
Informed consent for chiropractic care: Comparing patients' perceptions to the legal perspective
6
Original article Informed consent for chiropractic care: Comparing patients' perceptions to the legal perspective Melissa Winterbottom a, * , Heather Boon a , Silvano Mior b , Marcia Facey c a Leslie Dan Faculty of Pharmacy, University of Toronto, Canada b Canadian Memorial Chiropractic College, Canada c Dali Lana School of Public Health, University of Toronto, Canada article info Article history: Received 11 August 2014 Received in revised form 10 November 2014 Accepted 19 November 2014 Keywords: Informed consent Spinal manipulation Chiropractic abstract Purpose: This study explored chiropractic patients' perceptions of exchanging risk information during informed consent and compared them with the legal perspective of the informed consent process. Methods: Interviews were conducted with 26 participants, recruited from chiropractic clinics. Tran- scripts were analysed using a constant comparative method of analysis. Findings: Participants experienced informed consent as an on-going process where risk information informed their decisions to receive treatment throughout four distinct stages. In the first stage, infor- mation acquired prior to arriving at the clinic for treatment shaped perceptions of risk. In stage two, participants assessed the perceived competence of their practitioners. Participants then signed the consent form and discussed the risks with their practitioners. Finally, they communicated with their practitioners during treatment to ensure their pain threshold was not crossed. Conclusion: These findings suggest that chiropractic patients perceive informed consent as a process involving communication with their practitioners, and that it is possible to educate patients about the risks associated with treatment while satisfying the legal requirements of informed consent. © 2014 Elsevier Ltd. All rights reserved. 1. Background information The doctrine of informed consent outlines a practitioner's duty to disclose information about a medical treatment to his or her patients prior to providing care. This doctrine applies to all health care practitioners, including chiropractors. The information that must be disclosed includes: the nature of the treatment, potential benefits, associated material risks, and alternative treatment op- tions (Dickens and Cook, 2004). When a practitioner initially agrees to provide treatment to a patient, there is an imbalance of infor- mation about the proposed treatment (i.e., the practitioner has more information than the patient); this imbalance may compro- mise the patient's right to self-determination. Informed consent is intended to allow both parties to enter into dialogue and reach agreement as equals, thereby enhancing autonomous decision making for the patient (Snyder, 2012). According to the Supreme Court of Canada, practitioners must disclose all material informa- tion about a treatment. Material information is defined as infor- mation that a reasonable patient would require to make an informed decision about whether or not to receive that treatment (Dickens, 2002). What constitutes a reasonable patient is undefined and determined on a case-by-case basis. Risk disclosure is one element of informed consent that may be particularly challenging for chiropractors because high quality prospective data about risk are limited due to a lack of surveil- lance and reporting. The proposed legal requirements for risk disclosure include known effects, material risks, discomforts and side effects, the likelihood of occurrence, the limits of relevant knowledge, and areas where further information is required (Dickens and Cook, 2004). Research from the UK and the US suggests that chiropractors often omit serious risks from the disclosure discussion, potentially compromising patient autonomy when seeking chiropractic care (Langworthy and Cambron, 2007). These findings came from surveys with practitioners; whether or not patients felt that their autonomy was being compromised was not explored. * Corresponding author. 144 College Street, Toronto, ON M5S 3M2, Canada. Tel.: þ1 289 828 4698. E-mail address: [email protected] (M. Winterbottom). Contents lists available at ScienceDirect Manual Therapy journal homepage: www.elsevier.com/math http://dx.doi.org/10.1016/j.math.2014.11.009 1356-689X/© 2014 Elsevier Ltd. All rights reserved. Manual Therapy xxx (2014) 1e6 Please cite this article in press as: Winterbottom M, et al., Informed consent for chiropractic care: Comparing patients' perceptions to the legal perspective, Manual Therapy (2014), http://dx.doi.org/10.1016/j.math.2014.11.009
Transcript of Informed consent for chiropractic care: Comparing patients' perceptions to the legal perspective

lable at ScienceDirect
Manual Therapy xxx (2014) 1e6
Contents lists avai
Manual Therapy
journal homepage: www.elsevier .com/math
Original article
Informed consent for chiropractic care: Comparing patients'perceptions to the legal perspective
Melissa Winterbottom a, *, Heather Boon a, Silvano Mior b, Marcia Facey c
a Leslie Dan Faculty of Pharmacy, University of Toronto, Canadab Canadian Memorial Chiropractic College, Canadac Dali Lana School of Public Health, University of Toronto, Canada
a r t i c l e i n f o
Article history:Received 11 August 2014Received in revised form10 November 2014Accepted 19 November 2014
Keywords:Informed consentSpinal manipulationChiropractic
* Corresponding author. 144 College Street, ToroTel.: þ1 289 828 4698.
