INFLUENCE OF INITIAL NURSING EOUCATIONAL PREPARATION ...
264
INFLUENCE OF INITIAL NURSING EOUCATIONAL PREPARATION ON PATIENT ASSESSMENT BY CAROLYN JEAN YOCOM B.S.N., University of Pennsylvania, 1970 M.S.N., Case Western Reserve University, 1975 THESIS Submitted as partial fulfillment of the requirements for the degree of Doctor of Philosophy In Nursing Sciences In the Graduate College of the University of Illinois at Chicago Health Sciences Center, 1985 Chicago, Illinois
-
Upload
khangminh22 -
Category
Documents
-
view
4 -
download
0
Transcript of INFLUENCE OF INITIAL NURSING EOUCATIONAL PREPARATION ...
INFLUENCE OF INITIAL NURSING EOUCATIONAL PREPARATION
ON PATIENT ASSESSMENT
BY
CAROLYN JEAN YOCOM B.S.N., University of Pennsylvania, 1970
M.S.N., Case Western Reserve University, 1975
THESIS
Submitted as partial fulfillment of the requirements for the degree of Doctor of Philosophy In Nursing Sciences
In the Graduate College of the University of Illinois at Chicago Health Sciences Center, 1985
Chicago, Illinois
HI. i.̂ r .mi.iwijw i n ni •• •• I rotnin»mmu.iJi'j.;e*mTagJe3V- j
UNIVERSITY OF ILLINOIS AT CHICAGO HEALTH SCIENCES CENTER GRADUATE COLLEGE
Certificate of Approval
April 29, 1985 Date
I HEREBY RECOMMEND THAT THE THESIS PREPARED UNDER MY
SUPERVISION BY CAROLYN JEAN YOCQM
ENTITLED INFLUENCE OF INITIAL NURSING EDUCATIONAL
PREPARATION ON PATIENT ASSESSMENT
BE ACCEPTED IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR
THE DEGREE OF Doctor of Philosophy
In Charge of Thesis
Recommendation concurred in
Head of Department
Committee on
Final Examination
80173
?• T 3 - » n . -T y . - n w a T V •. ... T." - Jr.. Vti •<—- KU-t« * "J-.r- v '̂. i-R^acmmrurn:-I*..*; a wc ?r. r.z
Copyright by
Carolyn Jean Yocom
1985
ACKNOWLEDGMENTS
I wish to acknowledge the following Individuals for their
contributions to this dissertations
To my advisor and committee chair, Dr. Leona Peterson, for her
continued guidance, support, encouragement and understanding.
To the other members of my committee, Drs. Mary Bevls, Karyn
Holm, Margaret Grler, and Eta Berner, for their guidance.
To the panel members, Kathy Bronsteln, June Krawczak and Kathy
Czurylo, whose expert contributions were essential to the completion
of this dissertation.
To the Deans and Directors who facilitated access to their
students, and to the students who participated In the study. Without
them, the study could not have been completed.
Finally, to my family and friends. Their encouragement, support
and faith were essential and deeply appreciated.
This research was supported In part by a Research Support Award
from Alpha Lambda Chapter, Sigma Theta Tau, National Honor Society of
Nursing.
CJY
III
TABLE OF CONTENTS
chapter EASE
I INTRODUCTION 1 A. Background of the study 2
1. Definitions 3 2. Nursing process and nursing diagnosis 4 3. Cognitive processes..... 6 4. Characteristics of educational programs
and students that influence problem solving abilities..... 11
B. Conceptual framework....... 13 Cm Purpose of the study 15 D. Research Questions 15 E. Significance of the study 17
II LITERATURE REVIEW 21 A. The diagnostic process 21
1. The task environment. 22 a. Summary 25
2. Characteristics of the problem solver 26 a. Processing capabiI Itles 26 b. Short term memory 27 c. Long term memory 28
1) Organization of stored Information 29
2) Role of knowledge stored In LTM In problem solving... 31
d. Interaction of the processing system with the external environment 35
e. Summary 37 3. Diagnosis Identification 38
a. Concept attainment 38 b. Factors Influencing diagnostic
accuracy 40 4. Summary 44
B. Measurement of clinical problem solving ability.. 44 1. Observation-based methods 46 2. Record-based methods 46 3. Simulation methods..... 47
a. Oral format 48 b. Patient management problems 48
1) Psychometric properties 51 4. Summary 53
C. Nursing education 53
Iv
TABLE OF CONTENTS (continued)
CHAPTER BASSE
1. Historical overview 54 2. Differences In associate and
baccalaureate degree students and graduates 66 a. Demographic and pre-enrol Intent
educational characteristics 66 b. Characteristics related to nursing
program selection 70 1) Distance from home 70 2) Selection of type of
nursing program.. 70 3) Reason for selection of a
nursing career 71 c. Personal attributes of students... 71
1) Professional values 72 2) Leadership qualities 72 3) Other personality factors.. 72 4) Academic
aptitude/achievement 73 d. Clinical attributes of graduates.. 75
1) Competency ratings 75 a) Summary 84
2) Critical Incident reports.. 85 3) Problem solving ability.... 86 4) Summary 91
I I I METHOD 93 A. Research design 93 B. Population and sample selection 95
1. Rationale for sample selection 95 2. SamplIng procedure............. 96 3. Solicitation of Institutional agreement to
participate 97 4. Sample characteristics 98
a. Characteristics of participating programs..... 98
b. Characteristics of student participants 99
C. Operational IzatIon of the conceptual model 105 1. Independent variable 105 2. Covartates 105
a. Task setting 106 b. Task complexity 106 c. Critical thinking ability. 106 d. Post-high school education 107
v
TABLE OF CONTENTS (continued)
CHAPTER PAGE
e. Non-education related health care experience.. 107
f. Age and gender 107 g. Intellectual ability 107
3. Dependent variables 108 D. Instruments 108
1. Measurement of the covarlates 108 a. Background Inventory 108 b. Watson-Glaser Critical Thinking
Appraisal 109 1) Inference 110 2) Recognition of assumptions. 110 3) Deduction 110 4) Interpretation 110 5) Evaluation of arguments.... 111
2. Measurement of the dependent variable 112 a. Description 113 b. Content vaI IdIty 115 c. Construct va I Id Ity 116 d. Reliability 118
E. Procedure 119 1. Pilot testing 119 2. Data col lection 120
F. Protection of human subjects 121 G. Data reduction. 122
1. Covar I ates 122 2. Dependent variables 122
a. Patient Information 122 1) Scoring formulas...... 123
a) Efficiency score 123 b) Proficiency score.... 124 c) Psychosocial data
score 124 d) Percent psycho
social data score.. 124 b. Nursing diagnoses 125
1) Expert panel composition.... 125 2) Analysis of diagnostic
statements 126 3) Reliability 126
vl
TABLE OF CONTENTS (continued)
CHAPTER EASE
a) Inter-rater re11ab11-?ty 127
b) Intra-rater re I lab 11-Ity 127
4) Training of panel members 127
5) Scoring formulas... 129 3. Summary 130
IV ANALYSIS AND RESULTS 135 A. Influence of program type on assessment ability.. 135
1. Analysis and results 135 2. Conclusions 152
B. Data collection efficiency 152 C. Data co 11 ect I on proficiency 153 D. Amount of psychosocial patient data selected..... 158 E. Percent of psychosocial patient data selected.... 160 F. Nursing diagnosis Identification 163 G. Amount of plausible psychosocial nursing
diagnoses Identified 169 H. Percent of plausible psychosocial nursing
diagnoses Identified 171 I. Additional data analyses 174
1. Differential performance on PMPs 174 2. Proportion of AD and BD participants
selecting Individual data Items 175 3. Frequency of diagnostic statement
Identification 178 4. Type referent Identified for the nursing
diagnosis of Anxiety.... 181 5. Differences In learning experiences 182
J. Summary 183
V DISCUSSION 188 A. Conclusions 188
1. Assessment ability 189 2. Diagnostic ability 194 3. Data collection ability 195 4. Differential performance on the two
simulations 198 B. Implications 198 C. Recommendations 201 D. Summary 205
vll
TABLE OF CONTENTS (continued)
CHAPTER PAGE
VI APPENDICES 207 Appendix A . 208 Appendix B 210 Appendix C 211 Appendix D 213 Appendix E 220 Appendix F . 222
VII CITED LITERATURE 223
VIII VITA 240
vl II
LIST OF TABLES
IABJLE EASE
I CHARACTERISTICS OF ASSOCIATE DEGREE (AD) AND BACCALAUREATE DEGREE (BD) STUDENTS AS CITED IN THE LITERATURE, BY AGE, MARITAL STATUS, FAMILY RESPONSIBILITIES AND PRE-MATRICULATION ACADEMIC ACHIEVEMENTS 67
II DISTRIBUTION OF PARTICIPATING ASSOCIATE DEGREE (AD) AND BACCALAUREATE DEGREE (BD) PROGRAMS BY FINANCIAL SUPPORT AND NUMBER OF PARTICIPANTS 100
111 DEMOGRAPHIC CHARACTERISTICS OF STUDY PARTICIPANTS 101
IV ACADEMIC CHARACTERISTICS OF STUDY PARTICIPANTS 103
V SUMMARY OF THE INDEPENDENT VARIABLE, COVARIATES, AND DEPENDENT VARIABLES USED FOR DATA ANALYSIS 132
VI RELATIONSHIP BETWEEN THE LATENT VARIABLES OF KNOWLEDGE BASE, EDUCATION RELATED CLINICAL LEARNING EXPERIENCES, TASK COMPLEXITY AND ASSESSMENT ABILITY AND THEIR INDICATORS FOR THE MODEL EXPLAINING PERFORMANCE ON PMP-BROWN 138
VII RELATIONSHIP BETWEEN THE LATENT VARIABLES OF KNOWLEDGE BASE, EDUCATION RELATED CLINICAL LEARNING EXPERIENCES, TASK COMPLEXITY AND ASSESSMENT ABILITY AND THEIR INDICATORS FOR THE MODEL EXPLAINING PERFORMANCE ON PMP-ELLIS 139
VIII CORRELATION MATRIX: EXOGENOUS AND ENDOGENOUS VARIABLES IN THE MODEL FOR PMP-BROWN 141
IX CORRELATION MATRIX: EXOGENOUS AND ENDOGENOUS VARIABLES IN THE MODEL FOR PMP-ELL IS 142
X DIRECT EFFECT, INDIRECT EFFECT AND EFFECT COEFFICIENTS REPRESENTING INFLUENCE OF EDUCATIONAL PREPARATION ON PMP-BROWN ASSESSMENT PERFORMANCE 147
XI DIRECT EFFECT, INDIRECT EFFECT AND EFFECT COEFFICIENTS REPRESENTING INFLUENCE OF EDUCATIONAL PREPARATION ON PMP-ELL IS ASSESSMENT PERFORMANCE 148
ix
LIST OF TABLES (continued)
TABLE PAGE
XII GOODNESS OF FIT AND LEVEL OF SIGNIFICANCE FOR MODELS REPRESENTING ASSESSMENT PERFORMANCE ON PMP-BROWN AND PMP-ELLIS 150
XIII GOODNESS OF FIT AND TESTS OF SIGNIFICANCE FOR EACH ENDOGENOUS VARIABLE WITHIN THE PMP-BROWN MODEL 151
XIV GOODNESS OF FIT AND TESTS OF SIGNIFICANCE FOR EACH ENDOGENOUS VARIABLE WITHIN THE PMP-ELLIS MODEL 151
XV DESCRIPTIVE STATISTICS OF ASSOCIATE DEGREE (AD) AND BACCALAUREATE DEGREE (BD) PARTICIPANTS' PERFORMANCE ON DATA COLLECTION ACTIVITIES ON PMP-BROWN 154
XVI DESCRIPTIVE STATISTICS OF ASSOCIATE DEGREE (AD) AND BACCALAUREATE DEGREE (BD) PARTICIPANTS* PERFORMANCE ON DATA COLLECTION ACTIVITIES ON PMP-ELL IS 155
XVII ANALYSIS OF VARIANCE OF THE DATA COLLECTION EFFICIENCY SCORES OF ASSOCIATE DEGREE AND BACCALAUREATE DEGREE PARTICIPANTS ON PMP-BROWN 156
XVIII ANALYSIS OF VARIANCE OF THE DATA COLLECTION EFFICIENCY SCORES OF ASSOCIATE DEGREE AND BACCALAUREATE DEGREE PARTICIPANTS ON PMP-ELL IS 156
XIX ANALYSIS OF VARIANCE OF THE DATA COLLECTION PROFICIENCY SCORES OF ASSOCIATE DEGREE AND BACCALAUREATE DEGREE PARTICIPANTS ON PMP-BROWN 157
XX ANALYSIS OF VARIANCE OF THE DATA COLLECTION PROFICIENCY SCORES OF ASSOCIATE DEGREE AND BACCALAUREATE DEGREE PARTICIPANTS ON PMP-ELL IS 158
XXI ANALYSIS OF VARIANCE OF THE AMOUNT OF PSYCHOSOCIAL HISTORY DATA SELECTED BY ASSOCIATE DEGREE AND BACCALAUREATE DEGREE PARTICIPANTS ON PMP-BROWN 159
XXII ANALYSIS OF VARIANCE OF THE AMOUNT OF PSYCHOSOCIAL HISTORY DATA SELECTED BY ASSOCIATE DEGREE AND BACCALAUREATE DEGREE PARTICIPANTS ON PMP-ELL IS 160
x
LIST OF TABLES (continued)
TABLE PAGE
XXIII ANALYSIS OF VARIANCE OF THE PERCENT OF PSYCHOSOCIAL HISTORY DATA SELECTED BY ASSOCIATE DEGREE AND BACCALAUREATE DEGREE PARTICIPANTS ON PMP-BROWN 161
XXIV ANALYSIS OF VARIANCE OF THE PERCENT OF PSYCHOSOCIAL HISTORY DATA SELECTED BY ASSOCIATE DEGREE AND BACCALAUREATE DEGREE PARTICIPANTS ON PMP-ELLIS 162
XXV DESCRIPTIVE STATISTICS OF ASSOCIATE DEGREE (AD) AND BACCALAUREATE DEGREE (BD) PARTICIPANTS' PERFORMANCE ON NURSING DIAGNOSIS IDENTIFICATION ACTIVITIES ON PMP-BROWN 164
XXVI DESCRIPTIVE STATISTICS OF ASSOCIATE DEGREE (AD) AND BACCALAUREATE DEGREE (BD) PARTICIPANTS' PERFORMANCE ON NURSING DIAGNOSIS IDENTIFICATION ACTIVITIES ON PMP-ELLIS 165
XXVII ANALYSIS OF VARIANCE OF THE NUMBER OF PLAUSIBLE NURSING DIAGNOSES IDENTIFIED BY ASSOCIATE DEGREE AND BACCALAUREATE DEGREE PARTICIPANTS ON PMP-BROWN 166
XXVIII ANALYSIS OF VARIANCE OF THE NDXSCORES OF ASSOCIATE DEGREE AND BACCALAUREATE DEGREE PARTICIPANTS ON PMP-BROWN 166
XXIX ANALYSIS OF VARIANCE OF THE NUMBER OF PLAUSIBLE NURSING DIAGNOSES IDENTIFIED BY ASSOCIATE DEGREE AND BACCALAUREATE DEGREE PARTICIPANTS ON PMP-ELLIS 167
XXX ANALYSIS OF VARIANCE OF THE NDXSCORES OF ASSOCIATE DEGREE AND BACCALAUREATE DEGREE PARTICIPANTS ON PMP-ELLIS 168
XXXI ANALYSIS OF VARIANCE OF THE AMOUNT OF PLAUSIBLE PSYCHOSOCIAL NURSING DIAGNOSES IDENTIFIED BY ASSOCIATE DEGREE AND BACCALAUREATE DEGREE PARTICIPANTS ON PMP-BROWN 170
XXXII ANALYSIS OF VARIANCE OF THE AMOUNT OF PLAUSIBLE PSYCHOSOCIAL NURSING DIAGNOSES IDENTIFIED BY ASSOCIATE DEGREE AND BACCALAUREATE DEGREE PARTICIPANTS ON PMP-ELLIS 171
xl
LIST OF TABLES (continued)
TABLE EASE
XXXIII ANALYSIS OF VARIANCE OF THE PERCENT OF PLAUSIBLE PSYCHOSOCIAL NURSING DIAGNOSES IDENTIFIED BY ASSOCIATE DEGREE AND BACCALAUREATE DEGREE PARTICIPANTS ON PMP-BROWN 172
XXXIV ANALYSIS OF VARIANCE OF THE PERCENT OF PLAUSIBLE PSYCHOSOCIAL NURSING DIAGNOSES IDENTIFIED BY ASSOCIATE DEGREE AND BACCALAUREATE DEGREE PARTICIPANTS ON PMP-ELLIS 173
XXXV SUMMARY OF REPEATED MEASURES ANALYSES OF VARIANCE RESULTS FOR WITHIN SUBJECTS DIFFERENCES IN PERFORMANCE ON PMP-BROWN AND PMP-ELLIS FOR DATA COLLECTION AND NURSING DIAGNOSIS IDENTIFICATION TASKS 176
XXXVI SUMMARY OF DATA ITEMS WHERE STATISTICALLY SIGNIFICANT DIFFERENCES IN PERCENT OF AD AND BD PARTICIPANTS SELECTING ITEMS WERE DEMONSTRATED, BY PMP 177
XXXVII FREQUENCY DISTRIBUTION OF NURSING DIAGNOSIS STATEMENTS IDENTIFIED MOST FREQUENTLY ON PMP-BROWN 179
XXXVIII FREQUENCY DISTRIBUTION OF NURSING DIAGNOSIS STATEMENTS IDENTIFIED MOST FREQUENTLY ON PMP-ELL IS 180
XXXIX DESCRIPTIVE STATISTICS AND RESULTS OF ANALYSES OF VARIANCE COMPARING THE CLINICAL LEARNING EXPERIENCES OF ASSOCIATE DEGREE (AD) AND BACCALAUREATE DEGREE (BD) PARTICIPANTS, BY VARIABLE 184
XL CHARACTERISTICS OF INSTITUTIONS FROM WHICH THE STRATIFIED RANDOM SAMPLE OF ASSOCIATE DEGREE AND BACCALAUREATE DEGREE NURSING PROGRAMS WERE SELECTED 208
XL I RESULTS OF COCHRAN'S C TEST FOR HOMOGENEITY OF VARIANCE 222
xlf
LIST OF FIGURES
FIGURE EASE
1 Conceptual model 16
2 McClure's Model 1. 59
3 McClure's Model 2 59
4 McClure's Model 3 61
5 Spark's extension of McCture's Model 3 62
6 Path analysis results for PMP-Brown 144
7 Path analysis results for PMP-Ellls 144
xll I
SUMMARY
The purpose of this study was to examine the direct and Indirect
Influences of type of educational program attended on data collection
and nursing diagnosis Identification abilities of generic nursing
students within three months of graduation from associate degree and
baccalaureate degree nursing programs.
The primary research question qui ding this study was: Are the
patient assessment abilities of associate and baccalaureate degree
nursing students Influenced by the type of educational program
attended. Additional research questions addressed were differences
between the associate and baccalaureate degree students with regard to
data collection efficiency, data collection proficiency, amount and
percentage of psychosocial data collected, number of plausible nursing
diagnoses Identified, and amount and percentage of psychosocial nursing
diagnoses Identified.
A non-equivalent groups, post-test on Iy design was used. A
convenience sample of 91 associate degree and 86 baccalaureate degree
students was obtained from five randomly selected associate degree
programs and six randomly selected baccalareate degree programs within
a three state area In the mid-west. Participants completed the Watson-
Glaser Critical Thinking Appraisal (Form A), two latent Image,
branching type clinical simulations, and a background Inventory.
Analyses of variance, chl square and path analysis techniques were used
xlv
SUMMARY (CONTINUED)
to analyze the data. Performance on each simulation was analyzed
separately.
Analysis of performance on one simulation demonstrated
differences In the diagnostic abilities of the two groups <F (1,9) =
5.16; p<.05). No differences were found In data collection efficiency
or proficiency. In amounts or percent of psychosocial data collected,
or In amounts or percent of psychosocial nursing diagnoses Identified.
Path analyses revealed differential effects of the type of program
attended on the assessment abilities of the participants. On one
simulation, the effect coefficient was .411 while on the other It was
-.067.
On one simulation, baccalaureate degree participants Identified a
greater number of more complete nursing diagnosis statements than their
associate degree counterparts. Performance of all participants
differed across the two simulated patient encounters, demonstrating the
Influence of case specificity. Although not conclusive, findings
provide partial support for the claim that type of educational program
attended Influences diagnostic ablllltes of the participants. This has
Implications for differentiation of clinical practice of the two type
of graduates.
xv
I. INTRODUCTION
One question the nursing profession must address Is: What are the
differences. If any. In the nursing practice of graduates of associate
degree and baccalaureate degree nursing programs? Since the stated
goals and the course content Included In these two types of nursing
programs are different, the answer to this question has ramifications
for nurse educators, nursing service administrators, the profession as
a whole, and for the public the profession serves.
An example of the primacy of this concern Is the reluctance of
members of the New York State legislature to Introduce a bill revising
the state's nurse practice act to reflect the requirement of a
baccalaureate degree for the practice of professional nursing and the
associate degree for the practice of practical/technical nursing (New
York State Nurses' Association, 1983). The primary reason for this
reluctance Is the state nurses' association's Inability to demonstrate
that differences exist In the level of nursing care provided by
graduates of these two types of programs.
Previous research to distinguish between the nursing capabilities
of associate degree and baccalaureate degree graduates has been based,
primarily, on self-ratings, ratings of administrators and educators,
and on comparisons of self-ratings with the ratings of others (Chamlngs
and Teevan, 1979; Dlckerson, 1976; Hogstel, 1975; McKenna, 1971; Pitts,
1975; Schuyler, 1983; SchwIrian, 1979). A review of the results of
these studies has not demonstrated unequivocal evidence that
1
2
differences do exist. One threat to the validity of these studies Is
lack of control for the educational preparation of administrators who
rate staff members (McCloskey, 1981).
A different approach to demonstrating the existence of
differences In the level of nursing practice due to educational
preparation Is to focus on graduates' abilities to apply and use the
nursing process (Asplnall, 1976; Baumann and Bourbonnats, 1982; Davis,
1972; 1974; deTornyay, 1968; Gordon, 1980; Verhonlck et al., 1968. The
major focus of this research has been on decision making activities
associated with planning Interventions used for patients with specific
nursing problems or nursing diagnoses. Researchers have examined the
patient assessment abilities of the nurse In only a small proportion of
these studies. In addition, only 8 of these studies have compared,
directly or Indirectly, the capabilities of the associate degree
graduate or student with those of the baccalaureate degree graduate or
student CBassett, 1977; Frederlckson and Mayer, 1977; Gover, 1972; Gray
et al., 1977; Johnston, 1982; Retd, 1981; Sparks, 1979).
The remainder of this chapter Is focused on the background of the
present study, the conceptual framework, the purpose, the research
questions to be addressed, and the significance of the study.
Subsequent chapters Include a review of the literature, the methodology
used to conduct the study, the results, and a discussion of the results
and conclusions.
A. Background of the study
The provision of effective and efficient nursing care Is

3
dependent upon the nurse's cognitive ablIIty to define clearly a
patient's health problems and to select Interventions that have a high
probability of resolving those problems (Gordon, 1982). Such cognitive
activity Is an Integral part of nursing care and has been
conceptualized as the nursing process. The sections that follow
provide an overview of 1) the steps of the nursing process and the
Identification of a nursing diagnosis, 2) the cognitive processes
Involved In problem solving activity, and 3) the characteristics of
associate and baccalaureate degree students and programs that Influence
problem solving activity.
1 * Definitions
The terms used In this study are defined as follows:
1. Problem solving - A goal-dIrected sequence of
cognitive operations.
2. Problem solving process - The scientific method
utilized In problem solution which Includes encountering a problem,
collecting and analyzing the data In connection with a problem,
Identifying the exact nature of the problem, deciding on a plan of
action, carrying out the plan, and evaluation of the plan and the new
situation.
3. Nursing process - The problem solving process used by
nurses. An orderly systematic manner of determining the client's
problems, making plans to solve them, Implementing the plan or
assigning others to Implement ft, and evaluating the extent to which
the plan was effective In resolving the problems Identified. The four
4
phases of the process are: assessment, planning, Implementation, and
evaluation.
4. Assessment - A component of the nursing process that
encompasses Information gathering, a diagnostic Judgment, and the
labeling of a health problem.
5. Nursing diagnosis - A concise term representing a
cluster of signs and symptoms that describes responses to actual or
potential health problems or states-of-the-patlent which nurses by
virtue of their education and experience are able, licensed, and
legally responsible and accountable to treat.
6. Efficiency score - A measure of the degree to which a
participant's choices of data and procedural steps on a clinical
simulation are helpful In the resolution of a client's problem. A
ratio of the number of essential Items selected or steps taken to the
total number of Items and procedural steps selected (McGuIre et al.(
1976).
7. Proficiency score - A measure of the degree to which a
participant's selection of data and procedural steps corresponds with
those Judged optimal by experts In the field. A ratio of the number of
essential data and procedural steps taken minus the non-essential Items
selected to the optimal number of Items to be selected (McGuIre et at.,
1976).
2. Nursing, process, and. nursJng. diagnosis
The nursing process Is an application of scientific problem
solving to the management of patient care. This process consists of
5
the following steps: 1) assessment - which Includes data collection
and the Identification of nursing diagnoses; 2) formulation of a plan
of care; 3) Implementation of care; and 4) evaluation of outcomes
(Asplnall and Tanner, 1981; Carnevelli, 1983; Yura and Walsh, 1978).
The relevance of the plans for and the Implementation of specific
nursing care Is dependent upon the accuracy of the nursing diagnosis
statement. This statement must accurately reflect those problems
manifested by patients that can be dealt with and managed by nurses
working Independently or InterdependentIy with other health
professionals.
The diagnostic activity of the nurse was sanctioned by the
American Nurses' Association (ANA) when It published the Generic
Standard*; of Practice (1973). Additionally, the nurse practice acts In
all political Jurisdictions of the United States directly or Indirectly
address Incorporation of nursing diagnostic activity within the scope
of professional nursing practice (W. Young, persona! communication,
November 28, 1983).
The nursing diagnostic process has been described as being both
dynamic and cyclic In that diagnoses change with a patient's condition
(Mahomet, 1975). Abdellah and Beland (1965, p. 9) stated, "A nursing
diagnosis Is a determination of the nature and extent of the nursing
problems presented by Individual patients and families receiving
nursing care." Komortta (1963, p. 84) said: "A nursing diagnosis
should be a conclusion based on scientific determination of an
Individual's nursing needs, resulting from critical analysis of his
6
behaviour, the nature of his Illness, and numerous other factors which
affect his condition."
Other descriptions and definitions of nursing diagnoses and the
diagnostic process are very similar to that Identified by Komorlta
(1963) (Bonney and Rothberg, 19635 Carlson, 1972; Dodge, 1975b; Durand
and Prince, 1966; Gebble and Levlne, 1975; Kelly, 1966; Matheny et al.,
1972; McCain, 1965; Norrls, 1964; Roy, 1974a; 1974b). The common
element linking the various statements Is a conclusion that the
diagnostic process Is Inferential and culminates In a conclusive
statement of nursing Judgment; It recognizes patterns derived from the
nurse's Investigation of an individual's total condition.
3. Cognitive processes
The ability of Individuals to formulate nursing diagnoses is
limited by their Information processing abilities. Therefore, an
overview of the human Information processing system, and the use of
diagnostic hypotheses as a means of dealing with a problem solving task
within an open system will be discussed. In addition, characteristics
of the task environment and of the problem solver that Influence
problem solving ability also will be described.
Human problem solving behavior, which Includes problem
Identification (e.g., diagnosis), was described in terms of a theory of
human Information processing by Newell and others (Newell et al., 1958;
Simon and Newell, 1971; 1972). These Investigators described the
Information processing system as follows. Following the Initial
reception of Information via sense organs, subsequent processing occurs
7
in sensory memory where the Input either decays and Is lost from the
system or Is transferred to short term memory (STM). The STM Is a
working memory having rather limited capacity In terms of both the
quantity (Miller, 1956) and the length of time Information can be
retained (Simon and Newel 1, 1971; 1972). From the STM, Information to
be retafned Is transferred to long term memory (LTM) where It Is stored
along with the rules for Its processing (Simon and Newell, 1971; 1972).
The retrieval of Information from L7W entails Its transfer back to STM
(Bourne et a I., 1979).
Simon and Newell (1971; 1972) demonstrated that a problem solver,
when confronted with a task, defines It In terms of a problem space.
In searching memory for a solution to the problem, a promlnantly used
heuristic Is that of means-ends-analysis. This approach Is appropriate
when a specified goal or end-state Is present (Sweller and Levlne,
1982).
However, In clinical problem solving, an open, probabilistic
system prevails (Gordon, 1982; Grler, 1976; Hammond, 1966). A patient
presents with symptoms or a complex of symptoms representing the
presence of a problem of undefined nature. The clinician Is faced with
an Infinite number of possibilities from which to determine the cause
of the complaints and to prescribe a treatment plan. In order to limit
the problem space, the clinician formulates provisional hypotheses, or
diagnoses, and then tests these hypotheses (Elstein et al., 1978).
Research In medical problem solving has demonstrated that there
are four components of hypothesis generation (Elstein et al., 1978).
8
These components are: 1) attending to Initially available cues, 2)
Identifying problematic elements from among these cues, 3) associating
from problematic elements to LTM and back, generating hypotheses and
suggestions for further Inquiry, and 4) Informally rank ordering
hypotheses according to subjective estimation. The "problematic
element", referred to above, appears to serve as an Indexing key In an
associative process which links observations to prior knowledge.
Additional data are then collected In an attempt to confirm or reject
the set of provisional hypotheses (Elstein et aI., 1972).
At the current time, there Is no reason to reject this process as
the process by which nurses hypothesize and test out nursing diagnoses
(Gordon, 1982). This approach Is comparable to the sub-goal setting
strategies used to limit problem spaces, as described by Reed and
Abramson (1976), and sub-set sampling of hypotheses as described by
Levlne (1970).
The cognitive aspect of a diagnostic task Is one of concept
attainment (Bruner et al., 1956; Gordon, 1982). A diagnostic concept
consists of 1) observable facts or lower concepts; 2) an Idea or
pattern of the facts and their relationships which form a person's
recognlttonat capacity; and 3) a symbol or name which represents the
entire relationship (BIrcher, 1982).
A nursing diagnosis is a complex concept reflecting the actual or
potential health problems which nurses by vlrture of their education
are licensed, and legally responsible and accountable to treat
(BIrcher, 1982; Morltz, 1982). In relation to an Individual's
9
diagnostic ability, Gordon (1982, p. 46) Indicated that:
Diagnostic competence Includes the ability to collect, Interpret, and analyze clinical data and the ability to cluster data In the formulation of problems. These cognitive-perceptual abilities are basic to the diagnostic phase of the nursing process.
Gordon (1982) stated that the formulation of a nursing diagnosis
requires theoretical knowledge of a set of categories and their
critical defining characteristics. The possession and use of a network
of concepts, such that one or more cues may generate a set of
diagnostic hypotheses, then can be subjected to testing via further
clinical observation. However, If one does not know that the Incidence
of a specific nursing diagnosis Is Increased In the presence of a
particular disease entity or Its treatment, one may not search for cues
or attend to cues that are present. The formulation of appropriate
nursing diagnoses Is dependent upon the ability to generate multiple
hypotheses, recognize cue clusters, and permit these to control the
search for confirming or dI sconfirming Information.
One of the cognitive processes Involved In the diagnostic task Is
the exercise of Judgment. Newell and others (Newell, 1968; Newell and
Simon, 1971; 1972) stated that Judgment Is a cognitive process that
takes place between the Input of Information and output. Judgment Is
more than a simple transfer of Information. Prior to output, the
Individual, via Judgment, adds fnformtlon to that already available In
the situation. Depending upon the nature of the domain being Judged,
the output takes the form of an estimation, assertion, evaluation or
classification as to class membership.
10
Problem solving ability has been Investigated In terms of 1)
characteristics of the task environment and 2) characteristics of the
problem solver. Some of the characteristics of the task environment
that Influence problem solving ability are task complexity and task
setting (Bashook, 1976; Elsteln et al., 1978; McGuIre and Page, 1973;
Norman and Felghtner, 1981; Norman et al., 1983; Simon and Newell,
1971; 1972).
Characteristics of the problems solver reported to be associated
with problem solving ability are cognitive style,
Intelligence/aptitude, gender, age, creative ability, critical thinking
ability, and knowledge base (Bourne and Domlnowskl, 1972; Burke, 1965;
Burke and Maler, 1965; Laughlln, 1967, 1968; Laughlln et al., 1968;
Mater and Casselman, 1970; Maler and Jenson, 1969; Mendelsohn et al.,
1966; Ptshktn and Rosenblum, 1966; Plshkln and Wolfgang, 1965; Plshkln
et at., 1967). Kissinger and Munjas (1981) noted that historical
knowledge Influences application of acquired knowledge to problem
solving situations.
CharacterIstlcs of the nurse problem solver associated with
the exercise of clinical Judgment are theoretical knowledge, years of
clinical experience, and level of education (Broderlck and Ammentorp,
1979; Baumann and Bourbonnals, 1982; Davis, 1972; 1974; Grler and
Schnltzler, 1979). These characteristics were corroborated In medical
studies conducted by Burkett and Knafl (1974), Klelnmuntz (1968), and
Knafl and Burkett (1975). The relationship between problem solving
ability and characteristics of personality type, critical thinking and
11
Intellectual ability also were examined and Inconclusive results
reported (Kissinger and Munjas, 1981; Koehne-KapIan and Tilden, 1976;
Tanner, 1977).
A number of researchers Investigated the general problem solving
abilities and/or strategies used by nurses (Asplnall, 1976; 1979;
Baumann and Bourbonnals, 1982; Broderlck and Ammentorp, 1979; Dlncher
and Stldger, 1976; Farrand et at., 1982; Grler, 1972; Grler and
Schnltzler, 1979; Hammond, 1964; 1966; Hammond et al., 1967; Holzemer
et al., 1981; Johnston, 1982; Kelly, 1964a; 1964b; 1966; McLaughlin et
al., 1978; 1979; Sparks, 1979; Tanner, 1977). Of these researchers,
only a few have compared, either directly or Indirectly, the data
gathering and diagnostic capabilities of associate degree graduates or
students with their baccalaureate counterparts. In addition, the
results of some of these studies are suspect due to methodological
problems which Include small sample size and questions regarding
Instrument validity and reliability.
4. Characteristics of educational programs and S.tudfiRtS
that Influence problem sol v Ing ah I Mty
The ability of the nurse to Identify, analyze, and cluster
data and to Identify nursing diagnoses accurately Is dependent upon
knowledge acquired through formal education and clinical practice
(Gordon, 1982; McCarthy, 1981). Within nursing, there currently exist
three different types of formal educational programs through which an
Individual can become eligible for licensure to practice as a
registered nurse. The three types of programs are hospital-based
12
diploma programs, associate degree programs offered, primarily, by
junior and community colleges, and baccalaureate degree programs
offered by senior colleges and universities.
Although diploma programs were most prevalent prior to 1950
(I.e., prepared the vast majority of nurses), support for their
existence has waned. The reports of Goldmark (1923), Brown (1948) and
the Committee on the Function of Nursing (1950) all advocated moving
nursing education Into Institutions of higher learning. In a 1965
paper on the scope and nature of nursing practice In relationship to
educational requirements, the ANA took a position that the preparation
of Individuals for practice as professional nurses should take place
within Institutions of higher learning. The assumption underlying this
position Is that a baccalaureate education better prepares the nurse to
deliver professional nursing care than does associate degree or diploma
preparation (ANA, 1965).
This position has been reaffirmed by Individual state nurses'
associations (e.g., Illinois, Indiana, New York). Several states are
now working towards the Introduction of legislation to make the
necessary changes In their respective nurse practice acts.
The two levels of educational preparation supported by the ANA
are the associate degree for the practice of technical nursing, and the
baccalaureate degree for the practice of professional nursing. The
goals and objectives, and the scope and depth of the formal educational
content and the clinical learning experiences of these two types of
programs differ In many respects (Dowe, 1974; Dustan, 1964; Hartley,
13
1975; Johnston, 1982; Kramer, 1981; McClure, 1976; Melels and Farrell,
1974; Montag, 1951; National League for Nursing, 1967; 1978; 1979;
Richards, 1972; RInes, 1977a; 1977b; Schlotfeldt, 1977; Sparks, 1979;
Waters et at., 1972; Wren, 1971). These differences will be addressed
In the literature review.
The characteristics of the students In the two types of programs
have been found to differ In age (Dowe, 1974; Dustan, 1964; Hartley,
1975; Sparks, 1979; Wren, 1971), years of education between high school
and enrollment In nursing school (Dustan, 1964; Sparks, 1979), and
years of work experience In a health related discipline prior to
enrollment (Melels and Farrell, 1974; Richards, 1972; Wren, 1971).
These differences will be addressed In the literature review.
RInes (1977a; 1977b) theorized that differences should be evident
in the assessment abilities of associate degree and baccalaureate
degree graduates. The associate degree graduate Is expected by nurse
educators to use the following processes: observation, directed
questioning, physical examination, and measurement of bodily function.
The outcome or product of data collection Is the provision of
Information to the professional nurse, doctor, or other member of the
health team.
In contrast, the baccalaureate graduate Is expected by nurse
educators to perform data collection based on the following:
Interviewing, obtaining a patient history, Identification of questions
to be answered. Identification of sources of data, categorization of
data, and Interpretation of data. The expected outcome Is the
14
statement of nursing diagnoses and a plan for nursing care (RInesf
1977a; 1977b).
It Is clear that the baccalaureate graduate Is expected by nurse
educators to function differently than Is the associate degree graduate
with respect to data collection and Identification of nursing
diagnoses. Therefore, the major differences In the knowledge base of
graduates of the two types of programs should be reflected In the types
of data that they collect and the nursing diagnoses that they Identify.
B. Conceptual framework
Effective use of the nursing process for planning and delivering
nursing care Is highly dependent upon the cognitive Information
processing abilities of the nurse. The outcomes of the nursing process
are Influenced by task complexity, the environmental setting In which
the task occurs, and by the characteristics of the problem solver
(Gordon, 1980; Newell et a!., 1958; Simon and Newell, 1971; 1972).
Characteristics of the nurse problem solver that Influence
Information processing In a clinical setting, and that have been
Identified In the literature, are age , gender, theoretical knowledge
base, years of clinical experience, level of educational preparation.
Intellectual ability, creativity, critical thinking ability and
cognitive style. In addition, age (Knopf, 1975; Nash, 1975; Sparks,
1979), intellectual ability (Dustan, 1964; Schwirian, 1979; Sparks,
1979), the number of years of post-high school education prior to
enrollment (Sparks, 1979), and pre-nurslng experience In a clinical
environment (Sparks, 1979) have been found to differentiate between
15
students enrolled In associate degree and In baccalaureate degree
programs. Attributes which characterize the differences between
associate degree and baccalaureate degree education Include the scope
and depth of theoretical content and clinical practice, and the
specific goals and objectives of the programs.
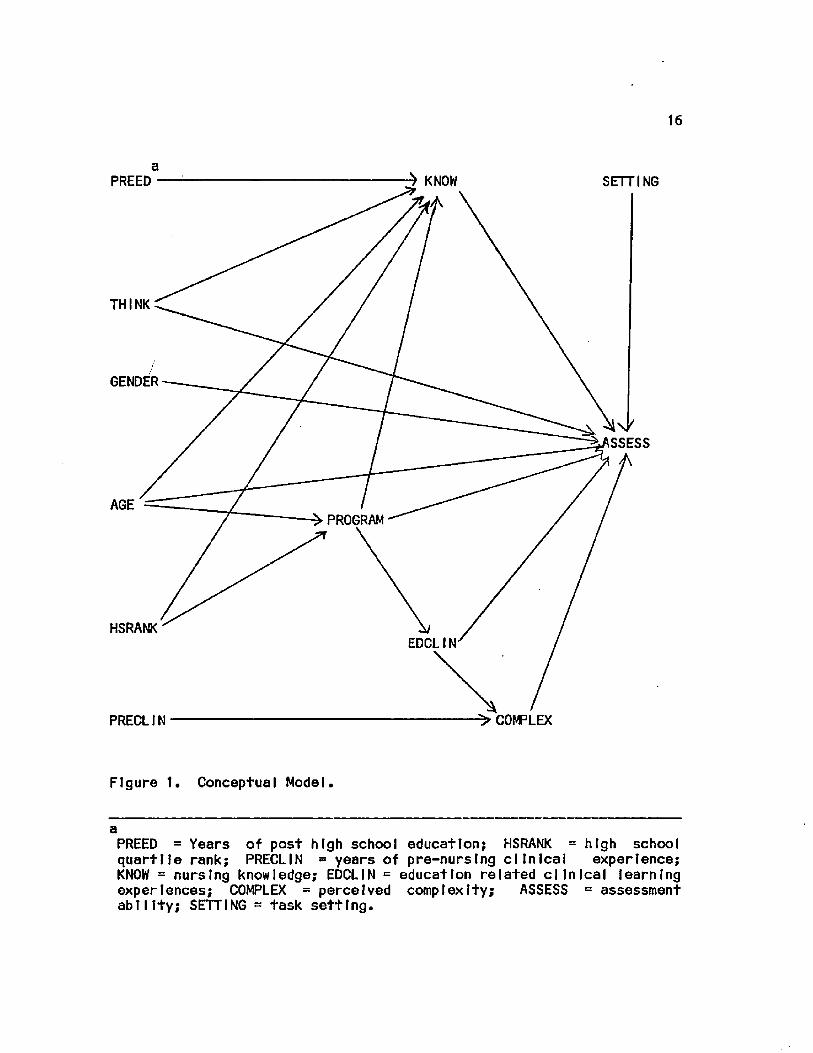
A determination of the Influence of the type of education
program attended on ab11Ity to collect patient data and Identify
diagnoses Is dependent on controlling the task environment and the
Influences of age, gender, knowledge base, critical thinking ability,
post high school education, and pre-nurslng experience on educational
preparation. A graphic description of this model Is depicted In Figure
1.
c. Purposfi af. .the study
The purpose of this study was to examine the direct and Indirect
Influence of the type of educational preparation on the data collection
and nursing diagnosis Identification abilities of generic nursing
students within three months of graduating from associate degree and
baccalaureate degree nursing programs.
D. Research questions
The primary research question was: Are the patient assessment
abilities of associate and baccalaureate degree nursing students, when
measured within three months prior to graduation from a program of
study accredited by the National League for Nursing, Influenced by type
of educational program?
16
a ^ KNOW PREED SETTING
THINK
GENDER
SSESS
AGE PROGRAM
HSRANK EDCLIN
-> COMPLEX PRECLIN
Figure 1. Conceptual Model.
a PREED = Years of post high school education; HSRANK = high school quartlle rank; PRECLIN = years of pre-nurslng clinical experience; KNOW = nursing knowledge; EDCLIN = education related clinical learning experiences; COMPLEX = perceived complexity; ASSESS = assessment ability; SETTING = task setting.
17
Additional questions addressed were:
1. When graduating associate and baccalaureate degree nursing
students are compared. Is there a difference In data collection
efficiency?
2. When graduating associate and baccalaureate degree nursing
students are compared, Is there a difference In data collection
proficiency?
3. When graduating associate and baccalaureate degree nursing
students are compared. Is there a difference In the amount of
psychosocial history data selected?
4. When graduating associate and baccalaureate degree nursing
students are compared, Is there a difference In the percent of
psychosocial history data selected?
5. When graduating associate and baccalaureate degree nursing
students are compared. Is there a difference In the amount and
completeness of nursing diagnoses Identified?
6. When graduating associate and baccalaureate degree nursing
students are compared. Is there a difference In the amount of
psychosocial nursing diagnoses Identified?
7. When graduating associate and baccalaureate degree nursing
students are compared, Is there a dlffernce In the percent of
psychosocial nursing diagnoses Identified?
E. SJg.n.1 -f.Icanca. of, tha_ study
Although the depth and breadth of course work and the major
objectives and goals of baccalaureate and associate degree nursing

18
programs differ, the graduates of both types of programs are eligible
to take the same licensing examination to practice as a registered
nurse, and are hired to fill similar. If not Identical, clinical
positions. The current licensing practices and the use of associate
degree and baccalaureate degree prepared graduates to fulfill similar
roles and functions tn nursing service settings also have been
identified as factors contributing to the confusion experienced by the
public and other health professionals as to the roles and functions of
nurses with different educational backgrounds (Gray et al., 1977;
McClure, 1976; Sweeney, 1980).
Since the ability to Identify relevant nursing diagnoses Is a
prerequisite for planning and Implementing nursing Interventions, the
results of this study will contribute to a further delineation of the
roles and responsibilities of the technical nurse from those of the
professional nurse.
The profession, as reflected In the ANA position paper on
educational preparation for nursing, has stated that baccalaureate
graduates should perform differently from associate degree graduates tn
terms of the scope of their practice and the complexity of the care
they provide patients and the patient's significant others. The
additional education obtained In a program of study leading to a
baccalaureate degree should prepare the graduate for a different level
of practice.
If differences can be demonstrated between the practice of the
associate and baccalaureate degree nurses, these will provide nursing
19
service administrators, nurse educators, state licensing boards and
legislatures, and the professional organization with a basis for
further clarification of the roles and responsibilities of the
technical nurse and the professional nurse. If differences can be
demonstrated, these results would aid In the delineation of specific
educational program objectives, and the types of assignments that
should be given to graduates of the different types of programs. If
the capabilities of the professional nurse and the technical nurse can
be distinctly differentiated and this Information disseminated to the
public at large, the expectations of other professionals and of
Individuals seeking health care from the nursing community may become
less confused and more realistic.
The number of Individuals currently graduating from associate
degree programs In nursing Is far greater than the number graduating
from baccalaureate programs (Vaughn, 1983). It Is an accepted fact
that the cost of two years of education Is cheaper, both for the
Individual student and for the public as a whole, than Is the cost of
four or five years of education necessary for a baccalaureate degree.
If there are no differences In the abilities of the associate degree
nurse and the baccalaureate degree nurse, It would be foolish for
society to support the more expensive baccalaureate program.
The cost of health care also could be Influenced by the
educational preparation of nurses. If the differences between the
roles and functions of the two levels of nursing practice were
delineated, it would facilitate the use of nursing personnel
20
appropriate to the care needs of the patient. On the other hand,
differential pay scales, as provided by some health care Institutions,
which acknowledge the additional preparation and enhanced capabilities
of the baccalaureate graduate would not be necessary If differences can
not be demonstrated between graduates of the two types of programs.
Therefore, additional public and private monies could be saved.
The following chapter contains a review of literature pertaining
to the diagnostic process, the measurement of clinical problem solving
ability and differences In associate and baccalaureate degree programs
and their students and graduates.
II. LITERATURE REVIEW
This study was based on the premise that the ability to collect
significant patient data and to formulate nursing diagnoses Is, In
part, dependent upon an Individual's knowledge base. The major focus of
this chapter Is a review of the literature relevant to a description of
the diagnostic process and a description of differences In the goals,
objectives, and content of associate and baccalaureate degree nursing
programs and characteristics of their students and graduates. An
additional section contains a review of the literature concerning the
measurement of clinical problem solving ability.
A. The dI agnostic prnrass
The diagnostic process refers to the analytical and evaluative
process aimed at determining the cause or nature of a patlent*s
problems (Barrows and Tamblyn, 1980). In the preceding chapter, It was
stated that the diagnostic process Is a problem solving task that
occurs In a probabilistic environment (Gordon, 1982j Grler, 1976;
Hammond, 1966). In addition, the cognitive aspect of a diagnostic task
also has been described as one of concept attainment (Blrcher, 1982;
Bruner et al., 1956; Gordon, 1980; 1982).
Information processing theory was chosen as the theoretical
framework for this study since this theory describes the cognitive,
problem solving processes that are used for Identification of nursing
diagnoses. The major focus of research within this paradigm has been
21
22
on a description of processes by which Information Is processed and
factors Imposing limitations on Information processing.
The theory, as developed by Newell et at. (Newell et al., 1958;
Simon and Newell, 1971; 1972) describes problem solving behavior as an
Interaction between a problem solver (the Information processing
system) and a problem or task (the task environment). How well a
problem solver utilizes the processing system Is dependent upon how
well one can adapt to constraints Imposed by the processing system
(Internal factors) and constraints Imposed by the task environment
(external factors) (Newell et al., 1958). Characteristics of the task
environment and characteristics of the problem solver that Impact on
diagnostic ability will be described In terms of Information processing
theory and research findings reported In nursing and medical
IIterature.
1. Task, environment
The nature of the task environment determines to a large
extent the behavior of the problem solver. Independently of the
detailed structure of the Internal Information processing system (Simon
and Newell, 1971; 1972). This subsection addresses environmental
factors that Influence clinical problem solving: setting,
characteristics of patient cues, and context of care.
The setting In which a clinical diagnostic task occurs has been
described as an open, probabilistic system (Gordon, 1980; Grler, 1976;
Hammond, 1966). As a result, clinical diagnoses are arrived at under
conditions that are Indeterminate In nature (Elstetn et al., 1978).
23
This situation has been described best by Hammond (1964; 1966)
and Kelly (1966) In their studies of clinical inference In nursing.
Signs and symptoms (cues) of a patient's condition from which a
clinician derives a diagnosis are not completely dependable. They are
probabilistically related to a given state of affairs. A specific
condition may be manifested by one cue one time and by a different one
on another occasion. In addition, a single cue may be produced by
several different conditions. The great majority of data are
uncertain, fallible, and Inter-substltutable (Hammond, 1966). Hammond
also noted that a nurse is faced with an uncertainty-geared task when
attempting to Infer the state of a patient. He stated that "The
nurse's problem is to Infer correctly the Impalpable state of the
patient from the uncertain, palpable data presented by the patient"
(1966, p.29). This conclusion also was reached by Kelly (1966) who
noted that data available from patients are Incomplete, probabilistic
In nature, and may have high Information value or be Irrelevant or
Inconsequential.
Additional evidence of the less than optimal conditions under
whtch diagnostic conclusions are arrived at Is related to findings that
data obtained directly from patients are characterized as
unstandardlzed and poorly quantified (Koran, 1975a; 1975b). Laboratory
test results also have been found to vary widely In sensitivity,
specificity, reliability, and accuracy (McNeil, 1975).
The characteristics of patient data have been examined In
relationship to their Impact on the diagnostic process. Cianfranl
24
(1982) examined the Influence of the amount and relevance of data on
the ability of 180 critical care nurses and students In graduate
nursing programs to Identify patient health problems. He found that
the accuracy of problem Identification was significantly less In the
presence of low relevant data than when high relevant data were
present. He also found that as the amount of available data Increased,
there was an Increase In the number of problems Identified, the time
necessary to Identify these problems, and In the number of errors
committed.
Archer et al. (1955) found that as the amount of Irrelevant
Information Increased, performance on a concept Identification task
decreased. This was corroborated by the findings of Walker and Bourne
(1961) who also found a decrease In performance related to an Increase
In the amount of Irrelevant data. In addition. Walker and Bourne (1961)
also found that as the amount of relevant data Increased, performance
on the concept attainment task decreased.
Bourne and Haywood (1959) examined performance on a concept
Identification task In relationship to different amounts and levels of
redundancy In relevant and Irrelevant data. They found that when non-
redundant Irrelevant data were added to available relevant data,
performance on the task diminished. In the presence of relevant and
Irrelevant data, the addition of redundant relevant data resulted In
Improved performance. The addition of redundant Irrelevant data to
varying levels of relevant data also Interfered with performance but
not as much as when non-redundant, Irrelevant data were added.
25
The results of these studies Indicate that both quantity and
quality of available data Influence diagnostic performance by adding
both to the amount of Information that needs to be processed and to the
level of complexity that needs to be dealt with.
An additional environmental characteristic that influences
diagnostic accuracy Is the context of care. Bashook (1976) noted that
problem solving In an emergency situation should be different than that
In a non-emergency situation due to the time constraints imposed on the
decision maker* Equivocal evidence has been accumulated In regard to
the performance of clinicians exposed to patients with different
problems. Elsteln et al. (1978) concluded that diagnostic competence
may be case related since they found considerable variation In the
diagnostic effectiveness of physicians and medical students across
patient problems. In contrast. Barrows et al. (1982) reported finding
little variation In physlcan performance across a variety of simulated
patient problems. Norman et al. (1983) found no support for "case
specificity" as an explanation for differences In diagnostic ability,
a. Summary
A diagnostic task is accomplished In an open
probabilistic system using data that are Incomplete and unstandardlzed,
probabilistic In nature, poorly quantified, and varying In sensitivity,
specificity, and reliability. In addition, the amount and relevancy of
the data available to the diagnostician also Influence diagnostic
outcomes. Variations In diagnostic accuracy are associated with the
context of care and also may be related to care specificity.
26
2. Character istics, of. the prob.l em salver
The focus of this section Is to describe the characteristics
of the human processing system. Simon and Newell (1971; 1972) described
the human Information processing system In terms analogous to
Information flow through an artificial Intelligence system.
Information obtained from the external environment Initially Is
processed through sensory memory where the Input, represented
symbol leally, either decays and Is lost from the system or Is
transfered to short term memory (STM). The STM Is a working memory
which Is the central processing unit of the system. Information can be
stored temporarily In STM but that which Is to be retained Is
transfered to long term memory (LTM) where It Is stored along with the
rules for Its processing. Use of Information stored In LTM for problem
solving Involves Its transfer back to STM for processing, the outcome
of which subsequently results In output. This output may take the form
of a problem solution, a search of the problem space for additional
Information, or the storage or retrieval of Information from LTM. The
processing capabilities and the characteristics of the STM and the LTM
wilt be described In detail.
a. Process, I no flanahMltles
The processing capability of a human Information
processing system Is dependent upon the number of processes It can do
simultaneously, the time It takes to perform each process, and the
amount of work done by each Individual process (Simon and Newell, 1971;
1972). The system operates In a serial as opposed to a parallel
27
fashion. It executes one elementary Information process at a time. As
the problem solver searches sequentially, small successive additions
are made to the store of Information about a problem and Its solution
(Simon and Newell, 1971; 1972). The processing rate Is dependent
upon the type of process being executed and Its complexity. The
results of rote memory experiments provided evidence that 5 to 10
seconds are required to store a symbol In LTM. In contrast, when
subjects were required to search down lists of simple arithmetic
problems, only milliseconds were found to be needed for the transfer of
Information Into and out of STM (Simon and Newell, 1971; 1972).
b. Short, teria memory
The processing of Information In STM significantly
Influences problem solving ability (Lindsay and Norman, 1977; Simon and
Newell, 1971; 1972). The major limitations of STM are Its capacity and
the amount of time that Information can be retained. The STM has a very
small capacity. Miller (1956), In a review of rote memory
experiments, concluded that the capacity of the STM Is 2.6 bits (s.d. =
0.6) of Information. This translates to a capacity for 7, plus or
minus 2 categories of Information that can be retained at any one time.
Elsteln et al. (1972; 1978) In Investigations of the reasoning
processes used by expert physicians, found that the number of
diagnostic hypotheses entertained at any one time was four, plus or
minus one. Although these estimates differ from those of Miller
(1956), they do depict the limited capacity that Is available.
The capacity of STM can be Increased through a process refered to
28
as "chunking" (Miller, 1956). Chunking refers to the grouping of
meaningful Items Into one category. However, as the number of Items
chunked together Increases, the qual Ity of the Information decreases
(Miller, 1956).
Shanteau and Phelps (1977), In an Investigation of the judgmental
processes used by IIvestock Judges, found that experts were able to
process larger amounts of Information than were non-experts. This
ability was attributed to the chunking of data In STM. Chase and Simon
(1973) found that grand master chess players were able to recreate
chess positions differently than were novices. The grand masters
replaced chess pieces In groupings that represented their relationships
under actual game positions. In contrast, novices replaced the pieces
Individually. The actions of the grand masters were Interpreted as
being representatIve of the chunking of Information In STM.
Long term retention of Information Is not a characteristic of
STM. Information not rehearsed Is generally lost within 30 seconds.
Rehearsal enhances the processing, but not the capacity of Information
held In STM. Repeated rehearsal of an Item Increases the likelihood
that It will be transfered to LTM from which It can be recalled
(Klatzkey, 1975; Lindsay and Norman, 1980; Simon and Newell, 1972).
c. Long term memory
Information to be retained for future use Is stored In
LTM. The organization of Information In LTM and Its role In problem
solving are discussed In the following subsections.
29
1) Organ teat-ton of stored Informat Ion
Through learning, certain stimuli or patterns of
stimuli are designated by particular symbols that can be stored In LTM.
The LTM has unlimited storage capacity and Is organized assocIat IveIy
with Its content being composed of symbols and structures of symbols
(also called chunks or nodes) that represent recognizable
configurations (Simon and Newell* 1972). The stored symbols serve as
the Internal representation for the corresponding stimulus patterns or
chunks. As new symbol structures are stored In LTM, they can be
embedded as symbols In other symbol structures, thus forming an
associative network of concepts and relations between concepts
(Anderson, 1980; Anderson and Bower, 1972; Simon and Newell, 1972).
Mayer (1975) noted that the extent to which new nodes are added
and linked to other nodes In LTM can vary along three dimensions.
First, the degree to which new nodes are acquired by a learner Is
reflected quantitatively by the amount of learning that takes place.
The second dimension Is the degree to which new nodes are connected
with one another In a single, well defined structure. The third
dimension Is the degree to which new nodes are connected with concepts
already existing In the learner's cognitive structure, thus forming an
Integrated network.
Mayer (1975) subsequently conducted an Investigation Involving
the use of different Instructional methods for teaching probability
theory. The results demonstrated that when there was no difference In
the amount of Information learned, a teaching method promoting the
30
Integration of new Information within existing knowledge resulted In
more flexible problem solving abl IIty than did a method focusing on
teaching procedural steps.
The results of several Investigations have provided Insight Into
the organization of Information stored In LTM. Collins and Quill Ian
(1969) used subject reaction times for the retrieval of Informtlon from
LTM In order to Judge the truth of assertions about concept
organization. Results of their Investigation supported the assumption
that a network of concepts and their associated properties are arranged
hierarchically. This finding was supported by the results of
Investigations of medical problem solving conducted by Kletnmuntz
(1968) and Wortman (1972).
Klelnmuntz (1968) used a variation of a 20 questions game to
examine the diagnostic skills of 12 neurologists who possessed varying
levels of experience. As the neurologists progressed through a
diagnostic task, they were encouraged to think aloud. The sessions
were recorded and the transcribed reports were used for analysis.
Klelnmuntz (1968) found that more experienced physicians tended to
start with general questions about the state of a patient and converged
on a diagnosis using progressively more specific questions. This
finding supports the hierarchical organization of Information In
memory.
Wortman (1972) used verbal protocol analysis and subsequent
computer simulations of a neurologist engaged In several diagnostic
tasks to test the hypothesis that medical knowledge Is organized
31
hierarchically. Results of the study provided support, but not
conclusive evidence for this type of organization. However, the
findings did corroborate those of Klelnmuntz.
Schwartz and Simon (1976) and Rubin (1975, cited In Tanner, 1977)
developed memory models that view the organization of medical knowledge
as a network of elements Interconnected by various relationships.
Rubtn (1975) Identified two major types of relationships. One type of
network Is represented by a hierarchical memory organization In which a
lower level concept Is related to an upper level concept (I.e., "X" Is
a type of "Y"). The second type of network refers to the organization
of concepts at a specific level within the hierarchy (I.e., "X" causes
"Y" or "Xw Is a complication of "Y"). The amount and organization of
knowledge stored In LTM has an essential role In determining the
outcomes of problem solving tasks.
2 ) Role of knowledge •storflri tn LTM In problem solving)
The role of knowledge In problem solving has been
addressed by Greeno (1980), Larkln (1980), and Simon (1980). All three
emphasized that all problem solving Is based on knowledge and that
without extensive and accessible knowledge, there can be no development
of expertise In problem solving. Greeno (1980) emphasized that any
task aiming to attain some goal constitutes a problem and the solution
of any such problem requires appropriate knowledge. A person may not
have learned exactly what to do In a specific problem situation, but
whatever the person Is able to do requires some knowledge, even If that

