International Trends in Cancer Mortality in France, West Germany, Italy, Japan, England and Wales,...
44
International Trends in Cancer Mortality in France, West Germany, Italy, Japan, England and Wales, and the United States” DEVRA LEE DAVIS,” DAVID HOEL,d JOHN FOX,” AND ALAN D. LOPEZ bNational Research Council Washington, D. C. dNational Institute of Environmental Health Sciences Research Triangle Park, North Carolina 27709 cOfjke of Population Censusesand Surveys London, England ‘Global Health Situation Assessment and Projections Unit World Health Organization Geneva, Switzerland In 1987, more than a half million Americans died from cancer and one million contractedthe disease. Similar patterns occurin a number of industrial countries. For instance, in Bologna, Italy, nearly two of every five deaths are due to cancer. We developed comparable data for the major industrial countries to examine trends in cancer. As a number of experts have noted, the interpretation of trends must be tentative and cautious, as artefacts can influence cancer rates. The papers in this volumescrutinize recent trendsin cancer over a relativelyrecent time period to reduce theroleof artifactsthat stemfromchangesinmedicalpractice,diagnostictechnology, and other shifting characteristics of modern society. Analyses of international patterns in cancer may well indicate opportunities for prevention, as well as future demands for health care in our aging society. lhis article was originally printed in LMcer 336 474-481 (1990). This version contains ECorrespondence to Dr. Devra Lee Davis, Scholar in Residence. National Academy of additional graphs and analyses. Sdcncca, 2101 Constitution Avenue, Washington, DC 20418. 5
Transcript of International Trends in Cancer Mortality in France, West Germany, Italy, Japan, England and Wales,...

International Trends in Cancer Mortality in France, West Germany, Italy, Japan,
England and Wales, and the United States”
DEVRA LEE DAVIS,” DAVID HOEL,d JOHN FOX,” AND ALAN D. LOPEZ
bNational Research Council Washington, D. C.
dNational Institute of Environmental Health Sciences Research Triangle Park, North Carolina 27709
cOfjke of Population Censuses and Surveys London, England
‘Global Health Situation Assessment and Projections Unit World Health Organization
Geneva, Switzerland
In 1987, more than a half million Americans died from cancer and one million contracted the disease. Similar patterns occur in a number of industrial countries. For instance, in Bologna, Italy, nearly two of every five deaths are due to cancer. We developed comparable data for the major industrial countries to examine trends in cancer. As a number of experts have noted, the interpretation of trends must be tentative and cautious, as artefacts can influence cancer rates. The papers in this volume scrutinize recent trends in cancer over a relatively recent time period to reduce theroleof artifactsthat stemfromchangesinmedicalpractice,diagnostictechnology, and other shifting characteristics of modern society. Analyses of international patterns in cancer may well indicate opportunities for prevention, as well as future demands for health care in our aging society.
l h i s article was originally printed in LMcer 336 474-481 (1990). This version contains
ECorrespondence to Dr. Devra Lee Davis, Scholar in Residence. National Academy of additional graphs and analyses.
Sdcncca, 2101 Constitution Avenue, Washington, DC 20418. 5
6 ANNALS NEW YORK ACADEMY OF SCIENCES
INTRODUCTION
Throughout the world, cancer patterns vary substantially and continue to change in important and interesting ways. Overall cancer mortality remains highest in developed countries,where it continues to increase. The World Health Organization estimates that in 1980 about half of all cases of cancer occurred in about one-fifth of the world's population-in industrial countries.' The range of cancer between and within countries is c~nsiderable:~ and common types also differ, although precise estimates are hard to obtain because of differences in access to diagnosis and related factors: Cancer linkedtocigarettesmoking,asbestos,anddietaryfat ismore frequent in the developed world, whereas cancer associated with food consumption, presex- vatives, and infectious diseases is more frequent in the developing world:
According to one estimate, women in North America had 30 times more breast cancerbut only halfasmuchuterinecervixcancerasdid theircounterpartsinwestern Africa and Central America.' Similarly, men in North America and northern Europe had a quarter as much liver cancer but 30 times more lung cancer than did men in western Africa and middle Africa? Japanese women who emigrate to Hawaii have half the risk of contractingstomach cancer than their grandmothers had at the same age, but twice the risk of getting breast cancer! Within and between industrial countries, rates of some common types of cancer can also vary by as much asfivefold- as, for instance, does the rate of breast cancer between U.S. and Japanese wome1i.S The importance of environmental factors in the development of cancer is confirmed by the observation that adopted children whose adoptive parents have died of cancer have a fivefold increased risk of getting the disease.'
Within the past two decades important variations in cancer have become evident in the industrial world. Stomach cancer continues to decline for reasons that are not ~lear;~*~lungcancerisstarting to decline formen under age85 in theunited Kingdom" andmen under age45in theunited States," but is stillrisinginoldermen and women in the United States." Several kinds of cancer not associated with cigarette smoking have also increased substantially in older persons in certain industrial c~untries. '~- '~ Cancer mortality in persons under age 45 has declined due to impressive improve- ments in treatment," while incidence continues to i n c r e a ~ e . ~ ~ * ' ~
In October, 1989, the Collegium Ramazzini sponsored a workshop of expertsfrom major cancer and statistical research organizations in Australia, Canada, China, Czechoslovakia, the Federal Republic of Germany, France, Israel, Italy, Japan, Norway, Poland, South Africa, Sweden, the United States, and the United Kingdom (see APPENDIX for list of participants). As part of the celebration of the 900th anniversary of the University of Bologna, and with the cooperation of the New York Academy of Sciences, the workshop assessed recent trends in some industrial coun- tries for specific age groups of males and females in overall cancer mortality and specific sites of cancer. It also considered evidence on diagnostic artifacts, changes in access tocare,codingshifts, and other factors that can affect the quality of ascertainment of recorded mortality trends.
The workshop convened researchers from 15 different countries and encouraged them to compare the patterns and trends of their own national data sets with those elsewhere. A central element in this activity is the idea of data exchange. The goals of the workshop were to: (I) increase awareness of what data are available interna- tionally and how these data might be used to generate hypotheses and to plan for

DAVIS ct at.: INTERNATIONAL TRENDS IN CANCER MORTALITY 7
health care needs; (2) discuss the problems ofworkingwith international cancer data and how these may be overcome; (3) provide an exchange of ideas about recent trends in cancer in industrial countries and the development of additional research on these trends;and (4) suggest additionalinter- andintra-nationaldata that might becollected to claxify some hypotheses and generate others. In particular wediscuss trends in age- and site-specific rates of cancer mortality, biases that can affect the quality of ascertainment over time, and the implications of the findings of trends in cancer mortality from 1968 to 1987. This focus on recent trends reduces, but does not eliminate, the effect of artifacts that can be introduced over longer periods.
METHODS AND MATERIALS
Data
Annual age-specific rates were calculated for cancer sites previously reported to increaseintheUnitedState~~~andforwhich thequality ofdetectionandconfirmation remain high. For the period from 1%8 through 1987, annual data on cancer deaths in 18 countries along with corresponding population data separated into five-year age groups were provided by the Global Health Situation Assessment and Projections Unit, World Health Organization, Geneva, to the chairmen of the workshop (Davis and Hoel), who developed and distributed data files to experts from different countries. To reduce the possibleinfluence of coding changes, the time studied spans a period during which a uniform system for classifying disease was in place in all countries-the Eighth and Ninth International Classification of Disease (ICD)?' Sweden wasexcludedfromthis analysis because achangein recordingdeath certificates in 1982introduced an artifactual decrease in cancer mortality;" malignant tumors were no longer listed as cause of death, except where they were the immediate cause.
Quality OfAscertainment
Regarding possible changes in the quality of ascertainment of cancer rates, the workshop reviewed evidence in selected large industrial countries on the following factors: necropsy and diagnosticconfirmation patterns, enumeration of older persons, access to care and diagnostic technology, and cultural and social factors.
Researchers from the U.S. National Cancer Institute estimated the rate of con- firmation from theU.S. Surveillance, Epidemiology, and End Result (SEER) data set, comparing death certificate diagnoses with histopathological confirmation, for the periods 1970-1971 and 1985-1986.= The SEERdataprovidecontinuouscoveragefor about 10% of the US . population since 1973. Other estimates of time trends in the quality of diagnoses were derived from provisional data obtained from the Radiation Effects Research Foundation (RERF) Autopsy Seriesz3+" and from a recent United Nations report.= To assess possible changes in the quality of enumeration over time, retrospective validations of population estimates for different age groups were examined in England and Wales for periods 1961-1970 and 1970-1981.26 The influ-

