
Financial Well-Being, Psycho-Social Abilities and Sale or ...

Journal of Abnormal Child Psychology, Vol .25, No. 2, 1997, pp. 133-144
Language Abilities in Children with Attention DeficitHyperactivity Disorder, Reading Disabilities, andNormal Controls
Karen L. Purvis1 and Rosemary Tannock2'3
Received August 22, 1995; revision received December 20, 1995;accepted March 4, 1996
Research has demonstrated a high prevalence of language impairments (LI) and readingdisabilities (RD) in children with attention deficit hyperactivity disorder (ADHD). Since RDis also associated with LI, it is unclear whether the language impairments are specific toADHD or associated with comorbid RD. The language abilities of ADHD children with andwithout RD were investigated in a task requiring recall of a lengthy narrative, and in testsassessing knowledge of the semantic aspects of language. The study was conducted with 50boys—14 ADHD, 14 ADHD + RD, 8 RD, and 14 normal controls, aged 7 to 11. Childrenwith ADHD (ADHD-only, ADHD + RD) exhibited difficulties in organizing and monitoringtheir story retelling. Children with RD (RD-only, ADHD + RD) demonstrated deficits inreceptive and expressive semantic language abilities on the language processing tests. Thecomorbid group (ADHD + RD) exhibited the deficits of both ADHD and RD children.The deficiencies of ADHD children are consistent with higher-order executive function defi-cits while the deficits of RD children are consistent with deficits in the basic semantics oflanguage processing.
KEY WORDS: Attention deficit hyperactivity disorder; reading disorder; language abilities; narratives.
Attention deficit hyperactivity disorder (ADHD)is characterized by persistent and developmentally in-appropriate levels of inattention, impulsivity, and hy-peractivity (American Psychiatric Association, 1994).However, ADHD is a heterogeneous disorder whichexhibits marked overlap with other disorders (see Bied-erman, Newcorn, & Sprich, 1991 for review). One classof disorders for which children with ADHD appear tobe at risk, yet which often remains unrecognized, is
1Doctoral candidate, University of Toronto, Toronto, Ontario,Canada.
2Department of Psychiatry Research, Hospital for Sick Children,Toronto, Ontario, Canada M5G 1X8.
3Address all correspondence to Rosemary Tannock, Ph.D., De-partment of Psychiatry Research, Hospital for Sick Children, 555University Avenue, Toronto, Ontario M5G 1X8 Canada.
communication/language disorders (Baker &Cantwell, 1992; Beitchman, Tuckett, & Batth, 1987;Cohen, Davine, Horodezky, Lipsett, & Isaacson,1993; Love & Thompson, 1988; Tannock & Schachar,1996).
Many of the studies of the language abilities ofchildren with ADHD have not distinguished betweenchildren with ADHD alone (ADHD-only) and thosewith comorbid disorders (e.g., Beitchman et al., 1987;Love & Thompson, 1988), making it difficult to de-termine whether the language impairments are spe-cific to ADHD or whether they are more a functionof the comorbid disorder. In particular, a substantialproportion of ADHD children also meet criteria fora diagnosis of reading disability (August & Garfinkel,1989; Dykman & Ackennan, 1991; Faraone et al.,1993; Lambert & Sandoval, 1980; Semrud-Oikeman
133<X»l-0627/97A>4aH>13»113<VO C 1997 Plenum Publishing Corporation

134 Purvis and Tannock
et al., 1992) which are also associated with languageimpainnents (Hallahan & Kaufman, 1976; Lapadat,1991).
The purpose of the present study was to examinethe pragmatic and semantic language abilities of chil-dren with ADHD and to examine the impact of con-current reading disabilities on their performance. Theinclusion of reading-disabled (RD) control groups(ADHD + RD, RD-only) permits an examination ofthe deficits due to ADHD and/or comorbidity withRD. As well, the separate language measures shouldpermit us to examine the pragmatic communicationversus semantic language difficulties of ADHD chil-dren. The task of story retelling was chosen becauseit requires attention to the incoming information, ex-traction of meaning and relevance, encoding of theinput into memory, and reconstruction from memoryusing effort and judgment so that the information isorganized, coherent, and sensitive to the needs of thelistener. The ability to fulfil and coordinate the on-going requirements while performing the task re-quires, in addition to linguistic abilities, effortfulorganization, planning, and self-monitoring, which in-volve higher-order cognitive skills, referred to as "ex-ecutive functions" (Douglas, 1988; Shallice, 1982).The two tests of receptive and expressive semanticlanguage abilities were chosen as language measureswhich do not have the additional executive functionrequirements of planning and organization.
METHOD
Subjects
A total of 50 boys, aged 7 to 11 years, partici-pated in the study. Of these, 14 boys had a confirmeddiagnosis of ADHD, 14 met the diagnosis of ADHDand reading disability (ADHD + RD), eight had adiagnosis of RD alone, and 14 children had no di-agnosis (normal comparison). The children were partof a larger study investigating the cognitive abilitiesof children with ADHD (Schachar, Tannock, Mar-riot, & Logan, 1995). The present study included70% of the sample from the larger study. Subjectswere selected for the current study based upon age,IQ, and diagnosis. Children with ADHD and/or RDwere recruited from children referred for behaviorproblems to the psychiatric or pediatric outpatientclinics at a children's hospital in a large metropolitanurban area. The normal comparison group (NC) con-
sisted of children recruited from other medical out-patient clinics at the same hospital for minor medicalproblems or routine health checks. Only those chil-dren without any history of behavioral or attentionalproblems, nor any current medical, behavioral, or at-tentional problems were eligible for the comparisongroup. Any child whose estimated full-scale IQ wasless than 80 or who showed evidence of a neurologi-cal disorder, poor physical health, uncorrected sen-sory impairments, or a history of psychosis wasexcluded. Four of the ADHD boys were receivingpsychostimulant medication. The remaining childrenwere being considered for an evaluation of stimulanttreatment. Medications were discontinued 48 hoursbefore the day of testing.
