
Diagnostic Decision Making in Oncology: Creating Shared Knowledge and Managing Complexity

KON3: a Clinical Decision Support System, in oncology environment, based on knowledge management
Michele Ceccarellia, Antonio Donatiellob, Dante Vitaleb
a University Of Sannio, RCOST (Research Centre On Software Technology), Benevento, 82100 Italy
b Unlimited Software S.r.l., Napoli, 80143 Italy
e-mail: [email protected], [email protected], [email protected]
Abstract
The application of scientific methodology to clinical practice is typically realized through recommendations, policies and protocols represented as Clinical Practice Guidelines (CPG). CPGs have the purpose to help the clinicians in their choices and to improve the patient care process.
The representation of Guidelines and their introduction in medical information system can lead to efficient Clinical Decision Support Systems (CDSS), however this poses several interesting challenges as it involves problems of knowledge representation, inference, workflow definition, access to unstructured databases of medical records and others.
In this paper we analyze the approaches and methods in computer-based CPG realization, and then we illustrate the choices (tools, architecture and clinical domain) to realize KON3 System.
KON3 purpose is to achieve a CDSS based on guideline and semantic information representation, in oncology environment.
Keywords: CDSS (Clinical Decision Support System), Ontology, OWL (Ontology Web Language), Protégé, SWRL (Semantic Web Rule Language) JESS (Java Expert System Shell), HER (Health Electronic Record), KON3 (Knowledge ON ONcology through ONtology), GLIF (Guideline Interchange Format)
1. Introduction The importance of clinical practice guidelines (CPG) has been widely recognized and clinicians are increasingly consulting such guidelines for decision support during patient encounters [1,2]. However, the main obstacle to the wide adoption of shared guidelines consists into the fact that most CPG are typically available as test (pdf files, web pages, charts, diagrams, etc…). Therefore, clinicians must consult the appropriate guideline and then determine how the guideline recommendations apply
to the patient at hand. In order to reducing the variability of care and by reducing omission of recommended best treatment practices the use of CPG should be encouraged and their use should be as simple and automated as possible [2,3]. Several studies have recently emerged in literature proposing decision support systems that use the guidelines as the knowledge base and the clinical information system as the source of instances for the inference engine [4] and several computer-based clinical decision support systems (CDSSs) embodying specific guidelines have been developed to facilitate timely decision support for clinicians. In order to be integrated into the clinical workflow, the guideline based approach should be depend on the specific patient and pathology at the hand. This implies that the CDSS should be an integral part of the clinical information system and the inference engine must be linked with all available clinical records of the patient [5]. Indeed, the wide-spread distribution and use of computable CPG content can be improved if the research community focuses on lack of standards for representing medical knowledge, and on the prohibitive complexity and expense required to adapt encoded guideline content across the heterogeneity of data structures, semantics, and medical vocabularies in use in the nation’s health care information systems. The main objective of the KON3, a joint effort among companies, university and regional government agencies is the development of technologies for a sharable knowledge based on CPG at a reasonable cost and effort, and in a form that can be integrated gracefully and supportively into the clinician’s workflow via functions of the local clinical information system. The main features of KON3 is the adoption an Ontology based on representation of the guidelines in addition to a registry, based healthcare information infrastructure, which is based on standard being implemented at a regional and national level in Italy. The paper is organized as follows: the next section reports some of the principal approaches proposed in literature to try to standardize and share
clinical knoin the third s 2. Approa
In litera
developing example theof a platforeffective an(EHRs). Threquirement
• Abincimapatins
• Arcsysdefof
• Mearc
These re
which is Alanguage ca
• De• De• Per• De
Fig. 1 – On
An examinformationthrough ADdefine someorder to get
The apprfigure 2.
