
Enhancing quality of life and contributing to a healthier future
Upload
independentCategory
view
2download
0
This article was downloaded by: [New York University]On: 11 October 2012, At: 09:37Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House,37-41 Mortimer Street, London W1T 3JH, UK
Journal of the American Planning AssociationPublication details, including instructions for authors and subscription information:http://www.tandfonline.com/loi/rjpa20
Interdisciplinary Planning for Healthier Communities:Findings from the Harlem Children's Zone AsthmaInitiativeSeth E. Spielman, Cynthia A. Golembeski, Mary E. Northridge, Roger D. Vaughan, RachelSwaner, Betina Jean-Louis, Katherine Shoemaker, Sandra Klihr-Beall, Eric Polley, Linda F.Cushman, Benjamin Ortiz, Vincent E. Hutchinson, Stephen W. Nicholas, Terry Marx, RogerHayes, Andrew Goodman & Elliott D. Sclar
Version of record first published: 26 Nov 2007.
To cite this article: Seth E. Spielman, Cynthia A. Golembeski, Mary E. Northridge, Roger D. Vaughan, Rachel Swaner, BetinaJean-Louis, Katherine Shoemaker, Sandra Klihr-Beall, Eric Polley, Linda F. Cushman, Benjamin Ortiz, Vincent E. Hutchinson,Stephen W. Nicholas, Terry Marx, Roger Hayes, Andrew Goodman & Elliott D. Sclar (2006): Interdisciplinary Planning forHealthier Communities: Findings from the Harlem Children's Zone Asthma Initiative, Journal of the American PlanningAssociation, 72:1, 100-108
To link to this article: http://dx.doi.org/10.1080/01944360608976727
PLEASE SCROLL DOWN FOR ARTICLE
Full terms and conditions of use: http://www.tandfonline.com/page/terms-and-conditions
This article may be used for research, teaching, and private study purposes. Any substantial or systematicreproduction, redistribution, reselling, loan, sub-licensing, systematic supply, or distribution in any form toanyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representation that the contentswill be complete or accurate or up to date. The accuracy of any instructions, formulae, and drug doses shouldbe independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims,proceedings, demand, or costs or damages whatsoever or howsoever caused arising directly or indirectly inconnection with or arising out of the use of this material.

Interdisciplinary Planningfor Healthier Communities
Findings from the Harlem Children’s ZoneAsthma Initiative
Seth E. Spielman, Cynthia A. Golembeski, Mary E. Northridge, Roger D. Vaughan,Rachel Swaner, Betina Jean-Louis, Katherine Shoemaker, Sandra Klihr-Beall, EricPolley, Linda F. Cushman, Benjamin Ortiz, Vincent E. Hutchinson, Stephen W.Nicholas, Terry Marx, Roger Hayes, Andrew Goodman, and Elliott D. Sclar
Crowded, unsanitary, and polluted living conditions in industrialized citiesof Europe and the United States in the middle of the th century led toinfectious disease outbreaks, social unrest, and class conflict (Krieger &
Higgins, ). These conditions also gave rise to the modern professions ofurban planning and public health. Both professions have historically attemptedto ameliorate urban environmental, social, and population health problems(Krieger & Birn, ). Understanding how physical structures and social factorscontribute to disparate environmental exposures and health inequalities could bea bridge reconnecting the fields (Schulz & Northridge, ).
This article describes the Harlem Children’s Zone Asthma Initiative(HCZAI), a community-based asthma intervention in Central Harlem, NewYork City, centered in a neighborhood located six blocks due north of CentralPark (see Figure ).
We begin by briefly describing the current epidemic of childhood asthma inU.S. cities and impoverished neighborhoods within cities; the concern for socialand environmental disparities in health that is reshaping contemporary publichealth research and practice; and the need for interdisciplinary, participatoryapproaches to understand and effectively address current urban health problems.Then we present background on asthma symptoms and triggers in home envi-ronments, HCZAI methods and management strategies, our preliminary results,and our conclusions, which relate these findings to an ecological model of socie-tal, community, and interpersonal determinants of individual and populationhealth and well-being.
The Epidemic of Childhood Asthma
Asthma is a chronic, episodic disease of the airways, which is best viewed asa single disease that exists in many forms. While the basic causes of asthma arenot fully understood, once a child or adult develops it (a new, or incident, case),much can be done to relieve the inflammation which, in susceptible individuals,leads to recurrent episodes of wheezing, breathlessness, chest tightness, andcoughing (National Heart, Lung, and Blood Institute, ). Exposure to irri-tants such as tobacco smoke and indoor and outdoor pollution, and allergens
Health disparities that affect wholecommunities may involve factors likehousing quality that lie at least partlywithin planners’ realm of policy influence.This article demonstrates a link betweenhousing and childhood asthma. The mag-nitude of the childhood asthma epidemicin Harlem in New York City and thecommitment of engaged communitypartners led to an interdisciplinary, par-ticipatory, and multifaceted approachto the planning, implementation, andevaluation of the Harlem Children’s ZoneAsthma Initiative. Here we present thefirst year’s data on environmental triggersin the homes of program participants,showing that intensive, community-basedprograms can reduce both home environ-mental triggers and adverse childhoodasthma outcomes. This provides an ex-ample of a community-wide public healthintervention that informs public policyand planning, and may provide a sus-tainable model for reducing childhoodasthma in impoverished communities.
