
Lampiran 1 CRITICAL APPRAISAL JURNAL 1 Effects of ...
66
Lampiran 1 CRITICAL APPRAISAL JURNAL 1 Effects of Auditory and Audiovisual Presentations on Anxiety and Behavioral Changes in Children Undergoing Elective Surgery Pertanyaan Fokus Yes No Unknown Bagian A : Apakah hasilnya valid? A. Apakah studi tersebut menjelaskan masalahnya secara fokus (studi populasi, intervensi, kelompok kontrol/intervensi, hasil) √ B. Apakah pembagian pasien kedalam kelompok intervensi dan kontrol dilakukan secara acak (bagaimana dilakukan, apakah alokasi pasien dilakukan secara tersembunyi dari penelitian dan penelitian) √ C. Apakah semua pasien yang terlibat dalam penelitian dicatat dengan benar di kesimpulan (apakah dihentikan lebih awal, apakah pasien dianalisis dalam kelompok untuk yang mereka acak) √ D. Apakah pasien, petugas kesehatan, dan responden pada penelitian ini “blind” terhadap intervensi yang dilaksanakan √ E. Apakah waktu pelaksanaan untuk setiap grup sama? √ F. Selain intervensi yang dilaksanakan, apakah setiap grup diperlakukan sama/adil? √ Bagian B : Apa hasilnya? A. Seberapa besar efek dari intervensi tersebut (outcome, hasilnya dijelaskan spesifik, hasil yang ditemukan, hasil dari setiap outcome yang diatur) √ B. Seberapa tepat dan akurat efek intervensi? √ Bagian C : Apakah hasil membantu secara lokal? A. Bisakah hasilnya diterapkan pada populasi lokal, atau konteks saat ini di lingkungan sekarang (apakah karakteristik pasien sama dengan tempat bekerja/populasi anda, jika berbeda apakah perbedaannya) √ B. Apakah hasil penelitian ini penting secara klinis untuk dipertimbangkan (apakah informasi yang anda inginkan sudah terdapat dalam penelitian, jika tidak apakah akan berpengaruh terhadap pengambilan keputusan) √ C. Apakah manfaatnya sepadan dengan bahaya dan biaya yang dibutuhkan (meskipun tidak tercantum dalam penelitian, bagaimana menurut anda?) √
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Lampiran 1 CRITICAL APPRAISAL JURNAL 1 Effects of ...

Lampiran 1
CRITICAL APPRAISAL JURNAL 1
Effects of Auditory and Audiovisual Presentations on Anxiety and Behavioral
Changes in Children Undergoing Elective Surgery
Pertanyaan Fokus Yes No Unknown
Bagian A : Apakah hasilnya valid?
A. Apakah studi tersebut menjelaskan masalahnya secara fokus
(studi populasi, intervensi, kelompok kontrol/intervensi, hasil)
√
B. Apakah pembagian pasien kedalam kelompok intervensi dan
kontrol dilakukan secara acak (bagaimana dilakukan, apakah
alokasi pasien dilakukan secara tersembunyi dari penelitian
dan penelitian)
√
C. Apakah semua pasien yang terlibat dalam penelitian dicatat
dengan benar di kesimpulan (apakah dihentikan lebih awal,
apakah pasien dianalisis dalam kelompok untuk yang mereka
acak)
√
D. Apakah pasien, petugas kesehatan, dan responden pada
penelitian ini “blind” terhadap intervensi yang dilaksanakan
√
E. Apakah waktu pelaksanaan untuk setiap grup sama? √
F. Selain intervensi yang dilaksanakan, apakah setiap grup
diperlakukan sama/adil?
√
Bagian B : Apa hasilnya?
A. Seberapa besar efek dari intervensi tersebut (outcome,
hasilnya dijelaskan spesifik, hasil yang ditemukan, hasil
dari setiap outcome yang diatur)
√
B. Seberapa tepat dan akurat efek intervensi? √
Bagian C : Apakah hasil membantu secara lokal?
A. Bisakah hasilnya diterapkan pada populasi lokal, atau
konteks saat ini di lingkungan sekarang (apakah
karakteristik pasien sama dengan tempat bekerja/populasi
anda, jika berbeda apakah perbedaannya)
√
B. Apakah hasil penelitian ini penting secara klinis untuk
dipertimbangkan (apakah informasi yang anda inginkan
sudah terdapat dalam penelitian, jika tidak apakah akan
berpengaruh terhadap pengambilan keputusan)
√
C. Apakah manfaatnya sepadan dengan bahaya dan biaya
yang dibutuhkan (meskipun tidak tercantum dalam
penelitian, bagaimana menurut anda?)
√

CRITICAL APPRAISAL JURNAL 2
Pengaruh Audiovisual Menonton Film Kartun terhadap Tingkat Kecemasan Saat
Prosedur Injeksi pada Anak Prasekolah
Pertanyaan Fokus Yes No Unknown
Bagian A : Apakah hasilnya valid?
A. Apakah studi tersebut menjelaskan masalahnya secara fokus
(studi populasi, intervensi, kelompok kontrol/intervensi, hasil)
√
B. Apakah pembagian pasien kedalam kelompok intervensi dan
kontrol dilakukan secara acak (bagaimana dilakukan, apakah
alokasi pasien dilakukan secara tersembunyi dari penelitian
dan penelitian)
√
C. Apakah semua pasien yang terlibat dalam penelitian dicatat
dengan benar di kesimpulan (apakah dihentikan lebih awal,
apakah pasien dianalisis dalam kelompok untuk yang mereka
acak)
√
D. Apakah pasien, petugas kesehatan, dan responden pada
penelitian ini “blind” terhadap intervensi yang dilaksanakan
√
E. Apakah waktu pelaksanaan untuk setiap grup sama? √
F. Selain intervensi yang dilaksanakan, apakah setiap grup
diperlakukan sama/adil?
√
Bagian B : Apa hasilnya?
A. Seberapa besar efek dari intervensi tersebut (outcome,
hasilnya dijelaskan spesifik, hasil yang ditemukan, hasil
dari setiap outcome yang diatur)
√
B. Seberapa tepat dan akurat efek intervensi? √
Bagian C : Apakah hasil membantu secara lokal?
A. Bisakah hasilnya diterapkan pada populasi lokal, atau
konteks saat ini di lingkungan sekarang (apakah
karakteristik pasien sama dengan tempat bekerja/populasi
anda, jika berbeda apakah perbedaannya)
√
B. Apakah hasil penelitian ini penting secara klinis untuk
dipertimbangkan (apakah informasi yang anda inginkan
sudah terdapat dalam penelitian, jika tidak apakah akan
berpengaruh terhadap pengambilan keputusan)
√
C. Apakah manfaatnya sepadan dengan bahaya dan biaya
yang dibutuhkan (meskipun tidak tercantum dalam
penelitian, bagaimana menurut anda?)
√

CRITICAL APPRAISAL JURNAL 3
Psychological Preparation Reduces Preoperative Anxiety in Children.
Randomized and Double-Blind Trial
Pertanyaan Fokus Yes No Unknown
Bagian A : Apakah hasilnya valid?
A. Apakah studi tersebut menjelaskan masalahnya secara fokus
(studi populasi, intervensi, kelompok kontrol/intervensi, hasil)
√
B. Apakah pembagian pasien kedalam kelompok intervensi dan
kontrol dilakukan secara acak (bagaimana dilakukan, apakah
alokasi pasien dilakukan secara tersembunyi dari penelitian
dan penelitian)
√
C. Apakah semua pasien yang terlibat dalam penelitian dicatat
dengan benar di kesimpulan (apakah dihentikan lebih awal,
apakah pasien dianalisis dalam kelompok untuk yang mereka
acak)
√
D. Apakah pasien, petugas kesehatan, dan responden pada
penelitian ini “blind” terhadap intervensi yang dilaksanakan
√
E. Apakah waktu pelaksanaan untuk setiap grup sama? √
F. Selain intervensi yang dilaksanakan, apakah setiap grup
diperlakukan sama/adil?
√
Bagian B : Apa hasilnya?
A. Seberapa besar efek dari intervensi tersebut (outcome,
hasilnya dijelaskan spesifik, hasil yang ditemukan, hasil
dari setiap outcome yang diatur)
√
B. Seberapa tepat dan akurat efek intervensi? √
Bagian C : Apakah hasil membantu secara lokal?
A. Bisakah hasilnya diterapkan pada populasi lokal, atau
konteks saat ini di lingkungan sekarang (apakah
karakteristik pasien sama dengan tempat bekerja/populasi
anda, jika berbeda apakah perbedaannya)
√
B. Apakah hasil penelitian ini penting secara klinis untuk
dipertimbangkan (apakah informasi yang anda inginkan
sudah terdapat dalam penelitian, jika tidak apakah akan
berpengaruh terhadap pengambilan keputusan)
√
C. Apakah manfaatnya sepadan dengan bahaya dan biaya
yang dibutuhkan (meskipun tidak tercantum dalam
penelitian, bagaimana menurut anda?)
√

CRITICAL APPRAISAL JURNAL 4
Video Distraction and Parental Presence for the Management of Preoperative Anxiety
and Postoperative Behavioral Disturbance in Children: A Randomized Controlled Trial
Pertanyaan Fokus Yes No Unknown
Bagian A : Apakah hasilnya valid?
A. Apakah studi tersebut menjelaskan masalahnya secara fokus
(studi populasi, intervensi, kelompok kontrol/intervensi, hasil)
√
B. Apakah pembagian pasien kedalam kelompok intervensi dan
kontrol dilakukan secara acak (bagaimana dilakukan, apakah
alokasi pasien dilakukan secara tersembunyi dari penelitian
dan penelitian)
√
C. Apakah semua pasien yang terlibat dalam penelitian dicatat
dengan benar di kesimpulan (apakah dihentikan lebih awal,
apakah pasien dianalisis dalam kelompok untuk yang mereka
acak)
√
D. Apakah pasien, petugas kesehatan, dan responden pada
penelitian ini “blind” terhadap intervensi yang dilaksanakan
√
E. Apakah waktu pelaksanaan untuk setiap grup sama? √
F. Selain intervensi yang dilaksanakan, apakah setiap grup
diperlakukan sama/adil?
√
Bagian B : Apa hasilnya?
A. Seberapa besar efek dari intervensi tersebut (outcome,
hasilnya dijelaskan spesifik, hasil yang ditemukan, hasil
dari setiap outcome yang diatur)
√
B. Seberapa tepat dan akurat efek intervensi? √
Bagian C : Apakah hasil membantu secara lokal?
A. Bisakah hasilnya diterapkan pada populasi lokal, atau
konteks saat ini di lingkungan sekarang (apakah
karakteristik pasien sama dengan tempat bekerja/populasi
anda, jika berbeda apakah perbedaannya)
√
B. Apakah hasil penelitian ini penting secara klinis untuk
dipertimbangkan (apakah informasi yang anda inginkan
sudah terdapat dalam penelitian, jika tidak apakah akan
berpengaruh terhadap pengambilan keputusan)
√
C. Apakah manfaatnya sepadan dengan bahaya dan biaya
yang dibutuhkan (meskipun tidak tercantum dalam
penelitian, bagaimana menurut anda?)
√

CRITICAL APPRAISAL JURNAL 5
Video Kartun dan Video Animasi dapat Menurunkan Tingkat Kecemasan Pre
Operasi pada Anak Usia Pra Sekolah
Pertanyaan Fokus Yes No Unknown
Bagian A : Apakah hasilnya valid?
A. Apakah studi tersebut menjelaskan masalahnya secara fokus
(studi populasi, intervensi, kelompok kontrol/intervensi, hasil)
√
B. Apakah pembagian pasien kedalam kelompok intervensi dan
kontrol dilakukan secara acak (bagaimana dilakukan, apakah
alokasi pasien dilakukan secara tersembunyi dari penelitian
dan penelitian)
√
C. Apakah semua pasien yang terlibat dalam penelitian dicatat
dengan benar di kesimpulan (apakah dihentikan lebih awal,
apakah pasien dianalisis dalam kelompok untuk yang mereka
acak)
√
D. Apakah pasien, petugas kesehatan, dan responden pada
penelitian ini “blind” terhadap intervensi yang dilaksanakan
√
E. Apakah waktu pelaksanaan untuk setiap grup sama? √
F. Selain intervensi yang dilaksanakan, apakah setiap grup
diperlakukan sama/adil?
√
Bagian B : Apa hasilnya?
A. Seberapa besar efek dari intervensi tersebut (outcome,
hasilnya dijelaskan spesifik, hasil yang ditemukan, hasil
dari setiap outcome yang diatur)
√
B. Seberapa tepat dan akurat efek intervensi? √
Bagian C : Apakah hasil membantu secara lokal?
A. Bisakah hasilnya diterapkan pada populasi lokal, atau
konteks saat ini di lingkungan sekarang (apakah
karakteristik pasien sama dengan tempat bekerja/populasi
anda, jika berbeda apakah perbedaannya)
√
B. Apakah hasil penelitian ini penting secara klinis untuk
dipertimbangkan (apakah informasi yang anda inginkan
sudah terdapat dalam penelitian, jika tidak apakah akan
berpengaruh terhadap pengambilan keputusan)
√
C. Apakah manfaatnya sepadan dengan bahaya dan biaya
yang dibutuhkan (meskipun tidak tercantum dalam
penelitian, bagaimana menurut anda?)
√

Lampiran 2
INSTRUMEN PENERAPAN EVIDENCE BASED PRACTICE (EBP)
MODIFIED YALE PREOPERATIVE ANXIETY SCALE (M‑YPAS)
I. Kuesioner Data Demografi
Petunjuk pengisian : Isilah data di bawah ini dengan lengkap dan berilah
tanda (√) pada tempat pilihan yang tersedia.
1. Nomor Responden :
2. Nama Responden :
3. Jenis Kelamin : ( ) Laki-Laki ( ) Perempuan
4. Umur : Tahun
5. Tanggal Pemeriksaan :
6. Pukul Pretest : Post test :
7. Diagnosa Penyakit :

II. Lembar Observasi Tingkat Kecemasan
Petunjuk : Lingkari satu kategori pada masing-masing domain yang paling
menggambarkan kondisi dan situasi anak.
A. Kegiatan
1. Memperhatikan sekeliling, ingin tahu, bermain, membaca (atau
kebiasaan lainnya).
2. Tidak mau melakukan kegiatan, menunduk, gelisah dengan
memainkan tangan, duduk dekat dengan orang tua.
3. Bergerak tanpa aktivitas yang jelas, menggeliat, memegang orang
tuanya.
4. Menghindari tenaga kesehatan, menolak perlakuan dengan kaki dan
tangan atau dengan seluruh tubuh, tidak mau bermain dan tidak mau
terpisah dari orang tua.
B. Pernyataan
1. Membaca (tanpa suara), bertanya, berkomentar, menjawab
pertanyaan, terlalu asyik bermain untuk merespon.
2. Menanggapi orang yang lebih dewasa dengan berbisik, hanya
menganggukkan kepala
3. Diam, tidak ada respon terhadap orang lebih dewasa
4. Merengek, mengerang, merintih
5. Menangis atau bahkan berteriak “tidak mau di operasi”
6. Menangis, berteriak keras terus menerus.

C. Luapan Emosi
1. Terlihat senang, tersenyum, atau asyik dengan kegiatannya
2. Netral, tidak terlihat emosi yang berarti pada wajah
3. Sedih, wajah ketakutam, terlihat tegang
4. Menangis, menjadi sangat marah
D. Keadaan Ingin Tahu
1. Berjaga-jaga, melihat sekeliling, melihat apa yang dilakukan tenaga
kesehatan
2. Anak berdiam diri dengan duduk tenang dan diam, menatap orang
yang lebih dewasa
3. Waspada melihat sekitarnya, terkejut akan suara-suara tertentu, mata
waspada, bahkan menegang
4. Panik dan merengek, menangis, mendorong orang di sekitarnya.
E. Peranan Orang Tua
1. Sibuk bermain atau sibuk dengan kebiasaannya, duduk tenang, tidak
membutuhkan orang tua, mau berinteraksi dengan oang tua apabila
orang tuanya yang memulai
2. Menggapai orang tua, mencari perlindungan dan kenyamanan,
bersandar pada orang tua.
3. Menatap orang tua, tidak ingin berhubungan dengan orang lain,
melakukan apa yang disuruh bila orang tua berada di dekatnya.
Rentang skor kecemasan
1. Cemas ringan = 30- 53
2. Cemas sedang = 54- 77
3. Cemas berat = 78-100
4. Tidak bisa jauh dari orang tua dan akan marah/menangis apabila
berpisah dengan orang tuanya, memegang erat orang tua dan tidak
melepaskannya, atau mendorong menjauhi orang tuanya.
SKOR TOTAL : (A/4 +B/6+C/4+D/4+E/4) x 100/5

Lampiran 3
STANDAR OPERASIONAL PROSEDUR (SOP)
DISTRAKSI MENONTON VIDEO KARTUN DAN ANIMASI
Pengertian Salah satu distraksi audiovisual yang merupakan jenis distraksi
gabungan dari distraksi audio dan distraksi visual menggunakan
media kartun dan animasi
Tujuan a. Mengurangi cemas (ansietas), setres hospitalisasi dan nyeri akut
skala ringan hingga sedang
b. Pengalihan perhatian klien terhadap sesuatu yang sedang
dihadapi
c. Rasa lebih nyaman, santai, dan merasa berada pada situasi yang
lebih menyenangkan
Indikasi Klien dengan kecemasan, setres hospitalisasi, nyeri akut ringan
hingga berat dan kondisi ketegangan yang membutuhkan distraksi
Kontraindikasi Klien anak yang memiliki kelainan congenital dan penyakit lainnya
seperti down sindrom, tuna netra, tuna rungu serta kondisi anak
sangat lemah sehingga tidak memungkinkan untuk menonton video
Persiapan
Klien
a. Membaca status kesehatan klien
b. Kontrak waktu, tempat, topik, dan kesediaan klien
c. Jelaskan tentang prosedur yang akan dilakukan
d. Atur posisi klien sesuai situasi, kondisi, dan kebutuhan
e. Menjaga privasi klien
Persiapan Alat a. Menyiapkan peralatan (media untuk menonton video kartun dan
animasi)
b. Modifikasi lingkungan senyaman mungkin termasuk suasana
dan kondisi ruangan agar tetap tenang dan jauh dari kebisingan
serta faktor pengganggu saat klien menonton video kartun dan
animasi

Fase Orientasi a. Salam Terapeutik
b. Perkenalan diri pada klien dan keluarga
c. Lakukan evaluasi/ validasi
d. Jelaskan tujuan dan menfaat distraksi video kartun dan animasi
e. Kontrak waktu, tempat, topik, dan prosedur tindakan
f. Minta izin dan kesediaan keluarga untuk mempraktikkan
Evidence Based Nursing Praktice berupa menonton video kartun
dan animasi dalam menurunkan tingkat kecemasan pre operasi
pada anak usia pra sekolah
g. Persilahkan klien jika ingin izin ke toilet atau menyiapkan
makanan dan minuman sebelum menonton video kartun dan
animasi dimulai
Fase Kerja 1. Cuci tangan menggunakan 6 langkah cuci tangan dengan sabun
antiseptik di bawah air mengalir atau menggunakan antiseptik
gel dan keringkan
2. Ciptakan suasana perasaan menenangkan
3. Mengatur posisi klien agar rileks
4. Memberikan salah satu teknik distraksi yaitu menonton video
kartun dan animasi. Anak diberikan kesampatan memilih salah
satu kartun (Upin Ipin, Doraemon, Bobo Boy dan Masha and the
Bear) kemudian dilakukan pemutaran video kartun selama 15
menit dan video animasi 15 menit
5. Menganjurkan keluarga klien untuk melakukan teknik distraksi
menonton video kartun dan animasi jika klien merasakan
ketidaknyamanan
6. Berikan reinforcement positif pada klien dan setelah
mempraktikkan Evidence Based Nursing Praktice berupa
menonton video kartun dan animasi
7. Cuci tangan menggunakan 6 langkah cuci tangan dengan sabun
antiseptik di bawah air mengalir atau menggunakan antiseptik
gel dan keringkan

Terminasi a. Melakukan evaluasi respon dengan menanyakan perasaan klien
setelah menonton video kartun dan animasi
b. Jelaskan rencana tindak lanjut
c. Kontrak waktu, tempat, dan topik untuk pertemuan berikutnya
d. Salam terapeutik
Dokumentasi a. Catat waktu pelaksanaan tindakan
b. Catat respon klien terhadap teknik distraksi dalam menurunkan
tingkat kecemasan pre operasi pada anak usia pra sekolah
Hal yang perlu
diperhatikan
Melakukan komunikasi terapeutik selama tindakan, menjaga
ketenangan, tidak ragu dan tidak tergesa-gesa selama tindakan,
memastikan keamanan dan kenyamanan klien dan peneliti selama
tindakan, serta memperhatikan respon klien.

Lampiran 4
CUPLIKAN TAMPILAN VIDEO KARTUN DAN ANIMASI
a. Cuplikan Tampilan Video Kartun
Video 1 : Upin Ipin – Kawan - Kawan Hilang?
Sumber : https://www.youtube.com/watch?v=51SCDlUDfx4
Video 2 : Doraemon - Pesawat UFO Alien & Beso Anjing Pengganti Manusia
Sumber : https://www.youtube.com/watch?v=nKEp-7xXK44

Video 3 : BoBoiBoy – Season 1 Episode 2 Part 1
Sumber : https://www.youtube.com/watch?v=t_H8fQZQUDM&t=18s
Video 4 : Masha and the Bear - Monkey Business
Sumber : https://www.youtube.com/watch?v=AxGlvetWIqc
b. Cuplikan Tampilan Video Animasi
Video 1 : Menjelaskan Anestesi pada Anak
Sumber : https://www.youtube.com/watch?v=FblP0vn3qxI
Lampiran 5

LEMBAR BIMBINGAN
PENYUSUNAN KARYA ILMIAH PROGRAM STUDI PROFESI NERS
JURUSAN KEPERAWATAN – POLTEKKES KEMENKES SEMARANG
Nama Mahasiswa : Nurus Suroya
NIM : P1337420919047
Program Studi : Profesi Ners
Pembimbing Utama : Ns. Anwar Adi P, S.Kep
Pembimbing Pendamping : Suharto, S.Pd., MN
Judul
: Video Kartun dan Animasi dalam Menurunkan Tingkat
Kecemasan Pre Operasi pada Anak Usia Pra Sekolah di
Ruang Prabu Kresna RSUD K.R.M.T Wongsonegoro
Kota Semarang
No Hari/Tanggal Materi Bimbingan Saran Bimbingan TTD
Pembimbing
4.
5.
6.
7.
Selasa, 18
Februari
2020
Rabu, 29
April 2020
Selasa, 05
Mei 2020
Kamis, 2 Juli
2020
Perbaikan (revisi)
pasca Proposal
KIN
Bab 3 dan 4
Kelengkapan KIN
Perbaikan (revisi)
pasca ujian hasil
KIN dan naskah
publikasi
Durasi pelaksanaan penerapan
EBP menonton video kartun
dan animasi lebih diperjelas
Perbaiki kesalah ejaan sesuai
kaidah penulisan KBBI
ACC dan lanjutkan ujian hasil
KIN
ACC dan lanjutkan publikasi
hasil Karya Ilmiah

Lampiran 5
LEMBAR BIMBINGAN
PENYUSUNAN KARYA ILMIAH PROGRAM STUDI PROFESI NERS
JURUSAN KEPERAWATAN – POLTEKKES KEMENKES SEMARANG
Nama Mahasiswa : Nurus Suroya
NIM : P1337420919047
Program Studi : Profesi Ners
Pembimbing Utama : Ns. Anwar Adi P, S.Kep
Pembimbing Pendamping : Suharto, S.Pd., MN
Judul
: Video Kartun dan Animasi dalam Menurunkan Tingkat
Kecemasan Pre Operasi pada Anak Usia Pra Sekolah di
Ruang Prabu Kresna RSUD K.R.M.T Wongsonegoro
Kota Semarang
No Hari/Tanggal Materi Bimbingan Saran Bimbingan TTD
Pembimbing
4.
5.
6.
7.
Selasa, 18
Februari
2020
Kamis, 26
Maret
Sabtu, 16
Mei 2020
Rabu, 01 Juli
2020
Perbaikan (revisi)
pasca Proposal
KIN
Bab 3 dan 4
Kelengkapan KIN
Perbaikan (revisi)
pasca ujian hasil
KIN dan naskah
publikasi
Laporan KIN tidak dilakukan
implementasi karena adanya
pandemic Covid 19
Bab hasil dan pembahan sesuai
dengan tujuan
ACC, persiapkan power point
dan lanjutkan ujian hasil KIN
ACC dan lanjutkan publikasi
hasil Karya Ilmiah

