Competencies and skills for remote and rural maternity care: a review of the literature
Upload
independentCategory
view
0download
0
Tropical Medicine and International Health
volume 5 no 9 pp 657–665 september 2000
Maternity care in rural Nepal: a health service analysis
Albrecht Jahn1, Maureen Dar Iang2, Usha Shah3 and H. J. Diesfeld1
1 Department of Tropical Hygiene and Public Health, Heidelberg University, Heidelberg, Germany
2 Okhaldunga Health Project, Nepal
3 Bheri Zonal Hospital, Nepalganj, Nepal
Summary This study assesses the performance of maternity care and its specific service components (preventive
interventions in antenatal care, antenatal screening, referral, obstetric care) in Banke District, Nepal, using a
set of structure, process, and output/outcome indicators. Data sources included health service documents in
14 first level health units and two hospitals, covering 1378 pregnancies and 1323 deliveries, structured
observations, antenatal exit interviews (n 5 136) and interviews with maternity users (n 5 146). Coverage of
antenatal care (28%) and skilled delivery care (16%) was low. In antenatal care, preventive interventions were
only partially implemented (effective iron supplementation in 17% of users). On average one minute was
spent on individual counselling per consultation. 41% of pregnancies were identified as high risk and 15%
received referral advice, which was followed in only 32%. Hospital deliveries accounted for 9.8% of all
deliveries. Hospital-based maternal mortality was 6.8/1000 births and the stillbirth rate 70/1000. High rates
of stillbirth were observed in breech delivery (258/1000 births), caesarean section (143/1000) and twin
delivery (133/1000). The risk of stillbirth was higher for rural women (RR 2.3; 95% CI 1.51–3.50) and
appeared to be related to low socio-economic status. Emergency admissions were rare and accounted for
3.4% of hospital deliveries or only 0.4% of all expected deliveries. There was hardly any accumulation of
high-risk pregnancies at hospital. The population-based rate of caesarean section was 1.1% (urban 2.3%,
rural 0.2%). The estimated unmet obstetric need was high (82 cases or 61% of expected live-threatening
maternal conditions did not receive appropriate intervention). The limited effectiveness of maternity care is
the result of deficiencies of all service components. We propose a two-pronged approach by starting quality
improvement of maternity care from both ends of maternity services: preventive interventions for all women
and hospital-based obstetric care. Antenatal screening needs to be rationalized by reducing inflated risk
catalogues that result in stereotypical and often rejected referral advice.
keywords safe motherhood, health systems research, maternity care, quality of care, Nepal
correspondence Dr Albrecht Jahn, Department of Tropical Hygiene and Public Health, Heidelberg
University, Im Neuenheimer Feld 324, 69120 Heidelberg, Germany. Fax: 149 6221 565 037, E-mail:
Introduction
Ten years of Safe Motherhood interventions have failed to
deliver a substantial reduction in the high maternal and
perinatal mortality in many developing countries. This casts
doubts on their health systems’ ability to provide effective
maternity care. Therefore we set out to identify possible causes
for this system failure by following the pathway in maternity
care from preventive interventions in antenatal care (ANC), to
screening and identification of high-risk pregnancies, referral
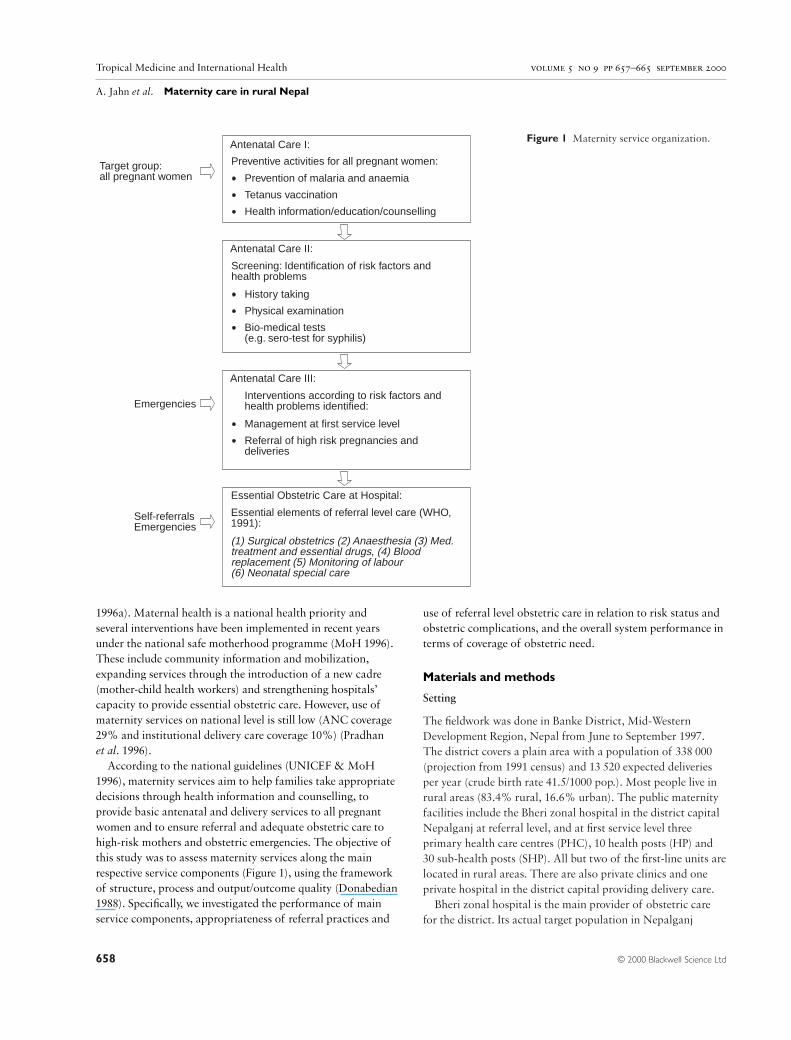
and hospital-based obstetric care (Figure 1). This approach is
based on the experience that substantial and sustainable
improvements in maternal health cannot be achieved with a
unifocal intervention, but depend on the co-ordinated function
of all service components (Fonn et al. 1998). Hence
identification of high-risk pregnancies and deliveries is only
meaningful in the presence of means for referral and
subsequent obstetric management according to quality
standards as outlined in WHO’s essential elements of referral
level care (WHO 1991a).
