Potentially inappropriate prescribing in elderly outpatients in Croatia
Upload
independentCategory
view
4download
0
European Neuropsychopharmacology (2014) 24, 499–509
0924-977X/$ - see frohttp://dx.doi.org/1
nCorresponding auE-mail addresses
[email protected]@imperia
www.elsevier.com/locate/euroneuro
Quality of prescribing for schizophrenia:Evidence from a national audit in Englandand Wales
Maxine X. Patela,n, Delia Bisharab, Simone Jayakumarc,Krysia Zalewskac, David Shiersc, Mike J. Crawfordd,Stephen J. Cooperc
aInstitute of Psychiatry, King's College London, Department of Psychosis Studies, Box 68,16 De Crespigny Park, London SE5 8AF, United KingdombPharmacy Department, South London and Maudsley NHS Foundation Trust, Denmark Hill,London SE5 8AZ, United KingdomcCollege Centre for Quality Improvement, Royal College of Psychiatrists, 21 Prescot Street,London E1 8BB, United KingdomdFaculty of Medicine, Imperial College London, Centre for Mental Health, Claybrook Centre. 37,Claybrook Road, London W6 8LN, United Kingdom
Received 27 November 2013; accepted 11 January 2014
KEYWORDSSchizophrenia;Antipsychotic;Dose;Prescribing
nt matter & 20140.1016/j.euroneur
thor. Tel.: +44 20: [email protected] (S. Jayl.ac.uk (M.J. Craw
AbstractThe National Audit of Schizophrenia (NAS) examined the quality of care received in England andWales. Part of the audit set out to determine whether six prescribing standards, set by thenational clinical guidelines for schizophrenia, were being implemented and to promptimprovements in care. Mental Health Trusts and Health Boards provided data obtained fromcase-notes for adult patients living in the community with schizophrenia or schizoaffectivedisorder. An audit of practice tool was developed for data collection. Most of the 5055 patientsreviewed were receiving pharmacological treatment according to national guidelines. However,15.9% of the total sample (95%CI: 14.9–16.9) were prescribed two or more antipsychoticsconcurrently and 10.1% of patients (95%CI: 9.3–10.9) were prescribed medication in excess ofrecommended limits. Overall 23.7% (95%CI: 22.5–24.8) of patients were receiving clozapine.However, there were many with treatment resistance who had no clear reason documented asto why they had not had a trial of clozapine (430/1073, 40.1%). In conclusion, whilst mostpeople were prescribed medication in accordance with nationally agreed standards, there was
Elsevier B.V. and ECNP. All rights reserved.o.2014.01.014
7848 0138; fax: +44 20 7848 0572.l.ac.uk (M.X. Patel), [email protected] (D. Bishara),akumar), [email protected] (K. Zalewska), [email protected] (D. Shiers),ford), [email protected] (S.J. Cooper).

M.X. Patel et al.500
considerable variation between service providers. Antipsychotic polypharmacy, high doseprescribing and clozapine underutilisation in treatment resistance were all key concerns whichneed to be further addressed.& 2014 Elsevier B.V. and ECNP. All rights reserved.
1. Introduction
Antipsychotic drugs have been the mainstay for the manage-ment of schizophrenia for over half a century. Their efficacy hasbeen established for the treatment of acute episodes (NationalInstitute for Clinical Excellence, 2009), and for maintenancetreatment by substantially reducing the risk of relapse (Leuchtet al., 2012b, 2012a). The benefits of these drugs must howeverbe weighed against their adverse effects (Carlson et al., 2006;Leucht et al., 2012b). Recommendations from the BritishAssociation for Psychopharmacology (Barnes, 2011) and theNICE guideline (National Institute for Clinical Excellence, 2009)recommend avoiding antipsychotic polypharmacy in the major-ity of cases. Also, there is no convincing evidence that doses ofantipsychotic drugs higher than the recommended maximumadvised in the BNF (British National Formulary) (BMJ Group andRPS Publishing, 2013) afford additional clinical benefit overstandard doses. High doses lead to greater risk of dose-relatedadverse effects such as cardiac sudden death (Barnes, 2011)and polypharmacy has been linked to higher rates of metabolicsyndrome and lipid markers of insulin resistance (Correll et al.,2007). Nevertheless, previous studies both in the UK (Patonet al., 2008) and worldwide (Agid et al., 2013; Faries et al.,2005; Ganguly et al., 2004; Kreyenbuhl et al., 2007; Procyshynet al., 2001; Sim et al., 2004) have shown that high doseantipsychotic prescribing and polypharmacy are common prac-tice. An audit of antipsychotic usage in New Zealand confirmedUK findings (Lelliott et al., 2002) that antipsychotic polyphar-macy is strongly associated with a combined daily dose inexcess of standard practice (Humberstone et al., 2004).Similarly, a Canadian study reported that a third of patientsare discharged on an antipsychotic polypharmacy regimen(Procyshyn et al., 2001). Studies in the US (Faries et al.,2005; Ganguly et al., 2004) and East Asia (Sim et al., 2004)found antipsychotic polypharmacy to be present for approxi-mately 50% of patients.
The term “treatment resistant” in schizophrenia is used todescribe people who have not adequately responded to med-ication despite adequate dose, duration and adherence(National Institute for Clinical Excellence, 2009). Since theaverage rate of non-adherence among patients with schizo-phrenia has been reported as 58% (range 24–90%) (Cramer andRosenheck, 1998) adherence should always be assessed in casesof non-response (National Institute for Clinical Excellence,2009). Furthermore, studies have shown that patients withpsychosis and coexisting substance misuse generally showpoorer response to treatment (National Collaborating CentreFor Mental Health, 2011). Where treatment resistance forschizophrenia does exist, the superiority of clozapine againstother agents has been established in large pragmatic clinicaltrials such as CATIE (McEvoy et al., 2006) and CUtLASS (Lewiset al., 2006) and yet, low rates of clozapine use are stillapparent in clinical practice (Weissman, 2002). Guidelines fromboth the UK (NICE (National Institute for Clinical Excellence,
2009)) and the US (Patient Outcomes Research Team —PORT(Buchanan et al., 2010)) recommend that clozapine should beoffered to all patients who continue to experience clinicallysignificant symptoms after two adequate trials of other anti-psychotics (National Institute for Clinical Excellence, 2009).Nevertheless, one study found that patients had received onaverage five antipsychotics before being prescribed clozapinewhich had been delayed for an average of five years longer thanis clinically desirable (Taylor et al., 2003). Clinician's knowl-edge, attitudes and preferences are likely predictive factors forthe variation in clozapine prescribing patterns (Patel, 2012).Furthermore, not all treatment resistant patients will respondadequately to clozapine and there is a lack of clear guidance onhow to manage those who fail to respond. Despite limitedevidence and modest improvement at best (Taylor et al., 2012),NICE suggests considering the addition of a second antipsychoticdrug to clozapine to augment its effects (National Institute forClinical Excellence, 2009). In contrast, the PORT guidelines donot support augmentation therapy due to insufficient efficacyand safety data (Buchanan et al., 2010).
