Management of acute mild gallstone pancreatitis under acute care surgery: should patients be...
7
Management of acute mild gallstone pancreatitis under acute care surgery: should patients be admitted to the surgery or medicine service? Narong Kulvatunyou, M.D.*, John Watt, M.D., Randall S. Friese, M.D., Lynn Gries, M.D., Donald J. Green, M.D., Bellal Joseph, M.D., Terence O’Keeffe, M.D., Andrew L. Tang, M.D., Gary Vercruysse, M.D., Peter Rhee, M.D. Division of Acute Care Surgery, Department of Surgery, University of Arizona, Room 5411, 1501 North Campbell Avenue, PO Box 245603, Tucson, AZ 85727-5063, USA KEYWORDS: Gallstone pancreatitis; Medicine service; Surgery service Abstract BACKGROUND: We hypothesized that patients with acute mild gallstone pancreatitis (GSP) admitted to surgery (SUR; vs medicine [MED]) had a shorter time to surgery, shorter hospital length of stay (HLOS), and lower costs. METHODS: We performed chart reviews of patients who underwent a cholecystectomy for acute mild GSP from October 1, 2009 to May 31, 2013. We excluded patients with moderate to severe and non-gallstone pancreatitis. We compared outcomes for time to surgery, HLOS, costs, and compli- cations between the 2 groups. RESULTS: Fifty acute mild GSP patients were admitted to MED and 52 to SUR. MED patients were older and had more comorbidity. SUR patients had a shorter time to surgery (44 vs 80 hours; P , .001), a shorter HLOS (3 vs 5 days; P , .001), and lower hospital costs ($11,492 6 6,480 vs $16,183 6 12,145; P 5 .03). In our subgroup analysis on patients with an American Society of Anesthesiologists score between 1 and 2, the subgroups were well matched; all outcomes still favored SUR patients. CONCLUSIONS: Admitting acute mild GSP patients directly to SUR shortened the time to surgery, shortened HLOS, and lowered hospital costs. Ó 2014 Elsevier Inc. All rights reserved. Several current reports in the literature 1–5 support an ‘‘early’’ cholecystectomy for patients who present with acute mild gallstone pancreatitis (GSP) because of an associated 18% readmission rate 1 due to biliary-related diseases. An ‘‘early’’ cholecystectomy usually implies one within the same initial hospital admission or what is often referred to as an ‘‘index cholecystectomy’’ (vs delayed-interval chole- cystectomy). Yet, many acute mild GSP patients have multi- ple concurrent comorbidities; these comorbidities may influence emergency department (ED) physicians’ decisions to choose the medicine service (MED) over the surgery service (SUR) for admission. Two previous studies 6,7 The authors declare no conflicts of interest. * Corresponding author. Tel.: 11-520-626-0889; fax: 11-520-626-5016. E-mail address: [email protected] Manuscript received March 29, 2014; revised manuscript September 8, 2014 0002-9610/$ - see front matter Ó 2014 Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/j.amjsurg.2014.09.003 The American Journal of Surgery (2014) -, -–-
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Management of acute mild gallstone pancreatitis under acute care surgery: should patients be...
Management of acute mild gallstone pancreatitisunder acute care surgery: should patients beadmitted to the surgery or medicine service?
Narong Kulvatunyou, M.D.*, John Watt, M.D., Randall S. Friese, M.D.,Lynn Gries, M.D., Donald J. Green, M.D., Bellal Joseph, M.D.,Terence O’Keeffe, M.D., Andrew L. Tang, M.D., Gary Vercruysse, M.D.,Peter Rhee, M.D.
Division of Acute Care Surgery, Department of Surgery, University of Arizona, Room 5411, 1501 NorthCampbell Avenue, PO Box 245603, Tucson, AZ 85727-5063, USA
KEYWORDS:Gallstone pancreatitis;Medicine service;Surgery service
AbstractBACKGROUND: We hypothesized that patients with acute mild gallstone pancreatitis (GSP)
admitted to surgery (SUR; vs medicine [MED]) had a shorter time to surgery, shorter hospital lengthof stay (HLOS), and lower costs.
METHODS: We performed chart reviews of patients who underwent a cholecystectomy for acutemild GSP from October 1, 2009 to May 31, 2013. We excluded patients with moderate to severeand non-gallstone pancreatitis. We compared outcomes for time to surgery, HLOS, costs, and compli-cations between the 2 groups.
RESULTS: Fifty acute mild GSP patients were admitted to MED and 52 to SUR. MED patients wereolder and had more comorbidity. SUR patients had a shorter time to surgery (44 vs 80 hours; P, .001),a shorter HLOS (3 vs 5 days; P , .001), and lower hospital costs ($11,492 6 6,480 vs $16,183 612,145; P 5 .03). In our subgroup analysis on patients with an American Society of Anesthesiologistsscore between 1 and 2, the subgroups were well matched; all outcomes still favored SUR patients.
CONCLUSIONS: Admitting acute mild GSP patients directly to SUR shortened the time to surgery,shortened HLOS, and lowered hospital costs.! 2014 Elsevier Inc. All rights reserved.