This study was conducted in Banke, a rural district in the
mid-west of Nepal. According to WHO, Nepal’s maternal
mortality ratio is among the highest in Asia with 1500/100 000
live births (WHO & UNICEF 1996); national data are lower
(539/100 000) but still high (Pradhan et al. 1996). Perinatal
mortality is also elevated with 75/1000 live births (WHO
TMIH611
© 2000 Blackwell Science Ltd 657
Tropical Medicine and International Health volume 5 no 9 pp 657–665 september 2000
A. Jahn et al. Maternity care in rural Nepal
1996a). Maternal health is a national health priority and
several interventions have been implemented in recent years
under the national safe motherhood programme (MoH 1996).
These include community information and mobilization,
expanding services through the introduction of a new cadre
(mother-child health workers) and strengthening hospitals’
capacity to provide essential obstetric care. However, use of
maternity services on national level is still low (ANC coverage
29% and institutional delivery care coverage 10%) (Pradhan
et al. 1996).
According to the national guidelines (UNICEF & MoH
1996), maternity services aim to help families take appropriate
decisions through health information and counselling, to
provide basic antenatal and delivery services to all pregnant
women and to ensure referral and adequate obstetric care to
high-risk mothers and obstetric emergencies. The objective of
this study was to assess maternity services along the main
respective service components (Figure 1), using the framework
of structure, process and output/outcome quality (Donabedian
1988). Specifically, we investigated the performance of main
service components, appropriateness of referral practices and
use of referral level obstetric care in relation to risk status and
obstetric complications, and the overall system performance in
terms of coverage of obstetric need.
Materials and methods
Setting
The fieldwork was done in Banke District, Mid-Western
Development Region, Nepal from June to September 1997.
The district covers a plain area with a population of 338 000
(projection from 1991 census) and 13 520 expected deliveries
per year (crude birth rate 41.5/1000 pop.). Most people live in
rural areas (83.4% rural, 16.6% urban). The public maternity
facilities include the Bheri zonal hospital in the district capital
Nepalganj at referral level, and at first service level three
primary health care centres (PHC), 10 health posts (HP) and
30 sub-health posts (SHP). All but two of the first-line units are
located in rural areas. There are also private clinics and one
private hospital in the district capital providing delivery care.
Bheri zonal hospital is the main provider of obstetric care
for the district. Its actual target population in Nepalganj
© 2000 Blackwell Science Ltd658
Figure 1 Maternity service organization.Antenatal Care I:
Preventive activities for all pregnant women:
Prevention of malaria and anaemia
Tetanus vaccination
Health information/education/counselling
Target group:all pregnant women
Antenatal Care II:
Screening: Identification of risk factors andhealth problems
History taking
Physical examination
Bio-medical tests(e.g. sero-test for syphilis)
Antenatal Care III:
Interventions according to risk factors andhealth problems identified:
Management at first service level
Referral of high risk pregnancies anddeliveries
Essential Obstetric Care at Hospital:
Essential elements of referral level care (WHO,1991):
(1) Surgical obstetrics (2) Anaesthesia (3) Med.treatment and essential drugs, (4) Bloodreplacement (5) Monitoring of labour(6) Neonatal special care
Emergencies
Self-referralsEmergencies

Tropical Medicine and International Health volume 5 no 9 pp 657–665 september 2000
A. Jahn et al. Maternity care in rural Nepal
extends to neighbouring districts, many of which lack
permanent obstetric services. Outflow of patients is likely to be
minimal, as the next reliable referral facilities are very far away
(Kathmandu 14 h drive, India 6 h drive). The zonal hospital
was staffed with doctors (one obstetrician) and six qualified
nurses. It offers comprehensive obstetric care including
emergency services on a 24-h basis and ANC on 5 days per
week.
Maternity services in first-line units (ANC and delivery care)
were provided by staff nurses (training 3 years) and auxiliary
nurse midwives (training 18 months). In primary health centres
(PHC) there were auxiliary nurse midwives, and in health posts
(HP) and subhealth posts (SHP) maternal child health workers
(training 10 weeks).
Study design
As suggested by St Leger et al. (1992), we pursued a pragmatic
study approach: based on our health service model (Figure 1),
we identified indicators along the categories of structure,
process and output/outcome (Donabedian 1988) and selected
the appropriate tools for data collection. These included the
analysis of health service data (Ronsmans et al. 1999),
structured observation with checklists and interviews with
health workers and their clients.
Indicators used for the assessment of ANC were
accessibility; availability of essential drugs and equipment;
coverage of ANC and delivery care; coverage of tetanus
immunization and anaemia prophylaxis; duration and content
of counselling; completeness of implementation and sensitivity
of screening; rate of referral advice in high-risk pregnancies;
referral compliance; and user satisfaction. Indicators used for
the assessment of hospital-based obstetric care were
availability of essential elements of obstetric care according to
WHO (WHO 1991a); rate of hospital deliveries; CS rate; time
lag in emergency management; stillbirth rate; maternal
mortality rate; and rate of obstetric emergency admissions.
