
Influence of Copper, Iron, Zinc and Fe 3 + Haemoglobin Levels on the Etiopathogenesis of Chronic...
11
Influence of Copper, Iron, Zinc and Fe 3 + Haemoglobin Levels on the Etiopathogenesis of Chronic Calcific Pancreatitis—A Study in Patients with Pancreatitis Geetha Arumugam & Monika Padmanaban & Dhanya Krishnan & Saranya Panneerselvam & Surendran Rajagopal Received: 11 July 2010 /Accepted: 11 August 2010 / Published online: 1 September 2010 # Springer Science+Business Media, LLC 2010 Abstract Chronic pancreatitis is a serious condition associated with severe abdominal pain, and a significant percentage of patients progresses to irreversible calcification in pancreas. The present study evaluates the degree to which the levels of trace elements, copper, iron, selenium, zinc and haemoglobin-Fe 3+ , in blood, serum and pancreas have any role to play in the calcification process associated with fibrosis in pancreas. Twenty-seven calcific (CCP) and 23 non-calcific chronic pancreatitis (CP) patients and equal number of age- and sex-matched normal volunteers (50) were enrolled in the study. Surgically removed pancreatic tissue and blood samples were analysed for copper, iron, selenium, zinc, protein, collagen and lipid peroxidation products in terms of malondialdehyde, protein carbonyls, glutathione, methemoglobin, methemoglobin reductase and ceruloplasmin activity levels. We could find that the pancreatic tissue levels of copper, iron, protein and collagen contents were significantly elevated in CCP patients when compared to CP patients. Serum levels of copper, free ionic copper and iron were also elevated in CCP patients. The serum and the pancreatic tissue level of zinc and selenium showed a significant decrease in CCP patients. The level of methemoglobin was elevated more significantly with the concomitant decline in the activity of methemoglobin reductase. There was a positive correlation between the pancreatic level of copper and iron with the collagen and protein levels. The results of the present study revealed that the levels of copper and iron, the pro-oxidants and zinc and selenium may influence calcification process in CCP patients. Hypoxia-related tissue injury due to the formation of oxidised haemoglobin may also contribute to the pathogenesis of calcification in pancreas. Keywords Chronic pancreatitis . Calcification . Copper . Iron . Zinc . Collagen . Methemoglobin . Methemoglobin reductase Biol Trace Elem Res (2011) 142:424–434 DOI 10.1007/s12011-010-8822-y G. Arumugam (*) : M. Padmanaban : D. Krishnan : S. Panneerselvam Department of Biochemistry, Bharathi Womens College (Affiliated to University of Madras), Chennai 600 108 Tamil Nadu, India e-mail: [email protected] S. Rajagopal Department of Surgical Gastroenterology, Stanley Medical College and Hospital, Chennai 600 108 Tamil Nadu, India
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Influence of Copper, Iron, Zinc and Fe 3 + Haemoglobin Levels on the Etiopathogenesis of Chronic...

Influence of Copper, Iron, Zinc and Fe3+ Haemoglobin
Levels on the Etiopathogenesis of Chronic CalcificPancreatitis—A Study in Patients with Pancreatitis
Geetha Arumugam & Monika Padmanaban &
Dhanya Krishnan & Saranya Panneerselvam &
Surendran Rajagopal
Received: 11 July 2010 /Accepted: 11 August 2010 /Published online: 1 September 2010# Springer Science+Business Media, LLC 2010
Abstract Chronic pancreatitis is a serious condition associated with severe abdominalpain, and a significant percentage of patients progresses to irreversible calcification inpancreas. The present study evaluates the degree to which the levels of trace elements,copper, iron, selenium, zinc and haemoglobin-Fe3+, in blood, serum and pancreas have anyrole to play in the calcification process associated with fibrosis in pancreas. Twenty-sevencalcific (CCP) and 23 non-calcific chronic pancreatitis (CP) patients and equal number ofage- and sex-matched normal volunteers (50) were enrolled in the study. Surgicallyremoved pancreatic tissue and blood samples were analysed for copper, iron, selenium,zinc, protein, collagen and lipid peroxidation products in terms of malondialdehyde, proteincarbonyls, glutathione, methemoglobin, methemoglobin reductase and ceruloplasminactivity levels. We could find that the pancreatic tissue levels of copper, iron, protein andcollagen contents were significantly elevated in CCP patients when compared to CPpatients. Serum levels of copper, free ionic copper and iron were also elevated in CCPpatients. The serum and the pancreatic tissue level of zinc and selenium showed asignificant decrease in CCP patients. The level of methemoglobin was elevated moresignificantly with the concomitant decline in the activity of methemoglobin reductase.There was a positive correlation between the pancreatic level of copper and iron with thecollagen and protein levels. The results of the present study revealed that the levels ofcopper and iron, the pro-oxidants and zinc and selenium may influence calcification processin CCP patients. Hypoxia-related tissue injury due to the formation of oxidisedhaemoglobin may also contribute to the pathogenesis of calcification in pancreas.
