
Adaptive Mechanisms of Niche Remodeling in Streptococcus ...
Upload
independentCategory
view
8download
0
For Peer Review O
nly
Intrapartum antibiotic prophylaxis failure and group-B
streptococcus early-onset disease
Journal: The Journal of Maternal-Fetal & Neonatal Medicine
Manuscript ID: DJMF-2010-0475.R2
Manuscript Type: Original Paper
Date Submitted by the Author:
20-Dec-2010
Complete List of Authors: Berardi, Alberto; Azienda Ospedaliero-Universitaria Policlinico, Scienze Ostetriche, Ginecologiche e Pediatriche Lugli, Licia; Azienda Ospedaliero-Universitaria Policlinico, Scienze Ostetriche, Ginecologiche e Pediatriche Rossi, Cecilia; Azienda Ospedaliero-Universitaria Policlinico, Scienze Ostetriche, Ginecologiche e Pediatriche China, Mariachiara; Azienda Ospedaliero-Universitaria Policlinico, Scienze Ostetriche, Ginecologiche e Pediatriche Chiossi, Claudio; Ospedale Civile, Unità Operativa di Pediatria Gambini, Lucia; Unità Operativa di Terapia Intensiva Neonatale, Azienda Ospedaliero-Universitaria, Parma, Italy Guidi, Battista; Ospedale Civile, Unità Operativa di Pediatria Pedna, Maria; Laboratorio di Microbiologia, Area Vasta Romagna, Pieve Sistina Piepoli, Marina; Ospedale G da Saliceto, Unità Operativa di Pediatria, Simoni, Angela; Ospedale B Ramazzini, Unità Operativa di Pediatria Ferrari, Fabrizio; Azienda Ospedaliero-Universitaria Policlinico, Scienze Ostetriche, Ginecologiche e Pediatriche
Keywords: Group B Streptococcus, Prophylaxis, Sepsis, Infant
URL: http://mc.manuscriptcentral.com/djmf Email: [email protected]
The Journal of Maternal-Fetal & Neonatal Medicine

For Peer Review O
nly
Page 1 of 25
URL: http://mc.manuscriptcentral.com/djmf Email: [email protected]
The Journal of Maternal-Fetal & Neonatal Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly
Intrapartum antibiotic prophylaxis failure and group-B streptococcus early-onset disease
Page 2 of 25
URL: http://mc.manuscriptcentral.com/djmf Email: [email protected]
The Journal of Maternal-Fetal & Neonatal Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly
Abstract
Objectives: To determine factors influencing intrapartum antibiotic prophylaxis (IAP) failure in the
prevention of group B streptococcus (GBS) early-onset disease (EOD)
Methods: GBS EOD case is defined as isolation of GBS from a normally sterile body site (e.g.,
blood or cerebrospinal fluid) in infants aged ≤7 days. During a consecutive 93 month period, GBS
EOD cases and care data were reviewed.
Results: Seventy-nine GBS EOD cases were registered; 67 infants were born to women who
received no i.v. antibiotics during labor. The 12 EOD cases exposed to IAP were more likely to be
associated with emergency caesarean section (P=0.0015), maternal obstetric risk factors (ORFs)
(P=0.0061), particularly intrapartum fever (P=0.0002), and to present with signs of illness at birth
(P=0.0015). Correct dosages, agents and timing were registered in 3 cases only; of which 2 were
associated with intrapartum fever.
Conclusions: ORFs, emergency caesarean section and signs of illness at birth are significantly
associated with GBS EOD in infants exposed to IAP. This study also suggests that recommended
IAP agents, dosages and timing are infrequently associated with EOD. Strict protocol adherence is
recommended in all cases.
Page 3 of 25
URL: http://mc.manuscriptcentral.com/djmf Email: [email protected]
The Journal of Maternal-Fetal & Neonatal Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly
Introduction
Group B streptococcus (GBS) is a major cause of severe bacterial infection in neonates [1].
Infection presenting within the first week of life (early-onset disease or EOD) is predominantly
caused by exposure to maternal GBS during childbirth. The risk of EOD increases for infants born
to GBS colonized mothers, with one or more obstetrical risk factors (ORFs: preterm birth, GBS
bacteriuria identified during the current pregnancy, previous infant with GBS infection, membrane
rupture ≥8 hours prior to delivery, maternal temperature ≥38° C during labour) [1,2].
EOD is mostly preventable through the administration of antibiotics during labour (intrapartum
antibiotic prophylaxis or IAP). The Centre for Disease Control and Prevention (CDC) guidelines
recommend maternal screening in late pregnancy (35-37 weeks of gestation) and the administration
of IAP to GBS screened culture-positive women, to women with GBS bacteriuria during current
pregnancy ant to women with a previous GBS infected infant [1].
As a result of prevention efforts, EOD rates have decreased over the past 15 years, but cases
continue to occur [3]. There is therefore a need to assess if further opportunities for preventing EOD
exist.
Culture-proven EOD is rare in infants exposed to IAP [4]. We compared all consecutive culture-
proven EOD cases over a period of 93 months in infants; they were classified according to the
administration or lack thereof of IAP. Individual patient demographic, clinical and infection
information were further analysed in infants who were exposed to IAP, in order to identify why
prophylaxis fails.
Methods
A prospective, population-based study has been ongoing in Emilia-Romagna since 2003 (a
northern region of Italy, population of 4,500,000). The GBS active surveillance network involves
regional neonatal and pediatric departments, and microbiologic laboratories [5].
