
Civil society or ‘comprador class’, participation or parroting?
Click here to load reader

ANTIMICROBIAL AGENTS AND CHEMOTHERAPY, Sept. 2010, p. 3884–3894 Vol. 54, No. 90066-4804/10/$12.00 doi:10.1128/AAC.01554-09Copyright © 2010, American Society for Microbiology. All Rights Reserved.
Liposomal Amphotericin B and Echinocandins as Monotherapy orSequential or Concomitant Therapy in Murine Disseminated
and Pulmonary Aspergillus fumigatus Infections
Jon A. Olson,1 Ancy George,1 David Constable,1 Peter Smith,1
Richard T. Proffitt,2 and Jill P. Adler-Moore1*D epartment of B iological Sciences, C alifornia State Polytechnic University, Pomona, C alifornia 91768,1
and RichPro Associates, 2095 L avender H ill C ourt, L incoln, C alifornia 956482
Received 3 November 2009/Returned for modification 28 January 2010/Accepted 21 June 2010
Monotherapy and combination therapy were compared using optimal doses of liposomal amphotericin B,micafungin, or caspofungin in Aspergillus fumigatus pulmonary and disseminated infections. Mice were chal-lenged intravenously (2.8 104 to 5.7 104 conidia) or intranasally (5.8 107 conidia) with A. fumigatus.Drugs (5, 10, or 15 mg/kg of body weight) were given for 3 or 6 days as single, concomitant, or sequentialtherapy (i.e., days 1 to 3 and then days 4 to 6). Mice were monitored for survival, and tissues were assayed forfungal burden and drug concentrations. Treatments starting 24 h postchallenge significantly prolongedsurvival in disseminated aspergillosis (P< 0.002), but only liposomal amphotericin B treatments or treatmentsbeginning with liposomal amphotericin B increased survival to 100% in the pulmonary aspergillosis model.Fungi in kidneys and spleens (disseminated) and lungs (pulmonary) were significantly decreased (P < 0.04)by liposomal amphotericin B, liposomal amphotericin B plus echinocandin, or liposomal amphotericin B priorto echinocandin. In the disseminated infection, liposomal amphotericin B andmicafungin (10 or 15mg/kg) hadsimilar kidney drug levels, while in the spleen, 5 and 15 mg/kg liposomal amphotericin B gave higher druglevels than micafungin (P < 0.02). In the pulmonary infection, drug levels in lungs and spleen with 5-mg/kgdosing were significantly higher with liposomal amphotericin B than with caspofungin (P < 0.002). Insummary, treatment of A. fumigatus infections with liposomal amphotericin B plus echinocandin or liposomalamphotericin B prior to echinocandin was as effective as liposomal amphotericin B alone, and a greaterdecrease in the fungal burden with liposomal amphotericin B supports using liposomal amphotericin B priorto echinocandin.
Invasive aspergillosis (IA) is a life-threatening fungal infec-tion that occurs in 10 to 28% of immunosuppressed patients(42, 43, 44), and the mortality rate for untreated IA is virtually100% (16, 34, 45). Aspergillus fumigatus is responsible for 66 to70% of IA infections (19, 36, 43). In a prospective, randomizedclinical trial comparing 3 mg/kg of body weight and 10 mg/kgAmBisome, a liposomal form of amphotericin B, the responserates for IA were reported to be 50% and 46%, respectively(14). These are similar to the response rate (53%) for voricon-azole reported in another prospective randomized clinical trialof IA comparing conventional amphotericin B and voricon-azole (22). In a more recent clinical trial for primary treatmentof IA, the investigators reported a 33% response rate forcaspofungin (Cancidas) at 50 mg/day with a 70-mg loadingdose on day 1 (53).
To further improve the treatment outcome for IA, combi-nation antifungal therapy of polyenes with the echinocandinshas begun to be investigated in nonclinical studies. Amphoter-icin B targets ergosterol in the fungal cell membrane, bindingwith ergosterol to create a pore in the membrane, which dis-rupts membrane integrity and leads to fungal-cell lysis (5, 15).
In comparison, the echinocandins target the enzyme 1,3- -glucan synthetase, required for the synthesis of 1,3- -glucan,an important fungal cell wall component (18, 20). The fungalspecificity of the echinocandins for the cell wall results in thesedrugs having minimal toxic side effects. Thus, by combining adrug which targets the cell wall with one directed at the cellmembrane, it is possible that there could be additive or syner-gistic antifungal effects.
Nonclinical studies have shown no antagonistic effects withthe combination of amphotericin B and the echinocandins forthe treatment of Aspergillus infections (10, 24, 47). In fact,improved efficacy has been reported in mice with chronic gran-ulomatous disease and pulmonary aspergillosis following ad-ministration of micafungin (Mycamine) and amphotericin B(17), as well as for murine systemic aspergillosis with a com-bination of caspofungin plus amphotericin B or amphotericinB-intralipid (2, 47). In contrast, although there was no antag-onism, Clemons and Stevens (10) reported no synergistic ac-tivity of micafungin and amphotericin B for pulmonary as-pergillosis in immunosuppressed DBA/2 mice.
Treatment of aspergillosis with the combination of lipid am-photericin B formulations and the echinocandins has also be-gun to be studied, but the reports are limited. This approachhas the added advantage of the reduced toxicity of the ampho-tericin B lipid formulations (2, 51). In one study of a systemicmurine aspergillosis model (21), the investigators reported lim-
* Corresponding author. Mailing address: Dept. of Biological Sci-ences, California State Polytechnic University, 3801 West Temple Av-enue, Pomona, CA 91768. Phone: (909) 869-4047. Fax: (909) 869-4078.E-mail: [email protected].
Published ahead of print on July 2010.
3884

ited additive effects of suboptimal doses of liposomal ampho-tericin B and micafungin with significantly reduced fungal bur-den in the spleens, but only when liposomal amphotericin Bwas given before micafungin.
The initial site of Aspergillus infection in humans is primarilythe lungs, with hematogenous dissemination of the fungus tothe spleen, kidneys, liver, and brain, which occurs as the dis-ease progresses, making the infection even more difficult totreat. Leenders et al. (33) reported that in a pulmonary as-pergillosis infection in rats, liposomal amphotericin B mono-therapy at 5 and 10 mg/kg was effective in preventing dissem-ination from the lungs to the kidneys, liver, and spleen. Toextend these observations, in the present study, we wanted todetermine if concomitant or sequential therapy with optimaldoses of liposomal amphotericin B and either caspofungin ormicafungin would be more or less effective than monotherapyin decreasing the fungal burden and increasing survival in an A .fumigatus pulmonary and/or disseminated infection. There areat least one randomized pilot clinical trial and several casereports in which clinicians have begun using combination reg-imens of liposomal amphotericin B and echinocandins for thetreatment of aspergillosis, although there are no publishedlarge-scale, randomized, double-blind clinical-trial data inwhich these combinations have been used. In the pilot ran-domized clinical trial (8), investigators compared concomitantliposomal amphotericin B (3 mg/kg) plus standard caspofungintherapy (70-mg/kg loading dose; 50 mg/kg daily) with high-dose (10-mg/kg) liposomal amphotericin B monotherapy. Theoverall response of the combination was significantly betterthan the monotherapy (P 0.028). In case reports, someinvestigators have used the drugs together as concomitant ther-apy (9), and in other case reports, the investigators have usedsequential treatment, with one drug replacing the other drug(25) or initiating treatment with one drug and then addinganother drug to the regimen (3, 26, 41). Thus, it is important toevaluate whether there will be any antagonism or synergismwhen liposomal amphotericin B and an echinocandin are usedtogether at optimal doses or if it is better to begin therapy withone class of drug and then switch to another class of drug. Toaddress these questions, we used two infection models. Wechallenged some groups of mice intranasally to produce a lunginfection, and for the disseminated model, we infected othermice intravenously (i.v.) to target the fungus to the nonlungtissues (i.e., kidneys and spleen). By using survival and fungalburden (i.e., tissue culturing and tissue galactomannan levels),we were able to evaluate the efficacy of the drugs given asmonotherapy or concomitant or sequential therapy in murinepulmonary and disseminated aspergillosis.
MATERIALS AND METHODS
Animals. Female Swiss Webster mice (7 weeks old; Harlan, Indianapolis, IN)were used in these studies. The animals were maintained in microisolator cageswith standard rodent diet (Teklad Laboratory Rodent diet 2918 [18% protein];Harlan/Teklad, Madison, WI) and water ad libitum. All animal research proce-dures were approved by the Institutional Animal Care and Use Committee ofCalifornia State Polytechnic University, Pomona, CA.