Keywords Chronic pancreatitis . Calcification . Copper . Iron . Zinc . Collagen .
Methemoglobin . Methemoglobin reductase
Biol Trace Elem Res (2011) 142:424–434DOI 10.1007/s12011-010-8822-y
G. Arumugam (*) :M. Padmanaban :D. Krishnan : S. PanneerselvamDepartment of Biochemistry, Bharathi Womens College (Affiliated to University of Madras), Chennai600 108 Tamil Nadu, Indiae-mail: [email protected]
S. RajagopalDepartment of Surgical Gastroenterology, Stanley Medical College and Hospital, Chennai 600 108Tamil Nadu, India

Introduction
Chronic pancreatitis is characterised by severe inflammation of the pancreas [1]. The mostcommon causes are alcoholism and cholithiasis [2, 3]. The other causes implicated in thedevelopment of inflammation are infection and exposure to chemical toxins, etc. In manycases, chronic pancreatitis progresses to calcification of the pancreas. During calcification,the precipitated proteins formed, plug the ductal system and tend to evolve into calculi andget distributed irregularly, affecting ducts of various sizes and may be associated withulceration that causes severe pain in the abdomen [4]. About 30–40% of the pancreatitispatients develop calcification in the pancreas, and the etiopathogenesis is not yet provencompletely with defined mechanisms.
Oxidative stress has been implicated in tissue inflammation and related complications inpancreatic disorders [5]. Trace elements such as copper and iron are closely associated withthe onset of oxidative insult in tissues, resulting in pathological conditions [6]. Zinc is thebeneficial trace element in regulating oxidative stress [7] and has a high turnover in thepancreas. Dominguez-Munoz et al. [8] have reported that quantification of the pancreaticoutput of zinc can be used as a measure of pancreatic function. Selenium is an essentialantioxidant involved in the activity of glutathione peroxidase and also influences theimmune status. Iron exists in two valency states, and the form Fe2+ is present in normalhaemoglobin (Hb) that delivers oxygen to tissues for biological oxidation and energyproduction. If iron in Hb is oxidised to Fe3+, the resulting metHb will not deliver oxygenefficiently to tissues, which manifests as hypoxia [9] and may lead to tissue injury orinflammation.
Since iron, copper, zinc and selenium are the trace elements which influence free radical-mediated reactions, the present study is undertaken to evaluate whether serum andpancreatic tissue levels of these elements can influence calcification and fibrosis of thepancreas in pancreatitis patients. Since blood circulation encounters oxidative stress inpancreatitis condition, the functional status of haemoglobin that delivers oxygen to tissueshas also been studied to find out whether hypoxia plays any role in the inflammation andcalcification of the pancreas in chronic pancreatitis.
Materials and Methods
Materials
Malondialdehyde, reduced and oxidised glutathione, NADH, sulphanilamide, N-(1-Naphthyl) ethylenediamine dihydrochloride, O-phenylene diamine, hydroxyproline, bovineserum albumin and sodium nitrite were purchased from Sisco Research Laboratories,Mumbai, India.
Subjects
The study included 50 chronic pancreatitis patients (27 calcific (CCP) and 23 non-calcific(CP)) and equal number of age- and sex-matched normal healthy volunteers. The patientswere in the age group of 30–50 years of both sexes registered as inpatients in thedepartment of Surgical Gastroenterology, Government General Hospitals and private clinicsat Chennai, Tamil Nadu. The patients were diagnosed with pancreatitis by abdominal X-ray,endoscopy and pancreatic exocrine and endocrine functional assay. The case history was
Cu, Fe, Zn and Fe3+ -Hb Levels on the Etiopathogenesis of CCP 425

recorded and the work protocol designed according to the suggestions given by the EthicalCommittee. The clinical history of the patients is presented in Table 1.
Blood sample was collected from each patient and the normal control subject with sterileequipment and processed for plasma and serum preparation and stored at 4°C until analysis.Surgically removed pancreatic tissue as a part of the treatment was collected in sterile salineand washed. A portion of the tissue was processed for the assay of copper, iron, zinc andselenium by atomic absorption spectrophotometry [10]. Another portion was used for thedetermination of total collagen [11, 12], protein [13], protein carbonyls [14], lipidperoxidation products [15] and reduced and oxidised glutathione [16] contents. Theremaining tissue was fixed in 10% formalin–saline and processed for histopathology andhistochemical study.