8 ANNALS NEW YORK ACADEMY OF SCIENCES
ences of changing access to care, diagnostic fashions, and technology and cultural factors were also explored.
Data Plotting
Plots of age-specific mortality rates from 1968 to 1987 were generated. Time is displayed on the x axis and rate per 100,OOO for specific age groups on they axis.
RESULTS
Mortality Trends
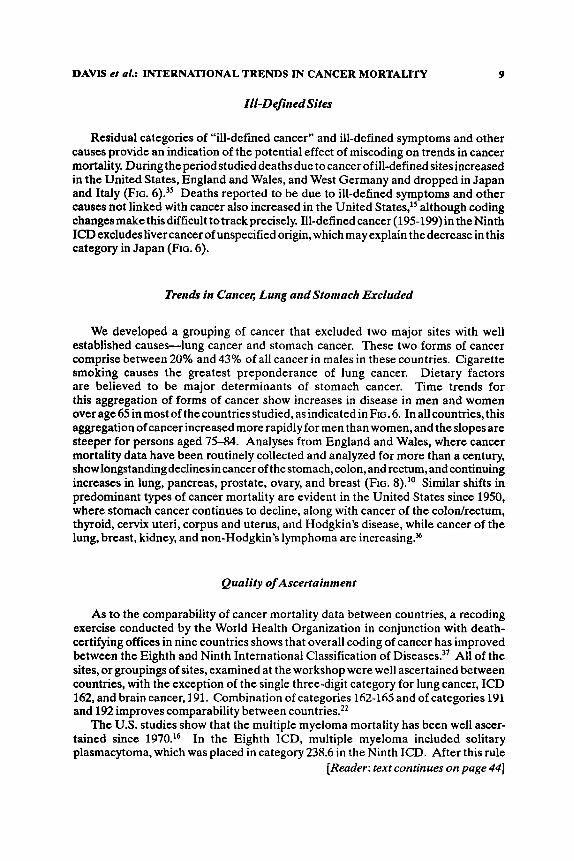
Some remarkable shiftsin patterns of cancer can be discerned across several major industrial countries. Stomach cancer continues to decline substantially in nearly all countriesstudied,althoughthe oldest groupsinItaly and Japan show somecontinuing increases (FIG. l).27928
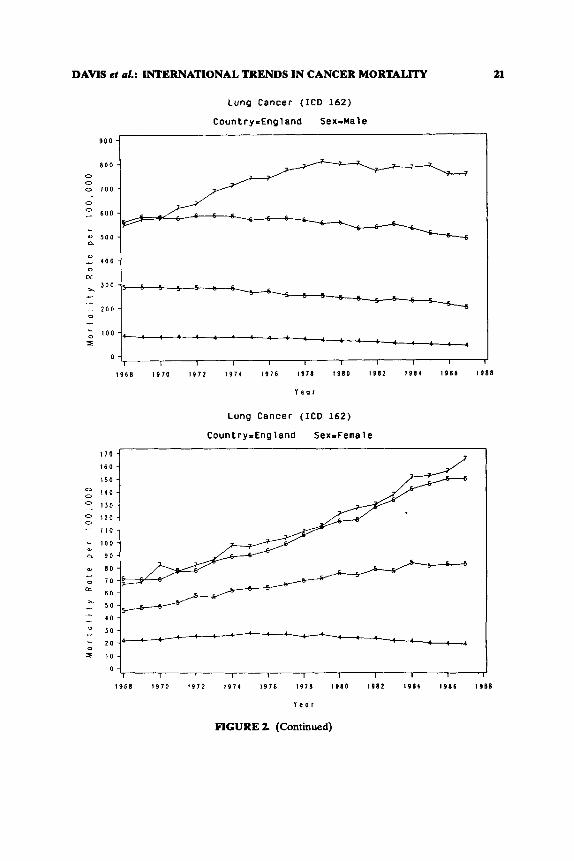
Lung cancer patterns show declines in England and Wales in men ages 35-38 and in women ages 45-69 and in the United States in men aged 35-44, and increases for all age groups in Italy, Japan, and France (FIG. 2). The highest rate of lung cancer mortality in the U.S. is in the cohort of men born at the turn of the century," although they were not the group who smoked the most cigarettes$
In all countries studied, brain and other nervous system cancer rates increased more than twofold in persons aged 75-84 and nearly doubled in those aged 65-74:' In Japan the rate of the increase is far greater, although the absolute levels are lower than in the other countries.
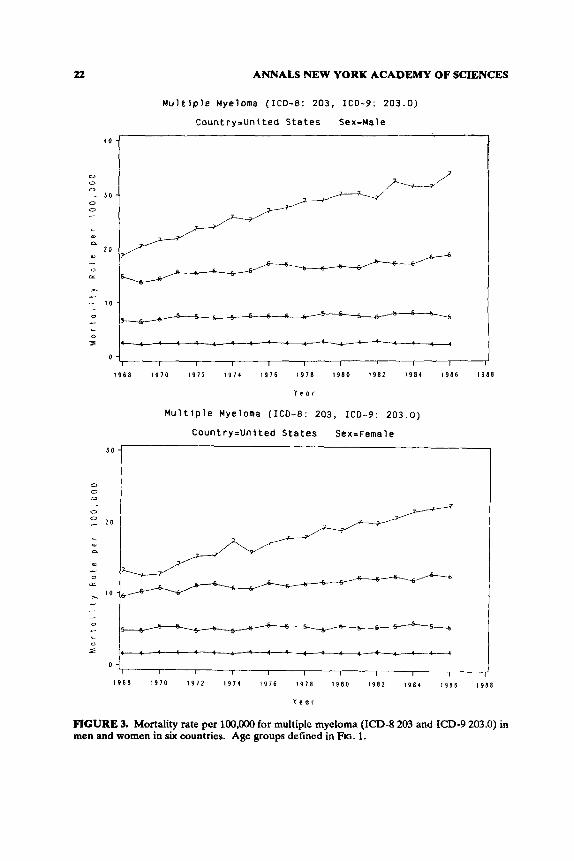
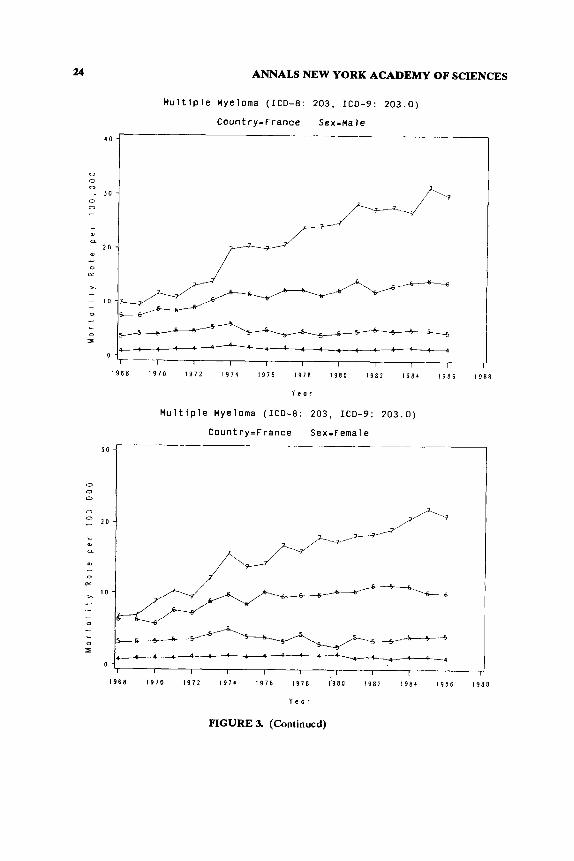
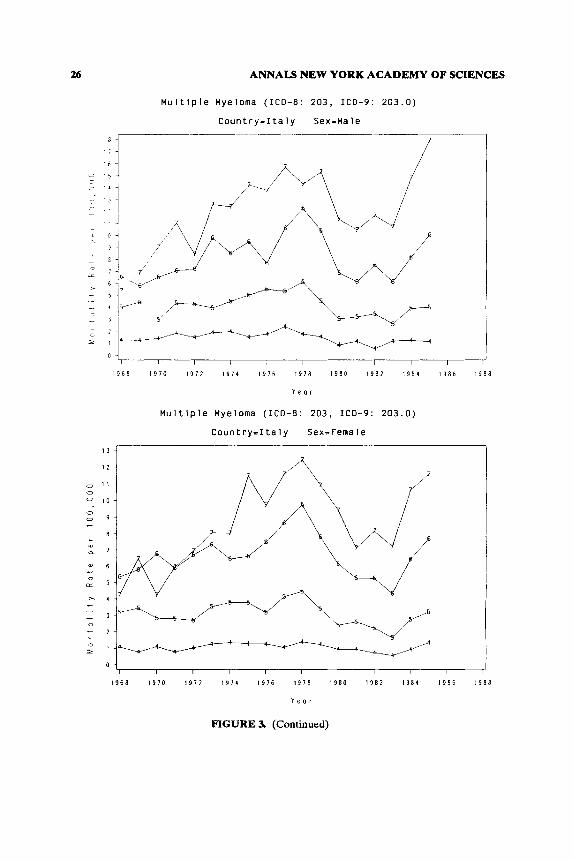
Patterns of multiple myeloma appear homogeneous between countries and within agegroups,withincreasingratesatincreasingagesforboth men a n d ~ o m e n . ~ ' In Italy andWest Germanyacodingchangeintroducedwith theNinthICDled toatransitory downturn in rates at all age groups; this disappeared in later years.32
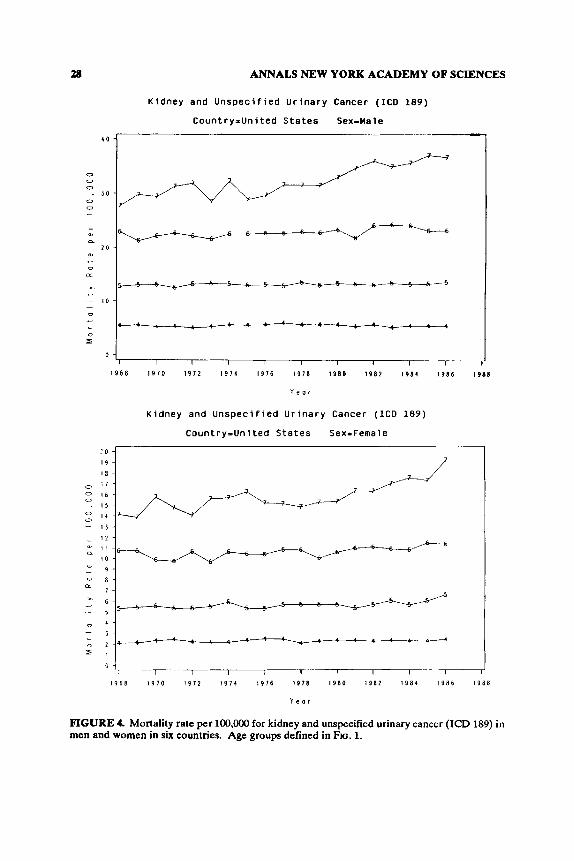
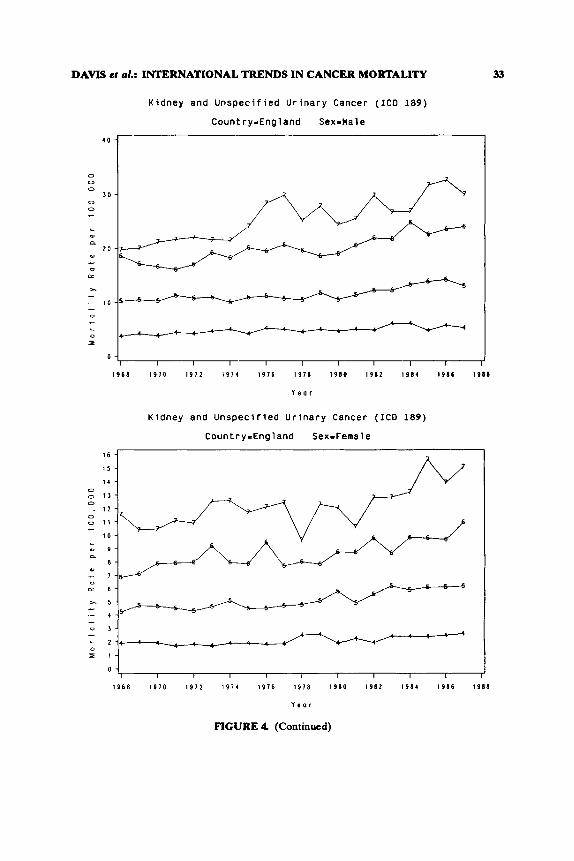
FIGURE 3 displays the trend in multiple myeloma mortality for men in several industrial countries. Kidney and unspecified urinary cancer appear similar to myeloma over time. Rates of increase are highest in the oldest age group, but also occur in younger persons (FIG. 4).
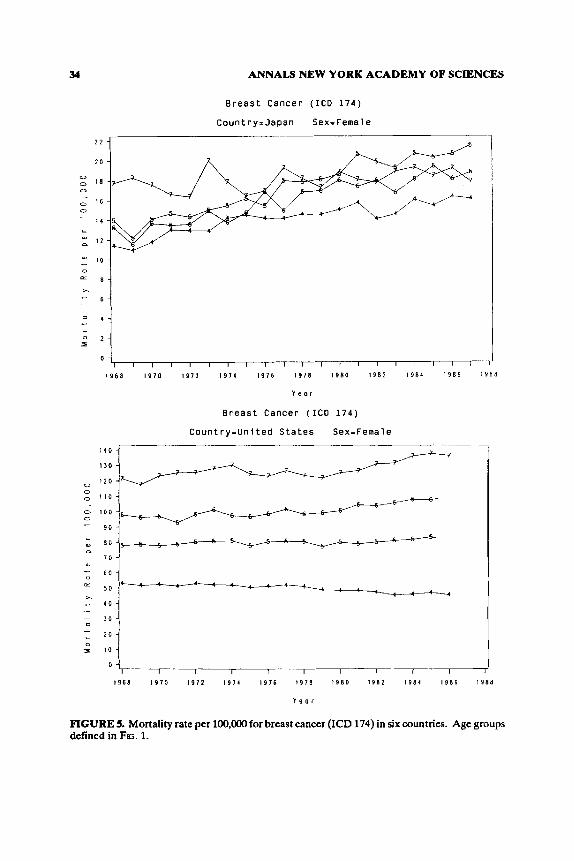
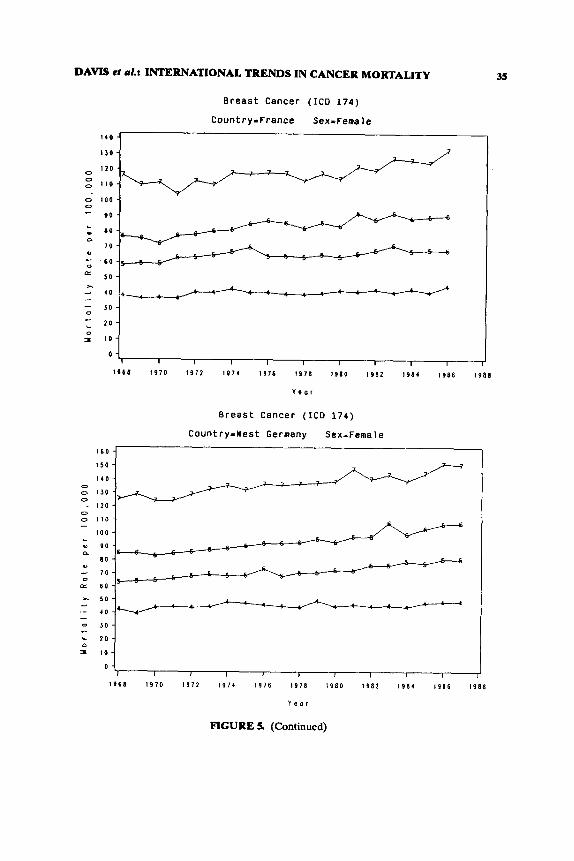
Breast cancer mortality rates are continuing to increase most in postmenopausal women, except in Japan (FIG. 5).33 In the industrialized world, with few exceptions, breast cancer is a leading cause of cancer deaths among premenopausal and post- menopausal women, with rates between countries varying most at the oldest age groups and continuing to increase in the past decade.
Although melanoma is an infrequently occurring cancer, mortality from mela- nomaisrisingrapidlyworldwide. Mortalityis higherin menoverage45 and inwomen under age 45. In the United States, melanoma rates have not changed appreciably in personsunder age 45 since 1970, but haveincreased annually between 2.8% and 3.1 YO for persons aged 45-84. Males aged 25-84 had a 40% greater rate of melanoma than did females in 1970-1973 and a 70% greater rate in 1982-1985, suggesting possible occupational factors.34