Several current reports in the literature1–5 support an‘‘early’’ cholecystectomy for patients who present with acutemild gallstone pancreatitis (GSP) because of an associated
18% readmission rate1 due to biliary-related diseases. An‘‘early’’ cholecystectomy usually implies one within thesame initial hospital admission or what is often referred toas an ‘‘index cholecystectomy’’ (vs delayed-interval chole-cystectomy). Yet, many acute mild GSP patients have multi-ple concurrent comorbidities; these comorbidities mayinfluence emergency department (ED) physicians’ decisionsto choose the medicine service (MED) over the surgeryservice (SUR) for admission. Two previous studies6,7
The authors declare no conflicts of interest.* Corresponding author. Tel.:11-520-626-0889; fax:11-520-626-5016.E-mail address: [email protected] received March 29, 2014; revised manuscript September 8,
2014
0002-9610/$ - see front matter ! 2014 Elsevier Inc. All rights reserved.http://dx.doi.org/10.1016/j.amjsurg.2014.09.003
The American Journal of Surgery (2014) -, -–-
comparing outcomes for acute mild GSP patients admitted toSUR vs MED drew differing conclusions.
Since the establishment of the field of acute care surgery(ACS),8–12 several studies have published its benefits of interms of improving ED work flow,13 along with decreasingsurgical evaluation time, shortening hospital length of stay(HLOS),14–18 and lowering hospital costs.14,18 With our cur-rent health care system’s continued financial constraint, it isimportant for clinicians to not only provide high-quality ofcare but also improve efficiency and lower hospital costs.
The evidence in the literature is limited regarding thepossible differences in outcomes for acute mild GSPpatients seen in the ED and then admitted to MED vsSUR. In this study, we hypothesized that admission directlyto SUR (instead of MED) will shorten the time to surgery,shorten HLOS, and perhaps lower hospital costs.
Methods
Study design and setting
We conducted this study at the University of Arizona(Tucson, AZ), a level I trauma center and a tertiary carecenter. The study was approved by our institutional reviewboard. Using our ongoing prospective ACS database, wereviewed the charts of patients who underwent a cholecys-tectomy for acute mild GSP from October 1, 2009 throughMay 31, 2013. Our hospital has about 73,000 annual patientvisits; our ACS service handles about 2,000 annualemergency general surgery consultations, both from theED and on an inpatient basis.
Patients
Patients were diagnosed with acute GSP if they had,according to the definition of the International Symposiumon Acute Pancreatitis in Atlanta in1992,19 acute upperabdominal pain and tenderness, an elevated serum amylaselevel (ie, at least 3 times the normal level), and imaging ev-idence of gallbladder stones. Acute mild GSP was definedas described previously plus minimal organ dysfunction
with less than 3 Ranson criteria20 or an Acute Physiologyand Chronic Health Evaluation II score , 8.21
All the patients in our study were initially seen andevaluated through the ED and subsequently admitted toeither MED or SUR. For patients admitted to MED, anACS consultation was obtained after they were admitted toMED. Excluded from our study were patients with mod-erate to severe pancreatitis, as well as patients withpancreatitis that was not related to gallstones.
Variables and outcomes