Indicators for the overall performance of maternity services
were coverage of obstetric care for specific risk groups (Jahn
et al. 1998) and major obstetric interventions (MOI) for
absolute maternal indications (AMI) according to the unmet
obstetric need approach (De Brouwere et al. 1996; Belghiti
et al. 1998). Many of these indicators were stratified for urban
and rural origin. The national maternity care guidelines of
Nepal (UNICEF & MoH 1996) were used as standard unless
specified otherwise.
Selection of health facilities
A stratified random sample of first-line units was done with
rural PHCs and HPs in one stratum and SHPs in another
stratum. The only urban HP was selected purposely. Five
PHC/HPs and nine SHPs were selected. Their distance from
Nepalganj ranged from 6 to 60 km.
Data sources
The data on structural quality were obtained by checklists
covering 14 tracer items for essential equipment, drugs and
consumables at first-line health facilities and 22 items at the
hospital. These checklists were developed along WHO
standards (WHO 1996b) and national maternity guidelines
(UNICEF & MoH 1996) jointly with health professionals in
Nepal. Antenatal care (ANC) and referral were assessed by
structured observation of first antenatal consultations
(n 5 58), exit interviews with users of ANC (n 5 136) and
analysis of antenatal registers in 14 first-line units, the hospital
and private clinics covering 1378, 772 and 873 first antenatal
consultations, respectively. Coverage of ANC in urban areas
was based on first antenatal visits recorded in all facilities
providing antenatal care there. In rural areas, coverage was
calculated based on first visits in the selected 13 rural health
units and their respective target populations.
Coverage of referral level obstetric care was assessed by
analysing hospital registers (delivery and theatre book,
discharge register) and case notes covering 1323 deliveries from
April 1996 to April 1997 of women residing in Banke District.
These sources were also used to estimate the unmet obstetric
need indicator (De Brouwere et al. 1996; Belghiti et al. 1998).
We interviewed the users of maternity services (n 5 146)
during a 3-month period (mid-June to mid-September 1997)
and reviewed their case notes to determine the cause for
admission, referral status, risk status, and cost incurred. These
interviews were also used to check the validity of register data
and revealed consistent information on place of residence, risk
factors and indications for caesarean section. The inpatient
interviews covered 90% of hospital deliveries in the study
period, as some women could not be interviewed because of
early discharge.
The data on the spatial population distribution was
obtained from the District Development Committee Office,
Nepalganj and from Village Development Committees.
Reference values for risk factor prevalence were derived from
the 1996 Nepal Family Health Survey (Pradhan et al. 1996) for
age, parity, previous caesarean section and the national
maternity care guidelines (UNICEF & MoH 1996) for breech
and twin pregnancies.
Results
Overall health infrastructure and accessibility of maternity
services
Forty-two first-line health units serve 338 000 population.
90% live within 5 km from a health facility. However, only
© 2000 Blackwell Science Ltd 659

Tropical Medicine and International Health volume 5 no 9 pp 657–665 september 2000
A. Jahn et al. Maternity care in rural Nepal
67% of first-line units offered ANC services at facility and/or
outreach points (usually 2–4 days per week) and only 38%
provided skilled assistance in home deliveries. There is no
facility-based delivery care in first-line units. Essential
obstetric care is provided at two hospitals in the district
capital. Almost half (45%) of the district population resides
within 10 km of the district capital, 43% within 11–30 km
and 12% beyond 30 km. But accessibility to referral level care
is hampered by irregular transport and seasonal flooding.
Most antenatal services are free of charge except fees for
medicine such as iron tablets and laboratory investigations
offered at hospital outpatient departments. Hospital care is
rather expensive with 300–3000 rupees (mean 600 5 11 US$)
for vaginal delivery and 1000–13000 rupees (mean 5360 5 96
US$) for a caesarean section (CS) in comparison to the 90
rupees (5 1.6 US$) minimum daily wage for an unskilled
labourer.
Quality of antenatal and delivery care in first line health
facilities
Overall, 69% of items from a tracer list for essential
equipment and drugs were available in the 14 selected
facilities. Availability was good for thermometers (100%),
sphygmomanometers (92%), foetoscopes (92%), and poor for
technical guidelines (7%), urinary catheter (7%), tape
measure (14%), sterile gloves (21%), ergometrine injection
(29%), and consultation room with privacy (43%).
Coverage of ANC was low with 28% (urban 50%; rural
24%). Only 37.5% of first consultations took place before
20 weeks of gestation. Coverage of ANC in rural areas,
stratified for distance from health facilities, was 32%
(# 5 km) and 10% (. 5 km). Health services were involved in
15.8% of deliveries: 9.8% being hospital deliveries and 6%
being home deliveries conducted by first-level health workers.
Most women delivered with a traditional birth attendant
(trained 18%, untrained 66.2% of total deliveries).
Direct observation of 58 antenatal consultations revealed
an average duration of 10 min (5–15). On average only one
minute was spent on health education and counselling . The
main topics were nutrition (85%), personal hygiene (71%)
and a general reassurance to women that ‘everything is all
right’ (86%). Other essential topics received little attention:
place of delivery and individual delivery plan (17%), danger
signs (12%) and family planning (7%). Communication was
mainly unidirectional and paid little attention to
interpersonal aspects. 65% of ANC users in exit interviews
complained that they were not given the time and
opportunity to ask questions. Although technical quality of
antenatal examinations was rated as satisfactory by most
clients (77%), only 43% were satisfied with counselling and
reassurance.
The observed low coverage of iron supplementation is the
result of a series of deficiencies (Figure 2): to start with, only
28% of pregnant women attended ANC. Only 32% of those
who attended for ANC (44 of 136), or 9% of all pregnant
women, got a prescription for iron tablets. Of those with a
prescription, only 65% received or bought iron tablets.
