
Attention deficit/hyperactivity disorder (ADHD): complex phenotype, simple genotype?
Upload
independentCategory
view
1download
0
Fax +41 61 306 12 34E-Mail [email protected]
Research Report
Eur Addict Res 2011;17:10–20 DOI: 10.1159/000321259
Influence of Attention Deficit Hyperactivity Disorder and Conduct Disorder on Opioid Dependence Severity and Psychiatric Comorbidity in Chronic Methadone-Maintained Patients
P.J. Carpentier a, b M.T. van Gogh a L.J.M. Knapen a J.K. Buitelaar c C.A.J. De Jong a, d
a Novadic-Kentron, Network for Addiction Treatment Services, Vught , b Reinier van Arkel groep, ’s-Hertogenbosch , c Department of Cognitive Neurosciences, Radboud University Nijmegen Medical Centre, Nijmegen , and d Nijmegen Institute for Scientist-Practitioners in Addiction (NISPA), Nijmegen , The Netherlands
CD. Conclusion: ADHD in MMT patients is characterised by greater addiction severity and more comorbid psychopa-thology, only partly explained by the influence of a coexist-ing CD. The presence of ADHD in a substantial minority of patients accentuates the need for early detection and treat-ment of this complicating disorder.
Copyright © 2010 S. Karger AG, Basel
Introduction
Attention deficit hyperactivity disorder (ADHD) is a common, highly heritable, neurobehavioural disorder that begins in childhood but often persists into adult-hood. It is associated with significant impairment in psy-chosocial functioning [1] . Worldwide prevalence of adult ADHD in the general population is estimated at 3.4% (range 1.2–7.3%) [2] . A much higher prevalence of ADHD has consistently been found in patients with substance use disorders (SUD) [3, 4] . More recent studies using strict DSM-IV criteria indicate a prevalence between 10 and 24% [5–8] in patients with different kinds of SUD. Although ADHD and SUD are highly comorbid disor-ders, adults with both together have a greater risk for oth-er psychiatric disorders than adults with either condition
Key Words
Attention deficit hyperactivity disorder � Conduct disorder � Opioid dependence � Methadone � Psychiatric comorbidity � Substance use disorders
Abstract
Background: Persistent attention deficit hyperactivity dis-order (ADHD) and a history of conduct disorder (CD) are highly prevalent among patients with substance use disor-ders (SUD). We examined the influence of both diagnoseson problem severity, psychiatric comorbidity, and quality of life in methadone-maintained patients. Methods: 193 pa-tients in long-term methadone maintenance treatment (MMT) were assessed for ADHD through a semi-structured interview. Psychiatric disorders and SUD were assessed with the MINI, the CIDI-SAM, and the SIDP-IV. Results: Childhood ADHD was diagnosed in 68 (35.2%) patients; 48 (24.9%) had persisting ADHD; a CD history was present in 116 (60.1%). Pa-tients with adult ADHD had significantly higher problem se-verity scores, lower quality of life scores, more comorbid SUD and more psychiatric comorbidity. Although both ADHDand CD contributed to problem severity, addictive patholo-gy and psychopathology, ADHD was found to substantially increase the risk of psychiatric comorbidity, independent of
Published online: September 25, 2010 European
AddictioncRe es ar h
P.J. Carpentier Nieuwe Erven 24 NL–5263 AR Vught (The Netherlands) Tel. +31 73 658 6715, Fax +31 73 658 6706 E-Mail pjcarpentier @ planet.nl
© 2010 S. Karger AG, Basel1022–6877/11/0171–0010$38.00/0
Accessible online at:www.karger.com/ear

Attention Deficit Hyperactivity Disorder in Methadone Maintenance Treatment
Eur Addict Res 2011;17:10–20 11
alone [9, 10] . A history of conduct disorder (CD) in these patients is common, with frequencies of up to 70% re-ported [6, 11] . Several studies have found higher rates of DSM-IV Axis I psychopathology (especially mood and anxiety disorders) in subjects with SUD + ADHD com-pared to patients with SUD or ADHD alone or controls [5, 8, 10, 12] . These differences have not been replicated in other studies [6] . Personality disorders were also more frequent in SUD patients with ADHD [5, 8, 11] .
The presence of ADHD in a substantial minority of SUD patients highlights its role as a risk factor for addic-tion. If untreated, children with ADHD have a higher risk than children without ADHD of developing problematic drug use. They also tend to start drug use at an earlier age, and they more rapidly transition to regular drug use, abuse, and dependence [11, 13, 14] . ADHD in SUD pa-tients has been linked to a more severe progression of substance abuse and a less favourable prognosis [15, 16] . It is still unclear whether ADHD is an independent risk factor for addiction and how much of this increased risk is mediated by comorbid externalising disorders. CD in childhood is a notorious risk factor for adult psychopa-thology and SUD [17] , and comorbid CD has been found in 30–50% of childhood ADHD cases [18, 19] . Most stud-ies tend to agree that CD is the more dominant influence and that the contribution of ADHD is minimal or absent when the high overlap between ADHD and CD is taken into account [20–23] . However a distinct influence of ADHD, and especially the hyperactive/impulsive symp-tomatology, on the development of addiction has been documented in a recent prospective study, using dimen-sional symptomatology scores [24] . There is evidence that the interaction between ADHD and CD augments the risk even more than either disorder alone [22, 25] .
Although there seems to be no specific relationship between ADHD and type of substance abuse [26] , and ADHD is associated with both stimulant and depressant psychoactive drug use disorders [7] , comparatively little is known about ADHD in opioid dependence. Of the few published studies, nearly half focused on a retrospective diagnosis of childhood ADHD rather than its adult man-ifestations ( table 1 ). In the first of these studies, 22% of 157 opioid-addicted patients reported a childhood his-tory of hyperactivity [27] . Along with symptomatology suggestive of adult ADHD, greater mood pathology and a higher prevalence of antisocial personality disorder were observed in this subgroup. The most comprehensive and detailed study used an extensive psychiatric assess-ment and found a 16.7% prevalence of adult ADHD in a group of 125 patients entering methadone maintenance
treatment (MMT) [8] . The ADHD patients were charac-terised by greater psychiatric comorbidity and a greater number of personality disorders, especially antisocial personality disorders. However, ADHD had no effect on the number of SUD or on treatment outcomes. This last finding was attributed to a strong psychiatric assessment and treatment focus in the treatment program studied. Studies with a more limited diagnostic assessment found a history of childhood ADHD in 11 and 29% of treat-ment-seeking opioid-dependent patients [28, 29] . ADHD has also been associated with more frequent antisocial behaviour [29] and negative treatment outcomes [30] . A recent study of 1,761 patients with a diagnosis of lifetime cocaine and/or opioid dependence found a relatively low lifetime ADHD prevalence of 5.2% [12] ; after controlling for the influence of a CD, the ADHD group showed an earlier age of first drug use and a greater number of sub-stance dependence and psychiatric disorders than the non-ADHD group. In all these studies, most patients with ADHD had never been previously diagnosed with ADHD nor treated for this disorder specifically.