Test substances. Liposomal amphotericin B (AmBisome; Gilead Sciences,Inc., San Dimas, CA), a lyophilized liposomal preparation of amphotericin B,was reconstituted with 12.5 ml sterile water for injection, shaken vigorously for1 min, and filtered through a 5- m filter according to the manufacturer’s in-structions. The resulting 4-mg/ml solution of amphotericin B was diluted in
sterile 5% dextrose for i.v. injection. Caspofungin (Cancidas; Merck and Co.,Inc., Whitehouse Station, NJ) was rehydrated in 10.5 ml sterile water to producea 5.0-mg/ml solution, which was then diluted in 0.9% sodium chloride for i.v.injection. Micafungin (Mycamine; Astellas Inc., Ltd., Osaka, Japan [formerlyFujisawa Pharmaceuticals Co.]) was rehydrated in 5.0 ml sterile water to give a10-mg/ml solution that was diluted in 0.9% sodium chloride for i.v. injection.Both caspofungin and micafungin were protected from light, according to themanufacturers’ instructions.In vitro testing for MICs. A . fumigatus (ATCC 13073) was cultured on potato
dextrose agar plates (Difco, Becton Dickinson & Co., Sparks, MD) at 35°Covernight and then at ambient room temperature for 9 to 10 days. Conidia weredislodged from the hyphal mats by dispersal in 0.9% saline with 0.05% Tween 80(Sigma Chemical Co., St. Louis, MO), filtered through sterile gauze to removehyphal fragments, and sonicated for 60 s in a water bath sonicator. The conidialcount was determined with a hemacytometer, and the conidial suspension wasadjusted to 2 104 spores/ml in RPMI-MOPS (morpholinepropanesulfonicacid). The viability of the conidia was assessed by plating 200 l of the suspensionon inhibitory mold agar plates (Hardy Diagnostics, Santa Maria, CA), followedby incubation at 35°C for 24 to 48 h. A series of 2-fold dilutions of liposomalamphotericin B, micafungin, or caspofungin (0.031 g/ml to 320 g/ml) wereprepared in RPMI-MOPS, and 100- l aliquots of each drug dilution and 100 lof the spore suspension were then dispensed into duplicate wells of a 96-wellround-bottom microtiter plate. A modified CLSI microtiter dilution assay wasperformed as previously described (38), since this method is a suitable alternativeprocedure for antifungal susceptibility testing of Aspergillus spp. (37) that uses acolorimetric endpoint rather than a visual endpoint.Galactomannan assay of infected tissues. To determine the galactomannan
levels in the tissues, the serum galactomannan assay was modified (7, 35). Otherinvestigators have reported successfully using the galactomannan assay for mea-suring fungal burden in the tissues (52), although the assay has been standardizedonly for serum galactomannan levels, not tissue levels. The galactomannan kitwas purchased from Bio-Rad Laboratories (Hercules, CA). To each tared tissuesample, 1 ml of phosphate-buffered saline (PBS) was added, and then the samplewas homogenized on ice using a mechanical homogenizer with a 7-mm-diameterprobe (Tissue Tearor; Biospec Products, Inc., Bartlesville, OK) for 30 s. Analiquot of 300 l of each sample was mixed 3:1 with EDTA solution and heatedat 100°C for 3 min, along with a positive control and a negative control. Allsamples were centrifuged at 10,000 g for 10 min, and 50 l of each supernatantwas added to a well of a plate coated with monoclonal anti-galactomannanantibody (EBA-2); 50 l of peroxidase-labeled anti-galactomannan antibody wasthen added to each well, and the plate was incubated for 90 min at 37°C. Afterincubation, the wells were washed, and 200 l of substrate-chromogen was addedto the wells and incubated for a half hour at room temperature in the dark. Thereaction was stopped by the addition of 1.5 N sulfuric acid. The optical density(OD) ratio of each sample was read in a spectrophotometer at 450 nm/620 nm,and the galactomannan index was calculated by dividing the sample OD by themean cutoff control OD.Monotherapy for disseminated and pulmonary aspergillosis. To assess the in
vivo activity of micafungin, caspofungin, or liposomal amphotericin B as mono-therapy against disseminated infection with A . fumigatus (ATCC 13073), SwissWebster female mice (7 weeks old) were immunosuppressed with 100 mg/kgcyclophosphamide (Sigma Chemical Co., St. Louis, MO) given intraperitoneally(i.p.) 3 days prior to fungal challenge. Maintenance i.p. doses of 100 mg/kgcyclophosphamide were given on the day of challenge and every third day for theduration of the study (40). The animals were infected via the tail vein with 2.8 104 conidia/mouse. Twenty-four hours later, intravenous drug therapy with oneof the following agents was initiated (n 12/group) and continued for 3 or 6days: liposomal amphotericin B (5, 10, or 15 mg/kg), micafungin (5, 10, or 15mg/kg), caspofungin (5 mg/kg), or 5% dextrose (D5W; controls). The animals(n 7/group) were monitored for morbidity (e.g., weight loss and activity level)for 28 days and then euthanized. The other 5 animals in each group weresacrificed 24 h posttreatment, and their kidneys and spleens, the targets of thisdisseminated infection (21), were harvested, weighed, homogenized on ice in 1.0ml PBS with a Tissue Tearor mechanical homogenizer, and diluted in 10-folddilutions with PBS for evaluation of the fungal burden. Aliquots of each dilution(200 l) were plated in duplicate on inhibitory mold agar (Hardy Diagnostics,Santa Maria, CA) with 0.05% chloramphenicol and incubated at 35°C for 96 h todetermine the number of CFU per g kidneys and spleens. A 96-h time point wasused throughout these studies because of the delay in visible growth of fungus onthe agar when the tissues were taken from the echinocandin-treated mice. Thelower limit of detection in this assay was 15 CFU/g tissue. The kidney homoge-nates were also analyzed for galactomannan levels according to the proceduredescribed above. In addition, the kidney and spleen homogenates of the mica-
VOL. 54, 2010 LIPOSOMAL AMPHOTERICIN B AND ECHINOCANDINS FOR ASPERGILLOSIS 3885

fungin and liposomal amphotericin B groups were evaluated for drug concen-trations using a previously described Paecilomyces variotii bioassay (48). Theintraday coefficient of variation for this bioassay ranged from 3.4% to 6.3%, andthe interday coefficient of variation ranged from 9% to 10%, with a minimumsensitivity of 0.03 g/ml.
For the pulmonary infection, mice were immunosuppressed with 6 mg/kgtriamcinolone acetonide (Bristol-Myers Squibb Co., Princeton, NJ) i.p. on days 3, 0, and 2. The animals were sedated i.p. with ketamine (80 mg/kg; BionicheAnimal Health USA, Inc., Athens, GA) and xylazine (16 mg/kg; Phoenix Scien-tific, Inc., St. Joseph, MO) and then challenged intranasally with 5.8 107
conidia/mouse. Two hours postchallenge, intravenous drug therapy with one ofthe following agents was begun (n 7/group for CFU per g and drug concen-trations, and n 7/group for survival) and continued daily for a total of 6treatments: liposomal amphotericin B (5 or 10 mg/kg), caspofungin (5 mg/kg),and D5W. Animals (n 7/group) were monitored for morbidity for 14 days asdescribed above and then euthanized. The lungs, kidneys, and spleens werecollected 24 h after the sixth (n 7/group) treatment and analyzed for thenumber of CFU/g (lungs only) and the drug concentrations in lungs, kidneys, andspleen using a C andida albicans bioassay modified from the P. variottii bioassaydescribed above (48). Initial screening indicated that caspofungin, unlike mica-fungin, did not inhibit P. variotii in the bioassay, but like liposomal amphotericinB, it readily inhibited C . albicans in the bioassay, with a minimum sensitivity of0.25 g/ml. The drug concentrations in the tissue from liposomal amphotericinB-treated mice were comparable whether the fungus used in the bioassay was P.variotii or C . albicans.Combination therapy for disseminated and pulmonary aspergillosis. For dis-
seminated aspergillosis (n 14/group), the challenge was 5.0 104 to 5.7 104
A . fumigatus conidia/mouse. When the drugs were given on the same day (i.e.,concomitant therapy), they were given as separate intravenous injections into thetail vein, and the regimen was 10 or 15 mg/kg i.v. liposomal amphotericin B plus5.0 mg/kg i.v. micafungin or caspofungin daily for 3 or 6 days. When the drugswere given sequentially, 10 or 15 mg/kg i.v. liposomal amphotericin B was givenon days 1 through 3 or days 4 through 6. Conversely, the other drug (5 mg/kg i.v.caspofungin) was administered on days 4 through 6 or days 1 through 3. Asdescribed above, kidneys and spleens were collected 24 h posttreatment from 7mice/group for determination of CFU per g. Kidney homogenates were alsoevaluated for galactomannan levels in the caspofungin and liposomal amphoter-icin B sequentially treated mice. The other animals (n 7/group) were moni-tored for morbidity for 27 or 28 days.
For pulmonary aspergillosis (n 14/group), the challenge was 5.8 107 A .fumigatus conidia/mouse. In the concomitant treatment, 5 or 10 mg/kg i.v. lipo-somal amphotericin B plus 5 mg/kg caspofungin was given daily for 6 days. Withthe sequential treatment, 5 mg/kg i.v. caspofungin was administered on days 1through 3, followed by 5 or 10 mg/kg i.v. liposomal amphotericin B on days 4through 6; conversely, 5 or 10 mg/kg i.v. liposomal amphotericin B was given ondays 1 through 3, followed by 5 mg/kg caspofungin on days 4 through 6. One dayafter the sixth treatment, lungs from 7 mice/group were collected and processedas described above for CFU per g. The other animals (n 7/group) weremonitored for morbidity for 14 days. It should be noted that drug concentrationsusing the bioassays were not done with any of the tissues from animals treatedwith drug combinations because, in the bioassays, both micafungin and liposomalamphotericin B inhibited P. variotii growth and caspofungin and liposomal am-photericin B inhibited C . albicans growth to the same extent.
Statistical analysis. Statistics for comparisons of tissue drug concentrationsand CFU per g were performed using GraphPad Prism, version 4.0 (GraphPadSoftware, Inc., San Diego, CA). The Kruskal-Wallis test was applied to comparethe control to all groups in each experiment, and where significant differencesoccurred, a two-tailed Mann-Whitney test was done between paired groups.Survival curves were compared using the log rank test. A P value of 0.05 wasconsidered significant.