Page 4 of 25
URL: http://mc.manuscriptcentral.com/djmf Email: [email protected]
The Journal of Maternal-Fetal & Neonatal Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly
Standardized forms are used to collect both, maternal (antenatal colonization, gestational age,
ethnicity, mode of delivery, hours since membrane rupture, antibiotic administration) and neonatal
data (Apgar scores, sex, birth weight, health status, laboratory evaluation).
A GBS case is defined as the isolation of GBS from a normally sterile body site (e.g., blood or
cerebrospinal fluid) in infants aged ≤90 days. Bacteraemia is a GBS positive blood culture in infants
without any signs of illness. Proven sepsis is the growth of GBS from blood culture associated with
clinical symptoms consistent with sepsis [6]. A detailed description of most EOD cases has recently
been reported by the GBS active surveillance network [5].
Antenatal maternal GBS recto-vaginal screening is performed between 35-37 weeks of gestation.
CDC guidelines recommend penicillin (or ampicillin) as the first line agents for prophylaxis [1].
Ampicillin is routinely administered in Italy, as penicillin is not produced in this country. We
recommend a standard dose of ampicillin (2 g intravenously plus 1 g intravenously every 4 hours
until delivery) during active labor. Prophylaxis is considered adequate, according to the CDC
guidelines, if penicillin (or ampicillin) is administered at least 4 hours prior to delivery.
Alternative agents, recommended for penicillin-allergic women, include cefazolin for women
without a consistent risk of anaphylaxis [1], as cases of resistance to group B streptococcus have
not been reported in literature to date, and its activity is most similar to that of penicillin.
In cases of anaphylaxis risk, GBS isolates testing of susceptibility should be performed prior to the
administration of erythromycin or clindamycin [1].
Wider spectrum antibiotics are recommended for women with intrapartum fever or
chorioamnionitis.
A full diagnostic evaluation for infants exhibiting signs of sepsis, and a limited diagnostic
evaluation (blood count and blood culture) for healthy appearing newborns who did not receive
adequate IAP (administration <4 hours prior to delivery) are recommended as standard clinical
practice [5].
Page 5 of 25
URL: http://mc.manuscriptcentral.com/djmf Email: [email protected]
The Journal of Maternal-Fetal & Neonatal Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly
Statistical analysis was performed according to the χ2 test and Mann-Whitney U test when
appropriate. A p value <0.05 was used as a threshold for statistical significance and 0.10<p<0.05 as
an indication of a trend. Data are presented as mean ± SD with ranges.
Results
Between 1st January 2003 to 31 August 2010, 307,148 live births were recorded, from which 79
EOD cases were registered (incidence rate of 0.26 per 1,000 live births).
Twenty-five mothers (31.6%) delivered by emergency caesarean section, whereas no cases of
EOD with planned caesarean section were identified. Maternal ORFs were found in 34 (43.0%) of
cases.
Clinical signs of illness were observed in 83.5% (66) of patients, whereas 16.5% (13) were
asymptomatic (bacteraemia). Mean gestational age was 37.1 weeks ± 4.6 (range 23-42), mean birth
weight was 2,936.8 gr ± 884.8.
Of the 79 EOD cases, 15.2% (12) were exposed to IAP and the remaining 85.8% (67) were not
(Table I). Characteristics of infants with and without IAP exposure are compared in Table 1.
Infants exposed to IAP
A significantly higher proportion of newborns exposed to IAP were delivered by emergency
caesarean section (p=0.0015), had identified ORFs (p=0.0061), particularly intra-partum fever
(p=0.0002), and presented with symptoms (p=0.0015) immediately (p=0.0031), compared with
EOD infected patients who had no exposure to IAP. The 12 individual patient characteristics,
management of IAP administration and EOD diagnosis are outlined in Table II.
Maternal ORFs were documented in 83.3% (≥2 ORFs were documented in 7 cases). Preterm
delivery was noted in 33.3%.
Page 6 of 25
URL: http://mc.manuscriptcentral.com/djmf Email: [email protected]
The Journal of Maternal-Fetal & Neonatal Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly
All cases of non protocol specified agent (azythromycin) administration (case 1-3) occurred in the
same maternity unit.
Inadequate protocol specified agents were administered in 3 cases (<4 hours prior to delivery;
cases 4-6), GBS isolates were resistant in 2 cases (cases 7, 11), and narrow spectrum antibiotics
were administered in 2 cases (cases 11-12).
Overall, 7 mothers were treated with alternative agents to ampicillin. Erythromycin or
clindamycin were administered in 3 cases, but no susceptibility testing was performed prior to
administration. Timing and agents administered prior to delivery are illustrated in the Table II.
Four newborns had no signs of illness (bacteraemia). According to protocol, these infants were
culture tested because of maternal ORF identification and/or inadequate antibiotics administration.
Two newborns (case 4, 7) were mechanically ventilated and 3 (cases 4,8-9) received
cathecolamine support.
Brain lesions were documented at hospital discharge in one case (case 9). One infant, born
severely preterm with inadequate IAP administration (case 4), died 8 days after birth caused by
acute respiratory failure.
Discussion
GBS prevention has been adopted extensively and the rate of EOD incidence have decreased to
0.26 per 1,000 live birth. In this population (>300.000 live births), only 15.2% of infants with EOD
were exposed to IAP.
