Informal carer activities, carer burden and health status in multiple sclerosis
14
http://cre.sagepub.com Clinical Rehabilitation DOI: 10.1177/0269215507075035 2007; 21; 563 Clin Rehabil Angus Forbes, Alison While and Lucia Mathes Informal carer activities, carer burden and health status in multiple sclerosis http://cre.sagepub.com/cgi/content/abstract/21/6/563 The online version of this article can be found at: Published by: http://www.sagepublications.com can be found at: Clinical Rehabilitation Additional services and information for http://cre.sagepub.com/cgi/alerts Email Alerts: http://cre.sagepub.com/subscriptions Subscriptions: http://www.sagepub.com/journalsReprints.nav Reprints: http://www.sagepub.com/journalsPermissions.nav Permissions: http://cre.sagepub.com/cgi/content/abstract/21/6/563#BIBL SAGE Journals Online and HighWire Press platforms): (this article cites 21 articles hosted on the Citations © 2007 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. at King's College London on July 6, 2007 http://cre.sagepub.com Downloaded from
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Informal carer activities, carer burden and health status in multiple sclerosis

http://cre.sagepub.comClinical Rehabilitation
DOI: 10.1177/0269215507075035 2007; 21; 563 Clin Rehabil
Angus Forbes, Alison While and Lucia Mathes Informal carer activities, carer burden and health status in multiple sclerosis
http://cre.sagepub.com/cgi/content/abstract/21/6/563 The online version of this article can be found at:
Published by:
http://www.sagepublications.com
can be found at:Clinical Rehabilitation Additional services and information for
http://cre.sagepub.com/cgi/alerts Email Alerts:
http://cre.sagepub.com/subscriptions Subscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
http://cre.sagepub.com/cgi/content/abstract/21/6/563#BIBLSAGE Journals Online and HighWire Press platforms):
(this article cites 21 articles hosted on the Citations
© 2007 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. at King's College London on July 6, 2007 http://cre.sagepub.comDownloaded from
Clinical Rehabilitation 2007; 21: 563–575
Informal carer activities, carer burden and healthstatus in multiple sclerosisAngus Forbes, Alison While and Lucia Mathes King’s College London, The Florence Nightingale School of Nursing &Midwifery, London, UK
Received 4th August 2006; returned for revisions 10th October 2006; revised manuscript accepted 13th November 2006.
Objective: To explore the contribution of carer characteristics, activities and disease impact to care burden and health in the multiple sclerosis caregiver population.Design: A prospective postal survey (24 months).Setting: The study was conducted in seven treatment centres within England.Subjects: Two hundred and fifty-seven caregivers of people with multiple sclerosis.Measures: Carer activity, the Caregivers Reaction Assessment Scale (CRA), theShort Form General Health Survey (SF-36), version 2, and care-related health problems. The carer data were linked to a comprehensive patient data set whichpermitted dyadic variables to be created measuring shared health.Results: Carers were engaged in a wide spectrum of physical care activities; liftingwas the most frequent, 74% (n �192). Patient disease impact scores were positively correlated (P �0.01) with higher carer activity levels (r �0.66). The careractivity level increased over time (P �0.001) by around 5% with a mean increaseof 0.22 (95% confidence interval (CI) 0.12–0.3) in the carer activity summary score(scale 0–4). Disease impact was negatively correlated (P �0.01) with carer burdenr ��0.44 (CRA composite scale), physical health status r ��0.27 (SF-36 physicalcomponent score) and mental health status r ��0.21 (SF-36 mental componentscore); and positively correlated with care-related health problems r �0.44.Hierarchical regression models explaining 39% and 49% of the variance in careburden and health problem respectively showed that disease impact and dyadichealth explained most of the variance, with carer activity contributing an additional2% to 4% of the variance (P �0.001).Conclusion: The analysis demonstrated that greater disease impact, lower dyadichealth, high carer activity and greater carer burden are related to the level of carer-related health problems. The data suggested the need to developinterventions for assessing carers and reducing their activity levels and careburden (objective and subjective).
Address for correspondence: Angus Forbes, King’s CollegeLondon, Florence Nightingale School of Nursing & Midwifery,James Clerk Maxwell Building, 57 Waterloo Road, London SE18WA, UK. e-mail: [email protected]
© 2007 SAGE Publications 10.1177/0269215507075035
© 2007 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. at King's College London on July 6, 2007 http://cre.sagepub.comDownloaded from

564 A Forbes et al.
Introduction
Informal caregivers make a substantial contribution tothe care and well-being of people with multiple sclero-sis.1 However, very few studies have been undertakenexamining this population.2 The available literaturesuggests that the carer population is heterogeneous(parents, partners, children and friends), with a prepon-derance of middle-aged male carers (spouses/partners)reflecting the gender bias in the disease.3 The multiplesclerosis caring role is reported as transitional (devel-oping as the person with multiple sclerosis becomesmore functionally dependent) and dynamic (marked byperiods of instability/distress and periods of stability).4,5
Interest in the caregiving role from a clinical perspec-tive has focused on carer burden; the impact of the car-ing role on health; and convergent and divergent healthin the carer patient relationship (dyad).
Carer burden in multiple sclerosis is both anobjective (what the carer does) and subjective (theexperience of and feelings toward the caring role)phenomenon.6 A number of factors have beenobserved to affect carer burden in multiple sclerosis,including: disease severity (severity more importantthan duration); the complexity and severity ofsymptoms (bowel problems and cognitive changes);the health and age of the carer; the availability of asupportive social network (isolation); the amount oftime spent away from the caring role (more is bet-ter); the number of additional (conflicting) roles(e.g. working or being a parent); the number ofhousehold members (the fewer the greater the bur-den); and the level of perceived uncertainty (worry-ing about the future).7–10 Female carers often faceadditional burden as they tend to have multiple car-ing roles and take on more caring duties.11
The multiple sclerosis caring role has been associ-ated with negative impact on: physical health; psy-chological health; social and economic well-being;and quality of life.2,6,12,13 These effects have beenfound to increase with the level of burden and thepatient’s level of disability, suggesting an interactionbetween carer health and carer burden.2,14
As the caring role exists in the context of a relation-ship with the person with multiple sclerosis,5 there is aninteractive or dyadic component to the role. A centralelement of this dyadic component is the collectivehealth capacity of the patient and carer, considering thehealth of the patient and carer as a shared unit rather
than each in isolation. Therefore, in studying the caringrole in multiple sclerosis it is important to considercoping at the relationship or dyadic level. Pakenham15
noted that in examining dyadic data (common data forboth patient and carer) it is necessary to examine boththe differences in the common measures (e.g. physicaland psychological health status) and the collectivemean of such measures, providing a dyad or meanpatient/carer couple score. Such an approach ensuresthat the effects of any disequilibrium in the overalldyad health status level are included in any examina-tion or prediction of carer burden. In the analysis pre-sented in this paper Pakenham’s method has beenadopted so that further reference to the term dyad with-in the paper is related to the level of similarity/dissimi-larity between the patient and carer scores on the com-mon measure of health status used in the study.