32
knowledge may be In the form of general strategies for analyzing
situations and for attempting solutions to the problem.
In relation to clinical problem solving, Hammond (1964; 1966)
stated that the nurse needs to be competent In Information seeking and
must have a thorough background of theoretical knowledge to conduct a
search for cues and to evaluate evidence. El stein et al. (1978) noted
that the possession of relevant bodies of Information and a
sufficiently broad experience with related problems Impacts on the
determination of what Information In the clinical situation Is
pertinent, which findings are significant, and how these findings can
be Integrated Into appropriate diagnostic hypotheses and conclusions.
In their studies. El stein et al. (1978) concluded that the effective
clinician has knowledge of the relation of findings, the relative
frequencies of different possible patient conditions, and the
particular characteristics of those conditions.
The results of Investigations In clinical problem solving In
nursing have shown that differences In problem solving ability can be
attributed to differences In knowledge (Asplnall, 1976: Baumann and
Bourbonnals, 1982; Davis, 1972; 1974; Verhonlck et al., 1968).
Verhonlck et ai. (1968) used a filmed, simulated patient care situation
to determine what observations were made, what types of nursing actions
were planned and what rationales were used for planned actions. The
study sample consisted of a large, diverse group of nurses attending
two national conventions. Included In the study were 43 nurses with
doctorates, 559 with masters degrees, 495 with baccalaureate degrees,
33
and 479 who had no degree. Analysis of the data revealed that
educational level was related to performance regarding the frequency of
Identifying relevant observations. Irrelevant observations, and
Inappropriate observations. The frequency and percent of both relevant
and Irrelevant observations made by each educational group Increased
with each higher degree. Conversely, an Inverse relationship was found
between the highest degree and the frequency and percent of
Inappropriate data selection. Nurses with no degree selected more
Inappropriate data than those with successively higher degrees.
Davis (1972; 1974) conducted two studies examining the
relationship between level of education and clinical expertise. These
studies were based on the assumption that through advanced knowledge
the nurse can make more complete, complex, thorough assessments and
carry through the appropriate required and designated Interventions.
Davis replicated the methodology of Verhonlck et at. (1968) using the
same taped simulations and data collection procedures. in the first
study, the respondents were 20 clinical specialists and 20
baccalaureate prepared nurses who were matched for years of clinical
experience. Analysis of the results demonstrated that the clinical
specialists made significantly more relevant observations, suggested a
greater number of relevant actions based on their observations, and
gave more appropriate reasons for their actions than did the
baccalaureate prepared nurses.
In the 1974 extension of the study, data were collected from an
additional 20 clinical specialists and 27 diploma prepared nurses. As
34
In the first study, analysis of the results demonstrated that In all
three areas, the performance of the clinical specialists was superior
to that of the baccalaureate prepared nurses, whose performance was
superior to that of the diploma nurses. An additional finding In this
study was that education and not years of experience was found to be
the determining factor In both the quality and quantity of patient
care.
Asplnall (1976) used a written case study of a patient exhibiting
an Impairment In the ability to process thoughts In order to determine
the ability of nurses with varying levels of education and experience
to Identify the cause of the patient's problem. The respondents were
6 nurses with masters degrees, 43 with baccalaureate degrees, 87 with
diplomas, and 51 with associate degrees. Of the 12 possible problems
that could be Identified, masters prepared nurses Identified a mean of
4 problems; baccalaureate nurses, 3.93; diploma nurses, 3.23; and
associate degree nurses, 3.35. Analysis of the data revealed
statistically significant differences between the number of problems
Identified by the baccalaureate and associate degree nurses and between
the baccalaureate and diploma nurses„ When the mean number of problems
Identified by nurses with less than 10 years of experience was
compared with that for nurses with 10 or more years of experience, a
statistically significant difference was demonstrated; those with less
experience Identified more problems.
Baumann and Bourbonnals (1982) used a convenience sample of 50
nurses working In critical care settings to explore decision making In
35
crisis situations and to determine factors nurses considered relevant
In making rapid patient care decisions under crisis conditions. A
semi-structured Interview was used In conjunction with a critical care
case study for data collection.
Participants In the study were 49 females and 1 male who ranged
between 20 and 50 years of age. Forty-three participants were
graduates of diploma schools and 7 had baccalaureate degrees. Analysts
of responses revealed that, Irregardless of the differences In
educational preparation, the factors most frequently cited as having
the greatest Influence on rapid decision making were knowledge and
experience.
The amount and organization of knowledge In LTM plays an
Important role In a diagnostic concept attainment task and the
subsequent search for cues In the environment. The learning histories
of students enrolled In associate and baccalaureate degree programs Is
also relevant to the amount and structure of Information stored In LTM.
These relationships will be addressed in subsequent subsections.
d. Interaction, of the, process ing, system, w ith, tha. - external
envlronmant
When faced with a problem solving task, the problem
solver is goal directed In the search for a solution (Simon and Newell,
1972). Attainment of a solution Is achieved through the development
of an Interface between the Internal processing system and the task
environment. This Interface Is represented In STM by a problem space.
The problem space can be thought of as a state of knowledge to which
36
the problem solver can attain. A search Is conducted through the
Information available In the problem space until a knowledge state Is
attained that Includes the problem solution (Simon and Newell, 1971;
1972). The process an Individual uses to achieve the problem solution
Is dependent upon whether the problem exists In a closed or an open
system.
In a closed system, the problem solver has knowledge of the
specific goals to be attained and compares knowledge of this goal to
the current knowledge state. Following each successive comparison, an
additional piece of Information Is added or deleted depending upon a
decrease or Increase In the distance between the current and the
desired state. This process continues until the two states are
synonymous. This process Is refered to as means-ends analysis (Simon
and Newell, 1971; Sweller and Levlne, 1982).
In contrast, a clinical diagnostic problem represents an open
system In which there are an Infinite number of possible end states;
the desired end state Is the Identification of a specific diagnosis.
In order to deal with the vagaries of an open system, problem solvers
transform It Into a series of hypothetical closed systems which can be
tested either serially or simultaneously (Bartlett, 1958). Using
verbal protocol analyses, El stein et al. (1972; 1978), Gordon (1980),
and Klelnmuntz (1968) demonstrated that clinicians Involved In a
diagnostic process utilize this approach. Based on Initially available
Information, the LTM Is searched for diagnostic labels that may
explain the data. The hypothesized diagnoses, which may be at the
37
level of "ideas", "guesses", or "Impressions" are then tested using a
hypothetIco-deductlve approach (Elstetn et al., 1978). Etsteln et al.
(1978) characterized the diagnostic process as one which entails
repetitive stages of cue acquisition, hypothesis generation, cue
Interpretation, and hypothesis testing.
Gordon (1980), In an Investigation of the hypothesis testing
strategies used by 60 graduate nursing students, found that they used a
mixed hypothesis-testing strategy. Under unlimited and limited (I.e.,
12 trials to solution) Information conditions, the use of multiple
hypothesis testing diminished significantly as the diagnostic tasks
progressed. As the use of multiple-hypothesis testing decreased, there
was a concomitant Increase In the use of single hypothesis testing.
This finding Indicates that while a hypothetIco-deductlve process Is
utilized, the process changes from one of simultaneous hypothesis
testing to single hypothesis testing as the field of possible diagnoses
Is narrowed. The Initial use of multiple hypothesis testing helps to
limit the subsequent search much more efficiently than would the
Initial use of single hypothesis testing.
e. Summary
Short term memory has a significant Influence on
problem solving ability due to limited capacity and low retention time.
These limitations can be compensated for by using data chunking
techniques. In contrast, LTM has an unlimited storage capacity. It
contains the symbolic representations of stimulus patterns, organized
In hierarchical associations as networks of concepts and relations
38
between concepts. The development of expertise In problem solving Is
dependent upon the amount and organization of Information acquired
through learning, that Is stored In LTM.
To deal with the open probabilistic system representative of a
diagnostic task. Initially available data are used to search LTM for
diagnostic labels that may account for this data. The potential
diagnoses are then transferred to STW where they help limit the scope
of the environment to be searched. A hypothetlco-deductlve approach Is
then used to test out the diagnostic hypotheses. An application of the
Interaction between the Internal processing system and the external
environment, as represented by the problem space, to a diagnostic task
Is addressed In the next subsection.
3. Diagnosis triantIfIratIon
The process of determining which diagnostic label best
represents a given cluster of patient data and factors which Influence
the accuracy of the diagnostic process are discussed In the following
subsections.
a. Concept, attainment
Arrival at a Judgment concerning which diagnoses best
explain the pattern of patient cues ts a concept attainment task
(Bruner et at., 1956; Gordon, 1980; 1982; Klelnmuntz, 1968). Bruner et
al. (1956) stated that diagnoses are examples of disjunctive concepts.
The presence of one attribute or another attribute, or both. Is
sufficient to define the concept. This Is consistent with the
39
previously described relationships existing between patient cues and
the diagnoses which they define.
A nursing diagnosis Is a symbol or name of a complex concept that
Is composed of lower-level concepts (I.e., observable facts) and their
relationship with each other (Blrcher, 1982). As discussed previously,
learned symbolic representations of concepts are stored In LTM and are
transferred selectively to SIM during problem solving tasks. In a
diagnostic task, the Initially perceived patient characteristics In the
problem space are used as the basis for a search of LTM for concepts
that Include these characteristics. Those concepts in LTM that Include
one or more of the characteristics become the hypothesized diagnoses
that are transferred to STM and serve as the goal against which
Information obtained from the problem space Is compared (Barrows and
Tamblyn, 1980; Simon and Newell, 1972).
Since diagnostic categories are disjunctive concepts, a concept
formation theory needs to take this Into account. Rosch and Mervls
(1975) demonstrated support for using "family resemblances" as a
structural basis for making comparisons. Using this approach, the
diagnostic categories (concepts) retrieved from LTM are used as
prototypical models against which groupings of currently available
Information are compared. The more attributes an Information grouping
has In common with one diagnostic category, the less tt will have In
common with others. The diagnosis Is Identified based on a subjective
appraisal and Informal rank ordering of the hypothesized diagnoses
(Elstein et at., 1972; 1978).
40
The accuracy of a diagnosis Is Influenced by the constraints
Imposed by both the Internal processing system and cognitive biases.
These will be addressed In the next subsection.
b. Factors. InfI imnrTnp diagnostic accuracy
The formulation of early diagnostic hypotheses has been
used to transform an open system Into a series of hypothetical closed
systems In which the clinician operates. The formulation of multiple
early hypotheses provides Insurance against premature closure about a
patient's problem (Elsteln et al., 1972; 1978). This formulation
forces consideration of possible alternative explanations for the
aval lable data.
Barrows et al. C1978) noted that the efficiency, effectiveness,
and quality of a clinician's evaluation of a patient are dependent
largely upon the hypotheses generated. The results of Klelnmuntz's
(1968) study demonstrated that patient Information not directly related
to hypothesized diagnoses Is usually forgotten. When data do not seem
to fit any hypothesis, they need to be challanged In terms of
reliability and the hypotheses need to be challenged In terms of their
adequacy (Barrows and Tamblyn, 1980).
Tanner (1977), In an Investigation designed to evaluate the
effects of different teaching strategies on early hypothesis generation
and diagnostic accuracy, found significant, positive relationships
between the formulation of diagnostic hypotheses and both the quality
of an Information search and diagnostic accuracy. The qualtty of
Information search was related to the validity and dependabllty of cues
41
sought and the search strategy employed. The correlation coefftcents
between the number of early hypotheses generated and diagnostic
accuracy ranged between 0.57 and 0.75 (p<.001). However when this
relationship was re-examined while controlling for Information quality,
a much lower correlation was demonstrated between the two factors (r
=0.256, p < .05).
Another factor contributing to diagnostic accuracy problems Is
that of cognitive strain due to the capacity limitations of the STW.
The value of chunking data to deal with this problem was previously
discussed. Another approach that can Increase the amount of Information
available for processing at any one time Is the use of an external
memory (Simon and Newell, 1972).
Aspfnall (1979) evaluated the use of decision trees for Improving
the diagnostic abilities of nurses. Thirty triads of nurses matched
for basic education, length of experience, and performance In a
previous study (Asplnaii, 1976) were exposed to three levels of
treatment prior to measurement of diagnostic ability on a written case
study. One group, the control, received only the written case study;
the second group received the case study and a list of the 18 possible
diagnoses; the third group received the case study, the list of
diagnoses, and a decision tree for each diagnosis, it was hypothesized
that the decision trees would facilitate the systematic use of data to
rule In or out each diagnosis.
Analysis of the data demonstrated that those nurses who received
the decision tree Identified a significantly greater number of correct
42
diagnoses and were more accurate than either of the other two groups
of nurses. In addition, those who received the list of diagnoses
Identified a significantly greater number of correct diagnoses than did
those In the control group. Further analysis demonstrated that use of
th© decision tree was most effective In aldtng those nurses who had the
least amount of education (I.e., diplomas and associate degrees).
Early hypothesis generation and the use of data chunking and
decision trees have been found to Influence diagnostic accuracy
positively. This accuracy can be Influenced negatively by one or more
types of Inductive biases. Kahneman and Tversky (1972; 1973; Tversky,
1977; Tversky and Kahneman, 1973) proposed a theory that described
people's dependence on a limited number of heuristic principles to
simplify cognitive processing. However, the use of these principles,
as demonstrated In Asp Inail's (1979) study, can lead to errors and
bIases In Judgement.
Asplnall (1979) reported that one nurse, who had access to the
decision trees, diagnosed the presence of renal failure when the
patient In fact had none of the criteria for this problem. When
questioned, the nurse replied that based on her past experience,
patients with hepatic disease also had renal failure. This example
demonstrates one of the heuristics, availability, described by Tversky
and Kahneman (1973). This refers to a strategy by which people assess
the frequency of a class or the probability of an event by the ease
with which It Is brought to mind.
Use of the availability heuristic can be biased by a number of
43
factors besides frequency and probability. The retrlevablIIty of
Instances Is one such bias where the recall of similar Instances
Influenced current judgment (Tversky and Kahneman, 1973). Evidence of
the use of this heuristic In the retrieval of diagnostic hypotheses
also has been Identified In physicians (Elsteln et al., 1972).
A second heuristic Is that of representativeness (Tversky and
Kahneman, 1974). According to this heuristic, the probability of an
event Is determined by "the degree to which It: 1) Is similar In
essential characteristics to the parent population, and 2) reflects
the salient features of the process by which It Is generated" (p. 430).
Biases occur when base rates, IIkelIhood of occurrance, and degree of
similarity are not taken Into consideration (Tversky and Kahneman,
1972).
Additional errors In diagnoses can occur as a result of the
misuse or tack of use of available Information. Bruner et al. (1956)
demonstrated that hypotheses are formed on the basis of positive
Information even though negative Information may have greater
diagnostic value. Information confirming hypotheses also are used more
effectively than Information which disproves them (Bruner et a!., 1956;
Kozleleckl, 1972). Diagnostic biases also can occur as a result of
overestimating the diagnostic value of the earliest obtained
Information (Kozleleckl, 1972) and of falling to revise diagnoses on
receipt of additional Information. In their clinical Inference
studies, Hammond et al. (1967) found evidence of the failure of nurses
.pa
44
to revise appropriately their Judgments of a patient's condition as
new Information was obtained.
4. Summary
Arrival at a Judgment regarding which diagnoses best explain
patient cues Is a concept attainment task made difficult by the fact
that diagnostic categories are examples of disjunctive concepts. The
Initially perceived Information, defined by the problem space. Is used
as a basis for searching LTW for concepts that include this
Information. Use of a "family resemblance" approach, as described by
Rosch and Mervls (1975) has received support as a structural basis for
making comparisons between available cue patterns and the attributes of
a diagnostic category, as stored In LTM.
Diagnostic accuracy is Influenced by the number of hypothesized
diagnostic categories Initially generated, the validity and reliability
of the available data, and cognitive strain related to STM limitations.
To cope with these limitations, data chunking, early hypothesis
formulation, external memory devises, and heuristics have been used.
An examination of the cognitive aspects of a diagnostic task
demonstrates that the characteristics of the environment, as
represented by the problem space In Internal memory, the limitations of
the STM and the processing system, the amount and organization of
Information stored In LTM, and the subjective analysis of patient cues
all influence diagnostic accuracy.
B. Measurement, of. cl inical. probJem soJvlng. ab i l ity
Boshuizen and Claessen (1982) stressed the Importance of
45
differentiating between the task of problem solving and the ability to
problem solve. They suggested that the term "problem solving" be used
to signify the activity and that "problem solving ability" be used to
signify the trait or ability to problem solve. Subsequently, In
discussing research In medical problem solving, they stated that
"Medical problem solving refers to the thinking processes that take
place In the course of finding an answer to the question: 'What Is
wrong with this patient and what should be done with him/her?1" Cp.
82). Within a nursing context, the measurement of problem solving
ability then becomes one of assessing " how well" a nurse Is able to
define and propose solutions to those patient problems that are
amenable to nursing Intervention.
Selection of an Instrument to measure clinical problem solving
ability and, specifically, assessment ability, must be based on
evaluations of appropriateness of an Instrument's format and mode of
administration; Its validity and reliability; Its cost; and the degree
of difficulty associated with Its preparation and administration In
relation to the explicit purpose of a study (McGuIre, 1980a; Vu, 1979).
Several different approaches have been used to assess problem solving
ability. These approaches have been characterized as observation-based
methods, record-based methods, and simulation methods (Vu, 1979). A
brief overview of the characteristics of the observation- and record-
based methods and a more comprehensive examination of one form of the
simulation method are Included In the following sections.
46
1. Ohserva-Hrin-hasftri rntH-hnHg
Observation of Individuals engaged In the performance of
various aspects of clinical problem solving Incorporates the use of
rating scales* written reports, and observer Impressions. These
observations may occur In actual clinical settings utilizing real
patients or Involve the use of trained actors.
Use of actual clinical settings and patients for the purpose of
making comparisons of problem solving abilities across Individuals has
several disadvantages. Difficulty Is encountered due to Inability of
the observer to control patient cooperation and environmental activity
In a testing situation. An additional potential problem, If the
problem solver Is a student, Is the occurrence of events to occur that
might endanger the patient and/or the student (McGuIre, 1980by McGuIre
et al., 1976).
Observer related variables also Influence the quality of the
data obtained. Factors that may Influence reliability and validity of
data are associated with problems in delineating the specific versus
the global activity to be evaluated, observer definition of "good"
versus "bad" performance, and weighting assigned to various performance
categories (Barro, 1973; Vu, 1979). McGuIre (1980b) advised that
considering time and cost associated with use of observation methods.
It should be reserved for assessment of Interpersonal and psychomotor
techniques.
2. Recorri-haseri methods
A retrospective, Indirect approach to the assessment of
47
problem solving ability Involves examination and evaluation of written
patient records. Factors contributing to questionable validity of
conclusions based on this method Include qualifications of the
reviewer. Inability of the measurement process to determine the problem
solving process utilized, and Influence of potential review on the
performance of the Individual being evaluated (Barro, 1973; Vu, 1979).
Evidence also has accumulated that Indicates clinicians do not always
completely record history and physical examination data that they have
collected (Barro, 1973; Norman and Felghtner, 1981; Norman and
Wakefield, 1978; Page and Fielding, 1980; Vu, 1979).
3. Simulation methods
Clinical problem solving tasks can be simulated through the
use of several different methods. One method already mentioned Is the
use of trained actors to portray a patient. As an alternative, several
other methods have been developed to assess how, or how well.
Individuals perform In a given clInlcal problem solving situation.
These Include the use of paper and pencil exercises, computer-managed
exercises, and/or an oral format (McGuIre, 1980b).
The common element Itnklng these formats Is use of a
predetermined description of a patient situation. The extent of this
description depends upon the purpose of the assessment and may be a
written, verbal, or audio-visual account. The problem solver Is
directed through the simulated experience according to the specific
method adopted for use.
48
a. OraJ, format
In the oral format, an examiner Is provided with all of
the data about a case and supplies this to the examinee upon specific
Inquiry or In response to a management decision (McGuIre, 1980b).
During the exercise, each Inquiry and management decision made by the
examinee Is recorded on a checklist (McGuIre, 1980b) or recorded on
tape (Tanner, 1977).
Use of this format permits ongoing extraction, by the examiner,
of the examinee's explanations of the reason for requesting specific
data, the meaning of those data regarding diagnosis and management
decisions, and why specific actions were Implemented (Tanner, 1977). A
major advantage of this format Is the examinee Is not prompted In the
selection of data, diagnoses, or management selections by the presence
of lists of written options (McGuIre, 1980b). However, this method Is
not useful for group testing and, therefore, Is a time consuming
enterprise when the object of a study Is to determine how well an
Individual performs or when a large number of participants are to be
evaluated. In addition, the use of another Individual to supply the
responses and to query the examinee Imposes a high degree of
artificial IIty on the testing situation.
b. Patient management problems
A number of variations of the paper-and-pencl1 format
have been developed for use In the evaluation of problem solving skills
(McGuIre, 1980b; Vu, 1979). One variation, the Patient Management
Problem (PMP) pioneered at the University of Illinois at Chicago, uses
49
a branching technique which requires the use of sequential analysis and
decision making (McGufre and Babbott, 1967). The branched format
permits alternative approaches and a variety of pathways through which
a solution can be reached. The technique also Involves the use of a
special answer sheet on which the examinee reveals sequentially the
results of decisions by erasing an opaque overlay or by developing
Invisible printing, thus, permitting access to only that Information
which has been requested (McGuIre, 1968).
The content of a PMP simulation Is presented In a series of
sections that permit the examinee freedom to select an Individual
course In resolving the problem presented. The simulation begins with
an opening scene which describes the problem to be solved, but contains
no more Information than that which Is usually evident during an
Initial encounter with a patient. A series of sections, corresponding
to different stages In the evaluation and resolution of the problem
follow the opening scene. Each section may contain an option segment,
which Includes a list of specific Inquiries or options available, and a
bridging segment that directs the examinee to the next appropriate
section or to a list of strategic alternatives. The beginning of each
segment contains Instructions regarding the type of response that Is
required (McGuIre, 1980b; McGuIre et al., 1976).
Quantitative measurement of performance on a PMP Is achieved
through the assignment of a weighted score to each Item. The weighting
system used and the summary performance scores to be reported are based
on the purpose of the study and the number of Items that can be grouped
50
together to obtain a summary score. The summary scores suggested by
M c G u I r e a n d o t h e r s ( M c G u I r e a n d B a b b o t t , 1 9 6 7 ; M c G u I r e e t a 1 9 7 6 )
Include measures of proficiency, efficiency, errors of ommlston and
commission, and overall competence.
Several characteristics of this type of written simulation make
It suitable for assessing problem solving skills. These
characteristics are freedom to select an Individual approach to
problem resolution, provision of Immediate feedback regarding the
Information desired or the outcomes of actions, and Inability to
retract a selection that proves to be unwarranted or unwise (McGuIre et
al., 1976).
Additional advantages Include ability to predetermine and
standardize the task to be performed while eliminating Irrelevant
complexities that would affect the evaluation process and/or the level
of difficulty. The PMP format also enables the sampling of a broad,
representative sample of problems and provides for the pre
determination of criteria to be used for performance (McGuIre et a I.,
1976).
One criticism of the PMP format Is based on the presence of lists
of decision options. Neuble and others (1982), Martin (McGuIre, 1980b)
and McCarthy (1966) reported that the cueing effects of these lists
result In artificial Inflation of patient history and physical
examination proficiency scores. When performance on cued and non-cued
tests was compared, substantial Increases were seen, on the cued test.
51
In both the total number of Items selected and In the number of correct
Items selected (McCarthy, 1966).
A concern related to the use of complex scoring systems and the
use of Item weighting, as proposed by McGuIre, Is related to the
masking of qualitative differences that may exist between decisions.
The selection of an action that results In patient death Is weighted no
differently than one causing discomfort or financial difficulty (Vu,
t979). Reliance on only the summary scores suggested by McGuIre also
masks differences In the type of patient Information selected and/or In
the areas of data selection concentration.
(1). Psychometric, properties
The psychometric properties of various PMPs have
been reported and although It is generally concluded that the content
validity of well constructed PMPs Is supported (Page and Fielding,
1980), the results of construct vaI Id Ity, criterion validity and
reliability estimations are highly test dependent. Various methods
have been used to estimate the validity of various PMPs. These Include
factor analysis (Juul et al., 1979), analysis of variance techniques
(Farrand et al., 1982; Norman et al., 1983; Norman and Felghtner,
1981), and correlational analyses. Including multi-trait, multi-method
procedures using Pearson product moment correlation coefficients
(Donnelly and Galagher, 1978; Farrand et al., 1982; Holzemer et al.,
1981; Norman et al., 1983; Page and Fielding, 1980; Sedlack and
Nattress, 1972; Sherman et a I., 1979; Wolf et a I., 1983), Spearman's
52
rank order correlation coefficients (DIncher and Stldger, 1976;
Holzemer et al., 1981), and cannonlcal correlation (Reld, 1981).
The stability of measures over time and the Internal stability
have been estimated using test-retest procedures (deTornyay, 1968;
Farrand et al.f personal communication, January, 1984) and Cronbach's
coefficient alpha (McGuIre and Babbott, 1967; Norlclnl, 1983).
Modifications In the use of Cronbach's coefficient alpha are
necessitated by the branching nature of PMPs and the ability to reach
an end-point In the exercise via different pathways and different
numbers of Items. Therefore, use of this statistic has been extended to
a comparison of composite scores measuring the same concepts within
tests or across multiple tests.
Problems that have been Identified with estimating the
reliability of PMPs are related to the use of a branching technique, as
discussed above, the Interdependence of Items (McGuIre and Babbott,
1967) the content and case specificity of each PMP (Norman et al.,
1983, Norlclnl et al., 1983), and knowledge of outcomes which can
Influence Item selection when a test-retest approach Is used (McGuIre
et al., 1976). An example of problems that can occur with test-retest
procedures was described by deTornyay (1968). She reported that the
unfamiliar content matter of one PMP so piqued the Interest of a group
of study participants, that they Investigated the area between the time
of the original testing and post-testing. This resulted In a
significant Increase In scores on the retest.

53
4. Summary
Three different approaches have been used to assess problem
solving ability. Observational approaches utilizing rating scales,
written reports and observer Impressions have been used In both actual
and simulated clinical settings. Comparisons of Individual performances
are made difficult due to uncontrollable events In the setting and
observer biases. Record review provides a retrospective and Indirect
approach to the assessment of clinical problem solving ability. The
validity of conclusions based on this approach are questionable
secondary to the Influence of potential review on the performance of
the Individual to be rated. In addition, evidence exists Indicating
clinicians do not always completely record all Information collected
and used for diagnostic and management purposes.
One type of paper and pencil simulation that Is appropriate for
testing large groups of Individuals In the patient management
problem (PMP). It provides for a standardized task environment,
permits alternative approaches and a variety of pathways through which
a solution can be achieved, and uses a pre-determlned, objective
scoring system. This method has received some criticism because It
provides the examinee with lists of available data which, through a
cueing effect, can lead to score Inflation. The validity and
reliability of PMPs can be estimated via a number of statistical and
review procedures.
'This section contains an overview of the historical evolution of
54
associate degree (AD) and baccalaureate degree (BD) programs In the
United States, the differences In the currlcular content of the two
programs, and differences In characteristics of AD and BD students and
graduates.
1. Historical overview
The 1965 American Nurses' Association (ANA) postlon
statement calling for the baccalaureate degree as the minimum
requirement for entry Into the practice of professional nursing was a
culmination of five years of formal deliberations within the
professional organization (ANA, 1965). However, If one goes back to
the beginning of formal nursing education, Florence Nightingale
envisioned nursing education being conducted In schools of nursing that
were Independent of service agencies (ANA, 1965). Within the United
States, the earliest nursing schools were Independent and adhered to
the Nightingale pattern. However, by the end of the 19th Century, the
number of hospital sponsored and controlled schools mushroomed In
response to desperate staffing problems (ANA, 1965; Brown, 1948);
Goldmark, 1923).
For over 100 years, nursing leaders In the United States have
been campaigning for the placement of nursing education In degree
granting Institutions. Wooley, In A Century of Nursing written In
1876, stressed the desirability of elevating nursing to an educated and
honorable profession and expressed the opinion that nursing education
should be located In Institutions of higher education (ANA Commission
on Nursing Education, 1979).
55
In 1923, the Committee for the Study of Nursing Education (1923)
(commonly referred to as the Wins low - Goldmark Report) noted that
nursing was one of the few fields of professional life that still used
an apprentice type of training. The report called for the movement of
nursing education Into "Independent Institutions organized and endowed
for a specifically educational purpose" (p.17). Additionally, It was
noted that the "development and strengthening of university based
programs for the training of nursing leaders was of fundamental
Importance for the furtherance of nursing education" (p.26).
These sentiments have been echoed by others. The most prominent
voices were the Report of the Committee on the Grading of Nursing
Schools (1934), Brown's (1948) report to the National Nursing Council,
and the report of the Committee on the Functioning of Nursing (1950).
The first collegiate nursing programs In the United States were
offered at Teachers College, Columbia University, and at the University
of Minnesota. Teachers College first admitted "properly qualified
graduate nurses" In 1899. These students were admitted Into the Junior
class; thus, they were automatically awarded two years of college
credit for their hospital training (Committee for the Study of Nursing
Education, 1923). It was, however, the University of Minnesota that
pioneered university education for nurses when. In 1910, It established
a school of nursing as part of the general university system. Upon
completion of the program of study. Its graduates were granted a
special professional degree (Commtttee for the Study of Nursing
Education, 1923). Although this program did not lead to a college
56
degree, Jt represented the first basic nursing program In the country
to be completely under the control of an educational Institution. The
first nursing programs leading to a college degree as well as a nursing
diploma were established between 1916 and 1920 and Included the
programs at Teachers College and at the University of Cincinnati
(PI Ileplch, 1962).
A movement developing parallel to the one calling for the
placement of nursing education within educational Institutions was one
concerned with the development of two levels of nursing practice.
Goldmark (1923), In her report to the Committee for the Study of
Nursing Education, called for formal training and licensure of a
subsidiary grade of nursing service worker who would practice under the
direction of a physician or a trained nurse. She envisioned this group
of Individuals working with the mild or chronically III or with
convalescents, and, thereby, freeing the trained nurse to care for the
more acutely III. Goldmark referred to these Individuals as practical
or household nurses or as attendants.
Brown (1948) Indicated that two types of nursing functions
existed: technical and professional, and that It would require less
time to prepare a person to perform the technical aspects of care than
to perform the professional aspects. She noted that practical nurses,
orderlies, and aides represented a large core of the system of
assistant nursing service and that they performed an Important role In
releasing nurses to give medication, treatments, and other "more true Iy
nursing care" (p.59).
57
Brown's (1948) recommendation that the services provided by non
professional workers be formalized Into a functional system was
Instrumental to Montag's development of a program to prepare nurses who
would perform predominantly technical functions (Montag, 1956). Montag
(1956) proposed the preparation of technically prepared nurses In two-
year colleges. She envisioned this type of practitioner functioning on
a level between that of the nursing assistant and that of the
professional nurse.
The two premises upon which the AD program was developed were
that 1) the function of nursing can and should be differentiated and
2) that these functions lie along a continuum differentiated at three
different levels with professional nursing at one end, the assisting
personnel at the other end, and the technical, or semi-professional,
personnel between the two. At that point on the continuum where the
functions of the professional and technical nurse meet, the roles of
the two become similar. However, Montag (1980) never saw the technical
and professional roles as replacements for each other. Nor did she
see the AD program as a stepping stone Into or preparation for a BD
program. The AD nursing program was seen as a terminal program.
Montag (Montag and GotkIn,1959) proposed and developed a two year
sample curriculum that Incorporated both general education and nursing
education courses that could be offered In Junior and community
colleges. A pilot project was Implemented In 1952 and extended through
1957 (Montag and Gotkln, 1959). The curriculum Implemented In these
programs was to be different from that offered In diploma and
58
baccalaureate programs and was to be based on "a clear picture of the
product to be produced by the educational program and the functions
this product should perform" (Montag and Gotkln, 1959, pp 342-343).
In the final report of the cooperative five year project that
Implemented and evaluated the Initial AD programs, Montag (Montag and
Gotkln, 1959) stated that the objectives of both associate degree and
baccalaureate degree programs needed to be stated clearly. Programs
claiming to prepare practitioners of the same competency should not
differ In length, content, and method since there can be little
Justification for a program requiring four years for Its completion
unless It prepares a practitioner who Is different In competence from a
graduate of the Junior college program. How the graduates of BD and AD
programs differ Is a question that has led to confusion and conflict
(Johnson, 1966; Tschudln, 1964; Waters et al., 1972).
McClure (1976) pointed out that the difficulty experienced In
differentiating the practice competencies of AD and BD programs may be
due to misconceptions In Interpretation of Montag*s model. Using Venn
diagrams, she proposed that a literal transformation of Montag's work,
as Illustrated In Model 1 (Figure 2), views professional and technical
nursing as adjoining one another although carrying out separate,
discrete, and easily Identifiable function. Educational components of
the two programs would, therefore, be equally separate, discrete, and
easily Identifiable. An alternative conceptualization, as represented
by Model 2 (Figure 3), depicts an overlap In the functioning of the two
levels of nursing practice. This model depicts some patient needs
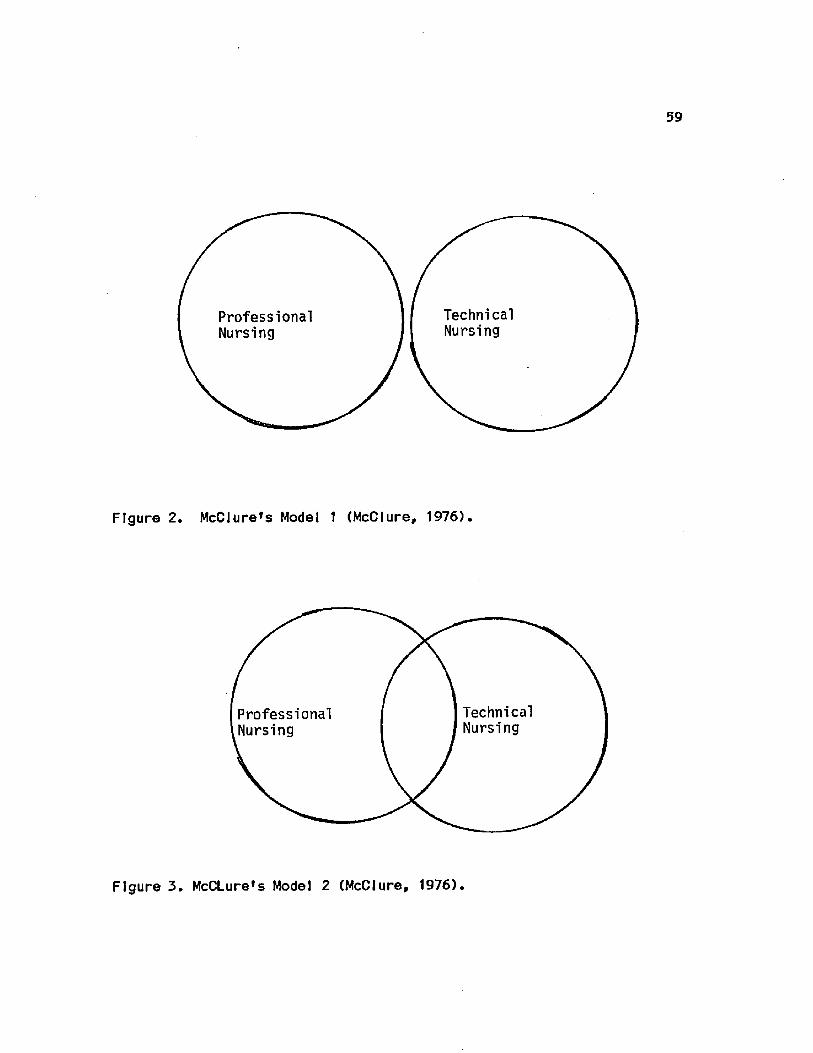
59
Professional Nursing
Technical Nursing
Figure 2. McClure's Model 1 (McClure, 1976).
Technical Nursing
Professional Nursing
Figure 3. McCLure's Model 2 (McClure, 1976).
60
falling within the purely professional realm, some within the purely
technical realm, and some within an area that can be met by either
level of practitioner. Since large portions of practice are still
conceived of as separate, discrete, and easily Identifiable, the
curricula should reflect these differences.
However, McClure (1976) found little support for either Model t
or Model 2 and concluded that a large number of the problems
encountered In differentiating the two levels of practice were due to
trying to Impose a Model 1 or Model 2 concept on a Model 3 world.
Model 3 (Figure 4) Illustrates the technical aspects of care as being
part of the professional nurse's realm but which also can be delegated
to the technical nurse. The curriculum patterns consistent with Model
3 would result In the AD program preparing Individuals to assist In
carrying out selected aspects of care that also could be performed by
graduates of BD programs.
Sparks (1979) extended McClure's Model 3 to Incorporate
differences In "knowledge base and intellectual skills gained.
Including problem solving, critical thinking, and/or decision making'
(p.42). Her conceptualization of McClure's model (Figure 5)
illustrates that the differences between technical and professional
nursing are knowledge base, responsibility, and role. This model Is
consistent with the ANA's position (1965) that theory base and depth of
knowledge differentiate technical from professional nursing practice.
From Inception, the goals of AD and BD programs have
differed. The objective of the BD program Is to prepare liberally
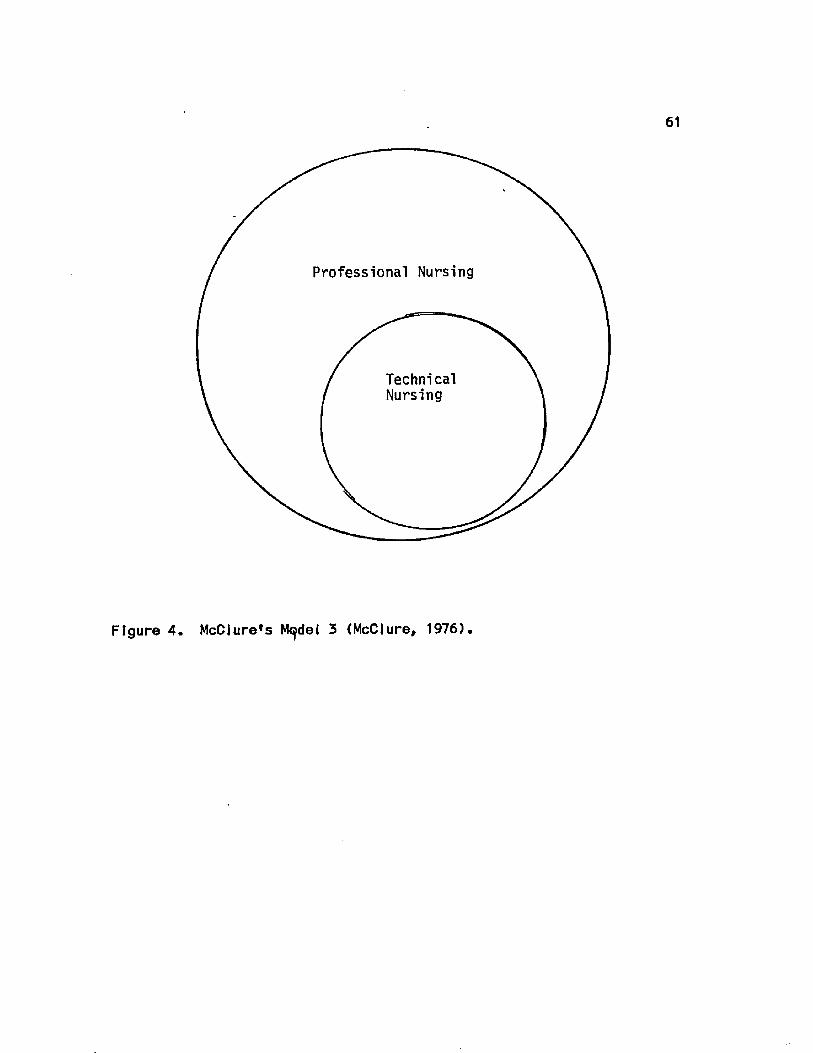
61
Professional Nursing
Technical Nursing
Figure 4. McClure*s M^del 3 (McClure, 1976).
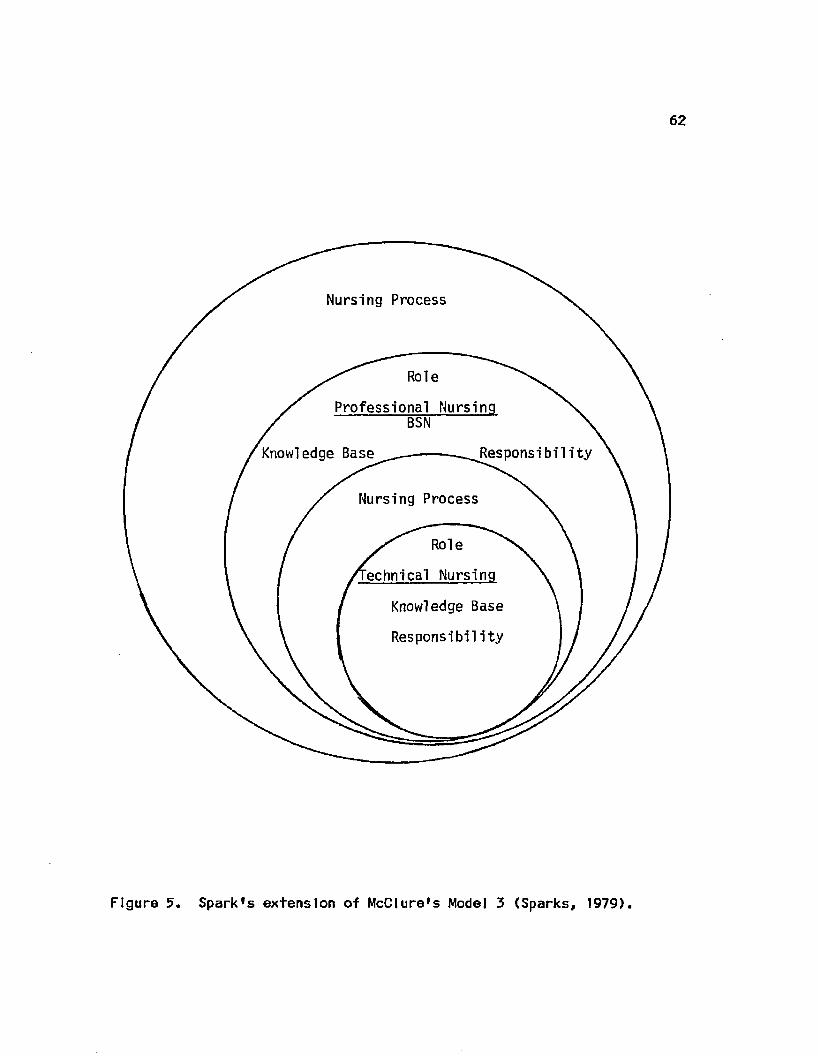
62
Nursing Process
Role
Professional Nursing BSN
Responsibility Knowledge Base
Nursing Process
Role
echnical Nursing
Knowledge Base
Responsibility
Figure 5. Spark's extension of McClure's Model 3 (Sparks, 1979).

63
educated IndFvtduals capable of functioning as professional nurses In a
variety of roles and settings. In contrast, the objective of the AD
program Is to prepare technical nurses capable of functioning In a
caregiver role within a structured, hospital setting (Bensman, 1977;
DeChow, 1967; Kramer, 1981; Montag, 1956; 1980; Montag and Gotkln,
1959; Schlotfeldt, 1967). Accomplishment of these objectives, via
currlcular content was addressed by DeChow (1967), Johnson (1966),
Kramer (1981), Schlotfeldt (1967; 1977) and the NLN Task Force on
Competencies of Graduates of Nursing Programs (1982).
In addition to the obvious difference In program length
(generally two years for the AD and four years for the BD) differences
exist In the proportion of total course work alloted to nursing courses
and liberal arts and science courses, and In the focus of course work.
Johnson (1966) examined differences In the level of knowledge to which
students In the two types of programs were exposed. She found that the
AD student's background In the physical and social sciences and In the
humanities was generally limited to Introductory survey courses which
provide for the acqulslslon of practical, but limited knowledge.
Since the content offered Is often from the perspective of practicality
or applicability to the solution of everyday affairs. Its usefulness
regarding the practice of knowledge may be limited since the depth of
knowledge of underlying principles Is limited.
In contrast, the BD student's background Included Introductory
level and upper division courses that provided for the understanding of
major concepts and principles and the ability to see relationships
64
between facts and among facts, concepts and theories. Acquisition of
theoretical knowledge at this level provides the student with the
ability to manipulate acquired knowledge, to seek new relationships,
and to move between empirical findings and abstract conceptualizations.
In nursing courses, Johnson (1966) noted that the content In AD
programs focused on the knowledge required to Identify and take
appropriate action In common, concrete, and specific problems
experienced by patients. Content was characterized as largely
empirical In nature and directly related to the anticipated actions and
activities associated with care delivery. Focus of theoretical
explanations was on specific bases for recognition of problems and on
the rationale for action In particular situations.
Nursing courses for BD students differed from the AD courses In
relation to organization and treatment of content. Focus In BD
programs was on theoretical explanations for responses to Illness or
factors leading to Illness. In addition, principles, concepts, and
theories of basic sciences were examined In the BD programs with
relation to ability to explain or predict patient responses or modes of
nursing Intervention.
Schlotfeldt (1977) contrasted the foci of baccalaureate and
associate degree education. She noted that while technical study
focuses on the development of particular skills and mastery of selected
essential concepts, programs of professional study focus Initially on
the behavioral sciences through which students gain mastery of concepts
about man. Subsequently, In the nursing program, professional
65
study focuses on the study of man In various states of health and
functional levels, and on development of Judgment and decision making.
Other dichotomies between technical and professional education
noted by Schlotfeldt (1977) were, for the technical program student,
related to a focus on accepted ways of performing. For the student In a
professional program, the focus was on the use of knowledge In the face
of uncertainty. Other dichotomies mentioned were a cumulative
repertoire of skills versus a holistic approach to the study of persons
who are served In a variety of ways; the mastery of skills and of
relevant existing knowledge versus the mastery of existing knowledge
and skills, the ability to Identify gaps In knowledge, and the value of
systematic Inquiry; and a focus on accountability to others within the
field versus the estab11shment and maintenance of Interprofessional
relationships.
These aforementioned findings were corroborated by a task force
of the the National League for Nursing (NLN). Following a review of NLN
documents and a review of the literature, the NLN Task Force on
Competencies of Graduates of Nursing Programs (1982) concluded thai-
differences do exist In the knowledge base among the different types of
nursing education programs. They also estimated the distribution of
course work within programs. In AD programs. It was estimated that
approximately 5Q% of course work was In the basic physical and social
sciences and 50% was In the nursing program. In addition, content
relative to legal Issues, ethics, nutrition, and pharmacology usually
was Integrated In the nursing courses. Within the four year BD

