Medication Therapy Management Guide - Portland, TX
68
MTMP Guide 2018-2019 2018-2019 Medication Therapy Management Guide Choice and Select MTMP Plan Options, Effective June 1, 2019 The Medication Therapy Management approach is a progressive model of prescription utilization and consumer centered purchase options. The program offers the consumer a variety of options for prescription access and out of pocket cost management. Over the Counter, vaccines/immunizations, generic, best brand, non-best brand, and cost share prescriptions are available. Step therapy, prior authorization, and cost share prescriptions (Choice MTMP) are management tools incorporated into the program to assist in managing evidence-based prescription cost. Enclosed are the prescription resources to assist in effective prescription purchasing. ● Prescription Flowsheet ● OptumRx Single Sign-On Access ● Step Therapy/RxResults ● OptumRx Consumer Portal ● Clinical Prior Authorization/RxResults ● OptumRx Mail Order Service ● OptumRx Vaccine/Immunization Network ● OptumRx Mobile Friendly Website: m.optumrx.com ● Value Based Benefits for Chronic Conditions (Diabetes, ● OptumRx Mobile Application Hypertension & High Cholesterol) ● Covered and Non-Covered Drugs BriovaRx, The OptumRx Specialty/Biotech Pharmacy ● Qualified High Deductible Health Savings Account ● Cost Share Prescription Copays/Sample Cost Share Letter Benefit Plans Wellness Drug List ● OptumRx Accessing the Pharmacy Locator - ● Political Subdivision Preferred/Formulary ● Internet Direct Access (IDA) » Choice MTMP: Select Formulary » Select MTMP: Premium Formulary and Cost Share Medications Excluded The popularity of pharmacy compounding has grown in recent years due to significant sterilization requirements and profit potential for pharmacies. When combining ingredients to make a “customized” medication, pharmacies may price the final product at a premium - which can result in additional plan costs. There are legitimate clinical reasons for compounding, such as dye allergies or difficulty in swallowing pills. However, there is growing concern about the quality of compound medications, which are not monitored by the Food and Drug Administration (FDA). A thoughtful and comprehensive approach is needed to help members address the safety and rising costs of compound prescriptions. As a result, OptumRx has enhanced the Pharmacy Compound Network Management Strategy - effective January 1, 2017. Compound claims filled at non-credentialed pharmacies will no longer be covered. Members may continue to fill covered compound medications at a broad range of credentialed pharmacies. To locate a credentialed pharmacy, members can access the NCCP Pharmacy Locator Guide or call the OptumRx phone number on the ID card.
-
Upload
khangminh22 -
Category
Documents
-
view
3 -
download
0
Transcript of Medication Therapy Management Guide - Portland, TX

MTMP Guide 2018-2019
2018-2019
Medication Therapy Management Guide
Choice and Select MTMP Plan Options, Effective June 1, 2019
The Medication Therapy Management approach is a progressive model of prescription utilization and
consumer centered purchase options. The program offers the consumer a variety of options for prescription
access and out of pocket cost management. Over the Counter, vaccines/immunizations, generic, best brand,
non-best brand, and cost share prescriptions are available. Step therapy, prior authorization, and cost share
prescriptions (Choice MTMP) are management tools incorporated into the program to assist in managing
evidence-based prescription cost. Enclosed are the prescription resources to assist in effective prescription
purchasing.
● Prescription Flowsheet ● OptumRx Single Sign-On Access
● Step Therapy/RxResults ● OptumRx Consumer Portal
● Clinical Prior Authorization/RxResults ● OptumRx Mail Order Service
● OptumRx Vaccine/Immunization Network ● OptumRx Mobile Friendly Website: m.optumrx.com
● Value Based Benefits for Chronic Conditions (Diabetes, ● OptumRx Mobile Application
Hypertension & High Cholesterol) ● Covered and Non-Covered Drugs
BriovaRx, The OptumRx Specialty/Biotech Pharmacy ● Qualified High Deductible Health Savings Account
● Cost Share Prescription Copays/Sample Cost Share Letter Benefit Plans Wellness Drug List
● OptumRx Accessing the Pharmacy Locator - ● Political Subdivision Preferred/Formulary
● Internet Direct Access (IDA) » Choice MTMP: Select Formulary
» Select MTMP: Premium Formulary and Cost Share
Medications Excluded
The popularity of pharmacy compounding has grown in recent years due to significant sterilization
requirements and profit potential for pharmacies. When combining ingredients to make a “customized”
medication, pharmacies may price the final product at a premium - which can result in additional plan
costs. There are legitimate clinical reasons for compounding, such as dye allergies or difficulty in
swallowing pills. However, there is growing concern about the quality of compound medications, which
are not monitored by the Food and Drug Administration (FDA).
A thoughtful and comprehensive approach is needed to help members address the safety and rising costs of
compound prescriptions. As a result, OptumRx has enhanced the Pharmacy Compound Network
Management Strategy - effective January 1, 2017. Compound claims filled at non-credentialed pharmacies
will no longer be covered. Members may continue to fill covered compound medications at a broad range
of credentialed pharmacies. To locate a credentialed pharmacy, members can access the NCCP Pharmacy
Locator Guide or call the OptumRx phone number on the ID card.

MTMP Guide 2018-2019 2
Healthcare Services for our Bilingual (English and Spanish) Membership
Translation Line: (800) 385-9952 [email protected]
Current Documents in Spanish Spanish Translation Support Per Request
» Benefit Documents » Enrollment/Change/Termination Forms
Summary of Benefits and Coverage (SBC) » Online Enrollment System (OES)
Enrollment Poster » Medical Intelligence Denials
Teladoc FAQs » Explanation of Benefits (EOB)
Teladoc Getting Started
» Forms
Right of Recovery Form (Subrogation)
Other Insurance Form
Protected Health Information Authorization
Form
» Medical Intelligence Documents
CM and DM Welcome Letter
Health Coach Flyer
CM and DM Education Letter
CM and DM Outreach Letter
Call Letter
CM-Self-Management Plan Letter
CM-Transition in Care for Parent Letter
CM-Transition in Care for Unable to Reach
Letter
Wellbeing Assessment

MTMP Guide 2018-2019 3
Helpful Resources
Please visit our website at tmlhealthbenefits.org for current benefit information 24 hours/7days a
week.
Address: PO Box 149190, Austin, Texas 78714-9190
Secured Customer Care E-mail: Login at tmlhealthbenefits.org >> "Contact Us" >> "I have a
general question"
Mobile Access: iPhone App Store, Android Google Play, or
tmlhealthbenefits.org for all other phones
Medical Information
Customer Care Helpline (800) 282-5385 7:00 AM - 6:00 PM Central
Translation Line (800) 385-9952 [email protected]
Medical Authorizations (800) 847-1213 8:30 AM - 5:00 PM Central
Where to Mail Paper Medical Claims TML Health, PO Box 149190, Austin, Texas 78714-9190
Telehealth (Teladoc) 1-800-Teladoc or (800) 835-2362 member.teladoc.com/signin
Prescription Information
Prescription Authorizations
(RxResults)
Toll Free
(844) 853-9400
Local
(501) 367-8402
Fax
(855) 856-3291
7:00 AM - 7:00 PM
Central
Where to Mail Paper OptumRx Claims OptumRx, PO Box 29044 Hot Springs, AR 71903
OptumRx Member Customer Service (888) 543-1369 optumrx.com
OptumRx Pharmacy Help Desk -
Pharmacist and Mail Customer Service (800) 788-7871 (TTY 711) optumrx.com
BriovaRx, The OptumRx
Specialty/Biotech Pharmacy (866) 218-5445 or (855) 4BRIOVA | Fax: (800) 491-7997

MTMP Guide 2018-2019 4
Table of Contents
Helpful Resources ............................................................................................................................... 3
How to get the most out of your Medication Therapy Management Program (MTMP) ......................... 5
MTMP Alliance Partners .............................................................................................................................5
TML Health will offer two MTMP Plans as Employer Choice .....................................................................5
MTMP MAC Options ...................................................................................................................................6
Covered Individual Copayments/Financial Responsibility .........................................................................7
Step Therapy ..................................................................................................................................... 10
Clinical Prior Authorization ................................................................................................................ 11
OptumRx Vaccine/Immunization Network Services ........................................................................... 16
Value Based Benefits for Chronic Conditions (Diabetes, Hypertension & High Cholesterol) ................. 19
BriovaRx Specialty/Biotech Pharmacy ............................................................................................... 20
Cost Share Prescription Copays for Choice MTMP .............................................................................. 25
Prescription Benefits ......................................................................................................................... 28
Covered and Non-Covered Drugs ....................................................................................................... 30
Drugs Covered under this Benefit ............................................................................................................30
Drugs Not Covered under this Benefit .....................................................................................................30
Miscellaneous Exclusions .........................................................................................................................32
Qualified High Deductible Health Savings Account Benefit Plans Wellness Drug List ........................... 34
Political Subdivision Choice Select Formulary .................................................................................... 39
Political Subdivision Select Premium Formulary ................................................................................. 51
OptumRx Pharmacy Resources .......................................................................................................... 65
Mobile Application ...................................................................................................................................65
Mobile Friendly Website ..........................................................................................................................65
Consumer Portal .......................................................................................................................................67
Mail Order Service ....................................................................................................................................68

MTMP Guide 2018-2019 5
How to get the most out of your Medication Therapy Management Program (MTMP)
MTMP Alliance Partners
Pharmacy Benefit Manager Network: OptumRx Membership: (888) 543-1369 | optumrx.com | 24 hours
a day/7 days a week
OptumRx Online Pharmacy Locator Tool: Members can locate a Value Network pharmacy near them
by using the OptumRx Online Pharmacy Locator Tool at optumrx.com.
OptumRx Pharmacy and Mail Service Customer Service: (800) 788-7871 (TTY 711) | optumrx.com
BriovaRx, The OptumRx Specialty Pharmacy: (866) 218-5445 or (855) 4BRIOVA | Fax: (800) 491-
7997
Submit OptumRx Paper Prescription Claims to: OptumRx | PO Box 29044 | Hot Springs, AR 71903
Evidence-Based Medication Review: RxResults | Toll Free: (844) 853-9400 | Local: (501) 367-8402 |
Fax: (855) 856-3291
RxResults provides both clinical and economical evaluations of drugs through its Pharmacy and
Therapeutics (P&T) Committee.
TML Health will offer two MTMP Plans as Employer Choice
1. Select MTMP Plan: MAC A Only
A. Premium Formulary (Exclusive Formulary)
B. Cost Share Prescriptions Excluded
C. New to Market Medications OptumRx Pharmacy and Therapeutic Committee Release
2. Choice MTMP Plan: MAC A or MAC C Options
A. Select Formulary (Broad Formulary)
B. Cost Share Prescriptions Copays: 1-30 days $150.00/31-60 days $300.00/61-90 days $450.00
C. New to Market Medications OptumRx and RxResults Pharmacy and Therapeutic Committee
Review and Release
Note: Consumer Centered Plans are MAC A only.

MTMP Guide 2018-2019 6
MTMP MAC Options
1. MAC A Plan
If a brand name drug is dispensed and a generic alternate drug exists, the Covered Individual pays the
difference between the brand name and generic price in addition to the appropriate copayment for the
brand name. The cost difference between the brand name and generic price does not apply to any
individual deductibles or out of pocket amounts. The MAC differential applies to all prescriptions
purchased through this program when a generic alternate is available.
2. MAC C Plan
If a brand name drug is dispensed and a generic alternate drug exists, the Covered Individual pays the
appropriate brand copay.
3. Lessor of Benefit
Through the OptumRx network contract, the covered individual’s out of pocket expense is managed
by the pharmacy network agreement that the covered individual will receive the most advantageous
pricing. This would be determined by the lessor of pharmacy contracts, Usual & Customary cost
(U&C), copayments or the discounted cost the covered individual would be charged. Due to the Lessor
of Benefit, the OptumRx Reportal will be an important price transparency resource to ensure covered
individual is purchasing the prescription from the most cost effective pharmacy.
4. Eligible Prescriptions
Lessor of U&C, Market Price, and Copay
5. Ineligible Prescriptions
Lessor of U&C and Calculated Cost

MTMP Guide 2018-2019 7
Covered Individual Copayments/Financial Responsibility
Preferred Retail Pharmacies*
Benefit 1-30 Days Supply 31-60 Days Supply 61-90 Days Supply
Generic medications $5 $10 $15
Preferred/Formulary branded medications $38 $76 $114
Non-Preferred branded medications $60 $120 $180
* The OptumRx Preferred Network of Pharmacies includes HEB and Walmart (not Sam’s Club)
National/Broad Network Retail Pharmacies
Benefit 1-30 Days Supply 31-60 Days Supply 61-90 Days Supply
Generic medications $10 $20 $30
Preferred/Formulary branded medications $43 $86 $129
Non-Preferred branded medications $65 $130 $195
Value Based Benefits for Chronic Conditions (Diabetes, Hypertension & High Cholesterol)*
Benefit 1-30 Days Supply** 31-60 Days Supply 61-90 Days Supply
Generic medications $0 $5 $10
Preferred/Formulary branded medications $38 $76 $114
Non-Preferred branded medications $60 $120 $180
* Not all medications for diabetes, hypertension and high cholesterol qualify (e.g., Cost Share prescription copays
and medication exclusions). Refer to the Medication Therapy Management Guide for the value based prescription
list). The Qualified High Deductible Plans Wellness drug list will override the value tiered list.
** Value Based Benefit Copays are applicable at the preferred, national/broad network.
Prescription Mail Service
Benefit 31-90 Days Supply
Generic medications $15
Preferred/Formulary branded Medications $114
Non-Preferred branded Medications $180
Take advantage of home delivery by online registration: Visit optumrx.com: register and follow the simple step-by-
step instructions. You can manage your medication online, including filing new prescriptions and transferring other
prescriptions to home delivery. You can also set up text message reminders to help manage your medication schedule.
Be sure to have your ID card and medication bottles on hand to have the required information.

MTMP Guide 2018-2019 8
Retail/Mail Order Cost Share Prescriptions*
Benefit 1-30 Days Supply 31-60 Days Supply 61-90 Days Supply
Branded or generic Cost Share prescription
copays (regardless of pharmacy or pharmacy
network)
$150 $300 $450
* Cost Share prescription copays are certain branded and generic medications for which there are lower cost
therapeutic alternative medications. These therapeutic alternatives should provide equal or similar medication
therapy for a covered individual when properly dosed. Cost Share prescription copays are identified in the Cost
Share Prescription Copays section of this guide. Cost Share prescriptions are excluded from the Select Medication
Therapy Management Plan.
BriovaRx Specialty Pharmacy
Benefit 1-30 Days Supply 31-60 Days Supply** 61-90 Days Supply**
Specialty medications* $100 N/A N/A
Biosimilar and generic specialty medications $75 N/A N/A
* Specialty medications are typically medications requiring special storage, handling, administration and patient
monitoring; or is taken for complex or rare patient conditions. Some specialty medications are sometimes
biotechnology medications.
** Specialty medications are limited to no more than a 30-day supply of the medication per prescription fill.
Affordable Care Act Benefits*
Benefit 1-30 Days Supply 31-60 Days Supply 61-90 Days Supply*
Smoking cessation medications - Nicorette Gum,
Nicotine Replacement Lozenge, Nicotine
Replacement Patch, Nicotrol Inhaler, Nicotrol
Nasal Spray. Quantity limits apply (six month's
supply per plan year).
$0 $0 N/A
Preventative statin medications – Includes low to
mid-strength statin medications, atorvastatin,
lovastatin, and simvastatin. Lovastatin covered
without a prior authorization.
$0 N/A N/A
Other preventative medications – aspirin (men
aged 45-79, women aged 55-79); folic acid
(women of childbearing age); fluoride tablets
and solution (for children aged zero to five years
old – toothpastes and rinses do not qualify);
chemoprevention supplements, iron deficiency
supplements; vitamin D (65 years and over); and
bowel preparation medications OTC (Bisacodyl
EC Tab, magnesium citrate solution,
polyethylene glycol 3350).
$0 N/A N/A
* Over the counter medications covered with this benefit require a prescription from your provider.

MTMP Guide 2018-2019 9
Affordable Care Act Benefits – Women’s Preventative Health Services
Benefit
Retail Rx Medical Plan
Prescription
Plan
Oral Contraceptives Generic N/A $0 cost share
IUD Device $0 cost share $0 cost share
Implant Device $0 cost share $0 cost share
Permanent Implantable Contraceptive Coil and hysterosalpingography
services related to the fitting $0 cost share N/A
Insertion and/or Removal of Contraceptive Devices $0 cost share N/A
Urine Pregnancy Test, Urinalysis, Sonogram to Detect Placement of Device $0 cost share N/A
Injectable Contraceptives $0 cost share $0 cost share
Injectable Administration Fee $0 cost share N/A
Diaphragm (cervical), Hormone Vaginal Ring, Hormone Patch, Cervical
Cap, Spermicides, Sponges N/A $0 cost share
Diaphragm (cervical) Instruction and Fitting Fee $0 cost share N/A
Emergency Contraceptives N/A $0 cost share
Over-The-Counter (OTC) Contraceptives (contraceptive films, foams, gels) N/A $0 cost share
Contraceptive Management $0 cost share N/A
Female Condoms N/A $0 cost share
Female Surgical Sterilization $0 cost share N/A
Medications for risk reduction of breast cancer in women (age thirty-five
(35) or older) who are at increased risk for breast cancer and at low risk for
adverse medication effects: Tamoxifen or Raloxifene
N/A $0 cost share
Women found to be at increased risk using a screening tool designed to identify a family history that may be
associated with an increased risk of having a potentially harmful gene mutation must receive coverage w/o cost-
sharing for genetic counseling, and, if indicated, testing for harmful BRCA mutations. This is true regardless of
whether the woman has previously been diagnosed with cancer, as long as she is not currently symptomatic of
receiving active treatment for breast, ovarian, tubal, or peritoneal. Jan 1, 2016 genetic counseling for BRCA
testing is covered 100% as a preventive benefit.
Mandate to provide a list of the lactation counseling providers available within the network under the plan or
coverage. Grandfathered plans cannot apply cost-share expenses for OON lactation services. Services for lactation
support services w/o cost-sharing must extend for the duration of breastfeeding.

MTMP Guide 2018-2019 10
Step Therapy
For Clinical Authorization, doctor/prescription prescribers should call RxResults toll free: (844) 853-9400
or local: (501) 367-8402. Your doctor/prescription prescriber will be asked a series of questions and
RxResults will then approve or deny the authorization request.
Sample of what will occur at pharmacy: Claim is processing for Advair® & the following message will alert
the pharmacist: Step Therapy after inhaled steroid 1st or Prior Authorization call toll free: (844) 853-9400
or local: (501) 367-8402.
Asthma
Required for members <40 years of age who have not demonstrated adherence to an inhaled corticosteroid
(ICS) (at least 90 days of therapy in the past 120 days).
Category A
Inhaled corticosteroid (ICS) - Member must demonstrate adherence to an inhaled steroid and/or satisfy
specific clinical criteria as determined by RxResults prior to obtaining a Category B medication.
Category B
(Only after demonstrated compliance and/or failure with a Category A medication)
Advair® • fluticasone-salmeterol inhaler
Airduo® • Perforomist®
Breo Ellipta® • Serevent®
Brovana® • Symbicort®
Dulera® • Wixela Inhub®
Treatment Plan Adherence is required for authorization to be approved.
Note: All clinical programs (Clinical Prior Authorization, Step Therapy, Cost Share Prescription Copays,
etc.) are subject to change without notice to accommodate new drug entries to the marketplace and
adjustments in established medical and pharmacy practice guidelines.

MTMP Guide 2018-2019 11
Clinical Prior Authorization
The list of conditions below may change as appropriate for the plan. For prior authorization requests, please
have your doctor/prescription prescriber call RxResults toll free: (844) 853-9400 or local: (501) 367-8402.
Your doctor/prescription prescriber will be asked a series of questions and RxResults will approve or deny
the request. A prior authorization is active for no more than one year.
The following medications may be reimbursed when approved by prior authorization review:
Acne Medications Tretinoin all dosage forms (e.g. Retin-A, Differin, Tazorac) for individuals 26 years of age or older
Analgesics/Anti-inflammatory/Pain Agents Actiq® fentanyl lozenges Fentora®
Antifungals VFEND® voriconazole
Congestive Heart Failure Corlanor® Entresto®
Gastrointestinals Amitiza® Linzess® Movantik® Trulance® (excluded from the SELECT MTMP)
Gout Uloric®
Lipid Reducers Vascepa®
Major Specialty/Biotech Medications Refer to the Specialty/Biotech section in this guide.
Migraine Medications Aimovig® Ajovy® Emgality®
Narcolepsy Medications armodafinil modafinil Nuvigil® Provigil® Xyrem®
Topical Anesthetics 5% lidocaine patches 5% Lidoderm® patch
Note: All clinical programs (Clinical Prior Authorization, Step Therapy, Cost Share Prescription Copays,
etc.) are subject to change without notice to accommodate new drug entries to the marketplace and
adjustments in established medical and pharmacy practice guidelines.

