Is there a need for cervical collar usage post anterior cervical decompression and fusion using...
11
RESEARCH REPORT Is there a need for cervical collar usage post anterior cervical decompression and fusion using interbody cages? A randomized controlled pilot trial Allan Abbott, PhD, Marie Halvorsen, MSc and Åsa Dedering, PhD Physiotherapist, Department for Physiotherapy, Karolinska University Hospital, Stockholm, Sweden ABSTRACT Anterior cervical discectomy and fusion (ACDF) is a common surgical intervention for radiculopathy resulting from degenerative cervical spine conditions. Post-surgical cervical collar use is believed to reduce post-operative pain, provide the patient with a sense of security during activities of daily living and even reduce rates of non-fusion. This prospective randomized controlled pilot trial investigates trial design feasibility in relation to prospective physical, functional, and quality of life-related outcomes of patients undergoing ACDF with interbody cage, with (n = 17) and without (n = 16) post-operative cervical collar usage. Results show that the sample provides suf- ficient statistical power to show that the use of a rigid cervical collar during 6 post-operative weeks is associated with significantly lower levels of neck disability index after 6 weeks and significantly lower levels of prospective neck pain. To investigate causal quality of life or fusion rate outcomes, sample size needs to be increased at least fourfold and optimally sixfold when accounting for data loss in prospective follow-up. The study suggests that post-surgical cervical collar usage may help certain patients cope with initial post-operative pain and disability. INTRODUCTION Anterior cervical discectomy and fusion (ACDF) is one of the most commonly performed surgical inter- ventions for radiculopathy resulting from degenerative cervical spondylosis, intervertebral disc herniation, or degenerative disc disease. In Sweden, ACDF surgeries are performed at a rate of approximately six surgeries per 100,000 population (Swedish National Board of Health and Welfare, 2011). In the USA, surgical rates of approximately 157 surgeries per 100,000 population have been reported (Marawar et al, 2010). The indication for neck surgery is based on the severity of patient pain, clinical and radiological signs of degeneration and nerve root compression, and the lack of response to conservative treatment. The Smith–Robinson and the Cloward procedures developed in the late 1950s have been the most widely used methods for ACDF. The procedures use an interbody corticocancellous allograft for cervical inter- body fusion and have generally shown good clinical out- comes (Bishop, Moore, and Hadley, 1996; Cauthen et al, 1998). However, complications in the form of significantly increased focal kyphosis, significant loss of disc space height due to graft migration, and nonunion have been observed in up to 22% of cases (Graham, 1989; Jagannathan et al, 2008; Lowery, Swank, and McDonough, 1995; McConnell et al, 2003). Therefore, alternative instrumentation techniques such as the use of interbody cages requiring less structural bone graft to provide initial stability have become more common in later years with lower complication rates reported (Jacobs et al, 2011; Marawar et al, 2010). The use of a cervical collar during the first 2–3 post-operative months of healing is commonly implemented based on the belief that it may reduce the risk of graft/cage migration, graft nonunion, reduce post-operative pain levels, and provide the patient with a sense of security during activities of daily living. A recently published Delphi investigation on an international sample of orthopedic and neuro- surgeons described how cervical collars are used post-operatively in 55% of single level ACDF surgeries Address correspondence to Allan Abbott, Physiotherapist, Department for Physiotherapy, Karolinska University Hospital, Stockholm, Sweden. E-mail: [email protected] Accepted for publication 09 September 2012 Physiotherapy Theory and Practice, 29(4):290–300, 2013 Copyright © Informa Healthcare USA, Inc. ISSN: 0959-3985 print/1532-5040 online DOI: 10.3109/09593985.2012.731627 290 Physiother Theory Pract Downloaded from informahealthcare.com by Karolinska Institutet University Library on 11/24/13 For personal use only.
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of Is there a need for cervical collar usage post anterior cervical decompression and fusion using...

RESEARCH REPORT
Is there a need for cervical collar usage post anteriorcervical decompression and fusion using interbodycages? A randomized controlled pilot trial
Allan Abbott, PhD, Marie Halvorsen, MSc and Åsa Dedering, PhD
Physiotherapist, Department for Physiotherapy, Karolinska University Hospital, Stockholm, Sweden
ABSTRACT
Anterior cervical discectomy and fusion (ACDF) is a common surgical intervention for radiculopathy resulting fromdegenerative cervical spine conditions. Post-surgical cervical collar use is believed to reduce post-operative pain,provide the patient with a sense of security during activities of daily living and even reduce rates of non-fusion.This prospective randomized controlled pilot trial investigates trial design feasibility in relation to prospectivephysical, functional, and quality of life-related outcomes of patients undergoing ACDF with interbody cage,with (n = 17) and without (n = 16) post-operative cervical collar usage. Results show that the sample provides suf-ficient statistical power to show that the use of a rigid cervical collar during 6 post-operative weeks is associatedwith significantly lower levels of neck disability index after 6 weeks and significantly lower levels of prospectiveneck pain. To investigate causal quality of life or fusion rate outcomes, sample size needs to be increased atleast fourfold and optimally sixfold when accounting for data loss in prospective follow-up. The study suggeststhat post-surgical cervical collar usage may help certain patients cope with initial post-operative pain anddisability.
INTRODUCTION
Anterior cervical discectomy and fusion (ACDF) isone of the most commonly performed surgical inter-ventions for radiculopathy resulting from degenerativecervical spondylosis, intervertebral disc herniation, ordegenerative disc disease. In Sweden, ACDF surgeriesare performed at a rate of approximately six surgeriesper 100,000 population (Swedish National Board ofHealth and Welfare, 2011). In the USA, surgicalrates of approximately 157 surgeries per 100,000population have been reported (Marawar et al,2010). The indication for neck surgery is based onthe severity of patient pain, clinical and radiologicalsigns of degeneration and nerve root compression,and the lack of response to conservative treatment.
The Smith–Robinson and the Cloward proceduresdeveloped in the late 1950s have been the most widelyused methods for ACDF. The procedures use an
interbody corticocancellous allograft for cervical inter-body fusion and have generally shown good clinical out-comes (Bishop, Moore, and Hadley, 1996; Cauthenet al, 1998). However, complications in the form ofsignificantly increased focal kyphosis, significant loss ofdisc space height due to graft migration, and nonunionhave been observed in up to 22% of cases (Graham,1989; Jagannathan et al, 2008; Lowery, Swank, andMcDonough, 1995;McConnell et al, 2003). Therefore,alternative instrumentation techniques such as theuse ofinterbody cages requiring less structural bone graft toprovide initial stability have become more common inlater years with lower complication rates reported(Jacobs et al, 2011; Marawar et al, 2010).
The use of a cervical collar during the first 2–3post-operative months of healing is commonlyimplemented based on the belief that it may reducethe risk of graft/cage migration, graft nonunion,reduce post-operative pain levels, and provide thepatient with a sense of security during activities ofdaily living. A recently published Delphi investigationon an international sample of orthopedic and neuro-surgeons described how cervical collars are usedpost-operatively in 55% of single level ACDF surgeries
Address correspondence to Allan Abbott, Physiotherapist, Departmentfor Physiotherapy, Karolinska University Hospital, Stockholm,Sweden. E-mail: [email protected]
Accepted for publication 09 September 2012
Physiotherapy Theory and Practice, 29(4):290–300, 2013Copyright © Informa Healthcare USA, Inc.ISSN: 0959-3985 print/1532-5040 onlineDOI: 10.3109/09593985.2012.731627
290
Phys
ioth
er T
heor
y Pr
act D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y K
arol
insk
a In
stitu
tet U
nive
rsity
Lib
rary
on
11/2
4/13
For
pers
onal
use
onl
y.

