
INFORMATION TO USERS - American University
228
INFORMATION TO USERS This manuscript has been reproduced from the microfilm master. UMI films the text directly from the original or copy submitted. Thus, some thesis and dissertation copies are in typewriter face, while others may be from any type of computer printer. The quality of this reproduction is dependent upon the quality of the copy submitted. Broken or indistinct print, colored or poor quality illustrations and photographs, print bleedthrough, substandard margins, and improper alignment can adversely affect reproduction. In the unlikely event that the author did not send UMI a complete manuscript and there are missing pages, these will be noted. Also, if unauthorized copyright material had to be removed, a note will indicate the deletion. Oversize materials (e.g., maps, drawings, charts) are reproduced by sectioning the original, beginning at the upper left-hand comer and continuing from left to right in equal sections with small overlaps. Each original is also photographed in one exposure and is included in reduced form at the back of the book. Photographs included in the original manuscript have been reproduced xerographically in this copy. Higher quality 6" x 9" black and white photographic prints are available for any photographs or illustrations appearing in this copy for an additional charge. Contact UMI directly to order. University Microfilms International A Bell & Howell Information Company 300 North Zeeb Road. Ann Arbor. Ml 48106-1346 USA 313/761-4700 800/521-0600 Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of INFORMATION TO USERS - American University

INFORMATION TO USERS
This manuscript has been reproduced from the microfilm master. UMI films the text directly from the original or copy submitted. Thus, some thesis and dissertation copies are in typewriter face, while others may be from any type of computer printer.
The quality of this reproduction is dependent upon the quality of the copy submitted. Broken or indistinct print, colored or poor quality illustrations and photographs, print bleedthrough, substandard margins, and improper alignment can adversely affect reproduction.
In the unlikely event that the author did not send UMI a complete manuscript and there are missing pages, these will be noted. Also, if unauthorized copyright material had to be removed, a note will indicate the deletion.
Oversize materials (e.g., maps, drawings, charts) are reproduced by sectioning the original, beginning at the upper left-hand comer and continuing from left to right in equal sections with small overlaps. Each original is also photographed in one exposure and is included in reduced form at the back of the book.
Photographs included in the original manuscript have been reproduced xerographically in this copy. Higher quality 6" x 9" black and white photographic prints are available for any photographs or illustrations appearing in this copy for an additional charge. Contact UMI directly to order.
University Microfilms International A Bell & Howell Information C om p an y
3 0 0 North Z e e b R oad. Ann Arbor. Ml 4 8 1 0 6 -1 3 4 6 USA 3 1 3 /7 6 1 -4 7 0 0 8 0 0 /5 2 1 -0 6 0 0
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

O rder N um ber 9422770
The effects of a 36-hour Marine Corps substance abuse awareness seminar on supervisors’ knowledge and perceptions of an employee alcoholism program
Baker, Kay Louise, Ph.D.
The American University, 1993
C opyright ©1993 by B aker, K ay Louise. All righ ts reserved.
UMI300 N. Zeeb Rd.Ann Arbor. MI 48106
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

THE EFFECTS OF A 36-HOUR MARINE CORPS SUBSTANCE ABUSE AWARENESS SEMINAR ON SUPERVISORS' KNOWLEDGE AND PERCEPTIONS OF AN EMPLOYEE ALCOHOLISM PROGRAM
byKay L. Baker
submitted to the Faculty of the College of Arts and Sciences
of The American University in Partial Fulfillment of
the Requirements for the Degree of
Doctor of Philosophy in
Counseling and Student DevelopmentSignaty,res of Conys^tjbee:, Chair:
Jean of Ithe ColleenDean of *the College4> - 30-93
Date1993
The American University Washington, D.C. 20016
iTHE AMERICAN UNIVERSITY LIBRARY
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

© COPYRIGHT by
KAY L. BAKER 1993
ALL RIGHTS RESERVED
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
THE EFFECTS OF A 36-HOUR MARINE CORPS SUBSTANCE ABUSE AWARENESS SEMINAR ON SUPERVISORS' KNOWLEDGE AND PERCEPTIONS OF AN EMPLOYEE ALCOHOLISM PROGRAM
BYKay L. Baker
ABSTRACTThis study investigated the effects of the 36-hour
Marine Corps Substance Abuse Awareness Seminar on the knowledge and perceptions of supervisors, as assessed by the Baker Knowledge Inventory and the Demographic Information Inventory, before and after substance abuse training, and compared these results with a similar group of supervisors who had not participated in the seminar. The primary component of knowledge assessed in this study was knowledge of the Marine Corps Substance Abuse Program, and the perceptions assessed in this study were perceptions of the confidentiality, staff competence, effectiveness, and management support for the Marine Corps Substance Abuse Program.
A quasi-experimental, pretest/posttest design, with a 126-subject experimental and 39-subject control group, was used. Four hypotheses were tested using dependent and independent one- and two-tailed t tests, with the following results: no significant difference existed between the mean
ii
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

pretest scores for the two groups; no significant difference existed between the mean pretest and posttest scores for the control group; the experimental group's mean posttest score was significantly higher than the control group's mean posttest score; and the experimental group's mean posttest score was significantly higher than their mean pretest score. Additional data analysis revealed that the experimental group's mean posttest scores on the knowledge scale and the perception scale, taken separately, were significantly higher than its mean pretest scores on the same scales, taken separately. From the results of hypothesis testing and ad hoc data analysis, the researcher concluded that supervisory training was a means of significantly improving supervisors' knowledge and perceptions of an Employee Assistance Program.
111
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

ACKNOWLEDGMENTS
This research project could not have been undertaken without the support and assistance of many others. First, doctors Hodinko, Messersmith, and Selden, my dissertation committee members, gave their unflagging support to this project from the very beginning. Through their expert guidance and determined efforts, this project reached completion. My committee chairperson, Dr. Hodinko, will retain a warm spot in my heart forever. His prodding at critical points and his faith in my abilities made all the difference to me. Mr. McHugh and Dr. Smith from the Marine Corps Human Resources Division receive a special thanks for giving their permission to use Marines in the study. Dr. Hamilton and Mr. Redd of the Drug and Alcohol Training Associates assisted in innumerable ways. They developed a superb training program, provided copies of their training manual, and provided moral support when it was much needed. Mr. Jackson and Ms. Tracy, from Systems Management Associates, Inc., helped in the initial stages of the project by evaluating the survey instruments and providing suggestions and support in its final development. The staff at the American University Library and the Social Sciences Computer Lab were very patient and helpful during the literature search and
iv
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

the data analysis. Each survey participant deserves a special thanks for taking the time to respond honestly and thoughtfully to the survey questions. And finally, my wonderful husband, Jim, receives a great big thanks for reading and rereading several renditions of the various chapters contained in this project. His computer expertise proved invaluable when it came time to load and analyze data, and his faith in my ability to complete this project endured when my own nearly vanished.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

TABLE OF CONTENTS
ABSTRACT................................................. iiACKNOWLEDGMENTS.......................................... ivLIST OF T A B L E S ............................................viiiChapter
I. THE PROBLEM AND ITS S E T T I N G .................... 1Introduction ................................... 1Statement of the P r o blem...................... 13Rationale for the Hypotheses.................. 13Hypotheses...................................... 14Definition of T e r m s .......................... 15Delimitations ................................. 20
II. LITERATURE REVIEW ............................... 22Overview........................................ 22The History of E A P s ........................... 22Role of the Supervisor........................ 29Supervisors' Perceptions ...................... 32
Knowledge of E A P s ...................... 33Program confidentiality ................ 34Program effectiveness .................. 37EAP staff competence .................... 40Management support for the E A P ......... 41
Supervisory Training ........................... 44S u m m a r y ........................................ 52
III. M E T H O D O L O G Y ...................................... 54Research Design ............................... 54Setting: The Substance Abuse Awareness
Seminar (SAAS) ............................. 55Subjects........................................ 62i n s t r u m e n t s ................................... 68
The Baker Knowledge Inventory ......... 68Val i d i t y ........................... 68R e l i a b i l i t y ...................... 69
vi
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
The Demographic Information Inventory . 71The perception question— demo
graphic information inventory(PQ-DII) .................... 72
V a l i d i t y ........................ 74Reliability...................... 75
Data Collection............................... 75Data Analysis................................. 78
Hypothesis 1 ............................. 79Hypothesis I I ........................... 80Hypothesis III........................... 80Hypothesis I V ........................... 80
Ethical Considerations........................ 81IV. RESULTS AND DISCUSSION........................... 83
Experimental and Control Group Pretest Scores 83Control Group Pretest and Posttest Scores . . 84Experimental Group Pretest and Posttest Scores 86Experimental and Control Group Posttest Scores 90Post Hoc Analysis............................. 92
V. SUMMARY, CONCLUSIONS, IMPLICATIONS ANDRECOMMENDATIONS ................................. 96
S u m m a r y ........................................ 96Experimental and Control Group Pretest Scores 98Control Group Pretest and Posttest Scores . . 99Experimental Group Pretest and Posttest Scores 99Experimental and Control Group PosttestS c o r e s ........................................ 100Conclusions and Implications ............... 101Recommendations ............................... 102
AppendixA. MARINE CORPS SUBSTANCE ABUSE AWARENESS
SEMINAR SYLLABUS ............................. 105B. STUDY INSTRUMENTS ........................... 202C. STUDY CORRESPONDENCE ........................ 207
BIBLIOGRAPHY .......................................... 210
vii
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

LIST OF TABLES
1. Distribution of 210 Subjects by Experimental andControl Group Classification on Certain Demographic Characteristics and Chi-square Test of Differences Between Groups .................. 64
2. Pearson's Correlation Test Comparing Five Demographic Variables and BKI/PQ-DII PosttestScores For 165 Subjects By Experimental andControl Group Classification .................. 67
3. Agreement and Disagreement of 35 Item Responsesof Ten Subjects in Two Administrations of the Baker Knowledge Inventory and the Demographic Information Inventory .......................... 70
4. Test of the Significance of the DifferenceBetween BKI and PQ-DII Mean Pretest forMarine Supervisors Who Did and Did NotAttend the S A A S ................................. 85
5. Test of the Significance of the DifferenceBetween BKI and PQ-DII Mean Pretest andPosttest Scores of Marine SupervisorsWho Did Not Attend the S A A S .................... 86
6. Test of the Significance of the Difference BetweenBKI and PQ-DII Mean Pretest and Posttest Scores of Marine Supervisor Who Did Attend the SAAS . 87
7. Test of the Significance of the Difference Betweenthe Mean Posttest Scores on the BKI and PQ-DIIfor Marine Supervisors who did and Did NotAttend the S A A S ................................. 91
8. Test of the Significance of the Difference Betweenthe BKI and PQ-DII (Taken Separately) MeanPretest and Posttest Scores of MarineSupervisors Who Did Attend the S A A S ........... 93
viii
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
CHAPTER I
THE PROBLEM AND ITS SETTING
IntroductionEmployers in business and industry have been con
cerned with employee alcoholism for decades. In the 1940s, several large companies began to assist alcoholic employees by offering medical treatment as an alternative to dismissal. By 1950, 50 organizations had employee alcoholism programs. The establishment of the National Institute on Alcohol Abuse and Alcoholism (NIAAA) in 1971 was the major impetus for the spread of industrial alcoholism programs. NIAAA funded and trained occupational program consultants (OPCs), who consulted with public and private employers in each state, and assisted in developing employee alcoholism programs (Roman, 1983). During the 1970s, the growth in employee alcoholism programs was impressive. A 1981-82 survey revealed over 1,000 persons acting as OPCs and approximately 8,000 formal employee alcoholism programs in various stages of development (Kinman & Roman, 1982).Recent estimates indicate that in 1987 there were over 12,000 programs in the United States (Cannon, 1988;Stackel, 1987).
1
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.
2
From the beginning, NIAAA promoted broadening the employee alcoholism program model. They supported a broadbrush program which would address not only alcohol abuse, but drug abuse, marital and family problems, child and spouse abuse, and mental illness. The resulting employee assistance program (EAP) format made services available to all employees seeking help for personal problems (Wrich, 1974).
Like their civilian counterparts, military alcoholism programs began in response to an increased awareness of the negative effects of alcohol abuse and alcoholism. A 1980 survey showed that 31 percent of military respondents suffered impairment (lowered performance, late for work or left early, did not come to work, drunk while working) due to alcohol abuse (Beary, Mazzuchi, & Richie, 1983). Initial rehabilitation efforts were informal. For example, the Navy's Alcohol Rehabilitative Service at the Naval Hospital in Long Beach, California, began as an Alcoholics Anonymous (AA) meeting (Pursch, 1976). Eventually these efforts were sanctioned by the services, and formal programs grew out of the informal beginnings. Finally, Title 10 United States Code, Section 1090, mandated the establishment and operation of alcoholism treatment programs within the military environment. In 1983, there were fifty-five Department of Defense residential alcoholism treatment facilities, and four hundred twenty-two
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

3
nonresidential and referral facilities worldwide to assist with prevention, education, and rehabilitation efforts (Beary, Mazzuchi, & Richie, 1983).
The military programs have maintained the employee alcoholism program format but, because they work in conjunction with military mental health, family program, and medical services to provide total EAP coverage, research and literature pertaining to Employee Assistance Programming is pertinent to the military programs, as well. The Marine Corps Substance Abuse Program is one such military program. It is the subject of this research project.
Formalized in 1984 with the publication of Marine Corps Order P5300.12 (THE MARINE CORPS SUBSTANCE ABUSE PROGRAM), the Marine Corps Substance Abuse Program addresses both alcohol and drug abuse. It consists of a proactive and a reactive phase. The proactive phase includes preventive education and deterrent measures. The reactive phase includes identification, discipline, treatment, rehabilitation, and return to full duty or separation from the service. The Marine Corps Substance Abuse Program relies heavily on supervisory identification of substance abuse problems and subsequent referral to Substance Abuse Counseling Officers (SACOs) for screening and treatment (MCO P5300.12, 1984).
The Marine Corps Substance Abuse Program is an in- house program manned almost entirely by Marines. Substance
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

4
Abuse Counseling Officers (SACOs), Substance Abuse Counseling Staff Noncommissioned Officers (SACNCOs), and Level II Program Directors are assigned from the supervisory ranks of the Marine Corps into their substance abuse program positions. No previous background or education in substance abuse is required for assignment as a SACO, SACNCO, or program director. Substance Abuse Counselors, also Marines, attend a ten-week Alcohol Counselors School at the Naval Base, San Diego, California. Upon completion of the school, these Marines are assigned an additional military occupational specialty of 8538 (Substance Abuse Counselor), and they spend three years in the counseling field. At the end of their three-year tour, these Marines return to their original occupational specialties. Substance Abuse Counselors are volunteers who are carefully screened prior to assignment to the counseling school. They may or may not have a previous background or education in substance abuse. Some are recovering alcoholics or addicts, others are not.
The Marine Corps Substance Abuse Program functions at three levels. Level I is conducted at the lowest unit level. A Level I program is staffed by a SACO and/or a SACNCO. A Level I program provides screening for Marines who have been referred or who have self-referred with a substance abuse problem. Preventive education is also conducted at Level I. Level II is conducted at the higher command level. A Level II program is staffed by a Level II
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

Program Director, substance abuse counselors, urinalysis and administrative clerks. Level II programs provide in-depth evaluation of Marines whose substance abuse problems exceed the capabilities of the Level I program. Substance Abuse Counselors refer Marines exhibiting symptoms of addiction/alcoholism, per the DSM IIIR, to a Medical Officer for diagnosis. Level II programs conduct more advanced preventive education than the Level I programs, and the Level II Program Director is responsible for monitoring the functioning of the Level I programs. The substance abuse counselors at Level II conduct outpatient treatment programs for Marines diagnosed as mildly dependent or chronic abusers. Upon diagnosis of moderate to severe addiction or alcoholism, Marines are sent to a Level III Treatment Program. The Level III program is conducted on an inpatient basis at a Naval Medical Center. Level III treatment is usually six weeks in length. Upon completion of either the Level II or the Level III treatment program, Marines are assigned to an aftercare program for 12 months (MCO P5300.12).
Confidentiality is protected by substance abuse program policy. All alcohol case files are maintained, under lock and key, by the SACOs, SACNCOs, or Program Directors. Information contained in the case file is releasable to others inside or outside the Command only when it is to be used as a diagnostic tool by an authorized
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

6
medical authority or when the Marine expressly releases the information. The information cannot be used in disciplinary transactions. The information is considered confidential, and disclosure is monitored directly by the Marine's Commanding Officer (MCO P5300.12).
Command, or management, support for the Marine Corps Substance Abuse Program is also a matter of program policy. Commanders are encouraged to set an example of responsible drinking behavior and to provide suitable alternatives to traditional "drinking functions" for their Marines. The use of alcohol is to be deglamorized verbally, in print, and in practice (MCO P5300.12). The fact that the Marine Corps invests over $600,000 dollars in substance abuse training is evidence that there is command support for the program from the highest echelons. However, local commanders may show their indifference to the program by sending only lower-ranking Marines to the training, or by operating only a minimum Level I or Level II program. Individual supervisors can adversely influence program success by neglecting to refer Marines exhibiting substance abuse problems to their SACOs for screening.
Because Marines are assigned from the rank and file of the Marine Corps to fill substance abuse program positions, supervisory training is especially important to the success of the program. A Marine never knows when he or she will be assigned one of these positions, or when one of
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

7
their Marines will have a substance abuse problem. Consequently, the Marine Corps invests approximately $600,000 in supervisory substance abuse training every year, thereby attesting to the important role Marine supervisors play in the success of the program.
In general, EAP professionals believe supervisors play a significant role in the success of all EAPs. From the beginning, first-line supervisors have been key referral agents in industrial alcoholism programs. The attitude of the immediate supervisor is cited as one of the most important factors in employees' acceptance of the EAP (Wright, 1984). Consequently, if employees believe their immediate supervisors support the program, it may influence their use of the program.
Ideally, supervisors identify problem employees and refer them for help before a serious problems arise.Despite the obvious wisdom of early intervention, supervisors tolerate substandard performance for long periods of time, and often refer employees only after a critical incident occurs (Harley, 1990a). One study found that the typical supervisor in a public agency covered up for a troubled employee for about 12 years before taking action and that the average private-sector supervisor covered up for 8 years (Ralfs & Morley, 1990). This reluctance to confront alcoholic employees has been labeled the "policy- practice gap" (Trice & Belasco, 1969).
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

8
Various reasons have been offered to explain supervisors' reluctance to refer troubled employees. These include negative attitudes toward alcoholism (Trice & Belasco, 1969); lack of knowledge about the EAP (Young, Reichman, & Levy, 1987); confusion as to their role in the referral of troubled employees (De Rosa & Zare, 1991;Harley, 1990b); psychosocial factors (Bayer & Gerstein, 1988); personality traits (Googins, 1979); and judgments about the EAP's effectiveness (Young, Reichman, & Levy,1987). This last reason warrants further examination.
An EAP's acceptance by groups within an organization is influenced by the program's perceived legitimacy, professionalism, neutrality, and confidentiality (Steele,1988). In light of its importance to EAP success, it is surprising to discover that limited empirical data have been collected on supervisors' perceptions of EAPs. In one study, Young, Reichman, and Levy (1987) predicted that supervisors' positive judgements of EAP effectiveness would be associated with identification of drinkers. Their prediction was substantiated in their analyses. They found that judging the EAP effective was especially important in the identification of male drinkers. McKirnan (1980) found that employees' perceptions of EAP effectiveness seemed to be related to their reported willingness to seek help with their drinking problems from various sources. Despite the paucity of empirical research in this area, EAP literature
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

9
provides some valuable insights into other elements critical to supervisors' trust of EAPs.
The perception of confidentiality is an issue raised by many EAP professionals (Gerstein & Bayer, 1988; Levine, 1985; Wright, 1984). In his article "Trust Me: EarningEmployee Confidence," Stuart Feldman (1991, p. 7), says that
trust in the confidentiality of the program is the cornerstone of a successful EAP, many experts say.Having a confidential program is not enough; employees must perceive it to be so. "Perception is 90 percent of it," said George Watkins, publisher of EAP Digest.
Supervisors as well as employees are concerned that information provided to EAP staff members is protected. Sensitive to this issue, most EAPs report special handling of EAP records. A Personnel survey of 39 corporate EAPs showed that tactics employed to ensure confidentiality of EAP records include keeping EAP records separate and under lock and key, limiting access to only the EAP administrator or similarly authorized personnel, and employing sign-out and tracking procedures. Confidentiality is related to "trust," a tone set by management, and indicative of their commitment to the EAP function (Levine, 1985).
Perceptions of staff competence or professionalism greatly affect an EAP's success; however, some controversy exists about who is best qualified to staff EAPs. Several schools of social work are actively training industrial social workers to augment the staff of corporate EAPs
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

1 0
(McClellan, 1982). Gerstein and Bayer (1988) urge counselors to establish their profession's role in the EAP system. Some practitioners argue that an understanding of Alcoholics Anonymous and personal experience with alcoholism are necessary prerequisites (McClellan, 1982). So important is perception of staff competence that some companies have set up oversight committees with representatives from key departments— human resources, benefits, medical, security, employee relations, union— to interview and hire the EAP staff or provider. Gerstein and Bayer (1991) suggest that additional research is needed to examine how EAPs and their staff are perceived by supervisors.
Perceptions of management support for the EAP program impact significantly on EAP success. In one study, Sonnenstuhl (1986) discovered that having a discussion with a supervisor who condoned or legitimated the concept of self-referral was a stimulus to employee self-referral.Ralfs and Morley (1990) found that training improved supervisors' perceptions of management support for EAP programs. They quote Dan Smith, EAP Manager at McDonnel Douglas, as saying that, "Although our EAP proved successful, we know now that getting supervisors and managers to collaborate with the program was the key to even greater success." Gerstein and Bayer (1991) suggested that additional research be done on the effect of management's support of the EAP.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

1 1
EAP literature shows that supervisors' training is one way of increasing knowledge and improving the effectiveness of the EAP. Ralfs and Morley (1990), in their article "Turning Employee Problems Into Triumphs," warn against trying to train supervisors to be counselors, but they say that "if supervisors lack the skills they need, an EAP's effectiveness and its value to the organization can suffer." They go on to say that with the right kind of training, supervisors can play a critical role by boosting the rate of successful referrals. Their interview with John Connor, EAP Manager at Torrington Company in Torring- ton, CT, revealed that training more than doubled referrals from supervisors in his organization. In another interview, Dan Smith, EAP Manager at McDonnel Douglas, revealed to them that he credits training with a boost in supervisors' confidence and increased referrals to the EAP at McDonnel Douglas. Smith said his company spends more than 15 hours preparing its supervisors to use the EAP as a management tool. IBM considers supervisory training essential to its EAP's success, and has trained more than 50,000 supervisors since 1984 (Ralfs £> Morley, 1990).
The Marine Corps Substance Abuse Program stresses the importance of supervisory training. Each Marine Corps command is required to conduct supervisory substance abuse training on an annual basis (MCO P5300.12, 1984). In addition, the Substance Abuse Awareness Seminar is offered
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

1 2
by the Drug, Alcohol and Health Affairs Branch of Headquarters, U.S. Marine Corps. The seminar is designed to train Marines who will become or are currently serving as administrators of the Marine Corps Substance Abuse Program. Supervisors serving in key leadership positions are also invited to attend the seminar. Reaching over 400 supervisors per year over the past 10 years, the seminar has been and remains a major training investment for the Marine Corps.
Considering the corporate and military investments in supervisory training, it is surprising how little empirical research has been conducted on supervisory EAP training.One study (Trice & Belasco, 1969) indicated that supervisory training had little affect on supervisors' attitudes, but that it did increase supervisors' knowledge and their tendency to take constructive action in the case of an alcoholic employee. This researcher found no data on how training affects supervisors' perceptions of EAPs. A study assessing supervisors' knowledge of EAP rules and procedures and their perceptions of EAP effectiveness, confidentiality, management support, and staff competence added to the knowledge about supervisors' perceptions of EAPs. Assessing training's affect on these variables, the focus of the present study, added to the sparse body of existing knowledge about the effectiveness of supervisors' EAP training to influence supervisors' perceptions.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

Statement of the Problem This study determined the effects of a 36-hour super
visory substance abuse training seminar (The Substance Abuse Awareness Seminar) on Marine Corps supervisors' knowledge of the Marine Corps Substance Abuse Program, as assessed through the Baker Knowledge Inventory (BKI). Supervisors' perceptions about the confidentiality, effectiveness, management support, and staff competence of the Marine Corps Substance Abuse Program were ascertained, using direct questions contained in the Demographic Information Inventory (Appendix B). These questions, 7, 8, 9, and 10, will be hereafter referred to as the PQ-DII.
Rationale for the Hypotheses Supervisors are an integral part of EAP success.
Their attitudes toward the EAP can affect their own and their employees' use of the program. Though several studies have investigated the effect of various factors on supervisors' referral of employees to an EAP, the writer found only one major study (Belasco & Trice, 1969) on the effect of EAP supervisory training on knowledge and attitudes, and that study found very minimal training effects. When you consider that only about two to three percent of troubled employees take advantage of their EAP through self-referral, and that supervisors tolerate substandard performance for years (Gerstein & Bayer, 1988), it is no wonder that companies are beginning to pour more time and
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

1 4
money into supervisors' EAP training. Training for supervisors is expensive and very difficult to conduct, however. Based on the limited research conducted in this area, it is not at all clear at this time what training content, how much, how often, and with whom such effort would be most effective. Research into the effects of supervisors' EAP training is called for. This study contributes to the base of knowledge about supervisors' knowledge and perceptions of various aspects of the EAP and about the effect of training on these perceptions.
Hypotheses1. No significant difference, at the .05 level,
would be found between mean pretest scores of Marine supervisors who attended and those who did not attend the Substance Abuse Awareness Seminar, as measured by the Baker Knowledge Inventory (BKI) and questions 7, 8, 9, and 10 of the Demographic Information Inventory (DII), referred to as the PQ-DII.
2. No significant difference, at the .05 level, would be found between mean pretest and posttest scores for Marine supervisors who did not attend the Substance Abuse Awareness Seminar, as measured by the BKI and PQ-DII.
3. The mean BKI and PQ-DII posttest scores for the experimental group of Marine supervisors would be significantly higher than their mean pretest scores on the BKI and PQ-DII.
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

15
4. The mean BKI and PQ-DII posttest scores for the experimental group of Marine supervisors would be significantly higher than the mean posttest scores on the BKI and PQ-DII for the control group.
Definition of Terms The terns used in this study on a recurring basis
which have special meaning are the following:Marine Corps Substance Abuse Program— The Substance
Abuse portion of the Marine Corps Employee Assistance Program. The program is outlined in Marine Corps Order P5300.12. It includes a proactive (preventive) and a reactive (treatment/punitive) phase, and is administered by Substance Abuse Counseling Officers, Staff Noncommissioned Officers, and Level II Program Directors. The main thrust of the program is to hold Marines responsible for their actions regarding the use of alcoholic beverages and drugs. The program relies heavily on supervisor awareness of the symptoms of substance abuse and their ability to constructively confront and refer Marines exhibiting those symptoms. Marines who have substance abuse problems are screened by a Level I SACO who will determine the extent of the problem. Depending on the degree of chemical dependency, as defined in the DSM III R, the Level I SACO will assign the Marine to an educational program to prevent further abuse, or if dependency is evident, will refer the Marine to a Level II SACO for in-depth evaluation. The
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

1 6
Level II SACO, as a result of his evaluation, will assign the Marine to outpatient treatment or will refer the Marine to a Medical Officer for subsequent diagnosis of chemical dependency and Level III inpatient treatment at a Naval Medical Center. Twelve-month aftercare programs follow both the Level II, outpatient treatment, and the Level III, inpatient treatment programs.
Substance Abuse Counseling Officer (SACO)— An administrator of the Marine Corps Substance Abuse Program at either the Unit or Command level. He or she is usually a warrant or commissioned officer. No previous background or training in substance abuse is required to be assigned duties as a SACO. Training within three months of assignment is required.
Substance Abuse Counseling Staff Noncommissioned Officer (SACNCO)— An administrator of the Marine Corps Substance Abuse Program at either the Unit or Command level. He or she is usually subordinate to the SACO, and holds a noncommissioned officer's rank. No previous background or training in substance abuse is required to be assigned duties as a SACO. Training within three months of assignment is required.
Level II Program Director— An administrator of the Marine Corps Substance Abuse Program at the Division, Base, or Group level. He or she holds the rank of warrant or commissioned officer. The Level II Program Director
R eproduced with perm ission of the copyright owner. Further reproduction prohibited without perm ission.

17
oversees the operation of the Substance Abuse Counseling Center, which is staffed by substance abuse counselors, and is responsible for providing in-depth screening and counseling for substance abuse problems. No previous training or background in substance abuse is required for assignment as a Level II Program Director; however, training within three months of assignment is required.
Substance Abuse Awareness Seminar (SAAS)— A 36-hour substance abuse training seminar in which SACOs, SACNCOs, and Level II Program Directors are trained to assume administrative positions within the Marine Corps Substance Abuse Program. Supervisors holding key leadership roles also attend the seminar. Participants are drawn from every Marine Corps command, worldwide. Participants either volunteer to attend or are assigned. The seminar was specifically designed for the Marine Corps and has been in operation for over ten years. The seminar is divided into nine learning modules with specific learning objectives ascribed to each module. The seminar is conducted at the Xerox Training Center, Leesburg, Virginia, which provides a self-contained, retreatlike setting isolated from distractions of every kind. Each class contains up to 40 participants. The seminar is divided into Junior and Senior classes. Marines holding the ranks of E-6 (staff sergeant) through 0-3 (captain) usually attend a Junior class.Marines in the ranks of E-8 (master sergeant) through 0-6
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 8
(colonel) usually attend a Senior class. Course content does not differ significantly between the Junior and Senior classes. The differentiation is made in order to put participants at ease and to encourage their sharing of personal information. Additionally, dividing the Juniors and Seniors enables each class to work on problems inherent at their particular level of command responsibility. The classes provide a forum for debate about the philosophies, ethics and purposes of the Marine Corps Substance Abuse Program (see Appendix A).
Alcoholism— A medically recognized disease manifested by the continued abusive use of alcohol and characterized by the development of psychological and/or physical dependency. It is a disease with recognizable symptoms and predictable behavior. It is a progressive disease that, if left untreated, may prove fatal (MCO P5300.12).
Alcoholic— An individual who suffers from the disease of alcoholism.
Alcohol abuse— Any use of alcohol that adversely affects individual performance, debilitates physical or mental health, interferes with financial responsibilities, deteriorates personal relationships, leads to the violation of military regulations or civil laws, or contributes to disorderly conduct (MCO P5300.12).
Alcohol abuser— A person who abuses alcohol, but is not dependent upon alcohol.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.
1 9
Supervisor— A person who is responsible for managing, leading or overseeing the conduct and performance of subordinate workers. For the purposes of this study, a military supervisor holds the rank of E-6 or higher or is a warrant or commissioned officer. A civilian supervisor holds the paygrade of GS-10 or above.
Perception— A direct or intuitive recognition, intelligent discernment, appreciation, insight, a capacity for comprehension, or intellectual grasp (Webster's Third International Dictionary).
Supervisory Training— Training which targets supervisors as its audience and is designed to help supervisors learn information or skills that will enhance their performance .
Employee Assistance Program (EAP)— Social services programs within the structure of businesses designed to encourage and assist employees with personal problems such as alcoholism, drug abuse, mental illness, stress, child care, etc.
Demographic Information Inventory (DII\— A ten-item inventory containing questions pertaining to age; gender; rank; education; previous experience with the Marine Corps Substance Abuse Program; perceptions about program confidentiality, staff competence, program effectiveness, and command support for the program (see Appendix B).
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

20
Perception Question-Demographic Information Inventory (PQ-DII)— Questions 7, 8, 9, and 10 of the DII which relate directly to supervisors' perceptions of the confidentiality, staff competence, program effectiveness, and command support for the Marine Corps Substance Abuse Program.
Baker Knowledge Inventory (BKI)— A 25-question, multiple choice and true/false testing instrument designed to ascertain the knowledge gained by supervisors attending the Substance Abuse Awareness Seminar. The instrument specifically measures knowledge of the Marine Corps Substance Abuse Program, its functions, procedures, and regulations (see Appendix B).
DelimitationsGeneralizations of the findings and conclusions of
this study may have been limited by the following considerations. The subjects were Marine Corps supervisors who either volunteered or were assigned to the Substance Abuse Awareness Seminar, or who were assigned to the Human Resources Division of Headquarters, U.S. Marine Corps, as opposed to a random selection of subjects. All data was self-report type data. Validity of the data was dependent on the subjects' ability and willingness to report true feelings. The knowledge and perceptions being measured were selected by the researcher, rather than including all areas of knowledge and perceptions relevant to the broad topic of Employee Assistance Programs. Marine Corps
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

21
supervisors were from one branch of the military service, and hence, may not have been representative of the universe of military or civilian supervisors in general. Supervisors were from a wide range of backgrounds having either a great deal or possibly little exposure to alcoholics, alcoholism, Employee Assistance Programs, or the Marine Corps Substance Abuse Program. When using Likert-type scales, the error of central tendency is always a peril.And, the Hawthorne effect may have been present, i.e., supervisors may have tried to guess the researcher's purpose and respond accordingly.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

CHAPTER I I
THE LITERATURE REVIEW
OverviewThis study explored the effects of a 36-hour super
visory substance abuse training seminar on Marine supervisors ' knowledge and perceptions of the Marine Corps Substance Abuse Program. This review of the current relevant literature addresses four specific areas: the historyof Employee Assistance Programs (EAP), especially military alcoholism programs; the role of supervisors in the success of the EAP; supervisors' perceptions of the confidentiality, staff competence, program effectiveness, and management support for the EAP; and supervisory EAP training.
The History of EAPs The custom of drinking on the job was brought to
America from the "old" country. The practice became popular among the working class and continued, unhampered, for many years. With the beginnings of the industrial age, and the dramatic increase in industry in America, the detrimental effects of alcohol on production soon became apparent. From the 1880s to the 1920s, a movement arose to remove drinking from the work environment. Its purpose was to
22
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

2 3
produce a reliable, dependable, and predictable workforce.It soon became known as the Temperance Movement and, with the help of people like Carry Nation, gained momentum in American society. In an effort to control their workforces, employers joined forces with others who fought drinking on the job. Some employers even threatened to fire employees caught drinking; for example, the railroads, by the early 1900s, required total abstinence, both on and off the job (Anderson & Ball, 1978).
During the 1920s and 1930s, the work ethic became a strong motivator in American society. Personal goals of discipline, self-reliance, and hard work coincided with organizational goals of profitmaking and efficient utilization of resources. Productivity was of paramount importance, and workers who used alcohol during work hours could no longer be tolerated. They came to be looked upon as a detriment to productivity (Trice & Beyer, 1982). Workman's Compensation laws added fuel to the fire by placing the financial responsibility for on-the-job injuries on the employer. Concern for employee safety heightened. Employers began to realize that alcohol users suffered more accidents and filed more grievances than nonusers (Spicer, Owen, & Levine, 1983).
The birth, in 1935, of Alcoholics Anonymous (A.A.) offered the common man a practical solution to his drinking problems. The beginning of World War II, with its
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