E-mail address: [email protected] (M. Winter
http://dx.doi.org/10.1016/j.math.2014.11.0091356-689X/© 2014 Elsevier Ltd. All rights reserved.
Please cite this article in press as: Winterbotperspective, Manual Therapy (2014), http://
a b s t r a c t
Purpose: This study explored chiropractic patients' perceptions of exchanging risk information duringinformed consent and compared them with the legal perspective of the informed consent process.Methods: Interviews were conducted with 26 participants, recruited from chiropractic clinics. Tran-scripts were analysed using a constant comparative method of analysis.Findings: Participants experienced informed consent as an on-going process where risk informationinformed their decisions to receive treatment throughout four distinct stages. In the first stage, infor-mation acquired prior to arriving at the clinic for treatment shaped perceptions of risk. In stage two,participants assessed the perceived competence of their practitioners. Participants then signed theconsent form and discussed the risks with their practitioners. Finally, they communicated with theirpractitioners during treatment to ensure their pain threshold was not crossed.Conclusion: These findings suggest that chiropractic patients perceive informed consent as a processinvolving communication with their practitioners, and that it is possible to educate patients about therisks associated with treatment while satisfying the legal requirements of informed consent.
© 2014 Elsevier Ltd. All rights reserved.
1. Background information
The doctrine of informed consent outlines a practitioner's dutyto disclose information about a medical treatment to his or herpatients prior to providing care. This doctrine applies to all healthcare practitioners, including chiropractors. The information thatmust be disclosed includes: the nature of the treatment, potentialbenefits, associated material risks, and alternative treatment op-tions (Dickens and Cook, 2004). When a practitioner initially agreesto provide treatment to a patient, there is an imbalance of infor-mation about the proposed treatment (i.e., the practitioner hasmore information than the patient); this imbalance may compro-mise the patient's right to self-determination. Informed consent isintended to allow both parties to enter into dialogue and reachagreement as equals, thereby enhancing autonomous decisionmaking for the patient (Snyder, 2012). According to the Supreme
nto, ON M5S 3M2, Canada.
bottom).
tom M, et al., Informed consedx.doi.org/10.1016/j.math.201
Court of Canada, practitioners must disclose all material informa-tion about a treatment. Material information is defined as infor-mation that a reasonable patient would require to make aninformed decision about whether or not to receive that treatment(Dickens, 2002).What constitutes a reasonable patient is undefinedand determined on a case-by-case basis.
Risk disclosure is one element of informed consent that may beparticularly challenging for chiropractors because high qualityprospective data about risk are limited due to a lack of surveil-lance and reporting. The proposed legal requirements for riskdisclosure include known effects, material risks, discomforts andside effects, the likelihood of occurrence, the limits of relevantknowledge, and areas where further information is required(Dickens and Cook, 2004). Research from the UK and the USsuggests that chiropractors often omit serious risks from thedisclosure discussion, potentially compromising patient autonomywhen seeking chiropractic care (Langworthy and Cambron, 2007).These findings came from surveys with practitioners; whether ornot patients felt that their autonomy was being compromised wasnot explored.
nt for chiropractic care: Comparing patients' perceptions to the legal4.11.009

Table 1Interview guide.
1. What brought you into the chiropractor's office on your first day oftreatment?⎕ How long were you feeling that way?⎕ How was it interfering with your life?⎕ Was this the first chiropractor that you saw?
2. What else have you tried for your (back pain/neck pain etc.)?⎕ If yes: Are you still taking that/seeing them/doing that?⎕ If no: Did you consider trying other options than the chiropractor?⎕ How did you decide that the chiropractor was the best option?
3. Before you had your first visit what were you expecting it to be like?⎕ Did you have any concerns about seeing the chiropractor?
4. What happened at your first visit with the chiropractor?⎕ What did you talk about with them?⎕ How did this compare with what you were expecting?
5. What did you and the chiropractor talk about during your first visit?⎕ Did they explain how the treatment was going to help you?⎕ Did they discuss any down sides of the treatment?⎕ Did you ask any questions/what were they/how were they answered?
