Interventions to Increase Physical Activity in Middle-Age Women at the Workplace
39
“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review” by Ling J, Robbins LB, Wen F, Peng W Pediatric Exercise Science © 2015 Human Kinetics, Inc. Note. This article will be published in a forthcoming issue of the Pediatric Exercise Science. The article appears here in its accepted, peer-reviewed form, as it was provided by the submitting author. It has not been copyedited, proofread, or formatted by the publisher. Section: Review Article Title: Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review Authors: Jiying Ling 1 , Lorraine B. Robbins 1 , Fujun Wen 2 , and Wei Peng 3 Affiliations: 1 College of Nursing; 2 Department of Kinesiology; 3 Department of Telecommunication, Information Studies, and Media; Michigan State University, East Lansing, MI. Journal: Pediatric Exercise Science Acceptance Date: February 2, 2015 ©2015 Human Kinetics, Inc. DOI: http://dx.doi.org/10.1123/pes.2014-0148
-
Upload
michiganstate -
Category
Documents
-
view
4 -
download
0
Transcript of Interventions to Increase Physical Activity in Middle-Age Women at the Workplace

“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
Note. This article will be published in a forthcoming issue of the
Pediatric Exercise Science. The article appears here in its accepted,
peer-reviewed form, as it was provided by the submitting author. It has
not been copyedited, proofread, or formatted by the publisher.
Section: Review
Article Title: Interventions to Increase Physical Activity in Children Aged 2-5 Years: A
Systematic Review
Authors: Jiying Ling1, Lorraine B. Robbins1, Fujun Wen2, and Wei Peng3
Affiliations: 1College of Nursing; 2Department of Kinesiology; 3Department of
Telecommunication, Information Studies, and Media; Michigan State University, East Lansing,
MI.
Journal: Pediatric Exercise Science
Acceptance Date: February 2, 2015
©2015 Human Kinetics, Inc.
DOI: http://dx.doi.org/10.1123/pes.2014-0148

“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
Interventions to Increase Physical Activity in Children Aged 2-5 Years:
A Systematic Review
Jiying Ling
Michigan State University College of Nursing
Lorraine B. Robbins
Michigan State University College of Nursing
Fujun Wen
Michigan State University Department of Kinesiology
Wei Peng
Michigan State University Department of Telecommunication, Information Studies, and Media
Ling and Robbins are with the College of Nursing, Wen is with the Department of Kinesiology,
and Peng is with the Department of Media and Information, Michigan State University, East
Lansing, MI. Address author correspondence to Jiying Ling at [email protected].

“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
Abstract
Comprehensive evaluation of prior interventions designed to increase preschoolers’ physical
activity is lacking. This systematic review aimed to examine the effect of interventions on
objectively measured physical activity in children aged 2-5 years. We followed the Preferred
Reporting Items for Systematic Reviews and Meta-Analyses statement. In May 2014, we
searched PubMed, CINAHL, PsycINFO, ERIC, SPORTDiscus, Cochrane, and Embase. Two
reviewers independently identified and appraised the studies. Twenty-four articles describing 23
independent studies and 20 unique interventions met inclusion criteria. Of the eight interventions
resulting in a significant effect in objectively measured physical activity, all were center-based
and included a structured physical activity component, six included multiple components, five
integrated theories or models, and four actively involved parents. Seven of the eight were
randomized controlled trials. Due to the heterogeneity of the study designs, physical activity
measures, and interventions, drawing definitive conclusions was difficult. Although the overall
intervention effect was less than optimal, the review indicated that theory-driven, multi-
component interventions including a structured physical activity component and targeting both
parents and their children may be a promising approach for increasing preschoolers’ physical
activity and warrant continued investigation using rigorous designs to identify those that are
most effective.
Keywords: review, exercise, preschool, program evaluation

“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
From 1990 to 2010, the worldwide prevalence of overweight and obesity among
preschool children has increased from 4.2% to 6.7%, and is expected to reach 9.1% by 2020 (20).
In the U.S., 22.8% of children, aged 2-5 years, are overweight or obese (50). Children who are
overweight at age 5 are 4 times as likely as those of the same age with a healthy weight to
become obese in either later childhood or adolescence (17). These alarming findings indicate that
excess body weight early in a child’s life may be strongly correlated with subsequent obesity
risks. Children who participate in a physical activity (PA) and nutrition intervention at an earlier
age (< 5 years) have greater weight loss over 2 years than those who participate in the same
intervention at an older age (> 5 years) (15). Therefore, intervening before the start of elementary
school holds promise in reversing the current epidemic of childhood obesity.
PA is protective against obesity during the preschool years (57) and is essential for
children’s physical, cognitive, social, and emotional development at all ages (28). Children aged
3-5 years who are inactive are 3.8 times more likely to gain subcutaneous fat than those who are
active (43). Preschoolers’ accelerometer-measured vigorous PA is significantly associated with
their lower odds of being overweight (40). A recently conducted systematic review indicates that
a high level of PA not only reduces adiposity, but also improves motor skill development and
psychosocial and cardiovascular health in children aged 0-4 years (68). These studies support
that important health benefits are accrued from PA.
Although PA guidelines have been developed in several countries, the amount of daily
PA recommended is inconsistent. Recommendations in Australia and the United Kingdom
indicate that preschool children should participate in at least 3 hours of PA every day, including
light, moderate, and vigorous PA (62). The U.S. National Association for Sport and Physical
Education (NASPE) (45) guidelines call for 120 minutes of daily PA. Moreover, the U.S.

“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
Institute of Medicine (IOM) (35) recommends that preschool children should participate in 15 or
more minutes of PA per hour, approximately 3 hours per day. Based on accelerometer data,
preschool children actually participate in an average of 43 minutes of moderate to vigorous PA
(MVPA) daily (13). Regardless of the guideline discrepancies, the majority of preschool children
worldwide do not meet current PA recommendations (58, 62, 69).
Conducting interventions during early childhood may be a promising approach for
assisting children to establish a positive behavioral pattern that has the potential to continue into
adulthood (66). Although many interventions have been conducted to increase PA in preschool
children, current information on their overall impact, especially factors influencing the
intervention effect, is lacking. Two systematic reviews only focus on PA interventions conducted
in childcare center-based settings including daycare or childcare center, preschool, and nursery
(39, 70). One meta-analysis, including studies conducted before 2012, examined the effect of PA
interventions in preschool children (30). Although childcare center-based settings provide an
excellent location for PA interventions, examining interventions conducted at home or other
community settings (e.g., church, park, outpatient clinic, or hospital) is also essential to acquire
information for targeting children’s home and community environment. In all three reviews, PA
was operationally defined and measured in a variety of ways including proxy reports. Due to the
limited reliability and validity of proxy reports of PA (54), results of the three reviews may be
questionable.
Previous reviews focusing on identifying factors influencing the intervention effect have
yielded somewhat contradictory findings. One review of 19 studies conducted in childcare
center-based settings indicated that regular structured PA programs had a beneficial effect in
increasing PA among preschoolers (70). In contrary, a meta-analysis of 15 studies showed that

“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
short-term (< 4 weeks), teacher-led PA programs including outdoor activity and unstructured PA
were most effective (30). Finally, another review that included 23 studies conducted in childcare
center-based settings noted no effect of theory-based, multi-component interventions (39). The
inconsistent findings, possibly due to the heterogeneity of the included studies, limit the ability to
draw conclusions regarding factors that influence the intervention effect.
This paper adds to the existing body of knowledge by conducting a systematic review of
all relevant PA intervention studies up to May 2014 that involve preschool-age children and
include an objective measure of PA, such as pedometers and accelerometers. To efficiently
inform future research efforts directed toward preventing obesity among older children and
adolescents, effective and sustainable interventions and strategies targeting PA in preschool-age
children need to be identified. Less biased than a narrative review, a systematic review can assist
with achieving this objective by offering a rigorous and comprehensive examination of all
studies addressing a specific topic (26), such as PA interventions among preschoolers.
Objective
The aim was to examine the effect of interventions on objectively measured PA in
children of preschool age. In this study, preschoolers represent children aged 2-5 years. Research
questions were:
(a) What types of interventions have been conducted to increase objectively measured PA
in preschoolers?
(b) What is the overall effect of previously conducted interventions on objectively
measured PA?
(c) What factors may influence the effect of interventions on objectively measured PA?

