Mechanical properties of human bone-implant interface tissue in aseptically loose hip implants
10
www.elsevier.com/locate/jmbbm Available online at www.sciencedirect.com Research Paper Mechanical properties of human bone–implant interface tissue in aseptically loose hip implants Gert Kraaij a,b,n , Amir A. Zadpoor b , Gabrielle J.M. Tuijthof b,c , Jenny Dankelman b , Rob G.H.H. Nelissen a , Edward R. Valstar a,b a Biomechanics and Imaging Group, Department of Orthopaedics, Leiden University Medical Center, P.O. Box 9600, Leiden 2300RC, The Netherlands b Department of Biomechanical Engineering, Delft University of Technology, Mekelweg 2, Delft 2628CD, The Netherlands c Department of Orthopedic Surgery, Academic Medical Center, Meibergdreef 9, Amsterdam 1105 AZ, The Netherlands article info Article history: Received 17 January 2014 Received in revised form 3 June 2014 Accepted 18 June 2014 Available online 26 June 2014 Keywords: Hip Prosthesis Loosening Interface membrane Biomechanics abstract The main cause of failure in total hip replacement is aseptic loosening which is associated with the formation of a periprosthetic fibrous (interface) tissue. Despite important applications for finite element modeling of loose implants, the mechanical properties of the bone–implant interface tissue have never been measured in humans. In this study, we performed unconfined compression tests to characterize the mechanical properties of the interface tissue and to determine the parameters of various hyperelastic material models which were fitted to the measurements. Human interface tissues were retrieved during 21 elective revision surgeries from aseptically loosened cemented (N ¼10) and uncemented hip implants (N¼11). Specimens were tested at a fixed deformation rate of 0.1 mm/min up to a maximum force of 10 N. Elastic moduli for low and high strain regions of the stress– strain curves were determined. Interface tissue from aseptically loose cemented pros- theses shows higher elastic moduli (mean ¼1.85 MPa, 95% C.I. ¼1.76–1.95 MPa) in the high strain region as compared to that of the interface tissue from the cementless group (mean ¼1.65 MPa, 95% C.I. ¼1.43–1.88 MPa). The 5-terms Mooney–Rivlin model (W ¼ C 1 ½I 1 3þ C 2 ½I 2 3þ C 3 ½I 1 3½I 2 3þ C 4 ½I 1 3 2 þ C 5 ½I 2 3 2 ) described the stress– strain behavior the best. Large variations in the mechanical behavior were observed both between specimens from the same patient as between those of different patients. The material model parameters were therefore estimated for the mean data as well as for the curves with the highest and lowest strain at the maximum load. The model parameters found for the mean data were C 1 ¼0.0074 MPa, C 2 ¼0.0019 MPa, C 3 ¼0 MPa, C 4 ¼0.0032 MPa and C 5 ¼0 MPa in the cemented group and C 1 ¼ 0.0137 MPa, C 2 ¼ 0.0069 MPa, C 3 ¼0.0026 MPa, C 4 ¼0.0094 MPa and C 5 ¼0 MPa in the cementless group. The results of this study can be used in finite element computer. & 2014 Elsevier Ltd. All rights reserved. http://dx.doi.org/10.1016/j.jmbbm.2014.06.010 1751-6161/& 2014 Elsevier Ltd. All rights reserved. n Corresponding author at: Biomechanics and Imaging Group, Department of Orthopaedics, Leiden University Medical Center, P.O. Box 9600, Leiden 2300RC, The Netherlands. Tel.: þ31 71 2563606; fax: þ31 71 2566743. E-mail address: [email protected] (G. Kraaij). journal of the mechanical behavior of biomedical materials 38 (2014) 59–68
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Mechanical properties of human bone-implant interface tissue in aseptically loose hip implants

Available online at www.sciencedirect.com
www.elsevier.com/locate/jmbbm
j o u r n a l o f t h e m e c h a n i c a l b e h a v i o r o f b i o m e d i c a l m a t e r i a l s 3 8 ( 2 0 1 4 ) 5 9 – 6 8
http://dx.doi.org/101751-6161/& 2014 El
nCorresponding aP.O. Box 9600, Leide
E-mail address: g
Research Paper
Mechanical properties of human bone–implantinterface tissue in aseptically loose hip implants
Gert Kraaija,b,n, Amir A. Zadpoorb, Gabrielle J.M. Tuijthofb,c,Jenny Dankelmanb, Rob G.H.H. Nelissena, Edward R. Valstara,b
aBiomechanics and Imaging Group, Department of Orthopaedics, Leiden University Medical Center, P.O. Box 9600,Leiden 2300RC, The NetherlandsbDepartment of Biomechanical Engineering, Delft University of Technology, Mekelweg 2, Delft 2628CD, The NetherlandscDepartment of Orthopedic Surgery, Academic Medical Center, Meibergdreef 9, Amsterdam 1105 AZ, The Netherlands
a r t i c l e i n f o
Article history:
Received 17 January 2014
Received in revised form
3 June 2014
Accepted 18 June 2014
Available online 26 June 2014
Keywords:
Hip
Prosthesis
Loosening
Interface membrane
Biomechanics
.1016/j.jmbbm.2014.06.010sevier Ltd. All rights rese
uthor at: Biomechanicsn 2300RC, The [email protected] (G. Kraai
a b s t r a c t
The main cause of failure in total hip replacement is aseptic loosening which is associated
with the formation of a periprosthetic fibrous (interface) tissue. Despite important
applications for finite element modeling of loose implants, the mechanical properties of
the bone–implant interface tissue have never been measured in humans. In this study, we
performed unconfined compression tests to characterize the mechanical properties of the
interface tissue and to determine the parameters of various hyperelastic material models
which were fitted to the measurements. Human interface tissues were retrieved during 21
elective revision surgeries from aseptically loosened cemented (N¼10) and uncemented
hip implants (N¼11). Specimens were tested at a fixed deformation rate of 0.1 mm/min up
to a maximum force of 10 N. Elastic moduli for low and high strain regions of the stress–
strain curves were determined. Interface tissue from aseptically loose cemented pros-
theses shows higher elastic moduli (mean¼1.85 MPa, 95% C.I.¼1.76–1.95 MPa) in the
high strain region as compared to that of the interface tissue from the cementless
group (mean¼1.65 MPa, 95% C.I.¼1.43–1.88 MPa). The 5-terms Mooney–Rivlin model
(W¼ C1½I1�3� þ C2½I2�3� þ C3½I1�3�½I2�3� þ C4½I1�3�2 þ C5½I2�3�2 ) described the stress–
strain behavior the best. Large variations in the mechanical behavior were observed both
between specimens from the same patient as between those of different patients. The
material model parameters were therefore estimated for the mean data as well as for the
curves with the highest and lowest strain at the maximum load. The model parameters
found for the mean data were C1¼�0.0074 MPa, C2¼0.0019 MPa, C3¼0 MPa, C4¼�0.0032
MPa and C5¼0 MPa in the cemented group and C1¼�0.0137 MPa, C2¼0.0069 MPa,
C3¼0.0026 MPa, C4¼�0.0094 MPa and C5¼0 MPa in the cementless group. The results of
this study can be used in finite element computer.
