Marine Stingers: Review of an Under-Recognized Global Coastal Management Issue
21
PLEASE SCROLL DOWN FOR ARTICLE This article was downloaded by: [Gershwin, Lisa-ann] On: 10 November 2009 Access details: Access Details: [subscription number 916739145] Publisher Taylor & Francis Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37- 41 Mortimer Street, London W1T 3JH, UK Coastal Management Publication details, including instructions for authors and subscription information: http://www.informaworld.com/smpp/title~content=t713626371 Marine Stingers: Review of an Under-Recognized Global Coastal Management Issue Lisa-Ann Gershwin a ; Monica De Nardi b ; Kenneth D. Winkel c ; Peter J. Fenner d a Queen Victoria Museum and Art Gallery and Australian Marine Stinger Advisory Services, Launceston, Tasmania, Australia b School of Education, University of Queensland, Brisbane, Australia c Australian Venom Research Unit, Department of Pharmacology, University of Melbourne, Melbourne, Australia d Fenner Family Medicine, Mackay, Queensland, Australia First published on: 10 November 2009 To cite this Article Gershwin, Lisa-Ann, De Nardi, Monica, Winkel, Kenneth D. and Fenner, Peter J.(2009) 'Marine Stingers: Review of an Under-Recognized Global Coastal Management Issue', Coastal Management, 38: 1, 22 — 41, First published on: 10 November 2009 (iFirst) To link to this Article: DOI: 10.1080/08920750903345031 URL: http://dx.doi.org/10.1080/08920750903345031 Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf This article may be used for research, teaching and private study purposes. Any substantial or systematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply or distribution in any form to anyone is expressly forbidden. The publisher does not give any warranty express or implied or make any representation that the contents will be complete or accurate or up to date. The accuracy of any instructions, formulae and drug doses should be independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with or arising out of the use of this material.
-
Upload
independent -
Category
Documents
-
view
7 -
download
0
Transcript of Marine Stingers: Review of an Under-Recognized Global Coastal Management Issue

PLEASE SCROLL DOWN FOR ARTICLE
This article was downloaded by: [Gershwin, Lisa-ann]On: 10 November 2009Access details: Access Details: [subscription number 916739145]Publisher Taylor & FrancisInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Coastal ManagementPublication details, including instructions for authors and subscription information:http://www.informaworld.com/smpp/title~content=t713626371
Marine Stingers: Review of an Under-Recognized Global CoastalManagement IssueLisa-Ann Gershwin a; Monica De Nardi b; Kenneth D. Winkel c; Peter J. Fenner d
a Queen Victoria Museum and Art Gallery and Australian Marine Stinger Advisory Services,Launceston, Tasmania, Australia b School of Education, University of Queensland, Brisbane, Australia c
Australian Venom Research Unit, Department of Pharmacology, University of Melbourne, Melbourne,Australia d Fenner Family Medicine, Mackay, Queensland, Australia
First published on: 10 November 2009
To cite this Article Gershwin, Lisa-Ann, De Nardi, Monica, Winkel, Kenneth D. and Fenner, Peter J.(2009) 'MarineStingers: Review of an Under-Recognized Global Coastal Management Issue', Coastal Management, 38: 1, 22 — 41, Firstpublished on: 10 November 2009 (iFirst)To link to this Article: DOI: 10.1080/08920750903345031URL: http://dx.doi.org/10.1080/08920750903345031
Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf
This article may be used for research, teaching and private study purposes. Any substantial orsystematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply ordistribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representation that the contentswill be complete or accurate or up to date. The accuracy of any instructions, formulae and drug dosesshould be independently verified with primary sources. The publisher shall not be liable for any loss,actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directlyor indirectly in connection with or arising out of the use of this material.

Coastal Management, 38:22–41, 2010Copyright © Taylor & Francis Group, LLCISSN: 0892-0753 print / 1521-0421 onlineDOI: 10.1080/08920750903345031
Marine Stingers: Review of an Under-RecognizedGlobal Coastal Management Issue
LISA-ANN GERSHWIN,1 MONICA DE NARDI,2
KENNETH D. WINKEL,3 AND PETER J. FENNER4
1Queen Victoria Museum and Art Gallery and Australian Marine StingerAdvisory Services, Launceston, Tasmania, Australia2School of Education, University of Queensland, Brisbane, Australia3Australian Venom Research Unit, Department of Pharmacology, University ofMelbourne, Melbourne, Australia4Fenner Family Medicine, Mackay, Queensland, Australia
Dangerous marine stingers (jellyfish) are an emotive issue in tropical Australia, wherethey are widely regarded as the number one marine health threat. However, numeroussevere and fatal stings have been reported throughout the tropical and temperate seasof the world, indicating that marine stingers are a global health problem. Further,life-threatening jellyfish stings are more frequently reported globally now compared toearlier decades, possibly as a result of improved recognition and reporting, or increasedspatial and/or temporal distribution or densities. As stinging incidents may also havesignificant financial implications (lost tourism revenues and liability settlements), andthe treatment of envenomed patients comes at high cost to the taxpayer, this issueis also a management challenge. This article outlines suggested approaches, basedlargely on Australian experience, for dealing with this under-recognized global coastalmanagement issue.
Keywords coastal and marine stinger management, Cubozoa, jellyfish, liability andrisk management, local government, tourism
We sincerely thank Professor Jeff Wilks, former director of the Strategic Development Unit atSurf Life Saving Australia (SLSA), for facilitating development of this report. We also appreciatethe valuable contributions of Paul Stormon, former business and development manager at SLSA, forstimulating ideas in the early stages of this article, and Grant Small, former lifeguard supervisor forSLSA, for teaching us a lot about pro-active stinger safety. Although all of the people referencedherein, as well as three of the authors, have moved on from SLSA, we appreciate the opportunity todevelop these ideas. This article benefited from comments made by two anonymous reviewers; wesincerely thank them for their time and insights. The majority of this article was written while Dr.Lisa Gershwin was supported by a grant from Australian Biological Resources Study (Grant 207-63).Dr. Ken Winkel is supported by the Australian Government Department of Health and Ageing.
Address correspondence to Lisa-ann Gershwin, Curator of Natural Science, Queen VictoriaMuseum and Art Gallery, Launceston, Tasmania 7250, Australia. E-mail: [email protected]
22
Downloaded By: [Gershwin, Lisa-ann] At: 21:48 10 November 2009

Marine Stinger Management 23
Introduction
Aliens! Jellyfish are some sort of alien life form, a “mystery from the deep”that will attack unprovoked, make young children cry, and in some parts of theworld, kill people unmercifully in the span of a few heartbeats. Even in theirmildest forms, they prevent us from enjoying the beach, from having fun. Alltold, jellyfish are a bad thing.—Popular perception about jellyfish
Some of the above is true, and some is not. However, the element most often neglected inmarine stinger management is public perception and the runaway anxieties that result frominconsistent or untrue information. Some peoples’ anxieties lead them to deny the problemrather than seek clarification, while others avoid the water completely out of fear of theunknown. Misunderstanding both the risks and the practical means of prevention leads toinjuries or missed opportunities, and perpetuates the cycle of fear. Stingers and stings aremanageable; it is the public perception of stings, and the highly variable approaches tostinger management, that are in need of a more balanced view.
The purpose of this article is to present our view of the marine stinger problem throughthe prism of Australian experience. Australia has had a leadership role in addressing andrecognizing the issue of marine stingers, from first describing the species and stings ofChironex fleckeri and Irukandjis, to developing preventative mechanisms, beachside firstaid protocols, hospital management of envenomed patients (Williamson et al., 1996), andthe development of the world’s only jellyfish antivenom (Winkel et al., 2006). We recognizethat marine stingers are an emerging global problem, and propose an array of managementstrategies.
The Problem of Marine Stingers
While approximately 2000 species of jellyfishes are formally described, only 10–15 areconsidered life-threatening (Williamson et al., 1996; Fenner, 1997b; Gershwin, 2007);herein, we restrict our usage of the term “marine stinger” to mean any or all speciesof jellyfish capable of delivering a potentially life-threatening sting to previously wellpersons. Excluding very rare allergic (i.e., anaphylactic) reactions (Gollan, 1968; Togiaset al., 1985), two general groups of jellyfish in the Class Cubozoa are of primary concern(Figure 1), corresponding to two quite different types of envenomation reactions. The larger“multi-tentacled box jellyfish” are in the taxonomic order Chirodropida, and have multipletentacles on each of four corners; the lethal members of this group include Chironex fleckeriand C. yamaguchii, and reportedly (but probably erroneously!) Chiropsalmus quadrumanus(Southcott, 1956; Bengston et al., 1991; Lewis & Bentlage, 2009). The smaller “Irukandji-type box jellyfish” fall into the order Carybdeida, and have only a single tentacle on eachcorner; this group includes Carukia barnesi, C. shinju, Malo maxima, M. kingi, Gerongiarifkinae, Morbakka fenneri, Alatina mordens, and A. moseri, as well as numerous otherundescribed species (Southcott, 1967; Gershwin & Alderslade, 2005; Gershwin, 2005a,2005b, 2005c, 2007, 2008). Chironex species reach about 25 cm in bell height, whereasIrukandji species range from 1 cm to 50 cm in bell height; all are nearly transparent andcolorless in the water. Without doubt, the list of dangerous species will grow, as moreinformation becomes available on stings and species from additional regions.
Chironex and related species kill humans by massive envenomation—a searing hotsting, with death occurring in as little as 2–3 minutes (Williamson et al., 1996, 70). In
Downloaded By: [Gershwin, Lisa-ann] At: 21:48 10 November 2009

