
INDOMETHACIN - Open Collections
254
INDOMETHACIN: CAPILLARY GAS CHROMATOGRAPHIC - ELECTRON CAPTURE DETECTION ANALYSIS AND PHARMACOKINETIC STUDIES IN THE FETAL LAMB by RAJESH KRISHNA B. Pharm., University of Kerala, Trivandrum, India, 1990 M. Pharm., Banaras Hindu University, Varanasi, India, 1992 A THESIS SUBMITTED FN PARTIAL FULFILMENT OF THE REQUIREMENTS FOR THE DEGREE OF MASTER OF SCIENCE (Biopharmaceutics and Pharmacokinetics) in THE FACULTY OF GRADUATE STUDIES Faculty of Pharmaceutical Sciences (Division of Clinical Pharmacy) We accept this thesis as conforming to the required standard THE UNIVERSITY OF BRITISH COLUMBIA February 1995 © Rajesh Krishna, 1995
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of INDOMETHACIN - Open Collections

INDOMETHACIN: CAPILLARY GAS CHROMATOGRAPHIC - ELECTRON CAPTURE DETECTION ANALYSIS AND PHARMACOKINETIC STUDIES IN
THE FETAL LAMB
by
RAJESH KRISHNA
B. Pharm., University of Kerala, Trivandrum, India, 1990
M . Pharm., Banaras Hindu University, Varanasi, India, 1992
A THESIS SUBMITTED FN PARTIAL FULFILMENT OF
THE REQUIREMENTS FOR THE DEGREE OF
M A S T E R OF SCIENCE
(Biopharmaceutics and Pharmacokinetics)
in
THE F A C U L T Y OF G R A D U A T E STUDIES
Faculty of Pharmaceutical Sciences
(Division of Clinical Pharmacy)
We accept this thesis as conforming
to the required standard
THE UNIVERSITY OF BRITISH C O L U M B I A
February 1995
© Rajesh Krishna, 1995
In presenting this thesis in partial fulfilment of the requirements for an advanced
degree, at the University of British Columbia, I agree that the Library shall make it
freely available for reference and study. I further agree that permission for extensive
copying of this thesis for scholarly purposes may be granted by the head of my
department or by his or her representatives. It is understood that copying or
publication of this thesis for financial gain shall not be allowed without my written
permission.
Department of ^ ^ ^ ^ ' ( 4 S c u ^ c ^ A
The University of British Columbia Vancouver, Canada
Date
DE-6 (2/88)

A B S T R A C T
11
Indomethacin is currently used in the treatment of patent ductus arteriosus,
preterm labour, and for polyhydramnios. In order to investigate its clearance and
disposition in the chronically instrumented ovine fetus, a sensitive assay was
required.
The developed GC-ECD method involves the extraction of indomethacin and
a-methyl indomethacin, the internal standard, from acidified plasma, urine,
amniotic and tracheal fluids using a simple one-step liquid-liquid extraction
procedure with ethyl acetate. The organic extract is evaporated and the residue
derivatised with N-methyl-N-(tert-butyldimethylsilyl)-trifluoroacetamide
(MTBSTFA). The derivatised samples were reconstituted with toluene and aliquots
of 2 jxL injected into the GC. Calibration curves were linear over the working range
of 1-32 ng of indomethacin/mL with a coefficient of determination (r ) > 0.99,
following extraction of 0.1 mL of plasma, and 0.1-1.0 mL of urine, amniotic and
tracheal fluids. Mean recoveries from plasma and urine were 96.99 ± 9.25 % and
94.74 ± 6.75 %, respectively. The limit of quantitation is 1 ng/mL (< 10% C.V.,
S/N > 10).Inter- and intra-day variabilities at each concentration point were < 11 %
for concentrations between 2-32 ng/mL and < 20 % at the LOQ of 1 ng/mL.

Ill
The mean steady state fetal femoral arterial concentration of indomethacin
was 181.67 ± 45.05 ng/mL in the high dose group (n=5), and 41.29 ± 3.14 ng/mL in
the low dose group (n=2). The arterio-venous concentration difference for
indomethacin at apparent steady state was minimal but statistically significant,
suggesting a low placental permeability to indomethacin in sheep. The fetal total
body clearance was estimated to be 44.55 + 11.14 mL/min (n=7). The placental
clearance of indomethacin, as determined by the Fick principle, was calculated to be
8.85 ± 0.81 mL/min/kg. The renal clearance was estimated to be 0.015 + 0.009
mL/min (n=5). Indomethacin appeared in very low concentrations in amniotic fluid
and fetal urine in high dose group fetuses. It was not observed to accumulate in
tracheal fluid. The drug appeared to induce lactic acidosis and a reduction in fetal
urinary output in some fetuses of the high dose group.
K. Wayne Riggs, Ph.D.
Research Supervisor
iv
TABLE OF CONTENTS Page
ABSTRACT ii
TABLE OF CONTENTS iv LIST OF FIGURES ix LIST OF TABLES xiii LIST OF SCHEMES xv LIST OF ABBREVIATIONS xvi ACKNOWLEDGEMENTS xxi DEDICATION xxii
1. INTRODUCTION 1 1.1. Indomethacin 1
1.1.1. Pharmacology of indomethacin 1 A. Mechanism of action 1 B. Clinical uses 6 C. Renal effects of indomethacin 11 D. Fetal effects of indomethacin 14
1.1.2. Pharmacokinetics of indomethacin 15
1.1.2.1. Absorption 15
1.1.2.2. Protein binding 17 1.1.2.3. Distribution 18 1.1.2.4. Metabolism and fate 19 1.1.2.5. Elimination kinetics 24
1.1.3. Placental transfer 27
1.1.3.1. Pharmacokinetic characterisation 28
1.1.3.2. The chronically instrumented pregnant sheep model 28

1.1.3.3. Placental transfer of indomethacin
1.1.4. Analytical methods
V
30 32
1.2. Rationale and specific aims 35
1.2.1. Rationale 35 1.2.2. Specific aims 36
2. EXPERIMENTAL 37 2.1. Materials and supplies 37
2.1.1. Chemicals 37 2.1.2. Reagents 38 2.1.3. Solvents 38 2.1.4. Gases 39 2.1.5. Supplies 39
2.2. Instrumentation 40 2.2.1. Gas chromatography 40 2.2.2. Gas chromatography-Mass spectrometry 41 2.2.3. Columns 41 2.2.4. Liquid chromatography-mass spectrometry/
mass spectrometry 42 2.2.5. Differential scanning calorimetry 42 2.2.6. Nuclear magnetic resonance spectrometry 43 2.2.7. General equipment 43 2.2.8. Physiological monitoring 43
2.3. Preparation of stock solutions 44 2.3.1. Preparation of drug stock solution 44
2.3.1.1. Indomethacin 44
2.3.2. Preparation of internal standard solutions 45 2.3.2.1. Zomepirac sodium 45

VI
2.3.2.2. Sulindac 45
2.3.2.3. a-Methyl indomethacin 46
2.3.2.4. Other experimental internal standards 46 2.3.3. Preparation of reagent solutions 46
2.4. Sample preparation 48 2.4.1. Analysis of intact indomethacin levels 48 2.4.2. Analysis of glucuronide conjugates 50
2.5. Preparation of calibration curves 51
2.5.1. Calibration curve with a-methyl indomethacin 51
2.5.2. Calibration curve with zomepirac sodium 51 2.6. Chemistry 52
2.6.1. Derivatisation procedures for indomethacin 52 2.7. Optimisation of assay parameters 54
2.7.1. Derivatisation of indomethacin 54 2.7.2. Chromatography 55 2.7.3. Extraction 55 2.7.4. Validation 56
2.7.4.1. Extraction recovery studies 56 2.7.4.2. Inter- and intra-day variability 57 2.7.4.3. Linearity 57 2.7.4.4. Stability 57
2.8. Animal experiments 58 2.8.1. Animal handling and surgical preparation 59 2.8.2. Recording and monitoring procedures 60 2.8.3. Determination of organ blood flows 61
2.8.4. Experimental protocol for fetal infusion studies 62
2.9. Data analysis 63
2.9.1. Pharmacokinetic calculations 63 2.9.2. Statistical calculations 64

3. RESULTS 66 3.1. Development of a capillary GC-ECD method for
indomethacin 66
3.1.1. Purity assessment of indomethacin 66 3.1.2. Optimisation of derivatisation 71 3.1.3. Selection of internal standards 78 3.1.4. Optimisation of GC conditions " 86 3.1.5. Optimisation of drug extraction 101 3.1.6. Gas chromatography-mass spectrometry 108
3.2. Validation of the GC-ECD method 113 3.2.1. GC operating conditions 113 3.2.2. Drug extraction from biological fluids 118 3.2.3. Recovery studies 123 3.2.4. Stability studies 123 3.2.5. Inter-day and intra-day variability 129
3.2.6. Calibration curves 129 3.3. Fetal infusion studies 137
3.3.1. Analysis of plasma samples 137 3.3.2. Analysis of urine samples 150
3.3.3. Drug disposition in amniotic and tracheal fluid
compartments 151
4. DISCUSSION 156 4.1. Development of a capillary GC-ECD method 156 4.2. Disposition of indomethacin in sheep 179
4.2.1. Placental transfer of indomethacin in sheep 180
4.2.2. Placental clearance 182 4.2.3. Elimination of indomethacin by the fetal kidney 186

4 .3. Drug disposition in amniotic and tracheal fluids
4.3.1. Amniotic fluid
4 .3.2. Tracheal fluid
4.4. Effect of indomethacin on physiological factors
S U M M A R Y & C O N C L U S I O N S
R E F E R E N C E S

IX
LIST OF FIGURES page
1. Chemical structure of indomethacin 1
2. Inhibition of PG synthesis by indomethacin (Adapted from 3 Shen and Winter, 1977).
3. Proposed role of PG's in labour (Adapted from Miller, 5 1983)
4. Metabolism of indomethacin in the adult human (Adapted 21 from Vree etal, 1993).
5. NMR spectra of indomethacin 67-68
6. DSC scan of indomethacin: (a) open pan, and (b) closed 70 pan methods.
7. LC/MS/MS spectrum of indomethacin 72
8. GC-ECD chromatograms of indomethacin derivatised by 73 (a) BSA, and (b) MTBSTFA.
9. GC-ECD chromatogram of indomethacin derivatised by 74 PFBBr.
10. Determination of optimum derivatising temperature for 76 indomethacin with MTBSTFA (data are mean values + 1 S.D., n=4).
11. Determination of optimum reaction time between 77 indomethacin with MTBSTFA (data are mean values ± 1 S.D., n=4).
12. Chemical structures of tested internal standards. 79
13A Derivatisation of 5-fluoro DL tryptophan with PFBBr for 80 use as potential internal standard for indomethacin.
13B GC-ECD chromatograms of indomethacin analogs, 5- 81 fluoroindomethacin, and oc-methyl indomethacin, derivatised by MTBSTFA.

14. Illustration of a decomposition peak "X" associated with 83 sulindac. Chromatograms indicate: (1) indomethacin and sulindac, (2) sulindac only, and (3) blank.
15. DSC scan of sulindac and recrystallised sulindac. 84
16. GC-ECD chromatogram of indomethacin and zomepirac in 85 fetal plasma.
17. Chemical structures of indomethacin and a-methyl 87 indomethacin.
18. Effect of injection port temperature on the chromatography 88-89 of (A) 20 ng/mL, and (B) 100 ng/mL indomethacin concentrations (n=4).
19. Effect of various column temperatures on peak retention 91 times.
20. Chromatograms of indomethacin and zomepirac using a 92 narrow bore fused silica Ultra-2 column.
21. Chromatogram of indomethacin and zomepirac using a 93 narrow bore DB-1701 column.
22. Effect of purge delay times on the peak area counts of 95 indomethacin tBDMS derivative (n=4).
23. Effect of various detector temperatures on the peak area 96 counts of indomethacin tBDMS derivative.
24. Determination of optimum column head pressure: Effects 97-98 of (1) peak indomethacin area counts, (2) peak area ratio, (3) retention times, and (4) peak width.
25. Determination of optimum column head pressure with 99-100 reference to (A) peak retention time, and (B) peak width.
26. Extraction efficiency of various organic solvents (n=4), in 102 a volume of 2 mL, using tracheal fluid as the model biological fluid.
27. Effect of solvent volume on the extraction efficiency of 105

ethyl acetate.
28. Determination of optimum pH on the extraction of 106 indomethacin (n=4).
29 Determination of optimum extraction time for 107 indomethacin from sheep biological fluid matrix using ethyl acetate at pH 5.0 (data are mean values ± 1 S.D., n=4)
30. GC-MS spectra of indomethacin tBDMS in the EI (A), 109-111 NCI (B), and PCI (C) modes.
31. GC-MS spectra of indomethacin-TMS 114-115
32. GC-MS spectra of indomethacin-PFB 116-117
33. Representative chromatograms of indomethacin and a- 119 methyl indomethacin spiked in fetal plasma (the inset shows the magnified baseline).
34. Representative chromatograms of indomethacin and a- 120 methyl indomethacin spiked in fetal urine.
35. Representative chromatograms of indomethacin and a- 121 methyl indomethacin spiked in amniotic fluid.
36. Representative chromatograms of indomethacin and 122 zomepirac in amniotic fluid.
37. Stability study of indomethacin infusate formulation at 128 room temperature, and at standard refridgeration conditions.
38. Representative calibration curve for indomethacin in fetal 134 plasma.
39. Representative calibration curve of indomethacin in fetal 135 urine.
40. Representative calibration curve of indomethacin in 136 amniotic fluid.

xii
41. Effect of low dose (E 1137, E 1115), and high dose (E 139-141 2160, E 1221) indomethacin on fetal arterial blood gas parameters (A & B), glucuose and lactate concentrations (C & D), pH and base excess (E & F).
42. Mean concentration-time profiles of indomethacin in 143 plasma, urine, and amniotic fluid for high dose ewes (n=5).
43. Mean concentration-time profiles of indomethacin in FA 144 and UV plasma for low dose ewes (n=2).
44. Effect of indomethacin on the fetal urinary flow rate. 153
45. Representative plot for the determination of renal 154 clearance.
LIST O F T A B L E S
xiii
page 1. Metabolites of indomethacin. 22
2. Pharmacokinetics of indomethacin in neonates. 26
3. Chemical shift values of indomethacin and their respective 69 group assignment.
4. Extraction efficiency (%) of organic solvents used to extract 104 indomethacin at different concentrations using tracheal fluid as the model biological fluid.
5a. Extraction recoveries (n=4), inter-day variability (n=4), and 124 intra-day variability (n=3) for indomethacin in (A) fetal plasma, and (B) fetal urine.
5b. Inter- and intra-day variability parameters for indomethacin 125 in amniotic fluid of fetal sheep, with zomepirac as the internal standard.
5b. (Continued) Extraction recoveries of indomethacin spiked in 126 amniotic fluid using zomepirac as the internal standard.
6. Stability of indomethacin in acidified sample matrix, during 127 freeze-thaw cycles (with a-methyl indomethacin as the I.S.), and on the GC autosampler tray (with zomepirac as the I.S.).
7. Variability parameters for the limit of quantitation (LOQ) of 130 1 ng/mL.
8. Calibration curve data for indomethacin in fetal plasma 131 (n=4).
9. Calibration curve data for indomethacin in fetal urine (n=4). 132
10. Calibration curve data for indomethacin in amniotic fluid 133 (n=8).
11 A. Animal experiment sampling and dosing protocol. 138
11B. Determination of apparent steady state plasma concentration 138

xiv
12. Mean concentration-time data for indomethacin in fetal 142 femoral arterial (FA) plasma, umbilical venous (UV) plasma, and fetal urine samples in high dose ewes (n=5).
13. Arterio-venous concentration difference for indomethacin at 146 apparent steady state.
14. Arterio-venous concentration difference in high dose ewes: 147 statistical evaluation.
15. Determination of fetal total body clearance. 148
16. Calculation of placental and non-placental clearances for 149 indomethacin.
17. Concentration of indomethacin in fetal urine. 152
18. Determination of renal clearance for indomethacin in high 155 dose group fetuses.
19. Stability of indomethacin in aqueous solution (Adapted from 175 Shen and Winter, 1977).
20. Stability of indomethacin in surfactant solubilised systems 178 (Adapted from Ghanem et al., 1979).

XV
LIST OF SCHEMES
Page 1. Sample preparation protocol for indomethacin. 49
2. Resonance forms of indomethacin-tBDMS ester. 161
3. Degradation of indomethacin in alkali. 175

ABBREVIATIONS
xvi
ACS American Chemical Society
AMN amniotic fluid
AVP arginine vasopressin
[A-V]indo(sS) aterio-venous indomethacin concentration difference at apparent steady state
BE base excess
BSA bis (trimethylsilyl) acetamide
BSTFA N, O-Bis (trimethylsilyl) trifluoroacetamide
°C degree Celsius
C.V. coefficient of variation
cAMP cyclic adenosine monophosphate
CBF cerebral blood flow
Cfa concentration of drug in fetal femoral arterial blood at steady
state
CLf 0 fetal non-placental clearance
CL P placental clearance
CL r renal clearance
CL t b total body clearance
C s s steady state plasma concentration
d m concentration of drug in umbilical venous blood at steady
state
DA ductus arteriosus
DBI N-deschlorobenzoyl indomethacin
DCM dichloromethane

DMF dimethyl formamide
DMI O-desmethyl indomethacin
DPMA diphenylmethoxyacetic acid
DSC differential scanning calorimetry
EA ethyl acetate
ECD electron capture detection
EI electron-impact ionisation
eV electron volts
F fetal
F-T freeze-thaw
F/M fetal-to-maternal ratio
FA fetal femoral arterial
[FA] i n d o ( S S) fetal arterial plasma indomethacin concentration at apparent steady state
FDA Food and Drug Administration
F E N a + fractional excretion of sodium ion
F s s fetal steady-state concentration
g acceleration due to gravity
g gram
GC gas chromatography, gas chromatograph
GC-MS gas chromatography-mass spectrometry
GFR glomerular filtration rate
h hour
H 2 hydrogen gas
HCO"3 bicarbonate ion

XV111
HETP
HP
HPLC
i.d.
I.U.
i.v.
IND
IPA
kg
ko
kPa
L
LC/MS/MS
LOQ
M
m/z
MA
MAO
meq
mg
min
mL
MLCK
MS
M.,
height equivalent to a theoretical plate
Hewlett-Packard
high performance liquid chromatography
internal diameter
international units
intravenous
indomethacin
isopropyl alcohol
kilogram
infusion rate
kilopascal
liter
liquid chromatography/mass spectrometry/mass spectrometry
limit of quantitation
maternal
mass to charge ratio
maternal arterial
monoamine oxidase
milliequivalents
milligram
minute
milliliter
myosin light chain kinase
mass spectrometry
maternal steady-state concentration

MSTFA N-methyl-N-trimethylsilyl trifluoroacetamide
MTBSTFA N-methyl-N-(tert-butyldimethylsilyl) trifluoroacetamide
M« microgram
|lL microliter
N normal
n sample size
NCI negative ion chemical ionisation
ND not detectable
ng nanogram
NMR nuclear magnetic resonance spectrometry
NSAID non-steroidal anti-inflammatory drug
o 2 oxygen
PCI positive ion chemical ionisation
pC0 2 partial pressure of carbon dioxide
PDA patent ductus arteriosus
PFB pentafluorobenzyl
PFBBr pentafluorobenzyl bromide
PFP pentafluoropropanol
PG prostaglandin
pH negative logarithm (base 10) of the hydrogen ion concentration
p0 2 partial pressure of oxygen
psi pounds per square inch
PTFE polytetrafluoroethylene
Qum umbilical blood flow
r correlation coefficient

coefficient of determination
RBF
RIA
rpm
Rt
S/N
SD
sec
SEM
T1/2
TBDM-SIM
TBDMCS
tBDMS
TEA
TMS
TR
UHP
UR
UTV
UV
[UV ] i n d o ( S S )
VP y=mx + c
renal blood flow
radioimmunoassay
revolutions per minute
retention time
signal-to-noise ratio
standard deviation
second
standard error of the mean
half life
N-t-butyldimethylsilylimidazole
t-butyldimethylchlorosilane
tert-butyldimethylsilyl
triethylamine
trimethylsilyl
tracheal fluid
ultra-high purity
fetal urine
uterine vein
umbilical venous
umbilical venous plasma indomethacin concentration at apparent steady state
vasopressin
linear regression statistics of a straight line

ACKNOWLEDGEMENTS
xxi
I would like to thank my research supervisor, Dr. Wayne Riggs, for his guidance, constructive criticism, and friendship. His constant encouragement is sincerely appreciated. Thanks also to my committee members, Dr. Frank Abbott, Dr. James E. Axelson, Dr. Dan W. Rurak, Dr. Martin P.R. Walker, and Dr. Jack Diamond, for their expert scientific input and constructive criticism.
I would like to thank Dr. Andras Szeitz for initial help during method development and friendship throughout the program. Mr. Eddie Kwan is thanked for his assistance with the experimental studies. Mr. Roland Burton is thanked for his help during mass spectrometric studies.
I am thankful to Dr. Rob Thies for his help in the preparation and
development of slides for the oral presentation.
Many thanks also to my colleagues, Mr. John Gordon, Dr. George Tonn, Ms.
Judit Orbay, Dr. Wei Tang, Dr. Anthony Borel, Dr. Weiping Tan, Mr. Sanjeev
Kumar, Mr. John Kim, Ms. Eva Law, Mr. Nanda Kumar, and Dr. Sarvajna Dwivedi,
for their constructive suggestions and friendship.
I gratefully acknowledge the award of Stanley Pharmaceuticals (Novopharm group) Scholarship by Stanley Pharmaceuticals, North Vancouver and UBC, and the Graduate Student Travel Award of the Faculty of Graduate Studies for poster presentation at the 9th annual meeting and exposition of AAPS at San Diego. I am thankful to Ms. Jennie Campbell and Mr. Frank Wang of International House, UBC, for their support. Award of a Graduate Teaching Assistantship and a Graduate Research Assistantship by the Faculty is acknowledged. Financial support for the research project was from the BC Health Research Foundation.

DEDICATION
'This thesis
is
dedicated
to my
parents
for their
Cove, support, and patience.

1. INTRODUCTION 1
1.1 Indomethacin
Indomethacin (l-[p-chlorobenzoyl]-5-methoxy-2-methyl-indole-3-acetic
acid), introduced as a non-steroidal antiinflammatory drug (NSAID), is a potent
prostaglandin synthetase inhibitor used in the treatment of gouty arthritis (O'Brien et
al., 1968), ankylosing spondylitis (Kass, 1965), osteoarthritis (Bilka et al, 1964),
rheumatoid arthritis (O'Brien et al, 1968), patent ductus arteriosus (Friedman et al.,
1976), and preterm labour (Zuckerman et al., 1974).
CH2COOH
Figure 1: Chemical structure of indomethacin.
1.1.1 Pharmacology Of Indomethacin
A. Mechanism Of Action

2 General Pharmacological Activity
Since its introduction in 1963, a number of mechanisms have been proposed
®
to account for indomethacin's (and other Aspirin like drugs) mode of action.
These include uncoupling of oxidative phosphorylation, mucopolysaccharide
biosynthesis inhibition, inhibition of platelet function, stabilisation of cellular and
lysosomal membranes, and effects on leukocyte migration (Morsdorf, 1964;
Schonhofer, 1967; Whitehouse, 1968; Bryant et al., 1963). Structural-activity
relationship studies at that time indicated the presence of a hypothetical
antiinflammatory receptor site consisting of a cationic core and two noncoplanar
hydrophobic regions (Shen, 1965; Shen, 1967). In the early 70s, the inhibition of
®
prostaglandin (PG) synthetase by indomethacin and Aspirin at therapeutically
effective concentrations was established (Vane, 1971; Smith and Willis, 1971;
Ferreira et al., 1971). Following this discovery, Ham et al., 1972, screened a series
of substituted aryl acid compounds in a PG synthetase system. However, the
elucidation of the exact mechanism of action was hindered largely due to the fact
that PG synthesis systems in different tissues possess markedly dissimilar
pharmacological and biochemical profiles, and that NSAIDs may inhibit the enzyme
system at different sites in the biosynthetic pathway. At that time, it was also
determined that the inactivation of PG synthetase was reversible and time-dependent
(Smith and Lands, 1971; Raz et al., 1973). Indomethacin was observed to be a
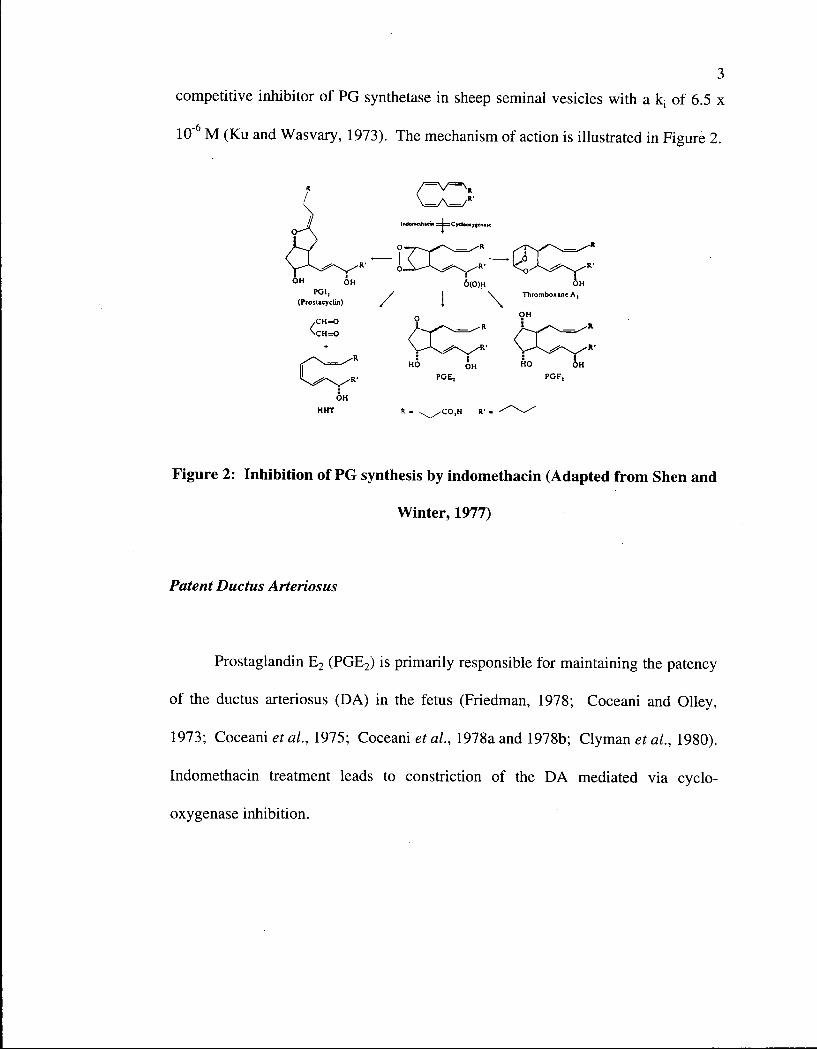
competitive inhibitor of PG synthetase in sheep seminal vesicles with a kj of 6.5 x
10"6 M (Ku and Wasvary, 1973). The mechanism of action is illustrated in Figure 2.
Figure 2: Inhibition of PG synthesis by indomethacin (Adapted from Shen and
Winter, 1977)
Patent Ductus Arteriosus
Prostaglandin E 2 (PGE2) is primarily responsible for maintaining the patency
of the ductus arteriosus (DA) in the fetus (Friedman, 1978; Coceani and Olley,
1973; Coceani et al, 1975; Coceani et al., 1978a and 1978b; Clyman al, 1980).
Indomethacin treatment leads to constriction of the DA mediated via cyclo-
oxygenase inhibition.

4 Premature Labour
Prostaglandins, PGE l 5 PGE2, and PGF2a, all stimulate uterine contractions in
pregnant subjects and are hence suitable candidates for the induction of labour
(Embrey, 1970; Beazley and Gillespie, 1971; Roth-Brandel et al, 1970). Of these,
prostaglandins, PGF2rx and PGE 2 are potent compounds used therapeutically for the
induction of labour (Thiery and Amy, 1975). The two common formulations are
PGE 2 gel for intracervical application and PGF 2 a for slow i.v. infusion. If the gel
cannot be employed or if the patient experiences primary dysfunctional labour
(Andersson et al., 1983), then the i.v. PGF 2 a formulation may be used. The exact
mechanism by which these PGs stimulate uterine contractions is unclear.
It has been shown that during labour there is a rise in PG concentrations in
blood (Karim, 1968) and amniotic fluid (Karim and Devlin, 1967; MacDonald and
Casey, 1993). A subsequent paper reported that exogenously administered PG's can
induce labour (Karim et al., 1969). These reports suggested a physiological role of
the PG's in uterine motility. The critical step in the initiation of labour is the local
production of PG's, i.e., production of PGE 2 in the amnion, which then reaches the
decidua. In the decidua, PGE 2 can either undergo conversion to PGF 2 a or initiate
the synthesis of further PGE 2 and PGF 2 a (Nakala et al., 1986; McCoshen et al.,
1990; Casey and McDonald, 1988; McDonald et al, 1991). Although the exact
mechanism by which PGs stimulate uterine contractions is unclear, there is some

5 evidence to suggest that they affect transmembrane calcium flow (Huszar, 1989). It
is speculated that PCs may activate smooth muscle cell contractile protein and that
the process involves an increase in calcium transport through the plasma membrane.
PGF2a stimulates Ca + + influx into the smooth muscle cell. This influx of Ca + +
results in the activation of myosin light-chain kinase (MLCK) initiating
phosphorylation. Shortening of smooth muscle cells is facilitated by actin-myosin
interactions (Figure 3). Indomethacin inhibits PGF2a production and thereby
interferes with its modulatory action on transmembrane calcium flow. This results
in an inhibition of uterine muscle activity. Therefore, by inhibiting uterine activity,
PG synthetase inhibitors like indomethacin are indicated for tocolysis (Zuckerman
etal., 1974; Wiquist et al, 1975; Niebylera/., 1980).
SARCOPLASMIC RETICULUM colcium pool
ff-udrimgw; agonists noprotere»«4
calmodulin
0 phosphorylation
| cAMP| '
(5 • acetylcholine^ | theophylline a - adrenergic^ papaverine
colcium
phosphodiesterase
/ \ MYOSIN LIGHT-CHAIN
KINASE CAMP
ACT1N • MYOSIN-P ACTOMYOSIN-P
Figure 3: Proposed role of PG's in labour (Adapted from Miller, 1983).

6 B. Clinical Uses
Anti-inflammatory, Analgesic, and Antipyretic Uses
As previously mentioned, indomethacin is effective in rheumatic disorders
(ankylosing spondylitis, osteoarthritis, rheumatoid arthritis) as well as for moderate
pain such as dysmenorrhoea. The anti-inflammatory, analgesic, and antipyretic
effects of indomethacin are the subject of several research papers: uses in Bartter's
syndrome (Zancan et al., 1976; Haluska a/., 1977; Donker et al., 1977; Rado et
al., 1978), in fever (Silberman et al., 1965; Kieley et al, 1969; Engerrall et al,
1986), in hypercalcaemia (Elliot and McKenzie, 1983; Dindogru et al., 1975;
Blum, 1975), in osteoarthritis (Zachariae, 1966; Harth and Bondy, 1969; Woolf et
al, 1978; Gordin et al, 1985), in pain (Holmlund and Slodin, 1978; Elder and
Kapadia, 1979; Mattila et al, 1983; Ebbehoj et al, 1985; Jonsson et al, 1987),
and in rheumatoid arthritis (Donnelly et al, 1967; Wright et al, 1969; Baber et al,
1979; Ekstrand et al, 1980).
Patent Ductus Arteriosus
The ductus arteriosus (DA) is a vascular shunt in the fetal circulation that
diverts about 90% of the right ventricular output past the lungs into the descending
aorta. PGE 2 is one of the most important determinants in the patency of the DA.
7 Closure of the ductus is imperative in the neonate as failure results in the
development of a left-to-right shunt from the aorta to pulmonary artery. Other
complications include hepatomegaly, hyperactive precordium, and congestive
cardiac failure. The incidence of patent ductus arteriosus (PDA) is about 80% in
neonates weighing less than lOOOg and 10-15% in those weighing between 1500-
2000g (Douider et al, 1988). PDA closure has been postulated to be age related
(McCarthy etal, 1978).
Surgical ligation (Gay et al., 1973) and treatment with a prostaglandin
synthetase inhibitor, such as indomethacin (Friedman et al., 1976), are two
commonly used methods of correcting PDA. Increased oxygen tension and
decreased prostaglandin concentrations are two common determinants of ductal
closure at birth (Noerr, 1991). Intravenous indomethacin, in the sodium trihydrate
form, is the drug of choice for neonatal PDA. However, renal dysfunction is
claimed to be a prominent side effect of such a therapy. Decreased urine output and
free water clearance, increased serum creatinine and blood urea nitrogen have all
been reported during indomethacin use (Betkerur et al., 1981; John et al., 1984). A
mean reduction in cerebral blood flow (CBF) by 24% has also been reported in a
study involving pharmacological closure of the DA at an i.v dose of 0.2 mg/kg in
human premature infants (Pryds et al, 1988). Changes in regional blood flow
velocity have also been observed following indomethacin infusion in preterm
infants with symptomatic PDA. These changes include a reduction in time-

8 averaged mean velocity, peak systolic velocity, and end-diastolic velocity in the
anterior and middle cerebral artery (Austin et al, 1992). Reductions in CBF
velocity to the extent of 50% in adult humans and 30% in newborn pigs have been
observed (Wennmalm et al, 1981; Leffler et al., 1985). The apparent volume of
distribution of indomethacin appears to be a useful marker of permanent PDA
closure since it varies significantly pre- and post-PDA closure (Gal et al., 1991).
Polyhydramnios
Polyhydramnios is a complication arising from excess amniotic fluid and is
determined by several methods including the maximum-vertical pocket technique
(Chamberlain et al., 1984), amniotic fluid index (Phelan et al., 1987), and
gestational age adjusted amniotic fluid index (Moore and Cayle, 1990). A 30% fetal
mortality rate due to premature rupture of the membranes as a result of
polyhydramnios has been reported (Cabrol et al., 1987). Conventionally, the
management of polyhydramnios incorporates repeated transabdominal
amniocentesis under tocolytic therapy and fluid withdrawal. Puncture
complications include infection and membrane rupture. Prostaglandin synthetase
inhibitors reduce amniotic fluid volume as well as inhibit premature labour (Cabrol
et al., 1987). The reduction of amniotic fluid volume is thought to be due to a
decrease in urinary flow (Cifuentes et al., 1979; Kirshon et al., 1988; Rosen et al.,
1991; Kirshon et al, 1991; Walker et al., 1992a). One risk of such therapy,

9 however, is the possibility of oligohydramnios (Nordstorm et al., 1992; Hendricks
etal, 1990; Krishon^a/., 1991; Goldenberg et al, 1989).
Indomethacin is recommended in the treatment of symptomatic
polyhydramnios (Krishon et al., 1990; Smith et al., 1990). The mechanism by
which indomethacin's effects are thought to be mediated in polyhydramnios is
through a reduction in fetal urinary output. The underlying mechanism by which
indomethacin reduces amniotic fluid volume by a fall in urinary output, however,
remains unclear. Suppression of vasodilatory renal PG's by indomethacin leading
to a fall in renal blood flow (Matson et al., 1981; Kover, 1980) is one proposed
mechanism for the reduction in fetal urinary output. However, recent results
indicate that indomethacin may interact with arginine vasopressin (AVP) at the V2
receptor level and augment the action of AVP; an increase in fetal AVP
concentration was observed when indomethacin reduced fetal urinary output at a
dose of 0.0025 mg/kg/min five hour infusion. (Walker et al., 1992a). When
indomethacin (0.05 mg/kg, 5 h) was co-administered with the AVP-V2 receptor
antagonist (d [CH2]5-D-Phe-Ile4, Arg8)-VP, the fetal oliguria that was observed with
indomethacin alone was inhibited by the antagonist, suggesting that V2 receptor
played a significant role (Walker et al., 1994). Indomethacin may increase
circulating AVP levels and enhance the peripheral effects of AVP in the fetus. It is
interesting to note that PGE 2 inhibits cAMP production (Levenson et al., 1982), and
this effect seems to be mediated via the V2 receptor of AVP (Levenson et al., 1982;

10 Somenburg et al, 1990). Considering the fact that PGE 2 is synthesised in the
kidney in response to AVP and oxytocin leads one to speculate that there exists a
negative feedback role for the PGs (Walker et al, 1993). Inhibition of PGE 2
synthesis by indomethacin will potentiate AVP action through release and
peripheral action of AVP (Walker etal., 1993; Levenson et al., 1982).
Studies by Walker et al., 1992b, have shown that short-term infusion of
indomethacin at a dose of 0.017 mg/kg/min for 5 hours leads to an increase in fetal
urinary output, urinary osmolality, sodium and chloride. However, when the dose
infused was reduced to 0.0025 mg/kg/min for 5 hours, there was a reduction in
urinary output, suggesting fetal antidiuresis at low levels of indomethacin (Walker
etal, 1992a).
Preterm Labour
One of obstetrics' major challenges lies in the therapy of preterm labour. The
only tocolytic drug approved to date by the U.S. FDA is the -sympathomimetic,
ritodrine hydrochloride. A potential therapeutic alternative to ritodrine are the
prostaglandin inhibitors as it is known that prostaglandins PGE,, PGE2, and PGF 2 c x
stimulate uterine contractions and induce labour (Embrey, 1970; Roth-Brandel et
al., 1970). In 1974, Zuckerman et al., demonstrated a marked inhibitory effect of
indomethacin on uterine contractions in premature labour. In a randomised

11 comparative trial of indomethacin and ritodrine, Besinger et al (1991) reported that
the two were equally effective in delaying preterm birth. In 1992, Carlan et al.,
compared two PG synthesis inhibitors, namely, indomethacin and sulindac for
efficacy in refractory preterm labour. Sulindac was equally effective as
indomethacin although the group that responded to indomethacin had a longer time
to delivery, higher birth weight, and a lower number of days in the intensive care
unit. The sulindac group, however, demonstrated a renal sparing effect speculated
to be due to minimal placental transfer. Several fetal risks have been identified
following indomethacin administration including premature ductal closure, renal
dysfunction, oligohydramnios, and pulmonary hypertension (Arcilla et al., 1969;
Manchester et al., 1976; Rudolph, 1977; Friedman et al., 1978; Cifuentes et al.,
1979). Other complications include tricuspid regurgitation, right ventricular
dysfunction, and pericardial effusion (Hallak et al., 1991). Maternal side effects
included perspiration, hypertension, gastritis, dizziness, and nausea (Grella and
Zanor, 1978).
C. Renal Eff ects Of Indomethacin
Production of large quantities of hypotonic urine (amniotic fluid), excretion
of sodium in large amounts, low renal blood flow (RBF), and low glomerular
filtration rate (GFR) with greater fractional blood flow to mature inner nephrons are
some of the characteristics of fetal renal function (Kleinman, 1978). As gestation

12 advances, there is a progressive increase in urinary flow rate, RBF, and GFR, and a
reduction in fractional excretion of Na + (FE N a+). Postnatal renal adaptation includes
increases in GFR and RBF, redistribution of intrarenal blood flow from inside to the
periphery of the cortex, reduction in FEjsf a +, and a greater ability to concentrate
urine. AVP levels are high at birth and during hypoxia and hemorrhage (Kleinman,
1978; Gleason et al, 1988; Robillard et al, 1982). Optimal urine concentrating
ability depends upon the GFR, the AVP level, and the ability of the renal collecting
tubule to respond to AVP. AVP enhances water resorption from the collecting
tubule leading to anti-diuresis. The exact role by which renal prostaglandins modify
A VP's effects is still unclear. In 1968, Grantham and Orloff proposed that AVP was
controlled by a negative feedback loop wherein it stimulates intrarenal biosynthesis
and production of PGs, and these PGs inhibit AVP's effects at the collecting tubule.
While the exact mechanism(s) remain to be elucidated, several studies have
demonstrated that the prostaglandin inhibitors enhance the anti-diuretic effect of
AVP (Anderson et al, 1975; Berl et al, 1977; Fejes-Toth et al., 1977; Gullner et
al, 1980; Lum etal:, 1977).
When indomethacin was administered to close the PDA, the observed
neonatal renal dysfunction was characterised by reduced urine output, decreased
free water clearance, and increased blood urea nitrogen and serum creatinine. Early
studies related these events to reduced renal PG production (Betkerur et al., 1981;
Cifuentes et al., 1979; Levenson et al, 1982; Terragno et al., 1977).