RESULTS
In vitro MIC testing. The MICs of caspofungin, micafungin,and liposomal amphotericin B for A . fumigatus (ATCC 13073)were 0.31 g/ml, 0.31 g/ml, and 0.625 g/ml, respectively.These MIC values are similar to previously published MICs forthese same drugs against A . fumigatus strains (4, 29, 30). Thus,low concentrations of the test drugs in vitro were able to mark-edly inhibit the growth of this strain of A . fumigatus.
Monotherapy with micafungin or liposomal amphotericin Bfor disseminated aspergillosis. Survival improved from 57% to86% as the dose of liposomal amphotericin B increased from5 to 15 mg/kg, whereas survival decreased from 86% to 57%with increasing doses of micafungin (5 to 15 mg/kg) (Fig. 1A),indicating a possible paradoxical effect for micafungin, as re-ported by other investigators in preclinical models (13, 23, 49,60). There are reports that the paradoxical effect may be as-sociated with increases in protein kinase C activity or chitincontent, but overall, the paradoxical effects in vivo with differ-ent fungal infections are not consistent (61). All drug treat-ments produced significantly better survival than the control(D5W) treatment (P 0.002), and there were no significantdifferences in survival among the drug treatment groups. Incomparison, the amount of fungus measured (CFU per g kid-ney) was significantly lower with 10 or 15 mg/kg liposomalamphotericin B than with micafungin dosing, 5 mg/kg liposo-mal amphotericin B, or control (P 0.008) (Fig. 1B), while 5mg/kg micafungin was more effective than the control (P 0.016) (Fig. 1B). It should be noted that the CFU data for thekidneys correlated with the galactomannan index (GI) results(Fig. 1C). In the spleen, as seen in the kidneys, 10 or 15 mg/kgliposomal amphotericin B decreased the fungal burden signif-icantly more than equivalent doses of micafungin (P 0.016and P 0.008, respectively) (Fig. 1D), but compared to thecontrol, the fungal burden in the spleen was significantly lowerwith all drug treatments (P 0.032). Thus, enhanced survivalcorrelated with decreased fungal burden when either drug wascompared to control mice. Drug concentrations in the kidneysof mice given comparable doses of liposomal amphotericin Bor micafungin were not significantly different from one anotheron the day that the kidneys were collected for determination ofthe fungal burden (Table 1). In contrast, the amphotericin Bdrug concentrations in the spleens of liposomal amphotericinB-treated mice were significantly higher than the micafunginconcentration when mice were treated with 5 or 15 mg/kgmicafungin (P 0.008 and P 0.016, respectively) (Table 1).Concomitant therapy versus monotherapy with liposomal
amphotericin B or micafungin for disseminated aspergillosis.Using the results from the monotherapy experiment, we se-lected the doses with the best efficacy in our model for thecombination therapies, i.e., 5 mg/kg micafungin with 10 or 15mg/kg liposomal amphotericin B. These doses are similar tothose used by other investigators in combination treatmentsfor disseminated aspergillosis (57). Monotherapy for 3 or 6days with liposomal amphotericin B (10 or 15 mg/kg), mica-fungin (5 mg/kg), or the combination of liposomal amphoter-icin B (10 or 15 mg/kg) plus 5 mg/kg micafungin significantlyincreased survival compared to the control if treatment wasbegun 1 day after A . fumigatus challenge (P 0.005 for 3 daysof therapy [Fig. 2A] and P 0.003 for 6 days of therapy [Fig.2B]). When initiation of the 3-day dosing regimen was delayeduntil day 4 postchallenge, none of the treatments improvedsurvival (Fig. 2A). Similarly, there was no reduction in fungalburden in the kidneys (Fig. 2C) or spleens (Fig. 2D) with 3 daysof dosing with 10 mg/kg liposomal amphotericin B or 5 mg/kgmicafungin if treatment was delayed until day 4 postinfection.In contrast, 15 mg/kg liposomal amphotericin B did reduce theCFU in the kidneys, even if the treatment was delayed (P 0.018). In comparison, if 3- or 6-day dosing was initiated 1 day
3886 OLSON ET AL. ANTIMICROB. AGENTS CHEMOTHER.

after infection, a significant decrease in fungal burden was seen inboth the kidneys and spleens following treatment with liposomalamphotericin B or liposomal amphotericin B plus micafungincompared to micafungin alone (P 0.001 for both kidneys andspleen). Combining micafungin with liposomal amphotericin B inthe 3-day treatment provided no additional benefit over usingliposomal amphotericin B alone. It should be noted that with theearlier initiation of treatment,micafunginwasmore effective thanthe control in reducing spleen CFU with 3 or 6 days of dosing(P 0.01 and P 0.001, respectively). Once again, there seemedto be a correlation between survival and fungal-burden outcomeswhen treatment groups were compared with the controls.Concomitant therapy versus monotherapy with liposomal
amphotericin B or caspofungin for disseminated aspergillosis.Six days of dosing with liposomal amphotericin B (10 or 15
TABLE 1. Mean drug concentrations in spleen and kidney afterintravenous monotherapy (days 1 to 7) with liposomal amphotericin
B or micafungin for treatment of murine disseminated aspergillosis
Drug Dosage(mg/kg/day)
Drug concn ( g/g tissue) mean (SD) a
Spleen Kidney
Liposomal amphotericin B 5 125 (111)b 23.9 (29.4)10 88.4 (58.7) 17.9 (9.5)15 227 (133)b,c 16.3 (9.5)
Micafungin 5 17.9 (18.1) 5.6 (5.2)10 33.6 (19.0) 25.2 (37.3)15 32.7 (30.4) 22.5 (23.3)
a n 5 mice per group; tissues were collected on day 8 postchallenge (24 hposttreatment).
b P 0.01 versus micafungin at 5 or 10 mg/kg/day.c P 0.02 versus micafungin at 15 mg/kg/day.
FIG. 1. (A) Survival following 6 days of monotherapy with liposomal amphotericin B (A) or micafungin (M) in cyclophosphamide-immunosup-pressed female Swiss Webster mice infected i.v. with 2.8 104 A . fumigatus conidia/mouse. Beginning 24 h postchallenge, the mice (n 7/group) weretreated i.v. with 6 daily doses of D5W, 5 mg/kg liposomal amphotericin B, 10 mg/kg liposomal amphotericin, 15 mg/kg liposomal amphotericin, 5 mg/kgmicafungin, 10 mg/kg micafungin, or 15 mg/kg micafungin (P 0.002 for all treatment groups versus D5W). (B) Scatterplot of fungal burden (log10CFU/g) in kidneys of mice taken 24 h after the final dose. Ten or 15 mg/kg liposomal amphotericin B versus D5W, 5 mg/kg liposomal amphotericin B,or 5, 10, or 15 mg/kg micafungin, P 0.008 for all comparisons of kidney fungal burden; 5 mg/kg micafungin versus D5W, P 0.016 for kidney fungalburden. (C) Scatterplot of GIs from kidneys taken 24 h after the final dose. Ten or 15 mg/kg liposomal amphotericin B versus D5W, 5 mg/kg liposomalamphotericin B, or 5, 10, or 15 mg/kg micafungin, P 0.008 for kidney GI. (D) Scatterplot of fungal burden (log10 CFU per g) in spleens of mice taken24 h after the final dose. All treatments versus D5W, for spleen fungal burden, P 0.032, 0.008, and 0.008 for 5, 10, or 15 mg/kg liposomal amphotericinB, respectively; P 0.016, 0.032, and 0.032 for 5, 10, or 15mg/kgmicafungin, respectively; 10 or 15mg/kg liposomal amphotericin B versus 10 or 15mg/kgmicafungin, P 0.016 and P 0.008, respectively. The horizontal lines indicate the median log10 CFU per g or galactomannan index for each group.