MTMP Guide 2018-2019 12
Sample Denial Member Letter
RxResults
320 Executive Ct, Ste 201
Little Rock, AR 7220
«Decision Date»
«Patient Name»
«Patient Address Line 1»«Patient Address Line 2»
«Patient City», «Patient State Code»«Patient Zip»
Dear Prescription Benefit Plan Participant:
RxResults is an organization that provides prior authorization services, or clinical reviews, for your prescription
benefit plan. This letter is to inform you that your physician, «Prescriber Name», recently requested plan coverage
authorization for «Drug Name» on your behalf. Unfortunately, the plan cannot provide plan coverage approval for
this drug at this time due to the following reason(s):
X Your plan’s coverage policy for this medication is associated with specific requirements. Based on your
medication history available to us, these requirements do not appear to have been met.
X «Patient Explanations»
We have communicated the denied authorization, or initial adverse benefit determination, for the above drug and the
reason(s) for the denial to your physician. Information located in the following clinical resources were used to make
this decision:
«General Explanation»
As a result of this denial, your physician may choose to prescribe a substitute medication for you that is covered by
the plan. However, he or she may believe that an alternative medication is not appropriate for you and may choose to
appeal this denial by providing additional clinical information. In our communication to your physician, we also
provided instructions for submitting an appeal to the RxResults Evidence-Based Prescription Drug Program (EBRx).
As a prescription benefit plan participant, you have the right to appeal our decision to deny coverage for the above
drug. If you wish to appeal, you may request your physician to submit a written clinical appeal request to RxResults.
If your physician has not submitted an appeal already and is in agreement that an appeal is appropriate, he or she may
submit their written appeal request by facsimile to:
Attn: Physician Appeals/Medical Director
Fax #: (501) 367-7672
If you have any questions about the appeals process, please contact RxResults Member Services at 844-853-9400.
What if my situation is urgent?
If your situation meets the definition of urgent under the law, your review will generally be conducted within 72
hours. Generally, an urgent situation is one in which your health may be in serious jeopardy or, in the opinion of your
physician, you may experience pain that cannot be adequately controlled while you wait for a decision on your appeal.
If you believe your situation is urgent, you may request an expedited appeal by following the instructions above for
filing an internal appeal and also you have the right to request an external review to be conducted by an independent
review organization for consideration of coverage for the above drug at the same time as this review. This request
may be submitted to your health plan administrator as explained in your health plan’s summary plan description.
Sincerely,
Clinical Pharmacist, PharmD
RxResults

MTMP Guide 2018-2019 13
Member Appeals Rights
Appeal Submission Options
Mail: TML Health, Medical Intelligence, 1821 Rutherford Lane, Austin, TX 78754-5151
Phone: (800) 847-1213 | Fax: (512) 719-6587 | Online: http://tmlhealthbenefits.org/
Appeals must be submitted twelve (12) months after receiving the denial.
Appeals may be submitted as Routine or Urgent/Emergent.
Appellant's clinician may request a peer-to-peer review with the physician or appropriate reviewer.
Appellant may request an independent review of the benefit denial.
Appellants are not required to bear costs of the independent review, including filing fees.
Appellant may request an Executive Director Appeal review.
Appellant may request an Executive Committee Board appeal review.
Appellant may request a copy of information used in denial process.
Covered Individual has the right to member representation of their choosing including an attorney and the
representative may act upon their behalf at all levels of appeals.
Covered Individual, Clinician, or designated Representative may submit written comments, documents or other
information relevant to the appeal.
Expedited external review can occur concurrently with internal appeals for urgent care.
For additional resources on appeals rights, you may contact the Texas Department Insurance consumer assistance
program at 1-855-839-2427 (1-855-TEX-CHAP).
Regulatory Timelines for Appeals
Appeal of Urgent/Emergent Request for Benefits (Adverse Pre-Determination/Notification Request) Prior to Claim
Submission
Type of Request for Benefits or Appeal
Internal/External Appeal
Process Hours/Calendar Days
If the appellant appeals the adverse notification
determination or declination of notification, the
appellant must appeal within: Internal
Twelve (12) months after receiving the
denial based on a completed review process
If the appellant’s request for emergent benefits is
incomplete TML Health will send the urgent/emergent
incomplete pre-determination/notification information
declination letter within:
Internal twenty-four (24) hours of receipt of
appellant’s information
The appellant must provide a completed information
request within: Internal
forty-eight (48) hours after receiving the
TML Health declination due to incomplete
information
If the request for urgent/emergent benefits is complete
and not approved, TML Health will send an
urgent/emergent pre-determination/notification denial
letter within:
Internal seventy-two (72) hours
If the request for concurrent review is complete and not
approved, TML Health will send a concurrent review
denial: Internal twenty-four (24) hours

MTMP Guide 2018-2019 14
Appeal of Urgent/Emergent Request for Benefits (Adverse Pre-Determination/Notification Request) Prior to Claim
Submission
Type of Request for Benefits or Appeal
Internal/External Appeal
Process Hours/Calendar Days
If the appellant requests an Independent Review
Organization (IRO), the external review appeal request
must be submitted for the review within:
External
one hundred twenty (120) calendar days of
receipt of the original denial or response to
your appeal
The IRO will complete the review and TML Health
will submit the response of an expedited
urgent/emergent pre-determination/notification of a
benefit appeal within:
External seventy-two (72) hours
Appeal of Non-Emergent Request for Benefits (Adverse Pre-Determination/Notification Request) Prior to Claim Submission
Type of Request for Benefits or Appeal
Internal/External Appeal
Process Hours/Calendar Days
The appellant must appeal the denial no later than: Internal Twelve (12) months after receiving the
denial based on a completed review process
If the request for a pre-determination/notification is
benefit information incomplete, TML Health will notify
the appellant within:
Internal five (5) calendar days
If the request for pre-determination/notification is
clinical information incomplete, TML Health will
notify you within:
Internal fifteen (15) calendar days
The appellant must then provide completed information
within: Internal
forty-five (45) calendar days after receiving
an extension notice*
TML Health will notify you of the first level appeal
decision within: Internal
fifteen (15) calendar days after receiving the
first level appeal
The appellant must appeal the first level appeal (file a
second level appeal) within: Internal
sixty (60) calendar days after receiving the
first level appeal decision
TML Health will notify you of the second level appeal
decision within: Internal
fifteen (15) calendar days after receiving the
second level appeal*
The appellant may request the appeal be submitted to
an IRO. The External Review Request must be
submitted within:
External
one hundred twenty (120) calendar days of
receipt of the original denial or response to
your appeal
The IRO must complete the review of a non-emergent
claim or benefit appeal within: External thirty (30) calendar days
* A one-time extension of no more than fifteen (15) days only if more time is needed due to circumstances beyond the appellant’s
control.
Post-Service Claims
Type of Claim or Appeal
Internal/External Appeal
Process Hours/Calendar Days
The appellant must appeal the claim denial no later
than: Internal
Twelve (12) months after receiving the
denial based on a completed review process
If the appellant’s claim is incomplete, TML Health will
notify the appellant within: Internal thirty (30) calendar days
The appellant must then provide completed claim
information within: Internal
forty-five (45) calendar days after receiving
an extension notice
TML Health will notify the appellant of the first level
appeal decision within: Internal
thirty (30) calendar days after receiving the
first level appeal
The appellant must file the second level appeal within: Internal sixty (60) calendar days after receiving the
first level appeal decision
The appellant will be notified of the second level
appeal decision generally within: Internal
thirty (30) calendar days after receiving the
second level appeal

MTMP Guide 2018-2019 15
Post-Service Claims
Type of Claim or Appeal
Internal/External Appeal
Process Hours/Calendar Days
The appellant may request an appeal be submitted to an
IRO. This request must be submitted for the review
within:
External
one hundred twenty (120) calendar days of
receipt of the original denial or response to
your appeal
The IRO must complete the review of a non-emergent
claim or benefit appeal within: External thirty (30) calendar days
The IRO must complete a requested expedited review
of an emergent claim or benefit appeal within: External seventy-two (72) hours

MTMP Guide 2018-2019 16
OptumRx Vaccine/Immunization Network Services
Get Your Flu Shot and Other Routine Vaccines
Flu Shots The flu affects millions of people each year and can lead to serious illness, or even death. The flu can be a
contagious illness caused by influenza viruses that infect the lungs, throat and nose. According to the
Centers for Disease Control and Prevention (CDC), one of the best ways to prevent the flu is by getting
vaccinated each year.1 The CDC recommends a yearly flu vaccine for everyone 6 months of age and older,
as the first and most important step in protecting against this serious disease.2
Routine Vaccines You can also keep yourself and your family members healthy with routine vaccines that prevent illnesses
like tetanus, pneumonia and shingles. Routine vaccines are available on most plans, and can help you and
your family maintain better overall health.
Easy Access to Flu Shots and Other Vaccines
OptumRx contracts with a variety of national pharmacy chains to provide members with easy access to flu
shots and other routine vaccines. Plus, members get the highest level of benefit coverage (100% for many
plans) for vaccines obtained from contracted pharmacies that participate in the Vaccine
Immunization/Injection Network administered by OptumRx.3
Many vaccines can be accessed on a walk-in network pharmacy basis. Show your ID card at an OptumRx
vaccine immunization/injection network pharmacy before getting your flu shot or vaccine and the 100%
benefit should apply. For a complete OptumRx vaccine immunization/injection network list, members will
need to register first, then log in to optumrx.com or call the number on their health plan or prescription ID
card.
Retail Pharmacies
This list represents the larger retail chain pharmacies in our network, but is not the full list. Pharmacists
administer the vaccines at these locations.
Ahold USA (Giant Food Stores, Giant of Maryland, Stop and Shop Supermarkets, Ukrop's Super
Markets)
Albertsons
CVS Pharmacy
Four B Corporation (Hen House, Price Chopper)
H-E-B Pharmacy
Hy-Vee Pharmacy
Kmart Pharmacy

MTMP Guide 2018-2019 17
The Kroger Co. (Dillons, King Soopers, Fry’s, Fred Meyer, Ralphs, QFC, Harris Teeter Roundy’s, Pick
N’ Save, Copps Food Center, Metro Market, Baker’s Pharmacy, City Market, Mariano’s, Pay Less,
Owens, Jay C Food Stores, Gerbes Pharmacy)
K-VA-T Food Stores, Inc. (Food City)
Marsh Drugs LLC
Meijer Pharmacies
Publix
Safeway Affiliated Pharmacies (Carr's, Pavilion’s, Randall's, Safeway, Tom Thumb, Vons)
Shopko Stores
SUPERVALU Affiliated Pharmacies (BIGGS, Osco, Sav-On, Shaw’s Supermarket)
Thrifty White Pharmacy
Tops Markets
Walgreens Pharmacy (Duane Reade, Rite Aid, featuring a Walgreens pharmacy)
Walmart Pharmacy
Wegmans
Routine Vaccines4
Most of the following routine vaccines are available at the OptumRx vaccine immunization/injection
network pharmacies. Age restrictions or limitations may apply. The Affordable Care Act requires most
health plans to cover routine vaccines under either the medical or pharmacy benefit.
Flu Shots Flu (Influenza)*
Afluria Afluria Quad Fluad Fluarix Quad Flublok Flublok Quad
Flucelvax Quad Flulaval Quad Fluvirin Fluzone HD Fluzone ID Quad Fluzone Quad
Fluzone Quad (pediatric dose)
Routine Adult Vaccines Hepatitis A* (Adult and Pediatric)
Havrix Vaqta
Hepatitis B* (Adult and Pediatric)
Engerix-B Heplisav-B (adult only) Recombivax-HB
Human Papilloma Virus (HPV)* – Vaccine prevents HPV related cancers
Gardasil Gardasil 9
Measles, Mumps, Rubella*
MMR-II
Meningococcal* – Vaccine prevents meningitis Groups A, C, Y and W-135
Menactra Menveo
Meningococcal* – Vaccine prevents meningitis Group B
Bexsero Trumenba
Pneumococcal* – Vaccine prevents pneumonia
Prevnar13 Pneumovax 23
Tdap* – Vaccine prevents tetanus, diptheria, pertussis
Adacel Boostrix
Tetanus Diptheria* – TD
Tenivac
Varicella* – Vaccine prevents chicken pox
Varivax

MTMP Guide 2018-2019 18
Zoster* – Vaccine prevents shingles
Shingrix
* Vaccine type
1 Sources: http://www.cdc.gov/flu/
2 http://www.cdc.gov/flu/protect/keyfacts.htm#flu-vaccination
3 There may be some instances where a particular location of one of the vaccine providers is not participating in the national
OptumRx Vaccine Immunization/Injection network.
4 Not all vaccines on this list are available at all participating pharmacies. Members should contact their participating
pharmacy of choice to confirm vaccine availability.
All trademarks are the property of their respective owners. © 2018 Optum, Inc. All rights reserved.

MTMP Guide 2018-2019 19
Value Based Benefits for Chronic Conditions (Diabetes, Hypertension & High Cholesterol)
Diabetes
Generic Copay
glimepiride
glipizide
glyburide
glyburide/metformin
metformin
metformin ER (generic Glucophage XR only)
pioglitazone
Insulin
Brand Copay
Humulin - vials only
Humalog - vials only
Lantus - vials only
High Blood Pressure
Generic Copay
amlodipine
atenolol
benazepril
benazepril/hctz
carvedilol
clonidine
diltiazem ER
doxazosin
furosemide
hydrochlorothiazide (hctz)
lisinopril
lisinopril/hctz
metoprolol
propranolol
verapamil
verapamil ER/SR
High Cholesterol
Generic Copay
atorvastatin
lovastatin
simvastatin

MTMP Guide 2018-2019
BriovaRx Specialty/Biotech Pharmacy
BriovaRx, The OptumRx Specialty Pharmacy is the Specialty/Biotech prescription alliance partner. Our
goal is to provide the highest quality pharmaceutical care, at lower costs.
BriovaRx Smart Fill Program
Specialty medications are an important component to managing complex diseases and conditions, and
sometimes it takes time for members to find the right dose and comfort level before they’re able to follow
their regimen. Forty-nine percent discontinue their oncology drug therapy within ninety days due to
incompatibility with medication. The Smart Fill program from BriovaRx, specialty pharmacy, offers two
strategies for dispensing specialty medications so that members get the medications they need, adhere to
their therapy, and reduce waste due to intolerance. The mandatory opt-in oncology drug therapy split fill
strategy enables twice-monthly prescription refills for the first 6 fills, while the 90-day fill program is a
voluntary offering that provides refills every three months.
BriovaRx Smart Fill Solution Overview
Split Fill
(1/2 Monthly Supply) 90-Day Supply
Conditions/Drugs Oral Oncology HIV, Multiple Sclerosis, Rheumatoid Arthritis, Transplant
Patient Stability Unstable on medication Stable on medication
Clinical Intent Adjust to medication Adherence
Program Intent Avoid waste Member convenience
Member Experience Increased clinical oversight Improved satisfaction
# Fills/Duration 6 fills over first 3 months 4 fills over 12 months
Copays 1/2 copay 3x copay
Opt in Mandatory Voluntary
Program Offering BriovaRx Exclusivity program required
No grace fills allowed
Steps Necessary for Specialty/Biotech Medication
For prior authorization requests, your provider will be required to call RxResults toll free: (844) 853-9400
or local: (501) 367-8402 for a prior authorization form.
RxResults Phone: Toll Free: (844) 853-9400 | Local: (501) 367-8402 | Fax: (855) 856-3291
BriovaRx, The OptumRx Specialty Pharmacy Phone: (866) 218-5445 or (855) 4BRIOVA | Fax: (800)
491-7997
Oncology Medication: (800) 847-1213

MTMP Guide 2018-2019 21
Ordering Specialty/Biotech Prescriptions
You can order directly from BriovaRx, The OptumRx Specialty Pharmacy by calling (866) 218-5445 or
(855) 4BRIOVA.
Disclaimer. Not all Biotech/Biosimilar medications are eligible under the MTMP. This Specialty
Pharmacy Drug List may not be a complete representation of all available specialty drugs; this list is subject
to change at any time without prior notice. Non-specialty alternatives may be a recommended first-line
therapy to treat your condition. Please consult your physician.
Generic specialty medications may not be included in the list below. Although it is not on the list, if the
brand name drug requires a prior authorization, the generic medication will require a prior authorization as
well.
Please note: Biotech = $100.00 copay, Biosimilar = $75.00 copay
Bold Underlined = non-covered
medication (Choice and Select Plan)
*Sample = Medication requires prior authorization through RxResults
(844) 853-9400
Bold Double-Underlined = non-covered
medication (Select Plan only)
*SampleDU (dual diagnosis utilization) = Oncology Diagnosis
Medication requires prior authorization through Medical Management
(800) 847-1213
Adult Incontinence
Solesta
Ammonia Detoxicants
*Ravicti
Anemia
*Aranesp DU
*Epogen DU
*Mircera DU
*Procrit DU
Anticoagulation
Arixtra
Enoxaparin
Fondaparinux
Fragmin
Lovenox
Anti-Gout Agent
*Krystexxa
Antihyperlipidemic
Juxtapid
Kynamro
*Praluent
*Repatha
*RepathaPushtro
nex System
*Repatha
Sureclick
Anti-Infective
*Daraprim
*Prevymis
Asthma
*Cinqair
*Fasenra
*Nucala
*Xolair
Birth Control
Nexplanon
Cardiovascular
*Northera
Central Nervous System Agents
*Austedo
*Brineura
*Hetlioz
*Radicava
*Sabril
*Tetrabenazin
*Vigabatrin
*Xenazine
Cystic Fibrosis
*Bethkis
*Cayston
*Kalydeco
*Kitabis Pak
*Orkambi
*Pulmozyme
*Symdeko
*Tobi Neb
*Tobi Podhalr
*Tobramycin Neb
Diagnostic
Acthrel
Duchenne Muscular Dystrophy
*Emflaza
Endocrine
*Crysvita
*Cuprimine DU
*Egrifta DU
*Firmagon
*Hydroxy Capr DU
*Jynarque
*Korlym DU
*Kuvan DU
*Lupaneta DU
*Makena
*Myalept DU
*Natpara DU
*Nityr
*Octreotide DU
*Parsabiv DU
*Procysbi
*Samsca DU
*Sandostatin DU
*Signifor DU
*Somatuline DU
*Somavert DU
*Supprelin LA DU
*Syprine DU
*Thiola DU
*Thyrogen DU
*Trientine DU
*Triptodur
*Vantas
*XuridenDU
Enzyme Therapy
Adagen
*Aldurazyme
*Aralast NP
Buphenyl
Carbaglu
*Cerdelga
*Cerezyme
*Cholbam
Cystagon

MTMP Guide 2018-2019 22
*Elaprase
*Elelyso
*Fabrazyme
*Glassia
*Kanuma
*Lumizyme
*Mepsevii
*Miglustat
*Naglazyme
*Orfadin
Phenylbutyra
*Prolastin-C
*Sodium Pheny
*Strensiq
Sucraid
*Vimizim
*Vpriv
*Zavesca
*Zemaira
Gastrointestinal Agents
*Gattex
*Ocaliva
*Xermelo
Growth Hormone Deficiency
*Genotropin
*Humatrope
*Increlex
*Norditropin
*Nutropin AQ
*Omnitrope
*Saizen
*Serostim
*Zomacton
*Zorbtive
Hematological Agents
*Fibryga
*Mozobil
*Nplate
*Panhematin
*Promacta
*Riastap
*Soliris
*Tavalisse
*Thrombat III
Hemophilia
*Advate
*Adynovate
*Afstyla
*Alphanate
*Alphanine SD
*Alprolix
*Bebulin
*Benefix
*Ceprotin
*Coagadex
*Corifact
*Eloctate
*Feiba
*Helixate FS
*Hemlibra
*Hemofil M
*Humate-P
*Idelvion
*Ixinity
*Koate
*Koate-DVI
*Kogenate FS
*Kovaltry
*Monoclate-P
*Mononine *Novoeight
*Novoseven RT
*Nuwiq
*Obizur
*Profilnine
*Rebinyn
*Recombinate
*Rixubis
*Tretten
*Vonvendi
*Wilate
*Xyntha
Hepatitis B
Adefov Dipiv
Baraclude
Entecavir
Epivir HBV
Hepsera
Lamivudine Vemlidy
Hepatitis C
Copegus
*Daklinza
Epclusa
Harvoni
*ledipasvir-sofosbuvir
Mavyret
Moderiba
*Olysio
*Pegasys
*Pegintron
Rebetol
Ribapak
Ribasphere
*Ribavirin
*sofosbuvir-velpatasvir
*Sovaldi
*Technivie
*Viekira
*Vosevi
*Zepatier
Hereditary Angioedema
*Berinert
*Cinryze
*Firazyr
*Haegarda
*Kalbitor
*Ruconest
HIV
ABACAV/LAMIV
Abacavir
Aptivus
Atazanavir
Atripla
Biktarvy
Cimduo
Combivir
Complera
Crixivan
Descovy
Didanosine
Edurant
Efavirenz
Emtriva
Epivir
Epzicom
Evotaz
Fosamprenavi
Fuzeon
Genvoya
Intelence
Invirase
Isentress
Juluca
Kaletra
Lamivud/zido
Lamivudine
Lexiva
Lopin/riton
Nevirapine
Norvir
Odefsey
Prezcobix
Prezista
Rescriptor
Retrovir
Reyataz
Ritonavir
Selzentry
Stavudine
Stribild
Sustiva
Symfi
Tenofovir
Tivicay
Triumeq
Trizivir
Trogarzo
Truvada
Tybost
Videx
Videx EC
Viracept
Viramune
Viread
Zerit
Ziagen
Zidovudine
Immune Globulin
*Atgam
*Bivigam
*Carimune NF
*Cuvitru
*Cytogam
*Flebogamma
*Gamastan S/D
*Gammagard
*Gammaked
*Gammaplex
*Gamunex-C
*Hizentra
*Hyperrab
*Hyperrab S/D
*Hyperrho S/D
*Hyqvia
*Imogam Rabie
*Kedrab
*Micrhogam
*Octagam
*Privigen
Immunological Agents
*Actimmune
*Arcalyst
*Benlysta
*Ilaris
*Lemtrada
Infertility
Bravelle
Cetrotide
Chor Gonadot
Follistim AQ
Ganirelix AC
Gonal-F
Menopur
Novarel
Ovidrel
Pregnyl

MTMP Guide 2018-2019 23
Inflammatory Conditions
*Actemra
*Cimzia
*Cosentyx
*Dupixent
*Enbrel
*Entyvio
*Humira
*Humira Pedia
*Humira Pen
*Inflectra *Kevzara
*Kineret
*Orencia
*Otezla
*Remicade
*Renflexis
*Siliq
*Simponi
*Simponi Aria
*Stelara
*Taltz
*Tremfya
*Xeljanz
*Xeljanz XR
Metabolic Bone Disease
*Reclast
*Zoledronic
*Zometa
Multiple Sclerosis
*Ampyra
*Aubagio
*Avonex
*Betaseron
*Copaxone
*Extavia
*Gilenya
*Glatiramer
*Glatopa
*Ocrevus
*Plegridy
*Rebif
*Tecfidera
*Tysabri
*Zinbryta
Musculoskeletal Agents
*Exondys 51
*Spinraza
*Xiaflex
Narcolepsy
*Xyrem
Neurological Agents
*Botox
*Dysport
*Myobloc
*Xeomin
Neutropenia
*Granix
H.P. Acthar
*Leukine
*Neulasta
*Neupogen
*Zarxio
Oncology - Injectable
*AbraxaneDU
*AdcetrisDU
*AdriamycinDU
*AdrucilDU
*Alferon NDU
*AlimtaDU
*AliqopaDU
*AlkeranDU
*ArranonDU
*ArzerraDU
*AvastinDU
*AzacitidineDU
*BavencioDU
*BeleodaqDU
*BendekaDU
*BesponsaDU
*BicnuDU
*BleomycinDU
*BlincytoDU
*BortezomibDU
*BusulfanDU
*BusulfexDU
*CampathDU
*CamptosarDU
*CarboplatinDU
*CisplatinDU
*CladribineDU
*ClofarabineDU
*ClolarDU
*CosmegenDU
*CyclophosphamideDU
*CyramzaDU
*CytarabineDU
*DacarbazineDU
*DacogenDU
*DarzalexDU
*DaunorubicinDU
*DecitabineDU
*DexrazoxaneDU
*DocetaxelDU
*DoxilDU
*DoxorubicinDU
*EligardDU
*EllenceDU
*EmplicitiDU
*EpirubicinDU
*ErbituxDU
*ErwinazeDU
*EtopophosDU
*EtoposideDU
*EvomelaDU
*FaslodexDU
*FloxuridineDU
*FludarabineDU
*Fluorouracil InjectableDU
*FolotynDU
*FusilevDU
*GazyvaDU
*GemcitabineDU
*GemzarDU
*HalavenDU
*HerceptinDU
*HycamtinDU
*IdarubicinDU
*IfexDU
*IfosfamideDU
*ImfinziDU
*ImlygicDU
*Intron ADU
*IrinotecanDU
*Istodax OVRDU
*Ixempra kitDU
*JevtanaDU
*KadcylaDU
*KepivanceDU
*KeytrudaDU
*KymriahDU
*KyprolisDU
*LartruvoDU
*LevoleucovorDU
*Lipodox 50DU
*Lupron DepotDU
*Lupron Depot PedDU
*MarqiboDU
*MelphalanDU
*MesnaDU
*MesnexDU
*MitomycinDU
*MitoxantronDU
*MustargenDU
*MutamycinDU
*MylotargDU
*NavelbineDU
*NipentDU
*OncasparDU
*OnivydeDU
*OpdivoDU
*OxaliplatinDU
*PaclitaxelDU
*PamidronateDU
*PerjetaDU
*PhotofrinDU
*PortrazzaDU
*ProleukinDU
*RituxanDU
*RomidepsinDU
*SylatronDU
*SylvantDU
*SynriboDU
*TaxotereDU
*TecentriqDU
*TemodarDU
*TeniposideDU
*TepadinaDU
*TheracysDU
*ThiotepaDU
*Tice BCGDU
*ToposarDU
*TopotecanDU
*ToriselDU
*TotectDU
*TreandaDU
*Trelstar mixDU
*TrisenoxDU
*UnituxinDU
*ValstarDU
*VectibixDU
*VelcadeDU
*VidazaDU
*VinblastineDU
*Vincasar PFSDU
*VincristineDU
*VinorelbineDU
*VyxeosDU
*XgevaDU
*YervoyDU
*YescartaDU
*YondelisDU
*ZaltrapDU
*ZanosarDU
*ZevalinDU
*ZinecardDU
*ZoladexDU
Oncology - Oral
*AfinitorDU
*AlecensaDU
*AlunbrigDU
*BexaroteneDU
*BosulifDU
*CabometyxDU
*CalquenceDU
*CapecitabineDU