Interestingly, most of them had identified maternal ORFs. Compared with EOD cases without
IAP administration, cases exposed to IAP were more likely to be associated with maternal
intrapartum fever, to be delivered by emergency caesarean section and to present clinical signs of
illness at birth. These are possibly characteristics of an advanced infection in utero.
In this region, nearly 90% of women treated with IAP receive ampicillin during labor; the
remaining 10% receive alternative agents.
Page 7 of 25
URL: http://mc.manuscriptcentral.com/djmf Email: [email protected]
The Journal of Maternal-Fetal & Neonatal Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly
Interestingly, most EOD cases exposed to IAP identified in this study were treated with
alternative agents to ampicillin. Resistant to these alternative agents by GBS is suspected, and
highlighted in this study was the question of the effectiveness of clindamycin and erythromycin.
Cefazolin, the recommended agent for women at risk of anaphylaxis, was only associated with 1
case of EOD, compared with 2 cases of clindamycin or erythromycin which were not tested for
susceptibility.
We do not know which was the actual risk of anaphylaxis for these penicillin-allergic mothers.
However, the choice of agent was guided mainly by the concern of adverse reactions. Having no
susceptibility testing, such agents were administered despite possible ineffectiveness.
Resistance of erythromycin and clindamycin to GBS isolates is increasingly reported in USA [7-
9]. Nevertheless, susceptibility testing to macrolides is rarely performed (<1% of colonized women
who are allergic to penicillin) and clindamycin is administered to 70% of women allergic to
penicillin [10].
In our case series, all non protocol specified agents were administered in the same maternity unit,
which was contacted and no further cases were registered.
Moreover, a protocol defined agent (ampicillin) was adequately administered in 3 mothers
according to correct dosages and timing. Strictly speaking, these cases only can be considered
failures of prophylaxis. Intrapartum fever (suspected chorioamnionitis) was observed in 2 cases and
all 3 newborns had severe disease at birth. Fetal acquisition of infection prior to initiation of IAP
was hypothesized. However, according to our local protocol and CDC guidelines, cases of
suspected chorioamnionitis should be treated with wider spectrum antibiotics rather than ampicillin
alone.
A limitation of this study is that we didn’t consider clinical sepsis (clinical course suggesting
sepsis with sterile blood culture). Sepsis may have been more common than this data shows, as
antibiotics may inhibit GBS growth in cultures.
Page 8 of 25
URL: http://mc.manuscriptcentral.com/djmf Email: [email protected]
The Journal of Maternal-Fetal & Neonatal Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly
Further, we documented the presence of histological chorioamnionitis in 2 preterm newborns.
Those patients were possibly already infected in uterus and prophylaxis should not be expected to
be effective, as infants needed treatment rather than IAP. However, information on the presence of
histological chorioamnionitis was very scanty, as only recently it has been routinely obtained.
Therefore we could not assess the exact proportion of infants with an underlying chorioamnionitis.
In conclusion, this study has an epidemiological relevance, as it reflects the data and GBS cases
of a large area. Correct dosages, agents and timing were infrequently associated with EOD. These
results highlight how valid is prophylaxis and the need of doing it well. Further, we emphasize the
importance of susceptibility testing before erythromycin or clindamycin administration and
continued clinical education regarding strict protocol adherence in all cases of GBS infection risk.
Acknowledgments
We thank dr. Johanna Chester, who kindly revised the manuscript and gave valuable suggestions
Declaration of Interest statement
The authors report no declarations of interest
Page 9 of 25
URL: http://mc.manuscriptcentral.com/djmf Email: [email protected]
The Journal of Maternal-Fetal & Neonatal Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly
References:
1. Schrag S, Gorwitz R, Fultz-Butts K, Schuchat A: Prevention of perinatal group B
streptococcal disease. Revised guidelines from CDC. MMWR Recomm Rep. 2002;
51(RR-11):1-22 .
2. Benitz WE, Gould JB, Druzin ML: Risk factors for early-onset group B streptococcal
sepsis: estimation of odds ratios by critical literature review. Pediatrics 1999;103:e77.
3. Jordan HT, Farley MM, Craig A, Mohle-Boetani J, Harrison LH, Petit S, Lynfield R,
Thomas A, Zansky S, Gershman K, Albanese BA, Schaffner W, Schrag SJ; Active
Bacterial Core Surveillance (ABCs)/Emerging Infections Program Network, CDC.
Revisiting the need for vaccine prevention of late-onset neonatal group B streptococcal
disease: a multistate, population-based analysis. Pediatr Infect Dis J. 2008;27:1057-64
4. Illuzzi JL, Bracken MB: Duration of intrapartum prophylaxis for neonatal group B
streptococcal disease: a systematic review. Obstet Gynecol. 2006;108:1254-65.
5. Berardi A, Lugli L, Baronciani D, Rossi C, Ciccia M, Creti R, Gambini L,Mariani S,
Papa I, Tridapalli E, Vagnarelli F, Ferrari F: Group B Streptococcus early-onset disease in
Emilia-romagna: review after introduction of a screening-based approach. Pediatr Infect
Dis J. 2010;29:115-21.
6. Gerdes JS. Clinicopathologic approach to the diagnosis of neonatal sepsis. Clin Perinatol.
1991;18:361-81.
7. Phares CR, Lynfield R, Farley MM, Mohle-Boetani J, Harrison LH, Petit S, Craig AS,
Schaffner W, Zansky SM, Gershman K, Stefonek KR, Albanese BA, Zell ER, Schuchat A,
Schrag SJ; Active Bacterial Core surveillance/Emerging Infections Program Network.
