Meaning perspective transformation following stroke: the process of change
10
RESEARCH PAPER Meaning perspective transformation following stroke: the process of change DOROTHY KESSLER 1 , CLAIRE-JEHANNE DUBOULOZ 2 , REG URBANOWSKI 3 & MARY EGAN 2 1 Occupational Therapy Service, Bruye `re Continuing Care, Ottawa, ON, Canada, 2 Faculty of Health Sciences, School of Rehabilitation Sciences, University of Ottawa, Ottawa, ON, Canada, and 3 Universities and Adult Learning, Ministry of Advanced Education, Employment and Labour, Regina, Saskatchewan, Canada Accepted August 2008 Abstract Purpose. Transformative Learning in an educational theory that posits that individuals learn and grow when their meaning perspectives (frames of reference for interpreting an experience based on knowledge, feelings, values and beliefs) are reformulated following a critical event. This theory has become quite influential in the exploration of adaptation to chronic illness. This study explored whether the change that occurs following stroke follows a process similar to transformative learning. Method. Grounded Theory approach was used to explore changes in meaning perspective among 12 people who were members of stroke support organisations, had a stroke at least 1 year prior to the study and described themselves as viewing life positively following stroke. Constant comparison analysis of interviews with these individuals was used to explore their experience following stroke. Results. Meaning perspective transformation occurred with four factors contributing to transformation: triggers, support, knowledge and choices to action. A substantive grounded theory of the process of meaning perspective transformation following stroke is presented, which illustrates the interaction of these contributing factors in initiating and facilitating the transformation process. Conclusion. Transformative learning can offer insight into how people who have experienced stroke learn, rebuild competence and re-engage in valued activities. Keywords: Stroke, transformative learning, grounded theory, rehabilitation Introduction Stroke is a major cause of disability, disrupting the lives of those who experience it. Studies indicate that many stroke survivors continue to experience de- pression [1,2], activity limitations [3,4], and reduced quality of life [3,5,6] despite the services provided. More knowledge of how people who have experienced stroke adapt, find meaning and reshape their lives is needed to assist in developing effective interventions and resources. Transformative Learning Theory [7] offers a framework for under- standing and facilitating change in how individuals living with chronic illness or disability ascribe mean- ing to experiences and therefore may have implica- tions for stroke recovery. The concept of transformative learning emerged from Mezirow’s [7] work in the area of adult learning. Mezirow [7] defines transformative learn- ing as ‘the process of learning through critical self- reflection, which results in the reformulation [or transformation] of a meaning perspective to allow a Correspondence: Dorothy Kessler, St. Vincent Hospital, Bruye `re Continuing Care, 60 Cambridge St. North, Ottawa, ON K1R 7A5, Canada. Tel: þ1 613 562 4262 ext. 2083. Fax: þ1 613 782 2785. E-mail: [email protected] Disability and Rehabilitation, 2009; 31(13): 1056–1065 ISSN 0963-8288 print/ISSN 1464-5165 online ª 2009 Informa UK Ltd. DOI: 10.1080/09638280802509512
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Meaning perspective transformation following stroke: the process of change

RESEARCH PAPER
Meaning perspective transformation following stroke: the process ofchange
DOROTHY KESSLER1, CLAIRE-JEHANNE DUBOULOZ2, REG URBANOWSKI3 &
MARY EGAN2
1Occupational Therapy Service, Bruyere Continuing Care, Ottawa, ON, Canada, 2Faculty of Health Sciences, School of
Rehabilitation Sciences, University of Ottawa, Ottawa, ON, Canada, and 3Universities and Adult Learning, Ministry of
Advanced Education, Employment and Labour, Regina, Saskatchewan, Canada
Accepted August 2008
AbstractPurpose. Transformative Learning in an educational theory that posits that individuals learn and grow when their meaningperspectives (frames of reference for interpreting an experience based on knowledge, feelings, values and beliefs) arereformulated following a critical event. This theory has become quite influential in the exploration of adaptation to chronicillness. This study explored whether the change that occurs following stroke follows a process similar to transformativelearning.Method. Grounded Theory approach was used to explore changes in meaning perspective among 12 people who weremembers of stroke support organisations, had a stroke at least 1 year prior to the study and described themselves as viewinglife positively following stroke. Constant comparison analysis of interviews with these individuals was used to explore theirexperience following stroke.Results. Meaning perspective transformation occurred with four factors contributing to transformation: triggers, support,knowledge and choices to action. A substantive grounded theory of the process of meaning perspective transformationfollowing stroke is presented, which illustrates the interaction of these contributing factors in initiating and facilitating thetransformation process.Conclusion. Transformative learning can offer insight into how people who have experienced stroke learn, rebuildcompetence and re-engage in valued activities.
Keywords: Stroke, transformative learning, grounded theory, rehabilitation
Introduction
Stroke is a major cause of disability, disrupting the
lives of those who experience it. Studies indicate that
many stroke survivors continue to experience de-
pression [1,2], activity limitations [3,4], and reduced
quality of life [3,5,6] despite the services provided.
More knowledge of how people who have
experienced stroke adapt, find meaning and reshape
their lives is needed to assist in developing
effective interventions and resources. Transformative
Learning Theory [7] offers a framework for under-
standing and facilitating change in how individuals
living with chronic illness or disability ascribe mean-
ing to experiences and therefore may have implica-
tions for stroke recovery.
