Intelligent image management in a distributed PACS and telemedicine environment
22
Intelligent Image Management in a Distributed PACS and Telemedicine Environment M. Tsiknakis 1 , D. Katehakis 1 , S. Orphanoudakis 1,2 1 Institute of Computer Science, Foundation for Research and Technology - Hellas, P.O. Box 1385, 711 10 Heraklion, Greece 2 Department of Computer Science, University of Crete, Heraklion, Greece Tel.: +30-81-391600, Fax.: +30-81-391601 IEEE Communications Magazine vol. 34(7), pp. 36-45 1996
Transcript of Intelligent image management in a distributed PACS and telemedicine environment

Intelligent Image Management in a DistributedPACS and Telemedicine Environment
M. Tsiknakis1, D. Katehakis1, S. Orphanoudakis1,2
1Institute of Computer Science, Foundation for Research and Technology - Hellas,P.O. Box 1385, 711 10 Heraklion, Greece
2Department of Computer Science, University of Crete, Heraklion, Greece
Tel.: +30-81-391600, Fax.: +30-81-391601
IEEE Communications Magazine
vol. 34(7), pp. 36-45
1996

-1 -
Intelligent Image Management in aDistributed PACS and Telemedicine
EnvironmentM. Tsiknakis1, D. Katehakis1, S. Orphanoudakis1,2
AbstractAdvances in information technology in the past decade have resulted in a proliferation of clinicalinformation systems dedicated to individual user groups and clinical functional areas. This, in turn,has led to the need for hospital-wide management and integration of information, and has triggeredmajor efforts towards the development of integrated hospital information systems.
A framework for developing an integrated regional health telematics system is presented, based on thefunctional and data integration of federated autonomous information systems. The concept of thepatient meta-record is introduced, as a central element in achieving integration in terms of content,structure, and access to information resources. Intelligent image management at the level of either asingle health care provider (hospital) or at the level of a regional health telematics network isaddressed and is achieved through event and model-driven strategies enabled by a distributedhierarchical storage management system. Intelligence, in this context, refers to methods of efficientand effective real-time resource management in the timely delivery of health care.
Keywords: computerized patient record, PACS, intelligent image management, telemedicine,hierarchical storage management, patient meta-record.
1. IntroductionThe health care organizational structure is naturally distributed, consisting of ageographical spread of medical centers in a hierarchy of regional hospitals down toindividual general practitioners. The objective of this structure is to offercomprehensive medical care at a local and regional level with continuity acrossdifferent levels of the hierarchy. Although each medical center is autonomous anddevoted to the delivery of a particular set of services, the desirable continuity of carerequires that different medical centers, offering complementary services or differentlevels of expertise, exchange relevant patient data and operate in a cooperativeworking environment. The sharing of information resources is generally accepted asthe key to substantial improvements in productivity and to better quality of service[[23] ].
The diversity of hospital organizations, the complexity of clinical protocols andprocedures, as well as the different preferences of various user groups make itextremely difficult for a single monolithic information system to effectively serve theneeds of an entire health care organizational structure. As a consequence, users mustbe allowed to select the applications most suitable for their needs and requirements. Inaddition, a number of applications are already available on the market that addressspecific aspects of the health care structure. Thus, information and
1Institute of Computer Science, Foundation for Research and Technology - Hellas, Heraklion, Crete, Greece.
2Department of Computer Science, University of Crete, Heraklion, Crete, Greece.
-2 -
telecommunications systems must primarily provide the infrastructure to permit theeffective integration of distributed and heterogeneous components, ensuring overallintegrity in terms of functional and information interworking.
The physically distributed resources of the health care sector and the diverserequirements of different medical facilities and clinical departments require thatspecialized autonomous information systems are used to support differentfunctionalities, while they interact transparently to the user as a federation ofautonomous systems. This approach to developing and managing regional healthtelematics applications ensures the transfer and integration of consistent informationthroughout a network of health care facilities, without imposing constraints on theoperation of individual units.
From the technological viewpoint, the adoption of standards and open architecturesrepresents the only viable solution to the problem of integrating diverse systemcomponents through an incremental approach, consistent with evolving requirements,while securing the investments already made. The definition and adoption of standards,not only as these concern the technical aspects, but mainly with respect to thefunctional interfaces between the various system components, represents a fundamentalrequirement which must be satisfied before different applications, developed bydifferent suppliers, can be integrated and used effectively in health care.
The purpose of this paper is to present the key design principles of a regional healthtelematics network and, specifically, to address the issue of intelligent imagemanagement in such a system. Section 2 introduces the patient meta-record concept asa means of integration of all patient related data and the activity concept as a formalismcapable of modeling a broad spectrum of healthcare processes. Section 3 presents thearchitecture of a hospital information system, integrated, through the patient meta-record. Section 4 presents the architecture of TelePACS 2.0, an extensible imagemanagement system, and its efficient and intelligent management and communicationof images, achieved through the implementation of a distributed hierarchical storagemanagement system. Section 0 presents some advanced added-value telematic servicesto be implemented within the framework of the regional health telematics network ofCrete. The final section concludes this phase of our R&D work and presents our futurework. A discussion of work to date and future work is included in Section 6.
2. The Patient Meta-Record ConceptThe integration of information and knowledge from different sources is increasinglybecoming a key to better quality of care. Achieving this integration, however, is achallenging problem mainly because the logic, knowledge and data structures used invarious systems are complex and often incompatible. Many tasks require a largevolume of data processing and communications across heterogeneous and distributedenvironments [[8] ].
Today, the problem of harnessing disparate information resources remains one of themost intensely contested information technology issue in the international researcharena [[14] ]. A promising approach to this integration problem is to gain control ofthe organization’s information resources at a meta-data level, while allowing autonomyof individual subsystems at the data instance level [[11] ]. The objective of the meta-
-3 -
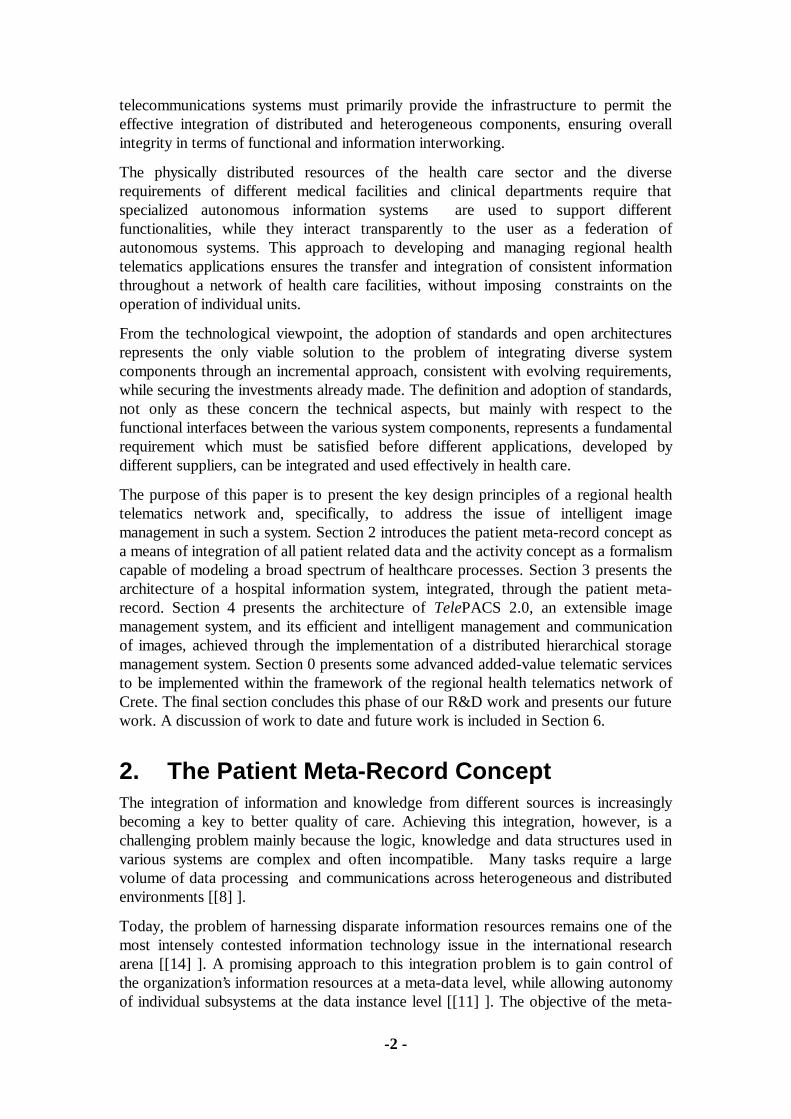
database model is to achieve enterprise information integration over distributed andpotentially heterogeneous systems while allowing these systems to operateindependently and concurrently [[12] ].