DAVIS el ol.: INTERNATIONAL TRENDS IN CANCER MORTALITY 9
Iil-Def inedsites
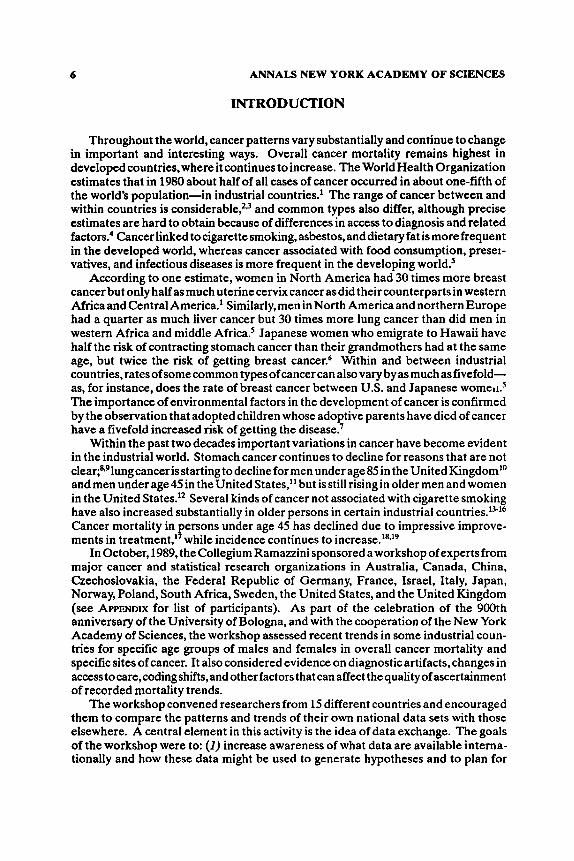
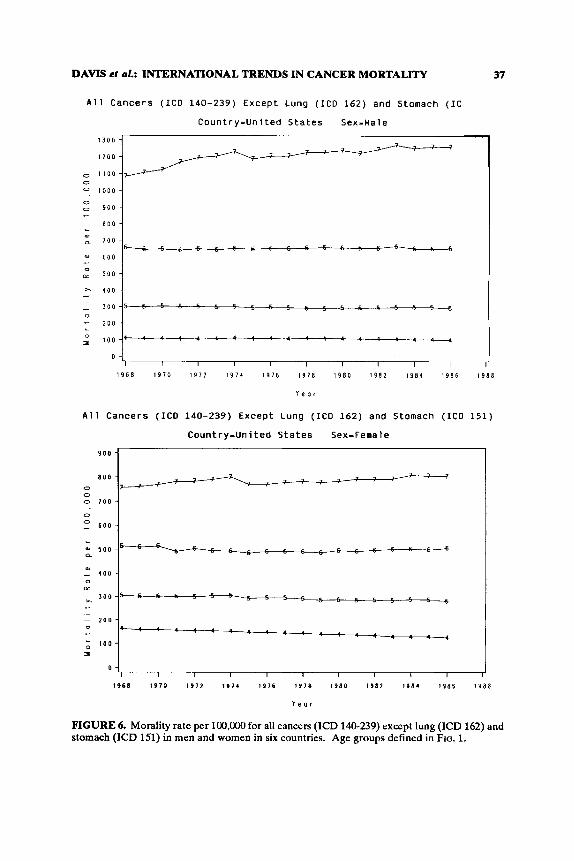
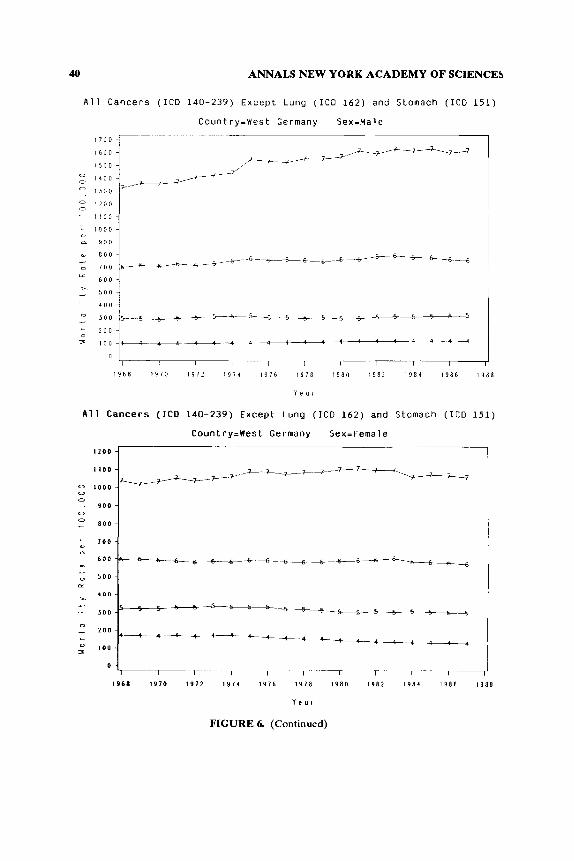
Residual categories of “ill-defined cancer” and ill-defined symptoms and other causes provide an indication of the potential effect of miscoding on trends in cancer mortality. During the period studied deaths due to cancer of ill-defined sites increased in the United States, England and Wales, and West Germany and dropped in Japan and Italy (FIG. 6).’s Deaths reported to be due to ill-defined symptoms and other causes not linked with cancer also increased in the United States,” although coding changesmake this difficult to track precisely. Ill-defined cancer (195-199) in the Ninth ICD excludesliver cancer of unspecified origin, which may explain the decrease in this category in Japan (FIG. 6).
Trenals in Cancer, Lung andStomach Excluded
We developed a grouping of cancer that excluded two major sites with well established causes-lung cancer and stomach cancer. These two forms of cancer comprise between 20% and 43% of all cancer in males in these countries. Cigarette smoking causes the greatest preponderance of lung cancer. Dietary factors are believed to be major determinants of stomach cancer. Time trends for this aggregation of forms of cancer show increases in disease in men and women overage65inmost ofthecountriesstudied, asindicatedinFIG.6. Inallcountries, this aggregation of cancer increased more rapidly for men than women, and the slopes are steeper for persons aged 75-84. Analyses from England and Wales, where cancer mortality data have been routinely collected and analyzed for more than a century, showlongstandingdeclinesincancerofthestomach,colon,and rectum,andcontinuing increases in lung, pancreas, prostate, ovary, and breast (FIG. 8).” Similar shifts in predominant types of cancer mortality are evident in the United States since 1950, where stomach cancer continues to decline, along with cancer of the colontrectum, thyroid, cervix uteri, corpus and uterus, and Hodgkin’s disease, while cancer of the lung, breast, kidney, and non-Hodgkin’s lymphoma are increasing.%
Quality of Ascertainment
As to the comparability of cancer mortality data between countries, a recoding exercise conducted by the World Health Organization in conjunction with death- certifying offices in nine countries shows that overall coding of cancer has improved between the Eighth and Ninth International Classification of Diseases?’ All of the sites, or groupings of sites, examined at the workshop were well ascertained between countries, with the exception of the single three-digit category for lung cancer, ICD 162, and brain cancer, 191. Combination of categories 162-165 and of categories 191 and 192 improves comparability between countries.22
The U.S. studies show that the multiple myeloma mortality has been well ascer- tained since 1970.16 In the Eighth ICD, multiple myeloma included solitary plasmacytoma, which was placed in category 238.6 in the Ninth ICD. After this rule
[Reader: text continues on page 44)