The concept of transformative learning emerged
from Mezirow’s [7] work in the area of adult
learning. Mezirow [7] defines transformative learn-
ing as ‘the process of learning through critical self-
reflection, which results in the reformulation [or
transformation] of a meaning perspective to allow a
Correspondence: Dorothy Kessler, St. Vincent Hospital, Bruyere Continuing Care, 60 Cambridge St. North, Ottawa, ON K1R 7A5, Canada.
Tel: þ1 613 562 4262 ext. 2083. Fax: þ1 613 782 2785. E-mail: [email protected]
Disability and Rehabilitation, 2009; 31(13): 1056–1065
ISSN 0963-8288 print/ISSN 1464-5165 online ª 2009 Informa UK Ltd.
DOI: 10.1080/09638280802509512

more inclusive, discriminating, and integrative un-
derstanding of one’s experience’. (p. xvi) Meaning
perspectives are frames of reference for interpreting
an experience based on knowledge, feelings, values
and beliefs [8]. Through critical reflection, a person
reassesses presuppositions on which beliefs are based
and develops new insights on which to base action.
Mezirow [9] identifies the following phases of
transformative learning with the end result being
transformation of meaning perspective: (a) a dis-
orienting dilemma, (b) self-examination of feelings,
(c) critical reflection, (d) recognising that others may
share similar discontent and have negotiated change,
(e) exploration and planning of new roles, relation-
ships and actions, (f) acquiring knowledge and skills,
(g) trying out new roles and actions, (h) negotiating
relationships, (i) building competence and (j) re-
integration into life with new perspective as a basis.
Although these phases are presented as occurring in
a linear manner, the process may proceed in a more
circular and spiraling fashion and may not include all
phases [10].
Examination of current models of adaptation to
stroke and Transformative Learning Theory applica-
tions in the areas of health and chronic illness
demonstrate support for potential application of
Transformative Learning Theory in the area of
stroke.
Models of adaptation following stroke
A number of qualitative studies have been
carried out to explore life post-stroke and
propose models for adaptation [11–15]. Included
in the results of most of these studies is
movement from shock, fear and hope in the acute
stage, to sadness at losses in functional abilities, to
acceptance of the remaining disability and re-
engagement in life with changed abilities. These
studies provide valuable information on the experi-
ences and feelings of people living with stroke but
offer little information about what facilitates
transition from one phase or stage to another. It
appears, though, that multiple comparisons [15],
changes in the perception of the situation [14,15],
movement from hope for total recovery to finding
new meaning and possibilities despite residual
disability [11,14], support from family and friends
[13,14], and taking increasing responsibility for
one’s health [11] may contribute to such adapta-
tion. These findings share similarities with
Mezirow’s stages in Transformative Learning
theory [9]. For example, initial feelings of loss
and fear fit with Mezirow’s disorienting dilemma,
and changes in perceptions and redefining
meaning suggest transformation of meaning
perspective.
Transformation and chronic illness
The process of transformation among people
with rheumatoid arthritis, cardiac conditions,
multiple sclerosis, Type I diabetes, spinal cord
injury (SCI), breast cancer and HIV/AIDS has
been explored in previous studies. A range of
transformation of meaning perspectives has been
uncovered. Shared themes among several of these
studies appear to be transformation of how one
evaluates the self [16–18]. For example, individuals
with arthritis who were receiving home-based reha-
bilitation shifted from a self-evaluation based on self-
reliance, activity and altruism to redefined values
within a self-caring framework [19,20]. Similarly, for
individuals who were receiving rehabilitation follow-
ing severe cardiac events, the importance of trans-
formation of self-definition was a key to adoption of a
new lifestyle that would allow them to care for their
health [16]. In a qualitative study of people with
Type I diabetes, the process of transformation
involved differentiating self from illness and body,
enabling the person to address challenges, maintain
self-integrity and learn new ways of doing and being
[21].
Other studies describe varying yet related concepts
in the transformation process and start to identify
contributors to transformation. Carpenter [22] ex-
plored the experience of people with SCI from a
transformative learning perspective and identified
themes of (a) rediscovering self, (b) redefining
disability and (c) establishment of a new identity.
Establishment of a new identity was facilitated by
realising potential in part through comparison with
others, and positive social experiences. In breast
cancer survivors, self-esteem and well-being have
been associated with self-transformation [23].
Baumgartner [24] observed transformational
learning among individuals living with HIV/AIDS
over a long period of time. Transformation included
increased appreciation of the human condition and
an expanded view of intimacy. Social interaction was
important in this process of transformation. Simi-
larly, Courtenay et al. [25] examined the process of
meaning making following a diagnosis of HIV/AIDS.
They identified a meaning-making process which
included development of new meaning which was
stabilised through opportunities to contribute to the
lives of others, heightened sensitivity to life and being
of service to others with HIV/AIDS.
Stroke is a chronic illness and therefore people
living with the consequences of a stroke may share
similar experiences with those described in the above
studies of transformation and chronic illness. This
study explored whether the change that occurs
following stroke follows a process similar to trans-
formative learning.
Meaning perspective change following stroke 1057

Methodology
A Grounded Theory approach was used as it is a
general methodology for developing theory that is
grounded in data systematically gathered and
analysed [26], and due to its focus on the day to
day life of people, understanding motivation,
action, interaction and how reality is constructed
[27] and its strength in providing a method for
systematic exploration of the potential phenomen-
on of meaning perspective transformation following
stroke.