& 2014 Elsevier Ltd. All rights reserved.
rved.
and Imaging Group, Department of Orthopaedics, Leiden University Medical Center,ds. Tel.: þ31 71 2563606; fax: þ31 71 2566743.j).

Table 1 – Demographic characteristics of the patients.
Parameter Total 21 patients
Age (years) 75.3 (61–88; sd 7.7)
GenderMen 9Women 12
j o u r n a l o f t h e m e c h a n i c a l b e h a v i o r o f b i o m e d i c a l m a t e r i a l s 3 8 ( 2 0 1 4 ) 5 9 – 6 860
1. Introduction
The main cause of failure in total hip replacements is asepticloosening (Garellick et al., 2011) which is associated with theformation of a fibrous interface membrane (Edwards et al., 2008;Jones et al., 1999; Neale et al., 2000; Quinn et al., 1992; Wang et al.,2005). This interface membrane has inferior mechanical proper-ties as compared to bone, resulting in subsequent mechanicalinstability of the implant within the bone. As a result, largedisplacements of the prosthesis relative to the host bone couldoccur that may result in walking difficulties as well as severepain and higher risk of pathological fractures. Currently, patientswith loose prostheses undergo open revision surgery, which is ahighly demanding procedure. In patients with poor generalhealth, the complication rate of this surgical procedure is high,with up to 60% complications and up to 20% mortality (Strehleet al., 2000). Therefore, it is important to develop a less demand-ing surgical procedure to refixate the loosened implant withsubsequent restoration of function.
Recently, a minimally invasive refixation procedure has beendeveloped (De Poorter et al., 2008). During this refixation proce-dure, the interface tissue is (partially) removed and bone cementis injected into the osteolytic areas. Andreykiv et al. (2012)analyzed whether this cement injection into the osteolytic areascontributed to the overall implant stability, by using a detailedfinite elementmodel. Regarding themechanical properties of theinterface tissue, Andreykiv et al. referred to the study of Hori andLewis (1982). This is the only study that reports such properties,however, interface tissue from dogs was used. Furthermore,most studies on interface tissue focus on the histo-morpho-logical properties (Boss et al., 1994; Bravo et al., 2011; Goldringet al., 1986, 1983; Shoji et al., 1983). No information regarding themechanical properties of human interface tissue is currentlyavailable. In order to develop a patient-specific refixation proce-dure and to determine where to inject bone cement to obtain anoptimal refixation, patient-specific finite element models ofimplanted joints are needed (Poelert et al., 2013) and this requiresthe evaluation of the human interface tissue.
In this study, we perform unconfined compression tests (Horiand Lewis, 1982; Miller, 2005; Miller and Chinzei, 1997; Miller-Young et al., 2002; Umale et al., 2013; Wu et al., 2007) on humaninterface tissues retrieved during revision surgeries from loosecemented and uncemented hip implants. Linear elastic modelsare not adequate for describing the mechanical behavior of suchsoft materials. Therefore, the obtained force–displacement datais analyzed within the context of hyperelastic material models.Six different types of hyperelastic material models are fitted tothe obtained experimental data to determine the parameters ofthe considered hyperelastic material models. The goodness of fitas well as the parameters of the material models are reportedand discussed.
Implant fixationCement 10Cementless 11
Time since implantation0–2 Years 2 (9.5%)2–5 Years 1 (4.8%)45 Years 17 (81%)Unknown 1 (4.8%)
2. Materials and methods
2.1. Specimens
We obtained interface tissue from 21 patients with asepti-cally loose hip prostheses who had elective revision surgery.
The demographic characteristics are listed in Table 1. Exclu-sion criterion was presence of a prosthetic infection as reasonfor revision. Stratification of the interface tissue was basedon whether the prosthesis was cemented or cementless.A certificate of no objection for this study was obtained fromthe local Medical Ethics Committee. Immediately after intrao-perative harvesting, the interface tissue was kept in salinesolution at room temperature and was transported to the lab.When the interface tissue was not immediately tested (N¼5)and had to be stored overnight, it was kept at 5–7 1C. A corepunch (diameter 6.2 mm) was used to cut at least threespecimens from the interface tissue of each patient.