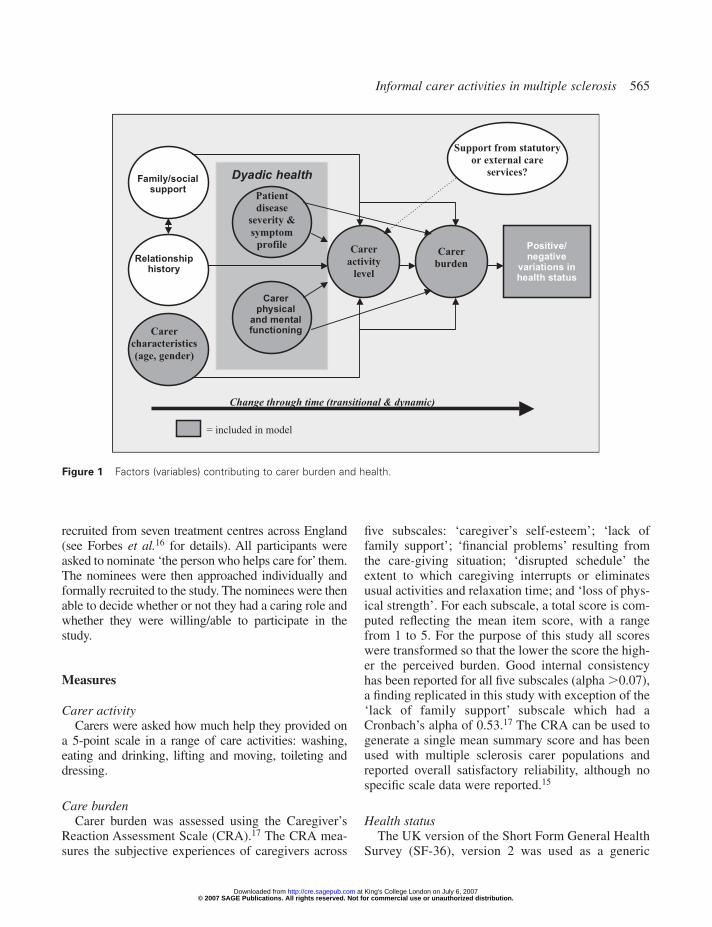
This paper provides an empirical assessment of someof the factors identified in the literature in the largest Eu-ropean multiple sclerosis carer data set presented to datewith paired patient data. The analysis aimed to explorethe relationship between care activities, care burden andthe health of multiple sclerosis carers. To provide afocus for this analysis, the factors (variables) identifiedfrom the literature were organised into a hypotheticalmodel (Figure 1). The model expresses a relationshipbetween the variables suggesting that high diseaseimpact effects care activity levels, which increases careburden and reduces carer health. The model also identi-fies other extraneous factors (e.g. carer age and supportfrom statutory services), although only the factors shad-ed in the figure are included in the analysis. The modelincludes a temporal dimension suggesting that theserelationships will fluctuate through time, such that careractivity and burden levels will rise as the severity of thedisease escalates.
Methods
Data were collected prospectively over a 24-monthperiod by postal survey. The study was approved by amulticentre research ethics committee.
SampleThe carers were identified by people with multiple
sclerosis (n �929) participating in a national evaluationof multiple sclerosis nurses. These patients were
© 2007 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. at King's College London on July 6, 2007 http://cre.sagepub.comDownloaded from
Informal carer activities in multiple sclerosis 565
recruited from seven treatment centres across England(see Forbes et al.16 for details). All participants wereasked to nominate ‘the person who helps care for’ them.The nominees were then approached individually andformally recruited to the study. The nominees were thenable to decide whether or not they had a caring role andwhether they were willing/able to participate in thestudy.
Measures
Carer activityCarers were asked how much help they provided on
a 5-point scale in a range of care activities: washing,eating and drinking, lifting and moving, toileting anddressing.
Care burdenCarer burden was assessed using the Caregiver’s
Reaction Assessment Scale (CRA).17 The CRA mea-sures the subjective experiences of caregivers across
five subscales: ‘caregiver’s self-esteem’; ‘lack offamily support’; ‘financial problems’ resulting fromthe care-giving situation; ‘disrupted schedule’ theextent to which caregiving interrupts or eliminatesusual activities and relaxation time; and ‘loss of phys-ical strength’. For each subscale, a total score is com-puted reflecting the mean item score, with a rangefrom 1 to 5. For the purpose of this study all scoreswere transformed so that the lower the score the high-er the perceived burden. Good internal consistencyhas been reported for all five subscales (alpha �0.07),a finding replicated in this study with exception of the‘lack of family support’ subscale which had aCronbach’s alpha of 0.53.17 The CRA can be used togenerate a single mean summary score and has beenused with multiple sclerosis carer populations andreported overall satisfactory reliability, although nospecific scale data were reported.15
Health statusThe UK version of the Short Form General Health
Survey (SF-36), version 2 was used as a generic
Positive/negative
variations inhealth status
Carer
burdenRelationship
history
Family/socialsupport
Carer
characteristics
(age, gender)
Dyadic health
Carer
activity
level
Carerphysical
and mentalfunctioning
Patient
disease
severity &
symptom
profile
Support from statutory
or external care
services?
Change through time (transitional & dynamic)
= included in model
Figure 1 Factors (variables) contributing to carer burden and health.
© 2007 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. at King's College London on July 6, 2007 http://cre.sagepub.comDownloaded from

566 A Forbes et al.
measure of health-related quality of life.18 The SF-36 provides a subjective measure of health acrosseight scales: physical functioning, social function-ing, role limitations due to physical problems, rolelimitation due to emotional problems, mental health,energy/vitality, bodily pain and general health per-ception. The scale scores from 0 to 100; the lowerthe score the lower the health status in each domain.The internal consistency findings reported byJenkins et al.18 were replicated in the dataset (alpharange 0.84–0.95). A change of �10 points in the SF-36 was adopted as the criteria for a clinically impor-tant change or difference.19 The SF-36 can providetwo summary scales detailing the physical and psy-chological components of the instrument. In additionparticipants were asked to identify the experience ofspecific care-related problems (feeling tired, a badback, feeling anxious or stressed, sleepless nights,feeling sad or depressed, shortness of breath and sex-ual or relationship problems) using 5-point ordinalscales (1 � ‘not at all’, 5 � ‘very’). These problemshave been previously associated with the multiplesclerosis caregiving role.20 The health problem vari-ables were used to create a composite health prob-lem score, the reliability of the score was assessedusing Cronbach’s alpha (0.87).
Disease impactThe carer and patient data had a common coding
enabling linkage across data sets. The patient data setcontained: demographic and disease-related data;measures of disease impact (Multiple SclerosisImpact Scale-29 (MSIS-29)21; and the SF-36. Thephysical scale of the MSIS-29 was used to determinefour groups of participants regarding the level of dis-ease impact. These four groups were defined as: min-imal (score �25), mild (score �25–49), moderate(score �50–74) and severe (score �74). The inclu-sion of the SF-36 meant that common (combinedpatient/carer) health scores could be calculated foreach of the SF-36 scales.
Data collectionThe questionnaire containing the measures was ini-
tially mailed in the autumn of 2000 to the consentingcarers, with two subsequent mailings at 12 and 24months. Two reminders were sent at three weeklyintervals to improve the response.
Data analysisThe Statistical Package for Social Sciences (SPSS
version 11.0) was used for carrying out statistical analy-ses. Preliminary analysis was undertaken to exploredata characteristics to check assumptions for statisticaltests. The short ordinal scales used for the carer activityand health problems were transformed into four cate-gories: those who did not undertake an activity or expe-rience the problem (no help/problem); those who gavea little help or had some experience of the problem,points 1–2 on the ordinal scales; those who providedhelp or experienced the problem moderately, point 3;and those who provided help a lot or experienced theproblem severely (points 4–5). Descriptive statistics ofparticipant characteristics were compiled and differ-ences between non-participant characteristics (patientand carer) identified (�2 and independent t-tests).
