
Maternal smoking during pregnancy predicts nicotine disorder (dependence or withdrawal) in young...
27
1 Maternal smoking during pregnancy predicts nicotine disorder (dependence or withdrawal) in young adults - a birth cohort study Frances V. O’Callaghan a , Abdullah Al Mamun b , Michael O’Callaghan c , Rosa Alati b , Jake M. Najman bd , Gail M. Williams b and William Bor c a School of Psychology, Griffith University, Gold Coast, QLD 4222, Australia, b School of Population Health, The University of Queensland, Brisbane, QLD 4072, Australia, c Mater Misericordiae Hospital, Brisbane, QLD 4101, Australia, d School of Social Science, The University of Queensland, Brisbane, QLD 4072 Address for correspondence: Dr Frances O’Callaghan School of Psychology, Griffith University, Gold Coast QLD, Australia, 4222 Ph: 61 7 555 28606 Fax: 61 7 555 28291 E-mail: [email protected] Funding: The core study was funded by the National Health and Medical Research Council (NHMRC) of Australia. This work was funded by the NHMRC grant number: 252834 and took place in Brisbane, Queensland, Australia.
Transcript of Maternal smoking during pregnancy predicts nicotine disorder (dependence or withdrawal) in young...
1
Maternal smoking during pregnancy predicts nicotine disorder (dependence or
withdrawal) in young adults - a birth cohort study
Frances V. O’Callaghana, Abdullah Al Mamunb, Michael O’Callaghanc, Rosa Alatib, Jake
M. Najmanbd, Gail M. Williamsb and William Borc
aSchool of Psychology, Griffith University, Gold Coast, QLD 4222, Australia, bSchool of
Population Health, The University of Queensland, Brisbane, QLD 4072, Australia, cMater
Misericordiae Hospital, Brisbane, QLD 4101, Australia, dSchool of Social Science, The
University of Queensland, Brisbane, QLD 4072
Address for correspondence:
Dr Frances O’Callaghan
School of Psychology,
Griffith University, Gold Coast
QLD, Australia, 4222
Ph: 61 7 555 28606
Fax: 61 7 555 28291
E-mail: [email protected]
Funding: The core study was funded by the National Health and Medical Research Council
(NHMRC) of Australia. This work was funded by the NHMRC grant number: 252834 and
took place in Brisbane, Queensland, Australia.

2
Abstract
Objective: To investigate whether maternal smoking during pregnancy predicts offspring
nicotine disorder (dependence or withdrawal) at 21 years.
Method: Participants comprised a prospective birth cohort involving 7223 singleton
children whose mothers were enrolled between 1981 and 1983 at the first antenatal visit to
the Mater Mothers’ Hospital, Brisbane, Queensland. The present sub-cohort consisted of
2571 youth who completed the Composite International Diagnostic Interview-computerized
version (CIDI-Auto) which assesses nicotine dependence and withdrawal according to
DSM-IV diagnostic criteria, at the 21-year follow-up.
Results: 12.8% of offspring met criteria for nicotine dependence and 8.5% met criteria for
withdrawal. 16.6% met criteria for either dependence or withdrawal. Smoking during
pregnancy resulted in offspring being more likely to have dependence or withdrawal at 21
years than offspring of mothers who never smoked (age adjusted odds ratio 1.53 (95%
confidence interval: 1.19, 1.96). The odds of nicotine disorder among offspring whose
mothers stopped smoking during pregnancy, but who then smoked at other times were
similar to those whose mothers had never smoked. This relationship was independent of
potential confounding and mediating factors including adolescent behaviour.
Conclusions. Findings emphasise the long-term adverse effects of maternal smoking
during pregnancy, including nicotine dependence in young adult offspring.
Implications. Public health approaches should strengthen arguments for mothers to cease
smoking during pregnancy in view of the long-term health implications for offspring, and
reinforce measures to help smokers among pregnant women and women of childbearing
age to stop.
Key words: nicotine disorder, nicotine dependence, maternal smoking, birth cohort, young
adult

3
Maternal smoking during pregnancy predicts nicotine disorder (dependence or
withdrawal) in young adults - a birth cohort study
Introduction
Nicotine dependence is a serious public health problem, with evidence suggesting that over
half of youth develop symptoms of nicotine dependence within weeks of the onset of
intermittent tobacco use.1 Since current nicotine dependence is a major indicator of
persistence of dependence and of chronic smoking,2 as well as a strong predictor of relapse
after cessation3, understanding its origins is an important issue. There has been growing
evidence suggesting that, apart from well-established predictors such as parental and peer
smoking,4 maternal smoking during pregnancy predicts the development of adolescent
smoking5 and smoking patterns of young adults.6 Yet little is known about the influence of
maternal smoking during pregnancy on the development of nicotine dependence.
To our knowledge, only two birth cohort studies have examined the association between
maternal smoking during pregnancy and the development of nicotine dependence in
offspring.7-8 The former study assessed offspring aged between 17 and 39 years and found
that the odds of progressing to nicotine dependence were almost twice as great for the
children of heavy smokers (one or more packs/day) compared to children of nonsmokers. 7
Although maternal smoking was assessed during pregnancy, subsequent maternal smoking,
maternal alcohol use and adverse parental and family factors were not controlled for. The
other study measured maternal smoking in pregnancy at offspring birth, and used a
questionnaire based on the Composite International Diagnostic Interview to assess 18-year
old offspring substance use during the previous two years.8 Adolescents whose mothers
smoked more than one pack/day during pregnancy had symptom rates that were between
1.4 and 2.5 times higher than offspring of mothers who did not smoke during pregnancy.
4
However, the relationship attenuated towards the null after adjustments were made for a
range of confounding factors.
In a study of offspring first assessed at 14-17 years of age, higher rates of nicotine
dependence were reported in offspring of mothers who retrospectively reported smoking
regularly during pregnancy compared to children of both nonsmokers and those who
retrospectively reported they did not smoke during pregnancy.9 Alcohol consumption and
adverse parental and family factors were not controlled for.
Of three studies,7-9 two reported maternal smoking during pregnancy predicted
offspring nicotine dependence and one reported the association attenuated to the null after
adjusting for potential confounders. These conflicting findings warrant further study with a
larger sample size and more measures of potential confounders and mediators. Furthermore,
the pathways underlying the association between maternal and offspring smoking remain
unclear. For example, the effect of maternal smoking during the developmental/teenage
years may be more important than the exposure during pregnancy. Familial transmission of
substance abuse risk may be involved.10-11 Also, a history of mental health disorders that
are known to be strongly correlated with regular tobacco use12-13 may fully or partly explain
the relationship. Another pathway may involve childhood behaviour problems, in
particular, externalizing behaviours that are associated with prenatal nicotine exposure and
may be linked with later smoking.14 Therefore, the association could be due to in-utero
biological modifications, genetic predisposition to mental health disorders or other
environmental/modelling exposures.
The objectives of this study were (1) to investigate whether maternal smoking during
pregnancy predicts offspring nicotine dependence in young adulthood, when smokers have
typically passed through the risk period for the onset of nicotine dependence (assessed
using DSM-IV criteria) and (2) to explore the mechanisms underlying the association,