VOL. 54, 2010 LIPOSOMAL AMPHOTERICIN B AND ECHINOCANDINS FOR ASPERGILLOSIS 3887
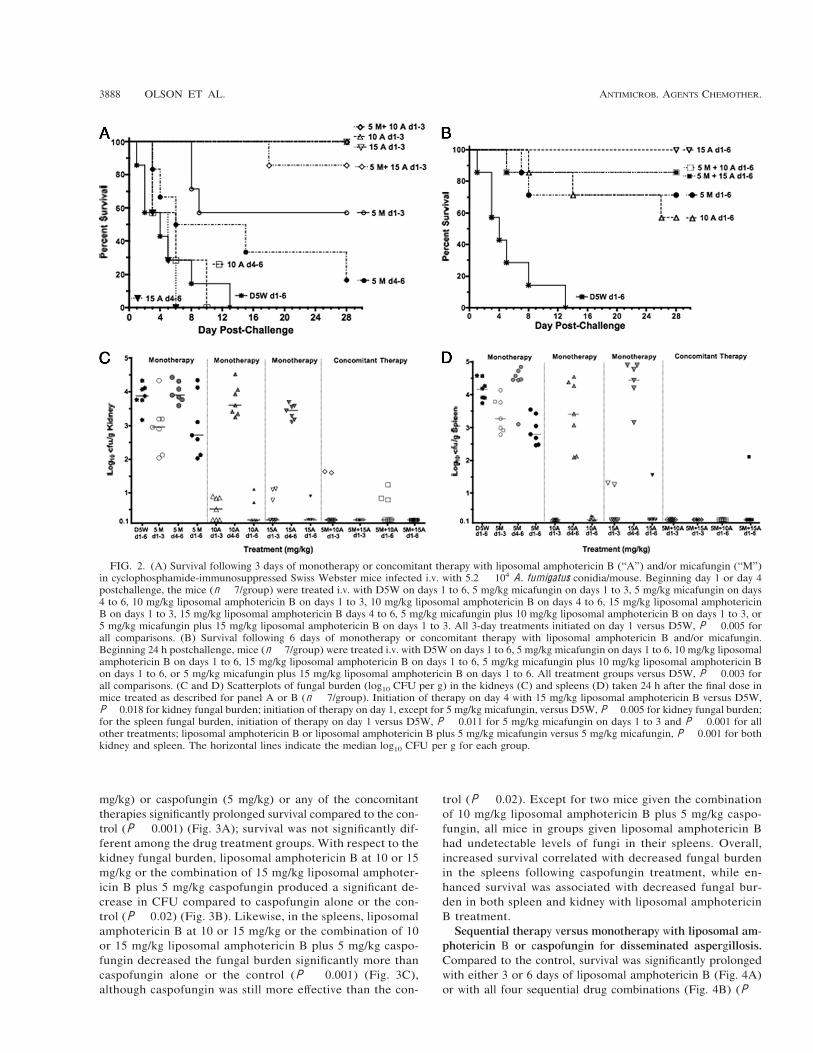
mg/kg) or caspofungin (5 mg/kg) or any of the concomitanttherapies significantly prolonged survival compared to the con-trol (P 0.001) (Fig. 3A); survival was not significantly dif-ferent among the drug treatment groups. With respect to thekidney fungal burden, liposomal amphotericin B at 10 or 15mg/kg or the combination of 15 mg/kg liposomal amphoter-icin B plus 5 mg/kg caspofungin produced a significant de-crease in CFU compared to caspofungin alone or the con-trol (P 0.02) (Fig. 3B). Likewise, in the spleens, liposomalamphotericin B at 10 or 15 mg/kg or the combination of 10or 15 mg/kg liposomal amphotericin B plus 5 mg/kg caspo-fungin decreased the fungal burden significantly more thancaspofungin alone or the control (P 0.001) (Fig. 3C),although caspofungin was still more effective than the con-
trol (P 0.02). Except for two mice given the combinationof 10 mg/kg liposomal amphotericin B plus 5 mg/kg caspo-fungin, all mice in groups given liposomal amphotericin Bhad undetectable levels of fungi in their spleens. Overall,increased survival correlated with decreased fungal burdenin the spleens following caspofungin treatment, while en-hanced survival was associated with decreased fungal bur-den in both spleen and kidney with liposomal amphotericinB treatment.Sequential therapy versus monotherapy with liposomal am-
photericin B or caspofungin for disseminated aspergillosis.Compared to the control, survival was significantly prolongedwith either 3 or 6 days of liposomal amphotericin B (Fig. 4A)or with all four sequential drug combinations (Fig. 4B) (P
FIG. 2. (A) Survival following 3 days of monotherapy or concomitant therapy with liposomal amphotericin B (“A”) and/or micafungin (“M”)in cyclophosphamide-immunosuppressed Swiss Webster mice infected i.v. with 5.2 104 A . fumigatus conidia/mouse. Beginning day 1 or day 4postchallenge, the mice (n 7/group) were treated i.v. with D5W on days 1 to 6, 5 mg/kg micafungin on days 1 to 3, 5 mg/kg micafungin on days4 to 6, 10 mg/kg liposomal amphotericin B on days 1 to 3, 10 mg/kg liposomal amphotericin B on days 4 to 6, 15 mg/kg liposomal amphotericinB on days 1 to 3, 15 mg/kg liposomal amphotericin B days 4 to 6, 5 mg/kg micafungin plus 10 mg/kg liposomal amphotericin B on days 1 to 3, or5 mg/kg micafungin plus 15 mg/kg liposomal amphotericin B on days 1 to 3. All 3-day treatments initiated on day 1 versus D5W, P 0.005 forall comparisons. (B) Survival following 6 days of monotherapy or concomitant therapy with liposomal amphotericin B and/or micafungin.Beginning 24 h postchallenge, mice (n 7/group) were treated i.v. with D5W on days 1 to 6, 5 mg/kg micafungin on days 1 to 6, 10 mg/kg liposomalamphotericin B on days 1 to 6, 15 mg/kg liposomal amphotericin B on days 1 to 6, 5 mg/kg micafungin plus 10 mg/kg liposomal amphotericin Bon days 1 to 6, or 5 mg/kg micafungin plus 15 mg/kg liposomal amphotericin B on days 1 to 6. All treatment groups versus D5W, P 0.003 forall comparisons. (C and D) Scatterplots of fungal burden (log10 CFU per g) in the kidneys (C) and spleens (D) taken 24 h after the final dose inmice treated as described for panel A or B (n 7/group). Initiation of therapy on day 4 with 15 mg/kg liposomal amphotericin B versus D5W,P 0.018 for kidney fungal burden; initiation of therapy on day 1, except for 5 mg/kg micafungin, versus D5W, P 0.005 for kidney fungal burden;for the spleen fungal burden, initiation of therapy on day 1 versus D5W, P 0.011 for 5 mg/kg micafungin on days 1 to 3 and P 0.001 for allother treatments; liposomal amphotericin B or liposomal amphotericin B plus 5 mg/kg micafungin versus 5 mg/kg micafungin, P 0.001 for bothkidney and spleen. The horizontal lines indicate the median log10 CFU per g for each group.
3888 OLSON ET AL. ANTIMICROB. AGENTS CHEMOTHER.

0.001). In contrast, in this experiment, six daily doses of caspo-fungin was less effective in prolonging survival than liposomalamphotericin B or the combinations in which liposomal am-photericin B was given prior to caspofungin (P 0.022). Li-posomal amphotericin B or liposomal amphotericin B givenbefore caspofungin was significantly more effective in reducingkidney CFU than dosing with caspofungin alone for 3 or 6days, caspofungin given before liposomal amphotericin B, orthe control (P 0.01, P 0.038, and P 0.001, respectively)(Fig. 4C), with galactomannan levels in the kidneys givingcomparable results (Fig. 4D). Thus, there was no benefit asso-ciated with adding 3 more days of caspofungin therapy if theanimals had already been treated with liposomal amphotericinB for the first 3 days. In comparison, in the spleens, liposomalamphotericin B or any of the sequential therapies significantly
lowered the fungal burden compared with caspofungin aloneor the control (P 0.001) (Fig. 4E).
Combination (concomitant or sequential) therapy versusmonotherapy with liposomal amphotericin B or caspofunginfor pulmonary aspergillosis. In the pulmonary infection, whichis representative of two experiments, 6 days of dosing with 5 or10 mg/kg liposomal amphotericin B alone, liposomal ampho-tericin B given prior to caspofungin (5 mg/kg), or liposomalamphotericin B plus caspofungin (5 mg/kg) prolonged survivalcompared to either control (58% survival; P 0.06), caspo-fungin given prior to 5 mg/kg liposomal amphotericin B (29%survival; P 0.006), caspofungin given prior to 10 mg/kg lipo-somal amphotericin B (0% survival; P 0.0001), or caspofun-gin alone (0% survival; P 0.0003) (Fig. 5A). In the lungs, thetarget of this infection, the liposomal amphotericin B treat-
FIG. 3. (A) Survival following 6 days of monotherapy or concomitant therapy with liposomal amphotericin B (“A”) and/or caspofungin (“C”)in cyclophosphamide-immunosuppressed Swiss Webster mice infected i.v. with 5.3 104 A . fumigatus conidia/mouse. Beginning 24 h postchal-lenge, the mice (n 7/group) were treated i.v. with D5W on days 1 to 6, 10 mg/kg liposomal amphotericin B on days 1 to 6, 15 mg/kg liposomalamphotericin B on days 1 to 6, 5 mg/kg caspofungin on days 1 to 6, 5 mg/kg caspofungin plus 10 mg/kg liposomal amphotericin B on days 1 to 6,or 5 mg/kg caspofungin plus 15 mg/kg liposomal amphotericin B on days 1 to 6. All treatment groups versus D5W, P 0.001. (B and C) Scatterplotsof fungal burden (log10 CFU per g) in the kidneys (B) or spleens (C) taken 24 h after the final dose in mice treated as described for panel A(n 7/group). Five or 10 mg/kg liposomal amphotericin B versus caspofungin or D5W, P 0.002 and P 0.001, respectively, for kidney fungalburden; combinations versus caspofungin or D5W, P 0.018 for kidney fungal burden; 5 mg/kg caspofungin versus D5W, P 0.018 for spleenfungal burden; 5 or 10 mg/kg liposomal amphotericin B or combinations versus 5 mg/kg caspofungin or D5W, P 0.001 for spleen fungal burden.The horizontal lines indicate the median log10 CFU per g for each group.