These studies suggest that ADHD is present in a sub-stantial minority of opioid-dependent patients and is as-sociated with more severe expressions of SUD and psy-chiatric disorders [10, 12] as well as antisocial personality disorders. However, the small number of studies, the var-ied and often limited ways in which ADHD was assessed, and the influence of a CD history preclude drawing for-mal conclusions ( table 1 ). The present study was designed to address these limitations by using an extensive and systematic psychiatric assessment to investigate ADHD and comorbid psychiatric disorders in a clinical popula-tion of opioid-dependent patients. By assessing both ADHD and a history of CD, we aimed to determine the influence of both disorders on psychiatric comorbidity and SUD severity. The high prevalence of psychiatric co-morbidity in opioid dependence [31–33] contributes to the low quality of life typical for these patients [34] , as was demonstrated in our previous work [35] . In an extension of this study we were interested to find out if the increased psychiatric comorbidity associated with ADHD would be reflected in a lower quality of life in these patients. In con-trast to the studies mentioned above, participants in the present study had been in long-term MMT.
We proposed the following hypotheses: (a) ADHD would be diagnosed in a sizable subgroup of MMT pa-tients; (b) the presence of ADHD would be associated with (i) a more severe course of addiction, (ii) greater fre-quency of co-occurring problematic substance use, (iii) a greater number of comorbid psychiatric disorders, (iv) a

Carpentier /van Gogh /Knapen /Buitelaar /De Jong
Eur Addict Res 2011;17:10–2012
higher level of dysfunctionality, and (v) a lower quality of life; (c) ADHD would be associated with more severe psy-chopathology even when the influence of a CD history is taken into account.
Methods
Participants The present study is part of a larger research project, the first
results of which have been published elsewhere [35] . All patients who registered in the MMT program at the Kanaaldijk, a low-threshold facility of the Novadic-Kentron in Eindhoven, The Netherlands, between March 1st and December 1st 2005 were in-vited to participate. Participation was voluntary, but the patients were repeatedly encouraged to take part. All patients were in-
formed that their personal data would be used for planning their further treatment. A small reward of EUR 5 per session was of-fered as an additional incentive to participate. As the study tar-geted the entire patient population, there were no formal exclu-sion criteria. However, the extensive interviews and rating scales included in the study required sufficient understanding of the Dutch language by the participants.
Procedure All participants gave their informed consent. In three or four
sessions, each lasting 60–90 min, an extensive evaluation of psy-chiatric comorbidity was conducted. The participants were each given access to a written or oral report of their results and, with their permission, the results were passed on to the treating physi-cian. The study was approved by the regional medical-ethical committee ( METIGG zuid : protocol 5.114, 2005).
Table 1. Prevalence studies of childhood and adult ADHD in patients with opioid dependence
Reference(first author)
n ADHD screeninginstruments
ADHD assessmentinstruments
Prevalencechildhood ADHD
Prevalenceadult ADHD
Additional findings in ADHD group
Eyre1982 [27]
157 Cantwell criteria 22% notassessed
Trend toward greater severity of drug useMore antisocial personality disordersSymptoms suggesting adult sequelae of the [ADHD] disorder
King1999 [8]
125 DIS-4.0 (Diagnostic Interview Schedule for DSM-IV)CPT: Continuous Performance Test
19.2% 16.7% No difference in number of lifetime substance use diagnosesSignificantly more comorbid psychiat-ric diagnosesSignificantly more personality disor-ders, especially antisocial personality disordersNo difference in treatment outcome
Modestin2001 [28]
100 Clinical question-naire for childhood ADHD, based on DSM-IV criteria
11% notassessed
Earlier start of drug abuse careerMore personality disorders
Davids2004 [29]
109 WURS-k (Wender-Utah Rating Scale): self-report
29% notassessed
No difference in substance use disorder characteristicsMore antisocial behaviour
Kolpe2007 [30]
687 ADDS (Attention Def-icit Disorder Screen)
notassessed
19% Less likely to achieve abstinence after 9 months
Arias2008 [12]
1,7611 SSADDA (Semi-structured Assess-ment for Drug Dependence and Alcoholism)
5.22% 4.15% Earlier age of first substance useMore substance use diagnosesMore psychiatric diagnoses
1 Non-treatment-seeking population with lifetime diagnosis of cocaine and/or opioid dependence.

Attention Deficit Hyperactivity Disorder in Methadone Maintenance Treatment
Eur Addict Res 2011;17:10–20 13
Measures To assess ADHD, psychiatric comorbidity, and problem sever-
ity, various instruments were administered by two researchers (M.v.G. and L.K.), who at the time of the study were training for their Master of Science in Mental Health, and by a nurse research-er (C.A.G. Verbrugge), who were supervised by the principal in-vestigator (P.J.C.). For this extensive examination of at least three sessions of more than 60 min, participants had to be sufficiently sober and alert. Multiple observation of each participant mitigated the influence of any drug use. The ADHD diagnoses were based on information obtained with the Semi-Structured Interview for ADHD in Adults , developed by Kooij et al. [36–38] . This instru-ment, available only in Dutch, is based on the DSM-IV definition of ADHD, and assesses both childhood and current presence of three symptom groups (inattention, restlessness, and impulsivity) and the resulting dysfunction. The instrument was developed pri-marily for clinical practice and its psychometric qualities have not been systematically validated. The resulting diagnosis is based pri-marily on information regarding lifetime and current symptom presence and functioning, and not on clinical symptom presenta-tion. If possible, and only with the permission of the participants, their partners or relatives were contacted to confirm the informa-tion. A diagnosis of definite ADHD was given only when the in-formation from the interview consistently confirmed the presence of invalidating ADHD symptoms from childhood to the present. Confirmation by other sources (partner, relatives) was considered as additional evidence, but not as necessary for the diagnosis. If the information was suggestive but inconsistent, a diagnosis of possible ADHD was made. If ADHD symptoms that were clear in childhood were no longer present or troublesome at the time of evaluation, a diagnosis of childhood ADHD was made. The choice for assessing ADHD in this way was based on the investigators’ experience with the patient group in question. The level of dys-function necessary for an ADHD diagnosis was better reflected by the semi-structured interview responses than they would have been by responses to symptom items on a rating scale. Thus, in our opinion the interview procedure we used allowed for a reliable di-agnosis of ADHD in this specific patient population. For retro-spective diagnoses of CD, the relevant section of the Diagnostic Interview Schedule (DIS-N) was used [39] .
Problem severity for seven life domains (general health, em-ployment and income, alcohol and drug use, legal problems, fam-ily and social relationships, psychiatric problems) was evaluated using the Europ-ASI, the European version of the Addiction Se-verity Index [40] . ASI scores, indicating the level of dysfunction in each domain, can range from 0 (no real problem) to 4–5 (mod-erate problem, some treatment indicated) to 8–9 (extreme prob-lem, treatment absolutely indicated). The general section of this instrument provided the sociodemographic characteristics of the participants.
