
INDIAN MEDICAL JOURNAL
83
E Notice —CME Notice ginal & nical Research 7t , v ber of WONCA 110 1h Yr. Publication INDIAN MEDICAL JOURNAL ure) al Journal AIGPA The Official Month y Scientific Journal of All India General Practitioners' Association Volume 109, No. 6 ISSN No. 0091-5871 June 2015 (Annexure) Idia C / BID! ICMR / JR /233 dt. 14.12.2012, INDEX MEDICUS by MC, New Delhi, Govt. of India ociation News —Dr Pina,ki Ghosh Ti Main Findings in Laboratory Tests Diagnosis of Acute Appendicitis: A Prospective Evaluation —Dr Bharat Prasad, Dr Subrat Prasad 408(A) A Comparative Study of Endometric Aspiration Biopsy, Curettage and Endometrial Thickness Measurement by USG in Cases of Pen i and Post-Menopausal Women with Abnormal Uterine Bleeding —Di: Nidhi Kumari. Dr Subrat Prasad 410(A) A Comparative Study of Intraoperative Retinoscopy and Biometry for Calculation of Power of Intraocular Lens —Dr. Archana Kumari 412(A) A Comparative Study of Labetalol Vs Methyldopa in the Treatment of Hypertensive Disorders of Pregnancy —Dr Shalini Sc/in, Dr Subrat Prasad 415(A) A Comparison of Intramedullary and Extramedullary Fixation Devices in Unstable Trochanteric Fractures t —Di: Anil Kumar Singh, Dr Laljee Chaudhaty 417(A) A Retrospective Study of Thrombocytopenia in Hypertensive Disorders During Pregnancy —Dr; Pragra, Shall Kumari Sinha 420(A) A Study of Normal P-R Interval in Children of Odisha —DI: Priyadarsini Samanta, Prof Dr Jayanti Mishra, Dr Anwesit Mohanty. DI: Magna Manjareeka. Dr Sudeep Satpathy, Dr Prakash kumar Nayak, Sounwa Mishra, Dr Swasti Batmerjee, DI: Thideep Kumar Sengupta, Prof DI: Prabhabati Mohanty, Dr Jyoti Prakash Mishra 422(A) A Study on Clinical Profile of Patients of Hepatic Abscess —Dr Rajesh Kumar Jha, Dr K K. Singh 424(A) Accuracy of Clinical Prediction Rules in Peptic Ulcer Perforation : An Observational Study , Bhuvanjee ilia, Dr: Rajeev Kumar Vatsa 427(A) Adenomatoid Odontogenic Tumor of the Mandible: Report of A Case with Literature Review —Dr Nupur Rannerjee, Dr Sanjay Dutta, Dr Prasanta Bandyopadhyay, Dr Anjan Chmtdhury 430(A) Cervical Ripening with Prostaglandin in Women with Previous One Caesarean Section —Dr Pratibha Prakash 432(A) Common Bile Duct Dilatation with Stones Indicates Requirement for Early Drainage in Patients with Or Without Cholangitis —Dr Rina KI1MCITi, Dr Mahender Prasad Rajak 434(A) Comparative Study of Trochanteric Fracture Fixation by D.H.S and Proximal Femoral Nailing —Di: Rajas!: Kumar RaMan 438(A) Comparision of Efficacy of Theophylline and Caffeine for Prevention and Treatment of Apnea of Prematurity —Dr As/it Kama,: Mayank Nilay Dr Ashok Kumar 440(A) &IMAM MEINCAL JOURNAL J June 2015 (Annexure), Vol. 109, No. 6 405(A) 409(A) 411(A)
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of INDIAN MEDICAL JOURNAL

E Notice —CME Notice
ginal & nical Research
7t,v
ber of WONCA 1101h Yr. Publication
INDIAN MEDICAL JOURNAL ure)
al Journal AIGPA
The Official Month y Scientific Journal of All India General Practitioners' Association Volume 109, No. 6
ISSN No. 0091-5871 June 2015 (Annexure)
Idia C / BID! ICMR / JR /233 dt. 14.12.2012, INDEX MEDICUS by MC, New Delhi, Govt. of India
ociation News —Dr Pina,ki Ghosh Ti
Main Findings in Laboratory Tests Diagnosis of Acute Appendicitis: A Prospective Evaluation
—Dr Bharat Prasad, Dr Subrat Prasad 408(A) A Comparative Study of Endometric Aspiration Biopsy, Curettage and Endometrial Thickness Measurement by USG in Cases of Pen i and Post-Menopausal Women with Abnormal Uterine Bleeding
—Di: Nidhi Kumari. Dr Subrat Prasad 410(A) A Comparative Study of Intraoperative Retinoscopy and Biometry for Calculation of Power of Intraocular Lens