“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
Methods
The Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA)
statement guided the literature search, conduct of the systematic review, and report of the
findings (42). The PRISMA statement, including a 27-item checklist and a 4-phase flow diagram,
specifies ways to ensure transparent and complete reporting of a review. The checklist addresses
the content to be included in each section of the review, including title, abstract, introduction,
methods, results, discussion, and funding. The flow diagram helps depict the number of records
identified, included, and excluded; and reasons for exclusion. Due to the need for a
comprehensive representation of evidence in the review, both randomized and non-randomized
quantitative studies incorporating a control or comparison group were analyzed (16).
Data Sources and Search Strategy
Assisted by a master-prepared university health science librarian, the first author
developed the initial search strategy to determine the general quantity and quality of published
studies testing PA interventions in children aged 2-5 years old in the PubMed database (from
1969). The following search terms and strategy were used: (("Motor Activity"[Mesh]) OR
("Exercise"[Mesh]) OR ("Play and Playthings"[Mesh]) OR "physical activity" OR "exercise*"
OR play*) AND (("Intervention Studies"[Mesh]) OR intervention* OR program*) Filters:
Humans; English; Preschool Child: 2-5 years. The procedure used for the PubMed database was
adapted to create a database-specific search strategy for CINAHL (from 1978), PsycINFO (from
1889), ERIC (from 1966), SPORTDiscus (from 1976), Cochrane database of systematic reviews
(from 1996), and Embase (from 1960). Because no filter or limit for age group existed in
databases of ERIC, SPORTDiscus, and Cochrane database of systematic reviews, (preschool*
OR toddler* OR child) was used to limit searching citations to children only. In May 2014, we

“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
carried out the full electronic search for published studies dating from their inception to 2014 in
these seven databases. To identify additional studies, we also reviewed reference lists of any
relevant reviews and original studies. The objective was to ensure an exhaustive search for all
international evidence associated with all disciplines and published in English.
Eligibility Criteria
Studies were included in the review if they: (a) primarily targeted children of preschool
age (2-5 years); (b) were original studies testing an intervention to increase PA or decrease
sedentary activity in any setting; (c) included a control or comparison group; and (d) reported
objectively measured PA as an outcome variable at baseline and post-intervention. In this study,
setting referred to the location where the intervention had been implemented. Exclusion criteria
were: (a) secondary analysis; (b) abstract only; (c) protocol only; (d) review study; (e) entire
population defined by a disease or a chronic condition such as autism, asthma, or obesity; and (f)
sample size less than 30 participants.
Study Selection
After exporting citations into the Endnote reference manager software, two authors (JL
and FW) independently screened all titles and abstracts against the inclusion and exclusion
criteria. After excluding citations that did not meet the inclusion criteria, they retrieved the full
text of the retained citations. They independently conducted a second screening by reading the
full version of each article and assessing whether or not the retained articles met the inclusion
criteria. They compared their findings and resolved any disagreement through discussion or, if
necessary, consultation with the second author (LR).

“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
Data Extraction
To simplify the analysis of each study, the first author developed a data extraction form
based on the Consolidated Standards of Reporting Trials (CONSORT) checklist (61). Details
about each study’s sample and setting, design, intervention, PA measure, and results were
extracted by the first author. All authors independently checked the extractions against the full
text for accuracy. Any discrepancies were discussed until all authors reached agreement.
Quality Appraisal and Risk of Bias
Each study was appraised based on the criteria adapted from the Cochrane Handbook for
Systematic Reviews of Interventions (33). Two authors (JL and LR) independently evaluated
each study and discussed any discrepancies until they agreed regarding the outcome. Risk of bias
(yes: low risk of bias, no: high risk of bias, and unclear: insufficient information) was evaluated
based on the following four quality indicators: (a) random sequence generation; (b) blinding of
PA outcome assessment; (c) valid PA measure (≥ 3 days of data) (1); and (d) clear explanation of
withdrawal. Only studies with no high risk of bias for all four indicators were considered low
risk of bias.
Data Synthesis
Examination of the included studies indicated substantial heterogeneity of the designs,
outcome measures, and intervention components. Therefore, a narrative summary technique
rather than a meta-analysis was used to report the findings according to the three research
questions.

“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
Results
Study Selection
A total of 11,559 citations were identified from the database searches and reference lists.
After screening titles and abstracts and removing duplicates, 191 articles were retained. The
second screening based on reading the full text yielded 24 articles focusing on increasing
objectively measured PA in children aged 2-5 years old. Two articles described the same study,
resulting in 23 independent studies; and four articles described one intervention but different
studies, resulting in 20 unique interventions. Figure 1 presents the flow diagram depicting study
selection results. Table 1 summarizes the 23 independent studies included in the review.
Risk of Bias
Table 2 presents the assessment of risk of bias for the 23 independent studies based on
the four quality indicators: random sequence generation, blinding of PA outcome assessment,
valid PA measure, and clear explanation of withdrawal. Several studies failed to provide details
to allow us to assess risk of bias, particularly concerning the random sequence generation
method (n = 16) and blinding of outcome assessment (n = 9). Only six studies clearly reported
the random sequence generation method including shuffling envelopes, using a computer random
number generator, or drawing of lots (18, 24, 36, 49, 52, 55); and one study did not use random
assignment (72). Seven studies reported taking measures to blind PA outcome assessment. Nine
studies did not use a valid PA measure (≥ 3 days of data). Most studies (n = 21) clearly explained
the reasons for missing PA data, but no study imputed missing data. Overall, based on the four
quality indicators, eight studies had low risk of bias.

“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
Study Characteristics
Publication dates for the 23 studies ranged from 2003 to 2014. As noted in Table 1,
studies were conducted in the U.S. (n = 11), United Kingdom (n = 2), Australia (n = 2), Belgium
(n = 2), Switzerland (n = 2), Canada (n = 1), Germany (n = 1), Scotland (n = 1), and Israel (n =
1). Eighteen studies were cluster RCTs, with clusters being preschools or childcare centers in 11
studies or classes in seven studies. Four studies were RCTs, and one study used quasi-
experimental non-equivalent group design. The sample size ranged from 32 (4) to 1,154 (6), with
a total sample size of 8,448 (mean age = 4.08). Eighteen studies enrolled children only aged 2-5
years, and one study involved children aged 1-3 (n = 40, M = 1.75; 32). In addition to including
children aged 2-5, four studies also involved children aged 6 (n = 2,034, M = 4.94; 18, 19, 23,
55). Details on children’s age were included in Table 1.
Physical Activity Measure. The most commonly used device for assessing PA was the
ActiGraph accelerometer: GT1M (n = 7), GT3X (n = 4), and CSA/MTI WAM-7164 (n = 3).
Four studies used pedometers to assess PA, with one study including Walk4Life (10), another
using Yamax (24), and two not reporting any particular model (23, 72). The remaining studies
used other types of accelerometers, including Actical (n = 1), Actiwatch (n = 1), TriTrac (n = 1),
and Actiheart (n = 1). The length of time for monitoring ranged from minutes (86-149 min.) to
seven days. The reported PA outcome variables included minutes or % of sedentary activity,
light PA (LPA), moderate PA (MPA), vigorous PA (VPA), MVPA, or overall PA.
Research Question 1: What types of interventions have been conducted to increase
objectively measured PA in preschoolers?
Among the 20 unique interventions, two interventions were home-based (32, 52), with
the remaining being center-based. Center-based interventions include interventions that were

“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
implemented in daycare or childcare centers, preschools, or nurseries. Intervention duration
ranged from 6 weeks (49) to 12 months (19, 63), with a mean duration of six months. Nine
interventions targeted both parents and children, with two having an environmental component
(19, 55). One intervention targeted only the preschools’ environment (14). Only two
interventions collected long-term follow-up data at either six months (49) or six and twelve
months after the intervention had ended (64).
Theoretical Framework. Of the 20 interventions, a single theory or model was used in
six; and two models or theories were integrated in three. Bandura’s (9) social cognitive theory
was integrated with self-efficacy theory in one intervention (7) and with self-determination
theory in another (25). One intervention was based on early childhood development theory and
general system theory (72). The socio-ecological model provided the theoretical foundation for
four interventions (12, 24, 48, 49). Other theories or models used alone included PRECEDE-
PROCEED model (19) and general system theory (18).
Research Question 2: What is the overall effect of previously conducted interventions on
objectively measured PA?
When compared to their respective control groups, eight of the 20 interventions
significantly increased PA or decreased sedentary activity at post-intervention (2, 5-8, 18-19, 23,
25, 63-64, 72). Among the eight interventions having a significant effect, two decreased
sedentary activity only (2, 18), three increased overall PA (23, 63-64, 72), and the remaining
three increased MVPA. One of the two interventions with long-term follow-up assessments
sustained the effect on PA six months, but not 12 months, after the intervention had ended (63-
64).

“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
Research Question 3: What factors may influence the effect of interventions on objectively
measured PA?
Risk of bias. Only three of the eight interventions with low risk of bias had a significant
effect (2, 18, 23). Two of the three decreased only accelerometer-measured sedentary activity (2,
18), and the remaining one increased overall pedometer-measured PA (23).
Study design. Seven of the 19 RCT interventions, including four RCTs and 15 cluster
RCTs, and one quasi-experimental study intervention had a significant intervention effect. Of the
eight interventions with a significant effect, two RCT interventions decreased only sedentary
activity (2, 18), whereas five RCT and one quasi-experimental interventions resulted in increased
MVPA or overall PA. One RCT, including 178 preschoolers offering 30 minutes of PA daily for
twelve months, had a significant intervention effect at 6-month, but not 12-month, follow-up (64).
Intervention Setting. Eight of the 18 center-based, teacher-delivered interventions had a
significant effect, while the two home-based interventions had no effect on PA. One 16-week
home-based intervention focusing on obesity prevention included 11 parenting lessons with 40
parent-child dyads (32). The other occurred across eight months and included monthly
interactive kits and a motivational interviewing session for parents among 400 parent-child dyads
(52).
Theoretical framework. Of the nine theory-based interventions, five had a significant
effect on sedentary activity, MVPA, or overall PA. Grounded in social cognitive theory and self-
efficacy theory, a 9-month Start For Life intervention, including 30 minutes of structured PA
daily, teacher training, and progress monitoring, resulted in a 2% increase in MVPA, compared
to a 1% decrease in the control group (5-8). Based on social cognitive theory and self-
determination theory, a 14-week teacher-delivered weight control intervention, including 20

“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
minutes of structured PA twice a week and weekly homework assignments for parents, increased
MVPA by 11 minutes/day, as compared to 4 minutes/day for the control group (25). Compared
to a state-sponsored PA program that decreased sedentary activity by 3 minutes/day, a 9-month
participatory PA intervention based on general system theory that involved parents through
parent-teacher meetings and a website decreased sedentary activity by 7 minutes/day (18). A 12-
month PRECEDE-PROCEED model-based ToyBox intervention including PA sessions for
children, newsletters for parents, and an environmental change increased MVPA by 1.2%,
compared to a 0.6% increase in the control group (19). Another study compared an 18-week
center-based with a home- and center-based intervention with both being grounded in early
childhood development theory and general system theory (72). Findings showed a significant
increase in PA assessed by pedometers in both intervention groups, but no between-group
differences.
Physical activity measure. Of the 11 interventions using 3-7 day accelerometer data to
assess PA, four had a significant effect. One non-theory-based structured PA program conducted
with 71 preschoolers decreased their sedentary activity by 3%, compared to a 4% increase in the
control group (2). The remaining three were theory-based, including Fitzgibbon’s (25) Weight
Control Intervention, De Bock’s (18) Participatory Physical Activity Intervention, and De
Craemer’s (19) ToyBox Intervention.
Significant difference between the intervention and control groups occurred in two of
three interventions measuring children’s PA using pedometers for at least three days (23, 72).
Yin’s (72) 18-week PA intervention increased PA by approximate 18 steps/minute in 252
preschoolers. Eliskim and colleagues’ (23) 4-month, center-based nutrition and PA intervention
with 101 children, ages 5-6, increased PA by 1,438 steps/day.