24 L. Gershwin et al.
Figure 1. Stinging jellyfish of primary concern. Left, chirodropid, i.e., multi-tentacled box jellyfish(Chironex fleckeri, 15 cm body height; up to 35 cm). Right, Irukandji, i.e., single-tentacled boxjellyfish (Carukia barnesi, 1 cm body height; other species up to 15 cm). Images copyright L.Gershwin.
general, about 1–2 meters of visible Chironex-type sting is enough to kill a small child(Currie & Jacups, 2005), or about 5 meters to kill an adult (Kinsey, 1986, 1988); not allstings are lethal, but even minor stings may leave deep scars (Williamson et al., 1996,269). The other serious sting type, causing the Irukandji syndrome, is currently thought toresult from at least 10 different species. Initially this sting is mild, but triggers a delayed-onset constellation of severe systemic signs and symptoms (with an onset of between 5–40minutes post-sting, depending on the species) (Gershwin, 2005a). Irukandji syndrometypically includes severe lower back pain plus any or many of the following: nausea,vomiting, difficulty breathing, profuse sweating, severe abdominal cramps, shooting limbspasms, coughing, headache, a feeling of impending doom, severe hypertension (Fenner etal., 1986), and severe toxic heart failure (Fenner & Carney, 2001). The syndrome itself isdebilitating: it almost always requires hospitalization, up to 30% of cases may have someform of cardiac damage (Fenner & Carney, 1999), some patients develop long-term orpermanent complications (Braidwood, unpublished; Australian Irukandji Sting Database,2009), and death can occur in otherwise healthy victims (Fenner & Hadok, 2002; Huynhet al., 2003).
Public Health Implications
It appears likely that lethal Irukandji stings have historically been mis-diagnosed as heartattack, stroke, drowning, or decompression illness, suggesting that the historical stingstatistics represent only a minimum dataset. Indeed as Irukandji stings leave little or nomark, and the syndrome presents no unequivocal findings at post-mortem (Barnes, 1964;Williamson et al., 1996), the diagnosis is highly dependent on the medical history. Forexample, as the syndrome may resembles “the bends” (decompression illness), it may beincorrectly treated (Kizer, 1984; Hadok, 1997; Williamson, 1985).
The mechanism of death in the two confirmed Australian Irukandji syndrome fatalitieswas brain haemorrhage caused by extremely high blood pressure (Fenner & Hadok, 2002;Huynh et al., 2003); furthermore, dozens of cases requiring life support have sufferedpulmonary oedema and heart failure (Fenner & Carney, 2001; Little et al., 2003; Corkeron,2003).
Downloaded By: [Gershwin, Lisa-ann] At: 21:48 10 November 2009

Marine Stinger Management 25
Hence, in view of the increasingly recognized potential for serious or even fatal com-plications (Fenner & Carney, 1999), it seems plausible that such cases may not have beenrecognized in the past. For example, in January 2004, a 58-year-old male suffered a ma-rine sting while swimming off his yacht anchored near Orpheus Island off Townsville,Queensland (Australian Irukandji Sting Database, 2009). Onset of symptoms was withinten minutes of the sting, and included severe lower back pain, nausea, difficulty breathing,sweating, abdominal cramps, and anxiety. Unfamiliar with the syndrome or its complica-tions, help was not sought; symptoms from his sting caused him to lapse into a coma andspend the next three days alone on the deck of his boat without treatment. Upon regainingconsciousness, he summoned medical care and spent several days in Townsville hospital.This extraordinary story of survival would have never been known had he suffered brainhaemorrhage or fatal cardiac failure. Without doubt, his friends would have found comfortthinking that he died doing what he loved, never realizing the underlying cause of his death.He did live to tell about it, and his case highlights the difficulties in accurate diagnosiswithout a good medical history.
Individual Vulnerability
Everyone is vulnerable to the invisible risk of marine stingers: recreational activities aremore about having fun than about being mindful of hazards. Local residents may believethat they fully understand local risks, or they may think that because they have practisedan activity in the past without incident, it is therefore safe. Tourists, in contrast, are oftenunfamiliar with local customs and the local environment, and may be more willing to adoptsafe behaviors, but may not receive adequate information (Wilks, 2006). Independent trav-ellers, in particular, are less likely to receive briefings on local risks and safety advice. Forexample, a tourist might arrive at night when signage is obscured, enter the beach withoutseeing warning signs, or see signage but not understand its wording or its importance.Either way, the risk may not be adequately communicated and the person may not beaware of stinger-resistant enclosures or other protective mechanisms. Similarly, perceivedresponsibility varies among cultures. For example, Americans tend to rely on governmentalintervention to keep them out of harm’s way, and may therefore not even think to ask aboutlocal hazards, believing instead that if a risk were to exist, they would be warned. SomeAsian cultures believe that if an accident occurs due to nature, it is fate; it is not in ourscope to prevent it, or in some cases, even treat it. Finally, in the Australian “she’ll be right”culture, it is assumed that everyone takes responsibility for their own safety, and shouldseek more information if there are concerns. As cultural expectations collide through in-ternational tourism, it is easy to imagine how safety may be compromised. Recent surveysin Queensland, Australia, indicated that only a small proportion of international touristsknow about Irukandji jellyfish, and that most tourists had not received information abouthow to protect themselves from Irukandji or Chironex box jellyfish (Leggat et al., 2005;Harrison et al., 2004). It is reasonable therefore to assume that marine stinger awareness iseven lower in other regions.
While the actual risk of being stung by a dangerous jellyfish and consequently dyingfrom the sting is statistically very low in relation to the number of people in the water peryear, to someone who experiences a severe sting, it may be a life-changing experience.With multi-tentacled box jellyfish, the sting itself is extremely painful and scarring maybe deep and permanent (Figure 2). With Irukandji, given the demonstrated potential forsignificant or serious acute morbidity, on-going cardiac and/or neurological problems mayrequire lifestyle modification.
Downloaded By: [Gershwin, Lisa-ann] At: 21:48 10 November 2009