Epidemiology of invasive group B streptococcal disease in the United States, 1999-2005.
JAMA. 2008;299:2056-65.
Page 10 of 25
URL: http://mc.manuscriptcentral.com/djmf Email: [email protected]
The Journal of Maternal-Fetal & Neonatal Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly
8. Castor ML, Whitney CG, Como-Sabetti K, Facklam RR, Ferrieri P, Bartkus JM, Juni
BA, Cieslak PR, Farley MM, Dumas NB, Schrag SJ, Lynfield R. Antibiotic resistance
patterns in invasive group B streptococcal isolates. Infect Dis Obstet Gynecol.
2008;2008:727505.
9. Blaschke AJ, Pulver LS, Korgenski EK, Savitz LA, Daly JA, Byington CL.
Clindamycin-resistant group B Streptococcus and failure of intrapartum prophylaxis to
prevent early-onset disease. J Pediatr. 2010;156:501-3.
10. Van Dyke MK, Phares CR, Lynfield R, Thomas AR, Arnold KE, Craig AS, Mohle-
Boetani J, Gershman K, Schaffner W, Petit S, Zansky SM, Morin CA, Spina NL, Wymore
K, Harrison LH, Shutt KA, Bareta J, Bulens SN, Zell ER, Schuchat A, Schrag SJ.
Evaluation of universal antenatal screening for group B streptococcus. N Engl J Med. 2009
18;360:2626-36
Page 11 of 25
URL: http://mc.manuscriptcentral.com/djmf Email: [email protected]
The Journal of Maternal-Fetal & Neonatal Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly
Page 12 of 25
URL: http://mc.manuscriptcentral.com/djmf Email: [email protected]
The Journal of Maternal-Fetal & Neonatal Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
For Peer Review O
nly
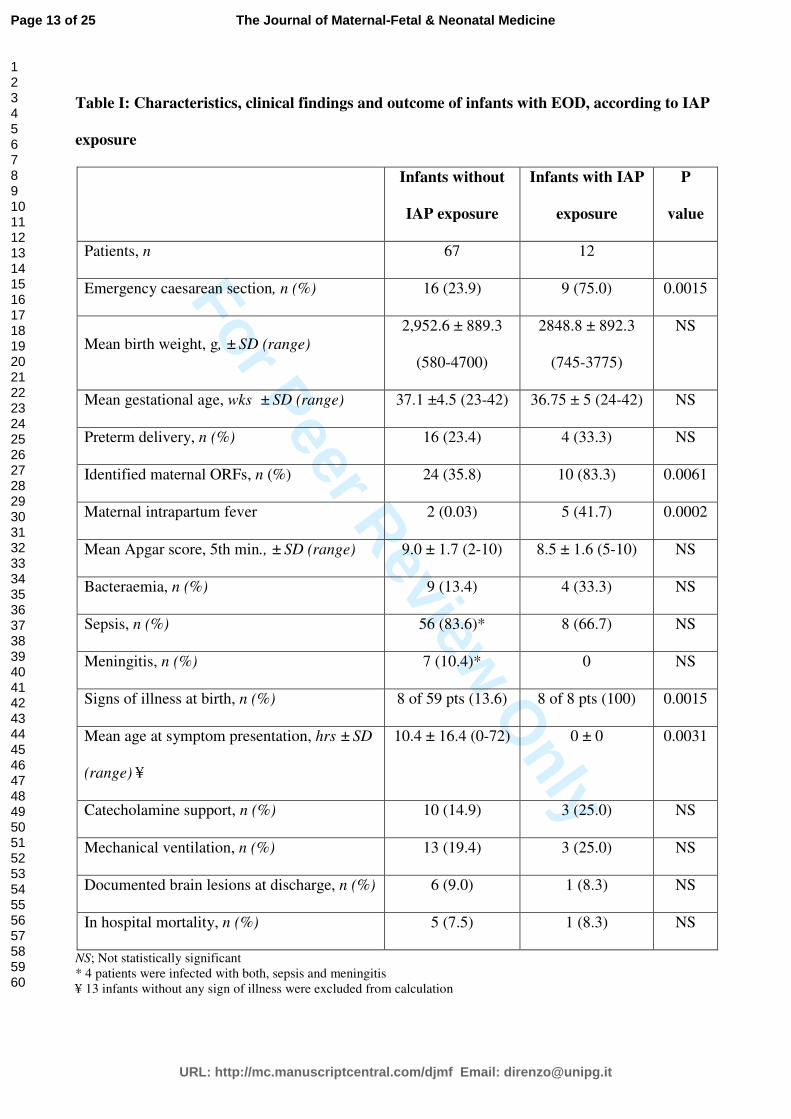
Table I: Characteristics, clinical findings and outcome of infants with EOD, according to IAP
exposure
Infants without
IAP exposure
Infants with IAP
exposure
P
value
Patients, n 67 12
Emergency caesarean section, n (%) 16 (23.9) 9 (75.0) 0.0015
Mean birth weight, g, ± SD (range)
2,952.6 ± 889.3
(580-4700)
2848.8 ± 892.3
(745-3775)
NS
Mean gestational age, wks ± SD (range) 37.1 ±4.5 (23-42) 36.75 ± 5 (24-42) NS
Preterm delivery, n (%) 16 (23.4) 4 (33.3) NS
Identified maternal ORFs, n (%) 24 (35.8) 10 (83.3) 0.0061
Maternal intrapartum fever 2 (0.03) 5 (41.7) 0.0002
Mean Apgar score, 5th min., ± SD (range) 9.0 ± 1.7 (2-10) 8.5 ± 1.6 (5-10) NS
Bacteraemia, n (%) 9 (13.4) 4 (33.3) NS
Sepsis, n (%) 56 (83.6)* 8 (66.7) NS
Meningitis, n (%) 7 (10.4)* 0 NS
Signs of illness at birth, n (%) 8 of 59 pts (13.6) 8 of 8 pts (100) 0.0015
Mean age at symptom presentation, hrs ± SD
(range) ¥
10.4 ± 16.4 (0-72) 0 ± 0 0.0031
Catecholamine support, n (%) 10 (14.9) 3 (25.0) NS
Mechanical ventilation, n (%) 13 (19.4) 3 (25.0) NS
Documented brain lesions at discharge, n (%) 6 (9.0) 1 (8.3) NS
In hospital mortality, n (%) 5 (7.5) 1 (8.3) NS
NS; Not statistically significant
* 4 patients were infected with both, sepsis and meningitis
¥ 13 infants without any sign of illness were excluded from calculation
Page 13 of 25
URL: http://mc.manuscriptcentral.com/djmf Email: [email protected]
The Journal of Maternal-Fetal & Neonatal Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly
Table II: Table II: Cases exposed to intrapartum antibiotics: doses, timing and agents administered
prior to delivery
Case Birth
weight,
gr (GA,
wks)
ORFs Antibiotic