2.2. Unconfined compression test
After harvesting, the specimens were mechanically testedwithin 48 h in unconfined uni-axial compression tests using astatic mechanical testing machine (LR5K, Lloyd Instrumentsltd, UK). A punch and anvil were constructed from stainlesssteel. The punch was attached to a 100 N load cell and theanvil was bolted to the table of the testing machine. Prior totesting, the punch was humidified with phosphate-bufferedsaline (PBS) solution to minimize friction between tissue andthe punch (Rashid et al., 2012). The specimens were not pre-conditioned, placed at an anvil (Fig. 1), and tested at a fixeddeformation rate of 0.1 mm/min up to a maximum force of10 N, with a data sampling rate of 8 kHz. The thickness of thespecimen was considered to be equal to the differencebetween the anvil surface and the position of the punch atthe load of 0.1 N. Each specimen was only tested once andwas subsequently discarded. During the tests, the specimenswere submerged in a standard saline solution bath at roomtemperature.
2.3. Material models and uni-axial compression tests
Soft tissues are often modeled as incompressible hyperelasticmaterials (Martins et al., 2006), because linear elastic materialmodels cannot sufficiently describe their mechanical beha-vior. Based on the results of the Hori and Lewis (1982) studyin the animal model, we expected a non-linear beha-vior in human interface tissue as well. The Ogden and Mooney–Rivlin material models are sophisticated hyperelastic material

Fig. 1 – Interface tissue sample in test setup.
j o u r n a l o f t h e m e c h a n i c a l b e h a v i o r o f b i o m e d i c a l m a t e r i a l s 3 8 ( 2 0 1 4 ) 5 9 – 6 8 61
models that are used to describe the non-linear mechanicalbehavior of rubbers, polymers, and biological tissues (Farshadet al., 1999; Miller, 2000, 2001; Miller and Chinzei, 1997; Millerand Chinzei, 2002; Snedeker et al., 2005).
In general, every hyperelastic material model is definedby a strain energy density function W, which is oftenconsidered to be a function of the principal stretch ratios λ1,λ2 and λ3
W¼ f ð λ1; λ2; λ3Þ ð1Þ
The prinicipal stretch ratios λi, i¼ (1, 2, 3), are defined asthe ratios of the thickness ti of a deformed sample to thethickness t0,i of the corresponding undeformed sample mea-sured along the xi axis
λi ¼tit0;i
ð2Þ
And for an incompressible material the principal stretchratios satisfy the constraint:
λ1λ2λ3 ¼ 1 ð3Þ
The principal Cauchy stresses σi, i¼ (1, 2, 3), defined perunit cross-sectional area normal to the xi axes in thedeformed configuration, for an incompressible material arerelated to stretches through W (Ogden et al., 2004)
σi ¼ λi∂W∂λi
–p ð4Þ
where p is an undetermined hydrostatic pressure introducedbecause of the incompressibility constraint which can bedetermined from the boundary conditions. Assuming thestress is applied along the x1 direction (which is the case inan uni-axial compression experiment), those boundary con-ditions are (Martins et al., 2006)
σ1 ¼ σ; σ2 ¼ σ3 ¼ 0 ð5Þ
which gives
σ ¼ λ1∂W∂λ1
–p ð6Þ
0¼ λ2∂W∂λ2
–p ð7Þ
0¼ λ3∂W∂λ3
�p ð8Þ
The prinicipal Cauchy stress for a hyperelastic incompres-sible material in an unconfined uni-axial compression testcan therefore be calculated as:
σ ¼ λ1∂W∂λ1
– λ3∂W∂λ3
ð9Þ
In order to compare theoretical and experimental forcevalues, the theoretical force values have to be obtained fromthe principal Cauchy stress σ.
Let A be the area of the deformed sample and A0 its initialarea, the theoretical force is given by
F¼ σA ð10Þ
Since the material is incompressible, conservation ofvolume dictates that
t0A0 ¼ tA ð11Þ
The ratio of areas is then given by
A0
A¼ t
t0¼ λ1 ð12Þ
and thus
A¼ A0
λ1ð13Þ
Combining Eqs. (9), (10) and (13), the theoretical reactionforce is given by
F¼ A0
λ1λ1
∂W∂λ1
–λ3∂W∂λ3
� �ð14Þ
As the theoretical force values must equal the experimen-tal force values, Eq. (14) was used to determine the para-meters of the hyperelastic material models to fit theexperimental data.
2.4. Determination of material model parameters
An overview of the six material models which were fitted tothe experimental data and the Cauchy stresses is presentedin Table 2. The fit function in the curve fitting toolbox ofMatlab (MATLAB and Statistics Toolbox Release 2012b, TheMathWorks, Inc., Natick, Massachusetts, United States) wasused to fit the models to the measured forces from eachindividual measurement. The initial guess for the materialmodel parameters was randomly chosen and the Trust-Region-Reflective algorithm (Byrd et al., 1988) was used for

j o u r n a l o f t h e m e c h a n i c a l b e h a v i o r o f b i o m e d i c a l m a t e r i a l s 3 8 ( 2 0 1 4 ) 5 9 – 6 862
the fitting procedure. The commonly used default fittingoptions, detailed in Table 3, were used. To compare thegoodness of fit between the models, the mean and the95% confidence interval of respectively the coefficient ofdetermination (R2) and the Root-Mean-Square-Error (RMSE)were determined for each fitted model. The RMSE wascalculated as:
RMSE¼ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi∑n
i ¼ 1ðσmeasured;i�σpredicted;iÞ2n
sð15Þ
2.5. Cemented vs cementless tissue
To determine a significant difference in the material proper-ties of tissue from cemented and cementless prostheses,the modulus of elasticity was determined for low-strain(up to 10%) and high-strain (last 10% of the deformationcurve) regions of the stress–strain curves. For each measure-ment, elastic moduli were calculated as the slope of the linearcurve fitted to the low-strain and high-strain parts of thedeformation curve (Fig. 2).