In order to turn a large, heterogeneous and distributed set of Computerized PatientRecord (CPR) components into a seemingly integrated and homogeneous patientrecord, the concept of the Patient Meta-Record (PMR) has been introduced [[18] ,[21] ]. The PMR concept permits the integration of CPR components, and alsoprovides aggregation and navigation facilities (which, in turn, can be fully configuredand customized) in order to assist in the appropriately personalized utilization of theCPR by the respective functional units or health care providers. The PMR manages, ata single logical point, references to all of the physical information related to a patientthroughout the Integrated Hospital regardless of where such information may reside.Therefore, it is an indexing system, providing access to all stored data for a particularpatient.
Physical CPR segments, distributed among several autonomous departmentalinformation systems are integrated by means of the institutional PMR. This PMRnotion can be extended at a regional, national or even transnational level (Figure 1).
The PMR may be seen as a central element in the provision of integrated computerassisted health care. The general approach relies
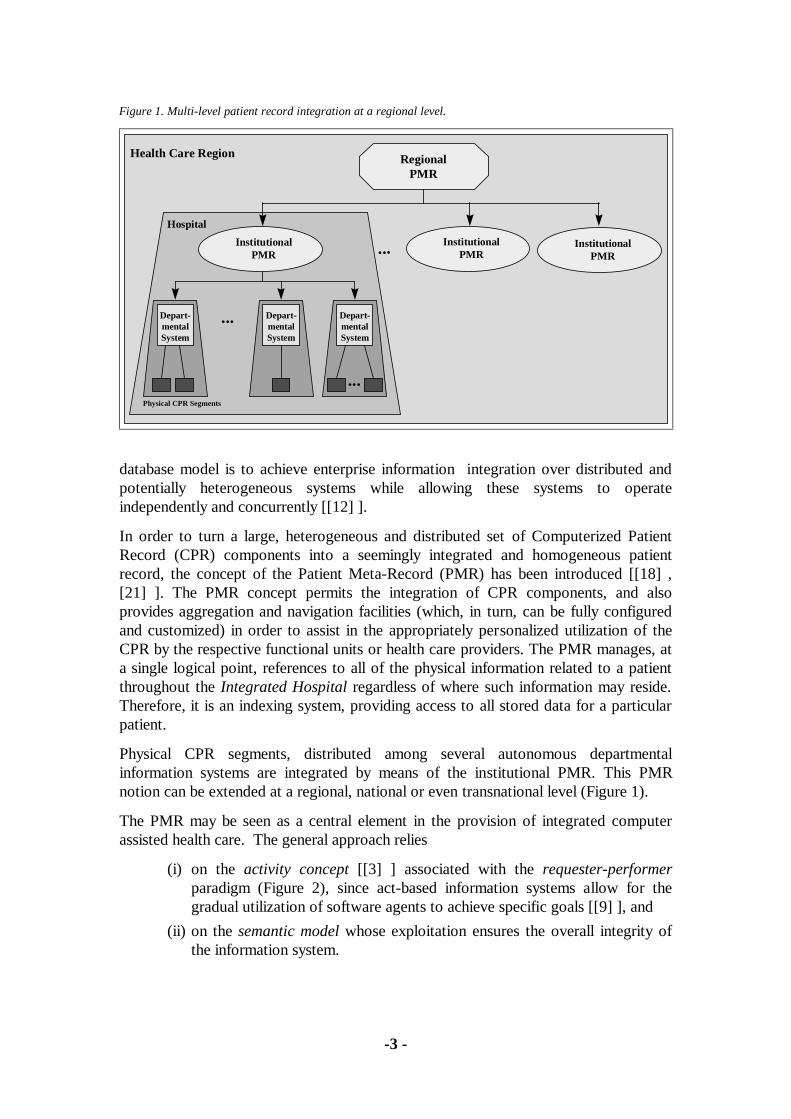
(i) on the activity concept [[3] ] associated with the requester-performerparadigm (Figure 2), since act-based information systems allow for thegradual utilization of software agents to achieve specific goals [[9] ], and
(ii) on the semantic model whose exploitation ensures the overall integrity ofthe information system.
Figure 1. Multi-level patient record integration at a regional level.
...
RegionalPMR
Physical CPR Segments
Depart-mentalSystem
Depart-mentalSystem
...
Depart-mentalSystem
...
Hospital
Health Care Region
InstitutionalPMR
InstitutionalPMR
InstitutionalPMR
-4 -
2.1. The Activity ConceptIn developing the architecture of an integrated hospital information system, ourobjective is to introduce a formalism that is capable of modeling a broad spectrum ofstructured and unstructured healthcare tasks, in a rigorous and comprehensive manner.The Activity Manager System (AMS) formalism [[3] ] is particularly suitable as arepresentation tool to describe the characteristics of the complex hospital tasks.
Acts and intelligent act management are central concepts in our approach. An act isany professional activity, which influences a patient’s status or augments theknowledge about a patient’s status. Acts have a life-cycle consisting of differentsuccessive states: demanded, established, accepted, canceled, performed, etc.As analyzed in [[3] ], three types of information are encapsulated by the activityconcept:
• the start-state, describing the precondition for performing the activity (e.g.authorization of user x to request examination y),
• the terminal-state, describing the effect (or the reached goal) caused by theexecution of the act, and
• the body, describing the way the activity is to be performed.
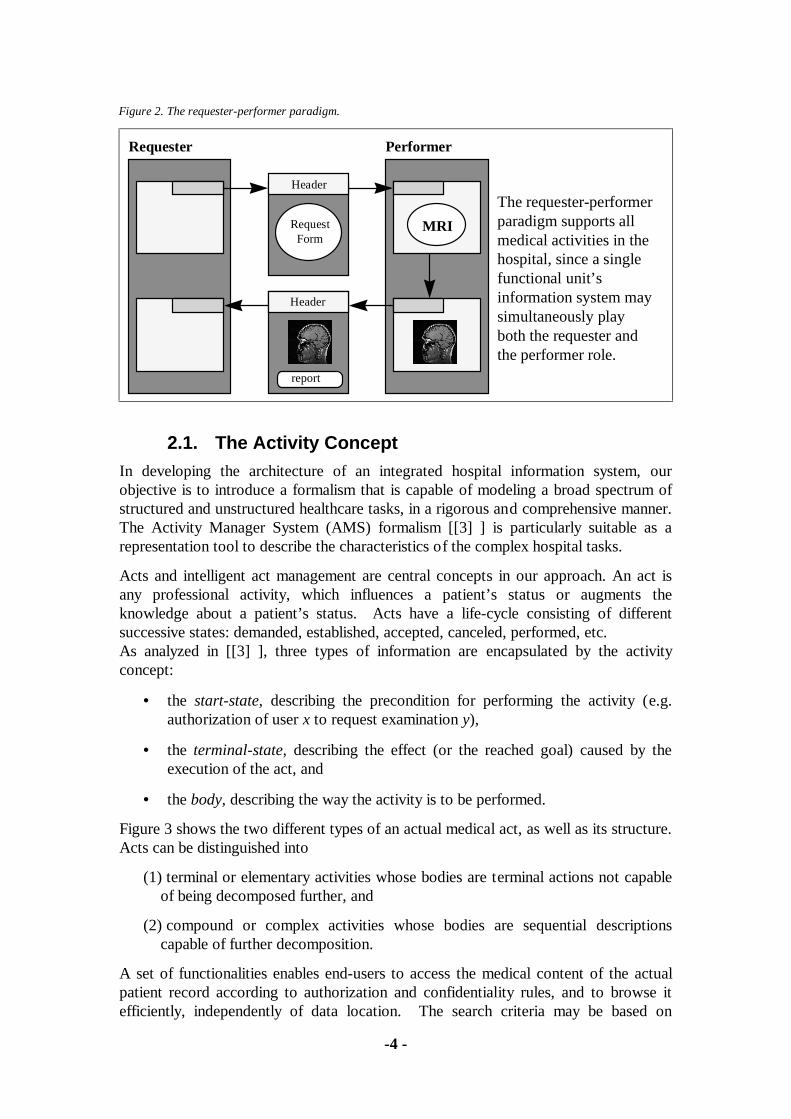
Figure 3 shows the two different types of an actual medical act, as well as its structure.Acts can be distinguished into
(1) terminal or elementary activities whose bodies are terminal actions not capableof being decomposed further, and
(2) compound or complex activities whose bodies are sequential descriptionscapable of further decomposition.