The EuroQol-5 (EQ-5D) was selected to measure patients’ health-related quality of life [41] . The EQ-5D assesses five different domains of general health and functioning (i.e. mobility, self-care, daily activities, presence of pain or discomfort, and presence of anxious or depressed mood) using a 3-point scale (1 = ‘no prob-lems’, 2 = ‘some problems’, 3 = ‘extreme problems’). The scores for the five domains are summed to create a single index, using a for-mula based on EQ-5D evaluations for the general population [42] . Scores on this summary EQ-5D index can range from –0.594 (a score of 3 for all domains) to 1.0 (perfect health). The EQ-5D also
employs a visual analogue scale on which respondents can indicate their overall state of health. The possible scores range from 0 to 100.
The Mini International Neuropsychiatric Interview (MINI), a brief diagnostic interview protocol based on DSM-IV-TR criteria, was used to screen for coexisting psychiatric disorders [43] . Re-cording current and past psychiatric symptomatology, this in-strument classifies psychiatric pathology, in general DSM-IV-TR categories.
Problematic substance use was examined in both a qualitative and a quantitative way. Comorbid SUD in addition to the opioid dependence were assessed using the Composite International Di-agnostic Interview – Substance Abuse Module (CIDI-SAM), a fully-structured interview protocol aimed at ascertaining DSM-IV-TR diagnoses representing problematic use of alcohol and five classes of psychoactive drugs (cannabis, stimulants, sedatives, co-caine, and other drugs) [44] . To provide more quantitative infor-mation about the use of these substances, independent of any di-agnosis, age at first use, years of regular use and current use (num-ber of days of substance use in the past 30 days) was assessed with the Alcohol & Drug section of the Europ-ASI.
The Social Conformism Scale (SCS), a screening instrument based on the Structural Interview for Personality Disorders (SIDP-IV), was used to screen for personality disorders [45, 46] . A score above the cut-off point does not indicate a definite per-sonality disorder but, rather, the possibility of a personality dis-order. Antisocial personality disorder was assessed using the rel-evant section of the SIPD-IV [45] .
Data Analysis The ADHD patients were compared with the non-ADHD pa-
tients on psychiatric comorbidity and dysfunction, using t tests for continuous variables and � 2 tests for categorical variables (degrees of freedom = N – 1). Patients diagnosed as only possibly having ADHD or who had ADHD only in childhood were excluded from these analyses. To differentiate the influence of ADHD and CD, linear and binary logistic regressions were carried out with ADHD and CD as the independent variables. The corresponding stan-dardised � coefficients and odds ratios were estimated. To com-pensate for the large number of analyses, a conservative � level of p ! 0.01, two-tailed, was adopted. All the statistical computations were performed using the Statistical Package for the Social Sci-ences 15.0.1, 2006 (SPSS Inc., Chicago, Ill., USA).
Results
From a total of 306 eligible patients, 193 (161 men and 32 women) volunteered to participate in the present study. Patient recruitment and participation have been de-scribed more extensively in a previous article [29] .
Prevalence of ADHD and CD History All 193 participants were assessed for the presence of
ADHD. For 19 participants, the partner provided addi-tional information on current symptomatology and func-tioning. For 50 participants, a family member supplied information on childhood symptomatology. A definite

Carpentier /van Gogh /Knapen /Buitelaar /De Jong
Eur Addict Res 2011;17:10–2014
diagnosis of childhood ADHD was made for 68 partici-pants (57 men, 11 women: 35.2% of the sample); 48 of them (38 men, 10 women: 24.9%) had persistent ADHD, whereas 19 no longer had significant ADHD symptom-atology at the time of assessment ( fig. 1 ). Most of the adult ADHD patients (89.6%) endorsed both inattentiveness and hyperactive/impulsive symptoms; only a few patients mentioned inattentiveness (2.1%) or hyperactive/impul-sive symptoms (8.3%) alone. For 14 patients, the infor-mation was suggestive but inconclusive for childhood ADHD, so they were given a diagnosis of possible child-hood ADHD. Ten continued to have some ADHD symp-tomatology in adulthood, but it was not severe enough to warrant a definite diagnosis. For the majority of patients, the ADHD diagnosis had not been made earlier; only 5 were currently being treated for ADHD.
A history of CD was confirmed in 116 participants (102 men, 14 women: 60.1%). For a majority of them (82 participants; 70.7%), CD symptomatology started only after the age of 10 years, whereas in 34 participants (29.3%) there was a history of childhood-onset CD. ADHD and CD frequently occurred together: 51 partici-pants with a history of CD had childhood ADHD (44.0%), whereas 37 (31.9%) had persistent ADHD. The prevalence of ADHD in the 77 participants without a CD history was
much lower: only 16 (20.8%) had childhood ADHD, and 11 (14.3%) had persistent ADHD.
Sociodemographic Characteristics The 48 participants with definite ADHD were com-
pared to the 111 participants without ADHD ( fig. 1 ). 15 participants with an unclear diagnosis and 19 patients with only childhood ADHD were excluded from theanalysis. The sociodemographic and opioid-dependence characteristics of both groups are listed in table 2 . The ADHD subgroup was significantly younger than the non-ADHD group, resulting in a significantly shorter mean duration of heroin use, but there were no differences be-tween the subgroups in age of first heroin and methadone
ADHD
diagnosis
Definite
Possible
No
Childhood
ADHD
68
(35.2%)
14
(7.2%)
111
(57.6%)
48
1
19
10
4
111
Adult
ADHD
48
(24.9%)
11
(5.7%)
134
(69.4%)
Fig. 1. Prevalence of childhood and adult ADHD in the study pop-ulation (n = 193). All participants were assessed for the presence of childhood and adult ADHD. Of 68 participants with childhood ADHD, 48 continued to have disabling ADHD symptoms at the time of assessment, 1 had questionable symptomatology, and 19 had remitted. For 14 participants, the history was suspect for childhood ADHD but the information was inconclusive; 10 of them continued to have some symptoms, but the symptoms were insufficient for a clear diagnosis of ADHD; the remaining 4 men-tioned no current ADHD symptoms.
Table 2. Opioid dependence and sociodemographic characteris-tics of 48 MMT patients with ADHD compared to 111 MMT pa-tients without ADHD
ADHD(n = 48)mean 8 SD
Non-ADHD(n = 111)mean 8 SD
t* Sig.
Age 37.886.5 41.887.0 –3.37 0.001Age first heroin use 21.785.6 21.985.6 –0.21 0.84Years of heroin use 12.187.4 16.187.6 –3.08 0.002Age first methadone use 24.885.8 26.886.9 –1.67 0.10Years of methadone use 10.887.1 12.487.4 –1.26 0.21
n (%) n (%) �2* Sig.
Gender –0.31 0.66Male 38 (79.1) 92 (82.9)Female 10 (20.9) 19 (17.1)
Land of birth –4.08 0.07The Netherlands 44 (91.7) 87 (78.4)Other 4 (8.3) 24 (21.6)
Nationality –1.25 0.44Dutch 47 (97.9) 104 (93.7)Other 1 (2.1) 7 (6.3)
Marital status –0.21 0.74Married 4 (8.3) 7 (6.3)Unmarried 44 (91.7) 104 (93.7)
Level of education –1.48 0.48Primary education 32 (66.7) 69 (62.2)Secondary education 14 (29.2) 31 (27.9)Higher education 2 (4.1) 11 (9.9)
Work situation –0.66 0.88Full-time employment 8 (16.7) 19 (17.1)Part-time employment 1 (2.1) 5 (4.5)Jobless 28 (58.3) 60 (54.0)Unfit for work 11 (22.9) 27 (24.3)
* d.f. = N – 1 = 158.

