Local cerebral blood volume response to carbon dioxide in man
9
JH Greenberg, A Alavi, M Reivich, D Kuhl and B Uzzell Local cerebral blood volume response to carbon dioxide in man 1524-4571 Copyright © 1978 American Heart Association. All rights reserved. Print ISSN: 0009-7330. Online ISSN: TX 72514 Circulation Research is published by the American Heart Association. 7272 Greenville Avenue, Dallas, 1978, 43:324-331 Circulation Research http://circres.ahajournals.org/content/43/2/324 located on the World Wide Web at: The online version of this article, along with updated information and services, is http://www.lww.com/reprints Reprints: Information about reprints can be found online at [email protected] 410-528-8550. E-mail: Kluwer Health, 351 West Camden Street, Baltimore, MD 21202-2436. Phone: 410-528-4050. Fax: Permissions: Permissions & Rights Desk, Lippincott Williams & Wilkins, a division of Wolters http://circres.ahajournals.org//subscriptions/ Subscriptions: Information about subscribing to Circulation Research is online at at VA MED CTR BOISE on July 9, 2011 http://circres.ahajournals.org/ Downloaded from
Transcript of Local cerebral blood volume response to carbon dioxide in man

JH Greenberg, A Alavi, M Reivich, D Kuhl and B UzzellLocal cerebral blood volume response to carbon dioxide in man
1524-4571 Copyright © 1978 American Heart Association. All rights reserved. Print ISSN: 0009-7330. Online ISSN:
TX 72514Circulation Research is published by the American Heart Association. 7272 Greenville Avenue, Dallas,
1978, 43:324-331Circulation Research
http://circres.ahajournals.org/content/43/2/324located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://www.lww.com/reprintsReprints: Information about reprints can be found online at [email protected]. E-mail: Kluwer Health, 351 West Camden Street, Baltimore, MD 21202-2436. Phone: 410-528-4050. Fax: Permissions: Permissions & Rights Desk, Lippincott Williams & Wilkins, a division of Wolters http://circres.ahajournals.org//subscriptions/Subscriptions: Information about subscribing to Circulation Research is online at
at VA MED CTR BOISE on July 9, 2011http://circres.ahajournals.org/Downloaded from

324
Local Cerebral Blood Volume Response toCarbon Dioxide in Man
JOEL H. GREENBERG, ABASS ALAVI, MARTIN REIVICH, DAVID KUHL,
AND BARBARA UZZELL
SUMMARY We used an emission tomographic brain scanner to investigate the relationship betweenlocal cerebral blood volume (LCBV) and arterial blood carbon dioxide tension (Pacoj) in normal awakeman. Measurements were made separately in three dimensions in various regions of grey and whitematter, and the resting LCBV as well as the difference in sensitivity among these regions werecompared. Over the range of PacO2 studied (20-42 torr), the response of both the grey matter and thewhite matter to carbon dioxide was linear. The LCBV sensitivity of the grey matter to changes in Paco2was 0.053 ml/100 g per torr Paco2 and in the white matter this sensitivity was 0.046 ml/100 g per torrPaco2. These sensitivities were found not to be significantly different, yielding a slope of 0.049 ml/100g per torr PacO2 for the LCBV-PacO2 curve for the entire brain. This is in excellent agreement with theother data for the whole brain. The resting cerebral blood volume of the grey matter at a Paco2 of 34.4torr, which was the average resting arterial carbon dioxide tension of the subjects, was 5.0 ml/100 gand was significantly higher than for white matter, which was 3.6 ml/100 g. At the local level, thecerebral blood volume of the frontal cortex is significantly less than that of the thalamus, whereas thefrontoparietal cortex in the region of the sylvian fissure has a local cerebral blood volume significantlygreater than that of the thalamus.
CEREBRAL blood volume (CBV) has been used as ameasure of cerebral hemodynamics in the study of thecerebral vasculature. Due to the difficulty in measuringcerebral blood volume experimentally, there is not a greatamount of data examining its relationship to alterationsin the physiological state. In particular, the correlationbetween cerebral blood volume and arterial carbon diox-ide tension (Paco2) lacks extensive documentation. Smithet al.1 calculated CBV from measurements of cerebralblood flow and mean cerebral transit time. These mea-surements were of global CBV only. To obtain regionalor local cerebral blood volume (LCBV), Ter-Pogossian etal.2 and Phelps et al.3 used an x-ray fluorescence techniqueto examine the local cerebral blood volume response toalterations in arterial carbon dioxide tension in rhesusmonkeys. This method, however, allows measurement ofLCBV in only one region of the brain at any one time.
To circumvent this problem, Kuhl et al.4 developed atechnique using emission tomography and "re-labeledred blood cells that is capable of measuring LCBV simul-taneously in multiple regions of the brain with a resolu-tion of 1.7 cm. An entire transverse section scan can bemade in less than 5 minutes. With this technique, LCBVresponse to alterations in Paco2 was obtained in a series
From the Cerebrovascular Research Center, Department of Neurology,and the Division of Nuclear Medicine, Department of Radiology, Hospitalof the University of Pennsylvania, Philadelphia, Pennsylvania.