VOL. 54, 2010 LIPOSOMAL AMPHOTERICIN B AND ECHINOCANDINS FOR ASPERGILLOSIS 3889
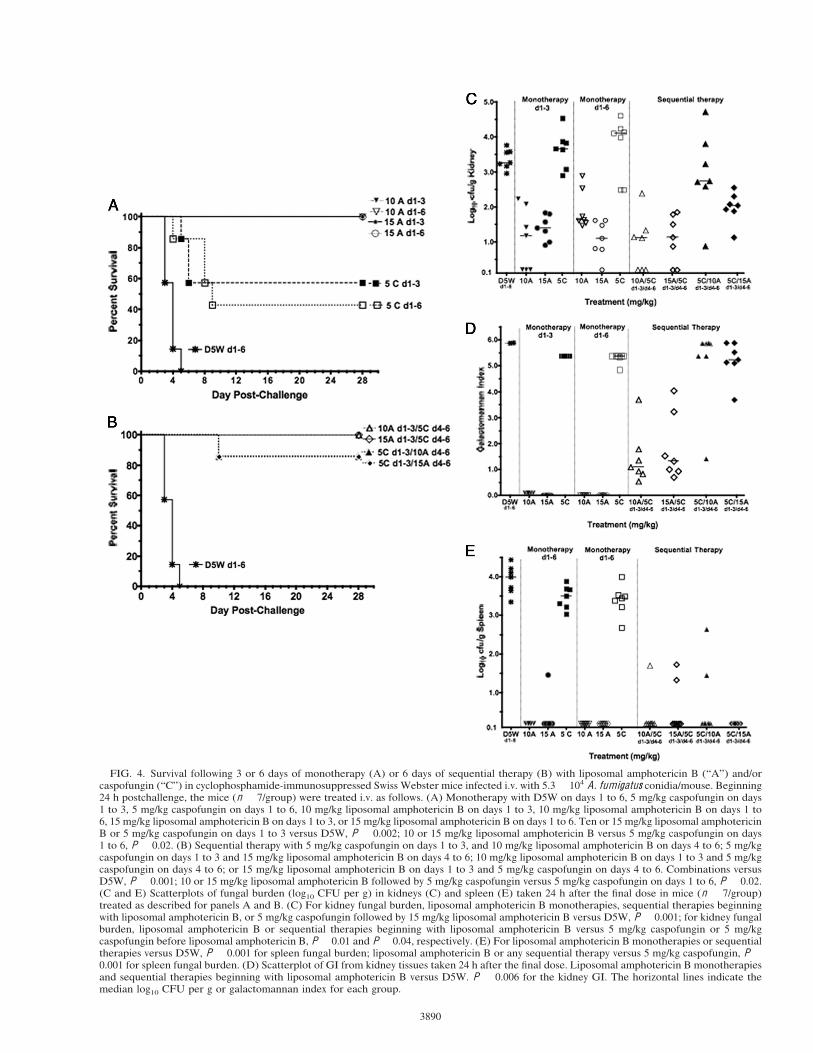
FIG. 4. Survival following 3 or 6 days of monotherapy (A) or 6 days of sequential therapy (B) with liposomal amphotericin B (“A”) and/orcaspofungin (“C”) in cyclophosphamide-immunosuppressed Swiss Webster mice infected i.v. with 5.3 104 A . fumigatus conidia/mouse. Beginning24 h postchallenge, the mice (n 7/group) were treated i.v. as follows. (A) Monotherapy with D5W on days 1 to 6, 5 mg/kg caspofungin on days1 to 3, 5 mg/kg caspofungin on days 1 to 6, 10 mg/kg liposomal amphotericin B on days 1 to 3, 10 mg/kg liposomal amphotericin B on days 1 to6, 15 mg/kg liposomal amphotericin B on days 1 to 3, or 15 mg/kg liposomal amphotericin B on days 1 to 6. Ten or 15 mg/kg liposomal amphotericinB or 5 mg/kg caspofungin on days 1 to 3 versus D5W, P 0.002; 10 or 15 mg/kg liposomal amphotericin B versus 5 mg/kg caspofungin on days1 to 6, P 0.02. (B) Sequential therapy with 5 mg/kg caspofungin on days 1 to 3, and 10 mg/kg liposomal amphotericin B on days 4 to 6; 5 mg/kgcaspofungin on days 1 to 3 and 15 mg/kg liposomal amphotericin B on days 4 to 6; 10 mg/kg liposomal amphotericin B on days 1 to 3 and 5 mg/kgcaspofungin on days 4 to 6; or 15 mg/kg liposomal amphotericin B on days 1 to 3 and 5 mg/kg caspofungin on days 4 to 6. Combinations versusD5W, P 0.001; 10 or 15 mg/kg liposomal amphotericin B followed by 5 mg/kg caspofungin versus 5 mg/kg caspofungin on days 1 to 6, P 0.02.(C and E) Scatterplots of fungal burden (log10 CFU per g) in kidneys (C) and spleen (E) taken 24 h after the final dose in mice (n 7/group)treated as described for panels A and B. (C) For kidney fungal burden, liposomal amphotericin B monotherapies, sequential therapies beginningwith liposomal amphotericin B, or 5 mg/kg caspofungin followed by 15 mg/kg liposomal amphotericin B versus D5W, P 0.001; for kidney fungalburden, liposomal amphotericin B or sequential therapies beginning with liposomal amphotericin B versus 5 mg/kg caspofungin or 5 mg/kgcaspofungin before liposomal amphotericin B, P 0.01 and P 0.04, respectively. (E) For liposomal amphotericin B monotherapies or sequentialtherapies versus D5W, P 0.001 for spleen fungal burden; liposomal amphotericin B or any sequential therapy versus 5 mg/kg caspofungin, P 0.001 for spleen fungal burden. (D) Scatterplot of GI from kidney tissues taken 24 h after the final dose. Liposomal amphotericin B monotherapiesand sequential therapies beginning with liposomal amphotericin B versus D5W. P 0.006 for the kidney GI. The horizontal lines indicate themedian log10 CFU per g or galactomannan index for each group.
3890

ments (5 or 10 mg/kg), alone or given with caspofungin eitherconcomitantly or sequentially, significantly decreased the fun-gal burden compared to the control (P 0.003) (Fig. 5B).Notably, both liposomal amphotericin B doses (5 or 10 mg/kg),as well as the concomitant and sequential combination regi-mens, were significantly more effective in reducing the fungalburden in the lungs than 5 mg/kg caspofungin (P 0.02) (Fig.5B). Furthermore, initial treatment with 10 mg/kg liposomalamphotericin B, followed by caspofungin, was more efficaciousin reducing the lung fungal burden than treatment with caspo-fungin first, followed by 10 mg/kg liposomal amphotericin B(P 0.038), supporting our previous observations in the dis-seminated model of aspergillosis.
Drug concentrations in the lungs of the infected mice fol-lowing 6 days of monotherapy were markedly elevated with 5or 10 mg/kg liposomal amphotericin B compared to 5 mg/kgcaspofungin (P 0.09 for 5 mg/kg liposomal amphotericin Band P 0.001 for 10 mg/kg liposomal amphotericin B) (Table2). In the kidneys, 10 mg/kg liposomal amphotericin B pro-duced significantly higher drug levels than either 5 mg/kg lipo-somal amphotericin B or 5 mg/kg caspofungin (P 0.01 andP 0.001, respectively) (Table 2), but in the spleen, the drugconcentrations with both 5 and 10 mg/kg liposomal amphoter-icin B were significantly higher than with 5 mg/kg caspofungin(P 0.0006 and P 0.001, respectively) (Table 2).
DISCUSSION
In humans, aspergillosis usually manifests first in the lungs,with subsequent spread to other organs. Therefore, in thepresent study, we compared the efficacies of the various drugtreatments in both murine disseminated aspergillosis and pul-monary aspergillosis. We used the murine pulmonary infectionbecause it produces primarily a lung infection (21), while thedisseminated murine infection was chosen to evaluate the drugefficacy in those organs to which the lung infection would likelyspread. In the latter case, the treatment was begun 24 h afterintravenous challenge, ensuring the dissemination of the infec-tion to the kidneys and spleen prior to drug treatment (46).
Survival is often used as an endpoint to determine antifungaldrug efficacy, but evaluation of the fungal burden in the tissuesis also needed to assess clearance or decreased fungal growth
FIG. 5. (A) Survival following 6 days of monotherapy or concom-itant therapy with liposomal amphotericin B (“A”) and/or caspofungin(“C”) in triamcinolone-immunosuppressed Swiss Webster mice in-fected intranasally with 5.8 107 A . fumigatus conidia/mouse. Begin-ning 2 h postchallenge, the mice (n 7/group) were treated i.v. withD5W on days 1 to 6, 5 mg/kg liposomal amphotericin B on days 1 to 6,10 mg/kg liposomal amphotericin B on days 1 to 6, 5 mg/kg caspofun-gin on days 1 to 6, 5 mg/kg liposomal amphotericin B plus 5 mg/kgcaspofungin on days 1 to 6, 10 mg/kg liposomal amphotericin B plus 5mg/kg caspofungin on days 1 to 6, 5 mg/kg caspofungin on days 1 to 3and 5 mg/kg liposomal amphotericin B on days 4 to 6, 5 mg/kg caspo-fungin on days 1 to 3 and 10 mg/kg liposomal amphotericin B on days4 to 6, 5 mg/kg liposomal amphotericin B on days 1 to 3 and 5 mg/kgcaspofungin on days 4 to 6, or 10 mg/kg liposomal amphotericin B ondays 1 to 3 and 5 mg/kg caspofungin on days 4 to 6. Liposomalamphotericin B monotherapies or concomitant or sequential therapiesbeginning with liposomal amphotericin B versus D5W, P 0.06; ver-sus 5 mg/kg caspofungin given before 5 mg/kg liposomal amphotericinB, P 0.006; versus 5 mg/kg caspofungin given before 10 mg/kgliposomal amphotericin B, P 0.0001; versus caspofungin alone, P 0.0003; D5W versus 5 mg/kg caspofungin monotherapy or sequentialtherapy beginning with 5mg/kg caspofungin, P 0.047. (B) Scatterplotof fungal burden (log10 CFU per g) in the lungs taken 24 h after thefinal dose in mice treated as described for panel A (n 7/group).Liposomal amphotericin B monotherapies or all combinations versusD5W, P 0.003 for lung tissue burden; liposomal amphotericin B orcombinations versus 5 mg/kg caspofungin, P 0.026 for lung tissueburden; 10 mg/kg liposomal amphotericin B followed by caspofunginversus caspofungin followed by liposomal amphotericin B, P 0.04.The horizontal lines indicate the median log10 CFU per g for eachgroup.