13
Maternal indomethacin administration often leads to adverse renal effects in
the human fetus and neonate (Mogilner et al, 1982; Veerema et al., 1983;
Vanhaesebrouk et al., 1988; VanDer Heijden et al., 1988). A reduction in fetal
urinary output has been demonstrated to be the underlying mechanism by which
indomethacin acts in polyhydramniotic states (Hickok et al., 1989; Krishon et al.,
1988; Krishon et al., 1991). These effects of indomethacin seem to be dose
dependent as fetal urinary output increased when indomethacin was administered at
a dose of 0.017 mg/kg/min, but decreased when the dose was reduced to 0.0025
mg/kg/min in the pregnant sheep model, suggesting fetal antidiuresis at lower
plasma indomethacin concentrations (Walker et al., 1992a, 1992b). This incidence
of fetal oliguria has been attributed to reduced RBF following inhibition of renal
prostaglandins (Matson et al, 1981; Millard et al, 1979). Walker et al (1994)
proposed, however, that this fetal oliguria is a result of an effect of AVP on the fetal
kidney and not due to RBF. Co-administration of indomethacin and the AVP-V2
receptor antagonist {(d[CH2]5-D-Phe-Ile4,-Arg8)-Vassopressin} resulted in
inhibition of oliguria due to indomethacin alone (Walker et al, 1993, 1994),
suggesting that oliguria was due to activation of the AVP-V2 receptor and not to a
reduction in RBF.

14 D . Fetal Effects Of Indomethacin
Indomethacin has been reported to exert marked fetal side effects following
either fetal or maternal drug administration. The latter scenario is widely perceived
as a consequence of easy and high degree of placental transfer. Indomethacin
increased fetal pulmonary arterial pressure at a dose of 0.05 mg/kg i.v in pregnant
ewes (Ohara et al, 1991). The study reported that ductal constriction by
indomethacin caused increases in the systolic pulmonary artery-aortic pressure
difference as well as fetal heart rate. A marked fall in placental blood flow was
noted after indomethacin was given in pregnant rabbits (Katz et al, 1981).
Indomethacin reduced CBF in the human fetus by about 40% (Vanbel et al, 1990).
A drastic decline in fetal urine output was noted when short term oral indomethacin
was used for therapy of preterm labour (Krishon et al, 1988). Indomethacin also
stimulates sleep state independent fetal breathing which is abolished by PGE 2
infusion in fetal lambs (Jansen et al, 1984). A similar study demonstrated that PG
synthesis inhibitors stimulated breathing movements in fetal sheep (Kitterman et al,
1979). Stevenson et al, 1992 evaluated the effects of indomethacin on the ovine
fetus. They administered indomethacin at a dose of 10 mg/kg i.v to the ewe and 12
mg/kg i.v to the fetus. Increases in fetal arterial P02, placental blood flow, and
urine osmolality, and decreases in lung liquid flow and free water clearance were
observed. Walker et al, 1992b, administered indomethacin as a 0.35 mg/kg bolus
followed by a 0.017 mg/kg infusion over 5 h in chronically catheterised ovine

15 fetuses and observed a marked increase in fetal urinary output (about 84%) and
urinary osmolality as well as sodium and chloride concentrations. Fetal heart rate
was also increased.
Though there are a number of studies illustrating fetal indomethacin effects
there does not exist a comprehensive database on the drug's dose-response
characteristics which would rationalise the continued use of the drug to a
therapeutic advantage.
1.1.2 Pharmacokinetics Of Indomethacin
1.1.2.1. Absorption
Following oral administration, indomethacin is readily and almost completely
absorbed from the gastrointestinal tract with peak plasma concentrations appearing
within 120 minutes (Duggan et al., 1972; Alvan et al., 1975). Dissolution of
indomethacin capsules was observed to be greater in a low acidity condition
compared to a more acidic environment (Aoyagi et al., 1985). Bioavailability of
indomethacin is markedly altered by various diets; absorption being faster with a
high protein and a high lipid diet compared to a high carbohydrate diet (Wallusch et
al., 1978). Bioequivalence studies have indicated that the bioavailability of many
indomethacin formulations are far from being equal. A 30% variation in

16 bioavailability was observed from formulations marketed in Finland (Turakka and
Airakinsen, 1974) and in India; two out of ten products studied were found to be
bioinequivalent (Chaudhari et al., 1984). However, this bioavailability information
should take into account the extensive enterohepatic recirculation indomethacin
undergoes as approximately half an intravenous dose of indomethacin is subjected
to biliary recycling (Kwan et al., 1976). Bile facilitates the dissolution of poorly
soluble indomethacin, due to micellar solubilisation, and thereby increases its rate of
absorption (Miyazaki et al, 1980; Miyazaki et al., 1981).
Significant species differences exist in the pharmacokinetics of intravenously
(bolus) administered indomethacin. Plasma levels of 14C-indomethacin were
markedly higher in dogs and rats than in guinea pigs and rhesus monkeys, and tissue
levels of 1 4C were greater in the guinea pig than in the rat (Baer et al., 1974).
Indomethacin can easily penetrate the skin of humans (Snyder, 1975; Eckard,
1982), rabbits (Naito and Tsai, 1981), rats (Shima et al, 1981; Wada et al, 1982),
and guinea pigs (Inagi et al.,-1981), from various formulations (gels, ointments,
etc.) indicating the potential for transdermal delivery. Indomethacin is detected in
the aqueous fluid, iris, and cornea following ocular absorption in the rabbit (Hanna
and Sharp, 1972; Green et al, 1983). Circadian changes, as a determinant of drug
administration time, have been observed with indomethacin; its
chronopharmacokinetics being well studied in humans (Clench et al., 1981) and in
rats (Guissou et al, 1987). The former study indicated that indomethacin

17 administered in the morning had the highest plasma concentration, and shortest time
to peak in addition to greater elimination (Clench et al, 1981).
1.1.2.2. Protein Binding
Indomethacin, a weakly acidic organic compound, binds strongly with
plasma proteins, the binding being in the order of 90% as determined by equilibrium
dialysis (Hucker et al., 1966; Hvidberg et al., 1972). An association constant of
0.86 x 10 L/mol with a total number of binding sites of 15 has been determined for
human serum albumin (Hvidberg et al., 1972). An ultracentrifugation method
yielded a considerably higher value of about 99%, with an association constant of 3
x 105 L/mol and an indication of a single primary binding site and seven secondary
binding sites with association constants in the order of 1.4 x 104 L/mol (Mason and
McQueen, 1974). Binding of indomethacin was reduced by aspirin and cinmetacin,
and increased by phenylbutazone (Mason and McQueen, 1974; Montero et al.,
1986). In another study, using indomethacin as a model drug, Zona et al., 1986,
suggested that the conformation of the protein in plasma played a key role in drug-
protein interaction, and that binding was favoured when human serum albumin
adopted a "loose" structure. Binding of indomethacin to human serum albumin,
studied by the dynamic dialysis method, yielded an association constant of 1.4 x
106/M with 2.71 as the number of primary binding sites (Montero et al., 1986).
Indomethacin was bound to proteins in the human cerebrospinal fluid in the order of

18 40%, as determined by equilibrium dialysis, with albumin being the protein of
importance (Muller et al., 1991).
Protein binding studies using radiolabeled indomethacin in maternal and fetal
plasma ultrafiltrates in sheep have revealed that 97.6% of the fetal and 98.5% of the
maternal drug is bound to plasma proteins (Anderson et al., 1980c). In another
study involving unlabeled indomethacin and an equilibrium dialysis procedure, the
binding in maternal, fetal, and nonpregnant control was determined to be 85.6%,
43.8%, and 92.1%, respectively (Harris and Van Petten, 1981). Binding of
indomethacin in the postnatal stage is speculated to be related to bilirubin levels
while levels of albumin in the mother and fetus appear to be responsible for the
maternal-to-fetal binding gradient (Nau et al., 1983).
1.1.2.3. Distribution
Indomethacin appears in synovial fluid, peak concentrations ocurring about a
hour later than in serum in patients with rheumatoid arthritis (Emori et al., 1973).
Similar results have been obtained with intraarticularly administered indomethacin
(Neander et al., 1992). Following intramuscular administration, the levels of
indomethacin in synovial fluid and blood were identical after an hour (Dittrich et
al., 1984). Indomethacin was not detected in spinal fluid in the same study, while
minimal amounts were detected in another study (Hucker et al., 1966).

19 Indomethacin was detected in saliva following intravenous administration to dogs,
the levels in parotid saliva and mandibular-sublingual saliva being 7.4 and 4.4% of
the levels in plasma respectively (Watanabe et al, 1981). Binding of indomethacin
to salivary proteins was greater in parotid saliva. Indomethacin appears in breast
milk; the milk:plasma ratio being 0.37 (Lebedevs et al., 1991). Indomethacin
readily and rapidly crosses the placental membrane in humans (Moise et al., 1990),
rabbits (Parks et al., 1977; Harris and Van Petten, 1981), and rats (Klein et al.,
1981). Transfer in sheep, however, appears to be more limited (Harris and Van
Petten, 1981; Anderson etal, 1980c).
1.1.2.4. Metabolism and Fate
Metabolism of Indomethacin in The Adult
The metabolism of indomethacin in several species (monkey, guinea pig,
dog, rats, and humans) has been the subject of numerous reports (Harman et al.,
1964; Duggan et al, 1972; Hucker et al, 1966; Yesair et al, 1970; Baer, 1972;
Vree et al., 1993). Two major metabolites of indomethacin are N-
deschlorobenzoyl-indomethacin (DBI) and O-desmethyl-indomethacin (DMI)
(Harman et al, 1964). Both are excreted in unconjugated as well as glucuronide
conjugated forms. Therefore, the metabolic pathways in man appear to be O-
desmethylation and N-deacylation as well as conjugation with glucuronic acid. The

20 major pathway, however, appears to be desmethylation mediated via the hepatic
microsomal enzyme system which is followed by a deacylation step that is
extramicrosomal in nature (Duggan et al., 1972). These metabolites are found in
high concentrations in plasma. Metabolites of indomethacin are devoid of
prostaglandin synthesis inhibiting activity (Shen, 1965).
Significant species variation has been observed with the metabolism of
indomethacin. The glucuronide of N-deschlorobenzoyl-indomethacin is primarily
eliminated in the urine of monkeys and guinea pigs. The primary product of
excretion in rabbit urine was indomethacin glucuronide. O-desmethyl-indomethacin
was not detected. Neither free nor conjugated indomethacin was detected in rat
urine (Harman et al., 1964). There was also minimal urinary excretion of
indomethacin or its metabolites in the dog. In another study (Yesair et al., 1970), it
was found that dogs excreted most of the drug given i.v. unchanged in the feces. In
monkeys indomethacin was extensively metabolised to DBI and excreted in the
urine, while in rats DMI was equally excreted in urine and feces.
In human subjects, less than 33% of the administered dose is excreted as
indomethacin with 50% of that as the conjugate. Unconjugated desmethyl-
indomethacin and desmethyl-desbenzoyl indomethacin contributed to total fecal
excretion which was in the order of 21-42% of the dose (Duggan et al., 1972).
Following the oral administration of indomethacin (100 mg) in a single human

21
subject (Vree et al, 1993), the percentage of the dose excreted can be individualised
as follows: indomethacin (0.76%), DMI (0.58%), indomethacin acyl glucuronide
(32.1%), DMI acyl glucuronide (7.3%), and DMI ether glucuronide (29.8%) (Figure
4).
NKJ«schkvobmzcr/<HrKkMTwUucin -«cy( g lucuronKte
r s o g l u c u r o n t d e
Indomethacin Indomethacin-acyl glucuronide
etfior glucuronide
O^esmethylHndoniethacin (J^esraettiyWrKtomettwcin-acyt fltucufonide
Figure 4: Metabolism of indomethacin in the adult human (Adapted from
Vree et al., 1993)

22
Hucker et al., 1966, reported that less than 5% of an oral dose of
indomethacin was excreted unchanged in the urine. In other studies (Duggan et al.,
1972; Kwan et al., 1976), the amount of indomethacin recovered in urine was in the
order of 27%, half of which was in the form of glucuronide conjugate. Urinary free
metabolites recovered were about 18% and 13% of the dose administered
respectively, with the remainder as conjugates. Indomethacin, desmethyl-
indomethacin, and deschlorobenzoyl-indomethacin are found in human plasma and
urine in high quantities while desmethyl-N-deschlorobenzoyl-indomethacin appears
primarily in the feces (Shen and Winter, 1977; Duggan et al., 1972). Indomethacin
and its metabolites undergo enterohepatic circulation in humans, rats, dogs, and
monkeys (Kwan et al., 1976; Yesair et al, 1970). The metabolic pathway for
indomethacin in humans is summarised in Figure 4, while the routes of formation
are presented in Table 1.
Table 1: Metabolites of Indomethacin
Pathway Product of Metabolism Location of Metabolic Enzymes
O-Demethylation DMI Microsomal oxidation involving cytochrome
P450 Deacylation DBI Cytosol
Glucuronidation Glucuronides (acyl, ether) Endoplasmic reticulum

23 Maternal/Fetal/Neonatal Indomethacin Metabolism
In rabbits, there is a significant increase in the production of DMI after 2
weeks of life (Evans et al, 1981). In the same study, indomethacin was found to be
mainly metabolised to DBI in neonatal rabbit hepatocytes by non-microsomal
deacylation. The major components of eliminated drug in adults were the
glucuronides of indomethacin and its metabolites, however, less than 8% of the total
metabolites were conjugated in hepatocytes from 25 day old rabbits indicating that
glucuronidation was not the major metabolic pathway in the neonate (Evans et al,
1981). The rate of production of DBI and DMI in fetal rabbits is in the order of
0.23 and 0.13 nmoles/106/min, respectively. A very high maturational increase in
DBI production was determined on day 12 of postnatal life with a value of 1.3
nmole/106/min (Evans et al, 1981). In newborn rats the metabolism of
indomethacin is minimal and has been attributed to reduced affinity between
enzyme and substrate as well as to the presence of competitive inhibitors. There is,
however, a progressive increase in the formation of DMI from day 1 of postnatal
life to 60 days of age (Clozel et al, 1986). Endogenous cytosolic factors appear to
selectively inhibit microsomal oxidation of indomethacin in neonatal rabbit liver
(Evans et al., 1981). This finding is consistent with the changes in K m observed in
the neonatal rat study (Clozel et al, 1986).

24 1.1.2.5. Elimination Kinetics
Pharmacokinetic reports on indomethacin have been extensive ever since its
introduction in 1962. However, early studies depended heavily on
spectrophotometric and spectrofluorimetric methods of analysis and reported
elimination half-lives were in the range of 1.5-2.3 hours (Duggan et al., 1972;
Hucker et al, 1966; Hvidberg et al, 1972; Traeger et al, 1972). Given the
sensitivity limitations of these assay methods it seems highly probable that the true
elimination phase was not accurately determined. Using a more sensitive mass
fragmentographic method, however, the mean elimination half-life of indomethacin
was found to be in the range of 6-7.6 hours following either oral, i.v., or rectal
administration (Alvan et al., 1975).
While differences in assay methods and sensitivity account for some of the
inter- and intra-individual variability in elimination kinetics of indomethacin, the
majority of this is considered to be due to extensive enterohepatic recycling and the
irregularity of biliary discharge (Helleberg, 1981).
Plasma concentration-time data obtained from single dose studies were fit to
a two compartment open model (Alvan et al., 1975). Decay of indomethacin from
plasma was characterised by a rapid initial phase (t 1 / 2 ~ 90 min) and a slower
elimination phase (t 1 / 2 ~ 10 hours). The apparent volume of distribution of

25 indomethacin was in the order of 0.34 L/Kg - 1.57 L/Kg, and plasma clearance
varied from 0.044 - 0.109 L/Kg (Alvan et al., 1975). Steady state concentrations in
plasma ranged from 0.3-0.6 |ig/mL. The long elimination phase was speculated to
be due to enterohepatic recycling of the drug. There is no indication of dose-
dependent elimination (Alvan et al., 1975; Duggan et al., 1972).
Using fluorimetric methods, the half-life of indomethacin in adults and
newborns was found to be 2.2 h and 14.7 h respectively (Traeger et al., 1973).
Using a gas chromatographic (GC) method, Friedman et al., 1978, determined the
half-lives of indomethacin in two premature infants with patent ductus arteriosus to
be 21 and 24 h respectively, with a volume of distribution of 4.4 L/Kg and plasma
clearance of 0.145 L/Kg/h in one of the infants. While drug elimination in urine
was not determined, it was suggested that the prolonged half-life could be due to
renal immaturity. In another study involving nine preterm infants, the half-life
following oral administration was found to be 11-20 hours (Bhat et al., 1979).
These same authors report that protein binding of indomethacin was in the order of
95%. The kinetic parameters obtained for indomethacin in neonates from various
studies are summarised in Table 2.

26
Table 2: Pharmacokinetics of Indomethacin in Neonates
Postnatal Age (days)
Birth Weight (g)
hn (h) Varea (L/Kg) CI (mUKg/h)
Reference
7-14 1301+72 14.5 + 3 0.80 38 Thalji et al, 1979
10.8 + 6.0 1253 ± 389 20.7 ± 8 0.35+0.21 13+9.5 Thalji et al, 1980
9.5 + 2.2 1300 + 200 33.9 + 11.7 0.35 + 0.16 7.6 + 3.0 Vert et al, 1980
8.8 ±6.8 1213 + 309 32 0.19-0.61 7.0 Brash et al, 1981
10.2 + 2.2 1200 + 400 21.6 0.3 9.2 Yeh et al, 1985
5.7+4.2 1125 + 399 - 0.280 2.63 Wiest et al, 1991
9.5 + 1.3 1455 + 119 16.2 + 2.9 0.36 + 0.01 17.1+2.8 Bhat et al, 1980
The elimination half-life is markedly prolonged in neonates when compared
to adults and is related inversely to gestational age (Vert et al, 1980; Evans et al,
1979). Data, however, is severely lacking for indomethacin in-utero
pharmacokinetics in the fetus.
Following a single oral dose of indomethacin, the total clearance in the
elderly (79.5 ± 1.3 y) was 0.8 mL/min/Kg compared to 1.4 mL/min/Kg in younger
subjects (36.9 ± 3 y) with an elimination rate constant of 0.23 h"1 and 0.32 h"1 ,
respectively (Oberbaur et al, 1993). The fall in clearance in the elderly has been
attributed to a decline in renal function and a reduced renal excretion of
indomethacin since about 27% of the dose is eliminated through the kidneys

27 (Duggan et al, 1972; Kwan et al., 1976; Traeger et al., 1973; Oberbaur et al.,
1993).
1.1.3. Placental Transfer
The maternal-placental-fetal unit is a complex pharmacokinetic system
comprised of two independent circulations. The lipoprotein nature of the placenta
is, however, very similar to other biological membranes in the body and plays an
important role in controlling drug transfer. The unbound lipophilic drug in the
unionised form can easily cross the placenta by passive diffusion while other
mechanisms such as facilitated diffusion, active transport, and pinocytosis are more
prevalent for placental passage of nutrients and other endogenous substances. The
mechanisms of placental transfer and subsequent degree of fetal drug exposure have
been the subjects of numerous reviews over the years (Moya and Thorndike, 1962;
Green et al, 1979; Krauer et al, 1980; Levy, 1981; Szeto et al, 1982b, 1982d;
Mihaly and Morgan, 1984; Reynolds and Knott, 1989; Szeto, 1993).
Several factors may potentially affect maternal-fetal drug exchange and fetal
exposure during the progression of normal pregnancy including the following: (i)
physico-chemical properties such as lipophilicity, molecular weight, and ionisation,
(ii) placental permeability, stage of gestation, and type of placentation, (iii)
orientation of maternal and fetal placental blood flows, (iv) placental metabolism of
28 drugs, (v) fetal circulation, (vi) pH, (vii) uterine and umbilical blood flows, and
(viii) protein binding.
1.1.3.1. Pharmacokinetic Characterisation
Pharmacokinetic evaluation of maternal/fetal drug disposition generally
involves consideration of the mother and fetus each as a single compartment. Such
a system assumes quick equilibration of the drug. If the drug enters fetal tissues
slowly with concurrent elimination from the maternal compartment, a deep
compartment is presumed to exist. The pharmacokinetic data of meperidine was
treated using the mother and fetus each as a single compartment (Szeto et al., 1978).
Such a system assumes fetal and maternal drug concentrations to be at steady state.
If a biexponential decay of the drug is observed in the fetus, then the fetus should be
considered as a two compartmental model to account for fetal distribution kinetics
(Szeto, 1982). The placenta (Krauer and Krauer, 1977) and the amniotic fluid
(Brien and Clarke, 1988) have also been considered as distinct kinetic
compartments.
1.1.3.2. The Chronically Instrumented Pregnant Sheep Model
Several experimental animal models, such as rats, guinea pigs, baboons,
goats, pigs, sheep, and monkeys, have been used in placental transfer studies due to

29 ethical and technical constraints precluding such studies in humans. The commonly
used animal models in fetal medicine have been reviewed (Nathanielsz, 1980).
Small animal models such as rats and guinea pigs are often inadequate when serial
sampling is required due to low blood volume. Of the available models, the
anatomy and physiology of the monkey closely parallels the human situation and
theoretically would seem to be the best to conduct studies on placental transfer.
However, several complications such as the cost of the preparation, ease of
handling, and size limitation of the fetus restrict the use of this model.
Sheep, on the other hand, are docile, have large fetuses conducive for chronic
preparation and similar physiology and biochemistry (Comline and Silver, 1974)
compared to humans. Both sheep and primate models demonstrate similar fetal
behavioural states (viz. fetal breathing movements, eye movements, etc) in the last
trimester of gestation (de Vries et al., 1982; de Vries et al., 1985; Nijhuis et al.,
1982). They have been used to study in-utero fetal physiology and placental
transfer of a number of endogenous compounds (Szeto et al., 1978; Van Petten et
al., 1978; Rurak et al., 1991). Sheep do, however, possess a different type of
placentation, and care must be excercised when extrapolating data to the human
situation, as is necessary with any animal model.

1.1.3.3. Placental Transfer of Indomethacin 30
Indomethacin has been reported to traverse the placental membrane in rabbits
(Parks et al, 1977; Harris and Van Petten, 1981), rats. (Klein et al, 1981), sheep
(Harris and Van Petten, 1981; Anderson et al, 1980c), and humans (Moise et al,
1990), however, detailed information is lacking.
When indomethacin was given orally at a dose of 2 mg/kg in pregnant
rabbits, in a study period of two hours, the drug was detected in maternal (M) and
fetal (F) blood and amniotic fluid within 15 minutes; the F/M ratio at the end of the
study being 0.568. Although indomethacin did appear in the amniotic fluid, its
concentration relative to maternal and fetal blood levels was much lower. At the
end of the study period detectable concentrations of free drug were seen in maternal
urine, i.e., 19.2 |i.g/mL, and bile, i.e., 0.35 |ig/mL (Parks et al, 1977). In another
study involving pregnant rabbits, indomethacin was administered subcutaneously in
a dose of 10 mg/kg for a study period of six hours (Harris and Van Petten, 1981). In
contrast to the former study where fetal plasma levels remained lower than maternal
levels throughout the experiment, fetal plasma indomethacin concentrations
exceeded maternal levels and remained elevated over a period of time before falling.
At the end of the 1st hour, the F/M ratio was 0.795. Indomethacin was detected in
the amniotic fluid 2 hours after dosing and its concentration at the end of six hours
was comparable to that of maternal plasma. A major concern as to the reliability of

31 these data is the analytical methodology involved, namely, spectrophotometric and
spectrofluorimetric methods of analysis.
In a study with pregnant rats, indomethacin was administered at a dose of 4
mg/kg by gastric intubation. At the end of the 3rd hour, maternal and fetal plasma
indomethacin concentrations were 16.8 ± 1.6 |ig/mL and 4.6 ± 0.3 |Lig/mL,
respectively, with a F/M ratio of 0.274 (Klein et al, 1981).
In 1980c, Anderson et al, were the first group to attempt description of
placental transfer in quantitative terms. Their study involved simultaneous
administration of 14C-indomethacin as bolus in the fetus and 3H-indomethacin as an
infusion in the ewe. Maternal and fetal blood were analysed for radioactivity in a
scintillation counter and placental blood flows measured using radiolabeled
microspheres. Placental clearance (Clp) was determined by the formula, C l p = Ctot x
Fss/Mss, where Ctot is the total clearance, and F s s and M s s are fetal and maternal
steady state concentrations. Fetal and placental tissue clearances were estimated to
be 3.63 ± 0.58 ml/min/kg and 2.10 + 0.32 ml/min/kg, respectively, with a F/M ratio
of 0.28. Major criticisms of this method include: (a) the requirement that steady
state conditions prevail, (b) it only provides single point estimation, (c) the model
is limited to cases where fetal clearance is zero and simultaneous solving of the
equations is impossible (Szeto, 1982b), (d) it is applicable only in instances where
drug clearance by the placenta from mother and fetus are equal, (e) the issue of an

: 32
isotope effects not addressed, and (f) the method cannot differentiate intact drug
from its metabolites.
When indomethacin was administered as an intravenous infusion at a dose of
10 mg/kg into pregnant ewes, maternal and fetal plasma levels at the end of infusion
were 13.5 ± 0.7 Lig/mL and 0.6 ± 0.1 pig/ml with a F/M ratio of 0.04 (Harris and
Van Petten, 1981). Indomethacin concentrations in amniotic fluid were markedly
higher than fetal and maternal plasma levels at the end of the study period. A major
concern is again the non-specific analytical methodology involved.
Moise et al., 1990, administered 50 mg of indomethacin orally to pregnant
human patients. Maternal and fetal indomethacin levels (cordocenteses) were 218 +
21 ng/ml and 219 ± 13 ng/ml, respectively, with a F/M ratio of 1.004. The fetal
plasma to amniotic fluid concentration ratio was 10.0 ± 1.2.
1.1.4. Analytical Methods
Indomethacin has been analysed in biological fluids, for a variety of study
requirements, by several methods including liquid chromatography (HPLC), gas
chromatography (GC), mass fragmentography, radioimmunoassay (RIA), and
spectrophotometric methods. The detection limits of most HPLC assays fall in the
range of 10 - 100 ng/mL, GC assays in the range of 1-50 ng/mL, and RIA methods

33 in the range of 50 ng/mL. Spectrophotometric methods of analysis are sensitive in
the |ig range with poor selectivity.
Major disadvantages of available methods include:
1. Radioimmunoassay is highly cross reactive to glucuronide conjugates of
indomethacin and its metabolites (Hare et al., 1977).
2. HPLC assays with fluoresence detection require post-column in-line hydrolysis
necessitating auxiliary pump setups (Bernstein and Evans, 1982; Mawatari et
al., 1989), and those with UV detection are not sensitive in the lower nanogram
range.
3. GC methods are plagued by long retention times (Nishioka et al., 1990), multi-
step derivatisation, lack of internal standards (Helleberg et al., 1976; Ferry et
al., 1974), long derivatisation reaction times (Nishioka et al., 1990), use of
hazardous and corrosive derivatising agents (Evans, 1980; Helleberg et al.,
1976), and inadequate internal standards (Evans, 1980; Guissou et al., 1983).
Other complications include large sample size (>1 mL), inadequate recovery,
multiple extractions, and high variability at lower concentrations.
Of the available methods, GC with electron-capture detection would appear
to provide the best sensitivity and selectivity; only one GC method has applied

34 fused silica capillary column technology to indomethacin measurement to date
(Nishioka et al, 1990).
Several derivatising reagents have been investigated for GC assays, viz.,
diazomethane (Guissou et al, 1983; Giachetti et al, 1983; Plazonnet and Van den
Heuvel, 1977), diazopropane (Arbin, 1977), l-ethyl-3-p-tolyltriazine (Nishioka et
al, 1990), pentafluorobenzyl bromide (Sibeon et al, 1978), hexafluoroisopropanol
and trifluoroacetic anhydride (Matsuki et al, 1983), bis (trimethylsilyl) acetamide
(Plazonnet and Van den Heuvel, 1977), ethyl iodide and extractive alkylation
(Jensen, 1978), pentafluoropropanol and pentafluoropropionic anhydride (Evans,
1980), and diazoethane (Helleberg, 1976). The simplest of the derivatisation
reactions is with bis (trimethylsilyl) acetamide, a silylating agent producing
trimethylsilyl esters of indomethacin.
Selection of internal standards for indomethacin, by either HPLC or GC, is
yet another problem encountered in the literature. Several reports incorporate
internal standards with no structural similarity to indomethacin including
phenylbutazone (Mehta and Calvert, 1983), phenacetin (Avgerinos and
Malamataris, 1989), testosterone (Kwong et al, 1982), itraconazole (Al-Angary et
al, 1990), and penfluridol (Guissou et al, 1983). Others use inappropriate internal
standards such as indomethacin propyl ester (Nishioka et al, 1990) and
indomethacin methyl ester (Arbin, 1977), and still others do not use any at all

35 (Helleberg, 1976; Ferry et al, 1974). Some suitable internal standards include di
methyl indomethacin (Stubbs et al., 1986; Bayne et al, 1981), and 5-fluoro
indomethacin (Sibeon et al., 1978).
1.2. Rationale and Specific Aims
1.2.1. Rationale
Available analytical methods for indomethacin were impractical for use in
the current study design with respect to sensitivity, selectivity, speed, sample
volumes, and variability at lower concentrations. Therefore, there is a need to
develop a sensitive, selective, and rapid analytical procedure.
Available data on placental transfer were limited and may be unreliable
because of the analytical methodology used and inadequate experimental design.
The chronically instrumented pregnant sheep modelis a versatile animal model for
studying placental drug transfer and maternal/fetal drug pharmacokinetics. The
model closely simulates the human system with respect to fetal renal,
cardiorespiratory, and behavioural states (de Vries et al., 1982; de Vries et al.,
1985) and fetal biochemistry and physiology (Van Petten et al., 1978). The model
also allows for serial sampling to an extent which is impractical in small animal
models such as rats, rabbits, and guinea pigs.

36
Reports on the limited placental transfer of indomethacin in sheep preclude
the use of the Szeto model (Szeto et al., 1982b) where measurable steady-state
concentrations of drug must be obtained in both the ewe and fetus following
individual maternal and fetal infusion. This coupled with the disadvantages of the
Anderson method (Anderson et al., 1980c) of clearance estimation illustrate the
need to determine placental clearance values by an alternate technique. The Fick
diffusion model, employing direct fetal administration to provide plasma
concentrations corresponding to those observed in studies of human tocolysis
(Moise et al., 1990), appeared then, to be a more suitable and reliable method for
our studies.
1.2.2. Specific Aims
1. To develop and optimise a sensitive and selective gas chromatographic method
with electron-capture detection for indomethacin in sheep biological fluids using
fused-silica capillary column technology.
2. To apply the developed method for the determination of plasma, urine, amniotic
and tracheal fluid indomethacin concentrations following long term infusion of
the drug in chronically instrumented sheep fetuses, and to calculate placental,
non-placental, and renal clearances.

37
2. EXPERIMENTAL
2.1 Materials and Supplies
2.1.1 Chemicals
Phenylbutazone (4-butyl-l,2-diphenyl-3,5-pyrazolidinedione, lot 110H0632),
acemetacin (1 -[p-chlorobenzoyl]-5-methoxy-2-methylindole-3-acetic acid
carboxymethyl ester, lot 38F0022), sulindac ([Z]-5-fluoro-2-methyl-l-[p-
(methylsulfinyl) benzylidene] indene-3-acetic acid, lot 101H0643), indomethacin
(l-[p-chlorobenzoyl]-5-methoxy-2-methylindole 3-acetic acid, lot 60H0448),
carprofen (lot 28F0440), zomepirac sodium (5-[p-chlorobenzoyl]-l,4-dimethyl-
pyrrole-2-acetic acid [sodium salt], lot 13H0228) and flufenamic acid (lot 61H3562)
were obtained from Sigma Chemicals Co., St. Louis, MO, USA. 5-Fluoroindole-2-
carboxylic acid (lot 10130DF) was purchased from Aldrich Chemicals Co.,
Milwaukee, WI, USA. 5-Fluoroindomethacin (Merck Research Laboratories, West
Point, PA, USA) and a-methylindomethacin (Merck-Frosst Inc., Kirkland, Quebec)
were generous gifts. Injectable ampicillin (PenbritinR), injectable gentamicin
sulphate (GaramycinR), injectable atropine sulphate, halothane (FluothaneR), and
injectable heparin (HepaleanR), were obtained from the Pharmacy Department of
Women's Hospital, Vancouver, BC. Sodium chloride for injection USP was

38 obtained from Abbott Laboratories, Montreal, Quebec. The enzyme, p-
glucuronidase (Bovine liver, type B-l), lot 117F7256, was purchased from Sigma
Chemicals Co., St. Louis, MO, USA.
2.1.2 Reagents
Sodium acetate (anhydrous, analytical reagent grade) was obtained from
BDH (Toronto, Ontario) and glacial acetic acid (American Chemical Society, ACS
reagent) from Allied Chemical (Pointe Claire, Quebec). Triethylamine was
purchased from Pierce Chemical Co., Rockford, Illinois, USA.
Pentafluorobenzylbromide (PFBBr, lot 930413082), N-methyl-N-(tert-
butyldimethylsilyl) trifluoroacetamide (MTBSTFA, lot 930817150), and N,0-Bis-
(trimethylsilyl) acetamide (BSA), were purchased from Pierce Chemical Co.
(Rockford, Illinois, USA). 2,2,3,3,3-Pentafluoro-l-propanol (97%) and
pentafluoropropionic anhydride (99%) were obtained from Aldrich Chemical Co.,
Milwaukee, WI, USA.
2.1.3 Solvents

39
The following (distilled in glass) were purchased from Caledon Laboratories
Ltd., Georgetown, Ontario: ethyl acetate, ethyl ether, hexane, toluene,
dichloromethane, and acetonitrile. Deionised, high-purity water (hereafter refered
to as water) was produced on-site by reverse osmosis using a Milli-Q® water system
(Millipore, Mississauga, Ontario).
2.1.4. Gases
Hydrogen, carrier gas for G C - E C D , and argon-methane (95:5), make-up gas
for E C D , and ultra-pure helium, carrier gas for G C - M S , were obtained from
Matheson Gas Products, Edmonton, Alberta. Nitrogen N F was obtained from
Praxair Canada Inc., Mississauga, Ontario.
2.1.5. Supplies
Membrane filters (0.45) (Millipore, Mississauga, Ontario); disposable plastic
pipet tips (National Scientific, San Rafael, C A , USA); needles and disposable
plastic syringes (Luer-LokR) for drug administration and sample collection
(Beckton-Dickinson Canada, Mississauga, Ontario); borosilicate glass pasteur
pipets (John Scientific, Toronto, Ontario); heparinised blood gas syringes
(Marquest Medical Products Inc., Englewood, C O , USA); heparinised VacutainerR

40 tubes (Vacutainer Systems, Rutherford, NJ, USA); PyrexR 15 mL disposable
culture tubes (Corning Glass Works, Corning, NY, USA); polytetrafluoroethylene
(PTFE) lined screw caps (Canlab, Vancouver, British Columbia); polystyrene tubes
(Evergreen Scientific International Inc., Los Angeles, CA, USA); polyvinyl tubing
for catheterisation (Dow Corning, Midland, MI, USA).
2.2 Instrumentation
2.2.1 Gas Chromatography
A HP (Hewlett-Packard, Avondale, PA, USA) model 5890 series II gas
chromatograph equipped with a HP model 7673 autosampler, split-splitless capillary
inlet system, model HP 3365 chemstation, and a 6 3Ni electron-capture detector, was
used for all analyses. A PyrexR glass inlet liner (78 mm x 4 mm, i.d.) and
ThermogreenR LB-2 silicone rubber septum (Supelco, Bellefonte, PA, USA) were
used for all analyses.
The optimised operating conditions for routine analyses were: column,
Ultra-2® fused silica capillary column cross-linked with 5% phenylmethylsilicone,
25m x 0.31 mm x 0.52p:m film thickness, (Hewlett-Packard, Avondale, PA, USA);
injection mode, splitless; injection port temperature, 200 °C; initial column
41 temperature, 210 °C (1 min); oven programming rate, 40 °C/min; final oven
temperature, 300°C (6 min); detector temperature (ECD), 330 °C; carrier gas, ultra
high purity hydrogen; column head pressure, 10 psi (i.e., 70 kPa, flow rate ~1
ml/min); purge delay time, 0.75 min; make-up gas, argon-methane, 95:5 (flow rate,
65 mL/min).
2.2.2. Gas Chromatography-Mass Spectrometry
A HP model 5890 series II gas chromatograph (Hewlett-Packard, Avondale,
PA, USA) equipped with a HP 7673 automatic injector system, and an HP model
5989A mass spectrometer, HP 59827A vacuum gauge controller, and an HP
98789A on-line computer, with a HP Ultra-2® fused silica capillary column (25 m x
0.31 mm x 0.52|im film thickness) was used for mass spectrometric studies. The
carrier gas, helium, was operated at a column head pressure of 3 psi. In the
chemical ionisation mode, methane was used as the reagent gas. The electron-
impact-MS ionisation energy was 200 eV, emission current 250 |iA, and source
pressure, 1.2 torr.
2.2.3. Columns

42 Ultra-2® fused silica capillary column cross-linked with 5%
phenylmethylsilicone (25 m x 0.31 mm, i.d., x 0.52 |um film thickness) and Ultra-2®
(25 m x 0.2 mm x 0.33 \im film thickness) narrow-bore columns were obtained
from Hewlett-Packard, Avondale, PA, USA; a DB-1701 column (30 m x 0.25 mm,
i.d., x 0.25 \im film thickness) was obtained from J & W Scientific, Folsom, CA,
USA.
2.2.4. Liquid Chromatography-Mass Spectrometry/Mass Spectrometry
A Varian VG Biotech LC/MS/MS system (Fisons Instruments, VG Biotech,
Altrincham, UK) equipped with an electrospray interface, VG Quattro triple
quadrupole mass spectrometer (two high performance quadrupole mass analysers,
and a hexapole collision cell between the two mass analysers), a Dynolite™ detector
system, with a PC-compatible computer to run the VG MassLynx software system
(Mass Spectrometry Data System, VG Biotech, Fisons Instruments, Pointe Claire,
Quebec, Canada).
2.2.5. Differential Scanning Calorimeter

43 A 910 Differential Scanning Calorimeter module interfaced to a Du Pont
Series 99 Thermal Analyzer (Du Pont, Wilmington, DE, USA) was used for
indomethacin melting point and water content determinations.
2.2.6. Nuclear Magnetic Resonance Spectrometry
Proton NMR spectra were obtained on a Briiker WH-200 spectrometer (200
Mhz) in the Department of Chemistry, University of British Columbia, Vancouver,
BC. D6-dimethylsulfoxide was used as the dissolution solvent.
2.2.7. General Equipment
Vortex-type mixer (Vortex-GenieR), incubation oven (IsotempR 500 series),
AccumetR pH meter 915, Fisher Scientific Industries, Springfield, MA, USA; IEC
Model HN-SII centrifuge, Damon/IEC Division, Needham Hts. MA, USA;
rotating-type tube mixer (LabquakeR Tube Shaker, model 415-110), Labindustries,
Berkeley, CA, USA; infusion pump (Harward model 944), Harvard Apparatus,
Millis, MA, USA.
2.2.8. Physiological Monitoring

44 Polygraph recorder to monitor fetal arterial pressure, venous pressure,
amniotic fluid pressure, heart rate, and breathing rate (Sensormedics Inc., Anaheim,
CA, USA); Apple He computer and computer data acquisition system consisting of
Interactive Systems (Daisy Electronics, Newton Square, PA, USA), analog to digital
converter and clock card (Mountain Software, Scott's Valley, CA, USA);
Instrument Laboratory System 1306 pH/blood gas analyser (Instrument Laboratory
System, Lexington, MA, USA); Advanced Digimatic Osmometer 3D2 to measure
urine osmolality, Needham Heights, MA, USA; American Optical hand-held
refractometer to measure plasma protein concentration (American Optical); YSI
Glucose/Lactate Analyser (Yellow Springs Instruments, Yellow Springs, CO, USA)
to measure glucose and lactate concentrations; Nova 5 Electrolyte Analyser
(Newton, MA, USA) to measure urine electrolyte concentrations.
2.3. Preparation of Stock Solutions
2.3.1. Preparation of Drug Stock Solution
2.3.1.1 Indomethacin
Approximately 10 mg of indomethacin was accurately weighed, transfered to
a 50 mL volumetric flask and made up to volume with methanol. A 0.5 mL aliquot
of solution was diluted with water to volume in a 50 mL volumetric flask. One mL

45 of the latter solution was further diluted to volume with water in a 50 mL volumetric
flask to give a final working stock solution with a concentration of 0.04 |ig/mL.
Volumes of 25, 50, 200, 400, and 800 |iL were used to prepare the calibration curve.
2.3.2 Preparation of Internal Standard Solutions
2.3.2.1. Zomepirac Sodium
Approximately 27.04 mg of zomepirac sodium (equivalent to ~ 25 mg of
zomepirac free acid) was accurately weighed and transfered to a 250 mL volumetric
flask and made up to volume with water. A 1 mL aliquot of this solution was
transfered to a 100 mL volumetric flask and made up to volume with water to
produce a working stock solution with a concentration of 1000 ng/mL. A 100 |iL
aliquot of this solution was used in the assay.
2.3.2.2. Sulindac
Approximately 10 mg of sulindac was accurately weighed and transfered to a
50 mL volumetric flask and made up to volume with methanol. A 0.5 mL aliquot of
solution was diluted with water to volume in a 50 mL volumetric flask producing a

46 concentration of 2 jig/mL. A volume of either 100 |iL (200 ng) or 50 |iL (100 ng)
was used.
2.3.2.3 a-Methyl Indomethacin
Approximately 5 mg of alpha-methyl indomethacin was accurately weighed
and made up to 1 mL with methanol. An aliquot of 100 p:L was transfered to a 10
mL volumetric flask and made up to volume with methanol. A 100 uX aliquot of
the latter solution was transfered to another 10 mL volumetric flask and made to
volume with water to produce a working solution with a concentration of 500
ng/mL. A volume of 50 \ih (25 ng) was used in the assay.
2.3.2.4 Other Experimental Internal Standards
Working solutions of 2 |ig/mL were separately prepared for: 5-fluoro indole-
2-carboxylic acid, 5-fluoro DL tryptophan, 5-fluoro indole-3-acetic acid, flufenamic
acid, carprofen, acemetacin, phenylbutazone, and 5-fluoro-indomethacin.
2.3.3. Preparation of Reagent Solutions

47 Acetate buffer pH 5.0 was prepared according to British Pharmacopoeia
standards by dissolving 13.6 g of sodium acetate and 6 mL of glacial acetic acid in
sufficient water to produce 1000 mL. An aliquot of 2 mL (excess) was used in the
assay to produce an aqueous phase pH of ~ 5.00.
Acetate buffer pH 2.45, B.P., was prepared by mixing 200 mL of 1M
hydrochloric acid with 200 mL of 1 M sodium acetate and diluting to 1000 mL with
water. The pH of the final solution was adjusted to 2.45 with 1 M hydrochloric
acid.
Acetate buffer pH 3.5 was prepared by dissolving 25 g of ammonium acetate
in 25 mL of water and adding 38 mL of 7 N hydrochloric acid.
Acetate buffer pH 4.6 was prepared by dissolving 5.4 g of sodium acetate in
50 mL of water, adjusting to pH 4.6 with glacial acetic acid and diluting to 100 mL
with water.
Acetate buffer pH 6.0 was prepared by dissolving 100 g of ammonium
acetate in 300 mL of water, adjusting to pH 6.0 with 4.1 mL of glacial acetic acid
and diluting to 500 mL with water.
48 2.4. Sample Preparation
2.4.1. Analysis of Intact Indomethacin Levels
Ovine fetal fluids (plasma, urine, etc.), typically 0.1 mL, were pipeted into
clean 15 mL borosihcate Kimax culture tubes with polytetrafluoroethylene
(PTFE)-lined screw caps. To the biological fluid were added 50 fiL of internal
standard, cx-methyl indomethacin, and 2 mL of acetate buffer pH 5.0 and the
mixture adjusted to a final volume of 3.0 mL with water (final pH of the aqueous
phase ~ 5.00). The mixture was gently vortex-mixed and 5 mL of ethyl acetate was
added. The aqueous phase was extracted for 20 minutes on a rotary shaker. The
samples were then placed in a freezer at -5 °C for 10 minutes to facilitate breakage
of any emulsion formed in the extraction step. This was followed by centrifugation
for 10 minutes at 3000 g. The upper organic layer was transfered to clean 15 mL
tubes and evaporated to dryness in a water bath maintained at 37 °C under a gentle
stream of nitrogen gas. To the residue was added 100 |iL of toluene containing 8
|iL of MTBSTFA. This was vortex-mixed and placed in an oven at 60 °C for 50
minutes. The samples were allowed to cool to room temperature after which 200
|iL of toluene was further added, vortex-mixed, and transfered to automatic sampler
injection vials. Aliquots of 2 |iL were injected into the gas chromatograph.
Scheme-I summarises the sample preparation protocol.

