LOW DOSE HYDROXYUREA IS EFFECTIVE IN REDUCING THE INCIDENCE OF PAINFUL CRISIS AND FREQUENCY OF BLOOD...
12
Hemoglobin, 2012; 36(5): 409–420 Copyright © Informa Healthcare USA, Inc. ISSN: 0363-0269 print/1532-432X online DOI: 10.3109/03630269.2012.709897 ORIGINAL ARTICLE LOW DOSE HYDROXYUREA IS EFFECTIVE IN REDUCING THE INCIDENCE OF PAINFUL CRISIS AND FREQUENCY OF BLOOD TRANSFUSION IN SICKLE CELL ANEMIA PATIENTS FROM EASTERN INDIA Dilip K. Patel, 1 Ranjeet S. Mashon, 2 Siris Patel, 3 Bhabani S. Das, 4 Prasanta Purohit, 5 and Subasa C. Bishwal 5 1 Department of Medicine, Veer Surendra Sai Medical College, Burla, Orissa, India 2 Indian Council of Medical Research (ICMR), New Delhi, India 3 Department of Medicine, Sickle Cell Research Project, Veer Surendra Sai Medical College, Burla, Orissa, India 4 Institute of Life Sciences, Bhubaneswar, Orissa, India 5 Sickle Cell Clinic, Department of Medicine, Veer Surendra Sai Medical College, Burla, Orissa, India Û There are several questions pertaining to dosage, duration and potential long-term toxicity of hydroxyurea (HU) therapy. Use of HU is extremely limited in eastern India because of its high cost and apprehension of its toxicities. We undertook this study to assess the clinical, biochemical and hemato- logical efficacy of minimal dose HU (10 mg/kg/day) in 118 sickle cell anemia patients (27 pediatric and 91 adults). The frequency of painful crises reduced significantly in 71.5 and 92.2% in pediatric and adult cases, respectively. Ninety-five percent of the patients became transfusion independent. The baseline Hb F, total hemoglobin (Hb), MCV, MCH and MCHC levels increased significantly, whereas the WBC, platelet count and total serum bilirubin values decreased significantly. This is the first study of minimal dose HU therapy in eastern India that showed impressive improvement in clinical and hematological parameters with minimal toxicity. Keywords Hydroxyurea (HU), Fetal hemoglobin (Hb F), Sickle cell anemia, Maximum tolerated dose (MTD), Low dose, Toxicity, Painful crises Received 3 July 2011; Accepted 24 April 2012. Address correspondence to Dr. Dilip K. Patel, Associate Professor, Qr. 3R/27, Doctors Colony, P.O. Burla, Dist Sambalpur, Orissa 768017, India; Tel.: þ91-943-706-2273; Fax: þ91-663-243-0768; E-mail: [email protected] 409 Hemoglobin Downloaded from informahealthcare.com by International Centre for Genetics Engineering and Biotechnology on 01/12/14 For personal use only.
Transcript of LOW DOSE HYDROXYUREA IS EFFECTIVE IN REDUCING THE INCIDENCE OF PAINFUL CRISIS AND FREQUENCY OF BLOOD...

Hemoglobin, 2012; 36(5): 409–420Copyright © Informa Healthcare USA, Inc.ISSN: 0363-0269 print/1532-432X onlineDOI: 10.3109/03630269.2012.709897
ORIGINAL ARTICLE
LOW DOSE HYDROXYUREA IS EFFECTIVE IN REDUCING THE
INCIDENCE OF PAINFUL CRISIS AND FREQUENCY OF BLOOD
TRANSFUSION IN SICKLE CELL ANEMIA PATIENTS FROM
EASTERN INDIA
Dilip K. Patel,1 Ranjeet S. Mashon,2 Siris Patel,3 Bhabani S. Das,4
Prasanta Purohit,5 and Subasa C. Bishwal5
1Department of Medicine, Veer Surendra Sai Medical College, Burla, Orissa, India2Indian Council of Medical Research (ICMR), New Delhi, India3Department of Medicine, Sickle Cell Research Project, Veer Surendra Sai Medical College, Burla, Orissa,India4Institute of Life Sciences, Bhubaneswar, Orissa, India5Sickle Cell Clinic, Department of Medicine, Veer Surendra Sai Medical College, Burla, Orissa, India
� There are several questions pertaining to dosage, duration and potential long-term toxicity ofhydroxyurea (HU) therapy. Use of HU is extremely limited in eastern India because of its high cost andapprehension of its toxicities. We undertook this study to assess the clinical, biochemical and hemato-logical efficacy of minimal dose HU (10 mg/kg/day) in 118 sickle cell anemia patients (27 pediatricand 91 adults). The frequency of painful crises reduced significantly in 71.5 and 92.2% in pediatricand adult cases, respectively. Ninety-five percent of the patients became transfusion independent. Thebaseline Hb F, total hemoglobin (Hb), MCV, MCH andMCHC levels increased significantly, whereasthe WBC, platelet count and total serum bilirubin values decreased significantly. This is the first studyof minimal dose HU therapy in eastern India that showed impressive improvement in clinical andhematological parameters with minimal toxicity.