Measures
Diagnostic Measures
The diagnosis of ADHD was based on informa-tion obtained from semi-structured interviews con-ducted with the child's parents [Parent Interview forChild Symptoms—Revised (PICS-R); Schachar &Wachsmuth, 1989] and teacher [Teacher TelephoneInterview (TTI); Schachar & Tannock, 1990]. In boththe PICS-R and TTT, informants provided descrip-tions of the child's behavior in various situationsspecified by the interview (e.g., playing out of doors,while watching television). The interviewer, ratherthan the informant, made decisions about the pres-ence of absence of symptoms by referring to specificcriteria regarding severity, frequency, age-appropri-ateness, and level of disability resulting from the be-havior. Interrater reliability for the PICS is high, withagreement for diagnoses at 100%. Substantial inter-rater agreement has also been obtained for diagnosesbased on the TTI: ADHD (K = .76), oppositional de-fiant disorder (ODD) (K = .76), and conduct disorder(CD) (K = .83) (Schachar et al., 1995). To be classi-fied as ADHD, children had to meet the severity andage-of-onset criteria in the Diagnostic and statisticalmanual of mental disorders (3rd ed., rev.) (DSM-III-R;American Psychiatric Association, 1987). ADHD wasdiagnosed if eight or more ADHD symptoms werereported by either parents (PICS) or teacher (TTI)with onset before 7 years of age and with persistenceof more than 6 months.
The diagnosis of reading disability was based ona combined formula approach recommended by

Language Abilities in ADHD and RD
Barkley (1990), which requires an achievement scoreof at least 1.5 SD below the mean for age, plus adiscrepancy of at least 1.0 SD between that achieve-ment score and the child's full scale IQ score. Allsubjects were administered the Vocabulary and BlockDesign subtest of the Wechsler Intelligence Scale forChildren—Revised (WISC-R; Wechsler, 1974) as anestimate of verbal and nonverbal intelligence (Sat-tler, 1988) as well as all three subtests of the WideRange Achievement Test—Revised (WRAT-R; Jastak& Wilkinson, 1987). In this study, the Reading sub-test of the WRAT-R was used to define reading dis-ability.
Language Measures
Three measures of language ability were se-lected. The first was a story retelling task which re-quired the comprehension and use of extendedstretches of language. The other two measures werestandardized measures of receptive and expressiveabilities involved in the semantic aspects of language.
Story Retelling Task. One folk tale was selectedas stimulus material for this task. This story was un-familiar to the children in the study but had beenused in prior studies on story recall in normal chil-dren (Brown, Day, & Jones, 1983; Brown & Smiley,1977; Smiley, Oakley, Worthen, Campione, & Brown,1977) and ADHD children (Tannock, Purvis, &Schachar, 1993). The folk tale, "The Father, His Sonand Their Donkey," originated from an oral traditionand was intended to be read aloud to children. Thestory was audiotaped at a normal rate for speakingor reading aloud, at approximately 100 words/minuteand narrated by a female voice. The story was 2 min,56 s, in length and involved multiple characters andsequences of events which made it too long and de-tailed to be recalled verbatim. Thus retelling re-quired the selection and organization of relevantinformation.
The story had been divided into individual units.A unit was defined as one which contained an ideaand/or represented a pausal unit. Each unit was rated(using a 4-point scale) for its importance to the struc-ture and theme of the story as a whole by Brownand colleagues in a previous study (Brown et al.,1983), following a procedure used by Brown andSmiley (1977), developed by Johnson (1970).
The story contained 427 words, and 63 pausalunits, and scored 5.2 on the Dale-Chall Readability In-
dex (Dale & Chall, 1948). The number of units at eachof the four levels, from most to least important were16,16,16, and 15, respectively, and occurred approxi-mately equally often in each quarter section of thestory. Recall of important units would therefore notbe contaminated by primacy or recency effects (Brown& Smiley, 1977).
Story Measures. Retelling a story involves two ba-sic steps. First the child must attend and comprehendthe story. Second, he or she must try and reproducethe narrative. For this reason, the children's perform-ances were assessed along these two basic dimen-sions, comprehension and production.
• Comprehension. Two measures were used to as-sess children's comprehension of the story. Thefirst was selective recall as a function of the pre-judged thematic importance of the story units.The second was a comprehension score basedon children's responses to a series of factual andinferential questions which were derived fromunits of information central to the theme of thestory.
Selective recall was defined as the num-ber of idea units correctly recalled at each ofthe four levels of importance. This was con-verted to a proportion of the total number ofunits at each level, to remain consistent withprevious research. The ability to focus on im-portant aspects of the story rather than non-essential material is an essential cognitiveprocess for comprehension of written or audi-torily presented information (Smiley et al.,1977). Thus it is the pattern of recall (ratherthan the absolute amount) which indicatescomprehension.
Responses to the comprehension ques-tions were rated as correct (score 2),partiallycorrect (score 1), or incorrect (score 0), yield-ing a maximum score of 10. The questionswere included as a supplement to the selec-tive recall measure because it was consideredpossible that the children could exhibit com-prehension by answering when prompted witha question but not spontaneously produce theinformation during free recall of the story.Production. Two aspects of children's produc-tion of narratives were assessed. The first wasoverall productivity (total amount recalled) andthe second was the adequacy of the children'sorganization and self-monitoring of their output.
135

136 Purvis and Tannock
Organization and self-monitoring were assessedin terms of unrepaired errors made by childrenduring their story reconstructions. Errors left un-repaired reflect a lack of ongoing self-monitor-ing of the accuracy of the child's own output.Four types of errors were analyzed: (a) errorsin sequencing story events, (b) ambiguous ref-erences, (c) misinterpretations, and (d) inappro-priate word substitutions. The number of errorsof a specific type were computed as a proportionof the total number of story units recalled bythe child to control for differences in total out-put. Definitions and examples of each of thesecoding categories are provided in the appendix.
Retelling story events out of sequence re-flects a breakdown in the global organizationof the story theme. Referring back to priorevents via the use of pronominal referencesrequires a complex organization of ideas tomaintain the distinction between characters,events, and their relationships, for the clari-fication of the listener (Liles & Purcell, 1987).Ambiguous references thus reflect cohesionproblems with the local organization of infor-mation across sentences (Fine, 1985; Liles &Purcell, 1987). Misinterpretations are seman-tic departures from the original text that vio-late text veracity (i.e., inaccurate informationthat alters the text's primary meaning). Thesereflect a breakdown in the process of self-monitoring the accuracy of the information.However, they must be interpreted in light ofthe child's comprehension of the story. Thatis, if comprehension is poor, misinterpreta-tions may in fact be due to poor comprehen-sion. However, if comprehension is adequate,misinterpretations may be viewed as deficitsin self-monitoring of the output at the propo-sition level. Inappropriate word substitutions(e.g., nuns substituted for maidens) also re-flect a breakdown in self-monitoring of theaccuracy of information but is at the wordlevel rather than the proposition level. Leav-ing unrepaired these inaccuracies that violatetext veracity reflects a failure to activelymonitor meanings within and across sen-tences (Liles & Purcell, 1987).