MTMP Guide 2018-2019 24
*CaprelsaDU
*CometriqDU
*CotellicDU
*ErivedgeDU
*ErleadaDU
*EtoposideDU
*FarydakDU
*GilotrifDU
*GleevecDU
*Gleostine HycamtinDU
*IbranceDU
*IclusigDU
*IdhifaDU
*Imatinib MesDU
*ImbruvicaDU
*InlytaDU
*IressaDU
*JakafiDU
*KisqaliDU
*LenvimaDU
*LonsurfDU
*LynparzaDU
*MatulaneDU
*MekinistDU
*MercaptopurineDU
*MesnexDU
*NerlynxDU
*NexavarDU
*NilandronDU
*NilutamideDU
*NinlaroDU
*OdomzoDU
*PomalystDU
*PurixanDU
*RevlimidDU
*RubracaDU
*RydaptDU
*SprycelDU
*StivargaDU
*SutentDU
*TabloidDU
*TafinlarDU
*TagrissoDU
*TarcevaDU
*TargretinDU
*TasignaDU
*TemodarDU
*TemozolomideDU
*ThalomidDU
*TretinoinDU
*TykerbDU
*VenclextaDU
*VerzenioDU
*VotrientDU
*XalkoriDU
*XelodaDU
*XtandiDU
*ZejulaDU
*ZelborafDU
*ZolinzaDU
*ZydeligDU
*ZykadiaDU
*ZytigaDU
Oncology - Topical
*Valchlor
Ophthalmic Agents
Bevacizumab
Cystaran
Eylea
Iluvien
Jetrea
Keveyis
Lucentis
Luxturna
Macugen
Ozurdex
Retisert
Visudyne
Opioid Antagonists
*Sublocade
Osteoarthritis
*Durolane
*Euflexxa
*Gel-one
*Gelsyn-3
*Genvisc 850
*Hyalgan
*Hymovis
*Monovisc
*Orthovisc
*Supartz
*Synvisc
*Synvisc One
*Visco-3
Osteoporosis
*Forteo
*Prolia
*Tymlos
Pain Management
*Prialt
Parkinson's Disease
*Apokyn
Pulmonary Fibrosis
*Esbriet
*Ofev
Pulmonary Hypertension
*Adcirca
*Adempas
*Epoprostenol
*Flolan
*Letairis
*Opsumit
*Orenitram
*Remodulin
*Revatio
*Sildenafil
*Tadalafil
*Tracleer
*Tyvaso
*Uptravi
*Veletri
*Ventavis
RSV
*Ribavirin inhal
*Synagis
*Virazole
Substance Abuse Treatment
*Vivitrol
Transplant
Astagraf XL
Cellcept
Cellcept IV
Cyclosporine
Envarsus XR
Gengraf
Mycophenolat
Mycophenolic
Myfortic
Neoral
Nulojix
Prograf
Rapamune
Sandimmune
Sirolimus
Tacrolimus
Zortress

MTMP Guide 2018-2019 25
Cost Share Prescription Copays for Choice MTMP
COST SHARE PRESCRIPTIONS ARE EXCLUDED FROM SELECT MTMP
We will impose a higher copayment for drugs for which there is no clinical evidence to show that non-preferred
Cost Share prescriptions perform any better than therapeutic doses of less costly preferred "Alternative Drugs".
Drugs on the Cost Share list may also be on the OptumRx formulary. Always check the Cost Share Prescriptions
section of the Prescription Drug Plan booklet first. The Cost Share copay will apply to the drug regardless of
where it is located on the OptumRx formulary.
Drugs starting with an Upper-case letter or that have the ® symbol are brand name drugs. Drugs starting with a
lower-case letter are generic drugs.
Analgesics/Anti-Inflammatory/Pain Agents
Impacts utilization on: Duragesic®, Lazanda®, Subsys®
Alternative Drugs: fentanyl patch, fentanyl lozenge
Impacts utilization on: Anaprox®, Arthrotec®, Celebrex®, celecoxib, Daypro®, diclofenac/misoprostol
combination, Feldene®, indomethacin ER, Ketoprofen ER®, Meclofen Sod®, mefenamic acid, Mobic®,
Naprelan®, naproxen sodium 550mg, Naproxen CR®, oxaprozin, piroxicam, Ponstel®, Tivorbex®, Vivlodex®,
Zipsor®, Zorvolex®
Alternative Drugs: diclofenac, ibuprofen, meloxicam, naproxen
Impacts utilization on: Allzital®, Bupap®, butalbital/acetaminophen tablet, butalbital/acetaminophen/caffeine
capsule, Esgic® tablet, Fioricet®, Fiorinal®, Tencon®, Vanatol LQ® Solution
Alternative Drugs: anolor, butalbital/acetaminophen 50-325mg tablet (for Bupap® and Allzital®),
butalbital/acetaminophen/caffeine tablet, butalbital/aspirin/caffeine tablet (for Fiorinal®), capacet, esgic
capsule, marten tablet, zebutal
Impacts utilization on: Conzip®, tramadol ER, Ultracet®, Ultram®, Ultram ER®
Alternative Drug: tramadol, tramadol/acetaminophen
Antibiotics/Anti-Infective Agents
Impacts utilization on: Acticlate®, Adoxa®, Amoxicillin® (brand only), Doryx®, doxycycline monohydrate
capsules (except 50 and 100mg), doxycycline monohydrate tablets 150mg, doxycycline hyclate, doxycycline
hyclate DR, Minocin®, minocycline tablets, minocycline ER, Minolira®, Monodox®, Moxatag®, Oracea®,
Solodyn®, Targadox®, Vibramycin®, Xepi® cream, Ximino ER®
Alternative Drugs: amoxicillin, doxycycline, doxycycline monohydrate capsules 50 or 100mg, doxycycline
monohydrate tablets (except 150mg), minocycline capsules, mupirocin ointment

MTMP Guide 2018-2019 26
Anticonvulsants
Impacts utilization on: Sympazan® oral film
Alternative Drugs: clobazam
Antidepressants/Fibromyalgia
Impacts utilization on: Aplenzin tab
Alternative Drugs: bupropion, citalopram, duloxetine, escitalopram, fluoxetine, paroxetine, sertraline,
venlafaxine, venlafaxine ER (capsules only)
Antihypertensive Agents
Impacts utilization on: amlodipine/olmesartan, amlodipine/olmesartan/HCTZ, amlodipine/valsartan,
amlodipine/valsartan/HCTZ, Atacand®, Atacand HCT®, Avalide®, Avapro®, Azor®, Benicar®, Benicar HCT®,
Coreg CR®, Cozaar®, Diovan®, Diovan HCT®, Edarbi®, Edarbyclor®, Eprosartan®, Exforge®, Exforge HCT®,
Hyzaar®, Inderal LA, Inderal XL, InnoPran XL®, Micardis®, Micardis HCT®, olmesartan, olmesartan HCTZ,
Tekturna®, Tekturna HCT®, telmisartan/amlodipine, Tribenzor®, Twynsta®
Alternative Drugs: Any generic ACE Inhibitor; Generic ARB Agents: candesartan, candesartan HCTZ,
losartan, losartan/HCTZ, Irbesartan, irbesartan/HCTZ, telmisartan, telmisartan HCTZ, valsartan,
valsartan/HCTZ; Generic Beta Blocker Agents: carvedilol for Coreg CR; propranolol IR/ER for Inderal LA/XL
and InnoPran XL
Central Nervous System: Sedative Hypnotics
Impacts utilization on: Ambien®, Ambien CR®, Belsomra®, Edluar®, Intermezzo®, Lunesta®, Rozerem®,
Silenor®, Sonata®, zolpidem ER®, zolpidem sublingual, Zolpimist®
Alternative Drugs: doxepin, zaleplon, zolpidem immediate release
Lipid-Lowering Agents (Statins)
Impacts utilization on: Altoprev®, amlodipine/atorvastatin combination, Caduet®, Crestor®, ezetimibe,
ezetimibe-simvastatin, Lescol®, Lescol XL®, Lipitor®, Livalo®, Mevacor®, Pravachol®, Vytorin®, Zetia®,
Zocor®
Alternative Drugs: atorvastatin, lovastatin, pravastatin, rosuvastatin, simvastatin
Migraine Headaches
Impacts utilization on: almotriptan, Amerge®, Axert®, Frova®, frovatriptan, eletriptan, Imitrex® (brand),
Imitrex® Spray, Maxalt®, Maxalt-MLT®, naratriptan, Onzetra XSAI®, Relpax®, sumatriptan spray,
sumatriptan/naproxen, Sumavel®, Treximet®, Zembrace, zolmitriptan, Zomig®, Zomig® nasal spray, Zomig
ZMT®
Alternative Drugs: rizatriptan, sumatriptan

MTMP Guide 2018-2019 27
Osteoporosis Drugs
Impacts utilization on: Actonel®, Alendronate® (brand), Atelvia®, Binosto®, Boniva®, Fosamax®, Fosamax-
D®, ibandronate, risedronate
Alternative Drug: alendronate
Overactive Bladder Drugs
Impacts utilization on: darifenacin, Detrol®, Detrol LA®, Ditropan XL®, Enablex®, Gelnique®, Myrbetriq®,
oxybutynin ER®, Oxytrol® patches, tolterodine, tolterodine ER, Toviaz®, trospium CL, trospium CL ER,
Vesicare®
Alternative Drug: Generic: oxybutynin immediate release
Skeletal Muscle Relaxants
Impacts utilization on: Amrix®, carisoprodol 250mg tablet, Chlorzoxazone®, Fexmid®, Lorzone®, metaxalone,
Parafon Forte®, Robaxin®, Skelaxin®, Soma®, Tabradol®, tizanidine (capsules only), Zanaflex®
Alternative Drugs: Generic: carisoprodol (except 250mg tablet), chlorzoxazone, cyclobenzaprine,
methocarbamol, tizanidine tablets

MTMP Guide 2018-2019 28
Prescription Benefits
Coverage for eligible injectable and non-injectable biotech and/or biosimilar prescriptions that are available
through the MTMP, but are purchased from Medical Providers will be paid per the Medical Benefit Plan.
MTMP non-injectable prescriptions purchased outside of the Pharmacy Benefit Manager will not be an eligible
benefit under the Medical Benefit Plan other than the biotech/biosimilar prescriptions mentioned above.
MAC A Rx Plan
If a brand name drug is dispensed and a generic alternate drug exists, the Covered Individual pays the difference
between the brand name and generic price in addition to the appropriate copayment for the brand name. The
cost difference between the brand name and generic price does not apply to any individual deductibles or out
of pocket amounts. The MAC differential applies to all prescriptions purchased through this program when a
generic alternate is available.
MAC C Rx Plan
Covered individual will pay the appropriate copayment amount of the prescription.
Qualified High Deductible Health Savings Account (H.S.A.) Health Plans
The qualified high deductible H.S.A. health plan wellness drug list may be accessed at the copay out of pocket
cost. The qualified high deductible H.S.A. health plan deductible will have to be met prior to
non-wellness/preventive medications being accessed at the copay out of pocket cost. Please see the qualified
high deductible wellness drug list within this guide.
Authorized Generics
The use of authorized generics undermines the Hatch-Waxman Act by devaluing the 180 day exclusive patent
period incentive. Ultimately, consumers pay the prices as brand companies keep drug prices high and access to
affordable alternative medicine is delayed. Once a generic (single or multi source) medication alternative is
allowed on the market the generic copay will be applied. The generic company that is first to successfully
challenge a questionable brand patent, file an abbreviated new drug application with the FDA and receive
approval to market that drug is awarded 180 days exclusivity. During the 180 day period, that generic company
alone is permitted to compete with the brand company, allowing the generic company to bring affordable
medicines to consumers faster.
Patents are generally good for 20 years from the date of filing. The abbreviated new drug application approval
allows manufacturers to bring generic competitors to market which allows the generic to challenge the current
patent on the brand medication. Authorized generics are generally coded as brand drugs by Medispan and First
Databank due to single source classification and manufactured by the brand name manufacturer. This brand
coding is what causes the higher dollar out of pocket cost.

MTMP Guide 2018-2019 29
Maximum Out Of Pocket Accumulation
The Qualified High Deductible/H.S.A. Health Plan will require the individual and/or family out-of-pocket
maximum to be met before the plan pays at 100% medical and/or prescription. Medical and Prescription
copayments for most cost effective eligible Network benefit and services will accumulate to the Federal
Government H.S.A. or PPO maximum out-of-pocket (MOOP) amount. Once the Federal Government defined
MOOP is met, eligible network services within the scope of the benefit plan will be paid at 100%.
New Drugs to Market (NDTM)
NDTM drugs will be excluded until otherwise decided by the plan efficacy of medication. Quarterly Review
will be conducted and prescription eligibility will be decided by the sixth (6th) month and quarterly thereafter.

MTMP Guide 2018-2019 30
Covered and Non-Covered Drugs
Plan exclusions (Drugs Not Covered under this Benefit) apply to both the brand and generic version of the
medication unless otherwise noted. This is not a complete list and is subject to change as new drugs are added
to the market. The absence of a medication from the exclusions list does not guarantee payment by the plan.
Drugs Covered under this Benefit
1. Legend Drugs;
2. Insulin or oral diabetic prescription;
3. Disposable insulin needles/syringes and physician prescribed needles/syringes/supplies;
4. Disposable blood/urine/glucose/acetone testing agents (e.g. Acetest Tablets, Clinitest Tablets, Glucometer
(one per calendar year), Lancets, Diastix Strips, Tes-Tape and Chemstrips);
5. Diabetic supplies will be purchased with order for insulin or oral diabetic prescription. The plan will allow
needles, syringes, lancets and testing strips at no charge if ordered within 30 days of a prescription at the
same pharmacy;
6. Compound medication of which at least one ingredient is a legend drug to maximum $200.00 per
prescription payment;
7. Any other drug which under the applicable State Law may only be dispensed upon the written prescription
of a physician or other lawful prescriber;
8. Contraceptives: Oral, Brand Extended cycle (mail order only), Generic Extended cycle (Network at 90
days copay), Transdermal patches, Contraceptive devices, Levonorgestrel (Norplant), Prescription
Strength Only;
9. Depo Provera;
10. Prescribed smoking deterrent medications containing nicotine or any other smoking cessation aids, all
dosage forms;
11. Growth hormones (requires a prior authorization through RxResults);
12. Extended Release anti-depressive agents: Wellbutrin XL, Effexor XR;
13. Extended Release migraine prophylactic agents: Depakote ER.
Drugs Not Covered under this Benefit
This is not a complete list of medications excluded by the plan. This list is subject to change as new drugs are
added to the market. The absence of a medication from this list does not guarantee payment by the plan. The
exclusion applies to both the brand and generic (if available) versions of medications listed below as well as all
doses and dosage forms unless specifically noted otherwise.
1. Non-legend drugs other than those listed above;
2. Non-FDA approved medications;

MTMP Guide 2018-2019 31
3. Therapeutic devices or appliances, including support garments and other non-medicinal substances,
regardless of intended use;
4. Charges for the administration or injection of any drug;
5. Drugs labeled "Caution - limited by Federal Law to investigational use" or experimental drugs even
though a charge is made to the individual;
6. Medications which are to be taken by or administered to an individual, in whole or in part, while he or she
is a patient in a licensed hospital, rest home, sanitarium, extended care facility, convalescent hospital,
nursing home or similar premises which operates on its premises or allows to be operated on its premises,
a facility for dispensing pharmaceuticals;
7. Any prescription refilled more than the number specified by the physician or any refill dispensed after one
year from the physician’s original order;
8. Prescription which an eligible individual is entitled to receive without charges from any Workers’
Compensation Laws or which is prescribed for an injury or illness which is excluded from any medical
coverage which is provided in conjunction with this prescription benefit;
9. Prescribed prenatal vitamins are not covered under the prescription card. Claims for prescribed prenatal
vitamins with a pregnancy diagnosis may be submitted to us for payment consideration;
10. Immunization agents, biological sera blood or blood plasma;
11. Dietary supplements, vitamins or formulas, vitamins individually or in combination;
12. Nutritional supplements (i.e. Deplin®, Metanx®);
13. Fertility medications;
14. Anti-obesity medications;
15. Agents used for cosmetic purposes;
16. Male pattern baldness medications; hair growth stimulants;
17. Lifestyle convenience prescriptions (i.e. erectile dysfunction prescriptions);
18. All non-injectable testosterone (including pellet and buccal formulations), Brand injectable testosterone
is also excluded;
19. All nasal steroids (e.g. Beconase® AQ, Nasonex®, QNASL®, etc.);
20. All non-sedating/low-sedating antihistamines (e.g. Claritin®, Clarinex®, desloratadine, levocetirizine,
Zyrtec®, etc.);
21. All proton pump inhibitors (e.g. Dexilant®, Nexium®, Prilosec®, Protonix®, etc.);
22. All topical non-narcotic pain medications (e.g. Sinelee®, Flector®, Solaraze®, etc.);
23. Certain acne medications: Absorica®, all benzoyl peroxide, Altreno®, Cleocin-T® gel, Clindagel®,
Clindamycin® gel, Duac® gel, Fabior®, Refissa®, Renova®, tretinoin emulsion cream, Retin-A®, Riax®;
24. Certain analgesic/anti-inflammatory/pain agents: Acetaminophen/Caffeine/Dihydrocodone®,
Aspirin/Caffeine/Dihydrocodone®, Arymo® ER, Belbuca®, Bunavail®, Embeda®, Exalgo®,
hydromorphone ER (generic Exalgo only), Hysingla® ER, Kadian® CR/ER, Morphabond® ER,
morphine sulphate ER capsules (generic Kadian only), Nalocet®, Nucynta®, Nucynta® ER, Opana® ER,
Oxaydo®, Roxybond®, Sprix spray®, Suboxone®, bupren/naloxone (generic Suboxone®), Synalgos-DC®,
Trezix®, Zohydro® ER; Zubsolv®;
25. Certain combination analgesic and gastric reflux/stomach ulcer medications: Duexis®, Vimovo® and
Yosprala®;

MTMP Guide 2018-2019 32
26. Certain antibiotics: Impavido®, Furadantin® suspension and its generic if over 7 years old;
27. Certain anticonvulsants: Briviact®, Keppra® XR; Lamictal®, Lamictal® XR, levetiracetam ER, Qudexy
XR®, roweepra XR, Topiramate® ER, Trokendi® XR;
28. Certain antidiabetic medications: Glumetza®, metformin ER (certain 1000mg and certain 500mg
strengths), Fortamet®; Symlin®; Invokana®, Invokamet®, Invokamet® XR;
29. Certain antiemetics: Akynzeo®; Bonjesta®; Cinvanti®; Diclegis®; Emend® (suspension and tripack),
Emend® for injection, Sustol®; and Varubi®;
30. Certain antifungals: Cresemba®, Extina® Aer 2%, Jublia®, Kerydin®, Luliconazole®, Luzu®, Naftin®,
Onmel®, Tolsura ®, Vytone®, Xolegel®;
31. Certain antipsychotics: Abilify® Myci (only), Aristada®, Nuplazid®, Rexulti®;
32. Certain cholesterol/triglyceride-lowering agents: Lovaza®, Niaspan®, niacin ER, niacor; Flolipid®; all
Fenofibrates (e.g. Antara®, Lipofen®, Fenoglide®, Tricor®, etc.);
33. Certain COPD medications: Daliresp®, Lonhala Magn®, Trelegy®, Yupelri®;
34. Certain gastrointestinal agents: Mytesi®, Relistor®, Symproic®, Viberzi®, Xermelo®;
35. Certain gout agents: Duzallo®, Zurampic®;
36. Certain ophthalmic agents: Inveltys®, Rhopressa®, Vyzulta®;
37. Certain topical steroids: Enstilar®, Trianex®, Triderm®; Impoyz®; all brands with generics available; all
gels, aerosols, sprays, shampoos, tapes and lotions;
38. Most convenience kits and paks such as but not limited to: Flanax Pain Kit Relief, Morgidox Kit,
Naproxen Comfort Kit, Nutridox Kit, etc.;
39. Miscellaneous exclusions: See below for a list of the medications.
Miscellaneous Exclusions
This is not a complete list of medications excluded by the plan. This list is subject to change as new drugs are
added to the market. The absence of a medication from this list does not guarantee payment by the plan. The
exclusion applies to both the brand and generic (if available) versions of medications listed below as well as all
doses and dosage forms unless specifically noted otherwise. .
ADDYI
ALEVAMAX CRE
ALPAWASH OIN
ALZAIR NASAL SPR
ARAKODA
ATOPADERM CRE
ATOPICLAIR CRE
AUVI-Q
BALCOLTRA
BEAU RX GEL
CAROSPIR
CELACYN GEL
CERACADE EMU
COPASIL GEL
DERMACINRX PAK
DPN PAK
DERMACINRX PAK
INFLAMMA
DERMACINRX PAK
THERAZOL
DERMACINRX SOL
BASE
DERMASORB XM KIT
DEXAMETHASON
TAB 10-DAY
DEXAMETHASON
TAB 13-DAY
DEXAMETHASON
TAB 6-DAY
DEXERYL CRE
DEXPAK PAK 10 DAY
DEXPAK PAK 13 DAY
DEXPAK PAK 6 DAY
DILATRATE SR CAP
40MG
DOXEPIN HCL
CREAM
DURLAZA
ELETONE CRE
ELETONE CRE
TWINPACK
EMULSION SB EMU
EMVERM CHW

MTMP Guide 2018-2019 33
ENDOMETRIN SUP
100MG
ENTTY EMU SPRAY
EPICERAM EMU
EPIPEN 2-PAK
EPIPEN-JR
EPISIL LIQ
EVZIO INJ
FLEXIPAK PAK
GOCOVRI
GONITRO POW
GUANFACINE ER
HIDEX 6-DAY PAK
1.5MG
HPR PLUS CRE
HYLATOPIC CRE
PLUS
IMIQUIMOD CRE
PMP
INFLAMMACIN MIS
INTUNIV
ISORDIL TAB 40MG
ISORDIL TAB 5MG
ISOSORB DIN TAB
40MG ER
ISOSORB DIN TAB
40MG SA
KAMDOY EMU
KELARX GEL
LOCORT PAK 11-DAY
LOKELMA PAK
LOYON SOL
LUCEMYRA
MACRILEN PAK
60MG
MEMANT TITRA PAK
5-10MG
MEMANTINE HC ER
MEMANTINE HC SOL
MEMANTINE SOL
METOPIC CRE 41%
MIMYX CRE
NAMENDA TAB 5-
10MG
NAMENDA XR
NAMENDA XR CAP
TITRATION
NASCOBAL SPR
500MCG
NEOCERA CRE
NEOSALUS CP CRE
NEOSALUS CRE
NIVATOPIC CRE
PLUS
NOCDURNA SUB
NOCDURNA SUB
55.3MCG
NOCTIVA EMU
NOCTIVA SPR
NORITATE CRE
NUDICLO PAK
NUVAIL SOL
ORAFATE PST
OSMOLEX ER
PEG BASE OIN
PENLEN EMU SPRAY
PERTZYE
PHLAG SPR
POLYPEG OIN BASE
PREVIDOLRX PAK
PLUS
PREVYMIS
PROTHELIAL PST
PRUCLAIR CRE
PRUDOXIN CRE
PRUMYX CRE
QBREXZA PAD
RECEDO GEL
REMIGEN CREA CRE
RESTIZAN GEL
SCAR MANAGE GEL
SCARCIN GEL
SCARSILK GEL
SOLOSEC GRA 2GM
SUVICORT EMU
SYNERDERM EMU
TAPERDEX PAK 12-
DAY
TAPERDEX PAK 6
DAY
TAPERDEX PAK 7-
DAY
TDM SOLUTION SOL
TETRIX CRE
TIGLUTIK SUS
TOLAK CRE
UREA CRE 41%
UTOPIC CRE 41%
VALCHLOR GEL
XENAFLAMM PAK
XERALUX CRE
ZONACORT PAK 11
DAY
ZONALON CRE
ZOSTAVAX INJ
ZYCLARA