Attention Deficit Hyperactivity Disorder in Methadone Maintenance Treatment
Eur Addict Res 2011;17:10–20 15
use. Gender, nationality, level of education, and work sit-uation were similar in both groups. A marginal (p ! 0.10) difference was found for land of birth, with fewer ADHD diagnoses for foreign-born participants.
Problem Severity and Quality of Life The ADHD participants had a significantly higher
mean Europ-ASI score than the non-ADHD participants, reflecting increased problem severity in terms of Legal Status, Relationships, and Psychiatric Status ( table 3 ). Dif-ferences in Relationships and Psychiatric Status remained significant after controlling for CD, whereas CD explained most of the variance in Legal Status. The ADHD partici-pants had higher problem scores for Usual Activities and Anxiety/Depression on the EuroQol-5. This resulted in a significantly lower index score for the combined mea-sures, reflecting a lower quality of life ( table 3 ). The ADHD group also rated their general health as significantly poor-er than the non-ADHD group on the visual analogue scale. Adding CD as an independent variable in the regres-sion model had little influence on these differences.
Substance Use Disorders The mean number of SUD assessed by the CIDI-SAM
was significantly greater in participants with ADHD
than in those without ADHD ( table 4 ). A nearly signifi-cant difference between these groups (p ! 0.05) emerged for the numbers of diagnoses of substance dependence and substance abuse. To a large extent, these differences are attributable to a co-occurring CD history; however, ADHD still has a comparable and significant influence when CD was controlled for. There were no significant differences in the prevalence of the individual SUD, with the exception of cannabis abuse (31.3% of the ADHD group vs. 14.4% of the non-ADHD group).
Amphetamine use as measured with the Europ-ASI was similar in the two groups: 23 patients (47.9%) in the ADHD group and 40 patients (36.0%) in the non-ADHD group had been regular users ( � 2 = 0.22), but only 6 in the ADHD group and 3 in the non-ADHD group were cur-rent users. In general, the ADHD group started their use of psychoactive substances at an earlier age than the non-ADHD patients. However, this age difference was signif-icant only for heavy alcohol users (18.3 vs. 22.0 years)and those who consumed different drugs each day (19.1 vs. 22.0 years); this difference was marginally signifi-cant for cocaine use (21.0 vs. 24.0 years; p ! 0.10). The ADHD group included a higher percentage of (prescribed and unprescribed) benzodiazepine users than the non-ADHD group (79.2 vs. 61.3%).
Table 3. Mean 8 SD Europ-ASI problem severity and EQ-5D quality of life scores for patients with and without ADHD, combined with hierarchical linear regression modelling using ADHD and CD diagnoses*
ADHD (n = 48)
Non-ADHD(n = 111)
S tep I: ADHD Step II: CD � (p) in full model Prop. explained varianceR2
changeFch ange
p R2
changeFchange
p ADHD CD
Europ-ASIMedical status 3.282.2 2.682.2 0.01 2.29 0.13 0.01 2.12 0.15 0.15 (0.06) –0.12 (0.15) 0.03Employment/support status 4.981.6 4.581.8 0.01 2.10 0.15 0.02 2.61 0.11 0.08 (0.35) 0.13 (0.11) 0.03Alcohol use 2.582.5 2.082.1 0.01 2.00 0.16 0.00 0.01 0.93 0.11 (0.19) 0.01 (0.93) 0.01Drug use 5.381.7 5.181.4 0.01 0.65 0.42 0.01 0.59 0.44 0.05 (0.58) 0.06 (0.44) 0.01Legal status 4.582.3 3.482.3 0.04 6.92 <0.01 0.12 21.80 <0.001 0.11 (0.17) 0.36 (<0.001) 0.16Family/social relationships 4.681.6 3.481.8 0.10 17.79 <0.001 0.04 7.45 <0.01 0.26 (<0.01) 0.21 (<0.01) 0.14Psychiatric status 5.581.5 3.682.2 0.15 28.22 <0.001 0.01 1.37 0.24 0.36 (<0.001) 0.09 (0.24) 0.16
EQ-5DMobility 1.3180.47 1.2980.49 <0.01 0.08 0.77 <0.01 0.04 0.85 0.03 (0.74) –0.02 (0.85) <0.01Self-care 1.2180.41 1.0980.32 0.02 3.87 0.05 <0.01 0.44 0.51 0.17 (0.04) –0.06 (0.51) 0.03Usual activities 1.6580.64 1.3780.52 0.05 8.23 <0.01 <0.01 0.75 0.39 0.20 (0.01) 0.07 (0.39) 0.05Pain/discomfort 1.8580.68 1.6680.67 0.02 2.86 0.09 <0.01 0.09 0.77 0.13 (0.13) 0.02 (0.77) 0.02Anxiety/depression 1.9680.65 1.5980.64 0.07 11.27 <0.01 <0.01 0.64 0.42 0.24 (<0.01) 0.06 (0.42) 0.07Health 2.1380.84 1.9680.66 0.01 1.68 0.20 0.05 7.71 <0.01 0.17 (0.042) –0.22 (<0.01) 0.06Index 0.5680.34 0.7080.29 0.04 7.02 <0.01 <0.01 0.05 0.82 –0.20 (0.02) –0.02 (0.82) 0.04Visual analogue scale 55823 64820 0.05 7.09 <0.01 <0.01 0.57 0.45 –0.22 (<0.01) 0.06 (0.45) 0.05
* S ignificant at p < 0.01.