The data we collected included baseline characteristics,such as demographics, body mass index, comorbidities(specifically a history of diabetes, hypertension, and coro-nary disease), Acute Physiology and Chronic Health Eval-uation II score, American Society of Anesthesiologists(ASA) physical status score, and operative details andfindings (including the rate of conversion to an opencholecystectomy). We also identified outcomes, includingwhich patients underwent magnetic resonance cholangio-pancreatography (MRCP) or endoscopic retrograde cholan-giopancreatography (ERCP), either before or after theircholecystectomy.
We then compared outcomes between patients admittedto MED vs SUR. Our primary outcomes were time tosurgery (ie, the time interval from ED arrival to operatingroom arrival) and HLOS. Our secondary outcomes werehospital costs and complications. We obtained hospitalcosts from our hospital cost accounting system (EclipsysCorporation, Chicago, IL). These costs did not includethird-party professional fee, which included daily evalua-tion and management fee, and/or procedural physician fees.We reviewed the charts for all clinic follow-up visits, returnED visits, and readmissions. For postoperative complica-tions, we used the definition developed by Aboulian et al2
in their randomized controlled study of acute mild GSP pa-tients who underwent either an early cholecystectomy(,48 hours after ED arrival) or a delayed cholecystectomy;their definition of complications included bile duct injury,postoperative bleeding requiring blood transfusion, wound
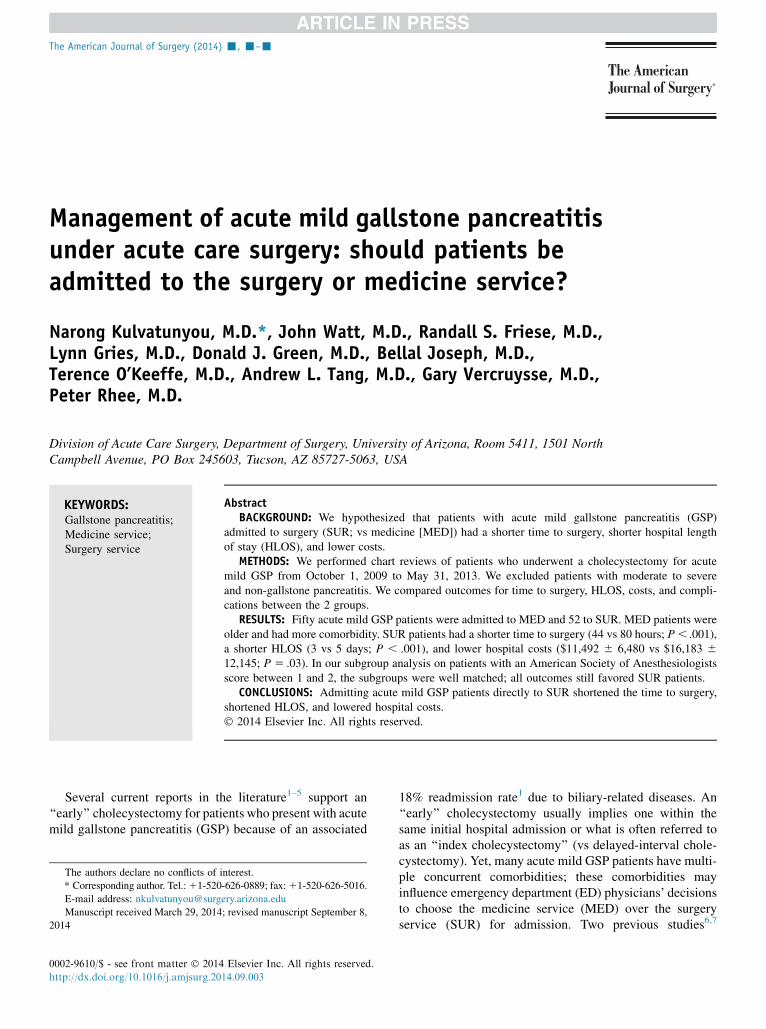
Table 1 Baseline characteristics for all patients
Characteristic MED (n 5 50) SUR (n 5 52) P
Age, mean 6 SD (years) 58 6 16 45 6 22 .001Male (%) 52 20 ,.001Body mass index, mean 6 SD (kg/m2) 32 6 8 31 6 8 .48History of diabetes, yes (%) 20 23 .71History of coronary disease, yes (%) 24 10 .05History of hypertension, yes (%) 56 37 .02APACHE II score, median (IQR) 7 (5–10) 5 (3–8) .02Cholecystectomy (%) 82 94 .10ASA score, median (IQR) 3 (2–3) 2 (2–2) ,.001
APACHE II 5 Acute Physiologic and Chronic Health Score; ASA 5 American Society of Anesthesiologists physical status; IQR 5 interquartile range;MED 5 admission directly to medicine service; SD 5 standard deviation; SUR 5 admission directly to surgery service.
2 The American Journal of Surgery, Vol -, No -, - 2014
infection, and pneumonia. In our study, we also consideredpostoperative biloma as a complication.
Statistical analysis
Continuous parametric data were expressed as the mean(6standard deviation), and nonparametric data were ex-pressed as the median (and interquartile range). Categoricaldata were expressed as a percentage. In our between-groupcomparisons, we used the Student t test for continuous para-metric data, the Wilcoxon rank sum test for nonparametricdata, and the chi-square test for proportional data. For our sta-tistical analysis, we used Stata 11 (StataCorp, College Sta-tion, TX); we considered a P value of% .05 significant.
Results
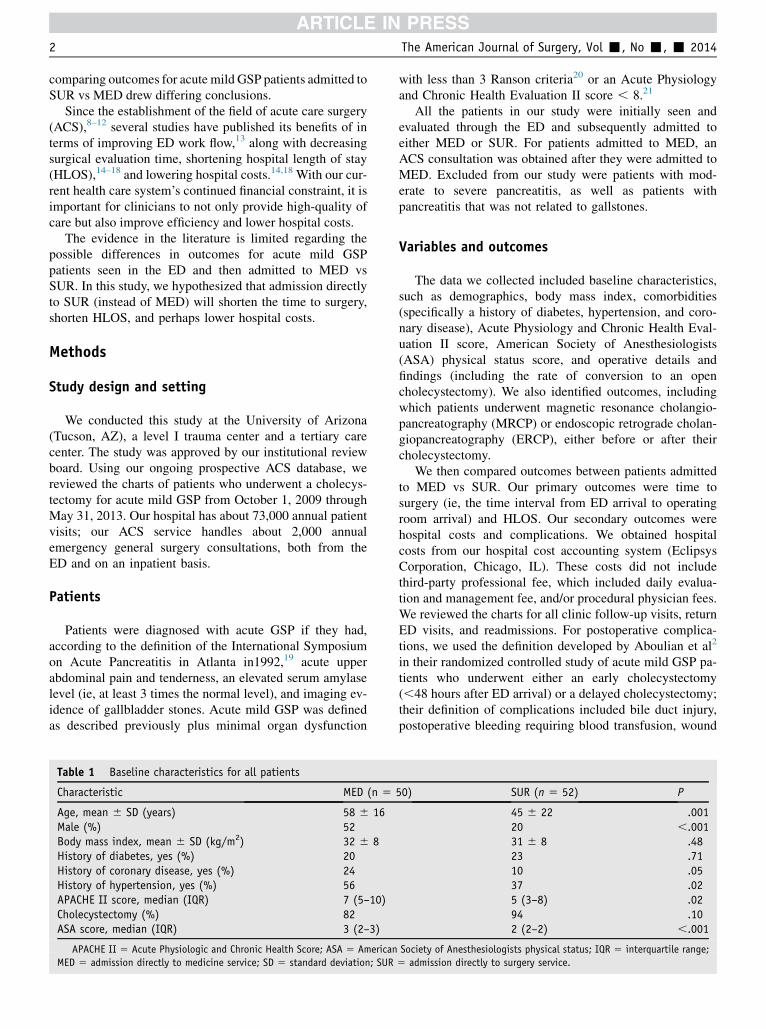
During the study period, 50 acute mild GSP patientswere admitted to MED and 52 to SUR. MED patients (vsSUR) were older, more likely to be male, and had morecomorbidities (Table 1). In all, 82% of MED and 94% ofSUR patients underwent cholecystectomy. Table 2 summa-rizes primary and secondary outcome comparison. SUR pa-tients had a shorter median time to surgery (44 vs 80 hours)and shorter median HLOS (3 vs 5 days). These shortertimes translated into mean hospital costs saving of about$5,000 per patient. The number of patients who requiredERCP interventions was similar. MED patients had highercomplication and readmission. Table 3 details the compli-cations and the reasons for patient readmission betweenthe 2 groups.