Keywords Hydroxyurea (HU), Fetal hemoglobin (Hb F), Sickle cell anemia, Maximumtolerated dose (MTD), Low dose, Toxicity, Painful crises
Received 3 July 2011; Accepted 24 April 2012.Address correspondence to Dr. Dilip K. Patel, Associate Professor, Qr. 3R/27, Doctors Colony,
P.O. Burla, Dist Sambalpur, Orissa 768017, India; Tel.: þ91-943-706-2273; Fax: þ91-663-243-0768; E-mail:[email protected]
409
Hem
oglo
bin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Inte
rnat
iona
l Cen
tre
for
Gen
etic
s E
ngin
eeri
ng a
nd B
iote
chno
logy
on
01/1
2/14
For
pers
onal
use
onl
y.

INTRODUCTION
Hydroxyurea (HU) remains the only approved disease-modifying therapyfor sickle cell anemia (1). However, there are several unanswered questionspertaining to its dosage, duration of therapy and potential long-term toxicity.In most studies, the maximum tolerated dose (MTD), ranging from 30 to 35mg/kg/day has been used, although it is unclear whether escalating dosage tothe MTD is essential to achieve a sustained clinical and hematologicalresponse (2–6). Several other studies have reported beneficial effects of HUtherapy at lower doses of 20 to 25 mg/kg/day, with no attempt to achieve theMTD (6–9).
Information on adverse drug reactions of HU at MTD is limited. Thepotential of HU to be an in vivomutagenic and even carcinogenic agent havenot been fully evaluated (10). Recent studies have reported significantlygreater DNA damage in leucocytes of sickle cell anemia patients treatedwith HU at a dose of 20-30 mg/kg/day (11). The possible deleterious effectof HU in human spermatogenesis, have recently been reported and warrantfurther evaluation (12,13).
Sickle cell anemia is a major public health problem in the state of Orissa,India (14). In a recent study, we found that in spite of high Hb F concentra-tions (22.3 � 6.9%; range 3.9-40.9%), 87.8% of patients had painful crises(15). Unfortunately, the use of HU is extremely limited in India, morespecifically in this part of the country, because of its high cost and theapprehension of its toxicities. We presume a low dose HU will be acceptableby a significant proportion of sickle cell anemia patients because of its lowercost and minimum adverse reactions, and therefore, wanted to assess theeffectiveness of HU at a dose of 10 mg/kg/day in reducing complications ofsickle cell anemia.
MATERIALS AND METHODS
The present study was undertaken on sickle cell anemia patients enrolledin the Sickle Cell Clinic and Molecular Biology Laboratory of the VeerSurendra Sai Medical College Hospital, Burla, in the state of Orissa locatedin eastern India. It is a tertiary care, referral hospital for 12 million peopleresiding in western Orissa and adjacent to the state of Chhattisgarh. Themajority of the inhabitants of these areas are tribal (aboriginals) and theprevalence of hemoglobin (Hb) disorders is very high.
This prospective open label observational study was carried out to assessthe effectiveness of HU with a very low and fixed dose of 10 mg/kg/day insickle cell anemia patients. One hundred and forty cases were enrolled start-ing July 2007 and were followed-up for 24 months. At the end of the study
410 D.K. Patel et al.
Hem
oglo
bin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Inte
rnat
iona
l Cen
tre
for
Gen
etic
s E
ngin
eeri
ng a
nd B
iote
chno
logy
on
01/1
2/14
For
pers
onal
use
onl
y.

period, 118 (84.3%) cases were under regular follow-up of 2 years and weretaken for the study.
Screening of sickle cell anemia was initially done by the sickling slide test.Those found positive were subjected to agarose gel Hb electrophoresis in analkaline medium (pH 8.6). Confirmation of sickle cell disease [codon 6(GAG>GTG) mutation] was done by amplification refractory mutationsystem-polymerase chain reaction (ARMS-PCR) using established protocols(16,17).