26 L. Gershwin et al.
Figure 2. Major Chironex envenomation to four-year-old female. Left, one day after sting. Center,scarring one year later. Right, scarring after 11 years. Images copyright P. Fenner.
Financial/Legal Implications
Marine stingers present a difficult position for local governments in the interplay betweenduty of care and legal liability. Duty of care liberally dictates that reasonably foreseeablerisks be pro-actively minimized; conversely, legal liability conservatively dictates thatresponsibility not be implied. This paradox may lead to a myriad of misinterpretationsand to highly variable management approaches, the inconsistencies of which may lead toanxiety in visitors, who just want to have a good time and do not want to have to thinkabout such problems.
Marine stingers also present an emotive threat to tourism. The number of documentedfatalities due to jellyfish is low in comparison to many other hazards, for example, roaddeaths (Wilks, 1999) or tourists’ preexisting medical conditions (Wilks et al., 2002). How-ever, the public perception of marine stingers, and how this affects people’s recreationalchoices, should not be under-estimated. For example, negative publicity about two stinger-related fatalities in Australia in early 2002 resulted in an estimated AU$65 million inlost tourist revenues (Williams, 2004). Northern Queensland currently boasts a AU$6 bil-lion/year tourism industry, with more than 9 million “people days” per year visiting theGreat Barrier Reef region (Access Economics, 2007). Thus, in an average year, the rate ofsting hospitalizations is about 1:200,000 users, but the medical and economic implicationsof stings are high. A decade ago, Fenner (1999) estimated the minimum annual cost to thecommunity in retrieval, treatment, and incidentals to be about $1–3 million; without evenaccounting for inflation. Other significant costs left out of original calculations include on-going medical care for complications, loss of worker productivity, including time off work,and impacted family activities, ruined holidays, and increased public anxiety. Thus, effec-tive stinger management is not only about saving lives, but also about saving livelihoods.
Tropical Australia is highly dependent on a world-class tourism industry, and there istension between those who want to manage the stinger problem pro-actively, and those whoprefer to keep the idyllic image of balmy breezes, inviting tropical waters, and secludedbeaches. Both can co-exist, and the idyllic image could be more realistic if stingers aremanaged pro-actively.
Not Just North Queensland
Chironex and Irukandji were both discovered in North Queensland, and the marine stingerproblem is often associated with this region; however, the deaths and injuries from marine
Downloaded By: [Gershwin, Lisa-ann] At: 21:48 10 November 2009

Marine Stinger Management 27
stingers extend well beyond. In all three primary tourist destinations across Australia’s North(tropical Queensland, Darwin, and Broome), safety personnel consider marine stingers to bethe number one aquatic health hazard (Surf Life Saving Queensland unpublished data; pers.comm. 2005, J. Gardiner, Director of Life Saving, Northern Territory; pers. comm. 2005, B.McCallum, CEO Pearl Producers Association, Western Australia). Australian physiciansand researchers have been documenting Chironex-related fatalities since 1884 and Irukandjihospitalizations since 1943. On average, northern Queensland records about 50 Irukandjihospitalizations per year (Australian Irukandji Sting Database, 2009) and approximately thesame number per year are recorded in northern Western Australia (Macrokanis et al., 2004).
While marine stingers are generally regarded as a tropical health problem, severalexamples in temperate Australia suggest that additional severe cases may be going unrec-ognized or undocumented. A single Irukandji case in Victoria, one near Perth at a Surf LifeSaving carnival in the 1980s and another near Rottnest Island off Perth in 2003, “dozensof cases” in the Sydney region in 1930, and at least one near Sydney in 2007, have allchallenged conventional thinking. In each of these cases, recognition and reporting wasthrough virtue of unusual circumstance. In the Victorian case (Cheng et al., 1999), a seniorclinician with experience in treating Irukandji syndrome made the diagnosis (K. Winkel,unpublished); in the 1980s Perth case, the diagnosis was made in retrospect, with the treat-ing physician unfamiliar with Irukandji syndrome at the time (P. Fenner, unpublished); inthe Rottnest case, the victim was a close friend of an Irukandji researcher (M. Corkeron,Townsville Hospital, pers. comm. 2005). Similarly, considering the 1930 Sydney cases,they were retrospectively diagnosed by later researchers (Cleland & Southcott, 1965); andthe 2007 Sydney case was brought to light by the victim who attended a seminar in whichIrukandji syndrome was described (N. Hood, Surf Life Saving National Medical Advisor,pers. comm. 2007). A similar event, involving the treating clinicians, triggered the retro-spective diagnosis of a probable Irukandji sting in Thailand of a Dutch tourist (de Penderet al., 2006). It is possible that other incidents have occurred which lacked the recognitionexpertise or the time or inclination for thorough and proper reporting.
Not Just Australia: An Emerging World Health Issue
While it might be tempting to dismiss marine stingers as “just an Australian problem,” stingdata over the last several decades certainly show otherwise. Fenner and Williamson (1996)stated their belief that current knowledge was “only the ‘tip of the iceberg’ and probablyan inadequate indication of the extent of the problem worldwide”; indeed, the data anddetails in their book spanned the globe. Fenner (1997b) titled his M.D. thesis, “The GlobalProblem of Cnidarian (Jellyfish) Stinging.” He clearly envisaged chirodropids as global;recognition of the Irukandji problem, however, was still embryonic. In particular, no deathshad yet been confirmed from Irukandji stings, and while Irukandji syndrome was known tooccur outside Australia, specific details were largely sketchy. We interpret recent increasesin recognition and reporting to indicate that marine stingers are a growing global healthissue, and that the scope of the problem is likely to continue to increase.
Irukandji envenomation was recently reported in continental U.S. waters for the firsttime (Grady & Burnett, 2003). Since these initial cases in Florida, Caribbean reports havecome from Guadeloupe (Pommier et al., 2005) and Cuba (R. Orduna, sting victim, pers.comm. 2005). Pommier and his colleagues (2005, 367) stated that “jellyfish envenomationmay not be unusual in the Caribbean.” In fact, cases of Irukandji syndrome have been de-scribed from many disparate locations, including Hawaii (Yoshimoto & Yanagihara, 2002),Thailand (de Pender et al., 2006), Philippines (Old, 1912), and even North Wales in the
Downloaded By: [Gershwin, Lisa-ann] At: 21:48 10 November 2009

28 L. Gershwin et al.
United Kingdom (Lord & Wilks, 1918). The species responsible for these stings remain un-known, with the diagnosis being made on the basis of syndrome. However, in most of thesecases, species related to known Irukandjis have been reported from these regions (Mayer,1910; Kramp, 1961; Gershwin, 2005a), and, with at least nine different Australian species intwo families and five genera apparently capable of causing Irukandji syndrome (Gershwin,2007), it seems highly likely that additional new non-Australian species will be described.
Chironex-type box jellyfish are widely regarded as the world’s deadliest venomousanimal (Cropp & Cropp, 1984; Endean, 1988), with rapid death following a searing stingsometimes compared to the intense pain of boiling oil. Fatalities from chirodropids havebeen documented throughout the Pacific, including Thailand, the Philippines, Papua NewGuinea, Malaysia, and Japan, as well as in the United States (Cleland & Southcott, 1965;Fenner & Williamson, 1996; Williamson et al., 1996), as summarized graphically in Fig-ure 3. One recent event, which may set a precedent, is an alleged fatal envenomation,which is said to have involved a massive out of court settlement. Only scant informationis available, but our hope is that its inclusion herein will facilitate the emergence of moredetail: the sting was in the summer of 2002, at Montego Bay, Jamaica; the victim was a maletourist from Ohio or Illinois (USA), and his family secured a US$35 million settlement witha confidentiality clause (Anonymous, 2006). Information on the nature of envenomation isunavailable, but a local marine safety source believed the jellyfish to be a chirodropid (i.e., amulti-tentacled box jellyfish). Indeed Chirodropids have been repeatedly documented fromnumerous localities throughout the Caribbean and adjacent regions (Beebe, 1928; Guest,1959; Kramp, 1961; Larson, 1982).
So, one may ask, why the problem of marine stingers is not more widely reported?Stings may go unreported for a variety of reasons, including lack of local knowledgeor recognition, fear of legal or financial ramifications, or time or logistical constraintson publication. Quite simply, not everyone recognizes the problem accurately, and noteveryone has the time or inclination to publish possible cases. Box jellyfish themselves arecommon throughout tropical regions of the world, and it is therefore likely that the paucityof recorded incidents reflects a lack of reporting rather than lack of stings. However, aparadox exists. It is clear that stings are under-reported, and the problem is therefore likelyto be worse than current estimates. However, as distressing as Irukandji syndrome is, andas rapidly lethal as chirodropids may be, deaths from either are nonetheless rare comparedwith the numbers of stings, which are in turn rare compared to the number of people in thewater as potential sting events. The real problem, therefore, is not the frequency of stings, oreven their severity when they do occur, but rather, the special challenge of communicatingan accurate and balanced prevention message about a low probability/high drama problemto people who may not want to hear it.
Deadly Jellyfishes versus Nuisance Jellyfishes
While the importance of the prevention of life-threatening jellyfish stings might seemobvious, there exists a general apathy about pro-active minimization of “nuisance” stings.We herein define nuisance stings as those causing pain and/or discomfort, but not requiringurgent medical assistance. Regardless, even non–life-threatening marine stings should beprevented; rarely, they can present with anaphylaxis, but more commonly they are acutelypainful and may leave scars.
Despite significant advancements in technology, techniques, and knowledge, marinestings still occur, and indeed, comprise an overwhelming majority of the injuries thatAustralian lifesavers and lifeguards attend to each year (Surf Life Saving Australia, 2005).
Downloaded By: [Gershwin, Lisa-ann] At: 21:48 10 November 2009