The National Audit of Schizophrenia (NAS) set out toobtain a comprehensive picture of the quality of carereceived by individuals with schizophrenia and schizoaffec-tive disorder in England and Wales. Since a national guide-line already exists (National Institute for ClinicalExcellence, 2009), the audit objective was to examinewhether this was being implemented and to promptimprovements in the care of patients with these conditions.Specifically it aimed to quantify the degree of prescribing ofantipsychotics at high dose, the rates for antipsychoticpolypharmacy, and also the nature of clozapine prescribingat a national level, thereby overcoming concerns aboutsampling and generalisability of smaller scale studies.
2. Experimental procedures
2.1. Setting
NAS is a cross-sectional survey of patients involving retrospectiveexamination of clinical records and collection of specific contem-poraneous data. It is an audit of practice at the level of individualTrusts and does not allow conclusions to be drawn at the level ofindividual clinical teams. The term 'Trust' has been used to refer toboth English Trusts and Welsh Health Boards throughout. All Trustsin England and Wales were expected to participate if they providedcare or treatment in the community for adults with schizophrenia.Sixty of the 64 organisations identified as being eligible by the NASteam submitted data. Further details are available in the nationalreport (Royal College of Psychiatrists, 2012).
2.2. Development
Standards and outcome indicators were developed in June-August2010 and the audit tools were then developed. Six Mental Health

501Quality of prescribing for schizophrenia: Evidence from a national audit in England and Wales
Trusts in England signed up to the pilot phase of NAS (October 2010March 2011) including data collection based on case notes reviewfor 50 patients. The main purpose of the pilot was to test all aspectsof the audit before the main audit was launched. In June 2011,based on the findings from the pilot phase, the standards, outcomeindicators, tools and methodology were refined and finalised. Priorto the start of the main audit, the Trust audit leads were given cleartimelines for identification of their individual case sample andpreparation of their clinical teams for data collection. Eachparticipating Trust identified a NAS audit lead to co-ordinate datacollection. Each NAS audit lead was sent a comprehensive pack ofmaterials to support them and a flow diagram of the process.
2.3. Six antipsychotic prescribing standards
2.3.1. Antipsychotic monotherapyThe patients are currently only prescribed a single antipsychoticdrug (unless they are in a short period of overlap while changingmedication or because clozapine is co-prescribed with a secondantipsychotic).
2.3.2. DoseThe current total daily dose of antipsychotic drug does not exceedthe upper limit of the dose range recommended by the BritishNational Formulary (BNF). If it does, the rationale for this has beendocumented.
2.3.3. Adherence and substance misuseIf there was no or inadequate response to the first antipsychoticdrug prescribed after a minimum of four weeks at the optimumdose: (i) medication adherence was investigated and documented;(ii) the potential impact of alcohol or substance misuse on responsewas investigated and documented.
2.3.4. Adequate trialsIf there was no or inadequate response to the first antipsychoticdrug after a minimum of four weeks at optimum dose the firstantipsychotic drug should be stopped and a second antipsychoticdrug given. At least one of the first two drugs should be a secondgeneration antipsychotic.
2.3.5. ClozapineIf there was no or inadequate response to the second anti-psychotic drug after a minimum of four weeks at optimum dose,clozapine was offered.
2.3.6. Clozapine augmentationIf there was no or inadequate response to treatment despite anadequate trial of clozapine, a second antipsychotic was given inaddition to clozapine for a trial period of at least eight weeks atoptimum dose.
2.4. Main sample
Patients were eligible for inclusion if they met the followingcriteria: (i) aged 18 years or over; (ii) being treated in thecommunity (not inpatients) and been under the care of the Trustfor at least 12 months; (iii) current ICD-10 diagnosis of F20.0–F20.9(schizophrenia) or F25.0–F25.9 (schizoaffective disorder), withdiagnosis established for at least 12 months and made before theage of 60 years. Patients were excluded from the sample if thepatient was receiving inpatient treatment at the time of the audit,known to live in a nursing home, residential home or continuingcare, or they had requested that they must be contacted viaanother person. To increase the generalisability of the sample,those on community treatment orders were not excluded.
Each Trust was asked to identify all patients meeting theeligibility criteria for the audit on a locally agreed census date.One of two sampling options was selected by the Trust (or acombination of both where sampling proved more difficult): eitheridentification of patients centrally or identification through thecommunity mental health teams. The Trust then had to randomlyselect 100 of these patients using established randomisationtechniques, the online randomisation tool suggested by NAS, or toask the NAS team to generate these random numbers.
The sample size was based on the ability to detect a differencein compliance with audit standards between different serviceproviders. Findings from a pilot study indicated that each Trustwould need to submit data on 73 patients, for 80% power to detecta 12% difference in compliance with standards between Trusts at a5% significance level. To take account of incomplete responses wetherefore asked Trusts to complete 100 audit forms.
2.5. Tools
The NAS Audit of Practice Tool was developed to collect data forindividual patients regarding demographics, antipsychotic prescrib-ing practice, physical health monitoring, physical health interven-tions and psychological therapies offered. This information was tobe gleaned largely from a patient's case notes but also fromconsultants and general practitioners (GPs) if required. Onlyregularly prescribed antipsychotics were recorded as it was antici-pated that community patients are unlikely to receive PRN pre-scriptions. The Audit of Practice Tool was developed from audittools designed by the Prescribing Observatory for Mental Health(POMH-UK), the Health of the Nation Outcomes Scale (HoNOS)(Royal College of Psychiatrists, 1996) and included bespoke ques-tions developed specifically to measure some NAS standards andoutcome measures. The tool was developed in conjunction with theNAS advisory group, tested and refined through the NAS Pilot andfurther tested and refined with consultant psychiatrists.
2.6. Data capture and statistical analysis
Data were collected between August and November 2011. All datawere entered using SNAP 9 Professional Surveys via secure web-pages and then analysed using PASW Statistics 18 (SPSS) or MicrosoftExcel 2007. Data cleaning was conducted to check for any duplica-tion of data, missing data, unexpected values and that the samplingcriteria were followed correctly. Any suspected data errors wereemailed back to Trusts along with their datasets for clarification andamendments were made as necessary. If an antipsychotic PRN wasrecorded under “other antipsychotic medication” (n=6, all had aregular antipsychotic recorded), this information was not includedin this dataset as PRN medication was not consistently captured forall patients and thus would in all likelihood lead to substantialunderestimation of the magnitude of such prescribing. Each dose ofantipsychotic medication that a patient was receiving was con-verted into a percentage of the maximum licensed dose for thatdrug as described in the British National Formulary (%BNF) (BMJGroup and RPS Publishing, 2013). For antipsychotic polypharmacy,the %BNF was calculated for each drug dose and the values werethen summated. High dose prescribing was defined as being 4100%BNF. If a short-acting intramuscular antipsychotic was recorded, thisinformation was not considered in the analysis as it not possible tonot calculate %BNF due to lack of ongoing frequency of doseadministration data. Descriptive statistics including frequencieswith 95% Confidence Intervals (CI) as well as cross tabulations wereconducted. After receiving their NAS Trust Level Report, Trusts weregiven the opportunity to alert the NAS team to any errors intheir data.