The Word Test. The Word Test (WT, Jorgeson,Barrett, Huisingh, & Zachman, 1981) is a stand-ardized measure of children's expressive vocabulary
and semantic abilities. Five of the six available sub-tests were administered to the children. These in-cluded (1) Associations, where the subject mustchoose the one word from four that does not belongand then explain his/her choice in relation to thecategory of the other three words; (2) Synonyms,where the subject must express a one-word synonymfor each stimulus item; (3) Semantic Absurdities,which measures the ability to identify and expresswhat is wrong with an absurd statement; (4) Anto-nyms, where the child must give a one-word oppositefor each stimulus item; and (5) Multiple Definitions,where the child must give two meanings for each testword.
Language Processing Test. The Language Process-ing Test (LPT, Richard & Hanner, 1985) is a stand-ardized measure of the semantic aspects of languagewhich taps the ability to analyze, organize, and asso-ciate linguistic units. Three of the six available sub-tests were chosen, including (1) Similarities, where thesubject must compare the properties of two items,identity the primary common aspects, and describehow they are alike; (2) Differences, which taps theability to contrast two items by identifying the primaryaspects of item variance and tell how the two objectsare not alike; and (3) Multiple Meanings, which re-quires the child to recognize and define a word invarying contexts using language strategies to select ap-propriate synonyms or definitions by giving up to fourdefinitions for each stimulus word.
Procedure
Children were tested individually in one sessionin a small quiet room. The instructions for the storyretelling task were to listen carefully to the story sothat each child could retell it in his or her own wordsfor the next child coming to the study. The childrenwere also told that their stories would be recordedand that afterwards they would be asked questionsabout the story. Details of the procedure and datapreparation including transcription and coding can befound in Tannock et al. (1993). Interrater agreementfor the story units, based on point-to-point correspon-dence and averaged across importance levels, was .91.Interrater reliability for story errors was .95. All dis-agreements were resolved through discussion prior todata entry and analysis. The children were then ad-ministered the subtests of The Word Test and Lan-guage Processing Test. Diagnostic interviews with

Language Abilities in ADHD and RD 137
Table I. Selection Criteria and Clinical Characteristics of the Sample0
F-values and significance(df = 1,46)"
Age
WISC-REstimated IQVocabularyBlock Design
WRAT-RReadingSpellingArithmetic
Controls(14)
9.2 (1.4)
109.0 (8.1)11.6 (1.8)11.6 (Zl)
100.9 (9.8)91.1 (11.9)95.3 (13.9)
RD(8)
9.3 (1.9)
102.8 (11.4)8.1 (2.8)
12.9 (3.3)
71.0 (7.1)74.2 (6.5)87.2 (7.3)
ADHD(14)
8.7 (1.4)
104.9 (9.4)10.6 (2.2)11.1 (2.1)
101.1 (9.5)92.6 (14.3)93.3 (7.6)
ADHD + RD(14)
8.7 (1.3)
101.6 (12.2)9.2 (2.6)
11.4 (2.7)
68.9 (9.4)68.6 (9.3)81.6 (15.7)
ADHDxADHD RD RD
12.5d
129.5*40.0"7.T1
Parent and Teacher Diagnostic Variables and Cutoff Scores
ParentHyperactivityOppositional defiantConduct disorder
TeacherHyperactivityOppositional defiantConduct disorder
0.6 (0.7)0.7 (1.1)0.1 (0.3)
0.7 (1.0)0.8 (1.9)0.0 (0.0)
1.8 (2.5)0.6 (1.5)0.1 (0.4)
3.7 (1.7)0.5 (1.2)0.0 (0.0)
11.0 (2.4)4.7 (2.O)1.6(1.4)
11.4 (2.2)3.6 (2.3)1.4 (1.6)
9.1 (4.2)32 (Z8)1.8(1.7)
9.4 (Z8)3.1 (3.4)1.5 (1.9)
92.4'25.5*16.4B
130.8* ViSf-"14.6'8.&
'Values given as means and standard deviations (in parentheses). ADHD = attention deficit hyperactivity disorder, RD = readingdisability.
6Missing data for some subjects; for parent ratings (df = 1,40), controls, n = 9, RD, n = 7, ADHD, n = 14, ADHD + RD, « = 14;for teacher ratings; (df = 1,38), controls, n = 9,, RD, n = 6, ADHD, n = 14, ADHD + RD, n = 13.
cPost hoc comparison of RD and contro groups, and post hoc comparison of ADHD and ADHD + RD groups not significant.dp < .01.'p < .001.
parents were conducted on the same day as the chil-dren's testing. Telephone interviews with teacherswere conducted within 1 to 2 weeks before or afterthe testing session. Testing was conducted blind toeach child's diagnosis.
Analysis
Diagnostic and sample characteristics were ana-lyzed using the analysis of variance (ANOVA) pro-gram in the windows version of the StatisticalPackage for the Social Sciences with two between-subjects factors: 2 (ADHD) x 2 (RD). Analysis ofcomprehension (proportion of idea units recalled asa function of their structural level of importance) wasanalyzed using a 2 (ADHD) x 2 (RD) x 4 (Impor-tance Level) ANOVA with repeated measures on the
last factor. Story errors were analyzed using a 2(ADHD) x 2 (RD) multivariate analysis of variance(MANOYA) on the four error types. Scores on thetwo standardized language tests were analyzed sepa-rately in 2 (ADHD) x 2 (RD) x 5 (WT subtests) and2 (ADHD) x 2 (RD) x 3 (LPT subtests) MANOVAS.Univariate analyses and post-hoc comparisons ofpairs of group means (Tukey Honestly SignificantDifference Test; Keppel, 1982) were conducted toclarify any main effects and interactions.
