
Interstitial Fluid Pressure in Normal and Inflamed Pulp
9
INTERSTITIAL FLUID PRESSURE IN NORMAL AND INFLAMED PULP K.J. Heyeraas* E. Berggreen Department of Physiology, University of Bergen, Arstadveien 19, N-5009 Bergen, Norway; *corresponding author ABSTRACT: Tissue pressure is the hydrostatic pressure in the interstitial fluid which surrounds the pulpal cells. This pressure outside the vessels is normally considerably lower than the blood pressure inside the vessels. The dental pulp has a relative- ly low interstitial compliance due to its enclosure between rigid dentin walls. Accordingly, even a modest increase in pulpal fluid volume will raise the tissue pressure, which may compress blood vessels, leading to ischemia and necrosis. Inflammation may lead to an increase in both interstitial fluid volume and blood volume in the low-compliant pulp and thereby increase the tissue pressure. However, the increased tissue pressure may, in turn, initiate increased lymph flow and absorption of fluid into capillaries in nearby non-inflamed tissue. Both of these latter factors will transport fluid out of the affected area and subse- quently out of the tooth and consequently lower the tissue pressure. Increased tissue pressure, whether caused by increased blood volume or increased capillary filtration, will promote outward flow of fluid through exposed dentin tubules and thereby help to protect the pulp against entry of harmful substances. It seems physiologically beneficial, therefore, for the pulp to have a high tissue pressure, which promptly increases when blood flow increases due to its low compliance. Key words. Dental pulp, circulation, tissue pressure, inflammation. Introduction The cells in the dental pulp, in common with all cells in the body, are dependent on the extracellular fluid, i.e., blood plasma and interstitial fluid, to remain vital and function normally. Every cell must have nutrition and the means to rid itself of waste products, and these meta- bolic requirements depend on the extracellular fluid. All cells, including the pulpal cells, are surrounded by inter- stitial fluid (Fig. 1). The concentrations of all plasma solutes except protein are virtually the same in the inter- stitial fluid as in plasma. In health, plasma proteins do not essentially permeate the capillary wall and have a very low concentration in the interstitial fluid. Blood is brought to the tissues through the vessels, and substances are transported between the blood and the interstitial fluid by diffusion (Fig. 1). The smallest vessels, i.e., the capillaries, are so widely distributed that no cells are more than 50-100 microns distant from the circulatory system. Due to this short distance, the exchange of substances between blood and interstitial fluid may take place rapidly by simple diffusion. The main function of the interstitial fluid is to be a suitable transport medium for nutrients and waste products between cells and capillary blood. Accordingly, the inter- stitial fluid provides a means of communication between cells and blood, or as an extension of the plasma. At the same time that the diffusional exchange of substances occurs across capillaries, another, complete- ly distinct, process is also taking place, i.e., the bulk flow of fluid across the capillary wall. The function of this bulk flow of fluid is not the exchange of nutrients and waste products, but the distribution of the extracellular fluid, which is governed by the hydrostatic pressure difference and the colloid osmotic pressure difference across the capillary wall. The difference in protein concentrations between plasma and interstitial fluid is important, because it creates a higher colloid osmotic pressure in plasma than in interstitial fluid, thus favoring bulk fluid movement into the capillary. The hydrostatic pressure in the interstitial fluid surrounding the cells is the intersti- tial fluid pressure, or so-called tissue pressure (Fig. 1). The interstitial fluid pressure outside the vessels is nor- mally considerably lower than the blood pressure inside the capillaries. This difference in hydrostatic pressure favors filtration, or bulk flow of fluid out of the vessels. This article will focus on the role of the interstitial fluid pressure (Pi) in normal tissue function and during inflammation. Interstitial Fluid Pressure In principle, all the methods used for measurement of hydrostatic pressure in the interstitial fluid are fluid- equilibration techniques (Guyton et al., 1971). By these 328Grit Rev Oral Biol Med lO(3):328-336 328 Crit Rev Oral Biol Med 10(3):328-336 (1999) by guest on October 1, 2015 For personal use only. No other uses without permission. cro.sagepub.com Downloaded from
-
Upload
independent -
Category
Documents
-
view
3 -
download
0
Transcript of Interstitial Fluid Pressure in Normal and Inflamed Pulp

INTERSTITIAL FLUID PRESSUREIN NORMAL AND INFLAMED PULP
K.J. Heyeraas*E. BerggreenDepartment of Physiology, University of Bergen, Arstadveien 19, N-5009 Bergen, Norway; *corresponding author
ABSTRACT: Tissue pressure is the hydrostatic pressure in the interstitial fluid which surrounds the pulpal cells. This pressureoutside the vessels is normally considerably lower than the blood pressure inside the vessels. The dental pulp has a relative-ly low interstitial compliance due to its enclosure between rigid dentin walls. Accordingly, even a modest increase in pulpalfluid volume will raise the tissue pressure, which may compress blood vessels, leading to ischemia and necrosis. Inflammationmay lead to an increase in both interstitial fluid volume and blood volume in the low-compliant pulp and thereby increase thetissue pressure. However, the increased tissue pressure may, in turn, initiate increased lymph flow and absorption of fluid intocapillaries in nearby non-inflamed tissue. Both of these latter factors will transport fluid out of the affected area and subse-quently out of the tooth and consequently lower the tissue pressure. Increased tissue pressure, whether caused by increasedblood volume or increased capillary filtration, will promote outward flow of fluid through exposed dentin tubules and therebyhelp to protect the pulp against entry of harmful substances. It seems physiologically beneficial, therefore, for the pulp to havea high tissue pressure, which promptly increases when blood flow increases due to its low compliance.
