Endemic and epidemic dynamics of cholera - BMC Infectious ...
Upload
universityfordevelopmentstudiesCategory
view
3download
0
AARJMD VOLUME 1 ISSUE 29 (JANUARY 2015) ISSN : 2319 - 2801
Asian Academic Research Journal of Multidisciplinary
www.asianacademicresearch.org
465
A Peer Reviewed International Journal of Asian
Academic Research Associates
AARJMD
ASIAN ACADEMIC RESEARCH
JOURNAL OF MULTIDISCIPLINARY
MALONGZA’S PRINCIPLE OF DISSOCIATION TO STOP EBOLA HEMORRHAGIC
FEVER EPIDEMIC
FRANCIS ISSAHAKU MALONGZA BUKARI1; NYAABIIRE NSOBILLA
ATINDAANA2; GLORIA TWUMASI
3; ADWOA NYANTAKYIWAA
4
1Department of Environment and Resource Studies, Faculty of Integrated Development
Studies, University for Development Studies, P. O. Box 520,Wa, Upper West Region, Ghana. 2Ghana Health Service, Achimota Hospital,
P. O. Box AH 15, Greater Accra Region, Accra,Ghana. 3Department of Biomedical and Forensic Sciences, School of Biological Sciences, University of
Cape Coast, University Post Office, Cape Coast, Ghana. 4Institute for Educational Planning and Administration, University of Cape Coast, University
Post Office, Cape Coast, Ghana.
Abstract
Despite numerous efforts to control the Ebola Virus Disease in West Africa since the beginning of the
2014 epidemic, there is still no hope that the disease could be stopped within the shortest possible time.
Hence, the main objective of this study is to present a global plan of action to stop the Ebola epidemic.
The disease, which reached the status of an epidemic in March 2014, has caused several socio-economic
mishaps, including loss of lives, crippling local economies, discouraging international movement of
goods and persons, and increasing dependency. The major challenge is the lack of approved drugs and
vaccines to deal with the disease. Being the outcome of a basic research, and identifying its niche from
content analysis of available data, this study proposes an alternative way of stopping the strive and spread
of the disease by a principle known as the Malongza’s Principle of Dissociation. This hypothesizes that
the incidence of the Ebola Virus Disease could be discontinued if the elements in the mediums that
support its occurrence are identified and eliminated. It also paves the way for applied research into the
practical relevance of the proposed principle to the control of hemorrhagic fever related diseases.
Key Descriptors: Ebola Virus Disease, epidemic, Malongza’s Principle of Dissociation, West Africa, the
World.
AARJMD VOLUME 1 ISSUE 29 (JANUARY 2015) ISSN : 2319 - 2801
Asian Academic Research Journal of Multidisciplinary
www.asianacademicresearch.org
466
Introduction:
The Ebola virus disease (EVD), formerly known as the Ebola hemorrhagic fever is a severe and
very fatal disease which is transmitted to people from infected wild animals, such as fruit bats. It
then spreads in human populations through human-to-human transmission. The case-fatality rate
of the disease has varied between 25% and 90% in past outbreaks (WHO, 2014). It is fatal
because at its advanced stage, it is symptomatically associated with excessive dehydration
through vomiting, diarrhea, and internal and external bleeding. Others include rash and malaria-
like symptoms such as fever, headache, muscle pain and nausea. Once it attains the status of an
epidemic, the EVD becomes an issue of global concern because it causes high case-fatality rate,
crippling of local economies, risk of transmission across international boundaries,
discouragement of international movement of goods and persons and heavy expenditure on the
management of the disease, as some of the negative socio-economic problems (Dixon & Schafer,
2014; World Bank, 2014).
Historically, the EVD is said to have originated from villages around the rainforests of
Central Africa, and was first detected in Nzara of South Sudan and Yambuku of the Democratic
Republic of Congo by a microbiologist called Peter Piot, in 1976. Spickler (2014), however
reports that earlier in 1967 hemorrhagic fever outbreak occurred among laboratory workers in
the Marburg city of Germany, due to contact with infected vervets. The virus responsible for the
disease was accordingly called the ‘Marburgvirus’. This is a virus of the same family with the
Ebola virus (Filoviridae). The virus responsible for the EVD was also named Ebola, because
Yambuku is located near the Ebola River in the Democratic Republic of Congo.
The recent EVD epidemic is better described as being disease relocation diffusion. This is
because some countries of origin, such as South Sudan are no longer involved (Haggett, 2000).
The EVD diffused to West Africa for the first time at Guinea in December 2013. After a
contagious diffusion in this country, it was reported as attaining an epidemic of international
significance in March 2014, as it spread by expansion diffusion to neighboring Liberia and Sierra
Leone. The EVD claimed 4,033 lives out of a total of 8,399 cases with a case-fatality rate of
about 48% reported from these three hardest hit West African countries by October 8, 2014. By
16 November 2014, 14,409 cases and 5,174 deaths with a case-fatality rate of about 37% (To the
nearest percentage figure) had occurred in the world, as the EVD spread further to Nigeria,
Senegal, USA, Spain and Mali, according to the World Health Organisation and the Center for
Disease Control (CDC) (2014).
The authors of this article argue that, the present situation has arisen because the initial
attempts to control the disease either did not foresee the possibility of its present rates of
transmission and fatality, or efforts made to manage the outbreak within the affected countries
and across international borders by the associated governments and the international community
have not been effective enough. The approaches used so far, focused on the identification of
infected persons and contact tracing and quarantining of suspects, restricted movements,
treatment of patients with experimental drugs, management of infected dead bodies, the safety of

AARJMD VOLUME 1 ISSUE 29 (JANUARY 2015) ISSN : 2319 - 2801
Asian Academic Research Journal of Multidisciplinary
www.asianacademicresearch.org
467
health personnel, foreign support in terms of skilled personnel, experimental vaccines and
protective gear, and public sensitization.
Despite the adoption of all the possible means of controlling and preventing the incidence
of the EVD at various locations in response to the situations in situ, there has been no uniformity
in the processes. In other words, the ongoing approaches lack the deliberate adoption of a theory
that organizes all the ongoing control and preventive practices in a coherent manner, to protect
the unaffected populations of the Ebola endemic countries and the world at large from the risk of
infection. This explains the persistence and continuing spread of the disease. This has led to a
situation where heavy financial and material resources are being injected into the affected
countries to the extent that the United Nations (UN), reports that aid pledges to fight Ebola have
fallen short of $1billion (800 million Euros) (Parry & Bazinet, 2014).
In view of the above, this study presents the Malongza‟s Principle of Dissociation (MPD)
to explain how the Ebola virus disease could be stopped from spreading both within the affected
countries and across international boundaries. It seeks to present a more uniform and effective
way to stop the epidemic within a specified period of seven weeks. The characteristic of the
EVD to be transmitted in human populations, presents the idea that the incidence of the disease
is dependent on contacts between people. This inspires the authors of this study that such human
contacts are made possible by the prevalence of the mediums of human associations. These refer
to all the possible means by which an infected individual relates to others. These include
households, friendships, schools, workplaces, markets, play grounds, hospitals/clinics,
passengers in a transport, congregational worships, festivals, outdoor inter-group sports, among
other forms of social gatherings. The risk of transmission starts once an initial contact with
infected wild animals by an individual, belonging to any of these mediums has occurred. The
principle presented in this piece of work therefore poses the dictum that once an infected case is
recorded, further infections would continue in human populations as long as the contacts
between individuals and the mediums that facilitate the contacts remain unaltered.
From the above, it is apparent that any action to eliminate the direct effects of human
contacts and the level of human associations would discontinue further occurrences and spread
of the EVD. This is so for any hemorrhagic fever related disease that has a known incubation
period for symptoms to be identified and treated, or creates little chances of survival of victims
such that the possibilities of further transmissions as carriers are eliminated. This is the premise
of the Malongza‟s Principle of Dissociation, postulated by Bukari Francis Issahaku Malongza, a
lecturer at the Department of Environment and Resource Studies, University for Development
Studies, Ghana, and a doctoral student at the Institute for Development Studies, University of
Cape Coast, Ghana in October 2014.
The article employs a simple mathematical approach to explain how dissociation could be
used to control the disease. The study derives its arguments from the theory of disease diffusion,
and identifies the Ebola epidemic as the dependent factor and the influence of infected wildlife in
the environment, human contacts and the mediums of human associations as the independent