This work was supported in part by U.S. Public Health Service GrantNS10939-05, NIGMS Grant GM16248, and ERDA Contract (#11-0-3399.
Dr. Kuhl's present address is: Division of Nuclear Medicine, UCLASchool of Medicine, Los Angeles, California.
Address for reprints: Dr. Joel Greenberg, Cerebrovascular ResearchCenter, 428 Piersol Building, Hospital of the University of Pennsylvania,3600 Spruce Street, Philadelphia, Pennsylvania 19104.
Received August 8, 1977; accepted April 13, 1978.
of baboons. We have employed this emission tomographicmethod to measure the LCBV response to carbon dioxidein a series of normal human volunteers.
MethodsTen male volunteers (18-22 years) were studied. Insti-
tutional and HEW resolutions for the protection of hu-man subjects were observed. With the subject lying com-fortably on the scan table, a short catheter was insertedin the left (for right-handed subjects) brachial artery afterpretreatment of the injection site with a local anesthetic.This catheter was joined through an Intraflo (SorensonResearch Co.) continuous flush system to a pressurizedsaline bag containing 1 U of heparin/ml which allowed aslow (3 ml/hour) flow through the catheter to preventclotting. Also attached to the Intraflo was a Stathamblood pressurre transducer. After catheterization, thesubject's head was placed in a foam cast that previouslyhad been fabricated individually to fit the subject snuglyand prevent head motion. This cast then was placed intothe center of the detector assembly of the Mark IVscanner which was used to obtain the transverse sectionscan.s The litter on which the subject was resting was onrollers and could be moved relative to the scanner detec-tors. This allowed the desired position to be obtainedwith reference to the orbital-meatal line.
After head positioning, the subject's nose was clampedwith a respiratory nose clamp and a mouthpiece (Collins)inserted in his mouth. This mouthpiece was connected toa two-way respiratory valve the input of which was joinedto an air bag. The air bag could be filled with the desiredgas mixture from prepared, premixed gas cylinders. Thesubject's tidal carbon dioxide concentration was moni-tored with an infrared CO2 analyzer (Beckman Instru-
at VA MED CTR BOISE on July 9, 2011http://circres.ahajournals.org/Downloaded from

CEREBRAL BLOOD VOLUME AND CARBON DIOXIDE/Greenberg et al. 325
ments—LB2) and recorded, along with blood pressure, ona Hewlett-Packard polygraph.
With the subject comfortable, 20 mCi of """Tc-labeledred blood cells were injected into the subject's arm vein.This tracer was produced by drawing 10 ml of venousblood from the subject approximately 1 hour previous tothis time and labeling the red blood cells with "mTc.4
Protocol
Approximately 15 minutes after the injection of "mTc-labeled red blood cells, the study began. Two separateprotocols were used, with five subjects included in each.In protocol A, the first two scans were obtained with thesubject breathing room air. These two scans were madeas close together as was possible (usually less than 1minute elapsed between the end of the first scan and thebeginning of the second scan). Following the second scan,the inhalation mixture was switched from room air to amixture of 3% CO2 and 21% O2, with the balance N2; thesubject breathed this gas mixture for 10 minutes. Thenthe third scan was obtained. The inspired gas then waschanged to 5% CO2, 21%, O2 with the balance N2. Thesubject breathed this for 10 minutes preceding the nextscan (scan number 4). At this point the respiratory tubingwas disconnected from the valve at the subject's mouth-piece and he was instructed to hyperventilate to bring hisend-tidal carbon dioxide concentration (ETCO2) down tobetween 3.0% and 3.2%. This end-tidal CO2 concentrationwas displayed on a large analog meter placed above thescanner in clear view of the subject. With the aid of visualfeedback from this meter, the subject was instructed tokeep his end-tidal CO2 concentration steady at this leveluntil after the next scan. The subject hyperventilated for10 minutes and then brain scan number 5 was obtained.Following this scan, the subject was instructed to breathenormally, and brain scan number 6 was obtained after hisend-tidal CO2 concentration had been stable for 10 min-utes at a value close to that of the first two (room air)scans.
Protocol B was identical to protocol A except that theorder of CO2 administration and hyperventilation wasreversed. Thus the scan sequence was: scan numbers 1and 2, room air; scan number 3, hyperventilation to3.0-3.2% ETCO2; scan number 4, 3% CO2; scan number 5,5% CO2; scan number 6, room air breathing.