Because MED patients were older and had morecomorbidities than SUR patients, we were concerned thatour initial findings might have been skewed. Therefore, weperformed a subgroup analysis of only those patients withan ASA score of either 1 or 2 (Tables 4 and 5). The groupswere well matched in terms of comorbidities (Table 4). Butboth primary and secondary outcomes still favored SUR
patients. Even costs were lower in SUR patients, althoughthe difference was not statistically significant (Table 5).
Comment
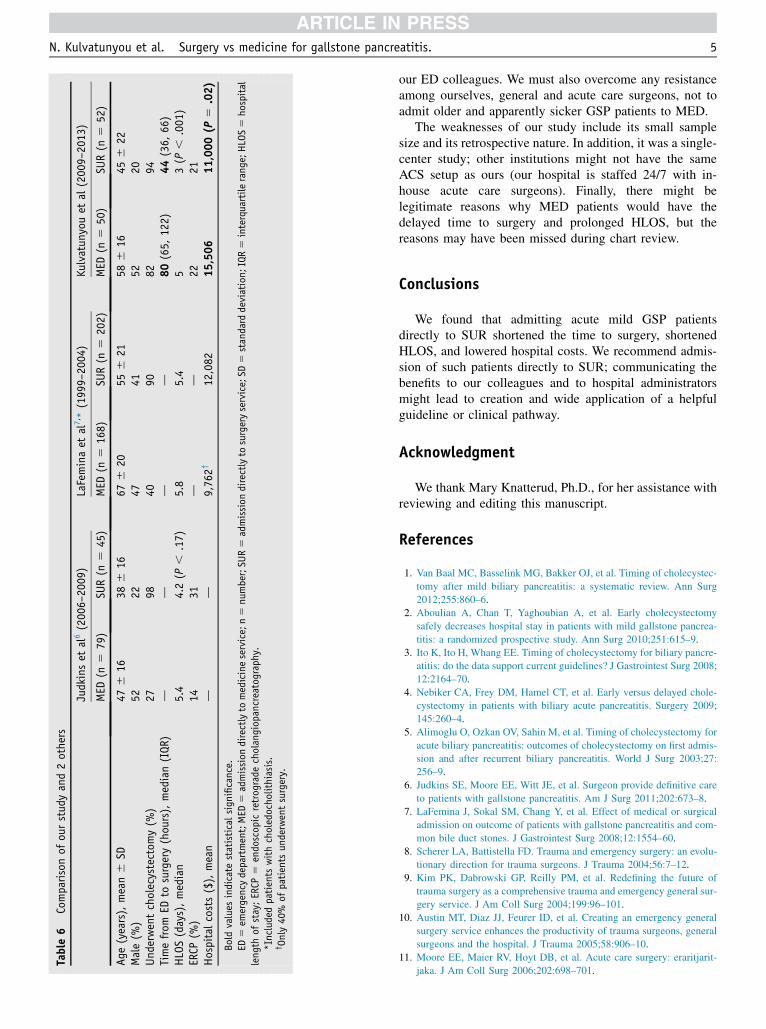
Our main finding supported our hypothesis: When acutemild GSP patients were admitted directly to SUR (insteadof MED), they were more likely to undergo surgery sooner.This shorter time to surgery, in turn, shortens the HLOS andperhaps lowers the hospital costs. Two previous studiessimilar to ours reached different conclusions (Table 6). Inboth those studies and ours, MED patients were older andhad more comorbiditiesdprobably the driving reason thatED physicians might decide to admit them to MED, despiterecognizing that GSP is a surgical disease and that surgicalintervention will likely be required.
Judkins et al6 drew a conclusion similar to ours in thattheir GSP patients, when admitted directly to SUR, had ashorter HLOS (by 1 day, although their finding did notreach statistical significance). Although they did notperform a between-group comparison of hospital costs,they were able to show that SUR patients required fewerlaboratory tests, imaging studies, and consultations; as aresult, admission directly to SUR lowered hospital costs.