Lampiran 6
LEMBAR PERBAIKAN (REVISI)
UJIAN KARYA ILMIAH NERS
NAMA MAHASISWA : NURUS SUROYA
NIM : P1337420919047
JUDUL KIN : VIDEO KARTUN DAN ANIMASI DALAM
MENURUNKAN TINGKAT KECEMASAN PRE OPERASI PADA ANAK
USIA PRA SEKOLAH DI RUANG PRABU KRESNA RSUD K.R.M.T
WONGSONEGORO KOTA SEMARANG
TELAH DIREVISI DAN DISETUJUI DENGAN PERBAIKAN SEBAGAI
BERIKUT :
NO. PERBAIKAN/ POIN REVISI TANDA TANGAN
1. 1. Perbaiki karya ilmiah sesuai masukan dari
pembimbing II
2. Klarifikasi mengenai risiko hambatan dalam
penerapan intervensi menonton video kartun
dan animasi di ruang Prabu Kresna
K.R.M.T Wongsonegoro Kota Semarang
PENGUJI I
Ns. Anwar Adi P, S.Kep
NIP. 198005032005011007
2. 1. Tambahkan studi pendahuluan pada latar
belakang
2. Bab 3 pada sub bab hasil dan pembahan
dipisah dan disesuaikan dengan tujuan
khusus dan sesuai conclution abstrak
3. Simpulan mengacu pada hasil dan saran
mengikuti simpulan
PENGUJI II
Suharto, S.Pd., MN
NIP. 196605101986031001
LEMBAR PERSETUJUAN PERBAIKAN (REVISI)
UJIAN KARYA ILMIAH NERS
NAMA : NURUS SUROYA
NIM : P1337420919047
TANGGAL UJIAN : KAMIS, 21 MEI 2020
PROGRAM STUDI : PROFESI NERS
JUDUL KIN : VIDEO KARTUN DAN ANIMASI DALAM
MENURUNKAN TINGKAT KECEMASAN PRE OPERASI PADA ANAK
USIA PRA SEKOLAH DI RUANG PRABU KRESNA RSUD K.R.M.T
WONGSONEGORO KOTA SEMARANG
TELAH DIREVISI DAN DISETUJUI OLEH TIM PENGUJI/ TIM
PEMBIMBING
NO. NAMA PENGUJI TANDA TANGAN
1. PENGUJI I
Ns. Anwar Adi P, S.Kep
NIP. 198005032005011007
2. PENGUJI II
Suharto, S.Pd., MN
NIP. 196605101986031001

788 © 2018 Nigerian Journal of Clinical Practice | Published by Wolters Kluwer ‑ Medknow
Background: Preoperative anxiety is a critical issue in children, and associated with postoperative behavioral changes. Aims: The purpose of the current study is to evaluate how audiovisual and auditory presentations about the perioperative period impact preoperative anxiety and postoperative behavioral disturbances of children undergoing elective ambulatory surgery. Materials and Methods: A total of 99 patients between the ages of 5–12, scheduled to undergo outpatient surgery, participated in this study. Participants were randomly assigned to one of three groups; audiovisual group (Group V, n = 33), auditory group (Group A, n = 33), and control group (Group C, n = 33). During the evaluation, the Modified Yale Preoperative Anxiety Scale (M‑YPAS) and the posthospitalization behavioral questionnaire (PHBQ) were used. Results: There were no significant differences in demographic characteristics between the groups. M‑YPAS scores were significantly lower in Group V than in Groups C and A (P < 0.001 and P < 0.001, respectively). PHBQ scores in Group C were statistically higher than in Groups A and V, but, no statistical difference was found between Groups A and V. Conclusion: Compared to auditory presentations, audiovisual presentations, in terms of being memorable and interesting, may be more effective in reducing children’s anxiety. In addition, we can suggest that both methods can be equally effective for postoperative behavioral changes.
Keywords: Anxiety, audiovisual aids, behavioral rating scale, child behavior
Effects of Auditory and Audiovisual Presentations on Anxiety and Behavioral Changes in Children Undergoing Elective SurgeryZ Hatipoglu, E Gulec, D Lafli, D Ozcengiz
Address for correspondence: Dr. Z Hatipoglu, Department of Anesthesiology and Reanimation, Faculty of Medicine, Cukurova University, Adana 01260, Turkey.
E‑mail: [email protected]
systems, preoperative information programs, hypnosis, music, and acupuncture.[2]
Behavioral interventions that are used as preoperative preparation programs are applied through coping skills, modeling, and play therapy.[2] The aim of behavioral programs is to teach coping skills through modeling for anxiety to children and also to provide information about the perioperative process. These interventions should be prepared taking into consideration a child’s age, developmental stage, and previous experience.[2,6]
Original Article
Introduction
Hospitalization and surgery are a serious and memorable event for children and their parents.
Children undergoing surgery and their parents can be anxious in the preoperative period, and it occurs up to 65% of children.[1] Preoperative anxiety is associated with postoperative pain, emergence delirium, and postoperative behavioral changes (e.g., general anxiety, appetite changes, sleep disturbances, enuresis, and temper tantrums).[2‑4]
Pharmacological and nonpharmacological methods are utilized to treat preoperative anxiety in children. In the recent years, nonpharmacological methods are preferred due to possible adverse effects (e.g., excessive sedation and delayed discharge) of pharmacological methods.[5] Nonpharmacological methods are as follows: the presence of parents, distraction techniques, fun transportation
Department of Anesthesiology and Reanimation, Faculty of Medicine, Cukurova University, Adana, Turkey A
bstr
act
Access this article onlineQuick Response Code:
Website: www.njcponline.com
DOI: 10.4103/njcp.njcp_227_17
PMID: *******
Date of Acceptance: 22-Nov-2017
How to cite this article: Hatipoglu Z, Gulec E, Lafli D, Ozcengiz D. Effects of auditory and audiovisual presentations on anxiety and behavioral changes in children undergoing elective surgery. Niger J Clin Pract 2017;XX:XX-XX.
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution‑NonCommercial‑ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non‑commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
For reprints contact: [email protected]
[Downloaded free from http://www.njcponline.com on Sunday, January 26, 2020, IP: 118.96.98.61]

Hatipoglu, et al.: Preoperative anxiety in children
789Nigerian Journal of Clinical Practice ¦ Volume 21 ¦ Issue 6 ¦ June 2018
There are three methods which are known to be effective in learning; i.e., visual (pictures, images, demonstrations), auditory (reading, words, listening), and kinesthetic (touch, taste). Visual images are important to visual learning, in which body language is also used. It is also important to be informed by listening to auditory learning.[7] Most people learn best using a combination of both, although visual learning is usually the prominent component.[8] To the best of our knowledge, an auditory‑related (listening) study outside of music therapy is not available for preoperative anxiety management while there are limited audiovisual studies involving children in the literature.[9‑11]
The current study was designed to compare the effects of audiovisual and auditory presentations on preoperative anxiety and postoperative behavioral disturbances of children undergoing elective ambulatory surgery. The primary end point was the preoperative anxiety levels of patients. The secondary end point was the behavioral changes of children in the postoperative period.
Materials and MethodsPatientsThe study protocol was approved by the Institutional Ethics Committee of the Cukurova University, Faculty of Medicine (no: 45/2015). We enrolled patients between March 2015 and February 2016. Written informed consent was obtained from all the parents. Ninety‑nine patients with the American Society of Anesthesiologists physical Status I‑II, aged 5–12 years old and scheduled for outpatient surgery (e.g., orchiopexy, hypospadias surgery, inguinal hernia, tonsillectomy, adenoidectomy, and strabismus surgery) were accepted in the present study. Children with chronic illness, undergoing emergency surgery, cognitive disorders, and parents who refuse to participate were excluded from this study.
Study designThe study participants were allocated to the groups using a computer‑generated randomization list at preoperative visit: audiovisual group (Group V, n = 33), auditory group (Group A, n = 33), and the standard of care group (Group C, n = 33).
After all patients were examined by an anesthesiologist at hospital admission 1 week before surgery, the following applications were presented: the patients in Group V were shown an audiovisual presentation to inform about preoperative preparation and postoperative period [Appendix 1]. The sound recording of this video was listened to by the patients in Group A without the visual element of the audiovisual presentation. The patients in Group C were verbally informed on usual the anesthesia practice of our hospital (e.g., anesthesia and
analgesia management, preoperative fasting, and regular use of the drug to be administered after surgery). Parents accompanied their children during this time. Patient’s age, gender, history of previous surgery, type of surgery, and parent’s age, gender, and educational level were recorded.
MeasurementsThe children in all groups were admitted with one of the parents into the preoperative holding room. The preoperative anxiety levels of children were measured with the Modified Yale Preoperative Anxiety Scale (M‑YPAS) at induction of anesthesia after being taken into the operating room. This assessment was made by an anesthesiologist who was blinded to the groups. In brief, the M‑YPAS is used to measure children’s anxiety in the preoperative holding area and during induction of anesthesia. The M‑YPAS contains 22 items in five categories (activity, emotional expressivity, state of arousal, vocalization, and use of parents). The scoring in each category is done with a different number of items (either four or six). A total adjusted score is calculated with a formula after evaluating partial weight ([activity/4+ emotional expressivity/4+ state of arousal/4+ use of parents/4+ vocalization/6] ×100/5). The cutoff point of 30 on the M‑YPAS leads to balance in which the sensitivity and specificity are high, and the predictive value is 79%.[12]
Postoperative maladaptive behaviors of children were assessed using the posthospitalization behavioral questionnaire (PHBQ). Parents were contacted by telephone 7 days after hospital discharge, and this assessment was performed by the same anesthesiologist. In brief, the PHBQ contains a total of 27 items in the following six subscales: general anxiety and regression, separation anxiety, eating disturbance, aggression toward authority, apathy/withdrawal, and anxiety about sleep. The PHBQ is scored by parents using five response options: much less than before (1), less than before (2), same as before (3), more than before (4), and much more than before.[13] Psychometric properties of the PHBQ have been shown in a study of Vernon et al.[14] We considered the negative behavioral change as a response of 4 or 5 for an item of the PHBQ.[15]
Anesthesia managementAfter 6 h of fasting, the children were taken into a preoperative holding area and none of the children used any premedication. The children were taken accompanied by their parents into the operating room from the preoperative holding area. Standard monitoring was applied to patients (electrocardiogram, pulse oximeter, and noninvasive blood pressure). Anesthesia induction was provided with 6%–8% sevoflurane and
[Downloaded free from http://www.njcponline.com on Sunday, January 26, 2020, IP: 118.96.98.61]

Hatipoglu, et al.: Preoperative anxiety in children
790 Nigerian Journal of Clinical Practice ¦ Volume 21 ¦ Issue 6 ¦ June 2018
the statistical hypotheses were fulfilled or not. For normally distributed data, regarding the homogeneity of variances, Bonferroni, Scheffe, Tamhane tests were used for multiple comparisons of groups. For abnormally distributed data, a Bonferroni adjusted Mann–Whitney U‑test was used for multiple comparisons of groups. To evaluate the correlations between measurements, the Pearson correlation coefficient was used. Multivariate logistic regression analysis was used to determine the predictors of postoperative maladaptive behaviors. According to the “cutoff points,” patients were divided into two subgroups; a calm group that included patients who scored <30th percentile of the M‑YPAS and an anxious group that included patients who scored >30th percentile of the M‑YPAS.[12] The statistical level of significance for all tests was considered to be 0.05.
ResultsFlow diagram for the study is shown in Figure 1. The demographic characteristics of patients and parents were similar between the three groups [Table 1]. No significant differences were found in terms of surgical data between the three groups [Table 2].
a gas mixture of (40%–60%) oxygen/nitrous oxide. After placing intravenous (IV) cannula on the hand, rocuronium 0.6 mg/kg was administered and all patients were intubated. Fluid resuscitation was accomplished with Ringer’s lactate solution (3–5 ml/kg/h). After anesthesia induction, the parents were taken out of the operating room with a nurse. Maintenance of anesthesia was provided with 1%–2% sevoflurane and a gas mixture of (40%–60%) oxygen/nitrous oxide. For intraoperative analgesia, fentanyl 1 µg/kg was given. Tramadol (2 mg/kg, IV) was administered for postoperative analgesia in all patients. After the end of the surgery, anesthesia was terminated, and the neuromuscular blockade was antagonized with atropine (0.015 mg/kg, IV) and neostigmine (0.05 mg/kg, IV). The awakened patients were transferred to the recovery room accompanied by their parents. After recovery, the children were transported to their clinical wards.
Statistical analysisSample size analysis was performed using G*Power version 3.1.9.2 (G*Power Software, Kiel, Germany). We calculated the sample size with a power of 0.80 and an α of 0.05 as 24 patients for each group to detect 10 points difference in M‑YPAS scores between the groups. A control mean M‑YPAS score of 50 with an SD of 12 was reported in a previous study.[16] All analyses were performed using IBM SPSS Statistics software package (IBM SPSS Statistics for Windows, Version 20.0; IBM Corp., Armonk, New York, USA). Categorical variables were expressed as numbers and percentages, whereas continuous variables were summarized as a mean and standard deviation and as median and range where appropriate. The normality of distribution for continuous variables was confirmed with the Kolmogorov–Smirnov test. For comparison of continuous variables between two groups, the Student’s t‑test was used. For comparison of three groups, the One‑way ANOVA or Kruskal–Wallis test was used depending on whether
Table 1: Patients and parents’ demographic dataGroup V Group A Group C P
PatientsAge (years)a 7.6±2.0 7.4±1.9 7.6±2.3 0.93Gender (female/male) 16/17 17/16 15/18 0.88Birth order (first born/middle/later) 16/10/7 23/4/6 15/13/5 0.37Previous surgery (yes/no) 10/23 10/23 17/16 0.12
Time of previous surgeryLast 1 year 6 4 6 0.21Last 1 years ago 4 6 11
ParentsAge (years)a 36.9±5.4 34.6±5.1 36.7±5.3 0.13Gender (female/male) 19/14 21/12 20/13 0.88Education (literate/primary school/higher/university) 1/10/22 0/11/22 0/17/16 0.28
aOne‑way ANOVA test was used. Values are presented as number or mean±SD. SD=Standard deviation
Table 2: Surgical dataGroup V Group A Group C P
SurgeryENT (other) 19 15 7 0.55Ear tube insertion 3 5 2Strabismus 4 6 11Dental surgery 2 2 3Circumcision 2 3 1Other 3 2 9
Time of surgery (min)a 50.0±14.3 46.1±14.2 51.9±21.8 0.38aOne‑way ANOVA test was used. Values are presented as number or mean±SD. ENT=Ear‑nose‑throat; ENT (other)=Adenoidectomy, tonsillectomy, adenoidectomy and tonsillectomy; SD=Standard deviation
[Downloaded free from http://www.njcponline.com on Sunday, January 26, 2020, IP: 118.96.98.61]

Hatipoglu, et al.: Preoperative anxiety in children
791Nigerian Journal of Clinical Practice ¦ Volume 21 ¦ Issue 6 ¦ June 2018
Table 4: Predictors for postoperative maladaptive behavioral changes
Predictors OR 95% CI PM‑YPASa 1.03 1.01‑1.06 0.002Parent gender (female/male)b 4.05 1.39‑1.06 0.01Agec 0.40 0.13‑1.16 0.09aAnxious children (>30%) compared to less anxious (<30%); bMale compared to female; c<7 years of age compared to >7 years of age. OR=Odds ratio; CI=Confidence interval; M‑YPAS=Modified Yale Preoperative Anxiety Scale
Table 3: The means of the Modified Yale Preoperative Anxiety Scale and Posthospitalization Behavioral
QuestionnaireGroup V Group A Group C P
M‑YPAS 27.4±7.1 39.3±19.2 73.1±18.0 <0.001a,b,c
PHBQ 81.4±2.6 82.1±1.8 87.6±3.4 <0.001a,b
aP<0.001 for Group C versus Group V; bP<0.001 for Group C versus Group A; cP<0.001 for Group A versus Group V. PHBQ=Posthospitalization Behavioral Questionnaire; M‑YPAS=Modified Yale Preoperative Anxiety Scale
The M‑YPAS scores were significantly lower in Group V than Groups C and A (P < 0.001) [Table 3]. When comparing the three groups, there were no statistically relationships among age, previous surgery, type of surgery, the education level, and gender of parents on the M‑YPAS scores. However, on the basis of the evaluation
of all patients, preschool children (<7 years old) had more anxiety (43.0 ± 23.3 vs. 52.3 ± 26.6, P = 0.071). Similarly, the M‑YPAS scores of 37 children who underwent a previous surgery were compared with 62 nonoperated children, nonoperated children had lower M‑YPAS scores (42.2 ± 23.9 vs. 54.0 ± 25.1, P = 0.022).
Figure 1: Flow diagram of the study
[Downloaded free from http://www.njcponline.com on Sunday, January 26, 2020, IP: 118.96.98.61]

Hatipoglu, et al.: Preoperative anxiety in children
792 Nigerian Journal of Clinical Practice ¦ Volume 21 ¦ Issue 6 ¦ June 2018
The patients in Group C had statistically higher PHBQ scores than those in Groups A and V (P < 0.001) [Table 3]. For all patients, no correlation was found between PHBQ and children’s age, whereas there was a correlation between PHBQ and parent gender (P = 0.01). In addition, anxious child (<30th percentile) had 1.03 times greater risk of adopting negative behaviors than a calm child (>30th percentile) [Table 4]. Especially, in anxious children, there was a significant correlation between M‑YPAS and general anxiety, separation anxiety, apathy, and sleep disturbances (P < 0.05), and the number of new postoperative maladaptive behavioral changes is summarized Table 5.
DiscussionThe results of the present study showed that audiovisual presentation related to preanesthetic information in children is an effective approach in reducing preoperative anxiety. Furthermore, children who were informed with audiovisual and audio presentation had less behavioral changes 1 week after discharge.
In the literature, there are some trials that used audiovisual presentations for providing information to patients.[17‑19] Gaskey showed that the addition of audiovisual presentation to the routine preoperative anesthesia visit did not produce a significant reduction in preoperative anxiety levels in adult patients. However, patients were less nervous and had higher levels of knowledge about anesthesia procedures.[18] In contrast, the study findings demonstrated exposure to an audiovisual presentation significantly reduced anxiety at anesthesia induction. In this regard, Kain et al. stated that behavioral preparation program (ADVANCE: Anxiety‑reduction, Distraction, Video modeling, Adding parents, No excessive reassurance, coaching, and exposure/shaping) is efficient in the reduction of children’s anxiety.[20] Similarly, Web‑Based Tailored
Intervention for Preparation of Parents and Children for Outpatient Surgery (WebTIPS) is a web‑based preoperative preparation program with features, including information provision, modeling, and coping skills. The study showed that WebTIPS reduces the anxiety of children in the preoperative settings.[21] Although both studies are comprehensive programs and effective on preoperative anxiety, the cost of these programs is quite expensive. In another study, Batuman et al. concluded that informational videos about preoperative preparation help to decrease children’s preoperative anxiety.[22] Unlike our study, they evaluated the effects on the preoperative anxiety of only audiovisual presentation. The result of these studies shows that an audiovisual presentation about preoperative information produces improved outcomes on children’s anxiety, and it is considered a low‑cost method.
A systematic review reported that music therapy might be an ineffective method for coping with anxiety, and an audiovisual presentation is more effective than music therapy in reducing preoperative anxiety in children.[9] Similar to the findings in our study, preoperative information video has a stronger impact on children’s anxiety than an auditory presentation. Although both methods include the same information, an audiovisual presentation may be more memorable and interesting to children. Since children have broad imaginations, the mental visualization in an auditory presentation will be unique for each child. This may cause them to misperceive the given information from auditory methods in unfavorable ways and become afraid of the upcoming surgery.
In this study, there is no relationship between the children’s age and M‑YPAS. This is consistent with the study by Vagnoli et al.[23] Although there was no statistical difference, children under the age of 7 years were more anxious. Surgery creates a greater emotional stress in younger children due to poorer comprehension increased dependency on the mother, less communication with the social environment, and decreased the ability to manage anxiety.[24] The study also shows that children without any previous operations had less anxiety. This should be noted as preoperative information programs may adversely affect the emotional status in previously hospitalized children.[6]
Risk factors for negative postoperative behavior changes have been reported to include the following; preoperative anxiety, younger age, previous anesthesia experiences, premedication, and increased parental anxiety.[1,4] In this study, the children who received a standard information had more PHBQ scores. Similarly, Hilly et al. indicated that workshops for preoperative preparation decrease
Table 5: New postoperative maladaptive behavioral changes
Behavioral changes Calm group (n=44)
Anxious group (n=55)
Difficulty about going to bed at night 3 20*When left alone for a few minutes, upset 1 11*Need help to do things 1 8*Avoid or afraid of new things 0 6*Temper tantrums 2 13*Negative reaction to doctors or hospitals 2 28*Follow you everywhere around the house 1 8*Sleeping problems 0 19**P<0.05 between the groups. Anxious children (M‑YPAS >30%) compared to calm children (M‑YPAS <30%). n=Number of patients; M‑YPAS=Modified Yale Preoperative Anxiety Scale
[Downloaded free from http://www.njcponline.com on Sunday, January 26, 2020, IP: 118.96.98.61]

Hatipoglu, et al.: Preoperative anxiety in children
793Nigerian Journal of Clinical Practice ¦ Volume 21 ¦ Issue 6 ¦ June 2018
both preoperative anxiety levels and postoperative behavioral changes in children.[3] Regardless of the format of presentation, we demonstrated a positive effect on behavioral changes in children in the postoperative period. In addition, we found that there is an association between preoperative anxiety and postoperative maladaptive behaviors such as separation anxiety, general anxiety, apathy, and sleep disturbances, which is consistent with the results of previous studies.[1] This study also shows that maternal presence may prevent the development of postoperative negative behavioral changes, regardless of other personal information of the parents. This situation can be explained by the emotional bond between mother and child.[25,26]
The present study has a number of limitations. First, the anxiety levels of parents were not evaluated. Parental anxiety has an effect on the child in the preoperative period.[2] McEwen et al. have reported that preoperative information videos can lessen the anxiety of parents.[27] Cassady et al. also agree with this study, but Chundamala et al. presented a different viewpoint that parental presence does not reduce the parents’ or the children’s anxiety.[28,29] Considering these results, we cannot eliminate the effect of parental anxiety on children. Second, the relationship between pain and behavioral changes is a controversial issue.[4,30] Pain may have a negative effect on a child’s behavior; however, we did not evaluate the children’s pain scores as an indicator of postoperative behavioral changes. Thus, we recommend the evaluation of pain in future studies. Third, M‑YPAS was measured only at the point of anesthesia induction. We do not know anxiety levels of the children in the preoperative waiting room or at hospital admission. Finally, there was no validity and reliability of the Turkish version of the M‑YPAS and PHBQ.
ConclusionAudiovisual presentation is an effective and inexpensive method to preoperative anxiety reduction in children. It is a more memorable and interesting approach compared to auditory presentations for children. Both audiovisual and auditory presentations have equal effects on postoperative behavioral changes.
AcknowledgmentsThe authors would like to thank Ilker UNAL (PhD, from Cukurova University, Faculty of Medicine, Department of Biostatistics) for the statistical analysis of this study.
Financial support and sponsorshipNil.
Conflicts of interestThere are no conflicts of interest.
References1. Kain ZN, Caldwell‑Andrews AA, Maranets I, McClain B,
Gaal D, Mayes LC, et al. Preoperative anxiety and emergence delirium and postoperative maladaptive behaviors. Anesth Analg 2004;99:1648‑54.
2. Ahmed MI, Farrell MA, Parrish K, Karla A. Preoperative anxiety in children risk factors and non‑pharmacological management. Middle East J Anaesthesiol 2011;21:153‑64.
3. Hilly J, Hörlin AL, Kinderf J, Ghez C, Menrath S, Delivet H, et al. Preoperative preparation workshop reduces postoperative maladaptive behavior in children. Paediatr Anaesth 2015;25:990‑8.
4. Stargatt R, Davidson AJ, Huang GH, Czarnecki C, Gibson MA, Stewart SA, et al. A cohort study of the incidence and risk factors for negative behavior changes in children after general anesthesia. Paediatr Anaesth 2006;16:846‑59.
5. Manyande A, Cyna AM, Yip P, Chooi C, Middleton P. Non‑pharmacological interventions for assisting the induction of anaesthesia in children. Cochrane Database Syst Rev 2015;14:CD006447.
6. Kain ZN, Mayes LC, Caramico LA. Preoperative preparation in children: A cross‑sectional study. J Clin Anesth 1996;8:508‑14.
7. Gilakjani AP. Visual, auditory, kinesthetic learning styles and their impacts on English language teaching. J Stud Educ 2011;2:104‑13.
8. Felder RM, Soloman BA. Learning Styles and Strategies. Available from: http://www4.ncsu.edu/unity/lockers/users/f/felder/public/ILSdir/styles.htm
9. Chow CH, Van Lieshout RJ, Schmidt LA, Dobson KG, Buckley N. Systematic review: Audiovisual interventions for reducing preoperative anxiety in children undergoing elective surgery. J Pediatr Psychol 2016;41:182‑203.
10. Bradt J, Dileo C, Shim M. Music interventions for preoperative anxiety. Cochrane Database Syst Rev 2013;6:CD006908.
11. Millett CR. The Effect of Music Therapy Interaction on Child and Parental Preoperative Anxiety in Parents of Children Undergoing Day. Theses and Dissertations‑Music. Student, University of Kentucky, Lexington, Kentucky, USA; 2015. p. 42.
12. Kain ZN, Mayes LC, Cicchetti DV, Bagnall AL, Finley JD, Hofstadter MB, et al. The Yale preoperative anxiety scale: How does it compare with a “gold standard”? Anesth Analg 1997;85:783‑8.
13. Jenkins BN, Kain ZN, Kaplan SH, Stevenson RS, Mayes LC, Guadarrama J, et al. Revisiting a measure of child postoperative recovery: Development of the post hospitalization behavior questionnaire for ambulatory surgery. Paediatr Anaesth 2015;25:738‑45.
14. Vernon DT, Schulman JL, Foley JM. Changes in children's behavior after hospitalization. Some dimensions of response and their correlates. Am J Dis Child 1966;111:581‑93.
15. Faulk DJ, Twite MD, Zuk J, Pan Z, Wallen B, Friesen R. Hypnotic depth and the incidence of emergence agitation and negative postoperative behavioral changes. Paediatr Anaesth 2010;20:72‑81.
16. Kain ZN, Caldwell‑Andrews AA, Krivutza DM, Weinberg ME, Gaal D, Wang SM, et al. Interactive music therapy as a treatment for preoperative anxiety in children: A randomized controlled trial. Anesth Analg 2004;98:1260‑6.
17. Rice M, Glasper A, Keeton D, Spargo P. The effect of a preoperative education programme on perioperative anxiety in children: an observational study. Paediatr Anaesth 2008;18:426‑30.
18. Gaskey NJ. Evaluation of the effect of a preoperative anesthesia
[Downloaded free from http://www.njcponline.com on Sunday, January 26, 2020, IP: 118.96.98.61]