Serum and tissue samples were wet-ashed by refluxing with a 70:21:9 mixture of nitric–perchloric–sulfuric acid in a 10-ml Erlenmeyer flask to dissolve the minerals. Samples weremade up to the volume with 0.1 N hydrochloric acid in deionized mineral-free water andanalysed for iron, copper, zinc and selenium concentrations by atomic absorptionspectrophotometry. Serum ceruloplasmin [17], total iron binding capacity [18] and freecopper levels were determined from the ceruloplasmin and total copper levels [19]. BloodHb, metHb [20] and metHb reductase [21] activity levels were also determined. Tenautopsied samples of similar regions of normal pancreas were obtained and processed foranalyses. The values were subjected to statistical analysis by ANOVA, and Spearman rankcorrelation test was conducted between the pairs of related parameters.
Results
The pancreatic tissue levels of copper, iron, zinc and selenium are presented in Table 2. Thepancreatic tissue resected from CCP patients showed a significant elevation in copper andiron and a decrease in zinc and selenium concentrations when compared to those of normalsubjects and CP patients. The protein and collagen levels are significantly high in thepancreas of CCP patients than in CP patients. Pancreatic tissue level of copper and iron canbe well correlated positively with the amount of collagen and protein content in the resectedpancreatic tissue. Table 3 shows the concentration of free and total copper, iron, ironbinding capacity, zinc, selenium and ceruloplasmin activity measured in the serum ofexperimental subjects. We could see a significant elevation in both the forms of copper andiron and a decrease in serum iron binding capacity, zinc and selenium in CCP patients.
Table 1 Clinical history of the patients
Particulars CP patients CCP patients
No. of patients 23 27
Male/female ratio 21:2 25:2
Age group 30–50 30–50
Alcoholic subjects 18 21
Gall stone occurrence 3 4
Tropical 2 2
Patients with hyperglycaemia 18 22
Patients with elevated serum lipase activity 18 20
426 Arumugam et al.

There is a significant elevation observed in the total iron binding capacity in CP patients.Ceruloplasmin activity is found to be decreased in CCP and increased in CP patients.
The total Hb concentration is found to be non-significantly low in both the group ofpatients, but the percentage of methemoglobin in total haemoglobin is found to be high inCCP cases. The concentration of total nitrite content in serum is found to have a positivecorrelation with the level of methemoglobin.
The activity of methemoglobin reductase is found to be significantly low in CCPpatients when compared to that of normal subjects and CP patients (Table 4).
The pancreatic tissue levels of lipid peroxidation products malondialdehyde and also theprotein carbonyl content are found to be elevated significantly in CCP cases than in CPpatients. The antioxidant protein glutathione (GSH) is found to be low in both the group ofpatients, and the ratio between GSH/GSSG is significantly low in CCP patients than in CPpatients (Table 5). Thiobarbituric acid-reactive substance (TBARS) level is found to have a
Table 2 Concentrations of copper, iron, zinc, selenium, collagen and protein in resected pancreatic tissue ofCP and CCP patients
Parameters Normal subjects CP patients CCP patients
Iron (ppm/g dry wt) 193.6±28.9 220.6±40.9a 261.8±46.9b
Zinc (ppm/g dry wt) 187.9±20.8 139.5±23.6a 120.9±19.9b
Copper (ppm/g dry wt) 12.5±23.5 20.6±3.0a 30.6±5.17b
Selenium (ppm/g dry wt) 0.634+0.097 0.46+0.07a 0.36+0.05b
Protein (mg/g wet wt) 123.5±19.9 143.7±23.6a 189.9±30.9b
Collagen (mg hydroxy proline/g wet wt) 87.9±12.4 100.5±15.6a 156.8±23.7b
Values are expressed as mean ± SD for 20 no. of patients in each groupa Statistically significant variations expressed as p<0.05 for the comparisons made between the controlsubjects and the CP patientsb Statistically significant variations expressed as p<0.001 for the comparisons made between CP and CCPpatients
Table 3 Serum levels of total copper, ionic copper, iron, total iron binding capacity, zinc, selenium andceruloplasmin in CP and CCP patients
Parameters Normal subjects CP patients CCP patients
Total copper (μmol/L) 2.12±0.31 2.69±0.36a 3.34±0.46b
Non-ceruloplasmin copper (μmol/L) 0.73±0.10 0.96±0.12a 2.5±0.30b
Ceruloplasmin (mg/L) 29.5±3.4 36.6±2.9a 17.8±2.0b
Iron (μmol/L) 3.0±0.41 3.65±0.48a 4.43±0.56b
Total iron binding capacity (μmol/L) 389.6±46.9 450.9±54.7a 300.7±36.9b
Zinc (μg/dL) 105.6±17.8 95.6±12.3a 79.5±9.6b
Selenium (μg/dL) 0.119±0.02 0.078±0.01a 0.059±0.009b
Values are expressed as mean ± SD for 20 no. of patients in each groupa Statistically significant variations expressed as p<0.05 for the comparisons made between the controlsubjects and the CP patientsb Statistically significant variations expressed as p<0.001 for the comparisons made between CP and CCPpatients
Cu, Fe, Zn and Fe3+ -Hb Levels on the Etiopathogenesis of CCP 427
negative correlation with the level of zinc and selenium and a positive correlation with ironin CCP patients (Table 6).
