
Increasing Disaster Medical Assistance Teams' Intent ... - MDPI

Journal of Surgical Oncology 47:121-130 (1991)
Major Amputations Done With Palliative Intent in the Treatment of Local Bony
Complications Associated With Advanced Cancer
MARTIN M. MALAWER, MD, FACS, RICHARD G. BUCH, M D , WILLIE E. THOMPSON, MD, A N D
PAUL H. SUGARBAKER, MD, FACS
From the Departments of Orthopedic Surgery (M. M. M.) and Orthopedic Oncology (R.G.B., W.E.T.), Children’s National Medical Center, and Department of Surgical Oncology (P.H.S.), Washington Hospital Center, Washington Cancer Institute, Washington, DC
Palliative amputations were performed on 11 patients (7 men, 4 women) with disseminated disease to control local bony complications. The average patient age was 54 years (range 14-78 years). The primary diseases were melanomdsarcoma (seven patients) and carcinoma (four patients). All had pain; eight had intractable pain that could not be controlled by analgesics. All 11 patients had additional severe local complications, which included recurrent pathological fracture (4), sepsis (2), hemorrhage (2), radiation necrosis (2), and iliofemoral thrombosis secondary to tumor (1). Previous attempts of palliation had been made in all 11 patients, and 8 had undergone previous operative procedures (5 had undergone two or more) prior to amputation. Three anterior hemipelvec- tomies, five posterior hemipelvectomies, two hip disarticulations, and one forequarter amputation were performed. All patients survived the surgery, and there were no intraoperative complications. All patients received dramatic relief of pain. Postoperative complications included two cases of flap necrosis and two infections; all resolved satisfactorily. The six patients who were nonambulatory before surgery ambulated postoperatively, and two eventually ambulated with a prosthesis. Six of 11 patients survived 1 year or longer, with a median postoperative survival period of 13 months (average 16 months). Although major amputations are viewed at times as offering little to already-compromised patients, they can improve dramat- ically the quality of life in selected patients.
KEY WORDS: palliation, metastatic cancer, hemipelvectomy, sarcomas
INTRODUCTION Major amputations (hip disarticulations, hemipelvec-
tomies , forequarter amputations) are rarely performed for patients with metastatic cancer. The usual indications for these extensive procedures are high-grade primary sar- comas of bone and soft tissue, recurrent low-grade sarcomas, and, occasionally, trauma [ 1-10]. Occasion- ally amputations have been performed as palliative procedures for metastatic tumors of the lower extremities 0 1991 Wiley-Liss, Inc.
(Table I) [3,5,7,11-171. Rarer still has been the decision to perform a higher level, palliative amputation for metastatic carcinoma, sarcoma, and/or melanoma involv- ing the pelvic or shoulder girdle or an extremity in a patient with advanced disseminated disease. Major am-
Accepted for publication January 27, 1991. Address reprint requests to Martin M. Malawer, M.D., Department of Orthopedic Surgery, Children’s National Medical Center, 11 1 Mich- igan Ave., N.W., Washington, DC 20010.

122 Malawer et al.
TABLE I. Literature Review: Radical Amputations for Palliation
lnvestigator publication Procedure reported Year of No. of procedures
Pack et al. 171 1947 Forequarter amputation 5 Hip disarticulation 2 Hemipelvectom y 2
Ravitch 1 121 1949 Hemipelvectomy 1 Lee and Alt 1 131 1953 Hemipelvectomy 1 Higinbotham and Coley [ 5 ] 1956 Hemipelvectomy 4 Miller 1271 1959 Hemipelvectomy 5 Ravitch and Wilson [ 141 1964 Hemipelvectomy 5
Deutsch et a]. [ 151 1984 Hemipelvectomy 1 Stener et al. [ 16) 1984 Forequarter amputation 1
Hip disarticulation 1 Hemipelvectomy 5
Douglas et al. [3] 1975 Hemipelvectomy 6
Karakousis et al. [ 171 1989 Hemipelvec tomy 23
putations are often looked upon as procedures employed out of desperation, associated with a high mortality rate and of doubtful benefit. Even after other modalities have failed, a large majority of the medical community does not consider that palliative major amputations may offer the patient an improved quality of life.