Table 2 Outcomes for patients who underwent surgery
MED (n 5 41) SUR (n 5 49) P
Time from ED to surgery, hours, median (IQR) 80 (65–122) 44 (36–66) ,.001HLOS, days, median (IQR) 5 (4–7) 3 (2–5) ,.001Hospital costs, $, mean 6 SD 16,183 6 12,145 11,492 6 6,480 .03ERCP, n (%) 8 (20) 11 (22) .73MRCP, n (%) 25 (61) 11 (22) , .001Conversion to open cholecystectomy, n (%) 3 (7) 1 (2) .23Mortality, n (%) 2 (5) 0 (0) .27Complications, n (%) 4 (10) 0 (0) .03Readmission, n (%) 4 (10) 2 (4) .28
Bold values indicate statistical significance.ED 5 emergency department; ERCP 5 endoscopic retrograde cholangiopancreatography; HLOS 5 hospital length of stay; IQR 5 interquartile range;
MED 5 admission directly medicine service; MRCP 5 magnetic resonance cholangiopancreatography; SD 5 standard deviation; SUR 5 admission directlyto surgery service.
Table 3 Complications and readmission reasons
Reason MED SUR
Complications, n 4 0Biloma 3 (1 required drain
placed by IR)Pneumonia 1
Readmission, nRecurrent pancreatitis 2 2Retained stones 1Biloma 1
IR 5 interventional radiologist; MED 5 admission directly tomedicine service; n 5 number; SUR 5 admission directly to surgeryservice.
N. Kulvatunyou et al. Surgery vs medicine for gallstone pancreatitis. 3
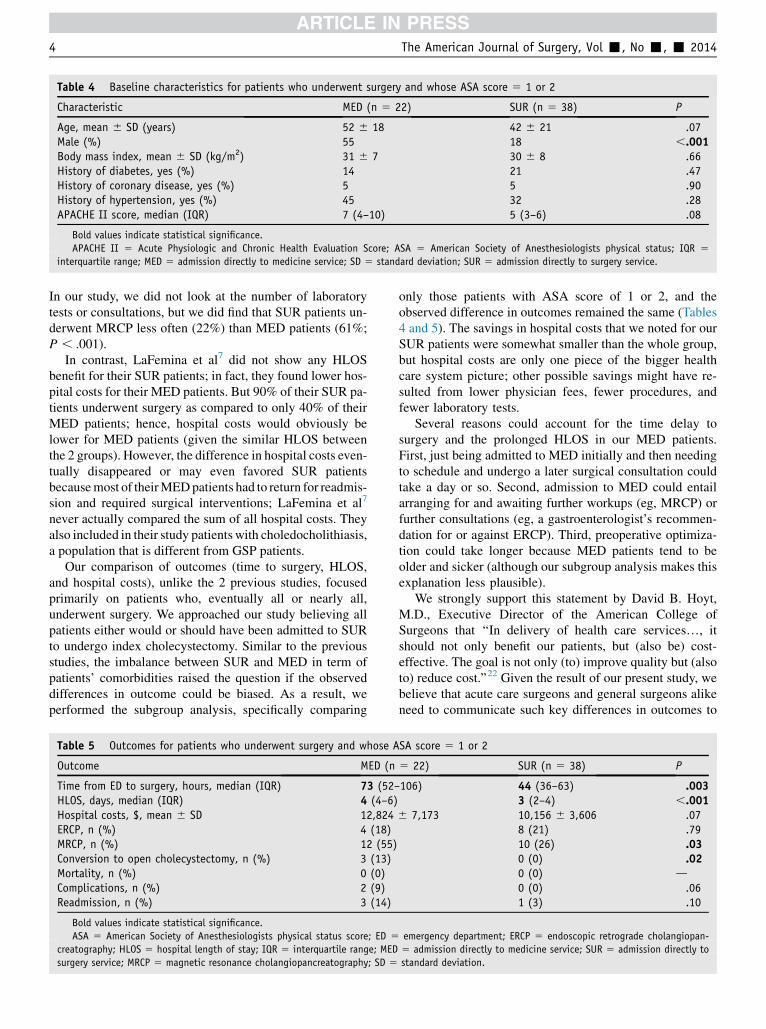
In our study, we did not look at the number of laboratorytests or consultations, but we did find that SUR patients un-derwent MRCP less often (22%) than MED patients (61%;P , .001).
In contrast, LaFemina et al7 did not show any HLOSbenefit for their SUR patients; in fact, they found lower hos-pital costs for their MED patients. But 90% of their SUR pa-tients underwent surgery as compared to only 40% of theirMED patients; hence, hospital costs would obviously belower for MED patients (given the similar HLOS betweenthe 2 groups). However, the difference in hospital costs even-tually disappeared or may even favored SUR patientsbecausemost of theirMEDpatients had to return for readmis-sion and required surgical interventions; LaFemina et al7
never actually compared the sum of all hospital costs. Theyalso included in their study patients with choledocholithiasis,a population that is different from GSP patients.
Our comparison of outcomes (time to surgery, HLOS,and hospital costs), unlike the 2 previous studies, focusedprimarily on patients who, eventually all or nearly all,underwent surgery. We approached our study believing allpatients either would or should have been admitted to SURto undergo index cholecystectomy. Similar to the previousstudies, the imbalance between SUR and MED in term ofpatients’ comorbidities raised the question if the observeddifferences in outcome could be biased. As a result, weperformed the subgroup analysis, specifically comparing
only those patients with ASA score of 1 or 2, and theobserved difference in outcomes remained the same (Tables4 and 5). The savings in hospital costs that we noted for ourSUR patients were somewhat smaller than the whole group,but hospital costs are only one piece of the bigger healthcare system picture; other possible savings might have re-sulted from lower physician fees, fewer procedures, andfewer laboratory tests.