Key words. Dental pulp, circulation, tissue pressure, inflammation.
Introduction
The cells in the dental pulp, in common with all cells inthe body, are dependent on the extracellular fluid, i.e.,
blood plasma and interstitial fluid, to remain vital andfunction normally. Every cell must have nutrition and themeans to rid itself of waste products, and these meta-bolic requirements depend on the extracellular fluid. Allcells, including the pulpal cells, are surrounded by inter-stitial fluid (Fig. 1). The concentrations of all plasmasolutes except protein are virtually the same in the inter-stitial fluid as in plasma. In health, plasma proteins donot essentially permeate the capillary wall and have avery low concentration in the interstitial fluid.
Blood is brought to the tissues through the vessels,and substances are transported between the blood andthe interstitial fluid by diffusion (Fig. 1). The smallestvessels, i.e., the capillaries, are so widely distributed thatno cells are more than 50-100 microns distant from thecirculatory system. Due to this short distance, theexchange of substances between blood and interstitialfluid may take place rapidly by simple diffusion. Themain function of the interstitial fluid is to be a suitabletransport medium for nutrients and waste productsbetween cells and capillary blood. Accordingly, the inter-stitial fluid provides a means of communication betweencells and blood, or as an extension of the plasma.
At the same time that the diffusional exchange ofsubstances occurs across capillaries, another, complete-ly distinct, process is also taking place, i.e., the bulk flowof fluid across the capillary wall. The function of this bulkflow of fluid is not the exchange of nutrients and wasteproducts, but the distribution of the extracellular fluid,which is governed by the hydrostatic pressure differenceand the colloid osmotic pressure difference across thecapillary wall. The difference in protein concentrationsbetween plasma and interstitial fluid is important,because it creates a higher colloid osmotic pressure inplasma than in interstitial fluid, thus favoring bulk fluidmovement into the capillary. The hydrostatic pressure inthe interstitial fluid surrounding the cells is the intersti-tial fluid pressure, or so-called tissue pressure (Fig. 1).The interstitial fluid pressure outside the vessels is nor-mally considerably lower than the blood pressure insidethe capillaries. This difference in hydrostatic pressurefavors filtration, or bulk flow of fluid out of the vessels.This article will focus on the role of the interstitial fluidpressure (Pi) in normal tissue function and duringinflammation.
Interstitial Fluid PressureIn principle, all the methods used for measurement ofhydrostatic pressure in the interstitial fluid are fluid-equilibration techniques (Guyton et al., 1971). By these
328Grit Rev Oral Biol MedlO(3):328-336
328 Crit Rev Oral Biol Med 10(3):328-336 (1999)
by guest on October 1, 2015 For personal use only. No other uses without permission.cro.sagepub.comDownloaded from

methods, a fluid-filleddevice, i.e., capsules, wicks,needles, or micropipettes,connects the interstitiumto a low-compliancemanometer, and thehydrostatic pressure at theinterstitial fluid interfaceis measured. The intersti-tial fluid pressure is part ofthe so-called Starlingforces (Starling, 1896),which determine the rateof bulk flow across themicrovascular endotheli-um, i.e., how much of thetotal extracellular fluidshall be located within thetissues as interstitial fluidand how much shall residein the blood vessels asplasma. In accordancewith Starling (l1896), netcapillary filtration will bezero when the hydrostaticpressure difference acrossthe capillary equals thetranscapillary difference inprotein concentration:
Capillary
Plasma -
Blood prel
Blood cell
Interstitialfluidpressure
j/
Blood flowFigure 1. Schematic drawing illustrating capillary, cells, and interstitial fluid. The interstitial fluid pressureis the hydrostatic pressure in the interstitial fluid surrounding the cells.
Pc - Pi = (COPp -COP)o)a
where PC is the capillary blood pressure, Pi is the inter-stitial fluid pressure, and COPp and COPi are the colloidosmotic pressures in capillary plasma and interstitialfluid, respectively, whereas aT is the osmotic reflectioncoefficient for plasma proteins at the capillary wall. If themicrovascular wall is impermeable to proteins, the u- = 1,and if the vessels are freely permeable to proteins, the a-= 0. Although the capillary wall is not completely imper-meable to proteins, recent studies indicate that c- is near1 in most undamaged capillaries (Renkin et al., 1988,1989). Normally, there is a positive net capillary filtrationpressure in most tissues, leading to a net filtration offluid from the vessels into the interstitium. This net fil-tration is balanced by an equal lymph flow during controlconditions. Thus, normally, the tissues have a relativelyconstant interstitial fluid volume (IFV). However, if lymphflow is different from net capillary filtration, a change inIFV will occur.