Seth Spielman is an adjunct associateresearch scholar at the Graduate Schoolof Architecture, Planning and Preserva-tion at Columbia University and a Na-tional Science Foundation IGERT Fellowin geographic information science at theNational Center for Geographic Infor-mation and Analysis at the University ofBuffalo. Mary Northridge and ElliottSclar are also on the faculty of the Grad-uate School of Architecture, Planningand Preservation at Columbia Univer-sity, and Northridge is also affiliated withthe Mailman School of Public Health atColumbia, as are Cynthia Golembeski,Roger Vaughan, Eric Polley, and LindaCushman. Rachel Swaner, Betina Jean-Louis, and Katherine Shoemaker are withthe Harlem Children’s Zone, Inc. SandraKlihr-Beall, Benjamin Ortiz, VincentHutchinson, and Stephen Nicholas areaffiliated with the Harlem Hospital Cen-ter at Columbia University. Terry Marxworks for the New York City Departmentof Education, and Roger Hayes andAndrew Goodman are with the East andCentral Harlem District Public HealthOffice of the New York City Depart-ment of Health and Mental Hygiene.
Journal of the American Planning Association,
Vol. , No. , Winter .
© American Planning Association, Chicago, IL.
Dow
nloa
ded
by [
New
Yor
k U
nive
rsity
] at
09:
37 1
1 O
ctob
er 2
012

Spielman et al.: Interdisciplinary Planning for Healthier Communities
Figure : Children with severe asthma screened by the HCZAI, by address.Source: Data from the Harlem Children’s Zone Asthma Initiative Screening Survey, April , . New York City DOF, COGIS File, NYCMAP.
Number of severe asthma cases
• 1 100
Dow
nloa
ded
by [
New
Yor
k U
nive
rsity
] at
09:
37 1
1 O
ctob
er 2
012

such as house dust mites, mold, and cockroach and animaldander may increase asthma symptoms in sensitized indi-viduals (National Heart, Lung, and Blood Institute, ).In this article, we refer to both irritants and allergens asasthma triggers. Asthma symptoms can be managed bytaking both preventive and “quick relief” medications(Swartz, Banasiak, & Meadows-Oliver, ), and byreducing irritants and allergens in the home (Gold &Wright, ).
The number of individuals with asthma in the UnitedStates has risen over the past several decades (Mannino etal., ). A recent study estimated that .% of U.S. chil-dren under the age of had physician-diagnosed asthma(Rodriguez, Winkleby, Ahn, Sundquist, & Kraemer, ).In New York City, % of children have experiencedasthma-like symptoms (New York City Department ofHealth and Mental Hygiene, ). Asthma prevalencevaries by neighborhood, with a disproportionate burden incommunities of color and impoverished neighborhoods.Over % () of the , children screened by theHCZAI as of this writing have asthma. Central Harlem,the site of the HCZAI, has the third highest rate of pedi-atric asthma hospitalizations among New York City’s
neighborhoods (New York City Department of Health andMental Hygiene, ). Poor housing conditions, expo-sures to environmental pollutants such as diesel exhaust,and lack of access to preventive care may contribute to thehigh prevalence of asthma symptoms in urban neighbor-hoods (Northridge et al., ; Kinney, Aggarwal, North-ridge, Janssen, & Shepard, ; Kinney et al., ).
Social and Environmental Disparitiesin Health
Public health’s recent focus on the elimination ofhealth disparities (Satcher, ) represents an importantadvance in conceptualizing, understanding, and addressingdifferences in disease rates at the individual, community,and societal levels. It is based on the principle that differ-ences in health and disease are linked to economic, social,and political inequalities (Fagan et al., ). For instance,unequal housing conditions, indoor environmental expo-sures (including allergens from dust mites, mold, and pestssuch as cockroaches and mice), treatment and access toquality health care, and environmental tobacco smokeexposure (Gold & Wright, ; Swartz et al., )contribute to disparities in asthma rates between racialand economic groups in the U.S.
Reducing disparities in hospitalizations, emergencyroom visits, and missed school days due to asthma will
depend in part on programs that reduce exposure to trig-gers, as well as those that improve access to education andmedical care. However, the long-term success of any ofthese is likely to depend on more general improvements inliving conditions and life opportunities (Gold & Wright,).
Community-Based, Participatory,Interdisciplinary Interventions
Problems at the intersection of the physical environ-ment and population health require approaches that crossdisciplinary and organizational boundaries (Sclar, North-ridge, & Karpel, ). Building upon the seminal workof Friere (), recent public health research demonstratesrenewed interest in participatory research and practiceapproaches (Green et al., ; Israel, Schulz, Parker, &Becker, ; Minkler & Wallerstein, ). Planning alsohas a long history of involving affected communities indevising solutions to urban ills.