Selection Criteria
Sickle cell anemia patients associated with one or more of the followingcomplications were included in the study: a) painful crises (more than threeepisodes in the previous 12 months); b) more than two blood transfusions inthe last 12 months. Painful crisis was defined as an acute painful event thatrequired oral/injectable analgesics and that lasted for at least 4 hours when noother cause could explain the symptom (3,18).
Patients with the following criteria were excluded from the study: a) patientswith other sickle cell syndromes such as Hb S/ β-thalassemia (Hb S-β-thal), HbS/ Hb E [codon 6/codon 26 (GAG>AAG)], Hb S/ Hb C [codon 6/codon 6(GAG>AAG)], Hb S/ Hb D-Punjab [codon 6/codon 121 (GAA>CAA)] andothers; b) children under 3 years and adults above 60 years of age; c) patientswho were a part of special program/trial that may have affected their clinical/hematological status; d) patients who could not be followed-up regularlybecause of the long distance that they would have to travel to and from theirresidence to the hospital, and those who refused to come for regular check-ups; e) patients who had taken HU for less than 80.0% of days, and f) patientswho refused to consent to being part of the study.
A control group of 45 sickle cell anemia cases, matched for age, wereselected, who had more than three vaso-occlusive crises per year and werefollowed every 3 months for 2 years. There were two groups of patients: GroupI (27 pediatric sickle cell anemia cases, 3-14 years old, 18 males and ninefemales) and Group II (91 adult sickle cell anemia cases, 15-45 years old, 64males and 27 females). The mean age of Group I cases was 9.3 � 4.1 years,while for Group II, the mean age was 27.3 � 8.7 years.
The objective of this trial was to assess the efficacy of low dose HU therapyin sickle cell anemia patients. The primary indicator was the reduction infrequency of painful crises (18). The patients who had 50.0% or more reduc-tion in painful crises were designated as responders. The secondary indicatorwas the reduction in blood transfusion requirements. Patients who becamecompletely transfusion independent were also designated as responders. Thestudy was approved by the Institutional Ethical Committee of Veer SurendraSai Medical College, Burla, Orissa, India.
Low Dose HU Therapy for Sickle Cell Anemia Patients 411
Hem
oglo
bin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Inte
rnat
iona
l Cen
tre
for
Gen
etic
s E
ngin
eeri
ng a
nd B
iote
chno
logy
on
01/1
2/14
For
pers
onal
use
onl
y.

Hematological Investigation
At entry, detailed baseline studies were done on all patients. Venous blood(5mL)was collected in EDTAand 3mL in a plain vacutainer for further analysis.A complete blood count was done on an automated hematology analyzer(Sysmex pocH-100i; Sysmex Corporation, Kobe, Japan). Quantitation of variousHbs including Hb F was done by high performance liquid chromatography(HPLC) using the VARIANT™ Hemoglobin Testing System (Bio-RadLaboratories, Hercules, CA, USA) on the principle of cation exchange HPLCaccording to the manufacturer’s guidelines. Biochemical parameters such asserum bilirubin, creatinine, urea, aspartate transaminase (AST) and alaninetransaminase (ALT) were done in a semi autoanalyzer (Erba Chem 7; ErbaDiagnostics Mannheim GmbH, Mannheim, Germany) as per the manufac-turer’s instructions.
Molecular Analysis
DNA extraction was done by QIAamp DNA Blood Midi Kit (Qiagen,Hilden, Germany). XmnI polymorphism and β-globin cluster haplotype analysisfor theHincII ε,HindIII Gγ,HindIII Aγ,HincII ψβ,HincII 30ψβ, AvaII β andHinfI30β polymorphic restriction sites was done as per the established protocol (19).
Follow-Up and Toxicity Monitoring
The patients in both control and HU groups were administered folic acid(5 mg/day) and counseled to increase their fluid intake and avoid extremetemperatures to decrease the risk of vaso-occlusive crises. Patients who suf-fered a vaso-occlusive crisis were offered standard management with analge-sics, fluid (oral or intravenous). The patients were followed-up at the SickleCell Clinic (Veer Surendra Sai Medical College, Burla, Orissa, India) at 3-monthly intervals, or earlier if they developed any health problems warrantingmedical attention. They were provided a health diary for documentation ofany medical problem and treatment received outside. The health diary wasverified at each visit. Patients who did not turn up for the scheduled follow-upwere contacted by a personal visit from one of the staff of the Sickle Cell Clinic.During each visit, patients were evaluated for HU toxicity. Laboratory investi-gations such as absolute neutrophil counts (ANC), platelet counts, Hb, liverfunction test, estimation of urea and creatinine were carried out at each visit.