Carpentier /van Gogh /Knapen /Buitelaar /De Jong
Eur Addict Res 2011;17:10–2016
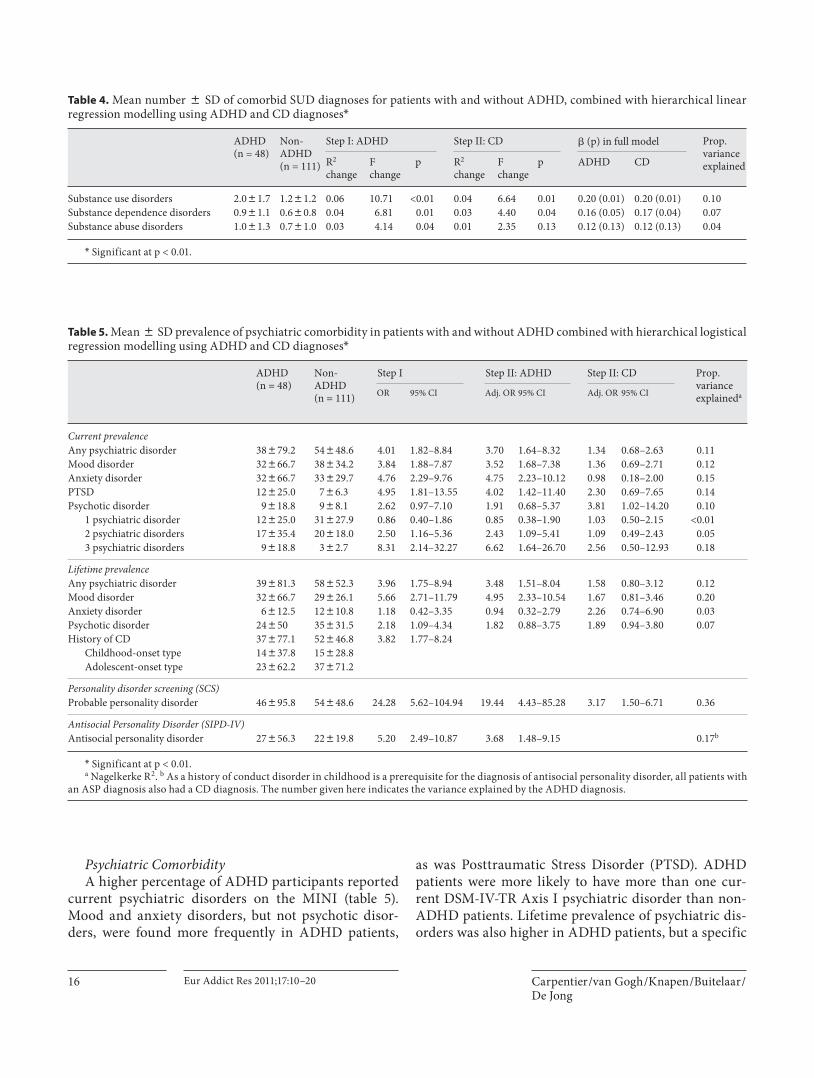
Psychiatric Comorbidity A higher percentage of ADHD participants reported
current psychiatric disorders on the MINI ( table 5 ). Mood and anxiety disorders, but not psychotic disor-ders, were found more frequently in ADHD patients,
as was Posttraumatic Stress Disorder (PTSD). ADHD patients were more likely to have more than one cur-rent DSM-IV-TR Axis I psychiatric disorder than non-ADHD patients. Lifetime prevalence of psychiatric dis-orders was also higher in ADHD patients, but a specific
Table 4. Mean number 8 SD of comorbid SUD diagnoses for patients with and without ADHD, combined with hierarchical linear regression modelling using ADHD and CD diagnoses*
ADHD (n = 48)
Non-ADHD(n = 111)
Step I: ADHD Step II: CD � (p) in full model Prop.variance explainedR2
changeFchange
p R2
changeFchange
p ADHD CD
Substance use disorders 2.081.7 1.281.2 0.06 10.71 <0.01 0.04 6.64 0.01 0.20 (0.01) 0.20 (0.01) 0.10Substance dependence disorders 0.981.1 0.680.8 0.04 6.81 0.01 0.03 4.40 0.04 0.16 (0.05) 0.17 (0.04) 0.07Substance abuse disorders 1.081.3 0.781.0 0.03 4.14 0.04 0.01 2.35 0.13 0.12 (0.13) 0.12 (0.13) 0.04
* Significant at p < 0.01.
Table 5. Mean 8 SD prevalence of psychiatric comorbidity in patients with and without ADHD combined with hierarchical logistical regression modelling using ADHD and CD diagnoses*
ADHD(n = 48)
Non-ADHD(n = 111)
Step I Step II: ADHD S tep II: CD Prop. variance explaineda
OR 95% CI Adj. OR 95% CI Adj. OR 95% CI
Current prevalenceAny psychiatric disorder 38879.2 54848.6 4.01 1.82–8.84 3.70 1.64–8.32 1.34 0.68–2.63 0.11Mood disorder 32866.7 38834.2 3.84 1.88–7.87 3.52 1.68–7.38 1.36 0.69–2.71 0.12Anxiety disorder 32866.7 33829.7 4.76 2.29–9.76 4.75 2.23–10.12 0.98 0.18–2.00 0.15PTSD 12825.0 786.3 4.95 1.81–13.55 4.02 1.42–11.40 2.30 0.69–7.65 0.14Psychotic disorder 9818.8 988.1 2.62 0.97–7.10 1.91 0.68–5.37 3.81 1.02–14.20 0.10
1 psychiatric disorder 12825.0 31827.9 0.86 0.40–1.86 0.85 0.38–1.90 1.03 0.50–2.15 <0.012 psychiatric disorders 17835.4 20818.0 2.50 1.16–5.36 2.43 1.09–5.41 1.09 0.49–2.43 0.053 psychiatric disorders 9818.8 382.7 8.31 2.14–32.27 6.62 1.64–26.70 2.56 0.50–12.93 0.18
Lifetime prevalenceAny psychiatric disorder 39881.3 58852.3 3.96 1.75–8.94 3.48 1.51–8.04 1.58 0.80–3.12 0.12Mood disorder 32866.7 29826.1 5.66 2.71–11.79 4.95 2.33–10.54 1.67 0.81–3.46 0.20Anxiety disorder 6812.5 12810.8 1.18 0.42–3.35 0.94 0.32–2.79 2.26 0.74–6.90 0.03Psychotic disorder 24850 35831.5 2.18 1.09–4.34 1.82 0.88–3.75 1.89 0.94–3.80 0.07History of CD 37877.1 52846.8 3.82 1.77–8.24
Childhood-onset type 14837.8 15828.8Adolescent-onset type 23862.2 37871.2
Personality disorder screening (SCS)Probable personality disorder 46895.8 54848.6 24.28 5.62–104.94 19.44 4.43–85.28 3.17 1.50–6.71 0.36
Antisocial Personality Disorder (SIPD-IV)Antisocial personality disorder 27856.3 22819.8 5.20 2.49–10.87 3.68 1.48–9.15 0.17b
* S ignificant at p < 0.01.a Nagelkerke R2. b As a history of conduct disorder in childhood is a prerequisite for the diagnosis of antisocial personality disorder, all patients with
an ASP diagnosis also had a CD diagnosis. The number given here indicates the variance explained by the ADHD diagnosis.

Attention Deficit Hyperactivity Disorder in Methadone Maintenance Treatment
Eur Addict Res 2011;17:10–20 17
difference in lifetime occurrence was found only for mood disorders. An ADHD diagnosis carried an in-creased likelihood of psychiatric comorbidity (not in-cluding psychotic disorders). This increased risk was only slightly reduced after a history of CD was taken into account.
CDs and Personality Disorders A history of CD was significantly more frequent in
ADHD patients than in non-ADHD patients (77.1 vs. 46.8%; p ! 0.001) ( table 5 ). There was no significant dif-ference in CD subtype between the two groups. The SCS screening instrument revealed a very high percentage of probable personality disorders in the ADHD group, with nearly all patients in this group scoring positive. The di-agnosis of antisocial personality disorder was also more frequent in the ADHD group. The presence of a personal-ity disorder was much more likely to be influenced by ADHD than by a CD history (OR 19.44 vs. 3.17).