There are several clinical situations in which an extensive lesion of an extremity severely limits a pa- tient’s activities (and possibly accelerates his or her demise) and in which a palliative amputation may be beneficial. When the cancer involves a proximal limb or a major joint, resulting in intractable pain, sepsis, fungation, or radiation-induced necrosis, or when previ- ous treatment has resulted in a nonfunctional extremity, major ablative surgery may be indicated. We report our experience with 11 patients with advanced local bony disease along with disseminated cancer involving the extremities who have undergone major palliative ampu- tations within the past 10 years. All patients survived the surgical procedures and improved significantly from their preoperative status. We urge that amputation not be denied to the rare patient for whom it may be beneficial.
MATERIALS AND METHODS Seven men and four women, ranging in age from 14 to
78 years (average age 54 years), were included in the study. The diagnoses at the time of initial presentation were sarcomdmelanoma (seven patients) and carcinoma (four patients). There were three melanomas, two meta- static renal cell carcinomas, and one osteosarcoma, Ewing’s sarcoma, fibrosarcoma, synovial cell sarcoma, squamous cell carcinoma, and metastatic colon carci- noma. At the time of amputation, all patients had metastatic disease. The primary site of the tumor was unknown in three patients (one with melanoma, one with adenocarcinoma, and one with squamous cell carci-
noma). Primary bony sarcomas involved the humerus (one patient), ilium (one patient), and proximal femur (one patient).
Indications for Major Amputation All patients complained of pain; eight patients had
unrelenting, intractable pain not relieved by analgesics. All 11 patients had additional severe local complications, including sepsis (2), hemorrhage (2), radiation-induced necrosis (2), iliofemoral thrombosis due to tumor with secondary muscle ischemia (l), and pathological frac- ture (4).
Illustrative Cases Case no. 1. This case demonstrates the value of
palliative hemipelvectomy in a patient with a large, bony metastasis with recurrent fracture, local recurrence, and tumor fungation despite multiple attempts at surgical control and stabilization (Fig. 1).
A 60-year-old man underwent radical neck surgery in 1980 for a histologic diagnosis of adenocarcinoma. The primary tumor site was undetermined. He sustained a pathologic fracture of a solitary left proximal femoral lesion in 198 1 and was treated with internal fixation (Fig. lA,B). In 1983, there was continued nonunion at the fracture site and the fixation device failed. The implant was removed and the fracture treated with an intramed- ullary (IM) rod. Chemotherapy was begun in May 1984 and completed in March 1985. The patient developed severe pain in the left hip in September 1984. At the same time, he noticed a soft-tissue mass in his buttock along the previous operative site. A biopsy revealed adenocar- cinoma. He had progressive pain unrelieved by narcotics for the following 8 months. The pain was continuous, even when the patient was at rest; he was nonambulatory.

Palliative Major Amputations 123
lesion in the right femur required rerodding and cement fixation. After surgery, the patient remained symptom- atic and was able only to transfer from bed to chair. He also had metabolic problems, including electrolyte im- balances and hypercalcemia. He was confused and dis- oriented most of the time.
On evaluation in 1987, the right lower extremity was extremely painful, and a large soft-tissue mass was shown to involve the middle third of the thigh. Plain radiographs showed destruction of the entire mid-diaphy- seal area and a large soft-tissue mass with cement within the mass. The IM rod was loose at the distal end. The patient and family were advised that surgery was indi- cated and that amputation was the best option. They opposed amputation and sought consultation elsewhere. The patient underwent a trial of intra-arterial chemother- apy (DTIC), by isolation-perfusion, with non response. In July 1987, he returned for surgery. There was a marked increase in pain and tumor size, and he was bedridden. The patient underwent a modified hemipel- vectomy in August 1987. His postoperative course was uneventful. His electrolyte and calcium levels returned to normal, and his confusion and disorientation resolved. He was transferred to a rehabilitation hospital 3 weeks after surgery, where he was fitted with a temporary prosthesis and began ambulation with a walker. He was discharged 4 weeks later, able to transfer and walk to the bathroom. Twenty-eight months after surgery, he is pain-free and is a home ambulator with his prosthesis.
RESULTS The clinical data, type of surgery, and results of
treatment of 11 patients are summarized in Table 11.
Types of Surgery Eight patients had hemipelvectomies, two had hip
disarticulations, and one had a forequarter amputation. Three of the hemipelvectomies were done using an anterior flap and five used posterior flaps.