Community-based, participatory, interdisciplinaryinterventions such as the HCZAI fundamentally restruc-ture planning and public health practice, promoting civilsociety and working against disparities in health and healthcare for those with limited resources (Northridge et al.,).
Housing and Asthma
Recent evidence suggests that intervening to alter theindividual’s home environment may decrease exposure toindoor allergens, reducing illness among urban childrenwith atopic asthma (Morgan et al., ). Exposure toallergens has been identified as a major source of airwayinflammation; thus efforts to control asthma have focusedon avoiding allergens. Approaches relying on communityhealth workers have effectively reduced exposure to indoorasthma triggers (Takaro, Krieger, & Song, ) and pro-moted community-wide efforts to reduce home environ-mental hazards (Kinney et al., ). The types of housinginterventions that have been found to work consistentlyinvolve home visitation programs and home modification,elements that were incorporated into the HCZAI (Sandel,Phelan, Wright, Hynes, & Lanphear, ). Indeed, asChaudhuri () concluded in a recent review, interven-tions to improve housing are essential to advancing chil-dren’s health. Yet, as we show, intervening to try to controlcockroaches and mice in individual apartments does notwork in poor-quality, ill-maintained, multifamily struc-
Journal of the American Planning Association, Winter , Vol. , No.
Dow
nloa
ded
by [
New
Yor
k U
nive
rsity
] at
09:
37 1
1 O
ctob
er 2
012

tures where enforcement of existing ordinances is lax,conditions common in impoverished communities (Kinneyet al., ).
In Central Harlem, low vacancy rates, high rents, weaktenant protection laws, and politically influential landlordsmean tenants often lack the power to improve their hous-ing conditions. Over % of households receive housingassistance in the form of public housing or Section vouchers, and % of households report serious housingaffordability or quality problems (Bhalla, Voicu, Meltzer,Ellen, & Been, ).
Background and Methods ofthe HCZAI
The HCZAI was established in to reduce asthma-related deaths through improved surveillance, health-careutilization, and health-care service delivery for childrenaged years or younger living in a -block area of Harlemknown as the Harlem Children’s Zone, or HCZ. TheHCZAI is led by a community-based organization, HCZ,Inc., and the Department of Pediatrics at Harlem HospitalCenter, which partnered with local institutions and agen-cies for advice and services as needs and opportunitiespresented themselves, notably: the Mailman School ofPublic Health and the Graduate School of Architecture,Planning and Preservation at Columbia University; theNew York City Department of Health and Mental Hy-giene; the New York City Department of Education; theBrazelton Touchpoints™ Center, a child and family de-velopment training program; and the law firm of LaBoeuf,Lamb, Greene & MacRae through Volunteers of Legal Ser-vices (Northridge, ). The initiative is interdisciplinaryand participatory, and takes an iterative approach, devel-oping initial protocols on the basis of existing scientificevidence and then revising them based on experience. Theinitiative’s approach to the management of home environ-mental triggers was modeled on the Seattle–King CountyHealthy Homes Project (Krieger et al., ).
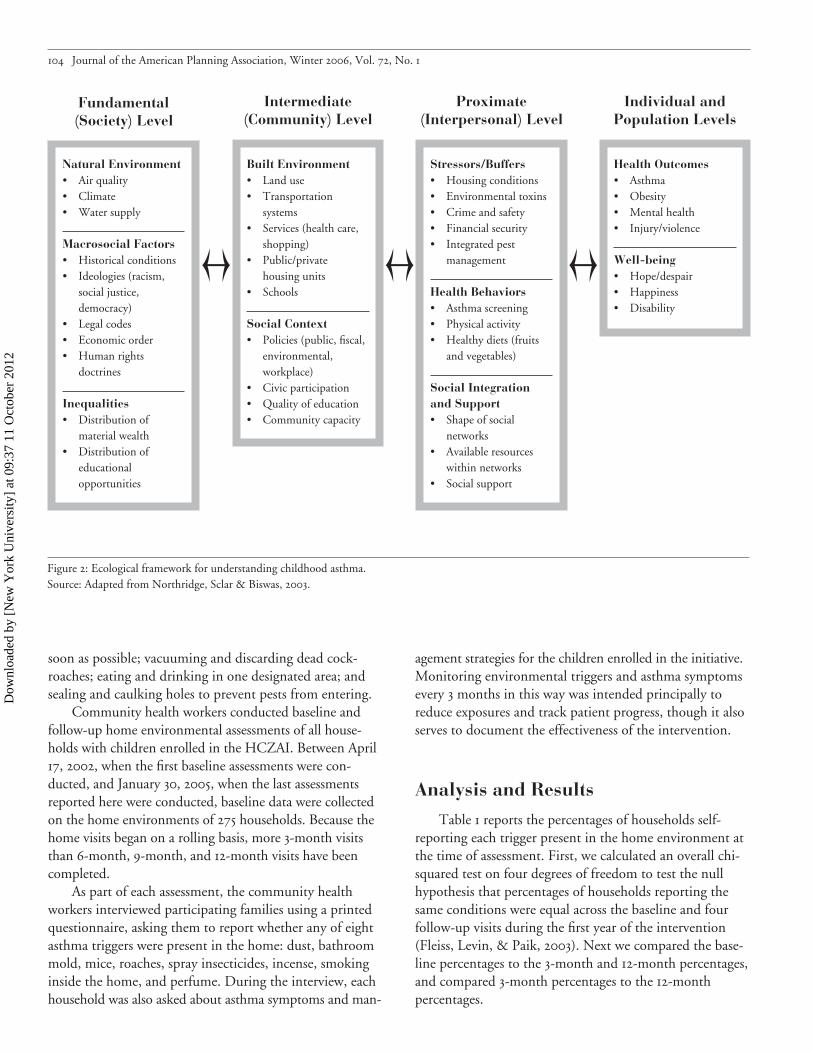
Figure demonstrates an ecological model useful forunderstanding childhood asthma. To reflect our emphasison childhood asthma and the built environment (notablyhousing and schools), we modified the original model inNorthridge, Sclar, and Biswas () to examine relation-ships among racial, ethnic, and social inequalities at thesocietal level, the built environment and social context atthe community level, stressors and buffers at the interper-sonal level, and disparities in health and well-being amongindividuals and across populations. Though the modelillustrates various levels of potential intervention (societal,