AARJMD VOLUME 1 ISSUE 29 (JANUARY 2015) ISSN : 2319 - 2801
Asian Academic Research Journal of Multidisciplinary
www.asianacademicresearch.org
468
factors. These influence the momentum of the disease incidence as the premise of the disease
diffusion theory. The study argues that any effort to control the independent factors could
positively impact on the control of the epidemic. It goes further to present suggested activity
schedules for remedy in the affected countries and all others at risk of infection, based on an
adopted ranking criterion. Its scope does not emphasise the practical aspects of medication and
vaccination. It is the result of a basic research, with the main objective to explain how to stop the
continuing spread of the disease and its negative effects within a minimum period of seven
weeks.
Theoretical basis of the study
The theory that gives direction to this study is the disease diffusion theory. Central to the
Malongza’s Principle of Dissociation are the tenets of contagion, expansion and relocation of the
diffusion theory.
Theory of disease diffusion
Leo Frobenius is the earliest scholar to conceptualize diffusion as a social phenomenon in his
1897/98 publication. It was however, related to the spread of elements of culture, such as belief
systems, technology, food and language (Frobenius, 1897/97). It has since been applied in other
social sciences to explain the spread of social phenomena, such as disease. Thus, health
geographers see disease diffusion as the occurrence and expansion of the incidence of a disease
within a location, and its spread to other locations from the original source. The expansionary,
relocation and contagious aspects of disease diffusion are central to the scientific method
adopted by this study.
Contagious diffusion occurs when the disease spreads through person-to-person contact
at a given destination.
Expansionary diffusion concerns the development and intensification of the incidence of
a disease at an original location and includes the possibility of spread to new locations.
Relocation diffusion is concerned with the trans-boundary or spatial spread of a disease,
as its original source becomes free of the disease (See Haggett, 2000).
Empirically, WHO (2014) and Dixon and Schafer (2014) explain the initial spread of the EVD
by contagious diffusion from the Districts of Gueckedou, Macenta, and Kissidougou in the
recent outbreak in Guinea. This was due to spatial interaction between the districts. The accounts
reveal that on March 21, 2014, there were only 49 reported cases with a case-fatality rate of 59%.
This reached 1,919 cases, with a case-fatality rate of about 41% by November 16, 2014.
Expansionary diffusion of the EVD began when on March 30, 2014, cases were reported in the
Foya District of neighboring Liberia. By May 2014, Sierra Leone also recorded its first case and
as of June 18, the total number of Ebola cases had increased to 528. It was however, disclosed
that the earlier victims of the disease in both Liberia and Sierra Leone had travelled to Guinea
(Ng & Cowling, 2014).
AARJMD VOLUME 1 ISSUE 29 (JANUARY 2015) ISSN : 2319 - 2801
Asian Academic Research Journal of Multidisciplinary
www.asianacademicresearch.org
469
In terms of the relocation diffusion of the EVD, since it started from the DR. Congo and
Sudan in 1976, Uganda is remembered for recording the highest number of 425 cases with a
case-fatality rate of 53% between 2000 and 2001 (Dixon & Schafer, 2014). Despite the breaking
of this Ugandan EVD record by June 2014, it is interesting to note that some of the countries
previously affected by the disease are no longer involved in the recent epidemic. This implies
disease relocation diffusion, as it moves from Central Africa to West Africa.
The contextual relevance of the theory of disease diffusion is that, from the contagious to
the relocation stages, certain conditions provide the mediums of spread. The continued spread of
the diseases within and across countries generates an enquiry into the efforts made so far, why
they failed and what could be done to stop the incidence and spread of the Ebola virus disease.
Ebola as a Hemorrhagic Fever Related Disease
According to WHO (2014), hemorrhagic fever related diseases refer to severe illnesses caused by
a number of viruses, and are sometimes characterised by bleeding. Some viral families
associated with such diseases include Arenaviridae (Lassa fever, Junin and Machupo),
Bunyaviridae (Crimean-Congo hemorrhagic fever, Rift Valley Fever, Hantaan hemorrhagic
fevers) and Flaviviridae (yellow fever, dengue, Omsk hemorrhagic fever, Kyasanur forest
disease). The Ebolaviruses and Marburgviruses belong to the Filoviridae family, which are
responsible for the Ebola virus disease (EVD) and Marburg virus disease (MVD) respectively
(Spickler, 2014). Specifically, WHO, reports that the dominant species of the 2014 EVD
outbreak is the Zaire ebolavirus.
Disease vectors
The viruses responsible for the EVD and other hemorrhagic diseases are believed to be carried in
fruit bats, which have antibodies to the viruses and so remain asymptomatic or unaffected by the
EVD or MVD. These Filoviridae have been found in ill or dead antelopes and chimpanzees
among other wild animals (Ng & Cowling, 2014; Spickler, 2014).
Mode of transmission
Ebola and other hemorrhagic fever related diseases are zoonotic. This means they are transmitted
to persons by contact with ill or dead infected animals identified above, either accidentally or
during wildlife care services. Hunting or contact with infected game meat could be a major
source of animal-to-human transmission from carrier asymptomatic animals such as fruit bats.
Human-to-human transmission then follows once an infected person begins to show symptoms,
through direct contact with the body fluids of that person, such as tears, blood, sweat, saliva,
urine, semen, vaginal fluids, excreta, vomit. Men who have recovered from the disease can also
still infect their sexual partners within 7 weeks after recovery by their semen (Spickler, 2014).
AARJMD VOLUME 1 ISSUE 29 (JANUARY 2015) ISSN : 2319 - 2801
Asian Academic Research Journal of Multidisciplinary
www.asianacademicresearch.org
470
Incubation period
The incubation period for the Filoviridae is between 3 to 16 days for nonhuman primates
(Spickler, 2014) and about 2 to 21 days for humans, and until signs of the disease appear, carriers
are not infectious within the incubation period (WHO, 2014).
Symptoms
According to the World Health Organization (2014), the symptoms or signs of EVD include
sudden onset of fever, intense weakness, muscle pain, headache and sore throat. This is followed
by vomiting, diarrhea, rash, impaired kidney and liver function, and in some cases, both internal
and external bleeding, which could result into death within a few days.
Persons most at risk of infection
The EVD affects all persons irrespective of sex, age or race. However, persons at higher risk of
infection include health workers, family members or others in close contact with infected people,
and mourners who have close contact with bodies of the diseased as part of burial ceremonies,
hunters and farmers working in forest areas believed to be hosting the disease vectors.
Treatment
There is no cure or vaccine for the EVD at the moment except experimental drugs such as
ZMapp, which is being developed by Leaf Biopharmaceutical Inc, of San Diego in USA.
However, according to WHO (2014) and the Center for Disease Control and Prevention (CDC)
(2014), in view of the fact that affected patients are frequently dehydrated, they need intensive
and supportive care, intravenous fluids or oral rehydration with solutions that contain
electrolytes.
From the literature above, it is obvious that Ebola is a hemorrhagic fever disease which is
Transmitted from wild animals within the environment of a human population;
Infection is by contact with infected animals and humans; and
In human-to-human transmission, the risk of infection increases with the level of
association or relationships with infected people.
These are the independent variables that this study seeks to examine in a mathematical
relationship, identify the gaps in the existing practices in efforts to control the disease in the
context of the variables, and design schedules of activities as policy recommendations to address
the challenge
Ebola Virus Disease as an Epidemic
According to Tsai and Koerner (2009) an epidemic occurs when a country considers the
incidence of a disease as causing a state of public emergency in terms of the number of people
being infected and dying from the disease. The writers state further that the Center for Disease
Control classifies a disease as being epidemic, when the number of deaths exceeds 7.7% of the
total number of reported cases.
Tsai and Koerner (2009), however opined that the CDC’s definition of an epidemic, as
―The occurrence of more cases of disease than expected in a given area or among a specific
group of people over a particular period of time" (CDC, cited in Tsai & Koerner, 2009, in State
AARJMD VOLUME 1 ISSUE 29 (JANUARY 2015) ISSN : 2319 - 2801
Asian Academic Research Journal of Multidisciplinary
www.asianacademicresearch.org
471
27/04/2009 ed.) does not stand the test of time since the prevalence rates of various diseases are
not the same. Furthermore, the 7.7% fatality rate is not static for all periods within a year. They
accordingly urge the CDC to come out with statistical figures on what it describes as being ‘more
than expected’ with reference to the various diseases.
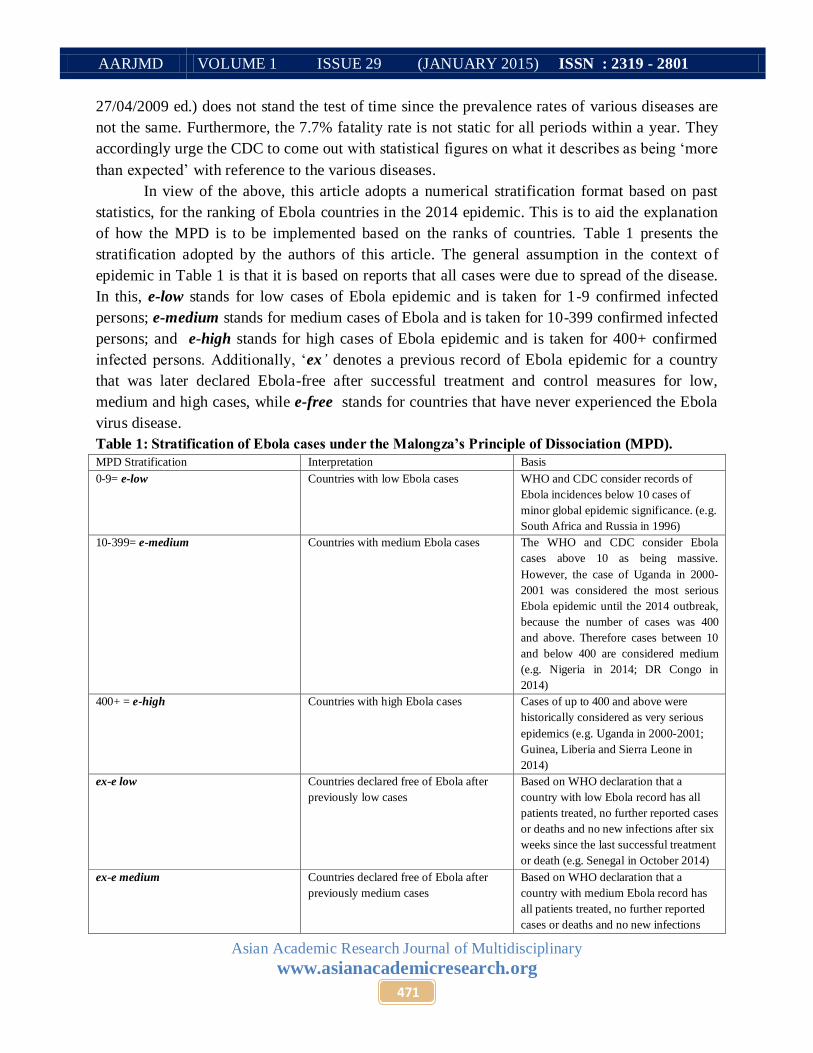
In view of the above, this article adopts a numerical stratification format based on past
statistics, for the ranking of Ebola countries in the 2014 epidemic. This is to aid the explanation
of how the MPD is to be implemented based on the ranks of countries. Table 1 presents the
stratification adopted by the authors of this article. The general assumption in the context of
epidemic in Table 1 is that it is based on reports that all cases were due to spread of the disease.
In this, e-low stands for low cases of Ebola epidemic and is taken for 1-9 confirmed infected
persons; e-medium stands for medium cases of Ebola and is taken for 10-399 confirmed infected
persons; and e-high stands for high cases of Ebola epidemic and is taken for 400+ confirmed
infected persons. Additionally, ‘ex‟ denotes a previous record of Ebola epidemic for a country
that was later declared Ebola-free after successful treatment and control measures for low,
medium and high cases, while e-free stands for countries that have never experienced the Ebola
virus disease.
Table 1: Stratification of Ebola cases under the Malongza’s Principle of Dissociation (MPD).
MPD Stratification Interpretation Basis
0-9= e-low Countries with low Ebola cases WHO and CDC consider records of
Ebola incidences below 10 cases of
minor global epidemic significance. (e.g.
South Africa and Russia in 1996)
10-399= e-medium Countries with medium Ebola cases The WHO and CDC consider Ebola
cases above 10 as being massive.
However, the case of Uganda in 2000-
2001 was considered the most serious
Ebola epidemic until the 2014 outbreak,
because the number of cases was 400
and above. Therefore cases between 10
and below 400 are considered medium
(e.g. Nigeria in 2014; DR Congo in
2014)
400+ = e-high Countries with high Ebola cases Cases of up to 400 and above were
historically considered as very serious
epidemics (e.g. Uganda in 2000-2001;
Guinea, Liberia and Sierra Leone in
2014)
ex-e low Countries declared free of Ebola after
previously low cases
Based on WHO declaration that a
country with low Ebola record has all
patients treated, no further reported cases
or deaths and no new infections after six
weeks since the last successful treatment
or death (e.g. Senegal in October 2014)
ex-e medium Countries declared free of Ebola after
previously medium cases
Based on WHO declaration that a
country with medium Ebola record has
all patients treated, no further reported
cases or deaths and no new infections