Fig
ure
3.G
ener
aliz
edpa
ttern
ofw
orld
wid
ede
aths
attr
ibut
edto
jelly
fish,
plus
wor
ldw
ide
Iruk
andj
ien
veno
mat
ions
repo
rted
toda
te.
Dat
afr
omC
lela
ndan
dSo
uthc
ott
(196
5),F
enne
ran
dW
illia
mso
n(1
996)
,Will
iam
son
etal
.(19
96),
and
refe
renc
esth
erei
n,as
wel
las
pers
onal
com
mun
icat
ions
with
Drs
.J.W
illia
mso
nan
dR
.H
artw
ick,
and
num
erou
sSo
uthe
ast
Asi
anhe
alth
and
safe
tyre
pres
enta
tives
.Si
zeof
circ
les
indi
cate
sre
lativ
enu
mbe
rof
repo
rted
ores
timat
edst
ings
.W
eem
phas
ise
that
abse
nce
ofev
iden
cesh
ould
notb
ein
terp
rete
das
evid
ence
ofab
senc
e.
29
Downloaded By: [Gershwin, Lisa-ann] At: 21:48 10 November 2009

30 L. Gershwin et al.
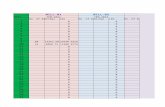
Table 1Beach injuries treated by Australian lifesavers and lifeguards in 2004–2005.
States & Suspected Major Minorterritories Stings spinal injuries Fractures wound cuts/abrasions
NSW 15,779 72 99 293 4114QLD 8,135 59 51 290 2193VIC — — — 90 1510SA 379 2 17 — 359WA 1061 14 15 — 466TAS 69 — — 6 132NT 22 — 2 5 19Total 25,445 147 184 684 8793
Source: Surf Life Saving Australia (2005).
Table 1 outlines stings noted by Australian Surf Lifesaving relative to other beach injuriesfor the 2004–2005 summer season. While most of these are not life-threatening, they arenonetheless distressing to those involved.
While Australia has a pro-active reporting system for sting events, and has for decades,it is clear that many non–life-threatening stings go unreported. Medically minor stingssuch as blue bottles (Physalia spp.—although some may rarely cause death or Irukandjisyndrome) and jimbles (Carybdea spp.) might be considered a public health hazard duringswarming conditions. Documented statistics range from 25,445 nationally reported stingtreatments in 2004–2005 (N. Hood, Surf Life Saving National Medical Advisor, pers.comm. 2006), to 17,029 in New South Wales alone in 1993/1994 (Fenner, 1997b), to upto 40,000 sting treatments in a year in eastern Australia (P. Fenner, unpublished data), andup to a half million stings per year on the east coast of America (Fenner, 1997a). Thesefigures should be regarded as minimum estimates, because not every person stung will seektreatment, and it is likely that not every treatment is reported.
Long-Term Outlook
Historical increases in sting statistics have generally been attributed to increases in reportingrather than increases in sting incidents. However, concerns have arisen on the potential effectof global warming in increasing both the population densities and latitudinal distribution ofmarine stinger species (Cheng et al., 1999; Roberts, 2002; Oiso et al., 2005; Andersen, 2006;Fenner, 2006); however, the long-term outlook for highly venomous species under changingclimatic conditions has not been rigorously examined. While evidence to support or refutethis hypothesis is lacking, available data indicate that many other kinds of jellyfish flourishin disturbed ecosystems (Mills, 1995, 2001; Parsons & Lalli, 2002; Purcell, 2005; NationalScience Foundation, 2008; Williams, 2009). It is therefore conceivable that dangerous jelly-fish may similarly respond to environmental stimuli by broadening their spatial and/or tem-poral distribution, or increasing in population densities. Thus, it may be more prudent to findways to co-exist with marine stingers rather than simply waiting to see if they will go away.
Managing Marine Stingers: Current Response
Both Irukandji and Chironex-type box jellyfish were originally described from Australia(Southcott, 1956, 1967); the knowledge base and research capability have remained
Downloaded By: [Gershwin, Lisa-ann] At: 21:48 10 November 2009