community, and interpersonal), this effort began by ad-dressing the immediate needs of children with asthma andtheir families.
Screening and EnrollmentThe methods used to screen and enroll children with
asthma in the HCZAI have been reported previously(Nicholas, Hutchinson, et al., ; Nicholas, Jean-Louis,et al., ). The HCZAI is an ongoing effort, but the datareported here were collected between April and Jan-uary . During this time, potential participants in theHCZAI were identified by screening all children aged years or younger who lived or attended school in the HCZ(Figure shows these boundaries) or who participated inHCZ, Inc. programs. Screening consisted of asking thechild’s parent or guardian to complete a written surveyand to consent to a physical examination of the child bya physician or nurse, although the latter was not required.(Overall, % of parents and guardians consented to phys-ical examinations of their children.) Participation rates forthe various sites (schools, day care centers, etc.) rangedfrom % to %.
Of the , children who were screened, (%)had asthma, asthma-like symptoms, or physical findingsconsistent with asthma, and were invited to enroll in theprogram. Because of the large number of children identi-fied to have asthma or asthma-like symptoms, participationwas initially limited to children with recent symptoms. Atthe time of this writing, of the eligible childrenwere enrolled in the asthma initiative. Over time, the goalof the initiative is to reach all children in need. As part ofthe HCZAI, a pediatric asthma team (including four com-munity health workers, a social worker, a nurse, and threephysicians) offered medical, educational, environmental,and social services to families of enrolled children.
MonitoringCommunity health workers monitor selected indicators
of home environmental triggers, asthma symptoms, andmanagement strategies by interviewing parents or guardiansof enrolled children during home visits approximately everythree months. They offer families with cockroach and/orrodent problems integrated pest management services,which use a combination of prevention strategies andinsecticides (gel and/or crack and crevice treatment, bothof which have a “caution” rating, the lowest rating forinsecticides) to reduce cockroaches. They demonstratetechniques to reduce and prevent pests, including cleaningup food spills and washing dirty dishes as soon as possible;not leaving pet food and water out overnight; containingfood products and clutter in plastic bins; repairing leaks as
Spielman et al.: Interdisciplinary Planning for Healthier Communities
Dow
nloa
ded
by [
New
Yor
k U
nive
rsity
] at
09:
37 1
1 O
ctob
er 2
012
soon as possible; vacuuming and discarding dead cock-roaches; eating and drinking in one designated area; andsealing and caulking holes to prevent pests from entering.
Community health workers conducted baseline andfollow-up home environmental assessments of all house-holds with children enrolled in the HCZAI. Between April, , when the first baseline assessments were con-ducted, and January , , when the last assessmentsreported here were conducted, baseline data were collectedon the home environments of households. Because thehome visits began on a rolling basis, more -month visitsthan -month, -month, and -month visits have beencompleted.
As part of each assessment, the community healthworkers interviewed participating families using a printedquestionnaire, asking them to report whether any of eightasthma triggers were present in the home: dust, bathroommold, mice, roaches, spray insecticides, incense, smokinginside the home, and perfume. During the interview, eachhousehold was also asked about asthma symptoms and man-
agement strategies for the children enrolled in the initiative.Monitoring environmental triggers and asthma symptomsevery months in this way was intended principally toreduce exposures and track patient progress, though it alsoserves to document the effectiveness of the intervention.