owledge from section the KO
aches and m
ature, there of computer
e system in [6rm, of which nd interoperabhe platform ts: bility to reccluding comaging, diagnostient educatistructions; chetype and stems, empowfine the contesystems indepessaging basedchetypes” and
quirements arADL (ArchTyan: efine ontologyefine constrainrform query;
efine HL7 tem
ntology based ap
mple of this appn are organiDL language. e constraints, a decision suproach propos
evidence basON3 overview
methods
are a lot r-based guide] is dedicated a major com
ble electronicshould supp
cord any climplex time-b
ses, care pon material,
template-enabwering clinicalent, semantics pendently fromd on HL7, viasystematic m
re based on a ype Definition
y; nts;
mplate;
pproach: architelanguage
proach is showized in sem
With ADL that they’re pport. ed in [7] is
sed medicine,w is reported.
of approacheline systemsto the develo
mponent is clin healthcare rorts the foll
inical informased lab r
plans, evalua workflow
bling of all c professionalsand user inte
m the softwarea the use of “l
mapping definit
new languagen Language)
ecture based on A
wn in figure 1mantic relatio
is also possidefine as ru
sketched sho
while
hes in s. For
opment nically ecords lowing
mation, results, ations, based
clinical s to erfaces e; legacy tions;
e type, . This
ADL
1. User nships ible to les, in
own in
F
fo
oneninenmelspac
ar
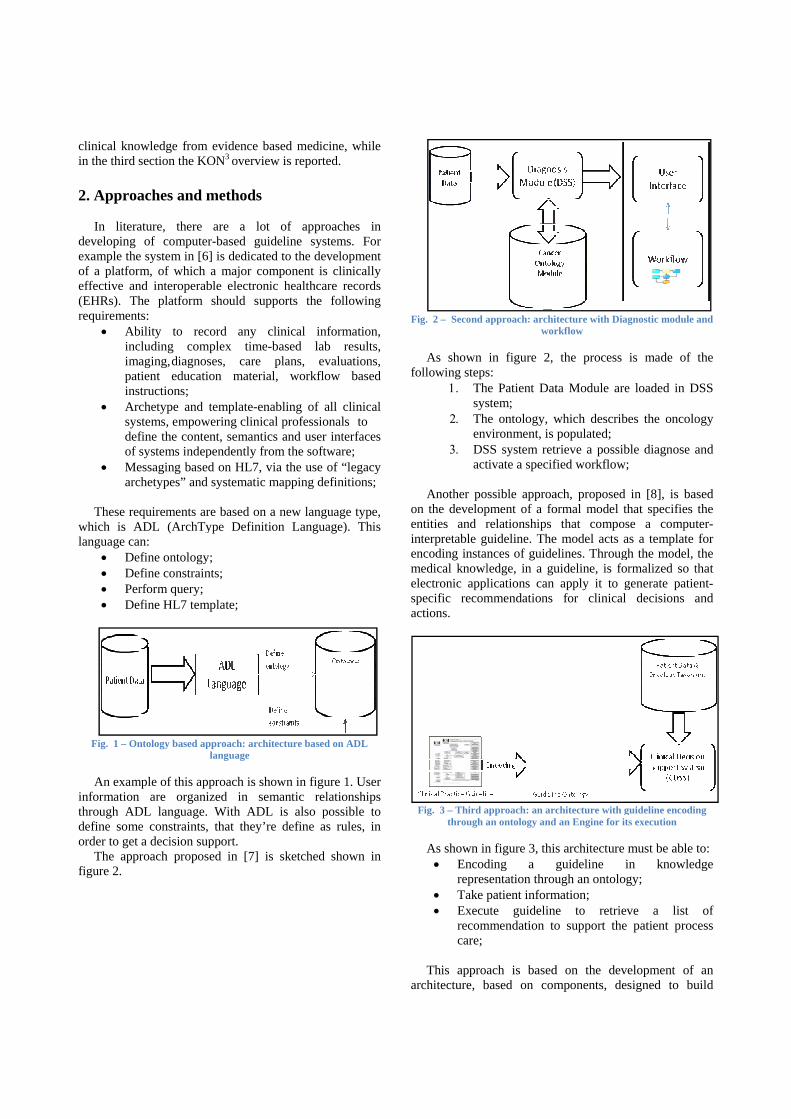
ig. 2 – Second a
As shown ollowing steps
1. Thsys
2. Thenv
3. DSact
Another po
n the developntities and rnterpretable gncoding instan
medical knowllectronic applpecific recomctions.