Discussion
Chronic pancreatitis is a relapsing condition in 30–40% of the cases that present withabdominal pain due to pseudocyst formation and fibrotic calcification in various regions ofthe pancreas. The role of protein trypsin and calcium in the stone formation and in thepathogenesis of pain in CCP patients has been studied [22]. We could find a significantelevation in copper and iron levels in the pancreas of CCP patients. Copper and iron arewell known for their pro-oxidant action at higher concentrations. The levels of seleniumand zinc were found to be decreased in CCP patients and have a negative correlation withthe lipid peroxidation products measured in pancreatic tissue. These trace element levelscan be correlated with the amount of collagen and protein content in the affected part of thepancreas. Along with the free radical mechanism, the defective collagen and proteinturnover has been implicated in the pathogenesis of chronic pancreatitis. Leung and Chan[5] have observed that ROS/RNS generation in the pancreatitis condition may be attenuatedby targeting the enzymes involved in their formation. Zinc has been reported to regulate
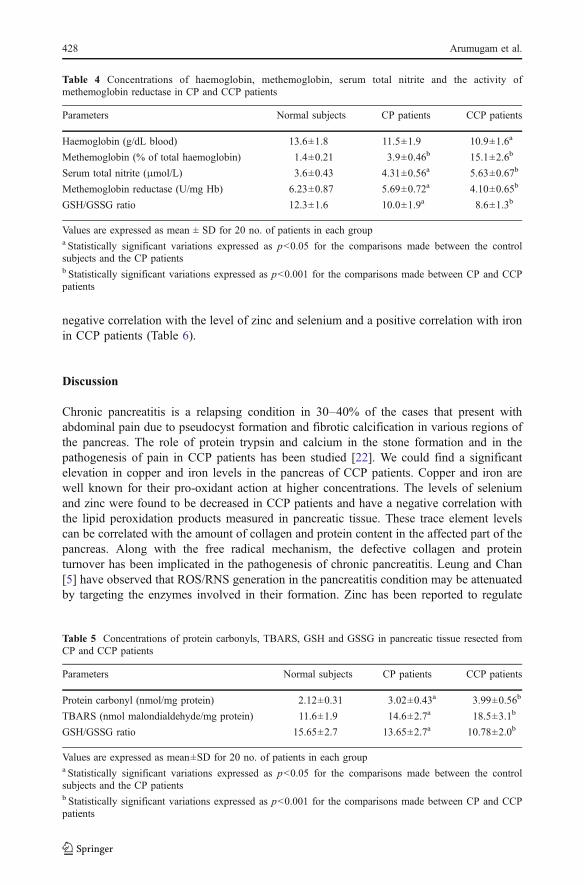
Table 4 Concentrations of haemoglobin, methemoglobin, serum total nitrite and the activity ofmethemoglobin reductase in CP and CCP patients
Parameters Normal subjects CP patients CCP patients
Haemoglobin (g/dL blood) 13.6±1.8 11.5±1.9 10.9±1.6a
Methemoglobin (% of total haemoglobin) 1.4±0.21 3.9±0.46b 15.1±2.6b
Serum total nitrite (μmol/L) 3.6±0.43 4.31±0.56a 5.63±0.67b
Methemoglobin reductase (U/mg Hb) 6.23±0.87 5.69±0.72a 4.10±0.65b
GSH/GSSG ratio 12.3±1.6 10.0±1.9a 8.6±1.3b
Values are expressed as mean ± SD for 20 no. of patients in each groupa Statistically significant variations expressed as p<0.05 for the comparisons made between the controlsubjects and the CP patientsb Statistically significant variations expressed as p<0.001 for the comparisons made between CP and CCPpatients
Table 5 Concentrations of protein carbonyls, TBARS, GSH and GSSG in pancreatic tissue resected fromCP and CCP patients
Parameters Normal subjects CP patients CCP patients
Protein carbonyl (nmol/mg protein) 2.12±0.31 3.02±0.43a 3.99±0.56b
TBARS (nmol malondialdehyde/mg protein) 11.6±1.9 14.6±2.7a 18.5±3.1b
GSH/GSSG ratio 15.65±2.7 13.65±2.7a 10.78±2.0b
Values are expressed as mean±SD for 20 no. of patients in each groupa Statistically significant variations expressed as p<0.05 for the comparisons made between the controlsubjects and the CP patientsb Statistically significant variations expressed as p<0.001 for the comparisons made between CP and CCPpatients
