
Qatar achieved high rankings in scientific education: Minister

Is more better? The relationship between outcomes achieved by problem gamblers and the number of counselling d o n s attended Beth R Crisp,’, Alun C Jackson’, Shane A Thomas’, Neil Thomason’, Serena Smith’, Jennifer Borrell’, Wei-ying Ho’ and Tangerine A Hol f
This paper addresses the question of how much intervention is necessary for the effective treatment of problem gambling by exploring the relationship between the number of counselling sessions attended and the degree of problem resolution achieved for 613 individuals who attended problem gambling counselling services in Victoria. While those who achieved partial or full resolution of presenting problems attended more sessions than those who finished counselling with their problems still unresolved, problems were typically reported as being resolved in fewer than five sessions. It is concluded that for some problem gamblers a relatively brief intervention may be sufficient.
Keywords problem gambling, counselling, outcomes
Introduction The question of how much treatment is required has long been an issue for funders, providers and recipients of counselling services. While conventional wisdom has been that counselling outcomes and the number of sessions attended are positively associated (Orlinsky and Howard 1986), the exact nature of the
* Dr Beth R Crisp, Department of Social Policy and Social Work, University of Glasgow, Lilybank House, Bute Gardens, Glasgow G12 ERT, Scotland. ’ School of Social Work, The University of Melbourne, Victoria 3010.
Department of History and Philosophy of Science, The University of Melbourne, Victoria 3010
University of Louisville, Kentucky, USA
relationship is open to question. It is presumed that there are points beyond which additional sessions or therapeutic input may be ineffective. Further responses to counselling in terms of speed and level of improvement may be idiosyncratic. For example, one study found that half of all psychotherapy patients make marked improvements within eight sessions, and although improvement rates increase beyond that number of sessions, one quarter had not made any marked progress after six months of weekly sessions, and 15 percent had not made progress after a year of counselling (Howard, Kopta, Krause and Orlinsky 1986). However, while such data provide some support for the proposition that more counselling leads to better outcomes, the research literature is somewhat more equivocal. In one of the very few experiments which has allocated
Australian Social Work/September 2001, Vol. 54. No. 3 83 I

clients to either brief time limited counselling or long-term time unlimited contact, clients allocated to the time limited condition were not only less likely to withdraw prematurely from treatment, but obtain outcomes which were comparable with, if not better than, those who were offered a long-term intervention (Reid and Shyne 1969).
In fiscal climates which place a premium on efficiency, the possibility of effectively treating clients in a relatively limited number of sessions is an attractive option (Neff, Lambert, Lunnen, Budman and Levenson 1996; Plouffe 1980). Once viewed as a stop gap measure until long- term treatment could begin (Wells and Phelps 1990), or as a last-ditch attempt, when long term therapies have failed (Breit, Im and Wilner 1983), brief treatments have become the norm for a wide range of psychosocial problems (Department of Human Services 1997; Wells and Phelps 1990) due to a growing body of evidence that short-term therapy may be as effective as long-term interventions (Hoyt 1995). Furthermore, with some clients, minimal interventions not involving attendance for face to face counselling including telephone counselling (Hetzel, Wilkins, Carrig, Thomas and Senior 1993), interactive computer programs (Barber, 1990; Eltringham and Barber 1990) or self help manuals (Barber and Gilbertson 1998) have been found to be effective.
effectiveness, brief therapies are attractive to many clients. When entering counselling, most clients expect their problems will require only a few sessions of therapy (Garfield 1978) and given the choice between short or long-term treatment opt for a brief intervention (Cummings 1988).