Prior Procedures Eight of 11 patients had undergone previous surgery
prior to amputation, and 5 patients had undergone two or more surgical procedures. Two patients had IM rod fixation of a pathologic fracture and two had prosthetic replacement for tumor recurrence prior to hemipelvec- tomy. Two patients with melanoma had multiple exci- sions of these lesions before hip disarticulation.
Survival, Clinical Response, and Functional Status All 11 patients survived the operative procedure. Six
survived 1 year or longer (median 13 months, range 1-52 months). One patient died from widespread metastatic disease 1 month after a forequarter amputation. One patient died 2 years after surgery from unrelated causes.
In April 1985, he was admitted to the hospital with intractable pain. A large, fungating buttock and thigh mass was evident (Fig. lC,D). He underwent an anterior flap hemipelvectomy (Fig. 1E). A portion of the flap became necrotic, requiring debridement. The wound was secondarily closed and there were no further complica- tions. He was discharged 3 weeks later, walking inde- pendently with crutches. He was able to tend his garden. He remained ambulatory and pain-free until his death 13 months following amputation.
Case no. 2. This case illustrates the use of a pallia- tive forequarter amputation for severe radiation-induced necrosis and pain control in a patient with widespread metastasis (Table 11).
A 14-year-old girl with Ewing’s sarcoma of the right proximal humerus with bony and pulmonary metastases was admitted to the Surgery Branch of the National Cancer Institute (NCI) in May 1982 for evaluation of recurrent swelling and pain in the right arm. The initial diagnosis of Ewing’s sarcoma had been made in August 1980. Treatment at that time was a combination of chemotherapy and radiation to the primary site and total body irradiation. She developed local recurrence in March 198 1, with evidence of metastases to the skull and pelvis, and was treated with an additional 4,000 rads to the involved humerus at that time. In March 1982, she was hospitalized for recurrent pain and swelling in the right upper extremity. Intravenous morphine did not relieve the pain. Clinical examination showed a “petri- fied” upper extremity without a pulse or sensation. Venography showed almost complete lack of drainage due to venous thrombosis. A forequarter amputation was performed. The patient was discharged after 14 days with complete resolution of her preoperative pain. She died 1 month later of progressive disease.
Case no. 9. This case illustrates the value of hemi- pelvectomy in a man with a massive tumor recurrence, complete failure of internal fixation of a metastatic renal carcinoma, and subsequent debilitating pain, inability to ambulate, and progressive metabolic abnormalities (Table 11).
A 44-year-old man presented in March 1987 with an extremely painful lower extremity. He was unable to walk and had been almost completely bedridden for more than 1 year. In 1974, he had undergone a right nephrec- tomy for hypernephroma at another institution. He re- mained disease-free until 1984, when he was found to have metastases to the brain, lungs, and right femur. The patient was treated with resection of a solitary brain metastasis and lung metastasis. He received radiation therapy to the brain and lung. The solitary bony metasta- sis to the midshaft of the femur was treated with IM rod and polymethylmethacrylate (PMMA). The patient’s right lower extremity remained symptomatic and painful, but he was able to walk. In 1985, progression of the