428 Arumugam et al.

collagen biosynthesis by influencing the activity of lysyl and prolyl hydroxylase and tomaintain the turnover of collagen in tissues [23, 24]. So the reduced level of zinc may beaccounted for the defective turnover of tissue collagen to influence calcification in thepancreas. Selenium is essential for the activity of glutathione peroxidase that neutralise thetoxic by-products of oxygen metabolism. It has been shown that the intravenousadministration of selenium prevented pancreatic injury in experimental animals [25]. Chenet al. [26] have proven that selenium could promote RNA synthesis with an increase inglutathione peroxidase activity in the pancreas. Selenium depletion may be accounted forthe low antioxidant status in the pancreas of CCP patients.
We could see a significant elevation in the level of serum total copper, free ionic copperand iron in both groups of patients, but the elevation was more significant in the CCPcondition. Copper is associated with a number of metalloproteins involved in oxidation–reduction reactions [27], but the excess level is always associated with the uncontrolledproduction of oxygen and nitrogen free radicals [28]. About 15% of the copper is present inthe free ionic form, whereas the rest is bound to ceruloplasmin (CPL), a copper bindingprotein. CPL is an abundant serum glycoprotein containing >90% of copper found in theplasma of vertebrates and prevents the availability of copper in the ionic form, whichotherwise acts as pro-oxidant [29]. The low level of CPL may be the reason for the highlevel of free ionic copper in the CCP condition, which might lead to deposition in tissues.The high level of ceruloplasmin in CP patients may be due to the compensatory mechanismto bind copper as much as possible before proceeding to calcification. In general, elevatedcopper and decreased zinc levels in serum have been shown in inflammation associatedwith many diseases [30, 31].
Iron concentration was non-significantly elevated in CP patients, whereas it wassignificantly high in the CCP condition. This might be due to low serum iron [32].Generally, the chronic pancreatitis patients present low serum protein content due toexocrine insufficiency, which results in reduced food digestion and absorption.
Table 6 Spearman rank test conducted for related parameters
Parameters rs value p value
Copperp vs proteinp +0.5436 <0.01
Copperp vs collagenp +0.4563 <0.01
Ironp vs proteinp +0.5432 <0.01
Ironp vs collagenp +0.6098 <0.01
Zincp vs collagenp −0.4530 <0.01
Zinc p vs TBARSp −0.5098 <0.01
Iron p vs TBARSp +0.6300 <0.01
Non-ceruloplasmin coppers vs CPLs −0.5112 <0.01
Irons vs CPLs −0.5231 <0.01
Irons vs MetHb +0.6543 <0.01
Met Hb vs metHb reductase −0.6321 <0.01
Ironp vs protein carbonylp +0.5432 <0.01
Total nitrite(s) vs metHb +0.4999 <0.01
Seleniump vs TBARSp −0.534 <0.01
Based on the critical values of the rank correlation (Spearman’s rho-rs), null hypothesis of no correlation wasrejected and concluded that the aforementioned parameters have correlations
Cu, Fe, Zn and Fe3+ -Hb Levels on the Etiopathogenesis of CCP 429
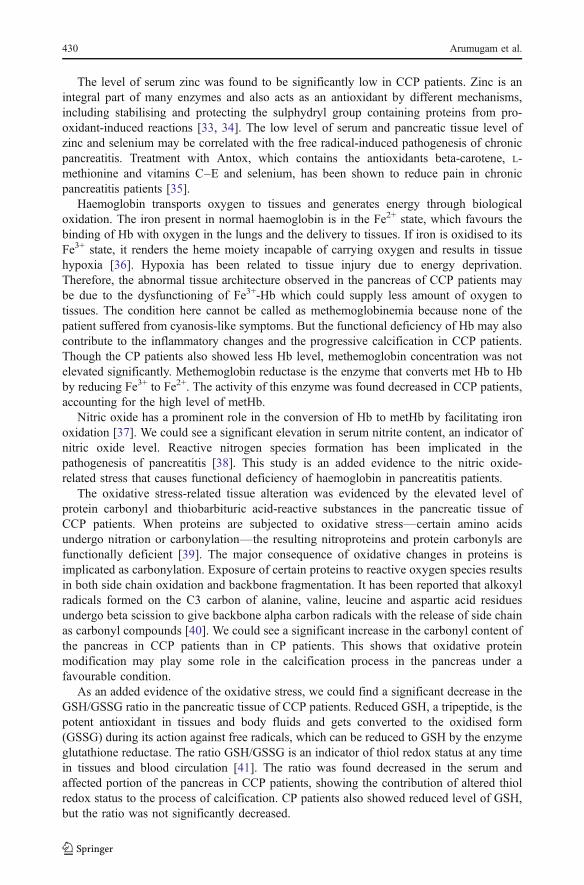
The level of serum zinc was found to be significantly low in CCP patients. Zinc is anintegral part of many enzymes and also acts as an antioxidant by different mechanisms,including stabilising and protecting the sulphydryl group containing proteins from pro-oxidant-induced reactions [33, 34]. The low level of serum and pancreatic tissue level ofzinc and selenium may be correlated with the free radical-induced pathogenesis of chronicpancreatitis. Treatment with Antox, which contains the antioxidants beta-carotene, L-methionine and vitamins C–E and selenium, has been shown to reduce pain in chronicpancreatitis patients [35].