Hatipoglu, et al.: Preoperative anxiety in children
794 Nigerian Journal of Clinical Practice ¦ Volume 21 ¦ Issue 6 ¦ June 2018
videotape. AANAJ 1987;55:341‑5.19. Cumino DO, Vieira JE, Lima LC, Stievano LP, Silva RA,
Mathias LA. Smartphone‑based behavioural intervention alleviates children's anxiety during anaesthesia induction: A randomised controlled trial. Eur J Anaesthesiol 2017;34:169‑75.
20. Kain ZN, Caldwell‑Andrews AA, Mayes LC, Weinberg ME, Wang SM, MacLaren JE, et al. Family‑centered preparation for surgery improves perioperative outcomes in children a randomized controlled trial. Anesthesiology 2007;106:65‑74.
21. Fortier MA, Bunzli E, Walthall J, Olshansky E, Saadat H, Santistevan R, et al. Web‑based tailored intervention for preparation of parents and children for outpatient surgery (WebTIPS): Formative evaluation and randomized controlled trial. Anesth Analg 2015;120:915.
22. Batuman A, Gulec E, Turktan M, Gunes Y, Ozcengiz D. Preoperative informational video based on model making reduces preoperative anxiety and postoperative negative behavioral changes in children. Minerva Anestesiol 2016;82:534‑42.
23. Vagnoli L, Caprilli S, Robiglio A, Messeri A. Clown doctors as a treatment for preoperative anxiety in children: a randomized, prospective study. Pediatrics 2005;116:563‑7.
24. McGraw T. Preparing children for the operating room:
Psychological issues. Can J Anaesth 1994;41:1094‑03.25. Messeri A, Caprilli S, Busoni P. Anaesthesia induction in
children: a psychological evaluation of the efficiency of parents’ presence. Paediatr Anaesth 2004;14:551‑6.
26. Rancourt KM, Chorney JM, Kain Z. Children’s immediate postoperative distress and mothers’ and fathers’ touch behaviors. J Pediatr Psychol 2015;40:1115‑23.
27. Mc Ewen A, Moorthy C, Quantock C, Rose H, Kavanagh R. The effect of videotaped preoperative information on parental anxiety during anesthesia induction for elective pediatric procedures. Paediatr Anaesth 2007;17:534‑9.
28. Cassady JF, Wysocki TT, Miller KM, Cancel DD, Izenberg N. Use of a preanesthetic video for facilitation of parental education and anxiolysis is before pediatric ambulatory surgery. Anesth Analg 1999;88:246‑50.
29. Chundamala J, Wright JG, Kemp SM. An evidence‑based review of parental presence during anesthesia induction and parent/child anxiety. Can J Anaesth 2009;56:57‑70.
30. Kotiniemi LH, Ryhänen PT, Moilanen IK. Behavioral changes in children following day‑case surgery: A 4‑week follow‑up of 551 children. Anaesthesia 1997;52:970‑6.
AppendicesAppendix 1: The content of the audiovisual presentationThe total duration of the video recording was 344 s and it consisted of two sections: Part 1 and 2. Doctors, nurses, an 11‑year‑old female, and her mother took part in the video and special permission was received from them to be recorded. The audiovisual presentation was recorded in the anesthesia clinic and operating room of our hospital.
Part 1: This section is 300 s long and includes the verbal explanation by the anesthesiologist of preoperative information, anesthesia management, and the postoperative period. Three people were involved in this section: the anesthesiologist, the child, and her mother. The teddy bear was used as model. The child and her mother visit the anesthesiologist for preoperative information in the anesthesia clinic. The anesthesiologist meets with them and then informs them about the surgery and the anesthesia methods. First, the child asks “What is surgery?” and then she mentions “I am afraid of the pain.” The doctor explains that “You will not be in any pain” and continues by saying, “The duties of the anesthesiologist are to apply anesthesia to patients, to reduce their pain and ensure their well‑being during operation.” After the child relaxes, the anesthesiologist describes how anesthesia is administered by two methods. The first method is to insert a small plastic tube into a vessel on the hand and some anesthetic drugs are administered via the small tube. The anesthesiologist uses a teddy bear for the second method. The doctor explains “This is a face mask and it smells nice.” She puts a small face mask on the face of the teddy bear and says, “It is connected to the anesthesia machine by a plastic tube. Anesthetic gases are given through the plastic tube.” The doctor pretends to tell the teddy bear to take deep breaths and says, “This will help you fall asleep quickly and after that the surgery will be performed. At the end of surgery, you will be awakened by the administering of some drugs. Furthermore, I will administer drugs for pain relief.” After explaining anesthesia, the doctor says to the child’s mother “Your child will be safe and you should not feel restlessness related to the surgery or anesthesia.” The anesthesiologist explains that preoperative fasting is six hours and postoperative drugs are given regularly. They leave and plan to meet again the next day for the operation.
Part 2: This section is 44 s long and contains preoperative preparation, anesthesia induction, and a recovery period. The child and mother come into the operating room with the personnel. The nurse meets them in the preoperative holding area. The anesthesiologist comes into the preoperative holding area and takes the child and mother into the operating room. The doctor inserts a device in the child’s finger and explains that “The device measures the amount of oxygen in the blood.” The doctor performs anesthesia with the face mask and says, “Take deep breaths and have a good sleep.” After completing the operation, the doctor wakes the child and takes her into the recovery room. The anesthesiologist talks with the child and mother and leaves from the recovery room.
[Downloaded free from http://www.njcponline.com on Sunday, January 26, 2020, IP: 118.96.98.61]

Pengaruh Audiovisual Menonton Film Kartun Terhadap Tingkat Kecemasan Saat
Prosedur Injeksi Pada Anak Prasekolah
Lilis Fatmawati, Yuanita Syaiful, Diyah Ratnawati
Universitas Gresik, [email protected]
Abstrak
Anak usia prasekolah menganggap sakit adalah sesuatu hal yang menakutkan. Anak
mempunyai keterbatasan dalam mekanisme koping mengatasi krisis tersebut. Intervensi
audiovisual menonton film kartun merupakan teknik distraksi untuk menurunkan
kecemasan pada anak. Tujuan penelitian untuk menganalisis pengaruh audiovisual
menonton film kartun terhadap tingkat kecemasan saat prosedur injeksi pada anak
prasekolah. Penelitian ini Pre-experimental dengan jenis pretest and posttest one group
design. Pengambilan data dengan mengunakan teknik purposive sampling pada 28
responden. Variabel independen audiovisual menonton film kartun, sedangkan variabel
dependen tingkat kecemasan. Instrumen yang digunakan SOP dan skala kecemasan
HAR-S. Uji statistik menggunakan uji Paired Sample T-Test, dengan signifikasi p< 0,05.
Hasil analisis statistik didapatkan nilai sig (p = 0.001, t = 11,71) yang berarti ada
pengaruh audiovisual menonton film kartun terhadap tingkat kecemasan saat prosedur
injeksi pada anak prasekolah. Diharapkan intervensi audiovisual menonton film kartun
dapat diterapkan sebagai salah satu intervensi keperawatan untuk menurunkan kecemasan
saat prosedur injeksi pada anak prasekolah.
Kata kunci : Anak Prasekolah, Audiovisual, Kecemasan, Prosedur Injeksi
Abstract
Among preschoolers, illness is a scary thing. Children have limitations in coping
mechanisms to overcome the crisis. Audiovisual intervention in watching cartoons is a
distraction technique to reduce anxiety in children. The purpose of the study was to
analyze the effect of audiovisual cartoon movie on anxiety levels during injection
procedures in preschool children. The design of this study was using Pre-experimental
pretest and posttest one group design. The research collecting the data using purposive
sampling technique on 28 respondents. Independent variable audiovisual watching
cartoons, while dependent variable is anxiety level. The instrument used is SOP and
HAR-S anxiety scale. Statistical tests using the Paired Sample T-Test, with significance p
<0.05. From the results of the statistical analysis, the sig value was obtained (p = 0.001,
t=11.71) which means an audiovisual intervention by on watching cartoons movie was
effective to reduce anxiety levels during the injection procedure in preschool children.
We suggest that audiovisual intervention by watching cartoons movie can be applied as
one of the nursing interventions to reduce anxiety during injection procedures in
preschool children.
Keywords: Anxiety, Audiovisual, Injection Procedure, Preschool Children
PENDAHULUAN
Anak-anak adalah suatu awal kehidupan
untuk masa-masa berikutnya (Nursalam,
2013). Anak prasekolah (3-6 tahun)
merupakan masa yang menyenangkan,
dipengaruhi dengan segala macam hal
yang baru. Anak prasekolah memiliki
ketrampilan verbal dan perkembangan
menjadi lebih baik untuk beradaptasi di
berbagai situasi, tetapi penyakit dan
15

16 Jurnal Ilmiah Kesehatan (Journal of Health Sciences), Vol. 12, No. 2, Agustus 2019, Hal. 15-29
hospitalisasi bisa menyebabkan stress.
Tetapi kenyataaannya tidak semua anak
mengalami masa-masa menyenangkan,
anak juga mengalami sakit yang
mengharuskan mereka dirawat di rumah
sakit (Utami, 2014). Sakit dan
hospitalisasi terjadi pada anak bisa
mengakibatkan stress dan kecemasan
disemua tingkat usia. Penyebab kecemasan
dipengaruhi oleh banyak faktor, dari
petugas rumah sakit (dokter, perawat, serta
tenaga kesehatan lainnya), lingkungan
baru, reaksi keluarga yang mendampingi
anak selama perawatan (Nursalam, dkk,
2013). Seringkali mereka harus menjalani
intervensi medis atau tindakan invasive
yang dapat menimbulkan ketakutan pada
anak seperti prosedur injeksi, pengambilan
atau tes sampel darah, operasi, medikasi
dan intervensi keperawatan lainnya.
WHO (2012) bahwa 3-10 % anak
dirawat di Amerika Serikat baik anak usia
toddler, prasekolah ataupun anak usia
sekolah, di Jerman sekitar 3 - 7% anak
toddler dan 5 - 10% anak prasekolah yang
menjalani hospitalisasi (Purwandari, 2013
dalam Carla, 2017). UNICEF jumlah anak
usia prasekolah di 3 negara terbesar dunia
mencapai 148 juta, 958 anak dengan
insiden anak yang dirawat di rumah sakit
57 juta anak setiap tahunnya dimana 75%
mengalami trauma berupa ketakutan dan
kecemasan saat menjalani perawatan
(James, 2010 dalam Saputro H dan Intan
Fazrin, 2017). Di Indonesia sendiri jumlah
anak yang dirawat pada tahun 2014
sebanyak 15,26% (Susenas, 2014). Anak
usia prasekolah, anak usia sekolah
merupakan usia rentan terhadap penyakit,
sehingga banyak anak usia tersebut harus
dirawat di rumah sakit, serta menyebabkan
populasi anak yang dirawat di rumah sakit
mengalami peningkatan sangat dramatis
(Wong, 2009).
Miller (2002) kecemasan anak saat
menjalani hospitalisasi berkisar 10%
mengalami kecemasan ringan, itu
berlanjut, sekitar 2% mengalami kece-
masan berat. Penelitian dilakukan untuk
melihat respon hospitalisasi terjadi anak
usia 3-12 tahun didapatkan bahwa 77%
anak mengatakan nyeri serta takut saat
dilakukan pengambilan darah, 63% anak
mengalami kekakuan otot, 63% anak
menangis sampai berteriak (Burnsnader,
2014 dalam Carla, 2017). Diperkirakan 35
per 100 anak menjalani hospitalisasi 45%
diantaranya mengalami kecemasan saat
menjalani perawatan di Rumah Sakit
(Depkes, 2010 dalam Widiatmoko, 2018).
Berdasarkan data dari Badan Pusat
Statistik (BPS) Jawa Timur dapat
dijelaskan bahwa anak usia prasekolah dari
tahun ke tahun semakin meningkat, data
tahun 2013 menunjukkan jumlah anak usia
prasekolah yang ada di Jawa Timur

Lilis Fatmawati, Yuanita Syaiful, Diyah Ratnawati
Pengaruh Audiovisual Menonton Film Kartun Terhadap Tingkat Kecemasan Saat Prosedur Injeksi Pada Anak
Prasekolah
17
2.485.218 dengan angka kesakitan
1.475.197, mengalami kecemasan saat
menjalani perawatan akibat sakitnya
sebanyak 85% (Dinkes Propinsi Jawa
Timur, 2014 dalam Saputro H dan Intan
Fazrin, 2017). Data yang di Rumah Sakit
Semen Gresik tahun 2017 terdapat 3043
anak yang dirawat, diantaranya 758 anak
usia prasekolah. Pada bulan Januari - April
2018 terdapat 1173 anak yang dirawat,
terdapat 262 anak usia prasekolah.
Data tingkat kecemasan anak yang
diukur dengan menggunakan kuisioner
Hamilton Rating Scala for Anxiety (HRS-
A) yang dilakukan pada tanggal 21 - 27
Mei 2018 di Rumah Sakit Semen Gresik
terdapat 10 anak usia prasekolah (3-5 th)
yang dirawat dan dilakukan tindakan
pemberian injeksi, terdapat 3 (30%) anak
mengalami kecemasan sedang, 5 (50%)
mengalami kecemasan berat, sedangkan 2
(20%) anak mengalami kecemasan ringan,
dari data tersebut menunjukkan anak yang
mengalami kecemasan berat di ruang anak
rawat inap Rumah Sakit Semen Gresik
masih cukup banyak. Selama ini perawat
maupun tenaga kesehatan lainnya hanya
menggunakan teknik komunikasi langsung
(direct) berupa instruksi sederhana maupun
modeling. Namun pemberian audiovisual
terhadap tingkat kecemasan saat dilakukan
prosedur pemberian injeksi pada anak
prasekolah belum bisa dijelaskan.
Anak usia prasekolah menganggap sakit
adalah sesuatu hal yang menakutkan,
kehilangan lingkungan yang aman dan
penuh kasih sayang, serta tidak
menyenangkan (Supartini, 2014). Asuhan
keperawatan pada anak biasanya
memerlukan tindakan invasif seperti
injeksi atau pemasangan infus, hal ini
merupakan stresor kuat yang dapat
membuat anak mengalami kecemasan.
Perawat biasanya akan menjelaskan
prosedur ini kepada orangtua dan
melakukan komunikasi terapeutik kepada
anak sebelum melakukan prosedur
tersebut, kondisi ini juga membuat anak
menjadi panik dan biasanya melakukan
perlawanan atau menolak untuk dilakukan
posedur pemasangan infus atau injeksi
obat, yang biasanya akan memaksa petugas
kesehatan untuk sedikit melakukan
paksaan kepada anak yang mengakibatkan
timbulnya trauma pada anak. Reaksi anak
terhadap tindakan invasive ini ditunjukkan
dengan agresi fisik dan verbal
(Hockenberry, Wilson & Winkelstein,
2008).
Oleh karena itu anak seringkali
menunjukkan perilaku tidak kooperatif
seperti sering menangis, marah-marah,
tidak mau makan, rewel, susah tidur,
mudah tersinggung, meminta pulang dan
tidak mau berinteraksi dengan perawat dan
seringkali menolak jika akan diberikan

18 Jurnal Ilmiah Kesehatan (Journal of Health Sciences), Vol. 12, No. 2, Agustus 2019, Hal. 15-29
pengobatan. Kondisi cemas yang terjadi
pada anak akan menghambat dan
menyulitkan proses pengobatan yang
berdampak terhadap penyembuhan pada
anak sehingga memperpanjang masa rawat
dan dapat beresiko terkena komplikasi dari
infeksi nosokomial serta menimbulkan
trauma pada anak. Untuk mengatasi
memburuknya tingkat kecemasan pada
anak, seorang perawat dalam memberikan
intervensi kepada anak harus
memperhatikan kebutuhan anak sesuai
dengan pertumbuhan anaknya.
Beberapa tindakan yang pernah
dilakukan untuk menurunkan tingkat
kecemasan pada anak antara lain: bermain
boneka, bermain clay, bermain puzzle,
aktivitas mewarnai, terapi musik, juga
tehnik komunikasi terapeutik, serta tehnik
pengalihan perhatian (distraksi).
Kombinasi antara distraksi pendengaran
(audio) dan distraksi penglihatan (visual)
disebut distraksi audiovisual, yang
digunakan untuk mengalihkan perhatian
pasien terhadap sesuatu yang membuatnya
tidak nyaman, cemas atau takut dengan
cara menampilkan tayangan favorit berupa
gambar-gambar bergerak dan bersuara
ataupun animasi dengan harapan pasien
asik terhadap tontonannya sehingga
mengabaikan rasa tidak nyaman dan
menunjukkan respon penerimaan yang
baik.
Audiovisual yang digemari oleh anak-
anak usia prasekolah adalah kartun atau
gambar bergerak, merupakan media yang
sangat menarik bagi anak-anak terutama
anak usia prasekolah yang memiliki daya
imajinasi tinggi. Anak juga dapat
mengeksplorasi perasaan, emosi, dan daya
ingat melalui audio visual, audio visual
juga dapat membantu perawat dalam
melaksanakan prosedur infus dan injeksi,
memudahkan perawat dalam mendistraksi
agar anak kooperatif dalam pelaksanaan
prosedur terapi (Tamsuri, 2007). Cara yang
dilakukan yaitu dengan memfokuskan
perhatian pada suatu hal yang disukai oleh
anak, misalnya menonton film kartun
(Maharezi, 2014 dalam Hapsari 2016).
Berdasarkan latar belakang di atas, maka
peneliti tertarik melakukan penelitian
tentang pengaruh audiovisual menonton
film kartun terhadap tingkat kecemasan
saat prosedur injeksi pada anak prasekolah.
METODE
Penelitian ini menggunakan desain pra-
experimental dengan rancang bangun one-
grup pra-post test design. Penelitian
dilaksanakan pada 5-28 Januari 2019.
Populasinya adalah seluruh anak usia
prasekolah yang masuk di Ruang Anak
Rumah Sakit Semen Gresik. Pengambilan
sampel menggunakan teknik purposive
sampling, sebanyak 28 responden.

Lilis Fatmawati, Yuanita Syaiful, Diyah Ratnawati
Pengaruh Audiovisual Menonton Film Kartun Terhadap Tingkat Kecemasan Saat Prosedur Injeksi Pada Anak
Prasekolah
19
Variabel independen (audiovisual
menonton film kartun), Upin Ipin,
Doraemon dan Frozen The Snow yang
diputar dengan menggunakan tablet phone.
Variabel dependen (tingkat kecemasan).
Intervensi menonton film kartun diberikan
selama minimal 10 menit, sedangkan
prosedur injeksi durante menonton film
kartun. Alat ukur yang digunakan pada
penelitian ini adalah kuesioner HAR-S
yang merupakan pengukuran kecemasan
didasarkan pada munculnya simptom pada
individu yang mengalami kecemasan.
Prosedur penelitiannya yaitu peneliti akan
melakukan pre test kepada responden pada
hari kedua rawat inap saat diberikan
prosedur injeksi. Kemudian kuesioner
(tingkat kecemasan HAR-S) diisi oleh
keluarga berdasarkan hasil observasi saat
itu, pada hari yang sama saat jadwal
pemberian injeksi selanjutya, peneliti akan
memberikan intervensi audiovisual
menonton film kartun, berupa salah satu
film kartun anak Upin Ipin, Frozen the
snow, Doraemon, sesuai kesediaan pasien.
Pemberian intervensi film kartun tersebut
diberikan minimal 10 menit. Sedangkan
prosedur injeksi diberikan durante
menonton film kartun. Dalam memberikan
intervensi audiovisual film kartun perawat
juga melibatkan keluarga dan teman
perawat dalam satu ruang rawat inap
tersebut, demikian juga dalam proses
dokumentasi. Peneliti melakukan post test
untuk pengambilan data tingkat kecemasan
responden menggunakan ceklis kuesioner
kecemasan skala HAR-S yang diisikan oleh
keluarga/orangtua responden.
Dalam penelitian ini menggunakan analisa
univariat dan bivariat menggunakan uji
Paired T-test untuk mengamati ada
tidaknya perbedaan dari dua data yang
merupakan sebuah sampel tetapi
mengalami perlakuan yang berbeda.
Tabel 1. Tingkat Kecemasan Sebelum dan Sesudah Intervensi Audiovisual Menonton Film
Kartun Saat Prosedur Injeksi Pada Anak Prasekolah di Ruang Anak Rumah Sakit
Semen Gresik pada tanggal 5-28 Januari 2019
Tingkat
Kecemasan
Sebelum Interensi Sesudah Intervensi
Frekuensi Persentase (%) Frekuensi Persentase (%)
Tidak cemas 2 7.1 23 82.1
Ringan 6 21.4 3 10.7
Sedang 2 7.1 1 3.6
Berat 17 60.7 1 3.6
Panik 1 3.6 0 0
Total 28 100.0 28 100.0
Sumber: Data Primer 2019

64 Jurnal Ilmiah Kesehatan (Journal of Health Sciences), Vol. 12, No. 2, Agustus 2019, Hal. 15-29
Tabel 2. Pengaruh Audiovisual Terhadap Tingkat Kecemasan Saat Prosedur Injeksi Pada
Anak Prasekolah di Ruang Anak Rumah Sakit Semen Gresik pada tanggal 5-28
Januari 2019
Tingkat Kecemasan
Intervensi Audiovisual Menonton Film Kartun
Sebelum intervensi Sesudah intervensi
F % F %
Tidak cemas 2 7.1 23 82.1
Ringan 6 21.4 3 10.7
Sedang 2 7.1 1 3.6
Berat 17 60.7 1 3.6
Panik 1 3.6 0 0.0
Total 28 100.0 28 100.0
Mean 28.67 11.75
Std.Deviation 9.03 5.00
Paired Sample T-Test nilai sig (2-tailed) p = 0.000 t = 11.61
Sumber: Data Primer 2019
PEMBAHASAN
1. Tingkat Kecemasan Sebelum Inter-
vensi Audiovisual Menonton Film
Kartun Saat Prosedur Injeksi Pada
Anak Prasekolah
Berdasarkan tabel 1 menunjukkan bahwa
hasil penelitian sebelum intervensi
audiovisual menonton film kartun saat
prosedur injeksi pada anak prasekolah
sebagian besar mengalami kecemasan
berat sebanyak 17 (60.7%). Sama dengan
penelitian sebelumnya mengenai pengaruh
terapi audiovisual terhadap tingkat
kecemasan anak usia prasekolah yang
dilakukan pemasangan infus sebagian
besar mengalami kecemasan berat 55.6%
(Ganda, 2017).
Kondisi cemas yang terjadi pada anak
yang menjalani hospitalisasi dan
mendapatkan tindakan invasif harus
mendapat perhatian khusus dan segera
diatasi. Bagi anak usia prasekolah (3-6
tahun) menjalani hospitalisasi dan
mengalami tindakan invasif merupakan
suatu keadaan krisis disebabkan karena
adanya perubahan status kesehatan,
lingkungan, faktor keluarga, kebiasaan
atau prosedur yang dapat menimbulkan
nyeri dan kehilangan kemandirian pada
anak (Wong, 2009). Lingkungan rumah
sakit, petugas kesehatan dan alat-alat yang
berada di rumah sakit yang baru dilihat
oleh anak menyebabkan anak menjadi
takut dan cemas. Penyebab stress dan
kecemasan pada anak dipengaruhi oleh
banyak faktor, diantaranya perilaku yang
ditunjukkan petugas kesehatan (dokter,
perawat dan tenaga kesehatan lainnya),
pengalaman hospitalisasi anak, support
system atau dukungan keluarga yang
mendampingi selama perawatan. Faktor-
faktor tersebut dapat menyebabkan anak

64 Jurnal Ilmiah Kesehatan (Journal of Health Sciences), Vol. 12, No. 2, Agustus 2019, Hal. 15-29
menjadi semakin stress dan hal ini
berpengaruh terhadap proses penyembuhan
(Nursalam dkk., 2013).
Peneliti mengambil sampel usia 3-6
tahun atau rentang perkembangan anak
usia prasekolah. Berdasarkan karakteristik
responden didapatkan umur responden
adalah anak usia 3-4 tahun sebanyak 46%,
usia 4,1-5 tahun 25%, usia 5,1-6 tahun
29%, dan usia 6 tahun 23%. Pengumpulan
data penelitian yang dilakukan anak yang
berada pada usia 3 tahun memiliki tingkat
kecemasan yang tinggi. Menurut Lau
(2002) dalam Apriliawati (2011) anak usia
infant, toodler, preschool lebih me-
mungkinkan mengalami stress akibat
perpisahan karena kemampuan kognitif
anak yang masih terbatas untuk memahami
hospitalisasi.
Beberapa penelitian menyatakan bahwa
semakin muda usia anak, kecemasan
hospitalisasi akan semakin tinggi (Mahat
& Scoloveno, 2003). Menurut Utami
(2014), anak merupakan populasi yang
sangat rentan terutama saat menghadapi
situasi yang membuat stress. Hal ini
dikarenakan kondisi koping yang
digunakan oleh orang dewasa belum
berkembang sempurna pada anak-anak.
Anak usia prasekolah menerima keadaaan
masuk rumah sakit dengan rasa ketakutan.
Jika anak sangat ketakutan dapat
menampilkan perilaku agresif, dari
menggigit, menendang-nendang bahkan
berlari ke luar ruangan.
Selain umur, jenis kelamin juga dapat
mempengaruhi kecemasan dan stress pada
anak, dimana anak perempuan prasekolah
yang menjalani hospitalisasi memiliki
tingkat kecemasan yang lebih tinggi
dibandingkan laki-laki. Distribusi dalam
penelitian ini didapatkan 57% responden
adalah perempuan. Demikian juga dalam
penelitian (Stubbe, 2008 dalam
Apriliawati, 2011) menyebutkan bahwa
anak perempuan yang menjalani
hospitalisasi memiliki kecemasan yang
lebih tinggi dibandingkan dengan anak
laki-laki.
Pengalaman hopitalisasi pada anak akan
mempengaruhi kecemasan yang dialami
oleh anak. Sebagaimana yang dijelaskan
oleh Tsai (2007) dalam Apriliawati (2011)
anak yang memiliki pengalaman menjalani
hospitalisasi memiliki kecemasan lebih
rendah dibanding anak yang belum
memiliki pengalaman hospitalisasi. Namun
dalam penelitian ini didominasi oleh anak
yang sebelumnya pernah dirawat di rumah
sakit sebanyak 18 anak (64%). Hal ini
dimungkinkan terkait dengan tindakan atau
prosedur medis yang pernah didapat
sebelumnya mungkin menyebabkan
trauma walaupun anak pernah dirawat
tetapi memiliki pengalaman tidak
menyenangkan sehingga anak tetap

Lilis Fatmawati, Yuanita Syaiful, Diyah Ratnawati
Pengaruh Audiovisual Menonton Film Kartun Terhadap Tingkat Kecemasan Saat Prosedur Injeksi Pada Anak
Prasekolah
65
mengalami kecemasan. Hal ini sesuai
dengan penelitian yang menyatakan bahwa
pengalaman hospitalisasi tidak
berpengaruh terhadap tingkat kecemasan
anak (Stubbe, 2008 dalam Apriliawati,
2011).
Berdasarkan teori dan hasil penelitian
yang didapat, terdapat keselarasan dimana
terdapat beberapa faktor yang dapat
mempengaruhi tingkat kecemasan pada
anak. Pada anak usia prasekolah penyebab
kecemasan berkaitan dengan umur,
pengalaman dirawat sebelumnya, yang
dapat menuyebabkan tinggi atau rendahnya
tingkat kecemasannya. Tingkat kecemasan
saat prosedur injeksi sebelum intervensi
audovisual sebagian besar mengalami
kecemasan berat 17 responden (60.7%),
dan didapatkan rata-rata skor tertinggi
pada gejala menangis, merengek, berteriak
dan memberontak. Hal ini selaras dengan
teori Supartini (2014) dimana anak usia
prasekolah menganggap sakit adalah
sesuatu hal yang menakutkan, kehilangan
lingkungan yang aman dan penuh kasih
sayang, serta tidak menyenangkan. Anak
menganggap tindakan dan prosedur rumah
sakit menyebabkan rasa sakit dan luka di
tubuhnya.
Ketakutan anak muncul karena anak
menganggap tindakan dan prosedurnya
mengancam intregitas tubuhnya. Oleh
karena itu, menimbulkan reaksi agresif
dengan marah, dan berontak. Demikian
pula disebutkan oleh Stuart (2009) anak
yang dirawat di rumah sakit dengan
kecemasan yang tinggi memiliki
kecenderungan menjadi hiperaktif dan
tidak kooperatif terhadap petugas
kesehatan serta menimbulkan gangguan
psikologik berupa perubahan perilaku
seperti gelisah, menangis, dan
memberontak.
2. Tingkat Kecemasan Sesudah Intervensi
Audiovisual Menonton Film Kartun
Saat Prosedur Injeksi Pada Anak
Prasekolah
Berdasarkan tabel 1 menunjukkan bahwa
hasil penelitian sesudah dilakukan
audiovisual menonton film kartun saat
prosedur injeksi pada anak prasekolah,
hampir seluruhnya tidak mengalami
kecemasan yaitu sebanyak 23 (82.1%).
Penelitian ini sesuai dengan
Wahyuningrum (2015) dalam pengaruh
cerita melalui audiovisual terhadap tingkat
kecemasan anak usia prasekolah yang
mengalami hospitalisasi setelah dilakukan
intervensi sebagian besar mengalami
kecemasan dengan kategori ringan
(59.1%). Penelitian Patma (2017) dalam
penelitiannya tingkat kecemasan setelah
diberikan terapi audiovisual pada pasien
yang dilakukan pemasangan infus,
sebagian besar mengalami kecemasan
ringan yaitu 6 responden (66.7%).