Descriptive statistics of care activities were com-piled and a hierarchical cluster analysis was employedusing Ward’s cluster method to identify groups of car-ers based on their overall level of activity. Compositeactivity scores were also calculated (the mean activitylevel for all five care activities) to provide an addition-al summary of the overall activity level. The reliabili-ty of these scores was assessed using Cronbach’s alphaand found to be 0.92, 0.93 and 0.94 at baseline, 12 and24 months respectively. Trends in the activity levelswere then explored through time to determine groupsof participants who had either increased, decreased orstabilized care activity levels.
Descriptive statistics for the CRA and SF-36 sub-scales were compiled and compared with normativedata. The CRA scales were compared with data fromcarers with rheumatoid arthritis.22 The SF-36 scoresof the patients and carers were used to generate dyadicdata of health status following the method ofPakenham15 which generates a ‘congruent functioning’variable representing the dyad’s index of similarity/dis-similarity between the caregiver’s and patient’s scoreon the SF-36 scale. Multivariate analysis of covari-ance (MANCOVA) was used to compare the level ofcare burden and health status between the diseaseimpact groups (controlling for age of person withmultiple sclerosis). The age of the person with multi-ple sclerosis was chosen as the covariate as it corre-lated with the caregiver’s age (r �0.71) and diseaseduration (r �0.38). Descriptive statistics were alsocompiled for the discrete health problems and com-parisons between disease impact groups were undertaken using �2. Change through time was assessed by
© 2007 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. at King's College London on July 6, 2007 http://cre.sagepub.comDownloaded from

Informal carer activities in multiple sclerosis 567
comparing baseline to 24-month values (using eitherpaired t-tests or Wilcoxon signed ranks tests).
The relationship between carer activity, health andcare burden was examined in relation to the followinghypotheses (based on the model expressed in Figure 1):
1) Greater care activity will impact negatively onhealth status and carer burden (independent ofthe effect of disease impact and age).
2) Increased care activity will lead to reduced healthstatus and increased care burden through time (in-dependent of the effect of disease impact and age).
These hypotheses were tested using MANCOVA.The independent factor for hypothesis I was the careactivity cluster with the CRA, SF-36 and compositehealth problem score as the dependent variables (withcarer age and the patients MSIS-29 physical as a covari-ate). For this stage of the analysis the composite physi-cal and mental health scores for the SF-36 were usedrather than all the base scales. The independent factorfor hypothesis II was the change in care activity (basedon two groups defined as a change score �0.5 on thecomposite activity scale compared with change �0.5)with the CRA, SF-36 and composite health problemscore as the dependent variables (with carer age and thepatients MSIS-29 physical as a covariate). Assumptionsfor normality, outliers, linerarity, homogeneity andmulticollinearity were met for all tests. Confirmatorypost-hoc procedures were used to explore hypothesis IIand included: ANCOVA analyses of single dependentvariables; correlations between mean activity changeand change in dependent variables; and absolute com-parisons between groups showing clinically importantchanges in scores and care activity change.
Finally, a hierarchical multiple regression was per-formed to explore the model described in the introduc-tion (Figure 1). Two models were constructed. The firstaimed to explain variance in carer burden (mean totalCRA score) and comprised the following blocks: dis-ease impact; carer age; SF-36 coupled (dyad) compo-nent scores mental and physical scales (reflecting thereshared physical and mental health); and care activitylevel (composite activity score). The second aimed toexplain the variance in health status (composite healthproblem variable) using the same variables as model1 but including carer burden as a predictor. Variableswere correlated prior to modelling to explore collinear-ity and variables within the model blocks with a corre-lation r �0.5 were eliminated. Collinearity diagnostics
were also considered for each model with the variance-inflation factors (VIF) and tolerance both being wellwithin acceptable limits.
Results
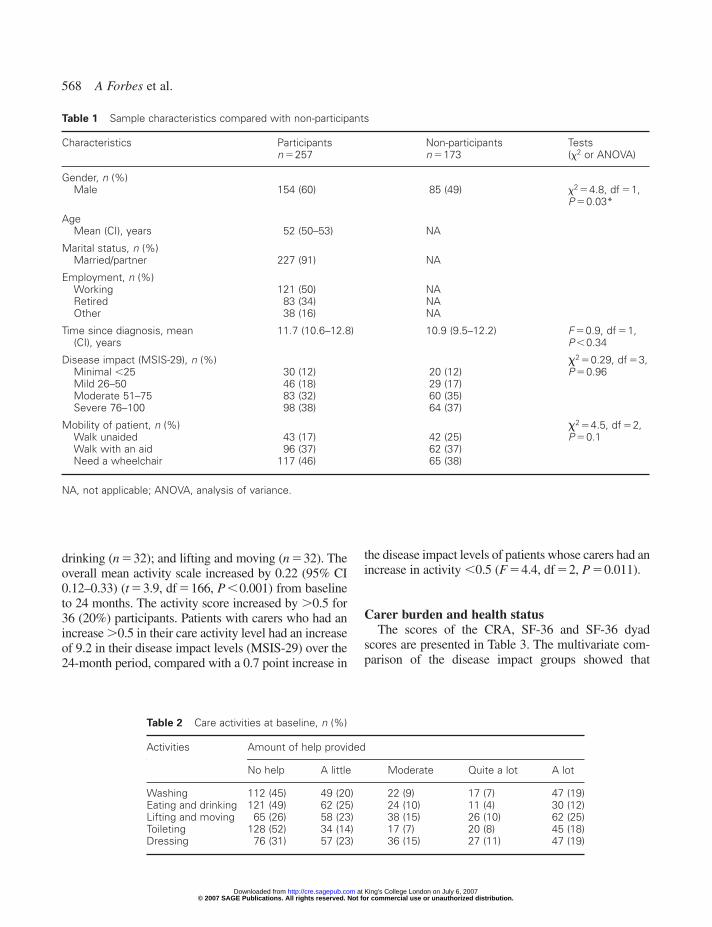
The patients nominated 430 carers and 257 agreed toparticipate (60% participation). The characteristicsof the sample together with the data available fornon-participants are presented in Table 1. There wasa preponderance of carers of patients with moderateor severe disease impact. After the 24-month periodthere was an attrition level of 28% (n �72), no sig-nificant differences in carer or patient characteristicswere found between the attrition group and partici-pants with complete data.
Carer activity levelsThe most common care activity undertaken was
lifting and moving, followed by help with: dressing,washing, eating and drinking, and toileting (Table 2).
Following the hierarchical cluster analysis, a three-cluster solution was accepted to determine the over-all activity level ratings: cluster 1: the ‘minimal activ-ity’ group (n �85, 33%); cluster 2:the ‘moderateactivity’ group (n �95, 37%); and cluster 3: the ‘highactivity’ group (n �63, 25%). The overall mean activi-ty score was 1.4 (SD 1.2) (scale 0–4). There were cleardifferences in the level of disease impact and careractivity. The MSIS-29 physical scores were 40.8 (95%confidence interval (CI) 36.6–45.0), 69.9 (95% CI65.9–73.9) and 82.4 (95% CI 77.5–87.4) for the low(n �84), medium (n �94) and high (n �61) activitygroups respectively (F �89, df �2, P �0.001). Thelow activity group with a mean age of 48.8 (95%CI 46.0–51.5) years were also significantly youngerthan the high activity group (mean age 54.8 (95% CI51.5–58.0) years) (F �4, df �2, P �0.02). The onlysignificant differences in care activities between maleand female carers was dressing, which was more fre-quent in the female group (�2�13, df �4, P �0.011).