6. Were you asked to sign any forms at this visit?⎕ Did you have an opportunity to read the forms?⎕ Do you remember anything that was on them?⎕ Did anyone talk to you about them/Who?/What was discussed?⎕ Where were you given them/where did you sign them?⎕ What do you think the purpose of these forms was?
7. How could your chiropractor have better prepared you?⎕ Was there anything that happened that you weren't expecting?⎕ After talking to your chiropractor did you feel like you knew what you
were getting into?8. What advice would you give to someone else who was thinking of going to
see a chiropractor?9. Is there anything you would like to talk about that we haven't discussed
yet?10. Is there anything that you would like to ask me?
M. Winterbottom et al. / Manual Therapy xxx (2014) 1e62
In addition to the goal of protecting patient autonomy,informed consent is also viewed as serving the purpose of pro-tecting practitioners from litigation. Although both of these ob-jectives are important, it is unclear whether they can both beaccomplished using the same approach. In the literature, informedconsent is often described as a social process of dialogue betweenpatients and their practitioners (Langworthy and Cambron, 2007;Brenner et al., 2009; Giuseppe & D'Angio, 2010). Historically, it isdescribed as a static event that consists of patients reading andsigning a form (Lidz et al., 1988). Although informed consent is nolonger defined as a static event, research suggests that it issometimes still treated that way in practice (Delany, 2007;Langworthy and Cambron, 2007; Brenner et al., 2009). It ispossible that these two approaches to informed consent mayfunction to achieve different objectives. For example, informedconsent when treated as a process may be more effective atenhancing patient autonomy, while treating informed consent as astatic event would likely be perceived as a way to protect practi-tioners from litigation. Despite the important role of the patient,no research explores whether patients perceive informed consentas a process or a discrete act.
Patients' voices are underrepresented in the literature aboutinformed consent for health care, particularly for chiropractic care.To address this gap, this study explored patients' perceptions ofinformed consent when seeking chiropractic care at teachingclinics and one private clinic in Ontario. Specific objectives were todescribe patients' experiences of exchanging risk information andto explore how those experiences compared to the legal perspec-tive of informed consent.
2. Methods
2.1. Design
A qualitative descriptive study (Sandelowski, 2000) was used toanswer the research question: how do chiropractic patients' per-ceptions of exchanging risk information during informed consentcompare with the legal requirements of informed consent for chi-ropractors? Participant recruitment, data collection, and dataanalysis occurred in an iterative manner, such that emergingthemes and concepts influenced the direction of inquiry. Approvalwas obtained from the research ethics boards at the X and theChiropractic College.
2.2. Participants
A purposive sampling strategy (Patton, 2005) was used to re-cruit participants who were receiving chiropractic care fromregulated chiropractors or chiropractic students at one privateclinic and three teaching clinics, respectively, in Ontario, Canada.Clinics were chosen to represent a range of chiropractic patientsfrom different geographical areas likely to have different de-mographic characteristics. Receptionists at participating clinicsdistributed a letter of invitation and study information to patients.Those who were interested contacted the researcher by email ortelephone to determine if they were eligible to participate. Pa-tients were eligible if they were over the age of 18, and receivedtheir first treatment within three weeks of being interviewed. Itwas assumed that new patients would be more likely toremember the consent forms and accompanying discussion thattook place before the first treatment. Patients who were healthcare workers or studying to become health care professionals wereexcluded from the study due to their specialized knowledge ofinformed consent. Participants received a $25 gift card in recog-nition of their time.
Please cite this article in press as: Winterbottom M, et al., Informed conseperspective, Manual Therapy (2014), http://dx.doi.org/10.1016/j.math.201
2.3. Data collection
Data were collected through interviews conducted by oneresearcher (MW) over the telephone and in-person. A semi-structured interview guide was used to help the interviewerfocus on the research objectives while remaining open to the par-ticipants' stories (Table 1). The interview guide was developedbased on the research objectives and related concepts in the liter-ature; it was adapted throughout data collection in response tocodes, categories, and themes that were identified during analysis.Interviews were audio recorded and transcribed by a professionaltranscriber. Transcripts were checked for accuracy and labelledwith pseudonyms chosen by the participants to protect theirconfidentiality. Initial interviews were conducted with patientsfrom teaching clinics; when thematic saturation was achieved,some interviews were conducted at a private clinic for comparison.