66 Jurnal Ilmiah Kesehatan (Journal of Health Sciences), Vol. 12, No. 2, Agustus 2019, Hal. 15-29
Demikian pula dalam penelitian ini
setelah intervensi audiovisual menonton
film kartun saat prosedur injeksi pada anak
prasekolah, masih didapatkan nilai rata-
rata ketakutan pada skor tertinggi yaitu,
takut diinjeksi dan takut pada orang
asing/perawat. Hal ini selaras dengan teori
yang dikemukakan Kozlowski dkk.,
(2013), salah satu kecemasan yang
dirasakan oleh pasien anak ketika harus
mendapatkan perawatan di rumah sakit
adalah tindakan invasif, seperti pemberian
obat injeksi yang dilakukan oleh tim
kesehatan. Tindakan invasif pemberian
obat injeksi, baik menyakitkan atau tidak
merupakan suatu ancaman bagi anak usia
prasekolah karena mereka menganggap
tindakan invasif merupakan sumber
kerusakan terhadap integritas tubuhnya.
Mott (2005) lingkungan rumah sakit yang
dianggap asing oleh anak akan
meningkatkan kecemasan anak pada saat
dirawat di rumah sakit (Apriliawati, 2011).
Kondisi cemas yang terjadi pada anak
yang menjalani hospitalisasi dan
mendapatkan tindakan invasif harus
mendapat perhatian khusus dan segera
diatasi (Wong, 2009). Intervensi
audiovisual menonton film kartun adalah
sebuah proses yang akan membentuk
imajinasi pada anak, memberikan
kesempatan pada anak untuk lebih
menangkap informasi, edukasi dan hiburan
serta dapat mengekspresikan perasaannya
(Koller dan Goldman, 2012, dalam Patma,
2017).
Anak-anak menyukai unsur-unsur
seperti gambar, warna, cerita pada film
kartun animasi. Unsur-unsur seperti
gambar, warna dan cerita dan emosi
(senang, sedih, seru, bersemangat) yang
terdapat pada film kartun merupakan unsur
otak kanan dan suara yang timbul dari film
tersebut merupakan unsur otak kiri. Unsur
grafis pada sajian anak prasekolah adalah
unsur yang paling penting karena pada
anak prasekolah unsur lisan dan audio
hanya mendapatkan perhatian sebesar 2%
dan 98% sisanya diporsikan pada unsur
visual statis (Evans dkk., 2008 dalam
Wahyuningrum, 2015). Sehingga dengan
menonton film kartun animasi seperti Upin
Ipin, Doraemon ataupun Frozen the Snow,
otak kanan dan otak kiri anak pada saat
bersamaan digunakan dua-duanya secara
seimbang dan anak fokus pada film kartun
(Wahyuningrum, 2015).
Dengan memberikan sajian interaktif
visual (gambar statis) dan video (gambar
dinamis) maka konsentrasi anak terhadap
audiovisual yang dilihat akan meningkat.
Sehingga audiovisual menonton film
kartun dapat memudahkan anak untuk
mendapatkan pembelajaran dengan basis
yang menyenangkan. Sehingga peman-
faatan audiovisual dapat membantu dan

Lilis Fatmawati, Yuanita Syaiful, Diyah Ratnawati
Pengaruh Audiovisual Menonton Film Kartun Terhadap Tingkat Kecemasan Saat Prosedur Injeksi Pada Anak
Prasekolah
67
memudahkan perawat dalam mendistraksi
agar anak kooperatif dalam pelaksanaan
prosedur injeksi (Taufik, 2007).
3. Pengaruh Audiovisual Terhadap
Tingkat Kecemasan Saat Prosedur
Injeksi Pada Anak Prasekolah
Hasil uji analisa Paired T Tes untuk
mengetahui Pengaruh Audiovisual
Menonton Film KartunTerhadap Tingkat
Kecemasan Saat Prosedur Injeksi Pada
Anak Prasekolah, pada penelitian ini
didapatkan hasil sig (2-tailed) p = 0.000,
p< 0.05 maka H0 ditolak dan H1 diterima
yang berarti ada pengaruh audiovisual
menonton film kartun terhadap tingkat
kecemasan saat prosedur injeksi pada anak
prasekolah di Ruang Anak Rumah Sakit
Semen Gresik. Hasil penelitian ini sejalan
pada penelitian Wahyuningrum (2015),
bahwa pemberian cerita melalui
audiovisual efektif dalam menurunkan
tingkat kecemasan pada anak usia
prasekolah yang mengalami hospitalisasi.
Berdasarkan tabel 3 tingkat kecemasan
anak sesudah diberikan audiovisual
menonton film kartun saat prosedur injeksi
pada anak prasekolah hampir seluruhnya
tidak mengalami kecemasan, yaitu
sebanyak 23 responden (82,1%). Tingkat
kecemasan yang berbeda pada tiap anak
disebabkan pula karena respon setiap
manusia terhadap stressor memang
berbeda. Hal ini sesuai dengan model
kognitif kecemasan yang menyebutkan
bahwa respon yang berbeda pada tiap
individu antara lain dipengaruhi oleh
adanya kelemahan dalam berbagai proses
informasi (Blackburn, 1990, dalam Juanita,
2017. Namun masih didapatkan 1 respon-
den mengalami kecemasan berat sesudah
intervensi audiovisual menonton film
kartun, meskipun responden kooperatif
saat diberikan intervensi audiovisual
menonton film kartun, dan masih
menunjukkan rasa takut saat akan
diinjeksi, takut pada perawat, gelisah,
tegang, menangis, berteriak dan
memberontak hingga menunjukkan muka
merah dan penurunan nafsu makan. Hal ini
dimungkinkan karena pasien mempunyai
riwayat sudah pernah dirawat dua kali
sebelumnya, sehingga pernah mempunyai
pengalaman yang masih menjadi sumber
kecemasan baginya, diantaranya penga-
laman mendapatkan prosedur injeksi serta
pemasangan infus.
Apabila anak mengalami kecemasan
tinggi saat dilakukan tindakan invasif,
kemungkinan besar tindakan yang
dilakukan menjadi tidak maksimal dan
tidak jarang harus mengulangi beberapa
kali sehingga akan menghambat proses
penyembuhan anak. Kondisi ini memper-
sulit perawat dalam melakukan tindakan
keperawatan (Supartini, 2014). Perlu
adanya upaya dalam menurunkan tingkat

68 Jurnal Ilmiah Kesehatan (Journal of Health Sciences), Vol. 12, No. 2, Agustus 2019, Hal. 15-29
kecemasan terutama saat prosedur injeksi,
diantaranya dengan distraksi audiovisual
(Tamsuri, 2007).
Koller dan Goldman (2012) dalam
studinya menyatakan bahwa pemberian
cerita melalui audiovisual guna menurun-
kan kecemasan termasuk teknik distraksi
kecemasan dengan teknik audiovisual.
Perhatian anak yang terfokus kepada cerita
audiovisual yang disimaknya mendis-
traksikan atau mengalihkan persepsi
kecemasan anak dalam korteks serebral.
Dengan intervensi audiovisual menonton
film kartun akan memberikan rangsangan
distraksi berupa visual, auditory dan
tactile. Perasaan aman dan nyaman yang
dirasakan anak akan merangsang tubuh
untuk mengeluarkan hormon endorphine.
Melalui pemberian audiosivisual
menonton film kartun yang diberikan oleh
perawat diharapkan dapat membantu anak
dalam mengatasi permasalahan dengan
meminta mereka ikut terlibat tentang
kegiatan atau tindakan injeksi yang
diberikan oleh petugas sehingga dapat
membantu membangun pikiran dan
kemungkinan dapat menyelesaikan
masalah yang berhubungan dengan
penyakit, perpisahan selama dirawat,
kecacatan dan keterasingan. Hal ini terlihat
pada saat penelitian anak menjadi fokus
dengan tayangan audiovisual menonton
film kartun dibandingkan prosedur injeksi,
walaupun anak masih tetap harus di
dampingi dan tetap dekat dengan
orangtuanya. Hasil uji analisis statistik
didapatkan adanya perbedaan tingkat
kecemasan pada pre test dan post test pada
anak yang diberikan audiovisual menonton
film kartun saat prosedur injeksi. Ini
berarti bahwa ada pengaruh audiovisual
menonton film kartun dalam menurunkan
tingkat kecemasan saat prosedur injeksi
pada anak prasekolah, baik secara
subyekstif maupun obyektif. Hal tersebut
sesuai dengan teori bahwa salah satu cara
yang dapat dilakukan untuk pengendalian
kecemasan adalah tehnik distraksi
audiovisual untuk mengalihkan perhatian
anak (Tamsuri, 2007, dalam Agustina
2015). Perhatian anak menjadi teralihkan
pada film kartun yang disukai anak, yang
menyebabkan anak tidak lagi memikirkan
prosedur injeksi, anak menjadi rileks dan
nyaman sehingga menurun kecemasannya.
KESIMPULAN
Sebelum diberi intervensi sebagian
responden memiliki kecemasan berat,
sedangkan sesudah diberi intervensi
hampir seluruh responden tidak mengalami
kecemasan. Sehingga Ada pengaruh
pemberian audiovisual menonton film
kartun terhadap penurunan tingkat
kecemasan saat prosedur injeksi pada anak
prasekolah.

Lilis Fatmawati, Yuanita Syaiful, Diyah Ratnawati
Pengaruh Audiovisual Menonton Film Kartun Terhadap Tingkat Kecemasan Saat Prosedur Injeksi Pada Anak
Prasekolah
69
DAFTAR PUSTAKA
Agustina, H, (2015). Pengaruh Distraksi
Audiovisual Terhadap Respon
Penerimaan Injeksi Intravena Pada
Anak Prasekolah di RSD Kalisat
Jember. Skripsi PSIK FIK Universitas
Muhammadiyah Jember Indonesia.
Apriliawati, A. (2011). Pengaruh
Biblioterapi Terhadap Tingkat
Kecemasan Anak Usia Sekolah Yang
Menjalani Hospitalisasi di Rumah Sakit
Islam Jakarta. Tesis Pogram Magister
Ilmu Keperawatan Anak Universitas
Indonesia Depok.
Ardiyanto, Kurniawan. (2011). Hubungan
Dukungan Sosial Terhadap Kecemasan
Keluarga Pasien di Ruang HND RSUP
Dr. Kariadi Semarang. Skripsi PSIK
FIK Universitas Muhammadiyah
Semarang.
Arikunto, Suharsimi (2010). Prosedur
Penelitian: Suatu Pendekatan Praktis,
Jakarta: Rineka Cipta.
Asmadi. (2008). Teknik Prosedural
Konsep & Aplikasi Kebutuhan Dasar
Klien. Jakarta: Salemba Medika.
Bossert. (1994) Factor influencing the
coping of hospitalization school- age
children. Journal of Pediatric Nursing.
9 (5): 299-306
Coyne, I. (2006). Children’s experiences of
hospitalization. Journal of Child
Health, 10 (4): 326-336
Dimyati dan Mudjiono (2006). Belajar dan
Media Pembelajaran. Jakarta: Rineka
Cipta, h .78
Fosson, Abe., Martin, Judi. & Haley, John.
(2010). Anxiety Among Hospitalized
Latency-Age Children. Journal of
Developmental & Behavioral Pediatric,
11(6), 28-339
Hanum, SA. (2015). Pengaruh
Biblioterapi Terhadap Kecemasan Anak
Usia Sekolah yang di Rawat Inap di
RSUD Dr. Pirngadi Medan. Skripsi
Fakultas Keperawatan Universitas
Sumatera Utara Medan Indonesia.
Hapsari, AY. (2016). Pengaruh Distraksi
Video film Kartun Terhadap
Kecemasan Anak Usia 6-8 Tahun
Selama Tindakan Dental di RS Tk IV
04.07.02 Slamet Riyadi Surakarta.
Publikasi Ilmiah Program Studi
Pendidikan Dokter Gigi FK Gigi
Universitas Muhammadiyah Surakarta.
Hartini, Sri. (2014). Pengaruh Biblioterapi
Dengan Buku Cerita Bergambar
Terhadap Tingkat Kecemasan Pada
Anak Prasekolah Saat Pemasangan
Infus di RS Telogorejo Semarang.
Skripsi PSIK STIKES Telogorejo
Semarang.
Journal/index.php/ilmukeperawatan/ari
cle/view/290/314
Hawari, D. (2008). Menajemen Stres
Cemas Dan Depresi. Fakultas
Kedokteran Universitas Indonesia:
Jakarta.
Hidayat, Aziz Aimul.(2008), Pengantar
Ilmu Keperawatan. Jakarta : Salemba
Medika.
Hockenberry, MarilynJ.,& Wilson, David
(2011). Wong’s Clinical Manual of
Pediatric Nursing 7th Ed.USA: Mosby
Elseiver
Jainar, Rahmatika. (2016). Perbandingan
Efektifitas Menonton Film Dengan
Terapi Bermain Terhadap Penurunan
Kecemasan Anak Umur 6-8 Tahun
Selama Perawatan Gigi. Skripsi S1
Pendidikan Dokter Gigi Fakultas
Kedokteran Gigi Universitas
Muhammadiyah Surakarta.
Juanita, Farida. (2017). Teknik Distraksi
Audiovisual Menurunkan Tingkat
Kecemasan Anak Usia Sekolah Yang
Menjalani Sirkumsisi. Jurnal Ners. Vol
2. No 2 (2007).
http://dx.doi.org/10.20473/jn.v2i2.4962.
Kautsar, F., Dayal, G & Fuad, A. (2015).
Uji Validitas dan Reliabilitas Hamilton
70 Jurnal Ilmiah Kesehatan (Journal of Health Sciences), Vol. 12, No. 2, Agustus 2019, Hal. 15-29
Anxiety Rating Scale Terhadap
Kecemasan dan Produktivitas Pekerja
Visual Inspection PT. Widatra Bhakti.
Seminar Nasional Teknologi 2015
Institut Teknologi Nasional Malang
ISSN: 2407– 7534.
email:[email protected]_
[email protected],fuadachmadi@g
mail.com. Diakses 6 Agustud 2018.
Kirkpatrick, T., & Tobias, K. (2013).
Pediatric age specific: self learning
module. Dari
http://hr.uclahealth.org/workfiles/AgeS
pecificSLM-Peds.pdf. Diperoleh pada
tanggal 28 Mei.
Koller dan Goldman, 2012. Pediatric
Psychosocial Oncology: Textbook for
Multidisciplinary Care, USA: Springer
Kusumadewi, Sri. (2008). Aplikasi Fuzzy
Total Integral Pada Hamilton Anxiety
Rating Scale (HAR-S). Jurusan Teknik
Informatika, Universitas Islam
Indonesia, Yogyakarta Jl. Kaliurang K,
14,5 Yogyakarta. Seminar Nasional
Aplikasi Teknologi Informasi 2008
(SNATI 2008) Yogyakarta, 21 Juni 2008
ISSN: 1907-5022. E-mail:
[email protected]. Diakses 10 Agustus
2018
Kurniawati, Rizka. (2016). Pengaruh
Terapi Bermain Mewarnai terhadap
tingkat kecemasan akibat Hospitalisasi
pada Anak Usia Prasekolah di Bangsal
Cempaka RSUD WATES. Skripsi, PSIK
Jendral A. Yani, Yogyakarta.
Kozlowski, Lori J, & Monitto, C. L.
(2013). Pain in hospitalized children.
Pediatrics for Parents.
http://search.proquest.com/d ocview/
diakses pada tanggal 5 Maret 2018.
Kristina, (2017). Pengaruh Kegiatan
Mewarnai Pola Mandala Terhadap
Tingkat Kecemasan Mahasiswa
Akademi Keperawatan Dirgahayu
Samarinda. Nurse Line Journal Vol. 2
No. 1 Mei 2017 p-ISSN 2540-7937 e-
ISSN 2541-464X. e-mail:
Kurniawan, Ardiyanto. (2011). Hubungan
dukungan sosial terhadap kecemasan
keluarga pasien di ruang HND RSUP
Dr. Kariadi Semarang. Skripsi PSIK
Fakultas Kesehatan Universitas
Muhammadiyah Semarang.
Kyle, Terry dan Susan Carman. (2016).
Buku Ajar Keperawatan Pediatri.
Jakarta: EGC.
Latifah, ON. (2014). Hubungan
Komunikasi Terapeutik Perawat dengan
Tingkat Kecemasan Anak Usia
Prasekolah Di RSUD Panembahan
Senopati Bantul. Skripsi PSIK Sekolah
Tinggi Ilmu Kesehatan Jendral Achmad
Yani, Yogyakarta.
Lemos, I. C. S., Silva, L. G. D.,
Delmondes, G. D. A., Brasil, A. X.,
Santos, P. L. F., Gomes, E., Silva, K. V.
L. G. D., Oliveira, D. D., Oliveira, J. D.
D., Fernandes, G. P., & Kerntopf, M. R.
(2016). Therapeutic Play Use in
Children under the Venipucture: A
Strategy for Pain Reduction. American
Journal of Nursing Research, 4(1), 1-5.
Lumiu, S.E., Tuda, J.S.B., & Ponidjan, T.
(2013), Hubungan Dukungan Keluarga
dengan Tingkat Kecemasan Akibat
Hospitalisasi pada Anak di Usia Pra
Sekolah di Irina E Blu RSUD Prof. Dr.
R. D Kandau Manad, Ejurnal
Keperawatan (e-kep), Vol 1 no 1,5.
Email: [email protected]
Miller. (2002). Clinical Pathology Edisi 2.
Jakarta: EGC.
Munadi, Y., 2011, Media Pembelajaran
Sebuah Pendekatan Baru, Jakarta:
Gaung Persada Press.
Muscari, E. M. (2013). Keperawatan
Pediatrik. Jakarta: EGC
Nasbar, Carla. (2017). Pengaruh
Penerapan Atraumatic Care Medial
Play Terhadap Respon Kecemasan

Lilis Fatmawati, Yuanita Syaiful, Diyah Ratnawati
Pengaruh Audiovisual Menonton Film Kartun Terhadap Tingkat Kecemasan Saat Prosedur Injeksi Pada Anak
Prasekolah
71
Anak Usia Prasekolah yang
Hospitalisasi di Ruang Rawat Inap
Anak RSUD Dr. M. Zein Painan Tahun
2017. Skripsi PSIK Fakultas
Keperawatan Universitas Andalas
Padang Sumatera Barat.
Notoatmodjo, S. (2012). Metodologi
Penelitian Kesehatan, Peneltian Ilmiah.
Jakarta: Rineka Cipta.
Nursalam, Susilaningrum, R & Utami, S.
(2013). Asuhan Keperawatan Bayi
dan Anak (Untuk Perawat dan Bidan).
Jakarta: Salemba Medika.
Nursalam. (2016). Metodologi Penelitian
Ilmu Keperawatan: Pendekatan Praktis.
Edisi 3 Salemba Medika.
Patma GN, Mohammad Nofiyanto 2017
Pengaruh Terapi Audio Visual
Terhadap Penurunan Tingkat
Kecemasan Pada Anak Preschool Yang
dilakukan Tindakan Pemasangan Infus
di UGD RSUD Wates. Skripsi S1
Keperawatan Program Studi
Keperawatan STIKES Jenderal Achmad
Yani Yogyakarta. Email:
Pillitteri, A., 2010, Maternal & Child
Health Nursing: Care of the
Childbearing & Childrearing Family,
New York: Lippincott Williams &
Wilkins.
Potts, Nicki L., & Mandleco, Barbara L.
(2012). Pediatric Nursing: Caring for
Children and Their Families. USA:
Delmar.
Potter, A., & Perry, A. G. (2010). Buku
ajar fundamental keperawatan: Konsep,
proses, dan praktik (edisi 4). Jakarta:
EGC.
PSIK FIK UNGRES. (2018). Pedoman
Penyusunan Proposal dan Skripsi.
Gresik
Rahayuningrum, Madyastuti, L &
Mafulah. (2015). Hubungan Peran
Orangtua dengan Kecemasan
Hositalisasi pada anak Prasekolah
(Correlation of Parent Roles and
Hospitalization Anxiety to The
Preschoole Age Children Patients).
Journal of News Community. Volume
06, Nomor 02. Hal. 158-165.
Ramdaniati, S., Hermaningsih, S. &
Muryati. (2016). Comparison Study of
Art Therapy in Reducing Anxiety on
Pre-School Children Who Experience
Hospitalization. Open Journal of
Nursing, 6, 46-52.
Rusdi AE. (2015) Pengaruh Tehnik
Distraksi Menonton Film Kartun Untuk
Menurunkan Stress Hospitalisasi Pada
Anak Prasekolah di RSUD Tugurejo.
ejournal.stikestelogorejo.ac.id/index.ph
p/ilmukeperawatan/article/viewFile/569
/568
Saputro, Heri & Fazrin, Intan. (2017).
Penurunan Tingkat Kecemasan Anak
Akibat Hospitalisasi dengan Penerapan
Terapi Bermain. Jurnal Konseling
Indonesia. Vol.3 No. 1. Hal. 9-12
Sarfika Rika, Nova Yanti, Ruspita Winda
(2015). Pengaruh Teknik Distraksi
Menonton Kartun Animasi Terhadap
Skala Nyeri Anak Usia Prasekolah Saat
Pemasangan Infus Di Instalasi Rawat
Inap Anak RSUP DR.M.Djamil Padang.
Ners Jurnal Keperawatan, 11 (1). 32-
40. Email: [email protected]
Soetjiningsih. (2012). Tumbuh Kembang
Anak, Jakarta: EGC.
Supartini. (2014). Buku Ajar Konsep
Dasar Keperawatan Anak. Jakarta:
EGC.
Sureskiarti E. (2017). Perbedaan
Kecemasan Anak Usia Prasekolah Pada
Tindakan Injeksi Dengan Diterapkan
Dan Tanpa Diterapkan Pemakaian
Rompi Bergambar Di Ruang Melati
Rsud Abdul Wahab Sjahranie
Samarinda. Program Studi Ilmu
Keperawatan STIKES Muhammadiyah:
Samarinda. Jurnal Ilmiah Manuntung.
72 Jurnal Ilmiah Kesehatan (Journal of Health Sciences), Vol. 12, No. 2, Agustus 2019, Hal. 15-29
Vol. 3 No. 1. Vol. 3 No. 1 (2017).
http://jurnal.akfarsam.ac.id/index.php/jl
m_akfarsam/article/view/98
Sutrisno, Widodo, G.G, Susanto, H.,
(2017). Kecemasan Anak Usia Sekolah
Sebelum dan Sesudah Mendapatkan
Informasi Saat Pemberian Obat Injeksi
di RSUD Ambarawa. Journal Ilmu
Kesehatan 2 (2) 2017, 99-106. http://
ejournal.stikesaisyah.ac.id/index.php/jik
a/
Stuart, Gail W. (2016). Keperawatan
Kesehatan Jiwa. Singapore: Elsevier.
Stubbe, D. A. (2008). A focus on reducing
anxiety in children hospitalized for
cancer and diverse pediatric medical
disease through a self-enganging art
therapy. Dissertation. The Faculty of
the School of Professional Psychology.
Chestnut Hill Colleege.
Tamsuri. (2007). Konsep dan
Penatalaksanaan Nyeri. Jakarta: EGC
Townsend, Mary C. (2009), Buku Saku
Diagnosa Keperawatan pada
Keperawatan Keperawatan Psikiatri
Edisi 6. Jakarta: EGC.
Tsai, C. (2007), ‘The effect of animal
assisted therapy on children’s stress
during hospitalization’. Doctoral
Disttertasi of Phylosopy. University of
Marylan, School of Nursing.
Utami, Yuli. (2014). DampakHospitalisasi
Terhadap Perkembangan Anak. Jurnal
Ilmiah Widya Volume 2, Nomor 2. Hal.
9-20.
Wahyuningrum I, (2015). Pengaruh Cerita
Melalui Audiovisual TerhadapTingkat
kecemasan Anak Usia Prasekolah Yang
Mengalami Hospitalisasi Di RSU PKU
Muhmmadiyah Bantul. Skripi S1
Program Studi Ilmu Keperawatan
STIKES ‘Aisyiyah Yogyakarta. Email:
Wong, D. L. et.al. (2009). Buku Ajar
Keperawatan Pediatrik, vol 1. Jakarta:
EGC
Yongblut, J.M. (2010). “Alternate Child
Care, History of Hospitalization, And
Preschool Child Behavior”. Nurs Res,
48 (1), 29-34.

