INTESTINAL SYSTEM - TaiLieu.VN
155
tahir99 - UnitedVRG 12 INTESTINAL SYSTEM Contd... HIRSCHSPRUNG’S DISEASE ○ Male : female = 4 : 1 ○ Absence of ganglion cells in both myenteric and submucous plexus ○ Accompanying hypertrophy of nerve trunks ○ Rectal full thickness biopsy—diagnostic ○ May present as acute intestinal obstruction to chronic constipation in later life ○ Absence of fecal soiling differentiates it from other types of constipation ○ Surgeries done: Duhamel, Swenson, Soave MECKEL DIVERTICULUM ○ Meckels is true diverticulum, located in antimesentric border ○ M/c congenital anomaly of gastrointestinal tract (GIT) ○ M/c ectopic mucosa: m/c is gastric (60%), pancreatic, colonic, Brunner's glands, endometriosis ○ Rule of 2: Prevalence 2%, 2 inch length, located 2 feet proximal to ileocecal (IC) valve, presents m/c in < 2 year age ○ M/c complication in adults: Obstruction, children—bleeding, overall— bleeding ○ Littre's hernia: Meckel's as content in the sac (Amyand’s hernia—appendix) ○ Tc-99 m pertechnate scan: Diagnosis ectopic gastric mucosa, angiography can diagnose active bleed ○ Surgery: Simple excision, wide mouth during other surgeries leave it ○ Resection of ileum with anastomosis is done if—peptic ulcer in ileum, gan- grene affecting base, rarely if malignancy associated
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of INTESTINAL SYSTEM - TaiLieu.VN

tahir99 - UnitedVRG
12IntestInal system
Contd...
HIRSCHSPRUNG’S DISEASE
○ Male:female=4:1○ Absenceofganglioncellsinboth myenteric and submucous plexus○ Accompanyinghypertrophyofnervetrunks○ Rectalfullthicknessbiopsy—diagnostic○ Maypresentasacuteintestinalobstructiontochronicconstipationinlaterlife
○ Absenceoffecalsoilingdifferentiatesitfromothertypesofconstipation○ Surgeriesdone:Duhamel,Swenson,Soave
MECKEL DIVERTICULUM
○ Meckelsistruediverticulum,locatedinantimesentricborder○ M/ccongenitalanomalyofgastrointestinaltract(GIT)○ M/c ectopic mucosa:m/cisgastric(60%),pancreatic,colonic,Brunner'sglands,endometriosis
○ Rule of 2:Prevalence2%,2inchlength,located2feetproximaltoileocecal(IC)valve,presentsm/cin<2yearage
○ M/c complication in adults:Obstruction,children—bleeding,overall—bleeding
○ Littre's hernia:Meckel'sascontentinthesac(Amyand’shernia—appendix)○ Tc-99 m pertechnate scan:Diagnosisectopicgastricmucosa,angiographycandiagnoseactivebleed
○ Surgery:Simpleexcision,widemouthduringothersurgeriesleaveit○ Resectionofileumwithanastomosisisdoneif—pepticulcerinileum,gan-greneaffectingbase,rarelyifmalignancyassociated

tahir99 - UnitedVRG
119Intestinal System
DIVERTICULAR DISEASE○ Diverticulosis:Multiplediverticula○ Diverticulitis:Perforateddiverticulumduetoinflamma-tion
○ Diverticulosis:Bestdiagnosedbybariumenema(Saw-toothappearance).Shouldnotbedoneinacutesettings
○ Diverticulitis:Bestdiagnosedbycomputedtomography(CT)scan
○ False divericula:Arem/c○ Leftside(sigmoid)colon:M/csite○ Bleedingm/cfromrightside:Suppliedbysuperiormes-entricartery
○ In small bowel—Duodenum is m/c site, m/c on mesen-tric side, false diverticula.
○ Most sensitive test—Enteroclysis○ Smallboweldiverticulaareassociatedwithblindloopsyndrome:Bacterialovergrowth,B12deficiency—megalo-blasticanemia
POLYPS○ Pseudopolypsarenotpremalignant○ Non-neoplasticpolyps:Hyperplastic,juvenile,Peutz-Jegherspolyps
○ Neoplasticpolyps:Tubularadenomas,�illousadenomas,�a- Neoplasticpolyps:Tubularadenomas,�illousadenomas,�a-milialpolyposiscoli,Gardner'ssyndrome,Turcotsyndrome
○ Familial adenomatous polyposis (FAP): Autosomaldomi-nant(AD)disorder,5q*—colorectalcancerdevelopsinallpatientsatagebefore40yearsifuntreated.Prophylacticcolectomyneeded
○ Turcot syndrome:�amilialpancreaticcancer(�PC)+braintumorslikeglioma,medulloblastoma—AR
○ Gardner's syndrome: �PC+osteomas,epidermoidcysts,congenitalhypertrophyofretinalpigmentepithelium,desmoidtumor,retroperitonealfibrosis,polypsofstomach,smallintestine,adenomasinpan-creas,thyroid,adrenal,parathyroid
○ Peutz-Jeghers syndrome: Hamartomatous polyps in jejunum*andotherpart,pigmentationoflips,tumorsofovary,breast,endometrium,pancreas
○ Cronkhite canada syndrome: Juvenilepolypsarenotedalongwithalopecia,cutaneouspigmentation,atrophyofnailsandtoenail.
COLONIC CANCERRisk factors
○ Geographicvariation:HighestriskinWesterncoun-triesandlowestriskindevelopingcountries
○ Age:Riskincreasesharplyafterthe5thdecade○ Diet:Increasedwithtotalandanimalfatdiets○ Physicalinactivity:Increasedwithobesityandseden-tarylifestyle
○ Adenoma:Riskdependentontypeandsize�APpen-etranceingenecarriers100%
○ Hereditarynon-polyposiscolorectalcancer(HNPCC)penetranceingenecarriers80%
○ Hamartomatous syndromes: RiskincreasedwithPeutz-Jegherssyndromeandjuvenilepolyposis,butnotisolatedjuvenilepolyps
○ Previoushistoryofcoloncancer:Increasedriskforrecurrentcancer
○ Ulcerativecolitis:10%–20%after20year○ Radiation:Associatedwithamucinoushistologyandpoorprognosis
○ Ureterosigmoidostomy:100–200timesincreasedriskatoradjacenttotheureterocolonicanastomosis
Contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery120
PERCENTAGES○ M/c—rectosigmoid○ Rectum—38%○ Sigmoid—21%○ Caecum—12%○ Ascending—5%○ Descending—4%○ Transverse—5.5%Peak age:60-80years98%casesareadenocarcinomaSymptoms:�agueandnonspecific
MANAGEMENT○ MalignantobstructionistheM/c cause of large bowel obstruction○ Theprimarygoaloftreatmentisdecompressionofobstructedsegmenttopreventperforation
○ Removalofdiseasedsegmentissecondgoal
○ Bothshouldbedonewheneverpossible
○ Iflesionisunresectableadiver-sioncolostomyisdone
Right colon Left colon1.Stablecase—resectionandileocolicanasto-mosisinasinglestage
2.Unstable/perforatedcolon—twostage,resectionwithileostomy,lateranastomosis
1.Traditionallyandmostcommonlyperformedsurgeryisresectionoflesionandproximaldiversion(Hartmanns)
2.Stablepatientwithnoperitonitis,resectabletumors—primaryresectionandanastomosisorsubtotalcolectomyandileorectalanastomosis
Staging Dukes classification○ T1—Limitedtomucosaandsubmu-cosa
○ T2—Extendstomusculariso T3—ExtendsintoorthroughserosaDepthofpenetranceisanimpor-tantpredictorfordistantmets
Carcinoembryonicantigen(CEA)—markerforrecurrence
○ StageA:Limitedtomucosa○ StageB1:Extendingintomuscularispropria,butnotpenetratingthroughit;nodesnotinvolved
○ StageB2:Penetratingthroughmuscularispropria;nodesnotinvolved○ StageC1:Extendingintomuscularispropria,butnotpenetratingthroughit.Nodesinvolved
○ StageC2:Penetratingthroughmuscularispropria.Nodesinvolved○ StageD:Distantmetastaticspread
tahir99 - UnitedVRG
121Intestinal System
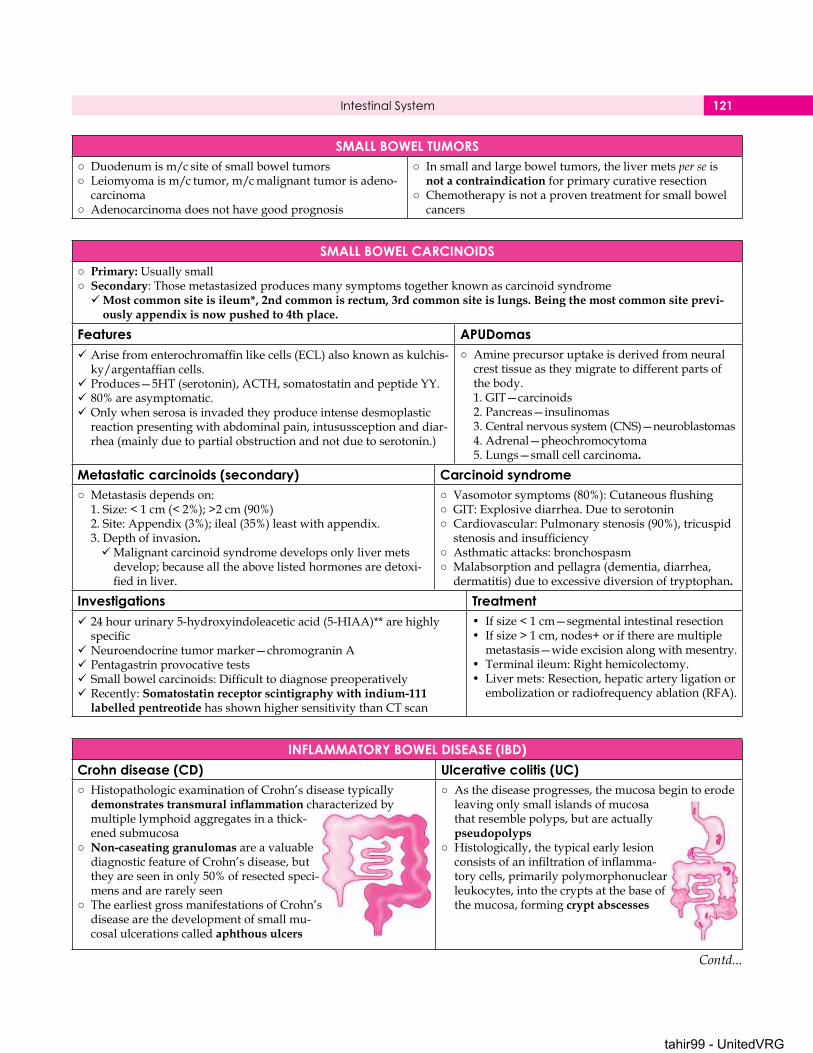
SMALL BOWEL TUMORS○ Duodenumism/csiteofsmallboweltumors○ Leiomyomaism/ctumor,m/cmalignanttumorisadeno-carcinoma
○ Adenocarcinomadoesnothavegoodprognosis
○ Insmallandlargeboweltumors,thelivermetsper seisnot a contraindicationforprimarycurativeresection
○ Chemotherapyisnotaproventreatmentforsmallbowelcancers
SMALL BOWEL CARCINOIDS○ Primary:Usuallysmall○ Secondary:ThosemetastasizedproducesmanysymptomstogetherknownascarcinoidsyndromeMost common site is ileum*, 2nd common is rectum, 3rd common site is lungs. Being the most common site previ-
ously appendix is now pushed to 4th place.
Features APUDomasArisefromenterochromaffinlikecells(ECL)alsoknownaskulchis-ky/argentaffiancells.
Produces—5HT(serotonin),ACTH,somatostatinandpeptideYY.80%areasymptomatic.Onlywhenserosaisinvadedtheyproduceintensedesmoplasticreactionpresentingwithabdominalpain,intusussceptionanddiar-rhea(mainlyduetopartialobstructionandnotduetoserotonin.)
○ Amineprecursoruptakeisderivedfromneuralcresttissueastheymigratetodifferentpartsofthebody.1.GIT—carcinoids2.Pancreas—insulinomas3.Centralnervoussystem(CNS)—neuroblastomas4.Adrenal—pheochromocytoma5.Lungs—smallcellcarcinoma.
Metastatic carcinoids (secondary) Carcinoid syndrome○ Metastasisdependson:1.Size:<1cm(<2%);>2cm(90%)2.Site:Appendix(3%);ileal(35%)leastwithappendix.3.Depthofinvasion.Malignantcarcinoidsyndromedevelopsonlylivermetsdevelop;becausealltheabovelistedhormonesaredetoxi-fiedinliver.
○ �asomotorsymptoms(80%):Cutaneousflushing○ GIT:Explosivediarrhea.Duetoserotonin○ Cardiovascular:Pulmonarystenosis(90%),tricuspidstenosisandinsufficiency
○ Asthmaticattacks:bronchospasm○ Malabsorptionandpellagra(dementia,diarrhea,dermatitis)duetoexcessivediversionoftryptophan.
Investigations Treatment24hoururinary5-hydroxyindoleaceticacid(5-HIAA)**arehighlyspecific
Neuroendocrinetumormarker—chromograninAPentagastrinprovocativetestsSmallbowelcarcinoids:DifficulttodiagnosepreoperativelyRecently:Somatostatin receptor scintigraphy with indium-111
labelled pentreotidehasshownhighersensitivitythanCTscan
• Ifsize<1cm—segmentalintestinalresection• Ifsize>1cm,nodes+oriftherearemultiplemetastasis—wideexcisionalongwithmesentry.
• Terminalileum:Righthemicolectomy.• Livermets:Resection,hepaticarteryligationorembolizationorradiofrequencyablation(R�A).
INFLAMMATORY BOWEL DISEASE (IBD)Crohn disease (CD) Ulcerative colitis (UC)○ HistopathologicexaminationofCrohn’sdiseasetypically
demonstrates transmural inflammationcharacterizedbymultiplelymphoidaggregatesinathick-enedsubmucosa
○ Non-caseating granulomasareavaluablediagnosticfeatureofCrohn’sdisease,buttheyareseeninonly50%ofresectedspeci-mensandarerarelyseen
○ TheearliestgrossmanifestationsofCrohn’sdiseasearethedevelopmentofsmallmu-cosalulcerationscalledaphthous ulcers
○ Asthediseaseprogresses,themucosabegintoerodeleavingonlysmallislandsofmucosathatresemblepolyps,butareactuallypseudopolyps
○ Histologically,thetypicalearlylesionconsistsofaninfiltrationofinflamma-torycells,primarilypolymorphonuclearleukocytes,intothecryptsatthebaseofthemucosa,formingcrypt abscesses
Contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery122
INFLAMMATORY BOWEL DISEASE (IBD)Crohn disease Ulcerative colitis○ Serpiginous network of linear ulcerationsthatsurroundis-landsofedematousmucosaproducingtheclassic‘cobblestone’appearance.Mucosalulcerationsmaypenetratethroughthesubmucosatoformintramuralchannelsthatcanboredeeplyintothebowelwallandcreatesinuses,abscessesorfistulas.
○ Althoughulcerativecolitisisgenerallyconfinedtothemucosa and submucosa,inthemostsevereformsofthedisease,suchasfulminantcolitisortoxicmegacolon,thediseaseprocessmayextendtothedeepermuscularlayersofthecolonandeventotheserosa
Clinical features Ulcerative colitis Crohn diseaseLocation ○ Colononly • Anywhereinthealimentarytract
Anatomic distribution ○ Continuous,beginningdistally • Asymmetricalskip lesions
Rectal involvement ○ >90% • Occasionally
Diarrhea/gross bleeding ○ Severe,oftenbloodywithmucus • Lesssevere,infrequentbleeding
Abdominal pain ○ Yes • Occasionally
Perianal fistulas ○ Rare • Common
Abdominal mass (palpable) ○ Rare • Common
Strictures and obstructions ○ Uncommon • Common
Fistulas and perforations ○ Rare • Common
Extraintestinal manifestations ○ Common • Common
Recurrence after surgery ○ Ifretainedrectalmucosa • Yes
Endoscopic features Ulcerative colitis Crohn diseaseMucosal involvement ○ Contiguous • Discontinuous
Discrete ulcers (aphthous) ○ Rare • Common
Surrounding mucosa ○ Abnormal • Relativelynormal
Longitudinal ulcers (serpiginous) ○ Rare • Common
Cobblestoning ○ No • Inseverecases
Rectal involvement ○ >90% • Sparingcommon
Mucosal friability ○ Common • Uncommon
Vascular pattern ○ Distorted • Normal
Radiographic featuresSmall bowel abnormalities ○ No • Yes
Terminal ileum abnormalities ○ Rare • Yes
Segmental colitis ○ No • Yes
Asymmetric colitis ○ No • Yes
Stricturing ○ Occasionally • �requently
Contd...

tahir99 - UnitedVRG
http:/
/vip.p
ersian
ss.ir/
123Intestinal System
LOCAL COMPLICATIONS OF IBD
TREATMENT FOR IBDUlcerative colitis Crohn disease○ Conservative○ Surgical—Electiveandemergency○ Indicationsforsurgery
○ RememberUCcanbecuredbyresectionofaffectedsegment,butCDneedsonlypalliativecare
Emergency ElectiveProvenorsuspectedperforationofcolon
Intractabledisease
Massivehemorrhage Dysplasticchanges/cancerToxicmegacolonnotrespondingtomedicaltreatment
Chroniccolitis>10years
Emergency• Fulminant colitis:Totalcolectomywithendileostomyratherthanatotalproctocolectomy(rectumalsoremoved).Thisisbecauserectumsymptomsimproveinvariablyandalsofirstprocedureavoidsunnecessarytimewasteinpelvisdissectionincriticallyillpatient.
• Iftoounstable:Loopileostomyanddecompressingcolostomy
Elective Indications of surgery• Restorativeproctocolectomywithilealpouchanalanastomosis(procedureofchoice)
• Totalproctocolectomywithendileostomy• Totalproctocolectomywithcontinentileostomy(Kock’spouch)
�istulasIntra-abdominalabscessPerianalabscessStrictures
○ Toxicmegacolon○ Massivebleed○ Dysplasia/cancer○ Intractability
EXTRAINTESTINAL MANIFESTS1. Dermatologic
• Erythemanodosum• Pyodermagangrenosum(m/cinUC)
Contd...
tahir99 - UnitedVRG
http:/
/vip.p
ersian
ss.ir/
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery124
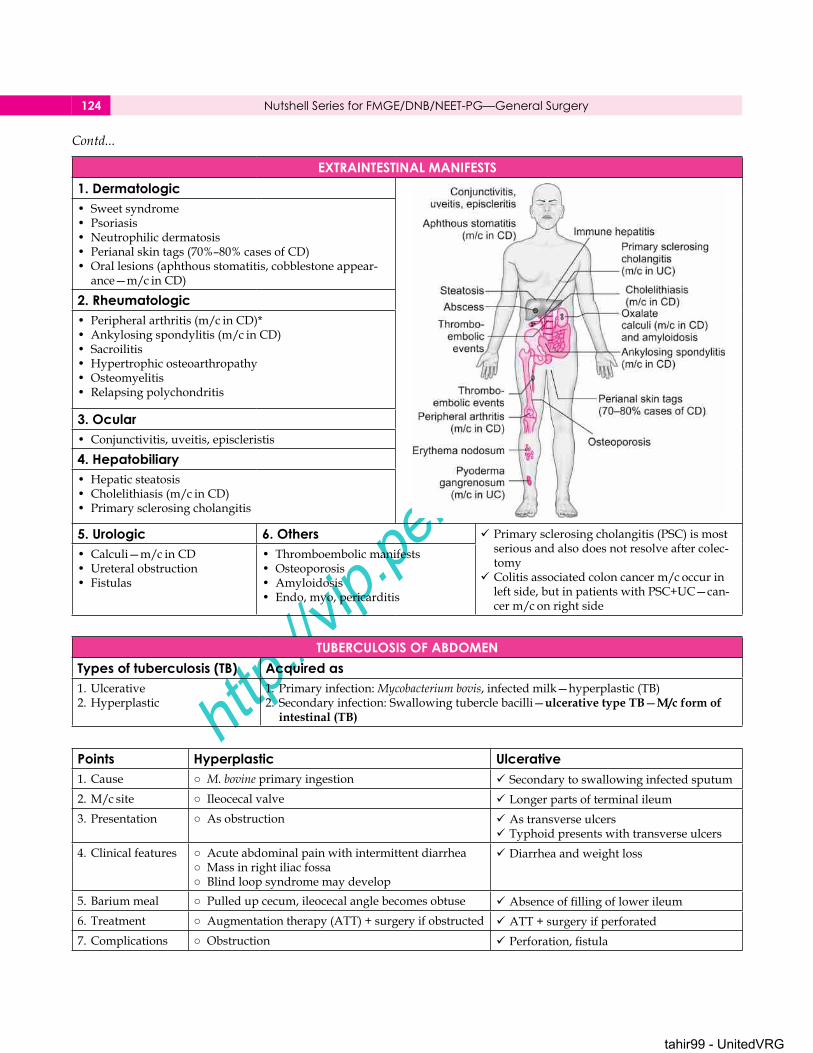
EXTRAINTESTINAL MANIFESTS1. Dermatologic• Sweetsyndrome• Psoriasis• Neutrophilicdermatosis• Perianalskintags(70%–80%casesofCD)• Orallesions(aphthousstomatitis,cobblestoneappear-ance—m/cinCD)
2. Rheumatologic• Peripheralarthritis(m/cinCD)*• Ankylosingspondylitis(m/cinCD)• Sacroilitis• Hypertrophicosteoarthropathy• Osteomyelitis• Relapsingpolychondritis
3. Ocular• Conjunctivitis,uveitis,episcleristis
4. Hepatobiliary• Hepaticsteatosis• Cholelithiasis(m/cinCD)• Primarysclerosingcholangitis
5. Urologic 6. Others Primarysclerosingcholangitis(PSC)ismostseriousandalsodoesnotresolveaftercolec-tomy
Colitisassociatedcoloncancerm/coccurinleftside,butinpatientswithPSC+UC—can-cerm/conrightside
• Calculi—m/cinCD• Ureteralobstruction• �istulas
• Thromboembolicmanifests• Osteoporosis• Amyloidosis• Endo,myo,pericarditis
TUBERCULOSIS OF ABDOMENTypes of tuberculosis (TB) Acquired as1.Ulcerative2.Hyperplastic
1.Primaryinfection:Mycobacterium bovis,infectedmilk—hyperplastic(TB)2.Secondaryinfection:Swallowingtuberclebacilli—ulcerative type TB—M/c form of
intestinal (TB)
Points Hyperplastic Ulcerative1.Cause ○ M. bovineprimaryingestion Secondarytoswallowinginfectedsputum2.M/csite ○ Ileocecalvalve Longerpartsofterminalileum3.Presentation ○ Asobstruction Astransverseulcers
Typhoidpresentswithtransverseulcers4.Clinicalfeatures ○ Acuteabdominalpainwithintermittentdiarrhea
○ Massinrightiliacfossa○ Blindloopsyndromemaydevelop
Diarrheaandweightloss
5.Bariummeal ○ Pulledupcecum,ileocecalanglebecomesobtuse Absenceoffillingoflowerileum6.Treatment ○ Augmentationtherapy(ATT)+surgeryifobstructed ATT+surgeryifperforated7.Complications ○ Obstruction Perforation,fistula
Contd...

tahir99 - UnitedVRG
http:/
/vip.p
ersian
ss.ir/
125Intestinal System
SHORT BOWEL SYNDROME○ Removalofsignificantportionofsmallbowel○ M/ccauses—mesentricinfarction,Crohndisease,trauma
○ Resectionofterminalileum—malabsorptionofbilesaltsandvitaminB12
Results in:1.Megaloblastic anemia2. Watery diarrhea—unabsorbedbilesaltsintocolon3. Malabsorptionoffatsolublevitamins4. Steatorrhea—reductioninbilesaltpool5. Oxalate kidney stones—unabsorbedfattyacidsbindwithcalcium6. Cholesterol gallstones—decreasedbilesaltinbile7. Increased gastrin secretion: duetoreducedhormonalinhibition
Risk factors for short gut syndrome• Smallbowellength<200cm• Absenceofileocecalvalve• Absenceofcolon• Diseasedbowelremaining(Crohndisease)• Ilealresection
TreatmentMedical treatment Non-transplant surgeries • Intestinal transplantation
H2antagonists/Protonpumpinhibitors(PPI)toreducegastricsecretion
Antimotilityagents—LoperamideOcterotideTotalparenteralnutrition(TPN)
Bianchiintestinallengtheningopera-tions
Serialtransverseenteroplasty
SUPERIOR MESENTERIC ARTERY (SMA) SYNDROME○ Wilkie’s syndrome○ Rareconditioninwhichthe3rdpartofduodenumcompressedbetweenSMAandaorta
Factors that precipitate the syndrome1.Suddenweightloss2.Rapidgrowthinheight3.Bodycastsapplication4.Supineimmobilization
Clinical features Treatment○ M/cseeninthinyoungfemale○ Presentswithgastricoutletobstruction(GOO)symptoms
○ Conservative/posturaltherapy○ Ifnotresponding—duodenojejunostomy
ENTEROCUTANEOUS FISTULA○ M/ccauseofenterocutaneous(EC)fistulaisiatrogenic○ Othercauses—Crohn’sdisease,diverticulitis,carcinomacolon
○ Highfistulasdrain>500mL/day
Complications of fistula1.�luidandelectrolytedisturbance2.Malnutrition3.Necrosisofskin4.Sepsisleadingtomultipleorganfailureanddeath
TreatmentCorrectionoffluidandelectrolyteimbalanceAntibioticsSkinprotection
TPNSurgeryindicated,iffistulafailstohealafter4-6week�istuloustractexcisionalongwithinvolvedsegmentandreanastomosis
Megacolon Toxic megacolon○ Megacolondescribeschronicallydilated,elongated,hypertrophiedlargebowel
○ Definedastransversecolondiameter>5–6cmwithlossofhaustration
Contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery126
Megacolon Toxic megacolon○ Congenital:Hirschsprungs,○ Acquired:1.Chagasdisease:T. cruziinfection2.Medications:Anticholinergics3.Neurological:Polio,paraplegia,multiplesclerosis,motorneurondisease
4.Rectalcancer
○ Causedby:1.Ulcerativecolitis2.Crohndisease3.Salmonellosis4.Amebiccolitis5.Pseudomembranouscolitis6.Ischemiccolitis
Treatmentoftoxicmegacolon: Surgery is a must as it may go for perfora-tion.
Points• UnlikeUC,whichstartswithrectumandalmostalwaysinvolvesrectum,rectal sparing is seen in Crohn disease• AngiodysplasiaisavascularmalformationassociatedwithageingItoccursm/cinascendingcolonandcecum
• ApatientpresentswithlowerGIbleeding,biopsyfromsigmoidcolonulcersareflask-shaped-amoebiccolitisulcers—treatment:I�Metrogyl
APPENDIX
ACUTE APPENDICITISNormal position of appendix Etiology factors○ Retrocecal:70%○ Pelvic:20%○ Preilealandpostileal
○ Subcecal○ Paracecal○ Subhepatic
○ Idiopathic○ �ecolithsandworms○ �alveofGerlach:�alveatbaseofappendix
○ First symptom:Anorexiafollowedbypain○ Murphy’s triad:Pain,vomitingandfever○ Blumberg sign—reboundtenderness○ Rovsing’s sign (American):Palpationofleftiliacfossaproducespaininrightiliacfossabyshiftofbowels.
○ Rovsing’s sign (Europe):Retrogradestrikeoutsofleft-sidedcolonleadstopainintheascendingcolonandcecum
○ Douglas sign:Right-sidedpaininrectalorvaginalexamination
○ Sherren’s triangle hyperesthesia:TriangleformedbyASIS,umbilicusandpubicsymphysisduetoirritationoflowerabdominalnerves
○ Bastede’s sign:Paininrightiliacfossa,ifairisinsuf-flatedintorectum
Investigations• Clinicalexaminationisthediagnostic• Ultrasonography(USG)andCTscanareusedtocon-firmthediagnosis
• Onthebasisofclinicalexaminationnormalappendixisfoundin15%–30%cases
TestsCope’s psoas test:Retrocecalappendicitisonextensionofhipproducespainduetoirritationoverpsoasmajor
Cope’s obturator test:Pelvicappendicitis,flexionandfedialrotationproducespain.
Contd...
Contd...
ENTEROCUTANEOUS FISTULA

tahir99 - UnitedVRG
127Intestinal System
ACUTE APPENDICITISAlvarado scoring
• M—Migratorypain• A—Anorexia• N—Nauseaandvomiting• T—Tenderness
• R—Reboundtenderness• E—Elevatedtemperature• L—Leukocytosis• S—Shifttoleft,segmentedneutrophils
Score of > 7 is strongly suggestive of appendicitisComplications
1. Perforation 2. Appendicular mass○ Earlyantibioticsdonotpreventrupture○ Occursmostfrequentlydistaltoobstructionalongtheantimesen-tericborder
○ Suspectruptureifthereishighgradefever>39degrees○ Riskfactorsofperforation—extremesofage,immunosuppression,diabetesmellitus,fecolithobstruction,pelvicappendix,previousabdominalsurgery
○ Infectionsealedoffbygreateromentum,cecum,terminalileum,whichresultsinatendersofttofirmmassinRI�
○ Ochsner-Sherrensconservativeregimenfol-lowed
○ Intervalappendicectomydoneafter6weeks
3. Appendicular abscess○ Ifinfectionisnotproperlycontrolledabscessresultspresent-ingwithhighgradefeverandchills
○ Drainpelvicabscessviarectum,drainretrocecalabscessex-traperitoneally,preandpostilealabscessbylaparotomy.Inallcases,electiveappendicectomydoneinalaterdate
○ Diffuseperitonitisfollowingappendicitisoccurif per-foration occurs in < 24 hours of onset.Inlaterstagestheomentumandsmallbowelsusuallysurroundtheinflammedappendixandpreventspread
Incisions Special situations• McBurney’s grid iron incision• Lanz incision:Cosmetichorizontalskininci-sion
• Rutherford-Morrison incision:Musclecut-tingincisionandnotaskinincisionextend-ingupwardsandlaterally
• Iliohypogastricnerveisinjuredingridironincision
• Resultsindirectherniarightside
○ Cecal wall edematous and inflamed:Stumpmustnotbeinvaginatedandpursestringnotused
○ Base of appendix inflamed:Baseisnotcrushed,ligatedclosetocecumandstumpinvaginated
○ Base is gangrenous:Neithercrushednorligatedremovetheappendixclosetobaseandapplytwolayerstitchesatthececalwall
○ OnopeningappendixisnormalpatientishavingCrohndisease:IfCrohndiseaseisnotinvolvingbaseofappendixdoappendicectomy,ifitinvolvesleaveitassuch
MUCOCELESHistological types ○ Intraluminalaccumulationofmucoidsubstance
○ Benigntumor,lowgrademalignancy:Hencesimpleap-pendicectomyisenoughRetentioncysts
MucoushyperplasiaCystadenomaCystadenocarcinoma
CARCINOID APPENDIX○ Argentaffinomasorcarcinoidtumorsarethem/cneoplasmofappendix
○ M/cindistalthird○ Rarelymetastasistoliver
TreatmentDependsonsizeoftumor<2cm—plainappendicectomy>2cm—righthemicolectomy
Ifcecalwallormesoappendixorlymphnodesinvolveddorighthemicolectomy
Contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery128
INTESTINAL OBSTRUCTIONIntusussception
○ Enteringtube—intussusceptum○ Returning—middletube○ Outertube—intussuscipiens○ M/ccauseofintestinalobstruction:age3monthsto6years
Causes• PediatricIdiopathic(70%–90%)Hypertrophiedpeyerspatch(m/c)Respiratoryinfection,gastroenteritis,urinaryinfectionareassociatedin30%
Rarely:Henoch-SchonleinPurpura•Older infants: Meckels diverticulum (M/C)•Adults: Tumours,polyps,submucosallipomas.•Colocolicvarietyiscommoninadults
TypesIleocolic(77%)Ileoileocolic(12%)Ileoileal(5%)
Colocolic(2%)MultipleRetrograde
Clinical features Investigation Treatment○ M/ctype:Ileocolic○ Characterizedby—severecrampyab-dominalpain
○ �omiting○ Red currant jelly stool○ P/A: Sausage-shapedmass○ Le dance sign: Emptyrightiliacfossa○ P/R: Apexmayseenprotruding
Bariumenema—Claw-sign,coiled-springsign
Ultrasound—Targetsign,pseudo-kidneysignandBullseyesign
X-rayplain—Targetsign(softtissuemasswithconcentricareaoflucencyduetomesentricfat)
• Hydrostaticreductionbycontrastagentorairenemaisdiagnosticandtherapeutic
• Suchprocedureiscontraindi-catedinperitonitisandhemody-namicinstability
MECONIUM ILEUS○ Neonatalmanifestofcysticfibrosis○ Pancreaticenzymedeficiencyandabnormalchloridesecretionresultsinviscouswaterpoormeconium
○ Obstruction of thick meconium occurs in ileum○ Presentsimmediatelyafterbirthwithprogressiveabdominaldistensionandinter-mittentbiliousvomiting
Plain X-ray○ Air fluid levels do not form in spite of complete small bowel obstruction be-
cause enteric contents are viscous and thick○ Dilatedloopsofsmallintestine○ Incaseofmeconiumileusinwhichperforationhasoccurred,intraperitonealeggshellcalcificationsarenoted
Management○ Conservative:GastrografinorMypaqueenema,whengivenwilleasilypasstoileumandmaydispersetheobstructionduetoitshighosmolarityanddetergentaction
○ Ifthismethodfailssurgeryindicated.
○ Bishop Koop operation resectionofmostdilatedseg-mentwithanendtosideanastomosisofcolontoileum.Thedistalilealopeningisformedintoanileostomythroughwhichthemeconiumisirrigatedpostopera-tively

tahir99 - UnitedVRG
129Intestinal System
CONGENITAL ATRESIAS○ Duodenalatresia(35%)○ Jejunalatresia(15%)○ Ileum(25%)○ Ascendingcolon(10%)○ Multiple(15%)Doublebubble—duodenalatresiaTriplebubble—jejunalatresia
SMALL BOWEL OBSTRUCTIONS1.Adhesions(60%):M/cfollowsappendicitisorotherpelvicopera-tions
Avoidimmediatesurgeryandobservefor<24hours
2.Malignancy(20%):M/cmetastasis.3.Hernias(10%)4.Crohn’sdisease(5%)○M/Ccauseofsmallbowelobstruction:Adhesions
Clinical features1.Abdominalcrampypain:Whenthebowelisstrangulatedpainbecomessteadyandmorelocalizedwithoutacolickycomponent
2.�omiting(followsonsetofpain)3.Obstipation4.Abdominaldistension5.�ever6.Bloodinstool(intussusception)
CAUSE OF DISTENSION1.Swallowedgas(m/c)2.�ermentationgasbybacteria
3.Extracellularfluidloss4.Gastrointestinalsecretions
ADHESION: CAUSES1. Ischemia 3. Infections—tuberculosis,
peritonitis4. Inflammatoryconditions—Crohn’sdisease
5.Radiationenteritis6.Drugs—practololSitesofanastomosis
RetroperitonealizationofrawareasTrauma�ascularocclusion
2.�oreignmaterial—talc,starch,gauze,silkRadiography To minimize adhesions○ Normal fluid levels ; 3–5 each < 2.5 cm is normal○ Fluid levels > 5 indicates small bowel obstruction○ Step ladder pattern: Small bowel obstruction
1.Goodsurgicaltechnique2.Washingperitonealcavitywithsalinetoremoveclots3.Minimizingcontactwithgauze4.Coveringanastomosisandrawperitonealsurfaces
Recurrent adhesions○ Repeatadhesiolysis○ Nobleplication
○ Charlesphillipsoperation○ IntraluminalBakerstubeviajejunostomy

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery130
PARALYTIC ILEUS (INORGANIC CAUSE)○ M/c—Postoperative○ Infections1.Peritonitis2.Intra-abdominalabscess3.Sepsis4.Pneumonia
○ Electrolyteabnormalities1.Uremia2.Hypokalemia3.Hyponatremia4.Hypomagnesemia5.Hypermagnesemia
○ Hypothyroidism○ MI○ Spinalcordinjury○ Retroperitonealhemorrhage
○ Mesentricischemia
○ Drugs1.Anticholinergics2.Opiates3.Phenothiazines4.Calciumchannelblockers5.Tricyclicantidepressants
Clinical features Differential diagnosis of organic and inorganic obstruction
○ Stateinwhichthereisfailureoftransmissionofperistalticwavessec-ondarytoneuromuscularfailure
○ Resultantstasisleadstoaccumulationfluidandgasinthebowelasso-ciatedwithdistension,vomiting,absentordiminishedbowelsounds.
○ Multipleairfluidlevel.
○ Onlydifferentiatingpointisgasincolonandrectuminparalyticileus
○ Otherclinicalpointsinfavorofparalyticileus 1.Diminishedbowelsounds 2.Nopaininabdomen
Management○ Usuallyresolvein3–5days○ Treatthecause
○ Ifprolongedbeyond5–7daysinterventionneededlaparoto- Ifprolongedbeyond5–7daysinterventionneededlaparoto-laparoto-mytor/ohiddencause
LARGE BOWEL OBSTRUCTIONS○ Twistingofasegmentoftheintestineonanaxisformedbyitsmesentryisvolvulus○ M/ccauseofcolonobstruction:Carcinomacolon.○ 2ndcommoncause:�olvulus○ M/csiteofvolvulus:Sigmoidcolon○ Coffeebeanappearance:Sigmoidvolvulus○ Clockwise:Cecalvolvulus○ Anticlockwise:Sigmoidvolvulus
Treatment○ �luidresuscitationfollowedbyendoscopicdecompressionusingsigmoidoscope○ Rectaltubeisinsertedtomaintainit○ Thisprocedureiscontraindicatedinevidenceofperforationorstrangulation○ Recurrencerateishigh○ Definitive treatment is—sigmoid colectomy
SALIENT POINTS IN LARGE BOWEL OBSTRUCTION○ M/csiteis:Sigmoidcolon○ Patentileocecalvalve—closedloopobstruction○ Closedloopobstruction:Colondistendsprogressivelyresultingingangreneandperfora- Closedloopobstruction:Colondistendsprogressivelyresultingingangreneandperfora-tion(m/csitebeingcecum)
Symptoms and signs○ Abdominaldistension—mostprominentinitialfinding○ Painislessseverecrampy○ �omitingislateandoccursifileocecalvalveisincompetent○ Obstipation○ Faeculent vomiting is seen in distal ileum obstruction and very rare in colon obstruction.
Resections○ Paul-Mikulicz operation—Proximalcolostomydistalbowelbroughtoutasfistulathatcanbeclosedextraperitoneallyinfuture.
○ Hartmann’s operation—Ifdistalbowelcannotreachthesurfaceitisclosedandreturnedtoperitonealcavityafterclosure.○ Secondstagecolorectalanastomosisisdoneifthepatientisfit

tahir99 - UnitedVRG
131Intestinal System
ACUTE MESENTERIC ISCHEMIA
1.SuddenocclusionofSMA(50%)AtherosclerosisEmbolism(m/ccause—90%cases)�asculitis(PAN)�ibromusculardysplasia
2.Mesentericveinocclusion(25%)Thrombosis:OCP,polycythemia,neoplasminfiltrating
3.Nonocclusiveobstruction(25%)Severeshock
Clinical features• Suddensevereabdominalpain,vomiting,abdominaldistension• �unctionalobstructionwithabsentbowelsounds• Shockandperitonitisisrapid• 100%mortalityifuntreated. Treatment
○ Resectionofnonviablebowelwithitsmesentery○ Secondlookoperation
MucosaisleastresistanttoischemiaIfmaintrunkofSMAisinvolvedinfarctionoccursfromduodenojeunalflexuretosplenicflexure
Classicallythepainiscentralandoutofproportiontophysicalfindings
Presenceofgasbubblesinmesentricveinispathognomonic
ISCHEMIC COLITIS○ M/csite:Splenicflexure○ Thumb print signonplainX-ray
X-ray finding○ Priortoinfarct:Plainabdominalfilm—normal.○ Adynamicileus,gaslessabdomen,smallbowelpseudo-obstruction.○ Pinkyprinting:�ormlessloopsofsmallintestine.○ Thumbprintingofrightcolon.○ Rarelypneumatosisorgasinportalvenoussystem.
Investigations○ UpperGIseries:Dilatedloops,thickenedfolds,mucosalulceration,scallopedbowelborder.
○ Duplex,CT,magneticresonanceimaging(MRI),positronemissiontomography(PET)scans.
○ Laparoscopy:Usefulonlyforserosallesions,mucosanotvisualized.
Management�luidresuscitationHeparinanticoagulationMesentricveinthrombosisisusuallyduetosmallperiph-eralveinthrombosis(SM�orIM�thrombosisisrare)
Hencethrombectomyisnotneeded(notindicated)If peritoneal signs are present—urgentlaparotomyneededIf peritoneal signs absent—heparin(5days),oralanticoag-ulationlifelongalongwithbowelrestandfluidsisenough.
PSEUDO-OBSTRUCTIONS○ Isaconditioninwhichtherearesignsandsymp-tomsofintestinalobstructionintheabsenceofactualphysicalcauseofobstruction
Types○ Acute : Ogilviesyndrome○ Chronic: Suspectthisinmedicalillpatient,withtympanicabdomenandnontender.
Contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery132
PSEUDO-OBSTRUCTIONSEtiological classification
Primary Secondary [m/c]Motilitydisorder�amilialandsporadicvis-ceralmyopathy
Endocrine: Hypothyroidism,hypoparathy-roidism,diabetes
Neurological: Chagasdisease,Parkinson,spinalcordinjury
Smooth-muscle disorders:Collagenvasculardisorders,amyloidosis,musculardystrophy
Drugs: Phenothiazines,tricyclicantidepressants,opiates
Miscellaneous: Uremia,viralinfection,radiationenteritis,retroperitonealhematomas
○ Air fluid levels are unusual and should think of other causes
○ AcuteforminvolvesonlycolonwhereaschronicinvolvesotherpartsofGITalso
TreatmentColonoscopicdecompression(recurrence—25%)Whencolonoscopyfails:Subtotalcolectomyandileorectalanastomosis
RECTUM AND ANUSCANCER RECTUM
○ Earliestandm/csymptom—bleeding*○ Secondm/csymptomalterationinbowelhabits○ Earlymorningspuriousdiarrheaischaracteristicallyseen*○ Annularcanceratpelvirectaljunctionpresentswithconstipationandobstruction
○ Bestinvestigationfordiagnosis—Sigmoidoscopicbiopsy
○ Bestinvestigationforlocalspread—TransrectalUSG○ BestinvestigationforlocalTandNstaging—Tran-srectalMRI
Treatment part• Rectumlength—12cmisdividedintoupper,middleandlower1/3rd.Analcanal4cm
• Dentatelineisabout2.5cmfromanalverge• Internalsphincterisanorectaljunctionformedbypuborec-talismuscle.
• Rectal cancer needs a clearance atleast 2 cm distally.• Abdominoperinealresection(APR)isperformedwhenthesphinctercannotbepreservedCompleteexcisionofrectumandanusalongwithpermanentcolostomy
AlsoknownasMile’sprocedure
Anatomy of rectum �ortumorsinvolvingupper1/3rdanteriorresectionandfortumorsinvolvingmiddle1/3rdlowanteriorresection
Inotherwords…anteriorresectionisdonefortumorscon-finedtorectumhavingperitonealreflectionandlowanteriorresectionfortumorsinrectumwithoutperitonealreflection.Withtheadventinventionofstaplerslowanteriorresectionhasbecomeeasier
○ Upper1/3rd:Coveredbytheperitoneuminthefrontandthesides
○ Middle1/3rd:Coveredonlyinthefront.○ Lower1/3rd:Noperitonealcovering.○ Peritonealreflectionsformrectovesicalpouchinmalesandrectouterinepouchinfemalesanteriorly
Evenlower1/3rdtumorsaretakenupforsphinctersavinglowanteriorresection
Hartmann’sprocedureisdoneifthereistoomuchsepsisorobstruction,alsoifthepatientisveryelderlyandunsuitableforanytypeofresection.
Transanal excision of cancer rectum• T1N0orT2N0lesion<4cmindiameter• <40%circumferenceofthelumen• <10cmfromdentateline• Welltomoderatelydifferentiatedhistology• Noevidenceoflymphaticorvascularinvasiononbiopsy
ANAL CANCER○ M/c type:Squamouscellcarcinoma(alsoknownasepidermoidcarcinoma)
○ Second m/c type :Basalcellcarcinoma.
Contd...
Contd...

tahir99 - UnitedVRG
133Intestinal System
ANAL CANCER○ Chemoradiationisthetreatmentofchoice(Nigro
regimen)○ Morethan80%casesarecuredbychemoradiation.IfanyresidualtumorispresentAPRisdone
○ Chemousedare5-�U,mitomycinc○ Otheragentsarebleomycin,cisplatin,doxorubicin
Types of anal carcinomaAnal margin—distal to dentate line Anal canal—proximal to dentate line• Bowen’sdisease• Paget’sdisease• Basalcellcarcinoma• Analmarginsquamouscellcarcinoma• �errucouscarcinoma(Buschke-lowenstein)
• Epidermoidcarcinoma—tumorsarisingintransitionalzoneshareasimilarbehavior—cloacogenic,basaloid,squamouscellormucoepidermoidepithelial.
• Melanoma• Adenocarcinoma
Malignant melanoma anal canalAnalcanalisthirdm/csiteformelanomaafterskinandeyeRadioandchemoresistanttumorAge—50–60yearsNonspecificsymptoms—bleeding,painandmass
Only surgery—wide excision (treatment of choice) or APR (if wide area of anal canal in-volved). Both carry same survival and prognosis)
Recurrenceiscommon,butnotinthelocalarearesected.Occurssystemicallyratherthanlocally
HEMORRHOIDS○ Internalhemorrhoids—painless,locatedproximaltodentateline
○ Externalhemorrhoids—painful,locateddistaltodentateline
○ Recenttheoriesstatethathemorrhoidsarenormalanatomicalstruc-turesandtheyarecushionsofsubmucosaltissuecontainingvenules,arterioles,smoothmusclefibers,andelasticconnectivetissues.
○ Threehemorrhoidalcushionsarethereat3,7,11O’clockposition
Contd...
Contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery134
HEMORRHOIDSTreatment
• Medical:1and2degreerespondstosoftfibrediet,stoolsofteners,dietregulation
• Rubber band ligation:1,2andselected3rddegree
• Sclerotherapy injec-tion:1,2,3rddegree
• Infrared photocoagula-tion:for1,2nddegreehemorrhoids
Surgery:4thdegree,mixedinternalandexter-nal,failureofnonoperativemanagement.
TheBarron’s bander isacommonlyavailabledeviceusedtosliptightelasticbandsontothebaseofthepedicleofeachhemorrhoid.
Injection sclerotherapy,thesubmucosalinjec-tionof5% phenol in arachis oil or almond oil,maybeadvisedusingGabriel syringe
TheopentechniqueismostcommonlyusedintheUKandisknownastheMilligan–Morgan operation:Namedafterthesurgeonswhodescribedit
FISSURE-IN-ANO○ Tearinanalmucosa,accompaniedbyseverepainattimeofdefecation
○ Characterizedbyfreshbleedingperanum.○ Perrectalexaminationiscontraindicated
○ M/csite:Midlineposterior○ M/csymptom:Pain○ Chronicfissureisaccompaniedbysentineltag○ Inpregnancy,itiscommonanteriorly
TreatmentConservative:Lignocaineandsteroidgellocalapplication
Surgery:Lateralsphincterotomy,whereinternalsphincteriscut
Maximumanaldilatationundergeneralanesthesiapreviouslydoneisnotallowednowadays
FISTULA-IN-ANO○ Dividedintotwotypeshighandlow,dependingwhethertheinternalopeningisaboveorbelowtheanorectalring
○ Highfistulasneedstagedoperationsasthereishigh-riskofincompetency
○ M/ctypeisintersphincteric○ Othertypesare—trans,supra,extrasphincteric○ Causesare:M/cfromcryptoglandularabscess(anorectalabscess).OthercausesareCrohn’sdiseasemalignancy,radiation,tuberculosis,actinomycosis
Goodsall’s rule• Anteriorlylocatedfistulasdraindirectlyintoanalcanal,whereasposteriorlylocatedfistulasdrainviaahorseshoetract.
ExceptiontoGoodsall’sisanteriorfistulalocatedgreaterthan3.5cmfromanalvergewillalsoformhorseshoetract
Treatment of fistula-in-ano○ �istulotomy○ Inhighanalfistulathereisriskofinjurytosphincter,hencesurgerymustbedonecarefully.
○ Inhighanalfistulas:Setons arespecialmaterials,whichareusedtohealthehighfistulaswithoutriskofinjurytosphincter
○ Asetonmaybeahorsehair,proleneareanyinertmaterial,whichisinsertedintothefistuloustractandbroughtviatheanalcanalandtiedtoallowfibrosis.
Contd...

