
ADHD Comorbidity Findings From the MTA Study: Comparing Comorbid Subgroups
Upload
khangminh22Category
view
1download
0
1
UNIVERSITY OF ZIMBABWE
Faculty of Medicine
College of Health Sciences
DEPARTMENT OF NURSING SCIENCE
A study to determine the relationship between
prevalence of late stage diagnosis of cervical cancer and
number of comorbid illnesses in women aged 65 years
and above in Zimbabwe.
Submitted by Yvonne Kagura in partial fulfilment of the
Masters in Nursing Science Degree Program
June 2015

2
ABSTRACT
The elderly are currently the fastest growing population worldwide. Illnesses arising
with advancing age, like hypertension, diabetes mellitus, dementia, Alzheimer’s and vascular
disorders are complicating cervical cancer diagnosis in elderly women. This descriptive,
correlational study was done to explore the relationship between prevalence of late stage
diagnosis of cervical cancer and number of comorbidities in women aged 65 years and above
in Zimbabwe guided by Betty Neuman’s Systems Model. Non-probability sampling was used
to recruit and interview 68 women aged 65 years and above with cervical cancer from
Parirenyatwa Hospital and Spilhause Clinic at Harare Hospital. Data analysis was done using
the Statistical Package for Social Sciences (SPSS), The Pearson’s Correlation coefficient and
simple regression to describe demographic characteristics and dependent and independent
variables. Study findings indicated that the average number of comorbidities suffered by
elderly women before late stage cervical cancer diagnosis was 2.03 with a mean comorbidity
score of 9.03 out of 38 using a modified Charleson Comorbidity Index. The prevalence of
late stage diagnosis was 0.661. Pearson’s correlation coefficient showed a positive and
significant relationship between prevalence of late stage diagnosis of cervical cancer and
number of comorbidities (r = .431, p < 0.01). This result means that the higher the number of
comorbidities in elderly women, the later the stage of presentation with cervical cancer.
There is need to focus early screening of cervical cancer efforts on elderly women to promote
early detection and treatment. The effect of the independent variable is indicated by
significant R² = 0.186 (b = 0.289). This result explains that the number of comorbidities
suffered before cervical cancer diagnosis causes 18.6% of the prevalence of late stage
diagnosis of cervical cancer. Further research is needed to clarify other factors leading to late
stage diagnosis of cervical cancer in elderly women aged 65 years and above in Zimbabwe.

3
ACKNOWLEDGEMENTS
I would like to thank my supervisor, Dr H. Zvinavashe, Mrs Nyamakura my mentor
and the whole nursing science department staff for their support during the time this study
was conducted. My gratitude also goes to Professor Rusakaniko, Mr V. Chikwasha and Mrs
M. Kaiyo-Utete from the Department of Medicine for their assistance in data entry and
analysis.
I am thankful to the respective clinical directors at Parirenyatwa Hospital and
Spilhause Clinic for granting permission to carry out the study and the sisters-in-charge of the
various departments from where the research participants were selected from, for ensuring a
peaceful and quiet environment. Special mention goes to the participants without whose
permission; this study would not have been done.
I am grateful to my parents, my brothers Albert and Kudzie, and wonderful sisters
who are all too numerous to mention but were nevertheless psychologically and financially
supportive during the course of this study. God bless you all.

4
TABLE OF CONTENTS ABSTRACT ............................................................................................................................... 2
ACKNOWLEDGEMENTS ....................................................................................................... 3
TABLE OF CONTENTS ........................................................................................................... 4
LIST OF FIGURES ................................................................................................................... 7
LIST OF TABLES ..................................................................................................................... 8
LIST OF APPENDICES ............................................................................................................ 9
CHAPTER 1 ............................................................................................................................ 10
BACKGROUND AND ORGANISING FRAMEWORK ................................................... 10
1.1. Introduction ............................................................................................................... 10
1.2. Background ................................................................................................................ 10
1.3. Problem statement ..................................................................................................... 14
1.4. Purpose of the study .................................................................................................. 17
1.5. Research Objectives .................................................................................................. 17
1.6. Research Questions.................................................................................................... 17
1.7. Significance to nursing .............................................................................................. 17
1.8. Theoretical framework .............................................................................................. 19
1.9. Conceptual definition of terms .................................................................................. 23
1.1.0. Summary ................................................................................................................. 24
CHAPTER 2 ............................................................................................................................ 25
LITERATURE REVIEW ..................................................................................................... 25
2.1. Introduction ............................................................................................................... 25
2.2. The cervix .................................................................................................................. 25
2.3. Cervical cancer .......................................................................................................... 26
2.4. Staging ....................................................................................................................... 27
Late stage presentation of cervical cancer............................................................................ 30
2.5. Comorbidity ............................................................................................................... 31

5
2.6. Cervical cancer and comorbidity ............................................................................... 35
The Comorbidity Index .................................................................................................... 37
Theoretical framework ..................................................................................................... 39
2.7. Summary .................................................................................................................... 39
CHAPTER 3 ............................................................................................................................ 40
METHODS........................................................................................................................... 40
3.1. Introduction ............................................................................................................... 40
3.2. Research design ......................................................................................................... 40
3.3. Sampling Plan ............................................................................................................ 41
3.4. Study site ................................................................................................................... 41
3.5. Target population ....................................................................................................... 42
3.6. Accessible Population................................................................................................ 42
3.7. Sampling Criteria ....................................................................................................... 42
3.8. Sample Size ............................................................................................................... 43
3.9. Sampling Procedure ................................................................................................... 44
3.1.0. Variables ................................................................................................................. 46
3.1.1. Instrument ............................................................................................................... 47
3.1.2. Validity ................................................................................................................... 47
3.1.3. Reliability ............................................................................................................... 48
3.1.4. Data collection plan ................................................................................................ 48
3.1.5. Data collection procedure ....................................................................................... 49
3.1.6. Human Rights Consideration .................................................................................. 49
3.1.7. Pilot study ............................................................................................................... 50
3.1.8. Data Analysis Plan.................................................................................................. 50
Chapter 4 .................................................................................................................................. 51
Results .................................................................................................................................. 51
4.1. Demographic data ...................................................................................................... 51
6
4.2. Cervical cancer .......................................................................................................... 58
4.3. Comorbidity ............................................................................................................... 59
4.4. Correlation ..................................................................................................................... 68
4.5. Regression analysis (n = 68) ......................................................................................... 69
Chapter 5 .................................................................................................................................. 70
Discussion of findings .......................................................................................................... 70
5.1. Demographic data ...................................................................................................... 70
5.2. Late stage cervical cancer diagnosis .......................................................................... 72
5.3. Comorbidity ............................................................................................................... 73
5.4. Study limitations ........................................................................................................ 74
5.5. Recommendations ..................................................................................................... 75
References ............................................................................................................................ 78
APPENDIX I: English Consent form .................................................................................. 83
APPENDIX II: Shona Consent Form .................................................................................. 85
APPENDIX I11: English Interview Guide .......................................................................... 88
APPENDIX 1V: Shona Interview Guide ............................................................................. 92
APPENDIX V: PERMISSION LETTERS .......................................................................... 96

7
LIST OF FIGURES
Fig 1: Adaptation of Betty Neuman Systems Model ........................................................................ 23

8
LIST OF TABLES
Table 2.0: The FIGO Clinical Staging for Cancer of the Cervix ...................................................... 29
Table 2.1: Modified Charleson Comorbidity Index .......................................................................... 38
Table 4.1.Demographic data (1): Age in years ................................................................................. 52
Demographic data (2): Age when married .................................................................................... 53
Demographic data (3): Number of children .................................................................................. 54
Demographic data (4): .................................................................................................................. 56
Demographic data (5): .................................................................................................................. 57
Table 4.2.1. Diagnosis ...................................................................................................................... 59
Table 4.2.2. Awareness ..................................................................................................................... 61
Table 4.3.0. Comorbidities ................................................................................................................ 62
Table 4.3.1. Comorbidities in elderly women with cervical cancer in Zimbabwe ........................... 63
Table 4.3.1. Score of comorbidities before cancer............................... Error! Bookmark not defined.
Table 4.3.2. Score of comorbidities after the cancer diagnosis......................................................... 65
Table 4.3.3. Total comorbidity score ................................................................................................ 64
Table 4.3.4. Comorbidity scoring summary ..................................................................................... 66
4.4. Correlation ................................................................................................................................. 68

9
LIST OF APPENDICES APPENDIX I: English Consent form ............................................................................................... 83
APPENDIX II: Shona Consent Form ............................................................................................... 85
APPENDIX I11: English Interview Guide ....................................................................................... 88
APPENDIX 1V: Shona Interview Guide .......................................................................................... 92
APPENDIX V: PERMISSION LETTERS ....................................................................................... 96

10
CHAPTER 1
BACKGROUND AND ORGANISING FRAMEWORK
1.1. Introduction
Cancer is a major cause of morbidity and mortality in Zimbabwe with over 5000 new
diagnoses being made and over 1000 deaths per year National Cancer registry, 2014). The
number of people developing cancer is expected to increase due to an increasing aging
population, HIV and AIDS, and unhealthy lifestyle choices in the population (National
Cancer Prevention and Control Strategy, 2014-2018). Cervical cancer is the number 1 cancer
among women in Zimbabwe, with an estimated 1 855 cases diagnosed and 1 286 deaths
recorded annually due to the disease (National Cancer Registry Annual Report, 2013).
Cervical cancer contributed 19% of all cancer deaths in 2007 (Chokunonga et al, 2010).
Cervical cancer is highly preventable with proper screening and early treatment (Alliance for
Cervical Cancer Prevention, 2014). The average elderly woman in Zimbabwe is living with at
least 1 or 2 chronic illnesses and is prone to frequent contact with the health care provider,
yet there is reduced screening of cervical cancer in these women leading to late diagnosis of
cervical cancer (Nhongo, 2014). It is worthwhile to discover the effect of comorbidity on
prevalence of late stage cervical cancer diagnosis in elderly women in Zimbabwe.
1.2. Background
The elderly are the fastest growing population today. Latest statistics from the Global
Cancer Network (GLOBOCAN) indicate that there were 506 million people aged 65 years
and older in 2008, a number expected to increase to 1.3 billion by 2040 worldwide including
the developing countries (GLOBOCAN, 2012). In the majority of countries, women
constitute 55% of the elderly population with 65% of them aged 80 years and above
(Nhongo, 2014). According to the 2012 population census in Zimbabwe, 758 000 people are

11
elderly, which is 6% of the entire population (Zimbabwe National Statistical Agency, 2014).
This increased population ageing is occurring due to several reasons some of which are cited
by Nhongo as declining fertility rates (from 4.5 children per woman in 1994 to 2.7 in 2002),
increased average life expectancy worldwide projecting from 45 years in 1945 to 69 years in
2000 and to an expected 73 years in 2050. In addition, there is improved nutrition, lifestyle
and healthcare in general.
However, with the adoption of cancer causing lifestyles like smoking and fast foods,
the effects of which are evident in the elderly, more elderly people are now living with
malignant conditions which will eventually transition into end of life stages requiring
palliative care and straining an already exhausted health care system especially in poor
resource countries (Jemal et al., 2011).Cancer incidence increases exponentially with
advancing age (Berger, 2006).According to GLOBOCAN, there were about 12.7 million
cancer cases and 7.6 million cancer deaths worldwide in 2008, and approximately 56% of the
cases and 64% deaths occurring in developing countries (Ferlay et al., 2010).Cervical cancer
is the third most commonly diagnosed cancer and the fourth leading cause of female cancer
deaths worldwide (Jemal et al., 2011; WHO, 2014). It accounted for 9% of the total new
cancer cases and 8% of the total cancer deaths among females in 2008 with more than 85% of
these cases and deaths occurring in developing countries (Ferlay et al, 2010; WHO, 2014).
The highest incidence rates are in Eastern, Western and Southern Africa as well as South-
Central Asia and South America (Jemal et al., 2011). In 2011, there were an estimated 249
632 women living with cervical cancer in the United States (Howlader et al, 2013).
According to the American Cancer Association, cervical cancer represents 0.7% of all new
cancer cases in 2014 and 0.7% of all cancer deaths of which more than 15% of the cases are
found in women aged 65 years and above. Records from the national cancer registry have the

12
prevalence of cervical cancer in Zimbabwe at 33.5% with 15.6% of that being in elderly
women aged 65 years and above (Zimbabwe National Cancer Registry, 2014).
Early stage cervical cancer can develop over a number of years (between 5-35 years)
without initial symptoms to accompany it (Cancer Association of Zimbabwe, 2014). Cervical
cancer is highly preventable with proper screening and early treatment (Alliance for Cervical
Cancer Prevention, 2014). Qualitative screening techniques in developing countries include
visual inspection using Lugol’s iodine or acetic acid and testing for human papillomavirus
(HPV) DNA in cervical cell samples (Sherris, Withet & Kleine, 2009). This is associated
with about 50% reduction in risk of developing advanced cervical cancer according to a
clinical trial done in rural India (Sankaranarayan et al., 2009). A study done in America found
that cervical cancer screening in women aged 55-79 years is associated with a 77-79%
reduction in cervical cancer incidence (Rustagi et al., 2014). A case only analysis of
Sweden’s cervical cancer screening registry found that women aged 66 years and above
experienced a 36% increase in long term survival if their cancers were detected by screening
rather than clinically. Despite increasingly widespread use of Papanicoloau (Pap) smears,
almost half of all women with invasive cervical cancer are diagnosed at a late stage (Ferrante,
Gonzalez, Roetzheim, Pal & Woodard, 2013). Little is known about factors associated with
late stage diagnosis of cervical cancer. The study by Ferrante et al. (2013) found that women
who are elderly, unmarried and without insurance are more likely to be diagnosed at a late
stage.
Sixty percent of Zimbabwe’s women risk dying from cervical cancer (Chigariro,
2014). Detection is usually late after presentation of uncontrolled or abnormal bleeding and
pain in the 3rd
and 4th
stage when the cancer has already spread to nearby tissue surrounding
the cervix (Cancer Association of Zimbabwe, 2014). Reasons for late diagnosis are lack of
awareness, low risk self-perception, inadequate financial resources, general myths

13
surrounding promiscuity, belief that cancer is caused by witchcraft thus delaying in seeking
health care and belief that the excision of cancerous masses result in death (Chigariro &
Nyemba, 2014).
Comorbidities play an important role in survival of women with cervical cancer
(Hatch, Samper-Tement, Zang, Yong-Fang & Freeman, 2014). Patients with comorbid
conditions have greater odds of late stage diagnosis of cancer (Gonzalez, Ferrante, Van
Durme, Naazneen & Roetzheim, 2013). Comorbidity generally increases with advancing age
and may be the reason behind age-related differences in cancer diagnosis, treatment and
outcome. Cancer stage at diagnosis determines treatment options and has strong influence on
length of survival (The American Cancer Association, 2014). The 5 year survival for
localised cervical cancer is 90.9% (Surveillance Epidemiology and End Results Program
[SEER], 2014). Regional or distant stage which occurs when the cancer has spread to other
parts of the body is presented by 53% of the cases and survival rate is low (SEER, 2014). In
developing countries like Zimbabwe, limited access to effective screening means that the
disease is often not identified until it is further advanced and clinical symptoms develop.
Treatment prospects are poor in such cases resulting in higher mortality rate from cervical
cancer in these countries (WHO, 2014). Findings from a study done by Berger (2006) in
America indicated that cancer screening decreases among the elderly and is particularly
deficient among those with comorbid conditions. A survey done by Nhongo in 2014 in
Zimbabwe indicated that more than 75% of rural elderly women are not considered for
cervical cancer screening as they come into clinics or hospitals for any health concern.
Screening efforts in Zimbabwe have focused on the 15-49 year age group as it is considered
the one at highest risk of contracting cervical cancer from the risky lifestyles undertaken
including early onset of sexual activity and douching (Nhongo, 2014). This has resulted in
side-lining of the older age groups who then present with late stage cervical cancer later