For ease of recruitment, participants were identi-
fied through community organisations and facilities
that offered programs for stroke survivors.
Semi-structured interviews were used to gather
information related to personal experience of stroke
(Table I). Probing questions were asked to capture
information related to meaning perspectives (feel-
ings, knowledge, values and beliefs) related to
participation, identity and illness, and factors con-
tributing to change following stroke. The interviews
were conducted by the first author, an occupational
therapist with 20 years experience working with
stroke survivors. The interviews were audio taped
and transcribed verbatim. A copy of the complete
transcribed interview was sent to participants for
their review.
Data analysis was completed using the constant
comparative method according to the procedures for
Grounded Theory outlined by Strauss and Corbin
[28]. These procedures included coding (open, axial
and selective), memo writing and constant compar-
ison. Transcribed interviews were analysed line by
line to identify and define key participant ideas,
actions and meanings as concepts or categories.
Initial concepts and categories were then analysed
and grouped during axial coding. In particular,
concepts and categories were grouped to compare
experiences pre-stroke to those post-stroke. Rela-
tionships between categories were identified and
story lines developed, using selective coding. These
story lines were integrated through further examina-
tion of relationships into a substantive Grounded
Theory on the process of transformation following
stroke. Analysis from all of the above steps was
presented to and discussed with the second author
during regular meetings where findings were con-
firmed or further developed.
Results
Twelve participants, 10 men and 2 women, con-
sented to participate in the study. The average age at
onset of stroke was 54 years with a range of 44–74.
Eight of the participants had experienced right brain
strokes, three had experienced left brain strokes and
one reported bilateral involvement. All participants
were able to walk with or without an aid but reported
some limitations in movement and/or balance. Four
participants had deficits in communication. Nine
reported or were observed to have mild-to-moderate
cognitive deficits. The average time since onset of
stroke at the time of the interview was 6.5 years with
a range of 3–11 years.
Meaning perspectives, as frames of reference
for interpreting the dimensions of work, family
role, illness/health, identity, living and recovery,
transformed or emerged following stroke [29]. The
processes of transformation of these meaning
perspectives were interconnected based on
four main contributing factors that moved partici-
pants towards transformation: triggers, support,
knowledge and choices to action. A substantive
Grounded Theory based on these four contributing
factors is presented in this article. Each contributing
factor is considered first separately and then
the interconnections between these factors are
described.
Triggers
Two triggers to the process of meaning perspective
transformation were identified. These were experi-
ence of limitations, and feelings of vulnerability. For
all transformed and new meaning perspectives, the
experience of limitations following stroke was a
trigger, which started the transformation process.
Participants could no longer participate in their lives
as they had done prior to stroke. They were faced
with challenges and the need for assistance from
others.
‘Before the stroke there’s nothing that I couldn’t tackle. I
could tackle anything that came along, you know what I
mean? After the stroke, I’m very limited.’
‘ . . . it [having a heart attack] didn’t hit home as hard as
having the stroke because I had to sort of adapt and do
things differently, or I became more tired.’
Table I. Semi-structured interview guide.
1. Could you tell me about your life before you had a stroke?
What did you used to do? What activities would you do on an
average day?
How would you describe yourself before the stroke?
What did you know about stroke?
2. Could you tell me about what your life has been like since you
had the stroke?
What do you do now? What do you do on an average day?
How would you describe yourself now?
What is your knowledge of stroke now?
1058 D. Kessler et al.

Along with the experience of limitations, the feelingof
being vulnerable was a trigger to start the transformation
process. Feelings of vulnerability were reflected through
concerns about health, having another stroke, the
possibility of death and loss of control.
‘But it wasn’t like there was any pain or anything. You
know, you are just going and going. And then one of the
pipes bursts. Your brain is bleeding and you’re going to
maybe die.’
‘It was the fact that I was absolutely helpless.’
Experience of limitations and feelings of vulner-
ability led participants to start to seek control, and to
examine their definition of self, their approach to life
and the priorities in their lives.
Support
Support received from others, including family,
friends, peers and health professionals, was an
overarching contributing factor that facilitated move-
ment towards meaning perspective transformation.
Support came in several forms: being there, provid-
ing assistance, providing encouragement and moti-
vation, shared experience or belonging, and instilling
feelings of value and competence.
‘As I say, that support, giving me a job that was not just
sanding, it was a little more stimulating.’
‘My daughter she gets a day about every two weeks,
she’ll call me and say, ‘‘Next Wednesday I have the day
off, Dad. It’s father-daughter day. Where’d you like to
go?’’ So I plan where we go, she drives and so we go.’
Support had an impact on work, family role,
illness/health, identity, recovery and living. For
example, participants reported strengthened family
relationships following stroke based on assistance
and encouragement received from them and on
instilled feelings of competence and value as a family
member. This support contributed to transformed
value of family with redefined family role.
Peer support was particularly important for trans-
formation of identity. Peer support developed as a
result of participants choosing recovery-related activ-
ities, which led to connection with others who had
experienced stroke. The opportunity to engage with
others who shared the experience of stroke and
develop a sense of belonging was important for
redefining self with stroke.
‘Someone comes in and says, ‘‘I’m crazy, I keep falling
over all the time’’. And you reassure them that so you
fell down, well we all fell down. Big deal. And it’s not
coming from a professional who didn’t have the stroke.’