(doses)
Administration,
complete hrs
before delivery
Loading
dose
Diagnosis Protocol
violation
1 2730
(36)
P Azythromycin (1) § 1 500 mg Bacteraemia NPSA
2 3650
(40)
F Azythromycin (1) § 4 500 mg Bacteraemia NPSA
3 3775
(40)
B Azythromycin (1) § 3 500 mg Bacteraemia NPSA
4 745
(24)
P, B Ampicillin (1) 2 2 gr, Sepsis,
Pneumonia
/
5 1900
(32)
P,
ROM
Cefazolin (1) 0 ¥ 2 gr Sepsis /
6 2140
(33)
P, B,
ROM
Ampicillin (1) 3 2 gr Bacteraemia /
7 2710
(38)
/ Clindamycin (1) §§ 3 900 mg Sepsis,
EA
/
8 2920
(39)
F,
ROM
Ampicillin (2) 5 2 gr Sepsis,
Pneumonia
/
9
3210
(40)
/ Ampicillin (1) 4 2 gr Sepsis,
Intrapartum
asphyxia
/
10 3270
(42)
F Ampicillin (2) 8 2 gr Sepsis /
11 3215
(40)
F,
ROM
Erythromycin (2) §§ 10 600 mg Sepsis NSA
12 3730
(40)
F Erythromycin (1) 2 600 mg Sepsis NSA
GA= gestational age. Wks = weeks. ORFs= obstetrical risk factors. P= prematurity. ROM= prolonged membrane
rupture (> 18 hours). B= bacteriuria. F= Intrapartum fever. IVH= intraventricular haemorrhage. NPSA=Non protocol
specified agent. OA= oral administration. EA= esophageal atresia. NSA=narrow spectrum antibiotics.
§ GBS sensitivity to azythromycin undetermined
¥ 20 minutes
§§ GBS resistant
Page 14 of 25
URL: http://mc.manuscriptcentral.com/djmf Email: [email protected]
The Journal of Maternal-Fetal & Neonatal Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly
Intrapartum antibiotic prophylaxis failure and group-B streptococcus early-onset disease
Page 15 of 25
URL: http://mc.manuscriptcentral.com/djmf Email: [email protected]
The Journal of Maternal-Fetal & Neonatal Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly
Abstract
Objectives: To determine factors influencing intrapartum antibiotic prophylaxis (IAP) failure in the
prevention of group B streptococcus (GBS) early-onset disease (EOD)
Methods: GBS EOD case is defined as isolation of GBS from a normally sterile body site (e.g.,
blood or cerebrospinal fluid) in infants aged ≤7 days. During a consecutive 93 month period, GBS
EOD cases and care data were reviewed.
Results: Seventy-nine GBS EOD cases were registered; 67 infants were born to women who
received no i.v. antibiotics during labor. The 12 EOD cases exposed to IAP were more likely to be
associated with emergency caesarean section (P=0.0015), maternal obstetric risk factors (ORFs)
(P=0.0061), particularly intrapartum fever (P=0.0002), and to present with signs of illness at birth
(P=0.0015). Correct dosages, agents and timing were registered in 3 cases only; of which 2 were
associated with intrapartum fever.
Conclusions: ORFs, emergency caesarean section and signs of illness at birth are significantly
associated with GBS EOD in infants exposed to IAP. This study also suggests that recommended
IAP agents, dosages and timing are infrequently associated with EOD. Strict protocol adherence is
recommended in all cases.
Comment [MSOffice1]: Added to
text
Page 16 of 25
URL: http://mc.manuscriptcentral.com/djmf Email: [email protected]
The Journal of Maternal-Fetal & Neonatal Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly
Introduction
Group B streptococcus (GBS) is a major cause of severe bacterial infection in neonates [1].