Lapses in compliance resulted in a further drop of the
coverage of effective anaemia prophylaxis, defined as
continuous supplementation for at least 30 days, to 4.8% of
expected pregnancies or 17% of ANC attendees. Coverage of
tetanus vaccination (at least two doses) was 51.4%.
Physical examinations and blood pressure measurements
were performed in 85% to 95% of the consultations, but no
biochemical tests (urine analysis, sero-testing for syphilis)
were performed. Taking the women’s history focused on the
present pregnancy; complications in previous pregnancies
were never asked after. 15% of antenatal attendees received
referral advice in the course of ANC, while 41.5% of
attendees were documented to be high risk according to the
national risk catalogue. Most referral advice (52%) was based
on the demographic risk factors young age (, 19 years),
nulliparity and multiparity. However, referral practices were
inconsistent and even in these risk groups, the majority (65%
to 75%) did not receive a referral advice.
© 2000 Blackwell Science Ltd660
Figure 2 Stepwise loss of coverage of
anaemia prophylaxis.
0Received
effective dosage
30 28.0
% o
f exp
ecte
d de
liver
ies
ANC coverage
25
20
15
10
5
Received irontablets
Received ironprescription
9.0
5.4 4.8
Tropical Medicine and International Health volume 5 no 9 pp 657–665 september 2000
A. Jahn et al. Maternity care in rural Nepal
Referral advice because of risk factors and symptoms of
higher clinical relevance, such as previous stillbirth, breech
presentation, twin pregnancy, clinical pallor, weakness, and
high blood pressure were rare and covered less than 10% of the
respective risk groups. No referral was documented for risk
factors such as bleeding in pregnancy, history of previous CS
and previous post-partum haemorrhage (PPH). A cross-check
with hospital data revealed that ANC attendees’ compliance
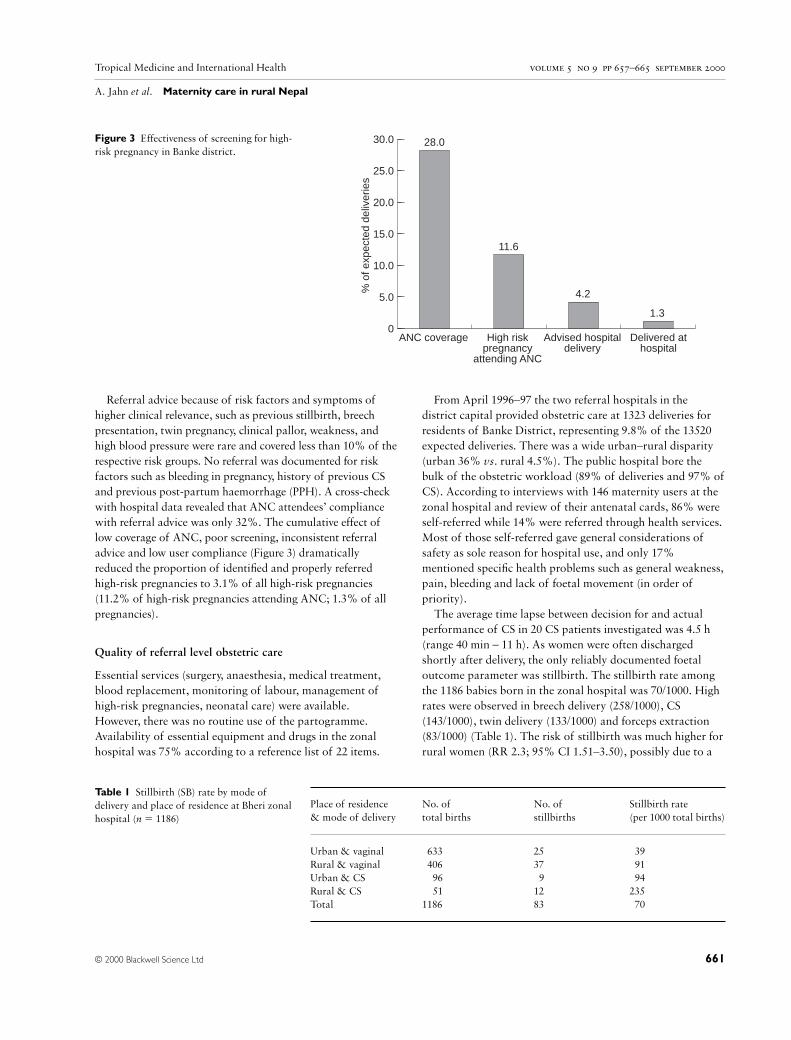
with referral advice was only 32%. The cumulative effect of
low coverage of ANC, poor screening, inconsistent referral
advice and low user compliance (Figure 3) dramatically
reduced the proportion of identified and properly referred
high-risk pregnancies to 3.1% of all high-risk pregnancies
(11.2% of high-risk pregnancies attending ANC; 1.3% of all
pregnancies).
Quality of referral level obstetric care
Essential services (surgery, anaesthesia, medical treatment,
blood replacement, monitoring of labour, management of
high-risk pregnancies, neonatal care) were available.
However, there was no routine use of the partogramme.
Availability of essential equipment and drugs in the zonal
hospital was 75% according to a reference list of 22 items.
From April 1996–97 the two referral hospitals in the
district capital provided obstetric care at 1323 deliveries for
residents of Banke District, representing 9.8% of the 13520
expected deliveries. There was a wide urban–rural disparity
(urban 36% vs. rural 4.5%). The public hospital bore the
bulk of the obstetric workload (89% of deliveries and 97% of
CS). According to interviews with 146 maternity users at the
zonal hospital and review of their antenatal cards, 86% were
self-referred while 14% were referred through health services.