ARTICLE IN PRESS+Model
J Pediatr (Rio J). 2018;xxx(xx):xxx---xxx
www.jped.com.br
ORIGINAL ARTICLE
Psychological preparation reduces preoperativeanxiety in children. Randomized and double-blindtrial�,��
Dânia P. Meletti a,∗, José Fernando A. Melettib, Rodrigo P.S. Camargoc,Leopoldo M. Silvad, Norma S.P. Módoloe
a Faculdade de Medicina de Jundiaí, Ciências da Saúde, São Paulo, SP, Brazilb Faculdade de Medicina de Jundiaí, Departamento de Anestesiologia, São Paulo, SP, Brazilc Faculdade de Medicina de Jundiaí, Departamento de Ginecologia e Obstetrícia, São Paulo, SP, Brazild Universidade Estadual Paulista ‘‘Júlio de Mesquita Filho’’ (UNESP), Departamento de Anestesiologia, São Paulo, SP, Brazile Universidade Estadual Paulista ‘‘Júlio de Mesquita Filho’’ (UNESP), Faculdade de Medicina de Botucatu, Departamento deAnestesiologia, Botucatu, SP, Brazil
Received 26 September 2017; accepted 26 April 2018
KEYWORDSChild;Anxiety;Psychologicalpreparation;Anesthesia;Surgery
AbstractObjective: To verify the effect of psychological preparation on the relief of preoperative anxietyin children and to correlate parents’ and children’s levels of anxiety.Method: After the approval of the institutional Research Ethics Committee and written consentof the children’s parents or guardians, 118 children of both genders were prospectively selected,aged between 2 and 8 years, physical condition classification ASA I, who were treated in thepre-anesthetic evaluation ambulatory of the University Hospital and who underwent ambula-tory surgeries at the same hospital. Two controlled groups of 59 children were randomized:control group basic preparation and psychological preparation group. On the day of surgery,all selected children were evaluated regarding their level of anxiety using the modified YalePreoperative Anxiety Scale and their parents were evaluated regarding their level of anxietythrough the Visual Analog Scale. The evaluator was blinded to which study group the child andfamily member belonged to.
Results: Nine children and their family members were excluded per group when the resultswere analyzed. Children from the prepared group showed significant reductions in their levelof anxiety in relation to the control group (p = 0.04). There was no correlation between thelevel of anxiety of children and their parents’ levels (p = 0.78).� Please cite this article as: Meletti DP, Meletti JF, Camargo RP, Silva LM, Módolo NS. Psychological preparation reduces preoperativeanxiety in children. Randomized and double-blind trial. J Pediatr (Rio J). 2018. https://doi.org/10.1016/j.jped.2018.05.009
�� Study conducted at the Master’s Degree Program of Faculdade de Medicina de Jundiaí, São Paulo, SP, Brazil∗ Corresponding author.
E-mail: [email protected] (D.P. Meletti).
https://doi.org/10.1016/j.jped.2018.05.0090021-7557/© 2018 Sociedade Brasileira de Pediatria. Published by Elsevier Editora Ltda. This is an open access article under the CC BY-NC-NDlicense (http://creativecommons.org/licenses/by-nc-nd/4.0/).
JPED-686; No. of Pages 7

ARTICLE IN PRESS+Model
2 Meletti DP et al.
Conclusion: The psychological preparation was effective in reducing the level of anxiety ofchildren. However, there was no relation between the level of anxiety of children and theirparents’ level.© 2018 Sociedade Brasileira de Pediatria. Published by Elsevier Editora Ltda. This isan open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
PALAVRAS-CHAVECrianca;Ansiedade;Preparacãopsicológica;Anestesia;Cirurgia
Preparacão psicológica reduz ansiedade pré-operatória de criancas. Ensaiorandomizado e duplamente encoberto
ResumoObjetivos: Verificar o efeito da preparacão psicológica no alívio da ansiedade pré-operatóriade criancas e avaliar se há correlacão com a ansiedade dos pais.Método: Após a aprovacão do Comitê de Ética e Pesquisa da Faculdade de Medicina e obtencãodo consentimento pelos responsáveis dos pacientes, foram selecionadas prospectivamente 118criancas, de ambos os sexos, com idade entre dois e oito anos, classificacão de estado físico ASAI, atendidas no ambulatório de avaliacão pré-anestésica do Hospital Universitário e submetidasa cirurgias ambulatoriais. Foram randomizados dois grupos controlados de 59 criancas: grupo depreparacão básica e grupo preparacão psicológica. No dia da cirurgia, todas as criancas foramavaliadas em relacão ao seu grau de ansiedade através da Escala de Ansiedade Pré-operatóriade Yale Modificada e seus pais, avaliados quanto ao seu nível de ansiedade pela Escala VisualAnalógica. O avaliador era cego sobre qual grupo do estudo a crianca e seu familiar pertenciam.Resultados: Na análise dos resultados, foram excluídas 9 criancas e familiares de cada grupo.As criancas do grupo preparado tiveram reducões significativas no grau de ansiedade em relacãoao grupo controle, (p = 0,04). Não houve correlacão entre os graus de ansiedade das criancas eseus pais (p = 0.78).Conclusão: A preparacão psicológica foi eficaz na reducão do grau de ansiedade das criancasno momento da cirurgia. Não houve, entretanto, relacão entre os graus de ansiedade dos paise seus filhos.© 2018 Sociedade Brasileira de Pediatria. Publicado por Elsevier Editora Ltda. Este éum artigo Open Access sob a licença de CC BY-NC-ND (http://creativecommons.org/licenses/by-nc-nd/4.0/).
I
Aupspiptloscfioiac
wtiia
tancaiaf
cmipt
M
C
A
ntroduction
nxiety is present in approximately 50% of patients whondergo an anesthetic-surgical procedure.1 The prospect ofostoperative pain, separation from family members, expo-ure to strangers, fear of the surgery and anesthesia, and theossibility of becoming incapacitated are factors that mayncrease the degree of anxiety in pediatric patients.2 In thereoperative period, anxiety tends to manifest as feelings ofension, nervousness, worry, apprehensiveness, or psycho-ogical stress.3 Some children verbalize their dreads, whilethers demonstrate anxiety through behavioral changes,uch as becoming restless, trembling, breathing deeply,easing to speak, crying, or becoming, in some cases, dif-cult to control.4 In relation to anesthesia, high levelsf anxiety can have negative effects, such as difficultyn achieving anesthetic induction, reduction in defensesgainst infections, and increase in intraoperative anestheticonsumption and postoperative analgesics.5
Diverse ways to alleviate preoperative anxiety have beenidely studied, such as preanesthetic medications, dis-
raction techniques, presence of parents during anesthesianduction, and preoperative psychological and educationalnterventions.6 The non-pharmacological management ofnxiety has advantages when compared to anxiolytics, as
dapd
hey do not have adverse events; however, further studiesre required to demonstrate the efficacy of distraction tech-iques such as the use of medical clowns, videogames, andartoons, among others.7,8 Psychological preparation is seens expensive due to the need for several sessions;9 however,t has good results in reducing preoperative anxiety, as wells in the psychological recovery of the children and theiramily members after the surgery.10,11
Thus, the authors propose a single-session model of psy-hological preparation for parents and children, with theain objective of verifying the effect of anxiety reduction
n children at the time of the surgery. Moreover, the authorsroposed to investigate whether there would be a correla-ion between parents’ and children’s anxiety.
ethods
linical study description and participants
fter approval by the Research Ethics Committee of Facul-
ade de Medicina de Jundiaí (CAEE: 16288513.2.0000.5412)nd after the informed consent form was signed by theatients’ parents or guardians, 118 children of both gen-ers, aged between 2 and 8 years, with physical status
IN+Model
P
FfaeftsfIrsfeonaussg
M
Adtpsttaosae4
gctTfiarsartbofb
i
ARTICLEPreparation reduces preoperative anxiety in children
classification according to the American Association ofAnesthesiologists (ASA) I, treated at the pre-anestheticoutpatient clinic of the University Hospital of Faculdadede Medicina de Jundiaí, and who underwent outpatientsurgeries at that hospital were selected. A randomized,parallel-controlled, prospective, and double-blinded trialwas carried out to evaluate the effect of psychologicalpreparation on the preoperative anxiety levels of childrenand their parents. The methodology was not changed afterthe study was started.
Allocation
Participants were randomly allocated using the List random-izer program (Randomness and Integrity Services Ltd, Schoolof Computer Science and Statistics at Trinity College, Dublin,Ireland). This allocation was implemented by two anesthe-siologists responsible for the pre-anesthetic consultation:they enrolled the participants, applied the exclusion cri-teria and directed the participants to intervention whennecessary. The exclusion criteria were children with provenbehavioral and cognitive alterations; history of previoussurgeries and general anesthesia; users of psychoactivemedications; and history of seizures, mental illness, orchronic pain. Five children were excluded for these reasonsand three patients were excluded because their parents didnot agree to their participation in the study (Fig. 1).
Interventions
From November 6, 2014 to October 5, 2015, two groupsof children and their parents or guardians were randomlyassigned, as described below:
Basic preparation group (BPG): a group that receivedthe standard preparation at the pre-anesthetic consulta-tion, where parents could have their questions answered andreceive explanations from the anesthesiologist; as for thechildren, on the day of surgery, they waited for the momentof surgery in the toy library, a place with toys and booksreserved for them and their family members.
Psychological preparation group (PPG): a group that, inaddition to the basic preparation, underwent a psycholog-ical interview always performed by the same psychologist,after the pre-anesthetic consultation, with the presence ofthe family member and the child. Parents were briefed onthe aspects of the surgery and the separation that wouldoccur when the child entered the operating room, aiming tohelp them cope with these situations. A story was told to thechild, with the support of a children’s book entitled ‘‘Gasparin the hospital’’ by Anne Gutman and Georg Hallensleben,published by Cosacnaif. Gaspar is a child character whosuffers an accident and needs to undergo an emergencysurgery.12 He was at school and is taken to the hospital byambulance alone. He needs to be operated on and duringanesthesia he sleeps and has a good dream. The book high-lights Gaspar’s courage and independence, how happy he
is with his dream and when he wakes up, how happy he isto see his mother. The approach used with the child is thatof coping with a new situation without the presence of theparents.6llt
PRESS3
sychological preparation
our main questions were addressed with the parents oramily members present in the psychological session using
semi-open interview model, i.e., the questions were nec-ssarily the same, but the interview varied according to theamily responses and demands. The first question addressedhe feelings about the surgery by the parent and the child;pecifically asking for the verbalization of feelings such asear, anxiety, concern and others as an initial approach.n the second question, adult aspects were questionedegarding the mother-child, or father-child separation, fromimple separations such as leaving the child with a relativeor a few hours, adaptation to school, and other separationxperiences. The third question addressed how the motherr father perceived and dealt with the child’s health and ill-ess situations, and the last question addressed the child’sttachment to objects. This session with the parents wassed to guide and to calm them down regarding the anesthe-ia and surgery aspects, as well as to support the children’separation from their parents, so they would feel confidentoing into the operating room.
easures
t the pre-anesthetic evaluation outpatient clinic, on theay of the consultation, the following tools were applied tohe parents: a questionnaire to assess the sociodemographicrofile, a questionnaire about the role of the anesthe-iologist, the parents’ apprehensions and fears relatedo anesthesia and assessment of their degree of anxietyhrough the visual analogue scale (VAS). Such scale, used as
secondary outcome measure, was also applied to parentsr guardians at the time of the surgery. The scale mea-ured 100 mm, where 0 (zero) was equivalent to ‘‘calm’’nd 100 mm meant ‘‘very anxious.’’13 Mild anxiety wasxpressed by the scores 0, 1, and 2; moderate anxiety, 3,, 5, 6, and 7; and intense anxiety, 8, 9, and 10.
On the day of the surgery, all children selected from bothroups were referred to the toy library attached to the surgi-al center, where their anxiety levels were assessed throughhe modified Yale Preoperative Anxiety Scale (m-YPAS).his observational scale consists of 27 items divided intove categories: activity, vocalization, emotional expression,pparent awakening state, and family interaction. The scoreanges from 23.5 to 100; when above 30, the higher thecore, the greater the anxiety.14 The m-YPAS Scale waspplied continuously, from the pre-anesthetic preparationoom at the time of the child’s separation from the parentso the moment of anesthetic induction, and was performedy a single and the same resident physician in anesthesiol-gy, under the supervision of the anesthesiologist in chargeor the division, after previous training. The evaluator waslinded to the child’s group.
The basic protocol of anesthetic induction was performedn a closed-loop anesthesia delivery system with 33% O2 and
6% N2O, with a total flow of 5 L.min-1 for one minute, fol-owed by administration of sevoflurane at 8%. After the childost consciousness, the gas flow was reduced to 2 L min−1 andhe anesthetic concentration, to 2---3%.
ARTICLE IN PRESS+Model
4 Meletti DP et al.
50 children were ana lyz ed for thebasic preparation group
Eligible patients: 118
Excluded: 8
Did not meet the inclusioncriteria: 5
Refused to participate: 3
Randomized: 110
Allocated to the psychologicalpreparation group (PPG): 55
Allocated to the BasicPreparation Group (BPG): 55
Exclu ded aft er all ocation:
Yale scale was not applied: 4
Surgery was cancelled: 1
Exclude d aft er all ocation:
Yale sc ale was not applied: 3
Surgery was cancelled: 2
50 chil dren were analyz ed for thepsychological prepa ration group
T ran
S
Acsot
aiaoCgs
w-mmtaaSd
fpuot
a
R
Tolp
pgim(se
ftdpt
tg
(ca
Figure 1 Flowchart according to the CONSOR
ample size determination and statistical analysis
fter the 110 children were allocated in both groups, fivehildren from each group were lost to follow-up due tourgery cancellation or non-application of the anxiety scalen the day of the surgery. The final analysis was restrictedo 50 children from each studied group.
Considering that the prevalence of anxiety in the oper-ting room in children is 50%1 and that the proposedntervention was able to reduce children’s anxiety by 20%fter a pilot study with 20 children, and using an �-errorf 5%, �-error of 20%, and 95% confidence interval (95%I), the number of patients was determined at 42 in eachroup, totaling a number of 84 participants in the proposedtudy.
The statistical analysis was performed using the soft-are Stata/SE version 9.0 for Windows (Stata Corporation
-- College Station, Texas, USA). In the analysis of groups,edians and the 25---75% percentiles were used as aeasure of central tendency and variability due to
he non-normal distribution trend of the sample sep-rated in groups. Categorical variables were shown asbsolute values and percentages. Histograms and thehapiro---Wilk test were used to verify the symmetry of dataistribution.
The chi-squared test and Fisher’s exact test were usedor categorical variables, and the chi-squared partition waserformed if p-value was less than 0.05 (significance levelsed). The comparisons between two groups for continuous
r ordinal variables were performed using the Mann-Whitneyest.Spearman’s correlation was used to evaluate the associ-tion intensity of ordinal variables in the same individual.
D
Tp
domization guidelines and participants’ study.
esults
he groups were homogeneous regarding gender, age, levelf schooling, and type of surgery. In both groups, a preva-ence of boys for both groups and children attendingreschool was observed (Table 1).
No significant differences were found regarding thearents’ characteristics (chi-squared test) when the tworoups were compared regarding gender (p = 0.76), school-ng (p = 0.39), income (p = 0.32), occupation (p = 0.20), andarital status (p = 0.36). Most interviewees were women
87%), who were generally the mothers, had finished highchool (39%), belonged to the middle class (57%), and weremployed (58%) and married (77%).
When comparing the groups, both parents and childrenrom the PPG group had significantly lower anxiety levels athe time of surgery when compared with parents and chil-ren from the BPG. There was no difference between thearents’ level of anxiety assessed by the VAS at the time ofhe preanesthetic consultation (Table 2).
There was no correlation between parental anxiety at theime of surgery and the children’s anxiety the two studiedroups (r = 0.0276, p = 0.78; Fig. 2).
None of the children’s demographic data, such as genderp = 0.20), age (p = 0.88), and level of schooling (p = 0.52;hi-squared test) presented a significant association withnxiety.
iscussion
his clinical trial demonstrated that the children and theirarents who received psychological preparation care in a

ARTICLE IN PRESS+Model
Preparation reduces preoperative anxiety in children 5
Table 1 Characteristics of the study children: comparison by group.
Variables Basic Preparation GroupBPGFrequency and percentage
Psychological PreparationGroupPPGFrequency and percentage
p-value
Gender 0.76a
Male 44(88) 43(86)Female 6 (12) 7 (14)
Child’s age 0.19a
≥2 and ≤4 27 (54) 18 (36)>4 and ≤6 1 5(30) 21 (42)>6 and ≤8 8 (16) 11 (22)
Child’s level of schooling 0.59a
No schooling 5 (10) 5 (10)Daycare 10 (20) 5 (10)Pre-school 21 (42) 20 (40)First grade 8 (16) 12 (24)Second grade 6 (12) 8 (16)
Type of surgery performedPostectomy 19 (38) 22 (44) 0.684a
Thyroglossal cyst correction 0 3 (6) 0.242b
Inguinal herniorrhaphy 4 (8) 7 (14) 0.523a
Umbilical herniorrhaphy 7 (14) 5 (10) 0.758a
Nevus excision 3 (6) 1 (2) 0.617b
Adenoamigdalectomy 17 (34) 12 (24) 0.378a
a Yates’ chi-squared test.b Fisher’s exact test.
Values expressed as frequency and percentage (%); p < 0.05.
Table 2 Parents’ and children’s anxiety: comparison bygroup.
Scales BPGMedian andpercentiles
PPGMedian andpercentiles
p-value
VAS (consulta-tion)
8 (6.75---10) 7 (5---10) 0.12
VAS (surgery) 9 (7---10) 7 (5---10) 0.01m-YPAS 33.4
(23.4---45.85)26.6(23.4---33.4)
0.04
120
100
80
60
40
201 3 5
Visual Analogue Scale – Anxiety before the surgery
Mod
ified
Yal
e P
reop
erat
ive
Anx
iety
Sca
le
7 9 11
Figure 2 Correlation between the parents’ anxiety (VAS)scale at the time of surgery and the modified Yale Preoper-ac
si
In his review article, Moro discusses the question of age
Mann---Whitney test.Values expressed as medians and percentiles (25---75%).
single session had their preoperative degree of anxiety sig-nificantly reduced when compared with the group that didnot receive this care (p = 0.04 for the children and = 0.01 forparents at the time of surgery).
The preparation was focused on alleviating separationanxiety in young children. According to the care protocolused at the University Hospital where this study was per-formed, the parents did not accompany their children duringanesthetic induction, and the separation took place at thetoy library attached to the surgical ward. The authors con-
sider the age limit of 8 years as a predisposing factor to thisanxiety,15 due to the peculiar fact that children between 6months and 4 years of age manifest a greater intensity ofrss
tive Anxiety Scale (m-YPAS) applied in children. Spearman’sorrelation: p = 0.78.
eizures and the fear of separation from parents still remainn some children between the ages of 4---8 years.15
16
elated to preoperative anxiety and concludes that there istill no consensus on the subject. The literature containsome assertions that younger children, up to 6 years of age,

IN+Model
6
atctnnwotrt1yttt
Ivaepars
ppatw
owgatptdssfpft
dtsotsttwpmc
em
pltstmpapih
dctteca
artpttss
F
TB
C
T
R
ARTICLE
re more likely to suffer from preoperative anxiety relatedo separation. Older children, however, would be more con-erned with the surgery itself. Some studies have reportedhat older children are more anxious, and other authors didot find any evidence related to age.16 In the present study,o differences regarding an age-related degree of anxietyere observed; younger children between 2 and 4 years,r those aged 5 and 6 years, were no more anxious thanhose aged 7 and 8 years (p = 0.08). Similarly to the presentesults, Wollin et al.17 found no significance in the associa-ion between anxiety and the children’s age between 5 and2 years --- they divided the children into age groups: 5---6ears, 7---10 years, and 11---12 years. The present authorsherefore believe that maintaining the focus on the separa-ion anxiety approach for the age group of 2---8 years reducedhe number of consultations to a single session.
Kain et al. performed a family-centered preparation.9
n this intervention, parents received counseling throughideos, booklets, or by telephone, and the children received
surprise box at the time of anesthetic induction; their par-nts were monitored by a researcher who asked them to uselanned distraction strategies for children, if necessary. Thisdvanced preparation group presented superior results ineducing the children’s anxiety in comparison with the othertudy groups that were not submitted to this preparation.
Although the trial concluded that the psychologicalreparation significantly contributed to the reduction ofreoperative anxiety in children, the program was expensivend feasible only in large hospitals. Moreover, because ofhe complexity involved, it was not clear which componentould be essential in this preparation.
Another study, comparing children who underwent a pre-perative psychological preparation to a group of childrenho did not receive this type of care showed that theroup of children trained by the psychologist had lowernxiety levels than those who underwent only distractionechniques.18 Another trial19 evaluated the psychologist’sresence at the time of anesthetic induction and concludedhis method was more effective in reducing anxiety in chil-ren when compared with distraction techniques. In thattudy, it was necessary to have the presence of a profes-ional psychologist, who is part of the surgical team, onlyor this in-person support during anesthetic induction. In theresent study, the preparation aimed to enable the child toace the moment of surgery alone, but with the support ofhe existing team.
Regarding the aspect of an association between theegree of anxiety of the parents and their children inhe preoperative period, the present* study did not showuch correlation. Another clinical trial20 also failed tobserve such association, but its result was attributed tohe restricted number of participants. Cui et al.21 demon-trated a correlation between the anxiety of parents andheir children younger than 4 years during anesthetic induc-ion. It could be suggested that this difference in resultsas due to the fact that the mean age of the children in theresent study was higher. According to Nascimento,22 thereay be differences in the correlations between parents’ and
hildren’s anxiety levels regarding their age group.The present study had some limitations. In the postop-
rative period, the children’s behaviors and need for painedication were not assessed and, therefore, it was not
PRESSMeletti DP et al.
ossible to verify the extent of the benefits in this psycho-ogical preparation model. It was also not possible to matchhe genders in the studied groups, which predominantly con-isted of boys, due to the high frequency of postectomies inhe service. The psychological preparation for preanestheticedication use was not compared, and ethical reasonsrevented the creation of a control group without any pre-nesthetic preparation. Children who received psychologicalreparation were compared with children awaiting surgeryn a toy library, since it has already been shown that toyselp reduce anxiety.3,23,24
Finally, the study could have selected parents and chil-ren with a high risk of anxiety based on the informationollected during the psychological consultation and comparehem to the anxiety assessed by VAS and YALE scale at theime of surgery. This prognosis would have been useful instimating which parents and children would need a moreomprehensive approach with more than one session. Theuthors suggest this approach for future studies.
Children in the PPG and their parents benefited from thenxiety reduction when compared to the group that did noteceive this preparation. Therefore, the authors concludehat a single psychological session was effective in preparingarents and children for separation anxiety and coping withhe surgical procedure in most cases. This result has prac-ical and clinical importance and thus, this approach washown to be as effective as programs that rely on multipleessions.
unding
he study was registered in the Registro de Ensaios Clínicosrasileiros. Primary Identifier: RBR-5jh9sf.
onflicts of interest
he authors declare no conflicts of interest.
eferences
1. Davidson AJ, Shirivastava PP, Jansen K, Huang GH, CzarnekiC, Gibson MA, et al. Risk factors for anxiety at induction ofanesthesia in children: a prospective cohort study. PaediatricAnaesth. 2006;16:919---27.
2. Maranets I, Kain ZN. Preoperative anxiety and intraoperativeanesthetic requirements. Anesth Analg. 1999;89:1346---51.
3. Weber FS. The influence of playful activities on children’s anx-iety during the preoperative period at the outpatient surgicalcenter. J Pediatr. 2010;86:209---14.
4. Kain ZN, Mayes LC. Anxiety in children during the perioperativeperiod. In: Borenstein M, Genevro JL, editors. Child devel-opment and behavioral pediatrics. Mahwah, New Jersey: L.Erlbaum Associates; 1996. p. 85---103.
5. Guaratini AA, Marcolino JA, Teixeira AB, Bernardis RC, PassarelliML, Mathias L. Estudo transversal de ansiedade pré-operatóriaem criancas: utilizacão da Escala de Yale modificada. Rev Bras
Anestesiol. 2006;56:591---601.6. Ahmed MI, Farrel MA, Parrish K, Karla A. Preoperative anxiety inchildren --- risk factors and non-pharmacological management.M E J Anesth. 2011;21:153---70.