Through time comparisons it was revealed that thelevel of activity increased in relation to all five careactivities. The activity with the greatest increase waswashing with 28% (n �49) of participants moving upby one or more points on the self-rated scale, followedby: toileting (n �42); dressing (n �40); eating and
© 2007 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. at King's College London on July 6, 2007 http://cre.sagepub.comDownloaded from
568 A Forbes et al.
drinking (n �32); and lifting and moving (n �32). Theoverall mean activity scale increased by 0.22 (95% CI0.12–0.33) (t �3.9, df �166, P �0.001) from baselineto 24 months. The activity score increased by �0.5 for36 (20%) participants. Patients with carers who had anincrease �0.5 in their care activity level had an increaseof 9.2 in their disease impact levels (MSIS-29) over the24-month period, compared with a 0.7 point increase in
the disease impact levels of patients whose carers had anincrease in activity �0.5 (F �4.4, df �2, P �0.011).
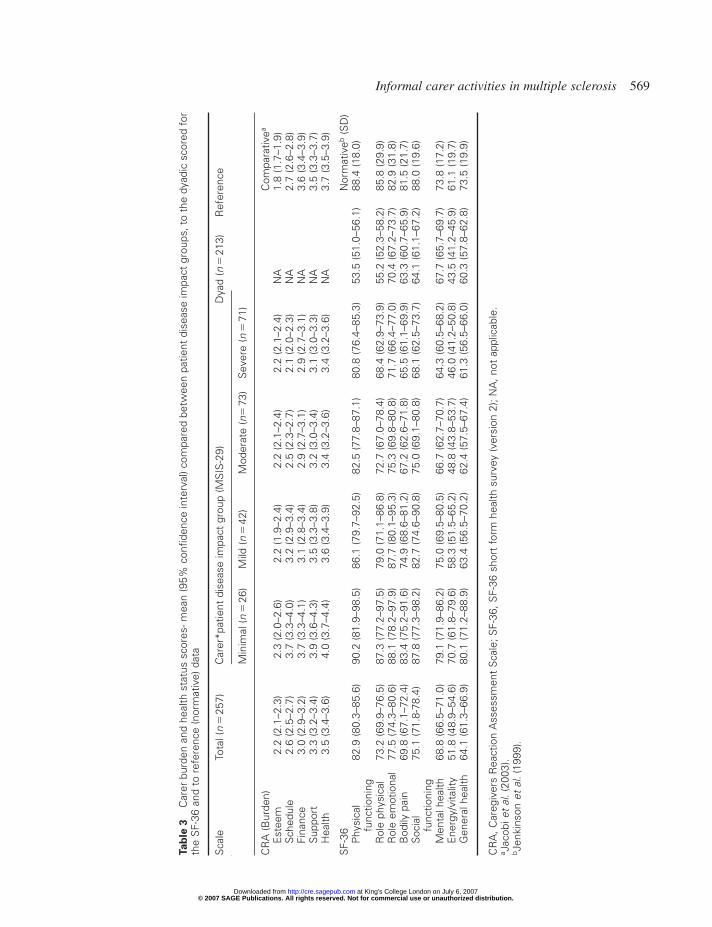
Carer burden and health statusThe scores of the CRA, SF-36 and SF-36 dyad
scores are presented in Table 3. The multivariate com-parison of the disease impact groups showed that
Table 1 Sample characteristics compared with non-participants
Characteristics Participants Non-participants Testsn �257 n �173 (�2 or ANOVA)
Gender, n (%)Male 154 (60) 85 (49) �2 �4.8, df �1,
P �0.03*
AgeMean (CI), years 52 (50–53) NA
Marital status, n (%)Married/partner 227 (91) NA
Employment, n (%)Working 121 (50) NARetired 83 (34) NAOther 38 (16) NA
Time since diagnosis, mean 11.7 (10.6–12.8) 10.9 (9.5–12.2) F �0.9, df �1,(CI), years P �0.34
Disease impact (MSIS-29), n (%) �2 �0.29, df �3,Minimal �25 30 (12) 20 (12) P �0.96Mild 26–50 46 (18) 29 (17)Moderate 51–75 83 (32) 60 (35)Severe 76–100 98 (38) 64 (37)
Mobility of patient, n (%) �2 �4.5, df �2,Walk unaided 43 (17) 42 (25) P �0.1Walk with an aid 96 (37) 62 (37)Need a wheelchair 117 (46) 65 (38)
NA, not applicable; ANOVA, analysis of variance.
Table 2 Care activities at baseline, n (%)
Activities Amount of help provided
No help A little Moderate Quite a lot A lot
Washing 112 (45) 49 (20) 22 (9) 17 (7) 47 (19)Eating and drinking 121 (49) 62 (25) 24 (10) 11 (4) 30 (12)Lifting and moving 65 (26) 58 (23) 38 (15) 26 (10) 62 (25)Toileting 128 (52) 34 (14) 17 (7) 20 (8) 45 (18)Dressing 76 (31) 57 (23) 36 (15) 27 (11) 47 (19)
© 2007 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. at King's College London on July 6, 2007 http://cre.sagepub.comDownloaded from
Informal carer activities in multiple sclerosis 569
Tab
le 3
Car
er b
urde
n an
d he
alth
sta
tus
scor
es- m
ean
(95%
con
fiden
ce in
terv
al) c
ompa
red
betw
een
patie
nt d
isea
se im
pact
gro
ups,
to
the
dyad
ic s
core
d fo
rth
e S
F-36
and
to
refe
renc
e (n
orm
ativ
e) d
ata
Sca
leTo
tal (
n�
257)
Car
er*p
atie
nt d
isea
se im
pact
gro
up (M
SIS
-29)
Dya
d (n
�21
3)R
efer
ence
Min
imal
(n�
26)
Mild
(n�
42)
Mod
erat
e (n
�73
)S
ever
e (n
�71
)
CR
A (B
urde
n)C
ompa
rativ
ea
Est
eem
2.2
(2.1
–2.3
)2.
3 (2
.0–2
.6)
2.2
(1.9
–2.4
)2.
2 (2
.1–2
.4)
2.2
(2.1
–2.4
)N
A1.
8 (1
.7–1
.9)
Sch
edul
e2.
6 (2
.5–2
.7)
3.7
(3.3
–4.0
)3.
2 (2
.9–3
.4)
2.5
(2.3
–2.7
)2.
1 (2
.0–2
.3)
NA
2.7
(2.6
–2.8
)Fi
nanc
e3.
0 (2
.9–3
.2)
3.7
(3.3
–4.1
)3.
1 (2
.8–3
.4)
2.9
(2.7
–3.1
)2.
9 (2
.7–3
.1)
NA
3.6
(3.4
–3.9
)S
uppo
rt3.
3 (3
.2–3
.4)
3.9
(3.6
–4.3
)3.
5 (3
.3–3
.8)
3.2
(3.0
–3.4
)3.
1 (3
.0–3
.3)
NA
3.5
(3.3
–3.7
)H
ealth
3.5
(3.4
–3.6
)4.
0 (3
.7–4
.4)
3.6
(3.4
–3.9
)3.
4 (3
.2–3
.6)
3.4
(3.2
–3.6
)N
A3.
