflict of interest)
2 Atosiben
In protocol it is specifically mentioned that the patients should be followed up to 7 days. However, the firm failed to present the followed up data for 7 days as per protocol. Further the trial was conducted at single centre on 100 patients only.
The committee opined that the clinical trial report should include the followed data as per the protocol. Trial should also be conducted in at-least 500 patients at geographically distributed multispecialty hospitals/medical college in which 50 % should be government hospital/medical college clinical trial sites. Accordingly protocol should be submitted to the office of DCG (I) to review and approved.
3Mirabegrontablets
The Firm presented Global clinical studies in which India was also the part of global clinical trial and 114 patients was included from India. The committee noted that drug has low side effects as compare to comparative drug used in trail and it would increase the patient compliance. After deliberation the committee recommended for the approval of drug for import and marketing on the basis of presented clinical study reports subject to the condition that firm should conduct Phase IV clinical trial in at-least 500 patients at multispecialty hospitals/medical college having emergency facilities and registered institutional ethics committee with CDSCO geographically distributed in the country and 50 % of trial sites should be government hospital/medical college. Accordingly protocol should be submitted to the
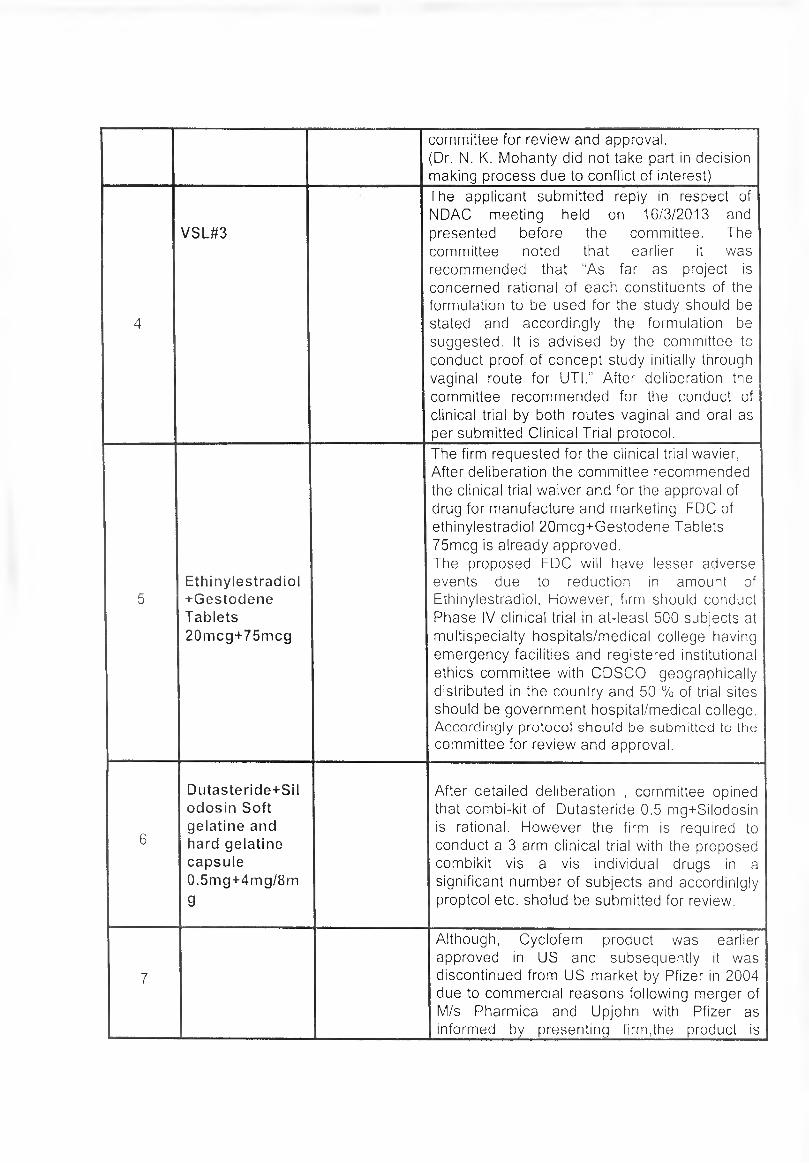
committee for review and approval.(Dr. N. K. Mohanty did not take part in decision making process due to conflict of interest)
4
VSL#3
The applicant submitted reply in respect of NDAC meeting held on 16/3/2013 and presented before the committee. The committee noted that earlier it was recommended that “As far as project is concerned rational of each constituents of the formulation to be used for the study should be stated and accordingly the formulation be suggested. It is advised by the committee to conduct proof of concept study initially through vaginal route for UTI.” After deliberation the committee recommended for the conduct of clinical trial by both routes vaginal and oral as per submitted Clinical Trial protocol.