IN+Model
1
1
1
1
2
2
2
2
ARTICLEPreparation reduces preoperative anxiety in children
7. Yip P, Middleton P, Cyna AM, Carlyle AV. Non-pharmacologicalinterventions for assisting the induction of anaesthesia in chil-dren. Evid Based Child Health. 2011;6:71---134.
8. Manyande A, Cyna AM, Yip P, Chooi C, Middleton P. Non-pharmacological interventions for assisting the inductionof anaesthesia in children. Cochrane Database Syst Rev.2015:CD006447.
9. Kain ZN, Caldwell-Andrews AA, Mayes LC, Weinberg ME, WangSM, MacLaren JE, et al. Family-centered preparation for surgeryimproves perioperative outcomes in children. Anesthesiology.2007;106:65---74.
10. Gorayeb RP, Petean EB, Pileggi FO, Tazima MF, Vicente YA,Gorayeb R. Importance of psychological intervention for therecovery of children submitted to elective surgery. J PediatrSurg. 2009;44:1390---5.
11. Hilly J, Hörlin A-L, Kinderf J, Ghez C, Menrath S, DelivetH, et al. Preoperative preparation workshop reduces postop-erative maladaptive behavior in children. Paediatr Anaesth.2015;25:990---8.
12. Gutman A, Hallensleben G. Gaspar no Hospital. 2nd ed. SãoPaulo: Cosac Naify; 2010.
13. Kindler CH, Harms C, Amsler F, Ihde-School T, Scheidegger D.The visual analog scale allows effective measurement of pre-operative anxiety and detection of patients. Anesth Analg.2000;90:706---12.
14. Kain ZN, Mayes LC, Cicchetti DV, Bagnall AL, Finley JD, Hofs-
tadter MB. The Yale Preoperative Anxiety Scale: does it comparewith a ‘‘gold standard’’? Anesth Analg. 1997;85:783---8.15. Ghazal EA, Mason LJ, Coté CJ. Preoperative evaluation pre-medication and induction of anesthesia. In: Cote CJ, Lerman
2
PRESS7
J, Anderson B, editors. A practice of anesthesia for infants andchildren. 5th ed. Canada: Saunders; 2013.
6. Moro ET, Módulo NS. Children, parents and anxiety. Rev BrasAnestesiol. 2004;54:728---38.
7. Wollin SR, Plummer JL, Owen H, Hawkins MF, Materazzo F. Pre-dictors of preoperative anxiety in children. Anaesth IntensiveCare. 2003;31:69---74.
8. Cuzzocrea F, Costa S, Gugliandolo MC, Larcan R. Psychologistsin preoperative programmes for children undergoing surgery. JChild Health Care. 2016;20:164---73.
9. Cuzzocrea F, Gugliandolo MC, Larcan R, Romeo C, Turi-aco N, Dominici T. A psychological preoperative program:effects on anxiety and cooperative behaviors. Paediatr Anaesth.2013;23:139---43.
0. Vagnoli L, Caprilli S, Robiglio A, Messeri A. Clown doctors as atreatment for preoperative anxiety in children: a randomized,prospective study. Pediatrics. 2005;116:563---7.
1. Cui X, Zhu B, Zhao J, Huang Y, Luo A, Wei J. Parental state anx-iety correlates with preoperative anxiety in Chinese preschoolchildren. J Paediatr Child Health. 2016;52:649---55.
2. Nascimento CR [dissertation] Relacões entre a resposta deansiedade de pais e a resposta de ansiedade de seus filhos. PortoAlegre (RS): Universidade Federal do Rio Grande do Sul; 1998.
3. Golden L, Pagala M, Sukhavasi S, Nagpal D, Ahmad A, MahantaA. Giving toys to children reduces their anxiety about receivingpremedication for surgery. Anesth Analg. 2006;102:1070---2.
4. Aydin GB, Yuksel S, Ergil J, Polat R, Akelma FK, Ekici M,et al. The effect of play distraction on anxiety before pre-medication administration: a randomized trial. J Clin Anesth.2016;36:27---31.

Copyright © 2015 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.778 www.anesthesia-analgesia.org September 2015 • Volume 121 • Number 3
Copyright © 2015 International Anesthesia Research SocietyDOI: 10.1213/ANE.0000000000000839
Preschool children undergoing surgery are particularly vulnerable to separation anxiety before anesthesia because they are dependent on their parents and are
old enough to recognize parental absence.1–3 Furthermore, the placement of a mask on the face and the inhalation of volatile anesthetics in the absence of parents further dis-tresses young children, sometimes to the extent of refusal of mask induction.1,2,4,5 A more anxious state preoperatively results in poor cooperation at anesthetic induction and may be associated with emergence delirium and negative behavioral change after surgery.6,7 Therefore, the transfer of children from a preoperative holding area to the operating
room (OR) and the smooth induction of anesthesia without heightened anxiety may be of paramount importance in terms of minimizing perioperative distress and improving behavioral outcome.
Portable multimedia devices, such as smart phones, tablet computers, and handheld DVD players, are readily available at low cost. Age-appropriate video clips and video games are commonly used as effective distraction tools for medical and surgical procedures in children.8,9 In anesthetic practice, active distraction by a handheld video game with parental presence was found to be more effective than pre-medication or parental presence only for reducing anxiety and improving cooperation during mask induction in chil-dren aged 4 to 12 years.10 In younger children, whose cog-nitive and motor development were not advanced enough to play interactive video games, passive viewing of an animated cartoon also proved a more effective distraction than traditional storytelling, game-playing, nonprocedural talking, or humor during mask induction.11 However, pre-vious studies did not completely control for parental pres-ence or used parents to keep children relaxed during video distraction.9–11
Thus, we performed this study to determine whether video distraction per se is capable of alleviating preoperative
BACKGROUND: The anxiolytic efficacy of video watching, in the absence of parents, during the mask induction of anesthesia in young children with high separation anxiety has not been clearly established. We performed this study to determine whether the effect of video distrac-tion on alleviating preoperative anxiety is independent of parental presence and whether a combination of both interventions is more effective than either single intervention in alleviating preoperative anxiety and postoperative behavioral disturbance in preschool children.METHODS: In this prospective trial, 117 children aged 2 to 7 years scheduled for elective minor surgery were randomly allocated to 1 of 3 groups, a video distraction group (group V), a parental presence group (group P), or a combination of video distraction plus parental presence group (group VP) during induction of sevoflurane anesthesia. The Modified Yale Preoperative Anxiety Scale (mYPAS) was used to assess anxiety in the preoperative holding area (baseline), immediately after entry to the operating room, and during mask induction. Compliance during induction, emergence delirium during recovery, and negative behavioral changes at 1 day and 2 weeks postoperatively were also assessed.RESULTS: The mYPAS scores were comparable (P = 0.558), and the number of children exhibit-ing baseline anxiety (an mYPAS score > 30) were not different among the 3 groups in the preop-erative holding area (P = 0.824). After intervention, the changes in mYPAS scores from baseline to induction were not different among the 3 groups (P = 0.049). The proportion of children with increased mYPAS scores was higher in group P compared with group V from baseline to operat-ing room entry (Bonferroni-adjusted 95% confidence interval for difference, 2 to 49) but similar from baseline to induction in all 3 groups. Although children in group V were more cooperative during mask induction than those in the other 2 groups (P < 0.001 versus group P and P = 0.001 versus group VP), no significant intergroup differences were observed in the incidence of emergence delirium or new-onset negative behavioral change after surgery.CONCLUSIONS: Video distraction, parental presence, or their combination showed similar effects on preoperative anxiety during inhaled induction of anesthesia and postoperative behav-ioral outcomes in preschool children having surgery. (Anesth Analg 2015;121:778–84)
From the Department of Anesthesiology and Pain Medicine, Yeungnam University School of Medicine, Daegu, Republic of Korea.
Accepted for publication April 15, 2015.
Funding: This work was funded by Yeungnam University Grant-in-Aid of 2012.
The authors declare no conflicts of interest.
Reprints will not be available from the authors.
Address correspondence to Sung Mee Jung, MD, Department of Anesthe-siology and Pain Medicine, Yeungnam University School of Medicine, 170, Hyeonchung-ro, Nam-gu, Daegu 705-703, Republic of Korea. Address e-mail to [email protected].
Video Distraction and Parental Presence for the Management of Preoperative Anxiety and Postoperative Behavioral Disturbance in Children: A Randomized Controlled TrialHyuckgoo Kim, MD, Sung Mee Jung, MD, Hwarim Yu, MD, and Sang-Jin Park, MD, PhD
Section Editor: James DiNardo
Society for Pediatric Anesthesia

Copyright © 2015 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.
September 2015 • Volume 121 • Number 3 www.anesthesia-analgesia.org 779
anxiety and improving cooperation independent of paren-tal presence and whether a combination of video distrac-tion and parental presence is more effective than either intervention in preschool children during mask induction of anesthesia. The primary end point of this study was a change in anxiety level from baseline to induction. In addi-tion, we investigated the effect of each proactive interven-tion on postoperative behavioral outcomes, that is, on the incidences of emergence delirium and new-onset maladap-tive behavioral changes.
METHODSThis prospective, randomized study was approved by the IRB of Yeungnam University Hospital in South Korea and was registered with ClinicalTrials.gov on the December 30, 2013 (NCT02027844). One hundred seventeen children aged between 2 and 7 years, ASA physical status I or II scheduled for elective minor surgery under general anesthesia were enrolled. Children with a chronic illness, developmental delay, a neuropsychiatric disease, cancer, experience of a recent stressful life event, previous anesthetic experience, sedative medication, or emergency surgery were excluded. Written informed consent was obtained from parents, and verbal assent was obtained from children older than 6 years before the day of surgery.
No participant received sedative premedication before anesthesia. After arriving in the preoperative holding area, participants were allocated to 1 of the 3 study groups: group V (distraction by watching an animated cartoon video), group P (parental presence), or group VP (video distraction plus parental presence), throughout induction of anesthesia, using a computer-generated random assignment scheme. In group V, children were allowed to select 1 animated cartoon video in a smartphone offered by the researcher or parents and started to watch it with or without parents while wait-ing in the preoperative holding area. Children in group V were separated from their parents in the preoperative hold-ing area and transported to the OR. Anesthesia was induced while children continued to view the chosen video. In group P, 1 parent accompanied the child to the OR and stayed dur-ing the induction of anesthesia, and in group VP, children watched a cartoon video with their parents throughout the whole anesthesia induction process.
After arrival in the OR, children were given the choice to sit up or lie down on the operating table. All participants were introduced to the facemask, which was detached from the anesthetic circuit, before induction. The anesthesiolo-gist explained the anesthesia induction process to children and gently asked them to breathe deeply. A pulse oximeter and electrocardiogram were used for continuous monitor-ing during induction. Anesthesia was induced by mask inhalation with incrementing sevoflurane up to 8% with N2O (4 L/min) and oxygen (2 L/min). The anesthesiologist carefully positioned the facemask/anesthesia circuit so as not to interfere with video watching or the parent. When a participant closed his/her eyes and failed to respond to his/her name, the video was discontinued and the parent was escorted out of the OR by a nurse. Noninvasive arte-rial blood pressure was measured as soon as possible. After endotracheal intubation, anesthesia was maintained by sevoflurane inhalation at an end-tidal concentration of 1.5%
to 3.0% in 50% oxygen and by IV remifentanil infusion at a rate of 0.05 to 0.1 μg/kg/min during surgery. At the end of surgery, sevoflurane administration was discontinued, and after awakening with adequate spontaneous ventila-tion, children were tracheally extubated and transferred to the postanesthesia care unit (PACU). Heart rate, Spo2, and respiratory rate were monitored in the PACU. Parents were allowed to rejoin their children in the PACU. If a child com-plained of pain or exhibited signs or symptoms of pain, IV fentanyl 1 μg/kg was administered in the PACU. All clinical management decisions were made by the anesthesiologist responsible for the care of the patients.
Children’s anxiety levels throughout anesthesia induc-tion were assessed using the modified Yale Preoperative Anxiety Scale (mYPAS) at 3 time points, that is, while wait-ing in the preoperative holding area (T0; baseline), on enter-ing the OR (T1), and during mask induction (T2). mYPAS scores are obtained by summing the scores of 22 items in 5 behavioral categories: activity, state of apparent arousal, vocalization, emotional expression, and the use of parents.12 In group V, the interaction with the parent was assessed by slightly modifying the original components of the “use of parents” because of parental absence.
An mYPAS score of >30 indicates the presence of signifi-cant anxiety.12 The induction compliance checklist (ICC) was used to assess cooperation during induction.13 Both mYPAS and ICC scores were assessed by a trained observer in real time during the perioperative period. Before patients were enrolled in this study, the observer was trained in how to perform mYPAS and ICC scoring by reviewing videotapes of children at induction of anesthesia until 80% agreement with the scores allocated by a psychologist was achieved consistently, as suggested by Sadhasivam et al.14
Parental anxiety was assessed using the Korean version of Spielberger’s State-Trait Anxiety Inventory (STAI), which evaluates trait (baseline) and state (situational) anxiety.15 In the preoperative holding area, both trait and state anxiety scores were measured to investigate the effect of parental anxiety on child anxiety. State anxiety scores after induction were obtained to assess the effect of the 3 interventions on situational anxiety changes in parents.
After surgery, postoperative pain was assessed using the Children’s Hospital of Eastern Ontario Pain (CHEOP) scale.16 Emergence delirium was evaluated using the Pediatric Anesthesia Emergence Delirium (PAED) scale at 10-minute intervals for 30 minutes after arrival in the PACU.17 When the highest PAED score recorded at any time exceeded 10, emergence delirium was deemed to be present.
An investigator, unaware of group assignments, con-tacted parents and requested that they complete the Post-Hospitalization Behavior Questionnaire (PHBQ) at 1 and 14 days postoperatively by phone. The PHBQ contains 27 items in 6 categories: general anxiety, separation anxiety, anxiety about sleep, eating disturbance, aggression toward author-ity, and apathy/withdrawal.18 Negative behavioral change development after anesthesia and surgery was recorded. Both CHEOP and PAED scores and PHBQ interviews were performed by an independent observer unaware of group assignments.
Power analysis was conducted using G*Power ver. 3.1.5. An effect size of 0.31 was estimated from the variance of

Copyright © 2015 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.780 www.anesthesia-analgesia.org aNeStheSia & aNalgeSia
Video Distraction and Parental Presence in Children
mean mYPAS differences between the baseline and the induction of anesthesia among the 3 groups and the square of the common SD within each group based on the results of a pilot study conducted on 27 children. The data of the pilot study were not included in data analysis in the current study. A sample size of 35 participants per group was calculated by 1-way analysis of variance (ANOVA) to yield an 80% power to detect this effect size at a set α value of 0.05 among the 3 groups. Thirty-nine participants per group were recruited to account for a 10% dropout rate due to withdrawal of con-sent, a change in anesthetic/surgical plan, or follow-up loss.
Statistical analysis was performed using SPSS version 19 (SPSS Inc., Chicago, IL). The Kolmogorov-Smirnov Lilliefors goodness-of-fit test was used to verify normalities of the residuals of all continuous variables. When P values of the data were >0.05, they were considered normally distrib-uted. The normally distributed continuous variables, such as age, weight, and duration of anesthesia, were presented as the means ± SDs and were compared using the 1-way ANOVA. Statistical significance was accepted for P values <0.05. Nonnormally distributed continuous variables, such as mYPAS scores at each time point and ICC, were presented as medians and ranges and compared using the nonpara-metric Kruskal-Wallis test. The test was followed the Mann-Whitney U test with Bonferroni adjustment for multiple pairwise comparisons (3 comparisons) if a significant inter-group difference was found. A Bonferroni-adjusted P value <0.017 (0.05/3) was considered statistically significant. The change in mYPAS scores over time among the 3 groups was compared using the repeated measures ANOVA.
Categorical variables were analyzed using the χ2 test or the Fisher exact test. Wilson score interval without continu-ity correction19 was used to compare Bonferroni-adjusted 95% confidence interval for differences in proportion of participants with increased anxiety from baseline to OR entry and induction of anesthesia among interventions. Statistical significance was considered for P < 0.017 after Bonferroni adjustment for 3 comparisons (0.05/3). The McNemar test was used to compare the incidence of newly developed maladaptive behavior 1 day and 2 weeks after surgery. Correlations between mYPAS score during induc-tion of anesthesia and PAED scores or numbers of patients exhibiting a postoperative negative behavioral change were assessed using the Pearson correlation or the Spearman rank correlation coefficients, respectively. Statistical signifi-cance was accepted for P values <0.05.
RESULTSOne hundred seventeen children were initially enrolled. Eleven children were excluded because of withdrawal of consent, incomplete data, or loss to follow-up (Fig. 1). Two children in group P were excluded because they viewed an animated cartoon with their parents while waiting in the preoperative holding area after random allocation. Thus, 104 participants completed the study, and they were included in the data analysis. No significant intergroup dif-ferences in demographic or surgical characteristics were observed (Table 1). Mothers predominantly accompanied children to the OR and stayed during anesthesia induction in groups P (n = 27, 81.8%) and VP (n = 26, 70.3%).
Eligibility
(n = 125)
Not meeting inclusion criteria (n = 6)
Decline to participate (n = 2)
Randomization
(n = 117)
Group V
(n = 39)
Group P
(n = 39)
Group VP
(n = 39)
Withdrawal of consent (n = 3)
Incomplete data (n = 2)
Withdrawal of consent (n = 2)
Noncompliance to protocol
(n = 2)
Loss of follow-up (n = 2)
Withdrawal of consent (n = 1)
Loss of follow-up (n = 1)
Completion of the study
(n = 34)
Completion of the study
(n = 33)
Completion of the study
(n = 37)
Data analysis
(n = 104)
Figure 1. Flow diagram of participants. Group V = video distraction; group P = parental presence; group VP = com-bination of video distraction and parental presence.

Copyright © 2015 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.
September 2015 • Volume 121 • Number 3 www.anesthesia-analgesia.org 781
The median mYPAS scores were comparably lower than 30 at T0 (P = 0.558), and the number of children exhibiting baseline anxiety (an mYPAS score > 30) was not different among groups (Table 2, P = 0.824) before intervention. After intervention, mYPAS scores were different among the 3 groups at T1 (P = 0.002) and T2 (P = 0.012). Specifically, chil-dren in group V exhibited lower mYPAS scores compared with the other 2 groups at both T1 (P < 0.001 versus group P and P = 0.015 versus group VP) and T2 (P = 0.012 ver-sus group P and P = 0.008 versus group VP). However, the overall changes in mYPAS scores from baseline to induc-tion of anesthesia were not different among the 3 groups (P = 0.049). The proportion of children who increased their mYPAS scores was higher in group P compared with group V from T0 to T1 (Bonferroni-adjusted 95% confidence inter-val for difference 2 to 49) but was similar in all groups from T0 to T2 (Fig. 2, Table 3).
The compliance of children at mask induction was signif-icantly different among groups (P = 0.001; Table 2). Children in group V were more cooperative during mask induction than children in the other 2 groups (P = 0.0005 versus group P and 0.001 versus group VP). ICC scores were found to be significantly correlated with mYPAS scores at each time point (P < 0.001, r = 0.338, 0.531, and 0.869 at T0, T1, and T2, respectively) and with the amount of mYPAS score change (P = 0.042, r = 0.199 from T0 to T1; P < 0.001, r = 0.702 from T0 to T2).
Parent anxiety was assessed using STAI before interven-tion and after completing anesthesia induction in all groups. Both trait and state anxiety scores in the preoperative hold-ing area and changes in state and anxiety scores over the peri-induction period were not different in the 3 groups (Table 2). Parent state anxiety score changes were found to be weakly correlated with the mYPAS score changes from T0 to T2 (P = 0.025, r = 0.221) and with ICC scores at mask induction (P = 0.035, r = 0.207). However, parent trait anxiety scores were not found to affect children’s anxiety
scores during the perioperative period. The majority of par-ents (75%) stated that they would prefer to be present dur-ing anesthesia induction in the future if their child had to undergo surgery. However, a significant intergroup differ-ence was found in this respect (P < 0.001), and fewer parents of group V children (39.1%) favored parental presence at the induction of anesthesia for any future surgery than parents of group P (95.8%, P < 0.001) or group VP (86.2%, P < 0.001) children.
Emergence statuses were comparable except for pain scores among groups (P = 0.041). Postoperative pain scores were weakly correlated with changes in anxiety scores among children between T0 and T2 (P = 0.041, r = 0.200). Median PAED scores and incidences of significant emer-gence delirium were comparable in the 3 groups and were not linked to the anxiety levels of children or parents at any of the 3 time points (Table 4). Number of children who developed new-onset negative behavior over the 2 weeks after surgery were comparable in all groups. Eating distur-bance (31.7%), separation anxiety (14.9%), and aggression toward authority (13.9%) were common on the first post-operative day but decreased significantly with time over the next 2 weeks (7.0%, P < 0.001, 7.0%, P = 0.02 and 8.0%, P = 0.07, respectively). The incidence of newly developed negative behavior was not found to be related to the anxi-ety levels of children or parents, postoperative pain scores, or the number of children who experienced emergence delirium in the PACU.
DISCUSSIONIn the present study, video distraction, parental presence, or a combination of both had a similar effect on preoperative anxiety during inhaled induction of anesthesia in preschool children undergoing surgery. We found that the overall changes in anxiety levels from preoperative holding area to induction of anesthesia were not different among the 3 groups although children with video distraction had lower anxiety levels compared with those with parental presence only or their combination at entry to the OR and during induction of anesthesia.
Our results suggest that video distraction and paren-tal presence appeared to have different anxiolytic mecha-nisms in the perioperative setting. Video distraction makes children oblivious to the unfamiliar OR environment and absorbs them in a familiar imaginary world, whereas parental presence simply relieves the distress associated with separation from parents. Previous studies demon-strated that the addition of viewing age-appropriate video provided greater reduction of anxiety than control or con-ventional distraction techniques in children accompanied by their parents during induction of general anesthesia.11,20 However, the changes in anxiety levels from holding area to anesthetic induction were similar not only between parental presence and video distraction, but also between each single intervention and combination of both interven-tions in the present study. This inconsistency in the results may be explained by different study designs. Allowing that parental presence and type of anesthetic induction were different. Mifflin et al.11 demonstrated that video distraction more effectively reduced preoperative anxi-ety compared with control during inhaled induction of
Table 1. Demographic and Surgical Characteristics of Patients
Group V Group P Group VP P(n = 34) (n = 33) (n = 37)
Age (y) 5.5 ± 1.0 5.3 ± 1.4 5.0 ± 1.3 0.097Sex (M/F) 15/19 12/21 18/19 0.581Weight (kg) 20.7 ± 4.1 22.4 ± 6.5 20.6 ± 6.0 0.372Height (cm) 114.9 ± 10.6 114.0 ± 10.1 111.7 ± 9.3 0.494ASA PS (I/II) 34/0 32/1 37/0 0.317Type of surgery,
n (%)0.250
Eye surgery 17 (50.0) 21 (63.6) 23 (62.2) Tonsillectomy 9 (26.5) 8 (24.2) 10 (27.0) Herniorrhaphy 5 (14.7) 0 3 (8.1) Excision of
neck mass3 (8.8) 4 (12.1) 1 (2.7)
Duration of surgery (min)
37.0 ± 16.5 40.9 ± 10.1 39.1 ± 10.6 0.449
Duration of anesthesia (min)
60.0 ± 19.3 62.9 ± 14.5 61.7 ± 11.5 0.748
Values are mean ± SD and number of patients (%).V = video distraction; P = parental presence; VP = combination of video distraction and parental presence; ASA PS = American Society of Anesthesiologist physical status.
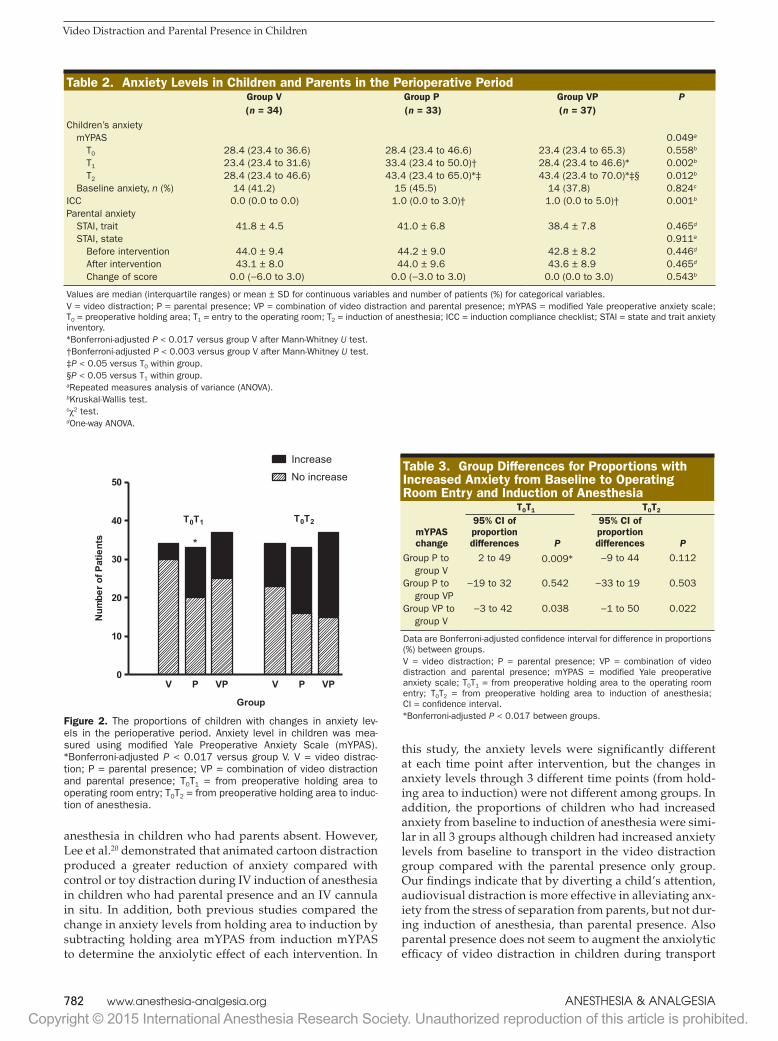
Copyright © 2015 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.782 www.anesthesia-analgesia.org aNeStheSia & aNalgeSia
Video Distraction and Parental Presence in Children
anesthesia in children who had parents absent. However, Lee et al.20 demonstrated that animated cartoon distraction produced a greater reduction of anxiety compared with control or toy distraction during IV induction of anesthesia in children who had parental presence and an IV cannula in situ. In addition, both previous studies compared the change in anxiety levels from holding area to induction by subtracting holding area mYPAS from induction mYPAS to determine the anxiolytic effect of each intervention. In
this study, the anxiety levels were significantly different at each time point after intervention, but the changes in anxiety levels through 3 different time points (from hold-ing area to induction) were not different among groups. In addition, the proportions of children who had increased anxiety from baseline to induction of anesthesia were simi-lar in all 3 groups although children had increased anxiety levels from baseline to transport in the video distraction group compared with the parental presence only group. Our findings indicate that by diverting a child’s attention, audiovisual distraction is more effective in alleviating anx-iety from the stress of separation from parents, but not dur-ing induction of anesthesia, than parental presence. Also parental presence does not seem to augment the anxiolytic efficacy of video distraction in children during transport
Table 2. Anxiety Levels in Children and Parents in the Perioperative PeriodGroup V Group P Group VP P(n = 34) (n = 33) (n = 37)
Children’s anxiety mYPAS 0.049a
T0 28.4 (23.4 to 36.6) 28.4 (23.4 to 46.6) 23.4 (23.4 to 65.3) 0.558b
T1 23.4 (23.4 to 31.6) 33.4 (23.4 to 50.0)† 28.4 (23.4 to 46.6)* 0.002b
T2 28.4 (23.4 to 46.6) 43.4 (23.4 to 65.0)*‡ 43.4 (23.4 to 70.0)*‡§ 0.012b
Baseline anxiety, n (%) 14 (41.2) 15 (45.5) 14 (37.8) 0.824c
ICC 0.0 (0.0 to 0.0) 1.0 (0.0 to 3.0)† 1.0 (0.0 to 5.0)† 0.001b
Parental anxiety STAI, trait 41.8 ± 4.5 41.0 ± 6.8 38.4 ± 7.8 0.465d
STAI, state 0.911a
Before intervention 44.0 ± 9.4 44.2 ± 9.0 42.8 ± 8.2 0.446d
After intervention 43.1 ± 8.0 44.0 ± 9.6 43.6 ± 8.9 0.465d
Change of score 0.0 (−6.0 to 3.0) 0.0 (−3.0 to 3.0) 0.0 (0.0 to 3.0) 0.543b
Values are median (interquartile ranges) or mean ± SD for continuous variables and number of patients (%) for categorical variables.V = video distraction; P = parental presence; VP = combination of video distraction and parental presence; mYPAS = modified Yale preoperative anxiety scale; T0 = preoperative holding area; T1 = entry to the operating room; T2 = induction of anesthesia; ICC = induction compliance checklist; STAI = state and trait anxiety inventory.*Bonferroni-adjusted P < 0.017 versus group V after Mann-Whitney U test.†Bonferroni-adjusted P < 0.003 versus group V after Mann-Whitney U test.‡P < 0.05 versus T0 within group.§P < 0.05 versus T1 within group.aRepeated measures analysis of variance (ANOVA).bKruskal-Wallis test.cχ2 test.dOne-way ANOVA.
V P VP V P VP0
10
20
30
40
50 No increase
Increase
Group
T0T1 T0T2
*
Num
ber o
f Pat
ient
s
Figure 2. The proportions of children with changes in anxiety lev-els in the perioperative period. Anxiety level in children was mea-sured using modified Yale Preoperative Anxiety Scale (mYPAS). *Bonferroni-adjusted P < 0.017 versus group V. V = video distrac-tion; P = parental presence; VP = combination of video distraction and parental presence; T0T1 = from preoperative holding area to operating room entry; T0T2 = from preoperative holding area to induc-tion of anesthesia.
Table 3. Group Differences for Proportions with Increased Anxiety from Baseline to Operating Room Entry and Induction of Anesthesia
T0T1 T0T2
mYPAS change
95% CI of proportion differences P
95% CI of proportion differences P
Group P to group V
2 to 49 0.009* −9 to 44 0.112
Group P to group VP
−19 to 32 0.542 −33 to 19 0.503
Group VP to group V
−3 to 42 0.038 −1 to 50 0.022
Data are Bonferroni-adjusted confidence interval for difference in proportions (%) between groups.V = video distraction; P = parental presence; VP = combination of video distraction and parental presence; mYPAS = modified Yale preoperative anxiety scale; T0T1 = from preoperative holding area to the operating room entry; T0T2 = from preoperative holding area to induction of anesthesia; CI = confidence interval.*Bonferroni-adjusted P < 0.017 between groups.

