Julie K - Institute of Lifestyle Medicine
506
Lifestyle Medicine 2015: Tools for Promoting Healthy Change Agenda Saturday, June 27, 2015 7:00–7:45 Registration/Continental Breakfast 7:15–7:45 Meet and Greet 7:45–8:45 Lifestyle Medicine: True Healthcare Reform David L. Katz, MD, MPH 8:45–10:15 The Lifestyle Medicine Dream Team Physician Social Worker Exercise Physiologist Health Coach Dietitian Elizabeth P. Frates, MD, Moderator Kriston Kent, MD, MPH Karen Lane, LICSW Cedric Bryant, PhD Heidi Duskey, MA Debra Wein, MS, RDN, LDN, NSCA-CPT*D, CWPD 10:15–10:30 Invigoration Break 10:30–11:45 Practitioner-to-Practitioner: Lessons Learned and Successes Earned by Early Adopters Elizabeth P. Frates, MD, Moderator Amira Aly, MD Reza Antoszewska, NP-C Karyn Bender, RPh, CHHC Barbara Brown, MD and Lynn Kossow, MD Rebecca Brown, MD and Larry Schmidt, MD Lilach Malatskey, MD, MHA Krutika Parasar, SciB Karen M. Sherritt, MD 11:45–12:45 Lunch (on your own) 12:00–12:45 Optional Lunch-and-Learn Forum: Billing and Coding for Lifestyle Medicine Nancy M. Enos, FACMPE, CPMA,CPC-I, CEMC 12:45–1:45 Motivational Interviewing: The Evidence-Based Strategies that Produce the Best Results Joji Suzuki, MD 1:45–2:45 Sleep Sat Bir Singh Khalsa, PhD 2:45–3:00 Meditation break (optional) Sat Bir Singh Khalsa, PhD 3:00–4:00 Obesity and Sleep Fatima Cody Stanford, MD, MPH 4:00–5:00 What Really Gets Patients (Even Reluctant Ones) to Effect Healthy Change Cheri Blauwet, MD
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Julie K - Institute of Lifestyle Medicine

Lifestyle Medicine 2015: Tools for Promoting Healthy Change Agenda
Saturday, June 27, 2015
7:00–7:45 Registration/Continental Breakfast
7:15–7:45 Meet and Greet
7:45–8:45 Lifestyle Medicine: True Healthcare Reform
David L. Katz, MD, MPH
8:45–10:15 The Lifestyle Medicine Dream Team
Physician Social Worker
Exercise Physiologist Health Coach
Dietitian
Elizabeth P. Frates, MD, Moderator Kriston Kent, MD, MPH Karen Lane, LICSW Cedric Bryant, PhD Heidi Duskey, MA Debra Wein, MS, RDN, LDN, NSCA-CPT*D, CWPD
10:15–10:30 Invigoration Break
10:30–11:45 Practitioner-to-Practitioner: Lessons Learned and Successes Earned by Early Adopters
Elizabeth P. Frates, MD, Moderator Amira Aly, MD Reza Antoszewska, NP-C Karyn Bender, RPh, CHHC Barbara Brown, MD and Lynn Kossow, MD Rebecca Brown, MD and Larry Schmidt, MD Lilach Malatskey, MD, MHA Krutika Parasar, SciB Karen M. Sherritt, MD
11:45–12:45 Lunch (on your own)
12:00–12:45
Optional Lunch-and-Learn Forum: Billing and Coding for Lifestyle Medicine
Nancy M. Enos, FACMPE, CPMA,CPC-I, CEMC
12:45–1:45 Motivational Interviewing: The Evidence-Based Strategies that Produce the Best Results
Joji Suzuki, MD
1:45–2:45 Sleep Sat Bir Singh Khalsa, PhD
2:45–3:00 Meditation break (optional) Sat Bir Singh Khalsa, PhD
3:00–4:00 Obesity and Sleep Fatima Cody Stanford, MD, MPH
4:00–5:00 What Really Gets Patients (Even Reluctant Ones) to Effect Healthy Change
Cheri Blauwet, MD

David L. Katz, MD, MPH
Lifestyle Medicine:
True Healthcare Reform

Lifestyle as Medicine: a GLiMMER of hope?
David L. Katz, MD, MPH, FACPM, FACP
Director, Prevention Research Center
Yale University / Griffin Hospital
President, American College of Lifestyle Medicine
Editor-in-Chief, Childhood Obesity
Author, Disease Proof
Harvard
6-15

The Blind Men and the Elephant
-John Godfrey Saxe

Out of the Woods-
The Elephant in the Room
The Peril, Promise, & Problem
…and the other problem
A Fork in the Road
The Right Metaphor
Sandbagging
Not Just Waitin’ on the World to Change
The Big Spoon
The Fork in the Road, Revisited
The Forest through the Trees

Death, in the dark wood…
McGinnis JM, Foege WH. Actual causes of death in the United States. JAMA. 1993;270:2207-12
Mokdad AH, Marks JS, Stroup DF, Gerberding JL. Actual causes of death in the
United States, 2000. JAMA. 2004;291:1238-45

The People in Potsdam-
Ford ES, Bergmann MM, Kröger J, Schienkiewitz A,
Weikert C, Boeing H. Healthy living is the best revenge:
findings from the European Prospective Investigation
Into Cancer and Nutrition-Potsdam study. Arch Intern
Med. 2009 Aug 10;169(15):1355-62
Or the UK: Kvaavik E, Batty GD, Ursin G, Huxley R, Gale CR. Influence of individual and combined
health behaviors on total and cause-specific mortality in men and women: the United
Kingdom health and lifestyle survey. Arch Intern Med. 2010;170:711-8
Or the US McCullough ML, Patel AV, Kushi LH, Patel R, Willett WC, Doyle C, Thun MJ, Gapstur SM.
Following cancer prevention guidelines reduces risk of cancer, cardiovascular disease, and
all-cause mortality. Cancer Epidemiol Biomarkers Prev. 2011;20:1089-97

Fresher still-
Akesson A, Larsson SC, Discacciati A, Wolk A. Low-
Risk Diet and Lifestyle Habits in the Primary
Prevention of Myocardial Infarction in Men: A
Population-Based Prospective Cohort Study. J Am
Coll Cardiol. 2014 Sep 30;64(13):1299-306

Fresher-er…
Aleksandrova K, et al. Combined impact of healthy
lifestyle factors on colorectal cancer: a large
European cohort study. BMC Med. 2014 Oct
10;12(1):168. [Epub ahead of print]

Fresher-er-er…
Chomistek AK, Chiuve SE, Eliassen AH, Mukamal KJ,
Willett WC, Rimm EB. Healthy lifestyle in the
primordial prevention of cardiovascular disease
among young women. J Am Coll Cardiol. 2015 Jan
6;65(1):43-51

rePercussions…
…to our pith and marrow; the case for nurturing nature:
Ornish D, Magbanua MJ, Weidner G, Weinberg V, Kemp C, Green C, Mattie MD,
Marlin R, Simko J, Shinohara K, Haqq CM, Carroll PR. Changes in prostate gene
expression in men undergoing an intensive nutrition and lifestyle intervention.
Proc Natl Acad Sci U S A. 2008 Jun 17;105(24):8369-74
Hietaniemi M, Jokela M, Rantala M, Ukkola O, Vuoristo JT, Ilves M, Rysä J, Kesäniemi Y. The effect
of a short-term hypocaloric diet on liver gene expression and metabolic risk factors in obese
women. Nutr Metab Cardiovasc Dis. 2009 Mar;19(3):177-83
Freedland SJ, Aronson WJ. Dietary intervention strategies to modulate prostate cancer risk and
prognosis. Curr Opin Urol. 2009 May;19(3):263-7
Ujvari U, Hulchiy M, Calaby A, Nybacka Å, Byström B, Hirschberg AL. Lifestyle intervention up-
regulates gene and protein levels of molecules involved in insulin signaling in the endometrium of
overweight/obese women with polycystic ovary syndrome. Hum Reprod. 2014 Jul;29(7):1526-35

The Master Levers of Destiny-
Feet
Forks
Fingers
But….

Lost in translation…
Knowledge, alas, isn’t power…
Katz DL. Life and death, knowledge and power:
why knowing what matters isn’t what's the
matter. Arch Intern Med. 2009 Aug 10;169(15):1362-3

Obesity Trends* Among U.S. AdultsBRFSS, 1985
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” person)
No Data <10% 10%–14%
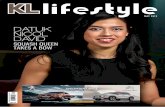
Obesity Trends* Among U.S. AdultsBRFSS, 1995
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” person)
No Data <10% 10%–14% 15%–19%

Obesity Trends* Among U.S. AdultsBRFSS, 2010
(*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person)
No Data <10% 10%–14% 15%–19% 20%–24% 25%–29% ≥30%
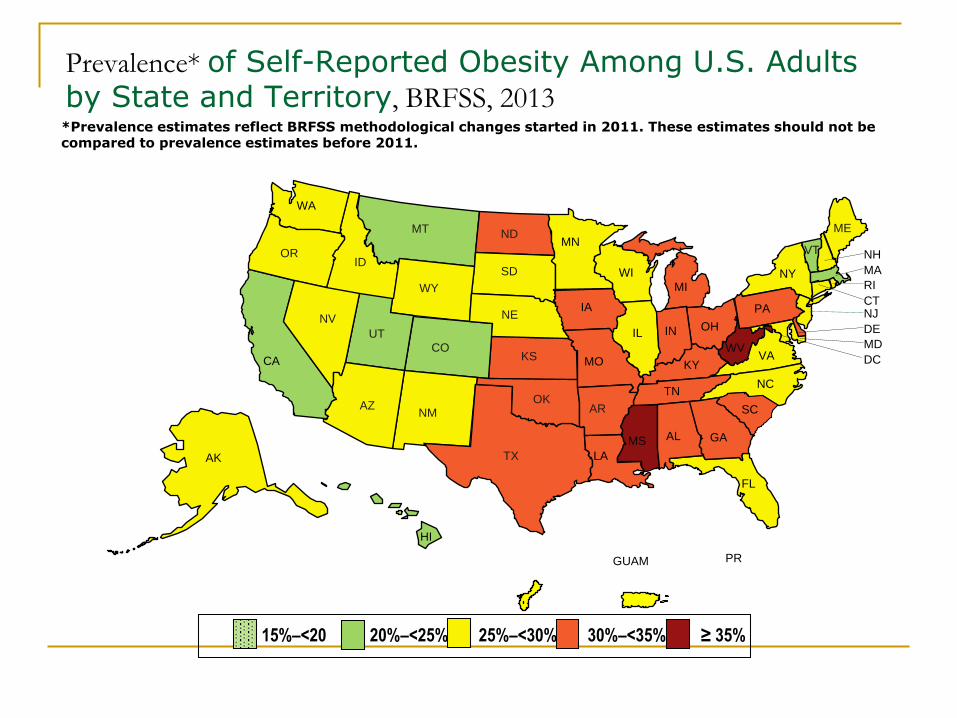
15%–<20 20%–<25% 25%–<30% 30%–<35% ≥ 35%
Prevalence* of Self-Reported Obesity Among U.S. Adults by State and Territory, BRFSS, 2013*Prevalence estimates reflect BRFSS methodological changes started in 2011. These estimates should not be compared to prevalence estimates before 2011.
CA
MT
ID
NV
UT
AZNM
WY
WA
OR
CO
NE
ND
SD
TX
OK
KS
IA
MN
AR
MO
LA
MI
IN
KY
ILOH
TN
MS AL
WI
PA
WV
SC
VA
NC
GA
FL
NY
VT
ME
HI
AK
NH
MA
RI
CTNJ
DE
MD
DC
PRGUAM

Age-adjusted Percentage of U.S. Adults Who Had
Diagnosed Diabetes
<4.5%Missing data
4.5 - 5.9% 6.0 - 7.4%
7.5 - 8.9% ≥9.0%
CDC’s Division of Diabetes Translation. National Diabetes Surveillance System
available at http://www.cdc.gov/diabetes/statistics
1994
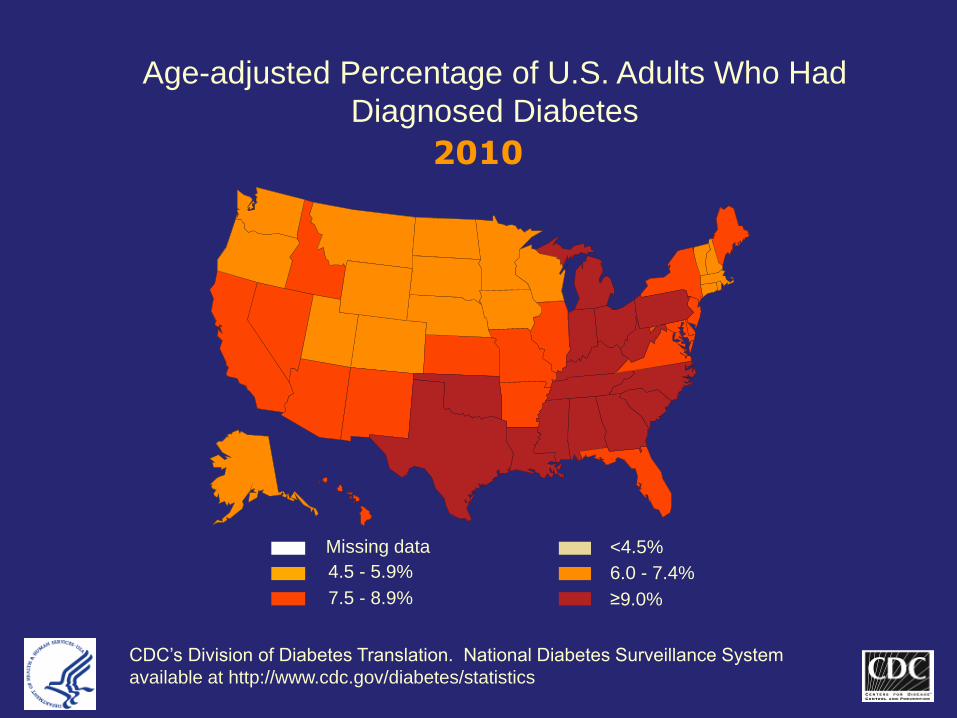
Age-adjusted Percentage of U.S. Adults Who Had
Diagnosed Diabetes
<4.5%Missing data
4.5 - 5.9% 6.0 - 7.4%
7.5 - 8.9% ≥9.0%
CDC’s Division of Diabetes Translation. National Diabetes Surveillance System
available at http://www.cdc.gov/diabetes/statistics
2010

From the frying pan…
http://www.pophealthmetrics.com/content/8/1/29
Projection of the year 2050 burden of diabetes in the US
adult population: dynamic modeling of incidence,
mortality, and prediabetes prevalence
One-Third of U.S. Adults Could Have Diabetes by 2050:
CDC 'Alarming numbers' point to importance of healthier lifestyles in reversing the
trend, experts say
HealthDay News, October 22, 2010
By 2050, between one-fifth and one-third of all adults could have diabetes -- with virtually all the
increase attributed to type 2 diabetes, which is largely preventable.
U.S. Diabetes Rates Soaring: CDC
Numbers have doubled over 15 years across
18 states, and all states now have rates of 6
percent or more
By Steven Reinberg
HealthDay ReporterLast Updated: Nov. 15, 2012
Masters RK, Reither EN, Powers DA, Yang YC,
Burger AE, Link BG. The Impact of Obesity
on US Mortality Levels: The Importance of
Age and Cohort Factors in Population
Estimates. Am J Public Health. 2013 Aug 15.
[Epub ahead of print]
Dabelea D, Mayer-Davis EJ, Saydah S, Imperatore G, Linder B, Divers J, Bell
R, Badaru A, Talton JW, Crume T, Liese AD, Merchant AT, Lawrence JM,
Reynolds K, Dolan L, Liu LL, Hamman RF; SEARCH for Diabetes in Youth
Study. Prevalence of type 1 and type 2 diabetes among children and
adolescents from 2001 to 2009. JAMA. 2014 May 7;311(17):1778-86
Diabetes in young people up 30% to 35% in past decade
By Steven Ross Johnson
May 6, 2014

Cooked?
40 Percent of Americans Will Develop
Diabetes, CDC Projects
Rates for black women and Hispanics even higher
at 50 percent
By Dennis Thompson
HealthDay Reporter
TUESDAY, Aug. 12, 2014 (HealthDay News) –
Aug. 13, 2014, The Lancet Diabetes & Endocrinology, online

The Writing is on the Wall-
November 12, 2008
Child Obesity Seen as Warning of Heart Disease By PAM BELLUCK
February 10, 2011, 2:27 pm
Stroke Rising Among Young People By TARA PARKER-POPE

The Promise of Public Health,
in Private Parts-

What lifestyle can do…
80% reduction in heart disease
90% reduction in diabetes
60% reduction in cancer
and so on…
4 Healthy lifestyle factors help ward off chronic disease. Diet, exercise, low body mass index and not smoking
can reduce the incidence of heart disease, diabetes, stroke and cancer. Duke Med Health News. 2009;15:4-5
Knoops KT, de Groot LC, Kromhout D, Perrin AE, Moreiras-Varela O, Menotti A, van Staveren WA.
Mediterranean diet, lifestyle factors, and 10-year mortality in elderly European men and women: the HALE
project. JAMA. 2004;292:1433-9

The Public-
in private parts…
Katz DL. Facing the facelessness of public health:
what’s the public got to do with it? Am J Health
Promotion. 2011 Jul-Aug;25(6):361-2

The Problem-







When clear where “there” is-
(Can We Say What Diet Is "Best"? David L. Katz; Huffington Post, 9/7/11: http://www.huffingtonpost.com/david-katz-md/best-diets_b_950672.html)
-it may still seem…
you can’t get there from here:

…& the other problem:
Is it clear where “there” is?

Fingers…Feet…Forks...
Health Diet/Nutrition
Low-Carb Diet Beats Low-Fat for Weight Loss
•Mandy Oaklander @mandyoaklander
Sept. 1, 2014

Bird’s (Katz’?) eye view-
Katz DL et al. Can we say what diet is best for
health? Annu Rev Public Health. 2014 Mar 18; 35:83-
103
Science Compared Every Diet, and the Winner Is Real Food
Researchers asked if one diet could be crowned best in terms of health outcomes.
If diet is a set of rigid principles, the answer is a decisive no. In terms of broader
guidelines, it's a decisive yes.
James Hamblin Mar 24 2014, 1:14 PM ET
Katz DL et al. Nutrition in Clinical Practice, 3rd Edition. Wolters
Kluwer/Lippincott Williams & Wilkins. September, 2014

Other eyes, on the same prize -
Mann J et al. Low carbohydrate diets: going against the
grain. Lancet. 2014 Oct 25:384;1479-80
Ley SH, Hamdy O, Mohan V, Hu FB. Prevention and
management of type 2 diabetes: dietary components and
nutritional strategies. Lancet. 2014 Jun 7;383:1999-2007
Katz DL, Hu F. Knowing what to eat, refusing to swallow it. Huffington
Post. 7/2/14

Macronutrients, Misrepresentations, &
Mayhem-
Chowdhury R et al. Association of Dietary,
Circulating, and Supplement Fatty Acids With
Coronary Risk: A Systematic Review and Meta-
analysis. Ann Intern Med. 2014;160:398-406
Bazzano LA et al. Effects of low-carbohydrate
and low-fat diets: a randomized trial. Ann Intern
Med. 2014;161:309-318

Low fat vegan
Low GL
DASH
DPP Paleo
Low Carb Mediterranean

“Eat food, not too much, mostly plants.”
-Michael Pollan

Much the same, in 572 pages…
Scientific Report of the 2015 Dietary
Guidelines Advisory Committee
http://www.health.gov/dietaryguidelines/2015-
scientific-report/

Mostly plants? Fuggedaboudit!...
Blanck HM, Gillespie C, Kimmons JE, Seymour JD, Serdula MK. Trends in
fruit and vegetable consumption among U.S. men and women, 1994-2005.
Prev Chronic Dis. 2008 Apr;5(2):A35. Epub 2008 Mar 15
Kimmons J, Gillespie C, Seymour J, Serdula M, Blanck HM. Fruit and
vegetablei ntake among adolescents and adults in the United States:
percentage meeting individualized recommendations. Medscape J Med.
2009;11(1):26. Epub 2009 Jan 26
Katz DL. Plant foods in the American diet? As we
sow... Medscape J Med.2009;11(1):25. Epub 2009
Jan 26


EVEN when clear where “there” is-
(Can We Say What Diet Is "Best"? David L. Katz; Huffington Post, 9/7/11: http://www.huffingtonpost.com/david-katz-md/best-diets_b_950672.html)
-it may seem…
you can’t get there from here:



A sandbagger…
and proud of it!