2 4
burgeoning and unique workforce, provided a superb laboratory to test its effectiveness. Medical directors in industrial settings saw the wisdom, both medically and economically, of helping problem drinkers. Their influential leadership, combined with the growth of A.A. and the trials of World War II, added impetus to the growth of industrial alcoholism programs (Anderson & Ball, 1978).
Military history often refers to the prevalence of alcohol consumption in the military forces. To soldiers of Rome, medieval knights (Windrow & Wilkinson, 1971), 15th- century French and English soldiers at Agincourt (Keegan, 1976), Civil War soldiers of the 6th Pennsylvania Cavalry, and soldiers of the modern U.S. military (Ingraham, 1978), alcohol consumption served important individual and group functions. Its importance continues today.
Numerous military traditions surround alcohol consumption. The Marine Corps Mess Night, for instance, has very detailed rules governing the serving and consuming of alcohol during a very formal dining occasion. Despite the traditional use of alcohol in the military, the Temperance Movement fostered a reaction within the military similar to that mushrooming in the civilian community. One example was President Rutherford B. Hayes banning the sale of alcohol at all military posts on February 22, 1881.
Employers began the fight against employee alcohol abuse by established company rules and policies forbidding
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

2 5
alcohol use on the job. Rules, though, had little impact on actual worker behavior. Consequently, some industrial and military leaders realized that more constructive solutions were needed.
The first occupational alcoholism programs attempted to help employees identify and overcome their alcohol problems. These programs were informal and usually operated under the direction of the medical department. Examples of early programs were those at Du Pont under Dr.George Gehrmann; at Eastman Kodak under Dr. John Norris; and at New England Telephone Company, thought to be the first ever, under Dr. Daniel Lynch (Spicer, Owen, & Levine,1983). One of the first formal civilian programs was at Caterpillar Tractor Company, which in 1945 developed a comprehensive companywide mental health program, which included alcoholism treatment (Harley, 1990b). In the late 1940s, even the unions began to acknowledge the need for such programs to help their members (Shipp, 1984).
Though similar informal programs were operating in the military, for instance, the U.S. Naval Alcoholism Rehabilitation Program at Long Beach, California, under Captain J.J. Zuska and Commander R. Jewell (Pursch, 1976), no formal alcoholism programming appeared until the mid- 1960s. Deterrent efforts abounded, however, as evidenced by the outlawing, again, of hard liquors at all Army establishments in February 1943.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

2 6
Over time, and with experience, occupational alcoholism programs became more sophisticated. The precursor of modern industrial alcoholism programs, the Yale Program, was distributed in 1953 by Henderson and Bacon. It introduced the concept of the "half-man" who is at work but unproductive and unsafe, as well as the "half-person," the woman who lives with an alcoholic husband who drives her to distraction with worry and repeated domestic crises. The program was very progressive for its time. It advocated changing the attitudes of management as well as employees, assigning responsibility for the program to the medical or personnel department, giving supervisors a leading role as liaison between the employee and the program, conducting education programs, and conducting needs assessments.
In 1969, the National Institute on Alcohol Abuse and Alcoholism (NIAAA) was formed with the passing of the Hughes Act. Roman and Trice (1976) consider this the "major event" for the growth of occupational alcoholism programming. Since then, the federal government has actively disseminated EAP program models and has stimulated program adoption in both government agencies and in private business and industry.
An equally important advance for the military took place in 1971, when President Nixon launched the "War on Drugs." The response from the Department of Defense was enormous. Programs requiring thousands of full-time
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

2 7
workers involved in drug detection, treatment, and rehabilitation were established around the world (Goodwin,Davis, & Robins, 1975). Before long, however, program administrators and counselors began to see that Southeast Asian heroin, which had produced intense public fear, was not the most serious drug problem; indeed, alcohol had become the number-one drug problem in the military. Alcohol was used by military personnel of all ranks, officer and enlisted alike, and resulted in the most damage to the greatest number of servicemembers. At the time, an estimated 19% of officers and 37% of the enlisted personnel were heavy drinkers and had serious problems as a result (Pursch, 1976). Consequently, the programs which were formed to deal with drug abuse slowly shifted emphasis toward alcohol abuse.
The 1970s saw a significant increase in both civilian and military alcoholism programming. In 1972, the states were given grant money, by NIAAA, to train and employ "occupational program consultants" whose task was to organize alcoholism programming within their states. A 1981-82 survey revealed over 1,000 persons acting as OPCs and approximately 8,000 formal employee alcoholism programs in various stages of development (Kinman & Roman, 1982). By 1983, there were 55 Department of Defense residential alcoholism treatment facilities, and 422 nonresidential and referral facilities worldwide to assist with prevention,
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

2 8
education, and rehabilitation efforts (Beary, Mazzuchi, & Richie, 1983).
From the beginning, NIAAA promoted broadening the employee alcoholism program model. The resulting broadbrush employee assistance program (EAP) format made services available to all employees seeking help for many different personal problems including mental illness, drug abuse, marital discord, and child and spouse abuse (Wrich, 1974).
The Marine Corps embraced the concept of employee assistance programming, and established Family Service Centers to meet the varied needs of the Marine Corps community through counseling and education. However, it maintained the Substance Abuse Program as an independent program, much like the employee alcoholism programs of the past. The Program works in conjunction with the Family Service Centers and the Naval Medical Facilities to provide a full range of mental health and family oriented programs. Consequently, literature pertaining to Employee Assistance Programs is relevant to the Marine Corps Substance Abuse Program, as well. Especially important is material about the changing role of the supervisor in the Employee Assistance Program, which took place along with the broadening focus of the EAP.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

2 9
Role of the SupervisorSupervisors are the key to success for the Employee
Assistance Program. The supervisors, because of their routine interaction with employees, are in a perfect position to observe problem drinking behavior. Early Occupational Alcoholism Programs concentrated more on the symptoms of alcoholism than on job performance. Thus, supervisors were trained specifically to be on the lookout for personal behavior that indicated excessive drinking either on the job or outside the workplace. While this made sense theoretically, it was a problem in practice. Supervisors were put in a position to conduct witch-hunts, trying to catch employees with alcohol on their breath or with bleary eyes. Because the supervisor was not trained to diagnose alcoholism and because identifying alcoholics was just one more thing he had to do during the work day, the early alcoholism programs were fairly ineffective at identifying or assisting the alcoholic employee in any meaningful way (Roman & Trice, 1976).
Over time, a new model was introduced that focused specifically on job performance. The job performance model emphasized the identification of poor work performance over symptoms. The workplace provided a stable background against which alcohol-related behavior, such as patterned absenteeism and chronic tardiness, could be highlighted. These behaviors, it was determined, provided a stronger and
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

3 0
more effective indicator of problem drinking than did the more elusive diagnostic symptomatology (Lotterhos &Waldrop, 1972).
Along with the job performance model came constructive intervention. Constructive intervention is a coercive strategy which includes the threat of disciplinary action or termination unless the drinker voluntarily improves his/ her work performance. It has proved an effective approach toward motivating alcoholics to stop drinking. EAP literature abounds in studies of the constructive intervention and its effectiveness in getting alcoholics to accept treatment.
Roman (1972) concluded that the constructive intervention was more effective than other strategies used under other conditions in the rehabilitation of alcoholics.Schramm and Defillippi (1975) believe that the constructive intervention may be even more important to the successful recovery of the alcoholic than the treatment program, because of the motivating influence it has on the alcoholic employee.
EAP research also supports the use of constructive confrontation in the work setting. Heyman (1976), in interviews with 180 randomly sampled alcoholics from four industrial alcoholism programs in the New York City area, discovered that employees who are strongly coerced into entering treatment because of their job performance
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

3 1
reported a higher proportion of work improvement than those entering treatment for other reasons. Another study that compared treatment results of alcoholic employees referred by supervisors and by other sources supported the hypotheses that (a) an industrial setting allows for early identification of problem drinkers; and (b) constructive coercion (intervention) is an effective approach in the sense that it enables the employer to force the worker to comply with rehabilitation (Chopra, Preston, & Gerson (1977). And a study by Freedburg and Johnston (1980) compared two groups of employed alcoholics, one which voluntarily sought treatment and one which sought treatment after being threatened with dismissal. Findings strongly supported confrontation of the employee by supervisors with the threat of job action for unsatisfactory performance or behavior.
Another study by Sherwood, Davidson, and Aharan (1979) compared 87 participants in a 26-day residential alcohol treatment program in Victoria, Canada. Forty-two participants had been strongly coerced into the treatment program by their employers. The remaining participants were referred either by doctors or social agencies, or self-referred. Fifty-seven percent of the employer- referred participants believed that their employment was conditional on program attendance; only 15% of those referred by other agencies or self-referred had the same
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

3 2
perception. Results indicated that 46% of the employer- referred participants were completely abstinent in the year following treatment. Only 32% of the other-referred participants remained abstinent. The researchers believe that their study supports the effectiveness of the constructive intervention process, and they conclude that it may not be important who confronts the alcoholic but that it be done and done strongly.
Considering the pivotal role supervisors play in the workplace, and the detrimental affects of alcohol abuse on productivity, one would expect supervisors to immediately refer problem drinkers as soon as deviant work-related behaviors arise. This is not the case, however. Trice and Belasco (1969) identified what they call a "policy-practice gap." They discovered that supervisors will tolerate poor performance from employees for a long time before referring them to an EAP. Much research has been conducted to determine the reasons for this gap.
Supervisors' PerceptionsVarious reasons have been offered by researchers to
explain supervisors' reluctance to refer troubled employees . They include their negative attitudes toward alcoholism (Trice & Belasco, 1969); confusion as to their role in the referral of troubled employees (Harley, 1990b;De Rosa & Zare, 1991); psychosocial factors (Bayer & Gerstein, 1988); and personality traits (Googins, 1979).
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

3 3
This section will explore the barriers to supervisory EAP referral posed by lack of knowledge about the EAP (Beyer & Trice, 1978; Googins, 1979; Riediger, 1979; Young, Reichman, & Levy, 1987); judgments about the EAP's effectiveness (Googins, 1979; Wilcox, 1984/1985; Young,Reichman, & Levy, 1987); and perceptions of confidentiality, staff competence, and management support for the EAP program (Gerstein & Bayer, 1988; Levine, 1985; Wright,1984).
Knowledge of EAPsKnowledge about the EAP, though it seems elemental,
cannot be taken for granted. Supervisors will not use a program that they know little or nothing about. Trice and Roman (1978) observed that publication and wide dissemination of a written organizational policy is important to EAP success. Supervisors translate these actions by management into EAP referrals. Kurtz (1982) stated that "neither supervisors nor employees are likely to use a plan or program that they do not know about" (p. 276). Googins (1979) discovered that 21% of the first-line supervisors he surveyed did not know of the existence of the company EAP, even though it had been there for over 12 years. "It is clear", he said, "from these data that absence of familiarity acts as a powerful barrier" (p. 148).
Beyer and Trice's (1978) study of occupational alcoholism policy and programs in federal agencies supported
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

3 4
these findings. They found that "for past use, familiarity is the most important predictor, or equally important with assessed need" (p. 64). And Nord (1988), in her study of 493 Iowa Department of Transportation supervisors, found that more knowledge of the EAP would be associated with referral. Harley's (1990b) study of 415 supervisors in 25 business locations found that 51.8% of his referring supervisors agreed that procedures for making an EAP referral were clear to them, and that 80.7% knew whom to contact if they wanted to refer an employee to the EAP.
Though Riediger (1979) found that 27% of the supervisors he studied knew how to use the EAP, 23%, a comparable percentage, reported not knowing how to use it. Ultimately, his findings regarding the importance of knowledge as a factor were ambiguous. He stated, "Knowledge of the program does not appear to be associated with program utilization" (p. 177). He did, however, discover a negative association between program knowledge and number of employees supervised which suggested that supervisors who needed the program most had learned the least about it.
Program ConfidentialityThe perception of confidentiality is an issue raised
by many EAP professionals (Braun & Novak, 1986; Harley, 1990b; Levine, 1985; Wright, 1984). In his article "EAP:An Important Supervisory Tool," Wright (1984) stressed the importance of confidentiality. He said that
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

confidentiality should be protected, and that "any hint that the program is not totally confidential, and that the supervisor is receiving information about referrals, will have a lasting negative impression on the program" (p. 20).
Levine (1985), in his telephone survey of 39 corporate EAPs, found that confidentiality was a major factor in inspiring employee confidence in the EAP program. He found that nine companies keep EAP records separate and generally under lock and key; eight noted that only the EAP administrator or similarly authorized personnel had access to the records; five reported that the EAP staff were professionals and adhered to professional standards of confidentiality; four attribute confidentiality to company policy; two companies broach the confidentiality issue by keeping no records; and two companies use only case numbers to identify cases. Some companies related that employees alone can release the EAP information to the personnel or other departments, and others indicated that EAP information is reported in a purely statistical manner with no names or individual identification possible.
In a study done by Braun and Novak (1986) of 145 EAP directors from the United States and Canada, it was found that 6% believed employees who do not use the EAP feared that their EAP was not confidential. Harley (1990b) found that the majority of his referring supervisors believed
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

3 6
that their EAP kept personal matters totally confidential (55.9%).
Bloom (1987) surveyed 213 organizations having EAPs, and discovered that 93% of the respondents reported complete confidentiality maintained between employee assistance staff and employees. When supervisors made the referrals, 87% required a release of information form signed by the employee before information was provided to other parties. Forty-two percent of respondents reported abridging confidentiality policies only at times when there was a threat of danger to self or others (suicide, homicide, child abuse, incest) and when program participation had been initiated by court order or was under court supervision. Bloom also discerned that the development and maintenance of employee awareness and trust appeared to be a central issue in EAP operation.
Several respondents cited employee reluctance to use program services due to fears regarding confidentiality. The issue of confidentiality appeared to greatly impact the development of employee assistance program credibility with unions as well as in individual cases, (p. 71)
Some respondents reported problems developing policies and procedures which would maintain employee confidentiality and still align with employer liability standards and goals. Others reported problems developing and maintaining confidential record-keeping systems.
Plavan (1989), in her study of 15 Fortune 500 companies, found that confidentiality was a prime factor
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

3 7
(equally as important as money saving) in the companies' selection of either an internal or an external EAP program. Fifty-six percent of respondents said they chose their particular EAP because it would ensure confidentiality.She found that confidentiality may be a doubled-edged sword in that from 22% to 25% of companies surveyed indicated that confidentiality constraints limited access to user information, thereby acting as a barrier to program evaluation.
Program EffectivenessPerceptions of the effectiveness of an intervention
and referral action appear related to the supervisor's readiness to refer an employee to the EAP. Supervisors who believe strongly in the effectiveness of EAP intervention and subsequent treatment are more likely to confront and refer the impaired worker (Googins, 1979; Love, 1989; Sonnenstuhl S> Trice, 1989; Wilcox, 1984; Young, Reichman, & Levy, 1988). Braun and Novak (1986), in their study, found that of the 145 EAP supervisors surveyed, 20% believed that EAP users had confidence in the services provided by the EAP. This perception has been substantiated by other EAP researchers.
Love (1989) studied 88 supervisors/managers in the U.S. Postal Service's Southern Region and found that referring supervisors were more impressed with the performance
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

3 8
of employees following EAP enrollment-treatment than werenonreferring supervisors. He stated that
supervisors who find the EAP to be effective are more likely to refer employees with impaired productivity. Supervisors with low EAP referral rates may have supervised an employee who relapsed following temporary improvement or no improvement. Thus, the supervisor's faith in the EAP system can be decreased. (p. 87)
Wilcox (1984) conducted a study with 167 federal supervisors from nine federal agencies located in the Washington, D.C., metropolitan area in order to determine the hindrances and facilitators to supervisory constructive intervention in federal government EAPs. He discovered that, in addition to the hindrances he suggested, supervisors reported they lacked confidence in the EAP's ability to deal effectively with employees' personal problems.
Harley (1990b) found that 63.9% of his referring supervisors were ambivalent about the success rate of their EAP, and about the improvement experienced by the referred employee (48.9%). He did, however, find that the majority of referring supervisors felt that counseling and other forms of treatment for the various types of personal problems was usually quite effective (57.5%), and that 60.3% believed that most people are really helped by counseling or "therapy" programs like the EAP. Over 58% had confidence in the ability of their EAP to deal with the really hard problems employees may have. And Nord (1988), in her study of 493 Iowa Department of Transportation supervisors,
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

3 9
found that referrers rated the EAP as significantly more effective than did nonreferrers.
Googins (1979) showed that supervisors who had a more positive outlook on the effectiveness of the program referred more employees to it. In his study, 35.7% of the referring supervisors gave an excellent rating to the program; only 13.5% of the nonreferring supervisors felt the same way. He further discovered that 36% of the referring supervisors view the program as very helpful for employees as compared to only 13.5% of the nonreferring supervisors. He found differences on other items such as effectiveness of program location, ease in dealing with the program staff, and the degree of qualifications of the program staff.
Closely linked with the perception of program effectiveness is the competence of the EAP staff. There are various schools of thought on what qualifications EAP professionals should possess. Counselors believe EAPs should be manned by counselors. Psychologists support a psychological base to EAP operations. EAP specialists believe that industry deserves a cadre of specially trained EAP staff members. Even recovering alcoholics want in on the action, indicating that EAP staff members must have knowledge and background in alcoholism rehabilitation and treatment. Regardless of the approach taken, it is evident
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

4 0
that without trust and confidence in the abilities of the EAP staff, the program will not be successful.
EAP Staff CompetenceIn their quest to determine the barriers to supervi
sory use of EAPs, researchers have explored supervisors' attitudes toward the EAP staff. Googins (1979), for instance, believed that negative attitudes might serve as barriers to referral. These negative attitudes, he said, might be directed toward the staff of the Alcoholism Program.
Roman and Trice (1976) reported that a reluctance of supervisors to consult with and interact with the staff (including EAP staff) resulted in a decrease of referrals by supervisors. Increased visibility and prestige of the EAP staff, though, are believed to cause supervisors to doubt their competence to deal with the troubled employee and to develop a greater reliance on the "experts" reducing their use of constructive confrontation.
O'Connell (1987) argued that supervisors resist referring an employee for several reasons, not the least of which are that they may doubt the ability of "outsiders"(EAP staff) to know what really happens on the job, and they may "distrust or feel threatened by mental health counselors."
Wilcox (1984) developed the Wilcox Holistic Inventory of Supervisory Personnel Employee Referrals (WHISPER),
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

4 1
which he used with 167 federal supervisors to determine hindrances and facilitators to supervisory constructive intervention. He listed hindering factors mentioned by authorities in the EAP field and grouped them as related to identification, confrontation, and referral. He also gave his respondents an opportunity to identify beliefs or attitudes which may have hindered them but which were not mentioned in his list. He found among the hindrances to referral lack of understanding of the staff functions of the EAP personnel and reluctance to refer because of lack of confidence in the competency of the EAP staff. Conversely, among the facilitators of confrontation and documentation were feelings of trust and confidence toward the EAP staff; and of referral, respect for EAP staff professionalism and EAP staff's willingness to assist. Obviously, confidence in EAP staff competence is a factor worth considering.
Management Support for the EAP Management's support or lack of support for the EAP
program can be shown in many ways. Weakly stated EAP policies reflect ambivalence on the part of management. A poorly organized EAP program or unqualified EAP staff also indicate a lack of support. By circumventing the EAP program and overriding EAP decisions, management shows not only a lack of support, but contempt for the program. Even a lack of commitment on the part of management to make
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

4 2
supervisors and employees available for EAP training portrays a lack of support. Any perceived lack of support can be detrimental to the success of the EAP.
One study, conducted by Schramm (1977) with a consortium of companies in the Baltimore area, isolated three factors that effect the supervisors' referral practices, one of which was the company policy and how it is perceived by supervisors. He determined that the absence of a company policy designed to provide uniform treatment for all employees referred will cause supervisors to ignore the referral process because of a lack of perceived support by the company.
Heyman's study (1976) suggests that the attitudes of supervisors toward their employees and the program are crucial to their use of referral. She found that, of those programs having strongly worded policies and training for supervisors, approximately 64% of all referrals were made by supervisors. The one company which showed only a moderate expression of support in its company policy and no supervisory training had only 22% of its referrals made by supervisors.
Love (1989), in his study of 88 supervisors from the United States Postal Service's Southern Region Field Division, found that referring supervisors perceived the upper management to be supportive of EAP operations significantly more than nonreferring supervisors. This finding probably
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

4 3
is a result of the Equal Employment Opportunity (EEO) and organized labor complaints filed against supervisors who refer employees to the EAP. In cases where employees, angered by a mandatory EAP referral, resort to EEO or discrimination complaints, supervisors are reassured by management commitment to the EAP and supervisor utilization.
Wilcox (1984) discovered that management support for the EAP was a significant facilitator of supervisory referrals. In his study of 167 federal supervisors he discovered that belief that the EAP was an "official" management system and should be used, and that being directly ordered (or encouraged) by one's own supervisor to make the referral, helped supervisors to make a positive referral decision.
Harley (1990b), in his study of 415 supervisors in 25 locations, found that among factors that encouraged supervisors to "approach" referral was a sense of organizational support for the EAP program. The majority of his referring supervisors did not believe that their organization subtly discouraged supervisors from using the EAP (68.2%), and did believe that their own supervisors expected them to refer employees to the EAP (55.5%).
Nord (1988) found that having an opinion about the degree of management support or lack of support for the EAP is associated with referral, and that not knowing how much
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

4 4
support the management gives the EAP was associated with nonreferral. Based on current research, it is evident that management support is an important ingredient in the success of an EAP, and that supervisors' perceptions of management support for the program may be just as important as the actual support. One important way to display support for an EAP is to provide supervisory training. The cost of such training and the workhours required to conduct it are often barriers to its implementation. The fact that supervisory training is conducted in an organization, regardless of its length or content, indicates that there is support for the EAP program.
Supervisory TrainingMost EAP professionals agree that supervisory train
ing is an important component of an EAP and that it can overcome some of the barriers to referral. To this end, a good deal of supervisory EAP training is conducted every year, as evidenced by Plavan's (1989) study of 15 Fortune 500 industries, which found that 78% of industrial and 75% of service companies conducted some sort of supervisory EAP training. Reporting on an extensive telephone survey of EAP practitioners, Googins, Schneider, and Colan (1989) provide evidence that the training currently being provided in organizations is "fairly homogenous."
Bloom (1987) found that in 90% of EAP programs responding to her survey, union and management training was
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

4 5
provided by the EAP staff. Training was also provided by outside consultants (20%), personnel department staff (8%), medical department staff (3%), and human relations department staff (4%). Seventy-five percent of the respondents indicated that they provided specialized training for development of supervisory personnel's referral skills. Training was also provided in identification (85%), confrontation techniques (76%), and assertive training (27%). Under three hours of training was reported by 40% of respondents, and 37% reported between three and ten hours of training. Only 4% reported conducting no EAP training at all.
Plavan (1989) discovered that the length of training varied from one to four hours and the content from educating employees of the EAP services and how to use them, to information on alcohol and drug abuse, symptoms of alcoholism, problem solving, and job performance evaluation. Many companies reported using films and videos in their training programs. "These presentations seem to occur on an ad hoc basis, and lack a consistent format and content" (p. 140).
Supervisory training objectives usually include introducing supervisors to the EAP, clarifying their role in its operation, dissipating resistance to EAP use, and gaining support for the program. Other objectives have been suggested. Gam, Sauser, Evans, and Lair (1983) advocated training supervisors to help them accurately assess
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

4 6
performance, to increase their awareness of stress disorders, and to school them in constructive confrontation procedures. Brownell (1973) recommended educating supervisory levels regarding the characteristics, costs, and other effects of alcohol abuse in his study of Navy alcoholism programs.
Beyer and Trice (1982) encouraged EAP trainers to incorporate general supervisory skills training into their training sessions. As a consequence, EAP implementation and training would afford supervisors an opportunity to upgrade and refine their supervisory skills. "Supervisory training about job-based intervention strategies provides an excellent opportunity to train line managers how to be more generally effective, by being concerned about both task performance and employee welfare" (Beyer & Trice,1982, p. 198). They also identified elements in EAP training which might possibly affect supervisory use of the program. These included familiarity with the underlying policy statements and specific knowledge of the existence of the EAP and its accessibility.
Still other objectives and strategies have been suggested. Hawthorne and Davidson (1983) believed that supervisors are receptive to training about the EAP only after they have failed with the alcoholic and have reached an emotional crisis themselves. They recommended targeting those supervisors feeling an immediate need for EAP
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

4 7
assistance, consisting of a period of "catharsis" followed by redirection of their efforts into positive behaviors of confrontation and referral.
Similarly, Older, Phillips, and Purvis (1978) suggested that an "immediacy of need" on the part of supervisors would motivate the trainees to assimilate and later use the training received. They advocated having supervisors label and accept their own feelings about problem employees, and encourage them to seek out the EAP staff whenever dealing with an employee with job problems.
O'Connell (1987) recommended EAPs go beyond "one-shot training" experiences. He suggested follow-up contacts and rehearsals with each supervisor, or small groups of supervisors . He sees this as an opportunity to answer individuals ' questions about the program and to deal with their resistances.
Googins (1979) observed that contact with and knowledge of other supervisors and employees using the EAP can develop program awareness and familiarity. Googins and Kurtz (1979) proposed building the training program around a core of supervisors who have successfully used the EAP. This "supervisory network" of peer models and satisfied users would influence fellow supervisors to accept and use the EAP. They believed that peer pressure, behavior modeling, and a supportive reference group might increase the impact of program information.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

4 8
Roman stated that EAP staff members may overestimate supervisors' willingness to identify and refer problem employees. In his opinion, "the implementation of programs which involve substantial use of constructive confrontation requires an orientation to organizational change rather than individual change" (1983, p. 372). This provides yet another objective of supervisory training, to help create and maintain organizational support for the supervisor in the routine use of the EAP through referrals.
The effectiveness of EAP training is another hotly debated issue. Following supervisory training, supervisors should be able confront employees who appear to have job- related problems, possibly due to alcohol abuse. However, Roman (1983) states that supervisory training only appears to close the gap between the EAP's goals and supervisors' readiness to confront and refer employees. He thinks this may be based upon faith in the "deeply respected American panacea of education" rather than upon sound evidence.
Conversely, Gerstein, Eichenhofer, Bayer, Valutis, and Jankowski (1989) reported that EAP-related training is beneficial in helping supervisors more accurately and more confidently identify job-impaired employees. Supervisors who participated in from zero to two hours of training were slightly more likely to identify behaviors and attitudes consistent with job impairment than supervisors who received no training. A correlation was also noted among
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

4 9
supervisors with favorable attitudes toward the EAP and those who received training. They were able to identify "industriousness," one of the four impairment factors studied, more often than the other supervisors.
Belasco and Trice (1969), in their research with 222 front-level supervisors, determined that the training sessions did, to a degree, cause supervisors to feel more prepared to confront workers. "The differences, however, between the trained and untrained groups were small"(p. 91). After training, the supervisors had increased knowledge, more favorable evaluations of employees, a view of problem employees as more potent and active attitude objects, and a more constructive orientation toward them.
They did, however, discover a positive correlation between training and pretesting. They concluded that the pretesting "sensitized" the supervisors to the training content, which made the training more potent for the pretested group. "In short, training is relatively impotent in producing change, while the change it does produce can be traced to the content of the training experience and the visibility of the change sought" (Belasco & Trice, 1969,p. 110).
Another important finding involved the attitudes of supervisors about alcoholics. They were surprised to discover that strongly negative attitudes toward alcoholics did not exist, and that tolerant attitudes were really the
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

barrier to confrontation and referral. When the supervisor's tolerant attitudes toward deviant behavior were reduced by training, there was significant increase in their intent to refer. This study of the effects of super visory training suggested that the emphasis in EAP supervi sory training should be on general management and supervisory issues and strategies, not on the problem employees and their conditions. Training which refines supervisors' job performance expectations and strengthens their orienta tion to actively manage their workers, using all available staff resources, should result in increased use of the EAP by supervisors (Belasco & Trice, 1969; Trice & Belasco, 1968).
Shoemaker (1983), reporting on a 1979-1980 Rand Corporation study into the effects of alcohol abuse seminars on 606 Air Force supervisors' knowledge, attitudes, and behaviors, found that the seminars had no effect on behavior and only limited impact on attitudes and knowledge. He stated, "Few significant changes in attitude or knowledge were found at the six-month point, including attitudes towards responsible drinking and the Air Force alcohol abuse control program in general" (p. 112). He suggested that targeting high-risk populations (married, living in quarters without a spouse, and not intending to reenlist) for alcohol abuse education would save significant training costs.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

5 1
Beyer and Trice (1978) found only a slight relationship between hours of supervisory training and EAP use by supervisors in the federal sector. Training hours did not predict future use of the EAP, nor did they impact the assessed need for the program. They concluded that training affected the "familiarity" with the program and was an essential, but not sufficient, factor in program use.After their training, supervisors did not accurately remember the alcoholism policy. In spite of their training, supervisors frequently endorsed job actions beyond the intent of the EAP policy.
Shain and Groeneveld (1980) studied over 300 Canadian organizations and found that the number of supervisors trained had no effect on reported rates of referral. They suggested changing the focus of EAP training to highlight behavioral changes in supervisors and upon dealing with organizational barriers to program use. Shain and Groeneveld observed that
although the EAP consultant may be frustrated, the client (industry) may be getting as much as it wanted out of the policy (and EAP). That is, the consultant may want a policy that gets down to early identification [of substance abusers]; the industry may simply want to clean up a backlog of problem employees. (p.18)
It is still not conclusive if or how much training affects supervisors' knowledge, attitudes, or referral behaviors. It is, however, agreed by most EAP researchers that though training may serve to familiarize supervisors
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

5 2
with the procedures for using the EAP, training may not be the cure-all EAP professionals seek. Researchers also agree that more clearly defined training objectives and evaluations are needed.
SummaryTrice and Belasco’s research (1969), the most exten
sive found on the topic of this study, examined the effects of training on supervisor's behaviors. And, although they reported that training produced little overall change, they noted that when training lowered the supervisor's tolerance for or attitude toward deviant behavior, the supervisor demonstrated a greater willingness to engage in confrontation and referral. This study suggested that the knowledge and attitudes of the supervisor could be influenced by training and that his/her decisions to identify, confront, and refer could be modified by that training.
The research of EAP professionals like Googins,Harley, Bayer, and Gerstein demonstrates the importance of supervisors' perceptions of the EAP on its success. Concepts such as confidentiality, program effectiveness, staff competence, and management support for the EAP program have been shown to influence supervisors' EAP use. Their research, coupled with the findings of Trice and Belasco and others that training can influence supervisors' attitudes and knowledge, clearly indicated that further study needed to be done in the area of EAP supervisory training
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

5 3
and its effects on supervisors' perceptions of the EAP program.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

CHAPTER III METHODOLOGY
Research Design The purpose of this study was to determine the effects
of the 36-hour Substance Abuse Awareness Seminar (SAAS) on Marine supervisors' knowledge and perceptions of The Marine Corps Substance Abuse Program.
The study utilized a quasi-experimental, pretest- posttest nonequivalent control group design. Quasi- experimental research involves the use of intact groups of subjects in experiment, rather than assigning subjects at random to experimental treatments. According to Wiersma (1991), "The pretest-posttest, nonequivalent control group design aids in checking the extent of group similarity, and the pretest scores may be used for statistical control or for generating gain scores" (p. 137). This design was used because the SAAS is a previously organized seminar, and participants are nonrandomly selected to attend the seminar. The experimental group of Marine supervisors was drawn from participants in the SAAS. The participants are considered to be a reasonable cross-section of Marine Corps supervisors. A control group consisting of nonrandomly selected Marine and civilian supervisors assigned to the Human
54
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

5 5
Resources Division of Headquarters Marine Corps in Clarendon, Virginia, were used.
The experimental group was exposed to the SAAS, which covers Marine Corps Substance Abuse Program policy and procedures as well as basic alcoholism and drug information. They were tested prior to and immediately following the seminar. The control group received no substance abuse training during the three weeks between the pretest and posttest administrations. The independent variable in the study was participation in the SAAS. Knowledge and perceptions about the Substance Abuse Program were assessed and quantified via two research instruments developed by the researcher, the Baker Knowledge Inventory (BKI) and the Demographic Information Inventory (DII).
Setting: The Substance AbuseAwareness Seminar (SAAS)
The SAAS (Appendix A) was developed and conducted by the Drug and Alcohol Training Associates, Inc., Arlington, VA. It was designed to train Marine Corps supervisors to administer the Marine Corps Substance Abuse Program as Substance Abuse Control Officers (SACOs), Staff Noncommissioned Officers (SACNCOs), and Level II Program Directors.It also provides supervisory awareness training for Officers/Staff Noncommissioned Officers in Charge of Marine work sections and for Commanders/First Sergeants/Sergeant Majors of Marine Units.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

5 6
The SAAS is conducted at the Xerox Training Center in Leesburg, Virginia. The Training Center is a self-contained training facility complete with residential and training rooms, common lounge areas, dining facility, cocktail lounge, and fitness facilities. Students do not have television sets in their rooms, but one is provided in a common lounge shared by six rooms. This fact in itself encourages participants to mingle and network. The fact that the training center is located in a very rural setting, approximately five miles from downtown Leesburg, and that most participants fly to the center via Dulles International Airport further isolates participants from outside distractions and encourages networking. Seminar participants are required to remain in training until it is complete. Only in extreme emergencies (death or serious injury to a family member) is one permitted to leave training. Further, participants are completely separated from their work environments and their associated distractions, a luxury many companies cannot or will not afford. This retreatlike setting is considered to be a major component of the program, as it enables participants to thoroughly digest what has been taught during the training and to share their thoughts and feelings with other participants.
The SAAS utilizes audio-visual materials, lecture presentations, experiential exercises, class discussions, and written exercises designed to educate Marine supervisors
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

5 7
about the Marine Corps Substance Abuse Program. The SAAS is divided into nine modules with distinct learning objectives.
Module I, Welcome and Overview, introduces the Substance Abuse Program staff and trainers to the class participants . It attempts to determine the expectations of the participants and enables modification of seminar material to meet the participants' expectations. It also introduces the participants to the training manual. Student learning objectives for Module I include introducing trainers and participants, reviewing course elements and aims, and developing a learning contract.
Module II, The Marine Corps Substance Abuse Program, begins with the Program staff leader explaining the basic philosophy of the Program, as presented in Marine Corps Order P5300.12 (THE MARINE CORPS SUBSTANCE ABUSE PROGRAM).He describes the proactive and reactive phases of the program, explains the extent to which alcohol and drugs are a problem for the Marine Corps, explains how supervisors can influence the success of the program, and motivates participants to ask questions about implementation of the Program at their locations. Often, during the open discussion portion of Module II, participants confront the Program staff leader with their misgivings about the programs effectiveness, the disease concept of alcoholism/addiction, and the Marine Corps' mandate to treat substance abusers. A legal officer from the Judge Advocate General's Office of
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

5 8
the Marine Corps provides insights into the legal aspects of the Marine Corps Substance Abuse Program. Nonpunitive and administrative procedures are explained and discussed. Punitive measures of the program are presented and discussed, as are the finer points of drug detection using urinalysis testing. Student learning objectives for Module II include knowing the elements of a successful drug program, understanding key legal processes and issues, being familiar with Levels I through III, and being familiar with the United States Marine Corps Drug Demand Reduction Strategy.
Module III, Patterns of Use, Abuse and Control, gives participants an overview of the laws, practices of substance use, and the reaction to the laws and substance use by our society through history. An open discussion concerning the possible consequences of legalizing marijuana highlights this module. Student learning objectives for Module III include receiving an overview of the history of substance abuse and being conversant with the control measures that have been employed in society and the Marine Corps.
Module IV, Values and Goals, is an experiential module in which participants are introduced to La Platica: An Approach to Cultural Clarification. In the first exercise, participants are asked about their personal impressions of the dominant culture of the United States, beliefs, concepts, and lifestyles toward drugs. These impressions are
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