“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
Length of intervention. Of the eight interventions having a significant effect, one was
implemented for either 8 weeks or 9 months (due to heterogeneous reporting of findings,
intervention effect was not able to be compared) (5-8). The duration of the remaining seven
interventions were: 14 weeks (25), 4 months (23), 18 weeks (72), 6 months (2), 9 months (18),
and 12 months (n = 2) (19, 63). The average duration for the interventions with a significant
effect was 6.55 months, compared to 6 months for the 20 included unique interventions.
Parental involvement. Five of nine interventions including a child component and a
parental component had a significant effect, with four of five actively involving parents through
goal setting, lecturing, group discussion, or homework assignment (18, 23, 25, 72), and one of
four passively involving parents through sending home handouts, CD/DVDs, flyers, leaflets,
books, or text messages (19). Two interventions that targeted only parents through motivational
interviewing, monthly newsletter, or educational lessons, had no beneficial effect (32, 52). One
intervention significantly increased PA when targeting both children and parents, compared to
only targeting parents through lectures (23). Two interventions evaluated the unique contribution
of involving parents to children’s PA (18, 72). One 9-month intervention adding a parental
component through a parent-teacher meeting and website resulted in a significant greater
decrease in children’s accelerometer-measured sedentary activity than a state-sponsored PA
program (18). The other intervention involving parents through peer-education and posters did
not change children’s PA, when compared to a regular center-based PA program (72).
Intervention components. Six of 12 multi-component interventions and two of eight
single-component interventions had a significant effect. Of the six multi-component
interventions, five involved both children and parents (18-19, 23, 25, 72), and one targeted only
children (8). The intervention components for children included: (a) structured PA (8, 18-19, 23,

“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
25, 72); (b) PA education (25); and (c) recess (72). The two effective single-component
interventions provided 30-60 minutes of structured PA daily for six or twelve months (3, 63).
Summary. Eight of the 20 unique interventions significantly decreased sedentary activity
or increased PA at post-intervention compared to a control group, and one of the two with
follow-up assessments sustained the effect six months after intervention had ended. Of the eight
interventions with a significant effect, all were center-based and included a structured PA
component, seven were RCTs including one RCT and six cluster RCTs, six used accelerometers
to assess PA, six involved more than one component, five integrated theories or models, four
actively involved parents, and three had low risk of bias. In summary, compared to other
approaches, center-based, theory-driven, multi-component interventions that include a structured
PA component and target both parents and their children hold a promise for increasing PA.
Discussion
This systematic review, which provided a critical synthesis and evaluation of 20 unique
interventions described in 23 independent studies targeting preschoolers to increase their PA, had
both strengths and limitations. All studies assessed PA objectively, and 19 were RCTs. The
majority (n = 16) had sample sizes greater than 200. Participants included diverse ethnic and
racial groups from several countries. Despite strengths, drawing conclusions from the review by
comparing the interventions was challenging due to some methodological limitations and
heterogeneity of the included studies, including varied wear time for pedometers and
accelerometers, and intervention durations ranging from six weeks to twelve months. Only two
studies had long-term (≥ 6 months) follow-up data, precluding any comprehensive synthesis of
results on whether or not an intervention effect can be sustained after an intervention has ended.
Overall, the review indicated that the effect of interventions conducted to date on objectively

“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
measured PA in preschoolers is not nil, as evidenced by significant improvement in the behavior
resulting from eight of 20 interventions. Additionally, four (n = 2,034) of the 20 interventions (N
= 8,448) enrolled children up to 6 years old with three reporting a significant effect, so results
from this review may be applicable to this age group of preschool children. However, of the
eight interventions with significant findings on PA, risk of bias was low for only three. Therefore,
continued investigation involving rigorous study designs is needed to accurately determine the
effect of interventions on preschoolers’ PA.
Study Design
Only one quasi-experimental intervention and seven of 19 RCT interventions had a
significant effect. Even though the preferred design of RCT was used, intervention effect can be
influenced by outcome measures (60) and implementation fidelity (21). Because only one of two
studies employing long-term follow-up measures had a sustained intervention effect in this
review, no definitive conclusion can be drawn about sustainability. Some researchers propose
that an intervention effect is delayed in health-promotion studies. An 8-week PA intervention
with 50 preschoolers did not increase MVPA after intervention, but did so at 4-month follow-up
(56). Another intervention did not show a significant effect until 12-month follow-up, and the
effect was sustained for 36 months (27).
Employing long-term follow-up measurements is not only essential in evaluating the
sustainability of an intervention effect, but also necessary in determining the duration of an effect
and identifying a delayed intervention effect. We found several studies involving adults only that
explored strategies or influencing factors for sustaining the behavioral intervention effect. One
study with 1,032 overweight or obese adults showed monthly personal contact had a modest
benefit in sustaining the effect, while an interactive technology-based intervention had an early

“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
but transient benefit (65). A systematic review concluded that maintenance in adults is
influenced by their internal motivation, social support, coping strategies, self-efficacy, and
autonomy (22). To better understand intervention sustainability and strategies for promoting it in
preschoolers, follow-up efforts for a minimum of 6-12 months after the last intervention contact
is essential (29).
Intervention Setting
Consistent with reports from other researchers (30), the review indicated that
interventions for preschoolers are mostly center-based and teacher-delivered. This approach
makes sense for the following reasons: (a) worldwide, about 33% of children aged 0-3 and 70%
of children aged 3-5 attend an organized childcare program (67); (b) the majority of children’s
waking hours are spent in the setting; (c) conducting an intervention can be cost-effective when
delivered by teachers in a school (71); and (d) sustaining an intervention effect needs
implementation of the intervention under real-world conditions that can be continued after the
researchers remove the resources (31). This information indicates that preschool teachers are
ideal interventionists for delivering center-based healthy lifestyle programs. Unfortunately, the
influence of interventionist and intervention setting on the intervention effect cannot be fully
evaluated due to the limited number of home-based interventions for comparison. With
approximately 67% of children aged 0-3 and 30% of children aged 3-5 not attending an
organized childcare program (67), family- and community-based interventions are essential to
target this group of children.

“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
Theoretical Framework
The majority of theory- or model-based interventions and less than one-third of the non-
theory-based interventions resulted in a beneficial effect. Although theory-based interventions
have been recommended for preventing obesity in children, a recent systematic review concludes
that use of appropriate behavioral change strategies (e.g., develop skills and behavioral capacity,
increase self-efficacy, educate parents and children, and model healthful behaviors) rather than
theoretical models is the key for managing obesity in preschoolers (46). Although tailoring a
theory or model to a specific population and behavior is important for enhancing intervention
effect, few theories or models have been developed for or tested in preschoolers (29). To capture
the variance of a behavior, the theory or model should be applied in a manner that is
developmentally appropriate for children’s age (11). Studies are needed to examine ways to
appropriately apply theories or models in interventions for preschoolers so that any benefit
concerning their use with this young population can be identified.
Physical Activity Measure
The most commonly used devices were ActiGraph GT1M or GT3X accelerometer,
consistent with other study findings (69). However, only 11 of 16 interventions met the
minimum requirement for assessing PA via accelerometers with four having a significant effect.
To obtain a reliability of .75 when estimating preschoolers’ PA via accelerometers, 5.5 days of
monitoring are needed (1). In this review, only nine used 5-days as a cut point, and four of them
had a significant effect on PA.
Although two of four interventions that included pedometers to assess PA showed a
significant effect, the reliability and validity of using pedometers to estimate preschoolers’ PA
are problematic (44, 51). Pagels and colleagues (53) reported a weak correlation (r = .19)

“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
between pedometer steps and MVPA assessed by accelerometer. One plausible explanation is
that preschoolers’ intensity of steps taken can be detected only by the more sensitive
accelerometer and are not strong enough for detection by pedometer. In addition, the types of PA
behaviors young children engage in may also not be detected by conventional pedometers.
Therefore, to accurately assess PA in preschoolers and compare the effect of different
interventions, researchers need to use standardized measurement protocols and accelerometers,
as opposed to pedometers.
Length of Intervention
Based on this review, the average duration for effective interventions on PA is 6.55
months, much longer than the four weeks reported by Gordon and colleagues (30). Little
evidence exists regarding the influence of intervention duration on intervention effect among
preschoolers. A meta-analysis of 32 studies involving individuals aged 7 or older showed that the
mean effect sizes of pedometer-based PA interventions differed according to intervention
duration (< 8 weeks: .68, 8-15 weeks: .65, >15 weeks: .76; 37). Another review including 31
studies noted no influence of intervention duration on intervention effect on objectively
measured PA among children (41). As can be determined from this information, the evidence on
the intervention duration effect is limited and inconsistent.
Parental Involvement
Although evidence on the effect of parental involvement in increasing children’s PA is
inconsistent, actively involving parents through goal setting, lecturing, group discussion, or
homework assignment may hold some promise. Research suggests that involving parents through
a family visit or via a phone to provide training, counseling, or preventive messages offers some