RESULTS
Age and IQ
The four groups did not differ in age, estimatedIQ, or Block Design scores of the WISC-R. A sig-
138 Purvis and Tannock
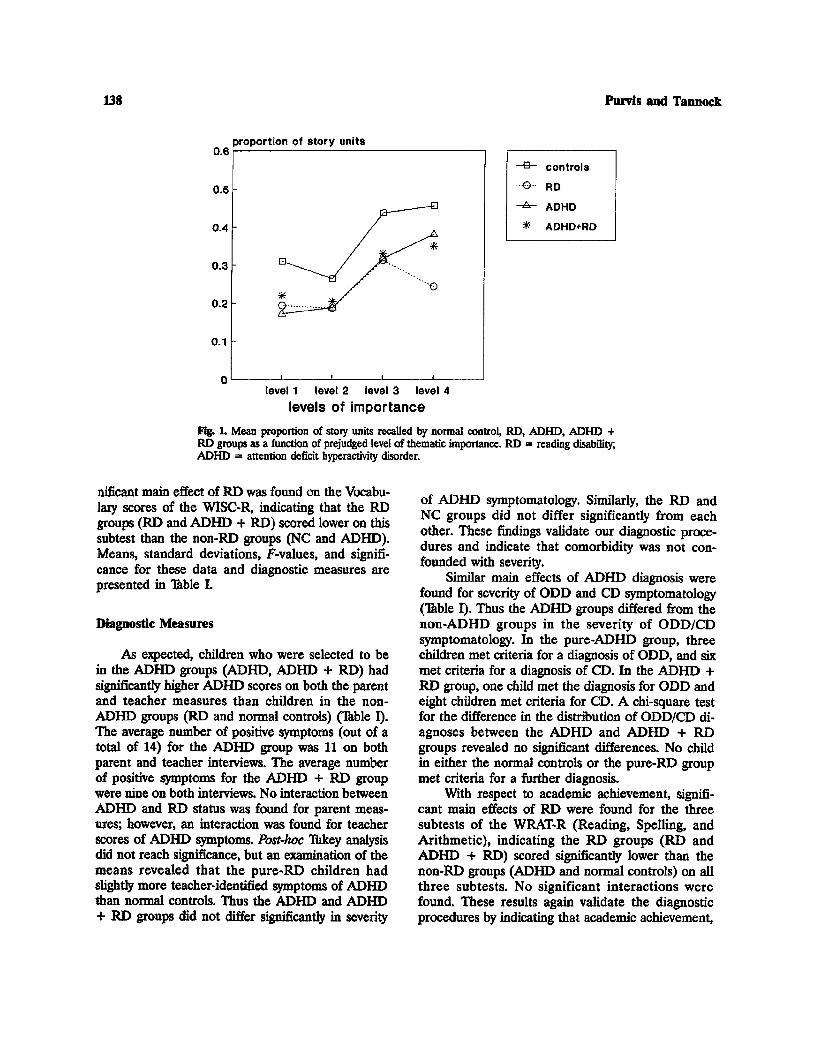
Fig. 1. Mean proportion of story units recalled by normal control, RD, ADHD, ADHD +RD groups as a function of prejudged level of thematic importance. RD = reading disability,ADHD = attention deficit hyperactivity disorder.
nificant main effect of RD was found on the Vocabu-lary scores of the WISC-R, indicating that the RDgroups (RD and ADHD + RD) scored lower on thissubtest than the non-RD groups (NC and ADHD).Means, standard deviations, F-values, and signifi-cance for these data and diagnostic measures arepresented in Table I.
Diagnostic Measures
As expected, children who were selected to bein the ADHD groups (ADHD, ADHD + RD) hadsignificantly higher ADHD scores on both the parentand teacher measures than children in the non-ADHD groups (RD and normal controls) (Table I).The average number of positive symptoms (out of atotal of 14) for the ADHD group was 11 on bothparent and teacher interviews. The average numberof positive symptoms for the ADHD + RD groupwere nine on both interviews. No interaction betweenADHD and RD status was found for parent meas-ures; however, an interaction was found for teacherscores of ADHD symptoms. Post-hoc Tukey analysisdid not reach significance, but an examination of themeans revealed that the pure-RD children hadslightly more teacher-identified symptoms of ADHDthan normal controls. Thus the ADHD and ADHD+ RD groups did not differ significantly in severity
of ADHD symptomatology. Similarly, the RD andNC groups did not differ significantly from eachother. These findings validate our diagnostic proce-dures and indicate that comorbidity was not con-founded with severity.
Similar main effects of ADHD diagnosis werefound for severity of ODD and CD symptomatology(Table I). Thus the ADHD groups differed from thenon-ADHD groups in the severity of ODD/CDsymptomatology. In the pure-ADHD group, threechildren met criteria for a diagnosis of ODD, and sixmet criteria for a diagnosis of CD. In the ADHD +RD group, one child met the diagnosis for ODD andeight children met criteria for CD. A chi-square testfor the difference in the distribution of ODD/CD di-agnoses between the ADHD and ADHD + RDgroups revealed no significant differences. No childin either the normal controls or the pure-RD groupmet criteria for a further diagnosis.
With respect to academic achievement, signifi-cant main effects of RD were found for the threesubtests of the WRAT-R (Reading, Spelling, andArithmetic), indicating the RD groups (RD andADHD + RD) scored significantly lower than thenon-RD groups (ADHD and normal controls) on allthree subtests. No significant interactions werefound. These results again validate the diagnosticprocedures by indicating that academic achievement,

Language Abilities in ADHD and RD 139
fig. 2. Mean proportion of errors produced by all groups during story recall. RD =reading disability; ADHD = attention deficit hyperactivity disorder.
particularly reading, was equated within the RD andnon-RD groups.
Story Retelling—Comprehension
The primary measure of comprehension was se-lective recall. The mean proportion of units recalledby the four groups of children at each level of im-portance are illustrated in Fig. 1. This figure showsthat the control, ADHD, and ADHD + RD groupsexhibited a similar pattern of recall, although thenormal children tended to recall more at each levelof importance. Thus these three groups recalledmore of the theman'calry important information thanthe minor details. The pure-RD group, as shown inFig. 1, appeared to have a different pattern of recallfrom the other three groups, recalling fewer of themost important units of information (level 4). Theydid not recall increasingly more information units asimportance level increased.
Statistical analysis of these results revealed nosignificant interactions or main effects for group. Asexpected, a significant effect of level [F(3, 138) =29.00, p < .001] was found. Post-hoc Tukey compari-sons among the means for importance levels revealedthat children recalled proportionately more of themost important units (levels 4 and 3) than the leastimportant (levels 2 and 1) but there was no signifi-
cant difference in the recall of levels 4 and 3, or be-tween levels 2 and 1.
The mean comprehension question scores (outof a possible 10) for the ADHD, ADHD + RD, RD,and control groups were 5.4,5.8, 4.9, and 6.4, respec-tively. Although the RD-only children obtained thelowest scores, the analysis revealed no significant dif-ferences between the groups.