2.4. Data analysis
A constant comparative method (Corbin and Strauss, 1990) wasused to analyse the transcripts, searching for concepts that wererelevant to participants' perceptions of informed consent and riskinformation. In the initial stages, the data were explored forrecurring concepts and ideas that were relevant to the researchquestion and objectives. These ideas and concepts were givendescriptive labels or codes. Codes were derived directly from thetext; definitions were developed and recorded for all codes to refertowhen analysing subsequent transcripts. Two independent coders(MW and HB) met weekly to compare and discuss codes untilconsensus was reached. A coding framework was developed bycomparing and contrasting codes and grouping similar codestogether to create categories. Hypotheses were then developedabout relationships between categories. Codes, categories, themes,and relationships between themwere tested against the data from
nt for chiropractic care: Comparing patients' perceptions to the legal4.11.009

M. Winterbottom et al. / Manual Therapy xxx (2014) 1e6 3
on-going interviews. Towards the end of the coding process, cate-gories were integrated to develop major themes that representeddistinct phases of the participants' processes of informed consent.NVivo® (Version xx, QSR International, Burlington, MA, USA) wasused to help organize the data and an audit trail of the study pro-cesses and decisions was recorded.
3. Findings
3.1. Participants characteristics
A total of 26 interviews were conducted; 14 with females and 12with males. When permission was granted, demographic infor-mation was recorded for each participant including gender,ethnicity, highest level of education, clinic where treatment wasreceived and year of birth (Table 2). There was a wide range ofethnicity, age, and education; however there were very few par-ticipants between the ages of 30 and 49. No relevant differenceswere observed between interviews conducted with participantsfrom private clinics and teaching clinics.
3.2. Overview
Participants perceived informed consent as a social processconsisting of ongoing information exchange with their practi-tioners and informed by interactions with family, friends, and themedia. When asked about their perceptions of informed consent,participants described a process that consisted of four stages whererisk information was incorporated into their decision making(Fig. 1). The four themes presented in this paper represent fourstages where participants incorporated risk information into theirdecision making processes. These themes include: 1) preconceivedideas about safety/risk; 2) perceived practitioner competence; 3)risk discussion & consent form; and 4) patient-practitioner feed-back loop. The findings presented here describe how contextualfactors influenced participants' perceptions of risk, and informedtheir decisions to receive treatment. Since these factors informed
Table 2Participant characteristics (n ¼ 26).
n %
GenderFemale 14 53.8Male 12 46.2
Educationa
High School Diploma 1 3.8College Diploma 7 26.9Bachelor's Degree 13 50.0Master's Degree 2 7.7Doctor of Philosophy 2 7.7
EthnicityNorth America 12 46.2Asia 7 26.9Europe 6 23.8Africa 1 3.8
Treatment clinicTeaching clinic 13 50.0Satellite teaching clinic 1 8 30.8Satellite teaching clinic 2 1 3.8Satellite teaching clinic 3 0 0.0Private clinic 4 15.4
Agea
19e29 10 38.530e39 2 7.740e49 2 7.750e59 7 26.960þ 3 11.5
a Category does not add up to n¼ 26 or 100% because participants did not discloseinformation.
Please cite this article in press as: Winterbottom M, et al., Informed conseperspective, Manual Therapy (2014), http://dx.doi.org/10.1016/j.math.201
decision making, they were conceptualized as stages of the par-ticipants' informed consent processes. The themes are described inthe chronological order that they were experienced by participantsthroughout their treatment. Most participants appeared to weighthis risk information against the potential benefits of receivingtreatment. However, the interviewer did not probe this part of thedecision-making process because it did not speak directly to theresearch objectives.
3.3. Stage 1: preconceived ideas about risk
The process of informed consent often began before participantsmade the decision to go to their practitioners' offices to receivetreatment. Participants received risk information about the treat-ment from non-clinical sources such as the media, family, andfriends. As a result, many participants arrived at treatment withspecific concerns about the consequences of receiving treatment. Insome cases, this information along with their previous experiencesof receiving chiropractic care, had a greater impact on their decisionmaking process than the risk information provided by their chiro-practors during risk disclosure. This was evident because manyparticipants had alreadymade the decision about whether or not toreceive treatment prior to arriving at the clinic and none of the risksdisclosed during the formal consent changed their minds:
The actual risk is very, very, small, but the headlines kind of stickwith you no matter how small the risks are. So in my mind Iknow the risk is extremely small, but sometimes what yourmind knows and the way you act are completely differentthings. e Logan
I was aware from co-workers about how negative the professionis from their perspective and I was also aware how positive it isfrom a friend of my wife's, right? So I had already made up mymind as to have the treatment [before arriving at the clinic]. eTheodore
Participants' predetermined ideas about risk are conceptualizedas the first stage in their perceived process of informed consentbecause these preconceptions appeared to inform their decisionsabout whether or not to consent to treatment.