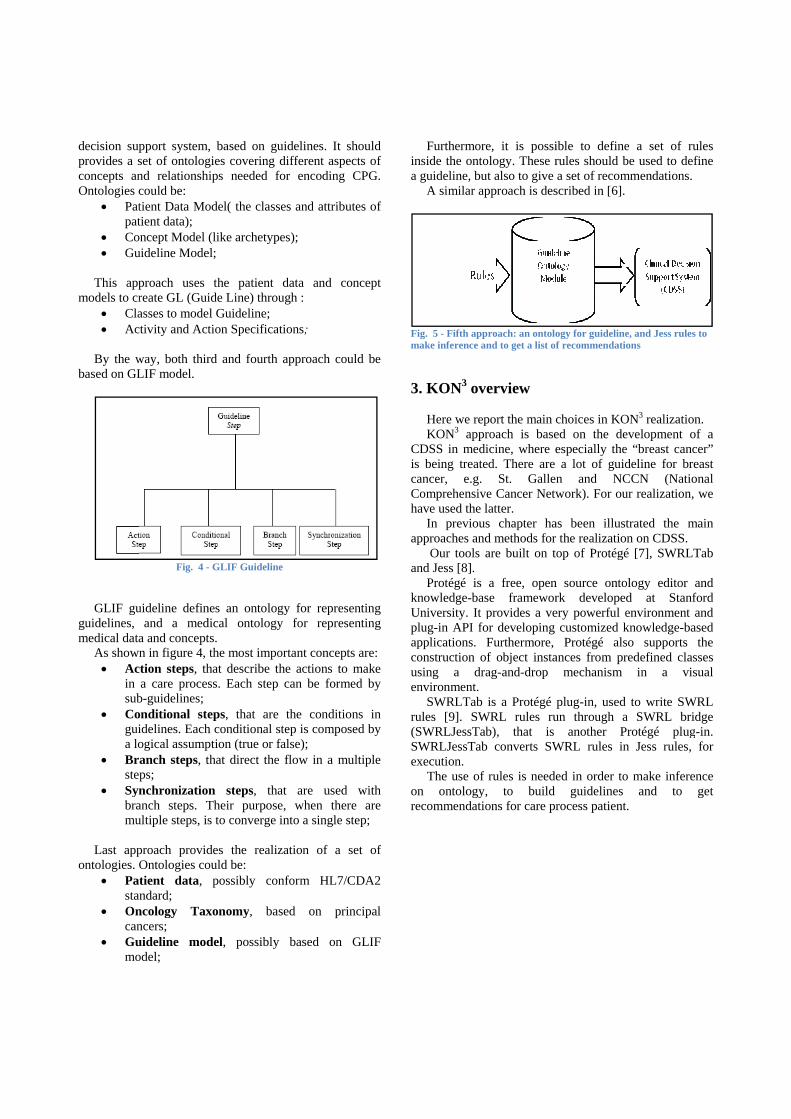
Fig. 3 – Third athrough a
As shown in• Encod
repres• Take p• Execu
recomcare;
This appro
rchitecture, b
approach: archiwor
in figure 2, s:
he Patient Datstem;
he ontology, wvironment, is SS system retrtivate a specif
ssible approapment of a forelationships
guideline. Thences of guideledge, in a gulications can mmendations
approach: an arcan ontology and
n figure 3, thisding a gsentation throupatient inform
ute guidelinemmendation to
ach is basedbased on com
tecture with Diarkflow
the process
ta Module are
which describpopulated; rieve a possib
fied workflow
ach, proposed ormal model t
that compose model acts aelines. Througuideline, is fo
apply it to gfor clinical
chitecture with gan Engine for it
s architecture guideline iugh an ontolo
mation; e to retrieo support the
d on the devmponents, de
agnostic module
is made of
e loaded in D
bes the oncolo
ble diagnose a;
in [8], is bathat specifies se a compuas a template gh the model, ormalized so tgenerate patiel decisions a
guideline encodits execution
must be able in knowledgy;
eve a list e patient proc
velopment of esigned to bu
and
the
DSS
ogy
and
ased the ter-for the
that ent-and
ng
to: dge
of cess
an uild
decision supprovides a sconcepts anOntologies c
• Patpat
• Co• Gu
This app
models to cr• Cla• Ac
By the w
based on GL
GLIF gu
guidelines, medical data
As shown• Ac
in sub
• Coguia lo
• Brste
• Synbramu
Last app
ontologies. O• Pa
sta• On
can• Gu
mo
pport system,set of ontolognd relationshicould be: tient Data Motient data);
oncept Model (uideline Mode
proach uses reate GL (Guiasses to modectivity and Act
way, both thirLIF model.