MTMP Guide 2018-2019 34
Qualified High Deductible Health Savings Account Benefit Plans Wellness Drug List
In addition to a healthy lifestyle, preventive medications can help people avoid many illnesses and conditions.
Preventive medications are defined as those prescribed to prevent the occurrence of a chronic disease or condition
for those individuals with risk factors, or to prevent the recurrence of a disease or condition. Some examples of
the medications listed are for high blood pressure, high cholesterol, diabetes, asthma, osteoporosis, and heart
disease.
This list provides examples of your preventive medications by drug category/therapeutic classification.
Medications may be added to or removed from the list, depending on different factors, including the intended
purpose of the medication and new medications.
To help you tell generic and brand drugs apart, all generics start with a lowercase letter.
SP Oral and self-injectable Specialty medications may be subject to limitations based on plan benefit design.
+ Products excluded from the Select Premium Formulary
‡ Where differences are noted between this Formulary and your benefit plan documents, the benefit plan
documents will rule.
This list is intended as a reference and may not be all-inclusive. Brand or generic availability may not be current
due to changes in the market. Use of generics may be required depending upon plan design.
Antipsychotics
ABILIFY
ADASUVE
aripiprazole
ARISTADA
chlorpromazine
clozapine
CLOZARIL
EQUETRO
FANAPT
FAZACLO
fluphenazine
GEODON
haloperidol
INVEGA
LATUDA
loxapine
molindone
NUPLAZID
olanzapine
olanzapine / fluoxetine
paliperidone ER
perphenazine
prochlorperazine
quetiapine
REXULTI
RISPERDAL
risperidone
SAPHRIS
SEROQUEL
SEROQUEL XR
SYMBYAX
thioridazine
thiothixene
trifluoperazine
VRAYLAR
VERSACLOZ
ziprasidone
ZYPREXA
Asthma and COPD
ACCOLATE
ADVAIR DISKUS
ADVAIR HFA
AEROSPAN
AIRDUO +
albuterol neb / syp / tab
albuterol ER
ALVESCO +
ANORO ELLIPTA
ARCAPTA
ARMONAIR +
ARNUITY ELPT
ASMANEX +
ASMANEX HFA +
ATROVENT HFA
BEVESPI +
BREO ELLIPTA
BROVANA
budesonide suspension
COMBIVENT RESPIMAT
cromolyn nebulizer solution
DALIRESP
DULERA +
ELIXOPHYLLIN
FLOVENT DISKUS
FLOVENT HFA
FLUTICASONE INH SALMETER
FORADIL
INCRUSE ELPT
ipratropium inhalation solution

MTMP Guide 2018-2019 35
ipratropium / albuterol
isoproterenol
LEVALBUTEROL AER +
levalbuterol neb
LONHALA MAGNAIR
metaproterenol
montelukast
PERFOROMIST NEB
PROAIR HFA
PROAIR RESPICLICK
PROVENTIL HFA +
PULMICORT +
PULMICORT FLEXHALER
QVAR +
SEEBRI NEOHALER +
SEREVENT DISKUS
SINGULAIR +
SPIRIVA
STIOLTO RESPIMAT
STRIVERDI RESPIMAT
SYMBICORT
terbutaline
THEO-24 CR / ER
theochron CR
theophylline
theophylline CR / ER
TRELEGY ELLIPTA
TUDORZA PRES +
UTIBRON NEOHALER +
VENTOLIN HFA
VOSPIRE ER
XOPENEX HFA +
XOPENEX SOLUTION
zafirlukast
zileuton ER
ZYFLO
ZYFLO CR
Cancer
anastrozole
ARIMIDEX
AROMASIN SP
EVISTA
exemestane SP
FARESTON
FEMARA SP
letrozole SP
raloxifene
SOLTAMOX
tamoxifen
Cardiovascular/Heart Disease
Anti-Anginal Agents
DILATRATE SR
GONITRO
ISORDIL
isosorb dinitrate
isosorbide dinitrate ER
isosorbide mononitrate
isosorbide mononitrate ER
minitran
NITRO-BID
NITRO-DUR
nitroglycerin
NITROLINGUAL SPR
NITROMIST
NITROSTAT +
nitro-time
petn
RANEXA
Anticoagulants
AGGRENOX
ARIXTRA SP
ASA / dipyridamole
BEVYXXA
BRILINTA
cilostazol
clopidogrel
COUMADIN
dipyridamole
DURLAZA
EFFIENT
ELIQUIS
enoxaparin SP
fondaparinux SP
FRAGMIN SP
heparin
jantoven
LOVENOX SP
PERSANTINE
PLAVIX
PLETAL
PRADAXA
prasugrel
SAVAYSA
ticlopidine
warfarin
XARELTO
YOSPRALA
ZONTIVITY
Cardiac Glycosides
digitek
digox
digoxin
LANOXIN
High Blood Pressure
ACCUPRIL
ACCURETIC
acebutolol
ACEON
ADALAT CC
afeditab CR
ALDACTAZIDE
ALDACTONE
ALTACE
amiloride
amiloride / hctz
amlodipine
amlodipine / atorvastatin
amlodipine / benazepril
amlodipine / olmesartan
amlodipine / valsartan
ATACAND
ATACAND HCT
atenol / chlorthalidone
atenolol
AVALIDE
AVAPRO
AZOR +
benazepril
benazepril / hctz
BENICAR +
BENICAR HCT +
BETAPACE
BETAPACE AF
betaxolol
BIDIL
bisoprolol
bisoprolol / hctz
bumetanide
BUMEX
BYSTOLIC
BYVALSON
CADUET
CALAN
CALAN SR
candesartan
candesartan / hctz
captopril
captopril / hctz
CARDIZEM
CARDIZEM CD
CARDIZEM LA
CARDURA
cartia XT
carvedilol
CATAPRES
CATAPRES TTS
chlorothiazide
chlorthalidone
clonidine
CLORPRES
COREG
COREG CR
CORGARD
CORZIDE
COZAAR
DEMADEX
DEMSER
DIBENZYLINE
dilt-XR
diltiazem
diltiazem CD
diltiazem ER

MTMP Guide 2018-2019 36
DIOVAN +
DIOVAN HCT +
DIURIL
doxazosin
DUTOPROL
DYAZIDE
DYRENIUM
EDARBI
EDARBYCLOR
EDECRIN
enalapril
enalapril / hctz
EPANED
eplerenone
eprosartan
ethacrynic acid
EXFORGE
EXFORGE HCT
ezide
felodipine ER
fosinopril
fosinopril / hctz
furosemide
guanfacine
HEMANGEOL
hydralazine
hydrochlorothiazide
HYZAAR
indapamide
INDERAL LA
INDERAL XL
INNOPRAN XL
INSPRA
irbesartan
irbesartan / hctz
isradipine
labetalol
LASIX
lisinopril
lisinopril / hctz
LOPRESSOR
LOPRESSOR HCT
losartan
losartan / hctz
LOTENSIN
LOTENSIN HCT
LOTREL
matzim LA
MAVIK
MAXZIDE
MAXZIDE-25
methyclothiazide
methyldopa
methyldopa / hctz
metolazone
METOPRO / HCTZ
metoprolol
metoprolol ER
metoprolol / hctz
MICARDIS
MICARDIS HCT
MICROZIDE
MINIPRESS
minoxidil
moexipril
moexipril / hctz
nadolol
nadolol / bendroflumethiazide
nicardipine
nifedical XL
nifedipine
nifedipine ER
nimodipine
nisoldipine
nisoldipine ER
NORVASC +
NYMALIZE
olmesartan
olmesartan / amlo / hctz
olmesartan / hctz
perindopril
phenoxybenzamine
pindolol
prazosin hcl
PRESTALIA
PRINIVIL
PROCARDIA
PROCARDIA XL
propranolol
propranolol ER
propranolol / hctz
QBRELIS
quinapril
quinapril / hctz
ramipril
SECTRAL
sotalol
sotalol AF
SOTYLIZE
spironolactone
spironolactone / hctz
SULAR
TARKA
taztia XT
TEKTURNA
TEKTURNA HCT
telmisartan
telmisartan / amlodipine
telmisartan / hctz
TENEX
TENORETIC
TENORMIN
terazosin
TIAZAC
timolol (tablet)
TOPROL XL +
torsemide
trandolapril
trandolapril / verapamil
triamterene / hctz
TRIBENZOR +
TWYNSTA
valsartan
valsartan / hctz
VASERETIC
VASOTEC
VECAMYL
verapamil
verapamil ER / SR
VERELAN
VERELAN PM
ZEBETA
ZESTORETIC
ZESTRIL
ZIAC
High Cholesterol
ALTOPREV
ANTARA
atorvastatin
cholestyramine
cholestyramine lite
COLESTID
colestipol
CRESTOR +
ezetimibe
ezetim / simva
fenofibrate
fenofibric
fenofibric DR
FENOGLIDE
FIBRICOR
FLOLIPID
fluvastatin
gemfibrozil
JUXTAPID SP
KYNAMRO SP
LESCOL XL
LIPITOR +
LIPOFEN
LIVALO
LOFIBRA
LOPID
lovastatin
LOVAZA +
MEVACOR
niacin ER (Rx)
niacor
NIASPAN ER
omega-3-acid (Rx)
PRALUENT SP
PRAVACHOL
pravastatin
prevalite
QUESTRAN
QUESTRAN LITE
REPATHA SP

MTMP Guide 2018-2019 37
rosuvastatin
simvastatin
TRICOR
TRIGLIDE
triklo
TRILIPIX
VASCEPA
VYTORIN +
WELCHOL
ZETIA +
ZOCOR
ZYPITAMAG
Contraceptives ‡
This section lists contraceptive categories.
Please note that brands and generics are
eligible.
CONTRACEPTIVE PATCH
CONTRACEPTIVE RING (NUVARING)
EMERGENCY CONTRACEPTIVES
IMPLANT CONTRACEPTIVE
INJECTABLE CONTRACEPTIVE
IUDs
ORAL CONTRACEPTIVES
Diabetes
Insulin
ADMELOG +
AFREZZA
APIDRA +
BASAGLAR +
FIASP +
HUMALOG
HUMALOG KWIKPEN
HUMALOG MIX
HUMULIN
LANTUS
LANTUS SOLOSTAR
LEVEMIR +
NOVOLIN +
NOVOLIN RELION +
NOVOLOG +
NOVOLOG MIX +
TOUJEO
TRESIBA FLEX +
Non-Insulin
acarbose
ACTOPLUS MET
ACTOPLUS MET XR
ACTOS
ADLYXIN +
ALOGLIPTIN +
ALOGLIPTIN / METFORMIN +
ALOGLIPTIN / PIOGLITAZONE +
AMARYL
BYDUREON
BYETTA
chlorpropamide
CYCLOSET
DIABETA
DUETACT
FARXIGA +
FORTAMET +
glimepiride
glipizide
glipizide / metformin
glipizide ER
glipizide XL
GLUCOPHAGE
GLUCOPHAGE XR
GLUCOTROL
GLUCOTROL XL
GLUCOVANCE
GLUMETZA +
glyburide
glyburide / metformin
glyburide micronized
GLYNASE
GLYSET
GLYXAMBI
INVOKAMET
INVOKAMET XR
INVOKANA
JANUMET
JANUMET XR
JANUVIA
JARDIANCE
JENTADUETO
JENTADUETO XR
KAZANO +
KOMBIGLYZE XR +
metformin
metformin ER
miglitol
nateglinide
NESINA +
ONGLYZA +
OSENI +
OZEMPIC
pioglitazone
pioglitazone / glimepride
pioglitazone / metformin
PRANDIN
PRECOSE
QTERN +
repaglinide
RIOMET
SOLIQUA
SEGLUROMET
STEGLATRO
STEGLUJAN
STARLIX
SYMLIN
SYNJARDY
SYNJARDY XR
TANZEUM +
tolazamide
tolbutamide
TRADJENTA
TRULICITY
VICTOZA
XIGDUO XR +
XULTOPHY
Estrogens
ACTIVELLA
ALORA
amabelz
ANGELIQ
CLIMARA
CLIMARA PRO
COMBIPATCH
covaryx
covaryx HS
DIVIGEL
DUAVEE
eemt
eemt HS
ELESTRIN
est estrogen mtest
est estrogen mtest HS
estra / noreth
ESTRACE (ORAL TAB)
estrad val
estradiol (oral tabs, patch)
estrog / mtest
ESTROGEL
estropipate
EVAMIST
FEMHRT
fyavolv
jevantique
jinteli
lopreeza
MENEST
MENOSTAR
mimvey
mimvey lo
MINIVELLE
noreth / ethin
PREFEST
PREMPHASE
PREMARIN (ORAL TAB)
PREMPRO
VIVELLE-DOT +
Gastrointestinal-Ulcer Drugs‡
ACIPHEX +
AXID
CARAFATE +
cimetidine
CYTOTEC
DEXILANT
Esomeprazole +

MTMP Guide 2018-2019 38
ESOMEPRAZOLE 24.65MG AND
49.3MG +
famotidine
lanso / amox / clarith
lansoprazole
misoprostol
NEXIUM +
nizatidine
OMECLAMOX
omeppi
omepra / bicar +
omeprazole
pantoprazole
PEPCID
PREVACID +
PREVPAC
PRILOSEC
PROTONIX
PYLERA
rabeprazole
ranitidine
sucralfate
ZANTAC
ZEGERID +
HIV/AIDS
abacavir / lamivudine SP
abacavir SP
abacavir / lamivudine / zidovudine SP
APTIVUS SP
atazanavir SP
ATRIPLA SP
BIKTARVY SP
COMBIVIR SP
COMPLERA SP
CIMDUO SP
CRIXIVAN SP
DESCOVY SP
didanosine SP
EDURANT SP
efavirenz SP
EMTRIVA SP
EPIVIR SP
EPZICOM SP
EVOTAZ SP
fosamprenavir SP
FUZEON SP
GENVOYA SP
INTELENCE SP
INVIRASE SP
ISENTRESS SP
JULUCA SP
KALETRA SP
lamivudine SP
lamivudine / zidovudine SP
LEXIVA SP
lopinavir / ritonavir sol SP
nevirapine SP
nevirapine ER SP
NORVIR SP
ODEFSEY SP
PREZCOBIX SP
PREZISTA SP
RESCRIPTOR SP
RETROVIR SP
REYATAZ SP
ritonavir SP
SELZENTRY SP
stavudine SP
STRIBILD SP
SUSTIVA SP
SYMFI LO SP
tenofovir SP
TIVICAY SP
TRIUMEQ SP
TRIZIVIR SP
TRUVADA SP
TYBOST SP
VIDEX SP
VIDEX EC SP
VIRACEPT SP
VIRAMUNE SP
VIRAMUNE XR SP
VIREAD SP
VITEKTA SP
ZERIT SP
ZIAGEN SP
zidovudine SP
Osteoporosis
ACTONEL
alendronate
ATELVIA
BINOSTO
BONIVA
calcitonin spray
etidronate
EVISTA
FORTEO SP
FOSAMAX
FOSAMAX + D
ibandronate
MIACALCIN SPRAY
raloxifene
risedronate
Smoking Deterrents ‡
bupropion
CHANTIX
NICODERM CQ
NICORETTE
nicotine gum / lozenge / patch
NICOTROL INH / NS
ZYBAN
Transplant
ASTAGRAF XL SP
AZASAN
azathioprine
CELLCEPT SP
cyclosporine SP
cyclosporine modified SP
ENVARSUS XR SP
gengraf SP
IMURAN
mycophenolate SP
mycophenolic DR SP
MYFORTIC SP
NEORAL SP
PROGRAF SP
RAPAMUNE SP
SANDIMMUNE SP
sirolimus SP
tacrolimus cap SP
ZORTRESS SP
Vitamins & Electrolytes
Pediatric vitamins with fluoride
(for example; POLY-VI-FLOR, tri-vit / fl)
generic products
BRAND NAME PRODUCTS
Prenatal multivitamins with iron and
folic acid
(for example; OB COMPLETE, prenatabs
RX)
generic products
BRAND NAME PRODUCTS

MTMP Guide 2018-2019 39
Political Subdivision Choice Select Formulary
The most up to date formulary may be located at https://tmlhealthbenefits.org/.
The most effective way to control costs is through the use of generic drugs and a drug formulary.
Drug Tier Includes
Tier 1:
Preferred Network Tier
* The OptumRx Preferred Network of Pharmacies includes HEB and Walmart (not Sam’s
Club). Use Tier 1 drugs for the lowest out-of-pocket costs.
Tier 2:
Value Tiered
Not all medications for diabetes, hypertension, and high cholesterol qualify (e.g., Cost Share
prescription exclusions). Copays are applicable. Use Tier 2 drugs, instead of Tier 3, to
help reduce your out-of-pocket costs.
Tier 3 Most commonly used generic drugs. Some low-cost brands may be included. Many Tier 3
drugs have lower cost options in Tier 1 or 2. Ask your doctor if they could work for you.
Tier 4:
Mid-range Cost
Many common brand-name drugs, called preferred brands. Lower cost alternative drugs are
listed in the Cost Share prescriptions section of this booklet.
Tier 5:
High Cost Mostly higher cost brand drugs, also known as non-preferred brands.
Tier 6:
Highest Cost
High cost brand and generic drugs that have very similar or equivalent low cost alternative
drugs.
Tier 7:
Biotech/Biosimilar
Specialty Prescriptions
Biotech drugs differ from pharmaceutical drugs in that they use biotechnology as a means for
manufacturing, which involves the manipulation of microorganisms, such as bacteria, or
biological substances, like enzymes, to perform a specific process. Biosimilar prescriptions
are biologic medical products which are almost identical to the original product.
Tier E
Excluded
May be excluded from coverage or subject to prior authorization. Lower-cost options are
available and covered.
Tier i-P Preferred specialty injectables
Check your benefit plan documents to find out your specific prescription plan costs.
Tier i-NP Non-preferred specialty injectables
Check your benefit plan documents to find out your specific prescription plan costs.
* Drugs may transition from tier to tier within benefit plan year impacting your out of pocket expense.

MTMP Guide 2018-2019 40
Some of the medications on this list may NOT be covered by your plan or have additional restrictions. Their
presence on this list does NOT guarantee coverage.
SP = Specialty Medication – Medication is designated as specialty. 3P = Tier 3 preferred
DRUG NAME DRUG
TIER NOTES
ANALGESICS - DRUGS FOR PAIN
acetaminophen-codeine #2 1
acetaminophen-codeine #3 1
acetaminophen-codeine #4 1
acetaminophen-codeine oral tablet 1
butalbital-apap-caffeine oral capsule 1
butalbital-apap-caffeine oral tablet 50-
325-40 mg
1
EMBEDA E
fentanyl 1
hydrocodone-acetaminophen oral tablet
10-300 mg, 10-325 mg, 2.5-325 mg, 5-
300 mg, 5-325 mg, 7.5-300 mg, 7.5-325
mg
1
hydromorphone hcl oral tablet 1
HYSINGLA ER E
methadone hcl oral tablet 1
morphine sulfate er oral tablet extended
release
1
oxycodone hcl oral tablet 1
oxycodone-acetaminophen oral tablet
10-325 mg, 2.5-325 mg, 5-325 mg, 7.5-
325 mg
1
OXYCONTIN ORAL TABLET ER 12
HOUR ABUSE-DETERRENT
2
tramadol hcl ir 1
tramadol-acetaminophen 1
ZOHYDRO ER ORAL CAPSULE ER
12 HOUR ABUSE-DETERRENT
E
ANALGESICS - DRUGS FOR PAIN AND INFLAMMATION
celecoxib oral 4
diclofenac potassium 1
diclofenac sodium oral 1
diclofenac sodium transdermal gel 1 % E
etodolac oral tablet 1
FLECTOR E
ibuprofen oral tablet 400 mg, 600 mg,
800 mg
1
indomethacin oral 1
ketorolac tromethamine oral 1
meloxicam oral tablet 1
nabumetone oral 1
naproxen oral tablet 1
naproxen sodium oral tablet 275 mg, 550
mg
1
sulindac oral 1
DRUG NAME DRUG
TIER NOTES
ANESTHETICS
lidocaine external ointment E
lidocaine external patch 5 % 1 PA
ANTI-ADDICTION / SUBSTANCE ABUSE TREATMENT AGENTS
BUNAVAIL E
buprenorphine hcl sublingual 1
buprenorphine hcl-naloxone hcl 1
CHANTIX STARTING MONTH PAK 3
naltrexone hcl oral 1
NARCAN 2
SUBOXONE SUBLINGUAL FILM 2
ZUBSOLV 2
ANTIBACTERIALS
amoxicillin oral capsule 1
amoxicillin oral suspension reconstituted 1
amoxicillin oral tablet 1
amoxicillin-potassium clavulanate oral
suspension reconstituted 200-28.5
mg/5ml, 250-62.5 mg/5ml, 400-57
mg/5ml, 600-42.9 mg/5ml
1
amoxicillin-potassium clavulanate oral
tablet 250-125 mg, 500-125 mg, 875-
125 mg
1
azithromycin oral suspension
reconstituted
1
azithromycin oral tablet 250 mg, 500
mg, 600 mg
1
BETHKIS 2 SP
cefdinir 1
cefuroxime axetil oral tablet 1
cephalexin oral capsule 1
cephalexin oral suspension reconstituted 1
ciprofloxacin hcl oral 1
clarithromycin oral tablet 1
clindamycin hcl oral 1
clindamycin phosphate external gel 1
clindamycin phosphate external lotion 1
clindamycin phosphate external solution 1
CLINDESSE 3
DORYX MPC 4
doxycycline hyclate oral capsule 1
doxycycline hyclate oral tablet 100 mg,
150 mg, 20 mg, 75 mg
4
doxycycline monohydrate oral capsule 1
doxycycline monohydrate oral tablet 1
levofloxacin oral tablet 1

MTMP Guide 2018-2019 41
DRUG NAME DRUG
TIER NOTES
metronidazole oral tablet 1
metronidazole vaginal 1
minocycline hcl oral capsule 1
mupirocin external 1
nitrofurantoin macrocrystal oral 1
nitrofurantoin monohydrate
macrocrystals
1
penicillin v potassium oral tablet 1
SOLODYN ORAL TABLET
EXTENDED RELEASE 24 HOUR 105
MG, 115 MG, 55 MG, 65 MG, 80 MG
4
sulfamethoxazole-trimethoprim oral
suspension 200-40 mg/5ml
1
sulfamethoxazole-trimethoprim oral
tablet
1
ANTICOAGULANTS
ELIQUIS 2
enoxaparin sodium i-NP SP
PRADAXA 2
SAVAYSA 3
warfarin sodium oral 1
XARELTO 2
XARELTO STARTER PACK 2
ANTICONVULSANTS - DRUGS FOR SEIZURES
carbamazepine oral tablet 1
divalproex sodium er oral tablet
extended release 24 hour
1
divalproex sodium oral tablet delayed
release
1
gabapentin oral capsule 1
gabapentin oral tablet 1
lamotrigine oral tablet 1
levetiracetam oral tablet 1
oxcarbazepine oral tablet 1
phenytoin sodium extended 1
topiramate oral tablet 1
VIMPAT 3
zonisamide oral 1
ANTIDEMENTIA AGENTS - DRUGS FOR ALZHEIMER'S DISEASE
AND DEMENTIA
donepezil hcl oral tablet 1
memantine hcl oral tablet 10 mg, 5 mg 1
NAMZARIC ORAL CAPSULE
EXTENDED RELEASE 24 HOUR 14-
10 MG, 28-10 MG
2
ANTIDEPRESSANTS
amitriptyline hcl oral 1
bupropion hcl er (sr) 1
bupropion hcl er (xl) 1
bupropion hcl oral 1
citalopram hydrobromide oral tablet 1
DRUG NAME DRUG
TIER NOTES
desvenlafaxine succinate er 1
doxepin hcl oral capsule 1
duloxetine hcl oral capsule delayed
release particles 20 mg, 30 mg, 60 mg
1
DULOXETINE HCL ORAL CAPSULE
DELAYED RELEASE PARTICLES 40
MG
3
escitalopram oxalate oral tablet 1
fluoxetine hcl oral capsule 1
fluoxetine hcl oral tablet 1
FORFIVO XL 2
mirtazapine oral tablet 1
nortriptyline hcl oral capsule 1
paroxetine hcl er 1
paroxetine hcl oral tablet 1
sertraline hcl oral tablet 1
trazodone hcl oral 1
TRINTELLIX 3
venlafaxine hcl 1
venlafaxine hcl er 1
VIIBRYD ORAL TABLET 3
VIIBRYD STARTER PACK 3
ANTIEMETICS - DRUGS FOR NAUSEA AND VOMITING
meclizine hcl oral tablet 25 mg 1
metoclopramide hcl oral tablet 1
ondansetron hcl oral tablet 1
ondansetron odt 1
prochlorperazine maleate oral 1
VARUBI ORAL E
ANTIFUNGALS
fluconazole oral tablet 1
GYNAZOLE-1 3
JUBLIA E
KERYDIN E
ketoconazole external cream 1
ketoconazole external shampoo 1
nystatin external cream 1
nystatin mouth/throat 1
terbinafine hcl oral 1
terconazole vaginal cream 1
ANTIGOUT AGENTS
allopurinol oral 1
COLCHICINE ORAL TABLET 3
COLCRYS 2
ULORIC 2 PA
ZURAMPIC E
ANTIMIGRAINE AGENTS
MIGRANAL 3
ONZETRA XSAIL 4
rizatriptan benzoate 1