7 (3
.5–3
.9)
SF-
36N
orm
ativ
eb(S
D)
Phy
sica
l82
.9 (8
0.3–
85.6
)90
.2 (8
1.9–
98.5
)86
.1 (7
9.7–
92.5
)82
.5 (7
7.8–
87.1
)80
.8 (7
6.4–
85.3
)53
.5 (5
1.0–
56.1
)88
.4 (1
8.0)
func
tioni
ngR
ole
phys
ical
73.2
(69.
9–76
.5)
87.3
(77.
2–97
.5)
79.0
(71.
1–86
.8)
72.7
(67.
0–78
.4)
68.4
(62.
9–73
.9)
55.2
(52.
3–58
.2)
85.8
(29.
9)R
ole
emot
iona
l77
.5 (7
4.3–
80.6
)88
.1 (7
8.2–
97.9
)87
.7 (8
0.1–
95.3
)75
.3 (6
9.8–
80.8
)71
.7 (6
6.4–
77.0
)70
.4 (6
7.2–
73.7
)82
.9 (3
1.8)
Bod
ily p
ain
69.8
(67.
1–72
.4)
83.4
(75.
2–91
.6)
74.9
(68.
6–81
.2)
67.2
(62.
6–71
.8)
65.5
(61.
1–69
.9)
63.3
(60.
7–65
.9)
81.5
(21.
7)S
ocia
l75
.1 (7
1.8-
78.4
)87
.8 (7
7.3–
98.2
)82
.7 (7
4.6–
90.8
)75
.0 (6
9.1–
80.8
)68
.1 (6
2.5–
73.7
)64
.1 (6
1.1–
67.2
)88
.0 (1
9.6)
func
tioni
ngM
enta
l hea
lth68
.8 (6
6.5–
71.0
)79
.1 (7
1.9–
86.2
)75
.0 (6
9.5–
80.5
)66
.7 (6
2.7–
70.7
)64
.3 (6
0.5–
68.2
)67
.7 (6
5.7–
69.7
)73
.8 (1
7.2)
Ene
rgy/
vita
lity
51.8
(48.
9–54
.6)
70.7
(61.
8–79
.6)
58.3
(51.
5–65
.2)
48.8
(43.
8–53
.7)
46.0
(41.
2–50
.8)
43.5
(41.
2–45
.9)
61.1
(19.
7)G
ener
al h
ealth
64.1
(61.
3–66
.9)
80.1
(71.
2–88
.9)
63.4
(56.
5–70
.2)
62.4
(57.
5–67
.4)
61.3
(56.
5–66
.0)
60.3
(57.
8–62
.8)
73.5
(19.
9)
CR
A, C
areg
iver
s R
eact
ion
Ass
essm
ent
Sca
le; S
F-36
, SF-
36 s
hort
for
m h
ealth
sur
vey
(ver
sion
2);
NA
, not
app
licab
le.
a Jac
obi e
t al
.(20
03).
b Jen
kins
on e
t al
.(19
99).
© 2007 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. at King's College London on July 6, 2007 http://cre.sagepub.comDownloaded from
570 A Forbes et al.
people caring for patients in the moderate and severedisease impact groups had significantly poorer SF-36(F �2.0, df �24, P �0.003) and CRA (F �5.8,df �15, P �0.001) scores (adjusted for age) than thosecaring for patients in the minimal and mild impactgroups. Only the esteem and physical function scaleswere not significant in the CRA and SF-36 modelsrespectively. Minimal variation through time wasobserved with only the SF-36 physical functioning(mean change �4.3, 95% CI �1.7 to �6.8) and bodilypain (mean change �3.3, and 95% CI �0.5 to �6.1)the CRA esteem (mean change 0.1, 95% CI �0.04 to0.2) and health (mean change �0.2, 95% CI �0.25 to�0.04) scales, demonstrating a statically significant(P �0.01) change.
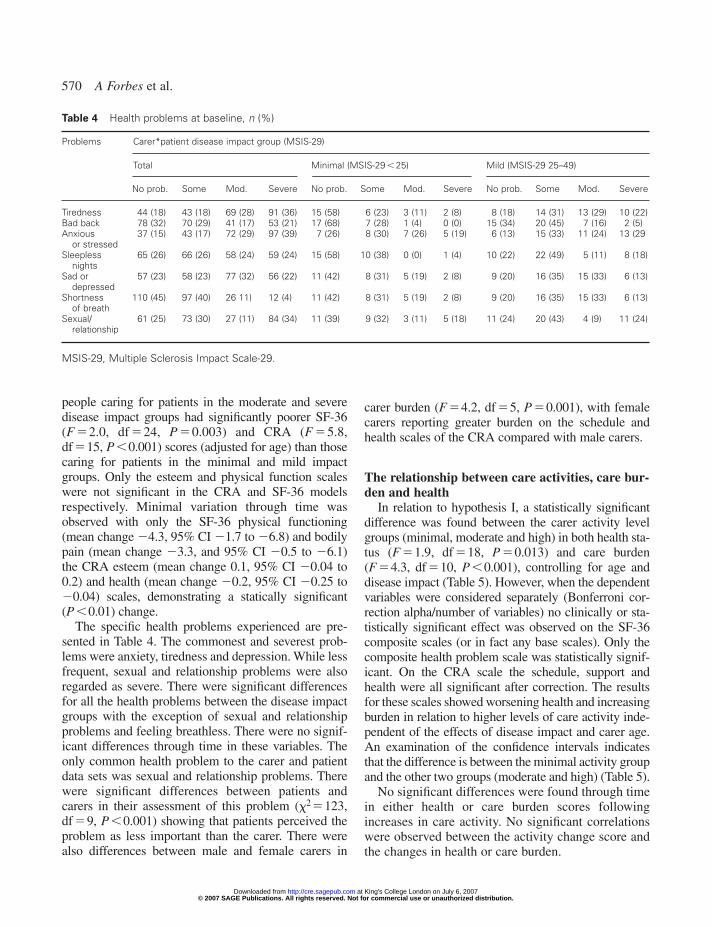
The specific health problems experienced are pre-sented in Table 4. The commonest and severest prob-lems were anxiety, tiredness and depression. While lessfrequent, sexual and relationship problems were alsoregarded as severe. There were significant differencesfor all the health problems between the disease impactgroups with the exception of sexual and relationshipproblems and feeling breathless. There were no signif-icant differences through time in these variables. Theonly common health problem to the carer and patientdata sets was sexual and relationship problems. Therewere significant differences between patients andcarers in their assessment of this problem (�2�123,df �9, P �0.001) showing that patients perceived theproblem as less important than the carer. There werealso differences between male and female carers in
carer burden (F �4.2, df �5, P �0.001), with femalecarers reporting greater burden on the schedule andhealth scales of the CRA compared with male carers.