66
programs, It was estimated that 35J6 to 4056 of course work was In the
physical and social sciences, 30$ to 55% was In nursing courses, and an
additional 25JS to 35j8 met degree area distributive requirements.
2. Differences, in associate, and, baccalaureate degree students
and graduates
The characteristics of AD and BD students and graduates have
been reported by a number of Investigators. Their findings will be
reported In terms of demographic and pre-enrolIment educational
characteristics, factors related to nursing program selection,
personality attributes of students, and clinical performance attributes
of graduates.
a. Demographic and pre-enrolJ ment. educational
characteristics
The characteristics of AD and BD students regarding
their ages, marital status, family responsibilities, high school
performance, and educational experiences between high school and
nursing program matriculation were reported In a number of studies
(Dustan, 1964; Gray et at., 1977; Knopf, 1975; Melels and Farrell,
1974; Nash, 1975; Richards, 1972; Schwerlan, 1979; Sparks, 1979; Wren,
1971). Their findings are summarized In Table I
In general, all Investigators reported that the AD student was
older than the BD student, was married as opposed to single, and had
more family responsibilities than did the BD student. Three out of four
investigators found that the BD student had a higher high school rank
than did the AD students. While one study (Wren, 1971) found no
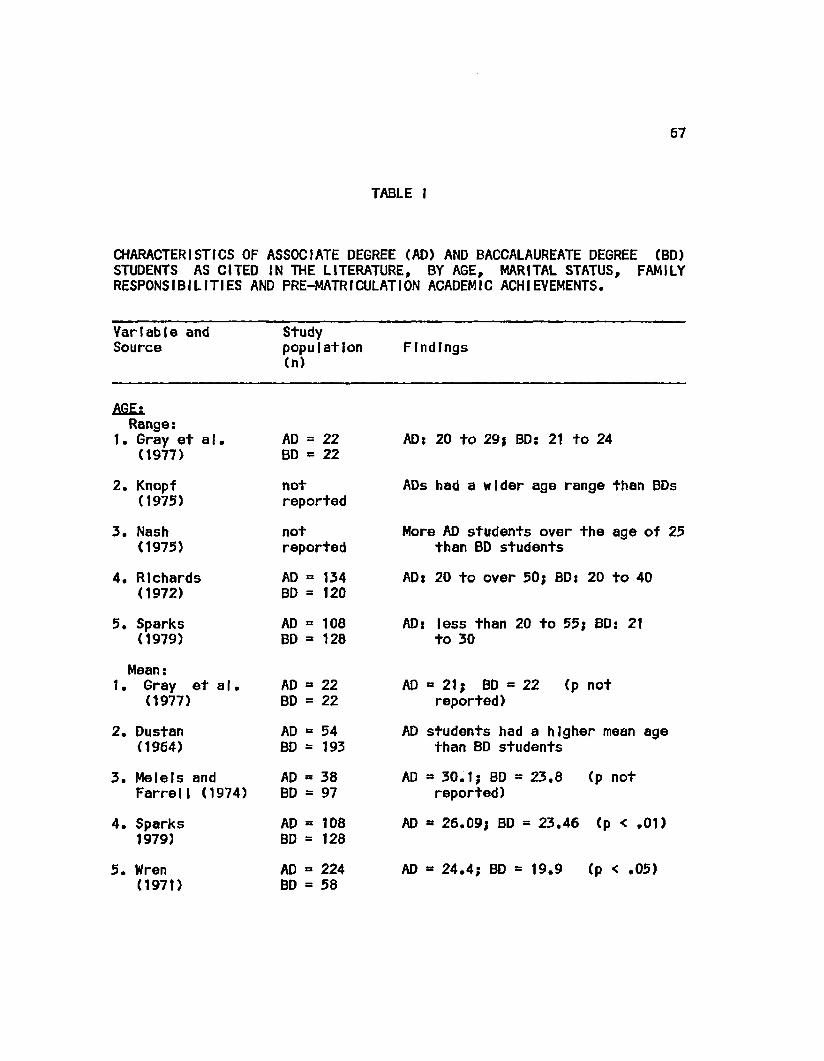
67
TABLE I
CHARACTERISTICS OF ASSOCIATE DEGREE (AD) AND BACCALAUREATE DEGREE (BD) STUDENTS AS CITED IN THE LITERATURE, BY AGE, MARITAL STATUS, FAMILY RESPONSIBILITIES AND PRE-MATRICULATION ACADEMIC ACHIEVEMENTS.
Variable and Source
Study population (n)
Findings
AGE; Range:
1. Gray et al. (1977)
2. Knopf (1975)
3. Nash (1975)
4. Richards (1972)
5. Sparks (1979)
Mean: 1. Gray et a I.
(1977)
2. Dustan (1964)
3. Melels and Farrell (1974)
4. Sparks 1979)
5. Wren (1971)
AD = 22 BD = 22
not reported
not reported
AD = 134 BD = 120
AD = 22 BD » 22
AD = 54 BD = 193
AD BD
AD BD
AD BD
38 97
108 128
224 58
AD: 20 to 29} BD: 21 to 24
ADs had a wider age range than BDs
More AD students over the age of 25 than BD students
AD: 20 to over 50; BD: 20 to 40
AD = 108 AD: less than 20 to 55; BD: 21 BD = 128 to 30
AD = 21; BD = 22 (p not reported)
AD students had a higher mean age than BD students
AD =30.1; BD = 23.8 (p not reported)
AD = 26.09; BD = 23.46 (p < .01)
AD = 24.4; BD = 19.9 (p < .05)
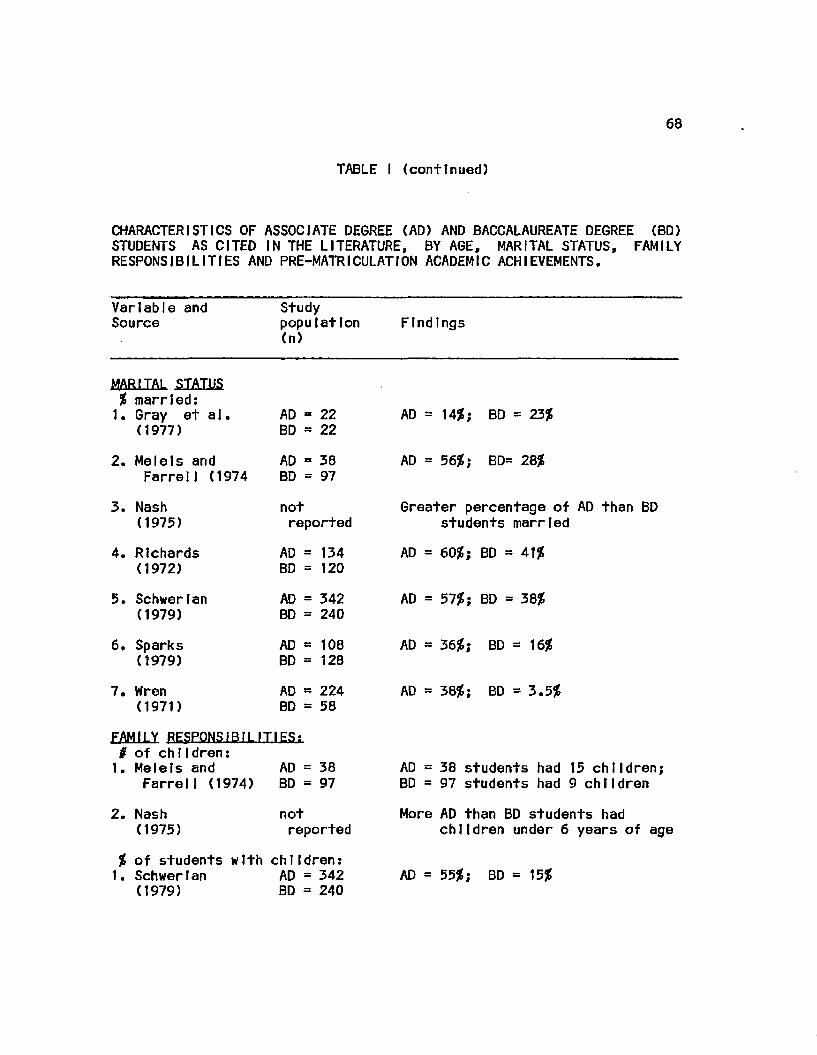
68
TABLE I (continued)
CHARACTERISTICS OF ASSOCIATE DEGREE (AD) AND BACCALAUREATE DEGREE (BD) STUDENTS AS CITED IN THE LITERATURE, BY AGE, MARITAL STATUS, FAMILY RESPONSIBILITIES AND PRE-MATRICULATION ACADEMIC ACHIEVEMENTS.
Variable and Source
Study population (n)
Findings
MARITAL STATUS % married: 1. Gray et a I.
(1977) AD = 22 BD = 22
2. Melels and AD = 38 Farrell (1974 BD = 97
AD = 1456; BD = 23%
AD = 5656; BD= 28j6
3. Nash (1975)
4. Richards (1972)
5. Schwerlan (1979)
6. Sparks (1979)
7. Wren (1971)
not reported
AD = 134 BD = 120
AD = 342 BD = 240
AD = 108 BD = 128
AD = 224 BD = 58
Greater percentage of AD than BD students married
AD = 60%} BD = 4156
AD = 57%; BD = 3 856
AD = 36/6; BD - 16J6
AD = 3856; BD = 3.556
FAMILY RESPONSIBILITIES; 0 of chIIdren: 1. Melels and AD = 38
FarrelI (1974) BD = 97 AD = 38 students had 15 children; BD = 97 students had 9 children
2. Nash (1975)
not reported
J6 of students with children: 1. Schwerlan AD = 342
(1979) BD = 240
More AD than BD students had children under 6 years of age
AD = 5556; BD = 15J6
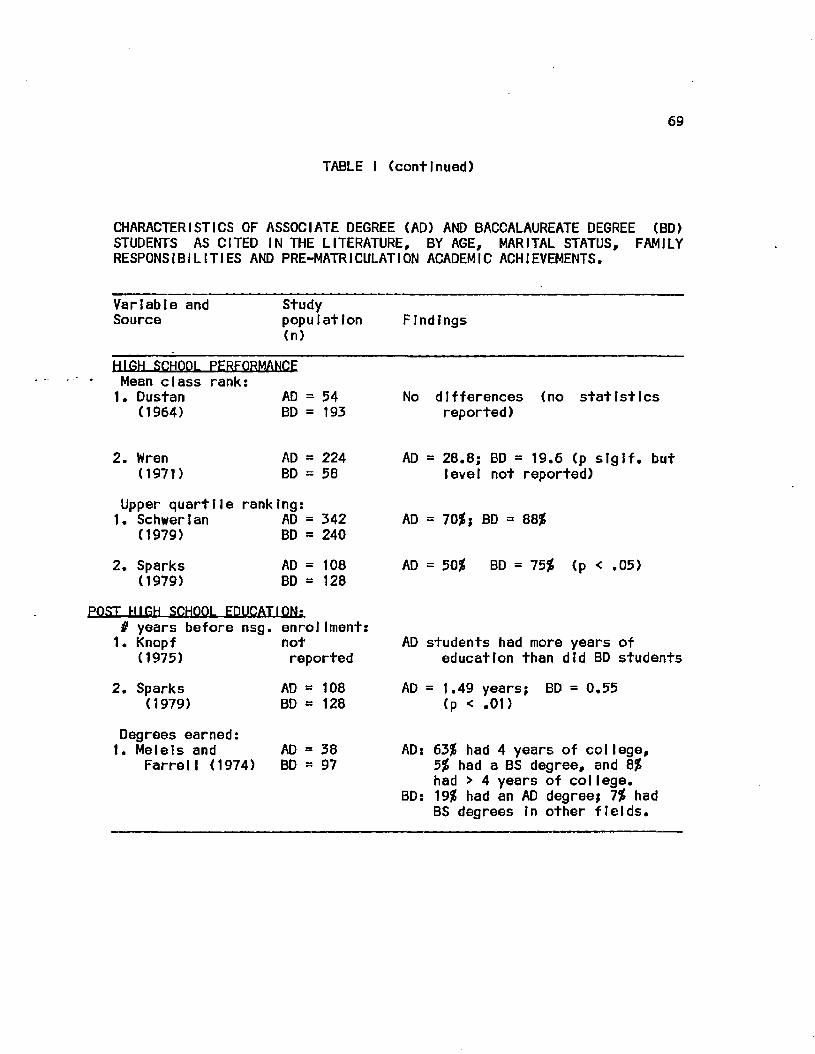
69
TABLE I (continued)
CHARACTERISTICS OF ASSOCIATE DEGREE (AD) AND BACCALAUREATE DEGREE (BD) STUDENTS AS CITED IN THE LITERATURE, BY AGE, MARITAL STATUS, FAMILY RESPONSIBILITIES AND PRE-MATRICULATI ON ACADEMIC ACHIEVEMENTS.
Variable and Study Source population Findings
(n)
HIGH SCHOOL PERFORMANCE Mean class rank: 1. Dustan AD = 54
(1964) BD = 193 No differences (no statistics
reported)
2. Wren (1971)
AD = 224 BD = 58
Upper quartlle ranking: 1. Schwerlan AD = 342
(1979) BD = 240
2. Sparks (1979)
AD = 108 BD = 128
AD = 28.8; BD = 19.6 (p slglf. but level not reported)
AD = 70j8; BD = 88J6
AD = 5056 BD = 7556 (p < .05)
POST HIGH SCHOOL EDUCATION; # years before nsg. enrolIment: 1. Knopf
(1975)
2. Sparks (1979)
Degrees earned: 1. Melels and
Farre11 (1974)
not reported
AD = 108 BD = 128
AD = 38 BD = 97
AD students had more years of education than did BD students
AD = 1.49 years; (p < .01)
BD = 0.55
AD: 63J6 had 4 years of col lege, 5{6 had a BS degree, and 8J6 had > 4 years of college.
BD: 19j6 had an AD degree; 7% had BS degrees In other fields.
70
difference In the number of years of post high school education before
entering a nursing program. Investigations by Knopf (1972) and Sparks
(1979) revealed that AD students had more years of post-high school,
pre-nurslng education than did the BD students. Melets and Farrell
(1974) found that more BD students had prior degrees than did AD
students.
b. Characteristics, related to nursing, program selection
Differences In characteristics that Influence the
selection of a nursing program by a prospective student have been
reported by several Investigators. These factors Include the distance
between home and the school, factors Influencing the selection of a
nursing program, and reasons for selecting nursing as a career.
1) Dlstence. from home
Dustan (1964) discovered that AD students attended
"more locally based" schools than did BD students. Wren (1971) found a
statistically significant difference In the mean number of miles
between home and school (AD = 39.5; Bd = 91.4), but concluded that this
was a function of school location within the state In which her study
was conducted.
2) Se.lect.lQfi. of. type, of. nursing, program
Differences have been reported In the factors
students Identified as Influencing their selection of a nursing
program. Dustan (1964) found that AD students cited cost, program
length, opportunity to live at home, and maintenance of family
responsibilities as having major Influences on program selection. The
71
BD students cited opportunities for personal and professional
development as most Influencing their decisions. Proximity to home
and/or economic considerations were found to be the most frequently
cited factor by AD students participating In studies conducted by
Sparks (1979), Wren (1971), Schwlrtan (1979), Nash (1975), Bui lough
and Sparks (1975), and Knopf (1975). Program length was cited by AD
students participating In studies conducted by Knopf (1975), Wren
(1971), Bui lough and Sparks (1975) and Schwertan (1979).
The most frequently cited reasons for the selection of a BD
program were program quality and location (Sparks, 1979), program
quality and career advancement (Schwerlan, 1979), and a desire for a
collegiate degree and a nursing program (Knopf, 1975).
3) Reason..for sblent,ton of, a, nurslnc. career
Dustan (1964) found no differences between AD and
BD students tn the reasons they cited for entering nursing. The reasons
cited most frequently were: Interest In and liking people, Interest In
caring for the sick, and Interest In the medical field. Sparks (1979)
also reported no differences In cited reasons. Those most frequently
cited were wanting to help people, past health related work experience,
and Job security. Wren (1971) reported that helping people was cited
most frequently by both AD and BD students, followed by "always wanted
to be a nurse" for AD students and "self Improvement" for BD students,
c. PsrsofiaJ_ attrJbutcs. of. students
The personal attributes of students enrolled In AD and
72
BD programs that have been studied are their professional values, their
leadership qualities, and various personality factors.
1) Professional, values
Attributes regarding professional orientation have
been examined by Eller (1976), Simons (1982), Archer (1976), Blaney
(1974), Watson (1983), and Davis (1973). All except Blaney and Archer
found BD students achieved significantly higher professionalism scores
than did AD students. Archer reported statistically significant
differences on subscale scores on an unidentified Instrument, but
concluded that no specific pattern could be Identified. Blaney
concluded there was no "great" difference In the professional values
held by AD and BD students.
2) Leader skip, tmn 1.1 .ties
The leadership opinion questionnaire used by
Melels and Farrell (1974) and Carrel I (1977) demonstrated no
statistically significant differences between AD and BD students on the
consideration subscale. However, AD students In both studies had
statistically significant higher scores on the structure subscale than
did the BD students. Richards reported no differences In the leadership
abilities of AD and BD students.
3) Other persona 1,1 ty. factors
Dowe (1974) found that analysis of reponses on the
Omnibus Personality Inventory (OPI) demonstrated statistically
significant higher scores for AD students than for BD students for
thinking Introversion and esthetlcism. Richards (1972) found no

73
statistically significant differences regarding social ability*
responsibility, or emotional stability for students In the two types
of programs. Ventura (1975) stated that AD and BD students differed on
some measures of social behavior but that all groups were similarly
high In some areas and low In others. She did not Identify what these
specific areas were. Melels and Farrell (1974) determined that AD and
BD students were similar In their levels of self esteem but that BD
students had slgnlflcanly higher scores for communication when tested
with the Satisfactory Achievement Scale.
4) Academic aptitude/achievement
In addition to comparing ratings of high school
performance, a number of other measures have been used to compare the
Intellectual abilities of AD and BD students. These measures Include
the Scholastic Aptitude Test (SAT) (Dustan, 1964; Gray et al., 1977;
Wren, 1971), Quick Word Test (Sparks, 1979), State Board Test Pool
Examination (SBE) results (Archer, 1976; Counts, 1975; McQuald and
Kane, 1979), OPI (Melels and Farrell, 1974), and IPAT test of general
Intelligence (Richards, 1972).
No significant differences In measures of Intellectual ability
were Identified by Counts (1975), Melels and Farrell (1974), Richards
(1972) or Sparks (1979). Differences In performance on the SAT varied.
In Dustan's study (1964), AD students had statistically higher mean
scores than did the BD students. The opposite was demonstrated by Wren
(1971). Gray et a|. (1977) found that more BD students than AD
students were In the upper decile and the upper quartlle of their high
74
school classes and had SAT scores greater than 1000, and that more AO
students than BD students were In the upper quartlle but had SAT scores
of less than 1000.
Comparisons of performance on the SBE also produced equivocal
results. Counts (1975) found no differences In the mean scores of AD
and BD graduates for both the medical and surgical nursing sections of
the exam* McQuald and Kane (1979) reported that AD graduates had
higher mean scores on the medical and surgical nursing sections than
did the BD graduates. Graduates of BD programs had higher mean scores
for the psychiatric, obstetric, and pediatric nursing sections. Further
analyses by McQuId and Kane (1979) revealed that BD graduates had
higher subscores than did AD graduates for the categories of
"understanding of mental health", "human relations; and "causes of
disease". No clear pattern of performance could be Identified for AD
students but the pattern was closer to that for diploma (DP) graduates
than to that for the BD graduates. They also found that, for all
programs, within school differences In performance were greater than
between school differences. Archer (1976) reported that AD graduates'
scores for obstetric and psychiatric nursing examinations were
significantly different from those of BD students. However, multiple
regression analysts demonstrated that age, ethnicity, and
Intelligence, rather than type of education, explained these
differences.
75
d. Ql ln lcaL attrthii+p^ nf grafhiatfis
An examination of differences In clinical competencies
of AD and BD graduates has been approached from several different
perspectives. Included are ratings by nursing educators and
administrators, comparisons of ratings regarding what the competencies
should be versus actual differences, and comparisons of self-ratings by
staff nurses with those of nursing educators, nursing service
administrators, and others. Analyses of critical Incident reports and
problem solving performance as measured on clinical simulations have
also been used to differentiate between the graduates of the AD and BD
programs.
1) Competency, rat ings
Chamlngs and Teevan (1979) examined differences In
AD and BD nurse educators' perceptions regarding differences In
conceptual, human, and functional competencies of graduates of AD and
BD programs. An 80 Item Instrument, based on a taxonomy of
competencies developed by the Southern Regional Education Board (Haase,
1976) was distributed to 222 randomly selected nurse educators
representing programs In a wide geographic area of the United States.
Data analysis was based on questionnaires returned by 57^ (n=63) of the
BD educators and by 50% (n-56) of the AD educators. Chi square and t-
test results Indicated that expectations for BD graduates were higher
but not clearly different In kind from those held for AD graduates.
Analysis of subscale scores demonstrated higher expectations for BD
graduate on the conceptual and human scales than for AD graduates.

76
Therefore, Ft was concluded that BD graduates were expected to
demonstrate greater competence In the ability to reason, to know and
use theoretical content, to recognize, analyze, synthesize, and
evaluate situations (conceptual competencies), and In the conduct of
Interpersonal and Intrapersonal Interactions (human competencies).
Differences In nursing educators' and admlnstrators' expectations
of the clinical competencies of beginning practitioners were examined
by Dlckerson (1976). She distributed an Investigator designed
scale composed of 36 competency statements to 127 nursing service
administrators and 165 nursing education administrators. Data analysts
was based on the 178 (60S?) returned questionnaires. Significant
differences were found between the ratings of nursing educators and
nursing service administrators of expected competencies for a beginning
nurse practitioner. Nursing service administrators rated Interpersonal
relationships and effective group functioning as more Important than
did the educational administrators. Educational administrators
considered patient safety, evaluation of patient care, continuity of
care, need for establishing priorities In planning care, alteration In
care necessitated by a patient's changing condition, and problem
solving more Important than did the nursing service administrators.
Although not elaborated on by the Investigator, significant differences
also were demonstrated between the ratings of some competencies when
the ratings of educational administrators were analyzed by type of
program (I.e., AD or BD). These Indicate different competency
expectations for graduates of AD and BD programs.

77
Pttts (1975) examined differences In actual versus Ideal
differences In the outcome goals of AD and BD programs. A mall survey
was conducted using a sample selected from physicians, hospital nursing
service administrators, nursing educators, and practicing nurses In the
state of Washington. Analysis of differential responses to a 37 Item
questionnaire revealed differences In perceptions of different
occupational groups regarding both Ideal and actual program goals.
Further analysis demonstrated that nursing educators perceived little
difference did exist but that they believed It should exist between the
outcome goals of AO and BD programs; nursing service administrators
perceived that a small difference did exist but that none should.
Practicing nurses perceived some differences existed and some should
exist. The responses of physicians Indicated that they perceived little
difference In the outcome goals and believed little should exist.
Schuyler (1983) examined perceived Importance of specific
critical requirements expected of beginning practloners for AD, diploma
(DP), and BD programs, and performance capab11 Itles of these new
graduates as perceived by nursing educators, nursing service
supervisors, and recent graduates. Methodology was not described.
Findings Indicated general agreement existed among groups regarding
perceived Importance of the areas under study to a common core of
knowledge and skills possessed by all beginning practitioners. Rank
order comparisons of Item ratings of perceived Importance demonstrated
agreement among nursing educators, nursing supervisors, and graduates
78
of DP and BD programs, but not among the AD students, educators, and
nursing service supervisors.
Comparisons of mean ability ratings Indicated that supervisors
perceived AD graduates as less than adequately prepared to function In
9 of 10 areas; DP graduates In 6 of 10 areas; and BD graduates, In 2 of
10 areas. In contrast, comparisons of graduates' self-ratings revealed
that they perceived themselves as adequately prepared In all areas.
Educators rated their students as adequately prepared In 8 of 10 areas.
Hogstel (1975) used an Investigator designed Instrument for an
analysis of differences between AD and BD graduates In relation to the
functions they were performing. Questionnaires were mailed to 109 AD
graduates, 236 BD graduates, and 100 employers. A A0% response rate
was attained In each group. Analysis of variance and t-test were used
to determine the existence of differences In function In 5 areas:
physical care and technical skills. Interpersonal relationships,
leadership, decision making, and community health care.
Based on self-ratings, the only function In which the BD
graduates were performing to a significantly greater extent than the AD
graduates was In community health. In terms of preparation, AD
graduates perceived themselves significantly better prepared than BD
graduates In the area of physical care and technical skills. Employers
rated BD graduates as significantly better than AD graduates In 4 of
the 5 functional areas, but reported that they did not discriminate
between the two types of graduates on orientation, position, promotion,

79
or assignment to nursing activities. A small majority of the employers
differentiated between AD and GD graduates In salary.
McKenna (1971) used 4 BD and a total of 6 AD and DP graduates,
from one clinical unit, who had been working according to job
descriptions delineating professional and technical nursing activities,
to examine components of tasks, knowledge, basic skills, and sources of
decisions. Over a period of seven consecutive work periods, staff
recorded the tasks they performed. Judgments concerning the type of
worker who should perform each task, the decision source, and the basic
skill and knowledge source for each task.
Analysis of 2801 tasks revealed the performance of 334 different
tasks. Of the total tasks, 73J6 were performed by either AD/DP or BD
graduates. In addition, BD graduates performed more of their tasks
with people while the AD/DP graduates performed more of their tasks
with things. It was concluded that 1) even though the BD graduates
performed tasks appropriate for their group, they did not do so with
the consistency of the AD/DP groups; 2) there were differences In
function, knowledge sources, and basic skills reported by the two
groups; and 3) the two groups perceived no differences In the sources
of their decisions.
Stanton (1982) Investigated differences In clinical competency of
AD and BD graduates within their Initial 3 to 12 months of employment
after licensure. Head nurses used the Slater Nursing Competencies
Rating Scale to evaluate retrospectively the performance of 90 AD and
143 BD graduates working In 35 Colorado hospitals. Analysis of the
80
results Indicated that new BD graduates displayed greater clinical
competence than did AD graduates.
tn a national study designed to operational Ize and measure
nursing performance, Schwerlan (1979) used an Investigator designed
Instrument (the Schwertan 6-D[mensIon Scale of Nursing Performance) (6-
D Scale) to obtain self-ratings and supervisor ratings of 3004
graduates of AD, DP, and BD programs. The respondent group of graduates
consisted of 342 AD, 332 DP, and 240 BD graduates; the overall
response rate was 30Jf. Supervisors returned questionnaires for 687
graduates. The six areas that were rated were: Interpersonal
relationships and communications, leadership, critical care, planning
and evaluation of care, teaching and collaboration, and professional
development. Results Indicated that AD graduates rated themselves
lower than DP and BD graduates on all six scales; BD graduates rated
themselves higher than AD and DP graduates on the
teaching/collaboration and planning of care scales.
The 6-D Scale also was used by two additional Investigators.
Chance (1982) used a modified version to compare self and supervisor
perceptions of the nursing performance of 34 AD, 35 DP, and 36 BD
graduates employed as staff nurses tn seven hospitals In a Southeastern
metropolitan area. No significant differences were demonstrated between
the self-perceptions of graduates from the three types of programs.
Supervisors rated BD graduates significantly higher than other
graduates In critical care performance. Additional analyses revealed
that hospital, type of unit, and shift were significant predictors of
81
components of nursing performance and that s e l f a n d supervisor ratings
were significantly correlated on over half of the Items.
McCloskey (1981) conducted a study to determine whether nurses
with different educational preparation differed In their Job
effectiveness. She hypothesized that Job effectiveness was a function
of formal education, continuing education. Job skills. Job
responsibility, and aptitude. A random sample of 402 nurses stratified
by type of education (practical, AD, DP, BD), size of hospital employed
In, and type of unit, was drawn from 12 general hospitals In the
Chicago area. A total of 53 practical nurses, 63 AD, 134 DP, and 49 BD
graduates participated In the study (75$ return rate). Self and head
nurse ratings on the 6-D Scale and Indicators of continuing education,
formal education, and Job responsibility were used to predict Job
effectiveness. Analysis of the results led to the conclusion that years
of nursing education had a significant but small effect on Job
performance, accounting for only 1 -2$ of the variance. It also was
found that the effects of nursing education on Job performance were
Indirect rather than direct.
Waters et al. (1972) explored and described evidence of
differences In nursing practice of graduates of AD and BD programs In
the San Francisco area. Data collection methods consisted of Interviews
with 12 nursing service directors, observations of and Interviews with
each of 22 AD and 22 BD graduates, and an Interview with the 22 head
nurses who were the subjects'Immediate supervisors. Observations were
designed to provide data regarding varieties of nursing actions
82
Implemented by the subjects. Follow-up Interviews were used to
substantiate observed nursing actions and to elicit examples of
critical or highly significant nursing problems worth remembering.
Ten of the 12 directors Interviewed reported specific differences
between the practice of BO graduates and of AD graduates. Analysis of
staff nurse activities and attitudes revealed that AD graduates*
performances appeared to be consistent with technical nursing practice
as described In the literature. In most cases nursing problems AD
graduates dealt with were concrete and specific, and nursing actions
had fairly predictable outcomes. Problems and Interventions were more
often physiological and physical than psychological or social In
nature.
The practice of BD graduates was found to be more technical than
professional In nature when Judged according to criteria cited In the
literature. Only 6 of 24 BD graduates were Judged to be practicing
professional nursing more consistently than the others. The practice
of these 6 Individuals was described as being wider In scope, less
common, having more alternatives to solutions, and often psychological
In nature.
All of the head nurses, with one exception. Indicated that
differences did exist between the practice of the two groups. The AD
graduates were characterized as working with more basic problems of
patient care; their practice was based on sound principles of nursing
care. In contrast, BD graduates were seen to have more depth for
83
solving problems, were more aggressive In trying to reason why, and
examined the psychological aspects of patient care.
Bui lough and Sparks (1975) conducted a survey of 201 AD students
and 192 BD students who were graduating from 3 AD and 4 BD programs In
the Los Angeles area. They used a questionnaire designed to ascertain
one of two basic orientations of the nursing role: one focused on
curing a patient's Illness and the other focused on caring for
patients. Based on the results of responses to both single Items and
parallel Items, the Investigators concluded that although the dominant
response of all respondents was one of a caring orientation, a
significant difference In orientation was found between the AD students
and the BD students. The AD students were more cure oriented while the
BD students were more care oriented.
Nelson (1978) conducted a study to determine If graduates of AD,
DP, and BD programs differed In perceptions of their competencies, If
supervisors differed In their perceptions of competencies of graduates
of the three programs, and If there were differences between the
perceptions of graduates and supervisors.
The Nurse Competency Inventory (NCI), an Investigator designed
Instrument containing 35 competency statements, was used to collect
data within three broad areas: technical skills, communication skills,
and administrative skills. The NCI was mailed to 429 graduates of 2 AD,
3 DP , and 4 BD programs. A 75^ return rate was achieved. Analysis of
the results Indicated that significant differences existed between the
competency perceptions of AD, DP, and BD graduates In each competency
84
area and across all areas combined. In overall competence and In
communication skills, BD graduates rated themselves higher than AD
graduates. There were no significant differences between AD and BD
self-ratings for technical skills and administrative skills.
Supervisors also rated the three groups significantly different with
regard to overall competence and competence In each of the three areas.
Supervisors of BD graduates rated BD nurses as more competent than AD
nurses In all three areas. Significant differences also were found
between perceptions of graduates and supervisors of overalI competency.
Ratings of BD graduates and their supervisors were significantly less
different than those of AD and DP graduates and their supervisors In
the areas of administrative skill and overall competence.
a) Summary
Thirteen Investigators have compared and
contrasted the clinical competencies of AD and BD graduates. A wide
variety of Instruments and data sources were used to obtain
measurements of expected and/or actual competencies. The majority of
ratings were based on retrospective analyses of a graduate's
performance or from the perspective of the actual and/or Ideal
competencies of all AD graduates, considered as a whole, and all BD
graduates considered as a whole. Data analyses led to varied
conclusions; although a majority of the Investigators stated there were
differences In the competencies of the two groups, others concluded no
differences existed. Although the results of these studies provide
Insight Into the various aspect of the roles and functions assumed by
85
the AD and BD graduates, the results do not provide direct Information
as to the assessment abilities of graduates.
2) Critical Incident reports
Jacobs (1980), as part of a larger study,
performed a content analysis of 9884 critical Incidents provided by
over 2000 nurses In a nationwide sample to determine the relationship
between educational preparation and number of effective and Ineffective
critical Incidents reported. Both self-reports and reports of observed
nursing performance were utilized.
Significant differences Mere found both between and within
behavioral areas In types of behaviors reported by and/or about AD, DP,
and BD graduates. Nurses from BD programs were most often Involved In
Incidents concerning leadership and professional responsibility;
patient teaching and the promotion of psychological well-being;
exchanging and recording Information about patients; and planning
nursing care. Significant differences also were demonstrated among the
three types of graduates In overall amount of effective and Ineffective
Incidents reported. More effective Incidents were reported about BD
graduates than about the AD and DP graduates. The greatest percentage
of Ineffective Incidents Involved AD graduates. Content analysts
failed to reveal consistent patterns of differences among the three
types of graduates In the following areas: degree of self-determination
by the nurse; degree of Judgment versus rote behavior; reasons for
Ineffective behaviors or close calls; and factors contributing to
success or lack of success of a reported Intervention.

86
3) Problem. goJyJng. abl i,lt.y
Studies designed to differentiate between how AD
and BD students problem solve In specific clinical situations have been
conducted by Bassett (1973), Fredertckson and Mayer (1977), Gover
(1972), Gray et al. (1977), Johnston (1982), and Sparks (1979). Gray
et at. (1977) used open-ended short essay questions based on cl(nlca)
situations to determine If there were differences In the performance of
techntcal skills, teaching, leadership, the provision of support to
patients and their families. In Interviewing for assessment purposes,
actions In structured situations, and actions following observations.
Participants In this study were a random sample of 27 AD and 22 BD
students graduating from the University of Vermont. Student responses
to questionnaire Items were coded by panel members acting In concert,
to reflect whether the performance of stated activities was to be
expected of technical level, professional level, or of all nurses.
Responses subsequently were assigned a point value. Significant
differences were demonstrated between mean technical skill,
professional, and total scores. BD students had higher mean total and
professional scores; AD students had higher technical skill scores.
Individual Item analyses revealed differences In scope of
functioning In the areas of teaching, provision of anticipatory
guidance, leadership, emotionally supportive actions, nursing process,
use of knowledge, use of extra time, and relationships with co-workers.
In the areas of nursing process and use of knowledge, BD students
provided responses representing the following actlvlltes: actively
87
seeks Information, evaluation of the adequacy of a plan of care, health
promotion and maintenance, prevention of health problems, and use of
knowledge as a base for assessment and planning.
The Investigators also noted that a comparison of nursing actions
that all nurses would take with those taken only by BD nurses helped to
explain why the general public and nursing have difficulty describing
differences In professionally and technically prepared nurses. Those
actions specific to the BD nurse are not readily visible because they
Involve use of knowledge In assessment prior to action and In planning
for and Implementing of preventive nursing actions. In contrast,
actions of AD nurses were readily vtslble and could be performed by
all nurses.
The generalIzablIIty of the findings of this study Is limited
due to the small sample size and the fact that all participants were
obtained from one Institution. In addition, the Instruments used to
collect data did not provide direct measures of students' abilities to
collect data and to formulate nursing diagnoses. Therefore, the study's
results provide no direct Information regarding any differences that
might exist In the assessment abilities of these two types of students.
Johnston (1982) conducted a study to delineate strategy
differences In the use of the nursing process by AD, DP, and BD
graduates. Using a theoretical model developed by Rtnes (1977a),
Johnston (1982) developed a questionnaire In which each Item
exemplified one of the theorized process strategies used by either
technical (AD, DP) or professional graduates. The final form of the
88
questionnaire was distributed to 60 staff nurses working full time In
one of 7 units within a hospital. A 10$ return rate was attained and
Included 8 AD, 5 DP, and 29 BD graduates. The AD and DP graduates were
treated as one group.
Results Indicated partial support for the hypothests that
different strategies were used by the two groups of nurses. In the
assessment phase, BD graduates preferred the use of analytical
questioning techniques more so than did the AD/DP graduates who
preferred the measurement of bodily functioning. Both groups equally
preferred the use of direct questlonnlng and the Identification of
alternative sources of data. As a product of the assessment phase, BD
graduates were found to prefer Identification of nursing diagnoses as
opposed to production of Information for other health team members, as
was preferred by the AD/DP graduates. There were no Identifiable
differences In strategies used In the planning and Intervention phases.
Different strategies again were demonstrated In the evaluation phase.
BD graduates preferred the strategy of Interpreting outcome of care
while AD/DP graduates preferred the strategy of reporting outcome of
care to others.
Johnston's (1982) study demonstrated that AD and BD graduates
used different strategies In their use of the nursing process by having
subjects Indicate which of several alternatives they wouJd take given a
specific situation. Although this methodology provides Insight Into
projected differences In behavior, It does not provide any Information
89
regarding what patient Information was considered relevant and what
problems were Identified as a result of having access to those data.
Frederlckson and Mayer U977) utilized a filmed clinical sequence
developed by Verhonlck et al. (1968) to Investigate the processes used
by graduates of AD and BD programs. Responses to the filmed situation
were categorized as follows: problem definition, data collection,
postulatton of solutions, and evaluation of solutions. Results
Indicated that both groups used primarily the first three steps
enumerated above. No significant differences were found between the
problem solving process used by AD and BD students.
The methodology used In this study provided the participants with
an opportunity to Identify relevant data. However, It did not provide
for the Initiation of data collection activity In those Instances when
the participant might have desired more Information. The participant
was.a passive observer. Therefore, although the results of this study
provide Insight Into the assessment capabilities of participants. It
does not provide a picture of what they would do If they had some
control over data collection activities.
Gover (1972) designed and used the Nursing Performance
Simulation Instrument (NPSI) to measure the problem solving abilities
of technical and professional nurses. The NPSI consists of four
clinical simulations In which specific patient care situations are
described. The respondent then chooses among a number of forced-choice
alternative actions that could be Implemented. Results Indicated no
90
significant differences In problem solving ability. Further
Information was not available about this study.
Bassett (1977) also used the NPSI to determine the existence of
differences In problem solving abilities of last term AD and BD
students. No significant differences were demonstrated between
performances of the two groups of students. Further Information was not
available about this study.
Sparks (1979) used the NPSI and an Investigator designed
Instrument, the Nursing Process Utilization Inventory (NPUI), to
evaluate problem solving abilities of AO and BD students. The NPUI
consists of two client situations In which a narrative description of a
client, Including relevant data, Is provided. Using an open ended Item
format, the student Is directed to Indicate each client's nursing
problem, the substantiating data, and, for the three priority problems
Identified by each participant, to Indicate objectives for care and
outcome evaluation criteria, nursing actions to be taken, and rationale
for each stated action.
Participants In the study were 128 AD and 108 BD senior level
students In programs located In three mid-western states. Analysis of
the NPSI scores demonstrated no significant differences In problem
solving abilities of the two groups of students. Analysis of the NPUI
revealed that BD students had significantly higher scores than did AD
students for the composite scores on each of the two simulations and
for problem Identification and care planning scores. Sparks suggested
that an explanation for the difference In outcomes, as measured by the
91
NPUI and the NPSI possibly could be related to the NPSI not measuring
nursing process ability.
Re Id (1981) designed a study to examine the psychometric
properties of the NPSI and the Clinical Nursing Simulation Instrument
(CNSI), a branching type simulation developed by the nursing faculty at
the University of St. Thomas. These Instruments were administered to
96 AD and 45 BD students from three AD and three BD programs In
Tennessee. The results of analyses lent support to Spark's conclusion
that the NPSI did not measure problem solving ability. Rather, Reld
(1981) concluded. It tests nursing knowledge. Analysis of student
performance on the two tests resulted In the demonstration of no
significant difference In performances of AD and BD students.
The NPSI used by Gover (1972), Bassett (1973), Sparks (1979) and
Reld (1981) and the NPUI used by Sparks (1979) do not provide an
opportunity for the participant to select patient data. As In several
of the previously described studies, data are presented and the
participant Is expected to react. The use of this type of Instrument
yields artificial Information regarding the overall assessment
abilities of the participant. A second concern regarding the
conclusions of Gover (1972), Bassett (1973), and Sparks (1979) Is
related to Sparks' (1979) question and Reld's (1981) conclusion that
the NPSI tests knowledge rather than problem solving ability.
4) Summary
Differences In the problem solving ability of AD
and BD graduates or students have been addressed directly by seven
92
Investigators. They have used a variety of Instruments designed to
address the question: What would you do In this situation? Although
the work of Frederlckson and Mayer (1977) best exemplifies the need to
look at what data are used to formulate nursing diagnoses or problems,
none of the studies addresses the need to examine the entire range of
activities encompassed In the assessment phase. Included should be
determinations of what data are Identified as relevant to collect,
what conclusions are drawn as a result of having access to specific
data, and are correct Judgments arrived at based on the data collected.
The methodology necessary to obtain Information regarding data
collection and nursing diagnosis Identification abilities of
graduating AD and BD students will be addressed In the next chapter.
III. METHOD
The primary research question to be addressed by this study wast
Are the patient assessment abilities of associate and baccalaureate
degree nursing students, when measured within three months prior to
graduation from a program of study accredited by the National League
for Nursing, Influenced by type of educational program? The secondary
questions addressed were: When graduating associate and baccalaureate
degree nursing students are compared. Is there a difference In 1) data
collection efficiency and proficiency?; 2) amount and percent of
psychosocial history data selected?; 3) number and completeness of
nursing diagnoses Identified?; and 4) amount and percent of
psychosocial nursing diagnoses Identified?
This chapter is focused on the methodological processes used In
conducting the study. The following sections Include descriptions of
the design of the study, population of Interest and sample selection
procedure, operational IzatIon and measurement of the conceptual model,
and data collection procedures.
A. Research design
Influence of type of nursing education program attended on
graduating students' abilities to collect patient data and Identify
nursing diagnoses was examined using a non-equivalent groups, post-test
only design (Cook and Campbell, 1979), This design was selected since
potential participants could not be assigned to treatment groups (I.e.,
93
94
either an associate or a baccalaureate degree program) and naturally
occurring groupings thus were studied.
A major weakness of this design Is lack of pre-test Information.
Therefore, It was Impossible to compare pre-nurslng education problem
solving abilities of participants, attribute any post-test differences
to type of educational program attended, or rule out selection bias
(Cook and Campbell, 1979). For these reasons, Cook and Campbell (1979)
classified the non-equivalent groups, post-test only design as a non-
experimental design.
To arrive at plausible causal Inferences regarding the total
Influence of type of nursing education program attended on data
collection and nursing diagnosis Identification abilities of the study
participants, several procedures were used to overcome the lack of
pretest measures. These Included measurement of additional variables
(covarlates) that are associated with performance on outcome measures
and selection of a nursing program, and use of selected statistical
analysis procedures. These covarlates and stattslttcal analysis
procedures will be discussed subsequently.
To prevent hypothesis guessing by the participants, a threat to
the Internal validity of the study (Cook and Campell, 1979), the Deans
and Directors of schools solicited for participation In the study and
potential participants were Informed only that the purpose of the study
was to explore the Influence of various educational factors and
Individual characteristics on clinical decisionmaking abllltes of
graduating students.
95
B. Population and sample selection
The target population was all National League for Nursing (NLN)
accredited associate and generic baccalaureate degree nursing programs.
Stratified random sampling, with replacement, was used to select 6
Institutions offering AD programs and 6 Institutions offering BD
programs located In three mtdwestern states and within a 150 mile
driving distance of a large mldwestern city. The population of
Institutions offering BDs was stratified so that two programs from
public supported Institutions and four programs from private
Institutions would be Included In the sample In proportion to their
representation In the population. A convenience sample of students
enrolled In their first nursing education program then was obtained.
It was anticipated that a minimum of 100 AD and 100 BD students who
were within 3 months of graduation would agree to participate In the
study.
1. Rationale for sample selection
The rationale for the sampling frame was as follows.
Limitation of the sample to only those Institutions which have attained
NLN accreditation was a quality control factor. The attainment of NLN
accreditation Indicates that a program has met standards of quality
that have been established for a specific level of educational
preparation for nursing.
A three state area was selected to provided a broader
representation of programs than would be provided by confinement of the
sample to one state. Confinement of the sample to within one hundred
96
fifty miles was Imposed due to travel time and financial considerations
associated with data collection.
Only students enrolled In AD and BD programs were Included In the
study since these two levels of programs were endorsed by the ANA
(1965) as appropriate for the preparation of technical and professional
nurses. To prevent confounding the study results due to the completion
of other nursing programs, only generic nursing students enrolled In
their first nursing education program were Included In the study.
Students with a degree In another area of study but enrolled In their
first nursing program also were eligible for Inclusion. Additionally,
only students within 3 months of graduation were Included to allow
students to gain maximum benefit from their educational program while
still providing for flexibility In the scheduling of data collection.
2. Sampling procedure
The State Approved Schools of Nursing - RN (NLN, 1983) was
used to Identify alt NLN accredited AD and BD degree nursing programs
In the designated geographic area. The Identified Institutions were
stratified Into three groups depending upon type of program offered and
the source of funding (private, public) for those Institutions offering
baccalaureate programs In nursing. Within each group, each Institution
was assigned a number.
A table of random numbers was used to compile lists of randomly
ordered associate degree granting Institutions, private baccalaureate
degree granting Institutions, and public baccalaureate degree granting
Institutions. The characteristics of the 19 AD and the 6 public BD and

97
15 private BD nursing programs from which the stratified random sample
was drawn are summarized In Table XL (Appendix A).
The convenience sample of participants was to be acquired from
the first six AD programs, the first two public BD programs, and the
first four private BD programs, on the respective lists, whose
Dean or Director was willing to participate In the study and who would
allow the Investigator access to the student population.
3. Solicitation of Institutional agreement to participate
A letter (Appendix B) was sent to the Dean or Director of
the first 6 AD, the first 2 public BD and the first 4 private BD
programs on the randomly ordered lists of programs. The letter
explained the purpose of the study, described the level of
participation required, and requested participation In the study. A
follow-up phone call, approximately one week after the anticipated
receipt of the letter, was made to ascertain willingness to participate
In the study.
If there were agreement to participate, arrangements subsequently
were made for a mutually agreeable time and place for student testing.
In addition, at the Dean's or Director's discretion, a liaison person
from the program was Identified to facilitate communication and
arrangements.
After all preliminary arrangements were made for testing,
sufficient copies of a letter (Appendix C) addressed to graduating
students was disseminated to all those generic students within 3
months of graduating. This letter described the general purpose of the
98
study, the extent of participation required and requested participation
In the study. In addition, the arrangements for testing were announced
and those students who desired to participate were requested to sign up
for a testing session. These lists were returned by program personnel
to the Investigator. Several days prior to the Investigator's visit to
the campus, those students Indicating a desire to participate received
a memo reminding them of the study and the arrangements that had been
made.
If a school declined to participate In the study, the next school
on the appropriate randomly ordered list was contacted using the same
procedure as described above. This procedure was repeated until the
Deans or Directors of 6 AD and 6 BD (2 public and 4 private) programs
agreed to participate.
The Director of 1 AD program, who Initially Indicated a desire to
permit the program's students to participate, eventually withdrew this
permission. Notification arrived at a point In time when the academic
calenders of the programs remaining on the random list of schools made
It Impossible to obtain a replacement. For this reason, the AD
students who participated In the study were obtained from 5 different
schools rather than the Initially planned 6 schools.
4. Sample characteristics
The following sections Include descriptions of the programs
and the students that participated In the study.
a. Characteristics of participating programs
Selected characteristics of the 11 schools from which
99
student participants were obtained and number of participants from each
school are summarized In Table II. All BD programs were located In
4-year colleges or In universities. Each required 4 academic years for
completion of course work. The modal curriculum pattern was one of 1
1/2 years of liberal arts and science (LAS) courses and 2 1/2 years of
nursing courses with at least one LAS course within each academic
semester or quarter. Four nursing programs reported that they had an
"Integrated" nursing curriculum pattern; the other two had a
"traditional" curricula. The required and elective LAS coursework
Included both Introductory and upper level (I.e., advanced) courses. A
review of the required courses for each program revealed that
approximately 30% to 45JS of the total credits required for graduation
were nursing courses.
The AO programs were located In community colleges or technical
Institutes. Three programs required 2 academic years for program
completion; 2 required an additional summer term In addition to the two
academic years. The modal curriculum pattern was a mix of nursing and
LAS courses throughout the program. The LAS courses can be described
best as single, Introductory level courses (I.e., Introduction to
sociology, anatomy and physiology, etc.) Nursing course work accounted
for 40J6 to 50J6 of the total number of courses required for graduation,
b. Characteristics of student participants
Of the 177 participants In the study, 86 were from BD
programs and 91 were from AD programs. The demographic characteristics
of the participants are summarized In Table III. Academic performance
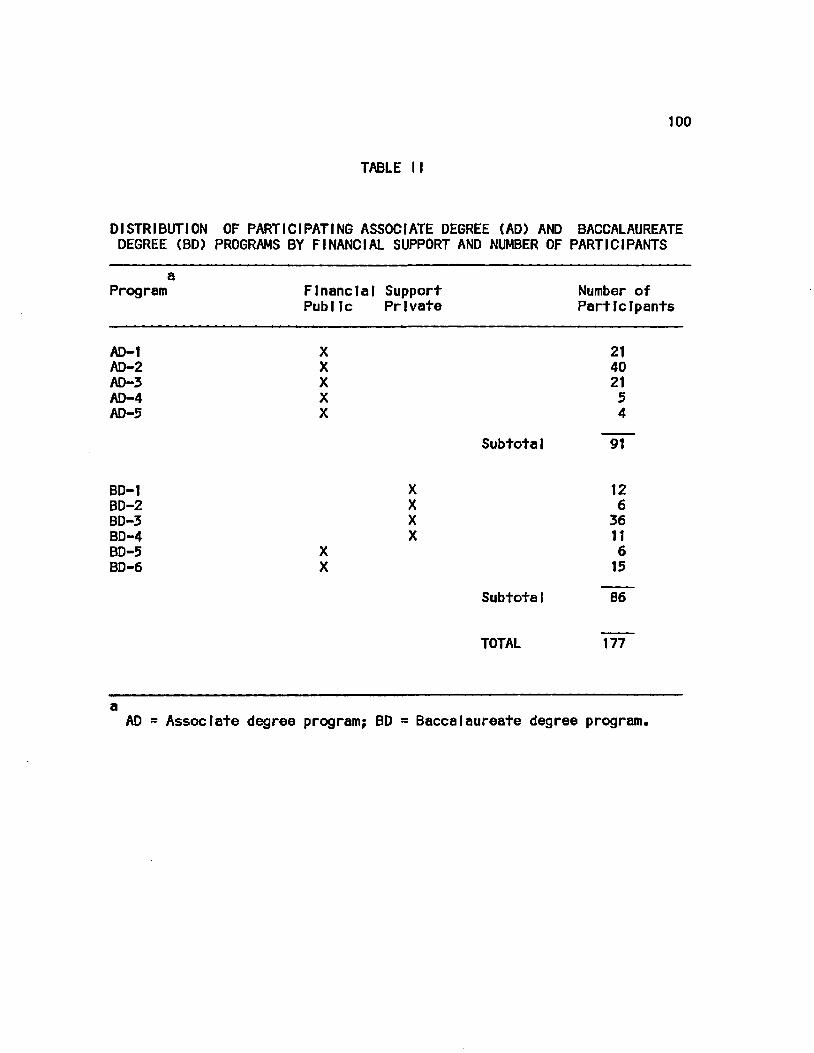
100
TABLE II
DISTRIBUTION OF PARTICIPATING ASSOCIATE DEGREE (AD) AND BACCALAUREATE DEGREE (BD) PROGRAMS BY FINANCIAL SUPPORT AND NUMBER OF PARTICIPANTS
a Program Financial Support Number of
Public Private Participants
AD-1 X AD-2 X AD-3 X AD-4 X AD-5 X
BD-1 BD-2 BD-3 BD-4 BD-5 X BD-6 X
21 40 21 5 4
SubtotaI 91
X 12 X 6 X 36 X 11
6 15
SubtotaI 86
TOTAL 177
a AD = Associate degree program; BD s Baccalaureate degree program.
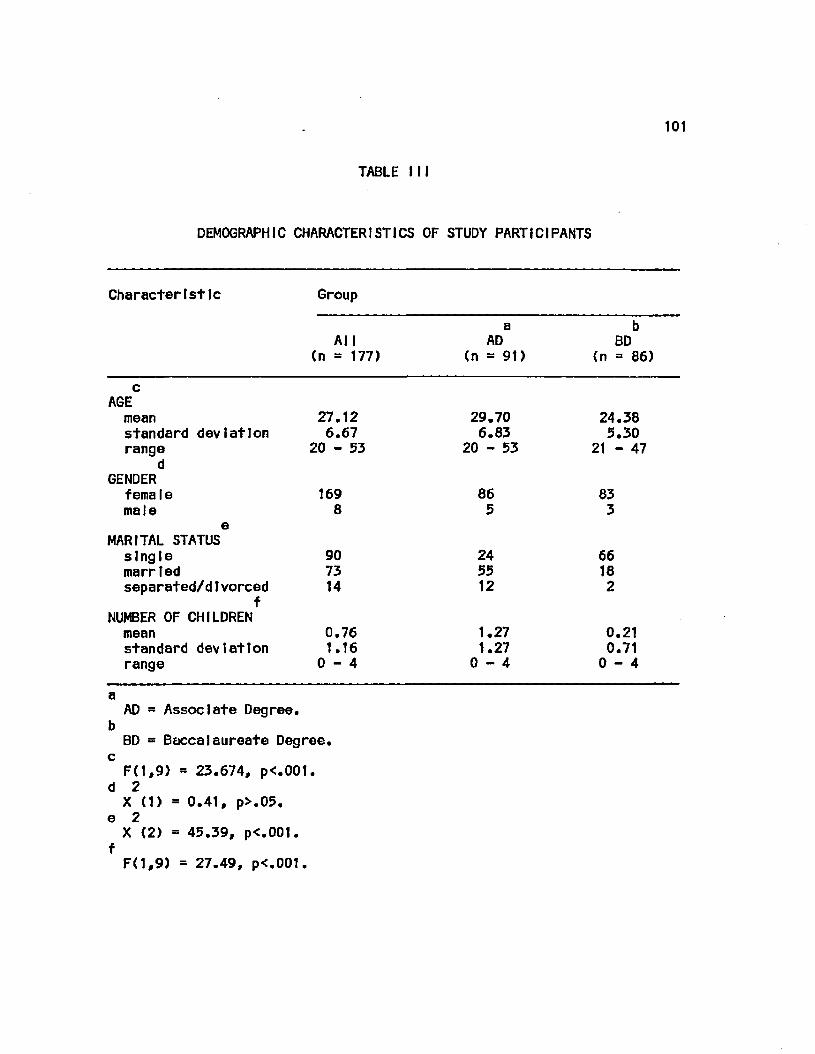
t o t
TABLE 111
DEMOGRAPHIC CHARACTERISTICS OF STUDY PARTICIPANTS
Characteristic Group
a b AJI AD BD
(n = 177) <n = 91) <n = 86)
c AGE mean standard deviation range
d GENDER femaIe male
e MARITAL STATUS single married separated/dIvorced
f NUMBER OF CHILDREN mean standard deviation range
a AD = Associate Degree.
b BD = Baccalaureate Degree.
c F(1,9) = 23.674, p<.00t.
d 2 X (1) = 0.41, p>.05.
e 2 X (2) = 45.39, p<.001.
f F(1,9) = 27.49, p<.001.
27.12 29.70 24.38 6.67 6.83 5.30
20 - 53 20 - 53 21 - 47
169 86 83 8 5 3
90 24 66 73 55 18 14 12 2
0.76 1.27 0.21 1.16 1.27 0.71 0 - 4 0 - 4 0 - 4