Myelotoxicity was defined when the ANC was <2500/μL, platelet countwas <80,000/μL or Hb level was lower than 4.5 g/dL. Renal toxicity wasdefined as an increase above the 50.0% baseline value of serum creatinine.Hepatic toxicity was defined as a 2-fold increase of the initial value of ALT(20). If the patients developed any of the above toxicities HU was temporarydiscontinued and was restarted after normalization of the hematological
412 D.K. Patel et al.
Hem
oglo
bin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Inte
rnat
iona
l Cen
tre
for
Gen
etic
s E
ngin
eeri
ng a
nd B
iote
chno
logy
on
01/1
2/14
For
pers
onal
use
onl
y.

parameters. The patients were followed up for 24 months after initiation ofHU therapy.
Statistical Methods
Paired t-test was done for comparing the baseline clinical and hematologicaldata to those after HU therapy. The Mann-Whitney unpaired test was used forcomparing non parametric data. Statistical analysis was done using GraphPadInStat Version 3.00 for Windows.
RESULTS
A total of 118 patients were enrolled in the study. The βS gene was linkedto the Asian haplotype [þþ –þþþþ –] in 89.0% cases of sickle cell anemia.Painful crisis was indication for treatment in 21 (77.7%) and 77 (84.6%) casesin Group I and Group II, respectively, while blood transfusion requirementwas the indication in six (22.2%) and 14 (15.3%) cases in Group I and GroupII, respectively. Painful crisis was themost common indication forHU therapy.
Clinical Response
The frequency of painful crises reduced significantly in both groups. InGroup I and Group II, there were 15/21 (71.5%) and 71/77 (92.2%)responders, respectively (Table 1). At the end of 2 years, the crisis ratesdiffered in the control and HU therapy groups with median rates of 4.8 crisesper year in the control group and 0.5 crises per year in the HU therapy group;an 89.6% difference (p ¼ 0.008) (Table 2). Following HU therapy, 19/20(95.0%) patients became transfusion independent (Table 1).
Hb F Response
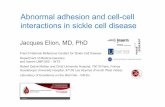
The baseline Hb F levels ranged from 19.0� 6.9% and 18.2� 6.4%, whichincreased to 22.5 � 7.3% and 22.5 � 6.7% following HU therapy in Group Iand Group II, respectively (Table 3). The rise in Hb F concentration was notuniform. The proportionate rise of Hb F varied from case to case, as evidencedby Figure 1. Moreover, on comparison of the Hb F response of the respondersand non responders for painful crisis, it was found that both in Group I andGroup II patients, the rise was insignificant in non responders (Table 4).
Hematological Response
The hematological parameters were compared before and after 24months of commencement of HU therapy. In both the groups, Hb, MCV,
Low Dose HU Therapy for Sickle Cell Anemia Patients 413
Hem
oglo
bin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Inte
rnat
iona
l Cen
tre
for
Gen
etic
s E
ngin
eeri
ng a
nd B
iote
chno
logy
on
01/1
2/14
For
pers
onal
use
onl
y.

MCH and MCHC increased significantly, whereas WBC, platelet and totalserum bilirubin decreased significantly (Table 3).
Toxicity
None of the patients had reduced ANC. Ten (7.5%) cases had transientthrombocytopenia (platelet <80,000/μL) that recovered after temporary dis-continuation of HU. There was no hepatic or renal toxicity. Two cases eachdeveloped pigmentation of skin and nail, and drug rash; HU was temporarilydiscontinued in these patients, and was restarted after normalization of theadverse effect.
TABLE 1 Clinical Response Following Hydroxyurea Therapy
Reduction in Painful Crises (%) Transfusion Independent (%) Total (%)
Group I (n ¼ 27)responders 15/21 (71.5) 6/6 (100.0) 21/27 (77.8)non responders 6/21 (28.5) 0/6 (0.0) 6/27 (22.2)
Group II (n ¼ 91)responders 71/77 (92.2) 13/14 (92.8) 84/91 (92.3)non responders 6/77 (7.8) 1/14 (7.2) 7/91 (7.3)
Total (n ¼ 118)responders 86/98 (87.2) 19/20 (95.0) 110/118 (90.2)non responders 12/98 (12.2) 1/20 (5.0) 13/118 (9.8)
Group I: pediatric sickle cell anemia cases (under 14 years of age); Group II: adult sickle cell anemia cases(over 14 years of age).
Responders (painful crises): sickle cell anemia cases who had 50.0% or more reduction in painful crisesfollowing HU therapy; non responders (painful crises): sickle cell anemia cases who did not have 50.0% ormore reduction in painful crises following HU therapy.