14
whilst they are now burdened with other comorbid illnesses like hypertension, diabetes,
cardiac failure or other malignancies like breast cancer as this research sought to find out.
Museveni & Tshuma did a cohort study in 198 people with malignant conditions including
colorectal, prostate, breast and lung cancer which indicated that survival rate was
considerably reduced in patients with comorbidities scoring 6 or higher on the Charleson
comorbidity scale (Museveni & Tshuma, 2002). The Zimbabwe National Health Policy does
look at elderly people as deserving of free medical attention but sadly, there is little
implementation in terms of cancer treatment as all ages are expected to fork out large
amounts of money and therefore treatment is unaffordable. There is little research done on
elderly people with cervical cancer and comorbidities and this researcher aimed at adding to
the body of knowledge already existing as the elderly population rises each year.
1.3. Problem statement
Globally cancer is the third leading cause of death and 12 million new cancer cases and 7.6
million cancer related deaths were recorded worldwide in 2008 (WHO, 2014). These figures
are projected to increase to 26 million cases and 17 million deaths by 20130 (WHO, 2014).
Cancer is an emerging public health problem in Africa. According to the International
Agency for Research on Cancer (IARC), about 681,000 new cancer cases and 512,400 cancer
deaths occurred in 2008 in Africa. These numbers are projected to nearly double (1.28
million new cancer cases and 970,000 cancer deaths) by 2030 simply due to the aging and
growth of the population, with the potential to be even higher because of the adoption of
behaviours associated with western lifestyles, such as smoking, unhealthy diet, and physical
inactivity.
There is an increase in elderly women with cervical cancer in the developing world. It is the
leading cancer among women in Zimbabwe (National Cancer Prevention and Control
Strategy, 2014 - 2018). The total number of new cancer cases recorded among Zimbabweans

15
in 2012 was 6 107 comprising 2 621 (42.9%) males and 3 486 (57.1%) females. The five
most common cancers among Zimbabwean black women were cervical cancer (33.5%),
breast (11.7%), Kaposi sarcoma (8.9%), eye (6.5%) and non-Hodgkin lymphoma (4.9%)
(National Cancer Prevention and Control Strategy 2014 – 2018).
With the Human Immuno-deficiency Virus (HIV) pandemic leaving orphans and ill spouses,
it is increasingly befalling the elderly to care for them thus leaving little to no time for self-
care, thus forfeiting early and regular cervical cancer screening. According to Ward (2011)
who did a research on the elderly in rural Zimbabwe, he postulated that they were so
encumbered with subsistence farming and sourcing funds for medication for their orphaned
grandchildren and ill children that there are little funds left for themselves and their health.
For those with relatives abroad life becomes a bit easier but then comes the fear factor; fear
of drug-drug interactions, fear of unknown side-effects due to lack of knowledge and fear of
polypharmacy, the elderly who are on treatment for other chronic illnesses believe that they
are taking enough medication already and do not need to add more perceived strain to their
bodies (Chigariro & Nhongo, 2014). In low resource settings like Zimbabwe, unavailability
of the required drugs and memory loss from the normal ageing process add to the resulting
non-adherence leading to development of complications which keep adding to the vicious
cycle of health resource strain. The 2015 National Budget has set aside 13.1 million for the
ministry of health for direct health care with a special mention to the fight against HIV and
AIDS, TB and malaria (Chinamasa, 2014).Whilst the scourge of these illnesses is real there is
need to recognise cancer and especially cervical cancer as a potential pandemic if left
unchecked. It will be a major drain on health resources as most cases are treated in their late
stages thus requiring more aggressive but futile intervention resulting in unprecedented and
unnecessary marginal utilities. Reasons for late cervical cancer diagnosis are cited as lack of
awareness, low risk self-perception and inadequate financial resources (Chigariro, 2014).

16
Major barriers to early diagnosis also include general myths surrounding promiscuity, belief
that cancer is caused by witchcraft in case of traditionalists or that it represents possession by
demonic spirits in case of Christians and belief that excision of the cancerous tumour results
in death (Nyemba, 2014).Despite improved screening methods, most women present late with
3rd
and 4th
stage clinical symptoms when the cancer has spread to other tissues and expensive
palliative care is required. Also most of the resources on cervical cancer programs have been
focused on younger women whilst keeping the elderly in the side-lines. Reduced parity and
HIV/AIDS killing more of the younger generation means that there are more elderly people
in the economically productive population of Zimbabwe which has seen the retirement age
moving beyond 65 years. This researcher postulated that comorbidities arise as ageing
advances. In addition to polypharmacy which is confounded by drug-drug interactions, non-
adherence, and unavailability and non- affordability of overall treatment, there is under
reporting of symptoms and delayed treatment of cervical cancer. As comorbidity increases,
there is a tendency to focus more on them by the patients themselves and their health care
providers resulting in non-referral for early screening of cervical cancer. A study done in
America indicated that cancer screening decreases among the elderly and is particularly
deficient among those with comorbid conditions (Berger, 2006).In Zimbabwe, survival rate is
particularly reduced in patients suffering from malignant conditions with added
comorbidities. No studies have been done to assess effect of comorbidity in elderly women
with cervical cancer therefore this researcher sought to establish the relationship between
number of comorbid conditions suffered by elderly women in Zimbabwe and stage at which
cervical cancer is diagnosed.

17
1.4. Purpose of the study
The purpose of this study was to determine the relationship between prevalence of
late stage diagnosis of cervical cancer and number of comorbidities in women aged 65 years
and above in Zimbabwe.
1.5. Research Objectives
The objectives of the research were:
1. To determine the prevalence of late stage diagnosis of cervical cancer in women aged
65 years and above in Zimbabwe.
2. To ascertain the number of comorbid illnesses suffered by women aged 65 years and
above presenting with late stage cervical cancer in Zimbabwe.
3. To establish the relationship between prevalence of late stage diagnosis of cervical
cancer and number of comorbidities in women aged 65 years and above in Zimbabwe.
1.6. Research Questions
1. What is the prevalence of late stage diagnosis of cervical cancer in women aged 65
years and above in Zimbabwe?
2. What is the number of comorbid illnesses suffered by women with late stage cervical
cancer aged 65 years and above in Zimbabwe?
3. What is the relationship between prevalence of late stage diagnosis of cervical cancer
and number of comorbidities?
1.7. Significance to nursing
Cervical cancer is fast becoming a pandemic in Zimbabwe. The majority of cases are
late diagnosis cases, reasons which were attributed to low risk self-perception, lack of
financial resources and myths surrounding cancer in general by Chigariro and Nyemba in
2014. No studies have been done to find out the effect of comorbidities on prevalence of late
18
stage cervical cancer diagnosis which is relevant in order to assist health care workers to
focus more on identified problem areas. It has been proven in India and America that geriatric
patients are referred less frequently for cervical cancer screening, meaning that only when
clinical symptoms manifest are they diagnosed. By then the cancer will have spread to other
organs, leading to expensive palliative care for the health-care institution and the patient and
loss of economically viable manpower. In less developed countries like Zimbabwe, the
referral may be even lesser than previously determined due to economic challenges. In 2014,
a survey done by Nyemba in rural Zimbabwe indicated that more than 75% of elderly women
are not screened for cervical cancer in the clinics or hospitals they would have attended for
other health concerns. Elderly women suffering from other chronic illnesses will refrain from
early screening and even delay treatment should they recognise symptoms due to reluctance
to become a burden to already strained funds.
Multi-parity has been cited as a predisposing factor to development of cervical cancer
(WHO, 2014). Findings from this study are of interest to women of child-bearing age and
their health as they impact on their life as they grow older. At a time that the Zimbabwe
National Health Research Agenda Strategy is vouching for reduction in maternal and child
deaths, findings from this research will ensure early screening of cervical cancer and prevent
the death of pivotal dependent carers which are the elderly women.
Stakeholders investing in women’s health should know the outcome of this study as it
brings out results of efforts put in place to combat cervical cancer. Also new areas of
investment are revealed, like providing Pap smear kits to every health institution in the
country and more focus on geriatric oncology. Investments in nursing curriculum
development are necessary to address evolving societal changes especially in geriatric
nursing.

19
Establishing a relationship between prevalence of late stage diagnosis of cervical
cancer and number of comorbidities is essential for nursing practice, nursing education as
well as nursing research. In nursing practice, clinicians will be interested to know whether
frequent contact with elderly women with chronic conditions delays referral for early
screening of cervical cancer as more focus is put on other conditions. The frequent contact
needs to be put to maximum use and actually help in increasing awareness of cervical cancer
screening leading to early diagnosis.
Nurse educators interested in curriculum adjustment in issues involving the elderly,
chronic conditions and malignancies as the elderly population continues to increase will be
given these results. The pap smear is a basic test for screening cervical cancer that can be
taught from neophyte nurses to advanced clinical practitioners so that it can be offered on a
regular basis in all health care settings including walk-in clinics. Nurse researchers will need
to identify areas of further scientific enquiry in order to establish evidence-based findings
which support or refute existing evidence and further advance the evolving profession of
geriatric nursing. They can then advocate for a more comprehensive health assessment
package for women with comorbid conditions which include regular pap smears along with
their usual blood pressure, blood sugar or cholesterol checks. Nurse Managers need to
advocate for more funding for their budget in order to provide palliative care and to educate
the community in a more aggressive manner to combat late diagnosis of cervical cancer.
They can also attract funding into installing cervical cancer screening equipment in their
respective health institutions to cater for all women clinicians come into contact with.
1.8. Theoretical framework
A framework is an abstract and logical structure of meaning that guides the
development of a study and enables the researcher to link study findings and nursing’s body

20
of knowledge (Burns & Grove, 2009). The Betty Neuman’s Systems model was used as the
theoretical framework for this study.
Theoretical frameworks in nursing are based on the nursing meta-paradigm which
Fawcett (1989) describes as person, environment, health and nursing.
Neuman, views a client as an open system which is composed of five variables. These
include physiological, psychological, socio-cultural, spiritual and developmental and are
surrounded by lines of defence and resistance which attempt to combat the effect of stressors.
The environment is viewed as a source of stressors and provides resources for managing the
same stressors (Neuman, 2011). Stressors can be intrapersonal, occurring within the
individual including feelings such as anger or fear. Interpersonal stressors occur between the
individual and others including health care providers, support groups, relatives and any other
people they come in contact with whilst extra-personal stressors occur outside the individual
like a job, financial pressures and comorbid illnesses. Neuman states that health or wellness is
a state in which all parts and sub-parts are in harmony or a steady state with the whole of the
person. Optimum wellness occurs when all needs are met. Illness conversely is a state of
insufficiency or instability. She therefore implies that health is on a continuum with wellness
at one end and extreme variables from wellness up to death at the other end of the continuum.
The term reconstitution is used to describe the process of adaptation to stressors.
Nursing is described as a unique profession that is concerned with all variables
affecting an individual’s response to stressors (Neuman, 2011). The goal of nursing is to
maintain, regain or attain client system stability. Neuman then goes ahead to describe the
nursing process which contains three basic parts namely the nursing diagnosis, nursing goal
and nursing outcome as an intervention at any point when a stressor is suspected, detected or
identified. Intervention before a reaction to a stressor occurs is described as a primary
21
intervention while intervention after a reaction has occurred is termed secondary intervention.
Tertiary intervention is appropriate only when reconstitution has occurred. This study focuses
on the four central concepts as defined by Neuman.
Betty Neuman’s System Model was chosen because of its open characteristics. The
major client variables which influence the individual’s observable reaction are going to be
considered. This study proposed that comorbidity influences stage at which cervical cancer is
diagnosed in elderly women aged 65 years or above leading to a health outcome on a
continuum with optimal wellness on one end as early diagnosis late diagnosis on the other
end. Comorbidity is part of the environmental stressors that have an influence on the
diagnosis of cervical cancer and is placed in the reaction phase. The environment is a source
of stress for the client’s system in the cancer patient. The patient with comorbidities might be
able to have early diagnosis of cervical cancer due to constant or frequent contact with health
care providers but may also not be able to do so due to overwhelming stressors which come
with comorbid illness including drug-drug interactions, non-adherence, availability and
affordability of treatment. Patients who are overwhelmed are unable to adapt to stressors
effectively leading to late stage diagnosis of cervical cancer and thus tertiary intervention.
The model was adapted to guide the nursing care of elderly women with chronic
illnesses on the continuum of care from early and regular screening to palliative treatment of
late presenters. The diagram illustrates the interaction of stressors from the extra-personal
(environmental), intra-personal and inter-personal stressors which eventually lead to the
diagnosis of cervical cancer. Early or late diagnosis will depend on the nursing intervention s
applied at the 3 different level of stress.

22
CLIENT SYSTEM
Lines of defence
Intra-personal
stressors –
genetics and
repeated HPV
infections
Inter-
personal
stressors –
lifestyle e.g.
diet and
exercise
Extra-personal
stressors –
environment,
carcinogens

23
Fig 1: Adaptation of Betty Neuman Systems Model
In clients with chronic illnesses, the role of the medical-surgical nurse is to provide
education on risk factors of developing cervical cancer, assess client scores on the risk factor
scale and encourage early screening to promote early detection and treatment. Clients who
are fully alert and are on treatment for other chronic illnesses must be fully aware of the
implications of constant cervical screening and must have at least undergone cervical
screening once a year. The medical-surgical nurse requires a body of knowledge to impart to
the client and to make observations, understanding the events and conditions and possible
courses of actions which will be beneficial to the client (Orem, 1991).
In terms of environmental stressors the nurse is mainly an advocate for safer
environment. With interpersonal stressors the nurse includes health education and in terms of
intra-personal stressors, clinical intervention is a key component.
1.9. Conceptual definition of terms
A conceptual definition provides a variable with an abstract of theoretical meaning
and it is reached through concept analysis (Burns & Grove, 2009). The following definitions
will be used in this study:
Client – synonymous with the term patient is used interchangeably in this study to mean an
elderly woman aged 65 years and above with cervical cancer.
Cancer – a malignant, autonomous and uncontrolled growth of cells and tissues forming
tumours.
Cervical cancer – a tumour of the cervix caused by the human papillomavirus (HPV).