In addition to their potential
Indeed this may be quite appropriate if the client’s treatment goal is symptom removal (Herron, Eisenstadt, Javier, Primavera and Schultz 1994) or to obtain information to assist the process of decision-making (Forster 1996). On attaining their treatment goals, clients may well terminate their counselling, irrespective of professional opinions as to the wisdom of such action (Rosenbaum 1990). On this basis, although there may be some variation depending on the type and severity of problems (Howard et al 1986) estimates of the median number of sessions of psychotherapy attended being in the vicinity of five or six (for example, Garfield 1978; Johnson and Shaha 1996; Phillips 1988) are hardly surprising. Nevertheless, the issues for which help is sought may be extremely serious such in Farrant’s (1979) study which found one-quarter of clients attending a rape crisis centre were seen once, and a further 50 percent attended for between two and four sessions.
is necessary has not been addressed explicitly but is implicitly present in the literature concerning the treatment of problem gambling. Interventions which have been advocated range from self help manual (Dickerson, Hinchy and Legg England 1990), a very limited number of counselling sessions (for example, (Ladouceur, Sylvain, Duval, Gaboury and Dumont 1989) through to hospitalisation (for example, Adkins 1988; Russo, Taber, McCormick and Ramirez 1984), and have frequently replicated existing modalities for treating clients who are alcohol dependent (for example, Blume 1986; Orford 1985).
When a statewide network of problem gambling counselling services, known as ‘Break Even’, was established in Victoria in
The question of how much intervention
1 84 Australian Social Work/September 2001, Vol. 54, No. 3

1995, the model of service delivery adopted involved placing professional counsellors (predominantly social workers and psychologists) in existing health and welfare agencies such as community health centres who would provide assistance on a nonresidential basis. As with other health and welfare services funded by the Victorian state government, brief interventions are favoured wherever appropriate (People Care Australia 1997). A further guiding principle is:
The fact that many problem gamblers seek treatment when least able to afford the financial cost indicates that prolonged psychoanalysis and group therapy are prohibitive treatment options. Consequently there is a need for a variety of treatment techniques which have shown to be both costeffective and outcome effective. (Marjanovic 1995, pp. 183).
A requirement of the funded Break Even services is that comprehensive deidentified records of service clients and their consultations are maintained and pooled to form a Minimum Dataset. This paper explores the relationship between client outcomes and the number of counselling sessions attended for the 613 problem gamblers whose cases were both opened and closed between 1 July 1996 and 30 June 1997 and who attended at least one session of facetcface session of problem gambling counselling.
have contact with a service. Data collected on the registration form includes gender, date and place of birth, marital status and household structure, income and occupation of clients. For clients who seek assistance because of concerns about their own gambling, a client assessment form should also be completed. Usually this data is obtained at the same time as the registration data, although in some situations counsellors may defer this to a subsequent session. This includes information about gambling practices including types of gambling and problems which are associated with gambling, including the degree of indebtedness.
Data pertaining to the ten diagnostic criteria which comprise the DSM-IV (American Psychiatric Association 1994) definition of a pathological gambler are also collected and this forms an indicator of the extent to which gambling is impacting on the lives of clients. After sessions in which a deliberate decision to terminate treatment has been made, counsellors are supposed to complete a case closure summary form. This provides an analysis of the interventions used and an indication of client outcomes. In accordance with their funding agreements, all services are required to provide these data to the Department of Human Services for analysis by the Problem Gambling Research Program at The University of Melbourne. The analyses described in this paper were conducted using SPSS for Windows software.
Overview
All 18 Break Even problem gambling counselling services in Victoria use a common set of forms for recording the characteristics of clients when they first
Subjects
Subjects for this study comprised all 613 problem gamblers who began and completed treatment involving at least one session of facetc-face counselling at a
Australian Social Work/September 2001, Vol. 54, No. 3 85 I

Break Even problem gambling counselling service in Victoria between 1 July 1996 and 30 June 1997. Summary characteristics of this population are presented in Table 1. This reveals a diverse range of people seeking help because of their gambling.
Measures Degree of problem resolution
Counsellors were required to rate, in their opinion based on their interactions with the client, the extent of problem resolution achieved when the case is closed for each of the problems which they considered were associated with the client's gambling. These included financial issues, employment/work role issues, gambling behaviour, and leisure use issues. interpersonal issues (relationship), intrapersonal issues (mood, anxiety etc), family issues, legal issues and physical symptoms. Possible responses on the rating scale are that the issue remains unresolved, has been partially resolved or has been fully resolved.