3.4. Stage 2: perceived practitioner competence
During introductions and medical history taking, participantsassessed the perceived competence of their practitioners. Practi-tioners were more likely to be perceived as competent if they spenttimewith participants, and explained what theywere doing as theywere doing it. Perceived practitioner competence appeared to bedirectly related to perceived risk; participants often felt safer pro-ceeding with treatment if their practitioner appeared competentand capable of safely performing the procedure:
He did a good job of explaining everything he was doing, so youcould sort of tell. Just cause he was talking out his process, and Ithought he knew what he was doing so I felt confident abouthim giving me treatment. e Amanda
Yah, things can go wrong but I know that she's doing what shecan to minimize the risks and she's a competent professional, soI shouldn't have anything to worry about. e John
For some participants, the amount of trust they had in theirpractitioners to safely perform the treatment contributed to theirdecisions to receive treatment. For example, Janis was adamant that
nt for chiropractic care: Comparing patients' perceptions to the legal4.11.009
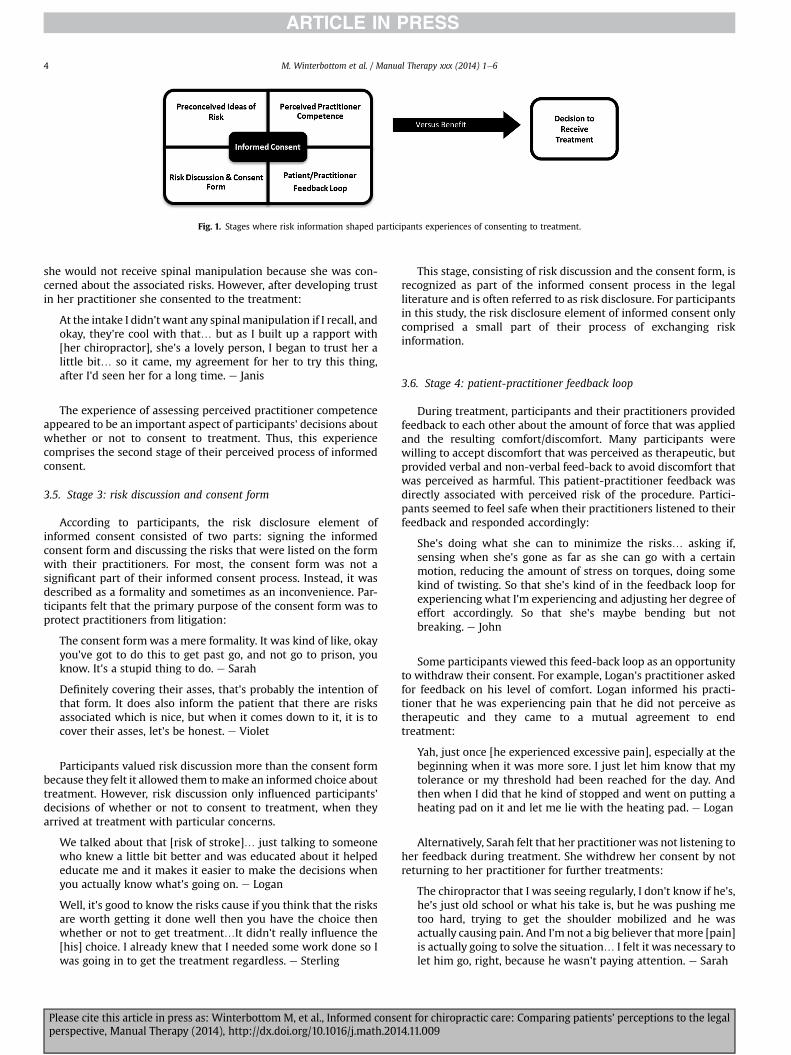
Fig. 1. Stages where risk information shaped participants experiences of consenting to treatment.