5 9
then discussed. The second exercise asks participants to write down what they have learned about drugs from their family experiences and their experiences in the Marine Corps, both positive and negative. Open disclosure of exercise results and discussion enables participants to become aware of some of their values and attitudes. Student learning objectives for Module IV include being exposed to value clarification and how values differ, and determining what students' attitudes are toward drugs and alcohol and their abusers.
Module V, Physiological and Sociological Implications of Alcohol Use, through lecture and open discussion, provides the participants with an understanding of the effects of alcohol on the behaviors of individuals who use them.The difference between alcohol abuse and alcoholism is discussed, and several perspectives (psychological, sociological, medical) are explored. During discussions of the disease concept of alcoholism, participants are encouraged to compare the disease of alcoholism to other chronic, progressive diseases like diabetes and heart disease. Several visual aids are used to illustrate the progressive nature and the various stages of the disease. The effects of alcohol on the human body are discussed at length. Student learning objectives for Module V include understanding the disease concept of alcoholism; understanding that the disease is progressive, maybe fatal; being aware of societal
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

6 0
and Marine Corps pressures and rewards regarding drinking; exposure to societal, racial, and cultural influence theories; differentiating among use, abuse, and addiction; knowing the blood alcohol content (BAC) required to be considered legally drunk in different states; understanding the relationship of individual weight, amount of alcohol, and time in which it was consumed on BAC levels; awareness of toxicity of alcohol and the process of physical addiction; understanding blackouts and tolerance as related to alcohol and physical aspects of its use, abuse, and addiction; knowing the physical symptoms of hangovers from alcohol use; and knowing what actions to take with alcohol abusers within their work sections.
Module VI, Physiological and Sociological Implications of Drug Use, through lecture and open discussion, provides the participants with a model to familiarize them with the process of addiction. It acquaints participants with the warning signs of increased dependency and potential addiction. Several visual aids are used to illustrate the cyclic nature of addiction. Discussion of the pharmacology and physiology of drug use provides participants information about the different classifications of psychoactive drugs and their potential for abuse. The psychological and physiological effects of drugs are also discussed. Various visual aids illustrating the effects of drugs on the nervous system are used. Participants are introduced to the most
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

6 1
popular drugs— alcohol, crystal meth (ice), crack, cocaine, PCP, etc. They become aware of how the drug effects an individual's behavior, and what an overdose looks like so they are able to identify abuse among their Marines. Urinalysis testing for drug identification is also discussed. This provides participants with general knowledge about the different types of urinalysis testing procedures, the effectiveness of the various testing procedures, and the periods of time during which substances can be detected in the urine. Student learning objectives for Module VI include recognizing the psychoactive substance in marijuana; being familiar with trends of marijuana usage and its relationship with the legal system; being aware of the major classes of drugs; being familiar with the physiological and psychological effects of each drug; and knowing the street names associated with each drug.
Module VII, Applying the Information, provides participants with a practical and useful technique for intervention. It also provides information regarding how alcoholism affects the family. Effective treatment strategies within and outside the Government are discussed. The student learning objective for Module VII is to provide an opportunity for participants to discuss the implications that new information has in shaping activities on their bases, from pretreatment through relapse prevention.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

6 2
Module VIII, Understanding Nutrition in Recovery, provides participants with a thorough understanding of the effects of sugar, caffeine, nicotine, and other addictive substances in the recovery process. Sugar's effect on brain chemistry is stressed, and the disease of hypoglycemia is explained in relation to recovery. The student learning objective for Module VIII is being aware of nutrition and its impact on recovery.
During Module IX, participants discuss their experiences attending mandatory Twelve Step meetings, and they listen to the testimony of a panel of recovering alcoholic/ addicted Marines. Instructors and Program staff members are available to answer questions participants may have saved to ask at the end of the seminar. Student learning objectives for Module IX include being aware of personal recovery issues and discussing 12-step meetings and attendance at them.
SubjectsThe experimental group of Marine supervisors was drawn
from the participants in the Substance Abuse Awareness Seminar (SAAS). The SAAS reaches approximately 700 Marine supervisors per year. One hundred twenty-six participants were used for this study. Each 35-member (approximate) class comprises of volunteers and designated attendees from every major Marine Corps command worldwide— a reasonable cross-section of Marine Corps supervisors. Though the
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

6 3
seminar was designed to train Marines to supervise the Marine Corps Substance Abuse Program, other Marines and civilians attend the seminar for its awareness components. Participants in seminars conducted on January 11-15, February 8-12, and March 1-5 and 22-26, 1993, were subjects for the study, and constituted the experimental group.
Nonrandomly selected supervisors from the Human Resources Division, Headquarters, U.S. Marine Corps constituted the control group. The control group received no substance abuse training during the three weeks between the first administration on February 5, 1993, and the last administration of the test on February 26, 1993. The control group subjects were selected from a roster provided by the Administrative Chief of the Human Resources Division.The researcher decided to use military supervisors with pay grades of E-5 (sergeant) and above, and civilian supervisors with pay grades of GS-10 and above. These criteria would produce 70 qualifying supervisors in the Human Resources Division. The researcher approached all 70 qualifying supervisors in order to obtain an adequate number of usable survey results. Thirty-nine usable surveys were obtained from the control group members.
Table 1 reports the distribution of experimental and control group subjects and the chi-square test of the difference between groups on each characteristic.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

6 4
TABLE 1
DISTRIBUTION OF 210 SUBJECTS BY EXPERIMENTAL AND CONTROL GROUP CLASSIFICATION ON CERTAIN DEMOGRAPHIC
CHARACTERISTICS AND CHI-SQUARE TEST OF DIFFERENCES BETWEEN GROUPS
Characteristic
Experimental (n = 126)
Control (n = 39)
n % n %
GenderMale 117 92.8 24 61.5Female 9 7.1 15 38.5
Total 126 99.9a 39 100.0Chi square = 23.502. df = 1. prob = .000
AgeUnder 25 4 3.2 1 2.625-30 21 16.6 3 7.731-35 51 40.4 8 20.536-40 23 18.2 10 25.6Over 40 27 21.4 17 43.5
Total 126 99. 8a 39 99. 9aChi square = 11.302. df = 4. prob = .023
EducationNon-high school grad 4 3.2 0 0.0Grad equiv degree (GED) 7 5.5 0 0.0High school grad 63 50.0 14 35.9Assoc. degree 11 8.7 4 10.2Bachelor's degree 33 26.2 11 28.2Master's degree 8 6.3 10 25.6
Total 126 99.9a 39 99. 9aChi square = 14.956. df = 5. prob = .011
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

TABLE 1— Continued6 5
Experimental Control(n = 126) (n = 39)
Characteristic n % n %
Pay GradeE-6 - E-7 56 44.4 6 15.4E-8 - E-9 22 17.5 1 2.60-1 - 0-3 30 23.8 8 20.50-4 4 3.2 5 12.80-5 - 0-7 4 3.2 1 2.6Other 9 7.1 18 46.2
Total 126 100.2a 39 100.laChi square = 42.324. df = 5. prob = .000
Previous ExperienceLevel I SACO 46 36.5 4 10.2Level II SACO 9 7.1 0 0.0Level II Program Dir. 0 0.0 3 7.7Substance Abuse Counselor 7 5.5 2 5.1None 64 50.8 30 76.9
Total 126 99.9a 39 100.0Chi square = 17.801. df = 4. prob = .001
aTotal does not equal 100.0 due to rounding.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.
66
Comparing the control group and experimental group subjects on five demographic factors (gender, age, pay grade, education, and previous experience) revealed differences on all of the variables. The experimental group was overwhelmingly male (93%), while the control group was more balanced on gender (62% male and 38% female).
The experimental group was significantly younger than the control group, with the majority of its members (56%) falling in the 25-35 years of age range. Only 28% of the control group was 25-35 years of age. Forty-three percent of the control group was over 40, while only 21% of the experimental group was over 40.
The experimental group was made up, almost entirely, of Marines (97%), while the control group contained almost half (46%) civilians. The members of the experimental group were massed in the lower pay grades, with 44% being E-6 through E-7 and 24% 0-1 through 0-3. Forty-six percent of the control group was civilians with pay grades of GS-10 or above. This pay grade grouping corresponds with the age grouping in that the younger people fall into the lower pay grades.
The education levels and the levels of previous experience with the Marine Corps Substance Abuse Program were matched better, but still were different.
It does not appear that the demographic differences had a significant effect in terms of different test scores
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.
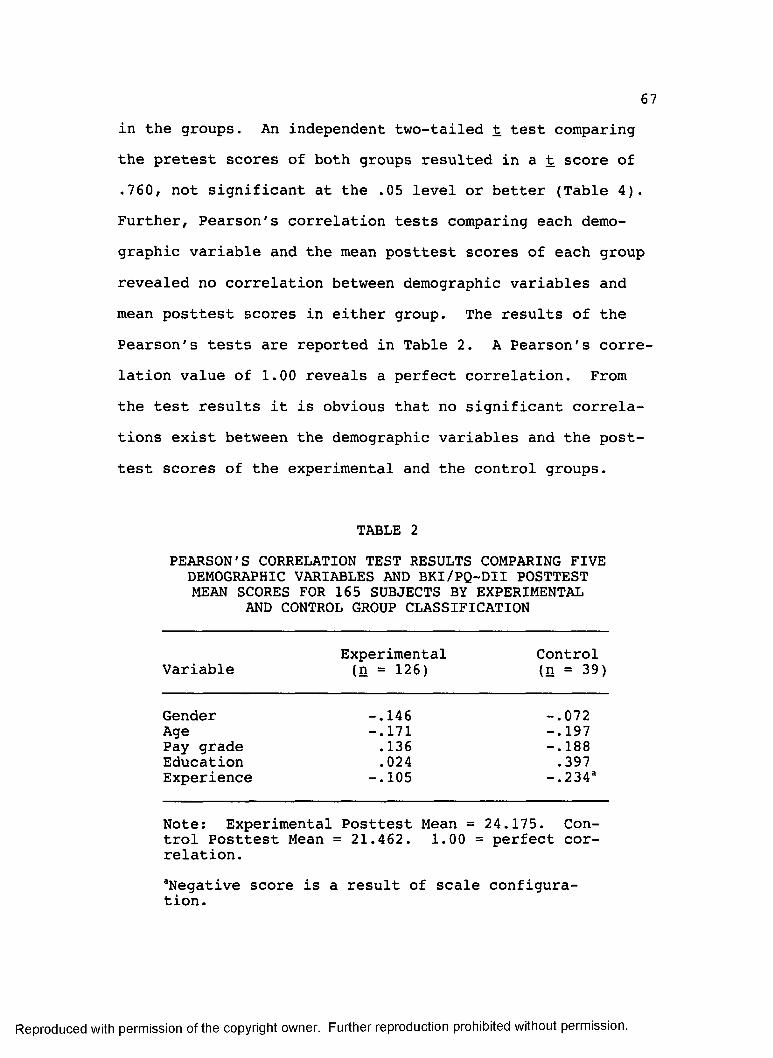
6 7
in the groups. An independent two-tailed t test comparing the pretest scores of both groups resulted in a t score of .760, not significant at the .05 level or better (Table 4). Further, Pearson's correlation tests comparing each demographic variable and the mean posttest scores of each group revealed no correlation between demographic variables and mean posttest scores in either group. The results of the Pearson's tests are reported in Table 2. A Pearson's correlation value of 1.00 reveals a perfect correlation. From the test results it is obvious that no significant correlations exist between the demographic variables and the posttest scores of the experimental and the control groups.
TABLE 2PEARSON'S CORRELATION TEST RESULTS COMPARING FIVE
DEMOGRAPHIC VARIABLES AND BKI/PQ-DII POSTTEST MEAN SCORES FOR 165 SUBJECTS BY EXPERIMENTAL
AND CONTROL GROUP CLASSIFICATION
VariableExperimental (n = 126)
Control (n = 39)
Gender -.146 -.072Age -.171 -.197Pay grade .136 -.188Education .024 .397Experience -.105 -. 234a
Note: Experimental Posttest Mean = 24.175. Control Posttest Mean = 21.462. 1.00 = perfect correlation.aNegative score is a result of scale configuration.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

68
InstrumentsSupervisors' knowledge and perceptions about the
Marine Corps Substance Abuse Program prior to and immediately after the seminar were assessed and quantified via two research instruments, the Baker Knowledge Inventory (BKI) and the Demographic Information Inventory (DII). Each instrument is located in Appendix B and is detailed in a following subsection.
The Baker Knowledge InventoryThe BKI, developed by the investigator, consists of 25
true/false and multiple-choice questions. The questions are designed to ascertain supervisors' knowledge of various aspects of the Marine Corps Substance Abuse Program.Sources used in this instrument's development were books and articles written by experts in the field of alcoholism and Employee Assistance Programs. Of special consideration was the issue of lack of knowledge of the EAP cited in various articles as a barrier to supervisory EAP referrals. The Marine Corps Order P5300.12 (THE MARINE CORPS SUBSTANCE ABUSE PROGRAM) and the Substance Abuse Awareness Seminar manual provided material for policy and procedure questions (See Appendix A).
ValidityThe face validity of the BKI was reviewed and found
adequate for use in this study by a panel of five experts
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.
6 9
through an examination for clarity of wording, content, and directions. This panel was composed of a psychologist familiar with the Marine Corps Substance Abuse Program and Marine supervisors' perceptions of the program through having taught the Substance Abuse Awareness Seminar for ten years; the director of the Marine Corps Substance Abuse Program staff; the Marine Corps Substance Abuse Program Training Officer; the developer of the Substance Abuse Awareness Seminar; and the current instructor of the seminar. The draft copies of the BKI that were sent to the expert panel contained 40 program knowledge questions. Fifteen questions were rejected from the BKI because either they didn't test material taught during the seminar or they were misleading or confusing. The BKI was hand scored by the researcher. Each BKI question received one point for a correct response, and zero points for an incorrect response.
ReliabilityThe test-retest procedure was used to determine the
reliability of the BKI. A sample of ten Marine supervisors from the Human Resources Division completed the BKI. It was administered again to the same individuals three weeks later. Pretest and posttest results were compared to determine the percentage of agreement. Items were considered to agree if the response on the posttest compared exactly with that for the same item on the pretest. They are reported in Table 3. The percentage of agreement was 84.8%. That is,
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.
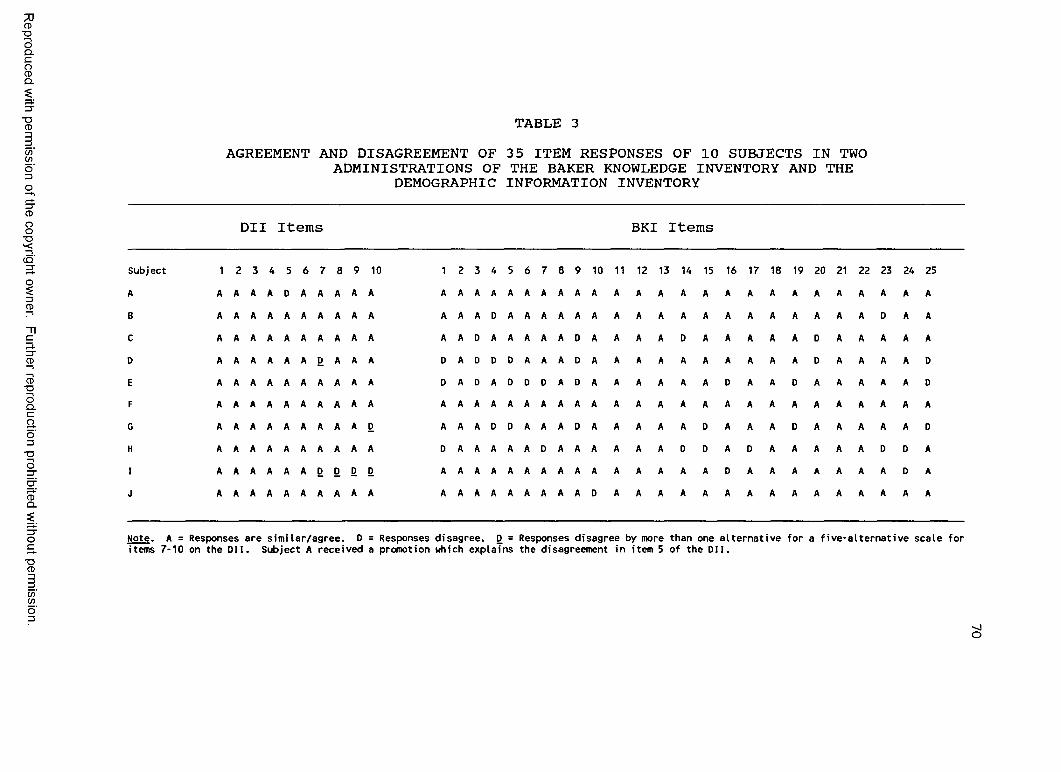
Reproduced
with perm
ission of the
copyright ow
ner. Further
reproduction prohibited
without
permission.
TA B L E 3
AGREEMENT AND DISAGREEMENT OF 35 ITEM RESPONSES OF 10 SUBJECTS IN TWO ADMINISTRATIONS OF THE BAKER KNOWLEDGE INVENTORY AND THE
DEMOGRAPHIC INFORMATION INVENTORY
DII Items BKI Items
Subject 1 2 3 4 5 6 7 8 9 10 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25A A A A A D A A A A A A A A A A A A A A A A A A A A A A A A A A A A A AB A A A A A A A A A A A A A D A A A A A A A A A A A A A A A A A A D A AC A A A A A A A A A A A A D A A A A A D A A A A D A A A A A D A A A A AD A A A A A A D A A A D A D D D A A A D A A A A A A A A A A D A A A A DE A A A A A A A A A A D A D A D D D A D A A A A A A D A A D A A A A A DF A A A A A A A A A A A A A A A A A A A A A A A A A A A A A A A A A A AG A A A A A A A A A D A A A D D A A A D A A A A A D A A A D A A A A A DH A A A A A A A A A A D A A A A A D A A A A A A D D A D A A A A A D D AI A A A A A A D D D D A A A A A A A A A A A A A A A D A A A A A A A D AJ A A A A A A A A A A A A A A A A A A A D A A A A A A A A A A A A A A A
Wote. A = Responses are similar/agree. D = Responses disagree. D = Responses disagree by more than one alternative for a five-alternative scale for items 7-10 on the DII. Subject A received a promotion which explains the disagreement in item 5 of the DII.
O

7 1
for the ten subjects responding to the 25 BKI items, all ten subjects agreed on seven of the items, only one subject disagreed on four items, two subjects disagreed on seven items, three subjects disagreed on five items, and four subjects agreed on one item. Of the 250 total items, 84.8% elicited the same response on the test as on the retest. On this basis, the reliability is considered sufficient for this study.
Item nine, a true/false question stating "As far as the Marine Corps is concerned, following treatment for alcoholism, a Marine may return to responsible social drinking," received the most disagreement (four subjects out of ten showed disagreement between test and retest responses). The item was considered to be poorly worded and was reworded as follows: "Though it is not condoned, following Level IIItreatment for alcoholism, a Marine may return to responsible social drinking without suffering any disciplinary action."
The Demographic Information InventoryTo obtain demographic data on this study's population,
the researcher developed a ten-item inventory titled the Demographic Information Inventory (DII). The DII items pertain to age; gender; education; rank; pervious experience with the Marine Corps Substance Abuse Program; and perceptions of program confidentiality, staff competence, program effectiveness, and command support for the program. These
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

7 2
demographic data were felt to be necessary to describe the sample of Marine supervisors studied.
The Perception Question— Demographic Information Inventory (PO-Dlli
Questions 7, 8, 9, and 10 of the DII elicit supervisors' perceptions of the Marine Corps Substance Abuse Program. Perceptions are reported on a five-alternative Likert-type response continuum for each item. The responses to these items were quantified and analyzed as part of this study. These four items were put into a separate section titled the Perception Question-Demographic Information Inventory (PQ-DII).
Information from various articles and studies on EAPs were used to develop the PQ-DII items. Item 7 addresses the issue of lack of confidentiality which has been shown to deter supervisors from referring employees to the EAP. Item 7 states: Considering the alternatives below, indicate yourperception of the confidentiality of the Marine Corps Substance Abuse Program.
Very confidential Somewhat confidential Neutral Not very confidential Not at all confidential
Item 8 addresses the issue of a lack of confidence in the EAP staff's competence, which has been shown to reduce
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.
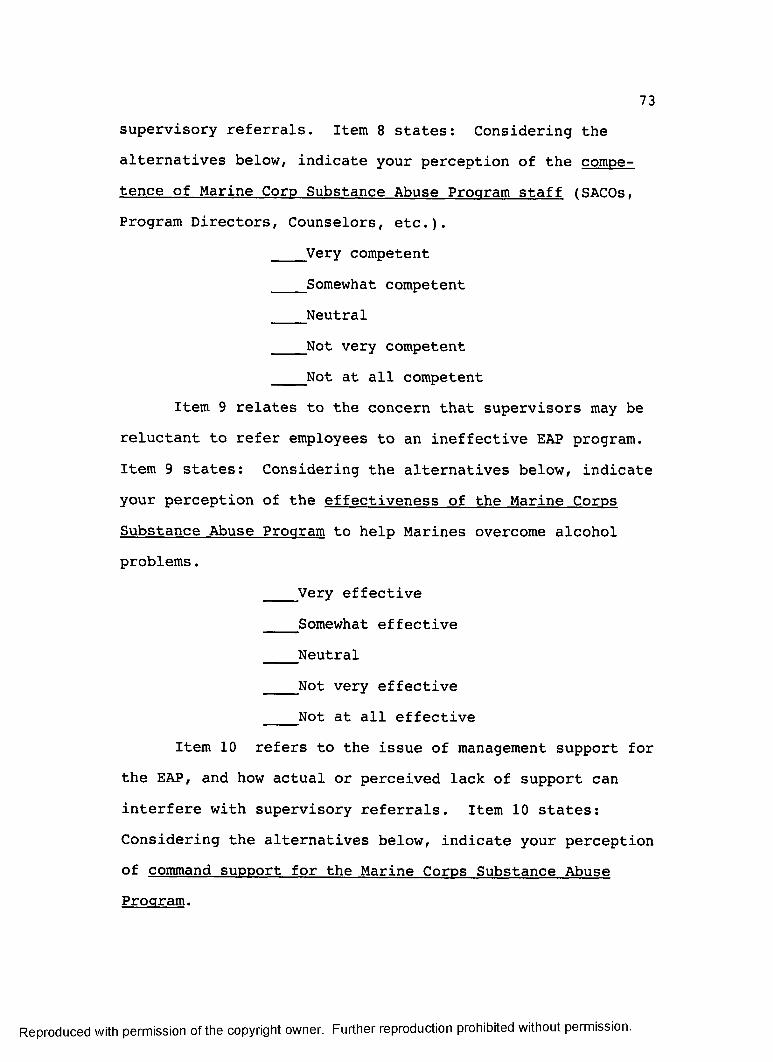
7 3
supervisory referrals. Item 8 states: Considering thealternatives below, indicate your perception of the competence of Marine Corp Substance Abuse Program staff (SACOs, Program Directors, Counselors, etc.).
Very competent Somewhat competent Neutral Not very competent Not at all competent
Item 9 relates to the concern that supervisors may be reluctant to refer employees to an ineffective EAP program. Item 9 states: Considering the alternatives below, indicateyour perception of the effectiveness of the Marine Corps Substance Abuse Program to help Marines overcome alcohol problems.
Very effective Somewhat effective Neutral Not very effective Not at all effective
Item 10 refers to the issue of management support for the EAP, and how actual or perceived lack of support can interfere with supervisory referrals. Item 10 states: Considering the alternatives below, indicate your perception of command support for the Marine Corps Substance Abuse Program.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

Very supportive Somewhat supportive Neutral Not very supportive Not at all supportive
The PQ-DII was hand scored by the researcher. Each item was scored using the following scale:
Very favorable response receives +2 Somewhat favorable response receives +1 Neutral response receives 0 Not very favorable response receives -1 Not at all favorable response receives -2
ValidityThe face validity of the DII was reviewed and found
adequate for use in this study by the same panel of five experts who reviewed the BKI. The draft copies of the perception inventory that were distributed to the expert panel contained 36 statements reflecting various perceptions supervisors might have about the Marine Corps Substance Abuse Program. All members of the panel agreed that only the direct perception questions should be maintained, so 32 perception questions were eliminated, and the four remaining questions, the PQ-DII, were added to the demographic information to form the DII. The rejected questions contained either leading or confusing wording. Accepted questions were, in some cases, reworded for clarity.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

lb
ReliabilityThe reliability of the DII was tested using the test-
retest method to determine percentage of agreement between test and retest responses. Items were considered to agree if the response on the posttest compared exactly with that for the same item on the pretest. For items 7-10 of the DII, responses that disagreed by more than one alternative for a five-alternative scale were considered to disagree. Table 3 reports the results of such testing. The percent agreement for the DII was 85%. That is, for the ten DII items, all ten subjects agreed on five items; one subject disagreed on three items; and two subjects disagreed on two items. Of the 100 total responses, 85% of the responses on the second administration of the test were in agreement with those on the first administration. Subjects did not disagree more on any one item than on any other. Consequently, no items were altered.
Data CollectionData were collected using two questionnaires, the
Baker Knowledge Inventory (BKI) and the Demographic Information Inventory (DII) (Appendix B). Participants received the questionnaires upon arriving at the Substance Abuse Awareness Seminar on Monday morning. The questionnaires were distributed by the researcher. The following script was read after the questionnaires were distributed:
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

7 6
Good morning, I am Kay Baker. I have just handed you two questionnaires that I would like you to complete now, before class begins. These questionnaires are part of a research project that will ascertain the impact of this training seminar on your knowledge and perceptions about the Marine Corps Substance Abuse Program. Please read the questions carefully, answer them honestly and to the best of your ability. Be sure to put the last four digits of your social security number on the questionnaire so pretest results can be matched with the posttest. You will be given these questionnaires again at the end of the week. When you have completed the questionnaires, please pass them to your right. The person at the end of the row will collect them. I will pick them up when everyone is finished. I appreciate your participation. Have a good week. Thank you.
The posttreatment BKI and DII questionnaires were distributed by the researcher to the class participants on Friday, following completion of all seminar material. The following script was read once the questionnaires were distributed:
Good morning. I trust you have had a good week and have learned a lot about substance abuse and the Marine Corps Substance Abuse Program. I have just distributed two questionnaires for you to complete. They are the same two questionnaires you were given at the beginning of the seminar. Please read the questions carefully.Answer the questions honestly and to the best of your ability. Be sure to put the last four digits of your social security number on the questionnaire. Persons who would like a report of the results of this research may receive one by writing your name and mailing address on the back of the questionnaire or on a separate sheet of paper. Please pass the questionnaires to the right when you are done. The person at the end of the row will collect them. When all participants are done, I will pick up the questionnaires. Thank you again for your participation, and have a safe trip home.
The researcher hand delivered the two questionnaires to control group participants at their work area. The following script was read to each participant:
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

7 7
Good morning, I am Kay Baker. You have been chosen as a member of the control group for a research project being conducted by myself with the help of the Drug, Alcohol and Health Affairs Branch. Your participation has been sanctioned by the Head, Human Resources Division. Do you have approximately 30 minutes to complete two short questionnaires? [If the participant indicated he/she had time to complete the questionnaire, the script continued.]I have just handed you two questionnaires that I would like you to complete now. These questionnaires are part of a research project that will ascertain the effects of the Substance Abuse Awareness Seminar on supervisors' knowledge and perceptions about the Marine Corps Substance Abuse Program. Your scores will be compared with those of participants in the seminar. Please read the questions carefully, answer them honestly and to the best of your ability. Please do not collaborate with anyone on the answers, and please do not attempt to look up the answers. Be sure to put the last four digits of your social security number on the questionnaire so pretest results can be matched with the posttest.You will be given these questionnaires again in three weeks. When you have completed the questionnaires, please place them on the corner of your desk. I will be back in 30 minutes to pick them up. I appreciate your participation. Thank you.
The researcher retrieved the questionnaires directly from the participants. Any participant who indicated he/she did not have time to participate at this time was given another opportunity at a later date. For these participants, the same process was repeated when time to participate was available. The majority of members completed the questionnaires on the first day they were offered. Several persons indicated they did not desire to participate in the survey, and their wishes were honored. A total of 51 useable surveys were collected from members who participated in the pretest administration.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

7 8
Posttests were administered to the control group inthe same fashion, three weeks later. The following scriptwas read to each participant:
Good morning. It is time for the second administration of the Substance Abuse Survey. Do you have time to complete the questionnaires at this time? [If members indicated they did have time to participate, the script was continued.]Please complete the questionnaires I have just given you. Please be sure to put the last four digits of your social security number on the questionnaire. Please answer the questions honestly and to the best of your ability. I will be back in approximately 30 minutes to collect the questionnaires. Do you have any questions?
Several posttest questionnaires were considered unusable due to missing demographic data, failure to answer perception questions, and failure to provide the last four digits of the social security number. Useable posttest questionnaires were collected from 39 control group members. The social security numbers on the useable posttest questionnaires were matched with those from the pretest, and only 39 control group members' pretest and posttest results were used in the study.
Data AnalysisFollowing data collection and test scoring, study
hypotheses were tested using paired and independent onetailed t tests. These tests were appropriate because the researcher is comparing sets of subjects or two measures from the same subject. When a large sample of n (n a 30) is taken from a normally distributed population with mean u and
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

7 9
standard deviation a , then the probabilities for the random variable
X - ut = ------
s / n
are equal, at least approximately, to areas under the standard normal curve (Weiss & Hassett, 1991). In this study, n = 126 for the SAAS participants and 39 for the control group. The significance level .05 was used. A .01 significance level or higher was not required, since this study was exploratory, and interpretation error would not cause dire consequences.
Hypothesis IThe first hypothesis stated that no significant dif
ference, at the .05 level, would exist between mean pretest scores of supervisors who attended and those who did not attend the SAAS, as measured by the Baker Knowledge Inventory (BKI) and questions 7, 8, 9, and 10 of the Demographic Information Inventory (DII), referred to as the PQ-DII. To test this hypothesis, an independent two-tailed t test was used. Stated symbolically, the hypothesis was:
Hx: TlE = T1Critical value of t .05 (x) = 1.96
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

8 0
Hypothesis II The second hypothesis stated that no significant
difference would exist, at the .05 level, between pretest and posttest scores for managers who did not attend the SAAS, as measured by the BKI and PQ-DII. To test this hypothesis, a paired two-tailed t test was used to determine if no significant difference exists between pretest and posttest scores. Stated symbolically, the hypothesis tested was:
H2: TjC = T2CCritical value of t .05 (x) = 1.96
Hypothesis III The third hypothesis states that the mean BKI and
PQ-DII posttest scores for the experimental group would be significantly higher than their mean pretest scores on the BKI and PQ-DII. For this hypothesis, a paired one-tailed t test was used to determine if the posttest scores were significantly higher than pretest scores. Stated symbolically, the hypotheses tested were:
H3: TjE < T2EH0: T3E = T2E
Critical value of t .05 (x) = 1.96
Hypothesis IV The fourth hypothesis states that the mean BKI and
PQ-DII posttest scores for the experimental group would be
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

8 1
significantly higher than the mean posttest scores on the BKI and PQ-DII for the control group. After calculating posttest mean scores for each group, an independent onetailed t test was used to determine the significance of the difference between the groups' posttest scores. Stated symbolically, the hypothesis tested was:
^4* ^ PcH0: Pg ~ Pc
Critical value of t .05 (x) = 1.96
Ethical Considerations The main risk in this study was breach of confidenti
ality. Several steps were taken to reduce this risk. All subjects in this study were advised of the study procedures in a script read prior to each administration of the questionnaires. The researcher felt that the study might be compromised if too much information about the purpose and expected outcomes of the study were divulged to the participants prior to the study. Consequently, little was said about the purpose or expected outcome of the study.
Participants' confidentiality was safeguarded by using only the last four digits of their social security number to identify their responses. Other identifying information was formatted to reduce the probability of matching specific responses with specific persons.
A summary of results of the study was offered to each participant upon completion of the study. At this time, a
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

8 2
full disclosure of the purpose and expected outcome of the study would have been made, as well as a discussion about how divulging the purpose prior to the study might have jeopardized the results; however, no participants requested copies of the study results.
Results of the study were provided to the Head, Drug, Alcohol and Health Affairs Branch, Headquarters, U.S. Marine Corps and to Drug and Alcohol Training Associates, the organization responsible for conducting the training.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

CHAPTER IV RESULTS AND DISCUSSION
This quasi-experimental study examined the effects of a 36-hour substance abuse awareness seminar on the knowledge and perceptions of Marine Supervisors about the Marine Corps Substance Abuse Program. Data were collected from an experimental group of 126 Marine Corps supervisors attending the Marine Corps Substance Abuse Awareness Seminar at the Xerox Training Center in Leesburg, VA, and from 39 Marine and civilian supervisors from the Human Resources Division of Headquarters, U.S. Marine Corps in Clarendon, VA, who constituted the control group. The Baker Knowledge Inventory and the Demographic Information Inventory were used to gather the data.
Four hypotheses were tested in the study. This chapter is developed around these hypotheses, resulting in four subsections. Each subsection presents the results of hypothesis testing, statistical analysis, and a related discussion.
Experimental and Control Group Pretest ScoresIt was hypothesized that no significant difference
would exist between mean pretest scores of Marine
83
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

8 4
supervisors who attended and those who did not attend the Substance Abuse Awareness Seminar as measured by the Baker Knowledge Inventory and questions 7,8, 9, and 10 of the Demographic Information Inventory, hereafter referred to as the PQ-DII. Symbolically, this was stated as follows:
Hl: TxE = TiCAn independent two-tailed t test was used to determine
the difference between BKI and PQ-DII pretest scores of the experimental group and the control group. Table 4 reports the test of the significance of the difference of mean BKI/PQ-DII pretest scores of 126 supervisors who attended and 39 who did not attend the Substance Abuse Awareness Seminar. As reported in Table 4, the mean difference was0.547. This difference was not significant at the .05 level or better. Therefore, the null hypothesis was not rejected. This means that no significant difference existed between the mean pretest scores of supervisors who attended and those who did not attend the Substance Abuse Awareness Seminar, as measured by the BKI and PQ-DII.
Control Group Pretest and Posttest Scores It was hypothesized that no significant difference
would exist between pretest and posttest scores for Marine supervisors who did not attend the Substance Abuse Awareness Seminar, as measured by the Baker Knowledge Inventory (BKI) and the Perception Questions of the Demographic Information
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

8 5
TABLE 4TEST OF THE SIGNIFICANCE OF THE DIFFERENCE BETWEEN BKI
AND PQ-DII MEAN PRETEST FOR MARINE SUPERVISORS WHO DID AND DID NOT ATTEND THE SAAS
GroupSampleSize X
MeanDifference t
Experimental 126 22.1110.547 0.760
Control 39 21.564
Inventory (PQ-DII). Symbolically, this was stated as follows :
H2: T ^ = T2CA paired two-tailed t test was used to determine the
difference between BKI/PQ-DII pretest and posttest scores of the control group. Table 5 presents the results of the t test of the significance of the difference between BKI/ PQ-DII mean pretest and posttest scores for 39 Marine Supervisors who did not attend the Substance Abuse Awareness Seminar. As reported in Table 5, this difference was -.161. This difference was not significant at the .05 level or better. Therefore, the null hypothesis was not rejected. This means that no significant difference existed between pretest and posttest scores for Marine Supervisors who did not attend the Substance Abuse Awareness Seminar, as measured by the BKI/PQ-DII. Testing confirmed that the knowledge and perceptions of the control group did not change
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