49 Biological Sample
(fetal plasma, urine, amniotic, or tracheal fluid) 0.1-1.0 mL
Internal Standard (a-methyl indomethacin, 50 pL, 25 ng)
2.0 mL pH 5.0 Acetate Buffer +
Distilled Water, q.s. to 3.0 mL total aqueous phase +
5.0 mL Organic Solvent (Ethyl Acetate)
Mix 20 minutes on rotary shaker
Freeze at -5 C for 10 minutes
Centrifuge at 3000 g for 10 minutes
Aqueous Organic (Waste)
T Evaporate to dryness under
nitrogen gas at 37 C
i
Derivatise residue with MTBSTFA (8 pL) and toluene (92 uL) at 60°C for 50 minutes
i Cool to room temperature and add toluene
to obtain a final reconstitution volume of 300 uL
I 2.0 uL for injection
Scheme 1: Sample Preparation Procedure For Indomethacin

50 2.4.2. Analysis of Glucuronide Conjugates
The glucuronide conjugates in urine and amniotic fluid samples were
analysed by enzyme hydrolysis using ( -glucuronidase. The method for preparation
of samples is similar to that described above. About 200 mg of (3-glucuronidase
was accurately weighed and made to volume in a 25 mL volumetric flask with pH
5.00 acetate buffer, resulting in a concentration of 5000-Units/mL. Prior to
extraction with ethyl acetate, 0.5 mL of the enzyme solution was added to the
buffered urine samples, and incubated at 37°C for 3 hours. Due to limited volume
of urine samples, it was not possible to conduct a rigorous study to determine
optimum hydrolytic conditions (incubation time and amount of enzyme) with a
satisfactory "n" value. However, a study was carried out with these limitations
along with input from Bayne et al, 1981, and Vree et al, 1993 (Vree et al., 1993,
determined optimum conditions for indomethacin conjugates in urine to be 10,000
Units of enzyme activity and an incubation time of 2 hours, while the conditions
reported by Bayne et al., were 1500 Units and 30 minutes, respectively). The
concentration of glucuronide-conjugated indomethacin was calculated by
subtracting the non-conjugated indomethacin concentration (as determined by the
method described in section 2.4.1 above) from the samples measured following
hydrolysis.
51
2.5. Preparation of Calibration Curve
2.5.1. Calibration Curve with ex-Methyl Indomethacin
Serial quantities of the working indomethacin stock solution (1, 2, 8, 16, and
32 ng) were added to 0.1 mL of blank fetal sheep biological fluid (plasma, urine,
amniotic, or tracheal fluid). A 50 p:L aliquot of the internal standard (a-methyl
indomethacin) was added, and the solution made up to a fixed volume of 1 mL. The
samples were then extracted and derivatised as described previously. Determination
of indomethacin concentration was made by plotting the peak area ratios of the tert-
butyldimethylsilyl derivatives of indomethacin and a-methyl indomethacin against
the known amount of indomethacin added to each sample.
2.5.2. Calibration Curve with Zomepirac Sodium
Serial quantities of the working indomethacin stock solution (1, 2, 8, 16, and
32 ng) were added to 0.1 mL of blank fetal sheep biological fluid (plasma, urine,
amniotic or tracheal fluid). A 100 jiL aliquot of the internal standard (zomepirac
sodium) was added, and the solution made up to a fixed volume of 1 mL. The
samples were then extracted and derivatised as described previously. Determination

52 of indomethacin concentrations was made by plotting the peak area ratios of the
terf-butyldimethylsilyl derivatives of indomethacin and zomepirac against the
known amount of indomethacin added to each sample.
2.6. Chemistry
2.6.1. Derivatisation Procedures For Indomethacin
[1] Reaction with bis (trimethylsilyl') acetamide (BSA): Method of Plazonnet
and vanden Heuvel, 1977.
A specified amount of indomethacin (1 (J-g/mL) was evaporated to dryness
under oxygen-free nitrogen in a water bath maintained at 40 °C. The residue was
dissolved in 90 |iL of ethyl acetate and 10 |iL of BSA added. The contents were
derivatised for 15 min at 60 °C in a hot air oven, cooled to room temperature and
diluted to 1 mL with ethyl acetate before injecting 1 jiL into the GC.
[2] Reaction with N-methvl-N-(tert-butyldimethvlsilvl)-trifluoroacetamide
(MTBSTFA)
53
A methanolic solution of indomethacin (0.5 (Xg/mL) was evaporated to
dryness under oxygen-free nitrogen gas in a water bath maintained at 40 °C. The
residue was derivatised with 100 | i L of toluene containing 8 \iL of M T B S T F A at 60
°C for 30 minutes. The solution was cooled to room temperature and 1 or 2 | i L
injected into the G C .
[3] Reaction with pentafluorobenzyl bromide (PFBBr): Method of Sibeon et al.,
1978)
A methanolic solution of indomethacin (0.5 |i.g/mL) was evaporated to
dryness under oxygen-free nitrogen gas in a water bath maintained at 40 °C. To
each tube about 25 mg of potassium carbonate (catalyst) and 0.5 m L of a stock
solution of PFBBr (10 |J,L of supplied solution is made up to 10 mL with acetone)
were added. The reaction was carried out at 60 °C for 30 minutes. Excess
derivatising agent was removed using a stream of nitrogen gas at room temperature.
To each tube was then added 1 mL of distilled water and 1 mL of hexane. The
tubes were mixed on a shaker for 10 minutes and centrifuged at low speed for a
further 10 minutes. About 2 | i L of the upper hexane layer was injected into the G C .
[4] Reaction with a mixture of pentafluoropropanol in pentafluoropropionic
anhydride (PFP): Method of Evans. 1980.

54
A methanolic solution of indomethacin was evaporated to dryness under
oxygen-free nitrogen in a water bath maintained at 40 °C. To the residue was added
10 p:L of a mixture of 2,2,3,3,3,-pentafluoro-l-propanol in pentafluoropropionic
anhydride (1:4, v/v) and derivatised at 75 °C for 20 min. The solution was allowed
to cool to room temperature, evaporated to dryness under nitrogen, and reconstituted
in 10 (J.L of ethyl acetate and 1 or 2 \xL injected into the GC.
2.7. Optimisation of Assay Parameters
2.7.1. Derivatisation of Indomethacin
The following derivatisation parameters were examined:
1. Selection of a suitable derivatising agent: reaction with BSA, MTBSTFA,
PFBBr, or PFP (see section 2.6.1.).
2. Volume of derivatising agent-2 |iL to 100 (J,L.
3. Temperature of derivatisation-27 to 90 °C.
4. Time course of derivatisaton-10 min-1 hour.
5. Selection of derivatisation solvent (toluene, acetonitrile, etc.)
6. Reconstitution volume (0.1-1.0 mL)

55
2.7.2. Chromatography
1. Selection of a suitable internal standard (sulindac, indole derivatives, zomepirac,
carprofen, acemetacin, phenylbutazone, 5-fluoroindomethacin, a-methyl
indomethacin).
2. Injection mode (split vs splitless).
3. Injection port temperature (140-300 °C).
4. Oven temperature programming (various initial temperatures, ramp rates, and
final temperatures and times were examined).
5. Column (nonpolar vs polar, wide bore narrow bore).
6. Column head pressure (5-15 psi).
7. Injector port liner configuration (packed vs unpacked inlet liner).
8. Purge activation time (10-120 seconds).
9. Detector temperature (300-360 °C).
2.7.3. Extraction
1. Solvent for extraction (ethyl acetate, hexane, hexane-ethyl acetate mixtures,
toluene, toluene-triethylamine (0.0125M) mixtures, hexane-isopropylalcohol
(10%) mixtures, diethyl ether, dichloromethane).

5 6
2. Volume of solvent (1-5 mL).
3. pH of extraction medium (pH 2-6.00, acetate buffers).
4. Time of extraction (5-60 minutes).
2.7.4. Validation
2.7.4.1. Extraction Recovery Studies
Extraction recoveries of indomethacin were determined at five concentration
points, i.e., 1, 2, 8, 16, and 32 ng/ml. Two groups of samples were used in this
study, namely the test and the control group. Samples in both groups contained
blank ovine fetal biological matrix (plasma, urine, amniotic or tracheal fluid), and
the internal standard, a-methyl indomethacin. Only samples from the test group
were spiked with IND to produce final concentrations of 1, 2, 8, 16, and 32 ng/ml.
Both test and control group samples were subjected to the liquid-liquid extraction
procedure (see section 2.4.1.) after which, aliquots of indomethacin, prepared in
methanol, were added to the control samples to produce concentrations of 1, 2, 8,
16, and 32 ng/ml. Control and test group samples were dried under nitrogen,
derivatised with MTBSTFA, reconstituted with toluene, and chromatographed as
described earlier (section 2.4.1.). Extraction recovery at each concentration point

57 was calculated as the ratio of peak area counts observed with test (extracted) to that
in control (unextracted) and expressed in percentage.
2.7.4.2. Inter-day & Intra-day Variability
Intra-day and inter-day variability were determined at five concentration
points, namely, 1, 2, 8, 16, and 32 ng/ml. For evaluating intra-day variability, three
calibration curves were prepared on the same day, and for inter-day variability,
calibration curves were prepared on three separate days (values are reported as %
C.V.).
2.7.4.3. Linearity
The linearity of the calibration curves was investigated over the
concentration range of 1-500 ng/mL for plasma and urine samples.
2.7.4.4. Stability Studies
Studies were performed periodically to assess the stability of the samples
during storage and analysis. Freezer storage stability was determined at one
concentration point (8 ng/ml): a batch of biological matrices (plasma and urine)

58 were spiked with a known amount of indomethacin, stored at - 2 0 ° C , removed
periodically (over 14 months) and analysed. In order to assess the stability of
indomethacin during freeze-thaw cycles, blank biological samples (plasma) were
spiked with indomethacin (8 ng/ml), frozen at standard freezer temperatures (-
20°C) , and thawed at room temperature on the bench-top for four consecutive
cycles, and analysed. A bench-top stability study (ambient conditions) was
performed which involved spiking plasma and urine samples with a known amount
of indomethacin, and allowing them to stand at room temperature for 0, 12, and 24
h. At the end of each study, the internal standard, oc-methyl indomethacin, was
added and the samples extracted and analysed as described above. The stability of
indomethacin in acidified biological matrix (pH 5.00) was investigated by adding an
excess of pH 5.00 acetate buffer to the biological fluid (plasma/urine), spiking with
a known amount of indomethacin and allowing the samples to remain on the bench-
top for 0, 6, 12, and 24 h. The internal standard, a-methyl indomethacin, was then
added and the samples processed as before. Finally, the stability of processed
samples on the G C autosampler tray was investigated by repeatedly injecting the
sample vials at 24 h intervals for ten days. Stability studies were also performed on
the indomethacin formulation used in the fetal infusion studies, at room temperature
and at 4 °C.
2.8. Animal Experiments

59
2.8.1. Animal Handling & Surgical Preparation.
Ten time dated pregnant sheep of Dorset/Suffolk breeds were used. These
pregnant ewes were kept in the animal unit at the Children's Variety Research
Center in groups of two or more in different but adjacent pens in full view of one
another. The animals were placed on a standard diet and water. Ethical approval
for these studies was obtained from the UBC Animal Care Committee and the
guidelines of the Canadian Council on Animal Care were followed.
The sheep were operated on between 124 and 125 days of gestation (term =
145 days). Atropine (6 mg) was administered as an intravenous bolus to control
salivation followed by (-15 min later) induction of anaesthesia with sodium
pentothal (1 g). The ewes were intubated with an endotracheal tube and anaesthesia
maintained using a mixture of halothane (1-2%), nitrous oxide (60%), and oxygen.
The abdominal area was shaved and the surgical area swabbed with a 10%
povidone-iodine topical solution following which the animal was draped with sterile
sheets. Following a midline abdominal incision, access to the fetus was gained
through an incision of the uterine wall free of placental cotyledons and major blood
vessels. The fetal hind limbs were extracted and polyvinyl catheters were placed in
the inferior vena cava and descending aorta through the femoral and tarsal vessels,
60
respectively. The fetal bladder was cannulated through a suprapubic incision,
followed by non-occlusive catheterisation of the common umbilical vein at the
umbilicus. Two catheters were placed in the amniotic cavity and anchored to the
abdominal skin of the fetus. A carotid artery was also catheterised, via a separate
uterine incision, and a non-occlusive catheter was inserted into the trachea, via an
incision below the larynx. A catheter was also placed in the amniotic cavity, and
anchored to the skin on the neck. The hysterotomy and laparotomy incisions were
then closed. The maternal inferior vena cava and descending aorta were cannulated
via maternal femoral vessels. All catheters were passed subcutaneously to a small
incision in the maternal abdominal wall on the left flank where they exited. They
were stored in a denim pouch attached to the flank. Postoperatively, ampicillin (500
mg) was adminsitered as an intramuscular prophylactic antibiotic for three days to
the ewe, and ampicillin (500 mg) intra-amniotically to the fetus at the time of
surgery and daily into the amniotic fluid for the duration of the preparation.
2.8.2. Recording and Monitoring Procedures
The analog signals were also processed by an on-line computerised data
acquisition system, which stored one minute averages of the variables on floppy
diskettes. Fetal arterial pressure, amniotic fluid pressure, heart rate, and fetal
tracheal pressure were continuously monitored using a polygraph recorder
(Sensormedics Inc.). Fetal arterial and venous pressures were adjusted to zero

61
reference by subtracting amniotic fluid pressure continuously using the computer.
Initial studies involved determination of urinary flow rate twice daily using an
intermittant measurement system. In later studies, fetal urine flow rate was
measured continuously by the computer by means of a bladder catheter which
drained by gravity into a sterile reservoir, the hydrostatic pressure of which was
monitored by the computer. When the preset pressure was exceeded, a calibrated
peristaltic pump was activated to pump urine from the reservoir into the amniotic
cavity via an amniotic catheter. The volume pumped each minute was stored on
diskette and provided a measurement of urine flow. Fetal arterial blood (0.7 mL)
samples were collected for measuring pH, pC02, p02, HC0 3, and base excess at
39.5 °C (Instrument Laboratory System 1306 pH/Blood Gas Analyser, Lexington,
Mass., USA). Glucose and lactate concentrations in fetal blood samples were also
determined using a YSI 2300 Glucose/Lactate Analyser. Hematocrit was estimated
using a micro-capillary centrifuge. Blood 0 2 saturation and hemoglobin
concentrations were determined using an OSM-2 Hemoximeter. Plasma protein
concentration was determined using an American Optical hand-held refractometer.
2.8.3. Determination of Organ Blood Flows
Fetal organ blood flows were determined by injecting 15+3 \im diameter
microspheres containing either 153Gd, 85Sr, 5 1Cr, 46Sc, or 9 5Nb radioisotopes

62 incorporated in their structure and suspended in 10% dextran. A different isotope
was used on each day of the 5-day protocol. Before injection, the microspheres
were mixed and placed in an ultrasonic bath for 5 min to minimize aggregation of
the spheres. Immediately after collecting the second (pm) sample of the day, 0.5
mL of the microsphere solution containing 1.2 x 106 microspheres was injected via
the fetal tarsal venous catheter and the catheter flushed with 3 mL of heparinised
saline. Lower and upper body reference blood samples via the fetal aortic and
carotid catheters were obtained during three minutes, begining about 30 sec prior to
injecting microspheres, at a 2.2 mL/min withdrawal rate using a Harvard pump.
Animals were euthanised after each experiment with pentobarbital sodium (100
mg/Kg) and the operated fetus removed and weighed. Fetal tissues and organs of
interest were obtained at autopsy, weighed and carbonised in an oven at 300°C for
3-5 days. The gamma emission generated by the radioactive microspheres was
measured from the fetal organs (kidneys, brain, adrenals, bone, liver, placenta,
amnion, chorion, gut, atria, ventricles, spleen, fetal aortic and carotid reference
samples) using a multi-channel gamma counter, isotope separation being achieved
using computer software.
2.8.4. Experiment Protocol For Fetal Infusion Studies

63
At least 24 h before each experiment, the ewe was placed in an experimental
pen in full view of companion ewes with access to standard diet and water. Each
experiment was composed of five days with the first day being the control day when
no drug was given. Indomethacin in a solution of 1.1% ethanol and 0.75% sodium
bicarbonate in normal saline was infused into the fetal vein at a dose of 0.0025 (high
dose) or 0.0006 (low dose) mg/Kg/min (2 mL/h) or vehicle alone (control) on days
2 through 4. The infusion was terminated on day 5 and the fetus also monitored
during this 24 h recovery period. Samples (2 mL) of fetal arterial blood, umbilical
venous blood, amniotic and tracheal fluids, and fetal urine were collected twice
daily at six hour intervals and stored at -20 °C pending assay. Blood samples were
collected in heparinised VacutainerR collection tubes, centrifuged at 3000 g for 10
minutes at -10 °C and the plasma transfered into PyrexR 15 mL culture glass tubes
for storage and analysis. Withdrawn fetal blood was promptly replaced with an
equal volume of heparinised drug-free maternal blood via the tarsal vein catheter.
2.9. Data Analysis
2.9.1. Pharmacokinetic Calculations
[1] Fetal total body clearance (Cltb) of indomethacin was estimated as:
Cltb = V C ss
64 where k<j was the infusion rate and C s s the apparent fetal arterial steady-state
indomethacin concentration.
[2] Placental clearance (Clp) was estimated as:
Clp — Qum X (Cf a-C u m)/Cf a
where Q u m is the umbilical blood flow rate, C f a the fetal femoral arterial
indomethacin concentration, and Cm the umbilical venous indomethacin
concentration at apparent steady state.
[3] Fetal non-placental indomethacin clearance (Clfo) was then calculated as:
Clfo = Cltb-Clp
[4] Renal clearance (Clr) was estimated by plotting the average urinary excretion
rate versus the drug concentration at the midpoint of the collection interval and
fitting the least squares straight line forced through the origin. The slope of the line
provided the renal clearance value in mL/min.
2.9.2. Statistical Calculations

65 Statistical evaluations were performed on analytical, physiological, and
pharmacokinetic parameters using established statistical tests as outlined in each
section. Data are expressed as the mean ± S.E.M. or 1 S.D as indicated. Coefficient
of variation is reported in percentage. Linear regression statistics are presented for
analytical data, and the paired Mest was used to determine whether fetal umbilical
venous and femoral arterial indomethacin concentrations were significantly
different. A significance level of P<0.05 was used.

66
3. RESULTS
3.1. Development of a capillary GC-ECD method for indomethacin.
3.1.1. Purity assessment of indomethacin
A proton NMR spectrum of indomethacin in deuterated dimethylsulfoxide
was taken at 200 Mhz (Figure 5). The spectrum was compared to a spectrum
obtained with an authentic (Merck standard) sample (O'Brien et al., 1984). The
chemical shift values of the test indomethacin sample (Table 3) compare well with
Merck standard indomethacin sample.
A differential scanning calorimetry (DSC) analysis of indomethacin is
illustrated in Figure 6. Indomethacin was observed to melt at a temperature of
162°C. The melting point of indomethacin has been reported to be 153-154 °C
(Shen et al., 1963). However, official monographs indicate the melting point to be
155 and 162 °C for two polymorphic forms of indomethacin (NF XIII), while the
BP (1980) specifies a m.p. of 158-162°C. There are two crystalline forms of
indomethacin, Form I which melts at 160-162°C, and Form II which melts at 153-
155°C, the former being more stable than the latter (O'Brien et al., 1984).

67
PRA12 HI FT HUN IN DMSO-06 WITH EXPANS R. KRISHNA
HA060S.11S AU PR06: XOO.AU
DATE 6-5-93 SF SY 01 SI TD SW HZ/PT PH RD AO RG NS TE
200.133 80.0 4390.000
32768 32768 4000.000
.244 0.0 0.0 4.096 10 32
298 FH 5000 02 4080.000 DP 63L PO LB GB CX CY F l F2
.300
. 100 25.00 15.00 U.500P -l.OOOP
HZ/CM 100.063 PPH/CH .500 SR 3290.15
' I ' 9.0 11.0 10.0 6.0 5.0
PPM
Figure 5a: NMR spectrum of indomethacin in DMSO
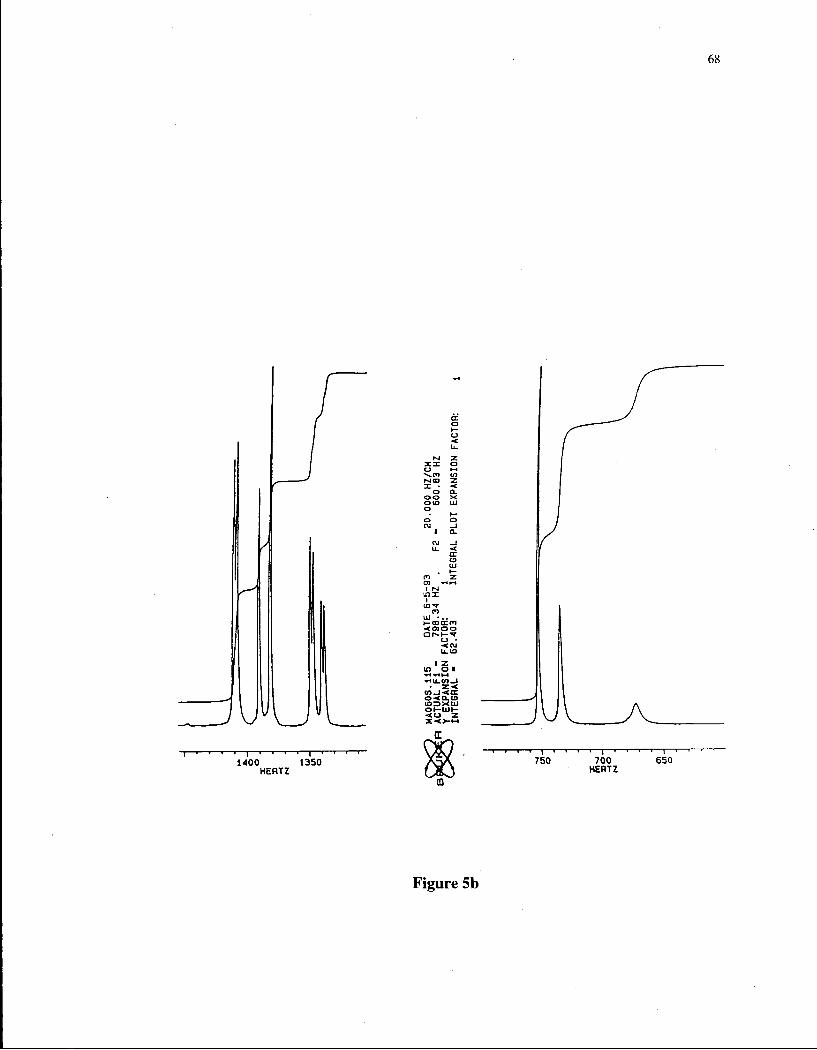
68
Figure 5b

69
Table 3: Chemical shift values of indomethacin and their respective group
assignment
Chemical Shift (ppm)
Indomethacin Sigma Chemical Co.
Indomethacin Merck Standard*
Assignment
2.2 (s) 2.22 (s) 2-CH3
3.62 (s) 3.67 (s) 3-CH2CO2H
3.78 (s) 3.74 (s) OCH3
6.7-6.9 (m) 6.55-7.10 (m) H4, H 6 , H 7
7.6-7.8 (m) 7.45-7.80 (m) c i - ( yi
+ Proton NMR spectrum of Indomethacin Merck Standard 6375-66-1 (Adapted
from O'Brien et al, 1984).

70
u o so
(a)
(b)
Temperature (°C) ->
Figure 6: DSC scan of indomethacin: (a) open pan, and (b) closed pan
methods

71
The LC/MS/MS spectra of indomethacin is illustrated in Figure 7. The
salient features of the spectrum are: m/z 139-141 due to the /?-chlorobenzoyl group,
and molecular ion at m/z 358.
3.1.2. Optimisation of Derivatisation
Derivatising Agents
Indomethacin was derivatised with four different derivatising reagents to
determine the most suitable agent with respect to reaction time, chemical safety of
the agent, completeness of the reaction, chromatographic behaviour of the resulting
derivative, as well as peak geometry and shape. The type of reactions selected were
(I) silylation (with BSA, MTBSTFA), and (ii) fluorination (PFBBr, PFP).
The chromatographic behaviour of the resulting derivatives following
derivatisation with BSA, MTBSTFA, and PFBBr is illustrated in Figures 8 and 9.
Derivatisation with PFP was incomplete and was, therefore, not pursued further.
The silylation reactions were much easier to perform. Peak response was best with
MTBSTFA and PFBBr. Derivatisation with PFBBr afforded compounds with high
volatility and short retention times (Figure 9). The response was slightly greater
than that obtained using MTBSTFA, however, the procedure was comparatively
more cumbersome and time consuming involving the use of a catalyst. Overall, the

72
312 357
CH 3 0
139
H
201 I 293 311
358
357J
J. 100 120 140 160 ISO ZOO 220 240 260 280 300 320 340 360 380 400 420 440 460 480 500
Figure 7: LC/MS/MS spectrum of indomethacin

73
Figure 8: GC-ECD chromatograms of indomethacin derivatised by (a) BSA,
and (b) MTBSTFA.

74
Retention time (minutes)
Figure 9: GC-ECD chromatogram of indomethacin derivatised by PFBBr.
75 reaction with MTBSTFA was quick, safe, complete and produced peaks of superior
geometrical shape and integrity.
Reaction Conditions
The effect of temperature on the derivatisation reaction was examined, from
room temperature (27°C) to 90°C and is shown in Figure 10. Maximum variability
was noted with lower temperatures (27°C, 45°C). Area counts were maximal at
60°C and did not increase following any further increase in temperature, and thus
this was chosen as the optimal temperature for derivatisation.
Different reaction times were also examined, from 10 min to 60 min, at a
constant temperature of 60°C (Figure 11). Mean area counts increased as
derivatisation time was prolonged from 10 min to an hour, with a plateau appearing
at 50 minutes. Keeping sample preparation time in mind as well as noting the least
variability at 50 minutes, the reaction time was set at 50 min.
Various concentrations of MTBSTFA were also examined, i.e., from 2% to
100% solution, the solvent being toluene (from 2 \\L in 100 |iL toluene to 100 |iL
MTBSTFA). The area counts did not differ significantly over the volume range,
however, an effect on peak height was observed. The optimal volume was

76
60
20 40 60 80 100
Temperature of Derivatisation (degree C)
Figure 10: Determination of optimum derivatising temperature for
indomethacin with MTBSTFA (data are mean values ± 1 S.D., n=4).

77
Reaction Time (Minutes)
Figure 11: Determination of optimum reaction time between indomethacin
and MTBSTFA (data are mean values ± 1 S.D., n=4).

78
determined as 8 fiL MTBSTFA in 100 |0,L toluene (8%), since this afforded the
greatest peak response in terms of peak height.
3.1.3. Selection of Internal Standards
Ideally, the internal standard should possess close structural resemblance to
the analyte, have similar chromatographic behaviour, and elute in a region free from
endogenous interference. Several compounds were screened, viz., sulindac, 5-
fluoro indole 2 carboxylic acid, 5-fluoro dl tryptophan, 5-fluoro indole 3 acetic acid,
zomepirac, acemetacin, carprofen, 5-fluoroindomethacin, and oc-methyl
indomethacin (Figure 12).
The indole analogs (Figure 12) are chemicals of fairly low molecular weight
and did not appear on the chromatogram when derivatised with MTBSTFA. When
these same compounds were derivatised with PFBBr, retention times of the
resulting derivatives were very short with interfering bridged peaks as shown in
Figure 13a. The indomethacin analogs, namely, 5-Fluoroindomethacin and a-
methyl indomethacin produced excellent peaks with MTBSTFA as shown in Figure
13b. Sulindac produced a satisfactory peak when derivatised with either MTBSTFA
or PFBBr with good retention times as well as pilot calibration curves yielding an
r>0.999. However, an unidentified peak of significant magnitude eluted with

79
CH2C00H
5-Fluoro Indole 3-acetic acid
1 COOH
5-Fluoro Indole 2 Carboxylic Acid
• CH2-CH-COOH I
NH2
5-Fluoro DL Tryptophan
Carprofen
C H 3
< N
CH2COOH
\ C H 3
C=0
[6 CL
Zomepirac
•CH2COOH
I
C=0
CL
5-Fluoroindomethacin
CH3O
9H3 CH-COOH
I c = o
CL
Alpha-Methyl Indomethacin
CH
SO I
C H 3
Sulindac
Figure 12: Chemical structures of tested internal standards
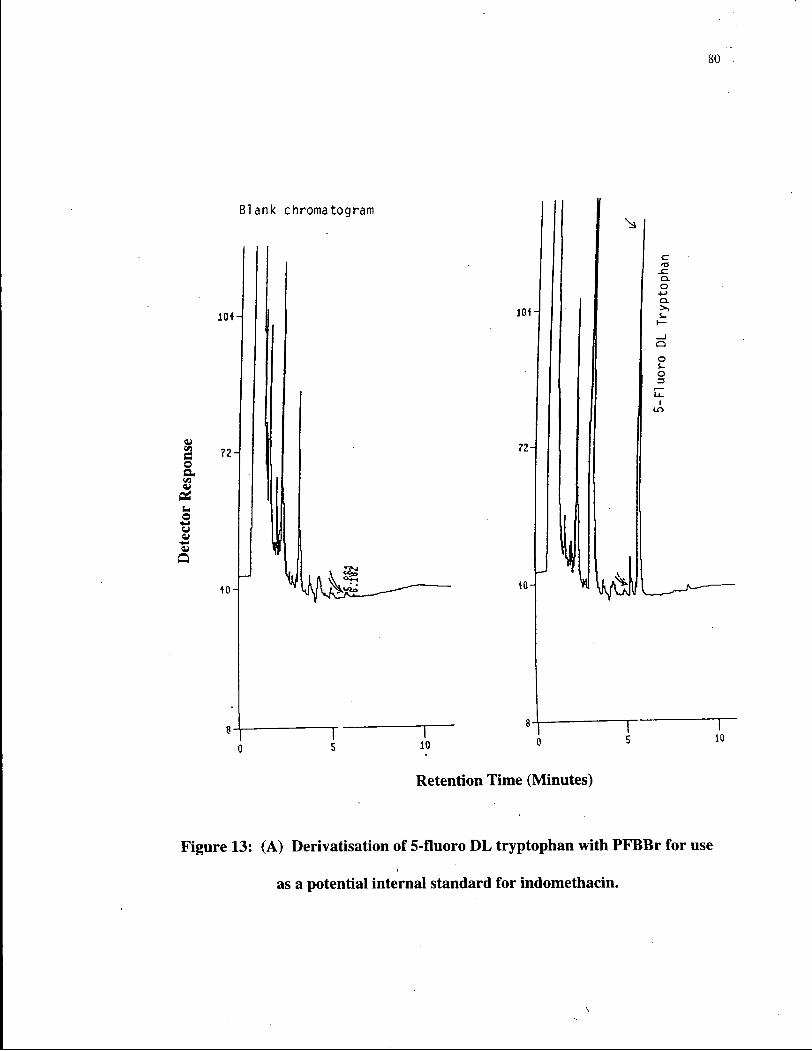
80
Blank chromatogram
Vi tt © a Vi
<u 04 u o
u
Q
?2 H
*0 L v ^l
10
10H
72
J 40-
c O-
o 4-> C L >>
s_
o s-o 3
Retention Time (Minutes)
10
Figure 13: (A) Derivatisation of 5-fluoro DL tryptophan with PFBBr for use
as a potential internal standard for indomethacin.

81
Figure 13: (B) GC-ECD chromatograms of indomethacin analogs, 5-
fluoroindomethacin, and a-methyl indomethacin, derivatised with MTBSTFA.

82
sulindac. Association of this peak with sulindac was confirmed by injecting
indomethacin alone, indomethacin and sulindac, sulindac alone, and blank plasma
(Figure 14). Oven temperature programming changes did not affect the presence of
peak "X", nor did recrystallising sulindac help. Figure 15 illustrates the DSC scan
of sulindac and its recrystallised form. It is speculated that sulindac may be oxidised
to a sulphone in the injection port, and this might have eluted as peak 'X' on the
chromatogram. Because of this additional peak we were unable to use this
compound as an internal standard for this assay.
Zomepirac is closely related to indomethacin and provided a fairly good
response with MTBSTFA (Figure 16). However, an extraneous peak in
experimental fetal plasma samples co-eluted with it, precluding the use of this
compound as the internal standard. This interference was not observed in fetal or
maternal plasma samples stored beyond two years (blank samples), amniotic and
tracheal fluids, or in fetal or maternal urine samples. Following analysis of samples
collected from the present infusion studies, however, the interference was detected,
leading to a re-examination of chromatographic conditions (oven temperature
programming, column stationary phase [polar/nonpolar], column diameter
[wide/narrow bore]), use of PFBBr as a potential derivatising agent, as well as
screening of additional internal standards.

83
Figure 14: Illustration of a decomposition peak "X" associated with sulindac.
Chromatograms indicate: (1) indomethacin and sulindac, (2) sulindac only,
and (3) blank.

84
Sulindac
recrystallised sulindai
(open pan)
! ; . ;L I. recrystallised sulindac
*P~^ (closed pan)
Figure 15: DSC scan of sulindac and recrystallised sulindac.
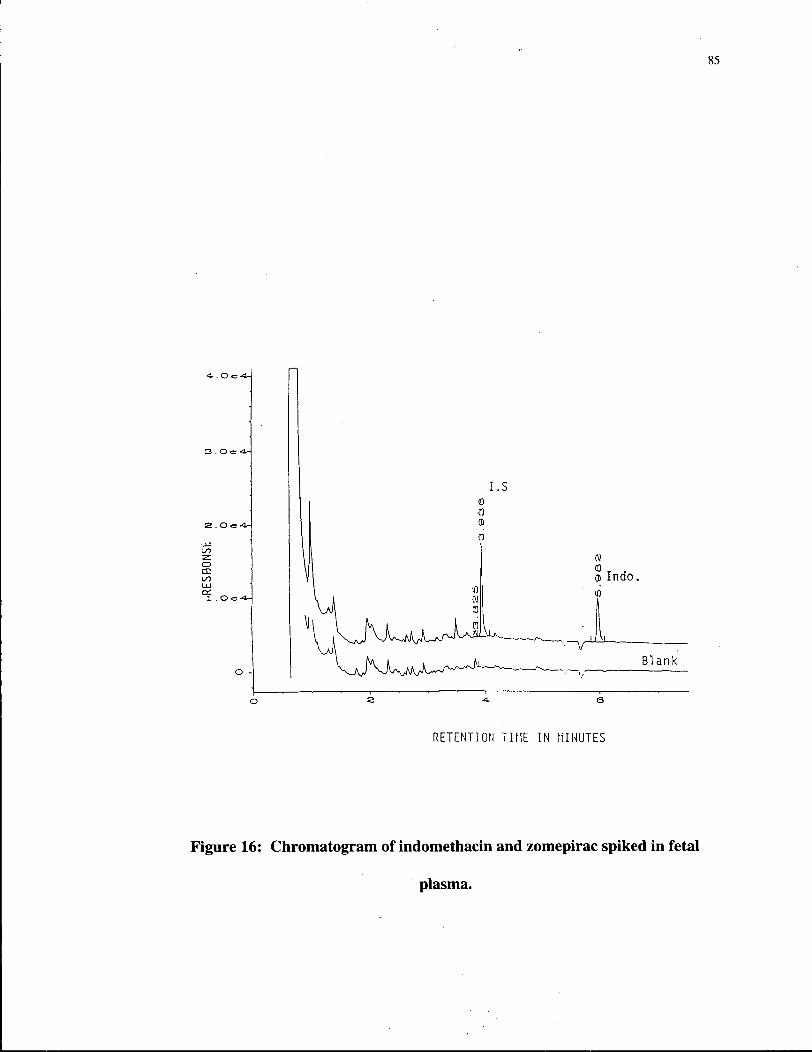
85
3 . O <= <A
•SI
o CE 00
1 .
N
Q Indo.
Blank
RETENTION TIME IN MINUTES
Figure 16: Chromatogram of indomethacin and zomepirac spiked in fetal
plasma.