AARJMD VOLUME 1 ISSUE 29 (JANUARY 2015) ISSN : 2319 - 2801
Asian Academic Research Journal of Multidisciplinary
www.asianacademicresearch.org
472
after six weeks since the last successful
treatment or death (e.g. Nigeria in
October 2014)
ex-e high Countries declared free of Ebola after
previously high cases
Based on WHO declaration that a
country with high Ebola record has all
patients treated, no further reported cases
or deaths and no new infections after six
weeks since the last successful treatment
or death (e.g. Uganda in 2001).
e-free Countries with no record Ebola All countries with no history of Ebola
virus disease.
Source: Authors’ modification of data from the National Center for Infectious Diseases & Centers for Disease
Control and Prevention (2014)
Distribution of the Recent Ebola Virus Disease Outbreak (2014)
Table 2, presents a summary of the distribution of reported cases, deaths and calculated case-
fatality rates for the EVD, based on a summation of published data (From March 21, 2014) up to
November 16, 2014, by the Centers for Disease Control and Prevention and the World Health
Organisation.
Table 2: Distribution of the recent Ebola virus disease outbreak as of November 16, 2014
Country Number of
reported cases
Number of deaths Case-fatality rate MPD ranking
Guinea 1,919 1,166 70% e-high
Liberia 6,878 2812 41% e-high
Sierra Leone 5,586 1,187 21.25% e-high
Nigeria 20 8 40% ex-e medium
Senegal 1 0 0% ex-e low
United States 4 1 25% e-low
Spain 1 0 0% e-low
Mali 4 3 75% e-low
Sources: CDC (2014); WHO (2014)
The data in Table 2 shows that apart from the diffusion of the disease from the Guinea, Liberia
and Sierra Leone as the initial sources of the 2014 Ebola epidemic, all other affected countries
except Spain, has met the CDC’s condition for the declaration of an epidemic. In other words,
they have case-fatality rates of more than 7.7%. Even though countries such as Senegal and
Nigeria managed to control the spread of the EVD after recording ex-e low and ex-e medium
cases on the MPD ranking, the prevailing incidences in the e-high countries is a warning that no
country is free forever until the EVD is all over (BBC, 2014).
As of November 16, 2014, there were a total world record of 14, 409 cases and 5,174
deaths (CDC, 2014; WHO, 2014). The associated world case-fatality rate was about 36%, which
also signifies that a global epidemic exists, since it exceeds the 7.7% limit. These rankings are
considered in the dissociation schedules of the MPD in the results and discussions section of this
article.

AARJMD VOLUME 1 ISSUE 29 (JANUARY 2015) ISSN : 2319 - 2801
Asian Academic Research Journal of Multidisciplinary
www.asianacademicresearch.org
473
The Socio-economic Effects of the Ebola Virus Disease Epidemic
Since the recent out-break of the Ebola virus disease in December 2013 in Guinea, and its
subsequent spread to other West African countries and beyond, some negative and positive
socio-economic effects have been realised. One of the negative effects includes increasing loss of
lives. About 4,033 persons died by October 8, 2014 and by November 16, 2014, the figure
increased to 5,174 on world record. Guinea, Liberia and Sierra Leone were the most affected
countries. The increasing level of mortality further has the effects of increasing the number of
orphaned children, widows and the aged as bread winners of households die. This increases the
vulnerability of the orphans to poor human development, while dependent widows and the aged
are also exposed to poverty, stigmatization and marginalisation, including the children as well
(World Bank, 2014).
The increasing risk of transmission of the EVD across international border has compelled
other countries to institute preventive measures such as bans on flights to, and from the Ebola
affected countries. This discourages international movement of goods and persons, while some
citizens of the affected countries who travelled to other countries temporally become exiled, as
they remain stranded in foreign lands. Furthermore, apart from the effects of restricted cross-
border movements, as the energetic labour force of the affected countries fall sick of the EVD
and internal movements are restricted due to scare and preventive measures, agricultural and
local business activities are also negatively impacted, which cripple the local economies. Such
economies become exposed to problems of food insecurity, reduced sources of income to
governments, businesses and households.
The situation becomes exacerbated as the already constrained governments have to spend
their limited financial resources on the management of the disease. This affects other aspects of
state responsibilities, such as the provision of basic infrastructure and the payment of salaries of
public sector workers, including health staff with additional overtime and risk allowances. In
Liberia for instance, President Ellen Johnson Sirleaf’s administration threatened to lay off
government employees who failed to report to work on the excuse of attending to sick family
members due to Ebola (The Analyst, October 2014). In Nigeria, President Goodluck Jonathan
sacked 16,000 resident doctors in August 2014, for striking during the outbreak of EVD in that
country (Kover, 2014).
One major positive effect of the EVD outbreak is that it has influenced some level of
international cooperation between countries that were initially in conflict. For instance, despite
the antagonism between USA and Russia over the latter’s interference in the political affairs of
Ukraine, the two countries collaborated in the production of an experimental vaccine called
Triazoverin. The scientists of the two countries produced the drug in Russia, and tested in USA.
This collaborative process is seen as an element of peace building (Specia, 2014). Furthermore, it
could be said that the widespread nature of the 2014 Ebola outbreak contributed to more serious
international alertness and innovation, which made it possible for the discovery of the EVD
vaccine, since the disease started in 1976. Another aspect of international solidarity, include
AARJMD VOLUME 1 ISSUE 29 (JANUARY 2015) ISSN : 2319 - 2801
Asian Academic Research Journal of Multidisciplinary
www.asianacademicresearch.org
474
financial assistance. For instance European countries have contributed about 500m euros for the
control of the EVD in Africa in October 2014 (BBC, 2014).
It has also led to the training and acquisition of skills for Ebola treatment and control by
health and military personnel of countries that are experiencing the EVD for the first time, as
well as those that have never even experienced it, as they prepare against a future outbreak.
Additionally, the management of the EVD provides additional income in the form of allowances
to health personal, as well as increased employment and market opportunities to industries
engaged in the production of the drugs, vaccines and protective gear for the epidemic. For
example Weiqun (2014), reports that the Weifang Lakeland Safety Products factory in China,
with only 100 employees was producing up to 6,000 protective plastic suits in October 2014, and
planned to increase its capacity in terms of employees and output in January 2015.
The high levels of morbidity and mortality associated with the EVD 2014 epidemic, as
well as the increasing levels of vulnerability of the masses to socio-economic mishaps, makes the
negative effects to out-weigh the positive effects of the disease. This therefore calls for the need
to explore more stringent methods of stopping the incidence of the disease in order to save
human lives.
Methodology
Typically the study has a basic research orientation, since it seeks to provide the knowledge base
and understanding in the explanation of how the Ebola virus disease epidemic could be
controlled in a systematic manner, through the postulation of the Malongza’s Principle of
Dissociation. The applicability of the principle also means that the study lays a foundation for
applied research if its principle becomes of practical relevance (See Kumar, 1999). In other
words, it is directed towards the use of knowledge gained by basic research to explain the
necessary conditions and situations that serve as a practical or utilitarian purpose for the control
of the Ebola epidemic in the affected countries in West Africa and the world at large (See Parker,
1984).
Philosophically its presents a positivistic argument expressed by mathematical models,
and then employs basic information from available research findings to identify the knowledge
gaps and establish the alternatives approaches for addressing the problem of controlling the
Ebola virus disease epidemic. This is by analysing the acquired information based on the
relationships between the variables of the mathematical basis of the principle. It is therefore a
combination of both objective and subjective realities for establishing the truth about the
management of the disease. This is achieved by a content study of existing information on
current practices on the subject to support and shape the focus of the idea behind what is
described as the Malongza’s Principle of Dissociation (MPD) to stop the Ebola virus disease.
Results and Discussions
From the contexts of the background information, the theories and empirical data on the Ebola
virus disease epidemic presented earlier, we now focus attention on the proposed principle and
the schedule of activities to stop the EVD.