Infection presenting within the first week of life (early-onset disease or EOD) is predominantly
caused by exposure to maternal GBS during childbirth. The risk of EOD increases for infants born
to GBS colonized mothers, with one or more obstetrical risk factors (ORFs: preterm birth, GBS
bacteriuria identified during the current pregnancy, previous infant with GBS infection, membrane
rupture ≥8 hours prior to delivery, maternal temperature ≥38° C during labour) [1,2].
EOD is mostly preventable through the administration of antibiotics during labour (intrapartum
antibiotic prophylaxis or IAP). The Centre for Disease Control and Prevention (CDC) guidelines
recommend maternal screening in late pregnancy (35-37 weeks of gestation) and the administration
of IAP to GBS screened culture-positive women, to women with GBS bacteriuria during current
pregnancy ant to women with a previous GBS infected infant [1].
As a result of prevention efforts, EOD rates have decreased over the past 15 years, but cases
continue to occur [3]. There is therefore a need to assess if further opportunities for preventing EOD
exist.
Culture-proven EOD is rare in infants exposed to IAP [4]. We compared all consecutive culture-
proven EOD cases over a period of 93 months in infants; they were classified according to the
administration or lack thereof of IAP. Individual patient demographic, clinical and infection
information were further analysed in infants who were exposed to IAP, in order to identify why
prophylaxis fails.
Methods
A prospective, population-based study has been ongoing in Emilia-Romagna since 2003 (a
northern region of Italy, population of 4,500,000). The GBS active surveillance network involves
regional neonatal and pediatric departments, and microbiologic laboratories [5].
Page 17 of 25
URL: http://mc.manuscriptcentral.com/djmf Email: [email protected]
The Journal of Maternal-Fetal & Neonatal Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly
Standardized forms are used to collect both, maternal (antenatal colonization, gestational age,
ethnicity, mode of delivery, hours since membrane rupture, antibiotic administration) and neonatal
data (Apgar scores, sex, birth weight, health status, laboratory evaluation).
A GBS case is defined as the isolation of GBS from a normally sterile body site (e.g., blood or
cerebrospinal fluid) in infants aged ≤90 days. Bacteraemia is a GBS positive blood culture in infants
without any signs of illness. Proven sepsis is the growth of GBS from blood culture associated with
clinical symptoms consistent with sepsis [6]. A detailed description of most EOD cases has recently
been reported by the GBS active surveillance network [5].
Antenatal maternal GBS recto-vaginal screening is performed between 35-37 weeks of gestation.
CDC guidelines recommend penicillin (or ampicillin) as the first line agents for prophylaxis [1].
Ampicillin is routinely administered in Italy, as penicillin is not produced in this country. We
recommend a standard dose of ampicillin (2 g intravenously plus 1 g intravenously every 4 hours
until delivery) during active labor. Prophylaxis is considered adequate, according to the CDC
guidelines, if penicillin (or ampicillin) is administered at least 4 hours prior to delivery.
Alternative agents, recommended for penicillin-allergic women, include cefazolin for women
without a consistent risk of anaphylaxis [1], as cases of resistance to group B streptococcus have
not been reported in literature to date, and its activity is most similar to that of penicillin.
In cases of anaphylaxis risk, GBS isolates testing of susceptibility should be performed prior to the
administration of erythromycin or clindamycin [1].
Wider spectrum antibiotics are recommended for women with intrapartum fever or
chorioamnionitis.
A full diagnostic evaluation for infants exhibiting signs of sepsis, and a limited diagnostic
evaluation (blood count and blood culture) for healthy appearing newborns who did not receive
adequate IAP (administration <4 hours prior to delivery) are recommended as standard clinical
practice [5].
Page 18 of 25
URL: http://mc.manuscriptcentral.com/djmf Email: [email protected]
The Journal of Maternal-Fetal & Neonatal Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly
Statistical analysis was performed according to the χ2 test and Mann-Whitney U test when
appropriate. A p value <0.05 was used as a threshold for statistical significance and 0.10<p<0.05 as
an indication of a trend. Data are presented as mean ± SD with ranges.
Results
Between 1st January 2003 to 31 August 2010, 307,148 live births were recorded, from which 79
EOD cases were registered (incidence rate of 0.26 per 1,000 live births).
Twenty-five mothers (31.6%) delivered by emergency caesarean section, whereas no cases of
EOD with planned caesarean section were identified. Maternal ORFs were found in 34 (43.0%) of
cases.
Clinical signs of illness were observed in 83.5% (66) of patients, whereas 16.5% (13) were
asymptomatic (bacteraemia). Mean gestational age was 37.1 weeks ± 4.6 (range 23-42), mean birth
weight was 2,936.8 gr ± 884.8.
Of the 79 EOD cases, 15.2% (12) were exposed to IAP and the remaining 85.8% (67) were not
(Table I). Characteristics of infants with and without IAP exposure are compared in Table 1.
Infants exposed to IAP
A significantly higher proportion of newborns exposed to IAP were delivered by emergency
caesarean section (p=0.0015), had identified ORFs (p=0.0061), particularly intra-partum fever
(p=0.0002), and presented with symptoms (p=0.0015) immediately (p=0.0031), compared with
EOD infected patients who had no exposure to IAP.
Of the EOD cases, 15.2% (12) were exposed to IAP and the remaining 85.8% (67) did not receive
IAP. (Table I).
Characteristics of all infants with EOD.