TABLE 2. Mean drug concentrations of indicated drugs in lungs,kidneys, and spleen after intravenous monotherapy (days 0 to 5)
for treatment of murine pulmonary aspergillosis
Drug Dosage(mg/kg/day)
Tissue drug concn ( g/g tissue) after 6treatments mean (SD) a
Lung Kidney Spleen
Liposomalamphotericin B
5 8.3 (3.7) 15.0d (6.5) 420e (41)10 23.7 (16.8)c 65.6 (31.5) 497e (426)
Caspofungin 5 Blqb (0) 14.4d (5.1) 31.6 (16.4)
a n 7 mice per group, except for 5 mg/kg/day caspofungin, which had 6mice per group; tissues were collected on day 6 postchallenge (24 h post-treatment).
b Blq, below limit of quantitation.c P 0.001 versus 5 mg/kg/day caspofungin.d P 0.01 versus 10 mg/kg/day liposomal amphotericin B.e P 0.001 versus 5 mg/kg/day caspofungin.
VOL. 54, 2010 LIPOSOMAL AMPHOTERICIN B AND ECHINOCANDINS FOR ASPERGILLOSIS 3891

in the tissues. Because several investigators have noted that theuse of more than one parameter (e.g., CFU per g, GI, andquantitative PCR [qPCR]) gives a better indication of theextent of the fungal growth in the host (52), we used both theCFU assay and the GI assay in some of our experiments. Thesetwo parameters produced similar results in our studies. It isimportant to underscore the importance of using a combina-tion of both survival and fungal burden as a means of evalu-ating drug efficacy, and in our studies, we observed a correla-tion between prolonged survival and reduction in the tissuefungal burden when the drug treatments were compared withthe D5W controls.
For the disseminated and pulmonary murine infections thatwe investigated, administering liposomal amphotericin B con-comitantly with micafungin or caspofungin, was neither antag-onistic, additive, nor synergistic with respect to improved sur-vival or fungal-burden reduction. However, in a rat model ofdisseminated A . fumigatus infection, Wasan et al. reportedadditive effects for the concomitant administration of liposo-mal amphotericin B (5 mg/kg) plus caspofungin (3 mg/kg) (58).In this disseminated study, the investigators showed that thecombination significantly decreased CFU (by 98%) comparedto untreated controls, while liposomal amphotericin B orcaspofungin alone decreased the CFU by 69% and 80%, re-spectively, compared to the untreated controls. Furthermore,in a preliminary report of liposomal amphotericin B in com-bination with echinocandins for the treatment of a nonfumiga-tus, murine disseminated infection, i.e., Aspergillus flavus, thedata suggested that concomitant treatment in this dissemi-nated model had additive effects (D. S. Constable, J. A. Olson,P. J. Smith, J. P. Adler-Moore, presented at the Third Ad-vances Against Aspergillosis Meeting, Miami, FL, 2008). Thus,additional studies of concomitant therapy using different ani-mal models and other Aspergillus species are needed to furtherour understanding of this therapeutic approach.
In contrast to the concomitant therapy, we found that thereduction of kidney fungal burden in the disseminated infec-tion, was significantly better if the liposomal amphotericin Bwas given prior to caspofungin than if caspofungin was givenfirst (sequential therapy). In previous work using the samedisseminated A . fumigatus model, we observed that liposomalamphotericin B given before the echinocandin micafungin wasalso more effective in reducing kidney fungal burden than ifmicafungin was given first (40a). Similarly, in the pulmonary A .fumigatus infection reported here, both survival and reductionin the lung fungal burden were significantly better if liposomalamphotericin B was given prior to caspofungin therapy. Apossible explanation for these results is that liposomal ampho-tericin B is a fungicidal drug (6, 15) that lyses and kills most ofthe fungus within the first 3 days of treatment. This is sup-ported by our data showing that when liposomal amphotericinB, unlike the echinocandins, was given as monotherapy for just3 days, it was very effective. The echinocandins are fungistaticagainst Aspergillus species (6), and although they slow hyphalgrowth and cause hyphal fragmentation during the first 3 daysof treatment, there is still enough viable fungal material in thetissues so that switching treatment to liposomal amphotericinB on day 4 postinfection is not effective. The sequence in whichdrugs are administered is particularly important, since the timeof initiation of antifungal treatment for aspergillosis in the
clinic is critical in terms of the patient outcome. von Eiff et al.(54) reported that if treatment was started within the first 10days, the mortality rate was 41%, but if it was initiated after10 days, the mortality rate was 90%. Similarly, in our animalmodel, if we waited until day 4 postchallenge to initiatetreatment with either liposomal amphotericin B or micaf-ungin, the mice did not survive, given that the fungal burdenat this time was probably just too extensive for effective drugtreatment.
Although drug levels in the tissues were higher with liposo-mal amphotericin B than with the echinocandins, one cannotconclude that this would result in better efficacy for liposomalamphotericin B. In fact, in these studies, we showed that 5, 10,or 15 mg/kg liposomal amphotericin B delivered similar levelsof amphotericin B to the kidneys and spleens, and yet 5 mg/kgliposomal amphotericin B was not as effective as the higherdoses in reducing the fungal burden in these tissues. It ispossible that drug localization within the target tissue was notequivalent and that the drug in animals given a lower dose ofliposomal amphotericin B did not reach the same levels at thefungal infection site as did the higher liposomal amphotericinB doses. Given that the echinocandins and liposomal ampho-tericin B have marked variations in their pharmacokinetics (25,31, 53, 55, 56), modes of action against Aspergillus (1, 2, 6, 59),and MICs (4, 29, 30), the differences in survival and/or fungalburden between the echinocandins and liposomal amphoteri-cin B reported in our studies cannot be attributed directly tothe differences in their tissue drug levels. Tissue drug levels arejust one of several important variables that have to be consid-ered in evaluating differences in drug efficacy between drugclasses.
We selected the liposomal amphotericin B doses for ourmurine studies based on their clinical relevance (14, 28, 32, 56)and because in previously published mouse studies of aspergil-losis (11, 12, 39, 50), these doses were effective. In clinicalaspergillosis trials (14, 32), doses of 3 to 5 mg/kg had efficacyrates of 50 to 60%, and doses as high as 15 mg/kg were welltolerated in patients with invasive mold infections (56). Instudies of murine disseminated aspergillosis (50), other au-thors reported that both 3 and 10 mg/kg of liposomal ampho-tericin B were efficacious, although 10 mg/kg was the mostprotective. In our previous work using the same immunosup-pressed murine pulmonary aspergillosis model that was used inthis study (39), we determined that doses of 3 to 15 mg/kg ofliposomal amphotericin B produced 100% survival, althoughthe optimum treatment was achieved with 15 mg/kg, reducingthe lung fungal burden by 100-fold and causing no significantnephrotoxicity in the mice. For the echinocandins, we useddoses similar to those used by other investigators who evalu-ated combination treatments for disseminated aspergillosis(58).
Our use of optimal drug doses is in contrast to a study byGraybill et al. (21) in which suboptimal doses of liposomalamphotericin B (0.15 mg/kg) and micafungin (1 mg/kg) wereused to study combination therapy for murine aspergillosis.These investigators reported an additive reduction in spleenCFU in murine disseminated aspergillosis, but only if liposo-mal amphotericin B was given 1 day before micafungin, fol-lowed by the drugs administered together. The authors did notdetermine kidney CFU in their disseminated model. It is pos-
3892 OLSON ET AL. ANTIMICROB. AGENTS CHEMOTHER.

sible that no additive effects were observed in our study ineither the kidneys or spleens in the disseminated infectionbecause we used higher doses of each drug. It should be noted,however, that, similar to our findings with caspofungin andliposomal amphotericin B, Greybill et al. did not observe anyadditive effects with the combination of micafungin and lipo-somal amphotericin B in the treatment of murine pulmonaryaspergillosis.
In conclusion, treatment of A . fumigatus disseminated orpulmonary infection in mice with the combination of liposomalamphotericin B plus an echinocandin or liposomal amphoter-icin B given prior to the echinocandin was as effective asliposomal amphotericin B treatment alone with respect to pro-longing survival and decreasing fungal burden in the targettissues. In comparison, echinocandin monotherapy prolongedsurvival in the disseminated infection, but not in the pulmonaryinfection, and, in general, did not significantly reduce the fun-gal burden in either model compared to liposomal amphoter-icin B. Given that in both models there was significantly betterefficacy when liposomal amphotericin B was given prior to theechinocandins, these observations provide a strong rationalefor using liposomal amphotericin B first if sequential drugtherapy is used for aspergillosis.
ACKNOWLEDGMENTS
Support for this research was provided by a research grant fromGilead Sciences, Inc.
J.P.A.-M. has received funds for speaking at symposia organized onbehalf of Gilead Sciences, Inc. All of the authors have received fundsfor research support from Gilead Sciences, Inc.
REFERENCES
1. Adler-Moore, J., and R. T. Proffitt. 2002. AmBisome: liposomal formulation,structure, mechanism of action and pre-clinical experience. J. Antimicrob.Chemother. 49(Suppl. A):21–30.
2. Adler-Moore, J. P., and R. T. Proffitt. 2008. Amphotericin B lipid prepara-tions: what are the differences? Clin. Microb. Infect. 14(Suppl. 4):25–36.