Fig. 4 -
uideline definand a med
a and conceptn in figure 4,
ction steps, tha care proces
b-guidelines; onditional steidelines. Eachogical assumpanch steps, tps; nchronizationanch steps. Tultiple steps, is
proach providOntologies cotient data,
andard; ncology Taxncers; uideline mododel;
, based on gugies covering ips needed f
odel( the class
(like archetypel;
the patient ide Line) throul Guideline; tion Specifica
rd and fourth
- GLIF Guidelin
nes an ontologdical ontologyts. the most impo
hat describe tss. Each step
eps, that areh conditional sption (true or fthat direct the
n steps, thaTheir purposes to converge
des the realizould be:
possibly con
xonomy, ba
del, possibly
uidelines. It sdifferent aspe
for encoding
ses and attribu
pes);
data and cough :
ations;
approach cou
e
gy for represy for repres
ortant conceptthe actions to can be form
e the conditiostep is compofalse); e flow in a m
at are used e, when therinto a single s
zation of a
nform HL7/C
sed on pri
y based on
should ects of
CPG.
utes of
oncept
uld be
senting senting
ts are: make
med by
ons in sed by
multiple
with re are step;
set of
CDA2
incipal
GLIF
ina
Fim
3
CiscaCh
ap
an
knUpapcouen
ru(SSex onre
Furthermorenside the ontoguideline, bu
A similar ap
ig. 5 - Fifth appmake inference an
3. KON3 ove
Here we repKON3 appr
CDSS in medis being treateancer, e.g.
Comprehensiveave used the l
In previouspproaches and
Our tools and Jess [8].
Protégé is knowledge-basUniversity. It plug-in API fopplications. Fonstruction osing a dranvironment.
SWRLTab ules [9]. SWSWRLJessTabWRLJessTabxecution. The use of
n ontology,ecommendatio
e, it is possiology. These rut also to give pproach is des
proach: an ontolond to get a list of
erview
port the main croach is baseicine, where eed. There are
St. Gallene Cancer Netwlatter. s chapter had methods for are built on to
a free, opense frameworprovides a ve
or developing Furthermore, f object instaag-and-drop
is a Protégé pWRL rules ru
b), that is b converts SW
rules is neede, to build ons for care pr
ible to definerules should ba set of recom
scribed in [6].
ogy for guidelinef recommendati
choices in KOed on the deespecially thea lot of guid
n and NCwork). For ou
as been illustthe realizatio
op of Protégé
n source ontork developeery powerful e
customized kProtégé als
ances from prmechanism
plug-in, used un through a
another PWRL rules in
ed in order toguidelines
rocess patient
e a set of rube used to defmmendations.
e, and Jess rulesons
ON3 realizationevelopment oe “breast cancdeline for breCCN (Natiour realization,
trated the mon on CDSS. é [7], SWRLT
ology editor ad at Stanfenvironment aknowledge-baso supports redefined clas
in a vis
to write SWa SWRL bridProtégé plugn Jess rules,
o make infereand to
t.