MTMP Guide 2018-2019 42
DRUG NAME DRUG
TIER NOTES
sumatriptan succinate oral 1
SUMAVEL DOSEPRO
SUBCUTANEOUS SOLUTION JET-
INJECTOR
4
ANTINEOPLASTICS - DRUGS FOR CANCER
anastrozole oral 1
CABOMETYX 2 SP
capecitabine 1 SP
IBRANCE 3 SP
letrozole oral 1
mercaptopurine oral 1 SP
REVLIMID 3 SP
SPRYCEL 2 SP
tamoxifen citrate oral 1
XTANDI 3 SP
ZYTIGA 3 SP
ANTIPARASITICS
EMVERM E
hydroxychloroquine sulfate oral 1
permethrin external cream 1
SOOLANTRA 2
ANTIPARKINSON AGENTS
benztropine mesylate oral 1
carbidopa-levodopa oral tablet 1
pramipexole dihydrochloride 1
ropinirole hcl 1
ZELAPAR 3
ANTIPLATELETS
BRILINTA 2
cilostazol 1
clopidogrel bisulfate oral 1
ANTIPSYCHOTICS - DRUGS FOR MOOD DISORDERS
aripiprazole oral tablet 1
ARISTADA INTRAMUSCULAR
PREFILLED SYRINGE 441
MG/1.6ML, 662 MG/2.4ML, 882
MG/3.2ML
3
haloperidol oral 1
INVEGA SUSTENNA 3
INVEGA TRINZA 3
LATUDA 3
olanzapine oral tablet 1
quetiapine fumarate 1
REXULTI E
risperidone oral tablet 1
SAPHRIS 2
ziprasidone hcl 1
DRUG NAME DRUG
TIER NOTES
ANTIVIRALS
abacavir sulfate-lamivudine 1 SP
acyclovir oral capsule 1
acyclovir oral tablet 1
ATRIPLA 2 SP
COMPLERA 2 SP
DESCOVY 3 SP
entecavir 1 SP
EPCLUSA 2 SP
GENVOYA 2 SP
HARVONI 2 SP
INTELENCE 2 SP
ISENTRESS ORAL TABLET 2 SP
MAVYRET 2 SP
NORVIR ORAL TABLET 2 SP
ODEFSEY 2 SP
oseltamivir phosphate oral capsule 1
PREZCOBIX 2 SP
PREZISTA ORAL TABLET 150 MG,
600 MG, 75 MG, 800 MG
2 SP
REYATAZ ORAL CAPSULE 150 MG,
200 MG, 300 MG
3 SP
STRIBILD 2 SP
TIVICAY 2 SP
TRIUMEQ 2 SP
TRUVADA 2 SP
valacyclovir hcl oral 1
VIREAD ORAL TABLET 150 MG, 200
MG, 250 MG
2 SP
VIREAD ORAL TABLET 300 MG 3 SP
VOSEVI 2 SP
ZOVIRAX EXTERNAL CREAM 2
ZOVIRAX EXTERNAL OINTMENT 3
ANXIOLYTICS - DRUGS FOR ANXIETY
alprazolam oral tablet 1
buspirone hcl oral 1
clonazepam oral tablet 1
diazepam oral tablet 1
hydroxyzine hcl oral tablet 1
hydroxyzine pamoate oral 1
lorazepam oral tablet 1
triazolam 1
BIPOLAR AGENTS - DRUGS FOR MOOD DISORDERS
lithium carbonate er 1
lithium carbonate oral capsule 1

MTMP Guide 2018-2019 43
DRUG NAME DRUG
TIER NOTES
BLOOD PRODUCTS / MODIFIERS / VOLUME EXPANDERS - DRUGS
FOR BLEEDING DISORDERS
AFSTYLA i-P SP
ARANESP (ALBUMIN FREE)
INJECTION SOLUTION 100
MCG/ML, 200 MCG/ML, 25 MCG/ML,
300 MCG/ML, 40 MCG/ML, 60
MCG/ML
i-P SP
ARANESP (ALBUMIN FREE)
INJECTION SOLUTION PREFILLED
SYRINGE
i-P SP
GRANIX i-P SP
NEUPOGEN INJECTION SOLUTION
300 MCG/ML, 480 MCG/1.6ML
i-P SP
NEUPOGEN INJECTION SOLUTION
PREFILLED SYRINGE
i-P SP
NUWIQ i-P SP
PROCRIT i-P SP
ZARXIO i-P SP
CARDIOVASCULAR AGENTS - DRUGS FOR HEART AND
CIRCULATION CONDITIONS
amiodarone hcl oral 1
amlodipine besylate oral 1
amlodipine besylate-benazepril hcl 1
amlodipine besylate-valsartan 1
atenolol oral 1
atenolol-chlorthalidone 1
atorvastatin calcium oral 1
benazepril hcl oral 1
benazepril-hydrochlorothiazide 1
bisoprolol fumarate 1
bisoprolol-hydrochlorothiazide 1
bumetanide oral 1
BYSTOLIC 2
BYVALSON 2
cartia xt 1
carvedilol 1
chlorthalidone oral tablet 25 mg, 50 mg 1
choline fenofibrate 1
clonidine hcl oral 1
CRESTOR 4
digox 1
digoxin oral tablet 1
diltiazem hcl er beads 1
diltiazem hcl er coated beads oral
capsule extended release 24 hour
1
diltiazem hcl oral 1
doxazosin mesylate 1
EDARBI 4
EDARBYCLOR 4
enalapril maleate oral 1
ezetimibe 1
ezetimibe-simvastatin 1
DRUG NAME DRUG
TIER NOTES
fenofibrate micronized oral capsule 134
mg, 200 mg, 67 mg
E
fenofibrate oral tablet E
fenofibric acid oral capsule delayed
release
E
flecainide acetate 1
furosemide oral tablet 1
gemfibrozil oral 1
guanfacine hcl oral 1
hydralazine hcl oral 1
hydrochlorothiazide oral 1
irbesartan 1
irbesartan-hydrochlorothiazide 1
isosorbide mononitrate er 1
labetalol hcl oral 1
LIPOFEN E
lisinopril oral 1
lisinopril-hydrochlorothiazide 1
LIVALO 4
losartan potassium 1
losartan potassium-hctz 1
lovastatin 1
metoprolol succinate er 1
metoprolol tartrate oral 1
MULTAQ 3
nadolol oral tablet 20 mg, 40 mg, 80 mg 1
niacin er (antihyperlipidemic) E
nifedipine er 1
nifedipine er osmotic release 1
nitroglycerin sublingual 1
olmesartan medoxomil oral 4
olmesartan medoxomil-hctz 4
omega-3-acid ethyl esters E
pentoxifylline er 1
PRALUENT SUBCUTANEOUS
SOLUTION PEN-INJECTOR
E SP
pravastatin sodium 1
prazosin hcl oral 1
propranolol hcl er 1
propranolol hcl oral tablet 1
quinapril hcl 1
ramipril 1
RANEXA 2
REPATHA E SP
REPATHA PUSHTRONEX SYSTEM E SP
REPATHA SURECLICK E SP
rosuvastatin calcium 1
simvastatin oral 1
sotalol hcl oral 1
spironolactone oral 1
TEKTURNA 4
TEKTURNA HCT 4
telmisartan 4
torsemide oral 1

MTMP Guide 2018-2019 44
DRUG NAME DRUG
TIER NOTES
triamterene-hctz 1
valsartan 1
valsartan-hydrochlorothiazide 1
VASCEPA E
verapamil hcl er oral tablet extended
release 120 mg, 180 mg, 240 mg
1
verapamil hcl oral 1
WELCHOL 2
CENTRAL NERVOUS SYSTEM AGENTS - DRUGS FOR ATTENTION
DEFICIT DISORDER
ADDERALL XR 3
amphetamine-dextroamphetamine 1
amphetamine-dextroamphetamine er 1
atomoxetine hcl 1
CONTEMPLA XR-ODT 3
dexmethylphenidate hcl 1
dexmethylphenidate hcl er 1
guanfacine hcl er E
methylphenidate hcl er 1
methylphenidate hcl er oral tablet 1
methylphenidate hcl oral tablet 1
VYVANSE 2
CENTRAL NERVOUS SYSTEM AGENTS - DRUGS FOR MULTIPLE
SCLEROSIS
AMPYRA 2 SP
AUBAGIO 3 SP
AVONEX PEN INTRAMUSCULAR
AUTO-INJECTOR KIT
i-P SP
AVONEX PREFILLED
INTRAMUSCULAR PREFILLED
SYRINGE KIT
i-P SP
AVONEX VIAL INTRAMUSCULAR
KIT
i-P SP
BETASERON SUBCUTANEOUS KIT i-P SP
COPAXONE SUBCUTANEOUS
SOLUTION PREFILLED SYRINGE
i-P SP
GILENYA 3 3P; SP
TECFIDERA 2 SP
CENTRAL NERVOUS SYSTEM AGENTS - MISCELLANEOUS
CONTRAVE E
GRALISE 4
GRALISE STARTER 4
LYRICA ORAL CAPSULE 4
phentermine hcl oral tablet E
DENTAL AND ORAL AGENTS - DRUGS FOR MOUTH AND THROAT
CONDITIONS
chlorhexidine gluconate mouth/throat 1
lidocaine viscous 1
DERMATOLOGICAL AGENTS - DRUGS FOR SKIN CONDITIONS
ABSORICA E
DRUG NAME DRUG
TIER NOTES
ACZONE 2
adapalene external gel 1
ATRALIN 3
claravis 1
clindamycin phosphate-benzoyl peroxide
external gel 1-5 %
1
clotrimazole-betamethasone external
cream
1
COSENTYX 150 MG/ML i-P 3P; SP
COSENTYX 300 DOSE i-P 3P; SP
COSENTYX SENSOREADY 300
DOSE
i-P 3P; SP
COSENTYX SENSOREADY PEN
SUBCUTANEOUS SOLUTION
AUTO-INJECTOR 150 MG/ML
i-P 3P; SP
DIFFERIN EXTERNAL GEL 0.3 % 3
DIFFERIN EXTERNAL LOTION 3
DUPIXENT i-P SP
ELIDEL 2
ENSTILAR E
EPIDUO 3
EPIDUO FORTE 3
EUCRISA 2
FLUOROPLEX 3
METROGEL EXTERNAL GEL 3
metronidazole external gel 1
MIRVASO 2
ONEXTON 3
ORACEA 4
OXSORALEN ULTRA 2
RETIN-A MICRO GEL 0.04 %, 0.1 % E
RETIN-A MICRO PUMP EXTERNAL
GEL 0.04 %, 0.1 %
E
RETIN-A MICRO PUMP EXTERNAL
GEL 0.06 %, 0.08 %
E
STELARA SUBCUTANEOUS
SOLUTION PREFILLED SYRINGE
i-P SP
TACLONEX E
TAZORAC 3
tretinoin external cream 1
VECTICAL 3
ZYCLARA 3
ZYCLARA PUMP 3
DIABETES - ANTIDIABETIC AGENTS
BYDUREON BCISE AUTOINJECTOR 2
BYDUREON PEN 2
BYDUREON VIAL 2
BYETTA 10 MCG PEN 2
BYETTA 5 MCG PEN 2
FARXIGA 3
glimepiride 1
glipizide er 1
glipizide ir 1
glipizide xl 1

MTMP Guide 2018-2019 45
DRUG NAME DRUG
TIER NOTES
glyburide oral 1
glyburide-metformin 1
INVOKAMET E
INVOKAMET XR E
INVOKANA E
JANUMET 2
JANUMET XR 2
JANUVIA 2
JARDIANCE 2
JENTADUETO 2
JENTADUETO XR 2
KOMBIGLYZE XR ?
metformin hcl er 1
metformin hcl er (mod) E
metformin hcl er (osm) oral tablet
extended release 24 hour 1000 mg, 500
mg
E
metformin hcl ir 1
ONGLYZA 3
pioglitazone hcl 1
SOLIQUA 2
SYNJARDY 2
SYNJARDY XR 2
TRADJENTA 2
TRULICITY 2
VICTOZA 2
DIABETES - GLUCOSE MONITORING
ACCU-CHEK AVIVA CONNECT KIT
W/DEVICE
2
ACCU-CHEK AVIVA PLUS 2
ACCU-CHEK COMPACT PLUS
CARE KIT
2
ACCU-CHEK COMPACT PLUS TEST
STRIPS
2
ACCU-CHEK FASTCLIX LANCET
KIT
2
ACCU-CHEK FASTCLIX LANCETS 2
ACCU-CHEK GUIDE 2
ACCU-CHEK MULTICLIX LANCET
DEVICE KIT
2
ACCU-CHEK MULTICLIX LANCETS 2
ACCU-CHEK NANO SMARTVIEW
KIT W/DEVICE
2
ACCU-CHEK SMARTVIEW TEST
STRIPS
2
ACCU-CHEK SOFT TOUCH
LANCETS
2
ACCU-CHEK SOFTCLIX LANCET
DEVICE KIT KIT
2
ACCU-CHEK SOFTCLIX LANCETS 2
DEXCOM G4 PLATINUM
PEDIATRIC RECEIVER DEVICE
3
DRUG NAME DRUG
TIER NOTES
DEXCOM G4 PLATINUM
RECEIVER, SENSOR,
TRANSMITTER DEVICE
3
DEXCOM G5 SENSOR,
TRANSMITTER, MOBILE RECEIVER
3
ONETOUCH ULTRA 2 KIT
W/DEVICE
2
ONETOUCH ULTRA BLUE TEST
STRIPS
2
ONETOUCH ULTRA MINI KIT
W/DEVICE
2
ONETOUCH VERIO 2
ONETOUCH VERIO FLEX SYSTEM
KIT W/DEVICE
2
ONETOUCH VERIO TEST STRIPS 2
ONETOUCH VERIO IQ SYSTEM KIT
W/DEVICE
2
ONETOUCH VERIO SYNC SYSTEM
KIT W/DEVICE
2
DIABETES - INSULINS
HUMALOG U-100 AND U-200
KWIKPEN
2
HUMALOG MIX 50/50 KWIKPEN 2
HUMALOG MIX 50/50 VIAL 2
HUMALOG MIX 75/25 KWIKPEN 2
HUMALOG MIX 75/25 VIAL 2
HUMALOG U-100 JUNIOR
KWIKPEN
2
HUMALOG U-100 VIAL AND
CARTRIDGE
2
HUMULIN 70/30 KWIKPEN 2
HUMULIN 70/30 VIAL 2
HUMULIN N KWIKPEN 2
HUMULIN N VIAL 2
HUMULIN R U-500 KWIKPEN 2
HUMULIN R U-500 VIAL
(CONCENTRATED)
2
HUMULIN R VIAL 2
LANTUS U-100 SOLOSTAR 2
LANTUS U-100 VIAL 2
LEVEMIR U-100 FLEXTOUCH 2
LEVEMIR U-100 VIAL 2
NOVOFINE AUTOCOVER PEN
NEEDLE
2
NOVOFINE PEN NEEDLE 2
NOVOFINE PLUS PEN NEEDLE 2
NOVOLIN 70/30 VIAL 2
NOVOLIN N VIAL 2
NOVOLIN R VIAL 2
NOVOLOG U-100 FLEXPEN 2
NOVOLOG MIX 70/30 FLEXPEN 2
NOVOLOG MIX 70/30 VIAL 2
NOVOLOG U-100 PENFILL 2
NOVOLOG U-100 VIAL 2

MTMP Guide 2018-2019 46
DRUG NAME DRUG
TIER NOTES
NOVOTWIST PEN NEEDLE 32G X 5
MM
2
TOUJEO SOLOSTAR 2
TRESIBA FLEXTOUCH 2
ELECTROLYTES / MINERALS / METALS / VITAMINS
cyanocobalamin injection 1
folic acid oral tablet 1 mg 1
klor-con m20 1
ludent 1
potassium chloride crys er 1
potassium chloride er 1
potassium citrate er 1
VELTASSA 3
vitamin d (ergocalciferol) 1
GASTROINTESTINAL AGENTS - DRUGS FOR ACID REFLUX AND
ULCER
DEXILANT E
esomeprazole magnesium E
famotidine oral tablet 20 mg, 40 mg 1
lansoprazole oral capsule delayed release E
omeprazole oral capsule delayed release E
pantoprazole sodium oral E
rabeprazole sodium E
ranitidine hcl oral capsule 1
ranitidine hcl oral syrup 1
ranitidine hcl oral tablet 150 mg, 300 mg 1
sucralfate oral tablet 1
GASTROINTESTINAL AGENTS - DRUGS FOR BOWEL, INTESTINE
AND STOMACH CONDITIONS
AMITIZA 3
dicyclomine hcl oral capsule 1
dicyclomine hcl oral tablet 1
diphenoxylate-atropine oral tablet 1
gavilyte-g 1
LINZESS 2
MOVIPREP 3
OMECLAMOX-PAK E
polyethylene glycol 3350 oral powder 1
PREPOPIK 3
PYLERA E
RELISTOR SUBCUTANEOUS
SOLUTION 12 MG/0.6ML
E
SUPREP BOWEL PREP KIT 3
VIBERZI 3
GENETIC OR ENZYME DISORDER: DRUGS FOR REPLACEMENT,
MODIFIERS, TREATMENT
CERDELGA 3 SP
CREON 2
ZENPEP ORAL CAPSULE DELAYED
RELEASE PARTICLES 10000 UNIT,
15000 UNIT, 20000-63000 UNIT,
2
DRUG NAME DRUG
TIER NOTES
25000 UNIT, 3000-10000 UNIT, 5000
UNIT
GENITOURINARY AGENTS - DRUGS FOR BLADDER, GENITAL
AND KIDNEY CONDITIONS
CIALIS E
DEPEN TITRATABS 2 SP
MYRBETRIQ 4
oxybutynin chloride er 4
oxybutynin chloride oral tablet 1
phenazopyridine hcl oral tablet 100 mg,
200 mg
1
RENVELA ORAL TABLET 3
tolterodine tartrate er 4
TOVIAZ 4
VELPHORO 3
VESICARE 4
VIAGRA E
GENITOURINARY AGENTS - DRUGS FOR PROSTATECONDITIONS
alfuzosin hcl er 1
finasteride oral tablet 5 mg 1
RAPAFLO 2
tamsulosin hcl 1
terazosin hcl oral 1
HORMONAL AGENTS - ADRENAL
betamethasone valerate external cream 1
clobetasol propionate external cream 1
clobetasol propionate external ointment 1
clobetasol propionate external solution 1
CLOBEX SPRAY E
dexamethasone oral tablet 1
fluocinonide external cream 1
hydrocortisone external cream 2.5 % 1
hydrocortisone external ointment 2.5 % 1
hydrocortisone oral 1
methylprednisolone oral 1
mometasone furoate external cream 1
prednisolone oral solution 1
prednisolone oral syrup 15 mg/5ml 1
prednisolone sodium phosphate oral
solution 10 mg/5ml, 15 mg/5ml, 20
mg/5ml, 25 mg/5ml, 6.7 (5 base)
mg/5ml
1
prednisone oral tablet 1
prednisone oral tablet therapy pack 1
triamcinolone acetonide external cream 1
triamcinolone acetonide external
ointment
1
HORMONAL AGENTS - MEN'S HEALTH
ANDRODERM TRANSDERMAL
PATCH 24 HOUR
E

MTMP Guide 2018-2019 47
DRUG NAME DRUG
TIER NOTES
ANDROGEL PUMP TRANSDERMAL
GEL 20.25 MG/ACT (1.62%)
E
ANDROGEL TRANSDERMAL GEL
20.25 MG/1.25GM (1.62%), 40.5
MG/2.5GM (1.62%)
E
testosterone cypionate intramuscular
solution 100 mg/ml, 200 mg/ml
1
HORMONAL AGENTS - OSTEOPOROSIS
OSPHENA 3
raloxifene hcl 1
HORMONAL AGENTS - PITUITARY
CETROTIDE SUBCUTANEOUS KIT
0.25 MG
i-P SP
GONAL-F i-P SP
GONAL-F RFF i-P SP
GONAL-F RFF REDIJECT i-P SP
HP ACTHAR E SP
LUPRON DEPOT (1-MONTH)
INTRAMUSCULAR KIT 7.5 MG
i-P SP
LUPRON DEPOT (3-MONTH)
INTRAMUSCULAR KIT 22.5 MG
i-P SP
LUPRON DEPOT (4-MONTH)
INTRAMUSCULAR KIT 30MG
i-P SP
LUPRON DEPOT (6-MONTH)
INTRAMUSCULAR KIT 45MG
i-P SP
NORDITROPIN FLEXPRO i-P SP
NUTROPIN AQ NUSPIN 10 i-P SP
NUTROPIN AQ NUSPIN 20 i-P SP
NUTROPIN AQ NUSPIN 5 i-P SP
OMNITROPE i-P SP
OVIDREL i-P SP
HORMONAL AGENTS - SEX HORMONES AND BIRTH CONTROL
apri 1
aviane 1
blisovi 24 fe 1
blisovi fe 1.5/30 1
blisovi fe 1/20 1
CLIMARA PRO 2
cryselle-28 1
DIVIGEL 3
drospirenone-ethinyl estradiol 1
DUAVEE 2
ELESTRIN 3
ENDOMETRIN E
enskyce 1
ESTRACE VAGINAL 3
estradiol oral 1
estradiol transdermal 1
jolivette 1
junel 1/20 1
junel fe 1.5/30 1
junel fe 1/20 1
DRUG NAME DRUG
TIER NOTES
levonorgestrel-ethinyl estrad oral tablet
0.1-20 mg-mcg, 0.15-30 mg-mcg
1
LO LOESTRIN FE 3
loryna 1
low-ogestrel 1
MAKENA INTRAMUSCULAR i-P SP
medroxyprogesterone acetate
intramuscular
1
medroxyprogesterone acetate oral 1
microgestin 1.5/30 1
microgestin 1/20 1
microgestin fe 1.5/30 1
microgestin fe 1/20 1
MINIVELLE 3
mono-linyah 1
mononessa 1
NATAZIA 2
nikki 1
norethindrone acet-ethinyl est oral tablet 1
norethindrone oral 1
norgestimate-ethinyl estradiol triphasic 1
nortrel 1/35 (21) 1
nortrel 1/35 (28) 1
NUVARING 2
ocella 1
portia-28 1
PREMARIN ORAL 2
PREMARIN VAGINAL 2
PREMPHASE 2
PREMPRO 2
progesterone micronized oral 1
SAFYRAL 3
sprintec 28 1
tri-estarylla 1
tri-linyah 1
tri-lo-marzia 1
tri-lo-sprintec 1
trinessa (28) 1
trinessa lo 1
tri-sprintec 1
vienva 1
viorele 1
xulane 1
yuvafem 1
HORMONAL AGENTS - THYROID
ARMOUR THYROID 3
levo-t 1
levothyroxine sodium oral 1
levoxyl 1
liothyronine sodium oral 1
methimazole oral 1
NATURE-THROID ORAL TABLET
113.75 MG, 130 MG, 146.25 MG, 16.25
MG, 195 MG, 260 MG, 32.5 MG, 325
3