102
characteristics of the participants are summarized In Table IV.
Analyses of Variance (ANOVA), with schools nested within program type,
and Chi square were used to determine the presence of any
statistically significant differences between the two groups. These
analyses demonstrated that the AD participants were significantly older
than the BD participants. Also, a significantly greater percentage of
the AD participants were married and had greater family
responsibilities than did BD participants. These findings demonstrate
that the sample was demographlcally similar to those used in other
studies contrasting AD and BD students (Dustan, 1964; Gray et al.,
1977; Knopf, 1975; Melets and Farrell, 1974; Nash, 1975; Richards,
1972; Schwerlan, 1979; Sparks, 1979; Wren, 1971).
Analysis of the academic characteristics demonstrated only one
statistically significant difference. A greater percentage of the BD
participants reported graduation from high school In the highest
quart!le, while the greater proportion of AD participants reported they
were In the second quart 11e. This finding Is consistent with those
reported by Schwerlan (1979) and Sparks (1979). Although no
statistically significant difference was demonstrated, the AD
participants reported having experienced more years of post-high school
education than had the BD participants. This difference Is In the same
direction as that reported by Knopf (1975) and Sparks (1979).
Although not statistically different, AD participants achieved a
higher score on the NCLEX-RN examination than did the BD participants.
This finding Is consistent with national results reported by the
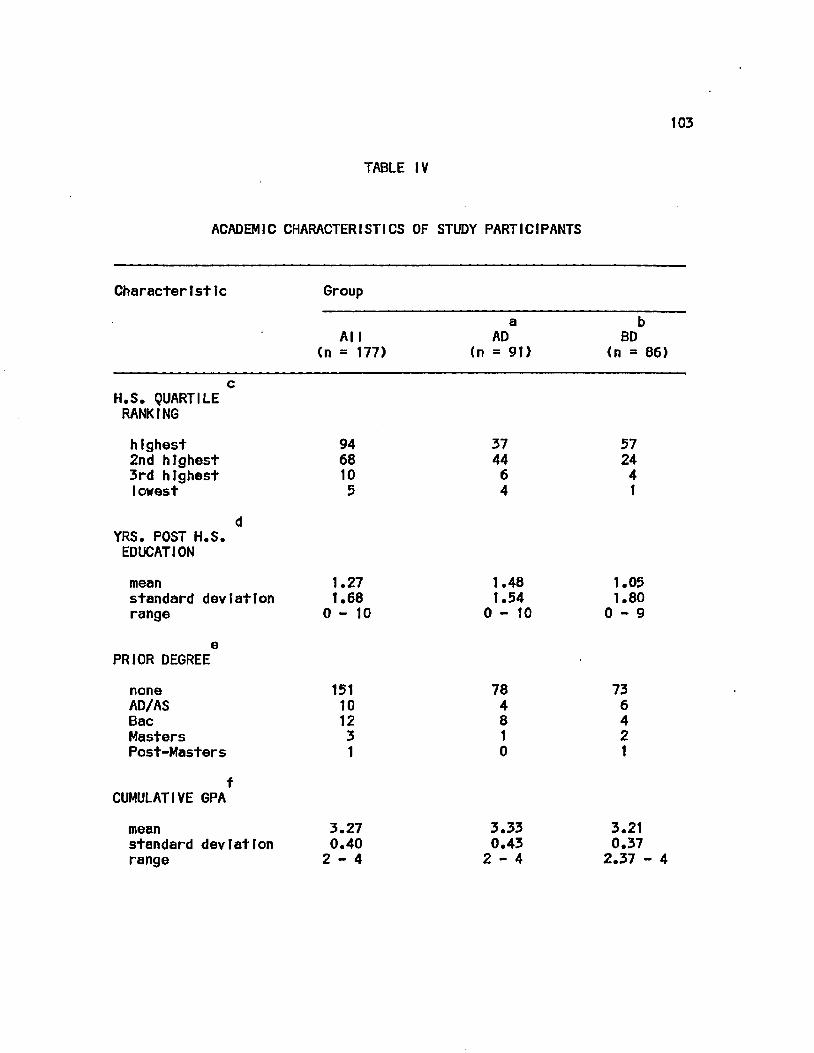
103
TABLE IV
ACADEMIC CHARACTERISTICS OF STUDY PARTICIPANTS
Characteristic Group
All (n = 177)
a AD
(n = 91)
b BD
<n = 86)
H.S. QUARTILE RANKING
highest 2nd highest 3rd highest lowest
94 68 10 5
37 44 6 4
57 24 4 1
YRS. POST H.S. EDUCATION
mean 1.27 standard deviation 1.68 range 0-10
1.48 1.54
0 - 1 0
1.05 1.80 0 - 9
PRIOR DEGREE
none AD/AS Bac Masters Post-Masters
151 10 12 3 1
78 4 8 1 0
73 6 4 2 1
CUMULATIVE GPA
mean 3.27 standard deviation 0.40 range 2-4
3.33 0.43 2 - 4
3.21 0.37 2.37 - 4
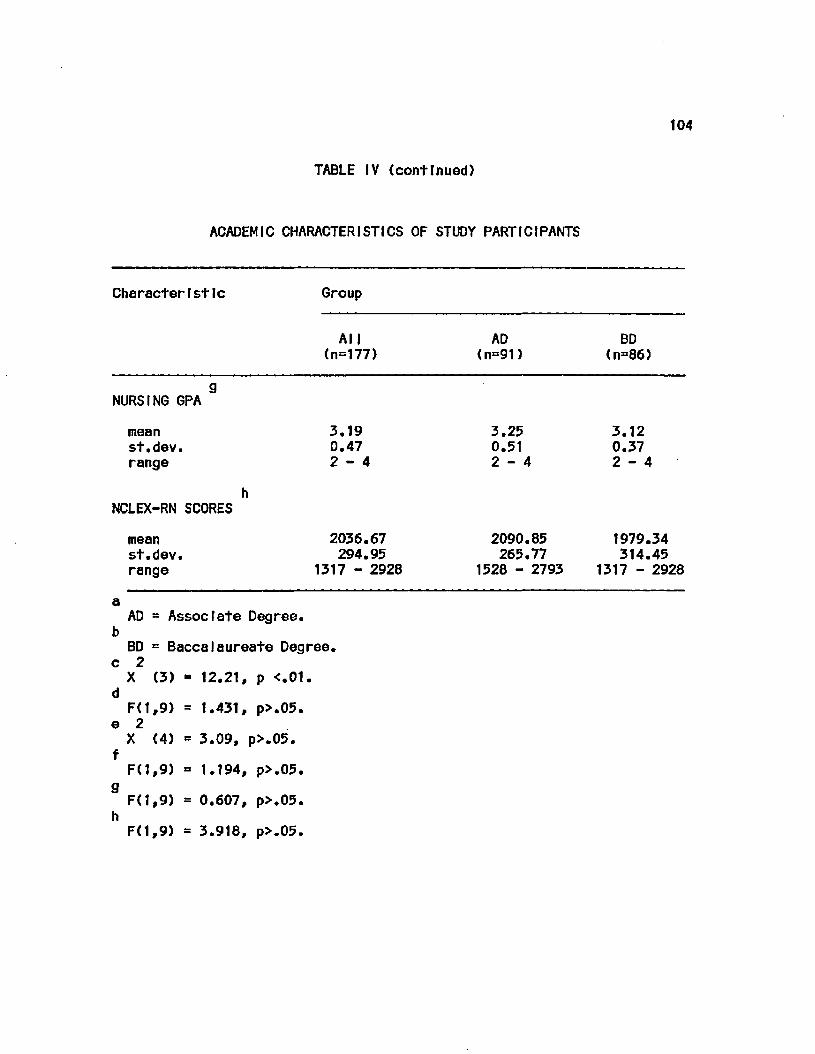
104
TABLE IV (continued)
ACADEMIC CHARACTERISTICS OF STUDY PARTICIPANTS
Characteristic Group
All (n=177)
AD (n=91)
BD (n=86)
NURSING GPA
mean st.dev. range
3.19 0.47 2 - 4
3.25 0.51 2 - 4
3.12 0.37 2 - 4
NCLEX-RN SCORES
mean st.dev. range
2036.67 294.95
1317 - 2928
a AD = Associate Degree.
b BD = Baccalaureate Degree,
c 2 X (3) = 12.21, p <.01.
d F< 119) = 1.431, p>.05.
e 2 X (4) = 3.09, p>.05.
f F(1,9) = 1.194, p>.05.
9 F(1,9) = 0.607, p>.05.
h F(1,9) = 3.918, p>.05.
2090.85 265.77
1528 - 2793
1979.34 314.45
1317 - 2928
105
National Council of State Boards of Nursing (Personal communication,
January, 1985) for the July, 1984 examination. The AD participants also
reported higher nursing and cumulative GPAs than did BD participants.
It Is difficult to arrive at any conclusions regarding the meaning of
this finding due to the Influence of the grading policies and practices
of Individual programs.
C. OperationalFzatlon of the conceptual model
The conceptual model, as previously described, stated that when
confronted with a nursing problem, Information processing capabilities
of the nurse, as reflected by the Implementation of the assessment
phase of the nursing process, Is dependent upon task setting and
complexity, type of educational program attended, and Individual
characteristics that affect cognitive, Information processing abilities
and/or the selection of a specific type of nursing education program.
Subsequent sections contain descriptions of the variables Included In
the model.
1. Independent variable
The Independent variable was the type of educational program
attended: an AD nursing program or a BD program.
2. Covarlates
The covarlates were those factors which Influence
cognitive, Information processing capability and/or the selection of a
nursing education program. The factors Influencing Information
processing were: task setting and complexity, and critical thinking
ability and gender of the problem solver. Those factors related to the
106
selection of a nursing education program were: number of years of pre-
nurslng work experience In health care settings, and number of years of
post-htgh school education prior to entering a nursing program. Factors
associated with both program selection and cognitive Information
processing were: age and Intellectual ability. Indicators selected to
represent each of these are described below.
a. Task setting
Two paper and pencil latent Image clinical simulations
(PMP-Brown and PMP-Ellls) were used to standardize and, therefore,
control the setting In which the clinical nursing problem was
experienced. Performance on the two simulations was analyzed
separately.
b. Task complexity
Task complexity was assessed from two different
perspectives. Each participant was requested to rate the level of
difficulty encountered In completing each simulated clinical problem
and to Indicate the degree of preparation that the nursing education
program provided for dealing with the simulated situation.
c. Critical thinking abtlIty
Critical thinking ability of a participant as reflected
by the general reasoning processes and problem solving processes used
to deal with problems encounterd In everyday life, was Indicated by the
total score on the Watson-Glaser Critical Thinking Appraisal (CTA)
(1980).
107
d. Post-high school education
Each participant was requested to Indicate the total
number of years of higher education completed prior to entering the
current nursing program. For descriptive purposes, the degree or
certificate earned, If any, was also to be Indicated.
e. Nnn—wdiiratton related health care experience
Each participant was requested to Indicate the number
of years worked In a clinical setting prior to entry Into a nursing
program and for descriptive purposes, the job title. The same
Information was obtained regarding work experience (non-education
related) In a clinical setting during program matriculation.
f. Age and gender
Each participant was requested to Indicate the current
age. In years, and sex.
g. Intellectual ability
Academic achievement was used as an Indirect measure of
Intellectual ability. An Indicant of pre-matIculatton achievement was
a participant's self-report of the high school quartlle ranking at the
time of graduation. Indicants of post-mat IcuIat Ion academic achlevment
were self-reports of the current cumulative GPA for all course work and
the cumulative GPA for all nursing course work. An additional measure
of academic achievement was a participant's score on the NCLEX-RN.
This score was obtained from the board of nursing In the political
Jurisdiction where the participant took the NCLEX-RN In July, 1984.
108
3. Dependent variables
The assessment phase of the nursing process Involves the
collection and analysis of patient Information and culminates In the
Identification of relevant nursing diagnoses. For the purposes of this
study, dependent variables were: efficiency of data collection,
proficiency of data collection, types of data collected (psychosocial
data and physiological data), total number of plausible nursing
diagnoses Identified, completeness of nursing diagnostic statements,
and types of plausible nursing diagnoses Identified (psychosocial
nursing diagnoses and physiological nursing diagnoses).
D. Instruments
The four Instruments used to gather data were: 1) the Background
Inventory (Bt), 2) the Watson-GIaser Crlttcal Thinking Appraisal, Form
A (CTA), and 3) two latent Image clinical simulations. The Bl and CTA
provided data relevant to the covarlates selected. The simulations were
selected to provide data pertaining to a participant's data gathering
and nursing diagnosis skill, the dependent variables. Each of these
Instruments Is described In subsequent sections.
1. Measurement of the covarlates
a. Background Inventory
The Background Inventory (Bl) (Appendix D) Is a
modification of one used by Sparks (1979) to collect demographic
Information and assess those characteristics Identified In the
literature as factors contributing to the selection of a nursing
education program and/or cognitive problem solving ability.
109
Mod If feat Ions Included changes In the structure of several Items In
order to Increase thetr clarity, expansion of the number and/or type of
response options available within several Items, and addition of Items
to assess a participant's famlllartty with nursing diagnosis
terminology, classroom and clinical learning experiences related to the
types of situations depicted In the simulations, and perceptions
regarding the difficulty of the simulations.
Prior to use, the Bl was reviewed by 3 nurse educators for Item
clarity and ease of completion. In addition, It was administered to
students who participated In the pilot testing of the procedural steps
of data collection. Information obtained from the review and use of
the Bl was used to make minor modifications In the layout of the
Instrument and In wording of the directions.
b. Watson-GIaser Critical Thinking Appraisal
The Watson-GIaser Critical Thinking Appraisal (CTA) Is
an 80 Item Instrument composed of five, sixteen Item subtests (Watson
and GIaser, 1980). This unttmed Instrument requires approximately 40
minutes for completion and can be handscored. The Instrument measures
general reasoning processes used on a dally basis. As conceptualized
by Watson and Glaser (1980), critical thinking ability Is one aspect of
general reasoning and problem solving processes necessary for the
Interpretation of Information, formation of Judgments, and decision
making In everyday life.
The authors viewed critical thinking ability as a composite of
attitudes, knowledge and skills, each of which Is estimated by measures
110
of the five subtests. A high level of competency In critical thinking,
as measured by the CTA, was operationally defined by Watson and Glaser
(1980) as the' ab11Ity to perform correctly the universe of tasks
represented by the 5 subtests. This Instrument was selected to provide
a measure of critical thinking ability based on the assumption that
activities represented In this Instrument are similar to those used In
a diagnostic task. The five subtests are as follows:
1) Inference
The Inference subtest samples ability to
discriminate among degrees of truth or falsity or probability of
certain Inferences drawn from given facts or data.
2 ) Recognition of assumptions
This subtest samples ability to recognize unstated
assumptions from given facts or data.
3) Deduction
The deduction subtest samples ability to reason
deductively from given premises; recognize the relation of Implication
between propositions and delineate whether what seems to be an
Implication or necessary Inference between one proposition and another
Is Indeed so.
4) Interpretation
The Interpretation subtest samples ability to
weigh evidence and distinguish between unwarranted generalizations and
probable Inferences which, although not conclusive or necessary, are
warranted beyond a reasonable doubt.
111
5) Evaluation of arguments
The evaluation subtest samples ability to
distinguish between arguments which are strong and Important to the
question at Issue and those which are weak and unimportant or
Irrelevant.
The authors reported that content va11dIty of the Instrument was
supported by the Judgments of qualified persons and the results of
research studies that supported the authors* beliefs that the Items In
the CTA represented an adequate sample of the five abllltes, as
represented by Items In the different subtests. Additionally, the total
score yielded by the test represents a valid estimate of the
proficiency of Individuals with respect to these aspects of critical
thinking.
Watson and Glaser (1980) reported that claims for construct
validity of the Instrument were supported by research results that
demonstrated that students who had participated In programs aimed at
developing critical thinking ability showed greater change In CTA
scores than did those exposed to course content delivered by
traditional lecture methods. The CTA also has been shown to relate to
various measures of academic achlevemnt and traditional measures of
general Intelligence. Although the CTA was found to correlate with
general Intelligence, factor analyses of the CTA subtests with other
measures of Intelligence were reported to demonstrate that the CTA
measured a dimension of ability that was distinct from overall
Intellectual ability.
112
The authors measured degree of Internal consistency In the CTA by
calculating split-half reliability coefficients for 10 different norm
groups. Samples chosen for reliability studies Included at least one
representative from each of the kinds of groups used for normlng the
responses. Reliability coefficients for Form A (used In this study)
ranged between .69 and ,85; for Form B, between .70 and .82
The stab 11Ity of responses over time was assessed using a group
of college students (n = 96) via test-re-test procedures with a 3 month
Interval between testing periods. The .73 correlation between
responses at the two times Indicated reasonable stability over time
(Watson and Glaser, 1980).
Alternate form ret fab!IIty was calculated by correlating the
responses of 228 high school seniors who took both Forms A and B of the
CTA. The correlation coefficient was .75. These results were reported
to be consistent with those observed on previous forms of the test
(Watson and Glaser, 1980).
2. Measurement of the dependent variable
Portions of two patient management problems (PMPs) developed
by Schleutermann and others (1979) and Farrand and others (1979) were
used to measure data collection and nursing diagnosis Identification
abilities of participants. These Instruments are latent Image,
branched simulations In which the participant Is presented with a brief
patient description and asked to demonstrate an approach to data
collection and nursing diagnosis Identification.
113
a. Description
The PMPs, "Mr. Ellis, a 48 year old man complaining of
chest pain and difficulty breathing" (PMP-Ellls) (Schleuterman et a I.,
1979) and "Mr. Brown, an adult male with frequent episodes of
eplstaxls" (PMP-Brown) (Farrand et a I., 1979), are 2 of 3 PMPs
developed for use In the education and evaluation of graduate students
enrolled In a nurse practlttoner program (Holzemer et al., 1981). For
this study, only the patient assessment sections, which Included a
brief opening statement (patient description) and lists of potentially
available history data, physical findings, and Iaboratory/dlagnostic
test results, and the patient problem Identification sections were
utilized. Patient problem sections were located at the conclusion of
the opening statement, at the conclusion of the three data collection
components, and In the management section. This last sect ton served as
a logical conclusion to the simulation since It directed the
participant to Identify the three highest priority nursing diagnoses to
which nursing care would be directed.
The medical management and follow-up sections of these PMPs were
not used because they were deemed Inappropriate for use with
undergraduate students (e.g., they required decisions regarding the
selection and dosage of medications to be used In treatment). Of the
276 total Items In PMP-Ellls, 148 Items were distributed across the
three assessment sections as follows: history = 68 Items, physical
findings = 38 Items, and laboratory/diagnostic test results = 42 Items.
Distribution of 140 assessment Items, out of 276 total Items, In PMP-

114
Brown was as follows: history = 63 Items, physical findings = 37 Itmes,
and laboratory/diagnostic test results = 40 Items.
In order to adapt the settings In which the patient encounters
occurred Into ones more familiar to AD and BD students, statements In
the opening scenes that read "You are a nurse practitioner...." were
modified to state: "You are a nurse...,". The opening scene for PMP-
EMIs was modified further to reflect a more likely setting - I.e., one
In which both AD and BD students would likely find themselves employed
In the near future. Therefore, the statements nurse
(practitioner) employed In a walk-In clinic of a city health
department..." and "...arrives In your office complaining..." were
changed to: "...nurse employed on a general medical-surgical unit of a
community hospital..." and "...Is admitted to your unit
complaining...".
Additional modifications were made In each PMP on the pages where
a participant was directed to select one of several actions that could
be Initiated. One of these options was "Consult with a physician"; the
response to which was "Physician feels you can work up this patient.
Make another selection In this section." For PMP-Ellls, this response
was changed to: "Physician on call does not answer his page. Make
another selection In this section." On PHP-Brown, the original
response was modified to read: "Physician has been called to the
emergency room. Make another selection In this section."
The final modification on both PMPs Involved the statements
directing a participant to record the problems and/or possible
115
diagnoses being considered at that time. These statements were changed
so that the participant was directed to Indicate the nursing diagnoses
that were being considered. A discussion with the primary author of
PMP-Brown, and co-author of PMP-EMIs concerning these modifications
led to the conclusion that the modtflcatons would not alter outcomes of
the assessment sections (Farrand, personal communication, January,
1983).
b. Content valIdlty
In support of the content validity of the PMPs, Farrand
et al. (1982) cited construction by several nurse practitioners and an
educator. Included In the development phase were delineation of
learning objectives, a blueprint, the opening scene, and section
options. Content for each section was developed according to nursing,
medical and educational principles. Branching techniques were
constructed to allow for variation In management styles and emphasis
was placed on patient safety and quality care with a focus on both
effectiveness and efficiency In the delivery of care. Following their
Initial construction, the PMPs were examined for content omissions,
clarity, structural flaws, Implausible alternatives, redundancy,
allowance for variation In managment styles, format and directional
clarity.
A panel of experts, which Included an educational evaluator with
experience In the construction of latent-Image simulations, a master's
prepared adult nurse practitioner, a doctorally prepared nurse-
physlolog 1st, and two physicians with specialties In preventive
116
medicine and family practice, critiqued the format and content, and
scored each Item for appropriateness for Inclusion In the PMP. Each
Item was reviewed for Its applicability to the problem, fidelity to a
real patient encounter, and possible variations In management. The
panel also critiqued the PMPs for Item clarity and construction,
c. Construct valIdlty
The construct validity of the PMPs as a measure of
clinical problem solving was explored using several different
approaches. Following the development of PMP-Ellls, a multi-method,
multi-trait correlation matrix, a multivariate analysis of covarlance,
and stepwise multiple regression analysis were used to assess constract
validity (Holzemer et al«, 1981). The multiple methods utilized were
self-chart audit, colleague evaluation, self-evaluation, and a
cognitive examination. The traits were: cognitive knowledge, problem
solving skill, and perception of clinical practice. It was
hypothesized that the validity of the PMP would be supported If:
"Significant correlations were observed between the PMP scores and the
self-audit, self-evaluation, and colleague evaluation; moderate
correlations were observed between the PMP scores and the cognitive
examination; and significant differences were demonstrated between
certificate and masters-prepared nurse practitioners" (p.140).
A total of 79 nurse practltoners completed the PMP and self
evaluation, 68 supplied colleague evaluation data, 60 completed the
cognitive examination, and 33 completed the self chart audit. Of the
117
60 practitioners completing the cognitive examination, 26 were master's
prepared and 34 were certificate prepared.
Holzemer et al. (1981) concluded that the results of the
Investigation provided "moderate evidence" (p. 139) supporting the
claim that the PMP simulation was a valid measue of the construct:
clinical problem solving. Findings supporting this conclusion were: a
Pearson product moment correlation of .54 (Spearman's rho = .56)
between performance on the cognitive examination and overall
proficiency score on the PMP, and significant correlations between PMP
proficiency score and self evaluation scores (r =.23, rho = .19). In
addition, step-wise multiple regression analysis, with PMP proficiency
score as the dependent variable, demonstrated that after the Influence
of performance on the cognitive examination was removed (31.89!? of the
variance), only 5.65f of the variance In PMP proficiency could be
explained by the Inclusion of four additional variables (self-
evaluation of management skill, col league evaIuatIon of management
skill, master's preparation, and self-evaluation of data-gathering
skill). No difference was demonstrated between the performance of
certificate and master's prepared Individuals on the PMP.
Additional work to Investigate the construct validity of PMP-Ellls
and PMP-Brown and an additional PMP was reported by Farrand and others
(1982). It was hypothesized that a claim for the construct validity of
the simulations would be warranted If significant differences were
found between the performance of nurse practitioners and nurses (I.e.
118
not nurse-practIt loners) on simulations designed for use with nurse
practitioners.
A sample of 34 nurses and 53 nurse practitioners completed the
three PMPs, a demographic survey, and a cognitive examination
constructed to test knowledge that paralleled the content of the three
PMPs. Data analysis procedures utilized multivariate analyses of
variance and co-variance, and Pearson product moment correlations.
The analysis of variance demonstrated that significant differences
in performance on the PMPs existed for the type of preparation
(p=.0001). The pooled test of the covarlate was not significant.
However, further examination of the correlations between examination
subscores and the respective PMPs demonstrated that significant,
moderate correlations were present for PMP-EII Is (r - .49) and for PMP-
Brown (r = .32)j for the third PMP, the correlation was .12.
Therefore, overall, the covarlate was not of sufficient magnitude to be
significant.
Based on the demonstration that meaningful differences were found
In the performance of nurses and nurse practitioners, Farrand et al.
(1982) concluded that support for the construct validity of the
clinical simulations was warranted.
d. Reliability
Overall reliability of each PMP and reliability of the
sections to be used for this study were supported based on results of
test-re-test procedures (Farrand, personal communication, January,
1983). Estimations of Internal consistency of various sections of the

119
PMPs could not be assessed due to the dependent nature of Items and
absence of additional similar sections within each PMP.
E. procedure
1. PMot testing
Prior to Initiation of formal data collection, the Bl and
and PMPs were administered to a convenience sample of 6 undergraduate.
Junior students enrolled In the nursing program of a large mid-western
university. All students had completed a course In the care of adults
with acute medical-surgical nursing problems. The purpose of the pilot
testing was to determine the clarity of Instructions regarding
completion of the Bl and the PMPs and the amount of time necessary to
complete the Instruments.
Following completion of these instruments, the pilot subjects
were requested to Indicate those areas where they were unsure of the
Intent of an Item or directions for Its completion. When pilot subjects
returned the completed Instruments to the Investigator, the Instruments
were reviewed to determine If the correct procedures had been followed.
All participants completed the Bl and the PMP according to the written
and verbal directions that were provided. In addition, pilot subjects
were questioned Individually to determine If anything was unclear to
them during test completion.
All pilot subjects were able to complete the 2 PMPs and the Bl
within 75 minutes; this Included the time required to distribute the
Instruments and review the directions for their completion. Therefore,
It was concluded that the entire set of Instruments (the Bl, CTA, and

120
the two PMPs) could be completed within a 2-hour period. Based on the
pilot subjects' comments, the content of the written Instructions was
expanded to Include Information regarding the order In which the
Instruments were to be completed.
2. Data col lection
Procedures used for formal data collection were as follows.
At the agreed upon times and locations, the Investigator met with those
students Indicating an Interest In participating In the study.
Following an explanation of the study, those desiring to participate
were requested to sign a consent form (Appendix E) Indicating that they
were participating voluntarily In the study, that confidentiality would
be maintained, and that the Investigator could have access to their
Individual scores on the NCLEX-RN examination following Its
administration In July, 1984. Those Interested In receiving a written
report of their performance on the PMPs and the CTA were requested to
provide mallIng Instructions.
Each participant received an envelope containing a complete set of
pre-coded Instruments, developing pens for use with the PMPs, a pencil,
and written Instructions for completing all Instruments. Order of the
Instruments In the envelope was as follows: 1) one of the PMPs, 2)
the CTA, 3) the second PMP, and 4) the Bl. The order In which the
PMPs were Included In the set was alternated In order to control for a
possible fatigue factor. The PMP-Ellls was the first Instrument I n
the evenly numbered sets and PMP-Brown was the first Instrument In the
odd numbered sets.
12!
To provide for Instruction and practice In using the latent Image
simulations, the first page of the first slmulatton In each set of
Instruments was Identical to those In all other sets. Following a
practice session, answering of questions from partlciants, and a review
of the written Instruction page, the participants were Instructed to
beg In.
Although no strict time limit was Imposed on completion of any
one Instrument, suggestions for self-timing were provided. It was
anticipated that completion of the entire set of Instruments would
require approxlmatley 2 hoars. All participants completed the task
within the alloted time period.
Upon completion of all Instruments, participants were Instructed
to return all Instruments to the envelope and to give the envelope to
the Investigator. Participants were thanked Individually for their
participation and provided with a written summary of expected outcomes
for each PMP. Following scoring of the CTA and the PMPs, all
participants who provided a mailing address received a written report
of their performance and, for the purpose of comparison, the means
scores for all participants, the AD participants, and the BD
participants.
F. Protection of human subjects
This study was approved by the Institutional Research Review
Board, Health Sciences Center, University of Illinois at Chicago
(exempt status) and by the Research Committee of the College of
Nursing, University of Illinois at Chicago.

122
The Deans and Directors of all programs permitting access to
students were assured that the school would not be Identified. In
addition, all participants were assured that their responses and the
degree of their participation In the study would remain confidential.
All participants In the study were requested to sign a consent to
participate form (Appendix E) and Informed of their right to withdraw
from the study, without penalty, at any time during the testing period.
G. Data rerinrtlnn
All Instruments were precoded with an Identification number to
Insure proper matching of responses on various Instruments. Following
completion, each participant's Instruments were coded to Indicate the
specific program attended and whether It was an AD or BD program.
1. Covarlates
All responses on the B| were coded and entered Into a
computer file for further analysis. Responses on the CTA were hand
scored according to the directions provided In the manual (Watson and
Glaser, 1980) and subscores, total score, and percentile score were
entered Into the computer file. Percentile score for BD participants
was based on a normative sample of 182 nursing students In mldwestern
university baccalaureate nursing programs; that for AD participants, on
a normative sample of 388 students In Junior and community colleges
(Watson and Glaser, 1980).
2. Dependent variables
a. Patient Information
Each Item within the history, physical, and
123
diagnostic/laboratory test result sections on each PMP was scored to
Indicate If a participant had or had not selected It. This Information
was entered Into the computer file. Furthermore, each Item within each
of these sections was weighted to reflect Its contribution to the
Identification of the simulated patients' nursing diagnoses. The three
point scale, developed by a panel of experts (Holzemer et al., 1981),
ranges from a +1 to a -1s +1 Indicated patient Information or a data
collection step that was essential to data collection and/or diagnosis,
0 Indicated Information or a step that was contributory but not
essential, and -1 Indicated Information or a step that was
Inappropriate, unsafe, of low quality, unreasonably costly, or delayed
proper treatment.
In addition to the weighting system described above, an expert
panel of 3 nurses (to be described In a subsequent section) classified
alt patient Information options In the history sections as having
primary relevance to either a physiological or a psychosocial nursing
diagnosis. Each panel member Independently Judged the Items; the focus
of each Item was then designated according to the majority opinion.
1) Scoring formulas
Following the computer Input of Individual
responses to each Item and the coding system to be used for score
computation, the following scores were generated for each participant
for each PMP.
a) Efficiency score
The Efficiency Score (E) was a measure of the
124
degree to which a partlclpantts choices of data and procedural steps
are helpful In the resolution of a cllent*s problems. It was computed
as a ratio of the number of essential (+1) Items selected to the total
number of Items selected.
Number of +1 Items selected E = X 100
Total number of Items selected
b) Proficiency score
The Proficiency Score (P) was a measure of
the degree to which a participant's selection of data and procedural
steps corresponds with those Judged optimal by experts In the fteld. It
was computed as a ratio of the number of essential (+1) items selected
minus the npn-essentlal (-1) Items selected to the total number of
essential (+1> Items available.
Number of +1 Items - number of -1 Items selected
P = X 100
Total number +1 Items available
c) Psychosocial data score
The Psychosocial Data Score was a measure of
the total number of psychosocial history data selected by each
participant.
d) Percent psychosocial data ££££&
The Percent Psychosocial Data Score (J&PSDS)
was a measure of the percentage of all data selected that had a
psychosocial focus. It was computed as a ratio of the number of
125
psychosocial history data Items (PSI) selected to the total number of
history data Items selected.
Total number PSI selected *PSDS = X 100
Total number of history Items selected
b. Nursing diagnoses
All diagnostic statements generated by each participant
at the completion of each phase of each PMP (I.e., following reading
the opening scene, the selection of history data, etc.) were compiled
and submitted to an expert panel for review. The majority opinion of
the panel was used to determine If a participant generated diagnostic
statement was a nursing diagnosis, whether the focus of a nursing
diagnosis statement was physiological or psychosocial, and the
plausibility of each nursing diagnosis statement. A nursing diagnosis
was plausible If a majority of panel members agreed that given the
patient data available to the participant, the nursing diagnosis could
exist.
These Judgments were used as a basis for determining the
diagnostic ability of the participants. The following sections
describe panel composition, the analysis procedure used by panel
members, reliability estimates, and procedures used to train panel
members. An additional section Includes a description of the procedure
used for scoring the diagnostic statements.
1) Expert panel composition
The panel of experts was composed of 3 master's
prepared nurses who were recognized by their peers as "experts In the

126
use of nursing diagnoses". All currently were using nursing diagnoses
In their nursing practice.
One member of the panel was a nurse educator with clinical
expertise In the nursing care of Individuals with respiratory problems.
A second member was a clinical specialist In cardiovascular nursing at
a large mid-western hospital. The third was a clinical specialist In
neurology at a large mldwestern medical center. AM panel members
received remuneration for their services.
2) Ana?ysIs of diagnostic statements
Each panel member independently reviewed and
classified each diagnostic statement to determine whether It was a
nursing diagnosis. If It were not, the panel member went on to the
next statement. If the statement was a nursing diagnosis, the panel
member Indicated Its focus: physiological, psychosocial, or mixed.
Each nursing diagnostic statement then was divided Into a maximum of
three components: stem (I.e., alteration In comfort), modifier (I.e.,
acute, chronic, potential, mild, severe, etc.) and referent or
etiology (I.e., related to tissue trauma). Each of the nursing
diagnosis statement components then was Judged as falling within one of
three categories: 1) incomplete or non-ex Istant statement; 2) complete
and plausible statement; or 3) complete, but Implausible statement.
3) Reliability
Inter-rater and Intra-rater reliability
coefficients were calculated upon completion of the Independent
evaluation, by each panel member, of the 3151 participant generated
127
diagnostic statements. The reliability coefficients were calculated
as the percent of agreement among panel members and were based on a
minimum of 1 or a maximum of 5 judgments per diagnostic statement
(I.e., 1) a nursing diagnosis?, 2) focus, and presence and plausibility
of the 3) modifier, 4) stem, and 5) referent).
a) Inter-rater reliability
A!I three panel members agreed on the
classification of 84.32£ of the statement components. At least two
panel members agreed on the rating of 97.55% of the statement
components.
b) Intra-rater reI lability
Prior to distributing the participant
generated statements to the panel members, 50 of the statements were
reproduced and coded with a bogus Identification code; these duplicate
statements were Included In the entire set of statements distributed to
each panel member. Percent of agreement for the classification of the
original and duplicate statement components was calculated for each
panel member. The Intra-rater reliability for one panel member was
94%f for a second member, 96and for the third member, 98?.
4) Training of panel members
Prior to analyzing the entire set of diagnostic
statements generated by the study participants, each panel member
received a list of essential and contributory patient Information that
participants could select. Based on this Information, each panel member
was Instructed to generate a list of nursing diagnoses that could be
128
present given the Information available following each phase of data
collection (I.e., following the opening scene, the history data, the
physical data, the laboratory/diagnostic data, and the final priority
listing). The panel generated lists of nursing diagnoses then were
compiled Into one master list and reviewed Jointly by the panel
members. At this time, redundancies were eliminated, diagnostic
statements refined and consensus reached regarding the plausibility of
each diagnostic statement. This master list served as a guide In
evaluation of participant generated diagnostic statements.
Panel members were Introduced to the diagnostic statement
evaluation task during a 2-hour training session. Diagnostic
statements representative of all those generated by study participants
were used to describe the evaluation process and to provide the panel
members with practice In using the rating form. Following the Joint
review of several diagnostic statements and discussions regarding areas
of actual or potential disagreement, the members were given 25
statements to evaluate Independently. At the completion of this task,
the ratings of each panel member, for each statement, were discussed.
When the panel members and the Investigator concluded that the
panel had reached consensus on decision rules to be used to Judge each
diagnostic statement, a final I 1st of 50 diagnostic statements was
distributed to each panel member. Following Independent, written
evaluations of these statements by panel members, the extent of Inter-
rater reliability for the training session, calculated as the percent
of agreement, was determined. All three members agreed 69.6% of the
129
time regarding the various levels of analysis of a diagnostic
statement. At least two panel members agreed 97.6% of the time. These
results were considered sufficiently high to discontinue training.
5) Scoring formulas
Following analysis of the diagnostic statements by
each panel member, the results were collated and the majority opinion
of the classification of each component of a statement was coded and
entered Into the computer file. To deal with those statements where
the panel could not agree on a classification, or were Inconsistent In
their classifications, the panel was reconvened as a group to discuss
the statements In question and arrive at a consensus. Following
discussion, all areas of disagreement or Inconsistency were resolved.
The Joint decision of the panel regarding the classlflcatlon(s) In
question then were used to code these statements.
Diagnostic statement stems were coded to reflect If they were a
non-nursing diagnosis, a plausible nursing diagnosis, or an Implausible
nursing diagnosis. The referent component for each nursing diagnosis
was coded to reflect If It were plausible or not, given the nursing
diagnosis stem's level of plausibility: If the nursing diagnosis stem
were plausible, the referent was coded as either plausible or
Implausible; If the stem were Implausible, the referent was also
Implausible. This coding system also was used to code the nursing
diagnosis stem's modifiers.
A NursIng Diagnosis Score (NDXSCORE), for each PMP, was computed
based on the following weighting system:
130
A non-nursing diagnosis statement = 0 points
An Implausible nursing diagnosis stem = 0 points
A plausible nursing diagnosis stem without a plausible referent = 1 point
A plausible nursing diagnosis stem and referent = 2 points
NDXSCORE = Sum of all points accrued for each diagnostic statement Identified within a PMP
All nursing diagnosis statements also were coded to reflect their
focus: physiological, psychosocial or mixed. The total number of
psychosocial nursing diagnoses (PSDX) Identified was computed as the
sum of the psychosocial and mixed nursing diagnoses Identified within a
PMP.
PSDX = Total number of psychosocial and mixed nursing diagnoses Identified
The percent of psychosocial nursing diagnoses (jfPSDX) Identified
was based on the following formula:
PSDX JSPSDX =
Total number of all diagnostic statements identIf led
3. Summary
A non-equivalent groups, post-test only design was used to
examine the data collection and diagnostic abilities of a convenience
sample of 91 AD and 86 BD students graduating from 5 randomly selcted
AD programs and 6 randomly selected BD programs. Instruments used for
data collection were Watson and Glaser's (1980) Critical Thinking
Appraisal (Form A), 2 PMPs (Farrand et al., 1979; Schleutermann et al.,
131
1979) and a background Inventory. The specific variables used for data
analysis, their Indicators and source are summarized In Table V. Data
analysis procedures and results of the study are described In the next
chapter.
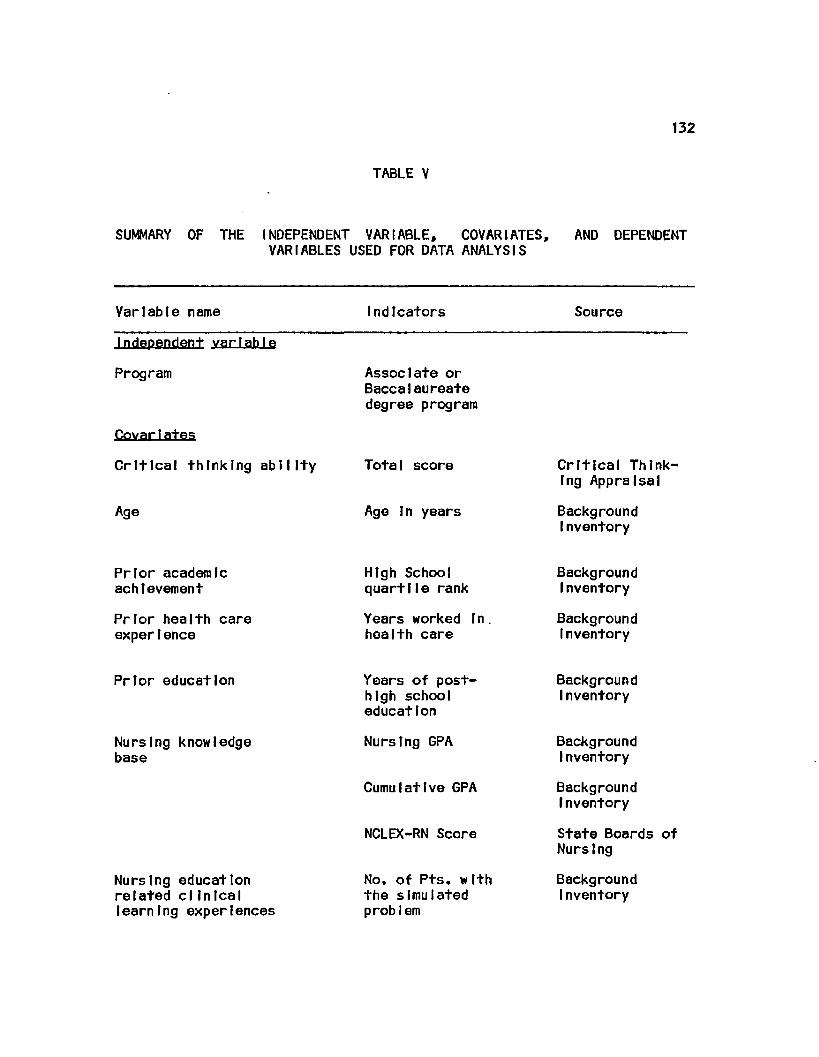
132
TABLE V
SUMMARY OF THE INDEPENDENT VARIABLE, COVARIATES, VARIABLES USED FOR DATA ANALYSIS
AND DEPENDENT
Variable name Indicators Source
Independent variable
Program
Covar1ates
Critical thinking ability
Age
Associate or Baccalaureate degree program
Total score
Age In years
Critical Thinking Appraisal
Background Inventory
Prior academic achievement
Prior health care experience
High School quart 11e rank
Years worked In health care
Background Inventory
Background Inventory
Prior education
Nursing knowledge base
Nursing education related clIn lea I learning experiences
Years of post-high school education
Nursing CPA
Cumulative GPA
NCLEX-RN Score
No. of Pts. with the simulated probI em
Background I nventory
Background Inventory
Background Inventory
State Boards of Nursing
Background Inventory
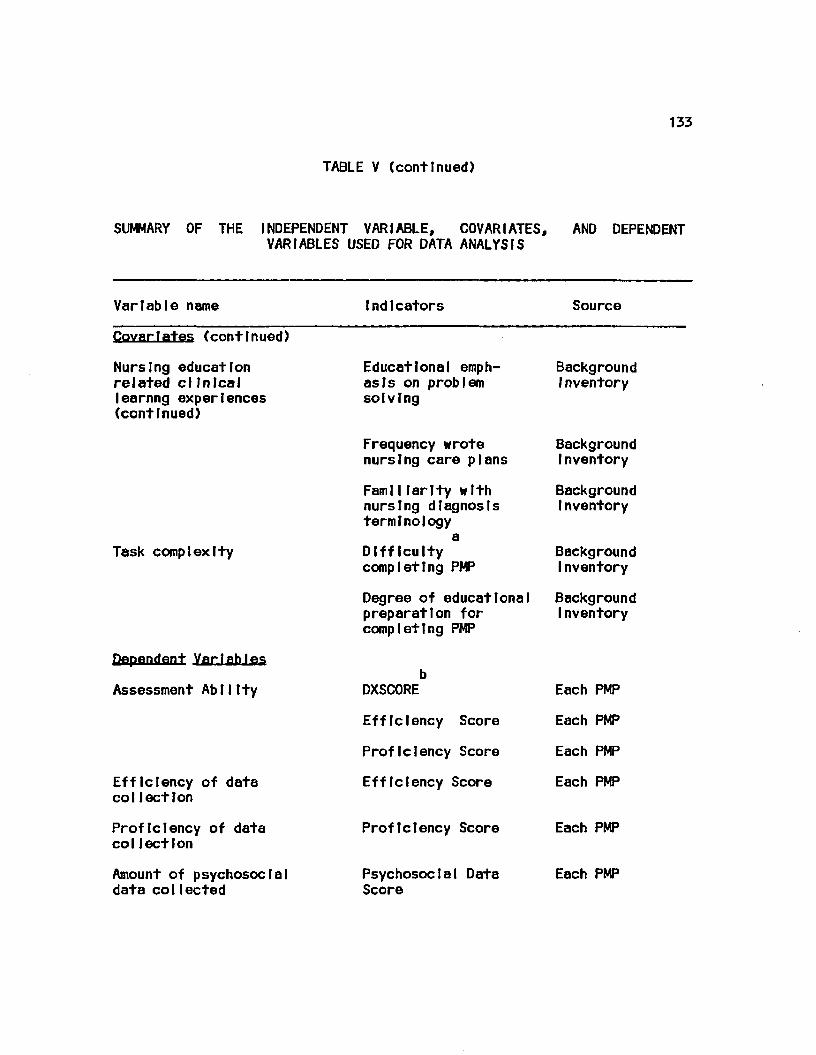
133
TABLE V (continued)
SUMMARY OF THE INDEPENDENT VARIABLE, COVARIATES, AND DEPENDENT VARIABLES USED FOR DATA ANALYSfS
Variable name Indicators Source
CovarIates (continued)
Nursing education related clinical learnng experiences (continued)
Task complexity
Dependent Variables
Assessment Ablltty
Efficiency of data col lection
Proficiency of data col lection
Amount of psychosocial data collected
Educational emphasis on problem solving
Frequency wrote nursing care plans
FamlIlarlty with nursing diagnosis terminology
a Difficulty completing PMP
Degree of educational preparation for completing PMP
Background Inventory
Background Inventory
Background Inventory
Background Inventory
Background Inventory
DXSCORE Each PMP
Efficiency Score Each PMP
Proficiency Score Each PMP
Efficiency Score Each PMP
Proficiency Score Each PMP
Psychosocial Data Each PMP Score
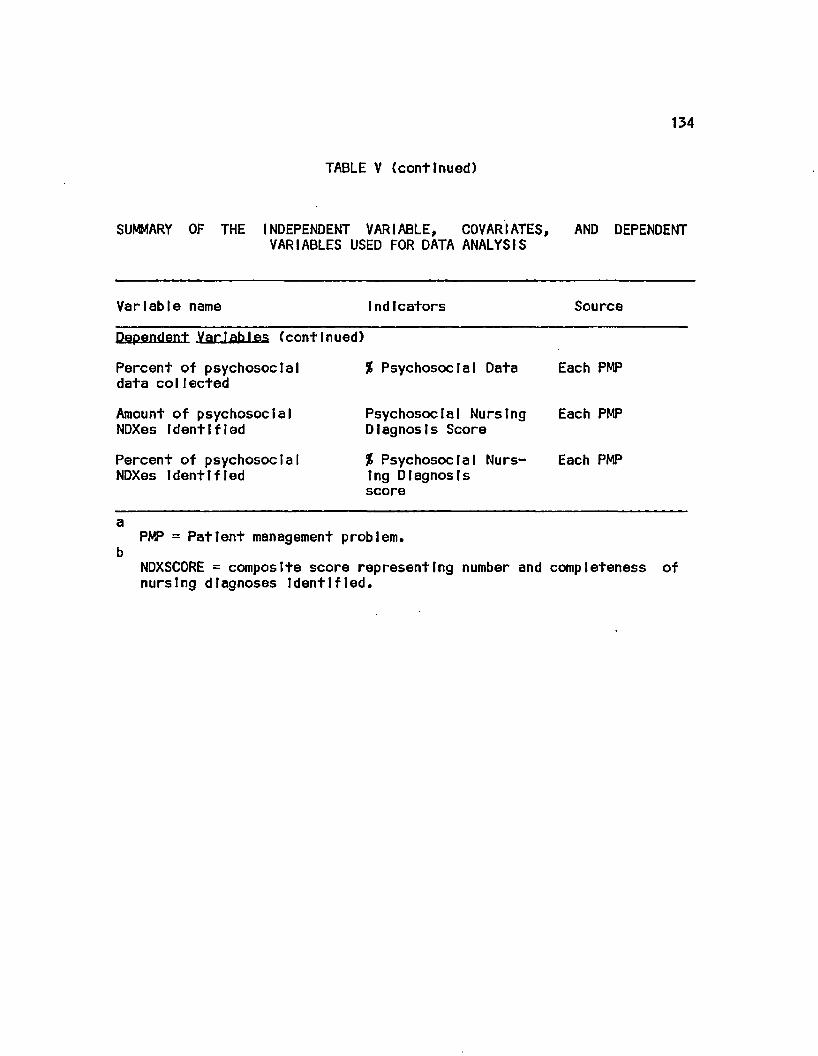
134
TABLE V {continued)
SUMMARY OF THE INDEPENDENT VARIABLE, COVARIATES, AND DEPENDENT VARIABLES USED FOR DATA ANALYSIS
Variable name Indicators Source
Dependent Variables (continued)
Percent of psychosocial data collected
Amount of psychosocial NDXes Identified
Percent of psychosocial NDXes Identified
% Psychosocial Data Each PMP
Psychosocial Nursing Each PMP Diagnosis Score
% Psychosocial Nurs- Each PMP Ing Diagnosis score
PMP = Patient management problem.
NDXSCORE = composite score representing number and completeness of nursing diagnoses Identified.
IV. ANALYSIS AND RESULTS
The purpose of this chapter fs to report the procedures used for
data analysis and the results. The research questions which guided the
study will be used as an organizational framework for reporting these
results. Although the data collected regarding performance on each PMP
were analyzed separately, findings will be presented Jointly within
the parameters represented by each research question. An additional
section Includes results of secondary data analyses.
A. Influence of program type on assessment ability
The primary research question to be answered by this study was:
Are the patient assessment abilities of associate degree (AD) and
baccalaureate degree (BD) nursing students, when measured within three
months prior to graduation from a program of study accredited by the
National League for Nursing, Influenced by type of educational program
attended?
t. Analysis and results
A path analytic approach was used to address this question.
Within the fields of sociology, economics, and political science, this
approach has gained acceptance as a technique useful for drawing
Inferences regarding causal relationships In non-experimental studies
(Cook and Campbell, 1979; Hanushek and Jackson, 1977; Pedhazur,1982).
The model used to explain assessment ability (Figure 1) was constructed
so It consisted of a series of hypotheses about how endogenous
135
136
variables are related to one or more exogenous variables and additional
endogenous variables (Hanushek and Jackson, 1977). The exogenous
variables, those which have their values determined outside the model
and are taken as given, were Critical Thinking Ability, Age, Gender,
Prior Academic Achievement, Prior Education, and Prior Health Care
Experience. The endogenous variables, representing events explained by
the model, were Type Program Attended, Nursing Knowledge Base, Nursing
Education Related Clinical Learning Experiences, Task Complexity and
Assessment AblIIty.
Prior to testing the model and determining the Influence of
educational preparation on assessment ability, correlation coefficients
were estimated between and among the latent variables (Nursing
Knowledge Base, Education Related Clinical Learning Experiences,
Assessment Ability) and the directly observed variables (Type Program
Attended, Age, Gender, Prior Academic Achievement, Prior Clinical
Experience, Critical Thinking Ability, and Prior Education) In the
model. As a preliminary step to determining these coefficients,
Pearsonlan correlation coefficients were computed between all possible
combinations of all Indicator variables, with program type treated as a
dummy variable (0 = ADj 1 = BD). In addition, an observed variable,
gender was dropped from Inclusion In the model since only 8 of the 177
participants were male. A visual Inspection of the respective scatter
plots revealed the existence of linear relationships or non-
relattonshlps between the various pairs of variables; no non-lInear
relationships were Identified.
137
The measurement model of LISREL VI (Joreskog and Sorbom, 1984)
was used to specify the relationships between the unobserved, latent
variables and their respective observed. Indicator variables and
between and among the exogenous and endogenous variables In the model.
The parameters representing the relationships between a latent variable
and Its Indicator variables (lambda) were estimated using maximum
likelihood estimates. The maximum tlkllhood estimates were obtained by
an Iterative procedure which minimizes a definite fitting function by
successively Improving the parameter estimates beginning with the
Initial estimates which the program computes using Instrumental
variables methods and least squares methods. The maximum 11k11 hood
estimates of the lambda values between the latent variables and their
respective Indicators for PMP-Brown are reported In Table VI. Those
for PMP-EIMs are reported In Table VII. Also Included In these
Tables are the standard errors and the t-values for each of the
lambdas.
A review of these Intermediate results for the PMP-Brown model
revealed that all t-values except three (familiarity with nursing
diagnosis terminology with Education Related Clinical Learning
Experiences; perceived difficulty of the simulation with Task
Complexity; and Data Proficiency Score with Assessment Ability) were
above 2.0. A t-value above 2.0 Indicates that a specific observed
variable is a significant predictor of the latent variable (Joreskog
and Sorbom, 1984). The modification Indices provided by the LISREL VI
program revealed the non-existence of any theoretically significant

138
TABLE VI
RELATIONSHIP BETWEEN THE LATENT VARIABLES OF KNOWLEDGE BASE, EDUCATION RELATED CLINICAL LEARNING EXPERIENCES, TASK COMPLEXITY AND ASSESSMENT ABILITY AND THEIR INDICATORS FOR THE MODEL EXPLAINING PERFORMANCE ON
PMP-BROWN
Latent Indicator Lambda Standard t-value variables variables coefficients error
Knowledge NCLEX .671 .070 9.577 Base Nsg. GPA .835 .065 12.844
Cum. GPA .877 .064 13.772
Education # of pts. .406 .089 4.571 Re1ated Emph. prob. .301 .086 3.485 CI In leal solving Learning NCP freq. .166 .092 1.80 Experience NDX faml1. .481 .085 1.960
Task Difficulty - .568 .101 - 5.617 Comp1 ex Ity Prepared .642 .107 5.989
Assessment DXSCORE .928 .159 1.115 AbllIty ProfIclency .276 .086 3.190
Efficiency .091 .081 5.851
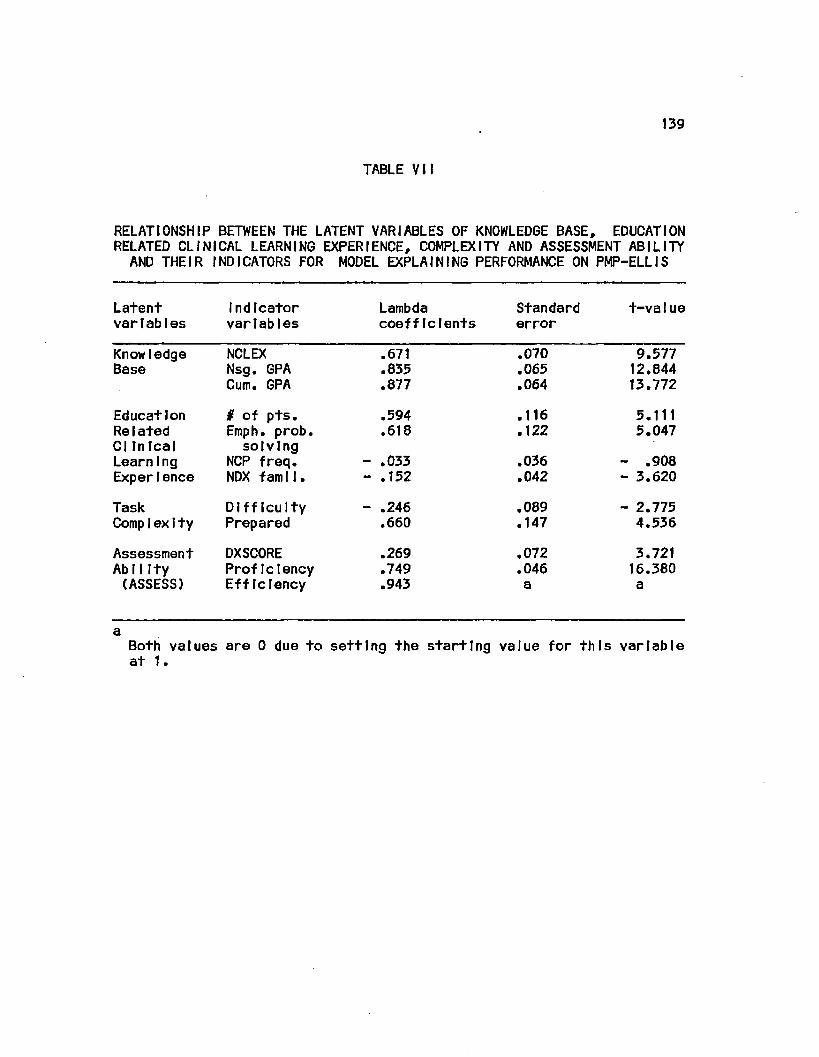
139
TABLE VII
RELATIONSHIP BETWEEN THE LATENT VARIABLES OF KNOWLEDGE BASE, EDUCATION RELATED CLINICAL LEARNING EXPERIENCE, COMPLEXITY AND ASSESSMENT ABILITY AND THEIR INDICATORS FOR MODEL EXPLAINING PERFORMANCE ON PMP-ELLIS
Latent variables
Indicator variables
Lambda coefficients
Standard error
t-va1ue
Knowledge NCLEX .671 .070 9.577 Base Nsg. GPA .835 .065 12.844
Cum. GPA .877 .064 13.772
Education # of pts. .594 .116 5.111 Re 1ated Emph. prob. .618 .122 5.047 CI In leal solving LearnIng NCP freq. - .033 .036 - .908 Experience NDX famll. - .152 .042 - 3.620
Task Difficulty - .246 .089 - 2.775 Comp1 exIty Prepared .660 .147 4.536
Assessment DXSCORE .269 .072 3.721 AbllIty Proficiency .749 .046 16.380 (ASSESS) Efficiency .943 a a
a Both values at t.
are 0 due to setting the starting value for this variable

140
relationships between any one observed variable and the remaining
latent variables. Therefore, the originally conceived models
representing the relationship of the Indicator variables to the latent
variables were retained for the next step of the analysis.
The Intermediate results for the PMP-EIIIs model revealed only
one t-value below the 2.0 level (frequency that care plans were written
with Education Related Clinical Learning Experiences). A review of the
modification Indices revealed the non-extstence of any theoretically
significant relationship between any one observed variable and the
remaining latent variables. Therefore, the originally conceived models
representing the relationship of the Indicator variables to the latent
variables were retained for the next step of the analysis.
Using the LISREL VI program, first-order correlation coefficients
were computed between and among all exogenous and endogenous variables
In the models for PMP-Brown and PMP-EIIIs. These are reported In Tables
VIII and IX, respectively. These coefficients were used to determine
the parameters for each hypothesized path In each of the two models.
The following regressions were run, using SPSS-X (SPSS, Inc., 1983)
regression procedure, to obtain the pertinent path coefficients:
1. Type Program Attended was regressed on Prior Academic
Achievement and Age.
2. Nursing Knowledge Base was regressed on Critical Thinking
Ability, Age, Prior Academic Achievement, Prior Education and Type
Program Attended.
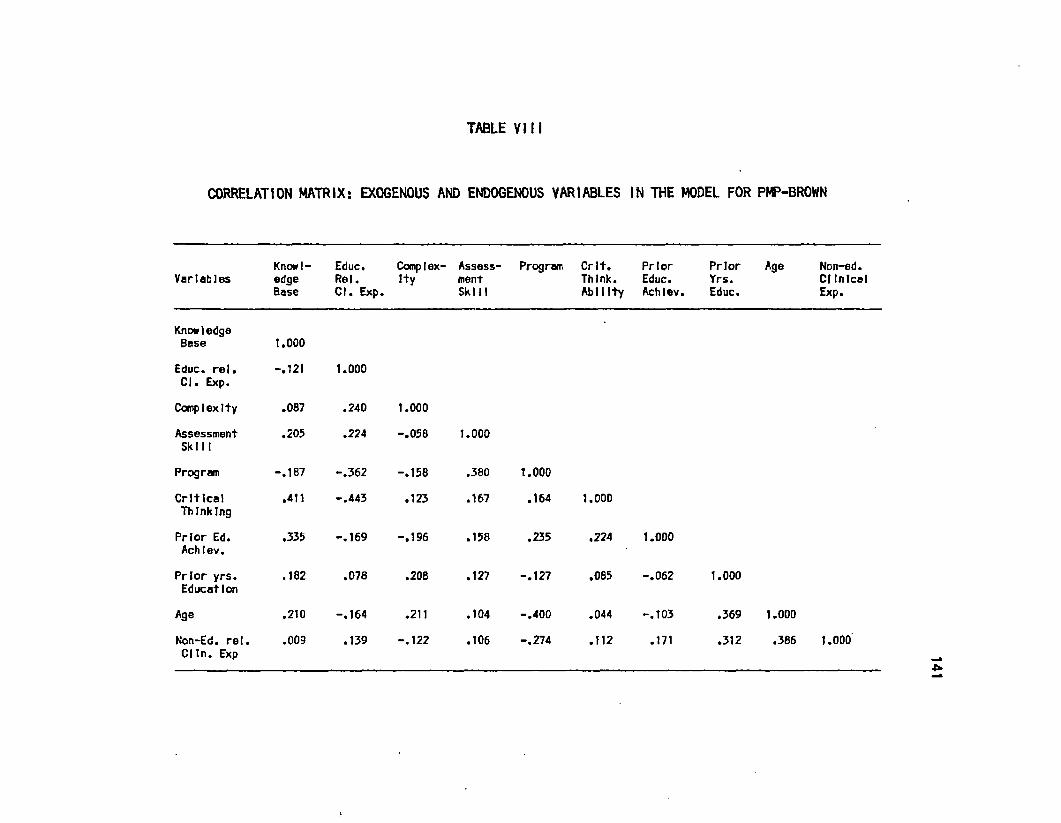
TABLE VIM
CORRELATION MATRIX: EXOGENOUS AND ENDOGENOUS VARIABLES IN THE MODEL FOR PMP-BROWN
Knowl- Educ. Complex- Assess- Program Crlt. Prior Prior Age Non-ed. Variables edge Rel. I+y ment Think. Educ. Yrs. Clinical
Base CI. Exp. Skill Ability Achlev. Educ. Exp.
Know ledge Base
Educ. rel. CI. Exp.
Complexity
Assessment Ski 11
Program
Critical Thinking
Prior Ed. Achlev.
Prior yrs. Education
Age
Non-Ed. rel, Cltn. Exp
1.000
-.121 1.000
.087 .240 1.000
.205 .224 -.058 1.000
-.167 -.362 -.158 .380 1.000
.411 -.443 .123 .167 .164 1.000
.335
.182
-.169 -.196
.078
.158
.208
.210 -.164 .211
.009 .139 -.122
.235
.127 -.127
.224 1.000
.085 -.062
.104 -.400 .044 -.103
.106 -.274 .112 .171
1.000
.369 1.000
.312 .386 1.000