86
a-methyl indomethacin (Figure 17), a generous gift of Merck Frosst Inc,
provided all the qualities required for an ideal internal standard, i.e., it was a very
close structural analog of indomethacin, eluted close to the analyte in a region free
from endogenous interference (Figure 13B), and produced a response factor of
-1.00 at a concentration equal to that of indomethacin. On this basis it was chosen
as the internal standard for all further studies.
3.1.4. Optimisation of G C conditions
In order to obtain maximal sensitivity, the splitless mode of injection
(suitable for trace level analyses) was used throughout. Injection port temperature is
another critical parameter since it influences greatly the thermal stability of the
derivatised compound as well as the degree of drug transfer onto the head of the
column. Hence, the effect of various temperatures (140-300 °C) on indomethacin's
response were examined. This evaluation was conducted using a low (20 ng/mL)
and a high (100 ng/mL) sample concentration of indomethacin. As illustrated in
Figure 18, maximal absolute area counts were obtained at injection port
temperatures in the range 180-200 °C. A drastic decline in area counts was
observed when the temperature was increased from 200-300 °C. The profile was
similar at both concentrations likely indicating thermal decomposition at higher

87
C H 3 0 ^ ^ C H 2 C O O H
B
c=o
Indomethacin
CI
C H 3
^ C H - C O O H
a-methyl indomethacin (Internal Standard)
Figure 17: Chemical structures of indomethacin and a-methyl indomethacin.

88
1500
0) 375 h
100 175 250 325 400
Injection Port Temperature (degree C)
Figure 18A: Effect of injection port temperature on the peak area counts of
(A) 20 ng/mL, and (B) 100 ng/mL indomethacin concentrations (n=4).

89
8000
Injection Port Temperature (degree C)
Figure 18B

90
temperatures. While a temperature of 180 °C resulted in the highest response the
chromatogram contained many peaks from endogenous compounds. The
chromatograms, however, were much cleaner at 200 °C and therefore, this
temperature was selected for use in the assay. Figure 19 illustrates the effect of
various initial column temperatures on the retention time of indomethacin at a
constant programming rate of 8 °C/min. An initial column temperature of 210 °C
and a final temperature of 300 °C with a programming rate of 40 °C/min provided
optimal resolution, peak geometry, run times, and response and were therefore,
chosen for the final assay.
Various column types were also investigated, viz., an Ultra-2 wide bore non-
polar column [stationary phase: 5% phenylmethylsilicone], Ultra-2 narrow bore
column, and a DB-1701 polar column [stationary phase: methyl (7% phenyl, 7%
cyanopropyl) silicone]. Use of the DB 1701 column was observed to be more
appropriate with PFBBr derivatised samples, and did not appear to be useful for
MTBSTFA derivatised samples as illustrated in Figure 21. Representative
chromatograms obtained for the narrow bore Ultra-2 column are illustrated in
Figure 20 and for the wide bore column in Figures 13B and 16. While both Ultra-2
non-polar columns provided rapid run times and excellent chromatography, the
wide-bore column allows for a greater volume of sample to be injected (Figures
13B, 16) and was therefore, selected for use in the assay.

91
Figure 19: Effect of various initial column temperatures on peak retention
times.

92
Figure 20: GC-ECD chromatograms of indomethacin and zomepirac using a
narrow bore fused silica Ultra-2 column.

Figure 21: GC-ECD chromatogram of indomethacin and zomepirac using
narrow bore DB-1701 column.

94
The time delay following injection for inlet purging to occur is critical in
determining the degree of sample transfer onto the column and, therefore, needs to
be optimised. To examine this, purge delay times ranging from 10-120 seconds
were examined (Figure 22). A plateau was reached at 40-120 seconds. Therefore, a
purge delay time of 0.75 min was chosen.
Various detector temperatures were also examined, ranging from 300-360 °C
(Figure 23). Detector temperature had no effect on overall indomethacin peak area
counts over the range studied so 330 °C was selected, since at lower temperatures
the ability to maintain an uncontaminated detector was in question. There was no
significant effect of make-up gas (argon-methane; 95/5) flow rate on the detector
response, therefore a flow rate of 65 mL/min was used.
Various column head pressures (5-15 psi) were also investigated (Figures 24
and 25). Maximal peak area counts and area ratios were noted at a column head
pressure of 10 psi. Furthermore, as column head pressure was increased from 5 to
15 psi, there was a proportionate fall in retention time and peak width. Hence, a
column head pressure of 10 psi was chosen since this afforded maximum peak area
counts and intermediate peak width and peak retention time.

95
Figure 22: Effect of purge delay times on the peak area counts of indomethacin
tBDMS derivative (n=4).

96
5000
4000
3000 h
2000
1000 h
250 300 350 400
Detector Temperature (degree C)
Figure 23: Effect of various detector temperatures on the peak area counts of
indomethacin tBDMS derivative (n=4).
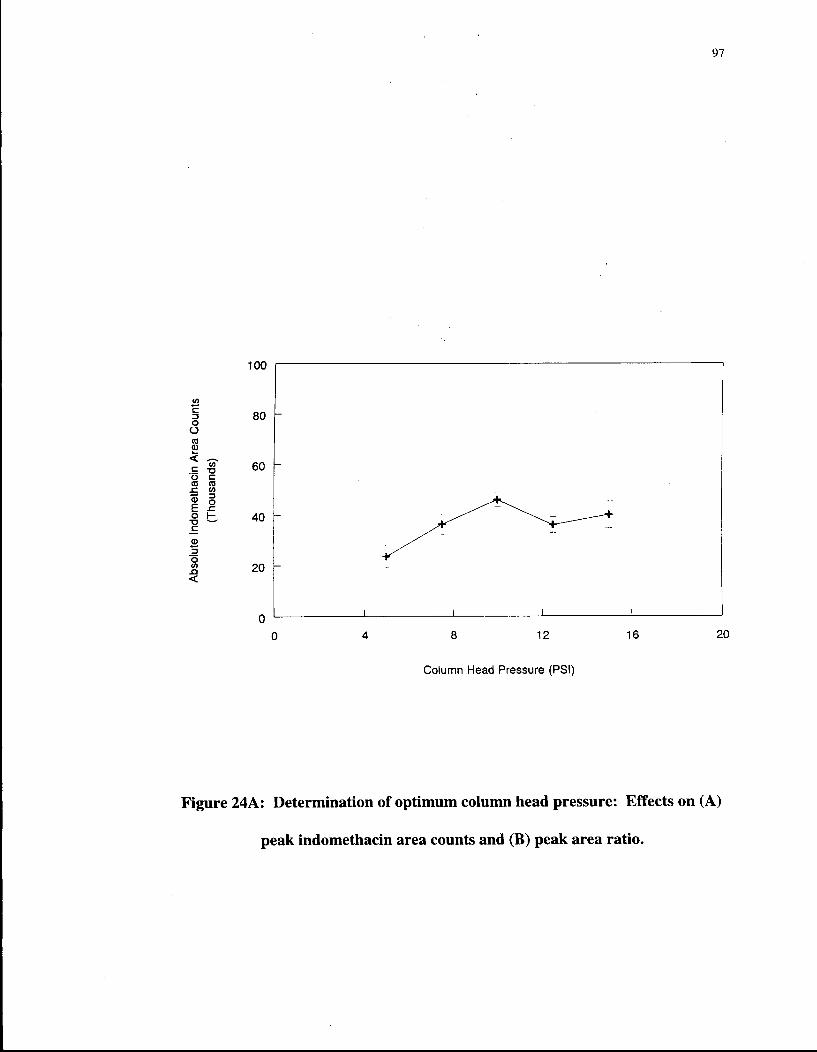
Figure 24A: Determination of optimum column head pressure: Effects on (A)
peak indomethacin area counts and (B) peak area ratio.

Figure 24B

99
Figure 25: Determination of optimal column head pressure with reference to
peak retention time (A), and peak width (B).

100'
1.00
0.80 h
0.20 h
0 4 8 12 16 20
Column Head Pressure (PSI)
Figure 25B

101
3.1.5. Optimisation of drug extraction
The extraction efficiency of various organic solvents was examined by
comparing the ratio of extracted samples/control samples following extraction from
a model biological fluid matrix (tracheal fluid) using acetate buffer pH 5.00 (Figure
26 and Table 4). Of the solvents examined, only ethyl acetate and dichloromethane
were able to extract 1 ng indomethacin effectively. Solvent mixtures were also
examined, namely, (a) toluene-TEA (0.0125M), (b) hexane-IPA (10%), and (c)
hexane-ethyl acetate (1:4, 2:3, 3:2, 4:1). As expected, the addition of triethylamine
(TEA) to toluene reduced extraction efficiency drastically. This is contrast to the
fact that addition of TEA to toluene markedly improves the recovery of basic
compounds (Wright, 1992). While the addition of isopropyl alcohol (IPA, 10%) to
hexane improved the overall extractability of indomethacin recoveries were still not
satisfactory with this solvent system. The addition of hexane to ethyl acetate was
observed to reduce the recovery of indomethacin (Table 4). For ethyl acetate (EA),
extraction efficiency improved with increasing volume (Figure 27), but increasing
solvent volume had no effect with dichloromethane. The recoveries following
extraction with 2 mL EA, 4 mL EA, and 5 mL EA, were 53.66 ± 4.32%, 73.01 ±
2.76%, and 84.59 ± 5.63%, respectively (Table 4). Based on these observations,
ethyl acetate, in a volume of 5 mL, was selected for use in the assay since maximal
recovery and extraction efficiency were noted at these conditions.
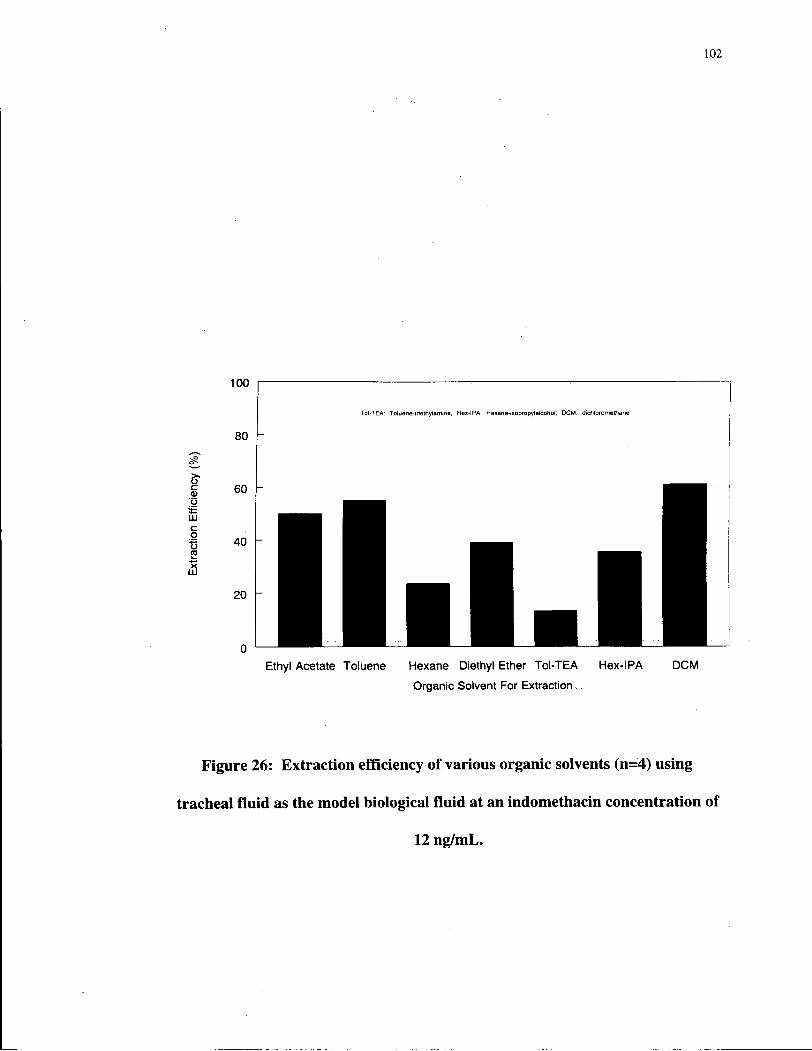
102
Figure 26: Extraction efficiency of various organic solvents (n=4) using
tracheal fluid as the model biological fluid at an indomethacin concentration of
12 ng/mL.
103
Helleberg (1976), and Ou and Frawley (1984) suggested that attainment and
maintenance of an aqueous phase pH of 5.00 was essential for optimal recovery of
indomethacin. To examine this, a series of acetate buffers were prepared in the pH
range 2-6 (BP, 1988). As shown in Figure 28, attainment of pH 5.00 was essential
for optimal extraction; a lower pH reduced extraction efficiency considerably. This
pH aggrees well with the pKa of 4.5-4.7 for indomethacin.
The effect of extraction times ranging from 5-60 min on indomethacin
response were also examined (Figure 29). The highest variability was observed at 5
min and the lowest at 20 min. Maximal area counts were also observed at 20 min
and hence an extraction time of 20 minutes was chosen.

104
Table 4: Extraction efficiency (%) of organic solvents used to extract
indomethacin at different concentrations using tracheal fluid as the
model biological fluid.
Solvent Volume Indomethacin Concentration [ng/mL] [mL] 1 6 12
Ethyl Acetate 2 58.43 52.56 50.00 Toluene 2 - 52.56 55.25 Hexane 2 - 20.26 23.57
Ethyl Acetate 4 75.90 70.38 72.75 Diethyl Ether 2 - 49.66 39.05
Toluene-TEA* 2 - 16.90 13.30 Hexane-IPA** 2 - 36.25 35.66
Dichloromethane 2 80.72 55.79 61.11 Ethyl Acetate 5 91.04 80.60 82.13
Dichloromethane 4 - 55.94 61.58 * Triethylamine (0:0125 M) ** Isopropyl alcohol (10%)

105
2 4 5
Volume of Ethyl Acetate (mL)
Figure 27: Effect of solvent volume on the extraction efficiency of ethyl
acetate.
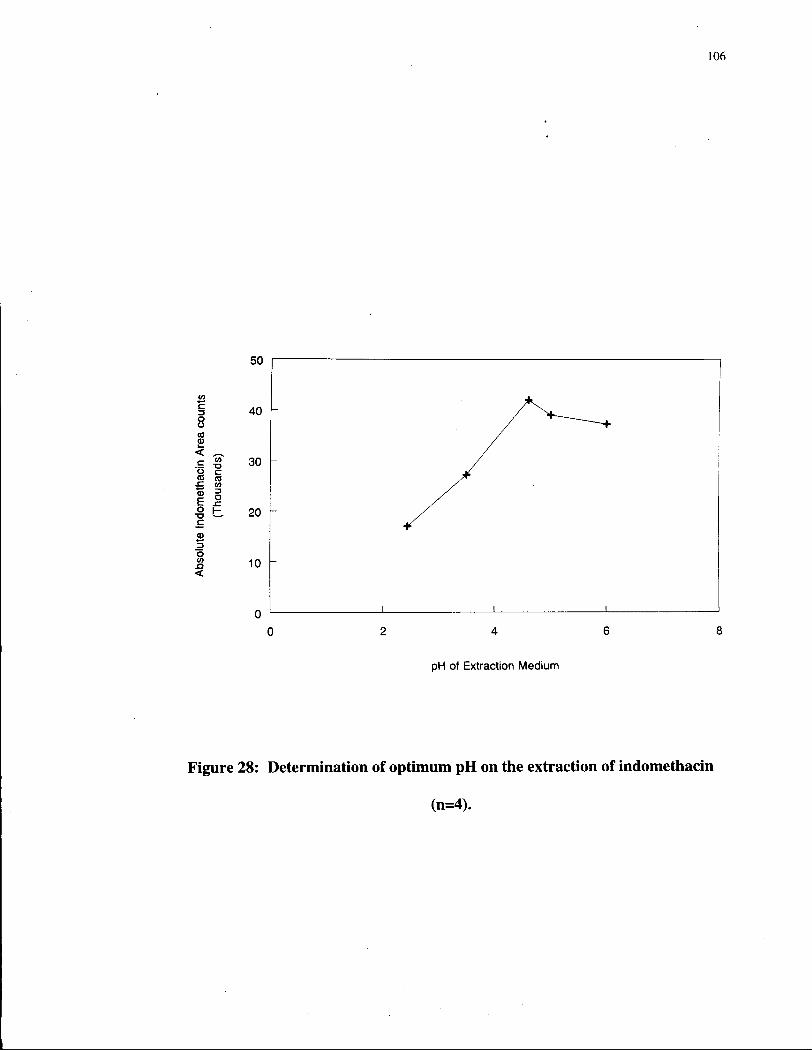
106
pH of Extraction Medium
Figure 28: Determination of optimum pH on the extraction of indomethacin
(n=4).

107
Figure 29: Determination of optimum extraction time for indomethacin from
tracheal fluid matrix using ethyl acetate at pH 5.00 (data are mean ± 1 S.D.,
n=4).

108
3.1.6. Gas chromatography-Mass spectrometry (GC-MS)
GC-MS was performed on the tBDMS, TMS, and PFB derivatives of
indomethacin in the EI, NCI, and the PCI modes (Figures 30-32) to confirm
chemical structure. The GC-MS of indomethacin-TMS has been previously
reported (Plazonnet and Vandenheuvel, 1977), but no data exits for indomethacin-
tBDMS.
Following derivatisation of indomethacin with MTBSTFA and PFBBr, both
GC-ECD and GC-MS demonstrate the formation of a single species as evidenced by
a single, symmetrical sharp peak in the respective GC-ECD and total ion
chromatogram (GC-MS), Figures 8 and 9. Derivatisation with BSA produced a
single peak, however, the peak geometry was poor compared to the tBDMS and
PFBBr derivatives (Figure 8).
The tBDMS derivative of indomethacin was subjected to detailed GC-MS
analysis to obtain the EI, NCI, and PCI spectrums (Figure 30). Following EI, the
most intense peak occurs at m/z 139 due to the p-chlorobenzoyl fragment. The
characteristic [M-57]+ peak at m/z 414 represents the loss of the C(CH 3) 3+ fragment.
The EI scan also shows a molecular ion peak at m/z 471. The spectrum following
chemical ionisation shows the molecular ion peak at m/z 471 (NCI, M+), and m/z
472 (PCI, MFT).

109
Abundance
1 B0OOO0 -|
]
1139
1
312
CH 30.
CH3
^ j S ^ _ _ ^ - C H ^ C O O — Si --(j; — C H 3
W^~-NT^-CH3 C H 3 C H 3
139 c=o
CH3
111 9 CI
370 /
312
216 275 \ 1_ L
333
414 /
L i —r 100 200 300
[— 400
MassVCharge
Figure 30A: GC-MS spectra of the indomethacin tBDMS derivative in the EI
(A), NCI (B), and PCI (C) modes.

110
ce 357
C H 3 C H 3
, M 0 0 <H C H 3 0 ~ ^ = ^ _ _ ^ C H 2 C O O - S i — C — C H 3
^ ^ - N T ^ - C H s C H 3 C H 3
I
c=o
100000-! a
20000-
357 J12 81 192 231 299 332 /
l 1 1 1 1 1 1 1 1 1 1 1 1 r- -i 1 1 ,— 100 200 300 400
Mass/Charge
Figure 30B

I l l
456
139
CH3O
XXX CH 3
312
• C H j C O O - S i - -
139 + c=o
6 CI
C H 3
C H 3 |
r CH3I
C H 3
357
M + H: 472
174
312
207
-I**1—<-
231
/ 300
\ L A 360
300
Mass/Charge
400 500
Figure 30C
112
The GC-MS of indomethacin-TMS derivative (Figure 31) is similar to that of
the tBDMS derivative. There is extensive fragmentation under EI conditions, and
the base peak at m/z 139 is again due to the /?-chlorobenzoyl fragment. The
molecular ion was observed, with significant abundance, at m/z 429. The spectrum
following chemical ionisation shows a molecular ion peak at m/z 429 (NCI, M+) and
m/z 430 (PCI, MFT).
In EI-MS, indomethacin-PFB ester produces a base peak of m/z 139
corresponding to the p-chlorobenzoyl fragment. Pentafluorobenzyl esters undergo
dissociative electron capture under NCI conditions as a part of the electron-
molecule interaction. The characteristic [M-l81]" is observed at m/z 356 which is
the base peak in the NCI spectrum (Figure 32). The molecular ion peak under PCI
conditions(MH+, PCI) is observed at m/z 538. A mass spectrometric assay operated
in the negative-ion chemical ionisation mode would appear to provide the best
sensitivity for indomethacin derivatised by PFBBr.

113
3.2. Validation of the GC-ECD method
3.2.1. GC Operating Conditions
The optimised operating conditions for routine analyses were: column,
Ultra-2 fused silica capillary column cross-linked with 5% phenylmethylsilicone (25
m x 0.31 mm x 0.52 \im film thickness); injection mode, splitless; injection port
temperature, 200 °C; initial column temperature, 210 °C (1 min); oven
programming rate, 40 °C/min; final oven temperature, 300 °C (6 min); detector
temperature (ECD), 330 °C; carrier gas, ultra-high purity hydrogen at a column
head pressure of 70 kPa (column flow rate, ~1 mL/min); purge delay time, 0.75
min; and detector make-up gas, argon-methane (95/5, 65 mL/min).

114
EI
141
/
73
• A . . I 327
/
370
— 200
i — i — 300 Masi/Charge
NCI
i 100
111 148
— i 1 (-218 265
299
200 300
Mi i l /Chi fgt
443
/ —I—
500
Figure 31A: GC-MS spectra of the indomethacin-TMS derivative.

115
Abundance
Average of 15.207 to 15.437 min. from USepOlOlOOt d ( _ K H , I K / * - T M S )
PCI
B0O0- |
iU.ii.-ii
207 223
200
312
300
Mass/Charge
340
J r - A -
370
Figure 31B

A b u n d a n c e
IGOOOO- EI
75 181 207 398
/ — r
400 300
Miss/Charge
—I— 500
Abundance Average of213fi9 to 21.810 min. from lxSep02010O2.d £_PC', l-do-?^)
279
\ 400
PCI
538
\
300
Mass/Charge
Figure 32A: GC-MS spectra of the indomethacin-PFB derivative.

117
Avenge of21 J2S lo 21.741 min. from lxSepO2010O4.d(k*:/ -real
111 148 246 322
->—i—'—r 300
Mass/Charge
•V-384
NCI
493
479/
—I— 200 500
Figure 32B

118
3.2.2. Drug extraction from biological fluids
The extraction and derivatisation procedure for indomethacin is summarised
in Scheme 1. Figures 33-36 illustrate the representative chromatograms of extracts
of biological fluids from the chronically instrumented ovine fetus. Both the tBDMS
derivatives of indomethacin and a-methyl indomethacin elute in regions free from
endogenous interference (Figures 33-35). The retention time of the internal
standard a-methyl indomethacin (Figure 33, peak a) is -4.8 min and that of
indomethacin (Figure 33, peak b) is -5.0 min. Figure 36 is a representative
chromatogram of indomethacin and zomepirac (the retention time of zomepirac
being -3.5 min and that of indomethacin -5.1 min) spiked in amniotic fluid
obtained during initial testing of zomepirac as a possible internal standard.

119
w c o a. w
o OJ O Q
4 - . O e - a - J
3 . O <= 4 - 1
1 . O .
a 4 , e s
Retention Time [minutes]
Figure 33: Representative chromatograms of the tBDMS derivative of
indomethacin and alpha-methyl indomethacin spiked in fetal plasma (the inset
shows the magnified baseline). The superimposed blank indicates no
interference from endogenous components.

Figure 34: Representative chromatograms of the tBDMS derivatives of
indomethacin and a-methyl indomethacin spiked in fetal urine.

121
C o a <M <U L.
U © w
Q
. O e 4-;
3 . O eS—
2.0e4H
1 . O <s 4-!
S .Oe4i
I i
U CQ JS
E o •a >>
S •
i 1
OS 5 s o -a s
Blank
Retention time (minutes)
Figure 35: Representative chromatograms of the tBDMS derivative of
indomethacin and a-methyl indomethacin spiked in amniotic fluid along with
the superimposed control.

122
1 . 4 e 5 H
1 : 2 e S J
1 .Oe£H
C 8.0e4-J o a
£ 6 . 0 e 4 j u 4)
4.0e4H
2 . 0 e 4 H
es a E o N
"3 CQ
S o •a fi
.... jv...i£i!Ai~. _.._JV.
Blank
Retention Time (Minutes)
Figure 36: Representative chromatograms of indomethacin and zomepirac
spiked in amniotic fluid.

123
3.2.3. Recovery studies
The extraction recoveries for plasma and urine of the fetal lamb, determined
by the matrix-compensation method, are presented in Table 5a. Mean recoveries
from plasma and urine were 96.99 ± 9.25% and 94.74 ± 6.75% respectively. This is
greater than the solid-phase extraction procedure of Nishioka et al., 1990 (about
87%), and the liquid-liquid extraction procedure, with ethylene dichloride, of
Sibeon et al., 1978 (about 85%), reported for plasma. However, recoveries
comparable to the present study have also been reported: viz 95% from serum using
dichloromethane (Jensen, 1978), and ~ 92% from plasma with ethyl acetate (Evans,
1980). In amniotic fluid, the recovery of indomethacin averaged 78.42 ± 2.57%
(Table 5b).
3.2.4. Stability studies
Indomethacin was found to be stable for at least four freeze/thaw cycles, at
least 24 h on bench-top, at least 24 h in acidified plasma and urine, and at least 1
week on the autosampler tray (Table 6). Indomethacin is also stable in plasma and
urine samples stored in the freezer following sampling in the time periods examined
to date (14 months). Indomethacin is also stable in the formulation prepared for the
infusion studies (pH 7.8) for at least 96 h as illustrated in Figure 37.

124
Table 5a: Extraction recoveries (n=4), inter-day variability (n=4) and intra-day variability (n=3) for indomethacin in (A) fetal plasma, and (B) fetal urine,
using cc-methyl indomethacin as the internal standard.
(A) Fetal Plasma
Concentration Inter-day Intra-day Recovery % (ng/mL) variability variability (S.D.2)
% C V 1 % C V 2 7.54 4.10 101.77
(2.05) 8 1.49 3.66 104.82
(3.24) 16 5.44 1.94 97.52
(3.33) 32 4.18 1.03 83.85
(1.29) slope 4.00 1.13 -
1 Coefficient of Variation; 2 One Standard Deviation
(B) Fetal Urine
Concentration Inter-day Intra-day Recovery % (ng/mL) variability variability (S.D.2)
% C V 1 % C V 2 9.05 11.14 100.71
(9.41) 8 7.75 1.09 100.35
(12.51) 16 7.01 0.37 87.83
(3.09) 32 3.92 3.56 90.07
(3.44) slope 3.11 4.11 -
1 Coefficient of Variation; 2 One Standard Deviation

125
Table 5b: Inter- and intra-day variability parameters for indomethacin in amniotic fluid of fetal sheep, with zomepirac as the internal standard.
Intra-day variability
Cone. ng/mL
Calibration curve 1
Calibration curve 2
Calibration curve 3
Mean % c . v .
1 0.0172 0.0169 0.0165 0.01686 2.08 2 0.0315 0.0334 0.0330 0.03263 3.09 . 8 0.125 0.1228 0.1250 0.1242 1.02 16 0.2238 0.2139 0.2223 0.2200 2.42 32 0.4324 0.4168 0.4247 0.4247 1.84 r 0.999 0.999 0.999 0.999 -Intercept 0.0086 0.0099 0.0100 0.0095 8.22 Slope 0.0133 0.0127 0.01307 0.01304 2.04
Inter-day variability
Cone. ng/mL
D A Y 1 DAY 2 DAY 3 DAY 4 D A Y 5 % C.V.
1 0.0174 0.0184 0.0207 0.0164 0.0164 10.02 2 0.0321 0.0333 0.0324 0.0323 0.0297 4.18 8 - 0.1120 0.1157 0.1167 0.1057 4.43 16 0.1998 0.2019 0.2065 0.2081 0.1836 4.87 32 0.3778 0.4100 0.3751 0.3995 0.3280 8.36 r 0.999 0.999 0.998 0.999 0.997 -slope 0.0116 0.0125 0.0115 0.0123 0.0100 8.48

126
Table 5b (Continued): Extraction recoveries of indomethacin spiked in amniotic fluid using zomepirac as the internal standard.
Concentration (ng/mL) % Recovery 2 80.24 8 80.87 16 75.34 32 77.42 Mean 78.42 Standard Deviation 2.57

127
Table 6: Stability of indomethacin in acidified sample matrix, during freeze-thaw cycles (with a-methyl indomethacin as the I.S.), and on the G C
autosampler tray (with zomepirac as the I.S.).
(A) Acidified biological sample (urine) matrix at pH 5.0 (n=2)
Time -> Area Ratio Mean
(% C V . ) Time -> Control 6 hours 12 hours 24 hours Mean (% C V . )
8 ng/mL 0.2187 0.2371 0.2468 0.2183 0.2302 (6.13)
(B) Freeze-thaw (F-T) cycle stability of indomethacin in plasma (n=2)
Cycles Control 1st F-T 2nd F-T 3rd F-T 4th F-T Mean (% C V . )
8 ng/mL 0.2307 0.2774 0.2491 0.2742 0.2618 0.2586 (7.43)
(C) GC autosampler tray stability of indomethacin (n=6)
Cone. ng/mL
A R E A RATIO Mean % C V .
Cone. ng/mL t=0h t=24h t=60h t=6d t=10d Mean % C V . 1 0.0114 0.0146 0.0153 0.0163 0.0129 0.0140 14.53 2 0.0230 0.030 0.0289 0.0304 0.0250 0.0274 11.94 4 0.044 0.051 0.0541 0.0567 0.0478 0.0507 9.92 6 0.076 0.079 0.0781 0.0803 0.0774 0.0781 2.09 8 0.0902 0.1065 0.1013 0.1006 0.0929 0.0983 6.75 10 0.119 0.134 0.1248 0.1228 0.1214 0.1244 4.64 20 0.249 0.2694 0.2402 0.2250 0.2240 0.2415 7.78 30 0.313 0.3607 0.3389 0.3061 0.3044 0.3246 7.53 40 0.485 0.5529 0.4769 0.3833 0.4392 0.4674 13.35 r 0.999 0.996 0.999 0.997 0.998 - -slope 0.0122 0.0132 0.0115 0.0099 0.0105 0.0115 11.26

128
+ — room temp 4 Deg. C
1000
100 t
100
Figure 37: Stability study of indomethacin infusate formulation at room
temperature, and at standard refridgeration conditions.
129
3.2.5. Inter-day and intra-day variability
Inter-day and intra-day variabilities (as % C.V.) for plasma were less than
8% (less than 4% for slope), and 5% (less than 1.5% for slope) at all concentration
points studied, respectively (Table 5a). For urine (Table 5a), the values were below
10% and 11% for inter- and intra-day variability, respectively. In amniotic fluid,
respective CV's for intra- and inter-day variability were < 4% and 11% (Table 5b).
The variability parameters for the LOQ are presented in Table 7: In urine and
plasma, respective CV's for inter- and intra-day variability parameters were below
10% and 20%, respectively, for both fluids.
3.2.6. Calibration Curves
The calibration curve parameters of indomethacin from plasma, urine, and
amniotic fluid of fetal sheep are presented in Tables 8-10 and Figures 38-40.
Working calibration curves of 1-32 ng/mL were linear with coefficients of
determination (r2) > 0.99 [linear regression statistics were: Y=0.05042X + 0.00543
for plasma, Y=0.03574X + 0.05947 for urine and Y=0.02637X + 0.03694 for
amniotic fluid]. The coefficient of variation at each concentration point as well as
for the slope, were below 11% for all three fluids. The limit of quantitation in both
fluids was 1 ng/mL with a signal-to-noise ratio of >10.

130
Table 7: Variability parameters for the limit of quantitation (LOQ) of 1 ng/mL
(A) Inter-day variability (n=10)
Biological Fluid*
Day 1 Day 2 Day 3 Mean % C . V . #
Urine 0.03260 (10.435%)
0.03415 (7.58%)
0.03338 (7.99%)
0.03337 2.32%
Plasma 0.05732 (13.269%)
0.08356 (15.51%)
0.07175 (11.744%)
0.07087 18.54%
* blank fluid samples are from the fetal lamb. NB: Numbers in paranthesis indicate the coefficient of variation in %. # Coefficient of variation for days 1, 2, and 3.
(B) Intra-day variability (n=3)
Biological Fluid*
Set l Set 2 Set 3 Mean % c . v . #
Urine 0.03486 (15.47%)
0.03160 (1.574%)
0.03048 (6.137%)
0.03231 7.04%
Plasma 0.05928 (5.081%)
0.05991 (14.41%)
0.05739 (14.291%)
0.05886 2.23%
* blank fluid samples are from the fetal lamb. NB: Numbers in paranthesis indicate the coefficient of variation in %. # Coefficient of variation for sets 1,2, and 3.
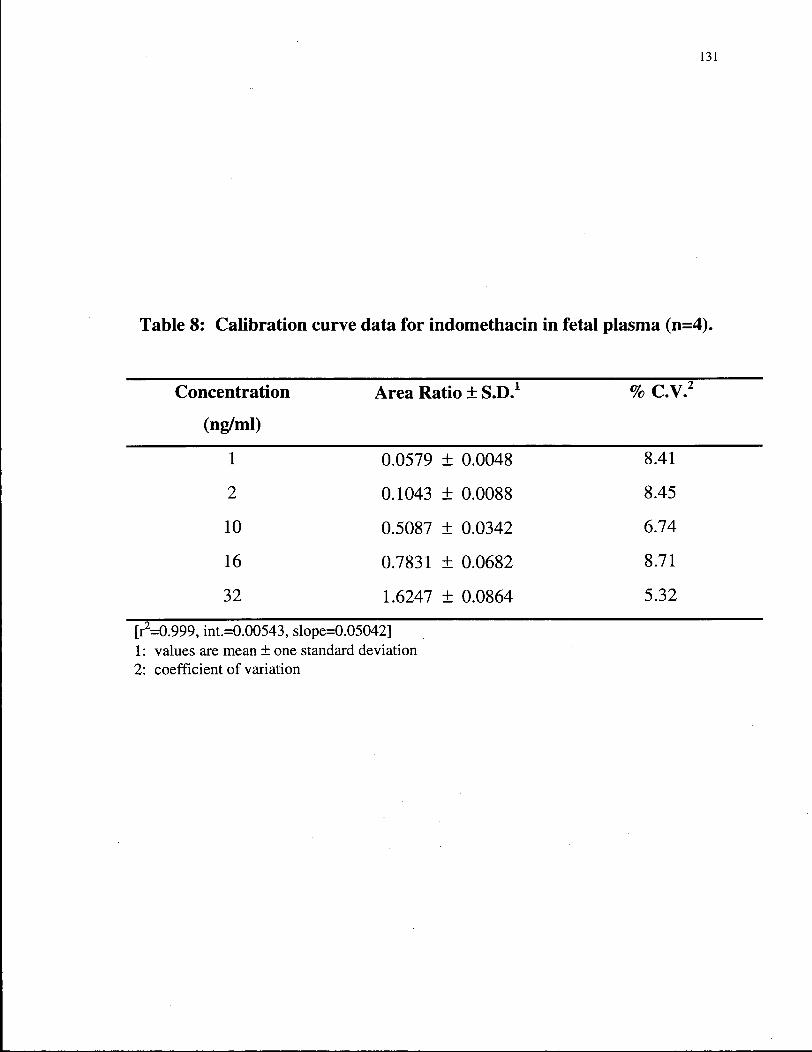
131
Table 8: Calibration curve data for indomethacin in fetal plasma (n=4).
Concentration Area Ratio ± S.D.1 % C V . 2
(ng/ml)
1 0.0579 ± 0.0048 8.41
2 0.1043 ± 0.0088 8.45
10 0.5087 ± 0.0342 6.74
16 0.7831 + 0.0682 8.71
32 1.6247 ± 0.0864 5.32
[r2=0.999, int.=0.00543, slope=0.05042] 1: values are mean ± one standard deviation 2: coefficient of variation
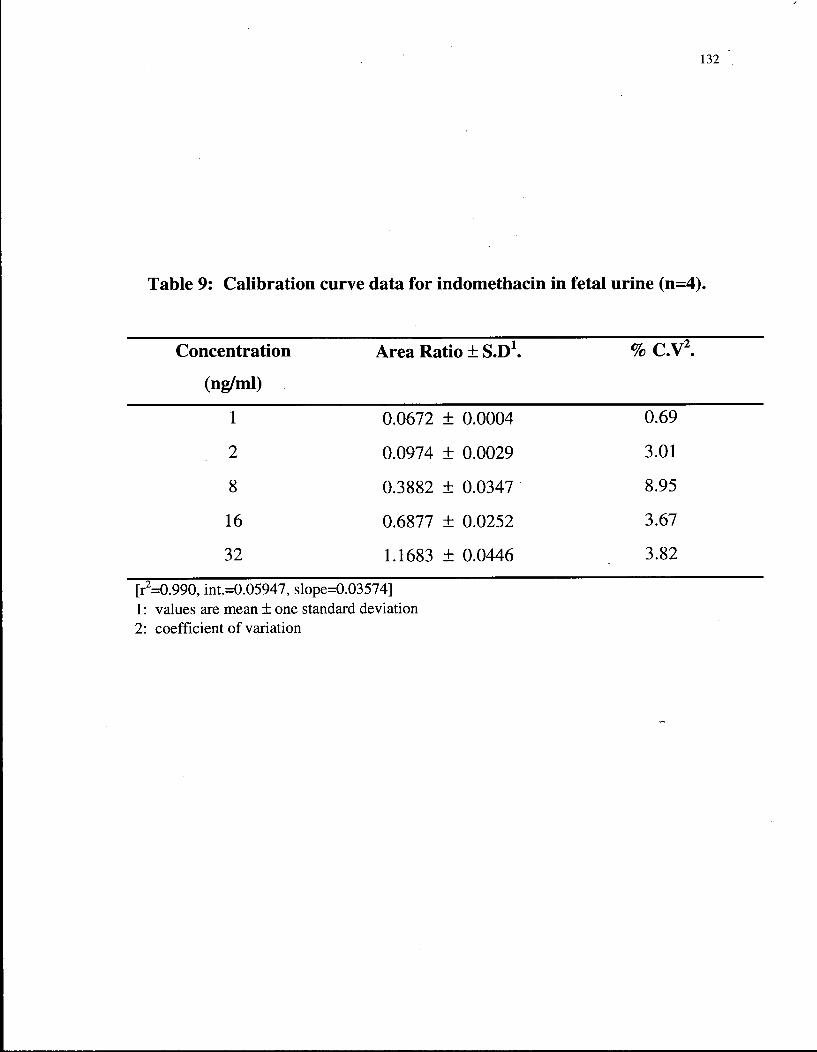
132
Table 9: Calibration curve data for indomethacin in fetal urine (n=4).
Concentration Area Ratio ± S.D1. % c . v 2 .
(ng/ml)
1 0.0672 ± 0.0004 0.69
2 0.0974 ± 0.0029 3.01
8 0.3882 ± 0.0347 8.95
16 0.6877 ± 0.0252 3.67
32 1.1683 ± 0.0446 3.82
[r2=0.990, int.=0.05947, slope=0.03574] 1: values are mean ± one standard deviation 2: coefficient of variation

133
Table 10: Calibration curve data for indomethacin in amniotic fluid (n=8).
Concentration Area Ratio ± S.D.1 % C V . 2
(ng/mL)
1 0.05429 ±0.00338 6.24
2 0.08985 ± 0.00945 10.52
8 0.24974 ± 0.00456 1.82
16 0.47369 ±0.01367 2.88
32 0.87350 ±0.01983 2.27
1 values are mean ± one standard deviation 2 Coefficient of variation [r = 0.9996, r 2 = 0.999, int. = 0.03694, slope = 0.02637]

134
CO
rr CO <D
3.00
2.40
1.80
1.20
0.60 h
0.00 10 20 30 40
Concentration (ng/mL)
Figure 38: Representative calibration curve for indomethacin in fetal plasma.