Throughout each scan a number of blood samples weredrawn from the indwelling arterial catheter. At the begin-ning of the scan, 7-8 ml of blood were drawn for analysisof "mTc activity in the blood at scan time. This wasfollowed immediately by two 1-ml blood samples foranalysis of Pco2, Po2, and pH. Toward the end of thescan, two additional blood samples were taken for Pco2,Po2, and pH determination, the mean of the four samplesdetermining the blood gas status of the subject during theparticular scan. Blood gas was analyzed with appropriateelectrodes at 37°C, corrections being made for glycolysisduring the time between obtaining the blood sample andperforming the analysis.6
LCBV was calculated by the methods outlined previ-ously.4 All scans were obtained approximately 5 cm abovethe orbital-meatal line. A scan was comprised of five
revolutions of the detector assembly around the subject'shead for a total scan time of 250 seconds. This producedapproximately 750,000 total counts in a picture, and thishas been shown by Kuhl et al.5 to be necessary for astatistically satisfactory scan. The subject was instructedto keep his head still throughout the entire procedure,which lasted about 90 minutes. The volumes of tissueexamined (both grey and white matter) were consideredlarge enough for the hematocrit to be assumed equal tothe average hematocrit for the whole brain (0.85 X pe-ripheral venous hematocrit.
Data Analysis
The output of each scan was a 64 X 64 matrix array ofthe reconstructed counts.5 For ease of analysis, this wasreduced to a 32 X 32 array which also was output on acomputer display oscilloscope as a local cerebral bloodvolume picture. Regions of interest in this picture wereidentified on a neuroanatomic basis, and the correspond-ing local cerebral blood volume was obtained from the 32X 32 array by multiplying the counts in the region byappropriate scale factors representing, among other fac-tors, radioactive decay (from the time of isotope injec-tion). These cerebral regions were identified neuroana-tomically, and efforts were made to analyze the samestructures in all the subjects.
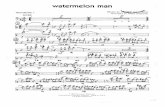
Three grey matter areas were selected for analysis.They were the thalamus, the frontal cortex, and theinsular cortex in the region of the sylvian fissure. Thewhite matter areas examined were the frontal white,internal capsule, and occipital white. In Figure 1, a typicalreconstructed scan and the areas of interest are shown.The local blood volume of each area was obtained byaveraging the counts in at least 20 picture elements for atotal cross-sectional area of approximately 3.2 cm2. Thesemeasurements usually were obtained in both hemispheresso that the regional cerebral blood volume of each regionwas based on a cross-sectional area of at least 6.4 cm2.For a given cerebral region, only the most central pels inthat region were used, to minimize possible contaminationof adjacent tissues. Thus the blood volume of the thala-mus was obtained using pels only in the central region ofthe thalamus to minimize contamination by the surround-ing white matter. For analysis of some of the data, all ofthe grey matter structures examined were averaged to-gether and taken to be representative of the cerebral greymatter; the white matter structures were averaged andtaken as representative of cerebral white matter.
ResultsIn all of the subjects, inhalation of carbon dioxide
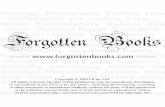
caused an increase in cerebral blood volume and moder-ate hyperventilation caused a decrease in cerebral bloodvolume from the normal levels. This can be seen in Figure2, where cerebral blood volumes of both the grey and thewhite matter are plotted as a function of arterial carbondioxide tension for each subject. Although these data doexhibit some scatter, especially in the absolute value ofblood volume between subjects at a given arterial carbondioxide tension, the response to CO2 of the individualsubjects is very consistent. The LCBV response to CO2
at VA MED CTR BOISE on July 9, 2011http://circres.ahajournals.org/Downloaded from

326 CIRCULATION RESEARCH VOL. 43, No. 2, AUGUST 1978
FRONTAL FRONTAL INSULARWHITE CORTEX CORTEX
THALAMUS OCCIPITAL FftRIETALWHITE WHITE
FIGURE 1 Section scan of subject 9 at a normal arterial carbondioxide tension. The outlines of the six areas of interest areshown indicating the minimal size of tissue comprising thelocal blood volume measurement. When possible, the valuesfrom both hemispheres were used to increase the tissue volumecontributing to the blood volume determination. The size of theparticular region was chosen individually for each subject andarea to be as large as possible and still be within the homoge-neous section of the structure.
appears linear; a polynomial regression of degree higherthan first order is not a statistically significant improve-ment as a representation of these data. The linear regres-sion parameters are tabulated for each subject in Table1.
Five of the subjects were asked to hyperventilate priorto the CO2 administration (protocol B) and the other fivesubjects hyperventilated after CO2 administration (pro-tocol A). These are indicated in Table 1. To see if theorder of study influenced the results, both the slope andthe constant of the linear regression were examined forstatistical differences between the two groups using apaired "t" parameter. No significant difference in thesensitivity of cerebral blood volume to alterations incarbon dioxide was found. This indicates that all 10subjects could be examined together without regard forthe order of study.