Analysis and Results
Table reports the percentages of households self-reporting each trigger present in the home environment atthe time of assessment. First, we calculated an overall chi-squared test on four degrees of freedom to test the nullhypothesis that percentages of households reporting thesame conditions were equal across the baseline and fourfollow-up visits during the first year of the intervention(Fleiss, Levin, & Paik, ). Next we compared the base-line percentages to the -month and -month percentages,and compared -month percentages to the -monthpercentages.
Journal of the American Planning Association, Winter , Vol. , No.
Figure : Ecological framework for understanding childhood asthma.Source: Adapted from Northridge, Sclar & Biswas, .
Natural Environment• Air quality• Climate• Water supply
Macrosocial Factors• Historical conditions• Ideologies (racism,
social justice,democracy)
• Legal codes• Economic order• Human rights
doctrines
Inequalities• Distribution of
material wealth• Distribution of
educationalopportunities
Fundamental(Society) Level
Built Environment• Land use• Transportation
systems• Services (health care,
shopping)• Public/private
housing units• Schools
Social Context• Policies (public, fiscal,
environmental,workplace)
• Civic participation• Quality of education• Community capacity
Intermediate (Community) Level
Stressors/Buffers• Housing conditions• Environmental toxins• Crime and safety• Financial security• Integrated pest
management
Health Behaviors• Asthma screening• Physical activity• Healthy diets (fruits
and vegetables)
Social Integrationand Support• Shape of social
networks• Available resources
within networks• Social support
Proximate(Interpersonal) Level
Health Outcomes• Asthma• Obesity• Mental health• Injury/violence
Well-being• Hope/despair• Happiness• Disability
Individual andPopulation Levels
Ö Ö Ö
Dow
nloa
ded
by [
New
Yor
k U
nive
rsity
] at
09:
37 1
1 O
ctob
er 2
012

Spielman et al.: Interdisciplinary Planning for Healthier Communities
Table shows that over the first year of enrollmentin the HCZAI, the percentage of parents or guardians ofenrolled children who reported dust in the living roomdecreased significantly, from .% at the baseline to .%at months. Similarly, the percentage of parents or guar-dians who reported mold in the bathroom decreased sig-nificantly from .% at the baseline to .% at months.Self-reported use of spray insecticide (from .% to .%),incense (from .% to .%), smoking inside the home(from .% to .%), and perfume (from .% to .%)all decreased significantly over the first year of enrollment.Table suggests that the greatest reduction in these triggersoccurred in the first three months, and that these reductionswere then sustained over the remainder of the -monthmonitoring period. Those aspects of home environmentsthat were within residents’ control changed significantly.On the other hand, there was no significant change inreported problems with mice or cockroaches during any ofthe monitored time intervals. While the HCZAI providedenvironmental education and integrated pest managementservices to families who reported problems with mice andcockroaches, these efforts had no measurable effect, sug-gesting that pest management at the scale of the individualhousehold is not effective in multifamily buildings.
Table presents data on the effectiveness of theHCZAI in reducing asthma as measured by nine selectedindicators of asthma symptoms and management strategies,as described in Nicholas, Hutchinson, et al. (). Afterone year of participation in the program, there were statis-tically significant reductions in school absences generally
(from .% to .%) and school absences due to asthma(from .% to .%) in the days before the home visit.Statistically significant decreases in emergency departmentand unscheduled physician office visits (from .% to.%) and hospital stays due to asthma (from .% to .%)were also reported for the three months preceding the homevisit. These reductions continued between the -month and-month visits, resulting in significant reductions in theuse of hospital emergency rooms for asthma treatment andsignificant reductions in school absences, both for asthmaand other reasons. In general, asthma symptoms (wheezingor tightness in chest, slowing down or stopping play be-cause of asthma, and waking up because of asthma) occur-ring in the days before the home visit also diminishedover the course of the first year, though these reductionswere not statistically significant. Finally, while the use ofany asthma medications (both preventive and “quickrelief”) showed little change from baseline to months,the use of preventive medications increased significantlyfrom .% at the baseline to .% at months.
The results presented here indicate that the vast ma-jority of improvement in measured indicators occurred be-tween baseline and the first follow-up visit, after monthsin the program. As the statistical tests indicate, there is sig-nificant change between the baseline and months, andbetween the baseline and months, but in general notbetween and months, suggesting that the interventioneffects occur quickly, and are sustained over time.
These preliminary data underscore the effectiveness ofintensive, community-based programs in reducing both
Table . Percentages of parents or guardians of enrolled children reporting asthma triggers in home environmental assessments.