AARJMD VOLUME 1 ISSUE 29 (JANUARY 2015) ISSN : 2319 - 2801
Asian Academic Research Journal of Multidisciplinary
www.asianacademicresearch.org
475
The Malongza’s Principle of Dissociation
The Malongza’s Principle of Dissociation (MPD) states that a phenomenon strives and spreads
as long as the conditions that support its medium remain unaltered. Therefore, the elimination of
the conditions that constitute its medium discontinues the phenomenon.
From our definition of the MPD above, we assume that
1. The dependent phenomenon (E) = Incidence of Ebola virus disease
2. Independent conditions (C) = {C1=Environmental factors (infected animals); &
C2=human contacts (hand shaking, hugging, etc.)} and
3. Independent mediums (M)= Presence of structural arrangements that promote human
contacts through association e.g. markets, schools, homes/ households, workplaces,
hospitals, commercial passenger transport, places of worship and all forms of social
or public gatherings.
Deriving from points 1-3 above, E = C+M
But C= C1 + C2
∴ E= C1 + C2 + M
In other words Ebola virus disease (E) is dependent on the presence of infected
animals in the environment (C1); human contacts (C2); and the mediums that
promote human contacts (M).
Let’s assume C1 cannot be changed within the shortest possible time with the best
available technology and medical practices.
⇒ E= C2 + M……………………………………………. (1)
The law of the MPD is that any action to eliminate C2 or M would reduce the
incidence of Ebola virus disease by the magnitude of the independent factor that is
removed. E.g. let’s remove human contact (C2),
Then we obtain E - C2 = C2 – C2 + M
⇒ E - C2= M………………..………………………… (2)
What this means is that the level of prevalence of Ebola virus disease is now determined by the
level of mediums (M) of human associations but with minimal level of contacts. In other words,
households, schools, workplaces, churches and mosques will continue to operate but with
controlled levels of human contacts, such as all people wearing protective clothing and gloves.
If we take away M also, then have
E - C2 - M= M – M
Such that the incidence of the Ebola virus disease is now reduced to
E - C2 - M= 0……………………………………… (3)
This does not mean Ebola ends completely, but the incidence of Ebola would be weakened by
dissociation. That is by reducing both human contacts and the mediums that promote human
associations. This does not also mean that society ceases to exist before Ebola is controlled. In
other words, the dissociation process is completed by equation 3, such that the strive and spread

AARJMD VOLUME 1 ISSUE 29 (JANUARY 2015) ISSN : 2319 - 2801
Asian Academic Research Journal of Multidisciplinary
www.asianacademicresearch.org
476
of the EVD through all possible means of human contacts and association are discontinued.
Whether the Ebola epidemic would continue or not, in a given society where the MPD is
implemented depends on how effective and efficient the stages of dissociation are carried out.
Duration and Dissociation Procedures According to MPD Ranking of Countries
This section discusses the duration and schedule of activities marking the procedures for the
implementation of the proposed MPD.
Duration of the implementation of the MPD
In the individual country cases, the World Health Organization and the Centers for Disease
Control and Prevention, adopt a standard period of 46 days or six weeks, for determination of
whether a country should be declared Ebola free. This depends on whether or not new cases are
reported since the last case of Ebola confirmed. The principle behind the duration is by doubling
the incubation period of 21 days for the Ebola virus. Being proposed for a global exercise, the
MPD suggests an additional one week to be distributed over the preparatory, effective
coordination, collation and communication activities. Seven weeks are therefore proposed for the
execution of the MPD schedules.
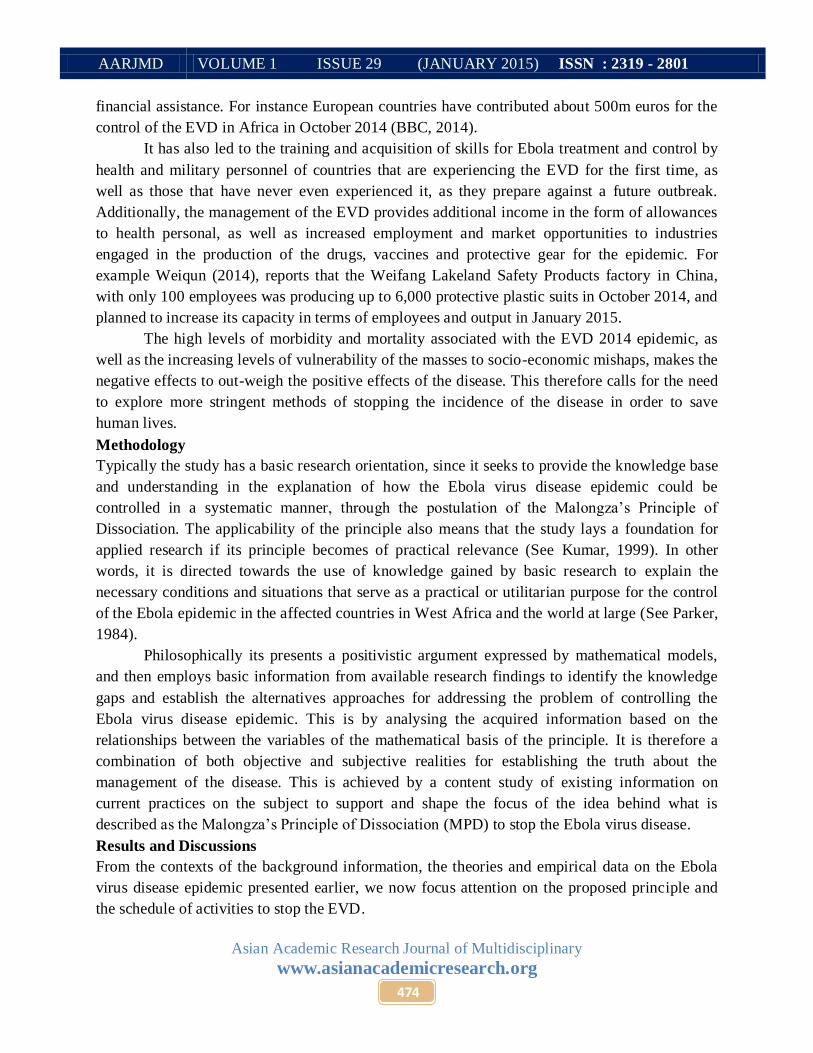
Scheduling for Dissociation Procedure by MPD Ranks of Countries
We now present activity schedules for the execution of what the MPD describes as
‘dissociation’. This involves the policy implications of ‘eliminating’ C2 (human contacts) and M
(Mediums of human associations) in the MPD equations 2 and 3 based on the ranking methods
described in Tables 1 and 2. Once approved for implementation, a commencement date is
declared by the World Health Organisation for all participating countries. This implies that the
legal consent of countries, especially e-free countries should be sought by the signing of an
agreement to stop the Ebola virus disease epidemic universally.
Table 3: Schedule of activities for dissociation by the elimination of C2 (Human contacts)
e-high countries
Activity Target persons Responsibility Monitoring &
Evaluation
Remarks
International
agreement and
declaration of
intention to
implement the MPD
and the purpose
Governments and
peoples of all e-
high countries
WHO, health
departments and
social media of e-
high countries
WHO and health
ministries of e-high
Countries
Screening of all
citizens for Ebola
symptoms
Members of all
households in e-high
countries
Health departments
of e-high countries,
trained military
personal, Red Cross
Society and
volunteers
Health ministries of
e-high countries and
WHO
representatives
Immediate
quarantine of
Members of all
households in e-high
Health departments
of e-high countries
Health ministries of
e-high countries and