ules fine
s to
n. of a cer” east onal
we
main
Tab
and ford and
ased the
sses sual
WRL dge
g-in. for
nce get
3.1 KON3
In figuredistinguish f
• Disdisinffor
• Semont
• Knknolay
• Wogui
• Intcon
3.2 KON3
In this pa
As show
the ontology
architecture
Fig. 6 - K
e 6 is shownfour levels: stributed Dstributed databformation canrmat; mantic layertologies:
o Patient o Oncoloo Guideli
nowledge Seowledge from
yer, is to run tho Make ino Create o Get rec
orkflow systeideline; terface layenfiguration int
ontology
aragraph is pre
Fig. 7 - Guide
wn in figure 7, y.
e
KON3 architectu
n a KON3 ar
ata Layer, base of patienn be represe
r, that repre
ontology; ogy Taxonomyine Model; ervice layer,
m ontology. Anhe rules in ordnference; guideline;
commendationem, is an alter
er, as a wterface.
esented the re
line concept in o
there’s a “Gu
ure
chitecture. W
that represnt informationent in HL7/C
sent the foll
y;
, used to enother scope, der to:
ns; rnative to the
web interface
ealized ontolog
ontology
uideline” conc
We can
ent a n. The CDA2
lowing
extract of this
single
e and
gy.
cept in
AacprP“Dd
Ta ca
an
A guideline• contex• tasks:
o
o
Therefore,
Actions and Dctions to be rincipal phas
Primary treatDecision” coecision”. This
In figure 8There’s a “sup
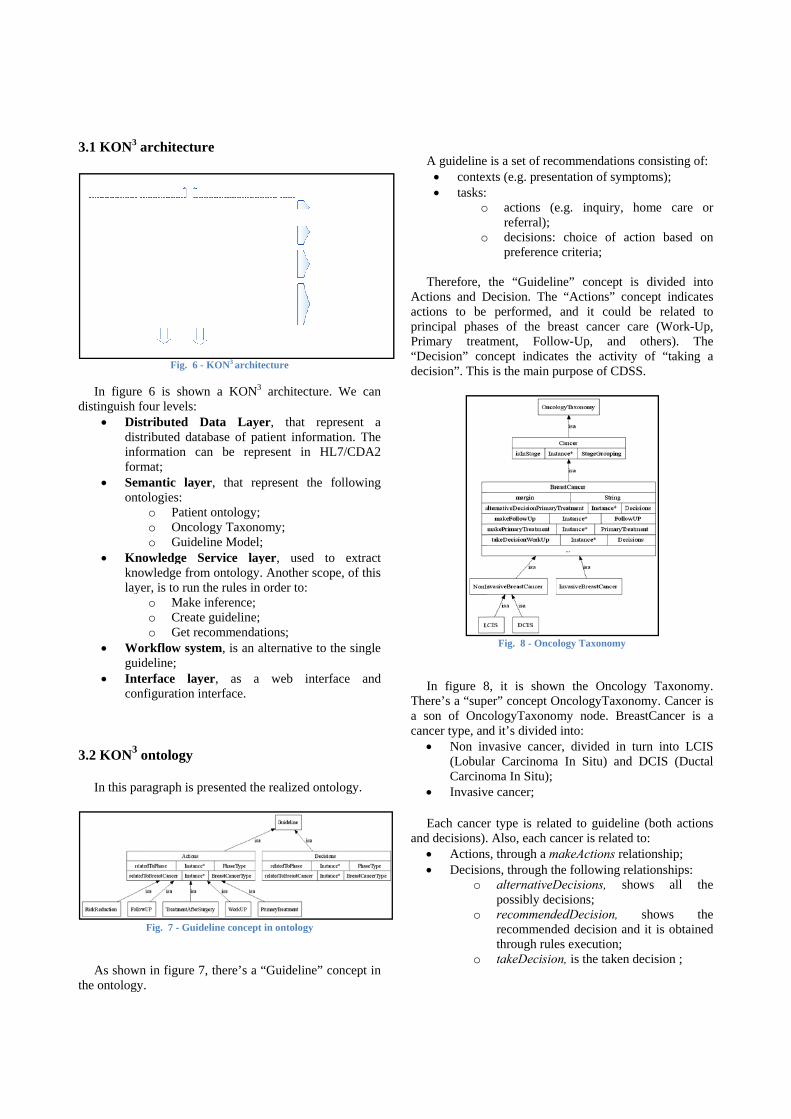
son of Oncancer type, an• Non in
(LobulaCarcino
• Invasiv
Each cancend decisions).• Actions• Decisio
o
o
o
e is a set of recxts (e.g. prese
o actions (ereferral);
o decisions: preference
the “GuideliDecision. The
performed, ses of the brtment, Follo
oncept indicats is the main p
Fig. 8 - Onco
8, it is shower” concept O
cologyTaxonond it’s dividednvasive cancear Carcinomaoma In Situ);ve cancer;
r type is relat. Also, each cas, through a mons, through th
alternativeDpossibly decrecommendrecommendthrough ruletakeDecisio
commendationentation of sym
e.g. inquiry,
choice of ae criteria;
ne” concept e “Actions” c
and it couldreast cancer ow-Up, and tes the activipurpose of CD
ology Taxonomy
wn the OncolOncologyTaxomy node. Br
d into: er, divided in a In Situ) an
ted to guideliancer is relate
makeActions rehe following rDecisions, scisions;
dedDecision, ded decision aes execution; on, is the taken
ns consisting omptoms);
home care
action based
is divided iconcept indicad be related care (Work-U
others). Tity of “taking
DSS.
logy Taxonomonomy. CancereastCancer i
turn into LCd DCIS (Duc
ine (both actied to: elationship; relationships:shows all
shows and it is obtain
n decision ;
of:
or
on
into ates
to Up, The g a
my. er is s a
CIS ctal
ons
the
the ned

3.3 KON3 rules in DCIS domain
As stated in the previous paragraph, it’s necessary, now, to develop a set of rules in order to create guideline, both for actions and decisions. The domain is DCIS.