5Ethinylestradiol+GestodeneTablets20mcg+75mcg
The firm requested for the clinical trial wavier, After deliberation the committee recommended the clinical trial waiver and for the approval of drug for manufacture and marketing. FDC of ethinylestradiol 20mcg+Gestodene Tablets 75mcg is already approved.The proposed FDC will have lesser adverse events due to reduction in amount of Ethinylestradiol. However, firm should conduct Phase IV clinical trial in at-least 500 subjects at multispecialty hospitals/medical college having emergency facilities and registered institutional ethics committee with CDSCO geographically distributed in the country and 50 % of trial sites should be government hospital/medical college. Accordingly protocol should be submitted to the committee for review and approval.
6
Dutasteride+Sil odosin Soft gelatine and hard gelatine capsule 0.5mg+4mg/8mg
After detailed deliberation , committee opined that combi-kit of Dutasteride 0.5 mg+Silodosin is rational. However the firm is required to conduct a 3 arm clinical trial with the proposed combikit vis a vis individual drugs in a significant number of subjects and accordingly proptcol etc. sholud be submitted for review.
7
Although, Cyclofem product was earlier approved in US and subsequently it was discontinued from US market by Pfizer in 2004 due to commercial reasons following merger of M/s Pharmica and Upjohn with Pfizer as informed by presenting firm,the product is

Estradiol Cypionate + Medroxyproges terone Acetate Injection 0.5mg+4mg/8m g5mg/0.05ml+2 5mg
presently marketed in countries like Latin America, Hongkong & Indonesia etc. The drug is also listed in WHO model list of essential medicines (18th list April 2013). ICMR has already conducted the clinical trial with the cyclofem in 1275 subjects who were followed up for 10934 women- months of use. The clinical data has been found satisfactory. The use of combined progesterone and estrogen (Cyclofem) has not been found associated with change in BMD. The committee recommended that the product Estradiol Cypionate + Medroxyprogesterone Acetate Injection 0.5mg+4mg/8mg5mg/0.05ml+25mg may be approved for marketing in the country subject to de-notification of banning of drug. The recommendation may be placed before DTAB for further consideration.
8
Desogestrel +Ethinylestradi ol tablet 0.15mg+0.03mg
The product is already approved as contraceptive pill and firm has proposed for marketing the imported product for additional indication- DUB. It was informed by the firm that the product is not approved in country of origin for the proposed additional indication. Accordingly the committee did not recommend for the proposed additional indication.
9 PergoverisThe committee recommended that a Phase III trial shal be conducted and accordingly protocol etc. shall be submitted
10.Estradiol Vaginal Tablets
After deliberation, committee recommended for grant of permission for conduct of clinical trial as per submitted protocol.
Experts Group meeting to review the status of monthly injectable contraceptive ‘Cyclofem’ held on 25th October, 2017 in R. No. 309,
Committee Room, ICMR Hqrs
The following members participated in the meeting:
Expert Members
Dr. Soumya Swaminathan, Secretary DHR, MoHFW & DG, ICMR - ChairpersonDr. S. K. Sikdar, Deputy Commissioner & OIC (FP), DHFW, MoHFWDr. A. K. Pradhan, Deputy Drugs Controller (India), FDA Bhavan, DelhiDr. Alka Kriplani, Prof and Head OBGyn, AIIMS, DelhiDr. Bikash Medhi, Professor Pharmacology, PGIMER, ChandigarhDr. Ankit Sharma, Asst Drugs Controller (India), FDA Bhavan, Delhi
ICMR
Dr. R. S. Sharma, Sci. ‘G’ & Head RBMCH Dr. Shalini Singh, Sci. ‘F’, RBMCH Dr. Malabika Roy, Consultant, RBMCH
Dr. Jagdish Prasad, DGHS and Dr Y. K. Gupta, Prof. and Head, Pharmacology, AIIMS, Delhi, were unable to attend due to other commitments.