Follow-up visits Significance of differencesa
p of Chi-squaredBaseline 3 mos. 6 mos. 9 mos. 12 mos. Baseline 3 mos. Baseline on overall(n = 275) (n = 171) (n = 140) (n = 129) (n = 104) vs. 3 mos. vs. 12 mos. vs. 12 mos. differencesa
Dust (living room) 60.7% 31.6% 32.1% 33.3% 32.7% *** *** < .0001Mold (bathroom) 29.1% 7.6% 5.0% 8.5% 8.7% *** *** < .0001Mice 28.5% 25.7% 15.7% 27.9% 26.0% 0.068Roaches 65.6% 64.0% 66.4% 61.2% 58.7% 0.657Spray bombs 14.8% 2.3% 0.7% 0.8% 1.9% *** *** < .0001Incense 19.3% 8.2% 12.1% 6.2% 4.8% ** *** < .0001Smoking in home 21.8% 12.9% 8.6% 5.4% 9.6% * ** < .0001Perfume 25.1% 5.8% 2.1% 2.3% 3.8% *** *** < .0001
* p < .05; ** p < .01; ***p < .001
Note:a. Calculated with 4 degrees of freedom. Significance levels replicated using repeated measures random effects models, Proc Mixed, SAS.
Dow
nloa
ded
by [
New
Yor
k U
nive
rsity
] at
09:
37 1
1 O
ctob
er 2
012

Journal of the American Planning Association, Winter , Vol. , No.
Table . Percentages of parents or guardians of enrolled children reporting asthma symptoms and management strategies.
Follow-up visits Significance of differencesa
p of Chi-squaredBaseline 3 mos. 6 mos. 9 mos. 12 mos. Baseline 3 mos. Baseline on overall(n = 362) (n = 187) (n = 150) (n = 141) (n = 119) vs. 3 mos. vs. 12 mos. vs. 12 mos. differencesa
Asthma symptoms in child last 14 days
Wheezing or tightness in chest 62.2% 47.6% 43.3% 45.4% 47.9% *** ** < .001
Had to slow down or stop play or activities because of asthma 50.8% 44.4% 40.0% 41.8% 46.2% .15
Woke up because of asthma, wheezing, cough, or tightness in chest 51.7% 40.6% 38.7% 39.7% 42.0% ** .015
Missed school forany reason 33.4% 24.6% 12.7% 10.6% 10.9% * ** *** < .001
Missed school due to asthma 23.5% 17.6% 10.0% 7.8% 6.7% ** *** < .001
Asthma symptoms in child last 3 months
Visited the emer-gency room or made unscheduled visit for treatment of asthma 36.5% 19.8% 16.8% 12.1% 11.8% *** * *** < .001
Admitted to a hospital floor and stayed overnightfor asthma 8.3% 3.2% 3.3% 3.5% 1.7% * ** < .01
Took any medi-cations for asthmab 82.6% 88.8% 88.7% 80.1% 84.9% * .10
Use of asthma management strategies
Took any medic-ations prescribed for asthma every day, even when s/he was well, to prevent asthma symptomsc 34.0% 42.8% 44.7% 45.4% 48.7% * ** .01
* p < .05; ** p < .01; ***p < .001
Notes:a. Calculated with degrees of freedom. Significance levels replicated using repeated measures random effects models, Proc Mixed, SAS.b. Asthma medications include both preventive and quick relief medications. Quick relief medications include: Albuterol, Proventil®, Proventil® HFA
(albuterol sulfate), Maxair™ (pirbuterol acetate) and Xopenex® (levalbuterol HCl). Preventive asthma medications include: Flovent® (fluticasonepropionate), Advair Diskus® (fluticasone propionate and salmeterol), Pulmicort Respules/ Turbuhaler® (budesonide), Singulair® (montelukastsodium), and Intal® (cromolyn sodium).
c. Preventive asthma medications include: Flovent® (fluticasone propionate), Advair Diskus® (fluticasone propionate and salmeterol), PulmicortRespules/ Turbuhaler® (budesonide), Singulair® (montelukast sodium), and Intal® (cromolyn sodium).
Dow
nloa
ded
by [
New
Yor
k U
nive
rsity
] at
09:
37 1
1 O
ctob
er 2
012

home environmental triggers and adverse childhood asthmaoutcomes through multifaceted interventions that targetthe built environment. Our findings confirm that com-munity health workers are an important complement topediatric asthma teams involving physicians, nurses, andsocial workers. Nonetheless, the program design does notallow us to link reduced asthma triggers to improvedoutcomes directly, nor to draw definitive conclusionsabout which specific aspects of the program contributed tothe successes demonstrated here.
Conclusions and Next Steps
Successfully eliminating childhood asthma disparitiesacross class and color lines will require multiple theories,methods, and tools to better design and implement inter-ventions that inform public policy and contribute to sus-tainable improvements in health in impoverished commu-nities. The HCZAI demonstrates that community-basedinterventions that target elements of the built environment,such as poor housing conditions, may have great potential.Community influences may be especially amenable to pol-icy manipulation, possibly offering planning practitionersnew opportunities to directly affect human health andwell-being.
Figure showed a clustering of severe childhoodasthma cases in a large public housing complex. Does thisreflect important connections between housing and child-hood asthma? Is it evidence of social disparity between thebetter off and the worse off, even within an impoverishedneighborhood? Clearly the answers to these questions haveimportant implications for the practices of both urbanplanning and public health, and argue for further researchand integration of the disciplines.