No Child Left (on their) Behind-Square Peg, Round Hole?
As easy as “ABC” for Fitness-
Activity Bursts in the Classroom
Katz DL, Cushman D, Reynolds J, Njike V, Treu JA, Walker J,
Smith E, Katz C. Putting physical activity where it fits in the
school day: preliminary results of the ABC (Activity Bursts in the
Classroom) for fitness program. Prev Chronic Dis. 2010
Jul;7(4):A82. Epub 2010 Jun 15

A Katz & Katz Production
2002 David & Catherine Katz
Katz DL, Katz CS, Treu JA, Reynolds J, Njike V, Walker J,
Smith E, Michael J. Teaching healthful food choices to
elementary school students and their parents: the Nutrition
Detectives™ program. J Sch Health. 2011 Jan;81(1):21-8




The ONQI Algorithm-
Numerator Denominator
FiberFolateVitamin AVitamin CVitamin DVitamin EVitamin B12Vitamin B6PotassiumCalciumZincOmega-3 fatty acidsTotal bioflavanoidsTotal carotenoidsMagnesiumIron
Saturated fatTrans fatSodiumSugarCholesterol
•Macronutrient Adjustors
Fat quality
Protein quality
Glycemic load
Energy density
•Trajectory Scores
•Weighting Coefficients
Categorical stipulations
• Pure foods vs.
processed
• Intrinsic vs. added
sugars
• Artificial
sweeteners
• Etc.

Katz DL, Ayoob KT, Decker EA, Frank GC, Jenkins DA, Reeves RS, Charmel P. The
ONQI Is Not a Black Box. Am J Prev Med. 2011 Sep;41(3):e15-6
Chiuve S, Sampson L, Willett WC. The association between a nutritional quality
index and risk of chronic disease. Am J Prev Med. 2011;40(5):505-13
Katz DL, Njike VY, Rhee LQ, Reingold A, Ayoob KT. Performance characteristics
of NuVal and the Overall Nutritional Quality Index (ONQI). Am J Clin Nutr.
2010;91:1102S-1108S
Katz DL, Njike VY, Faridi Z, Rhee LQ, Reeves RS, Jenkins DJ, Ayoob KT. The
stratification of foods on the basis of overall nutritional quality: the overall nutritional
quality index. Am J Health Promot. 2009;24:133-43
Jacobson MF. An important new way to rate the nutritional quality of foods. Am J Health
Promot. 2009;24:144-5

Measuring what matters…
RR of all-cause mortality, top vs. bottom quintile of
NuVal scores
NHS: RR = 0.88; p<0.001 (n ~ = 70,000)
HPFS: RR = 0.87; p = 0.001 (n ~ = 40,000)
Chiuve S, Willett WC et al. Harvard School of Public Health
Abstract presented: Experimental Biology 2010; Anaheim, CA
Am J Prev Med 2011 May;40(5):505-13

NuVal Mom of the Month for January, 2012:
Sally Galvin of Olathe, KS

NuVal con tempo >100,000 foods scored and audited
In >2000 supermarkets in 33 states, coast to coast
Reaching ~40 million shoppers every week

Sandbags…
on the assembly line:
http://www.yalegriffinprc.org/
www.turnthetidefoundation.org

Not just waitin’ on the world to change…

OWCH: On-line Weight Management Counseling
for Healthcare Professionals
http://www.turnthetidefoundation.org/OWCH/index.htm
Katz DL, Shuval K, Comerford BP, Faridi Z, Njike VY. Impact of an educational
intervention on internal medicine residents' physical activity counselling: the
Pressure System Model. J Eval Clin Pract. 2008 Apr;14(2):294-9
Katz DL. Behavior modification in primary care: the pressure system model.
Prev Med. 2001 Jan;32(1):66-72
O'Connell M, Comerford BP, Wall HK, Yanchou-Njike V, Faridi Z, Katz DL.
Impediment profiling for smoking cessation: application in the worksite. Am J
Health Promot. 2006 Nov-Dec;21(2):97-100
Katz DL, Boukhalil J, Lucan SC, Shah D, Chan W, Yeh MC. Impediment profiling
for smoking cessation. Preliminary experience. Behav Modif. 2003
Sep;27(4):524-37
O'Connell M, Lucan SC, Yeh MC, Rodriguez E, Shah D, Chan W, Katz DL.
Impediment profiling for smoking cessation: results of a pilot study. Am J Health
Promot. 2003 May-Jun;17(5):300-3

Medicine Lifestyle


The big spoon…
is culture.
Katz DL. Is obesity cultural? US News & World Report,
Eat + Run Blog; 10/4/12;
http://health.usnews.com/health-news/blogs/eat-
run/2012/10/04/is-obesity-cultural

Lifestyle Medicine
is
CULTURAL Medicine

GLiMMER
Global Lifestyle Medicine Movement to Effect Revolution
http://glimmerinitiative.org/
Lighting the World’s Way to Health

GLiMMER: Vision
The Earth is both a beautiful Blue Planet, and a
universal Blue Zone

LiM
Global coalition of lifestyle medicine organizations;
ACLM as convener
Development, Refinement, Dissemination of best
practice models
Contributions to medical education (all levels)
Engagement of payers and policy makers to
advance reimbursement models
Participant in the True Health Coalition (aid, out)
Able to leverage cultural supports (aid, in)

LaM

The True Health Coalition
Designed to advance the #UseWhatWeKnow
principle


Ship & Sail, Wind & Wave
Project components are “ship & sail,” specific to a
given destination
The True Health Coalition generates a wind to fill
all sails by establishing consensus, repudiating
distractions and discord

Join us -
True Health Coalition
One Voice, United
A global voice devoted to disseminating and applying
what we know for sure about health promotion and
disease prevention.
Sign up today to become a member of the True Health
Coalition. Your voice matters!
sign me up!
http://glimmerinitiative.org/#coalition



The Road Not Taken
-Robert Frost


Thank you!
David L. Katz, MD, MPH, FACPM, FACPDirector, Yale Prevention Research Center
President, Turn the Tide Foundation, Inc.
130 Division St.
Derby, CT 06418
(203) 732-1265
www.davidkatzmd.com

The Lifestyle Medicine Dream Team
Physician
Kriston Kent, MD, MPH Social Worker
Karen Lane, LICSW Exercise Physiologist
Cedric Bryant, PhD Health Coach
Heidi Duskey, MA Dietitian
Debra Wein, MS, RDN, LDN, NSCA-CPT*D, CWPD

Lifestyle Medicine in the Real
World
Kriston Kent MD MPH
The Kent Center for LIFE
Naples, FL

The Lifestyle Medicine Dream Team:
Physician, Nurse, Exercise Physiologist,
Health Coach, Dietician
Kriston Kent MD MPH
The Kent Center for LIFE
Naples, FL

No Disclosures
Kriston Kent MD MPH
The Kent Center for LIFE
Naples, FL

Objectives
• Describe how I arrived at Lifestyle Medicine
practice
• Essential components of a Lifestyle
Medicine practice
• Additional components/Adjuncts to a
Lifestyle Medicine practice
• Challenges of a Lifestyle Medicine practice

Introduction to:
The Kent Center for LIFE
My background:
• Raised on a cattle farm by 2 college
professors in the deep South
• Grew most of our fruits and vegetables (and
fried most of the vegetables)
• In late 1970s: read “the aerobics way” by
Kenneth Cooper MD MPH

Introduction to:
The Kent Center for LIFE
My background:
• Aging well and extending “health span”
became a passion by age 20
• 10 years of medical school and surgical
residency(little time for health habits)
• 1990:Started solo Facial Plastic Surgery
practice in Naples Florida with wife, 3 young
children, and lots of debt

Introduction to:
The Kent Center for LIFE
My background:
• Grew a successful practice helping people
“Age well on the outside” for 20+ years
• Empty nest and renewed passion for healthy
aging led to major personal/professional
lifestyle change
• Obtained MPH in Lifestyle Medicine from
Loma Linda University

Introduction to:
The Kent Center for LIFE
My Additional background:
• Attended: Active Lives: Transforming
Ourselves and Our Patients
• Attended: Healthy Kitchens, Healthy Lives
• Completed externship with the Institute of
Lifestyle Medicine – Harvard Medical School
• Completed externship with St. Helena
Center for Health

Introduction to:
The Kent Center for LIFE
KCL program development:
• Chose key team members
• Nutritionist/licensed clinical dietitian
• Fitness professionals/physical therapists
• Behavior professionals/LMHC
• Certified health and wellness coaches
• Developed protocols for each area with the
specific team member

Introduction to:
The Kent Center for LIFE
KCL program development:
• Taught entire team curriculum for each
critical area
• Lifestyle medicine evaluation
• Advanced nutrition evaluation
• Advanced fitness evaluation
• Advanced health behavior evaluation
• Advanced health and wellness coaching
protocols

Introduction to:
The Kent Center for LIFE
KCL program development:
• Chose patients for beta testing/focus
group
• Performed overall Lifestyle Medicine
Advanced Assessment for each beta
group patient
• Started beta group on one year “journey to
improved health and chronic disease
treatment/prevention”

Squaring Off the CurveThe Kent Center for LIFE

"Health Span"
• Dr. Kenneth Cooper's concept of:
• "Squaring off the Curve"

Squaring Off the Curve?
• More Life
• Better Life - "Health Span"
–Happier
–Healthier
–Freedom
– Independence

Increased Health SpanExamples:
• Reduced doctors visits for sickness
• Greatly reduced/remove need for medications, surgery, medical procedures
• Greatly increased time of feeling well/enjoyed life
• Greatly increased time of independent living
• Greatly reduced chance of assisted/nursing home living

"Health Span"• i.e. increase quality of life
• Jack Lelane :
–“People thought I was a charlatan and a nut. The doctors were against me – they said that working out with weights would give people heart attacks and they would lose their sex drive”

"Health Span"

LIFE• L- Living
• I- Inspiration
• F- Food
• E- Exercise

L- Living

LIFE• L- Living
– a physician supervises, guides, and inspires the individual towards Optimal health :• Reducing medications
• Improving health values
• Improving the quality and quantity of life
-- by helping them change their lifestyle habits!

Lifestyle Medicine MD Advanced Assessment
• Targeted health history
• Biometric evaluation
– Bio impedance
– Vital signs
– Basal metabolic rate eval
• Targeted lab evaluation
– Advanced cardiovascular lipid/lipoprotein eval
– Advanced cardiovascular inflammatory eval
– Advanced metabolic eval
– Intracellular micronutrients testing
– Screening for major organ/endocrine function

Lifestyle Medicine MD Advanced Assessment
• Key health habits evaluation – baseline score
• Diet score – establish baseline score
• Health Risk Appraisal(HRA)
• Nutrition screening form
• Physical activity screening form
• Framingham risk score
• Development/presentation of key health successes and challenges

Lifestyle Medicine MD : Ongoing Care
• Basic plan: Individualized 6 month or 12 month package with lifestyle medicine physician
• Upgraded plans include:
– Predetermined visits with health and wellness coach
– Predetermined package of advanced nutrition visits
– Predetermined package of advanced fitness visits
– Predetermined package of health behavior visits
• Regardless of plan, 6 month and 1 year programs involve:
– Follow-up Biometric and lab evaluations
– Follow-up health habits evaluation, diet score evaluation…

I- Inspiration
LIFE
• I- Inspiration– a behavior specialist/professional
counselor helps the individual with the stages of change and guiding the person towards their goals
– while the lifestyle coach keeps them on track, motivates, and inspires them to continue with change

LIFE
• I- Inspiration– Advanced Health behavior module includes:
• Advanced health behavior assessment by LMHC
• Recommendations regarding challenges identified during assessment
• At least 3 sessions with a certified health and wellness coach

LIFE
• F- Food– Advanced Nutrition module includes:
• Nutrition assessment by our licensed clinical dietitian
• Individualized Nutrition plan formulated by the dietitian and lifestyle medicine physician using challenges identified during assessment
• At least 2 follow-up visits with the nutritionist
• These visits are customized according to patient desire and needs

LIFE• F- Food
– the nutritionist individualizes and personalizes their food plan, increasing functional foods in the diet, to improve the health from the inside out
– helping to reverse disease and improve quality of life through the foods that they choose
– Pantry “clean out”, grocery shopping field trips, food prep assistance, eating out field trips

LIFE
• F- Food– our-base diet is a Mediterranean diet
emphasizing plant-based, whole food choices
– Full Plate Diet
– For patients with moderate/high cardiovascular risk• Esselstyn diet
• Ornish diet

E- Exercise

LIFE• E- Exercise
– Advanced Fitness module includes:• In depth assessment by a physical therapist
• Includes evaluation of gait, posture, balance, muscular strength, muscular endurance, aerobic capacity, and flexibility
• Fitness recommendations and plan are developed by physical therapist and lifestyle medicine physician based on the evaluation and patient desires
• At least 2 follow-up visits with physical therapist or personal trainer

LIFE
• E- Exercise
– the physical therapists and personal trainers help guide the individual towards physical activity and exercises to help correct alignment & balance, increase strength and flexibility, increase aerobic capacity and design a program that is fun, challenging, and sustainable for life

“The Real Cause” - Example:
• US soldiers atherosclerosis
• Middle aged atherosclerosis
• Mother-in-law example
• Don’t wait for symptoms and then only treat the symptoms
• TREAT THE CAUSE!

The Real Solution
• Bob
– Cardiac risk: TC dropped from 375 to 148 (227 points)
• Triglycerides dropped from 3721 to 202
• Weight dropped from 222 to 202(20 lbs.)
– Stroke risk: BP dropped from 138/88 to 110/72
– Diabetes risk: Blood sugar dropped from 186 to 95 (91 pt. drop)
• HA1c dropped from 7.6 to 5.3
– MD reduced/stopped 4 of his medications!
– All in a matter of 12 weeks!!

Same Patient – 115 # lighter
The Real Solution• Kathy
– Cardiac risk: TC dropped from 205 to 120( 85 points)
• LDL Cholesterol dropped from 92 to 47
• Weight dropped from 200 to 180 (20 lbs.)
– Stroke risk: BP dropped from 154/82(on BP meds) to107/74( off BP meds) (47 pt. sys BP drop!)
– Diabetes risk: Blood sugar dropped from 102 to 90( 12 pt. drop)
• HA1c dropped from 5.8 to 5.5
– All in a matter of 16 weeks!!

The Real Solution
• Others
– C/V & DM risk:
• Weight dropped 19 lbs., 16 lbs.
– Stroke risk: • BP dropped from 154/82 to 124/75 (30 pt. sys BP drop!)
• Another patient experienced 17 Pt. drop in Sys BP
– Diabetes risk:
• Blood sugar dropped 27 pts. (126 to 97)
• HA1c dropped from 6.0 to 5.8
– All in a matter of 12 weeks!!

Thomas Edison once said:
"The doctor of the future will give no medicine, but will interest her or his patients in the care of the human frame, in a proper diet, and in the cause and prevention of disease"

Value of Investment
• What is feeling better worth?
• What is more energy worth?
• What is looking better worth?
• What’s an additional year of Health worth?

Kent Center for LIFE: Plans available
• Basic plans:
– Silver: Major lifestyle medicine evaluation and 6 months working with lifestyle medicine physician and staff
– Gold: Major lifestyle medicine evaluation and 12 months working with lifestyle medicine physician and staff
• Advanced plans:
– Platinum: Major lifestyle medicine evaluation and 12 months working with lifestyle medicine physician and staff plus: Advanced nutrition module/Advanced fitness module/advanced health behavior module (2 of 3)
– Diamond: Major lifestyle medicine evaluation and 12 months working with lifestyle medicine physician and staff plus: Advanced nutrition module/Advanced fitness module/advanced health behavior module with health and wellness coaching(all 3)

Kent Center for LIFE: Plans available
• All plans are fee-for-service
• Global fee i.e. not charged per visit with physician
• Patients on basic plan purchase additional modules as desired and indicated
• Most lab test are covered by insurance
The Lifestyle Medicine Dream Team: Social Worker







Healthy Cooking Classes
Self-Compassion Yoga Community Acupuncture




www.lifeideals.net
Online Trainings•Health Coaching •Motivational Interviewing •Non-Violent Communication
Webinars•Guest Speakers •Blog













1
The Lifestyle Medicine Dream Team
The Health Coach
Heidi Duskey, MA, MS, PCC

2
Disclosures
Atrius Health
o Health Coach
Innosight
o Consultant
Objectives
o Outline the opportunities and considerations of
adding a health coach to your care team.
o Provide a brief sampling of the literature supporting
the effectiveness of health coaching across a
variety of behaviors and morbidities.
o Broaden this sampling with practical tips from my
own experience and practice.
o Enroll you in the possibility of hiring a health coach
for your team.
o Offer one tool for empowering behavior change
conversations with your patients.
3

4
Atrius Health
© 2014 Atrius Health, Inc. All rights reserved. Not for distribution.
The Northeast’s largest nonprofit independent multi-
specialty medical group. A national leader in delivering
high-quality, patient-centered coordinated care.
Dedham Medical Associates
Granite Medical Group
Harvard Vanguard Medical Associates
VNA Care Network
Providing care for ~ 675,000 adult and pediatric
patients with 750 physicians across more than 35
specialties

Atrius Health Core Competencies
5
Corporate Data Warehouse integrates single platform, electronic health record data with multi-payer claims data
Widespread extensive Population Health Management including disease-based and risk-based rosters, population managers
Long history with and majority of revenue under Global Payment across commercial and public payers
Sophisticated development and reporting of Quality and Performance Measures leading to high achievement
Patient-Centered Medical Home foundation, achieving level 3 NCQA across all primary care practices
© 2014 Atrius Health, Inc. All rights reserved. Not for distribution.

