Legal Provisions and Management Perspectives of Biomedical and Hospital Waste in India
26
ISSN No : 2394 - 3033, V – 1, I – 2, 2014 Journal Club for Management Studies (JCMS) Manuscript No: JCMS/RES/2014/12, Received On: 27/10/2014 , Accepted On : 07/11/2014, Published On: 20/11/2014 RESEARCH ARTICLE © All Rights Reserved by “Journals Club & Co.” 11 Legal Provisions and Management Perspectives of Biomedical and Hospital Waste in India Dr. Prashant Mehta 1 * 1 Assistant Professor, Faculty of Science, National Law University, Jodhpur, Rajasthan ABSTRACT Medical care is vital for our life, health and wellbeing. But the waste generated from medical activities can be hazardous, toxic and even lethal because of their high potential for diseases transmission. The hazardous and toxic parts of waste from healthcare establishments comprising infectious, medical, and radioactive material as well as sharps constitute a grave risks to mankind and the environment, if these are not properly treated /disposed or are allowed to be mixed with other municipal waste. In India, practical information on this aspect is slowly developing and research on the public health implications because of poor management of medical wastes (both Hospital and Biomedical) is hardly any and limited in scope. Findings drawn from literature particularly from the developing economies and more so India, highlights range of issues like lack of adequate finance, lack of awareness of the risks involved in handling medical wastes (both Hospital and Biomedical), lack of appropriate legislation or in other words poorly enforced legislation, and lack of specialized staff to handle and dispose medical wastes (both Hospital and Biomedical). The paper recommends how medical wastes (both Hospital and Biomedical) practices can be improved in medical facilities all across the country and how legislation will be helpful in handling this problem of great magnitude. KEYWORDS Biomedical Wastes, Hospital Waste, Waste Management, Infections, Sustainability, Waste Related Legislation INTRODUCTION Healthcare is vital for our life, health, and wellbeing. Healthcare activities are a means of protecting health, curing patients, and saving lives. However the waste generated from medical activities is hazardous, toxic, and even lethal because of their high potential for disease transmission (20 percent of which entails risk either of infection, of trauma, of chemical or radiation exposure). Although the risks associated with hazardous medical waste and the ways and means of managing that waste are relatively well Address for Correspondence: Dr. Prashant Mehta, Assistant Professor, Faculty of Science, National Law University, Jodhpur, Rajasthan Email: [email protected]
-
Upload
nlujodhpur -
Category
Documents
-
view
2 -
download
0
Transcript of Legal Provisions and Management Perspectives of Biomedical and Hospital Waste in India
ISSN No : 2394 - 3033, V – 1, I – 2, 2014 Journal Club for Management Studies (JCMS)
Manuscript No: JCMS/RES/2014/12, Received On: 27/10/2014 , Accepted On : 07/11/2014, Published On: 20/11/2014
RESEARCH ARTICLE
© All Rights Reserved by “Journals Club & Co.” 11
Legal Provisions and Management Perspectives of Biomedical and Hospital Waste in India
Dr. Prashant Mehta 1*
1 Assistant Professor, Faculty of Science, National Law University, Jodhpur, Rajasthan
ABSTRACT Medical care is vital for our life, health and wellbeing. But the waste generated from medical activities can be hazardous, toxic and even lethal because of their high potential for diseases transmission. The hazardous and toxic parts of waste from healthcare establishments comprising infectious, medical, and radioactive material as well as sharps constitute a grave risks to mankind and the environment, if these are not properly treated /disposed or are allowed to be mixed with other municipal waste. In India, practical information on this aspect is slowly developing and research on the public health implications because of poor management of medical wastes (both Hospital and Biomedical) is hardly any and limited in scope. Findings drawn from literature particularly from the developing economies and more so India, highlights range of issues like lack of adequate finance, lack of awareness of the risks involved in handling medical wastes (both Hospital and Biomedical), lack of appropriate legislation or in other words poorly enforced legislation, and lack of specialized staff to handle and dispose medical wastes (both Hospital and Biomedical). The paper recommends how medical wastes (both Hospital and Biomedical) practices can be improved in medical facilities all across the country and how legislation will be helpful in handling this problem of great magnitude.
KEYWORDS
Biomedical Wastes, Hospital Waste, Waste Management, Infections, Sustainability, Waste Related Legislation
INTRODUCTION
Healthcare is vital for our life, health, and
wellbeing. Healthcare activities are a
means of protecting health, curing patients,
and saving lives. However the waste
generated from medical activities is
hazardous, toxic, and even lethal because
of their high potential for disease
transmission (20 percent of which entails
risk either of infection, of trauma, of
chemical or radiation exposure). Although
the risks associated with hazardous
medical waste and the ways and means of
managing that waste are relatively well
Address for Correspondence: Dr. Prashant Mehta, Assistant Professor, Faculty of Science, National Law University, Jodhpur, Rajasthan Email: [email protected]

Legal Provisions and Management Perspectives of Biomedical and Hospital Waste in India
© All Rights Reserved by “Journals Club & Co.” 12
known and described in various manuals
and other literature, the effective treatment
(waste handling and management) and
elimination / disposal methods advocated /
described requires an considerable
technical, financial resources, and strong
legal framework, which are often lacking
in most situations. The staff is often
unequipped / untrained for coping with this
task of handling and disposing bio-medical
wastes.
A healthcare activity for instance,
immunizations, diagnostic tests, medical
treatments, surgical procedures, and
laboratory examinations helps protect,
restore health, and save lives but at the
same time the obvious question is what
about the wastes and by-products they
generate. From the total of all wastes
generated by healthcare activities, almost
80 percent is general waste which is nearly
comparable to domestic waste, remaining
20 percent of wastes is considered highly
hazardous that may be infectious, toxic,
and radioactive in nature. Thus such
hazardous waste represents a threat to the
environment and human health if not
handled or disposed of properly.
In addition, the inappropriate treatment or
disposal of that medical (hospital and
biomedical) waste can lead to
environmental contamination or pollution
of air, water, and soil. Surface and ground
water contamination takes place when
waste reach water bodies. Residues from
waste can change the water chemistry,
which can affect all levels of an
ecosystem. The health of animals and
humans are affected when they drink the
contaminated water. A specific
environmental hazard caused by waste is
leachate, which is the liquid that forms, as
water trickles through contaminated areas
leaching out the chemicals. Thus poor
waste management practice can jeopardize
life of medical or paramedical care staff,
hospital employees who handle medical
(hospital and biomedical) waste, patients,
their families, and also impact population
living in vicinity of hospitals. In
unfavorable contexts, the risks associated
with hazardous medical (hospital and
biomedical) waste can be significantly
reduced through simple and appropriate
measures.
DEFINITION OF BIO-MEDICAL
WASTES
‘Bio-medical waste’ means any solid and
or liquid waste including its container and
any intermediate product, which is
generated during the diagnosis, treatment
or immunization of human beings or
animals or in research pertaining thereto or
in the production or testing thereof. All
biomedical waste is hazardous. In hospital
it comprises of 20 percent of total hospital
waste. The physiochemical, biological
nature of these components, their toxicity,
Legal Provisions and Management Perspectives of Biomedical and Hospital Waste in India
© All Rights Reserved by “Journals Club & Co.” 13
and potential hazard are different,
necessitating different methods / options
for their treatment / disposal. In Schedule I
of the Bio-medical Waste (Management
and Handling) Rules, 1998, therefore, the
waste originating from different kinds of
such establishments, has been categorized
into 10 different categories (as mentioned
in the box below) and their treatment and
disposal options have been indicated.
Handling, Segregation, Mutilation,
Disinfection, Storage, Transportation, and
Final disposal are vital steps for safe and
scientific management of biomedical waste
in any establishment1.
Components of Bio-Medical Waste
1. Human Anatomical Waste (tissues, organs, body parts etc.)
2. Animal Waste (as above, generated during research/experimentation, from veterinary hospitals etc.)
3. Microbiology and biotechnology waste, such as, laboratory cultures, micro-organisms, human and animal cell cultures, toxins etc.
4. Waste sharps, such as, hypodermic needles, syringes, scalpels, broken glass etc.
5. Discarded medicines and Cytotoxic drugs
6. Soiled waste, such as dressing, bandages, and plaster casts, material contaminated with blood etc.
7. Solid waste (disposable items like tubes, catheters etc. excluding sharps)
8. Liquid waste generated from any of the infected areas
9. Chemical Wastes and 10. Incineration Ash Waste
Bio-medical waste needs to be properly
managed due to various hazards it poses to
health of people, environment besides
legal, aesthetic reasons, and ethical
reasons. The ethical aspect is more
important as it is related to the social
responsibilities, which the health
professions have, as a result of their status,
knowledge, and skills and an obligation to
alert those who are at risk. This is reflected
by the compulsory notification of
infectious and notifiable diseases as a
measure of public Hospital Management.
The issue of indiscriminate Bio-Medical
Waste disposal and management in India
has attracted the attention of the highest
judicial body at the level of Hon’ble.
Supreme Court of India which has time to
time issued instructions regarding
management of Bio-Medical Waste and its
proper management.
INFECTIOUS WASTE
Infectious waste is suspected to contain
pathogens (bacteria, viruses, parasites, or
fungi) in sufficient concentration or
quantity to cause disease in susceptible
hosts. This category includes:
Cultures and stocks of infectious agents
from laboratory work.
Waste from surgery and autopsies on
patients with infectious diseases (e.g.
tissues, and materials or equipment that
have been in contact with blood or other
body fluids).
Waste from infected patients in isolation
wards (e.g. excreta, dressings from
infected or surgical wounds, clothes