TABLE IX
CORRELATION MATRIX: EXOGENOUS AND ENDOGENOUS VARIABLES IN THE MODEL FOR PW-ELLIS
Variables Knowl- Educ, Complex- Assess- Program Crlt. Prior Prior edge Rel. Ity ment Think. Educ. Yrs. Base CI. Exp. Skill Ability Achlev. Educ.
Age Non-ed. CI Inlcol Exp.
Know I edge Base
Educ. rel. CI. Exp.
Complexity
Assessment Ski 11
Program
Critical Thinking
Prior Ed. Achlev.
Prior yrs. Education
Age
Non-Ed. rel. Clin. Exp
1.000
-.217
-.141
'.090
-.187
.411
.335
.182
.210
.009
1.000
.669 1.000
-.154 .015 1.000
-.148 -.117 -.076 1.000
-.286 -.194 -.036 .164 1.000
-.235
-.008
-.200 .026
.055
.235
.092 -.127
.224 1.000
.085 -.062
.060 .017 .014 -.400 .044 -.103
.120 -.089 .076 -.274 .112 .171
1.000
.369 1.000
.312 .386 1.000

143
3. Education Related Clinical Learning Experiences was
regressed on Type Program Attended.
4. Task Complexity was regressed on Education Related Clinical
Learning Experiences and Prior Clinical Experience.
5. Assessment Ability was regressed on Critical Thinking
Ability, Nursing Knowledge Base, Type Program Attended, Education
Related Clinical Learning Experiences, Task Complexity and Age.
All Independent variables within each of the above regression
models, for each PMP, were entered as a block. With forced entry, all
variables that satisfied the tolerance criterion (0.01) were entered
one at a time In order of decreasing tolerance. However, they were
treated as a single block for computing the requested statistics. The
tolerance of a variable Is the proportion of Its variance not accounted
for by other Independent variables In the equation. All Independent
variables met the criterion for Inclusion.
Figures 6 and 7 report the results of the regression equations In
terms of path coefficients and residuals (u) for the models
explaining performance on PMP-Brown and PMP-Ellls, respectively.
Examination of path coefficients for the PMP-Brown model revealed that
all were greater than 0.05, a generally accepted level Indicating the
existence of a meaningful causal relationship (Pedhauser, 1982). The
path coefficient between Type Program Attended and Assessment Ability
(.7397) Indicates that the type of program attended had a large direct
Influence on assessment ability, as measured by performance on PMP-
Brown, The residual associated with the endogenous variable
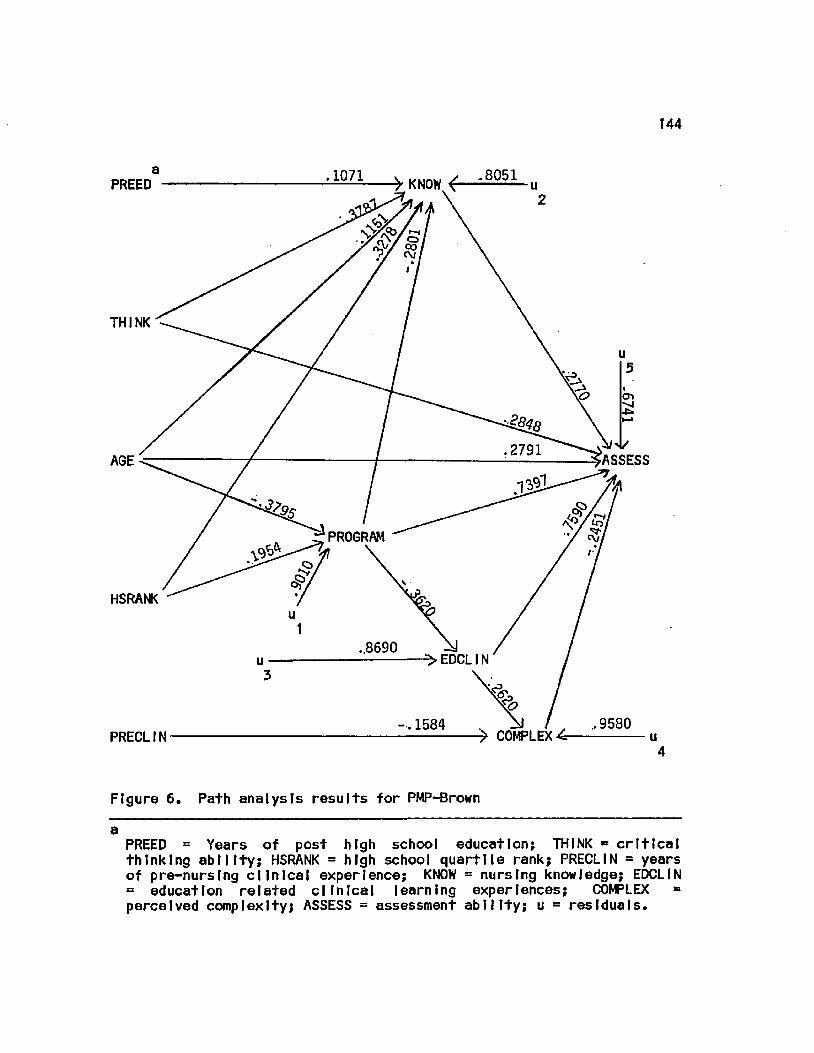
144
> KNOW {— .1071
PREED
CO cv
THINK
ASSESS AGE
PROGRAM
HSRANK
..8690 ^EDCLIN
.9580 1584 ^ COMPLEX PRECLIN
4
Figure 6. Path analysts results for PHP-Brown
a PREED = Years of post high school education; THINK = critical thinking ability; HSRANK = high school quartlte rank; PRECLIN = years of pre-nursing clinical experience; KNOW = nursing knowledge; EDCLIN = education related clinical learning experiences; COMPLEX = perceived complexity; ASSESS = assessment ability; u - residuals.
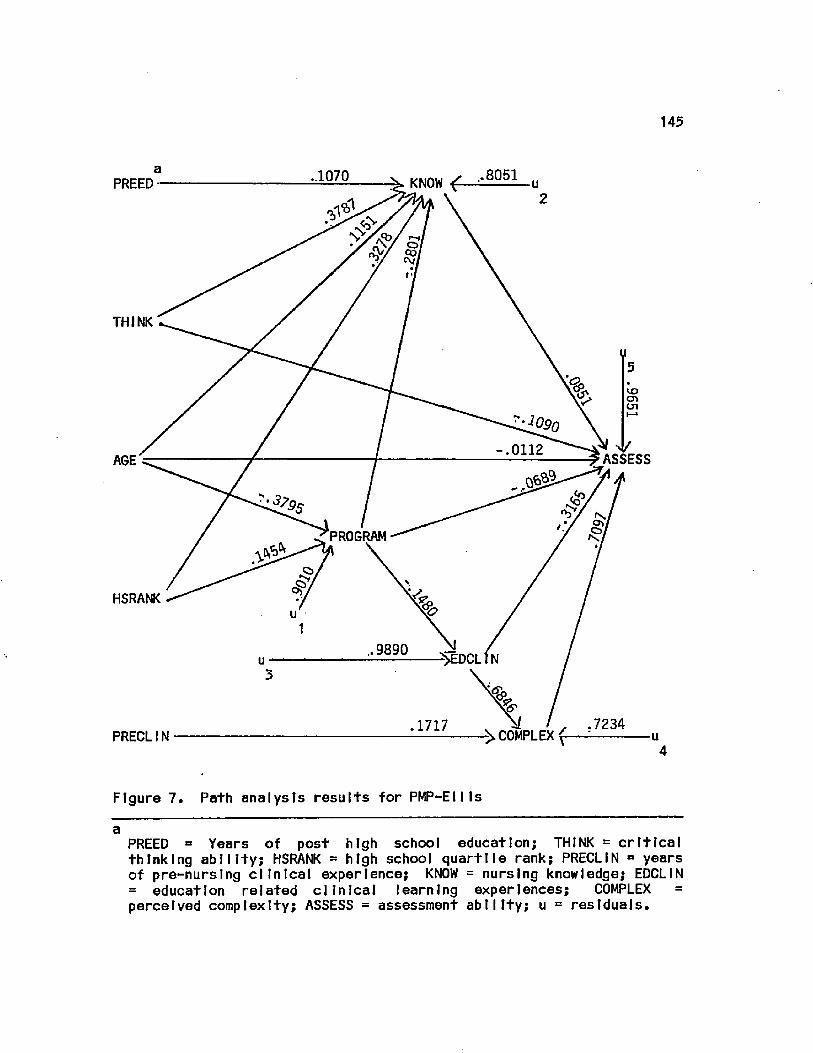
145
.1070 KNOW £ PREED
r~'i oi col <V/
THINK
vo CTl cn
-.,0112 ASSESS AGE
PROGRAM
HSRANK
.7234 .1717 >COMPLEXf PRECLIN
Figure 7. Path analysis results for PMP-Ellls
a PREED a Years of post high school education; THINK - critical thinking ability; HSRANK = high school quartlle rank; PRECLIN = years of pre-nurslng clinical experience; KNOW = nursing knowledge; EDCLIN = education related clinical learning experiences; COMPLEX = perceived complexity; ASSESS = assessment ability; u = residuals.
146
Assessment Ability (.6791) Is large. Indicating that variables not In
the model exerted major Influence on the assessment ability of AD and
BD graduates. It should be noted that residuals for other endogenous
variables In the PMP-Brown model also were large and, therefore,
Indicate that these attributes were explained by variables not In the
modeI.
Examination of path coefficients and residuals In the PMP-EII Is
model revealed that the explanatory capacity of program attended on
assessment ablliity was small and also has a negative effect
(-.0689). In addition, the residual (u = .9651) associated with
Assessment ability Is of great magnitude, thus Indicating that
assessment ability Is best explained by variables not In the model.
The amount of Influence exerted by type of program attended on
overall assessment skill for each model was determined. These effects
are expressed In terms of direct effects, Indirect effects and an
effect coefficient, representing the total direct and Indirect effects.
Results for the Influence of program attended on PMP-Brown assessment
performance are reported In Table X and those for PMP-EII Is assessment
performance. In Table XI. 2
A goodness of fit test with a X distribution (Sprecht, 1975)
was used to determine If the models fit the data. The statistical
evidence for rejection of the null hypothesis Indicated that the model
did not fit. However, a conclusion as to acceptability of a model
also must be based on a review of theoretical and experiential
evidence. To test the multi-stage, over I dent I fled model, goodness of
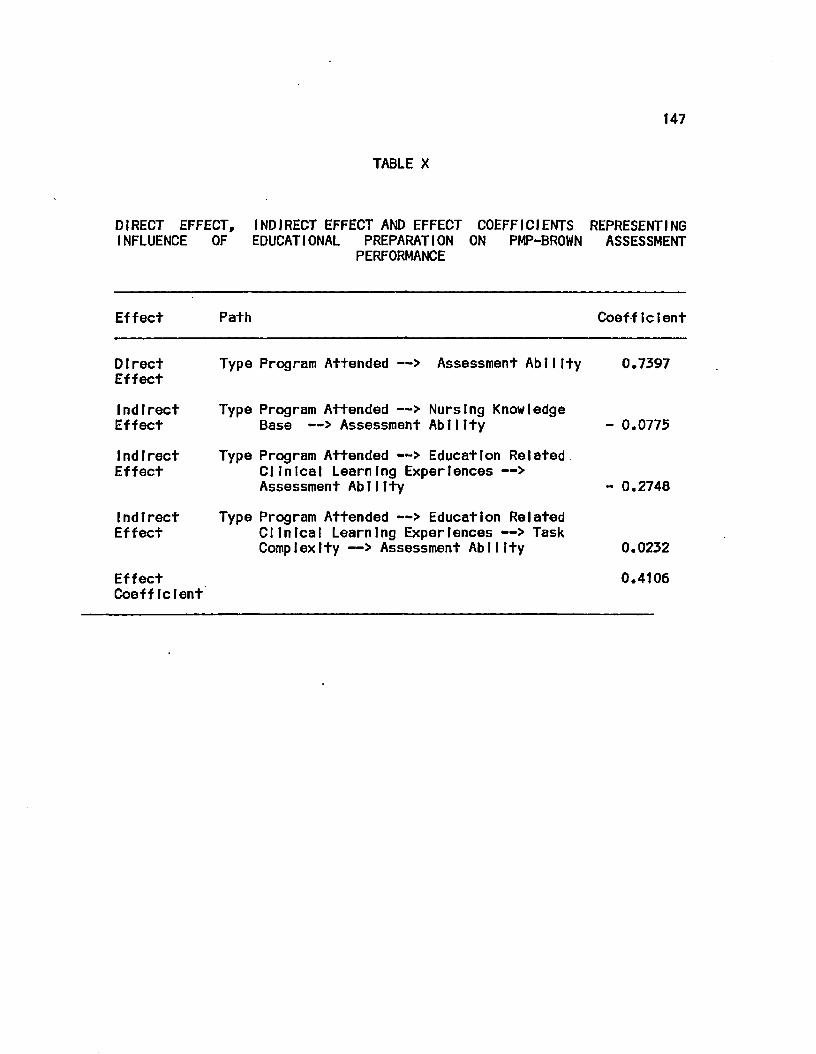
147
TABLE X
DIRECT EFFECT, INFLUENCE OF
INDIRECT EFFECT AND EFFECT COEFFICIENTS REPRESENTING EDUCATIONAL PREPARATION ON PMP-BROWN ASSESSMENT
PERFORMANCE
Effect Path Coefficient
DIrect Effect
Type Program Attended —> Assessment Ability 0.7397
Indirect Type Program Attended —> Nursing Knowledge Effect Base —> Assessment Ability - 0.0775
Indirect Type Program Attended —> Education Related Effect Clinical Learning Experiences —>
Assessment Ability - 0.2748
Indirect Type Program Attended —> Education Related Effect Clinical Learning Experiences —> Task
Complexity —> Assessment Ability 0.0232
Effect Coefficient
0.4106
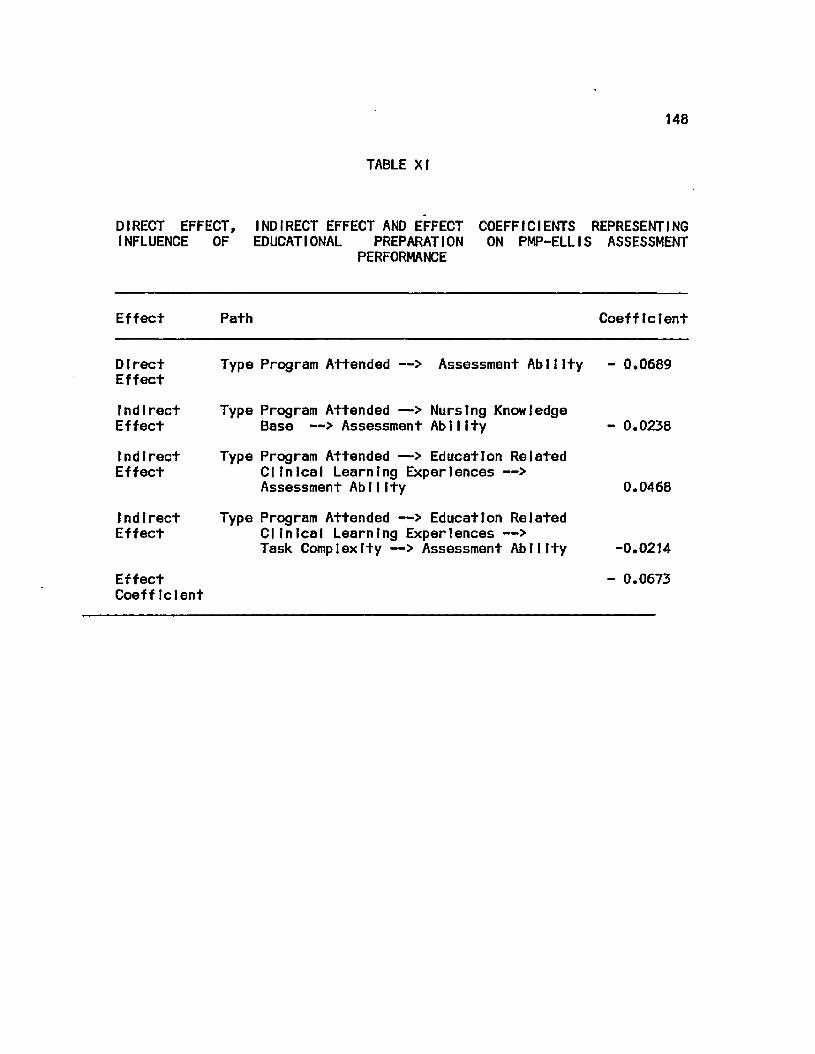
148
TABLE XI
DIRECT EFFECT, INDIRECT EFFECT AND EFFECT COEFFICIENTS REPRESENTING INFLUENCE OF EDUCATIONAL PREPARATION ON PMP-ELLIS ASSESSMENT
PERFORMANCE
Effect Path Coefficient
DIrect Effect
Indirect Effect
Indirect Effect
Indirect Effect
Effect Coeff tclent
Type Program Attended —> Assessment Ability - 0.0689
Type Program Attended —> Nursing Knowledge Base —> Assessment Ability
Type Program Attended —> Education Related Clinical Learning Experiences —> Assessment AblIIty
Type Program Attended —> Education Related Clinical Learning Experiences —> Task Complexity —> Assessment Ability
- 0.0238
0.0468
-0.0214
- 0.0673
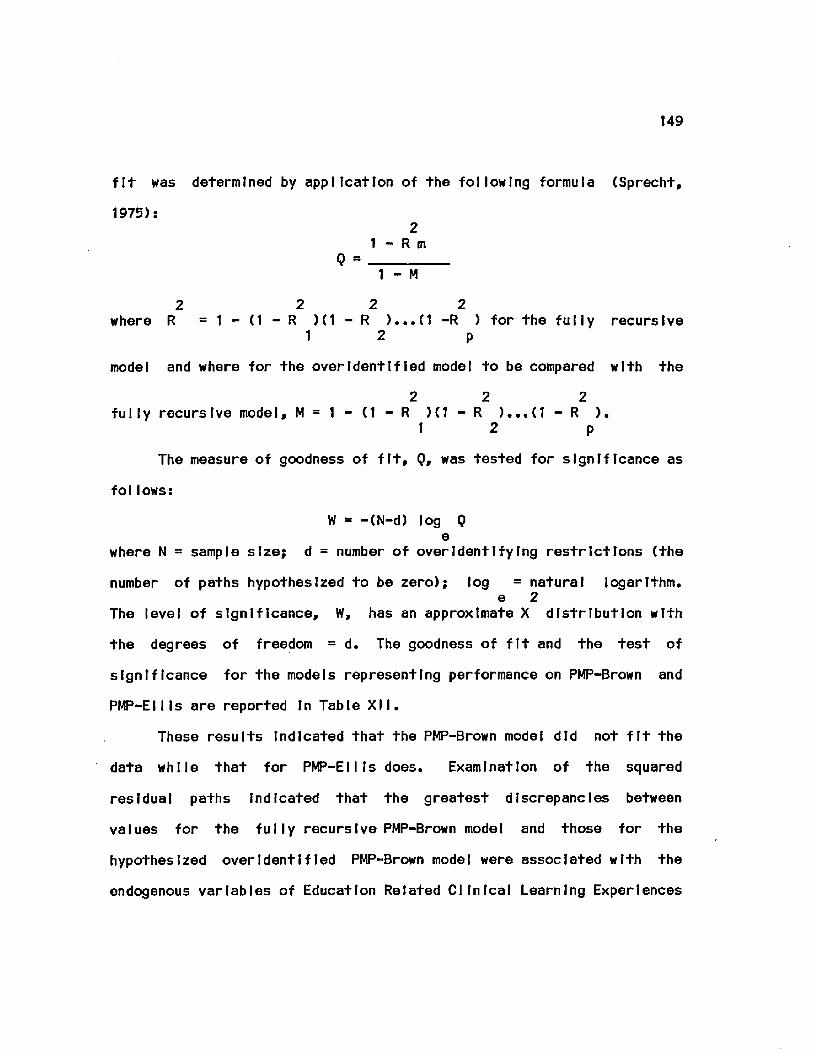
149
fit was determined by application of the following formula (Sprecht,
1975): 2
1 - R m Q =
1 - M
2 2 2 2 where R = 1 — (1 — R )(1-R )...(! —R ) for the fully recursive
1 2 p
model and where for the over Ident IfIed model to be compared with the
2 2 2 fully recursive model, M = 1 - (1 - R H1-R )...(1 - R ).
1 2 p
The measure of goodness of fit, 0, was tested for significance as
follows:
W = -(N-d) log Q e
where N = sample size; d = number of overIdentifying restrictions (the
number of paths hypothesized to be zero); log = natural logarithm. e 2
The level of significance, W, has an approximate X distribution with
the degrees of freedom = d. The goodness of fit and the test of
significance for the models representing performance on PMP-Brown and
PMP-Ellls are reported In Table XII.
These results Indicated that the PMP-Brown model did not fit the
data while that for PMP-Ellls does. Examination of the squared
residual paths Indicated that the greatest discrepancies between
values for the fully recursive PMP-Brown model and those for the
hypothesized over I dent I fled PMP-Brown model were associated with the
endogenous variables of Education Related Clinical Learning Experiences

150
TABLE XII
GOODNESS OF FIT AND LEVEL OF SIGNIFICANCE FOR MODELS REPRESENTING ASSESSMENT PERFORMANCE ON PMP-BROWN AND PMP-ELLIS
Model 2 R m
2 M Q W
PMP: Brown
PMP: El 1 Is
.9199
.8800
.8065
.7492
.4137
.7995
a 60.195
b 15.258
a df=20; p < .05.
b df=20; p > .05.
and Task Complexity. In order to explore these relationships further,
the fit of the model for each endogenous variable was examined
separately using the formulas described previously. Results of these
calculations are reported In Table XIII and XIV for the models
explaining performance on PMP-Brown and PMP-Ellls, respectively.
These results Indicated that, within the overall PMP-Brown model,
the models for the Individual endogenous variables of Education Related
Clinical Learning Experiences, Task Complexity, and Assessment Ability
did not, statistically, fit the data. Within the overall PMP-Ellls
model, the Individual models for all endogenous variables fit the data.
A review of the theoretfcal framework on which the complete models were
based and the hypothesized relationships among the variables In the
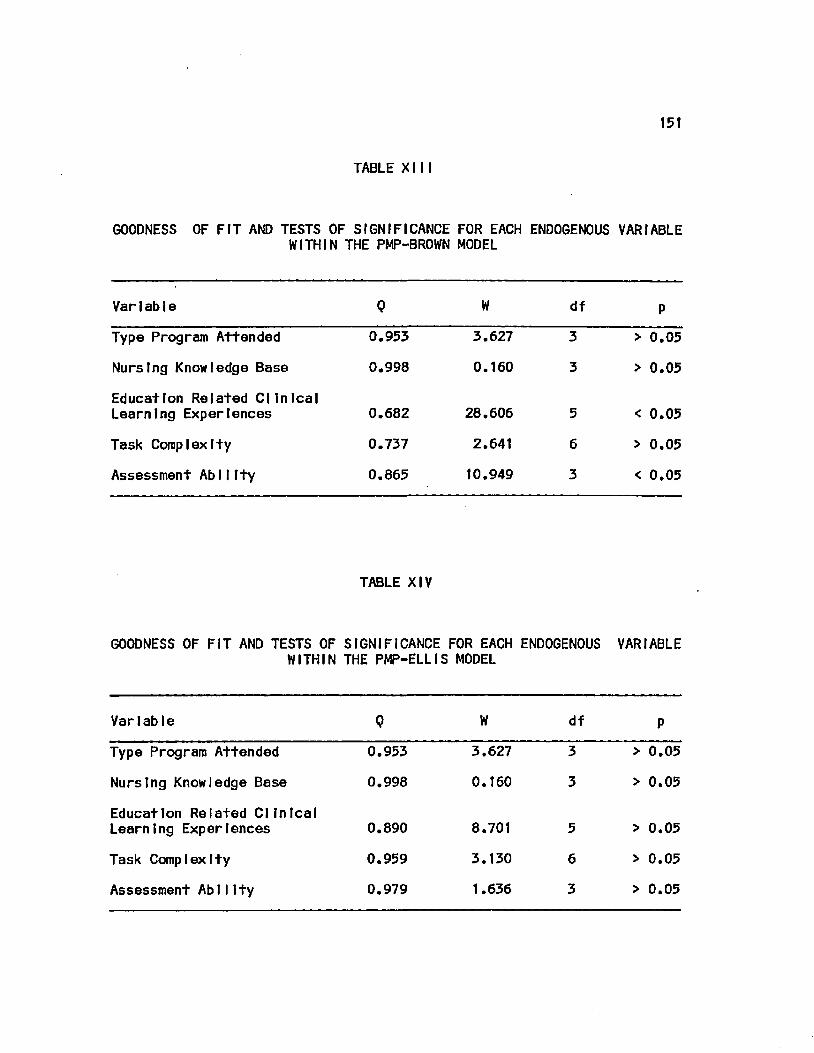
151
TABLE XIII
GOODNESS OF FIT AND TESTS OF SIGNIFICANCE FOR EACH ENDOGENOUS VARIABLE WITHIN THE PHP-BROWN MODEL
Variable 0 W df P
Type Program Attended 0.953 3.627 3 > 0.05
Nursing Knowledge Base 0.998 0.160 3 > 0.05
Education Related Clinical Learning Experiences 0.682 28.606 5 < 0.05
Task Complexity 0.737 2.641 6 > 0.05
Assessment Ability 0.865 10.949 3 < 0.05
TABLE XIV
GOODNESS OF FIT AND TESTS OF WITHIN
SIGNIFICANCE THE PMP-ELLIS
FOR EACH MODEL
ENDOGENOUS VARIABLE
Variable 0 W df P
Type Program Attended 0.953 3.627 3 > 0.05
Nursing Knowledge Base 0.998 0.160 3 > 0.05
Education Related Clinical Learning Experiences 0.890 8.701 5 > 0.05
Task Complexity 0.959 3.130 6 > 0.05
Assessment AblIIty 0.979 1.636 3 > 0.05