Table 1 Sample characteristics (n=5055).
n %
SociodemographicsGenderMale 3277 64.8Female 1774 35.1Not stated 4 0.1Age bands (years)18–24 220 4.425–34 984 19.535–44 1389 27.545–54 1268 25.155–64 774 15.365+ 420 8.3EthnicityWhite 3945 78.1Black 428 8.5Asian 410 8.1Mixed 93 1.8Other 76 1.5Not stated 103 2.0
Clinical FactorsDiagnosisSchizophrenia 4295 85.0Schizoaffective disorder 760 15.0Current mental health statusFull Remission 1082 21.4Partial remission with minimal symptoms/
disability2539 50.2
Partial remission with substantial symptoms/disability
1137 22.5
Not in remission 297 5.9Time since diagnosis (years)1–2 252 5.02–4 489 9.74–10 1296 25.6410 3018 59.7Team typeAssertive Outreach Team 610 12.1Community Mental Health Team 3533 69.9
M.X. Patel et al.502
3. Results
3.1. Sample characteristics
The mean number of records returned per Trust was 85(SD 20, range 17–134); 83% of included Trusts achieved at least73 records; 27% of Trusts achieved 100 records. Twenty-eight Trusts reported that they used the central identifica-tion of patients sampling option, and 10 reported that theyused the identification through the community mentalhealth teams sampling option, Four used other samplingmethods, which included a combination of the two samplingoptions. The remaining 18 Trusts did not provide informa-tion regarding the sampling method.
There were 5091 patient records submitted using the Auditof Practice Tool originating from 60 Trusts, from which 23 wereexcluded as they had antipsychotics recorded which were notlicensed in the UK (penfluridol (n=1), oral fluphenazine (17),thioridazine (1), zotepine (4)). Also 13 patients were excludeddue concerns about data quality as the dose for a singleantipsychotic was greater than four times the maximumlicensed dose as this was highly suggestive of a dose recordingerror. Of the 5055 patients included in the analysis set, 4792(94.8%) were prescribed regular antipsychotics (including 57for whom a short-acting intramuscular antipsychotic was alsorecorded in addition to a regular antipsychotic but not thosefor whom the only antipsychotic recorded was a short-actingintra-muscular antipsychotic (n=100). Short-acting intramus-cular antipsychotic data was disregarded for the remainder ofthe analysis.
The majority were male (64.8%) and 85.0% had a diagnosisof schizophrenia. The proportion of females with a diagnosis ofschizoaffective disorder was significantly higher than for males[405/1774 (22.8%) vs 354/3277 (10.8%), po0.001]. The meanage was 45 years (SD 13, range 18–93 years) and the majority(59.7%) had an illness duration greater than 10 years. Themajority were seen by community mental health teams(69.9%) although some were seen by specialist teams such asearly intervention (5.7%) or assertive outreach (12.1%). At thetime of the audit, 1434 (28.4%) were classified as being not inremission or in partial remission but with substantial symp-toms/disability (see Table 1).
Crisis Resolution Team 10 0.2Early Intervention 287 5.6Other 615 12.2
3.2. Choice of antipsychotic(s) and dose
Of the 5055 cases included in the analysis set, 5.2% were notprescribed a regular antipsychotic either in oral or long-acting injection formulation. Of the total sample, 36.5%were prescribed only one non-clozapine oral antipsychotic,24.0% were prescribed only one long-acting injection (pre-dominantly first generation antipsychotic, 17.5%), and 18.4%were prescribed clozapine as monotherapy. Overall, 1590patients (31.5%, 95%CI: 30.2–32.7) were prescribed anantipsychotic long-acting injection with comparativelyhigher rates for assertive outreach (240/610, 39.3%) andlower for early intervention teams (46/287, 16.0%).
Of the total sample, antipsychotic polypharmacy occurredin 15.9% (95%CI: 14.9–16.9, Trusts range 5.9–32.8%); thisinvolved only non-clozapine antipsychotics for 10.6% andincluded clozapine for 5.3% of the sample. Much of theantipsychotic polypharmacy, either with or without clozapine,
involved combination with a first and/or second generationantipsychotic long-acting injection (7.5%). For polypharmacywith clozapine, amisulpride and aripiprazole were mostcommonly chosen (see Table 2). Documentation of therationale for polypharmacy was not evaluated.
For the total sample, the mean total dose (includingantipsychotic polypharmacy) was 59.1%BNF (95%CI: 57.7–60.4, range 0.2–550.0). High dose prescribing occurredfor 511 (10.1%, 95%CI: 9.3–10.9%) patients with variationbetween Trusts (range 1.0–24.1%). The rationale for highdose prescribing was documented for only 129/511 (25.2%)patients overall. For those exceeding 100%BNF, the meanantipsychotic total dose was 150.2%BNF (SD 57.1). Findings

503Quality of prescribing for schizophrenia: Evidence from a national audit in England and Wales
also revealed that patients with antipsychotic polypharmacyhad a higher total mean dose than those prescribed only oneantipsychotic (98.8% vs 51.0% t=22.7 po0.001). Of all thecategories of monotherapy and polypharmacy in Table 2which included more than 5 patients, only clozapine mono-therapy was not associated with high dose prescribing asboth the mean dose and the range did not exceed 100%BNF.
3.3. Medication non-adherence and impact ofsubstance misuse on response
There were 1434 patients either not in remission or inpartial remission with substantial symptoms/disability. Med-ication adherence was reported as having been investigatedin 85.6% of those not on clozapine and in 87.8% of those onclozapine. The investigation of alcohol or other substancemisuse as a factor for poor response was less well reported,with only 77.7% of patients not on clozapine having hadthese factors considered and 80.6% of cases prescribedclozapine. Some degree of variation between Trusts wasevident (see Table 3).
Table 2 Means and ranges of doses for antipsychotic monothe
Number and type of antipsychotics Total
n %
No antipsychotic 263 5.21 Antipsychotic, not clozapine 3060 60.5FGA oral 184 3.6SGA oral 1663 32.9FGA-LAI 884 17.5SGA-LAI 329 6.5
2 Antipsychotics, not clozapine 519 10.3orals: FGA+SGA 60 1.2orals: SGA+SGA 94 1.9orals: FGA+FGA 7 0.1FGA-LAI+oral FGA 71 1.4FGA-LAI+oral SGA 198 3.9SGA-LAI+oral SGA 77 1.5SGA-LAI+oral FGA 7 0.1FGA-LAI+FGA-LAI 3 o0.1FGA-LAI+SGA-LAI 2 o0.1
Z3 Antipsychotics, not clozapine 17 0.3FGA-LAI+any Z2 orals, not clozapine 11 0.2SGA-LAI+any Z2 orals, not clozapine 3 o0.1Any Z3 orals, not clozapine 3 o0.1
Clozapine only 930 18.42 Antipsychotics, including clozapine 264 5.2Clozapine+aripiprazole 68 1.3Clozapine+amisulpride 112 2.2Clozapine+any other oral SGA 33 0.7Clozapine+oral FGA 46 0.9Clozapine+FGA-LAI 2 o0.1Clozapine+SGA-LAI 3 o0.1
Z3 Antipsychotics, including clozapine 2 o0.1
FGA first generation antipsychotic; SGA second generation antipsyclicensed dose in the British National Formulary.