Marine Stinger Management 31
strong domestically. The following recommendations derive from decades of experiencein Queensland. Current focus is on prediction (e.g., routine monitoring to identify highrisk days), prevention (e.g., education programs and barrier methods), and treatment (e.g.,clinical innovations and first aid).
While both are within in the same taxonomic class, Irukandji and chirodropid specieshave quite different lifestyles in terms of their biology and ecology, and their stings presentquite different health hazards; managing them requires different strategies.
Managing Multi-Tentacled Box Jellyfish: Still the Primary Concern
Chirodropids are documented to have killed many people (Cleland & Southcott, 1965;Williamson et al., 1996; see Figure 3 herein). In cases of severe envenomation, deathtypically occurs in 3–5 minutes caused by an irreversible contraction of the heart muscles(Endean, 1988); in medical terms, the heart locks in systole, or fails to relax, such that CPRis ineffective because the contracted heart chambers cannot be further compressed. While anantivenom exists, it cannot always be delivered quickly enough to be effective. Neverthelessit should be noted that CPR and antivenom are still recommended, because, to echo themotto of the Australian Resuscitation Council (2007), any attempt at resuscitation is betterthan no attempt at resuscitation. Indeed, numerous cases of successful resuscitation afterserious chirodropid stings exist (Williamson et al., 1980; Williamson et al., 1984; Lumleyet al., 1988; Williamson et al., 1996).
In response to the recognized public health threat from chirodropid box jelly-fish, stinger-resistant swimming enclosures were installed at popular swimming beachesthroughout tropical Queensland beginning in 1982 (Moss & Stark, 1983). These nets arecurrently used at 23 locations from November to May/June of each year. The 2.5 cm meshis sufficient to exclude Chironex, which are not considered a serious health hazard untilthey reach approximately 6–8 cm body size. Consequently, no serious Chironex stings haveoccurred within the stinger nets.
While the number of serious or lethal Chironex stings has dropped since implementationof the stinger-resistant swimming enclosures (L. Gershwin, unpublished data), the publichas become more relaxed. Specifically, many residents of North Queensland no longerregard Chironex as a major threat (L. Gershwin, unpublished data), possibly due to theeffective management practices applied by tourism operators and land managers. Thus, astrange paradox has developed: because Chironex is being successfully managed, fewerfatalities occur to reinforce the need for safe swimming practices. However, from a riskmanagement standpoint, a focus on Chironex preventative measures needs to be maintained.It remains a reality that these jellyfish swarm in large numbers and death typically occurstoo rapidly for medical intervention. Preventative measures include but are not limited toswimming within the stinger-resistant swimming enclosures, wearing protective clothing,and in building general public awareness.
Recommendation: In regions where multi-tentacled box jellyfish are present, stingernets should be considered as a primary means of keeping jellyfish away from human skin;if nets are impractical, protective clothing should be emphasized.
Managing Irukandji Jellyfish: An Emerging Important Issue
Irukandj stings hospitalize approximately 50 people per year in tropical and subtropicalQueensland, and have done so for decades, but were not widely regarded as a signifi-cant health hazard until two confirmed fatalities in early 2002. The following summer(2002–2003), lifeguards in the Cairns region began an on-going program of routine water
Downloaded By: [Gershwin, Lisa-ann] At: 21:48 10 November 2009
32 L. Gershwin et al.
sampling in order to monitor for the presence of jellyfishes and associated zooplankton (G.Small, former Cairns Lifeguard Supervisor, pers. comm. 2003). Monitoring is performedat each patrolled beach 2–3 times per day (depending on the tides) with specially designedone-man sampling nets, developed by Uninet Enclosure Systems. Identification charts weredeveloped for different regions by one of us (LG), to assist lifeguards in interpreting thevarious zooplankton, “jelly-buttons,” and “sea lice” that are commonly associated withIrukandjis. Salps (pelagic tunicates, phylum Urochordata) have long proven to be a keyindicator of the presence of Irukandjis (Barnes, 1964), and are now used routinely to signalthe highest risk conditions.
The most common coastal Irukandji, Carukia barnesi, grows to only a little overa centimeter in bell height, and thus readily penetrates the stinger-resistant swimmingenclosures. Indeed, it has been noted that more than 60% of reported stings occur inside theenclosures (Little & Mulcahy, 1998; Fenner & Carney, 1999; Mulcahy, 1999). It should alsobe noted, however, that the majority of coastal swimmers and bathers in these regions stayinside the enclosures. Finer mesh enclosures have proven problematical, either cloggingrapidly or catching the wind and sailing dangerously (K. Moss, Manager Uninet EnclosureSystems, pers. comm. 2005). For this reason, prediction remains a high priority, in order toidentify when and where Irukandjis are present and close affected beaches to prevent stingson these days.
Irukandji-type stings are documented to have killed at least two people (Fenner &Hadok, 2002; Huynh et al., 2003), plus a third possibility that remains ambiguous (Old,1908). However, it is highly likely that other deaths have occurred and been mis-diagnoseddue to the aforementioned lack of diagnostic physical signs. Some species cause extremelyhigh blood pressure—previously reported as high as 280/180 (Fenner & Carney, 1999),and recently recorded as high as 300 systolic (pers. comm. 2005, M. Corkeron, TownsvilleHospital), substantially increasing the chances of a cerebrovascular accident. The onsetof severe illness may be rapid once the sequence begins, making it difficult to swim tosafety if necessary, thus conceivably resulting in drowning (Old, 1912; Houghton, 1997).Furthermore, Irukandji syndrome has been confused for decompression illness, delayingappropriate treatment (Hadok, 1997; Williamson, 1985).
Protective clothing is effective in preventing Irukandji stings (Gershwin & Dabinett,2009), and is now in wide usage throughout the Whitsunday region of the Great Barrier Reef.Since its implementation in early 2006, stings in this region have dropped dramatically,from a historical average of about 25 hospitalizations per year, to seven in the first year, fourin the next, and three the next (Australian Irukandji Sting Database, 2009); all the while,the tourism industry has remained strong (D. Lewis, Whitsunday Charter Boat IndustryAssociation, pers. comm. 2009).
Recommendation: Wearing of protective clothing is the most effective measure ofprotection from Irukandji stings. In regions or activities where protective clothing is notused, predictive sampling to determine the highest risk times and places should be used.
Managing Public Perceptions: The Hardest Part
Managing stings and stingers has become easier through knowledge and experience; how-ever, managing public perceptions remains difficult.
In 2002, a multi-organizational entity, the Queensland Government Irukandji TaskForce (ITF), was formed, along with two operational legs, a Prevention and ResponseWorking Group and a Research Working Group. The primary aims of the ITF and its workinggroups were defining and refining policies and procedures, supporting research projects,
Downloaded By: [Gershwin, Lisa-ann] At: 21:48 10 November 2009

Marine Stinger Management 33
and disseminating information to raise public awareness. Collectively, they sponsored sevenlarge research projects, activated an information website, created posters and brochures,produced a widely distributed DVD, and established a cooperative working relationshipamong major stakeholder groups (e.g., state and regional tourism, local governments, healthand emergency organizations, and researchers). The strategy was to make the public awareof the problem, and offer clear, simple treatment guidelines in the event of a sting.
To complement the work of the ITF by creating a practically focused comprehensivecoastal management plan incorporating offshore divers, fishermen, and remote aquaticactivities, the Whitsunday Marine Stinger Management Committee (WMSMC) was formedin early 2006. Recognizing the importance of sting prevention and the damaging effect ofthe fear of the unknown, the strategy of the Committee was simple: their objective was100% adoption of protective clothing within three years, and their methodology was pro-active dissemination of a balanced and accurate safety message. By telling the truth aboutboth the positive and negative aspects of the stinger problem (i.e., they are deadly, butuncommon, and easy to prevent), delivered in a credible scientific context, combined withstrong and practical prevention advice, stings rapidly dropped while business rapidly grew.For the first time in a long time, sting prevention made sense to the aquatic recreationalpublic.
A similar organization was developed in 2004 in Broome, Western Australia, in aneffort to manage the stinger problems there; and in early 2009, the Whitsunday model wasused as the basis for developing a stinger management plan for Thailand.
The current strategies of marine stinger management are still largely based on coastalspecies and coastal issues; however, the Whitsunday approach has proven effective inmanaging the offshore problem in that region. The current challenges include pro-activeprevention of offshore stings in other regions, and the particular problems associated withprediction, remote identification, patient monitoring, and air evacuation.
In regions where marine stingers have only recently become recognized as a serioushealth problem (e.g., Thailand, Malaysia, Japan, Hawaii, Pacific Islands, Caribbean), thecurrent primary challenges include species identification, appropriate treatment procedures,data tracking, and public safety education.
Recommendation: State-wide or nation-wide management strategies are effective inoverseeing a consistent safety message; local management strategies are effective in meetingthe particular regional needs associated with species differences, ecological and environ-mental effects, and local expectations. At all levels, awareness of the problem and treatmentadvice is necessary, but not sufficient, for effective management; practical prevention advicemust be included.
Recommendation: While the basis of effective marine stinger management must beprevention, the essential first aid for tropical marine stings distills down to four basiccomponents following the standard first aid principles of “DRABC”: summon help, treatthe patient, treat the sting, and seek further medical care (Figure 4).
Managing Marine Stingers: On-Going Challenges
According to De Nardi and Wilks (2008) “Beach safety is the limitation or mitigation ofrisks and hazards that expose the public to danger or harm while in a beach environment.. . .” As marine stingers are becoming internationally recognized as an emerging healthhazard, the obligation increases for beach managers and tourism operators to demonstratemitigation planning.
Downloaded By: [Gershwin, Lisa-ann] At: 21:48 10 November 2009

34 L. Gershwin et al.
Figure 4. The core message for marine stinger first aid.
Local governments and tourism bodies around the world are now faced with legalresponsibilities to ensure that their duty of care has been met in providing a safe recreationalenvironment for the public. Many have chosen to do this through the provision of lifeguardservices, while others have chosen to sponsor predictive or preventative research, whilesome have chosen to sit and wait and see what happens.
Because the actual incidence of serious envenomation is low but unpredictable, man-agement strategies should be based on minimizing the randomness of envenomation; thatis, creating a barrier in time or space between the hazard and the victim, and increasing theawareness of safety options so that individuals can make better choices, for example, dailyrelative risks, protective clothing options (Table 2).
We assert that simply making the public aware of the problem is insufficient; goodmanagement should aim for keeping the public safe while simultaneously growing thetourism industry in these regions. We have often been told by members of the public, “Agreat way to keep people from getting stung is to generate fear so that they won’t go in thewater”; we assert that a better way is to educate people so that they have the tools to enjoythe water safely. Nonetheless, a certain amount of preventative action needs to be driven byland managers, who should have the depth of knowledge and local continuity to implementsafe practices.
StingSafe—A Marine Stinger Risk Management Model
Marine stings occur most often when the interplay of four factors (anticipation, preparation,calculation, and attention) are not properly managed (Figure 5). The first, anticipation, isthe expectation by the visitor to have an enjoyable experience. Without it, they wouldnot come to the beach in the first place; however, the stronger their anticipation, theweaker their attention to risk management is likely to be. The remaining three factors arethe tools and actions used by councils and others concerned with stinger management,in order to fulfill the safety and enjoyment expectations of the visitor. Preparation isthe pro-active planning and available infrastructure that provides awareness, offers riskminimization solutions, and manages accidents. Calculation is the compiling and analysisof sting and visitation statistics to assess relative risk in time and space. Attention is theprovision of signage and lifesaving services to ensure visible and understandable safetyadvice.
A somewhat antagonistic relationship exists between the anticipation of the visitorand the risk minimization measures of management. The visitor’s focus on enjoymentmay preclude them from readily embracing the necessary risk awareness and preventionstrategies. Likewise, as more risk management responsibility is placed on the visitor, the
Downloaded By: [Gershwin, Lisa-ann] At: 21:48 10 November 2009