Results A series of 3 X 2 analyses of variance (ANOVAs) were conducted in which the dependent measure was the number of counselling sessions attended. Factor 1 had three levels which related to the three degrees of problem resolution for each of the client's presenting problems. Factor 2, which had two levels, was an indicator of whether or not this problem was the primary presenting problem. As the distribution of the number of counselling sessions attended was positively skewed, this variable was logarithmically
TABLE 1. POPULATION CHARACTERISTICS
Characteristic
Mean age (years) 37.0
Percent
Sex Male Female
58.8 41.2
~~
Birthplace Australia Overseas
Marital status Never married Married Separated Divorced Widowed Other
73.8 26.2 -
35.7 35.5 10.1 11.3
2.5 4.9
Household structure Lives alone 22.9 Couple or family 62.8 Single parent family 5.8 Other 8.6
Has dependent children 40.4
Types of gambling Electronic gaming machines Totaliser Agency Board (off course betting) Cards Lotteries Races (on course betting) Bingo Numbers Other
69.5
17.2 6.2 3.3 2.9 1.8 1.5 2.0
Primary reason for attending Break Even Gambling behaviour 70.1 Legal issues 5.5 lntrapersonal issues 3.4 Interpersonal issues 2.9 Financial issues 2.6 Other 15.3
86 Australian Social Work/September 2001, Vol. 54, No. 3

transformed for the purpose of analysis. Because three outcomes were entered into each analysis, it was necessary to follow up a main effect of problem resolution with post hoc analysis (Boneferroni). Given previous findings that for brief interventions individual and group counselling is similarly effective (Piper and Joyce 1996) separate analyses were not conducted according to whether clients were treated individually or not. Table 2 presents the mean scores for the number of sessions attended by type of problem and degree of problem resolution, for those problem areas in which there were sufficient cases to conduct this form of analysis.
Analysis of variance produced a main effect of degree of problem resolution in respect of the number of counselling sessions attended by those whose problems included financial issues (f(2,382) = 4.42, p < .05), gambling behaviour (E(2,502) = 9.45, p < .05), interpersonal problems (E(2,341) = 10,54, p < .001), intrapersonal problems (E(2,377) = 6.54, p < .01) and legal
oblems (f(2,210) = 5.26, p < .01). Post j c tests revealed that for each problem
type, clients whose problems remained unresolved attended less counselling sessions than did those who achieved a degree of problem resolution. However, with the exception of clients who sought help in relation to their gambling behaviour for whom the number of sessions attended by those who achieved full resolution was greater than those who achieved partial resolution, there were no significant differences in the number of sessions attended by those with full and partial problem resolution.