The relationship between care activities, care bur-den and health
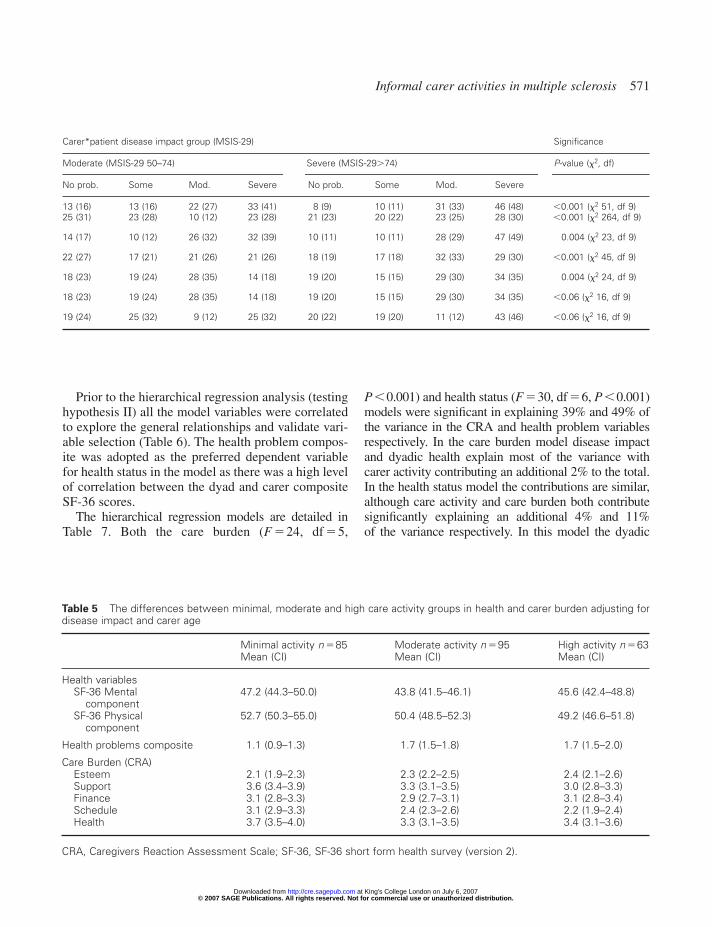
In relation to hypothesis I, a statistically significantdifference was found between the carer activity levelgroups (minimal, moderate and high) in both health sta-tus (F �1.9, df �18, P �0.013) and care burden(F �4.3, df �10, P �0.001), controlling for age anddisease impact (Table 5). However, when the dependentvariables were considered separately (Bonferroni cor-rection alpha/number of variables) no clinically or sta-tistically significant effect was observed on the SF-36composite scales (or in fact any base scales). Only thecomposite health problem scale was statistically signif-icant. On the CRA scale the schedule, support andhealth were all significant after correction. The resultsfor these scales showed worsening health and increasingburden in relation to higher levels of care activity inde-pendent of the effects of disease impact and carer age.An examination of the confidence intervals indicatesthat the difference is between the minimal activity groupand the other two groups (moderate and high) (Table 5).
No significant differences were found through timein either health or care burden scores followingincreases in care activity. No significant correlationswere observed between the activity change score andthe changes in health or care burden.
Table 4 Health problems at baseline, n (%)
Problems Carer*patient disease impact group (MSIS-29)
Total Minimal (MSIS-29 � 25) Mild (MSIS-29 25–49)
No prob. Some Mod. Severe No prob. Some Mod. Severe No prob. Some Mod. Severe
Tiredness 44 (18) 43 (18) 69 (28) 91 (36) 15 (58) 6 (23) 3 (11) 2 (8) 8 (18) 14 (31) 13 (29) 10 (22)Bad back 78 (32) 70 (29) 41 (17) 53 (21) 17 (68) 7 (28) 1 (4) 0 (0) 15 (34) 20 (45) 7 (16) 2 (5)Anxious 37 (15) 43 (17) 72 (29) 97 (39) 7 (26) 8 (30) 7 (26) 5 (19) 6 (13) 15 (33) 11 (24) 13 (29
or stressedSleepless 65 (26) 66 (26) 58 (24) 59 (24) 15 (58) 10 (38) 0 (0) 1 (4) 10 (22) 22 (49) 5 (11) 8 (18)
nightsSad or 57 (23) 58 (23) 77 (32) 56 (22) 11 (42) 8 (31) 5 (19) 2 (8) 9 (20) 16 (35) 15 (33) 6 (13)
depressedShortness 110 (45) 97 (40) 26 11) 12 (4) 11 (42) 8 (31) 5 (19) 2 (8) 9 (20) 16 (35) 15 (33) 6 (13)
of breathSexual/ 61 (25) 73 (30) 27 (11) 84 (34) 11 (39) 9 (32) 3 (11) 5 (18) 11 (24) 20 (43) 4 (9) 11 (24)
relationship
MSIS-29, Multiple Sclerosis Impact Scale-29.
© 2007 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. at King's College London on July 6, 2007 http://cre.sagepub.comDownloaded from
Informal carer activities in multiple sclerosis 571
Prior to the hierarchical regression analysis (testinghypothesis II) all the model variables were correlatedto explore the general relationships and validate vari-able selection (Table 6). The health problem compos-ite was adopted as the preferred dependent variablefor health status in the model as there was a high levelof correlation between the dyad and carer compositeSF-36 scores.
The hierarchical regression models are detailed inTable 7. Both the care burden (F �24, df �5,
P �0.001) and health status (F �30, df �6, P �0.001)models were significant in explaining 39% and 49% ofthe variance in the CRA and health problem variablesrespectively. In the care burden model disease impactand dyadic health explain most of the variance withcarer activity contributing an additional 2% to the total.In the health status model the contributions are similar,although care activity and care burden both contributesignificantly explaining an additional 4% and 11%of the variance respectively. In this model the dyadic
Carer*patient disease impact group (MSIS-29) Significance
Moderate (MSIS-29 50–74) Severe (MSIS-29�74) P-value (�2, df)
No prob. Some Mod. Severe No prob. Some Mod. Severe
13 (16) 13 (16) 22 (27) 33 (41) 8 (9) 10 (11) 31 (33) 46 (48) �0.001 (�2 51, df 9)25 (31) 23 (28) 10 (12) 23 (28) 21 (23) 20 (22) 23 (25) 28 (30) �0.001 (�2 264, df 9)
14 (17) 10 (12) 26 (32) 32 (39) 10 (11) 10 (11) 28 (29) 47 (49) 0.004 (�2 23, df 9)
22 (27) 17 (21) 21 (26) 21 (26) 18 (19) 17 (18) 32 (33) 29 (30) �0.001 (�2 45, df 9)
18 (23) 19 (24) 28 (35) 14 (18) 19 (20) 15 (15) 29 (30) 34 (35) 0.004 (�2 24, df 9)
18 (23) 19 (24) 28 (35) 14 (18) 19 (20) 15 (15) 29 (30) 34 (35) �0.06 (�2 16, df 9)
19 (24) 25 (32) 9 (12) 25 (32) 20 (22) 19 (20) 11 (12) 43 (46) �0.06 (�2 16, df 9)
Table 5 The differences between minimal, moderate and high care activity groups in health and carer burden adjusting fordisease impact and carer age
Minimal activity n �85 Moderate activity n �95 High activity n �63Mean (CI) Mean (CI) Mean (CI)
Health variablesSF-36 Mental 47.2 (44.3–50.0) 43.8 (41.5–46.1) 45.6 (42.4–48.8)
componentSF-36 Physical 52.7 (50.3–55.0) 50.4 (48.5–52.3) 49.2 (46.6–51.8)
component
Health problems composite 1.1 (0.9–1.3) 1.7 (1.5–1.8) 1.7 (1.5–2.0)
Care Burden (CRA)Esteem 2.1 (1.9–2.3) 2.3 (2.2–2.5) 2.4 (2.1–2.6)Support 3.6 (3.4–3.9) 3.3 (3.1–3.5) 3.0 (2.8–3.3)Finance 3.1 (2.8–3.3) 2.9 (2.7–3.1) 3.1 (2.8–3.4)Schedule 3.1 (2.9–3.3) 2.4 (2.3–2.6) 2.2 (1.9–2.4)Health 3.7 (3.5–4.0) 3.3 (3.1–3.5) 3.4 (3.1–3.6)
CRA, Caregivers Reaction Assessment Scale; SF-36, SF-36 short form health survey (version 2).