3.4. Adequate trials of antipsychotic treatmentprior to clozapine
For those currently prescribed clozapine and either not inremission or in partial remission with substantial symptoms/disability (n=361), there were 277 cases (76.7%) who had atleast two antipsychotics for at least 4 weeks prior toclozapine, which usually included at least one SGA(n=263). However there were 34 cases (9.4%) who appearedto have only received one antipsychotic prior to commencingclozapine, most commonly an SGA (n=32) (see Figure 1).Furthermore there were 13 cases (3.6%) prescribed cloza-pine who have not had a previous inadequate response toantipsychotic treatment and were presumably commencedon clozapine due to significant adverse effects of theirprevious treatment(s).
For those currently not prescribed clozapine and eithernot in remission or in partial remission with substantialsymptoms/disability (and yet under the care of the Trust forat least 12 months), 774/1073 (72.1%) cases had beenreceiving their current antipsychotic at optimal dose forat least four weeks. Of these, 656/774 (84.8%) had receiveda different antipsychotic at optimal dose for at least four
rapy and polypharmacy combinations (n=5055).
Range across Trusts Prescribed dose (% BNF)
% Mean Range
0.0–11.4 – –
40.5–75.6 53.3 0.2–400.00.0–10.5 43.7 0.3–400.0
15.5–53.4 57.9 0.2–312.54.1–37.1 34.1 0.3–350.00–14.8 87.3 6.7–224.0
2.6–27.0 103.5 8.3–550.00.0–4.8 108.3 13.3–400.00.0–5.7 112.8 22.1–245.80.0–1.4 76.7 24.5–130.00.0–3.7 75.8 8.3–241.7
0.0–14.0 99.0 9.2–550.00.0–5.8 131.0 50.0–406.30.0–2.0 94.1 40.0–133.30.0–1.2 79.3 29.0–105.00.0–1.4 54.8 24.7–85.00.0–2.0 185.5 56.7–390.00.0–2.0 192.2 56.7–390.00.0–1.4 184.0 148.1–218.80.0–1.7 162.6 149.4–180.0
6.2–31.5 43.5 1.4–100.00.0–17.6 84.0 23.3–188.90.0–17.6 91.4 44.4–100.00.0–10.5 83.6 27.8–188.90.0–3.9 88.9 40.0–163.30.0–6.2 72.8 36.1–122.20.0–1.4 44.8 25.6–63.90.0–1.3 72.1 23.3–133.30.0–5.9 124.7 107.8–141.7
hotic, LAI long-acting injection; %BNF percentage of maximum

Table 3 Subgroup of patients not in remission or in partial remission with substantial symptoms/disability (n=1434) andassessments regarding adherence and alcohol or substance misuse.
Sub-group Adherence investigated Substances/alcohol considered
N N % Trust range% n % Trust range %
Not on clozapine 1073 919 85.6 58.3–100.0 834 77.7 50.0–100.0On clozapine 361 317 87.8 50.0–100.0* 291 80.6 33.3–100.0
nExcludes one Trust where only 1 patient was on clozapine and not in remission and adherence was not investigated.
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
10 15 20 34 36 39 42 44 48 56 60 61 63 64 05 69 06 52 04 19 45 49 14 17 53 54 01 29 65 33TNS 12 31 28 08 35 50 13 41 03 11 16 24 30 47 68 07 21 26 67 09 25 37 38 46 51 70 59 43
Had at least two antipsychotics, one of which was a second-generation antipsychoticHad at least two antipsychotics, neither of which was a second-generation antipsychoticHad one second-generation antipsychoticHad one first-generation antipsychoticPatient did not have an inadequate response to previous medicationsMissing data
Figure 1 Inadequate response to treatment trials, each of at least 4 weeks at optimal dose prior to clozapine, for patients who arenot in remission or in partial remission with substantial symptoms/disability (n=361). TNS total national sample.
M.X. Patel et al.504
weeks, thus exceeding the guidance for minimum time tointroduction of clozapine.
3.5. Clozapine
Overall, 1196 cases were receiving clozapine (23.7%, 95%CI:22.5–24.8), and there was evidence of evidence of variationacross Trusts (range 7.2–42.0%). Clozapine was prescribed asmonotherapy (n=930, 18.4%) and also with augmentationby other antipsychotics (n=266, 5.3%). Of 1196 cases onclozapine, 361 were considered as being treatment resistantto clozapine as they were either not in remission or theywere in partial remission with substantial symptoms/dis-ability (see Table 4). Of all of those receiving clozapine andanother antipsychotic as augmentation, 111/266 (41.7%)remained treatment resistant to clozapine. Further, therewere 1073 cases who were not prescribed clozapine and
were not in remission or were in partial remission withsubstantial symptoms/disability (21.2%, 95%CI: 20.1–22.4)who were therefore considered as treatment resistantcases. Of these, 430/1073 (40.1%) cases had no clear reasondocumented for them as to why they had not had a trial ofclozapine.
4. Discussion
4.1. Principal findings
The National Audit for Schizophrenia provides the largestsystematically collected UK database of antipsychotic pre-scribing for people with schizophrenia and schizoaffectivedisorder. It builds on former national (Paton et al., 2008)and international (Faries et al., 2005; Humberstone et al.,2004; Procyshyn and Zerjav, 1998) antipsychotic prescribing
505Quality of prescribing for schizophrenia: Evidence from a national audit in England and Wales
audits by examining several key standards directly asso-ciated with NICE guidance (National Institute for ClinicalExcellence, 2009) which are also largely similar to otherinternational guidelines (e.g. PORT (Buchanan et al., 2010)).Our findings highlight that although the appropriate pre-scribing guidelines were followed for most patients, this wasnot the case for all, and there was a significant degree ofvariation in achievement of the individual standardsbetween Trusts. Differences in patient populations or sever-ity of illness are unlikely to fully account for these largevariations, thus indicating that prescribing practice may beimproved in some Trusts. Key areas of concern included:15.9% of the total sample being prescribed more than oneantipsychotic at a time (95%CI:14.9–16.9); 10.1% receivinghigh dose prescribing (95%CI:9.3–10.9, highest recordedtotal dose 550%BNF); and 23.7% were receiving clozapine(95%CI: 22.5–24.8) despite there being significant numbersof patients with treatment resistance who were not pre-scribed clozapine and who also had no clear reason docu-mented as to why (430/1073, 40.1%).