and 76% of multilevel ACDF surgeries (Bible et al,2009). It has been reported that cervical range ofmotion (CROM) in healthy asymptomatic subjects isreduced on average by 62.9% with rigid cervicalcollars while soft cervical collars reduce cervical move-ment on average by 17.4% (Whitcroft, Massouh,Amirfeyz, and Bannister, 2010) Despite this, CROMrestriction may be unnecessary when consideringthat most functional activities of daily living apartfrom backing up a car require well less than half ofthe normal cervical range of movement to be per-formed (Bible et al, 2010; Miller et al, 2010).
It has been reported that cervical radiculopathyimpairs balance performance on posturography, whichlater improves after surgical decompression (Persson,Karlberg, and Magnusson, 1996). Studies suggest thathealthy subjects after 5 days of rigid cervical collarusage demonstrate decreased velocity of voluntary eyemovementand subtledeterioration inanterior–posteriorbodysway inducedby vibrationat the calfmuscles (Burl,Williams, and Nayak, 1992; Karlberg, Magnusson, andJohansson, 1991). Taking this into consideration, onecan hypothesis that a prolonging of cervical movementrestriction by cervical collar use may have a greatereffect on static postural control and potentially disturbbalance during dynamic movement. In addition tothis, other adverse effects of cervical collar usage canoccur, such as pressure ulcers, nerve palsy, skin reac-tions, dysphagia, and respiratory complications (Stam-bolis et al, 2003; Totten and Sugarman, 1999;Webber-Jones, Thomas, and Bordeaux, 2002).
There are no published studies to our knowledgeinvestigating if the restriction of cervical movement pro-vided by a rigid cervical collar actually improves clinicaloutcomesafterACDFwith interbody cages.Wehypoth-esize that the use of rigid cervical collar post ACDFwithinterbody cage may not benefit patient-rated pain, dis-ability, or quality of life outcomes or even fusion rates.We hypothesize, however, that rigid cervical collarusage may potentially affect patients static anddynamic balance negatively. The study aims to investi-gate prospective physical, functional, and quality oflife-related outcomes of patients undergoing ACDFwith interbody cage, with and without post-operativecervical collar usage. The purpose of using a pilotstudy design was to assess feasibility in terms of samplesize requirements for hypothesis testing and resourcesneeded for patient recruitment and follow-up.
MATERIALS AND METHODS
The study is a prospective randomized controlled pilottrial with preoperative baseline measures and post-
operative measures at 6 weeks as well as 3, 6, 12,and 24 months post-surgery.
Recruitment of participants
Research ethics was obtained from the committee formedical research in the Stockholm health region.The primary diagnosis and selection of patients forACDF surgery were assessed and determined by neu-rosurgeons at the Karolinska University Hospital’sNeurosurgery Clinic, Stockholm, Sweden. Patientswere recruited over a 1-year period between 2003and 2004. The inclusion criteria for patients were: 1)ages between 18 and 65 years, 2) clinical and radio-logical signs of cervical root compression with corre-sponding pain distribution for more than 3 monthsof which conservative treatment had failed toimprove, 3) a primary diagnosis of cervical spondylo-sis, disc herniation, or degenerative disc disease,and 4) patients selected for ACDF. Patient’s inabilityto fully understand the Swedish language andpatients who had previously undergone ACDF wereexcluded.
Study conduct
The patients were consecutively and randomlydivided into two groups after they had fulfilledinclusion/exclusion criteria and signed the informedconsent forms. Random concealed allocation wasthe method used to form the groups. Patients andinvestigators were not blinded to post-operative treat-ment allocation. One group received no post-operat-ive neck movement restrictions while a second groupreceived a rigid cervical collar (Philadelphia Collarand Camp Scandinavia AB). During the first daysafter surgery, for all patients in both groups, the phy-siotherapists instructed respiratory and circulatoryexercises, training of transfers, walking, as well asother activities of daily living relevant for thepatient. Before discharge from the hospital, patientsreceived instruction of a home training program con-taining general exercises promoting shoulder andthoracic mobility, static isometric stabilizing functionof the cervical spine, and walking. The patients wereinstructed to wear the collar at daytime only over a6-week period. During the first 3 weeks the collarwas used both in and outdoors. After 3 weeks, thepatient could remove the collar when sitting indoorswith the neck supported. Patients were restrictedfrom activities such as contact sports, running,heavy lifting, driving, and outer-range cervical spinemovements during the first 3 months after theoperation.
Physiotherapy Theory and Practice 291
Physiotherapy Theory and Practice
Phys
ioth
er T
heor
y Pr
act D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y K
arol
insk
a In
stitu
tet U
nive
rsity
Lib
rary
on
11/2
4/13
For
pers
onal
use
onl
y.

Outcome measures
The patient’s background and demographic data aswell as a radiologist’s and neurosurgeon’s qualitativeanalysis of segmental fusion on X rays were collectedusing the University Hospital’s medical recordssystem. Radiological follow-up was conducted on allpatients 3 months post-surgery with standing lateralas well as flexion/extension radiographs. Fusion wasdefined as lack of qualitative motion of the interbodycage on post-operative flexion/extension radiographs.Sagittal alignment was also considered through quali-tative observation of potential focal kyphotic interver-tebral changes. All other outcome data were collectedwith self-reported questionnaires and clinical-basedphysical measurements.
Average pain intensity over 24 hours in the neck andshoulder/arm regions was assessed by using aBorgCR-10 scale ranging 0–10 with associated subjective cat-egories of pain description ordered from least to mostintense pain (Borg, 1982). The Borg CR-10 scale hasbeen shown to correlate strongly with visual analogscales ranging 0–10 with no significant differencereported for rating of pain during experimental jointloading experiments (Harms-Ringdahl et al, 1986).Neck disability was quantified by the neck disabilityindex (NDI) (Vernon and Mior, 1991). It is presentedas a 0–50 score where lower scores represent lowerlevels of neck pain-related disability. Health-relatedquality of life was measured with the MedicalOutcome Study Short Form-36 (SF-36) (Ware andSherbourne, 1992). The questionnaire’s multidimen-sionality is represented by eight subscales which are lin-early transformed to individual 0–100 scores. TheSF-36 is also presented as a 0–100 mental compositescore (MCS) and physical composite score (PCS) ac-cording to standard calculation procedures (Ware,Snow, Kosinski, and Gandek, 1993). Patient’s confi-dence in performing dynamic activities of daily livingwithout falling was measured with the Falls EfficacyScale (FES) ranging from 0 to 10, ordered from notconfident to totally confident (Tinetti, Richman, andPowell, 1990). Swedish versions of the Borg CR-10,NDI, SF-36, and FES have been shown to be validand reliable in Swedish conditions (Harms-Ringdahlet al, 1986; Helmerson-Ackelman and Lindgren,2002; Hellström and Lindmark, 1999).
The sitting CROM in degrees was measured withthe cervical measurement system (David SwedenAB) according to recommended procedures thathave shown to be valid and reliable (Peolsson,Hedlund, Ertzgaard, and Öberg, 2000). Six move-ment directions were performed in the followingorder: lateral flexion (to both sides), flexion,
extension, and rotation (to both sides) always startingtoward the right side and thereafter toward the left forlateral flexion and rotation. For each movement, themean of three measurements is presented.