‘So it’s a nice feeling when, sometimes when
they [others in swim program] feel that they can’t
quite do it they’ll ask me because we understand each
other.’
Participants’ environments of support enabled
them to seek knowledge and make choices to action
throughout the transformation process.
Knowledge
Knowledge facilitated transformation of values,
beliefs and meaning related to work, family role,
illness/health, identity, recovery and living. Partici-
pants in this study sought knowledge through read-
ing and other sources following stroke to understand
what had happened to them, to learn about how to
prevent another stroke, and to learn about possibi-
lities for recovery and living.
One source of knowledge was the experience of
others with stroke. Knowledge gained through
interaction with others who had experienced stroke
enabled participants to use comparison with others
as a strategy for establishing an optimistic perspective
on their lives. This strategy seemed to involve
reflection on the situations and choices of others
related to their strokes.
‘I saw that amongst the people that I was dealing with.
There were those who said ‘‘Yes, I ‘m going to learn all I
can about what I am doing and accommodate to the best
extent possible.’’ Then there were the people who had
already given up before they had gone out the door of
their hospital room.’
Knowledge seeking appeared to be a way in which
participants could take action and feel a sense of
control over the illness.
‘I’ve done a lot of reading since I had a stroke to try and
understand more about it and what happens to the
brain, what are the limitations that it has.’
Knowledge related to recovery provided hope,
motivation and a sense of control, and helped to
guide choice of activities. Knowledge also offered
evidence for reflection. Through reflection, partici-
pants were able to gain insight into what recovery
and life with stroke meant and to re-examine
priorities. Participants re-examined their priorities
in the areas of illness/health, work and family role.
Knowledge of health risk factors, combined with the
triggers identified above, contributed to a reconfi-
guration of priorities where health became a high
priority, family became more highly valued, and the
value of work decreased.
Meaning perspective change following stroke 1059

‘I think, yes, there was a definite change in my attitude
towards my mortality. I quickly decided that you’re only
here for a limited time so there were changes in my life
and my attitude toward taking care of myself properly.’
‘I probably care more for the family so I’ll put them first
instead of the work.’
Knowledge facilitated transformation by helping
participants gain understanding and a sense of
control, which in turn promoted decision making
and action.
Choices to action
Choices to action facilitated transformation of the
meanings of work, family role, illness/health, iden-
tity, recovery, and living. Participants responded to
their feelings of loss of control imposed by stroke by
seeking control. This was done through making
choices and taking action on these choices. When the
result of such decision-making was a success,
increased competence was felt. This, in turn,
promoted ongoing decision-making and action.
Two of the choices made early on following the
experience of stroke were to seek knowledge (as
described earlier) and to try to recover from the
stroke. Participation in recovery-related activities
increased feeling of competency by providing a sense
of purpose, challenge, stimulation, and feelings of
accomplishment when goals were achieved.
‘After 5 years I’m beginning to be able to use my left
hand more.’
‘It [ongoing recovery] is an important mental part
because it’s nice to see that things are getting better.’
Other choices that resulted in action include acting
on new priorities, choosing a different approach to
life, finding new ways to participate, and engaging
with others who experienced stroke.
Choices to action offered a means for re-establish-
ing a sense of control and building competence, and
therefore were an important facilitator of movement
towards transformation.
The interconnection of support, knowledge and choices
to action
It is important to note that support, knowledge
and choices to action were interconnected in
facilitating movement towards meaning perspective
transformation. There appears to be a cyclical
relationship between knowledge and choices
to action that is enabled by an overarching
environment of support. For example, knowledge
was gained as a result of participants choosing to
seek knowledge and acting on this choice. Partici-
pants then gained more knowledge through their
actions. Support facilitated acquisition of knowl-
edge and enabled action.
These interconnections are further illustrated by
the relationship between the meaning perspective
transformations of recovery, living and identity.
From the knowledge that participants gained about
stroke, they learned that some aspects of their
functional abilities would improve whereas others
would continue to be limited. Participants appeared
to make two choices related to this knowledge
which resulted in the emergence of the meaning
perspective of recovery and the transformation of
living. One choice was to pursue recovery, which
led to ongoing learning, building of competence
and connection with others with stroke. The other
choice involved examination of approach to living
with limitations, where participants were able to
learn about their abilities and limitations and build
competence through participating in valued activ-
ities. Connection with others with stroke, rebuilding
competence and learning about self were all
important for transformation of identity, where self
was redefined to include stroke. The choices and
actions described above were enabled by the
presence of support.
In summary, the process of transformation started
with the contributing factors defined as triggers:
experience of limitations and feeling vulnerable.