A set of functionalities enables end-users to access the medical content of the actualpatient record according to authorization and confidentiality rules, and to browse itefficiently, independently of data location. The search criteria may be based on
Figure 2. The requester-performer paradigm.
MRI
Performer
The requester-performerparadigm supports allmedical activities in thehospital, since a singlefunctional unit’sinformation system maysimultaneously playboth the requester andthe performer role.
Requester
RequestForm
Header
Header
report

-5 -
information contained in an act’s header or in its medical content. A search may alsoexploit the semantic model, which provides information on the structure of an act, itspossible links to other acts, etc.
2.2. The Semantic ModelWe base our PMR on the Semantic Indexing System (SIS) [[7] ]. The SIS is a tool fordescribing and documenting large evolving varieties of highly interrelated data,concepts and complex relationships. The SIS consists of a persistent storagemechanism based on an object-oriented semantic network data model, and a genericinteractive user interface to insert and retrieve information in various ways. The SISoffers significantly richer referencing mechanisms than relational or ordinary object-oriented systems. Together with the very high query speed, these mechanisms allowthe data and schema to be kept free of redundancies. An interesting feature of the SISis that its data entry mechanism, query system and user interface treat data and schemain a uniform manner.
The SIS will also be employed for the development of a context mediator in the sensedescribed in [[22] ]. The context mediator is an agent that directs the exchange ofvalues, from one autonomous information system to another, using domain knowledge,and provides services such as local-to-global schema translation, intersystem attributemapping, and consistency checking. All data exchange goes through the contextmediator. The context mediator in our approach is an example of the mediator conceptof Wiederhold [[26] ]. As we can see in Figure 4, each subsystem provides pairs ofconversion functions for the two-way mapping between its local values and the globalvalues, as used by the PMR. This way subsystems export communications methods andallow for dynamic schema definition and modification at runtime. Moreover, theschema is visible to the user, supporting the explanation and exploration of itsstructure.
Figure 3. Structure of an actual medical act.
Header
MedicalContent
• Act HeaderPatient ID, Act ID, Class of Act, Requester ID, Performer ID, Date, Current Status, History, ...
• Medical ContentImage, Bio-signal, Lab Results, Report, ...
Decomposition of a compoundact into its components.
Compound Medical Act
check up
CT
ECG
Elementary Medical Act

-6 -
Our approach enforces an important trend towards decoupling of applications fromother applications and data sources, thus simplifying the interface among systemcomponents [[22] ].
3. Architecture of an Integrated HospitalInformation System
A hospital is by far the most complex organization in the health care hierarchy.Therefore, a primary objective in developing a regional health telematics network is todesign and develop an Integrated Hospital Information System (IHIS) capable ofeffectively and efficiently supporting all patient related clinical processes within ahospital. The IHIS development is based on the definition and implementation of anopen architecture where the individual modules:
• are autonomous and self-consistent, supporting specific functional units;
• interwork through stable, public interfaces;
• are configurable, able to operate in a distributed environment, and can adapt tothe specific requirements and characteristics of an individual organization.
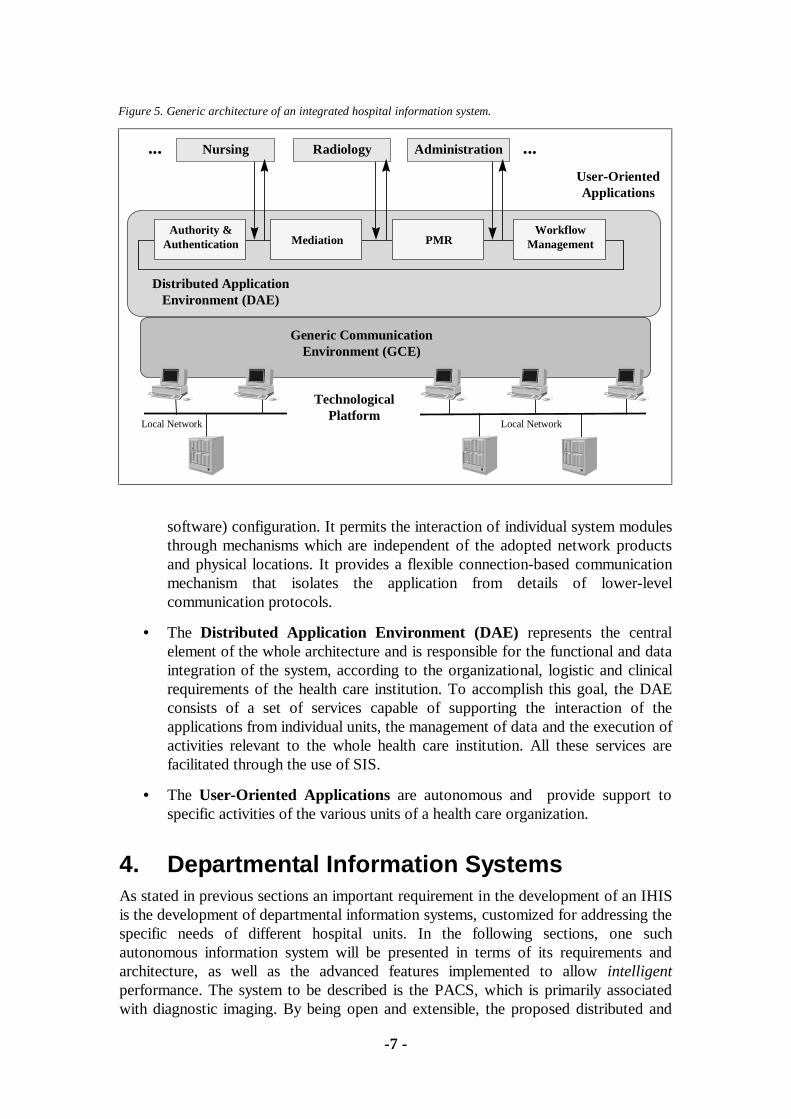
The key characteristic of the proposed architecture is its layered structure, based onfour fundamental layers, as shown in Figure 5.
• The Technological Platform is responsible for the transparent integration ofdistributed heterogeneous technological environments.
• The Generic Communication Environment (GCE) is responsible forensuring the transparency of the actual technological (both hardware and
Figure 4. Conversion routing implemented by means of the SIS.
mediator
PMRSIS
HL7LIS
DICOM 3.0
PACS
HL
7/S
CP
-EC
G
,&8
-7 -
software) configuration. It permits the interaction of individual system modulesthrough mechanisms which are independent of the adopted network productsand physical locations. It provides a flexible connection-based communicationmechanism that isolates the application from details of lower-levelcommunication protocols.