124 Malawer et al.
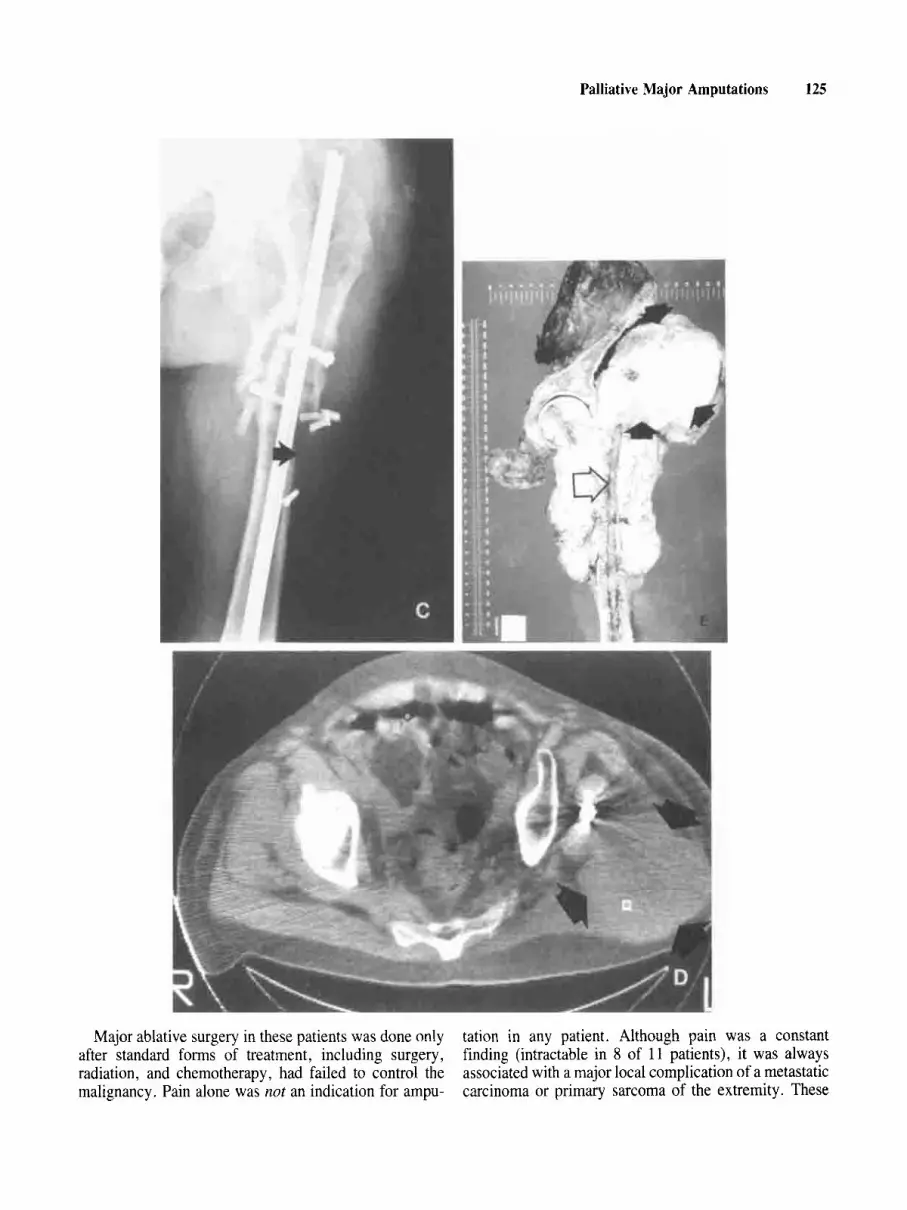
Fig. 1 . A 60-year-old man with metastatic adenocarcinoma from the head and neck region to the femur. A: Plain radiograph demonstrating the original solitary metastatic femoral lesion prior to fracture. The patient sustained a comminuted fracture that was fixed with a compression screw and plate. B: Two years following fixation, there was a recurrent pathological fracture, pain, and nonunion. The patient underwent revision with an IM rod. Fig. I . C-E appears on page 125. C: Plain radiograph 2 years following revision with an IM rod and 4 years following fracture. There is progressive destruction of the diaphysis of the femur (solid arrow), shortening, and fragmentation. A
Confusion, obtundation, and transitory problems with calcium, potassium, and glucose levels in three patients resolved after surgery. The two cases of sepsis resolved following surgery and the two cases of hemorrhage were controlled by the surgical procedures. Six patients who had been nonambulatory because of their tumor walked with crutches postoperatively; two of these used prosthe- ses.
Complications There were iio intraoperative complications. Postop-
erative complications included two cases of flap necrosis (both posterior flaps) and infection, (one superficial, one deep). All four patients healed following debridement.
large soft-tissue tumor component in the medial thigh and the buttock is evident. D: CAT of the proximal femur and pelvis prior to hemipelvectomy demonstrates a large soft-tissue tumor extending from the hip into the buttocks (solid arrows). There is no tumor extension into the pelvis. The area of the sciatic notch is free of tumor. E: Gross specimen following an anterior flap hemipelvectomy. The tumor completely surrounds the proximal one third of the femur. There is a large posterior extraosseous component (solid arrows) adjacent to the hip joint and ilium. Tumor extends along the nail tract (open arrow) into the femoral head and neck.