Given that most clients present to Break Even counselling services with a number of problems for which they are seeking solutions, an overall measure of problem resolution could arguably provide a more comprehensive measure of problem resolution than examining the outcome measures for specific problems. Thus, threeway (degree of problem resolution) ANOVAs were performed for both the problem which was reportedly the primary reason for attendance, and for the problem which individuals had achieved the greatest degree of resolution. The number of sessions attended by degree of problem
ABLE 2. MEAN NUMBER OF COUNSELLING SESSIONS AITENDED BY DEGREE OF .ROBLEM RESOUITION AND WHETHER PROBLEM WAS THE PRIMARY REASON -OR AITENDANCE
~~~
Unresolved Partially resolved Fully resolved
Problem Primary Other Primary Other Primary Other problem problem problem problem problem problem
Financial issues 1.40 2.48 2.00 4.00 2.67 4.64
Gambling behaviour 2.30 2.56 3.38 3.21 4.33 3.84
Interpersonal issues (relationshbs) 1.50 2.20 5.00 4.14 3.00 3.73
lntrapersonal issues (for example. mood, anxiety) 2.00 2.06 2.83 3.76 5.00 4.37
Legal issues 3.56 2.12 3.90 4.43 2.20 3.54
Australian Social Work/September 2001, Vol. 54, No. 3 87
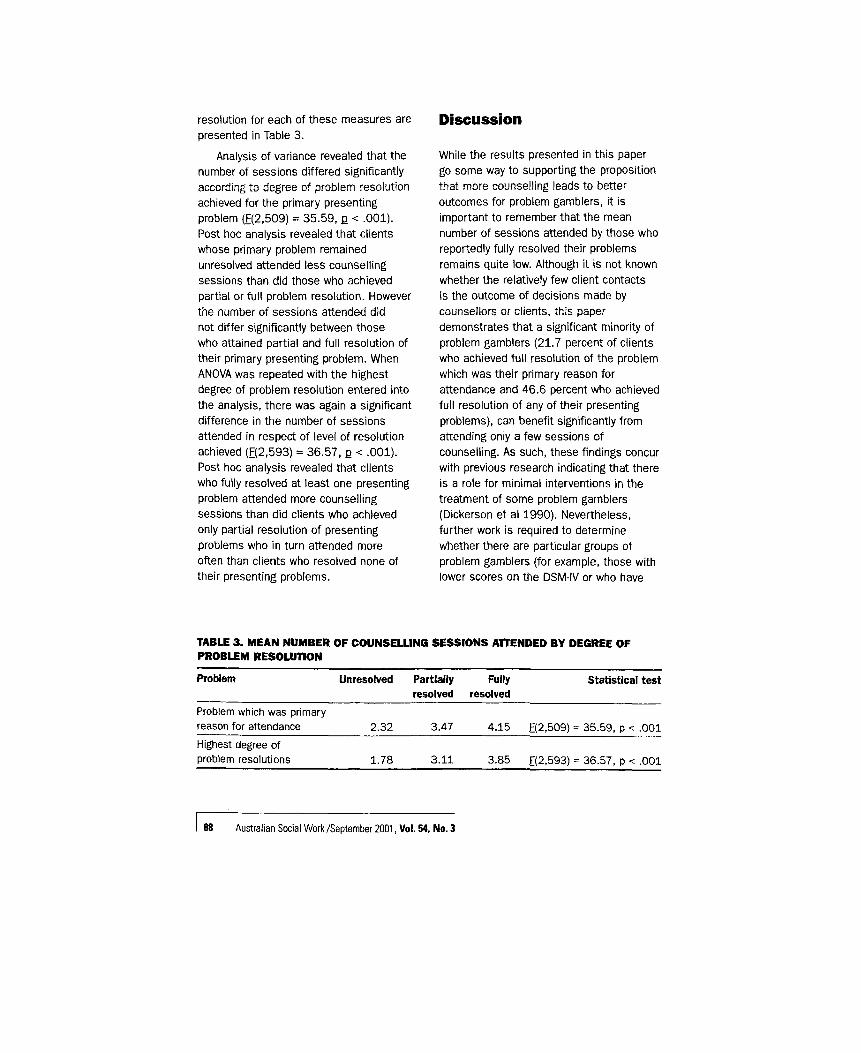
resolution for each of these measures are presented in Table 3.
Analysis of variance revealed that the number of sessions differed significantly according to degree of problem resolution achieved for the primary presenting problem (E(2,509) = 35.59, e < ,001). Post hoc analysis revealed that clients whose primary problem remained unresolved attended less counselling sessions than did those who achieved partial or full problem resolution. However the number of sessions attended did not differ significantly between those who attained partial and full resolution of their primary presenting problem. When ANOVA was repeated with the highest degree of problem resolution entered into the analysis, there was again a significant difference in the number of sessions attended in respect of level of resolution achieved (E(2,593) = 36.57, p < .001). Post hoc analysis revealed that clients who fully resolved at least one presenting problem attended more counselling sessions than did clients who achieved only partial resolution of presenting problems who in turn attended more often than clients who resolved none of their presenting problems.