The unipedal standing balance test was performedwith the eyes open both on hard and soft surface andwith the eyes closed only on hard surface. The softsurface was an 8 cm thick foam mat. The tests wereperformed without the cervical collar and subjectswere asked to stand with their arms folded acrosstheir chest. Failure was defined as touching the floorwith the non-stance foot or hopping/shifting on thestance foot. All tests were performed for right andleft leg, respectively, with a maximum time of 45seconds recorded. The mean time in seconds ofthree tests is presented. The test procedure has beenshown to be valid and reliable (Springer et al, 2007).
Statistical analysis
Statistical comparison between the study groups at 6weeks, 3, 6, and 12 months, and 2 years after the oper-ation was conducted using analysis of covarianceadjusted for baseline score, sex, and age as covariates.Theeffect of the surgeryalongwithpossible complimen-tary effects of the post-operative routine over all timepoints were assessed with repeated measure analysis ofcovariance. Effect sizes of the surgery and post-operativeinterventions were assessed with Cohen’s d where d=0.20 is considered a small effect, d= 0.50 a mediumeffect, and d= 0.80–infinity a large effect size (Cohen,1992). Data are presented with means scores and stan-dard deviations. Statistical significance was tested atthe5%level forall tests. Sensitivityofmissingdata impu-tation was considered satisfactory after comparison toper protocol analysis of data exclusively from patientssuccessfully followed up. An intention to treat principlewas used for continuous and discrete data, meaning theall patients, regardless of their loss to follow-up, drop-out, or non-compliance, remained in the analysis ofthe group to which they were randomized (Hollis andCampbell, 1999).No a priori sample size power analysiswas performed but post-hoc analysis was used to explainresults and study feasibility. For each analysis, IBMSPSS 20.0 for windows was used.
RESULTS
Patient recruitment and follow-up
A total of 33 patients planned for elective ACDFsurgery fulfilled the study’s inclusion and exclusion
292 Abbott et al
Copyright © Informa Healthcare USA, Inc.
Phys
ioth
er T
heor
y Pr
act D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y K
arol
insk
a In
stitu
tet U
nive
rsity
Lib
rary
on
11/2
4/13
For
pers
onal
use
onl
y.

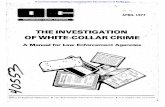
criteria and agreed to participate in the study. Afterbaseline measures were collected, the randomizationprocess resulted in 17 patients allocated to thecervical collar group and 16 patients to the groupwithout cervical collar. The randomization processproduced even group distributions for backgroundcharacteristics of the patients and baseline variables(Table 1).
All patients complied with the post-surgical inter-ventions and received clinical and radiologicalfollow-up by the neurosurgeon within 3 month post-surgery. Questionnaire and physical measure follow-up rates 6 weeks as well as at 3 and 6 months post-surgery occurred; however, ranged between 65% and75% for the groups. At 1-year follow-up rates averaged60% while at 2-years post-surgery follow-up rates
TABLE 1 Background patient data and baseline variable measures.
Patient characteristics Cervical collar (n = 17) No cervical collar (n = 16)
Malea 53 (9) 69 (11)Age – mean years 53.4 SD 13 47.3 SD 11Diagnosisa
Cervical spondylosis 47 (8) 31 (5)Cervical disk herniation 24 (4) 25 (4)Cervical degenerative disc disease 29 (5) 44 (7)
Classification of ACDFa
One levelC3–4 6 (1) 0C4–5 0 (0) 6 (1)C5–6 47 (8) 31 (5)C6–7 6 (1) 19 (3)
Two levelsC4–5 and C5–6 6 (1) 13 (2)C5–6 and C6–7 35 (6) 31 (5)
NDI – mean 31.12 SD 9.9 33.31 SD 6.2SF-36 – mean
PF 49.71 SD 29.7 56.25 SD 16.2RP 13.26 SD 29.5 6.25 SD 25.0BP 24.59 SD 24.8 26.69 SD 16.6GH 57.18 SD 24.6 53.88 SD 14.2VT 29.12 SD 26.4 25.94 SD 16.3SF 42.65 SD 32.5 50.00 SD 25.0RE 45.09 SD 44.0 45.83 SD 45.3MH 48.24 SD 26.5 61.00 SD 24.4PCS 31.00 SD 9.9 29.95 SD 6.6MCS 34.34 SD 15.0 37.86 SD 14.0
FES – mean 94.29 SD 31.8 98.81 SD 30.7Borg CR-10 – mean
Neck pain 5.12 SD 2.5 5.69 SD 1.9Arm pain 4.94 SD 2.7 5.13 SD 2.1
CROM – meanFlexion 34.74 SD 12.7 32.17 SD 10.4Extension 41.71 SD 13.7 40.62 SD 14.8Right lateral flexion 29.03 SD 8.6 27.35 SD 7.4Left lateral flexion 27.18 SD 8.4 27.81 SD 7.1Right rotation 51.01 SD 13.0 53.48 SD 11.5Left rotation 48.98 SD 13.0 50.25 SD 12.2
Unipedal balance – meanRight foot hard surface 28.23 SD 17.9 32.65 SD 16.9Left foot hard surface 28.27 SD 19.1 32.73 SD 18.4Right foot soft surface 13.88 SD 14.2 14.38 SD 14.1Left foot soft surface 18.25 SD 17.8 15.85 SD 15.6Right foot eyes closed 6.12 SD 8.2 5.71 SD 8.2Left foot eyes closed 8.37 SD 10.3 6.54 SD 8.2
aPercent of patients (number of patients).
Physiotherapy Theory and Practice 293
Physiotherapy Theory and Practice
Phys
ioth
er T
heor
y Pr
act D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y K
arol
insk
a In
stitu
tet U
nive
rsity
Lib
rary
on
11/2
4/13
For
pers
onal
use
onl
y.

averaged 45% between groups. A flow diagram withdetails on enrollment, allocation, follow-up rates at 6weeks, 3, 6, and 12 months, and 2 years after the oper-ation is presented in Figure 1.
Clinical outcomes
Mean score changes from baseline with correspondingeffect sizes aswell as analysis of covariance and repeatedmeasures analysis of covariance between groups withcorresponding effect sizes are shown in Tables 2–4.Both groups improved in all outcome measures andintermittently showed statistically significant improve-ments ( p < 0.05) from baseline to 2 years aftersurgery. These results are reflected in the generallymedium (0.50–0.80) to large effect sizes (>0.80) forreduced neck and arm pain as well as the NDI forboth groups. Notably large effect sizes occurred forthe non-collar group in the reduction of neck pain(1.57) and NDI (1.75), likewise the collar group inthe reduction of neck pain (1.34) after 2 year post-surgery. Similarly the FES, CROM as well as theSF-36 physical functioning (PF), role physical (RP),bodily pain (BP), and vitality (VT) subscales generallyhad medium to large effect sizes for improvements inboth groups. Smaller effect sizes were observed inboth groups for improvements in unipedal balance aswell as SF-36 general health (GH) and role emotional(RE) subscales. The SF-36 social functioning (SF)and mental health (MH) subscales in the collar group
showed medium to large effect sizes for improvementcompared to the smaller effect sizes in the non-collargroup. Generally small effect size differences wereobserved in the comparison of groups. Medium effectsize differences in favor of the cervical collar groupwere however observed for neck pain, SF-36 BP sub-scale, SF-36 physical component score as well asinitial NDI scores. Analysis of covariance showed thatthe cervical collar group scores for NDI at 6 weeks,SF-36 BP subscale at 6 and 12 months, SF-36 SF at12 months as well as the physical component scale at6 weeks, 3, 6, and 12 months improved significantlymore than for the non-collar group after the operation.Repeated measures analysis of covariance showed thatcontrolling for the combined effects of all prospectivemeasures gave significantly better outcome for the cer-vical collar group in neck pain, SF-36 BP subscale aswell as the physical component scale. Radiographicfusion rates were 100% in both groups. Radiologistand neurosurgeons noted no qualitative differencesin radiologically determined post-operative fusionrates or sagittal alignment between the cervical collargroup and those not prescribed a post-operativecervical collar.