AcknowledgmentsFinancial and ongoing program support for the Harlem Children’sZone Asthma Initiative is provided by the Robin Hood Foundation(grant RHF CU), the Anne E. Dyson Community PediatricsTraining Initiative, the National Institute of Environmental HealthSciences (grant R ES-), the American Legacy Foundation(grant ), the Centers for Disease Control and Prevention throughthe Harlem Health Promotion Center (grant U/CCU-), andthe Kellogg Scholars in Health Disparities Program.
Past and present participants in the Harlem Children’s Zone AsthmaInitiative include the authors of this article, as well as (in alphabeticalorder) Luisa Borrell, T. Berry Brazelton, Carol Brock, Denise Campbell,Geoffrey Canada, Jason Corburn, Jazmine Credell, Linda Cushman,Lisa Desrochers, Daouda Diarrassouba, Cynthia Dunbar, Sara Effron,Miriam Falconi, Shannon Farley, Lee Farrow, Keith Faulkner, Jacque-line Fox-Pascal, Regina Garrett, Katrina Gonzalez, Marilyn Joseph,Daniel Kass, Renuka Kher, Helen Kwon, Lucille Lebovitz, Rasuli Lewis,
Marty Lipp, Victor Marte, Jones Maxi, Cara McAteer, Brian McClen-don, Robert Mellins, Dennis Mitchell, Serina Moya, Carolyn Nash,Yvonne Pradier, Doris Prester, David Saltzman, Gwendolyn Scott,Carron Sherry, Donna Shelley, Caressa Singleton, Mike Smith, JoshuaSparrow, Gabriel Stover, Denise Sutton, Dawn Sykes, Bernard Wash-ington, Michael Weinstein, Mizetta Wilson, and Candace Young.
Notes. See Moloughney () and Saegert, Klitzman, Freudenberg,Cooperman-Mroczek, and Nassar ( ) for thoughtful reviews of thehousing and health literature from the planning and public healthperspectives, respectively.. See http://www.hcz.org for a description of the HCZ Project..Participants in the following HCZ programs were screened: BabyCollege, a program for parents of - to -year-old-children; CommunityPride, a community-building initiative; Employment and TechnologyCenter, a community computer lab; Family Support Center, a preventiveprogram working to strengthen families at risk for foster care placement;TRUCE, youth development through media arts; and TRUCE Fitnessand Nutrition Center, youth development through health and fitness.
ReferencesBhalla, C. K., Voicu, I., Meltzer, R., Ellen, I. G., & Been, V. ().State of New York’s housing and neighborhoods. New York: FurmanCenter for Real Estate and Urban Policy, New York University.Chaudhuri, N. (). Interventions to improve children’s health byimproving the housing environment. Reviews of Environmental Health, (–), –.Fagan, P., King, G., Lawrence, D., Petrucci, S. A., Robinson, R. G.,Banks, D., et al. (). Eliminating tobacco-related health disparities:Directions for future research. American Journal of Public Health, (),–.Fleiss J. L., Levin B., & Paik, M. C. (). Statistical methods for ratesand proportions, rd ed. New York: Wiley.Friere, P. (). Pedagogy of the oppressed. New York: Continuum.Gold, D., & Wright, R. (). Population disparities in asthma. AnnualReviews of Public Health, , –.Green, L., George, M. A., Daniel, M., Frankish, C. J., Herbert, C.P., Bowie, W. R., et al. (). Study of participatory research in health pro-motion: Review and recommendations for the development of participatoryresearch in health promotion in Canada. Vancouver, British Columbia:Royal Society of Canada.Israel B. A., Schulz, A. J., Parker, E. A., & Becker, A. B. (). Reviewof community-based research: Assessing partnership approaches toimprove public health. Annual Reviews of Public Health, , –.Kinney, P. L., Aggarwal, M., Northridge, M. E., Janssen, N. A. H., &Shepard, P. (). Airborne concentrations of PM(.) and dieselparticles on Harlem sidewalks: A pilot study. Environmental HealthPerspectives, (), –.Kinney, P. L., Northridge, M. E., Chew, G. L., Gronning, E., Joseph,E., Correa, J. C., et al., (). On the front lines: An environmentalasthma intervention in New York City. American Journal of PublicHealth, (), –.Krieger, J., Allen, C., Cheadle, A., Ciske, S., Schier, J. K., Senturia, K.,et al. (). Using community-based participatory research to addresssocial determinants of health: Lessons learned from Seattle partners forhealthy communities. Health Education and Behavior, (), –.
Spielman et al.: Interdisciplinary Planning for Healthier Communities
Dow
nloa
ded
by [
New
Yor
k U
nive
rsity
] at
09:
37 1
1 O
ctob
er 2
012

Journal of the American Planning Association, Winter , Vol. , No.