At the outset, Dr. Soumya Swaminathan, Secretary, DHR and DG, ICMR welcomed the members and informed that this Expert group meeting was convened to review the status of combined injectable contraceptive ’Cyclofem’ placed for approval to DCGI In 2009 for a multisite Pre-programme Introductory study at 40 sites throughout the country. One such combined injectable contraceptive Cyclofem has been evaluated in a Phase-Ill trial and the report was submitted to DCGI in 2007. Based on these results the Phase IV-Pre-Programme Introductory study was proposed at the behest of the MoHFW in 2008. It was envisaged to evaluate the logistics, training requirement, demand for the method and also validate the Phase III study findings in the field situation and for Cyclofem’s probable inclusion in the National Family Welfare Programme. She felt that since no decision has been taken by the DCGI since 2013 on injectable contraception Cyclofem therefore there is an urgent need to review the status of injectable contraceptive Cyclofem in presence of representatives from DCGI, DGHS, Dept of HFW, MoHFW and subject Experts so that a decision can be taken to take this product forward.
Page 1 of 4

Dr Sikdar appreciated that ICMR over the years has evaluated various newer contraceptive methods including progesterone only and combined hormonal methods for their safety, efficacy and acceptability in order to increase the contraceptive choices available to women or couples in reproductive age desiring family planning methods.
Dr. Y. K. Gupta conveyed through e-mail to DG, ICMR that it is unfortunate that such huge effort has not been deliberated enough to arrive at a decision, He stated that he was not aware of receiving any notification of the proposed committee by DTAB, nor any meeting to discuss the issue and that he will be happy to contribute in any possible manner to see that such a study does not go waste.
Dr. Roy presented the study findings of the Phase III study which was carried out in controlled clinical trial'settings in 16 tertiary level multispecialty facilities regarding efficacy, safety, acceptability and return of fertility in Cyclofem users. She infpjmed that the report was evaluated by expert committees at ICMR and report submitted to DCGI in 2007 with a suggestion for conducting pre-programme Introduction study. She stated that the subsequent Phase IV Pre-programme Introductory study proposal was approved by Research Advisory Council (RAC) of MOHFW in 2008 with financial support for being carried out at 31 Districts hospitals and 9 Mother NGO (MNGO) clinics having written MOU with Tertiary level multispecialty hospitals for back-up facilities. Following this ICMR obtained approval of ICMR Toxicology Review Panel (TRP) and ICMR’s Ethics committee (IEC) in 2008 along with Institutional Ethics committee approval from the participating sites. The proposal of the Phase IV study along with TRP and IEC approvals was submitted to DCGI in 2009 for approval to conduct the study.
A comngunication received from the office of DCGI to ICMR on 17th December 2013, informed'about the recommendations of NDAC held on 17th September 2013 and the 65th meeting of DTAB held on 25th November 2013.
The NDAC recommended that a) the study be titled as an extended Phase III trial and conducted through multi speciality hospitals having emergency facilities and registered ethics committees, b) undertaking by Investigators and Informed consent documents as per Appendix V of Schedule Y to be submitted, c) undertaking as per Rule 122DAB for compensation^ and medical management as per rule in case of injury /Death, d) denotification of Cyclofem ban i.e Fixed dose combination injectable preparations of synthetic oestrogen and progesterone and that the recommendation of NDAC be placed in the Drug Technical Advisory Board (DTAB) for further consideration.