Responders (blood transfusion requirement): sickle cell anemia cases who became completely transfu-sion independent after HU therapy; non responders (blood transfusion requirement): sickle cell anemiacases who did not become completely transfusion independent after HU therapy.
TABLE 2 Annual Rates of Painful Crises in the Control and Hydroxyurea-Treated Groups
Control Group HU Groups
25th percentile 3.1 0.050th percentile 4.8 0.575th percentile 5.6 1.090th percentile 8.5 1.095th percentile 9.4 1.5Median 4.8 0.5
There is a significant reduction (p¼ 0.008 by theMann-Whitney test) in the frequency of painful crises inthe sickle cell anemia cases treated with HU as compared to those sickle cell anemia cases where HUtherapy was not given (control group).
414 D.K. Patel et al.
Hem
oglo
bin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Inte
rnat
iona
l Cen
tre
for
Gen
etic
s E
ngin
eeri
ng a
nd B
iote
chno
logy
on
01/1
2/14
For
pers
onal
use
onl
y.

TABLE3
Hem
atolog
ical
Respo
nse
Follo
wingHydroxyurea
Therap
y
Group
I(n
¼27
)Group
II(n
¼91
)Con
trols(n
¼45
)
Indices
Pre
Post
pValue
Pre
Post
pValue
Pre
Post
pValue
HbF(%
)19
.0�
6.9
22.5
�7.3
<0.00
0118
.2�
6.4
22.5
�6.7
<0.00
0119
.3�
6.0
19.7
�5.7
0.10
HbS(%
)73
.2�
8.7
69.0
�8.0
<0.00
0174
.1�
7.3
69.5
�7.2
<0.00
0174
.8�
5.9
74.8
�4.0
0.13
WBC(103/μ
L)
10.0
�2.9
7.0�
1.5
<0.00
0111
.3�
6.8
7.9�
3.0
<0.00
0111
.1�
10.9
8.2�
1.6
0.08
Hb(g/d
L)
8.0�
1.6
9.1�
1.2
0.00
708.6�
1.8
10.1
�1.6
<0.00
019.0�
2.2
9.3�
2.0
0.31
MCV(fL)
80.7
�8.7
85.4
�8.8
<0.00
0180
.7�
7.3
86.1
�7.9
<0.00
0178
.8�
10.5
77.8
�9.5
0.78
MCH
(pg)
26.1
�3.8
29.2
�3.6
<0.00
0126
.4�
3.8
28.4
�4.0
<0.00
0125
.7�
4.0
26.1
�3.9
0.70
MCHC(g/d
L)
32.0
�3.8
34.1
�2.7
0.01
0031
.9�
3.6
33.7
�3.0
<0.00
0132
.7�
3.6
33.5
�2.4
0.60
Platelets(105/μ
L)
2.4�
1.1
2.2�
1.1
<0.00
012.7�
1.3
2.3�
1.2
<0.00
011.9�
0.8
2.1�
0.4
0.50
Bilirubin(m
g/dL
)2.8�
1.7
2.1�
1.5
0.00
603.1�
2.6
1.8�
1.4
<0.00
012.1�
5.9
1.5�
2.6
0.50
WBC:w
hite
bloo
dcells;M
CV:m
eanco
rpuscu
larvolume;
MCH:m
eanco
rpuscu
larHb;
MCHC:m
eanco
rpuscu
larHbco
ncentration.
Group
I:pe
diatricsicklecellan
emiacases(
unde
r14
yearso
fage
);Group
II:adu
ltsicklecellan
emiacases(
over
14yearso
fage
);co
ntrols:sicklecellan
emiacases
whereHU
therap
ywas
not
given.
Preindices:values
before
startin
gHU
therap
y;po
stindices:values
after2yearsof
HU
therap
y.pValue
swerecalculated
bypa
ired
t-testinprean
dpo
stindices.
Hem
oglo
bin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Inte
rnat
iona
l Cen
tre
for
Gen
etic
s E
ngin
eeri
ng a
nd B
iote
chno
logy
on
01/1
2/14
For
pers
onal
use
onl
y.

DISCUSSION
This study was designed tomeasure the clinical efficacy and hematologicalresponse in sickle cell anemia patients treated with minimal doses of HU (10mg/kg/day). At this dose, there was significant decrease in the frequency ofpainful crises in both the pediatric and adult groups. Moreover, there was asignificant rise of Hb F level in both groups. The baseline value of 19.0 and18.2% in pediatric and adult sickle cell anemia patients increased to 22.5 and
A. B.
C.