As we tested multiple specimens from the same patient inthe unconfined compression tests, a mixed linear (regression)model was used to analyze the effect of implant fixation(cemented or cementless) on the elastic moduli (low-strainand high-strain), with patient ID as a random factor. P valuesless than 0.05 were considered significant. SPSS Statistics
Table 2 – Overview of hyperelastic incompressible material m
Fit Model Strain-energy density functiona C
1 Neo–Hookean(Holzapfel, 2000;Yang et al., 2000)
W¼ c1ðI1�3Þ σ
2 2-Terms Mooney–Rivlin (Mooney,1940; Rivlin, 1948;Yang et al., 2000)
W¼ c1ðI1�3Þ þ c2ðI2�3Þ σ
3 3-Terms Mooney–Rivlin (Mooney,1940; Rivlin, 1948;Yang et al., 2000)
W¼ c1ðI1�3Þ þ c2ðI2�3Þ þ c3ðI3�3Þ σ
4 4-Terms Ogden(Ogden, 1984; Ogdenet al., 2004)
W¼ c1c2ðλc21 þ λc22 þ λc23 �3Þ
þ c3c4
ðλc41 þ λc42 þ λc43 �3Þ
þ c5c6
ðλc61 þ λc62 þ λc63 �3Þ
þ c7c8
ðλc81 þ λc82 þ λc83 �3Þ
σ
5 CombinedLogarithmic andOgden (Gao et al.,2010)
W¼ �c1 ln ½1�c2ðλc31 þ λc32 þ λc33 �3Þ�þ c4ðλc51 þ λc52 þ λc53 �3Þ σ
6 5-Terms Mooney–Rivlin (Mooney,1940; Rivlin, 1948;Umale et al., 2013)
W¼ c1ðI1�3Þ þ c2ðI2�3Þþc3ðI1�3ÞðI2�3Þ
þc4ðI1�3Þ2 þ c5ðI2�3Þ2σ
a I1¼ (λ1)2þ(λ2)
2þ(λ3)2, I2¼ (λ1)
2(λ2)2þ(λ2)
2(λ3)2þ(λ3)
2(λ1)2, ci are the material p
b Materials are assumed to be isotropic.
version 20 (IBM Corporation, Armonk, New York, USA) wasused for the analysis.
3. Results
3.1. Experimental results
No significant barrelling was observed during the compres-sion tests. This justifies the use of the frictionless contactassumption. The results of all unconfined compression testsare presented in the form of engineering stress–engineeringstrain plots in Fig. A1 (see Supplementary material). In Fig. 3,the experimental data is compared with the data presentedin the study by Hori and Lewis (1982) where they performedcompression tests on interface tissue harvested from dogs.The deformation curves are clearly non-linear with lowelastic moduli and large strains at low initial loads (Fig. 3).The interface tissue becomes stiffer as the load increases,resulting in higher elastic moduli for higher strains (Fig. 3).The interface tissue undergoes very large strains during thetests. Although the shape of the stress–strain curves issimilar for all specimens, the curves have different exten-sions along the strain-axis, with the cementless groupshowing a larger variation in general, i.e. a larger range incompression ratio at maximum applied load of 10 N (Fig. 4).In both groups (cemented and cementless), the variation incompression ratio can also be seen within specimens fromthe same patient in the associated group (Fig. 4).
odels.
auchy stressb
¼ 2c1 λ2� 1λ
� �
¼ 2c1 λ2� 1λ
� �þ 2c2 λ� 1λ2
� �
¼ 2c1 λ2� 1λ
� �þ 2c2 λ� 1λ2
� �þ2c3 λ� 1
λ2
3λ2 þ 3
λ�3λ�3
¼ c1 λc2 �λ� c22
� �þ c3 λc4 �λ
� c42
� �þc5 λc6 �λ
� c62
� �þ c7 λc8 �λ
� c82
� �
¼ c1c2c3 ðλc3 � λ� c32 Þ
1� c2 ðλc3þ2λ� c32 �3Þ
þ c4c5ðλc5 �λ� c52 Þ
¼ 2 λ2� 1λ
� �c1 þ c2
λ þ 3c3 1λ2�1
� �ð1�λÞ þ 2c4 λ2 þ 2
λ �3� �þ 2c5
λ1λ2þ 2λ�3
� �h i
arameters.

Table 3 – Fit options used for hyperelastic model fitting.
Fit option Value
Start point Initial values for the coefficients Random chosen by MatlabAlgorithm Algorithm to use for fitting procedure Trust-Region-ReflectiveDiffMaxChange Max change in coefficients 10�8 (Default)DiffMinChange Min change in coefficients 10�8 (Default)MaxFunEvals Max number of evaluations of model allowed 600 (Default)MaxIter Max number of iterations allowd for fit 400 (Default)TolFun Termination tolerance on model value 10�6 (Default)TolX Termination tolerance on coefficient values 10�6 (Default)
Fig. 2 – Engineering stress–engineering strain plot of onespecimen, indicating how the low and high strain E-moduliare calculated.
Fig. 3 – Engineering stress–engineering strain plots of allhuman interface tissue specimens compared to stress–strain curves of interface tissue harvested from dogs (Horiand Lewis, 1982).