86
TABLE 5TEST OF THE SIGNIFICANCE OF THE DIFFERENCE BETWEEN BKI AND PQ-DII MEAN PRETEST AND POSTTEST SCORES OF MARINE
SUPERVISORS WHO DID NOT ATTEND THE SAAS
TestingSampleSize X
MeanDifference t
Pretest 39 21.564-.103 -.161
Posttest 39 21.462
during the three-week period between the first and second administration of the BKI/PQ-DII. Because the control group did not participate in any substance abuse training, their knowledge and perceptions about the Marine Corps Substance Abuse Program did not significantly change. This suggests that normal events taking place during the course of the study did not significantly alter the knowledge or perceptions measured by the BKI/PQ-DII.
Experimental Group Pretest and Posttest Scores It was hypothesized that the mean BKI/PQ-DII posttest
scores for the experimental group would be significantly higher than their mean pretest scores on the BKI/PQ-DII. Symbolically this was stated as follows:
H3: TXE < T2E H0: TjE = T2E
A paired one-tailed t test was used to determine the difference between the posttest scores and pretest scores of
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

8 7
the experimental group at the .05 significance level. Table 6 reports the comparison between BKI/PQ-DII mean pretest and posttest scores for 126 experimental subjects. As reported in Table 6, the mean difference was 2.063. This difference was significant at the .001 level or better. Therefore, the null hypothesis was rejected, and the main hypothesis was confirmed. This means that the mean BKI/PQ-DII posttest scores for the experimental group was significantly higher than their mean pretest scores on the study instruments, BKI and PQ-DII. A significant increase in Marine supervisors' knowledge and perceptions of the Marine Corps Substance Abuse Program was achieved as ascertained by the BKI/PQ-DII.
A review of the literature reveals that one previous study (Trice and Belasco, 1969), found that supervisory training had little effect on supervisors' attitudes, but that it did increase supervisors' knowledge. Further,
TABLE 6TEST OF THE SIGNIFICANCE OF THE DIFFERENCE BETWEEN BKI AND PQ-DII MEAN PRETEST AND POSTTEST SCORES OF MARINE
SUPERVISORS WHO DID ATTEND THE SAAS
TestingSampleSize X
MeanDifference t
Pretest 126 22.1112.063 7.280*
Posttest 126 24.175
*p < .001.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

88
Shoemaker (1983) reported on a 1979-1980 Rand Corporation study into the effects of alcohol abuse seminars on 606 Air Force supervisors' knowledge, attitudes, and behaviors that the seminars had no effect on behavior and only limited impact on attitudes and knowledge. He stated, "Few significant changes in attitude or knowledge were found at the six- month point, including attitudes towards responsible drinking and the Air Force alcohol abuse control program in general" (p. 112). The results of this study counter the findings of both the Trice and Belasco study and the Shoemaker study. The researcher poses the following explanations .
First, the training program studied in this research was more extensive and intensive than the majority of supervisory EAP training programs. The Substance Abuse Awareness Seminar contains 36 hours of instruction conducted over a one-week period, in an isolated, retreatlike setting. As evidenced by Plavan's (1989) study of 15 Fortune 500 industries, under three hours of training was reported by 40% of respondents, and 37% reported between three and ten hours of training.
Second, the study instruments were especially designed to ascertain the results of the Substance Abuse Awareness Seminar. The training program has clearly stated learning objectives, and the study instruments were designed to
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

8 9
measure the attainment of those specific learning objectives .
Third, pretesting the experimental group before administering the Substance Abuse Awareness Seminar may have had a positive effect on posttest scores. Belasco and Trice (1969), in their research with 222 front-level supervisors, discovered a positive correlation between training and pretesting. They concluded that the pretesting "sensitized" the supervisors to the training content, which made the training more potent for the pretested group. "In short, training is relatively impotent in producing change, while the change it does produce can be traced to the content of the training experience and the visibility of the change sought" (Belasco & Trice, 1969, p. 110).
Fourth, Older, Phillips, and Purvis (1978) suggested that an "immediacy of need" on the part of supervisors would motivate the trainees to assimilate and later use the training received. The fact that the majority of the Marine supervisors attending the Substance Abuse Awareness Seminar either were recently assigned to positions administering the Marine Corps Substance Abuse Program or would shortly be assigned to such a position may have produced such an "immediacy of need" situation which, according to Older, Phillips and Purvis, would motivate them to be attentive to and retain information presented in the seminar.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

9 0
Finally, conversation with the developers/instructors of the Substance Abuse Awareness Seminar, who are strong proponents of the Pygmalion Effect, indicate that participants in the program are expected and encouraged to increase their knowledge and perceptions of the Marine Corps Substance Abuse Program. They believe that when expectations for learning and attitude change are high, then learning and attitude change will be high as a result of those expectations. The researcher, having extensive experience with the Substance Abuse Awareness Seminar and having seen almost miraculous changes in attitude as a result of the seminar, believes that the high expectations of the developers/ instructors does have a positive effect on the participants' degree of learning and attitude change. Whether these attitudinal changes can be extended to include attitudes toward alcoholics and alcoholism is not revealed by this study. This, and whether expectations effect training results, would be fertile ground for further research.
Experimental and Control Group Posttest Scores It was hypothesized that the mean posttest scores for
the experimental group would be significantly higher than the mean posttest scores for the control group. Symbolically, the hypothesis was stated as follows:
H4: Pg Pc H q : Pg = Pq
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

9 1
An independent one-tailed t test was used to determine the significance of the difference between the mean posttest scores for the experimental and control groups at the .05 significance level. Table 7 reports the t-test results for the significance of the difference between the mean posttest scores on the BKI/PQ-DII for 126 Marine supervisors who did and 39 Marine supervisors who did not attend the Substance Abuse Awareness Seminar. As reported in Table 7, the mean difference was 2.713. This difference was significant at the .001 level or better. Therefore, the null hypothesis was rejected, and the main hypothesis was confirmed. This means that the mean BKI/PQ-DII posttest scores for the experimental group were significantly higher than the mean posttest scores of the control group on the study instruments, BKI and PQ-DII.
TABLE 7TEST OF THE SIGNIFICANCE OF THE DIFFERENCE BETWEEN THE MEAN
POSTTEST SCORES ON THE BKI AND PQ-DII FOR MARINE SUPERVISORS WHO DID AND DID NOT ATTEND THE SAAS
TestingSampleSize X
MeanDifference t
Experimental 126 24.1752.713 4.139*
Control 126 21.462
* P < .001.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

9 2
The researcher hypothesized that the experimental group would score higher on the posttest than the control group would. Since the hypothesis was supported, a significant difference exists between the knowledge and perceptions as measured by the BKI/PQ-DII, for supervisors who attended the Substance Abuse Awareness Seminar, following the seminar, and those supervisors who did not attend the seminar, after three weeks during which no substance abuse training was received. This finding was logically based on the assumption that the control group, not having received any substance abuse awareness training during the three-week period between administrations of the BKI/PQ-DII, would not have a significant increase in its test scores. Consequently, the experimental groups' posttest scores would logically exceed those of the control group.
Post Hoc AnalysisFurther examination of the data indicates that the
posttest scores of the experimental group on both the BKI (knowledge scale) and the PQ-DII (perception scale) (taken separately) were significantly higher than the two scores (taken separately) on the pretest. Paired one-tailed t tests were used to determine if the posttest scores on each aspect were significantly higher than pretest scores.Stated symbolically, the hypotheses tested were
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

9 3
H5: TlE < T2EH0: = T2E
Critical value of t .001 (x) = 3.160 H6: TtE < T2EH0: TlE = T2E
Critical value of t .001 (x) = 3.160 The results of these tests (see Table 8) indicate that
both the knowledge and the perceptions of the supervisors were favorably effected by the Substance Abuse Awareness Seminar. This supports the conclusion that supervisory training can be a means of changing supervisors' knowledge and attitudes about Employee Assistance Programs.
TABLE 8TEST OF THE SIGNIFICANCE OF THE DIFFERENCE BETWEEN BKI AND PQ-DII (TAKEN SEPARATELY) MEAN PRETEST AND POSTTEST SCORES
OF MARINE SUPERVISORS WHO DID ATTEND THE SAAS
GroupSampleSize X
MeanDifference t
BKIPretest 126 18.317
1.365 5.949*Posttest 126 19.683
PQ-DIIPretest 126 3.794
0.706 3.424*Posttest 126 4.500
*p < .001.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

9 4
The most significant change in experimental group perceptions following the Substance Abuse Awareness Seminar was observed in the perceptions about the effectiveness of the Marine Corps Substance Abuse Program. A dependent onetailed t test comparing the experimental group's pretest and posttest perceptions of effectiveness resulted in a t score of 4.166, significant at the .001 level, or better. Another dependent one-tailed t test comparing the experimental group's pretest perceptions of confidentiality and their posttest perceptions of confidentiality resulted in a t score of 3.383 (significant at the .001 level). A third dependent one-tailed t test comparing the experimental group's pretest perceptions of program staff competence resulted in a t score of 2.586 (significant at the .01 level), and a dependent one-tailed t test comparing their pretest perceptions of management support for the Marine Corps substance Abuse Program and their posttest perceptions of management support resulted in a negative t score of -1.547 (insignificant at the .05 level). This indicates that the Substance Abuse Awareness Seminar improved Marine supervisors' perceptions of program effectiveness, program confidentiality, and program staff competence, while it diminished, though insignificantly, their perceptions of management support for the program.
The fact that the control group showed diminished, though insignificant, perceptions of program staff
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

9 5
competence (t = -1.312) and program effectiveness (t = -.334), only a slight increase (t = .416) in perception of program confidentiality, and no change in perception of management support (t = -.000) for the Marine Corps Substance Abuse Program in dependent one-tailed t tests comparing their mean pretest and posttest scores for these variables further supports the conclusion that the Substance Abuse Awareness Seminar did improve the perceptions of Marine Supervisors who attended it.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

CHAPTER V SUMMARY, CONCLUSION, IMPLICATIONS,
AND RECOMMENDATIONS
The purpose of this study was to determine the effects of the 36-hour Substance Abuse Awareness Seminar on the knowledge and perceptions of Marine supervisors, as assessed by the Baker Knowledge Inventory and the Demographic Information Inventory, before and after substance abuse training, and to compare these results with a similar group of supervisors who had not participated in the seminar. The primary component of knowledge assessed in this study was knowledge of the Marine Corps Substance Abuse Program, and the perceptions assessed in this study were perceptions of the confidentiality, staff competence, effectiveness, and management support for the Marine Corps Substance Abuse Program.
SummaryThe Substance Abuse Awareness Seminar was a 36-hour
course of instruction designed to train Marines to administer the Marine Corps Substance Abuse Program. It was taught over a five-day period in a retreatlike environment at the Xerox Training Center in Leesburg, Virginia. Topics covered during the seminar include an overview of the Marine Corps
96
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

9 7
Substance Abuse Program, a historical perspective of substance abuse, psychological and physiological aspects of substance abuse, self-awareness of attitudes about substance abuse, pharmacological aspects of substance abuse, effects of substance abuse on the family, intervention into substance abuse, mandatory attendance at a 12-step meeting, and nutritional aspects of substance abuse recovery. The materials presented during the Substance Abuse Awareness Seminar are intended to promote a better understanding of the Marine Corps Substance Abuse Program and to prepare Marines and supervisors to administer the program effectively.
This study used a quasi-experimental design, with a pretest and posttest administered to both experimental and control group subjects. Supervisors attending the Substance Abuse Awareness Seminar, a preexisting training program of nonrandomly volunteered and nonrandomly assigned participants, consistuted the experimental group. Supervisors who worked at the Human Resources Division of Headquarters, U.S. Marine Corps in Clarendon, Virginia, constituted the control group. Control group participants received no substance abuse training between administrations of the pretest and posttest.
The study was developed around four hypotheses. Each related to the experimental and control groups and the effectiveness of the Substance Abuse Awareness Seminar to alter knowledge and perceptions of the Marine Corps
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

Substance Abuse Program as ascertained by the Baker Knowledge Inventory (BKI) and the Perception Questions of the Demographic Information Inventory (PQ-DII). They were tested using dependent and independent one-tailed and two- tailed t tests. The .05 level of statistical significance was used. The study instruments were designed by the researcher and tested for both reliability and validity.
Experimental and Control Group Pretest Scores The first hypothesis stated that no significant dif
ference would exist between mean pretest scores of Marine supervisors who attended and those who did not attend the Substance Abuse Awareness Seminar as measured by the Baker Knowledge Inventory and questions 7,8, 9, and 10 of the Demographic Information Inventory, hereafter referred to as the PQ-DII. The mean pretest score for the experimental group was 22.111, and for the control group it was 21.462. The mean difference was 0.547, which resulted in a t value of .760 (p = .05). This difference was not significant at the .05 level or better. Therefore, the null hypothesis was not rejected which means that no significant difference existed between the mean pretest scores of supervisors who attended and those who did not attend the Substance Abuse Awareness Seminar.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

9 9
Control Group Pretest and Posttest Scores The second hypothesis stated that no significant
difference would exist between pretest and posttest scores for Marine supervisors who did not attend the Substance Abuse Awareness Seminar, as measured by the Baker Knowledge Inventory (BKI) and the Perception Questions of the Demographic Information Inventory (PQ-DII). A paired two-tailed t test was used to determine the difference between BKI/ PQ-DII pretest and posttest scores of the control group.The mean pretest score for the control group was 21.564, and their posttest score was 21.462, a decrease from the pretest score. The difference between the means was -.130, which resulted in a t value of -.161. This difference was not significant at the .05 level or better; therefore, the null hypothesis was not rejected. This means that no significant difference existed between pretest and posttest scores for Marine Supervisors who did not attend the Substance Abuse Awareness Seminar.
Experimental Group Pretest and Posttest Scores The third hypothesis stated that the mean BKI/PQ-DII
posttest scores for the experimental group would be significantly higher than their mean pretest scores on the BKI/ PQ-DII. A paired one-tailed t test was used to determine the difference between the posttest scores and pretest scores of the experimental group at the .05 significance level. The mean pretest score for the experimental group
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

100
was 22.111, and their mean posttest score was 24.175. The mean difference was 2.063 which resulted in a t value of 7.280. This difference was significant at the .001 level or better. Therefore, the null hypothesis was rejected, and the main hypothesis was confirmed. This means that the mean BKI/PQ-DII posttest scores for the experimental group were significantly higher than their mean pretest scores on the study instruments, BKI and PQ-DII.
Experimental and Control Group Posttest Scores
The final hypothesis stated that the mean posttest scores for the experimental group would be significantly higher than the mean posttest scores for the control group. An independent one-tailed t test was used to determine the significance of the difference between the mean posttest scores for the experimental and control groups at the .05 significance level. The mean of the experimental posttest was 24.175 and that of the control group was 21.462. The mean difference was 2.713 which resulted in a t value of 4.139. This difference was significant at the .001 level or better. Therefore, the null hypothesis was rejected and the main hypothesis was confirmed. This means that the mean BKI/PQ-DII posttest scores for the experimental group were significantly higher than the mean posttest scores of the control group on the study instruments, BKI and PQ-DII.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

101
Conclusion and ImplicationsFindings of the present study supported the theoreti
cal proposition that the knowledge and perceptions of supervisors, as assessed by the Baker Knowledge Inventory and the Perception Questions of the Demographic Information Inventory, would be improved by attendance at the Substance Abuse Awareness Seminar. Significant increases were noted in a combined score of knowledge and perceptions, and also in knowledge scores and perceptions scores taken separately. Based on the findings of the present study, the writer concludes that supervisory training is an effective means of improving supervisors' knowledge and perceptions of an Employee Assistance Program.
Significant changes in experimental group perceptions following the Substance Abuse Awareness Seminar were observed. A dependent one-tailed t test comparing the experimental group's pretest perceptions of program effectiveness, confidentiality, staff competence, and management support resulted in t scores of 4.166, 3.383 (significant at the .001 level or better), 2.586 (significant at the .01 level or better), and -1.547 (insignificant at the .05 level or better), respectively. This indicates that the Substance Abuse Awareness Seminar improved Marine supervisors' perceptions of program effectiveness, program confidentiality, and program staff competence, while it diminished, though
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 02
insignificantly, their perceptions of management support for the program.
The fact that the control group showed diminished, though insignificant, perceptions of program staff competence (t = -1.312) and program effectiveness (t = -.334), only a slight increase (t = 0.416) in perception of program confidentiality, and no change in perception of management support (t value = -.000) for the Marine Corps Substance Abuse Program in dependent one-tailed t tests comparing their pretest and posttest scores further supports the implication that the Substance Abuse Awareness Seminar did improve the perceptions of Marine Supervisors who attended it.
RecommendationsIn the development of this study, the researcher saw
the need for further research, as follows:1. The present study sought evidence that perceptions
about program confidentiality, staff competence, program effectiveness, and command support for the program would increase as a result of supervisory training. Other attitudes about Employee Assistance Programs have been proven to influence supervisors' use of the program. Further research should investigate the effects of supervisory training on those attitudes.
2. The Substance Abuse Awareness Seminar was conducted in an intensive, retreatlike environment. Further
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 0 3
research should investigate if this isolation from the normal work environment had a favorable impact on the training results.
3. Various aspects of the Substance Abuse Awareness Seminar appear to have a positive impact on participants. These include the use of interactive discussion formats, the credentials of the instructors, the high expectations of the instructors, the presentation styles of the instructors, the use of original materials produced and developed by the instructors, the mandatory attendance at 12-step meetings, the use of a peer panel discussion format to discuss the effects of alcoholism/drug abuse in the military, and others. The present study did not isolate the effect of the individual aspects of the program. Further research needs to be conducted in which aspects of the program are studied separately to identify those that contribute most to the increase of knowledge and improvement of attitudes.
4. The present study was a quasi-experimental study with nonrandomly selected participants. The Substance Abuse Awareness Seminar should be isolated and tested in another study with an experimental design using random selection and assignment of subjects to the experimental or control groups. This should result in a study that exercises greater control over confounding factors which might result in a more valid interpretation of the Substance Abuse Awareness Seminar.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 0 4
5. The present study used a pretest/posttest format for collecting data. Previous studies have shown that a pretest may positively influence posttest results. The Substance Abuse Awareness Seminar should be evaluated using only a posttest format to determine if the pretest had any effect on the posttest results.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

APPENDIX A MARINE CORPS SUBSTANCE ABUSE AWARENESS SEMINAR SYLLABUS
1 0 5
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 0 6
Table of ContentsSchedule At-A-Glance.................................. 108
DAY 1 - MONDAYModule I - Welcome & Overview........................ 109Module II - The Marine Corps Drug & Alcohol Program 110 DAY 2 - TUESDAYModule III - History of Substance Abuse ........... 121Module IV - Values and G o a l s ......................... 141Module V - Physiological and Sociological
Implications of Alcohol A b u s e ............145DAY 3 - WEDNESDAYDAY 4 - THURSDAYModule VI - Physiological & Sociological
Implications of Drug U s e ................ 167Module VII - Applying the Information............... 185Module VIII - Understanding Nutrition
In Recovery............................ 187DAY 5 - FRIDAYDiscuss 12 Step M e e t i n g .............................. 200P a n e l ...................................................200Individual Stories ................................. 200Question and Answer Period ........................ 200Wrap Up and Evaluations.............................. 200
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 0 7
IllustrationsThe Marine Corps Model Program .................. IllRepresentation of an Historical Cultural Patternof Dealing with Substance Abuse .................. 122Breakdown of Alcohol in the B o d y .................. 150Alcohol's Effect on the Brainas a Depressant D r u g ................................151Drugs and Their Classification.................... 178Points to Consider In Definingthe Effect of D r u g s ................................. 179Internal and External Drugs ...................... 180Eating/Food Disorders ............................. 197Hypoglycemia: A Response to Imbalance ........... 198General Evaluation Form ........................... 199
ArticlesSummary: US Marine Corps Order P5300.12 ......... 112Legal Aspects of Marine CorpsSubstance Abuse Program ........................... 114An Annotated History of the Use, Promotion and
Prohibition of Mood-Altering Drugs ......... 123La P l a t i c a ...........................................142The Disease of A l c o h o l i s m ......................... 146A Test for Addictiveness........................... 152BAC Handling Characteristics.......................166Definitions of Terms and C o n c e p t s ................ 169Marijuana............................................ 170Principles in Defining the Effects of Drugs . . . 172C o c a i n e .............................................174Internal and External Drugs ...................... 17 5Drugs: Incidence and Prevalence .................. 176NSCA Position Statement: Use and Abuse
of anabolic steroids............................... 181The Use of Anabolic-Androgenic Steroids in Sports 183 Anabolic-Androgenic Steroids, Body Compositionand Athletic Performance........................... 184Warning Signs of Relapse........................... 186Nutrition: Its Relationship toAddiction and Recovery............................. 188Our Love Affair With S u g a r .........................191Books for Developing a NutritionalRecovery P r o g r a m ....................................192Treatment of Addiction and Food Disorderswith Nutrient Supplements ........................ 194
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

Reproduced
with perm
ission of the
copyright ow
ner. Further
reproduction prohibited
without
permission.
SCHEDULE - SUBSTANCE ABUSE AWARENESS SEMINAR 1992 -1993
MONDAY_____________ TUESDAY____________WEDNESDAY THURSDAY FRIDAY
0100
0900
M O D V L E 1
WELCOME 4 OVERVIEW• INTRODUCTION• CONTRACTS• OVERVIEW
MODULE I I I
PATTERNS OF USE, ABUSE AND CONTROL
MODULE V (CONT.)
PHYSIOLOGICAL & SOCIOLOGICAL
IMPLICATIONS OF ALCOHOLISM
MODULE VI
PHYSIOLOGICAL * SOCIOLOGICAL IMPLICATIONS OF DRUG USE
M O D U L E IX
• DISCUSS 12-STEP MEETING
• DISCUSSION PANEL
)000MODULE I IA
THE MARINE CORPS DRUG AND ALCOHOL PROGRAM
MODULE IV
VALUES AND GOALS
• PERSONAL VALUES AND
• DISEASE CONCEPT
• SOCIAL, GENETIC
• DRUG EFFECTS• TERMS* CONCEPTS• CLASSES OF DRUGS• BRAIN* BODY
INDIVIDUAL STORIES
QUESTION AND ANSWER
1100
1200
1330
• ILLEGAL• REPORTS
GOALS
• MARINE CORPS GOALS
AND
CULTURAL RISK FACTORS• CHEMISTRY• SOCIAL EFFECTS
W RAP■ UP AND
EVALUATIONS
LUNCH LUNCH LUNCH LUNCH LUNCH
MODULE I I BPROVIDING TREATMENT
MODULE IV (CONT.)VALUES AND GOALS
ATTENDANCE AT A.A. MEETINGS
12 STEP PREPARATIONM O D U L E V I I
APPLYING THE INFORMATIONBUSES LEAVE
2:00 - NATIONALMODULE I I C
LEGAL ASPECTS OF THE DRUG AND ALCOHOL
PROGRAM
• SUMMARY OFALCOHOLANDDRUG INFORMATION
• LAPSE/RELAPSE PREVENTION
1430MODULE V
PHYSIOLOGICAL & SOCIOLOGICAL
IMPLICATIONS OF ALCOHOL ABUSE
AFTERNOON TO2 :0 0 - D U L L E S
1530 MODULE I I D
THE USMC DRUG OEMAND TASK FORCE
BEGIN FIELD TRIPS AND
M O D U L E V I I IUNDERSTANDING NUTRITION IN
RECOVERY
1700 WRAP - UP
• PROGRESSION
• TOXICITY12-STEP MEETINGS • INTERCEPTIVE
GENETICS• HYPOGLYCEMIA
108

1 0 9
Module I - Welcome & Overview Student Oriented Objectives
♦ To introduce Trainers and Participants.♦ To review course elements and aims.♦ To develop learning contract.
Time: 2 hoursMethodology: Group Discussion/LectureOutline: ► Introduce Name Game as tool for
instruction;► Negotiate Learning Expectations
► ►Break (10 minutes)► Review Elements and Aims
Materials: ► List of Course Aims
Module I sets the tone for the seminar. As introductions are being made and expectations for the course established, we get to know each other as trainers and students. These seminars are designed to provide a forum for a free exchange of ideas and opinions. The course aims have been standardized by Drug, Alcohol and Human Affairs Branch,USMC. Staff from the Branch and Military Justice and the Drug Demand Reduction Task Force will team with D.A.T.A. to provide lectures specific to Marine Corps protocol and USMC P5300.12.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 1 0
Module II - The Marine Corps Drug & Alcohol ProgramStudent Oriented Objectives
♦ Students will know the elements of a successfuldrug program.
♦ Students will understand key legal processes &issues.
♦ Students will be familiar with levels 1 thru 3.♦ Students will be familiar with USMC Demand
Reduction Strategy.
Time: 5 hoursMethodology:Outline:
Materials:
Lecture/discussionFacilitator will provide overview of the Marine Corps Drug and Alcohol strategies:(a) The Marine Corps Drug &
Alcohol Program(b) Providing Treatment(c) Legality of the Drug & Alcohol
Program(d) The USMC Drug Demand Reduction
Task ForceQuestion & Answer/clarification period.Entire MCO P5300.12 with changes, andOverhead — The Marine Corps Model Program.
The second Module focuses on the MCO P5300.12 which provides the legal framework for the seminars and for the entire Marine Corps strategy to confront substance abuse. We will not focus on drug and alcohol materials until questions about procedure are explained. This module, then, utilizes Headquarters staff to cover important aspects of the Commandant's program and to answer questions and concerns of seminar participants.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

I l l
THE MARINE CORPS MODEL
Proactive Measures
L Prevention
IV. Recovery
/ Troop Education
" N . I
ln terven tion /\ Referral / \
/ Urinalysis
\ Aftercare Level I /\ and Recovery Level II J
Level HI /
IIA.. Intervention
116. Interdiction
III. Treatment
Reactive Measures
The SACO Office has direct responsibility for three of these quadrants:Troop EducationIntervention and Referral/Urinalysis Aftercare
And, has direct responsibility for Level I treatment in the fourth quadrant
There is a growing sense of responsibility in the Commands for more involvement with the Marine while in Level II and Level HI treatment, especially the latter. Many Commands are now attending graduation ceremonies and keep the Marine up to date with what is going on in the unit.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

112
Summary: US Marine Corps Order P5300.12D.A.T.A. has coined the term "Marine Corps Model Program" which has become part of the standard lexicon, depicted in graphic form in Module 1, page 5. The four parts of the order are summarized below.The Alcohol Program1. The Alcohol program consists of two phases: the Proactive Phase and the Reactive Phase. Proactive involvement states that "every attempt should be made to [curb] alcohol abuse/alcoholism through proactive actions. Any positive action taken by a commander that is preventive in nature is considered proactive" (Reference: The Marine Corps Substance Abuse Program, pp.1-5, Chapter 1, Part 1, paragraph 1101). The MCO P5300.12 places commanders at the vanguard of the proactive thrust. Commanders are expected to model responsible drinking and thereby dispel the myth that "hard chargers" are "hard drinkers." Alcohol consumption is not tied to Marine Corps pride and alcohol abuse constitutes unacceptable Marine behavior. Within the proactive component, commanders institute policies which support responsible consumption of alcohol. In doing this, the commanders' responsibility reaches beyond the military installation. They initiate alternative leisure time activities as a means of reducing stress and combating boredom; and are advised to make full use of local, community public/human service opportunities.2. Also included are preventive education programs, professional training (SAIC, Xerox seminars, etc.), overseas alcohol awareness orientation, and deterrent measures (urinalysis, check points). These education, training, awareness, and orientation sessions provide Marines with "requisite knowledge of alcohol and its effect to assist them in making responsible decisions on personal use." The difference between alcohol abuse and alcoholism are outlined, in accordance with Navy/Marine Corp Order NAVMC 2662.3. In the effort to prevent alcohol abuse, deterrent measures often help identify possible alcohol abusers, but should not include or become tools for harassment, as a good deterrent program includes positive and/or punitive measures.4. The Reactive component recognizes that alcoholism is a disease and, therefore, a health issue. Alcohol abuse on the other hand is a behavioral issue. "Regardless of whether diagnosed as an alcohol abuser or an alcoholic, Marines remain responsible for their actions and standards
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 1 3
of performance an conduct" (Reference: ibid, pp. 1-11, Chapter 1, Part 2, paragraph 1200/2). Since, however, a developing alcohol problem manifests itself in a series of acts of misconduct and/or steadily deteriorating performance, the Reactive phase includes disciplinary and administrative measures as well as treatment and rehabilitation.5. The Marine Corps Substance Abuse Program established three levels of treatment services: Level I, Unit Programs;Level II, Major Command Programs; and Level III, Navy Residential Treatment Programs. The management of the alcohol and the drug programs components are different. "Drug" in Marine jargon refers to illicit and illegal substances. In both instances commanders are encouraged to expand their leadership skills to deal with the entire range of behaviors related to addiction. We see the Xerox seminars, proposed herein, as a tool for continuing this upgrade in skills. Residential Programs.The Urinalysis Program1. The Urinalysis Program is a means of deterrence and reinforcement of command level drug programs (I & II).Often cited as one of the more efficient corporate systems of its kind, the Marine Corps Urinalysis Program links with DoD certified laboratories in ensuring that urine samples are given careful scrutiny, so that careers are not harmed through false reports.2. The order explicitly details how samples are collected and tested within the unit and finally sent to a DoD approved lab for final confirmation. Ledgers and records documenting the specimen's movement through thisconfirmation-events chain ensures that the primary reasons for testing (inspections, search and seizure, medical examinations and fitness for duty) get accurate results.3. A Urine Sample Custody Document accompanying the journey of samples from unit to lab is the primary ledger/report that maintains the above cited quality control.4. When specimens of urine are tested and found positive, the order provides directive to the Command about options available, which can be either administrative or disciplinary.Additional Reports
1. Whereas the urine sample custody document accompanies the specimen to the laboratory, there is a standard format for informing the Command about samples that test positive.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 1 4
This format includes the following:a. Name of Command;b. Reporting period;c. Geographic area;d. Occasion for testing;e. Number of specimens tested; andf. Name and title of individual preparing report.
2. When the Marine is deemed eligible for treatment, a rehabilitation report is also filed. The format for this report includes:
a . Command;b. Reporting period;c. Type of report (drug or alcohol);d. Geographic area;e. Initial screening;f. Rehabilitation level (I - III);g. Dependant rehabilitation; andh. Name and title of person preparing the report.
New Reporting Procedures1. In 1988 (OPNAV 5350-2) introduced a change to reporting procedures through the development of an automated machine readable Drug and Alcohol Abuse Report (DAAR) format. The DAAR consolidates other report formats, and gives SACOs an even more efficient method for logging and tracking information about Marines identified as having substance abuse problems.
Legal Aspects of Marine Corps Substance Abuse ProgramI. INTRODUCTION
A. Non Punitive/Administrative MeasuresB. Punitive MeasuresC. Detection
II. NON PUNITIVE MEASURES -- ADMINISTRATIVE ACTIONA. Counseling. (MCO P1070.12E, IRAM, para. 4013).
Page 11 entry.1. MCO P1900.16D, MARCORSEPMAN, para. 6105,
counseling prerequisite for some type of administrative separations.
2. Entries concerning alcohol related incidents must be in form of counseling with an opportunity to rebut.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 1 5
B. Fitness Report. (MCO P1610.7C, PES, para.3009/4006). No reference to pending matters. Special report upon completion of action and appeals (Don't have to wait for completion of appeals of courts-martial.).
C. Pro/Con MarksD. Denial of privileges. (JAGMAN 0111) (Housing, On
Base Driving, etc.)1. Preliminary suspension of driving privileges
mandatory upon DUI/DWI arrest. Mandatory 1 year + suspension, plus mandatory treatment upon final adjudication or administrative finding of guilt. DOD Dir 1010.7, SECNAVINST 5300.29, MCO 5110.1C.
2. First offender "Courtesy ride" programs unauthorized.
E. Administrative Reduction. (MCO P1400.32, MARCORPROMAN, para. 5002).
F. Administrative Separation. (MC) P1900.16D, MARCORSEPMAN, para. 6210).
1. Separation processing mandatory for all ranks upon first instance of confirmed illegal drug use.
2. Voluntary drug exemption program has been cancelled.
3. Recent change permits discharge higher than OTH if recommended by discharge board or if approved by CMC.
4. Process under multiple bases when possible, for example misconduct and alcohol rehabilitation failure in the case of a second DUI after Level III.
5. Diagnosis of alcohol dependence does not preclude separation under other bases, i.e. misconduct.
6. For Reservists, conduct in the civilian community while not on active duty for training generally may not form the basis for characterization of separation. Such conduct may form the basis for separation.
G . Concepts1. Lower forum of resolution than courts-martial.2. Option to be considered if legal issues may effect
the admissibility of otherwise reliable evidence.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 1 6
3. Try to make decisions up-front, vice after a lost court, or refusal of NJP. Second shots by Government more susceptible to attack at BCNR, Federal District Court, NDRB.
4. Documentation and notice in accordance with applicable orders.
5. Document opportunity for rebuttal/appeal. (Even if not utilized).
6. Opportunity to correct deficiencies.7. Command utilization of available treatment options.8. Administrative actions must be corrective, vice
punitive in nature. Couch your language accordingly.III. PUNITIVE MEASURES
A. NJPB. SCM
1. Advantages to command:Quick and clean.E-4 and below can be reduced to E-l.E-5 and above can be reduced one grade.Can follow up with admin, separation.
2. Advantages to Accused:No federal conviction.No BCD potential.Max confinement is 30 days.Max forfeiture is 2/3 pay per month for 1 month.
3. Command should obtain pretrial agreement to plead guilty in exchange for sending the case to a SCM vice a SPCM. Stipulation of fact concerning guilty should be part of the agreement.
C. SPCMD. GCM
IV. DETECTIONA. Inspections
1. Military Rule of Evidence 313(a) An examination of the whole or part of a unit,
organization, installation, vessel, aircraft or vehicle, including an examination conducted at entrance and exit
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 1 7
points, conducted as an incident of command and the primary purpose which is to determine and to ensure the security military fitness or good order and discipline of the unit, etc.
(b) An inspection also includes an examination to locate and confiscate unlawful weapons and other contraband.
(c) An order to produce body fluids, such as urine is permissible in accordance with the rule.
(d) However/ an examination made for the primary purpose of obtaining evidence for use at trial or in other disciplinary proceeding is not an inspection.
2. Keys(a) Do not target individuals.(b) It's not an inspection if it is directed
immediately following a specific incident. (Subterfuge).(c) All those subject to inspection must be
treated the same.3. Who can order?
(a) Any person placed in a command or appropriate supervisory position may inspect the personnel and property within his/her control.
(b) Key: Inspections should by conducted in strict compliance to a pre-established procedure and very little, or no discretion should be left in the hands of the individual inspectors.
B. Inventories1. Administrative in nature.
C. Searches1. Searches not requiring probable cause
(a) Border searches(b) Searches upon entry to or exit from United
States installations, aircraft, and vessels.(c) Searches of government property...Unless the
person to whom the property is issued or assigned has a reasonable expectation of privacy therein at the time of the search. There is normally no reasonable expectation or
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 1 8
privacy if the property was not issued for personal use.Wall or floor lockers in living quarters issued for the purpose of storing personal possessions normally are issued for personal use; expectation of privacy depends of facts and circumstances at the time of the search.
(d) Consent search. . . must be voluntary; may be withdrawn at any time.
(e) Search incident to lawful stop.(f) Search incident to a lawful apprehension.(g) Searches within jails.(h) Emergency searches.
2. Probable cause searches(a) Who can order? Commander or miliary judge.(b) Probable cause: A reasonable belief that an
offense has been committed and the person, property, or evidence sought is located in the place or on the person to be searched. A search may be based upon hearsay evidence in whole or in part.
(c) Key: No Fishing...Be able to articulate thefactors which caused the reasonable belief...Write them down so you don't forget.
D. Dogs. Can be used in inspection or searches.E. Urinalysis
1. Types. Can be an inspection or a search. Make sure all parties know what is taking place.
(a) Random Sweeps, Unit Sweeps, Command directed(i) Welcome aboard, UA returns, leave returns(ii) Sticks in hat, sealed letters, CO
involvement(b) Probable Cause: Use for all purposes.(c) Fitness for duty and/or Surveillance: Not for
UCMJ purposes; OK for basis for separation but not as basis for characterization.
2. Trouble spots(a) Not really remote, subterfuge
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 1 9
(b) Chain of custody. Not every little mistake will cause suppression, but little mistakes add up in eyes of court.
(c) Administrative procedures not followed. Government bound by its own regulations.
(d) D & A personnel (Pop-up targets for defensecounsel)
Squeaky cleanKnowledge of orders, Strict compliance.No zealotsThey must know what job they are performing,i.e., Unit coordinator, observer, etc.
F. Miscellaneous* Good character. Evidence of good character may tend
to establish that a person was less likely to commit misconduct.
* Unknowing Ingestion. To be wrongful, drug use must be knowing. Knowledge may be presumed from presence, however this presumption may be rebutted by defense evidence.
* Polygraphs - Primarily investigation tool, inadmissible at courts-martial.QUESTIONS?
1.Your local Legal Service Center or Staff Judge Advocate2.HQMC (Code JAM) AV 224-4250 Comm (703) 614-4250E-Mail GIWMOB:HQMC
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 2 0
Daily Evaluation FormDay 1
For each day's work at the seminar, please circle the number, Module by Module, that best represents how valuable you consider the information. Please feel free to write additional comments on the back of the page.
Module I: Welcome and OverviewNot Valuable 1 2 3 4 5 Very ValuableHow can this module be improved?____________________________
Module II A: The Marine Corps Drug & Alcohol ProgramNot Valuable 1 2 3 4 5 Very ValuableHow can this module be improved?____________________________
Module II B: Providing TreatmentNot Valuable 1 2 3 4 5 Very ValuableHow can this module be improved?____________________________
Module II C: Legal Aspects of the Drug and Alcohol ProgramNot Valuable 1 2 3 4 5 Very ValuableHow can this module be improved?_______________________________
Module II D: The USMC Drug Demand Task ForceNot Valuable 1 2 3 4 5 Very ValuableHow can this module be improved?____________________________
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 2 1
DAY 2 - TUESDAYMODULE III
History Time: 08:00 - 10:00MODULE IV
Values and Goals Time: 10:00 - 14:30MODULE V
Physiological & Sociological
* Lunch: 12:00 - 13:30Implications of Alcohol Abuse 14:30 -17:00
Module III - History of Substance Abuse ____________ Student Oriented Objectives:________________♦ Students will have an overview of the history of
substance abuse.♦ Students will be conversant with the control
measures that have been employed.Time: 2 hoursMethodology:Outline:
Materials:
Lecture/discussionLecture: Patterns in the Promotion, Prohibition, and Institutionalization of Drugs.► ►Break (15 minutes) ■*<Question & Answer/Discussion"An Annotated History of Drug Abuse in the US"Representations of an Historical Cultural Pattern
The history module follows next. It gives participants a broader view of the drug problem and how it has taken different forms in different eras or generations but has always evolved socially and legally along certain lines and patterns. Understanding these historical patterns of drug/alcohol control, helps us to gain perspective on whether or not these patterns have worked or compounded the problem.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