MTMP Guide 2018-2019 48
DRUG NAME DRUG
TIER NOTES
MG, 48.75 MG, 65 MG, 81.25 MG, 97.5
MG
SYNTHROID 3
TIROSINT 3
IMMUNOLOGICAL AGENTS - DRUGS FOR IMMUNE SYSTEM
STIMULATION OR SUPPRESSION
azathioprine oral 1
CIMZIA PREFILLED KIT i-P SP
CIMZIA STARTER KIT i-P SP
CIMZIA VIAL KIT i-P SP
cyclosporine modified oral capsule 1 SP
ENBREL SUBCUTANEOUS
SOLUTION PREFILLED SYRINGE
i-NP SP
ENBREL SURECLICK
SUBCUTANEOUS SOLUTION
AUTO-INJECTOR
i-NP SP
HAEGARDA i-P SP
HUMIRA PEDIATRIC CROHNS
START SUBCUTANEOUS
PREFILLED SYRINGE KIT 40
MG/0.8ML
i-P SP
HUMIRA PEN SUBCUTANEOUS
PEN-INJECTOR KIT
i-P SP
HUMIRA PEN-CROHNS STARTER
SUBCUTANEOUS PEN-INJECTOR
KIT
i-P SP
HUMIRA PEN-PSORIASIS STARTER
SUBCUTANEOUS PEN-INJECTOR
KIT
i-P SP
HUMIRA SUBCUTANEOUS
PREFILLED SYRINGE KIT
i-P SP
methotrexate oral 1
methotrexate sodium oral 1
mycophenolate mofetil oral capsule 1 SP
mycophenolate mofetil oral tablet 1 SP
mycophenolate sodium 1 SP
ORENCIA SUBCUTANEOUS
SOLUTION PREFILLED SYRINGE
i-NP SP
OTEZLA ORAL TABLET 2 SP
OTEZLA ORAL TABLET THERAPY
PACK
2 SP
PROGRAF ORAL 3 SP
RASUVO SUBCUTANEOUS
SOLUTION AUTO-INJECTOR 10
MG/0.2ML, 12.5 MG/0.25ML, 15
MG/0.3ML, 17.5 MG/0.35ML, 20
MG/0.4ML, 22.5 MG/0.45ML, 25
MG/0.5ML, 30 MG/0.6ML, 7.5
MG/0.15ML
2
REMICADE i-P SP
SIMPONI ARIA i-P SP
SIMPONI SUBCUTANEOUS
SOLUTION AUTO-INJECTOR
i-P SP
SIMPONI SUBCUTANEOUS
SOLUTION PREFILLED SYRINGE
i-P SP
DRUG NAME DRUG
TIER NOTES
STELARA INTRAVENOUS i-P SP
tacrolimus oral 1 SP
TREMFYA i-P SP
XELJANZ XR 3 SP
IMMUNOLOGICAL AGENTS - DRUGS FOR VACCINATION
AFLURIA PRESERVATIVE FREE
INTRAMUSCULAR SUSPENSION
PREFILLED SYRINGE
3
BOOSTRIX INTRAMUSCULAR
SUSPENSION 5-2.5-18.5
3
FLUARIX QUADRIVALENT
INTRAMUSCULAR SUSPENSION
PREFILLED SYRINGE
3
FLUCELVAX QUADRIVALENT
INTRAMUSCULAR SUSPENSION
PREFILLED SYRINGE
3
FLUVIRIN INTRAMUSCULAR
SUSPENSION
3
FLUVIRIN INTRAMUSCULAR
SUSPENSION PREFILLED SYRINGE
3
FLUZONE HIGH-DOSE
INTRAMUSCULAR SUSPENSION
PREFILLED SYRINGE
3
FLUZONE QUADRIVALENT
INTRAMUSCULAR SUSPENSION
3
FLUZONE QUADRIVALENT
INTRAMUSCULAR SUSPENSION
PREFILLED SYRINGE
3
ZOSTAVAX SUBCUTANEOUS
SUSPENSION RECONSTITUTED
E
INFLAMMATORY BOWEL DISEASE AGENTS
APRISO 2
CANASA 2
DELZICOL 3
DIPENTUM 3
mesalamine oral tablet delayed release
1.2 gm
1
MESALAMINE ORAL TABLET
DELAYED RELEASE 800 MG
3
PENTASA 3
PROCTOFOAM HC 2
sulfasalazine oral tablet 1
UCERIS RECTAL 3
METABOLIC BONE DISEASE AGENTS - DRUGS FOR
OSTEOPOROSIS
alendronate sodium oral tablet 1
BINOSTO 4
calcitriol oral capsule 1
FORTEO SUBCUTANEOUS
SOLUTION 600 MCG/2.4ML
i-P SP
ibandronate sodium oral 4
TYMLOS i-P SP
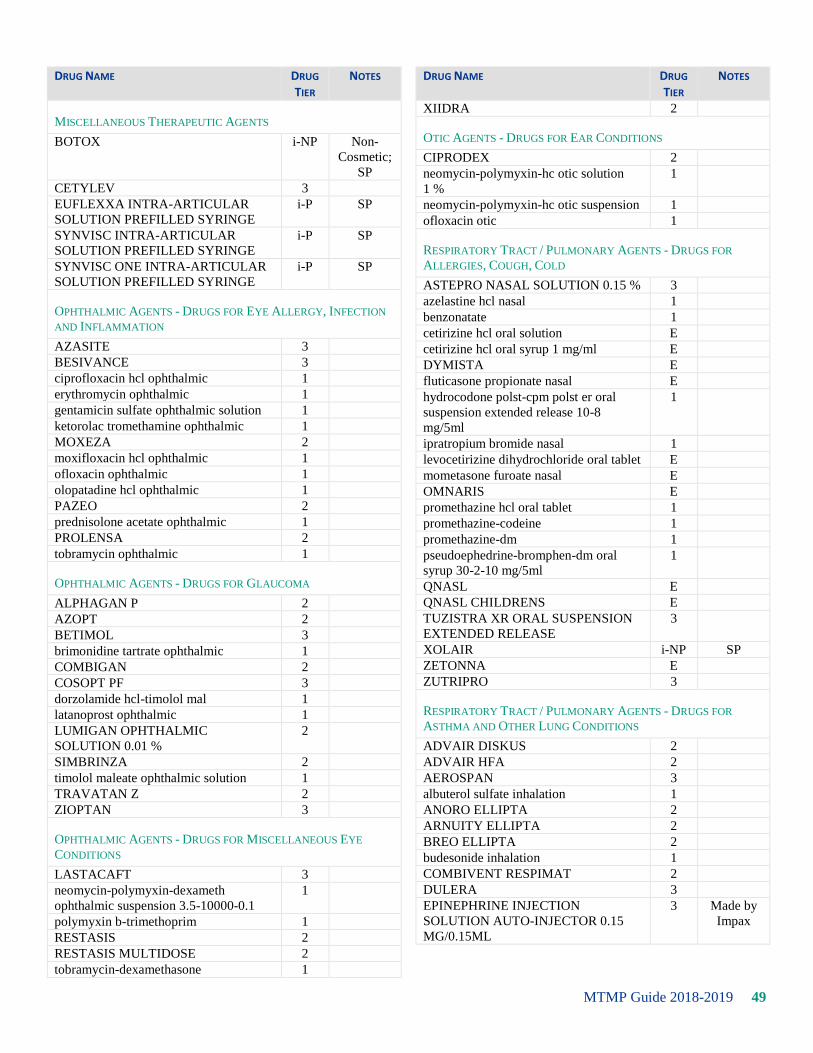
MTMP Guide 2018-2019 49
DRUG NAME DRUG
TIER NOTES
MISCELLANEOUS THERAPEUTIC AGENTS
BOTOX i-NP Non-
Cosmetic;
SP
CETYLEV 3
EUFLEXXA INTRA-ARTICULAR
SOLUTION PREFILLED SYRINGE
i-P SP
SYNVISC INTRA-ARTICULAR
SOLUTION PREFILLED SYRINGE
i-P SP
SYNVISC ONE INTRA-ARTICULAR
SOLUTION PREFILLED SYRINGE
i-P SP
OPHTHALMIC AGENTS - DRUGS FOR EYE ALLERGY, INFECTION
AND INFLAMMATION
AZASITE 3
BESIVANCE 3
ciprofloxacin hcl ophthalmic 1
erythromycin ophthalmic 1
gentamicin sulfate ophthalmic solution 1
ketorolac tromethamine ophthalmic 1
MOXEZA 2
moxifloxacin hcl ophthalmic 1
ofloxacin ophthalmic 1
olopatadine hcl ophthalmic 1
PAZEO 2
prednisolone acetate ophthalmic 1
PROLENSA 2
tobramycin ophthalmic 1
OPHTHALMIC AGENTS - DRUGS FOR GLAUCOMA
ALPHAGAN P 2
AZOPT 2
BETIMOL 3
brimonidine tartrate ophthalmic 1
COMBIGAN 2
COSOPT PF 3
dorzolamide hcl-timolol mal 1
latanoprost ophthalmic 1
LUMIGAN OPHTHALMIC
SOLUTION 0.01 %
2
SIMBRINZA 2
timolol maleate ophthalmic solution 1
TRAVATAN Z 2
ZIOPTAN 3
OPHTHALMIC AGENTS - DRUGS FOR MISCELLANEOUS EYE
CONDITIONS
LASTACAFT 3
neomycin-polymyxin-dexameth
ophthalmic suspension 3.5-10000-0.1
1
polymyxin b-trimethoprim 1
RESTASIS 2
RESTASIS MULTIDOSE 2
tobramycin-dexamethasone 1
DRUG NAME DRUG
TIER NOTES
XIIDRA 2
OTIC AGENTS - DRUGS FOR EAR CONDITIONS
CIPRODEX 2
neomycin-polymyxin-hc otic solution
1 %
1
neomycin-polymyxin-hc otic suspension 1
ofloxacin otic 1
RESPIRATORY TRACT / PULMONARY AGENTS - DRUGS FOR
ALLERGIES, COUGH, COLD
ASTEPRO NASAL SOLUTION 0.15 % 3
azelastine hcl nasal 1
benzonatate 1
cetirizine hcl oral solution E
cetirizine hcl oral syrup 1 mg/ml E
DYMISTA E
fluticasone propionate nasal E
hydrocodone polst-cpm polst er oral
suspension extended release 10-8
mg/5ml
1
ipratropium bromide nasal 1
levocetirizine dihydrochloride oral tablet E
mometasone furoate nasal E
OMNARIS E
promethazine hcl oral tablet 1
promethazine-codeine 1
promethazine-dm 1
pseudoephedrine-bromphen-dm oral
syrup 30-2-10 mg/5ml
1
QNASL E
QNASL CHILDRENS E
TUZISTRA XR ORAL SUSPENSION
EXTENDED RELEASE
3
XOLAIR i-NP SP
ZETONNA E
ZUTRIPRO 3
RESPIRATORY TRACT / PULMONARY AGENTS - DRUGS FOR
ASTHMA AND OTHER LUNG CONDITIONS
ADVAIR DISKUS 2
ADVAIR HFA 2
AEROSPAN 3
albuterol sulfate inhalation 1
ANORO ELLIPTA 2
ARNUITY ELLIPTA 2
BREO ELLIPTA 2
budesonide inhalation 1
COMBIVENT RESPIMAT 2
DULERA 3
EPINEPHRINE INJECTION
SOLUTION AUTO-INJECTOR 0.15
MG/0.15ML
3 Made by
Impax

MTMP Guide 2018-2019 50
DRUG NAME DRUG
TIER NOTES
EPINEPHRINE INJECTION
SOLUTION AUTO-INJECTOR 0.15
MG/0.3ML
2 Made by
Mylan
EPINEPHRINE SOLUTION AUTO-
INJECTOR 0.3 MG/0.3ML INJECTION
2 Made by
Mylan
EPINEPHRINE SOLUTION AUTO-
INJECTOR 0.3 MG/0.3ML INJECTION
3 Made by
Impax
FLOVENT DISKUS 2
FLOVENT HFA 2
INCRUSE ELLIPTA 2
ipratropium bromide inhalation 1
ipratropium-albuterol 1
montelukast sodium oral tablet 1
montelukast sodium oral tablet chewable 1
PERFOROMIST 3
PROAIR HFA 2
PROAIR RESPICLICK 2
PROVENTIL HFA 3
PULMICORT FLEXHALER 2
QVAR INHALATION AEROSOL
SOLUTION
2
SEREVENT DISKUS 2
SPIRIVA HANDIHALER 2
SPIRIVA RESPIMAT 2
STIOLTO RESPIMAT 2
SYMBICORT 2
VENTOLIN HFA 2
DRUG NAME DRUG
TIER NOTES
RESPIRATORY TRACT / PULMONARY AGENTS - DRUGS FOR
PULMONARY HYPERTENSION
ADCIRCA 3 SP
ADEMPAS 2 SP
LETAIRIS 2 SP
OPSUMIT 2 SP
ORENITRAM 3 SP
sildenafil citrate oral tablet 20 mg 1 SP
TRACLEER 2 SP
SKELETAL MUSCLE RELAXANTS - DRUGS FOR MUSCLE
TENSION AND SPASM
baclofen oral 1
carisoprodol oral 1
cyclobenzaprine hcl oral 1
LORZONE 4
metaxalone 1
methocarbamol oral 1
orphenadrine citrate er 1
tizanidine hcl oral tablet 1
SLEEP DISORDER AGENTS
eszopiclone 1
modafinil 1
SILENOR 4
temazepam 1
zolpidem tartrate er 4
zolpidem tartrate oral 1

MTMP Guide 2018-2019 51
Political Subdivision Select Premium Formulary
The most up to date formulary may be located at https://tmlhealthbenefits.org/.
The most effective way to control costs is through the use of generic drugs and a drug formulary.
Drug Tier Includes
Tier 1:
Preferred Network Tier
Lower-cost generics and some brand-name. Use Tier 1 drugs for the lowest out-of-pocket
costs.
Tier 2:
Value Tiered
Mid-range cost preferred brand-name. Use Tier 2 drugs, instead of Tier 3, to help reduce
your out-of-pocket costs.
Tier 3 Highest-cost non-preferred. Many Tier 3 drugs have lower cost options in Tier 1 or 2. Ask
your doctor if they could work for you.
Tier E
Excluded
May be excluded from coverage or subject to prior authorization. Lower-cost options are
available and covered.
* Drugs may transition from tier to tier within benefit plan year impacting your out of pocket expense.
Some medications are noted with letters next to them to help you see which ones may have coverage requirements
or limits. Your benefit plan determines how these medications may be covered for you.
Some of the medications on this list may NOT be covered by your plan or have additional restrictions. Their
presence on this list does NOT guarantee coverage.
M = Authorized generic or co-branded product SP = Specialty Medication – Medication is designated as specialty.
3P = Tier 3 preferred
DRUG NAME DRUG TIER
NOTES
ANALGESICS - DRUGS FOR PAIN
ABSTRAL E
acetaminophen-codeine #2 1
acetaminophen-codeine #3 1
acetaminophen-codeine #4 1
acetaminophen-codeine oral tablet 1
ARYMO ER E
butalbital-apap-caffeine oral capsule 1
butalbital-apap-caffeine oral tablet 50-
325-40 mg
1 generic Fioricet
excluded
DURAGESIC-100 E
DURAGESIC-12 E
DURAGESIC-25 E
DURAGESIC-50 E
DURAGESIC-75 E
EMBEDA 2
DRUG NAME DRUG TIER
NOTES
fentanyl 1
FENTORA BUCCAL TABLET 100
MCG, 200, MCG, 400 MCG, 600
MCG, 800 MCG
E
hydrocodone- acetaminophen oral tablet
10-300 mg, 10-325 mg, 2.5-325 mg, 5-
300 mg, 5-325 mg, 7.5-300 mg, 7.5-325
mg
1
hydromorphone hcl oral tablet 1
HYSINGLA ER 2
KADIAN ORAL CAPSULE
EXTENDED RELEASE 24 HOUR 10
MG, 100 MG, 20 MG, 200 MG, 30 MG,
40 MG, 50 MG, 60 MG, 80 MG
E
LAZANDA E
methadone hcl oral tablet 1
morphine sulfate er oral tablet extended 1

MTMP Guide 2018-2019 52
DRUG NAME DRUG TIER
NOTES
release
NORCO E
NUCYNTA E
NUCYNTA ER E
OPANA ER ORAL TABLET ER 12
HOUR ABUSE-DETERRENT
E
oxycodone hcl oral tablet 1
oxycodone- acetaminophen oral tablet
10-325 mg, 2.5-325 mg, 5-25 mg, 7.5-
325 mg
1
OXYCONTIN ORAL TABLET ER 12
HOUR ABUSE-DETERRENT 2
PERCOCET ORAL TABLET 10-325
MG, 2.5-325 MG, 5-325 MG, 7.5-325
MG
E
SUBSYS E
tramadol hcl ir 1
tramadol-acetaminophen 1
XTAMPZA ER E
ZOHYDRO ER ORAL CAPSULE ER
12 HOUR ABUSE-DETERRENT
E
ANALGESICS - DRUGS FOR PAIN AND INFLAMMATION
CAMBIA E
CELEBREX E
celecoxib oral E
diclofenac potassium 1
diclofenac sodium oral 1
diclofenac sodium transdermal gel 1 % E
DUEXIS E
etodolac oral tablet 1
FLECTOR E
ibuprofen oral tablet 400 mg, 600 mg,
800 mg
1
indomethacin oral 1
ketorolac tromethamine oral 1
meloxicam oral tablet 1
nabumetone oral 1
naproxen oral tablet 1
naproxen sodium oral tablet 275 mg,
550 mg
1
PENNSAID TRANSDERMAL
SOLUTION 2 %
E
sulindac oral 1
VIMOVO E
VOLTAREN GEL 1% E
ZORVOLEX E
ANESTHETICS
lidocaine external ointment E
lidocaine external patch 5 % 1
LIDODERM E
DRUG NAME DRUG TIER
NOTES
ANTI-ADDICTION / SUBSTANCE ABUSE TREATMENT AGENTS
BUNAVAIL 3
buprenorphine hcl sublingual 1
buprenorphine hcl- naloxone hcl 1
CHANTIX STARTING MONTH PAK 3
naltrexone hcl oral 1
NARCAN 2
SUBOXONE SUBLINGUAL FILM 2
ZUBSOLV 2
ANTIBACTERIALS
ACTICLATE E
amoxicillin oral capsule 1
amoxicillin oral suspension
reconstituted
1
amoxicillin oral tablet 1
amoxicillin-potassium clavulanate oral
suspension reconstituted 200-28.5
mg/5ml, 250-62.5 mg/5ml, 400-57
mg/5ml, 600-42.9 mg/5ml
1
amoxicillin-potassium clavulanate
oral tablet 250-125 mg, 500-125
mg, 875-125 mg
1
azithromycin oral suspension
reconstituted
1
azithromycin oral tablet 250 mg, 500
mg, 600 mg
1
BETHKIS 2 SP
cefdinir 1
cefuroxime axetil oral tablet 1
cephalexin oral capsule 1
cephalexin oral suspension
reconstituted
1
ciprofloxacin hcl oral 1
clarithromycin oral tablet 1
clindamycin hcl oral 1
clindamycin phosphate external gel 1
clindamycin phosphate external lotion 1
clindamycin phosphate external
solution
1
CLINDESSE 3
DORYX MPC E
doxycycline hyclate oral capsule E
doxycycline hyclate oral tablet 100 mg,
150 mg, 20 mg, 75 mg
E
doxycycline monohydrate oral capsule 1 50 and
100mg only
doxycycline monohydrate oral tablet 1 50, 75, and
100 only
KITABIS PAK E SP
levofloxacin oral tablet 1
metronidazole oral tablet 1
metronidazole vaginal 1

MTMP Guide 2018-2019 53
DRUG NAME DRUG TIER
NOTES
minocycline hcl oral capsule 1
mupirocin external 1
nitrofurantoin macrocrystal oral 1
nitrofurantoin
monohydrate
macrocrystals
1
penicillin v potassium oral tablet 1
SOLODYN ORAL TABLET
EXTENDED RELEASE 24 HOUR
105 MG, 115 MG, 55 MG, 65 MG, 80
MG
E
sulfamethoxazole- trimethoprim oral
suspension 200-40 mg/5ml
1
sulfamethoxazole- trimethoprim oral
tablet
1
TOBI NEBULIZER E SP
TOBI PODHALER E SP
tobramycin nebulization solution 300
mg/5ml inhalation
1 SP
TOBRAMYCIN NEBULIZATION
SOLUTION 300 MG/5ML
INHALATION
E M; SP
ANTICOAGULANTS
ELIQUIS 2
enoxaparin sodium 1 SP
PRADAXA 2
SAVAYSA 3
warfarin sodium oral 1
XARELTO 2
XARELTO STARTER PACK 2
ANTICONVULSANTS - DRUGS FOR SEIZURES
carbamazepine oral tablet 1
DILANTIN INFATABS E
DILANTIN ORAL CAPSULE 100 MG E
DILANTIN ORAL SUSPENSION E
divalproex sodium er oral tablet
extended release 24 hour
1
divalproex sodium oral tablet delayed
release
1
gabapentin oral capsule 1
gabapentin oral tablet 1
lamotrigine oral tablet 1
levetiracetam oral tablet 1
oxcarbazepine oral tablet 1
phenytoin sodium extended 1
topiramate oral tablet 1
TROKENDI XR E
VIMPAT 3
zonisamide oral 1
DRUG NAME DRUG TIER
NOTES
ANTIDEMENTIA AGENTS - DRUGS FOR ALZHEIMER'S DISEASE AND
DEMENTIA
donepezil hcl oral tablet 1
memantine hcl oral tablet 10 mg, 5 mg 1
NAMZARIC ORAL CAPSULE
EXTENDED RELEASE 24 HOUR
14-10 MG, 28-10 MG
2
ANTIDEPRESSANTS
amitriptyline hcl oral 1
bupropion hcl er (sr) 1
bupropion hcl er (xl) 1
bupropion hcl oral 1
citalopram hydrobromide oral tablet 1
CYMBALTA E
desvenlafaxine succinate er E
doxepin hcl oral capsule 1
duloxetine hcl oral capsule delayed
release particles 20 mg, 30 mg, 60 mg
E
DULOXETINE HCL ORAL
CAPSULE DELAYED RELEASE
PARTICLES 40 MG
E
EFFEXOR XR E
escitalopram oxalate oral tablet 1
fluoxetine hcl oral capsule 1
fluoxetine hcl oral tablet 1
FORFIVO XL 2
LEXAPRO ORAL TABLET E
mirtazapine oral tablet 1
nortriptyline hcl oral capsule 1
paroxetine hcl er 1
paroxetine hcl oral tablet 1
PRISTIQ E
PROZAC ORAL CAPSULE E
sertraline hcl oral tablet 1
trazodone hcl oral 1
TRINTELLIX 3
venlafaxine hcl 1
venlafaxine hcl er 1 capsules only
VIIBRYD ORAL TABLET E
VIIBRYD STARTER PACK E
WELLBUTRIN SR E
WELLBUTRIN XL E
ZOLOFT E
ANTIEMETICS - DRUGS FOR NAUSEA AND VOMITING
meclizine hcl oral tablet 25 mg 1
metoclopramide hcl oral tablet 1
ondansetron hcl oral tablet 1
ondansetron odt 1
prochlorperazine maleate oral 1
VARUBI ORAL E