Transformation was then facilitated by knowledge,
and choices to action that occurred in a cyclical
manner with support creating an environment
that enabled knowledge seeking and acquisition,
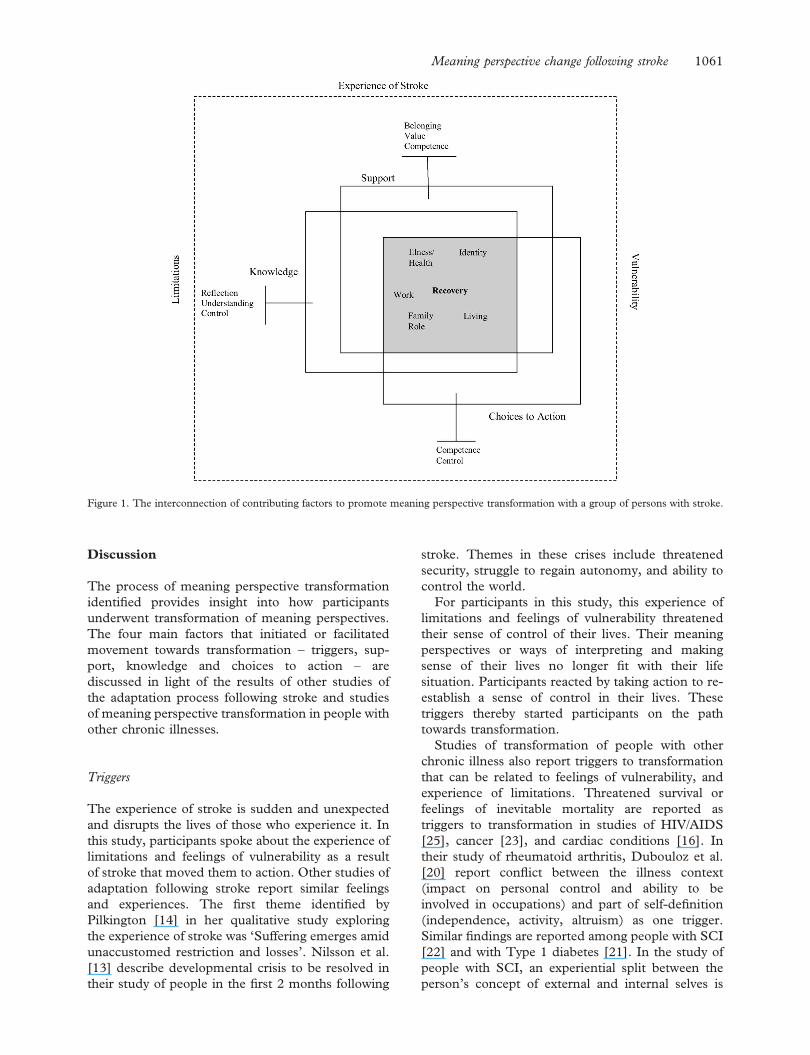
decision-making and action. Figure 1 illustrates
the interconnection of the contributing factors
in the process of meaning perspective transforma-
tion. The outside dashed square represents the
context of the experience of stroke that initiates
transformation. This context includes experience of
limitations and feelings of vulnerability. The factors
of support, knowledge and choices to action that
facilitate movement towards transformation are
represented by squares. The interconnection of
support, knowledge and choices to action is repre-
sented by the overlap of these squares creating a
central square where meaning perspective transfor-
mation occurs. The dimensions of meaning perspec-
tive transformation identified in this study are
located in this central square. Associated with each
of the contributing factors of support, knowledge and
choices to action are the important aspects that each
of these bring to the transformation process. For
example, belonging, value and competence are
associated with support.
1060 D. Kessler et al.
Discussion
The process of meaning perspective transformation
identified provides insight into how participants
underwent transformation of meaning perspectives.
The four main factors that initiated or facilitated
movement towards transformation – triggers, sup-
port, knowledge and choices to action – are
discussed in light of the results of other studies of
the adaptation process following stroke and studies
of meaning perspective transformation in people with
other chronic illnesses.
Triggers
The experience of stroke is sudden and unexpected
and disrupts the lives of those who experience it. In
this study, participants spoke about the experience of
limitations and feelings of vulnerability as a result
of stroke that moved them to action. Other studies of
adaptation following stroke report similar feelings
and experiences. The first theme identified by
Pilkington [14] in her qualitative study exploring
the experience of stroke was ‘Suffering emerges amid
unaccustomed restriction and losses’. Nilsson et al.
[13] describe developmental crisis to be resolved in
their study of people in the first 2 months following
stroke. Themes in these crises include threatened
security, struggle to regain autonomy, and ability to
control the world.
For participants in this study, this experience of
limitations and feelings of vulnerability threatened
their sense of control of their lives. Their meaning
perspectives or ways of interpreting and making
sense of their lives no longer fit with their life
situation. Participants reacted by taking action to re-
establish a sense of control in their lives. These
triggers thereby started participants on the path
towards transformation.
Studies of transformation of people with other
chronic illness also report triggers to transformation
that can be related to feelings of vulnerability, and
experience of limitations. Threatened survival or
feelings of inevitable mortality are reported as
triggers to transformation in studies of HIV/AIDS
[25], cancer [23], and cardiac conditions [16]. In
their study of rheumatoid arthritis, Dubouloz et al.
[20] report conflict between the illness context
(impact on personal control and ability to be
involved in occupations) and part of self-definition
(independence, activity, altruism) as one trigger.
Similar findings are reported among people with SCI
[22] and with Type 1 diabetes [21]. In the study of
people with SCI, an experiential split between the
person’s concept of external and internal selves is
Figure 1. The interconnection of contributing factors to promote meaning perspective transformation with a group of persons with stroke.
Meaning perspective change following stroke 1061

described. The external self represents the experi-
ence of disability, physical changes and sense of loss.
The internal self is the sense of remaining the same
person as represented by personal life history and
experience. For those with Type 1 diabetes, a
threatened balance between self with diabetes and
self wanting to live a normal life is presented. These
three studies speak of the experience of limitations
imposed by illness and the conflict this creates with
the person’s sense of self.