DISCUSSION
In assessing the value of major palliative amputations, success should not be measured by the rate of cure but by the number of months or years they enable the patient to live comfortably with lessened disability. All the patients in the present series benefited from their procedures. A11 had remarkable pain relief and improvement in lifestyle after surgery; all were gratified with the results. As cancer treatments improve, offering increased survival, the frequency of problems associated with widespread metastatic lesions is increasing. We believe that major amputations have a role in palliative treatment of certain metastatic lesions.
Palliative Major Amputations 125
Major ablative surgery in these patients was done only after standard forms of treatment, including surgery, radiation, and chemotherapy, had failed to control the malignancy. Pain alone was not an indication for ampu-
tation in any patient. Although pain was a constant finding (intractable in 8 of 11 patients), it was always associated with a major local complication of a metastatic carcinoma or primary sarcoma of the extremity. These

TABL
E 11
. C
linic
al D
ata
of 1
1 Pa
tient
s Tre
ated
by
Mai
or A
mpu
tatio
n fo
r Pa
lliat
ion
With
Kno
wn
Met
asta
tic D
isea
se*
Mon
ths
Cas
e Ty
pe o
f sy
mpt
omat
ic
Follo
w-u
p no
. A
ge
Site
Pr
imar
y tu
mor
su
rger
y In
dica
tion
Prio
r tre
atm
ent
Stat
us
resu
lt co
mm
ent
I 60
14
31
4 5
Hip
/fem
ur
Prox
imal
hu
mer
us
Hip
Squa
mou
s ce
ll A
nter
ior
H/P
Pa
in, l
arge
tum
or
Unk
now
n pr
imar
y in
abili
ty t
o tra
nsfe
r/ ca
rcin
oma
mas
s, re
curr
ent
frac
ture
,
ambu
late
Ewin
g’s
sarc
oma
Fore
quar
ter
Post
-rad
iatio
n Pr
imar
y he
mer
us
necr
osis
, pai
n,
Fibr
osca
rcom
a Po
ster
ior
H/P
Li
fe-th
reat
enin
g se
psis
, Pr
imar
y hi
p tu
mor
fun
gatio
n an
d
func
tionl
ess
extre
mity
hem
orrh
age
36
Ilium
/pel
vis
Mel
anom
a A
nter
ior
H/P
U
nkno
wn
prim
ary
62
Ilium
O
steo
sarc
oma
Ant
erio
r H
/P
Seve
re p
ain,
lar
ge tu
mor
, pa
thol
ogic
al f
ract
ure
of il
ium
, sac
ral
plex
us in
volv
emen
t Pa
in, f
unct
ionl
ess
extre
mity
RT,
CT
D
13
Exc
elle
nt
IM ro
d fix
atio
n Pl
ate/
scre
w f
ixat
ion
MS
Perc
orda
n (ia
troge
nic
MS,
RT,
CT
D
1 Ex
celle
nt
addi
tion)
RT,
CT
D
24
Exc
elle
nt
Prox
imal
fem
ur
repl
acem
ent (
2)
Rese
ctio
n an
d de
brid
emen
t M
S (ia
troge
nic
addi
tion)
M
S
Embo
lizat
ion
CT
Com
mun
ity a
mbu
lato
r, m
inim
al a
nalg
esic
s
Pain
-fre
e un
til d
eath
Seps
is re
solv
ed,
com
mun
ity a
mbu
lato
r
NED
52
Exc
elle
nt
Com
mun
ity a
mbu
lato
r, co
mpl
etel
y pa
in-f
ree,
im
mun
othe
rapy
11
2-LA
K c
ells
D
12 G
ood
Cle
aran
ce o
f m
etab
olic
ab
norm
aliti
es a
nd

conf
usio
n, p
ain-
free
an
d co
mm
unity
am
bula
tor,
pros
thet
ic
wea
rer
6 7 8 9 10
11
50
Leg
61
Leg,
foot
23
Thig
h,
groi
n 44
Fe
mur
69
Ilium
78
Mid
fem
ur
Mel
anom
a H
ip d
isar
ticul
atio
n Pa
in, s
ever
e se
psis
Mel
anom
a H
ip d
isar
ticul
atio
n Pa
in, h
emor
rhag
e,
Prim
ary
foot
tu
mor
fun
gatio
n Sy
novi
al s
arco
ma
Post
erio
r H
/P
Seve
re p
ain
Ren
al c
ell
Post
erio
r H
/P
Seve
re p
ain,
lar
ge
carc
inom
a tu
mor
, mas
sive
sof
t- tis
sue
invo
lvem
ent,
func
tionl
ess
extre
mity
Ade
noca
rcin
oma
Post
erio
r H
IP
Unc
ontr
olla
ble
pain
, U
nkno
wn
prim
ary
iliof
emor
al t
hrom
bosi
s, co
mpa
rtm
enta
l ne
cros
is
(but
tock
, qua
dric
eps)
, m
assi
ve s
oft-t
issu
e ex
tens
ion
Col
on c
arci
nom
a Po
ster
ior
H/P
Pa
thol
ogic
al fr
actu
re,
mas