DISCUSSION
The pilot design of this study initially aimed to deter-mine the feasibility of proceeding to a larger study. Arecent research methodology paper published byThabane et al (2010) advocated the publishing ofwell-structured pilot studies analyzing the feasibilityof a larger trial. Pilot studies should assess feasibilityin terms of recruitment flow, resources needed forprospective data collection as well as give estimatesof treatment effects and variance in treatment effectsfor sample size calculation (Thabane et al, 2010).
When considering feasibility in terms of recruit-ment flow, sample size calculation based on effectsize estimates and their clinical importance is required(Chmura Kraemer et al, 2006). To evaluate treatmenteffectiveness after ACDF, Carreon, Glassman, Camp-bell, and Anderson (2010) have reported the minimalclinical important difference (MCID) for the NDI tobe 7.5, the SF-36 PCS to be 4.1, and 0–10 painrating scales for arm and neck pain to be 2.5. This rep-resents the smallest difference between pre-operativeand prospective outcome measure scores in a largepatient sample reporting GH improvement. In apost-hoc sample size calculation based on an 8-pointMCID in NDI and a common standard deviation of8 point observed between our study groups, 80%power, and an alpha level of 0.05, this would require
FIGURE 1 Patient flow.
294 Abbott et al
Copyright © Informa Healthcare USA, Inc.
Phys
ioth
er T
heor
y Pr
act D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y K
arol
insk
a In
stitu
tet U
nive
rsity
Lib
rary
on
11/2
4/13
For
pers
onal
use
onl
y.

TABLE 2 Effect of cervical collar on pain, functional activities, and quality of life.
Outcome
Cervical collar (n = 17) No collar (n= 16) Between group p-Value
Mean changefrom baseline
Effectsizea
Mean changefrom baseline
Effectsizea
Mean difference(95% CI)b
Effectsizea
Analysis ofcovarianceb
Repeatedmeasuresanalysis ofcovarianceb
Neck pain6 weeks −2.69∗ SD 0.3 1.02 −1.78∗ SD 1.3 0.69 −1.4 (−3.4 to 0.6) −0.50 0.150 0.038∗
3 months −2.24∗ SD 0.6 0.80 −1.33 SD 1.1 0.54 −1.9 (−4.1 to 0.4) −0.43 0.1036 months −1.65∗ SD 0.1 0.56 −1.93∗ SD 0.2 0.99 −1.0 (−2.7 to 0.7) −0.47 0.22812 months −2.75∗ SD 0.1 1.10 −1.34 SD 1.1 0.54 −1.9 (−3.9 to 0.01) −0.73 0.05124 months −3.19∗ SD 0.3 1.34 −2.73∗ SD 0.3 1.57 −1.2 (−2.8 to 0.2) −0.52 0.093
Arm pain6 weeks −1.75 SD 0.5 0.69 −1.13 SD 0.5 0.49 −0.9 (−2.7 to 0.8) −0.28 0.292 0.1683 months −1.34 SD 0.3 0.47 −0.69 SD 0.9 0.27 −0.8 (−3.0 to 1.4) −0.28 0.4506 months −1.47 SD 0.4 0.48 −1.07 SD 0.1 0.52 −0.7 (−2.7 to 1.3) −0.21 0.48512 months −1.56 SD 0.3 0.54 −0.03 SD 1.3 0.01 −2.0 (−4.4 to 0.4) −0.54 0.09824 months −2.29∗ SD 0.5 0.92 −1.73∗ SD 1.8 0.93 −1.0 (−2.3 to 0.3) −0.39 0.132
NDI6 weeks −3.13 SD 1.5 0.34 −0.40 SD 2.7 0.08 −4.4 (−8.6 to −0.2) −0.77 0.042∗ 0.1683 months −5.81∗ SD 1.0 0.62 −4.43 SD 2.1 0.61 −2.1 (−8.0 to 3.8) −0.42 0.4696 months −6.42∗ SD 0.2 0.64 −5.24 SD 1.9 0.73 −3.1 (−9.8 to 3.5) −0.37 0.34212 months −7.47∗ SD 0.4 0.74 −5.14∗ SD 0.8 0.78 −4.3 (−10.1 to 1.5) −0.52 0.13824 months −7.94∗ SD 2.7 0.92 −9.93∗ SD 1.1 1.75 −1.2 (−5.7 to 3.3) −0.03 0.584
FES6 weeks 13.13∗ SD 10.0 −0.48 9.17 SD 8.7 −0.35 1.5 (−11.1 to 14.1) −0.03 0.814 0.5953 months 18.61∗ SD 17.9 −0.76 12.55 SD 9.9 −0.49 1.7 (−10.9 to 14.3) 0.09 0.7876 months 21.18∗ SD 16.5 −0.85 14.00∗ SD 9.8 −0.54 3.7 (−8.8 to 16.1) 0.09 0.55312 months 17.24∗ SD 14.1 −0.67 9.59 SD 6.6 −0.35 5.3 (−7.9 to 18.4) 0.15 0.41824 months 18.27∗ SD 18.4 −0.75 13.18 SD 13.4 −0.54 1.7 (−9.3 to 12.7) 0.04 0.757
SF-36 PF6 weeks 17.30∗ SD 11.7 −0.71 5.05 SD 6.0 −0.37 7.7 (−1.9 to 17.2) 0.39 0.110 0.1603 months 21.90∗ SD 12.9 −0.91 5.65 SD 5.0 −0.30 11.2 (−2.8 to 25.1) 0.51 0.1126 months 17.09∗ SD 7.3 −0.65 10.02 SD 1.1 −0.60 3.8 (−8.5 to 16.0) 0.03 0.53212 months 18.56∗ SD 5.8 −0.70 9.22 SD 0.9 −0.65 6.9 (−7.2 to 21.0) 0.14 0.32424 months 18.09∗ SD 12.5 −0.75 11.60∗ SD 3.9 −0.81 4.2 (−5.9 to 14.3) 0.00 0.402
SF-36 RP6 weeks 9.06 SD 8.4 −0.27 −3.35 SD 18.0 0.18 16.4 (−4.4 to 37.3) 0.71 0.118 0.0823 months 17.48∗ SD 6.5 −0.53 11.45 SD 5.7 −0.41 13.7 (−9.8 to 37.2) 0.39 0.2446 months 30.87∗ SD 8.1 −0.92 21.55∗ SD 14.2 −0.66 13.7 (−6.1 to 8.8) 0.43 0.28612 months 25.66∗ SD 4.4 −0.81 17.97 SD 8.3 −0.61 19.3 (−4.6 to 43.1) 0.44 0.10924 months 31.92∗ SD 2.7 −1.03 29.19∗ SD 0.9 −1.15 14.1 (−7.5 to 35.8) 0.33 0.192
SF-36 BP6 weeks 14.79∗ SD 6.3 −0.53 2.30 SD 4.0 −0.15 11.3 (−1.7 to 24.3) 0.44 0.085 0.029∗
3 months 14.74∗ SD 7.7 −0.51 9.43 SD 1.5 −0.54 6.7 (−9.7 to 23.1) 0.12 0.4096 months 30.22∗ SD 6.2 −1.08 8.01 SD 6.7 −0.39 21.4 (4.4–38.5) 0.73 0.016∗
12 months 21.65∗ SD 1.3 −0.85 6.34 SD 3.2 −0.35 17.5 (1.7–33.2) 0.57 0.031∗
24 months 26.10∗ SD 0.4 −1.04 17.81∗ SD 11.0 −1.45 10.8 (−2.0 to 23.6) 0.34 0.095
SF-36 GH6 weeks −1.60 SD 0.7 0.06 3.48 SD 0.6 −0.24 −3.4 (−17.0 to 10.3) −0.09 0.617 0.6943 months −0.33 SD 0.6 0.01 −1.51 SD 0.3 0.11 3.0 (−9.7 to 15.8) 0.23 0.6296 months 0.25 SD 1.6 −0.01 −2.43 SD 1.2 0.18 3.1 (−8.2 to 14.5) 0.29 0.57412 months 1.07 SD 4.1 −0.05 1.53 SD 1.4 0.11 6.0 (−6.3 to 18.3) 0.35 0.32624 months 2.22 SD 4.0 −0.10 2.46 SD 5.0 −0.21 0.5 (−10.3 to 11.3) −0.09 0.924
Continued
Physiotherapy Theory and Practice 295
Physiotherapy Theory and Practice
Phys
ioth
er T
heor
y Pr
act D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y K
arol
insk
a In
stitu
tet U
nive
rsity
Lib
rary
on
11/2
4/13
For
pers
onal
use
onl
y.