Several reasons could account for the time delay tosurgery and the prolonged HLOS in our MED patients.First, just being admitted to MED initially and then needingto schedule and undergo a later surgical consultation couldtake a day or so. Second, admission to MED could entailarranging for and awaiting further workups (eg, MRCP) orfurther consultations (eg, a gastroenterologist’s recommen-dation for or against ERCP). Third, preoperative optimiza-tion could take longer because MED patients tend to beolder and sicker (although our subgroup analysis makes thisexplanation less plausible).
We strongly support this statement by David B. Hoyt,M.D., Executive Director of the American College ofSurgeons that ‘‘In delivery of health care services., itshould not only benefit our patients, but (also be) cost-effective. The goal is not only (to) improve quality but (alsoto) reduce cost.’’22 Given the result of our present study, webelieve that acute care surgeons and general surgeons alikeneed to communicate such key differences in outcomes to
Table 4 Baseline characteristics for patients who underwent surgery and whose ASA score 5 1 or 2
Characteristic MED (n 5 22) SUR (n 5 38) P
Age, mean 6 SD (years) 52 6 18 42 6 21 .07Male (%) 55 18 ,.001Body mass index, mean 6 SD (kg/m2) 31 6 7 30 6 8 .66History of diabetes, yes (%) 14 21 .47History of coronary disease, yes (%) 5 5 .90History of hypertension, yes (%) 45 32 .28APACHE II score, median (IQR) 7 (4–10) 5 (3–6) .08
Bold values indicate statistical significance.APACHE II 5 Acute Physiologic and Chronic Health Evaluation Score; ASA 5 American Society of Anesthesiologists physical status; IQR 5
interquartile range; MED 5 admission directly to medicine service; SD 5 standard deviation; SUR 5 admission directly to surgery service.
Table 5 Outcomes for patients who underwent surgery and whose ASA score 5 1 or 2
Outcome MED (n 5 22) SUR (n 5 38) P
Time from ED to surgery, hours, median (IQR) 73 (52–106) 44 (36–63) .003HLOS, days, median (IQR) 4 (4–6) 3 (2–4) ,.001Hospital costs, $, mean 6 SD 12,824 6 7,173 10,156 6 3,606 .07ERCP, n (%) 4 (18) 8 (21) .79MRCP, n (%) 12 (55) 10 (26) .03Conversion to open cholecystectomy, n (%) 3 (13) 0 (0) .02Mortality, n (%) 0 (0) 0 (0) dComplications, n (%) 2 (9) 0 (0) .06Readmission, n (%) 3 (14) 1 (3) .10
Bold values indicate statistical significance.ASA 5 American Society of Anesthesiologists physical status score; ED 5 emergency department; ERCP 5 endoscopic retrograde cholangiopan-
creatography; HLOS 5 hospital length of stay; IQR 5 interquartile range; MED 5 admission directly to medicine service; SUR 5 admission directly tosurgery service; MRCP 5 magnetic resonance cholangiopancreatography; SD 5 standard deviation.
4 The American Journal of Surgery, Vol -, No -, - 2014
our ED colleagues. We must also overcome any resistanceamong ourselves, general and acute care surgeons, not toadmit older and apparently sicker GSP patients to MED.
The weaknesses of our study include its small samplesize and its retrospective nature. In addition, it was a single-center study; other institutions might not have the sameACS setup as ours (our hospital is staffed 24/7 with in-house acute care surgeons). Finally, there might belegitimate reasons why MED patients would have thedelayed time to surgery and prolonged HLOS, but thereasons may have been missed during chart review.
Conclusions
We found that admitting acute mild GSP patientsdirectly to SUR shortened the time to surgery, shortenedHLOS, and lowered hospital costs. We recommend admis-sion of such patients directly to SUR; communicating thebenefits to our colleagues and to hospital administratorsmight lead to creation and wide application of a helpfulguideline or clinical pathway.
Acknowledgment
We thank Mary Knatterud, Ph.D., for her assistance withreviewing and editing this manuscript.
References
1. Van Baal MC, Basselink MG, Bakker OJ, et al. Timing of cholecystec-tomy after mild biliary pancreatitis: a systematic review. Ann Surg2012;255:860–6.
2. Aboulian A, Chan T, Yaghoubian A, et al. Early cholecystectomysafely decreases hospital stay in patients with mild gallstone pancrea-titis: a randomized prospective study. Ann Surg 2010;251:615–9.
3. Ito K, Ito H, Whang EE. Timing of cholecystectomy for biliary pancre-atitis: do the data support current guidelines? J Gastrointest Surg 2008;12:2164–70.
4. Nebiker CA, Frey DM, Hamel CT, et al. Early versus delayed chole-cystectomy in patients with biliary acute pancreatitis. Surgery 2009;145:260–4.
5. Alimoglu O, Ozkan OV, Sahin M, et al. Timing of cholecystectomy foracute biliary pancreatitis: outcomes of cholecystectomy on first admis-sion and after recurrent biliary pancreatitis. World J Surg 2003;27:256–9.
6. Judkins SE, Moore EE, Witt JE, et al. Surgeon provide definitive careto patients with gallstone pancreatitis. Am J Surg 2011;202:673–8.
7. LaFemina J, Sokal SM, Chang Y, et al. Effect of medical or surgicaladmission on outcome of patients with gallstone pancreatitis and com-mon bile duct stones. J Gastrointest Surg 2008;12:1554–60.