Fig. 4 – Scatterplot of stretch at 10 N load in the cementedand cementless group, indicating the range of compressionratio measured in this study. On the x-axis different samplegroups are indicated: (A) all samples in cementless group,((B)–(D)) samples from three individual patients incementless group, (E) all samples in cemented group and((F)–(H)) samples from three individual patients incemented group.
j o u r n a l o f t h e m e c h a n i c a l b e h a v i o r o f b i o m e d i c a l m a t e r i a l s 3 8 ( 2 0 1 4 ) 5 9 – 6 8 63
3.2. Hyperelastic model fitting
The Neo–Hookean model was found to be incapable ofcapturing the non-linear mechanical behaviour of the
interface tissue (Fig. 5). For the combined Logarithmic–Ogdenmodel and 4-terms Ogden model, the optimisation algorithmwas unable to converge to a global minimum, as for thismaterial model different initial guesses of the model para-meters resulted in different final model parameters (Fig. 6).The Mooney–Rivlin model could adequately describe themechanical behavior of the interface tissue under compres-sion (Fig. 5). The best fit was obtained with the 5-termsMooney–Rivlin model (Table 4), as fitting this model resultedin the highest R2 and lowest RMSE values. Applying thismodel to each individual stress–strain curve resulted in agood description of the mechanical behavior.
For the Cauchy stresses, the mean of the associatedstrains was calculated for the specimens in both groups(cemented and cementless). The mean stress–strain curveand the deformation curves with respectively the highest andlowest strain at the maximum load for the cemented andcementless group are plotted in Fig. 7. As the 5 termsMooney–Rivlin material model gave the best fit, it is fitted(in the same way as described in Section 2.4) to the meanstress–strain curve. The following material model parameters

j o u r n a l o f t h e m e c h a n i c a l b e h a v i o r o f b i o m e d i c a l m a t e r i a l s 3 8 ( 2 0 1 4 ) 5 9 – 6 864
were obtained: C1¼�0.0074 MPa, C2¼0.0019 MPa, C3¼0 MPa,C4¼�0.0032 MPa and C5¼0 MPa in the cemented groupand C1¼�0.0137 MPa, C2¼0.0069 MPa, C3¼0.0026 MPa, C4¼�0.0094 MPa and C5¼0 MPa in the cementless group. Thecoefficient of determination between the measured andmodel forces (goodness of fit) was calculated as 0.99. .
3.3. Elastic modulus
The elastic modulus of the human interface tissue in thecemented group was 0.036 MPa (0.024–0.048 MPa, 95% C.I.) for
Fig. 5 – The 6 different non-linear material models from Table 2fitted to an experimental deformation curve of one specimenfrom a patient with a loosened cemented prosthesis.
Fig. 6 – The combined Logarithmic and Ogden model and the 4-tcoefficients, as is demonstrated by fitting the combined Logarithboth five times with a different initial guess of model coefficienFig. 5.
the low-strain region and 1.85 MPa (1.76–1.95 MPa, 95% C.I.)for the high strain region of the stress–strain curves. Inthe cementless group, the elastic modulus was 0.043 MPa(0.014–0.071 MPa, 95% C.I.) for the low-strain region and1.65 MPa (1.43–1.88 MPa, 95% C.I.) for the high strain regionof the stress–strain curves. According to the linear mixedmodel, the high strain elastic modulus of the cementlessgroup was significantly higher than that of the cementedgroup (P¼0.004).
4. Discussion
This study was performed to characterize the mechanicalbehavior of human interface tissue in aseptically loose hipprostheses using unconfined uni-axial compression tests and toobtain the parameters of hyperelastic material models thatcould be used for the description of the mechanical behavior ofthe interface tissue in computational studies. The experimentaldata do show large variations between cemented and cement-less loose prostheses and also between and within patients. Inthe current study, the in-situ location and orientation of theharvested interface tissue was not known and specimens weretaken randomly from the harvested tissue. Consequently, itwas not possible to investigate if and how location andorientation contributed to the scatter of the data. It wasobserved that the specimens taken from adjacent areas showedsimilar mechanical behavior (Fig. 4). A common finding ofstudies focusing on the histo-morphological properties of theinterface membrane (Boss et al., 1994; Bravo et al., 2011;Goldring et al., 1986, 1983; Shoji et al., 1983), is the presence ofwear particles e.g. metal, polyethylene or PMMA. Because wear
erms Ogden model are sensitive to the initial guess of modelmic and Ogden model (A) and the 4-terms Ogden model (B)ts to the same experimental deformation curve as shown in

Table 4 – 95% Confidence intervals of R2 and RMSE.
Model MeanR2 [N/mm2]
95% Confidenceinterval R2 [N/mm2]
MeanRMSE [N/mm2]
95% Confidenceinterval RMSE [N/mm2]
Neo–Hookean 0.831 0.820–0.843 0.012 0.0111–0.01282-TermsMooney–Rivlin
0.987 0.987–0.989 0.0029 0.0027–0.0031
3-TermsMooney–Rivlin
0.991 0.990–0.993 0.0024 0.0023–0.0025
4-Terms Ogden 0.796 0.725–0.868 0.0103 0.0090–0.0116Combined Ogden 0.653 0.533–0.774 0.0129 0.0107–0.01515-TermsMooney–Rivlin
0.992 0.991–0.993 0.0023 0.0022–0.0025
Fig. 7 – The mean Cauchy stress–principal stretch curve andthe Cauchy stress–principal stretch curves with respectivelythe highest and lowest stretch at the maximum load of 10 Nfor (A) the cemented group and (B) the cementless group.
j o u r n a l o f t h e m e c h a n i c a l b e h a v i o r o f b i o m e d i c a l m a t e r i a l s 3 8 ( 2 0 1 4 ) 5 9 – 6 8 65
particles originate from the articulating surfaces, proximallydeveloped interface tissue might contain more wear particles.Since the interface tissue was harvested after the removal ofthe prosthesis, small bone and or bone cement particles couldhave been introduced into the tissue. The presence of wearparticles and bone or bone cement fragments might influencethe mechanical properties. As it is not possible to perform bothhistological evaluation and compression test on the samespecimen, histological evaluation was not performed. It istherefore unknown whether such particles were present inthe specimens.