Copyright © 2015 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.
September 2015 • Volume 121 • Number 3 www.anesthesia-analgesia.org 783
and induction of anesthesia. Thus, each intervention or a combination of both interventions may result in similar effects on preoperative anxiety in children undergoing inhaled induction of anesthesia.
The similar changes in anxiety levels from baseline to induction among the 3 interventions in the present study sug-gest 2 interesting possibilities. First, contrary to the general belief, separation from parents may not be the most important cause of preoperative anxiety in preschool children. Although children accompanied by their parents did not experience sep-aration anxiety, their changes in anxiety levels until induction of anesthesia were similar to children with video distraction (parental absence) in this study. In fact, parental presence was shown to be briefly effective in reducing a child’s anxiety only at separation from parents but not at induction of anesthesia.21 Our data are consistent with previous reports that placement of a mask for anesthetic induction caused the greatest distress to children undergoing surgery.5,6,22 Next, the anxiety levels at the separation time point (transport to the OR) were lower in children with video distraction than parental presence only or a combination of both despite similar changes in anxiety lev-els over time. In addition, the proportion of children who had increased anxiety levels from baseline to OR entry was higher in children with parental presence than video distraction. Our data suggest that parental presence is unlikely to be a more effective intervention to reduce separation anxiety than video distraction even in preschool children at greatest risk of devel-oping a separation anxiety reaction.3 Lee et al.20 demonstrated that, in preschool children accompanied by their parents, the cartoon distraction group showed less change in anxiety lev-els at separation from parents compared with a control group. In contrast, the addition of video distraction did not provide additional benefit in reducing separation anxiety in children with parental presence in this study.
Increased parental anxiety can increase child anxiety and prolong anesthetic induction by generating interactions between children and parents.23,24 We found that a change in parent situational anxiety was influenced by a change in child anxiety or compliance at anesthetic induction and vice versa. Although no significant differences in parental anxiety change were found with respect to intervention, a few parents in both groups that had a parent present (group P and VP) left the OR in tears. However, no parent in the video distraction group
showed an emotional reaction at separation. In this study, the number of parents who reported their presence helped their child during transport to the OR and induction of anesthesia and would be present during the induction of anesthesia if required in the future was significantly higher in both paren-tal presence groups than in the video distraction group. These findings suggest that parental anxiety interacts with child anx-iety during induction of anesthesia and that a more objective instrument may be required to measure parental anxiety.
Although the pathogeneses of postoperative emergence delirium and negative behavioral changes remained unde-fined, preschool children, sevoflurane anesthesia, and high anxiety levels in the preoperative holding area and at induc-tion of anesthesia are considered potential risk factors.6,7,22 This means that postoperative emergence delirium and negative behavioral change might be reduced by a preoper-ative intervention targeting anxiety reduction. The addition of active distraction with a handheld video game effectively reduced the change of anxiety from holding area to mask induction of anesthesia but did not improve postoperative behavioral change compared with children accompanied by their parents.10 In this study, emergence delirium occur-ring within the first 30 minutes after anesthesia occurred similarly among the 3 groups and largely resolved in 10 to 20 minutes. New-onset negative behavior occurred in 49% of children on the first day after surgery and persisted for 2 weeks after surgery in 14%.
Several limitations related to this study should be dis-cussed. First, parental anxiety was assessed using a self-report-ing rating scale. Although the state-trait anxiety inventory is a validated anxiety assessment instrument for adults, we found some discrepancies between subjective reports and objective behaviors. Second, we did not measure the baseline temperament of children using a validated behavioral assess-ment tool, and baseline temperament characteristics can affect the effectiveness of an anxiolytic intervention by influencing how a child will respond emotionally in a stressful situation. Third, blinding was impossible in this study because video watching and parental presence were visible to investigators and participants, and thus, observer bias may have influenced assessments of anxiety levels and compliance at induction of anesthesia. Fourth, we were unable to calculate the use of par-ents’ item of the mYPAS accurately because parental presence
Table 4. Postoperative Emergence Delirium and Negative Behavioral Changes in ChildrenGroup V Group P Group VP
P(n = 34) (n = 33) (n = 37)Awakening time (min) 9.0 ± 3.9 12.2 ± 7.0 10.7 ± 5.0 0.056CHEOP score 7.0 (6.0–8.3) 8.0 (6.5–9.5) 9.0 (7.0–10.0)* 0.041Peak PAED score 7.9 ± 6.3 8.0 ± 5.5 9.3 ± 6.0 0.517Emergence delirium, n (%) 13 (38.2) 13 (39.4) 20 (43.5) 0.324Negative PHBC, n (%) ≥1 1 d 17 (50.0) 19 (57.6) 15 (40.5) 0.354 2 wk 7 (21.2) 5 (15.2) 3 (5.2) 0.299 ≥4 1 d 1 (2.9) 1 (3.0) 4 (11.4) 0.224 2 wk 2 (6.1) 1 (3.0) 0 0.551
Values are median (interquartile ranges) or mean ± SD for continuous variables and number of patients (%) for categorical variables.V = video distraction; P = parental presence; VP = combination of video distraction and parental presence; CHEOP = Children’s Hospital of Eastern Ontario Pain Scale; PAED = Pediatric Anesthesia Emergence Delirium scale; PHBC = post-hospital behavior change.*Bonferroni-adjusted P < 0.017 versus group V.

Copyright © 2015 International Anesthesia Research Society. Unauthorized reproduction of this article is prohibited.784 www.anesthesia-analgesia.org aNeStheSia & aNalgeSia
Video Distraction and Parental Presence in Children
was lacking in group V. Although we matched children’s responses in group V with the components of the use of par-ents, this may have affected the psychometric integrity of the mYPAS. Finally, the inability to relate the anxiolytic effects of video distraction and parental presence on the short- and long-term postoperative behavioral outcomes in children may be related to sample size. We calculated sample size based on a change in anxiety levels from baseline to induction of anesthesia, the primary end point of this study, and thus, the number of children recruited may have been insufficient to detect the effects of the 3 different interventions on postop-erative behavioral changes.
In conclusion, we found that video distraction, parental presence, or combination of both interventions had a simi-lar effect on preoperative anxiety during inhaled induction of anesthesia and postoperative behavioral outcomes such as emergence delirium and new-onset negative behavioral changes in preschool children. A further large-scale study is required to determine the ability of video distraction to improve postoperative behavioral outcomes. E
DISCLOSURESName: Hyuckgoo Kim, MD.Contribution: This author helped design and conduct the study, acquire the data, review and analyze the data, and draft and revise the manuscript.Attestation: Hyuckgoo Kim has seen the original study data, reviewed the analysis of the data, and approved the final manuscript.Name: Sung Mee Jung, MD.Contribution: This author helped design and conduct the study, acquire data, analyze and interpret the data, draft and revise the manuscript, and is the corresponding author.Attestation: Sung Mee Jung has seen the original study data, reviewed the analysis of the data, approved the final manu-script, and is the archival author.Name: Hwarim Yu, MD.Contribution: This author helped design and conduct the study, acquire the data, and prepare the manuscript.Attestation: Hwarim Yu has seen the original study data and approved the final manuscript.Name: Sang-Jin Park, MD, PhD.Contribution: This author helped design the study, analyze and interpret the data, and revise the data.Attestation: Sang-Jin Park has seen the original study data, analyzed and interpreted the data, and approved the final manuscript.This manuscript was handled by: James A. DiNardo, MD.
ACKNOWLEDGMENTSThe authors thank Ji Eun Jang, Department of Statistics, Yeungnam University, for assistance with statistical analysis.
REFERENCES 1. Kain ZN, Mayes LC, O’Connor TZ, Cicchetti DV. Preoperative
anxiety in children. Predictors and outcomes. Arch Pediatr Adolesc Med 1996;150:1238–45
2. Kain ZN, Mayes LC, Caramico LA, Silver D, Spieker M, Nygren MM, Anderson G, Rimar S. Parental presence during induction of anesthesia. A randomized controlled trial. Anesthesiology 1996;84:1060–7
3. Vetter TR. The epidemiology and selective identification of children at risk for preoperative anxiety reactions. Anesth Analg 1993;77:96–9
4. Przybylo HJ, Tarbell SE, Stevenson GW. Mask fear in children presenting for anesthesia: aversion, phobia, or both? Paediatr Anaesth 2005;15:366–70
5. Fortier MA, Del Rosario AM, Martin SR, Kain ZN. Perioperative anxiety in children. Paediatr Anaesth 2010;20:318–22
6. Kain ZN, Caldwell-Andrews AA, Maranets I, McClain B, Gaal D, Mayes LC, Feng R, Zhang H. Preoperative anxiety and emergence delirium and postoperative maladaptive behaviors. Anesth Analg 2004;99:1648–54
7. Kain ZN, Mayes LC, Caldwell-Andrews AA, Karas DE, McClain BC. Preoperative anxiety, postoperative pain, and behavioral recovery in young children undergoing surgery. Pediatrics 2006;118:651–8
8. Low DK, Pittaway AP. The ‘iPhone’ induction—a novel use for the Apple iPhone. Paediatr Anaesth 2008;18:573–4
9. Burk CJ, Benjamin LT, Connelly EA. Distraction anesthe-sia for pediatric dermatology procedures. Pediatr Dermatol 2007;24:419–20
10. Patel A, Schieble T, Davidson M, Tran MC, Schoenberg C, Delphin E, Bennett H. Distraction with a hand-held video game reduces pediatric preoperative anxiety. Paediatr Anaesth 2006;16:1019–27
11. Mifflin KA, Hackmann T, Chorney JM. Streamed video clips to reduce anxiety in children during inhaled induction of anesthe-sia. Anesth Analg 2012;115:1162–7
12. Kain ZN, Mayes LC, Cicchetti DV, Bagnall AL, Finley JD, Hofstadter MB. The Yale Preoperative Anxiety Scale: how does it compare with a “gold standard”? Anesth Analg 1997;85:783–8
13. Kain ZN, Mayes LC, Wang SM, Caramico LA, Hofstadter MB. Parental presence during induction of anesthesia versus sedative premedication: which intervention is more effective? Anesthesiology 1998;89:1147–56
14. Sadhasivam S, Cohen LL, Hosu L, Gorman KL, Wang Y, Nick TG, Jou JF, Samol N, Szabova A, Hagerman N, Hein E, Boat A, Varughese A, Kurth CD, Willging JP, Gunter JB. Real-time assessment of perioperative behaviors in children and parents: development and validation of the periopera-tive adult child behavioral interaction scale. Anesth Analg 2010;110:1109–15
15. Spielberger CD, Gorsuch RL, Lushene PR, Vagg PR, Jacobs GA. Manual for the State-Trait Anxiety Inventory STAI (Form Y) (“Self-Evaluation Questionnaire”). Palo Alto, CA: Consulting Psychologists Press, Inc., 1983
16. McGrath PJ, Johnson G, Goodman JT, Schillinger J, Dunn J, Chapman J. CHEOPS: A Behavioral Scale for Rating Postoperative Pain in Children. New York, NY: Raven Press, 1985
17. Sikich N, Lerman J. Development and psychometric evalu-ation of the Pediatric Anesthesia Emergence Delirium scale. Anesthesiology 2004;100:1138–45
18. Vernon DT, Schulman JL, Foley JM. Changes in children’s behavior after hospitalization. Some dimensions of response and their correlates. Am J Dis Child 1966;111:581–93
19. Newcombe RG. Interval estimation for the difference between independent proportions: comparison of eleven methods. Stat Med 1998;17:873–90
20. Lee J, Lee J, Lim H, Son JS, Lee JR, Kim DC, Ko S. Cartoon dis-traction alleviates anxiety in children during induction of anes-thesia. Anesth Analg 2012;115:1168–73
21. Wright KD, Stewart SH, Finley GA. When are parents helpful? A randomized clinical trial of the efficacy of parental presence for pediatric anesthesia. Can J Anaesth 2010;57:751–8
22. Kain ZN, Wang SM, Mayes LC, Caramico LA, Hofstadter MB. Distress during the induction of anesthesia and postoperative behavioral outcomes. Anesth Analg 1999;88:1042–7
23. Kain ZN, Caldwell-Andrews AA, Maranets I, Nelson W, Mayes LC. Predicting which child-parent pair will benefit from paren-tal presence during induction of anesthesia: a decision-making approach. Anesth Analg 2006;102:81–4
24. Kain ZN, Caldwell-Andrews AA, Mayes LC, Weinberg ME, Wang SM, MacLaren JE, Blount RL. Family-centered preparation for surgery improves perioperative outcomes in children: a randomized controlled trial. Anesthesiology 2007;106:65–74

Jurnal Keperawatan Silampari
Volume 3, Nomor 1, Desember 2019
e-ISSN: 2581-1975
p-ISSN: 2597-7482
DOI: https://doi.org/10.31539/jks.v3i1.837
332
VIDEO KARTUN DAN VIDEO ANIMASI DAPAT MENURUNKAN TINGKAT
KECEMASAN PRE OPERASI PADA ANAK USIA PRA SEKOLAH
Ajeng Dwi Retnani1, Titin Sutini2, Suhendar Sulaeman3
Program Studi Magister Keperawatan, Universitas Muhammadiyah Jakarta1
Program Studi Keperawatan, Universitas Muhammadiyah Jakarta2
Program Studi Manajemen, Universitas Muhammadiyah Jakarta3
ABSTRAK
Tujuan penelitian ini ialah menganalisis pengaruh video kartun dan video animasi
terhadap penurunan tingkat kecemasan pre operasi pada anak usia pra sekolah. Metode
penelitian ini menggunakan quasiaeksperimental dengan pendekatan pre and post-
testawithout control. Hasil penelitian menunjukkan bahwa penurunan tingkat
kecemasan pre operasi pada anak usia pra sekolah setelah diberikan intervensi video
kartun sebesar 4,20, setelah diberikan intervensi video animasi sebesar 4,70 dan setelah
diberikan intervensi kombinasi antara video kartun+video animasi sebesar 7,20.
Berdasarkan hal tersebut, tingkat kecemasan pre operasi menggunakan intervensi
kombinasi video kartun+video animasi menunjukkan penurunan paling besar. Hasil
penelitian juga didapatkan p value > 0,000. Simpulan, adanya pengaruh video kartun
dan video animasi terhadap penurunan tingkat kecemasan pre operasi pada anak usia pra
sekolah.
Kata Kunci: Animasi, Kecemasan, Pre Operasi, Video Kartun
ABSTRACT
The purpose of this study was to analyze the effect of cartoon videos and animated
videos on reducing preoperative anxiety levels in pre-school age children. This
research method uses quasi-experimental with a pre and post-test approach with out
control. The results showed that the reduction in preoperative anxiety levels in pre-
school children after being given a cartoon video intervention by 4.20, after being given
an animated video intervention by 4.70 and after being given a combination
intervention between cartoon videos + animated videos by 7.20. Based on this, the level
of preoperative anxiety using a cartoon video + animated video combination
intervention showed the greatest decrease. The results of the study also obtained p
value> 0,000. Conclusions, the influence of cartoon videos and animated videos on the
reduction of preoperative anxiety levels in pre-school age children.
Keywords: Animation, Anxiety, Pre Operation, Cartoon Video

2019. Jurnal Keperawatan Silampari 3 (1) 332-341
333
PENDAHULUAN
Anak usia pra sekolah merupakan anak yang berusia 3 sampai 5 tahun yang
memiliki kemampuan berinteraksi dengan sosial dan lingkungannya sebagai tahap
menuju perkembangan selanjutnya (Astarani, 2017). Anak usia pra sekolah memiliki
resiko besar untuk mengalami masalah kesehatan jika dikaitkan dengan respon imun
dan kekuatan pertahanan dirinya yang belum optimal (Papalia, et al, 2010). Alini (2017)
juga menyatakan bahwa pada masa usia pra sekolah aktifitas anak yang meningkat
menyebabkan anak kelelahan dan menjadikan anak rentan terhadap penyakit akibat
daya tahan tubuh yang lemah sehingga anak diharuskan menjalani hospitalisasi,
termasuk operasi.
Menurut Utami (2014) anak merupakan populasi yang sangat rentan terutama saat
menghadapi situasi yang membuat stress. Hal ini dikarenakan kondisi koping yang
digunakan oleh orang dewasa belum berkembang sempurna pada anak-anak. Anak usia
prasekolah menerima keadaaan masuk rumah sakit dengan rasa ketakutan. Jika anak
sangat ketakutan dapat menampilkan perilaku agresif, dari menggigit, menendang-
nendang bahkan berlari ke luar ruangan.
Tindakan operasi merupakan hal yang sangat beresiko. Lebih dari 230 juta operasi
mayor dilakukan setiap tahun di dunia yang menyebabkan keadaan pasien saat operasi
akan lemah, meningkatkan komplikasi setelah operasi dilakukan bahkan dapat
menyebabkan kematian (Priece, Moreno, 2012). Tindakan operasi memerlukan sebuah
tindakan keperawatan pre operasi yang merupakan tahapan awal dari keperawatan
operatif yang dimulai sejak pasien diterima masuk di ruang terima pasien dan berakhir
ketika pasien dipindahkan ke meja operasi untuk dilakukan tindakan pembedahan
(Wijayanti, 2011). Salah satu persiapan pre operasi ialah persiapan mental/psikis.
Persiapan mental merupakan hal yang tidak kalah pentingnya dalam proses
persiapan operasi karena mental pasien yang tidak siap atau labil dapat berpengaruh
terhadap kondisi fisiknya dan kelancaran proses operasi. Perawat perlu mengkaji
mekanisme koping pasien dalam menghadapi stres, dimana tindakan operasi merupakan
salah satu keadaan pemicu kecemasan dan stress pada pasien terutama pada pasien anak
(Sjamsuhidajat, De Jong, 2010). Terdapat sekitar 50%-70% dari anak-anak yang
menjalani operasi mengalami kecemasan dan kesusahan yang parah sebelum operasi
(Alini, 2017).
Kecemasan merupakan suatu kondisi yang tidak menyenangkan yang dapat
mempengaruhi perilaku pasien yang melakukan perawatan (Gracia, 2012). Kecemasan
dental pada pasien anak usia 6-8 tahun biasanya timbul karena belum adanya
pengalaman ke dokter gigi. Kecemasan dental pada anak tersebut menyebabkan anak
sering menunda bahkan menolak untuk dilakukan perawatan di dokter gigi yang juga
mengakibatkan betambah parahnya kondisi kesehatan gigi dan mulut pada anak
(Rehatta dkk, 2014). Kecemasan pada tindakan dental disebabkan oleh banyak hal, di
antaranya penggunaan alat dental yang dimasukan secara berurutan dan bergantian ke
mulut dan suara yang ditimbulkan dari alat-alat tersebut (Gracia, 2012). Setiap orang
menunjukkan tanda-tanda kecemasan berbeda-beda, di antaranya ditandai dengan
meningkatnya denyut nadi (Pontoh dkk, 2015). Penelitian yang dilakukan oleh Collip’s,
menyatakan bahwa terjadi peningkatan denyut nadi pada saat anak diberikan tindakan
medis (Stuart, Laira, 2005).
Kecemasan yang dialami anak usia pra sekolah jika tidak segera ditangani akan
mengakibatkan tubuh menghasilkan hormon yang menyebabkan kerusakan pada
seluruh tubuh termasuk menurunkan kemampuan sistem imun (Putra, 2011). Anak yang