WHYadd a health
coach to my
team?
6

Current State: how daily choices impact health
+
=+
=+
=+
+
+ +
=
=
+

Health coaches . . .
o Provide expertise as behavior change specialists
o Behavior is the leading determinant of health,
resulting in 40% of premature deaths. Leading
causes of death are tobacco use, poor diet, and
physical inactivity (Mokdad et al., 2004) .
o Preserve capacity of other team members, permitting
them to serve patients at the top of their licenses
o Improve patient outcomes in diabetes mgmt (McGloin et
al., 2015), smoking cessation (Sforzo et al., 2014), the health
of cancer survivors (Galatino et al., 2009), obesity (Schwarz,
2013) and other chronic diseases (Margolius et al., 2012)
8

Health coaches . . .
o Improve provider satisfaction
“I would estimate that at least ¾ of the medical issues I address at
each patient visit are heavily influenced by lifestyle. Having an
available health coach is a potent resource to help patients make
important lifestyle changes.”
“A health coach has become an enormous asset to the care delivery
team . . . We would be the poorer in our practice without this
complementary component and skill.”
“Health coaching provides a forum for the patient to really explore
their personal concerns, fears, and worries – as well as their
motivations.”
9

Health coaches . . .
o Increases patient satisfaction
“I am no longer overwhelmed with life. I make choices! Plus, my
cholesterol is normal.” (LDL decrease: 152 to 94)
“I’ve learned that smaller incremental changes make a big difference.
Also, I can still eat what I’ve always eaten, just smaller portions.”
(Weight loss: 25 lbs)
“Coaching has helped me take responsibility for my own health with
no guilt.” (Weight loss: 13 lbs, A1C decrease: 7.5 to 7.1)
“[I’m most proud of ] my attitude adjustment: Learning to take on
what's mine and let go of what isn't. No longer judging myself.“ Weight
loss: 21 lbs, career change, improved mgmt of Barret’s esophagus
10

WHICHbehaviors can
the coach help
my patients
change?
11

A health coach can help your patients . . .
o Stop smoking
o Modify their diet
o Increase their level of physical activity and exercise
o Improve their sleep hygiene
o Manage stress more effectively
o Take their medication as prescribed
These changes inform
o Improved self esteem and self awareness
o Increased energy and well-being
12

WHOdo I choose
to be the
health coach
on my team?
13

Professional Health Coaches . . .
o Are credentialed through a recognized coach training
organization
o Wellcoaches, Wisdom of the Whole Coaching
Academy, Duke Integrative Medicine, MentorCoach,
California Institute of Integral Studies
o National Consortium for the Credentialing of Health
and Wellness Coaches
o International Coaches Federation
o Have an additional expertise in an area useful to the
clinical team (e.g., nursing, nutrition, exercise physiology,
behavioral health, health psychology)
14

Professional Health Coaches . . .
o Can also provide training to other team members
o Medical Assistants (Willard-Grace et al., 2015)
o Nurses (Margolis et al., 2012)
o Patients who serve as peer coaches (Thorn et al.,
2013)
o Can work with individuals or groups as facilitators with
or without other team members
o Can serve as behaviorists at Shared Medical
Appointments
15

HOWdoes the
health coach
collaborate
with my team?
16

Collaboration . . .
o Describes the coach’s relationship to the primary care
physician or clinical team lead
o Referral-based relationships are coordinated.
The patient has two care plans.
o Consultative relationships are integrated. The
patient receives a unified care plan.
o In addition, the coach can be co-located within the
practice, the department, or the lead clinician’s office
to facilitate warm hand-offs and informal
communication.
Source: Blount, 200317
WHATother logistics
do I need to
consider?
18

Logistic considerations include . . .
o Template structure
o Frequency and length of service
o Choosing panel size and patient cohort
o Charting responsibilities
o Accessing the organization’s electronic medical
record and sharing of chart notes with other team
members
o Referral protocols to the coach and from the coach
to other team members
o Providing patients with the option of telephonic
appointments in addition to face-to-face encounters
19

HOWcan I improve
my ability to
promote healthy
lifestyles for my
patients today?
20

Change the question. Change the conversation.
o Some behavior change conversations are not informed
by lack of knowledge.
“Doctor, I know what to do.”
“I feel stuck.”
“Why do I do this?”
o What are the questions your patient is not asking?
What perspectives do they never question?
Change “Why?” questions to “What?” or “How?”
How do they know their thinking is accurate?
What shifts when the question shifts?
21

Thank you!
22

References
Blount, A. (2003). Integrated primary care: Organizing the evidence.
Families, Systems, & Health, 21(2), 121-133. doi: 10.1037/1091-
7527.21.2.121
Galatino, M. L., Schmid, P., Milos, A., Leonard, S., Botis, S., Dagan, C.,
Albert, W., Teixeira, J., & Mao, J. (2009). Longitudinal benefits of wellness
coaching: Interventions for cancer survivors. International Journal of
Interdisciplinary Social Sciences; 4(10).
Margolius, D., Bodenheimer, T., Bennett, H., Wong, J., Ngo, V., Padilla, G.,
& Thom, D. H. (2012). Health Coaching to Improve Hypertension Treatment
in a Low-Income, Minority Population. Annals Of Family Medicine, 10(3),
199-205. doi:10.1370/afm.1369
23

References
McGloin, H., Timmins, F., Coates, V. and Boore, J. (2015). A case study
approach to the examination of a telephone-based health coaching
intervention in facilitating behaviour change for adults with Type 2 diabetes.
Journal of Clinical Nursing, 24, 1246–1257. doi: 10.1111/jocn.12692
Mokdad, A. H., Marks, J. S., Stroup, D. F.,Gerberding, J. L. (2004). Actual
causes of death in the United States, 2000. The Journal of the American
Medical Association, 291(10), 1238-1245. doi: 10.1001/jama.291.10.1238
Schwartz, J. (2013). Wellness coaching for obesity: A case report. Global
Advances in Health and Medicine, 2(4). doi: 10.7453/gahmj.2013.029
Sforzo, G. A., Kaye, M., Ayers, G. D., Talbert, B., & Hill, M. (2014). Effective
tobacco cessation via health coaching: An institutional case report. Global
Advances in Health and Med, 3(5), 37 -44.
24

References
Thorn, D. H., Ghorob, A., Hessler, D., De Vore, D., Chen, E., &
Bodenheimer, T. A. (2013). Impact of peer health coaching on glycemic
control in low-income patients with diabetes: A randomized controlled trial.
Annals Of Family Medicine, 11(2), 137-144. doi:10.1370/afm.1443
Willard-Grace, R., Chen, E. H., Hessler, D., DeVore, D., Prado, C.,
Bodenheimer, T., & Thom, D. H. (2015). Health coaching by medical
assistants to improve control of diabetes, hypertension, and hyperlipidemia
in low-income patients: A randomized controlled trial. Annals Of Family
Medicine, 13(2), 130-138. doi:10.1370/afm.1768
25

+
The Lifestyle Medicine Dream Team:
Dietitian
Debra Wein, MS, RDN, LDN, NSCA-CPT, CWPD

+
No disclosures

+Who is a Dietitian?
■ Common credentials
■ RD: Registered Dietitian
■ RDN: Registered Dietitian Nutritionist
■ LDN: Licensed Dietitian Nutritionist
■ The food and nutrition experts. Dietitians translate the science of
nutrition into practical solutions for healthy living.
Academy of Nutrition and Dietetics. What is an RDN? http://www.eatright.org/Public/landing.aspx?TaxID=6442452104. Accessed on August 22, 2014.

+Education and Training
■ Dietitians must hold a BS, MS (2017), or PhD
■ Didactic Program of Dietetics
■ ACEND-Accredited Dietetic Internship
■ National Dietetic Examination
■ Continuing Education (75 credits over 5 years)

+ Board Certified RDN SpecialistsCertified professionals complete at least 4,000 hours of practice
experience and pass the Board Certification as a Specialist in Dietetics
Examination.
Examples
■ Board Certified Specialist in Renal Nutrition (CSR)
■ Board Certified Specialist in Sports Nutrition (CSSD)
■ Board Certified Specialist in Oncology Nutrition (CSO)
■ Board Certified Specialist in Pediatric Nutrition (CSP)
■ Board Certified Specialist in Gerontological Nutrition (CSG)

+Certificate of Training
■ Certified Eating Disorders Registered Dietitian (CEDRD)
■ Certified Diabetes Educator (CDE)
■ Adult Weight Management
■ Childhood Weight Management
■ National Board of Nutrition Support Certification (NBNSC)

+Using Evidence-Based Research
in the Nutrition Care Practice

+Nutritional Counseling, Typical Session
60-75 minutes
■ Detailed subjective and objective questions to gather specific information on patient.
■ Discuss/clarify: chief concerns, medical history, social history, anthropometrics, typical food intake, allergies / intolerances, medications, OTC, vitamin/mineral supplements, herbs, physical activity, lifestyle –stress, alcohol, smoking, cravings, past history with diets, barriers to change, etc.
20-45 minutes
■ Follow up questions assessing
the patient’s change
■ Review successes, barriers, goals,
further education
■ Weave education throughout
session
■ Goal setting
■ Don’t forget maintenance!
Initial Session Follow-Up

+Partnering with an RDN
■ People may be more inclined to see you as the expert, if you lead
a healthy lifestyle.
■ Understand a wide variety of situations
■ Shop in a different grocery stores to know what is/is not available
■ Know local resources: food banks, food assistance programs
■ Consider different cultures, ethnicities, and socioeconomic status

++

+

+
+
Why see an RDN?

+10 Reasons to Visit an RDN
1. You have diabetes, cardiovascular problems or high blood pressure.
2. You are thinking of having or have had gastric bypass surgery. Since your stomach can only manage small servings, it's a challenge to get the right amount of nutrients in your body.
3. You have digestive problems. A registered dietitian nutritionist will work with your physician to help fine-tune your diet so you are not aggravating your condition with fried foods, too much caffeine or carbonation.
4. You're pregnant or trying to get pregnant.
5. You need guidance and confidence for breast-feeding your baby. A registered dietitian nutritionist can help make sure you're getting enough iron, vitamin D, fluoride and B vitamins for you and your little one.
6. Your teenager has issues with food and eating healthfully.
7. You need to gain or lose weight.
8. You're caring for an aging parent.
9. You want to eat smarter. A registered dietitian nutritionist can help you sort through misinformation; learn how to read labels at the supermarket; discover that healthy cooking is inexpensive, learn how to eat out without ruining your eating plan and how to resist workplace temptations.
10. You want to improve your performance in sports.
Source: http://www.eatright.org/resource/food/resources/learn-more-about-rdns/10-reasons-to-visit-an-rdn,
last accessed, June 11, 2015.


+
Conclusion
Dietitians are…
■ The experts on nutrition
■ A member of the patient’s lifestyle medicine dream team
■ Able to offer exclusive time talking about diet and ways to
achieve nutrition goals
+
+

Practitioner to Practitioner Lessons Learned and Successes Earned by
Early Adopters
Amira Aly, MD Reza Antoszewska, NP-C Karyn Bender, RPh, CHHC
Barbara Brown, MD and Lynn Kossow, MD
Rebecca Brown, MD and Larry Schmidt, MD
Lilach Malatskey, MD, MHA Krutika Parasar, SciB Karen M. Sherritt, MD

Amira Aly, MD
Coming Back to our Bodies:how the Body’s Wisdom can Guide Lifestyle
Transformation

• No relevant financial relationships.
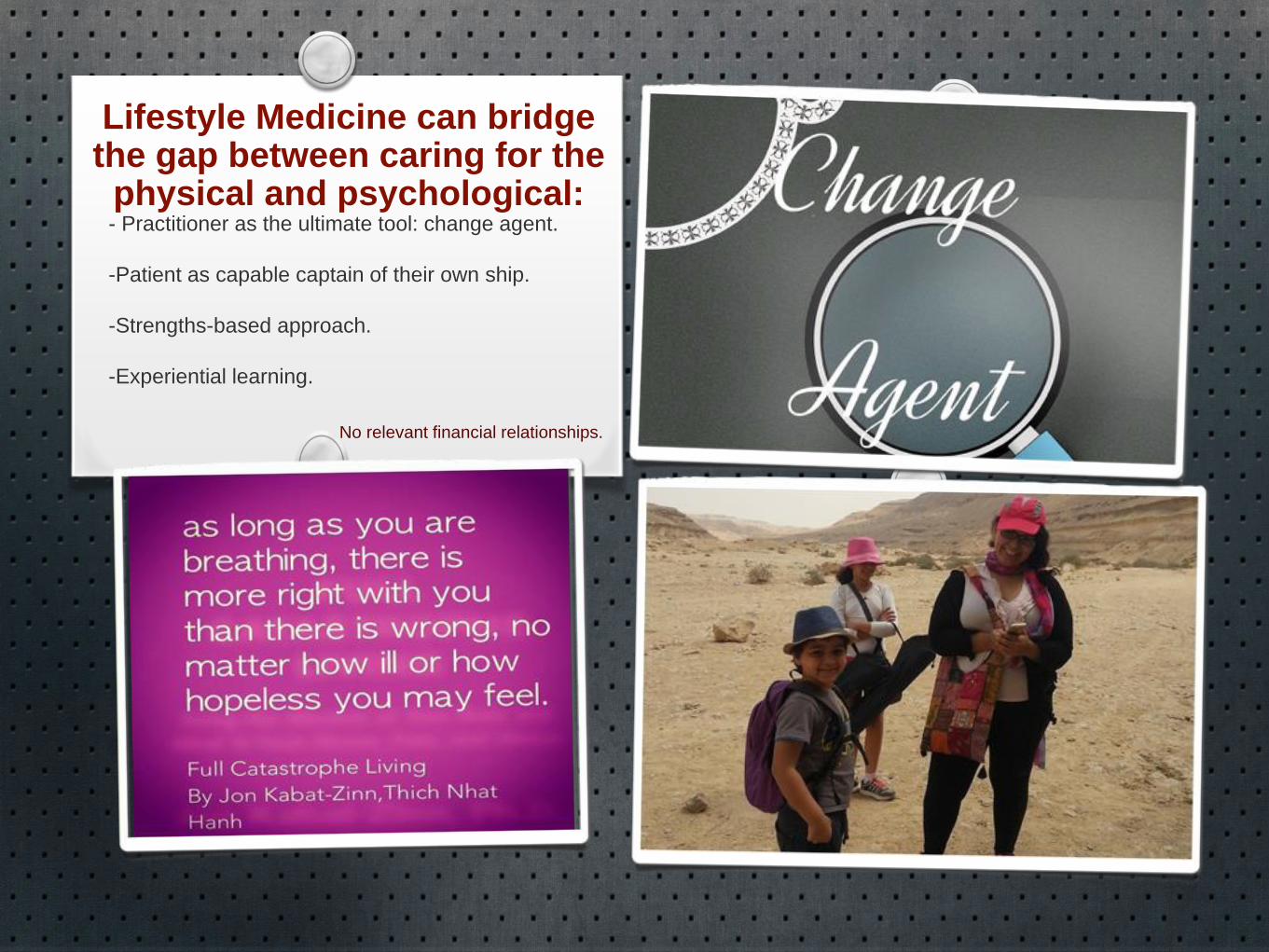
No relevant financial relationships.
Lifestyle Medicine can bridge the gap between caring for the
physical and psychological:- Practitioner as the ultimate tool: change agent.
-Patient as capable captain of their own ship.
-Strengths-based approach.
-Experiential learning.
References:1.KABAT-ZINN, J. (1991). Full catastrophe living: using the wisdom of your body and mind to face stress, pain, and illness. New York,
N.Y., Pub. by Dell Pub., a division of Bantam Doubleday Dell Pub. Group.
2.FRANKL, V. E. (1984). Man's search for meaning: an introduction to logotherapy. New York, Simon & Schuster.
3. HEFFERON, K. (2013). Positive psychology and the body: the somatopsychic side to flourishing.
4. Edward Phillips, MD. CME ONLINE: Lifestyle Medicine Competencies Case Study. Available from
<http://cmeonline.med.harvard.edu/course_descriptions.asp?Course_id=156> [14 May 2015]
Lifestyle Medicine Prescription:
Co-creating Self-Care Routine with Patients• Physical self-care:(habit-based nutrition, exercise prescription).
• Emotional self-care: (mindfulness practice, mind-body integration
skills).
• Social self-care (plan based on filling out a social support form
inspired by the one provided in HMS CME—Lifestyle Medicine
competencies +/- joining mind-body skills groups.)

Lifestyle Medicine In OncologyReza Antoszewska MS ANP-C
Legacy Cancer Institute
Portland OR
1

I have nothing to disclose
Disclosure
2

Describe Lifestyle Medicine’s Role at Legacy cancer Institute
Provide information on lifestyle Medicine Resources used in the clinic
Objectives
3

Diet
Exercise
Restorative sleep
Emotional resilience
Sense of connection
Environment
Lifestyle Medicine in Oncology
4
Symptom management
Prevention of sx
Cancer Risk Reduction

Plan for menopausal sx:
Hot flashes and Night Sweats
Sm protein meal before bed time
Mind/Body type exercise such as Tai Chi or Chi Gong
Daily ½ hour exercise or more
Trigger reduction: sugars, caffeine, ETOH spicy foods
Mindful activity during hot flashes
Stressors identified and managed
Fish oil and flax seed
Lifestyle Medicine in Oncology
5

Anticancer: A New Way of life, by David Servan-Schreiber
www.aicr.org Lifestyle medicine for cancer risk reduction- great patient resources
The Cancer Fighting Kitchen, by Rebecca Katz
www.lumosity.com web site offers games and activities to strengthen memory. It is a brain gym.
Selected Resources
6

Move a Little, Lose a Lot by James A. Levine MD.
www.strongwomen.com/fitness/fitness-eprograms
www.strongwomen.com/fitness/fitness-eprograms/strong-bones-overview/
http://www.mayoclinic.com/health/mediterranean-diet/CL00011
www.ewg.org – environmental considerations
Marc.ucla.edu/body.cfm?id=22 UCLA Mindfulness podcasts. Free podcasts to help with relaxation and sleep
http://www.huffingtonpost.com/2014/01/21/meditation-apps-stress-positive-thinking-mood_n_4639232.html
Selected Resources
7

https://www.functionalmedicine.org/
http://www.cityofhope.org/center-for-cancer-survivorship
http://www.harvardhealthbooks.org/book/mind-over-menopause-the-complete-mindbody-approach-to-coping-with-menopause/
http://www.legacyhealth.org/health-services-and-information/health-services/for-adults-a-z/cancer/all-cancer-services/survivorship-services.aspx
References
8

The Healing
Power of
SimplicityKaryn Bender RPh CHHC CMI
Integrative Pharmacist, Holistic Health & Nutrition Coach, Medical Intuitive,
Herbalist

Dislcosures
None

Objectives
Start from where you are
Know your own first step in healthy
change
Help your patients discover their first step
Trust in the power of one step at a time

Personal story We all have our life and health stories
Healing life with Lupus, thyroid disease, cancer
Lupus: Stress reduction and self esteem
Thyroid: Diet, exercise, stress reduction, sleep
Cancer: Value every moment of life
Easy diet changes came first, other lifestyle changes followed. Fueling for success & healing
Noticeable results
Grateful for my body and life every step of the way

Simple Powerful Steps
Menagerie of information – keep it simple
Witness results
Create your healthy life tool kit: make it
personal, simple, do-able, familiar, fun
Reach out, inspire others
Karyn Bender RPh CHHC CMI

References McCarty. It Works: Doing One Thing at a Time. Life Saving
Philosophy Blog [Internet]. January 7, 2012. URL: https://www.psychologytoday.com/blog/life-saving-philosophy/201201/it-works-doing-one-thing-time. Accessed: May 01, 2015
O’Connell A. The Pros and Cons of Doing One Thing at a Time. Harvard Business Review. January 20, 2015. URL: https://hbr.org/2015/01/the-pros-and-cons-of-doing-one-thing-at-a-time. Accessed: May 01, 2015
Lipman F, Claro D. The New Health Rules: Simple Changes to Achieve Whole-Body Wellness. New York, NY: Artisan; 2015
LowDog T. Life is Your Best Medicine: A Woman’s Guide to Health, Healing and Wholness at Every Age. Washington,DC: National Geographic Society; 2012

Dr. Lynne B. Kossow
Dr. Barbara A. Brown
1.0 hour initial consultation to begin the process of developing your own customized Lifestyle Medicine program for which you will be receiving on going lifestyle coaching throughout the year.
Direct doctor/patient e-mail communication for non-urgent issues.
Doctor phone time 7-9am and 5-6pm Monday-Friday when you can call in and speak directly to your doctor.
A private phone line connecting you directly to our administrative assistant so that your calls can be answered promptly and efficiently throughout the day.