Interstitial ComplianceThe manner by which Pi changes with alterations in tis-sue volume (V) is characterized by the tissue's interstitial
compliance (C). Interstitial compliance plays a centralrole in the regulation of the fluid volume in tissues andis defined as:
Ci = AV/APi
In other words, the change in Pi resulting from a givenchange in volume is determined by compliance. The den-tal pulp has a relatively low interstitial compliance dueto its enclosure between rigid dentin walls, a featurewhich limits its chances for expansion. In the dentalpulp, even modest changes in fluid volume will bereflected in the Pi. Accordingly, any increase in fluid vol-ume will increase Pi, and a decrease will act conversely.There are only two circumstances which may increase theextracellular fluid volume in any tissue: (1) increasedblood volume (due to venous stasis or increased bloodflow), and (2) increased IFV (caused by a net increase incapillary filtration compared with lymph flow).
In the low-compliant pulp, a nearly simultaneousincrease in Pi as a result of vasodilation (Heyeraas et al.,1994) and/or venous stasis (Tonder and Kvinnsland,1983) has been recorded, showing that vascular disten-sion with an increase in blood volume compresses thepulpal tissue. Thus, a rapidly responding hydrostaticcounter-pressure develops which tends to lower the
10(3) 328 336 (1999) Crit Rev Oral Biol Med 32910ot3 ) 328-336 (1 999) Crit Rev Oral Biol Med 329 by guest on October 1, 2015 For personal use only. No other uses without permission.cro.sagepub.comDownloaded from

20
16
cmI 12EE
.8
050
00 0
000
20 r0
0
12p-0
*- 05 0
100
IEEa.
.
150
PA mmHgFigure 2. Interstitial fluid pressure (IFP) in the dental pulp 7 daysaher experimentally induced pulpitis (open circles) and in con-trol teeth (closed circles) with simultaneously measured systemicarterial pressure (PA). (Reproduced from Tonder andKvinnsland, 1 983, with permission from the Journal ofEndodontics.)
transmural hydrostatic pressure difference.Consequently, capillary filtration will be reduced orabsorption will occur, according to the Starling equation.This is in line with other low-compliant tissues, such asrat tail and brain, where it has been shown that vasculardistension, whether caused by vasodilation or venousstasis, causes an abrupt rise in P. which counteracts arise in net capillary filtration pressure (Wiig and Reed,1983; Aukland and Wiig, 1984).
As should be obvious from the Starling equation,any increase in capillary blood pressure or protein con-centration in the interstitial fluid will increase capillaryfiltration and therefore the IFV. In the low-compliant den-tal pulp, both increased net filtration and augmentedblood volume will be counteracted by a marked increasein Pi, with only a modest rise in volume. Contrary to tis-sues with high compliance (Aukland and Nicolaysen,1981), i.e., skin and muscle, the Pi in the pulp is thereforean important variable, because the pulp resists progres-sive edema formation by a compensatory rise in Pi, thuskeeping pulpal volume relatively stable.
Interstitial Fluid Pressure in the PulpThe Pi in the dental pulp has been measured by severalinvestigators using fluid equilibration techniques. Themost commonly used method for Pi measurements inthe pulp has been the close cannulation technique, or
41
50 100 150
PA mm HgFi ure 3. Interstitial fluid pressure (IFP) measured in the locallyinfamed area (open circles) and 1 to 2 mm from the inducedpulpitis (closed circles). Measurements from the same tooth con-nected with solid line. (Reproduced from T6nder andKvinnsland, 1 983, with permission from the Journal ofEndodontics.)
so-called tap technique, involving a low-compliant pres-sure transducer connected to the pulp tissue by a saline-filled tube (Wynn et al., 1963; Weatherred, 1965; Beveridgeand Brown, 1965; Van Hassel, 1971; Stenvik et al., 1972).Another approach to the measurement of Pi is the tono-metric method, where an ultra-miniature tonometricpressure transducer is positioned next to the pulpal tis-sue (Christiansen et al., 1977). By applying a counter-pressure on exposed dentin, Vongsavan and Matthews(1992a) have measured the Pi in cat pulp. The micro-puncture technique developed by Wiederhielm et al.(1964) has been used to measure Pi in the dental pulp ofcats and ferrets (Heyeraas et al., 1994; Jacobsen andHeyeraas, 1997). This technique allows for measure-ments of interstitial fluid pressure through glass capil-laries with tip diameters in the range of 0.2-10 tim andhas been tested for possible inflammatory responsecaused by pipette insertion in several tissues (Wiig, 1985;Johannessen et al., 1987; Kristiansen and Heyeraas, 1989).It was concluded that the pressure measurements didnot induce any inflammatory response (Wiig, 1990). Therecorded pulpal P. measured by all these fluid equilibra-tion techniques was pulsatile and consistently wellabove atmospheric pressure. Positive values of Pi havealso been measured in other low-compliant tissues, suchas bone marrow (Michelsen, 1967; Christiansen et al.,1977), kidney (Tucker and Blantz, 1978; Granger et al.,1988), and brain (Wiig and Reed, 1983). In contrast, Pi is
330 Crit Rev Oral Biol Med10(3)328-336 (1999)
I I I I
330 Crit Rev Oral Biol Med 10(3):328-336 (1999)
I
by guest on October 1, 2015 For personal use only. No other uses without permission.cro.sagepub.comDownloaded from

close to zero or even subatmospheric inmore high-compliant tissues, such aslung, intestine, skin, and skeletal muscle(for refs., see Aukland and Reed, 1993)
Reported values of Pi in the dentalpulp during control conditions have var-ied considerably, and it cannot beregarded as settled Measurementsranging from zero (Kawamura et al., 1967)and up to 60 mm Hg (Brown andYankowitz, 1964) have been made bymeans of the close cannulation tech-nique. With the micropuncture tech-nique, a P, of 6 to 10 mm Hg has beenrecorded in the cat and ferret pulp dur-ing resting conditions (Heyeraas et al.,1994; Jacobsen and Heyeraas, 1997).Recently, Vongsavan and Matthews(I 992b) found that a counter-pressure of -about II mm Hg stopped dentinal fluid +flow in cat teeth. At present, no meth- Figure 4. Longiods are available for measurements of p. exposure in thein the intact tooth Furthermore, all tive to calcitonirtFr,.a tissue locoted ameasuring devices require some fluid dis- distal and middplacement if a pressure is to be detect-ed, Thus, the wide range of control pres-sure values is most likely explained by the low interstitialcompliance of the pulp, which allows small variations involume, caused by the pulp/dentin exposure or the mea-suring device, to create large changes in Pi.