In DCIS, a possible set of actions is the following:
Fig. 9 - An action lists in DCIS Work-Up phase
In figure 9 is shown an action lists in DCIS Work-Up
phase. If there’s a patient, who was diagnosed a DCIS, then in Work-Up phase is necessary to make:
• Medical history and physical exam; • Diagnostic mammogram; • Pathology review; • Measure hormone receptor of tumor;
After Work-Up action, it’s necessary to take decision
among the following options: • Complete surgical excision; • Patient prefers mastectomy; • DCIS in two or more separate areas of the breast;
A possible SWRL rule is the following:
PatientData(?patient) hasDiagnosed(?patient, ?cancer) DCIS(?cancer) isInStage(?cancer, Stage0)
→ makeWorkUp(?cancer, H&P) makeWorkUp(?cancer, Diagnostic Mammogram) makeWorkUp(?cancer, Measure hormone receptor of tumor) makeWorkUp(?cancer, Pathology review) alternativeDecisionWorkUp(?cancer, Complete surgical excision) alternativeDecisionWorkUp(?cancer, Patient prefer mastectomy) alternativeDecisionWorkUp(?cancer, DCIS in two or more separate area of the breast)
In SWRL rule, it’s possible to notice that if exist a Patient (PatientData (?patient)), who was diagnosed a DCIS cancer, then it’s necessary to make some actions (through makeWorkUp relationship) and take some decisions among those illustrated in alternativeDecisionWorkUp relationship.
In DCIS, a possible list of recommendations is the
following: A. The NCCN recommends a pathology review
(another pathologist to look at the biopsy sample) to be certain that you have DCIS and not an invasive cancer or other condition;
B. If DCIS is present in only one area and no cancer is found at the edges of the first surgical excision, the surgical options are either a total mastectomy or a lumpectomy;
C. If a lumpectomy is chosen, then radiation therapy to the whole breast with a boost to the site of the tumor may or may not be done depending on several factors, such as woman’s age, other health problems, certain characteristics of the tumor, and the woman’s preference;
D. Mastectomy is recommended if the margins of the excision contain cancer and, even with repeat surgery, the DCIS cannot be completely removed;
E. If the mammogram, physical examination or biopsy results show that two or more separate areas of the breast contain DCIS, mastectomy is recommended;
F. After lumpectomy, a mammogram is suggested to ensure that the entire tumor has been removed;
PatientData(?patient) hasDiagnosed(?patient, ?cancer) DCIS(?cancer) isInStage(?cancer, Stage0) StageGrouping(Stage0) takeDecisionWorkUp(?cancer, ?decision) margin(?cancer, "positivo") numeroRipetizioniChirurgia(?cancer, ?numRip) swrlb:greaterThan(?numRip, 2) → recommendedDecisionPrimaryTreatment(?cancer, Total Mastectomy)
In this rule is mapped D recommendation.