Priority appointment times to accommodate your schedule
Added time to all follow-up office visits to discuss your Lifestyle Medicine Program
Hospital social visits at The University of Princeton Medical Center during the week if you are admitted to the hospital for an extended stay. This will allow us to stay better connected with you during your hospitalization.
Priority in-office laboratory testing for your convenience.

Lifestyle Coaching Private phone line Cellphone hours with your doctor Emailing with your doctor Extra time at office visits Hospital Social Visits

Larry Schmidt, BSc, MD, CCFP, FCFP
Rebecca Brown, MSW, RSW, CHWC
Larry Schmidt – I have no disclosures to declare
Rebecca Brown – I have no disclosures to declare
How
Lifestyle
Medicine
Changed
our
Lives

What a difference
a year makes:
• Attended America College of Life
Medicine Conference in San Diego
• Decided we needed to do something!
• Integrated Lifestyle Medicine into daily
practice
• Started a national organization in
Canada to promote the
implementation of Lifestyle Medicine
into the health care system
• A grass roots approach


Lifestyle Medicine in our lives
Rebecca
Certified Health & Wellness Coach (Wellcoaches)
Private practice coaching
Conferences/Workshops on Vicarious Trauma & Resilience
Focus on Lifestyle Choices: stress, mindfulness, nutrition & exercise
Larry
Integrated Lifestyle Medicine into every patient visit
Talks on LM to faculty, residents, students & community
Changing practice location to Advanced Medical Group
Medical Director Canada’s 1st Lifestyle Medicine based medical center


• Describe our Lifestyle medicine course
• Feedback from participants
• Describe the essence of the syllabus
• Offer the syllabus as a tool for promoting LSM
teaching for medical students and doctors

• Lectures on nutrition, exercise, sleep medicine, sexuality and
health, personal health, smoking cessation and stress
• Workshops and experiential learning of behavioral
change techniques such as coaching and motivational
interviewing, yoga and exercise lessons
• Practical clinical project: accompanying and supporting a
patient in the process of lifestyle health behavior change
The courses were co- directed with Dr Adva Zuk Onn, Family medicine and geriatric specialist

Available to the audience ( English version )
Please contact:
Dr. Lilach Malatskey
Primary editor of the syllabus,
Head of the Israeli Society of Lifestyle Medicine,
Email: [email protected]
Acknowledgements to the team of writers and editors of the syllabus: Executive Members of the Israeli Society of Lifestyle Medicine
The panel of experts consulting and support team

• Prof. Amnon Lahad and Dr. Eli Rosenberg; Program initiative for a healthy future 2020 The Israeli Ministry of Health
• Lianov L, Johnson M; Physician competencies for prescribing lifestyle medicine. JAMA 2010;
• Dacey M, Arnstein F, Kennedy M A, Wolfe J & Phillips E; 2013. The impact of lifestyle medicine continuing education on provider knowledge, attitudes, and counseling behaviors; Medical Teacher
• Polak R, Tzuk Onn A, Shani M, Malatskey L; Family Physician Prescribing Lifestyle Medicine – Implementing a national training program; Unpolished data.
• The syllabus English translation was sponsored by the Israeli Association of Family Physicians

EXERCISE AS MEDICINE
Krutika Parasar
3rd Year Medical Student at Rutgers Robert
Wood Johnson Medical School

I HAVE NO DISCLOSURES

Topics:
The Exercise is Medicine Movement
The Importance of Introducing Exercise into
the Medical School Curriculum
Steps We Have Taken to Achieve this Goal!

ROBERT WOOD
JOHNSON
PACEMAKERS

SPREADING
THE WORD!
EXERCISE, SLEEP, AND STRESS
IN FIRST AND SECOND YEAR MEDICAL SCHOOL STUDENTS

A Journey Towards WellnessA Journey Towards Wellness
Karen Sherritt, MDPrimary Care InternistInstructor in MedicineInstructor in Medicine Harvard Medical School

“The Journey of a thousand miles begins with a single step.”
‐Lao Tzu

DisclosuresDisclosures
• NoneNone

ObjectivesObjectives
• Share the story of my journey• Share the story of my journey–Life as it was–The crisis The first step–The first step
–One step follows another

Lif A It WLife As It Was
•High achiever
•Doing it all
l l•People pleaser
•Working hardWorking hard
•Looking good
The CrisisThe Crisis
•Exhaustion
A i t•Anxiety
•AngerAnger
•Desire to quit

The First StepThe First Step
•Intentional change of attitude/perspectiveattitude/perspective
•Practice of•Practice of Gratefulness
One Step Followspthe Next
Commitment to self careE i⁻Exercise⁻Sleep⁻Low Carbohydrate DietLow Carbohydrate Diet⁻Reconnecting with GFs⁻Counselingg⁻Mindfulness Meditation

Tools/Tips/ p
Compassionate self‐care:
•Awaken to now•Note the effect of attitude• Take small steps• Be kind to yourself• Seek support• Seek support• Share with others

Courage, Integrity, Connectedness, Hope, Vision

ReferencesReferences
H l Th S lf•Heal ThySelf, Saki Santorelli
•www.Gratefulness.org,Brother David Steindl‐Rast
•I Thought It Was Just Me (b i i ' ) B B(but it isn't), Brene Brown

“Instructions for living a life.P tt tiPay attention.Be astonished.Tell about it ”Tell about it.
Mary Olivery

Nancy M. Enos, FACMPE, CPMA, CPC-I, CEMC
Billing and Coding for
Lifestyle Medicine

Approved
Instructor
Approved instructorApproved instructor
Coding and Billing for Lifestyle Medicine
Presented by:
Nancy M. Enos, FAMPE, CPC-I, CPMA, CEMC CPC
Tools for Healthy Change
June 27, 2015

Approved
Instructor
Approved instructor
Disclosures
• Enos Medical Coding does not provide legal advice and the information in this presentation is based on the coding guidelines in the Current Procedural Terminology (CPT) Manual published by the American Medical Association (AMA) and Evaluation and Management Coding Guidelines from the Centers for Medicare and Medicaid (CMS)
• CPT codes, descriptions and material only are copyright 2015 American Medical Association. All Rights Reserved.
• No fee schedules, basic units, relative values or related listings are included in CPT.
• The AMA assumes no liability for the data contained herein.

Approved
Instructor
Approved instructor
Objectives
• Understanding Documentation Guidelines and key components of E/M Services– History, Exam, Medical Decision Making– Time based E/M Services
• Understanding coding guidelines and identify risk areas for E/M services with: – Patient Status– Billing for Time Spent Counseling– Obesity Counseling – diagnosis and CPT codes– Preventative with Sick Visits– Welcome to Medicare Physicals– Medicare Annual Wellness Visit– E/M Modifiers

Approved
Instructor
Approved instructor
New versus Established
• E/M codes are divided on the patient status
• A new patient is one who has not received any face-to-face professional service from a provider of the same specialty or exact same subspecialty in the same group practice, within three years
– New group
– New Specialty
• If a provider is covering, the encounter is classified as it would have been by the patient’s provider.

Approved
Instructor
Approved instructor
TIME For coding purposes, face-to-face time for
office/outpatient visits or consult services is defined as only that time that the physician spends face-to-face with the patient and/or family.
When greater than 50% of the face-to-face time is spent in counseling or coordination of care, time may be considered in selecting the code level for the encounter
Tip: If the visit does not include any interval history ( “S” of SOAP note), no Physical Exam (“A”), such as a return visit to discuss test results, treatment options, compliance with treatment plan, etc. this lengthy visit would qualify for the “Time” component for code selection.

Approved
Instructor
Approved instructor
Time and Counseling Coding Issues
Physicians will often need to utilize the “Time” factor and frequently undercode counseling types of services
Diagnosis code sequencing is essential for follow-ups; avoid denials……..
– After Depression or any other mental health diagnosis, etc. is determined, what physicians are actually providing is medication management. Use the V code for the subsequent encounters.
V58.83 Encounter for therapeutic drug monitoring or if it is a long term current use drug, use the appropriate V58 code series
Nancy Enos, FACMPE CPC CPC-I

Approved
Instructor
Approved instructor
Time Spent Counseling
• Does the note state the total time of the visit?
• Does the note describe the content of counseling/coordination of care?
• Does the note reveal that more than half of the time was spent counseling and/or coordinating care?
Nancy Enos, FACMPE CPC CPC-I

Approved
Instructor
Approved instructor
Time and Counseling Diagnosis Coding Issues- Signs and Symptoms
• Anorexia - 783.0 (loss of appetite)
• Abnormal loss of weight 783.2X
• BMI V85.0-V85.54
• Excludes:anorexia nervosa (307.1)
• Anorexia is an unexplained loss of appetite. Do not use this code to report anorexia nervosa, which is found in category 307
Nancy Enos, FACMPE CPC CPC-I
Approved
Instructor
Approved instructor
Overweight and Obesity
• ICD-9 code is 278.00
– Morbid Obesity 278.01
– Overweight 278.02
– Obesity hypoventilation syndrome 278.03
– Localized adiposity 278.1
– Use Additional Code to identify Body Mass Index (BMI) if known, with V85.0-V85.54

Approved
Instructor
Approved instructor
Body Mass Index (BMI)
• V85.0 BMI less than 19, adult
• V85.1 BMI between 19-24, adult
• V85.2 BMI between 25-29, adult
• V85.3 BMI between 30-39, adult
• V85.4 BMI 40 and over, adult

Approved
Instructor
Approved instructor
Weight Management
• Health and Behavior Assessment or Intervention:
– For dietitians, certified diabetes counselors, nurses, or behavioral health professionals for identifying the psychological, behavioral, emotional, cognitive, and social factors important to the prevention, treatment, or management of physical health problems. These services do not represent and should not be reported on the same day as preventive medicine counseling services.
Nancy Enos, FACMPE CPC CPC-I

Approved
Instructor
Approved instructor
Weight Management
• CPT 96150 - Health and behavior assessment (e.g. health-focused clinical interview, behavioral observations, psycho-physiological monitoring, and health-oriented questionnaires) each 15 minutes face-to-face with the patient, initial assessment
• CPT 96151 - Health and behavior reassessment (e.g. health-focused clinical interview, behavioral observations, psycho-physiological monitoring, and health-oriented questionnaires) each 15 minutes face-to-face with the patient, initial assessment
• CPT 96152 - Health and behavior intervention, each 15 minutes, face-to-face, individual• CPT 96153 - Health and behavior intervention, each 15 minutes, face-to-face, group (2
or more)• CPT 96154 - Health and behavior intervention, each 15 minutes, face-to-face, family
(patient present)• CPT 96155 - Health and behavior intervention, each 15 minutes, face-to-face, family
(patient not present)• *Use of the appropriate E&M service code should be filed when these services are
performed by a physician.
Nancy Enos, FACMPE CPC CPC-I

Approved
Instructor
Approved instructor
Prolonged Services Face-to-Face
• 99354-99355 Outpatient
• 99356-99357 Inpatient
– minimum of 60 minutes
– Beyond the normal time frame
– Actual treatment vs. Counseling
– Add on to E&M code at any level
– Document time

Approved
Instructor
Approved instructor
Code SelectionCODE Office Visit Est. 2/3 HISTORY EXAM MDM Time
99211 Office visit, No. Phys. Required N/A N/A minimal 5 min
99212 Office visit, Est. (Prob focused) Problem Focused 1 Straightforward 10 min
99213 Office visit, Est (Low) Exp. Problem Focused 2-4 Low 15 min
99214 Office visit, Est. (Mod.) Detailed 5-7 Moderate 25 min
99215 Office visit Est. (High Comprehensive 8 High 40 min
CODE Office Visit New 3/3 HISTORY EXAM MDM Time
99201 IOV (No Referral) Problem Focused 1 Straightforward 10 min
99202 IOV (No Referral) Exp. Problem Focused 2-4 Straightforward 20 min
99203 IOV (No Referral) Detailed 5-7 Low 30 min
99204 IOV (No Referral) Comprehensive 8+ Moderate 45 min
99205 IOV (No Referral) Comprehensive 8+ High 60 min
Office Consults 3/3 HISTORY EXAM MDM Time
99241 Office Consult minimal Problem Focused 1 Straightforward 15
99242 Office Consult Prob. Focused Exp. Problem Focused 2-4 Straightforward 30
99243 Office Consult (Low) Detailed 5-7 Low 40
99244 Office Consult (Mod.) Comprehensive 8+ Moderate 60
99245 Office Consult (High) Comprehensive 8+ High 80
Prolonged Services Time
99354 Office Prolonged Service add on to base code 60
99355 Each Additional 30 minutes 1 unit each 30 min 30
Nancy Enos, FACMPE CPC CPC-I

Approved
Instructor
Approved instructor
Is the Service a Consultation?
Was the advice or opinion of the provider requested? Was the opinion issued as per guidelines? Are these facts clearly documented in the medical record? “Six R’s”
Request (From whom?) Reason for consultation Review of previous records Render patient evaluation (H&P) Recommendation for plan of treatment Report (separate if not shared record)

Approved
Instructor
Approved instructor
Consultations –not covered by Medicare and others following Medicare rule
• 99241 – 99245: Outpatient Consultations
– Office consults must be requested by another physician
– Example- Medicare will pay for surgical clearance
– Use if patient is considered observation status or consult is requested in ED and patient is discharged
• 99251 – 99255: Initial Inpatient Consultations
– Use if patient status is inpatient admission

Approved
Instructor
Approved instructor
Preventative Medicine
Codes are based on New vs. Established New and Established Patient
Solely for the purposes of distinguishing between new and established patients, professional services are those face-to-face services rendered by a physician and reported by a specific CPT code(s). A new patient is one who has not received any professional services from the physician or another physician of the same specialty who belongs to the same group practice, within the past three years.
An established patient is one who has received professional services from the physician or another physician of the same specialty who belongs to the same group practice, within the past three years.
In the instance where a physician is on call for or covering for another physician, the patient's encounter will be classified as it would have been by the physician who is not available.
Nancy Enos Medical Coding

Approved
Instructor
Approved instructor
Preventative Medicine Issues
The extent and focus of the service will vary based on the age of the patient
If an abnormality/ies is encountered or a preexisting problem is addressed in the process of performing this preventive medicine evaluation and management service, and if the problem/abnormality is significant enough to require additional work to perform the key components of a problem-oriented E/M service, then the appropriate Office/Outpatient code 99201-99215 should also be reported

Approved
Instructor
Approved instructor
Preventative Medicine Issues
• Modifier 25 should be added to the Office/ Outpatient code to indicate that a significant, separately identifiable Evaluation and Management service was provided by the same physician on the same day as the preventive medicine service. The appropriate preventive medicine service is additionally reported.
• An insignificant or trivial problem or abnormality that is encountered in the process of performing the preventive medicine evaluation and management service and which does not require additional work and the performance of the key components of a problem-oriented E/M service, should not be reported.

Approved
Instructor
Approved instructor
Preventative or Sick?
• A 72 year old established patient presented for a well check-up. The patient’s daughter claimed the patient had been walking with a limp and complaining of lower leg pain for the past 3 days after falling from the bed.
• The provider focused on further (extensive) evaluation of these symptoms and indicated a plan of x-ray and possible referral to orthopedics. The preventative exam was completed. The bill would look something like this:

Approved
Instructor
Approved instructor
Preventative Medicine and E/M
CPT: 99397
(Est.) Preventive medicine, 65+ years
DX 1: V70.0 Physical Exam
and also
CPT: 99213-25 E/M Service-(EPF,EPF,LC)
DX 2: 729.5 Pain in limb
DX 3: E880.9 Fall-Other stairs or steps
Approved
Instructor
Approved instructor
Nurse Visits 99211
• According to the CPT manual, a 99211 is an office or other outpatient visit "that may not require the presence of a physician. Usually, the presenting problem(s) are minimal. Typically, five minutes are spent performing or supervising these services."
• Unlike the rest of the office visit codes, 99211 does not have any documentation requirements for the history, physical exam or complexity of medical decision making. The nature of the presenting problem need be only "minimal," such as monthly B-12 injections, suture removal, dressing changes, allergy injections with observation by a nurse, and peak flow meter instruction
• Do not use for “shot visits” the administration codes include the work of 99211
• Remember, if you bill a 99211 you must collect a copay
Approved
Instructor
Approved instructor
Counseling/Risk Factor
99401 (weight management)
Preventive medicine counseling and/or risk factor reduction intervention(s) provided to an individual without a specific illness for which the counseling might otherwise be part of a treatment- 15 minutes
99402
30 minutes
99403
45 minutes
99404
60 minutesNancy Enos Medical Coding
Approved
Instructor
Approved instructor
Behavior Change/Interventions
• 99406 Smoking and tobacco use cessation counseling visit; intermediate, greater than 3 minutes up to 10 minutes
– 99407 greater than 10 minutes
• 99408 Alcohol and/or substance (other than tobacco) abuse structured screening (eg, AUDIT, DAST), and brief intervention (SBI) services; 15 to 30 minutes
– 99409 greater than 30 minutes Nancy Enos Medical Coding

Approved
Instructor
Approved instructor
Medicare Screening Services
The Patient Protection and Affordable Care Act (PPACA) changed coverage of preventative care services to Medicare
Since January 1, 2011 CMS covered Annual Wellness Visits
Other screening services may be covered based on frequency and patient risk
Check Medicare’s billing guide for G-Codes to report screening procedures and V-codes allowed as diagnoses
http://www.medicarenhic.com/providers/pubs/REF-EDO-0002_Preventive_Services_Billing_Guide.pdf

Approved
Instructor
Approved instructor
Medicare Covered Screening Services
• Bone Mass Measurement
• Cardiovascular Screening
• Colorectal Cancer Screening
• Diabetes Screening
• Flu (Influenza) Injections
• Glaucoma Screening
• Hepatitis B Injections
• Initial Preventive Physical Examination
• Mammography Screening
• Medical Nutrition Therapy
• Pneumococcal Pneumonia
Vaccination (PPV)
• Prostate Cancer Screening
• Screening Pap Smears
• Screening Pelvic Examinations
• Smoking and Tobacco-Use
Cessation
• Ultrasound Screening for
Abdominal Aortic
Aneurysm

Approved
Instructor
Approved instructor
Advanced Beneficiary Notice (ABN) Requirements
• A physician should obtain an Advanced Beneficiary Notice (ABN) when services provided fall outside of Medicare coverage requirements. The ABN can be found on the CMS website at: http://www.cms.gov/cmsforms/downloads/cmsr-131-g.pdf.
• Physicians, practitioners and hospitals will be liable for Screening services unless they issue an appropriate Advanced Beneficiary Notice

Approved
Instructor
Approved instructor
Medicare Preventative Services
• Under PPACA (Patient Protection and Affordable Care Act, or Healthcare Reform) coverage for preventative services has been expanded.
• Medicare continues to define the conditions of coverage of preventative services
• Not all commercial plans will follow the Medicare Guidelines

Approved
Instructor
Approved instructor
Welcome to Medicare” Exam (IPPE)
Once in a lifetime exam
Covered within the first 12 months of enrollment in Medicare Part B
Includes: Height, weight, body mass index
Referrals for necessary diagnostic testing
Blood Pressure
Education, counseling and health risk assessment

Approved
Instructor
Approved instructor
Welcome to MedicareCode Definition
G0402 “Welcome to Medicare” – Initial Preventative Physical Exam
G0403 Electrocardiogram, routine ECG w/12 leads; screening for the initial preventative PE
G0404 ……”tracing only, without interpretation and report
G0405 ……”interpretation and report only
G0403, G0404, G0405 can be billed in addition to G0402. EKG is no
longer a required part of IPPE. No specific diagnosis (ICD-9) is
required.
Co-insurance, co-pay and/or deductible waived only for G0402.
Approved
Instructor
Approved instructor
Annual Wellness Visit (AWV)
Once in a lifetime exam including Personalized Prevention Plan Services (PPPS)
Person Covered-
One who is no longer within 12 months after the effective date of first Medicare Part B Coverage
One who has not received either an initial preventative physical exam or an AWV within the past 12 months.