Interstitial Fluid Pressure in the Inflamed PulpSeveral studies have shown that inflammation increasesthe Pi in the dental pulp As early as 1971, van Hassel hadfound that, during the first stages of inflammation, Pi inthe pulp increased by an average of 15 mm Hg. One yearlater, Stenvik et al. ( 1972) reported Pi measurements of upto 50-60 mm Hg in inflamed monkey pulps.Micropuncture measurements of Pi in experimentallyinflamed and contralateral non-inflamed cat pulps withsimultaneously measured systemic arterial pressure areshown in Fig. 2 (Tonder and Kvinnsland, 1983). The tis-sue pressure in the inflamed pulps was significantlyincreased compared with that in the contralateral con-trols-about 3 times higher in inflamed than in controlteeth. It should also be noted (Fig. 2) that the tissuepressure in the control teeth was relatively high-onaverage, about 5 to 6 mm Hg in these experiments, whichis a high tissue pressure compared with that in mostother tissues
However, experiments have also shown that thepressure increase during pulpitis may be a localized phe-nomenon, one which does not necessarily involve the
tudinal section of rat molar showing locally inflamed area after pulpmesial pulp horn (C). Extensive sprouting of nerve fibers immunoreac-gene-related peptide is seen in the mesial pulp horn (arrow) and in the
t the periphery of the abscess (a), whereas the pulp tissue beneath thele pulp (P) horn seems uninflamed. (Courtesy of Dr. 1. Fristad.)
entire pulp (van Hassel, 1971; Tonder and Kvinnsland,1983). Paired measurements from inflamed and non-inflamed areas in the same pulps are shown in Fig. 3. Afew mm from the inflamed area, the tissue pressure wasdecreased and was only slightly higher than in normalnon-inflamed pulps (Figs. 2 and 3). The absolute magni-tude of the pressure increase in the locally inflamed areawas found to vary considerably (Fig. 3). This is due to thefact that the increase in Pi simply reflects the local pulpalvolume increase, which may vary depending on thedegree, severity, and state of the pulpitis. Also,histopathology of severe pulp inflammation often showsrelatively well-defined local borders of the inflamed area,indicating that a pulpitis may persist locally for long peri-ods of time without apparent pathological changes inthe surrounding adjacent pulp tissue (Fig. 4).
The initial, or the first, vascular reactions during anyacute inflammation are vasodilation and increased ves-sel permeability, which may increase both the blood vol-ume and the IFV in the inflamed area (Fig. 5). In the den-tal pulp, these inflammatory vascular reactions takeplace in special conditions, in a rigid dentin chamber,which makes the pulp vulnerable. Due to the rigidencasement of the pulp, even a modest increase in vol-ume may increase the tissue pressure. The drawback isthat a significant increase in tissue pressure may seri-ously impede the blood circulation. Compared with ves-sels of the same size in other tissues, the pulpal vessels
lO.3j 328 336 (19991 Grit Rei Oral Biol Med331
.,i
33 1Crit Rev Oral Biot Metd10(3):328-336 (I 999) by guest on October 1, 2015 For personal use only. No other uses without permission.cro.sagepub.comDownloaded from

VASODILATION
Increased capillaryblood pressure
Increased venousblood pressure
ICompression of venules
INCREASED VESSEL PERMEABILITY
1IIncreased capillary
filtration
\~+Dvolume
Absorption innon-inflamed area
LymphFigure 5. Schematic build-up of a so-called vicious circle during pulpal inflammation. The edema-preventing mechanisms that serve tokeep the pulpal fluid volume relatively constant, therefore opposing a rise in tissue pressure and breaking the vicious circle, are indicat-ed with open arrows. This "vicious circle" was the basis for the former self-strangulation theory of pulpal inflammation. (Modified fromHeyeraas, 1 990.)
are especially thin-walled (Dahl and Mjor, 1973, Hals andTonder, 1981) If the tissue pressure outside the vesselrises to the same level as the blood pressure inside thevessel, the vessel may be pinched off or strangled, thuscausing stagnation of the blood circulation, with resul-tant ischemia and necrosis. These changes will counter-act any beneficial blood flow increase during pulpitis.This has led to the general speculation that the inflam-matory process in the pulp has a particularly seriouscourse. Some studies have indeed shown that inflamma-tory agents may cause a dramatic sustained fall in pulpalblood flow (Okabe et all, 1989; Kim et al, 1992).