—Dr. Archana Kumari 412(A) A Comparative Study of Labetalol Vs Methyldopa in the Treatment of Hypertensive Disorders of Pregnancy
—Dr Shalini Sc/in, Dr Subrat Prasad 415(A) A Comparison of Intramedullary and Extramedullary Fixation Devices in Unstable Trochanteric Fractures t
—Di: Anil Kumar Singh, Dr Laljee Chaudhaty 417(A) A Retrospective Study of Thrombocytopenia in Hypertensive Disorders During Pregnancy
—Dr; Pragra, Shall Kumari Sinha 420(A) A Study of Normal P-R Interval in Children of Odisha
—DI: Priyadarsini Samanta, Prof Dr Jayanti Mishra, Dr Anwesit Mohanty. DI: Magna Manjareeka. Dr Sudeep Satpathy, Dr Prakash kumar Nayak,
Sounwa Mishra, Dr Swasti Batmerjee, DI: Thideep Kumar Sengupta, Prof DI: Prabhabati Mohanty, Dr Jyoti Prakash Mishra 422(A)
A Study on Clinical Profile of Patients of Hepatic Abscess —Dr Rajesh Kumar Jha, Dr K K. Singh 424(A)
Accuracy of Clinical Prediction Rules in Peptic Ulcer Perforation : An Observational Study , Bhuvanjee ilia, Dr: Rajeev Kumar Vatsa 427(A) Adenomatoid Odontogenic Tumor of the Mandible: Report of A Case with Literature Review
—Dr Nupur Rannerjee, Dr Sanjay Dutta, Dr Prasanta Bandyopadhyay, Dr Anjan Chmtdhury 430(A) Cervical Ripening with Prostaglandin in Women with Previous One Caesarean Section
—Dr Pratibha Prakash 432(A) Common Bile Duct Dilatation with Stones Indicates Requirement for Early Drainage in Patients with Or Without Cholangitis
—Dr Rina KI1MCITi, Dr Mahender Prasad Rajak 434(A) Comparative Study of Trochanteric Fracture Fixation by D.H.S and Proximal Femoral Nailing
—Di: Rajas!: Kumar RaMan 438(A) Comparision of Efficacy of Theophylline and Caffeine for Prevention and Treatment of Apnea of Prematurity
—Dr As/it Kama,: Mayank Nilay Dr Ashok Kumar 440(A)
&IMAM MEINCAL JOURNAL J June 2015 (Annexure), Vol. 109, No. 6 405(A)
409(A)
411(A)

Comparison between Conventional Radiography and High Resolution Computed Odginal & Tomography in Interstitial Diseases of the Lungs Clinical Research
—Dr. Subrat Prasad, Dr Bharat Prasad 441(A)
CT Scan Finding of Intracerebral Haemorrhagic Stroke and its Outcome in a Referral Hospital —Dr. Kh. Mani Singh, Dr Th. Rajendra Singh
443(A)
Estimation of Serum Lipoprotein (a) in Young Individuals as a Marker of Presence of Coronary Artery Disease
—Dr. Shobha Kumar Prasad, Dr C. M. Jha 447(A)
Evaluated to Medical Termination in Early Fetal Demise by using Mifepristone+ Sublingual Vs Oral Misoprostol
—Dr. Rau Kumari 450(A)
Generalized Peritonitis Secondary to Typhoid heal Perforation : Assessment of
V' Severity using Moditied Apache II Score
—Dr. Amjad Zia Ma/ilk, Dr Kahkashan Akluer 453(A)
Hepatic Dysfunction in Patients of Diabetes Mellitus Presenting in the Outdoor and Indoor Wards of Darbhanga Medical College & Hospital, Laberiasarai, Darbhanga
—Dr Shobha Kumar Prasad, Dr C. M. Jha 456(A)
Incidence of Angle Closure Glaucoma in Hypermetropic Patients above 40 Years of Age —Dr Archana Kumari
458(A)
Insight into the Management of Non-Traumatic Perforation of the Small Intestine —Dr. Md. Wahhaj
461(A)
Li raglutide Effect in Reducing HbAlc and Weight in Indian Population with Type 2 Diabetes, a Prospective Observational Trial
—Dr Manish Kutnar Prasad, Dr And: Kumar Prasad 464(A)
Management of Adhesive Intestinal Obstruction
Nutrient & Anti-Nutrient Changes in Finger Millet (E1ensine Coracana) During Germination 468(A) —Dr Shishir Kumar
—Dr Binata Nayak t 470(A)
Observation of Serum Uric Acid Level in Pregnancy —Dr. Shaltzadi Khatoon, Dr; Salina Khatun
473(A)
Observation of the Effect of Newer Calcium Channel Blocker Drugs (Amlodipine, Cilnidipine, Nitrendipine) on High Density Lipoprotein (1-101) Level of Rabbit's Serum