Approved
Instructor
Approved instructor
AWV Includes
Establish or update the individual’s medical and family history.
List the individual’s current medical providers and suppliers and all prescribed medications.
Record measurements of height, weight, body mass index, blood pressure and other routine measurements.
Detect any cognitive impairment.
Establish or update a screening schedule for the next 5 to 10 years including screenings appropriate for the general population, and any additional screenings that may be appropriate because of the individual patient’s risk factors.
Furnish personalized health advice and appropriate referrals to health education or preventive services.

Approved
Instructor
Approved instructor
Annual Wellness Visit (AWV)
Review of individual’s potential for depression
Including current or past experiences
Review functional ability and level of safety based on direct observation or screening questions/questionnaire
Approved
Instructor
Approved instructor
Annual Wellness Visit (AWV)
• Establish a written screening schedule for
the individual, such as a checklist for the
next 5-10 years, as appropriate
• Patient’s health status
• Screening History
• Age appropriate preventive services
Approved
Instructor
Approved instructor
Annual Wellness Visit (AWV)
• Community-based lifestyle interventions to reduce health risks and promote self-management and wellness
– Weight loss
– Physical activity
– Smoking cessation
– Fall prevention
– Nutrition

Approved
Instructor
Approved instructor
Annual Wellness Visit (AWV)
• Any other element(s) determined appropriate by the Secretary of
• Health and Human Services through the National Coverage Determination (NCD) process
• Not subject to “incident-to”
• Who may perform?
– Doctor of medicine, – Doctor of osteopathy
– Nurse practitioner, – Physician assistant, – Clinical nurse specialist
– Health professional, which includes:
– Health educator, • Registered dietitian
– Nutrition professional, • Team of such medical professionals who are working under the direct supervision of a physician

Approved
Instructor
Approved instructor
Subsequent Wellness Visit (SWV)
• Performed 11 months after AWV & includes
– Update to medical/family history
– Measurements of weight (or waist circumference), blood pressure and routine measurements as deemed appropriate
– Update to list of current medical providers/suppliers
– Detection of any cognitive impairment
– Update to written screening schedule
– Update to list of risk factors
– Furnish appropriate health advice and referral as appropriate

Approved
Instructor
Approved instructor
Annual & Subsequent Wellness Codes
HCPCS Code Description
G0438 Annual Wellness Visit, includes Personalized Prevention Plan of Service (PPPS), first visit
G0439 Annual Wellness Visit, includes PPPS, Subsquent Visit
No specific diagnosis (ICD-9) is required. Co-insurance, co-pay and/or
deductible waived. When a significant, separately identifiable medically
necessary E/M service in addition to the SWV, use 99201-99215 with
modifier -25; however co-pay, deductible, co-insurance required for E/M
Service.
E/M Service must be separately documented, no “double dipping” in
history or exam.

Approved
Instructor
Approved instructor
Guidance from the CDC on Health Risk Assessment
• At the request of the Centers for Medicare and Medicaid Services (CMS), the Centers for Disease Control and Prevention (CDC) is providing initial guidance on the development of a health risk assessment tool.
• http://www.cms.gov/coveragegeninfo/downloads/healthriskassessmentsCDCfinal.pdf

Approved
Instructor
Approved instructor
Insurance Coverage Issues
• Insurance plans vary on the range of services covered by a patient’s policy
• High deductibles, copays, co-insurance should be verified before providing a service
• Medical Necessity is key
• Preventive services are often covered but research your contacted payers for their reimbursement policies

Approved
Instructor
Approved instructor
References
CMS Evaluation and Management Guide
http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/downloads/eval_mgmt_serv_guide-ICN006764.pdf
CMS Annual Wellness Visit
http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/downloads/AWV_chart_ICN905706.pdf
Risk Assessment
http://www.cms.gov/coveragegeninfo/downloads/healthriskassessmentsCDCfinal.pdf
CMS Preventive Services Guide
http://www.cms.gov/Medicare/Prevention/PrevntionGenInfo/Downloads/MPS_QuickReferenceChart_1.pdf

Approved
Instructor
Approved instructorApproved instructor
Nancy M Enos, FACMPE, CPMA CPC-I, CEMC is an independent consultant with the MGMA Health Care Consulting Group. Mrs. Enos has 35 years of experience in the practice
management field. Nancy was a practice manager for 18 years before she joined LighthouseMD in 1995 as the Director of Physician Services and Compliance Officer. In July 2008 Nancy established an independent consulting practice, Nancy Enos Medical Coding.
As an Approved PMCC and ICD-10 Instructor by the American Academy of Professional Coders, Nancy provides coding certification courses, outsourced coding services, chart
auditing, coding training and consultative services and seminars in CPT and ICD-9and ICD-10 Coding, Evaluation and Management coding and documentation, and Compliance Planning.
Nancy frequently speaks on coding, compliance and reimbursement issues to audiences including National, State and Sectional MGMA conferences, and at hospitals in the provider
community specializing in primary care and surgical specialties.
Nancy is a Fellow of the American College of Medical Practice Executives. She serves s as a College Forum Representative for the American College of Medical Practice Executives. She is
on the board of Eastern Section MGMA and serves as Past President.
About the Speaker

Joji Suzuki, MD
Motivational Interviewing: The Evidence-Based Strategies that
Produce the Best Results

Talking about change:
Principles of motivational interviewing Joji Suzuki MD
Instructor in Psychiatry, Harvard Medical School
Department of Psychiatry, Brigham and Women’s Hospital
Member, Motivational Interviewing Network of Trainers

A typical conversation about behavior change can
quickly turn into an argument
You need to stop
using drugs. If you don’t stop using
drugs you will end up
dead.
I know why I need to
stop, but right now it’s
just not my priority.
Yes, I know I
need to stop, but
it’s so hard….
Change!
Yes but no!

How do conversations about behavior change* make you feel?
*reducing or stopping alcohol, drugs, or tobacco, changing dietary habits, exercising, taking medication,
checking blood sugar, keeping appointments, going to psychotherapy, flossing, getting a colonoscopy...
This is
frustrating
It feels futile
to even try
He obviously doesn’t
care about his own
health
This feels like
a waste of
time I don’t like
this
I feel
powerless

You would rather feel less frustrated and be
more effective in helping patients change

Psychotherapy
Stages of change model
Decisional balance (pros and cons)
For every patient in every situation
Easy to attain competence

British J Gen Practice 55: 305-312, 2005
Meta-analysis of 72 randomized controlled trials of MI
MI outperformed traditional advice giving in 80% of studies
Positive outcomes in 64% of studies (7/11) with encounters <20 minutes
Proportion of studies with positive outcomes obtained when MI delivered by:
Physician: 83% (19/23)
Psychologist: 79% (33/42)
Other: 46% (5/11)

Weak Comparison
groups
Strong Comparison
groups
Effect
Size
Difference
in success
rate (%)
Effect
Size
Difference in
success rate
(%)
Burke et al 2003 0.35 17 0.04 2
Hettema et al 2005 0.27 13 0.32 15
Vasilaki et al 2006 0.40 19 0.27 13
Lundahl et al 2009 0.28 14 0.09 5

Engaging
Focusing
Evoking
Planning

Engaging The relational foundation
and patient-centered communication

Spirit of MI
Acceptance
Evocation
Partnership
Compassion

Reflections

Reflective listening

I know how you must feel.
It must have been difficult
for you.

What the
speaker actually
meant to say
What the
speaker said
What the listener
thinks the speaker
meant to say
What the
listener heard
Reflectio
n


Simple reflections stay close to what the patient
said
I think I should
quit drinking.
You want to quit
drinking.

Simple reflections stay close to what the patient
said
I don’t know if I’m
ready to quit
drinking.
You’re not sure if
you’re ready.

Complex reflections add substantial meaning
I nned to stop
drinking.
Losing your job was
a wake-up call.

Complex reflections add substantial meaning
I’m not sure I can
quit drinking.
You’re not as
confident as you’d
like to be.
Complex reflections add substantial meaning
I’d like to get
sober.
On the one hand you like
your beer, and on the
other hand you want to
be there for your family.

Using reflections to “Roll with resistance”
I know I need to
stop heroin, but
cocaine is not a
big deal.
You’re not sure if cocaine
use is really that much of
a problem, although you
know heroin has ruined
your life.

Using reflections to “Roll with resistance”
I’m not going to
stop smoking pot. For now, changing how
you smoke marijuana is
not your priority.

Affirmations

Affirmations
Statements of appreciation for patient’s efforts or strengths
Genuine words of understanding
“You” statements, not “I”
Focus on specific behaviors
Nurture a competent self

I’m here to detox.
You’ve been to detox
five times already, and
you’re willing to try
again. It takes a lot of
courage to do that.

I can’t continue to
drink like this.
It’s important for
you to be a
responsible
husband.
Engaging
Focusing
Evoking
Planning

Focusing Agreeing what to talk about and
agenda setting

Focus clear
Several options
No clear path

Ask-Tell-Ask

1) Ask permission, or what they already know
2) Provide information or give advice
3) Ask what they think of that information
Ask
Tell
Ask
Ask-Tell-Ask

1) “What is the most important issue for us to
discuss today?”
2) “Great, we will definitely address your concerns
about the pain. I also want to make sure we
have a chance to discuss your blood test from
last visit.”
3) “Would that be ok with you?”
Ask
Tell
Ask
Skill #1: Giving Information or Advice (Ask-Tell-
Ask)

1) “Would it be ok if I shared some thoughts I have
the importance of exercise?”
2) “Increasing your physical activity level can
provide a lot of health benefits by reducing your
risk for a variety of illnesses, such as diabetes,
heart disease, and certain types of cancer.”
3) “What are your thoughts about that?”
Ask
Tell
Ask
Giving Information or Advice (Ask-Tell-Ask)


Engaging
Focusing
Evoking
Planning

Evoking Increasing motivation

External motivations are imporant, and sometimes
they are crucial
You should
stop smoking.

But ultimately, patients themselves have to find the
internal motivation to change
But we can’t directly see internal motivation

Most patients are ambivalent about most
unhealthy behaviors.
Most patients are ambivalent about most
unhealthy behaviors.
I don’t want
to change I want to
change
This side of the
ambivalence is
called Change Talk
This side of the
ambivalence is
called Sustain Talk

If pushed to change, patients who are ambivalent
often go to the other side of the ambivalence
I don’t want
to change I want to
change
You need to
change!

Instead, the goal of MI is to evoke change talk
I don’t want
to change I want to
change
We want patients
to argue for this
themselves

Change Talk (DARN-CAT)
D: Desire I want to…, I wish…, I’d like to….
A: Ability I could…, I know I can…., I could try….
R: Reason I want to change because…..
N: Need I should…, I need to…., I must….
C: Commitment I will…., I promise to…., I guarentee…
A: Activating I am ready to…., I am willing to…
T: Steps Taken I’ve tried…

Evoking change talk

Taste of MI questions
1) Is there something you would like to do for your health in the
next 1-2 weeks?
2) If you were to stop using cocaine, how would you go about
doing it?
3) What are the 3 most important reasons to stop using cocaine?
4) On a scale of 1 to 10, 10 being completely ready, 1 being not
at all ready, how ready are you to cut stop using cocaine?
Followup with: Why did you pick that, and not a lower number?

Selective responding to strenghten change talk
I don’t drink any more
than my friends. Sure I
sometimes feel a little
foggy the next day, but its
no big deal.
You feel a little
foggy the next
day. Tell me more
about that.
I don’t drink any more
than my friends. Sure I
sometimes feel a little
foggy the next day, but its
no big deal.
You are worried about
how it’s affecting your
work. What do you
already know about
how alcohol impacts
the brain?

Selective responding to strenghten change talk
It’s such a hassle to take
Prozac. I know I’m
supposed to take them,
but I don’t even have
them with me half the
time. There are good
reasons to be on them,
but it’s just not possible.
You have good
reasons to take them.
Tell me about that.
It’s such a hassle to take
the medication. I know
I’m supposed to take
them, but I don’t even
have them with me half
the time. There are good
reasons to be on them,
but it’s just not possible.
Despite the hassle,
you find a way to take
them some of the
time. How are you
successful half the
time?
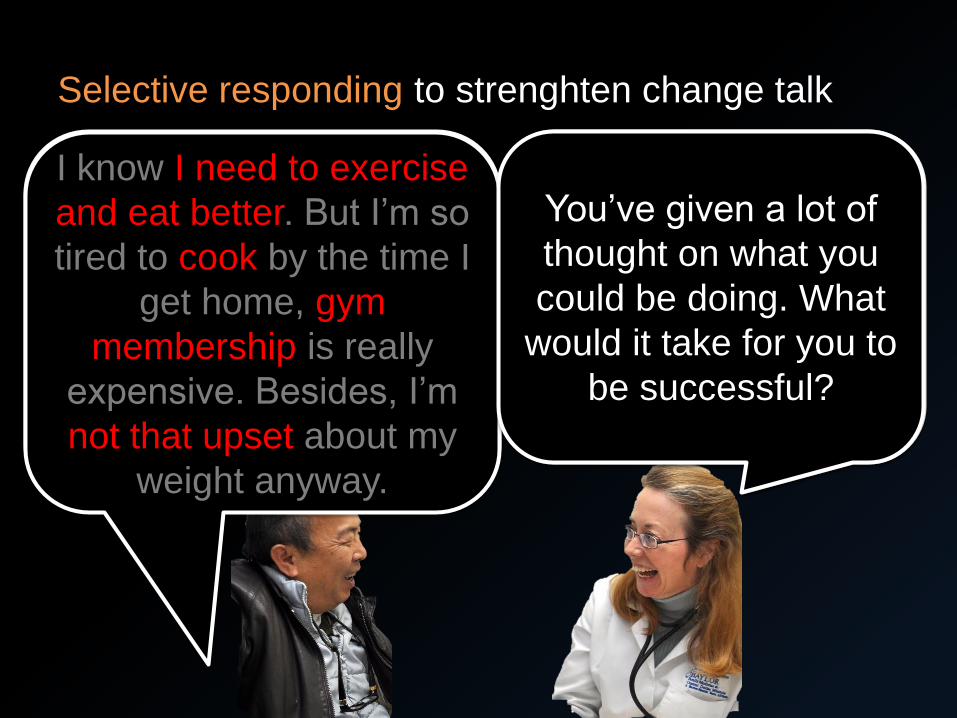
Selective responding to strenghten change talk
I know I need to exercise
and eat better. But I’m so
tired to cook by the time I
get home, gym
membership is really
expensive. Besides, I’m
not that upset about my
weight anyway.
You’re ok with your
weight, and yet a part
of you is still bothered
by it.
I know I need to exercise
and eat better. But I’m so
tired to cook by the time I
get home, gym
membership is really
expensive. Besides, I’m
not that upset about my
weight anyway.
You’ve given a lot of
thought on what you
could be doing. What
would it take for you to
be successful?
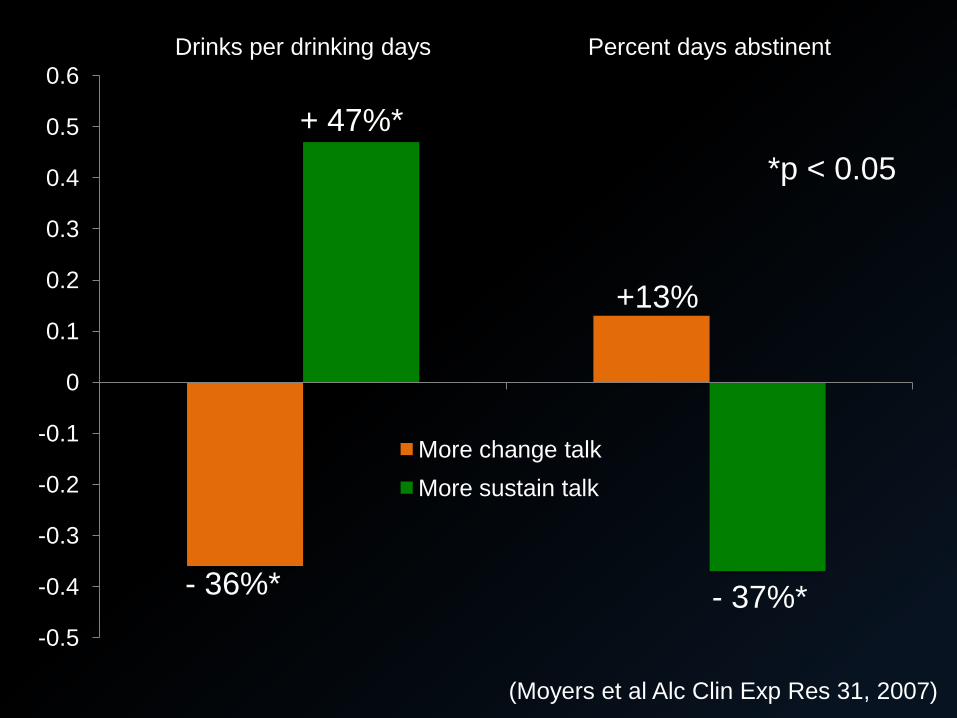
(Moyers et al Alc Clin Exp Res 31, 2007)
-0.5
-0.4
-0.3
-0.2
-0.1
0
0.1
0.2
0.3
0.4
0.5
0.6
Drinks per drinking days Percent days abstinent
More change talk
More sustain talk
*p < 0.05
- 36%*
+ 47%*
+13%
- 37%*

(Moyers et al Alc Clin Exp Res 31, 2007)
0
5
10
15
20
25 Likelihood of evoking Change Talk Likelihood of evoking Sustain Talk
MI Consistent behaviors
MI Inconsistent behaviors + 17%
+ 9%
+ 0.02% 0%

More
Sustain Talk Less change
MI inconsistent
behaviors
More
Change Talk More change
MI consistent
behaviors
You are in full control here. Patients are in full control
here.