• The Distributed Application Environment (DAE) represents the centralelement of the whole architecture and is responsible for the functional and dataintegration of the system, according to the organizational, logistic and clinicalrequirements of the health care institution. To accomplish this goal, the DAEconsists of a set of services capable of supporting the interaction of theapplications from individual units, the management of data and the execution ofactivities relevant to the whole health care institution. All these services arefacilitated through the use of SIS.
• The User-Oriented Applications are autonomous and provide support tospecific activities of the various units of a health care organization.
4. Departmental Information SystemsAs stated in previous sections an important requirement in the development of an IHISis the development of departmental information systems, customized for addressing thespecific needs of different hospital units. In the following sections, one suchautonomous information system will be presented in terms of its requirements andarchitecture, as well as the advanced features implemented to allow intelligentperformance. The system to be described is the PACS, which is primarily associatedwith diagnostic imaging. By being open and extensible, the proposed distributed and
Figure 5. Generic architecture of an integrated hospital information system.
...
Distributed ApplicationEnvironment (DAE)
Nursing Radiology Administration...
User-OrientedApplications
Local Network
TechnologicalPlatform
Generic CommunicationEnvironment (GCE)
PMR
Local Network
MediationAuthority &
AuthenticationWorkflow
Management
-8 -
modular architecture provides the basis for developing not only a hospital wide PACS,but ultimately an integrated regional Image Management and Communication System(IMACS) covering all of medical imaging including microscopy, endoscopy, etc.
4.1. The Diagnostic Imaging and CommunicationProcess
Medical images are one of the most important sources of diagnostic information. Theinformation flow involved, from the actual request for a radiological examination bythe referring physician to obtaining the radiologist’s report, requires considerablemovement of people, paper, and film with all of the attendant possibilities for delay andloss. The actual acquisition of diagnostic images is only one element in the chain. Themost important elements from the viewpoint of patient care are the following :
• the referral process, in which the attending physician requests an examination,
• the acquisition process, in which diagnostic imaging takes place,
• the reporting process, in which the radiologist reads the films and reports hisfindings,
• the image management process, in which diagnostic images and other patientrelated data are properly stored for future reference, and
• the consultation process, in which the radiologist and one or more attendingphysicians review the case.
4.2. PACS Storage and Communication RequirementsIn designing a PACS network architecture, selecting the appropriate type of networkand developing adequate communication mechanisms, the PACS imagecommunication pattern has to be determined. Estimates of the anticipated imagecommunication load and its temporal patterns can be found in [[17] ], whererepresentative figures, derived from observations and statistical evaluations at severalhospitals, are presented.
A first estimate of the mean image data transmission load was based on the total imageproduction and image consumption at reporting sites versus time. For example, theradiology department of the Aachen University Hospital (1500 beds) produces about20 Tbytes of image data per year. Similarly, the annual volume of images generated ina medium-size hospital of 600 beds is reported as 1.15 million images or 1.9 Tbytes in[[15] ].
In order for PACS to be effective in its role as a added-value service for theimprovement of patient care, image data must be delivered to their destination withnegligible delay. An image latency time of 1-2 seconds or data rates of 65-335 Mbpsare considered adequate for typical clinical situations [[13] ].
In a more recent publication on a PACS testbed installation [[27] ], the effectivetransfer rate was reported to be 3 Mbps with an Ethernet (disk-to-disk) and 14.4 Mbpswith an FDDI network (RAM-to-RAM). Therefore, FDDI with its 100 Mbps physicaldata rate may also result in a communication bottleneck. Intelligent image management

-9 -
[[16] ] provides solutions to the problem of timely delivery of image data in a PACSenvironment, given such a communication bottleneck. In this context, intelligence orintelligent behavior is characteristic of a system capable of achieving near real-timeperformance by selective exploitation of tools and strategies, given limitedcommunication and computational resources.
4.3. The TelePACS Image Management SystemThe Medical Information Systems Laboratory of the Institute of Computer Science(ICS), Foundation for Research and Technology - Hellas (FORTH), has designed andimplemented TelePACS 1.0, a system for the acquisition, management, andcommunication of medical images and related patient information (see Figure 6). Thissystem has been installed at the Radiology Clinic of the University of Athens, variousimaging clinics of the University Hospital in Heraklion, Crete and the VenizelionRegional Hospital, also in Heraklion. TelePACS 1.0 forms the basis of a pilottelemedicine network connecting these three hospitals, which is currently undergoingclinical evaluation.
In this Section, we present the architecture of TelePACS 2.0 [[21] ], which is currentlybeing implemented and supports the intelligent management of images at a local(hospital) and regional level.
Figure 6. Typical screen from TelePACS 1.0.
-10 -
4.3.1. TelePACS 2.0 Servers
The architecture of TelePACS 2.0 is open, distributed and modular, based on a largenumber of file servers which are distinguished according to their function. TheTelePACS 2.0 servers and their corresponding functions are:
• The Acquisition Server, which is connected to medical imaging modalities andis responsible for the acquisition of multimedia medical data. A singleacquisition server can be configured to serve one or multiple imagingmodalities.
• The Archive Server, which manages the permanent storage of images in atransparent hierarchical storage structure. One such server is normally presentin each hospital department.
• The Central Hospital Server, that holds meta-information on patient data andacts as a gateway among heterogeneous information systems. This is where thecontext resolution takes place. One such server is normally present in eachhospital.
• The Departmental Server, which is the front end to the intra-hospitalnetwork. One per department or cluster of servers.
• The Display Server, which is connected to a set of display workstations withadvanced Graphical User Interfaces (GUI). Caches patient related data.Schedules examination requests on acquisition servers.
• The Key Server, which is responsible for encryption and authentication. Oneper Hospital.
• The Name Server, which holds the directory of both the local TelePACS 2.0clusters and all remote TelePACS 2.0 systems. Manages both incoming andoutgoing communication. Each TelePACS 2.0 System has one primary nameserver.
4.3.2. TelePACS 2.0 Clusters
TelePACS 2.0 clusters form the basic components of the system in the intra-hospitalenvironment. Each cluster usually covers a hospital department and consists of morethan one servers. Departmental servers are responsible for cluster coordination. Thus,all intra-hospital communication is managed by departmental servers (placement ofservice requests, monitoring of outstanding requests, etc.).
4.3.3. TelePACS 2.0 Systems
TelePACS 2.0 systems form the nodes of the regional medical image managementsystem and are intended for autonomous hospital environments. Inter-hospitalcommunications are managed by the central hospital server that holds the mostimportant information (e.g. PMR, local TelePACS addresses, availability of resources,etc.).
-11 -
4.4. Work Flow ScenariosThe AMS formalism as a theoretical tool for the development of knowledge-basedsystems has been demonstrated in [[1] ], where an office model, using office operators(e.g. request, approve, perform, answer, circulate) as basic building blocks toconstruct office procedures, has been presented. These procedures can then be definedby creating activities, which are then implemented by using these operators and therequester-performer matching mechanism.
The AMS formalism together with the requester-performer paradigm was employedfor analyzing and modeling several medical acts to be supported by TelePACS 2.0. Thedescription of some acts, and the resulting information flow among informationsystems involved follows.