24
Comorbidity – a chronic illness or illnesses being suffered from in conjunction with the
cervical cancer in the elderly woman.
Condition – a state of unwellness, also synonymous with the term: illness. Will be used
interchangeably in this study.
Staging – classification of the cervical cancer according to histology.
Human papillomavirus – a most common sexually transmitted infection causing cervical
cancer if persistent.
Late stage presentation – stage 3 and 4 of cervical cancer.
Prevalence of late stage presentation of cervical cancer – percentage or fraction of elderly
women aged 65 years and above presenting with stage 4 cervical cancer in Zimbabwe.
Stressors – include intra-, inter-and extra-personal stressors that affect the client system
directly or indirectly.
Reconstitution – the nursing system put in place to ensure
Palliative care – end of life care for patients with stage 3 and 4 cervical cancer. Tab these
1.1.0. Summary
Cervical cancer is the fourth leading cause of all cancer deaths worldwide and the
number one cancer in females in Zimbabwe. With increasing age comes a host of chronic
illnesses which elderly women have to deal with as comorbidity generally increases with
advancing age. Cancer stage at diagnosis determines treatment options and has influence on
length of survival. Betty Neuman’s Systems Model was modified to illustrate the effect of
stressors on the continuum of care for elderly women from early and regular screening of
cervical cancer to those presenting with late stage symptoms requiring palliative care. There
is an urgent need therefore to determine the relationship between comorbidity and diagnosis

25
of cervical cancer in elderly women aged 65 years and above in Zimbabwe in order to adjust
the nursing care accordingly.
CHAPTER 2
LITERATURE REVIEW
This chapter looks at literature review concerning the independent and dependent
variables. This was a study to determine the relationship between late stage cervical cancer
diagnosis and number of comorbidities in women aged 65 years and above in Zimbabwe.
2.1. Introduction
Polit & Hungler (2008) defined literature review as a critical summary of findings on
a topic of interest generally prepared to put a research problem in perspective. Literature
review in nursing serves a number of purposes in the research process one of which is to refer
to scientific sources that are important in providing the in-depth knowledge that is needed to
make changes in education, practice and research and to assist the researcher in finding out
what is already known about an existing problem. The purpose of literature review in this
study was to identify, scrutinise, summarise and integrate previous work done globally,
regionally and locally on cervical cancer and comorbidity among elderly women presenting
with late stage cervical cancer in order to answer the posed research questions.
2.2. The cervix
The cervix constitutes the lower third of the uterus. In a non-pregnant fertile woman,
it is 3cm long and 2.5cm wide (Berek, 2011). The ectocervix is the lower part of the cervix
whilst the endocervix forms the upper two thirds. The ectocervix is lined by stratified,
squamous epithelium and the cervical canal by the columnar epithelium which is thinner and
more fragile (Berek, 2011). The area where the 2 types of epithelia meet forms the squamo-

26
columnar junction (SCJ). The cervix undergoes striking changes from birth to menopause
(Shaw, 2003).
From birth up to pre-puberty, the original SCJ remains intact. At puberty the cervix
grows in size in response to oestrogen. As the woman becomes more fertile, squamous
metaplasia occurs giving rise to a second SCJ, called the transformation zone, located
between the original and the new SCJ, cells of which are particularly vulnerable to persistent
HPV infection. It is here that most squamous cell carcinoma develops (WHO, 2014).
As women advance in age and the effects of oestrogen lessen and the cervix shrinks.
In post-menopausal women, the new SCJ and a variable portion of the metaplastic epithelium
of the transformation zone retreat into the cervical canal (Berek, 2011).
2.3. Cervical cancer
Cancer results from malignant, autonomous and uncontrolled growth of cells and
tissues forming tumours which invade surrounding normal tissue competing for nutrients and
oxygen thus destroying them (Tortora, 2012). Cervical cancer is caused by persistent
infection with cancer-causing HPV types 16 and 18(WHO, 2014). These types are
responsible for 70% of all cervical cancer cases throughout the world. The virus exclusively
pervades epithelium, produces new viral particles thus causing genetic damage and tumour
formation (Crosbie, Einstein, Franceschi & Kitchener, 2013). Ninety percent of cervical
cancers are squamous cell cancers and the other 10% are adenocarcinomas beginning in the
glandular columnar layers of the endocervix (WHO, 2014). Cervical precancer is a distinct
change in the epithelial cells of the transformation zone where cells start developing in an
abnormal fashion in the presence of persistent HPV infection (Crosbie et. al., 2013). This
precursor stage, stage 0, can last years before becoming invasive cancer; providing ample
opportunity for detection and treatment. Cervical cancer screening in Zimbabwe is aiming at

27
the 15-49 age group who may be in stage 0 so that they do not present later in life when they
are older and the cancer is at an advanced stage. In women, during puberty and pregnancy,
the transformation zone of the ectocervix is enlarged and exposure to HPV at these
vulnerable times facilitates infection (Basu et. al., 2011; WHO, 2014). This may explain the
association between squamous cell cervical cancer and early sexual activity, young age at
first birth and a history of multiple pregnancies. Behaviours that can also increase the risk of
HPV infection (and thus cervical cancer) include having multiple partners and having
partners with multiple partners (Gyenwali, Pariyar & Onta, 2013). This study aimed at
screening elderly women age 65 years and above with cervical cancer for all the above-
mentioned risk factors.
Conditions leading to HPV infection are not well understood but risk factors that play
a role include HPV type, oncogenicity or cancer-causing strength; immune status: those
living with HIV are more likely to have persistent HPV infection and a more rapid
progression from pre-cancer to invasive cancer; co-infection with other sexually transmitted
illnesses such as herpes simplex, Chlamydia and gonorrhoea; parity and young age at birth;
tobacco smoking and lastly use of oral contraceptives for over 5 years (WHO, 2014).
2.4. Staging
Cervical cancer is a progressive disease that is staged according to histology
(McCance & Huether, 2006).It is a process that can take weeks or months depending on
diagnostics done (Chitsike, 2015). Classification is done on a continuum from cervical
intraepithelial neoplasia or cervical dysplasia to cervical carcinoma in situ to invasive
carcinoma. Initially, there is cervical dysplasia. The patient is asymptomatic and only a pap
smear can detect changes in cell characteristics. Eventually, there is progression to invasive
cancer and this can take place over a period of 10-12 years (Gyenwali, Pariyar & Onta,
2013).

28
Four routes are taken by the invasive cancer progressing within the cervix. Spread
occurs from a tiny focus of microinvasive cancer until it covers the entire cervix and
enlarging to 8cm or more in diameter (WHO, 2014). Direct spread then occurs, downwards to
the vagina, upwards to the uterus, sideways into the tissues supporting the uterus in the pelvis
and ureters, backwards to the rectum and forwards to the bladder. Thirdly, there are lymph
node metastases which at first, are confined to the pelvis and then later up to the aorta.
Cervical cancer cells fourthly spread through the blood stream and lymphatic system to
develop distant metastases in the liver, bone, lung and brain producing symptoms related to
these regions. Patients are staged using the International Federation of Gynaecology and
Obstetrics (FIGO) clinical classification which remains the gold standard (WHO, 2014) and
is illustrated in Table 2.0. In addition to a clinical examination, use is made of radiological
investigations, which include a chest radiograph, a pelvic and abdominal ultrasound,
computed tomography (CT) and magnetic resonance imaging (MRI) to aid in the staging
process (Sauer, Simonds, Van der Merwe & Hatingh, 2013).

29
Table 2.0: The FIGO Clinical Staging for Cancer of the Cervix
Stage Characteristics
0 Cancer in situ, intraepithelial carcinoma, earliest stage of cancer,
cancer confined to its original site.
1
1A
1B
1A1
1A2
1B1
1B2
Carcinoma confined to cervix (extension to corpus disregarded)
Earliest form of stage 1, very small amount of cancer visible only
under the microscope
Area of invasion is < 3mm deep and < 7mm wide.
Area of invasion is between 3-5mm deep and < 7mm wide
Includes cancers that can be seen without a microscope and cancers
that can be seen only with a microscope that have spread deeper than
5mm into connective tissue of the cervix and are wider than 7mm.
A 1B cancer that is no larger than 4cm
A 1B cancer that is larger than 4cm
11
11A
11B
Cancer has spread beyond the cervix to the upper part of the vagina
but does not involve the lower third of the vagina.
Cancer has spread beyond the cervix to the upper 2/3 of the vagina.
Cancer has spread to the tissue next to the cervix (parametrical
tissue).
111
111A
111B
Cancer has spread to the lower part of the vagina or the pelvic wall;
cancer may be blocking the ureters
Cancer has spread to the lower third of the vagina but not the pelvic
wall
Cancer extends to the pelvic wall. Bocks urine flow to the bladder
from both ureters.
1V
1VA
1VB
Most advanced stage of cervical cancer, cancer has spread to other
parts of the body
Cancer has spread to the bladder or rectum, which are organs close
to the cervix
Cancer has spread to distant organs beyond the pelvic area such as
the lungs.
Adapted with permission from McCance & Huether (2006), 5th
edition, page 795.

30
2.4.1. Late stage presentation of cervical cancer
According to the Zimbabwe Ministry of Health, most women present late with
cervical cancer, in stage 3 and 4 (Zimbabwe National Cancer Strategy, 2014). The prevalence
of cervical cancer in women in Zimbabwe was 33.4% in 2009 with 15.6% being in elderly
women aged 65 years and above. A study done by Ferrante et al in 2009 indicated that older
patients in Florida had a 10.9% more likelihood of being diagnosed in the 3rd
0r 4th
stage of
cervical cancer than their younger counterparts. In India, a study done to assess screening
behaviours showed that elderly women in rural India were the least regularly screened and
presented with late clinical symptoms of cervical cancer (Gynewali, 2013).
Late stage presentation means that the focus of health resources is expended
fruitlessly. The current early cervical cancer screening drive has been focused on the 15-49
year age group whilst neglecting the elderly. Little research has been done in Zimbabwe
about the elderly and the researcher feels that more should be done to this vulnerable group.
We are in the age where people are striving to stay younger for longer but eventually old age
catches up with everyone. A survey done in 2011 in Europe about all research done
concerning late presentation of disease and co-infection related factors found that less than
2% of the studies concerned the elderly (Sangha et al, 2011). African literature is even
scantier. This research seeks to close that gap and pose questions for researchers to branch
more into geriatric research.
31
2.5. Comorbidity
Comorbidity is defined in relation to a specific index condition, as any distinct
additional entity or illness that has existed or may occur during the clinical course of a patient
who has the index disease under study (Valderas, Starfield, Sibbald, Salisbury & Roland,
2009). The question of which condition should be designated the index varies in relation to
the research question, the disease that prompted a particular episode of care, or of the
specialty of the attending physician. In this study, the index condition is cervical cancer.
Comorbid health problems are classified in terms of their relevance to clinical management.
For example, ischemic heart disease, cardiovascular risk factors (hypertension, hyper-
cholesterolemia), and diabetes are commonly managed within the same cardiovascular clinics
in primary care because they share important aspects of disease management (Valderas et al.
2009). Drawing together patients who have similar clinical management needs is efficient,
but runs the risk of interaction in relation to diagnosis, prognosis, treatment, and management
(including self-management) or outcomes. Even for the same pair of comorbid conditions
(e.g., diabetes and chronic pulmonary disease), some interventions can be antagonistic (e.g.
the effect of hypoglycaemic drugs and corticosteroids on blood glucose), others may be
agonistic (physical activity), and others may be neutral. Improved understanding of such
interactions among comorbid diseases is important to improving clinical care by promoting
early detection and treatment.
Understanding patterns and identifying common clusters of chronic diseases may help
policymakers, researchers, and clinicians to understand the needs of the care process better
and potentially save both provider and patient time and cost. However, only limited research
has been conducted in this area, and ambiguity remains as those limited previous studies used
different approaches to identify common clusters and findings may vary with approaches.
This study seeks to identify comorbid illnesses suffered by elderly women presenting with

32
late stage cervical cancer in Zimbabwe. A study in Australia estimated the prevalence of
common chronic diseases and examined co-occurrence of diseases using four approaches: (i)
identification of the most occurring pairs and triplets of comorbid diseases; performing (ii)
cluster analysis of diseases, (iii) principal component analysis, and (iv) latent class analysis
(Islam M.M., Valderas J.M., Yen L., Dawda P., Jowsey T., et al., 2014). Data were collected
using a questionnaire mailed to a cross-sectional sample of senior Australians, with 4574
responses. Eighty-two percent of respondents reported having at least one chronic disease and
over 52% reported having at least two chronic diseases. Respondents suffering from any
chronic diseases had an average of 2.4 comorbid diseases. Female respondents reported a
significantly higher number of diseases than male respondents. Of those respondents aged
over 75 years, 93% experienced at least one chronic disease and 73% more than one chronic
disease. Overall, 27% reported at least three chronic diseases, 11% at least four and 3% at
least five diseases. High blood pressure (HBP) (43.1%), arthritis (32.2%) and cancer (17.9%)
were three most prevalent diseases (Islam et al., 2014).
Three defined groups of chronic diseases were identified, asthma, bronchitis, arthritis,
osteoporosis and depression forming 1 group; high blood pressure and diabetes forming the
second and cancer, with heart disease and stroke either making a third group or attaching
themselves to different groups. The consistency of the findings suggests there is co-
occurrence of diseases beyond chance, and patterns of co-occurrence are important for
clinicians, patients, policymakers and researchers.
The National Institute on Aging (NIA) Geriatrics and Clinical Gerontology (GCG)
Program in Europe convened an interdisciplinary Task Force on Comorbidity to foster the
development of a research agenda on the multiple concurrent health problems that often
occur in older persons (Yancik R., Ershler W., Satariano W., Hazzard W., Cohen H. J., &
Ferrucci J., 2009).The risk of developing concomitant chronic illnesses and physiological

33
limitations escalates with aging. Diabetes, respiratory diseases, cancer, cardiovascular
problems, arthritis, hypertension, and certain other chronic conditions are more common in
older than in younger persons (Karlamangla A., Tinetti M., Guralnik J., Studenski S., Wetle
T., Reuben D., 2007). As a consequence, a new diagnosis of any common chronic health
condition is likely to be made in the context of pre-existing health problems.
A study done in England reviewed literature relating to comorbidity and dementia
(Bunn et al., 2014). Findings noted that comorbidity amongst patients with dementia
represented complex challenges in their primary and secondary care. Certain comorbid
conditions exacerbate the progression of dementia for example, they found out that cognitive
decline is accelerated in elderly patients with type 2 diabetes mellitus (Bunn et al., 2014).
Cervical cancer is a defining illness of acquired immune-deficiency syndrome (AIDS)
in patients with HIV (WHO, 2014). Immunocompromised women have a higher prevalence
of persistent infection with multiple high risk HPV types increasing susceptibility leads to a
stronger risk of developing precancer and cancer at younger ages. The degree of immune-
suppression increases risk of developing invasive disease up to 10 years earlier than in
uninfected women (WHO, 2014). They also have more frequent presentation with advanced
disease and a smaller chance of survival for 5 years (WHO, 2014).
As the elderly population expands, many diseases that predominantly affect older
people are also on the increase (Berger et. al., 2006). Many conditions that affect the elderly
are occurring in combination thereby complicating care of any single condition. The
incidence of cancer in those over 65 years is 10 times greater than in those younger and
cancer death rate is 16 times higher as well(Berger et. al., 2006). Since patients are likely to
acquire an increasing number of maladies with increasing age, strategies to prevent, screen or
prevent cancer and the need for physicians and caretakers to have expertise in both oncology

34
and geriatrics. A new approach established at the Case Western Reserve University uses a
Cancer-Aging Linked Database (CALD) for patients in the state of Ohio (Berger et. al.,
2006). The CALD accesses and merges information from a series of databases including the
Ohio Cancer Incidence Surveillance System (as cancer is a reportable disease in Ohio), the
Ohio death certificate file, Census block data and Long term care minimum data set amongst
others. Using the CALD, they were able to identify the following comorbidities in patients
aged 65 years and above with breast, prostate and colorectal cancers respectively: geriatric
syndromes such as incontinence, depression and dementia as well as disabilities leading to
functional impairment. The preliminary findings indicate that geriatric syndromes such as
depression and dementia are associated with late stage diagnosis of breast cancer. Also of
interest is the observation that older patients with breast cancer are less likely to be
recommended for therapy. These results clearly indicate that health care providers involved
in care of the elderly must be made aware of these disparities to more effectively orient their
cancer screening and treatment strategies (Berger et. al., 2006).
A study in Cleveland and Florida conducted to ascertain the impact of comorbidity on
cancer screening and prevention (Berger et. al., 2006) indicate that cancer screening
decreases among the elderly in general and is particularly deficient among those with
comorbid health problems. However, age was found to be a greater predictor than
comorbidity for health care providers not referring elderly patients for screening. In
Zimbabwe, for elderly women aged 65 years and above with cervical cancer, some are living
with hypertension, diabetes mellitus, arthritis, gout and HIV among another comorbid
conditions in rural areas (Ward, 2011). The elderly population in Zimbabwe especially in the
rural setting are already living with debilitating illness such as chronic backache and the
burden of taking care of orphaned grandchildren and sick children due to the AIDS

35
pandemic. These women present with late stage diagnosis of cervical cancer and reduced
survival rate due to comorbidities (Tshuma, 2002).
According to the World Health Organisation (2014), cervical cancer is the number
one cancer among women in Zimbabwe; with an estimated 1855 new cases and 1 280 deaths
due to the disease annually (WHO, 2014). Figures from the Zimbabwe National Cancer
Registry indicate the highest incidence of cervical cancer to be in women aged 65 years and
above. Of the 680 cases attended in 2006, 107 of them were 65 years and above, placing their
incidence at 15.6% out of the 32.5% total for all women in Zimbabwe (ZNCR, 2010).
A social study done in 2009 by Chinhamora & Trent linked multiple comorbidities in
the elderly population of Zimbabwe with a lesser tendency to seek professional healthcare for
serious or life-threatening conditions like cancer and cardiac anomalies. The recent economic
meltdown posed a threat especially to women’s health. They neglected themselves in favour
of their children or other family members and viewed general annual check-up as an
unaffordable luxury (Chinhamora, 2009).
2.6. Cervical cancer and comorbidity
Cervical cancer is a common malignancy in developing countries, in particular those
with a high prevalence of human papillomavirus and human immunodeficiency virus
(HIV).The incidence rate in black women is 11.2 per 100 000, exceeds the rate in white
women which is 7.3 per 100 000 and mortality risks for black women continue to be two
times higher than for white women (McCance & Huether, 2006). According to the South
African National Cancer Registry’s 2001 published report, cervical cancer was the third most
common malignancy (16%) after breast cancer (19%) and basal cell carcinoma of the skin
(17%) in female patients, and the most common malignancy in black African women (31%)
(Sauer, et. al., 2013).