© 2007 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. at King's College London on July 6, 2007 http://cre.sagepub.comDownloaded from

572 A Forbes et al.
mental health component also becomes more active.The direction of the relationships (positive and nega-tive) in the standardized �values are consistent with theunderlying hypotheses (that is �diseaseimpact, �dyadic health, �carer activity and the lowercarer burden score �health problem score).
Discussion
The findings extend previous studies in providingknowledge regarding the characteristics of the multiplesclerosis carer population, namely that most were male,
Table 6 Correlations between model variables
1 2 3 4 5 6 7 8 9
1) Carer age (years) 1.002) Disease impact 0.24** 1.00
(MSIS-29)3) Care activity 0.21** 0.66** 1.00
Dyadic data4) Physical �0.30** �0.57** �0.44** 1.00
component5) Mental 0.15* �0.31** �0.21** 0.06 1.00
component6) Carer Burden �0.05 �0.43** �0.40** 0.50** 0.37** 1.00
(CRA)
Health status7) SF-36 Physical �0.29** �0.27** �0.27** 0.76** 0.10 0.47** 1.00
component8) SF-36 Mental 0.19** �0.21** �0.19** 0.06 0.76** 0.51** 0.07 1.00
component9) Health problem �0.04 0.42** 0.44** �0.36** �0.46** �0.62** �0.34** �0.60** 1.00
composite
Pearson correlations *P �0.05, **P �0.01.MSIS-29, Multiple Sclerosis Impact Scale-29; CRA, Caregivers Reaction Assessment Scale; SF-36, SF-36 short form healthsurvey (version 2).
Table 7 Hierarchical regression models predicting carer burden (CRA) and health status (health problem)
Models Variable statistics Model statisticsfull model
Stand. � Sig. Block �R2 adj. R2 R2 change F-change P-value
Model 1 Care burdenCarer age (years) 0.07 0.3 1 0.00 0.00 0.00 0.5 0.47Disease impact (MSIS-29) 0.00 0.9 2 0.19 0.18 0.19 45.5 �0.001Dyadic data 3 0.37 0.36 0.18 28.5 �0.001Physical component 0.43 �0.001Mental component 0.30 �0.001Care activity �0.17 0.03 4 0.39 0.37 0.02 4.9 0.028
Model 2 Health statusCarer age (years) �0.09 0.1 1 0.00 0.00 0.00 0.35 0.56Disease impact (MSIS-29) 0.02 0.8 2 0.20 0.19 0.19 46.57 �0.001Dyadic data 3 0.34 0.33 0.15 21.70 �0.001Physical component �0.07 0.4Mental component �0.24 �0.001Care activity 0.20 0.01 4 0.38 0.37 0.04 12.11 �0.001Care burden (CRA) �0.42 �0.001 5 0.49 0.48 0.11 40.36 �0.001
MSIS-29, Multiple Sclerosis Impact Scale-29; CRA, Caregivers Reaction Assessment Scale.
© 2007 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. at King's College London on July 6, 2007 http://cre.sagepub.comDownloaded from

Informal carer activities in multiple sclerosis 573
married or in a partnership and that half were stillworking.2 The preponderance of patients with moder-ate and severe disease is consistent with other carer sur-veys14 and confirms that the caring role is generallyassociated with a reduction in the physical capacity ofthe patient.
The findings also show that informal carers con-tribute a high level of care to support people with mul-tiple sclerosis. The pattern of reported activity wasvery similar to the findings of Aronson et al.14 whoreported a significant proportion of carers were rou-tinely providing help of more than 90 minutes/daywith washing, lifting, bowel/bladder care and eating.The level of care activity was strongly associated withdisease impact and increased through time.
The level of carer burden (as measured by theCRA) was very similar to that reported for a rheuma-toid arthritis sample,22 although the finance subscaleshowed lower scores and the esteem subscale slightlyhigher scores. This comparison suggests that theeffects of the caring role are likely to be similar acrosschronic disorders. Care burden was significantly relatedto disease impact, with the interrupted schedule scaleshowing the greatest difference between the diseaseimpact groups. The data also confirm previous reportsthat the burden of care is greater in female care-givers.11
The data show that participants’ SF-36 scores werelower than the normative reference values with thedifferences in the role physical, role emotional, socialfunctioning and energy/vitality scales being clinicallysignificant (�10 scale points). For those carers ofpeople in the severe multiple sclerosis impact group,all SF-36 scores were clinically significantly lowerthan the normative data.
The data relating to specific carer health problems(tiredness, bad back, anxiety, insomnia, depression,shortness of breath and sexual/relationship problems)suggested that these are common problems thatadvance with increased disease impact. Sexual andrelationship problems were evident across all the dis-ease impact groups and were rated more severe bycarers than patients, reflecting previous evidence sug-gesting that patients and carers have divergent viewson the nature and severity of problems.7
The dyadic SF-36 scores showed that when patientand carer data are combined, they are significantlylower than the carers’ scores in isolation. The excep-tion to this pattern was the ‘mental health’ scale,which had greater congruity between the carers
(mean �68, SD 18) and the patients (mean �65, SD15). The lower dyadic physical scorers illustratea divergence in health status between carers andpatients, explained by the severe physical effects ofmultiple sclerosis on the patient. Conversely, thesimilarity in the mental health scores suggest a con-vergence in mental health status, explained either by ashared psychological effect of multiple sclerosis onboth the patient and the carer (multiple sclerosis caus-es anxiety and depression in both) or that mutualpositive psychological functioning is compensatory.Along with the patients’ disease impact level, dyadichealth contributed most to the explained variance incarer burden and carer health in the regression mod-els. While in the care burden model both the physicaland mental dyadic health were contributory, in thecarer health model only dyadic mental health showeda significant contribution. These data suggest that theshared health status (physical and mental) of the carerand patient is an important factor to consider in bothcarer burden and carer health, independent of theeffect of disease impact.
The central focus of this analysis was to examinethe relationship between care activities, care burdenand the health of multiple sclerosis carers. While it isclear that disease impact and dyadic health explainmuch of the variation in carer health, the amount ofactivities performed and the level of burden are alsovery important indicators for carer health. In terms ofcarer burden post-hoc analyses suggest that the inter-rupted schedule scale is particularly important, suchthat when the base scales for the CRA are used in themodel separately (after Bonferroni correction) onlyinterrupted schedule is significant, � �0.13.Additional post-hoc analysis showed that carers withpoor interrupted schedules (scores �3 on the sched-ule scale) scored 12 points lower on the SF-36 mentalscale compared with those with better schedulescores; and that SF-36 mental health scores for carerswhose schedule burden reduced (n �46) over the 24-month period improved by 5 points compared with a2-point reduction in those whose schedule burdenincreased (n �63) (F �2.6, df �2, P �0.08).
In summary, the analysis generally confirms the rela-tionships expressed in the hypothetical model detailedat the outset (Figure 1). While changes through timewere not significantly expressed in the data, the post-hoc analysis did show temporal trends showing a rela-tionship between fluctuations in carer burden andmental well-being. Therefore, interventions that can
© 2007 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. at King's College London on July 6, 2007 http://cre.sagepub.comDownloaded from

574 A Forbes et al.
reduce overall care activity, reduce interruptions inschedule and liberate personal time for carers may leadto improvements in mental and physical well-being.