Childhood ADHD Nineteen participants with clear childhood ADHD
but without significant ADHD symptomatology at the time of their assessment were identified ( fig. 1 ). A com-parison between this childhood ADHD group and the non-ADHD group (n = 111) revealed only a few signifi-cant differences. A history of CD was more frequent in the childhood ADHD patients than in the non-ADHD patients (73.7 vs. 46.8%). There also was a greater likeli-hood of personality disorders (78.9 vs. 48.6%; p ! 0.05) and antisocial personality disorders (42.1 vs. 19.8%; p ! 0.05) in the childhood ADHD group.
Discussion
A substantial presence of childhood and adult ADHD was found in this sample of MMT patients. The preva-lence of ADHD is generally higher than that found in less extensive studies [12, 27–29] but comparable to that found in recent studies of patients having other SUD [5–7] . The best documented study to date in a similar group of American patients with opioid dependence en-tering treatment found a somewhat lower but still com-parable prevalence [8] ; this dissimilarity can probably be attributed to methodological and assessment differ-ences.
Nearly all our results confirmed our hypotheses that MMT patients with ADHD have a more serious addic-tion, more comorbid SUD, greater severity of current
problems and a diminished quality of life than MMT pa-tients without ADHD. These findings are consistent with a growing body of literature showing that ADHD is as-sociated with more severe expressions of SUD and psy-chiatric disorders [10, 12] . As in previous studies [12, 13, 24] , our ADHD participants generally began using drugs at an earlier age than our non-ADHD participants. As expected, psychiatric comorbidity (both DSM-IV-TR Axis I and Axis II) was significantly more prevalent in the ADHD patients. Particularly noteworthy is the increased prevalence of PTSD in the ADHD patients, indicating a more specific association between these two disorders [47, 48] . The greater benzodiazepine use in the ADHD group, compared to the non-ADHD group, can be attrib-uted both to the higher prevalence of psychiatric comor-bidity and a more specific influence of benzodiazepines on ADHD symptoms.
The increase in problem severity and psychiatric co-morbidity found in the ADHD patients can be explained only partially by the frequent co-occurrence of a history of CD (present in 77.1% of ADHD patients). Indeed, most of the differences between the ADHD and non-ADHD patients (in functioning and quality of life, in SUD prev-alence and in psychiatric Axis I and Axis II comorbidity) remained significant when the influence of CD was con-trolled for. Although the cross-sectional and retrospec-tive design of the study limits the conclusions that can be drawn about a possible causal link between ADHD and addiction, the high prevalence of ADHD in childhood and the increased psychiatric comorbidity in adulthood suggest that ADHD is an influential factor in the origin and development of SUD, especially in conjunction with CD [23] .
Although both ADHD and CD contributed to the se-verity of the addiction, as reflected in the number of di-agnoses of SUD, the additional results suggest that these influences are mediated through different pathways. In the present study, a CD history explained most of the variance in social dysfunctioning. On the other hand, ADHD was associated with a much higher prevalence of Axis I psychiatric comorbidity and personality disor-ders. This finding suggests that, while CD is the more influential risk factor, ADHD has a unique contribution to the development and severity of SUD, possibly medi-ated through an increased risk for comorbid psychiatric pathology [10, 12, 24] . This influence of ADHD only be-comes more apparent retrospectively when psychiatric comorbidity is taken into account [8, 31] ; this may help to explain why the influence of ADHD was not detected in earlier studies focusing on the development of addic-

Carpentier /van Gogh /Knapen /Buitelaar /De Jong
Eur Addict Res 2011;17:10–2018
tion, as CD remains the more influential risk factor. Moreover, the increase in psychiatric comorbidity con-tributes to the negative prognosis associated with ADHD in SUD patients [15, 16] . This could result in an accumu-lation of this combination of disorders among chroni-cally addicted patients, offering a possible explanation for the somewhat higher prevalence in the present sam-ple of long-term MMT patients. In contrast, the study of King et al. [8] failed to identify any negative influence of an ADHD diagnosis on treatment outcome; this discrep-ancy with the present findings could be resulting from both a difference in study population and treatment set-ting and the somewhat smaller sample size of the King et al. study. Lastly, the psychiatric comorbidity adds to the decrease of quality of life of ADHD patients in our study group.
The repeated occurrence of a CD history in the total sample attests to the importance of this childhood diag-nosis as a risk factor for and precursor of adult psychopa-thology [17] . In this respect, the presence of a substantial subgroup with childhood-onset CD, which is known to be associated with a poor prognosis for adult psychopa-thology, cannot be considered a coincidence [6, 49] . The frequent co-occurrence of ADHD and CD in this sample of MMT patients confirms that the combination of dis-orders carries the greatest risk for the development of se-vere psychopathology and addiction [25, 50–52] . Opioid dependence in patients with both ADHD and CD can be considered the adult expression of a chronic psychiatric disorder starting in childhood [28, 53, 54] . More effort should be made to prevent this negative prognosis by de-veloping and implementing specific therapeutic strate-gies for children with this combination of disorders. The fact that ADHD can be detected and treated early in life offers a possible strategy for reducing the risk for SUD in later life [55–57] .
No greater problem severity and comorbidity was found in the small group of patients with childhood ADHD only compared to the other MMT patients with-out ADHD. This result may be due to the small size of this subgroup. Another possible explanation is that the risk of increasing psychopathology from ADHD diminishes as the severity of the ADHD lessens during adolescence and young adulthood. The increased personality pathology in the childhood ADHD group is probably accounted for by the high co-occurrence of a CD.
A strength of the present study is that a large group of MMT patients, frequently considered the ones with the most complex and difficult SUD, participated in an ex-tensive assessment protocol, allowing us to confirm the
substantial prevalence of ADHD, and to illustrate its siz-able influence in comorbid psychopathology, problem se-verity and quality of life. A limitation of the study is that the assessment of ADHD was not carried out with an in-ternationally validated instrument. Furthermore, collat-eral information could be obtained for only a minority of the participants, illustrating the impoverished social re-lationships of this patient group. In our opinion, the as-sessment procedure yielded sufficient information allow-ing reliable diagnoses in accordance with the DSM-IV-TR diagnostic criteria.
A further limitation of the present study is that the in-fluence of an ADHD diagnosis on treatment efficacy was not explored. In view of the higher psychiatric comorbid-ity and problem severity reported here, as well as in pre-vious studies, a diagnosis of ADHD would seem to carry a negative prognosis. However, as in earlier studies, most of our participants had never been diagnosed or treated for ADHD before, so the treatment options were not ful-ly explored. ADHD treatment is less successful in pa-tients with SUD than in ADHD adults without comor-bidities [4] . Treatment of ADHD in MMT patients has rarely been investigated, and results in the few studies that have been reported have been disappointing [58] . Standard ADHD treatment will probably be ineffective for this patient group due to the complexity of their psy-chopathology. On the other hand, a regimen integrating treatment for opioid dependence and for psychiatric co-morbidity with ADHD treatment can potentially make a significant contribution to the restoration of psychiatric stability and to an improved quality of life [59] . The prev-alence found in this study makes systematic screening for ADHD worthwhile and relevant in this patient group [60] .