Thus, the triggers to transformation identified in
this study are similar to those found in studies of
transformation of other chronic illnesses. However,
triggers may vary depending on the type of illness
and the person’s experience of it.
Support
Support was integral to the transformation process.
Support came in the form of assistance to accomplish
daily needs and valued activities and in the form of
social support – encouragement and belonging.
Participants received support from family, friends,
health professionals and/or other stroke survivors.
Through this support, participants experienced feel-
ings of being valued, of being competent and of
belonging.
Support has been widely identified in the stroke
literature as an important factor for adaptation
following stroke. Nilsson et al. [13] describe a crisis
to be resolved of ‘intimacy vs. isolation’ where
supportive relationships were identified as important.
The theme of ‘consoling relationships uplift the self’
as identified by Pilkington [14] also relays the
importance of social environment which includes
family, friends and caregivers.
Other studies that explore different aspects of
adaptation following stroke report the influence of
social support on well-being and quality of life
[6,30,31], continuity of self [32], and return to work
[33]. The present study adds to the literature by
describing in more detail the nature of support
needed for transformation following stroke.
Several studies of transformation in people living
with chronic illness also identity support as playing a
role in the transformation process. In her study of
people diagnosed with HIV/AIDS, Baumgartner
[24] identifies social interaction as integral to the
transformative learning process. Through social
interaction, people realised they were not alone and
they had control over the disease. A common source
of support was a support group. Support groups not
only provided support and encouragement; but also
the opportunity for relational discourse, destigmati-
sation of the disease, personal empowerment, trying
of new roles and gaining confidence. Similarly,
Carpenter [22] presents the importance participants
identified of being associated with others who shared
the experience of SCI. She also talks about the role of
accumulated positive social experience and the
reassertion of relationships with friends, family and
partners as important factors in restoring a sense of
continuum and identity. Courtenay et al. [25]
describe the support system (family, friends, support
group) as contributing to a catalytic experience that
moves people beyond their initial reaction to
diagnosis of HIV/AIDS.
Dubouloz et al. [20], in their study of people with
rheumatoid arthritis, and Paterson et al. [21], in their
study of Type 1 diabetes, both discuss the role of a
health professional in creating an environment that
supports transformation of the way participants
viewed management of their disease. Conversely,
lack of environmental support appeared to be a
barrier to transformation in a study of women
following diagnosis of breast cancer [23]. This study
found that those who reported feeling stuck and
unable complete transformation lacked the support
of health care providers, family and friends.
Based on the results of this study and the above,
support plays a role in moving a person with chronic
illness towards transformation through providing a
sense of shared experience, of continuity, of being
valued and through building feelings of competence.
Knowledge
Participants sought control in their lives following
stroke. One way that they did this was through
seeking knowledge that would help them understand
what had happened to them, why it may have
happened (risk factors) and what this meant in terms
of possibilities for recovery and living their lives.
Inherent in seeking and gaining knowledge was the
aspect of reflection on the information obtained and
its relevance to their reality.
Lack of knowledge and low satisfaction related to
provision of information of people who have experi-
enced stroke and their carers has been reported in the
literature [34]. Yet a review of the literature reveals
little benefit of information provision and education
in the area of stroke [35]. Perhaps, lack of benefit
arising from education programmes may relate to
how well these programmes correspond to the stroke
survivors’ underlying purpose for knowledge acquisi-
tion – one of re-establishing control. One other study
was found that mentions, but does not elaborate on,
knowledge as a source of control for participants
following stroke [11]. Programmes that provide
information but do not encourage participants to
use this information to enable them to regain control
of their lives may be viewed as ineffective.
1062 D. Kessler et al.

The role of knowledge in studies of transformation
with other chronic illnesses is not specifically
discussed but is mentioned in a few studies. Knowl-
edge of illness was described by Dubouloz et al. [20]
as a key element for critical reflection and the
resultant transformation of participants with rheu-
matoid arthritis receiving occupational therapy ser-
vices. Similarly, Paterson et al. [21] describe
participants with Type 1 diabetes as developing a
new understanding of health in a process where they
discover that they can respond to challenges and
manage their disease. Viewing self as in control of the
disease allowed the person to focus on life goals
despite limitations posed by effects of the disease.
In the present study, participants used knowledge
gained through reading and through comparison
with others to make decisions related to recovery,
health and living. In this way they established
themselves as being in control of their health and
their lives with stroke. Knowledge related to illness
and its management/expected course appears to
facilitate movement towards transformations for
participants with some chronic illnesses.
Choices to action
Participants in this study appeared to use knowledge
to re-establish a sense of personal control, which
then promoted making choices and taking action to
regain more control in their lives. Through choices
and actions that resulted in a positive outcome, such
as improvements in abilities, participants rebuilt their
feelings of competence.
In other studies of the experience of stroke themes
arise related to control, competence, choice and
action. Three of the crises experienced by people
following stroke, which Nilsson et al. [13] identified,
reflect choices and actions related to control and
competence. These are ‘autonomy vs. shame/doubt,’
‘initiation vs. guilt’ and ‘industry vs. inferiority’. In
these themes, participants talked about the ability to
control the world, regaining autonomy, courage to
act and regaining competence. George et al. [36]
examined impact of emotional changes following
stroke. One subject in their study reported the
positive impact of participating in activities where
he felt a sense of control. Conversely, ongoing
depression following stroke has been associated with
lower levels of perceived control over recovery as
well as a greater degree of communication
impairment [37].