122
REPRESENTATION OF AN HISTORICAL CULTURAL PATTERN IN DEALING
WITH SUBSTANCE USE
PROMOTE
INSTITUTIONALIZE PROHIBIT<-------
This pattern can be seen with many drugs, previously illegal, now legal. The drug is first discovered and exalted for its particular properties. Subsequently, some people begin to fear it and espouse its prohibition. Years of struggle ensue and tne drug eventually becomes accepted and institutionalized with some rules or rituals attached. Examples include alcohol, nicotine, and caffeine. Marijuana may be in a transitional period between prohibition and institutionalization.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.
1 2 3
An Annotated History of the Use, Promotion and Prohibitionof Mood-Altering DrugsBy William Lee White
Human history is an unending process of stepping beyond the consciousness of everyday reality through the aid of drugs, drama, ideologies, religions, and rituals, each promising a transfer and pleasurable vacation from the humdrum of one's existence or deliverance to the promised land. The following annotated record of human use of mood altering drugs and the efforts to promote and prohibit such use is a modest attempt to summarize one facet of this history. A synopsis of such an extensive history is unavoidably an interpretation. Implicit in the choice to include or exclude events is the author's view of which themes are crucial in understanding the evolution of our response to the use of intoxicating substances.The historical account presented here depicts religious and moral definitions of good and evil substances and good and evil people. It is a social history depicting the manner in which "in-groups" and "out-groups" are determined through the definition of normalcy and deviance. It is a cultural history demonstrating the immense power of cultural mores and social policies to shape our experiences with chemicals both positively and negatively. It is an economic ability to influence national policies. It is a history of bureaucracies with their innate tendencies to justify their existence and expand the scope of their influence. One also finds a personal history in the lives of those men and women who, for whatever reasons, ingest substances that are not sanctioned by their culture.This material is presented in the hope that it will be both informative and thought provoking. Extensive footnoting has been used for the benefit of those who may wish to explore it in greater depth.5000 BC Earliest historical record of opium use is by
Someri3500 BC Earliest recording of the production of an
alcohol, a description of a brewery on an Egyptian papyrus.
2737 BC First reference to medical use of marijuana in a pharmacy book is written by Shen Nung, a Chinese emperor, he recommends it for female weakness, gout, rheumatism, malaria, beriberi, constipation, and absent-mindedness.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 2 4
2000 BC Earliest prohibitionist teaching by an Egyptian Priest to his pupil: "I, thy superior, forbidthee to go to the taverns. Thou art degradable like the beast."
1134-256 BC During the Chou Dynasty in china, laws against the production, sale and consumption of alcohol are passed and repealed forty-one times.
624-584 BC Cyaxares reclaims Persia from the Scythians by inviting them to feast, getting them drunk, and then slaughtering them - one of the first references to the use of alcohol as a weapon in war.
565-478 BC Buddha in his teaching stressed the importance of total abstinence from alcohol. A number of the Sutras make reference to its disadvantages and the evils befalling one who partakes of strong drink. Among those Buddha listed were loss of reputation, disturbance of temper and loss of wisdom. After Buddhism became the national religion of Japan, prohibition of alcohol is decreed by several emperors from AD 646 to 770.
427-347 BC Plato recommends that wine be withheld from children under 18, slaves, magistrates,
judges, and councilors while on duty. He also suggests that drinking parties be regulated by appointing a supervisor for each affair.
350 BC Proverbs 31:6-7 "Give strong drink to him who isperishing, and wine to those in bitter distress; let them drink and forget their poverty and remember their misery no more."
300 BC First extensive description of the pharmacology ofopium appears in the writings of Theopovastus.
300 BC The Greek Physician Eclesiastus warns of theaddictive properties of opium.
AD 200 Earliest evidence of tobacco smoking among ArizonaIndians.
1327 First national legislation in England to control intemperance. It attempts to limit the number of places alcohol can be sold. It is rapidly repealed.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 2 5
1493 Tobacco is introduced into Europe by Columbus and his crew after their return from America.
1494 England enacts a law requiring establishments that sell alcohol to be licensed by a Justice of the Peace.
1500 Coffee is prohibited in Egypt; supplies of coffee are confiscated and burned.
1525 Paracelsus (1490-1541) introduces laudanum, acombination of alcohol and opium that becomes one of the most common sedatives through the 19th century; it is also used to treat coughing and diarrhea.
1528 The first commercial tobacco plantation is begun on the island of Santo Domingo.
1553 After their conquest of Peru, the Spanish in Lima prohibit use of the coca plant as heathenish and sinful. They later change this position when it is discovered that the natives cannot continue the heavy labor in the mines without use of the plant. A system is established whereby coca leaves are distributed three or four times a day to the workers.
1554 First coffee house in the world is opened inConstantinople.
1565 Dr. Nicholas Monrodes publishes first description of coca (cocaine) in Europe and in 1569 advocates and praises use of the plant in combatting hunger and fatigue.
1600 Drinking of coffee is forbidden in the Moslem EasternMediterranean Region. The penalty for owning orvisiting a coffee house is death. (Behind this ruling was the fact that political malcontents had begun using the coffee houses as a meeting place.)
1600 Czar Michael Federovitch sets execution as the penalty for possession of tobacco in Russia. Later, Czar Alexei Mikhailovitch rules that anyone caught with tobacco should be tortured until he reveals the name of his supplier.
1611 First American crop of Indian hemp (marijuana) is planted near Jamestown, Virginia.
1612 First commercial tobacco plantation in North America is started in jamestown, Virginia by John Rolfe. Within 25 years it becomes the primary export of the English Colonies.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.
1 2 6
1619 Twelve years after alcohol is brought to the Colony of Virginia a law is enacted against drunkenness with penalties as follows: first offenders to be rebuked inprivate by a minister; second offenders to be rebuked in public; third offenders to be sentenced to "lie in hot tar" for 12 hours and pay a fine. The same year Virginia passes laws encouraging the production of wine and distilled spirits.
1650 Connecticut enacts a law that places a fine of $5.00 for drunkenness in one's own home.
1664 Virginia passes a law forbidding ministers from drinking in excess.
1674 The Women's Petition Against Coffee reports among other things that the use of coffee diminishes sexual excitability and results in sterility.
1690 A law encouraging distillation of brandy and spirits from corn is enacted in England.
1691 The penalty for smoking tobacco in Luneberg, Germany is death.
1791 New Hampshire enacts an ordinance to publicly post the names of drunkards and forbids anyone to sell them liquor.
1729 Emperor Yung Cheng of China issues an imperial ban onopium and sets the punishment for keeping an opium shop at strangulation after brief imprisonment. China thus becomes the first country in the world to prohibit the sale and smoking of opium.
1753 The indian hemp plant is named Cannabis Sativa by Linnaeus.
1760 Virginia passes a law prohibiting ministers from "Drinking to excess and inciting riot."
1762 "Dover's Powder" is introduced in England and becomes one of the most common opium preparations for 150 years.
1762 Virginia imposes penalties upon farmers who do not produce hemp.
1768 Captain James Cook reports the use of Kava Kava inPolynesia. Kava Kava, a mild euphoriant, is used in the native religious rituals. Western missionaries attempt to stamp out its use and where they are
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 2 7
successful, alcohol replaces it in the religious ceremonies.
1789 The first American temperance society is formed in Litchfield, Connecticut.
1790 First US Federal law is passed regarding alcohol: this law authorizes giving every soldier a daily ration of a quarter pint of rum, brandy, or whiskey. This ration continued in the army until 1830, and in the Navy until 1862.
1791 Federal Government imposes an excise tax on whiskey.1794 In the "Whiskey Rebellion," a large number of
Pennsylvania rebels threaten insurrection challenging the government’s right to tax whiskey.
1789 Benjamin Rush publishes Essays Literary. Moral andPhilosophical in which he includes the first serious anti-tobacco tract, commenting on the effects of tobacco, Rush states: "A desire of course is excitedfor strong drinks, and these when taken between meals soon lead to intemperance and drunkenness." Tobacco is also associated with idleness, uncleanliness, and poor manners.
1839-42 The first opium war. The British force the trade of opium on China, a trade the Chinese want prohibited.
1841 Dr. Jacques Joseph Moreau uses hashish in treatment of mental patients.
1842 Sons of Temperance organizes in New York for a variety of purposes, a primary one being suppression of the liquor trade. By 1920 the report a membership of 600,000.
1844 Le Club des Haschischins - established in France by Avant-garde artists and writers is named and becomes knows for the use of hashish and marijuana.
1845 The hypodermic syringe is invented by Alexander Wood.1845 Dr. Horace Wells demonstrates the use of nitrous oxide
as an anesthetic in surgery. Although nitrous oxide had been discovered in 1776 by Sir Joseph Priestly and known for its intoxicant effects, its anesthetic properties remain unknown until Wells attends a meeting in 1844 where Gardner Colton demonstrates the intoxicating effects of nitrous oxide as the beginning
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 2 8
of his marketing N20 in competition with alcohol.Wells notes at the meeting that a person, while under the influence of N20 fall and cut his leg but experienced no pain. Wells' experiments with N20 as an anesthetic agent begin the following day. Nitrous Oxide is still taken as an anesthetic and reports of its use as an intoxicant continue.
1851 First prohibitionist law (alcohol) takes effect in Maine. By 1855 thirteen states have prohibitionist laws, although by 1863, they are repealed in eight states and modified in four others.
1860 Anti-tobacco forces denounce men who smoke aseffeminate and warn women that they would become sterile, grow a mustache and get TB if they smoke.
1860 Albert Niemann isolates an alkaloid from the coca leaves and calls it cocaine.
1861 The United States Brewers Association is organized to lobby nationally for the liquor interests.
1861-65 Morphine is used extensively during the Civil War, about 45,000 soldiers become addicted. Morphine addiction subsequently becomes known as the "soldier's disease."
1862 The Internal Revenue Act of 1862 levies a heavy tax on alcohol, thus making it an important source of government income. This law is a result of needed additional revenue to finance the Civil War.
1864 Adolf von Baeyer in Ghent synthesizes barbituric acid.1864 Nusbaum is first practitioner to mention increased
dangers of abuse of hypodermic injunction of morphine.1870 The Oberlin, Ohio Temperance Alliance organizes and
builds strategies that culminate in the creation of the Anti-Saloon league of America, the most powerful of all lobbying forces for prohibition.
1870 Dr. Clifford Allbutt of Britain publishes one of the first warnings about the addictive nature of morphine found in the English language.
1874 Women's Christian Temperance Union is founded in Cleveland.
1874 Heroin is first discovered by C. R. Alder Wright, a London chemist.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 2 9
1875 San Francisco passes the first narcotics control act in the US for the purpose of suppressing opium smoking.In all but one state opiate distribution is regulated by law between 1897 and 1922.
1880 All importation of opium is banned in China and the death penalty is imposed for its use.
1880 Cocaine is an official drug in the US Pharmacopeia.1880 A second wave of prohibitionist legislation (alcohol)
occurs; eight states pass prohibitory laws. Most of these states repeal the legislation by 1904.
1880 The use of cocaine in the treatment of morphine addiction is reported in the Detroit Therapeutic Gazette by Bently and Palmer.
1882 From H.H. Kane's Opium Smoking in America and China: "Many females are so much excited sexually by the smoking of opium during the first few weeks that older smokers with the sole objective of ruining them have taught them how to smoke. Many innocent and overcurious girls have been thus seduced."
1885 The first mention of opium use by blacks appears in an article in the North Carolina Medical Journal. The article reports three well documented cases of opium use by blacks, one in North Carolina, and others in South Carolina.
1885 Freud publishes Remarks on Craving for and Fear ofCocaine in which he responds to increasing criticism of the use of cocaine. On reports of cocaine abuse and addiction, Freud maintains that the only reported cases have been morphine addicts who simply replaced one addiction with another. He maintains that it its not habit forming in other cases. This is Freud's last publication specifically on uses of cocaine.
1885 Dr. W. H. Halstead, who himself had used cocaine agreat deal, injects cocaine into a nerve and discovers the process of nerve blocking for surgery.
1885 The Journal of the American Medical Association reports the case of Robert Louis Stevenson who was treated with cocaine for tuberculosis. Stevenson, while under this treatment, wrote the first draft of Dr. Jekvll and Mr. Hvde in three days.
1885 Park, Davis, and Company manufactures 15 preparations of coca and cocaine, including Wine of Coca and Coca
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 3 0
Cigarettes. The following is the first paragraph from their 1885 promotional brochure: "A simple narrativeof facts regarding the coca shrub and its derivatives, and especially its alkaloid cocaine and the wonderful role its preparations now play in practice, it is believed, form a chapter in the history of medicine and surgery full of interest...to all who recognize the importance of a drug which through its stimulant properties, can supply the place of food, make the coward brave, the silent eloquent, free bondage, and as an anesthetic, render the sufferer insensitive to pain, and make attainable to the surgeon heights of what may be called 'aesthetic surgery,1 never reached before."
1886 First mention of Sherlock Holmes' use of cocaine appears in "A Scandal in Bohemia" by Sir Arthur Conan Doyle.
1887-1914 "Forty-six states pass laws to regulate the use and distribution of cocaine, whereas only twenty-nine states pass such laws against the opiates."
1887 Amphetamine is first synthesized.1887 Congress passes a law prohibiting the Chinese from
importing opium. It did, however, remain a legal activity for Americans.
1888 Coca Cola introduced by Asa G. Chandler, contains cocaine and is advertised to "cure your headache" and "relieve fatigue for only 5C."
1888 The actions of peyote and mescaline are first described by Louis Lewin, a German pharmacologist and toxicologist.
1888 The National Formulary is started, it is acomprehensive listing of available medicinal drugs, their forms, dosage, etc.
1893 The Anti-Saloon League is founded as the political arm of the protestant push for prohibition.
1893-4 Report of the Indian Hemp Drug Commission concludes that there is no connection between the use of marijuana and crime, violence or bad character.
1899 Oklahoma becomes the first state to outlaw peyote. The law is repealed in 1908 after comanche Chief Quanan Parker testifies on its use in the worship of the Native American Church.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.
1 3 1
1903 Cocaine is removed from Coca Cola and is replaced by caffeine.
1906 Squibb's Materia Medica lists heroin as "a remedy ofmuch value...it is also used as a mild anodyne and as a substitute for morphine in combating the morphine habit."
1906 The Right Reverend Charles H. Brent, Episcopal Bishop and former member of Philippine Opium Commission, writes President Roosevelt suggesting that due to US interests in the Philippines and growing concern over opium use at home, that it would be an opportune time to call for international action to stop trafficking in opium.
1906 First Pure Food and Drug Act takes effect. The law requires that medicines containing morphine, heroin, cocaine be so labeled. Later amendments require standards of purity and require quantity of drugs be labeled accurately.
1907-1919 Thirty-four states enact statewide alcoholprohibition laws. During this period consumption of distilled liquor increases 16 percent in per capita consumption to the highest point in 45 years.
1908 New York enacts a law prohibiting women from using tobacco publicly.
1908 A report by the Federal Government on soft drinks states that more than 40 brands contain cocaine.
1908 Prohibition of drugs is established in the Philippines after the US takes over the islands from Spain.
1908 The media spread racial associations between blacks and cocaine use is highly prejudicial to the American public. In addition, the New York Times comments in an article on the growing cocaine "menace" that: "there is little doubt that every Jew peddler in the South carries the stuff."
1909 At the instigation of the US primarily, the International Opium Conference convenes in Shanghai.The US dominates the meeting with an inflexible position that all countries should aim at the immediate prohibition of opium. Several nations do not agree with extreme position but some agreements are reached on efforts to control opium traffic.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 3 2
1913 Congress passes the Webb-Kenyon Act forbidding shipment of alcohol into states which prohibit its sale.
1914 In January, Congress amends the 1909 opium prohibition law by adding a prohibitive tax of $300 per pound of opium prepared for smoking in the US.
1914 Edward Huntington Williams, MD, reports in the Medical Record: (dope refers here to cocaine) "Once the Negrohas reached the stage of being a 'dope taker'...he is a constant menace to his community until he is eliminated. ...sexual desires are increased and perverted, peaceful Negroes become quarrelsome, and timid Negroes develop a degree of 'Dutch courage' that is sometimes almost incredible... in the language of the police officer, 'the cocaine nigger is sure hard to kill'...a fact that has been demonstrated so often that many of these officers in the South have increased the caliber of their guns for the express purpose of •stopping' the cocaine fiend when he runs amuck."
1914 the Literary Digest speaking of cocaine: "Under itsinfluence are most of the daring crimes committed...most of the attacks upon white women of the South are the direct result of a cocaine crazed Negro brain."
1941 July 1 - First strong anti-narcotic law in America takes effect in New York. The Town-Boylan Act provides criminal penalties for nonmedical drug trafficking.
1914 The Harrison Act, controlling sale of opium and its derivatives becomes law. Opposition to the bill is quieted by presenting the act as necessary to meet US international treaty obligations resulting form the 191 international opium conference.The Harrison Act states: "Nothing contained in thissection (prohibiting distribution of opium, opiates, and cocaine) shall apply a) to the dispensing and distribution of any of the aforesaid drugs to a patient by a physician, dentist, or veterinary surgeon registered under this act i n the course of his professional practice..."
1914 "If our Republic is to be saved the liquor traffic must be destroyed." Quote from Purley A. Boker, Anti-Saloon League Yearbook.
1914 December 22 - The Hobson resolution calling for a national prohibition amendment to the Constitution
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 3 3
falls short of the two-thirds needed by a vote of 197 of to 190 against in the House of Representatives.Also through failing to get the needed two-thirds, the prohibitionists demonstrate their increasing political strength.
1915 Six weeks after passage of the Harrison Act, thefollowing appears as an excerpt from an editorial in the New York Medical Journal: "The really seriousresults of this legislation (the Harrison Act), however, will only appear gradually and will not always be recognized as such. These will be the failures of promising careers, the disrupting of happy families, the commission of crimes which will never be traced to their real causes and the influx into hospitals for the mentally disordered of many who would otherwise live competent lives."
1915 US v Jin Fuev Mov. the US Supreme Court rules that possession of smuggled drugs by an addict is a violation of the Harrison act and therefore illegal. This decision makes physicians the only legal source of narcotics left to the addicts.
1915 Tragedies of the Opium Traffic is published and include the following:"A crusade in some of the larger cities of the country against the illegal sale of opium, cocaine and kindred drugs gathered speed when more than a dozen dealers were fined or sent to prison for selling 'dope.1 Several of the fines were for $1,000, and no doubt this will stop considerable of the illegal traffic."
1915 "The very latest sort of drunkenness is that which, it has been discovered, comes from the constant inhalation of smelling salts. So great a hold has the smelling salts habit gained upon the modern woman that when she is deprived of them she experiences all the cravings that afflict the person who dearly loves liquor and finds himself deprived of it..."
1917 A third wave of alcohol prohibitionist legislationresults in about 25 states having some prohibitory laws by the beginning of World War I.
1917 The president of American medical Association endorses prohibition; the house delegates of the AMA pass the following resolution:"Resolved, the American Medical Association opposes the use of alcohol as a beverage; and be it further
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 3 4
resolved, that the use of alcohol as a therapeutic agent should be discouraged." By 1928, physicians make an estimated $40 million a year writing prescriptions for whiskey.
1918 A number of articles in the New York Times during this year charged that German agents were smuggling drugs to American army bases and public schools. The following excerpt form a December 18 issue is typical of the tone: "Into well-known German brands of toothpaste andpatent medicines...naturally for export only...habit forming drugs were to be introduced; at first a little, then more, as the habit grew on the non-German victim and his system craved ever increasing quantities...in a few years Germany would have fallen upon a world which cried for its German toothpaste and soothing syrup...a world of 'cokeys' and 'hop fiends' which would have been absolutely helpless when a Berman embargo shut off the supply of its pet poison."
1919-1938 25,000 physicians are indicted for violation ofthe Harrison Act, and 3,000 serve prison sentences. Thousands more lose their medical licenses.
1919 The Association against the Prohibition Amendment is organized as a lobbying force against passage of the 18th amendment. The Association is successful i getting the repeal of a number of State prohibition enforcement laws.
1919 "Prohibition was presented as 'first and foremost apatriotic program of win the war.' An incessant volley of dry propaganda preached that all patriots must be prohibitionists to save food for the starving allies; that German-Americans were guilty of spying and treason and drinking beer; that the German armies had committed their atrocities under the influence of alcohol; that the worst Kaiser of all was the liquor Kaiser; and that peace without victory and a land fit for heroes were only possible in an earth free from the jack boots of Sun brewers. Indeed, not only would the war bring about national and international prohibition, but lack of the ideology of prohibition had brought about the World War."
1919 The 18th Amendment (prohibition) is added to the constitution.
1919 The Volstead Act, the enforcement arm of nationalprohibition, is passed over President Woodrow Wilson's veto and becomes law.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 3 5
1919 In the first six months after the Volstead Act, some 15,000 doctors and 57,000 druggists and drug suppliers apply for licenses to prescribe and sell alcohol.
1920 Jin Fuev Mov v US. The US Supreme court rules that aphysician could not legally prescribe morphine "tocater to the appetite or satisfy the craving of one addicted to the use of the drug."
1920 Native American Church is established, with the use ofpeyote cactus as a religious sacrament.
1920 The US Department of Agriculture published a pamphlet urging Americans to grow marijuana for profit.
1921 Cigarettes are illegal in 14 states.1925 In Linder v US, the US Supreme Court rules that
addiction is a disease worthy of medical treatment and that it is not illegal for a physician acting in good faith and according to fair medical standards to prescribe moderate amounts of narcotics for the purpose of alleviating withdrawal symptoms. This ruling has minimal effect as the Treasury Department continues to threaten physicians with prosecution under the earlier Behrman decision. Dr. Linders exoneration costs him $30,000 and his medical license for 2 years.
1925-late 30s Earle Albert Rosell and his son Robert, probably the most famous of the anti-marijuana crusaders, assert that the "weed of madness"corrupts all morality, induces violent crimes and leads to insanity. They also warn that the increased use of tobacco could lead to a takeover of America by the reefer peddlers. They continually assert that the use of tobacco nourishes an appetite for "something stronger."
1931 From an anti-tobacco publication "Fifty percent of our insanity is inherited from parents who were users of tobacco; sometimes the victim is a smoker himself which hastens it on. Thirty percent of insanity cases are caused directly from cigarette smoking and the use of tobacco..."
1932 Amphetamine is first marketed under the trade name Benzedrine.
1932 Aldous Huxley's Brave New World is released describing a mechanized future world in which a drug called 'soma' is used to tranquilize all restlessness and discomfort.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 3 6
1933 John Collier, US commissioner of Indian Affairs, and Harold L. Ickes, Secretary of the Interior, jointly prohibit "absolutely an interference by the Indian Bureau with the religious practices of the Native American Church (Peyote Society).
1933 Dec. 5 - The 21st Amendment is officially in effect. Alcohol prohibition is ended.
1935 May 25 - A Federal narcotics farm opens in Lexington, Kentucky.
1935 The first group of Alcoholics Anonymous is formed in Akron, Ohio.
1937 Hearings on the Marijuana Tax Act took up parts of five days, consisted of information from 12 witnesses, three of which represented the Treasury Department which was proposing the law. The essence of the supportive testimony is summed up in the following interaction: Senator Davis; "How may (marijuana) cigarettes would you have to smoke before you got this vicious mental attitude toward your neighbor?"Mr. Anglinger; "I believe in some cases one cigarette might develop a homicidal maniac, who probably would kill his brother...probably some people could smoke five before it takes effect, but experts agree that the continued use leads to insanity."
1937 The Marijuana Tax Act becomes law.1937 Aug 2 - President Roosevelt signs the marijuana Tax
Act.1937 Of the 48 States, 46 have laws against possession and
sale of marijuana. Most penalties were similar to those for heroin, cocaine, and most states erroneously designated it a narcotic.
1939 Meperidine (Demerol) is introduced as a synthetic narcotic that is thought to be free of the risk of addiction. But it joins Hycodan, Alvodine, and Leritine which follows it in an endless list of effective synthetic narcotics all of which carry the potential for addiction.
1938 Dr. Albert Hoffmann, a chemist at Sandoz Laboratories in Switzerland synthesizes LSD. Five years later he accidentally ingests some and reports on its effects.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 3 7
1939 The "Big Bock" - Alcoholics Anonymous is published outlining the tenets of AA.
1941 A March 1 issue of Saturday Evening Post includes the Jack Anderson article on Alcoholics Anonymous. This article more than any other event sparks national and international interest in AA and results in a dramatic increase in AA groups all over the US. Membership jumps from 2,000 to 8,000 by the end of 1941.
1941 Nalline is first synthesized. A semisynthetic derivative of morphine, nalline reverses the effects of morphine and other opiates making it useful in the treatment of opiate overdoses. When nalline is administered to an addict, withdrawal symptoms occur.
1942 Dec. 11 - The Opium Poppy Control Act is approved.This act forbids production of the opium poppy in the US except under license for medical and scientific needs.
1951 The Boggs Act establishes mandatory minimum sentenceson all narcotic offenses and also eliminates parole for drug offenses. Many State legislatures follow with "little Boggs Acts."
1953 A Texas law is passed making possession of a"contrivance used in smoking a narcotic drug" (pipes, roach clips) a felony punishable by penalty of 2-10 years.
1955 Texas drug laws are revised to make first offensepossession of marijuana punishable by 2 years to life imprisonment. This law remains on the books until 1973. During this period possession of marijuana is deemed more serious than assault with intent to murder (maximum 25 years), kidnapping (maximum 25 years), castration (maximum 15 years), arson (maximum 25 years), administering poison (maximum 5 years), assault with a prohibited weapon (maximum 5 years), murder without malice (maximum 5 years), and burglary (maximum 12 years).
1955 The New York Academy of Medicine proposes "taking the profit out of the illicit trade by furnishing drugs to addicts at low cost under Federal control." A Senate subcommittee headed by Price Daniel, rejects this proposal and suggests that in light of the small percentage of addicts cured in treatment that the incurable should be permanently confined, an approach the committee admits would require additional prisons to accommodate 50,000 persons.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 3 8
1956 July 18 - The Narcotic Drug Control Act becomes law.Among other provisions, is one calling for the death of a person over 18 for selling heroin to people under 18.
1958 Synanon, the first therapeutic community for thetreatment of drug dependence operated by ex-addicts is established in California by Charles Dederion and will subsequently provide the initial model for other such therapeutic communities across the US.
1960 The Narcotic Manufacturing Act takes effect. Itspurpose is to provide a system for licensing narcotics manufacturers and to establish manufacturing quotas on all narcotic drugs.
1960 April 17 - New York Governor Rockefeller signslegislation providing for involuntary commitment of narcotic addicts to State hospitals.
1960-61 Professors Leary and Alpert begin experiments on Harvard graduate students using psilocybin.
1962 In Robinson v California, the US Supreme court rulesthat a California law making it a crime "to be addicted to the use of narcotics" is unconstitutional and in violation of the 8th and 14th Amendments.
1965 February - The first large scale methadone maintenance program is established at the Bernstein Institute in New York. This program is based on the research of Vincent Dole, MD, and Marie Nyswander, MD, which has been conducted under a grant for the Health Research Council of New York City since 1963.
1969 Gross sales for alcoholic beverage industry total $12 billion.
1969 Congress appropriates $17 million for drug law enforcement.
1969 Americans spend over $1.2 billion on 2.3 billion pounds of coffee.
1970 "No research demonstrates that any ingredient as found in cigarette smoke causes cardiovascular, respiratory or other illnesses in humans. No research has demonstrated any physiological process through which cigarette smoke results in disease."
1970 In Alabama, the penalty for possession of one marijuana cigarette is minimum of 5 years. Suspended sentences and probation are not allowed.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 3 9
In Colorado, first offense sale of marijuana is a minimum of 10 years.In Georgia, first offense sale of marijuana is punishable by life imprisonment; second offense by death.In Illinois, sentence for first offense sale of marijuana is 10 years to life.In Louisiana, sentence for possession of marijuana for persons over 21 for first offense is a minimum of 5 years at hard labor and first offense sale of marijuana to persons under 21 is 30 years of hard labor and could be the death sentence.In Rhode Island, first sale of marijuana is a minimum of 10 years.In Utah, a life sentence is possible for first sale of Marijuana.
1970 By the end of 1970, 32 states reduce penalties for possession of marijuana.
1970 Dr. Jerome H. Jaffe, Director of Special Action Office for Drug Abuse Prevention: "The addict who is able toobtain an adequate supply of drugs through legitimate channels and has adequate funds usually dresses properly, maintains his nutrition, and is able to discharge his social and occupational obligations with reasonable efficiency. He usually remains in good health, suffers little inconvenience, and is, in general, difficult to distinguish from other persons."
1970 US Department of Health Education and Welfare reports "An estimated 1.3 billion prescriptions were filled in 1970 at a consumer cost of $5.6 billion. Of these, 17 percent, or 217 million, were for anti-anxiety agents, anti-depressants, anti-psychotics, stimulants, hypnotics, and sedatives.
1970 Passage of Comprehensive Drug Abuse Prevention andControl Act replaces previous acts governing control of narcotics, marijuana, sedatives and stimulants and places them under the control of the Department of Justice. Charges for possession of some drugs are reduced to a misdemeanor and penalties are reduced. Provisions are included for rehabilitation, research, and education. The "no-knock" law is part of the act.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 4 0
1971 Eight billion doses of 31 different amphetaminesand meta-amphetamine preparations are manufactured by 15 drug companies.
1971 June - Special Action Office for Drug Abuse Prevention is established to coordinate Federal action in research, prevention, training, education, and treatment. (excluding alcohol and tobacco)
1971 Charles Dederich, founder of Synanon, estimates therelapse rate for Synanon graduates in the neighborhood of 90 percent.
1971 June - President Richard M. Nixon states that "The problem has assumed the dimensions of a national emergency... America's Public Enemy No. 1 is drug abuse."
1972 Edward Brecher - "The only possible conclusion is that the overwhelming majority of patients on the Done- Nyswandar program, after years as criminals on heroin, lead a law abiding life on methadone maintenance and the longer they stay on methadone, the more law abiding they become."
1972 Drug Abuse Office and Treatment Act provides for the establishment of Special Action Office for Drug Abuse Prevention (SACDAP) to coordinate nine Federal agencies involved in drug abuse activities. Provisions are made for the creation of the National Institute on Drug Abuse to carry on work of SACDAP. NIDA begins functioning in April, 1974.
1972 The Knapp commission investigation of widespread corruption in the New York City Police Department reveals that the disappearance of the 50 pounds of pure heroin from the NYCPD which had been seized in the famous "French Connection: case was only part of a total of 400 pounds of illicit drugs that had vanished.
1973 December - The National Institute of Drug Abuse is created by reorganization within HEW. NIDA assumes all of SACDAP's functions except coordination.
1974 The US has an estimated nine million alcoholics and problem drinkers. Each year 30,000 highway deaths are related to alcohol. Half of all homicides and a third of the suicides are alcohol related. Over 5.5 million arrests a year are for misuse of alcohol at a cost to the taxpayer of $100 million a year. A cost of $10 billion yearly is attributed to lost work related to
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 4 1
alcohol. The total cost to the nation has been calculated at 15 billion dollars a year.
1975 Federal support for treatment and rehabilitation of drug users reaches $241.3 million for FY 1975. By contrast the 1967 figure was $18 million.
1975 "Of 115 US medical schools, fewer than five require course work in drug dependency and less than 20 offer an elective in alcoholism and/or drug abuse."
1976 Eight States: Alaska, California, Colorado, Maine, Minnesota, Ohio, Oregon, and South Dakota, have laws approaching the decriminalization of marijuana for personal use.
1977 March 15 - The Carter Administration asks Congress to decriminalize the possession of marijuana and says that it is carefully reexamining its position on penalties for possessing cocaine.
Module IV - Values and Goals Student Oriented Objectives:
♦ Students will be exposed to value clarification (how values differ).
♦ Students will be asked to determine what their own attitudes are toward drugs and alcohol and their abusers.
Time: 2 hours.Methodology: Buzz Group/FishbowlOutline: Provide instruction for setting up small
Buzz Groups with observers.► Conduct La Platica.
► ►Break (15 minutes)► Conduct Fishbowl for observers.
Materials: ► La Platica: an approach to understanding cultural conflict and values from the Marine Corps perspective.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 4 2
The module on Values and Goals is an opener to major discussion among participants. Until now we have been involved in large group discussion, now we are given a chance to participate in small group discussions about your personal values and goals and those of the Marine Corps. Through group exercises, you are given a chance to see how personal values influence decision making and may conflict with the Marine Corps goals outlined in the Order. Learning to resolve conflicts that occur between one's own values and the goals of USMC programs is the purpose of the exercise:La Platica.
La Platica:An Approach to Cultural Clarification
John R. Moore, ASCW and Delfino Sanshez, MSW, M.Ed. The Worden School of Social Service Our Lady of the
Lake University San Antonio, TX
La Platica is designed to assist each of you in identifying and becoming aware of your culture and values. It will also help identify some of the cultural conflicts which you may have experienced. Your group as a whole will be able to identify its cultural make-up. This approach will be helpful in assessing needs of clients or staff.The culture with which we identify plays an extremely vital role in our relationships with others. Our values, which come from that culture, form the basis for our goals, motivations, and interactions.Culture is ever changing. If the culture you were born into is not identified as the dominant culture, or if the culture you identify with is changing rapidly, you may feel in conflict. The anger, guilt, and frustration that result can impair growth and development.Culture is reflected through language, dress, art music, food, manner, and appearance. All of our cultural traits are influenced by the Church, our philosophy, politics, and education.
La Platica workshop will help you:► experience your own cultural identity► identify conflicts relating to your own culture► surface your own values
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 4 3
► recognize other cultures► discover differences and similarities between
cultures (for example, your family culture and the Marine Corps culture) develop more satisfying relationships with people from different cultures through better understanding of and respect for other cultures
UNIVERSALLY ACCEPTED CULTURAL CONCEPTS AND TERMSDefinition of CultureCulture is the integrated system of learned behavior patterns which are characteristic of the members of a society and which are not the result of biological inheritance.According to anthropologist Edward B. Taylor, "culture is that complex whole which includes knowledge, belief, art, morals, law, custom, and any other capabilities and habits acquired by man as a member of a society. In short, cultures is an entire way of life of a people which is transmitted along general lines.Real Culture vs. Culture constructThe culture construct presents the real culture as accurately as scientific methodology permits. The real culture is what all the members of a society do and think in all their activities in their total round of living.The real culture is never sensed by anyone in its entirety. It can only be partially perceived as it is ordered and translated into understandable terms.Cultural Integration and Inter-Cultural DiversificationThe members of any given culture never exhibit all the behaviors of which we now know human beings are capable.Many people think that what they do is ipso facto an expression of human nature. Little do they realize that other humans have found quite different ways of doing the same things or perhaps they do not do it at all.Fundamental Cultural PostulatesBehavior typically associated with any given culture reflects two kinds of underlying assumptions:
Existential Postulates - assumptions about the nature of the external world and the nature of man himself; and
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 4 4
Normative Postulates - assumptions about what things or acts are good and to be sought after, and which are bad and to be rejected.
Both existential and normative postulates are the reference points that color a people's view of things, giving them their basic orientation toward the world around them and toward one another. They provide the frame of reference for a people's world view.
PRINCIPAL EXERCISE - PHASE 11. What is your personal impression or viewpoint of the dominant culture of the US, beliefs, concepts, and life styles toward drugs?2. You will now have 20 minutes to discuss (platica) your impressions with others. Please note below, during the group discussion, which of the above impressions you now feel to be myths, and which represent reality.
PRINCIPAL EXERCISE - PHASE 21. On your own, write down what you have learned about drugs based on your family experience (positive and negative) - 5 minutes.2. On your own, write down what you have learned about drugs based on your experience in the Marine Corps (positive and negative) - 5 minutes.3. Have a discussion (platica) concerning your past and present information and attitudes about drugs. Make notes of the key points - 20 minutes.4. Indicate below the drug-related information and attitudes you feel are positive and that you would like to continue, attitudes you would like to change, or new information or attitudes you would like to acquire - 5 minutes.
OBSERVER FORMThe purpose of your observing is to give you an
opportunity to develop skills in listening, to observe group process and discipline. You are asked to record similarities within you group so that the entire group will be able to discuss them following the three exercises.Below are some suggestions to assist you in your observation of the group and s\assist you in your presentation to the entire group. Keep these points in mind as you observe the group at each phase.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 4 5
1. What kind of interaction do you observe?2. Does any one speak noticeably more than the others?3. Was anyone left out of the discussion?4. Did anyone move closer to or away from other members?
5. Did voices change tone, volume or pitch? When?6. How do you feel observing this phase?
Module V - Physiological and Sociological Implications of Alcohol AbuseStudent Oriented Objectives:
♦ Students will understand the disease concept of alcoholism.
♦ Students understand the disease is progressive, maybefatal.
♦ Students are aware of societal and Marine Corpspressures and rewards regarding drinking.
♦ Students are exposed to societal, racial and culturalinfluence theories.
♦ Students will differentiate use, abuse, and addiction.♦ Students know the blood alcohol content (BAC) required
to be considered legally drunk in different states.♦ Students understand the relationship of individual
weight of amount of alcohol consumed to BAC.♦ Students become aware of toxicity of alcohol and the
process of physical addiction.♦ Students understand "blackouts" and "tolerance" as
related to alcohol, and physical aspect of its use, abuse and addiction.
♦ Students know the physical symptoms ofhangovers/alcohol.
♦ Students know what actions to take with alcohol abuserswithin their work parts.
Time: 6 1/2 hoursMethodology:Outline:
Lecture/Video/DiscussionLectureVideo: The Feeling Chart►Break (25 minutes) «•«
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 4 6
► Discussion/lecture/clarificationMaterials: ► Video: The Feeling Chart
► The Disease of Alcoholism► Comparison of Alcoholism and Heart
Disease► Breakdown of Alcohol in the Body
The Alcohol Module is presented separately from that of other drugs because alcohol is typically the drug in which there is the most interest. It is a long module because there are three important goals:► To change attitudes toward the problem drinker per
the recent Marine Corps policies about use and abuse;
► To help understand the progressive nature of thedisease and thus able to better identify potential problem drinkers; and
► To provide information about how alcohol affectsthe family, the workplace, etc., and to show how alcohol consumption is reflected in blood alcohol levels, and biochemical changes.
The Disease of AlcoholismBy Gayle R. Hamilton
This article is a description of the multiple factors determining alcoholism and how they might work together. Through this information, one can make a possible assessment of his or her likelihood of someday experiencing problems with alcohol. The research has been available for many years, but is still not generally available to the public.One of the most overlooked aspects of man's relationship to alcohol is the variability in that relationship: someexperience more of the depressant effects of alcohol, while others experience more of the stimulant effect; some get intoxicated on small quantities, while others have what we call a "hollow leg"; some get sick easily, while others seem to experience no negative side effects; some feel euphoric when they drink, while others feel little or nothing. Some can take it or leave it; others seem unable to leave it. In other words, we cannot judcre another's experience with alcohol bv our ownl Of course we do judge others' experience all the time. But that is largely because the general public knows few of the facts about this disease, particularly the facts about its biochemistry.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 4 7
The fact is we probably know more about the causes of this disease that we do about heart disease or cancer. It is a complex disease, with multiple causative factors that come together to form a variety of "recipes" for alcoholism, each of which gives its own expression and each of which requires its own emphasis in treatment and recovery. There are three basic categories of factors: genetic/biochemical;social/environmental; and psychological. Each category, discussed below, has many factors, some, none, or all of which may be pertinent to each individual.Genetic/Biochemical. Studies of the past two decades on adopted children have concluded that biological factors are greater predictors of alcoholism than are environmental factors. In other words, alcoholism includes hereditary factors. Some of these factors we know about; others are in various stages of discovery. We know, for example, that there are two enzymes in the liver which we inherit in different forms: alcohol dehydrogenase, which regulates howmuch we are able to consume; and acetaldehyde dehydrogenase, which regulates how we feel when we consume alcohol. Those that inherit forms of these enzymes that enable them to drink large quantities with minimal intoxication, and which enable them to drink without feeling "paying a price", are generally those who are at higher risk for developing a drinking problem. Why? Because they metabolize alcohol so efficiently that they lack mechanisms within them that say "it's time to stop!" And these are the very people whom we describe, with pride, as being able to "handle their liquor"!! In addition to these enzyme properties, there is also good evidence that diets deficient in the B vitamins increase the chances of our abusing alcohol AND that some of us are more vulnerable to this problem because we have inherited a greater need for B vitamins than have others. From emerging research over the past five years, we now understand that our nutrients are required to manufacture the neurotransmitters (brain chemicals responsible for communication within the body), which regulate our "craving" for outside drugs. Researchers are also currently exploring the possibility that some people break down alcohol in an unusual way, resulting in an end-product chemically related to the opiates. The presumption is that such a process would produce stronger euphoria for the drinker.Social/Environmental. Marines traditionally identify this category of factors as a crucial one for them, though major changes have taken place in recent years. Some factors to be included here are: availability (it is highly availableat low cost in the Marine Corps); peer pressure; social activities centered around alcohol (the Club, Wet Downs, etc.); absence of other things to do (particularly during family separations); and, role models who use alcohol to
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 4 8
cope with stress. Additionally, advertisements and commercials link alcohol use to numerous desirable qualities. This groupof factors shifts with the generation, with sub-cultural mores, and in relationship to other drug use.Psychological. Twenty years ago, one of our most prestigious alcohol research centers, the Menninger Clinic, concluded that psychological factors do not distinguish between alcoholics and non-alcoholics. However, for any individual, psychological or physical stresses may increase the incentive to drink and thus increase the risk for abuse. These factors might include: depression, shyness, death ofa loved one, fear, conflict, etc. Marines in particular tend to experience loneliness on deployment, the depression or disorientation associated with family separations, high pressure for job achievement, the pressure of extra duty due to being short staffed, pressures due to frequent moves, etc.Now the question is: how do these factors come together toexpress the disease of alcoholism in an individual? Imagine that each of us is making a soup and we have 3 varieties of spices to choose from: hot spices, such as chili peppers,hot paprika, black pepper; pungent spices, such as basil, oregano, tarragon; and, sweet spices, such as nutmeg, cinnamon, cloves. Each of the soups will be different because different combinations of the spices will be used.In addition, some of the soups will be more weighted with one category of spices — some on the hot spices, some on the pungent spices, and some on the sweet spices.Alcoholism gets expressed in a similar way. Additionally, each individual might have a different weighing of the categories of factors — some will have a form of alcoholism primarily determined by his or her genetics, some may be more environmentally induced, and still others might be heavily weighted with psychological stresses.Where the analogy breaks down, however, is that there is one set of factors that has to be at least partially present in order for alcoholism to express itself: the biochemical.A person lacking all of the biochemical factors discussed on the previous page would be someone who might: getintoxicated on a single glass of wine; get sick or have a hangover after very little drinking; never experience euphoria or even an elevation of mood. At best, the experience might provide minimal pleasure; at worst, the experience might be very unpleasant. The likelihood of this person drinking a sufficient amount of alcohol to become dependent is very slim! This person will have to find another way to deal with his or her psychological problems.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 4 9
Alcoholism Defined. The ways in which people express this disease can be quite different: some drink daily all theirlives, never appearing really drunk, but rarely sober either; some go for periods of time without drinking and then binge drink for a period of time; some never seem to have visible consequences while others get into lots of legal or social trouble; some people are more pleasant to be with when they are drinking while others are unpleasant to be with when they are drinking. To reconcile these differences, the standard, very simple, definition of a drinking problem used today is: "If the person has aproblem in any aspect of his or her life because of drinking,then he or she has a drinking problem". Thus, social problems, marital problems, job problems, or health problems that are related to the use of alcohol all indicate that a drinking problem exists.New Definition of Alcoholism. The National Council on Alcoholism and Drug Dependence and the American Society of Addiction Medicine approved the following definition of alcoholism in 1990. The major change in the definition is that it now specifically includes the presence of genetic factors.
Alcoholism is a primary, chronic disease with genetic, psychosocial, and environmental factors influencing its development and manifestations.The disease is often progressive and fatal. It is characterized by continuous or periodic impaired control over drinking, preoccupation with the drug alcohol, use of alcohol despite adverse consequences, and distortions in thinking, most notably denial.
ReferencesGoodwin, D.W. Genetic determinants of alcoholism. In Diagnosis and Treatment of Alcoholics. (Eds.) Mendelson, J.& Mello, Nancy, McGraw Hill, 1979, Ch. 3, pp.59-82.Collins, Michael. (Ed.), Aldehyde Adducts in Alcoholism. Alan R. Liss, Inc.: New York, 1985.Blum, K. The Alcoholic Gene: DNA research may prove majorbreakthrough in search for genetic link. Professional Counselor. September - October, 1990
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