10 ANNALS NEW YORK ACADEMY OF SCIENCES
Stomach Cancer (ICD 151)
Country=United States Sex=Hale
1968 1 9 7 0 1 9 7 2 1 9 7 4 1 9 7 6 1 9 7 8 1 9 8 0 1 9 8 2 1 9 8 4 1 9 8 6 1 9 8 8
Y e a r
Stomach Cancer (ICD 151)
Country=United States SexXFemale
0 I I I I I I I I r-
1 9 6 8 I 9 7 0 1 9 7 2 1 9 7 1 I 9 7 6 1 9 7 s 1 9 8 0 1 9 8 2 1 9 8 1 I 9 8 6 1 9 8 8
Y e a r
FIGURE 1. Mortality rate per 100,OM) for stomach cancer (ICD 151) in men and women in six countries. Age groups: 4.45 to 54 years old; 5,55 to 64 years old; 6,65 to 74 years old; and 7.75 to 84 years old.

DAVE3 er d.: INTERNATIONAL TRENDS IN CANCER MORTALITY 11
700
6 0 0 0 0
0 5 0 0 0 -
400 LI
a# a 3 0 0
OL
Stomach Cancer (ICD 151)
Country-Japan Sex-Uale
Stomach Cancer (1CD 151)
CountryEJapan Sex-Female
0 I I I I I I I 1 I
1968 1970 1972 197t I976 1978 1980 1 9 8 2 198) 1 9 3 6 1988
Y q o r
FIGURE 1. (Continued)

ANNALS NEW YORK ACADEMY OF SCIENCES
Stomach Cancer (ICD 151)
Country=France Sex=Hale
1 9 6 8 1 9 7 0 1 9 1 2 1 9 7 4 1 9 7 6 1 9 7 8 I980 1 9 8 2 1 9 8 4 1 9 8 6 1 9 8 8
Y e a r
Stomach Cancer (ICD 151)
Country=France Sex=Female
I 7 0
I 6 0
1 5 0
I 4 0
I30
I 2 0
I 1 0
1 0 0
90
8 0
7 0
6 0
5 0
40
30
2 0
I 0
0
1 3 6 8 1 9 1 0 1 9 7 2 1 9 7 4 1 9 7 6 I978 1 9 8 0 1 9 8 2 1 9 8 4 1 9 8 6 1 9 8 8
Y e o r
FIGURE 1. (Continued)
DAMS et ol.: INTERNATIONAL TRENDS IN CANCER MORTALITY
5 0 0
0
0 0 400
400
0 0 0
0 0
. 3 0 0
- L
w 0
Y
0 (L
2 0 0 - - - i a a - 0 - L
0 = 0
Stomach Cancer ( I C D 151)
Country-West Germany Sexlaale
4
I I I I I I I I I
1 9 6 8 1970 1972 1974 I976 1978 1980 1982 1984 1986 I988
Y e a r
Stomach Cancer (ICO 151)
Country-nest Germany Sex-Female
13
3

14 ANNALS NEW YORK ACADEMY OF SCIENCES
Stomach Cancer (ICD 151)
Country-Italy Sex=Hale
1 9 6 8 1 9 7 0 1 9 7 2 1 9 7 4 1 9 7 6 I 9 7 8 I 9 8 0 I 9 8 2 1 9 8 4 1 9 8 6 I 9 8 8
Y e a r
Stomach Cancer (ICD 151)
Country=Italy Sex-Female
I I I 1 I I 1 I I
1 9 6 8 1 9 7 0 1 9 7 2 1 9 7 4 1 9 7 6 1 9 1 8 I 9 8 0 1 9 8 2 1 9 1 1 1 9 8 6 I 9 8 8
Y e a r
FIGURE 1. (Continued)

DAYIS ct d.: INTERNATIONAL TRENDS IN CANCER MORTALITY
Stomach Cancer (ICD 151)
Country-England Sex-Hale
3 0 0 1 j
0 I I I I I I I I I
1 9 6 8 1910 I 9 7 2 I 9 7 4 1 9 7 6 1 9 7 8 I 9 8 0 19112 1 9 8 4 1 9 8 1 1 9 8 8
Y e a r
1 5 0
I 4 0
0 1 J O
- 1 2 0
0 1 1 0
1 0 0
0
0
0
c
Stomach Cancer (ICO 151)
Country-England Sex-Female
l!5
D I 1 I I I I I 1 I 1 I
1 9 6 8 I970 1 9 7 2 1 9 7 4 1 9 1 6 I 9 7 8 1 9 8 0 I 9 8 2 1 9 8 4 1 9 8 6 1 9 8 8
Y e o f
FIGURE 1. (Continued)

16 ANNALS NEW YORK ACADEMY OF SCIENCES
Lung Cancer (ICO 162)
Country-United States Sex=Hale
6 o o 1 0 5 0 0 0 0
0 0 - 1 0 0
* a
100
._
64 I
1968 1970 1972 l97k 1976 1978 1980 1982 1984 1986 1988
Y e u r
Lung Cancer (ICO 162)
Country=United States Sex=Female
:l0:L : : 1 1 : : 1 : I50
I40
I J O
0 1 2 0
o- 1 1 0
O - 1 0 0
0
0
9 0
a 8 0
a) 70
0 60
S O
4 0
a)
- LL
A - ._ - 0 '0
L 2 0
I 1 0
0
0
1968 1970 1 9 7 2 1974 1976 1978 1 9 8 0 1982 I984 1986 I988
Y e o i
FIGURE 2 Mortality rate per 100,000 for lung cancer (ICD 162) in men and women in six countries. Age groups defined in FIG. 1.