In some studies of transformation with other
chronic illnesses, making choices and taking action
were reported as being associated with transforma-
tion. In the study of people with cardiac conditions
[16], clients were finally able to apply what was
taught in their rehabilitation program to their daily
living after having transformed their meaning of work
which had been a barrier to new learning. Namely,
clients integrated different ways of cooking and
eating, and a certain number of minutes of physical
activity into their daily schedule. In her study of
women with breast cancer, Carpenter et al. [23]
describe a difference between those with positive
transformation and those with minimal transforma-
tion or described as stuck. Those with positive
transformation made the choice to review their lives
and had courage and strength to take action and
make changes. Those with minimal transformation
had a high degree of self-acceptance and did not
make similar choices. Those who were stuck were
not able to describe what changes were desired. They
lacked a clear decision to guide action. In her
description of how people redefine disability follow-
ing SCI, Carpenter [22] talks about building con-
fidence and self-esteem through exploring options,
getting involved and meeting self-determined goals.
Courtenay et al. [25] also talk about people with
HIV/AIDS making choices and taking action
through exploring options, modifying activities and
choosing alternate perceptions.
These studies support the role of making choices
and taking action in the transformation process. To
make these choices and take action people may
require some feeling of control, courage and
strength.
The interconnection of support, knowledge and choices
to action
This study introduces an interconnection between
support, knowledge and choices to action within the
transformation process that is not presented else-
where in the literature exploring adaptation following
stroke or meaning perspective transformation in
people with other chronic illnesses. Further research
exploring transformation by following people who
have experienced stroke through the process of
change could provide more information on the
interplay of contributing factors and the progression
of meanings perspective transformation.
Limitations
It is important to point out that the participants in
this study were recruited primarily from a stroke
support organisation. Therefore, they may have been
inclined towards finding meaning in information,
action and support from others. As well, their
perceptions of their processes of adjustment come
from retrospective reflection on the preceding 3–11
Meaning perspective change following stroke 1063

years. These perceptions may have changed over
time and may still be open to change. However, we
believe that the in-depth interviews focussing on the
transformation process provide a unique and helpful
view of the process of making a good recovery from
stroke.
The individuals interviewed were a relatively
young group of stroke survivors. The experience of
older individuals, who make up the majority of stroke
survivors, may be quite different. As well, to
participate in the study, a certain level of ability to
comprehend and express thoughts and ideas was
needed. Therefore, this study was not able to provide
insight into the experience of those with more
significantly impaired cognition and communication.
This study was also limited to those who could
communicate in English thereby excluding a wide
range of cultural backgrounds. As well, the bound-
aries of this study limited participants to those who
are community dwelling and did not include the
experiences of those living in long term care facilities
or retirement homes. This study provides insight into
the experience of a small number of people who have
experienced stroke and describe themselves as view-
ing life post-stroke in a generally positive way.
Conclusion
The results of this study show that transformation
of meaning perspective can occur following stroke.
The process of meaning perspective transformation
presented in this article involved two triggers that
disrupted the personal paradigms of participants.
These were experience of limitations and feelings of
vulnerability. Transformation was then facilitated by
an evolving interaction between knowledge and
choices to action, within an overarching presence of
support that instilled feelings of value, competence
and belonging. Important aspects of knowledge and
choices to action in the transformation process were
(a) knowledge of health with the choice to take
control and responsibility for one’s health, (b)
knowledge of the potential for recovery and for living
with stroke and (c) the choice of an optimistic
approach to life which led to ongoing learning about
abilities and limitations and to building competence
through participating in valued activities. At least the
first two of these aspects, knowledge regarding health
and potential for recovery, could be facilitated during
the rehabilitation process and this may enhance
adjustment following stroke.
Further research to build on the substantive theory
of the transformation of meaning perspective follow-
ing stroke presented in this paper is needed. This
research could include exploring transformation with
those who have experienced strokes of differing
severity, or exploring the experience of transforma-
tion from a temporal perspective.
Declaration of interest: The authors report no
conflicts of interest. The authors alone are respon-
sible for the content and writing of the paper.
References
1. Hacket ML, Chaturangi Y, Parag V, Anderson CS. Frequency
of depression after stroke: a systematic review of observational
studies. Stroke 2005;36:1330–1340.
2. King RB, Shade-Zeldow Y, Carlson C, Feldman JL, Philip M.
Adaptation to stroke: a longitudinal study of depressive
symptoms, physical health, and coping process. Top Stroke
Rehabil 2002;9:46–66.
3. Mayo NE, Wood-Dauphine S, Cote R, Durcam L, Carleton J.
Activity, participation and quality of life 6 months post stroke.
Arch Phys Med Rehabil 2002;83:1035–1042.
4. Pound P, Gompartz P. A patient-centered study of the
consequences of stroke. Clin Rehabil 1998;12:338–347.
5. Robinson-Smith G. Self-efficacy and quality of life after
stroke. J Neurosci Nurs 2002;34:91–98.
6. Wyller TB, Kirkevold M. How does a cerebral stroke affect
quality of life? Towards an adequate theoretical account.
Disabil Rehabil 1999;21:152–161.
7. Mezirow J. Fostering critical reflections in adulthood. San
Francisco, CA: Jessey-Bass, 1990.