a sample size of 16 patients per group. Similarly in apost-hoc sample size calculation based on a 2.5point decrease in 0–10 pain rating scales and 2 pointcommon standard deviation between groups observedin the study, a sample size of 11 patients per group isrequired. Considering a MCID of 4.1 points forSF-36 PCS and the study group’s common standarddeviation of 8, at least 60 patients per group arerequired to attain 80% statistical power.
Our initially recruited sample size is adequate forusing NDI and pain rating scales as primary outcomemeasures but due to loss to follow-up, only data forpain rating holds 80% power for data collected up to6 months post-surgery. Use of intention to treat prin-ciple and multiple imputations, however, allow the cal-culation of causal outcomes in NDI and pain rating inthis study. The main results of this study with sufficientstatistical power suggests therefore that the use of a rigid
TABLE 2 Continued
Outcome
Cervical collar (n = 17) No collar (n= 16) Between group p-Value
Mean changefrom baseline
Effectsizea
Mean changefrom baseline
Effectsizea
Mean difference(95% CI)b
Effectsizea
Analysis ofcovarianceb
Repeatedmeasuresanalysis ofcovarianceb
SF-36 VT6 weeks 13.56∗ SD 3.1 −0.55 8.91 SD 2.4 −0.60 5.9 (−6.6 to 17.5) 0.41 0.361 0.3843 months 21.27∗ SD 2.9 −0.76 21.37∗ SD 5.0 −1.14 2.2 (−13.9 to 18.3) 0.12 0.7816 months 18.98∗ SD 0.5 −0.73 15.72∗ SD 9.1 −0.75 4.7 (−12.5 to 22.0) 0.25 0.58012 months 15.58∗ SD 0.1 −0.59 10.07 SD 4.6 −0.55 8.6 (−7.1 to 24.3) 0.36 0.27424 months 18.17∗ SD 4.8 −0.76 17.85∗ SD 3.7 −1.23 4.6 (−7.5 to 16.8) 0.20 0.439
SF-36 SF6 weeks 8.86 SD 6.5 −0.30 −4.24 SD 6.4 0.19 9.7 (−3.3 to 22.7) 0.25 0.139 0.1123 months 19.73∗ SD 3.1 −0.64 11.56 SD 4.8 −0.42 6.7 (−13.0 to 16.3) 0.03 0.4946 months 22.35∗ SD 0.6 −0.69 8.72 SD 5.5 −0.31 13.3 (−6.4 to 33.0) 0.20 0.17712 months 25.20∗ SD 7.3 −0.87 6.87 SD 1.5 −0.28 16.5 (0.1–32.9) 0.45 0.049∗
24 months 28.07∗ SD 9.3 −0.86 16.41∗ SD 8.8 −0.78 9.1 (−5.5 to 23.7) 0.22 0.212
SF-36 RE6 weeks −5.45 SD 3.4 0.13 5.62 SD 1.4 −0.12 −14.1 (−47.4 to 19.3) −0.27 0.394 0.2023 months 3.48 SD 0.3 0.08 9.54 SD 4.1 −0.22 −16.6 (−46.4 to 13.2) −0.32 0.2636 months 5.49 SD 3.9 −0.13 18.49 SD 2.7 −0.42 −13.5 (−40.2 to 13.2) −0.33 0.31012 months 3.33 SD 6.0 −0.15 9.71 SD 6.5 −0.23 −9.9 (−34.8 to 14.8) −0.19 0.42224 months 10.48 SD 11.8 −0.35 21.29 SD 20.5 −0.58 −9.8 (−31.6 to 11.9) −0.40 0.363
SF-36 MH6 weeks 11.58 SD 0.02 −0.44 3.51 SD 2.6 0.15 3.0 (−12.4 to 18.4) −0.19 0.694 0.4843 months 15.53∗ SD 1.1 −0.60 7.63 SD 3.5 −0.34 3.3 (−11.5 to 18.1) −0.21 0.6526 months 14.50∗ SD 3.1 −0.58 7.68 SD 4.6 −0.35 1.0 (−13.3 to 15.3) −0.27 0.88612 months 16.11∗ SD 2.0 −0.63 0.36 SD 6.6 −0.02 9.0 (−6.8 to 24.9) 0.14 0.25324 months 18.72∗ SD 9.8 −0.84 6.28 SD 16.1 −0.34 3.8 (−5.8 to 13.4) −0.02 0.429
SF-36 PCS6 weeks 6.04 SD 1.1 −0.65 0.98 SD 1.2 −0.16 5.8 (0.8–10.7) 0.84 0.025∗ 0.010∗
3 months 7.20∗ SD 0.6 −0.71 2.32 SD 1.6 −0.31 6.8 (0.4–13.1) 0.63 0.038∗
6 months 10.02∗ SD 0.1 −1.01 3.24 SD 3.0 −0.39 7.4 (1.4–13.4) 0.80 0.017∗
12 months 8.65∗ SD 0.6 −0.85 3.50 SD 1.6 −0.47 7.5 (0.3–14.6) 0.66 0.041∗
24 months 8.11∗ SD 0.8 −0.85 6.28∗ SD 0.1 −0.95 4.9 (−0.8 to 10.5) 0.37 0.088
SF-36 MCS6 weeks 1.94 SD 1.8 −0.14 1.54 SD 0.1 −0.11 −1.9 (−11.1 to 7.4) −0.24 0.683 0.7073 months 4.19 SD 0.6 −0.28 6.16∗ SD 1.3 −0.46 −3.5 (−12.6 to 5.6) −0.40 0.4366 months 5.01 SD 1.4 −0.35 4.69 SD 1.7 −0.36 −1.3 (−9.6 to 7.1) −0.25 0.75912 months 5.14 SD 0.6 −0.35 1.95 SD 3.1 −0.16 1.3 (−7.4 to 10.1) −0.03 0.75924 months 7.44∗ SD 5.2 −0.59 5.69 SD 7.7 −0.52 −0.8 (−7.0 to 5.2) −0.22 0.769
aCohen’s d.bAdjusted for score at baseline, sex, and age.∗p ≤ 0.05.