DAVIS er al.: INTERNATIONAL TRENDS IN CANCER MORTALITY 17
Lung Cancer (ICD 162)
Country-Japan Sex-Hale
x &
.- z o a l l Lung Cancer (ICD 162)
Country-Japan Sex-Female
110 -
1 0 0 - 0
0 0 9 0 -
0
7 0 - -

18 ANNALS NEW YORK ACADEMY OF SCIENCES
Lung Cancer (ICD 162 )
Count ry=France Sex=Male
1 I I I 1 9 6 8 1 9 7 0 1 9 7 2 I 9 7 1 I 9 7 6 I 9 7 8 1 9 8 0 1 9 8 2 1 9 8 1 1 9 8 6
Y e a r
Lung Cancer ( I C D 162)
Count ry=France Sex=Female
5 0 1
--T. 1 9 8 8
I I I I I I
1 9 6 8 1 9 7 0 1 9 1 2 1 9 1 4 1 9 7 6 1 9 7 8 1 9 8 0 1 9 8 2 1 9 8 1 1 9 8 6 1 9 8 8
Y e a r
FIGURE Z (Continued)

DAWS el 81.: INTERNATIONAL TRENDS IN CANCER MORTALITY
w - D CX
2 0 0 - I .- - 2 1 0 0 - .. 0 I
0 -
Lung Cancer (ICD 162)
Country-West Germany Sex-Male
6 0 0
5 1 : : ' : i 6
+ : : i ' : . : : " " ~ - " : '
Lung Cancer ( I C O 162)
Country-West Germany Sex-Female
1 0

20 ANNALS NEW YORK ACADEMY OF SCIENCES
Lung Cancer (ICD 162)
Country-Italy Sex-Hale
0 5 0 0 0 0
0 0
4 0 0
a, (I
300 a, I
0 G=
2 0 0 A
I
.-
0 I I I I I I I I I
IS68 1910 1 9 7 2 1 9 7 4 1 9 1 6 I 9 7 8 1 9 8 0 1 9 8 2 1 9 8 4 1 9 8 6 I 9 8 8
Y e a r
Lung Cancer (ICD 162)
Country-Italy Sex-Female
0 I I I I I I I I I 1
I 9 6 8 1910 1 9 1 2 I 9 1 4 I 9 1 6 1 9 1 8 1 9 8 0 1 9 8 1 I 9 8 4 1 9 8 6 I 9 8 8
Y e a r
FIGURE 2 (Continued)
DAVIS et 01.: INTERNATIONAL TRENDS IN CANCER MORTALITY 21
Lung Cancer (ICO 162)
Country-England Sexdlale
900
8 0 0 - 0 0 0 7 0 0 -
0 0 6 0 0 - L
n, 5 0 0 - a
0 1 I 1 I I I I I I I
1 9 6 8 1970 1972 1974 1976 1978 1980 19112 I984 I9116 1 9 8 8
Y e a r
Lung Cancer (ICO 162)
Country-England SexIFernale
22
30 -
0 0 0
'O 1 0 0 0
0 0
- 3 0
c
L
w &
20 * - 0 (I
M u l t i p l e Myeloma (ICO-8: 203, ICD-9: 203.0)
Country=Unlted States Sex-Hale
ANNALS NEW YORK ACADEMY OF SCIENCES
1
1
1968 1970 1971 1974 1976 1978 1980 1911 1984 1986 I988
0 I I 1 1 1 1 1 1 1
i 17:: ; := 0
1968 1970 1972 1974 1976 1978 1980 1982 I984 1986 I988
Y e a r
FIGURE 3. Mortality rate per 100,OOO for multiple myeloma (ICD-8 203 and ICD-9 203.0) in men and women in six countries. Age groups defined in FIG. 1.

DAVIS el 41.: INTERNATIONAL TRENDS IN CANCER MORTALITY 23
Multiple Myeloma (ICO-8: 203, ICD-9: 203.0)
Country-Japan Sex=Hale
I 1 - 16 - 1 5 -
0 0 I + -
I 3 - 0 1 2 - 0
1 1
L 1 0
a 9 -
w 8 -
0 7 -
- -
u
E
x - 5 - ._
3 -
L 2 -
I 1 -
0 -
c
1 I I I I I I I I I
Country-Japan Sex=Hale
I 3
0 1 2 0
1968 I970 1972 1971 1916 1978 1980 I982 1981 1986 1988
Y e a r
Multiple Myeloma (ICD-8: 203, ICD-9: 203.0)
Country-Japan Sex-Female
1
4
0 I I I I I I I I I
1 9 6 8 1970 1972 1974 1 9 7 6 I978 1980 1982 1 9 8 4 1986 1 9 8 8
Y e a r
FIGURE 3, (Continued)
24 ANNALS NEW YORK ACADEMY OF SCIENCES
Multiple Myeloma (ICO-8: 203, ICO-9: 203.0)
Country=France Sex=Male
4 0
I
a
-c--c4
1 9 6 8 1 4 7 0 1 5 7 2 1 9 7 4 I 9 7 6 1 9 1 8 1 9 8 0 1 9 8 2 1 9 8 4 1 9 8 6 1 9 8 8
Y e a r
Multiple Myeloma (ICD-8: 203, ICD-9: 203.0)
Country=France Sex-Female ~ _ _
5 0 J
0 0 0
0 0 - 2 0 -
PI
2_ -
I +--- I ' I ' -- 7 I I I I I I I I I
1 9 6 8 I 9 7 0 1 9 7 2 1 9 7 4 1 9 7 6 1 9 7 8 1 5 8 0 1 9 8 2 1 9 8 1 1 5 8 6 1 9 8 8
Y e a r
FIGURE 3. (Continued)

DAMS el al.: INTERNATIONAL TRENDS IN CANCER MORTALITY 25
M u l t i p l e Myeloma (ICD-8: 203, ICD-9: 203.0)
Country=West Germany Sex-Hale
j0 1-
1 9 6 8 1 9 7 0 1 9 1 2 1 9 1 4 I 9 7 6 1 9 1 8 1 9 8 0 I982 1 9 8 1 1 9 8 6 1 9 8 8
Y e a !
M u l t i p l e Myeloma (ICD-8: 203, ICD-9: 203.0)
Country=West Germany Sex-Female
M u l t i p l e Myeloma (ICD-8: 203, ICD-9: 203.0)
Country=West Germany Sex-Female
1 9 6 8 1 9 7 0 1 9 7 2 1 9 7 1 I 9 7 6 1 9 7 8 1 9 8 0 1 9 8 2 I 9 8 4 1 9 8 6 1 9 8 8
Y e a r
FIGURE 3. (Continued)
26 ANNALS NEW YORK ACADEMY OF SCIENCES
M u l t i p l e Myeloma (ICD-8: 203, ICD-9: 203.0)
Country-Italy Sex=Male
1 9 6 8 1 9 7 0 1 9 7 2 1 9 7 1 1 9 7 8 1 3 7 8 1 5 8 0 1 3 8 2 1 9 8 4 1 3 8 6 1 9 8 8
Y e o r
Multiple Myeloma (ICD-8: 203, ICD-9: 203.0)
Country-Italy SexsFemale
1 2 -
I 1 -
1 0 - 9 -
a
7 -
I I I I I I I I I
1 9 6 8 1 5 7 0 1 9 7 2 1 9 7 1 1 9 7 6 1 9 7 8 1 9 8 0 1 9 8 2 I 9 8 q 1 5 8 6 1 9 8 8
Y e a r
FIGURE 3 (Continued)

DAVIS et ul.: INTERNATIONAL TRENDS IN CANCER MORTALITY
Multiple Myeloma (ICD-8: 203, ICD-9: 203.0)
Country-Enpland Sex-Wale
0 0 0
0 0
. 30
c
L
u a
2 0 0, L - n
A L
1 0 .-
I 9 6 8 1970 1972 1974 1976 1978 1 9 8 0 1982 19114 1 9 8 6 I 9 8 8
Y e a r
Multiple Myeloma (ICD-8: 203, ICD-9: 203.0)
Country-England Sex-Female
30
ANNALS NEW YORK ACADEMY OF SCIENCES
Kidney and Unspeci f ied U r i n a r y Cancer ( I C D 189)
Country-United S t a t e s Sex=Hale I
4 0
a 20 ]I”--
1 9 6 8 1 9 1 0 1 9 1 2 1 9 7 1 1 9 7 6 1 9 1 8 1 9 8 0 1 9 8 2 1 9 8 1 1 9 8 6
Y e o r
Kidney and Unspeci f ied Ur inary Cancer ( ICD 189)
C o u n t r y 4 n i t e d States Sex=Female
1988
I 1 I I I I
1 9 6 8 I S 7 0 1 9 7 2 1 9 7 1 1 9 7 6 1 9 7 8 1 9 8 0 I982 1 9 8 4 1 9 8 6 1 9 8 8
Y e a r
FIGURE 4. Mortality rate per 1OO.OOO for kidney and unspecified urinary cancer (ICD 189) in men and women in six countries. Age groups defined in FIG. 1.

DAVIS et 01.: INTERNATIONAL TRENDS IN CANCER MORTALITY 29
Kidney and unspecified Urinary Cancer (ICD 189)
Country-Japan Sex-Hale
0 I I I I I I I I I I
1 9 6 8 1 9 7 0 1972 I974 I976 1978 1 9 8 0 1982 1 9 8 4 I986 I988
Y e o r
Kidney and Unspecified Urinary Cancer (ICD 189)
Country-Japan Sex-Female
1 1
1968 1970 1972 I974 1 9 7 6 I978 I 9 8 0 1982 1984 1 9 8 6 1988
Y e a r
FIGURE 4 (Continued)

ANNALS NEW YORK ACADEMY OF SCIENCES
Kidney and Unspecified Urinary Cancer (ICO 189)
Country-France Sex-Male
5 0 -
0
0
0 0
4 0 -
-
0 2 0 CL
0 I I I I I I 1 I I
1 9 6 8 1 9 7 0 1 9 7 2 I 9 7 4 1 9 7 6 I 9 7 8 1 9 8 0 I 9 8 2 1 9 8 4 1 9 8 6 1 9 8 8
Y e a r
Kidney and Unspecified Urlnary Cancer (ICD 189)
Country-France Sexsfemale
0 I I I I 1 I I I I I
1 9 6 8 I 9 7 0 1 9 7 2 1 9 7 4 1 9 7 6 1 9 7 8 1 9 8 0 I 9 8 2 19114 1 9 8 6 I 9 8 4
Y e o r
FIGURE 4 (Continued)