8. Mezirow J. Transformative dimensions of adult learning. San
Francisco, CA: Jessey-Bass, 1991.
9. Mezirow J. Understanding transformation theory. Adult Educ
Q 1994;44:222–232.
10. Taylor E. The theory and practice of transformative learning:
a critical review. Information series No. 374. Columbus:
ERIC Clearinghouse on Adult, Career, and Vocational
Education, 1998.
11. Easton KL. The poststroke journey: from agonizing to
owning. Geriatr Nurs 1999;20:70–76.
12. Kirkevold M. The unfolding illness trajectory of stroke.
Disabil Rehabil 2002;24:887–898.
13. Nilsson I, Jansson L, Norberg A. To meet with a stroke:
patients’ experiences and aspects seen through a screen of
crises. J Adv Nurs 1997;25:953–963.
14. Pilkington FB. A qualitative study of life after stroke.
J Neurosci Nurs 1999;31:336–347.
15. Rochette A, St-Cyr Tribble D, Desrosier J, Bravo G, Bourget
A. Adaptation and coping following a first stroke: a qualitative
analysis of a phenomenological orientation. Int J Rehabil Res
2006;29:247–249.
16. Dubouloz CJ, Chevrier J, Savoie-Zajc L. Processus de
transformation chez un groupe de personnes cardiaques
suivies en ergotherapie pour une modification de leur
equilibre du fonctionnement occupationnel. Can J Occup
Ther 2001;68:171–185.
17. Dubouloz CJ, Vallerand J, Laporte D, Ashe B, Hall M.
Internet. 2008. Electronic citation. Occupational performance
modification and personal change among clients receiving
rehabilitation services for rheumatoid arthritis. http://
www.blackwell-synergy.com/toc/aot/0/0. Last accessed 2008
January 29.
18. Dubouloz CJ, Vallerand J, Lachaine C, Castonguay A,
Gingras C, Rabow R. Processus de transformation des
perspectives de sens chez un groupe de quatre personnes
atteintes de la sclerose en plaques: La definition de soi.
REFLETS: Revue Ontaroise d’Intervention Sociale et Com-
munautaire 2002;8:28–46.
1064 D. Kessler et al.

19. Ashe B, Taylor M, Dubouloz CJ. Enabling occupation
through client experiences in arthritis education groups. Can
J Occup Ther 2005;72:280–288.
20. Dubouloz CJ, Laporte D, Hall M, Ashe B, Douglas Smith C.
Transformation of meaning perspectives in clients with
rheumatoid arthritis. Am J Occup Ther 2004;58:398–407.
21. Paterson B, Thorne S, Crawford J, Tarko M. Living with
diabetes as a transformational experience. Qualitative Health
Research 1999;9:786–802.
22. Carpenter C. The experience of spinal cord injury: the
individual’s perspective – implications for rehabilitation
practice. Phys Ther 1994;74:614–628.
23. Carpenter JS, Brockopp DY, Andrykowski MA.
Self-transformation as a factor in the self-esteem and well-
being of breast cancer survivors. J Adv Nurs 1999;29:1402–
1411.
24. Baumgartner LM. Living and learning with HIV/AIDS:
transformational tales continued. Adult Educ Q 2002;53:44–
59.
25. Courtenay BC, Merriam SB, Reeves PM. The centrality of
meaning-making in transformation al learning: how HIV-
positive adults make sense of their lives. Adult Educ Q
1998;48:65–84.
26. Strauss A, Corbin J. Grounded theory methodology: an overview.
In: Denzin NK, Lincoln YS, Editors. Handbook of qualitative
research. Thousand Oaks, CA: Sage; 1994. pp 262–272.
27. Grbich C. Qualitative research in health: an introduction.
Thousand Oaks, CA: Sage; 1999.
28. Strauss A, Corbin J. Basics of qualitative research: grounded
theory procedures and techniques. Newbury Park, CA: Sage,
1990.
29. Kessler D. Transformation of meaning perspective following
stroke [dissertation]. Halifax, Nova Scotia: Dalhousie
University; 2007. pp 108. Available from: Library and
Archives Canada, Ottawa.
30. Clarke P, Black SE. Quality of life following stroke: nego-
tiating disability, identity and resources. J Appl Gerontol
2005;24:319–336.
31. Bays CL. Quality of life of stroke survivors: a research
synthesis. J Neurosci Nurs 2001;33:310–316.
32. Secrest JA, Thomas SP. Continuity and discontinuity: the
quality of life following stroke. Rehabil Nurs 1999;24:240–246.
33. Medin J, Baraja J, Ekberg K. Stroke patients’ experiences of
return to work. Disabil and Rehabil 2006;28:1051–1060.
34. Rodgers H, Bond S, Curless R. Inadequacies in the provision
of information to stroke patients and their families. Age Aging
2001;30:129–133.
35. Forster A, Smith J, Young J, Knapp P, House A, Wright J.
Information provision for stroke patients and their caregivers.
Cochrane Database of Systematic Reviews 2001;3:Art. No.:
CD001919.
36. George S, Wilcock A, Stanley M. Depression and liability: the
effects on occupation following stroke. B J Occup Ther
2001;64:455–461.
37. Thomas SA, Lincoln NB. Factors relating to depression after
stroke. B J Clin Psychol 2006;45:49–61.
Meaning perspective change following stroke 1065