36
A study done in Denmark in 2014 found large variations in cancer awareness
between individuals of different socioeconomic status supporting findings from previous
studies which show that people of low economic status are less aware of cancer symptoms
than their counterparts of higher economic status leading to late diagnosis (Hvidberg,
Fischer-Pederson, Nielsen-Wulff & Vedstead, 2014). Also supported by a study done by
Gyenwali in India in 2013. Poor socioeconomic status was linked to heavy burden of
comorbid conditions which demand polypharmacy and place financial constraints leading to
women bypassing cervical cancer screening and waiting for clinical manifestations to occur
of which the cancer would be advanced to stage 1V at that time.
Another study done in India revealed that economic constraints prioritises women
towards social responsibilities and self-neglect towards their health issues (Singh & Badaya,
2012). The most untouched population is in the rural areas, availability of facilities there
would increase compliance to cervical cancer screening (Singh & Badaya, 2012).
The Eve Appeal Survey carried out in England in 2010 was a study to ascertain
awareness of cervical cancer in women. Women aged 60 years and above were more able to
recognise clinical symptoms such as persistent bleeding post-menopause but cited fear of the
unknown as a barrier to seeking early cervical screening in the absence of those clinical
symptoms.
In Zimbabwe, cervical cancer screening is widespread but hardly offered to the
elderly woman with the regular check-up package due to health worker misconception,
reluctance for the invasive screening technique and focus on other comorbidities (Tshuma,
2002; Trent, 2009).A study done by Chipfuwa in 2012 indicated that the most focus of
cervical cancer screening was on the 15-49 year age group showing that the elderly are
neglected in cancer research but they are important members of our society. This study was

37
done to establish awareness and compliance in Zimbabwean women about early cervical
cancer screening.
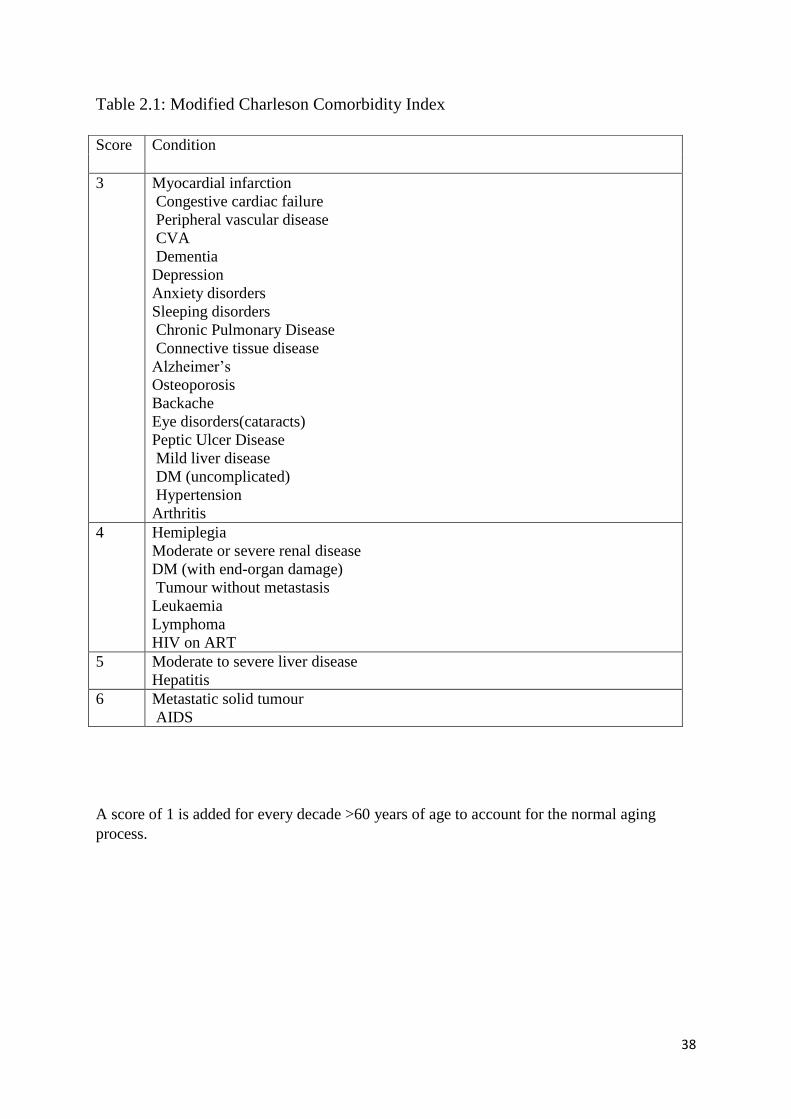
The Comorbidity Index
The Charleson Comorbidity Index is used to measure or predict prognosis and quality
of life in patients living with co-existing conditions. It was used successfully by Fadem in
2013 to predict or estimate the prognosis of elderly patients on dialysis by scoring the
comorbidities and estimating remaining survival rate. It has been modified for the purpose of
this research as illustrated in Table 2.1. A scoring system based on the quality or nature of
comorbidities was used in tailoring it to suit the Zimbabwean population according to the
chronic illnesses commonly found in the population. This researcher hypothesizes that elderly
women often present at health care institutions with late stage cervical cancer and most of
them suffer from a number of other diseases which could have developed either before or
after the cervical cancer diagnosis. The scoring system was used as a comparison system
against actual number of comorbidities to rule out gravity of the illnesses as the actual
contributor to late stage diagnosis of cervical cancer.
38
Table 2.1: Modified Charleson Comorbidity Index
A score of 1 is added for every decade >60 years of age to account for the normal aging
process.
Score Condition
3 Myocardial infarction
Congestive cardiac failure
Peripheral vascular disease
CVA
Dementia
Depression
Anxiety disorders
Sleeping disorders
Chronic Pulmonary Disease
Connective tissue disease
Alzheimer’s
Osteoporosis
Backache
Eye disorders(cataracts)
Peptic Ulcer Disease
Mild liver disease
DM (uncomplicated)
Hypertension
Arthritis
4 Hemiplegia
Moderate or severe renal disease
DM (with end-organ damage)
Tumour without metastasis
Leukaemia
Lymphoma
HIV on ART
5 Moderate to severe liver disease
Hepatitis
6 Metastatic solid tumour
AIDS

39
Theoretical framework
Betty Neuman’s Systems Model has been used in this study as a framework guide.
This conceptual framework is an open systems model, fitting well with the wholistic concept
of optimising a dynamic, yet stable interrelationship of mind, body and spirit of the client in a
constantly changing environment and society (Neuman, 1989).
White, Richter & Fry (1992), examined the impact of potential stressors, coping
strategies and perceived social support in the psychological adaptation of women with
diabetes mellitus using Betty Neuman’s model. Diabetes mellitus was selected as the
prototype of a chronic illness because of its prevalence as a chronic disease and the necessity
for significant lifestyle changes. In this study, cervical cancer is the prototype, studied in a
complex context of comorbidity adding to external stressors leading to delayed screening and
late stage diagnosis of cervical cancer.
A study done by Ladd in 1999 also used Betty Neuman’s Systems Model to study the
effect of social support on the psychological adaptation of an individual receiving an
alternative form of nutritional therapy in cancer patients. An interesting finding was that the
coexistence of 2 or more diseases in the same individual affects clinical care of the index
condition. One other major clinical question is whether there would be a common aetiological
pathway which then ties the index condition to external and internal stressors (Piccirillo &
Feinstein, 1996).
2.7. Summary
There have been various studies undertaken locally, regionally and internationally
concerning cervical cancer in women but none have focused on whether comorbidity plays a
role in diagnosis of cervical cancer in elderly women which is what this researcher has sought
to find out.

40
CHAPTER 3
METHODS
3.1. Introduction
Research methods incorporate all procedures that are used to pursue knowledge
(Burns & Grove, 2009). This study examined the relationship between prevalence of late
stage diagnosis of cervical cancer and number of comorbid conditions in women aged 65
years and above in Zimbabwe. This chapter will address the research design, setting,
sampling procedure, sample size, variables, development of research study instrument, data
collection plan, ethical issues and data analysis.
3.2. Research design
Research design is a blueprint for conducting the study that maximises control over
factors that may interfere with validity of findings (Burns & Grove, 2009). The descriptive,
correlational design was used to examine the relationship between late stage diagnosis of
cervical cancer and comorbidity in elderly women aged 65 years and above. It is a
retrospective study looking at medical records from previous hospital visits. The purpose of
this design was to guide the researcher in planning and implementing the study in the most
likely way to achieve the intended goal.
According to Polit & Hungler, descriptive, correlational study designs describe
relationships among variables rather than infer cause and effect. The variables under study
were prevalence of late stage diagnosis of cervical cancer as the dependent variable and
number of comorbidities as the independent variable. Descriptive research aims at observing,
describing and documenting aspects of a situation as it currently exists whilst correlational
research examines relationships among variables as they naturally occur (Polit & Hungler,

41
2008; Burns & Grove, 2009). Aspects of both descriptive and correlational research are
therefore combined. The research has no control over the independent variable but describes
rather how it is related to another. It is an efficient and useful method of collecting data in a
problem area in nursing over a short period of time. A quantitative, descriptive, correlational
study is appropriate for this study as the researcher seeks to describe the relationship between
number of comorbidities and prevalence of late stage diagnosis of cervical cancer in
Zimbabwe.
3.3. Sampling Plan
Sampling is a process of selecting a portion of the population as a representative of
the entire population (Polit & Beck, 2014). A sampling plan is a process of making the
selection (Burns & Grove, 2009). It describes the process for selecting the study site and
sample and specifies in advance how study participants are to be selected and how many are
to be included. The aim is to increase representativeness, decrease systematic bias and
determine sampling error. In this study, non-probability method of sampling is going to be
used. All patient records of women who are 65 years and above at Parirenyatwa Group of
Hospitals and Spilhause Clinic based at Harare Hospital who have cervical cancer were
reviewed in a process of convenience sampling as rate of patient attendance and time limit for
submission of study results did not correlate. A sample represents the entire population (Polit
& Beck, 2014). The element is the basic unit of a sample; in this study elements are referred
to as subjects as they are people, therefore sample will refer to elderly women aged 65 years
and above with cervical cancer with records at Parirenyatwa Hospital and Spilhause Clinic at
Harare Hospital.
3.4. Study site
Patients were selected from Parirenyatwa Radiography Department and Ward A6 and
at Spilhause Clinic at Harare Hospital. These are referral centres from council clinics,
42
provincial and district hospitals and private practitioners. The researcher also reviewed
patient records from the Parirenyatwa records department to confirm initial staging.
3.5. Target population
According to Burns & Grove (2009), a target population refers to all elements i.e.
individuals, objects or substances that meet the sample criteria for inclusion in a study. The
target population for this study were all cervical cancer patients aged 65 years and above in
Zimbabwe who were able to understand Shona or English.
3.6. Accessible Population
Accessible population is the aggregate of cases that meet the sampling criteria and are
accessible to the researcher (Polit & Hungler, 2008). One can generalise findings from
accessible population to the target population. The accessible population was the population
of elderly women with cervical cancer, attending Parirenyatwa Cancer Clinic and
radiotherapy clinic, Harare Hospital Spilhause clinic and with medical records at
Parirenyatwa Hospital.
3.7. Sampling Criteria
Sampling criteria is the essential characteristics of the target population (Burns &
Grove, 2009). Sampling criteria refers to inclusion and exclusion criteria which help to
control extraneous variables. It ensures homogeneity and provides a guideline for sample
recruitment. Inclusion criteria refer to specific characteristics the investigator wishes to
include in the study whereas exclusion criteria refer to characteristics not included in the
study.
3.7.1. Inclusion Criteria
The inclusion criteria included those subjects diagnosed with cervical cancer, whether
on treatment or recently diagnosed. The subjects should have been currently aged 65 years

43
and above and be able to communicate in English and Shona. Medical records had to be
available for elderly women diagnosed with cervical cancer dating back 2 years.
3.7.2. Exclusion Criteria
Exclusion criteria included those who could not communicate in English or Shona and those
aged below 65 years. The study also excluded those elderly women without a confirmed
diagnosis of cervical cancer and those not staged.
3.8. Sample Size
A sample is a fraction of the population that is selected for a study (Burns & Grove,
2009). The sample size is the minimum number of subjects needed to complete a study. It is
important to determine the sample size in order to yield adequate precision or power and is
calculated by considering significance level or alpha, then power and effect size (Burns &
Grove, 2009). The significance level is an index of how probable or reliable the study
findings are. The level of significance used in this study was 0.05, indicating the probability
that the relationship of the observed magnitude would be found by chance only 5 times out of
100 (Polit & Beck, 2014). The significance level will give the researcher an indication and
confidence that the findings are reliable.
According to Polit &Beck (2014), the effect size highlights the magnitude of the
differences between 2 groups or the magnitude of the relationship between 2 variables with
regard to some attribute of interest. It is a quantitative measure of the strength of a
phenomenon (Thalheimer & Cook, 2002). Sample based effect size estimates the strength or
magnitude of an apparent relationship (Kelly & Preacher, 2012). The effect size used in this
study was 0.50.
Polit &Beck (2014) defined power as the ability to detect existing relationships among
variables through use of a design. The power of .80 was used. The power assists the
44
researcher to avoid a type 2 error where conclusions can be made that there is no relationship
between the variables and yet a relationship actually exists. The sample size calculation was
based on the outcome: late stage diagnosis for cervical cancer. The sample outcome was
based on the proportion of women presenting late for cervical cancer diagnosis and using the
formula by A. Dobson: n = Z2pq⁄d
2
Where:
: p is the proportion of women aged 65 years and above presenting with cervical
cancer in Zimbabwe.
: q = (1-p)
: d is the precision which is presumed to be 5%
: Z is 1.96 based on a 95% confidence interval.
In this calculation, p was assumed to be 0.156 based on previous literature from the
Zimbabwe National Cancer Registry. Using the above formula, the sample size, n = 203.
Adjusting for a 75% response rate, the sample size was adjusted to 270. The researcher
utilised a sample of least 68, a quarter of the calculated sample size due to financial and time
constraints.
3.9. Sampling Procedure
The sampling procedure indicates how a group of people with whom to conduct a
study are selected. Non-probability sampling was used to recruit the study sample due to the
decreased number of elderly women being admitted in ward A6 or attending the Parirenyatwa
Hospital Radiography Department and Spilhause Clinic located at Harare Hospital Cancer
Clinics and the high death rate. Medical records dating back 2 years were reviewed. There is
no way to ensure that every member of the population is going to be selected thus introducing

45
a certain element of bias. Commonly used non-probability sampling methods are
convenience, quota and purposive sampling. In this study, convenience sampling was used to
select 68study participants (Polit & Beck, 2014). The interviews were carried out in Shona or
English with those subjects who met the inclusion criteria. An informed consent was sought
verbally after explaining the procedure and permission given to print names and hospital
numbers on the consent form in order to review medical records. A written consent was
obtained from the research sites heads of departments to recruit study participants and to
review medical records for elderly women with cervical cancer at the Records Department to
verify stage at diagnosis.
The investigator ensured privacy by using a counselling room and confidentiality by using a
coding system to label participant responses, real names and hospital numbers were only used
in order to retrieve medical records from the Parirenyatwa Database to confirm initial staging
and the record destroyed immediately after confirmation. The investigator visited the clinics
from 0700hrs weekdays, an hour before the actual clinic began in order to prepare stationery
and the counselling room. A list of potential subjects was drawn from the day’s Outpatients
Department Record book at the Radiography Department at Parirenyatwa and Spilhause
Clinic at Harare Hospital. The admission book and kardex were used in ward A6 at
Parirenyatwa and hospital notes for clarification. Medical records were reviewed from
1400hrs weekdays. Once candidates were identified, they were taken to the interview room
with the knowledge of the sister in charge of the clinic, made comfortable and introductions
made. Study purpose and approximate length of interview were explained to the subject. If it
was then established that the subject was competent and willing to participate, a verbal
informed consent was obtained and name printed on a written consent for records.