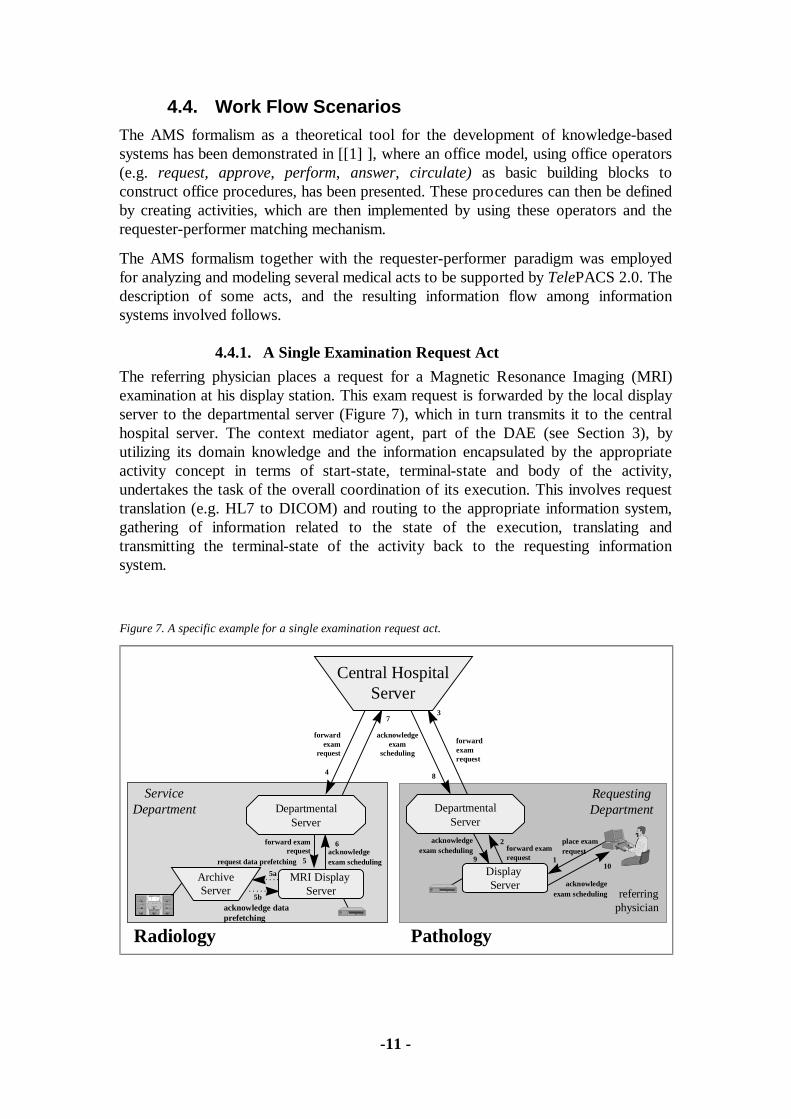
4.4.1. A Single Examination Request Act
The referring physician places a request for a Magnetic Resonance Imaging (MRI)examination at his display station. This exam request is forwarded by the local displayserver to the departmental server (Figure 7), which in turn transmits it to the centralhospital server. The context mediator agent, part of the DAE (see Section 3), byutilizing its domain knowledge and the information encapsulated by the appropriateactivity concept in terms of start-state, terminal-state and body of the activity,undertakes the task of the overall coordination of its execution. This involves requesttranslation (e.g. HL7 to DICOM) and routing to the appropriate information system,gathering of information related to the state of the execution, translating andtransmitting the terminal-state of the activity back to the requesting informationsystem.
Figure 7. A specific example for a single examination request act.
RequestingDepartment
forward examrequest
Departmental Server
referringphysician
Pathology
ServiceDepartment Departmental
Server
ArchiveServer
Radiology
Central HospitalServer
request data prefetching
MRI Display Server
Display Server
acknowledge dataprefetching
place examrequest
forward examrequest acknowledge
exam scheduling
acknowledgeexam scheduling
acknowledgeexam scheduling
forwardexam
request
forwardexamrequest
acknowledgeexam
scheduling
1
2
3
4
5
6
7
8
910
5a
5b
-12 -
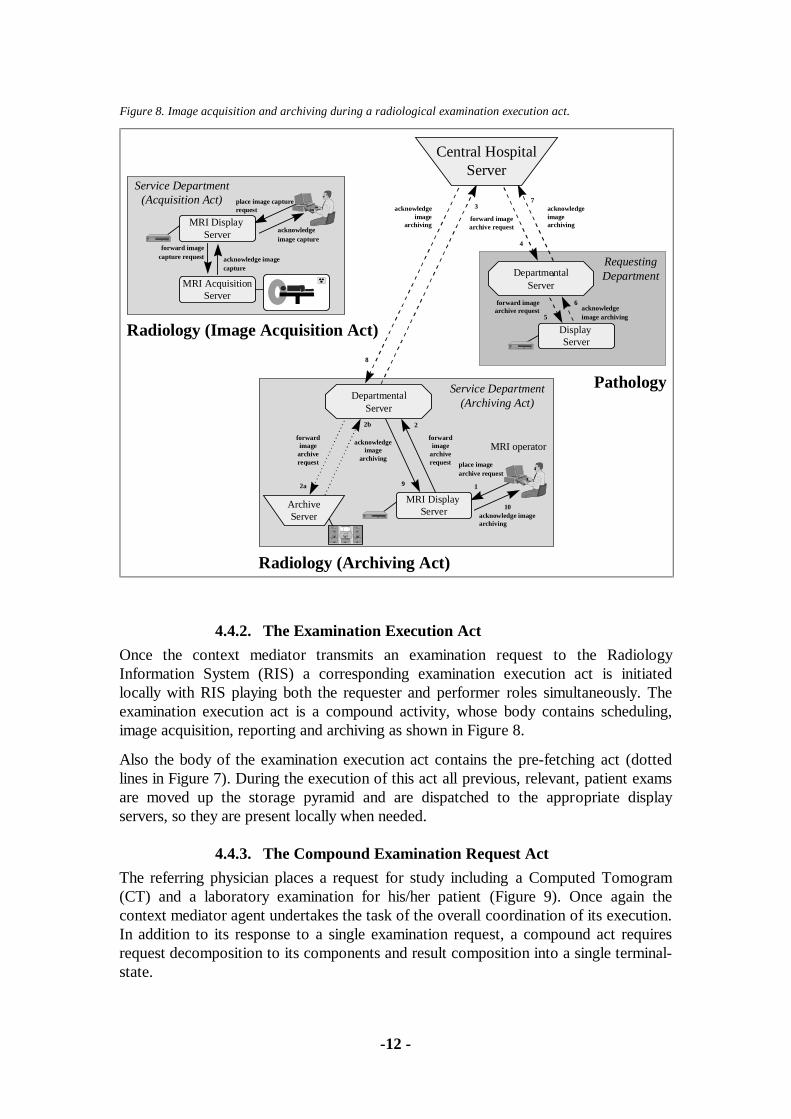
4.4.2. The Examination Execution Act
Once the context mediator transmits an examination request to the RadiologyInformation System (RIS) a corresponding examination execution act is initiatedlocally with RIS playing both the requester and performer roles simultaneously. Theexamination execution act is a compound activity, whose body contains scheduling,image acquisition, reporting and archiving as shown in Figure 8.
Also the body of the examination execution act contains the pre-fetching act (dottedlines in Figure 7). During the execution of this act all previous, relevant, patient examsare moved up the storage pyramid and are dispatched to the appropriate displayservers, so they are present locally when needed.