4.2. Adherence, polypharmacy and high dose
For patients not in remission or in partial remission but withsubstantial symptoms/disability, medication adherence wasinvestigated in the majority (86%) but substance or alcoholmisuse was investigated slightly less frequently. Alcohol and
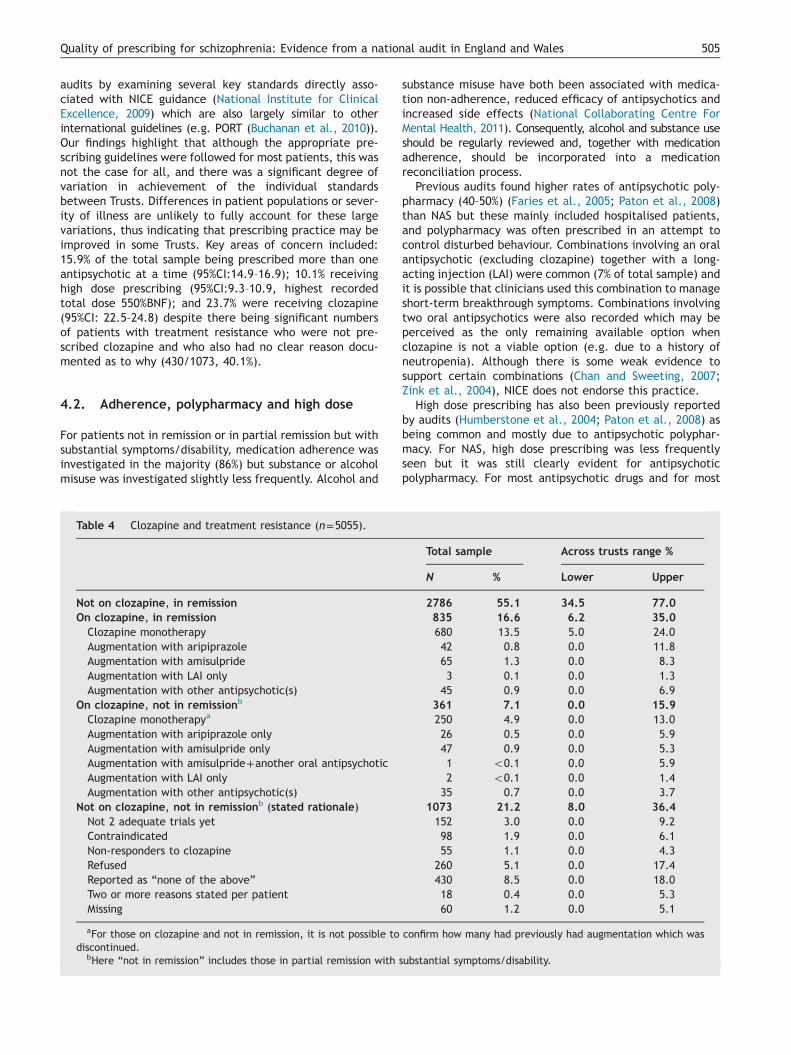
Table 4 Clozapine and treatment resistance (n=5055).
Not on clozapine, in remissionOn clozapine, in remissionClozapine monotherapyAugmentation with aripiprazoleAugmentation with amisulprideAugmentation with LAI onlyAugmentation with other antipsychotic(s)
On clozapine, not in remissionb
Clozapine monotherapya
Augmentation with aripiprazole onlyAugmentation with amisulpride onlyAugmentation with amisulpride+another oral antipsychoticAugmentation with LAI onlyAugmentation with other antipsychotic(s)
Not on clozapine, not in remissionb (stated rationale)Not 2 adequate trials yetContraindicatedNon-responders to clozapineRefusedReported as “none of the above”Two or more reasons stated per patientMissing
aFor those on clozapine and not in remission, it is not possible todiscontinued.
bHere “not in remission” includes those in partial remission with s
substance misuse have both been associated with medica-tion non-adherence, reduced efficacy of antipsychotics andincreased side effects (National Collaborating Centre ForMental Health, 2011). Consequently, alcohol and substance useshould be regularly reviewed and, together with medicationadherence, should be incorporated into a medicationreconciliation process.
Previous audits found higher rates of antipsychotic poly-pharmacy (40–50%) (Faries et al., 2005; Paton et al., 2008)than NAS but these mainly included hospitalised patients,and polypharmacy was often prescribed in an attempt tocontrol disturbed behaviour. Combinations involving an oralantipsychotic (excluding clozapine) together with a long-acting injection (LAI) were common (7% of total sample) andit is possible that clinicians used this combination to manageshort-term breakthrough symptoms. Combinations involvingtwo oral antipsychotics were also recorded which may beperceived as the only remaining available option whenclozapine is not a viable option (e.g. due to a history ofneutropenia). Although there is some weak evidence tosupport certain combinations (Chan and Sweeting, 2007;Zink et al., 2004), NICE does not endorse this practice.
High dose prescribing has also been previously reportedby audits (Humberstone et al., 2004; Paton et al., 2008) asbeing common and mostly due to antipsychotic polyphar-macy. For NAS, high dose prescribing was less frequentlyseen but it was still clearly evident for antipsychoticpolypharmacy. For most antipsychotic drugs and for most
Total sample Across trusts range %
N % Lower Upper
2786 55.1 34.5 77.0835 16.6 6.2 35.0680 13.5 5.0 24.042 0.8 0.0 11.865 1.3 0.0 8.33 0.1 0.0 1.3
45 0.9 0.0 6.9361 7.1 0.0 15.9250 4.9 0.0 13.026 0.5 0.0 5.947 0.9 0.0 5.31 o0.1 0.0 5.92 o0.1 0.0 1.4
35 0.7 0.0 3.71073 21.2 8.0 36.4152 3.0 0.0 9.298 1.9 0.0 6.155 1.1 0.0 4.3
260 5.1 0.0 17.4430 8.5 0.0 18.018 0.4 0.0 5.360 1.2 0.0 5.1
confirm how many had previously had augmentation which was
ubstantial symptoms/disability.

M.X. Patel et al.506
cases, high dose prescribing is reported as providing noadditional benefit in terms of efficacy (Barnes, 2011). Whilstsome evidence exists for 420 mg olanzapine for treatmentresistance, this may be associated with an increased risk ofmetabolic adverse effects (Meltzer et al., 2008). Howeverfor some cases, genetic factors can result in fast metabolismof some antipsychotics, and here therapeutic drug monitor-ing of drug plasma concentrations may be appropriate(Bishara et al., 2013). When prescribing high doses orantipsychotic polypharmacy, the rationale should be docu-mented and regularly reviewed with pro-active side effectmonitoring.
4.3. Clozapine and augmentation
Both the US (PORT (Buchanan et al., 2010)) and the UK(NICE (National Institute for Clinical Excellence, 2009))guidelines recommend 2 adequate trials of different anti-psychotics followed by clozapine as the accepted pathwayfor managing schizophrenia. Thus, if two different antipsy-chotics did not yield an adequate response, starting a thirdother than clozapine is difficult to justify (Patel et al., 2004;Patel, 2012). Overall, it is expected that 30% of patientswith schizophrenia will have treatment resistance to stan-dard antipsychotics and that about half of these willrespond to clozapine (Meltzer, 1997). In this sample, 23.7%were prescribed clozapine but variation between Trusts washigh, suggesting likely clozapine underutilisation in someTrusts. Notably, this sample did not include patients solelyunder primary care services or who were hospitalised.Further, 40% of patients who appeared to be treatmentresistant had not had a trial of clozapine, and had no clearreason documented as to why. For some it seems likely thatclozapine was offered and refused and that this reason wasnot documented. However, the rest remain unexplained.Where reasons were documented, refusal was the mostcommonly recorded reason.