4. Conclusions
In this paper, we have shown the main approaches to realization, computer based, of a CDSS. Our approach is based on development of an ontology for patient data, guideline and oncology taxonomy. The ontology includes a set of rules to build both specifies guideline and decision support systems, in order to get recommendations, and to help clinicians in their choices. 5. References
[1] J. A. Muir Gray, Evidence Based Healthcare, W.B. Saunders Company, 1997
[2] E. A. McGlynn , S.M. Asch, J. Adams, J. Keesey, J. Hicks, A. DeCristofar, and E.A. Kerr, “The quality of health care delivered to adults in the United States,” New England Journal of Medicine. 348(26), 2003, 2635-2645.
[3] M. Peleg, S. Tu, J. Bury, P. Ciccarese, J. Fox, R.A. Greenes, R. Hall, P.D. Johnson, N. Jones, A. Kumar, S. Miksch, S.Quaglini, A. Seyfang, E.H. Shortliffe, and M. Stefanelli, “Comparing computer-interpretable guideline models: a case-study approach,” Journal of the American Medical Informatics Association, 10(1), 2003, 52-68
[4] S. Quaglini, M. Stefanelli, A. Cavallini, G. Micieli, C. Fassino and C. Mossa, “Guideline based careflow systems,” Artificial Intelligence in Medicine, 20(1) 2000, 5-22.
[5] M. K. Goldstein, et al. “Translating Research into Practice: Organizational Issues in Implementing Automated Decision Support for Hypertension in Three Medical Centers”, Journal of Am. Med. Informatics Assoc., vol. 11, pp. 368-376, (2004).
[6] T. Beal, S. Heard, “An Ontology-based Model of Clinical Information”, MEDINFO2007, IOS Press.
[7] J. Siddiqi et al. “Towards and Automated Diagnosys for the Treatment of Colon Cancer: Position and Progress”, IEEE AICS2006, IEEE Press. http://www.match-project.com/
[8] Tu SW, Campbell JR, Musen MA. “SAGE Guideline Modeling: Motivation and
Methodology”. In: Kaiser K, Miksch S, Tu SW, editors. Computer-Based Support for Clinical Guidelines and Protocols: Proceedings of the Symposium on Computerized Guidelines and Protocols (CGP-2004): IOS Press; 2004. pp. 167-171.http://sage.wherever.org
[9] R. D. Shankar, S. W. Tu, S. B. Martins, L. M. Fagan, M. K. Goldstein, M. A. Musen. “Integration of Textual Guideline Documents with Formal Guideline Knowledge Bases”. AMIA 2001, 2001, http://www.smi.stanford.edu/projects/eon/
[10] Chiehfen Chen, Kung Chen, Chung-Hsin Chen, Welen Tsai, and Yu-Chuan Li: “Synthesizing Guideline-Based Decision Support System using Protégé and Jess”, Proceedings of Medical Information Systems in taiwan, 2005.
[11] N. F. Noy, R. W. Fergerson, M. A. Musen, “The knowledge model of Protege-2000: Combining interoperability and flexibility,” 2nd International Conference on Knowledge Engineering and Knowledge Management (EKAW'2000), France, 2000.
[12] Jess, the Rule Engine for the Java Platform. http://herzberg.ca.sandia.gov/jess/
[13] W3C, SWRL (Semantic Web Rule Language). http://www.w3.org/Submission/SWRL/
Copyright © 2022 FDOKUMEN




