46
3.1.0. Variables
3.1.0.1. Conceptual and operational definitions
A conceptual definition provides a variable with a connotative meaning (Burns &
Grove, 2009). It refers to how the variable is defined. An operational definition describes
how the variable or concept will be measured in a study. The investigator was able to observe
the variables in their natural setting.
3.1.0.2. Demographic Variables
Demographic variables describe the characteristics or attributes of the sample (Burns
& Grove, 2003). These include, age, marital status, educational status, rural or urban
background and household type (whether nuclear or extended family). The rationale for using
demographic variable was that when the investigator completed the study, demographic
information would be analysed to provide a picture of the sample characteristics (Polit &
Beck, 2014). The demographic variable was measured by the demographic section devised by
the investigator.
3.1.0.3. Late stage cervical cancer
This is the dependent variable. Conceptually, cervical cancer has been defined as
autonomous and uncontrolled growth of cells of the cervix forming tumours which may
invade the tissues surrounding the cancer and cause metastases. Cervical cancer can be
diagnosed in its pre-cancer phase via a pap smear or may progress to stage IV where
metastasis has occurred and the cancer will have spread to distant organs beyond the pelvic
area such as the lungs and clinical manifestations of lungs damage then lead to late diagnosis
of the cervical cancer. Staging was measured from 1-4 with late stage cervical cancer being
stage 3 and 4.

47
3.1.0.4. Comorbidity
This is the independent variable. Comorbidity refers to other chronic illnesses subjects
will be suffering from besides cervical cancer which was the index condition. Comorbidity
was determined at time of diagnosis. Comorbid illnesses include hypertension, diabetes
mellitus, epilepsy, asthma, chronic obstructive pulmonary disease (COPD), arthritis, gout,
ulcers, chronic renal failure (CRF), backache, geriatric symptoms like dementia,
schizophrenia, depression and Alzheimer’s or Parkinsonism. Comorbidity will be
operationalised by measuring it with a comorbidity scale designed by the investigator based
on the Charleson Comorbidity Index to find out the number of comorbid illnesses in elderly
cervical cancer women. This index was used to devise a scoring system based on the quality
of the comorbid illness so that not only the number of illnesses is considered, but their weight
on survival as well. This has greater impact on whether comorbid illnesses affect the stage at
which cervical cancer is diagnosed.
3.1.1. Instrument
An instrument is a device or technique that an investigator uses to collect data, e.g.
questionnaire and observable schedules (Polit & Hungler, 2008). The instrument designed for
this study was an interview guide which consisted of a demographic data section, a cervical
cancer diagnosis section, and comorbidity scale section. This instrument was devised by the
investigator, translated into Shona then pretested at the cancer clinic at the Radiography
Department at Parirenyatwa Hospital to establish reliability and validity. It was used to
conduct a 30 minute interview with the participants.
3.1.2. Validity
Validity refers to the degree with which an instrument measures what it is intended to
measure (Burns & Grove, 2009). The instrument was translated into Shona and checked by
experts in the Nursing Science Department and consultants at the cancer clinic.

48
3.1.3. Reliability
Reliability refers to the degree of consistency and accuracy with which the instrument
measures what it is supposed to measure (Burns & Grove, 2009). To ensure reliability, the
instrument was pretested on 8 patients only due to time constraints. A research assistant was
used to test consistency of responses in 4 of the pilot participants if the interviewer was
different.
3.1.4. Data collection plan
Polit & Hungler (2008) explain that data collection should normally follow a pre-
established plan to minimise confusion, delays and mistakes. The investigator plan should
specify where, when and how data will be collected paying particular attention to human
rights consideration and the actual data collection procedure.
Approval for the study was sought and granted by the Joint Research and Ethics
Council of Parirenyatwa Group of Hospitals and the College of Health Sciences (JREC) after
submission of this proposal before data collection. Permission from the study site such as
Parirenyatwa Hospital and Spilhause at Harare Hospital were also obtained. Pre-testing of the
research instrument was done on 8 patients who were then excluded from the study. Non-
probability sampling used to recruit subjects. The clinic staff continued their usual schedule
and duties to minimise bias. Once a subject was selected, they were taken into a prepared
counselling room with adequate lighting, good ventilation and comfortable chairs. The
investigator made a self-introduction with the sister-in-charge present at initial contact only
and gave information to the subject to obtain an informed consent. A structured interview
was usually completed in 30 minutes or less using the interview guide whilst answers were
entered into a code book. Data collection took place from 1 – 28 May 2015.
49
3.1.5. Data collection procedure
After obtaining permission from JREC and the clinical director of Parirenyatwa
Group of Hospitals and Harare Hospital, the investigator visited the sites for familiarization
and to make prior arrangements for data collection. On interview days, the investigator was
introduced to the subjects by the sister in charge before proceeding to do face to face
interviews which lasted about 30 minutes. Data collected as well as written consent forms
were kept locked in a briefcase that the only investigator had access in order to maintain
privacy and confidentiality.
3.1.6. Human Rights Consideration
Protection of the rights of human subjects is of paramount importance and was
prioritised in this study by using the JREC template for informed consent which ensured that
all rights were observed. Permission to carry out the study was sought from the Nursing
Science Department, JREC and the clinical director of Parirenyatwa Group of Hospitals and
Spilhause Clinic at Harare Hospital to ensure that ethical requirements were met. The
subjects were informed of the purpose of the study, length of interview, potential benefits and
risks in a language they understood. Privacy and confidentiality was maintained by locking
up consents where subjects’ actual names were recorded and using a coding system
decipherable only by the investigator instead when recording responses to study questions.
The right of the subject to withdraw from the study without any adverse effects was fully
explained. The principle of respect for human dignity encompasses peoples’ right to make
informed voluntary decision about their participation in the study (Polit & Hungler, 2008).
The signed consent forms and coded answers to the interview were kept locked by the
investigator and destroyed upon completion of the study to ensure that no information will be
linked to the subjects whatsoever.

50
3.1.7. Pilot study
A pilot study is frequently defined as a smaller version of a proposed study
undertaken to refine the methodology (Burns &Grove, 2008). This is done to assess the
clarity of the research study questions, time required to complete the questionnaire and the
extent to which the instrument answers the research study questions. Due to time and
financial constraints, an instrument pre-test was conducted on eight subjects who met the
inclusion criteria at the Radiography Department at Parirenyatwa Hospital. These were
excluded from the study. The pre-test assisted the researcher to become familiar with the
instrument and correct any foreseeable problems before the major study and use of a different
site could have been used to rule out bias. In this case, the pre-test was done on different days
to prevent repeating patients.
3.1.8. Data Analysis Plan
Data analysis is conducted to reduce, organise and give meaning to data (Burns &
Grove, 2009). After obtaining raw data, it was entered into a code book using the Statistical
Package for The Social Sciences (SPSS PC) which was then used to analyse that data.
Descriptive statistics were used to describe the sample characteristics, the dependent and the
independent variables. The Pearson’s correlational coefficient was computerised to show
whether there is a relationship between late stage cervical cancer diagnosis and number of
comorbidities in elderly women in Zimbabwe using a modified Charleson Comorbidity Index
and simple regression used to explain the relationship.

51
Chapter 4
Results
This section presents the results obtained from this study done to determine the
relationship between prevalence of late stage diagnosis of cervical cancer and number of
comorbidities in elderly women above 65 years in Zimbabwe.
4.1. Demographic data
Results from the demographic section are summarised as follows. Thirty-one women
(45.6%) were aged between 65-70 years, 17 (25%) aged between 71-75 years, 13 (19.1%)
between 76-80 years and 7 (10.3%) were aged above 80 years. The mean age was 72.57
years. On marital status, 6 (8.8%) women were single, 25 (36.8%) married, 9 (13.2%)
divorced and 28 (41.2%) were widowed. Of those who were married, 38 (55.9%) married in
their teens, 23 (33.8%) between the ages of 20-35 years and 1(1.5%) married beyond 35 years
of age. The mean age at marriage was 18.74. In terms of parity, 9 women (13.2%) were
nulliparous, 18 (26.5%) gave birth to 1-3 children, 23 (33.8%) had 4-6 children and 18
(26.5%) had more than 6 children. The mean parity was 4.66.
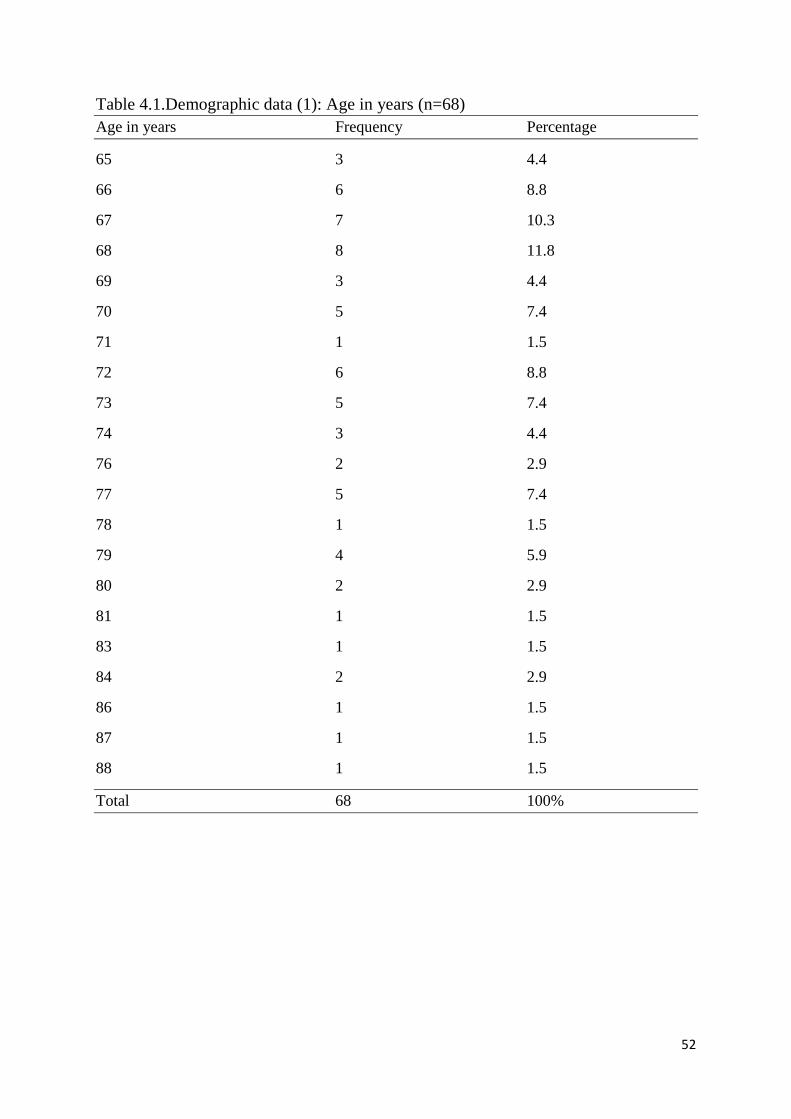
52
Table 4.1.Demographic data (1): Age in years (n=68)
Age in years Frequency Percentage
65 3 4.4
66 6 8.8
67 7 10.3
68 8 11.8
69 3 4.4
70 5 7.4
71 1 1.5
72 6 8.8
73 5 7.4
74 3 4.4
76 2 2.9
77 5 7.4
78 1 1.5
79 4 5.9
80 2 2.9
81 1 1.5
83 1 1.5
84 2 2.9
86 1 1.5
87 1 1.5
88 1 1.5
Total 68 100%

53
Demographic data (2): Age when married (n=68)
Age when married Frequency Percentage
12 1 1.5
13 4 5.9
14 8 11.8
15 6 8.8
16 8 11.8
17 4 5.9
18 5 7.4
19 2 2.9
20 2 2.9
21 3 4.4
22 4 5.9
23 6 8.8
24 3 4.4
25 2 2.9
27 1 1.5
28 1 1.5
30 1 1.5
36 1 1.5
Not applicable 6 8.8
Total 68 100%
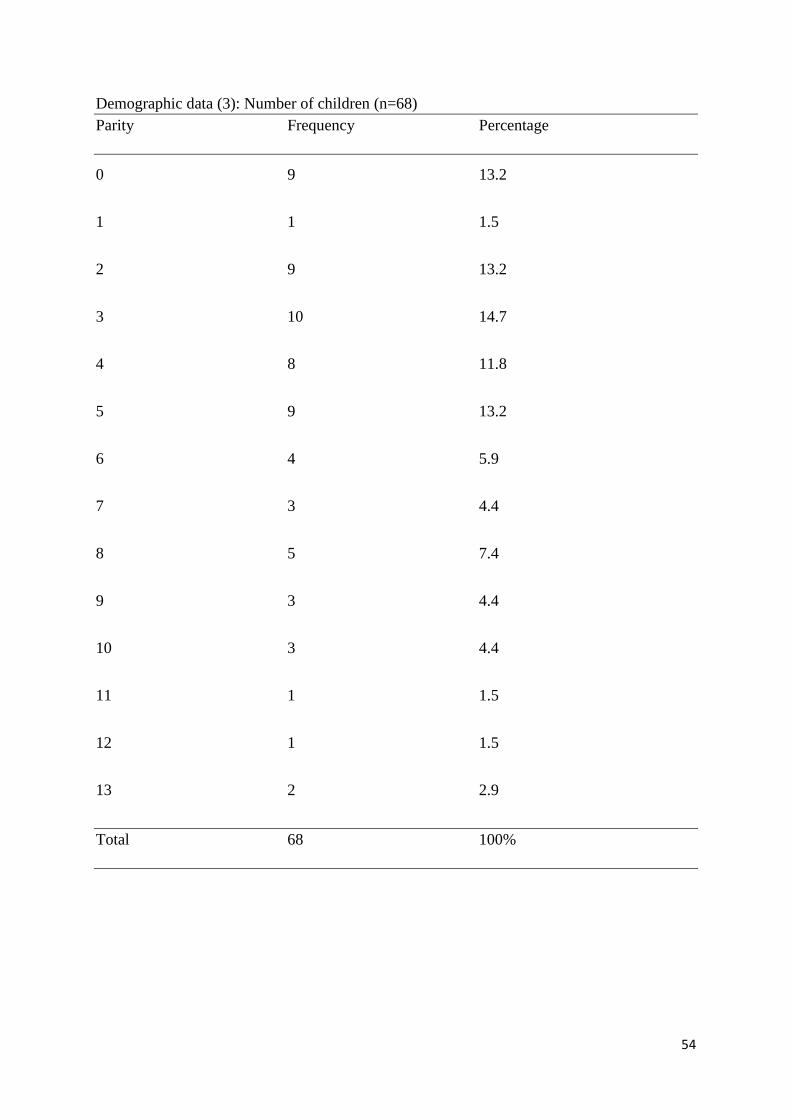
54
Demographic data (3): Number of children (n=68)
Parity Frequency Percentage
0 9 13.2
1 1 1.5
2 9 13.2
3 10 14.7
4 8 11.8
5 9 13.2
6 4 5.9
7 3 4.4
8 5 7.4
9 3 4.4
10 3 4.4
11 1 1.5
12 1 1.5
13 2 2.9
Total 68 100%

55
Forty-five (66.2%) lived in the rural areas whilst 23 (33.8%) were urban dwellers. Two
women (2.9%) lived alone, 29 (42.6%) lived in a nuclear family with their husband, children
and/or grandchildren, 31 (45.6%) lived in an extended family with other relatives and 6
(8.8%) live with friends or workers.
Seventeen women (25%) had never worked, 18 (26.5%) were retired from
professional employment whilst 9 (13.2%) were still employed, 1 (1.5%) was informally
employed and 23 (33.8%) were farmers. In terms of education, 4 (5.9%) had none, 10
(14.7%) had below primary education, 22 (32.4%) were educated up to primary level, 19
(27.9%) up to secondary level and 13 (19.1%) up to tertiary level. Three women (4.4%) cited
no religious affiliation, 9 (13.2%) were traditionalists, 55 (80.9%) were Christians and 1
(1.5%) admitted to both traditional and Christian beliefs and practices.
For 10 women (14.7%), the nearest health care facility was less than 2 km from their
home, for 46 (67.6%), it was between 2-10 km and for 12 (17.6%), the distance was greater
than 10 km. In terms of usual health care provider, 3 women (4.4%) cited home based carers,
31 (45.6%) went to a clinic, 22(32.4%) went to a hospital, 11 (16.2%) went to a private
practitioner and 1 (1.5%) had none.