Legal Provisions and Management Perspectives of Biomedical and Hospital Waste in India
© All Rights Reserved by “Journals Club & Co.” 14
heavily soiled with human blood or other
body fluids).
Waste that has been in contact with
infected patients undergoing
haemodialysis (e.g. dialysis equipment
such as tubing and filters, disposable
towels, gowns, aprons, gloves, and
laboratory coats).
Infected animals from laboratories.
Any other instruments or materials that
have been in contact with infected persons
or animals.
Note: Infected "Sharps" are a subcategory
of infectious waste.
All these institutions produce waste, which
is increasing in its amount and type, due to
advances in scientific knowledge and is
creating its impact2. The hazardous and
toxic waste from healthcare establishments
comprising infectious, bio-medical, and
radio-active material as well as sharps
(hypodermic needles, knives, scalpels etc.)
constitute a grave risk to human health
both for patients and personnel who handle
these wastes poses a threat to public health
and environment3, if these are not properly
treated or disposed off and are allowed to
get mixed with other municipal waste. Its
propensity to encourage growth of various
pathogen and vectors besides its ability to
contaminate other nonhazardous / non-
toxic municipal waste jeopardizes the
efforts undertaken for overall municipal
waste management. The rag pickers and
waste workers are often worst affected,
because unknowingly or unwittingly, they
rummage through all kinds of poisonous
material while trying to salvage items
which they can sell for reuse.
At the same time, this kind of illegal and
unethical reuse can be extremely
dangerous and even fatal. Diseases like
cholera, plague, tuberculosis, hepatitis
(especially HBV), AIDS (HIV), diphtheria
etc. in either epidemic or even endemic
form, pose grave public health risks.
Unfortunately, in the absence of reliable
and extensive data, it is difficult to
quantify the dimension of the problem or
even the extent and variety of the risk
involved. With a judicious planning and
management, however, the risk can be
considerably reduced.
Hospital waste is a potential health hazard
to the health care workers, public, flora,
and fauna of the area where it is discarded.
Hospital acquired infection, transfusion
transmitted diseases, rising incidence of
Hepatitis B, and HIV, increasing land and
water pollution lead to increasing
possibility of catching many diseases
which reoccurs. Hospitals are known for
the treatment of sick persons but we are
unaware about the adverse effects of the
garbage and filth generated by them on
human body and environment. Now it is a
well-established fact that there are many
adverse and harmful effects to the
environment including human beings

Legal Provisions and Management Perspectives of Biomedical and Hospital Waste in India
© All Rights Reserved by “Journals Club & Co.” 15
which are caused by the "Hospital waste"
generated during the patient care.
DESCRIPTION OF MEDICAL WASTE
The term "medical waste" covers all
wastes produced in health-care or
diagnostic activities. 75 percent to 80
percent of hospital wastes are similar to
household refuse or municipal waste and
do not entail any particular hazard. Refuse
similar to household waste can be put
through the same collection, recycling and
processing procedure as the community's
municipal waste. The other 20 percent to
25 percent is called hazardous medical
waste or special waste. This type of waste
entails health risks. Emissions from
incinerators or other waste burning devices
and landfills can cause air contamination.
Incinerators routinely emit dioxins
(Dioxins are known to increase the
likelihood of cancer and are considered a
serious threat to public health.
Environmental campaigners describe
dioxins as among the most dangerous
poisons known), furans(Furan is a
colorless, flammable, highly volatile liquid
with a boiling point close to room
temperature. It is toxic and may be
carcinogenic), and polychlorinated bi-
phenyls (Also called PCBs, these were
used as coolants and insulating fluids for
transformers and capacitors, stabilizing
additives in flexible PVC coatings of
electrical wiring and electronic
components etc. PCB production was
banned in the 1970s due to the high
toxicity of most products containing PCBs.
PCBs are classified as persistent organic
pollutants which bio-accumulate in
animals). The wastes and by-products
cover a diverse range of materials, as the
following list illustrates4:
Infectious Wastes - Waste suspected to
contain pathogens e.g. laboratory cultures;
waste from isolation wards; tissues
(swabs), materials, or equipment that have
been in contact with infected patients,
excreta, wastes contaminated with blood
and its derivatives, discarded diagnostic
samples, infected animals from
laboratories, and contaminated materials
(swabs, bandages), and equipment
(disposable medical devices etc.)
Anatomic Wastes / Pathological Wastes -
Human tissues or fluids e.g. body parts;
blood and other body fluids; fetuses.
Recognizable body parts and animal
carcasses. Infectious and anatomic wastes
together represent the majority of the
hazardous waste, up to 15percent of the
total waste from healthcare activities.
Pathological waste consists of tissues,
organs, body parts, human fetuses and
animal carcasses, blood, and body fluids.
Within this category, recognizable human
or animal body parts are also called
anatomical waste. This category should
be considered as a subcategory of
infectious waste, even though it may also
include healthy body parts.

Legal Provisions and Management Perspectives of Biomedical and Hospital Waste in India
© All Rights Reserved by “Journals Club & Co.” 16
Sharps - Sharp waste e.g. needles;
infusion sets; scalpels; knives; blades;
broken glass. Sharps are items that could
cause cuts or puncture wounds, including
needles, hypodermic needles, scalpel and
other blades, knives, infusion sets, saws,
broken glass, and nails. Whether or not
they are infected, such items are usually
considered as highly hazardous health-care
waste
Chemical Wastes - Waste containing
chemical substances e.g. laboratory
reagents; film developer; disinfectants that
are expired or no longer needed; solvents.
Chemical waste consists of discarded
solid, liquid, and gaseous chemicals, for
example from diagnostic and experimental
work and from cleaning, housekeeping,
and disinfecting procedures. Chemical
waste from health care may be hazardous
or non-hazardous; in the context of
protecting health, it is considered to be
hazardous if it has at least one of the
following properties viz Toxic, Corrosive
(e.g. Acids of pH < 2 and Bases of pH >
12); Inflammable, Reactive (Explosive,
Water- Reactive, Shock- Sensitive);
Genotoxic (e.g. Cytostatic Drugs). Non-
hazardous chemical waste consists of
chemicals with none of the above
properties, such as sugars, amino acids,
and certain organic, and inorganic salts.
Pharmaceuticals Wastes - Waste
containing pharmaceuticals e.g.
pharmaceuticals that are expired or no
longer needed; items contaminated by or
containing pharmaceuticals (bottles,
boxes). Pharmaceutical waste includes
expired, unused, spilt, and contaminated
pharmaceutical products, drugs, vaccines,
and sera that are no longer required and
need to be disposed of appropriately. The
category also includes discarded items
used in the handling of pharmaceuticals,
such as bottles or boxes with residues,
gloves, masks, connecting tubing, and drug
vials.
Radioactive Matter / Waste - Waste
containing radioactive substances: radio-
nuclides used in laboratories or nuclear
medicine, urine or excreta of patients
treated. Glassware contaminated with
radioactive diagnostic material or radio-
therapeutic materials. Waste containing
radioactive substances e.g. unused liquids
from radiotherapy or laboratory research;
contaminated glassware, packages, or
absorbent paper; urine and excreta from
patients treated or tested with unsealed
radio-nuclides; sealed sources Cultures and
stocks of highly infectious agents, waste
from autopsies, animal bodies, and other
waste items that have been inoculated,
infected, or in contact with such agents are
called highly infectious waste.
Wastes with High Heavy Metal Content
Batteries; broken thermometers; blood-
pressure gauges; etc. heavy metals. Wastes
with a high heavy-metal content represent
a subcategory of hazardous chemical