152
models led to the conclusion that the models for PMP-Brown and PMP-
Ellts were acceptable as originally conceived In spite of the lack of
statistical fit for the PMP-Brown model.
2. Conclusions
Based on the magnitudes of the effect coefficients, the
following conclusions about the theoretical acceptability of the 2
models and the statistical fit of the PMP-Ellis model were drawn. On
PMP-Brown, which simulates the clinic visit of a patient with
hypertenion and complaints of eplstaxls, the type of program attended
by participants had a strong causal effect on assessment ability. This
causal relationship was demonstrated by both the direct effect
coefficient (.74) and the total effect coefficient (.41).
In contrast, on PMP-Ellls, which simulates the admission of a
patient with chronic obstructive pulmonary disease and pneumonia and
complaining of chest pain, the type of program attended by the
participants had a neglIglble causal effect on assessment ability.
This was demonstrated by both the direct effect coefficient (-.07) and
the total effect coefficient (-.07).
Specific differences In the performance of the AD and BD
participants with regard to the data collection and nursing diagnosis
Identification abilities are addressed In the following sections.
B. Data col I artIon efficiency
The second research question to be answered was: When graduating
associate and baccalaureate degree nursing students are compared. Is
there a difference In data collection efficiency? A one way analysis
153
of variance (ANOVA), with schools nested within program, was used to
answer this question and the remaining research questions. The
statistical null hypotheses tested were that: mean = mean . An AD BD
alpha of 0.05 was set as the level of statistical significance for all
tests. Cochran's C was used to test the assumption that the variance
In scores for the two groups was equal. This assumption was met except
where noted otherwise. Table XL I (Appendix F) summarizes the Cochran's
C results for each set of score variances tested.
Data collection efficiency scores of AD and BD participants and
for all participants combined are summarized In Tables XV and XVI for
PMP-Brown and PMP-Ellls, respectively.
For PMP-Brown, ANOVA results (Table XVII) demonstrated no
statistically significant differences in data collection efficiency of
the two groups (F (1,9) = 1.94; p>.05). Therefore, the null hypothesis
was not rejected.
The ANOVA results (Table XVIII) for data collection efficiency
on PMP-Ellls demonstrated no statistically significant differences In
the performance of the two groups (F (1,9) = .77; p>.05). Therefore
the null hypothesis could not be rejected.
These results demonstrate that AD and BD participants selected
the same ratio of essential data to total data selected In both PMP-
Brown and In PMP-Ellls.
C. Data collection proficiency
The third research question to be answered was: When graduating
associate and baccalaureate degree nursing students are compared. Is
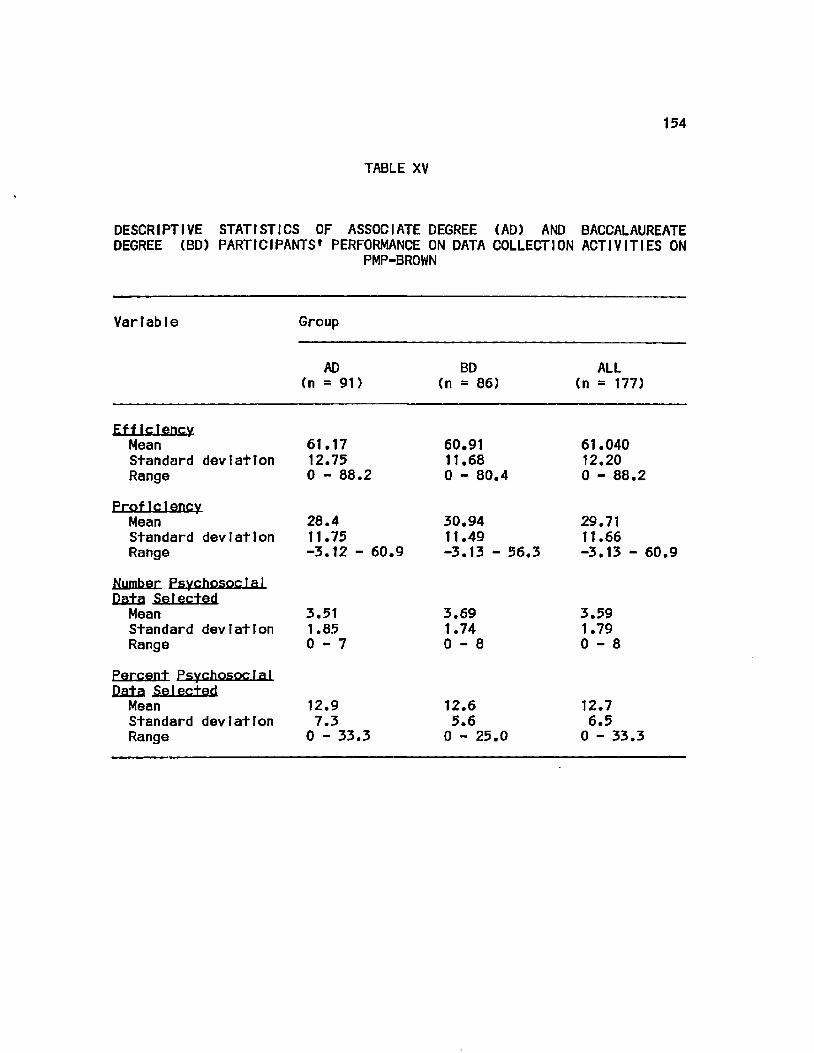
154
TABLE XV
DESCRIPTIVE STATISTICS OF ASSOCIATE DEGREE (AD) AND BACCALAUREATE DEGREE (BD) PARTICIPANTS' PERFORMANCE ON DATA COLLECTION ACTIVITIES ON
PMP-BROWN
Variable Group
AD (n = 91)
BD (n = 86)
ALL (n = 177)
Eff tctency Mean 61.17 Standard deviation 12.75 Range 0 - 88.2
Proficiency Mean Standard deviation Range
Number Psychosocial Data Selected Mean Standard deviation Range
28.4 11.75 -3.12 - 60.9
3.51 1.85 0 - 7
Percent Psychosocial Data Selected Mean 12.9 Standard deviation 7.3 Range 0 - 33.3
60.91 11.68 0 - 80.4
30.94 11.49 -3.13 - 56.3
3.69 1.74 0 - 8
12.6 5.6 0 - 25.0
61.040 12.20 0 - 88.2
29.71 11.66 -3.13 - 60.9
3.59 1.79 0 - 8
12.7 6.5 0 - 33.3
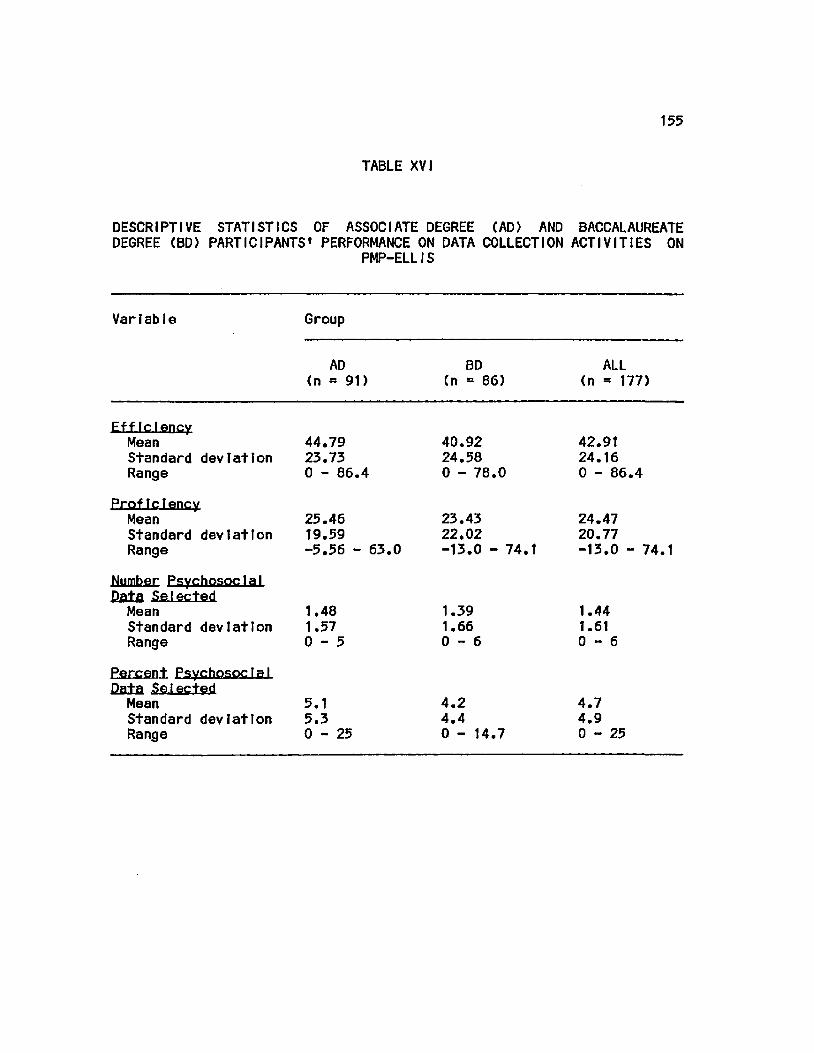
155
TABLE XVI
DESCRIPTIVE STATISTICS OF ASSOCIATE DEGREE (AD) AND BACCALAUREATE DEGREE (BD) PARTICIPANTS' PERFORMANCE ON DATA COLLECTION ACTIVITIES ON
PMP-ELLIS
Variable Group
AD (n = 91)
BD (n = 86)
ALL (n = 177)
Efficiency
Mean 44.79 Standard deviation 23.73 Range 0 - 86.4
Proficiency
Mean Standard deviation Range
25.46 19.59 -5.56 - 63.0
Number Psychosocial Data Selected
Mean 1.48 Standard deviation 1.57 R a n g e 0 - 5
Percent Psychosocial
Dfl±a Selected Mean 5.1 Standard devlatton 5.3 Range 0-25
40.92 24.58 0 - 78.0
23.43 22.02 -13.0 - 74.1
1.39 1.66 0 - 6
4.2 4.4 0 - 14.7
42.91 24.16 0 - 86.4
24.47 20.77 -13.0 - 74.1
1.44 1.61 0 - 6
4.7 4.9 0-25
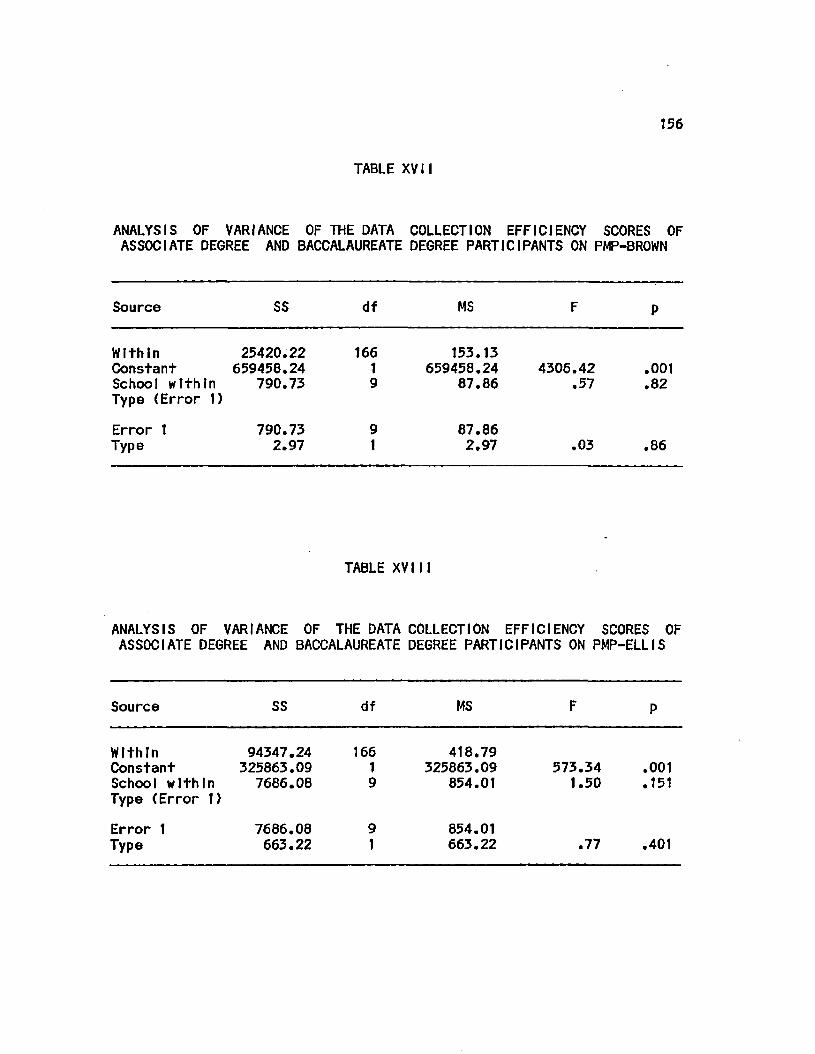
156
TABLE XVII
ANALYSIS OF VARIANCE OF THE DATA COLLECTION EFFICIENCY SCORES OF ASSOCIATE DEGREE AND BACCALAUREATE DEGREE PARTICIPANTS ON PMP-BROWN
Source SS df MS
Within 25420.22 166 153.13 Constant 659450.24 1 659458.24 4306.42 .001 School within 790.73 9 87.86 .57 .82 Type (Error 1)
Error 1 790.73 9 87.86 Type 2.97 1 2.97 .03 .86
TABLE XVIII
ANALYSIS OF VARIANCE OF THE DATA COLLECTION EFFICIENCY SCORES OF ASSOCIATE DEGREE AND BACCALAUREATE DEGREE PARTICIPANTS ON PMP-ELLIS
Source SS df MS
Within 94347.24 166 418.79 Constant 325863.09 1 325863.09 573.34 .001 School within 7686.08 9 854.01 1.50 .151 Type (Error 1)
Error 1 7686.08 9 854.01 Type 663.22 1 663.22 .77 .401
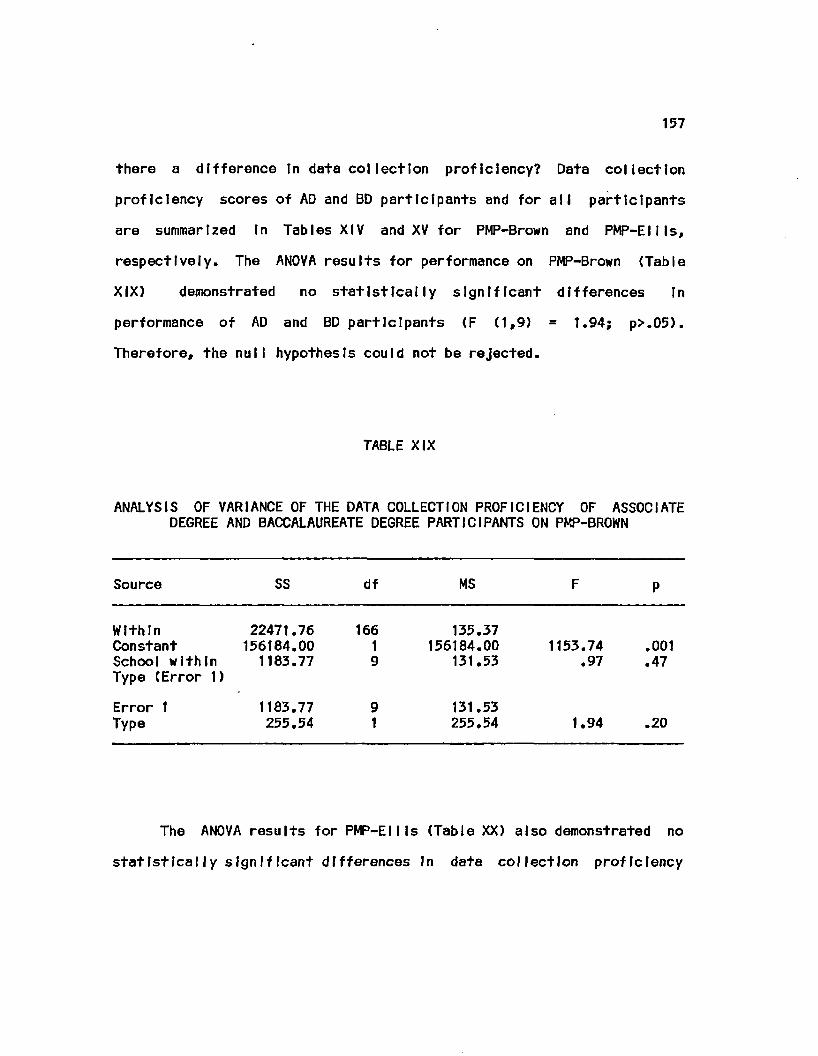
157
there a difference In data col lection proficiency? Data collection
proficiency scores of AD and BD participants and for all participants
are summarized In Tables XIV and XV for PMP-Brown and PMP-EUIs,
respectively. The ANOVA results for performance on PMP-Brown (Table
XIX) demonstrated no statistically significant differences In
performance of AD and BD participants £F £1,9) = 1.94; p>.05).
Therefore, the null hypothesis could not be rejected.
TABLE XIX
ANALYSIS OF VARIANCE OF THE DATA COLLECTION PROFICIENCY OF ASSOCIATE DEGREE AND BACCALAUREATE DEGREE PARTICIPANTS ON PMP-BROWN
Source SS df MS F P
Within 22471.76 166 135.37 Constant 156184.00 1 156184.00 1153.74 .001 School within 1183.77 9 131.53 .97 .47 Type fError 1)
Error 1 1183.77 9 131.53 Type 255.54 1 255.54 1.94
o
IN •
The ANOVA results for PMP-Ellls £Table XX) also demonstrated no
statistically significant differences In data collection proficiency
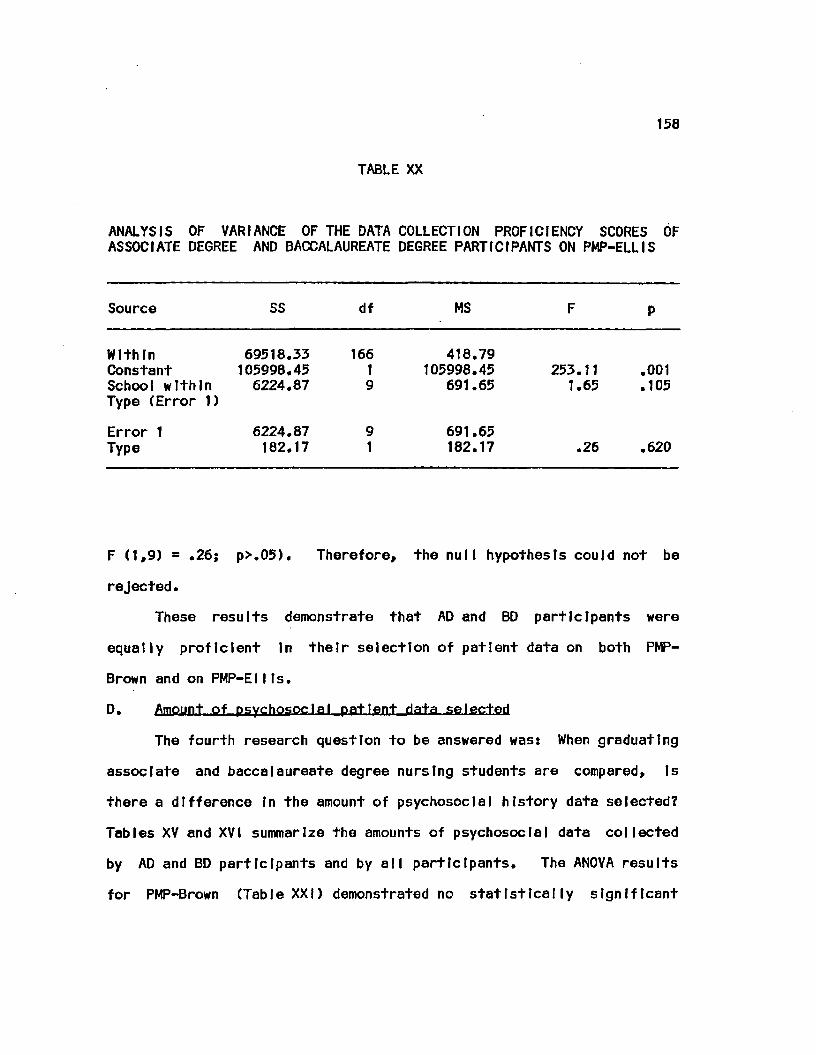
156
TABLE XX
ANALYSIS OF VARIANCE OF THE DATA COLLECTION PROFICIENCY SCORES OF ASSOCIATE DEGREE AND BACCALAUREATE DEGREE PARTICIPANTS ON PMP-ELLIS
Source SS df MS F P
Within 69518.33 166 418.79 Constant 105998.45 1 105998.45 253.11 .001 School within 6224.87 9 691.65 1.65 .105 Type (Error 1)
Error 1 6224.87 9 691.65 Type 182.17 1 182.17 .26 .620
F (1,9) = .26; p>.05). Therefore, the null hypothesis could not be
rejected.
These results demonstrate that AD and BD participants were
equally proficient In their selection of patient data on both PMP-
Brown and on PMP-EIIIs.
D. Amount of psychosocial patient data selected
The fourth research question to be answered was: When graduating
associate and baccalaureate degree nursing students are compared, Is
there a difference In the amount of psychosocial history data selected?
Tables XV and XVI summarize the amounts of psychosocial data collected
by AD and BD participants and by all participants. The ANOVA results
for PMP-Brown (Table XXI) demonstrated no statistically significant
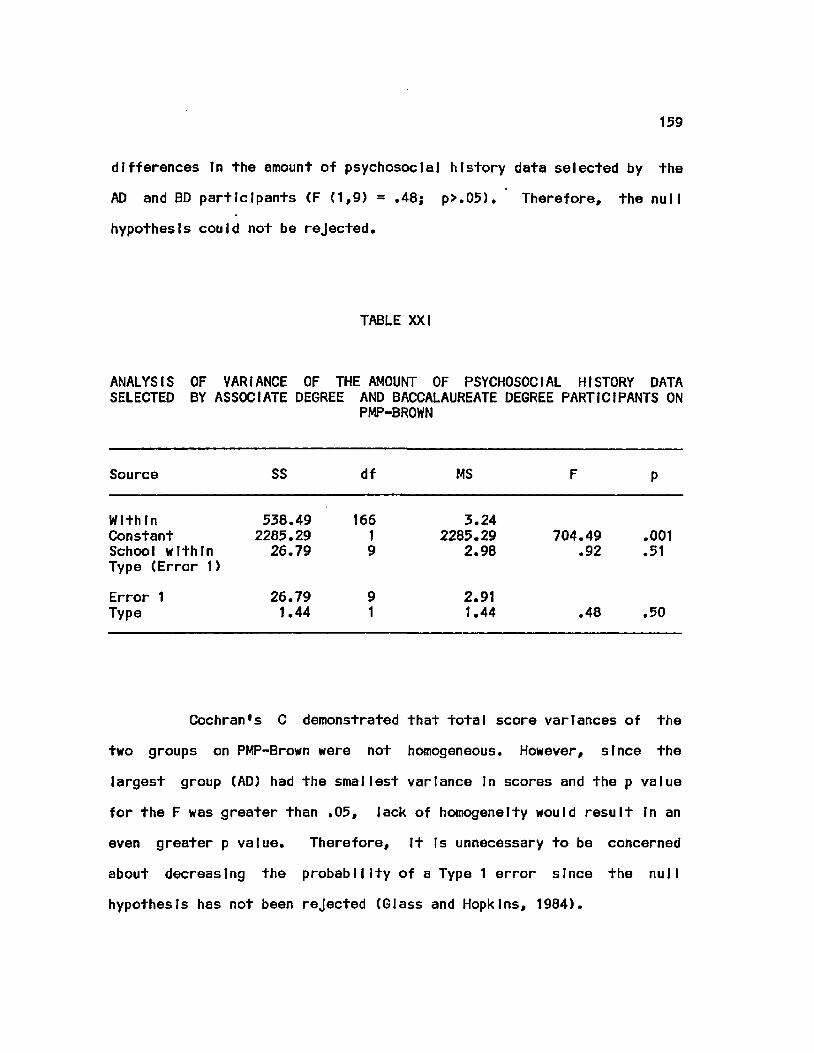
159
differences In the amount of psychosocial history data selected by the
AD and BD participants (F (1,9) = .48; p>.05). Therefore, the null
hypothesis could not be rejected.
TABLE XXI
ANALYSIS OF VARIANCE OF THE AMOUNT OF PSYCHOSOCIAL HISTORY DATA SELECTED BY ASSOCIATE DEGREE AND BACCALAUREATE DEGREE PARTICIPANTS ON
PMP-BROWN
Source SS df MS F P
Within 538, .49 166 3, .24 Constant 2285, .29 1 2285, .29 704.49 .001 School within 26. .79 9 2, ,98 .92 .51 Type (Error 1)
Error 1 26, ,79 9 2, ,91 Type 1. ,44 1 1. ,44 .48 .50
Cochran's C demonstrated that total score variances of the
two groups on PMP-Brown were not homogeneous. However, since the
largest group (AD) had the smallest variance In scores and the p value
for the F was greater than ,05, Jack of homogeneity would result In an
even greater p value. Therefore, It Is unnecessary to be concerned
about decreasing the probability of a Type 1 error since the null
hypothesis has not been rejected (Glass and Hopkins, 1984).
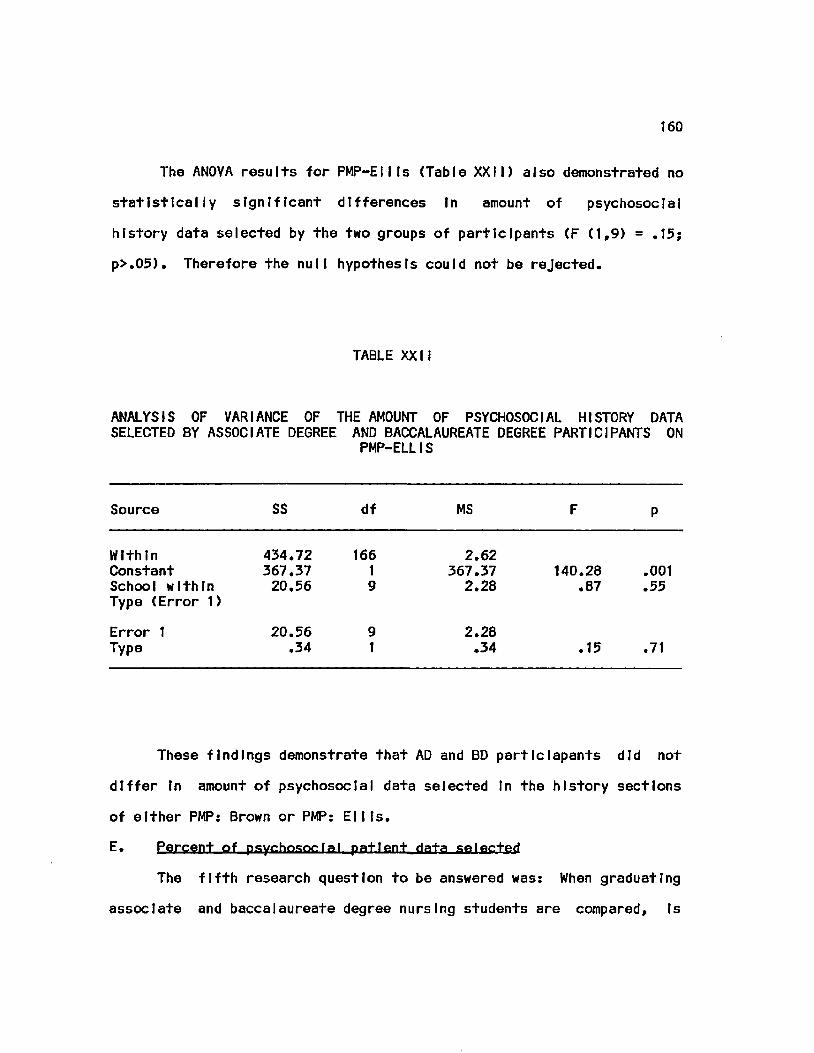
160
The ANOVA results for PMP-Etlts (Table XXII) also demonstrated no
statistically significant differences In amount of psychosocial
history data selected by the two groups of participants (F (1,9) = .15;
p>.05). Therefore the null hypothesis could not be rejected.
TABLE XXII
ANALYSIS OF VARIANCE OF THE AMOUNT OF PSYCHOSOCIAL HISTORY DATA SELECTED BY ASSOCIATE DEGREE AND BACCALAUREATE DEGREE PARTICIPANTS ON
PMP-ELLIS
Source SS df MS F P
Within 434.72 166 2.62 Constant 367.37 1 367.37 140.28 .001 School within 20.56 9 2.28 .87 .55 Type (Error 1)
Error 1 20.56 9 2.28 Type .34 1 .34 .15 .71
These findings demonstrate that AD and BD participants did not
differ In amount of psychosocial data selected In the history sections
of either PMP: Brown or PMP: Ellis.
E. Percent of psychosocial patient data selected
The fifth research question to be answered was: When graduating
associate and baccalaureate degree nursing students are compared. Is
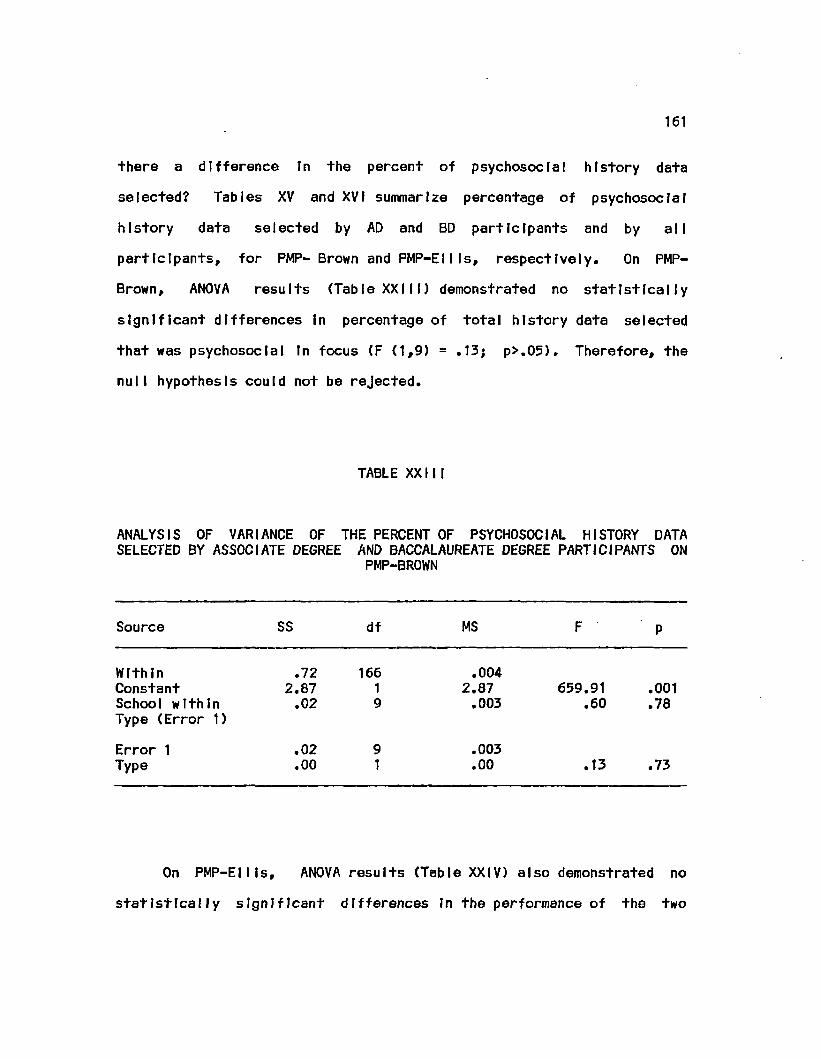
161
there a difference In the percent of psychosocial history data
selected? Tables XV and XVI summarize percentage of psychosocial
history data selected by AD and BD participants and by all
participants, for PMP- Brown and PMP-Ellls, respectively. On PMP-
Brown, ANOVA results (Table XXIII) demonstrated no statistically
significant differences In percentage of total history data selected
that was psychosocial In focus (F (1,9) = .13; p>.05). Therefore, the
null hypothesis could not be rejected.
TABLE XXIII
ANALYSIS OF VARIANCE OF THE PERCENT OF PSYCHOSOCIAL HISTORY DATA SELECTED BY ASSOCIATE DEGREE AND BACCALAUREATE DEGREE PARTICIPANTS ON
PMP-BROWN
Source SS df MS F P
Within .72 166 .004 Constant 2.87 1 2.87 659.91 .001 School within .02 9 .003 .60 .78 Type (Error 1)
Error 1 .02 9 .003 Type .00 1 .00 .13 .73
On PMP-EII Is, ANOVA results (Table XXIV) also demonstrated no
statistically significant differences In the performance of the two
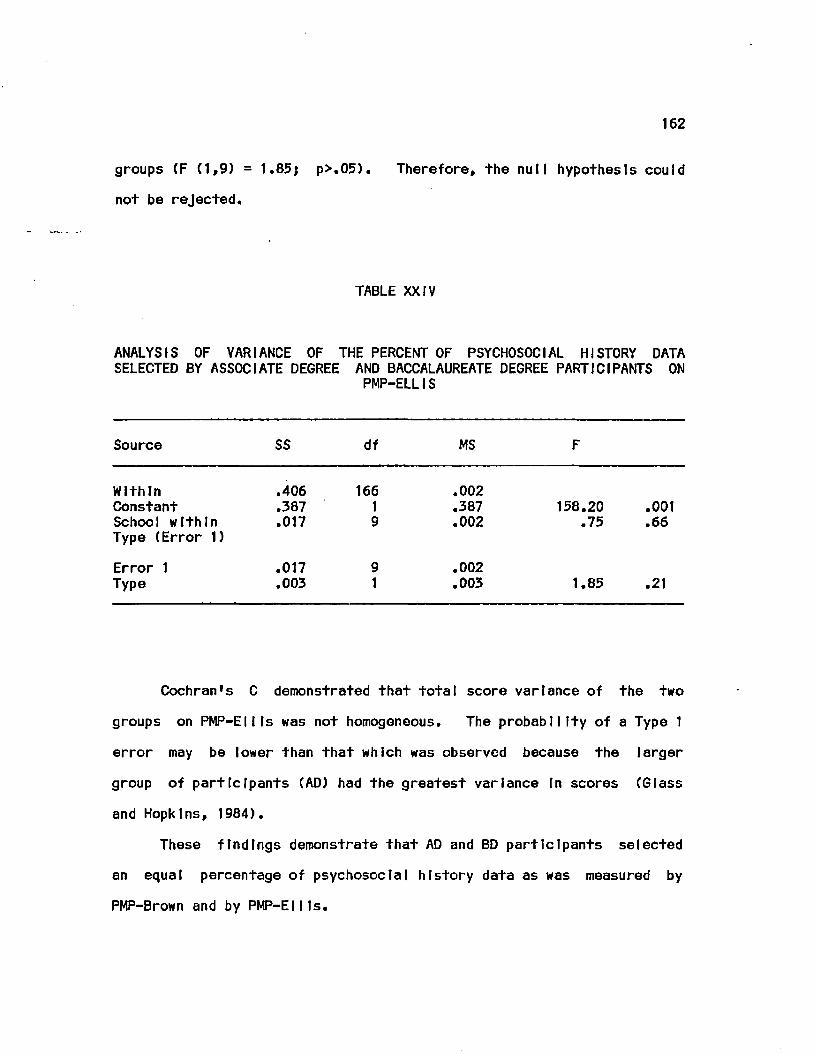
162
groups CF (1,9) = 1.85; p>.05). Therefore, the null hypothesis could
not be rejected.
TABLE XXIV
ANALYSIS OF VARIANCE OF THE PERCENT OF PSYCHOSOCIAL HISTORY DATA SELECTED BY ASSOCIATE DEGREE AND BACCALAUREATE DEGREE PARTICIPANTS ON
PMP-ELLIS
Source SS df MS F
Within .406 166 .002 Constant .387 1 .387 158.20 .001 School within .017 9 .002 .75 .66 Type (Error 1)
Error 1 .017 9 .002 Type .003 1 .003 1.85 .21
Cochran's C demonstrated that total score variance of the two
groups on PMP-Ellls was not homogeneous. The probability of a Type 1
error may be lower than that which was observed because the larger
group of participants (AD) had the greatest variance In scores (Glass
and Hopkins, 1984).
These findings demonstrate that AD and BD participants selected
an equal percentage of psychosocial history data as was measured by
PMP-Brown and by PMP-Ellls.
163
F. Nursing diagnosis Identification
The sixth research question to be answered was: When graduating
associate and baccalaureate degree nursing students are compared. Is
there a difference In the number of plausible nursing diagnoses
Identified? This question was answered based on results of two
different scores: number of plausible nursing diagnoses Identified and
NDXSCORE - a composite score reflecting the type of each diagnostic
statement Identified (a symptom, medical diagnosis or a nursing
diagnosis) and completeness of the Identified nursing diagnosis
statements. Performances of AD and BD participants In the diagnostic
tasks are summarized In Tables XXV and XXVI for PMP-Brown and PMP-
ElI Is, respectively.
Statistically significant differences In number of plausible
nursing diagnosis statements Identified on PMP-Brown were not
demonstrated by ANOVA results (Table XXVII) (F (1,9) = 4.27j p>.05).
Cochran's C demonstrated that total score variance of the two
groups on PMP-Brown was not homogeneous. Probability of a Type 1
error may be greater than what was observed because the larger group of
participants (AD) had the least variance In scores (Glass and Hopkins,
1984).
In contrast, ANOVA results (Table XXVIII) did demonstrate a
significant difference In NDXSCOREs (F (1,9) - 5.16); p<.05). The BD
participants Identified a greater number of plausible nursing diagnoses
that were stated more completely than those Identified by AD
participants on PMP-Brown.
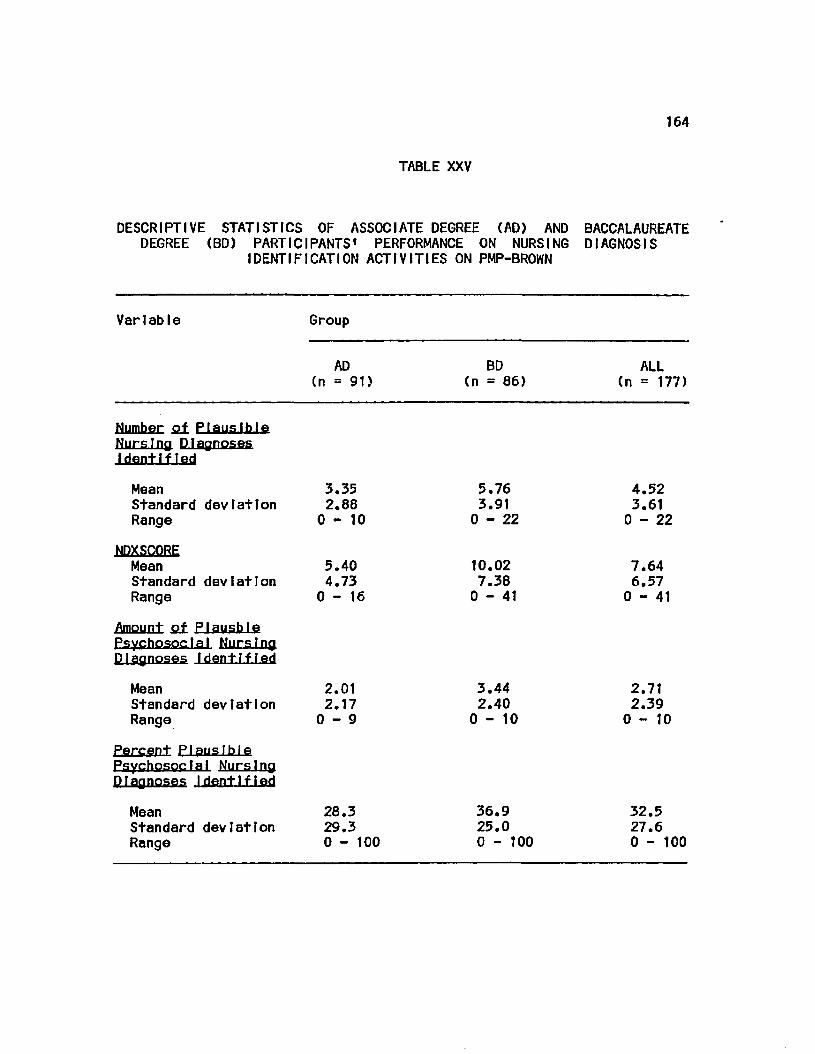
164
TABLE XXV
DESCRIPTIVE STATISTICS OF ASSOCIATE DEGREE (AD) AND BACCALAUREATE DEGREE (BD) PARTICIPANTS' PERFORMANCE ON NURSING DIAGNOSIS
IDENTIFICATION ACTIVITIES ON PMP-BROWN
Variable Group
AD (n = 91)
BD (n = 86)
ALL (n = 177)
Number oi Plausible Nursing Diagnoses I dent IfIed
Mean 3.35 Standard deviation 2.88 R a n g e 0 - 1 0
5.76 3.91
0 - 2 2
4.52 3.61
0 - 2 2
NDXSCORE
Mean 5.40 Standard deviation 4.73 Range 0-16
10.02 7.38 0 - 4 1
7.64 6.57 0 - 4 1
Amount q± Plausfale Psychosocial Nursing Diagnoses Identified
Mean Standard Range
devIatIon 2.01 2.17 0 - 9
3.44 2.40
0 - 1 0
2.71 2.39
0 - 1 0
Percent Plausible Psychosocial Nursing D1agnoses I dent 1f1ed
Mean Standard Range
deviation 28.3 29.3 0 - 100
36.9 25.0 0 - 100
32.5 27.6 0 - 100
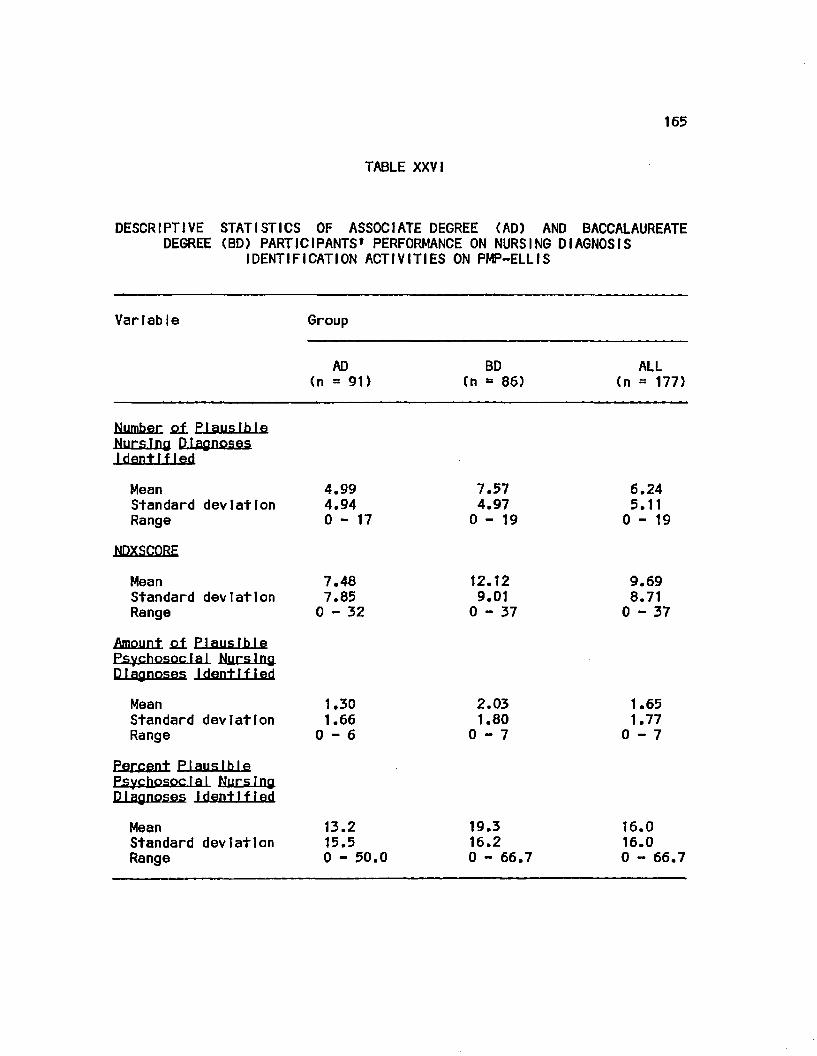
165
TABLE XXV!
DESCRIPTIVE STATISTICS OF ASSOCIATE DEGREE (AD) AND BACCALAUREATE DEGREE (BD) PARTICIPANTS* PERFORMANCE ON NURSING DIAGNOSIS
IDENTIFICATION ACTIVITIES ON PMP-ELLIS
Variable Group
AD BD ALL (n = 91) (n - 86) (n = 177)
Numher Q± Plausible Nursing Diagnoses Identified
Mean 4.99 7.57 6.24 Standard deviation 4.94 4.97 5.11 Range 0-17 0-19 0-19
NDXSCQRE
Mean 7.48 12.12 9.69 Standard deviation 7.85 9.01 8.71 Range 0-32 0-37 0-37
Amount Plausible Psychosocla I Nurs1ng
D. lag noses Identified
Mean 1.30 2.03 1.65 Standard deviation 1.66 1.80 1.77 Range 0-6 0-7 0-7
Percent Plausible Psychosocial Nursing Diagnoses Identified
Mean 13.2 19.3 16.0 Standard deviation 15.5 16.2 16.0 Range 0 - 50.0 0 - 66.7 0 - 66.7
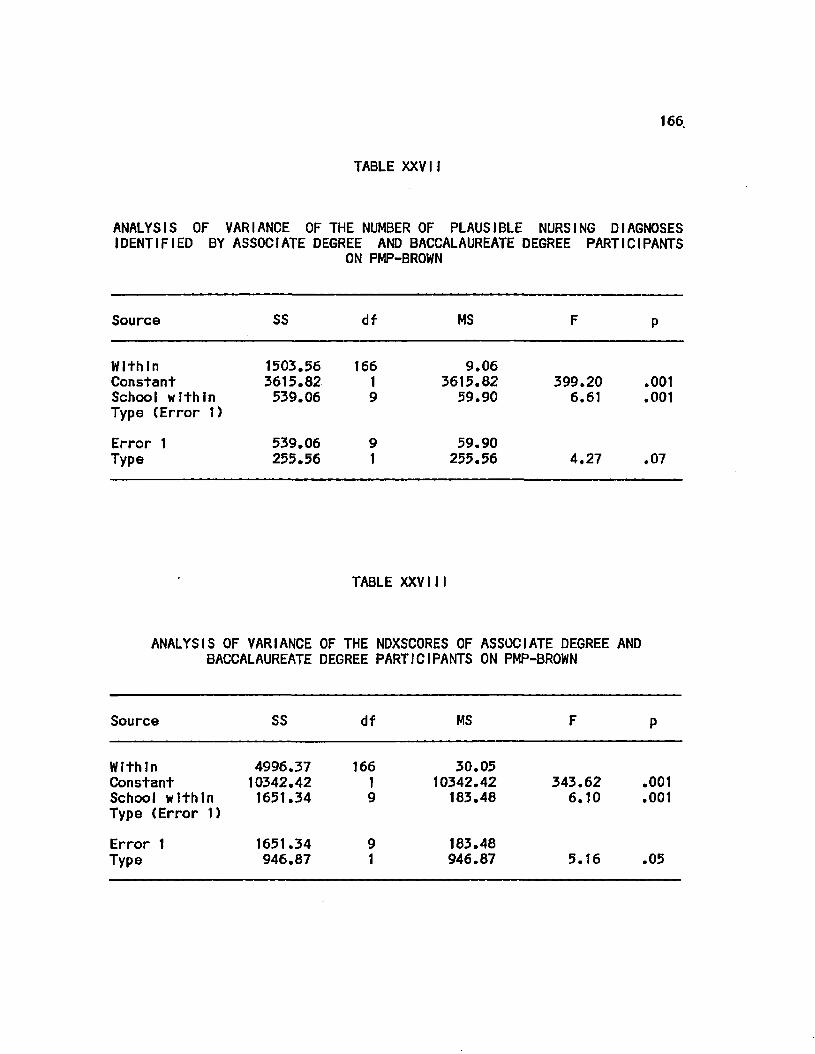
166.
TABLE XXVII
ANALYSIS OF VARIANCE OF THE NUMBER OF PLAUSIBLE NURSING DIAGNOSES IDENTIFIED BY ASSOCIATE DEGREE AND BACCALAUREATE DEGREE PARTICIPANTS
ON PMP-BROWN
Source SS df MS
Within Constant School within Type (Error 1)
1503.56 3615.82 539.06
166 1 9
9.06 3615.82 59.90
399.20 6.61
.001
.001
Error 1 Type
539.06 255.56
9 1
59.90 255.56 4.27 .07
TABLE XXVIII
ANALYSIS OF VARIANCE OF THE NDXSCORES OF ASSOCIATE DEGREE AND BACCALAUREATE DEGREE PARTICIPANTS ON PMP-BROWN
Source SS df MS
Within 4996.37 166 30.05 Constant 10342.42 1 10342.42 343.62 .001 School within 1651.34 9 183.48 6.10 .001 Type (Error 1)
Error 1 1651.34 9 183.48 Type 946.87 1 946.87 5.16 .05
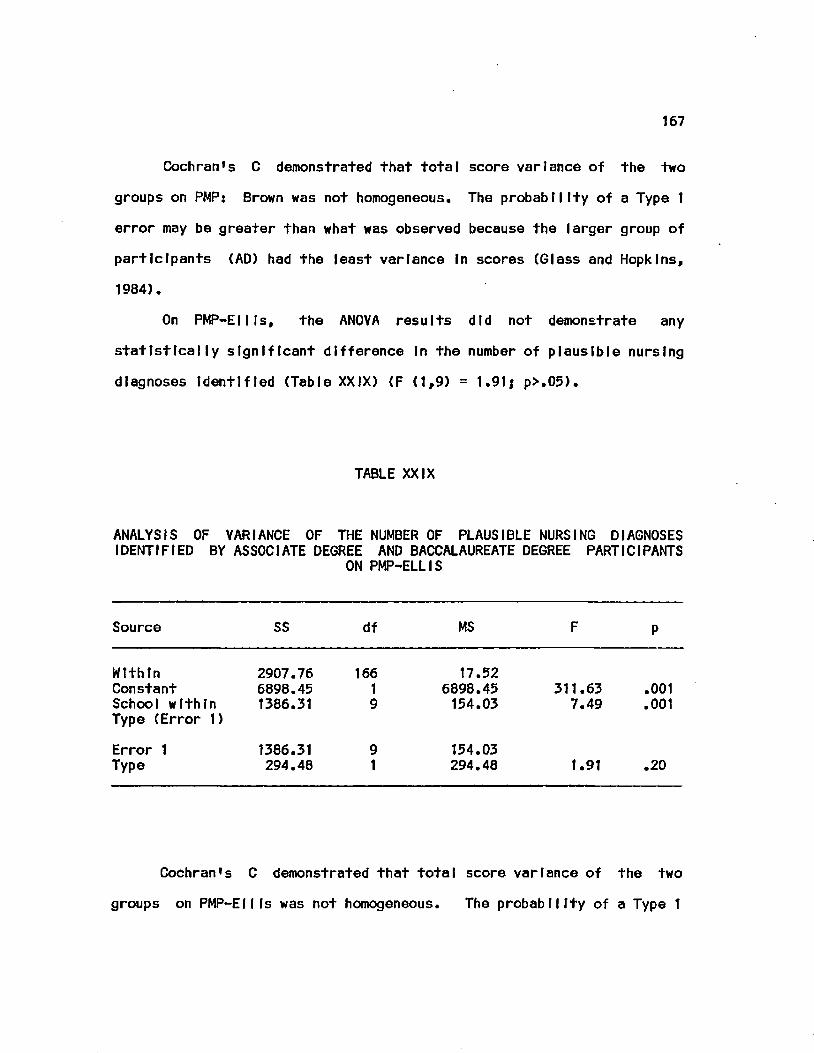
167
Cochran's C demonstrated that total score variance of the two
groups on PMP: Brown was not homogeneous. The probability of a Type 1
error may be greater than what was observed because the larger group of
participants (AD) had the least variance In scores (Glass and Hopkins,
1984).
On PMP-EII Is, the ANOVA results did not demonstrate any
statistically significant difference In the number of plausible nursing
diagnoses Identified (Table XXIX) (F (1,9) = 1.91j p>.05).
TABLE XXIX
ANALYSIS OF VARIANCE OF THE NUMBER OF PLAUSIBLE NURSING DIAGNOSES IDENTIFIED BY ASSOCIATE DEGREE AND BACCALAUREATE DEGREE PARTICIPANTS
ON PMP-ELLIS
Source SS df MS F P
Within 2907.76 166 17.52 Constant 6898.45 1 6898.45 311.63 .001 School within 1386.31 9 154.03 7.49 .001 Type (Error 1)
Error 1 1386.31 9 154.03 Type 294.48 1 294.48 1.91 .20
Cochran's C demonstrated that total score variance of the two
groups on PMP-Ellfs was not homogeneous. The probability of a Type 1
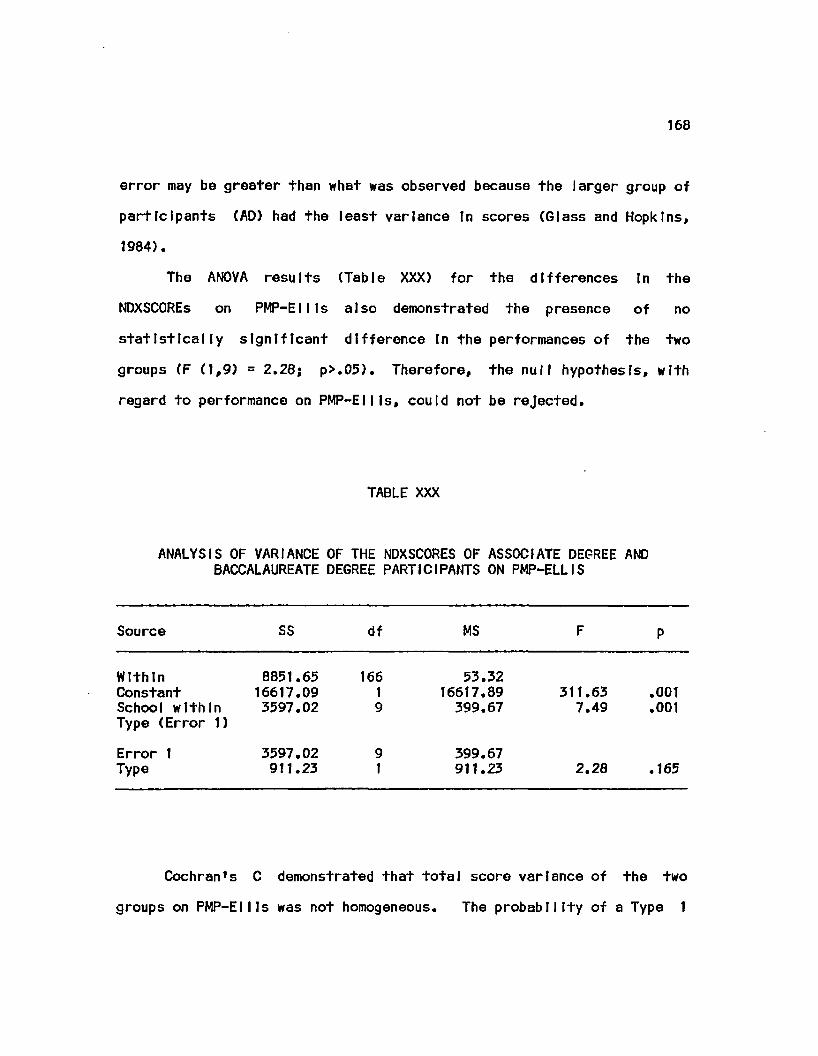
168
error may be greater than what was observed because the larger group of
participants (AD) had the least variance In scores (Glass and Hopkins,
1984).
The ANOVA results (Table XXX) for the differences In the
NDXSCOREs on PMP-EII Is also demonstrated the presence of no
statistically significant difference In the performances of the two
groups (F (1,9) = 2.28; p>.05). Therefore, the null hypothesis, with
regard to performance on PMP-EII Is, could not be rejected.
TABLE XXX
ANALYSIS OF VARIANCE OF THE NDXSCORES OF ASSOCIATE DEGREE AND BACCALAUREATE DEGREE PARTICIPANTS ON PMP-ELLIS
Source SS df MS F P
Within 8851.65 166 53.32 Constant 16617.09 1 16617.89 311.63 .001 School within 3597.02 9 399.67 7.49 .001 Type (Error 1)
Error 1 3597.02 9 399.67 Type 911.23 1 911.23 2.28 .165
Cochranfs C demonstrated that total score variance of the two
groups on PMP-EII Is was not homogeneous. The probability of a Type 1
169
error may be greater than what was observed because the larger group of
participants (AD) had the least variance In scores (Glass and Hopktnsf
1984).
Comparisons of the diagnostic ablliitles of the AD and BD
participants yielded contradictory findings. Both groups Identified
simtlar numbers of plausible nursing dtagnosls statements on both PMP-
Brown and on PMP-EII Is. However, on PMP-Brown, the BD participants
achieved a higher NDXSCORE than did the AD participants. This
Indicated that the BD participants Identified a significantly higher
number of more complete nursing diagnosis statements than the AD
participants. Therefore, for PMP-Brown, there was evidence supporting
rejection of the null hypothesis that there Is no difference In the
number and completeness of nursing diagnosis statements Identified by
the two groups. In contradiction to this finding, no statistically
significant difference was demonstrated between the performance of the
AD and BD participants on PMP-Ellls. Therefore, for performance on this
PMP, the null hypothesis could not be rejected.
G. Amount of plausible psychosocial nursing diagnoses Identified
The seventh research question to be answered was: When
graduating associate and baccalaureate degree nursing students are
compared. Is there a difference In the amount of psychosocial nursing
diagnoses Identified? Tables XXV and XXVI summarize the amount of
psychosocial nursing diagnoses Identified by AD and BD participants and
by all participants. On PMP-Brown, ANOVA results (Table XXXI)
demonstrated no statistically significant differences In amount of
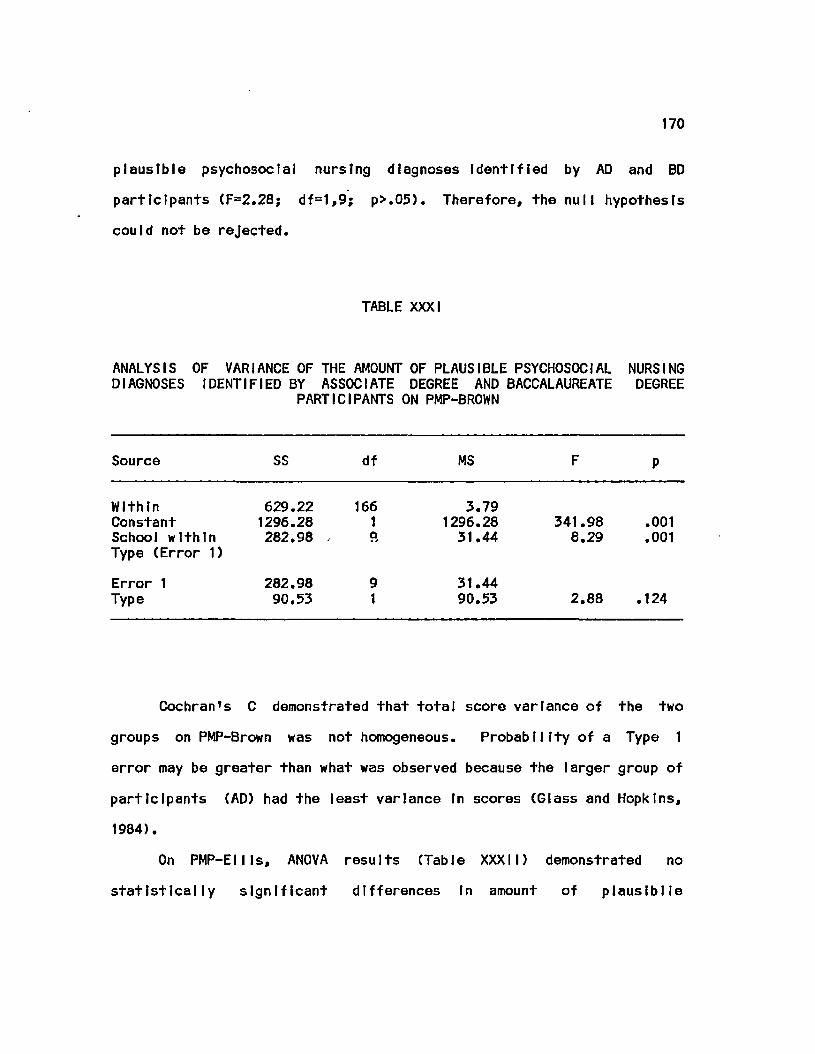
170
plausible psychosocial nursing diagnoses Identified by AD and BD
participants (F=2.28; df=1,9; p>.05). Therefore, the null hypothesis
could not be rejected.
TABLE XXXI
ANALYSIS OF VARIANCE OF THE AMOUNT OF PLAUSIBLE PSYCHOSOCIAL NURSING DIAGNOSES IDENTIFIED BY ASSXIATE DEGREE AND BACCALAUREATE DEGREE
PARTICIPANTS ON PMP-BROWN
Source SS df MS F P
Within 629.22 166 3.79 Constant 1296.28 1 1296.28 341.98 .001 School within 282.98 - 9, 31.44 8.29 .001 Type (Error 1)
Error 1 282.98 9 31.44 Type 90.53 1 90.53 2.88 .124
Cochran's C demonstrated that tota1 score variance of the two
groups on PMP-Brown was not homogeneous. Probability of a Type 1
error may be greater than what was observed because the larger group of
participants (AD) had the least variance In scores (Glass and Hopkins,
1984).
On PMP-ElI Is, ANOVA results (Table XXXII) demonstrated no
statistically significant differences In amount of plauslblle
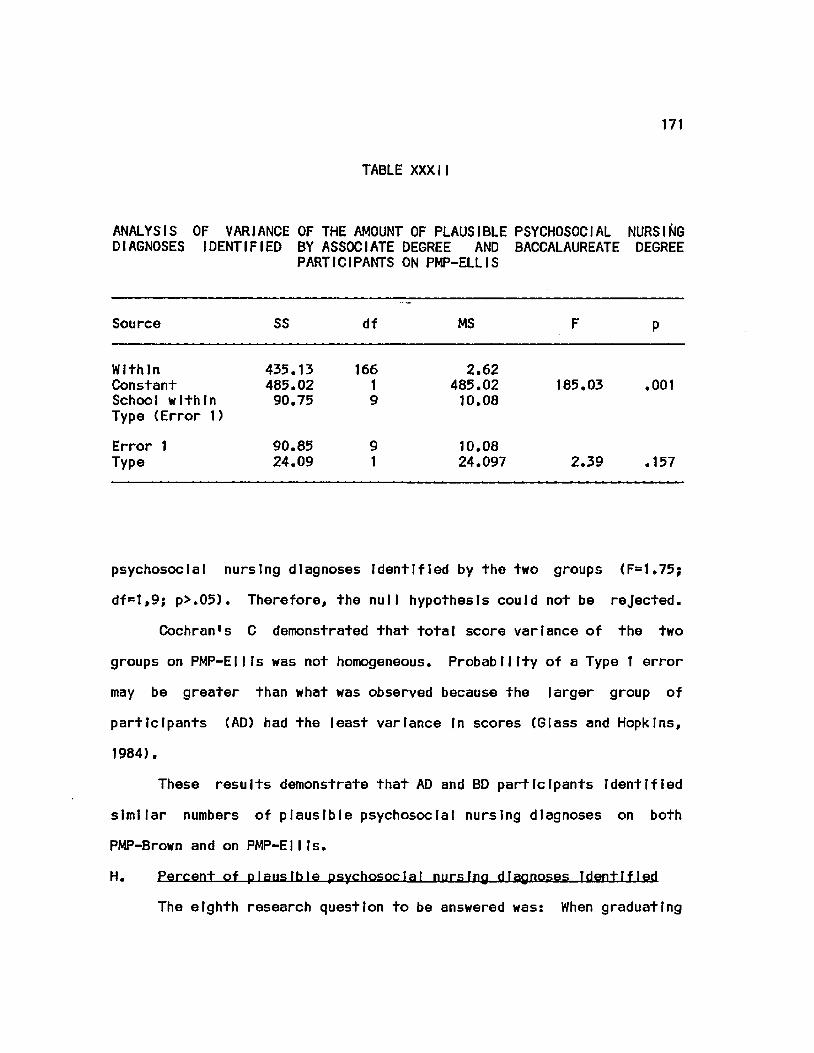
171
TABLE XXXII
ANALYSIS OF VARIANCE OF THE AMOUNT OF PLAUSIBLE PSYCHOSOCIAL NURSING DIAGNOSES IDENTIFIED BY ASSOCIATE DEGREE AND BACCALAUREATE DEGREE
PARTICIPANTS ON PMP-ELLIS
Source SS df MS F P
Within Constant School within Type (Error 1)
435.13 485.02 90.75
166 1 9
2.62 485.02 10.08
185.03 .001
Error 1 Type
90.85 24.09
9 1
10.08 24.097 2.39 .157
psychosocial nursing diagnoses Identified by the two groups (F=1.75;
df=l,9; p>.05). Therefore, the null hypothesis could not be rejected.
Cochran's C demonstrated that total score variance of the two
groups on PMP-EII Is was not homogeneous. Probability of a Type 1 error
may be greater than what was observed because the larger group of
participants (AD) had the least variance In scores (Glass and Hopkins,
1984).
These results demonstrate that AD and BD participants Identified
simitar numbers of plausible psychosocial nursing diagnoses on both
PMP-Brown and on PMP-EII Is.
H. Percent of plausible psychosoctal nursing diagnoses Identified
The eighth research question to be answered was: When graduating
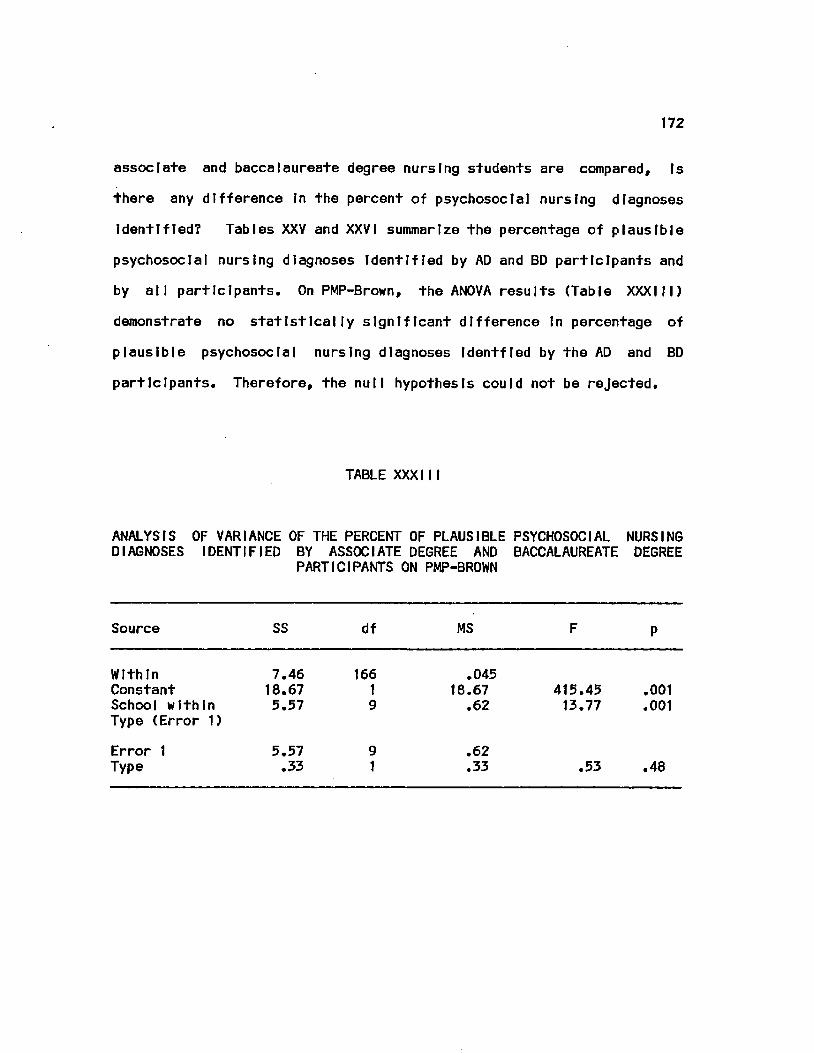
172
associate and baccalaureate degree nursing students are compared. Is
there any difference In the percent of psychosocial nursing diagnoses
Identified? Tables XXV and XXVI summarize the percentage of plausible
psychosocial nursing diagnoses Identified by AD and BD participants and
by all participants. On PMP-Brown, the ANOVA results (Table XXXIII)
demonstrate no statistically significant difference In percentage of
plausible psychosocial nursing diagnoses Identfled by the AD and BD
participants. Therefore, the null hypothesis could not be rejected.
TABLE XXXII I
ANALYSIS OF VARIANCE OF THE PERCENT OF PLAUSIBLE PSYCHOSOCIAL NURSING DIAGNOSES IDENTIFIED BY ASSOCIATE DEGREE AND BACCALAUREATE DEGREE
PARTICIPANTS ON PMP-BROWN
Source SS df MS F P
Within 7.46 166 .045 Constant 18.67 1 18.67 415.45 .001 School within 5.57 9 .62 13.77 .001 Type (Error 1)
Error 1 5.57 9 .62 Type .33 1 .33 .53 .48
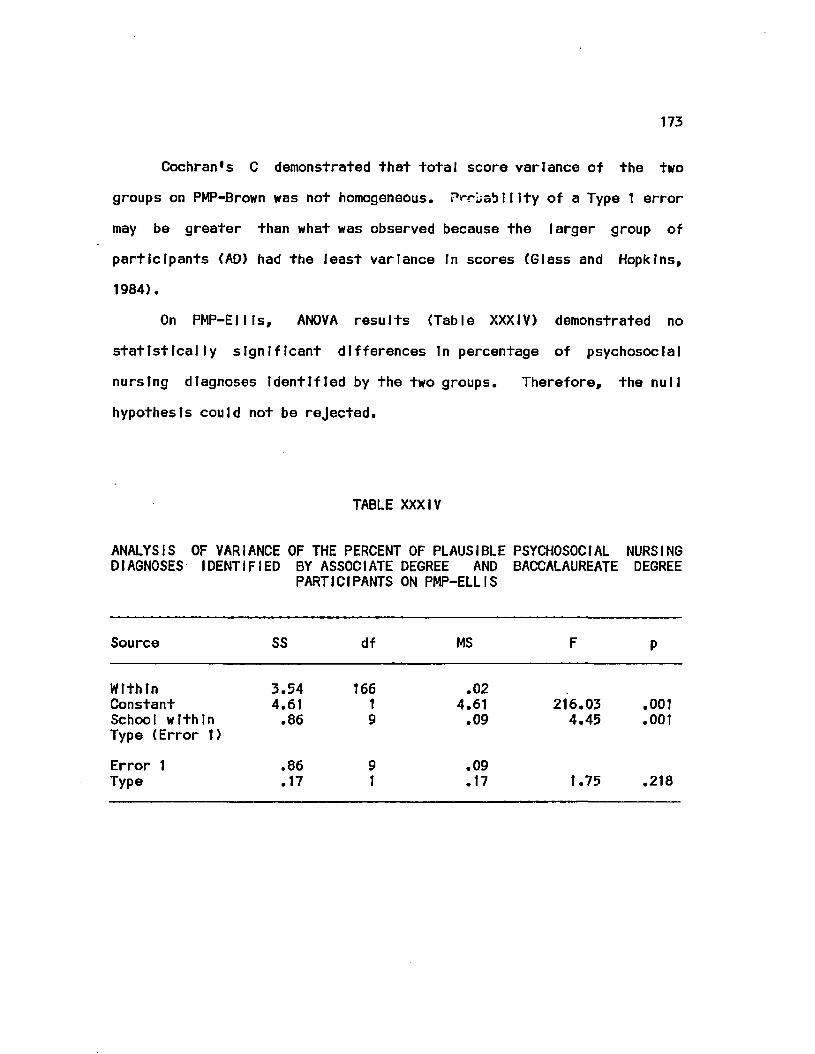
173
Cochran's C demonstrated that total score variance of the two
groups on PMP-Brown was not homogeneous. Prrbablllty of a Type 1 error
may be greater than what was observed because the larger group of
participants (AD) had the least variance In scores (Glass and Hopkins,
1984).
On PMP-Ellls, ANOVA results (Table XXXIV) demonstrated no
statistically significant differences In percentage of psychosocial
nursing diagnoses Identified by the two groups. Therefore, the null
hypothesis could not be rejected.
TABLE XXXIV
ANALYSIS OF VARIANCE OF THE PERCENT OF PLAUSIBLE PSYCHOSOCIAL NURSING DIAGNOSES IDENTIFIED BY ASSOCIATE DEGREE AND BACCALAUREATE DEGREE
PARTICIPANTS ON PMP-ELLIS
Source SS df MS F P
Within 3.54 166 .02 Constant 4.61 1 4.61 216.03 .001 School within .86 9 .09 4.45 .001 Type (Error t)
Error 1 .86 9 .09 Type .17 1 .17 1.75 .218
174
Cochran's C demonstrated that total score variance of the two
groups on PMP-EII Is was not homogeneous. Probability of a Type 1
error may be greater than what was observed because the larger group of
participants (AD) had the least variance In scores (Glass and Hopkins,
1984).
These results demonstrated that AD and BD participants Identified
similar percentages of plausible psychosocial nursing diagnoses on PMP-
Brown as we 11 as on PMP-EII Is.
I. Additional data analyses
The data were examined further and submitted to additional
analyses to determine 1) differences In participant performance on the
2 PMPs; 2) differences In the proportions of AD and BD participants
selecting Individual patient data Items; 3) frequencies of diagnostic
statement identification on each PMP; 4) differences In the proportions
of AD and BD participants citing Job or family stress as an etiology
for anxiety; and 5) differences In the types of learning experiences
engaged In by AD and BD patlclpants. The following subsections contain
the results of these analyses.
1. Differential performance on PMPs
A visual Inspection of the 8 Individual data collection and
nursing diagnosis Identification scores for PMP-Brown and PMP-EII Is
(Tables XV, XVI, XXV, and XXVI) revealed that In all but 1 Instance
(Number of psychosocial nursing diagnoses Identified) the differences
between the PMP-Brown and PMP-EII Is scores appeared to be disparate. To
175
explore this further, the data were submitted to a series of repeated
measures, one-way ANOVAs.
The within subjects results of these ANOVAs are reported In Table
XXXV. Statistically significant differences were observed across all 8
scores. The scores for data collection efficiency and proficiency,
amount and percent of psychosocial data selected, and amount and
percent of psychosocial nursing diagnoses Identified were higher on
PMP-Brown than on PMP-Ellls. Scores for number of plausible nursing
diagnoses Identified and NDXSCORE were higher on PMP-EIHs than on PMP-
Brown. These results Indicate that the participants performed
differently on the two PMPs.
2. Proportion of AD and BP participants selecting Individual
data Items
The efficiency and proficiency scores only provide an
Indication of the quantities of essential, contributory, and non
essential data that were selected by participants. To determine If
AD and BD participants differed In their selection of Individual data
Items, the proportions of AO and BD participants selecting each Item 2
was subjected to X analysis.
Statistically significant differences were demonstrted for 9 of
the 140 Items In PMP-Brown and for 4 of the 147 Items In PMP-Ellls. 2
The proportions of participants selecting these Items and the X
statistics are reported In Tables XXXVI. Of the 9 Items In PMP-Brown,
1 Item Is from the history section (family history of similar symptoms;
2 from the physical examination section (observation and palpation of
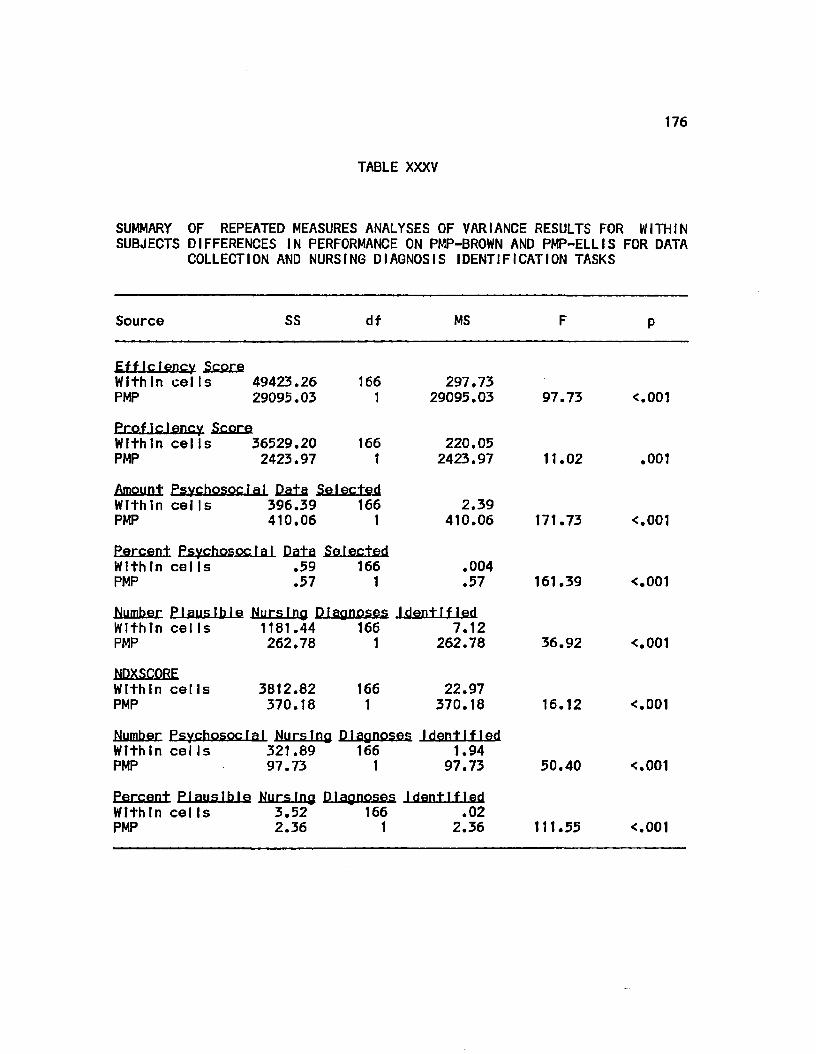
176
TABLE XXXV
SUMMARY OF REPEATED MEASURES ANALYSES OF VARIANCE RESULTS FOR WITHIN SUBJECTS DIFFERENCES IN PERFORMANCE ON PMP-BROWN AND PMP-ELLIS FOR DATA
COLLECTION AND NURSING DIAGNOSIS IDENTIFICATION TASKS
Source SS df MS
EffIclency SCSFB Within celts 49423.26 166 297.73 PMP 29095.03 1 29095.03 97.73 <.001
ProfIclency Score Within cells 36529.20 166 220.05 PMP 2423.97 1 2423.97 11.02 .001
Amount Psychosocial Data Selected Within cells 396.39 166 PMP 410.06 1
2.39 410.06 171.73 <.001
Percent Psychosocrai Data Selected Within cells .59 166 PMP .57 1
.004
.57 161.39 <.001
Number Plausible Nursing Diagnoses .l.dmt.liJsd Within cells 1181.44 166 7.12 PMP 262.78 1 262.78 36.92 <.001
NDXSCORE Within eel Is PMP
3812.82 370.18
166 1
22.97 370.18 16.12 <.001
Number PsychesocI a I Nursing Diagnoses Identified Within cells 321.89 166 1.94 PMP 97.73 1 97.73 50.40 <.001
Percent Plausible Nursing Diagnoses Identified Within cells 3.52 166 .02 PMP 2.36 1 2.36 111.55 <.001
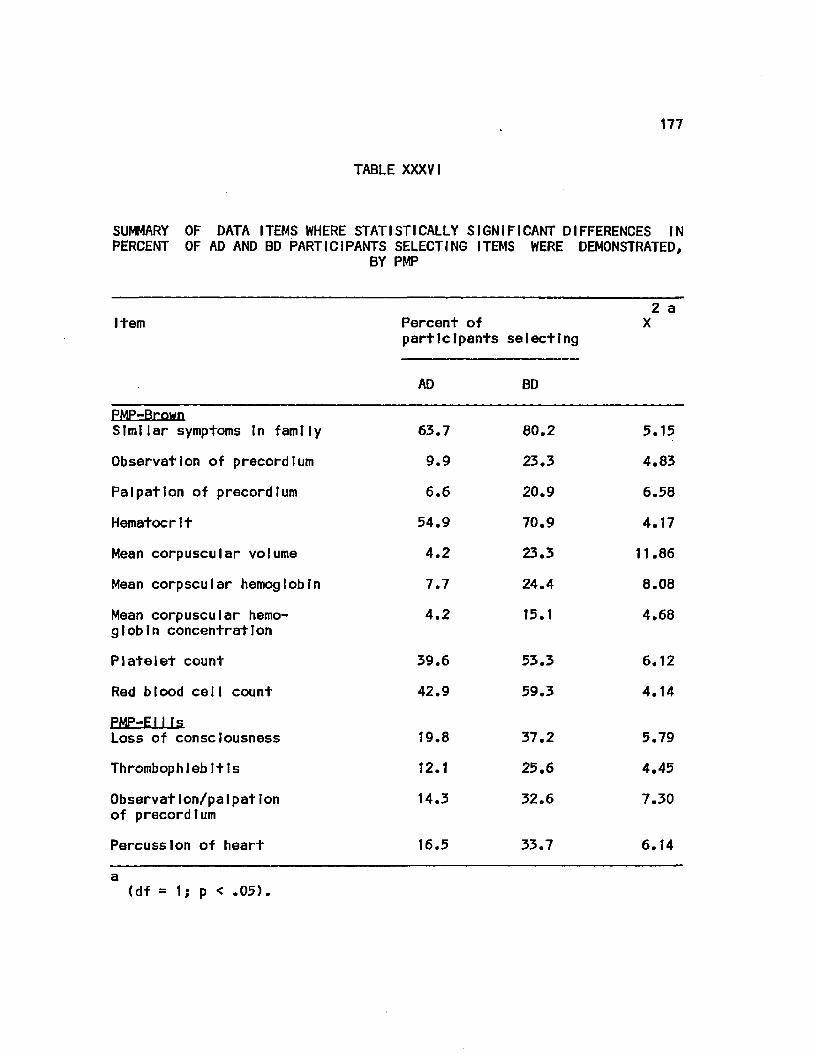
177
TABLE XXXVI
SUMMARY OF DATA ITEMS WHERE STATISTICALLY SIGNIFICANT DIFFERENCES IN PERCENT OF AD AND BD PARTICIPANTS SELECTING ITEMS WERE DEMONSTRATED,
BY PMP
Item Percent of participants selecting
2 a X
AD BD
PMP-Brown Similar symptoms In family 63.7 80.2 5.15
Observation of precordtum 9.9 23.3 4.83
Palpation of precordfum 6.6 20.9 6.58
Hematocrit 54.9 70.9 4.17
Mean corpuscular volume 4.2 23.3 11.86
Mean corpscular hemoglobin 7.7 24.4 8.08
Mean corpuscular hemoglobin concentration
4.2 15.1 4.68
Platelet count 39.6 53.3 6.12
Red blood ceil count 42.9 59.3 4.14
PMP-E11 Is Loss of consciousness 19.8 37.2 5.79
Thrombophlebitis 12.1 25.6 4.45
Observation/palpation of precordlum
14.3 32.6 7.30
Percussion of heart 16.5 33.7 6.14
a (df = 1; p < .05).
178
the precordlum); and 6 from the laboratory section (hematocrit, mean
corpuscular volume, mean corpuscular hemoglobin, mean corpuscular
hemoglobin concentration, platelet count, and red blood cell count).
In all Instances, a greater proportion of BD than AD participants
selected these Items. With the exception of the history Item, all data
had been classified previously, by a panel of experts, as essential
data.
Of the 4 Items In PMP-EII Is, 2 Items were In the history section
(loss of consciousness and thrombophlebitis) and 2 were In the physical
examination section (observation and palpation of the precordlum and
percussion of the heart). However, only one of these (observation and
palpation of the precordlum) was classified as essential data.
Overall, these results Indicate there was very little dlffernce In the
proportions of AD and BD participants selecting each Item on either
PMP-Brown or on PMP-EII Is.
3. Frfiquftnry of diagnostic statement 1denttflcatTon
The participants Identified a total of 23 different nursing
diagnoses on PMP-Brown and 26 different nursing diagnoses on PMP-EII Is.
Frequency distributions of the 10 most frequently Identified nursing
diagnoses on PMP-Brown and PMP-EII Is, by all participants and by AD and
BD participants, are reported In Tables XXXVII and XXXVIII,
respectively. On PMP-Brown, the most frequently Identified nursing
diagnosis was Anxiety (n = 339). The most frequently Identified
nursing diagnosis with a physiological focus was Alteration In
Circulation (n = 98). On PMP-EII Is, the most frequently Identified