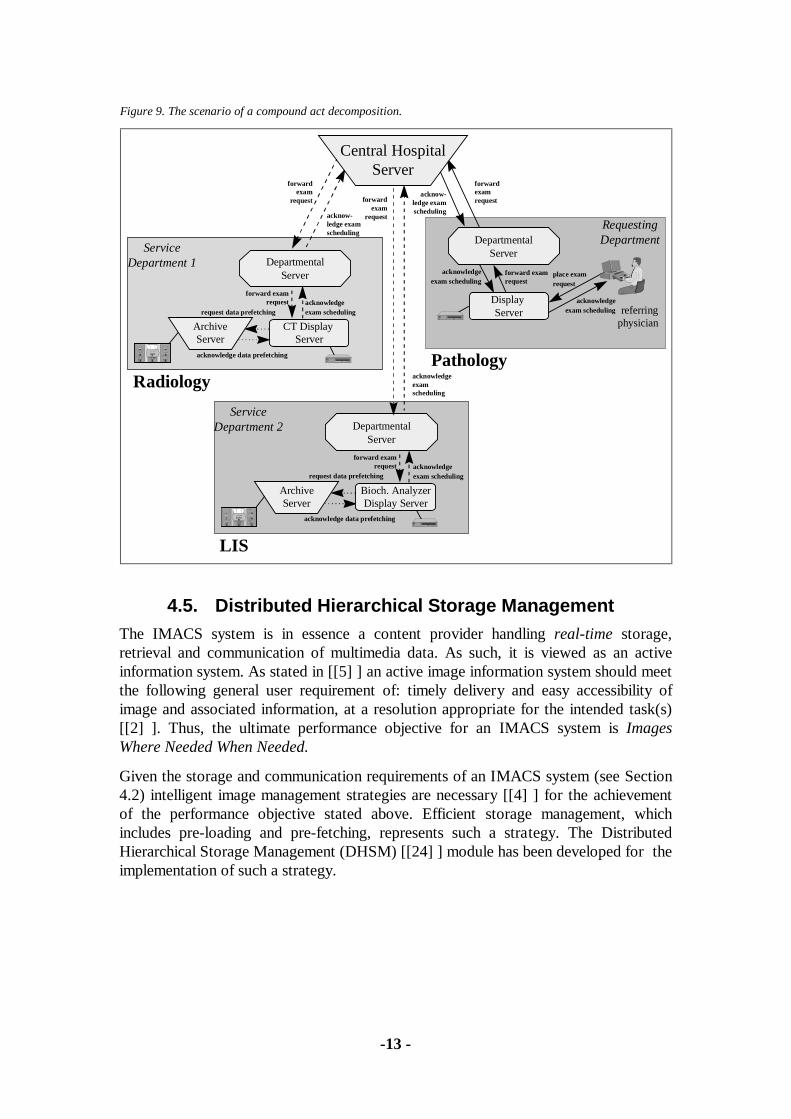
4.4.3. The Compound Examination Request Act
The referring physician places a request for study including a Computed Tomogram(CT) and a laboratory examination for his/her patient (Figure 9). Once again thecontext mediator agent undertakes the task of the overall coordination of its execution.In addition to its response to a single examination request, a compound act requiresrequest decomposition to its components and result composition into a single terminal-state.
Figure 8. Image acquisition and archiving during a radiological examination execution act.
RequestingDepartment
acknowledgeimage archiving
Departmental Server
Pathology
Display Server
forward imagearchive request
Radiology (Archiving Act)
Service Department(Archiving Act)
ArchiveServer
place imagearchive request
Departmental Server
MRI operator
MRI AcquisitionServer
forward imagecapture request acknowledge image
capture
place image capturerequest
acknowledgeimage capture
Service Department(Acquisition Act)
Radiology (Image Acquisition Act)
acknowledge imagearchiving
MRI Display Server
Central HospitalServer
MRI Display Server
acknowledgeimagearchiving
acknowledgeimage
archiving
acknowledgeimage
archivingforward imagearchive request
forwardimage
archiverequest
forwardimage
archiverequest
1
2
2a
2b
3
4
7
6
4
5
8
9
10
-13 -
4.5. Distributed Hierarchical Storage ManagementThe IMACS system is in essence a content provider handling real-time storage,retrieval and communication of multimedia data. As such, it is viewed as an activeinformation system. As stated in [[5] ] an active image information system should meetthe following general user requirement of: timely delivery and easy accessibility ofimage and associated information, at a resolution appropriate for the intended task(s)[[2] ]. Thus, the ultimate performance objective for an IMACS system is ImagesWhere Needed When Needed.
Given the storage and communication requirements of an IMACS system (see Section4.2) intelligent image management strategies are necessary [[4] ] for the achievementof the performance objective stated above. Efficient storage management, whichincludes pre-loading and pre-fetching, represents such a strategy. The DistributedHierarchical Storage Management (DHSM) [[24] ] module has been developed for theimplementation of such a strategy.
Figure 9. The scenario of a compound act decomposition.
acknowledgeexam schedulingService
Department 1
ArchiveServer
Radiology
request data prefetching
CT Display Server
acknowledge data prefetching
forward examrequest acknowledge
exam scheduling
ServiceDepartment 2
ArchiveServer
LIS
request data prefetching
Bioch. AnalyzerDisplay Server
acknowledge data prefetching
forward examrequest acknowledge
exam scheduling
Departmental Server
Departmental Server
RequestingDepartment
forward examrequest
referringphysician
Pathology
Display Server
place examrequest
acknowledgeexam scheduling
Departmental Server
Central HospitalServer
acknowledgeexam scheduling
forwardexam
request
forwardexamrequestforward
examrequest
acknow-ledge examscheduling
acknowledgeexamscheduling
acknow-ledge examscheduling

-14 -
4.5.1. Hierarchical Storage Management
The key characteristic of storage media necessitating the introduction of a storagehierarchy are access, speed, capacity and cost [[6] ]. The overall objective inintroducing a storage hierarchy is to provide average access speed almost as fast as thefastest level, the High Speed Buffer (HSB), with an average cost per bit of on-linedata almost as low as the least expensive level, the Direct Access Storage Device(DASD). This performance requirement can only be achieved if the majority of on-linedata are resident on DASD while almost all of the Central Processing Unit’s (CPU)storage accesses are satisfied by high-speed buffers. Figure 10 shows such a storage
pyramid.
4.5.2. Image Management Strategies
The DHSM allows for the intelligent management of storage, according to pre-definedmodels (model-driven) or in response to trigger events (event-driven).
Model-Driven Image Management: Image data is automatically moved downwardaccording to a Least Recently Used (LRU) algorithm and the corresponding settings(e.g. a third of the HSB capacity must always be empty to satisfy requirements forevent driven upward migration of required data).
Event-Driven Image Management: As stated in Section 0, an examination executionact initiates the prefetching act which has as a precondition the successful scheduling ofthe requested examination. The DHSM prefetching algorithm identifies all previouspatient data managed by the IMACS system and transfers them to the appropriatedisplay server, to be available during the reporting phase of the process together withthe currently generated examination image data. Additionally, the DHSM pre-fetchingalgorithm not only retrieves past examinations into the highest storage level of thearchive server but also dispatches them to distributed caches at the correspondingdisplay servers.
Figure 10. The hierarchical storage management pyramidwith respect to the physical medium.
HSB
DASD
User ShortAccessTime
LargeStorage
Capacity

-15 -
4.5.3. The DHSM System Architecture
The DHSM system introduces an additional layer of cache memory on disk betweenthe application and the information managed by distant, slow-to-access, archive servers(Table 1). Upward and downward migration through the storage hierarchy is based onreference activities. The management approach is based on an LRU algorithm forreplacing an inactive data element by a more active one. The element replaced ismoved downward in the hierarchy, while the requested element rises to the top of thehierarchy. Figure 11 illustrates the proposed architecture through a possible scenario ofthree applications running in three different locations (e.g. departments) and sharingimages of the same modality, stored in tables A1, A2, and A3. The role of the dhsm-deamon is to maintain the loose-consistency among the distributed caches.
5. Telematic ServicesHealth care is an important telematics application domain in the emerging informationsociety. In recent years, we have all been witnesses to the gradual transformation ofhealth informatics into health telematics, a process which continues. For thistransformation to be successful a strategy is needed for the creation of an integrated
Figure 11. Data sharing through the use of the DHSM module.
Hierarchical Storage Management
Application 3(shares its data with site 2)
RDBMS 3 dhsm-deamon
Site 3
Cache of A2
Table A3
Hierarchical Storage Management
Application 2(shares its data with site 3)
RDBMS 2 dhsm-deamon
Site 2
Cache of A1
Table A2
Cache of A3
Hierarchical Storage Management
Application 1(shares its data with site 2)
RDBMS 1
Site 1
Table A1
dhsm-deamon
Table 1. The DHSM pyramid.
Layers of StorageManagement
Location Maximum Capacity
User Application Display Server Limited by the size of RAMCache Local Archive Server A fraction of the total locally kept dataStorage Medium Remote Archive Server Practically unlimited
-16 -
health care information infrastructure. A fundamental problem for the establishment ofa scaleable regional health telematics network is the development of an architectureand tools for the integration of specialized autonomous applications that, together witha shared patient record, will support the interoperability of functions and serviceswithin a health care institution, the interconnection of different institutions, and theintelligent management of medical data within such a network.