296 Abbott et al
Copyright © Informa Healthcare USA, Inc.
Phys
ioth
er T
heor
y Pr
act D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y K
arol
insk
a In
stitu
tet U
nive
rsity
Lib
rary
on
11/2
4/13
For
pers
onal
use
onl
y.

cervical collar during 6 weeks post ACDFwith interbodycage is associated with significantly lower levels of NDIafter 6 weeks and significantly lower levels of prospectiveneck pain. One must however keep in mind when con-sidering these results that sample size is a limitation ofthis study. Optimally, for designing of a larger study itwould be beneficial to recruit 50% more patients pergroup to account for prospective loss to follow-up inpain rating and NDI outcome measures.
Significantly lower prospective levels of BP andgreater improvements in PF at clinically importantlevels were seen during the first post-operative yearfor the cervical collar group. However, a much largersample is required to assure that these results are notfalse positive. Radiologist and neurosurgeons notedno qualitative differences in radiologically determinedpost-operative fusion rates or sagittal alignmentbetween the groups. A limitation of these findings is
TABLE 3 Effect of cervical collar on unipedal balance test.
Outcome
Cervical collar (n = 17) No collar (n = 16) Between group p-Value
Mean changefrom baseline
Effectsizea
Mean changefrom baseline
Effectsizea
Mean difference(95% CI)b
Effectsizea
Analysis ofcovarianceb
Repeatedmeasuresanalysis ofcovarianceb
Right foot6 weeks 1.12 SD 3.5 −0.07 1.04 SD 5.1 −0.07 −1.6 (−8.1 to 4.9) −0.33 0.625 0.3713 months 4.07 SD 3.8 −0.25 3.68 SD 2.3 −0.23 −2.6 (−12.8 to 7.6) −0.28 0.6086 months 8.91∗ SD 7.0 −0.60 5.34 SD 3.6 −0.35 0.2 (−7.0 to 7.5) −0.07 0.94812 months 1.84 SD 5.7 −0.12 4.29 SD 5.8 −0.30 −4.9 (−13.2 to 3.4) −0.59 0.23824 months 5.04 SD 6.8 −0.34 6.13 SD 12.6 −0.50 −4.4 (−10.5 to 1.7) −0.65 0.153
Left foot6 weeks 3.26 SD 6.1 −0.20 1.90 SD 5.4 −0.12 0.1 (−5.7 to 5.8) −0.24 0.986 0.6193 months 7.49 SD 5.3 −0.44 5.66 SD 4.0 −0.34 −1.6 (−11.4 to 8.3) −0.19 0.7496 months 8.96∗ SD 6.3 −0.55 6.49 SD 7.2 −0.76 4.7 (−8.2 to 6.7) −0.17 0.83512 months 3.99 SD 4.8 −0.24 3.48 SD 6.6 −0.23 −2.2 (−10.4 to 5.9) −0.30 0.58424 months 7.03 SD 7.9 −0.45 6.20 SD 14.3 −0.47 −3.0 (−9.3 to 3.3) −0.43 0.335
Right foot soft surface6 weeks 4.12 SD 0.3 −0.29 2.44 SD 0.9 −0.18 1.6 (−5.8 to 9.0) 0.09 0.656 0.7773 months 5.10∗ SD 0.6 −0.37 4.32 SD 1.8 −0.31 1.6 (−6.5 to 9.8) 0.02 0.6876 months 7.71∗ SD 0.8 −0.56 6.47 SD 5.7 −0.47 −0.4 (−8.7 to 7.9) 0.06 0.92112 months 7.68∗ SD 1.4 −0.57 7.05 SD 4.8 −0.59 −0.08 (−8.2 to 8.1) 0.01 0.98424 months 4.03 SD 4.7 −0.33 2.44 SD 10.2 −0.23 0.9 (−4.5 to 6.5) 0.15 0.716
Left foot soft surface6 weeks 1.56 SD 0.2 −0.25 3.10 SD 6.7 −0.27 0.9 (−6.0 to 7.7) 0.16 0.796 0.8283 months 3.80 SD 2.3 −0.28 3.60 SD 4.0 −0.32 0.9 (−8.2 to 10.1) 0.16 0.8356 months 3.54 SD 1.9 −0.37 11.20 SD 5.8 −0.41 1.3 (−6.1 to 8.8) 0.24 0.72112 months 3.88 SD 0.3 −0.26 7.50 SD 3.7 −0.24 2.5 (−6.9 to 11.9) 0.26 0.59624 months 1.82 SD 3.9 −0.20 5.55 SD 10.3 −0.48 −2.6 (−8.8 to 3.7) −0.03 0.411
Right foot eyes closed6 weeks 1.56 SD 0.2 −0.19 0.89 SD 4.0 −0.14 2.3 (−0.4 to 4.9) 0.45 0.090 0.0563 months 3.80∗ SD 2.3 −0.40 0.71 SD 5.2 0.11 4.7 (−0.04 to 9.4) 0.64 0.0526 months 3.54∗ SD 1.9 −0.38 1.75 SD 3.8 −0.58 1.7 (−3.1 to 6.5) 0.28 0.47412 months 3.88∗ SD 0.3 −0.48 1.01 SD 3.9 −0.15 3.5 (−0.9 to 7.8) 0.51 0.11424 months 1.82 SD 3.9 −0.28 4.30 SD 5.8 −0.15 1.6 (−1.1 to 4.3) 0.37 0.236
Left foot eyes closed6 weeks 1.96 SD 1.3 −0.53 0.70 SD 4.9 0.12 3.3 (−1.2 to 7.8) 0.53 0.140 0.1803 months 2.89 SD 3.0 −0.76 0.20 SD 2.6 −0.03 1.9 (−3.9 to 7.7) 0.45 0.5106 months 4.66∗ SD 2.5 −1.10 3.90 SD 0.1 −0.48 0.9 (−5.0 to 6.8) 0.24 0.76612 months 6.91∗ SD 3.3 −0.97 2.55 SD 2.9 −0.37 5.0 (−0.8 to 10.8) 0.60 0.09124 months 5.22∗ SD 1.1 −0.86 3.47 SD 3.6 −0.34 1.8 (−3.1 to 6.7) 0.51 0.457
aCohen’s d.bAdjusted for score at baseline, sex, and age.∗p ≤ 0.05.
Physiotherapy Theory and Practice 297
Physiotherapy Theory and Practice
Phys
ioth
er T
heor
y Pr
act D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y K
arol
insk
a In
stitu
tet U
nive
rsity
Lib
rary
on
11/2
4/13
For
pers
onal
use
onl
y.

however the lack of objective measurement of inter-body cage motion on flexion and extension radio-graphs as well as sagittal alignment. The study isalso substantially underpowered to detect differencesbetween groups in fusion rates considering studiessuggesting that non-fusion occurs at rate of approxi-mately 2% when modern ACFD techniques are used(Marawar et al, 2010).
Therewere no indications that use of a cervical collarfor 6 weeks affected the static balance tests or self-per-ceived confidence to manage dynamic activitieswithout falling.Therefore, the tendencies toward cervi-cal collar usage causing decreased velocity of voluntaryeye movement and subtle deterioration in anterior–posterior body sway observed in earlier studies couldnot be seen in static and dynamic balance after
TABLE 4 Effect of cervical collar on CROM.