tahir99 - UnitedVRG
135Intestinal System
NORMAL FECAL CONTINENCE REQUIRE○ Adequaterectalwallcompliance○ Appropriateneurogeniccontrol○ �unctionalinternalandexternalsphincters○ Anorectalanglemaintainsanacuteangle
○ Hemorrhoidalcushionsactsmechanicallybyblockinganalcanal
○ Anorectalring(puborectalis,deepexternalsphincter,internalsphincter)isveryimportantforcontinence
ANORECTAL ABSCESS○ Usually produces a painful, throbbing swelling in
the anal region.•Thepatientoftenhasswingingpyrexia• Subdividedaccordingtoanatomicalsiteintoperi-anal,ischiorectal,submucousandpelvirectal
•Underlyingconditionsincludefistula-in-ano (mostcommon),Crohndisease,diabetes,immunosup-pression
•Treatment isdrainageofpusinfirstinstance,togetherwithappropriateantibiotics
•Alwayslookforapotentialunderlyingproblem
Mostcommontypeofanalabscessisperianalab-scess.
Ischiorectalabscessspreadsfromonesidetootherinahorse-shoe-shapedtract.
PILONIDAL SINUS○ Thetermpilonidalsinusdescribesaconditionfoundinthenatalcleftoverlyingthecoccyx,consistingofoneormore,usuallynon-infected,midlineopenings,whichcommunicatewithafibroustracklinedbygranulationtissueandcontaininghairlyinglooselywithinthelumen.
○ ItiscommoninjeepdrivershencecalledJeeper’s bottom○ Itisthoughtthatthecombinationofbuttockfrictionandshearingforcesinthatareaallowsshedhairorbrokenhairs,whichhavecollectedtheretodrillthroughthemidlineskinorthatinfectioninrelationtoahairfollicleallowshairtoentertheskinbythesuctioncreatedbymovementofthebuttocks,socreatingasubcutaneous,chronicallyinfected,midlinetrack
Treatment• Manymethodsarethereforsurgery.�orthefirsttimewecanexcisethesinuswidelocallyandal-lowittohealbysecondaryintention.(Disadvan-tageisthehealingofwoundtakesalongtime)
• Excision of all tracks and then closure by some other means designed to avoid a midline wound (Z-plasty, Karydakis procedure)
• Bascom’s procedure involves an incision lateral to the midline to gain access to the sinus cavity, which is rid of hair and granulation tissue
PRURITUS ANI○ Thisisintractableitchingaroundtheanus,acommonandembarrassingcondition.Usually,theskinisreddenedandhyperkeratoticanditmaybecomecrackedandmoist.
○ Thecausesarenumerous.○ Ausefulmnemonicis‘pus,polypus,parasites,piles,psyche’
Causes• Lackofcleanliness• Perianaldischargeduetofistula,hemorrhoidsandfis-sure
Infectiouscauses:• Trichomonasvaginalis• Parasitecauses:Threadworms,scabies,etc.• Epidermatophytosis• Bacterialinfection:Corynebacterium diphtheriae
• Allergy:Hayfever• Skindiseases:Psoriasis,lichenplanus,contactdermatitis
• Psychosis• Diabetes
Contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery136
PRURITUS ANITreatment
HygienicmeasuresStrappingbuttock
HydrocortisoneUnlessthereisconcomitantlesioninanusandrectumnoneedofsurgery.
IMPERFORATE ANUS○ Imperforateanus(strictly,itshouldbeanal‘agenesis’or‘atresia’)hashistoricallybeendividedintotwomaingroups○ Highandlow:Dependingonthelevelofterminationoftherectuminrelation to the pelvic floor
Boys Girls○ Themostfrequentdefectinboyswithimperforateanusisoneinwhichthedistalrectumissitedwithinthepuborectalissling,butterminatesasafistulaintothe bulbar urethra or prostatic urethraabovethemainanalsphinctercomplex.
○ Boyswithafistulaintothebladderneck(ahighdefect)havethepoorestprognosis,becauseoftheunderdevelopmentofthesacrumandpelvicandanalmusculature
○ Themostcommondefectingirlsisarectovestibularfistulainwhichthefis-tulaopensintotheposterior vestibule (not the vagina)
Investigation to diagnoseLateralproneradiographwithoutcontrastistakenat24hours,whenintestinalgasreachesrectum.
Invertogram*withbabyupsidedownX-rayshowsairindistalrec-tumat6hourswithacoinattheanalorificeplace.
TreatmentLowanomalieswithaperinealfistulacanbetreatedbyananoplasty.Morecomplexmalformationsrequireearlycolostomy,withdefinitiverepairperformedseveralmonthslater.
Thismayinvolveposterior sagittal anorectoplasty (PSARP,Pena,withorwithouttransabdominalmobilizationoftheleftcolonanddivisionofanycommunicationwiththeurinarytract)
RECTAL PROLAPSE○ Partial:Onlymucosaandsubmucosaprotrudesout○ Complet:Wholerectalwallprotrudes
Treatment of partial prolapseInchild—digitalreposition,submucousinjnof5%phenolInadults—submucousinjnofalmondoil,exciseprolapsedmucosa
Treatment of complete prolapseAdults
Perineal approach Abdominal approach Children:1.Thierschoperation2.Lockhart-Mummeryrectopexy Delormesoperation
ThierschoperationAltemeier’sprocedure
RipsteinsanteriorrectopexyWell’sposteriorrectopexy
Contd...

tahir99 - UnitedVRG
137Intestinal System
SOLITARY RECTAL ULCER○ Usuallyinanteriorrectum○ Causes:Intussusceptions,anteriorrectalwallprolapse,increasedintrarectalpressure
○ Increasedstrainingduetoconstipation
○ Pain,bleeding,mucusdischarge,outletobstruction○ Treatment:Diet(highfiberdiet,laxatives,avoidstraining)○ Surgeryreservedformedicallyfailedcases
ABDOMINAL COMPARTMENT SYNDROME○ Definitionofabdominalcompartmentsyndrome(ACS):○ Organdysfunctioncausedbyintra-abdominalhypertension(IAH)
Category• PrimaryoracuteACS:Intra-abdominalpathologyisdirectlyandproximallyresponsibleforthecom-partmentsyndrome.
• SecondaryACS:Novisibleintra-abdominalinjuryispresent,butin-juriesoutsidetheabdomencausefluidaccumulation.
Itisduesplanchnicreperfusionaftermassiveresus-citation.
• ChronicACS:Thisoccursinthepres-enceofcirrhosisandascites,ofteninthelaterstagesofthedisease.
Pathophysiology
Compression of kidneys Decreased venous return Increased intrathoracic pressure ○ Decreasedrenalbloodflow
○ Decreasedurineoutput.
○ Decreasedcardiacoutput,ventricularenddiastolicvol-umeandstrokevolume
○ Increasedvascularresistance
○ Hypoxemiadueto:1.Increasedairwaypressure2.Decreasedcompliance3.Increasedcentralvenouspressure(C�P)
4.Increasedpulmonaryarterypressure
o Increased intra-cranial pressure
CausePrimary (i.e. acute) Secondary ChronicPenetratingtraumaIntraperitonealhemorrhagePancreatitisExternalcompressingforces,suchasdebrisfromamotorvehiclecollisionorafteralargestructureexplosion
PelvicfractureRuptureofabdominalaorticaneurysmPerforatedpepticulcer
○ Occurinpatientswithoutanintra-abdominalinjury (�luidaccumulatesinvolumessufficienttocauseIAH)Large-volumeresuscitation:Theliteratureshowsasig-nificantlyincreasedriskwhenmorethan3Lareinfused.
Largeareasoffullthicknessburns:PenetratingorblunttraumawithoutidentifiableinjuryPostoperativePackingandprimaryfascialclosure,whichincreasesincidence
Sepsis
Peritonealdialysis
Morbidobesity
CirrhosisMeigssyn-drome
Contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery138
ABDOMINAL COMPARTMENT SYNDROMEClinical Complication○ Physicalexaminationreveals•Distendedabdomen•Wheezes,rales,increasedrespiratoryrate•Cyanosis
○ Renalfailure○ Respiratorydistressandfailure○ Bowelischemia(bacterialtranslocation)○ Increasedintracranialpressure○ �ailingcardiacoutputandrefractoryshock○ Hypotensionandasystole:Reperfusionsyndromeandde-creasedS�R
Reperfusion syndrome Image studies• Suddenlossofbloodpressureafterabdominaldecompression
• Noclearetiologyexists• Maybeduetoacombinationoffactors,includingthefollowing:○Washoutofproductsofanaerobicmetabolism(e.g.lacticacid),whichmaybedirectlytissuetoxic
○ SuddenlossofS�R○Prevention:I�resuscitationwithmannitolandNaHCO3immediatelybeforedecompression
• Examinetheabdominalseriesforevidenceoffreeairorbowelobstruction.
• (Realizeplainabdominalradiographicstudiesareoftenuselessinidentifyingabdominalcompartmentsyndrome)
• AbdominalCTscanningcanrevealmanysubtlefindings:Round-bellysignAbdominaldistentionwithanincreasedratioofanteroposterior-to-transverseabdominaldiameter(ratio>0.80;P<0.001)
CollapseofthevenacavaBowelwallthickeningwithenhancementBilateralinguinalherniation
• Abdominalultrasonography
Diagnosis○ ThefollowinggradingsystemhasbecomeacceptedifIAHispresent○ (NormalIAP:0–7cmH2O)•GradeI,13–20cmH2O•GradeII,21–35cmH2O•GradeIII,36–47cmH2O•GradeI�,greaterthan48cmH2O
Bladder pressure grading I. 10–15mmHg II. 16–25mmHg III. 26–35mmHgI�. >35mmHg
Measurement○ Direct:Needlepuncturetoperitonealcavity○ Indirect:a.Intermittent(commonlyperformed): Intraluminalbladderpressureb.Continuous:Balloontipcatheterintostomach
Management outlineGenerallynospecificbladderpressureneedsactiveinterventionunlessthepressureexceeds>35mmHg
Decompressionitselfmayleadtodangerifdonepresumptively60%mortalityifdonepresumptively70%mortalityifnotdoneatappropriatetime.
Treatment In ICU○ GIdecompression(mechanical,drugs)○ Diureticswithalbumin○ Sedationandmusclerelaxant○ Percutaneousfluiddrainage○ Laparoscopicdecompression:○ Surgicaldecompression
○ Inintensivecareunit(ICU),thecauseoftheseeventsmighteasilybemistakenforotherpathologiceventssuchashypov-olemiaiftheclinicianisnotalertedtothemorbidityassociatedwithACS.
○ TwotypesofdecompressioninICU1.OperativelyinICUitselfinhemodynamicallyunstable2.IncasesofprimaryACS—percutaneousdrainisbest.
Decompression by surgery○ Longmidlinelaparotomyistheproceduredone○ Thoughopenedfullmidlinemonitorbladderpressureevery4hoursassomepatientsmayneedrepeatdecom-pression
○ Theopenwoundmaybecoveredbymanyways:1.�ascialclosurewithmesh2.Splitskingrafts3.Methodofchoiceisvacuum-assistedclosure(�AC)devices.
Contd...

tahir99 - UnitedVRG
139Intestinal System
FMGE QUESTIONS
1. Routine management of paralytic ileus include all of the following, except: (Sep 2009, 2007)
a. Electrolytecorrection b. Nasogastricaspiration c. Parasympathomimetics d. IntravenousfluidsAns: c (Parasympathomimetics)Parasympathomimetics is used only in resistant casesandnotroutinely.Management of paralytic ileus:Bailey and Love (Page 1201, 25th edition)State inwhich there is failureof transmissionofperi-statlticwavessecondarytoneuromuscularfailure.�arieties: 1. Postoperative’—remainsfor24–72hours 2. Infection 3. Reflexileus—�ractureribs,spineorretroperitoneal
hemorrhagemayresultinileus 4. Metabolic—uremiaandhypokalemiaO/E:• Nobowelsounds(DD:Mechanicalobstruction—in-creasedbowelsounds)
• Obstipation(Notpassingstoolsaswellasflatus)Management:• Nasogastricsuction• Restrictionoforalintake• Correctelectrolytedisturbance• Intravenous(I�)fluids• Treatthecause• Noplaceforroutineperistalticstimulants*• Rarely in resistant cases—Cholinergic stimulants(e.g.neostigmine)canbeused—Catchpole regimen*
• Ifparalyticileusisprolongedweshoulddolaparoto-mytolookforanyhiddencauseforobstruction.
2. Ideal management in an old and frail patient pre-senting with intestinal obstruction with a mass situ-ated 15 cm away from anal orifice: (March 2010)
a. Abdominoperinealresection b. Colonoscopicremoval c. Hartmann’soperation d. AnteriorresectionAns: c (Hartmann’s operation)Explanation:• Thisisacaseofintestinalobstructionduetocancerrectuminupper-third.
• �orupper-thirdrectumcancersifthepatientisfitandhemodynamicallystableweoptforanteriorresection(explainedinmaterial).
• But,sincethispatientisoldandfrailwegoforHart-mann’s operation—proximal colostomy and distalclosure. Hartmann’s is a very useful procedure inemergencyconditions.
3. Which of the following is not associated with Crohn’s disease? (March 2010)
a. �istula b. Stricture c. Pseudopolyps d. GranulomaAns: c (Pseudopolyps)Explanation:inmaterial
4. Hirschsprung disease involves, which region of intestine commonly: (March 2007)
a. Colon b. Rectum c. Rectosigmoidpart d. TerminalileumAns: c (Rectosigmoid part)Explanation:BaileyandLove(Page86),25thedition• Theaganlionosisisrestrictedtorectumandsigmoidcolon(shortsegment)—75%
• Involvesproximalcolonalsoin15%(longsegment)• Entire colon and a portion of terminal ileum—10%(totalcolonicaganglionosis)
5. Hirschsprung disease in diagnosed by: (Sep 2006) a. USG b. CTscan c. Anogram d. RectalbiopsyAns: d (Rectal biopsy)Explanation:(BaileyandLovePage87,25thedition)• �amilial or associated with Down’s/other geneticdisorders
• Genemutationisidentifiedonchromosome10(RETprotooncogene*)andrarelyinchromosome13
• Definitive diagnosis is by Full thickness rectal biopsy*,whichwillshowabsenceofganglioncellsbothinauerbachandmyentericplexusandpresenceofhypertrophiednervetrunks.

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery140
6. Which of the following is the investigation of choice for diagnosing carcinoma colon? (Sep 2009)
a. X-rayabdomen b. CTscan c. Colonoscopy d. BariumenemaAns: c (Colonoscopy)Colonoscopyisthebestinvestigationtodiagnosecancerofcolonbecausewecantakebiopsyalso.
7. Uncommon complication of Meckel’s diverticu-lum is: (Sep 2007)
a. Intussusception b. Diverticulitis c. Malignancy d. IncreasedbleedingAns: c (Malignancy)• M/ccomplicationoverall—bleeding’• M/ccomplicationinadults—obstruction• M/ccomplicationinchildren—bleeding
8. Acute appendicitis is characterized by all of the following, except: (Sep 2005)
a. Anorexia b. Rovsing’ssign c. �ever>42degreecelsius d. PeriumbilicalcolicAns: c (Fever > 42 degree celsius)Explanation:Page1208(BaileyandLove,25thedition)• AcuteappendicitisischaracterizedbyMurphy’s triad* Pain(migratory) �omiting �ever• Patientgetspainfirstaroundtheumbilicus(Visceral
pain—Which is poorly localized)• Thepatientthengetsprogressiveinflammationandtheadjacentperitoneumgetsirritatedcalledsomatic pain—which is localised in the right iliac fossa.
• This classic visceral—somatic sequence of pain is seen in more than half of patients.
• Anorexiaisaconstantclinicalfeature• Fever:Pyrexiaisalwaysslight(37.2—37.7°C).Itwillnever reach beyond 38.5°C. If it goes beyond thattemperature other causes like mesenteric adenitismustbethought.
• Rovsing’s sign—PaininRI�oncompressingtheleftiliacfossaisafeatureofappendicitis
9. Enteroenteric fistula is found in all, except: (March 2005) a. Crohndisease b. Colorectalmalignancy
c. Actinomycosis d. UlcerativecolitisAns: d (Ulcerative colitis)Explanation:(Refermaterial)�istulaisafeatureofCrohndiseaseandnotseeninul-cerativecolitis.
10. Which of the following statement is false? (March 2011)
a. GranulomatousinflammationisfoundinCrohndisease.
b. PerianallesionsarecommoninCrohndisease. c. Strictureinvolvingthecolonisfoundinulcera-
tivecolitis. d. �istulaformationiscommoninCrohn’sdis-
ease.Ans: c (Stricture involving the colon is found in ulcera-tive colitis).Stricture isa featureofCrohndiseaseandnotseen inulcerativecolitis.
11. Which of the following is not a commoner cause of intestinal perforation (March 2004)
a. Gastriculcer b. Coloniccancer c. Typhoid d. CrohndiseaseAns: b (Colonic cancer)ExplanationAlltheabovecanproduceperforationandperitonitis.Butcoloniccancerveryrarelypresentwithperforation• Rightcoloncancerpresentswithmassandanemia• LeftcoloncancerpresentswithintestinalobstructionTyphoidcasespresentwithintestinalperforationon3rdweek.
12. A patient presents with history of mild diarrhea, blood in stools with multiple fistulas. What is the most probable diagnosis? (March 2007)
a. Intestinaltuberculosis b. Ulcerativecolitis c. Crohndisease d. TyphoidAns: c (Crohn disease) Explanation: Explained in material
13. Ochsner-Sherren regimen is used for: (March 2007, Sep 2010) a. Appendicularabscess b. Pelvicabscess c. Appendicularmass d. AcuteappendicitisAns: c (Appendicular mass) Explanation: Explained in material

tahir99 - UnitedVRG
141Intestinal System
14. Most common site of volvulus is: (Sep 2009, 2010) a. Ileum b. Appendix c. Sigmoidcolon d. CecumAns: c (Sigmoid colon)Explanation:• M/csiteofvolvulus—Sigmoidcolon• M/csiteforlargeintestinalobstruction—Malignancy(2ndcause—volvulus)
• Directionofsigmoidvolvulus—Anticlockwise• Directionofcecalvolvulus—Clockwise
15. The commonest cause of significantly lower gas-trointestinal bleed in a middle aged person with-out any known precipitating factor may be due to:
(Sep 2005) a. Ulcerativecolitis b. Ischemiccolitis c. Angiodysplasia d. DiverticulumofsigmoidcolonAns: d (Diverticulum of sigmoid colon)Explanation:MostcommoncauseoflowerGIbleedinginoldagepa-tientsisdiverticulumofcolon.Angiodysplasiaofcolon:• Itisavascularmalformationassociatedwithageing.• Incidencevariesfrom—5%–25%over60years• M/cinascendingcolonandcecumofelderlypatient.• Malformation consist of dilated tortuous vessels insubmucosaandinseverecasesmucosaisreplacedbymassivelydilateddeformedvessels.
16. Treatment of an incidentally detected appendicu-lar carcinoid measuring 2.5 cm is: (March 2008)
a. Righthemicolectomy b. Limitesresectionoftherightcolon c. Totalcolectomy d. AppendicectomyAns: a (Right hemicolectomy) (Refer: Bailey and Love- Page 1217)Carcinoid tumor of appendix:• Mostcommonindistalpartofappendix• Appendicealcarcinoidsrarelyproducemets.Treatment:• �ortumors<2cmandnotinvolvingcecalwall—ap-pendicectomyisenough
• �ortumors>2cm/baseinvolved/lymphnodesin-volved—righthemicolectomy.
17. A 26-year-old male presented with 4 day history of pain in the right sided lower abdomen with fre-quent vomiting. Patients GC is fair and clinically a tender lump was felt in the right iliac fossa. Most appropriate management for this case would be:
(Sep 2007) a. Exploratorylaparaotomy b. Immediateappendicectomy c. Ochsner-Sherrenregiman d. ExternaldrainageAns: c (Ochsner-Sherren regiman)ThiscaseofappendicularmassismanagedbyOchsner-Sherrenregimen
18. Lateral internal sphincterotomy is useful for: (Sep 2009, 2010) a. Analfistula b. Analcanalstrictures c. Hemorrhoids d. AnalfissureAns: d (Anal fissure)
19. Treatment of choice for 3rd degree hemorrhoids is: (March 2009, Sep 2010)
a. Sclerotherapy b. Bandligation c. Hemorrhoidectomy d. AlloftheaboveAns: d (All the above)
20. All of the following are true regarding pilonidal sinus, except: (March 2009)
a. Seenpredominantlyinwomen b. Occursonlyinsacrococcygealregion c. Tendencyforrecurrence d. ObesityisariskfactorAns: a (Seen predominantly in women)• Itsmostcommoninhairymalesnotinfemales.
21. Jeep disease is also known as: (March 2008) a. Analincontinence b. Hemorrhoids c. Pilonidalsinus d. AnalfissureAns: c (Pilonidal sinus)
22. Ideal investigation for fistula-in-ano is: (Sep 2005, 2007) a. Endoanalultrasound b. MRI c. �istulography d. CTscanAns: a (Endoanal ultrasound)

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery142
• EndoanalUSGisthemostaccurateinvestigationthanclinicalexamination
• ThoughMRI is acknowledged tobegold standard,becauseof its limitedavailability itsusefulonly forrecurrentfistula-in-ano.
23. Aim of surgery in carcinoma rectum is: (March 2004) a. Limitedexcisionoftherectum b. Sacrificinggastrointestinalcontinuity c. Preservingtheanalsphincter d. PreservingmesorectumAns. c (Preserving the anal sphincter)
24. A 10-month-old infant present with acute intesti-nal obstruction. Contrast enema X-ray shows the intussusception. Likely cause is: (March 2009)
a. Peyer’spatchhypertrophy b. Mekel’sdiverticulum c. Mucosalpolyp d. DuplicationcystAns: a (Peyer’s patch hypertrophy)
25. After undergoing surgery, for carcinoma of colon, a 44-year-old patient developed single liver metas-tasis of 2 cm. What do you do next? (Sep 2008)
a. Resection b. Chemoradiation c. Aceticacidinjection d. RadiofrequencyablationAns: a (Resection)
26. A 50-year-old male, working as a hotel cook, has four dependent family members. He has been di-agnosed with an early stage squamous cell cancer of anal canal. He has more than 60% chances of cure. The best treatment option is: (Sep 2008)
a. Abdominoperinealresection. b. Combinedsurgeryandradiotherapy. c. Combinedchemotherapyandradiotherapy. d. Chemotherapyalone.Ans: c (Nigro regimen—Chemoradiation)
27. The following is ideal for the treatment with in-jection of sclerosing agents: (Sep 2007)
a. Externalhemorrhoids b. Internalhemorrhoids c. Prolapsedhemorrhoids d. StrangulatedhemorrhoidsAns: b (Internal hemorrhoids)
28. In which of the following locations, carcinoid tu-mor is most common? (Sep 2003)
a. Esophagus b. Stomach c. Smallbowel d. AppendixAns: c (Small bowel)
29. Gardner’s syndrome is a rare hereditary disorder involving the colon. It is characterized by:
(Sep 2005) a. Polyposiscolon,cancerthyroid,skintumors b. Polyposisinjejunum,pituitaryadenomaand
skintumors c. Polyposisofcolon,osteomas,epidermalinclu-
sioncyst,fibroustumorsinskin d. PolyposisofGIT,cholangiocarcinomaandskin
tumorsAns: c (Polyposis of colon, osteomas, epidermal inclu-sion cyst, fibrous tumors in skin)
30. All of the following are true for patients of ul-cerative colitis associated with primary sclerosing cholangitis (PSC), except: (Sep 2006)
a. Theymaydevelopbiliarycirrhosis b. Mayhaveraisedalkalinephosphatase c. Increasedriskofcholangiocarcinoma d. PSCrevertsafteratotalcolectomyAns: d (PSC reverts after a total colectomy)
31. Patients of rectovaginal fistula should be initially treated with: (Sep 2008)
a. Colostomy b. Primaryrepair c. Colporrhaphy d. AnteriorresectionAns: a (Colostomy)
32. Most common cause of hepatic abscess in India is: (March 2007) a. Amebicabscess b. Infectedhematoma c. Ascendinginfection d. SecondarytocholelithiasisAns: a (Amebic abscess)
33. Not a complication of Crohn disease: (Sep 2005) a. Sclerosingcholangitis b. Granuloma c. �istula d. StrictureAns: None

tahir99 - UnitedVRG
143Intestinal System
• All the above mentioned complications can occurwithCrohndisease
• Ifyouwanttoexcludeyoucanexcludeprimaryscle-rosing cholnagitis—which is rare in Crohn’s com-paredtoulcerativecolitis.
34. Hirschsprung disease is most commonly involves: (Sep 2005) a. Rectosigmoidjunction b. Rectum c. Colon d. TransversecolonAns: b (Rectum)
35. Hirschsprung disease is diagnosed by: (Sep 2005) a. Rectalbiopsy b. USG c. CTscan d. BariumenemaAns: a (Rectal biopsy)
36. Brunners glands are seen in: (Sep 2006) a. Duodenum b. Ileum c. Stomach d. ColonAns: a (Duodenum)
37. Meckel’s diverticulitis associated with: (Sep 2006) a. Increasedbleeding b. Associatedwithinguinalhernia c. Pharyngealpouch d. AlltheaboveAns: a (Increased bleeding)
38. Acute appendicitis is not characterized by: (Sep 2006) a. �ever>42°C b. Anorexia c. Rightiliacfossapain d. �omitingAns: a (Fever >42°C)
39. Enterocutaneous fistula is found in: (March 2007) a. Crohndisease b. Ulcerativecolitis
c. Ischemiccolitis d. AmebiccolitisAns: a (Crohn disease)
40. Treatment of appendicular abscess are all, except: (Sep 2009) a. Intraperitonealdrainage b. Extraperitonealdrainage c. Emergencyappendicectomy d. ObservationAns: d (Observation)
41. Villous adenoma present as: (Sep 2010) a. Hypercalcemia b. Hypokalemia c. Hyperphosphatemia d. AlltheaboveAns. b (Hypokalemia)
42. Treatment of choice for small intestine carcinoma: (March 2011)
a. Radiotherpay b. Chemotherapy c. Surgery d. NoneoftheaboveAns. c (Surgery)
43. Which of the following is a dynamic cause of in-testinal obstruction: (March 2011)
a. Gallstone b. Paralyticileus c. Mesentericvascularobstruction d. OgilviesyndromeAns: a (Gallstone)• Dynamiccausemeansanymechanicalcauseforob-struction,e.g.hernia,adhesions,gallstones,etc.
• Adynamic orparalytic ileus there is nomechanicalcauseforobstruction
44. Enteoenteric fistula is seen in: (March 2011) a. Ulcerativecolitis b. Crohndisease c. Bothoftheabove d. NoneoftheaboveAns: b (Crohn disease)

tahir99 - UnitedVRG
13Hepatobiliary and pancreatic SyStem
Gallbladder and biliary tractAnatomy○ Capacity:50ml,7-12cm○ Cysticduct(CD):1-3mmdiameter○ CryptsofLuschka:mucousfoldsingallbladder(GB)○ Common hepatic duct: 2.5 cm○ Common bile duct: 7.5 cm and contains 4 parts1.Supraduodenal(SDP)(2.5cm)2.Retroduodenal(RDP)3.Infraduodenalorintrapancreatic(IfDP/IPP)4.Intraduodenal(InDP)
○ Enters duodenum at ampulla, located posteriorly 10 cm from py-lorus
○ Cystic artery arisesfromrighthepaticarterybehindcommonhepaticduct.Accessorycysticartery—fromgastroduodenalartery.
calot triangleo Formed between1. Inferior:CysticductandGB.2.Medial:Commonhepaticduct3.Above:Inferiorliversurface
Moynihans huMp and caterpillar turn○ Righthepaticarterytakesatortuouscourseinfrontoforiginofcysticduct○ MaybedamagedinCalot’striangle
lymphatic drainage○ CysticnodeofLund—sentinelnodeofGB○ PresentinCalot’striangle.

tahir99 - UnitedVRG
145Hepatobiliary and Pancreatic System
anoMalies of Gallbladder○ MCanomalyPhrygiancap(fundusisconstrictedandturnedbackonitself)○ OthersDoubleGB,septuminGB,diverticulosisinGBandHartmann’spouch.
cystic duct variations○ Lateralinsertion—15%to20%○ Anteriororposteriorinsertion—m/c40%
○ Spiralandmedial—35%○ Paralleltocommonbileductandinsertsdistally—5%.NormalsizeofCBD:6mm
functions of Gb1.Absorption:10timesconcentrationoccurs2.Secretion:SecretesH+ions,mucusdecreasesbilepHandhencekeepscalciumsaltssolubleinacid.
3.Motor:CCKstimulatescontractionofGBVagusnervestimulatescontractionInhibitionbyVIPandsomatostatin.
cholecystokinin causes biochemistry• Thegallbladdertocontract• Thehepatopancreaticsphinctertorelax• Asaresult,bileenterstheduodenum.
Cholesterolandphospholipidssynthesizedinliverareprincipallipidsinbile
Primarybilesalts(cholate,chenodoxycholate)aresynthe-sizedinliverconjugatedwithtaurineandglycine.
investiGationoral cholecystogram (Graham-cole test) plain X-ray• Dye used: Iopanoicacidbp• Mainlyusedfornonopaquestones.
• 10%gallstonesareradioopaque• Porcelain GB:CalcifiedGB(premalignant)
limey bile iv cholangiogram usG• Relatedtomultiplesmallgallstones• Notpremalignant.
• Biligrammeglumineioglyca-mate*
• First investigation for GB and bile duct.
hida scan ct scan• Tc 99m-labeled iminodiacetic acid• Secretedbyliverintobile,henceusefulincasesofobstruction
• Acutecholecystitis:mostaccuratetest—nonvisualizationofGB
• Tostudyjaundiceinneonates• Tolocateleaksandanastomoticpathology.
• Onlyincarcinomagallbladderandbileduct.Mrcp
• Mostaccuratenoninvasive.
ercp• Gold standard in gallstones• Inmodernworld,onlyusedforinterventionalpurposes*.Diagnosticpurposeisoutdated.

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery146
cholecystosis Gallbladder polyp risk of malignancy○ Chronic inflammatory changes with hyperpla-
siaCholesterosis—strawberry GB,associatedwithcholesterolstones
CholesterolpolyposisAdenomyomatosis—intramuraldiverticulosisDiverticulosisofGB—associatedwithblackpigmentstonesincryptsofluschka*.
Types:1.Cholesterolpolyps2.Adenomyomatosis3.Benignadenomas4.Malignantadenocarci-noma
1.Oldage2.Gallstonesassociated3.Documentedincreaseinsize4.Size>10mm○Cholecystectomyisdoneinsymp-tomaticpolypsandasymptomaticpolypswithanyofaboverisk.
Gallstones○ MC type of stone mixed stone○ Types of stonesCholesterolstonesBrownpigmentstonesBlackpigmentstonesMixed
Pathogenesis○ Lithogenicbile○ Nucleation○ Stasis
lithogenic bile○ Bilesaltsandphospholipidsinbilekeepcholesterolinsolutionbyform-ingmicelles
○ Normal ratioBileacids:cholesterol=20:1Criticalratio=<13:1atwhichcrystallizationoccurs.
○ Cholesterolisinsolubleinwater,whichismadesolublebybilesaltsandphospholipids
○ Increasedcholesterol1.Obesity2.High-cholesteroldiet3.Clofibratetherapy.
decreased bile salts1.Primarybiliarycirrhosis2.OCP/estrogens3.Geneticfactors○Decreased7-alpha-hydroxylase(Convertslivercholesteroltobileacids)
4.Decreasedenterohepaticcirculationa.Ilealdiseaseb.Ilealresectionc.Cholestyraminesd.Deoxycholates
nucleation stasis○ Processbywhichcholesterolmonohydratecrystalsformandagglomeratetobecomemacroscopiccrystals
○ Excesspronucleatingfactors—1.Mucins,2.Nonmucinglycoprotein,3.Infection.
○ DeficiencyofantinucleatingfactorsApolipoproteinsa1anda2
ProlongedTPNFastingPregnancyDrugs—OctreotidesOCPBurns,surgery.
predisposing factors• Fat,fertile,female,flatulent,fifty(5f’s)• Diabetesmellitus.
• Oldage○ Increasedcholesterollevel○Decreasedbileacidpool○Decreasedbladdermotility.
piGMent stones○ Namegivenwhencontainscholesterol<30% black pigment
Composition:Purecalciumbilirubinate+mucin predisposed by brown pigment
○ Geneticfactors○ Chronichemolysis○ Alcoholiccirrhosis○ Infection—E. coli,ascariasis,clonorchis○ Ilealresection/bypass○ Cysticfibrosis.
Composition:Calciumsaltsofunconjugatedbilirubin+cholesterol+calciumbilirubinate/palmitate/stearate.
black pigment○ MCinhemolyticstates1.Hereditaryspherocyto-sis,sicklecelldisease
2.Heartvalves(mechanical)
3.Livercirrhosis
4.Gilbertsyndrome5.Cysticfibrosis6. Ilealresection.
contd...

tahir99 - UnitedVRG
147Hepatobiliary and Pancreatic System
piGMent stonesbrown pigment acalculus cholecystitis
○ Rareingallbladder○ Primarybileductstoneformation
○ Duetobilestasisandinfection○ MCE. coli*
○ MCinpresenceofFB,stents,parasites○ E. colisecretesbetaglucuronidasethatdeconjugatesthesolubleconjugatedbilirubintoinsolublefreeunconjugatedbilirubin
○ Highestmortality*○ Mostcommonlymisseddiagnosis○ M/cinpatientsrecoveringfrommajorsurgeryandburns,trauma*
coMplications1.Silent2.Acutecholecystitis3.Chroniccholecystitis
4.Mucocele5.Empyema6.Gangrene
7.Carcinoma8.Fistula
Mucocele Mirrizzi syndrome○ Obstructionofstoneat
neckofgallbladder○ BiletotallyabsorbedandreplacedbymucousandsecretionofGB1.Empyema2.Perforation3.Gangrene.
○ Treatment:Earlycholecys-tectomy
○ Itreferstotheobstructionorstrictureofthecommonhepaticductasresultofextrinsiccompressionbyagall-stoneinthecysticduct.
typesType1:(11%)—extrinsiccompressionofCHDbyalargestoneinHartmann’spouch
Type2:(41%)—stonehasnowerodedintothehepaticducttoformafistulainvolvinglessthanone-thirdofcircumfer-ence
Type3:(44%)—lesionsinvolvetwo-thirdofcircumferenceType4:(<4%)—completelydestroyedhepaticduct.
fistulas from gallbladder saint triad• MCsiteduodenum(cholecystoentericfistula)• Diagnosissuspiciousbypresence of air in bile duct• Complication:Gallstoneileus• Othersitesoffistula:Colon.
○ Gallstones○ Diverticulosisofcolon○ Hiatushernia.
contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery148
liMey bile• OnX-ray—calciumprecipitationinthewallofgallbladderproducingdiffusehazy,opacificationduetocalciumsaltsecretion.Clinicallyasymptomatic,butcholecystectomytobedoneThisconditionoccurswhenthereisgradualobstructionofcysticductorCBDduetochronicpancreatitisorcapancreas.Toothpaste-likematerialinGB.
treatMent options○ Operate for symptomatic gallstones○ Forasymptomaticstone,surgerymustinfollowingsituationsonly3cmsizeMultiplesmallstones(canpasstoCBD)PolypassociatedwithstonePorcelaingallbladderCongenitallyabnormalgallbladderDiabeteswithgallstonesImmunocompromisedpatients:ComplicationsarehighTransplantcases.
Medical treatment○ Usefulonlyforcholesterolgallstonesnotforpigmentstones
○ Mechanismisbyinhibiting3-hydroxy-3-methylglutar-yl-coenzymeA(HMGCo-A)reductaseincholesterolsynthesis,thusdecreasecholesterolsupersaturation.
○ Usefulonlyin:RadiolucentSize<10mmFunctioninggallbladderNonacutesymptoms.
coMMon bile duct stonesprimary secondaryFormedinbileductitselfBrownpigmentstonesmostcommonly.
FormedingallbladderandentersCBDCholesterolstones.
clinical featurescharcot triad reynaud pentad○ CBDstonecausingcholangitis Pain+Jaundice+Rigors ○ Charcotstriad+Septicshock+Mentalstatuschangescholangitis Lab findingsEtiological factors:○ CBDstone○ Endoscopicretrogradecholangiopancreatography(ERCP)
○ Benignandmalignantstric-tures
○ ParasitesM/CorganismsE. coli,
Klebsiella,Streptococcus faecalis,Bacteroides
In absence of cholangitis In presence of cholangitis First investigation to be done—USG
Definitive investigation—ERCP(GoldstandardforgallstonesinCBD)
Best non-invasive investi-gation—MRCP.
• Increasedserumalkalinephosphatase
• IncreasedGGT• Increasedbilirubin• MildincreaseinSGOT,SGPT.
• IncreasedWBCcount• SevereincreaseinSGOT,SGPT.
treatMent optionsin presence of cholangitis in absence of cholangitis1.ERCPwithsphincterotomyandstoneextraction(treatmentofchoice)2.PTCdrainage:ERCPfailedcasesBiliaryentericanastomosisIfobstructionismoreproximal.
3.Surgicaltreatment:Onlywhenabovetwoproceduresnotpossible.Decompression of CBD with T tube.
• LapcholecystectomywithCBDexplo-ration
• LapcholecystectomywithERCPstoneremovallater
CBD exploration and T tube removal Unexpected ductal calculi after cholecystecto-my or routine intraoperative cholangiogram (4% to 10%)
Laparoscopiccysticductextractionorimmedi-atepostoperativeERCPretrieval.
○ Postoperative(OP)cholangiogram—day7thPOD○ RemoveTtube—10to14days○ RemoveTtubeon2weeksfordiabetesandimmunocompromised.

tahir99 - UnitedVRG
149Hepatobiliary and Pancreatic System
Missed/retained/residual stones (< 2 years)if t tube present if t tube absent○ Flushingwithheparinizedsaline○ DissolutionwithMTBE(methylter-butylether)○ PercutaneousstoneextractionviaTtubetractafter4-6weeks(Burhennetechnique)*
○ ERCPstoneremoval
recurrent stones (> 2 years)○ M/Cduetononabsorbablesuturematerials,clips.○ Theygetinternalizedandgetcoveredwithcalciumbili-rubinatetoformbrown*pigmentstones
○ ERCP—firstapproach○ Ifductdilated>2cm—choledochoduodenostomyortrans-duodenalsphincteroplasty
choledochal cysts○ Congenitaldilatationofintraandextrahepaticducts○ Associatedwithanomalouspancreaticandbiliaryductjunc-tion(APBDJ).
Clinical features○ M/cinfemales○ M/cageofpresentationinfancy.
classic triad (seen only in 10%) types of cystsPainLumpIntermittentjaundice
• Type1—mostcommon*.Fusiformdilatationofbileduct
• Type2—diverticulumfromCBD• Type3(choledochocele)—dilatationofbiliarytractwithinduodenum
• Type4a—multipledilatationofintraandextrahepaticducts
• Type4b—multipledilatationofextra-hepaticducts
• Type5—(Carolidisease)*Multipledilatationofintrahepaticducts
complicationsRecurrentcholangitisPancreatitisGallstonesCholecystitisCirrhosiswithportalhypertensionPortalveinthrombosisMalignancyRiskfactorforcarcinomabileduct,GB,pancreas,liver,duodenum
treatmento Types1&2:CystexcisionwithRoux-en-yreconstructionwithjejunum
o Type3:Transduodenalsphinctero-plasty
o Type4&5:Livertransplantation
eXtrahepatic biliary atresiaOcclusionorevencompletedestructionofpartorallofextra-hepaticbileducts:Accompaniedbyavariabledegreeofintrahepaticdamagethatprogressivelydamagestheliverleadingtocirrhosisandliverfailure
Mostcommoncauseofsurgicaljaundiceinnewborn*.
types of biliary atresia○ Type1:obstructionwithincommonbileduct(gall-bladderhencecontainsbile)—5%
○ Type2:obstructionwithincommonhepaticduct(gall-bladderhasnobile)—3%
○ Type3:Obstructionatportahepatis—90%.
contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery150
eXtrahepatic biliary atresia
clinical features○ Severeobstructivejaundiceduringfirstmonthoflifewithpaleacholicstools
○ Ifundiagnosedoruncorrectedleadstocirrhosisin3to6month.
differential diaGnosis of jaundice in infantsjaundice in newborn and infants (in india) pathology1.Hepatocellular cause:Neonatalhepatitis(47%),metabolic(4%),variedetiology
2.Obstructive:Biliaryatresia(34%),choledochalcyst(4%)3.Ductal paucity (3%)4.Idiopathic
○ InflammationandfibrosingstrictureofCBDandCHD○ Markedbileductularproliferationwithbileplugsonbiopsy
○ Inflammatorydestructionofhepaticductswithpaucityofbileducts
investigations treatment○ USG abdomen:tor/oothercausesofjaundice(choledochalcysts)○ Triangular cord sign:Fibrousconeofbileductremnantathepaticporta
○ TC99m-labeledradionuclidescan○ Liverbiopsy:Differentiatesneonatalhepatitisfromatresia(96%sensitive)
○ Goldstandardisintraoperativecholangiogram.
Kasai procedure:PortoenterostomyAnastomosisofportalplatethatcontainsmicro-scopicpatentbiliaryductuleswithRouxen-Yjejunumloop
Mostpatientswillprogressultimatelytolivertransplantation
Kasaiprocedureactuallyprovidessometimeforliverdonorarrangement.
prognosis after Kasai's procedure: after Kasai procedure prognosis depends on1.Ageofpatient(<6week—better)2.Absenceofcirrhosis
3.Microscopicductules>150microns4.Decreasednumberofcholangitisepisodes
•M/cindicationoflivertransplantininfants—EHBA
priMary sclerosinG cholanGitis• Fibrosingcholangitisofbileductulesleadingtoinflamma-torystrictureandobliterationofintraandextrahepaticductswithdilatationofpreservedsegments.
contd...
contd...

tahir99 - UnitedVRG
151Hepatobiliary and Pancreatic System
priMary sclerosinG cholanGitistype
Primary:Unknownetiology.AssociatedwithHLAB8,HLADR3,HLADQ2,DRW52A
Secondary:Ulcerativecolitis,Crohndisease.
clinical features pathology○ Agegroup:30–40year○ Male>females(2:1)○ Intermittentjaundice,weightloss,fatigue,pruritus,abdominalpain
○ AssociatedwithReidelthyroiditis,retroperitonealfibrosis
○ Fibrosingcholangitisofbileductswithlymphocyticinfiltrate,progressiveatrophyofbileductepitheliumandobliterationoflumen
○ Concentricperiductalfibrosisaroundobliteratedducts(onionskinappearance)
○ 10to20percentcasesdevelopcholangiocarcinomainvestigations treatment○ Asymptomaticpatientswillhaveincreasingserumalkalinephosphatase○ Clinicalcourseishighlyvariablewithcyclicremissionsandexacerbations○ Most sensitive:ERCP—multipledilatationandstrictureofintraandextrahepaticducts○ Noninvasive:MRCP
Livertransplantationonly.
vanishing bile duct syndrome bilhemia○ Adultbileductopenia○ Decreasednumberofbileductsonliverbiopsy○ Causes:1.Graftversushostdisease(GVHD)afterbonemarrowtransplant
2.Chronicgraftrejectionafterlivertransplant3.Sarcoidosis4.Drugslikechlorpromazine
○ Bileflowsintobloodstreameitherviaportalveinorhepaticartery○ Causes:HighintrabiliarypressureGallstoneerodingintoavesselAccidentaloriatrogenictrauma.
○ Investigationshowshighlyincreaseddirectbilirubinwithseptice-mia(despitenormalSGOTandSGPT)
○ Causesdeathiflargeamountbileemboliseslung
heMobilia○ Bleedingintobiliarytreefromanabnormalcommunicationbetweenabloodvesselandbileduct.classic triad causes ManagementBiliarycolickyObstructivejaundiceMelenaoroccultbloodinstool.
1.M/ccauseistrauma**(iatrogenic,PTCdrainage,surgeries,biopsy)
2.Gallstones3.Vascularcauses—aneurysms,angiod-ysplasia,hemangioma.
4.Malignancy5.Parasites(m/ccauseinoriental)
6.Liverabscess7.Cholangitis.
○ UGIscopy—bleed-ingfromampullaofvater
○ Investigation of choice—angiography.
carcinoMa Gallbladder○ M/cmalignancyofbiliarytract ○ M/cfemaleelderly ○ 70%to80%casesaregallstonesassociated
risk factorsGallstonesPolyps(>10mm)PorcelainGBCholedochalcyst
AnomalouspancreaticbileductjunctionTyphoidcarriers*SclerosingcholangitisUlcerativecolitis
CholecystoentericfistulaDrugs—estrogens(notOCP)*Carcinogens(nitrosamines,azodyes,rubberindustrychemicals).
clinical features• Pain(73%)• Anorexiaandweightloss(63%)
• Jaundice(54%)poorprog-nosticsign
• Fever
• Vomiting(mechanicalobstructionormalignantgastroparesis)
• O/E—masspalpable(50%),hepatomegaly,ascites
contd...
contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery152
carcinoMa Gallbladder○ Pathology:Adenocarcinoma(90%),undifferentiated,squamouscellcarcinoma.
investigations contraindications for surgery• USG:Localizedexcessivethickeningofgallbladder(normalGBthicknessis<3mm)• CTcontrast(CECT):lymphnodes>10mmvisible• MRI+MRCP+MRA:ismostusefulthanallabove—helpsinplanningmanagement• FNAC:contraindicatedinoperabletumors(riskofdisseminationviatract).FNACisindicatedonlyininoperabletumors
• Diagnostic laparoscopy:Beforecurativeresectionbylaparotomy38%casesfoundinoperableamongthemplannedforcurativeresectionafterallaboveinvestigations.
• TumormarkersCEA,CA19-9
○ Poorgeneralcondition○ Livermets○ Extrahepaticmets○ Peritonealspread○ Distantnodes(coeliac,superiormesenteric,para-aortic)
○ Portalveinorhepaticarteryinvolved
○ Bilateralinvolvementofsecond-arybiliaryradicles
○ Extensiveduodenalinvolvement.
treatment palliative treatment○ Limited to mucosa:Simplecholecystectomy○ Reaching muscle:Extended cholecystectomy ○ Perimuscular connective tissues:Extendedcholecystectomy+segment4band5resection○ Extendedrighthepatectomyisdonefortumorsextendingtoliver.
1.Radiotherapy—rolenotclear
2.Chemotherapy—gemcit-abine+cisplatinregimen.
cancers diagnosed in cholecystectomy specimenso Exceptfortumorsconfinedtomucosaredo-laparotomyisadvisedwithresectionasperstagingalongwithlapportsitesexcision.
Palliation for○ Pain:Celiacplexusblock○ Jaundice:• Endoscopicstent(patentconfluence)Percutaneousbilestenting(notpatentconfluence)Segment3bypassifsurgeryisdone.
○ Obstruction (GOO):•GastrojejunostomymustnotbedoneasitmayleadtononfunctioningofGBandstasisandcholangitis
• Feedingjejunostomyornasojejunaltubebeyondobstructionisadvised.
bile duct cancersrisk factors pathology types clinical features• Primarysclerosingcholangitis• Choledochalcyst• Ulcerativecolitis• Clonorchissinensis• Chronictyphoidcarriers• Biliaryentericanastomosis• Thorotrast,dietarynitrosamines• Liverflukes• Others—methyldopa,isoniazid,OCP,asbestos.
1.Sclerosingvariety(m/c)2.Nodular3.Papillary(betterprognosis)typeofadenocarcinomas2/3rdlocatedathepaticductbifurcation(Klatskintumors—tumorsatbifurca-tion)
• M/cpresentation—painlessjaun-dice
• Courvoisier law exemption.Non-palpableGBwithjaundice:Obstructionduetocholan-giocarcinomaathilarlevel(e.g.Klatskintumors)
Hence,palpablegallbladdersuggestsdistalobstruction.
○ CBD stone is not a risk factor.
Bismuth classification○ Type1:Atcommonhepaticductonly○ Type2:Involvingconfluencewithoutinvolvementofsecondaryducts○ Type3a:Involvingrightsecondaryintrahepaticducts○ Type3b:Involvingleftsecondaryintrahepaticducts○ Type4:Involvessecondaryductsonbothsides.
contd...
contd...

tahir99 - UnitedVRG
153Hepatobiliary and Pancreatic System
bile duct cancersinvestigations
○ USG:IHBRdilatation○ ContrastenhancedCT:Toruleoutvascularinvolvement○ Percutaneoustranshepaticcholangiogram(PTC)○ CA19-9tumormarker(follow-uprecurrence**)○ ERCP is not the best invasive investigation, but PTC is best ….
why? Ifcontrastisinjectedintotheobstructedsegmentandifobstruc-tionisnotcompletelyrelieveditwillinvariablyresultincholan-gitis.
treatmentoperable tumors inoperable cancersSurgery involves• ExtensiveclearanceneedscaudatelobectomyandremovalofCBDuptosuperiorborderofheadandneckofpancreas
• Hilar,portal,commonhepatic,posteriorpancreaticnodesandeliacnodesremoved• Portalveinremovedifinvolved.Contraindications:• Peritonealspread,livermets,para-aorticnodes+ve
• Brachytherapy• Gemcitabine+5-fluorouracil• Metallicstents.
bile duct injuries• AnatomiclvariationsVariationsinanatomyofductsandvessels
• SurgeonsinexperienceRetractioninjuries,thermalinjuries,previousscars
• LocalpathologyAcuteinflammationShrunkengallbladderMirrizzisyndromeMoynihanshump○laparoscopiccholecystectomyassociatedwithhigherpercentageofinjuries(0.16–2.31)comparedtoopensurgeries(0.1–0.1).
clinical features○ Patientmaypresentwithindaystoseveralmonthsdepend-ingontheinjury
○ Presentingwithabdominalpain,distension,cholangitis,sepsis,ileus,jaundice,excessivebilefromdrain—thinkofbileductinjury
investigations• USG—firstinvestigationtoconfirm• CTscan—moresensitiveinconfirmingleaksandcollections• Biliaryscintigraphy—diagnosisleak,butnotthesite• ERCP—diagnosisleak,butnotdelineatesintrahepaticductalanatomyinpresenceofCBDorhepaticductdisruption
• MRCP—besttodecidetherapeuticapproach.Classifications
Bismuth classification: (based on location) Strasberg classification (based on patterns of injury)
• Type1:Lowcommonhepaticductstricture.stump>2cm• Type2:Proximalstricture.Stump<2cm• Type3:Hilarstricture.Confluenceintact• Type4:Destructedconfluence.Rightandleftductsseparated• Type5:InvolvementofrightaberrantsectoralductaloneoralongwithstrictureatCHD.
• TypeA:minorhepaticductorcysticductleaks• TypeB:Aberrantrighthepaticductorsectoralductdividedandligated
• TypeC:SameasB,butbileleak• TypeD:lateralinjurytoCBDorCHD• TypeE:Circumferentialinjurytomainducts.
contd...
contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery154
bile duct injuriesManagement
Earlyrepairnotattempted.Onlydrainageprocedurescarriedout
Idealtimeofrepairis8to12weekstoallowinflammationtosubside**Roux-en-Yhepaticojejunostomyis ideal repair.
emphysematous cholecystitis chronic cholecystitis○ Acute cholecystitis associated with infection
by gas forming organisms like Clostridium welchii or perfringens.
○ Thisconditionoccursmostfrequentlyinelderlymenandinpatientswithdiabetesmellitus.
○ Can be seen on plain X-ray.○ The condition is very aggressive, may go for
gangrene and perforation.○ Emergency cholecystectomy must be done.
○ Ongoinginflammationwithrecurrentepisodesofbiliarycolicorpainfromcysticductobstructioniscalledchroniccholecystitis.
○ About2/3rdofthepatientswithgallstoneswillpresentwiththeserepeatedattacks.
○ Primarysymptom:○ Biliary colicky—constantpainthatbuildsinintensityandcanradiatetotheback,interscapularregionorrightshoulder.Painisconstantex-tendingfor1to5hours.Itusuallysubsidesbylessthan24,ifitpersistsbeyond24hoursthinkofacutecholecystitis.
○ Treatmentisnecessaryforsymptomaticcases—laparoscopiccholecys-tectomy.
pancreasanatomy
○ DuctofWirsung:Mainpancreaticduct○ DuctofSantorini:Minorpancreaticduct(accessoryduct)Mainduct—arisesfromtailandterminatesatpapillaofvaterliesposteriorlyMinorduct—extendsfrommainducttoenterduodenumatlesserpapillaly-ingmoreanteriorlyand2cmproximal.
physiology○ Secretin:Alkaline,bicarbonaterichfluid○ Cholecystokinin:Stimulatesenzyme.Serumamylase,lipase,ribonuclease.
pancreatic function test○ NBT-PABAtest ○ Pancreolauryltest ○ Fecalelastasetest
pancreatitisetiology (get smashed)
G-gallstonesE-ethanolT-traumaS-steroids
M-mumpsA-autoimmune(PAN,SLE,etc.)S-scorpionvenomH-hyperlipidemia,hypercalcemia,hypothermia
E-ERCP,emboliD-Drugs(azathioprine,thiazides,furosemide,tetracyclines,Lasparaginase,phenformin,procainamide,valproicacid,pentamidine,dideoxyinosine,etc.)
○ 4I’S infection/infestation/ischemia/idiopathic ○ Infectious causes: mumps,coxsackie,CMV.
M/c causesAdults:Gallstones(m/c)Alcohol(2ndcommon)
Children:Trauma.
contd...
contd...