135
Figure 39: Representative calibration curve of indomethacin in fetal urine.

136
0.00 ' 1
0 12 24 36
Amount of Indomethacin spiked (ng/mL)
Figure 40: Representative calibration curve of indomethacin in amniotic fluid.
i

137
3.3. Fetal Infusion Studies
Table 11A lists the ewes on which experiments were performed, samples
collected, and the dose of indomethacin administered. In two animals (E 1137 and E
1115), the dose of indomethacin infused was one-third of that normally administered
(i.e., low dose ewes). In all of the animals studied, hemodynamic and metabolic
parameters were within normal limits at the start of experimentation (Figures 41 A-F).
Indomethacin was observed to induce lactic acidosis in the high dose group of fetuses
(E 1221, E 2160), as evidenced by markedly high blood lactate levels (Figure 4ID),
and a reduction in pH (Figure 41E) and base excess (Figure 41F), while blood glucuose
levels remained constant (Figure 41C). This was not seen in low dose group (E 1137,
E 1115).
3.3.1. Analysis of Plasma Samples
The concentration of indomethacin was determined in FA and UV plasma
samples (Table 12) obtained following administration of indomethacin in seven
chronically instrumented ovine fetuses and the mean profiles are illustrated in Figures
42 and 43. Table 11B summarises the attainment of steady state concentrations, i.e.,
time achieved, samples used, the average concentrations and the variability. The
indomethacin concentrations in the fetus, in the high dose group, are similar to those
observed during human tocolysis (Moise et al., 1990) with mean values ranging

138
Table 11 A: Animal experiment sampling and dosing protocol.
Ewe No. Samples Collected Dose of Indomethacin (mg/min)
E796 UV, FA, MA, UTV, 0.0075 AMN, TR, UR
E984Y UV, FA, UR, AMN, TR 0.0075 E2160 UV, FA, UR, AMN, TR 0.0075 E 1221 UV, FA, UR, AMN, TR 0.0075 E 1211 UV, FA, UR, AMN, TR 0.0075 E 1137 UV, FA, UR, AMN, TR 0.0019 E 1115 UV, FA, UR, AMN, TR 0.0019 E562V UV, FA, UR, AMN, TR Vehicle only (Control) E2182 UV, FA, UR, AMN, TR Vehicle only (Control) E2221 UV, FA, UR, AMN, TR Vehicle only (Control)
Abbreviation: UV, umbilical venous; FA, fetal femoral arterial; UR, fetal urine; MA, maternal arterial; AMN, amniotic fluid; TR, tracheal fluid; UTV, uterine vein.
Table 11B: Determination of apparent steady state plasma concentration.
Ewe No. Sample Duration ofSS1
attained (h)
Mean2
(ng/mL) S.D.3 % C.V4.
E796 FA 5 23-69 195.07 16.83 8.63 E984Y FA 5-69 113.12 8.40 7.43 E2160 FA 5-69 222.25 13.05 5.87 E 1221 FA 23-69 161.69 16.58 10.25 E 1211 FA 23-69 216.21 45.02 20.82 E1137 6 FA 5-69 39.07 5.69 14.58 E1115 7 FA 5-69 43.51 7.93 18.22
1: steady state 2: mean steady state plasma indomethacin concentration 3: standard deviation 4: coefficient of variation 5: fetal femoral arterial plasma sample 6, 7: fetuses of the low dose group

CM O CL
CD c <
100
80
60
40
20
- A •
E 1137
E984
A E1115
E796
E2160
E 1211
E1221 1 3 9
-40 -20 20 40 60 80
Time (Hours)
CM o o Q.
0) r <
- + — E 1137 A E 1115 - • - E2160 • E 1221
— A — E984 E796 E 1211
100
80
60 A = A — — •
•
— f JL M-qp
• •< ... 40 t /
+ 20 _
i i
-40 -20 20 40 60 80
Time (Hours)
Figure 41A: Effect of indomethacin on fetal arterial blood gas parameters.

+ — E 1137
A - E 984
140 A E 1115
E796
E2160
E 1211
E 1221
4.00
3.50
3.00
2.50
2.00
1.50
1.00
0.50
0.00
I
/ N
+ *: A
-40 -20 0 20 40 60 80
Time (Hours)
• + - E1137 A E 1115 - • - • E2160 • E1221
A - E984 E796 E 1211
25
20 h
15
10
5 h
-40 -20 20
Time (Hours)
40 60 80
Figure 41B: Effect of indomethacin on fetal arterial glucose and lactate concentrations.

141 + •
• •
E 1137
E984
E 1115
E796
• - E2160
E 1211
E 1221
- + - E1137 * E 1115 E2160 • E1221
~ A - E 984 E 796 E 1211
10
6
2
-2
-6
-10
-14
-18
-22
-26
-30
- i * * * * J * . . 4 •
l . * Vv . \ \ \ \ •
\ A \ * \
\ \
\ \ •
I I I
-40 -20 20 40 60 80
Time (Hours)
Figure 41C: Effect of indomethacin on fetal arterial pH and base excess.

142
3 O
a
.a s s c
CQ S W3 II « s
fa a>
•2 «
CQ - s CQ
O
« CQ
.4>
fi S3
- ' C
.S 3
CQ w
S e 5 «• fi -a
CQ O
§. £ fi eo
c o CQ
CQ
£ Vi CQ
fi o at ^ e & o u c CQ
< N 1-1
CQ
H
Q
fa U "5k fi O
fa
"5k
< fa
N O N O
vol co i n N O
C O oo
00 I
N O
d CN co
N O C N
N O
in o C N
C N in I C M
O N C O
»n C N
C N
N O I co co
O N
C N C N
oo oo
C O
C N
1—I N O
d
N O in in o
oo O N N O
N O C O
| C N
C N O O
wo
co C O
o in oo N O
in in
N O C N
in
C O C N
C O O N
C N
O O
O N
d C N
O O C O
O N
C N
O N O N I in C O
C O
O O C O
CN N O I C O
N O N O
in in
r--N O
O N O N
O O I> N O co C O
C O
O N
O N
00 o C N
C N O
N O C O
co O N oo
oo
1—1 CN
fa t/5
in C N C N
C N
CN
O N
O O
in O N
O N I
in
C N
O N C O I oo CN
N O N O
N O O N N O
C O
oo
i n q oo I N O
O N
in
co p col O N
oo
O CN
O CN
O N O
00 N O
T t
N O
4>
& H
2 © in
co C N
O N C N
N O C N
i n O N N O
C N
N O O O
* o
1 _ L
C O
in O N
O N C N
C N C N
* N O I 1 -
O N
C N
C/3 QJ
cd
a o
* O N
O

Mean (S.E.M.) Concentration-Time Profile
— + — FA - O - U V - A - urine - • - A M N
1000 F ~
0 20 40 60 80 100
Time (Hours) ^ Post-Infusion
;ure 42: Mean concentration-time profiles of indomethacin in plasma, urine,
and amniotic fluid for high dose ewes (n=5).

144
Mean (S.E.M.) Concentration-Time Profile
0 20 40 60 80
Time (Hours)
Figure 43: Mean concentration-time profiles of indomethacin in FA and UV
plasma for low dose ewes (n=2).

145
from —111-208 ng/mL during the infusion period. MA and UTV samples from one
ewe (E796) were analysed but no drug was detected in them, i.e., the concentration
was below the detection limit of the assay. The arterio-venous concentration
difference for indomethacin at apparent steady state in the high dose ewes averaged
11.72 ± 1.53 ng/mL (mean ± 1 S.D.) (Table 13), and while small, was significantly
different (a=0.05, t-test, Table 14). These results suggest a low placental
permeability to indomethacin in sheep.
Fetal total body clearance was estimated to be 44.55 + 11.14 mL/min (n=7,
Table 15). It was only possible to calculate placental and non-placental clearances
in two animals because of incomplete umbilical blood flow data. The placental
clearance in E 796 was determined to be about 32.00 mL/min, and the non-placental
clearance to be 6.44 mL/min (Table 16). In a low dose ewe (E 1115), the values
were 26.47 mL/min and 22.16 mL/min, respectively. These values are much lower
than those reported for either diphenhydramine or metoclopramide (Rurak et al.,
1991). Ritodrine, on the other hand, had a fetal placental clearance of about 5
mL/min/kg and a markedly higher fetal non-placental clearance of 63 mL/min/kg
(Rurak et al, 1991).

146
Table 13: Arterio-venous concentration difference for indomethacin at
apparent steady state.
Ewe No. [ F A ] t a d o (ss) [UVJindo (SS) [A-VJindo (SS) Extraction
ng/mL 1 ng/mL 2 ng/mL 3 Ratio4
796 195.07 181.71 13.37 0.068
984Y 113.12 101.67 11.45 0.101
2160 222.25 - - -
1221 161.69 151.35 10.34 0.064
1211 216.21 - - -
1137* 39.07 36.67 2.39 0.061
1115* 43.51 - - -
* Low dose group 1: Mean apparent steady-state fetal arterial (FA) indomethacin concentration. 2: Mean apparent steady-state umbilical venous (UV) indomethacin concentration. 3: Mean arterio-venous (A-V) indomethacin concentration difference. 4: Extraction ratio = C F A - C U V / C F A , where C is the concentration of indomethacin at
apparent steady-state.
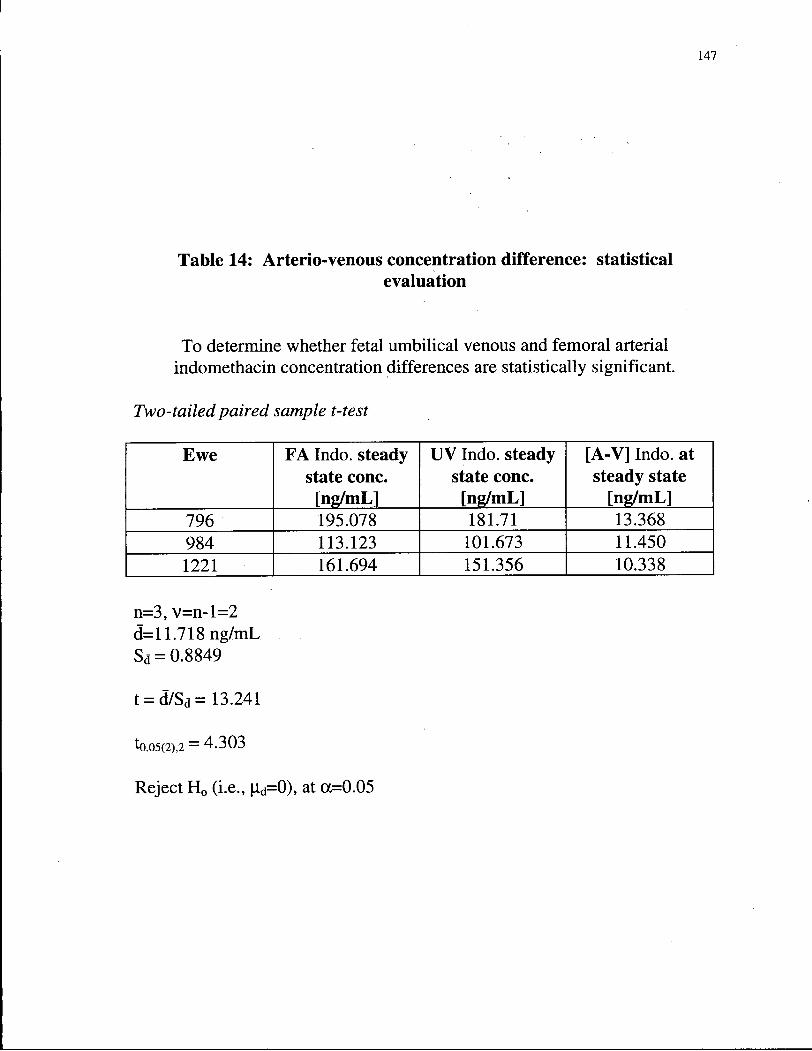
147
Table 14: Arterio-venous concentration difference: statistical evaluation
To determine whether fetal umbilical venous and femoral arterial indomethacin concentration differences are statistically significant.
Two-tailed paired sample t-test
Ewe FA Indo. steady UV Indo. steady [A-V] Indo. at state cone. state cone. steady state [ng/mL] [ng/mL] [ng/mL]
796 195.078 181.71 13.368 984 113.123 101.673 11.450 1221 161.694 151.356 10.338
n=3, v=n-l=2 d=l 1.718 ng/mL S d = 0.8849
t = d7Sa= 13.241
t0.05(2).2 = 4.303
Reject H 0 (i.e., p,d=0), at oc=0.05

148
Table 15: Determination of fetal total body clearance.
Ewe No. Infusion Rate
mg/min
[FA]i„d0 (ss) ng/mL*
CLtb mL/min**
796 0.0075 195.07 38.45
984Y 0.0075 113.12 66.29
2160 0.0075 222.25 33.75
1221 0.0075 161.69 46.38
1211 0.0075 216.21 34.69
1137 0.0019 39.07 48.63
1115 0.0019 43.51 43.67
* Mean steady-state fetal arterial (FA) concentration of indomethacin
** Total body clearance.
Mean total body clearance: 44.55±11.14 mL/min

Clfo
[mL
/min
] 6.445
22.159
Cl p
[mL/
min
] 32.001
26.467
S 38.446
48.626
O
* [m
L/m
in]
as as
<r>
O
* [m
L/m
in]
so so t-
i — i
co O
* [m
L/m
in]
[A-V]
[ng/
mL]
13.368
2.398
I S
195.078
39.073
ight
ta
l Wei
[kgl
3.393
3.194
Fel
Ewe *o
as i>
e'en
1/5
T3 O .—I U H
<D &
4 C / 3
CD 4-* fli > 4 o <D OH fi fli
X !
fli > O
T3 fli
a o ~3 o
5 S » 6 E * «« « u
^ ^ s o
T3
-a o > ~J3
£ E J

150
3.3.2. Analysis of Urine Samples
The results from the analysis of indomethacin in urine samples are
summarised in Table 17 and Figure 42. As Table 17 indicates, the levels of intact
indomethacin in fetal urine are, in general, very low. The urine samples were also
subjected to enzyme ((^-glucuronidase) hydrolysis to determine if there were
conjugates present. While there is considerable variability, the results indicate that
the fetal lamb does have some ability to conjugate indomethacin. Figure 44
illustrates the urine flow rate (mL/min) as a function of time during indomethacin
infusion. In three of the fetuses (E 2160, E 984Y, and E 796), there was a marked
reduction in urine flow rate within 23 hours (-50% reduction) of initiating the
indomethacin infusion. However, in the other two fetuses, urine flow was observed
to increase.
The estimated fetal renal clearance of indomethacin, in the high dose group,
is about 0.015 ± 0.009 mL/min (Table 18) (Figure 45), and is not significantly
different from zero. This finding is consistent with observations for other weak
organic acids in the fetal lamb, viz., diphenylmethoxyacetic acid, a metabolite of
diphenhydramine (Tonn et al., 1994), and valproic acid (Gordon et al., 1994).
Cumulative amounts of drug excreted could not be calculated since urine samples

151
were only collected over a one-half to one hour period at each blood sampling
interval.
3.3.3. Drug Disposition in Amniotic and Tracheal Fluid Compartments
The concentration of indomethacin in amniotic fluid, in the high dose
experiments, was significantly lower than the plasma concentrations and slightly
higher than fetal urine levels as illustrated in Figure 42. Amniotic fluid
indomethacin concentrations were below detection limits in E 1137 and E 1115, the
two low dose ewes. These findings are in sharp contrast to basic drugs such as
metoclopramide, labetalol, and ritodrine which have been shown to accumulate
considerably in amniotic fluid (Rurak et al., 1991). Conjugates were not measured
in amniotic fluid due to limitations in sample volume.
Indomethacin levels in fetal tracheal fluid samples were below the detection
limit of the assay. Again, this is in sharp contrast to basic drugs, such as
metoclopramide, ritodrine, and labetalol, wherein the levels in tracheal fluid far
exceeded those in fetal plasma, the extent of accumulation being the greatest for
metoclopramide (Rurak et al., 1991).

152
a *E s Is 4-t
cu OJ
cu s o TS a
CM O
e cs M
c CU CJ a ©
—
H
CN
o
1—I
T t 00 O S
p
V© ON f -
cu P
TJ J. S i 1
P «T
P TJ S.
P
p TJ
sis p
TJ J,
p TS S.
* I
TS P
P siT
cu
5 CN
CO
o *o
<u cd G O
o
c/3 c/5 cs-
5 00 <+H ' O
cu "3 S I
o fi o > <o ^ s
CU
o c
e l l — <u — O •—i G
CU S T3 « T j U - O fl cn CU
O ^ °
P Q
CU
CU
t rt
T3 (U H—» o CU H—» CU C O
rt 00
n3 cu rt 00
O o
o rt
O G
OH
o t-t 00 cu C/3 o
T3 OH £
(U . - I
cu
-2 P

153
Figure 44: Effect of indomethacin on the fetal urinary flow rate.
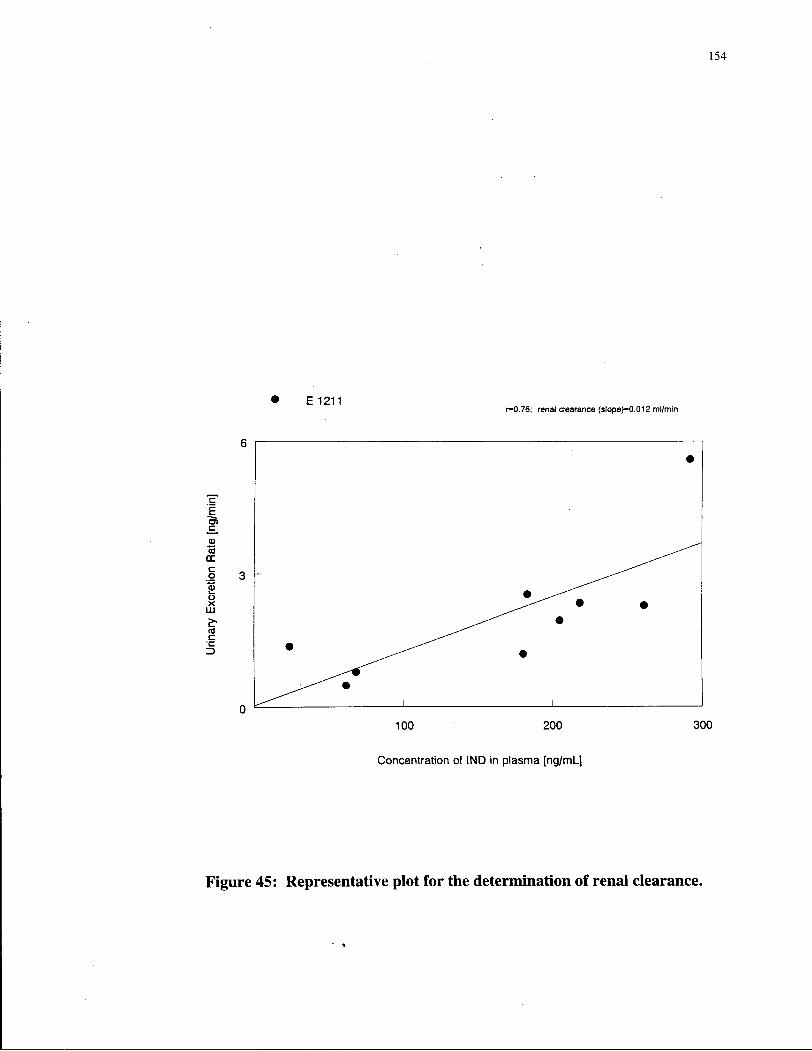
154
Figure 45: Representative plot for the determination of renal clearance.
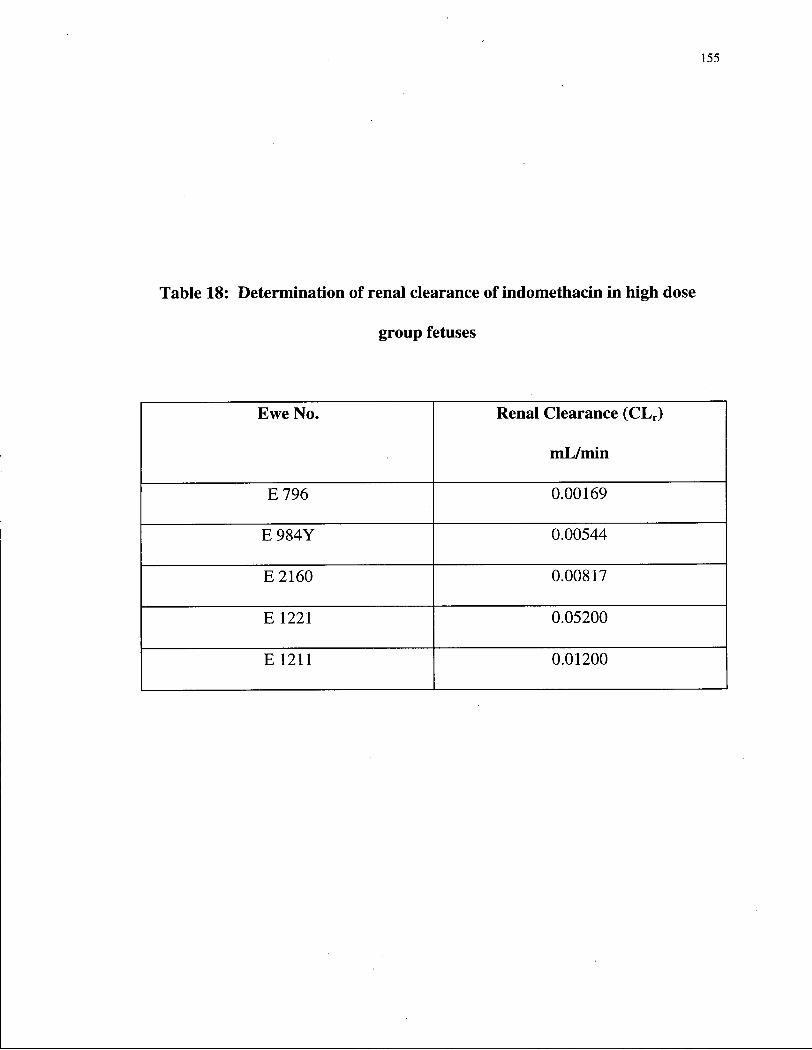
155
Table 18: Determination of renal clearance of indomethacin in high dose
group fetuses
Ewe No. Renal Clearance (CL r )
mL/min
E 7 9 6 0.00169
E 9 8 4 Y 0.00544
E2160 0.00817
E 1221 0.05200
E 1211 0.01200

156
4. DISCUSSION
4.1. Development of a capillary G C - E C D method
Purity assessment of indomethacin
According to O'Brien et ah, 1984, indomethacin is defined as the crystalline,
non-solvated free acid entity of the compound (Form I; see section 3.1.1.). The
indomethacin sample we procured from Sigma Chemical Co., St. Louis, MO, was
subjected to a variety of physical tests to authenticate its purity for our experimental
studies. NMR studies indicated that the chemical shift values obtained with our
sample compared well with those obtained with Merck reference standard (Table 3)
(O'Brien et al, 1984). DSC studies indicated that the melting point of our
indomethacin sample was at 162°C (Figure 6). The Form I (crystalline)
indomethacin has a melting point of 162°C (NF XIII). Since no other peak was
observed in the DSC scan, other than that which melted at 162°C, we can attribute
the melting temperature as observed to Form I. This is in full aggreement with that
observed with the Merck standard; the recorded temperature being 162°C (O'Brien
et al., 1984). The mass spectrum obtained in an LC/MS/MS system was
characterised by a molecular ion at m/z 358 (the molecular weight of indomethacin
is 357.81) and a characteristic base peak at m/z 139 corresponding to the p-

157
chlorobenzoyl group (Figure 7). These findings confirmed that indomethacin, as
obtained from Sigma, is comparable in its physical assessment to the Merck
standard. Indomethacin was therefore used in our experimental studies without
further purification.
Assay development
Several packed column GC assay procedures have been described for the
determination of indomethacin in human plasma/serum and urine (Guissou et ah,
1983; Sibeon et al, 1978; Matsuki et al, 1983; Plazonnet and Vandenheuvel,
1977; Jensen, 1978; Arbin, 1977; Evans, 1980; Ferry et al, 1974; Helleberg,
1976). These packed column methods suffer from serious limitations of poor
resolution and chromatography, since they are prone to interference from
endogenous peaks due to fewer theoretical plates compared to capillary columns.
There is also one report on the use of fused silica capillary column technology for
indomethacin (Nishioka et al, 1990) determination in plasma. However, this
method has a number of disadvantages including: high sample volume (1 mL),
lengthy derivatisation step with l-ethyl-3-p-tolyltriazine (i.e., 6 hours), lengthy
retention times (-20 min), a moderate recovery of 87% using a solid-phase
extraction procedure, and a detection limit of 2 ng/mL.

158
For our detailed pharmacokinetic studies with indomethacin there is the
potential for interference from components in biological matrices (e.g., tracheal and
amniotic fluids, plasma, and urine) as well as limitations on fetal fluid sampling
volume, in particular blood (-250-500 |iL of plasma). The existing analytical
methods were, therefore, not suitable and it was necessary to develop an analytical
method with high sensitivity, specificity, simplicity, reproducibility and robustness.
Selection of derivatising agent
Although the conjugated /?-chlorobenzoyl group in indomethacin affords the
inherent electron-capture property in the molecule, derivatisation is necessary to
increase volatility and thereby improve chromatography. This subsequently results
in enhanced sensitivity. A number of derivatising agents have been used for
indomethacin including the explosive diazoalkanes (Arbin, 1977; Giachetti et al.,
1983; Guissou et al, 1983; Helleberg, 1976; Plazonnet and Vandenheuvel, 1977),
and poisonous fluorine containing reagents (Matsuki et al, 1983; Evans, 1980;
Sibeon et al, 1978). There have been only two instances where the derivatising
agent is reportedly non-toxic, i.e., bis (trimethylsilyl) acetamide (Plazonnet and
Vandenheuvel, 1977), and l-ethyl-3-p-tolyltriazine (Nishioka et al, 1990).
However, bis (trimethylsilyl) acetamide (BSA) derivatisation produces
trimethylsilyl esters that are unstable to hydrolysis, and thus require protection from

159
moisture, and the use of freshly derivatised samples for GC runs. The use of ethyl
tolyltriazine is also not desirable since the derivatisation step is very lengthy, i.e., in
the order of 6 hours. Since BSA as a silylating agent provides the advantages of
safety and simplicity of the derivatisation step, further newer silylating agents were
explored.
Silylation of organic compounds improves volatility greatly by blocking
protic sites thereby reducing dipole-dipole interactions, as illustrated below:
H-Y + — I
Si I
6+ Y I H
V -S i -
8-X Y-SI- + HX
There is a nucleophilic reaction between the electronegative heteroatom and the
silicon atom of the silyl donor resulting in a bimolecular transition state. The
derivatisation proceeds to completion if the basicity of the leaving group (X) is
greater than that of Y. Silylation with MTBSTFA confers several advantages over
other silylating agents (BSA, MSTFA, BSTFA, TBDM-SIM, and TBDMCS) such
as:
(a) increased reactivity, especially its ability to silylate carboxyls,
(b) short derivatisation reaction times, and
(c) superior hydrolytic stability (while TMS derivatives need to be freshly prepared
and injected into the GC, tBDMS derivatives are stable to hydrolysis as was

160
observed in this study where the processed samples were stable on the GC
autosampler tray for at least one week)
Based on our studies, MTBSTFA derivatisation was rapid and produced
tBDMS derivatives with superior hydrolytic stability in agreement with previous
studies by Mawhinney and Madson, 1982, for other compounds with reactive
carboxyl groups.
Derivatising with PFBBr produced comparable sensitivity to MTBSTFA.
Because sample preparation was more cumbersome and time consuming with
PFBBr we chose to use MTBSTFA for our assay. This is the first instance wherein
a silylating agent like MTBSTFA has been used for indomethacin with high
sensitivity electron-capture detection.
The electron-capture properties of tBDMS-indomethacin derivatives can be
attributed to the conjugated p-chlorobenzoyl group, more specifically the carbonyl
group in resonance with an imide structure, i.e., the two aromatic ring systems
enhancing charge delocalisation (Plazonnet and Vandenheuvel, 1977; Matin and
Rowland, 1972). The carbonyl carbon acts as the first site of electron acceptance
while the final electron-capture response is dependent upon resonance stabilisation
as illustrated in Scheme 2.

161
Although the GC-MS spectra of indomethacin derivatised by BSA has been
reported (Plazonnet and Vandenheuvel, 1977), there are no detailed reports in the
literature of mass spectra of tBDMS derivatised indomethacin. The tBDMS
derivative of indomethacin was subjected to GC-MS analysis to obtain EI, NCI, and
PCI spectrums (Figure 30). Following EI, the most intense peak occurs at m/z 139
due to the />chlorobenzoyl fragment (Figure 30 A). The characteristic [M-57]+
peak at m/z 414 represents the loss of the C(CH 3) 3+ fragment. The EI scan also
shows a molecular ion peak at m/z 471. The spectrum following chemical

162
ionisation shows the molecular ion peak at m/z 471 (NCI, M+) and m/z 412 (PCI,
MH +) (Figure 30, B and C).
During optimisation of the extraction conditions for this assay, a number of
solvents were examined (viz., ethyl acetate, toluene, hexane, diethyl ether, toluene-
0.0125M TEA, hexane-10% IPA, hexane-ethyl acetate, and methylene chloride),
with ethyl acetate providing the highest extraction efficiency (Table 4). In order to
improve the selectivity of extraction, various mixtures of hexane-ethyl acetate were
examined. However, the addition of hexane markedly reduced the extraction
efficiency of ethyl acetate and provided only a marginal improvement in selectivity.
Of all of the solvents tested ethyl acetate alone was found to provide the best
recovery of indomethacin from sheep biological fluids and the cleanest
chromatograms.
A number of solvents have been used in existing assay procedures for
indomethacin, the most common being dichloroethane (Sibeon et al, 1978; Bayne
et al, 1981; Helleberg, 1976), ethyl acetate (Matsuki et al, 1983; Evans, 1980),
hexane-ethyl acetate (4:1), (Plazonnet and Vandenheuvel, 1977), dichloromethane
(Jensen, 1978), and hexane-amyl alcohol 10% (Ferry et al, 1974). Nishioka et al,
1990, are the only group who have attempted a solid-phase extraction procedure for
indomethacin, however, this method does not offer any advantages over the

163
conventional liquid-liquid extraction, either in extraction recovery (87%), or in
terms of cleanliness of the chromatogram.
The extractability of indomethacin is highly pH-dependent. Our results
indicated that attainment and maintenance of pH 5.00 was required for optimal
recovery. These results aggree well with similar observations of Helleberg (1976),
and Ou and Frawley (1984). Recovery is drastically reduced when pH is less than 4
or higher than 6. The pKa of indomethacin is 4.5-4.7 (O'Brien et al, 1984), and
this likely explains the optimal recovery around pH 5.00. Varying times of
extraction have been reported in the literature for indomethacin including 5 min
(Giachetti et al, 1983), 15 min (Ferry et al, 191 A; Helleberg, 1976), and as high as
40 min (Jensen, 1978). In the present study, however, extraction time was
optimised as 20 minutes.
Mean recoveries from plasma and urine in the present study were 96.99 ±
9.25% and 94.74 ± 6.75%, respectively. These values are comparable with those
reported in the literature: 95% from serum using dichloromethane (Jensen, 1978),
92% from plasma using ethyl acetate (Evans, 1980), 95% from serum with
dichloroethane (Helleberg, 1976), and 95% from plasma with a 50:50 mixture of
petroleum ether-dichloromethane (Johnson and Ray, 1992). The values are greater
than the solid-phase extraction procedure of Nishioka et al., 1990, i.e., about 87% in

164
plasma and the liquid-liquid extraction procedure with dichloromethane of Sibeon et
al., 1978, i.e., about 85% from plasma.
The column used in this assay is a fused silica wide bore capillary column
cross-linked with 5% phenylmethylsilicone (25 m x 0.32 mm x 0.52 pjn film
thickness). Chromatographic'behaviour of indomethacin and the internal standard,
in terms of resolution, retention times, sensitivity, and peak geometry, was optimal
with this relatively non-polar column stationary phase (Rtind0=~4.8 min). When a
narrow bore column with the same stationary phase was used (25 m x 0.2 mm x
0.33 |im film thickness), retention times (Rt) were longer and sensitivity was lower.
The decrease in sensitivity is likely in part due to the lower sample capacity of the
narrow column as only a 1 p i volume can be injected compared to 2 |iL for the
wide bore column. With a narrow bore column of the same phase, there is both a
reduction in internal diameter was well as in stationary phase thickness. Equation 1
illustrates the relationship between phase ratio, p\ internal radius, r, of a wall coated
open tubular column, and stationary phase film thickness, df.
P=r/2df (1)
From this equation, it can be observed that a decrease in df (if r is constant) will
result in a reduction in partition ratio and a decrease in component retention and
resolution with reduction in run times (Hyver and Sandra, 1989). However, with the
narrow-bore column, the internal diameter is also smaller, with run times being

165
dramatically longer. When a polar DB-1701 column was used (narrow-bore, methyl
[7% phenyl, 7% cyanopropyl] silicone) of dimensions, 30 m x 0.25 mm x 0.25 |im,
however, the elution behaviour of the analytes were reversed. Zomepirac, being the
more polar compound was retained longer in the column than was indomethacin.
The splitless mode of injection was used for all analyses since this method of
sample introduction is generally very suitable for trace level analysis. This is
because 100% of the injected sample is introduced into the column (Hyver and
Sandra, 1989).
The time delay following inlet purging to occur is critical for the following
reasons and was therefore optimised. The purge delay time is dependent upon the
solvent and solute characteristics, capacity of the vaporising chamber, sample
volume, speed of injection, and the velocity of the carrier gas. Short purge delay
times will prevent complete transfer of solute into the column while long delay
times will prevent venting of residual waste vapour resulting in their transfer onto
the column and solvent tailing. A purge delay time of 0.75 min was chosen from the
tested range of 10-120 seconds as this provided optimal peak response (Figure 22).
The overall peak characteristics (peak shape, geometry, etc.) of the analyte
are dependent upon the injection port temperature. Stability of the derivatised

166
compound is also important as it may decompose at higher temperatures resulting in
a loss of sensitivity. A very low injection port temperature may result in peak
broadening as a result of slower sample vapourisation with the time for transfer into
the column being longer. In this study, it was determined that maximal peak area
counts of indomethacin were observed over the 180-200°C range and that any
further increase in temperature resulted in a drastic decline in absolute indomethacin
area counts. Usually the injection port temperature is higher than the column
temperature. However, in the present study an injection port temperature of 200°C
and an initial column temperature of 210°C were chosen as these provided optimal
response.
The column temperature has a direct effect on run time and peak geometry.
It also has a marked effect on peak separation. The log of partition ratio (k) is
inversely related to the temperature. The lower the column temperature, the larger
the partition ratio, thereby increasing the time the analyte spends in the stationary
phase. This increased retention of the analyte in the liquid phase confers greater
selectivity. Various column temperatures were examined and an initial column
temperature of 210°C was selected with quick ramping at 40°C/min to 300°C, the
final column temperature. Maximal absolute indomethacin area counts were
observed at this final column temperature. These column temperatures also resulted

167
in short analysis times (~9 min) and are within the maximum 400 °C temperature
rating recommended for these columns.
The carrier gases commonly used in GC are hydrogen, helium, and nitrogen.
Nitrogen is a denser gas compared to either hydrogen or helium. Of the three gases,
the major advantage of using hydrogen is that the value for the theoretical plate
height increases very slowly when one increases the average linear gas velocity
through the column. This results in a in faster analysis with little loss in resolution.
In the current study, hydrogen was used as the carrier gas for these reasons. A
variety of carrier gases have, however, been used for the GC analysis of
indomethacin including nitrogen (Sibeon et al., 1978; Arbin, 1977; Evans, 1980;
Ferry et al., 197'4; Helleberg, 1976); argon-methane, 90:10 (Plazonnet and
Vandenheuvel, 1977; Jensen, 1978; Guissou et al., 1983); and helium (Nishioka
al., 1990). Except for the method of Nishioka et al., 1990, these assays involve the
application of packed column technology.
Make-up gases are frequently used in many capillary GC methods since the
low column flow rates (1-5 mL/min) employed do not sufficiently maintain cell
volume or effectively sweep the electron capture detector cell (ECD). The ECD is
a concentration sensitive detector, the sensitivity being inversely related to flow.
Flow through the cell then, must be sufficient to maintain ECD cell volume in order

168
to accomodate the high surface area of the 6 3Ni source as well as to efficiently
sweep the cell so that solute mixing does not occur. Use of the make-up gas also
assures an equlibrium concentrations of thermal electrons in the ECD. Argon^
methane (95:5) was chosen as a make-up gas at a flow rate of 65 mL/min, since this
provided the greatest sensitivity, the lowest S/N ratio, and minimal band spreading.
The length of the capillary column entering the detector cell appeared to
influence absolute indomethacin area counts markedly. In spite of the
recommended depth of 72 mm into the ECD cell (Hewlett-Packard support line), a
depth of about 40 mm provided maximal area counts and was therefore chosen for
the assay. This could be due to effective sweeping of the make-up gas at the
detector base.
In summary, the optimised operating conditions for routine analyses were:
column, Ultra-2 fused silica capillary column cross-linked with 5%
phenylmethylsilicone (25 m x 0.31 mm x 0.52 urn film thickness); injection mode,
splitless; injection port temperature, 200°C; initial column temperature, 210°C (1
min); oven programming rate, 40°C/min; final oven temperature, 300°C (6 min);
detector temperature (ECD), 330°C; carrier gas, ultra high purity hydrogen gas at a
column head pressure of 70 kPa (column flow rate ~1 mL/min); purge delay time,
0.75 min; make-up gas, argon-methane, 95:5, at a flow rate of 65 mL/min.

169
Internal Standards
Several compounds were screened as potential internal standards in this assay
(Figure 12 illustrates some of these). A variety of internal standards have been
reported in the literature including compounds that are not structurally related to
indomethacin, such as phenylbutasone (Mehta and Calvert, 1983), phenacetin
(Avgerinos and Malamataris, 1989), testosterone (Kwong et al., 1982), itraconazole
(Al-Angaary et al, 1990), penfluridol (Guissou et al., 1983), esters of indomethacin,
such as indomethacin propyl ester (Nishioka et al., 1990), and indomethacin methyl
ester (Arbin, 1977), and close structural analogs of indomethacin, such as a-methyl
indomethacin (Stubbs et al., 1986; Bayne et al., 1981), and 5-fluoroindomethacin
(Sibeon et al, 1978).
Ideally the internal standard should:
1. Be a close structural analog of indomethacin, so that it exhibits similar extraction
and chromatographic behaviour.
2. Possess an active carboxylic acid site for derivatisation like indomethacin.
3. Elute in a region free from endogenous interference and close to the analyte of
interest.

170
4. Produce a peak response equivalent to the analyte's, resulting in area ratio of
unity at equivalent concentrations.
5. Not exhibit any chemical interactions with indomethacin.
6. Possess good chemical stability following derivatisation.
With these requirements in mind several compounds were evaluated as potential
candidates. Sulindac, a close structural analog of indomethacin, was one of the first
compounds to be tested (Figure 12). Chemically, it had an ideal halogen (i.e.,
fluorine) function on the 5 th position of the heterocyclic ring and an acetic acid
function on the 3rd. It also produced a satisfactory peak when derivatised with
either MTBSTFA or PFBBr, and calibration curves when derivatised with the
former, were linear with r>0.999. However, it was speculated that sulindac was
oxidised to a sulphone in the injection port, due to the appearance of a coeluting
peak in the chromatogram (Figure 14). Use of lower injection port temperatures did
not affect peak "X" as it continued to elute. Recrystallising sulindac from
chloroform also did not help, although one polymorph was selectively isolated as
depicted in the DSC scan in Figure 15. The fact that there is no reported GC
method for sulindac in the literature would also appear to indicate that this
compound is not stable under these conditions. Based upon these observations this
compound was not considered further.