M. Winterbottom et al. / Manual Therapy xxx (2014) 1e64
she would not receive spinal manipulation because she was con-cerned about the associated risks. However, after developing trustin her practitioner she consented to the treatment:
At the intake I didn't want any spinal manipulation if I recall, andokay, they're cool with that… but as I built up a rapport with[her chiropractor], she's a lovely person, I began to trust her alittle bit… so it came, my agreement for her to try this thing,after I'd seen her for a long time. e Janis
The experience of assessing perceived practitioner competenceappeared to be an important aspect of participants' decisions aboutwhether or not to consent to treatment. Thus, this experiencecomprises the second stage of their perceived process of informedconsent.
3.5. Stage 3: risk discussion and consent form
According to participants, the risk disclosure element ofinformed consent consisted of two parts: signing the informedconsent form and discussing the risks that were listed on the formwith their practitioners. For most, the consent form was not asignificant part of their informed consent process. Instead, it wasdescribed as a formality and sometimes as an inconvenience. Par-ticipants felt that the primary purpose of the consent form was toprotect practitioners from litigation:
The consent formwas a mere formality. It was kind of like, okayyou've got to do this to get past go, and not go to prison, youknow. It's a stupid thing to do. e Sarah
Definitely covering their asses, that's probably the intention ofthat form. It does also inform the patient that there are risksassociated which is nice, but when it comes down to it, it is tocover their asses, let's be honest. e Violet
Participants valued risk discussion more than the consent formbecause they felt it allowed them tomake an informed choice abouttreatment. However, risk discussion only influenced participants'decisions of whether or not to consent to treatment, when theyarrived at treatment with particular concerns.
We talked about that [risk of stroke]… just talking to someonewho knew a little bit better and was educated about it helpededucate me and it makes it easier to make the decisions whenyou actually know what's going on. e Logan
Well, it's good to know the risks cause if you think that the risksare worth getting it done well then you have the choice thenwhether or not to get treatment…It didn't really influence the[his] choice. I already knew that I needed some work done so Iwas going in to get the treatment regardless. e Sterling
Please cite this article in press as: Winterbottom M, et al., Informed conseperspective, Manual Therapy (2014), http://dx.doi.org/10.1016/j.math.201
This stage, consisting of risk discussion and the consent form, isrecognized as part of the informed consent process in the legalliterature and is often referred to as risk disclosure. For participantsin this study, the risk disclosure element of informed consent onlycomprised a small part of their process of exchanging riskinformation.
3.6. Stage 4: patient-practitioner feedback loop
During treatment, participants and their practitioners providedfeedback to each other about the amount of force that was appliedand the resulting comfort/discomfort. Many participants werewilling to accept discomfort that was perceived as therapeutic, butprovided verbal and non-verbal feed-back to avoid discomfort thatwas perceived as harmful. This patient-practitioner feedback wasdirectly associated with perceived risk of the procedure. Partici-pants seemed to feel safe when their practitioners listened to theirfeedback and responded accordingly:
She's doing what she can to minimize the risks… asking if,sensing when she's gone as far as she can go with a certainmotion, reducing the amount of stress on torques, doing somekind of twisting. So that she's kind of in the feedback loop forexperiencing what I'm experiencing and adjusting her degree ofeffort accordingly. So that she's maybe bending but notbreaking. e John
Some participants viewed this feed-back loop as an opportunityto withdraw their consent. For example, Logan's practitioner askedfor feedback on his level of comfort. Logan informed his practi-tioner that he was experiencing pain that he did not perceive astherapeutic and they came to a mutual agreement to endtreatment:
Yah, just once [he experienced excessive pain], especially at thebeginning when it was more sore. I just let him know that mytolerance or my threshold had been reached for the day. Andthen when I did that he kind of stopped and went on putting aheating pad on it and let me lie with the heating pad. e Logan
Alternatively, Sarah felt that her practitioner was not listening toher feedback during treatment. She withdrew her consent by notreturning to her practitioner for further treatments:
The chiropractor that I was seeing regularly, I don't know if he's,he's just old school or what his take is, but he was pushing metoo hard, trying to get the shoulder mobilized and he wasactually causing pain. And I'm not a big believer that more [pain]is actually going to solve the situation… I felt it was necessary tolet him go, right, because he wasn't paying attention. e Sarah
nt for chiropractic care: Comparing patients' perceptions to the legal4.11.009

M. Winterbottom et al. / Manual Therapy xxx (2014) 1e6 5
Therefore, the ability of practitioners to receive and providefeedback to and from participants during treatment informedparticipants' decisions to return for subsequent care. If that is true,then this feedback loop represents the last stage in the participants'processes of informed consent.