Page 2 of 4
The DTAB recommended the constitution of an Expert Committee with Gynecologists, endocrinologists, pharmacologists under the Chairmanship of DGHS to look into the essentiality of the Clinical Trial as well as the requirement if any, of amendment of entry No 27 of the list of banned drugs in respect of fixed drug combinations of Injectable preparations containing synthetic oestrogen and progesterone in context of present day knowledge.
The Expert group deliberated on the study findings and historical scenario presented during the meeting and the following observations were made:
Observations and comments of the Review Committee
- Cyclofem is available worldwide and is an approved product. Injectable contraceptives are among the 4th most commonly used contraceptive in the world.
- Members noted that Cyclofem has been added to the WHO Model List of Essential Medicines in March 2007.
- Cyclofem has been approved by the US FDA in the year 2000 and was marketed as Lunelle.
\ V- Indian Medical eligibility criteria for Contraceptives (2015) include Cyclofem
as one of the products.
- Study data of Phase III study with Cyclofem carried out through 16 multispeciality hospitals indicates that Cyclofem is safe, efficacious (no inadvertent pregnancy reported during the study period of one year), and acceptable with continuation rate of 63.2 per 100 users at 12 months of use
Members noted that the return of fertility is 83% at the end of one year which is comparable to fecundity in the normal population of 70-80% (Srinivasan K. An application of a probability model to the study of inters live-birth intervals. Sankhya 1966, Series 28: 175-82).
There were 2 (0.16%) stillbirths and one spontaneous abortion (0.0007%) in women who became pregnant following discontinuation of Cyclofem use during the follow up period of one year. However, in general population the corresponding rates are much higher 10.0% (ACOG, 2015) for spontaneous abortion and 2.2.1 pe.&1000 live births (WHO-PMNCH-2011) for still births in India and, therefore these effects are unlikely to be related to product use.
Gynaecologists opined that the women in OPDs demand and prefer monthly injectables for contraception, also the compliance with OCPs is reported to be low, and therefore there is a great need for this product to be made available in the country.
Page 3 of 4

- NUVA ring which is also a combined hormonal contraceptive and is available in the country (pharmacies) however, it is not affordable to most women in India. Cyclofem is relatively inexpensive and will be affordable to the masses. Besides, Cyclofem does not need self insertion unlike the ring, and may be acceptable to some women.
- Combined oral and Injectable high dose preparations were banned in 1988 because of speculation of misuse and lack of diagnostic kits for pregnancy detection at that time.
- The ban on fixed dose combined hormonal preparations in 1988 was due to its misuse. Since then the scenario has changed and pregnancy detection kits are freely available now, the members strongly recommended that introduction of monthly injectable contraceptive is a national need and therefore the process for denotification may be initiated at the earliest.
- The DCGI officials informed that a follow up meeting would be held,soon in November, 2017.
Recommendations
• The Committee reviewed the entire sequence of application to the statutory regulatory bodies inclbdinig the Phase-Ill study findings and noted that Injectable contraceptive Cyclofem is safe, efficacious and acceptable to the women in India.
• The Committee was satisfied with the study study findings and hence unanimously recommended that the DCGI should denotify the monthly combined injectable contraceptive Cyclofem so that the product can be made available for the women in the country.
The meeting ended with vote of thanks to the Chair.
Page 4 of 4

MINUTES OF THE 65™ MEETING OF DRUGS TECHNICAL ADVISORY BOARD
HELD ON 25™ NOVEMBER, 2013 IN
BHAWAN, NEW DELHI - 110002
PRESENT
1. Dr. Jagdish Prasad,
Director General of Health Services,
Nirman Bhawan, New Delhi.
2. Shri C. Hariharan
Director in-charge,
Central Drugs Laboratory,
Kolkata-700016
3. Dr. J.A.S. Giri
815A, Road No. 41
Jublee Hills, Hyderabad-500033
4. Dr. C. Nath,
Central Drug Research Institute
Lucknow
5. Dr. Anshu Sethi Bajaj,
Medical Council of India,
New Delhi
6. Dr. B.P.S. Reddy,
CMD, Hetero Drugs Ltd.
Hyderabad
7. Dr. A. K. Tiwari
Indian Veterinary Research Institute
lzatnagar-243122 (U.P.)