AARJMD VOLUME 1 ISSUE 29 (JANUARY 2015) ISSN : 2319 - 2801
Asian Academic Research Journal of Multidisciplinary
www.asianacademicresearch.org
477
confirmed and
suspected persons
for treatment in
previously designed
isolated wards. All
persons sick of any
other disease other
than Ebola, shall
also be under
compulsory custody
of the health
department within
the MPD period.
countries WHO
representatives
Scheduled
temporary and
regulated stay off
from residential
homes while mass
disinfection takes
place in the homes
Members of all
households in e-high
countries
Trained military
personal, , Red
Cross Society and
volunteers
Health ministries of
e-high countries and
WHO
representatives
Provision of plastic
protective clothing,
gloves and foot
wears and enforcing
their use
Members of all
households in e-high
countries
WHO, through
globally mobilized
funds from Ebola
special levy on all
able adults in the
MPD participating
countries.
Health ministries
and social welfare
departments of e-
high countries,
military personnel,
volunteers and
WHO
representatives
Education of citizens
on how Ebola virus
spreads from person-
to-person contacts,
how they should use
the protective plastic
clothing, symptoms
of the disease, self
examination for
symptoms and
where to report in
the event of illness.
Members of all
households in e-high
countries
Departments of
education, health,
social welfare,
information and
social media of the
e-high countries
WHO, Ministries of
health, education
and communication
of all e-high
countries.
Self quarantine of all
households in their
disinfected homes
without individual
household member
interactions, except
persons under five
Members of all
households in e-high
countries
Health ministries
and social welfare
departments of e-
high countries,
military personnel,
Red Cross Society
and volunteers.
WHO, health
ministries, social
welfare departments
of e-high countries,
traditional
authorities

AARJMD VOLUME 1 ISSUE 29 (JANUARY 2015) ISSN : 2319 - 2801
Asian Academic Research Journal of Multidisciplinary
www.asianacademicresearch.org
478
with mothers. This is
after provisions for
food and water have
been considered.
Domestic animals
and pets should also
be quarantined
separately, and
examined for
infection, treatment
or euthanasia. The
duration should be
21 days (3 weeks)
e-medium
countries
International
agreement and
declaration of
intention to
implement the MPD
and the purpose
Governments and
peoples of all e-
medium
countries
WHO, health
departments and
social media of e-
medium
countries
WHO and health
ministries of e-
medium
Screening of al1
residents of towns
and villages that
have records of
EVD.
All households in
towns and villages
of e-medium
countries.
Health departments
of e-medium
countries, trained
military personal, ,
Red Cross Society
and volunteers
Health ministries of
e-medium countries
and WHO
representatives
Immediate
quarantine of
confirmed and
suspected persons
for treatment in
previously designed
isolated wards. This
is followed by
contact tracing for
all persons that had
contact with the
infected persons
outside the enlisted
towns and villages in
the country. The
locations of
identified persons
are included in the
screening process.
All households in
towns and villages
of e-medium
countries
Health departments
of e-medium
Health ministries of
e-medium countries
Scheduled Members of all Trained military Health ministries of

AARJMD VOLUME 1 ISSUE 29 (JANUARY 2015) ISSN : 2319 - 2801
Asian Academic Research Journal of Multidisciplinary
www.asianacademicresearch.org
479
temporary and
regulated stay off
from residential
homes of the
enlisted locations
while mass
disinfection takes
place in the homes
households of
enlisted locations in
e-medium countries
personal, , Red
Cross Society and
volunteers
e-medium countries
and WHO
representatives
Provision of plastic
protective clothing,
gloves and foot
wears and enforcing
their use
Members of all
households of
enlisted locations in
e-medium countries
WHO, through
globally mobilized
funds from Ebola
special levy on all
able adults in the
MPD participating
countries.
Health ministries
and social welfare
departments of e-
medium countries,
military personnel,
volunteers and
WHO
representatives
Education of all
citizens on Ebola
transmission, how
the protective gear
should be used by
those in enlisted
areas, and self
examination for
symptoms and
where to report in
the event of illness.
Members of
households in the
enlisted areas of e-
medium countries
Departments of
education, health,
social welfare,
information and
social media of the
e-medium countries
WHO, Ministries of
health, education
and communication
of e-medium
countries.
Self quarantine of
households of the
enlisted areas in
their disinfected
homes without
individual household
member interactions,
except persons under
five with mothers.
There should be
considerations for
food and water.
Domestic animal
management should
also be considered,
to prevent re-
infection of persons
after the MPD
period by the
animals.
Members of
households in the
enlisted areas of the
e-medium countries
Health ministries
and social welfare
departments of e-
medium countries,
military personnel ,
Red Cross Society
and volunteers.
WHO, health
ministries, social
welfare departments
of e-medium
countries and
traditional
authorities

AARJMD VOLUME 1 ISSUE 29 (JANUARY 2015) ISSN : 2319 - 2801
Asian Academic Research Journal of Multidisciplinary
www.asianacademicresearch.org
480
The duration should
be 21 days (3
weeks)
For towns and
villages without
Ebola cases in the e-
medium, countries,
there should
adequate public
education about
Ebola, conscious
change of culture
within the MPD
period. E.g. all
persons should
acquire and use
impermeable long-
sleeve clothing and
the use of plastic
hand gloves at
subsidised cost.
Men and boys
should were trousers
and women and girls
should wear long
skirts. The use of
open foot wears and
direct contacts with
other persons
outside their homes
should be avoided.
Members of
households in the
Ebola free areas of
the e-medium
countries
Military personnel ,
Red Cross Society
and volunteer groups
Ministries of health
and defense and
traditional
authorities.
e-low countries
International
agreement and
declaration of
intention to
implement the MPD
and the purpose
Governments and
peoples of e-low
countries
WHO, health
departments and
social media of e-
low countries
WHO and health
ministries of e-low
countries
Screening of al1
residents of the
particular residential
areas in the towns
and villages that
have records of
EVD. This should
include the locations
of persons identified
All households in
residential areas of
towns and villages
with Ebola cases in
the e-low countries.
Health departments
of e-low countries,
trained military
personal, , Red
Cross Society and
volunteers
Health ministries of
e-low countries and
WHO
representatives