Story Retelling—Production
Verbal Productivity. As illustrated in Fig. 1, thenormal controls appeared to recall proportionatelymore total idea units than the other three groups.The proportion of idea units for the ADHD, ADHD+ RD, RD, and NC groups were .27, .28, .24, and.36, respectively. This trend was indicated by a non-significant interaction between the ADHD and RDgroups [F(l, 46) = 3.40, p = .072].
Organization and Monitoring. The mean propor-tion of error types as a function of diagnostic groupare illustrated in Fig. 2. The overall MANOVA indi-cated a three-way interaction between ADHD, RD,and error type [F(3,138) = 4.69, p < .01]. Thereforeerrors were analyzed separately in 2 (ADHD) x 2(RD) ANOVAs. Significant main effects of ADHDdiagnosis were found for sequence errors [F(l, 46)= 5.7, p < .05], misinterpretations [F(l, 46) = 4.5,

140 Purvis and Tannock
Table II. Mean Scores on the Word Test (WT) and Language Processing Testa
F-values and significance (WT, df= 1,37; LPT, df = 1,36)
The Word TestAssociationsSynonymsSemantic AbsurditiesAntonymsMultiple Definitions
Mean scoreLanguage Processing Test
SimilaritiesDifferencesMultiple Meanings*
Mean score
Controls
51.9 (63)50.8 (6.0)51.6 (4.6)48.6 (4.3)50.4 (4.6)605 (3.9)
52.7 (65)50.9 (5.3)48.9 (10.3)50.8 (5.4)
RD
44.2 (8.8)43.8 (45)42.7 (6.1)44.0 (4.3)41.0 (5.4)43.2 (5.0)
45.0 (9.9)43.8 (9.4)40.5 (85)43.1 (8.6)
ADHD
50.1 (2.8)50.6 (4.0)49.8 (5.2)51.4 (4.4)48.4 (4.6)50.0 (22)
51.8 (6.8)50.8 (8.1)46.3 (5.2)49.6 (5.0)
ADHD + RD
47.8 (7.6)47.9 (4.0)47.8 (3.4)47.4 (2.8)46.6 (4.3)47.6 (3.2)
49.5 (9.9)46.5 (8.9)425 (3.6)46.2 (6.1)
ADHDxADHD RD RD
18.6e 45C
7.3d
"Values given as cans and standard deviations (in parentheses) T-scores, mean = 50, SD = 10 (WT); 15 (LPT. Missing data for somesubjects; the Word Test controls, n = 9., RD, n = 4, ADHD, n = 14, ADHD, n = 14; Language Processing Test ADHD + RD, n= 13. RD = reading disability; ADHD = attention deficit hyperactivity disorder.
^Scores on this test significantly lower than the combined scores of Similarities and Differences.cp < .05.*p < .01.'p < .001.
p < .05], and substitutions [F(l, 46) = 5.2, p < .05],indicating that the ADHD groups (ADHD, ADHD+ RD) made more of these errors than the non-ADHD groups. A significant ADHD x RD interac-tion was found for ambiguous references [F(l, 46) -7.6, p < .01]. Post-hoc analyses of the four groupsrevealed that the pure-ADHD and pure-RD groupsmade significantly more ambiguous references thannormal controls. No differences in ambiguous refer-ences were found between the two ADHD groups(ADHD and ADHD + RD) or between the two RDgroups (ADHD + RD and RD).
The Word Test and Language Processing Test
Word Test. Means and standard deviations forThe Word Test and Language Processing lest arepresented in Table II. The overall MANOVA for TheWord lest revealed a significant ADHD x RD inter-action [F(l, 37) = 4.5, p < .05]. Although post-hocTukey tests for this interaction did not reach signifi-cance, an examination of the means suggests that theinteraction occurred within the non-ADHD groups,
with the pure-RD children scoring lower than thenormal controls. A significant main effect for RD\F(1, 37) = 18.65, p < .001] was also found, indicat-ing that the RD groups (RD and ADHD + RD)scored significantly lower than the non-RD groups(normal controls and ADHD). No other main effectsor interactions were found.
Language Processing Test. Again, a significantmain effect for reading disability [F(l, 36) = 7.3, p< .05] was found, indicating that the RD groups (RDand ADHD + RD) scored significantly lower thanthe non-RD groups (normal controls and ADHD).No interactions between ADHD and RD diagnosticstatus or subtests were found. A significant main ef-fect of subtest was found [F(2, 72) = 6.0, p < .01].Post-hoc tests found that all children scored lower onthe Multiple Meanings subtest than on the Similari-ties and Differences subtests.
DISCUSSION AND CONCLUSIONS
The results revealed two central findings con-cerning the language abilities of ADHD children

Language Abilities in ADHD and RD 141
with and without reading disabilities. First, childrenwith ADHD, regardless of RD status, exhibited dif-ficulties in organizing and monitoring their verbalproductions. Second, children with RD, regardless ofADHD status, demonstrated deficits in receptive andexpressive semantic language abilities. In otherwords, difficulties in story organization and self-monitoring of the accuracy of the information as re-flected in story errors were affected by ADHD status,whereas deficits in semantic aspects of language wereaffected by RD status. The comorbid group (ADHD+ RD) generally exhibited the deficits of both puregroups (ADHD-only and RD-onty).
The difficulties of ADHD children in organizingtheir productions as reflected in story errors are con-sistent with previous research (Tannock et al., 1993).The ADHD groups exhibited a higher frequency ofsequence errors, which reflects a breakdown in theglobal organization of story theme. The pure-ADHDgroup had difficulties in local organization, reflectedin ambiguous references. These are failures in cohe-sion which make it difficult for the listener to followthe speaker's train of thought Ambiguous referencescan result from a failure to organize and monitor thecohesion between sentences, as well as from a failureto take into account the needs of the listener. Boththe pure-ADHD and ADHD + RD groups weremore likely to misinterpret information and to useinappropriate word substitutions. These two errortypes occurred in the absence of comprehensionproblems; therefore they are interpreted to reflect afailure to monitor the accuracy of the information.These errors reflect pragmatic difficulties with lan-guage use. The inability to relate ideas specificallyand accurately in a logical sequence results in dis-unity in discourse and makes comprehension by thelistener difficult (Prutting & Kirchner, 1987).