However, the fact that most pulps survive the life-long exposure to various noxious stimuli and also sur-vive our clinical procedures implies that a dramaticincrease and spread in tissue pressure followed by
decreased blood flow usually does not take place duringpulpitis. The theoretical implications for the lack of aspread and sustained increase in Pi during inflammationin the dental pulp are outlined in Fig. 5. As already men-tioned, inflammation induces two conditions, vasodila-tion and increased vessel permeability. Vasodilationcauses increased blood flow and therefore increasedblood volume. In addition, vasodilation is usually locat-ed in precapillary vessels, and this leads to an increasein capillary blood pressure, which causes increased cap-illary filtration and therefore an increase in IFV in thepulp (Fig 5). The other event, increased vessel perme-ability, leads to leakage of plasma proteins out into thetissue, thus increasing the protein concentration in thepulp, which contributes to increased fluid filtration and afurther rise in IFV (Fig. 5). This increased fluid volume in
Crit Rev Oral BiodMed1332 10(3):328-336 ( 1999) by guest on October 1, 2015 For personal use only. No other uses without permission.cro.sagepub.comDownloaded from
the pulp, caused by both increased blood volume andIFV, will raise the tissue pressure in the low-compliantpulp. The disadvantage is that the increased tissue pres-sure will tend to compress the thin-walled veins and thuslower blood flow and increase venous blood pressure. Arise in venous pressure will automatically increase thecapillary blood pressure and thereby capillary filtrationIn this way, a "vicious circle" with a constantly growingtissue pressure may develop. The former so-called self-strangulation theory by pulpitis was founded on thisvicious circle (Fig. 5). Theoretically, the tissue pressuremay soon reach a magnitude that results in compressionof the blood vessels and total pulp necrosis. However, aslong as the pulp is not so severely damaged that thelocal feedback mechanisms counteracting the volumeand thus the pressure increase are functioning, thevicious circle will be broken and the spread of theincreased tissue pressure will be limited. The main feed-back mechanisms counteracting a build-up and spreadin tissue pressure are shown with open arrows in Fig. 5.According to the Starling equation, any increase in Pi willlower the transcapillary hydrostatic pressure differenceand therefore oppose filtration. In addition, the locallyincreased Pi will most probably favor net absorption ofinterstitial fluid in capillaries in adjacent uninflamed tis-sue and increase the lymph flow (Aukland and Reed,1993). Both of these latter factors will transport fluid outof the affected area and then out of the tooth and conse-quently lower the pressure (Fig. 5). Accordingly, in spiteof vasodilation and increased vessel permeability, thepulpal volume during pulpitis may be kept relatively con-stant so that the tissue pressure does not rise to a levelthat will cause vessel compression with resultant necro-sis, Thus, local coronal pulpitis may persist withoutspreading to the root pulp Therefore, the pulp may heal,provided that the injurious agents are removed or arenot too extensive. However, in the case of severe persis-tent irritants, the increased tissue pressure may spreadin an apical direction and cause total pulp necrosis.
The lymphatics are important, however, because thelymphatic vessels drain away not only fluid, but alsomacromolecules such as plasma proteins that haveleaked out of the vessels due to the inflammatory-induced increased vessel permeability. In fact, the onlymechanism for removal of such macromolecules from theinterstitial fluid is the lymphatic vessels. In order torestore the protein concentration in the interstitial fluidin the inflamed tissue to a level lower thin that in theblood, which is of vital importance to making absorptionand therefore healing possible, plasma proteins must beremoved by the lymphatics. The capillaries in non-inflamed adjacent area may absorb fluid; however, thenormal permeability of the non-inflamed vessels will pre-vent the macromolecules from following into the circula-
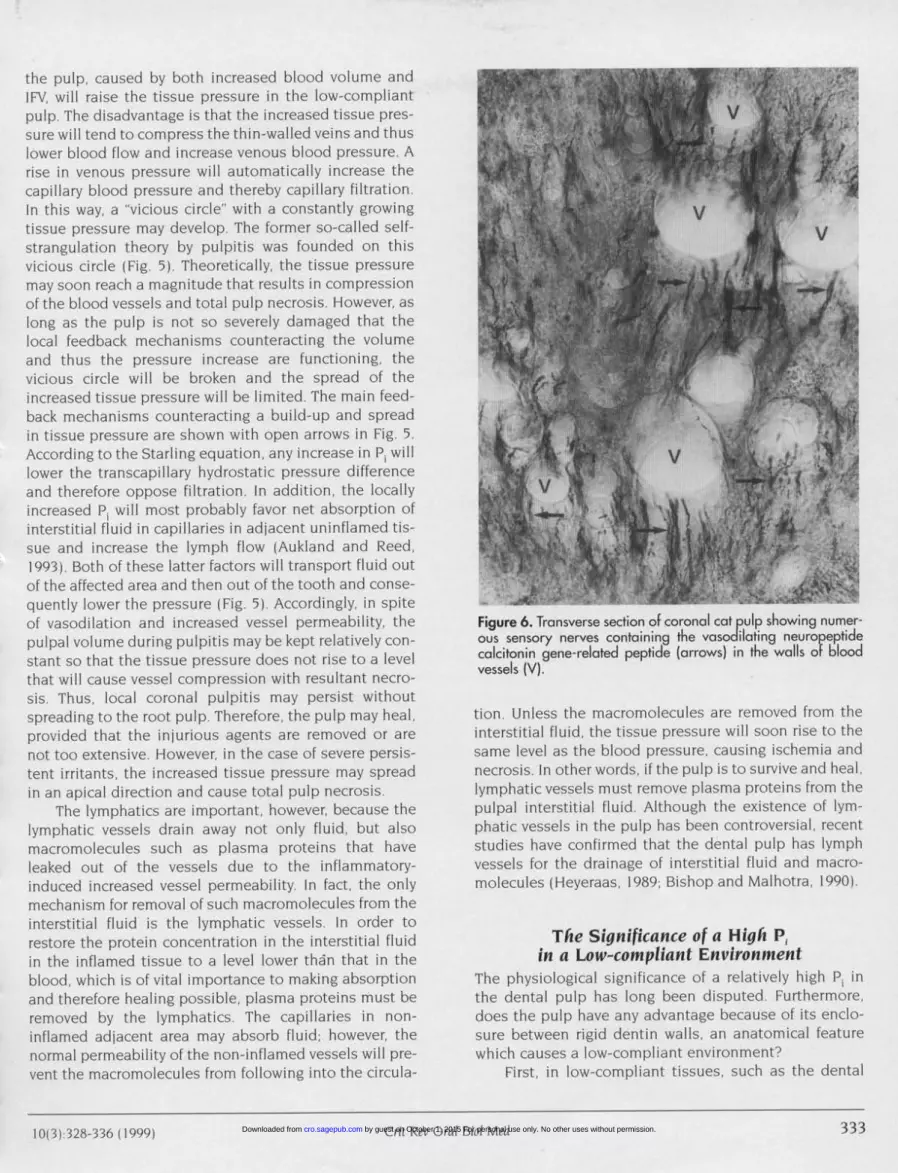
Figure 6. Transverse section of coronal cat pulp showing numer-ous sensory nerves containing the vasodilating neuro eptidecalcitonin gene-related peptide (arrows) in the walls ofbloodvessels (V).