Discussion
While the results presented in this paper go some way to supporting the proposition that more counselling leads to better outcomes for problem gamblers, it is important to remember that the mean number of sessions attended by those who reportedly fully resolved their problems remains quite low. Although it is not known whether the relatively few client contacts is the outcome of decisions made by counsellors or clients, this paper demonstrates that a significant minority of problem gamblers (21.7 percent of clients who achieved full resolution of the problem which was their primary reason for attendance and 46.6 percent who achieved full resolution of any of their presenting problems), can benefit significantly from attending only a few sessions of counselling. As such, these findings concur with previous research indicating that there is a role for minimal interventions in the treatment of some problem gamblers (Dickerson et al 1990). Nevertheless, further work is required to determine whether there are particular groups of problem gamblers (for example, those with lower scores on the DSM-IV or who have
TABLE 3. MEAN NUMBER OF COUNSELLING SESSIONS AlTENDED BY DEGREE OF PROBLEM RESOLUTION
~ ~ ~~
Problem Unresolved Partially Fully Statistical test
Problem which was primary reason for attendance 2.32 3.47 4.15 E(2,509) = 35.59, p c .001 Highest degree of problem resolutions 1.78 3.11 3.85 E(2,593) = 36.57, p <: .001
resolved resolved
88 Australian Social Work /September 2001, Vol. 54. No. 3

fewer problems associated with their gambling) who are more likely to achieve Positive outcomes from attending only a few sessions of counselling.
It is pertinent to note that despite a common name being adopted by problem gambling counselling agencies in Victoria, the type and length of counselling offered by the different Break Even services varies considerably. For example, one agency offers a lengthy single session of counselling to a substantial number of its clients, whereas in another agency clients and counsellors typcially contract for an initial six visits and may subsequently contract for further sessions.
Many Break Even services, however, have not formalised expectations as to how many sessions of counselling would be normal for treating problem gamblers, although individual counsellors may well have their own assumptions as to the number of counselling sessions typically required. Irrespective of whether these are formalised, differing assumptions as to the number of sessions required may well reflect different modes of counselling used in the various Break Even services (Jackson, Thomas, Thomason, Borrell, Crisp, Ho, Smith and Holt 1999). Further work is still required to determine whether more counselling leads to better outcomes for each of the main modes of counselling used by Break Even counsellors such as systemic therapies, supportive counselling, cognitive behavioural therapies and assessment or referral.
This study has the virtue that it involves a large number of participants across a wide range of settings, but this also means that control of the intervention is limited. It is also pertinent to note that the measures of problem resolution were
provided by counsellor ratings rather than by clients of counselling programs. This has both an inherent strength and weakness. The strength is that the ratings are independent of the clients. However, one might argue that clients could have a more relevant perspective than counsellors concerning counselling outcomes. Problem resolution data is only recorded by counsellors after sessions in which there has been a deliberate decision to terminate treatment by the client and/or the counsellor, rather than at the end of each counselling session.
Unlike those reporting on doseeffect studies in which outcome data is collected regularly and can be plotted over time (Howard et al 1986; Seligman 1995), our claims that more counselling leads to better outcomes must be more circumspect. Furthermore, our outcome measures are ostensibly subjective assessments by counsellors who may overestimate the extent of problem resolution (Gorey 1996). This is hardly surprising given that apparently successful outcomes from brief interventions bring hope to both counsellors and clients (Breit et al 1983). Yet paradoxically, less effective therapists have been found more likely to rate their work with clients as effective (Lafferty, Beutler and Crago 1989). Ratings of effectiveness may be further confounded by an implicit assumption that counsellors and their clients have shared treatment goals although this may not necessarily be so (Rosenbaum 1990). It may well be that clients have somewhat different ideas as to the degree of outcomes achieved.
in this paper is that no longer term outcomes of counselling are established.