To examine more clearly the sensitivity of cerebral
6/5- -
£ 6 0--
15 5--
§ 50--
4 5--
4.0- -
3 5--
20 25 30 35PoCO2 (torr)
40 45
4-Sr
3 5
O2 30
2 0 20 25 30 35PoCO2 (torr)
40 45
FIGURE 2 Local cerebral blood volume (LCB V) response of allsubjects to carbon dioxide inhalation and hyperventilation.The individual data points for each subject are joined forclarity. Grey matter (A) and white matter (B) are shown sepa-rately.
blood volume to changes in arterial carbon dioxide ten-sion, the data were normalized around a control carbondioxide tension. This control Pco2 (34.4 torr) was ob-tained by averaging all the subjects' arterial carbon diox-ide tensions for the first two scans when the subject wasbreathing only room air. With the regression equation foreach individual subject, a local cerebral blood volume wasobtained at this control Paco2. The local cerebral bloodvolumes measured in each subject were divided by thisbaseline control blood volume to compute a normalizedlocal cerebral blood volume. This procedure removes thebaseline blood volume differences that were present
at VA MED CTR BOISE on July 9, 2011http://circres.ahajournals.org/Downloaded from

CEREBRAL BLOOD VOLUME AND CARBON DIOXIDE/Greenberg et al. 327
TABLE 1 Regression of LCBVwith Paco2 I 2-r
Subject
1*2*3t4t5*
6t7*
8t9t
10*
MeanSE
a
0.0310.0730.0720.0550.0440.0530.0830.0330.0410.042
0.0530.0056
Grey matter
b
3.363.082.454.202.612.612.164.473.573.53
3.190.24
LCBV
4.445.604.916.104.154.425.005.604.974.97
5.020.192
Wh
a
0.0400.0360.0530.0700.0390.0600.0590.0380.0340.035
0.046.004
ite matter
b
2.122.641.380.731.881.081.131.922.432.07
1.760.19
LCBV
3.513.883.413.133.213.153.163.243.603.26
3.550.077
The relationship between local cerebral blood volume (LCBV) andarterial carbon dioxide tension (Paco2) in the range 20-42 torr for eachsubject for both grey and white matter. The coefficients (a, b) of a linearregression (LCBV = aPaco^ •+• b) performed on data of each subject aretabulated along with LCBV obtained from this regresion at Paco2 = 34.4torr which was the average arterial carbon dioxide tension of all subjectsbreathing room air.
* Hyperventilated prior to CO2 administration.f Hyperventilated following CO2 administration.
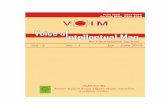
among subjects. The results of this normalization proce-dure are shown in Figure 3.
Heterogeneity of Cerebral Blood Volume
Table 1 summarizes the individual linear regressioncoefficients for each subject describing the relationshipbetween local cerebral blood volume and Paco2 for bothgrey matter and white matter. The average regressionequations are:
LCBV = 0.053 Paco2 + 3.19 (grey matter)LCBV = 0.046 Paco2 + 1.76 (white matter)
where coefficients are the means of the respective slopesand intercepts of the individual subjects. A paired t testusing these individual coefficients does not show anysignificant difference between the slopes of the tworegression equations. Consequently, the sensitivity of lo-cal cerebral blood volume to arterial carbon dioxide al-terations is not different for grey and white matter. Wethus can average them to obtain a mean blood volumesensitivity of cerebral tissue to carbon dioxide of 0.0495ml/100 g per torr PaCO2. The intercepts of the two regres-sion equations are significantly different (P < 0.001),indicating a difference in baseline cerebral blood volumebetween grey matter and white matter. This differencecan be determined more meaningfully by examining thelocal cerebral blood volumes at a typical arterial carbondioxide tension. Cerebral blood volumes at Paco2 = 34.4torr are tabulated in Table 1; the mean cerebral bloodvolume of grey matter (5.02 ml/100 g) is significantlygreater than the mean cerebral blood volume of whitematter (3.55 ml/100 g) (P < 0.001).
The specific areas comprising both grey and whitematter also were analyzed for differences in both baselineblood volumes and blood volume response to carbondioxide. Among the grey matter structures, there were no
i.o- •
i•g 0.9 • -
0 .8 - •
• .
*
*• «*• •
• •
• o
20 25 30 35PQCO2 (torr)
40 45
12 -r
II
I . 0 - -
8
I0.8 --
i
°.• • • J >
30 36PoC02 (torr)
40 45
FIGUKE 3 Normalized local cerebral blood volume (LCBV)response to carbon dioxide and hyperventilation. The datahave been normalized by setting the local cerebral blood volumeof each subject at an arterial blood carbon dioxide tensionlevel of 34.4 torr to unity and scaling all blood volumes accord-ingly (see text). The grey matter (A) and while matter (B) areshown separately.