5
especially whether it is mediated by adolescent behaviour. Our hypothesis was that
maternal smoking during pregnancy would predispose children to dependency as young
adults.
Methods
Participants were from the Mater-University of Queensland Study of Pregnancy
(MUSP).15 Initially, 8556 women attending their first antenatal clinic at the Mater
Misericordiae Mothers’ Hospital, Brisbane (1981-83), were invited to participate. At the
time of hospital discharge, 7223 singleton children were enrolled in an ongoing birth cohort
study.16 Mothers were interviewed at the first pregnancy visit (Mean = 19.8 + 6.0 weeks
gestation), several days after delivery, at 6 months, and at 5, 14 and 21 years. Offspring
were also assessed at 6 months and at 5, 14 and 21 years. The present cohort consisted of a
subgroup of 2546 youth (51.1 percent female) who completed the lifetime version of the
Composite International Diagnostic Interview-computerized version (CIDI-Auto)17 and
self-reported current smoking status at the 21-year follow-up. The study was approved by
the Mater Hospitals and University of Queensland Ethics Committees with written consent
being obtained from the mother at each stage of follow-up and from the youth at 21 years.
Participants who were lost to follow-up (i.e. did not attend the 21-year follow-up) were
more likely to be males, their mothers were more likely to be less educated, to be teenage
mothers, to be not married (single/defacto/other during pregnancy), from lower income
families at their birth, to use tobacco and alcohol during pregnancy and to be anxious and
depressed at their first antenatal visit (all p-values < 0.01; Table 1).
Nicotine dependence and withdrawal
6
The young adults completed the lifetime version of the CIDI-Auto.17 It has excellent
reliability and acceptable validity.18 Its use in a range of epidemiological studies has further
confirmed its reliability and validity as a survey instrument in this type of research.19 The
CIDI-Auto assesses psychiatric disorders according to DSM-IV diagnostic criteria.20 It was
used to assess current diagnoses of nicotine dependence and withdrawal at 21 years.
Subjects meeting criteria for either nicotine dependence or withdrawal were classified in
this study as having a nicotine disorder.
Maternal smoking
At the first clinical visit (FCV) when the women were on average 18-weeks of
gestation, then 3-5 days post-delivery, at 6-months, 5-years and 14-years follow-up,
mothers were asked to record whether they smoked (yes or no). If they smoked, they were
asked to report the frequency and quantity of tobacco use in the previous week. In addition,
at the FCV women were asked about whether and how much they smoked before they
became pregnant. At 3 to 5 days after delivery, mothers were asked to recall their smoking
level over the last trimester.
We defined maternal smoking status in three mutually exclusive categories: never
smoked (responded ‘no’ at all stages of the study), smoked throughout pregnancy and at
other times, and smoked before and/or after pregnancy but not during pregnancy (women
who responded ‘no’ throughout pregnancy but ‘yes’ either to smoking before pregnancy
and/or at any stage of follow-up to the 14 year follow-up) (Table 2).
Confounding and mediating factors
Measures at time of pregnancy consisted of maternal age, education (did not complete
secondary school, completed secondary school, completed further/higher education),

7
depression (using the Delusions Symptoms States Inventory),21 dyadic adjustment (using the
Dyadic Adjustment Scale),22 alcohol consumption (non drinker vs drinker),23 and
breastfeeding (never, less than 4 months, 4+ months). This categorisation of breastfeeding
has been used in previous research. 24 Breastfeeding information was collected at a 6-month
follow-up of the mothers, at which time some mothers were in fact between 4 and 6 months
postdelivery. The response options in the original question regarding breastfeeding duration
were: never, 2 weeks or less, 3-6 weeks, 7 weeks – 3 months, 4-6 months, and still
breastfeeding. Because women were at least 4 months post-delivery when they responded to
this question, the final two categories were combined into ‘breastfed for greater than 4
months’. As there were too few women in the categories from 2 weeks to 3 months to enable
meaningful analyses, the final categories used in the analyses were those noted above (i.e.
never, less than 4 months, 4+ months).
At 5 years, degree of parenting control25 and measures assessing number of children in
the household were considered as potential confounders. Family communication at 14
years, measured using the 20-item Parent-Adolescent Communication Scale26 (e.g. I have
trouble believing my child), was used as a confounder. Child externalizing and internalizing
behaviour problems were assessed with the Child Behaviour Checklist at 14-year follow-
up. 27 The externalizing behaviour subscale addresses aggression and delinquency while the
internalizing subscale addresses social withdrawal, anxiety/depression, and somatic
complaints. These were used as mediating factors. Potential confounders and mediators
were chosen because of their known or likely associations with smoking, and their
availability in the data set.2,4,28
Statistical analysis