Legal Provisions and Management Perspectives of Biomedical and Hospital Waste in India
© All Rights Reserved by “Journals Club & Co.” 17
waste, and are usually highly toxic.
Mercury wastes are typically generated by
spillage from broken clinical equipment
but their volume is decreasing with the
substitution of solid-state electronic
sensing instruments (thermometers, blood-
pressure gauges, etc.). Whenever possible,
spilled drops of mercury should be
recovered. Residues from dentistry have
high mercury content. Cadmium waste
comes mainly from discarded batteries.
Certain "reinforced wood panels"
containing lead is still used in radiation
proofing of X-ray and diagnostic
departments. A number of drugs contain
arsenic, but these are treated here as
pharmaceutical waste. Broken mercury
thermometers. Genotoxic waste,
radioactive matter and heavy metal content
represent about 1percent of the total waste
from health-care activities.
Pressurized Containers - Gas cylinders;
gas cartridges; aerosol cans. Many types of
gas are used in health care, and are often
stored in pressurized cylinders, cartridges,
and aerosol cans. Many of these, once
empty or of no further use (although they
may still contain residues), are reusable,
but certain types - notably aerosol cans -
must be disposed of. Whether inert or
potentially harmful, gases in pressurized
containers should always be handled with
care; containers may explode if incinerated
or accidentally punctured.
Genotoxic Wastes - Waste containing
substances with genotoxic properties e.g.
waste containing cytostatic drugs (often
used in cancer therapy); genotoxic
chemicals. Genotoxic waste is highly
hazardous and may have mutagenic,
teratogenic, or carcinogenic properties. It
raises serious safety problems, both inside
hospitals and after disposal, and should be
given special attention. Genotoxic waste
may include certain cytostatic drugs,
vomitus, urine, or faces from patients
treated with cytostatic drugs, chemicals,
and radioactive material. Cytotoxic (or
antineoplastic) drugs, the principal
substances in this category, have the
ability to kill or stop the growth of certain
living cells and are used in chemotherapy
of cancer. They play an important role in
the therapy of various neoplastic
conditions but are also finding wider
application as immunosuppressive agents
in organ transplantation and in treating
various diseases with an immunological
basis. Cytotoxic drugs are most often used
in specialized departments such as
oncology and radiotherapy units, whose
main role is cancer treatment; however,
their use in other hospital departments is
increasing and they may also be used
outside the hospital setting. Cytotoxic
wastes are generated from several sources
and can include the following:
Contaminated Materials from drug
preparation and administration, such as

Legal Provisions and Management Perspectives of Biomedical and Hospital Waste in India
© All Rights Reserved by “Journals Club & Co.” 18
syringes, needles, gauges, vials,
packaging;
Outdated Drugs, excess (leftover)
solutions, drugs returned from the wards;
Urine, faeces, and vomit from patients,
which may contain potentially hazardous
amounts of the administered cytostatic
drugs or of their metabolites and which
should be considered genotoxic for at least
48 hours and sometimes up to one week
after drug administration. In specialized
oncological hospitals, genotoxic waste
(containing cytostatic or radioactive
substances) may constitute as much as
1percent of the total healthcare wastes.
Harmful Cytostatic Drugs can be
categorized as follows:
Alkylating Agents: cause alkylation of
DNA nucleotides, which leads to cross-
linking and miscoding of the genetic stock;
Antimetabolites: inhibit the biosynthesis
of nucleic acids in the cell;
Mitotic Inhibitors: prevent cell
replication.
HAZARDOUS CHEMICALS USED IN
MAINTENANCE OF HOSPITALS
AND HEALTHCARE CENTERS
Formaldehyde - It is a significant source of
chemical waste in hospitals. It is used to
clean and disinfect equipment (e.g.
haemodialysis or surgical equipment), to
preserve specimens, to disinfect liquid
infectious waste, and in pathology,
autopsy, dialysis, embalming, and nursing
units.
Photographic Chemicals - Photographic
fixing and developing solutions are used in
X-ray departments. The fixer usually
contains 5-10 percent hydroquinone, 1-5
percent potassium hydroxide, and less than
1 percent silver. The developer contains
approximately 45 percent glutaraldehyde.
Acetic acid is used in both stop baths and
fixer solutions.
Solvents - Wastes containing solvents are
generated in various departments of a
hospital, including pathology and
histology laboratories and engineering
departments. Solvents used in hospitals
include halogenated compounds, such as
methylene chloride, chloroform,
trichloroethylene, and refrigerants, and
non-halogenated compounds such as
xylene, methanol, acetone, isopropanol,
toluene, ethyl acetate, and acetonitrile.
Organic Chemicals - Waste organic
chemicals generated in Health-Care
Facilities Include disinfecting and
cleaning solutions such as phenol-based
chemicals used for scrubbing floors,
perchlorethylene used in workshops and
laundries; oils such as vacuum-pump oils,
used engine oil from vehicles (particularly
if there is a vehicle service station on the
hospital premises); insecticides,
rodenticides.
Inorganic Chemicals - Waste inorganic
chemicals consist mainly of acids and
alkalis (e.g. sulfuric, hydrochloric, nitric,
and chromic acids, sodium hydroxide and

Legal Provisions and Management Perspectives of Biomedical and Hospital Waste in India
© All Rights Reserved by “Journals Club & Co.” 19
ammonia solutions). They also include
oxidants, such as potassium permanganate
(KMnO4) and potassium dichromate
(K2Cr2O7), and reducing agents, such as
sodium bisulfite (NaHSO3) and sodium
sulfite (Na2SO3). Chemicals and
pharmaceuticals amount to about
03percent of waste from healthcare
activities.
WASTE GENERATED IN INDIA
As per the Tenth Plan document, India
produces 48 million tonnes (MT) of urban
solid waste annually, with solid waste
generation being approximately 0.4 kg per
capita per day. The Director General of
Health Services estimates that 5.4 MT of
bio-medical waste is being generated in the
country every year; based on the
generation figure of 250 grams/capita/day.
The Tenth Plan document also estimates
that around 7.2 MT of hazardous waste is
being generated in the country. However,
no estimates exist for the other kinds of
wastes being generated in the country5.
A. RISKS AND IMPACT ON HEALTH
AND THE ENVIRONMENT
All persons who are in contact with
hazardous medical waste are potentially
exposed to the various risks it entails:
persons inside the establishment
generating the waste, those who handle it,
and persons outside the facility who may
be in contact with hazardous wastes or
their by-products, if there is no medical
waste management or if that management
is inadequate. The following groups of
persons are potentially exposed:
Inside the hospital: care staff (doctors,
nursing staff, auxiliaries), stretcher-
bearers, scientific, technical and logistic
personnel (cleaners, laundry staff, waste
managers, carriers, maintenance personnel,
pharmacists, laboratory technicians,
patients, families and visitors).
Outside the hospital: off-site transport
personnel, personnel employed in
processing or disposal infrastructures, the
general population (including adults or
children who salvage objects found around
the hospital or in open dumps).
B. RISKS ASSOCIATED WITH
HAZARDOUS MEDICAL WASTE
The health risks associated with hazardous
medical waste can be divided into four
categories:
1. RISKS OF TRAUMA AND
INFECTION
Health-care wastes are a source of
potentially dangerous micro-organisms
that can infect hospital patients, personnel
and the general public. There are many
different exposure routes: through injury
(cut, prick), through contact with the skin
or mucous membranes, through inhalation
or through ingestion.
Some accidental exposure to blood (AEB)
or to other body fluids are examples of
accidental exposure to hazardous medical
waste6.