With this in mind the Medical Information Systems Laboratory of ICS - FORTH isdeveloping a regional health telematics network based on an open, expandable andextensible architecture with various added-value autonomous systems supportingclinical decision making, medical training, and clinical research, which will eventuallyextend the functionalities and services supported. Examples of such subsystems whichare currently at various stages of development are: a computer supported conferencingapplication, an advanced image processing module and the Image Indexing by Content(I2C) system described below.
Synchronous teleconsultation is possible via a Computer Supported Cooperative Work(CSCW) application [[25] ], which allows interactive real-time cooperation amongseveral conference participants. This application provides a shared workspace for thedisplay, discussion and annotation of multimedia medical data which is multicasted toconference participants prior to the consultation session. A replicated architecture andtechniques for caching, data compression and screening of events allow its successfuloperation over heterogeneous, relatively slow networks.
Version 1.0 of TelePACS (see Section 4.3) has already been integrated with the I2Csystem [[20] ], an information system providing an object oriented environment for theindexing and retrieval of medical images by pictorial content (Figure 12). The I2Carchitecture integrates a set of tools and algorithms for the extraction, indexing andstorage of image descriptions. The interoperability of the two systems provides added-value capabilities to both systems, thus creating a powerful environment for clinical,educational and research activities.
I2C is currently being extended to I2Cnet [[19] ], so that it will operate over theevolving regional health telematics network. I2Cnet is a network of image descriptionservers based on I2C, which operate over the World Wide Web. Through the WWWbrowser, I2Cnet users are provided with reliable, network transparent content-basedaccess to a geographically distributed image collections maintained by I2C servers. Thearchitecture of I2Cnet brought out several new issues and challenges. Peer-to-peerserver communication, agent based computing, query formulation, incremental querymodification, query decomposition and result composition are but a few of them.
A Pre-Hospital Health Emergency Management System (PHEMS) is also beingdeveloped as a distributed real time system. The system allows prompt and efficientmanagement of the response to a health emergency and the efficient mobilization of theoperational resources at a regional level. Functional integration of the basic healthtelematics system, through the PMR, with the PHEMS allows the efficient transmissionof the physical patient record contents to relevant health care providers and/or experts,as required in intelligently and efficiently managing health emergencies.

-17 -
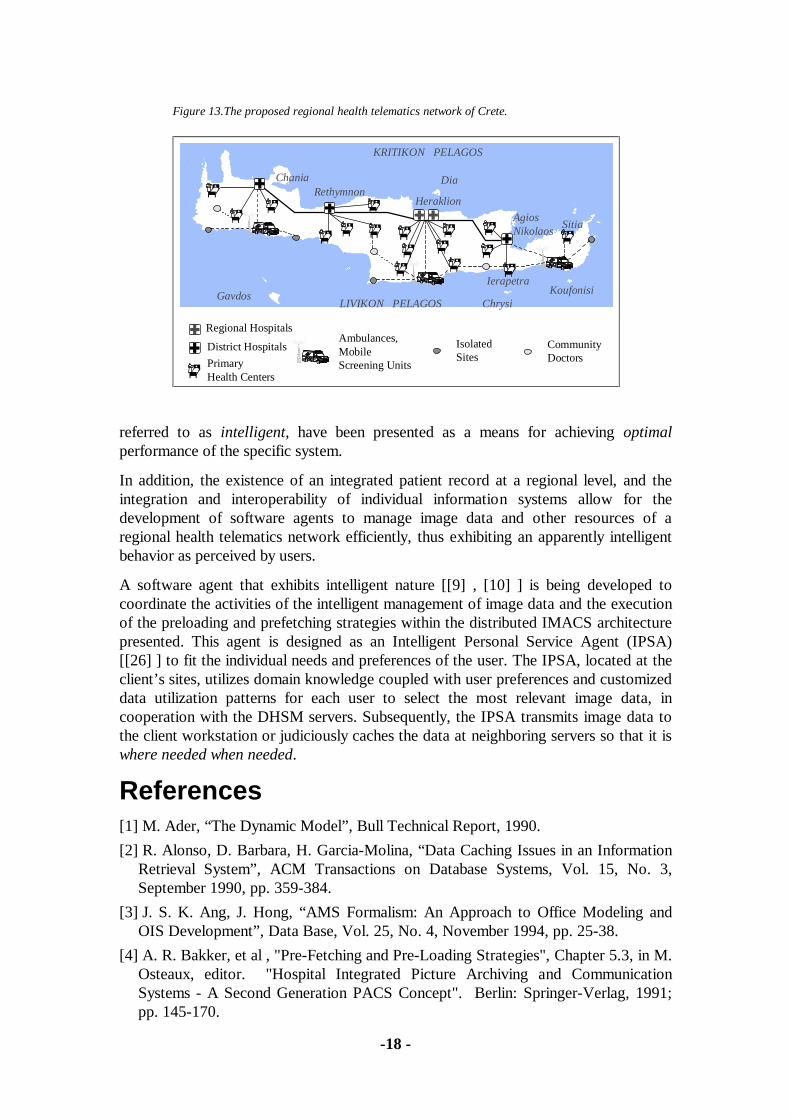
6. DiscussionThe ultimate goal of our R & D efforts is to design and develop an integrated healthtelematics network in the region of Crete (Figure 13), by developing and validatingtelematic services connecting health care professionals at all levels of care.
A fundamental problem for the establishment of such a network is the development ofan architecture and tools for the integration of specialized autonomous applications,that together with a shared patient record will support interoperability of function andservices within the health care institution, the interconnection amongst institutions, andthe intelligent management of medical data within such an integrated network.
This paper presents the PMR concept as a mean for integrating a large, heterogeneousand distributed set of CPR components (direct observations) into an unified andhomogeneous patient record. This allows for the medical record of a patient to beviewed in a variety of different ways, according to the needs and capabilities of theindividual customized information system.
Through this approach, individual information systems can be autonomouslycustomized, or even optimized as far as their independent operation is concerned,according to the specific requirements of the corresponding functional units. Thearchitecture of such a system, i.e. TelePACS 2.0, is presented. Effective and efficientimage management strategies, which in the context of this application domain are
Figure 12. The I2C user interface.
-18 -
referred to as intelligent, have been presented as a means for achieving optimalperformance of the specific system.
In addition, the existence of an integrated patient record at a regional level, and theintegration and interoperability of individual information systems allow for thedevelopment of software agents to manage image data and other resources of aregional health telematics network efficiently, thus exhibiting an apparently intelligentbehavior as perceived by users.
A software agent that exhibits intelligent nature [[9] , [10] ] is being developed tocoordinate the activities of the intelligent management of image data and the executionof the preloading and prefetching strategies within the distributed IMACS architecturepresented. This agent is designed as an Intelligent Personal Service Agent (IPSA)[[26] ] to fit the individual needs and preferences of the user. The IPSA, located at theclient’s sites, utilizes domain knowledge coupled with user preferences and customizeddata utilization patterns for each user to select the most relevant image data, incooperation with the DHSM servers. Subsequently, the IPSA transmits image data tothe client workstation or judiciously caches the data at neighboring servers so that it iswhere needed when needed.
References[1] M. Ader, “The Dynamic Model”, Bull Technical Report, 1990.
[2] R. Alonso, D. Barbara, H. Garcia-Molina, “Data Caching Issues in an InformationRetrieval System”, ACM Transactions on Database Systems, Vol. 15, No. 3,September 1990, pp. 359-384.
[3] J. S. K. Ang, J. Hong, “AMS Formalism: An Approach to Office Modeling andOIS Development”, Data Base, Vol. 25, No. 4, November 1994, pp. 25-38.
[4] A. R. Bakker, et al , "Pre-Fetching and Pre-Loading Strategies", Chapter 5.3, in M.Osteaux, editor. "Hospital Integrated Picture Archiving and CommunicationSystems - A Second Generation PACS Concept". Berlin: Springer-Verlag, 1991;pp. 145-170.