tahir99 - UnitedVRG
155Hepatobiliary and Pancreatic System
pancreatitisprognostic indicators symptoms• Ransonscoring• Apache2• Glasgow• CTseverityindex• C–rectiveprotein
PainNauseaVomitingRetchingHiccough
Suddenabdominalpain(Mohammedprayersign)
Mimics:Acutecholecystitis,myocar-dialinfarction,perforatedpepticulcer,pneumonia,etc.
signs○ Tachypnea○ Tachycardia○ Hypotension○ Icterus
○ Facialflushing○ Cyanoticmarblingofanteriorabdominalwall○ Grey-Turnersign—hemorrhagicpigmentationaroundtheflanks
○ Cullensign—pigmentationaroundumbili-cus
○ Tenderrednodulesinlimbs○ Abdominaldistension—ileus○ Ascites.
Radiology findings investigationsNospecificradiologicalsign,SentinalloopofjejunumColon cut-off sign (gasfilledhepaticandsplenicflexuresseparatedbygaslesstransversecolon)
Calcifiedgallstones.
SerumamylaseSerumlipase:mostspecificSerumtrypsin(exclusivelybypancreas)Hypocalcemia.
normal serum amylase is seen in following cases• Greaterthan3dayafterattack• Massiveglanddestruction
• Completelydestroyedglandbypreviousattacks.
chronic pancreatitis• Alcohol• Pancreasdivisum• Tropicalpancreatitis
• Hyperparathyroidism• Trauma• Obstructivepancreatitis
• Idiopathicchronicpancreatitis• Cysticfibrosis• Hereditarychronicpancreatitis.
surGeries○ Child procedure:Distalpancreatectomy+sple-nectomy
○ Puestow procedure :Duct>8mmanasto-mosedtoRoux-en-yjejunum
○ Frey procedure:Headcor-inganastomosis
○ Beger procedure:Duodenumpreservingpancreaticheadresectionandanastomosis
contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery156
pseudocyst pancreas• 6weekafterpancreatitis• Resolvesin6week
intervene ifPersists>6weekSize>6cm
ComplicationsdevelopSecondaryinfection
complications• Obstruction• Hemorrhage• Rupture• Pseudoaneurysmofsplenicartery• Infection
• Mostcommonsiteofpseudocyst—bodyandtail• Mostcommoncause—pancreatitis• Secondcause—trauma*• Mostcommoncauseinchildren—trauma.
ranson's criteriaon admission Within 48 hoursAge>55yearWBCcount>16,000/mm3
Bloodglucose>10mmol/lLDH>700u/lAST>250sigmafrankelunits %
BUN>5mg%ArterialO2saturationPaO2<60mmHgSerumcalcium<2.0mmol/lHematocritfall>10%Basedeficit>4mmol/lFluidsequestration>6l
pancreatic tuMors• Exocrine• Endocrine
o M/c type:Adenocarcinomao M/c site:Head
periampullary carcinoma• Tumorsinregionofampulla,lowerCBD,duodenum• M/cpresentationispainlessjaundice• Mostcommonsiteistheheadofthepancreas• Necroticpancreatictumorsincreasethromboplasticfactors• Thrombophlebitisseenasaresult• Nospecificbloodteststodiagnose
• Elevatedamylase,lipase,alkalinephosphatase,biliru-bin,CEA,C19-9
• CT,ultrasonography• Needlebiopsy• Paracentesis• ERCP: mostdefinitivediagnostictest
courvoisier law ○ Trousseau sign:migratorythrombophlebitis
○ Troisier sign:Leftsupra-clavicularnode
○ Inapatientwithjaundiceifthereisapalpablegallbladder,itisnotduetostones.
exceptionsDoubleimpactedstone(astonewhereGBpalpableduetomucuscollectioninit)
LargestoneinHartmannpouchKlatskintumor—alreadydescribed.
Whipple procedure○ Radicalpancreaticoduodenectomy○ Used for cancer of the pancreas head onlyRemoval ofPancreasheadDuodenumPartofstomachPortionofjejunumGallbladder.o Triple anastomosis:1—choledochojejunostomy,2—pan-creatojejunostomy,3—gastrojejunostomy.
o RememberportalveinisnotremovedinWhippleproce-dure

tahir99 - UnitedVRG
157Hepatobiliary and Pancreatic System
endocrine neoplasMs○ Thesearelesscommonthannon-endocrinetumorsandgenerallybenignandsometimesmultiple.Theyincludes:• Insulinoma(betacells)• Glucogonomas(alphacells)
• Others:Gastrinomas(Gcells)Somatostatatinomas(Dcells)Vipomas(vasoactiveintestinalpolypeptide)
insulinomas○ Mostcommontypeofendocrinetumorinpancreas.
○ Beta cell tumor:MostlysolitaryMostlybenign*(10%–15%malignant)m/csymptom—hypoglycemia(confu-sion,irritationanddisorientation)
Whipple triad• Signsandsymptomsofhypo-glycemia
• Bloodglucose<2.8mmol/l• ReliefofsymptomsbyIVglucose
Characteristicsymptomisweightgaininsteadofweightloss(onlymalignan-cy,wherethereisweightgain)
Most sensitive investigation:Intraop-erativeUSG
Treatment:Surgicalexcision
Gastrinomas○ Thetumorarisingfromtheisletscelloflangerhansinthepancreasandintheduodenalwall.
○ Themajority(60%)ofthesetumorsaremalignant.○ Theymaybeassociatedwith(MEN1),whichincludesparathyroidhyper-plasiaandpituitaryadenoma.
○ ThemostcommonpancreaticendocrinetumorinMEN1isgastrinoma.○ GastrinomagiverisetoZollinger-Ellisonsyndrome,whichconsistoftriad1.Hypersecretionofgastricacid2.Severepepticulceration3.Presenceofnonbetacelltumorofthepancreasorduodenum.
○ Presents with complaints of peptic ulcer:RefractoryUnusualsitesUnusualrecurrence
passaro triangleJunctionofCBDandcysticductJunctionofneckandbodyofpancreas Junctionof2ndand3rdpartofduodenum.
diagnosis ○ Investigation of choice: Somatostatinscintigraphy
○ Drug of choice:Protonpumpinhibitors.• Normalgastrinlevel<150pg/ml• BAO:>15mEq/h• Secretinstimulation:Increasesthegastrinsecretion>200pg/ml• Fastinggastrin>1,000pg/mlishighlysuggestive.
vipomas somatostatinomas Glucagonomas○ Verner-Morrison syndrome○ WDHA syndrome:Waterydiarrhea,hypokalemia,achlorhydria
○ Characterizedbysevereintermittentwaterydiarrhea
○ Mostsensitiveinvestigation:EUS
○ Inhibitoryhormonesomatostatinispro-ducedinexcess
○ Inhibitsbileandpancreaticsecretion○ HencepresentswithGallstonesDiabetesSteatorrhea
○ Diabetes+dermatitis○ Necrolyticmigratoryerythe-ma(perianal,lowerabdomen,perineum,foots)
eXtra points
Pancreatogenicdiabetesism/caftersurgicalresectionforchronicpancreatitis(alsoknownaspancreatogenicorTypeIIIdiabetes)
Doublebubblesign—duodenalatresia,annularpancreas Triplebubblesign—jejunalatresia.

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery158
fMGe questions
1. Which of the following is not a complication of pseudopancreatic cyst (Sep 2007)
a. Malignancy b. Rupture c. Hemorrhageintocyst d. InfectionAns: a (Malignancy)
2. All of the following are associated with the gall-stones, except: (Sep 2008)
a. Acutepancreatitis b. Acutecholecystitis c. Acuteappendicitis d. AcutecholangitisAns: c (Acute appendicitis)
3. Grey Turner sign is seen in: (Sep 2007) a. Acuteappendicitis b. Acutepancreatitis c. Acutecholecystitis d. AcutehepatitisAns: b (Acute pancreatitis)Explanation:Acute pancreatitis is characterized by the followingsigns:• Grey-Turnersign:Pigmentationinloin• Cullensign:Pigmentationaroundtheumbilicus• Mohammedprayersign:Painintheepigastricregionradiatingtotheback,whichisrelievedbysittingandleaningforwardlikeMuslimspraying.
• Colon cut off sign: A segment of intestinewithoutperistalsisseenonX-ray(plain)ascutoff.
4. Acute pancreatitis causes all of the following, except: (March 2007)
a. Hypercalcemia b. Increasedamylaselevel c. Subcutaneousfatnecrosis d. HyperlipidemiaAns: a (Hypercalcemia)Explanation:Metaboliccomplicationsofacutepancreatitis:• Hyperglycemia• Hypertriglyceridemia• Hypocalcemia• Encephalopathy• Suddenblindness(Purtscher retinopathy)*
5. Acute pancreatitis is associated with: (March 2005) a. Elevatedserumamylase b. Alcohol c. Gallbladderstones d. AlloftheaboveAns: d (All the above)
6. Investigation of choice for acute pancreatitis: (March 2008) a. X-rayabdomen b. CTscan c. USG d. ERCPAns: b (CT scan)• Investigation of choice for acute pancreatitis is CTscan.
• Balthazar,etalcriteriaiscriteriaforacutepancreatitisbasedonCTscan.
7. Charcoat triad is seen in: (Sep 2009, 2010, March 2008) a. Acutepancreatitis b. Acuteappendicitis c. Acutehepatitis d. CholangitisAns: d (Cholangitis)• Charcottriad:Pain,jaundiceandrigorisafeatureofacutecholangitis
• Reynaudpentad:Pain,jaundice,rigor+septicshockandmentalstatuschanges.
8. Investigation for assessing proper functioning of biliary system: (Sep 2008)
a. USG b. CTscan c. HIDAscan d. AlloftheaboveAns: d (All of the above)• ButHIDAscanisthebest**• Hydroxyiminodiaceticacid(HIDA)isgivenintrave-nously isabsorbedby the liverhepatocytesandse-cretedunchanged into the biliary radicles. ThedyeissecretedintothecommonhepaticductunchangedandcanbeseenonHIDAscan.
• HIDAscanisusedtostudythebiliarysystem.

tahir99 - UnitedVRG
159Hepatobiliary and Pancreatic System
9. Best way to diagnose gallbladder stones: (March 2007) a. USG b. Oralcholecystography c. Percutaneoustranshepaticcholangiography d. IntravenouscholangiogramAns: a (USG)
10. Charcot’s triad is defined by all of the following, except: (March 2007)
a. Fever b. Gallstones c. Jaundice d. PainAns: b (Gallstones)
11. Which of the investigation can itself lead to acute pancreatitis: (Sep 2003)
a. USG b. CTscan c. ERCP d. MRIscanAns: c (ERCP)
12. Most sensitive and specific for acute pancreatitis amongst the following is: (Sep 2007)
a. Serumamylase b. Serumalaninetransaminase c. serumlipase d. C-reactiveproteinAns: c (Serum lipase)
13. Pentad of pain, fever, jaundice, confusion and shock is seen in: (Sep 2010)
a. Pancreatitis b. Hepatitis c. Cholangitis d. AppendicitisAns: c (Cholangitis)
14. Most common type of gallstone in India is: (March 2007, 2009) a. Cholesterol b. Pigment c. Mixed d. BothAandCAns: c (Mixed)
15. Management of infected pancreatic necrosis in-cludes all of the following, except: (Sep 2010)
a. Percutaneousdrainage b. Pancreaticnecrosectomy
c. Manageconservativelywithantibioticsalone d. NutritionalsupportAns: c (Manage conservatively with antibiotics alone)
16. Investigation of choice for acute cholecystitis: (Sep 2007) a. Plainradiography b. USG c. CTscan d. HIDAscanAns: d (HIDA scan)
17. Calculous cholecystitis is associated with all of the following, except: (Sep 2007)
a. Oralcontraceptives b. Estrogen c. Obesity d. DiabetesAns: a (Diabetes)
18. Chronic calcific pancreatitis is associated with all of the following complications, except:
(March 2007) a. Hypercalcemia b. Diabetesmellitus c. Malabsorptionoffat d. SteatorrheaAns: a (Hypercalcemia)• Thoughhypercalcemiacanbecauseforchronicpan-creatitis,thecomplicationofpancreatitisishypocal-cemia*
19. Conjugated hyperbilirubinemia is seen in: (Sep 2006) a. Dubin-Johnsonsyndrome b. Gilbert’ssyndrome c. Crigler-NajjartypeI d. Crigler-NajjartypeIIAns: a (Dubin-Johnson syndrome)• Dubin-Johnson and Rotor syndrome are associatedwithconjugatedhyperbilirubinemia
(Pneumonic-DR-Conj)• Crigler-Najjar andGilbert are unconjugated hyper-bilirubinemia.
20. All of the following are seen with bile duct stone, except: (March 2009)
a. Obstructivejaundice b. Distendedandpalpablegallbladder c. Pruritis d. Clay-coloredstoolsAns: b (Distended and palpable gallbladder)

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery160
21. Reversed '3' sign on barium studies is seen in which condition: (Sep 2009)
a. Ampullarycarcinoma b. Carcinomastomach c. Carcinomaheadofpancreas d. InsulinomaAns: c (Carcinoma head of pancreas)
22. Investigation of choice for gallbladder stone is: (Sep 2009) a. OCG b. USG c. PTC d. X-rayAns: b (USG)
23. All of the following are false for gallbladder carci-noma, except, i.e which is true? (Sep 2006)
a. Carriesagoodprognosis b. Gallstonesmaybeapredisposingfactor c. Commonlysquamouscellcarcinoma d. JaundiceisrareAns: b (Gallstones may be a predisposing factor)
24. A 70-year-old male patient presented with history of chest pain and was diagnosed to have coro-nary artery disease. During routine evaluation, ultrasound of the abdomen showed presence of gallbladder stones. There was no past history of biliary colic or jaundice. What is the best treat-ment advice for such a patient for his gallbladder stones: (March 2003, Sep 2007)
a. Opencholecystectomy b. Laparoscopiccholecystectomy c. Nosurgeryforgallbladderstones d. ERCPandremovalofgallbladderstonesAns: c (No surgery for gallbladder stones)
25. Most common location of gastrinoma is: a. Duodenum b. Jejunum c. Stomach d. PancreasAns: a (Duodenum)
26. Acute pancreatitis cause all, except: (Sep 2005) a. Fatnecrosis b. Hypercalcemia c. Increasedamylase d. IncreasedlipaseAns: b (Hypercalcemia)
27. Amylase is increased in all the following, except: (Sep 2005) a. Acuteappendicitis b. Acutepancreatitis c. Duodenalperforation d. IntestinalobstructionAns: d (Intestinal obstruction)
28. Most common mode of spread of gallbladder can-cer: (Sep 2005)
a. Transcoelomicspread b. Lymphaticspread c. Hematogenicspread d. DirectextensionAns: d (Direct spread)
29. Chronic cholecystitis is associated with all, except: (Sep 2005) a. Palpablegallbladder b. M/cinwomen c. Associatedwithgallstones d. RokitanskycellsAns: a (Palpable gallbladder)• Incasesofchroniccholecystitisbecauseofchronicin-flammation,gallbladderwouldhaveshrunkenwiththickhypertrophiedmusculatureofgallbladderwall
• Rokitanksy aschoff sinuses are histologically out-pouchingsofgallbladdermucosaincasesofchroniccholecystitis.
30. The best way to diagnose gallstones in CBD intra-operatively: (March 2007)
a. Intraoperativecholangiogram b. CTscan c. MRI d. USGAns: a (Intraoperative cholangiogram)
31. Not a part of Charcot’s triad: (Sep 2009) a. Intermittentpain b. Intermittentvomiting c. Intermittentfever d. IntermittentjaundiceAns: b (Intermittent vomiting)
32. Pentad of pain, jaundice, fever, confusion and shock is seen in: (Sep 2009)
a. Acutepancreatitis b. Hepatitis c. Cholangitis d. CholecystitisAns: c (Cholnagitis)

tahir99 - UnitedVRG
14LIVER
Anatomy Blood supply○ Largestorganinthebody○ Barearea—posteriorsurface○ 5surfaces—anterior,pos-terior,right,superiorandinferior.
• 80%fromportalveinand20% from hepatic artery• Lefthepaticducthaslongestextrahepaticcourse2cmisaccessibleoutsideliver• TherightandlefthepaticveinsjointogetherandentertheIVC.TheinferiorhepaticveinsjointheIVCdirectlyonitsanteriorsurface
• Relationsintheportahepatisfrombehindforwards—Portalvein(posterior),hepaticartery(left)andhepaticducts(right)
• Commonhepaticarteryrunsoverthesuperiorborderofpancreasandrunsalongtherightsideofthelesseromentumanditascendstohilumandliesanteriortoportalveinandtoleftofhepaticduct.
○ Aberrant right hepatic arteryarisesfromsuperiormes-entricarteryandrunsposteriortothepancreashead
○ Replaced or accessory left hepatic arteryarisesfromleftgastricartery
○ An accessory cystic artery canoriginatefromgastrodu-odenalorpropercommonhepaticartery.
FunctionAl AnAtomy (couinAud's segments)○ Cantlie line:AnimaginarylinerunningfromgallbladdertoleftsideofIVC.○ Rightliversegments5,6,7,8○ Leftliversegments1,2,3,4○ Caudatelobeissegment1.Vascularinflowandbiliarydrainagetothecaudatelobeisfrombothrightandleftsystems
Contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery162
FunctionAl AnAtomy (couinAud's segments)○ Reidel lobe: A tongue-like extension from the right liver inferiorly○ Segmentstotheleftoffalciparumsegment:Segment2and3○ Caudate lobeisthelobethatisnotaffectedinBudd-Chiarisyndromeandcir-rhosisofliverbecauseofitsdirectdrainageintoIVC(segment1)
○ Quadratelobeisthefourthsegment.
• Removalofsegments2-4(lefthepa-tectomy)
• Removalofsegments5-8(righthepatectomy)
• Removalofsegments5-8alongwith4(extendedrighthepatectomy)
• Removalofsegments2-4alongwith5and8(extendedlefthepatectomy)
Functions of liver liver function tests○ Maintainscorebodytemperature○ pHbalanceandcorrectionoflacticacidosis○ Synthesisofclottingfactors○ Glucosemetabolism,glycolysisandgluconeogen-esis
○ Ureaformationfromproteincatabolism○ Bilirubinformationfromhemoglobindegradation○ Drugandhormonemetabolism○ Removalofgutendotoxinsandforeignantigens.
○ Humanwillsurvivefor24-48hoursinanhepaticstatedespitefullsupportivetherapy.
○ Serum alkaline phosphatase—elevatedincholestasisorbiliaryobstruction.
○ AST/ALT—reflectsacuteliverdamage○ GGT—reflectsliverinjuryduetoacutealcoholingestion*○ synthetic functions—albuminlevelandprothrombinlevel.○ Clearance tests:Indocyanine,aminopyrine,lidocaineclearancetestsaretodiagnosefunctionallivercapacity.
Few important points• TheextravascularfluidcompartmentinsidetheliveriscalledasSpaceofDisse• Hepatic stellate cells (ito cells) containhighlipidcontentanditsmajorfunctionistostorevitaminAandsynthesizeextracellularcollagen.
normal valuesBilirubin:5-17µmol/LALP:35-150IU/L
AST:5-40IU/LGGT:10-48IU/L
Albumin:35-50g/LProthrombin time:12-16second
Acute liver FAilure cAuses• Viralhepatitis(hepatitisA,B,C,D,E)• Drugreactions:Halothane,isoniazid,rifampic-in,antidepressants,NSAIDs,valproicacid.
• Paracetamoloverdose• Mushroompoisoning• Shockandmultiorganfailure
• AcuteBudd-Chiarisyndrome• Wilsondisease• Fattyliverofpregnancy
Contd...

tahir99 - UnitedVRG
163Liver
modiFied child-pugh clAssiFicAtionclinical 1 2 33
Encephalopathy None 1or2 3or4Ascites None Mild Moderate
Bilirubin(mg/dL) 1–2mg/dL 2.1–3mg/dL ≥3.1mg/dLAlbumin(g/dL) ≥3.5g/dL 2.8–3.4g/dL ≤2.7g/dL
Prothrombintime(increaseinseconds) 1–4 4.1–6 ≥6oGrade A: 5–6 oGrade B: 7-9 oGrade C: 10-15points
chronic liver diseAseMost useful clinical sign—flapping tremor Ascite is a late feature
investigAtions• Ultrasound:Firstlineinvestigation• SpiralCT:Anatomicalplanningforliversurgery(goldstandardforliverimaging)
• MRI—incasesofiodineallergy,whereCTcannotbedone.• MRCP—goldstandardforbiliarytractimaging• ERCP—Itisthegoldstandard,ifbileductstonesissuspectedorwheninterventionisneeded
ercp percutaneous transhepatic cholangiography○ indications InterventionneededBileductstonesBrushbiopsyfrombiliarytract
○ Pre-requisitesProphylacticantibioticsCoagulationprofileneedstobechecked
○ ComplicationsPancreatitisCholangitisBleeding/perforationofduo-denum
○ indications1.WhereERCPfailedorimpossiblelikepolyagastrec-tomy.
2.Intrahepaticduct/hilarbileductcancers,whereERCPcannotreach.
Angiography nuclear scan• Todiagnosebleedingfrombiletract(hemobilia)
• TC99mscan(IoDIDA)—ifbileleakorbiliaryobstructionissuspected• Sulphurcolloidliverscan—allowsKupffercellsactivitytobedeterminedAdenomasandhemangiomaslackKupffercellsandhencenouptakeofsulphurcolloid.
• FDGPET—basedontheprinciplethatcanceroustissuetakesuphighamountofglucosethannormaltissue.
portAl hypertension And cirrhosis• Micronodular—alcoholiccirrhosis• Macronodular—posthepatiticcirrhosis
Contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery164
portAl hypertension And cirrhosisrelated anatomy
Portalveinisformedbytheconfluenceofsuperiormesentricveinandsplenicveinbehindtheneckofpancreas.
Leftgastric(coronary)veinenterstheportalveinatitsorigin.Splenicveinisjoinedbyinferiormesentricveinjustbeforeitsconfluencewithsuperiormesentricvein.
Portalveinlength:6-8cmNormalpressureinportalvenoussystemis3-5mmHgand10–12cmH2o.
important points• M/ccauseofdeathinportalhypertension—hepaticfailure• 2ndcommoncauseofdeath—varicealhemorrhage
• M/ccauseofportalhypertension—alcoholiccirrhosis
left-sided portal hypertension• Duepancreaticneoplasmorinflammationofthesplenicveingetsthrombosedandresultsinleftsidedportalhypertension
• Thesuperiormesentricandportalvenouspressureisnormal.
• Leftgastroepiploicbecomesthemajorcollateralandhence,gastricvaricesdevelopratherthanesophageal
• Easilyreversedbysplenectomy
• What do you think, if there is an unexpected functional deterioration in a case of cirrhosis? Thinkofhepatocellularcarcinoma(elevatedafetoprotein)in60%cases.
• How will you take liver biopsy in a case of cirrhosis with coagulopathy or moderate ascites? Percutaneousliverbiopsymustnotbedone,transjugularorlaparoscopicbiopsyisadvised.
• What are the common serum electrolyte abnormalities in cirrhosis? Hyponatremia,hypokalemia,metabolicalkalosis• Therewillbehypersplenisminportalhypertension,whichresultsinplateletcount<50,000/cubicmm.• Becausemanycoagulationfactorsaresynthesizedinliver,thecoagulationfactorisalsoimpairedresultingincoagulopathy
sites oF portAcAvAl AnAstomosissite systemic portal1.Lowerendofesophagus
Accessoryhemiazygousvein
Leftgastricvein
2.Analcanal Middleandinferiorrectalveins
Superiorrectalvein
3.Umbilicus(caputmedusae)
Anteriorabdominalwallveins
Leftportalvein(viaparaumbilicalvein)
4.Bareareaofliver Phrenicandintercostalveins
Hepaticvenules
5.Liver IVC PatentductusvenosusconnectleftportalveintoIVC
6.Posteriorab-dominalwall
Retroperitonealveinsofabdominalwall
Veinsofretroperitone-alorganslikeduode-num,ascendingcolon,descendingcolon
Contd...
Contd...

tahir99 - UnitedVRG
165Liver
sites oF portAcAvAl AnAstomosismeasuring portal pressure gradient
1.Bytranshepaticorumbilicalvenouscannulationofportalvein2.Bytranscutaneouspuncturespleen•Portalpressurecanbeindirectlymeasuredbymeasuringhepaticvenouswedgepressuregradient(HVPG),butremem-berthepressurewillbenormalinpresinusoidalcausesofhypertension.
Bleeding in portal hypertension• ThemostcommoncauseofbleedinginPHTpatientsisfromesophago-gastricvarices(esophagus80%andgastric20%)
• Isolatedgastricvaricesmustraisethesuspicionofsplenicveinthrombosis
• Theonlynon-varicealcauseofportalhypertensivebleedingisportalhyperten-sivegastropathy(m/caftereradicationofvarices).
treatment○ Esophagogastricvariceswillnotbleeduntilthepressureexceeds12mmHg
• Resuscitation• Non-interventional
• Interventional• Surgical
resuscitation interventional• Isotoniccrystalloids,CVPmeasurement• About6unitscross-matched• IfPTisprolongedmorethan3secondsFFPtransfused
• Ifplateletcount<50,000—platelettransfusiondone
• Startprophylacticantibiotics
• Thefirstandforemosttreatmentnextisendoscopyandsclerotherapyorbanding
• othernon-interventionaltreatmentsstartedonlyifendoscopycouldnotbedoneduetobleeding
• Endoscopicbandingisadvantageousbecauseitdoesnotleadtonecrosisorulcerationofesophagus,butbothareequallyeffectiveincontrollingbleeding.
• Sclerosantsused—ethanolamineoleate,cyanoacrylate,sodiummorrhuateorsodiumtetradecylsulfate.
sengstAken-BlAkemore tuBe• Modifiedsengstakencontainsfour tubes(oldSengstaken-Blakemoretubecontainsthreetubes)• oneforaspirationfromstomach,onefromesophagus,oneforesophagealballoondilatationandlastoneforgastricbal-loondilatation.Thegastricballooninflatedto250mLofairandesophagealballoontoapressureof40 mm Hg.Thepotentiallylethalcomplicationisaccidentallyinflatinggastricballooninsidetheesophagusresultinginperforationofesophagus
Balloonsshouldbetemporarilydeflatedafter12hourstopreventesophagealnecrosis.
Contd...
Contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery166
pharmacotherapy○ octreotide(long-actinganalogueofsomatostatin)andsomatostatinareeffectivelikeendoscopy○ Vasopressinpreviouslyusedisalsoeffective,butnitroglycerinemustbegivenalongwithittopreventcoronaryvesselsconstriction
trAnsjugulAr intrAhepAtic portAl shunt (tips)• Short-termbridgetolivertransplant• Insertedviainternaljugularvein(IJV)byinterventionalradiologist• Accesstheportalveininsidetheliverviaabranchofhepaticveinanddilatethetractto10mmthroughwhichexpandablemetallicstentisinserted.
• Itisnotusedasinitialtherapy,butcanbeusedifendoscopyandpharmacotherapyfails.• Itisatypeofnon-selective shunt
complicationsMainearlycomplicationisperforationoflivercapsuleandfatalintraperitonealhemor-rhage
Postshuntencephalopathyistheconfusionalstateduetothetoxicmetabolitesbypassingthemetabolisminliver
Long-termcomplicationisshuntstenosis,whichmayoccurin<1year
contraindicationsAbsolute:RightsideheartfailurePolycysticliverdisease
Relative:PortalveinthrombosisHypervascularlivertumorsEncephalopathy
prevention oF recurrent Bleed• Drugusedisnon-selectivebeta-blockers—propranololhasshowntoreducerebleed
• CombinationofISDNandpropranololhasbeenshowntobemoreeffectivethanvaricealligation
shunting surgeriesnon-selective shunts
1.Endtosideportocavalshunt(Eckfistula)2.Sidetosideportocavalshunt
3.Largediameterinterpositionshunts(>16mm)4.Conventionalsplenorenalshunts
5.TIPS
ConventionalsplenorenalshuntInvolvesremovalofspleenandinsertionofproximalsplenicveinintorenalvein.Theonlyadvantageofthisshuntishyper-splenismbeingeliminatedbysplenectomy
complication Advantages○ Portalshuntencephalopa-thyismorecommoninthisprocedure.
○ Thisshuntcompletelydivertthebloodfromportalsystemtocavalsystem○ Thistypeofshuntalsodecompressesthesplanchnicvenoussystemandintrahepaticsinusoidalnetworkhence,sidetosideshuntsaretheeffectiveincontrollingascitesandpreventingrebleed
selective shunts○ Splenorenalshunt—distal(Warrens) ○ Inokuchi:Leftgastricvenacavalshunt.Veingraftinterposedbetween
theleftgastricveinandinferiorvenacava.
Contd...
Contd...

tahir99 - UnitedVRG
167Liver
shunting surgeriesdistal splenorenal shunt
• Anastomosisofdistalendofsplenicveintotheleftrenalveinalongwithinterruptionofallcollaterals
• This shunt aggravates the ascitebecausesinusoidalandmesentrichyper-tensionismaintainedandimportantlymphaticpathwaysaretransectedduringdissection.
• Contraindications:Previoussplenectomy(absolute)Splenicveindiameter<7mm(relative)
partial shunts non-shunt operations• Smallprostheticgraftsize<10mmusedtobehaveaspartialshunt.
• Simplestnon-shuntoperationistransectionandreanastomosisofthedistalesophaguswithastaplingdevice.
• Extensiveesophagogastricdevascularizationcombinedwithsplenectomyandesophagealtransection(Sugiura operation)
• Mainindicationforthissurgeryisdistalsplanchnicvenousthrombosisandforpatientswithdistalsplenorenalshuntthrombosis
trAnsplAnt cAndidAtes• Non-alcoholiccirrhosisandabstinentalcoholiccirrhoticswithchildBorC
• Patientswithpoorqualitylifestyleduetoencepha-lopathy,fatigueofchildAwillalsobeindicated
Non-cirrhotic portal fibrosis (ncpF) and extrahepatic portal venous obstruction (ehpvo)
ncpF vs extrahepatic portal venous obstruction
○ Thetwocommoncausesofnon-cirrhoticportalhypertensioninIndiaare•NCPF—meanageofpresentationis30.5years•EHPVo—mostcommonsiteofobstructionisatportalveinformation(90%)AscitesistransientorabsentEsophagealvaricesseenin90%-95%andgastricvaricesin35%-40%M/cpresentationisvaricealbleedandsplenomegaly
○ Both the conditions present with similar features:Massivevaricealbleed (m/cpresentationofNCPF)
ModeratetomassivesplenomegalyNormalliverhistologyAbsenceofascitesNormalliverfunction
differentiation pointsNCPF—age:Youngadults(2ndor3rddecade)Smaller3rdand4thorderbranchofPVinvolved
EHPVO—age:Children(1stor2nddecade)Mainor1storderbranchofportalveininvolved
important pointsin india• Inpediatricagegroup—EHPVo(70%),cirrhosis(30%),NCPF(4%),congenitalhepaticfibrosis(4%)andBudd-Chiari(3%)• InIndia—thereisequalincidenceofbothcases
Contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery168
pyogenic ABscess○ The potential routes of hepatic
exposure to bacteria follows:Biliarytree(mostcommonroute)Portalvein(pyelophlebitisduediverticulitis,appendicitis,PID,IBD,perforation,etc.)
Hepaticartery(systemicbacte-remia-associatedwithmultiplemicroabscess)
DirectextensionTrauma
clinical feature management○ M/cinrightlobe○ M/corganismsisolated–
E. coliandKlebseilla pneumo-niae.
○ M/cpresentingsymptom—fever,chills,abdominalpain.
○ ArarecomplicationofKleb-seillaabscessisendogenousendophthalmitis(3%),com-monindiabetics.
• USGandCTarethetwocommonlyusedtools.• CTscan95%-100%specific.• X-raychestshowselevatedrighthemidi-aphragm,pleuraleffusionandatelectasis.
• Treatment involvespercutaneouscatheterdrainagealongwithbroadspectrumantibi-otics.Surgeryisreservedforthosewhofailpercutaneoustechniqueandforthosewhomsurgeryisrequiredforsomeotherpathologylikeappendicectomy.
AmeBic ABscesspathogenesis
○ Entamoeba histolytica cystsareingestedthroughfeco-oralroute.○ Cystsarenotdegradedinstomachandtheypasstointestine,wherethetrophozoitesarereleased.○ Trophozoitespasstothecolonandcaninvadethemucosaresultinginthedisease.Fromwheretheyentertheportalsystem.○ Themajormechanismofabscessformationisenzymaticcellularhydrolysis.Theabscesscontainsacellularproteinaceousdebrissurrounded by a rim of invasive amoebic trophozoites
○ Duetoliquefactionnecrosisofliver,theabscessresultsanchovy sauce colored and odorless○ CharacteristicfeatureofamebicabscessisGLISoNcapsuleisresistanttoamoebicinvasion,henceabscessislimitedtoGlisoncapsule.
clinical feature investigation• M/cLFTabnormalityiselevatedprothrombintime• Enzymeimmunoassays(EIA)havesensitivity99%andspecificity>90%inpatientswithamebicabscess.
• USGcharacters:Hypoechoic and non homogenous rounded lesion abutting liver capsule without sig-nificant rim echoes.
• CT scan: Moresensitiveindifferentiatingpyogenicfromamebicbecausetherewillberimenhancementinpyogenicabscessoncontraststudy.
• Nuclear scan (Gallium or Tc):Helpsindifferentiatingbe-causeamebicabscessdoesnotcontainleukocytesandhencedoesnotlightuponthesescans
treatment percutaneous aspiration• Oral metronidazole—750mgthreetimes/10daysisthedrugofchoice.
• EmetineIMinjectionsisveryeffectiveforinvasiveamoebiasis.
• Aftertreatmentofliverabscess,luminalagentslikeiodoquinol,paromomycinanddiloxanidefuroateareadministeredtotreatcarrierstate.
• Therapeuticaspirationisusuallyavoided.Metrogylisthetreatmentofchoiceandabout90%casesrespondwell.
• Indicationsforaspiration:abscesswalldiameterlargerthan5cm(abscesswithhighriskofrupture)abscessintheleftlobeofliverfordiagnosticuncertaintyfailuretorespondin3-5days
○ Themostfrequentcomplicationofliverabscessisrupture.
diFFerentiAl diAgnosis oF AmeBic And pyogenic FeAturesFeatures Amebic pyogenicAge 20–40year >50yearMale : female ratio >10:1 1.5:1Solitary% 80% 50%Diabetes Uncommon CommonJaundice Uncommon CommonElevated alkaline phosphatase Common CommonPositive blood culture Negative PositivePositive amoebic serology Yes No

tahir99 - UnitedVRG
169Liver
hydAtid cyst○ Echinococcus granulosusisM/c.othersE. multilocularis,E. oligartus.○ Dogs are definitive hosts,inwhichadulttapewormisattachedinvilliofsmallintestine.
○ Sheeps are intermediate hoststhatconsumetheovapassedbythefecesofdogovergrasses.
○ Humansareaccidentalhostsconsumingtheseeggsthatcovertstoembryoinduodenumandreleasesanoncospherecontaininghookletsthatpenetratethemucosaandreachthebloodstream.
○ Theoncospherereachestheliver(m/c)orlungs,wheretheparasitedevelopsintolarvalstagecalledashydatidcyst.
○ Rememberhumansareend-stagehost.
pathogenesis clinical featureThreeweeksafteringestion,apericystderivedfromhosttissuewalldevelopssurroundingthehydatidcyst.
Thecystitselfhastwowalls:ectocyst (outergelatinous)andendocyst(innergerminal)layers.
Indefinitivehost,theydevelopintoadulttapeworm,butinintermediatehosttheydeveloponlyintonewhydatidcyst.
Daughtercystsaretruereplicaeofthemothercyst.
M/cinrightlobeofliver**Mostfrequentsign—hepatomegalyM/csymptoms—abdominalpain,dyspepsiaandvomiting.Complications:Ruptureintobiliarytree,bronchialtree,pleural,peritonealandpericardialcavity.
investigations• USG:Rosettelikeappearanceorwaterlilleyappearanceisseenwhendaughtercystsarepresent.Calcificationsinthewallarehighlydiagnostic
• Serologicaltests:ELISA,arc5test,IHAtest,immunoblasttest,whereavailableisthetestofchoice• Casoni test:Intradermalinjectionofsterilehydatidfluidproducesawhealof5cminhalfhourtreatment pAir○ Primarilysurgical,butintroductionofPAIRhastotallyreplacedit.
○ Duringsurgery,packingofftheabdomenfromthecystisveryimportantbecauseoftheanaphylacticreactionthatmayoccurifcystrupturesintoperitonealcavity
○ Surgicalprocedures:PericystectomyMarsupializationomentoplastyTotalcystectomyPartialhepatectomy
○ Remembersurgeryisnowpreferred,wherePAIRisnotpossibleorwhenitdoesnotrespondtoPAIRorwhenthereisanycommunicationtobiliarytree
• Percutaneous aspiration, infusion of scolicidal agents and reaspiraion (PAiR).
• Givenwithprophylacticcoverofalbendazole.• Scolicidalagents—20%hypertonicsaline,0.5%silvernitrate,95%ethanol,absolutealcohol,mebendazole2.4microgram/mL
• ContraindicationsforPAIR:1.Superficiallylocatedcyst(chanceofrupture)2.Honeycombingofcysts(multiplethickinternalseptae)3.Communicationwithbiliarytree4.Deadorinactivecysts
echinococcus multilocularis recurrent pyogenic cholangitis• Alwaysmultiloculated• Treatmentisalwayssurgicalresection
• Alsonamedasorientalcholangiohepatitisorhepatolithiasis.• Male:femaleissame.Age:20-40year• Usuallysecondarytobiliarystoneandstricture.
Benign liver tumorcharacter liver cell adenoma Focal nodular hyperplasia hemangiomaIncidence ○ Rare • Secondcommonbenigntumor ■ M/cincidentaloma
■ M/cbenigntumor
Contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery170
Benign liver tumorAgegroup/sex ○ Youngwomen
○ 20-40year• Middleagedfemales ■ About45years
■ M/cinfemalesEtiology ○ Benignproliferationof
hepatocytes• Developmentalvascularmal-formation
■ Congenitalvascularmalformations
Associatedfactors ○ oCPandsteroids • FemalehormonesandoCP ■ -------Complications ○ Rupture and malignant
transformation • Rupture/hemorrhage ■ Rupture/hemorrhage
Histology ○ Benignhistocytescon-tainingglycogenorfat
• Characteristicallycentralfi-brousscarwithradiatingsepta
■ Smallcapillarytypeandlargecavernoustypesarethere
Imagingstudies ○ CT—heterogenousmasswithearlyenhancement
○ MRI—welldemarcatedmasswithfatorhemor-rhage
• Homogenousmasswithcen-tralscar
• Sulfur colloid liver scan: KupffercellsinFNHonlytakeupthecolloid.
■ CT/MRI—slowcontrastenhance-mentduetosmallvesseluptake.Typicalnodularperipheralen-hancement
Treatment o Laparotomy and resec-tion
• Asymptomaticandtypicalcasesrequirenotreatment
■ Canbeleftassuchunlesssympto-maticordoubtexists
■ Enucleationwithproximalcontrol• Kassabach meritt syndrome:Liverhemangioma+thrombocytopenia+consumptivecoagulopathy• Complication of large hemangiomas in children:Congestivecardiacfailuresecondarytoarteriovenousshunting• Giant hemangiomas:Size>5cm
mAlignAnt tumor○ M/cprimarymalignanttumor—hepa-tocellularcarcinoma
○ M/cmalignanttumor—metastaticlivercancer
○ M/csiteofprimaryformetstoliver—colon
hepatocellular carcinoma (hcc)risk factors clinical features• infections:HepatitisBvirus,hepatitisCvirus• Cirrhosis:Alcoholinduced,autoimmunehepatitis,primarybiliarycirrhosis
• Environmental:AflatoxinspyrrolizidinealkaloidsThorotrastN-nitrosylatedcompounds
• Metabolic diseases:Hemochromatosis,alpha1-antitrypsindeficiency,Wilsondisease,porphyriacutaneatarda,Type1and3glycogenstoragedisease,galactosemia,citrullinemia,hereditarytyrosinemia,familialcholestaticcirrhosis
• Most important risk factor is cirrhosis
○ M/cinmales;50-60year○ Presentation:1.Rightupperquadrantpain2.Weightloss3.Palpablemass4.Inknowncirrhotics—suddendecompensationofliverthinkofHCC.
5.Rupture6.Lessthan1%casespresentwithparaneoplasticsyndromemostcommonlyhypercalcemia,hypogly-cemia,erythrocytosis
diagnosis• MCQpoint—hepatocellularcarcinomahasthetendencytoinvadetheportalvein• USG—playssignificantroleinscreeningandearlydetectionofHCC• CTandMRI—aredefinitelyneededforplanningsurgeries• Serum AFP—used in diagnosing HCC Duetorecentadvancesininvestigations,itismainlyusedasadjuncttoimagingtests. Value>400mg/dLishighlysuggestiveAFPismainlyusedtomonitor recurrences intreatedpatientsAFPlevelsareelevatedinabout70%–80%cases
Biopsy■ Biopsyiscontraindicatedinsuspectedcases.Biopsyisdoneonlyininoperablecases/cases,whicharetriedfornon-opera-tivetherapies
■ Percutaneousbiopsycarriestheriskoftumorspillage,ruptureandbleeding
Contd...
Contd...

tahir99 - UnitedVRG
171Liver
mAlignAnt tumorAssessment of liver function treatment○ LiverresectionisthetreatmentofchoiceforHCC○ Child(modifiedbyPUGH)isthemostcommonlyusedsystem○ ChildCarenotcandidatesforresection○ ChildAcandidatescanusuallytoleratesomedegreeofresection○ ChildBareconsideredborderline.
○ CompleteexcisionofHCCbypartialhepatectomyorbytotalhepatectomywithlivertrans-plantationarethetreatmentofchoices.
Ablative1.Percutaneousethanolinjection2.Percutaneousaceticacidinjection3.ThermalablativetechniquesCryotherapyRadiofrequencyablation(RFA)microwave
○ RFAandcryotherapycanbedonepercutaneously.○ Maindisadvantageisheatsinkeffect,limitingtheusenearmajorbloodvessels.
transarterial ○ External beam ra-diotherapy—roleislimitedbecauseofthesurroundingtissuedamage.
○ Systemic chemothera-py
○ Basedonthefactthatmostofthetumorbloodsupplyisfromthehepaticartery1.HAI(hepaticarterialinfusion)chemotherapyusing5flouorouracil,cisplatin,doxorubicin2. Chemoembolization:EmbolizationparticlesandlipoidaloilsaddedwithchemotherapyagentsselectivelytakenupbyHCC
3.Transarterialradiotherapy
FiBrolAmellAr vAriAnt oF hcccharacters hcc FhccMale:Femaleratio o 8:2 • 1:1Medianage o 55 • 25Tumor o Invasive • WellcircumscribedResectability o <25% • 50%-75%Cirrhosis o 90% • 5%Alphafetoprotein o 80%elevated • 5%elevatedHEPBpositive o 65% • 5%FHCCalsohasacentralfibrousscarmakingitdifficulttodifferentiateitfromfocalnodularhyperplasia.FHCCdoesnotproducefetoprotein,butproducesneurotensinFHCChasabetterprognosisthanHCC
Hepatoblastoma metastatic liver tumor○ M/cprimaryhepatictumorofchildhood○ Ageofpresentation:18month(almost<3year)
○ Tumorderivedfromfetalhepatocytes○ Serumalphafetoproteinlevelselevated
○ M/cmalignanttumorofliver○ M/cfromcolorectalcancers○ Nowitisfoundhepatectomyiscurativeforcolorectalmets○ Theonlycontraindicationforliverresectionisinabilitytoresectalldisease○ Thethreecancers,wheresecondaryinliverisresected—colorectal,smallintestineandcarcinoids
Budd-chiAri syndrome• Youngfemalesareaffectedcommonly• Venousdrainageisoccludedbyeitheravenousthrombosisorobstructionbyavenousweb
• M/cpresentation—ascites*andabdominaldiscomfort
• CTscan—asciteswithlargecongestedliverorasmallcirrhotic,liverinwhichthereisgross enlargement of segment 1 (caudate lobe),becauseonlysegment1hasdirectdrainagetoIVC.
Contd...
Contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery172
Budd-chiAri syndrome• Asaresultofvenousoutflowobstruction,thelivergetscon-gestedwithdevelopmentofimpairedliverfunctionwithsub-sequentportalhypertension,ascitesandesophagealvarices
• R/ounderlyingetiology—myeloprolifertaivedisorderorprocoagulantstatelikeproteinCSdeficiencyorantithrombindeficiency
• Confirmationofdiagnosis:Hepaticvenographyviatransjugularroute
• Treatment○Cirrhoticliver/fulminantliverfailure—livertrans-plant
○Non-cirrhotic—portocavalshunting
liver trAnsplAnt• M/cindicationinchildren:Biliaryatresia• M/cindicationinadults:Cirrhosis
indication in adult Absolute contraindications 1. Primarybiliarycirrhosis 2. Secondarybiliarycirrhosis 3. Primarysclerosingcholangitis 4. Carolisdisease 5. Cryptogeniccirrhosis 6. Chronichepatitiswithcirrhosis 7.Hepaticveinthrombosis 8. Fulminanthepatitis 9. Alcoholiccirrhosis10. Chronicviralhepatitis11. PrimaryhepatocellularCa12.Hepaticadenomas
1.Activeuntreatedsepsis2.Advancedcardiopulmonarydisease3.Extrahepaticmalignancy4.Metastasisinliver5.AIDS6.Life-threateningsystemicdiseases
indication in children1.Biliaryatresia2.Neonatalhepatitis3.Congenitalhepaticfibrosis4.Alagillesdisease5.Alpha1antitrypsindeficiency6. InheriteddisordersofmetabolismWilsons,tyrosinemia,glycogenandlysosomalstoragedisorders,hemophilia,oxalosis,etc.
types of graft○ Orthotopic graft—agraftplacedinitsnormalanatomicsite,e.g.liver
○ Heterotopic graft—agraftplacedinasitedifferentfromitsnormalloca-tion,e.g.kidneykeptiniliacfossa
important points in liver transplant• STARZLperformedfirstlivertransplant(1963)• Hepaticarterythrombosismayoccursponta-neouslyorasapartofacutegraftrejection.Itmaypresentasfever,bileleakorriseinserumtransaminaselevel.Thiscomplicationrequiresimmediateretransplantation.
• Portalveinthrombosisoccursinsidiouslyanddoesnotrequireretransplant
• Pediatriclivertransplantusingadultlateralsegmentofleftliver.• Chroniclivergraftrejectionoccursduetovanishingbileductsyn-drome
• Liverisresistanttohyperacuteandchronicrejection
Fmge questions
1. Which of the following statement is true regard-ing pyogenic liver abscess? (Sep 2005)
a. Diagnosiscanbeconfirmedbyserologicaltest b. Radiographicfeaturesarediagnostic c. Usuallyalargeandsingleabscessisseenin
casesofdirectspread d. SystemicmanifestationsareuncommonAns: c (Usually a large and single abscess is seen in cases of direct spread)Explanation:• Amebicliverabscessisdiagnosedbyserology*
• PyogenicliverabscessiscommonlycausedbyE. coli. Bloodculturemaybepositive
• If thespreadisbydirectmethod, it isusually largeand single, multiple abscess* seen only when thespreadisbyarterial(hepaticartery)route
• Systemicmanifestationsintheformfever,chillsandrigorsaresocommon.
2. investigation of choice for hydatid disease is: (March 2006) a. CTscan b. ELISA
Contd...