Comment [MSOffice2]: Revised
results presentation
Page 19 of 25
URL: http://mc.manuscriptcentral.com/djmf Email: [email protected]
The Journal of Maternal-Fetal & Neonatal Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly
Twenty-five mothers delivered by emergency caesarean section. No cases of EOD with planned
caesarean section were identified. Maternal ORFs were found in 43% of cases. Information
regarding histological or clinical chorioamnionitis was mostly unavailable.
Clinical signs of illness were observed in 83.5% of patients. Mean gestational age was 37.1
weeks ± 4.6 (range 23-42), mean birth weight was 2,936.8 gr ± 884.8. Characteristics of infants
with and without IAP exposure are compared in table 1.
A significantly higher proportion of newborns with EOD exposed to IAP were delivered by
emergency caesarean section (p=0.0015), had identified ORFs (p=0.0061), particularly intra-partum
fever (p=0.0002), and presented with symptoms (p=0.0015) immediately (p=0.0031), compared
with EOD infected patients who had no exposure to IAP.
Characteristics of infants exposed to IAP
The 12 individual patient characteristics, management of IAP administration and EOD diagnosis are
outlined in Table II.
Maternal ORFs were documented in 83.3% (≥2 ORFs were documented in 7 cases). Preterm
delivery was noted in 33.3%. Histological confirm of chorioamnionitis was available in 2 of 4
mothers (case 4 and 6).
All cases of non protocol specified agent (azythromycin) administration (case 1-3) occurred in the
same maternity unit.
Inadequate protocol specified agents were administered in 3 cases (<4 hours prior to delivery;
cases 4-6), GBS isolates were resistant in 2 cases (cases 7, 11), and narrow spectrum antibiotics
were administered in 2 cases (cases 11-12).
Overall, 7 mothers were treated with alternative agents to ampicillin. Erythromycin or
clindamycin were administered in 3 cases, but no susceptibility testing was performed prior to
administration. Timing and agents administered prior to delivery are illustrated in the Table II.
Comment [MSOffice3]: delete
Page 20 of 25
URL: http://mc.manuscriptcentral.com/djmf Email: [email protected]
The Journal of Maternal-Fetal & Neonatal Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly
Four newborns had no signs of illness (bacteraemia). According to protocol, these infants were
culture tested because of maternal ORF identification and/or inadequate antibiotics administration.
Two newborns (case 4, 7) were mechanically ventilated and 3 (cases 4,8-9) received
cathecolamine support.
Brain lesions were documented at hospital discharge in one case (case 9). One infant, born
severely preterm with inadequate IAP administration (case 4), died 8 days after birth caused by
acute respiratory failure.
Discussion
GBS prevention has been adopted extensively and the rate of EOD incidence have decreased to
0.26 per 1,000 live birth. In this population (>300.000 live births), only 15.2% of infants with EOD
were exposed to IAP.
Interestingly, most of them had identified maternal ORFs. Compared with EOD cases without
IAP administration, cases exposed to IAP were more likely to be associated with maternal
intrapartum fever, to be delivered by emergency caesarean section and to present clinical signs of
illness at birth. These are possibly characteristics of an advanced infection in utero.
In this region, nearly 90% of women treated with IAP receive ampicillin during labor; the
remaining 10% receive alternative agents.
Interestingly, most EOD cases exposed to IAP identified in this study were treated with
alternative agents to ampicillin. Resistant to these alternative agents by GBS is suspected, and
highlighted in this study was the question of the effectiveness of clindamycin and erythromycin.
Cefazolin, the recommended agent for women at risk of anaphylaxis, was only associated with 1
case of EOD, compared with 2 cases of clindamycin or erythromycin which were not tested for
susceptibility.
Page 21 of 25
URL: http://mc.manuscriptcentral.com/djmf Email: [email protected]
The Journal of Maternal-Fetal & Neonatal Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly
We do not know which was the actual risk of anaphylaxis for these penicillin-allergic mothers,
However, the choice of agent was guided mainly by the concern of adverse reactions. Having no
susceptibility testing, such agents were administered despite possible ineffectiveness.
Resistance of erythromycin and clindamycin to GBS isolates is increasingly reported in USA [7-
9]. Nevertheless, susceptibility testing to macrolides is rarely performed (<1% of colonized women
who are allergic to penicillin) and clindamycin is administered to 70% of women allergic to
penicillin [10].
In our case series, all non protocol specified agents were administered in the same maternity unit,
which was contacted and no further cases were registered.
Moreover, a protocol defined agent (ampicillin) was adequately administered in 3 mothers
according to correct dosages and timing. Strictly speaking, these cases only can be considered
failures of prophylaxis. Intrapartum fever (suspected chorioamnionitis) was observed in 2 cases and
all 3 newborns had severe disease at birth. Fetal acquisition of infection prior to initiation of IAP
was hypothesized. However, according to our local protocol and CDC guidelines, cases of
suspected chorioamnionitis should be treated with wider spectrum antibiotics rather than ampicillin
alone.
A limitation of this study is that we didn’t consider clinical sepsis (clinical course suggesting
sepsis with sterile blood culture). Sepsis may have been more common than this data shows, as
antibiotics may inhibit GBS growth in cultures.
Further, we documented the presence histological chorioamnionitis in 2 preterm newborns. Those
patients were possibly already infected in uterus and prophylaxis should not be expected to be
effective, as infants needed treatment rather than IAP.