Haemoglobin transports oxygen to tissues and generates energy through biologicaloxidation. The iron present in normal haemoglobin is in the Fe2+ state, which favours thebinding of Hb with oxygen in the lungs and the delivery to tissues. If iron is oxidised to itsFe3+ state, it renders the heme moiety incapable of carrying oxygen and results in tissuehypoxia [36]. Hypoxia has been related to tissue injury due to energy deprivation.Therefore, the abnormal tissue architecture observed in the pancreas of CCP patients maybe due to the dysfunctioning of Fe3+-Hb which could supply less amount of oxygen totissues. The condition here cannot be called as methemoglobinemia because none of thepatient suffered from cyanosis-like symptoms. But the functional deficiency of Hb may alsocontribute to the inflammatory changes and the progressive calcification in CCP patients.Though the CP patients also showed less Hb level, methemoglobin concentration was notelevated significantly. Methemoglobin reductase is the enzyme that converts met Hb to Hbby reducing Fe3+ to Fe2+. The activity of this enzyme was found decreased in CCP patients,accounting for the high level of metHb.
Nitric oxide has a prominent role in the conversion of Hb to metHb by facilitating ironoxidation [37]. We could see a significant elevation in serum nitrite content, an indicator ofnitric oxide level. Reactive nitrogen species formation has been implicated in thepathogenesis of pancreatitis [38]. This study is an added evidence to the nitric oxide-related stress that causes functional deficiency of haemoglobin in pancreatitis patients.
The oxidative stress-related tissue alteration was evidenced by the elevated level ofprotein carbonyl and thiobarbituric acid-reactive substances in the pancreatic tissue ofCCP patients. When proteins are subjected to oxidative stress—certain amino acidsundergo nitration or carbonylation—the resulting nitroproteins and protein carbonyls arefunctionally deficient [39]. The major consequence of oxidative changes in proteins isimplicated as carbonylation. Exposure of certain proteins to reactive oxygen species resultsin both side chain oxidation and backbone fragmentation. It has been reported that alkoxylradicals formed on the C3 carbon of alanine, valine, leucine and aspartic acid residuesundergo beta scission to give backbone alpha carbon radicals with the release of side chainas carbonyl compounds [40]. We could see a significant increase in the carbonyl content ofthe pancreas in CCP patients than in CP patients. This shows that oxidative proteinmodification may play some role in the calcification process in the pancreas under afavourable condition.
As an added evidence of the oxidative stress, we could find a significant decrease in theGSH/GSSG ratio in the pancreatic tissue of CCP patients. Reduced GSH, a tripeptide, is thepotent antioxidant in tissues and body fluids and gets converted to the oxidised form(GSSG) during its action against free radicals, which can be reduced to GSH by the enzymeglutathione reductase. The ratio GSH/GSSG is an indicator of thiol redox status at any timein tissues and blood circulation [41]. The ratio was found decreased in the serum andaffected portion of the pancreas in CCP patients, showing the contribution of altered thiolredox status to the process of calcification. CP patients also showed reduced level of GSH,but the ratio was not significantly decreased.
430 Arumugam et al.

The Spearmen test conducted between Fe(p)-protein(p), Cu(p)-protein(p),Zn(p)-collagen(p), Fe(p)-collagen(p), Cu(p)-collagen(p), serum total nitrite-metHb, iron(p)-TBARS(p)and Zn(p)-TBARS(p) revealed that the trace elements iron and copper have a positivecorrelation with protein, collagen and TBARS levels. Negative correlation was observedfor the paired values of CPL-free ionic copper, metHb-metHb reductase, Zn–TBARS andselenium–TBARS.