tahir99 - UnitedVRG
173Liver
c. Biopsy d. USGAns: a (CT scan)Explanation:• ThoughhydatidcystcanbediagnosedbyUSG,CTscanismuchmoreinformativeaboutthecommuni-cationwithbiliarytreeandregardingthesegmentofliverinvolved
• USGshowsWaterlillyappearance*• Calcificationsinthecystarealmostdiagnosticofhy-datidcyst
• Casoniintradermal*testwasonceusedtodiagnosehydatidcyst,butnotdonenowadays.
3. Number of lobes in liver as per Couinaud classifi-cation: (Sep 2009)
a. 3 b. 4 c. 6 d. 8Ans: d (8)Explanation:• Couinauddividedtheliverintotwolobesbyaline—Cantle’sline,whichisdrawnfromgallbladderfossatoleftofinferiorvenacava
• The classification isbasedon thehepaticveins fur-therinto8segments.
4. All of the following are true about fibrolamellar carcinoma of the liver, except: (Sep 2004)
a. Equalincidenceinmalesandfemales b. BetterprognosisthanHCC c. AFPlevelsalwaysgreaterthan>1000 d. occurinyoungerindividualsAns: c (AFP levels always greater than > 1000)Explanation:• Fibrolamellarvarietyofcancer in liverhaselevatedneurotensinB*astumormarker
• Commoninyoung individuals,goodprognosis, re-sectablerateisgood
• NotassociatedwithcirrhosisorhepatitisB*
5. Most common cause of liver abscess in india: (Sep 2005) a. Amebicabscess
b. Ascendinginfection c. Infectedhematoma d. SecondarytocholelithiasisAns: a (Amebic abscess)Explanation:• AmebicliverabscessisverycommoninIndia• Mostcommoninmales*.• Metronidazoleisthetreatmentofchoice*
6. Amebic abscess is commonly located in which part of liver? (March 2007)
a. Anteriorsuperior b. Posteriorsuperior c. Anteriorinferior d. PosteriorinferiorAns: d (Posterior inferior)
7. Most commonly ruptured organ in blunt trauma to abdomen is: (Sep 2010, March 2009)
a. Adrenals b. Kidney c. Liver d. SpleenAns: c (Liver)Explanation:Mostcommonorganinjuredinblunttraumaisliver.Mostcommonorganinjuredinblunttraumathatneces-sitateslaparotomyisspleen
8. Not a contraindication for doing percutaneous liver biopsy: (Sep 2009)
a. INR1.5 b. Hemangioma c. Biliaryobstruction d. PortalhypertensionAns: c. Biliary obstruction
9. Cause of hematemesis in a patient with mild sple-nomegaly: (Sep 2007)
a. Esophagealvarices b. Cancerstomach c. Pepticulcer d. GastritisAns: a. Esophageal varices

tahir99 - UnitedVRG
15Spleen
AnAtomy• Spleen size:12cmlength*7cmwidth*3-4cmthick• Weight:150g(75–250g)
• Longaxisliesalong10thrib• Parietalperitoneumadherestospleen:Exceptatsplenichilum.
Ligaments Splenophrenic and splenocolicligaments—relativelyavascular Splenorenalligamentextendsfromanteriorleftkidneytohilumofspleenastwolayer,enclosessplenicvesselsandtailofpan-creasinvested.
Theabovetwolayercontinuetothegreatercurvatureofstomachtoformtwoleavesofgastrosplenicligament
Blood supply• Splenic artery:Branchfromceliacarteryrunsalongsuperiorborderofpancreas
• Splenic vein:Fivemajortributariesjointoformsplenicveininsplenorenalligamentandrunsinferiortoarteryandposteriortothepancreatictailandbody
• Joinwithsuperiormesentricveintoformportalveinatneckofpancreas
• Rememberinferiormesentericveinoftenemptiesintothesplenicvein.
SpLenic function1. Mechanical filtration (most important function) Asplenic condition (peripheral blood)○ Removalofsenescenterythrocytes○ ClearingpathogenthatresideinRBC(malaria,bartonella)○ Ironisremovedfromdegradedhemoglobinandreturnedtoplasma(culling)**
○ Essentialtomaintainnormalerythrocytemorphologyandfunc-tion.
○ Thisfunctionresultsinanemiainconditionassociatedwithab-normalredcellmorphology(e.g.hereditaryspherocytosis,sicklecellanemia,thalassemia,etc.)
Targetcells(immaturecells)Howell-Jollybodies(nuclearremnant)Heinzbodies(denaturedHb)Pappenheimerbodies(irongranules)StipplingSpurcells
Contd...

tahir99 - UnitedVRG
175Spleen
SpLenic function2. Immune function 3. pitting
○ SynthesisofimmunoglobinM○ Synthesisofproperdin,tuftsin(theseantibodiesareofB&Tcelloriginandreactwithbacteriaandfungitorenderthemmoresusceptibletophagocytosis.
○ Particulateinclusionfromredcellsareremovedandrepairedredcellsarereturnedtocirculation.
4. Reservoir function 5. cytopoiesis○ Contain8%ofredcellmass. ○ From4thmonthofintrauterinelife,somedegreeof
hemopoiesisoccurinfetalspleen.
SpLenic trAumA○ M/corganinjuredinbluntabdomentrauma○ M/cindicationforlaparotomyafterbluntinjuryabdomen
○ M/cassociatedfindingisleftlowerribfracture(44%case)
Clinical features Radiological feature of splenic rupture○ Classictriadofacutesplenicinjury:ElevatedlefthemidiaphragmLeftlowerlobeatelectasisPleuraleffusion.
○ Balance sign unilateralshiftingdullness○ Kehrs sign painreferredtotipofleftshoulderduetoirrita-tionofundersurfaceofthediaphragmwithbloodandthepainisreferredtotheshoulderthroughtheaffectedfibersofphrenicnerve(c4&c5)
1.Obliterationofpsoasshadow2.Obliterationofsplenicshadow(mostimportantradiologicalsign)
3.Elevationofleftdiaphragm4.Medicaldisplacementofgastricairbubble*
Grades of splenic injury• Grade 1—subcapsularhematoma<10%surfacearea,laceration<1cmdeep
• Grade 2—subcapsularhematoma10%–50%surfacearea,laceration1–3cmdeep.
• Grade 3—subcapsularhematoma>50%surfaceareaorexpanding,laceration > 3 cm deep
• Grade 4—lacerationinvolvingsegmentalorhilarvesselswithmajordevascularization
• Grade 5—shatteredspleen,hilarvesselinjurywithdevascularizedspleen.
Treatment○ Conservativetreatmentofsplenicrupturehasgainedfavoroverrecentyears
Complication of conservative management• PresenceofvascularblushonCTscanafter3dayindicatesfalseaneurysmsofintraparenchymalbranchesofsplenicarteries(theseaneurysmscausedelayedruptureofspleen)
Non-operative managementindications Indications of splenectomy in trauma○ Canbetriedforhemodynamicallystablecases.○ Evengrade4,5injuriesarenowtakenupforcon-servativemanagement
○ Recently splenorrhaphy for grade 2, 3 and mesh wrapping for 4, 5 injuries are done.
UnstablepatientWhenotherinjuriesinabdomenrequirepromptattentionSpleenisextensivelyinjuredwithcontinuousbleedingBleedingassociatedwithhilarinjuryRuptureofpathologicalspleen
Contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery176
SpLenectomyindications
• Trauma:Immediate,delayed,spontaneousrupture• Neoplasms:Lymphomas,leukemias,hemangiomas• As part of other surgeries:D2resection(gastrectomy):pancreatectomy,splenorenalshunt:
• Miscellaneous:Abscess,infarct,aneurysm,cyst,topre-ventgraftrejection.
• Hematological:1.Foranemia2.Forpurpura3.Hypersplenism4.Myelofibrosis.
Splenectomy always indicated○ Primarysplenictumor○ Hereditaryspherocytosis
HemAtoLogicAL indicAtionSFor anemia
1. Intracellular defect•Membrane abnormality Hereditaryspherocytosis Hereditaryelliptocytosis
•Enzyme defect G6PDdeficiency Proteinkinasedeficiency
•HemoglobinopathiesThalassemiasSicklecelldisease(rarelyindicated3%)
2.Extracellular defect:Autoimmunehemolyticanemia○For purpuraIdiopathicthrombocytopenicpurpuraThromboticthrombocytopenicpurpura
○For primary hypersplenism ○For myelofibrosis
Splenectomy not indicated for:• Asymptomatichypersplenism• Splenomegalywithinfection• SplenomegalyassociatedwithelevatedIgM
• Hereditaryhemolyticanemiaofmoderatedegree• Acuteleukemias• Agranulocytosis.
○ MCindicationforsplenectomysplenictrauma○ MCindicationforsplenectomyinelectivesettingITP
compLicAtionS of SpLenectomy○ MCinfectionaftersplenectomyStreptococcus pneumonia
immediate Intermediate delayed• Hemorrhage• Gastricdilatation• Hematemesis
• Leftbasalatelectasis(MC complication after splenectomy—16%)
• Pancreaticfistula,pancreatitis,pseudocyst• Gastricfistula(duetoperforationassmallgastricvesselsarecutduringsurgery)
• Subphrenicabscess/hematoma.
• Thromboembolicepisodes(duetothrombo-cytosisasgreaterthansevenandhalflakhsplateletsgetsaddedaftersplenectomy)
• Overwhelmingpostsplenectomyinfection(OPSI)
• Portalveinthrombosis.
overwHeLming poStSpLenectomy infectionBacterial infection Protozoan infection after splenectomy• Streptococcus pneumonia• Haemophilus influenzatypeB• Meningococcus• GroupAStreptococcus
• Babesia• MalariaNo increased risk of viral infection
Contd...

tahir99 - UnitedVRG
http:/
/vip.p
ersian
ss.ir/
177Spleen
overwHeLming poStSpLenectomy infectionThe following vaccination are given:
Two week before planned splenectomy Postsplenectomy prophylaxis○ Pneumococcalvaccine:boostedevery5years○ H.influenzatypeB(Hib)vaccine○ Influenzavaccine—annually○ Meningococcalvaccine:
AntibioticprophylaxiswithpenicillinV250mgbd(or)erythromycin250mgbdforlongerofthefollowing1.2yearspostsplenectomy(or),2.Uptoageof16years.
RiskofdevelopmentofOPSIishighforhematologicindicationsthenthose,whoundergosplenectomyfortrauma.
HemAtoLogic effect of SpLenectomyImmediately after splenectomy Returntonormalwithin2–3week
• Leukocytosis• Thrombocytosis.
Chronic manifestationsAnisocytosisandpoikilocytosisHowel-Jollybodies(nuclearremnants)Heizbodies(denaturedhemoglobin)Basophilicstipling.
SpLenic tumorS○ M/cbenigntumorofspleen—hemangioma○ M/cmalignanttumorofspleen—hemangiosarcoma
Accessory spleen○ M/ccongenitalanomalyofspleen○ 80%accessoryspleenareinsplenichilumandvascularpedicle○ Otherlocationsaregastrocolicligament,tailofpancreas,greateromentum,greatercurvatureofstomach,splenocolicligament,smallandlargebowelmesentry,leftbroadligamentinwomen,leftspermaticcordinman.
Splenosiso Ruptureofspleenanddistributionofitstissueonperitoneum
SpLenic-gonAdAL fuSion• Rarecongenitalanomalyinwhichectopicsplenictissueuniteswithagonad(<200casesreported)• Continuousordiscontinuous.• Continuous:Spleenconnectedtoectopicsplenicmassbycordofsplenicandfibroustissue.
• Discontinuous:Noconnectionbetweenspleenandectopicsplenicmass.
20%ofcontinuoustypesassociatedwithothercongenitaldefects,includingperomelus(fetuswithmalformedlimbs)andmicrognathiaalsotesticularectopia,inguinalhernia.
Diagnosis:TechnetiumTc-99msulfurcolloidscan
Treatment:Surgicalexcisionofectopicsplenictissuetopreventtesticu-laratrophy,torsionorinfarctionandpreservefertility.
Contd...

tahir99 - UnitedVRG
http:/
/vip.p
ersian
ss.ir/
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery178
Splenorenal fusion Hypersplenism Felty syndrome• Maybeduetosplenosisaftersplenictraumaorsplenectomyorlesscom-monly,beadevelopmentalanomalyresultinginfusionofsplenicandrenaltissue
• Maypresentasarenalmassorwithsymptomsofhypersplenism
• Itisaconditioncharacterizedbysplenomegaly,cytopenia(anemia,leucopeniaandsplenomegaly)normalorhyperplasticbonemarrowandanexcellentresponsetosplenectomy.
• Rheumatoidarthritis+leucope-nia+splenomegaly
• Splenectomyproducesonlyatransientimprovementinbloodpicture,butrheumatoidarthritispreviouslyresistanttosteroidnowrespondswell.
SpLenic Artery AneurySm• Incidence:0.04%–1%• M/cinfemales;m/cin6thdecade*• M/csolitary(multipleaneurysmsareseenin1/4thcases)
etiology1. Intra-abdominalsepsis2.Pancreaticnecrosis3.Arteriosclerosis(elderly)
Clinical features TreatmentUsuallyasymptomatic(83%caser)½thecasesruptureinyoungage<45-year-old,¼ruptureinpregnantwomen(inthirdtrimesteroratlabor)
○ Notreatmentneededinasymptomaticandlesions<2cm○ Symptomaticlesionandlesions > 2 cmrequiresurgery○ Treatmentofchoice—splenectomyandremovalofdiseasedartery○ Ifexcisioninnotpossibletheproximalanddistalendsofthesacareligatedtoallowthrombosisofsplenicartery.
○ Embolizationofsplenicartery(inunfitcases)
SpLenic infArctionetiology CT scan:Perfusiondefectinenlargedspleen
MyeloproliferativesyndromePortalhypertensionPancreaticdiseaseSplenicveinthrombosisSicklecelldisease
TreatmentConservativeonlySplenectomyconsideredonlywhenasepticinfarctcausesanabscess*
IdIoPATHIC THRoMBoCyToPeNIC PuRPuRA (ITP)• Autoimmunedisorder• Presentwithlowplateletcountandmucocutaneousandpetechialbleeding• Lowplateletisduetotheantiplatelet IgG autoantibodiesproducedinspleen
• Plateletcountlessthan10,000/mmcubeareatriskofinternalbleeding• Inadditiontolowplateletcount,presenceofimmature(megathrombocytes)ispathognomonicofITP
• Most common indication for elective splenectomy • Forpatientswithlowplateletcountshouldhaveplateletsavailableatsur-gery,butshouldbeinfusedonly after ligating the pedicle
• Shouldnotbegivenpreoperatively• Thetreatmentofchoiceismedical—oral prednisolone 1 mg/kg producesdramaticresponsein50%–70%cases
• Intravenousimmunoglobinisindicatedforinternalbleeding.
Splenectomy is indicated for: 1.Failureofsteroids.2.Undesirableeffectsduetolonguseofsteroids.
3.Mostcasesoffirstrelapse.

tahir99 - UnitedVRG
http:/
/vip.p
ersian
ss.ir/
179Spleen
fmge queStionS
1. True regarding hemangioma of the spleen: (March 2006)
a. Leastcommonbenigntumorofthespleen b. Maytransformtohemangiosarcoma c. Malignanttransformationmaybemanaged
conservatively d. NoneoftheaboveAns: b (May transform to hemangiosarcoma)
2. Splenectomy can lead to: (Sep 2008) a. Leukopenia b. Thrombocytosis c. Thrombocytopenia d. ThrombocytopeniaandleukopeniaAns. b (Thrombocytosis)
3. Indications of splenectomy are all, except: (Sep 2007) a. Hereditaryspherocytosis b. Trauma c. Polycythemia d. IdiopathicthrombocytopenicpurpuraAns: c (Polycythemia)
4. Splenectomy is most useful in: (March 2007) a. Hemophilia b. Polycythemia c. Hereditaryspherocytosis d. ThalassemiaAns: c (Hereditary spherocytosis)
5. All of the following are common cause of post- splenectomy infections, except: (Sep 2006)
a. H. influenza b. E. coli c. Meningococcus d. Streptococcus Ans. b (E. coli)
6. All of the following are true regarding splenic rupture, except: (March 2005)
a. Elevationoftheleftdomeofdiaphragm b. Obliteratedpsoasshadow c. Obliteratedcolonicgasshadow d. ObliteratedsplenicoutlineAns. c (Obliterated colonic gas shadow)
7. In which of the following conditions splenectomy is not useful: (Sep 2008)
a. Hereditaryspherocytosis b. Porphyria c. Thalassemia d. SicklecelldiseasewithlargespleenAns. b (Porphyria)
8. Splenectomy is not done in: (March 2011) a. Trauma b. Tuberculosisofspleen c. Hereditaryspherocytosis d. SplenicabscessAns: b (Tuberculosis of spleen)

tahir99 - UnitedVRG
16Urological SUrgery
KIDNEY AND URETERSTypes of renal calculus
1. Calcium oxalate calculus (Most common) They have hard, small and jagged surface
2. Phosphate calculus Usually calcium phosphate, but sometimes is combined with
ammonium and magnesium to form the triple phosphate cal-culus ammonium magnesium phosphate
Also k/a struvite stone Smooth and dirty white and solitary Seen in alkaline urine especially with proteus infection, which
split urea to ammoniaThistypeofcalculusmayenlargetofillallormostofrenalcol-
lecting system forming a staghorn calculus*3. Uric acid and urate calculus These are radiolucent
4. Cystine stones Uncommon, seen in cystinuria Appear only in acid urine*Theyarepinktoyellowwhenfirstremoved,
but they change color to a greenish hue when exposed to air
6. Indinavir calculiIndinavirisproteaseinhibitorusedinacquiredimmunodeficien-
cy syndrome (AIDS) patients. It results in calculi in ~ 6% patient who use indinavir.
Indinavir calculi are radiolucent7. Phosphate or struvite stones They are infection stones associated with urea splitting organ-
isms, i.e Proteus, Pseudomonas, Providencia, Klebsiella, Staphylococ-cus and Mycoplasma
The high ammonium concentration derived from urea—split-ting organisms results in an alkaline urinary pH, required for the precipitation of phosphate crystals
5. Xanthine calculi These are radiolucent Thesearesecondarytoacongenitaldeficiency
of xanthine oxidase

tahir99 - UnitedVRG
181Urological Surgery
Dietl crisis: After an attack of acute renal pain, a swelling in the loin is found. Few hours later, following the passage of large amounts or urine, the pain is relieved and swelling disappears
Position of stone Site of pain At pelviureteric junction or
upper ureter Pain radiates to the testicles
At middle of the ureter (i.e. at crossing of gonadal ves-sels and ureter)
Pain is referred to McBurneys point on the right resembling appendicitis and on left simulates diverticulitis
At lower ureter or at pelvic brim
Pain is referred to inner side of thigh, groin
In the intramural ureter Strangury (painful and fruitless desire to micturate)
METHODS OF STONE REMOVALExtracorporeal shock wave lithotripsy (ESWL) Stones in calyceal diverticulum○ TheleastinvasiveandmostwidelyusedisESWL○ Conservativeapproachisusedwhenthestoneis4 or 5
mm in diameter○ Alsoknow•Steinstrasse: Is a new medical term, literally meaning ‘stone streetItiscondition,whichfollowstheuseofESWL Small pieces of fragmented calculi collect and
obstruct in the distal ureter, like sand occluding a straw
• Calycealdiverticulasarecongentialanomalies.Thesediverticula are usually drained by a narrow connection to the collecting system. So when a calyceal stone is broken by ESWL,thepassageoffragmentsishamperedbythenarrowconnection.ThishasleadtolowsuccessrateofESWL
• Percutaneous nephrolithotomy (PCNL) is more effective than ESWL for stones in calyceal diverticulum
Inference:• EventhroughESWLisnotverysuccessfulforstonesof
calyceal diverticulum. It is not a contraindicationContraindications for ESWL
Absolute contraindications Relative contraindications1. Uncorrected bleeding disorder2. Pregnancy
1. Urinary tract infection (UTI)2. Urinary tract obstruction distal to stone3. Cardiac pacemaker4. Severe orthopedic deformity5. It is a contraindication only if it prevents proper positioning of the stone at the F2
focal point6. Severe renal failure7.Cysteinestones,becauseofthephysicalpropertiesofitscrystallattice,ESWLisnot
effective in fragmenting it 8.Weight>300pound9.Lowerureteralstonesinwomenofchildbearingage
URETEROSCOPY• ‘Ureteroscopicstoneextractionishighlyefficaciousfor
lower ureteral calcui’, stones can be caught in baskets or endoscopic forceps. Those that cannot be removed via baskets or endoscopic forceps, are fragmented using ureteroscopic lithotrites
• Any renal calculi that is 4 mm or less in size, is allowed some time (approx 4 week) to pass spontaneously
Contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery182
URETEROSCOPYIndications for surgical removal of a ureteric
calculus Stone is too large to pass spontaneously Urine is infected Repeated attacks of pain and the stone is not moving It is enlarging
It causes complete obstruction Stone is obstructing solitary kidney or there is bilateral obstructions
PERCUTANEOUS NEPHROLITHOTOMY (PCNL)• PCNL:Shorthospitalstay• PCNL:Minimummorbidity
• PCNLsuccess:Similartoopenoperation• TheoverallcostmaynotbedifferentofopenandPCNLoperation
Indications Complications of pcnlLargecalculi>2.5cmsize Infected calculi Cystine calculi Obstructive uropathies FailedESWL Anatomic abnormalities Recurrent large calculi after open operation
Bleedingbloodtransfusion3%–10% Septicemia—more with struvite calculusPerforationandextravasationoffluid Pleural injury—upper calyceal puncture Duodenal Injury/colon injury (subcostal approach) Liverandspleeninjuries—rare Injury to vessels: Renal vein, renal artery or inferior vena cava (IVC)—rare
Contd...

tahir99 - UnitedVRG
183Urological Surgery
RENAL CELL CARCINOMA○ Arenalcellcarcinoma(RCC)thathasspreadtorenalvein,IVCorevenuptothethorax(heart)isoperable○ ApreopbiopsyisnotnecessaryasaRCC is the most common malignant neoplasm of kidney (90%–95%) and any solid
renal mass is considered to be RCC until unless proved otherwise○ AchestX-rayshouldbedonetoruleoutpulmonarymetastasisasitwillmaketheCaofstageIVwithworstprognosis
and also decide the t/t plan
More about renal cell carcinoma Risk factors• Itisthemeningalcoreinomatosis(MC)malignantneo-plasmofkidney(90%–95%)
• MCsiteoforiginisproximalconvolutedtubules*• RCCoriginatesinthecortexandtendstogrowoutinto
perinephric tissue • Usuallysituatedatpoles(commonlyatupperpole)*• Malefemaleratiois2:1*• Age—5thto6thdecade
• Cigarettesmoking*• Obesity*• Polycystickidneydisease• Tuberoussclerosis*• VonHippel-Lindau(VHL)syndrome (cerebellar hemangioblastoma, retinal angimatosis and B/l
renal cell Ca)
○ Histologically RCC is an adenocarcinoma.IthasbeenreclassifiedintosubtypesofwhichclearcellsCaistheMCtype
Cytogenetics of various subtypes of renal cell (Ca)Clear cell carcinoma Papillary carcinoma
○ Itisthemostcommontype(70–80)○ Thesetumorscanbe• Familial•AssociatedwithVHLdiseaseor• Sporadic(95%)
Almost all (98%) of clear cell carcinomas are associated with loss of se-quences on short arm of chromosome 3. The lost sequences include the VHLgene.
TheVHLgeneactsastumor-suppressorgenetheloss,ofwhichisassoci-ated with clear cell Ca
○ Alsooccursinbothfamilialandsporadicforms
○ Thecytogeneticabnormalitiesassociatedwith papillary Ca are: Trisomies 7, 16 and 17 and loss of Y is
male patients for sporadic form Trisomy 7 in the familial formFamilialformisassociatedwithMET
proto-oncogene.
Chromophobe carcinoma Oncocytoma○ Oncytogeneticexaminations,thesetumors
exhibit multiple chromosome losses and extreme hypoploid
○ Associatedwithlossofchromosome1andY○ Renal medullary Ca is a relatively new histologic subtype of RCC that
occurs almost exclusively in association with the sickle cell trait.
Contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery184
Classical triad of RCC consist of• Hematuria*• Flankpain*• Palpableflankmass*EarliestandMCpresentingfeatureis
hematuria*
Paraneoplasitc syndromes○ Feverofunknownorigin*○ Anemia*○ Erythrocytosis*(d/tsecretionoferythro-
poietin* by RCC) (butanemiaisamorecommonfinding)*
○ Hypertension○ Abnormalliverfunction
(stauffers syndrome, * i.e. nonmetastatic hepatic dysfunction)
○ Hypercalcemia*○ Neuromyopathy*○ Amyloidosis*○ Increased (ESR) (MC paraneoplastic syndrome)*○ Dysfibrinogenemia
○ Cushingsyndrome*○ Galactorrhea○ Feminizationandmasculinization
Important points in RCC• MCrouteofmetastasisishematogenous • MCsiteofdistantmetastasisislung* (canonball secondaries, secondaries may be
pulsatile)
• Investigationofchoice CT scan*• Treatmentofchoice Radical nephrectomy• Radiotherapy,chemotherapyorhormonaltherapyhavelittleroleinRCC
t/t
Treatment○ Partialnephrectomyisnowbeingusedasprimarysurgicaltherapyforpatientswithtumor<4cminsize. For tumor < 4 cm—partial nephrectomy For tumor > 4 cm—radical nephrectomy
Radical nephrectomy includes removal ofi. KidneyandGerota’sfasciaii. Ipsilateral adrenal
iii. Renal hilar lymph nodesiv. Proximal half of ureter
The renal cell Ca is prone to grow into the renal vein. Produce cannonball mets in lung and mets are highly vascular, which may pulsate (also in follicular Ca thyroid)
MC POINTS○ MCsiteofdistantmetastasisfromlungCa Adrenals *next is liver, brain○ MCsitefordistantmetastasisfrombreastCa Vertebrae ○ MCsitefordistantmetastasisfrombladderCaLung*○ MCsitefordistantmetastasisfromcolorectalCaLiver*○ MCsitefordistantmetastasisfrommelanoma(cutaneous) Skin/subcutaneous tissue lung*○ MCsitefordistantmetastasisfrommelanoma(ocular)Liver*○ MCsitefordistantmetastasisfromprostate bones*○ MCsitefordistantmetastasisfromsoft-tissuesarcomaLung*○ MCsitefordistantmetastasisfromtestisCaLung*○ MCsitefordistantmetastasisfromthyroidCaBone*,Lung*○ Metastasistolungismostcommonlyfrom Breast Ca*
RENAL CELL CARCINOMA
Contd...

tahir99 - UnitedVRG
185Urological Surgery
WILM’S TUMORAnomalies associated with Wilm’s tumor
○ ChromosomalanomaliesassociatedwithWilm’stumor 8th & 11th○ MCandearliestsymptom Abdominal lump○ MCsiteofdistantmetastasis Lung○ MCpresentationispainlessabdominalmassusuallydiscoveredbythe
mother while routinely bathing the baby other signs and symptoms are Abdominal pain, fever, abdominal distention, hematuria Anorexia, hypertension, nausea and vomiting
• Hemihypertorphy• Perlmansyndrome• Aniridia• WAGRsyndrome{Wilmstumor,aniridia,genitouri-
nary anomalies (horseshoe kidney), retardation of intellect}
• Beckwith–Wiedemannsyndrome*• Cryptorchidism• Denysdrashsyndrome• Hypospadias
○ Thisisamixedtumorcontainingepitheliumandconnectivetissueelementsarising from embryonic nephrogenic tissue
○ Triad of: Abdominal mass Pyrexia Hematuria
Treatment○ Theimmediatetreatmentforunilateraltumorsissurgical
removal of the affected kidney even if pulmonary metasta-sis are present
○ Wilm’stumorisbothchemo sensitive and radiosensi-tive tumor. So both chemotherapy and radiotherapy play significantroleinitstreatment (cf. Renal cell Ca is both chemoresistant and radiore-
sistant)
○ CombinationchemotherapyusedinvincristineandactinomycininlocalizeddiseaseandDoxorubicin added for advanced disease.
○ Radiotherapyisusedforadvanceddisease.ThepostoperativeradiotherapyinWilm’stumoris
started within 10 day of surgery Delay in starting radiotherapy beyond ten days leads to
tumor cells repopulation and increases the relapse rate
THE FOLLOWING ARE THE DIFFERENTIATING FEATURE BETWEEN NEUROBLASTOMA AND WILM’S TUMORa.Calcification:Therearefactofcalcificationvisible in neuroblastoma (about
85%), which are generally less common and less prominent in Wilm’stumor(<15%)
b. Location Wilm’stumorandneuroblastomcanbedifferentiatedonlocationtoo.Computedtomograpy(CT)findingswillconfirmtheintrarenallocationofwilm’swhereasneuroblastoma will be seen above the kidney pushing it downwards and outwards
c. Intraspinal extension: IntraspinalextensionisseeninneuroblastomanotinWilm’s
tumor d. Crossing midline Wilm’stumorsaretypicallyconfinedtoonesideofthe
abdomen, whereas neuroblastoma usually cross the midline
e. Aorta and IVC invasion Wilm’stumorinvadesaortaandIVC.Whereasneuroblastoma
does not invade these structures
ANGIOMYOLIPOMA OF KIDNEY○ Angiomyolipomaisabenigntumorofkidney(infact,itisahamartomaandcharac-
teristically presents with fat in the lesion)○ Itischaracterizedby3majorhistologicalcomponents.○ Thereareasthenamesuggests:Bloodvessels,smoothmuscleandfatcells Angiomyolipoma may occur as an isolated phenomenon or in association with
tuberous sclerosis. Angiomyolipoma occurs in 50% of patients with tuberous sclerosis
Signs and symptoms and angiomyolipomas• Hematuria • Hypovolemicshock• Flankpain • Hypertension• Palpablemass • Anemia
Contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery186
ANGIOMYOLIPOMA OF KIDNEY○ Sometimesitpresentswithspontaneous
retroperitoneal hemorrhage (k/a Wunderlich’s syndrome)
○ TheinvestigationofchoiceisCT scan, which shows the presence of fat within the lesion
Treatment• Inasymptomaticandlesionlessthan4cminsize observation and
follow-up with annual imaging • Inlesions>4cmwithnoormildsymptoms follow-up with biannual
imaging• Inlesionlargethan4cmwithmoderateorseveresymptomsuchaspain
and hemorrhage selectiveembolizationorpartialnephrectomy
GENITOURINARY TUBERCULOSIS (TB)• Genitourinarytuberculosisisalways
secondary to pulmonary infection, though in many cases has healed or is quiescent.
• Infectionoccursviathehematogenous route.
• Inearly renal tuberculosis, the only ra-diological abnormality may be irregular-ity or destruction of papillae.
• Most sensitive modality to detect it is intravenous urogram (IVU) as it can show detailed calyceal anatomy
Advanced changes are1.Calcification This may occur in any part of genitourinary tract, most commonly in kid-
ney, next in ureter2. Cavities 3. Fibrosis leading to obstruction Fibrotic strictures of the pelvis or ureters lead to hydronephrosis Strictures of the calyceal neck leads to hydro calyces (or hydrocalicosis)
4. Bladder changes Bladder wall may appear thickened and trabeculated and bladder may be
small, contracted (thimble bladder).Inlaterstagesvesicoureteralreflux(VUR)mydevelop
○ Computedtomography:Showsadvancedchangeswell,butislesssensitiveinearlystagesasitcannotdetailcalycealanatomy
○ ‘Sterilepyuria’istheruleButabout15%–20%ofpatientswithtuberculosishavesecondarypyogenicinfection,obscuringthecluepyuriaTheTuberclebacillicanbeidentifiedonAFBstainingof24hrurinespecimenorthefirstmorningurinecollectedon3
successive days. Acidfastbacilli(AFB)stainingispositiveinabout60%ofcases.
○ Mostcommonsiteofgenitourinarytuberculosisis Kidney ○ Commonestcauseofpyelonephritisis E. coli
RENAL TRAUMA○ Approachtokidneyshouldbetransperitoneal to exclude the pos-
sibility of damage to other abdominal organs ○ Approachshouldnotbelumbar.○ “Surgical exploration is needed in < 10% of closed injuries and
is indicated if either there is progressive blood loss or there is an expanding mass in the loin”
○ More than 90% of all blunt renal injuries are managed conserva-tively
• Anintravenouspyelogram(IVP) is done urgently to assess the damage to the kidney and to know the functioning of the other kidney
• Hematuria is the cardinal sign of a damaged kidney, but it may not appear until some hoursaftertheinjury.Thisispresentin>95%of patients with renal injury. The degree of hematuria does not precisely correlate with severity of injury
Closed renal injury almost always extraperitoneal. The exception is seen occasionally in young children with
very little extraperitoneal fat. Their peritoneum is in close contact to the kidney and can tear with the renal capsule.
Complications of renal trauma1. Pararenal pseudohydronephrosis2.Hypertensionresultingfromrenalfibrosismayoccur3
month or more after injury3. Aneurysm of renal artery
Contd...

tahir99 - UnitedVRG
187Urological Surgery
POLYCYSTIC KIDNEY DISEASE• Adultpolycystickidneydisease(PKD)• Inheritanceisautosomaldominant(AD)• Diseasemanifestsitselfinadultlife
• InfantilePKD• Inheritanceisautosomalrecessive(AR)• Diseasemanifestsininfancyassevererenalfailureandlifeexpectancyis
short
Adult PKD• Almostalwaysbilateral (95%)• Diseaseordinarilydoesnotmanifestitselfbefore40 yr of age.• Pathology The kidney is enlarged 3 to 4 time Cysts are distributed evenly throughout the cortex and medulla Content of the cyst varies, but it is not urine Renal tissue is progressively replaced by cysts leading to chronic renal failure (CRF)
Associated anomalies with ADPKD Clinical presentation Urine examination1. Cysts in liver, spleen, pancreas and
ovaries (lungs)2. Berry aneurysm3. Mitral valve proplase4. Colonic diverticulosis 5.Congenitalhepaticfibrosis
• Mass• Pain• Hypertension (70%–80% of cases)• Hematuria• Infection• Uremia
• Highoutputofurine• Lowspecificgravity• Itmaycontaintracesofalbu-
min
○ Three forms of ADPKD have been identified• ADPKD 1 Accounts for 85% cases Its gene is found on chromo-
some 16p
• ADPKD 2 Its gene has been mapped to chromosome 4q It appears to have a later age of onset of symp-
toms and renal failure than ADPKD 1
• ADPKD 3 It has not been mapped to
a gene up till now
Treatment○ Decompositionoruncappingofcysts(Rovsingoperation)isofnouseinpreservingtherenalfunction○ ItultimatelyleadstoCRFandrenaltransplantationistheonlydefinitet/t
ECTOPIC URETER• Inthemale,theposterior urethra is the most
common site of termination of an ectopic ureter • Locationofectopicureters(indecreasingorder)
○ More about ectopic ureters•Ectopicuretersareusuallyassoci-
ated with duplicate ureters (in 80% cases) but may also occur in single ureters systems
•More common in females•Theuretersfromtheupperpelvis
opens distally and medially to its fellow ureters
•Mostcommonsymptom In males recurrent UTI In females incontinence (para-
doxical incontinence)
In males In femalesPosterior urethraSeminal vesicleProstatic utricleEjaculatoryductVas deferens
UrethraVestibuleVaginaCervix or uterusGartnerductUrethral diverticulum
• Inamalepatient;theectopicuretersopensalwaysabovetheexternalurethralsphincter(thebulbarurethraisbelowtheexternal urethral sphincter)
• Infemalespatients;anectopicuretersmayopenaboveorbelowtheexternalurethralsphincterEctopicopeningbelowtheexternalurethralsphincterleadstourinaryincontinence,‘continuousincontinenceinagirlwithanotherwisenormalvoidingpatternaftertoilettrainingistheclassicsymptomofanectopicureteralorifice’

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery188
CONGENITAL PELVIURETERIC JUNCTION OBSTRUCTION (PUJ OBSTRUCTION)• Itwasearlierbelievedthattheaberrantrenalvesselsisresponsibleforcausingthecong. Pelvi ureteric junction (PUJ) obstruction Bailey writes that “aberrant vessels probably
do not cause hydronephrosis, although a hydronephrotic renal pelvis bulge between renal vessels”
• Cambellsurologywrites “whether the aberrant vessel causes obstruction or is a co-variable that exist alone with an intrinsic narrowing is unclear”
Important points about congenital PUJ obstruction• CongenitalPUJobstructionisthemostcommoncauseofsignificantdilatationofthecol-
lecting system in the fetal kidney• Incidenceismore in boys (2 : 1)• Usually unilateral,butbilateralin10%–40%cases
Associated anomalies• Renaldysplasia• Multicysticdysplastickidney• Renalagenesis(5%ofchildren)
• Vesicouretericreflux• PUJobstructionwasnotedin21%ofchildrenwiththeVATERgroupanoma-lies(VATERstandsforvertebraldefects,imperforateanus,tracheoesophagealfistula,radialandrenaldysplasia)
Most common presentation of cong PUJ obstruction is asymptomaticDiagnostic tools Surgical repair• Majorityofcasesarediagnosedprenatallywithhelpofultra-
sound•Whitakertest(pressureflowstudies)canbeusedtofindoutobstructiontoflowofurine.InWhitakertest,cathetersareplaced in renal pelvis and bladder. Fluid is infused into the kidney and the pressures are measured. A differential pres-sure between kidney and bladder could then be indicative of obstructiontotheflow
• Retrogradepyleographycanbeusefultolocatethesiteofobstruction
• CongenitalPUJobstructionarecorrectedbyeitheropen surgical techniques or endoscopic and laparo-scopic approaches
• Outoftheopentechniques,theAnderson-Hynes dismembered pyeloplasty is the most commonly employed technique
• EndoscopicapproachesincludeEndoscopicpyelotomy Balloon dilation Stent placement
MEDULLARY SPONGE KIDNEY• Medullary sponge kidneyisacongenitaldisordercharacterizedbycysticdilationofinner
medullary and papillary collecting ducts• Patientsgenerallypresentwith: Kidney stones Recurrent hematuria Infection (UTI)
• Mostcasesaresporadic,whilesomeshowautosomaldominantinheritance• Involvementisbilateralinmostcases
RENAL TRANSPLANTATION• First the type of grafts○Allograft—anorganortissuetransplantedfromoneindividualto
the other○ Isograft—atransplantbetweenidenticaltwins○Orthotopicgraft—atransplantplacedinitsnormalanatomicsite
• Types of donorDonors are of 3 types:○Livingdonor○ Braindead,heartbeatingcadavericdonors○Non-heart-beating(asystolicdonors)
Contd...

tahir99 - UnitedVRG
189Urological Surgery
RENAL TRANSPLANTATION○Heterotrophic—atransplantplacedinasitedifferentfromwheretheorgansisnormallylocated
• Renal transplant is a heterotrophic graft because the transplanted kidney is not placed in its normal anatomic position, but is placed in the iliac fossa in the retroperitoneal position leaving the native kidney in situ
Organ procurement○ Inbrainstemdeaddonor,theorgantobeprocuredshouldbe
preserved to maintain its functional integrity○ Forthispurposetheorganshouldbeperfusedwiththeorganpre-
servative solution twice, before it is transplanted to the recipient○ Thefirstperfusion is done just after the abdomen is opened at
laparotomy and the second perfusion is done just after the organs has been removed from the donor
○ CommonlyusedpreservativesolutionincludeUW solution (university of wisconsin) and Eurocol-lins solution
○ Afterremovalfromthedonor,theorganisplacedin two sterile bags and stored at 0–4°C by im-mersion in ice, while they are transported to the recipient centre
Immunosuppresive drug in renal transplant○ Calcineurin blockers are especially useful in renal transplant pa-
tients. These include cyclosporine and tacrolimus ○ Skin cancer is the commonest cancer on im-
munosuppression in renal transplant.
RENAL CASTS• Albuminsecretedfromtheglomerulidonotformcasts.Thiswe
know from our knowledge of various diseases, e.g. in nephritic syndrome there is hyperalbuminuria, but no casts are seen in urine
• Hyalinecast,whichmaybeseeninnormalindividualsareformedfrom Tamm-Horsfall proteins secreted by epithelial cells of loop of Henle
Types of casts • Waxycasts CRF• Broadcasts CRF• Browngranularcasts acute renal failure (ARF)• Whitebloodcells(WBC)cast pyelonephritis• Redbloodcells(RBC)cast glomerulonephritis
Some important appearancesRadiological features Seen in Spider leg appearance Polycystic kidney Cobra head appearance Ureterocele Flower vase appearance on ureters Horseshoe kidney Sandy patches Schistosomiasis of bladder Soap bubble appearance/Rim sign Hydronephrosis Apple-core lesion on barium enema Ca colon Claw appearance on barium enema Intussusceptions Saw tooth appearance Diverticula of colon Birds beak appearance of esophagus on barium meal Achalaisa Corkscrew appearance of esophagus on barium meal Diethylstilbestrol(DES) String sign of Kantor Crohn disease Thumb printing sign Ischemic colitis
XANTHOGRANULOMATOUS PYELONEPHRITIS○ Xanthomeanslipidfoamcells○ Xanthogranulomatouspyelonephritisisavariantof
chronic pyelonephritis that characteristically presents in middle aged patients with a poorly functioning kidney (as in diabetic)
○ Onhistologythereareareasofclearcellsthatarelipidladenmacrophages
○ Theseareasoflipidlaidenmacrophageappearasfatdensitylesion on U/S
○ Thispyelonephritisisoftenaccompaniedbyacalculus and proteus infection.
Contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery190
NEPHRECTOMY APPROACHES• Therearetwocommonmethodstoapproachkidneyfornephrectomyorotherwise:○ Thetransperitonealabdominalapproach○Theretroperitonealloinapproach
• Theretroperitoneal loin approach is preferred method except for two conditions: Malignant tumors Renal injury (peritoneum is opened to exclude other
injuries)
• InloinapproachfollowingmusclearecutLatissimusdorsi Serratus posterior inferior 3 lateral muscle of the abdominal wall○Externaloblique○ Internaloblique○Transverseabdominis
URETEROCELE• The‘adder head ’ or ‘cobra head ’appearance on excretory urography
is noted in ureteroceles Ureterocele is a ballooning of the distal submucosal ureters into the
bladder Ureterocele is thought to result from congenital atresia of the ureteric orifice
Although present from childhood the condition is often unrecog-nizeduntiladultlife
It may get large enough to obstruct the vesical neck or the contralat-eral ureters
It is more common in females10%ofcasesarebilateral Often associated with duplicate ureters (always involve the ureters
draining the upper renal pole) Almost always associated with significanthydroureteronephrosis
URINARY BLADDER
CARCINOMA BLADDER○ Therearethreecommonhistologicaltypesofbladdercancer:1.TransitionalcellCa—~90% 2.SquamouscellCa—~5%–10% 3. Adenocarcinoma—~ 2%
Risk factor for transitional cell Ca of bladder1. Cigarette smoking isthemainetiologicalfactorandaccountsforabout50%ofbladdercancers2. Occupational chemicals • Thefollowingcompoundsmaybecarcinogenic: 2 naphthylamine combustion gases and soot from
coal 4 aminobiphenyl chlorinated aliphatic hydrocar-
bons 4 nitrobiphenyl certain aldehydes such as acrolein 4-4 diaminobiphenyl aniline dyes
• Occupationreportedtobeassociatedwithincreasedriskofbladder cancer
Autoworker Painters Truck drivers Drill press operatorLeatherworkers Metal workers
Textile workers Dye workers Petrol workers Rodent exterminators and
sewage worker
3. Schistosoma hematobium Risk factor for both transitional cell Ca and squamous cell Ca4.Drugssuchasphenacetinandchlornaphazine5. Cyclophosphamide therapy6. Pelvic irradiation
Contd...

tahir99 - UnitedVRG
191Urological Surgery
CARCINOMA BLADDERRisk factor for squamous cell Ca of bladder
• Schistosomahemotobium○ ItisariskfactorforbothtransitionalcellCaandsqua-
mous cell Ca but more for squamous cell Ca
• Chronicirritationfromurinarycalculi,longtermin-dwelling catheters, chronic urinary infections
• Bladderdiverticula
Also remember• MCprimarytumor,whichgivessecondarytopenis blad-
der carcinoma• Commonesttumorofurinarybladder transitional cell Ca• CommonesttumorofUBinachild rhabdomyosarcoma• MCsymptomofrenalcellCa painless hematuria
• MCsymptomofWilm’stumor mass in abdomen• MCsymptomofbonymetastasis pain• MCsymptomofrenalstone pain• Earliestsymptomofvesicalcalculus frequency• Cardinalsymptomofrenaltrauma hematuria• MCsymptomofacutearterialocclusion pain
MANAGEMENT OF BLADDER CANCER• Cystoscopyandtransurethralresectionorbiopsy• Initiallyanypatientwithhematuriaisexamined
by cystoscopy and any tumor seen is removed by transurethral resection (if possible) or biopsied
• Furthertreatmentdecisionsaremadeaftertumorstaging on histology.
• Suchdecisionsarebasedontumorstagetumornodemetastasis(TNM),gradesize,multiplicityand recurrence pattern
Staging (TNM) • Nowthehistologicalgrading There are three histological grades—
grade I, II & III There is a strong correlation between
tumor grading and tumor recurrence progression and survival
Tis Ca in situTa Caconfined
to mucosa
T1 Caconfinedtosubmucosa
T2 muscle inva-sion
T3 perivesical fat invasionT4 invasion of adjacent struc-
tures (prostate, uterus, vagina, pelvic wall, abdominal wall)
Treatment options for bladder cancersCancer stage Initial treatment optionsTis Complete transurethral resection (TUR) followed by intravesical
bacilusCalmette-Guerin(BCG)Ta (single, low to moderate grade, not recurrent) Complete TURTa (large, multiple high grade or recurrent T1) Complete TUR followed by intravesical chemo or immunotherapy T2 –T4 1. Radical cystectomy
2.Neoadjuvantchemotherapyfollowedbyradicalcystectomy3. Radical cystectomy followed by adjuvant chemotherapy 4.Neoadjuvantchemotherapyfollowedbyconcomitantchemothera-
py and irritationAny T, N+, M+ Systemic chemotherapy followed by selective surgery or irradiation • Intravesical therapy: Common agents used for intravesical therapy are: Mitomycin C Doxorubicin Thiotepa BCG
• Amongtheseagents,BCG is the most effective
Contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery192
BLADDER CALCULI• Ingeneral,mostofthebladdercalculiareformedwithinthebladderitself.Onlysomestonesareformedinthekidney
and pass into the bladder, where they grow by additions of crystals• Etiology of bladder calculi○Bladderoutletobstructionisthemostcommon
cause of vesical calculi in adults○Othercausesare:■Neurogenicbladderleadingtourinarystasis■Aforeignbody,e.g.Foleycatheterandforgotten
double-J (DJ) stent, which serve as midi for stones■Bladderdiverticula
• Bladderstonesarecommonlyseeninolder men (> 50 yr) usu-ally because of bladder outlet obstruction
• Common vesical stones are○Uricacidstones○ Struvitestones
• Otherlesscommonstonetypeare:○Oxalatestones○Cysteinstones
• Struvite stones are also know as ‘jack stones’ because of their rough surface as against the smooth surface of uric acid stones.
Based on origin Clinical features• Primary bladder stone is one that develops in sterile urine and
originates in kidney and passes down the ureters to the bladder, where it enlarges
• Secondary bladder stones occur in presence of some infections, bladderoutflowobstruction,impairedbladderemptyingoraforeign body such as non-absorbable sutures, metal staples or catheter fragments
• Most of the bladder stones are secondary. Only some stones are primary. Kidney stones, which are small enough to pass through the ureters into bladder are easily passed out through the urethra
• Mostbladderstonescontaincalciumandarethereforeradiopaque
○ Frequency is the earliest symptom○ Hematuriaiscommonandthismaybecharacter-izedbyfewdropsofbloodattheendofmicturition
○ Pain(strangury)mayoccurbecauseofspeculatedoxalate stone. It usually occurs at the end of mictu-rition and is usually referred to the tip of penis or to the labia majora. In young boys, screaming and pulling at the end of penis with hand at the end of micturition are indicative of bladder stone. Uric acid stones are primarily formed in bladder. Its oxalate stones are dropped from above
• Treatment of vesical calculus○ Smallstonescanberemovedorcrushedtransurethrally(cystolitholapaxy)○ Largerstonesareoftendisintegratedbytransurethralelectrohydrauliclithotripsy(shockwavegeneratingprobe),or
may require suprapubic transvesical removal (vesiolithotomy)
RUPTURE OF BLADDER• Bladderruptureisoftwotypes:1.Extraperitoneal—80%ofcases2.Intraperitoneal—20%ofcases
• Urethralruptureisalsooftwotypes:1. Bulbar urethral injury is MC2. Membranous urethral injury
○ Extravasation of urine in bladder & urethral injuries• Extravasation of urine (+ blood) in bulbar urethral
injuryItisasuperficialextravasation If the Buck’s fascia remains intact, extravasation of bloodandurineareconfinedtothepenileshaft.However, disruption of Buck’s fascia allows extrava-sated contents into a space limited by Colle’s fascia formsascrotalandperinealbutterflyhematoma,which can extend up the abdominal wall.
• Extravasation of urine in membranous urethral injury and extraperitoneal bladder rupture.Extravasationissameinboth It is a deep extravasation Urine extravasates in the layer of the pelvic fascia and the
retroperitoneal tissues Urine collects in the perivesical spaceThetypicalfindingoncystogramisextravasationofthe
contrast material into the pelvis around base of the bladder• Intraperitoneal rupture Usually occurs with a direct blow to lower abdomen with full bladder Blood and urine will extravasate into the peritoneal cavity producing signs of peritonitis
More about bladder and urethral injuries• Bladderinjuriesareusuallyassociatedwithpelvic#• Bladderrupturesassociatedwithpelvic#isextraperi-
toneal type
○ Urethralinjassociatedwith#pelvis membranous urethral inj○ Urethralinjcausinghighflyingprostate membranous
urethral inj.
Contd...

tahir99 - UnitedVRG
193Urological Surgery
RUPTURE OF BLADDER
TUBERCULOSIS OF BLADDER• Bladdertuberculosisisalmostalways secondary to renal
tuberculosis• Thediseasestarts at the ureteric opening, the earliest evi-
dence being pallor of the mucosa due to submucosal edema• Subsequentlytinywhitetranslucenttuberclesdevelopallover.Graduallythesetuberclesenlargeandmayulcerate(butdo not cause bladder perforation)
• Thesetubercleslend‘cobblestone’ appearance on cystoscopy
• Thereisconsiderablesubmucousfibrosis,whichcaus-esdiminishedcapacityofbladder.Scarred&fibrosed,small capacity bladder is k/a thimble bladder
• Thefibrosis,whichusuallystartsaroundtheureters,contracts to cause a pull at the ureters. This either leads to a stricture or displaced, dilated and rigid wide mouthed ureters k/a golf hole ureters. This almost alwaysleadstoureteralreflux
PROSTATE AND SEMINAL VESICLES
ANATOMICAL DIVISION OF PROSTATEProstatehasfivelobes:○ Anterior lobes ○ Posterior lobes ○ Median lobes ○ Lateral lobes Is small isthmus con-
necting the two lateral lobes in front of the urethra.
It connects the two lateral behind the urethra. It lies behind the me-dian lobe and the ejaculatory ducts. Carcinomas are most common in this lobe.
Liesbehindtheupperpartof the urethra, in front of the ejaculatory ducts just below the neck of the bladder.
Benign prostatic hyperplasia (BHP) arises in this lobe.
Lieoneoneachside of the urethra.
Zonal or surgical division of prostate• Prostatehasthreedistinctzonesa.Theperipheralzone(PZ)—accountsfor70%ofvolumeof
young adult prostateb.Thecentralzone(CZ)—accountsfor25%c.Thetransitionzone(TZ)—accountsfor5%
• Carcinoma of prostate arises most commonly in the peripheralzone.
• Benignprostatic hyperplasia originates in the transi-tionzone.
Contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery194
COMPLICATIONS OF TURP1. Water intoxication is an important complication of TURP (transurethral resec-
tion of prostate)○ “Theabsorptionofwaterintothecirculationatthetimeoftransurethral
resection can give rise to congestive cardiac failure, hyponatremia and frequently confusion and other cerebral events often mimicking a stroke.
○Theincidenceofthisconditionhasbeenreducedsincetheintroductionofisotonic glycine for performing the resections and the use of isotonic saline for postoperative irrigation.Thetreatmentconsistsoffluidrestrictions”.
2. Perforation of bladder is one of the complications of TURP. It can present with periumblical pain after recovery from spinal anesthesia○ {Meteorism – is distention of the
abdomen or intestines by gas. This is seen in renal injury but not in TURP}
ABSOLUTE INDICATIONS FOR SURGICAL TREATMENT OF BPH1. Refractory urine retention (failing at least one attempt at
catheter removal)2. Recurrent UTI from BPH3. Bladder stones d/t BPH
4.Renalinsufficiencyd/tBPH5.LargebladderdiverticulasecondarytoBPH6. Recurrent goes hematuria from BPH
• “Theholmium: Yttrium aluminium garnet (YAG) laser is excellent for stone fragmentation and tissue ablation and is now the most popular system in use”
• BothHo:AG&Nd:YAGlasersystemscanbeusedforBPH,but only Ho: YAG is used for stone fragmentation. For BPH, Ho: YAG is preferred over Nd: YAG
• Duringtransurethralresectionofprostatestripsoftissuearecutfromthebladderneckdowntothelevel of verumontanum
SOLUTIONS IN TURP• Weallknowthatnormal salineisaverygoodconductorofelectricity(asitcontainions–Na+ & Cl– ions)• SoifitisusedwhileperformingTURP,thediathermycurrentusedintheprocedurewillcauseelectrolytedissociationofnormalsalineandthecurrentwillnotbelocalizedintheloopandhencecuttingofthetissuewillnotbeproper.
• Hence normal saline should not be used in TURP○ Youcanputupaquestionthatthesamecanoccurwiththeuseofdistilled water too. Distilled water can also conduct electricity but the current used during TURP is not very strong and distilled water is
not good conductor of electricity as normal saline. (you must be aware that distilled water is a worse conductor of electric-ity than normal water)
Therewerealsoargumentsthatdistilledwatercausesfluidoverload and therefore should not be used in TURP
True,distilledwatercausesfluidoverloadorTURPsyn-drome, but this complication is not common.
Distilled water is being replaced by 1.5% glycine but still can be used for TURP (and is used in many center when glycine is not available)
MEDICAL TREATMENT OF BPH• TwoclassesofdrugsarecommonlyusedforBPHa.α-adrenergicblockers,e.g.prazosin,terazosin(α1blockers)andtamsulosin(α1a blocker)b.5α-reductaseinhibitors,e.g.finasteride
Contd...