FIGURE 1 Hb F levels before and after 2 years of HU therapy. Hb F levels in individual cases plotted beforestarting HU therapy and 2 years after HU therapy in the three groups. (A) Group I: pediatric patients (n ¼27); (B) Group II: adult patients (n ¼ 91) and (C) controls (n ¼ 45).
416 D.K. Patel et al.
Hem
oglo
bin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Inte
rnat
iona
l Cen
tre
for
Gen
etic
s E
ngin
eeri
ng a
nd B
iote
chno
logy
on
01/1
2/14
For
pers
onal
use
onl
y.

22.5%, respectively. Similar findings were reported in a recent study fromwestern India, where HU at the dose of 15 mg/kg/day was effective in themajority of sickle cell anemia patients (21).
Various trials with HU have aimed at increasing the Hb F level to approxi-mately 20.0%, a common therapeutic goal and threshold level suggested toprovide clinical benefits (24). In most US studies, this degree of rise of Hb Flevel has been achieved with MTD of HU, which is 30 to 35 mg/kg/day inadults and 25.4 � 5.4 mg/kg/day in the pediatric population (2–4,6,22). Inthe present study, the threshold level of 20.0% could be achieved with a lowerdose of HU, probably because of the fact that in our patients, the βS mutationis linked to the Asian haplotype in the majority of cases, and the baseline Hb Flevel was high both in pediatric and adult patients. In the American patients,the baseline Hb F level is low (5.0-5.2%), which necessitates dose escalation toMTD to achieve similar results (3). We did not escalate the dose of HU in anattempt to achieve myelosuppression as a treatment goal, as the majority ofour patients (90.2%) had a significant improvement in clinical parameterswith a dose of 10 mg/kg/day.
Several studies have attributed the beneficial effect of HU to increasedHbF concentration in responding patients (23). Additional effects of this druginclude reduction in the count of white cells and platelets, potentiallyreducing their roles in vascular injury, improving red cell hydration anddecreased red cell adhesiveness to the endothelium (24–27). However, datafrom a recent study in murine model of sickle cell anemia suggests thatinduction of Hb F is the essential mechanism for its clinical benefits (23). Inthe present study, we found that the Hb F increased significantly in respon-ders, whereas in non responders, the rise was insignificant.
TABLE 4 Level of Hb F in Responders and Non Responders for Painful Crises
Pre HU Hb F Post HU Hb F p Value
Group Iresponders (n ¼ 15) 20.6 � 7.8 23.9 � 8.7 0.0006non responders (n ¼ 6) 17.9 � 3.9 21.6 � 3.0 0.05
Group IIresponders (n ¼ 71) 18.0 � 6.4 22.5 � 6.8 <0.0001non responders (n ¼ 6) 18.6 � 4.6 19.9 � 5.5 0.23
Group I: pediatric sickle cell anemia cases (under 14 years of age); Group II: adult sickle cell anemia cases(over 14 years of age).
PreHUHb F:Hb F level before startingHU therapy; postHUHb F:Hb F level after 2 years of HU therapy.p Values were calculated by paired t-test in pre and post indices; responders (painful crises): sickle cell
anemia cases who had 50.0% or more reduction in painful crises following HU therapy; non responders(painful crises): sickle cell anemia cases who did not have 50.0% or more reduction in painful crisesfollowing HU therapy.
Low Dose HU Therapy for Sickle Cell Anemia Patients 417
Hem
oglo
bin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Inte
rnat
iona
l Cen
tre
for
Gen
etic
s E
ngin
eeri
ng a
nd B
iote
chno
logy
on
01/1
2/14
For
pers
onal
use
onl
y.

Blood transfusion requirement was the indication for HU therapy in16.0% of sickle cell anemia cases (Groups I and II). Following treatment,there was a significant rise in total Hb level and the patients became transfu-sion independent. The MCV and MCH increased significantly, whereas thetotal leucocyte count also decreased significantly in the adult sickle cellanemia cases. Similar findings were reported in a Brazilian study where HUwas used at the dose of 15 mg/kg/day (28).
The primary short term toxicity observed in our patients was mild bonemarrow suppression in 7.5% of cases that recovered following temporarydiscontinuation of HU. Other toxicities were rare. This is not surprising,considering the very low dose of HU administered to these patients. In tworecent studies, Berthaut et al. (13) and Lima et al. (29) reported that sicklecell anemia induced hypogonadism was exacerbated by a clinically relevantdose of HU (20–30 mg/kg/day), which was confirmed in an experimentalmodel of adult male transgenic sickle mice. Similarly, sickle cell anemiapatients who received HU at a mean dose of >20 mg/kg/day or received itfor more than 42 months, showed significantly more DNA damage thanthose who received it in lower doses or a shorter period of time (11). Arecent study in a Yemeni sickle cell anemia population (30) demonstrated anincrease in Hb and Hb F levels with low dose of HU (500 mg/day). However,the authors did not attempt to correlate the outcome of the treatment on theclinical presentation of the disease (30). The above findings justify the use ofHU in low doses in view of its clinical efficacy and reduction in mutagenicpotential. Moreover, this low dose HU is less likely to exacerbate hypogonad-ism in sickle cell anemia cases.