tion Unless the macromolecules are removed from theinterstitial fluid, the tissue pressure will soon rise to thesame level as the blood pressure, causing ischemia andnecrosis. In other words, if the pulp is to survive and heal,lymphatic vessels must remove plasma proteins from thepulpal interstitial fluid. Although the existence of lym-phatic vessels in the pulp has been controversial, recentstudies have confirmed that the dental pulp has lymphvessels for the drainage of interstitial fluid and macro-molecules (Heyeraas, 1989; Bishop and Malhotra, 1990).
The Significance of a High Piin a Low-compliant Environment
The physiological significance of a relatively high Pi inthe dental pulp has long been disputed Furthermore,does the pulp have any advantage because of its enclo-sure between rigid dentin walls, an anatomical featurewhich causes a low-compliant environment?
First, in low-compliant tissues, such as the dental
10131 328 336)19991 Crit Rev Orcil Biol Me.333
33310(3):328-336 ( 1999) Crit Rev Orcal Biol Med by guest on October 1, 2015 For personal use only. No other uses without permission.cro.sagepub.comDownloaded from

Cortex(pain)
Stimuli
Ggl. trigem.
Sensorynerves
1 - ,
Hvesse',uui Dentin tubulus%///ySPVasodilation
Figure 7. Diagram showing how dentin stimuli will excite nerves in the dentin-odontoblast area, causing pain, and at the same time bring-ing about release of sensory neuropeptides (CGRP, SP) from nerve endings in the pulp. The neuropeptides induce vasodilation, which inturn increases the tissue pressure locally in the low-compliant pulp. The increased tissue pressure wi l cause augmented outward flow offluid in the exposed dentin tubules (broken arrows) and thereby help protect the pulp against inward diffusion of harmful substances.
pulp, a rapid increase in tissue pressure will in itself actas a negative feedback mechanism and promote absorp-tion of fluid into capillaries. Thus, the pulp's inability toexpand is a favorable situation, since the fast rise in tis-sue pressure due to increased blood or interstitial fluidvolume serves as an efficient edema-preventing mecha-nism. Second, the high interstitial fluid pressure in thepulp has recently been linked to a sensory neurogenicdefense mechanism, which might protect the pulpagainst entry of harmful agents when the dentin isexposed (Matthews, 1992). Research during the lastdecade has shown that not only the autonomic sympa-thetic nerves but also the sensory nerves have a strongimpact on blood circulation in the dental pulp, due tothe liberation of vasodilating neuropeptides such as cal-citonin gene-related peptide (CGRP) and substance P(SP). In the cat pulp, most of the sensory nerve fiberscontain these neuropeptides (Heyeraas et al), 1993). Themajority of sensory nerve fibers containing the vasodilat-
ing neuropeptides CGRP and SP in the main pulp seemto be located in the walls of blood vessels (Fig. 6), a find-ing which implicates these neuropeptides in blood flowregulation. However, not only the nerves associated withblood vessels, but also most nerves in the subodonto-blast/odontoblast area (Casasco et al., 1990) and nervefibers penetrating the dentinal tubules show immunore-activity for CGRP and substance P (Byers, 1992; Heyeraaset al, 1993). These immunoreactive nerve fibers in dentinmay very well represent branches of nerves terminatingaround the pulpal blood vessels. It has been shown thatmechanical or electrical stimulation of dentin causespulpal vasodilation and therefore increased P, in the low-compliant dental pulp (Olgart et al, 1991; Heyeraas et al.,1994; Olgart, 1996; lacobsen and Heyeraas, 1997).Furthermore, a continuous outward flow of fluid throughexposed dentin has been demonstrated in cat teeth, andstimulation of the inferior alveolar nerve caused a signif-icant increase in the rate of outward flow of fluid from the
Grit Rev Oral Bid Med1013) 328 33n U999Crit Rev Oral Biot Medt 1000) 28-336 I 1999)
-\
by guest on October 1, 2015 For personal use only. No other uses without permission.cro.sagepub.comDownloaded from