In conclusion, the present findings confirm the high prevalence of ADHD in SUD patients. They also support the hypothesis that by influencing the expression of co-occurring psychopathology ADHD contributes to a more severe disorder in which the individual initiates sub-stance use at an early age and later experiences more se-vere addiction with more comorbid psychopathology [12] . The present study confirms the relevance of ADHD for opioid-dependent patients in MMT, and it emphasises the need for ADHD assessment and treatment in this pa-tient group.

Attention Deficit Hyperactivity Disorder in Methadone Maintenance Treatment
Eur Addict Res 2011;17:10–20 19
1 Biederman J, Faraone SV: Attention-deficit hyperactivity disorder. Lancet 2005; 366: 237–248.
2 Fayyad J, De Graaf R, Kessler R, et al: Cross-national prevalence and correlates of adult attention-deficit hyperactivity disorder. Br J Psychiatry 2007; 190: 402–409.
3 Kalbag AS, Levin FR: Adult ADHD and sub-stance abuse: diagnostic and treatment is-sues. Subst Use Misuse 2005; 40: 1955–1958.
4 Wilens TE: Attention-deficit/hyperactivity disorder and the substance use disorders: the nature of the relationship, subtypes at risk, and treatment issues. Psychiatr Clin North Am 2004; 27: 283–301.
5 Levin FR, Evans SM, Kleber HD: Prevalence of adult attention-deficit hyperactivity dis-order among cocaine abusers seeking treat-ment. Drug Alcohol Depend 1998; 52: 15–25.
6 Schubiner H, Tzelepis A, Milberger S, et al: Prevalence of attention-deficit/hyperactivi-ty disorder and conduct disorder among substance abusers. J Clin Psychiatry 2000; 61: 244–251.
7 Clure C, Brady KT, Saladin ME, Johnson D, Waid R, Rittenbury M: Attention-deficit/hyperactivity disorder and substance use: symptom pattern and drug choice. Am J Drug Alcohol Abuse 1999; 25: 441–448.
8 King VL, Brooner RK, Kidorf MS, Stoller KB, Mirsky AF: Attention deficit hyperac-tivity disorder and treatment outcome in opioid abusers entering treatment. J Nerv Ment Dis 1999; 187: 487–495.
9 Sobanski E: Psychiatric comorbidity in adults with attention-deficit/hyperactivity disorder (ADHD). Eur Arch Psychiatry Clin Neurosci 2006; 256(suppl 1):i26–i31.
10 Wilens TE, Kwon A, Tanguay S, et al: Char-acteristics of adults with attention deficit hy-peractivity disorder plus substance use dis-order: the role of psychiatric comorbidity. Am J Addict 2005; 14: 319–327.
11 Carroll KM, Rounsaville BJ: History and sig-nificance of childhood attention deficit dis-order in treatment-seeking cocaine abusers. Compr Psychiatry 1993; 34: 75–82.
12 Arias AJ, Gelernter J, Chan G, et al: Corre-lates of co-occurring ADHD in drug-depen-dent subjects: prevalence and features of sub-stance dependence and psychiatric disorders. Addict Behav 2008; 33: 1199–1207.
13 Wilens TE, Biederman J, Mick E, Faraone SV, Spencer T: Attention deficit hyperactiv-ity disorder is associated with early onset substance use disorders. J Nerv Ment Dis 1997; 185: 475–482.
14 Biederman J, Wilens TE, Mick E, Faraone SV, Spencer T: Does attention-deficit hyper-activity disorder impact the developmental course of drug and alcohol abuse and depen-dence? Biol Psychiatry 1998; 44: 269–273.
15 Wilens TE, Biederman J, Mick E: Does ADHD affect the course of substance abuse? Findings from a sample of adults with and without ADHD. Am J Addict 1998; 7: 156–163.
16 Levin FR, Evans SM, Vosburg SK, Horton T, Brooks D, Ng J: Impact of attention-deficit hyperactivity disorder and other psychopa-thology on treatment retention among co-caine abusers in a therapeutic community. Addict Behav 2004; 29: 1875–1882.
17 Kim-Cohen J, Caspi A, Moffitt TE, Har-rington H, Milne BJ, Poulton R: Prior juve-nile diagnoses in adults with mental dis-order: developmental follow-back of a prospective-longitudinal cohort. Arch Gen Psychiatry 2003; 60: 709–717.
18 Biederman J, Newcorn J, Sprich S: Comor-bidity of attention deficit hyperactivity dis-order with conduct, depressive, anxiety, and other disorders. Am J Psychiatry 1991; 148: 564–577.
19 Spencer TJ. ADHD and comorbidity in childhood. J Clin Psychiatry 2006; 67(suppl 8):27–31.
20 Lynskey MT, Hall W: Attention deficit hy-peractivity disorder and substance use disor-ders: is there a causal link? Addiction 2001; 96: 815–822.
21 Disney ER, Elkins IJ, McGue M, Iacono WG: Effects of ADHD, conduct disorder, and gen-der on substance use and abuse in adoles-cence. Am J Psychiatry 1999; 156: 1515–1521.
22 Roy A: The relationships between attention-deficit/hyperactive disorder, conduct disor-der and problematic drug use. Drugs Educ Prevent Policy 2008; 15: 55–75.
23 Flory K, Lynam DR: The relation between at-tention deficit hyperactivity disorder and substance abuse: what role does conduct dis-order play? Clin Child Fam Psychol Rev 2003; 6: 1–16.
24 Elkins IJ, McGue M, Iacono WG: Prospec-tive effects of attention-deficit/hyperactivity disorder, conduct disorder, and sex on ado-lescent substance use and abuse. Arch Gen Psychiatry 2007; 64: 1145–1152.
25 Flory K, Milich R, Lynam DR, Leukefeld C, Clayton R: Relation between childhood dis-ruptive behavior disorders and substance use and dependence symptoms in young adulthood: individuals with symptoms of attention-deficit/hyperactivity disorder and conduct disorder are uniquely at risk. Psy-chol Addict Behav 2003; 17: 151–158.
26 Biederman J, Wilens T, Mick E, Milberger S, Spencer TJ, Faraone SV: Psychoactive sub-stance use disorders in adults with attention deficit hyperactivity disorder (ADHD): ef-fects of ADHD and psychiatric comorbidity. Am J Psychiatry 1995; 152: 1652–1658.
27 Eyre SL, Rounsaville BJ, Kleber HD: History of childhood hyperactivity in a clinic popu-lation of opiate addicts. J Nerv Ment Dis 1982; 170: 522–529.
28 Modestin J, Matutat B, Wurmle O: Anteced-ents of opioid dependence and personali - ty disorder: attention-deficit/hyperactivity disorder and conduct disorder. Eur Arch Psychiatry Clin Neurosci 2001; 251: 42–47.
29 Davids E, von Bunau U, Specka M, Fischer B, Scherbaum N, Gastpar M: History of atten-tion-deficit hyperactivity disorder symp-toms and opioid dependence: a controlled study. Prog Neuropsychopharmacol Biol Psychiatry 2005; 29: 291–296.