8
We first tabulated the different patterns of maternal smoking into six, and then three
mutually exclusive exposure groups (Table 2). The relationship between maternal cigarette
smoking and the outcome of current diagnosis (based on CIDI-Auto lifetime criteria) of
nicotine disorder in 21 year-old offspring was examined using chi-square tests. Unadjusted
odds ratios and 95 percent confidence intervals were estimated using logistic regression,
with the reference categories being mothers who never smoked (Table 2) and offspring who
reported no nicotine disorder at 21 years (Table 3).
Factors that were statistically significant in the univariate analysis were included in a
series of multiple logistic regression models (see footnotes to Table 4) to assess the
association between maternal smoking status in the same three mutually exclusive
categories and offspring nicotine dependence at age 21 years, taking into account potential
confounding and mediating factors. These results are for the 2101 young adults and their
mothers with complete data on all variables included in the model.
To determine whether non-response affected the validity of our findings we undertook a
weighted analysis using inverse probability (of having missing outcome data) weights.29
Probability weights were computed by using a logistic regression model with the outcome
being complete data or not. The influence of all other covariates used in our primary
analyses on having complete data or not was assessed in combination in a logistic
regression model. The regression coefficients from this model were then used to determine
probability weights for the covariates in the main analyses (e.g. if the probability of non-
response was 0.7 for a mother who did not complete secondary school, the inverse
probability of weight would be 1.44). All analyses were undertaken using Stata version
10.0 (Stata Inc., Texas).
Results