DAVIS el aZ.: INTERNATIONAL TRENDS IN CANCER MORTALITY 31
Kidney and Unspecified Urinary Cancer (ICD 189)
CountryPWest Germany Sex-Male
70
1968 I970 1972 1971 1976 I978 1980 1982 1981 1986 1988
Y e a r
Kidney and Unspecified Urinary Cancer (ICD 189)
Country-nest Germany Sex-Female
1 0 7
1968 1970 1972 197k 1976 1978 1980 1982 1 9 8 4 I986 1988
Y e s r
FIGURE 4 (Continued)

32 ANNALS NEW YORK ACADEMY OF SCIENCES
Kidney and Unspecified Urinary Cancer (ICD 189)
Country=Italy Sex=Male
7
0 I I I I I I I I I
1 9 6 8 1910 1 9 7 2 1 9 7 4 1 9 7 1 I978 1 9 8 0 1 9 8 2 1 9 8 1 I986
Y e a r
Kidney and Unspecified Urinary Cancer (ICD 189)
Country=Italy Sex=Female
1 9 8 8
16 - 1 5 - I 4 -
0 I 3 -
- 1 2 ~
0
0
Lr- I I 1 - 1 I I I I 9 6 8 I 9 7 0 1 9 7 2 1 9 7 1 1 9 7 6 1 9 7 8 1 9 8 0 1 9 8 2 1 9 8 4 I 9 8 6 1 9 8 8
Y e a r
FIGURE 4 (Continued)
DAVIS er el.: INTERNATIONAL TRENDS IN CANCER MORTALITY 33
Kidney and Unspecified Urinary Cancer (ICO 189)
Country-England Sex-Male
1 9 6 8 1 9 7 0 1 9 1 2 l 9 J l 1 9 7 6 l 9 J 8 I 9 8 0 1 9 8 2 1 9 8 1 I 9 1 6 I 9 8 8
Y e a r
Kidney and Unspecified Urinary Cancer (ICO 189)
Country-England Sex-Female
I 9 6 8 1 9 7 0 1 9 7 2 1 9 7 1 1 9 7 6 1 9 7 8 I 9 8 0 1 9 8 2 1 9 8 1 1 9 8 6 19118
Y e o r
FIGURE 4 (Continued)
34
.v 6 0 -
5 0 -
I
0
e
A - 4 0 - 30 - -
0
~ 2 0 -
I 10 -
- 0
0 -
ANNALS NEW YORK ACADEMY OF SCIENCES
C . 4 / ! < ~
+ - - 4 ! < : 4 . ’ 4
I 1 I I 1 I I I I I
B r e a s t Cancer ( I C D 1 7 4 )
Country-Japan Sex-Female
0 - 1 1 1 1 1 1 1 1 1 1 1 1 1 1 1 I 1 1 1
1 9 6 8 1 9 7 0 I 9 1 2 1 9 7 4 1 9 7 6 1 9 7 8 I 9 8 0 1 9 8 2 1 9 8 1 1 9 8 6 1 9 8 8
Y e a 1
B r e a s t Cancer (ICO 174)
Count ry=Uni ted S t a t e s Sex=Female
9 0
DAVIS d d.: INTERNATIONAL TRENDS IN CANCER MORTALITY
5 0 - Lz
x - .-
J D - - c .. 2 0 -
I 1 0 -
0 -
0
Breast Cancer (ICD 174)
CountrylFrance Sex-Female
1 4 0
40.- . 4:-
0 1 0 0 4
35
.-'" ; 7 ? 1: ; a : 0 I 10
0
1 9 6 8 1 9 7 0 1 3 7 2 1 9 7 4 1 9 7 6 1 9 7 8 1 9 8 0 1 9 8 2 I 9 8 4 1 9 8 6 1 9 8 8
Y e a r
FIGURE 5. (Continued)

36
0 1 6 0 - - 1 5 0 -
1 4 0 -
0
: * a :::: 1 1 0
1 0 0 - ,”
I - 0 8 0 - ci
5 0 - .- - 0 1 0 -
3 0 - 0 2 0 -
L .. = 1 0 -
0 -
ANNALS NEW YORK ACADEMY OF SCIENCES
o ; ; ; ! d ~ ~~ / -- ------
9 0 - 5 - c s - - - - :::+z+---- + <-
I I I I I I 1 1 I
Breast Cancer (ICD 174)
Country-Italy Sex-Female
1 9 6 8 1 9 7 0 1 9 7 2 1 9 7 4 1 9 7 6 1 9 1 8 1 9 8 0 1 9 8 2 1984 1 9 8 6 I 9 8 8
Y e o r
FIGURE S (Continued)
DAVIS el al.: INTERNATIONAL TRENDS IN CANCER MORTALITY
0 :::: 1 1 0 0 - 0 0 1 0 0 0 -
0 9 0 0 -
8 0 0 - a 700 -
0
c - a
a 600 -
," 5 0 0 - 1 0 0 -
-
I
- - 3 0 0 5 0 - 2 0 0 - ; 1 0 0 - 4
0 -
37
:/--
6 E s P 5 5 $, $ 5 5 E c, 5 6 5 5 6
5 5 5 5 5 5 : 4 5 E 5 5 5 5 5 c, 5 5
1 5 : : ! : : ! 4 ! : 1 4
I I I I I I I I I
A l l Cancers (ICD 140-239) Except Lung (ICD 162) and Stomach (IC
Country=United States Sex-Hale
9 0 0 -
800 - 0 0 o 7 0 0 - 0
6 0 0 -
4 7 7
1968 1 9 7 0 1 9 7 2 1 9 7 4 1 9 7 6 1 9 7 8 1 9 8 0 19112 1 9 8 4 1 9 8 s 1 9 8 8
Y e a 1
FIGURE 6. Morality rate per 100,000 for all cancers (ICD 140-239) except lung (ICD 162) and stomach (ICD 151) in men and women in six countries. Age groups defined in FIG. 1.

38 ANNALS NEW YORK ACADEMY OF SCIENCES
A l l Cancers ( ICD 140-239) Except Lung ( ICD 162) and Stomach ( ICD 151)
Country-Japan Sex=Male
1 0 0 0
9 0 0
8 0 0
1 0 0
6 0 0
5 0 0
4 0 0
3 0 0
2 0 0
1 0 I
0
1968 1910 1972 I974 1976 I978 1980 1982 1981 1986 1988
Y e a r
A l l Cancers ( I C D 140-239) Except Lung ( ICD 162) and Stomach ( ICD 151)
600
Country=Japan Sex=Fenale
1968 1970 1972 1914 1916 1978 I980 1982 I984 1986 1988
Y e o r
FIGURE 6. (Continued)

1 8 0 0
1 1 0 0 -
0 0
O - 1 2 0 0 -
0 I 4 0 0 - 0 1 3 0 0 -
I 1 0 0 - w I O O O - L
Q a 9 0 0
8 0 0 - ," J O O -
I --- 1 9 6 8 I 9 1 0 1912 1 9 7 4 1976 I 9 1 8 1980 1982 1981 1986
Y e a r
4 ::::I-
.~&A+---a-b--
1988
0 7 0 0 -
6 0 0 - aJ a
W 5 0 0 -
I - 4 0 0 - n
3 0 0 - x - ~
~
200 -
All C a n c e r s (ICD 140-239) Except Lung (ICD 162) and Stomach (ICO 151)
Country=France Sex=Female
B C C 5 "W
- 5
I I I
1968 1970 1972 I 9 7 1 1916 1978 1980 1982 1981 1986 1988
Y e o r
FIGURE 6. (Continued)
40 ANNALS NEW YORK ACADEMY OF SCIENCES
A l l Cancers ( I C D 140-239) E x c e p t Lung ( ICO 162) and Stomach ( ICD 151)
Coun t ry=Wes t Germany Sex=Hale
1 7 0 0 ~
a)
1 6 0 0 -
i s 0 0 - 0 1 4 0 0 - ,---/ 0 I 3 0 0 - T_--
0 I 2 0 0 ~
t i t o -
L I 0 0 0 ~
0 -
a 9 0 0 ,
1 9 6 8 1 9 7 0 1 9 7 2 I 9 7 1 I 9 7 6 1 9 7 8 1 9 8 0 1 9 8 2 1 9 8 4 1 9 8 6 1 9 8 8
Y e a r
A l l Cancers (ICO 140-239) E x c e p t Lung (ICD 162) and Stomach ( ICD 1 5 1 )
Coun t ry=Wes t Germany Sex=Female
1200
700 a a
a
5 0 0 LL
1 9 6 8 1 9 7 0 1 9 7 2 1 9 7 1 1 9 7 6 1 9 7 8 I 9 8 0 1 9 8 1 1 9 R 1 1 9 8 6 1 9 8 8
Y e o r
FIGURE 6. (Continued)

DAVIS ct al.: INTERNATIONAL TRENDS IN CANCER MORTALITY 41
All C a n c e r s (ICD 140-239) Except Lung (ICD 162) a n d Stomach (ICO 151)
Country=Italy Sex=Male
0 1 1 0 0
0 1 0 0 0 0
9 0 0
Y e o r
All C a n c e r s ( I C D 140-239) Except Lung (ICD 162) and S t o m a c h
1 9 6 8 I970 1 9 7 2 1 9 1 4 1 9 7 6 1 9 7 8 1 9 8 0 I 9 8 2 1 9 8 1 1 9 8 6 1 9 8 8
I C D 151)
Country=Italy Sex=Female
9 0 0
0
a I I I I I I I I I
1 9 6 8 1 9 1 0 1 9 7 2 1 9 7 4 1 9 7 6 I 9 1 8 1 9 8 0 1 9 8 2 I 9 8 4 1 9 8 6 I 9 8 8
Y e a r
FIGURE 6. (Continued)