30 Kolpe M, Carlson GA: Influence of atten-tion-deficit/hyperactivity disorder symp-toms on methadone treatment outcome. Am J Addict 2007; 16: 46–48.
31 Brooner RK, King VL, Kidorf M, Schmidt CW Jr, Bigelow GE: Psychiatric and sub-stance use comorbidity among treatment-seeking opioid abusers. Arch Gen Psychiatry 1997; 54: 71–80.
32 Marsden J, Gossop M, Stewart D, Rolfe A, Farrell M: Psychiatric symptoms among cli-ents seeking treatment for drug dependence. Intake data from the National Treatment Outcome Research Study. Br J Psychiatry 2000; 176: 285–289.
33 Ross J, Teesson M, Darke S, et al: The char-acteristics of heroin users entering treat-ment: findings from the Australian Treat-ment Outcome Study (ATOS). Drug Alcohol Rev 2005; 24: 411–418.
34 Millson P, Challacombe L, Villeneuve PJ, et al: Determinants of health-related quality of life of opiate users at entry to low-threshold methadone programs. Eur Addict Res 2006; 12: 74–82.
35 Carpentier PJ, Krabbe PF, van Gogh MT, Knapen LJ, Buitelaar JK, De Jong CA: Psychi-atric comorbidity reduces quality of life in chronic methadone-maintained patients. Am J Addict 2009; 18: 470–480.
36 Kooij JJ: ADHD bij volwassenen. Inleiding in diagnostiek en behandeling (in Dutch). Lisse, Swets & Zeitlinger, 2002.
37 Kooij JJ, Burger H, Boonstra AM, Van der Linden PD, Kalma LE, Buitelaar JK: Efficacy and safety of methylphenidate in 45 adults with attention-deficit/hyperactivity disor-der. A randomized placebo-controlled dou-ble-blind cross-over trial. Psychol Med 2004; 34: 973–982.
38 Kooij JJ, Marije BA, Swinkels SH, Bekker EM, de Noord I, Buitelaar JK: Reliability, validity, and utility of instruments for self-report and informant report concerning symptoms of ADHD in adult patients. J At-ten Disord 2008; 11: 445–458.
39 Robins LN, Cottler L, Bucholz K, Compton W: The Diagnostic Interview Schedule, Ver-sion IV. St Louis/MO, Washington Univer-sity, 1995.
References
Carpentier /van Gogh /Knapen /Buitelaar /De Jong
Eur Addict Res 2011;17:10–2020
40 McLellan AT, Luborsky L, Woody GE, O’Brien CP: An improved diagnostic evalu-ation instrument for substance abuse pa-tients. The Addiction Severity Index. J Nerv Ment Dis 1980; 168: 26–33.
41 Brooks R: EuroQol: the current state of play. Health Policy 1996; 37: 53–72.
42 Dolan P: Modeling valuations for EuroQol health states. Med Care 1997; 35: 1095–1108.
43 Sheehan DV, Lecrubier Y, Sheehan KH, et al: The Mini-International Neuropsychiatric Interview (MINI): the development and val-idation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry 1998; 59(suppl 20):22–33.
44 Cottler LB, Robins LN, Helzer JE: The reli-ability of the CIDI-SAM: a comprehensive substance abuse interview. Br J Addict 1989; 84: 801–814.
45 Pfohl B, Blum N, Zimmerman M: Structured Interview for DSM-IV Personality Disor-ders. Washington, American Psychiatric Press, 1997.
46 Damen KF, De Jong CA, Van der Kroft PJ: Interrater reliability of the structured inter-view for DSM-IV personality in an opioid-dependent patient sample. Eur Addict Res 2004; 10: 99–104.
47 Adler LA, Kunz M, Chua HC, Rotrosen J, Resnick SG: Attention-deficit/hyperactivity disorder in adult patients with posttraumat-ic stress disorder: is ADHD a vulnerability factor? J Atten Disord 2004; 8: 11–16.
48 Ford JD, Racusin R, Ellis CG, et al: Child maltreatment, other trauma exposure, and posttraumatic symptomatology among chil-dren with oppositional defiant and attention deficit hyperactivity disorders. Child Mal-treat 2000; 5: 205–217.
49 Hill J: Early identification of individuals at risk for antisocial personality disorder. Br J Psychiatry Suppl 2003; 44:S11–S14.
50 Knop J, Penick EC, Nickel EJ, et al: Child-hood ADHD and conduct disorder as inde-pendent predictors of male alcohol depen-dence at age 40. J Stud Alcohol Drugs 2009; 70: 169–177.
51 Marshal MP, Molina BS: Antisocial behav-iors moderate the deviant peer pathway to substance use in children with ADHD. J Clin Child Adolesc Psychol 2006; 35: 216–226.
52 Hinshaw SP: Conduct disorder in childhood: conceptualization, diagnosis, comorbidity, and risk status for antisocial functioning in adulthood. Prog Exp Pers Psychopathol Res 1994: 3–44.
53 Soderstrom H, Sjodin AK, Carlstedt A, Fors-man A: Adult psychopathic personality with childhood-onset hyperactivity and conduct disorder: a central problem constellation in forensic psychiatry. Psychiatry Res 2004; 121: 271–280.
54 Dalsgaard S, Mortensen PB, Frydenberg M, Thomsen PH: Conduct problems, gender and adult psychiatric outcome of children with attention-deficit hyperactivity disor-der. Br J Psychiatry 2002; 181: 416–421.
55 Glantz MD, Anthony JC, Berglund PA, et al: Mental disorders as risk factors for later sub-stance dependence: estimates of optimal pre-vention and treatment benefits. Psychol Med 2009; 39: 1365–1377.
56 Wilens TE, Faraone SV, Biederman J, Gu-nawardene S: Does stimulant therapy of at-tention-deficit/hyperactivity disorder beget later substance abuse? A meta-analytic re-view of the literature. Pediatrics 2003; 111: 179–185.
57 Mannuzza S, Klein RG, Truong NL, et al: Age of methylphenidate treatment initiation in children with ADHD and later substance abuse: prospective follow-up into adulthood. Am J Psychiatry 2008; 165: 604–609.
58 Levin FR, Evans SM, Brooks DJ, Kalbag AS, Garawi F, Nunes EV: Treatment of metha-done-maintained patients with adult ADHD: double-blind comparison of methylpheni-date, bupropion and placebo. Drug Alcohol Depend 2006; 81: 137–148.
59 Blix O, Dalteg A, Nilsson P: Treatment of opioid dependence and ADHD/ADD with opioid maintenance and central stimulants. Heroin Addict Relat Clin Probl 2009; 11: 5–14.
60 Daigre Blanco C, Ramos-Quiroga JA, Valero S, et al: Adult ADHD Self-Report Scale (ASRS-v1.1) symptom checklist in patients with substance use disorders. Actas Esp Psiquiatr 2009; 37: 299–305.
Copyright © 2022 FDOKUMEN




