CONCLUSIONS
To the best of our knowledge, this is the first study of HU therapy provided ata minimal dose of 10 mg/kg/day dependent on the clinical and hematologicalparameters. With this dose, most of the patients showed an impressiveimprovement in clinical and hematological parameters. In addition to this,most of the patients achieved the threshold level of Hb F (20.0%), suggestedto provide the most clinical benefit. In view of this, MTD was not attempted inthese cases. There was no significant short term toxicity. In resource poorcountries like India, low dose HU therapy provides a suitable therapeuticoption for a vast number of untreated sickle cell anemia patients. In view ofthe recent reports of mutagenicity and deleterious effect on spermatogenesis,even with a clinically relevant dose of 20 mg/kg/day, it would be prudent tohave long term trials of low dose of HU therapy in a larger number of patients,to ascertain its efficacy and toxicity.
418 D.K. Patel et al.
Hem
oglo
bin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Inte
rnat
iona
l Cen
tre
for
Gen
etic
s E
ngin
eeri
ng a
nd B
iote
chno
logy
on
01/1
2/14
For
pers
onal
use
onl
y.

Declaration of Interest: This study was supported by the Department ofBiotechnology, Government of India, New Delhi; Indian Council for MedicalResearch (ICMR), New Delhi, India; Department of Science & Technology,New Delhi and National Rural Health Mission (NRHM), Orissa, India. Theauthors report no conflicts of interest. The authors alone are responsible for thecontent and writing of this article.
REFERENCES
1. Lanzkron S, Strouse JJ, Wilson R, et al. Systematic review: hydroxyurea for the treatment of adults withsickle cell disease. Ann Intern Med. 2008;148(12):939–955.
2. Charache S, Dover GJ, Moore RD, et al. Hydroxyurea: effects on Hemoglobin F production in patientswith sickle cell anemia. Blood. 1992; 79(10):2555–2565.
3. Charache S, Terrin ML, Moore RD, et al. Effect of hydroxyurea on the frequency of painful crises insickle cell anemia. N Engl J Med. 1995;332(20):1317–1322.
4. Kinney TR, Helms RW, O’Branski EE, et al. Safety of hydroxyurea in children with sickle cell anemia:results of the HUG-KIDS study, a phase I/II trial. Pediatric Hydroxyurea Group. Blood. 1999;94(5):1550–1554.
5. Ware RE, Aygun B. Advances in the use of hydroxyurea. Hematology Am Soc Hematol Educ Program.2009:62–69.
6. Zimmerman SA, Schultz WH, Davis JS, et al. Sustained long-term hematologic efficacy of hydroxyureaat maximum tolerated dose in children with sickle cell disease. Blood. 2004;103(6):2039–2045.
7. Ferster A, Vermylen C, Cornu G, et al. Hydroxyurea for treatment of severe sickle cell anemia: apediatric clinical trial. Blood. 1996;88(6):1960–1964.
8. Ferster A, Tariri P, Vermylen C, et al. Five years of experience with hydroxyurea in children and youngadults with sickle cell disease. Blood. 2001;97(11):3628–3632.
9. Maier-Redelsperger M, de Montalembert M, Flahault A, et al. Fetal hemoglobin and F-cell responses tolong-term hydroxyurea treatment in young sickle cell patients. The French Study Group on Sickle CellDisease. Blood. 1998;91(12):4472–4479.
10. Ware RE. Summary of the evidence regarding efficacy of hydroxyurea treatment for sickle cell diseasein children and adolescents. Proceedings of the Hydroxyurea Treatment for Sickle Cell Disease, AnNIH Consensus Development Conference, held at the William H. Natcher Conference Center,National Institutes of Health, Bethesda, MD, USA on February 25-27 2008. 2008:29–32.
11. Friedrisch JR, Prá D, Maluf SW, et al. DNA damage in blood leukocytes of individuals with sickle celldisease treated with hydroxyurea. Mutat Res. 2008;649(1–2):213–220.