A further limitation of the data reported
~~
Australian Social Work/September 2001, Vol. 54, No. 3 89 I

There is widespread agreement that problem gambling is a difficult behaviour to overcome and that reinstatement of the behaviour can occur after months or years of abstinence (Brown 1989; Marlatt 1985). So normal are relapses that Prochaska and DiClemente (1983) included this a part of the process in their now well-known model of people change. In their work with smokers, they found that individuals took an average of three attempts before achieving permanent extinguishment of the undesirable behaviour (Prochaska and DiClemente 1988) and subsequent studies have suggested this model to be applicable to a far wider range of behaviours (Prochaska et al 1994). Consequently, it is not unreasonable to expect that a proportion of clients at a problem gambling counselling service will seek help for problems associated with gambling on one or more times subsequent to a case closure at which some problems have apparently been resolved.
Not withstanding the potential for relapse, for some clients, even a single session may be sufficient to start a process of change which they can continue to work on by themselves (Hoyt 1995). Indeed, therapy is more likely to be brief when clients are highly aware of their problems and committed to change (Steenbarger 1992). Although high drop out rates before the completion of treatment are not unexpected (Baekland and Lundwall 1975; Silberfield and Glaser 1978), it should not be assumed that cases which are only partially resolved at the end of counselling will remain somewhat unresolved (Hoyt 1995).
Notwithstanding the limitations of the data and the need for further research, the findings presented in this paper have
immediate implications for the treatment of problem gambling. Although no treatment is 100 percent effective in alleviating any disorder (Howard et al 1986), brief work is only cost effective if desired outcomes are achieved (Johnson and Shaha 1996) and there may well be some clients for whom a more intensive form of intervention is necessitated than can be provided by a relatively few sessions of counselling (Johnson and Shaha 1996). Consequently, any attempts to impose strict limits on the number of sessions clients can attend for counselling may be counterproductive (Steenbarger 1994). Conversely, treatment programs which are based on the assumption that all problem gamblers need long-term treatment need to be open to the possibility that some clients may make substantial progress in far fewer than the standard number of sessions.
~ ~
Acknowledgement
This research was funded by the Victorian Government Community Support Fund through the Department of Human Services.
References ADKINS. B.J. (1988). 'Discharge Planning with Pathological Gamblers: An Ongoing Process', Journal of Gambling Behavior. Val. 4, pp. 208-218.
BAEKLAND, F. & LUNDWALL. L. (1975). 'Dropping Out of Treatment: A Critical Review', Psychological Bulletin. Vol. 82, pp. 738-783.
BARBER, J G. 11990). 'Computer-Assisted Drug Prevention', Journal of Substance Abuse Treatment, Vol. 7. pp. 125131
BARBER, J.G. & GILBERTSON, R. (1998). 'Evaluation of a Self- Help Manual for the Female Partners of Heavy Drinkers', Research on Social Work Practice. Vol. 8, pp. 141-151.
BARBER, S. & LANE, R.C. (1995). 'Efficacy Research in Psychodynamic Therapy: A Critical Review of the Literature', Psychotherapy in Private Practice, Val. 14. No. 3, pp. 43-69.
BLUME, S.B. 11986). 'Treatment for the Addictions. Alcoholism, Drug Dependence and Compulsive Gambling in a
90 Australian Social Work/Septernber 2001, Vol. 54, No. 3
Psychiatric setting', Journal of Substance Abuse Treatment Vol. 3, pp. 131-133
BREIT. M.. IM. W-G. & WILNER. R.S. (1983). 'Strategic Approaches with Resistant Families', The American Journal of Family Therapy. Vol. 11. pp. 51-58.
BROWN. R.I.F. (19891. 'Relapses from a gambling perspective', in Gossop. M. led), Relapse and Addictive Behaviour Tavistock/Routledge, London.
CUMMINGS. N. (1988). 'Emergence of the Mental Health Complex: Adaptive and Maladaptive Responses', Professional Psychology, Vol. 19, pp. 308-315.
DEPARTMENT OF HUMAN SERVICES (19971. The Redevelopment of VicforiaZ Yourh and Family Services- Strategic Directions, Victorian Department of Human Services, Melbourne.