Outcome
Cervical collar (n = 17) No collar (n = 16) Between group p-Value
Mean changefrom baseline
Effectsizea
Mean changefrom baseline
Effectsizea
Mean difference (95%CI)b
Effectsizea
Analysis ofcovarianceb
Repeatedmeasuresanalysis ofcovarianceb
Right lateral flexion6 weeks 0.73 SD 0.6 −0.09 0.71 SD 2.6 −0.11 1.2 (−2.9 to 5.4) 0.26 0.553 0.1853 months 2.97 SD 0.9 −0.36 0.54 SD 2.6 −0.09 4.3 (−0.9 to 9.1) 0.64 0.0546 months 2.10 SD 2.8 −0.28 3.14 SD 1.6 −0.47 0.5 (−3.6 to 4.7) 0.11 0.78812 months 5.20∗ SD 2.5 −0.71 5.00∗ SD 4.0 −0.86 2.0 (−1.4 to 5.4) 0.38 0.23024 months 5.28∗ SD 4.5 −0.78 6.10∗ SD 1.8 −0.93 1.3 (−2.3 to 4.9) 0.18 0.472
Left lateral flexion6 weeks 2.81 SD 1.4 −0.36 1.15 SD 0.9 −0.17 1.7 (−2.8 to 6.3) 0.16 0.436 0.6233 months 3.89∗ SD 2.5 −0.54 2.14 SD 0.4 −0.31 1.7 (−2.4 to 5.8) 0.18 0.3286 months 4.93∗ SD 2.6 −0.68 3.94∗ SD 0.1 −0.55 0.5 (−3.8 to 4.8) 0.06 0.81712 months 5.07∗ SD 1.7 −0.67 5.25∗ SD 0.8 −0.78 −0.5 (−5.0 to 4.0) −0.12 0.81424 months 4.06 SD 4.3 −0.62 3.06 SD 1.5 −0.48 0.7 (−3.1 to 4.5) 0.07 0.713
Flexion6 weeks 3.30 SD 6.9 −0.33 3.16 SD 2.1 −0.36 2.2 (−3.1 to 7.6) 0.38 0.397 0.6813 months 6.22 SD 7.6 −0.64 7.48∗ SD 3.8 −0.86 0.6 (−4.0 to 5.1) 0.22 0.8046 months 8.24∗ SD 8.6 −0.87 9.32∗ SD 3.2 −1.04 0.5 (−3.4 to 4.4) 0.25 0.79212 months 6.92 SD 8.5 −0.67 10.07∗ SD 2.8 −1.10 −1.2 (−6.0 to 3.6) −0.18 0.61124 months 3.79 SD 8.6 −0.40 5.8 SD 5.2 −0.70 1,1 (−2.5 to 4.8) 0.13 0.523
Extension6 weeks 2.88 SD 4.5 −0.25 3.1 SD 6.7 −0.26 0.3 (−5.6 to 6.3) 0.10 0.905 0.8023 months 6.27 SD 2.7 −0.50 3.6 SD 4.0 −0.28 2.9 (−5.0 to 10.8) 0.34 0.4586 months 9.81∗ SD 6.8 −0.91 11.2∗ SD 5.8 −0.91 −0.5 (−6.3 to 5.3) −0.03 0.85712 months 8.75∗ SD 3.8 −0.73 7.5 SD 3.7 −0.57 2.4 (−5.4 to 10.2) 0.23 0.54324 months 13.92∗ SD 5.9 −1.25 16.1∗ SD 6.7 −1.35 −1.6 (−7.3 to 4.2) −0.14 0.583
Right rotation6 weeks 5.9∗ SD 4.2 −0.53 3.7 SD 3.6 −0.37 0.3 (−5.6 to 6.2) −0.03 0.910 0.5253 months 9.5∗ SD 1.9 −0.78 5.0 SD 1.8 −0.50 3.4 (−3.3 to 10.2) 0.21 0.3076 months 11.4∗ SD 3.0 −0.99 9.9∗ SD 2.3 −0.97 0.2 (−6.9 to 7.3) −0.09 0.95212 months 13.1∗ SD 3.8 −1.16 7.6∗ SD 0.5 −0.63 3.8 (−4.0 to 11.6) 0.28 0.32624 months 12.4∗ SD 3.8 −1.10 10.5∗ SD 3.7 −1.07 0.8 (−6.1 to 6.5) −0.06 0.954
Left rotation6 weeks 6.0∗ SD 3.4 −0.53 4.2 SD 3.8 −0.40 1.2 (−4.7 to 7.2) 0.07 0.675 0.4943 months 9.7∗ SD 0.5 −0.76 7.6∗ SD 1.5 −0.66 1.2 (−6.5 to 9.0) 0.07 0.7496 months 14.4∗ SD 0.7 −1.10 10.9∗ SD 2.2 −0.98 2.2 (−4.8 to 9.2) 0.16 0.52712 months 11.2∗ SD 3.2 −0.97 7.6∗ SD 3.3 −0.55 2.7 (−5.7 to 11.0) 0.18 0.51724 months 9.8∗ SD 3.8 −0.86 7.1 SD 1.1 −0.61 2.0 (−5.2 to 9.1) 0.15 0.580
aCohen’s d.bAdjusted for score at baseline, sex, and age.∗p ≤ 0.05.
298 Abbott et al
Copyright © Informa Healthcare USA, Inc.
Phys
ioth
er T
heor
y Pr
act D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y K
arol
insk
a In
stitu
tet U
nive
rsity
Lib
rary
on
11/2
4/13
For
pers
onal
use
onl
y.

prolonged cervical collar use in subjects in our study(Burl, Williams, and Nayak 1992; Karlberg, Magnus-son, and Johansson, 1991). Improvements in balanceafter surgical decompression for cervical radiculopathyobserved byPersson,Karlberg, andMagnusson (1996)were however generally reflected in prospective balancemeasures seen in our study.
Whitcroft, Massouh, Amirfeyz, and Bannister(2010) reported that rigid cervical collar provideapproximately 62.9% CROM restriction. Thishowever did not seem to affect prospective CROMor fusion healing compared with the control group.Miller et al (2010) suggested that use of a rigid ortho-sis after procedures incorporating internal fixationmay be unnecessary because soft collar usage wasfound to be sufficient for restricting motion duringroutine activities. The lower levels of neck/BP andhigher levels of PF seen in our cervical collar groupmay have eventuated even if the patients had usedsoft collars. One can hypothesize that the initial im-provements in pain and function in the cervicalcollar group may be explained partly by the collar pro-viding a proprioceptive sense of security and partly bypsychological factors such as coping, functional self-efficacy, and less fear avoidance. This is the oppositeto recommendations for treatment of acute whiplashwhere randomized controlled trials have shown earlymobilization to be more effective than immobilizationwith a cervical collar (Muzin et al, 2008).
To recruit a large group of patients for sufficientpower to investigate causal outcomes using the SF-36or difference in fusion rates, sample size needs to beincreased at least fourfold and optimally sixfold whenaccounting for data loss in prospective follow-up. Thisis not feasible for our current single site patientrecruitment flow which would take up to 6 years toattain an adequate sample size. The only possible wayminimizing time required for patient recruitmentwould be to analyze pain, disability, quality of life, andfusion rates in cervical collar users compared to non-users post ACDF surgery on a regional or national level.
The feasibility of the current pilot design was ade-quate to show short-term greater improvements inNDI and pain reduction in the cervical collar group.These results indicate that the short-term use of a cer-vical collar may be beneficial in the post-operativeregime for ACDF with interbody cage.
CONCLUSION
This pilot study suggests that short-term cervical collaruse post ACDF with interbody cage may help certainpatients copewith initial post-operative pain anddisabil-ity. Larger data collections are required to investigate
health-related quality of life and fusion rates in patientswith and without rigid collar use post ACDF surgery.