9
Of the 2546 offspring who completed the CIDI-Auto, 12.8 percent met the criteria for
nicotine dependence and 8.4 percent met the criteria for nicotine withdrawal. 16.5 percent
met the criteria for either dependence or withdrawal and are the subjects described in
further analyses as having nicotine disorder. At 21 years, 25.7% of offspring reported
regular smoking, and of these, 65.3% showed either nicotine dependence or withdrawal. Of
the 25% who reported that they occasionally smoked or used to smoke, 34.2% showed
nicotine dependence or withdrawal.
Table 2 shows the prevalence of current diagnosis of nicotine disorder in offspring at 21
years by maternal smoking status categorised into three mutually exclusive groups from
pre-pregnancy to 14 years. In this unadjusted analysis, smoking during pregnancy added an
additional risk for later nicotine problems. Possible confounding factors and their
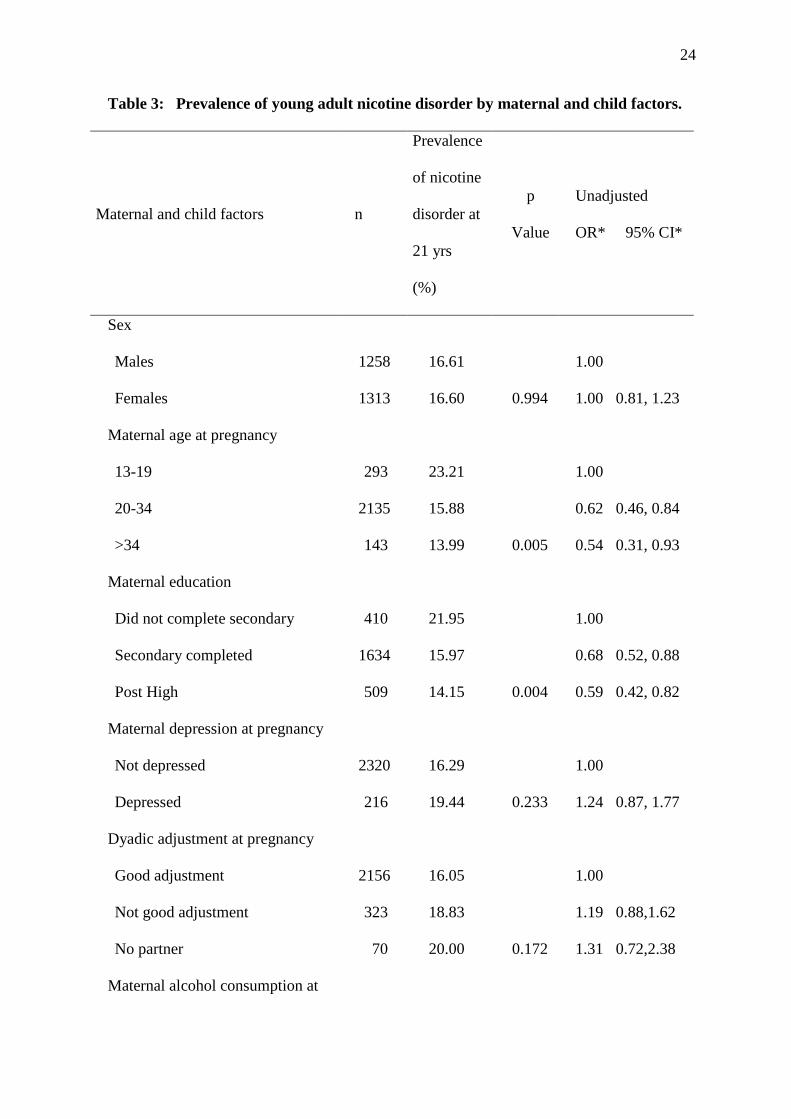
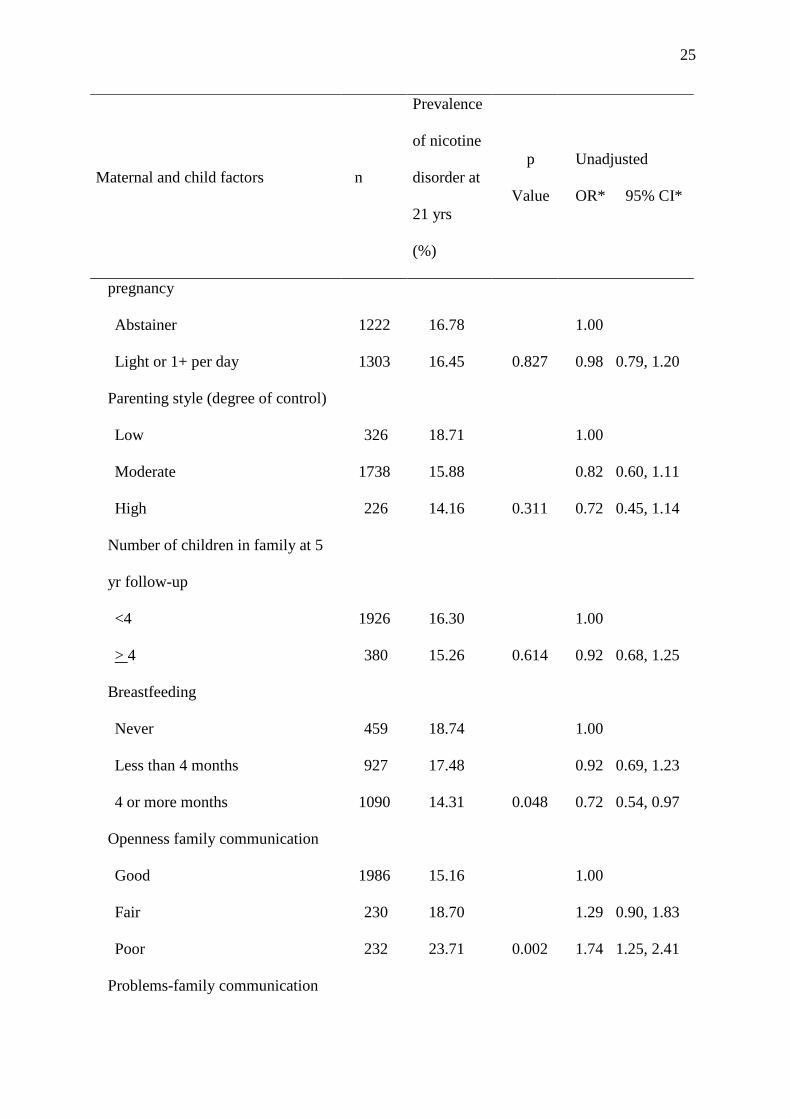
relationship to youth nicotine disorder are shown in Table 3. Maternal age at birth,
education, duration of breastfeeding, parental communication at 14 years and internalizing
and externalizing behaviour problems in adolescence were all associated with young adult
nicotine disorder.
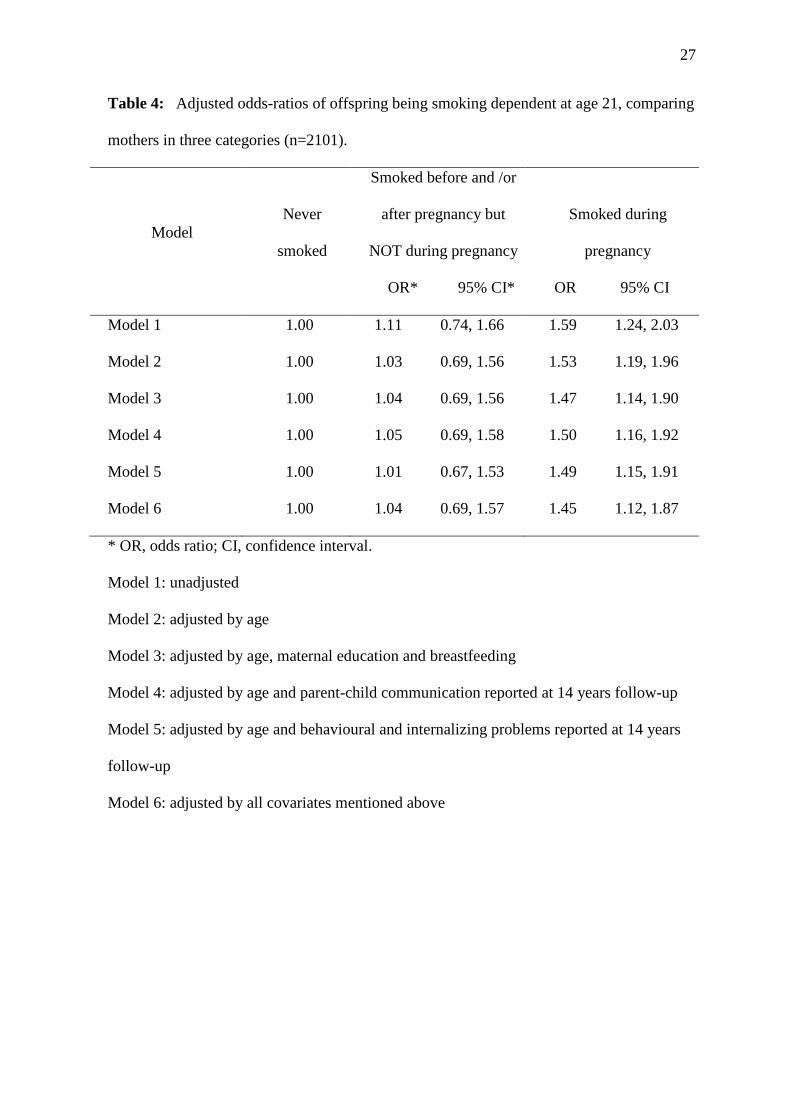
Table 4 shows the odds ratios for nicotine disorder at age 21years, comparing each
maternal smoking category to the reference group of never smoking. Potential confounders
and mediators were adjusted for in a series of multiple logistic regression models to
examine the effect of specific confounders. These results are for the 2101 young adults and
their mothers with complete data on all variables included in the model. The age adjusted
odds ratio for smoking in pregnancy was 1.53 (95 percent confidence interval (CI): 1.19,
1.96). This association remained consistent in the final model including all potential
confounders and mediators (Adj OR 1.45, 95% CI: 1.12,1.87). Smoking at other times but
not in pregnancy was 1.03 (95 percent CI: 0.69, 1.56).