“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
promise in increasing the PA of children (47). Similarly, interventions that engage parents
directly in activities, such as family counseling or training, have more positive effects on
children’s healthy eating behaviors than indirect methods, such as inviting parents to a healthy
behavior activity or providing messages without requesting a response (34). Therefore, actively
engaging parents in behavioral interventions with their children may be a fruitful approach for
promoting positive changes.
Intervention Components
A structured PA component ranging from 20 to 45 minutes/session was included in all
the interventions with a significant effect. Alhassan and colleagues (3) found that a structured PA
program significantly decreased sedentary activity more than an unstructured free-play program,
consistent with the finding from a systematic review (70). This information indicates that
providing structured PA may be an important strategy for increasing PA in preschoolers.
However, because free play is vital for child’s motor, emotional, and cognitive development (38),
interventions to increase PA should not be implemented at the cost of children’s free play time.
Therefore, opportunities for both structured (e.g., physical education) and non-structured (e.g.,
recess) PA are needed during a child’s school day. One possible approach is simply integrating
structured PA into a child’s daily routine or existing curriculum.
Conclusion
This review indicates that theory-driven, multi-component interventions including a
structured PA component and targeting both parents and preschoolers may be promising for
promoting positive behavior changes in this young age group, although definitive conclusions
regarding the overall effect of interventions conducted to date to increase preschoolers’ PA are

“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
difficult to draw due to varied settings, designs, outcome measures, and interventions. To reduce
the current childhood overweight and obesity problem, continuing investigation with well-
designed RCTs that incorporate long-term follow-up procedures and reliable measures is
warranted to identify the most effective approaches for increasing the PA of preschoolers.
Acknowledgment
The authors thank Ms. Heidi M. Schroeder for her consultation and assistance on developing the
search strategies.

“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
References
1. Addy CL, Trilk JL, Dowda M, Byun W, Pate RR. Assessing preschool children's
physical activity: How many days of accelerometry measurement. Pediatr Exerc Sci.
2014;26(1):103-109. doi:10.1123/pes.2013-0021
2. Alhassan S, Nwaokelemeh O, Ghazarian M, Roberts J, Mendoza A, Shitole S. Effects of
locomotor skill program on minority preschoolers' physical activity levels. Pediatr Exerc
Sci. 2012;24(3):435-449.
3. Alhassan S, Nwaokelemeh O, Lyden K, Goldsby T, Mendoza A. A pilot study to
examine the effect of additional structured outdoor playtime on preschoolers' physical
activity levels. Child Care in Practice. 2013;19(1):23-35.
doi:10.1080/13575279.2012.712034
4. Alhassan S, Sirard JR, Robinson TN. The effects of increasing outdoor play time on
physical activity in Latino preschool children. Int J Pediatr Obes. 2007;2(3):153-158.
doi:10.1080/17477160701520108
5. Annesi JJ, Smith AE, Tennant GA. Cognitive-behavioural physical activity treatment in
African-American pre-schoolers: Effects of age, sex, and BMI. J Paediatr Child Health.
2013;49(2):E128-E132. doi:10.1111/jpc.12082
6. Annesi JJ, Smith AE, Tennant GA. Effects of a cognitive-behaviorally based physical
activity treatment for 4- and 5-year-old children attending US preschools. Int J Behav
Med. 2013;20(4):562-566. doi:10.1007/s12529-013-9361-7
7. Annesi JJ, Smith AE, Tennant GA. Effects of the Start For Life treatment on physical
activity in primarily African American preschool children of ages 3-5 years. Psychol
Health Med. 2013;18(3):300-309. doi:10.1080/13548506.2012.712704
8. Annesi JJ, Smith AE, Tennant GA. Reducing high BMI in African American
preschoolers: effects of a behavior-based physical activity intervention on caloric
expenditure. South Med J. 2013;106(8):456-459. doi:10.1097/SMJ.0b013e3182a05bef
9. Bandura A. Social cognitive theory: An agentic perspective. Annu Rev Psychol.
2001;52:1-26. doi:10.1146/annurev.psych.52.1.1
10. Bellows LL, Davies PL, Anderson J, Kennedy C. Effectiveness of a physical activity
intervention for head start preschoolers: A randomized intervention study. Am J Occup
Ther. 2013;67(1):28-36. doi:10.5014/ajot.2013.005777
11. Bluford DA, Sherry B, Scanlon KS. Interventions to prevent or treat obesity in preschool
children: A review of evaluated programs. Obesity. 2007;15(6):1356-1372.
doi:10.1038/oby.2007.163
12. Bonvin A, Barral J, Kakebeeke TH, Kriemler S, Longchamp A, Schindler C, et al. Effect
of a governmentally-led physical activity program on motor skills in young children

“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
attending child care centers: A cluster randomized controlled trial. Int J Behav Nutr Phys
Act. 2013;10(1):90-101. doi:10.1186/1479-5868-10-90
13. Bornstein DB, Beets MW, Byun W, McIver K. Accelerometer-derived physical activity
levels of preschoolers: A meta-analysis. J Sci Med Sport. 2011;14(6):504-511.
doi:10.1016/j.jsams.2011.05.007
14. Cardon G, Labarque V, Smits D, De Bourdeaudhuij I. Promoting physical activity at the
pre-school playground: The effects of providing markings and play equipment. Prev Med.
2009;48(4):335-340. doi:10.1016/j.ypmed.2009.02.013
15. Cheng JK, Wen X, Coletti KD, Cox JE, Taveras EM. 2-year BMI changes of children
referred for multidisciplinary weight management. Int J Pediatr. 2014;152586.
doi:10.1155/2014/152586
16. Cochrane Effective Practice and Organisation of Care Group. EPOC Resources for
review authors [Internet]. 2013 [cited 2014 Jun]. Available from
http://epocoslo.cochrane.org/epoc-specific-resources-review-authors
17. Cunningham SA, Kramer MR, Narayan KM. Incidence of childhood obesity in the
United States. N Engl J Med. 2014;370(5):403-411. doi:10.1056/NEJMoa1309753
18. De Bock F, Genser B, Raat H, Fischer JE, Renz-Polster H. A participatory physical
activity intervention in preschools: A cluster randomized controlled trial. Am J Prev Med.
2013;45(1):64-74. doi:10.1016/j.amepre.2013.01.032
19. De Craemer M, De Decker E, Verloigne M, De Bourdeaudhuij I, Manios Y, Cardon G, et
al. The effect of a kindergarten-based, family-involved intervention on objectively
measured physical activity in Belgian preschool boys and girls of high and low SES: The
ToyBox-study. Int J Behav Nutr Phys Act. 2014;11:38. doi:10.1186/1479-5868-11-38
20. de Onis M, Blossner M, Borghi E. Global prevalence and trends of overweight and
obesity among preschool children. Am J Clin Nutr. 2010;92(5):1257-1264.
doi:10.3945/ajcn.2010.29786
21. Durlak JA, DuPre EP. Implementation matters: A review of research on the influence of
implementation on program outcomes and the factors affecting implementation. Am J
Community Psychol. 2008;41(3-4):327-350. doi:10.1007/s10464-008-9165-0
22. Elfhag K, Rossner S. Who succeeds in maintaining weight loss? A conceptual review of
factors associated with weight loss maintenance and weight regain. Obes Rev.
2005;6(1):67-85. doi:10.1111/j.1467-789X.2005.00170.x
23. Eliakim A, Nemet D, Balakirski Y, Epstein Y. The effects of nutritional-physical activity
school-based intervention on fatness and fitness in preschool children. J Pediatr
Endocrinol Metab. 2007;20(6):711-718. doi: 10.1515/JPEM.2007.20.6.711

“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
24. Finch M, Wolfenden L, Morgan PJ, Freund M, Jones J, Wiggers J. A cluster randomized
trial of a multi-level intervention, delivered by service staff, to increase physical activity
of children attending center-based childcare. Prev Med. 2014;58(1):9-16.
doi:10.1016/j.ypmed.2013.10.004
25. Fitzgibbon ML, Stolley MR, Schiffer LA, Braunschweig CL, Gomez SL, Van Horn L, et
al. Hip-hop to Health Jr. obesity prevention effectiveness trial: Postintervention results.
Obesity. 2011;19(5):994-1003. doi:10.1038/oby.2010.314
26. Garg AX, Hackam D, Tonelli M. Systematic review and meta-analysis: When one study
is just not enough. Clin J Am Soc Nephrol. 2008;3:253-260. doi: 10.2215/CJN.01430307
27. Gillham JE, Reivich KJ, Freres DR, Chaplin TM, Shatte AJ, Samuels B, et al. School-
based prevention of depressive symptoms: A randomized controlled study of the
effectiveness and specificity of the Penn Resiliency Program. J Consult Clin Psychol.
2007;75(1);9-19. doi:10.1037/0022-006x.75.1.9
28. Ginsburg KR. The importance of play in promoting healthy child development and
maintaining strong parent-child bonds. Pediatrics. 2007;119(1):182-191.
doi:10.1542/peds.2006-2697
29. Glanz K, Rimer BK, Viswanath K. Health behavior and health education: Theory,
research, and practice (4th ed.). San Francisco, CA: John Wiley & Sons, Inc., 2008.
30. Gordon ES, Tucker P, Burke SM, Carron AV. Effectiveness of physical activity
interventions for preschoolers: A meta-analysis. Res Q Exerc Sport. 2013;84(3):287-294.
doi:10.1080/02701367.2013.813894
31. Han SS, Weiss B. Sustainability of teacher implementation of school-based mental health
programs. J Abnorm Child Psychol. 2005;33(6):665-679. doi:10.1007/s10802-005-7646-
2
32. Harvey-Berino J, Rourke J. Obesity prevention in preschool Native-American children: A
pilot study using home visiting. Obes Res. 2003;11(5):606-611. doi:10.1016/S0749-
3797(99)00117-8
33. Higgins JP, Green A. Cochrane handbook for systematic reviews of interventions.
Chichester: Wiley-Blackwell, 2011.
34. Hingle MD, O'Connor TM, Dave JM, Baranowski T. Parental involvement in
interventions to improve child dietary intake: A systematic review. Prev Med.
2010;51(2):103-111. doi:10.1016/j.ypmed.2010.04.014
35. Institute of Medicine. Early childhood obesity prevention policies. Washington, DC: The
National Academies Press, 2011.