Study limitationsThe study findings need to be considered in rela-
tion to a number of potential biases, including selec-tion and response bias. The selection bias is related tothe selection of the patients from which the carerswere identified. Patients were identified from sevenneurological services from across the UK, excludingthose unknown to services (see Forbes et al.24). Theresponse bias relates to the discrepancy betweenpatient nominations and people’s perception of them-selves in the caring role. Not all nominees perceivedthemselves to be carers. The way someone in a rela-tionship with a person with multiple sclerosis definesthemselves and their transition into the carer role iscomplex and worthy of additional study. Neverthelessthis is a comparatively large sample of carers report-ing the views from a broad range of carers supportingpeople with multiple sclerosis from across the dis-ease spectrum. While there was a preponderance ofcarers of patients with more severe disease, this mir-rors previous studies and reflects the relationshipbetween patient functioning and the caring role. Nosignificant differences were observed between thecarer nominees and participants. Another potentialbias arises from the data being collected as part of anexperimental study examining the impact of special-ist nurses. However, no differences were observed inrelation to those who had contact with in an multiplesclerosis nurse (n �94, 36%) in any of the variablesconsidered in the analysis and those who had nocontact.
There were in addition some measurement issues.First, there are limitations in using composite orsummary scales (SF-36 physical/mental components,CRA mean total and health problem composite).However, the internal consistence of these summarieshas been reported and in the post-hoc analyses basescales or variables have been considered individually.More specific limitations in measurement include: afocus on the physical aspects of the care role ratherthan psychosocial support; the CRA is limited as itfocuses on subjective rather than objective burden;and the depression reported may not be clinicallydefinitive as a previous study showed that self-reportof depression was not supported by more objective
measurement such as the Hospital Anxiety andDepression Scale.13 Finally, the lack of variationthrough time in the main dependent variables limitedthe prospective predictive power of the analysis,although more subtle variations (trends) were observedand have been detailed.
Overall it is contended that the analysis was suffi-ciently robust (and cautious) to provide useful addi-tional knowledge about multiple sclerosis carers interms of what they do, their burden and how thisimpacts on their health. The next steps should be totest further the relationship between the variablesexpressed in Figure 1 and to identify and trial inter-ventions that may reduce carer burden and/or improvethe health of this important population.
Clinical messages
● The level of patient disease impact is the mostimportant factor in explaining carer activity,burden and health.
● The shared health (dyadic health) of the patientand carer together is a significant additionalfactor in explaining carer burden and health.
● Higher care activity and burden, particularlyinterruptions to the carer’s own schedule areassociated with poorer carer health.
AcknowledgementsThe research team is grateful to all the carers and
people with MS who participated, the sites which sup-ported the study, the MS Society for Great Britainwhich funded the research.
References
1 Carton H, Loos R, Pacolet J, Versieck K, Vlietinck R.A quantitative study of unpaid caregiving in multiplesclerosis. Multiple Sclerosis 2000; 6.
2 McKeown LP, Porter-Armstrong A, Baxter G. Theneeds and experiences of caregivers of individuals
© 2007 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. at King's College London on July 6, 2007 http://cre.sagepub.comDownloaded from
Informal carer activities in multiple sclerosis 575
with multiple sclerosis: a systematic review. ClinRehabil 2003; 17: 234–48.
3 Chesson R. Who’s there for carers? Report from theMS Society Scotland, Edinburgh, 2003.
4 Hind L. Challenging assumptions of care. Way Ahead(Multiple Sclerosis Trust) 2001; 5: 2.
5 Boeije H. Duijnstee M, Grypdonck M. Continuationof caregiving among partners who give total care tospouses with multiple sclerosis. Health Social CareCommunity 2003; 11.
6 DesRosier M, Catanzaro M, Piller J. Living withchronic illness: social support and the well spouseperspective. Rehabil Nurs 1992; 17: 87–91.
7 O’Brien R, Wineman N, Nealon N. Correlates of thecaregiving process in multiple sclerosis. ScholarlyInquiry Nurs Pract 1995; 9: 323–38.
8 Chipchase SY, Lincoln NB. Factors associated withcarer strain in carers of people with multiple sclero-sis. Disabil Rehabil 2001; 23: 768–76.
9 Cohen C, Colantonio A, Vernich L. Positive aspectsof caregiving: rounding out the caregiver experienceInt J Geriatr Psych 2002; 17: 184–88.
10 Good D, Bower D, Einsporn R. Social support: gen-der differences in multiple sclerosis spousal care-givers. J Neurosci Nurs 1995; 27: 305–11.
11 Aronson KJ. Quality of life among persons with mul-tiple sclerosis and their caregivers. Neurology 1997;48: 74–80.
12 Hakim EA, Bakheit A, Bryant T et al. The socialimpact of multiple sclerosis – a study of 305 patientsand their relatives. Disabil Rehabil 2000; 22: 288–93.
13 Hatch L, Hayes G, Griffith C, Burn J, Baker R. Carerstress scales: are they valid for the caregivers ofyounger disabled people? Way Ahead (MultipleSclerosis Trust) 2002; 6: 3.
14 Aronson KJ, Cleghorn G, Goldenberg E. Assistancearrangements and use of services among persons with
multiple sclerosis and their caregivers. DisabilRehabil 1996; 18: 354–61.
15 Pakenham KI. Couple coping and adjustment to mul-tiple sclerosis in care receiver-carer dyads. FamilyRelations 1998; 47: 269–77.
16 Forbes A, While A, Mathes L, Griffiths P. Evaluationof an MS specialist nurse programme. Int J Nurs Stud2006; 43: 985–1000.
17 Given B, Stommel M, Collins C. The caregiver reac-tion assessment (CRA) for caregivers to persons withchronic physical and mental impairments. Res NursHealth 1992; 15: 271–83.
18 Jenkinson C. Stewart-Brown S. Petersen S, Paice C.Assessment of the SF-36 version 2 in the UnitedKingdom. J Epidemiol Community Health 1999; 53:46–50.
19 Craig J, Young CA, Ennis M, Baker G, Boggild M. Arandomised controlled trial comparing rehabilitationagainst standard therapy in multiple sclerosis patientsreceiving intravenous steroid treatment. J NeurolNeurosurg Psychiatry 2003; 74: 1225–30.
20 White DM. Treating the family with multiple sclero-sis. Phys Med Rehabil Clin N Am 1998; 9: 675–87.
21 Hobart JC, Lamping DL, Fitzpatrick R, Riazi A,Thompson AJ. The Multiple Sclerosis Impact Scale(MSIS-29): a new patient-based outcome measure.Brain 2001; 124: 962–73.
22 Jacobi C, van den Berg B, Boshuizen H, Rupp I,Dinant H, van den Bos G. Dimension specific burdenof caregiving among partners of rheumatoid arthritispatients. Rheumatology 2003; 42: 1226–33.
23 Duijnstee M, Boeije H. Home care by and for rela-tives of MS patients. J Neurosci Nurs 1998; 30:356–60.
24 Forbes A While A, Mathes L, Griffiths P. Healthproblems and health related quality of life in peoplewith multiple sclerosis. Clin Rehabil 2006; 20: 67–78.
© 2007 SAGE Publications. All rights reserved. Not for commercial use or unauthorized distribution. at King's College London on July 6, 2007 http://cre.sagepub.comDownloaded from