However, information on the presence of chorioamnionitis was very scanty, as only recently it has
benn routinely obtained. Therefore, we could not assess the exact proportion of infants who had an
underlying chorioamnionitis. Formatted: Italian (Italy)
Deleted: but the concern of adverse
reactions was the main reason
Comment [MSOffice4]: add to text
Comment [MSOffice5]: delete
Deleted: primary motive for the agents
choice; having no susceptibility testing,
such agents were administered despite
possible ineffectiveness. ¶
Deleted: wa
Deleted: true
Comment [MSOffice6]: Added to
text
Page 22 of 25
URL: http://mc.manuscriptcentral.com/djmf Email: [email protected]
The Journal of Maternal-Fetal & Neonatal Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly
In conclusion, this study has an epidemiological relevance, as it reflects the data and GBS cases
of a large area. newborns exposed to IAP were more likely to be delivered by emergency caesarean
section, to have ORFs and to present with signs of illness at birth. Correct dosages, agents and
timing were infrequently associated with EOD. These results further highlight how valid is GBS
prophylaxis and the need of doing it well. Further, we emphasize the importance of susceptibility
testing before erythromycin or clindamycin administration and continued clinical education
regarding strict protocol adherence in all cases of GBS infection risk.
Acknowledgments
We thank dr. Johanna Chester, who kindly revised the manuscript and gave valuable suggestions
Declaration of Interest statement
The authors report no declarations of interest
Comment [MSOffice7]: New
sentence added to text
Comment [MSOffice8]: delete
Comment [MSOffice9]: added to
text
Page 23 of 25
URL: http://mc.manuscriptcentral.com/djmf Email: [email protected]
The Journal of Maternal-Fetal & Neonatal Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly
References:
1. Schrag S, Gorwitz R, Fultz-Butts K, Schuchat A: Prevention of perinatal group B
streptococcal disease. Revised guidelines from CDC. MMWR Recomm Rep. 2002;
51(RR-11):1-22 .
2. Benitz WE, Gould JB, Druzin ML: Risk factors for early-onset group B streptococcal
sepsis: estimation of odds ratios by critical literature review. Pediatrics 1999;103:e77.
3. Jordan HT, Farley MM, Craig A, Mohle-Boetani J, Harrison LH, Petit S, Lynfield R,
Thomas A, Zansky S, Gershman K, Albanese BA, Schaffner W, Schrag SJ; Active
Bacterial Core Surveillance (ABCs)/Emerging Infections Program Network, CDC.
Revisiting the need for vaccine prevention of late-onset neonatal group B streptococcal
disease: a multistate, population-based analysis. Pediatr Infect Dis J. 2008;27:1057-64
4. Illuzzi JL, Bracken MB: Duration of intrapartum prophylaxis for neonatal group B
streptococcal disease: a systematic review. Obstet Gynecol. 2006;108:1254-65.
5. Berardi A, Lugli L, Baronciani D, Rossi C, Ciccia M, Creti R, Gambini L,Mariani S,
Papa I, Tridapalli E, Vagnarelli F, Ferrari F: Group B Streptococcus early-onset disease in
Emilia-romagna: review after introduction of a screening-based approach. Pediatr Infect
Dis J. 2010;29:115-21.
6. Gerdes JS. Clinicopathologic approach to the diagnosis of neonatal sepsis. Clin Perinatol.
1991;18:361-81.
7. Phares CR, Lynfield R, Farley MM, Mohle-Boetani J, Harrison LH, Petit S, Craig AS,
Schaffner W, Zansky SM, Gershman K, Stefonek KR, Albanese BA, Zell ER, Schuchat A,
Schrag SJ; Active Bacterial Core surveillance/Emerging Infections Program Network.
Epidemiology of invasive group B streptococcal disease in the United States, 1999-2005.
JAMA. 2008;299:2056-65.
Page 24 of 25
URL: http://mc.manuscriptcentral.com/djmf Email: [email protected]
The Journal of Maternal-Fetal & Neonatal Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly
8. Castor ML, Whitney CG, Como-Sabetti K, Facklam RR, Ferrieri P, Bartkus JM, Juni
BA, Cieslak PR, Farley MM, Dumas NB, Schrag SJ, Lynfield R. Antibiotic resistance
patterns in invasive group B streptococcal isolates. Infect Dis Obstet Gynecol.
2008;2008:727505.
9. Blaschke AJ, Pulver LS, Korgenski EK, Savitz LA, Daly JA, Byington CL.
Clindamycin-resistant group B Streptococcus and failure of intrapartum prophylaxis to
prevent early-onset disease. J Pediatr. 2010;156:501-3.
10. Van Dyke MK, Phares CR, Lynfield R, Thomas AR, Arnold KE, Craig AS, Mohle-
Boetani J, Gershman K, Schaffner W, Petit S, Zansky SM, Morin CA, Spina NL, Wymore
K, Harrison LH, Shutt KA, Bareta J, Bulens SN, Zell ER, Schuchat A, Schrag SJ.
Evaluation of universal antenatal screening for group B streptococcus. N Engl J Med. 2009
18;360:2626-36
Page 25 of 25
URL: http://mc.manuscriptcentral.com/djmf Email: [email protected]
The Journal of Maternal-Fetal & Neonatal Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

For Peer Review O
nly
Page 26 of 25
URL: http://mc.manuscriptcentral.com/djmf Email: [email protected]
The Journal of Maternal-Fetal & Neonatal Medicine
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Copyright © 2022 FDOKUMEN




