In contrast to the RD groups (RD and ADHD+ RD), the ADHD-only group did not show deficitsin the receptive or expressive, semantic aspects oflanguage. Unlike the narrative task, The Word lestand the Language Processing lest did not requirelengthy responses with demands for self-organization.Thus the language deficits of ADHD children with-out RD seem to reflect difficulties with language use(i.e., pragmatics) rather than deficits in the basic sub-systems of language (i.e., phonology, semantics andsyntax). A wide range of pragmatic difficulties, suchas difficulties in maintaining a conversation or turntaking during conversations (Humphries, Koltun,
Malone, & Roberts, 1994; Zentall, Gohs, & Culatta,1983) have been demonstrated in ADHD children.
The pragmatic difficulties of ADHD childrenmay be related to the higher-order cognitive deficitsreferred to as "executive functions" (Barkley, 1994;Benson, 1991; Douglas, 1988; Hamlett, Pellegrini, &Connors, 1987; Mattes, 1980; Pennington, Groissser,& Welsh, 1993; Schachar, Tannock, & Logan, 1993;Shue & Douglas, 1992). Executive functions are self-regulatory processes which are responsible for the or-ganization and monitoring of information processing,mobilizing attention, and inhibiting respondingDouglas, 1988; (Goldman-Rakic, 1987; Luria, 1966).The problems in self-regulation are not problems ofknowing what to do, but rather in doing what is known(Kinsbourne, 1989). The story used in this study wascomplex (many characters and events) and was notlogically sequenced. This increases the demands onthe child's executive processes, requiring self-directedeffort, planning, and organization. Thus it may bedeficits in executive function rather than deficits inthe fundamental subsystems of language (i.e., pho-nology, semantics, and syntax) that accounted for thepragmatic difficulties of the ADHD children (Tan-nock & Schachar, 1996).
Impairments in these basic language subsystemsare more closely associated with RD than withADHD (Ackerman, Dykman, & Gardner, 1990; Au-gust, 1987; August & Garkinkel, 1989; Felton, Wood,Brown, Campbell, & Harter, 1987; Tannock, Corkum,Schachar, & Purvis, 1994; Tannock et al., 1993;). Thefindings of deficits on the language processing testssupported this general conclusion, since children witha diagnosis of RD (ADHD + RD, RD-onty), scoredsignificantly lower than children with adequate read-ing skills (normal controls, ADHD).
In this study, no differences were found betweengroups in comprehension of the story as reflected inthe selective recall of levels of importance or in thecomprehension questions scores. Previous narrativestudies have found a lack of sensitivity to the impor-tance of information in children with learning dis-abilities (Hansen, 1978; Smiley et al., 1977; Worden& Nakamura, 1982), but not in ADHD children(O'Neill & Douglas, 1991; Tannock et al., 1993; Zen-tall, 1988). The present findings are consistent withprevious research, with the pure-RD children recall-ing fewer of the most important units of information;however, the sample size may have been too smallto permit detection of differences.

142 Purvis and Tannock
In contrast to the language deficits on the lan-guage processing tests, the children with RD did notexhibit difficulties organizing their story retelling inan accurate, logical sequence. However, the pure-RDchildren did have particular difficulties with referen-tial cohesion as reflected in the number of ambigu-ous references. Previous research has supported thefinding that children with RD and language-disor-dered children have particular difficulties with refer-ential cohesion even in the absence ofcomprehension difficulties (Lapadat, 1991), but nodifficulties with sequencing story information whenthe story is meaningfully structured (Feagans &Short, 1984; Graybeal, 1981; Montague, Maddus, &Dereshivksy, 1990; Worden & Nakamura, 1982).
The deficits of the comorbid group (ADHD +RD) relative to the two pure groups allows for anexamination of the basis for comorbidity. There isconsiderable debate in the literature as to whetherthis group has the core cognitive deficits of RD-ontychildren, ADHD-only children, or both (i.e., Fergus-son & Horwood, 1992; Pennington et al., 1993; Shay-witz et al., 1995). In this study, the ADHD + RDchildren were found to have the most of the deficitsof both pure groups. However, there was some indi-cation that this group was less impaired on the lan-guage measures than pure-RD children. The ADHD+ RD group did not differ from normal controls inambiguous references and the pure-RD childrenseemed to be the most impaired on The Word lest.In addition, the RD group tended (albeit nonsignifi-cantly) to be the least sensitive to importance levelsin the story retelling task. It is possible that the basisfor the reading disability in ADHD + RD childrenis somewhat different than for its presence in pure-RD children. One limitation of this study was that itcould not measure phonological processing.Phonological abilities are widely recognized as thecore deficit in reading disabilities (e.g., Stanovich,1988) and may have differentiated between theADHD + RD and pure-RD groups.
A recent study which addressed issues relatingto classification and definition with a large cohort ofRD, ADHD, and ADHD + RD children found thatchildren with both ADHD and RD did indeed ex-hibit difficulties within the language system (includ-ing phonological awareness) characteristic ofchildren with RD only. Thus it appears that manychildren with comorbid ADHD and RD diagnosesexhibit the characteristics of both pure disorders.This issue is also being addressed by the authors in
a current study with a similar design and comparablepopulations.
From a clinical perspective, these results suggesta need to emphasize different aspects of language inthe instruction and remediation of children in thedifferent diagnostic categories. In particular, pure-ADHD children would benefit from instruction inself-monitoring and awareness of language use inlanguage contexts which are beyond the sentencelevel. Children with RD would benefit from instruc-tion in the semantic aspects of language, includingthe ability to analyze, categorize, and associate themeanings of words in a language. The finding thatchildren with both ADHD and RD exhibited thedeficits of both pure groups suggests that remedia-tion should be directed to both types of difficulties.
APPENDIK
Error code Explanation
Sequence error Idea unit is retold in a different order thanin the original story,so that the story theme is affected (e.g.,"The father gets off thedonkey and then hoists his son up behindhim"). It is not scoredif an item is simply omitted and the storycontinues in order.
Misinterpretation Meaning of an action or event isincorrectly interpreted, (e.g., inthe original story the father hoists his sonup behind him on thedonkey, whereas the child interprets theevent as the father getsoff and then the son gets on).
Substitution A word for an object, character, or eventin the original story isreplaced with an inappropriate word (i.e.,not a synonym). Forexample, nuns is substituted for maidens, pondis substituted for aver.
Ambiguous A pronoun is not linked to a specificreference character or event so that its
referent is ambiguous. For example, in thesentence "The fatherand son were on the donkey and then hegot off," it is notknown whether the pronoun "he" refers tothe father or the son.