10
We repeated the analysis considering maternal smoking before and/or after pregnancy
as the reference category to examine whether the relationship between smoking during
pregnancy and nicotine disorder was independent of maternal smoking either before or after
pregnancy. The point estimate did not attenuate substantially (unadjusted odds ratio 1.43
(95 percent CI: 0.96, 2.15) and the confidence interval became wider, as expected.
When we repeated the analyses removing the 69 women who reported smoking before
the birth of their child but at no other time the results did not differ from those presented
here. Similarly, when we repeated the analyses removing the 30 women who reported
smoking during their child’s pregnancy but then quit after the pregnancy, the results did not
alter. When we repeated the analyses using weights for factors that predicted non-response
the results did not differ from those presented here.
Discussion
Compared to mothers who did not smoke at all, offspring of mothers who smoked
during pregnancy and at other times had an age adjusted OR of 1.53 (95% CI: 1.19, 1.96)
for nicotine disorder (dependence or withdrawal) while offspring of mothers who smoked
at other times, but not during pregnancy, had an age adjusted OR of 1.03 (95% CI: 0.69,
1.56).
Both indirect and direct mechanisms may explain this relationship.30 Indirect
mechanisms from smoking during pregnancy include poor maternal nutrition, carbon
monoxide exposure, catecholamine constrictive effects, and the association between low
birth weight and behavioural problems that may be linked with a greater likelihood of
smoking among offspring. The addictive and neurotoxic effects of nicotine are well
documented.31 Direct effects include the action of nicotine on nicotine acetylcholine
receptors that are present from approximately eight weeks and prominent from mid-

11
gestation.32-33 Stimulation of these receptors in animal models can lead to disturbances in
neural development and in associated catecholamine systems of the fetal brain including
dopamine pathways.34 Drugs of abuse, including nicotine, may cause dependence by acting
on the mesolimbic dopamine system which is the natural reward system of the brain.31,36
The results are consistent with two previous studies7,9 but differ from another.8 Our
study differs to the latter in that it included various factors measured at birth (i.e. maternal
smoking, alcohol and other drug use during pregnancy), whereas similar factors taken into
account in the current study were measured during pregnancy. Further, our analyses were
based on DSM-IV diagnoses of dependence and withdrawal while previous research8
involved scale measures of the number of DSM-IV symptoms reported. Ferguson et al.8
however, adjusted also for measures of parental characteristics and childrearing practices,
all of which were not included in our database.
Measures that may mediate or confound the association between maternal smoking
during pregnancy and adult nicotine disorder, such as behavioural problems, parenting style
and family communication were also examined in this study. Addictions and other
psychiatric disorders have common neurobiological pathways that mediate factors such as
reward responses, behavioural control and the anxiety or stress response.36 When we
controlled for these characteristics, the relationship between maternal smoking during
pregnancy and adult nicotine disorder remained consistent and significant. The association
was also independent of parenting style characterised by physical punishment, maternal
depression and poor family communication, which may represent another potential pathway
from maternal smoking to adult nicotine disorder. Finally the relationship remained robust
even when we accounted for the modifying effect of externalizing behaviour. Although
young age at first pregnancy is associated with a range of potential adverse outcomes, in

12
this study, adjusting for age did not substantially alter the effect measure. This may reflect
the relatively small number of mothers in this group.
In previous research involving the present cohort, we found that the proportion of
young adults who smoked regularly at age 21, either with early (before age 14) or later
onset was greater among those whose mothers had smoked during pregnancy than those
whose mothers had never smoked or who smoked at other times but not during pregnancy.5
The association between maternal smoking during pregnancy and negative developmental
outcomes among offspring have also indicated a dose-response relationship8 and this issue
is being addressed in a subsequent investigation involving the current cohort. Although
higher levels of smoking are generally associated with a higher prevalence of nicotine
dependence37-38 there is only a modest association between cigarette consumption and
dependence,37 and no defined amount of smoking automatically leads to dependence.39
Recent studies showed that a substantial proportion of those engaging in daily and/or heavy
smoking were not nicotine dependent according to DSM-IV criteria,38,41 while some
smoking at relatively low levels were nicotine dependent.37 In the current study, we found
similar rates of regular smoking to those reported in national prevalence surveys (i.e. 23.7%
daily smokers among 20-29 year olds).42 According to DSM-IV criteria, dependence
involves a combination of physiological (e.g. tolerance, withdrawal symptoms), cognitive
(e.g. desire to quit) and behavioural symptoms (e.g. considerable time spent in smoking-
related activities) related to an individual’s continued use of a substance despite significant
substance related problems. As highlighted by the current and previous research, however,
failure to meet DSM-IV criteria does not imply that daily smoking poses a less serious
health risk or makes it easier for such individuals to quit smoking.
Overall, the current study has several important strengths. It is the first to examine
prospectively measured maternal smoking prior to and during pregnancy, and the

13
development of nicotine dependence and withdrawal in young adult offspring; diagnostic
interviews based on DSM-IV criteria were used to assess offspring dependence; offspring
were assessed in young adulthood, by which time the risk period for the onset of nicotine
dependence has generally passed; and a range of confounding factors including childhood
and family influences were controlled for. The findings support the importance of prenatal
exposure in predicting both regular smoking and actual smoking dependence among young
adult offspring.
Notwithstanding the strengths of the current study, caution is needed when interpreting
the findings since the relationship may be accounted for by common genetic factors
associated with both maternal smoking during pregnancy and nicotine disorder in
adulthood. If this were so, however, the association may also have been evident in those
who smoked at other times, though not in pregnancy. Also, we could not measure peer
influences, which have been found to be important in the development of youth
smoking,40,43 nor did we have information on the father’s smoking during pregnancy.
Further, mothers who give up smoking while pregnant may possess certain personality
factors that, in turn, may be related to styles of parenting or other family variables that were
not measured and that may have contributed to explanations of this association. The
accuracy of self-reported smoking has been discussed in a previous publication involving
this cohort. 44 Under-reporting and/or denial of smoking during pregnancy has been found
in previous research involving pregnant women45 and may have led to an underestimation
of the effects of smoking during pregnancy. It is therefore possible that outcomes relating to
nicotine disorder are greater than those reported here. It is also possible that over-estimation
of smoking may have contributed to some degree of error in the extent of outcomes
reported here, although efforts were made to maximize the accuracy of the information
provided by participants (e.g. assurances of confidentiality, the clinical setting, detailed