AARJMD VOLUME 1 ISSUE 29 (JANUARY 2015) ISSN : 2319 - 2801
Asian Academic Research Journal of Multidisciplinary
www.asianacademicresearch.org
481
by outcomes of
contact tracing.
Immediate
quarantine of
confirmed and
suspected persons
for treatment in
previously designed
isolated wards.
All households in
residential areas of
towns and villages
with Ebola cases in
the e-low countries
Health departments
of e-low
Health ministries of
e-low countries
Scheduled
temporary and
regulated stay off
from residential
homes of the
enlisted locations
while mass
disinfection takes
place in the homes
All households in
residential areas of
towns and villages
with Ebola cases in
the e-low countries
Trained military
personal, Red Cross
Society and
volunteers
Health ministries of
e-low countries
Provision of plastic
protective clothing,
gloves and foot
wears and enforcing
their use
All households in
residential areas of
towns and villages
with Ebola cases in
the e-low countries
WHO, through
globally mobilized
funds from Ebola
special levy on all
able adults in the
MPD participating
countries.
Health ministries
and social welfare
departments of e-low
countries, military
personnel and
volunteers
Education of all
citizens on Ebola
transmission, how
the protective gear
should be used by
those in enlisted
areas, and self
examination for
symptoms and
where to report in
the event of illness.
All households in
residential areas of
towns and villages
with Ebola cases in
the e-low countries
Departments of
education, health,
social welfare,
information and
social media of the
e-low countries
WHO, Ministries of
health, education
and communication
of e-low countries.
Self quarantine of
households of the
enlisted areas in
their disinfected
homes without
individual household
member interactions,
except persons under
five with mothers.
There should be
considerations for
All households in
residential areas of
towns and villages
with Ebola cases in
the e-low countries
Health ministries
and social welfare
departments of e-low
countries, military
personnel and
volunteers.
WHO, health
ministries, social
welfare departments
and traditional
authorities of e-low
countries.
AARJMD VOLUME 1 ISSUE 29 (JANUARY 2015) ISSN : 2319 - 2801
Asian Academic Research Journal of Multidisciplinary
www.asianacademicresearch.org
482
food and water.
Domestic animal
management should
also be considered,
to prevent re-
infection of persons
after the MPD
period by the
animals.
The duration should
be 21 days (3
weeks)
For towns and
villages without
Ebola cases in the e-
low, countries, there
should be adequate
public education
about Ebola,
conscious change of
culture within the
MPD period, as in
the case of e-
medium countries
above.
All households in
residential areas of
towns and villages
with Ebola cases in
the e-low countries
Military personnel
and volunteer groups
Ministries of health
and defense and
traditional
authorities.
e-free, ex-e high,
ex-e medium,
and ex-e low
countries
International
agreement and
declaration of
intention to
implement the MPD
and the purpose
Governments and
peoples of countries
with previous or no
record of Ebola virus
disease
WHO, health
departments and
social media of
countries with
previous or no
record of Ebola virus
disease
WHO and health
ministries of Ebola
free countries
Intensification of
education on the
causes, symptoms,
treatment, effects,
and prevention of
Ebola virus disease.
Citizens of all
countries with
previous or no Ebola
cases
WHO, health and
education
departments and
social media of
countries with
previous or no Ebola
cases
WHO and health
ministries of Ebola
free countries
Conscious change of
culture within the
MPD period. E.g. all
Citizens of all
countries with
previous or no Ebola
WHO, health and
education
departments and
WHO and health
ministries of Ebola
free countries
AARJMD VOLUME 1 ISSUE 29 (JANUARY 2015) ISSN : 2319 - 2801
Asian Academic Research Journal of Multidisciplinary
www.asianacademicresearch.org
483
persons should
acquire and use
impermeable long-
sleeve clothing and
the use of plastic
hand gloves at
subsidised cost.
Men and boys
should were trousers
and women and girls
should wear long
skirts. The use of
open foot wears and
direct contacts with
other persons
outside their homes
should be avoided.
cases social media of
countries with
previous or no Ebola
cases
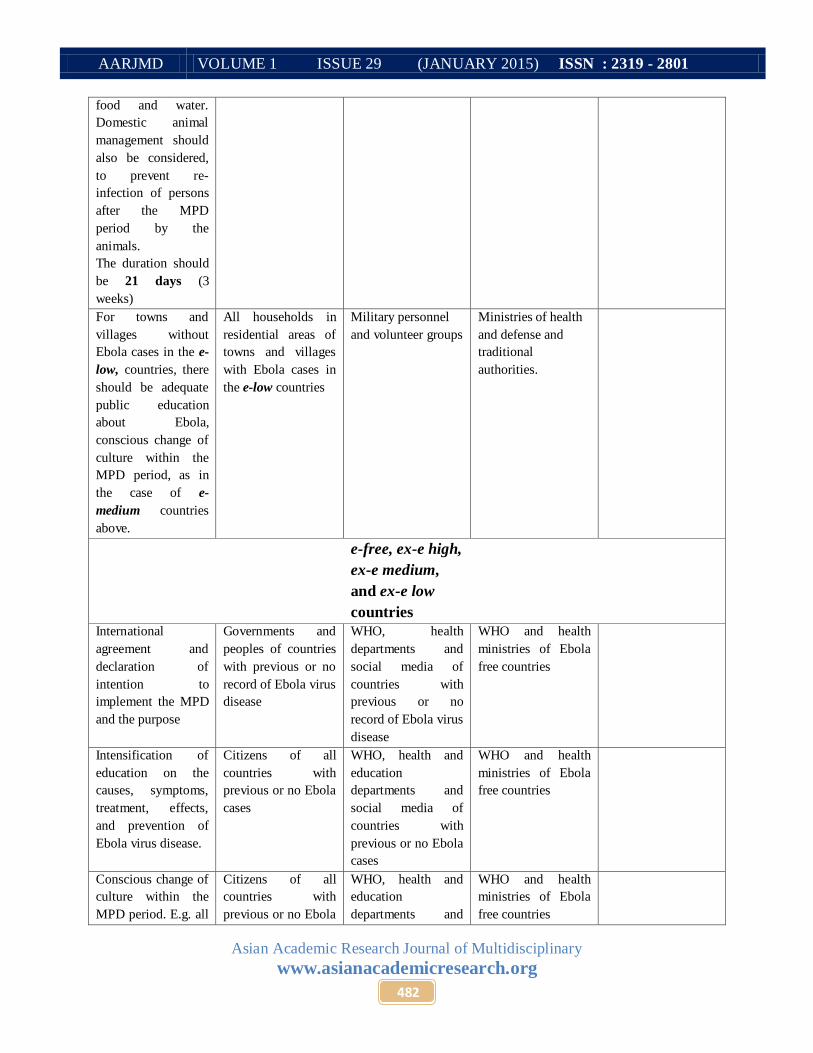
Interpretations of the MPD ranks of countries: e-low =1-9 Ebola cases; e-medium =10-399 Ebola cases; e-high= 400+ Ebola cases; ex- (high,
medium & low) = previously e-high, e-medium and e-low; e-free= Never had Ebola.
Source: Authors’ own construct
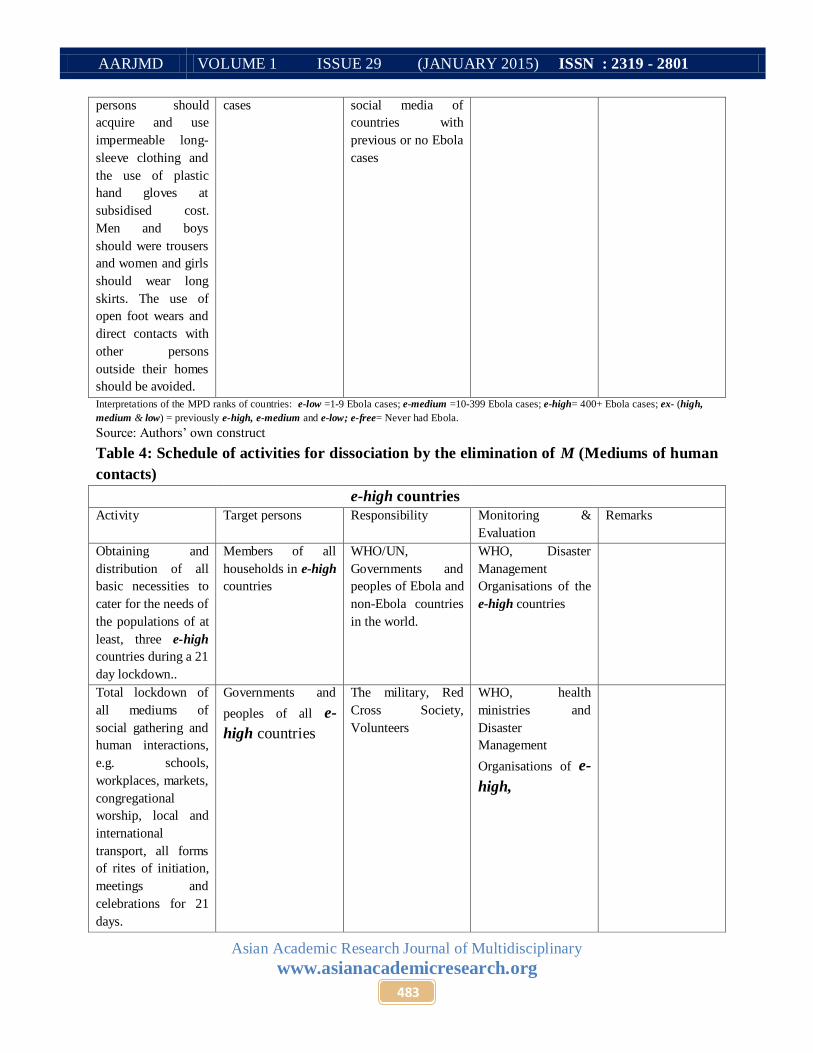
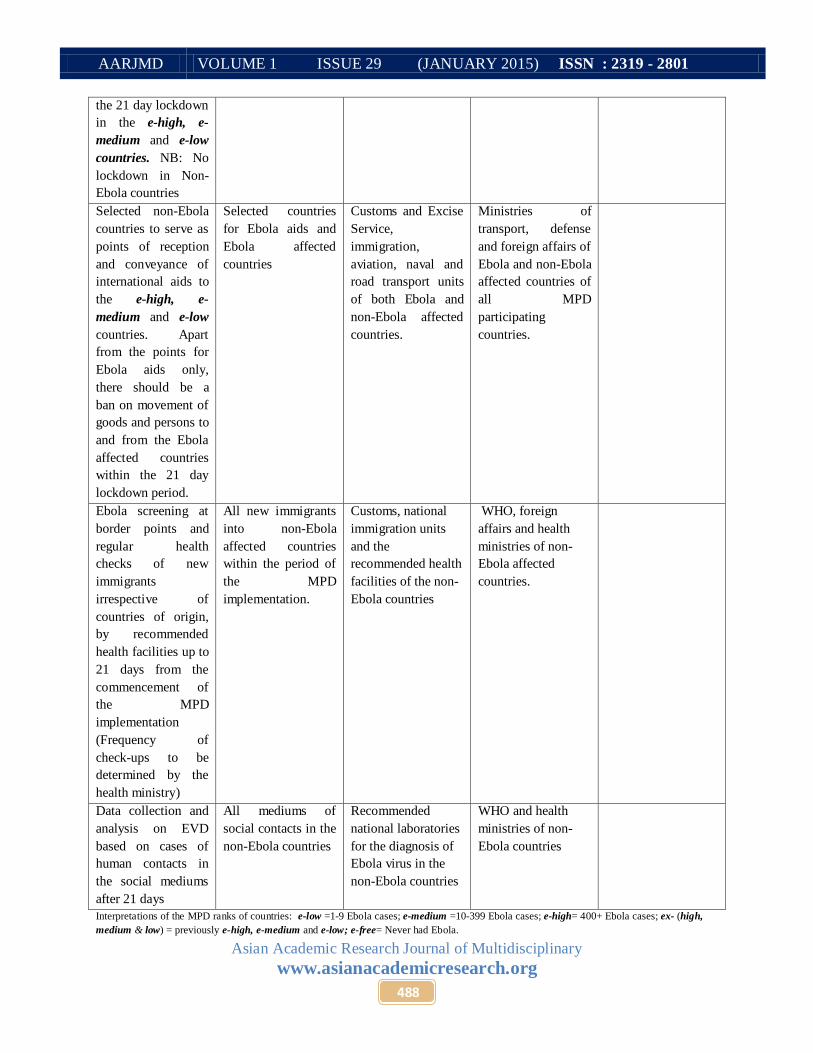
Table 4: Schedule of activities for dissociation by the elimination of M (Mediums of human
contacts)
e-high countries
Activity Target persons Responsibility Monitoring &
Evaluation
Remarks
Obtaining and
distribution of all
basic necessities to
cater for the needs of
the populations of at
least, three e-high
countries during a 21
day lockdown..
Members of all
households in e-high
countries
WHO/UN,
Governments and
peoples of Ebola and
non-Ebola countries
in the world.
WHO, Disaster
Management
Organisations of the
e-high countries
Total lockdown of
all mediums of
social gathering and
human interactions,
e.g. schools,
workplaces, markets,
congregational
worship, local and
international
transport, all forms
of rites of initiation,
meetings and
celebrations for 21
days.
Governments and
peoples of all e-
high countries
The military, Red
Cross Society,
Volunteers
WHO, health
ministries and
Disaster
Management
Organisations of e-
high,