Most of those self-referred gave general considerations of
safety as sole reason for hospital use, and only 17%
mentioned specific health problems such as general weakness,
pain, bleeding and lack of foetal movement (in order of
priority).
The average time lapse between decision for and actual
performance of CS in 20 CS patients investigated was 4.5 h
(range 40 min – 11 h). As women were often discharged
shortly after delivery, the only reliably documented foetal
outcome parameter was stillbirth. The stillbirth rate among
the 1186 babies born in the zonal hospital was 70/1000. High
rates were observed in breech delivery (258/1000), CS
(143/1000), twin delivery (133/1000) and forceps extraction
(83/1000) (Table 1). The risk of stillbirth was much higher for
rural women (RR 2.3; 95% CI 1.51–3.50), possibly due to a
© 2000 Blackwell Science Ltd 661
Figure 3 Effectiveness of screening for high-
risk pregnancy in Banke district.
0Delivered at
hospital
30.0 28.0
% o
f exp
ecte
d de
liver
ies
ANC coverage
25.0
20.0
15.0
10.0
5.0
Advised hospitaldelivery
High riskpregnancy
attending ANC
11.6
4.2
1.3
Place of residence No. of No. of Stillbirth rate
& mode of delivery total births stillbirths (per 1000 total births)
Urban & vaginal 633 25 39
Rural & vaginal 406 37 91
Urban & CS 96 9 94
Rural & CS 51 12 235
Total 1186 83 70
Table 1 Stillbirth (SB) rate by mode of
delivery and place of residence at Bheri zonal
hospital (n 5 1186)
Tropical Medicine and International Health volume 5 no 9 pp 657–665 september 2000
A. Jahn et al. Maternity care in rural Nepal
higher proportion of emergencies among rural women.
However, emergency admissions were rare and accounted for
only 3.4% of hospital deliveries or 0.4% of all deliveries in
the district. Four of the five emergency cases observed in the
study period were of urban residence. Risk profiles in urban
and rural women were similar except for a higher rate of
multiparity among rural women (13% vs. 20%). Eight
mothers died in 1171 deliveries (hospital-based MMR
683/100).
Overall maternity service performance in terms of care for
high-risk pregnancies and obstetric complications
The extent to which women in need are covered by adequate
obstetric care is influenced by all service components of
maternity care. Coverage of obstetric care is therefore a good
indicator of the overall performance of maternity services.
We measured this coverage using two approaches: (1) the
coverage of obstetric care for predefined risk groups
according to official risk factors and (2) the coverage of
major obstetric interventions (MOI) for absolute maternal
indications (AMI).
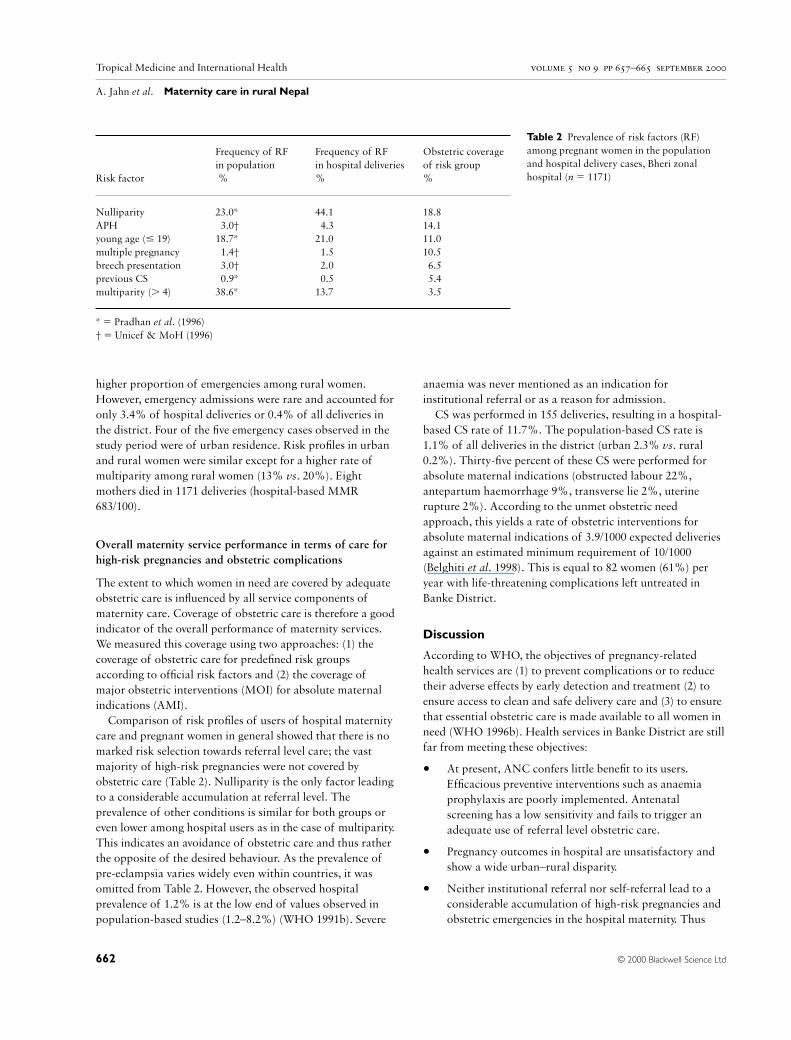
Comparison of risk profiles of users of hospital maternity
care and pregnant women in general showed that there is no
marked risk selection towards referral level care; the vast
majority of high-risk pregnancies were not covered by
obstetric care (Table 2). Nulliparity is the only factor leading
to a considerable accumulation at referral level. The
prevalence of other conditions is similar for both groups or
even lower among hospital users as in the case of multiparity.