171
Zomepirac, a structurally similar compound to indomethacin, provided a
fairly good chromatographic response when derivatised with MTBSTFA and
appeared to satisfy most of the requirements mentioned above. Figure 16 illustrates
a representative chromatogram of indomethacin and zomepirac spiked in fetal
plasma. When spiked in stored plasma, amniotic, tracheal fluids, and urine (fetal
and maternal) as well as freshly collected amniotic and tracheal fluids and fetal
urine, both indomethacin (Rt = 5.9 min) and zomepirac (Rt = 3.9 min) eluted in
regions free from any significant interference. However, the analysis of
experimental samples and use of freshly collected blank fetal plasma samples
resulted in a co-eluting endogenous peak that interfered with that of zomepirac. It
was, therefore, not possible to use zomepirac as an internal standard for the analysis
of experimental samples. Zomepirac was used, however, as the internal standard
during initial validation studies with amniotic fluid (Tables 5b and 6c). Figure 36
provides a representative chromatogram of indomethacin and zomepirac spiked in
amniotic fluid and illustrates that no interference was present for either compound.
A further re-examination of chromatographic conditions, columns,
derivatising agents, and screening of other internal standards (carprofen,
acemetacin, 5-fluoroindomethacin) was then conducted. However, none of these
proved to be satisfactory, a-methyl indomethacin, on the other hand, met all the
requirements of an ideal internal standard outlined above. It is a very close

172
structural analog of indomethacin (Figure 17), elutes in a region free from any
endogenous interference (Figure 33) and close to the analyte, and yields an area
ratio of about unity at equivalent concentrations, a-methyl indomethacin was
chosen, therefore, as the internal standard for the final assay procedure.
Using a-methyl indomethacin, calibration curves were linear over the
working range of 1-32 ng of indomethacin. mL"1 with a coefficient of determination
(r2) > 0.99, following extraction of 0.1 mL of plasma, and 0.1-1.0 mL of urine,
amniotic and tracheal fluids. Linearity was also observed over a concentration
range of 1-500 ng/mL (r2 > 0.99). Inter- and intra-day variabilities at each
concentration point were < 11 % for concentrations between 2-32 ng/mL and < 20
% at the L O Q of 1 ng/mL. The limit of quantitation is 1 ng/mL (< 10% C . V . , S/N >
10). The developed method is therefore reproducible and robust for accurate
determination of indomethacin concentrations in biological fluids.
Derivatisation Conditions
Derivatisation of indomethacin and a-methyl indomethacin with 100 u L of
toluene containing 8 uL of M T B S T F A (8% v/v) at 6 0 ° C for 50 minutes was found
to be rapid, constant, and reproducible with maximal indomethacin area counts. No
significant differences in peak response were observed between the temperatures of

173
60-90°C (Figure 10) and between reaction times of 50-60 minutes (Figure 11). A
reaction time of 50 minutes and temperature of 60 °C was chosen to ensure
complete derivatisation. This is the first reported use of MTBSTFA as a
derivatising agent for indomethacin. Plazonnet and Vandenheuvel, 1977, used BSA
to silylate indomethacin producing the trimethylsilyl ester. They derivatised
indomethacin with 10 |iL of BSA and 90 uL of ethyl acetate (10%), and
reconstituted the final samples with 3% BSA in ethyl acetate since the resulting
TMS esters were prone to hydrolysis. However, this problem is not evident for
MTBSTFA since this molecule contains sterically crowded alkyl substituents on the
silicon atom that confers hydrolytic stability. In this assay, 100 |iL of a 8% v/v
solution of MTBSTFA (8 |iL) in toluene (92 fiL) produced optimal reaction
conditions.
A solvent is usually used in the reaction medium for derivatisation and for
reconstitution, i.e., dilution prior to injection into GC. Some of the recommended
solvents in silylation reactions include pyridine, dimethylformamide (DMF),
dimethyl sulphoxide, tetrahydrofuran, and acetonitrile (Blau and Halket, 1993).
However, toluene appeared to be a better medium for MTBSTFA derivatisation and
for sample dilution than any of these solvents (DMF, Acetonitrile, or ethyl acetate),
and on this basis was selected for the assay.

174
It has been suggested that addition of t-butyldimethylchlorosilane
(TBDMCS, 1% v/v) as a catalyst improves the silylation power of MTBSTFA
(Mawhinney and Madson, 1982; Ballard et al, 1990; Lewis and Yudkoff, 1987).
However, addition of this agent did not have any effect on indomethacin area
counts.
MTBSTFA has been popularly used over the recent years to derivatise
various chemicals and drugs for GC determinations. The carboxy lie acid
derivatisations reported in the literature include: carboxylic and hydroxyl groups in
tartaric acid and y-resorcylic acid (Kim et al, 1989), and valproic acid and its
metabolites (Abbott et al, 1986).
Stability studies on indomethacin
Indomethacin is a pale yellow crystalline powder. It may exist in amorphous
or crystalline forms [Form I (mp 160-162 °C) and Form II (mp 153-155°C), with
Form I being more stable]. Form II converts to the more stable Form I on storage.
Indomethacin is sparingly soluble in water and early pharmaceutical formulations
incorporated a small amount of mild alkali (sodium carbonate or bicarbonate) to
improve solubility. However, in the presence of strong alkali such as sodium
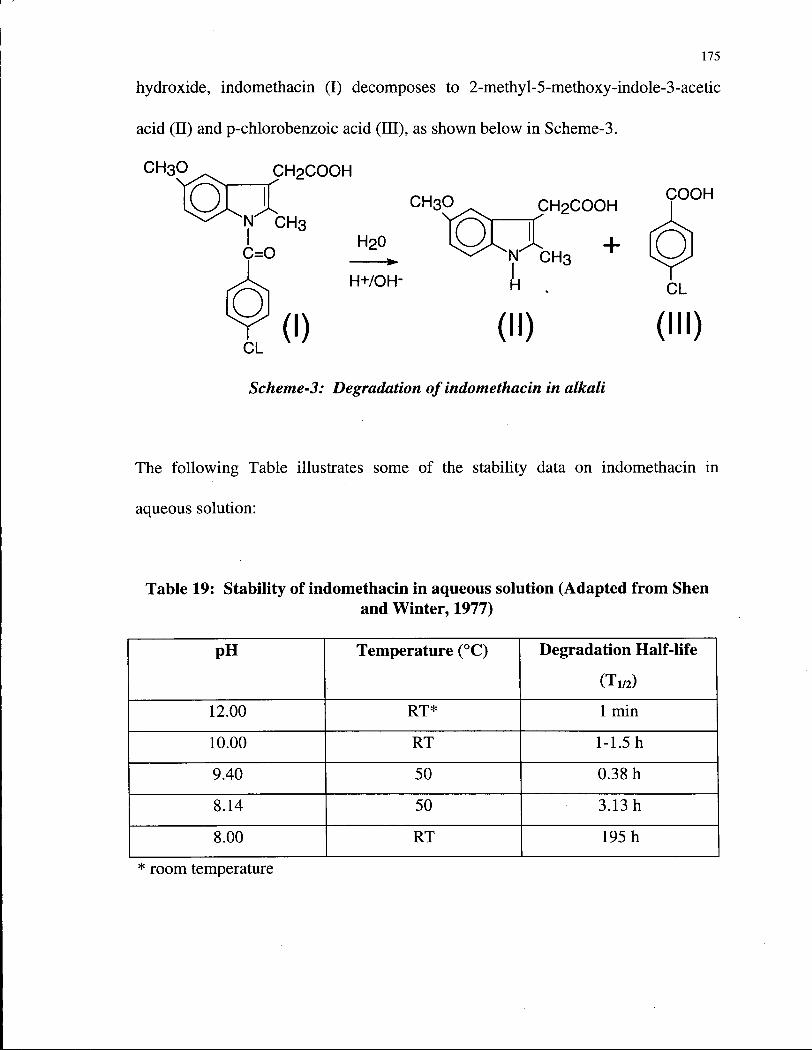
175
hydroxide, indomethacin (I) decomposes to 2-methyl-5-methoxy-indole-3-acetic
acid (II) and p-chlorobenzoic acid (III), as shown below in Scheme-3.
Scheme-3: Degradation of indomethacin in alkali
The following Table illustrates some of the stability data on indomethacin in
aqueous solution:
Table 19: Stability of indomethacin in aqueous solution (Adapted from Shen and Winter, 1977)
pH Temperature (°C) Degradation Half-life
(Tw) 12.00 RT* 1 min
10.00 RT 1-1.5 h
9.40 50 0.38 h
8.14 50 3.13 h
8.00 RT 195 h
* room temperature

176
In our study, indomethacin was administered in a vehicle of 1.1% ethanol
and 0.75% sodium bicarbonate in normal saline. The pH of this infusate is about
7.8-7.9. Stability studies on indomethacin in this vehicle indicated that the drug was
stable for at least 96 hours at both room temperature and standard regfrigerator
temperature (4°C) (Figure 37). This observation is consistent with that of Shen and
Winter, 1977, who determined the T i / 2 of indomethacin in an aqueous solution, at
pH 8.00, to be about 195 h at room temperature.
Several pharmaceutical formulations have been designed for indomethacin
administration in animal experimentation from the combined standpoints of stability
and solubility. It is strongly recommended that these solutions be freshly prepared
before each study. These indomethacin formulations usually contain sodium
carbonate, mannitol, and Emulphor-620, with the pH of the resulting solution being
between 8.4-9.1 (Shen and Winter, 1977).
Indomethacin powder solubilised in a vehicle of simple syrup with 10%
alcohol (pH 5.2) for pediatric administration appeared to be stable for at least 224
days at 24°C (Das Gupta et al, 1978). Curry et al, 1982, reported that a solution of
indomethacin in 0.1 M sodium carbonate (pH 10.7) lost 75% of its content in 80
minutes: Adjustment of the pH to 7.4 resulted in stability for at least 24 h. These
authors also found that a solution of indomethacin in polyethylene glycol, PEG 400,
1 7 7
was stable. However, Curry et al., 1982, also indicated that inclusion of sodium
carbonate in a vehicle can be potentially dangerous, and recommended that while
preparing a solution containing Na2C03, the sodium carbonate must be added very
slowly to the indomethacin slurry to avoid rapid degradation in a high alkalinity
environment. It appears that vehicles containing PEG or alcohol would be highly
desirable from the standpoint of stability, but not quite so from the pharmacological
perspective.
The maximal stability of indomethacin in aqueous solution at 25 °C is at pH
4.9, and solutions at this pH are predicted to be stable for at least 2.0 years (Kahns et
al., 1989). A 3% aqueous indomethacin solution was prepared in 30% each of ethyl
carbamate and ethylurea and the mixture boiled for 30 sees (pH 6.95) resulting in
stability for 25 months at 20°C (Pawelczyk and Knitter, 1978).
Indomethacin was observed to be most stable in surfactant systems
solubilised in Tween 80 or Brij 99. The T 1 / 2 in these solutions being more than 6
months (Ghanem et al., 1979). The following Table summarises some of these
vehicles:

178
Table 20: Stability of indomethacin in surfactant solubilised systems (Adapted from Ghanem et al., 1979)
Vehicle Condition T 5 0 (months) Tween 80 RT* 9.8 Tween 80 5°C 12.6
Brij 99 RT 10.7 Brij 99 5°C 15.5
Tween 80, 40% syrup, sodium benzoate
RT 6.8
Tween 80, 60% syrup, sodium benzoate
RT 12.4
Tween 80, 20% glycerol, 40% propylene glycol
RT 11.9
Tween 80, 10% ethanol, 10% glycerol
RT 11.9
Brij 99, chlorocresol 5°C 17.7 Brij 99, sodium thiosulphate 5°C 17.7 * room temperature
It appears then, that the following parameters are important to ensure drug
stability: p H of the infusate (it is preferable to keep the p H from exceeding 8.0
units); mode and order of ingredient mixing (as determined by Curry et al., 1982);
and use of surfactants (these wi l l aid against degradation). I also strongly
recommended that freshly prepared solutions be used. Use of the sodium trihydrate
salt of indomethacin, which is presently being employed in the treatment of patent
ductus arteriosus, however, may be preferable as it would be completely soluble in
aqueous solutions.
The stability of indomethacin in biological fluids and extracted samples was
also assessed. The drug was found to be stable for at least four freeze-thaw cycles,

179
at least 24 h on the bench-top, at least 24 h on the acidified sample matrix, and at
least one week on the autosampler tray (Table 6). Indomethacin is also stable in
plasma and urine samples stored in the freezer in the time periods studied to date
(over 14 months).
Data on the stability of indomethacin during analytical development in
existing assays have been sparse. Al-Angary et al., 1990, found that indomethacin
was stable for at least 1 month in serum at -20°C. Indomethacin was found to be
stable for at least 30 minutes in various extraction solvents including ethyl acetate,
hexane 2 propanol, chloroform, benzene-cyclohexane, and hexane-diethyl ether, all
acidified to pH 2.0 with HC1 (Catrula and Cusido, 1992).
4.2. Disposition of indomethacin in sheep
Following assay development and validation the method was applied to the
study of indomethacin disposition in the chronically instrumented pregnant sheep
model. The indomethacin concentrations in the fetus, obtained in the high dose
group, were similar to those observed during human tocolysis , i.e., ~ 200 ng/mL
(Moise et al., 1990). Steady state levels in fetal plasma were achieved over the 5-69
hour period following indomethacin infusion, while in some fetuses this was
delayed and was observed over the 23-69 hour period. Since samples were only

180
collected twice daily, six hours apart, it was not possible to determine the exact time
and/or duration of the steady state achieved. The mean steady state fetal femoral
arterial concentration of indomethacin was 181.67 + 45.05 ng/mL in the high dose
ewes (n=5), and 41.29 ± 3.14 ng/mL in the low dose ewes (n=2). Fetal total body
clearance was estimated to be 44.55 ± 11.14 mL/min (n=7). Indomethacin was
detected in very low levels in urine (Section 4.2.3.). The urine samples were also
subjected to enzyme hydrolysis with [ -glucuronidase, and the results indicate the
presence of glucuronide metabolites of indomethacin, suggesting that the fetal lamb
does have some ability to conjugate indomethacin (Table 17). This aspect of fetal
drug metabolism (i.e., conjugation), however, requires further investigation.
4.2.1 Placental transfer of indomethacin in sheep
Indomethacin is a polar and fairly medium molecular weight (MW 357.8)
organic acid that crosses the placental membrane easily in humans (Moise et al,
1990) and rabbits (Parks et al, 1977; Harris and VanPetten, 1981). In the present
study with the pregnant sheep model, however, there is a limited placental
permeability to indomethacin. The sheep placenta has been shown to be relatively
impermeable to polar compounds (Boyd et al., 1976). There is a low but
statistically significant arterio-venous indomethacin concentration difference at
apparent steady state indicating placental uptake of the drug (Figures 42, and 43;

181
Tables 13 and 14). Indomethacin levels were below detection limits in maternal
arterial and uterine vein plasma samples collected in one ewe suggesting little or
quantitatively insignificant placental transfer of indomethacin. In other studies, the
fetal-to-maternal (F/M) drug ratio has been reported to be 0.28 (Anderson et al,
1980c) and 0.04 (Harris and Vanpetten, 1981) in sheep, indicating limited placental
transfer of indomethacin in this species. The epitheliochorial placenta in sheep has
a placental pore radius of 4-5 A, while the hemochorial placenta in rabbits and
humans behaves as if it has a placental pore radius of -300 A. This difference could
explain, in part, the limited placental permeability in sheep. In general, the sheep
placenta has been reported to be relatively impermeable to polar compounds (Boyd
et al., 1976). The partition coefficient of the nonionised form of indomethacin and
that of the ionised form of the drug, between 1-dodecanol and water at 32°C, has
been determined to be 2400 and 1.1, respectively (De Vos et al., 1994). Ionised
indomethacin is also reported to form ion-pairs with such ions as Na+, K+, and NH 4+
(De Vos et al., 1994). It is likely that indomethacin partitions into a lipophilic phase
predominantly in the un-ionised form. Indomethacin could form ion-pairs with
cations in the physiological milieu, and thus its implication in absorption through
biological membranes may be underestimated (De Vos et al., 1994).
A relatively high degree of plasma protein binding has been reported for
indomethacin in maternal (98.5%) and fetal (97.6%) sheep (Anderson et al., 1980c).

182
This is markedly higher than that observed in pregnant rabbits, where the maternal
binding of indomethacin (85.6%) is significantly higher than fetal binding (43.8%)
(Harris and Vanpetten, 1981). However, these differences cannot be attributed
solely to species differences because: (a) the methods of protein binding used are
different; ultracentrifugation (Anderson et al., 1980c), and equilibrium dialysis
(Harris and Vanpetten, 1981), and (b) use of radiolabeled indomethacin (14C) by
Anderson et al., 1980c, and unlabeled indomethacin by Harris and Vanpetten, 1981.
4.2.2. Placental clearance
To date, three major methods have been reported in the literature for
determining placental clearance: the Fick principle (Meschia et al., 1967), the Szeto
(Szeto et al, 1982b) and the Anderson methods (Anderson et al., 1980c). Placental
clearance is defined as the ratio of flux in the concentration difference between the
maternal artery and fetal umbilical artery (Meschia et al., 1967), while fetal
clearance may be defined as the number of mL of plasma from which a drug is
completely removed per unit of time (Anderson et al., 1980c).
The Fick principle involves sampling of maternal arterial and uterine venous
blood or fetal femoral arterial and umbilical venous blood to determine drug
concentrations in these samples following a respective maternal or fetal steady state
infusion. It also requires quantitative data on uterine or umbilical blood flow,

183
respectively. Placental clearance is then calculated as a product of the blood flow
rate and the ratio of arterio-venous concentration difference to the arterial drug
concentration at apparent steady state. The Anderson method involves the
simultaneous administration of a fetal intravenous bolus dose of labeled drug and
maternal i.v. infusion of unlabeled drug. The total fetal body clearance (Ctot = C p +
Cf) can be determined from the fetal bolus. Placental clearance, then, is determined
as the product of the total body clearance (Ctot) and the ratio of steady state fetal to
maternal concentrations of the drug (F/M). However, a major limitation is the
inability of the method to differentiate between the intact drug and its metabolites.
Other limitations include the difficulty of procuring a stable isotope or radiolabeled
form of the drug and possibility of an "isotope effect" occuring, i.e., selectivity of
the placenta between the isotope and its natural element. The Szeto method
involves the representation of the maternal-fetal unit as a two compartment
pharmacokinetic system that requires paired drug infusions to steady state to both
the mother and the fetus. A potential limitation again, is the availiability of a stable
isotope labeled drug and an analytical method that will selectively quantitate the
unlabeled compound and the stable isotope. If the stable isotope labeled drug is not
available, then the experiments need to be performed on different days with a
suitable washout period between them. This may result in considerable variablility
due to time-dependent changes in both maternal and fetal physiology. The fetus, for
example, grows at the rate of about 5% per day (Kong et al., 1975). Apart from
these limitations, the requirement that detectable drug concentrations should be seen

184
in the maternal circulation across the placenta during fetal infusion studies, and vice
versa, must be met. In the current fetal indomethacin infusion studies, drug
concentrations were below detection limits in MA and UTV samples precluding
therefore, the application of the Szeto method to determine placental clearance.
The Fick principle is also not without problems. It requires more extensive
surgical catheterisation of the umbilical venous or uterine blood vessel apart from
either MA or FA vessels. It also requires determination of either the umbilical or
uterine blood flow. Another problem lies in the complexities of the fetal circulation
as there may be a difference between observed and actual concentrations leaving the
sites of exchange, e.g., uterine venous blood may be a mix of myometrical and
placental venous blood.
In spite of these potential problems the Fick principle may be used to
determine placental clearance. However, it must be borne in mind that the method
allows for the estimation of either the fetal to maternal placental clearance or vice
versa, at any given time. Examples of its use include the estimation of placental
clearance of glucose analogs (Stacey et al., 1978), sodium and chloride (Armentrout
et al, 1977), and ritodrine (Wright, 1992) in the fetal lamb.
In this study, there is a low but statistically significant difference between the
indomethacin concentrations in FA and UV plasma at apparent steady state (mean

185
difference: 11.718 + 0.8849 ng/mL; mean ± s.e.m., n=3), indicating placental
uptake of indomethacin (Tables 13 and 14). Placental clearance values were
determined only for two ewes, one at the high dose, and the other at the low dose.
This was due to surgical failures of cannulation, catheter failures during
experimentation (especially UV sampling), and the unavailability of umbilical blood
flow data. The placental clearance of indomethacin as determined by the Fick
method was calculated to be 9.43 mL/min/kg in E 796 and 8.28 mL/min/kg in E
1137. These values are only somewhat higher than the value of 2.10 ± 0.32
mL/min/kg reported by Anderson et al, 1980c. The mean placental clearance value
for indomethacin in this study, i.e., 8.85 mL/min/kg, is similar to that determined for
ritodrine, i.e., 9.2 + 2.7 mL/min/kg (Wright, 1992), but markedly lower than the
values reported for other drugs in the fetal lamb, namely, metaclopramide - 103 ± 13
mL/min/kg (Riggs et al., 1989), diphenhydramine - 124 ± 22 mL/min/kg (Rurak et
al, 1991), and methadone - 168 ± 29 mL/min/kg (Szeto et al, 1982a). The
observed placental clearance of indomethacin in E 796 (high dose ewe) accounts for
more than 80% of the total fetal body clearance while in the low dose ewe (E 1137)
it accounts for about 55%.

186
4.2.3. Elimination of indomethacin by the fetal kidney
It was evident from the present study that the pathway for elimination of
indomethacin, a weak acid, by the fetal kidney are not matured. Very low levels of
indomethacin were observed in fetal urine samples collected from the high-dose
ewes, and indomethacin concentrations were below detection limits in urine samples
from the low dose ewes. Similar observations have been reported for other weakly
acidic agents such as valproic acid (Gordon et al., 1994), diphenylmethoxy acetic
acid or DPMA (Tonn et al., 1994), and p-aminohippuric acid (Elbourne et al., 1990)
in the ovine fetus. It has been speculated that the pathways for the excretion of
organic acids by the fetal kidney mature after birth in contrast to that for organic
bases which appear to mature much earlier (Elbourne et al., 1990). The estimated
fetal renal indomethacin clearance value in this study (Table 18) was very low
(0.015 ± 0.009 mL/min) and not significantly different from zero. This is again,
consistent with findings for valproic acid (Gordon et al., 1994) and
diphenylmethoxy acetic acid, an acid metabolite of diphenhydramine (Tonn et al.,
1994), in the fetal lamb.

187
4.3. Drug disposition in amniotic and tracheal fluids
4.3.1. Amniotic fluid
Indomethacin concentrations in amniotic fluid were significantly lower than
FA plasma levels in the present study. Amniotic fluid indomethacin concentrations
were below detection limits in E 1137 and E 1115, the two low dose ewes. These
findings are also consistent with those observed for valproic acid and DPMA
(Gordon et al., 199»4; Tonn et al., 1994). However, they are in sharp contrast to
observations for basic drugs (metoclopramide, dyphenhydramine, labetalol, and
ritodrine) which have been shown to accumulate considerably in amniotic fluid
(Rurak et al., 1991). Renal excretion of drug and subsequent appearance in
amniotic fluid has been observed for meperidine (Szeto et al., 1978), lidocaine
(Morishima et al., 1979), and ethanol (Clarke et al., 1987) in the fetal lamb. It has
been suggested that basic drugs accumulate in amniotic fluid due to the mechanism
of "ion-trapping" due to the lower pH of amniotic fluid as compared to fetal plasma
(Szeto et al., 1978). The sources of drug appearance in the amniotic fluid are two
fold, i.e., fetal renal drug elimination (time delay in the appearance of drug in the
amniotic fluid following dosage is characteristic for this type), and diffusion across
chorio-allantoic membranes. The latter route was suggested to be a predominant
pathway for the appearance of meperidine in amniotic fluid (Szeto et al., 1978).
Renal elimination, on the other hand, has been suggested to be important for

1 8 8
compounds such as mannitol (Basso et al, 1977). Metabolites have also been
detected in amniotic fluid with the glucuronide conjugates of ritodrine serving as an
example (Wright et al., 1991). The presence of glucuronide conjugates in amniotic
fluid for indomethacin in the present study, however, could not be confirmed due to
limited sample volume.
4.3.2. Tracheal fluid
Indomethacin levels in fetal tracheal fluid samples were below assay
detection limits. While above detectable limits, the concentrations of valproic acid
(Gordon et al., 1994) and DPMA (Tonn et al., 1994), two other acidic compounds,
in tracheal fluid have been reported to be very low. This is in sharp contrast to basic
drugs, such as metaclopramide, ritodrine, labetalol, and dyphenhydramine, wherein
the drug levels in tracheal fluid were equivalent or even higher than those in fetal
plasma, the extent of accumulation being greatest for metoclopramide (Riggs, 1989;
Wright etal, 1991; Yoo, 1989; Yeleswaram, 1992).
Basic drugs are known to accumulate in the adult lung. Amphiphilic amines
are preferentially taken up by the lung which appears to be a major organ of
clearance for these agents. It has been suggested that molecules containing the
amino group and a lipophilic alkyl function are necessary for lung specificity and
uptake (Fowler et al., 1976) and that predictions can be made on the basis of drug

189
basicity and lipid solubility. Okumura et al., 1978, have implied the existence of
active transport system or a specialised binding system as a mechanism for
accumulation of basic drugs in the lung. There is also evidence to suggest that
mitochondrial monoamine oxidase (MAO) is a binding site for tertiary basic drugs
in the lung (Yoshida et al., 1989) and may hence act as a reservoir. Carrier-
mediated transport processess for the uptake of organic anions (Schanker, 1978) and
amino acids (Lin and Schanker, 1981) have been reported in the rat lung. However,
there is no reported accumulation of weakly acidic drugs in the tracheal fluid,
suggesting that the lung plays a minor role in the elimination of these compounds.
4.4. Effect of indomethacin on physiological factors
Indomethacin appears not to influence arterial p02 and arterial pC02 in both
high and low dose ewes, as they remain constant throughout the study period in
relation to control (Figures 41 A, B). Indomethacin also did not appear to affect
fetal arterial blood lactate levels in low dose ewes. However, in three high dose
ewes lactate levels were markedly higher than respective controls (Figure 41 D). It
was interesting to note that the drug did not influence arterial glucose levels in
either of the two dose groups (Figure 41 C). Significant decreases in arterial pH as
well as base excess were observed when indomethacin was given in higher doses,
whereas the values remained more or less constant in low dose ewes compared to
the respective controls (Figures 41 E, F). It can be observed that indomethacin

190
caused lactic acidosis in some high dose ewes (E 1221, E 984, and E 2160) and that
the effect might be dose related as the same was not observed in low dose ewes.
Further, a severe metabolic acidosis was observed when indomethacin was
administered as a 6 hour intravenous infusion at a dose of 17 jig/min in hypoxic
ovine fetuses (Hooper et al., 1992). The severe lactic acidosis observed in E 1221,
E 2160, and E 984 (high dose group fetuses) were characterised by markedly
reduced fetal pH. All the three fetuses died following cessation of drug infusion.
That the deaths of these fetuses was attributable solely to drug effect is
questionable, as death due to infectious etiology cannot be ruled out. Further, high
dose group fetuses that survived the experimental protocol demonstrate that the drug
does not cause significant lactic acidemia. Also, no significant reduction in arterial
pH, p02, pC02, or base excess was observed. Further investigation is underway to
elucidate the relationship between indomethacin and lactic acidemia.
In three of the high dose ewes (E 2160, E 984Y, and E 796), there was a
significant reduction in fetal urine flow rate, in the order of 50%, within 23 hours of
initiating indomethacin infusion (Figure 44). A similar reduction in urinary flow
rate, in the order of 55%, was observed within 2 hours of a 5 h indomethacin
infusion at an identical dose (Walker et al., 1992a). This effect on urinary flow rate
appears to be dose related. When indomethacin was infused at a rate of 0.017
mg/kg/min for 5 h, fetal urinary output significantly increased by an order of -85%

within 3 hours (Walker et al., 1992b). Further studies are being carried out to
elucidate the mechanism of oliguria and its physiological implications.

192
5 S U M M A R Y AND CONCLUSIONS
The following points summarise the salient features of the developed assay
method:
1. Simple one step liquid-liquid extraction procedure.
2. High efficiency fused silica capillary column technology.
3. Rapid run times (9.25 min)
4. Simple and rapid derivatisation with the relatively safer MTBSTFA.
5. Small sample volumes (0.1-1.0 mL).
6. Sensitivity of 1 ng/mL (Limit of quantitation, < 10% C.V., S/N >10).
7. Excellent chromatography with both the analyte, indomethacin, and the internal
standard, a-methyl indomethacin, eluting in regions free from endogenous
interference.
Overall the developed method offers several advantages over existing
analytical techniques for indomethacin in biological fluids, the most important
being: improved sensitivity, simpler sample preparation, improved selectivity, and a
smaller biological fluid sample requirement.
193
Application of the method to indomethacin measurement in plasma, urine,
tracheal and amniotic fluid samples was demonstrated by investigating its
disposition in the ovine fetus. The following observations were made:
1. The fetal plasma concentrations of indomethacin in the high dose animals were
similar to those seen during human tocolysis (Moise et al., 1990).
2. The low levels of indomethacin in amniotic fluid and fetal urine are consistent
with our observations for other organic acids (e.g., valproic acid,
diphenylmethoxyacetic acid) in the fetal lamb.
3. Unlike our observations with basic amine compounds (e.g., metoclopramide,
diphenhydramine), indomethacin was not observed to accumulate in tracheal
fluid.
4. The mean steady-state fetal femoral arterial concentration of indomethacin was
181.67 ± 45.05 ng/mL in the high dose group (n=5) and 41.29 ± 3.14 ng/mL in
the low dose group (n=2).
5. The arterio-venous concentration difference for indomethacin, at apparent steady
state, was minimal but statistically significant suggesting a low placental
permeability to indomethacin in sheep. This finding is consistent with
observations in other studies (Anderson et al., 1980; Harris and Vanpetten,
1981).

194
6. The fetal total body clearance of indomethacin was estimated to be 44.55 ±
11.14 mL/min (n=7).
7. The placental clearance of indomethacin as determined by the Fick principle was
calculated to be 8.85 ± 0.81 mL/min/kg.

1 9 5
6 REFERENCES
Abbott, F.S., Kassam, J., Acheampong, A., Ferguson, S., Panesar, S., Burton, R., Farrell, K., and Orr, J.: Capillary gas chromatographic-mass spectrometry of valproic acid metabolites in serum and urine using tert-butyldimethylsilyl derivatives. / Chromatogr. 375 (2): 285-298, 1986.
Ahuja, S.: Derivatisation in gas chromatography. JPharmSci. 65: 163-182,1976.
Al-Angary, A.A., El-Sayed, Y.M., Al-Meshal, M.A., Lutfi, K.M.: High-performance liquid chromatographic analysis of indomethacin in serum. / Clin Pharm Ther. 15: 257-265, 1990.
Alvan, G., Orme, M., Bertilsson, L., Ekstrand, R., and Palmer, L.: Pharmacokinetics of indomethacin. Clin Pharmacol Ther. 18: 364-373, 1975.
Alvan, G.: Individual differences in the disposition of drugs metabolised in the body•. Clin Pharmacokinet. 3: 155-175,1978.
Anderson, D.F., Phernetton, T.M., and Rankin, J.H.G.: Prediction of fetal drug concentrations. Am J Obstet Gynecol. 137: 735-738, 1980a.
Anderson, D.F., Phernetton, T.M., and Rankin, J.H.G.: The placental transfer of acetylsalicylie acid in near-term ewes. Am J Obstet Gynecol. 136: 814-818, 1980b.
Anderson, D.F., Phernetton, T.M., Rankin, J.H.G.: The measurement of placental drug clearance in near-term sheep: indomethacin. J Pharmacol Exp Ther. 213: 100-104, 1980c.
Anderson, D.F., Stock, M.K., and- Rankin, J.H.G.: Placental transfer of dexamethasone in near-term sheep. J Dev Physiol. 1: 431-436,1979.
Anderson, R.J., Berl, T., McDonald, K.M., Schrier, R.W., McCool, A., and Gilbert, L.: Evidence for an in-vivo antagonism between vasopressin and prostaglandin in the mammalian kidney. J Clin Invest. 56: 420-426, 1975.
Andersson, K. -E., Forman, A., and Ulmsten, U.: Pharmacology of labour. Clin Obstet Gynecol. 26(1): 56-77,1983.
Aoyagi, N., Ogata, H., Kaniwa, N., and Ejima, A.: Bioavailability of indomethacin capsules in humans. (II): Correlation with dissoluation rate. Int J Clin Pharmacol Ther Toxicol. 23: 529-534,1985.

196
Aoyagi, N., Ogata, H., Kaniwa, N., and Ejima, A.: Bioavailability of indomethacin capsules in humans. (I): Bioavailability and effects of gastric acidity. Int J Clin Pharmacol Ther Toxicol. 23: 469-47'4, 1985.
Aranda, J.V., Turmen, T., and Sasyniuk, B.I.: Pharmacokinetics of diuretics and methylxanthines in the neonate. Eur J Clin Pharmacol. 18: 55-63,1980.
Arbin, A.: Three alkylation methods for the determination of indomethacin in plasma by electron-capture gas chromatography. J Chromatogr. 144: 85-92, 1977.
Arcilla, R.A., Thilenius, O.G., and Ranniger, K.: Congestive heart failure from suspected ductal closure in utero. J Pediatr. 75: 74, 1969.
Armentrout, T., Katz, S., Thornburg, K.L., and Faber, J.J.: Osmotic flow through the placental barrier of chronically prepared sheep. Am J Physiol. 233: H 466-H 474, 1977.
Astier, A., and Renat, B.: Sensitive high-performance liquid chromatographic determination of indomethacin in human plasma, pharmacokinetic studies after single oral dose. J Chromatogr. (Biomed Appl.) 233: 279-288, 1982.
Austin, N.C., Pairandeau, P.W., Hames, T.K., and Hall, M.A.: Regional cerebral blood flow velocity changes after indomethacin infusion in preterm infants. Arch Disease Child. 67: 851-854, 1992.
Avgerinos, A and Malamataris, S: High-performance liquid chromatographic determination of indomethacin in human plasma and urine. J Chromatogr. (Biomed Appl.) 495: 309-313, 1989.
Baber, N., Halliday, L.D.C., van den Heuvel, W.J.A., Walker, R.W., Sibeon, R., Keenan, J.P., Littler, T., and Orme, M.L'e.: Indomethacin in rheumatoid arthritis: Clinical effects, pharmacokinetics, and platelet studies in responders and ononresponders. Annals Rheum Dis. 38: 128-137, 1979.
Baer, J.E., Hucker, H.B., and Duggan, D.E.: Bioavailability of indomethacin in man. Annals Clin Res. 6 (supp.ll): 44-46, 1974.
Baer, J.E.: Role of drug metabolism in drug research and development: basic considerations. J Pharm Sci. 61: 1674-1677,1972.
Bakke, O.M., and Haram, K.: Time-course of transplacental passage of diazepam: influence of injection-delivery interval on neonatal drug concentrations. Clin Pharmacokin. 7: 353-362, 1982.
Ballard, K.D., Knapp, D.R., Oatis, J.E.Jr., and Walle, T.: Resolution of the seven isomeric ring-hydroxylated propranolols as tert-butyldimethylsilyl derivatives by
197
capillary gas chromatography-mass spectrometry. J Chromatogr. 277: 333-339, 1983.
Bass, L.: Flow dependence of first-order uptake of substances by heterogenous perfused organs. J Theoret Biol. 86: 365-376,1980.
Basso, A., Fernandez, A., Althabe, O., Sabini, S., Piriz, H., and Belitzky, R.: Passage of mannitol from mother to amniotic fluid and fetus. Obstet Gynecol. 49: 628-631, 1977.
Bayne, W.F., East, T., Dye, D.: High-pressure liquid chromatographic method with postcolumn, in-line hydrolysis and fluorometric detection for indomethacin in biological fluids. JPharmSci. 70: 458-459, 1981.
Beaven, M.A., and Bayer, B.M.: Factors influencing the uptake and disposition of indomethacin-[14C] in cell cultures. Biochem Pharmacol. 29: 2055-2061,1980.
Beazley, J.M., and Gillespie, A.: Double-blind trial of prostaglandin E2 and oxytocin in the induction of labour. Lancet. 1: 152,1971.
Berl, T., Raz, A., Wald, H., Horowitz, J., and Czazkes, W.S.: Prostaglandin synthesis inhibition and the action of vasopressin: Studies in man and rat. Am J Physiol. 232: F529- F 537, 1977.
Berman, W., Friedman, Z., and Vidyasagar, D.: Pharmacokinetics of inhibitors of prostaglandin synthesis in the prenatal period. Sem Perinatol. 4: 67-72, 1980.
Bernstein, M.S., and Evans, M.A.: High-performance liquid chromatography-fluoresence analysis for indomethacin and metabolites in biological fluids. J Chromatogr. (Biomed Appl.) 229: 179-187,1982.
Besinger, R.E., Niebyl, J.R., Keyes, W.G., and Johnson, T.R.B.: Randomised comparative trial of indomethacin and ritodrine for the long-term treatment of preterm labour. Am J Obstet Gynecol: 164: 981-988,1991.
Betkerur, M.V., Yeh, T.F., Miller, K., Glasser, R.J., and Pildes, R.S.: Indomethacin and its effect on renal function and urinary kallikrein excretion in premature infants with patent ductus arteriosus. Pediatr. 68: 99-102, 1981.
Bhat, R., Vidyasagar, D., Fisher, E., Hastreiter, A., Ramirez, J.L., Burns, L., and Evans, M.: Pharmacokinetics of oral and intravenous indomethacin in preterm infants. Dev Pharmacol Ther. 1: 101-110,1980.

198
Bhat, R., Vidyasagar, D., Vadapalli, M., Whalley, C, Fisher, E., Hastreiter, A., Evans, M.: Disposition of indomethacin in preterm infants. J Pediatr. 95: 313-316, 1979.
Bianchetti, G., Monin, P., Marchal, F., Dubruc, C., Boutroy, M.J., Morselli, P.L., and Vert, P.: Pharmacokinetics of indomethacin in the premature infant. Dev Pharmacol Ther. 1: 111-124,1980.
Bilka, P.J., Wollheim, F., and Williams, R.C.Jr.: Indomethacin: a new antirheumatic agent. Minn Med. 47: 777-781,1964.
Blau, K., and Halket, J.: Handbook of derivatives for chromatography. John Wiley, New York, 1993.
Blum, I.: Indomethacin in hypercalcaemia. Lancet. 1: 866, 1975.
Bond, J.T., Bailie, M.D., and Hook, J.B.: Maturation of renal organic acid transport in vivo: substrate stimulation by penicillin. J Pharmacol Exp Ther. 199: 25-31, 1976.
Bonds, D.R., Anderson, S., and Meschia, G.: Transplacental diffusion of ethanol under steady state conditions. J Dev Physiol. 2: 409-416,1980.
Boyd, R.D.H., Haworth, C., Stacey, T.E., and Ward, R.H.T.: Permeability of the sheep placenta to unmetabolised polar non-electrolytes. J Physiol. 256: 617-634, 1976.
Brash, A.R., Hickey, D.E., Graham, T.P., Stahlman, M.T., Oates, J.A., and Cotton, R.B.: Pharmacokinetics of indomethacin in the neonate. Relation of plasma indomethacin levels to response of the ductud arteriosus. N Engl J Med. 305: 67-72, 1981.
Brash, A.R., Hickey, D.E., Graham, T.P., Stahlman, M.T., Oates, J.A., and Cotton, R.B.: Pharmacokinetics of indomethacin in the neonate. Relation of plasma indomethacin levels to response of the ductus arteriosus. ./V Engl J Med. 305: 67-72, 1981.
Brien, J.F., and Clarke, D.W.: Disposition and fetal effects of ethanol during pregnancy. In "Toxicologic and pharmacologic principles in pediatrics", Kacew, S., and Lock, S. (Eds.), Hemisphere, 1988.
British Pharmacopoeia, London, 1980.
British Pharmacopoeia, London, 1988.