8. Scherer LA, Battistella FD. Trauma and emergency surgery: an evolu-tionary direction for trauma surgeons. J Trauma 2004;56:7–12.
9. Kim PK, Dabrowski GP, Reilly PM, et al. Redefining the future oftrauma surgery as a comprehensive trauma and emergency general sur-gery service. J Am Coll Surg 2004;199:96–101.
10. Austin MT, Diaz JJ, Feurer ID, et al. Creating an emergency generalsurgery service enhances the productivity of trauma surgeons, generalsurgeons and the hospital. J Trauma 2005;58:906–10.
11. Moore EE, Maier RV, Hoyt DB, et al. Acute care surgery: eraritjarit-jaka. J Am Coll Surg 2006;202:698–701.
Table6
Comparisonof
ourstud
yand2others
Judkinset
al6(200
6–20
09)
LaFeminaet
al7, *
(199
9–20
04)
Kulvatun
youet
al(200
9–20
13)
MED
(n5
79)
SUR(n
545
)MED
(n5
168)
SUR(n
520
2)MED
(n5
50)
SUR(n
552
)
Age
(years),
mean6
SD47
616
386
1667
620
556
2158
616
456
22Male(%
)52
2247
4152
20Und
erwentcholecystectom
y(%
)27
9840
9082
94Timefrom
EDto
surgery(hou
rs),
median(IQR)
dd
dd
80(65,
122)
44(36,
66)
HLOS(days),median
5.4
4.2(P
,.17)
5.8
5.4
53(P
,.001
)ERCP
(%)
1431
dd
2221
Hospitalcosts($),mean
dd
9,76
2†12
,082
15,506
11,000(P
5.02)
Boldvalues
indicate
statisticalsign
ificance.
ED5
emergencydepartment;MED
5admission
directlyto
medicineservice;n5
number;SU
R5
admission
directlyto
surgeryservice;SD
5standard
deviation;
IQR5
interquartilerang
e;HLOS5
hospital
leng
thof
stay;ERCP
5endoscop
icretrog
rade
cholangiop
ancreatography.
*Includedpatients
withcholedocho
lithiasis.
†Only40%
ofpatients
underwentsurgery.
N. Kulvatunyou et al. Surgery vs medicine for gallstone pancreatitis. 5

12. Britt RC, Weireter LJ, Britt LD. Initial implementation of an acutecare surgery model: implications for timeliness of care. J Am CollSurg 2009;209:421–4.
13. Qureshi A, Smith A, Wright F, et al. The impact of an acute careemergency surgical service on timely surgical decision-makingand emergency department overcrowding. J Am Coll Surg 2011;213:284–93.
14. Cubas RF, Nephtali RG, Rodriguez S, et al. Outcomes in the manage-ment of appendicitis and cholecystitis in the setting of a new acute caresurgery service model: impact on timing and cost. J Am Coll Surg2012;215:715–21.
15. Lau B, Difronzo AL. An acute care surgery model improves timelinessof care and reduces hospital stay for patients with acute cholecystitis.Am Surg 2011;77:1318–21.
16. Britt RC, Bouchard C, Weireter LJ, et al. Impact of acute care surgeryon biliary disease. J Am Coll Surg 2010;210:595–601.
17. Lehane CW, Jootun RN, Bennett M, et al. Does an acute care surgicalmodel improve the management and outcome of acute cholecystitis.ANZ J Surg 2010;80:438–42.
18. Michailidou M, Kulvatunyou N, Friese RS, et al. Time and cost anal-ysis of gallbladder surgery under acute care surgery model. J TraumaAcute Care Surg 2014;76:710–4.
19. Bradley EL. A clinically based classification system for acute pancre-atitis. Summary of the International Symposium on Acute Pancreatitis,Atlanta, GA, September 11 through 13, 1992. Arch Surg 1993;128:586–90.
20. Ranson JHC, Rifkind RM, Roses DF. Prognostic signs and the role ofoperative management in acute pancreatitis. Surg Gynecol Obstet1975;139:69–80.
21. Knaus WA, Draper EA, Wagner DP, et al. APACHE II: a severity ofdisease classification system. Crit Care Med 1985;13:818–29.
22. Hoyt DB. Editorial forward. Bull Am Coll Surg 2011;96:4–6.
Discussion
Dr. Sarah Majercik (Murray, UT): In this study, the au-thors have examined whether patients admitted through theemergency department with mild gallstone pancreatitis arebetter served by being admitted to an acute care surgical vsmedical service. The study concluded that although patientsadmitted to the ACS service had similar outcomes to theirmedical counterparts, both time to surgery and HLOS wereshorter and hospital costs were lower for the surgical admitgroup. I have a few questions.
First, one of your major findings was that patientsadmitted to the ACS service got to surgery quicker, whichclearly helped to decrease hospital length of stay and costs. Inthemanuscript, you state that theACSconsult for themedicalpatients was obtained ‘‘after’’ admission to the medicalservice. Do you know how long after? Is it standard practicein your hospital for the ER doctor to initiate an ACS consultimmediately after themedical service accepts a patient?Or isthe surgical consult obtained by the hospitalist or medicalresident or whoever at their discretion at some point after thepatient lands on the floor? We all know that the timedifference between these might be many hours or evendays depending on the culture and workings of the medicaland surgical services in your hospital.