56
Demographic data (4): n = 68
Variable Frequency Percentage
Area lived
Rural
Urban
Total
45
23
68
66.2
33.8
100%
Family dynamics
Lives alone
Nuclear family
Extended family
Friends or workers
Total
2
29
31
6
68
2.9
42.6
45.6
8.8
100%
Occupation
Never worked
Retired
Professionally employed
Informal employment
Farmer
Total
17
18
9
1
23
68
25.0
26.5
13.2
1.5
33.8
100%
Level of education
None
Below primary schooling
Primary
Secondary
Tertiary
Total
4
10
22
19
13
68
5.9
14.7
32.4
27.9
19.1
100%
Religion
None
Traditional
Christianity
Both
Total
3
9
55
1
68
4.4
13.2
80.9
1.5
100%

57
Demographic data (5): n = 68
Variable Frequency Percentage
Nearest health care facility
< 2 km 10 14.7
2 – 10 km 46 67.7
>10 km 12 17.6
Total 68 100%
Usual health care provider
Home based carer 3 4.4
Clinic 31 45.6
Hospital 22 32.4
Private practitioner 11 16.2
None 1 1.5
Total 68 100%

58
4.2. Cervical cancer
4.2.0. Diagnosis
Results are summarised as follows: Eighteen women (26.5%) had been diagnosed less
than a year, 26 (38.2%) between 1-3 years and 24 (35.3%) greater than 2 years. The mean
duration of diagnosis was 1.09 years. Seven (10.3%) were diagnosed in Stage 1, 16 (23.5%)
in Stage 11, 26 (38.2%) in Stage 111 and 19 (27.9%) in Stage 1V. The mean stage was 2.84.
Sixty-three women (92.6%) were currently on treatment or had received treatment and 5
(7.4%) had no treatment. For those on treatment, the duration at the time when this study was
conducted was as follows: 4(5.9%) had weeks, 19 (27.9%) had months, 22 (32.4%) had years
of treatment and 18 (26.5%) had finished treatment. The mean duration of treatment was 2.01
years. In terms of treatment type, 8 women (11.8%) cited chemotherapy, 16 (23.5%)
radiotherapy, 7 (10.3%) cryotherapy, 3 (4.4%) traditional herbs, 6 (8.8%) had surgery and 23
(33.8%) had combined therapy. Those on combined therapy, 13 (56.5%) cited chemotherapy
and radiotherapy, 5 (21.7%) had chemotherapy then surgery, 4 (17.4%) had radiotherapy then
surgery and 1 (4.4%) was combining chemotherapy and traditional herbs from a registered
herbalist.

59
4.2.1. Awareness
Twenty-nine women (42.6%) were aware of the cervical cancer screening drive whilst
39 (57.4%) were not aware. Of those aware, 9 (13.2%) had been actually screened before
cervical cancer diagnosis, 8 of them (11.8%) more than annually and 1 (1.5%) annually.
Fifty-nine of the women (86.8%) were screened at diagnosis. Source of information for
cervical cancer screening awareness was directly from health care providers for 50 women
(73.5%), indirectly from peers, television or other source for 3 (4.4%) and 15 (22.1%) had
both as informants. These results are illustrated in table 4.3.0.
4.3. Comorbidity
A list of the comorbidities suffered by the women is listed in table 4.3.1. Fifty-four
women (79.4%) had comorbidities. Ten (14.7%) had 1 other chronic illness, 16 (23.5%) had
2 other illnesses, 19 (27.9%) had 3, 6 (8.8%) had 4 and 3 (4.4%) had 5 other illnesses. The
mean number of comorbidities was 2.03. The modified Charleson Comorbidity index showed
that 40 (74.1%) participants suffered from comorbidities before the cervical cancer diagnosis,
29 (53.7%) had them after the cervical cancer diagnosis and 13 (24.1%) had comorbidities
before and after the cervical cancer diagnosis. The scoring range was 0-38 sliding scale with
0 being no comorbidities and 38 being the largest number or most affected by other chronic
illnesses. Fourteen (26%) scored from 0-5 and 17 (31.5%) scored from 6-10 on comorbidities
before the cervical cancer diagnosis. The mean score before cervical cancer diagnosis was
5.16 out of 38. After the cervical cancer diagnosis 9 (16.7%) scored between 0-5, 10 (18.5%)
between 6-10 and 7 (13%) from 11-15. The mean score after the cervical cancer diagnosis
was 3.87 out of 38. The results are summarised in table 4.3.
Table 4.2.1. Diagnosis (n = 68)

60
Variable Frequency Percentage
Duration of diagnosis
< a year
1-3 years
>3 years
Total
18
26
24
68
26.5
38.2
35.3
100%
Stage at diagnosis
1
2
3
4
Total
7
16
26
19
68
10.3
23.5
38.2
28.0
100%
Treatment
Yes
No
Total
63
5
68
92.6
7.4
100%
Duration of treatment
Weeks
Months
Years
Finished treatment
Not treated
Total
4
19
22
18
5
68
5.9
27.9
32.4
26.5
7.4
100%
Type of treatment
Chemotherapy
Radiotherapy
Cryotherapy
Traditional herbs
Surgery
Combined treatment
Not treated
Total
8
16
7
3
6
23
5
68
11.8
23.5
10.3
4.4
8.8
33.8
7.4
100%

61
Table 4.2.2. Awareness (n=68)
Variable Frequency Percentage
Screening awareness before diagnosis
Yes
No
Total
29
39
68
42.6
57.4
100%
Actual screening before diagnosis
Yes
No
Total
9
59
68
13.2
86.8
100%
Screening frequency before diagnosis
>Annually
Annually
Stat (at diagnosis)
Total
8
1
59
68
11.8
1.5
86.8
100%
Source of information about screening
Direct
Indirect
Both
Total
50
3
15
68
73.5
4.4
22.1
100%

62
Table 4.3.0. Comorbidities
Variable Frequency Percentage
Comorbidity
Yes 54 79.4
No 14 20.6
Total 68 100%
Number of comorbidities
0 14 20.6
1 10 14.7
2 16 23.5
3 19 27.9
4 6 8.8
5 3 4.4
Total 68 100%
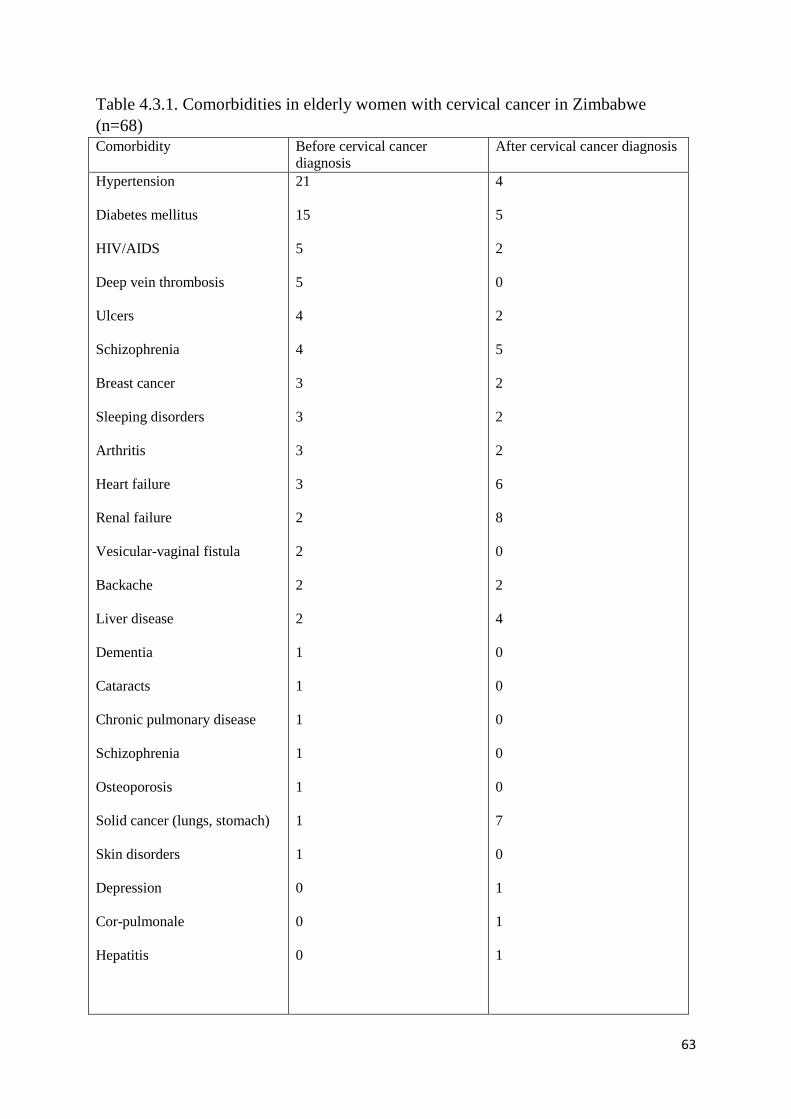
63
Table 4.3.1. Comorbidities in elderly women with cervical cancer in Zimbabwe
(n=68)
Comorbidity Before cervical cancer
diagnosis
After cervical cancer diagnosis
Hypertension
Diabetes mellitus
HIV/AIDS
Deep vein thrombosis
Ulcers
Schizophrenia
Breast cancer
Sleeping disorders
Arthritis
Heart failure
Renal failure
Vesicular-vaginal fistula
Backache
Liver disease
Dementia
Cataracts
Chronic pulmonary disease
Schizophrenia
Osteoporosis
Solid cancer (lungs, stomach)
Skin disorders
Depression
Cor-pulmonale
Hepatitis
21
15
5
5
4
4
3
3
3
3
2
2
2
2
1
1
1
1
1
1
1
0
0
0
4
5
2
0
2
5
2
2
2
6
8
0
2
4
0
0
0
0
0
7
0
1
1
1

64
Table 4.3.2. Comorbidity score before cervical cancer (n = 68. Mean = 9.03)
Score Frequency Percentage
0 14 20.6
3 3 4.4
4 4 5.9
5 2 2.9
6 4 5.9
7 1 1.5
8 8 11.8
9 5 7.4
10 1 1.5
11 8 11.8
12 2 2.9
13 1 1.5
14 4 5.9
15 2 2.9
17 2 2.9
18 3 4.4
19 1 1.5
20 1 1.5
21 1 1.5
28 1 1.5
31 1 1.5
Total 68 100%

65
Table 4.3.3. Score of comorbidities after the cancer diagnosis (n = 68. Mean = 3.87)
Score Frequency Percentage
0 39 57.4
3 1 1.5
4 6 8.8
5 2 2.9
6 3 4.4
7 3 4.4
8 1 1.5
9 2 2.9
10 1 1.5
11 1 1.5
12 2 2.9
13 1 1.5
14 1 1.5
15 2 2.9
18 1 1.5
20 1 1.5
21 1 1.5
Total 68 100%

66
Table 4.3.4. Comorbidity scoring summary (n=68.)
Score range Number of
participants with
chronic illnesses
before cancer
diagnosis
Number of
participants with
chronic illnesses
after cancer
diagnosis
Number of
participants who had
chronic illnesses
before and after the
cancer diagnosis
0-10 - low
11-20 - moderate
>20– high
31
7
3
19
9
1
27
24
3
67
4.4. Relationship between prevalence of late stage cervical cancer diagnosis and number of
comorbidities
Table 4.4shows the results of the Pearson correlation analysis to establish if there was
a relationship between prevalence of late stage cervical cancer diagnosis in elderly women
and number of comorbidities. The correlation coefficient is 0.431 and significance is
0.01.The results show a positive correlation (r = .431, p = 0.01), which shows a strong
relationship between prevalence of late stage diagnosis and number of comorbidities. As
number of comorbidities increase, the later the stage of diagnosis of cervical cancer.
Table 4.4.1 shows the regression analysis. R² is 0.186. which when expressed as a
percentage is 18.6%.This result implies number of comorbidities accounts for 18.6% of the
variance in late stage diagnosis of cervical cancer which is the dependent variable. Other
factors are involved in affecting late stage diagnosis besides number of comorbidities. The
significant F-test (F = 15.062, p = 0.01) indicates a linear relationship and that R² is
significant. The T-test for the unstandardized regression coefficient (b = 0.289) and is
significant at 0.01. It represents a change in the dependent variable which is late stage
diagnosis for every unit change in number of comorbidities significant at the level of 0.01.
Summary
This chapter presented the results of the study undertaken using frequencies and
percentages presented in tables as descriptive statistics. Pearson’s correlation analysis was
used to test the relationship between prevalence of late stage diagnosis of cervical cancer and
number of comorbidities. The regression coefficient was then used to analyse the change in
the prevalence of late stage diagnosis of cervical cancer against change in number of
comorbidities.