“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
36. Jones RA, Riethmuller A, Hesketh K, Trezise J, Batterham M, Okely AD. Promoting
fundamental movement skill development and physical activity in early childhood
settings: A cluster randomized controlled trial. Pediatr Exerc Sci. 2011;23(4):600-615.
37. Kang M, Marshall SJ, Barreira TV, Lee JO. Effect of pedometer-based physical activity
interventions: A meta-analysis. Res Q Exerc Sport. 2009;80(3):648-655.
doi:10.1080/02701367.2009.10599604
38. Kreichauf S, Wildgruber A, Krombholz H, Gibson EL, Vogele C, Nixon CA, et al.
Critical narrative review to identify educational strategies promoting physical activity in
preschool. Obesity Reviews. 2012;13:96-105. doi:10.1111/j.1467-789X.2011.00973.x
39. Mehtala MAK, Saakslahti AK, Inkinen ME, Poskiparta MEH. A socio-ecological
approach to physical activity interventions in childcare: A systematic review. Int J Behav
Nutr Phys Act. 2014;11. doi:10.1186/1479-5868-11-22
40. Metallinos-Katsaras ES, Freedson PS, Fulton JE, Sherry B. The association between an
objective measure of physical activity and weight status in preschoolers. Obesity.
2007;15(3):686-694. doi:10.1038/Oby.2007.571
41. Metcalf B, Henley W, Wilkin T. Effectiveness of intervention on physical activity of
children: Systematic review and meta-analysis of controlled trials with objectively
measured outcomes (EarlyBird 54). BMJ. 2012;345:e5888. doi:10.1136/bmj.e5888
42. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P. Preferred reporting items for
systematic reviews and meta-analyses: The PRISMA statement. PLoS Med.
2009;6(7):e1000097. doi:10.1371/journal.pmed.1000097
43. Moore LL, Nguyen US, Rothman KJ, Cupples LA, Ellison RC. Preschool physical
activity level and change in body fatness in young children: The Framingham Children's
Study. Am J Epidemiol. 1995;142(9):982-988.
44. Murray ME. Validity and reliability of using MVP 4 Function Walk4Life digital
pedometers to assess physical activity levels among preschool-aged Head Start children
[thesis]. Houston, TX: The University of Texas Health Science Center at Houston; 2009.
45. National Association for Sport and Physical Education. Active start: A statement of
physical activity guidelines for children from birth to age 5 (2nd ed.). Sewickley, PA:
American Alliance for Health, Physical Education, Recreation, and Dance, 2009.
46. Nixon CA, Moore HJ, Douthwaite W, Gibson EL, Vogele C, Kreichauf S, et al.
Identifying effective behavioural models and behaviour change strategies underpinning
preschool- and school-based obesity prevention interventions aimed at 4-6-year-olds: A
systematic review. Obes Rev. 2012;13(Suppl 1):106-117. doi:10.1111/j.1467-
789X.2011.00962.x

“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
47. O'Connor TM, Jago R, Baranowski T. Engaging parents to increase youth physical
activity: A systematic review. Am J Prev Med. 2009;37(2):141-149.
doi:10.1016/j.amepre.2009.04.020
48. O'Dwyer MV, Fairclough SJ, Knowles Z, Stratton G. Effect of a family focused active
play intervention on sedentary time and physical activity in preschool children. Int J
Behav Nutr Phys Act. 2012;9:117. doi:10.1186/1479-5868-9-117
49. O’Dwyer MV, Fairclough SJ, Ridgers ND, Knowles ZR, Foweather L, Stratton G. Effect
of a school-based active play intervention on sedentary time and physical activity in
preschool children. Health Educ Res, 2013;28(6):931-942. doi:10.1093/her/cyt097
50. Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of childhood and adult obesity in
the United States, 2011-2012. JAMA. 2014;311(8):806-814. doi:10.1001/jama.2014.732
51. Oliver M, Schofield GM, Kolt GS, Schluter PJ. Pedometer accuracy in physical activity
assessment of preschool children. J Sci Med Sport. 2007;10(5):303-310.
doi:10.1016/j.jsams.2006.07.004
52. Ostbye T, Krause KM, Stroo M, Lovelady CA, Evenson KR, Peterson BL, et al. Parent-
focused change to prevent obesity in preschoolers: Results from the KAN-DO study.
Prev Med. 2012;55(3):188-195. doi:10.1016/j.ypmed.2012.06.005
53. Pagels P, Boldemann C, Raustorp A. Comparison of pedometer and accelerometer
measures of physical activity during preschool time on 3- to 5-year-old children. Acta
Paediatr. 2011;100(1):116-120. doi:10.1111/j.1651-2227.2010.01962.x
54. Pate RR, O'Neill JR, Mitchell J. Measurement of physical activity in preschool children.
Med Sci Sports Exerc. 2010;42(3);508-512. doi:10.1249/MSS.0b013e3181cea116
55. Puder JJ, Marques-Vidal P, Schindler C, Zahner L, Niederer I, Burqi F, et al. Effect of
multidimensional lifestyle intervention on fitness and adiposity in predominantly migrant
preschool children (Ballabeina): Cluster randomised controlled trial. BMJ.
2011;343:d6195. doi:10.1136/bmj.d6195
56. Qiu W. Physical activity intervention in early care and education settings [dissertation].
Newark, DE: University of Delaware; 2008.
57. Reilly JJ. Physical activity, sedentary behaviour and energy balance in the preschool
child: Opportunities for early obesity prevention. ProcNutr Soc. 2008;67(3):317-325.
doi:10.1017/S0029665108008604
58. Reilly JJ. Low levels of objectively measured physical activity in preschoolers in child
care. Med Sci Sports Exerc. 2010;42(3):502-507. doi:10.1249/MSS.0b013e3181cea100
59. Reilly JJ, Kelly L, Montgomery C, Willianson A, Fisher A, McColl JH, et al. Physical
activity to prevent obesity in young children: Cluster randomised controlled trial. BMJ.
2006;333(7577):1041. doi:10.1136/bmj.38979.623773.55

“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
60. Savovic J, Jones H, Altman D, Harris R, Juni P, Pildal J, et al. Influence of reported study
design characteristics on intervention effect estimates from randomised controlled trials:
Combined analysis of meta-epidemiological studies. Health Technol Assess.
2012;16(35):1-82. doi:10.3310/hta16350
61. Schulz KF, Altman DG, Moher D, Consort Group. CONSORT 2010 Statement: Updated
guidelines for reporting parallel group randomised trials. J Clin Epidemiol.
2010;63(8):834-840. doi:10.1016/j.jclinepi.2010.02.005
62. Skouteris H, Dell'Aquila D, Baur LA, Dwyer GM, McCabe MP, Ricciardelli LA, et al.
Physical activity guidelines for preschoolers: A call for research to inform public health
policy. Med J Aust. 2012;196(3):174-177.
63. Specker B, Binkley T. Randomized trial of physical activity and calcium supplementation
on bone mineral content in 3- to 5-year-old children. J Bone Miner Res. 2003;18(5):885-
892. doi:10.1359/jbmr.2003.18.5.885
64. Specker B, Binkley T, Fahrenwald N. Increased periosteal circumference remains present
12 months after an exercise intervention in preschool children. Bone. 2004;35(6):1383-
1388. doi:10.1016/j.bone.2004.08.012
65. Svetkey LP, Collaborat WLM. Comparison of strategies for sustaining weight loss: The
weight loss maintenance randomized controlled trial. Am J Health Promot.
2008;23(2):152-153. doi:10.1001/jama.299.10.1139
66. Telama R, Yang X, Leskinen E, Kankaanpaa A, Hirvensalo M, Tammelin T, et al.
Tracking of physical activity from early childhood through youth into adulthood. Med
Sci Sports Exerc. 2014;46(5):955-962. doi:10.1249/Mss.0000000000000181
67. The Convention on the Organisation for Economic Co-operation and Development.
PF3.2: Enrolment in childcare and pre-schools. 2014 [cited 2015 Jan.]. Available from
www.oecd.org/social/family/database
68. Timmons BW, Leblanc AG, Carson V, Connor GB, Dillman C, Janssen I, et al.
Systematic review of physical activity and health in the early years (aged 0-4 years).
Appl Physiol Nutr Metab. 2012;37(4):773-792. doi:10.1139/h2012-070
69. Tucker P. The physical activity levels of preschool-aged children: A systematic review.
Early Child Res Q. 2008;3(4):547-558. doi:10.1016/j.ecresq.2008.08.005
70. Ward DS, Vaughn A, McWilliams C, Hales D. Interventions for Increasing Physical
Activity at Child Care. Med Sci Sports Exerc. 2010;42(3):526-534.
doi:10.1249/Mss.0b013e3181cea406
71. Wu S, Cohen D, Shi Y, Pearson M, Sturm R. Economic analysis of physical activity
interventions. Am J Prev Med. 2011;40(2):149-158. doi:10.1016/j.amepre.2010.10.029