DICKERSON. M.. HINCHY. J. & LEGG ENGLAND. S (19901, 'Minimal Treatments and Problem Gamblers: A Preliminary Investigation', Journal of Gambling Studies, Vol. 6.
ELTRINGHAM, A. & BARBER, J.G. (19901. 'Can Microcomputers Help the Problem Drinker?', Drug and Alcohol Review. Vol. 9. pp. 169-176.
FARRANT. P (19791. 'A Service for Victims of Rape and Sexual Assault'. Ausfralian Social Wart Vol. 32. No. 2, pp 2E-32
FORSTER. J. (1996). 'Helping Men to Cope with Marital Breakdown', in Cavanagh, K. & Cree, V.E. (eds). Working with Men: Feminism and Social Work, Routledge London.
GARFIELD. S.L. (1978). 'Research on Client Variables in Psychotherapy'. in Garfield, S.L. & Bergin. A.E. (eds). Handbook of Psychotherapy and Behavior Change (2nd edition). New York. Wiley.
GOREY, K M. 11996). 'Effectiveness of Social Work Intervention Research: Internal versus External Evaluations'. Social WorkResearch. Vol. 20, pp. 119-128.
HERRON. W.G.. EISENSTADT, E.N.. JAVIER. R.A.. PRIMAVERA. L.H. & SCHULTZ, C.L. (19941. 'Session Effects, Comparability. and Managed Care in the Psychotherapies'. Psychotherapy. Vol. 31, pp. 27S285.
HETZEL. S.. WILKINS, V.. CARRIG. H., THOMAS, J. & SENIOR, P (1993). 'An Evaluation of Caller Satisfaction with Solution-Focused Telephone Counselling'. Australian Social Work, Vnl. 46, No. 2, pp. 51-55.
HOWARD, K I.. KOPTA, S.M., KRAUSE, M.S & ORLINSKY, D.E. (19861. 'The Dose-Effect Relationship in Psychotherapy'. American Psychologist, Vol. 41, pp. 159-164.
HOYl, M.F. (1995). Brief Therapy and Managed Care. San Francisco: Jossey-Bass.
JACKSON, A C.. THOMAS, S.A.. THOMASON. N , BORRELL. J.. CRISP. B.R.. HO. W.. SMITH, S & HOLT, T.A. 119991. Analysis of Clients Presenring to Problem Gambling
pp. 87-102.
Counselling Services. July 1997 to June 7998, Department of Human Services, Melbourne.
JOHNSON, L 0 & SHAHA. S 11996). 'Improving Ruality in Psychotherapy'. Psychotherapy. Vol 33, pp. 225-236.
LADOUCEUR. R., SYLVAIN. C., OUVAL, C.. GABOURY. A & DUMONT. M. 119891. 'Correction des verbalisations irrationnelles chez des joueurs de poker-video', lnremational Journal of Psychology. Vol. 24, pp 43-56
LAFFERlY P.. BEUTLER. L.E. & CRAGO. M. (1989). 'Differences Between More and Less Effective Therapists: A Study of Select Therapist Variables', Journal of Consulting and Clinical Psychology. Vol 57. pp. 7 6 8 0 .
MARJANOVIC, E. (1995). 'Regaintng Control: Cue-Exposure with Problem Gamblers', in O'Connor. J (ed). High Stakes in the Nineties, Curtin University, Perth.
MARLAX, G.A (1985). 'Relapse prevention' Theoretical Rationale and Overview of the Model', in Marlan. G.A. & Gordon, J.R. (edsl. Relapse Prevention Maintenance Strategies in the Treatment of Addictive Behaviors, Guildford. New York.
NEFF, W.L.. LAMBERT, M.J.. LUNNEN. K.M.. BUOMAN. S.H. & LEVENSON. H. (19961. 'Therapists' Attitudes Toward Short- T e n Therapy. Changes with Training', Employee Assisrance Ouarterly, Vol 11. No 3. pp. 67-77.