sive
sof
t tis
sue
Com
Don
ent
RT
D
17 G
ood
Mul
tiple
exc
isio
n Li
mb
perf
usio
ns
Mul
tiple
exc
isio
n D
12
Exc
elle
nt
CT
R
T, C
T
D
7 G
ood
Wid
e ex
cisi
on
IM r
od w
ith c
emen
t (2)
L
WD
28
Exc
elle
nt
MS
CT
Li
mb
perf
usio
n, R
T
Pros
thet
ic re
plac
emen
t D
6
Goo
d C
T
Embo
lizat
ion
D
4 G
ood
RT
Com
plet
e pa
in r
elie
f, am
bula
tes
with
cr
utch
es, c
lear
ance
of
obt
unda
tion,
m
etab
olic
ab
norm
aliti
es,
hype
rcal
cem
ia
com
mun
ity a
mbu
lato
r, re
solu
tion
of
met
abol
ic
abno
rmal
ities
Mar
ked
relie
f of
pai
n,
Com
mun
ity a
mbu
lato
r
* H/P
, hem
ipel
vect
omy;
RT,
radi
atio
n th
erap
y; C
T, c
hem
othe
rapy
; IM
, int
ram
edul
lary
; MS,
mor
phin
e su
lfate
; D, d
ead;
LW
D, l
ivin
g w
ith d
isea
se;
NED
, no
evid
ence
of
dise
ase.

128 Malawer et al.
c. ELEVATION OF QUADRICEPS FLAP
Superficial Femoral A. & V.
Psoas m.
\
B.
/ Femur Tensor Fascia rn. Profundus Femoris A. & V. (ligated)
D. ROTATION CLOSURE Superficial Femoral A. & V.
External Iliac A. & V
Bladder
Peritoneum
Sacrum
Fig. 2. Technique of anterior myocutaneous flap hemipelvectomy as used by the author. This technique permits adequate removal of all contaminated posterior and lateral hip incisions following multiple failed orthopedic procedures for tumors of the hip and/or femur. A: The posterior incision follows the iliac crest and the sacroiliac joint. B: The anterior incision outlines the quadriceps muscle group and permits
ligation of the superficial femoral vessels at the level of the adductor hiatus. C: All or a portion of the quadriceps muscles is elevated with the anterior thigh skin. It is necessary to ligate the profunda vessels in order to get above the inguinal ligament. D: The amputation is then performed similar to the standard hemipelvectomy.

Palliative Major Amputations 129
an attempt at fixation of a pathologic fracture, surgical stabilization may not be possible. For these patients, major amputation may result in improved function and lifestyle. This is especially true for renal cell carcinomas, characterized by a wide variation in individual survival and often marked bony destruction associated with large extraosseous component. Stener et al. [16] reported 21 patients with metastatic renal cancer who underwent surgery for their disease. Eight patients underwent major amputations (five hemipelvectomies, one hip disarticu- lation, one interscapulothoracic , one modified hemipel- vectomy) [16]. All had relief of pain. Seven were ambulatory after surgery; six were fitted with prostheses.
The technique of an anterior myocutaneous flap hemi- pelvectomy based upon the external iliac vessels and preservation of the quadriceps mechanism, as described by Sugarbaker and Ackerman [20], has proved to be useful when tumor has involved the buttock musculature making a standard posterior flap difficult. It is important to ligate the profunda femoris vessels distal to the take-off of the circumflex vessel (Fig. 2). This is a common problem following multiple hip and femoral procedures, since posterior incisions are the standard surgical ap- proach to pathological fractures. The use of an anterior flap is also advisable because it heals relatively rapidly, will tolerate radiation if necessary, and is less likely to develop necrosis than is a posterior flap. An important technical aspect is that the profunda femoris vessels are ligated distal to the take-off of the circumflex vessels.