1 5 0 0 -
lk00 -
1 3 0 0 - 0
0 0 I 2 0 0 -
0 f I 0 0
I 0 0 0 -
9 0 0 -
0
a,
1 9 6 8 1 9 7 0 1 9 7 2 1 9 7 4 1 9 7 6 1 9 7 8 I 9 8 0 1 9 8 2 1 9 8 4 1 9 8 6 1 9 8 8
Y e 0 1
A l l Cancers (ICO 140-239) Except Lung (ICD 162) and Stomach (ICD 151)
Country=England Sex=Female
I 0 0 0
I 9 0 0 1
0
q 8 0 0 j2-;--/ 4 0
1
*w -&--
0 dr-rT-r ~~ -,--- 1 1 1 1
1 9 6 8 I 9 7 0 1 9 7 2 I 9 7 4 1 9 7 6 1 9 7 8 I 9 8 D 1 9 8 2 I 9 8 4 1 9 8 6 I988
Y e o r
FIGURE 6. (Continued)

(a) m
ales
(b) f
emal
es
e
IOM
X)'
loo0
100 10
All
ncop
lum
s -
/
-- -- - -
-- - - --
---
*.--
B
mrh
ur .- .-
,-
'7
1 A
ll n
wp
lm
_.
-l
#1
.1
11
1.
~.
-1
l
o!
@ '
'I
'1
'1
" " '
1921
- 19
26 1
931-
193
6.
1941
- 19
46-
1951
. 19
56 1
%1-
1
96
197
1- 1
976
1981
- 19
21-
1926
19
31-
1936
- 19
41-
1946
- 19
51-
19%
19
61-
1966
- 19
71-
1976
198
1-
1925
19
30 I935
1940
I9
45
l9W
19
55
1960
1%
5 19
70
1975
19
80
1965
19
25
19W
19
35
1940
I9
45
1954
I9
55
1960
1%
5 19
70
1975
19
80
1985
FIGURE 7.
Can
cer d
eath
s by
site
and
sex,
1921
to 1
985 (
age-
stan
dard
ized
deat
h ra
te p
er m
illio
n pop
ulat
ion)
. x a
xis =
yea
rs a
nd y
axis
= ra
te p
er m
illio
n (lo
g sc
ale)
. (Fr
om th
e Uni
ted
Kin
gdom
Offi
ce of
Cen
suse
s and
Pop
ulat
ion
Surv
eys.)

44 ANNALS NEW YORK ACADEMY OF SCIENCES
change in the Ninth ICD, an artifactual downturn occurred in recorded multiple myelomamortality inItaly and West Germany. In these countries about halfthe cases were classified as 2 3 8 . 6 a n d hence outside of 203. (The Tenth revision is expected to return to the practice of the Eight ICD, which should increase uniformity of coding regarding multiple myeloma.) In the U.S. SEER program multiple myeloma and breast cancer have the highest confirmation and detection rates of all specific sites of cancer assessed over time.16
The influences of diagnostic and technological changes on recorded cancer deaths are especially difficult to study quantitatively. Computed axial tomographic (CAT) studies and magnetic resonance (MR) imaging techniques only became widely availablein theearly 1980sin the countries studied.25 Moreover, theunited Kingdom and West Germany had longstanding systems of national health insurance, which effectively limit the use of MR and CAT scans. Japan has more CAT scanners per capita thandoestheUnitedStates,andon averagea Japanesecitizenvisitsaphysician three times more frequently than does the U.S. citizen.3s
What of changes in access to medical care? In the United States, Medicare and Medicaid have provided health care since the mid-l960s, while the United Kingdom, West Germany, and Japan have long-established national programs of coverage for basic health care, with special attention for the elderly. The Japanese system includes public and private financing for national health insurance, while those in West Germany and the United Kingdom rely extensively on public programs and rationing of services.
The longer experience with diagnostic radiography in the developed world may have a double-edged impact on recorded cancer mortality differences. The mass diagnostic radiological screening commonly employed in the late 1940s and 1950s was donewithfluoroscopes,which emitted doseequivalents of X-rays that are high by the standards of t0day.3~ To the extent that such screening was widespread, higher exposures could play a role in initiating cancer. In turn, improved capacity to detect cancer in the developed world may enhance the detection rate of some of the very forms of cancer that were caused by earlier radiographic exposures.m
Cultural values and norms can also exert important influences on mortality data. Forinstance,in Japan, thediagnosisof cancercarriesnegativeconnotations, asit once did in much of the developed world. Changes in public discussion of the disease itself can affect recorded trends. Japanese media accounts of the serious illness of the Emperor Hirohito in 1989 did not mention that he had pancreatic cancer until after his death. In contrast, in the United States the surgery for colon cancer of President Reagan was graphically discussed throughout the news media. While we cannot estimate the quantitative influence of such phenomena on recorded cancer mortality rates, it is clear that they do have animpact, aswasevidenced by therecorded increase in breast cancer incidence in the United States after the well-publicized surgery on Betty Ford!1
DISCUSSION
The cancer mortality trends noted here indicate major shifts in types of cancer in several industrial countries within the past two decades, especially in older persons. In the United States, West Germany, and England and Wales, age-specific mortality rates for men and women aged 55 to 84 due to cancer of ill-defined sites continued to increase, while these rates decreased in Italy and Japan. At the same time, in all

DAVIS ct al.: INTERNATIONAL TRENDS IN CANCER MORTALITY 45
countriesstudied, mortalityrates increased in personsover age 54 fromcancer at some specific sites not linked to cigarette smoking, including multiple myeloma, cancer of the breast, brain, and other central nervous system sites, and myeloma, and for all cancer except lung and stomach. Improved diagnosis, greater access to care, or cultural changes in willingness to put cancer on death certificates may account for some of the increases in cancer at specific sites recorded in these countries over the same time period, but are unlikely to explain all of it.
The workshop also discussed several uses of mortality statistics to look at trends in occupational cancer, including changing sex ratiosU and the quality of death cer- tificate data on occupation and longitudinal record linkage studies. Evaluating time trendsin theratioofmale tofemaleratesofcancer avoidsanydiagnosticartefactsthat may be involved since it is not likely that these would substantially vary with gender over the years.O
Concerningpotential occupational factors, for each non-sex-specific site (exclud- ing lung cancer, which is mostly due to smoking) and all types of cancer combined in allcountriesstudiedmen have higherrates of disease than do women. In addition, the ma1e:female ratio of the rates of many forms of cancer is increasing for a number of sites, indicating that the rate of increase is greater for men.u
Within the framework of this analysis it is not possible to quantify the extent to which these recent increases in specific cancers reflect changes in coding practices and diagnostic technology or real changes in environmental andlor occupational expo- sures some two decades past. However, it is unlikely that ascertainment biases are operatingin both men and women in all the major industrial countriesexamined here in the same way over the same time period.
Regardingincreasesin specificcancer in the age group 75-84, the critical questions to be investigated are whether these forms of cancer have been previously underdiagnosed and underreported in the elderly and whether the size of this population has beenconsistently well enumerated in industrial countries. Considering only trends since 1978 in this age group, multiple myeloma, and cancers of breast and brain and other central nervous system sites show continuing increases that merit careful study.
The search for environmental determinants of stomach cancer focuses mainly on diet,8although improvements in food storage9 and reduction of preservatives are also likely to be involved. Reduced use of high sodium preservatives and nitrates may also be factor sin thegeneralreduction of thisimportant cancer typeinindustrialcountries (it remains common in the developing world). While annual per capita consumption of fresh fruits and vegetables has declined,4’ daily availability of such anticarcinogen- containing food is greater year-round because of refrigeration and improved transpor- tation.
Whatever their causes, these shiftingcancer mortality patternsinolder personsin leading industrial countries have important implications for future demands for health care treatment. Worldwide projections include increasing aging of the popu- lation,urbanization, and need for access to medical care and diagnostic technology. In 1985 the world population was increasing at 1.7% per year-developed regions0.6%, developing countries about 2% ?5 Nearly one-fifth of the current U.S. population is over 65. In the Federal Republic of Germany, Italy, Switzerland, and Greece more than one-fifth of the population is expected to be over the age of 60 by the year 2000, with sizeable increases in urbanization as well.” Thus, whatever the causes of these increasedratesofcancer, they predict increasing demandsfor cancer care in industrial countries.