ORFORO. J. (19851. Excessive Appetites' A Psychological View ofAddictions. John Wiley & Sons Chichester.
ORLINKSY, D.E. & HOWARD, K.I. (1986). 'The Relation of Process to Outcome in Psychotherapy', in Garfield, S.L. & Bergin. A.E. (eds). Handbook of Psychotherapy and Behavior Change (3rd edition). Wiley. New York.
PEOPLE CARE AUSTRALIA (1997). A Framework for Counselling Casework. Melbourne: Department of Human Services.
PHILLIPS, E.L. (1988). 'Length of Psychotherapy and Outcome: Observations Stimulated by Howard, Kopta. Krause & Orlinsky'. American Psychologist, Vol. 43, pp. 669-670.
PIPER, W.E. &JOYCE, A.S. (1996). 'A Consideration of Factors Influencing the Utilization of Fme-Limited. Short-Term Group Therapy', lntemational Journal of Group Psychotherapy. Vol.
PLDUFFE. P. (1980). 'The Use of Brief Psychoanalytically- Oriented Psychotherapy by Clinical Social Workers', Smith College Studies in Social Work, Vol. 50, pp. 203-2313.
PRDCHASKA. J.O. & DICLEMENTE. C.C. (1983). 'Stages and Processes of Self-change in Smoking, Towards an Integrative Model of Change', Journal of Consulring and Clinical Psychology, Val. 51, pp 390-395.
PROCHASKA. J.O. & DICLEMENTE. C.C. (19881. 'Toward a Comprehensive Model of Change', in Miller, W.R. & Heather, N (eds). Treating Addictive Behaviors. New York. Plenum Press
46, pp. 31 1-328.
Australian Social Work/September 2001, Vol. 54, No. 3 91

PROCHASKA. J.O.. VELICER. W.F.. ROSSI. J.S.. GOLOSTEIN. M.G.. MARCUS, B.H., RAKOWSKI. W.. FIORE. C.. HARLOW. L.L. REDOING, C.A.. ROSENBLOOM. 0. & ROSSI, S.R. (1994). 'Stages of Change and Decisional Balance for 12 Problem Behaviours'. Health Psychology. Vol. 13. pp. 3946 .
REID, W. & SHYNE, A. (1969), Briefandfflended Casework Columbia University Press, New York.
ROSENBAUM. R. (1990). 'Strategic Psychotherapy'. in Wells. R.A. & Gianebi, V.J. (eds). Handbook of the Brief Psychotherapies. Plenum, New York.
RUSSO. A.M.. TABER. J.1.. MCCORMICK, R.A. & RAMIRU, L.F (1984). 'An Outcome Study of an Inpatient Treatment Program for Pathological Gamblers', Hospital and Community Psychtarry. Vol. 35. pp. 823-827.
SELIGMAN. M. (19951. 'The Effectiveness of Psychotherapy The Consumer Reports study'. American Psychologist, Vol 50. pp. 965-974.
SILBERFIELD. M. & GLASER. F. (1978). 'Use of the Life Table Method in Oelermining Attrition from Treatment', Journal of Srudies on Atcoho/, Vol. 39. pp 1582-1590.
STEENBARGER. B.N. (1994). 'Duration and Outcome in Psychotherapy: An Integrative Review', Professional Psychology Research and Practice, Vol. 25. pp. 11 1-1 19.
WELLS, R.A. & PHELPS. PA. (1990). 'The Brief Psychotherapies: A Selective Overview', in Wells, R.A. & Gianetti. V.J. (edsl. Handbook of rhe brief psychotherapies. Plenum, New York
Article accepted for publication March 2001.
For immediate atOention call Andrea h a g o n in Australia on:
61 2 6947 4606 t x ~ n . r U t m o / n s t r m l - ~
92 Australian Social Work/September 2001, Vol. 54, No. 3
Copyright © 2022 FDOKUMEN




