Tabl
e2
Seve
rity
ofst
ings
and
thei
rap
prop
riat
em
anag
emen
tbas
edon
freq
uenc
yof
occu
rren
ce
Type
ofst
ing,
orst
inge
rsth
atpr
oduc
eth
emR
arel
yoc
cur
Occ
asio
nally
occu
rFr
eque
ntly
occu
rR
elia
bly
occu
r
Mild
(e.g
.,se
alic
e)V
erba
ladv
ice
and
sign
age
for
awar
enes
sV
erba
ladv
ice
and
sign
age
for
awar
enes
sA
dvic
eof
risk
,con
side
rpr
otec
tive
clot
hing
Focu
son
pred
ictio
n;ac
tion
plan
inpl
ace
for
aler
teve
nts
Mod
erat
e(e
.g.,
blue
bottl
es;h
air
jelli
es)
Ver
bala
dvic
ean
dsi
gnag
efo
raw
aren
ess
Focu
son
pred
ictio
n;ac
tion
plan
inpl
ace
for
aler
teve
nts
Adv
ice
ofri
sk,
reco
mm
enda
tion
ofpr
otec
tive
clot
hing
Reg
ular
mon
itori
ngpl
anw
ithbe
ach
clos
ure
prov
isio
n
Seve
re(e
.g.,
Iruk
andj
is)
Focu
son
pred
ictio
n;ac
tion
plan
inpl
ace
for
aler
teve
nts
Adv
ice
ofri
sk,
avai
labi
lity
ofpr
otec
tive
clot
hing
Reg
ular
mon
itori
ngpl
anw
ithbe
ach
clos
ure
prov
isio
nR
egul
arm
onito
ring
plan
with
beac
hcl
osur
epr
ovis
ion
Let
hal(
e.g.
,C
hiro
nex-
type
box
jelly
fish)
Focu
son
pred
ictio
n;ac
tion
plan
inpl
ace
for
aler
teve
nts
Bar
rier
met
hods
inpl
ace,
e.g.
,stin
ger
nets
,pr
otec
tive
clot
hing
Bar
rier
met
hods
inpl
ace,
e.g.
,st
inge
rne
ts,p
rote
ctiv
ecl
othi
ng
Bar
rier
met
hods
inpl
ace,
e.g.
,st
inge
rne
ts,p
rote
ctiv
ecl
othi
ng
35
Downloaded By: [Gershwin, Lisa-ann] At: 21:48 10 November 2009

36 L. Gershwin et al.
Figure 5. StingSafe, a model illustrating the relationship between four factors that comprise aneffective marine stinger management plan.
awareness message must become stronger to ensure adoption; however, a stronger messagemay be perceived by the visitor as “scary.” Therefore, a risk control program provided bymanagement is likely to have better adoption than one that relies on the initiative of thevisitor. Conversely, too much risk minimization on the part of management could lead toprolonged beach closures or impractical protective clothing regulations.
One good comparison of a management-provided risk control program is in theaforementioned stinger-resistant swimming enclosures. The stingers are prevalent in bothQueensland and the Northern Territory. Many local governments in Queensland have cho-sen to manage their risk by installing stinger nets, whereas the official recommendationin the Northern Territory is to advise people to stay out of the water (Currie, 2002). Theformer is compatible with a growing beach-based tourism industry, whereas the latter isnot.
In another example, after 24 years of recommendations that the public wear lycrabody suits to protect from stingers in the summer months, less than 5% of beach-goersactually do. By contrast, in just a few years of providing lycra suits to passengers, manyreef operators are recording nearly 100% adoption (C. McKenzie, immediate past CEO,and D. Windsor, current CEO, Association of Marine Park Tourism Operators, pers. comm.2007; D. Lewis, Whitsunday Charter Boat Industry Association, pers. comm. 2009).
While anticipation is a feeling of the visitor rather than a responsibility of management,maintaining this emotion must be part of the management strategy; there must be balance toprovide a safe experience while not dampening the dream too much. A well-designed stingersafety management plan, therefore, balances these four factors to provide an enjoyable andsafe experience to the recreational public.
Downloaded By: [Gershwin, Lisa-ann] At: 21:48 10 November 2009

Marine Stinger Management 37
Who Needs a Marine Stinger Management Plan?
Any council with beach responsibilities, any tourism operator with beach or aquatic venues,or organization whose employees are exposed to marine stingers, needs a marine stingermanagement plan to meet social and legal responsibilities. Monitoring programs and man-agement plans are particularly important in regions at a heightened risk of marine stingerproblems, for example, regions with historical indications, recent ecosystem perturbations,or high recreational use. Also needed is support for scientific initiatives to improve pre-diction, prevention, and treatment of marine stingers and marine stings. Regular trainingprograms for lifeguards and lifesavers to identify marine stings and use appropriate first aid(recommendations vary greatly for different types of stings) are paramount, as are improvedreporting procedures so that concerned parties have access to the information required tomake better management decisions.
A further need exists for a team to coordinate such a program, to stay abreast ofscientific needs and outputs, to assist organizations in management strategies that meettheir needs, and pro-active information delivery to ensure that front-line personnel aretrained in best practice.
Reasons to Have a Stinger Management Plan
• pro-active sting prevention will reduce sting numbers;• to provide direct benefits to public health and local tourism;• a duty of care dictates that organizations and individuals must take action to reduce
foreseeable risk;• there is a corporate responsibility to protect assets and legal liability of the organi-
zation;• to minimize the adverse media consequences of sting events;• a good plan protects the organization in the event of an accident.
Four-Point Strategy for Pro-Active Marine Stinger Management
1. Risk Audit
The objectives of an initial marine stinger risk audit are to define the facilities where peoplemay be in danger, to assess existing control measures, and to compare the rate of incidentsagainst an established benchmark. Conditions of particular importance include the historyof incidents, latitude, presence, or absence of stinger resistant swimming enclosures, rateof local/domestic/foreign visitation, signage (including multi-lingual for certain areas),nature of public safety management, lifeguard/lifesaver monitoring, access to emergencycommunication, ambulance call-out time, and distance to hospitals/medical centers.
2. Development of Targeted Marine Stinger Management Plans for Councils
Each local government deals with slightly different marine stinger issues and public needs.Some regions rarely have Irukandji incidents, whereas others have them regularly; some re-gions are more prone to box jellyfish than Irukandji stings, or vice versa; some regions havea high through-put of offshore visitors and staff, whereas others have a higher coastal beachusage. Because of these nuances, a blanket approach is not ideal. Nevertheless a pro-activemanagement plan should ensure that the following elements are in place: standardized
Downloaded By: [Gershwin, Lisa-ann] At: 21:48 10 November 2009