Reluctance to perform major amputations is under- standable. They are difficult to perform and are consid- ered mutilating surgeries that result in considerable disability. The fact that the patients are already compro- mised increases the surgical risk. Nonetheless, as this study demonstrates, functional status and pain relief following amputation is routinely obtained. We believe that the risk/benefit ratio for these patients is similar to that of other patients commonly undergoing major sur- gery, e.g., an elderly patient with a hip fracture or a dysvascular patient requiring amputation. Our results- 13-month median survival--compare favorably with those of patients in these categories [ 10,26,28-311.
In summary, we believe that this study substantiates the value of palliative major amputation in carefully selected patients. Such procedures offer more comfort- able survival. We recommend, however, that major extirpation be considered only when other surgical or palliative treatments offer no effective resolution to the patient’s problem. Careful planning and execution are critical.
local problems were related either to bony or soft-tissue recurrence with local extension into adjacent structures, The most common problems were recurrent fracture and loss of stabilization, local vascular compromise (usually venous around the pelvis/groin) , secondary compartment necrosis syndrome, and fungation with hemorrhage and/ or infection.
Radical amputations are rarely performed in the United States. The incidence is approximately 1/1,000,000 per population per year [ 18,193. The mortality rate of such procedures has decreased dramatically over the years. Sugarbaker and Ackerman [20] reported that prior to 1935, the mortality rate was 56%. Between 1935 and 1945, it decreased to approximately 15% [4,20,21]. More recently, ’d rate of 0-7% has been reported [3,8- 10,13,14,19,22-261. We report no operative mortality in this study, despite the advanced systemic disease of all patients.
The efficacy of major palliative amputations has been shown in several previous studies (Table I>. In 1947, Pack et al. [7] reported one of the largest series of radical amputations for palliation for treatment of a wide range of lesions: five forequarter amputations, two hip disartic- ulations, and two hemipelvectomies. Similarly, Douglas et al. [3], Higinbotham et al. [ 5 ] , and Miller [27] with six, four, and five patients, respectively, reported sur- prisingly good results after palliative amputations. In general, results were gratifying unless the patient’s general condition had deteriorated prior to surgery. Other studies with fewer patients dealing with major amputa- tions for varied reasons also recommend these procedures as palliative measures [9,10,12,13,15,16]. Some authors have indicated that increased age is not a contraindication to these procedures. Sugarbaker and Ackerman [20] advised surgeons to treat patients on the basis of disease, not age. Coley and Higinbotham [22] had 7 patients over 60 years of age who did as well as their younger patients. We believe strongly that age should not be a factor in patient selection. Six of our 11 patients were over 50 years old.
Interestingly, the types of cancers in our series tended to be the less common malignancies. Breast, lung, and prostate cancers account for the majority of all metastatic cancers, and yet none of these was treated in this study. Renal cell carcinomas are well-known for their unpre- dictability; two were included in our group. Sarcomas, which account for less than 2% of all malignancies, accounted for 4 of 11 cases in this study. An interesting observation is that the patients in this study had survived with their underlying disease a relatively long period of time and only later developed severe local problems. This relative “symbiotic” relationship might also be reflected in the patients’ relatively long survival following pallia- tive amputation.
On those rare occasions when tumor recurs following
REFERENCES
1. Bailey RW, Steven DB: Radical exarticulation of the extremities for the curative and palliative treatment of malignant neoplasms. J Bone Surg 43-A:854, 1964.

130 Malawer et al.
2. Coley BL, Higinbotham NL: Indications for hemipelvectomy.
3. Douglas HO. Razack M, Holvoke ED: Hemipelvectomy. Arch Surgery 44:76&774, 1958.
Surc110:82, 1975.
Philadel~hia: Lea & Febieer, 1974. DD 1041-1051. 4. Francis KC: Radical amputations, In “Nora’s Operative Surgery.”
5 . Higinboiham NL, Coley BL! Hemipdvectomy: Experience in a series of thirty-nine cases. Cancer 9: 1233-1238, 1956.
6. Higinbotham NL, Marcove RC, Casson P: Hemipelvectomy: A clinical study of 100 cases with five-year follow-up on 60 patients. Surgery 59:706-708, 1966.