significant differences in sensitivity to arterial carbondioxide alterations. There were, however, statisticallysignificant differences in the baseline cerebral blood vol-umes of the three areas at a control carbon dioxidetension (Paco2 = 34.4 torr). The local blood volume ofthe frontal cortex (3.93 ml/100 g) is significantly less thanthat of the thalamus (5.00 ml/100 g) (P < 0.01), whereasthe insular cortex has a blood volume (5.86 ml/100 g)significantly higher than that of the thalamus (P < 0.001).The frontal cortex differs from the insular cortex at the
at VA MED CTR BOISE on July 9, 2011http://circres.ahajournals.org/Downloaded from

328 CIRCULATION RESEARCH VOL. 43, No. 2, AUGUST 1978
TABLE 2 Reproducibility of L CB V Determinations
Subject
123456789
10
LCBVscanno. 1
4.335.444.886.294.244.094.475.544.994.93
Grey matter
LCBVscanno. 2
4.405.014.906.584.144.324.665.715.104.94
AdjustedLCBVno. 2
4.445.154.896.564.144.284.635.665.104.95
LCBVscanno. 1
3.393.863.243.063.203.032.903.123.543.31
White matter
LCBVscanno. 2
3.503.733.383.013.143.122.913.023.433.28
AdjustedLCBVno. 2
3.533.853.372.993.143.092.882.983.433.29
Local cerebral blood volumes (LCBV) for grey and white cerebraltissue obtained from the first two section scans when the subject wasbreathing room air. Approximately 1 minute elapsed between the twoscans. The adjusted LCBV was obtained by correcting the LCBV data ofscan no. 2 for the difference in Paco? of the subject between the two scansusing relationships LCBV (grey) = 0.053 Paco2 + 3.19 and LCBV (white)= 0.046 Paco2+ 1.76.
P < 0.001 level. The white matter areas (frontal white,internal capsule, and occipital white) exhibited neitherdifferences of cerebral blood volume sensitivity to CO2
nor differences in baseline (PacO2 = 34.4 torr) local cere-bral blood volume.
Reproducibility of Technique
The protocol for all 10 subjects included two initialsequential section scans while breathing room air. Con-sequently, there was minimal change between the twoscans in arterial carbon dioxide tension, head position aswell as other physiological parameters. These back-to-back scans yield data on the reproducibility of the entiretomographic scanning technique for measuring local cer-ebral blood volume in man. Those data are shown inTable 2. The coefficient of variation of LCBV in this test-retest situation was 4.3% for grey matter and 3.0% forwhite matter. If the blood volumes obtained from thesecond scan are corrected for slight changes in the arterialcarbon dioxide tension that occurred between the twoscans, the coefficients of variation become 3.4% and 2.9%for grey and white matter, respectively.
Discussion
There is a variety of methods for cerebral blood volumemeasurement. One technique involves injecting 131I-la-beled serum albumin (RISA) into the blood.7 Approxi-mately 1 hour later a blood sample is drawn, the animalkilled, the brain frozen, and a representative brain tissuesample obtained. The ratio of the counts per minute perunit volume in the brain sample and the blood sampleyields the blood volume. A similar technique uses 51Cr-labeled red blood cells as the tracer. Sklar et al.5 obtaineda cerebral blood volume in cats of 2.7 ml/100 g usingRISA and 1.9 ml/100 g using 5ICr-labeled red blood cells.These values are significantly lower than those reportedby Weil et al.8 who measured the brain content of silverfollowing an intravenous injection of a hypertonic solu-tion (collargol) in dogs. Their value of 8.3 ml/100 g differsfrom that of Sklar et al.,7 probably because of differences
in methodology and species. These techniques, however,do not lend themselves to measurements in man, nor canrepeat volume determinations be made.
The red cell-labeling technique was modified for use inman9 by estimating the concentration difference of 32P-labeled erythrocytes across the brain from samples ofcarotid arterial and jugular venous blood following anintravenous injection of the tracer. This technique mea-sures total brain blood volume. Assuming the brainweight to be approximately 1400 g, the cerebral bloodvolume obtained was 7.0 ml/100 g.
Risberg et al.10 modified the RISA method of bloodvolume determination to measure regional cerebral bloodvolume using external scintillation detectors. An intervalof approximately 80 minutes was allowed for equilibrationfollowing an intravenous injection of 1-2 mCi of I31I-labeled serum albumin in cats. Knowledge of the volumeseen by each probe as well as the arterial blood RISAactivity allows calculation of regional cerebral blood vol-ume. When the brain was removed with minimal bloodloss, the extracerebral background blood pool was foundto comprise approximately 30% of the measured bloodvolume. Absolute values of blood volume are not re-ported. This technique is an improvement over the invitro methods in that it can be used in man, but suffersfrom the limitation of not being totally regional. Addi-tionally, the cerebral blood volume measurement is con-taminated by extracerebral contributions. Similarly, Mat-thew et al.11 calculated cerebral blood volume in manfrom cerebral blood flow measured by the intracarotid133Xe injection technique and from the mean cerebraltransit time using """Tc pertechnitate. These measure-ments were made with a gamma camera and so region-ality was obtained.