4. Discussion
This study identified that participants perceived informed con-sent as a social process rather than a discrete act. Moreover, it is thefirst study to describe that process as it relates to risk information,from the perspective of chiropractic patients. The four themes:preconceived ideas about safety/risk; perceived practitionercompetence; risk discussion and consent form; and patient-practitioner feedback loop, provide a detailed description of howpatients perceive the process of exchanging risk informationwithinthe context of informed consent. They provide a framework thatcan be used as a starting point for a more detailed investigation ofthe informed consent process.
For the participants in this study, preconceived ideas about riskinfluenced their decisions to receive treatment. Since these ideasoften came from non-clinical sources, the information theyreceived was at times conflicting, confusing, and/or inaccurate. Ifpractitioners ask patients what they already know about associatedrisks prior to disclosure, it may enhance the informed consentprocess by providing an opportunity to clarify conflicting infor-mation, correct misconceptions about the risks associated withtreatment, and address individual concerns. Furthermore, the in-clusion of personal experiences in patients' decisions demonstratesthat their perceptions are aligned with the reasonable patientstandard of informed consent outlined by the Supreme Court ofCanada (Dickens, 2002). Therefore, understanding this stage of theinformed consent process may enhance patient education and helpchiropractors fulfil the legal criteria of informed consent.
Participants in this study often developed trust in chiropractorswho took time to listen to their concerns and explained what theywere doing throughout treatment. Although it is unclear if estab-lishing trust between participants and the practitioners enhancedautonomous decision making, it had other benefits including pa-tients feeling comfortable and safe prior to treatment initiation.Moreover, other studies have shown that taking time with patientsand explaining the treatment process as it is carried outmay reducethe risk of malpractice lawsuits for practitioners (Stelfox et al.,2005; Cydulka et al., 2011). These findings suggest that whenpractitioners take time to address patient concerns, it will enhancerapport with their patients and may decrease the chance of litiga-tion if harm occurs. This is also an area where patients' perceptionsalign with the legal perspective, since addressing specific patientconcerns is one of the proposed legal requirements for disclosure(Dickens, 2002).
Many participants in this study did not read the consent form,and no one appeared to use it to inform their decision to receivetreatment. Since participants in this study perceived the consentform as a tool to protect practitioners from litigation, these findingssupport the notion that the informed consent form is not particu-larly useful for facilitating informed decisionmaking (Brenner et al.,2009). Although obtaining written consent is not a legal require-ment in Ontario, the chiropractic profession has placed a greatemphasis on the consent form compared to other practitioners whoperform spinal manipulation. For example, physiotherapists inOntario who practice SMT are required to obtain verbal consent,whereas the standard of practice for chiropractors requires them toobtain written consent (CCO, 2004). If patients view the form pri-marily as a waiver to protect practitioners from litigation, then thechiropractic profession may benefit by placing less emphasis on the
Please cite this article in press as: Winterbottom M, et al., Informed conseperspective, Manual Therapy (2014), http://dx.doi.org/10.1016/j.math.201
form. The findings of this study question the validity of the use of aform to educate patients suggesting that this may be betteraccomplished through communication and discussion.
Participants in this study experienced a communication feed-back loop with their practitioners to ensure the amount of forceapplied by themanipulation did not cause a level of discomfort theyperceived as harmful. Some participants in this study perceived thispatient-practitioner feedback loop as an opportunity to withdrawtheir consent to treatment if they felt that they were in danger ofbeing harmed. According to the Ontario Patients' Bill of Rights Act,all patients have the right to withdraw consent during treatment ifthey feel they are in danger of harm; however, this feedback loop isnot acknowledged as a method of withdrawing consent in the legalliterature (Smith, 2002). Likewise, not returning to treatment is notconsidered a form of withdrawing consent, yet some participants inthis study described their actions in this way. For some participants,engaging in this communication feedback loop was perceived tomitigate risk. The Agency for Health Care Research and Quality hasrecommended informed consent as one of 22 patient safety stra-tegies that are encouraged for adoption (Shekelle et al., 2013). Yet, itis unclear how informing patients of risks associatedwith treatmentcould mitigate those risks. If this feedback loop is in fact part of theinformed consent process, it could represent a direct link betweeninformed consent and patient safety.