This indicates an avoidance of obstetric care and thus rather
the opposite of the desired behaviour. As the prevalence of
pre-eclampsia varies widely even within countries, it was
omitted from Table 2. However, the observed hospital
prevalence of 1.2% is at the low end of values observed in
population-based studies (1.2–8.2%) (WHO 1991b). Severe
anaemia was never mentioned as an indication for
institutional referral or as a reason for admission.
CS was performed in 155 deliveries, resulting in a hospital-
based CS rate of 11.7%. The population-based CS rate is
1.1% of all deliveries in the district (urban 2.3% vs. rural
0.2%). Thirty-five percent of these CS were performed for
absolute maternal indications (obstructed labour 22%,
antepartum haemorrhage 9%, transverse lie 2%, uterine
rupture 2%). According to the unmet obstetric need
approach, this yields a rate of obstetric interventions for
absolute maternal indications of 3.9/1000 expected deliveries
against an estimated minimum requirement of 10/1000
(Belghiti et al. 1998). This is equal to 82 women (61%) per
year with life-threatening complications left untreated in
Banke District.
Discussion
According to WHO, the objectives of pregnancy-related
health services are (1) to prevent complications or to reduce
their adverse effects by early detection and treatment (2) to
ensure access to clean and safe delivery care and (3) to ensure
that essential obstetric care is made available to all women in
need (WHO 1996b). Health services in Banke District are still
far from meeting these objectives:
• At present, ANC confers little benefit to its users.
Efficacious preventive interventions such as anaemia
prophylaxis are poorly implemented. Antenatal
screening has a low sensitivity and fails to trigger an
adequate use of referral level obstetric care.
• Pregnancy outcomes in hospital are unsatisfactory and
show a wide urban–rural disparity.
• Neither institutional referral nor self-referral lead to a
considerable accumulation of high-risk pregnancies and
obstetric emergencies in the hospital maternity. Thus
© 2000 Blackwell Science Ltd662
Frequency of RF Frequency of RF Obstetric coverage
in population in hospital deliveries of risk group
Risk factor % % %
Nulliparity 23.0* 44.1 18.8
APH 3.0† 4.3 14.1
young age (# 19) 18.7* 21.0 11.0
multiple pregnancy 1.4† 1.5 10.5
breech presentation 3.0† 2.0 6.5
previous CS 0.9* 0.5 5.4
multiparity (. 4) 38.6* 13.7 3.5
* 5 Pradhan et al. (1996)
† 5 Unicef & MoH (1996)
Table 2 Prevalence of risk factors (RF)
among pregnant women in the population
and hospital delivery cases, Bheri zonal
hospital (n 5 1171)

Tropical Medicine and International Health volume 5 no 9 pp 657–665 september 2000
A. Jahn et al. Maternity care in rural Nepal
most women in need of obstetric care either because of
their risk status or because of delivery complications
give birth at home without skilled assistance.
• Coverage of modern maternity services is low, even in
comparison with other countries in the region.
Quality of antenatal care
ANC is an essential element of maternity care. A core set of
efficacious diagnostic and preventive interventions, including
the tracer interventions used in this study, are advocated by
WHO and others (Enkin et al. 1995; WHO 1996b, c; Villar &
Bergsjo 1997). However, turning their beneficial potential into
real health gains depends on the technical quality of
implementation, user compliance and the functioning of
corresponding parts of the health system such as the referral
system. This study reveals shortcomings in all of these areas:
The implementation of preventive interventions is rather
incomplete; only a minority of users receives iron
supplementation (Figure 2) and individual counselling is
almost absent. Only tetanus vaccination reaches a reasonable
level of implementation. While most ANC users had their
blood pressure checked and were physically examined, target
conditions of these procedures such as pre-eclampsia and
multiple pregnancy were hardly ever detected. Low sensitivity
of antenatal screening is a common problem in developing
and developed countries. It has contributed to a rethinking of
the risk approach and related screening procedures (Jahn &
Kowalewski 1998) and is discussed below in the context of
obstetric coverage of high-risk pregnancies.
Quality of obstetric referral level care
The stillbirth rate at the zonal hospital in Banke (7%) is
higher than hospital or population-based stillbirth rates
reported from Nepal previously (1.5–3.4%) (WHO 1996a).
However, hospital data are difficult to compare because of
differences in user profiles (Mancey-Jones & Brugha 1997),
e.g. hospitals with a good reputation may attract more
emergencies. Given the low proportion of emergencies and
the modest risk selection in our study, the observed high rates
of stillbirths and maternal mortality in hospital appear to
reflect inappropriate management at the hospital maternity.
This is confirmed by the observation that every seventh CS
(14.3%) and every 4th breech delivery (23.4%) ended in a
stillbirth, which is hardly acceptable in a referral level facility.
This is partly explained by the considerable time lag between
indication and obstetric intervention. The patient’s social
background may also contribute: rural women had a 2.3
times higher risk of stillbirth than urban women. Late arrival
at hospital and a higher proportion of emergencies would
offer a plausible explanation. However, risk profiles and CS
rates were rather similar in both groups. Obstetric emergency
admissions were rare and mainly from the urban population.
Therefore, eventual differences in biomedical risk factors do
not provide a satisfactory explanation for the grossly
divergent stillbirth rates. Thus we hypothesize that quality of
obstetric care is also related to the client’s socio-economic
status, putting low-status rural women at a disadvantage.
Referral and obstetric coverage of high-risk pregnancies and
obstetric emergencies
There are two approaches to assess coverage of obstetric care:
firstly, coverage can be assessed according to specific
predefined risk groups. Like most ANC programmes, the
Nepalese maternity care guidelines stipulate referral for high-
risk pregnancies in anticipation of complications (UNICEF
& MoH 1996). Only 3.5–18.8% of the respective risk groups
were covered by obstetric care (Table 2). It is particularly
worrying that the majority of women with a previous CS
deliver at home, instead of having a trial of labour in a
hospital setting. In other developing countries, this risk group
was found to have a significant preference for hospital
delivery, resulting in a coverage of obstetric care well above
50% (Voorhoeve et al. 1984; Jahn et al. 1998).