In order to obtain three-dimensional resolution of cer-ebral blood volume in man, Ter-Pogossian et al.,2 Phelpset al.3 and Grubb et al.12 developed a technique wherebythe characteristic x-ray fluorescence of iodine from aninjected contrast material is excited with a narrow (1 cmin diameter) x-ray beam. The resulting fluorescence isdetected with a collimated radiation spectrometer. Theintensity of the signal is proportional to the amount oflabel in the region of study. By placing a sample of thesubject's blood in a phantom, this instrument can becalibrated and an absolute value of local cerebral bloodvolume calculated. Using this technique, these investiga-tors obtained a value for local cerebral blood volume inman of 3.2 ml/100 g tissue.12 Their reported values forthe dog and monkey2 are slightly higher. The majordisadvantage of this technique is that cerebral bloodvolume can be measured only in one region of the brainat a time. Furthermore, since the contrast agent does notstay in the intravascular compartment in certain patho-logical conditions in which there is an altered blood brainbarrier (meningioma, glioblastoma, etc.),13 this techniquewill overestimate local cerebral blood volume in theseareas.
This objection has been circumvented by Kuhl et al.4' u
who developed a method for measuring local cerebralblood volume throughout a brain section with three-di-mensional resolution. They used a transverse section
at VA MED CTR BOISE on July 9, 2011http://circres.ahajournals.org/Downloaded from

CEREBRAL BLOOD VOLUME AND CARBON DIOXIDE/Greenberg et al. 329
scanner (Mark III, the predecessor of the Mark IV usedin this investigation) to measure the local activity of"""To-labeled red blood cells and studied patients as wellas examined the local cerebral blood volume response ofbaboons to carbon dioxide.4
Various attempts have been made to measure cerebralblood volume with a computerized transverse axial scan-ner.15' 16 Such a technique would be advantageous becauseof the excellent resolution (1.5 X 1.5 X 13 mm) of thisinstrument as well as the wide availability of transaxialtomographic scanners. Two separate scans are made ofthe subject's head. The first is a normal scan withoutintroduction of a contrast agent and the second sectionscan is obtained following the introduction of a highdensity contrast agent (diatrizoate sodium,15 sodium io-thalamate16). The two scans are subtracted to obtain theincrease in density due to blood content. Knowledge ofthe concentration of contrast agent in the blood allowslocal cerebral blood volumes to be quantitated. As wasdiscussed for the x-ray fluorescent technique, the contrastagent crosses the blood brain barrier in pathologicalsituations13 and so this technique cannot be used indisease states.
The technique used in this investigation has yieldeddata on local cerebral blood volume in an entire sectionof the human brain in vivo. The resolution of the MarkIV scanner has allowed us to obtain measurements ofLCBV in grey matter and white matter separately and toquantify further the LCBV in various specific cerebralareas. The cerebral blood volume of normal resting manobtained in this study, 5.02 ml/100 g for grey matter and3.55 ml/100 g for white matter, agrees well with thelimited data in the literature (Table 3). It can be seen inthis table that cerebral blood volume ranges from 1.9 to8.3 ml/100 g, depending on the study. This wide range ismost likely due to differences in techniques and species.Assuming that the brain is 50% grey matter and that themeasurements made in this study for grey and whitematter blood volumes are representative of average greyand white matter, respectively, then the mean cerebral
blood volume obtained in this study is 4.3 ml/100 g. Thisis approximately the midpoint of the values in the liter-ature obtained with in vivo measuring techniques. Theredo not exist any in vivo data on the blood volumes of greyand white matter separately since all of the previoustechniques for cerebral blood volume determinations(with the possible exception of the x-ray fluorescencetechnique) were not capable of imaging grey and whitematter separately. It has been shown17'18 that the volumeof capillaries in the grey matter is greater than in thewhite matter, although the actual values are lower thanhas been obtained for local blood volume in this study.This is due in part to blood vessels other than capillaries(veins, arterioles, etc). Additionally, the volume occupiedby capillaries determined by in vitro techniques mayunderestimate the actual in vivo capillary volume. Thestatistically significant difference in resting cerebral bloodvolume between grey and white matter obtained in thisstudy is consistent with the reports of relative vascularityand with what is known about blood flow in the differentcerebral tissues.
Table 3 also lists the sensitivity of cerebral blood vol-ume to alterations in Paco2 obtained by various previousinvestigations. The values obtained in this study, 0.053ml/100 g per torr Paco2 for grey matter and 0.046 ml/100g per torr Paco2 for white matter with an average wholebrain blood volume of 0.0495 ml/100 g per torr Paco2, arein excellent agreement with these prior measurements.
We can define a percentage volume change index(PVCI) as the percentage change in cerebral blood vol-ume of the tissue for a 1-torr change in arterial carbondioxide tension using 34.4 torr as the carbon dioxidetension for computing the percentage change. ComputingPVCI for grey and white matter separately, we obtain1.05 ± 0.11% change/torr and 1.40 ± 0.14% change/torr,respectively. Thus, PVCI is greater for white matter thanfor grey (P < 0.05), indicating that for a given increase(or decrease) of PacO2, the white matter increases itsblood volume by a greater percentage than does the greymatter.
TABLE 3 Summary of CB V and CB V-PaCO2 Sensitivities in the Literature
Species
CatCatHumanDogHumanHumanHuman
HumanGoatMonkeyBaboonHuman
C B V
2.71.97.08.34.23.25.7 (cortex)5.1 (thalamus)3.04.75.63.05.02 (grey)3.55 (white)
CO2 sensitivity!