The full process of informed consent was not explored in thisstudy. For example, the investigator did not explore how partici-pants weighed risk information against potential benefits whendeciding whether or not to proceed with treatment. Similarly, therewere some areas of inquiry, regarding the ‘patient-practitionerfeedback loop’ that were not investigated. For example, followingdata analysis it remained unclear to what extent participantsperceived the patient/practitioner feed-back loop as an opportunityto withdraw consent. Future research could consider exploringthese areas of inquiry, using purposive sampling to recruit patientswho chose to withdraw from treatment for the latter. Finally, futureresearch could explore if the phases noted herein are also foundamongst patients seeking care from other groups of health carepractitioners.
5. Conclusion
This descriptive study has provided the first insight into howchiropractic patients perceive the process of risk information ex-change within the context of informed consent. Four stages havebeen identified that represent their perceptions of how risk infor-mation shapes decisions about whether or not to receive treatment.These findings suggest that patients perceive informed consent as aprocess rather than a static event and that it is possible to educatechiropractic patients about the risks associated with treatmentwhile satisfying the legal requirements of informed consent.However, the informed consent form does not appear to be themost appropriate tool for patient education and may be moreuseful as a legal waiver.
Acknowledgements
This research is supported by The Canadian Institute of HealthResearch (492230), the University of Alberta, the Women andChildren's Health Research Institute and Alberta Innovates HealthSolutions. This work was part of a team grant. The authors wouldlike to thank their co-principal investigators, Drs. Caulfield, Vohra,Kawchuk, and O'Beirne, for their insightful comments and sug-gestions to improve the work, as well as the participants whoshared their stories. This work is attributed to Leslie Dan Faculty of
nt for chiropractic care: Comparing patients' perceptions to the legal4.11.009

M. Winterbottom et al. / Manual Therapy xxx (2014) 1e66
Pharmacy, University of Toronto 144, College St. Toronto, ON M5S3M2
References
Brenner LH, Brenner AT, Horowitz D. Beyond informed consent: educating thepatient. Clin Orthop Relat Res 2009;467:348e51.
College of Chiropractors of Ontario. Standard of practice: consent. 2004. http://www.cco.on.ca/site_documents/S-013.pdf.
Corbin J, Strauss A. Grounded theory research: procedures, canons, and evaluativecriteria. Qual Sociol 1990;13(1):3e21.
Cydulka R, Tamayo-Sarver J, Gage A, Bagnoli D. Association of patient satisfactionwith complaints and risk management among emergency physicians. J EmergMed 2011;41(4):405e11.
Delany CM. In private practice informed consent is interpreted as providing ex-planations rather than offering choices: a qualitative study. Aust J Physiother2007;53:171e7.
Dickens BM. Informed consent. In: Downie J, Caulfield T, Flood C, editors. Canadianhealth lawandpolicy. 2nded.Canada:ButtersworthsCanada Ltd; 2002. p.129e56.
Dickens BM, Cook RJ. Ethical and legal Issues in Reproductive health: dimensions ofinformed consent to treatment. Int J Gynecol Obstet 2004;85:309e14.
Please cite this article in press as: Winterbottom M, et al., Informed conseperspective, Manual Therapy (2014), http://dx.doi.org/10.1016/j.math.201
Giuseppe M, D'Angio G. How to improve the informed consent process. PediatrBlood Cancer 2010;55:10e1.
Langworthy JM, Cambron J. Consent: its practices and implications in UnitedKingdom and United States chiropractic practice. J Manip Physiol Ther 2007;30:419e31.
Lidz W, Appelbaum P, Meisel A. Two models of implementing informed consent.Archives Intern Med 1988;148(6):1385e9.
Patton MQ. Qualitative research. Encyclopedia of statistics in behavioral science.2005.
Sandelowski M. Whatever happened to qualitative description? Res Nurs Health2000;23:334e40.
Shekelle PG, Pronovost PJ, Wachter RM, McDonald KM, Schoelles K, Stevinson SM,et al. The top patient safety strategies that can be encouraged for adoption now.Ann Intern Med 2013;158:365e8.
Smith M. Patient's bill of rights e a comparative overview. Law and GovernmentDivision. 2002. Retrieved from:, http://publications.gc.ca/Collection-R/LoPBdP/BP/prb0131-e.htm#b. Ontariotxt.
Snyder L. ACP ethics manual 6th edition. Ann Intern Med 2012;156:73e104.Stelfox H, Gandhi T, Orav J, Gustafson M. The relation of patient satisfaction with
complaints against physicians and malpractice lawsuits. Am J Med 2005;118:1126e33.
nt for chiropractic care: Comparing patients' perceptions to the legal4.11.009




