Legal Provisions and Management Perspectives of Biomedical and Hospital Waste in India
© All Rights Reserved by “Journals Club & Co.” 20
As regards viral infections such as AIDS
and hepatitis B and C, it is nursing staff
that are most at risk of infection through
contaminated needles. Sharps and
pathogenic cultures are regarded as the
most hazardous medical waste. In 2000,
the World Health Organization (WHO)
estimated that at world level accidents
caused by sharps accounted for 66,000
cases of infection with the hepatitis B
virus, 16,000 cases of infection with
hepatitis C virus and 200 to 5,000 cases of
HIV infection amongst the personnel of
health-care facilities. Some wastes, such as
anatomical wastes, do not necessarily
entail a health risk or risk for the
environment but must be treated as special
wastes for ethical or cultural reasons. A
further potential risk is that of the
propagation of micro-organisms outside
health-care facilities which are present in
those facilities and which can sometimes
be resistant, a phenomenon that has not yet
been sufficiently studied.
2. SURVIVAL OF MICRO-ORGANISMS
IN THE ENVIRONMENT
Pathogenic micro-organisms have a
limited capacity of survival in the
environment. Survival depends on each
microorganism and on environmental
conditions (temperature, humidity, solar
Table 1: Examples of infections that can be caused by hazardous medical waste
Type of infection Infective agent Transmission agent
Gastrointestinal infections Enterobacteria (Salmonella, Vibrio cholerae, Shigella, etc.)
Feces, vomit
Respiratory infections
Mycobacterium tuberculosis, Streptococcus pneumoniae, SARS virus (Severe Acute Respiratory Syndrome),
measles virus
Inhaled secretions, saliva
Eye infections Herpes virus Eye secretions
Skin infections Streptococcus Pus
Anthrax Bacillus anthracis Skin secretions
Meningitis Neisseria meningitidis Cerebro-spinal fluid
AIDS Human Immunodeficiency Virus (HIV) Blood, sexual secretions, other body fluids
Haemorrhagic fever Lassa, Ebola, Marburg, and Junin viruses Blood and secretions
Viral hepatitis A Hepatitis A virus Feces
Viral hepatitis B and C Hepatitis B and C viruses Blood and other biological fluids
Avian influenza H5N1 virus Blood, feces
Legal Provisions and Management Perspectives of Biomedical and Hospital Waste in India
© All Rights Reserved by “Journals Club & Co.” 21
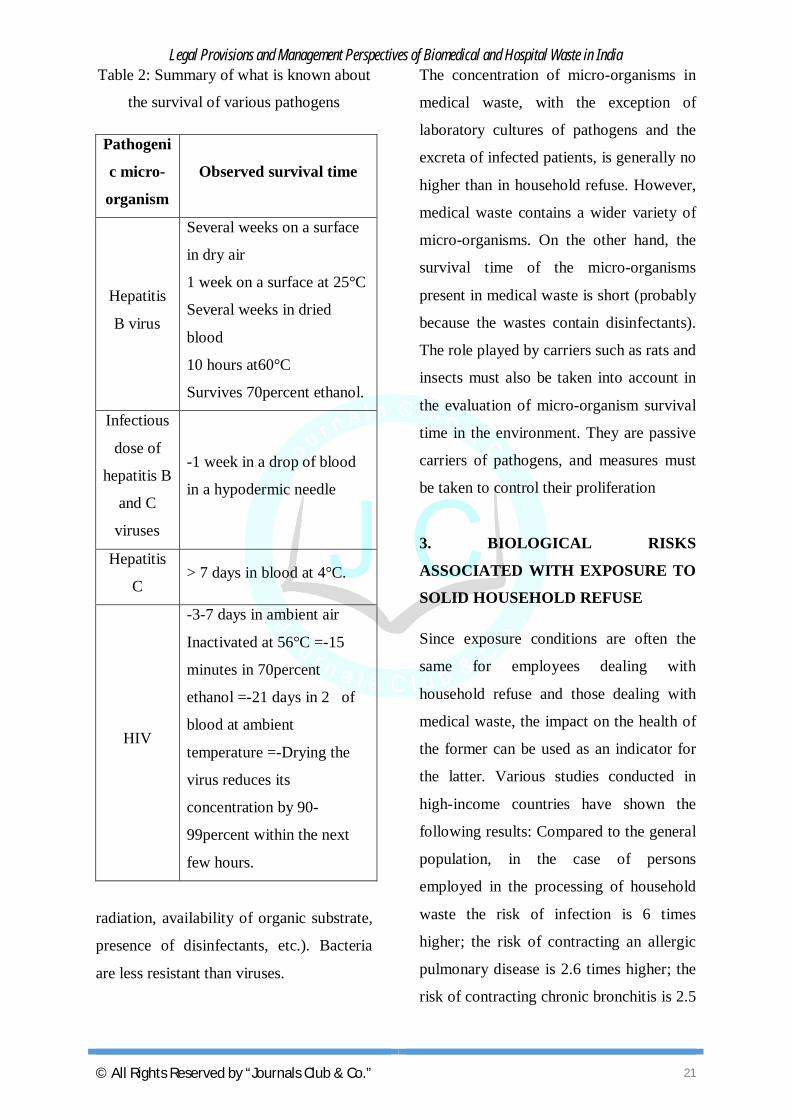
Table 2: Summary of what is known about
the survival of various pathogens
Pathogeni
c micro-
organism
Observed survival time
Hepatitis
B virus
Several weeks on a surface
in dry air
1 week on a surface at 25°C
Several weeks in dried
blood
10 hours at60°C
Survives 70percent ethanol.
Infectious
dose of
hepatitis B
and C
viruses
-1 week in a drop of blood
in a hypodermic needle
Hepatitis
C > 7 days in blood at 4°C.
HIV
-3-7 days in ambient air
Inactivated at 56°C =-15
minutes in 70percent
ethanol =-21 days in 2 of
blood at ambient
temperature =-Drying the
virus reduces its
concentration by 90-
99percent within the next
few hours.
radiation, availability of organic substrate,
presence of disinfectants, etc.). Bacteria
are less resistant than viruses.
The concentration of micro-organisms in
medical waste, with the exception of
laboratory cultures of pathogens and the
excreta of infected patients, is generally no
higher than in household refuse. However,
medical waste contains a wider variety of
micro-organisms. On the other hand, the
survival time of the micro-organisms
present in medical waste is short (probably
because the wastes contain disinfectants).
The role played by carriers such as rats and
insects must also be taken into account in
the evaluation of micro-organism survival
time in the environment. They are passive
carriers of pathogens, and measures must
be taken to control their proliferation
3. BIOLOGICAL RISKS
ASSOCIATED WITH EXPOSURE TO
SOLID HOUSEHOLD REFUSE
Since exposure conditions are often the
same for employees dealing with
household refuse and those dealing with
medical waste, the impact on the health of
the former can be used as an indicator for
the latter. Various studies conducted in
high-income countries have shown the
following results: Compared to the general
population, in the case of persons
employed in the processing of household
waste the risk of infection is 6 times
higher; the risk of contracting an allergic
pulmonary disease is 2.6 times higher; the
risk of contracting chronic bronchitis is 2.5