Furthermore, due to the viscous nature of the material, itwas difficult to prepare perfectly identically-shaped speci-mens, causing some variations in the specimen diameter(70.2 mm). For the same reason, it was not possible to createspecimen with absolutely flat and parallel faces, which mightinduce asperity-flattening effects.
Hori and Lewis (1982) tested tissue present betweenimplant and bone at the tibial plateau (subplate tissue) andthe tissue present between implant stem and bone (cavitytissue) of the canine stifle joint. They implanted a prosthesis
in six dogs in the same way, hence the interface tissue wasdeveloped under comparable circumstances in these dogs.The interface tissue may therefore have been more homo-geneous than in our study. Although the tested interfacetissue in dogs may not be fully representative of the humaninterface tissue, Hori and Lewis describe the same type ofnon-linear behavior.
Different hyperelastic models were fitted to each indivi-dual stress strain curve. In order to test the sensitivity of themodel to different initial guesses of the model coefficients,each model was fitted five times to the same stress straincurve with random initial guesses. This showed that for thecombined Logarithmic–Ogden model and 4-terms Ogdenmodel, the optimisation algorithm was unable to convergeto a global minimum most probably due to the interdepen-dence of the parameters (Fig. 6). In contrast to the otherfitted models, each time the combined Logarithmic–Ogdenmodel or 4-terms Ogden model was fitted to the same curve,different model coefficients were found. The mechanicalbehavior of the human interface tissue under compressionwas best described by the 5-terms Mooney–Rivlin model.Fitting this model to each individual stress–strain curveresulted in a good description of the mechanical behavior.The stress–strain curves showed variation between patients,which is almost the same as the variation of the stress–straincurves within patients (Fig. 4). The parameters of the 5 termsMooney–Rivlin model were estimated for the mean data aswell as for the curves with the lowest and highest strain at aload of 10 N, a summary of material model parameters ispresented in Table 5. Future patient-specific finite elementstudies that, for example, investigate the effects of the inter-face tissue layer on prosthesis movements, could considerthe influence of variation in the mechanical behavior ofthe interface tissue on the prosthesis movement using thedifferent sets of material model parameters presented here.
The variation of the stress strain curves is not seen in themodulus of elasticity. The 95% confidence intervals of the Emoduli are small. Therefore, it is not expected that includingmore specimens will result in different statistical outcome.
Even the material models that match the compressiontests very well may start to behave differently under otherloading modes or under multi-axial loading. In order to fullydescribe the material behaviour under multi-axial loading, itis important to perform more than one type of test. Sinceprostheses are loaded in shear as well as in compression, it isparticularly important to study the behaviour of the interface

Table 5 – Summary of model coefficients for the 5 terms Mooney–Rivlin model.
Cemented Cementless
Smallest strain Mean strain Highest strain Smallest strain Mean strain Highest strain
C1 �0.0253 �0.0074 �0.0234 �0.1493 �0.0137 0.0068C2 0.0144 0.0019 0.0179 0.1234 0.0069 �0.0068C3 0.2734 0 0 2.3580 0.0026 0C4 �0.2592 �0.0032 �0.0066 �1.8338 �0.0094 0.0016C5 �0.0816 0 0 �0.8252 0 0
j o u r n a l o f t h e m e c h a n i c a l b e h a v i o r o f b i o m e d i c a l m a t e r i a l s 3 8 ( 2 0 1 4 ) 5 9 – 6 866
tissue under shear loading. The material properties obtainedin different tests could then be combined into multi-axialconstitutive equations and be used for finite element model-ling of the implants surrounded by loose interface tissue.Even though the load applied on orthopaedic implants islarger than the range of loads used in the current study, notall the applied load is transmitted through the interfacetissue, since bone also transmits a significant portion of theapplied load. That is why in the current study, as well as inthe only other similar study (Hori and Lewis, 1982), smallerloads up to 10 N have been used.
Since the squeezing of water out of the material speci-mens contributes to the stiffness of the material, the appliedstrain rate plays an important role in unconfined compres-sion testing of soft tissues. Ideally, the tests should beperformed either very slowly close to equilibrium or veryquickly such that there is no time for significant fluid flow. Inthe present study, we performed the experiments very slowlyat 0.01 mm/min. Each experiment took on average about20 min to complete (i.e. to go from 0 N to 10 N). Observationsregarding the fluid flow and individual stress–strain curvessuggested that the experiments were performed under near-equilibrium conditions.
In principle, the fluid loss during unconfined compressionmay cause some deviations from the incompressibility con-ditions. When interpreting the load–displacement curves ofvery soft tissues tested under unconfined compression, thestandard practice, as noted by Miller (2005), is to assume theincompressibility condition holds true.
5. Conclusion
From our uni-axial unconfined compression test, we deductthat the elasticity modulus of tissue of the cemented group in
the high-strain region of stress–strain curves was signifcantlyhigher as compared to that of the tissue from the cementlessgroup. Among the six hyperelastic material models consid-ered here, the 5-terms Mooney–Rivlin model is found to bestdescribe the mechanical behavior of the interface tissueunder compression. As the results show large variations inthe mechanical behavior of the interface tissue, finite ele-ment modeling studies should not only use the meanmaterial model parameters but also the material modelparameters from the extreme deformation curves, for exam-ple, to investigate the effects of the mechanical behavior ofinterface tissue on the displacement of loose prostheses.
Acknowledgments
The authors would like to thank Piet Bakkenes at the LUMCDepartment of Instrumentation Development for producingthe parts of the experimental setup. The authors also thankthe orthopedic surgeons from MCHaaglanden, Haga Hospital,Reinier de Graaf Gasthuis, Rijnland Hospital and LeidenUniversity Medical Center for collecting the interface tissue.