38 L. Gershwin et al.
signage, life-saving provision, Occupational Health and Safety policies, information dis-semination, tourism organization support, cooperative inter-organizational media strategies,protective clothing availability, accurate/standardized data collection and reporting, and anevacuation plan.
3. Integrated Structured Communication among Providers
Recent information-sharing initiatives such as real-time SMS/phone incident notificationhave proven successful in enabling front-line entities to make on-the-spot decisions basedon current information. Future initiatives may include multi-access Web-based databasingof sting and condition information, such that various entities can access, in real time,relevant information and make updates as appropriate. The health application of geospatialresources, such as using GoogleEarth to develop “healthmap.org” as a real time monitor ofinfectious disease outbreaks is one example (see www.healthmap.org).
Access to information on how to recognize certain types of stings and stingers, high riskconditions, appropriate public communication, early incident management, and efficientreporting are essential to successful marine stinger management. A variety of tools suchas informational workshops, seminars, newsletters, websites, brochures, freecall numbers,and auditing services should be available to assist organisations in improving safety output.
4. Periodic Formal Re-Auditing
Assessment of existing facilities and control plans should occur, ideally, before and aftereach stinger season, or at a minimum, before each stinger season. In particular, weaknessesidentified against the benchmark should be addressed. Similarly, a method of assessingoutcomes should be incorporated.
References
Access Economics. 2007. Measuring the economic & financial value of the Great Barrier Reef MarinePark 2005/2006. Townsville: Great Barrier Reef Marine Park Authority.
Andersen, J. 2006. Talk of the town. Townsville Bulletin 10 January:8.Anonymous. 2006. Sting report from Jamaican safety professional (source anonymous by request).Australian Irukandji Sting Database. 2009. Collection of sting records and related information,
maintained by various researchers since 1943.Australian Resuscitation Council. 2007. Available at http://www.resus.org.au (accessed May 27,
2007).Barnes, J. H. 1964. Cause and effect in Irukandji stingings. Medical Journal of Australia 1 (51st Year)
(24):897–904.Beebe, W. 1928. Beneath tropic seas. New York and London: G.P. Putnam’s Sons.Bengston, K., M. M. Nichols, V. Schnadig, and M. D. Ellis. 1991. Sudden death in a child following
jellyfish envenomation by Chiropsalmus quadrumanus. Case report and autopsy findings. JAMA(Journal of the American Medical Association) 266(10):1404–1406.
Braidwood, S. Unpublished. Long-term notes of Irukandji syndrome experience with permanent heartdamage, from sting at Port Douglas, QLD, January 2002. Archived with the authors.
Cheng, A. C., K. D. Winkel, G. M. Hawdon, and M. McDonald. 1999. Irukandji-like syndrome inVictoria. Australian and New Zealand Journal of Medicine 29(6):835.
Cleland, J. B., and R. V. Southcott. 1965. Injuries to Man from Marine Invertebrates in the AustralianRegion. 282 pp. Canberra: Commonwealth of Australia.
Corkeron, M. A. 2003. Magnesium infusion to treat Irukandji syndrome. Medical Journal of Australia178:411.
Downloaded By: [Gershwin, Lisa-ann] At: 21:48 10 November 2009

Marine Stinger Management 39
Cropp, B., and I. Cropp. 1984. The deadliest creature on Earth. The Scuba Diver 3:42–48.Currie, B. J. 2002. Box jellyfish in tropical Australia—New findings and the treatment and prevention
of Chironex fleckeri stings. The Northern Territory Disease Control Bulletin 9(4):3–6.Currie, B. J., and S. P. Jacups. 2005. Prospective study of Chironex fleckeri and other box jelly-
fish stings in the “Top End” of Australia’s Northern Territory. Medical Journal of Australia183(11/12):631–636.
De Nardi, M., and J. Wilks. 2008. Beach safety. In Encyclopaedia of tourism and recreation in marineenvironments, ed. M. Luck, 57. London: Routledge.
de Pender, A. M. G., K. D. Winkel, and R. J. Ligthelm. 2006. A probable case of Irukandji Syndromein Thailand. Journal of Travel Medicine 13(4):240–243.
Endean, B. 1988. Venom of Chironex, the world’s most venomous animal. In Venoms and victims,eds. J. Pearn and J. Covacevich, 15–24. Brisbane: The Queensland Museum and Amphion Press.
Fenner, P. J. 1997a. Awareness, prevention and treatment of world-wide marine stings and bites.International Life Saving Federation Medical/Rescue Conference Proceedings, 1–13. Availableat www.usla.org/PublicInfo/library/Treatment of Marine Stings.pdf (accessed June 1, 2007).
Fenner, P. J. 1997b. The global problem of cnidarian (jellyfish) stinging, MD Thesis. 202 pp. London:London University.
Fenner, P. J. 1999. Comment on: Med J Aust. 1998 Dec 7–21; 169(11–12): 638–641. Irukandjienvenomation in far north Queensland. Medical Journal of Australia 170(10):512.
Fenner, P. J. 2006. Invited Review: Jellyfish stings—First aid and early medical treatments revisited.Annals of the Australasian College of Tropical Medicine 7:3–7.
Fenner, P. J., and I. Carney. 1999. The Irukandji syndrome: A devastating syndrome caused by anorth Australian jellyfish. Australian Family Physician 28:1131–1137.
Fenner, P. J., and I. Carney. 2001. The Irukandji syndrome: A devastating syndrome caused by anorth Australian jellyfish. An updated review with symptoms including cardiac failure. ACTMBulletin [Supplement] 10(1):3–4.
Fenner, P. J., and J. C. Hadok. 2002. Fatal envenomation by jellyfish causing Irukandji syndrome.Medical Journal of Australia 177(7):362–363.
Fenner, P. J., J. Williamson, V. I. Callanan, and I. Audley. 1986. Further understanding of, anda new treatment for, “Irukandji” (Carukia barnesi) stings. Medical Journal of Australia145(11–12):569, 572–574.
Fenner, P. J., and J. A. Williamson. 1996. Worldwide deaths and severe envenomation from jellyfishstings. Medical Journal of Australia 165(11–12):658–661.
Gershwin, L. 2005a. Taxonomy and phylogeny of Australian Cubozoa. PhD, School of MarineBiology and Aquaculture, James Cook University, Townsville, Queensland.
Gershwin, L. 2005b. Two new species of jellyfishes (Cnidaria: Cubozoa: Carybdeida) from tropicalWestern Australia, presumed to cause Irukandji Syndrome. Zootaxa 1084:1–30.
Gershwin, L. 2005c. Carybdea alata auct. and Manokia stiasnyi, reclassification to a new familywith description of a new genus and two new species. Memoirs of the Queensland Museum51(2):501–523.
Gershwin, L. 2007. Malo kingi: A new species of Irukandji jellyfish (Cnidaria: Cubozoa: Carybdeida),possibly lethal to humans. Zootaxa 1659:55–68.
Gershwin, L. 2008. Morbakka fenneri: A new genus and species of Irukandji jellyfish (Cnidaria:Cubozoa). Memoirs of the Queensland Museum 54(1):23–33.
Gershwin, L., and P. Alderslade. 2005. A new genus and species of box jellyfish (Cubozoa: Caryb-deida) from tropical Australian waters. The Beagle 21:27–36.
Gershwin, L., and K. Dabinett. 2009. Comparison of eight types of protective clothing againstIrukandji jellyfish stings. Journal of Coastal Research 25(1):117–130.
Gollan, J. A. 1968. The dangerous Portuguese Man-of-war. Medical Journal of Australia 1968:973.Grady, J. D., and J. W. Burnett. 2003. Irukandji-like syndrome in South Florida divers. Annals of
Emergency Medicine 42(6):763–766.Guest, W. C. 1959. The occurrence of the jellyfish Chiropsalmus quadrumanus in Matagorda Bay,
TX. Bulletin of Marine Science of the Gulf and Caribbean 9(1):79–83.
Downloaded By: [Gershwin, Lisa-ann] At: 21:48 10 November 2009