MTMP Guide 2018-2019 54
DRUG NAME DRUG TIER
NOTES
ANTIFUNGALS
fluconazole oral tablet 1
GYNAZOLE-1 3
JUBLIA E
KERYDIN E
ketoconazole external cream 1
ketoconazole external shampoo 1
nystatin external cream 1
nystatin mouth/throat 1
terbinafine hcl oral 1
terconazole vaginal cream 1
ANTIGOUT AGENTS
allopurinol oral 1
COLCHICINE ORAL TABLET 3
COLCRYS 2
ULORIC 2
ZURAMPIC E
ANTIMIGRAINE AGENTS
MIGRANAL 3
ONZETRA XSAIL E
rizatriptan benzoate 1
sumatriptan succinate oral 1
SUMAVEL DOSEPRO
SUBCUTANEOUS SOLUTION JET-
INJECTOR
E
ZOMIG ORAL E
ZOMIG ZMT E
ANTINEOPLASTICS - DRUGS FOR CANCER
anastrozole oral 1
CABOMETYX 2 SP
capecitabine 1 SP
IBRANCE 3 SP
letrozole oral 1
mercaptopurine oral 1 SP
REVLIMID 3 SP
SPRYCEL 2 SP
tamoxifen citrate oral 1
XTANDI 3 SP
ZYTIGA 3 SP
ANTIPARASITICS
EMVERM 2
hydroxychloroquine sulfate oral 1
permethrin external cream 1
SOOLANTRA 2
ANTIPARKINSON AGENTS
benztropine mesylate oral 1
carbidopa-levodopa oral tablet 1
pramipexole dihydrochloride 1
DRUG NAME DRUG TIER
NOTES
ropinirole hcl 1
ZELAPAR 3
ANTIPLATELETS
BRILINTA 2
cilostazol 1
clopidogrel bisulfate oral 1
ANTIPSYCHOTICS - DRUGS FOR MOOD DISORDERS
aripiprazole oral tablet 1
ARISTADA INTRAMUSCULAR
PREFILLED SYRINGE 441
MG/1.6ML, 662 MG/2.4ML, 882
MG/3.2ML
3
haloperidol oral 1
INVEGA SUSTENNA 3
INVEGA TRINZA 3
LATUDA 3
olanzapine oral tablet 1
quetiapine fumarate 1
REXULTI E
risperidone oral tablet E
SAPHRIS 2
ziprasidone hcl 1
ANTIVIRALS
abacavir sulfate- lamivudine 1 SP
acyclovir oral capsule 1
acyclovir oral tablet 1
ATRIPLA E SP
COMPLERA 2 SP
DESCOVY 3 SP
entecavir 1 SP
EPCLUSA 2 SP
GENVOYA 3 SP
HARVONI 2 SP
INTELENCE 2 SP
ISENTRESS ORAL TABLET 2 SP
MAVYRET 2 SP
NORVIR ORAL TABLET 2 SP
ODEFSEY 3 SP
oseltamivir phosphate oral capsule 1
PREZCOBIX 2 SP
PREZISTA ORAL TABLET 150
MG, 600 MG, 75 MG, 800 MG
2 SP
REYATAZ ORAL CAPSULE 150
MG, 200 MG, 300 MG
3 SP
STRIBILD 3 SP
TAMIFLU ORAL CAPSULE E
TAMIFLU ORAL SUSPENSION
RECONSTITUTED 6 MG/ML
2
TIVICAY 2 SP
TRIUMEQ 2 SP
TRUVADA 2 SP
valacyclovir hcl oral 1

MTMP Guide 2018-2019 55
DRUG NAME DRUG TIER
NOTES
VIREAD ORAL TABLET 150 MG,
200 MG, 250 MG
2 SP
VIREAD ORAL TABLET 300 MG 3 SP
VOSEVI 2 SP
ZOVIRAX EXTERNAL CREAM 2
ZOVIRAX EXTERNAL OINTMENT E
ZOVIRAX ORAL E
ANXIOLYTICS - DRUGS FOR ANXIETY
alprazolam oral tablet 1
buspirone hcl oral 1
clonazepam oral tablet 1
diazepam oral tablet 1
hydroxyzine hcl oral tablet 1
hydroxyzine pamoate oral 1
lorazepam oral tablet 1
triazolam 1
VALIUM E
XANAX E
XANAX XR E
BIPOLAR AGENTS - DRUGS FOR MOOD DISORDERS
lithium carbonate er 1
lithium carbonate oral capsule 1
BLOOD PRODUCTS / MODIFIERS / VOLUME EXPANDERS - DRUGS
FOR BLEEDING DISORDERS
AFSTYLA 3 SP
ARANESP (ALBUMIN FREE)
INJECTION SOLUTION 100
MCG/ML, 200 MCG/ML, 25
MCG/ML, 300 MCG/ML, 40
MCG/ML, 60 MCG/ML
E SP
ARANESP (ALBUMIN FREE)
INJECTION SOLUTION PREFILLED
SYRINGE
E SP
EPOGEN INJECTION SOLUTION
10000 UNIT/ML, 2000 UNIT/ML,
20000 UNIT/ML, 3000 UNIT/ML,
4000 UNIT/ML
E SP
GRANIX 2 SP
NEUPOGEN INJECTION SOLUTION
300 MCG/ML, 480 MCG/1.6ML
2 SP
NEUPOGEN INJECTION SOLUTION
PREFILLED SYRINGE
2 SP
NUWIQ 3 SP
PROCRIT 2 SP
ZARXIO 2 SP
CARDIOVASCULAR AGENTS - DRUGS FOR HEART AND
CIRCULATION CONDITIONS
amiodarone hcl oral 1
amlodipine besylate oral 1
amlodipine besylate- benazepril hcl 1
amlodipine besylate- valsartan 1
DRUG NAME DRUG TIER
NOTES
atenolol oral 1
atenolol-chlorthalidone 1
atorvastatin calcium oral 1
AZOR E
benazepril hcl oral 1
benazepril- hydrochlorothiazide 1
BENICAR E
BENICAR HCT E
bisoprolol fumarate 1
bisoprolol- hydrochlorothiazide 1
bumetanide oral 1
BYSTOLIC 2
BYVALSON 2
cartia xt 1
carvedilol 1
chlorthalidone oral tablet 25 mg, 50 mg 1
choline fenofibrate 1
clonidine hcl oral 1
CRESTOR E
digox 1
digoxin oral tablet 1
diltiazem hcl er beads 1
diltiazem hcl er coated beads oral
capsule extended release 24 hour
1
diltiazem hcl oral 1
DIOVAN E
DIOVAN HCT E
doxazosin mesylate 1
EDARBI E
EDARBYCLOR E
enalapril maleate oral 1
ezetimibe 1
ezetimibe-simvastatin 1
fenofibrate micronized oral capsule
134 mg, 200 mg, 67 mg
E
fenofibrate oral tablet E
fenofibric acid oral capsule delayed
release
E
flecainide acetate 1
furosemide oral tablet 1
gemfibrozil oral 1
guanfacine hcl oral 1
hydralazine hcl oral 1
hydrochlorothiazide oral 1
irbesartan 1
irbesartan- hydrochlorothiazide 1
isosorbide mononitrate er 1
labetalol hcl oral 1
LIPITOR E
LIPOFEN E
lisinopril oral 1
lisinopril- hydrochlorothiazide 1
LIVALO E
losartan potassium 1
losartan potassium-hctz 1

MTMP Guide 2018-2019 56
DRUG NAME DRUG TIER
NOTES
lovastatin 1
LOVAZA E
metoprolol succinate er 1
metoprolol tartrate oral 1
MULTAQ 3
nadolol oral tablet 20 mg, 40 mg, 80 mg 1
niacin er (antihyperlipidemic) E
nifedipine er 1
nifedipine er osmotic release 1
nitroglycerin sublingual 1
NITROSTAT E
NORVASC E
olmesartan medoxomil oral E
olmesartan medoxomil- hctz E
omega-3-acid ethyl esters E
pentoxifylline er 1
PRALUENT SUBCUTANEOUS
SOLUTION PEN- INJECTOR
2 SP
pravastatin sodium 1
prazosin hcl oral 1
propranolol hcl er 1
propranolol hcl oral tablet 1
quinapril hcl 1
ramipril 1
RANEXA 2
REPATHA 2 SP
REPATHA PUSHTRONEX SYSTEM 2 SP
REPATHA SURECLICK 2 SP
rosuvastatin calcium 1
simvastatin oral 1
sotalol hcl oral 1
spironolactone oral 1
TEKTURNA 2
TEKTURNA HCT 2
telmisartan E
TOPROL XL E
torsemide oral 1
triamterene-hctz oral capsule 37.5-25
mg
1
triamterene-hctz oral tablet 1
TRIBENZOR E
valsartan 1
valsartan- hydrochlorothiazide 1
VASCEPA 2
verapamil hcl er oral tablet extended
release 120 mg, 180 mg, 240 mg
1
verapamil hcl oral 1
VYTORIN E
WELCHOL 2
ZETIA E
CENTRAL NERVOUS SYSTEM AGENTS - DRUGS FOR ATTENTION
DEFICIT DISORDER
ADDERALL XR E
amphetamine- dextroamphetamine 1
DRUG NAME DRUG TIER
NOTES
amphetamine- dextroamphetamine er E
atomoxetine hcl 1
CONCERTA E
dexmethylphenidate hcl 1
dexmethylphenidate hcl er E
guanfacine hcl er E
methylphenidate hcl er oral tablet
extended release 10 mg, 18 mg, 20 mg,
27 mg, 36 mg, 54 mg
E
methylphenidate hcl er oral tablet
extended release 24 hour
E
methylphenidate hcl oral tablet 1
VYVANSE 2
CENTRAL NERVOUS SYSTEM AGENTS - DRUGS FOR MULTIPLE
SCLEROSIS
AMPYRA 2 SP
AUBAGIO 3 SP
AVONEX PEN
INTRAMUSCULAR AUTO-
INJECTOR KIT
2 SP
AVONEX PREFILLED
INTRAMUSCULAR PREFILLED
SYRINGE KIT
2 SP
AVONEX VIAL INTRAMUSCULAR
KIT
2 SP
BETASERON SUBCUTANEOUS KIT 2 SP
COPAXONE SUBCUTANEOUS
SOLUTION PREFILLED SYRINGE
2 SP
EXTAVIA SUBCUTANEOUS KIT E SP
GILENYA 3 3P; SP
PLEGRIDY E SP
PLEGRIDY STARTER PACK E SP
REBIF REBIDOSE SUBCUTANEOUS
SOLUTION AUTO- INJECTOR
3 SP
REBIF REBIDOSE TITRATION
PACK SUBCUTANEOUS SOLUTION
AUTO- INJECTOR
3 SP
REBIF SUBCUTANEOUS
SOLUTION PREFILLED SYRINGE
3 SP
REBIF TITRATION PACK
SUBCUTANEOUS SOLUTION
PREFILLED SYRINGE
3 SP
TECFIDERA 2 SP
CENTRAL NERVOUS SYSTEM AGENTS - MISCELLANEOUS
CONTRAVE E
GRALISE E
GRALISE STARTER E
LYRICA ORAL CAPSULE 2
phentermine hcl oral tablet E

MTMP Guide 2018-2019 57
DRUG NAME DRUG TIER
NOTES
DENTAL AND ORAL AGENTS - DRUGS FOR MOUTH AND THROAT
CONDITIONS
chlorhexidine gluconate mouth/throat 1
lidocaine viscous 1
DERMATOLOGICAL AGENTS - DRUGS FOR SKIN CONDITIONS
ABSORICA E
ACANYA E
ACZONE 2
adapalene external gel 1
AKTIPAK E
ATRALIN 3
BENZACLIN E
BENZACLIN WITH PUMP E
BENZAMYCIN E
claravis 1
clindamycin phosphate- benzoyl
peroxide external gel 1-5 %
1
clotrimazole- betamethasone external
cream
1
COSENTYX 150 MG/ML 3 3P; SP
COSENTYX 300 DOSE 3 3P; SP
COSENTYX SENSOREADY 300
DOSE
3 3P; SP
COSENTYX SENSOREADY PEN
SUBCUTANEOUS SOLUTION
AUTO- INJECTOR 150 MG/ML
3 3P; SP
DIFFERIN EXTERNAL GEL 0.3 % 3
DIFFERIN EXTERNAL LOTION 3
DUAC E
DUPIXENT 2 SP
ELIDEL 2
ENSTILAR E
EPIDUO 3
EPIDUO FORTE 3
EUCRISA 2
FLUOROPLEX 3
METROGEL EXTERNAL GEL 3
metronidazole external gel 1
MIRVASO E
ONEXTON 3
ORACEA E
OXSORALEN ULTRA 2
RETIN-A MICRO GEL 0.04 %,
0.1 %
E
RETIN-A MICRO PUMP
EXTERNAL GEL 0.04 %, 0.1 %
E
RETIN-A MICRO PUMP
EXTERNAL GEL 0.06 %, 0.08 %
2
STELARA SUBCUTANEOUS
SOLUTION PREFILLED SYRINGE
2 SP
TACLONEX EXTERNAL
OINTMENT
E
TACLONEX EXTERNAL 3
DRUG NAME DRUG TIER
NOTES
SUSPENSION
TALTZ E SP
TAZORAC 3
tretinoin external cream 1
VECTICAL 3
VELTIN E
ZIANA E
ZYCLARA 3
ZYCLARA PUMP 3
DIABETES - ANTIDIABETIC AGENTS
ADLYXIN E
ADLYXIN STARTER PACK E
ALOGLIPTIN BENZOATE E M
ALOGLIPTIN- METFORMIN HCL E M
ALOGLIPTIN- PIOGLITAZONE E M
BYDUREON BCISE
AUTOINJECTOR
2
BYDUREON PEN 2
BYDUREON VIAL 2
BYETTA 10 MCG PEN 2
BYETTA 5 MCG PEN 2
FARXIGA E
glimepiride 1
glipizide er 1
glipizide ir 1
glipizide xl 1
GLUMETZA E
glyburide oral 1
glyburide-metformin 1
INVOKAMET 2
INVOKAMET XR 2
INVOKANA 2
JANUMET 2
JANUMET XR 2
JANUVIA 2
JARDIANCE 2
JENTADUETO 2
JENTADUETO XR 2
KAZANO E
KOMBIGLYZE XR E
metformin hcl er 1
metformin hcl er (mod) E
metformin hcl er (osm) oral tablet
extended release 24 hour 1000 mg, 500
mg
E
metformin hcl ir 1
NESINA E
ONGLYZA E
OSENI E
pioglitazone hcl 1
SOLIQUA 2
SYNJARDY 2
SYNJARDY XR 2
TANZEUM E

MTMP Guide 2018-2019 58
DRUG NAME DRUG TIER
NOTES
TRADJENTA 2
TRULICITY 2
VICTOZA 2
XIGDUO XR E
DIABETES - GLUCOSE MONITORING
ACCU-CHEK AVIVA DEVICE E
ACCU-CHEK AVIVA CONNECT
KIT W/DEVICE
E
ACCU-CHEK AVIVA PLUS E
ACCU-CHEK COMPACT PLUS
CARE KIT
E
ACCU-CHEK COMPACT PLUS
TEST STRIPS
E
ACCU-CHEK FASTCLIX LANCET
KIT
2
ACCU-CHEK FASTCLIX LANCETS 2
ACCU-CHEK GUIDE E
ACCU-CHEK MULTICLIX
LANCET DEVICE KIT
2
ACCU-CHEK MULTICLIX
LANCETS
2
ACCU-CHEK NANO SMARTVIEW
KIT W/DEVICE
E
ACCU-CHEK SMARTVIEW TEST
STRIPS
E
ACCU-CHEK SOFT TOUCH
LANCETS
2
ACCU-CHEK SOFTCLIX LANCET
DEVICE KIT KIT
2
ACCU-CHEK SOFTCLIX LANCETS 2
DEXCOM G4 PLATINUM
PEDIATRIC RECEIVER DEVICE
3
DEXCOM G4 PLATINUM
RECEIVER, SENSOR,
TRANSMITTER DEVICE
3
DEXCOM G5 SENSOR,
TRANSMITTER, MOBILE
RECEIVER
3
ONETOUCH ULTRA 2 KIT
W/DEVICE
2
ONETOUCH ULTRA BLUE TEST
STRIPS
2
ONETOUCH ULTRA MINI KIT
W/DEVICE
2
ONETOUCH VERIO 2
ONETOUCH VERIO FLEX
SYSTEM KIT W/DEVICE
2
ONETOUCH VERIO TEST STRIPS 2
ONETOUCH VERIO IQ SYSTEM
KIT W/DEVICE
2
ONETOUCH VERIO SYNC
SYSTEM KIT W/DEVICE
2
DRUG NAME DRUG TIER
NOTES
DIABETES - INSULINS
APIDRA SOLOSTAR E
APIDRA VIAL E
BASAGLAR KWIKPEN E
FIASP E
FIASP FLEXTOUCH E
HUMALOG U-100 AND U-200
KWIKPEN
2
HUMALOG MIX 50/50 KWIKPEN 2
HUMALOG MIX 50/50 VIAL 2
HUMALOG MIX 75/25 KWIKPEN 2
HUMALOG MIX 75/25 VIAL 2
HUMALOG U-100 JUNIOR
KWIKPEN
2
HUMALOG U-100 VIAL AND
CARTRIDGE
2
HUMULIN 70/30 KWIKPEN 2
HUMULIN 70/30 VIAL 2
HUMULIN N KWIKPEN 2
HUMULIN N VIAL 2
HUMULIN R U-500 KWIKPEN 2
HUMULIN R U-500 VIAL
(CONCENTRATED)
2
HUMULIN R VIAL 2
LANTUS U-100 SOLOSTAR 2
LANTUS U-100 VIAL 2
LEVEMIR U-100 FLEXTOUCH E
LEVEMIR U-100 VIAL E
NOVOFINE AUTOCOVER PEN
NEEDLE
2
NOVOFINE PEN NEEDLE 2
NOVOFINE PLUS PEN NEEDLE 2
NOVOLIN 70/30 RELION E
NOVOLIN 70/30 VIAL E
NOVOLIN N RELION E
NOVOLIN N VIAL E
NOVOLIN R RELION E
NOVOLIN R VIAL E
NOVOLOG U-100 FLEXPEN E
NOVOLOG MIX 70/30 FLEXPEN E
NOVOLOG MIX 70/30 VIAL E
NOVOLOG U-100 PENFILL E
NOVOLOG U-100 VIAL E
NOVOTWIST PEN NEEDLE 32G X 5
MM
2
TOUJEO SOLOSTAR 2
TRESIBA FLEXTOUCH 2
ELECTROLYTES / MINERALS / METALS / VITAMINS
cyanocobalamin injection 1
folic acid oral tablet 1 mg 1
klor-con m20 1
ludent 1
potassium chloride crys er 1

MTMP Guide 2018-2019 59
DRUG NAME DRUG TIER
NOTES
potassium chloride er 1
potassium citrate er 1
VELTASSA 3
VITAFOL ORAL TABLET E
vitamin d (ergocalciferol) 1
GASTROINTESTINAL AGENTS - DRUGS FOR ACID REFLUX AND
ULCER
ACIPHEX E
CARAFATE ORAL TABLET E
DEXILANT 2
esomeprazole magnesium E
famotidine oral tablet 20 mg, 40 mg 1
lansoprazole oral capsule delayed
release
E
NEXIUM ORAL CAPSULE
DELAYED RELEASE
E
omeprazole oral capsule delayed release E
pantoprazole sodium oral E
PREVACID E
rabeprazole sodium E
ranitidine hcl oral capsule 1
ranitidine hcl oral syrup 1
ranitidine hcl oral tablet 150 mg, 300
mg
1
sucralfate oral tablet 1
ZEGERID E
GASTROINTESTINAL AGENTS - DRUGS FOR BOWEL, INTESTINE
AND STOMACH CONDITIONS
AMITIZA E
dicyclomine hcl oral capsule 1
dicyclomine hcl oral tablet 1
diphenoxylate-atropine oral tablet 1
gavilyte-g 1
LINZESS 2
MOTOFEN E
MOVANTIK 2
MOVIPREP 3
OMECLAMOX-PAK 2
polyethylene glycol 3350 oral powder 1
PREPOPIK 3
PYLERA 2
RELISTOR SUBCUTANEOUS
SOLUTION 12 MG/0.6ML
E
SUPREP BOWEL PREP KIT 3
VIBERZI E
GENETIC OR ENZYME DISORDER: DRUGS FOR REPLACEMENT,
MODIFIERS, TREATMENT
CERDELGA 3 SP
CREON 2
PANCREAZE E
PERTZYE E
VIOKACE E
DRUG NAME DRUG TIER
NOTES
ZENPEP ORAL CAPSULE
DELAYED RELEASE PARTICLES
10000 UNIT, 15000 UNIT, 20000-
63000 UNIT, 25000 UNIT, 3000-
10000 UNIT, 5000 UNIT
2
GENITOURINARY AGENTS - DRUGS FOR BLADDER, GENITAL AND
KIDNEY CONDITIONS
CIALIS 2
DEPEN TITRATABS 2 SP
LEVITRA E
MYRBETRIQ 2
oxybutynin chloride er E
oxybutynin chloride oral tablet 1
phenazopyridine hcl oral tablet 100 mg,
200 mg
1
RENVELA ORAL TABLET 3
STAXYN E
STENDRA E
tolterodine tartrate er E
TOVIAZ E
VELPHORO 3
VESICARE E
VIAGRA E
GENITOURINARY AGENTS - DRUGS FOR PROSTATE CONDITIONS
alfuzosin hcl er 1
finasteride oral tablet 5 mg 1
RAPAFLO 2
tamsulosin hcl 1
terazosin hcl oral 1
HORMONAL AGENTS - ADRENAL
betamethasone valerate external cream 1
clobetasol propionate external cream 1
clobetasol propionate external ointment 1
clobetasol propionate external solution 1
CLOBEX SPRAY E
dexamethasone oral tablet 1
fluocinonide external cream 1
hydrocortisone external cream 2.5 % 1
hydrocortisone external ointment 2.5 % 1
hydrocortisone oral 1
methylprednisolone oral 1
mometasone furoate external cream 1
prednisolone oral solution 1
prednisolone oral syrup 15 mg/5ml 1
prednisolone sodium phosphate oral
solution 10 mg/5ml, 15 mg/5ml, 20
mg/5ml, 25 mg/5ml, 6.7 (5 base)
mg/5ml
1
prednisone oral tablet 1
prednisone oral tablet therapy pack 1
triamcinolone acetonide external cream 1
triamcinolone acetonide external 1