tahir99 - UnitedVRG
195Urological Surgery
MEDICAL TREATMENT OF BPHα-adrenergic blockers 5α-reductase inhibitorSinceactivationofα1 reception in the blad-
der neck, prostatic urethra increases their smooth-muscle tone, their blockade relaxes these structures, reducing the dynamic obstructionandincreasingtheurinaryflowrate
These drugs prevent the conversation of testosterone into more active dihydrotestosterone responsible for androgen action in many tissues includingprostate.Theiruseresultsinreductioninthesizeoftheglandand improvement in symptom.
But 6 months of therapy is required to see the maximum effect on prostatesizeandsymptomaticimprovementisseenonlyinmenwithenlargedprostate(>40cm3)
Finasteride• UsesBPH—decreasesthesizeoflargeprostate(>40
cm3) and can retard disease progression. Male pattern baldness—in patients of male
pattern baldness, it promotes hair growth and prevents further hair loss.
• Sideeffects Impotence: It is a well documented although infrequent side
effect. Decreased libido Decreased volume of ejaculate Skin rashes Swelling of lips
CANCER PROSTATE○ Prostate is divided into following three
zones:Peripheralzone,whichliesintheouterpart
of prostate but mainly posterior.Centralzone,whichliesposteriortotheure-
thral lumen and above the ejaculatory ducts as they pass through the prostate
Periurethraltransitionalzone(TZ)
• As BHP arises from transitional zone and ‘prostatectomy’ one for BHP removes TZ leaving behind the PZ. The pt. is still at risk for prostatic carcinoma
• Prostaticcancerspreadstothebonesthroughbloodvessels;firstinto Batson’s periprostatic venous plexus and then into the internal vertebral plexus of veins. This metastasis is possible because of valve-less communication between the periprostatic and vertebral plexus of veins
• ApatientissuspectedtohaveCaprostateas: Prostatic Ca is the most common malignant tumor in men over 65
year of age Symptoms of bladder outlet obstruction and back pains (due
to bony metastasis in the pelvis and lumbar vertebra) indicate towards prostate Ca
TUMOR MARKERS IN CARCINOMA PROSTATE• SerumacidphosphataseisatumormarkerofprostateCa.• ButnowserumacidphosphataseassayhasbeensupersededbyPSAassay(prostatespecificantigen)
• Sinceprostatesepcificantigen(PSA)isnotspecificfor Ca,
• PSAvelocityandPSAdensityareusedtodetectprostate cancer
• PSAvelocityofmorethan75ng/mLyearissug-gestive of Ca
• PSA density is calculated by dividing the serum PSA by the estimated prostate weight (measured by TRUS). It was developed to correct for the con-tribution of BPH to the total PSA levelValues<0.10areconsistentwithBPH>0.15suggestcancer
• “Even so, the realities of clinical practice are that the combination of digital rectal examination and serum PSA monitoring is the most effective screening protocol”
Prostate specific antigen• Itisaglycoproteinproducedonlyintheprostaticcells(both
benign & malignant). It facilitates liquefaction of semen.• Itisneithersensitivenorspecificforearlyprostatecarcinoma,
nevertheless it gives some help in making a diagnosisNormalserumlevellessthan4ng/mL.4–10ng/mL this range is common for both BPH and CaMorethan10ng/mL approx 75% will have cancer More than 35 ng/mL is diagnostic of Ca
Contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery196
CLINICAL FEATURES• Mostcommonmetastaticsitesofprostatecarcinomaarelymphnodesand
bones• Lymphaticmetastasisoccursmostcommonlytoobturatorlymphnodes• Otherlymphnodesinvolvedare: Common iliac Presacral Periaortic
• Mostcommonbonymetastasisoccursin(in decreasing order)Lumbarspine(mostcommon) Proximal femur Pelvis Thoracic spine Ribs
Staging of prostate cancer○ Tis carcinoma in situ○ T1 these are incidentally found tumors in a clinically benign gland T1a ≤5%oftissueinresectionfor‘benign’diseasehascancer,digitalrectalexamination(DRE)isnormal T1b >5%oftissueinresectionforbenigndiseasehascancer,DREisnormal T1c CadetectedbyelevatedPSAalone,normalDREandTRUS
○ T2 tumorpalpablebyDREorvisiblebytransrectalultrasonography(TRUS)andconfinedtoprostate○ T3 extracapsular extension with or without seminal vesicle involvement○ T4 tumor directly extends into bladder neck, sphincter, rectum, pelvic side walls, etc. T1 & T2 are early disease T3 & T4 are advanced disease
MANAGEMENT PLAN• Curativet/tcanonlybeofferedtopatientswithearly disease (i.e. T1 & T2) radical prostatectomy or radical radio-
therapy (both are equally effective)• RadicalretropubicprostatectomyisperformedforCaprostate• Hemorrhageisthemostcommonintraoperativecomplicationandthemostcommonlyinjuredvesselisdorsalvenous
complex• Thet/tforadvanceddisease(i.e.T3,T4oranymetastasis)isonlypalliative.Hormoneablationisthefirstlinetherapy
for palliation
• T1a disease These tumors found incidentally at TURP is by thedefinitionlowvolume(≤5%)andusuallywell differentiated and associated with very slow growth rate
They are managed by watchful waiting (regu-larfollow-upisdonebyDREandPSA)
• T1b, T1c & T2 disease Management depends on patient’s age, life expectancy, perfor-
mance status, and patient’s preferences Inyounger,fittermen(<70year),Maybetreatedbyradicalpros-
tatectomy or radical radiotherapy. Watchfulwaitingisanoptionforelderlywithlowlifeexpectancy(<10year).Evenyoungerpatientsmaychoosewatchfulwaitingwhencounseledaboutriskversusbenefit.
• Advanced disease (T3, T4 or any metastasis)○Onlypalliativet/tistheoption■Androgenablationisthefirstlinetherapy
• Itcanbeachievedby Orchidectomy or Drugs (medical castration)
• Palliativeradiotherapy Androgen ablation is the mainstay of therapy
for advanced prostatic cancer (T3, T4 ds or any metastasis)
Most prostatic carcinomas are hormone dependent and large number of men with advanced disease show response to androgen ablation therapies
• Androgen ablation Surgical orchidectomy is the ‘gold standard’ approach, but least
acceptable. Medical castration
• Drugsusedare:○Gonadotropin-releasinghormone(GnRH)analogues■Leuprolide■Goserline
○Estrogenssuchasdiethylstilbestrol■Notusednowbecauseofhigh-riskofcomplications
○Antiandrogens■ Flutamide,bicalutamide,nilutamide
○Ketoconazole○Cyproteroneacetate

tahir99 - UnitedVRG
197Urological Surgery
SEMINAL VESICLES• Spermsareproduceintestisandthenstoredandmaturewithintheepididymis• Vasdeferenscarriesthespermsfromepididymistotheurethra,wheretheyopenbyseparateopeningsintotheprostatic
urethra• Justbeforeopeningvasdeferensisjoinedbyductsofseminalvesicles.Vasdeferensandseminalvesicleductsjointoform
the ejaculatory duct• Thesecretionsofseminalvesiclesformalargepartofseminalfluidandcontainfructoseandacoagulatingenzymecalled
the vesiculase
○ Semen analysis forms a important part of infertility assessment• Low ejaculatoy volume is caused by Retrograde ejaculation into the bladder
or Obstruction of the vas deferens or the
ejaculatory duct
■ Azoospermia may be seen in Testicular failure or Obstruction of vas deferens
■ Absence of fructose suggests Seminal vesicle agenesis or
obstruction
○ Semen that is low in volume with azoospermia and absence of fructose sug-gests either obstruction of the ejaculatory ducts or congenital absence of the vas deferens and seminal vesicles.
○ Theanatomyofthevasdeferensandseminalvesiclescanbevasography(wherecontrast medium is injected into the vas deferens) or TRUS (transrectal ultra-sonography) However TRUS is superior to vasography and is the investigation of choice.
• Alsoknow Semen specimen should be ob-
tained following at least 3 days of sexual abstinence and examined within 1 or 2 hour at least 2 speci-mens are examined several weeks apart.
PENIS AND URETHRA
HYPOSPADIAS• Hypospadiasisacondition,inwhichtheurethralmeatusopensontheunderside
of penis or the perineum (i.e. ventral surface of penis proximal to the tip of the glans penis.
• Thereareseveraltypesofhypospadiasaccordingtolocation
Types of hypospadiasa.Glandularopeningisintheglanspenis,proximaltothetipb. Coronal opening on the coronal sulcusc. Peniled. Penoscrotale. Perineal: This is the most severe abnormality. The scrotum is split and the ure-
thra opens between its two halves. There may be testicular maldescent, which maymakeitdifficulttodeterminethesexofchild.
• Glandular hypospadias is the most common type• Alsoknow Hypospadias is the most common congenital malformation of the urethra. In epispadias—the urethra opens on the dorsum of penis. It is a rare congenital anomaly that is commonly associated
with bladder exstrophy.• Besttimeforsurgeryforhypospadiasisbetween6–12 months of age
Contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery198
HYPOSPADIASClinical features Complications of hypospadias• Besidestheabnormalpositionofexternalurethralmeatustheotherassociated
abnormalities are: In the penile variety the urethra and corpus spongiosum distal to the ectopic openingareabsent,insteadafibrouscordispresent.Duetocontractureofthisfibrouscord,thepenisis curved ventrally (in a downward direction) this is known as chordee. So the more proximal the ectopic opening is placed the greater is the change of chordee. This curved penis causes problem in inter-course as well as micturition.
Inallcases,inferioraspectoftheprepuceispoorlydeveloped.While,thesuperior aspect is normally developed. This cause prepuce to take the form of hood and is called hooded prepuce.
○ Difficultyindirectingtheurinarystream
○ Duetopresenceofchordee,erec-tionisdifficultandpainfulandtheintercoursemaybedifficultorimpossible
○ Infertilitycanoccur(usuallyassoci-ated with penoscrotal and perineal variety)
Treatment of hypospadias○ Treatmentofhypospadiasisverycomplex.Hereare
some important points○ Treatment is not required in glandular variety. ○ Incaseofothervarieties,aplasticoperationisper-
formed to bring the external urethral meatus to its normal position, and remove the chordee to straight-en the curvature
○ Operationcanbedoneinonestageortwostagesurgeries.Nowadaysonestagesurgeriesaremorepopular.• Indicationsfortwostageoperations○ Scrotalorperinealvariety○Chordee(inthefirststagechrodeeiscorrectedthenthe
opening is corrected)■ Circumcision is not done in patients with hypospadias as the
prepuce can later be used in surgical repair
Consolidated○ Anabnormalventralopeningoftheurethralmeatus○ Anabnormalventralcurvatureofthepenis(chordee)○ Aabnormaldistributionofforeskinwitha‘hood’presentdorsallyanddeficientforeskinventrally(hoodedprepuce)
○ Rememberthatcryptorchidismisnotafeatureofhypospadias.But it may be seen associated with hypospadias in 8%–9% of cases
• Ventralchordeeisseeninhypospadias• Dorsalchordeeisafeatureofepispadias• Metalstenosismaybeassociatedwithhypospa-
dias and needs meatotomy for correction.• Bifidscrotummaybeseeninpenoscrotaland
perineal hypospadias
PHIMOSIS• Ballooningofprepuceduringmicturi-
tion is suggestive of phimosis• Whentheopeningoftheprepuceisso
small that it cannot be retracted over the glans penis, the condition called phimosis
Phimosis is of two types1. Congential2. Acquired—it usually presents late in life and is associated with:• Inflammation•Trauma•Balanitisxeroticaobliterans•Cancer
Clinical features• Difficultyinmicturition: It is the main symptom. In a case of typically congenital phimosis the
mother complains that when the child micturates the prepuce balloons out and the urine comes out in thin stream.
• Inoldcasespatientpresentwith:Recurrentbalanitis(inflammationofglans)causingpainandpurulentdischarge Paraphimosis (the tight foreskin gets retracted and stuck behind the glans penis)
Contd...
Contd...

tahir99 - UnitedVRG
199Urological Surgery
PHIMOSISComplications Treatment○ Balanoposthitis–(inflammationofglansandprepuce)○ Preputialstonesorcalculi○ Paraphimosis○ Hydroureter,hydronephrosis○ Carcinoma
The treatment is circumcisionNote,ifphimosisisassociatedwithconsiderable
infection dorsal slit is performed
PARAPHIMOSIS• EtiologyWhenaprepuceisforciblyretractedovertheglanspenis,itmaygetstuckbehindtheglans. Condition is k/a paraphimosis
• PathologyThisconstrictingbandofphimoticprepucecausesobstructiontothevenousflow,whichleadto
edema and congestion of the glansTheglansswellsleadingtomoredifficultyinretractingbacktheprepuce In neglected cases gangrene may result
Treatment○ Icebags,gentlemanualcompressionandinjectionofasolutionofhyaluronidaseinnormalsalinemayhelptoreducethe
swelling○ Ifconservativemethodfailsthenthepatientcanbetreatedbycircumcision• Itisuncommonfortheurethratobecompressed,sothemicturitionisnormallynotaffected.
INJURY TO URETHRA○ Thepartofurethramostlikelyinjuredinpelvicfractureis
membranous urethra (a part of posturethra) Posturethra includes prostatic + membranous urethra Anterior urethra includes bulbar + penile urethra
○ Theanteriorurethra(particularlybulbarurethra)isinjured due to direct blow to the perineum (straddle injuries)
○ Prostaticurethraismostdilatableandwidestpartofurethra (3 cm long)
○ Ejaculatoryductsopeninprostaticurethra.○ Membranousurethraisshortest(2cm)andleastdilat-
able part.
○ BulbourethralglandsofCowperthoughlocatedoneachsideof membranous urethra, their ducts open into penile urethra.
○ Externalurethralorificeismostnarrowestpartofurethra.
MCQ pointsa. Prostate is displaced superiorly (high lying prostate) in membranous urethral injury due to rupture of puboprostatic
fascia. Pelvic hematoma is seen in membranous urethral injuries (perineal hematoma is seen in bulbar urethral injury)b.OnceanurethralinjuryissuspectedthepatientisinstructednottopassurineandaRGUorascendingurethrogramis
performed to assess the injuryc. CatheterizationiscontraindicatedandispassedonlyiftheRGUisnormal
Contd...
tahir99 - UnitedVRG
http:/
/vip.p
ersian
ss.ir/
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery200
COMPARE THE TWO TYPES OF URETHRAL INJURIESBulbar urethral injury Membranous urethral injury
Common More commonMechanism of injury Direct blow to the perineum Blunt pelvic trauma with fracture pelvisSigns and symptoms • Retentionofurine
• Bloodaturethralmeatus• Perinealhematoma
• Retentionofurine• Bloodaturethralmeatus• Pelvichematoma• Highlyingprostate
Extravasation of urine
SuperficialextravasationUrinefirstcollectsintosuperficialperinealpouchandthenpassé into scrotum, penis and anterior abdominal wall
Deep extravasationUrine collects in the perivesical space
○ Thisisverywellknownthatinapatient of urethral injury, cathe-terizationisnotdoneb/citwouldconvert a partial tear into a com-plete transaction of the urethra
○ Blood at the urethral meatus is the single most important sign of urethral injury.
• Clinicalfeaturesseeninruptureofbulbarurethraoranteriorurethra: Patient usually presents with a history of fall on the perineum The triad of signs of a ruptured bulbar urethra is:○Retentionofurine○ Perinealhematoma○Bleedingfromtheexternalurinarymeatus Rectal examination in case of bulbar urethral injury reveals a normal situated
prostate (this differentiates it from membranous urethral rupture in prostate is displaced superiorly)
○ Bloodatthemeatusissuspiciousofurethralinjuryandanimmediateurethrographyisadvisedtoruleoutanyurethralinjury
Carcinoma of penis• Thecircumcisionthatisdonesoonafterbirthininfancy,
gives almost complete immunity against Ca penis • Butthatdoneinlaterinlifedoesnothavethesameeffect,
so muslims circumcised between the ages of 4 and 9 year still liable to the disease
• AboutCapenis○Mostcommonhistologicaltypeis squamous cell Ca
(98%) ○Erythroplasiaofqueretisprecancerousconditionitis
the in situ form of Ca penis
Premalignant lesions of Ca penisa. Penile cutaneous hornb. Balanitis xerotica obliteransc. Leukoplakiad. Viral (human papilloma virus) related dermatologic lesion■Condylomaacuminata(alsok/agenitalwarts)■Bowenoidpapulosis
• Theoneetiologicalfactormostcommonlyassociatedwithpenile carcinoma is poor hygiene
Clinical features• Age-penileCaoccursmostcommonlyinthe6th
decade of life, but its presentation in younger age not uncommon(‘40%ofpointsareunder40yearofage’—Bailey)
• Mostcommoncomplaintatpresentationisthelesionitself. Pain is rare
○ Most common site of involvement Glans ~ 48% Prepuce ~ 21% Both glans and prepuce 9% Coronal sulcus ~ 6% Shaft ~ 2%
○ Lymph node involvement Morethan50%ofpatientpresentwithaenlargedinguinallymphnodes(buthalfofthisarereactiveenlargementd/t
sepsis) The presence and the extent of metastasis to the inguinal region is the most important prognostic for survival in pa-
tients with Ca penis○ Distantmetastasisisinfrequent Diagnosis is made by biopsy of lesion Inguinal lymph nodes erode the skin of the groin and the death of patient may be due to involvement of the femoral or
external iliac artery with torrential hemorrhage
Contd...

tahir99 - UnitedVRG
http:/
/vip.p
ersian
ss.ir/
201Urological Surgery
COMPARE THE TWO TYPES OF URETHRAL INJURIESManagement of carcinoma penis
Small non-invasive lesion can be treated by○ Fluorouracilcream○ Nd:YAGlaser○ Radiotherapy○ Suchtreatmentpreservesthepenis,butclosefollow-upismandatory
Invasive penile carcinomas○ The goal of t/t invasive penile carcinomas is complete excision with adequate margins
a. For lesion involving the prepuce: – Simple circumcision is effectiveb. For lesion of glans or distal shaft: – Partial penectomy with a 2 cm marginc.Forlesioninvolvingtheproximalshaftorwhenpartialpenectomyresultsinapenilestumpofinsufficientlengthfor
sexual function or directing the urinary stream: – Total penectomy with perineal urethrostomy
Inguinal lymph nodes• Palpableinguinalnodeshouldbet/tbyantibodiesfor6weeksfollowingt/toftheprimarylesiontoeliminateinfections
(this is to cure reactive lymphadenopathy d/t sepsis). Persistent adenopathy following antibiotic t/t is considered to be metastatic disease and bilateral ilioinguinal node dissection is performed
POSTERIOR URETHRAL VALVE• Poorurinarystreamin3-year-oldboysuggestsurinarytractobstruction(usuallyinfravesical)
and the most common of obstructive uropathy in a male child is posterior urethral valve • Posteriorurethralvalve: These are symmetrical folds of urothelium extending distally from prostatic urethra to
external urinary sphincter It most commonly lies just distal to the verumontanum or at the verumontanum It occurs only in malesItbehavesasflapvalvesso,althoughurinedoesnotflownormallyaurethral catheter can bepassedwithoutdifficulty
Sometimes, the valves are incomplete and the patient remains without symptoms until adolescence or adulthood
Approximately30%ofpatientsexperienceend-stagerenaldisease Vesicoureteralrefluxoccursin50%ofpatients
• Diagnosisismadeby:a. Voiding cystourethrogram b.Endoscopy
• Bothoftheseinvestigationsclearlydepictinsiteofobstruction• Thediagnosiscanbeestablishedprenatallybytheultrasound
Management:○ Firstasmallpolyethylenefeedingtubeisinsertedinthebladderandleftforseveraldays.Thenfurthermanagementis
done according to serum creatinine levelWithnormalserumcreatininetransurethralablationofthevalveleafletsWithincreasedserumcreatinineandtheworseningofcondition vesicostomy to bypass the obstruction and when
normal creatinine levels are achieved, transurethral ablation is done“Themostreliablemethodtoconfirmthediagnosisofposteriorurethralvalvesisvoidingcystourethrographythatmeansradiographsaretakenduringtheactofmicturitionafterthebladderhasbeenfilledwiththecontrastmedia”
Contd...
Contd...

tahir99 - UnitedVRG
http:/
/vip.p
ersian
ss.ir/
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery202
POSTERIOR URETHRAL VALVERadiological studies in urethral stricture
○ Retrogradeurethrography It is the mainstay of radiographic of stricture disease
○ Voidingcystourethrogram/micturatingcystourethrogram(MCU) MCU demonstrates the segment of urethraproximal to the
stricture
○ Endoscopy Retrograde urethroscopy Antegrade cystrourethroscopy
○ Sonographicurethrogram•MRIhasnoroleinthediagnosisofurethralstric-
tures
PEYRONIE’S DISEASE○ Peyroniediseaseisusuallyseenover40yearsofage○ ImportantpointsaboutPeyroniediseaseare:Itisalsok/apenilefibromatosisItisduetofibrousplaquesinoneorbothcorpuscavernosum.They
may later calcify or ossify Fibrous plaques leads to pain and curvature of the penis on erection Palpable induration or mass appears usually on the dorsolateral
aspect of the penisPalmarfibromatosis(Dupuytrencontracture),plantarfibromatosisandpenilefibromatosis(Peyroniedisease)arecomponentsofthesamepathologicalprocesscalledsuperficialfibromatosis
○ Theetilogyisuncertain,butitmaybearesultofpasttrauma○ Treatmentisdifficult,butsomecasesmayshowspontaneous
regression
○ Inthepeniledeformityisdistressing,Nesbitt opera-tion can be performed to straighten the penis
MCQ pointsa. Commonest cause of stricture in posterior urethra trauma with fracture pelvisb. Commonest cause of stricture in anterior urethra straddle injuries (direct trauma to the perineal region)Voiding cystouethography is the best method to visualize posterior urethra: Urethra can be imaged radiographically in two ways1. Anterograde techniques bestforvisualizationofposteriorurethra
(This is done along with voiding cystourethrography or with voiding following excretory urography)2. Retrograde technique best for examining the anterior (penile) urethra
(Contrast is injected through tip of urethra)
TESTIS AND SCROTUM
TESTICULAR TUMORSTesticular cancer is mainly of two types:1.Germcelltumors(GCT)~95%2.Non-germinalneoplasms~5%(includeLeydigcells,Sertolicells,
gonadoblastoma)
Germ cell tumors are of two types• Seminomas(morecommon,betterprognosis)• Non-seminomas,i.e.EmbryonalCa Teratoma ChoriocarcinomaYolksac(Endodermalsinus)carcinoma
Contd...

tahir99 - UnitedVRG
203Urological Surgery
GERM CELL TUMOR STAGING AND TREATMENTExtent of disease Seminoma Non-seminoma Testis only, no vascular/lymphatic invasion (TI) Radiation therapy Retroperitoneallymphnodedissection(RPLND)or
observationTestis only, with vascular/lymphatic invasion (T2), or extension through tunica albuginea (T2), or involvement of spermatic cord (T3) or scrotum(T4)
Radiation therapy RPLND
Nodes<2cm Radiation therapy RPLNDorchemotherapyoftenfollowedbyRPLNDNodes2–5cm Radiation therapy RPLND+/-adjuvantchemotherapyorchemothera-
pyfollowedbyRPLNDNodes>5cm Chemotherapy Chemotherapy,oftenfollowedbyRPLNDDistant metastases Chemotherapy Chemotherapy, often followed surgery (biopsy or
resection)
MORE ABOUT TESTICULAR MALIGNANCY• Mostcommontesticulartumorabove50yearofage is lymphoma*
• Non-seminomasaremore malignant than seminomas *
Predisposing factors for testicular germ cell tumors (GCTs) are:a. Cryptorchidism b.Testicularfeminizationsyndromec. GCTofonetestisisariskfactorfortheothertestisd. Testicular Ca in a siblinge.KlienfeltersyndromeisassociatedwithmediastinalGCTf. Administrationofestrogens(e.g.DES)tothemotherduringpregnancyisassociated
SOME POINTS ARE WORTH MENTIONING ABOUT CRYPTORCHIDISM• Ofthepredisposingfactors,cryptorchidism
has the strongest association with testicular cancer
• Increasedriskisseenforboththetestis,i.ethe cryptorchid testes as well as the normally descended testis
• Abdominalcryptorchidtestesareatahigherriskthaninguinalcryp-torchid testis
• Seminoma is the most common type of testicular cancer seen in a cryptorchid testis
• Rememberthis:Placementofthecryptorchidtestisintothescrotum(orchiopexy) does not alter its malignant potential, however it facili-tates examination and tumor detection
TUMOR MARKERSSeminoma no marker Beta HCG
Alpha feto protein:Raised in: pure embryonal, terato carcinoma yolk sac tumor combined tumor
Raised in:100%choriocarcinoma60%embyonalcarcinoma 55% teratocarcinoma 25% yolk cell tumor 7% seminomas
Not raised in • purechoriocarcinoma• pureseminoma
○ Beta human chorionic gonadotropin (HCG): concentration is increased in both seminoma & non-seminoma
○ AFP: concentration is increased in only non-seminoma○ LDH:Itisincreasedinboth,itisnotasspecificaseitherofalphafetoprotein(AFP)orBetaHCG
Contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery204
○ Seminomas representabout50%ofallgermcelltumorsoftestis
○ Medianageis4thdecade(Non-seminomasaremostfre-quent in the 3rd decade).
○ Seminomasfollowamoreindolentcourse
○ Most seminomas (70%) present with stage I disease (disease limited to testis).
○ About20%withstageIIdisease(withretroperitonealmetastases).And10%withstageIIIdisease(spreadbeyond retroperitoneum)
Non-seminomas:1/3patientspresentwithstageIdisease,1/3withstageIIand1/3withstageIIIdiseaseseminomasaswellasnon-seminomastypicallymetastasizethroughlymphatics(exceptchoriocarcinomawhichdemonstratesearlyhematogenous spread)
Seminomasareoneofthemostradiosensitivetumors(Non-seminomasareinsensitivetoradiation)
○ “ Lymphoma is the most common testicular tumor in a patient over the age of 50 and is the most common secondary neoplasm of the testis”

tahir99 - UnitedVRG
205Urological Surgery
VARICOCELE TESTISIt is seen 95% of times on left side. A number of reasons are given for this left predilection, the main being = the valveless left testicular vein drains into the left renal vein at right angles whereas the right testicular vein (also valveless) drains obliquely into IVCThis drainage pattern creates high pressure in the left testicular vein.
Clinical picture • Age—youngadult• Tallthinmenarefrequentlyaffected*• Bagofworms*likefeelonpalpation• Theveinsemptyinsupineposition(soexaminationisalwaysdoneinstanding
position)• Infertility: Varicocele increases the temperature in the scrotum and this decreas-
es spermatogenesis (It must be confessed that at present there is no statistical support to this)
Varicocele may be secondary to renal cell carcinoma of the left kidney: The growth from renal cell carcinoma blocks the renal vein by venous permeation
So sudden onset of varicocele (left side) in middleaged man should arouse suspicion of a renal cell carcinoma of the left side In renal cell Ca, the variocele does not decompress in the supine position.
UNDESCENDED TESTIS • Inundescended testis, the testis is arrested in some part of its path to the scrotum
• Inectopic testis, the testis is abnormally placed outside its path
• Retractile testis,ininfancy80%ofinapparenttestis are retractile testis and required no t/t
• Approx70%–77%ofcryptorchidtestiswillspontaneously descend, usually by 3 months of age
• Morecommoninpreterm,smallforgestationalage,LBWandtwinneonates
• Morecommononright side• Secondarysexualcharacteristicsarenormal
Complications of incomplete descent• Torsionoftestis• Epididymo-orchitis• Anassociatedindirectinguinalherniaisfrequent• Atrophy
• Pain—atestissituatedintheingunialcanalisoftenliabletotrauma and give rise to pain in the groin
• Sterility—iftheconditionisbilateral• Malignancy—riskis40timesmorethananormallyplacedtestis
“Definitivetreatmentoftheundescendedtestisshouldoccur before 1 year of age”

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery206
Torsion of testis• Torsion of testis is the torsion of the spermatic cord caus-
ing strangulation of the blood supply to the testis and unless it is t/t within 3 to 4 hours, testicular atrophy is inevitable
• Itisseencommonlyinadolescent(10-25years)• Symptoms it presents sudden agonising pain in the groinandthelowerabdomen.Nauseaandvomitingarevery common
Predisposing factors Heavy straining often precipitates torsion due to vigorous contraction of cremaster muscle1. Inversion of testis
2. High investment of tunica vaginalis forming a mesentery like structure for testis (mesorchium), which makes the testishangdownhorizontally
3. Presence of gap between testis and epididymis makes testis hang and go for torsion
Signs in torsion testis○ Angel sign: It is a sign on the normal side (unaffected side).Oppositetestislieshorizontallybecauseofthepres-ence of mesorchium (the predisposing factor for torsion is same on both sides)
○ Deming sign: It is a sign on the affected side, where the affected testis is positioned high because of the twisting of the cord and spasm of muscles
• Itmustbedifferentiated from epididymo-orchitis by:○Prehns sign on elevation of testis the:■Painincreases in torsion■Paindecreases in epidydimo-orchitis
○Color Doppler detectsthedecreasedbloodflowtotestis in torsion.
It is the inv. Of choice to exclude torsion from the epididymo-orchitis○ Tc 99m pretechnate scan it demonstrates decreased bloodflow
• Treatment In the 1st hour the torsion can be treated by manipula-tion(butlateronsurgeryhastobedonetofixthetestis)
If not correctable by manipulation or more than one hour has passed then surgery has to be done. Surgery must be done within 4 hours. Otherwise the testis will be dead
Both the affected and unaffected testis should undergo orchiopexy because the anatomical variation responsible for torsion is likely to be bilateral
CONGENITAL HYDROCELE• “Congenitalhydroceleareaspecialformofindirectinguinalherniaandaretreatedbyherniotomy”• Congenitalhydrocele In this condition, the processus vaginalis remain patent so there is direct communication of the tunica vaginal with the peritonealcavity.Thecommunicatingorificeatthedeepinguinalringistoosmallforthedevelopmentofhernia
It is present since birth In contraindication to assumption. Congenital hydrocele is not easily reducible due to narrowness of the inguinal ring,
but when the child lies supine, it disappearsTreatment methods of hydrocele
• Forcongenitalhydrocele herniotomy• Forothertypes Jaboulay method forsmallandmedium-sized
hydroceleLordsprocedureforbig-sizedhydroceleExcisionofsac for hematocele, infected sac
• Alsoremember MC types of primary hydrocele is vaginal type Hydrocele en-bisac this type of hydrocele has two
intercommunicating sac one above and one below the neck of scrotum

tahir99 - UnitedVRG
207Urological Surgery
Types of hydrocele Some other typesa. Vaginal hydrocele (most common)Thereisabnormalaccumulationofserousfluidwithinthetunica
vaginalis b. Infantile hydroceleThefluidcollectswithinthetunicavaginalisandprocessusvagi-
nalis, which are continuous, but the vaginalis is not communicating with the peritoneal cavity
c. Congenital hydrocele The processus vaginalis is present so there is direct communicating
of the tunica vaginalis with the pelvic cavityThecommunicatingorificeatthedeepinguinalringistoosmallfor
the development of hydrocele of the cordd. Hydrocele of the cord Here the central portion of the processus vaginalis is patient, but its
upper and lower parts are oblitera
e. Funicular hydrocele Here the processus vaginalis remains patents
upto top of the testis, where it is shut off from the tunica vaginalis
f. Hydrocele en-basic or bilocular hydrocele Here the hydrocele has two intercommuni-
cating sacs—one above and one below the neck of the scrotum. Upper sac has no con-nection with the processus vaginalis and it is in fact the herniated tunica vagina
g. Hydrocele of the canal of nuck This is female counterpart of the hydrocele of
the cord. It is seen in relation to the ground ligament
TUBERCULOSIS OF TESTIS○ Thediseasefirsteffectstheepididymis*while causing orchitis. The body
of testis may remain uninvolved for years, but the contralateral epididymis often becomes diseased
○ TreatmentisATT
○ Ifthisdoesnotresolve,epididymec-tomy is indicated
o Note: Syphilis will not affect the epididymis, while causing orchitis.
INFECTIONS OF TESTIS○ Acuteepididymitisandacuteepididymo-orchitisareinflammationoftheepididymisand
testis due to infective pathology• Infectionreachestheepididymisthroughthevasfromurethra.Sometimesitmaybeblood
borne•MCinfectiveorganisminsexuallyactiveyoungmaleisGonococus and Chlamydia and in
children and older men are d/t urinary pathogen such as E. coli• Clinical symptoms○Thepatientspresentswithafever, very painful, swollen, red, tender scrotum○Theepididymisandthetestisarebothswollen○Theacutepainfulconditionhastobedifferentiatedfromtorsionoftestis
• Pyuria is associated with epidydimo-orchi-tis, not with torsion of testis
• Treatment Antibiotics Rest Lotsoffluid
TUBERCULOSIS OF KIDNEY AND BLADDER○ InTBofkidney,agroupoftuberculousgranulomasforminthe
renal pyramid. They coalesce and form an ulcer. Untreated the le-sions enlarges and a tuberculous abscess may form in the paren-chyma.Graduallythekidneyisreplacedbycaseousmaterial(putty kidney),itmaybecalcified(cement kidney).Calcificationsmayappear on X-ray as calculi (pseudo-calculi)
○ Renaltuberculosisisoftenassociatedwithtu-berculosis of the bladder. TB of bladder leads to fibrosisandthuscontractureofbladder(thimble bladder)
○ Golf hole ureters are seen in TB bladder
VESICOURETERAL REFLUX (VUR)○ Theretrogradeflowofurinefromthebladdertotheuretersandtherenalpelvis○ TwotechniquesarecommonlyusedtodetectVUR. The radiocontrast MCU is most commonly used (excellent anatomic
details)
Contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery208
VESICOURETERAL REFLUX (VUR) Isotope radionuclide cystography is more sensitive for detecting
VUR and causes less radiation exposure then the former, but pro-vides less anatomical details.
Most sensitive investigation for VUR is radionuclide cystography Investigation of choice for VUR is MCU
Grading of VUR is based on the appearance of the urinary tract on micturating cystourethrogramGradeI Refluxintoanon-dilateduretersGradeII RefluxintotheuppercollectingsystemwithoutdilationGradeIII Refluxintodilateduretersand/orbluntingofcalycealfornicesGradeIV RefluxintoagrosslydilateduretersGradeV Grossdilationoftheureters,renalpelvisandcalyces:calycesshowlossofpapillaryimpression
Complications of VURRefluxpredisposestorenalinfection(pyelonephritis) by facilitating the transport of bacteria from the bladder to the
upper urinary tractTheinflammatoryreactioncausedbyapyelonephriticinfectionmayresultinrenalinjuryorscarringExtensiverenalscarringimpairrenalfunctionandmayresultinreninmediatedhypertension,refluxnephropathy,renalinsufficiency,endstagerenaldisease,reducedsomaticgrowthandmorbidityduringpregnancy
Treatment○ Thegoalsoft/taretopreventpyelonephritis,renalinjuryandothercomplicationofreflux○ Treatmentmodalityiseithermedicalorsurgical
• MedicaltherapyIsbasedontheprinciplethatrefluxoftenre-
solves over time and the antibiotic maintain urine sterility and prevent infection and complication while awaiting spontaneous resolution
• Surgicaltherapy The basis for surgical therapy is that in selected children, ongo-ingrefluxhascausedorhassignificantpotentialforcausingrenal injury
The decision to do medical or surgical t/t is based on certain principles and parental, patient preference
Contd...
FMGE QUESTIONS
1. Investigationofchoiceinvesico-uretericrefluxis: (March 2005, Sep 2010)
a. CT scan b. Voiding cystourethrography c. Intravenous urography d. X-ray KUB Ans. b (Voiding cystourethrography)
2. Seminoma is carcinoma of: (March 2011) a. Kidney b. Urinary bladder c. Testes d. Penis Ans. c (Testes)
3. Reflexnephropathyisdiagnosedmainlyby: (Sep 2011) a. X-ray KUB b. Micturating cystourethrogram c. CT scan d. MRI scanAns. b (Micturating cystourethrogram)
4. Which one of the following is radiolucent stone: (March 2009)
a. Calcium oxalate b. Cystine c. Uric acid d. Phosphate Ans: c (Uric acid)

tahir99 - UnitedVRG
209Urological Surgery
5. True about incompletely descended testis are all of the following, except: (March 2008)
a. Earlyrepositioningcanpreservefunction b. It may lead to sterility, if bilateral c. Poorly developed secondary sexual characters d. May be associated with indirect inguinal her-
nia Ans. c (Poorly developed secondary sexual characters)
6. Most radiosensitive testicular tumor is: (Sep 2007) a. Seminoma b. Teratoma c. Interstitial tumors d. LymphomaAns: a (Seminoma)
7. Erythroplasia of Queyrat occurs in: (Sep 2011) a. Scrotum b. Testes c. Penis d. Bladder Ans: c (Penis)
8. A 25-year-old man presents with varicocele on the left side. Associated condition could be a:
(March 2007) a. Nephroma b. Hepatic malignancy c. Testicular tumor d. Penile malignancy Ans: a (Nephroma)
9. Treatment of stage I teratoma is: (Sep 2009) a. Chemotherapy b. Radiotherapy c. Surgery d. Observation Ans: c (Retroperitoneal lymph node dissection is done)
10. Fourniers gangrene is seen in: (Sep 2007) a. Scrotum b. Shaft of penis c. Base of penis d. GlanspenisAns: a (Scrotum)
11. Most common testicular tumor in 4th decade is: (Sep 2005)
a. Teratoma b. Dermoid c. Seminoma d. All of the above Ans: c (Seminoma)
12. Following urethral rupture, immediate procedure to be done is: (March 2006)
a. Urinarycatheterization b. Suprapubic cystostomy c. Referral to a urologist d. Observation Ans: b (Suprapubic cystostomy)
13. Delirium, mental confusion and nausea in pa-tients who had undergone transurethral resection of prostate suggests: (March 2006)
a. Hypernatremia b. Sepsis c. Hepatic coma d. WaterintoxicationAns: d (Water intoxication)
14. Associated with urinary bladder carcinoma are all of the following, except: (Sep 2005)
a. Smoking b. Human papilloma virus infection c. Schistosomiasis d. Cyclophosphamide Ans: b (Human papilloma virus infection)
15. All of the following are radio-opaque stones, ex-cept: (Sep 2008)
a. Calcium b. Struvite c. Uric acid d. CystineAns: c (Uric acid)
16. Features of carcinoma penis include all, except: (March 2007)
a. Metastasizetoinguinallymphnodes b. Surgery is the treatment of choice c. Hypospadias is a premalignant lesion d. Circumcision provides protection Ans: c (Hypospadias is a premalignant lesion)
17. Chyluria is caused by all, except: (Sep 2007) a. Pregnancy b. Childbirth c. Filariasis d. Bile duct stonesAns: d (Bile duct stones)
18. All of the following are features of carcinoma pe-nis, except: (Sep 2007)
a. Surgery is the treatment of choice b. Balanoposthitis may be a predisposing factor c. Metastaizestoinguinalnodes d. Histologically a transitional cell carcinomaAns: d (Histologically a transitional cell carcinoma)

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery210
19. A 65-year-old male smoker presents with gross to-tal painless hematuria the most likely diagnosis is: (Sep 2009)
a. Carcinoma urinary bladder b. Benign prostatic hyperplasia c. Carcinoma prostate d. CystolithiasisAns: a (Carcinoma urinary bladder)
20. A 10 mm calculus in the right lower ureter associ-ated with proximal hydrouretero-nephrosis is best treated with: (Sep 2009)
a. Extracorporealshockwavelithotripsy b. Antegrade percutaneous access c. Open ureterolithotomy d. Ureteroscopic retrievalAns: d (Ureteroscopic retrieval)
21. Most common type of hypospadias is: (Sep 2011) a. Glandular b. Penile c. Coronal d. PerinealAns: a (Glandular)
22. A 70-year-old patient with benign prostatic hyperplasia underwent transurethral resection of prostate under spinal anesthesia. 1 hour later, he developed vomiting and altered sensorium. The most probable cause is: (Sep 2007)
a. Overdosage of spinal anaesthetic agent b. Rupture of bladder c. Hyperkalemia d. WaterintoxicationAns: d (Water intoxication)
23. The commonest cause of an obliterative stricture of the membranous urethra is: (Sep 2007)
a. Fall astride injury b. Roadtrafficaccidentwithfracturepelvisand
rupture urethra c. Prolongedcatheterization d. GonococcalinfectionAns:b(Roadtrafficaccidentwithfracturepelvisandrupture urethra)
24. Which of the following is an absolute indication for surgery in cases of benign prostatic hyperpla-sia: (Sep 2007)
a. Bilateral hydroureteronephrosis b. Nocturnalfrequency c. Recurrent urinary tract infection d. Voidingbladderpressures>50cmofwaterAns. a (Bilateral hydroureteronephrosis)
25. A 27-year-old man presents with a left testicular tumor with a 10 cm retroperitoneal lymph node mass. The treatment of choice is: (March 2009)
a. Radiotherapy b. Immunotherapy with interferon and inter-
leukins c. Lefthighinguinalorchidectomypluschemo-
therapy d. Chemotherapy aloneAns: c (Left high inguinal orchidectomy plus chemo-therapy)
26. The best time for surgery of hypospadias is: (March 2011)
a. 1–4 months of age. b. 6–10monthsofage. c. 12–18 months of age. d. 2–4 years of age.Ans: c (12–18 months of age)Before age of 2
27. Which of the following is most troublesome source of bleeding during radical retropubic pros-tatectomy ? (Sep 2006)
a. Dorsal venous complex b. Inferior vesical pedicle c. Superior vesical pedicle d. Seminal vesicular arteryAns: a (Dorsal venous complex)
28. The most sensitive imaging modality for diagnos-ing ureteric stone in a patient with acute colic is:
(March 2008) a. X-ray KUB b. Ultrasonogram c. Non-contrastCTscanofabdomen d. Contrast enhanced CT scan of abdomenAns: d (Contrast enhanced CT scan of abdomen)
29. Which of the following is not used as a tumor marker in testicular tumors? (Sep 2003)
a. AFP b. LDH c. HCG d. CEAAns. d (CEA)
30. Not a premalignant lesion is: (Sep2005) a. Condyloma lata b. Bowen’s disease c. Balanoposthitis d. ErythroplasiaofQueyratAns. a (Condyloma lata)

tahir99 - UnitedVRG
211Urological Surgery
Premalignant conditions of cancer penis:Dermatologic conditions:Cutaneous horn: Develops from pre-existing skin lesion like warts, nevus, traumatic abrasion
or malignancy.Pseudo epitheliomatous Micaceous keratotic Balanitis :
Present as hyperkeratotic, micaceous growth on the glans and may have some microscopic features of verrucous carcinoma
Balanitis Xerotica obliterans : Genitalvariationoflichensclerosisetatrophicusthatpresentsaswhitepatchon the prepuce or glans, often involving the meatus extending into fossa navicularis M/C in uncircumcised makes of middle age and diabetics
Leukoplakia: Present as solitary/multiple whitish plaques that often involve the meatus.
1. Condyloma acuminatum (genital/veneral warts) ○ HPV6,11,42-44:LowgradedysplasiaandGrosscondylomata ○ HPV16&18;31,33,39:Highassociationwithmalignancy.
2. Bowenoid papulosis:
3. Kaposi sarcoma: ○ Cutaneousneovascularlesion,raised,painful,Bleedingpapule;orasanulcerwithBluishdiscoloration. ○ HHV–8isthecausativeorganism. ○ Kaposi’ssarcomaofpenisisthe2ndcommonmalignancyofpenisaftersquamouscelltype. ○ Kaposi’ssarcomaofpenishasbecomearelativelycommonlesioninpatientswithAIDS. Termed carcinomas: • BuschkeLowenstein tumor (Verrucous carcinoma, giant condyloma acuminatum) • Carcinomain situ: ○ ErythroplasiaofQueyra—involvesglanspenis,prepuce ○ Bowen’sdisease—involvespenileshaft. • Pagetsdiseaseofpenis o Paget’s disease: It may often herald a deeply seated cancer with pageti cells running through ducts or
lymphatics to epidermal surface o It is seen to develop after radiation therapy to transitional cell carcinoma of bladder. Invasive carcinoma of penis M/c sites: Glans (48%), prepuce (21%) and shaft and coronal sulcus
Viral conditions
31. Thimble bladder is seen in (March 2011) a. Acute TB b. Chronic TB c. Schistosomiasis d. All the aboveAns: b (Chronic TB)32. Refluxnephropathyisdiagnosedby: (March 2005, Sep 2006) a. Micturating cystogram b. CT scan c. USG d. All the aboveAns: a (Micturating cystogram)
33. Which of the following causes orchitis without epididymitis: (Sep 2009)
a. TB b. Gonorrhea c. Syphilis d. ChlamydiaAns. c (Syphilis) 34. Drainage of venous blood after varicocelectomy is
through (Sep 2009) a. Pampiniform plexus b. Cremasteric vein c. Iliac vein d. Internal pudendal veinAns: b (Cremasteric vein)

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery212
35. Not a complication of prostatic surgery in an el-derly man: (Sep 2009)
a. Urinary retention b. Constipation c. Rupture of urethra d. EjaculatoryfailureAns: b (Constipation)
36. Following urethral rupture the immediate proce-dure to be done is: (Sep 2009)
a. Rail road tracking b. Suprapubic cystotomy c. Urinarycatheterization d. NoneAns: b (Suprapubic cystotomy)
37. Most common testicular tumor in 4th decade of life: (Sep 2009)
a. Seminoma b. Dermoid cyst c. Teratoma d. DysgerminomaAns: a (Seminoma)
38. Erythroplasia of Queyrat occurs in: (Sep 2009) a. Glanspenis b. Shaft of penis c. Base of penis d. ScrotumAns: a (Glans penis)• Carcinoma in situ of penis that occurs in the glans,
prepuce and urethral meatus is called as erythropla-sia of Queyrat
39. All of the following are predisposing factors for cancer penis, except: (Sep 2010)
a. Pagets disease b. Phimosis c. Balanoposthitis d. PapillomaAns. d (Papilloma)
40. BPH is most common in which zone? (Sep 2008) a. Peripheralzone b. Centralzone c. Transitionzone d. NoneAns. b (Central zone)
41. BPH is most common in which lobe? (Sep 2008) a. Median lobe b. Laterallobe c. Posterior lobe d. NoneAns. a (Median lobe)
42. Lord’s and Jaboulay’s operation is done for: (March 2011)
a. Rectal prolapse b. Fistula-in-ano
c. Inguinal hernia d. HydroceleAns: d (Hydrocele)
43. Golf-holeuretericorificeisseenin: (March2011) a. Ureteric calculus b. Ureteral polyp c. Tuberculosis of urinary bladder d. RetroperitonealfibrosisAns: c (Tuberculosis of urinary bladder)
44. Cause of bladder cancer are all, except: (March 2011) a. Alcohol b. Naphthylamineexposure c. Cigarette smoking d. Schistosoma hematobium Ans: a (Alcohol)
45. Painless hematuria is seen in all of the following, except: (March 2011)
a. Hypernephroma b. Renal TB c. Bleeding disorders d. Renal infarctionAns: d (Renal infarction)
46. Which of the following is not a self-retaining uri-nary catheter: (March 2011)
a. Foley b. Malecot c. Gibbon d. Red rubberAns: d (Red rubber)
47. Which of the followings renal stones may be large and still be asymptomatic for years: (March 2011)
a. Urate b. Oxalate c. Staghorn d. CystineAns: c (Staghorn)
48. Myoglobinuria is associated with which of the following: (Sep 2011)
a. Tumors b. Electricalinjury c. Crush injury d. All of the aboveAns: d (All of the above)
49. Orchidopexy for incompletely descended testis is done after the age of: (Sep 2011)
a. At birth b. 1 year c. 2 years d. 5 yearsAns: b (1 year)Ideal age = 6 months

tahir99 - UnitedVRG
17Hernia, UmbilicUs, abdominal
Wall and PeritoneUm
Contd...
Hernia Prolapse Eventration• Passageofaperitonealsacwithorwithoutabdominalcontentsthroughasiteofcongenitaloracquiredweak-nessintheabdominalwall.
• Abnormaldescentofastructure,butwithoutaperitonealcovering(sac)
• Example:Rectalprolapsed,uterineprolapse
• Itisaprotrusionofthewholecontentbecauseofabsence/defectofwall/structurethatpreventsthem
• Example:Eventerationofdiaphragm
○Hernia consists of three parts:Thesac,thecontentsofthesacandthehernialringHernial sacisprotrusionofperitoneum,whichhasaneck,abodyandafundus
Hernial ringisaweakplacethroughwhichpassesthehernialsac
The narrowest part of sac is neck
AnAtomy of inguinAl cAnAl (HousE of bAssini)3.75cmlengthExtendsfromdeepringtosuperficialringDeepringisasemiovalopeninginthefasciatransversalisSuperficialringisatriangularopeningintheexternalobliqueaponeurosis,guardedbytwocruraofmusclefibres
openings• Deep ring (DI):Halfinchabovemidinguinalpoint*(betweenanteriorsuperioriliacspineandpubicsymphysis)
• Superficial ring (SI):Justabovepubictubercle• Saphenous opening (S):4cmbelowandlateraltopubictubercle*
Walls of canalAnterior wall Posterior○ Skin,superficialfascia(superficialfattylayerofcamper,deepmembranouslayerofscarpa),deepfascialata,externalobliqueaponeurosis
○ Formedlaterallybytheaponeurosisofthetransversusabdominismuscleandthetransversalisfascia;intheremainder,theposteriorwallistransver-salisfasciaonly.Mediallytheposteriorwallisreinforcedbytheinternalobliqueaponeurosis