This research is supported by the Dutch TechnologyFoundation STW, which is the applied science division ofNWO, and the Technology Programme of the Ministry ofEconomic Affairs (grant number LKG 7943).
Appendix A
See below for Fig. A1.
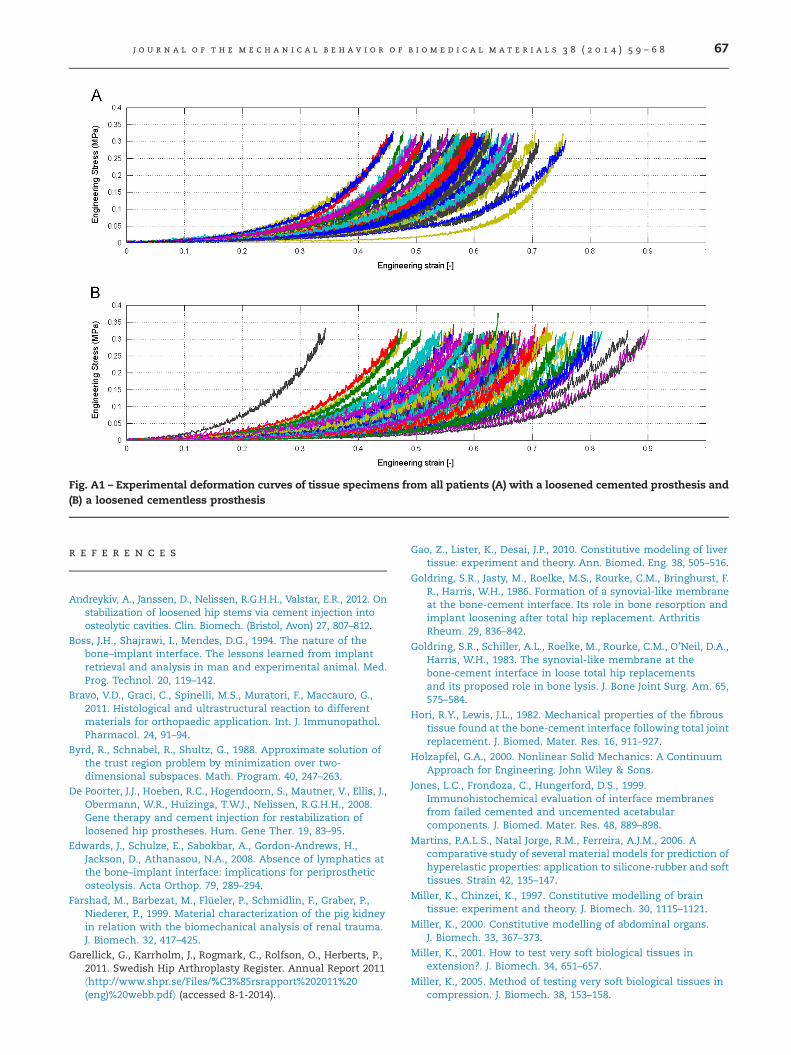
Fig. A1 – Experimental deformation curves of tissue specimens from all patients (A) with a loosened cemented prosthesis and(B) a loosened cementless prosthesis
j o u r n a l o f t h e m e c h a n i c a l b e h a v i o r o f b i o m e d i c a l m a t e r i a l s 3 8 ( 2 0 1 4 ) 5 9 – 6 8 67
r e f e r e n c e s
Andreykiv, A., Janssen, D., Nelissen, R.G.H.H., Valstar, E.R., 2012. Onstabilization of loosened hip stems via cement injection intoosteolytic cavities. Clin. Biomech. (Bristol, Avon) 27, 807–812.
Boss, J.H., Shajrawi, I., Mendes, D.G., 1994. The nature of thebone–implant interface. The lessons learned from implantretrieval and analysis in man and experimental animal. Med.Prog. Technol. 20, 119–142.
Bravo, V.D., Graci, C., Spinelli, M.S., Muratori, F., Maccauro, G.,2011. Histological and ultrastructural reaction to differentmaterials for orthopaedic application. Int. J. Immunopathol.Pharmacol. 24, 91–94.
Byrd, R., Schnabel, R., Shultz, G., 1988. Approximate solution ofthe trust region problem by minimization over two-dimensional subspaces. Math. Program. 40, 247–263.
De Poorter, J.J., Hoeben, R.C., Hogendoorn, S., Mautner, V., Ellis, J.,Obermann, W.R., Huizinga, T.W.J., Nelissen, R.G.H.H., 2008.Gene therapy and cement injection for restabilization ofloosened hip prostheses. Hum. Gene Ther. 19, 83–95.
Edwards, J., Schulze, E., Sabokbar, A., Gordon-Andrews, H.,Jackson, D., Athanasou, N.A., 2008. Absence of lymphatics atthe bone–implant interface: implications for periprostheticosteolysis. Acta Orthop. 79, 289–294.
Farshad, M., Barbezat, M., Flueler, P., Schmidlin, F., Graber, P.,Niederer, P., 1999. Material characterization of the pig kidneyin relation with the biomechanical analysis of renal trauma.J. Biomech. 32, 417–425.
Garellick, G., Karrholm, J., Rogmark, C., Rolfson, O., Herberts, P.,2011. Swedish Hip Arthroplasty Register. Annual Report 2011⟨http://www.shpr.se/Files/%C3%85rsrapport%202011%20(eng)%20webb.pdf⟩ (accessed 8-1-2014).
Gao, Z., Lister, K., Desai, J.P., 2010. Constitutive modeling of livertissue: experiment and theory. Ann. Biomed. Eng. 38, 505–516.