dentin (Vongsavan and Matthews, 1992b). An axon reflex,like that involved in cutaneous nociceptor stimulation(Lewis, 1927), might therefore also seem possible in thepulp, and might be of functional importance in the devel-opment of vasodilation observed by stimulation ofdentin as oulined in Fig. 7 (Matthews, 1992). It seemslogical to assume that any increase in P. caused byvasodilation will promote outward flow of fluid throughdentin tubules when dentin is exposed. The sensorynerve fibers in the odontoblast/dentin area, when excit-ed by, for example, the hydrodynamic mechanism(Brannstr6m, 1963), might cause pulpal vasodilation andconsequently increased Pi due to the release of neu-ropeptides via a so-called axon reflex (Fig. 7). Theincreased Pi will in turn promote outward flow of fluidthrough the exposed dentin tubules. This flow is impor-tant because it will affect the rate at which toxic sub-stances from outside the tooth will diffuse into thedentin tubules. Thus, the increased outward flow of fluidwill help to protect the pulp against entry of harmful sub-stances, as previously suggested by Matthews (1992). Itseems, therefore, physiologically beneficial for the pulpto have a high tissue pressure, which promptly increaseswhen blood flow increases due to its low compliance.
It is concluded that inflammation leads to a localincrease in both interstitial fluid pressure and blood flowin the low-compliant pulp. The locally increased tissuepressure may initiate increased lymph flow and absorp-tion of fluid into capillaries in nearby non-inflamed tissue.This will counteract a rise in volume and therefore a rise intissue pressure, thus preventing a spread and further risein interstitial fluid pressure. Increased tissue pressure,whether caused by increased blood volume or increasedcapillary filtration, will promote outward flow of fluidthrough exposed dentin tubules and thereby help to pro-tect the pulp against the entry of harmful substances.
AcknowledgmentsThis review is based upon valuable collaboration with many colleagues,to whom I am greatly indebted. This work was supported by theResearch Council of Norway and by the Colgate Research Foundation.
REFERENCESAukland K, Nicolaysen G (1981). Interstitial fluid volume:
local regulatory mechanisms. Physiol Rev 61:556-642.Aukland K, Reed RK (1993). Interstitial-lymphatic mech-
anisms in the control of extracellular fluid volume.Physiol Rev 73:1-78.
Aukland K, Wiig H (1984). Hemodynamics and interstitialfluid pressure in the rat tail. Am I Physiol 247:H80-H87.
Beveridge EE, Brown AC (1965). The measurement ofhuman dental intrapulpal pressure and its responseto clinical variables. Oral Surg 19:655-668.
Bishop MA, Malhotra M (1990). An investigation of lym-phatic vessels in the feline dental pulp. Am I Anat187:247-253.
Brannstrom M (1963). A hydrodynanic mechanism in thetransmission of pain-producing stimuli through den-tine. In: Sensory mechanisms in dentin. Anderson DI,editor. Oxford: Pergamon, pp. 73-79.
Brown AC, Yankowitz (1964). Tooth pulp tissue pressureand hydraulic permeability. Circ Res 15:42-50.
Byers MR (1992). Effects of inflammation on dental sen-sory nerves and vice versa. Proc Finn Dent Soc 88(SupplI):499-506.
Casasco A, Calligaro A, Casasco M, Springall DR, PolakIM, Poggi P, et al. (1990). Peptidergic nerves in humandental pulp. Histochemistry 95:115-121.
Christiansen RL, Meyer MW, Visscher MB (1977).Tonometric measurements of dental pulp andmandibular marrow blood pressures. I Dent Res56:635-645.
Dahl E, Mjor IA (1973). The fine structure of the vesselsin the human dental pulp. Acta Odontol Scand 31:223-230.
Granger lP, Haas JA, Pawlowska D, Knox FG (1988). Effectof direct increases in renal interstitial hydrostaticpressure on sodium excretion. Am I Physiol 255:F527-F532.
Guyton AC, Granger HI, Taylor AE (1971). Interstitial fluidpressure. Physiol Rev 51:527-563.
Hals E, Tonder KIH (1981). Elastic (pseudoelastic) tissuein arterioles of the human and dog dental pulp. ScandJ Dent Res 89:218-227.
Heyeraas KI (1989). Pulpal hemodynamics and intersti-tial fluid pressure: balance of transmicrovascular fluidtransport. I Endod 15:468-472.
Heyeraas Kl (1990). Interstitial fluid pressure and trans-microvascular fluid flow. In: Dynamic aspects of den-tal pulp. Inoki R, Kudo T, Olgart LM, editors. London:Chapman and Hall, pp. 189- 198.
Heyeraas KI, Kvinnsland 1, Byers MR, Jacobsen EB (1993).Nerve fibers immunoreactive to protein gene product9.5, calcitonin gene-related peptide, substance P, andneuropeptide Y in the dental pulp, periodontal liga-ment, and gingiva in cats. Acta Odontol Scand 51:207-221.