“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
72. Yin Z, Parra-Medina D, Cordova A, He M, Trummer V, Sosa E, et al. Miranos! Look at
us, we are healthy! An environmental approach to early childhood obesity prevention.
Child Obes. 2012;8(5):429-439. doi:10.1089/chi.2012.0125

“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
Figure 1 ─ Flow of literature search on physical activity interventions among children aged 2-5
“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
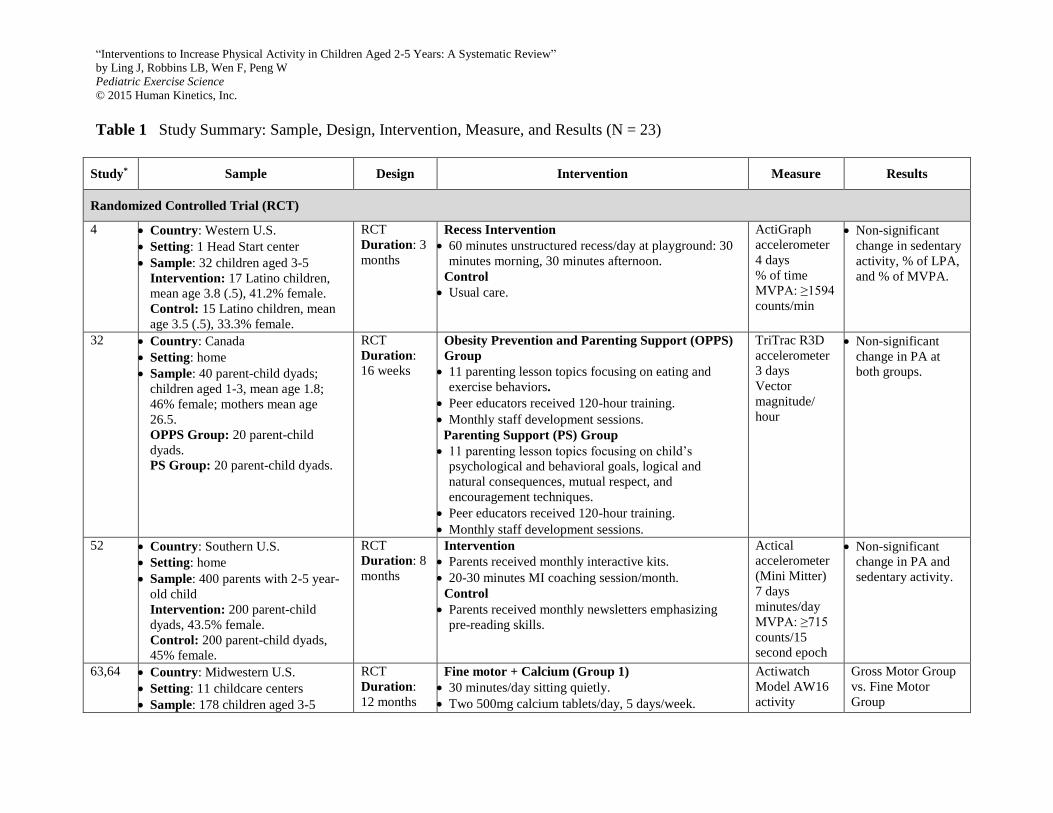
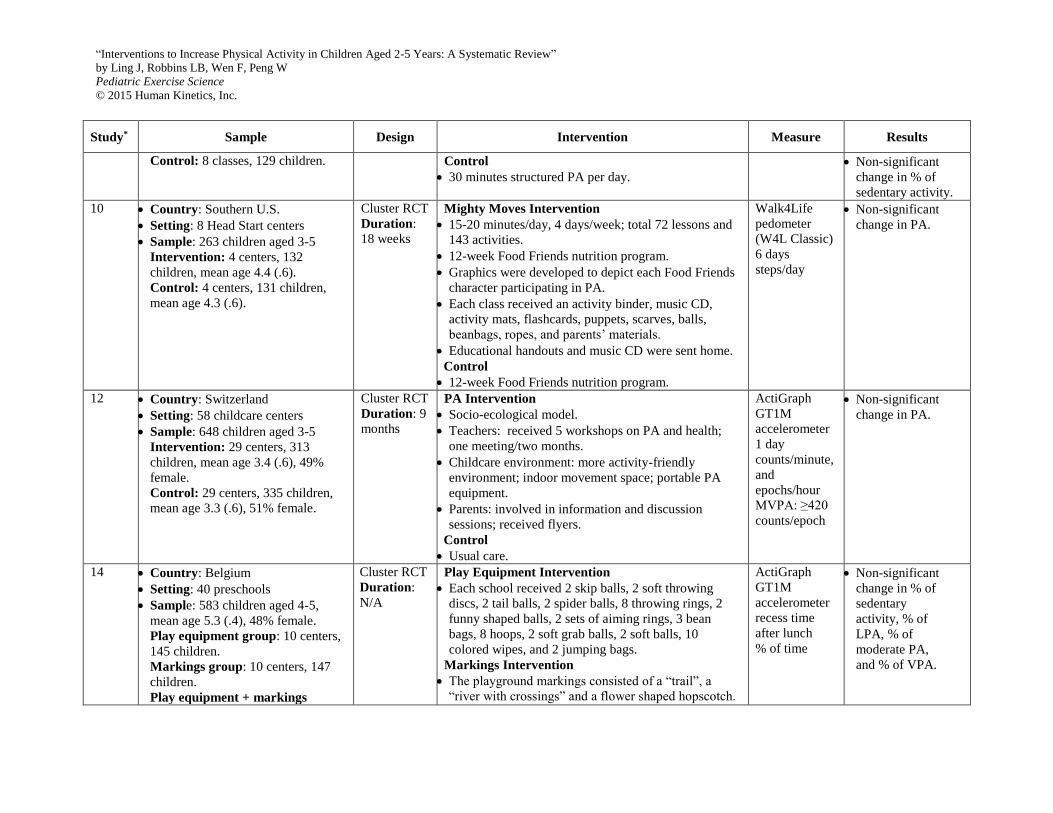
Table 1 Study Summary: Sample, Design, Intervention, Measure, and Results (N = 23)
Study* Sample Design Intervention Measure Results
Randomized Controlled Trial (RCT)
4 Country: Western U.S.
Setting: 1 Head Start center
Sample: 32 children aged 3-5
Intervention: 17 Latino children,
mean age 3.8 (.5), 41.2% female.
Control: 15 Latino children, mean
age 3.5 (.5), 33.3% female.
RCT
Duration: 3
months
Recess Intervention
60 minutes unstructured recess/day at playground: 30
minutes morning, 30 minutes afternoon.
Control
Usual care.
ActiGraph
accelerometer
4 days
% of time
MVPA: ≥1594
counts/min
Non-significant
change in sedentary
activity, % of LPA,
and % of MVPA.
32 Country: Canada
Setting: home
Sample: 40 parent-child dyads;
children aged 1-3, mean age 1.8;
46% female; mothers mean age
26.5.
OPPS Group: 20 parent-child
dyads.
PS Group: 20 parent-child dyads.
RCT
Duration:
16 weeks
Obesity Prevention and Parenting Support (OPPS)
Group
11 parenting lesson topics focusing on eating and
exercise behaviors.
Peer educators received 120-hour training.
Monthly staff development sessions.
Parenting Support (PS) Group
11 parenting lesson topics focusing on child’s
psychological and behavioral goals, logical and
natural consequences, mutual respect, and
encouragement techniques.
Peer educators received 120-hour training.
Monthly staff development sessions.
TriTrac R3D
accelerometer
3 days
Vector
magnitude/
hour
Non-significant
change in PA at
both groups.
52 Country: Southern U.S.
Setting: home
Sample: 400 parents with 2-5 year-
old child
Intervention: 200 parent-child
dyads, 43.5% female.
Control: 200 parent-child dyads,
45% female.
RCT
Duration: 8
months
Intervention
Parents received monthly interactive kits.
20-30 minutes MI coaching session/month.
Control
Parents received monthly newsletters emphasizing
pre-reading skills.
Actical
accelerometer
(Mini Mitter)
7 days
minutes/day
MVPA: ≥715
counts/15
second epoch
Non-significant
change in PA and
sedentary activity.
63,64 Country: Midwestern U.S.
Setting: 11 childcare centers
Sample: 178 children aged 3-5
RCT
Duration:
12 months
Fine motor + Calcium (Group 1)
30 minutes/day sitting quietly.
Two 500mg calcium tablets/day, 5 days/week.
Actiwatch
Model AW16
activity
Gross Motor Group
vs. Fine Motor
Group