Engaging
Focusing
Evoking
Planning

Planning Translating motivation into action

The KEY question

Building motivation
A B
What will you do?
Where should we
go from here?
Where does that
leave you?

Specific:
Measurable:
Achievable/Re
alistic:
Timely:
What will you do?
For how long? how much? how
many?
What have you done before that’s
worked?
When will you start?
Action Planning

Specific:
Measurable:
Achievable/Re
alistic:
Timely:
Walk to the park and back in the
evenings, Mondays and
Wednesdays
Walk for 10 minutes
Has done this before, and
confident about succeeding with
plan
Start tonight
Skill #6: Action Planning

Confidence scaling
On a scale of 1-10, 1 being not at all confident,
and 10 being completely confident, how
confident are you that this plan will work for
you?

Add some accountability
When can we meet again to discuss your
progress?
When would you like to meet with our care
manager to discuss how things are going?
If you’d like, we could talk more about this
during the next visit.


You would rather feel less frustrated and be
more effective in helping patients change

Further training
Practice, practice, practice
Listen to how patients respond
Introductory MI training (2 days)
Advanced MI training (1-2 days)
Feedback on your practice by coach/supervisor/peer/patients

Sat Bir Singh Khalsa, PhD
Sleep

Sleep
June 27, 2015
Lifestyle Medicine 2015
Harvard Medical School CME Course
Sat Bir S. Khalsa, Ph.D.
Assistant Professor of Medicine, Harvard Medical School
Research Associate, Benson Henry Institute for Mind Body Medicine
Brigham & Women’s Hospital Harvard Medical School

Conflicts of Interest / Disclosures
• I have no financial conflicts of interest with commercial entities
• I am funded in part by non-profit charitable organizations that support yoga practice
• I am strongly biased in favoring behavioral and mind-body medicine as a first-line treatment strategy

Objectives
• To describe the underlying characteristics of sleep and its importance
• To describe major sleep disorders, their etiology and their lifestyle implications
• To describe lifestyle behaviors and strategies for improving sleep and sleep disorders

Sleep
• A biological need
• Sleep : Wakefulness
• An active process
• A complex process

Physiologic Determinants
Sleep and Wakefulness
• Biological Time of Day (circadian phase)
• Number of Hours Awake & Nightly Sleep
Duration

Sleep Disorders
Three major categories:
• Parasomnias
• Disorders of excessive daytime
sleepiness
• Insomnia


Sleep DisordersSocioeconomic Consequences
• 40 million Americans suffer from chronic disorders of
sleep and wakefulness.
• 95% of these remain unidentified and undiagnosed.
• The annual direct cost of sleep-related problems is $16
billion, with an additional $50-$100 billion in indirect
costs (accidents, litigation, property destruction,
hospitalization, and death).
• More than 100,000 motor vehicle accidents annually
are sleep-related.
• Disasters such as Chernobyl, Three Mile Island,
Challenger, Bhopal, and Exxon Valdez were officially
attributed to errors in judgement induced by sleepiness
or fatigue.


Disorders of Excessive Daytime
Sleepiness
Defining Hypersomnolence
• Must be distinguished from fatigue.
• Is a tendency to fall asleep
unintentionally in passive situations:
– Reading
– Watching television
– Driving
– Lectures

Differential Diagnosis
of Excessive Daytime Sleepiness
Increased Sleep Drive:
• Narcolepsy
• Primary Central Nervous System Hypersomnolence
Sleep Disruption:
• Obstructive Sleep Apnea
• Periodic Limb Movement Disorder
• Restless Legs Syndrome
Inadequate Sleep:
• Self Imposed Sleep Restriction
• Shift Work
Other
Sleep Apnea

Sleep Apnea Recording

Sleep Apnea Recording

Hyoid Bone
Mandible
Maxilla
Nasal Passage
Trachea
Epiglottis
Tongue
(Genioglossus)
Soft Palate
Choanae
Anatomy of the Upper Airway

Sleep Apnea
Risk Factors and Consequences
From: Risk factors for obstructive sleep apnea in adults. Young T, Skatrud J,
Peppard PE. Journal of the American Medical Association 291:2013-2016, 2004.


Sleep Apnea
Treatments
From: Obstructive sleep apnea
syndrome: Diagnosis and management,
Goodday RHB, Precious DS, Morrison
AD, Robertson CG, Journal of the
Canadian Dental Association, 67:652-
658,2001

From: Norman JF, Von Essen SG, Fuchs RH, McElligott M., Exercise training
effect on obstructive sleep apnea syndrome. Sleep Res Online. 000;3(3):121-9.
Sleep Apnea
Behavioral Treatment

Self-Restricted Sleep

Self-Restricted Sleep
From: QuickStats: Percentage of Adults Aged >18 Years Who Reported an Average of <6
Hours of Sleep per 24-Hour Period, by Sex and Age Group --- National Health Interview
Survey, United States, 1985 and 2006, MMWR Morbidity and Mortality Weekly Report,
Centers for Disease Control and Prevention 57:209, 2008.

From: The cumulative cost of additional wakefulness: dose-response effects on neuro-
behavioral functions and sleep physiology from chronic sleep restriction and total sleep
deprivation. Van Dongen HP, Maislin G, Mullington JM, Dinges DF. Sleep 26:117-26, 2003.
Cumulative Sleep Deprivation
Cognitive Function
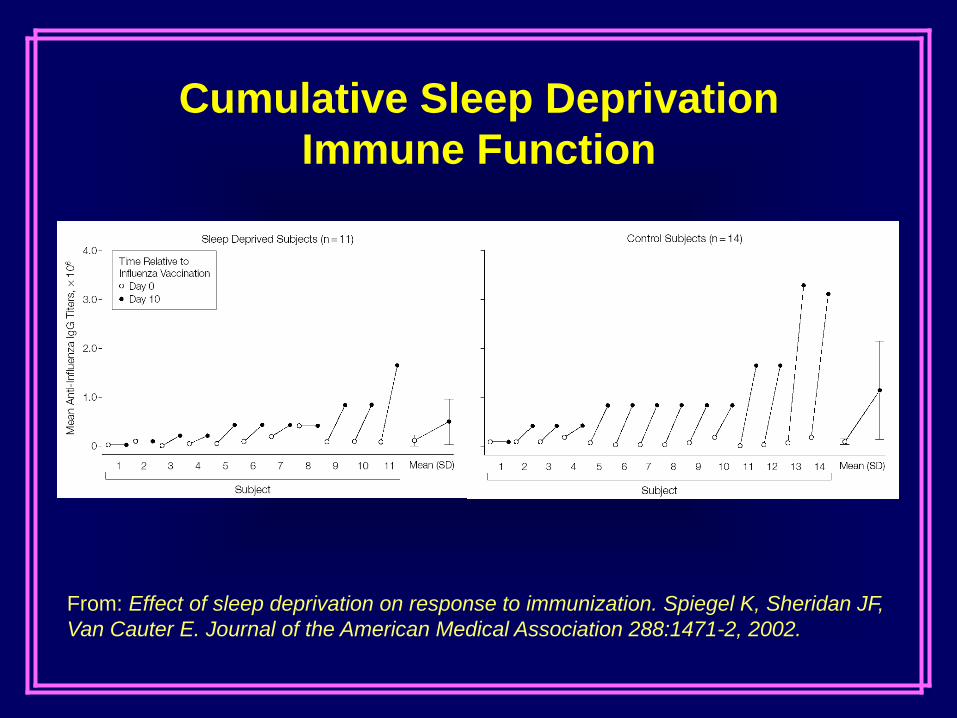
From: Effect of sleep deprivation on response to immunization. Spiegel K, Sheridan JF,
Van Cauter E. Journal of the American Medical Association 288:1471-2, 2002.
Cumulative Sleep Deprivation
Immune Function

From: Sleep loss: a novel risk factor for
insulin resistance and Type 2 diabetes,
Spiegel K, Knutson K, Leproult R, Tasali
E, Van Cauter E. Journal of Applied
Physiology 99:2008-19, 2005.
Cumulative
Sleep
Deprivation
Endocrine
Function
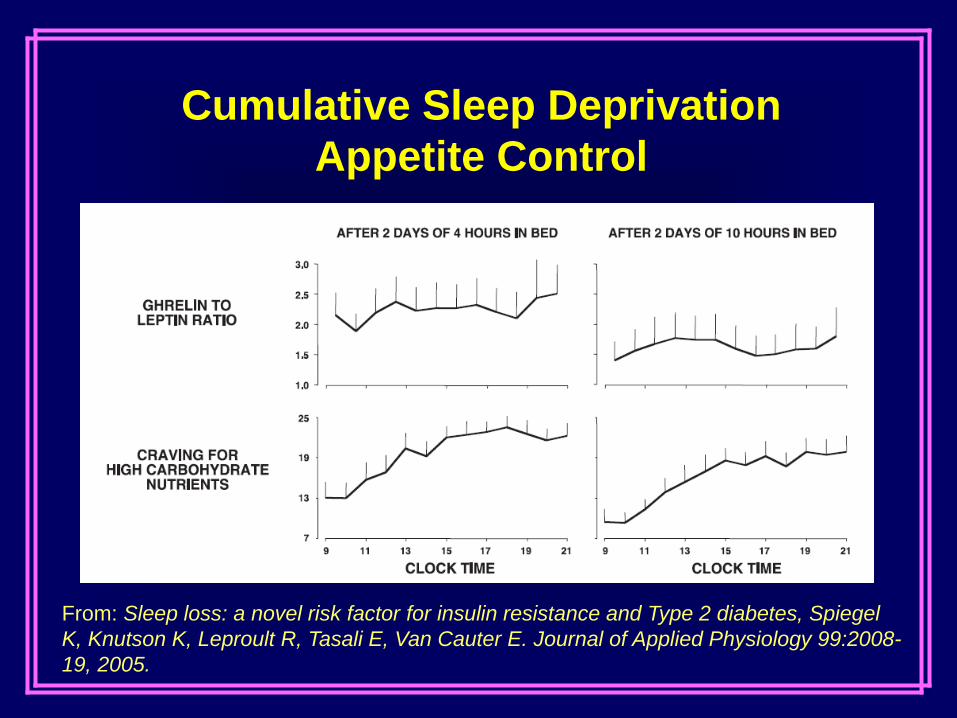
From: Sleep loss: a novel risk factor for insulin resistance and Type 2 diabetes, Spiegel
K, Knutson K, Leproult R, Tasali E, Van Cauter E. Journal of Applied Physiology 99:2008-
19, 2005.
Cumulative Sleep Deprivation
Appetite Control

ChronicSleep Deprivation
ObesityMetabolic SyndromeDiabetes
Sleep ApneaSelf-restricted Sleep
Impairment/Dysfunction- Cognitive- Immune- Autonomic

Insomnia



“…the overall prevalence estimate of broadly defined insomnia (23.6%)
is considerably higher than the 6% to 10% prevalence range widely
reported in reviews of previous epidemiological studies.”
“Insomnia is…associated with substantial decrements in perceived
health.
America Insomnia Study
From: Roth T et al., Prevalence and perceived health associated with insomnia based
on DSM-IV-TR; International Statistical Classification of Diseases and Related Health
Problems, 10th Rev.; and Research Diagnostic Criteria/ICSD, 2nd Ed. criteria: results
from the America Insomnia Survey, Biological Psychiatry 69(6):592-600, 2011.
“…insomnia is much more strongly related to presenteeism than
absenteeism. This means that workers with insomnia generally
put in the same number of work hours as other workers, but
that their on-the-job performance is lower than other workers.”
“…estimate of $59.8 billion annual lost productivity…”
From: Insomnia and the performance of US workers: results from the America insomnia
survey, Kessler RC, Berglund PA, Coulouvrat C, Hajak G, Roth T, Shahly V, Shillington
AC, Stephenson JJ, Walsh JK, Sleep, 34:1161-71, 2011.



Insomnia Presentation
Sleep onset insomnia
Sleep maintenance insomnia
Poor quality/non-restorative sleep

Insomnia Diagnostic Criteria
Sleep onset latency > 30 minutes
Wake time after sleep onset > 30 minutes
Frequency at least 3 times/week
Duration at least 6 months
Significant daytime impairment

Medicationsand substances
• Acute use• Chronic use• Withdrawal
Circadian Factors• Jet lag• Shift work• Advanced, delayed
sleep phases
Medical/NeurologicalFactors
• Pain, discomfort• Specific disorders
Psychiatric orPsychological Factors
• Depression or Anxiety • Bereavement• Acute stress
EnvironmentalFactors
• Physical discomfort• Noise• Light
PrimarySleep Disorders• Restless Legs Syndrome• Periodic limb movements• Respiratory arousals• Parasomnias
INSOMNIA
From: The evaluation and treatment of
insomnia, Buysse DJ, Perlis ML, Journal
of Practical Psychiatry and Behavioral
Health. 10:541-553, 1987.

Medicationsand substances
• Acute use• Chronic use• Withdrawal
Circadian Factors• Jet lag• Shift work• Advanced, delayed
sleep phases
Medical/NeurologicalFactors
• Pain, discomfort• Specific disorders
Psychiatric orPsychological Factors
• Depression or Anxiety • Bereavement• Acute stress
EnvironmentalFactors
• Physical discomfort• Noise• Light
PrimarySleep Disorders• Restless Legs Syndrome• Periodic limb movements• Respiratory arousals• Parasomnias
Behavioral,Psychophysiological,
and Conditioning Factors• Fear, frustration with insomnia• Sleep-incompatible behaviors• Increased arousal
INSOMNIA

Behavioral,Psychophysiological,
and Conditioning Factors• Fear, frustration with insomnia• Sleep-incompatible behaviors• Increased arousal
INSOMNIA

Models of Primary Insomnia
Conditioning
Emotional Arousal
Cognitive Arousal
Physiological Arousal

Insomnia Treatment
• Treat underlying cause (secondary insomnia)
• Pain, depression, anxiety, sleep disordered
breathing, RLS/PLMD
• Pharmacological Treatments
• Behavioral Treatments

Insomnia Treatment
Pharmacological Treatment
Antihistimines / Melatonin / Valerian (Over-the-counter)
• Little or no efficacy as nighttime hypnotics, mild sedation
• Antihistamines have daytime sedative effects (hangover) and
anticholinergic side effects
Hypnotics
• Recommended mostly as adjunctive therapy for transient or
intermittent insomnia with minimal dosing for brief periods
• Primarily benzodiazepines or a few non -benzodiazepines
• Half - life should be tailored to sleep disturbance
• Side effects include paradoxical insomnia or disruption of
sleep architecture, anterograde amnesia, withdrawal
symptoms
• Tolerance is common
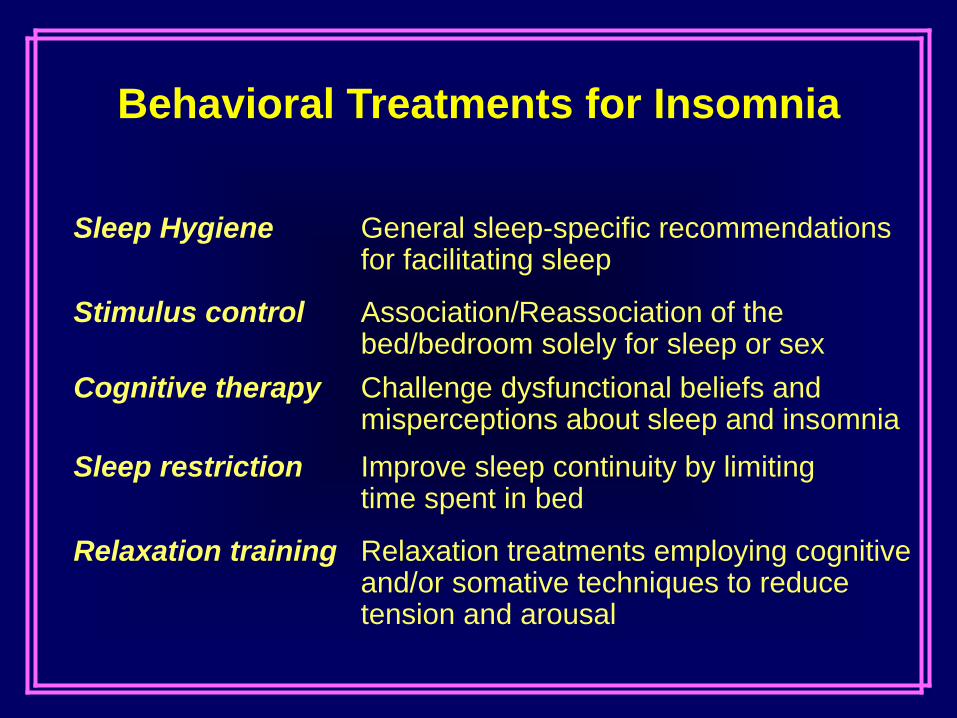
Behavioral Treatments for Insomnia
Sleep Hygiene General sleep-specific recommendations for facilitating sleep
Stimulus control Association/Reassociation of the bed/bedroom solely for sleep or sex
Cognitive therapy Challenge dysfunctional beliefs andmisperceptions about sleep and insomnia
Sleep restriction Improve sleep continuity by limitingtime spent in bed
Relaxation training Relaxation treatments employing cognitive and/or somative techniques to reduce tension and arousal



• Avoid stimulants such as caffeine 4-6 hours before bedtime.
• Avoid drinking alcohol 4-6 hours before going to bed.
• Eat a light, easily digestible snack before bed but avoid large
meals before bedtime.
• Adopt a regular exercise program
• Avoid exercising within 3-4 hours of bedtime.
• Give yourself a quiet period or calm time for at least one or two
hours before bed.
• Develop a regular pre-sleep routine.
• Improve the comfort of your bed if needed.
• Reduce noise and disruptions.
• Reduce light in the bedroom.
• Maintain a regular temperature.
Behavioral Treatments for Insomnia
Sleep Hygiene