Figure 13.The proposed regional health telematics network of Crete.
KRITIKON PELAGOS
AgiosNikolaos
RethymnonHeraklion
LIVIKON PELAGOS
Sitia
Chania
KoufonisiChrysi
Gavdos
Dia
Ambulances,Mobile Screening Units
IsolatedSites
CommunityDoctors
District Hospitals
PrimaryHealth Centers
Regional Hospitals
Ierapetra

-19 -
[5] S. Chang, A. Hsu, “Image Information Systems: where do we go from here?”,IEEE Transactions on Knowledge and Data Engineering, Vol. 4, No. 5, October1992, pp. 431-442.
[6] E. I. Cohen, G. M. King, J. T. Brady, "Storage Hierarchies", IBM Systems Journal,Vol. 28, No. 1, 1989.
[7] P. Constantopoulos, M. Doerr, “The Semantic Indexing System”, TechnicalReport, Institute of Computer Science, Foundation for Research and Technology -Hellas, 1995.
[8] D. M. Dilts, W. Wu, "Using Knowledge-Based Technology to Integrate CIMDatabases", IEEE Expert, Vol. 3, No. 2, June 1991, pp. 237-245.
[9] Oren Etzioni, D. S. Weld, "Intelligent Agents on the Internet: Fact, Fiction, andForecast", IEEE Expert, Vol. 10, No. 4, August 1995, pp. 44-49.
[10] M. R. Genesereth, S. P. Ketchpel, "Software Agents", Communication of theACM, Vol. 37, No. 7, July 1994, pp. 48-53.
[11] C. Hsu, M. Bouziane, W. Cheung, L. Rattner, L. Yee, "Meta-Database Modelingfor Enterprise Information Integration", Journal of Systems Integration, Vol. 2, No.1, 1992, pp. 5-37.
[12] C. Hsu and L. Rattner, "Metadatabase Solutions for Enterprise InformationIntegration Problems", Data Base, Vol. 24, No. 1, Winter 1993, pp. 23 - 35.
[13] G. Irie, T. Miyamoto, T. Kojim, I. Yamamoto, T. Kudo, "PACS experience at theUniversity of Hokkaido Medical School", SPIE 1990, No. 1234, pp. 26 - 32.
[14] V. S. Krishnamurthy, H. Lam, M. Mitchell , E. Barkmeyer, "IMDAS, AnIntegrated Manufacturing Data Administration System", Journal of Data andKnowledge Engineering, Vol. 3, No. 2, 1988, pp. 109-131.
[15] D. F. Leotta, Y. Kim, “Requirements for Picture Archiving AndCommunications”, IEEE Engineering in Medicine and Biology, Vol. 12, No. 1,March 1993, pp. 62-80.
[16] R. Mattheus, J. G. Tiberglien , "Network Management", Chapter 5.2 in M.Osteaux, editor, "Hospital Integrated Picture Archiving and CommunicationSystems- A Second Generation PACS Concept", Berlin: Springer-Verlag, 1991,pp. 120-140.
[17] D. Meyer-Ebrecht, "Digital image communication", European Journal ofRadiology, Vol. 17, No. 93, pp. 47-55.
[18] M. Ohly, L. Kleinholz, H. Oswald, B. Mahr, R. Felix, E. Fleck, "Integration in theBERMED Project: The Multimedia Patient Record", Proceedings of the CAR ‘95,Berlin, June 1995, pp. 542-547.
[19] S. Orphanoudakis, C. Chronaki, D. Vamvaka: "I2Cnet: Content-based SimilaritySearch in Geographically Distributed Repositories of Medical Images", TechnicalReport, Institute of Computer Science, Foundation for Research and Technology -Hellas, 1996. (Also to appear in the Journal of Computerized Medical Imaging andGraphics).
[20] S. Orphanoudakis, C. Chronaki, S. Kostomanolakis, “I2C: A System for theIndexing, Storage, and Retrieval of Medical Images by Content”, Journal ofMedical Informatics, Vol. 19, No. 2, April-June 1994, pp. 109-122.

-20 -
[21] S. Orphanoudakis, M. Tsiknakis, C. Chronaki, S. Kostomanolakis, M. Zikos, Y.Tsamardinos, “Development of an Integrated Image Management andCommunication System on Crete”, Proceedings of the CAR ‘95, Berlin, June 1995,pp. 481-487.
[22] E. Sciore, M. Siegel, A. Rosenthal, “Using Semantic Values to FacilitateInteroperability Among Heterogeneous Information Systems”, ACM Transactionson Database Systems, Vol. 19, No. 2, June 1994, pp. 254-290.
[23] J. T. C. Teng, W. J. Keffinger, “Bussiness Process Redesign and InformationArchitecture: Exploring the Relationships”, Data Base, Vol. 26, No. 1, February1995, pp. 30-42.
[24] Y. Tsamardinos, “DHSM: A Distributed Hierarchical Multimedia DatabaseManagement System”, Graduate Thesis, Department of Computer Science,University of Crete, Heraklion, July 1995.
[25] M. Tsiknakis, “CoMed - Cooperation in Medicine”, ERCIM - News, No. 21,April 1995, page 23.
[26] G. Wiederhold, “Mediators in the Architecture of Future Information Systems”,IEEE Computer Magazine, Vol. 25, No. 3, March 1992, pp. 38-49.
[27] A. W. K. Wong, H. K. Huang, "Subsystem Throughputs of a Clinical PictureArchiving and Communication System", Journal of Digital Imaging, No. 5, 1992,pp. 252-261.
-21 -
About the authors:
Manolis Tsiknakis (S’85 - M’89) received a B.Eng. degree in electronicengineering, a M.Sc. in microprocessor engineering and a Ph.D. in control systemsengineering from Bradford University, U.K.
He is at the Institute of Computer Science of Foundation for Research andTechnology - Hellas, where he is currently coordinating the activities of the MedicalInformation Systems Laboratory. His current research interests are in the areas ofmultimedia systems with emphasis on medical information systems, Picture Archiveand Communications Systems, CSCW and Telematics Engineering.
Dimitrios G. Katehakis (S’89 - M’93) received his Diploma in electricalengineering from the Technical University of Patras, Greece in 1991 and the M.S.degree also in electrical engineering from the University of Maryland at College Park in1993.
He is a Telecommunications Engineer of the Medical Information SystemsLaboratory at the Institute of Computer Science, Foundation for Research andTechnology - Hellas. He works on data integration analysis and the design of object-oriented systems and distributed architectures for medical telematics applications. Hisresearch focuses in the functional integration of heterogeneous information systems, aswell as the intelligent management and communication of multimedia data.
Stelios C. Orphanoudakis (S’72-M’76-SM’83) received the B.A. degree inengineering sciences from Dartmouth College, Hanover, NH, in 1971, the M.S. degreein electrical engineering from M.I.T., Cambridge, MA, in 1973, and the Ph.D. degreein electrical engineering from Dartmouth College in 1976.
He is Director of the Institute of Computer Science, Foundation for Researchand Technology - Hellas, and Professor of Computer Science, University of Crete,Greece. He held a faculty appointment in the Departments of Diagnostic Radiologyand Electrical Engineering at Yale University, USA from 1975 until 1991. Prof.Orphanoudakis has many years of academic and research experience in the fields ofcomputer vision and robotics, intelligent image management and retrieval by content,and medical imaging. He has served on various committees and working groups of theEuropean Commission and has been active in European R&D programs. He currentlyserves on the Board of Directors and is Vice President of the European ResearchConsortium for Informatics and Mathematics (ERCIM). He is also a member of theNatioal Telecommunications Commission and the National Advisory Research Councilof Greece.
Authors’ Present Address:
ICS-FORTHScience and Technology Park of CreteVassilika Vouton, P.O. Box 1385GR 711 10, Heraklion, Crete, Greece.Email: {orphanou, tsiknaki, katehaki}@ics.forth.gr