If you do know when the surgical consult was initiated, itwould be interesting to know the time from surgical consultto the operating room in the 2 groups. This information, if
nothing else, could be used as internal quality improvementdata to take to the medical service and say, ‘‘Hey, the earlieryou consult us, the better for everyone involved,’’ as well asadd something to the manuscript.
Furthermore, I would appreciate hearing some commentsabout how your ACS service functions, although I think I doknow the answer to this question. From previous publicationsand what you alluded to in this presentation, I am pretty sureyou have a 24/7 in-house ACS surgeon who does whatevercases need to be done no matter the hour of the day. So thatbeing said, what does these data mean for those of us whowork in an institution without such a mature ACS service?
My second question has to do with the decision aboutwho got admitted to surgery and who got admitted tomedicine. My take on your data is that the more typicalgallbladder patients, women, age in the 40s, tend to getadmitted to the surgical service. For that reason, thebaseline characteristics of the medical and surgical groupsturned out to be quite different. I understand you tried tomitigate this with the ASA 1 and 2 group.
Is there some sort of defined protocol about who goeswhere? Is this just how ED physicians think? Do they try tosell the less typical patients to the ACS service, maybe getpushback from a junior resident and end up admitting tomedicine? Or maybe there is, as you did allude to, a goodclinical reason for a particular patient to go to medicine, thatis, they have pulmonary edema or they have acute kidneyinjury or some other thing going on. If that is the case, theremay be sound clinical reasons why the group admitted tomedicine took an extra day and a half to get to surgery.
My third question has to do with hospital costs and howthey are calculated. What constitutes cost in your system?Are you talking about charges, Medicare-reimbursed costs,or something else? Do you use activity-based cost account-ing? What about third-party costs and the professional feesfor the surgeons, anesthesiologists, and radiologists? Arethey accounted for here? Are they captured in the dollarfigures you report? Finally, in economics and statistics, wetalk about a concept called endogeneity. It is kind of achicken-and-egg thing and asks is the predictor reliant onthe outcome variable? Another way to ask the question is, isone of the variables in this model caused by anothervariable? If the answer is yes, then the predictor is called anendogenous predictor and it becomes significantly lessvalid. Would you consider admission to a surgical servicean endogenous predictor for the time to get to the operatingroom? I would be interested to hear your opinion on thispossibility.
Dr. Narong Kulvatunyou: Regarding the first question,it was difficult and inconsistent from the chart review to saywhen surgical consultation was obtained and how long ittook. I assume most consultations were requested by themedical services but we did not specifically look at thisin our chart review. How long did it take from surgicalconsultation to surgery? Again, it was difficult to obtainbecause of the lack of documentation when the residentsaw the patient and staffed with the attending.
6 The American Journal of Surgery, Vol -, No -, - 2014

The comment about the function of the ACS, if you donot have the ACS system, and I understand that was one ofthe things I put in our limitation, was that if you do not havethe same setup as ours, it may not be as fast and efficient.No, we do not have a specific protocol regarding howpatients were triaged to us, surgery, vs medicine. This issomething we would like to take back and discuss with ourED colleagues. It could be when patient first presented; thediagnosis of acute gallstone pancreatitis was not clear-cutso they got triaged to medicine service.
As far as the costs calculation is concerned, this wasbased on total hospital costs (direct and indirect costs) andnot hospital charges (what hospital billed the patients),which tended to be much higher than the hospital costs.These costs did not include professional (physician) fees.
On your last philosophical question about ‘‘endogene-ity,’’ or was surgical admission an endogenous predictor forsooner surgery, my honest answer would be ‘‘yes,’’ but whywould not it be. Because as a surgeon, knowing that patientwill definitely need surgery, why would not we all try to getthe patient to surgery as soon as possible.
Dr. Charles Scoggins (Louisville, KY): I think you havesome very compelling data. I am curious, have you takenthis data to your ED folks and your hospitals and internists,showed them the data, and say, look, how can we use theseto now effect a change in our hospital that might have moreof these patients shift over to the surgical service, and then
measure that over time to see if you have improved costsand improved patient flow?
Dr. Narong Kulvatunyou: That was exactly my idea af-ter we completed the study that we would like to take thisstudy and show it to our ED colleagues. We have a verygood relationship with them, and I am sure they would bevery happy to help us out on this.
Dr. Alicia Mangram (Phoenix, AZ): Just to take that alittle bit further, is it really taking it to the ED colleagues oris it really getting the surgeons to say yes? I really enjoyedyour article because it speaks to my bias. I think most sur-gical anything should just be admitted to the surgical team.We tend to have this tendency to be very upset with medi-cine when they call us too late and wait until the patient isreally sick or there is ischemic bowel. But at the same time,we refuse to admit the patients.
My question is, is it the ER doctors that you need toeducate or do you need to convince the surgeons that we aregoing to accept the patient that may have gallstonepancreatitis, knowing that it could just be pancreatitis andwe may be stuck with the patient?
Dr. Narong Kulvatunyou: I agree with Dr. Mangram. Ido not know if the reason patient got admitted to medi-cine was due to the resistance from my surgical col-leagues. I am hoping when my partners have seen thestudy results, some who have been resistant will changetheir practice.
N. Kulvatunyou et al. Surgery vs medicine for gallstone pancreatitis. 7