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery214
AnAtomy of inguinAl cAnAl (HousE of bAssini)superior inferior○ Theroofofthecanalisformedbythearchedfibersoftheloweredge(roof)oftheinternalobliquemuscleandbythetransversusabdominismuscleandaponeurosis.
○ Thewallofthecanalisformedbytheinguinalligament(Poupart’s)andthelacunarligament(Gimbernat’s)
contents of inguinal canalmales females○ Spermaticcordandilioingui-nalnerve(notiliohypogastricnerve)
○ Roundligamentinfemalesandilioinguinalnerve(notiliohypogastricnerve)
contents of spermatic cordArteries:Testicularartery,arteryofvas,arterytocremas-ter
Veins:PampiniformplexusofveinsVeinscorrespondingtoarteriesLymphaticsoftestisTesticularplexusofsympatheticnervesGenital branch of genitofemoral nerveVasdeferens
tyPEs of HErniA○ Vaginal(complete)—descendsuptoscrotumbase,testisnotfelt(sepa-rately)
○ Funicular—testisfeltseparately,processusvaginalisclosedaboveepi-didymis
○ Bubonocele—inguinalswellingonly
HEssElbAcH triAnglE○ Weakspotinanteriorabdominalwallthroughwhichdirecther-niaappears•Medial: Outerborderofrectusabdominis•Lateral: Inferiorepigastricvessels•Below: Medialpartofinguinalligament•Floor:Fasciatransversalis
○ InguinalherniaMConrightside○ Directhernianeveroccursinfemalesandrarelygetsstrangulated○ FemoralherniaisMCinfemalesthanmales○ IndirectinguinalherniaistheMCtypeofherniainfemales○ Cryptorchidismisassociatedwithindirecthernia○ Ofallherniasfemoralistheonemostliableforstrangulationbecauseofnarrowneck
Contd...
Contd...

tahir99 - UnitedVRG
215Hernia, Umbilicus, Abdominal Wall and Peritoneum
HEssElbAcH triAnglEfemoral hernia
○ Femoral canal : 2 x 2 cm size○ Medialcompartmentoffemoralsheath
Walls of femoral canalAbove—femoralringBelow—saphenousopeningAnteriorly—inguinalligamentPosteriorly—Cooper’sligamentMedially—lacunarligamentLaterally—femoralveinContents: Cloquet’snode Lymphatics Areolartissue
surgEriEs for fEmorAl HErniAlothiessen’s inguinal approach High approach of mcEvedy low operation of lockwoodInguinalincisionmadesimilartoinguinalhernia
FasciatransversalisopenedApproximateinguinalligamentwithiliopec-tinealandalsoconjointtendonwithinguinalligament
Preventsinguinalherniaalso
Verticalincisionmadeoverthefemoralcanalcontinuedabovetoinguinalligament
Veryusefulforirreducibleandstrangulatedhernia
GroincreaseincisionIndicatedinuncomplicatedfemo-ralherniaonly
Justapproximateinguinalliga-mentandiliopectinealligament
Notpreventsinguinalhernia
sliding HErniA○ MConrightside:Caecum*○ MConleftside:Sigmoidcolon*○ Others—appendix,urinarybladder,uterus,fallopiantube,ovary○ Partoftheposteriorwallformednotonlybytheperitoneum,butalsobypartofretroperitonealstructures
during surgery1.Donotdissectthesacfromtheretroperitonealstructures,justpushpartofthesacalongwiththem
2.Hernioplastyisdone
spigelian hernia Epigastric hernia of linea alba○ Occursviaspigelianfascia,whichiscomposedofaponeu-roticlayerbetweenrectusabdominisandsemilunarlinelaterally
○ OccursatorbelowarcuatelineArcuatelineliesmidwaybetweenumbilicusandpubicsymphysis
○ It is a variety of intraparietal hernia○ Itoccursinoldage>50years○ Highincidenceofstrangulation
○ Epigastricherniaorfattyherniaoflineaalba○ Itoccursvialineaalbaanywherebetweenxiphoidproceesandumbilicus
○ Alsoknownassacless hernia,onlypreperitonealpadoffatentersthedefectinalba
○ Symptomsmimicgastriculcer,endoscopyneeded
Contd...
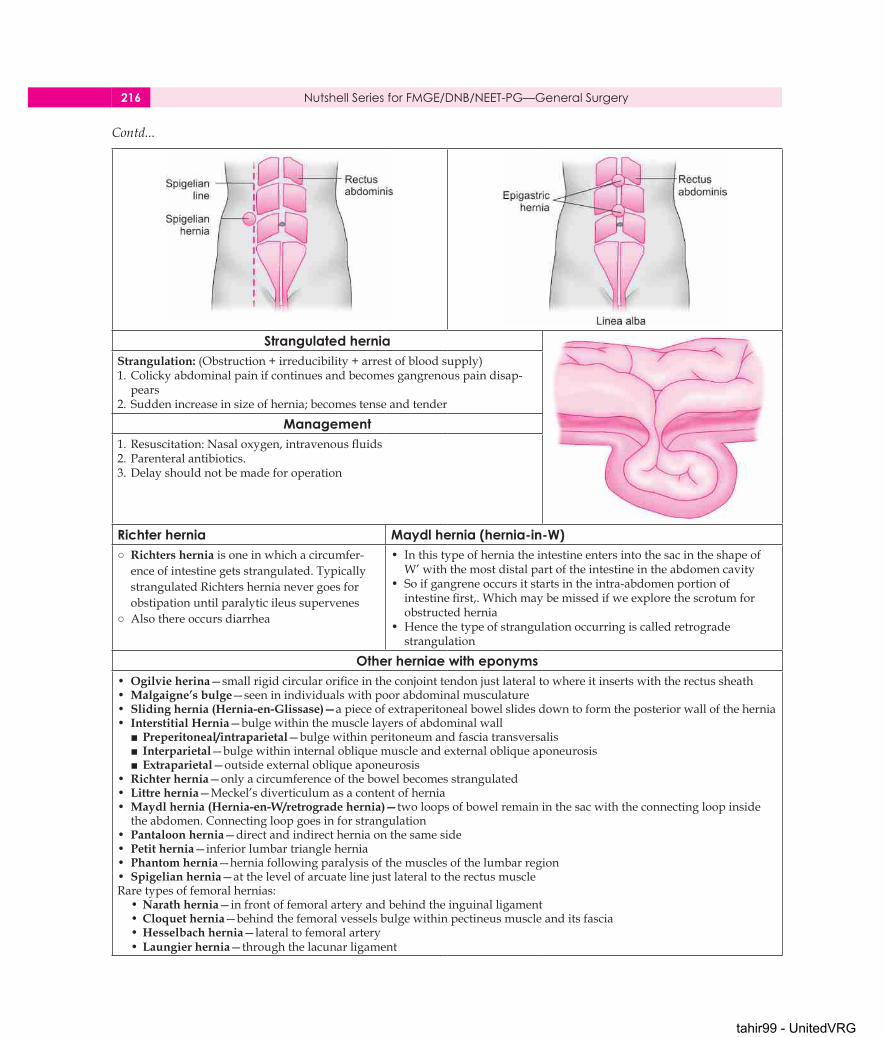
tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery216
strangulated herniaStrangulation:(Obstruction+irreducibility+arrestofbloodsupply)1.Colickyabdominalpainifcontinuesandbecomesgangrenouspaindisap-pears
2.Suddenincreaseinsizeofhernia;becomestenseandtender
management1.Resuscitation:Nasaloxygen,intravenousfluids2.Parenteralantibiotics.3.Delayshouldnotbemadeforoperation
richter hernia maydl hernia (hernia-in-W)○ Richters hernia isoneinwhichacircumfer-enceofintestinegetsstrangulated.TypicallystrangulatedRichtershernianevergoesforobstipationuntilparalyticileussupervenes
○ Alsothereoccursdiarrhea
• InthistypeofherniatheintestineentersintothesacintheshapeofW’withthemostdistalpartoftheintestineintheabdomencavity
• Soifgangreneoccursitstartsintheintra-abdomenportionofintestinefirst,.Whichmaybemissedifweexplorethescrotumforobstructedhernia
• Hencethetypeofstrangulationoccurringiscalledretrogradestrangulation
other herniae with eponyms• Ogilvie herina—smallrigidcircularorificeintheconjointtendonjustlateraltowhereitinsertswiththerectussheath• Malgaigne’s bulge—seeninindividualswithpoorabdominalmusculature• Sliding hernia (Hernia-en-Glissase)—apieceofextraperitonealbowelslidesdowntoformtheposteriorwallofthehernia• Interstitial Hernia—bulgewithinthemusclelayersofabdominalwall■Preperitoneal/intraparietal—bulgewithinperitoneumandfasciatransversalis■ Interparietal—bulgewithininternalobliquemuscleandexternalobliqueaponeurosis■Extraparietal—outsideexternalobliqueaponeurosis
• Richter hernia—onlyacircumferenceofthebowelbecomesstrangulated• Littre hernia—Meckel’sdiverticulumasacontentofhernia• Maydl hernia (Hernia-en-W/retrograde hernia)—twoloopsofbowelremaininthesacwiththeconnectingloopinsidetheabdomen.Connectingloopgoesinforstrangulation
• Pantaloon hernia—directandindirectherniaonthesameside• Petit hernia—inferiorlumbartrianglehernia• Phantom hernia—herniafollowingparalysisofthemusclesofthelumbarregion• Spigelian hernia—atthelevelofarcuatelinejustlateraltotherectusmuscleRaretypesoffemoralhernias:•Narath hernia—infrontoffemoralarteryandbehindtheinguinalligament•Cloquet hernia—behindthefemoralvesselsbulgewithinpectineusmuscleanditsfascia•Hesselbach hernia—lateraltofemoralartery•Laungier hernia—throughthelacunarligament
Contd...

tahir99 - UnitedVRG
217Hernia, Umbilicus, Abdominal Wall and Peritoneum
surgEriEs for HErniAHerniorrhaphy lichtensteins1.Herniotomy2.Narrowingofthedeepringwith2’0prolene(Lytle’srepair)3.Approximationofconjointtendonwithinguinalligamentusing1’polypropylenematerial
○ Weuseprolene mesh tobridgethegapbetweeninguinalligamentandconjointtendon
○ Thepreferredapproachforallhernia*
shouldice technique stoppas procedure○ Hegaveadditionalstrengthtotheposteriorwallbydoublebreastingthefasciatransversalis
○ Bestamongallanatomicalrepairs(herniorrha-phy)
○ Leastrecurrenceamongherniorrhaphy
○ Forbilateraldirecthernia’s,amodifiedpfannensteilincisionmadeinthelowerabdomenandahugemeshplacedinbetweentheperito-neumandthefasciatransversalis(preperitonealmeshrepair)
○ AlsocalledasGPVRS—giantprostheticvisceralreinforcementsur-gery
laparoscopic repair○ Transabdominalpreperitonealmesh(TAPP).Peritonealcavityenteredandapproachthepreperitonealspaceviaabdomencavity
○ Totalextraperitonealrepair(TEP).Peritoneumnotentered.Extraperitonealspaceentered
dEsmoid tumor○ Desmoidisatumourarisingfromthemusculoaponeuroticstructuresofab-dominalwall
○ Clinicalfeaturesofdesmoids:80%occurinfemales*SeenbelowumbilicusUnencapsulatedfibromaandtendstoinfiltratemuscleinneighbourhoodShowsslowgrowthNosarcomatouschangeseen*Alsoknownasrecurrentfibromaofpagets*
Treatment:• Widelocalexcision• Moderatelyradiosensitive
rEctus sHEAtH HEmAtomA○ ThisisduetosuddenhemorrhagefromruptureofInferiorepigastricartery○ Thesiteofthehematomaisusuallyatthelevelofthearcuateline,wheretheposteriorsheathoftherectusabdominisislacking
○ Commoninthreeagegroup:ElderlyYoungthinathletesPregnantfemales
• Itmayfollowasuddenboutofcough• Treatment—minimalhematomasleftassuchtoresolve,biggeronesneedtobeletoutbysurgery

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery218
divAricAtion of rEcti• Divaricationoftherectusabdominisisseenprincipallyinelderlymultiparouspatients
• Whenthepatientstrains,agapcanbeseenbetweentherectusabdominis,throughwhichtheabdominalcontentsbulge
• Whentheabdomenisrelaxed,thefingerscanbeintroducedbetweentherectus
• Anabdominalbeltisallthatisrequired.Thereisnoriskofstran-gulation
raspberry tumor omphalitis• PersistenceofdistalpartofVitellointestinalduct(proximalpartpersistenceiscalledasMeckel’sdiverticulum)
• AlsocalledasUmbilicaladenoma• Surgeryhastobedone.umbilectomyisindicatedifitrecursafterexcisionoftumoralone
• Infectionofumbilicalcord,resultingincrustformation
• Antibioticsandlocalsilvernitrateap-plicationisbeneficial
umbilical granuloma umbolith (umbilical calculus)• Chronicinfectionoftheumbilicalcicatrixthatcontinuesforweekscausesgranulationtissuetopoutattheumbilicus
• Differentialdiagnosis—umbilicaladenoma• Treatment—localapplicationofsilvernitrate
• Thisisoftenblackincolorandiscomposedofdesquamatedepithe-lium,whichbecomesinspissatedandcollectsinthedeeprecessoftheumbilicus
• Thetreatmentistodilatetheorificeandextractthecalculusbut,topreventrecurrence,itmaybenecessarytoexcisetheumbilicus
rEtroPEritonEAl fibrosis○ Fibroticprocessentrapsandconstrictstheureterstherebycausingobstructiveuropathy
○ Types1. Primary Idiopathic(ormondsdisease)2.Secondary
clinical features• MCinmen• Dullachingpain,nausea,anorexia• Compressionofureter,aorta,IVC• Diagnosis—intravenouspyelogram—showslater-allydeviatedureter
• CurrentlyCTScanistheprocedureofchoice• IfrenalfunctionimpairedMRIisthechoice• Rememberureterism/cobstructedatlower1/3rd
causes of secondaryInflammatory-chronicpancreatitis,histoplasmosis,tuberculosis,actinomycosis
Drugs–methysergide,alphamethyldopa,betablockers,hydralazine,
Malignancies-prostate,NHL,sarcoma,carcinoid,gastriccancerAutoimmune-ankylosingspondylitis,SLE,PAN
PEritonitis• SpontaneousbacterialperitonitisE. coli (most common)
Klebsiella(2ndmc)• SecondarybacterialperitonitisE. coli and bacterioids
Pneumoperitoneum Pseudopneumoperitoneum• Hollowviscusperforation• Postoperativeabdomen• Laparoscopy• Diagnosticproceduresinvolvingfemalegenitaltract
• Peritonealdialysis
• Distendedviscus• Chilaiditi’ssyndrome(interposition of colon with gas between liver and
diaphragm)• Subphrenicabscess• Subdiaphragmaticfat,omentalfat• Unevendiaphragm• Subpulmonarypneumothorax• Curvilinearpulmonarycollapse• Intramuralgasinpneumatosisintestinalis

tahir99 - UnitedVRG
219Hernia, Umbilicus, Abdominal Wall and Peritoneum
subPHrEnic AbscEssAnatomy
○ Thecomplicatedarrangementoftheperitoneumresultsintheformationoffourperitonealandthree*
○ extraperitonealspacesinwhichpusmaycollect.Extraperito-nealspacesareoneithersideofthebodyandoneisapproxi-matelyinthemidline
left superior (anterior) intraperitoneal (left subphrenic)Isboundedabovebythediaphragmandbehindbythelefttriangularligamentandtheleftlobeoftheliver
thegastrohepaticomentumandanteriorsurfaceofthestom-ach.Totherightisthefalciformligamentandtotheleftthespleen,gastrosplenicomentumanddiaphragm.Patientistoxic
Thecommoncauseofanabscesshereisanoperationonthestomach,thetailofthepancreas,thespleenorthesplenicflex-ureofthecolon
left inferior (posterior) intraperitoneal (left subhepatic)
right superior (anterior) intraperitoneal (right sub-phrenic)
Isanothernameforthe‘lessersac’Thecommonestcauseofinfectionhereiscompli-catedacutepancreatitis
Inpracticeaperforatedgastriculcerrarelycausesacollectionherebecausethepotentialspaceisoblit-eratedbyadhesions
LiesbetweentherightlobeoftheliverandthediaphragmItislimitedposteriorlybytheanteriorlayerofthecoronaryandtherighttriangularligaments,andtotheleftbythefalciformligament.Commoncauseshereareperforatingcholecystitis,aperforatedduodenalulcer,aduodenalcap‘blowout’followinggastrectomyandappendicitis
right inferior (posterior) intraperitoneal (right subhepatic)LiestransverselybeneaththerightlobeoftheliverinRutherfordMorison’spouchItisboundedontherightbytherightlobeoftheliverandthediaphragm.TotheleftissituatedtheforamenofWinslowandbelowthisliestheduodenum.Infrontaretheliverandthegallbladder,andbehind,theupperpartoftherightkid-neyanddiaphragm
Thespaceisboundedabovebytheliver,andbelowbythetransversecolonandhepaticflexureItisthedeepestspaceofthefourandthecommonestsiteofasubphrenicabscesswhichusuallyarisesfromappendicitis,cholecystitis,aperforatedduodenalulcerorfollowingupperabdominalsurgery
mEsEntric cyststypes—chylolymphatic (mc type) and enterogenous cyst
chylolymphatic cyst Enterogenous cystUsuallycongenitalasaresultofsequestrationoflymphatics Derivedfromdiverticulumofmesentricborderthat
hasbecomesequestratedCystwallisthin,lacksmuscularwall,notlinedbymucosa ThickwalllinedbymucosaUsuallysolitaryandoftenunilocularwithclearlymphorchyle ContentismucinousMostfrequentlyseeninmesentryofileumIndependentbloodsupply CommonbloodsupplyasadjacentbowelEnucleation is enough Resection anastomosis needed
tillaux triad ○ Recurrentattacksofabdominalpainwithorwithoutvomitingduetoobstruction
○ Acuteabdominalpainduetotorsionofmesentry,rup-tureofcyst,hemorrhageintocyst,infectionofcyst
1.Centralareaofdullnesswithzoneofresonanceallaround2.Swellingmovesperpendiculartomesentryfreely3.Softfluctuantswellingintheumbilicalregion

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery220
fmgE quEstions
1. Spigelian hernia is: (Sep 2005, 2007) a. Herniapassingthroughtheobturatorcanal b. Herniaoccurringthroughthelineaalba c. Herniathroughthetriangleofpetit d. HerniaoccurringatthelevelofarcuatelineAns: d (Hernia occurring at the level of arcuate line)
2. Strangulation most commonly occurs in: (Sep 2008) a. Femoralhernia b. Directinguinalhernia c. Indirectinguinalhernia d. LumbarherniaAns: a (Femoral hernia)
3. True regarding indirect inguinal hernia are all, except: (Sep 2009)
a. Mostcommontypeofhernia b. Alwaysunilateral c. Inguinalherniotomyisthebasicoperation d. Transilluminationdistinguishesitfromhydro-
celeAns: b (Always unilateral)
4. If caecum is involved as a part of the wall of herni-al sac and is not its content, then it will be known as: (Sep 2005)
a. Richter’shernia b. Spigelianhernia c. Slidinghernia d. InterstitialherniaAns: c (Sliding hernia)
5. Most common type of hernia in the young age group: (Sep 2006)
a. Femoralhernia b. Directinguinalhernia c. Indirectinguinalhernia d. UmbilicalherniaAns: c (Indirect inguinal hernia)
6. While operating upon strangulated hernia, the sac is opened at: (Sep 2009)
a. Neck b. Body c. Fundus d. MouthAns. c (Fundus)
7. Which of the following describes Richter’s hernia: (March 2009)
a. Thestrangulatedloopof‘W’lieswithintheabdomen
b. Herniaoccurringatthelevelofarcuateline c. Involvesonlyaportionofthecircumferenceof
thebowel d. HerniaoccurringthroughthelineaalbaAns: c (Involves only a portion of the circumference of the bowel)
8. Hernia which often simulates a peptic ulcer is: (March 2010)
a. Umbilicalhernia b. Incisionalhernia c. Strangulatedhernia d. FattyherniaoflineaalbaAns: d (Fatty hernia of linea alba)
9. Which of the following is the most pathognomon-ic sign of impending burst abdomen: (March 2007)
a. Fever b. Shock c. Pain d. SerosanguinousdischargeAns: d (Serosanguinous discharge)
10. All of the following regarding diagnosis of acute peritonitis are correc, except: (March 2006)
a. RaisedWBCcountinperitonealaspirate b. Moderatelyraisedamylaselevelsarediagnos-
ticofperitonitis c. CTscanmayaidindiagnosis d. Uprightfilmsshowsfreeairunderthedia-
phragmAns: a (Raised WBC count in peritoneal aspirate)(ReferPage995BaileyandLove,25thedition)Investigationsforperitonitis:• RaisedbloodWBCcountandCRP• Serumamylasemoderatelyelevated• Abdomen radiographs show free gas under dia-phragm,
• USGandCTaidindiagnosis• Peritonealdiagnosticaspirationmaybehelpful
11. A patient on antibiotics for treatment for peritoni-tis presents with mucus diarrhea. Most probable cause could be: (March 2008)

tahir99 - UnitedVRG
221Hernia, Umbilicus, Abdominal Wall and Peritoneum
a. Ulcerativecolitis b. Activationoflatenttuberculosis c. Antibioticassociateddiarrhea d. GastritisAns: c (Antibiotic associated diarrhea)
12. All of the following conditions are associated with raised amylase level, except: (March 2006)
a. Carcinomapancreas b. Perforatedulcer c. Acutepancreatitis d. AcuteappendicitisAns: d (Acute appendicitis)Increasedbloodamylaselevelsmayoccurdueto:• Acutepancreatitis• Cancerofthepancreas,ovariesorlungs• Cholecystitis• Gallbladderattackcausedbydisease• Gastroenteritis(severe)• Infectionofthesalivaryglands(suchasmumps)orablockage
• Intestinalblockage• Macroamylasemia• Pancreaticorbileductblockage• Perforatedulcer• Tubalpregnancy(mayhaveburstopen)Decreasedamylaselevelsmayoccurdueto:• Cancerofthepancreas• Damagetothepancreas• Kidneydisease• Toxemiaofpregnancy 13. Serum amylase level is increased in all of the fol-
lowing, except: (March 2005) a. Intestinalobstruction b. Perforatedulcer c. Acutepancreatitis d. AcuteappendicitisAns: d (Acute appendicitis)
14. Pneumoperitoneum is created by: (March 2009) a. O2 b. CO
c. CO2 d. N2OAns: c (CO2)
15. Painful, tender, non reducible sac through the inguinal canal with absent cough impulse. Diag-nosis is: (Sep 2008)
a. Strangulatedhernia b. Orchitis c. Irreduciblehernia d. TorsiontestisAns: a (Strangulated hernia)
16. Which is not a cause for burst abdomen: (March 2011) a. Abdominaloperationlastingmorethan2hours b. Incompletesuture c. Infection d. PoorgeneralconditionofpatientAns: a (Abdominal operation lasting more than 2 hours)
17. Non-metabolic cause of abdominal pain: (March 2011) a. DKA b. Sicklecellanemia c. Hyperparathyroidism d. PorphyriaAns: b (Sickle cell anemia)Metabolicandendocrinecausesofpainabdomen:• Diabetesketoacidosis• Hypercalcemia• Acuteintermittentporphyria• Adrenalinsufficiency• Poisonsanddrugs
18. Viscera, forms a wall in which of the following hernia: (March 2011)
a. Lumbarhernia b. Slidinghernia c. Epigastrichernia d. FemoralherniaAns: b (Sliding hernia)

tahir99 - UnitedVRG
18ElEctivE NEurosurgEry
Raised intRacRanial pRessuRe• Normalintracranialpressure(ICP)variesfrom5to15mmHgintheadultatrest
• Resultsinreducedcerebralperfusionandbrainherniation• ThemajorcausesofraisedICParehematomas,tu-morsandhydrocephalus
Monro-Kellie doctrine• Skull contains—brain, cerebrospinal guild (CSF) andblood to-gethermaintaintheICT.
• Ifoneincreasestheotheronecompensatesforpressurebydecreasing.
Theremayalsobediplopiaduetoasixthnervepalsy;thisnerveisvulnerabletodownwardscerebralshiftofanycauseduetoitslongintracranialcourse,sometimescalleda false localising sign.Theremaybeabnormalitiesofconjugategaze.
Inparticular,impairedupgazeorsun-settingmaybeseenaspartofParinaud syndrome,causedbypressureonthedor-salmidbrain.
Sun set sign—hydrocephalus
signs of raised ict in infants○ Papilledema○ Sixthnervepalsy○ Impairedupgaze○ Focalneurologicaldeficits○ Impairedconsciouslevel
• Progressivemacrocephaly• Bulginganteriorfontanelle• Dilatedscalpveins• Sun-settingeyes
Cerebrospinal fluid pathway• CSFflowsfromthelateralventricles,throughtheforamenofMonro,intothethirdventricle
• ThenintothecerebralaqueductandfourthventriclebeforeexitingintothesubarachnoidspaceviathemidlineforamenofMagendieandlateralforaminaofLuschka
Contd...

tahir99 - UnitedVRG
223Elective Neurosurgery
CSF physiology ProductionHydrocephalusisaconditioninwhichthereisdis-equilibriumbetweenCSFproductionandabsorp-tion,leadingtoraisedICPandisoftenassociatedwithdilatedventricles.
Volume:150mL
• 20mLh–1,80%bychoroidplexus• Activeprocess• Absorptionatarachnoidvilli• Pressuredependent• Relativetoplasma• ReducedK+andCa2+• IncreasedCl–andMg2+• pH7.33–7.35(slightlyacidiccomparedtoplasma)
Types of hydrocephalusObstructivehydrocephaluslesionswithintheventricle Communicatinghydrocephalus ExcessiveCSFproduction(rare)• Lesionsintheventricularwall• Lesionsdistantfromthe• Ventriclebutwithamasseffect
• Posthemorrhagic• CSFinfection• RaisedCSFprotein
• Choroidplexus• Papilloma/carcinoma
Block at I: Foramen of Monro and 3rd ventricle Gliosis ChiasmalgliomasColloidcyst Craniophryngiomas ArachnoidcystsBlock at II: AqueductPinealtumors/ParinaudsyndromeductalstenosisPeriductal/subependymalgliosisBlockatIII:4thventricleandbasilarobstructionMedulloblastoma/ArachnoiditisEpendymomas/Arnold-ChiarisyndromeAstrocytomasDandy-WalkersyndromeBlockatIV:WhenpassingbasalcisternArachnoiditis—Posthemorrhagic,postmeningiticBlockatV:AbsorptiveobstructionArachnoiditis—Posthemorrhagic,Postmeningiticvenousthrombosis
investigationsLumbarpunctureiscontraindicatedinobstructivehydrocephalusbecauseoftheriskofcausingtonsillarherniationanddeath.
Magneticresonanceimaging(MRI)
• CTscan• Inchildren,chronicraisedICPcanresultincopperbeatingoftheskull
• Copper-beating-chronic raised intracranial pressure.
Treatment of hydrocephalus○ Aventriculoperitonealshuntinvolvestheinsertionofacatheterintothelateralventricle(usuallyrightfrontaloroccipital)
○ Thecatheteristhenconnectedtoashuntvalveunderthescalpandfinallytoadis-talcatheter,whichistunnelledsubcutaneouslydowntotheabdomenandinsertedintotheperitonealcavity.
○ IftheCSFpressureexceedstheshuntvalvepressure,thenCSFwillflowoutofthedistalcatheterandbeabsorbedbytheperitoneallining.
○ Otheroptionsfordistalcatheterplacementincludetherightatriumviathedeepfacialandjugularvein(ventriculoatrialshunt)orthepleuralcavity(ventriculo-pleuralshunt)
Contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery224
intRacRanial tuMoRs○ Intracranialtumorsmaypresentwithseizures,focalneurologicaldeficit,raisedICPorendocrinedisturbanceCerebralmetastasesarethemostcommonintracranialtumorsBenigntumorsmaycauselife-threateningintracranialcomplicationsForaggressivetumours,managementoptionsincludesteroids,surgery,radiotherapyandchemotherapy
Feature of brain tumors• Intracranialtumorscanpresentwithseizures,focalneurologicaldeficits,raisedICP,seizuresorendocrinedysfunctionorcanbeincidentalfindings.
FND:• Withregardtothetime-courseofneurologicalsymptoms,asteadyprogressionofsymptomsovertimesuggestsastruc-turallesionmorethantheacutedeficitofvascularpathology.
• Anexceptiontothismaybetheacutedeficitproducedbyhemorrhageintoamalignantglioma,amelanomametastasisorpituitaryapoplexy.
• Frontal lobe lesions tendtopresentwithpersonalitychange,gaitataxiaandurinaryincontinence,contralat-eralhemiparesisifposteriorfrontalanddysphasiaifinvolvingtheleftinferiorfrontalgyrus.
• Parietal lesions areassociatedwithsensoryinatten-tion,dressingapraxia,astereognosisandifonthedominantside,acalculia,agraphia,left–rightdisorien-tationandfingeragnosia(Gerstmannsyndrome).
• Temporal lobe lesionsmaybeassociatedwithdisturbanceofmemory,contralateralsuperiorquadrantanopiaorhemipare-sisand,ifonthedominantside,dysphasia.
• Occipital lesions areoftenassociatedwithvisualfielddefi-cits,mostcommonlyanincompletecontralateralhomony-moushemianopia
• Otherclassicalfocaldeficitsassociatedwithtumorsinclude:bitemporalhemianopiawithapituitary macroadenoma;
• Anosmia,ipsilateralopticatrophyandcontralateralpapilledemawithananteriorskull base meningioma (Foster-Kenne-dy syndrome);
• Ipsilateralhearingloss,tinnitusanddysequilibriumwithavestibular Schwannoma.
ClassificationNeuroepithelial tumors○ Gliomas—astrocytomas,oligoden-drogliomas,ependymoma,choroidplexustumor
○ Pinealtumors○ Neuronaltumous—ganglioglioma,gangliocytoma,neuroblastoma
○ Medulloblastoma
Nerve sheath tumours—Vestibularschwannoma
Tumor-like malformations—Craniophar-yngioma,epidermoidtumor,dermoidtumorandcolloidcystMeningeal tumors:Meningioma
○ Pituitarytumors○ Germcelltumors—germinoma○ Lymphomasteratoma
Metastatic tumors○ Contiguousextensionfromregionaltumors,e.g.glomustumor

tahir99 - UnitedVRG
225Elective Neurosurgery
Supratentorial infratentorial (posterior fossa)• Astrocytoma(allgrades)(50%)• Craniopharyngioma(2%–5%)• Others:Pinealregiontumors,choroidplexustumors,ganglioglioma,DNET
• Medulloblastoma(15-20%)• Cerebellarastrocytoma(15%)• Ependymoma(9%)• Brainstemastrocytoma
Highgradeastrocytoma(e.g.glioblastomamultiforme(GBM)(12–15%)Metastasis(15%–30%,includesinfratentorial)Meningioma(15%–20%)Lowgradeastrocytoma(8%)Pituitaryadenoma(5%–8%)Oligodendroglioma(5%)Other:Colloidcyst,CNSlymphoma,dermoid/epidermoidcysts
MetastasisAcousticneuroma(Schwannoma)(5–10%)Hemangioblastoma(2%)Meningioma
age○ <15year○ Incidence:2–5/100,000/year○ 60%infratentorial
○ >15year○ 80%supratentorial
GlioMas○ Gliomasincludeastrocytomas,oligodendrogliomasandependymomas.TheyaregradedaccordingtotheWHOclassification.
○ AgradeItumor,suchasapilocytic astrocytoma,istheleastaggressive;agradeIVtumor,suchasaglioblastoma multiforme,isthemostaggressive
○ Pilocyticastrocytomaismostcommoninchildrenandyoungadults,withapeakincidenceattheageof10years.
○ Diffuse astrocytomas (WHOgradeII)aremostcommoninthe4thdecadeoflifeandoftenpresentwithseizuresorareincidentalfindings
○ High-gradegliomas,includinganaplastic astrocytomas (WHO grade III) and glioblastoma (WHO grade IV) aremostcommoninthe4thand6thdecadesofliferespec-tively.
○ Glioblastomaisthemostcommonadultglialtumor.
MC points from this area○ MCglioma—astrocytoma○ MCbraintumors—Metastasis(bailey) Astrocytomas(osbornneuro)○ MCastrocytomas—glioblastomamultiforme
treatmentSurgeryisusuallyfollowedbyhigh-dose(60Gy)focusedirradiationforthosepatientswithagoodperformancestatus.Chemotherapyoptionsincludeoraltemozolomide,eitherconcurrentlyorafterradiotherapy
ceRebRal Metastasis○ Cerebralmetastasesarebyfarthemost common intracranial tumorsandwillaffectapproximatelyoneineveryfourcancersufferers.
○ Themajorityofpatientswithcerebralmetastaseshavemultiplele-sionsandarenotsuitablecandidatesforsurgery.
○ Palliationwithsteroidsandwhole-brainirradiationremainoptions
Most common sites of primaryLung40Breast10–30Melanoma5–15Colon,renalUnknown15
MeninGioMa• Meningiomasarisefrommeningothelialcellsandrepresentaround15–20%ofallintracranialtumors.
• Meningiomasareusuallybenignalthoughatypicalandmalig-nantformscanoccur.Around80%aresupratentorial
• Meningiomasdisturbbrainfunctionbymasseffect,stimulationofvasogenicedema,directbraininva-sionorobstructivehydrocephalus.
• Treatmentisresection

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery226
Pituitary adenoma Pituitary tumors• Constituteabout10%–15%tumorsinbrain.• Themostcommonpituitaryadenomasareprolactinoma(30%),non-functioningadenoma(20%),growthhormonesecretingadenoma(15%)andadrenocorticotrophichormone(ACTH)—secretingadenoma(10%).
• Pituitary apoplexy resultsinthesuddenonsetofheadache,visualloss,ophthalmoplegiaandpossiblyalteredconsciouslevel.Itiscausedbyhemorrhagicinfarctionofapituitarytumor.ThesuddenheadacheandmeningismissimilartothepresentationofaneurysmalSAH.
• Mostcommonsellartumorsinadults• M/csellartumorinchildren—craniopharyn-gioma
• M/cpituitaryadenoma—prolactinoma• Theyarethem/ccauseofhyperpituitarism• Pituitarystone—duetodystrophiccalcifica-tionofprolactinoma.
pediatRic bRain tuMoRs○ Intracranialtumorsarethemostcommonsolidtumorsinchildren.○ In neonates,tumorstendtobeofneuroectodermaloriginandmost
are supratentorial.Tumortypesinclude:•Teratoma;•Primitiveneuroectodermaltumor;•High-gradeastrocytoma;•Choroidplexuspapilloma/carcinoma.
o Inolder children,themajorityoftumorsareinfratentorialandoneofthreetypes:•Medulloblastoma•Ependymoma•Pilocyticastrocytoma.
Othertumorsincludesupratentoriallow-gradegliomas,craniopharyngiomaandbrainstemgliomas
FMGe and dnb questions
1. TheCNStumorthatpresentwithcalcificationis: a. Oligodendroglioma b. Astrocytoma c. Medulloblastoma d. PheochromocytomaAns: a (Oligodendroglioma)
2. Suprasellarcalcificationwithpolyuriaisseenin: a. Medulloblastoma b. Pinealoma c. Craniopharygioma d. AstrocytomaAns: c (Craniopharygioma)
3. Which of the tumor is highly vascular in nature? a. Glioblastoma b. Meningioma c. Pituitaryadenoma d. EpidermoidatCPangle
4. Which of the following route is preferred for pi-tuitary surgery?
a. Transcranial b. Transethmoidal c. Transphenoidal d. TranscallosalAns: c (Transphenoidal)
5. Which of the following is the most common type of glial tumors?
a. Astrocytoma b. Medulloblastoma c. Neurofibroma d. EpendymomaAns: a (Astrocytoma):
6. Most common spinal tumor is: a. Meningioma b. Ependymoma c. Neurofibroma d. NeuroblastomaAnsc(Neurofibroma)M/c in spinal cord• M/cspinaltumor—metastasis• M/cprimaryspinaltumor—neurofibroma,schwan-noma(nervesheathtumor)
• M/cextraduraltumor—metastasis• Mostcommonintramedullarytumor—ependymoma• M/cintraduralextramedullarytumor—nervesheathtumor.
7. Raised intracranial pressure will cause:
(Sep 2007) a. Tachycardia b. Hypotension c. Papilledema d. NormallookinganteriorfontanelleininfantsAns: c (Papilledema)

tahir99 - UnitedVRG
19CardiothoraCiC Surgery
MediastinuMa. Superior mediastinumb. Anterior mediastinum c. Middle mediastinum d. Posterior mediastinum
anterior mediastinum• Thymoma(m/C)• Lymphoma• Germcelltumors• Mesenchymaltumors• Thyroidandparathyroidthymomas
Middle mediastinum• Cysts(m/c—pleuropericardial,bronchogenic,enterogenousandneuroenteric)
• Vascularmasses(aneurysm)• Lymphnodes• Mesenchymaltumors• pheochromocytoma
Posterior mediastinum Mostcommonanteriormediastinalmass—thymomaMostcommonmediastinalmass—neurogenictumorsMostcommonmalignantmassofmediastinum—lym-phomas
Mostcommonmediastinalmassinchildren—neuro-genictumor
• Neurogenictumors(m/coverall)• Meningoceles• Gastroentericcyst• Mesenchymaltumors• Pheochromocytoma• lymphoma
Bronchogenic cyst Congenitallunglesion,whicharisesfromtheanomalousdevelopmentofforegutortracheobronchialtree.
Contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery228
Bronchogenic cyst○ Mostofthemariseinmediastinum,but15%occurinpulmonaryparenchyma.
○ Inlungsmostcommoninrightlung,lowerlobes.○ Linedbycuboidalorciliatedepitheliumandareusuallyfilledwith
mucoid material
complications of bronchogenic cyst Infection Atelectasis Tensionpneumothorax
Lung sequestration○ Asequestrationconsistsofnormallydevelopedbronchiolesandalveolisuppliedbysystemicratherthanpulmonaryarteries95%oftimethisbloodsupplyisfromaorta.M/cinlowerlobes,leftmorecommonthanright.
extralobar sequestration intralobar sequestration25% 75%Drainviaazygousvein DrainviapulmonaryveinDonotcommunicatewithlung Theyareincommunicationwithtracheo-
bronchialtreeAssociatedwithcongenitaldia-phragmatichernia
Pronetoinfectionandlungabscess
Pancoast tuMor○ Itisatumoroftheapexoflung(squamouscellorepidermoidcancer)○ Causesdestructionoffirstandsecondribs.○ Maygrowtocause—shoulderpain,erosionofribsandHornersyndrome
Lungs and PLeuraempyema of lungs
○ Empyema(pusinlungs)istheendstageofpleuralinfectionfromanycause;thepathologicaldiagnosisrequiresthepres-enceofthickpuswithathickcortexoffibrinandcoagulumoverlung.
causes complications of empyema• Infectionofanycause—TB,pneumonia(m/ccause)*,bronchiectasis,fungalandlungabscess
• Traumatichemothoraxgettinginfected
• Pleuraleffusionontreat-ment
• Surgeriesinthorax• Extrapulmonarysources—subphrenicabscess
• Boneinfections—ribosteomyelitis
• Empyemanecessitans(spon-taneousdecompressionofpusthroughthechestwall)
• Chronicempyema(withen-trappedlungandpulmonaryrestrictivedisease)
• Osteomyelitis• Pericarditis• Mediastinitis• Bronchopleuralfistula• Disseminatedinfectionofcentralnervoussystem
treatment• Drainageofpus—drainmustbekeptatthebottomofcavityandmustexitanteriortomidaxillaryline
• Ifthedrainageisinsufficientdecorticationofthelungisperformed
Contd...

tahir99 - UnitedVRG
229Cardiothoracic Surgery
hydatid cyst of lung amebic lung abscess• Lungissecondcommonsiteafterliverforhydatidcystinfec-
tion• Only10%ofthehydatidcystsoflungshaveassociatedhe-paticcyst
• 20%casesarebilateral• M/csiteislowerlobe*• Calcificationisveryrare(Itisverycommoninliverhydatidcyst)
• Mayruptureintobronchialtree
• Infectionspreadsdirectlythroughdiaphragm• M/careaoflunginvolvedisrightlowerlobe*• Amebicliverabscessmayruptureintorightlung(m/c)*,leftlung,rightorleftpleuralcavity,pericar-diumorperitonealcavity
• Itisthesecondcommoncomplicationofamebicliverabscess(m/ccomplicationofliverabscessissecondarybacterialinfection)
Foreign Body in Lung• Mostcommonsiteofdislodgementinlungsisrightmainstembronchusorrightlowerlobe*(becausetherightmainstemiswider,shorterandverticallyplaced)
Most common lobes for aspirationsupine position sitting or erect position• Rightupperlobe—posteriorsegment*• Rightlowerlobe—superiorsegment• Leftlowerlobe—superiorsegment
• Rightbasilarsegmentoflowerlobe(rightlowerlobe—basalsegment)*
Bronchogenic canceretiological factors Pathological types• Cigarettesmoking(85%–95%)• Atmosphericpollution• Occupation(radioactiveoreandchromiummining)
• Smallcelllungcancer(Oatcellcancer)• Non-smallcelllungcancer(NSCLC)Ratioofsmallcelllungcancer:Non-smallcelllungcancer(1:4)Pathologicalstagingisveryimportantformanagement.
histological types• Small cell lung cancer—(oat cell cancers) 20%EarlymetastasistolymphnodesandbybloodbornespreadMediansurvivalinmonthsRespondtochemotherapySurgeryhaslittleplace
• Squamous cell cancer:Appearsaswellcavitatingcancer
• Large cell undifferentiated:TypeofNSCLCandisincludedinneuroendocrine
tumor• Adenocarcinoma:MostcommonofNSCLChavingovertakensquamouscellcancernow
Increasedincidenceinwomen
• Bronchioalveolar carcinoma:Groundglassappearance
squamous cell ca adenocarcinoma small cell ‘ca’ Large cell ‘ca’○ McvariantinIndian○ Subcontinent○ Pancoast tumor is histologi-
cally SCC○ Mostlycentralindistribution○ Itcancavitate○ Best prognosis ○ M/cassociatedparaneoplas-ticsyndromeishypercalce-miaandhypophosphatemia*
○ T/tbysurgicalexcision
○ Overall Mc histological type ○ Mctypeinnon-smoker,youngandfemale
○ Mostlyperipheralindistribu-tion
○ Overallprognosisisgood○ Maymetastasizetooppositelung(thisisduetoaerosoltransmission and is seen more frequentlyinbronchoalveolartype)
○ Most aggressive form of lung ‘Ca’ (rapidly growing)
○ Mostlycentralindistribution○ Itrespondbesttochemother-apyandradiotherapy
○ Worst prognosis (Least resectability)
○ Mctypecausingextrathoracicmetastasis
○ Strong association with smoking
○ Itmaycausegyne-comastia
○ Galactorrheadueto ectopic prolac-tin secretion.
Lung‘Ca’istheleadingcauseofcancerdeathinbothmaleandfemale
McsiteofmetastasisisliverMcendocrineorganinvolvedisadrenal
LungCaisMctumormetastasizingtoheartBrainmetastasismaypresentwithneurologicaldeficit
Contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery230
Bronchogenic cancerclinical features
• Hemoptysis—lessthan50%cases• Cough—commonsymptom,butnon-specific• Localizedpain—duetoinfiltrationofanintercos-talsnerve
• Pancoasttumor—invasionofapicalareamayinvolvebrachialplexus
• Dyspnea• Pleuraleffusion• Clubbingandhypertrophicpulmonaryosteoarthropathy(resolvewithexcisionofcancer)
• Hoarsenessofvoiceduetorecurrentlaryngealnerveinvolvement
• Dysphagia(esophaguscompression)
• Superiorvenacavalobstruction• Smallcellcarcinoma:DevelopmentofmyopathiesincludingEaton-Lambertsyndrome,whichissimilartomyastheniagravis
tumor, node, metastasis (tnM) staging○ T1:Tumor<3cm;notinvolvesmainbronchus○ T2:Tumor>3cm;involvesmainbronchus○ T3:Anysizeinvolvingchestwall,diaphragm,mediastinalpleura,parietalpericardium,ortumorsinmainbronchus <2cmfromcarina,butnotinvolvingcarina.
○ T4:Anysizeinvadesmediastinum,heart,greatvessels,tra-chea,esophagus,vertebralbody,carinaorpleuraleffusionorpericardialeffusion*orsatellitenodules
• N1:Ipsilateralperibronchialandipsilateralhilarnodesandintrapulmonarynodes
• N2:Ipsilateralmediastinalandsubcarinalnodes• N3:Contralateralmediastinalorhilar,ipsilateralorcontralat-eralscalenenodesorsupraclavicularnodes.
M1:Distantmetastasis.
Management modalitiescancer tnM staging small cell cancer non-small cell cancerEarlystage(IA/IB/IIA/IIB)
IA-T1N0M0 Radiotherapyandchemo-therapy
Preoperativechemotherapyfollowedbysurgery
IB-T2N0M0 “ “IIA-T1N1M0 “ “IIB-T2N1M0IIB-T3N0M0
“ “
Locallyadvanced,butsurgicallyresectable disease
IIIA-T3N1M0T1/2/3N3M0
Inoperable Combinedmodality(Chemotherapy+radiotherapy+Surgery)
Locallyadvanced,butsurgicallyunresectable
IIIB-T4N0/1/2M0T1/2/3/4N3M0
Inoperable Radiationtherapy+chemo-therapy
Metastatic disease IVM1
Inoperable Chemotherapyonly
Contd...
Contd...
tahir99 - UnitedVRG
231Cardiothoracic Surgery
Bronchogenic cancer5 year survival of each cancer
• Squamouscellcancer:35%–50%(Bestprognosis)• Adenocarcinoma:25%–45%• Adenosquamous:20%–35%
• Undifferentiated:15%–25%• Smallcellcarcinoma:0%–5%(badprognosis)*
Paraneoplastic syndrome (non-metastatic complication)small cell ‘cancer’ squamous cell ‘ca’ Large cell ‘ca’ adeno ‘ca’ExcessADHsecretioncausesSlADHandhyponatremia
EctopicACTHcauseshypokalemiaandCushingsyndrome
MyasthenicEaton-LambertsyndromeRetinalblindnessCerebellardegeneration
EctopicPTH’andPTHrelatedpeptideproductioncauses—hypercalcemiaand
hypophosphatemia#Clubbing—inallnon-smallcell‘Ca’
Gynecomastia Maycausehypertrophicpul-monaryosteoarthropathy.
Migratorythrombophlebitis (Trousseau’ssyndrome)DlCwithleukoerythroblasto-
sis.
other paraneoplastic manifestations• Peripheralneuropathies• Subacutecerebellarandcorticaldegeneration
• Polymyositisanddermatomyositis• Nephroticsyndromeandglomerulonephritis• Acanthosisnigricans
heartcardiac surgery
• Cardiopulmonarybypass(CPB)wasfirstsuccessfullyusedin1953byGibbon*• CPBmachinetakesovertheventilationandcirculation
coronary artery bypass graftinganatomy of coronary artery invasive methods of diagnosiso Coronaryarteriesarebranchesofascendingaorta.Rightfromanteriorsinusandleftfromleftposteriorsinus.
Gold standardforimagingiscoro-naryangiography
Demonstratesextent,severityandlocationofstenosis
Reductionindiameter>70%isconsideredassevere
EvaluatessuitabilityofsurgeryAidsinprognosticassessment
Left coronary artery:• Worstprognosisintermsofsurvivalwithoutsurgery• Leftmainstemdisease• Branches:Leftanteriordescending(LAD)oranteriorinterventriculararteryandObtuse/marginalbranchesofcircumflexartery
• LADisthemostfrequentlydiseasedarteryandmostoftenbypassedduringcoro-naryarterybypassgrafting(CABG)
right coronary artery:• Continuesasposteriordescendingarteryorinterventricularartery
indications for surgery: surgery is indicated for symptomatic or prognostic reasons• >50%stenosisoftheleftmainstem(criticalleftmaindisease)*• >70%stenosisoftheproximalleftanteriorinterventricularartery
• Allthreemaincoronaryarteriesdiseased(Triplevesseldisease)
• Poorventricularfunctionassociatedwithcoronarydisease.
conditions and surgerieschronic stable angina: Percutaneous transluminal coro-naryangioplasty(PTCA)andstent-ingismorecommonlyusedthanCABGnow.
acute coronary syndrome:Unstableanginabecomeasymptomaticwithin48hourofmedicalantianginadrugs
IfthepatientdevelopsrecurrentanginaandECGchanges—thrombolysisandPTCAisusedmorethansurgery
IfsurgeryistobedoneelectiveCABGtobedoneatleastafter6week
Contd...
Contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery232
heartcardiac surgery
Surgery for complication of myocardial infarction (MI): Myocyte necrosis and ventricular septal rupture:Presentsafter3to7daysofinfarctionwithpulmonaryedema,pansystolicmurmurandhypotension.RepairiswithapericardialorartificialDacronpatch.
Papillary muscle necrosis:Causesacutemitralregurgitation,apansystolicmurmurandpulmonaryedema.Mitralvalvereplacementisusuallynecessary.
Ventricular aneurysm:Partialthicknessnecrosisofventricularwall,iffreewallisreplacedwithnon-contractilefibroustissue.RepairisundertakenusingCPBandCABGisundertakenatthesametimeifnecessary.
contraindications for surgery• Smalldiffuselydiseasedarteries• Diffusediseaseandheartfailure
• AcuteMIover6hoursold• Moribundpatientsafterresuscitation
seLection oF conduitVenous grafts arterial graft○ Long saphenous vein*isthemostcom-monlyusedveinasaconduit
○ 10yearpatencyrateforlongsaphenousveingraftsisreportedtobe50%–60%with10%–15%occludingin1year
○ Alternativeveinsareshortsaphenousveinandcephalicvein
○ Left internal mammary artery or internal thoracic artery has become the conduit of choiceforLAD
○ 10yearpatencyratesare90%*○ Internalmammaryarterieshavesomelimitationslikesternalwoundinfec-
tions in diabetes○ Radialarteryisusedinthosecasesassecondoralternativearterialbypassgraft(Allens testhastobepeformedbeforeharvestingradialartery).Thistestlooksforthepatencyofulnararteryforpalmararch
Postoperative complications survival• Bleeding• Arrythmias(sinustachycardiaism/cfollowedbyatrialfibrillation)• Poorcardiacoutputstate• Neurologicaldysfunction• Woundinfection• Mortality(2%–3%)
• 95%at1year• 90%at5years• 75%at10years• 60%at15years.
MyxoMa•Mcprimarycardiactumor• Mostlyin3rdto6thdecade,withfemalepredilec-
tion. • Mostlysporadic,somefamilialAlzheimerdisease(AD)transmission
• Sporadicformsaresolitary,locatedmostlyinleftatria,arisingfrominteratrialseptumnearfossaovalis
• Familialformsaremultipleandventricularinloca-tionandisknownforrecurrence
clinical features• MCclinicalfeatureisthatofMSorMR• Ventricularformmaypresentwithobstructivefeature.• Embolicandconstitutionalsymptomsincludefever,weightloss,arthralgia,rash,clubbing,Raynaudphenomenon,hyper-gammaglobulinemia,anemia,polycythemia,thrombocytosisorthrombocytopenia,etc.
○ Diagnosis:2Decho,CTorMRItodeterminesize,shape○ Treatment:Surgicalexcision
Contd...