“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
Study* Sample Design Intervention Measure Results
Group 1: 45 children, mean age 4.0
(.6), 48.9% female, 2.2% Black.
Group 2: 45 children, mean age 4.0
(.6), 46.7% female, 11.1% Black.
Group 3: 43 children, mean age 3.9
(.6), 44.2% female, 7.0% Black.
Groups 4: 45 children, mean age
3.8 (.5), 48.9% female, 4.4% Black.
Follow-up:
6, 12
months
Fine motor + Placebo (Group 2)
30 minutes/day sitting quietly.
Cross motor + Calcium (Group 3)
30 minutes PA/day, 5 days/week; 5 minutes warm-up,
20 minutes jumping, hopping, and skipping activities,
5 minutes cool-down.
Two 500mg calcium tablets/day, 5 days/week.
Cross motor + Placebo (Group 4)
30 minutes PA/day, 5 days/week; 5 minutes warm-up,
20 minutes jumping, hopping, and skipping activities,
5 minutes cool-down.
monitor
2 days
% of time, and
counts/day
Significant increase
in % of VPA, and
counts/day after
intervention, and at
6-month follow-up.
Non-significant
change at 12-month
follow-up.
Cluster RCT
2 Country: Northeastern U.S.
Setting: 2 preschool centers
Sample: 71 children aged 2.9-5
Intervention: 4 classrooms, 43
children, mean age 4.5 (.6), 49%
female, 65% Hispanic, 35% Black.
Control: 4 classrooms, 28 children,
mean age 4.1 (.6), 54% female, 54%
Hispanic, 46% Black.
Cluster RCT
Duration: 6
months
Locomotor Skills-based Structured PA Program
30 minutes structured PA/day, 5 days/week.
Teachers received 8 hours training on structured PA.
Control: Unstructured free playtime
30 minutes free play PA/day, 5 days/week.
Teachers received 2 hours training on free play.
ActiGraph
GT1M
accelerometer
7 days
% of time
MVPA: ≥615
counts/ 15
second epoch
Significant
decrease in % of
sedentary activity,
76.2 (5.5) to 73.7
(8.0) vs. 70.6 (7.0)
to 74.7 (6.0), p=.01.
Non-significant
change in % of
LPA.
5 Country: Southern U.S.
Setting: 32 YMCA preschool
classes
Sample: 275 Black children aged
3.5-5.6, mean age 4.6 (.5), 55.6%
female.
Intervention: 21 classes, 154
children.
Control: 11 classes, 121 children.
Cluster RCT
Duration: 8
weeks
Start For Life Intervention
Self-efficacy theory and social cognitive theory.
30 minutes structured PA per day.
Teachers received 4-hour training, and a binder of
daily lesson plans.
Teachers used ‘achievement charts’ to monitor
children’s progress with stickers.
Control
30 minutes structured PA per day.
ActiGraph
GT3X
accelerometer
1 day
% of time
MVPA: ≥3
METs
Significant increase
in % of MVPA,
31.80 (8.37) to
33.92 (6.95) vs.
30.33 (6.69) to
29.80 (8.48),
p=.0130; and % of
VPA, 22.27 (6.65)
to 24 (5.72) vs.
21.13 (5.26) to
21.06 (7.3), p=.016.
Non-significant
change in % of
sedentary activity.

“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
Study* Sample Design Intervention Measure Results
6 Country: Southern U.S.
Setting: 98 YMCA preschool
classes
Sample: 885-1154 children aged 4-
5, mean age 4.4 (.5), 51.2% female,
86% Black.
Intervention: 60 classes.
Control: 38 classes.
Cluster RCT
Duration: 9
months
Start For Life Intervention
Self-efficacy theory and social cognitive theory.
30 minutes structured PA per day.
Teachers received 4-hour training, and a binder of
daily lesson plans.
Teachers used ‘achievement charts’ to monitor
children’s progress with stickers.
Control
30 minutes structured PA per day.
ActiGraph
GT3X
accelerometer
1 day
% of time
MVPA: ≥3
METs
Significant increase
in % of MVPA,
23.9 (6.9) vs. 22.5
(4.8), p=.016;
and % of VPA,
17.5 (5.5) vs. 15.7
(3.6), p<.001.
Non-significant
change in % of
sedentary activity.
7 Country: Southern U.S.
Setting: 19 YMCA preschool
classes
Sample: 338 children aged 3-5
Intervention: 11 classes, 202
children, mean age 4.6 (.6), 52.5%
female, 90.6% Black.
Control: 8 classes, 136 children,
mean age 4.7 (.3), 55.9% female,
94.1% Black.
Cluster RCT
Duration: 8
weeks
Start For Life Intervention
Self-efficacy theory and social cognitive theory.
30 minutes structured PA per day.
Teachers received 4-hour training, and a binder of
daily lesson plans.
Teachers used ‘achievement charts’ to monitor
children’s progress with stickers.
Control
30 minutes structured PA per day.
ActiGraph
GT3X
accelerometer
1 day
% of time
MVPA: ≥3
METs
Significant
decrease in % of
sedentary activity,
48.84 (11.1) to
48.54 (10.04) vs.
48.68 (10.81) to
50.68 (10.22),
p=.034.
Significant increase
in % of MVPA,
32.14 (8.33) to
33.03 (7.15) vs.
31.71 (7.83) to
29.83 (8.44),
p<.001; % of VPA,
22.58 (6.7) to 23.39
(6.05) vs. 22.34
(6.47) to 21.15
(7.35), p<.001.
8 Country: Southern U.S.
Setting: 17 YMCA preschool
classes
Sample: 273 Black children aged 4-
5, mean age 4.4 (.5), 47.6% female.
Intervention: 9 classes, 144
children.
Cluster RCT
Duration: 9
months
Start For Life Intervention
Self-efficacy theory and social cognitive theory.
30 minutes structured PA per day.
Teachers received 4-hour training, and a binder of
daily lesson plans.
Teachers used ‘achievement charts’ to monitor
children’s progress with stickers.
ActiGraph
GT3X
accelerometer
1 day
% of time
MVPA: ≥3
METs
Significant increase
in % of MVPA,
35.3 (7.7) vs. 33.3
(7.1), p=.031;
and % of VPA,
17.9 (4.4) vs. 15.8
(3.7), p<.001.
“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
Study* Sample Design Intervention Measure Results
Control: 8 classes, 129 children. Control
30 minutes structured PA per day.
Non-significant
change in % of
sedentary activity.
10 Country: Southern U.S.
Setting: 8 Head Start centers
Sample: 263 children aged 3-5
Intervention: 4 centers, 132
children, mean age 4.4 (.6).
Control: 4 centers, 131 children,
mean age 4.3 (.6).
Cluster RCT
Duration:
18 weeks
Mighty Moves Intervention
15-20 minutes/day, 4 days/week; total 72 lessons and
143 activities.
12-week Food Friends nutrition program.
Graphics were developed to depict each Food Friends
character participating in PA.
Each class received an activity binder, music CD,
activity mats, flashcards, puppets, scarves, balls,
beanbags, ropes, and parents’ materials.
Educational handouts and music CD were sent home.
Control
12-week Food Friends nutrition program.
Walk4Life
pedometer
(W4L Classic)
6 days
steps/day
Non-significant
change in PA.
12 Country: Switzerland
Setting: 58 childcare centers
Sample: 648 children aged 3-5
Intervention: 29 centers, 313
children, mean age 3.4 (.6), 49%
female.
Control: 29 centers, 335 children,
mean age 3.3 (.6), 51% female.
Cluster RCT
Duration: 9
months
PA Intervention
Socio-ecological model.
Teachers: received 5 workshops on PA and health;
one meeting/two months.
Childcare environment: more activity-friendly
environment; indoor movement space; portable PA
equipment.
Parents: involved in information and discussion
sessions; received flyers.
Control
Usual care.
ActiGraph
GT1M
accelerometer
1 day
counts/minute,
and
epochs/hour
MVPA: ≥420
counts/epoch
Non-significant
change in PA.
14 Country: Belgium
Setting: 40 preschools
Sample: 583 children aged 4-5,
mean age 5.3 (.4), 48% female.
Play equipment group: 10 centers,
145 children.
Markings group: 10 centers, 147
children.
Play equipment + markings
Cluster RCT
Duration:
N/A
Play Equipment Intervention
Each school received 2 skip balls, 2 soft throwing
discs, 2 tail balls, 2 spider balls, 8 throwing rings, 2
funny shaped balls, 2 sets of aiming rings, 3 bean
bags, 8 hoops, 2 soft grab balls, 2 soft balls, 10
colored wipes, and 2 jumping bags.
Markings Intervention
The playground markings consisted of a “trail”, a
“river with crossings” and a flower shaped hopscotch.
ActiGraph
GT1M
accelerometer
recess time
after lunch
% of time
Non-significant
change in % of
sedentary
activity, % of
LPA, % of
moderate PA,
and % of VPA.

“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
Study* Sample Design Intervention Measure Results
group: 10 centers, 145 children.
Control group: 10 centers, 146
children.
18 Country: Germany
Setting: 35 preschools
Sample: 809 children aged 4-6,
mean age 5.1, 48% female.
Intervention: 18 centers, 433
children.
Control: 19 centers, 376 children.
Cluster RCT
Duration: 9
months
Participatory Intervention
General system theory.
State-sponsored PA Program. PLUS
Three parent-teacher meetings.
Parent and preschools received:
An intervention-specific website.
An introductory video.
A book with 15 project ideas.
State-sponsored PA Program
Two 1-hour gym classes per week.
One parent-gym trainer meeting.
Actiheart
accelerometer
6 days
minutes/day
Significant
decrease in
sedentary activity,
631.3 (68.3) to
623.9 (66.8) vs.
631.4 (63.2) to
628.1 (67.1),
p=.014.
Non-significant
change in MVPA.
19 Country: Belgium
Setting: 27 daycare centers,
kindergartens, preschools
Sample: 472 children aged 4-6,
mean age 4.4 (.6), 44.9% female.
Intervention: 15 centers, 301
children.
Control: 12 centers, 171 children.
Cluster RCT
Duration:
12 months
ToyBox Intervention
PRECEDE-PROCEED model.
Teachers received 3 training sessions.
20-week structured PA.
Parents received 2 newsletters, 2 tip-cards, and one
poster through children.
Environmental change in classrooms.
Control
Usual care.
ActiGraph
GT1M, GT3X,
GT3X+
accelerometer
6 days
% of time
Significant change
in % of MVPA, 7.4
to 8.6 vs. 7.5 to 8.1,
p<.05.
Non-significant
change in % of
LPA.
23 Country: Israel
Setting: 4 preschool classes
Sample: 101 children aged 5-6
Intervention: 2 classes, 54 children,
mean age 5.5 (.1), 38.9% female.
Control: 2 classes, 47 children,
mean age 5.6 (.1), 46.8% female.
Cluster RCT
Duration: 4
months
Intervention
Parents received two orientation lectures on childhood
obesity and benefits of exercise in the first 2 months.
Nutrition: nutrition curriculum in class; dietary
information on working sheets/flyers.
PA: 45 minutes/day exercise training, 6 days/week;
encouraged to reduce sedentary activities and increase
PA after school.
Control
Parents received two orientation lectures on childhood
obesity and benefits of exercise in the first 2 months.
Pedometers
3 days
steps/day
Significantly
increase in PA,
6927 (364) vs. 5489
(284), p=.003.