Krieger, J., & Higgins, D. L. (). Housing and health: Time again forpublic health action. American Journal of Public Health, (), –.Krieger, N., & Birn, A. E. (). A vision of social justice as the foun-dation of public health: Commemorating years of the Spirit of .American Journal of Public Health, (), –.Mannino, D. M., Homa, D. M., Akinbami, L. J., Moorman, J. E.,Gwynn, C., & Redd, S. C. (). Surveillance for asthma—UnitedStates, –. Morbidity and Mortality Weekly Report, (SS-), –.Minkler, M., & Wallerstein, N. (). Introduction to community-based participatory research. In M. Minkler & N. Wallerstein (Eds.),Community-based participatory research for health (pp. –). SanFrancisco: John Wiley & Sons.Moloughney, B. (). Housing and population health: The state ofcurrent research and knowledge. Ottowa: Canadian Insititute for HealthInformation.Morgan W. J., Crain, E. F., Gruchalla, R. S., O’Connor, G. T., Meyer,K., Evans, R., et al. (). Results of a home-based environmentalintervention among urban children with asthma. New England Journalof Medicine, (), –.National Heart, Lung, and Blood Institute. (). National asthmaeducation program expert panel report II: Guidelines for the diagnosis andmanagement of asthma (National Institutes of Health Publication No.-A). Washington, DC: National Institutes of Health.New York City Department of Health and Mental Hygiene. ().NYC vital signs: Asthma can be controlled. Retrieved March , ,from http://home.nyc.gov/html/doh/pdf/survey/survey-asthma.pdfNicholas, S. W., Hutchinson, V. E., Ortiz, B., Klihr-Beall, S., Jean-Louis,B., Shoemaker, K., et al. (). Improving childhood asthma throughcommunity-based service delivery: The Harlem Children’s ZoneAsthma Initiative. Morbidity and Mortality Weekly Report, (SS-), –.Nicholas, S. W., Jean-Louis, B., Ortiz, B., Northridge M. E., Shoemaker,K., Vaughan, R. D., et al. (). Addressing the childhood asthma crisisin Harlem: The Harlem Children’s Zone Asthma Initiative. AmericanJournal of Public Health, (), –.Northridge, M. E. (). It takes lawyers to deliver health care.American Journal of Public Health, (), .Northridge, M. E., Sclar E., & Biswas, P. (). Sorting out theconnections between the built environment and health: A conceptualframework for navigating pathways and planning healthy cities. Journalof Urban Health, (), –.
Northridge, M. E., Shoemaker, K., Jean-Louis, B., Ortiz, B., Swaner,R., Vaughan, R. D., et al. (). What matters to communities? Usingcommunity-based participatory research to ask and answer questionsregarding the environment and health. Essays on the future of environ-mental health research: A tribute to Dr. Kenneth Olden. Environonmen-tal Health Perspectives , (Suppl. ), –.Northridge, M. E., Yankura, J., Kinney, P., Santella, S., Shepard, P.,Riojas, Y., et al. (). Diesel exhaust exposure among adolescents inHarlem: A community-driven study. American Journal of Public Health, (), –.Rodriguez, M. A., Winkleby, M. A., Ahn, D., Sundquist, J., & Krae-mer, H. C. (). Identification of population subgroups of childrenand adolescents with high asthma prevalence: Findings from the thirdnational health and nutrition examination survey. Archives of Pediatricsand Adolescent Medicine, (), –.Saegert, S., Klitzman, S., Freudenberg, N., Cooperman-Mroczek, J.,& Nassar S. (). Healthy housing: A structured review of publishedevaluations of US interventions to improve health by modifying housingin the United States, –. American Journal of Public Health, (), –.Sandel, M., Phelan, K., Wright, R., Hynes, H. P., & Lanphear, B. P.(). The effects of housing interventions on child health. PediatricAnnals, (), –.Satcher, D. (). Our commitment to eliminate racial and ethnichealth disparities. Yale Journal of Health Policy Law Ethics, , –.Schulz, A., & Northridge, M. E. (). Social determinants of healthand environmental health promotion. Health Education and Behavior, (), –.Sclar, E. D., Northridge, M. E., & Karpel, E. M. () Promotinginterdisciplinary curricula and training in transportation, land use, physicalactivity, and health. Retrieved January , , from www.TRB.org/downloads/srpapers/srpaperstoc.pdfSwartz, M., Banasiak, N., & Meadows-Oliver, M. () Barriers toeffective pediatric asthma care. Journal of Pediatric Health Care, (),–.Takaro, T. K., Krieger, J. W., & Song, L. (). Effect of environ-mental interventions to reduce exposure to asthma triggers in homes oflow-income children in Seattle. Journal of Exposure Analysis and Envi-ronmental Epidemiology, (Suppl. ), S–S.
Dow
nloa
ded
by [
New
Yor
k U
nive
rsity
] at
09:
37 1
1 O
ctob
er 2
012
Copyright © 2022 FDOKUMEN




