179
TABLE XXXVI I
FREQUENCY DISTRIBUTION OF NURSING DIAGNOSIS STATEMENTS IDENTIFIED MOST FREQUENTLY ON PMP-BROWN
Diagnosis Group
AD BD All
Anx1ety 145 194 339
Alteration In Circulation 68 30 98
Alteration In Cardiac Output: Decreased
29 51 80
Alteration In Individual Cop Ing
11 51 62
Fluid Volume Deficit 6 43 49
Knowledge Deficit 17 30 47
Alteration In Tissue Perfusion
9 29 38
Alteration In Comfort 2 35 37
Alteration In Nutrition: More than required
5 11 16
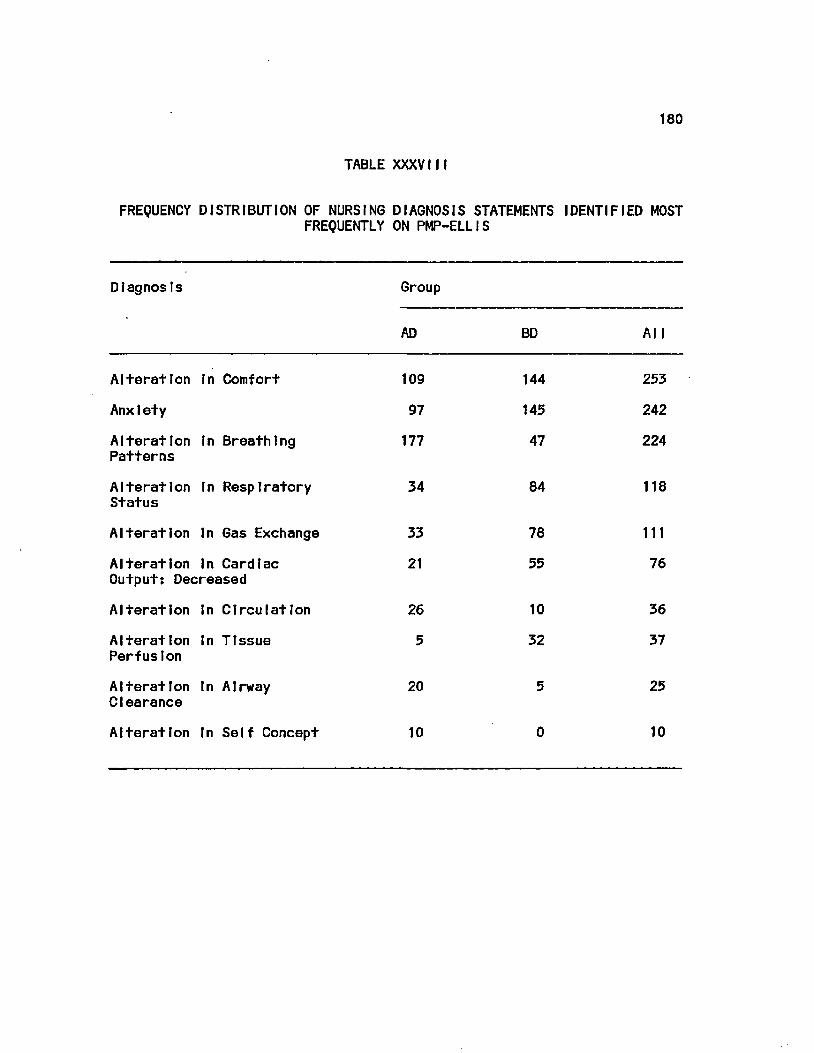
180
TABLE XXXVIII
FREQUENCY DISTRIBUTION OF NURSING DIAGNOSIS STATEMENTS IDENTIFIED MOST FREQUENTLY ON PMP-ELLIS
Diagnosis Group
A D B D A l l
Alteration In Comfort 109 144 253
Anxiety 97 145 242
Alteration In Breathing 177 47 224 Patterns
Alteration In Respiratory 34 84 118 Status
Alteration In Gas Exchange 33 78 111
Alteration In Cardiac 21 55 76 Output: Decreased
Alteration In Circulation 26 10 36
Alteration In Tissue 5 32 37 Perfusion
Alteration In Airway 20 5 25 Clearance
Alteration In Self Concept 10 0 10
181
nursing diagnosis was Alteration In Comfort (n = 252). The most
frequently Identified nursing diagnosis with a psychosocial focus was
Anxiety (n = 242).
A total of 112 different non-nursing diagnosis statements were
Identified on PMP-Brown and 124 on PMP-EIIIs. The most frequently
Identified non-nursing diagnosis on PMP-Brown was Hypertension or
descriptors Indicating this problem (I.e., elevated blood pressure,
etc) (n=185). Statements Indicating this problem were Identified a
total of 126 times by 22 AD participants (24?) and 59 times by 11
BD participants (13j0. Chi square analysis demonstrated no
statistically significant difference In the proportions of AD and BD
participants Identifying these statements.
On PMP-EIIIs, the most frequently Identified non-nursing
diagnosis statement was pneumonia or descriptors Indicating this
problem (I.e., resptratoy Infection, etc.) (n = 97). These statements
were Identified 76 times by 23 AD participants {25%) and 21 times by 3
BD participants (35?). Chi square analysis demonstrated a statistically
significant difference In the proportions of AD and BD participants 2
who Identified diagnostic statements representing pneumonia (X (1) =
16.63; p < .05).
4. Type referent Identified for the nursing diagnosis—Q±
Anxiety
On PMP-Brown, the nursing diagnosis, Anxiety was Identified
145 times by 45 AD participants <4956) and 194 times by 59 BD
participants (69JC). Chi square analysis demonstrated a statistically
182
significant difference in the proportions of AD and BD participants 2
Identifying this nursing diagnosis (X (1) = 7.39; p < .05). Further 2
analyses with X demonstrated that a greater proportion of the
diagnostic statements Identified by BD participants (26$) had a
referent indicting that anxiety was related to stress In the home or at 2
work than those Identified by AD participants (15j6) (X (1) = 3.99; p <
.05).
5. Differences in learning experiences
Differences In classroom and clinical learning experiences
of the AD and BD participants were examined. Two questions on the
Backgrond Inventory (Bl) requested participants to Indicate the number
of contact hours spent In various types of learning experiences where
the nursing care of patients similar to those represented by PMP-Brown
and PMP-Ellls were discussed. The types of learning experiences listed
on the Bl were: lecture, lecture-discussion, discussion, seminar, and
conference.
An examination of the descriptive statistics and the frequency
distributions demonstrated the unreliability of the data that were
collected. In 8 of the 11 programs, participants' time estimates
varied greatly (I.e., estimates ranged between 1 and 20 hours of
lecture within a single program). Therefore, additional analyses were
not undertaken.
Nine additional questions on the Bl requested participants to
Indicate the number of patients they had cared for with medical
diagnoses similar to the simulated patients, the level of difficulty
183
experienced completing each simulation, how well they felt their
educational program prepared them to deal with the simulated situations,
their familiarity with nursing diagnosis terminology, the frequency
that nursing care plans were Initiated or updated, and the degree of
emphasis on problem solving within their curriculum. The descriptive
statistics and the ANOVA results are reported In Table XXXIX. No
differences were found when the experiences of the AD and BD
participants were compared.
An examination of program catalogs and other available printed
materials from each program did not provide any additional Information
regarding the types and amounts of time spent In learning activities
related to the content of the 2 PMPs.
J. Summary
Influence of type of nursing educational preparation on the
assessment abilities of graduating AD and BD students was examined
using a path analytic procedure. Direct and indirect effects of type
program attended on assessment ability, on the hypothesized causal
model for PMP: Brown performance. Indicated a strong direct effect
(.74) and a moderate overall effect (.41). Although the fit of this
model was not supported statistically. It was accepted on theoretical
grounds.
In contrast, direct and Indirect effects of type program attended
on assessment ability, on the hypothesized causal model for PMP: Ellis
performance, indicated a negative and negligible Influence. Direct and
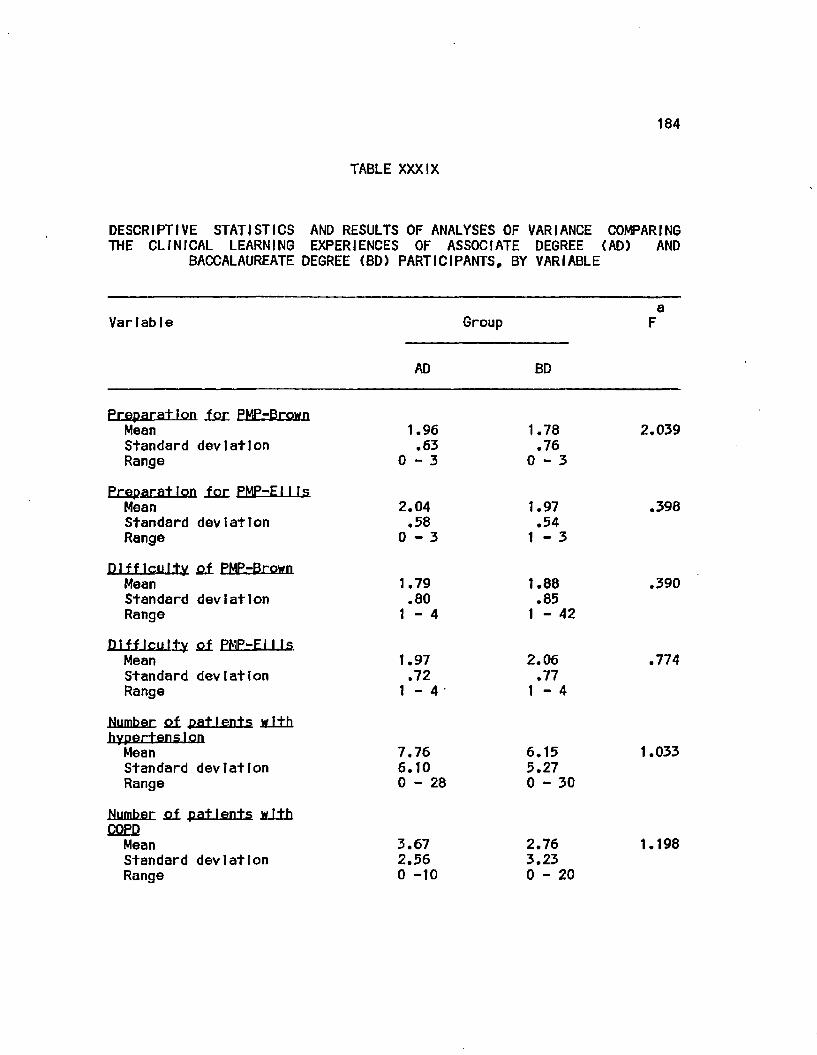
184
TABLE XXXIX
DESCRIPTIVE STATISTICS AND RESULTS OF ANALYSES OF VARIANCE COMPARING THE CLINICAL LEARNING EXPERIENCES OF ASSOCIATE DEGREE (AD) AND
BACCALAUREATE DEGREE (BD) PARTICIPANTS, BY VARIABLE
a Variable Group F
AD BD
Preparation ,f.or PMPrBrown Mean Standard deviation Range
Preparation ion PMP-EII Is Mean Standard deviation Range
Difficulty q± PMP-Brown Mean Standard deviation Range
Difficulty q± PMP-EII Is Mean Standard deviation Range
Number £f patients with hypertension Mean Standard deviation Range
Number M patients with COED
Mean Standard deviation Range
1.96 .63
0 - 3
2.04 .58
0 - 3
1.79 .80
1 - 4
1.97 .72
1 - 4
7.76 6.10 0 - 2 8
3.67 2.56 0 -10
1.78 .76
0 - 3
1.97 .54
1 - 3
1.88 .85
1 - 42
2.06 .77
1 - 4
6.15 5.27 0 - 3 0
2.76 3.23 0 - 2 0
2.039
.398
.390
.774
1.033
1.198
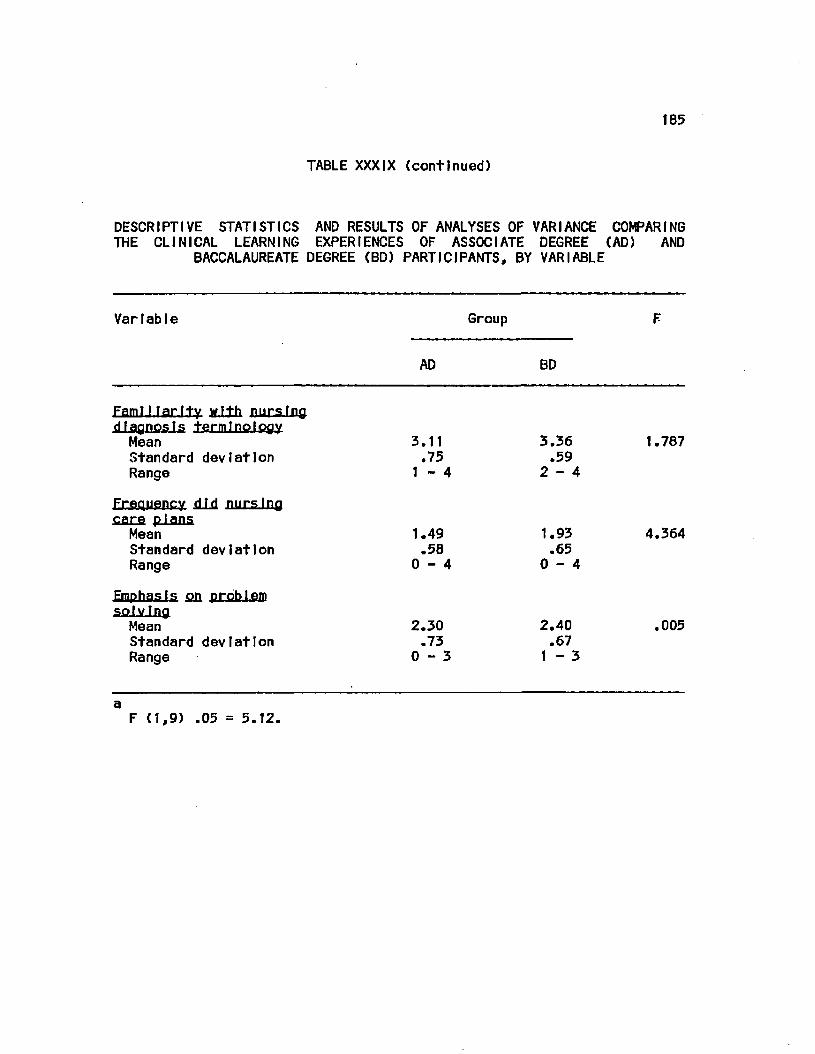
t85
TABLE XXXIX (continued)
DESCRIPTIVE STATISTICS AND RESULTS OF ANALYSES OF VARIANCE COMPARING THE CLINICAL LEARNING EXPERIENCES OF ASSOCIATE DEGREE (AD) AND
BACCALAUREATE DEGREE (BD) PARTICIPANTS, BY VARIABLE
Variable Group
AD BD
Famt I larity y.fth nursing diagnosis terminology Mean 3.11 3.36 1.787 Standard deviation .75 .59 Range 1-4 2-4
Frequency slid nursing care plans Mean 1.49 1.93 4.364 Standard deviation .58 .65 Range 0-4 0-4
Emphasis £& problem solving Mean 2.30 2.40 .005 Standard deviation .73 .67 Range 0-3 1-3
a F (1,9) .05 = 5.12.
186
effect coefflcents were both -.06. Fit of this model was supported on
statistical grounds In addition to theoretical grounds.
Differences In data collection and nursing diagnosis
Identification activities of AD and BD participants were examined using
a series of one-way, nested ANOVAs. The purpose of these analyses was
to determine If there were any differences between the two groups with
regard to data collection efficiency, data collection proficiency,
number and percent of psychosocial history data selected, number and
completeness of plausible nursing diagnosis statements Identified, and
number and percent of plausible psychosocial nursing diagnoses
Identified. Performance on each PMP was analyzed separately.
The only statistically significant (p<.05) difference
demonstrated was in the NDXSCORE for PHP: Brown. The BD participants
identified a significantly greater number of more complete nursing
diagnosis statements than did AD participants.
Additional analyses demonstrated that the 1) proportion of AD and
BD participants selecting individual data Items differed significantly
in only 9 Items on PMP-Brown and In 4 Items on PMP-Ellls; and 2) a
significantly greater proportion of BD participants Identified
stressors at home or at work as the etiology for Anxiety In PMP-Brown.
In addition, the most frequently Identified nursing diagnosis
statements on PMP-Brown were Anxiety and Alteration In Circulation;
those on PMP-Ellls were Alteration In Comfort and Anxiety. Repeated
measures ANOVAs demonstrated that participants performed differently on
187
PMP-Brown than on PMP-Ellls. Due to unreliable data, differences In
learning experiences of the two groups could not be Identified.
The following chapter Includes a discussion of the conclusions
that can be drawn from these findings, their Implications, and
recommendatIons for further study.
V. DISCUSSION
The purpose of this study was to examine the Influence of type of
educational preparation on data collection and nursing diagnosis
Identification abilities of generic nursing students within 3 months of
graduating from associate degree (AD) and baccalaureate degree (BD)
nursing programs. To achieve this goal, the performance of AD and BD
students on two simulated clinical situations was examined. The
primary research question addressed by this study was: Are the patient
assessment abilities of AD and BD nursing students, when measured
within 3 months prior to graduation from a program of study accredited
by the National League for Nursing, Influenced by type of educational
program? The seven, secondary questions addressed were: When
graduating AD and BD nursing students are compared. Is there a
difference In 1) data collection efficiency, 2) data collection
proficiency, 3) number of psychosocial data Items selected, 4) percent
of psychosocial data Items selected, 5) number and completeness of
plausible nursing diagnoses Identified, 6) number of psychosocial
nursing diagnoses Identified, and 7) percent of psychosocial nursing
diagnoses Identified.
A. Conclusions
The findings did not provide conclusive evidence that the type of
educational program attended influenced assessment ability.
Performance on one clinical simulation (PMP-Ellis) demonstrated that
type of program attended had a small and negative effect on assessment
188
189
ability and resulted In demonstration of no differences In performance
on data collection and diagnostic tasks. However, on a second
simulation (PMP-Brown), type of program attended had a strong, positive
Influence on overall assessment abllty. In addition, statistically
significant difference was demonstrated for one measure of diagnostic
ability. The BD participants Identified a greater number of more
complete nursing diagnosis statements than did AD participants. This
finding provided partial support for claiming a difference In the
diagnostic abilities of the two groups. This claim was further
supported by findings on PMP-Ellls; although not statistically
significant, the scores of the AD and BD participants were In the same
direction as those on PMP-Brown.
It also was demonstrated that the participants performed
differently on the two clinical simulations. They were less efficient
and proficient In data collection, but Identified a greater number of
plausible nursing diagnosis statement on PMP-Ellls than on PMP-Brown.
The purpose of this chapter Is to discuss the findings and their
Implications for nursing education and practice. Recommendations
for further study will also be discussed.
1. Assessment ability
Assessment ability was defined as a composite of three
variables: data collection efficiency score, data collection
proficiency score, and the NDXSCORE - an Indicator of the number and
completeness of plausible nursing diagnoses Identified. The
conceptual framework for the study stated that assessment ability was
190
Influenced by the level of educational preparation In nursing, age,
gender, theoretical knowledge base, critical thinking ability, post-
high school education, task complexity and task setting. The
conceptualized relationships among these factors was diagramed In
Figure 1. Due to the small number of men participating, the Influence
of gender was not considered during data analysis. Task setting was
controlled through use of 2 different clinical simulations.
Path analyses of models representing factors Influencing
assessment performance on PMP-Brown and PMP-ElI Is demonstrated
contradictory outcomes. On PMP-Brown, the magnitude of direct effect
(.74) and total effect (.41) coefficients Indicated that, when other
factors In the conceptual model were controlled, type of program
attended had a very strong, positive causal Influence on assessment
ability. The positive direction of these coefficients Indicated that
participants from BD programs performed at a higher level on the
outcome variable than did those from AD programs.
In contrast to these findings, the magnitude of direct effect (-
.06) and total effect (-.06) coefficients for the PMP-Ellls model
Indicated that type of program attended had a small, negative Influence
on assessment ability. The negative direction of these coefficients
Indicated that participants from AD programs performed at a higher
level on the outcome variable than did those from BD programs.
A factor contributing to differences In influence of program
attended on measures of assessment ability may be attributed to
learning histories of the participants. The goals, scope and depth of
191
format educational content and the clinical learning experiences of AD
and BD programs differ In many respects. Johnson (1966) noted that
content In AO programs focused on knowledge required to Identify and
take appropriate action In common, concrete and specific problems
experienced by patients. In BD programs, the focus was on theoretical
explanations for responses to Illness or factors leading to Illness.
In addition, principles, concepts and theories of basic sciences are
examined with relation to their ability to explain or predict patient
responses or modes of Intervention.
Information regarding the learning experience activities In
classroom and clinical settings was obtained. However, that related to
types and amounts of classroom activities was unreliable and could not
be used. Examination of reported clinical learning experiences (Table
XXXIX) revealed no statistically significant differences between the
two groups for: number of patients cared for with medical diagnoses
similar to those simulated; perceived difficulty of the simulated
experiences; level of perceived educational preparation for dealing
with the simulated patients* problems; frequency nursing care plans
were developed; familiarity with nursing diagnosis terminology; or
emphasis on problem solving behavior within the program of study.
It Is possible that the problems represented by the two
simulations may have some bearing on the differential performance of
the two groups when considered In relation to the focus of course
content In AD and BD programs. The opening scene for PMP-Brown
provides very little Information about the patient's problems. All
192
that Is known Is that a middle-aged black male comes to the clinic with
a history of eplstaxts and displaying minor symptoms of anxiety. There
Is no Information provided as to the possible cause of his problem.
Only through data collection Is It revealed that he has an elevated
blood pressure and Is under stress due to changes In Job and home
responslblIitles.
As demonstrated by the various data collection scores and the
number of plausible nursing diagnoses Identified (Tables, XV, XVII,
XIX, XXI, XXIII, XXV, XXVII, XXXI, AND XXXIII), AD and BD participants
collected similar amounts and types of data and Identified similar
numbers and types of nursing diagnosis statements. However, the
NDXSCOREs were significantly different (Table XXVIII). Further
examination of the referents for the nursing diagnosis, Anxiety (the
most frequently Identified nursing diagnosis) revealed that a greater
proportion of BD than AD participants were able to Identify that the
anxiety was related to occupational and domestic stressors.
When these findings are considered In relation to the academic
backgrounds of the two groups. It Is the BD program that contains a
greater concentration of course work In the behavioral sciences and an
emphasis on using this Information to determine the specific bases for
the recognition of problems (Johnson, 1966; National League for
Nursing, 1982).
In contrast, PMP-EIIIs represents a patient experiencing an acute
physiological problem (pneumonia supertmposed on chronic bronchitis)
manifested by complaints of chest pain and difficulty breathing. The
193
situation occurs In an acute medical-surgical unit. Examination of all
data collection and nursing diagnosis scores (Tables XVI, XVIII, XX
XXII, XXIV, XXVI, XXVII, XXVIII, XXX AND XXXII) demonstrated no
differences In the performance of the 2 groups. The similarity In
performance can be attributed to the type of patient situation
encountered and the focus of the learning activities In the 2 types of
educational programs.
The nature and severity of the patient's complaints. In addition
to the wife's plea to help her husband because "he Is having a heart
attack" Indicates the existence of a situation that needs to be dealt
with Immediately. The situation also represents the possible ex Istance
of 2 commonly occurring problems (acute respiratory and cardiac
diseases) (Luckman and Sorensen, 1980). The combination of 1) an
emergency situation, 2) a basic phystologcal problem, 3) a commonly
occurIng problem, and 4) the structured setting In which the situation
takes place may be responsible for the similarity In performance of the
AD and BD graduates. The objectives and content of BD programs are
directed towards preparing the graduate to perform In a variety of
settings, while those for AD programs are directed towards preparing an
Individual who Is capable of functioning In a care giver role within a
structured, hospital setting (DeChow, 1967} Kramer, 1981} SchlotfeJdt,
1967). Although no documentation could be found, It Is also highly
possible that both types of programs would Include similar content
regarding basic data to be collected and the nursing problems
experienced when a patient manifests respiratory and/or cardiac
194
distress. Whether this Is responsible for the lack of significant
differences In the data collection and nursing diagnosis scores, or for
the AD students demonstration of a slightly greater assessment ability
Is open to speculation.
2. Diagnostic ablIIty
One component of patient assessment Is the ability to
Identify nursing diagnoses. The statistically significant, higher
NDXSCORE of BD participants on PMP-Brown Indicated they were able
to Identify more complete diagnostic statements than AD participants.
Since there was no statlstlcaly significant difference In the number of
nursing diagnoses Identified, this finding reflects the ability to
determine plaslble referents (or etiologies) for the Identified nursing
diagnosis stems. Although not statistically significant, the findings
on PMP-EII Is were In the same direction.
The lack of differences In the numbers of nursing diagnoses
Identified, on both PMPs, can be related to the learning experiences
provided In both types of programs. Both groups of participants
reported similar levels of "familiarity" with nursing diagnosis
terminology.
Another factor contributing to Identification of similar numbers
of nursing diagnoses Is the frequency with which "Anxiety" was
Identified on both PMPs (Tables XXXVII and XXXVI11). The use of
"Anxiety" as both a medical diagnosis and a nursing diagnosis may be
responsible for the Inability to demonstrate any statistically
significant differences In either the number of plausible nursing

195
diagnoses Identified or In the number and percent of psychosocial
nursing diagnoses Identified. On PMP-Brown, Anxiety was the most
frequently Identified nursing diagnoses by all participants (n = 339)
and by AO (n = 145) and BD (n = 194) participants. This Is In
comparison to the second most frequently Identified nursing diagnosis,
Alteration In Circulation (all = 98; AO = 68; BD = 30). Similarly, on
PMP-EIils, Anxiety was Identified 242 times by all participants (AD =
97; BD = 145). The frequency with which this diagnosis was Identified
was exceeded only by Alteration In Comfort (All = 253; AD = 109; BD =
253).
The diagnostic statements were Identified on each PMP following
the selection of patient Information from the history, physical and/or
laboratory data sections. Data collection abilities of the AD and BD
participants will be addressed In the next section.
3. Data col lection ability
Performance on data collection activities will be discussed
In terms of differences In the efficiency and proficiency of the
partlcpants and differences In the proportions of participants
selecting Individual data Items. influence of a cueing effect on the
magnitude of all efficiency and proficiency scores also will be
Included.
Data collection efficiency and proficiency scores reflect the
amounts of essential, contributory, and non-essenttat data selected and
the order In which the history, physical and laboratory data were
selected. The findings demonstrated that the two groups used similar
196
ratios of essential data to total data selected (efficiency) and
similar ratios of essential and non-essential data to the total amount
of essential data available (proficiency).
Both groups were much more efficient than proficient.
Approximately 61$ of all PMP-Brown data and 43J6 of all PMP-EII Is data
that they selected previously had been determined, by a panel of
experts, as essential for the Identification of the patients' problems.
Proficiency scores of 30$ and 24$, for PMP-Brown, and PMP-EIIIs,
respectively, Indicated that participants selected relatively few
essential and even fewer non-essential Items In comparison to the
total number of essential Items available, or they selected a
relatively large number of non-essential Items In relation to the
number of essential Items selected and total number of essential Items
available. In view of the magnitude of the efficiency score for PMP-
Brown, the low proficiency score Is probably a reflection of selection
of relatively little data, overall In relation to the total amount of
essential data available. For PMP-EIIIs, the low proficiency score Is
problably related to the low efficiency score (I.e., < 50$) which Is a
reflection of the selection of a large ratio of non-essential data to
essential data. In addition. If relatively little data was collected,
this would also lower the proficiency score.
Lack of a difference In data collection efficiency and
proficiency scores Indicates that the two groups collected similar
ratios of essential data to total data selected and were not very
proficient In their data collection. They collected Inordinate amounts
197
of non-esentlal data (as demonstrated on PMP-Ellls); additionally, they
did not Identify what data were essential to collect.
Efficiency and proficiency scores only Indicate the quantities of
different types of data that were selected. An examination of
proportions of AD and BD participants selecting each data Item, on each
PMP, revealed the presence of some differences (Table XXXVI). On PMP-
Brown, a greater proportion of BD participants selected 8 essential
Items and 1 contributory Item. On PMP-Ellls, a greater proportion of
BD participants selected 1 essential Item and 3 contributory Items.
Six of the 8 essential Items selected by the BD partlcpants on PMP-
Brown reflected the status of the patients hematopoetlc status. That a
greater proportion of the BD participants Identified the need to
examine these Indicators, In light of the patient complaints of
frequent nosebleeds, probably Is Indicative of differences In content
of AD and BD programs.
One factor that may be obscuring actual data collection and
proficiency abilities of both groups of participants Is the cueing
effect provided by lists of available data. Neuble et al. (1982),
Martin (McGuIre, 1980b) and McCarthy (1966) reported that cueing
effects of such lists result In artificial Inflation of patient history
and physical examination scores. When performance on cued and non-cued
tests was compared, substantial Increases were seen on the cued test In
both the total number of Items selected and In the numer of correct
Items selcted (McCarthy, 1966). Therefore, the performances of the AD
198
and BD par+Icpants on PMP-Brown and on PMP-Ellls may be artificially
Inflated.
4. Differential performance on the two simulations
An additional finding of this study was a demonstration of
a differential performance on the two PMPs. Statistically significant
differences were demonstrated between all data collection and nursing
diagnosis Identification scores on PMP-Brown and those of PMP-Ellls
(Table XXXV). Elsteln et al. (1978) concluded that case specificity
may be responsible for differences In performances across patients.
Case specificity refers to those factors that differentiate one type
of patient diagnostic and management problem from others (I.e.,
validity and reliability of patient data, types of data available, and
areas of expertise of the problem solver (physician)). In addition,
Bashook (1976) noted that data collection and diagnostic performance In
an emergency situation should be different from performance In a non
emergency situation due to time constraints tmposed on the decision
maker. Therefore, the differences In the task environment (I.e., a non
emergency clinic setting vs. a potential emergency setting) and content
of the two PMPs were probably responsible for the observed differences
In performance.
The Implications of these findings for nursing education and
nursing practice are discussed In the next section.
B. Imp IIcatIons
The need to distinguish between the nursing practice of AD and BD
graduates Is of primary concern to nurse educators, nursing service
199
administrators, the nursing profession as a whole, state licensing
boards and legislatures, and the public served by the profession. If
differences can be demonstrated In the assessment abilities of
graduates from AD and BD educational programs, these differences can
serve as the basis for further clarification of the roles and
responsibilities of the technical and professional nurse. If
differences can not be demonstrated, the educational practices within
the two types of programs need to be re-examined and defined In terms
of expected outcomes.
Although path analyses of the models constructed to explain the
Influence of type educational program attended on overall assessment
abilities provided conflicting results, the demonstration of
statistically significant differences In the diagnostic ability of AD
and BD participants (on one PMP) does contribute to the differentiation
of the abilities of AD and BD graduates. Although no difference was
demonstrated In diagnostic ability on the second PMP, scores were In
the same direction; this finding adds support to a claim that BD
graduates Identify more complete nursing diagnosis statements than do
AD graduates.
If additional research findings can substantiate that BD
graduates are able to Identify more complete diagnostic statements
(I.e., Include a plausible etiological statement), this should have an
Impact on nursing practice. Such an etiological statement helps to
focus plans for Implementing nursing care that meets the specific needs
of Individual patients. Therefore, If the greater ability of BD
200
graduates to Identify complete, patient specific, nursing diagnoses can
be confirmed, this should result In nursing care that Is more specific
to the Individual needs of patients than that based on less complete
nursing diagnosis statements.
The use of non-nursing diagnosis statements by BD participants
does not comply with the Standards for Practice (ANA, 1973) or with the
Nurse Practice Acts In many polItlcal Jurisdictions (I.e., Illinois).
This finding has Implications for educators and administrators. If
nursing care Is to be based on the Identification of problems that
nurses are legally responsible and accountable to treat, terminology
used to describe these problems must reflect those problems and not
medical diagnoses. Students and graduates need to be Introduced to the
diagnostic task, and use of nursing diagnoses needs to be strongly
encouraged. In addition, all practicing nurses need to be Involved In
the ongoing processes of refining the diagnostic labels and validating
the defining characteristics that are essential for Identification of a
specific nursing diagnosis.
Although both groups of participants were equally proficient In
their data collection, the low magnitude of their scores Is cause for
concern. Mean proficiency scores ranged between 23.43 and 30.94.
Since the proficiency score was calculated as a ratio of essential data
Items minus the non-essential Items selected to the total number of
essential Items available, these low values Indicate that even though
the participants selected some essential data, they also were selecting
201
inordinate amounts of non-essential data, very few essential data In
relation to what were available, or both.
Given the unreliable and probabilistic nature of patient data
(Hammond, 1966; Koran, 1975a; 1975b; McNeil, 1975); collection of non-
esenttal data can contribute to diagnostic errors. Given the small
capacity of the short term memory (Miller, 1956), the collection of
non-essential data can lead to cognitive strain which In turn also can
contribute to diagnostic errors.
These findings have Implications for nurse educators, nursing
service administrators, and Inservlce educators. Efforts need to be
Initiated and/or continued to assist students and graduates In the
Identification of what data are essential to collect In a given
situation. Cognitive strain, also could be decreased by the use of
external memory aids such as decision trees. Such aids would reduce
the amount of information that needs to be retained and processed In
short term memory.
C. Recommendations
On the basis of this study, the following recommendations are
made for replication of the study and for additional study. The
recommendations pertaining to a replication of the study include
methodological Issues of sample selection. Instrumentation, and data
analysis.
Because participants in this study were a convenience sample
obtained from within randomly selected AD and BD programs, a selection
bias may have operated. Therefore, the findings can be generalized

202
only to comparable graduating students from AD and BD programs In the
three state region. It Is recommended that a random sample of
Individuals be used In future studies and that geographic boundaries be
enlarged.
The use of patient management problems that Incorporate a
branching type format should be continued In studies whose major
purpose Is to determine problem solving abilities. This format
provides a means whereby the study participant fs able to select an
approach to patient management while still providing the Investigator
with a means for controlling the study environment. In addition, as
reported In the literature review. It Is generally concluded that the
content validity of well constructed PMPs Is supported (Page and
Fielding, 1980.) The content, construct and criterion validity of the
PMPs used In this study were supported (Farrand et al., 1979; Holzemer
et al., 1981) as was the reliability (Farrand, personal communication,
1983).
In this study, performance on the clinical simulations was
analyzed using quantitative methods. Although this provided an
Indication of the performance abllftes of the two groups, additional
study also needs to be focused on the type of data collected by AD and
BD graduates. Data analysis In this study focused on the amounts of
essential, contributory, and non-essential data that were selected.
Although there were no statistically significant differences
demonstrated In the amounts of the data selected, this tells us nothing
about what data were specifically collected, what area(s) the data

203
collector focused on, or what data was used to support the Judgments
that specific nursing diagnoses were In fact present. Such measures
would provide greater Insight Into the data collection and nursing
diagnosis Identification abillltes of AD and BD graduates.
This study focused on only the assessment phase of the nursing
process. It Is recommended that future simulation studies be expanded
to Include goal setting. Identification of nursing Interventions and
evaluation of patient outcomes. Such an expansion would provide
Insight Into the abilities of AD and BD participants to apply these
processes. Because simulated clinical situations contain elements of
artificiality, consideration also needs to be given toward development
of reliable and valid methods of assessing performance in actual
clinical situations.
In this study, It Is possible that the long lists of available
data about each patient had a cueing effect on the participants and
resulted In score Inflation. As computerized technology becomes more
available It would appear that the next appropriate step would be to
move away from a latent Image format to a fully Interactive and
computerized simulation. If this type of format were used for testing,
the study participant would have to be provided with only the Initial
patient Information and would then be asked what type of Information
about the patient was desired. The participant then would have to
generate the categories of Information desired. In addition, the
computer could be programed to record each participant's progress thus
204
elImfna+lng the need for Inputlng this Information from hard-copy
formats.
The method of obtaining Information about participants' learning
histories and academic characteristics needs to be Improved. It was
found that self reports about previous experiences with situations
similar to those simulated were not a reliable source of estimated time
spent In related learning activities. It Is recommended that faculty
sources be used to obtain this type of data.
Depending upon the time available for testing, consideration
also should be given to administration of an Instrument designed to
test knowledge specific to the simulated situations. The cumulative
and nursing grade point averages and NCLEX - RN scores are general
Indicators of academic performance, and, with respect to GPAs, can not
be compared across Institutions.
The findings of this study also suggest several areas where
additional Investigation Is needed. The simulations used examined
performance only In relation to 2 different situations. Additional
study should be directed towards examining the performance of AD and BD
graduates on several different types of patient situations and In
several different settings. These replications would provide
additional Information relative to a differentiation of assessment
abilities of the two types of graduates.
Finally, this study examined performance only at one point In
time. The development and Implementation of longitudinal studies would
be beneficial In providing Information about whether performance
205
changes over time, what factors Influence any changes that occur, and
what direction do performance changes take.
C. Summary
The purpose of this study was to examine the direct and Indirect
Influences of type of educational program attended on data collection
and nursing diagnosis Identification abilities of generic nursing
students within three months of graduation from associate degree and
baccalaureate degree nursing programs.
The primary research question quldlng this study was: Are the
patient assessment abilities of associate and baccalaureate degree
nursing students Influenced by the type of educational program
attended. Additional research questions addressed were differences
between the associate and baccalaureate degree students with regard to
data collection efficiency, data collection proficiency, amount and
percentage of psychosocial data collected, number of plausible nursing
diagnoses Identified, and amount and percentage of psychosocial nursing
diagnoses Identified.
A non-equivalent groups, post-test only design was used. A
convenience sample of 91 associate degree and 86 baccalaureate degree
students was obtained from five randomly selected associate degree
programs and six randomly selected baccalareate degree programs within
a three state area In the mid-west. Participants completed the Watson-
Glaser Critical Thinking Appraisal (Form A), two latent Image,
branching type clinical simulations, and a background Inventory.
Analyses of variance, chl square and path analysis techniques were used

206
to analyze the data. Performance on each simulation was analyzed
separately.
Analysis of performance on one simulation demonstrated
differences In the diagnostic abilities of the two groups (F (1,9) e
5.16; p<.05). No differences were found In data collection efficiency
or proficiency, In amounts or percent of psychosocial data collected,
or In amounts or percent of psychosocial nursing diagnoses Identified.
Path analyses revealed differential effects of the type of program
attended on the assessment abilities of the participants. On one
simulation, the effect coefficient was .411 while on the other It was
-.067.
On one simulation, baccalaureate degree participants Identified a
greater number of more complete nursing diagnosis statements than their * t
associate degree counterparts. Performance of all participants
differed across the two simulated patient encounters, demonstrating the
Influence of case specificity. Although not conclusive, findings
provide partial support for the claim that type of educational program
attended Influences diagnostic ablllttes of the participants. This has
Implications for differentiation of clinical practice of the two type
of graduates.
APPENDICES
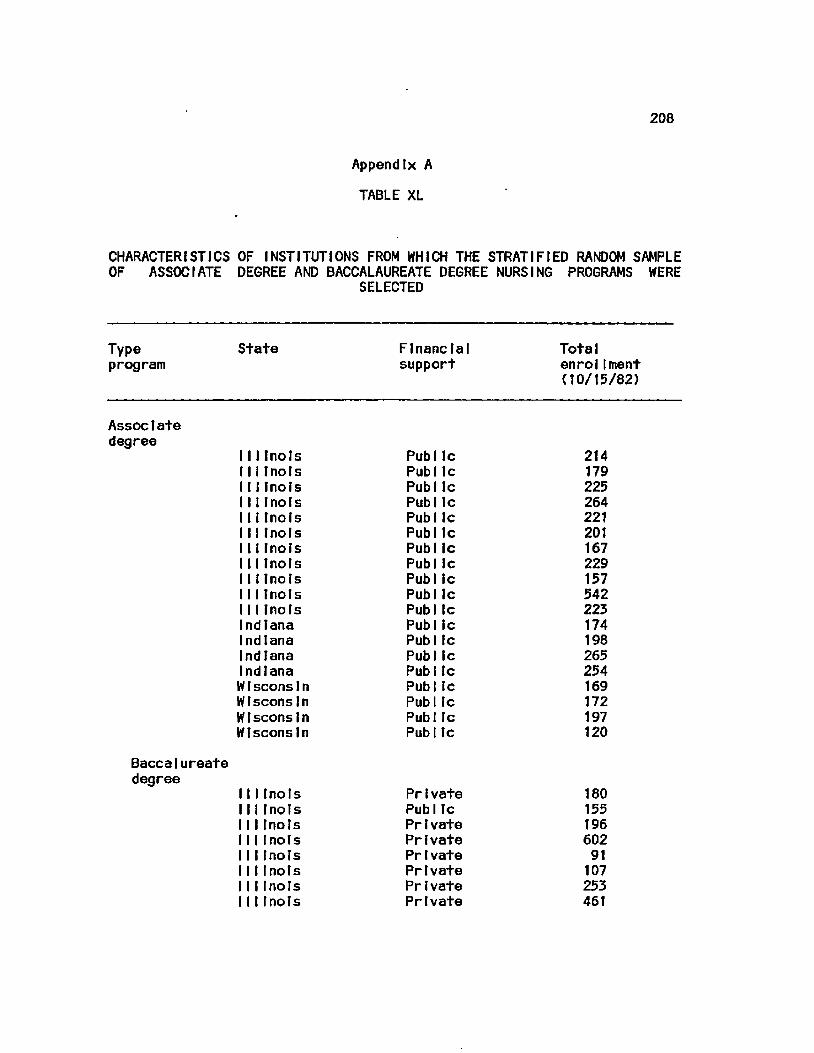
208
Appendix A
TABLE XL
CHARACTERISTICS OF INSTITUTIONS FROM WHICH THE STRATIFIED RANDOM SAMPLE OF ASSOCIATE DEGREE AND BACCALAUREATE DEGREE NURSING PROGRAMS WERE
SELECTED
Type State Financial Total program support enroltment
(10/15/82)
Assoc t ate degree
1111no Is Pub Ic 214 111Inots Pub Ic 179 1111noIs Pub Ic 225 1111 riots Pub Ic 264 111Inots Pub Ic 221 1111noIs Pub Ic 201 111Inots Pub Ic 167 1111noIs Pub Ic 229 1111no Is Pub ic 157 111tnols Pub Ic 542 111Inots Pub ic 223 Indiana Pub ic 174 Indiana Pub Ic 198 Indiana Pub ic 265 Indiana Pub Ic 254 W1 scons In Pub Ic 169 WIscons In Pub Ic 172 Wisconsin Pub Ic 197 Wisconsin Pub Ic 120
Baccalureate degree
Illinois Private 180 Illinois Public 155 Illinois PrIvate 196 Illinois Private 602 Illinois Private 91 Illinois PrIvate 107 Illinois Private 253 Illinois Private 461

209
Appendix A (continued)
TABLE XXXIX (continued)
CHARACTERISTICS OF INSTITUTIONS FROM WHICH THE STRATIFIED RANDOM SAMPLE OF ASSOCIATE DEGREE AND BACCALAUREATE DEGREE NURSING PROGRAMS WERE
SELECTED
Type State Financial Total program support enrolIment
(10/15/82)
Baccalaureate Degree (cont.)
111 Inols Pub 1 Ic 385 111Inols PrIvate 120 111Inols Private 119 111Inols PrIvate 216 111Inols PublIc 415 Indiana PrIvate 183 Indiana PrIvate 338 Indiana PublIc 134 WIscons In Public 1295 Wisconsin PrIvate 549 Wisconsin Pr1vate 199 Wisconsin PublIc 823 W1scons 1n Private 288
210
Append Fx B
LETTER TO DEANS AND DIRECTORS
Dear :
I seek your cooperation and that of your faculty to permit/encourage your senior students to participate In a study on clinical decision making. Student participation entails completion of two clinical sfmualatlons and related Instruments, a task that requires two hours of their time. It Is an educational experience since students will receive a copy of the optimal solutions to the simulations and an opportunity to receive feedback on personal performance In relation to group norms.
The use of decision making strategies within a nursing process framework Is an Important part of nursing today and Is receiving Increased emphasis as a means through which nursing can further establish Itself as an Independent profession. As part of my doctoral work In the College of Nursing at the University of Illinois at Chicago, I am conducting this Investigation of decision making strategies utilized by generic nursing students who are within three months of graduating from an NLN accredited nursing program. The findings from this Investigation will be useful to nurse educators and nursing service administrators who need Information to plan better utilization of new graduates.
To obtain a representative sample of Individuals entering the nursing profession, I have selected a stratified random sample of nursing programs from Illinois, Indiana, and Wisconsin and your program was Included In the sample. If you consent to participate, you will be asked to supply: a description of the parent Institution, the philosophy and conceptual framework of the nursing program and Its outcome objectives, a sample curriculum plan, the clock hour to credit hour ratio for classroom courses, and the average number of clock hours spent per week In clinical practice experiences for each term of the nursing program. I will need two hours with senior students either as a group or as a few groups at times, dates, and places of your choice during April through June, 1984. The experience Is such that It could be used as a clinical post-conference.
All Information Identifying students and nursing programs will be coded and kept confidential. If you desire, I shall supply your program with data summarizing the performance of your students.
In order to determine your Interest In helping with this study, I shall contact your office next week In order to make an appointment to speak with you.
Sincerely,
Carolyn J. Yocom R.N., M.S.N.
211
Appendix C
LETTER TO GRADUATING STUDENTS
Dear Graduating Student:
My name Is Carolyn Yocom and I am a doctoral candidate In the College of Nursing at the University of Illinois at Chicago. In conjunction with my dissertation, I am exploring the Influence of various educational factors and Individual characteristics on the clinical decision making abilities of new graduates. The results of this study should be useful to nurse educators In evaluating their curricula and to nursing service personnel In develop!Ing Inservlce programs.
As you approach graduation from your nursing program, I seek your participation In this study. Participation would Involve the completion of several questionnaires. Included are: (a) simulations of two different patient care situations In which you will be asked to select from IIsts of options, what approaches you would use to manage the patients' problems; (b) a questionnaire that assesses your critical thinking ability; and (c) a questionnaire that requests demographic and background Information. The amount of time required to complete these Is, approximately, two hours. A convenient time, between now and graduation, will be arranged for administration of these questionnaires.
All Information regarding Individual student participation and nursing programs will remain confidential and will be reported only In summary form without Identifying you or your Institution. Your participation or non-partIclpatlon will not affect your status within your own program since faculty will not have access to your responses.
I encourage you to participate In this research study. It provides you with a means of assessing your clinical decision making ability. The simulations permit you to work Independently through two different patient problems that occur In different clinical situations. They allow a means of assessing what you would do In a similar clinical situation without any risk associated with the outcomes, especially If you should take a less than beneficial approach to managing the patients' problems. Upon completion of the questionnaires, I will provide you with a summary of the optimal solutions to the patient management problems. In addition, following their scoring, I will provide you with your score and, for comparison, the group norms.
212
Appendix C (continued)
Your participation will make the results of this study more representative of all graduating nursing students and will permit broader conclusions and recommendations to be made. Participation would also fulfill a professional responsibility regarding your making a contribution to the Improvement of educational programs In schools of nursing and In the agencies and Institutions hiring new graduates.
If you are Interested In participating In this study, would you please sign your name on the sign-up sheet that Is available and indicate what day of the week and the times that you would have a two hour block of time available for me to administer the questionnaires. After I have looked at the responses, arrangements will be made for testing at one or two times that are convenient for the majority of those Indicating a desire to participate.
Thank you,
Carolyn J. Yocom R. N., M.S.N.

213
Appendix D
BACKGROUND INVENTORY
Directions!
The following Information about you Is requested to aid In summarizing and Interpreting your responses on the previous Instruments. Please provide as complete and accurate responses as possible. Study findings will be published only In summary form and no attempt will be made to Identify Individuals or specific schools.
Please respond by placing a check mark ( ) to the left of the appropriate response or by providing the requested Information.
A. Personal background:
1. Age:
2. Sex: (1) Female (2) Male
3. Current marital status:
(1) single (3) married (2) divorced (4) spouse deceased
4. Number of chtldren:
B. Educational Background
5. Check your approximate rank In your high school graduating class:
low / / / / / high BOTTOM 1/4 MID POINT TOP 1/4
6. What Is your current cumulative grade point average: .
7. What Is your current nursing grade point average: .
8. What scale Is your GPA calculated on:
(1) on a 4 point scale with nAM = 4 (2) on a 5 point scale with "A" = 5 (3) other (Specify)
214
Appendix D (continued)
9. Did you pursue any education beyond high school, but prior to entering your present educational program:
(0) No. Skip to question 12.
(1) Yes. If yes, number of years:
10. If answer above Is yes, what type of post high school Institution did you attend prior to your present program (excluding any pre-nurslng program): (check all that apply)
.(1) vocational or trade (5) military
.(2) hospital nursing program (6) business
.(3) Junior col lege (7) other (Specify).
.(4) senior college or university
11. If answer to question 9 was yes, what degree or certificate did you earn, If any: (check all that apply)
(0) none (4) BS or BA (1) LPN (5) MS or MA (2) RN (diploma) (6) Doctorate (3) AD, AAS, AA (7) Other (Specify)
12. What are your future educational plans:
(0) none (5) MS In other field (1) unsure (6) Doctorate in nursing (2) BS In nursing (7) Doctorate in other (3) BS In other field field (4) MS In nursing (8) Other (Specify)
13-15. Check highest level of educational attainment of:
13. Father I J J J J J J J J UJJJ tJJJJ UJJJ
14. Mother UJJJJJJJ UJJJ UJJJ UJJJ
15. Spouse UJJJJJJJ UJJJ UJJJ UJJJ
(years) 12345678 1234 1234 1234 elem. school h. sch. col. adv. ed.