AARJMD VOLUME 1 ISSUE 29 (JANUARY 2015) ISSN : 2319 - 2801
Asian Academic Research Journal of Multidisciplinary
www.asianacademicresearch.org
484
Ebola Preventive
training and
certification
exercises for
management and
employees of all
public and private
social service
institutions, e.g.
hospitals, beauty
salons, barber shops,
driver associations,
financial institutions,
, hotels and
restaurants, markets,
local food vendors,
hawkers, etc. (This
could be before or
immediately after
the 21 day
lockdown)
Management and
employees of social
service providing
institutions in e-high
countries
Health departments,
Red Cross Society
and Disaster
Management
Organisations of e-
high countries.
WHO, Health
ministries and
Disaster
Management
Organisations of
e-high countries
During the
lockdown, there
should be
disinfection of the
mediums of social
contacts. These
include the
structures involved
in the preventive and
certification
exercises specified
above.
All mediums of
social contacts in e-
high countries
Health departments,
Disaster
Management
Organisations,
trained military
personnel, Red
Cross Society and
volunteers of e-high
countries
WHO and Health
ministries of
e-high countries
Data collection and
analysis on EVD
based on cases of
human contacts in
the social mediums
after 21 days
All mediums of
social contacts in e-
high countries
Recommended
national laboratories
for the diagnosis of
Ebola virus in the e-
high countries
WHO and health
ministries of e-high
countries
e-medium
countries
Obtaining and
distribution of all
basic necessities to
cater for the needs of
the populations of
enlisted areas of
Members of
households in the
enlisted areas of e-
medium countries
WHO/UN,
Governments and
peoples of Ebola and
non-Ebola countries
in the world.
WHO, Disaster
Management
Organisations of the
e-medium countries

AARJMD VOLUME 1 ISSUE 29 (JANUARY 2015) ISSN : 2319 - 2801
Asian Academic Research Journal of Multidisciplinary
www.asianacademicresearch.org
485
countries during a 21
day lockdown..
Total lockdown of
all mediums of
social gathering and
human interactions,
e.g. schools,
workplaces, markets,
congregational
worship, local and
international
transport, all forms
of rites of initiation,
meetings and
celebrations for 21
days.
All mediums of
social contacts in the
enlisted areas of e-
medium countries
The military, Red
Cross Society,
Volunteers
WHO, health
ministries and
Disaster
Management
Organisations of e-
medium
Ebola Preventive
training and
certification
exercises for
management and
employees of all
public and private
social service
institutions, e.g.
hospitals, beauty
salons, barber shops,
driver associations,
financial institutions,
, hotels and
restaurants, markets,
local food vendors,
hawkers, etc. (This
could be before or
immediately after
the 21 day
lockdown)
Management and
employees of social
service providing
institutions in the
enlisted areas of e-
medium countries
Health departments,
Red Cross Society
and Disaster
Management
Organisations of e-
medium countries.
WHO, Health
ministries and
Disaster
Management
Organisations of
e-medium countries
During the
lockdown, there
should be
disinfection of the
mediums of social
contacts. These
include the
structures involved
in the preventive and
certification
All mediums of
social contacts in the
enlisted areas of e-
medium countries
Health departments,
Disaster
Management
Organisations,
trained military
personnel, Red
Cross Society and
volunteers of e-
medium countries
WHO and Health
ministries of
e-medium countries

AARJMD VOLUME 1 ISSUE 29 (JANUARY 2015) ISSN : 2319 - 2801
Asian Academic Research Journal of Multidisciplinary
www.asianacademicresearch.org
486
exercises specified
above.
Data collection and
analysis on EVD
based on cases of
human contacts in
the social mediums
after 21 days
All mediums of
social contacts in e-
medium countries
Recommended
national laboratories
for the diagnosis of
Ebola virus in the e-
medium countries
WHO and health
ministries of e-
medium countries
e-low countries
Obtaining and
distribution of all
basic necessities to
cater for the needs of
the populations of
enlisted areas of
countries during a 21
day lockdown..
All households in
residential areas of
towns and villages
with Ebola cases in
the e-low countries
WHO/UN,
Governments and
peoples of Ebola and
non-Ebola countries
in the world.
WHO, Disaster
Management
Organisations of the
e-low countries
Total lockdown of
all mediums of
social gathering and
human interactions,
e.g. schools,
workplaces, markets,
congregational
worship, local and
international
transport, all forms
of rites of initiation,
meetings and
celebrations for 21
days.
All mediums of
social contacts in the
residential areas of
towns and villages
with Ebola cases in
the e-low countries
The military, Red
Cross Society,
Volunteers
WHO, health
ministries and
Disaster
Management
Organisations of e-
low
Ebola Preventive
training and
certification
exercises for
management and
employees of all
public and private
social service
institutions, e.g.
hospitals, beauty
salons, barber shops,
driver associations,
financial institutions,
, hotels and
restaurants, markets,
local food vendors,
All mediums of
social contacts in the
residential areas of
towns and villages
with Ebola cases in
the e-low countries
Health departments,
Red Cross Society
and Disaster
Management
Organisations of e-
low countries.
WHO, Health
ministries and
Disaster
Management
Organisations of
e-low countries