40 L. Gershwin et al.
Hadok, J. C. 1997. “Irukandji” syndrome: A risk for divers in tropical waters. Medical Journal ofAustralia 167(11/12):649–650.
Harrison, S. L., P. A. Leggat, P. J. Fenner, D. N. Durrheim, and A. L. Swinbourne. 2004. Reportedknowledge, perceptions, and behavior of tourists and North Queensland residents at risk ofcontact with jellyfish that cause the “Irukandji syndrome.” Wilderness & Environmental Medicine15(1):4–10.
Houghton, D. 1997. Tiny jellyfish blamed for drownings. The Times, December 27. Availableat http://www.igorilla.com/gorilla/animal/Tiny jellyfish blamed for drownings.html (accessedJuly 31, 2004).
Huynh, T. T., J. Seymour, P. Pereira, R. Mulcahy, P. Cullen, T. Carrette, and M. Little. 2003. Severityof Irukandji syndrome and nematocyst identification from skin scrapings. Medical Journal ofAustralia 178(1):38–41.
Kinsey, B. E. 1986. Barnes on Box Jellyfish. 87 pp. Townsville: Sir George Fisher Centre for TropicalMarine Studies, James Cook University.
Kinsey, B. E. 1988. More Barnes on Box Jellyfish. 109 pp. Townsville: Sir George Fisher Centre forTropical Marine Studies, James Cook University.
Kizer, K. W. 1984. Case report: Decompression sickness or Portuguese Man-of-war envenomation?Wilderness Medicine 1(July–Aug):7–8.
Kramp, P. L. 1961. Synopsis of the medusae of the world. Journal of the Marine Biological Associationof the United Kingdom 40:1–469.
Larson, R. J. 1982. Medusae (Cnidaria) from Carrie Bow Cay, Belize. In The Atlantic Barrier ReefEcosystem at Carrie Bow Cay, Belize, I: Structure and communities, eds. K. Rutzler and I. G.Macintyre, 253–258. Washington DC: Smithsonian Contributions to the Marine Sciences.
Leggat, P. A., S. L. Harrison, P. J. Fenner, D. N. Durrheim, and A. L. Swinbourne. 2005. Healthadvice obtained by tourists travelling to Magnetic Island: A risk area for ‘Irukandji’ jellyfish inNorth Queensland, Australia. Travel Medicine and Infectious Disease 3(1):27–31.
Lewis, C., and B. Bentlage. 2009. Clarifying the identity of the Japanese Habu-kurage, Chironexyamaguchii, sp. nov. (Cnidaria: Cubozoa: Chirodropida). Zootaxa 2030:59–65.
Little, M., and R. F. Mulcahy. 1998. A year’s experience of Irukandji envenomation in far northQueensland. Medical Journal of Australia 169:638–641.
Little, M., P. Pereira, R. Mulcahy, P. Cullen, T. Carrette, and J. Seymour. 2003. Severe cardiac failureassociated with presumed jellyfish sting. Irukandji Syndrome? Anaesthesia and Intensive Care31:642–647.
Lord, R. E., and S. L. B. Wilks. 1918. A case of jelly-fish sting simulating an acute abdomen. TheLancet 192(4960):390.
Lumley, J., J. A. Williamson, P. J. Fenner, J. W. Burnett, and D. M. Colquhoun. 1988. Fatal enveno-mation by Chironex fleckeri, the north Australian box jellyfish: the continuing search for lethalmechanisms. Medical Journal of Australia 148(10):527–531, 533–534.
Macrokanis, C. J., N. L. Hall, and J. K. Mein. 2004. Irukandji syndrome in northern Western Australia:An emerging health problem. Medical Journal of Australia 181(11/12):699–702.
Mayer, A. G. 1910. Medusae of the world. Vol. 3, The Scyphomedusae, 499–735. Washington, DC:Carnegie Institution.
Mills, C. E. 1995. Medusae, siphonophores, and ctenophores as planktivorous predators in changingglobal ecosystems. ICES Journal of Marine Science 52(3–4):575–581.
Mills, C. E. 2001. Jellyfish blooms: Are populations increasing globally in response to changingocean conditions? Hydrobiologia (451):55–68.
Moss, K. H., and K. P. Stark. 1983. Development of a marine stinger resistant swimming enclosure. InProceedings 6th Australian Coastal & Ocean Engineering Conference. Gold Coast, July13–15,1983.
Mulcahy, R. 1999. A severe case of Irukandji syndrome. In Neurological Emergencies Handbook,Winter Symposium. Melbourne: Australasian College for Emergency Medicine.
National Science Foundation. 2008. Jellyfish gone wild! Available at http://www.nsf.gov/news/special reports/jellyfish/index.jsp (accessed May 26, 2009).
Downloaded By: [Gershwin, Lisa-ann] At: 21:48 10 November 2009

Marine Stinger Management 41
Oiso, N., K. Fukai, M. Ishii, T. Ohgushi, and S. Kubota. 2005. Jellyfish dermatitis caused by Porpitapacifica, a sign of global warming? Contact Dermatitis 52:232–233.
Old, H. H. 1908. A report of several cases with unusual symptoms caused by some unknown varietyof jellyfish. Philippine Journal of Science, B 3:329–333.
Old, H. H. 1912. Additional report of several cases with unusual symptoms caused by some unknownvariety of jellyfish. United States Naval Medical Bulletin 6:377–380.
Parsons, T. R., and C. M. Lalli. 2002. Jellyfish population explosions. La Mer 40:111–121.Pommier, P., M. Coulange, and L. D. Haro. 2005. Systemic envenomation by jellyfish in Guadeloupe:
Irukandji-like syndrome. Medecine Tropicale 65(4):367–369.Purcell, J. E. 2005. Climate effects on formation of jellyfish and ctenophore blooms: A review.
Journal of the Marine Biological Association of the United Kingdom 85(3):461–476.Roberts, G. 2002. Tiny harbinger of death lurking in our seas. Sydney Morning Herald, News and
Features 20 April:1.Southcott, R. V. 1956. Studies on Australian cubomedusae, including a new genus and species appar-
ently harmful to man. Australian Journal of Marine and Freshwater Research 7(2):254–280.Southcott, R. V. 1967. Revision of some Carybdeidae (Scyphozoa: Cubomedusae), including a
description of the jellyfish responsible for the “Irukandji syndrome.” Australian Journal ofZoology 15:651–671.
Surf Life Saving Australia. 2005. Valuing an Icon: 2005 Annual Report. 92 pp. Sydney: Surf LifeSaving Australia.
Togias, A. G., J. W. Burnett, A. Kagey-Sobotka, and L. M. Lichtenstein. 1985. Anaphylaxis aftercontact with a jellyfish. Journal of Allergy and Clinical Immunology 75:672–675.
Wilks, J. 1999. International tourists, motor vehicles and road safety: A review of the literature leadingup to the Sydney 2000 Olympics. Journal of Travel Medicine 6:115–121.
Wilks, J. 2006. Current issues in tourist health, safety and security. In Tourism in turbulent times:Towards safe experiences for visitors, eds. J. Wilks, D. Pendergast, and P. Leggat, 3–18. Oxford:Elsevier.
Wilks, J., D. Pendergast, and M. Wood. 2002. Overseas visitor deaths in Australia: 1997–2000.Current Issues in Tourism 5:550–557.
Williams, C. 2009. The next big fin: Seafood’s slimy future. New Scientist (2698):40–43.Williams, R. 2004. Update on Irukandji issues. In Report presented to the Queensland Government
Irukandji Task Force meeting. Townsville, Queensland. February 24.Williamson, J. 1985. “Irukandji” syndrome or decompression sickness or cerebral arterial gas em-
bolism? A differential diagnostic trap for practitioners of diving medicine in north Queensland.South Pacific Underwater Medicine Society Journal 15:38–39.
Williamson, J. A., V. I. Callanan, and R. F. Hartwick. 1980. Serious envenomation by the northernAustralian box-jellyfish (Chironex fleckeri). Medical Journal of Australia 1(1):13–16.
Williamson, J. A., V. I. Callanan, M. L. Unwin, and R. F. Hartwick. 1984. Box jellyfish venom andhumans. Medical Journal of Australia 140:444–445.
Williamson, J. A., P. J. Fenner, J. W. Burnett, and J. Rifkin. Eds. 1996. Venomous and poisonousm,arine animals: A medical and biological handbook. Sydney, Australia: NSW University Press.
Winkel, K. D., P. Mirtschin, and J. Pearn. 2006. Twentieth century toxinology and antivenom devel-opment in Australia. Toxicon 48:738–754.
Yoshimoto, C. M., and A. A. Yanagihara. 2002. Cnidarian (coelenterate) envenomations in Hawai‘iimprove following heat application. Transactions of the Royal Society of Tropical Medicine andHygiene 96(3):300–303.
Downloaded By: [Gershwin, Lisa-ann] At: 21:48 10 November 2009