215
Appendix D (continued)
C. Employment background and plans;
16. Years of health-care related work experience prior ±e present nursing education:
(If none, mark here: and skip to question 18)
17. This work was as a: (check all that apply)
(1) practical nurse (6) ward secretary (2) registered nurse (5) other (Specify) (3) nurses' aide
18. Years of non-education related health-care work experience during period of education: .
(If none, mark here and skip to question 20)
19* This work was as a: (check all that apply)
(1) practical nurse (6) ward secretary (2) registered nurse (5) other (Specify) (3) nurses' aide
20. After graduation do you plan (or hope) to be employed In a:
(1) hospital (5) nursing school (2) nursing home (6) physician's office (3) public/private (7) Industry
health agency (8) other (Specify) (4) public or private
school system
21. Five years from now, do you expect to be employed:
(1) full time In nursing (2) part time In nursing (3) outside of nursing (4) undecided (5) not at a 11
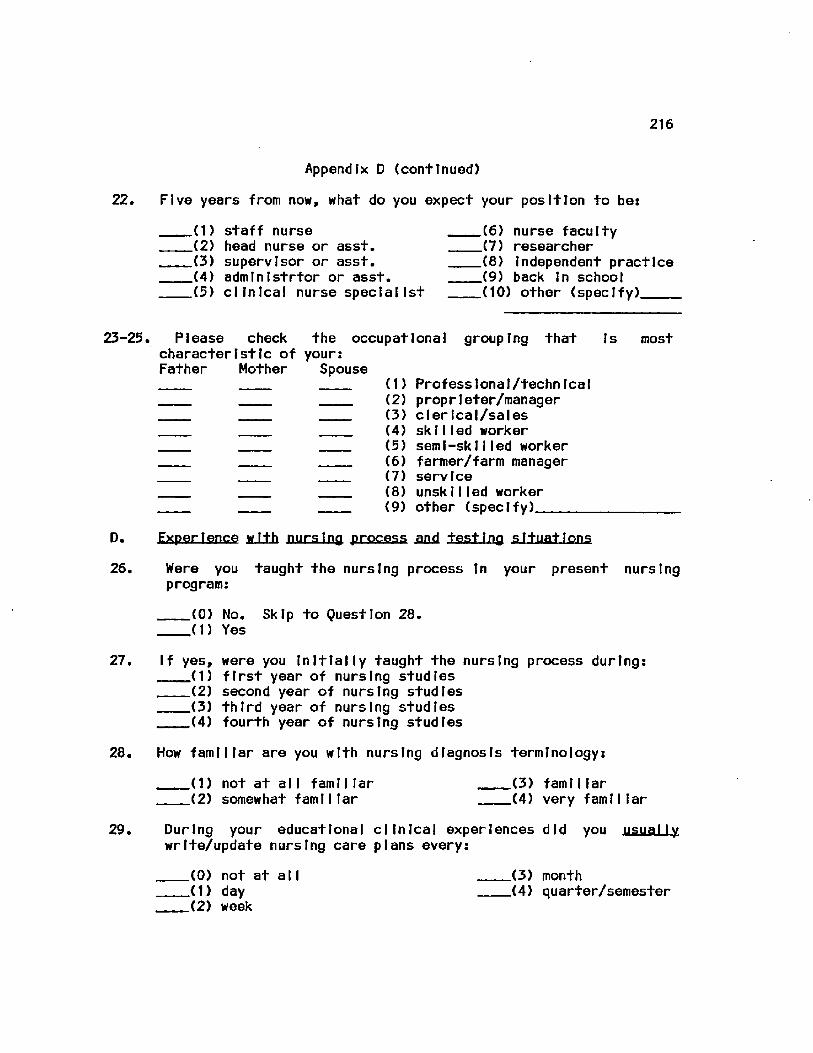
216
22.
Appendix D (continued)
Five years from now, what do you expect your position to be:
„(1) staff nurse .(2) head nurse or asst. .(3) supervisor or asst. .(4) adminIstrtor or asst. _(5) clinical nurse specialist
.(6) nurse faculty _(7) researcher .(8) Independent practice .(9) back In school .(10) other (specify)
23-25. Please check the occupational grouping that Is most characteristic of your: Father Mother Spouse
(1) Professional/technical (2) proprleter/manager (3) clerical/sales (4) skilled worker (5) semi-skilled worker (6) farmer/farm manager (7) service (8) unskilled worker (9) other (specify)
D. ExperIence w.I.th nursing process .and testing situations
26, Were you taught the nursing process In your present nursing program:
(0) No. Skip to Question 28. (1) Yes
27. If yes, were you Initially taught the nursing process during: first year of nursing studies second year of nursing studies third year of nursing studies fourth year of nursing studies
28. How familiar are you with nursing diagnosis terminology:
(1) not at all familiar (3) familiar (2) somewhat familiar (4) very familiar
29. During your educational clinical experiences did you usually write/update nursing care plans every:
(0) not at all (3) month (1) day (4) quarter/semester (2) week
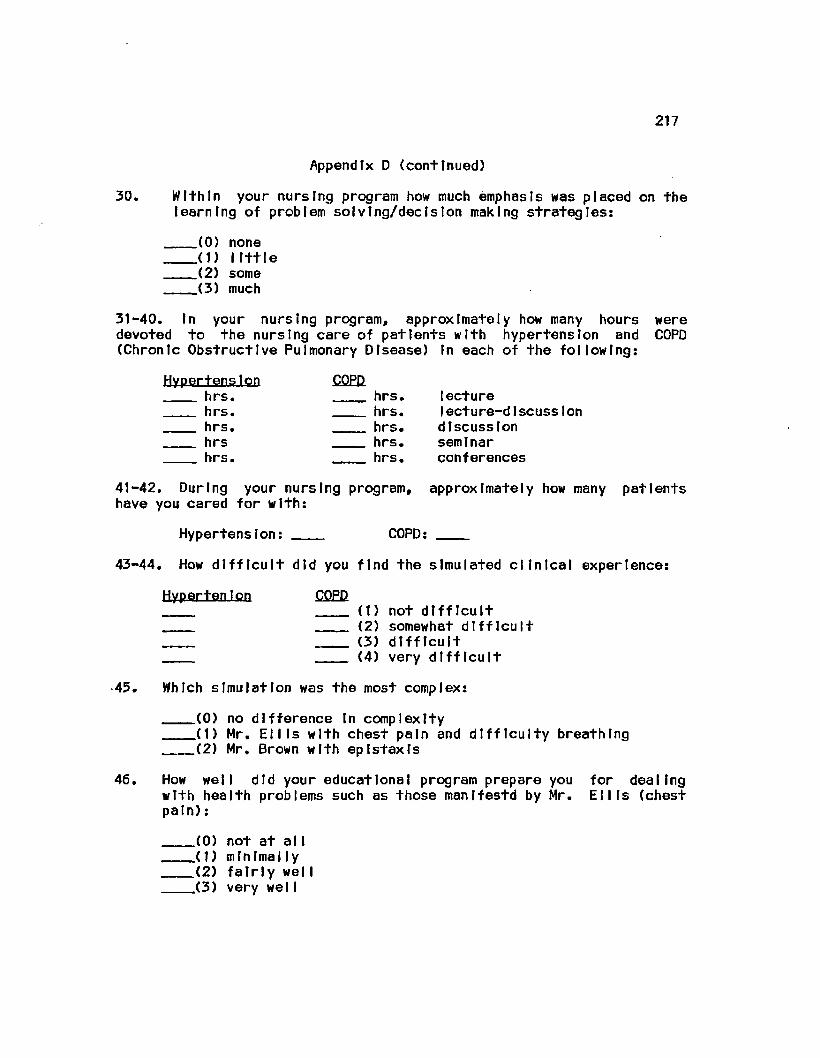
217
Appendix D (continued)
30. Within your nursing program how much emphasis was placed on the [earning of problem solving/decision making strategies:
(0) none (1) little (2) some (3) much
31-40. In your nursing program, approximately how many hours were devoted to the nursing care of patients with hypertension and COPD (Chronic Obstructive Pulmonary Disease) In each of the following:
Hypertension CQPD hrs. hrs. lecture hrs. hrs. Iecture-d1scuss1on hrs. hrs. discussion hrs hrs. seminar hrs. hrs. conferences
41-42. During your nursing program, approximately how many patients have you cared for with:
Hypertension: COPD:
43-44. How difficult did you find the simulated clinical experience:
HypertenIon CQED (1) not difficult (2) somewhat difficult (3) difficult (4) very difficult
•45. Which simulation was the most complex:
(0) no difference In complexity (1) Mr. Ellis with chest pain and difficulty breathing (2) Mr. Brown with eplstaxts
46. How well did your educational program prepare you for dealing with health problems such as those manifestd by Mr. Ellis (chest pain):
(0) not at a 11 (1) minimally (2) fairly welI (3) very welI
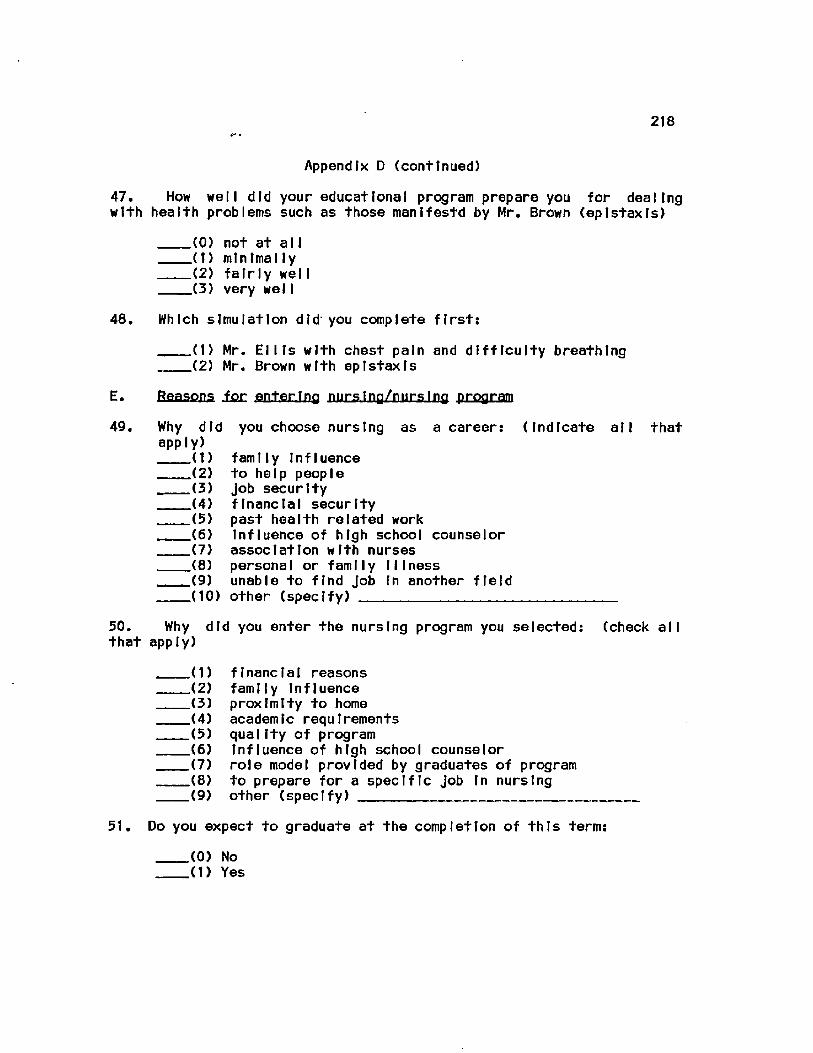
218
Appendix D (continued)
47. How well did your educational program prepare you for dealing with health problems such as those manlfestd by Mr. Brown (eplstaxls)
(0) not at all (1) minimally (2) fairly welI (3) very welI
48. Which simulation did' you complete first:
(1) Mr. Ellis with chest pain and difficulty breathing (2) Mr. Brown with eplstaxls
E. Reasons icc enter Ino nursing/nursing program
49. Why did you choose nursing as a career: (Indicate all that apply)
(1) family Influence (2) to help people (3) Job security (4) financial security (5) past health related work (6) Influence of high school counselor (7) association with nurses (8) personal or family Illness (9) unable to find Job In another field (10) other (specify)
50. Why did you enter the nursing program you selected; (check all that apply)
(1) financial reasons (2) family Influence (3) proximity to home (4) academic requirements (5) quality of program (6) Influence of high school counselor (7) role model provided by graduates of program (8) to prepare for a specific Job In nursing (9) other (specify)
51. Do you expect to graduate at the completion of this term:
(0) No (1) Yes
219
Appendix D (continued)
Is there any other Information that would help me In Interpreting your responses on any of the Instruments?
Thank you for your participation In this study
220
Appendix E
CONSENT FORM
CLINICAL DECISION MAKING INVESTIGATION
The use of decision making strategies within a nursing process framework Is an Important part of nursing today and Is receiving emphasis as a means through which nursing can further establish Itself as an Independent profession.
The purpose of this study Is to explore the Influence of various educational factors and Individual characteristics on the clinical decision making abilities of graduating students enrolled In entry level educational programs. The results of this study should be of benefit to nurse educators as they review their curricula and to nursing service personnel as they plan and review orientation programs for new graduates.
Participation Involves the completion of two clinical simulations, a questionnaire that assesses critical thinking ability, and a questionnaire that requests demographic and background Information about you. The amount of time necessary to complete these Instruments ts approximately two hours.
Participation also entails your granting me permission to have access to your score on the professional nursing licensure examination to be administered In July, 1984.
All Information regarding Individual student participation and their nursing programs will remain confidential and will be reported only In summary form without Identifying you or your school. Your participation or non-partIclaptIon will not affect your status within your own program since faculty will not have access to your responses.
Your participation will make the results of this study more representative of all graduating nursing students and will permit broader conclusions and recommendations to be made. Participation would also fulfill a professional responsibility regarding your making a contribution to the improvement of educational programs In schools of nursing and In the agencies and Institutions hiring new graduates.
If you are willing to participate In this study, please complete the following section and then place the consent form In the man I la envelope. If you do not wish to participate, replace all materials In the man!la envelope and return them to the test administrator.
221
Appendix E (continued)
I AGREE TO PARTICIPATE IN THIS RESEARCH STUDY ON CLINICAL
DECISION MAKING. I UNDERSTAND THAT MY PARTICIPATION IS VOLUNTARY AND
THAT I MAY WITHDRAW AT ANY TIME. MY DECISION TO PARTICIPATE OR NOT
WILL HAVE NO BEARING ON MY STATUS IN THIS EDUCATIONAL PROGRAM. FOR THE
PURPOSE OF THIS STUDY, I GRANT PERMISSION TO CAROLYN YOCOM TO OBTAIN
THE RESULTS OF MY PERFORMANCE ON THE PROFESSIONAL NURSING LICENSURE
EXAMINATION (NCLEX-RN) TO BE ADMINISTERED IN JULY, 1984.
Name (print) Soc. Sec. §
Name (signature)
State where plan to take licensing exam:
Permanent mailing address (complete only If you want your clinical
simulation and critical thinking appraisal scores reported to you):
Number & Street
City, State, Zip
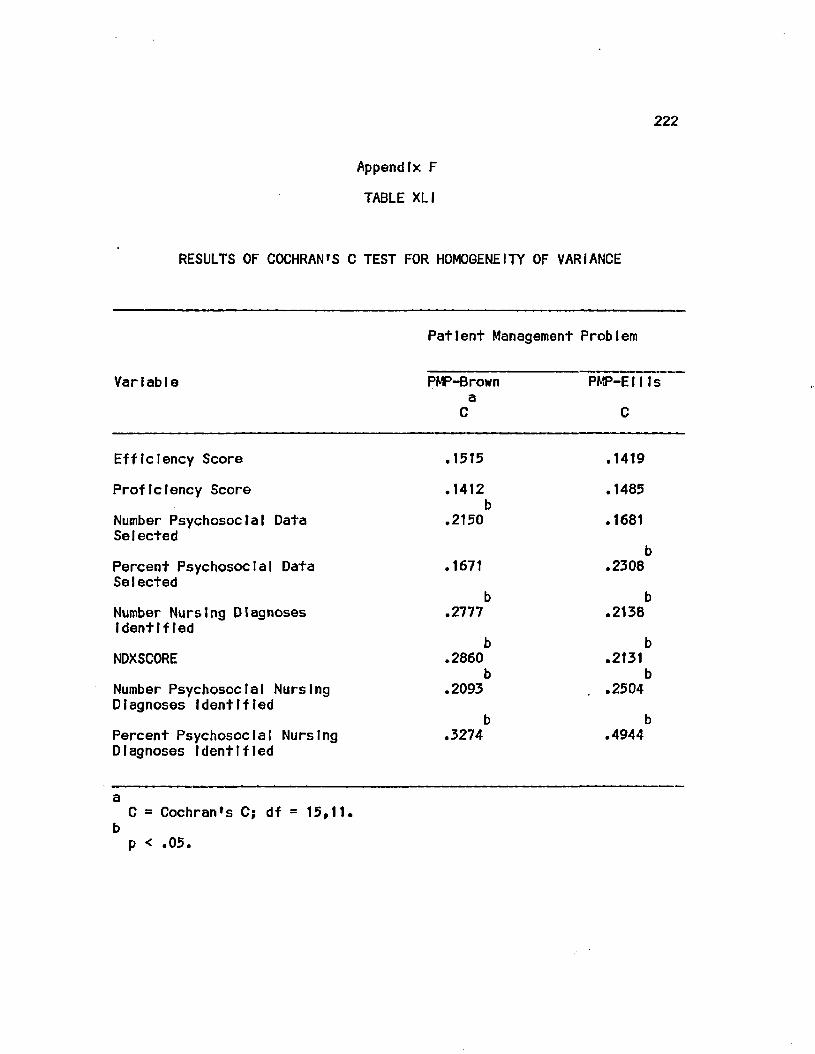
222
Appendix F
TABLE XL I
RESULTS OF COCHRAN'S C TEST FOR HOMOGENEITY OF VARIANCE
Patient Management Problem
VarIabIe PMP-Brown PMP-EIlls a C C
Efficiency Score .1515 .1419
Proficiency Score .1412 .1485 b
Number Psychosocial Data .2150 .1681 Selected
b Percent Psychosocial Data .1671 .2308 SeIected
b b Number Nursing Diagnoses .2777 .2138 Identified
b b NDXSCORE .2860 .2131
b b Number Psychosocial Nursing .2093 .2504 Diagnoses Identified
b b Percent Psychosocial Nursing .3274 .4944 Diagnoses Identified
a C = Cochran's C; df = 15,11,
b p < .05.
VII. CITED LITERATURE
Abdellah, F. G. and Beland, I. L.: Patient Centered Approaches to Nursing. New York, Macmlllan, 1965.
American Nurses' Association: First position on education for nursing. American Journal of Nursing 65 (12): 106-111, 1965.
American Nurses* Association: Standards of Nursing Practice. Kansas City, MO., American Nurses' Association, 1973.
American Nurses' Association: A Case for Baccalaureate Preparation In Nursing. Kansas City, MO., American Nurses' Association, 1979.
Anderson, J. R.: Cognitive Psychology and Its Implications. San Francisco, Freeman and Co., 1980.
Anderson, J. R. and Bower, B. H.: Conflgurat properties in sentence memory. Journal of Verbal Learning and Verbal Behavior 11: 595-
605, 1972.
Anderson, J. R. and Bower, G. H.: Interference In memory for multiple contexts. Memory A Cognition 2: 509-514, 1974.
Archer, E. J., Bourne, L. E. and Brown, F.: Concept Identification as a function of Irrelevant Information and Instructions. Journal of ExperImentaI Psycho Iogy 49 (3): 153-164, 1955.
Archer, M. L.: Establishing equivalency for nurses seeking admission to graduate nursing programs. Dissertation Abstracts International 37: 2161-B, 1976.
Asplnall, M. J.: Nursing diagnosis: The weak link. Nursing Outlook 24: 433-436, 1976.
Asplnall, M. J.: Use of a decision tree to Improve accuracy of diagnosis. Nursing Research 28: 182-185, 1979.
Asplnall, M. J. and Tanner, C. A.: Decision Making for Patient Care. New York, Appleton-Century-Crofts, 1981.
Barro, A. R.: Survey and evaluation of approaches to physician performance measurement. Journal of Medical Education 48: 1048-1093, 1973.
223
224
Barrows, H. S., Norman, G. R., Neufeld, V. R. and Felghtner, J. W.i The clinical reasoning of randomly selected physicians In general medical practice, ciintcal & Investigative Medicine 5: 49-55, 1982.
Barrows, H. S. and Tamblyn, R. M.: Problem-Based Learnings An Approach to Medical Education. New York, Springer, 1980.
Barrows, H. 5., Tamblyn, R. M., Sinclair, J. C. Watts, J. L., Mohlde, P. T., Kaufman, K. S., Leltch, R. E., Conltn, M. S., Mllner, R. S., Elliot, M. J. and Anderson, G. D.: A problem based, self directed educational program In neonatal respiratory disease for community hospital personnel. In Proceedings of the 17th Annual Conference on Research In Med leal Education, PP 111-116. Washington, D.C., Association of American Medical Colleges, 1978.
Bartlett, F. C.: ThInkIng. New York, Basic Books, 1958.
Bashook, P. G.: A conceptual framework for measuring clinical problem solving. Journal of Medical Education 51: 109-114, 1976.
Bassett, M. B.: The creative thinking ability and problem solving skill of associate and baccalaureate degree nursing students. D1ssertatIon Abstracts Internat1onaI 37: 6052-B, 1977.
Baumann, A. and Bourbonnals, F.: Nursing decision making In critical care areas. Journal of Advanced Nursing 7: 435-446, 1982.
Bensman, P. A.s Have we lost sight of the AD philosophy: Nursing Outlook 25: 511-513, 1977.
Berner, E. S., Hamilton, L. A. and Best, W. R.: A new approach to evaluating problem solving In medical students. Journal of Medical Friiicat Ion 49: 666-672, 1974.
Blrcher, A. U.: The concept of nursing diagnosis. In ClasslfIcatlon of Nursing JDJagHfiSfi&i Proceedings of the Third and Fourth National Conferences,, eds. M. J. Kim and D. A. Morltz, pp. 30-43. New York, McGraw-Hill, 1982.
Blaney, D. R.: Comparison of value systems of the graduates of two types of programs In nursing. Dissertation Abstracts International 34: 3877-B, 1974.
Bonney, V. and Rothberg, J: Nursing Diagnosis and Therapy; An Instrument for Eva I nation and Measurement. New York, National League for Nursing, 1963.
225
Boshulzen, H. P.A. and Claessen, H. F. A.: Problems of research Into medical problem solving: Some remarks on theory and method. Medical Education 16: 81-87, 1982.
Bourne, L. E. and DomlnowskI, R. L.: Thinking. Annual Review of Psychology 23: 105-112, 117-122, 1972.
Bourne, L. E., Domlnowskt, R. L. and Loftus, E. T.: Cognitive Processes. Englewood Cliffs, NJ, Prentice Hall, 1979.
Bourne, L. E. and Haywood, R. C.: The role of stimulus redundancy In concept Identification, Journal of Experimental Psychology 58: 232-238, 1959.
Broderlck, M. and Ammentorp, W.: Information stuctures: An analysis of nursing performance. Nursing Research 28: 106-110, 1979.
Brown, E. L.: Nursing for the Future. New York: Russell Sage Foundation, 1948.
Bruner, J. S., Goodnow, J. J. and Austin, G. A.: A Study of Thinking. New York, WHey, 1956.
Bui lough, B. and Sparks, C.: Baccalaureate vs. associate degree nurses: The care-cure dichotomy. Nursing Outlook 23: 688-692, 1975.
Burke, R. J.: Sex differences In recognizing the correct answer to a problem. Psychological Report 17; 532-534, 1965.
Burke, R. J. and Mater, N. R.: Attempts to predict success on an Insight problem. Psychologleal Report 17: 303-310, 1965.
Burkett, G. and Knafl, K.: Judgment and decision making In a medical specialty. Sociology of Work and Occupations 1 (1): 82-119, 1974.
Carlson, S.: A practical approach to the nursing process. American Journal of Nursing 72: 1589-1591, 1972.
Carnevelll, D. L.: Nursing Care Planning: Diagnosis and Management (3rd ed.). New York, Llpplncott, 1983.
Carrell, J.: An analysis of leadership abilities of senior nursing students. Dissertation Abstracts International 38: 590-B, 1977.
Chamlngs, P. A. and Teevan, J.: Comparisons of expected competencies of baccalaureate and associate degree graduates In nursing. Image 11: 16-21, 1979.
226
Chance, K. S.: Level of nursing education and perceptions of nursing performance. Dissertation Abstracts International 42: 2778-2779-B, 1982.
Chase, W. G. and Simon, H. A.: Perceptions In chess. CognItlve Psychology 4: 55-81, 1973.
CTanfranl, K.: The I n f l u e n c e Q± Amounts and Relevance of Data on Identifying Health Problems. Doctoral dissertation. Chicago, University of Illinois at Chicago, Health Sciences Center, 1982.
Collins, A. M. and Qui 11 Ian, M. R.: Retrieval time from semantic memory.. Journal of Verbal Learning and Verbal Behavior 8: 240-247, 1969.
Committee for the Study of Nursing Education: Nursing and Nursing Education In the United States. New York, Macmlllan, 1923.
Committee on the Function of Nursing: A Program for the Nursing Profess Ton. New York, Macmlllan, 1950.
Committee on the Grading of Nursing Schools: Nursing Schools Today and Tomorrow. Report jaf the Committee. New York, The Committee, 1934.
Cook, T. D. and Campbell, D. T.: Quasf-experImentatIon Design and Analysis issues for Field Settings. Boston, Houghton Mifflin, 1979.
Counts, M. M.: An analysis of a selected associate degree and baccalaureate degree nursing curriculum as related to graduates performance of functions In the medical-surgical area. Dissertation Abstracts International 36: 2152-B, 1975.
DavTs, B. C.: Clinical expertise as a function of educational preparation. Nursing Research 23: 530-534, 1972.
Davis, B. C.: Effects of levels of nursing education on patient care: A replication. Nursing Research 23: 150-153, 1974.
Davis, C. K.: Anticipatory socialization: Its effects on role conception, role deprivation and adaptive role strategies of graduating nurses In selected associate degree and baccalaureate degree programs. Dissertation Abstracts International 33: 4358-B, 1973.
DeChow, G. H.: Educatton for technical practice. In Proceedings Educational Conference for Members and Professional Employees of State Boards of Nursing - 1967. pp 23-36. New York, American Nurses1 Association, 1967.
227
deTornyay, R.: Measuring problem solving skills by means of the simulated cITnlcal nursing problem test. Journal of Nursing Education 7 (Aug.): 1-15, 1968.
Dickerson, T. M.: An examination of competency ratings for beginning nurse practitioners. Dissertation Abstracts International 36: 3870-B, 1976.
Dlncher, J. R. and Stldger, S. L.: Evaluation of a written simulation format for clinical nursing Judgment: A pilot study. Nursing Research 25: 280-285, 1976.
Dodge, G. H.: What determines nursing vs. medical diagnosis? AORN Journal 22: 23-24, 1975a.
Dodge, G. H.: Forces influence move toward nursing diagnosis. AORN Journal 22: 157-158, 1975b.
Donnelly, M. B. and Gallagher, R. E.: A study of the predictive validity of patient management problems, multiple choice tests and rating scales. In Proceedings 17th Annual Conference on Research In Medical EducationP pp. 117-123. Washington, D.C., Association of American Medical Colleges, 1978.
Dowe, M. C.: A study of the characteristics of two selected groups of student nurses. Dissertation Abstracts International 35: 1310-B, 1974.
Durand, M. and Prince, R.: Nursing diagnosis: Process and decision. Nursing Forum 5: 50, 1966.
Dustan, L.: Characteristics of students In three types of nursing education programs. Nursing Research 13: 159-166, 1964.
Eller, V. M.: Role orientation toward professional nursing of students completing associate degree, diploma, and baccalaureate nursing education programs. Dissertation Abstracts International 37: 2770-B, 1976.
Efstefn, A. S., Kagan, N., Shufman, L. S., Jason, H. and Loupe, M. J.: Method and theory In the study of medical inquiry. Journal of Medical Education 47: 85-92, 1972.
Elsteln, A. S., Shulman, L. S. and Sprafka, S. A.: Medical Problem Solving; An Analysis of CIInlcal Reasonfng. Cambridge, MA, Harvard University Press, 1978.
228
Farrand, L., AI banc, E. A., Schleutermann, J. A. and Holzemer, W. L.: Brown. an adult with frequent episodes of eplstaxls-
Chicago, University of Illinois at Chicago, Health Sciences Center, 1979.
Farrand, L., Holzemer, W., and Schleutermann, J.: A study of construct validity: Simulations as a measure of nurse practitioners problem solving skills. Nursing Research 3t s 37-42, 1982.
Frederickson, K. C. and Mayer, G. H. C.: Problem solving skills: What effect does education have? American Journal of Nursing 77: 1167-1169, 1977.
Gebble, K. M. and Levlne, M. A.: Proceedings of the First National Conference? Classification of Nursing Diagnosis. St. Louis, Mosby, 1975.
Glass, G. V. and Hopkins, K. D.: Statistical Methods In Education and Psychology,. 2nd ed. Englewood Cliffs, NJ, 1984.
Goldmark, V: Nursing and nursing education In the United States. In Nursing and Nursing Education In the United States. Report of the
Committee for the Study of Nursing Education. New York,
Macmlllan, 1923.
Gordon, M.s Predictive strategies In diagnostic tasks. Nursing Research 29: 39-45, 1980.
Gordon, M.: The diagnostic process. In Classification of Nursing Diagnoses? Proceedings of the Thfrd SJUl Fourth National Conference?, eds. M.J. Kim and D. Morltz, pp. 47-53. New York, McGraw-Hill, 1982.
Gover, V.: The NPSI: A nursing performance simulation Instrument. In Proceedings of the Eighth Nursing Research Conference,, pp. 9-44. Kansas City, MO, American Nurses Association, 1972.
Gray, J. E., Murray, B. L. S., Roy, J. F. and Sawyer, J. R.: Do graduates of technical and professional nursing programs differ In practice? Nursing Research 26: 368-373, 1977.
Greeno, J. G.: Trends In the theory of knowledge for problem solving. In Problem solving and education: Issues in teaching and researchf eds. D. T. Tuma and F. Relf, pp. 9-24. Hillside, NJ, Erlbaum Assoc., 1980.
Grler, M.: Decision making about patient care. Nursing Research 25: 105-110, 1976.

229
Grler, M. and Schnltzler, C.: Nurses' propensity to risk. Nursing Research 28: 186-190, 1979.
Haase, D. T.: A Proposed System for Nursing; Theoretical Framework, Part 2. Atlanta, Southern Regional Education Board, 1976.
Hammond, K.: An approach to the study of clinical Inference In nursing. Part II: Clinical Inference In nursing: A methodological approach. Nursing Research 13s 315-319, 1964.
Hammond, K: Clinical Inference In nursing. II. A psychologist's viewpoint. Nursing Research 15s 27-38, 1966.
Hammond, K., Kelly, K., Schneider, R. and Vanclnl, M.: Clinical Inference In nursing: Revising Judgments. Nursing Research 16: 38-45, 1967.
Hanushek, E. A. and Jackson, J. E.: Statistical Methods for Social
Scientists. New York, Academic Press, 1977.
Hartley, 6. E.i A comparison of baccalaureate and associate degree nursing students on selected personality characteristics. Dissertation Abstracts International 35: 4963-B, 1975.
Hogstel, M. 0.: Analysis of nursing functions and preparation. Dissertation Abstracts International 35: 4964-B, 1975.
Holzemer, W. L., Schleutermann, J. A., Farrand, L. L., and Miller, A. G.: A validation study: Simulations as a measure of nurse practitioners' problem solving skills. Nursing Research 30; 139-144, 1981.
Jacobs, A. M„: Clinical competencies of baccalaureate, associate degree, and diploma nurses - Are they different? Issues 1 (4):1-3,6, 1980.
Johnson, D. E.: Competence In practice: Technical and.professional. Nursing Outlook 14: 30-33, 1966.
Johnston, S.: The use of the RInes model In differentiating professional and technical nursing practice. Nursing and Health Care 3: 374-379, 1982.
Joreskog, K. G. and Sorbom, D.: LISREL JJ.L. Analysis of ULnasu: Structural Relationships by the Method of Maximum Likelihood,. 3rd ed. Upsala, Sweden, University of Upsala, 1984.
230
Juul, D. H., Noe, M. J, and Nerenberg, R. L.: A factor analytic study of branching patient managment problems. Medical Education 13: 199-203, 1979.
Kahneman, D. and Tversky, A.: Subjective probability: A Judgment of representativeness. Cognitive Psychology 3: 430-454, 1972.
Kahnemen, D. and Tversky, A.: On the psychology of prediction. Psychological Review 80: 237-251, 1973.
Kelly, K.: An approach to the study of clinical Inference In nursing. Part I. Introduction to the study of clinical Inference In nursing. Nursing Research 13: 314-315, 1964a.
Kelly, K.: An approach to the study of clinical Inference In nursing. Part III. Utilization of the "Lens Model" method to study the Inferential process of the nurse. Nursing Research 13: 319-322, 1964b.
Kelly, K.: Clinical Inference In nursing. I. A nurse's viewpoint. Nursing Research 15: 23-26, 1966.
Kissinger, J. F. and Munjas, B. A.: Nursing process, student attributes, and teaching methodologies. Nursing Research 30: 242-246, 1981.
Klatzkey, R. L.: Human memory; Structure and Processes. San Francisco, W. H. Freman, 1975.
Klelnmuntz, B.: The processing of clinical Information by man and machine. In Formal Representation of Human Judgment,, ed. B. Klelnmuntz, pp. 149-186. New York, Wiley & Sons, 1968.
Knafl, K. and Burkett, G.: Professional socialization In a surgical specialty. Sociology of Science and Medicine 9: 397-404, 1975.
Knopf, L.: RN's One and Five Years After Graduation. New York, National League for Nursing, 1975.
Koehne-Kaplan, N. S. and Tllden, V. : The process of clinical Judgment In nursing practice: The component of personality. Nursing Research 25: 268-272, 1976.
Komorlta, N.: Nursing diagnosis. American Journal of Nursing 63: 83-86, 1963.
Koran, L. J.: The reliability of clinical methods, data and Judgments, first of two parts. New England Journal of Medicine 293: 642-646, 1975a.
231
Koran, L. J.i The reliability of clinical methods, data, and Judgments, second of two parts. New England Journal of Medicine 293: 695-701, 1975b.
Kozleleckl, J.: A model for diagnostic problem-solving. Acta Psycholog lea 36: 370-380, 1972.
Kramer, M.: Philosophical foundations of baccalaureate nursing education. Nursing Outlook 29: 224-228, 1981.
Larkln, J. H.j Teaching problem solving In physics: The psychological laboratory and the practical classroom. In Problem Solving and Education: Issues in Teaching and Researchr eds. D. T. Tuma and F. Relf, pp. 111-126. Hillside, NJ, Erlbaum Assoc., 1980.
Laughlln, P. R.: Incidental concept formation as a function of creativity and Intelligence. Journal of Personality and Social Psychology 5; 115-119, 1967.
Laughlln, P. R.: Focusing strategies for eight concept rules. Journal of Experimental Psychology 77: 661-669, 1968.
Laughlln, P. R., Doherty, M. A. and Dunn, R. F.: Intentional and Incidental concept formation as a function of motivation, creativity. Intelligence and sex. Journal of Personality and Social Psychology 8: 401-409, 1968.
Levlne, M.: Human discrimination learning: The subset-sampling assumption. Psychological Bulletin 74: 397-404, 1970.
Lindsay, P. H. and Norman, D. A.: Human Information Processing (2nd ed.). New York, Academic Press, 1977.
Luckman, J. and Sorensen, K.C.: Medical Surgical Nursing: A Psychophysiological Approach. Philadelphia, Saunders,1980
McCain, F. P.: Nursing by assessment - not Intuition. American Journal of Nursing 65 (4): 82-84, 1965.
McCarthy, M.: The nursing process: Application of current thinking In clinical problem solving. Journal of Advanced Nursing 6: 173-177, 1981.
McCarthy, W. J.: An assessment of the Influence of cueing Items In objective examination. Journal of Medical Education 41: 263-266, 1966.
McCloskey, J. C.: Toward an Educational Model of Nursing Effectiveness. Chicago, Doctoral Dissertation, University of Chicago, 1981.

232
McClure, M. L.: Entry Into professional practice: The New York proposal. Journal of Nursing Administration 6 (June): 12-17, 1981.
McGuIre, C. H.: Testing In professional education. Review of Educational Research 38 (1): 49-60, 1968.
McGutre, C. H.: Assessment of problem solving skills, 1. Medical Isacjbsc 2: 74-79, 1980a.
McGuIre, C. H.: Assessment of problem solving skills, 2. Medical Teacher 2; 118-121, 1980b.
McGuIre, C. H. and Babbott, D: Simulation technique In the measurement of problems solving skills. Journal of Educational Measurement 4 (1): 1-10, 1967.
McGuIre, C. H. and Page, G.: The assessment of clinical performance by written and oral simulation. Report to the Faculty 1972-1973. Chicago, Center for Educational Development, University of Illinois College of Medicine, 1973.
McGuIre, S. H., Solomon, L., and Bashook, P.: Construction and Use of Written Simulations. New York, The Psychological Corporation, 1976.
McKenna, M. E.: Differentiating between professional nursing practice and technical nursing practice. Dissertation Abstracts International 31: 4157-B, 1971.
McLaughlin, F. E., Cesa, T., Johnson, H., Lemons, M., Anderson, S., Larson, P. and Gibson, J.: Primary Care Judgments of Nurses and Physicians. Vol. 1. San Francisco, Veterans Administration Hospital, 1978.
McLaughlin, F. E., Cesa, T., Johnson, H., Lemons, M., Anderson, S.f Larson, P. and Gibson, J.: Primary Care Judgments of Nurses and Phys1clans. Vol. 11. San Francisco, Veterans Administration Hospital, 1979.
McNeil, B. J., Keeler, E. and Adelsteln, S. J.: Primer on certain elements of medical decision making. New England Journal of Medicine 293: 211-215, 1975.
i
McQuald, E. and Kane, M.: How do graduates of different types ;of programs perform on state boards? American Journal of Nursing 79: 305-308, 1979.
233
Mahomet, A. D.: Nursing diagnosis for ther OR nurse. AORN Journal 22: 709-711, 1975.
Maler, N. R. and Casselman, G.: Locating the difficulty In Insight problems: Individual and sex differences. Psycho Iogleal Reports 26: 103-117, 1970.
Maler, N. R. and Jenson, J. C.: Are good problem solvers also creative? Psychological Reports 24: 139-146, 1969.
Matheny, R. V., Nolan, B. T., Hogan, A. E. and Griffin, G. J. (eds.): Fundamentals of Patient Centered Nursing (3rd ed.). St Louis, Mosby, 1972.
Mayer, R. E.: Information processing variables In learning to solve problems. Review of Educational Research 45: 525-541, 1975.
Mel els, A. I. and Farrell, K. M.: Operation concern: A study of senior nursing students In three nursing programs. Nursing Research 23 461-468, 1974.
Mendelsohn, G. A., Grlswald, B. B. and Anderson, M. L.: Individual differences In anagram-solving ability. Psychological Reports 19: 799-809, 1966.
Miller, G. A.: The magical number seven, plus or minus two: Some limits on our capacity for processing Information. Psychological Review 63: 81-97, 1956.
Montag, M. L.: The Education of Nursing Technicians. New York, Putnam, 1956.
Montag, M. L.: Looking back: Associate degree education In perspective. Nursing Outlook 28: 248-250, 1980.
Montag, M. L. and Gotkln, L. C.: Community College Education for Nursing. New York, McGraw-Hill, 1959.
Morltz, D.: Nursing diagnoses In relation to the nursing process. In Classification of Nursing Diagnoses: Proceedings of the Third and Fourth National Conferences,, eds. M. J. Kim and D. Morltz, pp. 53-58. New York, McGraw-Hill, 1982.
Nash, P. M.: Evaluation of Employment Opportunities for Newly Licensed Nurses. Washington, DC, DHEW. (Pub. No. (HRA) 75-12), 1975.
National League for Nursing: The Shifting Scene - Directions ffir Practice. New York, National League for Nursing, 1967.
234
National League for Nursing: Development of Competencies Fn Associate Degree Nursing: A New Perspective. New York, National League for Nursing, 1978.
National League for Nursing: Characteristics of BaccaI aureate Education In Nursing. New York, National League for Nursing, 1979.
National League for Nursing: Competencies of Graduates of Nursing Programs. New York, National League for Nursing, 1982.
Nelson, L. F.: Competence of nursing graduates In technical, communicative, and administrative ski I Is. Nursing Research 27: 121-125, 1978.
Neuble, D. I., Hoare, J. and Baxter, A.: Patient management problems. Issues of validity. Medical Education 16: 137-142, 1982.
New York State Nurses Association: Obstacles to moving entry Into practice bill. NYSNA Legislative Bulletin 23: 3, 1983.
Newell, A.: Judgment and Its representation: An Introduction . In Formal Representation of Human Judgment,, ed. B. Klelnmuntz, pp 1-16. New York, Wiley, 1968.
Newell, A., Shaw, J. C. and Simon, H. A.: Elements of a theory of human problem solving. Psychological Review 65: 151-166, 1958.
Norlclnl, J. J., Swanson, D. B. and Webster, G. D.: Reliability, validity and efficiency of various Item formats In assessment of physician competence. In Proceedings of the Twenty-second Annual Conference on Research In Medical Frinratlon. pp. 53-58. Washington, DC, Association of American Medical Colleges, 1983.
Norman, G. R. and Felghtner, J. W.: Behavior on the PMP and simulated patients. Medical Education 16; 26-32, 1981.
Norman, G. R., Felghtner, J. W., Tugwell, P., Muzz In, L. J. and Guyatt, G.: The generalIzabIIIty of measures of clinical problem-solving. In Proceedings of the Twenty-second Annual Conference on Research In Medical Education, pp. 110-114. Washington DC, Association of American Medical Colleges, 1983.
Norman, G. R. and Wakefield, J. G.s The validity of the medical record. In Proceedings of the 17th Annual Conference on Research La
Medical EducatIonr pp. 124-128. Washington, DC, Association of American Medical Colleges, 1978.
Norrls, C. M.: Towards a science of nursing: A method for developing unique content In nursing. Nursing Forum 3: 10-15, 1964.
235
Page, G. G. and Fielding, D. W.: Performance on PMP's and performance tn clinical practice: Are they related? Journal of Medical Education 55: 529-537, 1980.
Pedhazur, E. J.: Multiple Regression In Behavioral Research. 2nd ed. New York, Holt, RInehart and Winston, 1982.
PI Ileplch, M. K.: Development of General Education In Collegiate Nursing Programs: Role of the Administrator New York, Teachers College, Columbia University, 1962.
PIshkIn, V. and Rosenblum, E. S.: Concept Identification of auditory dimensions as a function of age and sex. PsychoneurologIc Science 4: 165-166, 1966.
PIshkIn, V. and Wolfgang, A: Number and type of available Instances In concept le rntng. Journal of Expertmental_£sychology
PIshkIn, V., Wolfgang, A. and Rasmussen, E: Age, sex, amount, and type of memory Information In concept learning. Journal of Experimental Psychology 73: 121-124, 1967.
Pitts, J. A.: An analysis of perceived nursing program outcome goals. Dissertation Abstracts International 35: 4004-4005-B, 1975.
Reed, S. and Abramson, A.: Effect of the problem space on subgoal facilitation. Journal of Educational Psychology 68; 243-248, 1976.
Re Id, B. J.: A COfnp.arJ.SOJ pf the Psychometric Properties and Relative Predlctlvce Abilities of Two Problem Solving Patient Care Simulations for Associate and Baccalaureate Degree Nursing Students. Doctoral Dissertation, Memphis State University, 1981.
Richards, M.A.: A study of differences In psychological characteristics of students graduating from three types of basic nursing programs. Nursing Research 21: 258-261, 1972.
RInes, A. P.: Associate degree education: History, development and rationale. Nursing Outlook 25: 496-502, 1977a.
RInes, A. P.: Development of objectives: Program, level, course and unit. In Preparing the Associate Degree Graduate, pp. 17-31. New York, The League, 1977b.
Rosch, E. and Mervls, C. B.: Family resemblances: Studies In the Internal stucture of categories. Cognitive Psychology 7: 573-605, 1975.
236
Roy, S. C.: A diagnostic classification: A system for nursing. Nursing Outlook 23: 90-94, 1974a.
Roy, S. C.: The Impact of nursing diagnosis. AORN Journal 21: 1023-1030, 1974b.
Rubin, A. 0.: Hypothesis Formation and Evaluation In Medical Diagnosis. Unpublished Master's Thesis, Massachusetts Institute of Technology, 1975.
Schleutermann, J. A., Albano, E. A., Miller, A. G., Farrand, L. L. and Holzemer, W. L.: Mr. Ellis, a 48 year old man complaining of chest pain and difficulty breathing. Chicago: University of Illinois at Chicago, Health Sciences Center, 1979.
Schlotfeldt, R. M.: Education for professional practice. In Proceedlnqsf Educational Conference for Members and Professional Employees of State Boards of Nursing - 1967. pp. 12-22. New York: American Nurses' Association, 1967.
Schlotfeldt, R. M.: Educational requirements for registered nursTng. In Entry Into Registered Nursing - Issues and Problems,, pp. 10-16. New York: National League for Nursing, 1977.
Schuyler, S. B.: An examination of critical requirements expected of beginning practitioners of nursing from associate degree, baccalaureate and diploma programs as perceived by supervisors, recent graduates, and nurse educators. Dissertation Abstracts International 44: 3923-B, 1983.
Schwartz, S. H. and Simon, R. I.: Systems approach to studying Information processing and decision making In medical diagnosis. In Health Research: The Systems ApproachP ed. H. Werley, pp. 225-248. New York: Springer, 1976.
Schwerlan, P. M.: Prediction of Successful Nursing Performance. Part 111 and Part IV. Washington, DC, DHEW, Division of Nursing, 1979.
Sedlack, W. E. and Nattress, L. W.: A technique for determining the validity of patient management problems. Journal of Medical FrinratIon 47: 263-2166, 1972.
Shanteau, J. and Phelps, P: Judgment and swine: Approaches and Issues In applied Judgment analysis. In Human Judgment and Decision Processes in Applied Settings,, eds. M. Kaplan and S. Schwartz, pp. 255-271. New York, Academic Press, 1977.
237
Sherman, J. E., Miller, A. G., Farrand, L. L. and Holzemer, W. H.: A simulated patient encounter for the family nurse practitioner. Journal of Nursing Education 18 (5): 5-15, 1979.
Simon, H. A.: Problem solving and education. In Problem Solving and Education! Issues In teaching and Research,, eds. D.T. Tuma and F. Reif, pp. 81-96. Hillside, NJ, Erlbaum Assoc, 1980.
Simon, H. A. and Newell, A.: Human problem solving: The state of the theory In 1970. American Psychologist 26: 145-149, 1971.
Simon, H. A. and Newell, A.; Human Problem Solving. Englewood Cliffs, NJ: Prentice-Hall, 1972.
Simons, B.J.: The relationship of education, work experience and position of employment to professionalism In nursing. Dissertation Abstracts International 43: 1045-B, 1982.
sparks, R. K.: Prohlem Solving Ability of Graduates from Associate and Baccalaureate Degree Nursing Programs. Doctoral Dissertation, University of Minnesota, 1979.
Sprecht, D. A.: On the evaluation of causal models. Social Science Research 4: 113-133, 1975.
SPSS, Inc.: SPSS-X User's Guide. New York: McGraw-Hl11,1983.
Stanton, C. J. M.: A comparison of ratings of the clinical competency of recent graduates of associate and baccalaureate degree programs In nursing. Dissertation Abstracts International 43: 3189-B, 1982.
Sweeney, J.: An associate degree educator supports the entry to practice resolution. Nurse Educator 5 (5): 28-29, 1980.
Sweller, J. and Levlne, M.: Effects of goal specificity on means-ends analysis and learning. Journal of Experimental Psychology; Human Learning,. Memoryf and Cognition 8: 463-474, 1982.
Tanner, C. A. W.: Ihfi Effects of Hypothesis Generation as an Instructional Method on the Diagnostic Processes of Senior
Baccalaureate Nursing Students. Doctoral Dissertation, University of Colorado at Boulder, 1977.
Tschudln, M. S.: Educational preparation needed by the nurse of the future. Nursing Outlook 12 (4): 32-35, 1964.
Tversky, A.: Features of similarity. Psychological Review 84: 327-349, 1977.
238
Tversky, A. and Kahneman, D.: Availability: A heuristic for Judging frequency and probability. Cognitive Psychology 5; 207-232, 1973.
Tversky, A. and Kahnemanfm D.: Judgment under uncertainty: Heuristics and biases. ScIence 185: 1124-1131, 1974.
Vaugh, J. C.: Educational preparation for nursing - 1982. Nursing and Health Care 4:. 460-464, 1983.
Ventura, M. S.: Creative thinking and related social behaviors of students In different nursing education programs. Dissertation Abstracts International 36: 653-Bk, 1975.
Verhonlck, P. J., Nichols, G. A., Glor, B. A., and McCarthy, R. T.: I came, f saw, I responded: Nursing observation and action survey. Nursing Research 17: 38-44, 1968.
Vu, N. V.: Medical problem solving assessment. A review of methods and Instruments. Evaluation and the Health Professions 2: 281-90, 1979.
Walker, C. and Bourne, L. E.: The Identification of concepts as a function of amounts of relevant and Irrelevant Information. The American Journal of Psychology 74: 410-417, 1961.
Waters, V., Chater, S. S., VIvler, M. L., Urrea, J. H. and Wilson, H. S.: Technical and professional nursing: An exploratory study. Nursing Research 21: 124-131, 1972.
Watson, A. B.: Professional socialization of the registered nurse as measured by attitudes and problem Identification skills. Dissertation Abstracts International 43: 3190-B, 1983.
Watson, G. and Glaser, E. M.: Manual.- Watson-G laser Critical Thinking Appraisal. Nlles, IL, The Psychological Corporation, 1980.
Wolf, F. M., Allen, N. P., Cassldy, J. T., Maxim, B. R. and Davis, W. K.: Concurrent and criterion-referenced validity of patient managment problems. In Proceedings of the Twenty-Second Annual Conference of Research In Medical Education,. pp 115-121. Washington, DC, Association of American Medical Colleges, 1983.
Woodward, C. A.: Simulated patients In evaluation of medical education
Research in Medical Educatlonfp 244. Washington, D.C., American Association of Medical Colleges, 1983.
Wortman, P. M.: Medical diagnosis: An Information-processing approach. Computers and Biomedical Research 5: 315-328, 1972.
239
Wren, G. P.: Some characteristics of freshman students In baccalaureate, diploma, and associate degree nursing programs. Nursing Research 20: 167-172, 1971.
Yura, H. and Walsh, M. B.: The Nursing Proces5.;-Aa5.e.&sIng, PlannJjuu Implementing,. Evaluating, 3rd ed. New York, App I eton-Century-Crofts, 1978.

VIII. VITA
NAME:
BIRTH DATE:
BIRTH PLACE:
EDUCATION:
1964
1970
1975
1985
PROFESSIONAL EXPERIENCE:
1964 - 1966
1966 - 1967
1967 - 1973
Carolyn Jean Yocom
Diploma In Nursing Ablngton Memorial Hospital School of Nursing Ablngton, Pennsylvania
B.S., Nursing University of Pennsylvania Philadelphia, Pennsylvania
M.S., Nursing Frances Payne Bolton School of Nursing Case Westrn Reserve University Cleveland, Ohio
Ph.D., Nursing Sciences University of Illinois at Chicago Health Sciences Center Chicago, MIT no I s
Staff Nurse Ablngton Memorial Hospital Ablngton, Pennsylvania
Inservice Education Instructor Ablngton Memorial Hospital Abngton, Pennsylvania
Instructor Ablngton Memorial Hospital School of Nursing Ablngton, Pennsylvania
240
241
VITA (continued)
1973 - 1974
1974 - 1975
1975 1977 1982
1977 1982 1985
1984 - 1985
PROFESSIONAL MEMBERSHIPS:
AWARDS AND HONORS:
Staff Nurse University Hospitals of Cleveland Cleveland, Ohio
Research Assistant Frances Payne Bolton School of Nursing Case Western Reserve University Cleveland, Ohio
Instructor Assistant Professor Research Assistant Col lege of NursIng University of Illinois at Chicago Health Sciences Center Chicago, Illinois
Assistant Professorial Lecturer Department of Nursing St. Xavler College Chicago, Illinois
American Association for the Advancement of Science
American Nurses Association Midwest Nursing Research Society National League for Nursing Sigma Theta Tau, Alpha Lambda Chapter Society for Research In Nursing Education
Professional Nurse Tralneeshlp Department of Health, Education, and Welfare Public Health Service, 1969 - 1970
Professional Nurse Tralneeshlp Department of Health, Education, and Welfare Public Health Service, 1974 - 1975
Sigma Theta Tau Frances Payne Bolton School of Nursing Case Western Reserve University, 1975
Graduate College Fellowship University of Illinois at Chicago, 1982 - 1983
242
VITA (continued)
Professional Nurse Traineeshlp Department of Health, Education, and Welfare Public Health Service, 1983 - 1984
Research Support Award Alpha Lambda Chapter Sigma Theta Tau, 1985
Student Recognition Award - Honorable Mention Alpha Lambda Chapter Sigma Theta Tau, 1985
Kim, M. J., Amoroso, R., Gulantck, M., Moyer, K., Parsons, E., Scherubel, J., Stafford, M., Suhayda, R., and Yocom, C.: Clinical use of nursing diagnoses (preliminary results). Regional Conference on Nursing Diagnoses, Milwaukee, Wisconsin, November 2, 1979.
Kim, M. J., Amoroso, R., Gulanlck, M., Moyer, K., Parsons, E., Scherubel, J., Stafford, M., Suhayda, R., and Yocom, C.: Clinical Identification and usefulness of nursing diagnoses for cardiovascular patients. Chicago Heart Association, Chicago, Illinois, March 4, 1980.
Kim, M. J., Amoroso, R., Gulanick, M., Moyer, Ku, Parsons, E., Scherubel, J., Stafford, M., Suhayda, R., and Yocom, C.: Agreement between clinical specialists and staff nurses on nursing diagnoses Identification. Fourth Midwest Nursing Research Conference, Kansas City, Kansas, April 14 - 15, 1980.
Kim, M. J., Amoroso, R., Gulanlck, M., Moyer, K., Parsons, E., Scherubel, J., Stafford, M., Suhayda, R., and Yocom, C.: Clinical testing of nursing diagnoses In cardiovascular nursing practice. Veterans Administration District § 17 Nursing Research Conference, North Chicago, Illinois, November 19, 1980.
243
VITA (continued)
Kim, M. J., Amoroso, R., Guianick, M., Moyer, K., Parsons, E., Scherubel, J., Stafford, M., Suhayda, R., and Yocom, C.: Clinical validation of nursing diagnoses In acute cardiovascular nursing. American Nurses Association Council of Nurse Researchers. Minneapolis, Minnesota, September 23, 1983.
Scherubel, J. C. and Yocom, C. J.: Academic performance as predictors of success on nursing licensure examinations. Graduate Student Exchange, Midwest Nursing Research Conference, Iowa City, Iowa, April 10 - 12, 1983.
Scherubel, J. C., Ellison, D. and Yocom, C. J.: Predictive validity of a tool used to evaluate baccalaureate nuring program applicants. Third Annual Scientific Meettng of the Society for Research In Nursing Education, San Francisco, California, January 9-11, 1985.
Yocom, C. J.: Nursing staff involvement In clinical research. Sixth Annual Research Conference. V. A. Medical District #17 Nursing Services and University of Illinois Nursing, Chicago, Illinois, October 21, 1983.
Yocom, C. J.: Nursing staff involvement In clinical research. Sigma Theta Tau, Beta Eta Chapter and University of Wisconsin -Madison, School of Nursing Research Day. Madison, Wisconsin, November 3, 1984.
Yocom, C. J.: Influence of Initial nursing educational preparation on patient assessment. Sigma XI Graduate Student Research Forum, University of Illinois at Chicago, Chicago, Illinois, April 1, 1985.
Yocom, C. J. and Scherubel, J. C.: Academic performance as predictors of success on nursing IIcensure examinations. 1983 Post Graduate Conference, Marquette University, Milwaukee, Wisconsin, June 10, 1983.
244
VITA (continued)
Yocom, C. J. and Scherubel, J. C.: Predictors of success on the NCLEX and SBE licensing examinations. Second Annual Scientific Meeting of the Society for Research In Nursing Education. San Francisco, California, January 18-20, 1984.
Yocom, C. J. and Scherubel, J. C.: Predictors of success on the NCLEX and SBE licensing examinations. Sigma Theta Tau, Beta Eta Chapter and University of Wisconsin Madison, School of Nursing Research Day, Madison, Wisconsin, November 3, 1984.
PUBLICATIONS: Ellison, D., Scherubel, J. C. and Yocom, C. J.: Evaluation of a process to evaluate baccalaureate nursing program applicants. Journal of Professional Nursing (In press).
Klm, M. J., Amoroso, R., Gulanlck, M., Moyer, K., Parsons, E., Scherubel, J., Stafford, M., Suhayda, R. and Yocom, C.: Clinical use of nursing diagnoses. In Classification of Nursing Diagnoses - Proceedings of the Third and Fourth National Conferences,, eds. M. J. Kim and A. M. McClaln, pp 184-190. St. Louis, Mosby, 1982.
Kim, M. J., Amoroso, R., Gulanlck, M., Moyer, K., Parsons, E., Scherubel. J., Stafford, M., Suhayda, R. and Yocom, C.: Clinical use of nursing diagnoses related to cardlovasuclar nursing. In Classification of Nursing Diagnoses - Proceedings of the Fifth National
Conferencef eds. M. J. Klm and A. M. McClaln, pp 128-138. St. Louts, Mosby, 1984.
Klm, M. J., Suhayda, R., Waters, L. and Yocom, C.: The effect of using nursing diagnoses In nursing care planning. In Classification of Nursing Diagnoses - Proceedings of the Third and Fourth National Conferences,, eds. M. J. Klm and A. M. McClaln, pp 158-165. St. Louis, Mosby, 1982.

245
VITA (continued)
Yocom, C. J.: Pre- and post-operative nursing. In Manual of Med lea I-Surg lea I Nursing, eds. E. HIncker and L. Malasanos, pp. 143-169, Boston, Little Brown, 1983.
Yocom, C. J.: Care of patients with peripheral vascular disease. In Manual of Med lea I-Surgical Nursing, eds. E. HIncker and L. Malasanos, pp. 505-520. Boston, Little, Brown, 1983.
Yocom, C. J.: Differentiation of fear and anxiety. In Classlf Icatlon af Nursing Diagnoses - Proceedings of the Fifth National
Conference,, eds. M. J. Kim and A. M. McClaln, pp 352-355. St. Louis, Mosby, 1984.
Yocom, C. J. and Scherubel, J. C.: Selected preadmission and academic correlates of success on state board examinations. Journal of Nursing Education (In press).
Kim, M. J., Amoroso, R., Gutanlck, M., Moyer, K., Parsons, E., Scherubel, J., Stafford, M., Suhayda, R., and Yocom, C.: Clinical use of nursing diagnoses (preliminary results). Regional Conference on Nursing Diagnoses, Milwaukee, Wisconsin, November 2, 1979.
Kim, M. J., Amoroso, R., Gulantck, M., Moyer, K., Parsons, E., Scherubel, J., Stafford, M., Suhayda, R., and Yocom, C.: Clinical Identification and usefulness of nursing diagnoses for cardiovascular patients. Chicago Heart Association, Chicago, Illinois, March 4, 1980.
Kim, M. J., Amoroso, R., Gulanlck, M., Moyer, K., Parsons, E., Scherubel, J., Stafford, M., Suhayda, R., and Yocom, C.: Clinical use of nursing diagnoses. Fourth National Conference on Classification of Nursing Diagnoses, St. Louis, Missouri, April 8 - 13, 1980.
PRESENTATIONS AND POSTERS:
246
VITA (continued)
Kim, M. J., Amoroso, R., Gulanlck, M., Moyer, K., Parsons, E., Scherubel, J., Stafford, M., Suhayda, R., and Yocom, C.: Agreement between clinical specialists and staff nurses on nursing diagnoses Identification, (poster) Fourth Midwest Nursing Research Conference, Kansas City, Kansas, April 14 - 15, 1980.
Kim, M. J., Amoroso, R., Gulanlck, M., Moyer, K., Parsons, E., Scherubel, J., Stafford, M., Suhayda, R., and Yocom, C.: Clinical testing of nursing diagnoses In cardiovascular nursing practice. Veterans Administration District #17 Nursing Research Conference, North Chicago, Illinois, November 19, 1980.
Kim, M. J., Amoroso, R., Gulanlck, M., Moyer, K., Parsons, E., Scherubel, J., Stafford, M., Suhayda, R., and Yocom, C.: Clinical use of nursing diagnoses In cardiovascular nursing. Fifth National Conference on Classification of Nursing Diagnoses, St. Louis, Missouri, April 14 - 17, 1982.
Kim, M. J., Amoroso, R., Gulanlck, M., Moyer, K., Parsons, E., Scherubel, J., Stafford, M., Suhayda, R., and Yocom, C.: Clinical validation of nursing diagnoses In acute cardiovascular nursing. American Nurses Association Council of Nurse Researchers. Minneapolis, Minnesota, September 23, 1983.
Kim, M. J., Suhayda, R., Waters, L. and Yocom, C.: The effect of using nursing diagnoses In nursing care planning. Third National Conference on Classification of Nursing Diagnoses. St. Louis, April 7 - 10, 1978.
Scherubel, J. C. and Yocom, C. J.: Academic performance as predictors of success on nursing licensure examinations. Graduate Student Exchange, Midwest Nursing Research Conference, Iowa City, Iowa, April 10 - 12, 1983.
247
VITA (continued)
Scherubel, J. C. Ellison, D., and Yocom, C. J.: Predictive validity of a tool used to evaluate baccalaureate nursing program applicants. Third Annual Scientific Meeting of the Society for Research In Nursing Education, San Francisco, California, January 9-11, 1985.
Yocom, C. J.s Differentiation of Fear and Anxiety. Fifth National Conference on Classification of Nursing Diagnoses, St. Louis, Missouri, April 14-17, 1982.
Yocom, C. J.: Nursing staff Involvement In clinical research. Sixth Annual Research Conference. V. A. Medical District #17 Nursing Services and University of Illinois Nursing, Chicago, Illinois, October 21, 1983.
Yocom, C. J.; Nursing staff Involvement In clinical research, (poster) Sigma Theta Tau, Beta Eta Chapter and University of Wisconsin - Madison, School of Nursing Research Day. Madison, Wisconsin, November 3, 1984.
Yocom, C. J.: Influence of Initial nursing educational preparation on patient assessment. Sigma XI Graduate Student Research Forum, University of Illinois at Chicago, Chicago, Illinois, April 1, 1985.
Yocom, C. J.: Influence of Initial nursing educational preparation on patient assessment. College of Nursing, University of Illinois at Chicago, April 29, 1985.
Yocom, C. J. and Scherubel, J. C.: Academic performance as predictors of success on nursing I(censure examinations.(poster) 1983 Post Graduate Conference, Marquette University, Milwaukee, Wisconsin, June 10, 1983.
248
VITA (continued)
Yocom, C. J. and Scherubel, J. C.: Academic performance as predictors of success on nursing licensure examinations. (poster) Illinois Nurses Assoclaton Biennial Convention, Chicago, Illinois, November 9, 1983.
Yocom, C. J. and Scherubel, J. C.: Predictors of success on the NCLEX and SBE licensing examinations. (poster) Second Annual Scientific Meeting of the Society for Research In Nursing Education. San Francisco, California, January 18-20, 1984,
Yocom, C. J. and Scherubel, J. C.: Predictors of success on the NCLEX and SBE licensing examinations, (poster) Sigma Theta Tau, Beta Eta Chapter and University of Wisconsin -Madison, School of Nursing Research Day, Madison, Wisconsin, November 3, 1984.