0.0430.0490.0490.053 (grey)0.046 (white)
Technique131RISA51Cr-RBC32P-RBCCollargolRCBF by l33Xe; f by ""TcX-ray fluorescenceCAT scanner
CAT scannerCBF by ^Kr; t by ICGX-ray fluorescence"Tc-RBC-Mark III"Tc-RBC-Mark IV
Reference
7798
111216
15134
Present study
Cerebral blood volumes (CBV) and sensitivities of CBV to carbon dioxide in this investigation and values fromthe literature. CBF = cerebral blood flow, RISA = radioactive iodine-labeled serum albumin, RBC = red blood cells,I = mean transit time, ICG = indocyanine green, CAT = computerized axial tomography.
* Cerebral blood volume (ml/100 g) adjusted when possible to an arterial carbon dioxide tension (Paco2) of 34.4torr.
t CBV sensitivity to carbon dioxide (ml/100 g per torr Paco2).
at VA MED CTR BOISE on July 9, 2011http://circres.ahajournals.org/Downloaded from

330 CIRCULATION RESEARCH VOL. 43, No. 2, AUGUST 1978
From the blood volume picture resulting from thesection scan, a few specific cerebral regions were identified(frontal cortex, thalamus, and insular cortex in the regionof the sylvian fissure). The resting blood volume of thefrontal cortex (3.93 ml/100 g) was significantly smallerthan that obtained for the thalamus (5.00 ml/100 g). Thevalue for the blood volume of the thalamus is very closeto that found by Ladurner et al.16 who measured localcerebral blood volume using a transmission-computerizedtomographic scanner. They obtain a value of 5.1 ml/100g with a standard deviation of 1.0 ml/100 g, whereas ourvalue is 5.0 ± 0.64 (SD) ml/100 g. These are not signifi-cantly different. The blood volume we obtain for thefrontal cortex (3.93 ± 0.52 ml/100 g) is less than thatfound by Ladurner et al.16 (6.3 ± 3.1 ml/100 g). This isprobably due to the fact that their data were obtained inpatients with a variety of brain disorders. As discussedby Phelps and Kuhl,19 transmission-computed tomogra-phy is not a valid technique for cerebral blood volumedetermination in pathological states. It will cause anoverestimation of the measured blood volume, which mayexplain the high value obtained by Ladurner et al.16 inthe frontal cortex. Although these investigators at-tempted to limit their tissue samples to the "normal"hemisphere of their patients, extrapolation of blood vol-umes obtained in patients with known neurological defi-cits to the normal individual is less than ideal. Addition-ally, the transmission tomographic technique requires thesubtraction of two scans (a scan without a contrast agentis subtracted from a scan in which a contrast agent hasbeen used). Since the EMI numbers of the two scans aresimilar, the difference is subject to considerable error. Forexample, in a series of 17 patients, Ladurner et al.16 obtaina mean EMI number in the thalamus of 17.7 beforeinjection of a contrast agent and 19.7 following an injec-tion of sodium iothalamate. An error only 1.0 of an EMInumber will produce an error of 50% in the computedblood volume. The technique used in our studies (radio-active labeled red blood cells detected with an emissiontomographic scanner) is not susceptible to this problem.
After hyperventilation in some of the subjects thecerebral blood volume did not return to its control levelin spite of a return of the arterial carbon dioxide tensionto its resting value. This suggests that the cerebral vas-culature may require more than 15 minutes to recoverfrom a stimulus causing a significant decrease in bloodvolume. This represents a longer response time than hasbeen found for the adjustment of cerebral blood flow tocarbon dioxide alterations.20"21 This may be due to thefact that cerebral blood flow alterations are caused byactive arteriolar diameter changes, whereas the mecha-nism for cerebral blood volume changes may include apassive component (dilation of capillaries and/or openingup of previously closed capillary beds).
It has been shown that cerebral blood volume changesare produced by alterations in arterial blood pressure.3'4
The data in this study have been analyzed for such arelationship by performing a multiple regression witharterial blood pressure and Paco2 as the independentvariables and LCBV as the dependent variable. Localcerebral blood volume and arterial blood pressure corre-
lated poorly due in large part to the very small bloodpressure changes observed in the subjects during thestudy. Blood pressure was altered only secondarily toalterations in arterial carbon dioxide tension. Since Paco2
was changed only over a relatively narrow range (20-42torr), the induced arterial blood pressure changes weresmall. Consequently, the correlation between local cere-bral blood volume and arterial blood pressure was poor.
This study has extended to man the observation pre-viously made only in animals that cerebral blood volumeis responsive to changes in arterial carbon dioxide tension.It also has examined for the first time the regional re-sponses of CBV to alterations in Paco2. We have dem-onstrated that grey matter and white matter have thesame sensitivities to carbon dioxide although they havedifferent resting local blood volumes. The data generatedin this study are being used as a normal baseline withwhich local cerebral blood volumes in various pathologi-cal conditions can be compared.