12. Grigg A. Effect of hydroxyurea on sperm count, motility and morphology in adult men with sickle cellor myeloproliferative disease. Intern Med J. 2007;37(3):190–192.
13. Berthaut I, Guignedoux G, Kirsch-Noir F, et al. Influence of sickle cell disease and treatment withhydroxyurea on sperm parameters and fertility of human males. Hematologica. 2008;93(7):988–993.
14. Kar BC. Sickle cell disease in India. J Assoc Phys India. 1991;39(12):954–96015. Mashon RS, Dash PM, Khalko J, et al. Higher fetal hemoglobin concentration in patients with sickle cell
disease in eastern India reduces frequency of painful crisis. Eur J Haematol. 2009;83(4):383–384.16. Wu DY, Ugozzoli L, Pal BK, Wallace RB. Allele-specific enzymatic amplification of β-globin genomic
DNA for diagnosis of sickle cell anemia. Proc Natl Acad Sci USA. 1989;86(8):2757–2760.17. Old JM, Varawalla NY,Weatherall DJ. Rapid detection and prenatal diagnosis of β-thalassaemia: studies
in Indian and Cypriot populations in the UK. Lancet. 1990;33(8719):834–837.18. Charache S, Terrin ML, Moore RD, et al. Design of the multicenter study of hydroxyurea in
sickle cell anemia. Investigators of the Multicenter Study of Hydroxyurea. Control Clin Trials.1995;16(6):432–446.
19. Mukherjee MB, Surve RR, Gangakhedkar RR, Ghosh K, Colah RB, Mohanty D. β-Globin gene clusterhaplotypes linked to the βS gene in western India. Hemoglobin. 2004;28(2):157–161.
Low Dose HU Therapy for Sickle Cell Anemia Patients 419
Hem
oglo
bin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Inte
rnat
iona
l Cen
tre
for
Gen
etic
s E
ngin
eeri
ng a
nd B
iote
chno
logy
on
01/1
2/14
For
pers
onal
use
onl
y.

20. Braga LB, Ferreira AC, Guimarães M, et al. Clinical and laboratory effects of hydroxyurea inchildren and adolescents with sickle cell anemia: a Portuguese hospital study. Hemoglobin.2005;29(3):171–180.
21. Italia K, Jain D, Gattani S, et al. Hydroxyurea in sickle cell disease—a study of clinico-pharmacologicalefficacy in the Indian haplotype. Blood Cells Mol Dis. 2009;42(1):25–31.
22. Noguchi CT, Rodgers GP, Serjeant GR, Schechter AN. Levels of fetal hemoglobin necessary fortreatment of sickle cell disease. N Engl J Med. 1988;318(2):96–99.
23. Ware RE, Eggleston B, Redding-Lallinger R, et al. Predictors of fetal hemoglobin response in childrenwith sickle cell anemia receiving hydroxyurea therapy. Blood. 2002;99(1):10–14.
24. Lebensburger JD, Pestina TI, Ware RE, Boyd KL, Persons DA. Hydroxyurea therapy requires Hb Finduction for clinical benefit in a sickle cell mouse model. Haematologica. 2010;95(9):1599–1603.
25. Platt OS. Hydroxyurea for the treatment of sickle cell anaemia. N Eng J Med. 2008;358(13):1362–1369.26. Orringer EP, Blythe DS, Johnson AE, Phillips G Jr, Dover GJ, Parker JC. Effects of hydroxyurea on
Hemoglobin F and water content in the red blood cells of dogs and of patients with sickle cell anaemia.Blood. 1991;78(1):212–216.
27. Hillery CA, Du MC, Wang WC, Scott JP. Hydroxyurea therapy decreases the in vitro adhesion of sickleerythrocytes to thrombospondin and laminin. Br J Haematol. 2000;109(2):322–327.
28. Wiles N,Howard J. Role of hydroxycarbamide in prevention of complications in patients with sickle celldisease. Ther Clin Risk Manag. 2009;5:745–755.
29. Lima CS, Arruda VR, Costa FF, Saad ST. Minimal doses of hydroxyurea for sickle cell disease.Braz J Med Biol Res. 1997; 30(8):933–940.
30. Al-NoodHA, Al-Khawlani MM, Al-Akwa A. Fetal hemoglobin response to hydroxyurea in Yemeni sicklecell disease patients. Hemoglobin. 2011;35(1):13–21.
420 D.K. Patel et al.
Hem
oglo
bin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Inte
rnat
iona
l Cen
tre
for
Gen
etic
s E
ngin
eeri
ng a
nd B
iote
chno
logy
on
01/1
2/14
For
pers
onal
use
onl
y.