THE CHAMBER OF DGHS, NIRMAN
Chairman
Member
Member
Member
Member
Member
Member
Admin
Typewriter
Annexure -6

value and having the end use for use in the human is considered as a drug. In view of
this the DTAB recommended that the class of drugs under item 1 of schedule D should
be amended to read as under:
“Substances not intended for medicinal use excluding those intended to be used
as drugs after further purification or rendering them sterile".
CONSIDEARTION OF THE PROPOSAL TO GRANT PERMISSION FOR
CONDUCTING THE CLINICAL TRIAL OF AN INJECTABLE CONTRACEPTIVE
CYCLOFEM AND NET-EN BY ICMR
The Member Secretary, briefed the members that the office of DCG(I) had
received an application from Dr. Malabika Roy, Scientist-F, Division of RHN, ICMR,
New Delhi for conducting study entitled “Pre-programme introduction of Injectable
Contraceptive Cyclofem and NET-EN through district hospitals and NGO clinics- An
ICMR Task Force study."The NET-EN is Norethisterone Enanthate 200 mg as a two
monthly injectable hormonal contraceptive.
The “Fixed Dose Combination of Oestrogen and Progestin (other than oral
contraceptive) containing per tablet estrogen content of more than 50 meg (equivalent
to Norethisterone Acetate) and fixed dose combination injectable preparations
containing synthetic Oestrogen and Progesterone” was prohibited by the Ministry of the
Health and Family Welfare under section 26A of the Drugs and Cosmetics Rules, 1945
under entry number 27 of the list of banned drugs vide Gazette Notification G.S.R.
743(E) dated 10.08.1989.
Earlier a proposal of ICMR to conduct clinical trial in the country with the
injectable preparations containing Medroxyprogesterone acetate and estradiol
cypionate (Cyclofem) as monthly contraceptive was recommended by the DTAB in its
48th meeting held on 08th July, 1999 for the reason that the clinical trial could continue
AGENDA NO. 13
23

without disturbing the present prohibitory status and the drugs would be imported for
limited purpose of clinical trial only.
The proposal was deliberated in 61st meeting of DTAB held on 24th July, 2012
also. The Board after deliberation recommended that an expert committee consisting of
Gynecologists, Pharmacologists may be constituted by the DCG(I) to examine the
safety and efficacy of Cyclofem especially in the light of the fact that such contraceptive
injections are prone to cause reduction in bone mineral density (BMD). The proposal of
was deliberated in New Drug Advisory Committee (NDAC) (Reproductive and Urology)
of the CDSCO on 17.09.2013. The Committee recommended for the grant of
permission of conducting clinical trial with Cyclofem and NET-EN subject to the
following condition:-
1. The study should be titled as extended phase III clinical trial.
2. The study should be conducted at multispecialty hospitals having
emergency facilities and Institutional Ethics Committee registered with
CDSCO.
3. Details of such sites along with Undertaking by Investigators as per
Appendix VII of Schedule Y should be submitted.
4. Informed Consent Documents as per appendix V of schedule Y should be
submitted.
5. Undertaking as per Rule 122DAB for compensation and providing medical
management as per the rule in case of injury/death in clinical trial.
6. Denotification of the banning of Cyclofem i.e. Fixed Dose Combination
Injectable preparations containing synthetic Oestrofen and Progesterone.
7. The recommendation may be placed before DTAB for further
consideration.
During deliberation the members were of the view that the proposal also
includes the requirement of the amendment of the entry number 27 of the list of
banned drugs also.
The DTAB recommended that an Expert Committee consisting of at least
three Gynecologists, three endocrinologists, Dr. Anoop Mishra and Dr. Y. K.
Gupta, HOD, Department of Pharmacology, AIIMS, New Delhi under the
24
Chairmanship of DGHS may be constituted to examine the essentiality of the
clinical trial as well as the requirement, if any, of the amendment of entry number
27 in respect of the FDC of injectable preprations containing synthetic oestrogen
and progesterone, in the context of present day knowledge.
Meeting ended with the vote of thanks to the Chair.
25




