Fig. 1 Photomicrograph of the pancreatic section from a CCP patient showing fibrotic inflammation inacinar cells, ductal hyperplasia and regions of calcification (b); inflammation with less fibrotic changes inpancreatic section of CP patients (c); and normal tissue architecture with acinar cells from a normal subject(a). H × E ×400
Cu, Fe, Zn and Fe3+ -Hb Levels on the Etiopathogenesis of CCP 431

Histological observation made with the thin sections of pancreas extracted from CCPpatients showed the ductal hyperplasia and dysplasia of the pancreatic duct, numerous celldivisions and fibrotic acinar cells with regions of calcified tissues (Fig. 1b). In Fig. 1c, wecould see the inflammation-rich portion of the pancreas without much fibrotic changes (CPcase).We could also observe the iron deposits in the tissue architecture of the pancreas ofthe CCP patients (Fig. 2b, c).
The results of this study show that the elevation in the levels of copper and iron in thepancreas have some role in influencing calcification. The reduced level of zinc may alsocontribute to collagen deposition during the process of calcification. The tissue injury andinflammation in pancreatitis may partly be due to the formation of metHb by ROS/RNS-related free radicals. The high collagen content in calcific pancreas directs us to study thedefect in collagen turnover with reference to the level of trace elements in pancreatitispatients that influence calcification.
Fig. 2 a Photomicrograph of apancreatic section of normalsubject showing normal tissuearchitecture. b, c CCP patientshowing iron deposits in thetissue architecture.Pearl stain ×400
432 Arumugam et al.

Acknowledgement The author (AG) thanks the University Grants Commission, New Delhi, India, for thefinancial support to the research work.
References
1. He SQ, Yao JR, Zhang FX et al (2010) Inflammation and nerve injury induce expression of pancreatitis-associated protein-II in primary sensory neurons. Mol Pain 26:23–36
2. Maisonneuve P, Lowenfels AB, Mullhaupt B et al (2005) Cigarette smoking accelerates progression ofalcoholic chronic pancreatitis. Gut 54:510–514
3. Aboulian A, Chan T, Yaghoubian A, Kaji AH et al (2010) Early cholecystectomy safely decreaseshospital stay in patients with mild gallstone pancreatitis: a randomized prospective study. Ann Surg 251(4):615–619
4. Nealon WH, Bhutani M, Riall TS et al (2009) A unifying concept: pancreatic ductal anatomy bothpredicts and determines the major complications resulting from pancreatitis. J Am Coll Surg 208(5):790–799
5. Leung PS, Chan YC (2009) Role of oxidative stress in pancreatic inflammation. Antioxid Redox Signal11(1):135–165
6. Geetha A, Saranya P, Annie Jeyachristy S et al (2009) Relevance of non-ceruloplasmin copper tooxidative stress in patients with hepatocellular carcinoma. Biol Trace Elem Res 130(3):229–240
7. Shevchuk IA, Sanduliak LI (2009) Relation between the concentration of zinc in the pancreas and thefunctional activity of the islets of Langerhans. Pancreas 38(6):681–688
8. Domínguez-Muñoz JE, Martinez SM, Leodolter A et al (2004) Quantification of pancreatic zinc outputas pancreatic function test: making the secretin–caerulein test applicable to clinical practice.Pancreatology 4(1):57–62
9. Poberezkina NB, Zadorina OV, Andriushchenko PI et al (1992) The role of peroxidation processes andantioxidant protection in nitrite-induced hypoxia and its correction with vitamins. Ukr Biokhim Zh 64(6):64–70
10. Carthew GW, Dey RL (1985) A rapid tissue extraction method for determining liver copper content byatomic absorption spectroscopy. N Z Vet J 33:168–170
11. Reddy GK, Envemaka CS (1996) A simplified method for the analysis of hydroxyl proline in biologicaltissues. Clin Biochem 29:225–229
12. Bornstein P, Kang AH, Piez KA (1996) The nature and location of intramolecular crosslinks in collagen.Proc Natl Acad Sci 55:417–424
13. Lowry OH, Rosebrough NJ, Farr AL (1951) Protein measurement with the Folin phenol reagent. J BiolChem 193:265–275
14. Abraham ZR, Packer L (1993) Oxidative damage to proteins: spectrophotometric method for carbonylassay. Methods enzymol Part C 233:357–363
15. Ohkawa H, Ohishi N, Yagi K (1979) Assay of lipid peroxide in animal tissue by thiobarbituric acidreaction. Anal Biochem 95:351–358