Language Abilities in ADHD and RD 143
ACKNOWLEDGMENTS
This research was supported by grants fromHealth and Welfare Canada (NHRDP) awarded toDrs. Schachar, Tannock, and Logan, and from theMedical Research Council of Canada awarded toDrs. lannock, Schachar, and Logan. The study isbased in part on a Master's thesis completed byKaren Purvis at the University of Toronto. Theauthors gratefully acknowledge Michael Marriott andPatricia Fulford for their assistance with data collec-tion.
REFERENCES
Ackerman, P. T., Dykman, R. A., & Gardner, M. Y. (1990). ADDstudents with and without dyslexia differ in sensitivity torhyme and alliteration. Journal of Learning Disabilities, 23,279-283.
American Psychiatric Association. (1987). Diagnostic and statisticalmanual of mental disorders (3rd ed., rev.). Washington, DC:Author.
American Psychiatric Association. (1994). Diagnostic and statisticalmanual of mental disorders (4th ed.). Washington, DC:Author.
August, C. J. (1987). Production deficiencies in free recall: A com-parison of hyperactive, learning disabled and normal children.Journal of Abnormal Child Psychology, 15, 429-440.
August, G. L., & Gaifinkel, B. D. (1989). Behavioral and cognitivesubtypes of ADHD. Journal of the American Academy of Childand Adolescent Psychiatry, 28, 739-748.
Baker, L., & Cantwell, D. £ (1992). Attention deficit disorder andspeech/language disorders. Comprehensive Mental HealthCare, 2, 3-16.
Barkley, R. A. (1990). Attention deficit hyperactivity disorder: Ahandbook for diagnosis and treatment (pp. 76-77). New York:Guilford Press.
Barkley, R. A. (1994). Delayed responding and attention deficithyperactivity disorder A unified theory. In D. K. Routh (Ed),Disruptive behavior disorders in children: Essays in honor ofHerbert Quay. New York: Plenum Press.
Beitchman, J. H., Tuckett, M., & Battb, S. (1987). Language delayand hyperactivity in preschoolers: Evidence for a distinct sub-group of hyperactives. Canadian Journal of Psychiatry, 32, 683-687.
Benson, D. F. (1991). The role of frontal dysfunction in attention-deficit hyperactivity disorder. Journal of Child Neurology, 6,9-12.
Biederman, J., Newcorn, J., & Sprich, S. E. (1991). Comorbidityof attention deficit hyperactivity disorder (ADHD). AmericanJournal of Psychiatry, 148, 564-577.
Brown, A. L., Day, J. D., & Jones, R. S. (1983). The developmentof plans for summarizing texts. Child Development, 54, 968-979.
Brown, A. L., & Smiley, S. S. (1977). Rating the importance ofstructural units of prose passages: A problem of metacognitivedevelopment. Child Development, 48, 1-8.
Cohen, N., Davine, M., Horodezky, N., Lipsett, L., & Isaacson, L.(1993). Unsuspected language impairment in psychiatricallydisturbed children: Prevalence and language and behavioralcharacteristics. Journal of the American Academy of Child andAdolescent Psychiatry, 32, 595-603.
Dale, E, & Chall, J. S. (1948). A formula for predicting readabil-ity. Educational Research Bulletin, 27, 11-21, 37-54.
Doughs, V I. (1988). Cognitive deficits in children with attentiondeficit disorder with hyperactivity. In L. M. Bloomingdale &G. Swanson (Eds.), Journal of Child Psychology and Psychiatry,5, (Book Suppl.), 65-81.
Dykman, R. A., & Ackerman, P. T. (1991). Attention deficit disorderand specific reading disability: Separate but often overlapping dis-orders. Journal of Learning Disabilies, 24, 96-103.
Faraone, S. V., Biederman, J., Lehman, B. K., Spencer, T, Norman,D., Seidman, L. J., Kraus, I., Perrin, J., Chen, W. J., & Tsuang,M. T (1993). Intellectual performance and school failure inchildren with attention deficit hyperactivity disorder and intheir siblings. Journal of Abnormal Psychology, 102, 616-623.
Feagans, L., & Short, E. (1984). Developmental differences in thecomprehension and production of narratives by reading-dis-abled and normally achieving children. Child Development, 55,1727-1736.
Felton, R. H., Wood, E B., Brown, I. S., Campbell, S. K., & Harter,M. R. (1987). Separate verbal memory and naming deficitsin attention deficit disorder and reading disability. Brain andLanguage, 31, 171-184.
Fergusson, D. M., & Horwood, L, J. (1992). Attention deficit andreading achievement. Journal of Child Psychology and Psychia-try, 33, 375-385.
Fine, J. (1985). Cohesion as an index of social-cognitive factors:Oral language of the reading disabled. Discourse Processes, 8,91-112.
Goldman-Rakic, P. S. (1987). Development of cortical circuitry andcognitive function. Child Development, 58, 601-622.
Graybeal, C (1981). Memory for stories in language-impaired chil-dren. Applied Psycholinguistics, 2, 269-283.
Hallahan, D. P., & Kaufman, J. M. (1976). Introduction to learningdisabilities: A psychobehavioral approach. Englewood Cliffs,NJ.: Prentice-Hall.
Hamlett, K. W., Pellegrini, D. S., & Conners, C. K. (1987). Aninvestigation of executive processes in the problem solving ofattention deficit disorder-hyperactive children. Journal of Pe-diatric Psychology, 12, 227-240.
Hansen, C L. (1978). Story retelling used with average and learn-ing disabled readers as a measure of reading comprehension.Learning Disability Quarterly, 1, 62-69.
Humphries, T, Koltun, H., Malone, M., & Roberts, W. (1994).Teacher-identified oral language difficulties among boys withattention problems. Developmental and Behavioral Pediatrics,15, 92-98.
Jastak, S., & Wilkinson, G. S. (1987). Manual for the Wide RangeAchievement Test (revised). Wilmington, DE: Jastak.
Johnson, R. & (1970). Recall of prose as a function of the struc-tural importance of the linguistic units. Journal of VerbalLearning and Verbal Behavior, 9, 12-20.
Jorgeson, C, Barrett, M., Huisingh, R., & Zachman, L. (1981).The Word Test: A test of expressive vocabulary and semantics.Moline, Illinois: Linguisystems Inc.
Keppel, G. (1982). Design and analysis: A researcher's handbook(2nd ed.). Englewood Cliffs, NJ: Prentice-Hall Inc.