Legal Provisions and Management Perspectives of Biomedical and Hospital Waste in India
© All Rights Reserved by “Journals Club & Co.” 22
times higher; and the risk of contracting
hepatitis is 1.2 times higher. Pulmonary
diseases and bronchitis are caused by
exposure to the bio-aerosols contained in
the air at the sites where the refuse is
dumped, stored or processed.
4. CHEMICAL RISKS - Many chemical
and pharmaceutical products are used in
health-care facilities. Most of them entail a
health risk due to their properties (toxic,
carcinogenic, mutagenic, repro-toxic,
irritant, corrosive, sensitizing, explosive,
flammable, etc.). There are various
exposure routes for contact with these
substances: inhalation of gas, vapor or
droplets, contact with the skin or mucous
membranes, or ingestion. Some substances
(such as chlorine and acids) are incom-
patible and can generate toxic gases when
mixed. The identification of potential
hazards caused by certain substances or
chemical preparations can be easily done
through labeling: symbols, warning
statements or hazard statements. More
detailed information is set out in the
material safety data sheet (MSDS).
Cleaning products and, in particular,
disinfectants are examples of dangerous
chemicals which are used in large
quantities in hospitals. Most are irritant or
even corrosive, and some disinfectants
(such as formaldehyde) can be sensitizing
and toxic.
Mercury is a heavy metal in liquid form at
room temperature and pressure and is
highly toxic. It is very dense (1 liters of
mercury weighs 13.5 kg). It evaporates
readily and can remain for up to a year in
the atmosphere. It accumulates in
sediments, where it is converted into
methyl mercury, a more toxic organic
derivative. Mercury is found mainly in
thermometers, manometers, dental alloys,
certain types of battery, electronic
components and fluorescent or compact
fluorescent light tubes. Health-care
facilities are one of the main sources of
mercury in the atmosphere due to the
incineration of medical waste. These
facilities are also responsible for the
mercurial pollution of surface water. There
is no threshold under which it does not
produce any undesirable effect. Mercury
can cause fatal poisoning when inhaled. It
is harmful in the event of transcutaneous
absorption and has dangerous effects on
pregnancy. Silver is another toxic element
that is found in hospitals (photographic
developers). It is bactericidal. Bacteria
which develop resistance to silver are also
thought to be resistant to antibiotics.
C. RISKS ASSOCIATED WITH THE
INAPPROPRIATE PROCESSING
AND DUMPING OF HAZARDOUS
MEDICAL WASTE
A. Incineration Risks - In some cases,
particularly when wastes are incinerated at

Legal Provisions and Management Perspectives of Biomedical and Hospital Waste in India
© All Rights Reserved by “Journals Club & Co.” 23
low temperature (less than 800°C) or when
plastics containing polyvinyl chloride
(PVC) are incinerated, hydrochloric acid
(which causes acid rain), dioxins, furans
and various other toxic air-borne pollutants
are formed. They are found in emissions
but also in residual and other air-borne ash
and in the effluent gases released through
incinerator chimneys. Exposure to dioxins,
furans and other coplanar polychlorinated
biphenyls can have effects that are harmful
to public health. These substances are
persistent, that is to say, the molecules do
not break down in the environment and
they accumulate in the food chain. The
bulk of human exposure to dioxins, furans
and coplanar polychlorinated biphenyls
takes place through food intake.
Even in high-temperature incinerators
(over 800°C) there are cooler pockets at
the beginning or the end of the incineration
process where dioxins and furans can
form. Optimization of the process can
reduce the formation of these substances if
it is ensured, for example, that incineration
takes place only at temperatures above
800°C and if the formation of combustion
gas is prevented at temperatures of 200 -
400°C. And lastly, the incineration of
metals or of materials with a high metal
content (especially lead, mercury and
cadmium) can result in metals being
released into the environment.
D. RISKS RELATED TO RANDOM
DISPOSAL OR UNCONTROLLED
DUMPING
In addition to the above-mentioned risks,
burial and random dumping on
uncontrolled sites can have a direct impact
on the environment in terms of soil and
water pollution which impacts nearly
everyone including animals.
E. RISKS RELATED TO THE
DISCHARGE OF RAW SEWAGE
Poor management of wastewater and
sewage sludge can result in the
contamination of water and soil with
pathogens or toxic chemicals. Pouring
chemical and pharmaceutical wastes down
the drain can impair the functioning of
biological sewage treatment plants or
septic tanks. These can end up polluting
the ecosystem and water sources.
Antibiotics and their metabolites are
excreted in the urine and feces of patients
under treatment and end up in sewage.
Hospital sewage contains 2 to 10 times
more antibiotic-resistant bacteria than
domestic wastewater, a phenomenon
which contributes to the emergence and
propagation of pathogens such as MRSA
(methicillin-resistant Staphylococcus
aurous).
LEGISLATIVE AND POLICY
IMPERATIVES
Legal Provisions and Management Perspectives of Biomedical and Hospital Waste in India
© All Rights Reserved by “Journals Club & Co.” 24
International agreement has been reached
on a number of underlying principles that
govern either public health or safe
management of hazardous waste. These
principles outlined below should be taken
into consideration when national
legislation or regulations governing
healthcare waste management are
formulated:
The “Basel Convention” signed by
more than 100 countries, concerns
transboundary movements of
hazardous waste; it is also applicable to
health-care waste. Countries that
signed the Convention accepted the
principle that the only legitimate
transboundary shipments of hazardous
waste are exports from countries that
lack the facilities or expertise to
dispose safely of certain wastes to
other countries that have both facilities
and expertise.
The “polluter pays” principle implies
that all producers of waste are legally
and financially responsible for the safe
and environmentally sound disposal of
the waste they produce. This principle
also attempts to assign liability to the
party that causes damage.
The “precautionary” principle is a
key principle governing health and
safety protection. When the magnitude
of a particular risk is uncertain, it
should be assumed that this risk is
significant, and measures to protect
health and safety should be designed
accordingly.
The “duty of care” principle stipulates
that any person handling or managing
hazardous substances or related
equipment is ethically responsible for
using the utmost care in that task.
The “proximity” principle
recommends that treatment and
disposal of hazardous waste take place
at the closest possible location to its
source in order to minimize the risks
involved in its transport. According to
a similar principle, any community
should recycle or dispose of the waste
it produces, inside its own territorial
limits.
LEGAL PROVISIONS
National legislation is the basis for
improving health-care waste practices in
any country. It establishes legal controls
and permits the national agency
responsible for the disposal of healthcare
waste, usually the ministry of health, to
apply pressure for their implementation.
The ministry of environment or national
environmental protection agency may also
be involved; there should be a clear
designation of responsibilities before the
law is enacted.
The law should be complemented by a
policy document, and by technical

Legal Provisions and Management Perspectives of Biomedical and Hospital Waste in India
© All Rights Reserved by “Journals Club & Co.” 25
guidelines developed for implementation
of the law. This legal “package” should
specify regulations on treatment for
different waste categories, segregation,
collection, storage, handling, disposal, and
transport of waste, responsibilities, and
training requirements; it should take into
account the resources and facilities
available in the country concerned and any
cultural aspects of waste-handling. A
national law on healthcare waste
management may stand alone or may be
part of more comprehensive legislation
such as the following:
Law on management of hazardous
wastes: application to health-care
waste should be explicitly stated;
Law on hospital hygiene and infection
control.
The law should include the following:
A clear definition of hazardous health-
care waste and of its various
categories;
A precise indication of the legal
obligations of the health-care waste
producer regarding safe handling and
disposal;
Specifications for record-keeping and
reporting;
Specifications for an inspection system
to ensure enforcement of the law, and
for penalties to be imposed for
contravention;
Designation of courts responsible for
handling disputes arising from
enforcement of or noncompliance with
the law.
DISPOSAL GUIDELINES AND
LEGISLATIONS
Environmental health policies formulated
by nation states are intended to eliminate
the effects of exposure to environmental
hazards. While hospitals and other related
institutions providing healthcare are
engaged in safeguarding and promoting
human health, these very institutions
generate a lot of waste, the disposal of
which has serious environmental
implications. Therefore scientific methods
and effective safeguards for handling and
disposal of biomedical and hospital waste
had to be codified.
Indiscriminate disposal of infected and
hazardous waste from hospitals, nursing
homes, and pathological laboratories has
led to significant degradation of the
environment, leading to spread of diseases
and putting the people to great risk from
certain highly contagious and transmission
prone disease vectors. This has given rise
to considerable environmental concern.
The first standard on the subject to be
brought out in India was by the Bureau of
Indian Standards (BIS), IS 12625:1989,
entitled ‘Solid Wastes Hospitals
Guidelines for Management’ (Annexure