199
Brown, Y.L., Kandrotas, R.J., Douglas, J.B., Gal, P.: High-performance liquid chromatographic determination of indomethacin serum concentrations. / Chromatogr. 459: 275-279, 1988.
Bryant, C, Smith, M.J.H., and Hines, W.J.W.: Effects of salicylate and y-resorcylate on the metabolism of radioactive succinate and fumarate by rat-liver mitochondria and on dehydrogenase enzymes. BiochemJ. 86: 391-396, 1963.
Buddingh, F., Parker, H.R., Ishizaki, G., and Tyler, W.S.: Long-term studies of the functional development of the fetal kidney in sheep. Am J Vet Res. 32: 1993-1998, 1971.
Buick, A.R., Doig, M.V., Jeal, S.C., Land, G.S., McDowall, R.D.: Method validation in the bioanalytical laboratory. J Pharm Biomed Anal. 8: 629-637, 1990.
Burrows, J.L.: Evaluation of calibration routines in pharmaceutical and bioanalytical separations, with reference to Monte Carlo simulations. / Pharm Biomed Anal. 11: 523-531, 1993.
Cabrol, D., Landesman, R., Muller, J., Uzan, M., Surean, C, and Saxena, B.B.: Treatment of polyhydramnios with prostaglandin synthetase inhibitor (indomethacin). Am J Obstet Gynecol. 157: 422-426, 1987.
Campbell, D.B.: The use of kinetic-dynamic interactions in the evaluation of drugs. Psychopharmacoldgy. 100: 433-450, 1990.
Cardone, M.J., Willavize, S.A., Lacy, M.E.: Method validation revisited: a chemometric approach. Pharm Res. 7: 154-160,1990.
Carlan, S.J., O'Brien, W.F., O'Leary, T.D., and Mastrogiannis, D.: Randomised comparative trial of indomethacin and sulindac for treatment of refractory preterm labour. Obstet Gynecol. 79 (2): 223-238, 1992.
Carmichael, M.C., and Kumar, R.: Molecular biology of vasopressin receptors. Sem Nephrol. 14: 341-348, 1994.
Carr, G.P., and Wahlich, J.C.: A practical approach to method validation in pharmaceutical analysis. J Pharm Biomed Anal. 8: 613-618,1990.
Casey, M.L., and MacDonald, P.C.: Bimolecular processes in the initiation of parturition: Decidual activation. Clin Obstet Gynecol. 31: 533, 1988.
Caturla, M.C., and Cusido, E.: Solid-phase extraction for the high-performance liquid chromatographic determination of indomethacin, suxibuzone,

200 phenylbutazone, and oxyphenbutazone in plasma, avoiding degradation of compounds. J Chromatogr (Biomed Appl). 581: 101-107,1992.
Causey, A.G., Hill, H.M., and Phillips, L.J.: Evaluation of criteria for the acceptance of bioanalytical data. J Pharm Biomed Anal. 8: 625-628, 1990.
Cerretani, D., Runci, F.M., Segre, G.: High-pressure liquid chromatographic (HPLC) determination of indomethacin in plasma. Eur Rev Med Pharmacol Sci. 10: 409-413, 1988.
Chamberlain, P.F., Manning, F.A., Morrison, I., et al.: Ultrasound evaluation of amniotic fluid volume. Am J Obstet Gynecol. 150: 250-254, 1984.
Chaudhari, G.N., Tipnis, H.P., Doshi, B.S., and Kulkarni, R.D.: Bioequivalence studies in humans of indomethacin capsules marketed in India. Eur J Clin Pharmacol. 26: 261-264, 1984.
Chiang, C.N., and Lee, C.C. (Eds.): Prenatal Drug Exposure: Kinetics and Dynamics. NIDA Research Monograph. 60: 1-147,1985.
Ching, M.S., Mihaly, G.W., Morgan, D.J., Date, N.M., Hardy, K.J., and Smallwood, R.A.: Low clearance of cimetidine across the human placenta. / Pharmacol Exp Ther. 241: 1006-1009, 1987.
Chiou, W.L., and Lam, G.: The significance of the arterial-venous plasma concentration difference in clearance studies. Int J Clin Pharmacol Ther Toxicol. 20: 197-203, 1982.
Chiou, W.L., Lam, G., Chen, M.-L., and Lee, M.G.: Instantaneous input hypothesis in pharmacokinetic studies. JPharmSci. 70: 1037-1039,1981.
Chremos, A.N., Shen, D., Gibaldi, M., Proctor, J.D., and Newman, J.H.: Time-dependent change in renal clearance of bethanidine in humans. J Pharm Sci. 65: 140-142, 1976.
Cifuentes, R.F., Olley, P.M., Balfe, J.W., Raddle, I.C., and Soldin, S.J.: Indomethacin and renal function in premature infants with persistent patent ductus arteriosus. J Pediatr. 95: 583-587,1979.
Clarke, D.W., Patrick, J., Wlodek, M.E., Smith, G.N., Richardson, B., and Brien, J.F.: The role of fetal urinary excretion in the transfer of ethanol into amniotic fluid after maternal adminstration of ethanol to the near-term pregnant ewe. Can J Physiol Pharmacol. 65: 1120-1124,1987.
201
Clarke, G.S.: The validation of analytical methods for drug substances and drug products in UK pharmaceutical laboratories. / Pharm Biomed Anal. 12: 643-652, 1994.
Clench, J., Reinberg, A., Dziewanowska, Z., Ghata, J., and Smolensky, M.: Circardian changes in the bioavailability and effects of indomethacin in healthy subjects. Eur J Clin Pharmacol. 20: 359-369,1981.
Clozel, M., Behary, K., and Aranda, J.V.: Indomethacin metabolism in liver microsomes during postnatal development in the rat. Biol Neonate. 50: 83-90, 1986.
Clyman, R.I., Mauray, F., Rudolph, A.M., and Heymann, M.A.: Age-dependent sensitivity of the lamb ductus arteriosus to indomethacin and prostaglandins. J Pediatr. 96: 94-98, 1980.
Coceani, F., and Olley, P.M.: The response of the ductus arteriosus to prostaglandins. Can J Physiol Pharmacol. 51: 220-225, 1973.
Coceani, F., Bishai, I., White, E., Bodach, E., and Olley, P.M.: Action of prostglandins, endoperoxides, and thromboxanes on the lamb ductus arteriosus. Am J Physiol. 234: H 117-H 122, 1978a.
Coceani, F., Olley, P.M., and Bodach, E.: Lamb ductus arteriosus: Effect of prostaglandin synthesis inhibitors on the muscle tone and the response to prostaglandin E2. Prostaglandins. 9: 299-308, 1975.
Coceani, F., Olley, P.M., and Lock, J.E.: Prostaglandins, ductus arteriosus, pulmonary circulation: current concepts and clinical potential. Eur J Clin Pharmacol. 18: 75-81, 1980.
Coceani, F., Olley, P.M., Bishai, I., Bodach, E., and White, E.P.: Significance of the prostaglandin system to the control of muscle tone of the ductus arteriosus. In: Coceani, F., and Olley, P.M. (Eds.). Prostaglandins and Perinatal Medicine, Advances in Prostaglandin and Thromboxane Research, Volume 4, Raven Press, New York, pp. 325-333, 1978b.
Colditz, P., Murphy, D., Rolfe, P., and Wilkinson, A.R.: Effect of infusion rate of indomethacin on cerebrovascular responses in preterm neonates. Arch Disease Child. 64: 8-12, 1989.
Collins, J.M., and Dedrick, R.L.: Contribution of lungs to total body clearance: linear and non-linear effects. J Pharm sci. 71: 66-70, 1982.
202 Comline, R.S., and Silver, M.: Recent observations on the undisturbed fetus in utero and its delivery. In "Recent advances in physiology", Linden, R.J. (Ed.). Churchill Livingstone, Edinburgh, pp. 406, 1974.
Conn, R.B., Sabo, A.J., Landes, D., and Ho, J.Y.L.: Inconstancy of renal clearance values with changing plasma concentrations. Nature. 203: 143-146,1964.
Cook, J.A., and Smith, D.E.: Theoretical limits of changes in plasma protein binding or renal clearance. J Pharm Sci. 74: 108-109,1985.
Cooper, J.K., McKay, G., Hawes, E.M., Midha, K.K.: High-performance liquid chromatographic assay of indomethacin and its application in pharmacokinetics in healthy volunteers. J Chromatogr. (Biomed Appl.) 233: 289-296, 1982.
Cowan, F.: Indomethacin, patent ductus arteriosus, and cerebral blood flow. J Pediatr. 109: 341-344, 1986.
Curry, S.H., Brown, E.A., Kuck, H., and Cassin, S.: Preparation and stability of indomethacin solutions. Can J Physiol Pharmacol. 60: 988-992,1982.
Czuba, M.A., Morgan, D.J., Ching, M.S., Mihaly, G.W., Ghabrial, H., Hardy, K.J., and Smallwood, R.A.: Disposition of the diastereoisomers quinine and quinidine in the ovine fetus. J Pharm Sci. 80: 445-448, 1991.
Das Gupta, V., Gibbs, C.W.Jr., and Ghanekar, A.G.: Stability of pediatric liquid dosage forms of ethacrynic acid, indomethacin, methyldopate hydrochloride, prednisone, and spironolactone. Am J Hosp Pharm. 35: 1382-1385,1978.
Dawes, G.S.: Foetal and Neonatal Physiology. Year Book Medical Publishers, Chicago, 1968.
De Vos, A., Vervoort, L., and Kinget, R.: Release of indomethacin from transparent oil-waters gels. J Pharm Sci. 83: 641-643,1994.
de Vries, J.I.P., Visser, G.H.A., and Prechtl, H.F.B.: The emergence of fetal behaviour. II Quantitative aspects. Early Hum Dev. 12: 99-120,1985.
de Vries, J.I.P., Visser, G.H.A., and Prechtl, H.F.R.: The emergence of fetal behaviour. I Qualitative aspects. Early Hum Dev. 7: 301-322,1982.
De Zeeuw, D., Brater, D.C., Jacobson, H.R.: Micro-HPLC and transfer techniques for directly measuring drug (indomethacin) transport across the isolated perfused renal proximal straight tubule. J Pharmacol Meth. 19: 275-282,1988.
De Zeeuw, D., Leinfelder, J.L., Bruter, D.C.: Highly sensitive measurement of indomethacin using a high-performance liquid chromatographic technique

203 combined with post-column in-line hydrolysis. J Chromatogr. (Biomed Appl.) 380: 157-162, 1986.
De Zeeuw, D., Jacobson, H.R., and Brater, D.C.: Indomethacin secretion in the isolated perfused proximal straight rabbit tubule. Evidence for two parallel transport mechanisms. J Clin Invest. 81: 1585-1592,1988.
Dindogru, A., Gailani, S., Henderson, E.S., Wallace, H.J.Jr., and Fitzpatrick, J.: Indomethacin in hypercalcaemia. Lancet. 2: 365, 1975.
Dittrich, P., Kohler, D.G., Primbs, P., and Kukovetz, W.R.: Pharmacokinetics of indomethacin i.m. in blood, synovial fluid, synovial membrane, muscle, fat, bone, and spinal cord. Eur J Rheum Inflamm. 7: 45-50, 1984.
Donker, A.J., de Jong, P.E., van Eps, L.W., Brentjens, J.R., Bakker, K., and Doorenbos, H.: Indomethacin in Bartter's syndrome: Does the syndrome represent a state of hyperprostaglandinism? Nephron. 19(4): 200-213,1977.
Donnelly, P., Lloyd, K., and Campbell, H.: Indomethacin in rheumatoid arthritis: An evaluation of its anti-inflammatory and side effects. BrMedJ. 1: 69-75,1967.
Douidar, S.M., Richardson, J., and Snodgrass, W.R.: Role of indomethacin in ductus closure: An update evaluation. Dev Pharmacol Ther. 11(4): 196-212, 1988.
Dousa, T.P.: Cyclic-3', 5'-nucleotide phosphodiesterases in the cyclic adenosine monophosphate (cAMP)-mediated actions of vasopressin. Sem Nephrol. 14: 333-340, 1994.
Dudley, D.K.L., and Hardie, M.J.: Fetal and neonatal effects of indomethacin used as a tocolytic agent. Am J Obstet Gynecol. 151: 181-184, 1985.
Duggan, D.E., and Kwan, K.C.: Enterohepatic recirculation of drugs as a determinant of therapeutic ratio. Drug Metab Rev, 9: 21-41,1979.
Duggan, D.E., Hogans, A.F., Kwan, K.C., and McMahon, F.G.: The metabolism of indomethacin in man. J Pharmacol Exp Ther. 181: 563-575,1972.
Duggan, D.E., Hooke, K.F., Noll, R.M., and Kwan, K.C.: Enterohepatic circulation of indomethacin and its role in intestinal irritation. Biochem Pharmacol. 25: 1749-1754, 1975.
Dutton, G.J.: Developmental aspects of drug conjugation with special reference to glucuronidation. Ann Rev Pharmacol Toxicol. 18: 17-35, 1978.

204 Dutton, G.J.: Glucuronide synthesis in fetal liver and other tissues. Biochem J. 71: 141-148, 1959.
Dvorchik, B.H.: Drug disposition during pregnancy. Biol Res Pregnancy. 3: 129-137, 1982.
Ebbehoj, N., Friis, J., Svendsen, L.B., Bulow, S., and Madsen, P.: Indomethacin treatment of acute pancreatitis. A controlled double-blind trial. Scand J Gastroenterol. 20 (7): 798-800, 1985.
Eckard, R.: Amuno S: Klinisch-pharmakologische grundlagen. Akt Rheumatol. 7: 20, 1982.
Edwards, A.D., Wyatt, J.S., Richardson, C, Potter, A., Cope, M., Delpy, D.T., and Reynolds, E.O.R.: Effects of indomethacin on cerebral hemodynamics in very preterm infants. Lancet. 335: 1491-1495,1990.
Ekstrand, R., Alvan, G., L'e Orme, M., Lewander, R., Palmer, L., and Sarby, B.: Double-blind dose-response study of indomethacin in rheumatoid arthritis. Eur J Clin Pharmacol. 17 (6): 437-442, 1980.
Elbourne, I., Lumbers, E.R., and Hill, K.J.: The secretion of organic acids and bases by the ovine fetal kidney. Experimental Physiol. 75: 211-221,1990.
Elbourne, I., Lumbers, E.R., and Hill, K.J.: The secretion of organic acids and bases by the ovine fetal kidney. Exp Physiol. 75: 211-221,1990.
Elder, M.G., and Kapadia, L.: Indomethacin in the treatment of primary dysmenorrhoea. Br J Obstet Gynecol. 86: 645-647,1979.
Elliott, G.T., and McKenzie, M.W.: Treatment of hypercalcemia. Drug Intel Clin Pharm. 17 (1): 12-22, 1983.
Embrey, M.P.: Induction of abortion by prostaglandins El, E2. Br Med J. 2: 256, 1970.
Emori, H.W., Champion, G.D., Bluestone, R., and Paulus, H.E.: Simultaneous pharmacokinetics of indomethacin in serum and synovial fluid. Ann Rheum Dis. 32: 433-435, 1973.
Engervall, P., Bjorkholm, M., Grimfors, G., and Holm, G.: Antipyretic effect of indomethacin in malignant lymphoma. Acta Med Scand. 219: 501-505, 1986.
Eronen, M., Pesonen, E., Kurki, T., Ylikorkala, O., and Hallman, M.: The effects of indomethacin and a -sympathomimetic agent on the fetal ductus arteriosus during

205 treatment of premature labour: a randomised double-blind study. Am J Obstet Gynecol. 164: 141-146, 1991.
Eronen, M.: The hemodynamic effects of antenatal indomethacin and (3-sympathomimetic agent on the fetus and the newborn. A randomised study. Pediatr Res. 33: 615-619, 1993.
Evans, D.H., Levene, M.I., and Archer, L.N.J.: The effect of indomethacin on cerebral blood-flow velocity in premature infants. Dev Med Child Neurol. 29: 776-782, 1987.
Evans, M.A., Bhat, R., Vidyasagar, D., Vadapalli, M., Fisher, E., and Hastreiter, A.: Gestational age and indomethacin elimination in the neonate. Clin Pharmacol Ther. 26: 746-751, 1979.
Evans, M.A., Papazafiratou, C., Bhat, R., Vidyasagar, D.: Indomethacin metabolism in isolated neonatal and fetal rabbit hepatocytes. Pediatr Res. 15: 1406-1410, 1981.
Evans, M.A.: GLC microdetermination of indomethacin in plasma. J Pharm Sci. 69: 19-220, 1980.
Evershed, R.P.: Advances in silylation. In "Handbook of derivatives for chromatography", Blau, K., and Halket, J (Eds.). John Wiley, New York, pp. 51-108, 1993.
Feely, J., and Wood, A.J.J.: Effect of inhibitors of prostaglandin synthesis on hepatic drug clearance. Br J Clin Pharmacol. 15: 109-111,1983.
Feigen, L.P., Klainer, E., Chapnick, B.M., and Kadowitz, P.J.: The effect of indomethacin on renal function in pentobarbital-anesthetised dogs. J Pharmacol Exp Ther. 198: 457-463, 1976.
Fejes-To'th, G., Magyar, A., and Walter, J.: Renal response to vasopressin after inhibition of prostaglandin synthesis. Am J Physiol. 232: F416-F423, 1977.
Ferreira, S.H., and Vane, J.R.: New aspects of the mode of action of nonsteroidal antiinflammatory drugs. Ann Rev Pharmacol. 14: 57-73, 1974.
Ferreira, S.H., Moncada, S., and Vane, J.R.: Indomethacin and aspirin abolish prostaglandin release from the spleen. Nature New Biol. 231: 237-239, 1971.
Ferry, D.G., Ferry, D.M., Moller, P.w., McQueen, E.G.: Indomethacin estimation in plasma and serum by electron capture gas chromatography. J Chromatogr. 89: 110-112,1974.

206
Flower, R.J.: Drugs which inhibit prostaglandin biosynthesis. Pharmacol Rev. 26: 33-67, 1974.
Fowler, J., Gallagher, B.M., MacGregor, R.R., and Wolf, A.P.: Carbon-11 labeled aliphatic amines in lung uptake and metabolism studies. J Pharmacol Exp Ther. 198: 133-145, 1976.
Friedman, N.F., Heymann, M.A., and Rudolph, A.M.: Commentary: New thoughts on an old problem-patent ductus arteriosus in the preterm infant. / Pediatr. 90: 338, 1977.
Friedman, W.F., Hirschklau, M.J., Printz, M.J., Pitlick, P.T., and Kirkpatrick, S.E.: Pharmacological closure of patent ductus arteriosus in the premature infant. New Engl J Med. 295: 526-529,1976.
Friedman, W.F.: Studies of responses of the ductus arteriosus in intact animals. In "The ductus arteriosus", Heymann, M.A., and Rudolph, A.M. (Eds.). Report of the seventy-fifth Ross conference on pediatric research. Ross Laboratories, Columbus, Ohio, pp. 35-43, 1978b.
Friedman, Z., and Berman, W.: Hematologic effects of prostaglandins and thromboxanes and inhibitors of their synthesis in the perinatal period. Sem Perinatol. 4: 73, 1980.
Friedman, Z., Whitman, V., Maisels, M.J., Berman, W., Marks, K.H., and Vesell, E.S.: Indomethacin disposition and indomethacin induced platelet dysfunction in premature infants. J Clin Pharmacol. 18: 272-279, 1978.
Gal, P., Ransom, J.L., Weaver, R.L., Schall, S., Wyble, L.E., Carlos, R.Q., and Brown, Y.: Indomethacin pharmacokinetics in neonates: the value of volume of distribution as a marker of permanent patent ductus arteriosus closure. Ther Drug Monit. 13: 42-45, 1991.
Garrett, E.R.: Pharmacokinetics and clearances related to renal processes. Int J Clin Pharmacol. 16: 155-172,1978.
Gay, J.H., Daily, W.J.R., Meyer, B.H.P., Trump, D.S., Cloud, D.T., and Moltham, M.E.: Ligation of the patent ductus arteriosus in premature infants: Report of 45 cases. J Pediatr Surg. 8(5): 677-683,1973.
Gerlowski, L.E., and Jain, R.K.: Physiologically based pharmacokinetic modelling: principles and applications. J Pharm Sci. 72: 1103-1127,1983.
Ghanem, A-H., El-Sabbagh, H., Abdel-Alim, H.: Stability of indomethacin solubilised system. Pharmazie. 34: 406-407, 1979.

207 Giachetti, C., Canali, S., Zanolo, G.: Separation of non-steroidal anti-inflammatory agents by high-resolution gas chromatography. Preliminary trials to perform pharmacokinetic studies. J Chromatogr. 279: 587-592, 1983.
Gibaldi, M., and Koup, J.R.: Pharmacokinetic concepts-drug binding, apparent volume of distribution, and clearance. Eur J Clin Pharmacol. 20: 299-305, 1981.
Gibaldi, M., Levy, G., and McNamara, P.J.: Effect of plasma protein and tissue binding on the biologic half-life of drugs. Clin Pharmacol Ther. 24: 1-4,1978.
Gillespie, W.R., and Veng-Pedersen, P.: Theorems and implications of model independent elimination/distribution function decomposition of linear and some non-linear drug dispositions. II Clearance concepts applied to the evaluation of distribution kinetics. J Pharmacokinet Biopharm. 13: 441-451, 1985.
Gines, P., Abraham, W.T., and Schrier, R.W.: Vasopressin in pathophysiological states. Sem Nephrol. 14: 384-397, 1994.
Gleason, C.A., Clyman, R.I., Heymann, M.A., Mauray, F., Leake, R., and Roman, C: Indomethacin and patent ductus arteriosus: Effect on renal function in preterm lambs. Am J Physiol. 254(23): F38-F44, 1988.
Goldenberg, R.L., Davis, R.D., and Baker, R.C.: Indomethacin-induced oligohydramnios. Am J Obstet Gynecol. 160: 1196-1197,1989.
Gordin, A., Sotka, S., and Nuutila, J.: Comparison of a slow-release indomethacin tablet and naproxen in osteoarthritis. Curr Med Res Opinion. 9(7): 500-504, 1985.
Gordon, J.G.: personal communication, 1994.
Grantham, J.J., and Orloff, J.: Effect of prostaglandin E l on the permeability response of the isolated collecting tubule to vasopressin, adenosine 3', 5'-monophosphate and theophylline. J Clin Invest. 47: 1154-1161,1968.
Green, K., Bowman, K., Luxenberg, M.N., and Friberg, T.R.: Penetration of topical indomethacin into phakic and aphakic rabbit eyes. Arch Ophthal. 101: 284-288, 1983.
Green, T.P., O'Dea, R.F., and Mirkin, B.L.: Determinants of drug disposition and effect in the fetus. Ann Rev Pharmacol Toxicol. 19: 285-322, 1979.
Grella, P., and Zanor, P.: Premature labor and indomethacin. Prostaglandins. 16: 1007-1017, 1978.

208
Guissou, P., Cuisinaud, G., Legheand, J., and Sassard, J.: Chronopharmacokinetics of indomethacin in rats. Arzneim Forsch. 37: 1034-1037, .1987.
Guissou, P., Cuisinaud, G., Sassard, J: Gas chromatographic determination of indomethacin and its O-desmethylated metabolite in human plasma and urine. / Chromatogr. (Biomed Appl.) 277: 368-373,1983.
Gullner, H.G., Gill, J.R., Bartler, F.C., and Dusing, R.: The role of the prostglandin system in the regulation of renal function in normal women. Am J Med. 69: 718-724, 1980.
Gund, P., and Shen, T.Y.: A model for the prostaglandin synthetase cyclooxygenation site and its inhibition by antiinflammatory arylacetic acids. J Med Chem. 20: 1146-1152, 1977.
Hall, S., and Rowland, M.: Influence of fraction unbound upon the renal clearance of furosemide in the isolated perfused rat kidney. / Pharmacol Exp Ther. 232: 263-268, 1985.
Hall, S., and Rowland, M.: Relationship between renal clearance, protein binding, and urine flow for digitoxin, a compound of low clearance in the isolated perfused rat kidney. J Pharmacol Exp Ther. 228: 174-179,1983.
Hallak, M., Reiter, A.A., Ayres, N.A., and Moise, K.J.Jr.: Indomethacin for preterm labor: fetal toxicity in a dizygotic twin gestation. Obstet Gynecol. 78: 911-913, 1991.
Halushka, P.V., Wohltmann, H., Privitera, P.J., Hurwitz, G., and Margolius, H.S.: Bartter's syndrome: Urinary prostaglandin E-like material and kallikrein: indomethacin effects. Annals Intern Med. 87 (3): 281-286,1977.
Ham, E.A., Cirillo, K.J., Zanetti, M., Shen, T.Y., and Kuehl, F.A.: Studies on the mode of action of non-steroidal, anti-inflammatory agents. In Prostaglandins in Cellular Biology, Ramwell, P.W., and Pharriss, B.B. (Eds), Plenum Press, New York, pp. 345-352, 1972.
Hanna, C, and Sharp, J.D.: Ocular absorption of indomethacin by the rabbit. Arch Ophthal. 88: 196-198, 1972.
Hare, L.E., Ditzler, C.A., Duggan, D.E.: Radioimmunoassay of indomethacin in biological fluids. J Pharm Sci. 66: 486-489,1977.
Harman, R.E., Meisinger, M.A.P., Davis, G.E., and Kuehl, F.A.: The metabolites of indomethacin, a new antiinflammatory drug. J Pharmacol Exp Ther. 143: 215-220, 1964.
209 Harris, W.H., and Van Petten, G.R.: Placental transfer of indomethacin in the rabbit and sheep. Can J Physiol Pharmacol. 59: 342-346,1981.
Harth, M., and Bondy, D.C.: Indomethacin and acetylsalicylic acid in the treatment of osteoarthritis of the hips and knees. Can Med Ass J. 101 (6): 311-316, 1969.
Heijden, A.J.v.d., Provoost, A.P., Nauta, J., Grose, W., Oranje, W.A., Wolff, E.D., and Sauer, P.J.J.: Renal functional impairment in preterm neonates related to intrauterine indomethacin exposure. Pediatr Res. 24: 644-648, 1988.
Hekman, P., and Van Ginneken, C.A.M.: Kinetic modelling of the renal excretion of isopyracet in the dog. J Pharmacokinet Biopharm. 10: 77-92, 1982.
Helleberg, L.: Clinical pharmacokinetics of indomethacin. Clin Pharmacokin. 6: 245-258, 1981.
Helleberg, L.: Determination of indomethacin in serum and urine by electron-capture gas-liquid chromatography. J Chromatogr. 117: 167-173,1976.
Hendricks, S.K., Smith, J.R., Moore, D.E., and Brown, Z.A.: Oligohydramnios associated with prostaglandin synthetase inhibitors in preterm labour. Br J Obstet Gynecol. 97: 312-316, 1990.
Hickok, D.E., Hollenbach, K.A., Reilley, S.F., and Nyberg, D.A.: The association between decreased amniotic fluid volume and treatment with non-steroidal antiinflammatory agents for preterm labour. Am J Obstet Gynecol. 160: 1523-1531, 1989.
Hill, K.J., and Lumbers, E.R.: Renal function in adult and fetal sheep. / Dev Physiol. 10: 149-159, 1988.
Holmlund, D., and Sjodin, J-G.: Treatment of ureteral colic with intravenous indomethacin. / Urol. 120: 676-677, 1978.
Honore, B., Brodersen, R., and Robertson, A.: Interaction of indomethacin with adult human albumin and neonatal serum. Dev Pharmacol Ther. 6: 347-355,1983.
Hooper, S.B., Harding, R., Deayton, J., and Thorburn, G.D.: Role of prostaglandins in the metabolic responses of the fetus to hypoxia. Am J Obstet Gynecol. 166: 1568-1575, 1992.
Hori, R., Sunayashiki, K., and Kamiya, A.: Pharmacokinetic analysis of renal handling of sulphamethizole. J Pharm Sci. 65: 463-465, 1976.
210
Hubert, Ph., Renson, M., Crommen, J: A fully automated high-performance liquid chromatographic method for the determination of indomethacin in plasma. J Pharm Biomed Anal. 7: 1819-1827, 1989.
Hucker, H.B., Stauffer, S.C., White, S.D., Rhodes, R.E., Arison, B.H., Umbenhauer, E.R., Bower, R.J., McMahon, F.G.: Physiologic disposition and metabolic fate of a new anti-inflammatory agent, cis-5-fluoro-2-methyl-l-[p-(methylsulfinyl)-benzylidenyl]-indene-3-acetic acid in the rat, dog, rhesus monkey, and man. Drug Metab Disp. 1: 721-736, 1973.
Hucker, H.B., Zacchei, A.G., Cox, S.V., Brodie, D.A., and Cantwell, N.H.R.: Studies on the absorption, distribution, and excretion of indomethacin in various species. J Pharmacol Exp Ther. 153: 237-249,1966.
Huszar, G.: Physiology of the myometrium, Chapter 7. In: Maternal-fetal medicine: Principles and practice. Creasy, R.K., and Resnik, R., pp. 141, 1989.
Hvidberg, E., Lausen, H.H., and Jensen, J.A.: Indomethacin. Plasma concentrations and protein binding in man. Eur J Clin Pharmacol. 4: 119-124, 1972.
Hyver, K.J., and Sandra, P.: High resolution gas chromatography. Hewlett-Packard, Avondale, 1989.
Inagi, T., Muramatsu, T., Nagai, H., et al.: Influence of vehicle composition on the penetration of indomethacin through guinea pig skin. Pharm Bull. 29: 1708-1714, 1981.
Jansen, A.H., De Boeck, C, Ioffe, S., and Chernick, V.: Indomethacin-induced fetal breathing: Mechanism and site of action. J Appl Physiol. 57: 360-365,1984.
Jensen, K.M.: Determination of indomethacin in serum by an extractive alkylation technique and gas-liquid chromatography. / Chromatogr. 153: 195-202, 1978.
John, E.G., Vasan, U., Hastreiter, A.R., Bhat, R., and Evans, M.A.: Intravenous indomethacin and changes in renal function in premature infants with patent ductus arteriosus. Pediatr Pharmacol. 4: 11-19, 1984.
Johnson, A.G., and Ray, J.E.: Improved high-performance liquid chromatographic method for the determination of indomethacin in plasma. Ther Drug Monit. 14: 61-65, 1992.
Juchau, M.R., Chao, S.T., and Omiecinski, C.J.: Drug metabolism by the human fetus. Clin Pharmacokinet. 5: 320-339, 1980.

211 Kahns, A.H., Jensen, P.B., Mork, N., and Bundgaard, H.: Kinetics of hydrolysis of indomethacin and indomethacin ester prodrugs in aqueous solutions. Acta Pharm Nord. 1 (6): 327-336, 1989.
Kamiya, A., Okumura, K., and Hori, R.: Quantitative investigation on renal handling of drugs in rabbits, dogs, and humans. J Pharm Sci. 72: 440-443, 1983.
Kanto, J.H.: Use of benzodiazepines during pregnancy, labour, and lactation with particular reference to pharmacokinetic considerations. Drugs. 23: 354-380, 1982.
Karim, S.M.M., and Derlin, J.: Prostaglandin content of amniotic fluid during pregnancy and labour. J Obstet Gynecol Br Commonw. 74: 230,1967.
Karim, S.M.M., Trussel, R.R., Hiller, K., and Patel, R.C.: Induction of labour with prostaglandin F2a- J Obstet Gynecol Br Commonw. 76: 769, 1969.
Karim, S.M.M.: Appearance of prostaglandin F 2 a in human blood during labour. BrMedJ. 4: 618, 1968. Karnes, H.T., and March, C: Calibration and validation of linearity in chromatographic biopharmaceutical analysis. J Pharm Biomed Anal. 9: 911-918, 1991.
Kass, E: Indomethacin in ankylosing spondylitis. Acta Rheum Scand. 11: 205-211, 1965.
Katz, M., and Creasy, R.K.: Uterine blood flow distribution after indomethacin infusion in the pregnant rabbit. Am J Obstet Gynecol. 140: 430-434, 1981.
Kazemifard, A.G., and Moore, D.E.: Liquid chromatography with amperometric detection for the determination of non-steroidal anti-inflammatory drugs in plasma. J Chromatogr. {Biomed Appl.) 533: 125-132, 1990.
Kennedy, R.L., Bell, J.U., Miller, R.P., Doshi, D., de Sousa, H., Kennedy, M.J., Heald, D.L., Bettinger, R., and David, Y.: Uptake and distribution of lidocaine in fetal lambs. Anesthesiol. 72: 483-489, 1990.
Kiely, J.M.: Symptomatic control of fever in lymphoma and leukemia. Mayo Clin Proc. 44: 272-280, 1969.
Kier, L.B., and Whitehouse, M.W.: Similarities in the interatomic distances of some anti-inflammatory agents and inflammagenic amines: A possible insight into their common receptors. J Pharm Pharmacol. 20: 793-795,1968.

212 Kill, F.: Dynamics of renal proximal tubular secretion. Nature. 189: 927-928, 1961.
Kim, K.R., Hahn, M.K., Zlatkis, A., Horning, E.C., and Middleditch, B.S.: Simultaneous gas chromatography of volatile and non-volatile carboxylic acids as tert-butyldimethylsilyl derivatives. J Chromatogr. 468: 289-301,1989.
Kirshon, B., Mari, G., and Moise, K.J.Jr.: Indomethacin therapy in the treatment of symtomatic polyhydramnios. Obstet Gynecol. 75: 202-205, 1990.
Kirshon, B., Moise, K.J.Jr., Mari, G., and Willis, R.: Long-term indomethacin therapy decreases fetal urine output and results in oligohydramnios. Am J Perinatol. 8: 86-88, 1991.
Kirshon, B., Moise, K.J.Jr., Wasserstum, N., Ou, C.-N., and Huhta, J.C.: Influence of short-term indomethacin therapy on fetal urine output. Obstet Gynecol. 72: 51-53, 1988.
Kirshon, B.: Fetal urine output in hydramnios. Obstet Gynecol. 73: 240-242, 1989.
Kitterman, J.A., Liggins, G.C., Clements, J.A., and Tooley, W.H.: Stimulation of breathing movements in fetal sheep by inhibitors of prostaglandin synthesis. / Dev Physiol. 1: 453-466, 1979.
Kitterman, J.A., Liggins, G.C., Fewell, J.E., and Tooley, W.H.: Inhibition of breathing movements in fetal sheep by prostaglandins. J Appl Physiol. 54: 687-692, 1983.
Klein, K.L., Scott, W.J., Clark, K.E., and Wilson, J.G.: Indomethacin-placental transfer, cytotoxicity, and teratology in the rat. Am J Obstet Gynecol. 141: 448-452, 1981.
Kleinman, L.I.: The Kidney. In "Perinatal physiology", Stave, U (Ed.). Plenum, New York, chapter 27, pp. 589-616, 1978.
Knepper, M.A., Nielsen, S., Chiou, C.-L., and DiGiovanni, S.R.: Mechanism of vasopressin action in the renal collecting duct. Sem Nephrol. 14: 302-321, 1994.
Kong, L.J., Garrett, W.N., and Rattray, P.V.: A description of the dynamics of fetal growth in sheep. J Animal Sci. 41: 1065-1243,1975.
Koppel, R., and Rabinovitch, M.: Regulation of fetal lamb ductus arteriosus smooth muscle migration by indomethacin and dexamethasone. Pediatr Res. 33: 352-358, 1993.
213
Kover, G.: The effect of indomethacin on renal function. Acta Physiol Acad Sci Hung. 55: 283-298, 1980.
Koyima, I.: Urine flow dependence of renal clearance and inter-relation of renal reabsorption and physicochemical properties of drugs. Drug Metab Disp. 14: 239-245, 1986.
Krauer, B., and Krauer, F.: Drug kinetics in pregnancy. Clin Pharmacokin. 2: 167-181, 1977.
Krauer, B., Krauer, F., and Hytten, F.E.: Drug disposition and pharmacokinetics in the maternal-placental-fetal unit. Pharmacol Ther. 10: 301-328, 1980.
Ku, E.C., and Wasvary, J.M.: Inhibition of prostaglandin synthetase by Su-21524. Fed Proc. 32: 3302, 1973.
Kuehl, F.A.Jr.: Prostaglandin research: clinical implication. Sem Arthritis Rheumat. 12 (supp.l): 119-125,1982.
Kullama, L.K., Ross, M.G., Lam, R., Leake, R.D., Ervin, M.G., and Fisher, D.A.: Ovine maternal and fetal renal vassopressin receptor response to maternal dehydration. Am J Obstet Gynecol. 167: 1717-1722,1992.
Kulmacz, R.J., Ren, Y., Tsai, A.L., and Palmer, G.: Prostaglandin H synthetase: Spectroscopic studies of the interaction with hydroperoxides and with indomethacin. Biochemistry. 29: 8760-8771, 1990.
Kumar, R.: Endocytosis of the vasopressin receptor. Sem Nephrol. 14: 357-367, 1994.
Kwan, K.C., Breault, G.O., Umbenhauer, E.R., McMahon, F.G., and Duggan, D.E.: Kinetics of indomethacin absorption, elimination, and enterohepatic circulation in man. J Pharmacokin Biopharm. 4: 255-280,1976.
Kwong, E., Pillai, G.K., McErlane, K.M.: HPLC analysis of indomethacin and its impurities in capsule and suppository formulations. J Pharm Sci. 71: 828-830, 1982.
Lam, G., and Chiou, W.L.: Determination of renal clearances using arterial and venous plasma: procainamide in rabbits. J Pharm Sci. 70: 1373-1375,1981.
Lang, J.R., and Bolton, S.: A comprehensive method validation strategy for bioanalytical applications in the pharmaceutical industry-1. experimental considerations. J Pharm Biomed Anal. 9: 357-361,1991.

214
Lang, J.R., and Bolton, S.: A comprehensive method validation strategy for bioanalytical applications in the pharmaceutical industry-2. statistical analyses. / Pharm Biomed Anal. 9: 435-442, 1991.
Lawrence, J.R., Bryson, S.M., Sumner, D.J., Campbell, B.C., and Whitby, B.: The renal clearance of disopyramide after bolus intravenous injection. Biopharm Drug Dispos. 1: 51-57, 1980.
Lebedevs, T.H., Wojnar-Horton, R.E., Yapp, P., Roberts, M.J., Dusci, L.J., Hackett, L.P., and Ilett, K.F.: Excretion of indomethacin in breast milk. Br J Clin Pharmac. 32:751-754,1991.
Leffler, C.W., Busija, D.W., Fletcher, A.M., et al.: Effects of indomethacin upon cerebral hemodynamics in newborn piglets. Pediatr Res. 19: 1160-1164, 1985.
Leffler, C.W., Mirro, R., Shibata, M., Parfenova, H., Armstead, W.M., and Zuckerman, S.: Effects of indomethacin on cerebral vasodilator responses to arachidonic acid and hypercapnia in newborn pigs. Pediatr Res. 33: 609-614, 1993.
Leichtweiss, H.-P.: Carrier-mediated placental transfer. Placenta (supp.l): 115-124, 1981.
Levenson, D.J., Simmons, C.E.Jr., and Brenner, B.M.: Arachidonic acid metabolism, prostaglandins, and the kidney. Am J Med. 72: 354-374,1982.
Levy, G.: Effect of plasma portein binding on renal clearance of drugs. J Pharm Sci. 69: 482-483, 1980.
Levy, G.: Pharmacokinetics of fetal and neonatal exposure to drugs. Obstet Gynecol. 58: 9S-16S, 1981.
Lewis, S., and Yudkoff, M.: Gas chromatographic-mass spectrometric determination of isotopic enrichment of 6-15NH2 in adenine nucleotides. Anal Biochem. 145 (2): 354-361, 1985.
Lin, J.H., Cocchetto, D.M., and Duggan, D.E.: Protein binding as a primary determinant of the clinical pharmacokinetic properties of non-steroidal antiinflammatory drugs. Clin Pharmacokin. 12: 402-432, 1987.
Lin, Y-J., and Schanker, L.S.: Active transport of foreign amino acids by rat lung slices. Biochem Pharmacol. 30(21): 2937-2943,1981.

215
Lum, G.M., Aisenbrey, G.A., Dunn, M.J., Berl, T., Schrier, R.W., and McDonald, K.M.: In vivo effect of indomethacin to potentiate the renal medullary cyclic AMP response to vasopressin. J Clin Invest. 59: 8-13, 1977.
MacDonald, P.C., and Casey, M.L.: The accumulation of prostaglandins (PG) in amniotic fluid is an aftereffect of labor and not indicative of a role for PGE 2 or PGF 2 a in the initiation of human parturition. J Clin Endocrinol Metab. 76: 1332-1339, 1993.
Machin, G.A.: Fetal indomethacin exposure and renal dysgenesis. Am J Med Genetics. 44: 112-113, 1992.
MacTaggart, D.L., and Farwell, S.O.: Analytical use of linear regression. Part I: regression procedures for calibration and quantitation. J AO AC Int. 75: 594-614, 1992.
Manchester, D., Margolis, H.S., and Sheldon, R.E.: Possible association between maternal indomethacin therapy and primary pulmonary hypertension of the newborn. Am J Obstet Gynecol. 126: 467, 1976.
Manning, M., Chan, W.Y., and Sawyer, W.H.: Design of cyclic and linear peptide antagonists of vasopressin and oxytocin: Current status and future directions. Regulatory Peptides. 45: 279-283, 1993.
Mari, G., Moise, K.J.Jr., Deter, R.L., Kirshon, B., and Carpenter, R.J.: Doppler assessment of the renal blood flow velocity waveform during indomethacin therapy for preterm labour and polyhydramnios. Obstet Gynecol. 75: 199-201,1990.
Martin, B.K.: Drug urinary excretion data-some aspects concerning the interpretation. Br J Pharmacol. 29: 181-193, 1967.
Mason, R.W., and McQueen, E.G.: Protein binding of indomethacin: binding of indomethacin to human plasma albumin and its displacement from binding by ibuprofen, phenylbutasone and salicylate in vitro. Pharmacol. 12: 12-19,1974.
Matin, S.B., and Rowland, M.: Electron-capture sensitivity comparison of various derivatives of primary and secondary amines. J Pharm Sci. 61: 1235-1240,1972.
Matson, J.R., Stokes, J.B., and Robillard, J.E.: Effects of inhibition of prostaglandin synthesis on fetal renal function. Kidney Int. 20: 621-627, 1981.
Matsuki, Y., Ito, T., Kojima, M., Katsumura, H., Ono, H., Nambara, T.: A gas chromatographic-mass spectrometric method for the evaluation of bioconversion of indomethacin prodrugs into the parent drug. Chem Pharm Bull. 31: 2033-2038, 1983.