AARJMD VOLUME 1 ISSUE 29 (JANUARY 2015) ISSN : 2319 - 2801
Asian Academic Research Journal of Multidisciplinary
www.asianacademicresearch.org
487
hawkers, etc. (This
could be before or
immediately after
the 21 day
lockdown)
During the
lockdown, there
should be
disinfection of the
mediums of social
contacts. These
include the
structures involved
in the preventive and
certification
exercises specified
above.
All mediums of
social contacts in the
residential areas of
towns and villages
with Ebola cases in
the e-low countries
Health departments,
Disaster
Management
Organisations,
trained military
personnel, Red
Cross Society and
volunteers of e-low
countries
WHO and Health
ministries of
e-low countries
Data collection and
analysis on EVD
based on cases of
human contacts in
the social mediums
after 21 days
All mediums of
social contacts in e-
low countries
Recommended
national laboratories
for the diagnosis of
Ebola virus in the e-
low countries
WHO and health
ministries of e-low
countries
e-free, ex-e high,
ex-e medium,
and ex-e low
countries
Ebola Preventive
training and
certification
exercises for
management and
employees of all
public and private
social service
institutions, e.g.
hospitals, beauty
salons, barber shops,
driver associations,
financial institutions,
, hotels and
restaurants, markets,
local food vendors,
hawkers, etc. This
could be before or
immediately after
All mediums of
social contacts in the
non-Ebola countries
Health departments,
Red Cross Society
and Disaster
Management
Organisations of
non-Ebola countries.
WHO, health
ministries and
Disaster
Management
Organisations of
non-Ebola countries
AARJMD VOLUME 1 ISSUE 29 (JANUARY 2015) ISSN : 2319 - 2801
Asian Academic Research Journal of Multidisciplinary
www.asianacademicresearch.org
488
the 21 day lockdown
in the e-high, e-
medium and e-low
countries. NB: No
lockdown in Non-
Ebola countries
Selected non-Ebola
countries to serve as
points of reception
and conveyance of
international aids to
the e-high, e-
medium and e-low
countries. Apart
from the points for
Ebola aids only,
there should be a
ban on movement of
goods and persons to
and from the Ebola
affected countries
within the 21 day
lockdown period.
Selected countries
for Ebola aids and
Ebola affected
countries
Customs and Excise
Service,
immigration,
aviation, naval and
road transport units
of both Ebola and
non-Ebola affected
countries.
Ministries of
transport, defense
and foreign affairs of
Ebola and non-Ebola
affected countries of
all MPD
participating
countries.
Ebola screening at
border points and
regular health
checks of new
immigrants
irrespective of
countries of origin,
by recommended
health facilities up to
21 days from the
commencement of
the MPD
implementation
(Frequency of
check-ups to be
determined by the
health ministry)
All new immigrants
into non-Ebola
affected countries
within the period of
the MPD
implementation.
Customs, national
immigration units
and the
recommended health
facilities of the non-
Ebola countries
WHO, foreign
affairs and health
ministries of non-
Ebola affected
countries.
Data collection and
analysis on EVD
based on cases of
human contacts in
the social mediums
after 21 days
All mediums of
social contacts in the
non-Ebola countries
Recommended
national laboratories
for the diagnosis of
Ebola virus in the
non-Ebola countries
WHO and health
ministries of non-
Ebola countries
Interpretations of the MPD ranks of countries: e-low =1-9 Ebola cases; e-medium =10-399 Ebola cases; e-high= 400+ Ebola cases; ex- (high,
medium & low) = previously e-high, e-medium and e-low; e-free= Never had Ebola.
AARJMD VOLUME 1 ISSUE 29 (JANUARY 2015) ISSN : 2319 - 2801
Asian Academic Research Journal of Multidisciplinary
www.asianacademicresearch.org
489
Source: Authors’ own construct.
The activities marking the elimination of the variables C2 and M in Tables 3 and 4 are supported
by some relevant empirical applications. For instance when Thomas Eric Duncan of Liberia
became the first man to contract EVD in Dallas city of USA, apart from himself as an EVD
patient, his family and over 100 others who had contact with him, identified by contact tracing
were also quarantined for 21 days. At the same time, Duncan’s home was power-washed or
disinfected (Stone, 2014). The news of Ebola outbreak in Dallas, following the infection of the
nurses who treated Duncan, prompted Ebola alertness on the part of the ordinary citizens, as they
changed their dressing style by wearing long-sleeve jackets, hand gloves and boots. Airline
flights to Ebola affected countries were also cancelled in the US and other parts of the World.
The Ebola control process also had to do with waste management. Thus, everything that
Thomas Eric Duncan used was packed and sealed in plastics and safely disposed. Stableford
(2014), also reports a similar situation for a female Spanish nurse who contracted Ebola in Spain.
Besides, a Spanish court ordered the euthanizing of the nurse’s dog, to prevent further zoonotic
(Animal-to-human) transmission of the EVD. Faul (2014), presents a case on the issue of total
lockdown, when she reports that following the death of 25 persons in 5 days, the authorities of
Sierra Leone ordered a two weeks lockdown of the eastern Kono District of the country. This
was to control further transmission of the EVD.
Despite the relevance of these strategies, the lack of global uniformity in their
applications has negatively impacted on the progress to control the disease. It is therefore argued
that a uniform adoption of theory such as the MPD for concurrent application all over the world
could stop the spread of the EVD and other hemorrhagic fever diseases. Thus, 21 days or three
weeks are required for the execution of the schedules in Tables 3 and 4 concurrently all over the
world. The expected outcomes are that within that period
There would be no chances of disease diffusion;
New cases occurring within a given household due to earlier contacts before the
MPD would have no chances of infecting other household members; and
All infected persons would have been identified and quarantined for treatment or
would have been dead.
An additional 21 days after the implementation of the MPD schedules are required to assess
whether new cases would, or would not occur. At the end, based on the distribution of the extra 7
AARJMD VOLUME 1 ISSUE 29 (JANUARY 2015) ISSN : 2319 - 2801
Asian Academic Research Journal of Multidisciplinary
www.asianacademicresearch.org
490
days or one week, analysed data on country-by-country bases are compiled, and the new MPD
rankings of countries declared by the World Health Organisation. This serves as feed-back for
policy review or project exit due to successful implementation.
Conclusion
The discussions have shown that it is possible to bring the Ebola virus disease under global
control. It simply requires the harmonization of the on-going but separate strategies at various
locations in the world to be implemented uniformly. Thus, a stratification of countries on the
basis of the prevalence of the disease, and identifying which existing practice is best suitable for
addressing the situation of each country in the interest of the whole world, is what is needed. The
Malongza’s Principle of Dissociation makes this simple by contributing to the stratification
criterion and identifying the independent variables as human contacts (C2) and the mediums that
promote human contacts (M). The comprehensive schedule of activities in the tabular form
serves as a global master plan on how the variables could be regulated through dissociation to
stop the spread of the disease.
It is however, expected that zoonotic researchers would be inspired by the mathematical
basis of the principle of this study, to determine how the influence of the vector of the disease
(bats and other animals or the C1 factor) could be controlled for a more permanent solution.
Already, practices such as euthanizing infected animals and the avoidance of contact with, or the
eating of meat of wild animals are ongoing. But a lot more need to be covered by zoonotic
researchers. Also, the challenge of overcoming the influence of socio-cultural factors as such the
performance of funeral rights and adaptation to the appropriate dressing styles within the limited
period of 21 days in typical traditional African societies stands to be dealt with, through intensive
education and the enforcement of associate regulations.
Although efforts have been made to indicate the sources and rational use of funding, the
cost implications of the MPD could also be considered with alternative options based on
situational analysis. It is however, far cheaper than the total cost of treating infected persons and
vaccinating the whole world, since the MPD has the potential to stop the Ebola virus disease
within seven weeks without emphasis on medications.

AARJMD VOLUME 1 ISSUE 29 (JANUARY 2015) ISSN : 2319 - 2801
Asian Academic Research Journal of Multidisciplinary
www.asianacademicresearch.org
491
References
BBC (2014). Ebola crisis: Nigeria declared free of virus. BBC news, October 20, 2014.
Bonnett, A. (2008) What is geography? London: SAGE.
Centers for Disease Control and Prevention (CDC) (2001). Outbreak of Ebola hemorrhagic
fever ---Uganda, August 2000--January 2001. Weekly, 50(05); 73-7
Centers for Disease Control and Prevention (2014). 2014 Ebola Outbreak. New York: CDC.
Centers for Disease Control and Prevention (CDC) (2014). Ebola in West Africa: impact on
health. New York Times, September 22, 2014.
Centers for Disease Control and Prevention (CDC) (2014). Ebola outbreaks
2000-2014. Accessed December 28, 2014.
http://www.cdc.gov/vhf/ebola/outbreaks/history/summaries.html.
Dixon, M.G. & Schafer, I.J. (2014). Ebola viral disease outbreak — West Africa, 2014.
Weekly, 63(25): 548-551.
Faul, M. (2014). Sierra Leone area to hold 2-week Ebola 'lockdown'. Associate Press,
December 10, 2014.
http://news.yahoo.com/sierra-leone-area-hold-2-week-ebola-lockdown-140920923.html.
Frobenius, L. (1897/98). Der westafrikanische Kulturkreis. Petermanns Mitteilungen, P. 43-44.
Haggett P. (2000). The geographical structure of epidemics. Clarendon; Oxford
Isaac, B. (2004). The invention of racism in classical antiquity. Princeton: Princeton University
Press.
Kover, C. (2014). Nigerian president sacks doctors on strike during the Ebola outbreak. Vice
News, August 15, 2014.
National Center for Infectious Diseases & Centers for Disease Control and Prevention (2014).
Known cases and outbreaks of Ebola hemorrhagic fever, in reverse chronological order.
New York: CDC.
Ng, S. &Cowling, B.J. (2014). Association between temperature, humidity and ebolavirus
disease outbreaks in Africa, 1976 to 2014. Euro Surveill, 19(35): ii. Accessed November
26, 2014. http://www.eurosurveillance.org/ViewArticle.aspx?
AARJMD VOLUME 1 ISSUE 29 (JANUARY 2015) ISSN : 2319 - 2801
Asian Academic Research Journal of Multidisciplinary
www.asianacademicresearch.org
492
Muanya, M. (2014). Hoe Nigeria contained Ebola virus disease. The Guardian, October 8, 2015.
Parker, S. (ed.) (1984). McGraw-Hill dictionary of science and technical terms. New York:
McGraw-Hall Book Company.
Parry, R.L & Bazinet, I. (2014). Ebola toll passes 4,000 as fears grow worldwide. Yahoo News,
October 10, 2014.
Specia, M. (2014). Russia claims to have ebola vaccine. Mashable, October 13, 2014
Spickler, A.R. (2014). Ebolavirus and Marburgvirus infections. Iowa: The Center for Food
Security & Public Health.
Stableford, D. (2014). Excalibur, Ebola nurse's dog, is euthanized in Spain.
Yahoo News, October 8, 2014.
http://news.yahoo.com/excalibur-spanish-ebola-nurse-dog-dead-175117255.html.
Stone, M. (2014). Four who hosted Dallas Ebola patient quarantined.
Al Jazeera America, October 2, 2014.
http://america.aljazeera.com/articles/2014/10/2/ebola-texas-fourquarantined.html
The Analyst (2014). No threat to „non-essential‟ civil servants-MICAT reacts. Liberian News
Agency, October 16, 2014.
Tsai, M. & Koerner, B. (2009). Outbreaks vs. epidemics. Sate, April 27, 2009.
http://www.slate.com/articles/news_and_politics/recycled/2009/04/outbreaks_vs_epidemi
cs.html.
Weiqun, Z. (2014). China factory whirs overtime to make Ebola suits. Accessed October 30,
2014. http://news.yahoo.com/china-factory-whirs-overtime-ebola-suits-070204145.html
World Bank (2014). Ebola: economic impact could be “catastrophic”- World Bank.
Washington DC: World Bank.
World Health Organisation (WHO) (2014). Ebola disease. Geneva: WHO.
World Health Organisation (WHO) (2014). Global alert and response: Frequently asked
questions on Ebola virus disease. Geneva: WHO.
World Health Organisation (WHO) (2014). Global alert and response: Ebola virus disease
outbreak news, November 16, 2014.
Copyright © 2022 FDOKUMEN