Time to clozapine commencement also exceeded guide-line recommendations for 85% of cases who had receivedthe current antipsychotic for at least 4 weeks and also oneprior antipsychotic for at least 4 weeks, and who werecurrently not in remission or were in partial remission butwith substantial symptoms/disability. Pharmacists are wellplaced to undertake comprehensive medication reviewsdocumenting clear reasons for stopping medication (e.g.lack of tolerability or response) which could then facilitatethe recognition of treatment resistance and need forclozapine initiation.
When faced with non-response to clozapine, measurementof therapeutic drug levels before adding a second antipsycho-tic is recommended by NICE (National Institute for ClinicalExcellence, 2009) and PORT (Buchanan et al., 2010) guide-lines. Augmentation with another antipsychotic is oftenconsidered despite evidence of only modest improvementsat best (Taylor et al., 2012). However this is only supported byNICE (National Institute for Clinical Excellence, 2009) and notPORT (Buchanan et al., 2010). Of the total sample, 250 (5%)were not in remission and were still prescribed clozapinealone. Thus it seems that augmentation was not attempteddespite inadequate response with clozapine monotherapy.Clozapine was being augmented at the time of the audit for
5% of the total sample (and 22% of those on clozapine), mostcommonly with amisulpride or aripiprazole. Amisulpride hashigh binding affinity to D3/D2-dopamine receptors, and thusmight provide supplementary dopamine blockade and thusclinical improvement (Assion et al., 2008; Matthiasson et al.,2001). Alternatively, augmentation with aripiprazole, may beprescribed solely in an attempt to minimise weight gain due toclozapine (Fleischhacker et al., 2008, 2010) and/or to enhancesymptom control. Both amisulpride and aripiprazole have beeninvestigated in augmentation to clozapine in RCTs as hasrisperidone and sulpiride (Barnes, 2011). On balance, if theaddition of the second antipsychotic does not afford anyadditional benefit after an adequate trial of about 8–10 weeks(National Institute for Clinical Excellence, 2009), it should bewithdrawn in order to minimise the risk of adverse effects.Where augmentation does provide benefit, this should beaccompanied by pro-active monitoring for side effects.
4.4. Limitations
The main limitations for the methodology of the NAS auditinclude Trusts providing unequal samples due to difficultiesidentifying and generating a random sample, difficultieswith involving consultants and difficulties with mandatoryinformation items where data were missing from the casenotes preventing the form from being returned. For some, alack of access to the full case notes from both thecommunity and hospital may have caused under-reportingof the full details of antipsychotic exposure. The samplewas limited to patients who had been under each Trust'scare for 12 months or more and comprised patients in thecommunity only. Further, the data collected is not long-itudinal in nature and so conclusions drawn are limited bydesign (Bitter et al., 2008). In this analysis set we furtherexcluded 36 cases (0.7% of the original sample of 5091patients) due to either being prescribed a non-licensed (UK)antipsychotic or concerns about data quality regarding theantipsychotic dose and so the estimates of prescribing ratesshould be considered bearing this in mind. We also dis-regarded information about short-acting intramuscular anti-psychotics as, not only was it not possible to calculate %BNFdue to lack of ongoing frequency of dose administrationdata but also, detailed examination of the data entriessuggested that many may be incorrectly entered data fororal prescriptions and it was not possible to subsequentlyconfirm this either way. Across the sample, patient data wascaptured at different stages of their illness and their currentclinical status with regard to whether or not “remission” hadbeen achieved was not operationally defined though waspartially validated by reference to HoNOS scores (RoyalCollege of Psychiatrists, 1996, 2012). The term “treatmentresistance” was not confirmed by clinicians, and was inferredwhere a case was either not in remission or was in partialremission with substantial symptoms/disability. Further, theresults cannot be extrapolated to in-patients, patients treatedsolely by primary care services (Reilly et al., 2012), nor maythey hold true for the population as a whole. Similarly,comparisons over time can only be considered with duecaution. That being said, the demography of the populationsample is similar to that which one might expect in terms ofage distribution, gender split and distribution of those with

507Quality of prescribing for schizophrenia: Evidence from a national audit in England and Wales
diagnoses of schizophrenia and schizoaffective disorder. Theproportions of different ethnic groups largely mirrors that ofthe general population of England & Wales, except for anexcess of patients of Black or Black British origin, whichmirrors other epidemiological findings for schizophrenia(Fearon et al., 2006).
4.5. Conclusions and implications
The National Audit of Schizophrenia (NAS), for England andWales, provides a snapshot of the current state of play forantipsychotic prescribing in the context of standardsdirectly derived from the national guidelines (NationalInstitute for Clinical Excellence, 2009). Whilst some aspectsof prescribing are meeting expectations of the set stan-dards, this is not true for all patients. Antipsychoticpolypharmacy, high dose prescribing and clozapine under-utilisation for treatment resistance were all key concernswhich need to be further addressed. These findings providea national benchmark and enable Trusts to compare theirperformance and highlight prescribing practices for indivi-dual clinicians to consider further. Moreover, these findingsallow prescribing practices in the UK to be comparedagainst the standards set by the equivalent US guidelinesand for international comparisons to be made amongstsimilar audits carried out worldwide.
Education in psychopharmacology includes the indica-tions for medicines and their risks and benefits. This needsto be improved and delivered to all professions withinmental health teams, including mental health nurses, andto staff in primary care, such as practice nurses. Forpsychiatrists in the UK and abroad, the Royal College ofPsychiatrists or equivalent institutions should ensure that
(1.) Psychiatrists must recognise that antipsychotic
used requires clear documentation of the reasons.
(2.) Psychiatrists should be aware of the upper dos
this level they should always document the reason.
polypharmacy or high dose should be highlighted in
to licensed doses and monotherapy as soon as po
used, additional monitoring should be undertaken e
(3.) Trusts should make sure health professionals a
prescribing of antipsychotics as well as the guidelin
indications. This includes ensuring that prescribers
(4.) Good systems are required for the identification
standard antipsychotics so that reviews can be und
through the use of a newly established Trust-wide
allow improved monitoring and detection of treatme
team.
(5.) Funding and facilities should be in places so th
antipsychotics may be offered clozapine. We would
staff training on how best to offer clozapine for both
patient refusal be clearly documented.
(6.) Trained clinical pharmacists should be availabl
professionals, particularly regarding monitoring and
decisions. Specifically, pharmacists could review th
with antipsychotics (including off label prescribing)
as appropriate.
Figure 2 NAS recommendations to
the curricula for both undergraduate and postgraduatetraining in psychiatry provide sufficient focus on psycho-pharmacology. This should enable psychiatrists to properlymonitor clinical response, recognise treatment resistanceand the onset of adverse effects. Education in psychophar-macology must extend in to continuing professional devel-opment (CPD) and can be facilitated by appropriateteaching programmes, such as those provided by the BritishAssociation for Psychopharmacology (BAP) in the UK.Responsibility for good prescribing performance also lieswith each Trust Board. Specific recommendations to improveantipsychotic prescribing are outlined in Figure 2. Data collec-tion for the second NAS audit cycle commenced in Autumn 2013and, in accordance with the Government's transparency agenda(Healthcare Quality Improvement Partnership, 2013) the parti-cipation and performance for each Trust will no longer beanonymised. Further information is available at: www.rcpsych.ac.uk/quality/NAS.