Declaration of interest: The authors report nodeclaration of interests.
REFERENCES
Bible JE, Biswas D,Whang PG, Simpson AK, Rechtine GR, GrauerJN 2009 Post-operative bracing after spine surgery for degenera-tive conditions: A questionnaire study. Spine Journal 9: 309–316
Bible JE, Biswas D,Miller CP, Whang PG, Grauer JN 2010 Normalfunctional range of motion of the cervical spine during 15 activi-ties of daily living. Journal of Spinal Disorders and Techniques23: 15–21
Bishop RC, Moore KA, Hadley MN 1996 Anterior cervical inter-body fusion using autogeneic and allogeneic bone graft sub-strate: A prospective comparative analysis. Journal ofNeurosurgery 85: 206–210
BorgGA1982Category scalewith ratio properties for intermodal andinterindividual comparisons. In: Geisler HG and Petzold P (eds)Psychophysical Judgment and the Process of Perception, pp 25–34. Berlin, VEBDeutscher Verlag der Wissenschaften
Burl MM, Williams JG, Nayak US 1992 Effects of cervical collarson standing balance. Archives of Physical Medicine and Rehabi-litation 73: 1181–1185
Carreon LY, Glassman SD, Campbell MJ, Anderson PA 2010 NeckDisability Index, Short Form-36 physical component summary,and pain scales for neck and arm pain: The minimum clinicallyimportant difference and substantial clinical benefit after cervicalspine fusion. Spine Journal 10: 469–474
Cauthen JC, Kinard RE, Vogler JB, Jackson DE, De Paz OB,Hunter OL, Wasserburger LB, Williams VM 1998 Outcomeanalysis of noninstrumented anterior cervical discectomy and in-terbody fusion in 348 patients. Spine 23: 188–192
Chmura Kraemer H, Mintz J, Noda A, Tinklenberg J, Yesavage JA2006 Caution regarding the use of pilot studies to guide powercalculations for study proposals. Archives of General Psychiatry63: 484–489
Cohen J 1992 A power primer. Psychology Bulletin 112: 155–159Graham JJ 1989 Complications of cervical spine surgery. A five year
report on a survey of the membership of the Cervical Spine Re-search Society by the Morbidity and Mortality Committee.Spine 14: 1046–1050
Harms-Ringdahl K, Carlsson AM, Ekholm J, Raustorp A, SvenssonT, Toresson HG 1986 Pain assessment with different intensityscales in response to loading of joint structures. Pain 27:401–411
Hellström K, Lindmark B 1999 Fear of falling in patients withstroke: A reliability study. Clinical Rehabilitation 13: 509–517
Helmerson-Ackelman B, Lindgren U 2002 Validity and reliability ofa modified version of the neck disability index. Journal of Reha-bilitation Medicine 34: 284–287
Hollis S, Campbell F 1999 What is meant by intention to treatanalysis? Survey of published randomised controlled trials.BMJ 319: 670–674
Jacobs W, Willems PC, Kruyt M, van Limbeek J, Anderson PG,Pavlov P, Bartels R, Oner C 2011 Systematic review of anteriorinterbody fusion techniques for single- and double-level cervicaldegenerative disc disease. Spine 36: E950–E960
Jagannathan J, Shaffery CI, Oskouian RJ, Dumont AS, Herrold C,Sansur CA, Jane JA 2008 Radiographic and clinical outcomesfollowing single-level anterior cervical discectomy and allograft
Physiotherapy Theory and Practice 299
Physiotherapy Theory and Practice
Phys
ioth
er T
heor
y Pr
act D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y K
arol
insk
a In
stitu
tet U
nive
rsity
Lib
rary
on
11/2
4/13
For
pers
onal
use
onl
y.

fusion without plate placement or cervical collar. Journal of Neu-rosurgery: Spine 8: 420–428
Karlberg M, Magnusson M, Johansson R 1991 Effect of restrainedcervical mobility on voluntary eye movements and posturalcontrol. Acta Oto-laryngologia 111: 664–670
Lowery GL, SwankML,McDonough RF 1995 Surgical revision forfailed anterior cervical fusions. Articular pillar plating or anteriorrevision? Spine 20: 2436–2441
Marawar S, Girandi FP, Sama AA, Ma Y, Gaber-Baylis LK, Bescu-lides MC, Mentsoudis SG 2010 National trends in anterior cer-vical fusion procedures. Spine 35: 1454–1459
McConnell JR, Freeman BJ, Debnath UK, Grevitt MP, Prince HG,Webb JK 2003 A prospective randomized comparison of coral-line hydroxyapatite with autograft in cervical interbody fusion.Spine 28: 317–323
Miller CP, Bible JE, Jegede KA, Whang PG, Grauer JN 2010Soft and rigid collars provide similar restriction in cervicalrange of motion during 15 activities of daily living. Spine 35:1271–1278
Muzin S, Zacharia I, Walker J, Abd OE, Baima J 2008When shoulda cervical collar be used to treat neck pain? Current Reviews inMusculoskeletal Medicine 1: 114–119
Peolsson A, Hedlund R, Ertzgaard S, Öberg B 2000 Intra- andinter-tester reliability and range of motion of the neck. Phy-siotherapy Canada 52: 233–242
Persson L, Karlberg M, Magnusson M 1996 Effects of differenttreatments on postural performance in patients with cervicalroot compression. A randomized prospective study assessingthe importance of the neck in postural control. Journal of Vestib-ular Research 6: 439–453
Springer BA, Marin R, Cyhan T, Roberts H, Gill NW 2007Normative values for the unipedal stance test with eyes open andclosed. Journal of Geriatric Physical Therapy 30: 8–15
Stambolis V, Brady S, Klos D, Wesling M, Fatianov T, Hildner C2003 The effects of cervical bracing upon swallowing in young,normal, healthy volunteers. Dysphagia 18: 39–45
Swedish National Board of Health and Welfare 2011. www.sos.seThabane L, Ma J, Chu R, Cheng J, Ismaila A, Rios LP, Robson R,
Thabane M, Giangregorio L, Goldsmith CH 2010 A tutorial onpilot studies: The what, why and how. BMC Medical ResearchMethodology 10: 1
Tinetti M, Richman D, Powell L 1990 Falls efficacy as a measure offear of falling. Journal of Gerontology 45: P239–P243
Totten VY, Sugarman DB 1999 Respiratory effects of spinal immo-bilization. Prehospital Emergency Care 3: 347–352
Vernon H, Mior S 1991 The neck disability index: A study ofreliability and validity. Journal of Manipulative PhysiologicalTherapeutics 14: 409–415
Ware J, Sherbourne C 1992 The MOS 36-item short-form healthsurvey (SF-36). I. Concept framework and item selection.Medical Care 30: 473–483
Ware J, Snow K, Kosinski M, Gandek B 1993 SF-36 Health Survey.Manual and Interpretation Guide. Boston, MA, New EnglandMedical Center
Webber-Jones JE, Thomas CA, Bordeaux RE 2002 The manage-ment and prevention of rigid cervical collar complications.Orthopedic Nursing 21: 19–25
Whitcroft KL, Massouh L, Amirfeyz R, Bannister G 2010 Compari-son of methods of measuring active cervical range of motion.Spine 35: E976–E980
300 Abbott et al
Copyright © Informa Healthcare USA, Inc.
Phys
ioth
er T
heor
y Pr
act D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y K
arol
insk
a In
stitu
tet U
nive
rsity
Lib
rary
on
11/2
4/13
For
pers
onal
use
onl
y.