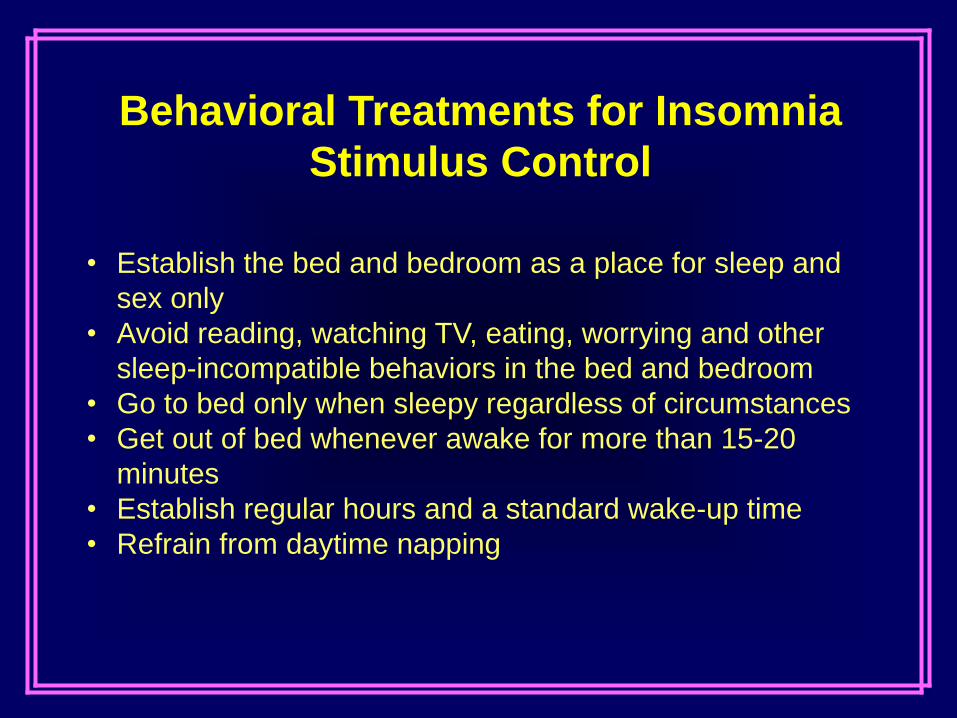
• Establish the bed and bedroom as a place for sleep and
sex only
• Avoid reading, watching TV, eating, worrying and other
sleep-incompatible behaviors in the bed and bedroom
• Go to bed only when sleepy regardless of circumstances
• Get out of bed whenever awake for more than 15-20
minutes
• Establish regular hours and a standard wake-up time
• Refrain from daytime napping
Behavioral Treatments for Insomnia
Stimulus Control



1. Identify thoughts about sleep that tend to make sleeping more difficult
2. Replace these thoughts with more constructive thoughts
The more important it is to get a good night's sleep, the less sleep is possible.
Belief that a poor night's sleep is a disaster only generates more anxiety
and worry about sleep. For example, beliefs such as "everyone needs 8
hours of sleep to function well during the day" or "insomnia is necessarily
detrimental to physical and mental health" only create performance anxiety
and worsen sleep problems. Challenge this thinking and consider
alternative thoughts that minimize the negative consequences of insomnia
(i.e. "It's no big deal", "I'll be a little tired and cranky tomorrow but nothing I
can't handle.").
The more you try to control your sleep, the less you sleep. Sleep is a natural
body response. Telling yourself that you must sleep and trying to force
yourself to sleep only puts pressure on you and makes your sleep worse.
Paradoxical Intention as a cognitive treatment.
Behavioral Treatments for Insomnia
Cognitive Restructuring
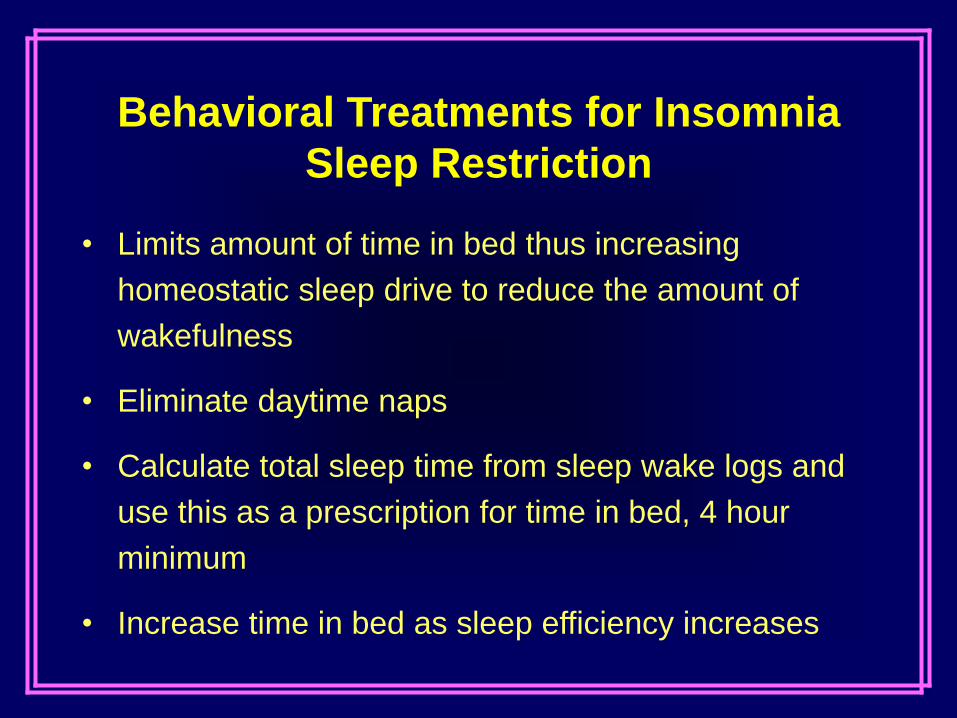
• Limits amount of time in bed thus increasing
homeostatic sleep drive to reduce the amount of
wakefulness
• Eliminate daytime naps
• Calculate total sleep time from sleep wake logs and
use this as a prescription for time in bed, 4 hour
minimum
• Increase time in bed as sleep efficiency increases
Behavioral Treatments for Insomnia
Sleep Restriction



Adam K et al, J Psychiatr Res, 1986
Physiological Arousal in Insomnia
Bonnet MH & Arand DL, Sleep, 1995
Johns MW et al., Psychosom Med, 1971 Bonnet MH & Arand DL, Psychosom Med, 1998

Insomnia as Disorder of Hyperarousal
“…primary insomniacs suffer from a disorder of
hyperarousal and that the elevated arousal produces
the poor sleep and other symptoms reported by
patients. It is therefore suggested that new treatment
strategies directed at reduction of arousal level be
considered in these patients.”
“Treatments for insomnia, such as relaxation, exercise
training, and some medications…may provide long-term
benefits over and above short-term improvement in
reported sleep quality.”
From: Heart rate variability in insomniacs and matched normal sleepers,
Bonnet MH & Arand DL, Psychosomatic Medicine 60:610-615, 1998.
From: Hyperarousal and insomnia, Bonnet MH & Arand DL, Sleep Medicine
Reviews 1:97-108, 1997.

Relaxation Treatments for Insomnia
• Progressive muscle relaxation
• Biofeedback
• Guided imagery
• Autogenic training
• Meditation
• Yoga

Mind-body interventions were able to improve sleep efficiency and total sleep
time. Most can ameliorate sleep quality; some can reduce the use of hypnotic
drugs in those who are dependent on these drugs.
According to the studies we selected, self-reported sleep was improved by all
mind-body treatments, among them yoga, relaxation, Tai Chi…



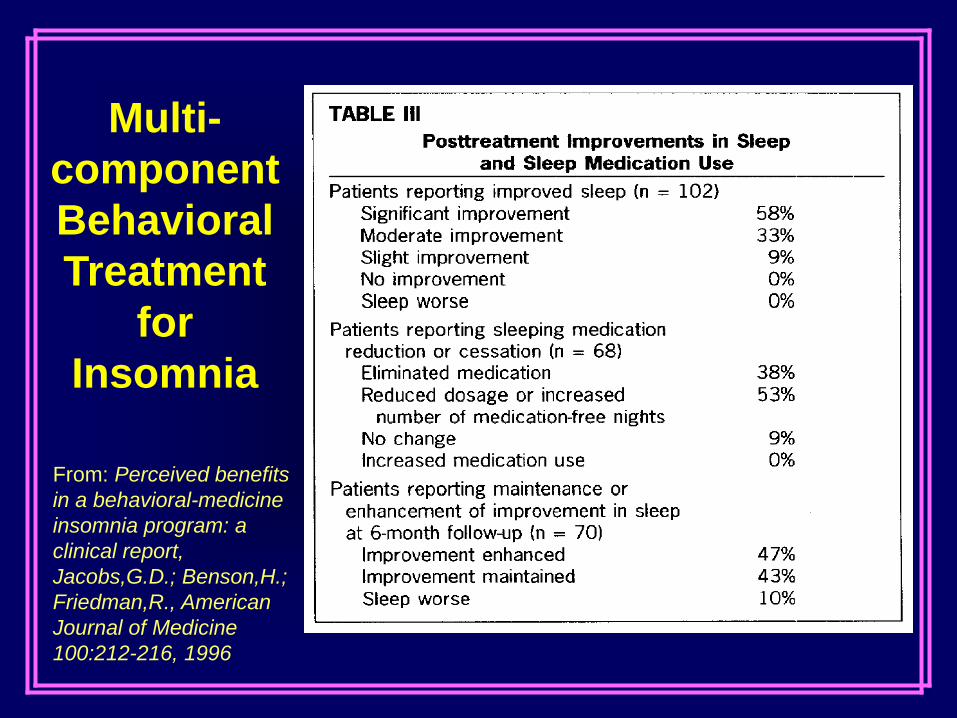
From: Perceived benefits
in a behavioral-medicine
insomnia program: a
clinical report,
Jacobs,G.D.; Benson,H.;
Friedman,R., American
Journal of Medicine
100:212-216, 1996
Multi-
component
Behavioral
Treatment
for
Insomnia


Yoga for
Sleep

Sleep in Yoga Practitioners
From: Subjective sleep quality and hormonal modulation in long-term yoga practitioners,
Vera FM, Manzaneque JM, Maldonado EF, Carranque GA, Rodriguez FM, Blanca MJ,
Morell M, Biological Psychology 81:164-8, 2009.

Sleep in Elderly Yoga Practitioners
From: Impact of long term Yoga practice on sleep quality and quality of life in the elderly,
Bankar MA, Chaudhari SK, Chaudhari KD, Journal of Ayurveda and Integrative
Medicine, 4:28-32, 2013.
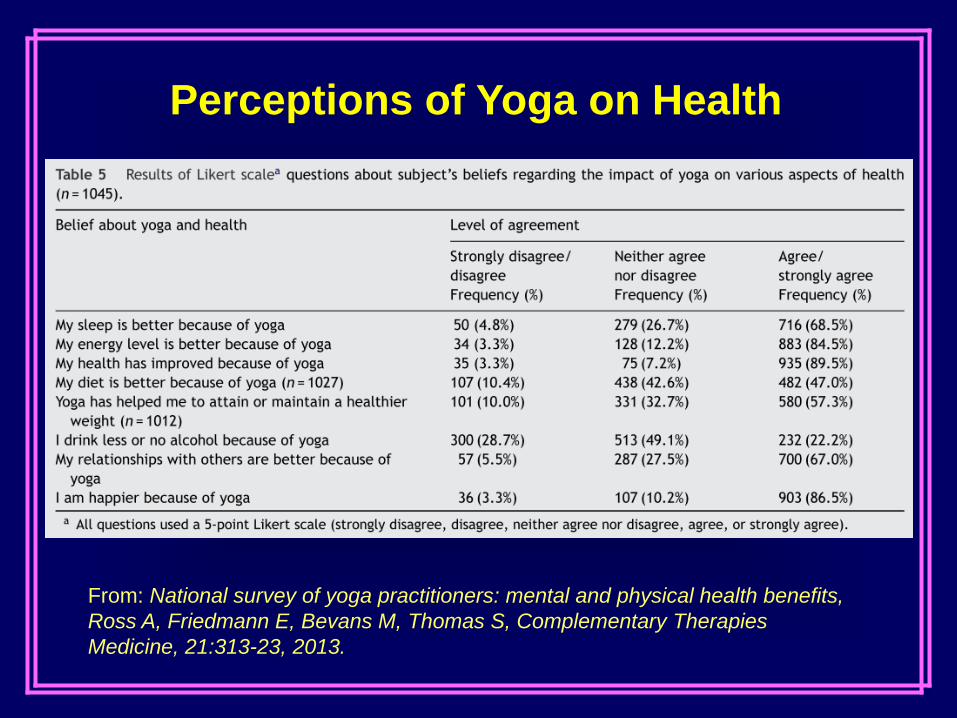
Perceptions of Yoga on Health
From: National survey of yoga practitioners: mental and physical health benefits,
Ross A, Friedmann E, Bevans M, Thomas S, Complementary Therapies
Medicine, 21:313-23, 2013.

Yoga Practice Associations
From: Frequency of yoga practice predicts health: results of a national survey of
yoga practitioners, Ross A, Friedmann E, Bevans M, Thomas S, Evidence
Based Complementary and Alternative Medicine, 983258, 2012.

Yoga on Sleep in the Elderly
From: Influence of Yoga & Ayurveda on self-rated sleep in a geriatric population,
Manjunath NK, Telles S, Indian Journal of Medical Research 121:683-690, 2005.
5.5
5.7
5.9
6.1
6.3
6.5
6.7
6.9
7.1
7.3
Pretreatment Posttreatment Followup
Sle
ep
Du
rati
on
(H
ou
rs) Yoga Controls
20
25
30
35
40
45
Pretreatment Posttreatment Followup
Sle
ep
On
se
t L
ate
nc
y (
Min
)
Yoga Controls

Sle
ep O
nset Late
ncy
0
30
60
90
120
Sle
ep Q
ualit
y
1
2
3
4
5N
um
ber
of A
wakenin
gs
0
1
2
3
4
Tota
l S
leep T
ime
0
2
4
6
8
Tota
l W
ake T
ime
0
2
4
6
Sle
ep E
ffic
iency
0
25
50
75
100
Subject CH
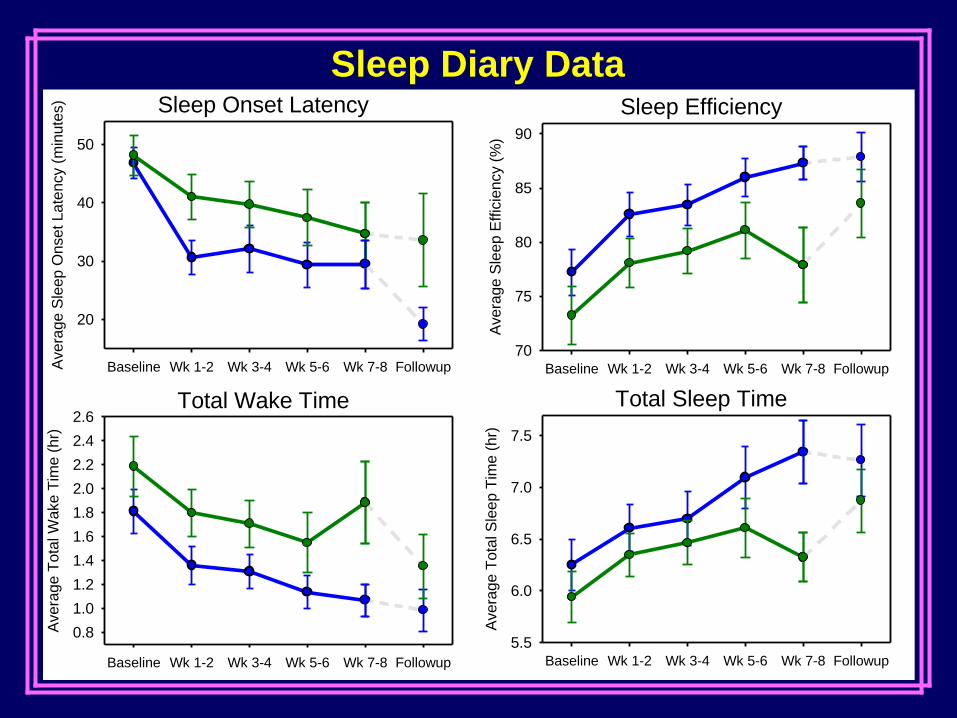
Sleep Onset Latency
Baseline Wk 1-2 Wk 3-4 Wk 5-6 Wk 7-8 FollowupAvera
ge S
leep O
nset Late
ncy (
min
ute
s)
20
30
40
50
Sleep Efficiency
Baseline Wk 1-2 Wk 3-4 Wk 5-6 Wk 7-8 Followup
Avera
ge S
leep E
ffic
iency (
%)
70
75
80
85
90
Total Wake Time
Baseline Wk 1-2 Wk 3-4 Wk 5-6 Wk 7-8 Followup
Avera
ge T
ota
l W
ake T
ime (
hr)
0.8
1.0
1.2
1.4
1.6
1.8
2.0
2.2
2.4
2.6Total Sleep Time
Baseline Wk 1-2 Wk 3-4 Wk 5-6 Wk 7-8 Followup
Avera
ge T
ota
l S
leep T
ime (
hr)
5.5
6.0
6.5
7.0
7.5
Sleep Diary Data



Kripalu | center for yoga & health


“Now, when I can’t sleep I can watch a little TV.”

http://www.aasmnet.org
American Academy of Sleep Medicine
http://www.nhlbi.nih.gov/health/public/sleep
National Heart Lung and Blood Institute
http://www.users.cloud9.net/~thorpy
Sleep Medicine Home Page
http://www.sleepnet.com
Sleepnet.com
http://www.sleepfoundation.org/default.cfm
National Sleep Foundation
Website Links

Fatima Cody Stanford, MD, MPH
Obesity and Sleep
Fatima Cody Stanford, MD, MPH, MPA
Obesity Medicine & Nutrition
Massachusetts General Hospital
Harvard Medical School
American Board of Obesity Medicine Diplomate

Disclosures
American Academy of Nutrition and Dietetics-Speaker
Medscape- Consultant

Objectives
• Define prevalence of obesity in the United States
• Learn obesity and sleep pathophysiology
• Evaluate the role of sleep in childhood obesity
• Evaluate the role of sleep in adult obesity
• Ascertain role of sleep on energy intake and expenditure
• Outline steps for good sleep hygiene

1 CDC.gov – All numbers from 2012 or 2013 summary data
Obesity Compared to other Diseases in US0 50 100 150 200 250
Prevalence in the US inmillions
Own a Smartphone
Own a TV
Obesity
NAFLD
Diabetes
All Cancers
Breast CA
Colon CA
HIV

Obesity: A Multi-factorial Disorder
Genetics Environment Development Behavior

Regulation of Food Intake
http://www.cellbiol.net/ste/alpobesity2.php

Regulation of Food Intake
Nature Reviews Genetics 10, 431-442 (July 2009)

Regulation of Food IntakeSubstance Production Site Effect
(Relevant for Feeding)
Ghrelin (grow) •Stomach (fundus region,entero-endocrine cells)
•Neurons in the hypothalamus
Appetite (orexigenic)
Anandamide(endocannabinoide, ananda;
bliss, delight + amide )
Small intestine Appetite (orexigenic)
Insulin(insula; island or islet)
Pancreas(β-cells in islets of Langerhans)
•Satiety (anorexigenic)•glycogen and lipid storage
Leptin(leptos, thin)
•Adipocytes (long term)•Stomach (short term)
Satiety (anorexigenic)
CCK(cholecystokinin,
“move the bile-sac”)
Small intestine •Early satiety (anorexigenic)•release of digestive enzymes from exocrine pancreas, bile
from the gallbladder andH+ from parietal cells in stomach
PYY(peptide tyrosine tyrosine)
•Ileum•colon
Satiety (anorexigenic)
http://www.cellbiol.net/ste/alpobesity4.php