14
questions, and trained interviewers). Finally, the attrition was substantial and greater than
the approximate 40 percent and 20 percent in two previous studies.8-9 This potentially may
lead to biased estimates, though the direction of the bias is likely to lead to our findings
being a modest underestimate of the strength of the association. As loss to follow-up and
nicotine disorder are both related to more adverse social circumstances and maternal
smoking in pregnancy, it is unlikely that the association would be less evident in those not
included, particularly given that we have found that those lost to follow-up are more likely
to be anxious/depressed, and to be smokers and drinkers.15
In conclusion, the current study suggests that smoking during pregnancy may
predispose offspring to nicotine disorder (dependence and withdrawal) in early adulthood.
Adjustment for confounding factors such as maternal age, education, breastfeeding and
family communication, and mediating factors such as externalizing behaviour and
internalizing problems of adolescents, did not alter the relationship materially, suggesting a
direct association between maternal smoking and offspring nicotine disorder in adulthood.
The results extend the public health significance of findings in this area and highlight the
importance of intensifying efforts to reduce maternal smoking during pregnancy.
Acknowledgments
We thank all participants in the study, the MUSP data collection team, and data manager,
University of Queensland who has helped to manage the data for the MUSP.
Funding: The core study was funded by the National Health and Medical Research Council
(NHMRC) of Australia. AAM and RA are funded by NHMRC Career Development Awards
in Population Health ( ID 519756 and ID 519721 respectively). The views expressed in the
paper are those of the authors and not necessarily those of any funding body and no funding
body influenced how the data were analysed and presented.

15

16
References
1. DiFranza JR, Savageau JA, Rigotti NA, Fletcher K, Ockene JK, McNeill AD, et al.
Development of symptoms of tobacco dependence in youths: 30 month follow up data
from the DANDY study. Tob Control. 2002;11(3):228-35.
2. Hu M, Davies M, Kandel DB. Epidemiology and correlates of daily smoking and
nicotine dependence among young adults in the United States. Am J Public Health.
2006;96(2):299–08.
3. Killen JD, Fortmann SP, Kraemer HC, Varady A, Newman B. Who will relapse?
Symptoms of nicotine dependence predicts long-term relapse after smoking cessation. J
Consult Clin Psychol. 1992;60(5):797-801.
4. Tyas SL, Pederson LL. Psychosocial factors related to adolescent smoking: a critical
review of the literature. Tob Control. 1998;7(4):409-20.
5. O’Callaghan FV, O’Callaghan M, Najman J, Williams G, Bor W, Alati R. Prediction
of adolescent smoking from family and social risk factors at 5 years, and maternal
smoking in pregnancy and at 5 and 14 years. Addiction. 2006;101(2):282-90.
6. Mamun AA, O’Callaghan FV, Alati R, O’Callaghan M, Najman J, Williams G, et al.
Does maternal smoking during pregnancy predict the smoking patterns of young adult
offspring? A birth cohort study. Tob Control. 2006;15(6):452-57.
7. Buka SL, Shenassa ED, Niaura R. Elevated risk of tobacco dependence among
offspring of mothers who smoked during pregnancy: A 30-year prospective study. Am J
Psychiatry. 2003;160(11):1978-84.
8. Fergusson DM, Woodward LJ, Horwood LJ. Maternal smoking during pregnancy and
psychiatric adjustment in late adolescence. Arch Gen Psychiatry. 1998;55(8):721-27

17
9. Lieb R, Schreier A, Pfister H, Wittchen H. Maternal smoking and smoking in
adolescents: A prospective community study of adolescents and their mothers. Eur
Addict Res. 2003;9(3):120-30.
10. Bierut LJ, Dinwiddie SH, Begleiter H, Crowe V, Hesselbrock V, Nurnberger JI Jr. et al.
Familial transmission of substance dependence: alcohol, marijuana, cocaine, and
habitual smoking. Arch Gen Psychiatry. 1998;55(11):982-88.
11. Dick DM, Bierut L, Hinrichs A, Fox L, Bucholz KK, Kramer J. et al. The role of
GABRA2 in risk for conduct disorder and alcohol and drug dependence across
developmental stages. Behav Genet. 2006;36(4):577-90.
12. Breslau N, Novak SP, Kessler RC. Daily smoking and the subsequent onset of
psychiatric disorders. Psychol Med. 2004;34(2):323-33.
13. Schumann A, Hapke U, Meyer C, Rumpf HJ, John U. Prevalence, characteristics,
associated mental disorders and predictors of DSM-IV nicotine dependence. Eur Addict
Res. 2004;10(1):29-34.
14. Niaura R, Bock B, Lloyd EE, Brown R, Lipsitt LP, Buka S. Maternal transmission of
nicotine dependence: Psychiatric, neurocognitive and prenatal factors. Am J Addiction.
2001;10(1):16-29.
15. Najman JM, Bor W, O’Callaghan M, Williams GM, Aird R, Shuttlewood G. Cohort
profile: the Mater-University of Queensland Study of Pregnancy (MUSP). Int J
Epidemiol. 2005;34(5):992-97.
16. Keeping JD, Najman JM, Morrison J, Western JS, Andersen MJ, Williams GM. A
prospective longitudinal study of social, psychological and obstetric factors in
pregnancy: response rates and demographic characteristics of the 8556 respondents. Br
J Obstet Gynaecol. 1989;96(3):289-97.