J BREAKDOWN OF ALCOHOL IN THE BODY
150
Pathway Through the Body1. Alcohol flows from the esophagus to the stomach,
duodenum and upper part of the small intestine.2. From there it flows out into the blood stream and,
from the blood stream, flows into the liver and pancreas.
3. The breakdown of alcohol takes place only in the liver.
Breakdown in the Liver
alooholdehydrogenase
1
acetaldehydedehydrogenase
1Alcohol -* acetaldehyde ■» acetic add -*■ HjO + C 02
iThis enzyme regulates how much alcohol we can drink-this is our tolerance.
This enzyme regulates how we feel (sick or hungover) after we drink. Antabuse blocks this breakdown and increases the amount of acetaldehyde (a toxic substance) in the system.
There are different methods of breakdown in the liver, which may include one in which the final products are opiate-like substances called enkephalins.
Enkephalins give us our sense of well-being. See below for speculated route.
alcohol acetaldehyde -*• dopamine -» enkephalins
STOMACH
PANCREAS
DUODENUM
LARGE
SMALL
M
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

ALCOHOL'S EFFECT O N THE BRAIN AS A DEPRESSANT DRUG\
151
4 DRINKS
1-2 DRINKS
3 DRINKS
PARIETAL LOBI?• R m rfin r t Hrrv* •Reaction time • Coordination SOMEWHAT AFFECTED
Vision Speech
FRONTAL LOBE
• Reason •Caution
Inhibitions Memory Judgment Ocdpital LOBE
• Vision Speech
• Balance Legally Drunk
TEMPORAL LOBE
BRAINSTEM Breathing and Pulse depressed GROSS MOTOR
£2t£EB2LWalking
• Standing• Balance
goneDI-ATI I MAY KTSULT
{M r
20 DRINKS OR MORE (VARIES)
5 DRINKS
(.10%)
6-8 DRINKS
CEREBELLEM • Loss of consciousness (passing-out)
10 DRINKS OR MORE
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 5 2
A Test for AddictivenessPhelps-Nourse
Are you an addictive person? As yet there is no single laboratory test that can provide you with a reliable, definitive, yes-or-no answer to that question. Nor is it really possible for most people to look at themselves objectively for possible clues to addictiveness and come up with a meaningful answer, no matter how sincere their motivation. It is part of the nature of addictiveness that even the most obviously addicted person may vigorously deny that any addiction exists.
General DescriptionMany factors are helpful in identifying a person's
addictiveness: The history of how one consumes andmetabolizes sugar-foods, the person's family history, the occurrence of a significant amount of depressions, personal history relevant to past or present drinking habits or prescription and street drug use, and certain aspects of the quality of one's life. This test seeks to uncover clues or risk factors in each of these areas. The test is not designed or intended for anyone to pass or fail. It is intended solely to help you discover some useful and important information about yourself, namely the risk factors that you have suggesting addictiveness.
This Profile is a self-administered test that will result in a numerical score. The different parts of the test deal with a number of addictiveness risk factors that may be present in your life. The test will not tell you whether or not you are an addictive person in absolute terms. What this Profile will do is suggest, with some validity, whether there is a high, moderate, or lowlikelihood that you are an addictive person.How to take this test - Answer each question in each part ofthe following test with the utmost honesty and objectivityyou can manage, and score each question on the separate score sheet provided according to the instructions with each individual question. Do not worry about interpreting the questions. If you feel that any question has absolutely no relationship to your life in any way, sore 0 for that question.PART I - DIETARY SUGAR - (Please mark all answers on score sheet)1. How often have you eaten the following foods?
Score
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 5 3
Less than once a week 0Once a week 1Once a day 2Twice a day 3Three Times a day 4More than three times a day 5List of foods - Question 1-4a. Sugar, Honey, or Syrupb. James or jelliesc. Chocolated. ice cream or sherbete. Cake, pie, or cookiesf. Doughnuts, sweet roles, or pastriesg. Other desserts (pudding, canned fruit in syrup,
fruited yogurt, ice cream toppings, etc.)h. White breads or dinner rollsi Soft drinks (non-diet)
2. Have you ever craved one of the foods on the above list so much that it distracts you?
ScoreLess than once a week 0Once a day 2More than three times a day 4
3. Has eating a moderate amount of one of the above foods made you lose your appetite for more? Has it made you want more immediately?
ScoreLose appetite 0Want More 3
4. Have you ever overeaten any of the foods listed about to the point of discomfort?
ScoreNever 0Once a month 1Once a week 3Once a day 5
5. Have you ever gone on food binges, eating many helpings of any kind of food?
ScoreRarely or never 0Once a month 1Once a week 3Once a day 5
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 5 4
6. How much sugar have you used a day?Score
0-2 Teaspoons a day 03-5 Teaspoons a day 26 or more teaspoons a day 4
7. Have you had trouble controlling your weight?Score
Never 0Occasional trouble 1Constant trouble 4
8. Have you had any of the following symptoms regularly (that is, daily or more than 3 times a week)?(No, score 0; yes, score 2 for each group of symptoms):a. Unexplained or undiagnosed stomachache, backache
or indigestion?b. Unexplained headache?c. Trouble sleeping?d. Low energy or fatigue?e. Trouble getting started, getting things
accomplished?f. Trouble concentrating or reading?g. Angry outbursts for trivial reasons?h. Daytime faintness, sleepiness, cold spells or
shakiness?8. If you have had any of the above symptoms, were they
noticeably or reliably relieved by eating sweets or starchy foods? (For each symptom that was, score 2 additional points).
9. How long have you been able to stay on a reducing diet that severely restricts or eliminates all sweets or starchy foods, including bread, pasta, potatoes, etc. (Indefinitely, these foods are not a problem, score 0 only one week, score 2; 1-2 days, score 3; less than a day, score 5.
PART II - FAMILY HISTORY (Please mark all answers on score sheet)
The questions in this section refer exclusively to blood relatives, both living and dead, in your immediate family. The relatives referred to are your parents, grandparents, brothers, sisters or your own children. The term does not include aunts, uncles, cousins, step-relatives, marital partners or in-laws.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 5 5
1. Have any blood relatives in your immediate family habitually consumed foods high in starch and sugar, to excess?
ScoreNone 0One or two 3Most of them 5
2. Have any relatives been "heavy" coffee or tea drinkersmore than three cups per day)?
ScoreNone 0One or more 2
3. Have any relative had serious trouble controlling their weight; are they 25 pounds overweight or more?
ScoreNone 0One 1Two 2More than two 4
4. Have any relatives been alcoholics or recovering alcoholics, including relatives who are no longer living?
ScoreNone 0Each one who qualifies 5
5. Have there been any relative who were no acknowledged alcoholics but who were probably alcoholic, who had four or more drinks of alcohol daily, from what you personally know about their drinking habits?
ScoreNone 0Each one who qualifies 5
6. Have there been any relatives you think were probably not alcoholics but who have had occasional or periodic episodes of heavy drinking or getting drunk?
ScoreNone 0Each one who qualifies 3
7. Have there been any relatives who, in your private opinion, may have been "problem drinker" or alcoholics, even though you have no specific evident to support this feeling?
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 5 6
9.
10.
11.
12.
13.
14.
ScoreNone 0Each one who qualifies 2Have any relative been hard narcotic addicts, using either prescribed or street drugs, now or in the past?
ScoreNone 0Each one who qualifies 5To your knowledge, have any relatives been regular (i.e. virtually every day) users of tranquilizers, such as Meprobamate, Valium, or Xanax?
ScoreNone 0Each one who qualifies 3Have any relative been long-term heavy smokers? (One pack or more a day)
ScoreNone 0Each one who qualifies 2Have any relatives been regular (i.e., virtually every night) users of sleeping pills whether prescribed or over-the-counter?
ScoreNone 0Each one who qualifies 3
Have any relatives been regular users of so-called recreational drugs (marijuana, cocaine, speed, peyote, LSD, etc.)?
ScoreNo 0Each one who qualifies 3Have any relatives been known to have suffered long or severe spells of depression?
ScoreNone 0Each one who qualifies 3If your answer to 13 is yes, have any of those relatives been treated with anti-depressant drugs, been hospitalized for treatment, or received electroshock therapy?
ScoreNone 0Each one who qualifies 3
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 5 7
15. Have any relatives ever been diagnosed as hyperactive during their childhood?
ScoreNone 0Each one who qualifies 3
16. Have any relatives committed suicide or made suicideattempts?
ScoreNone 0Each one who qualifies 5
PART III - DEPRESSION (Please mark all answers on scoresheet)1. Have you had trouble getting to sleep or staying asleep
at night?Score
None or infrequently 0Some 2Frequently 3
2. Have you cried easily or felt like crying a lot?Score
None or infrequently 0Some 2Frequently 3
3. Have you regularly had to push yourself to get things done?
ScoreNone or infrequently 0Some 2Frequently 3
4. Have you often felt fatigued or excessively drowsy during the day?
ScoreNo or infrequently 0Some 2Frequently 3
5. Has your sexual response changed for the worst?Score
No or infrequently 0Some 2Frequently 3
6. Have you often felt fearful, tense, or anxious?
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 5 8
ScoreNo or infrequently 0Some 2Frequently 3
7. Have you quickly lost interest or enthusiasm for what you are doing?
ScoreNo or infrequently 0Some 2Frequently 3
8. Have you found yourself looking for escapes?Score
No or infrequently 0Some 2Frequently 3
9. Have you often felt guilty about things that happen?Score
No or infrequently 0Some 2Frequently 3
10. Have you ever considered suicide?Score
Never 0Once or twice, vaguely 1Once or twice seriously 3More often and more detailed than that 5
11. All of the factors mentioned in question 1 through 10 above are frequently associated with depression. Do you feel that any of these factors have interfered with your life or achievements?
ScoreNo 0At one time but not now 2Repeatedly 5
12. Have you regularly eaten to relieve depression or because of a gnawing insatiable hunger?
ScoreNo or infrequently 0Some 2Frequently 3
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 5 9
13. Have you regularly used alcohol to relieve depression?Score
No or infrequently 0Some 2Frequently 5
14. Have you ever taken drugs or medicine other thanprescribed antidepressants to relieve depression?
ScoreNo or infrequently 0Some 2Frequently 5
15. Have you ever been subject to prolonged or serious episodes of depression?
ScoreNo 0Once Daily 1Two or three times that you can remember 3Frequently 5
16. Have you ever been hospitalized for depression, or had electroshock therapy?
ScoreNo 0Yes 5
17. Have you ever taken antidepressant drugs onprescription, for depression? (Some common anti-depressant drugs include Elavil, imipramine, Ludiomil, Norpramine, Tofranil, Asendin and Desyrel).
ScoreNo 0Yes, for one month or less, once 2Yes, for longer than a month or more than once 5
PART IV - ALCOHOL USE (Please mark all answers on scoresheet)1. Have you drunk alcohol regularly in the past, or do you
now?Score
Never 0Once a month 1Once a week 2Daily 4
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 6 0
2. If you drank, indicate the average quantity you drank in a day.
ScoreNot very much (up to 1 1/2 oz. of hard liquor or 1 beer or 1 glass of wine in a day) 0 A moderate amount (2-3 1/2 oz. of hard liquor or 2 beers or 2 glasses of wine in a day 2Quite a bit (4-6 oz. of hard liquor or 3-4 beers, or 3-4 glasses of wine in a day) 4
• Lots (8 or more oz. of hard liquor or 5 or more beers, or 5 or more glasses of wine in a day) 6
3. Have you ever suffered one or more of the following events because of over-drinking: Throwing up from drinking too much? Passing out? Being unable to remember what you did the night before? Hissing work on account or your drinking?
ScoreNever any of them 0One or more of them daily 2One or more of them occasionally 4One or more of them frequently 6
4. Has drinking made your home life unhappy or interfered with your gosils or achievements?
ScoreNot at all 0Maybe a little 2Quite a bit 4Very seriously 6
5. Have you ever felt remorseful, ashamed or guilty about drinking?
ScoreNever 0Occasionally 1Frequently 2
6. Have you craved a drink at a regular time each day?Score
No 0Yes 2
7. Have you drunk to relieve tension or escape pressure orunwind?
ScoreNo 0Yes 2
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 6 1
9 .
10.
11.
12.
13.
14.
15.
Have you drunk alone?Score
Never 0Very rarely 2Occasionally 4Frequently 6Have you wanted to drink in the morning?
ScoreNever 0Very rarely 2Occasionally 4Frequently 6Have you ever been medically treated, hospitalized, or admitted to an institution because of drinking?
ScoreNo 0Once 3More than once 6Have you ever been cited for DWI (Driving While Intoxicated)?
ScoreNo 0Yes, score for each time 4Have you ever drunk more than you intended to?
ScoreNo 0Rarely 1Occasionally 3Often 5Have other people (close friends, your children, employer, doctor or spouse) ever commented negatively on your drinking or urged you to cut down?
ScoreNo 0Yes, score 3 for one of the above 3Score 6 for two or more of the above 6Have most fun things and good times in your life now orin the past been associated with alcohol?
ScoreNo 0Yes 2Have you sometimes declined a drink or left your firstdrink unfinished?
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 6 2
ScoreSometimes or often 0Did once or twice 2Almost never 3
16. Have you been comfortable associating socially with people who do not drink at all?
ScoreYes 0No 2
PART V - DRUG USE (Please mark answers on score sheet)1. Have you regularly taken prescription drugs of any of
the following types for any reason? (No, score 0; yes, score 5 for each type)a. Sleeping pillsb. Tranquilizersc. Diet Pillsd. Pain pills (Rx only)
2. Have you taken any kink of pills on a daily basis to"feel better?" (Excluding vitamins)
ScoreYes 0No 2
3. Have you ever sought prescriptions from two or moredoctors simultaneously for the same pills?
ScoreYes 0No 5
4. Have you ever been addicted to a narcotic such as opium, morphine, heroin, Demerol, methadone, Dilaudid, codeine?
ScoreYes 0No 5
5. Have you ever used one or more of the following drugs:Marijuana, speed, downers, acid or cocaine?
ScoreNever 0Once 1Occasionally 2Frequently 3Daily (for each drug used) 4
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 6 3
6. Have you ever had medical or institutional treatment for a drug habit?
ScoreYes 0No 5
7. Have you personally known a ready source of marijuana,cocaine, heroin, or other street drugs?
ScoreNo 0Yes 2
8. How many cigarettes have you smoked daily?Score
None 0Less than a pack a day 2More than a pack a day 3
9. Have you ever chewed tobacco or smoked a pipe or cigars on a regular basis?
ScoreNo 0Yes 3
10. Have discussions of drug abuse made you uncomfortable?Score
No 0Yes 2
11. How much coffee, tea, or cola have you drunk daily?Score
Less than 16 ounces 0More than 17 ounces 2
12. Have you suffered a financial strain, family problems or work difficulties because of drug use?
ScoreNo 0Yes (for each one) 4
Interpreting Your TestA relatively low score indicates that the individual has comparatively few risk factors suggesting that he or she may be addictive. A high score suggests a large number of such clues or risk factors; a middle-range score suggests only a moderate likelihood that you are an addictive person.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 6 4
This means that the Individual Addictiveness Profile test will separate people into three large groups.Early experience with the test suggests that if you score under 50 on this test it is very unlikely that you are addictive, and this book probably will be of major interest to you only if other people close to you happen to be addictive. If yo score between 50 and 100, you should definitely be on guard and read this book for further information, because you may well be an addictive person with present or potential problems with addiction. If you score above 100, it is extremely likely that you are an addictive person and probably already have one or more active addictions whittling away at your vitality and reducing the quality of your life. People with a high score may or may not have known that they are addictive or addicted, so the test results may well come as a surprise to them.It has been my experience that addictive persons are very likely to have a number of qualities or traits in common, and the more such qualities or traits that a person exhibits, the more likely it is that he or she is an addictive person. It is these qualities and traits that the Individual Addictiveness Profile is designed to reveal or identify— the more of them identified, the higher the score.It is very important to evaluate the partial scores as well as the total score. It's conceivable that a score lower than 50 could be misleading and the person could be addictive or even addicted. For example, if the person eats little sugar and is unaware of depression, but has a heavy family history score and uses no alcohol or drugs, his/her total score could be below 50. He or she would well be addictive and should understand the risk present of becoming addicted to sugar, alcohol, or drugs in the future because of the heavy influence of family history.Another person could have a score around 50 or less with the points coming primarily from consumption of sugar. Even though there is a low scoring in family history and alcohol and drug use, one should take a serious look at the addictiveness risk if large quantities of sugar are being eaten.If the depression score is 12 or higher, regardless of the total score, the person should be evaluated for depression by a trained health professional. If the depression score is high, addictiveness is a risk even without any know family history.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 6 5
Occasionally, low scores may be obtained by persons with alcohol or drug problems if (1) those taking the test do not have adequate information about their family history, (2) depression is masked by regular alcohol and/or drug use, and/or (3) sugar intake is low because of alcohol consumption. In these cases low scores may result despite addictive use of alcohol and/or drugs.
PHELPS-NOURSE INDIVIDUAL ADDICTIVENESS PROFILE
SCORE SHEETPart 1 Part II Part III Part IV Part V1. a l.______ l.______ l._______ l.__
b 2.______ 2.______ 2._______ 2.__c_____ 3.______ 3.______ 3._______ 3.__d 4.______ 4.______ 4._______ 4.__e 5.______ 5.______ 5.______ 5.__f 6.______ 6.______ 6.______ 6.__g 7.______ 7.______ 7._______ 7.__h 8.______ 8.______ 8._______ 8.__i 9.______ 9.______ 9._______ 9.__
2. 10. 10. 10. 10.__3. ______ 11.______ 11.______ 11._______ 11.__4. ______ 12.______ 12.______ 12._______ 12.__5. ______ 13.______ 13.______ 13._______ 13.__6. ______ 14.______ 14.______ 14._______ 14.__7. ______ 15.______ 15.______ 15._______ 15.__8. a 16.______ 16.______ 16._______ Total
b Total______ 17._______Totc Total______d_____e_____f_____g_____h Total score for Parts I-V_i_____
9. ______10. ______Total _______
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 6 6
BAC HANDLING CHARACTERISTIC
0.00 — Sober as a judge0.03 — Mildly relaxed, existing mood slightly changed0.06 — Mentally relaxed, fine skills slightly decreased,
less concerned with surrounding environment, skin flushed, inhibitions begin to disappear, heart speeds up, gaiety
0.09 — Behaviors exaggerated, talkative, noisy, moody,loss of good judgment, remaining judgement slowed, giddiness, coordination a bit off
0.12 — Clumsy, serious loss of judgment, serious loss ofcoordination, vision blurred, speech fuzzy, reaction time slowed.
0.15 — Staggering, speech slurred, coordinated0.18 — Obviously intoxicated, grossly uncoordinated in
all behavior0.21 — Grossly intoxicated, all physical faculties
impaired, all mental faculties impaired, loss of balance, double vision
0.24 — Falling toward alcoholic stupor and coma0.30 — Semi-stupor, coma may occur0.35 — Surgical anesthesia, minimum death level for one
of 100 people.0.40 — Death level for 50 of 1000.50 to 0.80 Breathing and heart action slow; death occurs
Daily Evaluation Form _______________Day 2
For each day's work at the seminar, please circle the number, Module by Module, that best represents how valuable you consider the information. Please feel free to write additional comments on the back of the page.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 6 7
Module III: HistoryNot Valuable 1 2 3 4 5 Very ValuableHow can this module be improved?____________________________
Module IV: Values and GoalsNot Valuable 1 2 3 4 5 Very ValuableHow can this module be improved?____________________________
Module V: Physiological and Sociological Implications of Alcohol Abuse
Not Valuable 1 2 3 4 5 Very ValuableHow can this module be improved?____________________________
DAY 3 - WEDNESDAY MODULE V
Module V - Physiological & Sociological Implications of Alcohol Abuse (continued)
Time: 08:00 - 12:00
NOTE: The afternoon is being reservedto allow participants to begin attending 12 Step meetings (Time: 13:30 - 17:00).
* Lunch: 12:00 - 13:00
DAY 4 - THURSDAYMODULE VI
Physiological & Sociological Implications of Drug Use
Time: 08:00 - 12:00
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 6 8
MODULE VII Applying the Information The intervention Process
Time: 13:30 - 15:30
MODULE VIII Understanding Nutrition in Recovery
Strengthening Programs Nutrition and Recovery
Time: 15:30 - 17:00
* Lunch: 12:00 - 13:00Module VI - Physiological & Sociological
Implications of Drug UseStudent Oriented Objectives:
♦ Recognizing the psychoactive substance in marijuana.
♦ Students will be familiar with trends of marijuanausage and its relationship with the legal system.
♦ Students will be aware of the major classes ofdrugs.
♦ Students will be familiar with the physiologicaland psychological effects of each drug.
♦ Knowing the street names associated with drugs.
Methodology:Outline:
Materials: ►►►►►
Time: 2 hoursLecture/Discussion/Video
Instructor will introduce subject using videos.
► ►Break (15 minutes) <■*Question and Answerclarification/discussion period.Definitions of Terms and ConceptsMarijuana ArticleDefining the Effects of DrugsClasses of DrugsDefining the Effects of Drugs
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 6 9
Participants are given six principles for understanding pharmacological effects of other drugs (for example the crack phenomenon), explaining each drug or drug group's major psychological and physical effects, medical uses, withdrawal patterns, overdose effects, street names, and changing use patterns. Marijuana is emphasized, with focus on its increasing potency and current research on its effects. There is special emphasis on cocaine as well. Recently, the interest in cocaine is on a par with marijuana, thus the special emphasis. This is an entry module for the portion of the course that helps participants gain needed knowledge. It provides a birds' eye view of addictive behavior and lifestyles by providing:► An overview of the interrelationship of drugs— how
use of one leads to another, their similarities and differences;
► Current use patterns;► A theoretical model for how imbalance in one area
of our life makes the use of one drug more attractive (nicotine, caffeine), and how this use creates more imbalance, requiring another drug to temper existing effects;
► A biochemical model for the development ofdependency;
► An understanding of the lifestyles that developaround the use of a variety of drugs and howlifestyles (diet, exercise, stress) effect druguse.
Videos and slides are utilized here to illustrate very complex materials describing the psychoactive way drugs create brain chemical, metabolic and hormonal imbalance. Lectures and discussions will then focus on how these imbalances effect behavior and social institutions, such as the family.
Definitions of Terms and ConceptsDrug - A substance that by it's chemical nature affects the structure and functioning of a living organism. This seminar pertains to mood-altering drugs, used for:
relief of pain reduction of tensionincrease of energy or reduction of fatigue or depression
changes in perception euphoria (a sense of well-being)
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 7 0
Dependent Behavior - Any behavior that, if ceased, would produce discomfort ranging from uneasiness to objective, physical symptoms.Drug Use - Realizing the desired effects of a drug with minimal hazard and as part of legally and socially acceptable behavior.Drug Abuse - Taking a drug under circumstances and in doses that significantly increase their hazardous potential or are outside legally or socially acceptable behavior. In the Marine Corps, any use of an illegal drug is considered abuse.Drug Dependence - When one feels that one cannot live without the drug; and/or, when the body responds negatively to the withdrawal of a substance.Withdrawal - The symptoms which occur when a substance is removed from a person who has become either physically or psychologically dependent. In the case of physical dependence on alcohol, withdrawal symptoms can be life- threatening.Tolerance - The adaption of the body to frequent use of a substance so that it takes increasingly larger amounts of the substance to maintain the desired effect.Cross-Tolerance - When tolerance to one drug automatically applies to other drugs in the same classification whether used frequently or not.Drug Interactions► Independent Effect► Addictive Effect► Synergistic Effect► Antagonistic Effect► Blockade Effect► Idiosyncratic Effect► Placebo Effect
Kxamples1 + 1 = 1 + 1 Antibiotic + Aspirin 1 + 1 = 2 Nicotine + Caffeine1 + 1 = 3 , 5, 7...Alcohol + Valium 1 + 1 = +/- .001 Alcohol+Caffeine
1 + 1 = 0 Heroin + Naloxone1 + 1 = ? Alcohol + Marijuana
1 + Expectations = Expectations
MarijuanaGayle. R. Hamilton, Ph.D.
Effects• In low doses, is like a sedative-hypnotic (depressant)• In high doses, is hallucinatory in effect• Effects have been controversial for many years.
Problems:1. It takes many years for implications to
become clear — has only been 20 years for mj2. Early studies did not account for other drug
use and for reasonable dosage levels.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 7 1
Acute Effects;Heart rate increases; blood pressure decreases when standing. May be threat to those with hypertension; maybe not a threat for healthy young adult.Reddening of eyes.Hand steadiness reduced.Slow reaction time on complex tasks.
• Slow information processing on complex tasks.Increases body sway.
• No continuous attention for tracking ability — for up to 10 hours after smoking
• Reduced response to peripheral stimuli Reduced driving skills.
Chronic EffectsHarm to respiratory system.Mj more harmful, however, to the lungs Mj has 5 mg tar; cigarettes have 1.2 mg tar.
• Mild immune depression. Jury still out on this.No persistent EEG brain wave changes. No permanent change in brain structure, but behavioral changes are apparent.
BehaviorFelt to be related to a motivational system. But unclear which came first.1/2 of high school seniors who quit did so because of "loss of energy or motivation;" 40% quit because of lessened ability to think
Psychological and Psychosocial EffectsImpaired digit/symbol substitution, digit span, serial subtraction, reading comprehension and overestimation of time.Alters perception of sight, sound and touch.The more complex, unfamiliar and demanding the task, the greater is the impairment.Psychological tests currently available cannot detect significant differences between moderate users and nonusers of mj but show that chronic use correlates with those who are abusers of other drugs (psychological dependence, anxiety when supply is uncertain, and self-perceived inability to relate to the world in general when not high).Casual user = 1-4 times per month. Heavy user = 20-30 times per month.Heavy users judged to have poorer work adjustment, a self-reported inability to master new problems, and found to be more hostile toward society and to havemore anxiety than casual users.
• More recent longitudinal studies have shown that heavymj use is associated with poor academic performance and
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 7 2
motivation, various kinds of delinquent behavior, problems with authority, and lack of self-esteem.These descriptions are thought to precede the drug use. Those who are peer-oriented are more likely to use drugs.
Medicinal UseAncient Chinese and Indian texts show that it was recommended for hundreds of problems: insomnia, pain,anxiety, tension, etc.In recent years, was used for asthma, glaucoma, the nausea of chemotherapy, and epilepsy.
Principles in Defining the Effects of DrugsDrug Abuse Training Associates, Inc.
There are some principles to be used that guide us in determining how a drug, or a food, might effect someone. We will discuss seven of these below:Properties of the Drug. Each drug group, which we have discussed at the beginning of this chapter, induces a set of symptoms that generally effect people in ways that define the drug group. For example, all of the hallucinogens tend to produce large distortions in one's sense of reality; all of the stimulants tend to increase one's energy output; and, all of the narcotics tend to put one in a dreamy state where worries evaporate. Like groups of drugs tend to have these effects regardless of external circumstances.Characteristics of the individual. Even though drugs in the same groups tend to have identifiably different effects, individuals themselves can respond in uncharacteristic ways, or with different nuances to their responses. For example, some people become more relaxed when they drink alcohol and may sit alone drinking, while others, become more stimulated to party and engage in risky behaviors; some people seem to have a hollow leg and can drink enormous amounts without showing drunkenness, while others are what we might call "cheap dates"; and, some people enjoy the effects of smoking marijuana, while others do not.Context of use. Smokers of marijuana, or users of hallucinogens, know that the context in which they use their drug makes a difference in how they react. If in a trusting, safe environment, they may have a pleasant "trip". If alone, or in unusual circumstances, however, the trip may be characterized by paranoia or extreme fear. Studies have also indicated that the mood related to drinking alcohol are
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 7 3
more pleasurable when drinking in a social context rather than drinking alone, where the mood may become more morose for some. The context may even influence the extent of the drug reaction. For example, studies have shown that, if the subjects think they are getting alcohol or marijuana (when in fact they are not), they may react 'as if' they were under the drug's influence.Method of use. The method of use of the drug makes a difference in its rewarding effects. That is, when a drug, such as heroin, is injected directly into the vein so that the blood stream immediately carried it to the brain, addiction is more likely than if the heroin is snorted, a method often used by beginners. Likewise, cocaine is more reinforcing when either injected or smoked than if it is snorted. The most reinforcing method, and therefore the method with the most addictive potential, is when cocaine is smoked. Cigarettes, too, are very reinforcing, and probably the most addictive drug used, because of its method of use.Dosage. The dosage of a drug can alter the experience of the drug, but will not always bring simply more of the same response. Higher dosages may bring a different quality to the experience. For instance, small or moderate amounts of alcohol may produce a more sociable, caring, open friend or family member. Higher doses, however, might produce aggression and irritability. Low doses of marijuana might bring giddiness and playfulness, or increased sexual interest. Higher doses, however, may produce paranoia. Higher doses of many drugs also need to be approached carefully or lethal overdose might occur. This sometimes happens when a more pure batch of heroin hits the streets. The users inject the same amount, but, with the greater purity, receive more of the drug. If the difference is significant, there may be an overdose. On the other hand, if the person had gradually worked up to that same level, the body would have adapted, without overdosing.Means of preparation. Drugs are prepared in various ways to control the concentration and the method of use. For example, crack is not a new drug as some people think; it is cocaine that has been prepared to be in smokable form.Crack is also a more concentrated form of cocaine. Drugs can be deliberately diluted in order to increase the quantity that can be sold. For instance, heroin on the streets is usually about 3 - 5 % heroin; the rest includes a variety of fillers, such as milk sugar, or even various poisons. This is the way the middle dealers make their money. If a more pure batch of heroin hits the streets (say, 7%), there may be a string of overdoses.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 7 4
Distance from the plant. An important principle to understand is that the greater the distance from the original plant, the more damaging to the body and the more addictive is the drug. As an example, morphine is a natural substance extracted from the poppy plant. Though addictive, morphine has relatively benign effects on the body. When something is done to the morphine to make heroin, we now have a drug that does more damage to the body, which is a more potent pain killer, and which is more addictive than morphine. Methadone is a purely synthetic opiate. This drug does more damage than does heroin, is an even greater pain killer, and is more addictive than heroin. The same process describes what happens in the synthesis of sugar. And, yes, studies have already shown that the synthetic sugars do more damage to amino acid levels in the brain.
CocaineExcerpted from an Article Written for World Book Encyclopedia, Health and Science Annual 1992 by Gayle R. Hamilton, Ph.D.Teams of researchers from the National Institute of Drug Abuse (NIDA), the Johns Hopkins Medical Institutions, and the Oregon Health Sciences University reported in the October issue of Science magazine that they have isolated a gene in rat brains that makes the protein molecule that transports dopamine back into the cells from which it was released. The same gene is presumed to exist in human brains. Dopamine, released in the brain when cocaine and other drugs are consumed, is responsible for feelings of pleasure. After normal release, dopamine is then swiftly picked up by the transporter and safely stored. When cocaine is used, however, the cocaine blocks the ability of the transporter to take back the dopamine, thus allowing dopamine to reward brain cells willy nilly. Scientists are hoping that this new knowledge enables them to better understand the nature of addiction, depression, and other mental disorders.It is now known that these feelings of pleasure are magnified and last longer when cocaine is combined with alcohol, the second most common combination reported by the Drug Abuse Warning Network (DAWN) for substance abuse- related deaths. Dr. Deborah Mash, associate director of the Comprehensive Drug Research Center at the University of Miami School of Medicine, reports in the February 26 issue of JAMA, that this combination of alcohol and cocaine produces a third drug called cocaethylene which is more lethal and more addictive than cocaine.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 7 5
Dr. Elizabeth Brickner, author of a study reported in the September issue of Circulation (a journal of the American Heart Association), has demonstrated a link between chronic cocaine abuse and enlargement of the left ventricle of the heart. Comparing 30 chronic cocaine abusers with 30 age- and race-matched controls with no history of high blood pressure or heart disease, she found that hearts were heavier and heart muscle walls were thicker in those who used cocaine. She suggests these findings are caused by skyrocketing blood pressures from cocaine use.According to research reported by the Alcohol, Drug Abuse, and Mental Health Administration (ADAMHA) in the December issue of JAMA, there is increasing evidence that the binding of drugs or neurotransmitters to receptors may produce changes in genes that regulate other genes, with the result that lasting changes occur in components of cells, including neurotransmitters. These lasting changes found in animal studies may explain why drug craving exists months or years later and why greater vulnerability to the effects of stress is often seen in affective illnesses and progressing addiction.
Internal and External DrugsDrug Abuse Training Associates, Inc.
Research of the past five years has focused on brain chemistry to understand drug effects and the craving for excessive amounts of drugs that some people experience.This has been a very fruitful area of research and has led to a greater understanding both of the process of addiction and the genetics of addiction.The human brain is the world's largest pharmacy. The amino acids we eat in our foods, with the help of vitamins, minerals, and essential fatty acids, are formed by the body into neurotransmitters. These neurotransmitters (chemicals) are the messengers in the brain that allow for communication to occur between the many systems of the body — they serve to transmit impulses from one nerve cell to another. These are very complex systems and not yet fully understood. We do know, however, that neuro-transmitters are critical to all body functions.An impulse, or message, travels along a neuron (an electrical-like response caused by the exchange of sodium and potassium in and out of the cell walls), either on its way to the brain (to inform), or on its way back from the brain to another system (to produce a response). Along the
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 7 6
way, there are synapses, or gaps in the neurons, over which the impulse cannot travel. These synapses are like railway junctions where the impulse could go in many directions. It is the diffusion of the neurotransmitters (chemicals) across the synapse that enables the impulse to continue to its destination. If there are insufficient quantities of these neurotransmitters, then the impulse may be weak or may be unable to continue altogether.The relevance to drug and alcohol use and abuse is this: the drugs which we use and abuse in our culture have their counterparts in the brain; and, it is the activation of these neurotransmitters by the external drugs taken that give us the effects we are looking for (or trying to avoid, as the case may be). These neurotransmitters are, in effect "internal drugs".There are several dozen neurotransmitters in the brain. Of these, there are at least six with which the study of drug use concerns itself: Endorphins; Enkephlalins; Serotonin;Dopamine; GABA; and Norepinephrine. These are the internal drugs that regulate mood, feelings, and energy — precisely what our external drugs do for us. Inadequate amounts can disrupt normal impulses and influence subjective states, such as drug craving, anxiety, depression, insomnia, and tremulousness. One of the most important areas of inquiry is the relationship between these half-dozen neurotransmitters and the genetics of alcohol and other drug addiction.
Drugs: Incidence and PrevalenceCocaine. 6 million Americans. Since 1982, the number of users 26 and older has doubled. Approximately 10,000 more children, aged 12 to 17, used cocaine in 1985 than in 1982. At the American Academy of Pediatrics annual meeting later this week, Dr. Donald Ian MacDonald, head of Alcohol, Drug Abuse and Mental Health Administration, will report that 44 percent of cocaine users age 12 to 17 "freebased" or smoked the drug, which increases the potency of cocaine."I regard this as ominous and cause for urgent concern," MacDonald said. Hispanic youths are more likely than black or white youngsters to have tried cocaine. Among young adults, age 18 to 25, whites are more likely than either Black or Hispanics to have sampled cocaine. For those 26 and older, blacks are the most likely to have used cocaine in the past year, followed by whites and Hispanics.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.
1 7 7
Hallucinogens (LSD, PCP, mescaline, peyote). 960,000 Americans. Experimenting with hallucinogens remains largely a phenomenon of white youth; only 6 percent of Hispanics and 3 percent of blacks have ever tried these drugs, compared with 13 percent of whites.Heroin. About 500,000 Americans— no change in the number of users since 1982. But drug experts say these figures are deceptive because people who "use" heroin are probably addicted to it, unlike users of other drugs, who may take them just occasionally. Heroin addiction remains a largely urban problem— one that affects a disproportionate number of minorities.A key concern is acquired immune deficiency syndrome because heroin is commonly taken intravenously, and needles are shared. According to Dr. Sander Genser, a research psychiatrist in the National Institute of Drug Abuse's clinical medicine branch, heroin addicts and other i.v. drug users are the "the major vehicle of transmission" to pass AIDS to the heterosexual population.Marijuana and hashish. 18 million Americans. Since 1982, approximately 1.8 million Americans stopped using "grass." Only among those 12 to 17 did marijuana use increase. Some 15 million young people smoke marijuana monthly; 9 million daily. Among those 18 to 25 who smoke marijuana, about a quarter also use cocaine.Stimulants (Dexedrine, Benzedrine and others). 2.7 million Americans, sedatives (Seconal Phenobarbital and other) 2.2 million American. In general, nonmedical use of these legal drugs is declining. Only among adults 26 and older is therea slight increase in the use of tranquilizers and theanalgesics, such as codeine or Darvon.Alcohol. More than 100 million Americans. Of that number, 18 million are problem drinkers; 10.6 million are alcoholics. One third of those aged 12 to 17 drink. Nearly 60 percent of boys who drink also smoke marijuana, compared with only 10 percent of nondrinkers.Cigarettes. Approximately 60 million Americans— about one third of the population. Among adults, smoking has declinedslightly— 2 percent since 1982. But among those 12 to 17,the numbers are increasing. Almost 80 percent of boys who smoke also drink compared with just one quarter of nonsmokers. Close to half of all boys who smoke cigarettes also smoke marijuana, versus just 7 percent of nonsmokers. And 10 percent of boys who smoke cigarettes also use cocaine, compared with just 0.5 percent of nonsmokers.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