Role of funding source
The National Audit of Schizophrenia (NAS) is managed by the RoyalCollege of Psychiatrists' (RCPsych) College Centre for QualityImprovement (CCQI). It is commissioned by the Healthcare QualityImprovement Partnership (HQIP) as part of the National ClinicalAudit and Patient Outcomes Programme (NCAPOP), which is fundedby NHS England. HQIP had no further role in study design; in thecollection, analysis and interpretation of data; in the writing of thearticle; and in the decision to submit the article for publication.The views expressed in this publication are those of the authors andnot necessarily those of the NHS, the National Institute for HealthResearch, the Department of Health, National Collaborating Centrefor Mental Health (NCCMH) or National Institute for Health and CareExcellence.
polypharmacy is only rarely appropriate and if
e limits for antipsychotics. If they presc ribe above
We would add that short term use of antipsychotic
order to prompt review and patient should return
ssible. Whilst high doses or polypharmacy are
.g. ECG and metabolic parameters.
re aware of and understand the guidelines for the
es for prescribing outside the usual licensed
carefully document any off label use of a drug.
of patients who becom e treatment resistant to
ertaken and clozapine offered. This may be
case register for patients with schizophrenia to
nt with regular review by each relevant clinical
at those who have not responded to full trials of
add that the need should be evaluated for further
voluntary and detained patients and further, that
e to offer advice on prescribing to other
documentation of the rationale for key prescribing
e use of polypharmacy and high dose prescribing
and prompt the consideration of clozapine initiation
improve antipsychotic prescribing.

M.X. Patel et al.508
Contributors
MXP conducted the statistical analysis, interpreted the findings andco-wrote the first draft of the manuscript. DB managed theliterature search, interpreted the findings, and co-wrote the firstdraft of the manuscript. SJ managed the database and conductedthe statistical analysis. KZ, MJC and DS oversaw the project,including aspects of study design, tool design, and recruitment ofsites, and also contributed to interpretation of the findings. SJC co-wrote the first draft of the manuscript, interpreted the findings andoversaw the project, including aspects of study design, tool design,and recruitment of sites. All authors contributed to and haveapproved the final manuscript.
Conflict of interest
MXP holds a Clinician Scientist Award supported by the NationalInstitute for Health Research and has also received consultancyfees, lecturing honoraria, and/or research funding from Janssen,Lilly, Endo, Lundbeck, Otsuka and Wyeth and has worked or iscurrently working on clinical trials and studies for Janssen, Amgenand Lundbeck. DB has received consultancy fees or speakerhonorarium from Novartis, Astra Zeneca, Eli Lilly and Eisai. DS isa current member of the Guideline Development Group for NICEguidance for adults with psychosis and schizophrenia, member ofNCCMH board, and has received lecturing honoraria from Janssen.SJC has previously been Chair of the Psychiatry Expert Group of theNorthern Ireland Pharmaceutical Clinical Excellence Programmeand a member of the NI Health & Social Care Board Formularycommittee. Prior to the last 5 years he has received researchfunding, consultancy fees and lecturing honoraria from pharmaceu-tical companies involved in the manufacture of antipsychotic andantidepressant drugs. MC, SJ and KZ declare no conflicts of interest.
Acknowledgements
With grateful thanks to the participating 60 Trusts and HealthBoards including clinicians, support staff, medical directors, gov-ernance and audit personnel, as well as the patients and carers whocompleted the audit forms and members of the Advisory Group,especially TRE Barnes and C Paton for their guidance during datacleaning.
References
Agid, O, Schulze, L, Arenovich, T, Sajeev, G, McDonald, K, Foussias,G, Fervaha, G, Remington, G., 2013. Antipsychotic response infirst-episode schizophrenia: efficacy of high doses and switching.Eur. Neuropsychopharmacol. 23, 1017–1022.
Assion, HJ, Reinbold, H, Lemanski, S, Basilowski, M, Juckel, G.,2008. Amisulpride augmentation in patients with schizophreniapartially responsive or unresponsive to clozapine. A randomized,double-blind, placebo-controlled trial. Pharmacopsychiatry 41,24–28.
Barnes, TR., 2011. Evidence-based guidelines for the pharmacolo-gical treatment of schizophrenia: recommendations from theBritish Association for Psychopharmacology. J. Psychopharma-col. 25, 567–620.
Bishara, D, Olofinjana, O, Sparshatt, A, Kapur, S, Taylor, D, Patel,MX., 2013. Olanzapine: a systematic review and meta-regressionof the relationships between dose, plasma concentration,receptor occupancy, and response. J. Clin. Psychopharmacol.33, 329–335.
Bitter, I, Treuer, T, Dyachkova, Y, Martenyi, F, McBride, M,Ungvari, GS., 2008. Antipsychotic prescription patterns inoutpatient settings: 24-month results from the IntercontinentalSchizophrenia Outpatient Health Outcomes (IC-SOHO) study.Eur. Neuropsychopharmacol. 18, 170–180.
BMJ Group and RPS Publishing (2013) British National Formulary—65th ed..
Buchanan, RW, Kreyenbuhl, J, Kelly, DL, Noel, JM, Boggs, DL,Fischer, BA, Himelhoch, S, Fang, B, et al., 2010. The 2009schizophrenia PORT psychopharmacological treatment recom-mendations and summary statements. Schizophr. Bull. 36, 71–93.
Carlson, C, Hornbuckle, K, DeLisle, F, Kryzhanovskaya, L, Breier, A,Cavazzoni, P., 2006. Diabetes mellitus and antipsychotic treat-ment in the United Kingdom. Eur. Neuropsychopharmacol. 16,366–375.
Chan, J, Sweeting, M., 2007. Combination therapy with non-clozapine atypical antipsychotic medication: a review of currentevidence. J. Psychopharmacol. 21, 657–664.
Correll, CU, Frederickson, AM, Kane, JM, Manu, P., 2007. Doesantipsychotic polypharmacy increase the risk for metabolicsyndrome? Schizophr. Res. 89, 91–100.
Cramer, JA, Rosenheck, R., 1998. Compliance with medicationregimens for mental and physical disorders. Psychiatr. Serv.49, 196–201.
Faries, D, scher-Svanum, H, Zhu, B, Correll, C, Kane, J., 2005.Antipsychotic monotherapy and polypharmacy in the naturalistictreatment of schizophrenia with atypical antipsychotics. BMCPsychiatry 5, 26.
Fearon, P, Kirkbride, JB, Morgan, C, Dazzan, P, Morgan, K, Lloyd, T,Hutchinson, G, Tarrant, J, et al., 2006. Incidence ofschizophrenia and other psychoses in ethnic minority groups:results from the MRC AESOP Study. Psychol. Med. 36, 1541–1550.
Fleischhacker, WW, Heikkinen, ME, Olie, JP, Landsberg, W,Dewaele, P, McQuade, RD, Loze, JY, Hennicken, D, Kerselaers,W., 2010. Effects of adjunctive treatment with aripiprazoleon body weight and clinical efficacy in schizophreniapatients treated with clozapine: a randomized, double-blind,placebo-controlled trial. Int. J. Neuropsychopharmacol. 13,1115–1125.