Low effectiveness of antenatal risk assessment has also
been observed in other countries and many risk factors have
shown to be poor predictors of adverse outcomes (Maine
1991; McDonagh 1996; Geefhuysen et al. 1998; Jahn et al.
1998). The Safe Motherhood Initiative has thus
recommended abandoning the risk approach in ANC (Inter-
Agency Group for Safe Motherhood 1997). However,
national programmes are still built on it, and there is
reasonable evidence to justify antenatal identification and
referral for specific risk groups such as women with a history
of CS, breech presentation, multiple pregnancy and
hypertension (WHO 1996d; Villar & Bergsjo 1997). The
WHO trial, evaluating a new ANC programme restricted to
interventions with proven efficacy, includes screening
procedures in the intervention arm (Villar et al. 1998). Our
findings provide no definite answer to the current controversy
on risk assessment in ANC. However, we can conclude that
risk catalogues and related referral guidelines are often not
operational because they classify an unacceptably large
proportion of pregnancies (in our study above 40%) as high
risk and mask the wide differences in predictive properties
and clinical importance across risk factors.
The unmet obstetric need approach compares post hoc the
number of actually performed obstetric interventions (MOI
for AMI) with the estimated need for these life-saving
interventions (Belghiti et al. 1998). As delivery complications
are often unforeseeable, the observed difference is mainly an
indicator for emergency obstetric care. Our results show that
© 2000 Blackwell Science Ltd 663

Tropical Medicine and International Health volume 5 no 9 pp 657–665 september 2000
A. Jahn et al. Maternity care in rural Nepal
only 39% of the estimated minimal need for these life-saving
interventions is covered. This corresponds to the low rate of
intrapartum referrals (0.37% of home deliveries) against an
estimated prevalence of 5% of severe delivery complications
even in low-risk pregnancies (Rooks et al. 1989; WHO
1996b). Thus, antenatal as well as emergency obstetric care
miss the majority of their respective target groups.
Acceptability of maternity services
The majority of Nepalese women have no pregnancy-related
contact with modern health services. Coverage of ANC
(national 29%, Banke District 28%) and skilled delivery
assistance (national 10%, Banke District 16%) are at the
bottom end of global statistics and compare unfavourably
with the south-central Asia region (ANC 52%; skilled
assistance 34%) and with the developing world in general
(ANC 65%; skilled assistance 53%) (WHO 1997). Though
far from being satisfactory, geographical accessibility in
Banke with one static maternity care service outlet per 12 000
population plus about 100 outreach service points compares
well with neighbouring countries. Even within a 5-km range
from health facilities, coverage of ANC is only 32%. This
indicates that there are strong reasons for non-use of
maternity services beyond geographical accessibility. These
may include cultural barriers, perceived low quality of care,
perceived discrimination of rural people and lack of
perceived health gain (Annis 1981; Thaddeus & Maine 1994;
MacRorie 1998; Kowalewski et al. 2000). Further research is
needed to clarify this issue.
Implications for health services
The overall low effectiveness of maternity services is the
cumulative result of deficiencies throughout the pathway
from preventive interventions to hospital-based obstetric care.
As it is almost impossible to address all of these
simultaneously, we propose a two-pronged and stepwise
approach by starting from both ends of maternity care
(preventive interventions in pregnancy and hospital-based
obstetric care). Interventions in these two areas produce an
immediate health benefit and there is a wide scope for
improvement even within limited resources (Mbaruku &
Bergström 1995). Provision of obstetric care, offering a
substantially better survival chance for high-risk pregnancies
than home management, is a prerequisite for meaningful
antenatal screening interventions and referral. Preventive
interventions to be intensified would include tetanus
vaccination and anaemia prophylaxis. Obstetric care has
been shown to improve considerably after the introduction of
systematic participatory evaluation procedures, which may
include perinatal and maternal audit, team-based analysis of
routine data and a streamlining of organizational procedures
(Mbaruku & Bergström 1995; Mancey-Jones & Brugha
1997).
The focus of ANC needs to be shifted from schematic and
ineffective allocation of risk labels to competent and
individualized counselling in order to empower mothers and
their families to take informed decisions. Lack of counselling
is also a major complaint of ANC users in this study.
Screening still has a place in this process as women’s key
question ‘Is my pregnancy all right?’ requires a technically
competent answer. The proposed re-orientation of ANC
towards the individual client implies abandoning long-
standing ritualistic practices and adopting new attitudes and
skills. This includes a modification of policies and maternity
guidelines, which still operate on a risk concept that classifies
a large proportion of pregnant women as high risk in a self-
defeating manner and compromises the credibility of
compliant health workers. Risk catalogues and referral
guidelines should be restricted to a core set of locally defined
and accepted risk factors and symptoms.
Acknowledgements
We gratefully acknowledge the co-operation and invaluable
help of Dr M. Kidwai, District Medical Officer and all staff
at the Zonal Hospital Nepalganj and the first-line health
units in the district. Ms. A. de Graaf was very helpful in
organizing the field visits. Mr G. Falkenhorst participated in
the development of indicators and Ms. M. Kowalewski
reviewed earlier drafts. The study was supported by the
Federal Ministry of Research and Technology, Germany
(grant 01 KA 9301/3) and the German Academic Exchange
Service (DAAD).
References
Annis S (1981) Physical access and utilization of health services in
rural Guatemala. Social Science and Medicine 15, 515–523.