2019. Jurnal Keperawatan Silampari 3 (1) 332-341
334
mengalami cemas juga cenderung menolak perawatan dan pengobatan yang sedang
dijalani (tidak kooperatif). Anak yang tidak kooperatif akibat kecemasan akan
menyebabkan terjadinya delay terhadap tindakan operasi yang akan dilakukan.
Hasil studi pendahuluan di ruang rawat inap RS Islam A. Yani Surabaya melalui
wawancara dengan perawat ruang anak didapatkan data bahwa 4 dari 5 perawat ruangan
mengalami kesulitan dalam menghadapi pasien anak yang akan menjalani operasi. Anak
cenderung melakukan penolakan saat perawat akan mengukur tanda-tanda vital,
menginjeksi obat atau mengganti cairan infus. Hal lain juga dikemukakan oleh perawat
bedah RS Islam A. Yani Surabaya yaitu untuk melakukan tindakan operasi pada pasien
anak cenderung membutuhkan waktu yang sedikit lebih lama daripada pasien dewasa.
Mereka perlu menunggu hingga anak berhenti menangis dan mau untuk didekati
perawat. Kecemasan ini memberikan dampak negatif jangka panjang pada anak-anak
terhadap tindakan medis di kemudian hari. Kecemasan pre operasi pada anak usia pra
sekolah ini perlu diatasi dengan melakukan persiapan psikologis berbasis caring dan
diharapkan dapat menurunkan kecemasan pre operasi pada anak usia pra sekolah seperti
teori model keperawatan yang digambarkan oleh Kristen Swanson dalam teori caring.
Perawat memerlukan teknik komunikasi terapeutik yang efektif dalam setiap
tindakan yang akan diberikan kepada klien, selain itu diperlukan pula teknik non
farmakologis agar anak dapat bersikap kooperatif misalnya dengan teknik distraksi
(pengalihan) (Prasetyo, 2010). Salah satu teknik distraksi yang bisa dilakukan pada anak
adalah menonton kartun animasi (Wong, 2009). Ketika anak lebih fokus pada kegiatan
mononton film kartun, hal tersebut mengakibatkan impuls nyeri yang disebabkan
adanya cedera tidak mengalir melalui tulang belakang, pesan nyeri tidak tersampaikan
ke otak sehingga anak tidak merasakan nyeri (Brannon, 2013)
Terdapat beberapa macam persiapan psikologis guna mengurangi kecemasan pre
operasi pada anak pra sekolah, salah satunya ialah teknik non-farmakologi, seperti
kehadiran orang tua, musik, akupunktur, terapi bermain, bermain dengan mainan yang
sudah dikenal, dan menonton kartun (Potter, Perry, 2012). Amerika Academy of
Pediatrics merekomendasikan beberapa cara untuk mengurangi kecemasan dan
membantu anak-anak mengatasi stres rawat inap dan operasi, yaitu dengan pemberian
informasi, pendidikan kesehatan, dan membina hubungan saling percaya dengan anak-
anak dan orang tua mereka dengan menggunakan beberapa alat, seperti gambar,
diagram, boneka, orientasi tour area operasi atau ruang perawatan (Brown, 2012).
METODE PENELITIAN
Penelitian ini menggunakan desain quasi eksperimental dengan pendekatan pre
and post-test without control. Populasi yang digunakanadalam penelitian ini adalah
anak usia pra sekolah yang akan menjalani operasi di RS Islam A. Yani Surabaya.
Teknik pengambilan sampel menggunakan purposive sampling. Sampel dalam
penelitian ini ialah anak yang akan menjalani operasi di RS Islam A. Yani Surabaya
yakni sebanyak 30 anak yang dibagi menjadi 3 kelompok. Proses pengambilan data
dilakukan selama empat bulan. Instrumen yang digunakan ialah kuesioner HARS untuk
mengukur kecemasan anak usia pra sekolah.
Kriteria inklusi pada penelitian ini diantaranya anak usia 3-5 tahun, anak
menjalani rawat inap di rumah sakit minimal 1 hari sebelum jadwal operasi, anak yang
akan menjalani operasi sedang dan orang tua bersedia anak menjadi responden. Untuk
kriteria ekslusi pada penelitian ini adalah anak yang dilakukan operasi cito, anak yang
memiliki kelainan konginetal dan penyakit lainnya seperti sindrom down, tuna netra,

2019. Jurnal Keperawatan Silampari 3 (1) 332-341
335
dan sebagainya, serta kondisi anak sangat lemah sehingga tidak memungkinkan untuk
menonton video.
Penentuan kelompok kartun, animasi dan video+animasi dilakukan dengan cara
acak. Anak dengan jadwal operasi awal akan masuk dalam kelompok video kartun, anak
kedua akan masuk dalam kelompok video animasi, anak ketiga akan masuk dalam
kelompok video kartun+animasi, dan anak keempat akan masuk ke dalam kelompok
video kartun, begitu seterusnya. Sebelum dilakukan proses pengambilan data, orang tua
calon responden diberikan informasi tentang penelitian yang akan dilakukan,
keuntungan dan dampak yang mungkin dapat ditimbulkan selama proses penelitian, bila
orang tua calon responden menyetujuinya maka dilanjutkan dengan pengisian lembar
persetujuan menjadi responden. Kemudian dilakukan pengukuran kecemasan anak
sebelum intervensi menggunakan skala HARS 40 menit sebelum anak dibawa ke ruang
operasi.
Pada kelompok video kartun, anak diberi kesempatan memilih salah satu kartun
(bobo boy, tayo the little bus dan marsha and the bear) kemudian dilakukan pemutaran
video kartun selama 15 menit. Pada kelompok video animasi, dilakukan pemutaran
video animasi selama 15 menit. Pada kelompok kombinasi video kartun+video animasi,
anak diberi kesempatan memilih salah satu kartun (bobo boy, tayo the little bus dan
marsha and the bear) kemudian dilakukan pemutaran video kartun 15 menit dan video
animasi 15 menit. Setelah pemutaran video dilakukan pengukuran kecemasan anak
setelah dilakukan intervensi menggunakan skala HARS 5 menit sebelum anak masuk ke
ruang operasi.
HASIL PENELITIAN
Tabel. 1
Distribusi Frekuensi Responden (n=30)
No. Variabel Frekuensi Persentase (%)
1. Jenis Kelamin
- Video kartun
a. Laki-laki
b. Perempuan
- Video animasi
a. Laki-laki
b. Perempuan
- Video kartun+video animasi
a. Laki-laki
b. Perempuan
6
4
5
5
6
4
60
40
50
50
60
40
2. Riwayat operasi
- Video kartun
a. 0 b. 1
c. >1
- Video animasi
a. 0
b. 1
c. >1
- Video kartun+video animasi
a. 0
b. 1
c. >1
10 0
0
10
0
0
10
0
0
100 0
0
100
0
0
100
0
0

2019. Jurnal Keperawatan Silampari 3 (1) 332-341
336
Tabel 1 menunjukkan bahwa sebagian besar anak berjenis kelamin laki-laki. Pada
data riwayat operasi, seluruh responden belum memiliki riwayat operasi sebelumnya
yang artinya semua responden baru pertama kali menjalani operasi.
Tabel. 2
Distribusi Frekuensi Tingkat Kecemasan Sebelum Intervensi
Berdasarkan Jenis Kelamin (n=30)
Jenis
kelamin
responden
Kecemasan responden Total
Kecemasan sedang Kecemasan Berat
F % F % N %
Laki-laki 17 100 0 0 17 100
Perempuan 9 69,2 4 30,8 13 100
Total 26 86,7 4 13,3 30 100
Sumber : data primer, 2019
Tabel 2 menunjukkan terdapat 17 anak berjenis kelamin laki-laki termasuk dalam
kecemasan sedang. Pada anak yang berjenis kelamin perempuan, terdapat 9 anak
termasuk dalam kecemasan sedang dan 4 anak termasuk dalam kecemasan berat.
Tabel. 3
Perbedaan Rata-Rata Tingkat Kecemasan Pre Operasi pada Anak Usia Pra Sekolah
Sebelum dan Setelah Intervensi Menonton Video Kartun, Video Animasi,
Serta Kombinasi Video Kartun+Video Animasi (n=30)
Variabel Mean SD 95% CI p value n
a. Menonton video kartun
Tingkat kecemasan sebelum
Tingkat kecemasan setelah
Selisih
24,70
20,50
-4,20
2,111
2,506
3,258-5,142 0,000 10
b. Menonton video animasi
Tingkat kecemasan sebelum
Tingkat kecemasan setelah
Selisih
24,40
19,70
-4,70
1,767
2,058
3,529-5,871 0,000 10
c. Menonton video kartun+video animasi
Tingkat kecemasan sebelum
Tingkat kecemasan setelah Selisih
24,90
17.70 -7,20
1,729
1,567
5,947-8,453 0,000 10
Berdasarkan tabel 3 menunjukkan bahwa pada kelompok anak yang diberikan
intervensi menonton video kartun mengalami penurunan tingkat kecemasan pre operasi
sebesar 4,20. Hasil uji statistik didapatkan nilai p value = 0,000 dengan derajat
kepercayaan 95% (3,258-5,142), sehingga dapat disimpulkan bahwa ada perbedaan
antara tingkat kecemasan pre operasi pada anak sebelum dan setelah diberikan
intervensi menonton video kartun.
Tabel 3 juga menunjukkan bahwa pada kelompok yang diberikan intervensi
menonton video animasi terjadi penurunan tingkat kecemasan pre operasi sebesar 4,70.
Hasil uji statistik didapatkan nilai p value = 0,000 dengan derajat kepercayaan 95%
(3,529-5,871), sehingga dapat disimpulkan bahwa ada perbedaan antara tingkat
kecemasan pre operasi anak sebelum dan setelah diberikan intervensi menonton video
animasi.

2019. Jurnal Keperawatan Silampari 3 (1) 332-341
337
Tabel di atas juga menunjukkan bahwa pada kelompok anak dengan intervensi
kombinasi video kartun+video animasi terjadi penurunan tingkat kecemasan pre operasi
sebesar 7,20. Hasil uji statistik didapatkan nilai p value = 0,000 dengan derajat
kepercayaan 95% (5,947-8,453), sehingga dapat disimpulkan bahwa ada perbedaan
antara tingkat kecemasan pre operasi anak sebelum dan setelah diberikan intervensi
kombinasi video kartun+video animasi.
Berdasarkan penjelasan di atas, dapat diketahui bahwa penurunan tingkat
kecemasan pre operasi anak setelah diberikan video kartun lebih kecil daripada
penurunan tingkat kecemasan pre operasi anak setelah diberikan video animasi. Maka,
pemberian video animasi lebih efektif daripada video kartun dalam menurunkan tingkat
kecemasan pre operasi pada anak usia pra sekolah.
Untuk penurunan tingkat kecemasan pre operasi anak setelah diberikan video
kartun juga lebih kecil daripada penurunan tingkat kecemasan pre operasi anak setelah
diberikan kombinasi video kartun+video animasi. Maka, kombinasi video kartun+video
animasi lebih efektif daripada video kartun dalam menurunkan tingkat kecemasan pre
operasi pada anak usia pra sekolah. Untuk penurunan tingkat kecemasan pre operasi
anak setelah diberikan video animasi lebih kecil daripada penurunan tingkat kecemasan
pre operasi anak setelah diberikan kombinasi video kartun+video animasi. Maka,
kombinasi video kartun+video animasi lebih efektif daripada video animasi dalam
menurunkan tingkat kecemasan pre operasi pada anak usia pra sekolah.
Berdasarkan, ketiga intervensi di atas dapat disimpulkan bahwa intervensi
kombinasi video kartun+video animasi memiliki penurunan yang paling besar daripada
dua intervensi yang lain, sehingga intervensi kombinasi video kartun+video animasi
lebih direkomendasikan untuk digunakan dalam menurunkan tingkat kecemasan pre
operasi anak usia pra sekolah.
PEMBAHASAN
Jenis Kelamin
Hasil analisis didapatkan bahwa anak laki-laki yang termasuk dalam kecemasan
sedang ialah sebanyak 17 anak dan tidak ada yang termasuk dalam kecemasan berat,
sedangkan pada anak perempuan yang termasuk dalam kecemasan sedang ialah
sebanyak 9 anak dan yang termasuk dalam kecemasan berat sebanyak 4 anak. Potter,
Perry (2012) menyebutkan bahwa salah satu faktor yang mempengaruhi kecemasan
ialah jenis kelamin. Kecemasan lebih sering terjadi pada anak perempuan dibandingkan
anak laki-laki.
Hal ini karena laki-laki lebih aktif dan eksploratif sedangkan perempuan lebih
sensitif dan banyak menggunakan perasaan. Pada perempuan juga lebih mudah
dipengaruhi oleh tekanan-tekanan lingkungan daripada laki-laki, kurang sabar dan
mudah menggunakan air mata. Mudatsir (2010) menyatakan bahwa anak harus
mendapatkan penanganan medis dan tindakan operasi di rumah sakit yang mampu
menimbulkan kecemasan akan suasana rumah sakit.
Riwayat Operasi
Hubungan riwayat operasi dengan tingkat kecemasan pre operasi anak usia pra
sekolah dalam penelitian ini tidak dapat dianalisis karena semua responden belum
pernah menjalani operasi sehingga kali ini merupakan pengalaman pertamanya. Maka,
perlu adanya penelitian yang menggunakan responden yang variatif. Menurut Supartini
(2013) anak yang baru mengalami perawatan di rumah sakit akan berisiko menimbulkan

2019. Jurnal Keperawatan Silampari 3 (1) 332-341
338
perasaan cemas yang ditimbulkan baik oleh anak maupun orang tua. Berbagai kejadian
dapat menimbulkan dampak atraumatik terutama pada anak yang baru pertama kali
mengalami perawatan di rumah sakit, salah satunya karena adanya pengalaman interaksi
yang tidak baik dengan petugas kesehatan.
Hockberry, Wilson (2010) juga menyebutkan bahwa anak yang mempunyai
pengalaman sebelumnya akan mulai membentuk respon koping dibandingkan dengan
anak yang belum mempunyai pengalaman. Hal ini disebabkan karena anak yang pernah
dirawat sebelumnya di rumah sakit yang sama akan merasa lebih terbiasa dibandingkan
dengan yang baru pertama kali dirawat serta anak akan merespon sakitnya dengan lebih
positif. Hal ini juga didukung oleh Pelander, Leino-Kilpi (2010) menyebutkan bahwa
semakin sering anak berhubungan dengan rumah sakit maka semakin kecil bentuk
kecemasan atau sebaliknya.
Pengaruh Video Kartun terhadap Penurunan Tingkat Kecemasan Pre Operasi
pada Anak Usia Pra Sekolah
Hasil penelitian menunjukkan bahwa ada perbedaan tingkat kecemasan anak
sebelum dan setelah diberikan intervensi video kartun (p value = 0,000) dengan
penurunan nilai rata-rata tingkat kecemasan pre operasi anak sebesar 4,20. Video kartun
cocok digunakan untuk mendistraksi/mengalihkan rasa cemas anak menjelang operasi
(Noorlaila, 2010). Teknik distraksi yang dapat dilakukan untuk mengatasi kecemasan
anak yaitu melibatkan anak dalam permainan, karena bermain merupakan salah satu alat
komunikasi yang natural bagi anak-anak (Suryanti et al, 2011). Penelitian oleh Lee
(2012) menyatakan bahwa menonton video kartun oleh pasien bedah anak adalah
metode yang sangat efektif untuk mengurangi kecemasan pra operasi. Intervensi ini
merupakan metode yang murah, mudah dikelola, dan komprehensif untuk mengurangi
kecemasan dalam populasi bedah pediatrik.
Pengaruh Video Animasi terhadap Penurunan Tingkat Kecemasan Pre Operasi
pada Anak Usia Pra Sekolah
Hasil penelitian menunjukkan bahwa ada perbedaan tingkat kecemasan anak
sebelum dan setelah diberikan intervensi video animasi (p value = 0,000) dengan
penurunan tingkat kecemasan pre operasi anak sebesar 4,70. Penurunan tingkat
kecemasan pre operasi menggunakan video animasi ini lebih besar daripada pemberian
video kartun. Kecemasan pada anak timbul karena menghadapi sesuatu/lingkungan
yang baru dan belum pernah ditemui sebelumnya, serta ketidaknyamanan/ketakutan
terhadap sesuatu karena merasa bahaya dan menyakitkan (Townsend, 2009 dalam
Suprobo, 2017). Pada anak usia pra sekolah, ia akan beranggapan bahwa saat
dipindahkan ke ruang operasi hal tersebut merupakan sebuah hukuman baginya
sehingga timbul perasaan malu dan bersalah, merasa dipisahkan, merasa tidak aman dan
kemandiriannya terhambat (Hockenberry & Wilson, 2010).
Salah satu cara yang dapat digunakan perawat untuk mengurangi kecemasan pre
operasi anak ialah dengan pemberian informasi menggunakan beberapa alat, seperti
gambar, diagram, boneka, orientasi tour area operasi atau ruang perawatan (Brown,
2012). Tour area operasi yang dimodifikasi dengan menggunakan media video animasi
dapat memudahkan anak usia pra sekolah yang memiliki daya imajinasi tinggi untuk
mendapatkan informasi ringan berbasis menyenangkan, sekaligus menurunkan
kecemasan pre operasinya.

2019. Jurnal Keperawatan Silampari 3 (1) 332-341
339
Pengaruh Kombinasi Video Kartun+Video Animasi terhadap Penurunan Tingkat
Kecemasan Pre Operasi pada Anak Usia Pra Sekolah
Hasil penelitian menunjukkan bahwa ada perbedaan tingkat kecemasan anak
sebelum dan setelah diberikan intervensi video animasi (p value = 0,000) dengan
penurunan tingkat kecemasan pre operasi anak sebesar 7,20. Intervensi kombinasi video
kartun+video animasi ini memiliki penurunan tingkat kecemasan paling besar daripada
pemberian video kartun maupun video animasi.
Intervesi ini memiliki jenis video yang lebih bervariasi dan waktu penayangan
yang lebih lama, sehingga mampu lebih efektif dalam menurunkan tingkat kecemasan
pre operasi pada anak usia pra sekolah. Hal tersebut dikarenakan video kartun
menayangan tokoh kartun yang lucu dan disukai anak-anak sehingga membuat anak
merasa senang, terhibur dan melupakan rasa cemasnya menjelang operasi. Kemudian
penayangan video kedua yaitu video animasi tour area operasi dimana memudahkan
anak usia pra sekolah yang memiliki daya imajinasi tinggi untuk mendapatkan
informasi ringan mengenai situasi dan kondisi ruang operasi atau ruang perawatan
berbasis menyenangkan, sekaligus menurunkan kecemasan pre operasi anak dengan
mengatasi ketidaktahuan dan kewaspadaan anak terhadap ruang operasi/ruang
perawatan.
Sejalan dengan penelitian yang dilakukan oleh Fatmawati, Syaiful & Ratnawati
(2019) yang menyatakan bahwa ada pengaruh audiovisual menonton film kartun
terhadap tingkat kecemasan saat prosedur injeksi pada anak prasekolah. Hasil penelitian
ini juga sejalan dengan penelitian Wahyuningrum (2015) yang menyatakan bahwa
pemberian cerita melalui audiovisual efektif dalam menurunkan tingkat kecemasan pada
anak usia prasekolah yang mengalami hospitalisasi.
Apabila anak mengalami kecemasan tinggi saat dilakukan tindakan invasif,
kemungkinan besar tindakan yang dilakukan menjadi tidak maksimal dan tidak jarang
harus mengulangi beberapa kali sehingga akan menghambat proses penyembuhan anak.
Kondisi ini memper-sulit perawat dalam melakukan tindakan keperawatan (Supartini,
2014).
Koller, Goldman (2012) dalam studinya menyatakan bahwa pemberian cerita
melalui audiovisual guna menurun-kan kecemasan termasuk teknik distraksi kecemasan
dengan teknik audiovisual. Perhatian anak yang terfokus kepada cerita audiovisual yang
disimaknya mendis-traksikan atau mengalihkan persepsi kecemasan anak dalam korteks
serebral. Dengan intervensi audiovisual menonton film kartun akan memberikan
rangsangan distraksi berupa visual, auditory dan tactile. Perasaan aman dan nyaman
yang dirasakan anak akan merangsang tubuh untuk mengeluarkan hormon endorphine.
SIMPULAN
Berdasarkan hasil penelitian dapat disimpulkan bahwa terdapat perbedaan rata-
rata tingkat kecemasan pre operasi anak sebelum dan setelah diberikan video kartun (p
value = 0,000, selisih = 4,20), setelah diberikan video animasi (p value = 0,000, selisih
= 4,70), dan setelah diberikan kombinasi video kartun+video animasi (p value = 0,000,
selisih = 7,20).

2019. Jurnal Keperawatan Silampari 3 (1) 332-341
340
SARAN
Perawat diharapkan dapat menerapkan pemberian kombinasi video kartun+video
animasi untuk anak usia pra sekolah yang akan menjalani operasi. Intervensi ini
merupakan salah satu tindakan atraumatic care berbasis caring. Bagi peneliti
selanjutnya diharapkan dapat mempertimbangkan jumlah sampel yang lebih besar,
karakteristik responden yang lebih variatif dari sisi pengalaman operasi sebelumnya,
jenis operasi yang sama dan penggunaan instrumen lain untuk mengukur tingkat
kecemasan pada anak.
DAFTAR PUSTAKA
Alini, A. (2017). Pengaruh Terapi Bermain Plastisin (Playdough) terhadap Kecemasan
Anak Usia Pra Sekolah (3-6 Tahun) yang Mengalami Hospitalisasi di Ruang
Perawatan Anak RSUD Bangkinang. Jurnal Ilmu Kedokteran, 1(2), 4-7
Astarani, K. (2017). Hospitalisasi & Tempat Bermain pada Anak. Adjie Media
Nusantara, Nganjuk
Brannon, L., Feist, J., & Updegraff, J. A. (2013). Health Psychology: An Introduction to
Behavior and Health, Eight Edition. USA: Wadsworth
Brown, J. (2012). Effects of Group Medical Play on Reducing Stress, Fear, and Anxiety
in Children. Master’s thesis The University of Alabama
Ekawati, D., Rosyidah, I., Sumarsono. (2017). Pengaruh Distraksi Menonton Animasi
Kartun terhadap Tingkat Stress Hospitalisasi pada Anak Saat Dilakukan Injeksi
Bolus. Skripsi. Stikes Insan Cendekia Medika Jombang
Fatmawati, L., Syaiful, Y., & Ratnawati, D. (2019). Pengaruh Audiovisual Menonton
Film Kartun terhadap Tingkat Kecemasan saat Prosedur Injeksi pada Anak
Prasekolah. Jurnal Ilmiah Kesehatan (Journal of Health Sciences), 12(2), 15-29
Gracia, Mia. (2015). Hypnosis In Destistry. Jakarta: PT. Gramedia Pustaka Utama
Hockenberry, J. M. & Wilson D. (2010). Wong’s essentials of pediatric nursing. Mosby
Elsevier, Philadelphia
Koller & Goldman. (2012). Pediatric Psychosocial Oncology: Textbook for
Multidisciplinary Care, USA: Springer
Lee, J., Jihye L.S., Hyungsun L. S., & Jun-Rae L. (2012). Cartoon Distraction
Alleviates Anxiety in Children during Induction of Anesthesia. International
Anesthesia Research Society, 115(5), 1168-1173
Mudatsir. (2010). Spiritual Emotional Freedom Technique dan Nyeri Pasien Pasca
Operasi Fraktur Femur. Jurnal Terpadu Ilmu Kesehatan, 45-49
Noorlaila, I. (2010). Panduan Lengkap Mengajar PAUD. Yogyakarta: Pinus Book
Publisher
Papalia, D. E., Sally, W. O., & Ruth, D. F. (2010). Human Development (Psikologi
Perkembangan) Bag. I-IV. Jakarta: Salemba Humanika
Pelander & Leino. K. (2010). Empirical Studies: Children’s Best and Worst
Experiences during Hospitalization. Finland Scand Journal Caring Sci, 12(4),
347-356
Pontoh, B. I., Damajanti, H.C.P, & Ni Wayan, M., 2015. Hubungan Tingkat Kecemasan
dengan Perubahan Denyut Nadi Pada Pasien Ekstraksi Gigi di Puskesmas
Tuminting Manado, Jurnal e-GiGi, 3(1): 13-17
Prasetyo, S. N. (2010). Konsep dan Proses Keperawatan Nyeri. Jakarta: Graha Ilmu
Potter & Perry. (2012). Fundamental of Nursing. Jakarta: Salemba Medika
Priece & Moreno. (2012). At a Glance Ilmu Bedah. Edisi Ketiga. Jakarta: EGC

2019. Jurnal Keperawatan Silampari 3 (1) 332-341
341
Putra, S.T. (2011). Psikoneuroimunologi kedokteran. Surabaya: AUP
Rehatta, V.C., Joyce, K, & Paulina, N.G., 2014. Gambaran Kecemasan Tindakan Dental
Anak di Puskesmas Bahu Manado, Jurnal e-GiGi, 2(2), 1-6
Sjamsuhidajat, R., & De jong, W. (2010). Buku Ajar Ilmu Bedah. Jakarta: EGC
Stuart & Laraia. (2005). Buku Saku Keperawatan Jiwa, Edisi 5. Jakarta: EGC
Supartini, Y. (2013). Konsep Dasar Keperawatan Anak. Jakarta: EGC
Supartini. (2014). Buku Ajar Konsep Dasar Keperawatan Anak. Jakarta: EGC
Suprobo, G. N. P. (2017). Pengaruh Terapi Audio Visual terhadap Penurunan Tingkat
Kecemasan pada Anak Preschool yang Dilakukan Pemasangan Infus di UGD
RSUD Wates. Jurnal Keperawatan
Suryanti., Sodikin., & Yulistiani. (2011). Pengaruh Terapi Bermain Mewarnai dan
Origami terhadap Tingkat Kecemasan sebagai Efek Hospitalisasi pada Anak Usia
Pra Sekolah di RSUD Dr. R. Goetheng Tarunadibrata Purbalingga. Jurnal
kesehatan
Utami, Y. (2014). Dampak Hospitalisasi terhadap Perkembangan Anak. Jurnal Ilmiah
Widya, 2(2), 9-20
Wahyuningrum I, (2015). Pengaruh Cerita Melalui Audiovisual terhadap Tingkat
Kecemasan Anak Usia Prasekolah yang Mengalami Hospitalisasi di RSU PKU
Muhmmadiyah Bantul. Skripi S1 Program Studi Ilmu Keperawatan STIKES
‘Aisyiyah Yogyakarta
Wijayanti, R. (2011). Pengaruh Pemberian Terapi Murottal terhadap Tingkat
Kecemasan pada Pasien Pre Operasi di Ruang Rawat Inap Kelas III RS PKU
Muhammadiyah Yogyakarta. Jurnal STIKES
Wong, L. D. (2009). Pedoman Klinis Keperawatan Pediatrik. Jakarta: EGC




