Fleischhacker, WW, Heikkinen, T, Olie, JP, Landsberg, W, Dewaele,P, McQuade, RD, Hennicken, D., 2008. Weight change onaripiprazole-clozapine combination in schizophrenic patientswith weight gain and suboptimal response on clozapine: 16-week double-blind study. Eur. Psychiatry 23 (Suppl. 2),S114–S115.
Ganguly, R, Kotzan, JA, Miller, LS, Kennedy, K, Martin, BC., 2004.Prevalence, trends, and factors associated with antipsychoticpolypharmacy among Medicaid-eligible schizophrenia patients,1998–2000. J. Clin. Psychiatry 65, 1377–1388.
Healthcare Quality Improvement Partnership. 2013. The Transpar-ency Agenda and NCAPOP. ⟨http://www.hqip.org.uk/transparency-agenda-and-the-national-clinical-audit-and-patient-outcomes-programme/⟩.
Humberstone, V, Wheeler, A, Lambert, T., 2004. An auditof outpatient antipsychotic usage in the three healthsectors of Auckland, New Zealand. Aust. N. Z. J. Psychiatry38, 240–245.
Kreyenbuhl, JA, Valenstein, M, McCarthy, JF, Ganoczy, D, Blow,FC., 2007. Long-term antipsychotic polypharmacy in the VAhealth system: patient characteristics and treatment patterns.Psychiatr. Serv. 58, 489–495.
Lelliott, P, Paton, C, Harrington, M, Konsolaki, M, Sensky, T,Okocha, C., 2002. The influence of patient variables onpolypharmacy and combined high dose of antipsychotic drugsprescribed for in-patients. Psychiatr. Bull. 26, 411–414.
Leucht, S, Tardy, M, Komossa, K, Heres, S, Kissling, W, Davis, JM.,2012a. Maintenance treatment with antipsychotic drugs forschizophrenia. Cochrane Database Syst. Rev. 5, CD008016.

509Quality of prescribing for schizophrenia: Evidence from a national audit in England and Wales
Leucht, S, Tardy, M, Komossa, K, Heres, S, Kissling, W, Salanti, G,Davis, JM., 2012b. Antipsychotic drugs versus placebo forrelapse prevention in schizophrenia: a systematic review andmeta-analysis. Lancet 379, 2063–2071.
Lewis, S, Davies, L, Jones, P, Barnes, T, Murray, R, Kerwin, R,Taylor, D, Hayhurst, KP, et al., 2006. Randomised controlledtrials of conventional antipsychotic versus new atypical drugs,and new atypical drugs versus clozapine, in people with schizo-phrenia responding poorly to, or intolerant of, current drugtreatment. Health Technol. Assess. 10, 1–182.
Matthiasson, P, Costa, DC, Erlandsson, K, Waddington, W, Visvikis,D, Cullum, I, Cobb, AM, Ell, PJ, Kerwin, RW, Travis, MJ., 2001.Relationship between dopamine D2 receptor occupancy andclinical response in amisulpride augmentation of clozapinenon-response. J. Psychopharmacol. 15, S41.
McEvoy, JP, Lieberman, JA, Stroup, TS, Davis, SM, Meltzer, HY,Rosenheck, RA, Swartz, MS, Perkins, DO, et al., 2006. Effective-ness of clozapine versus olanzapine, quetiapine, and risperidonein patients with chronic schizophrenia who did not respond toprior atypical antipsychotic treatment. Am. J. Psychiatry 163,600–610.
Meltzer, HY., 1997. Treatment-resistant schizophrenia—the role ofclozapine. Curr. Med. Res. Opin. 14, 1–20.
Meltzer, HY, Bobo, WV, Roy, A, Jayathilake, K, Chen, Y, Ertugrul, A,nil Yagcioglu, AE, Small, JG., 2008. A randomized, double-blindcomparison of clozapine and high-dose olanzapine in treatment-resistant patients with schizophrenia. J. Clin. Psychiatry 69,274–285.
National Collaborating Centre For Mental Health (2011) PsychosisWith Coexisting Substance Misuse: Assessment and Managementin Adults and Young People, vol. 120: Rcpsych Publications.
National Institute for Clinical Excellence, 2009. Schizophrenia: coreinterventions in the treatment and management of schizophre-nia in adults in primary and secondary care (update). Clin. Guid.82 ⟨http://www.nice.org.uk/⟩.
Patel, MX, Young, C, Samele, C, Taylor, DM, David, AS., 2004.Prognostic indicators for early discontinuation of risperidonelong-acting injection. Int. Clin. Psychopharmacol. 19, 233–239.
Patel, MX., 2012. Clinician hesitation prior to clozapine initiation: isit justifiable? Br. J. Psychiatry 201, 425–427.
Paton, C, Barnes, TR, Cavanagh, MR, Taylor, D, Lelliott, P., 2008.High-dose and combination antipsychotic prescribing in acuteadult wards in the UK: the challenges posed by p.r.n. prescrib-ing. Br. J. Psychiatry 192, 435–439.
Procyshyn, RM, Kennedy, NB, Tse, G, Thompson, B., 2001. Anti-psychotic polypharmacy: a survey of discharge prescriptionsfrom a tertiary care psychiatric institution. Can. J. Psychiatry46, 334–339.
Procyshyn, RM, Zerjav, S., 1998. Drug utilization patterns andoutcomes associated with in-hospital treatment with risperidoneor olanzapine. Clin. Ther. 20, 1203–1217.
Reilly, S, Planner, C, Hann, M, Reeves, D, Nazareth, I, Lester, H.,2012. The role of primary care in service provision for peoplewith severe mental illness in the United Kingdom. PLoS One 7,e36468.
Royal College of Psychiatrists. 1996. Health of the Nation Out-come Scales (HoNOS). ⟨http://www.rcpsych.ac.uk/training/honos.aspx⟩.
Royal College of Psychiatrists, 2012. Report of the National Audit ofSchizophrenia (NAS). Healthcare Quality Improvement Partner-ship, London2012.
Sim, K, Su, A, Fujii, S, Yang, SY, Chong, MY, Ungvari, GS, Si, T,Chung, EK, et al., 2004. Antipsychotic polypharmacy in patientswith schizophrenia: a multicentre comparative study in EastAsia. Br. J. Clin. Pharmacol. 58, 178–183.
Taylor, D, Smith, L, Gee, SH, Nielsen, J., 2012. Augmentation ofclozapine with a second antipsychotic. A meta analysis. ActaPsychiatr. Scand. 125, 15–24.
Taylor, DM, Young, C, Paton, C., 2003. Prior antipsychotic prescrib-ing in patients currently receiving clozapine: a case note review.J. Clin. Psychiatry 64, 30–34.
Weissman, EM., 2002. Antipsychotic prescribing practices in theVeterans Healthcare Administration—New York metropolitanregion. Schizophr. Bull. 28, 31–42.
Zink, M, Henn, FA, Thome, J., 2004. Combination of amisulprideand olanzapine in treatment-resistant schizophrenic psychoses.Eur. Psychiatry 19, 56–58.
Copyright © 2022 FDOKUMEN