Belghiti A, De Brouwere V, Kegels G & van Lerberghe W (1998)
Monitoring unmet obstetric need at district level in Marocco.
Tropical Medicine and International Health 3, 584–591.
De Brouwere V, Laabid A & van Lerberghe W (1996) Estimation des
besoins en interventions obstétricales au Maroc. Une approche
fondée sur l’analyse spatiale des déficits. Revue d’Epidemiologie et
de Sante Publique 44, 111–124.
Donabedian A (1988) The quality of care – How can it be assessed?
Journal of the American Medical Association 260, 1743–1748.
Enkin M, Keirse MJNC, Renfrew M & Neilson JP (1995) A Guide to
Effective Care in Pregnancy & Childbirth, 2 edn. Oxford University
Press, Oxford.
Fonn S, Xaba M, Tint K, Conco D & Varkey S (1998) Maternal
health services in South Africa During the 10th anniversary of the
WHO ‘Safe Motherhood’ Initiative. South African Medical Journal
88, 697–702.
© 2000 Blackwell Science Ltd664

Tropical Medicine and International Health volume 5 no 9 pp 657–665 september 2000
A. Jahn et al. Maternity care in rural Nepal
Geefhuysen CJ, Isa AR, Hashim M & Barnes A (1998) Malaysian
antenatal risk coding and the outcome of pregnancy. Journal of
Obstetrics and Gynaecology Research 24, 13–20.
Inter-Agency Group for Safe Motherhood (1997) The safe
motherhood action agenda: Priorities for the next decade.
Colombo.
Jahn A & Kowalewski M (1998) The risk approach in antenatal care:
Pitfalls of a global strategy. Curare 15, 195–209.
Jahn A, Kowalewski M & Kimatta SS (1998) Obstetric care in
Southern Tanzania: Does it reach those in need? Tropical Medicine
and International Health 3, 926–932.
Kowalewski M, Jahn A & Kimatta SS (2000) Why do at-risk mothers
fail to reach referral level care? Barriers beyond distance and cost.
African Journal of Reproductive Health 4, 100–109.
MacRorie RA (1998) Births, deaths and medical emergencies in the
district: a rapid participatory appraisal in Nepal. Tropical Doctor
28, 162–165.
Maine D (1991) Safe motherhood programs: Options and Issues,
Columbia University, New York.
Mancey-Jones M & Brugha RF (1997) Using perinatal audit to
promote change: a review. Health Policy and Planning 12, 183–192.
Mbaruku G & Bergström S (1995) Reducing maternal mortality in
Kigoma, Tanzania. Health Policy and Planning 10, 71–78.
McDonagh M (1996) Is antenatal care effective in reducing maternal
morbidity and mortality? Health Policy and Planning 11, 1–15.
MoH (1996) Safe Motherhood Policy of His Majesty’s Government of
Nepal. Journal of the Nepal Medical Association 34, 162–164.
Pradhan A, Aryal RH, Regmi G, Ban B & Govindasamy P (1996)
Nepal Family Health Survey. FHD/MoH Nepal, Kathmandu.
Ronsmans C, Achadi E, Sutratikto G, Zazri A & McDermott J (1999)
Use of hospital data for Safe Motherhood programmes in South
Kalimantan, Indonesia. Tropical Medicine and International
Health 4, 514–521.
Rooks JP, Weatherby NL, Ernst EKM et al. (1989) Outcomes of care
in birth centers: The national birth center study. New England
Journal of Medicine 321, 1804–1811.
St Leger AS, Schnieden H & Walsworth-Bell JP (1992) Evaluating
Health Services’ Effectiveness. Open University Press, Milton Keynes.
Thaddeus SA & Maine D (1994) Too far to walk: Maternal Mortality
in Context. Social Science and Medicine 38, 1091–1110.
UNICEF & MoH (1996) National Maternity Care Guidelines, Nepal.
FHD/MoH Nepal & UNICEF, Kathmandu.
Villar J, Bakketeig LS, Donner A et al. (1998) The WHO Antenatal
Care Randomised Controlled Trial: rationale and study design.
Paediatric and Perinatal Epidemiology 12, 27–58.
Villar J & Bergsjo P (1997) Scientific basis for the content of routine
antenatal care. Acta Obstetricia et Gynecologica Scandinavica 76,
1–14.
Voorhoeve AM, Kars C & van Ginneken JK (1984) Modern and
traditional antenatal and delivery care. In: Maternal and Child
Health in Rural Kenya – an Epidemiological Study, 2nd edn (eds
JK van Ginneken & AS Muller) Croom-Helm and African Medical
Research Foundation, London and Nairobi, pp. 309–322.
WHO (1991a) Essential Elements of Obstetric Care at First Referral
Level. Macmillan Press Ltd, London.
WHO (1991b) Hypertensive Disorders of Pregnancy: Report of a
WHO/MCH interregional collaborative study. WHO, Geneva.
WHO (1996a) Perinatal Mortality. WHO, Geneva.
WHO (1996b) Mother-Baby-Package: Implementing Safe
Motherhood in Countries. Maternal Health and Safe Motherhood
Programme, WHO, Geneva.
WHO (1996c) Care in Normal Birth: a Practical Guide. Maternal and
Newborn Health / Safe Motherhood Unit, WHO, Geneva.
WHO (1996d) Report of the Technical Working Group on Antenatal
Care. WHO, Geneva.
WHO (1997) Coverage of Maternity Care: a Listing of Available
Information, 4th edn. WHO, Geneva.
WHO & UNICEF (1996) Revised 1990 Estimates of Maternal
Mortality: a New Approach by WHO and UNICEF. WHO,
Geneva.
© 2000 Blackwell Science Ltd 665
Copyright © 2022 FDOKUMEN