Central Nervous System regulates weight
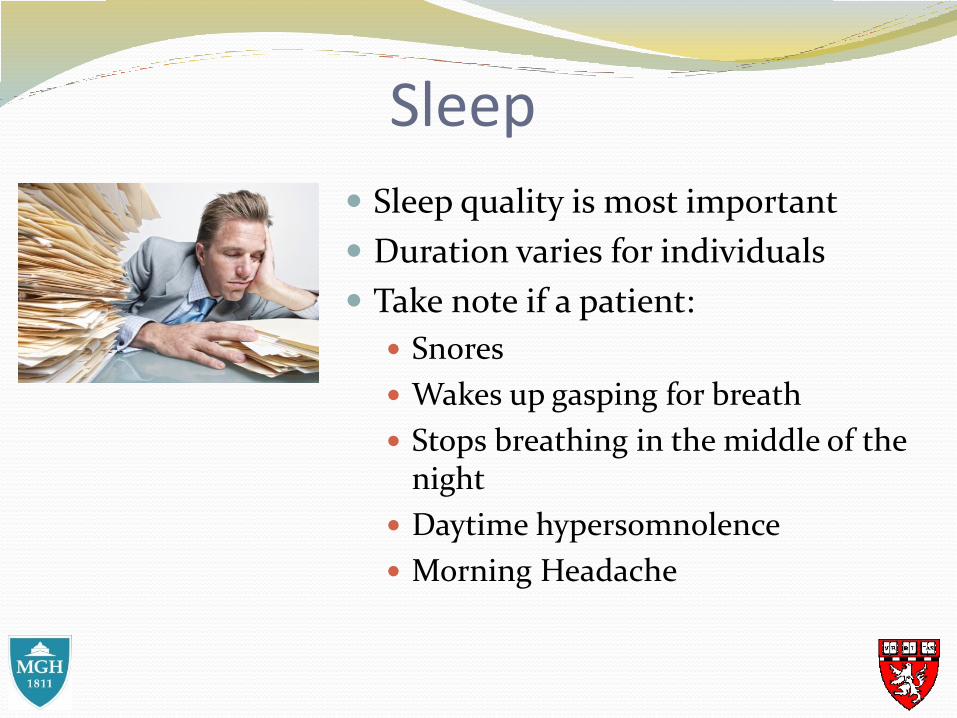
Sleep
Sleep quality is most important
Duration varies for individuals
Take note if a patient:
Snores
Wakes up gasping for breath
Stops breathing in the middle of the night
Daytime hypersomnolence
Morning Headache

Circadian Rhythm Disturbances Loss of circadian resonance appears
to contribute to human obesity
Availability of artificial light leads to progressive disintegration of rhythms of human sleeping
Circadian desynchrony (CD) leads to alterations in:
glucose homeostasis
feeding behavior
metabolic rate
Bioassays 35 :921-924(2012)
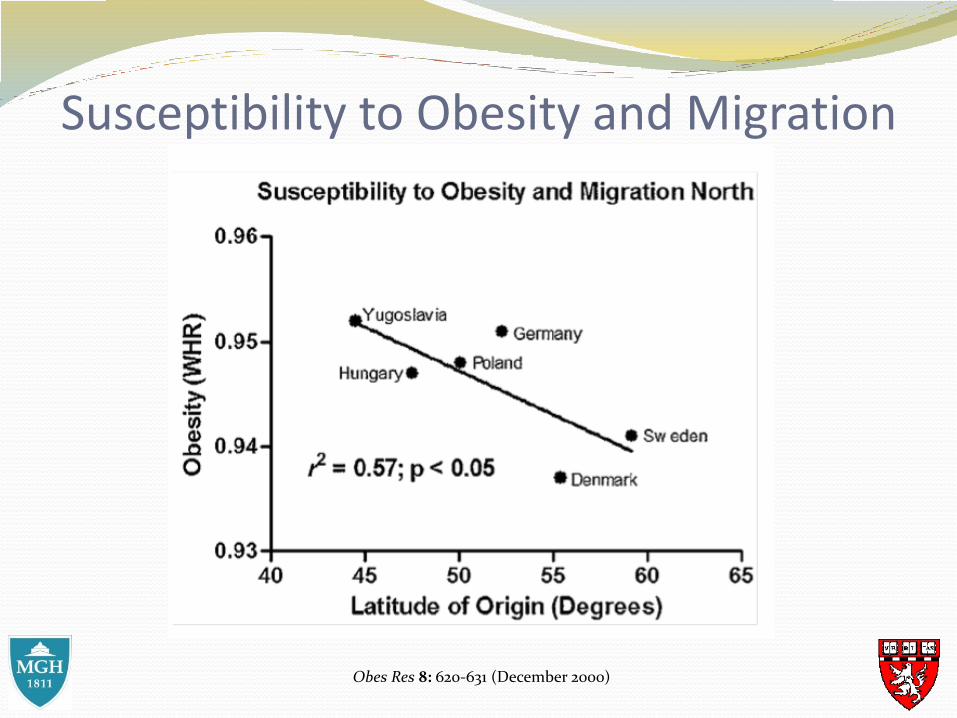
Susceptibility to Obesity and Migration
Obes Res 8: 620-631 (December 2000)

Circadian Rhythm and Metabolism
Journal of Applied Physiology 107 (6): 1972-1980(December 2009)

Circadian Rhythm Regulation
Nature 437 :1257-1263 (October 20o5)

Sleep needs across the lifespanAge Recommended Hours
of SleepAppropriate Range
Newborns (0-3 months) 14 to 17 hours 11 to 19 hours
Infants (4-11 months) 12 to 15 hours 10 to 18 hours
Toddlers (1-2 years) 11 to 14 hours 9 to 16 hours
Preschoolers (3-5 years) 10 to 13 hours 8 to 14 hours
School-Aged Children(6-13 years)
9 to 11 hours 7 to 12 hours
Teenagers (14-17 years) 8 to 10 hours 7 to 11 hours
Young Adults (18-25 years)
7 to 9 hours 6 to 10 hours
Adults (26-64 years) 7 to 9 hours 6 to 10 hours
Older Adults ≥ 65 years 7 to 8 hours 5 to 9 hours
Sleep Health Foundation

Sleep and Childhood Obesity Project Viva- a prospective observational cohort study
of gestational diet, pregnancy outcomes, and offspring health
1676 mother-infant pairs in a pre-birth cohort study
Evaluated mothers’ report of their infants’ average 24-hour sleep duration at 6 months, 1 year, and 2 years of age.
Infants slept mean (SD) durations of 12.2 (2.0) hours/day at 6 months, 12.8 (1.6) hours/day at 1 year, and 11.9 (1.3) hours/day at 2 years.
Acad Pediatr 10 (3):187-193(May-June 2010)
Sleep and Childhood Obesity
Shortened sleep duration at 1 and 2 years of age associated with:
Maternal antenatal depression
Introduction of solids < 4 months
Infant TV/video viewing were associated with shorter sleep durations at both 1 and 2 years of age
Variation in sleep apparent by racial and ethnic background
Acad Pediatr 10 (3):187-193(May-June 2010)

Sleep and Childhood Obesity
Acad Pediatr 10 (3):187-193(May-June 2010)

Sleep and Childhood Obesity
Obesity 19(2):353-361 (February 2011)

Long Term Impact of Childhood Sleep on Obesity

Sleep and Adult Obesity

Sleep and Adult Obesity

Sleep and Adult Obesity

Sleep and Adult Obesity

Sleep Deprivation and Energy Intake
PLoS Med. 2004 Dec; 1(3): e62.

Sleep Deprivation and Energy Intake
PLoS Med. 2004 Dec; 1(3): e62.

Sleep Deprivation and Energy Intake
Am J Clin Nutr 2008;89:126-133.

Sleep Deprivation and Energy Intake
J Physiol Anthropol Appl Human Sci. 2002; 21:115-20..

Sleep Deprivation and Energy Intake
J Physiol Anthropol Appl Human Sci. 2002; 21:115-20..

Sleep Deprivation and Energy Intake
J Physiol Anthropol Appl Human Sci. 2002; 21:115-20..

Sleep Deprivation and Energy Expenditure
May be a decrease in physical activity
May be a drop in body temperature
Conflicting results in studies

Case 44 year old woman Past medical history:
Hypertension Anxiety/ Depression Asthma Fibromyalgia Bipolar disorder Gastroesophageal reflux disease Obstructive sleep apnea Metabolic syndrome X
History of being on several weight promoting: Ziprasidone, Quetiapine, Duloxetine, Citalopram, Fluozetine, Zolpidem, Trazodone, Atenolol, Pregablin, and Nortriptyline
Postpartum weight retention of 20 pounds Poor sleep- daytime hypersomnolence, snoring, morning headache

BMI: 33.5
BMI: 26.5
CPAP
45 year old woman

Sleep Hygiene Tips
1. Avoid Caffeine, Alcohol, Nicotine, and Other Chemicals that Interfere with Sleep
2. Turn Your Bedroom into a Sleep-Inducing Environment
3. Establish a Soothing Pre-Sleep Routine
4. Go to Sleep When You’re Truly Tired
5. Don’t Be a Nighttime Clock-Watcher
6. Use Light to Your Advantage
http://healthysleep.med.harvard.edu/healthy/getting/overcoming/tips

Sleep Hygiene Tips
7. Keep Your Internal Clock Set with a Consistent Sleep Schedule
8. Nap Early—Or Not at All
9. Lighten Up on Evening Meals
10. Balance Fluid Intake
11. Exercise Early
12. Follow Through
http://healthysleep.med.harvard.edu/healthy/getting/overcoming/tips
Conclusion
Obesity is multifactorial disease process
There are different reasons why a person may struggle with weight
Sleep plays a role in weight regulation
Strategies should target individual to determine the best strategy that will help one to achieve a healthy weight

Thank you for your time!Fatima Cody Stanford, MD, MPH
Obesity Medicine & NutritionMassachusetts General Hospital
Harvard Medical SchoolAmerican Board of Obesity Medicine Diplomate

Cheri Blauwet, MD
What Really Gets Patients
(Even Reluctant Ones)
to Effect Health Change

What Really Gets Patients (Even Reluctant Ones)
to Effect Healthy Change
Cheri Blauwet, MDinstructor, Physical Medicine and Rehabilitation
Sports Medicine Service, SRH/BWHChair, Int’l Paralympic Committee Medical Commission

Disclosures
• My disclosures include:
– Travel and accommodation support from the International
Paralympic Committee in my role with the Medical Commission
– Grant reviewer for the Craig H. Neilsen Foundation (Quality of Life
Grant Review Board) and the Foundation for PM&R
– Associate Editor for the PM&R Journal and ad hoc reviewer for
several others

Objectives
• To discuss concepts of who is or is not “active” and
various barriers to physical activity for different populations
• To consider the paradigm of “Universal Design” as a
useful road forward in building opportunities for physical
activity and exercise
• To understand that we, as physicians, truly can make a
difference in effecting change for our patients

Overview – Key Points and Questions
• The beauty of human diversity– “If you have a body, you are an
athlete”
• “No Brakes” – my personal story
• Three principles for effecting change
• Example of the road forward -Universal Design
• Wrap up – and tools for you

The Beauty of Human Diversity
• We come in all shapes, sizes, and levels of ability …

The Paradigm Shift
• Nike slogan: “To bring innovation and inspiration to every athlete* in the world”
*If you have a body, you are an athlete
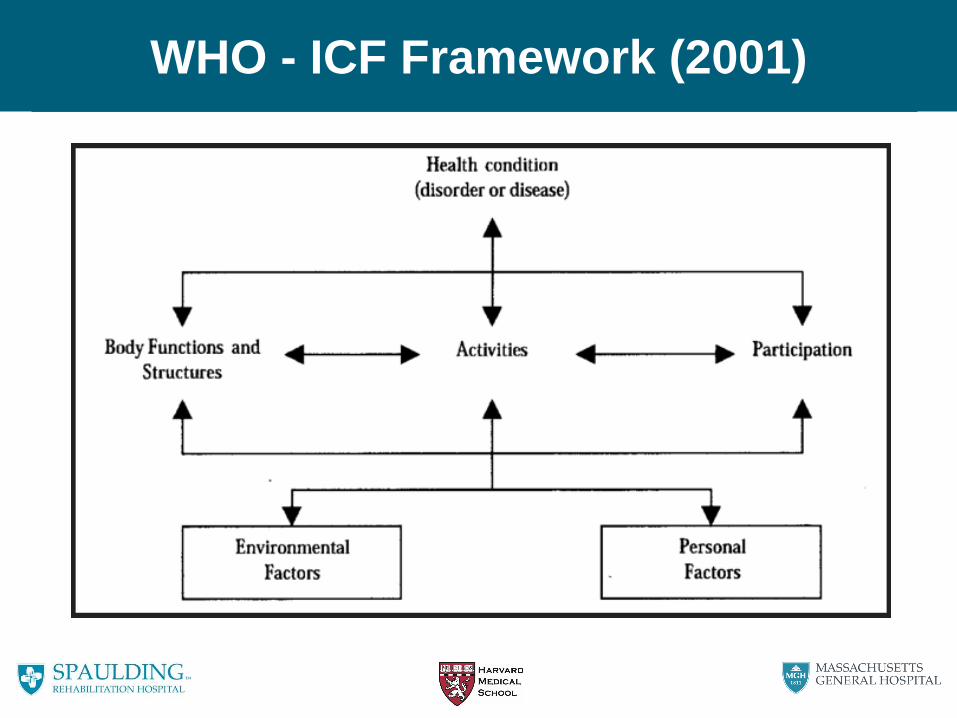
WHO - ICF Framework (2001)
CDC - Physical Activity Guidelines
• You’ve heard this before!
• Adults (age 18-64) need at least: – 150 minutes of moderate-intensity aerobic activity every week, and…
– Muscle strengthening activities 2 or more days a week that work all
major muscle groups
– Etc etc.
• For aerobic activity, generally-speaking the more the
better
… But, what are the barriers to involvement?

The Barriers are Real - Physical
• Survey of 83 adults with unilateral stroke
• Major barriers to exercise: – Cost of the program (61%)
– Lack of awareness of where to go (57%)
– No means of transportation (57%)
– Unaware of how to exercise (46%)
– Lack of interest (16%)
– Lack of time (11%)
– Fear it will worsen condition (1%)
(Rimmer J, Rehabil Res Dev 2008)

Barriers - Physical
• Accessibility of health clubs for people with mobility and visual disabilities
• Assessment of 35 facilities in 6 topic areas:
– Built environment
– Equipment
– Swimming pool
– Information
– Policies
– Professional behavior
(Rimmer J, Am J Pub Health, 2005)

Barriers - Physical
• Findings:
– Few facilities with accessible showers, power-assisted doors, ramps
meeting ADA specs
– <10% with cardio machines that offered anything aside from traditional
lower extremity modalities
– 50% with pool lifts
– <25% with information in accessible formats
– >85% asked person with disability if they would like help prior to
providing assistance
(Rimmer J, Am J Pub Health, 2005)

My Mantra - “No Brakes”
• No Brakes
– People with disabilities do not expect or want “breaks” or special exceptions – treat us as your equal
– Do not hold us back under the premise of false “brakes”
• Brakes may be necessary, but
they should be self-imposed

The Journey Begins

“Do the things you can be good at”

Introduction to Sport

Wait – I’m an “athlete?”

Taking it All the Way
Three Paralympic Games, Seven Paralympic Medals

Taking it All the Way
Three Paralympic Games, Seven Paralympic Medals

Taking it All the Way
Boston Marathon Wins – 2004, 2005

Taking it All the Way
Boston Marathon Wins – 2004, 2005

Taking it All the Way
One Epic Crash

And Then… This Happened

Through it All – Values of Olympism
• “The goal of the Olympic
Movement is to contribute to
building a peaceful and better
world by educating youth through
sport practiced without
discrimination of any kind and in
the Olympic spirit, which requires
mutual understanding with a spirit
of friendship, solidarity, and fair
play.” (Olympic Charter)

The Transformative Power of Sport
Confidence, Self-Respect
Physical Empowerment Expanded World View

Academic Pursuits

Rapid Growth of the Paralympic Movement
0
500
1000
1500
2000
2500
3000
3500
4000
4500
19
60
19
64
19
68
19
72
19
76
19
80
19
84
19
88
19
92
19
96
20
00
20
04
20
08
20
12
20
16
Summer Games
0
100
200
300
400
500
600
700
Winter Games
One of the fastest rates of growth in all of sport

A New Field: Paralympic Sports Medicine
• Athletes with disabilities remain underserved
• Many sports medicine physicians “fear” this population– Feel as though they lack expertise
• Extremely interesting work at the intersection of disability/rehabilitation and sports performance
• Compelling argument for public health impact

Paralympic Sports Medicine – IPC
• IPC Medical Committee– Standards for sports medicine services
– Therapeutic Use Exemptions (TUEs)
– Injury and Illness Surveillance Study
– Athlete and coach education

Bringing the Games to Boston?
Back To “No Brakes”
• No Brakes
– People with disabilities do not expect or want “breaks” or special exceptions – treat us as your equal
– Do not hold us back under the premise of false “brakes”
• Brakes may be necessary, but
they should be self-imposed
So – What’s the Bottom Line?
• We have a long road ahead, but we can get there
• The barriers have been defined
• It’s not impossible

Keys to Effecting Healthy Change
• Ultimately, it all boils down to this: 1. Tell people you believe in them
2. Meet them where they are at
• Not “us” vs. “them,” but “we”
3. Give them the tools to succeed
• The challenge – this will mean something slightly
different for everyone!
• The opportunity – the principles remain constant!

One Example - Universal Design
• Universal Design: Design that is usable by the widest
range of people without need for special or separate
programs
• Applies to
– Places
– Things
– Policies

Universal Design - Places
• “Places”: Applies to the built infrastructure– Full ADA Guidelines applied to fitness facilities
(www.adachecklist.org)

Universal Design - Things
• “Things”: Applies to the tools and materials we use within our
environment– Upper body spin class

Universal Design - Policy
• “Policies”: Applies to the laws we create that ensure universal
access…
Rehab Act
of 1973
ADA of
1990
DOE
Guidance
2013
IDEA of
1990
CRPD
2006
1970 1980 1990 2000 2010 2025

Universal Design – Elite Sport
• Policy in Sport: Eastern College Athletic Conference

A Paradigm Shift
Changing the paradigm…
And with it, changing society’s expectations

Back to the Three Principles
1. Tell people you believe in them
2. Meet them where they are at
3. Give them the tools to succeed
Example – Casey Martin

Take Home Points
• The beauty of human diversity
– “If you have a body, you are an athlete”– The barriers to change are real, but not
insurmountable
• Three principles for effecting change
• Example of the road forward -Universal Design
• The tools are now in your hands -let’s push the envelope together!

Thank You
• Many thanks to…
– Institute for Lifestyle Medicine
– Dr. Eddie Phillips and Dr. Beth Frates
– Mary Alice Hanford
– HMS/Spaulding Department of PM&R
– Brigham and Women’s Hospital
– International Paralympic Committee
– All of you!

References
Center for Disease Control and Prevention. 2008 Physical Activity Guidelines for Americans.
Atlanta: Center for Disease Control and Prevention; 2008.
Rimmer JH, Wang E, Smith D. Barriers associated with exercise and community access for
individuals with stroke. J Rehabil Res Dev 2008; 45:315-22.
Rimmer JH, Riley B, Wang E, Rauworth A. Accessiblity of health clubs for people with mobility
disabilities and visual impairments. Am J Pub Health. 2005 Nov 95(11);2022-8.
World Health Organization. International Classification of Functioning, Disability, and Health.
Geneva: World Health Organization; 2001.

Supplemental Material