Kinsboume, M. (1989). Control system instability in hyperactivechildren. In L M. Bloomingdale (Ed), Attention deficit disor-der (Vol. 3, pp. 104-106). New York: Pergamon Press.
Lambert, N. M., & Sandoval, J. (1980). The prevalence of learningdisabilities in a sample of children considered hyperactive.Journal of Abnormal Psychology, 8, 33-50.
Lapadat, J. C. (1991). Pragmatic language skills of students withlanguage and/or learning disabilities: A quantitative synthesis.Journal of Learning Disabilities, 24, 147-158.
Liles, B. Z., & Purcell, S. (1987). Departures in the spoken nar-ratives of normal and language-disordered children. AppliedPsycholinguistics, 8, 185-202.
144 Purvis and Tannock
Love, A. J., & Thompson, M. G. (1988). Language disorders andattention deficit disorders in young children referred for psy-chiatric services. American Journal of Orthopsychiatry, 58, 52-64.
Luria, (1966). Higher cortical function in man. New York: BasicBooks.
Mattes, J. A. (1980). The role of frontal lobe dysfunction in child-hood hyperkinesis. Comprehensive Psychiatry 21, 358-369.
Montague, M., Maddus, C. D., & Dereshrwsky, M. I. (1990). Storygrammar and comprehension and production of narrativeprose by students with learning disabilities. Journal of Learn-ing Disabilities, 23, 190-197.
O'Neill, M. E., & Douglas, V I. (1991). Study strategies and storyrecall in attention deficit disorder and reading disability. Jour-nal of Abnormal Child Psychology, 19, 671-692.
Pennington, B. F., Groisser, D., & Welsh, M. C. (1993). Contrast-ing cognitive deficits in attention deficity hyperactivity disor-der versus reading disability. Developmental Psychology, 29,511-523.
Prurting, C A., & Kirchner, D. M. (1987). A clinical appraisal ofthe pragmatic aspects of language. Journal of Speech andHearing Disorders, 52, 105-119.
Richard, G., & Hanner, M. (1985). Language Processing Test.Moline, Illinois: Linguisystems Inc.
Sattler, J. M. (1988). Assessment of Children (3rd. ed). San Diego,CA: J. M. Sattler.
Scbachar, R., & Tannock, R. (1990). Teacher Telephone Interviewfor Disruptive Behavior Disorders (DSM-III-R). Unpublishedmanuscript, Hospital for Sick Children, Department of Psy-chiatry Research, Toronto.
Schachar, R., Tannock, R., & Logan, G. (1993). Inhibitory control,impulsiveness and attention deficit hyperactivity disorder.Clinical Psychology Review, 13, 721-739.
Schachar, R, Thnnock, R., Marriott, M, & Logan, G. (1995). De-ficient inhibitory control in attention deficit hyperactivity dis-order. Journal of Abnormal Child Psychology, 23, 411-437.
Schachar, R. J., & Wachsmuth, R. (1989). Parent Interview for ChildSymptoms—Revised DSM-III-R. Unpublished manuscript,Hospital for Sick Children, Department of Psychiatry,Toronto.
Semrud-Clikeman, M., Biederman, J., Sprich-Buckminster, S.,Lehman, B., Faraone, S., & Norman, D. (1992). Comorbiditybetween ADDH and learning disability: A review and reportin a clinically referred sample. Journal of the American Acad-emy of Child and Adolescent Psychiatry, 31, 439-448.
Shallicc, T (1982). Specific impairments in planning. Royal Societyof London, B298, 199- 209.
Shaywitz, B. A., Fletcher, J. M., Holahan, J. M., Schneider, A. E.,Marchione, K. E., Stuebing, K. K., Francis, D. J., Shankweiler,D. P., Katz, L., Liberman, I. Y., & Shaywitz, S. E. (1995).Interrelationships between reading disability and attention-deficit/hyperactivity disorder. Child Neuropsychology, 1, 170-186.
Shue, K. L., & Douglas, V I. (1992). Attention deficit hyperactivitydisorder and the frontal lobe syndrome. Brain and Cognition,20, 104-124.
Smiley, S., Oakley, D, Worthen, D., Campione, J., & Brown, A.(1977). Recall of thematically relevant material by adolescentgood and poor readers as a function of written versus oralpresentation. Journal of Educational Psychology, 69, 381-387.
Stanovich, K. E. (1988). Explaining the differences between thedyslexic and the garden-variety poor reader: The phonologi-cal-core variable-difference model. Journal of Learning Dis-abilities, 21, 590-604.
Tannock, R., Corkum, P., Schachar, R., & Purvis, K. (1994).Phonological processing in children with attention deficit hyper-activity disorder. Poster presentation at the Annual Child Psy-chiatry Day, The Hospital for Sick Children, Children,
Tannock, R., Purvis, K. L., & Schachar, R. J. (1993). Narrativeabilities in children with attention deficit disorder and normalpeers. Journal of Abnormal Child Psychology, 21, 103-117.
Tannock, R., & Schachar, R. (1996). Executive dysfunction as anunderlying mechanism of behavior and language problems inattention deficit hyperactivity disorder. In J. H. Beitchman,N. Cohen, M. M. Konstantareas, & R. Tannock (Eds.), Lan-guage learning and behavior disorders: Developmental, biologi-cal, and clinical perspectives (pp. 128-155). Cambridge,England: Cambridge University Press.
Voelker, S. L, Carter, R. A., Sprague, D. J., Gdowski, C. L, &Lachar, D. (1989). Developmental trends in memory andmetamemory in children with attention deficit disorder. Jour-nal of Pediatric Psychology, 14, 75-88.
Wechsler, D. (1974). Manual for the Wechsler Intelligence Scale forChildren—Revised. New York: Psychological Corporation.
Worden, P. E., & Nakamura, G. V (1982). Story comprehensionand recall in learning disabled vs. normal college students.Journal of Educational Psychology, 74, 633-641.
Zentall, S. S. (1988). Production deficiencies in elicited languagebut not in the spontaneous verbalization of hyperactive chil-dren. Journal of Abnormal Child Psychology, 16, 657-673.
Zentall, S. S., Gohs, D. E., & Culatta, B. (1983). Language andactivity of hyperactive and comparison children during listen-ing tasks. Exceptional Children, 50, 255-266.
Copyright © 2022 FDOKUMEN




