Legal Provisions and Management Perspectives of Biomedical and Hospital Waste in India
© All Rights Reserved by “Journals Club & Co.” 26
7.1) but it was unable to bring any
improvement in the situation. In this
scenario, the notification of the
‘Biomedical BIO-MEDICAL WASTE
(MANAGEMENT & HANDLING)
RULES 1998 assumes great significance.
Accordingly all the hospitals in the public
and private sector are now bound to follow
these rules to evade legal action7. The
Biomedical Waste Management &
Handling) Rules, 1998 came into force on
1998. In exercise of the powers conferred
by section 6, 8, and 25 of Environment
Protection Act, 1986, the Central
Government notified these rules for the
Management and Handling of biomedical
wastes generated from Hospitals, clinics,
other institutions for scientific importance.
The Biomedical waste means any waste,
which is generated during the diagnosis,
treatment or immunization of human
beings or animals or in research activities
pertaining thereto or in the production or
testing of biological and including
categories mentioned in schedule I of the
Rules.
It shall be the duty of every occupier of
an institution generating bio-medical
waste which includes a hospital, nursing
home, clinic, dispensary, veterinary
institution, animal house, pathological
laboratory, blood bank by whatever
name called to take all steps to ensure
that such waste is handled without any
adverse effect to human health and the
environment. The Segregation,
Packaging, Transportation and Storage
shall be done as under:-
1. Bio-medical waste shall not be mixed with other wastes.
2. Bio-medical wast e shall be segregated into containers / bags at the points of generation in accordance with Schedule II prior to its storage transportation, treatment and disposal. The containers shall be labeled according to Schedule III.
Every occupier of an institution
generating, collecting, receiving, storing,
transporting, treating and /or handling
Biomedical Waste shall apply on Form 1
for Authorization to the Board. The Board
grants authorizations after satisfying
itself. Every occupier / operator shall
submit an annual report to the prescribed
authority in Form II by 31 January every
year, to include information about the
categories and quantities of bio-medical
wastes handled during the preceding year.
The prescribed authority shall send this
information in a complied form to the
Central Pollution Control board by 31
March every year.
When any accident occurs at any
institution or facility or any other site
where bio-medical waste is handled or
during transportation of such waste, the
authorized person shall report the
accident in Form III to the prescribed
authority forthwith. Any person aggrieved
by an order made by the prescribed

Legal Provisions and Management Perspectives of Biomedical and Hospital Waste in India
© All Rights Reserved by “Journals Club & Co.” 27
authority under these rules, may within
thirty days from the date on which the
order is communicated to him, prefer an
appeal to such authority as the
government of State / Union Territory
may think fit to constitute. Provided that
the authority may entertain the appeal
after the expiry of the period of thirty
days if it is satisfied that the appellant
was prevented by sufficient cause from
filing the appeal in time. For violating the
provisions of these Rules, the Board can
file a complaint under section 15 of
Environment Protection Act which
provide for imprisonment which may
extend upto 5 years with fine. The Board
can also have directions for closure of
any defaulting hospital / clinic /
institution under section 5 of Environment
Protection Act as per powers delegated by
the Central Government. The Central
Government has notified these rules on
20th July, 1998 in exercise of section 6, 8,
and 25 of the Environment (Protection)
Act, 1986. Prior to that, the draft rules
were gazetted on 16th October, 1997 and
Public suggestion / comments were
invited within 60 days. These suggestions
were considered before finalising the
rules.
SCOPE AND APPLICATION OF THE
RULES
These rules apply to all those who
generate, collect, receive, store, transport,
treat, dispose or handle bio-medical waste
in any form. According to these rules, it
shall be the duty of every occupier of an
institution generating bio-medical waste,
which includes hospitals, nursing homes,
clinics, dispensaries, veterinary institution,
animal houses, pathology laboratories,
blood banks etc., to take all steps to ensure
that such wastes are handled without any
adverse effect to human health and the
environment.
They have to either set up their own
facility within the time frame (Schedule
VI) or ensure requisite treatment at a
common waste treatment facility or any
other waste treatment facility. Every
occupier of an institution, which is
generating, collecting, receiving, storing,
transporting, treating, disposing and/or
handling bio-medical waste in any other
manner, except such occupier of clinics,
dispensaries, pathological laboratories,
blood banks etc., which provide Treatment
/ service to less than 1000 (one thousand)
patients per month shall make an
application in prescribed form to the
prescribed authority for grant of
authorisation to carry on the work.
The State Pollution Control Board /
Committees have been asked to take action
against the defaulting hospitals or nursing
homes under section 15(1) of the
Environment (Protection) Act, 1996 which
reads as “ Whoever fails to comply with or
contravenes any of this act, or the rules
made or orders or directions issued
Legal Provisions and Management Perspectives of Biomedical and Hospital Waste in India
© All Rights Reserved by “Journals Club & Co.” 28
hereunder in respect of each such failure or
contravention, be punishable with the
imprisonment for a term which may extend
to 5 years or with fine which may extend
to one lakh rupees, or with both, and in
case of failure or contravention continues,
with additional fine which may extend to
five thousand rupees for every day during
which such failure or contravention
continues after the conviction for the first
such failure or contravention”8.
CONCERN FOR ENVIRONMENT
The following are the main environmental
concerns with respect to improper disposal
of bio-medical waste:
a. Spread of infection and disease
through vectors (fly, mosquito, insects
etc.) which affect the in-house as well
as surrounding population.
b. Spread of infection through contact /
injury among medical/non-medical
personnel and sweepers / rag pickers,
especially from the sharps (needles,
blades etc).
c. Spread of infection through
unauthorised recycling of disposable
items such as hypodermic needles,
tubes, blades, bottles etc.
d. Reaction due to use of discarded
medicines.
e. Toxic emissions from defective /
inefficient incinerators.
f. Indiscriminate disposal of incinerator
ash / residues.
BIO MEDICAL WASTES
(MANAGEMENT AND HANDLING)
RULES 2011
Ministry of Environment and Forests has
revised the Bio Medical
Waste (Management and Handling) Rules
promulgated under the Environment
Protection Act of 1986. The Rules now
called the Bio Medical Wastes
(Management and Handling) Rules 2011
are made more stringent and has been
notified for information of the masses and
feedback received from all fronts would be
considered by the Central Government.
BIO-MEDICAL WASTE RULES 2011:
KEY PROVISIONS
The new Rules on BMW are elaborate,
stringent and several new provisions have
been added in it. The Rules are not
applicable for the radioactive waste,
hazardous waste, municipal solid waste
and battery waste which would be dealt
under the respective rules. One of the
features of the new rules is that now every
occupier, operator regardless of the
number of patients being serviced has to
seek prior authorization from the
prescribed authority which is the State
Pollution Control Board for States and
Pollution Control Committee for Union
Territories. Earlier hospitals serving
thousand or more patients only required to