18
17. World Health Organisation. Composite International Diagnostic Interview (CIDI),
version 2.1. Geneva (SWITZERLAND): World Health Organisation; 2002.
18. Andrews G, Peters L. The psychometric properties of the Composite International
Diagnostic Interview. Soc Psychiatr Psychiatr Epidemiol. 1998;33(2):80–88.
19. Teesson M, Hall W, Lynskey M, Degenhardt L. Alcohol- and drug-use disorders in
Australia: Implications of the National Survey of Mental Health and Wellbeing. Aust N
Z J Psychiatry. 2000;34(2):206−13.
20. American Psychiatric Association. Diagnostic and Statistical Manual of Mental
Disorders Fourth Edition. Washington (USA): American Psychiatric Association;
1994.
21. Bedford A, Foulds GA. Delusions-Symptoms-States Inventory of Anxiety and
Depression. Windsor (UK): National Foundation for Educational Research; 1978.
22. Spanier GB. Measuring dyadic adjustment: new scales for assessing the quality of
marriage and similar dyads. J Marriage Fam. 1976;38:15-28.
23. O’Callaghan FV, O’Callaghan M, Najman J, Williams GM, Bor W. Maternal alcohol
consumption during pregnancy and child outcomes in relation to birthweight, length
and head circumference: A longitudinal study. Early Hum Dev. 2003;71(2):137-48.
24. Mamun AA, Lawlor DA, O’Callaghan MJ, Williams GM, Najman JM. Family and
early life factors associated with changes in overweight status between ages 5 and 14
years: findings from the Mater University Study of Pregnancy and its outcomes. Int J
Obes. 2005;29(5):475-82.
25. Baumrind D, Black AE. Socialization practices associated with dimensions of
competence in preschool boys and girls. Child Dev. 1967;38(2):291-27.
26. Barnes HL, Olson DH. Parent-adolescent communication and the Circumplex model.
Child Dev. 1985;56(2):438-47.

19
27. Achenbach TM, Edelbrock C. Manual for the Child Behaviour Checklist and Revised
Child Behaviour Profile. Burlington (USA): University of Vermont Department of
Psychiatry; 1983.
28. Flay BR, Hu FB, Richardson J. Psychosocial predictors of different stages of cigarette
smoking among high school students. Prev Med. 1998;27(5):A9-18.
29. Hogan JW, Roy J, Korkontzelou C. Handling drop-out in longitudinal studies. Stat Med.
2004:23(9):1455-97.
30. Ernst M, Moolchan ET, Robinson ML. Behavioural and neural consequences of
prenatal exposure to nicotine. J Am Acad Child Adolesc Psychiatry. 2001;40(6):630-41.
31. Hyman SE. Addiction: a disease of learning and memory. Am J Psychiatry.
2005;162:1414-22.
32. Hagino N, Lee JW. Effect of maternal nicotine on the development of sites for
[3H]nicotine binding in the fetal brain. Int J Dev Neurosci. 1985;3:567–71.
33. Pauly JR, Slotkin TA. Maternal tobacco smoking, nicotine replacement and
neurobehavioural development. Acta Paediatr. 2008;97(10):1331-7.
34. Slotkin TA. If nicotine is a developmental neurotoxicant in animal studies, dare we
recommend nicotine replacement therapy in pregnant women and adolescents?
Neurotoxicol Teratol. 2008;30(1):1–19.
35. Shea AK, Steiner M. Cigarette smoking during pregnancy. Nicotine Tob Res.
2008;10(2):267-78.
36. Balfour DJ. The neurobiology of tobacco dependence: a preclinical perspective on the
role of the dopamine projections to the nucleus accumbens. Nicotine Tob Res.
2004;6:899-912. Review. Erratum in: Nicotine Tob Res. 2005;7(2):307.
37. Goldman D, Oroszi G, Ducci F. The genetics of addictions: uncovering the genes Nat
Rev Genet. 2005;6:521-32.

20
38. Dierker LC, Donny E, Tiffany S, Colby SM, Perrine N, Clayton RR et al. The
association between cigarette smoking and DSM-IV nicotine dependence among first
year college students. Drug Alcohol Depend. 2007;86(2-3):106–14.
39. Kandel DB, Chen K. Extent of smoking and nicotine dependence in the United States
1991-1993. Nicotine Tob Res. 2000;2(3):263-74.
40. Karp I, O’Loughlin J, Paradis G, Hanley J, Difranza J. Smoking trajectories of
adolescent novice smokers in a longitudinal study of tobacco use. Annu Epidemiol.
2005;15(6):445-52.
41. Reeder AI, Williams S, McGee R, Poulton R. Nicotine dependence and attempts to quit
or cut down among young adult smokers. N Z Med J. 2001;114(1139):403-6.
42. Australian Institute of Health and Welfare. 2007 National Drug Strategy Household
Survey. Canberra (AUST):AIHW; 2008.
43. Fergusson DM, Lynskey MT, Horwood JL. The role of peer affiliations, social, family
and individual factors in continuities in cigarette smoking between childhood and
adolescence Addiction. 1995;90(5):647-59.
44. O’Callaghan FV, O’Callaghan MJ, Najman J, Williams G, Bor W, Alati R. Prediction
of adolescent smoking from family and social risk factors at 5 years, and maternal
smoking in pregnancy and at 5 and 14 years. Addiction. 2006;101(2):282-290.
45. Ford, R.P.K., Tappin, D.M., Schluter, P.J. & Wild, C.J. Smoking during pregnancy:
how reliable are maternal self reports in New Zealand? J Epidemiol Community Health.
1997;51:246-251.