MTMP Guide 2018-2019 60
DRUG NAME DRUG TIER
NOTES
ointment
HORMONAL AGENTS - MEN'S HEALTH
ANDRODERM TRANSDERMAL
PATCH 24 HOUR
2
ANDROGEL PUMP
TRANSDERMAL GEL 20.25
MG/ACT (1.62%)
2
ANDROGEL TRANSDERMAL GEL
20.25 MG/1.25GM (1.62%), 40.5
MG/2.5GM (1.62%)
2
ANDROGEL TRANSDERMAL GEL
25 MG/2.5GM (1%), 50 MG/5GM
(1%)
E
DEPO-TESTOSTERONE
INTRAMUSCULAR SOLUTION
E
FORTESTA E
TESTIM E
testosterone cypionate intramuscular
solution 100 mg/ml, 200 mg/ml
1
TESTOSTERONE TRANSDERMAL
GEL 10 MG/ACT (2%)
E M
VOGELXO PUMP E
VOGELXO TRANSDERMAL GEL 50
MG/5GM (1%)
E
HORMONAL AGENTS - OSTEOPOROSIS
OSPHENA 3
raloxifene hcl 1
HORMONAL AGENTS - PITUITARY
BRAVELLE E SP
CETROTIDE SUBCUTANEOUS KIT
0.25 MG
2 SP
FOLLISTIM AQ SUBCUTANEOUS E SP
GENOTROPIN E SP
GENOTROPIN MINIQUICK E SP
GONAL-F 2 SP
GONAL-F RFF 2 SP
GONAL-F RFF REDIJECT 2 SP
HP ACTHAR 2 SP
HUMATROPE E SP
LUPRON DEPOT (1- MONTH)
INTRAMUSCULAR KIT 7.5 MG
2 SP
LUPRON DEPOT (3- MONTH)
INTRAMUSCULAR KIT 22.5 MG
2 SP
LUPRON DEPOT (4- MONTH)
INTRAMUSCULAR KIT 30MG
2 SP
LUPRON DEPOT (6- MONTH)
INTRAMUSCULAR KIT 45MG
2 SP
NORDITROPIN FLEXPRO 2 SP
NUTROPIN AQ NUSPIN 10 2 SP
NUTROPIN AQ NUSPIN 20 2 SP
NUTROPIN AQ NUSPIN 5 2 SP
OMNITROPE 2 SP
DRUG NAME DRUG TIER
NOTES
OVIDREL 3 SP
SAIZEN E SP
SAIZEN CLICK.EASY E SP
SAIZENPREP E SP
ZOMACTON E SP
HORMONAL AGENTS - SEX HORMONES AND BIRTH CONTROL
apri 1
aviane 1
BEYAZ E
blisovi 24 fe 1
blisovi fe 1.5/30 1
blisovi fe 1/20 1
CLIMARA PRO 2
cryselle-28 1
DIVIGEL 3
drospirenone-ethinyl estradiol 1
DUAVEE 2
ELESTRIN 3
ENDOMETRIN 2
enskyce 1
ESTRACE VAGINAL 3
estradiol oral 1
estradiol transdermal 1
jolivette 1
junel 1/20 1
junel fe 1.5/30 1
junel fe 1/20 1
levonorgestrel-ethinyl estrad oral
tablet 0.1-20 mg-mcg, 0.15-30 mg-
mcg
1
LO LOESTRIN FE 3
loryna 1
low-ogestrel 1
MAKENA INTRAMUSCULAR 2 SP
medroxyprogesterone acetate
intramuscular
1
medroxyprogesterone acetate oral 1
microgestin 1.5/30 1
microgestin 1/20 1
microgestin fe 1.5/30 1
microgestin fe 1/20 1
MINASTRIN 24 FE E
MINIVELLE 3
mono-linyah 1
mononessa 1
NATAZIA 2
nikki 1
norethindrone acet- ethinyl est oral
tablet
1
norethindrone oral 1
norgestimate-ethinyl estradiol triphasic 1
nortrel 1/35 (21) 1
nortrel 1/35 (28) 1
NUVARING 2

MTMP Guide 2018-2019 61
DRUG NAME DRUG TIER
NOTES
ocella 1
ORTHO TRI-CYCLEN (28) E
ORTHO TRI-CYCLEN LO E
portia-28 1
PREMARIN ORAL 2
PREMARIN VAGINAL 2
PREMPHASE 2
PREMPRO 2
progesterone micronized oral 1
SAFYRAL 3
sprintec 28 1
tri-estarylla 1
tri-linyah 1
tri-lo-marzia 1
tri-lo-sprintec 1
trinessa (28) 1
trinessa lo 1
tri-sprintec 1
VAGIFEM VAGINAL TABLET 10
MCG
E
vienva 1
viorele 1
VIVELLE-DOT E
xulane 1
YAZ E
yuvafem 1
HORMONAL AGENTS - THYROID
ARMOUR THYROID 3
CYTOMEL E
levo-t 1
levothyroxine sodium oral 1
levoxyl 1
liothyronine sodium oral 1
methimazole oral 1
NATURE-THROID ORAL TABLET
113.75 MG, 130 MG, 146.25 MG,
16.25 MG, 195 MG, 260 MG, 32.5
MG, 325 MG, 48.75 MG, 65 MG,
81.25 MG, 97.5 MG
3
SYNTHROID 3
TIROSINT 3
IMMUNOLOGICAL AGENTS - DRUGS FOR IMMUNE SYSTEM
STIMULATION OR SUPPRESSION
azathioprine oral 1
CIMZIA PREFILLED KIT 2 SP
CIMZIA STARTER KIT 2 SP
CIMZIA VIAL KIT 2 SP
cyclosporine modified oral capsule 1 SP
ENBREL SUBCUTANEOUS
SOLUTION PREFILLED SYRINGE
3 SP
ENBREL SURECLICK
SUBCUTANEOUS SOLUTION
AUTO- INJECTOR
3 SP
DRUG NAME DRUG TIER
NOTES
HAEGARDA 3 SP
HUMIRA PEDIATRIC CROHNS
START SUBCUTANEOUS
PREFILLED SYRINGE KIT 40
MG/0.8ML
2 SP
HUMIRA PEN SUBCUTANEOUS
PEN- INJECTOR KIT
2 SP
HUMIRA PEN-CROHNS STARTER
SUBCUTANEOUS PEN- INJECTOR
KIT
2 SP
HUMIRA PEN- PSORIASIS
STARTER SUBCUTANEOUS PEN-
INJECTOR KIT
2 SP
HUMIRA SUBCUTANEOUS
PREFILLED SYRINGE KIT
2 SP
INFLECTRA E SP
methotrexate oral 1
methotrexate sodium oral 1
mycophenolate mofetil oral capsule 1 SP
mycophenolate mofetil oral tablet 1 SP
mycophenolate sodium 1 SP
ORENCIA SUBCUTANEOUS
SOLUTION PREFILLED SYRINGE
3 SP
OTEZLA ORAL TABLET 2 SP
OTEZLA ORAL TABLET THERAPY
PACK
2 SP
PROGRAF ORAL 3 SP
RASUVO SUBCUTANEOUS
SOLUTION AUTO- INJECTOR 10
MG/0.2ML, 12.5 MG/0.25ML, 15
MG/0.3ML, 17.5 MG/0.35ML, 20
MG/0.4ML, 22.5 MG/0.45ML, 25
MG/0.5ML, 30 MG/0.6ML, 7.5
MG/0.15ML
2
REMICADE 2 SP
SIMPONI ARIA 2 SP
SIMPONI SUBCUTANEOUS
SOLUTION AUTO- INJECTOR
2 SP
SIMPONI SUBCUTANEOUS
SOLUTION PREFILLED SYRINGE
2 SP
STELARA INTRAVENOUS 2 SP
tacrolimus oral 1 SP
TREMFYA 2 SP
XELJANZ XR 3 SP
IMMUNOLOGICAL AGENTS - DRUGS FOR VACCINATION
AFLURIA PRESERVATIVE FREE
INTRAMUSCULAR SUSPENSION
PREFILLED SYRINGE
3
BOOSTRIX INTRAMUSCULAR
SUSPENSION 5-2.5-18.5
3
FLUARIX QUADRIVALENT
INTRAMUSCULAR SUSPENSION
PREFILLED SYRINGE
3

MTMP Guide 2018-2019 62
DRUG NAME DRUG TIER
NOTES
FLUCELVAX QUADRIVALENT
INTRAMUSCULAR SUSPENSION
PREFILLED SYRINGE
3
FLUVIRIN INTRAMUSCULAR
SUSPENSION
3
FLUVIRIN INTRAMUSCULAR
SUSPENSION PREFILLED
SYRINGE
3
FLUZONE HIGH-DOSE
INTRAMUSCULAR SUSPENSION
PREFILLED SYRINGE
3
FLUZONE QUADRIVALENT
INTRAMUSCULAR SUSPENSION
3
FLUZONE QUADRIVALENT
INTRAMUSCULAR SUSPENSION
PREFILLED SYRINGE
3
ZOSTAVAX SUBCUTANEOUS
SUSPENSION RECONSTITUTED
E
INFLAMMATORY BOWEL DISEASE AGENTS
APRISO 2
ASACOL HD E
CANASA 2
DELZICOL E
DIPENTUM E
LIALDA E
mesalamine oral tablet delayed release
1.2 gm
1
MESALAMINE ORAL TABLET
DELAYED RELEASE 800 MG
E M
PENTASA 3
PROCTOFOAM HC 2
sulfasalazine oral tablet 1
UCERIS RECTAL 3
METABOLIC BONE DISEASE AGENTS - DRUGS FOR OSTEOPOROSIS
alendronate sodium oral tablet 1
BINOSTO E
calcitriol oral capsule 1
FORTEO SUBCUTANEOUS
SOLUTION 600 MCG/2.4ML
2 SP
ibandronate sodium oral E
TYMLOS 2 SP
MISCELLANEOUS THERAPEUTIC AGENTS
BOTOX 2 Non-
Cosmetic;
SP
CETYLEV 3
EUFLEXXA INTRA- ARTICULAR
SOLUTION PREFILLED SYRINGE
2 SP
SYNVISC INTRA- ARTICULAR
SOLUTION PREFILLED SYRINGE
2 SP
SYNVISC ONE INTRA-
ARTICULAR SOLUTION
2 SP
DRUG NAME DRUG TIER
NOTES
PREFILLED SYRINGE
OPHTHALMIC AGENTS - DRUGS FOR EYE ALLERGY, INFECTION
AND INFLAMMATION
AZASITE 3
BESIVANCE 3
ciprofloxacin hcl ophthalmic 1
erythromycin ophthalmic 1
gentamicin sulfate ophthalmic solution 1
ketorolac tromethamine ophthalmic 1
MOXEZA 2
moxifloxacin hcl ophthalmic 1
ofloxacin ophthalmic 1
olopatadine hcl ophthalmic 1
PAZEO 2
prednisolone acetate ophthalmic 1
PROLENSA 2
tobramycin ophthalmic 1
OPHTHALMIC AGENTS - DRUGS FOR GLAUCOMA
ALPHAGAN P OPHTHALMIC
SOLUTION 0.1 %
2
ALPHAGAN P OPHTHALMIC
SOLUTION 0.15 %
E
AZOPT 2
BETIMOL 3
brimonidine tartrate ophthalmic 1
COMBIGAN 2
COSOPT PF 3
dorzolamide hcl-timolol mal 1
latanoprost ophthalmic 1
LUMIGAN OPHTHALMIC
SOLUTION 0.01 %
2
RESCULA E
SIMBRINZA 2
timolol maleate ophthalmic solution 1
TRAVATAN Z 2
ZIOPTAN E
OPHTHALMIC AGENTS - DRUGS FOR MISCELLANEOUS EYE
CONDITIONS
LASTACAFT 3
neomycin-polymyxin- dexameth
ophthalmic suspension 3.5-10000-0.1
1
polymyxin b-trimethoprim 1
RESTASIS 2
RESTASIS MULTIDOSE 2
TOBRADEX OPHTHALMIC
SUSPENSION
E
tobramycin- dexamethasone 1
XIIDRA 2

MTMP Guide 2018-2019 63
DRUG NAME DRUG TIER
NOTES
OTIC AGENTS - DRUGS FOR EAR CONDITIONS
CIPRODEX 2
neomycin-polymyxin-hc otic solution
1 %
1
neomycin-polymyxin-hc otic
suspension
1
ofloxacin otic 1
RESPIRATORY TRACT / PULMONARY AGENTS - DRUGS FOR
ALLERGIES, COUGH, COLD
ASTEPRO NASAL SOLUTION
0.15 %
3
azelastine hcl nasal 1
benzonatate 1
cetirizine hcl oral solution E
cetirizine hcl oral syrup 1 mg/ml E
DYMISTA 2
fluticasone propionate nasal E
hydrocodone polst-cpm polst er oral
suspension extended release 10-8
mg/5ml
1
ipratropium bromide nasal 1
levocetirizine dihydrochloride oral
tablet
E
mometasone furoate nasal E
NASONEX E
OMNARIS E
promethazine hcl oral tablet 1
promethazine-codeine 1
promethazine-dm 1
pseudoephedrine- bromphen-dm oral
syrup 30-2-10 mg/5ml
1
QNASL E
QNASL CHILDRENS E
TUZISTRA XR ORAL SUSPENSION
EXTENDED RELEASE
3
XOLAIR 2 SP
ZETONNA E
ZUTRIPRO 3
RESPIRATORY TRACT / PULMONARY AGENTS - DRUGS FOR
ASTHMA AND OTHER LUNG CONDITIONS
ADVAIR DISKUS 2
ADVAIR HFA 2
AIRDUO RESPICLICK 113/14 E
AIRDUO RESPICLICK 232/14 E
AIRDUO RESPICLICK 55/14 E
albuterol sulfate inhalation 1
ALVESCO E
ANORO ELLIPTA 2
ARNUITY ELLIPTA 2
ASMANEX 120 METERED DOSES E
ASMANEX 14 METERED
DOSES
E
DRUG NAME DRUG TIER
NOTES
ASMANEX 30 METERED
DOSES
E
ASMANEX 60 METERED
DOSES
E
ASMANEX 7 METERED DOSES E
ASMANEX HFA E
AUVI-Q INJECTION SOLUTION
AUTO- INJECTOR
E
BREO ELLIPTA 2
budesonide inhalation 1
COMBIVENT RESPIMAT 2
DULERA E
EPINEPHRINE INJECTION
SOLUTION AUTO-INJECTOR 0.15
MG/0.15ML
E Made by
Impax; M
EPINEPHRINE INJECTION
SOLUTION AUTO-INJECTOR 0.15
MG/0.3ML
2 Made by
Mylan
EPINEPHRINE SOLUTION AUTO-
INJECTOR 0.3 MG/0.3ML
INJECTION
2 Made by
Mylan
EPINEPHRINE SOLUTION AUTO-
INJECTOR 0.3 MG/0.3ML
INJECTION
E Made by
Impax; M
EPIPEN 2-PAK INJECTION
SOLUTION AUTO-INJECTOR
E
EPIPEN JR 2-PAK INJECTION
SOLUTION AUTO-INJECTOR
E
FLOVENT DISKUS 2
FLOVENT HFA 2
INCRUSE ELLIPTA 2
ipratropium bromide inhalation 1
ipratropium-albuterol 1
LEVALBUTEROL HFA
INHALATION AEROSOL 45
MCG/ACT
E M
montelukast sodium oral tablet 1
montelukast sodium oral tablet
chewable
1
PERFOROMIST 3
PROAIR HFA 2
PROAIR RESPICLICK 2
PROVENTIL HFA E
PULMICORT FLEXHALER 2
PULMICORT SUSPENSION E
QVAR INHALATION AEROSOL
SOLUTION
E
QVAR REDIHALER E
SEREVENT DISKUS 2
SINGULAIR E
SPIRIVA HANDIHALER 2
SPIRIVA RESPIMAT 2
STIOLTO RESPIMAT 2
SYMBICORT 2
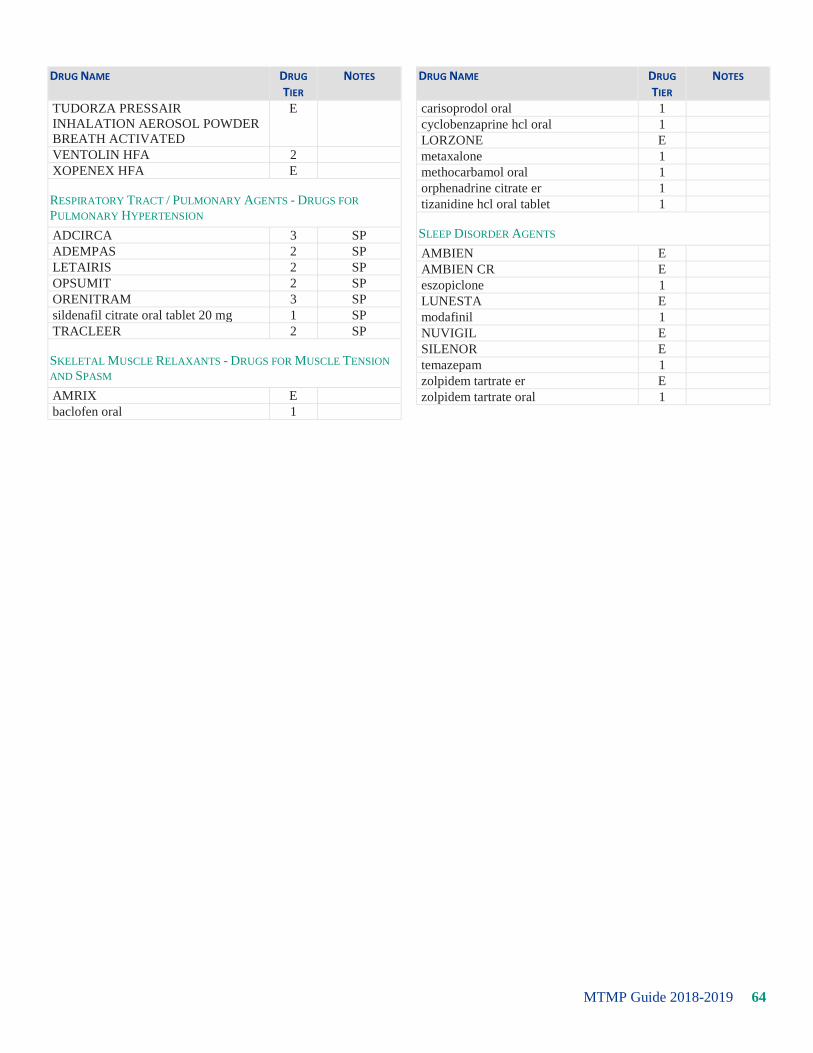
MTMP Guide 2018-2019 64
DRUG NAME DRUG TIER
NOTES
TUDORZA PRESSAIR
INHALATION AEROSOL POWDER
BREATH ACTIVATED
E
VENTOLIN HFA 2
XOPENEX HFA E
RESPIRATORY TRACT / PULMONARY AGENTS - DRUGS FOR
PULMONARY HYPERTENSION
ADCIRCA 3 SP
ADEMPAS 2 SP
LETAIRIS 2 SP
OPSUMIT 2 SP
ORENITRAM 3 SP
sildenafil citrate oral tablet 20 mg 1 SP
TRACLEER 2 SP
SKELETAL MUSCLE RELAXANTS - DRUGS FOR MUSCLE TENSION
AND SPASM
AMRIX E
baclofen oral 1
DRUG NAME DRUG TIER
NOTES
carisoprodol oral 1
cyclobenzaprine hcl oral 1
LORZONE E
metaxalone 1
methocarbamol oral 1
orphenadrine citrate er 1
tizanidine hcl oral tablet 1
SLEEP DISORDER AGENTS
AMBIEN E
AMBIEN CR E
eszopiclone 1
LUNESTA E
modafinil 1
NUVIGIL E
SILENOR E
temazepam 1
zolpidem tartrate er E
zolpidem tartrate oral 1

MTMP Guide 2018-2019 65
OptumRx Pharmacy Resources
Mobile Application
The convenient app makes the online pharmacy experience as simple as possible.
From your mobile phone, you can:
View all medications in a clear and concise format using the "Medicine Cabinet" feature
Refill and renew home delivery prescriptions
Transfer a retail prescription to home delivery
Find drug prices and lower cost options
View your prescription claims history or order status
Locate a pharmacy: Enjoy the convenience of our pharmacy locator to locate an in-network retail location at
any time.
Set up refill reminders: Set text message reminders for refills or taking a medication
Track your order
When you receive your physician's order, visit optumrx.com, register, and follow the simple step-by-step
instructions. You can manage your medication(s) online.
Mobile Friendly Website
Access your Account Anytime, Anywhere.
Manage your prescription drug benefits on your smartphone, iPad, Android tablet, or other handheld device.
OptumRx Mobile makes it easy to:
Refill mail service pharmacy prescriptions
Check the status of and track orders
Locate a pharmacy by ZIP code
View your prescription history
Set up text message medication reminders
Search your formulary by generic or brand-name drug, status, or class
How do I find the mobile site?
Open your smartphone browser and type in m.optumrx.com. You also can type in our full address, optumrx.com,
and you will automatically be directed to the mobile version of our site. Once the site is loaded on your phone,
you can bookmark it.

MTMP Guide 2018-2019 66
Can I use the mobile site on any smartphone?
Yes. Just enter m.optumrx.com into the web browser of your smartphone.
Can I use both the full site and the mobile site?
Yes. If you make a change to your account or manage your prescriptions on one site, that information will be
updated on the other site as well.
How to refill prescriptions
1. On the home page, click "My Prescriptions". Click "Refill Prescriptions". (If you are not logged in, you will
be prompted to log in first.)
2. Select the prescription(s) you would like refilled by checking the box(es).
3. Click "Add to Cart" to proceed to the shopping cart page.
4. Review your selections. You can remove items from your cart, keep shopping, or check out. When you are
finished, click "Check Out".
5. Review your shipping information and your order summary. You may change your shipping address or add
a new one.
6. Review your order summary. To make changes to your order, click "Back". If your order is complete, click
"Submit".
How to set up text message medication reminders
1. On the home page, click "My Prescriptions". Click "Medication Reminders". (If you are not logged in, you
will be prompted to log in first.)
2. Enter the mobile phone number where you want the text message reminder(s) to be sent.
3. Select your time zone.
4. Select your mobile carrier.
5. Choose the type of reminder you would like to receive. You can get reminders when mail order prescriptions
are ready for refill and renewal, when prescriptions are eligible for transfer to mail service, and when orders
have been shipped. You can also set reminders for specific times of day and for specific medications.
6. When you are done, click "Save".
MTMP Guide 2018-2019 67
Consumer Portal
The OptumRx® consumer portal empowers you to become an informed advocate of your own health by allowing
you to easily manage and gain deeper insight into your prescription benefits.
Simple: The responsive design makes it easy for you to access your complete profile to manage your
prescription benefits on any device.
Smart: With accurate drug pricing, proactive messaging on cost savings, and detailed order status
information, all of your real time benefits information is readily available.
Seamless: You can enroll in text message reminders for taking your medications as well as when you need to
refill or renew prescriptions, and when orders have shipped.
Register or sign in to optumrx.com to take advantage of these features.
My Medicine Cabinet
Upon login, you will see your My Medicine Cabinet dashboard. This makes it easy for you to view your real time
benefits and access the many tools and features to help you manage your medications and health from a single
page.
Once registered on the website, you can access:
1. Household prescriptions
Ability to manage prescriptions on behalf of
family members
2. Order status
You are able to track where your home
delivery order is within the process and view
order hold information if applicable
3. Proactive savings messaging
Advocates for you by providing proactive
ways to save such as transferring retail
prescriptions to home delivery
4. Member tools
Provides easy access to the most commonly
used member tools throughout the site
5. Medicine cards
Provides visibility to the most relevant information for medications

MTMP Guide 2018-2019 68
Single Sign-On Access
Re-registration is required.
The first time you click on the new SSO link from tmlhealthbenefits.org, you will be taken to OptumRx's
Portal to register. Registration will create a unique identifier that will recognize your access between websites
from that point forward.
The next time you click on the SSO link, you will be taken directly into the OptumRx Portal.
Mail Order Service
OptumRx state-of-the-art mail service pharmacy sends refrigerated injectable medications via express delivery to
your location of choice, or to your provider to administer to you in the office. Our goal is to meet and exceed your
needs when it comes to how, when, and where you receive your medications.
How do I use OptumRx mail service pharmacy for new prescriptions?
Ordering a new medication is easy with our website. Just log on to optumrx.com. From there go to "My Account"
then click on "Manage My Mail Service" to fill a new prescription through our easy-to-use online tools. Or, if
you prefer to speak to someone on the phone, call (800) 788-7871 (TTY 711) to order through home delivery
anytime.
How will I order refills from OptumRx mail service pharmacy?
Once you place your first order with OptumRx, you can choose from three different ways to order refills:
Online: Order refills by logging into optumrx.com, selecting "Manage my Prescriptions" and viewing your
refills.
Mail: Complete the reorder form included with each medication shipment and then mail it to us for processing.
Phone: Call customer service at (800) 788-7871 (TTY 711). You can choose to use our automated system or
speak with a representative.
Also, if you register at optumrx.com, you will receive e-mail reminders when it is time to refill your prescription.
How long will it take to receive my mail service prescription orders?
New prescription orders should arrive in about 10 business days after we receive complete order information,
while refills should arrive in about 7 business days.