Goldring, S.R., Jasty, M., Roelke, M.S., Rourke, C.M., Bringhurst, F.R., Harris, W.H., 1986. Formation of a synovial-like membraneat the bone-cement interface. Its role in bone resorption andimplant loosening after total hip replacement. ArthritisRheum. 29, 836–842.
Goldring, S.R., Schiller, A.L., Roelke, M., Rourke, C.M., O’Neil, D.A.,Harris, W.H., 1983. The synovial-like membrane at thebone-cement interface in loose total hip replacementsand its proposed role in bone lysis. J. Bone Joint Surg. Am. 65,575–584.
Hori, R.Y., Lewis, J.L., 1982. Mechanical properties of the fibroustissue found at the bone-cement interface following total jointreplacement. J. Biomed. Mater. Res. 16, 911–927.
Holzapfel, G.A., 2000. Nonlinear Solid Mechanics: A ContinuumApproach for Engineering. John Wiley & Sons.
Jones, L.C., Frondoza, C., Hungerford, D.S., 1999.Immunohistochemical evaluation of interface membranesfrom failed cemented and uncemented acetabularcomponents. J. Biomed. Mater. Res. 48, 889–898.
Martins, P.A.L.S., Natal Jorge, R.M., Ferreira, A.J.M., 2006. Acomparative study of several material models for prediction ofhyperelastic properties: application to silicone-rubber and softtissues. Strain 42, 135–147.
Miller, K., Chinzei, K., 1997. Constitutive modelling of braintissue: experiment and theory. J. Biomech. 30, 1115–1121.
Miller, K., 2000. Constitutive modelling of abdominal organs.J. Biomech. 33, 367–373.
Miller, K., 2001. How to test very soft biological tissues inextension?. J. Biomech. 34, 651–657.
Miller, K., 2005. Method of testing very soft biological tissues incompression. J. Biomech. 38, 153–158.

j o u r n a l o f t h e m e c h a n i c a l b e h a v i o r o f b i o m e d i c a l m a t e r i a l s 3 8 ( 2 0 1 4 ) 5 9 – 6 868
Miller, K., Chinzei, K., 2002. Mechanical properties of brain tissuein tension. J. Biomech. 35, 483–490.
Miller-Young, J.E., Duncan, N.A., Baroud, G., 2002. Materialproperties of the human calcaneal fat pad in compression:experiment and theory. J. Biomech. 35, 1523–1531.
Mooney, M., 1940. A Theory of Large Elastic Deformation. J. Appl.Phys. 11, 582–592.
Neale, S.D., Fujikawa, Y., Sabokbar, A., Gundle, R., Murray, D.W.,Graves, S.E., Howie, D.W., Athanasou, N.A., 2000. Humanbone-derived cells support formation of human osteoclastsfrom arthroplasty-derived cells in vitro. J. Bone Joint Surg. Br.82, 892–900.
Ogden, R.W., 1984. Non-Linear Elastic Deformations. DoverPublications Inc.
Ogden, R.W., Saccomandi, G., Sgura, I., 2004. Fitting hyperelasticmodels to experimental data. Comput. Mech. 34, 484–502.
Poelert, S., Valstar, E., Weinans, H., Zadpoor, A.A., 2013. Patient-specific finite element modeling of bones. Proc. Inst. Mech.Eng. Part H J. Eng. Med. 227, 464–478.
Quinn, J., Joyner, C., Triffitt, J.T., Athanasou, N.A., 1992.Polymethylmethacrylate-induced inflammatory macrophagesresorb bone. J. Bone Joint Surg. Br. 74, 652–658.
Rashid, B., Destrade, M., Gilchrist, M.D., 2012. Determination offriction coefficient in unconfined compression of brain tissue.J. Mech. Behav. Biomed. Mater. 14, 163–171.
Rivlin, R.S., 1948. Large elastic deformations of isotropic materialsIV. Further developments of the general theory. Philos. Trans.R. Soc. Lond. A 241, 379–397.
Shoji, H., Karube, S., D’Ambrosia, R.D., Dabezies, E.J., Miller, D.R.,1983. Biochemical features of pseudomembrane at the bone-cement interface of loosened total hip prostheses. J. Biomed.Mater. Res. 17, 669–678.
Snedeker, J.G., Niederer, P., Schmidlin, F.R., Farshad, M.,Demetropoulos, C.K., Lee, J.B., Yang, K.H., 2005. Strain-ratedependent material properties of the porcine and humankidney capsule. J. Biomech. 38, 1011–1021.
Strehle, J., DelNotaro, C., Orler, R., Isler, B., 2000. The outcome ofrevision hip arthroplasty in patients older than age 80 years:complications and social outcome of different risk groups.J. Arthroplasty 15, 690–697.
Umale, S., Deck, C., Bourdet, N., Dhumane, P., Soler, L.,Marescaux, J., Willinger, R., 2013. Experimental mechanicalcharacterization of abdominal organs: liver, kidney & spleen.J. Mech. Behav. Biomed. Mater. 17, 22–33.
Wang, J.S., Diaz, J., Sabokbar, A., Athanasou, N., Kjellson, F.,Tanner, K.E., McCarthy, I.D., Lidgren, L., 2005. In vitro andin vivo biological responses to a novel radiopacifying agent forbone cement. J. R. Soc. Interface 2, 71–78.
Wu, J.Z., Cutlip, R.G., Andrew, M.E., Dong, R.G., 2007.Simultaneous determination of the nonlinear-elasticproperties of skin and subcutaneous tissue in unconfinedcompression tests. Skin Res. Technol. 13, 34–42.
Yang, L.M., Shim, V.P.W., Lim, C.T., 2000. A visco-hyperelasticapproach to modelling the constitutive behaviour of rubber.Int. J. Impact Eng. 24, 545–560.