3. Aliff, T. B., P. G. Maslak, J. G. Jurcic, M. L. Heaney, K. N. Cathcart, K. A.Sepkowitz, and M. A. Weiss. 2003. Refractory Aspergillus pneumonia inpatients with acute leukemia: successful therapy with combination caspofun-gin and liposomal amphotericin. Cancer 97:1025–1032.
4. Antachopoulos, C., J.Meletiadis, T. Sein, E. Roilides, and T. J. Walsh. 2008.Comparative in vitro pharmacodynamics of caspofungin, micafungin, andanidulafungin against germinated and nongerminated Aspergillus conidia.Antimicrob. Agents Chemother. 52:321–328.
5. Barwicz, J., and P. Tancrede. 1997. The effect of aggregation state onamphotericin-B on its interactions with cholesterol- or ergosterol-containingphosphatidylcholine monolayers. Chem. Phys. Lipids 85:145–155.
6. Bowman, J. C., P. S. Hicks, M. B. Kurtz, H. Rosen, D. M. Schmatz, P. A.Liberator, and C. M. Douglas. 2002. The antifungal echinocandin caspofun-gin acetate kills growing cells of Aspergillus fumigatus in vitro. Antimicrob.Agents Chemother. 46:3001–3012.
7. Bretagne, S., A. Marmorat-Khuong, M. Kuentz, J. P. Latge, E. Bart-Delabesse, and C. Cordonnier. 1997. Serum Aspergillus galactomannan an-tigen testing by sandwich ELISA: practical use in neutropenic patients.J. Infect. 35:7–15.
8. Caillot, D., A. Thiebaut, R. Herbrecht, S. de Botton, A. Pigneux, F. Bernard,J. Larche, F. Monchecourt, S. Alfandari, and L. Mahi. 2007. Liposomalamphotericin B in combination with caspofungin for invasive aspergillosis inpatients with hematologic malignancies: a randomized pilot study (Combist-rat trial). Cancer 110:2740–2746.
9. Cesaro, S., T. Toffolutti, C. Messina, E. Calore, R. Alaggio, R. Cusinato, M.Pillon, and L. Zanesco. 2004. Safety and efficacy of caspofungin and liposo-mal amphotericin B, followed by voriconazole in young patients affected byrefractory invasive mycosis. Eur. J. Haematol. 73:50–55.
10. Clemons, K. V., and D. A. Stevens. 2006. Efficacy of micafungin alone or incombination against experimental pulmonary aspergillosis. Med. Mycol. 44:69–73.
11. Clemons, K. V., and D. A. Stevens. 2004. Comparative efficacies of four ampho-tericin B formulations—Fungizone, Amphotec (Amphocil), AmBisome, andAbelcet—against systemic murine aspergillosis. Antimicrob. Agents Che-mother. 48:1047–1050.
12. Clemons, K. V., M. Espiritu, R. Parmar, and D. A. Stevens. 2005. Compar-ative efficacies of conventional amphotericin B, liposomal amphotericin B(AmBisome), caspofungin, micafungin, and voriconazole alone and in com-bination against experimental murine central nervous system aspergillosis.Antimicrob. Agents Chemother. 49:4867–4875.
13. Clemons, K. V., M. Espiritu, R. Parmar, and D. A. Stevens. 2006. Assess-ment of the paradoxical effect of caspofungin in therapy of candidiasis.Antimicrob. Agents Chemother. 50:1293–1297.
14. Cornely, O. A., J. Maertens, M. Bresnik, R. Ebrahimi, A. J. Ullmann, E.Bouza, C. P. Heussel, O. Lortholary, C. Rieger, A. Boehme, M. Aoun, H. A.Horst, A. Thiebaut, M. Ruhnke, D. Reichert, N. Vianelli, S. W. Krause, E.Olavarria, R. Herbrecht, and the AmBiLoad Trial Study Group. 2007. Li-posomal amphotericin B as initial therapy for invasive mold infection: arandomized trial comparing a high-loading dose regimen with standard dos-ing (AmBiLoad Trial). Clin. Infect. Dis. 44:1289–1297.
15. Czub, J., and M. Baginski. 2006. Modulation of amphotericin B membraneinteraction by cholesterol and ergosterol—a molecular dynamics study. J.Phys. Chem. 110:16743–16753.
16. Denning, D. W. 1996. Therapeutic outcome in invasive aspergillosis. Clin.Infect. Dis. 23:608–615.
17. Dennis, C. G., W. R. Greco, Y. Brun, R. Youn, H. K. Slocum, R. J. Bernacki,R. Lewis, N. Wiederhold, S. M. Holland, R. Petraitiene, T. J. Walsh, andB. H. Segal. 2006. Effect of amphotericin B and micafungin combination onsurvival, histopathology, and fungal burden in experimental aspergillosis inthe p47phox / mouse model of chronic granulomatous disease. Antimicrob.Agents Chemother. 50:422–427.
18. Douglas, C. M. 2001. Fungal (1, 3)-D-glucan synthesis. Med. Mycol.39(Suppl. 1):55–66.
19. Enoch, D. A., H. A. Ludlam, and N. M. Brown. 2006. Invasive fungal infec-tions: a review of epidemiology and management options. J. Med. Microb.55:809–818.
20. Ghannoum, M., and L. B. Rice. 1999. Antifungal agents: mode of action,mechanism of resistance, and correlation of these mechanisms with bacterialresistance. Clin. Microb. Rev. 12:501–517.
21. Graybill, J. R., R. Bocanegra, G. M. Gonzalez, and L. K. Najvar. 2003.Combination antifungal therapy of murine aspergillosis: liposomal ampho-tericin B and micafungin. J. Antimicrob. Chemother. 52:656–662.
22. Herbrecht, R., D. W. Denning, T. F. Patterson, J. E. Bennett, R. E. Greene,J. W. Oestmann, W. V. Kern, K. A. Marr, P. Ribaud, O. Lortholary, R.Sylvester, R. H. Rubin, J. R. Wingard, P. Stark, C. Durand, D. Caillot, E.Thiel, P. H. Chandrasekar,M. R. Hodges, H. T. Schlamm, P. F. Troke, B. dePauw, and the Invasive Fungal Infections Group of the European Organi-sation for Research and Treatment of Cancer and the Global AspergillusStudy Group. 2002. Voriconazole versus amphotericin B for primary therapyof invasive aspergillosis. N. Engl. J. Med. 347:408–415.
23. Ibrahim, A. S., J. C. Bowman, V. Avanessian, K. Brown, B. Spellberg, J. E.Edwards, Jr., and C.M. Douglas. 2005. Caspofungin inhibits Rhizopus oryzae1,3- -D-glucan synthase, lowers burden in brain measured by quantitativePCR, and improves survival at a low, but not a high dose, during murinedisseminated zygomycosis. Antimicrob. Agents Chemother. 49:721–727.
24. Johnson, M. D., C. MacDougall, L. Ostrosky-Zeichner, J. R. Perfect, andJ. H. Rex. 2004. Combination antifungal therapy. Antimicrob. Agents Che-mother. 48:693–715.
25. Kartsonis, N. A., A. J. Saah, C. Joy Lipka, A. F. Taylor, and C. A. Sable.2005. Salvage therapy with caspofungin for invasive aspergillosis: resultsfrom the caspofungin compassionate use study. J. Infect. 50:196–205.
26. Krivan, G., J. Sinko, I. Z. Nagy, V. Goda, P. Remenyi, A. Batai, S. Lueff, B.Kapas, M. Reti, A. Tremmel, and T. Masszi. 2006. Successful combinedantifungal salvage therapy with liposomal amphothericin B and caspofunginfor invasive Aspergillus flavus infection in a child following allogeneic bonemarrow transplantation. Acta Biomed. 77(Suppl. 2):17–21.
27. Kurtz, M. B., I. B. Heath, J. Marrinan, S. Dreikorn, J. Onishi, and C.Douglas. 1994. Morphological effects of lipopeptides against Aspergillus fu-migatus correlate with activities against (1,3)-beta-D-glucan synthase. Anti-microb. Agents Chemother. 38:1480–1489.
28. Lanternier, F., and O. Lortholary. 2008. Liposomal amphotericin B: what isits role in 2008? Clin. Microbiol. Infect. 14(Suppl. 4):71–83.
29. Lass-Florl, C., M. Nagl, E. Gunsilius, C. Speth, H. Ulmer, and R. Wurzner.2002. In vitro studies on the activity of amphotericin B and lipid-basedamphotericin B formulations against Aspergillus conidia and hyphae. Myco-ses 45:166–169.
30. Lass-Florl, C., A. Mayr, S. Perkhofer, G. Hinterberger, J. Hausdorfer, C.Speth, and M. Fille. 2008. Activities of antifungal agents against yeasts andfilamentous fungi: assessment according to the methodology of the Euro-pean Committee on Antimicrobial Susceptibility Testing. Antimicrob.Agents Chemother. 52:3637–3641.
31. Lee, J. W., M. A. Amantea, P. A. Francis, E. E. Navarro, J. Bacher, P. A.Pizzo, and T. J. Walsh. 1994. Pharmacokinetics and safety of a unilamellarliposomal formulation of amphotericin B (AmBisome) in rabbits. Antimi-crob. Agents Chemother. 38:713–718.
32. Leenders, A. C., S. Daenen, R. L. Jansen, W. C. Hop, B. Lowenberg, P. W.Wijermans, J. Cornelissen, R. Herbrecht, H. van der Lelie, H. C. Hoogst-
VOL. 54, 2010 LIPOSOMAL AMPHOTERICIN B AND ECHINOCANDINS FOR ASPERGILLOSIS 3893
eden, H. A. Verbrugh, and S. de Marie. 1998. Liposomal amphotericin Bcompared with amphotericin B deoxycholate in the treatment of docu-mented and suspected neutropenia-associated invasive fungal infections.Br. J. Haematol. 103:205–212.