216
Mattila, M.A.K., Ahlstrom-Bengs, E., and Pekkola, P.: Intravenous indomethacin or oxycodone in prevention of post-operative pain. Br Med J. 287: 1026,1983.
Mawatari, K.-L, Iinuma, F., Watanabe, M: Fluorimetric determination of indomethacin in human serum by high-performance liquid chromatography coupled with post-column photochemical reaction with hydrogen peroxide. J Chromatogr. (Biomed Appl.) 491: 389-396,1989.
Mawhinney, T.P., and Madson, M.A.: N-methyl-N-(tert-butyldimethylsilyl) trifluoroacetamide and related N-tert-butyldimethylsilyl amides as protective silyl donors. J Org Chem. 47(17): 3336-3339,1982.
Mazzoni, M.R., and Lucacchini, A.: Evidence for the existence of a specific binding site for indomethacin on bovine vesicular gland microsomes. Biotech Appl Biochem. 9: 339-345, 1987.
McCarthy, J.S., Zies, L.G., and Gelband, H.: Age-dependent closure of the patent ductus arteriosus by indomethacin. Pediatr. 62: 706-712, 1978.
McCormick, D.C., Edwards, A.D., Brown, G.C., Wyatt, J.S., Potter, A., Cope, M., Delpy, D.T., and Reynolds, E.O.R.: Effect of indomethacin on cerebral oxidised cytochrome oxidase in preterm infants. Pediatr Res. 33: 603-608,1993.
McCoshen, J.A., Hoffman, D.R., Kredentser, J.V., et al.: The role of fetal membranes in regulating production, transport, and metabolism of prostaglandin E2 during labour. Am J Obstet Gynecol. 163: 1632,1990.
McCray, P.B., and Bettencourt, J.D.: Prostaglandins stimulate fluid secretion in human fetal lung. J Dev Physiol. 19: 29-36,1993.
McDonald, P.C., Koga, S., and Casey, M.L.: Decidual activation in parturition: examination of amniotic fluid for mediators of the inflammatory response. Ann NY Acad Sci. 622: 315, 1991.
McElnay, J.C., Passmore, A.P., Crawford, V.L.S., McConnell, J.G., Taylor, I.C., and Walker, F.S.: Steady state pharmacokinetic profile of indomethacin in elderly patients and young volunteers. Eur J Clin Pharmacol. 43: 77-80, 1992.
Mehta, A.C., and Calvert, R.T.: An improved high-performance liquid chromatographic procedure for monitoring indomethacin in neonates. Ther Drug Monit. 5: 143-145, 1983.
Meschia, G., Battaglia, F.C., and Bruns, P.D.: Theoretical and experimental study of transplacental diffusion. J Appl Physiol. 22: 1171-1178,1967.

217
Meschia, G.: Physiology of transplacental diffusion. Obstet Gynecol Ann. 5: 21-38, 1976.
Mihaly, G.W., and Morgan, D.J.: Placental drug transfer: effects of gestational age and species. Pharmacol Ther. 23: 253-266, 1984.
Millard, R.W., Baig, H., and Vatner, S.R.: Prostaglandin control of the renal circulation in response to hypoxemia in the fetal lamb in-utero. Circ Res. 45: 172-179, 1979.
Miller, F.C.: Uterine motility in spontaneous labour. Clin Obstet Gynecol. 26 (1): 78-85, 1983.
Mirkin, B.L.: Maternal and fetal distribution of drugs in pregnancy. Clin Pharmacol Ther. 14: 643-647, 1973.
Miyazaki, S., Yamahira, T., and Nadai, T.: Effect of bile flow on indomethacin absorption in rats. Acta Pharm Suec. 18: 135-138,1981.
Miyazaki, S., Yamahira, T., Inoue, H., and Nadai, T.: Interaction of drugs with bile components II Effect of bile on the absorption of indomethacin and phenylbutazone in rats. Chem Pharm Bull. 28: 323-326, 1980.
Mogilner, B.M., Ashkenazy, M., Borenstein, R., and Lancet, M.: Hydrops fetals caused by maternal indomethacin treatment. Acta Obstet Gynecol Scand. 61: 183-185, 1982.
Moise, K.J.Jr., Huhta, J.C., Sharif, D.S., Ou, C.-N., Kirshon, B., Wasserstrum, N., and Cano, L.: Indomethacin in the treatment of premature labor. Effects on the fetal ductus arteriosus. N Eng J Med. 319: 327-331, 1988:
Moise, K.J.Jr., Ou, C.-N., Krishon, B., Cano, L.E., Rognerud, C, and Carpenter, R.J.: Placental transfer of indomethacin in the human pregnancy. Am J Obstet Gynecol. 162: 549-554, 1990.
Montero, M.T., Pouplana, R., Vails, O., and Garcia, S.: On the binding of cinmetacin and indomethacin to human serum albumin. / Pharm Pharmacol. 38: 925-927, 1986.
Moore, T.R., and Cayle, J.E.: The amniotic fluid index in normal human pregnancy. Am J Obstet Gynecol. 162: 1168-1173, 1990.
Morel, A., Lolait, S.J., and Brownstein, M.J.: Molecular cloning and expression of rat V i a and V2 arginine vasopressin receptors. Regulatory Peptides. 45: 53-59, 1993.

218 Morishima, H.O., Finster, M., Pedersen, H., Fukunaga, A., Ronfeld, R.A., Vassallo, H.G., and Covino, B.G.: Pharmacokinetics of lidocaine in fetal and neonatal lambs and adult sheep. Anesthesiol. 50: 431-436, 1979.
Morsdorf, K.: In "Non-steroidal antiinflammatory drugs", Garattini, S., and Dukes, M.N.G., (Eds.), Excerpta Medica Foundation, Amsterdam, pp. 85-97, 1964.
Morselli, P.L., Franco-Morselli, R., and Bossi, L.: Clinical pharmacokinetics in newborns and infants. Age related differences and therapeutic implications. Clin Pharmacokinet. 5: 485-527, 1980.
Moya, F., and Thorndike, V.: Passage of drugs across the placenta. Am J Obstet Gynecol. 84: 1778-1798, 1962.
Muller, N., Lapicque, F., Monot, C, Payan, E., Gillet, P., Bannwarth, B., and Netter, P.: Protein binding of indomethacin in human cerebrospinal fluid. Biochem Pharmacol. 42: 799-804, 1991.
Naito, S-I., and Tsai, Y-H.: Percutaneous absorption of indomethacin from ointment bases in rabbits. Int J Pharm. 8: 263-276,1981.
Nakala, S., Skimmer, K., Mitchell, B.F., et al.: Changes of prostaglandin transfer across fetal membranes obtained after spontaneous labour. Am J Obstet Gynecol. 155: 1337, 1986.
Nathanielsz, P.W.: Monographs in fetal physiology 2: Animal models in fetal medicine (I). Elsevier/North-Holland Biomedical Press, Amsterdam, 1980.
Natochin, Y.V.: Renal Pharmacology: comparative, developmental, and cellular aspects. Ann Rev Pharmacol. 14: 75-90, 1974.
Nau, H., Luck, W., Kuhnz, W., and Wegener, S.: Serum protein binding of diazepam, desmethyldiazepam, furosemide, indomethacin, warfarin, and phenobarbital in human fetus, mother, and newborn infant. Pediatr Pharmacol. 3: 219-227, 1983.
Nau, H.: Clinical pharmacokinetics in pregnancy and perinatology. I Placental transfer and fetal side effects of local anaesthetic agents. Dev Pharmacol Ther. 8: 149-181, 1985.
National formulary, XIII.
Neander, G., Eriksson, L.O., Wallin-Boll, E., Ersmark, H., and Grahnen, A.: Pharmacokinetics of intraarticular indomethacin in patients with osteoarthritis. Eur J Clin Pharmacol. 42: 301-305,1992.

219
Niebyl, J.R., Blake, D.A., White, R.D., Kumor, K.M., Dubin, N.H., Robinson, J.C., and Egner, P.G.: The inhibition of premature labor with indomethacin. Am J Obstet Gynecol. 136: 1014-1019, 1980.
Nijhuis, J.G., Prechtl, H.F.R., Martin, C.B., and Bots, R.S.G.M.: Are there behavioural states in the human fetus? Early Hum Dev. 6: 177-195, 1982.
Nishioka, R., Harimoto, T., Umeda, I., Yamamoto, S., Oi, N.: Improved procedure for determination of indomethacin in plasma by capillary gas chromatography after solid-phase extraction. J Chromatogr. (Biomed Appl.) 526: 210-214,1990.
Nix, A.B.J., and Wilson, D.W.: Assay detection limits: concept, definition, and estimation. Eur J Clin Pharmacol. 39: 203-206,1990.
Noerr, B.: Indomethacin. Neonatal Network. 10: 81-83, 1991.
Nordstrom, L., and Westgren, M.: Indomethacin treatment for polyhydramnios-effective but potentially dangerous? Acta Obstet Gynecol Scand. 71: 239-241, 1992.
O'Brien, M., McCauley, J., Cohen, E.: Indomethacin. In Analytical Profiles of Drug Substances. Florey, K. (Ed.). Academic Press. 13: 211-238,1984.
O'Brien, WM: Indomethacin: a survey of clinical trials. Clin Pharmacol Ther. 9: 94-107, 1968.
Oberbaur, R., Krivanek, P., and Turnheim, K.: Pharmacokinetics of indomethacin in the elderly. Clin Pharmacokinet. 24: 428-434,1993.
Ohara, T., Ogata, H., and Tezuka, F.: Effects of indomethacin in-utero on the pulmonary vasculature of the newborn lambs. Tohoku J Exp Med. 164: 67-79, 1991.
Okumura, K., Yoshida, H., and Hori, R.: Tissue distribution and metabolism of drugs. Ill Accumulation of drugs by the isolated perfused rat lung. J Pharm Dyn. 1: 230-237, 1978.
Olkkala, K.T., Maunuksela, E.L., and Korpela, R.: Pharmacokinetics of postoperative intravenous indomethacin in children. Pharmacol Toxicol. 65: 157-160, 1989.
Ou, C.-N., and Frawley, V.L.: Liquid-chromatographic determination of indomethacin in blood from newborns with patent ductus arteriosus. Clin Chem. 30: 898-901, 1984.

220 Pacifici, G.M., Sawe, J., Kager, L., and Rane, A.: Morphine glucuronidation in human fetal and adult liver. Eur J Clin Pharmacol. 22: 553-558, 1982.
Parks, B.R., Jordan, R.L., Rawson, J.E., and Douglas, B.H.: Indomethacin: studies on absorption and placental transfer. Am J Obstet Gynecol. 129: 464-465,1977.
Paulick, R.P., Meyers, R.L., Rudolph, CD., and Rudolph, A.M.: Venous and hepatic vascular responses to indomethacin and prostaglandin Ei in the fetal lamb. Am J Obstet Gynecol. 163: 1357-1363,1990.
Pawelczyk, E., and Knitter, B.: Kinetics of drug degradation. Part 58: A method of preparation and the stability of 3% aqueous indomethacin solution. Pharmazie. 33: 586-588, 1978.
Pelkonen, O.: Xenobiotic metabolism in the maternal-placental-fetal unit: implications for fetal toxicity. Dev Pharmacol Ther. 7 (supp.l): 11-17, 1984.
Peng, G.W., and Chiou, W.L.: Analysis of drugs and other toxic substances in biological samples for pharmacokinetic studies. J Chromatogr. (Biomed Appl.) 531: 3-50, 1990.
Perucca, E., and Crema, A.: Plasma protein binding of drugs in pregnancy. Clin Pharmacokin. 7: 336-352, 1982.
Phelan, J.P., Smith, C.V., Broussard, P., et al.: Amniotic fluid volume assessment with the four-quadrant technique at 36-42 weeks' gestation. J Reprod Med. 32: 540-542, 1987.
Plazonnet, B., and Van den Heuvel, W.J.A.: Preparation, gas chromatography and mass spectrometry of methyl and trimethylsilyl esters of indomethacin, J Chromatogr. 142: 587-596, 1977.
Plotz, CM.: Clinical application of indomethacin: efficacy and tolerability. Sem Arthritis Rheumat. 12 (supp.l): 100-102,1982.
Pratzel, H., Dittrich, P., and Kukovetz, W.: Spontaneous and forced cutaneous absorption of indomethacin in pigs and humans. J Rheumatol. 13: 1122-1125, 1986.
Prietsch, V., Maier, R., Schmitz, L., and Obladen, M.: Long-term variability of heart rate increases with successful closure of patent ductus arteriosus in preterm infants, Biol Neonate. 61: 142-149,1992.
221 Pryds, O., Greisen, G., and Johansen, K.H.: Indomethacin and cerebral blood flow in premature infants treated for patent ductus arteriosus. Eur J Pediatr. 147: 315-316, 1988.
Rado, J.P., Simatupang, T., Boer, P., and Dorhout Mees, E.J.: Pharmacologic studies in Bartter's syndrome: Effect of DDAVP and indomethacin on renal concentrating operation. Part II. Int J Clin Pharmacol Biopharm. 16 (1): 22-26, 1978.
Rajadurai, V.S., and Yu, V.Y.H.: Intravenous indomethacin therapy in preterm neonates with patent ductus arteriosus. J Pediatr Child Health. 27: 370-375, 1991.
Raz, A., Stern, H., and Kenig-Wakshall, R.: Indomethacin and aspirin inhibition of PGE2 synthesis by sheep seminal vesicles microsome powder and seminal vesicle slices. Prostaglandins. 3: 337-352, 1973.
Reynolds, F., and Knott, C: Pharmacokinetics in pregnancy and placental drug transfer. Oxford Rev Reprod Biol. 11: 389-449,1989.
Riggs, K.W., Rurak, D.W., Yoo, S.D., McErlane, B.A., Taylor, S.M., McMorland, G.H., and Axelson, J.E.: Drug accumulation in lung fluid of the fetal lamb after maternal or fetal administration. Am J Obstet Gynecol. 157: 1286-1291, 1987.
Riggs, K.W.: Metoclopramide kinetics in sheep: Maternal-fetal disposition, fetal pharmacodynamics and a comparison between pregnant and non-pregnant ewes. PhD thesis, University of British Columbia, Vancouver, 1989.
Robertson, G.L.: The use of vasopressin assays in physiology and pathophysiology. Sem Nephrol. 14: 368-383, 1994.
Robillard, J.E., Weitzman, R.E., Fisher, D.A., and Smith, F.G.: Developmental aspects of renal tubular reabsorption of water and fetal renal response to arginine vasopressin. In "The kidney during development: Morphology and function." Spitzer, A (Ed.), Masson, New York, chapter 27, pp. 205-213, 1982.
Rosen, D.J.D., Fejgin, M.D., Rabinowitz, R., Regev, R.H., and Beyth, Y.: Indomethacin therapy and fetal urine production in twins with polyhydramnios. J Perinat Med. 19: 173-176,1991.
Roth-Brandel, U., Bygdeman, M., and Wiquist, N.: Effect of intravenous administration of prostaglandin E! and F 2 a on the contractility of the nonpregnant uterus in vivo. Acta Obstet Gynecol Scand. (Suppl.) 49: 1,1970.
222 Rowe, J.S., and Carless, J.E.: Investigations on the in vitro dose-related metabolism of indomethacin in four laboratory species. Eur J Drug Metab Pharmacokin. 7: 159-163, 1982.
Rowland, M., Benet, L.Z., and Graham, G.G.: Clearance concepts in pharmacokinetics. J Pharmacokin Biopharm. 1: 123-136,1973.
Rubaltelli, F.F., Chiozza, M.L., Zanardo, V., and Cantarutti, F.: Effect on neonate of maternal treatment with indomethacin. J Pediatr. 94: 161,1979.
Rudolph, A.M., and Heymann, M.A.: Hemodynamic changes induced by blockers of prostaglandin synthesis in the fetal lamb in-utero. Adv Prostaglandin Thromboxane Leukotriene Res. 4: 231,1978.
Rudolph, A.M.: The effects of nonsteroidal antiinflammatory compounds on fetal circulation and pulmonary function. Obstet Gynecol. 58: 63S-67S, 1981.
Rudolph, A.M.: The fetal circulation and its response to stress. / Dev Physiol. 6: 11-19, 1984.
Rurak, D.W., Wright, M.R., and Axelson, J.E.: Drug disposition and effects in the fetus. J Dev Physiol. 15: 33-44,1991.
Rurak, D.W.: Fetal behavioural states: pathological alterations with drug/alcohol abuse. Sem Perinatol. 16: 239-251,1992.
Sabik, J.F., Assad, R.S., and Hanley, F.L.: Prostaglandin synthesis inhibition prevents placental dysfunction after fetal cardiac bypass. J Thorac Cardiovasc Surg. 103: 733-742, 1992.
Saliba, E., Autret, E., Nasr, C, Sue, A.L., and Laugier, J.: Perinatal pharmacology and cerebral blood flow. Biol Neonate. 62: 252-257, 1992.
Schanker, L.S.: Drug absorption from the lung. Biochem Pharmacol. 27: 381-385, 1978.
Schoenfeld, A., Bar, Y., Merlob, P., Ovadia, Y.: NSAIDs: maternal and fetal considerations. Am J Reprod Immunol. 28: 141-147,1992.
Schonhofer, P., and Anspach, K.F.: Die aktivitat der L-glutamin-D-fructose-6-phosphat-aminotransferase im verlauf einer durch carrageenin induzierten entzundung und ihre hemmbarkeit durch phenylbutazon. Arch Int Pharmacodyn. 166 (2): 382-389, 1967.

223 Schooley, D.L., Kubiak, F.M., and Evans, J.V.: Capillary gas chromatographic analysis of volatile and non-volatile organic acids from biological samples as the tert-butyldimethylsilyl derivatives. J Chromatogr Sci. 23(9): 385-390, 1985.
Schwertschlag, U., Gerber, J.G., Barnes, J.S., and Nies, A.S.: A dual effect of nonsteroidal anti-inflammatory drugs on renal water handling in humans. / Pharmacol Exp Ther. 238: 653-658, 1986.
Shah, V.P., Midha, K.K., Dighe, S., McGilveray, I.J., Skelly, J.P., Yacobi, A., Layoff, T., Vishwanathan, C.T., Cook, C.E., McDowall, R.D., Pittman, K.A., Spector, S.: Analytical methods validation: bioavailability, bioequivalence, and pharmacokinetic studies. Int J Pharm. 82: 1-7,1992.
Shen, T.Y., and Winter, C.A.: Chemical and biological studies on indomethacin, sulindac, and their analogs. Adv Drug Res. 12: 89-245, 1977.
Shen, T.Y., Windholz, T.B., Rosegoy, A., Witzel, B.E., Wilson, A.N., Willet, J.D., Holtz, W.J., Ellis, R.L., Mattzuk, A.R., Lucas, S., Stammer, C.H., Holly, F.W., Sarett, L.H., Risley, E.A., Nuss, G.W., and Winter, C.A.: Non-steroidal antiinflammatory agents. J Am Chem Soc. 85: 488-489, 1963.
Shen, T.Y.: Synthesis and biological activity of some indomethacin analogs. In "International symposium of non-steroidal anti-inflammatory drugs", Garattini, S., and Dukes, M.N.G., (Eds.), International congress series No. 82, pp. 13-20, 1965.
Shen, T.Y.: The discovery of indomethacin and the proliferation of NSAIDs. Sem Arthritis Rheumat. 12 (supp.l): 89-93,1982.
Shima, K., Matsusaka, C, Hirose, M., et al.: Biopharmaceutical characteristics of indomethacin gel ointment. Chem Pharm Bull. 29: 2338-2344, 1981.
Sibeon, R.G., Baty, J.D., Baber, N., Chan, K., L'e Orme, M.: Quantitative gas-liquid chromatographic method for the determination of indomethacin in biological fluids. J Chromatogr. 153: 189-194,1978.
Silberman, H.R., McGinn, T.G., and Kremer, W.B.: Control of fever in Hodgkin's disease by indomethacin. J Am Med Ass. 194(6): 597-600,1965.
Simmons, M.A., Battaglia, F.C., and Meschia, G.: Placental transfer of glucose. / Dev Physiol. 1: 227-243, 1979.
Singh, A.K., Jang, Y., Mishra, U., Granley, K.: Simultaneous analysis of flunixin, naproxen, ethacrynic acid, indomethacin, phenylbutazone, mefenamic acid and thiosalicylic acid in plasma and urine by high-performance liquid chromatography

224 and gas chromatography-mass spectrometry. J Chromatogr. (Biomed Appl.) 568: 351-361, 1991.
Skeith, M.D., Simkin, P.A., and Healey, L.A.: The renal excretion of indomethacin and its inhibition by probenecid. Clin Pharmacol Ther. 9: 89-93, 1967.
Skellern, G. G., and Salole, E.G.: A high-speed liquid chromatographic analysis of indomethacin in plasma. J Chromatogr. 114: 483-485, 1975.
Smith, J.B., and Willis, A.L.: Aspirin selectively inhibits prostaglandin production in human platelets. Nature New Biol. 231: 235-237, 1971.
Smith, L.G., Kirshon, B., and Cotton, D.B.: Indomethacin treatment for polyhydramnios and subsequent infantile nephrogenic diabetes insipidus. Am J Obstet Gynecol. 163: 98-99, 1990.
Smith, P.C., and Benet, L.Z.: High-performance liquid chromatographic method for the determination of indomethacin and its two primary metabolites in urine. J Chromatogr. (Biomed Appl.) 306: 315-321,1984.
Smith, W.L., and Lands, W.E.M.: Stimulation and blockade of prostaglandin biosynthesis. JBiolChem. 21: 6700-6702,1971.
Snyder, D.S.: Cutaneous effects of topical indomethacin an inhibitor of prostaglandin synthesis on UV-damaged skin. J Invest Dermatol. 64: 322-325, 1975.
Sonnenburg, W.K., Zhu, J.H., and Smith, W.L.: A prostaglandin E receptor coupled to a pertussis toxin-sensitive guanine nucleotide regulatory protein in rabbit cortical collecting tubule cells. JBiolChem. 265: 8479-8483,1990.
Srivastava, M., Collins, M.D., Scott, W.J.Jr., Wittfoht, W., and Nau, H.: Transplacental distribution of weak acids in mice: accumulation in compartments of highpH. Teratology. 43: 325-329,1991.
Stacey, T.E., Weedon, A.P., Haworth, C, Ward, R.H.T., and Boyd, R.D.H.: Fetomaternal transfer of glucose analogs by sheep placenta. Am J Physiol. 234: E 32-E 37, 1978.
Stanford, N., Roth, G.J., Shen, T.Y., and Majerus, P.W.: Lack of covalent modification of prostaglandin synthetase (cyclo-oxygenase) by indomethacin. Prostaglandins. 13: 669-675, 1977.

225 Steele, A., and Ayromlooi, J.: Effects of indomethacin on the acid-base balance and hemodynamics of chronically instrumented pregnant sheep. Dev Pharmacol Ther. 11: 96-101, 1988.
Stein, G., Kunze, M., Zaumseil, J., and Traeger, A.: Zur pharmakokinetik von indomethazin und indomethazin-metaboliten bei wiederholter applikation an nierengesunden und nierengeschadigten patienten. Int J Clin Pharmacol. 15: 470-473, 1977.
Stevenson, K.M., and Lumbers, E.R.: Effects of indomethacin on fetal renal function, renal and umbilicoplacental blood flow and lung liquid production. / Dev Physiol. 17: 257-264, 1992.
Stubbs, R.J., Schwartz, M.S., Chiou, R., Entwistle, L.A., Bayne, W.F.: Improved method for the determination of indomethacin in plasma and urine by reversed-phase high-performance liquid chromatography. J Chromatogr. (Biomed Appl.) 383: 432-437, 1986.
Surborg, V.K.H.: Vergleichende metabolische studien von [14C]-markiertem indometacin und acemetacin bei rattess. Arzneim Forsch. 30: 1384-1391,1980.
Szeto, H.H., Mann, L.I., Bhaktharathsalan, A., Liu, M., and Inturisz, C.E.: Meperidine pharmacokinetics in the maternal-fetal unit. / Pharmacol Exp Ther. 206: 448, 1978.
Szeto, H.H., Umans, J.G., and McFarland, J.: A comparison of morphine and methadone disposition in the maternal-fetal unit. Am J Obstet Gynecol. 143: 700-706, 1982a.
Szeto, H.H., Umans, J.G., and Rubinow, S.I.: The contribution of transplacental clearances and fetal clearance to drug disposition in the ovine maternal-fetal unit. Drug Metab Disp. 10: 382-386, 1982b.
Szeto, H.H., Umans, J.G., Umans, H.R., and McFarland, J.W.: The relationship between maternal and fetal plasma protein binding of methadone in the ewe during the third trimester. Life Sci. 30: 1271-1279, 1982c.
Szeto, H.H.: Behavioural states and their ontogeny: animal studies. Sem Perinatol. 16: 211-216, 1992.
Szeto, H.H.: Kinetics of drug transfer to the fetus. Clin Obstet Gynecol. 36: 246-254, 1993.
Szeto, H.H.: Maternal-fetal pharmacokinetics and fetal dose-response relationships. Ann NY Acad Sci. 562: 42-55, 1989.

226 Szeto, H.H.: Pharmacokinetics in the ovine maternal-fetal unit. Ann Rev Pharmacol Toxicol. 22: 221-243, 1982d.
Tang-Li, D.D.-S., Tozer, T.N., Riegelman, S.: Dependence of renal clearance on urine flow: A mathematical model and its application. J Pharm Sci. 72: 154-158, 1983.
Terhaag, B., and Hermann, U.: Biliary elimination of indomethacin in man. Eur J Clin Pharmacol. 29: 691-695,1986.
Terragno, N.A., Terragno, D.A., and McGiff, J.C.: Contribution of prostaglandin to the renal circulation in conscious, anesthetised, and laparotomised dogs. Circ Res. 40: 590-595, 1977.
Terweij-Groen, G.P., Heemstra, S., Kraak, J.C.: Rapid determination of indomethacin and salicylic acid in serum by means of reversed-phase liquid chromatography. J Chromatogr. (Biomed Appl.) 181: 385-397,1980.
Thalji, A., Yeh, T.F., Raval, D., et al.: Pharmacokinetics of intravenous indomethacin in premature infants. Pediatr Res. 13: 374,1979.
Thalji, A.A., Carr, I., Yeh, T.F., Raval, D., Luken, J.A., and Pildes, R.S.: Pharmacokinetics of intravenously administered indomethacin in premature infants. J Pediatr. 97: 995-1000, 1980.
Thiery, M., and Amy, J-J.: Induction of labour with prostaglandins. In Karim, S.M.M. (Ed.), Prostaglandins and reproduction. Press Limited, pp. 149, 1975.
Tomson, G., Lunell, N.-O., Sundwall, A., and Rane, A.: Placental passage of oxazepam and its metabolism in mother and newborn. Clin Pharmacol Ther. 25: 74-81, 1979.
Tonn, G.R.: personal communication, 1994.
Traeger, A., Joschel, N., and Zamumseil, J.: Pharmacokinetics of indomethacin in pregnant and parturient women and in their newborn infants. Zentralbl Gynaekol. 95: 635-641, 1973.
Traeger, A., Stein, G., Kuntze, M., and Zaumseil, J.: Zur pharmakokinetik von indomethazin bei nierengeschadigten patienten. Int J Clin Pharmacol. 6: 237-242, 1972.
Tucker, G.T.: Measurement of the renal clearances of drugs. Br J Clin Pharmacol. 12: 761-770, 1981.

227 Turakka, H., and Airaksinen, M.M.: Biopharmaceutical assessment of phenylbutasone and indomethacin preparations. Annals Clin Res. 6 (Suppl. 11): 34-41, 1974.
van Bel, F., Van de Bor, M., Stijnen, T., Baan, J., and Ruys, J.H.: Cerebral blood flow velocity changes in preterm infants after a single dose of indomethacin: duration of its effect. Pediatrics. 84: 802-807,1989.
van Bel, F., van Zwieten, P.H.T., Lya, L., and Ouden, D.: Contribution of colour doppler flow imaging to the evaluation of the effect of indomethacin on neonatal cerebral hemodynamics. J Ultrasound Med. 9: 107-109,1990.
van der Heijden, A.J., Provoost, A.P., Nauta, J., et al.: Renal functional impairment in preterm neonates related to intrauterine indomethacin exposure. Pediatr Res. 24: 644-648, 1988b.
van der Heijden, A.J., Provoost, A.P., Nauta, J., Wolff, E.D., and Sauer, P.J.J.: Indomethacin as an inhibitor of preterm labour. Effect on postnatal renal function. Contrib Nephrol. 67: 152-154, 1988a.
van der Meer, M.J., and Hundt, H.K.L.: Estimation of serum indomethacin at therapeutic levels by means of thin-layer chromatography and spectrophotometry. J Chromatogr. 181: 282-285, 1980.
van Kreel, B.K.: A mathematical approach to the mechanisms of placental transfer. Placenta (supp.l): 81-100,1981.
van Petten, G.R., Mathison, H.J., Harris, W.H., and Mears, G.J.: Chronic preparation of the pregnant ewe and fetus for pharmacological research: The placental transfer and fetal effects of bunitrolol. / Pharmacol Meth. 1: 45-60, 1978.
van der Veyver, I.B., and Moise, K.J.: Prostaglandin synthetase inhibitors in pregnancy. Obstet Gynecol Survey. 48: 493-502, 1993.
Vane, J.R.: Inhibition of prostaglandin synthesis as a mechanism of action for aspirin-like drugs. Nature New Biol. 231: 232-239,1971.
Vanhaesebrouck, P., Thiery, M., Leroy, J.G., et al.: Oligohydramnios, renal insufficiency and ileal perforation in preterm infants after intrauterine exposure to indomethacin. J Pediatr. 113: 738-743, 1988.
Veersema, D., de Johng, P.A., van Wijck, J.A.M.: Indomethacin and the fetal renal nonfunctional syndrome. Eur J Obstet Gynecol Reprod Biol. 16: 113-121,1983.

228
Vert, P., Bianchetti, G., Marchal, F., Monin, P., and Morselli, P.L.: Effectiveness and pharmacokinetics of indomethacin in premature newborns with patent ductus arteriosus. Eur J Clin Pharmacol. 18: 83-88,1980.
Vree, T. B., Van den Biggelaar-Martea, M., Verwey-van Wissen, C. P. W. G. M.: Determination of indomethacin, its metabolites and their glucuronides in human plasma and urine by means of direct gradient high-performance liquid chromatographic analysis. Preliminary pharmacokinetics and effect of probenecid. J Chromatogr. (Biomed Appl.) 616: 271-282, 1993.
Wada, Y., Etoh, Y., Ohira, A., Kimata, H., Koide, T., Ishihama, H., and Mizushima, Y.: Percutaneous absorption and anti-inflammatory activity of indomethacin in ointment. J Pharm Pharmacol. 34: 467-468, 1982.
Waddell, W.J., and Marlowe, C.: Transfer of drugs across the placenta. Pharmacol Ther. 14: 375-390, 1981.
Waddell, W.J.: Localisation and metabolism of drugs in the fetus. Federation Proceedings. 31: 52-62, 1972.
Wade, J.B.: Role of membrane traffic in the water and Na + responses to vasopressin. Sem Nephrol. 14: 322-332, 1994.
Wahlich, J.C., and Carr, G.P.: Chromatographic system suitability tests-what should we be using? J Pharm Biomed Anal. 8: 619-623,1990.
Walker, M.P.R., Cheung, C.Y., and Brace, R.A.: Plasma atrial natriuretic factor and arginine vasopressin responses to indomethacin in the ovine fetus [Abstract]. Am J Obstet Gynecol. 166: 379,1992c.
Walker, M.P.R., Rurak, D.W., and Riggs, K.W.: Fetal consequences of prostaglandin synthesis blockade. BC Health Research Foundation grant, 1993.
Walker, M.P.R., Moore, T.R., and Brace, R.A.: Indomethacin and arginine vasopressin interaction in the fetal kidney: A mechanism of oliguria. Am J Obstet Gynecol. Ill: 1234-1241, 1994.
Walker, M.P.R., Moore, T.R., and Brace, R.A.: Urinary and cardiovascular responses to indomethacin infusion in the ovine fetus. Am J Obstet Gynecol. 167: 834-843, 1992b.
Walker, M.P.R., Moore, T.R., Cheung, C.Y., and Brace, R.A.: Indomethacin-induced urinary flow rate reduction in the ovine fetus is associated with reduced free water clearance and elevated plasma arginine vasopressin levels. Am J Obstet Gynecol. 167: 1723-1731, 1992.

229 Walker, R.W., Gruber, V.F., Rosenberg, A., Wolf, F.J., Vanden Heuvel, W.J.A.: computerised mass spectrometric assay for sulindac and its metabolites in human plasma. Anal Biochem. 95: 579-586, 1979.
Wallusch, W.W., Nowak, H., Leopold, G., Netter, K.J.: Comparative bioavailability: Influence of various diets on the bioavailability of indomethacin. Int J Clin Pharmacol. 16: 40-44, 1978.
Wang, L.H., Rudolph, A.M., and Benet, L.Z.: Comparative study of acetaminophen disposition in sheep at three developmental stages: the fetal, neonatal, and adult periods. Dev Pharmacol Ther. 14: 161-179,1990.
Wang, L.H., Rudolph, A.M., and Benet, L.Z.: Distribution and fate of acetaminophen conjugates in the fetal lambs in-utero. / Pharmacol Exp Ther. 235: 302-307, 1985.
Ward, R.M.: Maternal drug therapy for fetal disorders. Sem Perinatol. 16: 12-20, 1992.
Watanabe, J., Urasaki, Y., Nakase, Y., Ueda, H., Iwamoto, K., and Ozeki, S.: Excretion of indomethacin into saliva following intravenous administration to dogs. J Pharm Dyn. 4: 336-344,1981.
Weiner, I.M., and Mudge, G.H.: Renal tubular mechanisms for excretion of organic acids and bases. Am J Med. 36: 743-762.
Wells, P.G.: Analgesics: direct embryopathic effects and indirect biochemical effects modulating teratogenecity of other drugs and chemicals. In Toxicologic and Pharmacologic Principles in Pediatrics. Kacew, S., and Lock, S. (Eds.) Hemisphere Publishing Corporation, pp. 127-166, 1988.
Wennwalm, A., Eriksson, S., and Wahren, J.: Effect of indomethacin on basal and carbon dioxide stimulated cerebral blood flow in man. Clin Physiol. 1: 227-234, 1981.
Whitehouse, M.W.: The molecular pharmacology of anti-inflammatory drugs: Some possible mechanisms of action at the biochemical level. Biochem Pharmacol. Suppl.: 293-307, 1968.
Wiest, D.B., Pinson, J.B., Gal, P.S., Brundage, R.C., Schall, S., Ransom, J.L., Weaver, R.L., Purohit, D., and Brown, Y.: Population pharmacokinetics of intravenous indomethacin in neonates with symtomatic patent ductus arteriosus. Clin Pharmacol Ther. 49: 550-557,1991.
230 Wilkening, R.B., and Meschia, G.: Current topic: comparative physiology of placental oxygen transport. Placenta. 13: 1-15,1992.
Wilkening, R.B., Anderson, S., and Meschia, G.: Non steady state placental transfer of highly diffusible molecules. J Dev Physiol. 6: 121-129,1984.
Wilkening, R.B., Anderson, S., Martensson, L., and Meschia, G.: Placental transfer as a function of uterine blood flow. Am J Physiol. 242: H429-H436, 1982.
Wilkinson, G.R.: Clearance approaches in pharmacology. Pharmacol Rev. 39: 1-47,1987.
Winther, J.B., Hoskins, E., Printz, M.P., Mendoza, S.A., Kirkpatrick, S.E., and Friedman, W.F.: Influence of indomethacin on renal function in conscious newborn lambs. Biol Neonate. 38: 76-84,1980.
Wood, J.H., and Leonard, T.W.: Kinetic implications of drug resorption from the bladder. Drug Metab Rev. 14: 407-423,1983.
Woolf, D., Huskinsson, E.C., and Nicol, C.G.: Indomethacin and benorylate in osteoarthritis of the hip. Practitioner. 221 (1325): 791-792, 1978.
Wright, M.R., Rurak, D.W., van der Weyde, M.P., Taylor, S.M., and Axelson, J.E.: Clearance and disposition of ritodrine in the fluid compartments of the fetal lamb during and after constant rate fetal intravenous infusion. J Pharmacol Exp Ther. 258: 897-902, 1991.
Wright, M.R.: Ritodrine: Analysis, comparative maternal and fetal pharmacokinetics and pharmacodynamics in sheep, PhD thesis, University of British Columbia, Vancouver, 1992.
Wright, V., Walker, W.C., and McGuire, R.J.: Indomethacin in the treatment of rheumatoid arthritis. Ann Rheum Dis. 28: 157, 1969.
Wurtzel, D.: Prenatal administration of indomethacin as a tocolytic agent: effect on neonatal renal function. Obstet Gynecol. 76: 689-692, 1990.
Yaffe, S.J., and Juchau, M.R.: Perinatal Pharmacology. Ann Rev Pharmacol. 14: 219-238, 1974.
Yaffe, S.J., Friedman, W.F., Rogers, D., Lang, P., Ragni, M., and Saccar, C: The disposition of indomethacin in preterm babies. J Pediatr. 97: 1001-1006,1980.
Yeh, K.C.: Pharmacokinetic overview of indomethacin and sustained-release indomethacin. Am J Med. 79 (Supp. 4C): 3-12,1985.

231 Yeleswaram, K.: Analysis, pharmacokinetics, metabolism, and pharmacodynamics of labetalol in pregnant and non-pregnant sheep. PhD thesis, University of British Columbia, Vancouver, 1992.
Yesair, D.W., Callahan, M . , Remington, L . , and Kensler, C.J.: Role of the enterohepatic cycle of indomethacin on its metabolism, distribution in tissues and its excretion by rats, dogs, and monkeys. Biochem Pharmacol. 19: 1579-1590,1970.
Yoo, S.D.: Maternal-fetal disposition, fetal pharmacodynamics, and comparative pharmacokinetics of diphenhydramine in pregnant and non-pregnant sheep. PhD thesis, University of British Columbia, Vancouver, 1989.
Yoshida, H . , Kamiya, A . , Okumura, K. , and Hori, R.: Contribution of monoamine oxidase (MAO) to the binding of tertiary basic drugs in lung mitochondria. Pharm Res. 6 (10): 877-882, 1989.
Zachariae, E . : Osteoarthritis treated with indomethacin. Nordisk Medicin. 75 (14): 384-385, 1966.
Zancan, L . , Zacchello, F., and Mantero, F.: Indomethacin for Bartter's syndrome. Lancet. 2: 1354, 1976.
Zinic, M . , Kuftinec, J., Hofman, H . , Kajfez, F., Meic', Z.: Zomepirac sodium. In Analytical Profiles of Drug Substances. Florey, K . (Ed.). Academic Press. 15: 673-698, 1986.
Zona, C , Roscetti, G. , Venturelli, F., and Roda, L . G . : Effect of different parameters on the binding of two anti-inflammatory drugs to human serum albumin. Pharmacol Biochem Behav. 24: 1031-1037,1986.
Zuckerman, H . , Reiss, U . , and Rubinstein, I.: Inhibition of human premature labour by indomethacin. Obstet Gynecol. 44: 787-792, 1974.




