tahir99 - UnitedVRG
233Cardiothoracic Surgery
FMge questions
1. Which of the following subtype of lung carcinoma produces superior vena cava syndrome most com-monly: (Sep 2008)
a. Small cell carcinoma b. Adenocarcinoma c. Anaplastic carcinoma d. SquamouscellcarcinomaAns: a (Small cell cancer)
2. Vein used in bypass surgeries is: (Sep 2006)
a. Longsaphenousvein b. Shortsaphenousvein c. Cephalicvein d. none Ans: a (Long saphenous vein)

tahir99 - UnitedVRG
20Burns and CosmetiC surgery
Burns○ Effects of burns: Burnscausedamageinanumberofdifferentways,butbyfarthemostcommonorganaffectedistheskin
respiratory system○ WarningsignsofburnstotherespiratorysystemBurnsaroundthefaceandneckAhistoryofbeingtrappedinaburningroom
Changeinvoice Stridor
Dangers of smoke inhalationInhaledhotgasescancausesupraglotticairwayburnsandlaryngealedema
Inhaledsteamcancausesubglotticburnsandlossofrespiratoryepithe-lium
Inhaledsmokeparticlescancausechemicalalveolitisandrespiratoryfailure
Inhaledpoisons,suchascarbonmonoxide,cancausemetabolicpoisoning
Fullthicknessburnstothechestcancausemechanicalblockagetoribmovement
Metabolic problems following burns○ Burns produce an inflammatory reaction○ Thisleadstovastlyincreasedvascularpermeability○ Water,solutesandproteinsmovefromtheintratotheextravascularspace
○ Thevolumeoffluidlostisdirectlyproportionaltotheareaoftheburn
○ Above15%ofsurfacearea,thelossoffluidproducesshock
Contd...

tahir99 - UnitedVRG
235Burns and Cosmetic Surgery
BurnsOther complications of burns• Infectionfromtheburnsite,lungs,gut,linesandcatheters• Malabsorptionfromthegut
• Circumferentialburnsmaycompromisecircula-tiontoalimb
MajOr DeterMinants Of the OutcOMe Of a Burn• Percentageofsurfaceareainvolved • Depthofburns • Presenceofaninhalationalinjury
criteria for admission to a burns unit schwartz mentions the area○ Suspectedairwayorinhalationalinjury○ Anyburnlikelytorequirefluidresuscitation○ Anyburnlikelytorequiresurgery○ Patientswithburnsofanysignificancetothehands,face,feetorperineum○ Patientswhosepsychiatricorsocialbackgroundmakesitinadvisabletosendthemhome
○ Anysuspicionofnon-accidentalinjury○ Anyburninapatientattheextremesofage○ Anyburnwithassociatedpotentiallyserioussequelaeincludinghigh-ten-sionelectricalburnsandconcentratedhydrofluoricacidburns
○ Partialthicknessandfullthicknessburnstotaling>10%totalbodysurfacearea(TBSA)under10yearsage
○ Partialthicknessandfullthicknessburnstotaling>20%TBSAinotheragegroup.
○ Fullthicknessburns>5%TBSAinanyagegroup
○ Anyburnsinface,hands,feet,genitalia,perineumandmajorjoint
assessing the area of a burn
○ Thepatient’swholehandis1%TBSAandisausefulguideinsmallburns
○ TheLundandBrow-derchartisusefulinlargerburns
○ Theruleofninesisadequateforafirstapproximationonly
Ruleofnine(Alexander-Wallacerule)
o Eachupperlimb—9%TBSAo Eachlowerleg—18%TBSAo Anteriororposteriortrunk—18%TBSAo Headandneck—9%TBSAo Perineum—1%TBSAo Inchildrenheadandneckisrelativelylargemayaccountfor18%–21%
o Infants—21%TBSA
Contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery236
superficial Burns have capillary filling○ Deeppartialthicknessburnsdonotblanch,buthavesomesensation
○ Fullthicknessburnsfeelleatheryandhavenosensation
Degrees Of Burns○ First degree involvesonlyepidermis○ Second degree involvesepidermisandsomepartofdermis.(alsoknownaspartialthicknessburns)
○ Furtherdividedinto:Superficialseconddegreeorsuperficialpar-tialthicknessinvolvesupperpartofdermis
Deepseconddegreeordeeppartialthick-nessextendsuptoreticularlayerofdermis. ○ Third degree orfullthicknessburnsinvolvesfullthicknessofdermis
○ Fourth degree burnsinvolvessubcutaneousfatanddeepstructures
first degree second degreesuperficial
second degreedeep
third degree
NoblisterformationBlanchtotouchPainfulHealwithoutscarringin5–10days
Blisters formedBlanchtotouchPainfulHealwithoutscarringin7–14days
BlistersseenMottledpinkandwhitecolorbecauseofvaryingbloodsupplytodermis
Pain is absentHeals with scar 3-9 week
Eschar formationBlackorbrownPainlessHealswithwoundcontractureorbysplitskingraft(SSG)only.
ManageMent Of Burnsimmediate care follow-up care○ Sedation○ Analgesicsandantibiotics○ Fluidresuscitation○ Escharotomy
○ Dressing○ Woundcover○ Latecare○ Skingrafting○ Contracturerelease
fluids for resuscitation ideal fluid○ Inchildrenwithburnsover10%TBSAandadultswithburnsover15%TBSA,considertheneedforintravenousfluidresuscitation
○ Iforalfluidsaretobeused,saltmustbeadded○ Fluidsneededcanbecalculatedfromastandardformula○ Thekeyistomonitorurineoutput
○ Therearethreetypesoffluidused.ThemostcommoniscrystalloidsCrystalloids:RingerlactateorHartmannsolution;Colloids:Humanalbuminsolutionorfresh-frozenplasma
Somecentersusehypertonicsaline.
about crystalloids hypertonic saline colloids○ Ringerlactateisthemostcommonlyusedcrystalloid.Crystalloidsaresaidtobeaseffectiveascolloidsformain-tainingintravascularvolume
○ Hypertonicsalinehasbeeneffectiveintreatingburnsshockformanyyears.Itproduceshyperosmolarityandhypernatremia
○ Plasmaproteinsareresponsiblefortheinwardoncoticpressurethatcounteractstheoutwardcapillaryhydrostaticpressure
Contd...
tahir99 - UnitedVRG
237Burns and Cosmetic Surgery
ManageMent Of Burnsabout crystalloid hypertonic saline colloids○ Theyarealsosignificantlylessexpen-sive
○ Anotherreasonfortheuseofcrystal-loidsisthatevenlargeproteinmol-eculesleakoutofcapillariesfollowingburninjury;however,non-burntcapillariescontinuetosieveproteinsvirtuallynormally
○ Thisreducestheshiftofintracellu-larwatertotheextracellularspace
○ Advantagesincludelesstissueedemaandaresultantdecreaseinescharotomiesandintubations
○ Withoutproteins,plasmavolumeswouldnotbemaintainedastherewouldbeedema
○ Proteins should be given after the first 12 hours of burn because,beforethistime,themassivefluidshiftscauseproteinstoleakoutofthecells
parkland formula Muir and Barclay formula○ TBSA%×weight(kg)×4=volume(mL)needed○ Halfofthisvolumeisgiveninthefirst8hoursandthesecondhalfisgiveninthesubsequent16hours
○ Thevolumereplacementisbycrystalloid
○ Thecommonestcolloid-basedformulaistheMuirandBarclayformula:
0.5×percentageofbodysurfaceareaburnt×weight=oneportion;periodsof4/4/4,6/6and12hourrespectively;oneportiontobegivenineachperiod
Maintenance○ Thekeytomonitoringofresuscitationisurineoutput.○ Itshouldbebetween0.5and1.0mL/kg/1bodyweightperhour.○ Iftheurineoutputisbelowthis,theinfusionrateshouldbeincreasedby50%
escharotomy○ Circumferentialfullthicknessburnstothelimbsrequireemergencysurgery
○ Thetourniqueteffectofthisinjuryiseasilytreatedbyincisingthewholelengthoffullthicknessburns.
○ Thisshouldbedoneinthemidaxialline,avoidingmajornerves.
level of escharotomies • Upper limb: Midaxial,anteriortotheelbowmediallytoavoidtheulnarnerve• Hand: Midlineinthedigits• Lower limb midaxial:Posteriortotheanklemediallytoavoidthesaphenousvein
• Chest:Downthechestlateraltothenipples,acrossthechestbelowtheclavicleandacrossthechestatthelevelofthexiphisternum
tOpical treatMent• Wounddressing• Vaselinedressingimpregnatedinchlorhexidine• Fenestratedsiliconesheet• Hydrocolloid dressings: Hydrocolloiddressingsneedtobechangedevery3–5days.Theyareparticularlyusefulinmixed-depthburnasthehighproteaselevelsundertheocclusivedressingsaidwiththedebridementofthedeeperareasofburn.Theyalsoprovideamoistenvironment,whichisgoodforepithelialization
• Biological, synthetic (e.g. Biobrane) and natural (e.g. amniotic membrane) dressings alsoprovidegoodhealing,theywillbecomedetachedifappliedtodeepdermalwoundsastheescharneedstoseparate.Theyarethere-forenotasusefulinmixed-depthwoundsandbetteronlyforsuperficialburnsasonestopmanagement
healing of a third degree burns Management of deep burns Delayed reconstruction of burns• Collagendressing• Grafting• Earlydebridementandgraftingisthekeytoeffectivelytreatingdeeppartialandfullthicknessburnsinamajorityofcases
• Meshedgrafts
• Deepdermalburnsneedtangentialshavingandsplit-skingrafting
• All,butthesmallestfullthicknessburnsneedsurgery
• Theanesthetistneedstobereadyforsignificantbloodloss
• Topicaladrenalinereducesbleeding• All,burnttissueneedstobeexcised• Stablecover,permanentortempo-rary,shouldbeappliedatoncetoreduceburnload
• Eyelidsmustbetreatedbeforeexpo-surekeratitisarises
• TranspositionflapsandZ-plastieswithorwithouttissueexpansionareuseful
• Full-thicknessgraftsandfreeflapsmaybeneededforlargeordifficultareas
• Hypertrophyistreatedwithpressuregarments
• Pharmacologicaltreatmentofitchisimportant
Contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery238
cOsMetic surgeryMethods of wound closure
1.Graft: Itisone,whichistakenfromonesiteandkeptinanothersite,ithasnoownbloodsupplyandhastoderiveitsbloodsupplyfromtherecipientsite.
2.Flaps:Itisone,whichcarriesitsownbloodsupplywithittocovertherecipientsite.
facts aBOut skin grafts• Skingraftstakeswellovergranulationtissue,muscleandfat
• Itwouldnotadhereonbone,tendonandcartilagedevoidofperiosteum,paratenonandperichondriumrespec-tively.
two types of skin graft1.Fullthicknessuptothefulldermis—Wolfe graft2.Partialthickness:uptosuperficiallayerofdermis—Thiersch graftInpartialthicknessgraftasweareleavingapartofthedermis,skingrowsbyitselfandnoneedofanyclosureofthedonorsite
Infullthicknessgraftasthereisnodermisskincannotgrowtheresowehavetoclosethedonorsitebysomeway
partial thickness (thiersch) full thickness (Wolfe)• Easyuptakeandsurvival• Largegraftscanbederived• Samesitegraftcanbetaken• Cosmeticallyunacceptable• Donorsitehealswithoutcontarction• MCsiteisthigh
• Uptakeisdifficult• Onlysmallgraftscanbetaken• Cosmeticallygood• Donorsitehastobeclosedorelseitwillhealwithcontracture.• MCsiteisbehindear
cannOt We graft every WOunD? Why DO We neeD flaps?• Foragrafttosurviveavascularbedisamust• Ifawoundcangranulateandtheextrawaitingdoenotdamageexposedtissuesonecannotforagraft
• Ifwoundisincapableofgranulatingorifwaitingisharmfulaflapshouldbeused
• Exposedpacemaker• Radiationnecrosis• Heelpadavulsion—exposedcalcaneus
types Of flaps1.Pedicle flap:Theflap,whichhasitsownbloodsupplywithanamedbloodvesselisusedtocoveraexposedarea.
2.Free flap:Thisisatypeofflap,whichhasitsownbloodves-sel,buthastoundergomicrovascularanastomosiswithanybloodvesselneartherecipientarea
axial anD ranDOM flaps• Ifthebloodsupplyisnotderivedfromarecognizedartery,butrathercomesfrommanylittleunnamedvessels,theflapisreferredtoasarandom flap.Manylocalcutaneous(skin)flapsfallintothiscategory
• Ifthebloodsupplycomesfromarecognizedarteryorgroupofarteries,itisreferredtoasanaxial flap.Mostmuscleflapshaveaxialbloodsupplies
○ Rotation:Coverwoundsofvarioussizes○ Commonuse:Sacralpressuresores
○ Transposition:Usefulwhennotenoughlaxityofsurround-ingtissuetocreateothertypesofflaps
Contd...

tahir99 - UnitedVRG
239Burns and Cosmetic Surgery
axial anD ranDOM flaps○ Z-plasty:Usedtoreorientandlengthenascarattheex-penseofwidth(releasescarcontractures)
○ Commonuse:Dupuytrendisease
Advancement flaps (single/bipedicle, V-Y, Y-V)V-Yflaps:Woundswithlaxsurroundingtissue;thepedicleisthedeeptissueunderlyingtheflap
lOcal flap• Transpositionflap • Advancementflap • B/Lgluteusmaximusmyocutaneous
V-Yadvancementflap
terMs in plastic surgery• Plasma imbibition—graftsurvivesuptofirst48hourbyplasmaimbibition,absorptionofnutrientsintograft.
• Inosculation—designatestheperiodinwhichthedonorandrecipientcapillar-iesbecomealigned.
• Revascularization and angiogenesis—afterapproximately5dayrevasculari-zationoccursandgraftdemonstratesbotharterialandvenousoutflow.
time of each process • Plasmaimbibtion—upto24hours• Inosculation—24–72hours• Revascularization—after72hours
cleft lip/palate○ Thetypicaldistributionofclefttypesis:Cleftlipalone:15%Cleftlipandpalate:45%Isolatedcleftpalate:40%
• Cleftlipwithpalatepredominatesinmales • Whereascleftpalatealoneappearstobemorecommonin
females. • Inunilateralcleftlipthedeformityaffectstheleftsidein60%ofcases.
associated syndromes • PierreRobinsequenceremainsthemostcommonsyn-drome
• Stickler(ophthalmicandmusculoskeletalabnormalities),• Shprintzen(cardiacanomalies)• Downsyndrome• ApertandTreacher–Collinssyndromesaremostfrequentlyencountered
types
timing of surgery rule of 10 lip for cleft lip repair• Closureofcleftpalateshouldbedoneat6 month ageasitaidsinchildfeeding
• Pharyngealflapoperationisoperationofchoice• LangenbachoperationandWardilloperation
• Weightofbabyis10pound• Hemoglobinis10gm%• Ageof10week
Contd...
Contd...
tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery240
cleft lip/palatetiming of repair for cleft lip alone
cleft lip alone timing○ Unilateral (one side) Oneoperationat5–6months○ Bilateral (both sides) Oneoperationat4–5months
timing of repair for cleft palate alone○ Soft palate alone Oneoperationat6months○ Soft and hard palate Twooperations Softpalate—6months
Hardpalate—15–18months
cleft lip and palatetypes timingUnilateral Twooperations Cleftlipandsoftpalateat5–6months
Hardpalatewithgumswithorwithoutrevisionoflipat15–18monthsBilateral Twooperations Cleftlipandsoftpalateat4–5months
Hardpalatewithgumswithorwithoutrevisionoflipat15–18months
DnB questiOns
1. Late deaths in burns is due to: a. Sepsis b. Hypovolemia c. Contracture d. NeurogenicAns: a (Sepsis)
2. An adult with both lower limb charred with exter-nal genitalia the percentage of burns is:
a. 18% b. 19% c. 36% d. 37%Ans: d (37%)
3. Sepsis in burns cases is due to: a. Proteus b. Pseudomonas c. Pneumococci d. StaphylococciAns: b (Pseudomonas)
4. In burns heat loss is due to: a. Dilatationofveins b. Exposedareabyevaporation c. Shock d. NoneAns: b (Exposed area by evaporation)
5. In second degree burns, re-epithelialization oc-curs around:
a. 1week b. 2weeks c. 3weeks d. 4weeksAns: c (3 weeks)
6. Late deaths in burns is due to: a. Sepsis b. Hypovolemia c. Contracture d. NeurogenicAns: a (Sepsis)
7. An adult with both lower limb charred with exter-nal genitalia the percentage of burns is:
a. 18% b. 19% c. 36% d. 37%Ans: d (37%)
8. In burns, which of the following is the medium of choice:
a. Dextrose b. Ringerlactate c. IsolyteM d. GlucoseAns: b (Ringer lactate)

tahir99 - UnitedVRG
241Burns and Cosmetic Surgery
9. All of the following are true regarding fluid resus-citation in burnt patients, except:
a. ConsiderIVresuscitationinchildrenwithburnsgreaterthan15%
b. Oralfluidsmustcontainsalts c. MostpreferredisRingerlactate d. Halfthefluidcalculatedisgivenin8hours.Ans: a (Consider IV resuscitation in children with burns greater than 15%)At 10% in children and 15% in adults fluid must be given
10. Within 48 hours of transplantation the graft sur-vives due to:
a. Amountofsalineingraft b. Plasmaimbibition c. Newvesselsgrowfromdonorsite d. Connectionbetweendonorandrecepientcap-
illariesAns: b (Plasma imbibition)
11. Ideal graft for leg injury 10*10 cm raw area expos-ing bone is:
a. Amnioticmembranegraft b. Pedicleflap c. SSGfullthickness d. PartialthicknessflapAns: b (Pedicle graft)Skingraftisabsolutelycontraindicatedwithinfectionsofstreptococci
12. True statement of axial flap is: a. Carriesitsownvesselswithinit b. Keptinlimb
c. Transverseflap d. CarriesitsownnervesupplyAns: a (Carries its own vessels within it)
13. Full thickness grafts can be taken from the follow-ing sites, except:
a. Elbow b. Backofneck c. Supraclavicularfossa d. UppereyelidsAns: None Fullthicknessgraftforfaceistakenfrombehindearandsupraclavicularareaforcolormatch.
14. What is the appropriate age for repair of cleft pal-ate?
a. 6monthsto1year b. 12to15month c. Atpuberty d. JustbirthAns: a (6 month to 1 year)
15. A midline cleft palate is due to failure of fusion between:
a. Maxillaryprocess b. Medialnasalprocess c. Medialandlateralnasalprocess d. Medialnasalandlateralmaxillaryprocess.Ans: a (Maxillary process)EmbryologyPremaxilla—medialnasalprocessPalatineprocess—derivedfrommaxillaryprocessSecondary palate: Fusion of twopalatine process (de-rivedfrommaxillaryprocess)andpremaxilla.Defectofthisresultsincleftpalate.
fMge questiOns
1. All of the following are true regarding fluid resus-citation in bum patients, except: (Sep 2009)
a. Considerintravenousresuscitationinchildrenwithburnsgreaterthan15%TBSA
b. Oralfluidsmustcontainsalts c. MostpreferredfluidisRingerlactate d. Halfofthecalculatedvolumeoffluidshould
begiveninfirst8hours
Ans: a (Consider intravenous resuscitation in children with burns greater than 15% TBSA)Explanation:
• IVresuscitationforchildrenwithburnsgreaterthan10%andforadultsabove15%
• Parklandformula—halfthecalculatedvolumegivenin8hoursandremaininghalfin16hours

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery242
2. According to 'rule of nines', burns involving peri-neum are: (Sep 2002, 2009)
a. 1% b. 9% c. 18% d. 27%Ans:a(1%)Explanation:*Wallaceruleof9%–1%forperinealburns
3. Which of the following is not seen in third degree burns: (Sep 2009)
a. Lossofskinappendages b. Novesicles c. Redcolor d. ExtremelypainfulAns: d (Extremely painful)Explanation:Thirddegreeburns(fullthicknessburns)•Involvesfulldermis•Escharformationiscommon•Painlessburns
4. In second-degree burns, re-epithelialization oc-curs around: (Sep 2008)
a. 1week b. 2weeks c. 3weeks d. 4weeeksAns : c (3 weeks)(Ref: Bailey and Love, 25th Edn, Page 382)Explanation:*Superficialpartialthicknessburns(2degree)—healsat2weeks*Deeppartial, thickness (third degree)—heals at 3 ormoreweeks
5. Which of the following is false regarding deep second degree burns: (Sep 2011)
a. Healbyscardeposition b. Painless c. Damagetodeeperdermis d. LessblanchingAns: d (Less blanching) (Ref: Bailey and Love, 25th Edn, Page 382• Thecolorofdeeppartialthicknesswillnotblanchun-dertheexaminersfingersonpressureunderexamin-ersfingers
• Deepdermalthicknessburnshealswithhypertroph-icscar.
• Sensationisreduced.Patientisunabletodistinguishsharpfrombluntpressurewhenexaminedwithnee-dle.
6. In bums management, which of the following is the medium of choice: (Sep 2008)
a. Dextrose5% b. Normalsaline c. Ringerlactate d. Isolyte-MAns: c (Ringer lactate)(AlreadyexplainedinTopic)
7. Graft is not taken up by the following tissue: (Sep 2011) a. Fat b. Muscle c. Skullbone d. DeepfasciaAns: c (Skull bone)
8. Most common congenital anomaly of the face is: (Sep 2011) a. Cleftlipalone b. Isolatedcleftpalate c. Cleftlipandcleftpalate d. AllhaveequalincidenceAns: c (Cleft lip and cleft palate)
9. Not seen in third degree burns. (Sep 2009) a. Novesicle b. Redcolor c. Painful d. LossofskinappendagesAns: c (Painful)
10. Palmar surface of hand corresponds to: (Sep 2010) a. 1%oftotalbodysurfacearea b. 2%oftotalbodysurfacearea c. 3%oftotalbodysurfacearea d. 4%oftotalbodysurfaceareaAns: a (1% of total body surface area)
11. In burns management (within 24 hours), which of the following is the medium of choice:
(March 2011) a. Dextrose5% b. Normalsaline c. Ringerlactate d. Isolyte-MAns: c (Ringer lactate)

tahir99 - UnitedVRG
243Burns and Cosmetic Surgery
12. A patient with burns die within 24 hours. What could be the most probable cause: (Sep 2011)
a. Circulatoryshock b. Physicalburninjurytotheairwaysabovethe
larynx c. Physicalburninjurytotheairwaysbelowthe
larynx d. CircumferentialburnAns: a (Circulatory shock) 13. Initial method to prevent infection in burm pa-
tients: (Sep 2011) a. Physiotherapy
b. Intravenousantibiotics c. Handwashing d. TopicalantibioticsAns: b (Intravenous antibiotics)
14. False statement about cleft palate repair is: (March 2011) a. Hemoglobinshouldbe10gram% b. Weightshouldbe10pounds c. Repairedimmediatelyafterbirth d. 2stageprocedure,ifassociatedwithcleftlipAns: c (Repaired immediately after birth)
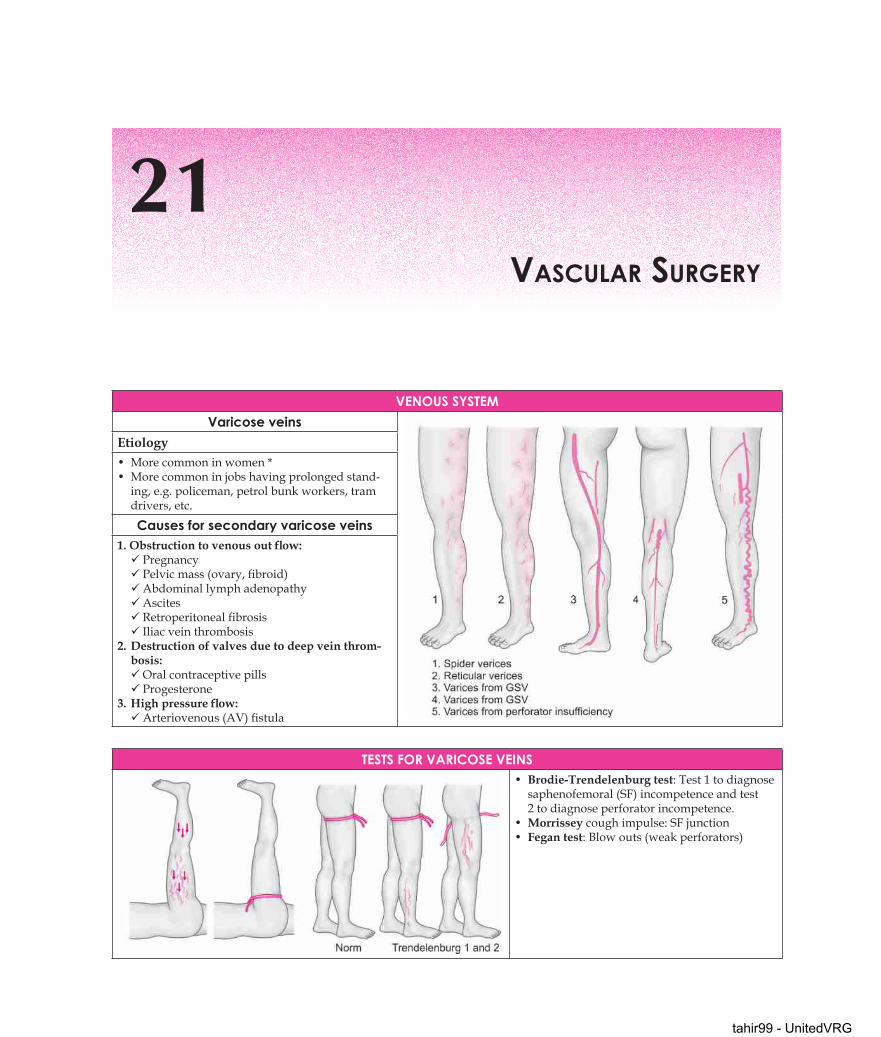
tahir99 - UnitedVRG
21Vascular surgery
Venous systemVaricose veins
Etiology• Morecommoninwomen*• Morecommoninjobshavingprolongedstand-ing,e.g.policeman,petrolbunkworkers,tramdrivers,etc.
Causes for secondary varicose veins 1. Obstruction to venous out flow:PregnancyPelvicmass(ovary,fibroid)AbdominallymphadenopathyAscitesRetroperitonealfibrosisIliacveinthrombosis
2.Destruction of valves due to deep vein throm-bosis:OralcontraceptivepillsProgesterone
3.High pressure flow:Arteriovenous(AV)fistula
tests for VariCose Veins• Brodie-Trendelenburg test:Test1todiagnosesaphenofemoral(SF)incompetenceandtest2todiagnoseperforatorincompetence.
• Morrissey coughimpulse:SFjunction• Fegan test:Blowouts(weakperforators)

tahir99 - UnitedVRG
245Vascular Surgery
short saphenous inCompetenCyKlippel-trenaunay sydnrome Venous ulcer : (stasis ulcer)1.Abnormallateralvenouscomplex(shortsaphenous)2.Capillarynevus3.Bonyabnormalities4.Aplasiaofdeepveins5.Limblengthening.○ It is a mesodermal abnormality and not familial
• Site: Lowerone-thirdmedialsideofleg• Size: Variable• Shape: Ovaltocircular • Margin: Well-defined • Edge: Slopingedge(healing) • Floor: Formed by deepfascia• Surrounding:Pigmentation,eczema,varicosity• Base: Extenduptoperiosteum. • Deformity: Talipesequinovarus
Lipodermatosclerosis Complications of venous ulcer• Progressivesclerosisoftheskinandsubcutaneoustissuemayoccurduetofibrindeposition,tissuedeathandscarringduetochronicvenoushyper-tension.
○ Ulcercomplicatesvaricoseveininabout5%ofthepeople.○ Marjolin’s ulcer*:Malignantchangeinlong-standingvenousulcertosqua-mouscellCa.
○ Periosteitis tibia:Occursinlong-standingulceronmedialsurfaceoftibia.○ Equinus deformity:Walkingontoerelievespain,sopatientcontinueswalkingresultinginshorteningoftendo-Achilles
perforator inCompetenCei. Subfascial ligation of Cockett and Dodd:PreferableincasesoflipodermatosclerosisLongincisionmadetoopenthedeepfasciaandtheperforatorsareligateddeeptodeepfascia
ii.Suprafascial ligation of Linton:Thereshouldnotbelipodermatosclerosis Perforatorsareligatedabovethedeepfasciaiii. Subfascialendoscopicperforatorsurgery(SEPS)○ Nerveatriskduringgreatsaphenousvein(GSV) stripping issaphenousnerve○ Toavoidinjurydonotstripbeyondthemidcalflevel○ Nerveatriskatstripping of small saphenous vein (SSV) issuralnerve
Deep Vein thrombosis• MCcause—hospitaladmissionformedicalorsurgicalconditions• E-thrombosis:Thrombosisdevelopinginpeoplesittingattheircomputerforlongtime.• Bilateraldeepveinthrombosis(DVT)isseenin30%cases.SignsofDVT• Homan’s sign—forceddorsiflexion • Mosse’s sign—calftenderness • Pratt’s sign—calftendernesson
pressingfromsides

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery246
• Modified Perthes test—elastocrepebandagetesttodiagnoseDVT.
VirChow’s triaD• Endothelialdamage• Stasis• Increasedcoagulabilityofblood
Clinical featuresMCpresentation—painandswellingincalf.
treatment• Startheparinimmediately,followedbywarfarin10mg/day1,2and5mgfromday3• Thrombolysisisindicatedifthereisiliacveininvolvement• Surgicaltreatment:Palma operationIncasesofDVToftheexternaliliacveinononeside,thecontralateralsaphenousveinisanastomosedtothefemoralveinontheaffectedsitebelowthelevelofocclusionorstenosis.
Latest treatments to varicose veins○ Endovenous ablation of the GSV using radiofrequency (RF) or laser without high ligation is becoming a less invasive
alternative to ligation and stripping. ○ Endoscopicvenouslaserablation:EVLA○ TheELAS:VNUSclosure○ Ultrasound-guidedfoamsclerotherapy
Contd...

tahir99 - UnitedVRG
247Vascular Surgery
VirChow’s triaDsclerosants used
• Ideallypolidocanolisusedforultrasonography(USG)guidedfoamsclerotherapy.
• Complicationsoffoamsclerotherapy:CutaneousulcerationDVTifitentersdeepveinSevereheadaches(duetoairenteringheartandthentobrain)
TransientblindnessStroke
few Line about DupLex sCan○ ThebestinvestigationtodiagnosethevenousincompetencyandDVTisduplex(B-modecolorUSG)○ OnpressingtheveinsinthecalfandhavingtheprobeattheSFjunction○ Inference:Upwardflowofveinsisindicatedbyblue colorOnreleasingthepressurethereisnoreflux,whichwhenpresentisindicatedbyred color.
points from baiLey anD LoVe• Thecompressionstockingsusedforvaricoseveins
Class 2 stockings with30mmHgatankleand10-15mmHgatkneelevel.
• MostcommonlyuseddrugforinjectionsclerotherapyisSodium tetradecyl sulfate
• BestagentforfoamsclerotherapyisPolidocanol • M/canomalyofGSV—doublesaphenousvein
• M/ccomplicationofvaricoseveinsurgeryrecurrence.• M/csiteofaplasiaofvenoussystemisIVC• M/csiteofdeepveinthrombosisiscalf veins• May-Thurner and Cockett syndrome alsocalledasiliacveincompressionsyndrome:Membranousocclusionofleftcommoniliacveinwhenitpassesbehindtherightcommoniliacartery.
arteriaL systemaneurysm abdominal aortic aneurysm• MCsiteoflargevesselaneurysmisabdominalaorticaneu-rysm
• MCsiteofperipheralaneurysmispoplitealartery
• 95%aneurysmsareinfrarenal• Siteofrupture:m/csite=posterolateral(80%)• 2ndm/csite=anterior
Contd...
Contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery248
arteriaL systemIndications for surgery • Allsymptomaticaneurysm(m/csymptomisbackandabdominaldiscomfort)• Aneurysmsizeis>55 mm* onUSGanteroposteriorly.
postoperative complication• MCisrespiratory—lowerlobeconsolidation,atelectasisandshocklungandcardiac—ischemiaandinfarction• Colonicischemiain10%cases—resolvesspontaneously*• Recentadvance—endovascularrepair
popLiteaL artery aneurysm• MCperipheralarteryaneurysm(70%)• Two-thirdbilateral• One-thirdaccompaniedbyaorticdilatation
• Complication—thrombosisfollowedbydistalischemiculceration• Indicationforsurgery—size>25mm• MCperipheralarteryaneurysm
○ Hunterian ligature: Ligationofthearteryproximaltotheaneurysmabovethefirstcollateral
myCotiC aneurysm• Misnomercausedbyinfectionduetostaphylococcal.• MCsiteisfemoralarteryfollowedbyaorta.
• MCcauseistraumafollowedbybacteremia• Falseaneurysm
amputationsConebearing(prosthesispossible)
Endbearing(wherelimbfittingfa-cilitiesarelimited)
• Belowknee(stump=8cmpreferably10-12cmbelowknee)
• Aboveknee(stump=20cmaboveknee)
• Gritti-stokes(transcondylaratlowerfemur)
• Throughknee• Symeamputation(tibiaandfibulaaresectionedabovetheanklejointpreserv-ingbloodsupplytocalcaneus)
Contd...
Contd...

tahir99 - UnitedVRG
249Vascular Surgery
amputations• ThroughAnkle(Syme)notsuitableforseverelyischemiclimbsbecauseofpoorhealingofflap• Lisfranc’s(tarso–metatarsal)
GanGrene• Wet (moist) Infectionandputrefactionarepresentwithinfectionpredominant,e.g.diabetic
• Drydryandwrinkledgangrene,e.g.atheromatous
arteriaL stenosis anD oCCLusion○ MCcauseatheromaIntermittentclaudication:• Broughtbywalking• Notpresentontakingfirststep(dd.Osteoarthrosis)• Relievedbystanding(dd.Lumbarandnerveproblems)
• MCsiteofclaudicationiscalf• Lerichsyndromebuttockclaudication+sexualimpotency
Choice of procedures Graft material• Aortofemoral• Femeropopliteal• Femorodistal• Axillobifemoral bypass:○ Salvageprocedureforpoorriskpatientswithbilateraliliacarteryocclusionusingalongprostheticgraft.
○Rememberitshouldnotbedoneforintermittentclaudica-tion.Itisadvisedonlyforimpendinggangrenecases
Best grafts• Superficialfemoralarteryocclusion—saphenousvein*• Infrapoplitealocclusions—saphenousvein*• AortoiliacDacron*Best materials• Aorta—2/0and3/0prolene• Femoral—4/0and5/0• Infrapopliteal—7/0prolenes
subCLaVian aneurysm• Occlusionoffirstpartofsubclavianarteryresultsinsubclavianstealsyndrome=vertebralarteryprovidingacollateraltoarmwithresultantcerebralischemia
ainhum• Usuallyaffectsblackmen• Barefootwalkers• Afissureappearsatthelevelofinterphalangealjointofatoe,littletoe• ComplicationNecrosis• Z-plastyandamputation.
seLDinGer’s teChnique• RetrogradeSeldingertechniqueisusedtoenterthevesselbypercutaneouspuncturetechnique• Usedforvariousdiagnosticandtherapeutictechniques• Especiallyforpercutaneoustransluminalangioplasty(PTA)forocclusionandstenosis
Contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery250
buerGer’s Disease/thromboanGitis obLiteransshionaya criteria Clinical features• H/osmoking• Onsetbeforeageof50year• Infrapoplitealarterialocclusion• Eitherarminvolvementorphlebitismigrans• Absenceofriskfactorsforatherosclerosisotherthansmoking
• M/cinyoungmales(40–45years)• Claudicationoffeet,legsorarms,hands• Superficialthrombophlebitis(40%)• There will be involvement adjacent veins and nerves*• Onexaminationpoplitealpulseispresentandtherewillbeabsentdorsalispedisandanteriortibialonbothsides(bilateral)
investigations• Absence of other risk factors likediabetes,hypertensionandhypercholesterolemiamustberuledout• Angiographyshowstreeroot/spiderlegorcorkscrewcollaterals.
Lumbar sympatheCtomyprinciples indications○ Increasebloodflow(byvasodilatation)○ Nutritivevalueforsmallulcers○ Reducesischemicrestpain○ Noeffectoncollateralcirculation
○ Restpain*○ Ulcers*○ Superficialgangrene*○ Notusefulforintermittentclaudication**○ ContraindicatedifABPI>0.3andindiabetics**(Diabeticshaveautonomicneuropathyalreadysotherewouldnotbeanybenefitonsympathectomy)
Ganglia removed Cervicodorsal sympathectomy• L2andL3ganglionectomyadvised• IfL1isremovedpreserveitforatleastforoneside(retrogradeejaculationoccurs)
• Treatmentofpalmarhyperhidrosis*• T1,T2andT3removedpreservingthestellateganglion*(Hornersyndrome—ptosis,miosis,enophthalmosisandanhydrosisonremovalofstellateganglion*)
raynauD Disease• Primary—Idiopathic(Raynauddisease)**• Secondary—Raynaud’sphenomenonsecondarytoscleroderma,SLEandrheumatoidarthritis.
• Vibratingwhitefinger—secondaryRaynaudsyndromefollowusingvibratingtoolsinfactory.
Clinical features:• 70%–90%inyoungfemales• Upperlimb*m/caffected• AbnormalsensitivitytocoldStages:1.Localsyncope—white,
2.Localasphyxia—blue3.Recovery—crimsonred
Treatment○ Raynaud disease:Protectfromcold,avoidnailinfections,nifedipine,cervicodorsalsympathectomy
○ Raynaud syndrome treatthecause
acrocyanosis• ConfusedwithRaynaud,buttheimportantdifferenceisitispainlessandnotepisodic**

tahir99 - UnitedVRG
251Vascular Surgery
arterioVenous fistuLa• Abnormalcommunicationbetweenarteryandveineithercongenitaloracquired.• MCcauseforacquiredAVfistula—penetratingtrauma**
• MCcauseoverallissurgicallycreated**• Localgigantism
Changes Clinical features○ Structurally:Veinsaredilatedandtortuouswiththickwalled(arterialized)
○ Physiologically:Increasedvenousreturn,increasedpulserate,increasedpulsepressure,increasedcardiacoutput.
○ Localgigantism,ulcersandbleeding
PulsatilesuperficialswellingContinuousthrill(machinerymurmur)Nicoladoni sign or Branham sign**:Pressureproximaltofistulacausestheswellingtodiminishinsize,thrillandbruittoceaseandpulse rate slows (bradycardia)*
points from bailey and LoveDisappearing pulse:Incasesofstenosisorocclusionofvesselwhenthepatientexercisesthealreadypalpablepulsesgoesimpalpable.Thisisduetodilatationofvesselsonexercises.
Renal artery stenosis:PTAisprocedureofchoiceFogarty catheter isusedtoremovetheintra-arterialemboli.Air embolism treatment:Trendelenburgheaddownposition,placethepatientinleftlateral,airaspirationvialeftcostalmarginandnasaloxygen.
Parasites causing embolus:OvaofTaenia echinococcusandfilariasanguinishominis.Materialsusedfortherapeutic embolization : Gelfoamsponge,plastic,balloons,ethylalcoholandmetalcoils.
LymphatiC systemLymph edema
• MCcauseoflymphedemainIndia/alloverworld=filariasis* • MCcauseofupperlimblymphedema=filarial*• Classifiedintoprimaryandsecondary
types of primary lymph edemaCongenital Lymph edema praecox Lymph edema tarda ○ Onset<1year○ MCbilateral*○ Involvewholeleg○ Milroy disease*
○ Onset1–35years○ MCprimarylymphedema○ MCinwomen○ MCunilateral*○ Mostlyinvolvebelowkneesonly○`Meig disease*
○ Onset>35years
features○ Stemmers sign*—inabilitytopinchsubcutaneoustissueinlymphedema
treatment of established lymph edematypes of stockings Drugs bypass proceduresClass3—40–50mmHgstockings
Class4—50–60mmHgstockings
InUKonlydrugapprovedforvenous disease isoxerutin (paroven)andnodrugisapprovedforlymphedema
Benzypyronesarenaturaldrugusedforlymphedema
Neibulouwitz—anastomosisofnodestovein(lymphovenousanastomosis)
Kinmonth—usingilealmucosalpatchGillies—skinbridge.

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery252
Limb reDuCtion proCeDures○ Charles—wholesubcutaneousandslimexcuseduptodeepfasciaandSSGdone
○ Sistrunk—wedgeexcisionofskinandsubcutaneoustissueandwoundclosedprimarily.
○ Homans—skinflapraised,subcutaneoustissueremovedMostsatisfactoryoperationMaincomplicationisskinflapnecrosisContraindicatedinpresenceofvenousobstructionandmalignancy
○ Thompson—burieddermalflap.Commoncomplicationofthisprocedureispilonidalsinus.
points for memory○ Butchersthighisduetoinjurytofemoralarteryinfemoraltriangle
aneurysms types of aneurysms• Mostcommontypeof‘trueaneurysm’isfusiformtype• Mostcommonsiteofarterialaneurysmisinfrarenalpartofabdominalaorta.
• Poplitealaneurysms*arethemostcommonperipheralaneu-rysms.
• Themostcommonsitefordissectinganeurysmsisascendingaorta*
• MCcauseforabdominalaorticaneurysmisatherosclerosis*• Cirsoidaneurysms”arecommoninsuperficialtemporalartery.
• Berryaneurysm:Occursincircleofwillis• Micro aneurysms:Seenindiabetesandhypertension• Mycoticaneurysms:Areseeninbacterialinfections.• Aorticdissectinganeurysms:Duetodegenerationoftunicamedia.OccurinMarfanssyndromeandhypertension.
• Syphiliticaneurysmsorlueticaneurysms:Involveascendingaorta’”
• Pseudoaneurysmsfollowtraumamostcommonly
fmGe questions
1. Superficial thrombophlebitis is seen in: (Sep 2009)
a. AVfistula b. Raynauddisease c. Buergerdisease d. AneurysmAns: c (Buerger disease)
2. Which of the following is associated with Vir-chows triad: (March 2011)
a. Hypercoagulability b. Disseminatedmalignancy c. DVT d. AlloftheaboveAns: d (All of the above)Virchow’s triad:• Hypercoagulability• Stasis• Endothelialdamage
3. Most common vessels to be affected in Buergers disease: (Sep 2009)
a. Femoralartery b. Iliacartery c. Poplitealartery d. AnteriorandposteriortibialarteryAns: d (Anterior and posterior tibial artery)
4. Drug used for sclerotherapy of varicose veins are all of the following, except: (Sep 2009)
a. Ethanolamineoleate b. Polidocanol c. Ethanol d. SodiumtetradecylsulfateAns: c (Ethanol)
5. Raynaud syndrome occurs in all of the following, except: (Sep 2011)
a. SLE b. Rheumatoidarthritis

tahir99 - UnitedVRG
253Vascular Surgery
c. Osteoarthritis d. ColdagglutinindiseaseAns: c (Osteoarthritis)Causes of secondary Raynaud syndrome Connectivetissuedisorders• Mixedorundifferentiatedconnectivetissuedisease• Polymyositis/dermatomyositis• RA• Sjögrensyndrome• SLE• SystemicsclerosisEndocrinedisorders• HypothyroidismHematologicdisorders• Coldagglutinindisease• PolycythemiaveraNeoplasticdisorders• Carcinoid• ParaneoplasticsyndromeNeurologicdisorders• CarpaltunnelsyndromeTrauma• Frostbite• VibrationVasculardisorders• ThoracicoutletsyndromeDrugs• β-blockers• Cocaine• Ergotpreparations• Nicotine• Sympathomimeticdrugs
6. All of the following are true regarding DVT, ex-cept: (March 2009)
a. Pulmonaryemboliistheimmediaterisk b. Mayleadtolunginfarction c. AssociatedwithdeficiencyofproteinC d. PriorhistoryofDVTisanimportantriskfactorAns: b (May lead to lung infarction)
7. Sequence of color changes observed in Raynaud disease: (Sep 2006)
a. Red,blue,white b. White,blue,red c. Blue,red,white d. White,red,blueAns: b (White, blue, red)(Pneumonic:WBC—white,blueandcrimsonred)
8. Buerger’s disease usually affects all of the follow-ing, except: (Sep 2005)
a. Small-sizedarteries b. Medium-sizedarteries
c. Largearteries d. DeepveinsAns: c (Large arteries)
9. Nicoladoni-Branham’s sign is seen in: (March 2011) a. Buergerdisease b. Arteriovenous(AV)fistula c. Raynaud’sdisease d. PeripheralaneurysmAns: b (AV fistula)
10. Which of the following is spared in lumbar sym-pathectomy: (Sep 2011)
a. L1 b. L2 c. L3 d. L4Ans. a (L1)
11. Seldinger needle is used for: (Sep 2010) a. Suturingmuscles b. Arteriography c. Pulmonarybiopsy d. LymphographyAns: b (Arteriography)
12. If a patient with Raynaud disease immersed his hand in cold water, the hand will: (2003)
a. Becomered b. Remainunchanged c. Turnwhite d. BecomeblueAns: c (Turn white)
13. The Hunterian ligature operation is performed for: (Sep 2003)
a. Varicoseveins b. Arteriovenousfistulae c. Aneurysm d. AcuteischemiaAns. c (Aneurysm)
14. Sympathectomy is indicated in all the following conditions, except: (Sep 2009)
a. Ischemiculcers b. Intermittentclaudication c. Anhidrosis d. AcrocyanosisAns. c (Anhidrosis)
15. Lumbar sympathectomy is of value in the man-agement of: (March 2011)
a. Intermittentclaudication b. Distalischemiaaffectingtheskinoftoes

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery254
c. Arteriovenousfistula d. BackpainAns: b (Distal ischemia affecting the skin of toes)
16. Drug used for sclerotherapy of varicose veins: (Sep 2007) a. Tetracycline b. Ethanolamineoleate c. Phenolinalmondoil d. AlltheaboveAns: b (Ethanolamine oleate)
17. Brodie-Trendelenburg test is positive in: (Sep 2010) a. Deepveinthrombosis b. Saphenofemoralincompetence c. Thromboangitisobliterans d. BelowkneeperforatorincompetencyAns: b (Saphenofemoral incompetence)
18. Buerger disease usually affects all the following, except: (Sep 2010)
a. Small-sizedarteries b. Medium-sizedarteries
c. Largearteries d. VeinsAns. c (Large arteries)
19. A 60-year-old male has been operated for carci-noma of cecum and right hemicolectomy has been done. On the 4th postoperative day, the patient develops fever, swelling and pain in the legs. The most important clinical entity one should look for is: (March 2011)
a. Urinarytractinfection b. Intravenouslineinfection c. Chestinfection d. DeepveinthrombosisAns: d (Deep vein thrombosis)
20. Test, which is not done for varicose veins: (March 2011 a. Perthes’test b. Tourniquettest c. Trendelenburgtest d. AdsontestAns: d (Adson test)

tahir99 - UnitedVRG
22OncOsurgery
EpidEmiology of common cancEr○ Overall,1:3peoplewilldevelopsomeformofcan-cerduringtheirlife
○ Therearemorethan200differenttypesofcancer○ Breast,lung,colorectalandprostatecanceraccountforover50%ofnewcases
ageCanceroccurspredominantlyinolderpeople65%casesarediagnosedovertheageof65yearLessthan1%occurinchildren Breastcanceraccountsfor50%ofallcancersdiag-nosed40–60year
men• Prostatecancerhasovertakenlungcancerasthecommonestcancerdiagnosedinmen
• IncidenceofprostatecancerisrisingduetothewidespreaduseofPSA
• Lungcanceristhesecondmostcommoncancer• Incidenceoflungcancerisfalling
WomenBreastcanceristhecommonestcancerinwomenAccountsfor30%ofallfemalecancerThesecondcommonestcancerinwomeniscolorectalcancer
TubErous sclErosis○ AlsoknownasBourneville’s disease* ○ Characterizedbycutaneouslesions,seizuresandmen-talretardation.
○ Calcifiedsubependymalnoduleischaracteristic.
○ Associatedlesionsinclude:Subependymalgiantcellastrocytoma.Rhabomyomasofthemyocardium.Angiomyomasofkidney,liver,adrenalandpancreas.