Heyeraas Kl, Kim S, Raab WH-R, Byers MR, Liu M (1994).Effect of electrical tooth stimulation on blood flowand interstitial fluid pressure and substance P andCGRP-immunoreactive nerve fibers in the low compli-ant cat dental pulp. Microvasc Res 47:329-343.
Jacobsen EB, Heyeraas KI (1997). Pulp interstitial fluidpressure and blood flow after denervation and elec-trical tooth stimulation in the ferret. Arch Oral Biol42:407-415.
Johannessen AC, Fieertoft M, Heyeraas KI (1987). Tissue
pressure in rat oral mucosa measured by micropunc-
33510(3)328-336 11999) CritBiol
Crit Rev Oral Biol Med10(3):328-336 (1999) by guest on October 1, 2015 For personal use only. No other uses without permission.cro.sagepub.comDownloaded from

ture technique. J Periodont Res 22:139-143.Kawamura Y, Kato Y, Kato 1 (1967). Studies on the dental
pulp pressure. J Osaka Univ Dent Sch 7:7-16.Kim S, Liu M, Simchon S, Dorscher-Kim JE (1992). Effects
of selected inflammatory mediators on blood flowand vascular permeability in the dental pulp. Proc FinnDent Soc 88(Suppl 1):387-392.
Kristiansen AB, Heyeraas Kl (1989). Micropuncturemeasurements of interstitial fluid pressure in the ratperiodontal ligament. Proc Finn Dent Soc 85:295-300.
Lewis T (1927). The blood vessels of the human skin andtheir responses. London: Shaw and Sons.
Matthews B (1992). Sensory physiology: a reaction. ProcFinn Dent Soc 88(Suppl 1): 529-532.
Michelsen K (1967). Pressure relationships in the bonemarrow vascular bed. Acta Physiol Scand 71:16-29.
Okabe E, Todoki K, Ito H (1989). Microcirculation: func-tion and regulation in microvasculature. In: Dynamicaspects of dental pulp. Inoki R, Kudo T, Olgart LM,editors. London: Chapman and Hall, pp. 151-166.
Olgart L (1996). Neural control of pulpal blood flow. CritRev Oral Biol Med 7:159-171.
Olgart L, Edwall L, Gazelius B (1991). Involvement ofafferent nerves in pulpal blood flow reactions inresponse to clinical and experimental procedures inthe cat. Arch Oral Biol 36:575-581.
Renkin EM, Gustafson-Sgro M, Sibley L (1988). Couplingof albumin flux to volume flow in skin and muscles ofanesthetized rats. Am J Physiol 255(Heart Circ Physiol24):H458-H466.
Renkin EM, Rew K, Wong M, O'Loughlin D, Sibley L(1989). Influence of saline infusion on blood-tissuealbumin transport. Am I Physiol 257(Heart Circ Physiol26):H525-H533.
Starling EH (1896). On the absorption of fluids from theconnective tissue spaces. I Physiol Lond 19:312-326.
StenvikA, Iversen J, Mjor IA (1972). Tissue pressure andhistology of normal and inflamed tooth pulps inMacaque monkeys. Arch Oral Biol 17:1501-1511.
Tonder KJ, Kvinnsland 1 (1983). Micropuncture measure-ments of interstitial fluid pressure in normal andinflamed dental pulp in cats. I Endod 9:105-109.
Tucker BI, Blantz RC (1978). Determinants of proximaltubular reabsorption as mechanisms of glomerulo-tubular balance. Am I Physiol 235:F142-F150.
Van Hassel HI (1971). Physiology of the human dentalpulp. Oral Surg 32:126-134.
Vongsavan N, Matthews B (1992a). Fluid flow through catdentin in vivo. Arch Oral Biol 37:175-185.
Vongsavan N, Matthews B (1992b). Changes in pulpalblood flow and in fluid flow through dentine pro-duced by autonomic and sensory nerve stimulation inthe cat. Proc Finn Dent Soc 88(Suppl I):491-497.
Weatherred JG (1965). Peripheral nervous system effectsin the dental pulp of the rat and dog (thesis).University of Texas.
Wiederhielm CA, Woodbury JW, Rushmer RF (1964).Pulsatile pressures in the microcirculation of frog'smesentery. Am I Physiol 207:173-176.
Wiig H (1985). Comparison of methods for measurementof interstitial fluid pressure in cat skin/subcutis andmuscle. Am I Physiol 249:H929-H944.
Wiig H (1990). Evaluation of methodologies for measure-ments of interstitial fluid pressure (Pi): physiologicalimplications of recent P, data. Crit Rev Biomed Eng18:27-54.
Wiig H, Reed R (1983). Rat brain interstitial fluid pressuremeasured with micropipettes. Am I Physiol 244:H239-H246.
Wynn W, Haldi I, Hopf MA, John K (1963). Pressure with-in the pulp chamber of the dog's tooth relative toarterial blood pressure. I Dent Res 42:1169-1177.
336 Grit Rev Oral Biol Med 10(3):328 336 (1999)336 Crit Rev Oral Biol Med 10(3):328-336 (1999) by guest on October 1, 2015 For personal use only. No other uses without permission.cro.sagepub.comDownloaded from




