46 ANNALS NEW YORK ACADEMY OF SCIENCES
Once artifacts have been adequately explored, several theoretical explanations for the rising mortality of site-specific cancer in the elderly in industrialized countries need to be studied further. As a cohort, the generation born in the decade spanning the turn of the twentieth century experienced several factors that may put them at increasedriskof contractingcancer. They smoked cigarettescontainingmore tarthan today;46 worked in dirtier workplace^;^' ate fewer fresh fruits and vegetables year- round;45 received doses per procedure of diagnostic r a d i a t i ~ n ; ~ ~ . ~ greater antigenic stimulationfromchronicpandemic diseases (such as the influenza epidemicof 1918); and longer and greater environmental exposures to carcinogenic substances and processes, including poorly controlled exposures from newly introduced household pesticides and chemicals in the 1940s and 1950s. Persons now over age 64 have experienced greater per capita exposure to workplace carcinogens than have younger age groups, not only because they have lived longer but also because they worked at a time when there were fewer environmental and occupational controls. In addition, the proportion of US. workers employed in blue-collar jobs has steadily declined since the late 1950s. Production of some synthetic carcinogens grew exponentially throughout the 1970~.~
In the 1940s, reports of increasing lung cancer deaths were dismissed as artifacts ofbetterdiagnoses." Thechangesreported hereincancerotherthan lung aresogreat that it would be imprudent not to investigate their causes aggressively. Their implications for the developing world should also be seriously weighed.
REFERENCES
5.
6.
7.
8.
9.
10.
11.
12. 13.
PARKIN, D. M., E. LARRA & C. MUIR 1988. Estimates of the worldwide frequency of sixteen major cancers in 1980. Int. J. Cancer 41: 184-197.
GREENBERG, M. 1983. Urbanization and Cancer Mortality. Oxford University Press. New York.
DOLL, R. 1967. Prevention of Cancer: Pointers from Epidemiology. The Nuffield Provincial Hospitals Trust. London.
JUNG, B. & H. HOFFMEISIER 1987. Das Mittler Sterbealter fur Ausgewahlte Todesurachen und die Mortalitatsstruktur in der Bundesrepublic Deutschland 1958 und 1978. Lebensversicherungsmedizin 39: 50-55.
WATERHOUSE, J., C. MUIX, K. SHANMUGARATNAM & J. POWELL, Eds. 1989. Cancer in Five Continents. IARC Sci. Pub. Vol. 5. Lyon.
STANLEY, K., J. STJERNSWARD & V. KOROLTCHOUK. 1988. Cancers of the stomach, lung and breast: Mortality trends and control strategies. World Health Stat. Q. 41: 107-114.
SORENSEN. T.. G. NIELSEN, P. K. ANDERSON & T. TEASDALE. 1988. Genetic and environmental influence on premature death in adult adoptees. N. Eng. J. Med. 318: 727-732.
HOWSON, C. P.,T. HIYAMA& E. L. WYNDER 1986.The decline in gastriccancer: epidemiology of an unplanned triumph. Epidemiol. Rev. 8: 1-27.
COGGON, D., D. J. P. BARKER, R. B. COLE & M. NELSON. 1989. Stomach cancer and food storage. J. Natl. Cancer Inst. 81: 1178-1182.
OFFICE OF CENSUSES AND POPULATION SURVEYS. 1990. Review of the National Cancer Reg- istration Scheme, Report on the Working Group, London. HMSO. London.
DEVESA, S. S.. W. J. BLOT& J. FRAUMENI, JR 1989. Declining lung cancer rates among young men and women in the United States: A cohort analysis. J. Natl. Cancer Inst. 81: 1568-1571.
SCHWARTZ, J. 1990. This volume. CUZICK, J.. R. VELEZ & R. DOLL. 1983. International variations and temporal trends in
mortality from multiple myeloma. Int. J. Cancer. 32 13-19.

DAVIS el d.: INTERNATIONAL TRENDS IN CANCER MORTALITY 47
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
TIJRESON, I., 0. ZEI?CRVALL., J. CLIUCK, J. G. WALDENSTROM & R. VELEZ. 1984. C o m p a h n of trends in the incidence of multiple myeloma in Malmo, Sweden. and other countries. 1950-1979. N. Eng. J. Med. 310: 421-424.
DAVIS, D. L, A. D. LILIENFELD, A. GTIT~~SOHN & M. E. SCHECKENBACH. 1986. Increasing trends in some cancers in older Americans: Fact or artifact? Toxicol. Ind. Hlth. 2
DAVIS, D. L. & J. SCHWARTZ. 1988. Trends in cancer mortality: US. white males and females.
DOLL, R. 1990. Are we winning the fight against cancer?: An epidemiological assessment.
U.S. NATIONAL CANCER INSITNTE. 1990. Cancer Statistics Review, 1973-1987. National
O ~ C E OF CENSUSES AND POPULATION SURVEYS. 1990. Cancer Statistics Registrations, 1985.
WHO Manual of the International Statistical Classification of Diseases, Injuries and
NATIONAL CENTRAL B u ~ u u OF STAnsncs. 1983. Dodsarsaker 1981-official Statistics of
PERCY, C.. E. STANEK & L. GLOCKLER 1981. Accuracy of cancer death certificates and its
JABLON, S., D. THOMPSON. M. M ~ N N E Y & K. MAFIUCHI. 1990. Accuracy of cause of death
HOEL, D. 1990.
127-144.
1968-1983. Lancet k 633-636.
Eur. J. Cancer 26e 500-508.
Institutes of Health. Bethesda, MD.
Series MBI, No. 18.
Causes of Death. 1977. Geneva.
Sweden. Statistics Sweden, S-11581. Stockholm 6,lO.
effect on cancer mortality statistics. Am. J. Pub. Hlth. 71: 242-250.
certification in Hiroshima and Nagasaki, Japan. Ann. N.Y. Acad. Sci. This volume.
25. UN SCXENIIFIC COMMITTEE ON THE E F F E ~ OF ATOMIC RADIATION. Sources, Effects and Risks of Ionizing Radiation. Rewrt to the General Assemblv, Geneva 1988.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38. 39.
40.
OFFICE OF POF&ATION CENSUS& AND SURVEYS. 1984. Final mid-1981 and revised mid-1961 to mid-1980 population estimates for England and Wales. OPCS Monitor p. 1-11.
KURIHARA, M., K. Aow & S. TOMINAGA, Eds. 19S4. Cancer Mortality Statistics in the World. University of Nagoya Press. Nagoya, Japan.
MACINUS, K., Ed. 1982. Trends in Cancer Incidence: Causes and Practical Implications. McGraw-Hill. New York.
I-huus, J. E. 1983. Cigarette smoking among successive cohorts of men and women in the United States during 1900-1980. J. Natl. Cancer Inst. 7k 473-479.
AHLBOM. A. 1990. Some notes on brain tumor epidemiology. Ann. N.Y. Acad. Sci. This volume.
Cvucrc, J. 1990. International time trends for multiple myeloma. Ann. N.Y. Acad. Sci. This volume.
SCHWARTZ, J. 1990. Multinational trends in multiple myeloma. Ann. N.Y. Acad. Sci. This volume.
KOHLMEIER, L. J. REHM & H. HOFFMEISTER 1990. Lifestyle and trends in worldwide breast cancer rates. Ann. N.Y. Acad. Sci. This volume.
W A O E N ~ D. 1990. Patterns of melanoma deathsin the United States. Ann. N.Y. Acad. Sci. This volume.
LOPEZ, A. 1990. Competing causes of death: a review of recent trends in mortality in industrialized countries with special reference to cancer. Ann. N.Y. Acad. Sci. This volume.
NATIONAL CANCER INSITNTE. 1990. Annual Cancer Statistics Review 1973-1987. National Institutes of Health. Bethesda. Md.
PERCY, C. & C. Mrnu 1989. The international comparability of cancer mortality data. Am. J. Epidemiol. l2% 934-946.
IOLEHART, J. K. 1988. Japan’s medical care system. N. Eng. J. Med. 319: 807-812. MORGAN, K. Z. 1967. History of damage and protection from ionizing radiation. I n Prin-
ciples of Radiation Protection: A Textbook of Health Physics. K. Z. Morgan & J. E. Turner, Eds. Wiley. New York.
MILLER, A. B., G. R. HOWE, G. J. SHERMAN ef al. 1989. Mortality from breast cancer after irradiation during fluoroscopic examinations in patients being treated for tuberculosis. N. Engl. J. Med. 32k 1285-1289.

48 ANNALS NEW YORK ACADEMY OF SCIENCES
41.
42.
43.
44. 45.
46.
47.
48. 49.
BETSILL, W. L., B. F. BYRD, JR. & W. H. HARTMANN. 1975. Breast cancer report. Cancer 36c
WWGARD, D. The sex differential in life expectancy at birth and its components. In World
NICHOLSON, W. J. 1988. IARC evaluation in the light of limitations of human epidemiologic
NICHOLSON, W. J. & D. L. Davis. 1990. This volume. NATIONAL RESEARCH COUNCIL, DIET AND HEALTH. 1989. National Academy Press. Wash-
ington, D.C. U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES. 1981. The health consequences of
smoking: the changing cigarette, a report of the Surgeon General. Washington, DC. KAZANTIS, G. & J. C. MCDONALD. 1986. Work, health and disease. In Epidemiology of
Occupational Health, M. Karvonen & Mikheev, Eds. World Health Organization Regional Publications, European Series no. 20. Copenhagen.
DAVIS, D. L. & B. MCGEE. 1979. Cancer and chemical production. Science #)6: 1356-1358. HEADY, J. A. & E. L. KENNAWAY. 1949. The increase in death attributable to cancer of the
305-307.
Population Trends and Policies: 1979. Monitoring Report, 1980. New York.
data. Ann. N.Y. Acad. Sci. 53a: 44-54.
lung. Br. J. Cancer 3 311-320.
APPENDIX
Collegium Ramazzini Attendees
Anders Ahlbom (Sweden) Stephen Levin (United States) Olav Axelson (Sweden) Alan Lopez (Australia) John Bailar (Canada) Jeffrey Lybarger (United States) Louis Beliczky (United States) Hans Malker (Sweden) Jan Carstensen (Sweden) Cesare Maltoni (Italy) Thomas Chalmers (United States) Berlin Mathas (Czechoslovakia) Jorge Chiriboga (Puerto R im) Anthony Mazzocchi (United States) Jack Cuzick (United Kingdom) David Muir (South Africa) Devra Lee Davis (United States) William Nicholson (United States) Anders Englund (Sweden) Anna Palazzini (Italy) Jacques Estbve (France) Carmentano Pasquale (Italy) Francesco Forrestiere (Italy) Constance Percy (United States) John Fox (United Kingdom) Elihu Richter (Israel) Larry Garfinkel (United States) Ermanno Rondini (Italy) Bernard Goldstein (United States) Marvin Schneiderman (United States) Fengsheng He (China) Joel Schwartz (United States) Clark Heath, Jr. (United States) Herbert Seidman (United States) David Hoe1 (United Stares) Irving Selikoff (United States) Hans Hoffmeister (Federal Republic of Germany) Tony Swerdlow (United Kingdom) Seymour Jablon (United States) Hirayama Takeshi (Japan) Howard Kelman (United States) Diane Wagener (United States) Lenore Kohlmeier (Federal Republic of Germany) Gun Wingren (Sweden) Philip Landrigan (United States) Songnian Yin (China) Audrey Lange (Poland)