178
DRUGS AND THEIR CLASSIFICATIONS
DEPRESSANTS Ethyl Alcohol Barbiturates: V7 -Minor Tranquilizers: Inhalants:
Anesthetics:
Second, Nembutal, Am y tal, Paraldehyde, Doriden, Chloral HydrateMiltown, Equanil, Librium, Valium, Serax, Meprospan Glue,Paintand Lacquer Thiimers, Freon, general household products (Huffing)Ether, Nitrous Oxide
OPIATESNatural:Semi-synthetic Synthetic (high potency): Synthetic Oow potency): Opiate Antagonists: (Blockers)
Morphine, Codeine, and Opium Heroin 7Dilaudid, Demerol, Prinadol, Lomotil, Methadone Darvon, Zactane, Talwin Nalline, Lorfan, Narcan, Naloxone
CNS STIMULANTSNatural:Synthetic
. Caffeine, Nicotine, Sugar .Amphetamines: Dexadrine, Benzedrine, Methadrine,
Desoxyn, Ritalin Amphetamine-like: Preludine, Tenuate, Tepanil,
Wyamine,Ice
Semi-Synthetic Cocaine
HALLUCINOGENSNatural:Semi-syntheticSynthetic
Psilosybin (Mushrooms, shrooms). Mescaline (cactus) LSD-25DMT, PCP, DET, DPT, DOM, MOA
CANNABIS (SATTVA & INDICA)Marijuana Hashish Hashish oil
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

179
rexMignra im laaiMaiTMBramb umbipmbiibub
imra rcmgragips m fmia ibimokb
PROPERTIES OF THE
CHARACTERISTICS OF THE IM B im iM M ,
CONTEXT OF HOT
MEANS OF
METHOD OF
>A©I§m m
U S K
Oj*, JdJtkljt-Mf
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

180
f INTERNAL AND EXTERNAL DRUGS:'X V THEIR ACTIONS AT THE SYNAPSE J
COCAINE EXAMPLE
; t t -J 'Dopamine
r r /Transmitting
'Cell
NORMAL IMPULSE SHORT-TERM EXCITEMENT LONG-TERM DEPLETION
EXTERNAL DRUGS INTERNAL DRUGS orNEURQIRANSM nXERSOpiates Beta-Endorphins; EnkephalinsStimulants AdrenalinAnti-Depressants Enkephalins; Serotonin; DopamineDepressants Serotonin; GABAHallucinogens DMTCocaine Dopamine
For every external drug, there is an internal drug that has a similar effect These internal drugs represent different kinds of neurotransmitters, which are the language of the body. Then tell the neurons when to fire and when to stop firing and dictate a variety of feelings and behaviors.
HEALTHY BRAIN CAN GET THESE FEELINGS BY:Has energy as needed Eating the right foodsCan think clearly Inheriting the right genesHas tolerance for discomfort Reducing stress in your lifeExperiences pleasure Having supportive friendsRelaxed - able to cope with stress Movement - such as dancingFeels good - Has feeling of well-being Different kinds of music
UNHEALTHY BRAIN is depressed Craves drugs/junk foodis anxious Fuzzy ThinkingLow energy Low interest in lifeInsomnia No tolerance for discomfortN o pleasure is irritable
CAN GET THESE FEELINGS BY: Eating poorly Specific genetic patterns Ongoing stressNo supportive friends/family Low physical activity
Drug Abuse Training Associates: Gayle R. Hamilton. Ph.D. and Bernard], Redd
Reproduced wild permission of the copyright owner. Further reproduction prohibited without permission

1 8 1
National Strength and Conditioning Association Position on Anabolic Steroids
The NSCA has based this position stand on a comprehensive survey and analysis of the scientific literature dealing with the effects of anabolic steroids on physiology and physical capacities and performance. Additional concerns for safely improving performance, promoting fair play, protecting health and protecting the future of amateur sport were also important factors.It is the position of the National Strength and Conditioning Association that:1) The administration of therapeutic doses of anabolic
steroids to healthy males has not been shown in itself to elicit significant improvement in the maximum strength, maximum oxygen intake, aerobic performance, lean body mass or weight.
2) When combined with resistance training, anabolic hormone administration generally results in an increased body weight gain as compared to training alone. Body composition may or may not change, although the majority of investigations suggest an increase in lean body mass with no change in fat, and thus a reduced percentage of body fat. The increasesin body fat may or may not be enhanced by higher drug dosages.
3) When combined with resistance training, anabolic steroid administration may increase maximum strength or power more than training alone. Facilitation of strength development occurs most often in experienced weight trainers and may be the result of physiological or psychological changes.
4) There is no conclusive scientific evidence regarding the effects of large doses or long term administration of anabolic steroids on the health or physical performance of athletes.
5) Anabolic steroid administration poses a threat, the extent of which over the long term remains undefined, to the liver, cardiovascular, immunological and endocrine systems, and thus to overall health and longevity.
6) Steroids and continuing effort would be made to educate athletes, coaches, trainers, physicians, physical educators and the general public regarding the limited benefits and potential risks of steroid use as
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 8 2
documented by the scientific method. An open dialogue between interested parties should be encouraged. Only by bridging the gap between all concerned can an environment of knowledge and understanding be created.
7) Based upon the limitations and deficiencies of our current data base and the universal and overwhelmingly positive empirical experience of the athletic community, concurrent efforts by the above groups should be directed toward resolving the disputed and outstanding issues.
8) If drug testing is to be the deterrent to steroid usage, then testing should eguitably encompass all levels of athletes.
9) All those concerned and supportive of athletic competition (coaches, fans, sports administrators, alumni, news media, etc.) should reevaluate their perspectives on sports. In this way, the accountability of anabolic steroid usage can more clearly be defined. A win-at-all-cost philosophy may create enormous pressure for the competitor. The competitor's response to this pressure may include anabolic steroid use, directly determining the type of role model projected to our youth — the athletes of tomorrow.
10) The NSCA should actively support research that will address questions concerning short-and long-term effects of steroids and take a responsible lead in research that may help cover methods performance enhancement through proper conditioning and restoration technique.
11) The use of anabolic steroids in an attempt to improve physical capacity or performance is contrary to the ethical principles and regulations of competition as established and set down by all athletic federations and sports governing bodies. The National Strength and Conditioning Association supports these ethical principles and regulations.
12) In summary, because sports governing bodies have uniformly rejected the use of anabolic-androgenic steroids on the basis of ethics and the ideals of fair play of competition and because their use gives possible competitive advantage harmful to the user, the National Strength and Conditioning Association joins these sports governing bodies in condemning the use of anabolic-androgenic steroids by athletes.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 8 3
The Use of Anabolic-Androgenic Steroids in SportsBased on a comprehensive literature survey and a careful analysis of the claim concerning the ergogenic effects and the adverse effects of anabolic-androgenic steroids, it is the position of the American College of Sports Medicine that:1. Anabolic-androgenic steroids in the presence of an adequate diet can contribute to increases in body weight, often in the lean mass compartment.2. The gains in muscular strength achieved through high- intensity exercise and proper diet can be increased by the use of anabolic-androgenic steroids in some individuals.3. Anabolic-androgenic steroids do not increase aerobic power or capacity for muscular exercise.4. Anabolic-androgenic steroids have been associated with adverse effects on the liver, cardiovascular system, reproductive system, and psychological status in therapeutic trials and in limited research on athletes. Until further research is completed, the potential hazard of the of the anabolic-androgenic steroids in athletes must include those found in therapeutic trials.5. The use of anabolic-androgenic steroids by athletesis contrary to the rules and ethical principles of athletic competition as set forth by many of the sports governing bodies. The American College of Sports Medicine supports these ethical principles and deplores the use of anabolic- androgenic steroids by athletes.
This document is a revision of the 1977 position stand of the American College of Sports Medicine concerning anabolic-androgenic steroids.Background
In 1935 the long-suspected positive effect of androgens on protein anabolism was documented. Subsequently, this effect was confirmed, and the development of 19 nortestosterone heralded the synthesis of steroids that have greater anabolic properties than natural testosterone but less of its virilizing effect. The use of androgenic steroids by athletes began in the early 1950s and has increased through the years, despite warnings about potential adverse reactions and the banning of these substances by sports governing bodies.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 8 4
ANABOLIC-ANDROGENIC STEROIDS. BODY COMPOSITION AND ATHLETIC PERFORMANCE
Body composition. Animal studies investigating the effect of anabolic-androgenic steroids on body composition have shown increases in lean body mass, nitrogen retention and muscle growth in castrated males and normal females.The effect of anabolic-androgenic steroids on body weights or normal, untrained, male animals, treadmill-trained or isometrically-trained rates, or strength-trained monkeys have been minimal to absent; however, the effects of steroids on animals undergoing heavy resistance training have not been adequately studied. Human males who are deficient in natural androgens by castration or other causes have shown significant increases in nitrogen retention and muscular development with anabolic-androgenic steroids therapy. Human males and females involved in experimental and therapeutic trials of anabolic steroids have shown increases in body weight.
The majority of the strength-training studies in which body weight was reported showed greater increases in weight under steroid treatment than under placebo. The weight gained was determined to be lean body mass in three studies that made this determination with hydrostatic weighing techniques. Four other studies found no significant differences in lean body mass between steroid and placebo treatments, but in two of those the mean difference favored the steroid treatment. The extent to which increased water retention accounts for steroid-induced changes in body composition is controversial and has yet to be resolved.
In summary, anabolic-androgenic steroids can contribute to an increase in body weight in the lean mass compartment of the body. The amount of weight gained in the training studies has been small but statically significant.
Muscular strength. Strength is an important factor in many athletic events. The literature concerning the efficacy of anabolic steroids for promoting strength development is controversial. Many factors contribute to the development of strength, including heredity, intensity of training, diet, and the status of the psyche. It is very difficult to control all of these factors in an experimental design. The additional variable of dosage is included when drug research is undertaken. Some athletes claim that doses greater than therapeutic are necessary for strength gains even though positive results have been reported using therapeutic (low-dose) regimen.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 8 5
ADVERSE EFFECTSAnabolic-androgenic steroids have been associated with
many undesirable or adverse effects in laboratory studies and therapeutic trials. The effects of major concern are those on the liver, cardiovascular, and reproductive systems, and on the psychological status of individuals who are using the anabolic-androgenic steroids.
Adverse effects on the liver. Impaired excretory function of the liver, resulting in jaundice, has been associated with anabolic-androgenic steroids in a number of therapeutic trials. The possible cause-and-effect nature of this association is strengthened by the observation of jaundice remission after discontinuance of the drug. In studies of athletes using anabolic androgenic steroids (65 athletes tested), no evidence of cholestasis has been found.
Structural changes in the liver following anabolic steroid treatment have been found in animals and in humans. Conclusions concerning the clinical significance of these changes on a short-long term basis have not been drawn. Investigations in athletes for these changes have not been performed, but there is no reason to believe that the athletes using anabolic-androgenic steroids is immune from these effects of the drugs.
The most serious liver complication associated with anabolic-androgenic steroids are peliosis hepatic (blood- filled cysts in the liver of unknown etiology) and liver tumors. Cases of peliosis hepatis have been reported in individuals treated with anabolic-androgenic steroids for various conditions. Rupture of the cysts or liver failure resulting from the condition is fatal in some individuals.In other case reports the condition was an incidental finding at autopsy. The possible cause-and-effect nature of the association between peliosis hepatis and the use of anabolic-androgenic steroids is strengthened by the observation of improvement in the condition in athletes using anabolic-androgenic steroids, but investigations specific for this disorder have not been performed in athletes.
Module VII - Applying the Information
♦ To provide opportunity for participants to discuss the implications that new information has in shaping activities on their base, from pre-treatment through relapse prevention.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 8 6
Time: Day 3 Day 4
Methodology:
3 1/2 hours 2 hours
Video\Discussion\ExperientialExercise
Outline: ►►
Video: "America in Jeopardy"Lecture: Relapse Prevention Planning
► ►Break (20 minutes) <■*Discussion Groups, Report out, Wrap-up
► Role Play: Conducting Interventions
Materials: Warning Signs of Relapse
Both the lecture and the video are a preface to a final exercise which will allow you to test the application of drug and alcohol information in Level I, II, and III programs. The final two hours of this module are completed on Day 4, and consist of role play on the intervention process.
Warning Signs of RelapsePhase I. Return of Denial
1. Concern about well-being2. Denial of concerns.
Phase II. Avoidance & Defensive Behavior.3. Believing I'll never drink/drug again. Loss
of one day at a time focus.4. Worrying about others instead of self.5. Defensiveness. Especially when not necessary.6. Compulsive behavior.7. Impulsive behavior.8. Tendency toward loneliness.
Phase III. Crisis Building9. Tunnel vision.10. Minor depression.11. Loss of constructive planning.12. Plans begin to fail.
Phase IV. Immobilization13. Daydreaming & wishful thinking.14. Feelings that nothing can be solved.15. Immature wish to be happy. Vague desires.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 8 7
Phase V. Confusion & Overreaction16. Periods of confusion.17. Irritation with friends.18. Easily angered.
Phase V I . Depression19. Irregular eating habits.20. Lack of desire to take action.21. Irregular sleeping habits.22. Loss of daily structure.23. Periods of deep depression.
Phase VII. Behavioral Loss of Control.24. Irregular attendance at AA/NA meetings.25. Development of "I don't care attitude."26. Open rejection of help.27. Dissatisfaction with life.28. Feelings of powerlessness & Helplessness.
Phase VIII. Recognition of Loss of Control29. Self pity.30. Thoughts of social drinking/drugging.31. Conscious lying.
Phase IX. Option Reduction.32. Complete loss of self-confidence.33. Unreasonable resentments.34. Discontinues all AA/NA meetings.35. Overwhelming loneliness, frustration, & anger
Phase X. Acute Relapse Episodes36. Loss of behavioral control in all areas of
life.37. Relapse episodes.
Module VIII - Understanding NutritionIn Recovery
Student Oriented Objectives
♦ To discuss nutrition and recovery.♦ To discuss personal recovery issues.♦ To discuss 12-step meetings and attendance at them.
Time: 5 1/2 hrsMethodology: Lecture/Discussion/PanelOutline: ► Discuss Impressions of 12-step Programs
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 8 8
► Lecture/Discuss Relapse Process andPrevention: Biological,Psychological
Materials: ► Nutrition: Relationship toAddiction/Recovery
► Dietary factors in preventing & treating addictions
► Our love affair with sugar► Books for developing a nutritional
recovery program► Overview of Addiction and Nutrition► Hypoglycemia: A Response to
ImbalanceMCO P5300.12 gives specific guidance to Commanders and SACOs to help them manage the aftercare of Marines "restored to full duty," who have completed treatment. Good management of Biochemical imbalances such as hypoglycemia is an aspect of a good aftercare/recovery program.Module X: Understanding Recovery, is introduced during the afternoon of Day 4 and is completed on the morning of Day 5. The first section deals with nutritional aspects of recovery.The panel of recovering alcoholics, 3-5 local Marines who are willing to discuss their recovery in the Marine Corps, is the last content module of the course. It is through hearing their stories and asking questions that participants can integrate the information they have received during the week.
Nutrition; Its Relationship to Addiction and RecoveryIncreasingly, drug addiction recovery programs are including nutritional support as an important aspect of recovery.Some even suggest that there exist nutritional deficits prior to addiction and prescribe improved diet and nutrition to prevent relapse. Peter Bell at the Minnesota Institute on Black Chemical Abuse strongly urges even prevention programs to include research on nutritional and chemical imbalance.There is little disagreement on the fact that most recovering people increase their intake of sugar, caffeine, and nicotine to alarming levels to manage the depression and low energy of recovery, due in part to the common condition in recovery, hypoglycemia. These drug increases, however, manage rather to exacerbate the existing depression and low energy and lead to further nutritional deficits.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 8 9
The theory behind these findings and proposals is that a critical factor in both becoming addicted and in recovering from addiction is the functioning of significant neurotransmitters in the brain — those neurotransmitters which regulate mood, energy and feelings. Those methods which best restore the functioning of these neurotransmitters are the most important to include in a treatment program. Increased nutrient intake has been shown to begin the restoration process (as has ear acupuncture).There have been several studies on the relationship of nutrition to recovery. Dr. Janice Phelps, in Washington state, divided patients in an inpatient treatment program into two groups: those receiving the standard inpatientprogram; and, those receiving the standard program, plus nutritional education and supplements. At the end of six months, 33% of the former group, and 81% of the latter group, were sober.Scientists at MATRIX Technologies in Houston, Texas have shown that recovery from the abuse of alcohol, cocaine and other drugs is helped significantly by using naturally occurring food-based nutrients to restore brain chemical deficits. The neuronutrients reduce the rate of inpatients leaving the treatment program against medical advice (AMA), drug craving, withdrawal tremors, and the need for tranquilizer medication.This is a very needed step in a direction that provides some consistency between our understandings of these diseases and the treatments we provide them. If we know these diseases to be biological in nature, then it might be appropriate to seek biological answers for solving the problem. However, our ability to manufacture needed neurotransmitters probably requires more than a few nutrients in a pill; we need to return to eating in the manner that nature designed.Nutrients are best absorbed from foods, not pills. These foods, however, have to be as fresh and free of chemicals as possible and they need to be eaten as nature provided them. Why is this? Because, when we eat foods that are grown and stored with the more than 500 approved chemicals on them (chemicals for preserving, retarding ripening, coloring, etc.), our bodies must use up valuable nutrients in order to detoxify these poisons out of the body. These are valuable nutrients that the body can use for making the needed levels of neurotransmitters in the brain!! As foods are picked, cooked, and packaged, they lose nutrients. Additionally, many of the packaged foods we eat are artificially made. We even eat artificial crab today.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 9 0
Here is the way in which our species utilize nutrients. The DNA for the human species (much like a computer disk, with finite space) does not include much space for making vitamins, minerals, amino acids, and essential fatty acids. Our DNA contains higher order programs — programs for making various proteins in the body that determine our functioning. What this means is that we must eat the vitamins, minerals, amino acids, and essential fatty acids in order for these programs to work. The manufacture of proteins, such as the neurotransmitters, requires all of these elements. It is thought that there are at least 40 such "essential" elements. "Essential" means that the capacity to reproduce is dependent upon these nutrients. Animals, fish, and plants in our environment provide these nutrients. The difficulty in these "modern" times is that we are no longer eating these nutrients in the quantities intended for making the proteins we need. This is a very serious problem, leading to many degenerative diseases in our species and recently observed brain dysfunction, such as alzheimer's disease, MS, lupus, etc. This condition may also be part of the explanation for the high level of addiction in our species today. Remember: craving for orinterest in external drugs appears to be related to the level of the internal drugs (neurotransmitters); neurotransmitters are manufactured from the 40 essential nutrients we consume through eating plants, animals, fish, seeds and nuts, legumes, and whole grains.Studies during the 20's and 30's of this century by Dr.Price provided evidence that our ancestors ate very differently than we do today: they ate 'unsophisticated'food in nature's packages; and, they consumed 5 to 20 times the nutrients which our modern nutritionists recommend. To make matters worse, the American Cancer Society has shown, through food surveys, that only 9% of our population consume what is recommended.While not an answer for all of our problems, we need to concern ourself with the overall functioning of our species, with "brain health". And this means protecting our environment so that needed foods are available! Such an understanding and approach would certainly add immeasurably to our ability to prevent substance abuse and our ability to treat those with the problem of addiction.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 9 1
Our Love Affair With SugarGayle R. Hamilton, Ph.D.
Sugar is accepted by many today as a stimulant drug. That is, it stimulates the central nervous system; some people respond to it addictively; and, there is usually some withdrawal syndrome if its use is suddenly discontinued.It is associated medically with diabetes, hypoglycemia, loss of bone minerals, and high cholesterol levels, as well as numerous behavioral problems.Our ancestors ate no refined sugar, but we are certainly making up for lost time! At the turn of the century, we consumed roughly 8 pounds of sugar per person per year. Today, we consume roughly 130 (13 teaspoons per day) pounds of sugar per person per year. One Nutritionist who works with youth offenders (Reed, 1982), says that the average dose of sugar for teenagers per day is 36 teaspoons. Note that this estimate was given 10 years ago and is surely much higher now.There is an additional major concern, however, with its effect on brain energy. The brain needs about 3 teaspoons of circulating glucose at any time. Our systems are set up to obtain that glucose from the complex carbohydrates that we eat. Instead, when we eat sugar, the body doesn't have to work to obtained the glucose — it is broken down already, into sucrose.What this situation does is bring about panic in the pancreas whose job it is to take excess glucose from the system and store it in the liver. In its panic, the pancreas releases too much insulin, thereby reducing the glucose to dangerously low levels. Glucose is so important for the brain that we can only live for four minutes without glucose on the brain without going into a coma. This low glucose condition also creates a crisis in the body! The adrenals now send out an S.O.S. to the liver, telling it to get some of the stored glycogen out of storage and up to the brain — pronto! This high and low glucose cycle is called hypoglycemia.When the glucose is low, the brain becomes starved and shuts down the frontal lobes — the area responsible for thought, learning, social, and moral behavior. The little glucose available is then reserved for the survival instincts (food and sex, aggressive instincts, and vital functions). This situation, then, gives primacy to aggressive and sexual behavior, exactly what is seen in the behavior of our teenagers in trouble with the law. The coincidence between hypoglycemia and aggression, depression, and anxiety has
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