Legal Provisions and Management Perspectives of Biomedical and Hospital Waste in India
© All Rights Reserved by “Journals Club & Co.” 29
Table 3: BMW Rules 2011 vs. 1998
2011 1998
Every occupier
generating BMW,
irrespective of the
quantum of wastes
comes under the
BMW Rules and
requires to obtain
authorization
Occupiers with
more than 1000
beds required to
obtain authorization
Duties of the
operator listed
Operator duties
absent
Categories of
Biomedical Waste
reduced to Eight
Biomedical waste
divided in ten
categories
Treatment and
disposal of BMW
made mandatory
for all the HCEs
Rules restricted to
HCEs with more
than 1000 beds
A format for
annual report
appended with the
Rules
No format for
Annual Report
Form VI i.e. the
report of the
operator on HCEs
not handing over
the BMW added to
the Rules
Form VI absent
obtain authorization from the concerned
authorities. The present Rules also
specifies that irrespective of the quantum
of wastes generated, every occupier such
as from the hospitals, nursing homes,
clinics, dispensaries, veterinary
institutions, animal houses, pathological
laboratories and blood banks generating,
collecting, receiving, storing, transporting,
disposing or handling bio medical wastes
needs to obtain authorization from the
prescribed authority. “Such a change has
been proposed because earlier hospitals
did not give a clear picture of the number
of patients being served and thus evaded
authorization and were exempted from
treating their wastes.
The Bio Medical Waste (Management and
Handling) Rules 1998 contained ten
categories of wastes which have been
reduced in the present rules to eight. The
2011 Rules have discarded Category No. 8
(containing liquid waste generated from
laboratory, cleaning, washing, and
disinfection activities) and Category No. 9
(containing incineration ash). However,
laboratory wastes listed in Category 8 has
been included in the present Category 3.
The current rules have also cleared the
confusion over the color coding of the
containers used for disposal of BMW. The
Schedule II of the 1998 Rules creates a
confusion regarding the disposal of
Category 3 and Category 6 wastes which
could either be disposed in yellow or red
colored bags. Similarly, Category 7 wastes
could also be disposed in red or blue bags.

Legal Provisions and Management Perspectives of Biomedical and Hospital Waste in India
© All Rights Reserved by “Journals Club & Co.” 30
The present Rules have thus clarified the
ambiguity and allotted one color code to
each category of waste.
Table 4: Color Coding and Type of
Container for Disposal of BMW
Color
Coding
Type of
Container to
be Used
Waste
Category
Number
Yellow
Non
Chlorinated
plastic bags
Category
1,2,5,6
Red
Non
Chlorinated
plastic
bags/puncture
proof container
for sharps
Category
3,4,7
Blue
Non
Chlorinated
plastic bags
container
Category 8
Black
Non
Chlorinated
plastic bags
Municipal
Waste
Apart from the various categories of
wastes, Schedule II of the Rules has also
incorporated the storage and disposal of
municipal solid waste (MSW) generated
from the hospitals. The Rules expounds
that the MSW such as paper waste, food
waste and other noninfectious wastes
generated from the hospitals should be
stored in black colored bags/containers and
disposed as per the Municipal Solid Waste
(Management and Handling) Rules 2000.
NEW / EMERGING TECHNOLOGY
FOR WASTE TREATMENT /
MANAGEMENT OF WASTE
Different methods have been developed
for rendering bio-medical waste
environmentally innocuous and
aesthetically acceptable but all of them are
not suitable for our condition. The ‘Bio-
Medical Waste (Management & Handling)
Rules, 1998’ has elaborately mentioned the
recommended treatment and disposal
options according to the 10 different
categories of waste generated in health
care establishments. Standards for the
treatment technologies are given in
Schedule V of the Rules, which must be
complied with.
A comparison of the advantages and
limitations of the different technologies for
treatment of bio-medical waste is given at
Annexure A review of the above schedule
would show that there is no single
technology, which can take care of all
categories of bio-medical waste. A
judicious package has to be evolved for
this purpose. For example, small and
medium hospitals can opt for local (in
house) disinfection, mutilation / shredding
and dedicated autoclaving plus off-site
incineration at a common treatment /

Legal Provisions and Management Perspectives of Biomedical and Hospital Waste in India
© All Rights Reserved by “Journals Club & Co.” 31
disposal facility followed by disposal in
sanitary and secured landfills.
1. Incineration - This is a high
temperature thermal process employing
combustion of the waste under controlled
condition for converting them into inert
material and gases. Incinerators can be oil
fired or electrically powered or a
combination thereof. Broadly, three types
of incinerators are used for hospital waste:
multiple hearth type, rotary kiln and
controlled air types. All the types can have
primary and secondary combustion
chambers to ensure optimal combustion.
These are refractory lined. In the multiple
hearth incinerators, solid phase
combustion takes place in the primary
chamber whereas the secondary chamber
is for gas phase combustion. These are
referred to as excess air incinerators
because excess air is present in both the
chambers. The rotary kiln is a cylindrical
refractory lined shell that is mounted at a
slight tilt to facilitate mixing and
movement of the waste inside. It has
provision of air circulation. The kiln acts
as the primary solid phase chamber, which
is followed by the secondary chamber for
the gaseous combustion. In the third type,
the first chamber is operated at low air
levels followed by an excess air chamber.
Due to low oxygen levels in the primary
chamber, there is better control of
particulate matter in the flue gas. In a
nutshell, the primary chamber has
pyrolytic conditions with a temperature
range of about 800 ± 50◦C. The secondary
chamber operates under excess air
conditions at about 1050 ± 50◦C. The
volatiles are liberated in the first chamber
whereas they are destroyed in the second
one. Some models are fitted with educator
mechanism, which maintains the system
under negative pressure and helps control
the flue gases more effectively. The
chimney height should be minimum 30
meters above ground level. Installation of
incinerators in congested area is not
desirable. In the Bio-medical Waste
(Management and Handling) Rules,
Incineration has been recommended for
human anatomical waste, animal waste,
cytotoxic drugs, discarded medicines and
soiled waste.
2. Autoclave Treatment - This is a
process of steam sterilisation under
pressure. It is a low heat process in which
steam is brought into direct contact with
the waste material for duration sufficient to
disinfect the material. These are also of
three types: Gravity type, Pre-vacuum type
and Retort type. In the first type (Gravity
type), air is evacuated with the help of
gravity alone. The system operates with
temperature of 121◦C and steam pressure
of 15 psi. for 60-90 minutes. Vacuum
pumps are used to evacuate air from the
pre-vacuum autoclave system so that the
Legal Provisions and Management Perspectives of Biomedical and Hospital Waste in India
© All Rights Reserved by “Journals Club & Co.” 32
time cycle is reduced to 30-60 minutes. It
operates at about 132◦C. Retort type
autoclaves are designed to handle much
larger volumes and operate at much higher
steam temperature and pressure. Autoclave
treatment has been recommended for
microbiology and biotechnology waste,
waste sharps, soiled and solid wastes .This
technology renders certain categories of
bio-medical waste innocuous and
unrecognizable so that the treated residue
can be land-filled.
3. Hydroclave Treatment – It is
innovative equipment for steam
sterilization process (like autoclave). It is a
double walled container, in which the
steam is injected into the outer jacket to
heat the inner chamber containing the
waste. Moisture contained in the waste
evaporates as steam and builds up the
requisite steam pressure (35-36 psi).
Sturdy paddles slowly rotated by a strong
shaft inside the chamber tumble the waste
continuously against the hot wall thus
mixing as well as fragmenting the same. In
the absence of enough moisture, additional
steam is injected. The system operates at
132◦C and 36 psi steam pressure for
sterilization time of 20 minutes. The total
time for a cycle is about 50 minutes, which
includes start-up, heat-up, sterilization,
venting, and depressurization and
dehydration. The treated material can
further be shredded before disposal. The
expected volume and weight reductions
are upto 85 percent and 70 percent
respectively. The hydroclave can treat the
same waste as the autoclave plus the waste
sharps. The sharps are also fragmented.
This technology has certain benefits, such
as, absence of harmful air emissions,
absence of liquid discharges, non-
requirement of chemicals, reduced volume
and weight of waste etc. Tata Memorial
Hospital in Mumbai has installed the first
hydroclave in India in September 1999.
4. Microwave Treatment - This again
is a wet thermal disinfection technology
but unlike other thermal treatment systems,
which heat the waste externally,
microwave heats the targeted material
from inside out, providing a high level of
disinfection. The input material is first put
through a shredder. The shredded material
is pushed to a treatment chamber where it
is moistened with high temperature steam.
The material is then carried by a screw
conveyor beneath a series (normally 4-6
nos.) of conventional microwave
generators, which heat the material to 95-
100◦C and uniformly disinfect the material
during a minimum residence time of 30
minutes and total cycle is of 50 minutes. A
second shredder fragments the material
further into unrecognizable particles before
it is automatically discharged into a
conventional / general waste container.
This treated material can be land-filled