68
4.4.0 Correlation (n = 68)
Pearson’s correlation matrix of late stage diagnosis of cervical cancer and number of
comorbidities (n = 68):
Y
1.000
X .431**
*p < 0.05 **p < 0.01 *** p < 0.001
Key
Y = Late stage diagnosis of cervical cancer
X = Number of comorbidities before cervical cancer diagnosis

69
4.5. Regression analysis (n = 68)
Variable B SEB BETA
X 2.251 0.184 0.431
Constant 12.211 0.075
R² 0.186
F = 15.062** 0
*p < 0.05 **p < 0.01 *** p < 0.001
Key
X = Independent variable
70
Chapter 5
Discussion of findings
5.1. Demographic data
The modal age group range was 65-70 years with the mean age at 72 years. Women
older than this could have been lost to follow up due to death or failure to honour review
dates. The commonest marital status was widowed followed by married women. This
supports findings by Gyenwali in India that women tend to look after themselves last after
taking care of everyone else. In this study’s demographic section, 42.6% of the participants
were from a nuclear family and 45.6% from an extended family thus having social support to
seek health treatment. This supports a study done by Mupepi et al (2011) to examine the
demographic factors influencing cervical cancer screening behaviours in Zimbabwe, results
indicated that younger women are more open to screening, and that older women need
support from their family.
One of the risk factors for development of cervical cancer is early sexual activity.
Fifty-five percent of the participants married in their teens commencing early sexual activity
and 60.5% had 4 or more children. Increased parity also increases the chances of developing
cervical cancer (WHO, 2014). The majority of women came from the rural areas where the
usual health care provider was on average 2-10 km away from home. Considering the aging
process and the burden of extended family that the elderly women has, this supports the
findings that 42.6% of the participants were aware of the cervical cancer screening drive but
unable to go for the actual screening process as only 13.2% of those aware were actually
screened before the cervical cancer diagnosis.
The official retirement age in Zimbabwe is 65 years (Zimbabwe Constitution, 2014).
Eighteen (26.5%) participants were retired from formal employment, 9 (13.2%) were still

71
formally employed and 33.8% were farmers as the country is a farming region. In a study by
Sagonda & Chamanga (2013), most employees who reach the retirement age continue in
formal employment and some branch out into unofficial employment to make ends meet.
They found that 69.3% of employees working in the public sector continue to do so beyond
65 years of age as well as 74.2% in other sectors due to various reasons, the most common of
which was backlog of paperwork followed by personal requests.
The findings of this study also show that literacy levels are high as 70.1% of
respondents had at least attained primary level education. More than 80% of participants
followed Christian beliefs and only 1.5% admitted to mixing both traditional and Christian
values. The traditional viewpoint has a large impact in Zimbabwe as treatment leans towards
herbs and away from hospital care due to traditional socialisation especially in elderly
patients. As 87% of those aware of cervical cancer screening were not actually screened, it
shows that level of education has little bearing on the screening drive. There is need to
disseminate information and offer a flexible cervical cancer screening package to elderly
women above 65 years of age to promote regular screening.
The usual health care provider is important in providing health education for early
cervical cancer screening. Only 1.5% of the participants had no usual heath care provider,
indicating that more than 90% of them had regular contact with health care workers. This is
supported by the finding that 73.5% of participants received screening information directly
from a health worker even though only a few them were actually screened. According to
studies done in America, physicians seldom refer elderly women for cervical cancer
screening using the assumption that it would not improve quality of life at that age. So
although most elderly women came in contact with health care workers, few of them were
referred for screening. In Zimbabwe, a lot of resources towards cervical cancer efforts have
been channelled to the 15-49 year age group whilst neglecting the elderly people (Chipfuwa,
72
2012). A survey done at the Visualisation and Acetic Testing screening clinic at Parirenyatwa
and Chinhoyi showed that 14 out of 23 health care providers did not refer elderly patients for
cervical cancer screening with 1 of the reasons being that they were perceived to now less
sexually active thereby at no risk of developing cervical cancer. This was part of a study to
assess knowledge levels about the cervical cancer screening package given to health care
workers (Chinhamora, 2009). Health care providers at VIAC centres verbalised that they
hardly refer elderly patients for cervical cancer screening as they perceive it to be a waste of
resources. There is a need for further research to find out other reasons for non-referral.
5.2. Late stage cervical cancer diagnosis
Respondents for the study had been diagnosed from 1999 – 2015. The duration of
diagnosis for 64.7% of respondents was within 3 years and 35.3% beyond 3 years.
Presentation by stage was normally distributed with most participants presenting at stage 111
(38.2%) and 27.9% presenting with stage 1V. Prevalence for late stage presentation was
0.661. The Zimbabwe National Cancer registry put the prevalence of cervical cancer
presentation at 0.154 in 2009; it stands to reason that the prevalence has increased since then
despite early detection awareness due to late stage presentation of patients. This supports
findings from a study done in Cleveland that more cancer causing lifestyles are affecting the
elderly now and leading to late diagnosis of cancers (Berger, 2011).
Fortunately, 92.6% of participants were on treatment, with 33.8% receiving combined
therapy. The most common combination was radiotherapy coupled with chemotherapy which
gave rise to a high development of comorbidities after cervical cancer diagnosis for these
elderly women.

73
5.3. Comorbidity
Fifty-four respondents (79.4%) suffered from comorbidities. From these, 35% had at
least 3 or more other chronic illnesses before the cervical cancer diagnosis. The average
number of comorbidities was 2.03. Hypertension and diabetes mellitus were the most
common comorbidities patients had before they were diagnosed with cervical cancer. After
diagnosis, respondents reported renal, heart and liver failure as the most common illnesses.
An interesting finding was that breast cancer occurred in 6% of respondents both before and
after cervical cancer diagnosis. Further research might be needed to find out if there is a link
between the 2.
The Pearson’s correlation coefficient showed a positive and significant relationship (r
= .431, p = 0.01) between prevalence of late stage presentation of cervical cancer and number
of comorbidities. Regression analysis showed a strong effect relationship (R² = 0.289). This
supported the hypothesis that the greater the number of comorbidities suffered by elderly
women, the later they presented with cervical cancer but at a smaller scale. Other factors are
also causing the late stage presentation in these elderly women. Other causes of late
presentation could be health-care provider lack of knowledge. This study showed that 45
(66.2%) of the participants hailed from the rural area. This could mean reduced accessibility
to health care facilities as well as delayed referral system.
Not much research has been done in Zimbabwe about the elderly in particular even
though we are all moving towards old age. According to Nhongo (2014), there are several
factors involved in the elderly who suffer from chronic illnesses. They are bombarded with
polypharmacy, fear of the unknown and drug-drug interactions of which they are then
reluctant to seek professional heath care therefore end up presenting with late symptoms.
Chigariro (2014), from the Cancer Association of Zimbabwe, postulated that elderly women
with cervical cancer are less likely to seek medical care as they are swamped with other
74
responsibilities. A study done by Ward in rural Zimbabwe in 2011 supported these findings
as he discovered that although heath care was within reach for the elderly woman, she was
bound to prioritise others first and she last especially when living with orphaned
grandchildren or with HIV/AIDS. In this study, there were 5 women who were on anti-
retroviral for years before the cervical cancer diagnosis and 2 who developed full blown
AIDS after the cervical cancer diagnosis.
The Eve Appeal study done in America in 2010 found out that although most elderly
women were aware of cervical cancer screening, few bothered to have it done due to fear of
the unknown (Singh & Badaya, 2012). There is a need to address fears of the elderly
population in particular if there is to be improved uptake of cervical cancer screening and
early detection in elderly patients, leading to early treatment.
Although figures from the Zimbabwe National Cancer Registry are available for
prevalence of cervical cancer in elderly women, there is need to define specific parameters on
the late diagnosis and to do studies specifically for the elderly.
5.4. Study limitations
A proper pilot study could not be done and the sample had to be quartered due to time
and financial constraints. The permission to carry out the study took 2 months to be granted
from JREC leaving little time for data collection and analysis. This led to use of a small
sample and bias as the pre-test of the study instrument had to be done at the same area as the
actual study. According to Polit & Hungler (2011), use of a different site in pre-testing or
piloting reduces the chance of a bias and increases validity and reliability of a research
instrument. There is a need to include reviewers in the ethical panel who are specific to
proposal review and not committed elsewhere in order to promote carrying out of timeous
research studies.

75
Most potential participants were not staged and therefore not eligible for the study.
There is need to identify ways of staging patients early on the diagnosis to monitor progress
and prevent delays in treatment.
5.5. Recommendations
Research
Further research needs to done in the area of cervical cancer screening uptake by elderly
women in Zimbabwe. Studies can also be done about the particular treatment combinations as there is
need for fine balance to prevent renal or liver failure from heavy chemotherapy agents especially with
the ageing process in effect.
Clinical practice
Rigorous patient follow-up measures need to be put in place so that patients are not
lost to follow up and to reduce time between contact with health care provider and treatment
commencement. Pap smears should be taught to all health care providers including
pharmacists and home based carers who must be able to perform cervical cancer screening at
the most basic level of contact so that elderly patients already saddled with other chronic
illnesses are not ferried from one carer to the next, which is not only tiring but time-
consuming as well. From this study, the most common comorbidity cluster was hypertension
and diabetes mellitus before diagnosis and renal failure with cardiac conditions after the
cervical cancer diagnosis. Elderly patients should be able to obtain BP, blood sugar,
cholesterol, weight and renal function tests together with pap smears at 1 place, be it a
pharmacy, clinic or mobile HBC team to promote early screening and treatment.
Education
Government efforts and foreign investors should aim at arming all women with
knowledge about their health and also make readily available and affordable cervical cancer
76
screening and treatment equipment; not focus on younger groups only. The nursing
curriculum should include a speciality in geriatric nursing in Zimbabwe to accommodate the
ever-increasing elderly population and keep up with international standards in care of the
elderly. As a nation. Zimbabwe is adopting cancer-causing lifestyles from the eastern and
western nations thus it follows that there is a surge of non-communicable diseases including
cancer in the new age pandemic.
Summary
This study presented a summary of findings, discussion and implications of the study
to medical-surgical nursing research, practice and education. Limitations and
recommendations were also discussed. The average number of comorbidities suffered before
the cervical cancer diagnosis in elderly women in Zimbabwe is 2.03 Number of comorbidities
in elderly women affect the way they interact with the health care system, discourages them
from seeking treatment for more serious conditions like cancer leading to presentation with
late stage symptoms.
The purpose of the study was to determine the relationship between prevalence of late
stage diagnosis of cervical cancer and number of comorbidities in elderly women aged 65
years and above in Zimbabwe. Betty Neuman’s Systems model was used to guide the study.
A number of environmental stressors affect the primary and secondary prevention of cervical
cancer in elderly women leading to tertiary prevention which leads to palliative care as the
disease will have progressed to stage 3 or 4. A quantitative, non-experimental, descriptive
correlational design was used to conduct the study. The design helped in the description of
variables and the relationship between them. Convenience sampling was used to select 68
participants from the Parirenyatwa Radiography department, ward A6 as well as Spilhause
clinic at Harare Hospital. Thirty minute structured interviews were conducted using an
interview guide. A power analysis of .80 and significance level of .05 were used to calculate

77
the sample size which was then quartered due to time and financial constraints. Power assists
in identification of relationships in populations, a positive, significant correlation was
identified between prevalence of late stage cervical cancer diagnosis and number of
comorbidities before the diagnosis (r = .431**, p < 0.01).
Regression analysis was used to predict the value of late stage cervical cancer
diagnosis based on the values of number of comorbidities. The R² of .186 supported that
number of comorbidities explains an 18.6% variance in late stage diagnosis of cervical
cancer. This indicates that there are other factors which actually contribute to late stage
diagnosis besides number of comorbidities. This alludes to further research.

78
References
Basu P., Roychowdhury S., Dasbafna U., Chaudry S., Kothari S., … Sekhon R.
(2009). Human papillomavirus genotype distribution in cervical cancer in India. Asian Pac J
10(1): 27-34
Berek J.S. (2011). Berek & Novak’s Gynaecology, 15th ed. Lippincott, Baltimore.
Berger N.A., Savvides P., Koroukian S.M., Kahana E.F., Deimling G.T., Rose J.H.,
Bowman K.F., Miller R.H. (2006). Cancer in the elderly. Trans American Clinical
and Climatology Association. 117 (147-156).
Blumenthal P.D., McIntosh N. (2014). Cervical cancer prevention guidelines for low-
resource settings. Baltimore (MD) http://www.jhpiego.org/files/CECAP_Manual.pdf;
accessed 8 January 2014.
Burns N., Grove S.K. (2009).The Practice of Nursing Research; 4th
Ed, Saunders,
Philadelphia
Cancer Association of Zimbabwe. www.cancerzimbabwe.org
Cancer Fact Sheets: Cervical Cancer Incidence: GLOBOCAN 2012: Estimated cancer
incidence mortality and prevalence worldwide in 2012 (obtained from International
Agency for Research on Cancer [IARC] and World Health Organisation [WHO]:
http://globocan.iarc.fr//pages/fact_sheets_cancer.aspxon 8 January 2014)
Chigariro T, Nyemba P. (2014). Cervical Cancer: Zimbabwe’s Silent Epidemic.
Cancer Journal (article written by Fungai Machirori)
Chinhamora O., Trent K. (2009). Factors associated with late presentation of disease
in society. Social Sciences Scene 2(3) 89-93.

79
Chipfuwa T., Gundani H. (2013). Awareness of cervical cancer in HIV positive
women aged 18-49 years in Bindura, Zimbabwe. Oriental Journal of Scientific Research
2(1): 30-34.
Chokunonga E., Borok M.Z., Chirenje Z.M., Nyakabau A.M., Makunike-Mutasa R.
(2014). Cancer incidence in Harare: Triennial report 2010 – 2012.
Crosbie E.J., Einstein M.H., Franceschi S., Kitchener H.C. (2013). Human
papillomavirus and cervical cancer. The Lancet, volume 382(9895), pg 889-899.
Fadem S.Z. (2014). Charleson Comorbidity Scoring System used to estimate the
prognosis for dialysis patients. Multimorbidity and comorbidity of chronic diseases in
senior Australians. [PubMed]
Ferlay J, Shin HR, Bray F, Forman D, Mathers CD, Parkin D (2010).Cancer
Incidence and Mortality Worldwide: GLOBOCAN 2008. http://globocan.iarc.fr. 2010.
Ferrante J.M., Gonzalez E.C., Roetzheim R.G., Pal N., Woodard L. (2013). Clinical
and demographic predictors of late stage cervical cancer. Arch Fam Med 9(5). Extracted
from PubMed Online
Gonzalez E., Ferrante J.M., Van Durme D.J., Naazneen P.A.L., Roetzheim R.G.
(2013). Comorbid illness and the early detection of cancer. South Med J. 94 (9).
Gyenwali D., Pariya J., Raj Onta S. (2013). Factors associated with late diagnosis of
cervical cancer in Nepal.
Hatch S.S., Samper-Tement R., Zang D., Yong-Fang K., Freeman J. (2014).
Comorbidities and senior oncology patients: How comorbidities affect older women with
cervical cancer. Journal ONCOLOGY.

80
Hivdberg L., Pederson A., Wulff C., Vedstead P. (2014). Cancer awareness and socio-
economic position: A population based study in Denmark. BMC Cancer 14: 581.
http://www.biomedcentral.com/1471-2407/14/581.
Howlader N., Noone A.M., Krapcho M., Garshell J., Neyman N., Alterkruse S.F.,
Kosary C.L., Yu M., Ruhl J., Tatalovich Z., Cho H., Mariotto A., Lewis D.R., Chen H.S.,
Feur E.J.Cronin K.A. (2013). SEER Cancer Statistics Review, 1975-2011. National
Cancer Institute, Bethseda.
Islam M.M., Valderas J.M., Yen L., Dawda P., Jowsey T., et al. (2014)
Multimorbidity and Comorbidity of Chronic Diseases among the Senior Australians:
Prevalence and Patterns. PLOS ONE 9(1): e83783. doi:10.1371/journal.pone.0083783
Jemal A, Center MM, Desantis C, Ward EM. (2010).Global patterns of cancer
incidence and mortality rates and trends. Cancer Epidemiol Biomarkers Prev. 2010; 19:
1893-190
Jemal A., Bray F., Centre M.M., Ferlay J.M.E., Ward E., Forman D. (2011). Global
Cancer Statistics. CA: A Journal for Cancer Clinicians. 61 (2).
Karlamangla A., Tinetti M., Guralnik J., Studenski S., Wetle T., Reuben D.
(2007).Comorbidity in older adults: nosology of impairment, diseases, and conditions. J
Gerontol A Biol Sci Med Sci. 2007; 62A:296–300. [PubMed]
McCance K. L., Heuther S.E. (2006). Path physiology. 5th edition. St Louis. Mosby.
Mupepi S.C., Sampselle C.M., Johnson, T. R. (2011) Knowledge, attitudes, and
demographic factors influencing cervical cancer screening behaviour of Zimbabwean
women. Women’s Health Journal 20(6):943-52.