21
Table 1: Comparison of study and non-study groups.
Non-Study
(n = 4426)
Study
(n = 2571)
p Value
n % n %
Maternal Education
Incomplete high 838 18.93 410 16.06
Complete high 2861 64.64 1634 64.00
Post high 727 16.43 509 19.94 <0.001
Maternal Age (years)
13-19 669 15.12 293 11.40
20-34 3562 80.48 2135 83.04
> 34 195 4.41 143 5.56 <0.001
Marital Status
Married 3191 72.10 2081 81.48
Single 494 11.16 208 7.14
Defacto 604 13.65 223 8.73
Other 137 3.10 42 1.64 <0.001
Gross Family Income
Low 1502 33.94 731 28.43
Medium 2230 50.38 1408 54.76
High 410 9.26 309 12.02
Missing 284 6.42 123 4.78 <0.001
Maternal Cigs Early
Preg
Nil 2662 60.14 1652 64.81

22
Non-Study
(n = 4426)
Study
(n = 2571)
p Value
n % n %
Light smokers (1-19
cigarettes per day)
1359 30.70 709 27.81
Heavy smokers (20 or
more cigarettes per day)
405 9.15 188 7.38 < 0.001
Maternal alcohol during
pregnancy
Abstainer 2278 51.47 1222 47.87
Light or 1 drink per day 2148 48.53 1331 52.13 0.004
Child Gender
Male 2374 53.64 1258 48.93
Female 2052 46.36 1313 51.07 <0.001
Maternal depression
Not depressed 4120 93.09 2441 96.25
Depressed 306 6.91 95 3.75 <0.001
Child birth weight
(gram)
<2500 203 4.59 111 4.32
2501-3000 737 16.65 413 16.07
3001-3500 1656 38.09 995 38.72
3501 and more 1800 40.67 1051 40.89 0.855

23
Table 2: Classification of maternal smoking behaviour and association with offspring
nicotine disorder.
Maternal smoking status in the three mutually exclusive categories used in main
analyses
Smoker classification n Prevalence p value Unadjusted
OR* 95% CI*
Never smoked 1118 13.60 <0.001 1.00
Smoked before and /or after
pregnancy but NOT during
pregnancy
231 15.15 1.13 0.76, 1.69
Smoked during pregnancy 779 20.03 1.59 1.25, 2.03
* OR, odds ratio; CI, confidence interval.
24
Table 3: Prevalence of young adult nicotine disorder by maternal and child factors.
Maternal and child factors n
Prevalence
of nicotine
disorder at
21 yrs
(%)
p
Value
Unadjusted
OR* 95% CI*
Sex
Males 1258 16.61 1.00
Females 1313 16.60 0.994 1.00 0.81, 1.23
Maternal age at pregnancy
13-19 293 23.21 1.00
20-34 2135 15.88 0.62 0.46, 0.84
>34 143 13.99 0.005 0.54 0.31, 0.93
Maternal education
Did not complete secondary 410 21.95 1.00
Secondary completed 1634 15.97 0.68 0.52, 0.88
Post High 509 14.15 0.004 0.59 0.42, 0.82
Maternal depression at pregnancy
Not depressed 2320 16.29 1.00
Depressed 216 19.44 0.233 1.24 0.87, 1.77
Dyadic adjustment at pregnancy
Good adjustment 2156 16.05 1.00
Not good adjustment 323 18.83 1.19 0.88,1.62
No partner 70 20.00 0.172 1.31 0.72,2.38
Maternal alcohol consumption at
25
Maternal and child factors n
Prevalence
of nicotine
disorder at
21 yrs
(%)
p
Value
Unadjusted
OR* 95% CI*
pregnancy
Abstainer 1222 16.78 1.00
Light or 1+ per day 1303 16.45 0.827 0.98 0.79, 1.20
Parenting style (degree of control)
Low 326 18.71 1.00
Moderate 1738 15.88 0.82 0.60, 1.11
High 226 14.16 0.311 0.72 0.45, 1.14
Number of children in family at 5
yr follow-up
<4 1926 16.30 1.00
> 4 380 15.26 0.614 0.92 0.68, 1.25
Breastfeeding
Never 459 18.74 1.00
Less than 4 months 927 17.48 0.92 0.69, 1.23
4 or more months 1090 14.31 0.048 0.72 0.54, 0.97
Openness family communication
Good 1986 15.16 1.00
Fair 230 18.70 1.29 0.90, 1.83
Poor 232 23.71 0.002 1.74 1.25, 2.41
Problems-family communication

26
Maternal and child factors n
Prevalence
of nicotine
disorder at
21 yrs
(%)
p
Value
Unadjusted
OR* 95% CI*
Few 1916 14.67 1.00
Some 313 19.81 1.44 1.06, 1.95
Many 219 25.57 <0.00
1
2.00 1.44, 2.78
Child externalizing behaviour
No 2231 15.33 1.00
Yes 215 26.51 <0.00
1
1.99 1.44, 2.76
Child internalizing behaviour
No 2215 15.53 1.00
Yes 231 23.81 0.001 1.70 1.23, 2.35
* OR, odds ratio; CI, confidence interval.
27
Table 4: Adjusted odds-ratios of offspring being smoking dependent at age 21, comparing
mothers in three categories (n=2101).
Model Never
smoked
Smoked before and /or
after pregnancy but
NOT during pregnancy
OR* 95% CI*
Smoked during
pregnancy
OR 95% CI
Model 1 1.00 1.11 0.74, 1.66 1.59 1.24, 2.03
Model 2 1.00 1.03 0.69, 1.56 1.53 1.19, 1.96
Model 3 1.00 1.04 0.69, 1.56 1.47 1.14, 1.90
Model 4 1.00 1.05 0.69, 1.58 1.50 1.16, 1.92
Model 5 1.00 1.01 0.67, 1.53 1.49 1.15, 1.91
Model 6 1.00 1.04 0.69, 1.57 1.45 1.12, 1.87
* OR, odds ratio; CI, confidence interval.
Model 1: unadjusted
Model 2: adjusted by age
Model 3: adjusted by age, maternal education and breastfeeding
Model 4: adjusted by age and parent-child communication reported at 14 years follow-up
Model 5: adjusted by age and behavioural and internalizing problems reported at 14 years
follow-up
Model 6: adjusted by all covariates mentioned above




