Legal Provisions and Management Perspectives of Biomedical and Hospital Waste in India
© All Rights Reserved by “Journals Club & Co.” 33
provided adequate care is taken to
complete the microwave treatment. In the
modern versions, the process control is
computerized for smooth and effective
control. Microwave technology has certain
benefits, such as, absence of harmful air
emissions (when adequate provision of
containment and filters is made), absence
of liquid discharges, non-requirement of
chemicals, reduced volume of waste (due
to shredding and moisture loss) and
operator safety (due to automatic hoisting
arrangement for the waste bins into the
hopper so that manual contact with the
waste bags is not necessary). However, the
investment cost is high at present.
According to the rules, category Nos, 03
(microbiology and biotechnology waste),
04 (waste sharps), 06 (soiled waste), and
07 (solid waste) are permitted to be
microwaved.
5. Chemical Disinfecting - This
treatment is recommended for waste
sharps, solid and liquid wastes as well as
chemical wastes. Chemical treatment
involves use of at least 01percent
hypochlorite solution with a minimum
contact period of 30 minutes or other
equivalent chemical reagents such as
phenolic compounds, iodine,
hexachlorophene, iodine-alcohol or
formaldehyde-alcohol combination etc.
Preceding of the waste is desirable for
better contact with the waste material. In
the USA, chemical treatment facility is
also available in mobile vans. In one
version, the waste is shredded, passed
through 10percent hypochlorite solution
(dixichlor) followed by a finer shredding
and drying. The treated material is land
filled.
6. Sanitary and Secured Land filling -
Sanitary and secured land filling is
necessary under the following
circumstances:
• Deep burial of human anatomical
waste when the facility of proper
incineration is not available (for towns
having less than 5 lakh population and
rural areas).
• Animal waste (under similar conditions
as mentioned above) - Secured landfill.
• Disposal of autoclaved / hydroclave /
microwaved waste (unrecognizable) -
Sanitary landfill.
• Disposal of incineration ash - Sanitary
land-fill.
• Disposal of bio-medical waste till such
time when proper treatment and
disposal facility is in place - Secured
land-fill.
• Disposal of sharps - Secured land-fill.
This can also be done within a hospital
premises as mentioned below.
• In case disposal facility for sharps is
not readily available in a town, health
care establishments, especially
hospitals having suitable land, can

Legal Provisions and Management Perspectives of Biomedical and Hospital Waste in India
© All Rights Reserved by “Journals Club & Co.” 34
construct a concrete lined pit of about
1m length, breadth and depth and
cover the same with a heavy concrete
slab having a 1-1.5m high steel pipe of
about 50mm diameter. Disinfected
sharps can be put through this pipe.
When the pit is full, the pipe should be
sawed off and the hole sealed with
cement concrete. This site should not
be water logged or near a bore well.
CONCLUSION
Hospital Management must understand the
gravity of the issue and they must be able
to differentiate between hospital waste and
general waste. They must ensure proper
identification, segregation at the source of
generation, collection in prescribed
colored containers, safe transportation,
appropriate treatment and environmentally
sound disposal of Bio-Medical Waste.
They should also provide health education
and training9 of everyone involved in the
management and handling of Bio-Medical
Waste.
While there a large number of technologies
available for the safe disposal of hospital
waste, a large number of health care
institutes are deterred from setting up a
sound waste disposal system owing to
misconceptions over the cost of such a
system. In India, hospital waste
management continues to be a largely
ignored area because of the lack of
awareness among the public and the health
care institutes. This lack of awareness can
be attributed to the lackadaisical attitude of
the administration to enforce the punitive
regime that has been provided for by the
regulations of the Central Government, in
cases of violation of these regulations.
While these regulations are adequate to
deal with the problem of waste
management, the continued lethargy on
part of the administration is the root cause
for the rampant mismanagement of
hospital waste.
It is agreed by the researcher that it is not
feasible for small clinics to set up their
own waste treatment plants, but their small
setup should not prevent them from
following the prescribed procedure for
segregation and packaging hospital waste
as per the color coding. The more viable
option for these small scale health care
institutes is that there should be a common
treatment plant for the waste that is
collected from these institutions.
In fact there are already initiatives in this
direction, for instance in the district of
Erode, 200 small clinics have jointly
acquired 20 acres of land for the purpose
of disposal and burial of hospital waste. If
the government is serious at implementing
its own regulations then initiatives like the
above ones should be furthered by
affording favorable treatment to such
institutions in the form of relaxed tax
norms and other such benefits.

Legal Provisions and Management Perspectives of Biomedical and Hospital Waste in India
© All Rights Reserved by “Journals Club & Co.” 35
REFERENCES
1. Sharma RK., Mathur S.K. (1989).
Management of Hospital Waste. Journal of
Academy of Hospital Administration, l(2),
55-57.
2. Rao SKM, Garg RK. (1994). A Study of
Hospital Wasted Disposal System in
Service Hospital. Journal of Academy of
Hospital Administration, 6(2), 27-31.
3. Singh, I. B., Sharma, R. K. (1996).
Hospital Waste Disposal System and
Technology. Journal of Academy of
Hospital Administration, 8(2), 44-48.
4. Muzaffar, Ahmad. Indian Journal for the
Practicing Doctor, 1(4), (2005-01 - 2005-
02)
5. CAG, Audit Report, Report No. PA 14 of
2008
6. A. E. Giroult., P. Rush. book Safe
management of wastes from health-care
activities, WHO.
7. Basu RN. (1995). Issues involved in
Hospital Waste Management, an
experience from a large teaching
institution. Journal of Academy of Hospital
Administration, 7(2), 79-83
8. The Bio-Medical Waste (Management and
Handling) Rules, 1998
9. Neera, Kewalramani. Brihan Mumbai
Palika Public Health Dept. Training
Module on Hospital Waste Management.
10. Acharya. D. B., Singh. Meeta. (2000). The
Book of Hospital Waste Management,
Minerva Press, New Delhi, 1st Edition, 15,
47.
11. Sharma. R. K., Mathur. S. K. (1989).
Management of Hospital Waste, Journal of
Academy of Hospital Administration, l(2),
55-57.
12. Pathak, S. (1998). Management of
Hospital Waste: A Jaipur Scenario.
Proceedings of National Workshop on
Management and Hospital Waste, 31-33
13. Singh. R., Mahajan. S. L. (1998).
Management of Hospital Waste in
Hospitals of Govt. Medical College,
Amritsar. Journal of Academy of Hospital
Administration, l0(1), 33-37
14. Sharma, R. K., Mathur, S.K. “Management
of Hospital Waste”, Journal of Academy of
Hospital Administration, 1989 July; l (2):
55-57
15. Mumbai Medwate Achar Group.
"Infecting Mumbai: A report for healthcare
professionals, govt. and citizens." (Jan.
2000)
16. Srishti. (2000). Emerging Experience in
Medical Waste Management.
17. Peter, A., Reinhardt., Judith, G. (1991).
Infectious and Medical Waste
Management. Lewis Publishers Michigan,
USA

Legal Provisions and Management Perspectives of Biomedical and Hospital Waste in India
© All Rights Reserved by “Journals Club & Co.” 36
18. Personal Communication to Dr. V. K. Iya
from Dr. Rohini Kelkar, Tata Memorial
Hospital, Mumbai; Dr. B. S. Srinath,
Bangalore, Institute of Oncology,
Bangalore
19. "Toxic Shock", (2000). Editorial, Times of
India, 21, 5.
20. Bio-Medical Waste. News Item, Danik
Bhaskar, Feb 23, 2005, Page No. 1
21. www.medind.nic.in
22. www.isebindia.com
23. www.toxicslink.org
24. www.maha-arogya.gov.in
25. www.cpcb.nic.in
26. www.health.delhigovt.nic.in
HOW TO CITE THIS ARTICLE Dr. Prashant Mehta. (2014). Legal Provisions and Management Perspectives of
Biomedical and Hospital Waste in India. Journal Club for Management Studies (JCMS), 1(II), 11-36.