AcknowledgmentsWe wish to thank Angelina Sylvestro, John Hoffman, Ilene Kasloff,
Joanne Miller, and Anthony Ricci for their invaluable assistance in theseexperiments.
References1. Smith AL, Neufeld GR, Ominsky AJ, Wollman H: Effect of arterial
CO2 tension on cerebral blood flow, mean transit time, and vascularvolume. J Appl Physiol 31: 701-707, 1971
2. Ter-Pogossian MM, Phelps ME, Grubb RL, Gado M: Measure ofregional cerebral blood volume in vivo by means of excited fluorescentx-radiation, and factors affecting this parameter. Eur Neurol 6:218-223, 1971-1972
3. Phelps ME, Grubb RL, Ter-Pogossian MM: Correlation betweenPaC02 and regional cerebral blood volume by x-ray fluorescence. JAppl Physiol 35: 274-280, 1973
4. Kuhl DE, Reivich M, Alavi A, Nyary I., Staum MM: Local cerebralblood volume determined by three-dimensional reconstruction ofradionuclide scan data. Circ Res 36: 610-619, 1975
5. Kuhl DE, Edwards RQ, Ricci AR, Yacob RJ, Mich TJ, Alavi A: TheMark IV system for radionuclide computed tomography of the brain.Radiology 121: 405-413, 1976
6. Severinghaus JW, Stupfel M, Bradley AF: Accuracy of blood pH andPco2 determinations. J Appl Physiol 9: 189-196, 1956
7. Sklar FH, Burke EF Jr, Langfitt TW: Cerebral blood volume: Valuesobtained with Cr-labelled red blood cells and RISA. J Appl Physiol24: 79-82, 1968
8. Weil A, Zeiss FR, Cleveland DA: The determination of the amount ofblood in the central nervous system after injection of hypertonicsolutions. Am J Physiol 98: 363-367, 1931
9. Nylen G, Hedlund S, Regnstrom O: Cerebral circulation studies withlabelled red cells in healthy males. Circ Res 9: 667-674, 1961
10. Risberg J., Ancri D., Ingvar DH: Correlation between cerebral bloodflow in the cat. Exp Brain Res 8: 321-326, 1969
11. Matthew NJ, Meyer JS, Bell RL, Johnson PC, Neblett CR: Regionalcerebral blood flow and blood volume measured with the gammacamera. Neuroradiology 4: 133-140, 1972
12. Grubb RL, Phelps ME, Ter-Pogossian MM: Regional cerebral bloodvolume in humans. Arch Neurol 28: 38-44, 1973
13. Gado MH, Phelps ME, Coleman RE: An extravascular component ofcontrast enhancement in cranial computed tomography. Part I: Thetissue-blood ratio of contrast enhancement. Radiology 117: 589-593,1975
14. Kuhl DE, Edwards RQ: The Mark HI scanner: A compact device formultiple view and section scanning of the brain. Radiology 96:560-570, 1970
15. Penn RD, Walser R, Ackerman L: Cerebral blood volume in man.Computer analysis of a computerized brain scan. JAMA 234:1154-1155, 1975
16. Ladurner G, Zilkha E, Ififf LD, DuBoulay GH, Marshall J: Measure-ment of regional cerebral blood volume by computerized axial tomog-raphy. J Neurol Neurosurg Psychiatry 39: 152-158, 1976
17. Lierse W: Zur Methodik quantitativer angioarchitektonischer Unter-
at VA MED CTR BOISE on July 9, 2011http://circres.ahajournals.org/Downloaded from

CEREBRAL BLOOD VOLUME AND CARBON BIOXIDE/Greenberg et al. 331
suchungen an Hirnstamm des Meerschweinschens. Z Mikrosk Anat 20. Shapiro W, Wasserman AJ, Patterson JL: Mechanism and pattern ofForsch 69: 439-455, 1963 human cerebrovascular regulation after rapid changes in blood CO2
18. Lierse W: Die Kapillardichte im Wirbeltiergehern. Acta Anat (Basel) tension. J Clin Invest 45: 913-922, 196654: 1-31, 1963 21. Severinghaus JW, Lassen N: Step hypocapnia to separate arterial
19. Phelps ME, Kuhl DE: Pitfalls in the measurement of cerebral blood from tissue Pco2 in the regulation of cerebral blood flow. Circ Res 20:volume with computed tomography. Radiology 121: 375-377, 1976 272-278, 1967
ErratumIn the article by Robert E. Mates, Ramji L. Gupta, Adam C. Bell, and Francis J. Klocke,
"Fluid Dynamics of Coronary Artery Stenosis," Circ Res 42: 152-162 (January), 1978, inparagraph 1, page 152, the statement, "approximately 80-84%" should read "approximately84-96%." In the last sentence on page 153, the statement should read "the basic frequencyof the system which is proportional to the heart rate." The authors are grateful to Dr.Robert L. Feldman of the University of Florida for pointing out these errors.
at VA MED CTR BOISE on July 9, 2011http://circres.ahajournals.org/Downloaded from