192
been thoroughly documented (Reed, 1982). Even so, there seems to be a tendency for physicians and many nutritionists to downplay its importance to everyday functioning.The primary principle to retain from our discussion of sugar is that it lowers the glucose in the brain, and this glucose is the primary fuel for the brain.
Books for Developing a Nutritional Recovery ProgramTHE HIDDEN ADDICTION AND HOW TO BE FREE
Janice Phelps, M.D. & Alan E. Nourse, M.D.Dr. Janice Helps is a physician whose private practice only serves addicted people. Her book is excellent and provides good guidelines for using nutrients to aid in the recovery process. It costs about $10.00 and can be obtained (ordered) from B. Dalton. Besides useful recovery information, it provides a scale which tests one's addictiveness potential covering: Diet; Family History; Depression; Alcohol Use; and Drug Use.Excerpts from BookAddiction and Sugar. She contrasts two types of people: those who eat some sugar-food and then feels satisfied for a prolonged period of time; and, those who eat same food, but immediately want more. Instead of being quieted, this physiological hunger is stimulated, sometimes turning into a binge.At MIT's Laboratory of Neuroendocrine Regulation, they have discovered that, in normal people, serotonin is released by cells deep in the brain after we have eaten a meal rich in sugars. Once released, this serotonin induces sleepiness, decreases sensitivity to pain, and suppresses the appetite for more carbohydrates. In some people, this carbohydrate- serotonin feedback mechanism may not work properly. No one yet knows why.Addiction and other drugs. Similar appetite distortions probably occur with the other neurotransmitters, creating an unfillable appetite for these drugs as well. That is, use creates the obsession to use.Addiction and Depression. She tests most of her clients for depression and finds that about one-third manifest biological depression. Most can be treated by diet alone. However, some need medication. Many may need antidepressants at the very beginning in order to provide
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 9 3
sufficient energy to start the recovery process and cooperate with treatment.Treatment ProgramThe foundation of her treatment program is nutrition! It emphasizes:
► Frequent sugar-free feedings to stabilize blood sugar;
► Large doses of vitamins and minerals to reverse the body's long-standing depression;
► Nutritious foods to counteract malnutrition;► Detoxification through the use of Vitamin C.
DetoxificationShe uses large amounts of Vitamin C. It is a safe detoxifier, it eliminates of modifies the withdrawal symptoms, and it is a powerful aid in rebuilding nutritional status. It is used in crystalline or powder form. She recommends taking 1 teaspoon (4000 mg) every tow to four hours while awake for three to seven days. This helps enormously with craving. She provides ordering information in her book.Restoring vitamin and mineral deficiencyShe provides supplements called Nutrabalance provided by JCM research (see her book).Body-building raw materialsClients need extra protein during withdrawal to help repair damaged tissues, particularly those of the brain. She suggest that, in addition to good foods, they need a protein powder made from mild protein with no extra sweeteners.This helps stabilize blood sugar.Specific symptomatic treatmentShe provides specific supplements for nervousness and agitation, for depression, for poor stress responses, for trouble sleeping, and for curbing craving for alcohol, drugs, and sugar.Frequent feedingsStop eating sugar foods. Eat three meals per day plus three snacks in mid-morning, mid-afternoon, and evening. Eat the foods that have been advocated throughout this material: whole grains, fresh fruits and vegetables, cheese, milk, and fish.NOTE: It is important to add nuts and seeds, raw andunsalted. These help the body make protein and aid in repair of the brain. It is also valuable to take extra lecithin, which you can get at the health food store and put
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 9 4
in juice. Lecithin actually makes up about a third of the brain mass.There are two additional books that provide more excellent about nutrition and recovery. They are:e a t i n g RIGHT TO LIVE SOBER: Katherine Ketcham & AnnMueller, M.D.A good diet will also control blood-sugar problems, restore chemical balance, and prevent such symptoms as depression, irritability, shakiness, headaches, and mental confusion. Otherwise, the addiction will remain in control Avoid sweets. Eat lots of nutrients: essential amino acids; essential fatty acids; minerals; vitamins. Avoid caffeine - - a damaged liver may make caffeine accumulate to toxic levels.RECOVERY FROM ADDICTION: John Finnegan and Daphne GrayAddiction leads to severe glandular weakness and nutritional deficiencies which it takes several months to correct. The book provides detailed descriptions of whole foods and medicinal herbs that are useful in restoring metabolic imbalances. However, it is more complicated then the proscriptions of the two foods above. An advantage of this book is that there are many nutritious recipes in the back.
Treatment of Addiction and Food Disorders with Nutrient Supplements
Excerpt from: Leoblich, Laurel. "Phencal for Overeaters". Matrix Today; New and Information from MATRIX Technologies. Inc.. a Subsidiary of NeuroGenesis. Inc. Issue 3/October 1990.Scientists at MATRIX Technologies in Houston Texas have shown that recovery from the abuse of alcohol, cocaine and other drugs is helped significantly by using naturally occurring food-based nutrients to restore brain chemical deficits. The neuronutrients reduce the rate of inpatients leaving the treatment program against medical advice (AMA), as well as drug craving, withdrawal tremors, and the need for tranquilizer medication.Neurotransmitters (brain chemicals) also have been shown to play a significant role in controlling amount of food eaten, as well as craving for specific foods. These findings have led to studies to determine if eating disorders can also be treated with nutrient therapy. The nutrients used are intended to modify the making of and release of, key neurotransmitters known to be associated with food
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 9 5
disorders. There have been two studies with a nutrient formula, PCAL-103, developed by MATRIX Technologies in Texas. In the smaller study, 27 overeaters with a history of bingeing on sugar lost 27 pounds over a 90-day period while the control not on PCAL-103 lost only 10 pounds. In the larger study of 247 overeaters, half were put on PCAL- 103 after losing their desired weight and half were not given the supplement. At the end of two years, the overeaters who had been given PCAL-103 had regained 13.5% of their lost weight, had reduced binge eating, and had reduced food craving. The control group had regained 51% of their lost weight, had no reduction in craving, and had about 3 times the food binges that those on PCAL-103 had.Matric Labs has an 800 where these products can be ordered either for your person use or for that of your clients: 1-800-345-9012
REFERENCE LIST1. Airola, Paavo. Hypoglycemia: A Better Approach.
Phoenix: Health Plus Publishers, 1977.2. Birch, Herbert and Gussow, Joan. Disadvantaged
Children. Health. Nutrition and School Failure. 1970.3. Conners, Keith C. Feeding the Brain: How Foods Affect
Children. New York: Plenum press, 1989.4. Crawford, M. & March, D. The Driving Force: Food.
Evolution and the Future. New York: Harper and Row, Publisher, 1989.
5. Davis, Adelle. Let's Get Well. Signet, 1972. (Old,but excellent.)
6. Dohan, F.C. "Wartime changes in admission for Schizophrenia." Acta Psychiatric Scandinavia. 42, 1966, p. 125.
7. Doll, R., Muir, C. & Waterhouse, J. Cancer incidence in Five Countries. New York, Springer-Verlag, 1968.
8. Doyle, W., Crawford, M.A. & Laurance, B.M. "Dietary survey during pregnancy in low socio-economic group.In J of Human Nutrition. 36A: 95-1061982.
9. Finnegan, John & Gray, Daphne. Recovery fromAddiction: A Comprehensive Understanding of SubstanceAbuse With Nutritional Therapies for Recovering Addicts and Co-dependents. Berkeley, CA: Celestial Arts, 1990.
10. Hornstra, G. et al, 1989. Was in press at the time of writing this book.
11. Ketcham, Katherine & Mueller, Ann, M.D. Eating Right to live Sober. Signet, 1986.
12. McCarrison, R. Nutrition and Health. London, Faber & Faber/McCarrison Society. 1953.
13. Miller, Saul & Miller, Jo Anne. Food for Thought: aNew Look at Food and Behavior. New Jersey: Prentice-Hall, 1979.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 9 6
14. Nubold, H.L., M.D. Mega-Nutrients for Your Nerves. H.L. Nubold, M.D., Berkley Publishing Corporation, 1980.
15. Phelps, J., M.D. The Hidden Addiction and How to Be Free. 1988. Excellent overview of all addictions; includes an addictiveness questionnaire.
16. Price, Weston A. Nutrition and Physical Degeneration.La Mesa CA, The Price Pottinger Nutrition Foundation, Inc. 1938. Can order from the Foundation: P.O. Box2614, La Mesa, CA 92044; 619-582-4168: $29.00
17. Rojas, N. and Sanchi, A.F. Archives of Legal Medicine.11, p. 29, 1941. Reported in Natural health. Sugar and the Criminal Mind, by J.I. Rodale, New York: PyramidBooks, 1968.
18. Smithels, R.W. Shepherd, S. & Schorah, S.J. "Possible prevent of neuraltube defects by preconceptual vitamin supplementation. In Lancet. i:339, 1980.
19. Williams, R. Nutrition Against Disease. N.Y.: Pitman, 1971.
20. Winick, Myron. Malnutrition and Brain Development. 1983.
21. Yudkin, John. Pure White and Deadly. London Davis-Poynter, 1972. Also, The Penguin Encyclopedia of Nutrition. London, Penguin., 1985.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

197
EATING/FOOD DISORDERS
1. COMPULSIVE OVEREATING (Bulemia- craving for food)
Obesity
THEORIES
Psychosocial
Bulemarexia (binging and purging)
Dr. Gayle R. Hamilton, D.A.T.A
2. STARVING
Anorexia Nervosa(nearly half develop bulamarexia)
No will power* Overemphasis on thinnessWants to draw attention Loathing of body
to self Need for perfectionWants to distanoe self Need for control
Society's emphasis on thinness
History of sexual abuse .
Biological
Endorphin high from both overeating and starving.Imbalance in neurotransmitters, both as a cause of the food disorder and as a response to the food disorder.Lack of satiety inhibition, that is, those who crave foods, or overeat, have been shown not to satiate on the taste of sucrose.Hypothalamic diseases, such as an imbalance in the food-regulating nuclei of the hypothalamus.Allergies (now called food addictions because one of the manifestations of food allergies is craving for the allergie substance).Chemical allergies, which may produce food cravings after exposure.General nutritional imbalances, which make the body feel that it is starving (which it is).
COMPLICATIONS of Starving and PurgingDehydrationElectrolyte disturbancesLow potassiumCardiovascular and kidney failure
Nutritional Disorders Cessation of menses Salivary gland enlargement Dental enamel erosion
NOTE: At present, those most susceptible to bulemarexia and anorexia nervosaare white, middle class, adolescent women in their 20's, with strong values toward academic achievement and traditional lifestyles.Obesity appears to be distributed more evenly among the sexes and races.
•NOTE O N WILLPOWER- The concept of willpower is still being used today to explain avariety of phenomenon. It has helped no one. The "will" to do is a function of the balance of body/m ind/spirit. With imbalance, we cannot "do". It is not something w e call forth.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

198
HYPOGLYCEMIA:A RESPONSE TO IMBALANCE
A VIEW OF INCREASING DEPENDENCE
PANCREAS. vs aNsuEnsr*HIGH GLUCOSE
LOW GLUCOSE
ADRENALGLANDS
When too much sugar goes into the system, the Pancreas panics. Then blood sugar falls.
The Adrenals then panic, sending an S.O.S. to the liver to get Glycogen converted to glucose and up to the brain.
Cigarettes, caffeine, and other drugs prod the liver to work faster, thus more quickly sending up the blood sugar.
Soon we need an increasing number of drugs to manage our glucose levels - Alcohol, morning coffee, cigarettes, and then —
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

1 9 9
Day 4
For each day's work at the seminar, please circle the number, Module by Module, that best represents how valuable you consider the information. Please feel free to write additional comments on the back of the page.
Module VI: Physiological & Sociological Implicationsof Drug Use
Not Valuable 1 2 3 4 5 Very ValuableHow can this module be improved?____________________________
Module VII: Applying the InformationNot Valuable 1 2 3 4 5 Very ValuableHow can this module be improved?____________________________
Module VIII: Understanding Nutrition in RecoveryNot Valuable 1 2 3 4 5 Very ValuableHow can this module be improved?____________________________
DAY 5 - FRIDAY MODULE IX
Discuss 12 Step MeetingTime: 08:00 - 09:30
Panel Individual Stories
Question and Answer Period Time: 09:30 - 11:30
Wrap Up and Evaluations Day 5
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

2 0 0
For each day's work at the seminar, please circle the number, Module by Module, that best represents how valuable you consider the information. Please feel free to write additional comments on the back of the page.
Module VIII USMC Recovery ProgramsNot Valuable 1 2 3 4 5 Very ValuableHow can this module be improved?___________________________
General Evaluation FormFor each item pertaining to the seminar, please circle the number that best represents your experience in the seminar. In each category the lowest score is 1 (one) and the highest is 5 (five). Please feel free to write additional comments on the back of the page.
1. How did you rate our Video/Library in terms of usefulness to Marines in your unit?
Not Valuable 1 2 3 4 5 Very ValuableHow can this module be improved?____________________________
2. Were Trainers prepared?Not Very Well 1 2 3 4 5 Very WellHow can this module be improved?:______________________
3. Were materials presented clearly, with humor and in an interesting fashion?
Not Very Well 1 2 3 4 5 Very WellHow can this module be improved?:_____________________________
4. Were the variety of techniques used sufficient (Video, Role Play, etc.)?
Not Sufficient 1 2 3 4 5 Very SufficientHow can this module be improved?:______________________________
5. Will you find materials in the workbook useful in your
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

2 0 1
command?Not Valuable 1 2 3 4 5 Very ValuableHow can this module be improved?:___________________________
6. Were Seminar leaders knowledgeable?Not Very 1 2 3 4 5 Very Much SoHow can this module be improved?:_________________________
7. Were training staff helpful with administrative and logistical matters?
Not Very 1 2 3 4 5 Very Much SoHow can this module be improved?:_________________________
8. Did you feel that training rooms were comfortable and conducive to learning?
Not Very 1 2 3 4 5 Very Much SoHow can this module be improved?:____________________________
9. How do you rate the facilities in general?Poor 1 2 3 4 5 Excellent
How can this module be improved?:_______________________
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

APPENDIX B STUDY INSTRUMENTS
202
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

2 0 3
DEMOGRAPHIC INFORMATION INVENTORY DIRECTIONS: Place an X on the blank before the selection which best describes you.1. Last Four Digits of SSN: _________________
(To match pre-test and post-test results, not for individual identification.)2. Gender
Male Female
3. Age Under 25 25 - 30 31 - 35 36 - 40 Over 40
4. Education Non High School Grad GED HSG Associates Degree Bachelors Degree Masters Degree
5. Paygrade E-6 - E-7 E-8 - E-9 0-1 - 0-3 0-4 0-5 - 0-7 Other
6. Previous experience with the Marine Corps Substance Abuse Program: Level I SACO Level II SACO Level II Program Director Substance Abuse Counselor Other (specify):_________________________
7. Considering the alternatives below, indicate your perception of the confidentiality of the Marine Corps Substance Abuse Program. Very confidential Somewhat confidential Neutral Not very confidential Not at all confidential
8. Considering the alternatives below, indicate your perception of the competence of Marine Corps Substance Abuse Program staff (SACOs, Program Directors, Counselors, etc.) Very competent Somewhat competent Neutral Not very competent Not at all competent
9. Considering the alternatives below, indicate your perception of the effectiveness of the Marine Corps Substance Abuse Program to help Marines overcome alcohol problems. Very effective Somewhat effective Neutral Not very effective Not at all effective
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

2 0 4
10. Considering the alternatives below, indicate your perception of command support for the Marine Corps Substance Abuse Program. Very supportive Somewhat supportive Neutral Not very supportive Not at all supportive
BAKER KNOWLEDGE INVENTORY
This questionnaire will test your knowledge of various aspects of the Marine Corps Substance AbuseProgram. Both multiple choice and true/false questions will be asked.DIRECTIONS: Indicate your choice by circling the letter which represents your selection.1. All of the following are examples of legal alcohol abuse deterrent measures except:
a) To conduct vehicle checks on all vehicles entering the front gate between the hours of 2000and 0300 on Friday night
b) To conduct a search for beer in the barracksc) To have military police cruise the base looking for moving vehicle violationsd) To conduct periodic health and welfare inspections of the barracks
2. Vehicle checks for possible DUI (Driving While Intoxicated) should be all of the following except:a) Randomb) Unannouncedc) Exclusive of Officers and Staff NCO'sd) Conducted at all points of entry
T F 3. Marines participating in both Level II and Level III alcohol treatment programs arerequired to take antabuse.
A. Which of the following should not be noted in a Marine's fitness report:a) Periods of hospitalization for the treatment of alcoholism dependencyb) Comments concerning alcohol abuse's effect on performancec) Failure to successfully complete a formal alcohol treatment programd) Return to responsible use of alcohol following alcohol treatment
T F 5. Attendance in an alcohol treatment program automatically precludes participation in thePersonnel Reliability Program (PRP).
6. After Level III treatment for alcoholism, a Marine's commander should do all the following except:a) Return the Marine to his former duties and responsibilitiesb) Support his attendance at AA meetingsc) Make sure he's not drinkingd) Ensure he participates in an aftercare program
T F 7. Each Marine Corps command is required to conduct supervisor level substance abusetraining at least annually.
8. A Level I Program is manned by a Substance Abuse Control Officer (SACO) who may be responsible for any of the following functions except:a) Alcohol abuse screeningb) Alcoholism treatmentc) Preventive substance abuse educationd) Maintaining records on each Marine who is involved in an alcohol related incident
T F 9. Though it is not condoned, following Level III treatment for alcoholism, a Marine mayreturn to responsible social drinking without suffering any disciplinary action.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

2 0 5
10. A Level II program is manned by substance abuse counselors (MOS 8538) who may be responsible for any of the following functions except:
a) Alcoholism treatmentb) Indepth evaluation and screening of Marines for alcohol related problemsc) Aftercare Program Managementd) Arrange medical evaluation for any Marine suspected of being alcohol or drug dependent
T F 11. Early intervention into a Marine's alcohol abuse is important because alcoholism is a progressive disease and the problem will probably get worse with time.
12. The director of a Level II program must be all of the following except:a) Assigned in writingb) Trained within 6 months of assignmentc) A commissioned or warrant officerd) A recovering alcoholic
T F 13. Disclosure of information made by a Marine during alcohol screening, counselingor treatment relating to past alcohol abuse is considered confidential providing the disclosure is made for the express purpose of seeking counseling, treatment or rehabilitation.
14. A medical officer's opinion is required for all of the following actions except:a) Assignment to a 12 Step programb) Diagnosis of alcohol dependencyc) Assignment to a Level III programd) Alcohol detoxification
T F 15. The Director of a Level II Program can call him/herself an alcohol/drug counselor ifhe/she possesses a degree in counseling or psychology.
16. A Level III treatment program may be all of the following except:a) 4 to 6 weeks in lengthb) Attended by a Marine's dependents on a space available basisc) Conducted on an outpatient basisd) Conducted at a Naval Medical Treatment Facility
T F 17. A Marine who is diagnosed as being alcohol dependent will not be available fordeployment until completion of Level III treatment.
18. A Marine will be placed in an aftercare status for ___ months following completion of Level IIIalcohol treatment:a) 6b) 12c) 2d) 9
T F 19. A Marine who has a problem with alcohol will exhibit poor rather than stellarperformance.
T F 20. Without adequate documentation, an alcoholism intervention will most likely fail.T F 21. If a Marine denies he has a problem with alcohol, you should believe him.22. The major thrust of the Marine Corps' policy toward the abuse of alcohol is:
a) Make individual Marines responsible for their actionsb) Make commanders responsible for the actions of their Marinesc) Discharge alcohol abusers as quickly as possibled) Deny alcohol abuse is a problem in the Marine Corps
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

2 0 6
23. Disclosure of confidential substance abuse files is permitted in all of the following cases, except:a) When the Marine gives written consent for disclosureb) When the Commanding Officer needs the information for matters pertaining directly to the
individual whose case is being requestedc) When the Adjutant needs the information to complete administrative documentsd) When the Medical Officer at the treatment facility needs them for diagnostic purposes
T F 24. A Commander may decide not to send a Marine, diagnosed alcohol dependent, to Level IIItreatment.
T F 25. Following screening by the Unit SACO, Level I action for alcohol abusers may include agood chewing out by the CO.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

APPENDIX C STUDY CORRESPONDENCE
207
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.
HAVMC HQ-33S (REV 5-09) 208
2. CPCRATIOM CODE
X • ORIGINATOR Of OFFICE AFFIXING ROUTING SHEET
A • APPROPRIATE ACTION S • GUIDANCE C • SIGNATURE D • CCHMENT E • RCCOKHEMOATION F ■ CONCURRENCE
C - INFORMATION N • RETURN TO HN_
CSB ROOM ___^INITIAL DISPOSITION OECTSION RETENTION
I •
0 • (OTHER)
ROUTING * Use nutters to show order of routing
G.ITC.
5.0P#| 6. AD0RESSEES CODE
7. OATEIN | OUT
8 . INITIALSCONCUR iNOMCOHnn
• t t t ICOMMANDANT CMC 1 1‘/ / / I 1 MILITARY SECY | | 1• m \V/ / I
ASST COMMANOANT I ACMCCHIEF OF STAFF
l SECY GEN STAFF SGS1 1 OIR SPL PROJ SPO 1 1 1 11 IOC/S HERA MIRA 1 1 1 1
DC/S III IOC/S PPIO P
I IOC/S AVM A | | | || IOC/S U P IP 1 I I1 AC/S CGI CGI1 FOHC FOI ISJA TO CMC JA 1 I I II ILEGIS ASST OLA 1 1 11 OIR PA PA1 DIR AR ARI 101R MCHlM NO I 11 1ONICMC 1C 1 11 COUNSEL FOR CMC a
"1 MEO OFF KEO1 tOEV OFF OEM 1 1 11 1 CHAPLAIN REl 1 1 1
iMClffl NCUB 1 1K gtkajkarcor SGTMAJI
1CG MCCDC MCCDC 1
1 COMMARCORSYSCOM1 CO H08NI ICO MARBCS 1 1 II I I I I
MIRA DEPARTMENT ROUTINGI IMPR ANAL E I C KA 1 11 OIR PERS MCT OIV t * 1 11 OIR HPR PINIPOL MP | | | |1 OIR PERS PROC OIV MR1 OIR HPRHGMTtHFOSYS Ml — '1 OIR MUR SPT ACTT MU 1
AUTHORIZATION TO USE KH D IV ISIO N PERSONNEL IN SUBSTANCE ABUSE STUDY
V. NATURE Of ACTION REQUIRS)
ORIGINATOR'SINITIALS
OUE OAIE (if »ny)
10.RCFEKEXCES HELD IT(N»tfte,Grade,Off ice Code, Telephone est)
J.H. MCHUGH, MHH
IPIR RES AFf 01V
H U A HLKAJ RESOURCES D IV IS IO N R INC (KH)
OIRECTORDEPUTY OIRECTORDIVISION AOMIN
IBUOCCT OFFICERIcoat g»
HKE \FOUAt QPTT BRFAN PROGS BR
ALCH BRNIL AVROS BRPERS AFF BRSAFETY BR
11.REKARCS AM) SICHATURE (If additional space is necessary, attach plain paper)
1. Purpose. To obtain authorization to use MH Division personnel in a substance abuse study.2. Background
a. The Drug, Alcohol and Health Affairs Branch is working on a study which will evaluate the effects of the Jr/Sr Substance Abuse Awareness Course on Marines' knowledge and perceptions of the Marine Corps Substance Abuse Program.
b. Participants in the Jr/Sr Course will comprise the experimental group. The participants will be surveyed prior to and immediately„ ter the Jr/Sr Course. Their "responses will be computed and analyzed to determine what impact, if any, pie course has on their knowledge and perceptions of the Maripe Corps Substance Abuse Program.
c. In order to add credibility to the study, a control group will also be surveyed. The control group will be surveyed and then
M- MH-
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

209
Subj: AUTHORIZATION TO USE MH DIVISION PERSONNEL IN DRUG ANDALCOHOL RESEARCH PROJECT
resurveyed three weeks later, without attending any substance abuse education in the interim.
d. Marines from the MH Division would be a convenient and representative population from which to draw control group subjects. Approximately 70 subjects will be needed. Subjects would be randomly selected from a roster of MH Division personnel.
e. Participation in the control group survey would require approximately 15 - 20 minutes of each member's time, twice within a three week period.
f. The study instrument is attached (TAB A). The instrument will be hand delivered to and picked up from each control group participant. Confidentiality will be protected by using only the last four digits of the social security number for identification purposes. Study results will be reported in groups. No individual results will be divulged.
g. The study will emphasize how the training changes Marines' perceptions of the Marine Corps Substance Abuse Program, if it does. Whether Marines generally hold positive or negative perceptions of the program is not a main consideration of the study.3. Action. That authorization be granted to use MH Division personnel in the study, and that a roster of personnel be provided to MHH for subject selection so the study can commence in January 1993.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

BIBLIO G RAPHY
Anderson, S. B., & Ball, S. (1978). The profession and practice of program evaluation. San Francisco: Jossey-Bass.
Bayer, G. A., & Gerstein, L. H. (1988). An adaptation of models of prosocial behavior to supervisor interventions with troubled employees. Journal of Applied Social Psychology. 18(1), 23-37.
Beary, J. F., Mazzuchi, J. F., & Richie, S. I. (1983).Drug abuse in the military: An adolescent misbehaviorproblem. Journal of Drug Education. 13(1), 83-93.
Belasco, J. A., & Trice, H. M. (1969). The assessment of change in training and therapy. New York: McGraw-Hill.
Bloom, S. (1987) . Employee assistance programs: Thestructure of counseling applications within organizational settings. Dissertation Abstracts International. 4£(4), 2269A-2270A. (University Microfilms No. 8712821)
Brownell, S. M. (1973) . Validated measurements of cost effectiveness in an alcoholism program. Labor Management and Alcoholism Journal. 7, 27-38.
Cannon, P. (1988). Drugs in the workplace: A discussionof issues (Informational Bulletin 88-1B-1). Madison, WI: Legislative Reference Bureau.
Cooke, G. (1975). Training paraprofessionals in the treatment of alcoholism. Journal of Studies on Alcohol. 36(7), 720-723.
DeRosa, C., & Zare, N. (1991, September). Supervisortraining may increase referrals. Employee Assistance, pp. 20-24; 42.
Feldman, S. (1991, February). Trust me: Earning employeeconfidence. Personnel. p. 7.
Freedberg, E. J., & Johnston, W. E. (1978). Effects ofvarious sources of coercion on outcome of treatment of alcoholism. Psychological Reports. 43. 1271-1278.
Gam, J., Sauser, W. I., Jr., Evans, K. L., & Lair, C. V.(1983). Implementing an employee assistance program. Journal of Employment Counselingf 20(2), 61-69.
210
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

2 1 1
Gerstein, L. H., & Bayer, G. A. (1988, February). Employee assistance programs: A systemic investigation of theiruse. Journal of Counseling and Development, pp. 294- 297.
Gerstein, L. H., Eichenhofer, D. J., Bayer, G. A., Valutis, W., & Jankowski, J. (1989). EAP referral training and supervisors' beliefs about troubled workers. Employee Assistance Quarterly. 4(4), 15-30.
Goodwin, D. W., David, D. H., & Robins, L. N. (1975).Drinking amid abundant illicit drugs: The Vietnamcase. Archives of General Psychiatry. 32., 230-233.
Googins, B. K. (1975). Employee Assistance Programs.Social Work. 20(6), 464-467.
Googins, B. K. (1979). The use and implementation ofoccupational alcoholism programs by supervisors: Ananalysis of barriers. (Doctoral dissertation, Brandeis University, 1979) . Dissertation Abstract on Disc. 1861-1980. (University Microfilms No. 79-22701)
Googins, B. K., Colan, N. B., & Schneider, R. J. (1989). Supervisor training in employee assistance programs. Research Presentations of the 18th Annual Conference of the Employee Assistance Professionals Association. 91-99.
Googins, B. K., & Kurtz, N. R. (1984). Discriminating participating and nonparticipating supervisors in occupational alcoholism programs. Journal of Drug Issues. 11(2), 199-216.
Harley, D. A. (1990a). Factors influencing supervisors'referrals to employee assistance programs. (Doctoral dissertation, Michigan State University, 1990). Dissertation Abstract on Disc. 1989-1991. (University Microfilms No. 90-11598)
Harley, D. A. (1990b, August). Impaired job performance and critical incidents: Factors influencingsupervisory EAP referrals. A Paper Presented at the 98th Annual Convention of the American Psychological Association, Boston, MA.
Harris, M. M., & Fennell, M. L. (1988). Perceptions of an employee assistance program and employees' willingness to participate. The Journal of Applied Behavioral Science. 24(4), 423-438.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

2 1 2
Hawthorne, W. B., & Davidson, B. N. (1983). Thealcoholic's supervisor: Another victim in need.Occupational Health and Safety. 52(2), 28-29.
Henderson, R., & Bacon, S. (1953). Problem drinking: TheYale Plan for business and industry. Quarterly Journal of Studies on Alcohol. 14, 247-262.
Heyman, M. (1976). Referral to alcoholism programs inindustry: Coercion, confrontation and choice. Journalof Studies on Alcohol. 37. 900-907.
Ingraham, L. H. (1978). The bovs in the barracks:Observations on American common soldiers in garrison. Washington, D.C.: Walter Reed Army Institute ofResearch.
Keegan, J. (1976). The face of battle. New York: Viking Press.
King-Kramer, M. M. (1990) . Behavioral cues that indicate the presence of debilitating issues which affect training programs, as perceived by training professionals. (Doctoral dissertation, Michigan State University, 1990). Dissertation Abstract on Disc. 1989-1991. (University Microfilms No. 90-02696)
Kinman, M., & Roman, P. (1982). EAP consultants in 1982:A profile. Labor and Management Journal on Alcoholism. 12, 65-76.
Levine, H. Z. (1985, April). Employee assistance programs, Personnel. 14-19.
Lotterhos, J. F., & Waldrop, J. H. (1972). A historical perspective of employee assistance programs.Investorv. North Carolina Department of Mental Health, 20, 24-28.
Love, G. A. (1989). Factors which influence supervisory referrals to industry-based employee assistance programs. (Doctoral dissertation, Vanderbilt University, 1989). Dissertation Abstract on Disc. 1989-1991. (University Microfilms No. 89-21127)
Machell, D. F. (1990). The lethality of the corporateimage to the recovering corporate executive alcoholic. Journal of Alcohol and Drug Education. 35. 1-5.
McClellan, K. (1982). An overview of occupationalalcoholism issues for the 80's. Journal of Drug Education. 12.(1) , 1-25.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

2 1 3
McKirnan, D. (1980). Community differences in conceptions of deviant behavior: An exploratory study of attitudestoward alcohol-related help sources. American Journal of Community Psychology. 8, 637-656.
Myers, D. W. (1984). Establishing and building employee assistance programs. Westport, CT: Quorum Books.
Nord, J. L. (1988). Predictors of supervisors' referrals of employees to an employee assistance program. (Doctoral dissertation, Iowa State University, 1988) . Dissertation Abstract on Disc. 1985-1988. (University Microfilms No. 88-09182)
O'Connell, V. C. (1987). A strategy for overcomingsupervisors' resistance. EAP Digest. 7(3), 63-66.
Older, H. J., Phillips, D. A., & Purvis, A. J. (1978). A new approach to the training of supervisors and union personnel. Labor-Management Alcoholism Journal. 8(1), 12-2 1 .
Phillips, D. A., & Older, H. J. (1977). A model forcounseling troubled supervisors. Alcohol Health and Research World. 1, 24-30.
Plavan, K.A. (1989). A descriptive study of significant characteristics and evaluation activities of employee assistance programs. (Doctoral dissertation,University of Pittsburgh, 1989). Dissertation Abstract on Disc. 1989-1991. (University Microfilms No. 90- 10055)
Pursch, J. A. (1976). From quonset hut to naval hospital: The story of an alcoholism rehabilitation service. Journal of Studies on Alcohol. 37(11), 1655-1666.
Ralfs, M., & Morley, J. (1990, November). Turning employee problems into triumphs. Training and Development Journal. pp. 73-76.
Roman, P. M. (1983). Employee assistance programs in australia and the united states: Comparisons oforigin, structure, and the role of behavioral science research. The Journal of Applied Behavioral Science. 19(3), 367-379.
Roman, P. M., & Trice, H. (1976). Alcohol abuse and workorganization. In B. Kissin and H. Begleiter (Eds.), The biology of alcoholism: Vol. 4. (445-517). New York: Pelenum Press.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

2 1 4
Schramm, C. J. (1977). Alcoholism and its treatment inindustry. Baltimore, MD: Johns Hopkins University Press.
Schramm, C. J., & Defillippi, R. J. (1975).Characteristics of successful alcoholism treatment programs for American workers. British Journal of Addiction. 70(3), 272-275.
Shain, M., & Groeneveld, J. (1980). Emplovee-assistanceprograms: Philosophy, theory, and practice. Lexington, MA: Lexington Books.
Sherwood, G. G., Davidson, P. 0., & Aharan, C. H. (1979). Constructive coercion: A comparison of treatmentresults with voluntary versus employer referred alcoholics. Proceeding of the 25th International Institute on the Prevention and Treatment of Alcoholism. Tours, France.
Shipp, T. (1984) . Financial evaluation of employee assistance programs. EAP Research, i, 110-112).
Shoemaker, G. L. (1983). Analysis of specific alcohol risk characteristics of participants in the United States Air Force Supervisor Alcohol Abuse Education.(Doctoral dissertation, The George Washington University, 1983). Dissertation Abstract on Disc. 1980-1984. (University Microfilms No. 83-24490)
Smart, R. (1974). Employed alcoholics treated voluntarily and under coercion. Quarterly Journal of Studies on Alcohol. 35. 196-209.
Sonnenstuhl, W. J. (1990). Inside an emotional health program. Ithaca, NY: ILR Press.
Sonnenstuhl, W.J. (1991, September). On a personal level: Using peers as an effective means of intervention. Employee Assistance, pp. 8-13.
Spicer, J., Owen, P, & Levine, D. (1983). Evaluating Employee Assistance Programs— A sourcebook for the administrator and counselor. Center City, MN:Hazelden Foundation.
Stackel, L. (1987). EAP's in the workplace. Employment Relations Today. 3 , 289-294.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.

2 1 5
Steele, P. D. (1988). Substance abuse and the work place, with special attention to employee assistance programs: An overview. The Journal of Applied Behavioral Science. 24.(4), 315-325.
Trice, H. M . , & Belasco, J. A. (1968). Supervisorytraining about alcoholics and other problem employees. Quarterly Journal of Studies on Alcoholism. 29. 382- 398.
Trice, H. M., & Roman, P. (1972). Spirits and demons at work: Alcohol and other drugs on the job. Ithaca,N.Y.: Cornell University Press.
Wilcox, J. E. (1984). Employee Assistance Programs in the federal government: Hindrances and facilitators tosupervisory constructive intervention. (Doctoral Dissertation, The George Washington University, 1984). Dissertation Abstract on Disc. 1980-1984. (University Microfilms No. 84-22782)
Windrow, M . , & Wilkinson, F. (1971). The universalsoldier: Fourteen studies in campaign life. A.D. 43-1944. Garden City, N.J.: Doubleday and Co.
Wood, S. P., & Steiner, J. R. (1989). Applyinginstructional technology to EAPs. EAP Digest. 9(6), 43-48.
Wrich, J. (1974). The employee assistance program. Center City, MN.: Hazelden Foundation.
Wright, J. (1984, December). EAP: An importantsupervisory tool. Supervisory Management, pp. 15-2 3.
Young, D. W., Reichman, W. R., & Levy, M. F. (1987).Differential referral of women and men to employee assistance programs: The role of supervisoryattitudes. Journal of Studies on Alcohol. 48.(1), 22- 28.
Reproduced with permission of the copyright owner. Further reproduction prohibited without permission.


