“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
Study* Sample Design Intervention Measure Results
24 Country: Australia
Setting: 20 childcare centers
Sample: 328 children aged 3-5
Intervention: 10 centers, 172
children, 46% female.
Control: 10 centers, 156 children,
40% female.
Cluster RCT
Duration: 6
months
Intervention
Social ecological model.
Daily structured fundamental movement skill
development sessions, 20 minutes/session.
Increased physical activity opportunities.
Staff role modeling.
Limited screen and sedentary time.
Provided a physical activity promoting physical
environment.
Control
Usual care.
Yamax
SW200 and
SW7000
pedometers
1 day
steps/minute
Non-significant
change in PA.
25 Country: Midwestern U.S.
Setting: 18 Head Start centers
Sample: 618 children aged 3-5
Intervention: 9 centers, 325
children, mean age 4.2 (.6), 52%
female, 1% Hispanic, 97% Black.
Control: 9 centers, 293 children,
mean age 4.3 (.5), 55% female, 5%
Hispanic, 91% Black.
Cluster RCT
Duration:
14 weeks
Teacher-delivered Weight Control Intervention
Social cognitive theory and self-determination theory.
Two 20 minutes lessons on nutrition and PA per week.
Two 20 minutes PA sessions per week.
Parents received weekly newsletters with a homework
assignment.
Control
One 20 minutes lesson on general health concepts per
week.
Parents received weekly newsletters without a
homework assignment.
ActiGraph
GT1M
accelerometer
7 days
minutes/day
MVPA: ≥420
counts/15
second epoch
Significant increase
in MVPA, 98.6
(30.2) to 109.9
(2.0) vs. 98.8 (26.0)
to 102.5 (2.0),
p=.02.
36 Country: Australia
Setting: 2 childcare centers
Sample: 97 children aged 3-5, mean
age 4.1
Intervention: 1 center, 52 children.
Control: 1 center, 45 children.
Cluster RCT
Duration:
20 weeks
Jump Start Intervention
Professional development for teachers: 4 30-minute
workshops.
Structured lessons and unstructured activities for
children: 20 minutes structured lesson, 3 times/week;
unstructured activities were in afternoons.
Control
Usual care.
ActiGraph
MTI/CSA
WAM-7164
accelerometer
2 days
counts/minute,
and % of time
MVPA: ≥3
METs
Non-significant
change in total
PA, % of sedentary
activity, LPA,
MPA, VPA.
48 Country: United Kingdom
Setting: 8 SureStart children’s
centers
Sample: 79 children aged 3-5, mean
Cluster RCT
Duration:
10 weeks
Active Play Intervention I
Social-ecological model.
Intervention occurred every other week and had 5
contact sessions, 70 minutes/session.
ActiGraph
GT1M
accelerometer
7 days
Non-significant
change in sedentary
activity, LPA, and
MVPA.

“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
Study* Sample Design Intervention Measure Results
age 3.7
Intervention: 4 centers, 34
children, 50% female.
Control: 4 centers, 45 children,
46.7% female.
20 minutes PA/session for children.
20 minutes workshop/session for parents.
40 minutes PA/session parents-children together.
Each family received a log book; an active dance
DVD; resources and instructional materials; 5 test
messages to provide support between sessions.
Control
Usual care.
minutes/day
49 Country: United Kingdom
Setting: 12 preschools
Sample: 240 children aged 3-5,
mean age 4.5 (.6), 48.3% female
Intervention: 6 preschools, 109
children, mean age 4.7 (.5).
Control: 6 preschools, 131 children,
mean age 4.5 (.6).
Cluster RCT
Duration: 6
weeks
Follow-up:
6 months
Active Play Intervention II
Socio-ecological model.
Active play 60 minutes/week.
Each preschool received a resource pack including 20
activity cards, user manual, exemplar lesson plans,
signposting information, and a poster.
Control
Usual care.
ActiGraph
GT1M
accelerometer
7 days
minutes/day
Non-significant
change in sedentary
activity, MVPA,
and VPA after
intervention or at
follow-up.
55 Country: Switzerland
Setting: 30 childcare centers
Sample: 40 preschool classes, 652
children aged 3.8-6.8
Intervention: 20 classes, 342
children, mean age 5.2 (.6), 49%
female.
Control: 20 classes, 310 children,
mean age 5.2 (.6), 51% female.
Cluster RCT
Duration:
12 months
Intervention
Children: 4 sessions of 45 minutes PA/week; 22
sessions on nutrition, media use, and sleep; received a
funny PA or nutrition activity card every other week;
received a CD with music for PA cards; stickers on a
classroom poster showed progress.
Teachers: 2 workshops on intervention; formal
meetings to exchange experiences.
Parents: 3 information and discussion evenings;
information leaflets.
Environment: installed fixed and mobile equipment;
poster hung up on classroom walls; each class
received a game on health behaviors.
Control
Usual care.
ActiGraph
MTI/CSA
WAM-7164
accelerometer
5 days
counts/minute
Non-significant
change in PA.
59 Country: Scotland
Setting: 36 nurseries
Sample: 545 children aged 4-5
Intervention: 18 centers, 268
Cluster RCT
Duration:
24 weeks
Intervention
Nursery element: PA program including 30
minutes/week for 24 weeks.
Teachers attended 3 training sessions.
ActiGraph
MTI/CSA
WAM-7164
accelerometer
Non-significant
change in PA
and % of sedentary
activity.

“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
Study* Sample Design Intervention Measure Results
children, mean age 4.2 (.3), 52.2%
female.
Control: 18 centers, 277 children,
mean age 4.1 (.3), 47.7% female.
6-week poster display at each center.
Home element: each family received a resource pack
with guidelines on linking PA at center and at home;
and two education leaflets on opportunities for
increasing PA and encourage families to seek
opportunities.
Control
Usual care.
6 days
% of time
MVPA: >3200
counts/minute
Quasi-experimental (QE) Design
72 Country: Southern U.S.
Setting: 4 Head Start centers
Sample: 252 children aged 3-5
Center-based Intervention: 2
centers, 118 children, mean age 4.2
(.6), 49% female.
Center- and home-based
intervention: 1 center, 66 children,
mean age 4.2 (.5), 58% female.
Control: 1 center, 69 children,
mean age 4.1 (.5), 49% female.
QE: non-
equivalent
groups
design
Duration:
18 weeks
Center-based Intervention
Early childhood development theory and general
system theory.
30-45 minutes structured outdoor play/day.
15-20 minutes PA during recess.
Classroom activities: Sesame Street Workshop
Healthy Habits for Life resource kit, including 9
modules, one module/2 weeks.
Teachers received 6-hour initial and 4-hour follow-up
training.
Center- and Home-based Intervention
Center-based intervention. PLUS
Seven peer educators.
Parents viewed posters.
Take-home bag including a storybook, family
activities, and games.
Control
Parents received monthly newsletters emphasizing
pre-reading skills.
Pedometer
3 days
steps/day
Significant increase
in PA in both
intervention groups.
Non-significant PA
differences between
the two intervention
groups.
Note. *=reference number. RCT=randomized controlled trials; QE=quasi-experimental; PA=physical activity; LPA=light physical activity; MPA=moderate
physical activity; VPA=vigorous physical activity; MVPA=moderate to vigorous physical activity; MI=motivational interviewing; N/A=not applicable.
Compared to RCT designs, QE designs lack random assignment of study participants. Head Start in the U.S. is federally-funded program serving low-income
families with children ≤ 5 years (4). SureStart children’s center in the United Kingdom provide free childcare services to families with children ≤ 5 years and are
located in disadvantaged parts of England (48).

“Interventions to Increase Physical Activity in Children Aged 2-5 Years: A Systematic Review”
by Ling J, Robbins LB, Wen F, Peng W
Pediatric Exercise Science
© 2015 Human Kinetics, Inc.
Table 2 Risk of Bias Assessment for Included Studies (N = 23)
Study* Random Sequence Generation Blinding of Outcome
Assessment
Valid PA Measure Clear Explanation of
Withdrawal
2 Unclear Yes Yes Yes
4 Unclear Yes Yes Yes
5 Unclear Unclear No Yes
6 Unclear Unclear No No
7 Unclear Unclear No Yes
8 Unclear Unclear No Yes
10 Unclear No Yes Yes
12 Unclear No No Yes
14 Unclear Unclear No Yes
18 Yes (envelops) Yes Yes Yes
19 Unclear No Yes Yes
23 Unclear Unclear Yes Yes
24 Yes (computer) No No Yes
25 Unclear No Yes Yes
32 Unclear Unclear Yes Yes
36 Yes (computer) Yes No Yes
48 Unclear No Yes Yes
49 Yes (drawing) No Yes Yes
52 Yes (computer) Unclear Yes Yes
55 Yes (envelops) Yes Yes Yes
59 Unclear Yes Yes Yes
63,64 Unclear Yes No Yes
72 No Unclear Yes No
Note. *=reference number. yes=low risk of bias, no=high risk of bias, unclear=insufficient information to permit judgment of ‘low risk’ or ‘high risk’. Studies 5,
6, 7, and 8 described the same intervention.