7. Pack GT, Ehrlich HE, Gentil FdeC: Radical amputations of the extremities in the treatment of cancer. Surg Gynecol Obstet 84: - . 1 105-1 116, 1947.
8. Pack GT. Miller TR: Exarticulation of the innominate bone and corresponding lower extremity (hemipelvectomy) for primary and metastatic cancer. A report of one hundred and one cases with analysis of the end results. J Bone Jt Surg 46-A:91-95, 1964.
9 . Miller TR: Hemipelvectomy in lower extremity tumors. Surg Clin North Am 8:903-919, 1977.
10. Taylor GW, Rogers WP: Hindquarter amputation: Experience with eighteen cases. N Engl J Med 249:963, 1953.
1 1 . Marcove RC, Milke V, Hutter RVP, Huvos AG, Shozi H, Miller TR, Kosloff R: Chondrosarcoma of the pelvis and upper end of the femur. J Bone Jt Surg 54-A:S61-572, 1972.
12. Ravitch MM: Hemipelvectomy. Surgery 26:199-214, 1949. 13. Lee CM, Alt LP: Hemipelvectomy and hip disarticulation for
malignant tumors of the pelvis and lower extremity. Ann Surg 137:704-7 17, 1953.
14. Ravitch MM, Wilson TC: Long-term results of hemipelvectomy. Ann Surg 159:667-682, 1964.
IS. Deutsch AA, Bachar A, Reiss R: Hemipelvectomy for liposar- coma: An unusual case and course. Postgrad Med J 60:70-72, 1984.
16. Stener B, Henriksson C, Johansson S, Gunterberg B, Peterson S: Surgical removal of bone and muscle metastases of renal cancer. Acta Orthop Scand 55:491-500, 1984.
17. Karakousis CP, Emrich LJ, Driscoll DL: Variants of hemipelvec- tomy and their complications. Am J Surg 158:404-408, 1989.
18. Murdock G: “Prosthetic and Orthotic Practice.” London: Edward Arnold, 1969, p 313.
19. Sneppan 0, Johansen T, Heerfordt J, Dissing I, Peterson I: Hemipelvectomy. Acta Orthop Scand 49: 175, 1978.
20. Sugarbaker ED, Ackerman LV: Disarticulation of the innominate bone for malignant tumors of the pelvic parietis and upper thigh. _ _ Surg GynecorObstet 81:36-52, 1’945.
21. Gordon-Tavlor G. Wiles P. Wamvick WT: The interinnomino-
- ~
abdominal’operatlon. Observation on a series of fifty cases. J Bone Jt Surg 34-B:1&21, 1952.
22. Coley BL, Higinbotham NL: Indications for hemipelvectomy . Surgery 44:766-774, 1958.
23. Lewis RC Jr, Bickel WH: Hemipelvectomy for malignant disease. - JAMA 165:8-12, 1957.
24. Pack GT: Exarticulations for malignant neodasms of the extrem- ities. Interscapulothoracic amputition, hip’-joint disarticulation, and interilio-abdominal amputation. A report of end results in 228 cases. J Bone Jt Surg 38-A:249, 1956.
25. Sim FH, Pritchard DJ, Ivins JC: Forequarter amputation. Or- thoped Clin North Am 8:921-931, 1977.
26. Kim GE, Imparato AM, Chu DS, Davis SW: Lower limb amputation for occlusive vascular disease. Am Surg 42598-601, 1976.
27. Miller TR: Interilio-abdominal amputation: A report of 32 cases. Acta Radio1 (Stockholm) 188 (Suppl):173-189, 1959.
28. Hunter G, Holliday P: Major amputation following vascular reconstructive procedures (including sympathectomy). Can J Surg 21:456-458, 1978.
29. Miller CW: Survival and ambulation following hip fracture. J Bone Jt Surg 60-A(2):930-934, 1978.
30. Robinson K: Limb ablation and limb replacement. Amputation in vascular disease. Ann R Coll Surg Engl 62:87-91, 1980.
31. Williams JW, Britt LG, Eades T, Sherman RT: Pulmonary embolism after amputation of the lower extremity. Surg Gynecol Obstet 140.246-248, 1975.
Copyright © 2022 FDOKUMEN




