tahir99 - UnitedVRG
http:/
/vip.p
ersian
ss.ir/
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery256
nEurofibromaTosis 1 (von rEcklinghausEn’s disEasE)○ Mchereditaryneurocutaneousdis-ease(Phakomatosis).
○ Autosomaldominant.○ Numerousneurofibromasinskinandperipheralnerves.
○ Cafealllaitspot(earliestmanifesta-tion).
○ Fordiagnosis≥6spotsof≥5mmprepubertal.≥15mmpostpubertal
○ Frecklinginseenexposedarea(mostcommonlyaxilla,Crowesign).○ MelanotichematomaofirisLISCHnodule○ Pseudoarthrosisoftibia○ PlexiformneurofibromatosisElephantmandisease○ Generallyasymptomaticbutmaypresentwithcompressiverediculopathy,aqueductalstenosis,shortstature,hypertension,mentalretardation,epilepsy.
○ Increasedriskofdevelopingnervoussystemneoplasmmorecommonlyopticnerveglioma
○ NeurofibromasareunencapuslatedbenignneoplasmcontainingSchwanncellandfibroblast.Thereisnoplaneofcleavage,socannotberemovedwith-outsacrificingnerve.
nEurofibromaTosis 2○ Characterizedbydevelopmentofbilateralvestibularschwannoma(oracousticneuroma)in90%cases.
○ Presentwithprogressivedeafness(unilateralin3rddecade)(vestibularsystemadaptstotheslowlygrowingtumor,hencenovestibularsymptoms)
○ AssociatedwithpostsubcapsularCATARACTandothernervouscyst.Neo-plasm.
○ NF2gene,referencodingschwannomin(merlin).
○ Schawannoma(neurilemmoma)areencapsulatedtumorswithaplaneofcleavageseparating:itfromnerveandhencecanberesectedsurgically.
skin cancErslayers of skin Epidermis dermis○ Theskinisdividedintotwomainlayers:Surfaceepitheium(epidermis)
Dermis
○ Keratinizedstratifiedsquamousepithelium1.Stratumcorneum2.Stratumlucidum3.Stratumgranulosum4.Stratumspinosum(malphigianlayer,pricklecelllayer)5.Stratumbasale
1.Superficialpapillary2.Deepreticularlayer•Melanocytesarefoundinthejunctionbetweenbasallayeranddermis
Acquired melanotic nevus classified as Junctional nevi○ Based on location of nevus cells1.Junctional:Epidermis(Str.Basale),i.e.junction (m/csiteoforiginofmelanoma)2.Compound:Epidermisandpartlydermis3.Dermal:Atdermis
○ Commoninchildren,malignantpotentialinadultBasalcellCa—mostcommonSquamouscellCa—2ndcommon
Basal Cell CarCinomaBasalcellcarcinoma(BCC)arisesfromstratumbasale.Occasionallyitarisesfromthebasalcellsofhairfolliclesandsweatglands.Suchtumorsaremostlyseeninscalpandadolescentsaretheusualvictims.Theyarecalled‘turbantumors’or‘epitheliomaadenoidescysticum’ ○ Mcskinmalignancy○ Mcagegroup—40–80years○ Mcinmen○ Mcsiteisface○ Exclusivelyaffectswhiteskinnedpeople.
○ Extremelylowmetastaticpotential○ Arisesfromstratumbasalelayer
Clinical features• m/c site:InnercanthusofeyeOutercanthusofeyeNoseOnandaroundnasolabialfoldOntheforehead
○ Tearcancer—asitislocatedalongtheinnercanthus.○ Rodentulcer—duetoitspropertyofdestroyingthetissueitcomesincontactwith.
Contd...

tahir99 - UnitedVRG
http:/
/vip.p
ersian
ss.ir/
257Oncosurgery
Basal Cell CarCinomaHistology shows:Peripheralpalisadingofcells*
Predisposing factors for BCC:Ultravioletlight—sunlight(strongestpredisposingfactor)Exposuretoarsenic,coaltar,aromatichydrocarbons.
subtypes of bccnodular bcc Superficial bccmost common subtype (50% of all)Nodularandnodulocysticvariantsaccountsfor90%UsuallyoccursinsunexposedareasUlcerationiscommon (rodent ulcer)
OftenmultipleUsuallyontrunkRedscalypatcheswithareasofbrown/blackpigmentation(DD:Actinickeratosis,psoriasis,eczema)
others spread of bcc○ Morpheaform○ Cysticform○ Geographicalvariety(Fieldfire/forestfire○ Superficialspreadingtype:Withadvancingedgeandhealingcenter,ithasanirregu-larraisededgearoundflatwhitescar.
○ Perineuralspread○ Nonodalspread(ifnodesarepresentthediagnosisshouldbequestioned)
○ Localspread:Slowgrowing,canerodelocaltissuesdeeplylikecartilage,bone(rodentlike)
○ Hematogenousmetastasis:Incidence0.0028%—0.1%
Treatment of choice• Excisionalbiopsyistreatmentofchoice
• ButifMOH’smicrographicsurgeryisthereinthechoice,optforit• Othermodes—topical5fluorouracilcreams,radiotherapy.
squamous cEll carcinoma○ Secondmostcommoncancer○ Males>Females
○ Itisthepricklecelllayer(St.Spinosum)fromwhichthetumorarisesandmigrateoutwardstothesurface(Baileymentionsitarisesfromstratumbasale)
premalignant conditions1. Bowen’s disease: Itisanintradermalprecancerouscondition.Itpresentsasbrownishindurationwithwell-definededge.(Erythroplasiaofqueyrat:Penis)
2.Paget’sdiseaseofnipple3.Leukoderma,erythroplakia4.Senile(or)solarkeratosis5.Radiation
6. Arsenic 7. Chronicscars:Marjolin’s 8. Xerodermapigmentosa 9. Chroniclupusvulgaris10. Prolongedirritationofskinbydyes,tar,soot,etc.11.HPV5and16
pathological types characteristic histology○ Thefirstclinicalevidenceofmalignancyisindura-tion
○ Thetissuearoundthegrowthishyperemic○ Macroscopictypes:Proliferative(Cauliflower-like)Ulcerative(MCtype)PlaguelikeVerrucous
○ Epithelialpearl(nest)formation.○ epithelial formation not seen in:RapidlygrowingtumorEsophagusSCCBladderSCCBroder’sgrading(1-4)basedonepithelialpearlformation.Thetumorstainspositiveforcytokeratin1and10
characteristic types variants of scc (without lymphatic spread) • Kangri cancer—Duetoconstantplacingofhotcharcoalpot(kan-gri)tocontrolcoldoverabdomenwallinKashmir.
• Kang cancer—SeeninButtockandheelofTibetans,duetosleep-ingoverovenbedtocontrolcold.
• Chimney sweeper cancer—Inscrotum duetoexposuretocon-stantirritationbytar.
○ Marjolinulcer:○ Verrucouscarcinoma
Contd...

tahir99 - UnitedVRG
http:/
/vip.p
ersian
ss.ir/
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery258
TrEaTmEnT of skin cancErs1. excision treatmentBCC: Surgicalexcisionisthemostcommonformoftreatmentover-allcurerate91%.Therefore, 4–6 mmmarginsforlesions>2cm.sCC: 4 mm marginisenoughfortumors<2cm.Largertumors>2cmrequirea1cmmargin.
2. moh’s micrographic surgery:3. Destructive management:1.Electrodissectionandcurette.2.Cryosurgery.3.CO2laser.4.Radiotherapy.
contraindications for rT prognostic factors for metastasis ○ Patientswithxerodermapigmentosum,epidermolysisverruciformis,basalcellnevussyndrome(maycausemoretumorinRTfield)
○ Verrucouscarcinoma(SCC)—mayconvertedtoaggressiveform.○ Closetotheeye.○ Lesionadherestoboneandcartilage(leadstoosteoradionecrosis)
○ Overallrateofmets=2%usuallytore-gionalnodes
○ Localrecurrence=20%1.Depth2.Size3.Grade
malignanT mElanoma○ 4%ofskincancer○ 79%ofskincancerdeaths○ 1.4%ofallcancerdeaths.○ IncidenceinIndia○ Male:0.5/lakh○ Female:0.2/lakh○ melanoma is the leading cause of death in women 25–35 year.○ mC cancer in age group from 20–39 year—malignant melanoma.
risk factors SunlightXerodermapigmentosaPast/familyhistoryofmelanomaDysplaticnevi(10%lifetimerisk)Immunocompromised—HIV,cyclosporinAtherapy,Hodgkindisease.
cutaneous melanoma subungual melanoma melanomaFeatures of melanoma:•a Asymmetry•B Borderirregularity•C Colorvariation •D Diameter>6mm•e Evolution,elevation,enlargement•F Funnylooking
○ Digitcommonlyinvolved(greattoe/thumb)
○ extension of pigment onto the proximal lateral nail fold (Hutchinson’s sign)
Superficialspreading—Mostcom-mon
Acrallentiginous—Mostcommonindarkskin
Nodular—WorstprognosisLentigomaligna—Bestprognosis
Superficial spreading (70%) Nodular melanoma (16%)○ M/ctypeoccurringinwhitepopulation○ Melanomasarisinginpre-existingdysplasticnevusareusu-allySSM.
○ MCSites:Males:TrunkFemales:Lowerlegsandback
○ Secondmostcommon○ Canoccuronanysurfaceofthebody,50–70years○ M/Csite:Head,neckandtrunk○ Onlyverticalgrowth,noradialspread.○ HighRiskgroupandpoorprognosis
Acral Lentiginous melanoma (10%)○ Palms, soles, mucosal surfaces, subungual○ Mostcommonindarkskinnedindividuals○ Becauseofthelocation,diagnosedverylate
subungual type:Arisefromnailmatrixm/c—greattoe/thumbnailsDiagnosticbiopsyincludesnailmatrix
poor prognosis: lentigo maligna melanoma (5%) Tumor markers for melanoma:• Melan-A• HMB-45(HydroxymethylBro-mide)
• S-100
Olderageindividuals.PreviouslycalledHutchinsonmelanoticfreckle.
Commoninface.
Mostcommonlyaffectswomenthanmen
Insituvariantiscalledlentigomaligna.Lowestmetastaticpotential
Contd...

tahir99 - UnitedVRG
259Oncosurgery
malignanT mElanomaspread
○ lymphatic: Regionallymphnodesbypermeation,embolization
○ Blood:Brain—Convulsion,raisedICPLung—Cannonballsecondaries,pleuraleffusion,hemoptysis,chestpainLiver—AscitesSkin—PigmentednodulesBones—Pathologicalfracture,paraplegia,neurologicaldeficit
○ in-transit or satellite nodules:Betweentheprimarylesionandregionallymphnodearea,duetoretrogradespreadtodermallymphatics
prognosTic facTorsDepth(mostimportant)UlcerationLymphnodestatus
SatellitelesionsDistantmets
othersSite—Extremities(good)Sex—Female(good)Histology—Lentigomaligna(good)
breslow thickness○ Basedonthicknessofinvasionbyopticalmicrometer I : Lessthan0.75mm II : Between0.76to1.5mm III : 1.51mmto4mm IV : Greaterthan4mm
clark level○ LevelI:Onlyinepidermis○ LevelII:Intopapillarydermis○ LevelIII:Fillingofpapillarydermiscompletelyuptothejunction.
○ LevelIV:Intoreticulardermis○ LevelV:Extensionintosubcutaneoustissue
saTElliTE nodulEs TrEaTmEnT○ Excisionbiopsywithpreferredmargins○ Sentinelnodebiopsy○ Blockdissectionifsentinelnodeispositive○ Reconstructionofdefects.○ Excisionclearance
Tumor thickness (mm) ‘T’ stage Excision margin In situ T0 0.5–1cm0–1 T1 1cm1–2 T2 1–2cm*2–4 T3 2cm>4 T4 Atleast2cm
sofT TissuE sarcomas• M/csofttissuetumorinachildisrhabdomyosarcoma.
• M/ctype:Embryonalrhabdo-myosarcoma.
• Resectionisthetreatmentofchoice.
• Softtissuesarcomasmostlyspreadhema-togeneously.
• Butlymphaticmetastasisisseeninembryo-nalrhabdomyosarcoma.
• Lowerextremityisthecommonestsite.• Gradeoftumordetectsprognosis
• Liposarcomaisthemcretroperito-nealtumor*.
• Lymphomaandretroperitonealsarcomaaremcretroperitonealmalignantlesions
Contd...

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery260
sponTanEous rEgrEssion is sEEn in○ Renalcellcarcinoma○ Retinoblastoma
○ Choriocarcinoma○ Neuroblastoma
○ Malignantmelanoma
radiaTion inducEd cancErsAcuteleukemia(MC)PappilaryCaofthyroidBreastcarcinoma
LungCa(Radon)Angisarcomaofliver(Thorotrast)Skincancers(BCC,SCC,melanoma)
BraintumorOsteosarcoma
sEnTinEl nodE biopsy is donE in○ Cabreast ○ Melanoma ○ Capenis
fmgE quEsTions
1. Basal cell carcinoma usually spreads by which route: (sep 2003)
a. Hematogenousroute b. Lymphaticroute c. Directspread d. Alloftheaboveans: c (Direct spread)
2. Which of the following is commonest site for ro-dent ulcer: (sep 2011)
a. Lips b. Outercanthusofeye c. Innercanthusofeye d. Cheekans: c (inner canthus of eye)
3. most common subtype of basal cell carcinoma is: (sep 2005)
a. Superficialbasalcellcarcinoma b. Nodularbasalcellcarcinoma c. Sclerosingbasalcellcarcinoma d. PigmentedbasalcellcarcinomaAns: a (Superficial basal cell carcinoma)
4. Which of the following soft tissue sarcomas fre-quently metastasizes to lymph nodes: (sep 2008)
a. Fibrosarcoma b. Osteosarcoma c. Embryonalrhabdomyosarcoma d. Alveolarsoftpartsarcomaans: c (embryonal rhabdomyosarcoma)explanation:Sarcomas are a heterogeneous group of tumors thatarise predominantly from the embryonic mesoderm,
but also can originate as does the peripheral nervoussystemfromtheectoderm.Incidence: 1%inadultcancers 7%inchildren’scancers.site of occurrence• Extremity(59%):Upperlimbs(15%)andlowerlimbs(45%)
• Trunk(19%)• Retroperitoneum(13%)• Headandneck(9%)occurrence of each types:• Malignantfibroushistiocytoma(28%)• Liposarcoma(15%)• Leiomyosarcoma(10%)• Synovialperipheralnervesheathtumors(6%)• Rhabdomyosarcoma(m/cinchildhood)lymph nodal metastasis: (sCerea)S—SynovialsarcomaC—ClearcellsarcomaE—EwingsarcomaR—RhabdomyosarcomaE—EpitheliodsarcomaA—Angiosarcoma
5. Prognosis of malignant melanoma depends upon: (march 2011)
a. Gradeoftumor b. Ageofthepatient c. Depthofinvasion d. Siteoflesionans: c (Depth of invasion)

tahir99 - UnitedVRG
23Pediatric Surgery
OmphalOcele• Congenitaldefectintheanteriorabdominalwallinwhichthebowelandsolidvisceraarecoveredbyperitoneumandamnioticmembrane.
• Umbilicalcordinsertsintosac• Incidence=1in5,000• Associatedcardiacanomaliesin20%–40%,withchromosomeanomalies
exomphalos minor exomphalos major• Defectissmall(<5cm)• Onlysmallbowelprotrudes• Umbilicalcordattachedtosummit• Strappingisenoughastreatment• Goodprognosis
• Defectis>5cm• Smallbowelandliverprotrudes• Umbilicalcordattachedtotheside• Treatmentisdifficultandneedsstagedoperation.
• Badprognosis
GastrOschisis• Congenitaldefectcharacterizedbydefectinanteriorabdominalwallvia,whichintes-tinalcontentsprotrude,nomembranecovering.
• Sizeofthedefectisusually<4cm• Defectisalmostalwaystotherightofumbilicus• Notassociatedwithcardiacanomalies,butmaybeassociatedwithintestinalatresia• NomembraneTreatment• Urgentsurgicalintervention• Reductionandcorrectionofintestinalatresia.
Gastroschisis OmphaloceleUmbilicalcordnormal UmbilicalcordgoestothedefectNoprotectivemembrane ThinmembranecoveringpresentAngrylookingbowel NormalbowelNeedsclosure Needsclosure

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery262
exstrOphy Of bladder (ectOpia vesicae)• Incidenceis1in50,000• M:F=4:1• Inmalesassociatedwith—broadandshortpenis,bilateralinguinalhernia*
• Infemalesassociatedwith—epispadias*andsplitclitoris
• otheranomalies–separationofpubicbone(Splitpelvis)
treatment• Closureofthedefectinthe1styearoflife.
• Osteotomyofiliacbones • Otheroptionsureterosigmoidos-tomy
cOnGenital diaphraGmatic hernia• Anteromedial:SpaceofLarrey(foramenofMor-gagni)MConrightsideCausesnosymptom.
• Posterolateral:CommonesttypeofCDHOccursviaforamenofBochdalekMConleftCauserespiratorydistressDeathofinfantduetoabdominalvisceralher-niation
pOints frOm cdh• Failureofdiaphragmaticdevelopmentleavesapos-terolateraldefectknownasaBochdalekhernia.Thisanomalyisencounteredmore commonly on the left(80%–90%).
• Prenatalultrasonographyissuccessfulinmakingthediagnosisofcongenitaldiaphragmatichernia(CDH)asearlyas15 week gestation○AusefulindexofseverityforpatientswithleftCDHisthelung-to-head ratio (LHR).
○AnLHRvalueof<1.0isassociatedwithapoorprognosis,whereasanLHR>1.4predictsamorefavorableoutcome
• Followingdelivery,thediagnosis of CDH is made by chest X-ray (CXR)
Contd...

tahir99 - UnitedVRG
263Pediatric Surgery
pOints frOm cdh• Overallmortalityinmostseriesisapproximately60%–70%.Itisinterestingthatthefirst24–48hourafterbirthareoftencharacterizedbyaperiodofrelativestability,withhighpartialpressureofarterialoxygen(PaO2)levelsandrelativelygoodperfusion
Thishasbeentermedthe‘honeymoonperiod’andisoftenfollowedbyprogressivecardiorespiratorydeteriorationinthemajorityofpatients
managementstep 1 step 2 Operative repair• Inthepast,correctionoftheherniawasfelttobeasurgicalemergency
• Itisnowacceptedthatthepresenceofpersistent pulmonary hypertensionthatresultsinright-to-leftshuntingacrosstheopenforamenovaleortheductusarteriosusandthedegreeofpulmonaryhypoplasia,aretheleading causes of cardiorespiratory insuffi-ciency*
• Therefore,currentmanagementisdirectedtowardpreventingorreversingthepulmonaryhypertensioninfantsareplacedonmechanicalventilation
• InfantswithCDHwhoremainseverelyhypoxicdespitemaximalventilatorycaremaybecandidatesfortreatmentoftheirrespira-toryfailurebyextracorpor-eal membrane oxygenation (ECMO)
• Thetimingofdiaphragmrepairiscontroversial.InpatientsthatarenotplacedonECMO,mostsurgeonsperformrepaironcethehemodynamicstatushasbeenoptimized
• Operativerepairofthedia-phragmaticherniaisbest ac-complished by an abdominal approach
Contd...
fmGe questiOns
1. Hernia of Morgagni passes through: (Sep 2006) a. Pleuroperitoneum b. DiaphragmviaLa c. Deepring d. ArcuatelineAns: b (Diaphragm via Larrey’s space)
2. Where does the diaphragmatic hernia of Boch-dalek occurs: (Sep 2008)
a. Leftsideanterior b. Rightsideanterior c. Posterolateral d. NoneAns: c (Posterolateral)Mostcommononleftposterolateral*

tahir99 - UnitedVRG
Index
AAbbe’s flap 36Abdominal aortic aneurysm 247 compartment syndrome 137 crampy pain 129 groans 72 injury 27 trauma 26Aberrant right hepatic artery 161 thyroid 56Abscess 3Absence of cholangitis 148Absorbable suture material 8Acalculus cholecystitis 147Accessory cystic artery 161 spleen 177Achalasia 98 cardia 98Acid urine 180Acinic cell tumor 51Acquired branchial sinus 44 immunodeficiency syndrome 180 melanotic nevus 256Acral lentiginous melanoma 258Acrocyanosis 250Actinomycosis 1Acute appendicitis 126 cholecystitis 154 coronary syndrome 231 gastric dilatation 112 liver failure 162 mesenteric ischemia 131 paronychia 4 subdural hematoma 22 submandibular sialadenitis 54
Adder head 190Adenocarcinoma 51, 100, 229 nodes 36Adenoid cystic carcinoma 51Adenolymphoma 51Adenoma 50, 76Adjustable banded gastroplasty 114Adrenal glands 70, 73 medulla 73Adriamycin 86Adson’s test 42Advanced gastric cancer 108 trauma life support 20Alexander-Wallace rule 235Alkaline urine 180Amebic abscess 168 colitis 126 lung abscess 229Anal canal 133 cancer 132 margin 133Anaplastic carcinoma 66Anatomical division of prostate 193Anatomy of coronary artery 231 inguinal canal 213, 214 rectum 132Anderson-Hynes dismembered pyeloplasty
188Anemia 107, 113, 176Angel sign 208Angelchik prosthesis 93Angiomyolipoma 185 of kidney 185Aniridia 185, 188Anomalies of gallbladder 145Anorectal abscess 135
Anterior dissection 36 gastric nerve 103 lesser curve seromyotomy 106 mediastinum 227 triangle of neck 44Antithyroid drugs 61Aphthous ulcers 121Appendicular abscess 127 mass 127Arterial graft 232 plane 48 stenosis and occlusion 249 system 247Arteriovenous fistula 251Artificial nutrition 4Askanazy cell 63Assessment of liver function 171Astley Cooper’s ligament 88Ataxia telangiectasia 83Auchincloss modification 85Auerbach’s plexus 92, 98Autogenous transplant 89Autosomal dominant mutation 83Axillary vessels 86Azoospermia 198
BBacterial infection 176Balance sign 175Balanced salt solution 8Bariatric surgery 114Barium enema 119Barrett esophagus 93, 94Barron’s bander 134Basal cell carcinoma 1, 256Bascom’s procedure 135Bastede’s sign 126

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery266
B-cell non-Hodgkin’s lymphoma 66Beckwith-Wiedemann syndrome 185Bell’s nerve 86Belsey mark intravenous operation 93Benign breast diseases 80 mixed tumor 50 thyroid disorders 58Beta cell tumor 157Bilateral breast cancer 83 neck dissection 35 subtotal thyroidectomy 66Bile duct cancers 152 injuries 153 vomiting 108Biliopancreatic diversion without duodenal
switch 114Bishop Koop operation 128Bismuth classification 152, 153Bladder calculi 192 cancers 191 pressure grading 138Bleeding in portal hypertension 165Block and replacement therapy 62Blood products 13 supply 57, 103, 161, 174 transfusion 11Blumberg sign 126Blunt myocardial injury 26 trauma 20Boerhaave syndrome 95Bone disease 107 marrow suppression 86Borchardt’s triad 114Bormann classification 108Bourneville’s disease 255Bowel injuries 27Bradycardia 251Brain tumors 224Branchial arches 43 cyst 44 fistula 2 sinus 44Branchiogenic carcinoma 44Branham sign 251Breast cancer syndrome 83 conservation surgery 89 disorders 78Breslow thickness 259Brodie-Trendelenburg test 244Bronchioalveolar carcinoma 229
Bronchogenic cancer 229 cyst 227, 228Brown pigment 147Buccal mucosa 34Buerger’s disease 250Bulbar urethra 136 urethral injury 201Burns produce inflammatory reaction 234Bypass procedures 251
CCalcineurin blockers 189Calcium homeostasis 71 oxalate calculus 180Called mixed tumor 50Calot’s triangle 144Calyceal diverticulum 181Cancer esophagus 100 prostate 195 rectum 132 stomach 108Carbimazole 61, 62Carbuncle 3Carcinoid appendix 127 syndrome 121Carcinoma 34, 50, 71 bladder 190 breast 81, 82 buccal mucosa 37 cheek 34 gallbladder 151 hard palate 35 in situ 82 lip 34, 36 lower alveolus 37 of penis 201 prostate 196 tongue 34Cardiac surgery 231Cardiogenic shock 11Cardiothoracic surgery 227Caroli disease 149Carotid body anatomy 40 tumor 40 triangle 47Caudate lobe 162Causes of distension 129 hypergastrinemia 113 recurrent ulcer 108 thoracic outlet syndrome 42Cellulitis 3, 4
Central neck dissection 66Cephalic vein 86Cerebral contusions 23 metastasis 225Cerebrospinal fluid pathway 222Cervical ribs 42Cervicodorsal sympathectomy 250Charcot triad 148Chemodectoma 40Chemoembolization 171Chemotherapy 65, 86Chimney sweeper cancer 257Choice of fluid 8Cholangitis 148Cholecystosis 146Choledochal cysts 149Cholesterol gallstones 125Chromophobe carcinoma 183Chronic breast abscess 81 cholecystitis 154 graft rejection 16 hyperplastic candidiasis 32 kidney graft rejection 16 liver disease 163 pancreatitis 155 paronychia 4 renal failure 187 stable angina 231 subdural hematoma 23 submandibular sialadenitis 54Chylolymphatic cyst 219Circadian rhythm 75Circulation 21Cirrhosis 170Classic radical neck dissection 35Classification of salivary gland tumors 50 shock 11Clear cell carcinoma 183Cleft lip and palate 239, 240Clonidine suppression test 74Cloquet hernia 216Clostridium perfringens 154 welchii 154Cobblestone’ appearance 122, 193Cobra head 190Cock peculiar tumor 3Cold abscess 4 in neck 46 storage time 17Colloids 7, 8, 236Colonic cancer 119Colovesical fistula 2Commando operation 35Common bile duct stones 148

tahir99 - UnitedVRG
267Index
hepatic duct 144 vesical stones 192Completion total thyroidectomy 64Complications of bronchogenic cyst 228 burns 235 conservative management 175 empyema 228 enteral nutrition 5 incomplete descent 207 parotid surgery 52 peptic ulcer disease 106 renal trauma 186 sclerotherapy 100 shock 12 splenectomy 176 surgery 107 venous ulcer 245 kidneys 137Computed tomography scan 119Congenital atresias 129 diaphragmatic hernia 262 hydrocele 208, 209 hypertrophic pyloric stenosis 113 pelviureteric junction obstruction 188 PUJ obstruction 188 torticollis 45Congestive cardiac failure 194Conn’s syndrome 76Contents of inguinal canal 214 spermatic cord 214Control of intracranial pressure 23Cope’s obturator test 126 psoas test 126Copper-beating-chronic raised intracranial
pressure 223Corecut biopsy 80Coronary artery bypass grafting 231Corynebacterium diphtheriae 135Costoclavicular compression 42Couinaud’s segments 161Course of branchial sinus tract 44Courvoisier law 152, 156Cowden disease 83Crile’s operation 35Crohn disease 121-123, 126Cronkhite Canada syndrome 119Crypt abscesses 121Cushing disease 75, 76 syndrome 75, 76, 184 ulcers 111Cutaneous melanoma 258Cyclophosphamide 86Cylindroma 51Cystic artery 144 duct variations 145 hygroma 2, 45
Cystosarcoma phyllodes 81, 88Cysts 2 of jaw 38Cytogenetics of various subtypes of renal
cell 183Cytopoiesis 175
DDalrymples sign 61Dangers of smoke inhalation 234De Quervain’s thyroiditis 63Deep palmar abscess 4 vein thrombosis 244, 245Deformities of stomach 106Degrees of burns 236Delayed reconstruction of burns 237Deming sign 208Dental cyst 38, 39Dentigerous cyst 38, 39Denys Drash syndrome 185Dercum disease 2Dermis 256Dermoid cyst 2 tumor 217Destruction of valves 244Diagnostic peritoneal lavage 26Diaphragmatic injury 26Diarrhea 108Diffuse esophageal spasm 97 hyperplastic goiter 59Diseases of esophagus 92Distal splenorenal shunt 167Distant metastasis 87Distributive shock 11Diurnal variation 75Diverticular disease 119Diverticulitis 119Diverticuloesophagectomy 99Diverticulosis 119Diverticulum esophagus 98 in stomach 112Dohlmann operation 99Douglas sign 126Down syndrome 95Duct ectasia 81Ductal anomalies 56 carcinoma 82Dukes classification 120Dumb bell tumor 50Dunhill’s classification of malignant thyroid
63Duodenal stricture 112 stump blow out 108, 110 ulcer 104-106
Duodenum 103Dupuytren’s contracture 4Dyspepsia 106Dysphagia 96 lusoria 96
EEarly gastric cancer 109, 113Echinococcus granulosus 169 multilocularis 169Ectocyst 169Ectopia vesicae 262Ectopic testis 207 thyroids 56 ureter 187Eczema 80Elevated arms test 42Emergency thoracotomy 26Emphysematous cholecystitis 154Empyema of lungs 228Endocrine neoplasms 157 shock 11Endocyst 169Enterocutaneous fistula 125, 126Enterogenous cyst 219Enzyme defect 176Epidemiology of common cancer 255Epidermis 256Epididymal cyst 2Epigastric hernia of linea alba 215Epithelial formation 257 polyps 113 tumors 50Epulis 38Equinus deformity 245Erysipelas 3, 4Erythroplakia 32Esophageal injury 26 varices 99Esophagogastric junction 93Estlander’s flap 36Estrogen receptor status 86Exogenous hormones 83Exomphalos major 261 minor 261Exstrophy of bladder 262Extended radical dissection 36 mastectomies 85, 86External beam radiotherapy 65, 171 fistula 2 laryngeal nerve 57

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery268
Extracorporeal membrane oxygenation 263 shock wave lithotripsy 181Extradural hematoma 22Extrahepatic biliary atresia 149 portal venous obstruction 167Extralobar sequestration 228
FFacial nerve involvement 52 trichilemmoma 83Faeculent vomiting 130False capsule 48 divericula 119Familial adenomatous polyposis 119Fascial planes 4Fegan test 244Feminization 184Femoral hernia 215Finasteride 195First bite syndrome 41Fistula 2Flail chest 25Flank pain 184Floor of mouth 34Fluid therapy 7, 12Focal nodular hyperplasia 169Focused abdominal sonogram of trauma 27Follicular adenoma 59 cancer 64, 65 infections 3 odontoma 38, 39Foramen of Monro 223Fordyce’s disease 3Foreign body in lung 229Foster-Kennedy syndrome 224Frey procedure 155 syndrome 52, 53Fries modification of Bernard flap 36Frontal lobe lesions 224
GGabriel syringe 134Galactorrhea 184Gallbladder and biliary tract 144 polyp 146Gallstones 146Gangrene 249Gardner’s syndrome 3, 119Gastric lymphoma 111
outlet obstruction 106, 112, 125 ulcer 105Gastrin secretion 125Gastrinomas 157Gastroduodenal artery 106Gastroenteric cyst 227Gastroesophageal reflux disease 93Gastrointestinal stromal tumors 111 tract 118Gastrojejunostomy 106, 108Gastroschisis 261Gastrostomy 5Genital branch of genitofemoral nerve 214Genitourinary anomalies 188 tuberculosis 186Germ cell tumors 185, 204Giant fibroadenoma 81, 88 hemangiomas 170Gifford’s test 61Glasgow coma scale 21 outcome score 23Gliomas 225Goodsall’s rule 134Grades of splenic injury 175Graft versus host disease 16Graham-Cole test 145Grave’s disease 61Great saphenous vein 245
HHair follicle infection 3Halstead radical mastectomy 86 test 42Hamartomatous polyps in jejunum 119 syndromes 119Hartley Dunhill procedure 66Hartmann’s operation 130 pouch 145Hashimoto’s thyroiditis 63Hay fever 135Head injury 21Healing of third degree burns 237 ulcer 1Heinke Mickulicz pyloroplasty 106Heinz bodies 188Helicobacter pylori infection 105Hemangioma 169Hematogenous metastasis 64 route 186
Hematoma 67Hematuria 184, 186Hemihypertorphy 151Hemobilia 151Hemoglobinopathies 176Hemorrhagic cystitis 86Hemorrhoids 133Hepatic artery 161Hepatobiliary and pancreatic system 144Hepatoblastoma 171Hepatocellular carcinoma 170Hereditary non-polyposis colorectal cancer
119Hernia 213, 216Herniorrhaphy 217Hesselbach hernia 216 triangle 214Heterotopic graft 172Hiatus hernia 94Hidradenitis 3 suppurativa 3High pressure flow 244 selective vagotomy 107Hill procedure 93, 106Hilton’s method 46Hirschsprung’s disease 98, 118Holmium:yttrium aluminium garnet laser
194Homan’s sign 245Hormone replacement therapy 84 therapy 86Horner syndrome 228Horseshoe kidney 188Howell-Jolly bodies 188Hunt-Larence pouch 110Hurthle cell 63 carcinoma 65Hydatid cyst 169 of lung 229Hydrocele 2 of cord 209Hydrocolloid dressings 237Hypercalcemia 7Hyperkalemia 6Hypernatremia 7Hyperplasia 71, 76Hypertension 75, 187Hypertonic saline 8, 236, 237Hypertrophic scar 6Hypocalcemia 7, 67, 110Hypokalemia 6Hyponatremia 7Hypospadias 185, 198Hypovolemia 12Hypovolemic shock 11

tahir99 - UnitedVRG
269Index
IIdiopathic thrombocytopenic purpura 178Immature cells 106Immunosuppression 17Impacted tooth 39Imperforate anus 136Implantation dermoid 3Incidence of carcinoma breast 82Infantile hydrocele 209Infective thyroiditis 63Inflammatory bowel disease 121 carcinoma breast 88Infraclavicular subclavian vein 5Inguinal lymph nodes 202Injection sclerotherapy 134Inoperable node 36 secondaries 36 tumors in cardiac end 111Insulinomas 157Intermittent dysphagia 96Internal fistula 2Interstitial hernia 216Intestinal obstruction 128 system 118 transplantation 125Intracellular defect 176Intracranial tumors 224Intralobar sequestration 228Intramammary abscess 80Intraperitoneal rupture 193Intraspinal extension 185Intrathoracic goiter 67 pressure 137Intravenous urogram 186Intravesical therapy 192Intusussception 128Invasive cancers 82 ductal carcinoma 82 lobular carcinoma 82, 83 penile carcinomas 202Iron granules 174Ischemic colitis 126, 131
JJack stones 192Japanese classification 109Jaundice in infants 150 newborn and infants 150Jeeper’s bottom 135Jejunal interposition 110Jejunostomy 5Jellinek’s sign 61
Joffroy’s sign 61Johansson step ladder 36Johnson classification 104
KKarydakis procedure 135Kasai’s procedure 150Kassabach Meritt syndrome 170Kehrs sign 175Keloid 6Kidney and ureters 180 stones 168Klebseilla pneumoniae 168Klippel-Trenaunay sydnrome 245Krukenberg’s tumor 81
LLanz incision 127Laparoscopic repair 217Large bowel obstruction 120, 130Laryngocele 45Larynopharyngeal reflux of
gastroesophageal reflux disease 93Lateral aberrant thyroid 56 neck dissection 35Latissimus dorsi 86Laungier hernia 216Laurens classification 109Layers of skin 256Left coronary artery 231 sided portal hypertension 164Lentigo maligna melanoma 258Leukemia 83Leukoplakia 32Level of escharotomies 237 nodes 33, 78 verumontanum 194Lid lag sign 61Li-Fraumeni syndrome 83Ligaments of Cooper 78Limb reduction procedures 252Limey bile 145, 148Lingual thyroid 56Lipodermatosclerosis 245Lipoma 2Lithogenic bile 146Littre hernia 118, 216Liver 161 cell adenoma 169 function tests 162 transplant 172Lobectomy 66Lobular carcinoma 82
Long sinus forceps 46Lothiessen’s inguinal approach 215Low ejaculatory volume 198 operation of Lockwood 215Lower esophageal sphincter zone 93Ludwig’s angina 38Lugol iodine 62Lumbar sympathectomy 250Lung abscess 99 sequestration 228Lymph edema 251 praecox 251 tarda 251 node metastasis 52Lymphatic drainage 34, 57, 78, 104, 144 system 251Lymphoma 50, 59, 227Lyre sign 40
MMacis scale 64Mackler triad 95Major vascular injuries 26Malabsorption 125Malgaigne’s bulge 216Malignant ascites 81 exophthalmos 61 melanoma 258 anal canal 133 pheochromocytoma 74 tracheoesophageal fistula 100 transformation 50 tumor 170Mallory-Weiss tear 95Mammography 79Management of bladder cancer 191 burns 236, 237 carcinoma penis 202 deep burns 237 oral cancers 36Mandibulectomy 36Manifestation of organs 16Manometry 97Marjolin’s ulcer 245Masculinization 184Massive hemothorax 25Maydl hernia 216Mayos operation 106McBurney’s grid iron incision 127Measuring portal pressure gradient 165Meckel diverticulum 118, 128Meconium ileus 128Medial abberant thyroid 56

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery270
Mediastinum 227Medullary carcinoma 65, 82, 83 sponge kidney 188Megaloblastic anemia 125Meissner plexus 98Melanoma 258Membranous urethral injury 201Menarche 84Menetrier’s disease 108, 112Meningeal tumors 224Meningioma 225Meningocele 2, 227Menopause 84Mesenchymal tumors 227Mesentric cysts 219Metabolic diseases 170Metastatic cancer thyroid 66 carcinoids 121 liver tumor 171Methods of stone removal 181 wound closure 238Middle mediastinum 227Midline swellings 46Milligan-Morgan operation 134Minor salivary gland tumor 51Mirrizzi syndrome 147Misnomers 56Modified child-Pugh classification 163 Perthes test 246 radical mastectomy 85 neck dissection 35, 66Moebius sign 61Mondor’s disease 81Monomorphic adenoma 50Monro-Kellie doctrine 222Morrissey cough impulse 244Mosse’s sign 245Motility disorders 96Moynihans hump 144MRI breast 79Mucinous carcinoma 82, 83Mucocele 127, 147Mucoepidermoid carcinoma 51Muir and Barclay formula 237Multiple adenomas 71 diverticula 119 hamartoma syndrome 83Mumps 54Murphy’s triad 126Muscular elements 43Mutilating surgery 86Mycobacterium bovis 124Mycotic aneurysm 248Myelofibrosis 176
Myenteric and submucous plexus 118 plexus 92, 98Myxoma 232
NNaffziger’s test 61National Institute for Health and Clinical
Excellence 22Near-total thyroidectomy 66Neck dissection for nodal metastasis 66Neoadjuvant chemotherapy 86Neoplasia 59Nerve plane 48 sheath tumors 224 supply of parotid gland 49Neuroepithelial tumors 224Neurofibromatosis 256Neurogenic tumors 86Nicoladoni sign 251Nigro regimen 133Nipple retraction 80Nissens partial fundoplication 93Nodular goiter 59 melanoma 258 swelling 60Non-caseating granulomas 121Non-cirrhotic portal fibrosis 167Nonepithelial tumors 50Non-small cell cancer 230Normal position of appendix 126 saline 8 serum amylase 155Nutcracker esophagus 97
OOat cell cancers 229Obesity 114, 183Obstruction to venous outflow 244Obstructive shock 11Odontogenic cyst 38Odynophagia 98Ogilvie herina 216Omphalitis 218Omphalocele 261Oncocytoma 183Oncosurgery 255Open pneumothorax 25Operable neck nodes 36 tumors 153Ophthalmoplegia 61Optimal storage time 17
Oral cavity 32 carcinoma 32 cholecystogram 145 contraceptives 84 lichen planus 32 submucosal fibrosis 32Organ donation 17 procurement 189 transplantation 11, 16Orocutaneous fistula 2Orthotopic graft 172Osteomalacia 107Osteomyelitis 1Osteosarcoma 83Otic ganglion 49Oxalate kidney stones 125
PPacked cell volume 107Paget disease 82 of nipple 82Palliative procedures 110Palpable flank mass 184Pancoast tumor 228, 229Pancreas 27, 154Pancreatic function test 154 tumors 156Pancreatitis 154Pantaloon hernia 216Papillary carcinoma 64, 82, 83 cystadenoma lymphomatosum 51Papilloma 83Pappenheimer bodies 174Paradoxical incontinence 187Paragangliomas 40Paraneoplastic syndrome 184, 231Paraphimosis 200Parathyroids 70Parenteral nutrition 5Parkland formula 237Parotid duct 49 gland 48, 49, 50 surgeries 52Paroxysmal spells 74Parts of ulcer 1Passaro triangle 157Paterson-Brown-Kelly syndrome 101Patey’s modification 85 pectoralis 85Pathology of oral cancers 34Paul-Mikulicz operation 130Peau d’orange 88Pectoralis major 86 minor 86

tahir99 - UnitedVRG
271Index
Pediatric brain tumors 226 surgery 261Peptic ulcer disease 104Percutaneous aspiration 168, 169 nephrolithotomy 181, 182 transhepatic cholangiography 163Perforator incompetence 245Periampullary carcinoma 156Pericardial tamponade 24Periductal mastitis 81Perimuscular connective tissues 152Periodontal cyst 38, 39Periosteitis tibia 245Peritonitis 218Perlman syndrome 227Persistent pulmonary hypertension 263Petit hernia 216Peutz-Jeghers syndrome 119Phantom hernia 216Pharyngeal pouch 46, 99Pheochromocytoma 40, 73, 227Phimosis 199Phyllodes tumor 88Pigment stones 146Pigmentation of lips 119Pilonidal sinus 1, 135Pituitary adenoma 76, 226 macroadenoma 224 tumors 226Plasma imbibition 239Pleomorphic adenoma 50, 51Plummer-Vinson syndrome 101Plunging ranula 53Pneumoperitoneum 218Polycystic kidney disease 183, 187Polyps 119Popliteal artery aneurysm 248Port-wine stain 6Postcibal syndrome 107Posterior gastric nerve 103 mediastinum 227 sagittal anorectoplasty 136 triangle 47 swelling 99 urethral valve 203 vestibule 136Posterolateral dissection 36Potato tumor 40Pott puffy tumor 3, 4Pratt’s sign 245Preauricular sinus 1Prehns sign 208Preparation of thyroid crisis 61Pretibial myxedema 61Prevention of recurrent bleed 166
Primary bladder stone 192 hemorrhage 13 hyperaldosteronism 76 hyperparathyroidism 71 hypersplenism 176 sclerosing cholangitis 150 survey 21 therapy 5 thyrotoxicosis 61Progressive dysphagia 96Propylthiouracil 61, 62Prostate and seminal vesicles 193 specific antigen 196Prostatic hyperplasia 193 urethra 136Proteus infection 180Proton pump inhibitors 93Protozoan infection after splenectomy 176Pseudoachalasia 98Pseudocyst pancreas 156Pseudomembranous colitis 126Pseudopneumoperitoneum 218Puestow procedure 155Pulmonary contusion 26Pulse rate slows 251Pyogenic abscess 4, 168
RRadiation induced cancers 260Radical excision of submandibular gland 53 mastectomy 86 parotidectomy 52Raised intracranial pressure 222Ranson’s criteria 156Ranula 2, 53Raspberry tumor 218Raynaud disease 250 syndrome 250Reactionary hemorrhage 13Reactive hypoglycemia 107Reconstruction of breast 89Rectal cancer 132 prolapse 136Rectum and anus 132Rectus sheath hematoma 217Recurrent adhesions 129 hematuria 174 infection 44 laryngeal nerve 57, 58 pyogenic cholangitis 169 stones 149Reflux esophagitis 93
Reidel lobe 162 thyroiditis 63Removal of breast tissue 86 internal mammary 86Renal casts 189 cell carcinoma 183, 184 medullary carcinoma 183 transplantation 188 trauma 186 tuberculosis 193Reperfusion syndrome 138Respiratory dyspnea 67 system 234Resuscitation 12Retractile testis 207Retroperitoneal fibrosis 218 loin 190Retrosternal goiter 60Richter hernia 216Right colon 120 coronary artery 231Ringer lactate 8Rodent ulcer 1Rolling hernia 94Roos test 42Roux-en-y gastric bypass 114Rovsing’s sign 126Rubber band ligation 134Rule of 10 lip for cleft lip repair 239 nine 235Rupture of bladder 192Rutherford-Morrison incision 127, 219
SSacless hernia 215Saint triad 147Salivary gland 48 tumors 49Salmon patch 6Salmonellosis 126Saphenous nerve 245 opening 213Sarcomas 88Satellite nodules treatment 259Saw-tooth appearance 119Scanlon modification 85Schatzki rings 101Schistosoma hematobium 190Sclerotherapy injection 134Seat belt injuries 20Sebaceous cyst 3 horn 3

tahir99 - UnitedVRG
Nutshell Series for FMGE/DNB/NEET-PG—General Surgery272
Secondary bladder stones 192 hemorrhage 13 hyperaldosteronism 76 hyperparathyroidism 72 thyrotoxicosis 61 varicose veins 244Seldinger’s technique 249Selective estrogen receptor modulators 87Seminal vesicles 197Seminomas 206Sengstaken-Blakemore tube 95, 165Sentinel node biopsy 260Serocystic disease of Brodie 88Serpiginous network of linear ulcerations
122Serum alkaline phosphatase 162Severity of shock 12Shamblin classifications 41Sherren’s triangle hyperesthesia 126Shionaya criteria 250Shock 11Short bowel syndrome 125 saphenous incompetency 245Shortening of esophagus 93Shouldice technique 217Shunting surgeries 166Sialadenitis 54Sideropenic dysphagia 32Significant hydroureteronephrosis 190Signs of base of skull fracture 21 inoperability 109Simple goiter 59 mastectomy 85Single adenoma 72Sinus 1Skeletal elements 43Skin cancers 256Skull base meningioma 224Sliding hernia 94, 215, 216Sloping ulcer 1Small bowel carcinoids 121Small bowel obstructions 129 tumors 121 cell cancer 230, 231 carcinoma 229 lung cancer 229 stomach syndrome 108Smooth muscle disorders 132Soft tissue sarcoma 81, 83, 259Solitary nodule thyroid 59 rectal ulcer 137Spigelian hernia 215, 216Spleen 27, 174
Splenectomy 176, 177 in trauma 175Splenic artery 106, 174, 178 gonadal fusion 177 infarction 178 trauma 175 tumors 177 vein 174Splenocolic ligaments 174Splenophrenic ligaments 174Splenorenal fusion 178 ligament 174Splenosis 177Spread methods 109Spur cells 174Squamous cell 92 cancer 229 carcinoma 1, 100, 229, 257, 231Stafne bone cyst 53Staghorn calculus 180Staphylococcus aureus 54, 80Starch iodine test 52Stauffers syndrome 184Steatorrhea 125Stellwag’s sign 61Stenson’s duct 48Stewart-Treves syndrome 88Stomach 27Stoppas procedure 217Strangulated hernia 216Strasberg classification 153Strawberry angioma 6Streptococcus pneumonia 176 pyogenes 4 viridans 54Stripping of small saphenous vein 245Structures within gland 48Struma ovary 56Struvite stone 180, 192Stylomandibular ligament 48Subarachnoid hemorrhage 23Subclavian aneurysm 249Subcutaneous tissue 4Subfascial endoscopic perforator surgery 245 ligation of Cockett and Dodd 245Sublingual duct 49Submandibular duct 49 gland 49, 50 excision 53 triangle 46Submucosal plexus 92Subphrenic abscess 219Subtotal thyroidectomy 66Subungual melanoma 258Sulfur colloid liver scan 170Superficial
parotidectomy 52 ring 213 spreading 258Superior laryngeal nerve 58 mesenteric artery syndrome 125Supraomohyoid block dissection 35Surgery in cyst 59 lymphoma 111Surgical division of prostate 193 removal of ureteric calculus 182Swellings in skin 2, 3Syphilitic glossitis 32 gumma ulcer 1
TTamoxifen 87Target cells 106Taylor procedure 106Temporal lobe 224Tension pneumothorax 25Teratomatous dermoid 3Testicular cancer 204 malignancy 205 tumors 204Testis and scrotum 204Thoracic aorta disruption 25 outlet syndrome 41 trauma 24Thoracotomy 26Thromboangitis obliterans 250Thumb print sign 131Thyroglossal cyst 46, 56 fistula 2Thyroid 59 acrobachy 61 adenoma 59 and parathyroid thymomas 227 cancers 63 carcinoma 59 disorders 56 storm 62Thyroiditis 59, 62Thyrotoxicosis 60Tillaux triad 219Time of absorption 8TNM staging of breast 84 oral cancer 35Torsion of testis 208Total conservative parotidectomy 52 extraperitoneal repair 217

tahir99 - UnitedVRG
273Index
gastrectomy 110 parenteral nutrition 5Toupet posterior fundoplication 93Toxic megacolon 125 multinodular goiter 61 nodular goiter 61Tracheobronchial injury 24Tracheoesophageal fistula 2, 95Traditional classification of hemorrhagic
shock 13Transabdominal preperitoneal mesh 217Transanal excision of cancer rectum 132Transjugular intrahepatic portal shunt 166Traumatic fat necrosis 81Treatment of complete prolapse 136 established lymph edema 251 fistula-in-ano 134 hydrocephalus 223 hypospadias 199 intraductal papilloma 80 partial prolapse 136 skin cancers 258 vesical calculus 192Triangles of neck 46Triangular cord sign 150Triple assessment of breast 79Troisier sign 156Trophic ulcer 1Trousseau sign 156True shortening of esophagus 96Trypanosoma cruzi 98Tuberculosis 1, 46 of bladder 193 of testis 209Tuberculuos sinus 1Tuberous sclerosis 183, 255Tubular carcinoma 83Tubulodermoid 2Tumor like malformations 224 localization 74 of ovary 119 of vagal body 40 thickness 259Turcot syndrome 119Types of allograft rejection 16 anal carcinoma 133 aneurysms 252 bariatric surgery 114 biliary atresia 149 casts 189 donor 188 emergency thoracotomy 26 enteral nutrition 5
flaps 238 graft 172 head injury 22 hernia 214 hydrocephalus 223 hypospadias 198 neck dissection 35 nutrition 4 of tuberculosis 124 primary lymph edema 251 renal calculus 180 skin graft 238 stockings 251 toxicosis 60 ulcer 1 urethral injuries 201 wound 8 suturing 8
UUlcer 1 of oral cavity 37Ulcerative colitis 121-123Ultimately inoperable tumors 111Umbilical calculus 218 granuloma 218Umbilicus 213Undescended testis 207Upper gastrointestinal bleeding 106, 112 limb 237 part of rectus abdominis 86Urea breath test 105Ureterocele 190Ureteroscopy 181Ureterosigmoidostomy 119Urethra 200Urethral injuries 193Uric acid stones 192Urinary bladder 190Urological injuries 27 surgery 180
VVaginal hydrocele 209Vagotomy 107Vagus nerve 92, 103Vanillymandelic acid 74Vanishing bile duct syndrome 151Varicella zoster 98Varicocele testis 207Varicose veins 244, 246
Variety of intraparietal hernia 215Vascular masses 227 surgery 244Vein of Mayo 103Venous drainage 57 grafts 232 plane 48 system 244Vigorous achalasia 97Virchow’s triad 246von Graefe’s sign 61von Hippel-Lindau syndrome 183von Recklinghausen’s disease 256
WWalls of canal 213 femoral canal 215Wardill operation 239Warthin tumor 51Water intoxication 194Watery diarrhea 125Weight loss 107Wharton submandibular duct 49Whipple procedure 156Whitaker test 188Whole blood 13Wilkie’s disease 112 syndrome 125Wilm’s tumor 185, 188Wolman’s classification 64Wunderlich’s syndrome 186
XXanthogranulomatous pyelonephritis 189
Yy loop 110
ZZenkers diverticulum 99Zollinger-Ellison syndrome 104Zona fasciculata 73 glomerulosa 73 reticularis 73Z-plasty 135, 239