16. Hansen RE, Østergaard H, Nørgaard P (2007) Quantification of protein thiols and dithiols in thepicomolar range using sodium borohydride and 4,4′-dithiodipyridine. Anal Biochem 363(1):77–82
17. Ceron JJ, Martinez SS (2004) An automated spectrophotometric method for measuring canineceruloplasmin in serum. Vet Res 6:671–679
18. Ramsay WN (1997) An improved technique for the determination of plasma iron binding capacity.Biochem J 20:1208–1211
19. Gaffiney D, Fell GS, O’Reilly DS (2000) ACP Best Practice no163. Wilson’s diseases: acute andpresymptomatic laboratory diagnosis and monitoring. J Clin Pathol 53:807–812
20. Matsuoka T (1978) Determination of methemoglobin and carboxyhemoglobin in blood by rapidcolorimetry. Nippon Ketsueki Gakkai Zasshi 41(4):695–704
21. Tanishima K, Takeshita M, Yubisui T et al (1978) A colorimetric method for the specific determinationof methemoglobin reductase activity in red blood cells. Nippon Ketsueki Gakkai Zasshi 41(4):695–704
22. Jin CX, Naruse S, Kitagawa M et al (2002) Pancreatic stone protein of pancreatic calculi in chroniccalcified pancreatitis in man. JOP 3(2):54–61
23. Camps J, Bargalio T, Gimenez A et al (1992) Relationship between hepatic lipid peroxidation andfibrogenesis in carbon tetrachloride treated rats: effect of zinc administration. Clin Sci 83:695–700
24. Anttinen H, Oikarinen A, Puristolo U et al (1985) Prevention by zinc of rat lung collagen accumulationin carbon tetrachloride injury. Am Rev Respir Dis 132:536–540
Cu, Fe, Zn and Fe3+ -Hb Levels on the Etiopathogenesis of CCP 433
25. Hardman J, Jamelav S, Sheilds C et al (2005) Intravenous selenium modulates L-arginine inducedexperimental acute pancreatitis. JOP J Pancreas 6:431–437
26. Chen FS, Zhao TG, Xu GL, Jia XA (1990) Effect of selenium on RNA synthesis and content in ratpancreas. Biofactors 4:259–261
27. Arredondo M, Núñez MT (2005) Iron and copper metabolism. Mol Aspects Med 26(4–5):313–32728. Repetto MG, Ferrarotti NF, Boveris A (2010) The involvement of transition metal ions on iron-
dependent lipid peroxidation. Arch Toxicol 84(4):255–26229. Cousins RJ (1985) Absorption, transport and hepatic metabolism of copper and zinc: special reference to
metallothionein and ceruloplasmin. Physiol Rev 65:1–430. Iskra M, Majewski W (1999) Oxidase activity of ceruloplasmin and concentration of copper and zinc in
chronic arterial occlusion of the lower limbs. J Trace Elem Biol Med 13:76–8131. Rogers JT, Lahiri DK (2004) Metal and inflammatory targets for Alzheimer’s disease. Curr Drug Targets
5:535–55132. Lu HZ, Yuan YS, Zhang WM et al (2006) Concentrations of serum iron and transferrin in children with
nephrotic syndrome. Zhongguo Dang Dai Er Ke Za Zhi 8(6):467–46933. Kojima-Yuasa A, Umeda K, Ohkita T et al (2005) Role of reactive oxygen species in zinc deficiency-
induced hepatic stellate cell activation. Free Radic Biol Med 39(5):631–64034. Powell SR (2000) The antioxidant properties of zinc. J Nutr 130:144–15435. Kirk JR, White JS, McKie L (2006) Combined antioxidant therapy reduces pain and improves quality of
life in chronic pancreatitis. J Gastrointest Surg 10:499–50336. Solheim L, Brun AC, Greibrokk TS (2000) Methemoglobinemia—causes, diagnosis and treatment.
Tidsskr Nor Laegeforen 120(13):1549–155137. Hamon I, Gauthier-Moulinier H, Grelet-Dessioux E et al. (2010) Methaemoglobinaemia risk factors with
inhaled nitric oxide therapy in newborn infants. Acta Paediatr (in press)38. Chvanov M, Petersen OH, Tepikin A (2005) Free radicals and the pancreatic acinar cells: role in
physiology and pathology. Philos Trans R Soc Lond B Biol Sci 360(1464):2273–228439. Levine RL (2002) Carbonyl modified protein in cellular regulation, aging and diseases. Free Radical Biol
Med 32:790–79640. Headlam HA, Davies MJ (2004) Markers of protein oxidation: different oxidants give rise to variable
yields of bound and released carbonyl products. Free Radical Biol Med 36:1175–118441. Ashfaq S, Abramson JL, Jones DP (2006) The relationship between plasma levels of oxidized and
reduced thiols and early atherosclerosis in healthy adults. J Am Coll Cardiol 47(5):1005–1011
434 Arumugam et al.




