81
National Cancer Institute. http://www.cancer.gov
National Cancer Prevention Control and Strategy (2014 – 2018).
Neuman B., Fawcett J. (2011). The Neuman Systems model, 5th
ed. Upper Saddle
River, New Jersey.
Nhongo T. (2014). The Changing Role of Older people in African Households and the
Impact of Ageing on African Family Structures. Help Age International Representative
for Africa: The Ageing in Africa Conference, 18-20 August 2004.
Orem D.E. (1991). Nursing Concepts in Practice, 4th
ed. Mosby’s Louis.
Parkin M.D., Bray F., Ferlay J., Jemal A. (2014). Cancer in Africa 2012. Cancer
Epidemiology Biomarkers Prev 23(6).
Polit D.F., Hungler B.P. (2008).Nursing Research Principles and Methods; 5th
edition,
J.B.Lippincott Company, Philadelphia.
Polit & Beck. (2014).Nursing Research Principles and Methods; 7th
Ed, J.B Lippincott,
Philadelphia
Rustagi A.S., Kamineni A., Weinman S., Reed S.D., Newcomb P., Weiss S. (2014).
Cervical screening and cervical cancer death among older women: A population based
case-control study. AJ Epidemiology. 179(9) 1107-1114.
Sangha O., Stuck G., Liang M.H., Fossel A.H., Katz J.N. (2003). The self-
administered comorbidity questionnaires: A new method to assess comorbidity for
clinical and health services. American College of Rheumatology. 49(2), 156-163.
Sankaranarayan R., Nerve B.M., Shatriss S.S.et al (2009). HPV screening for cervical
cancer in rural India. N Engle J Med. 360 (1385-1394).
82
Sauer J., Simonds H.M., Van der Merwe H., Hatingh S, M. (2013). A retrospective
analysis comparing clinical staging with magnetic resonance imaging in patients with
cervical cancer. South African Journal of Oncology 5(11): 11-15. Retrieved 8 January
2014.
SEER Cancer Statistics Fact Sheet: Cervix Uteri Cancer. National cancer Institute.
Bethseda, MD. Extracted fromhttp://seer.cancer.gov/statfacts/html/cervix.html
Sherries J., Withet S., Kleine A. (2009). Evidence based alternative cervical cancer
screening approaches in low resource settings. Int. Perspect. Sex Reprod. Health. 35(147-
154).
Shaw R.W., Swatter W.P., Stanten S.L. (2003). Gynaecology, 3rd
edn, Churchill
Livingstone, Edinburgh.
Singh S., Badaya S. (2012). Factors influencing uptake of cervical cancer screening
among women in India: A hospital based pilot study. J Community Med Health Educ
2:157.doi 10.4172/2161-0711.1000 157.
Tortora G.J.; Derrickson B.H. (2012). Principles of anatomy and physiology. 13th
edition. John Wilkins and Sons. Asia.
Tshuma P. (2002). Prognosis in elderly women with cancer and comorbidities in
Harare. ISBN 51324
Ward D. (2011). Cancer in Zimbabwe: Can we ease the suffering? Better HealthCare
for Africa, WordPress
WHO. (2014). Comprehensive Cervical Cancer Control: A guide to essential practice.
2nd
edition. Australia. ISBN 978 92 4 154895 3

83
APPENDIX I: English Consent form
PARTICIPANT INFORMED CONSENT
PROTOCOL TITLE: A study to determine the relationship between prevalence of late stage
diagnosis of cervical cancer and number of comorbidities in elderly women aged 65 years
and above in Zimbabwe.
NAME OF RESEARCHER: Yvonne Kagura
PHONE: 0772 393 036
PROJECT DESCRIPTION: This is a study looking at elderly women in Zimbabwe suffering
from cervical cancer, whether diagnosed recently or over years. Comorbidities or concurrent
illnesses in these women will also be looked at to find out if they have any effect on
prevalence of late stage diagnosis of cervical cancer.
YOUR RIGHTS: Before you decide whether or not to volunteer for this study, you must
understand its purpose, how it may help you, the risks to you, and what is expected of you.
This process is called informed consent.
PURPOSE OF RESEARCH STUDY: The purpose of the study is to determine the effect of
comorbidity on prevalence of late stage cervical cancer diagnosis. The results will be used to
further knowledge of health care providers and implement health conscious programs for
elderly women who suffer from chronic illnesses including cervical cancer.
PROCEDURES INVOLVED IN THE STUDY: A 30 minute interview will be conducted
with you being asked questions relating to your condition and how you are living with it.
DISCOMFORTS AND RISKS: The structured interview will take at most 30 minutes of your
time and will take place in a quiet, comfortable and private place to protect your
confidentiality. All measures have been taken to ensure minimal risk to your health.

84
POTENTIAL BENEFITS: There are no financial benefits for participating in this study. You
will be allowed time to ask all the questions you wish to and clarification will be made. You
are free to call me anytime if you have any further enquiries.
Initials ___________
STUDY WITH DRAWAL: You may choose not to enter the study or withdraw from the
study at any time without loss of benefits entitled to you.
CONFIDENTIALITY OF RECORDS: Your name or hospital number will not appear on any
of the documents which may tie the information back to you. The answers you give in the
interview will be entered in a database and cannot be traced back to you so feel free to answer
all questions.
PROBLEMS/QUESTIONS: Please ask questions about this research or consent now. If you
have any question in future please ask or call me on the given telephone number -
0772393036.
AUTHORIZATION: I have read this paper about the study or it was read to me. I understand
the possible risks and benefits of this study. I know being in this study is voluntary. I choose
to be in this study: I know I can stop being in the study and I will not lose any benefits
entitled to me. I will get a copy of this consent form. (Initial all the previous pages of the
consent form)
___________________________________________________________________________
Client Signature Date
___________________________________________ Client Name (Printed)
___________________________________________________________________________
Researcher Signature Date
___________________________________________________________________________
Witness Signature Date

85
APPENDIX II: Shona Consent Form
GWARO REBVUMO
MUSORO WETSVAKURUDZO: Tsvakurudzo yehukama huri pakati pekurwara nezvirwere
zvimwewo nekunonoka kubatwa kwechirwere chegomarara remuromo wechibereko
muvanhukadzi vane makore makumi matanhatu nemashanu kana kudarika muno
muZimbabwe.
ZITA REMUTSVAKURUDZI: Yvonne Kagura
MBOZHANHARE: 0772 393 036
TSANANGUDZO YETSVAKURUDZO: Ino itsvakurudzo iri kutarisa madzimai ane makore
makumi matanhatu nemashanu kana kudarika vari muZimbabwe zvisinei kuti vachangobatwa
negomarara remuromo wechibereko, kana kuti vave nemakore. Zvimwe zvirwere zvinenge
zvichirwariwa nemadzimai aya zvichange zvichiongororwa kuti zvine chekuita here
nekunonoka kubatwa kwegomarara remuromo wechibereko.
KODZERO DZENYU: Munofanira kunzwisisa chikonzero nei tsvakurudzo iyi iri kuitwa,
ingakubatsirei sei, chii chamunotarisirwa kuita uye kuti pangave nenjodzi here kuutano
hwenyu musati mafunga kuti mupinde mutsvakurudzo iyi. Urwu ruzivo runokubatsirai kuita
sarudzo yakakwana.
CHIKONZERO CHETSVAKURUDZO: Tsvakurudzo ino inotarisa ukama huri pakati
pezvimwe zvirwere pakunonoka kubatwa kwegomarara remuromo wechibereko.
Zvichawanikwa mutsvakurudzo iyi zvichabatsira kuwedzera zivo kune vakoti kuti vawane
mabatsiro avangaite madzimai echikuru ane zvimwewo zvirwere pamusoro pegomarara
remuromo wechibereko.

86
ZVAMUNOTARISIRWA KUITA: Muchabvunzwa mibvunzo pamusoro pechirwere
chegomarara chamuinacho uye kuti muri kurarama sei nacho. Zvichatora minhasvu
isingadarike makumi matatu.
NJODZI DZINGATARISIRWE: Mibvunzo ichaita minhasvu makumi matatu bedzi.
Muchabvunzirwa munzvimbo yakahwanda, inochengetedza nhau dzeutano hwenyu. Njodzi
kuutano hwenyu ichange iri shoma chose.
ZVAMUNGATARISIRWE KUWANA: Hapana mari yamunotarisirwa Kuwana nekuda
kwekunge muri mutsvakurudzo iyi. Munobvumirwa kubvunza mibvunzo chero nguva kana
kuchaya nhare kuti munzwisise nezvetsvakurudzo kana chirwere chenyu.
Mavara ekutanga emazita enyu ___________
KUREGEDZA TSVAKURUDZO:Munokwanisa kurega kuenderera mberi netsvakurudzo iyi
chero nguva pasina njodzi ingakuwirei.
KUCHENGETEDZWA KWENHAU DZEHUTANO HWENYU: Zita kana nhamba
yemuchipatara hazvisi kuzonyorwa chero pai hapo. Saka hapana nhau dzeutano hwenyu
dzingaburitswe kunze kwemutsvakurudzi. Mhinduro dzamuchapa dzichaiswa mudatabase
saka hadzingazodzoki kwamuri saka pindurai makasungunuka.
MIBVUNZO: Bvunzai mibvunzo pamusoro petsvakurudzo iyi kana gwaro rino rebvumo
izvozvi. Makasununguka henyu kuzobvunza pamberi apo kana kuchaya nhare panhamba
dzinotevera - 0772393036.
BVUMO:Ndaverenga gwaro rino rebvumo kana kuti ndariverengerwa. Ndanzwisisa njodzi
yandingasangane nayo kana zvandingabatsirike nazvo. Ndinoziva kuti kuve kwangu
mutasvakurudzo iyi kuzvipira kuzere. Ndasarudza kunge ndiri mutsvakurudzo iyi pasina
kugombedzerwa, hapana zvingandiwire ndikarega ndiri pakati. Ndichawanawo kopi yegwaro

87
rebvumo iri. (Nyorai mavara ekutanga emazita enyu pa bepa rega-rega regwaro rino).
___________________________________________________________________________
Runyoro rwemurwereZuva
___________________________________________ Zita remurwere (Printed)
___________________________________________________________________________
Runyoro rwemutsvakurudzi Zuva
___________________________________________________________________________
Runyoro rwemuchuchisi Zuva

88
APPENDIX I11: English Interview Guide
INTERVIEW GUIDE_____________
Section A: Demographic Data
1. Age 65 – 70______
71 – 75______
76–80______
>80______
2. Marital status Single_______
Married______
Divorced_____
Widowed_____
3. Age at marriage Teen_________
20 – 35_______
>35__________
N/A______
4. Parity Nulliparous____
1 -3__________
4-6___________
>6____________
5. Area Lived Rural_________
Urban ________
6. Family dynamics Lives alone_____
Nuclear family___
Extended family__
Friends or workers__
7. Occupation Never worked______
Retired___________
Professionally employed______
Informal employment_________
Farmer__________
89
8. Level of education None____
Below primary level____
Primary level____
Secondary level___
Tertiary level_____
9. Religion None_____________
Traditionalist_______
Christian__________
Combine_______
10. Nearest health care facility <2km________
2 – 10km_____
>10km_______
11. Usual health care provider HBC (home based carers)____
Council clinic_________
Gvt or mission Hospital______
Private Practitioner______
None________
Section B: Cervical cancer
12. Year diagnosed
13. Duration of diagnosis <a year_________
1-3 years____
>3years_____
14. Stage at diagnosis 1____
11___
111___
1V__

90
15. Treatment Yes___
No____
16. Duration of treatment so far Weeks ________
Months_________
Years__________
Finished treatment (remission)
N/A
17. Type of treatment Chemotherapy only___
Radiotherapy only____
Cryotherapy only_____
Traditional herbs only___
Surgery only______
Brachytherapy only____
Combined (specify) ______
N/A_____
18. Cervical cancer screening awareness Yes______
No______
19. Screening before diagnosis Yes_____
No______
20. How often >Annually___
Annually__
Stat (at diagnosis) ________
21. Source of information(screening) Direct from health care provider__
Indirect from TV, radio, peers__
Both_____

91
Section C: Comorbidity
22. Any other illness Yes__
No___
23. Comorbidity scoring
Note: for each decade > 60 years of age, a score of 1 will be added.
Score Condition When diagnosed Treatment
Before Ca
cervix
After Ca
cervix
Yes No
3 Myocardial infarction
Congestive cardiac failure
Peripheral vascular disease
CVA
Dementia
Depression
Anxiety disorders
Sleeping disorders
Chronic Pulmonary Disease
Connective tissue disease
Alzheimer’s
Osteoporosis
Backache
Eye disorders(cataracts)
Peptic Ulcer Disease
Mild liver disease
DM (uncomplicated)
Hypertension
Arthritis
4 Hemiplegia
Moderate or severe renal
disease
DM (with end-organ damage)
Tumour without metastasis
Leukaemia
Lymphoma
HIV on ART
5 Moderate to severe liver
disease
Hepatitis
6 Metastatic solid tumour
AIDS

92
APPENDIX 1V: Shona Interview Guide
MIBVUNZO YENHAURIRANO_____________
Section A: Demographic Data
1. Makore ekuberekwa 65 – 70______
71 – 75______
76 – 80______
>80______
2. Kuwanikwa Kwete_______
Hongu______
Vakarambana_____
Chirikadzi_____
3. Makore ekuwanika Teen_________
20 – 35_______
>35__________
N/A____
4. Vana vakaberekwa Hapana____
1 -3__________
4-6___________
>6____________
5. Nzvimbo inogarwa Kumusha _________
Mudhorobha________
6. Mhando yemhuri yavanogara nayo Vega____
Vemumba mavo bedzi__
Hama dzimwewo__
Shamwari kana vashandi__
7. Basa Havana kumboshanda______
Vari pamudyandigere___________
Vanoshanda pakambani ______
Vnozvishandira_________
Murimi__________
8. Dzidzo Kwete____

93
Pazasi pepuraimari____
Vakasvika kupuraimari____
Vakasvika kusekondari___
Vakasvika kuUnivhesiti_____
9. Chinamato Havana_____________
Vanoita zvemidzimu_______
MuKristu__________
Vanosanganisa_____
10. Panorapwa pedyo zvakadii <2km________
2 – 10km_____
>10km_______
11. Kwavanosirapwa Varapi vekumba____
Kiriniki yekanzuru_________
Chipatara chehurumende kana misheni______
Chiremba akazvimirira______
Hakuna_____
Section B: Gomarara remuromo wechibereko
12. Gore rabatwa gomarara
13. Gomarara rabatwa nguvai Pazasi pegore_________
1-3 years____
>3years_____
14. Rakabatwa panhamba ipi 1____
11___
111___
1V___

94
15. Vari kurapwa Hongu___
Kwete____
16. Varapwa nguva yakareba sei Mavhiki ________
Mwedzi_________
Makore__________
Vakatopedza kurapwa_____
17. Vari kurapwa nei Chemotherapy chete___
Radiotherapy chete____
Cryotherapy chete_____
Traditional herbs chete____
Surgery chete_____
Brachytherapy chete___
Zvakasangana (ndezvipi) ______
N/A______
18. Ruzivo nezvekuongororwa gomarara Hongu______
Kwete______
19. Kuongororwa vasati vabatwa negomarara Hongu_____
Kwete______
20. Vakaongororwa kangani Pasi pegore___
Gore negore__
Kamwe chete________
21. Vakaudzwa nani nezvekuongororwa Nanamukoti__
Nevamwewo__
Vose vari pamusoro___

95
Section C: Comorbidity
22. Zvimwe zvirwere zvisiri gomarara Hongu__
Kwete___
23. Comorbidity scoring
Note: for each decade > 60 years of age, a score of 1 will be added.
Chibo
dzwa
Chirwere Chakabatwa riini Kurapwa
Before Ca
cervix
After Ca
cervix
Hon
gu
Kwe
te
3 Myocardial infarction
Congestive cardiac failure
Peripheral vascular disease
CVA
Dementia
Depression
Anxiety disorders
Sleeping disorders
Chronic Pulmonary Disease
Connective tissue disease
Alzheimer’s
Osteoporosis
Backache
Eye disorders(cataracts)
Peptic Ulcer Disease
Mild liver disease
DM (uncomplicated)
Hypertension
Arthritis
4 Hemiplegia
Moderate or severe renal
disease
DM (with end-organ damage)
Tumour without metastasis
Leukaemia
Lymphoma
HIV on ART
5 Moderate to severe liver
disease
Hepatitis
6 Metastatic solid tumour
AIDS

96
APPENDIX V: PERMISSION LETTERS
Copyright © 2022 FDOKUMEN




