33. Leenders, A. C. A. P., S. deMarie,M. T. ten Kate, I. A. Bakker-Woudenberg,and H. A. Verbrugh. 1996. Liposomal amphotericin B (AmBisome) reducesdissemination of infection as compared with amphotericin B deoxycholate(Fungizone) in a rat model of pulmonary aspergillosis. J. Antimicrob. Che-mother. 38:215–225.
34. Lin, S.-J., J. Schranz, and S. M. Teutsch. 2001. Aspergillosis case-fatalityrate: systematic review of the literature. Clin. Infect. Dis. 32:258–366.
35. Maertens, J., J. Verhaegen, K. Lagrou, J. Van Eldere, and M. Boogaerts.2001. Screening for circulating galactomannan as a noninvasive diagnostictool for invasive aspergillosis in prolonged neutropenic patients and stem celltransplantation recipients: a prospective validation. Blood 97:1604–1610.
36. Marr, K. A., R. A. Carter, F. Crippa, A. Wald, and L. Corey. 2002. Epide-miology and outcome of mould infections in hematopoietic stem cell trans-plant recipients. Clin. Infect. Dis. 34:909–917.
37. Martín-Mazuelos, E., J. Peman, A. Valverde,M. Chaves,M. C. Serrano, andE. Canton. 2003. Comparison of the Sensititre YeastOne colorimetric anti-fungal panel and Etest with the NCCLS M38-A method to determine theactivity of amphotericin B and itraconazole against clinical isolates of As-pergillus spp. J. Antimicrob. Chemother. 52:365–370.
38. Olson, J. A., J. P. Adler-Moore, G. M. Jensen, J. Schwartz, M. C. Dignani,and R. T. Proffitt. 2008. Comparison of the physicochemical, antifungal, andtoxic properties of two liposomal amphotericin B products. Antimicrob.Agents Chemother. 52:259–268.
39. Olson, J. A., J. P. Adler-Moore, J. Schwartz, G.M. Jensen, and R. T. Proffitt.2006. Comparative efficacies, toxicities, and tissue concentrations of ampho-tericin B lipid formulations in a murine pulmonary aspergillosis model.Antimicrob. Agents Chemother. 50:2122–2131.
40. Olson, J. A., J. P. Adler-Moore, P. J. Smith, and R. T. Proffitt. 2005. Treat-ment of C andida glabrata infection in immunosuppressed mice by using acombination of liposomal amphotericin B with caspofungin or micafungin.Antimicrob. Agents Chemother. 49:4895–4902.
40a.Olson, J. A., D. S. Constable, P. J. Smith, and J. P. Adler-Moore. 2006.Abstr. 46th Annu. Intersci. Conf. Antimicrob. Agents Chemother., SanFrancisco, CA, poster M-1746. American Society for Microbiology, Wash-ington, DC.
41. Pancham, S., C. Hemmaway, H. New, E. Albert, I. Dokal, I. A. Roberts,and M. McCloy. 2005. Caspofungin for invasive fungal infections: com-bination treatment with liposomal amphotericin B in children undergoinghemopoietic stem cell transplantation. Pediatr. Transplant. 9:254–257.
42. Perfect, J. R., G. M. Cox, J. Y. Lee, C. A. Kauffman, L. de Repentigny, S. W.Chapman, V. A. Morrison, P. Pappas, J. W. Hiemenz, D. A. Stevens, and theMycoses Study Group. 2001. The impact of culture isolation of Aspergillusspecies: a hospital-based survey of aspergillosis. Clin. Infect. Dis. 33:1824–1833.
43. Pfaller, M. A., P. G. Pappas, and J. R. Wingard. 2006. Invasive fungalpathogens: current epidemiological trends. Clin. Infect. Dis. 43(Suppl. 1):S3–S14.
44. Richardson,M., and C. Lass-Florl. 2008. Changing epidemiology of systemicfungal infections. Clin. Microbiol. Infect. 14(Suppl. 4):5–24.
45. Shao, P.-L., L.-M. Huang, and P.-R. Hsueh. 2007. Recent advances andchallenges in the treatment of invasive fungal infections. Int. J. Antimicrob.Agents 30:487–495.
46. Sionov, E., S. Mendlovic, and E. Segal. 2006. Efficacy of amphotereicin B oramphotericin B-intralipid in combination with caspofungin against experi-mental aspergillosis. J. Infect. 53:131–139.
47. Sionov, E., S. Mendlovic, and E. Segal. 2005. Experimental systemic murine
aspergillosis: treatment with polyene and caspofungin combination and G-CSF. J. Antimicrob. Chemother. 56:594–597.
48. Smith, P. J., J. A. Olson, D. Constable, J. Schwartz, R. T. Proffitt, and J. P.Adler-Moore. 2007. Effects of dosing regimen on accumulation, retentionand prophylactic efficacy of liposomal amphotericin B. J. Antimicrob. Che-mother. 59:941–951.
49. Stevens, D. A., M. Espiritu, and R. Parmar. 2004. Paradoxical effect ofcaspofungin: reduced activity against C andida albicans at high drug concen-trations. Antimicrob. Agents Chemother. 48:3407–3411.
50. Takemoto, K., Y. Yamamoto, Y. Ueda, Y. Sumita, K. Yoshida, and Y. Niki.2004. Comparative studies on the efficacy of AmBisome and Fungizone in amouse model of disseminated aspergillosis. J. Antimicrob. Chemother. 53:311–317.
51. Torrado, J. J., R. Espada, M. P. Ballesteros, and S. Torrado-Santiago. 2008.Amphotericin B formulations and drug targeting. J. Pharm. Sci. 97:2405–2425.
52. Vallor, A. C., W. R. Kirkpatrick, L. K. Najvar, R. Bocanegra, M. C. Kinney,A. W. Fothergill, M. L. Herrera, B. L. Wickes, J. R. Graybill, and T. F.Patterson. 2008. Assessment of Aspergillus fumigatus burden in pulmonarytissue of guinea pigs by quantitative PCR, galactomannan enzyme immuno-assay, and quantitative culture. Antimicrob. Agents Chemother. 52:2593–2598.
53. Viscoli, C., R. Herbrecht, H. Akan, I. Baila, C. Doyen, A. Gallamini, A.Giagounidis, O. Marchetti, R. Martino, L. Meerts, W. Paesmans, M. R.Shivaprakash, A. J. Ullmann, J. Maertens, and the Infectious DiseasesGroup of the EORTC. 2007. Caspofungin © as first-line therapy of invasiveaspergillosis (IA) in haematological patients (pts): a study of the EORTCInfectious Disease Group, abstr. O12. J. Chemother. 19(Suppl. 3):36.
54. von Eiff, M., N. Roos, R. Schulten, M. Hesse, M. Zuhlsdorf, and J. van deLoo. 1995. Pulmonary aspergillosis: early diagnosis improves survival. Res-piration 62:341–347.
55. Walsh, T. J., V. Yeldandi, M. McEvoy, C. Gonzalez, S. J. Chanock, A.Freifeld, N. I. Seibel, P. Jarosinski, G. Boswell, I. Bekersky, A. Alak, D.Buell, J. Barret, and W. Wilson. 1998. Safety, tolerance, and pharmaco-kinetics of a small unilamellar liposomal formulation of amphotericin B(AmBisome) in neutropenic patients. Antimicrob. Agents Chemother.42:2391–2398.
56. Walsh, T. J., J. L. Goodman, P. Pappas, I. Bekersky, D. N. Buell, M. Roden,J. Barrett, and E. J. Anaissie. 2001. Safety, tolerance, and pharmacokineticsof high-dose liposomal amphotericin B (AmBisome) in patients infectedwith Aspergillus species and other filamentous fungi: maximum tolerateddose study. Antimicrob. Agents Chemother. 45:3487–3496.
57. Warn, P. A., G. Morrissey, J. Morrissey, and D. W. Denning. 2003. Activityof micafungin (FK463) against an itraconazole-resistant strain of Aspergillusfumigatus and a strain of Aspergillus terreus demonstrating in vivo resistanceto amphotericin B. J. Antimicrob. Chemother. 51:913–919.
58. Wasan, K. M., O. Sivak, M. Rosland, V. Risovic, and K. Bartlett. 2007.Assessing the antifungal activity, pharmacokinetics, and tissue distribution ofamphotericin B following the administration of Abelcet® and AmBisome®in combination with Caspofungin to rats infected with Aspergillus fumigatus.J. Pharm. Sci. 96:1737–1747.
59. Watabe, E., T. Nakai, S. Matsumoto, F. Ikeda, and K. Hatano. 2003. Killingactivity of micafungin against Aspergillus fumigatus hyphae assessed byspecific fluorescent staining for cell viability. Antimicrob. Agents Che-mother. 47:1995–1998.
60. Wiederhold, N. P., D. P. Kontoyiannis, C. Jingduan, J. Chi, R. A. Prince,V. H. Tam, and R. E. Lewis. 2004. Pharmacodynamics of caspofungin in amurine model of invasive pulmonary aspergillosis: evidence of concentra-tion-dependent activity. J. Infect. Dis. 190:1464–1471.
61. Wiederhold, N. P. 2009. Paradoxical echinocandin activity: a limited in vitrophenomenon? Med. Mycol. 47(Suppl. 1):S369–S375.
3894 OLSON ET AL. ANTIMICROB. AGENTS CHEMOTHER.
Copyright © 2022 FDOKUMEN




