—Dr Manish Kumar Prasad, Dr Amit Kumar Prasad 475(A)
Observation on Australia Antigen Positivity and Risk Factors of HBV Infection in a Sample of Apparently Healthy Mothers and their Infants
—DI: Shah-Lath Khatoon, Dr. I.-:har Nam 477(A)
Observations on Effects of Itopride, Gatifloxacin, and Desloratadine on Q-Tc Interval in Patients —Dr Manish Kumar Prasad, Dr Amit Kumar Prasad
479(A)
Retrospective Analysis of Post Neonatal Admissions to the Paediatric Emergency Ward of a Tertiary Care Hospital in Eastern India
—Dr Mayank Nilay, Dr As/it Kumar, Dr Ashok Kumar 481(A)
Role of Elisa Test (rk39) in Diagnosis of Kala-Azar —Dr. Rajesh Kumar Jha, Dr K. K. Singh
482(A)
Role of Multidetector Computed Tomography in Determining Conservative Vs. Operative Management in Cases of Blunt Abdominal Trauma
—Dr Subrat Prasad, Dr Bharat Prasad 485(A)
Role of Oral Nimodipine in Reducing the Incidence of Morbidity and Mortality in Patients of ICH (Intracerebral Haemorrhages)
—Dr Rajesh Kumar Jha, Dr K. K. Singh 487(A)
Screening of Neonatal Sensorineural Deafness by Otoacoustic Emissions —Dr. Md. ShartjAlam
489(A)
Short-Term Mortality and Complications in St Elevation Myocardial Infarction —Dr Kumar Soura DI: Kumar Gaurav
Small Bowel Obstruction : The Eternal Dilemma of When to Intervene 491(A)
v
—Dr. Rina Kaman. Dr Ma/lender Prasad Rajak 493(A)
Study of Clinical Presentation, Aetiological Profile, Immediate Outcome and Short Term Follow Up of Bleeding Neonates
—Dr Abhay Kumar Dr Nidhi Kuntari 495(A)
INDIAN MEDICAL JOURNAL' June 2015 (Annexure), Vol. 109, No. 6 406(A)

Generalized Peritonitis Secondary to Typhoid Ilea! Perforation : Assessment of Severity using
Modified Apache II Score
Dr. Ainjad Zia Mal likl, Dr. Kahkashan Akhter2
IGINAL gr. CLINICAL RESEARCH
-hat ; nett iota
m .ation Mt; 1
2. Sm of m
ncy.
Smtt it of asop
g Ho do
Mat a : e od.
S, C 44-1 stud
s of vs anage as. Hu
ang ( for M
(Jul. leath
Isson onion
RACT
GROUND t• Generalized peritonitis from Heal perforation is a common cause of emergency in the developing countries,
ed with high morbidity and mortality. The assessment of a disease condition is often
to prioritise treatment and reduce morbidity roortality. High severity scores are usually
•ed with high morbidity and mortality; , these patients may require more intensive t than those with low severity scores.
: The purpose of this study was to assess ty of generalized peritonitis from typhoid
oration using modified APACHE II score.
TER1ALS AND h1ETI-SODS :Over a period of Patients had severity of illness assessed
modified APACHE II score. Demographic, preoperative, operative and postoperative each patient were entered into a prepared
Each patient had postoperative outcome rity of illness were compared to determine
goificance of the severity of illness on live outcome.
ITS The mean age was of 23.6 + 15.5 'th 4:1 male: female ratio. Morbidity rate from 8.8-713% and mortality in 17.5%.
APACHE II score ranged from 0-19, with a 8.2 + 4, 7.6 + 4 for survivors and 9.4 + 2 who died. There was no death among the
scored 0-4, whereas mortality was 13% who scored 5-9, 41.2% in those who scored and 50% in patients who scored 15-19
The modified APACHE II Score significantly mortality, but did not influence the
of other postoperative complications.
USION : A high APACHE II score was with high mortality, but did not predict
rate in the patients studied. More study is involving a larger number of patients to lidate our findings
UCTION
generalized peritonitis from typhoid deal is a potentially life-threatening condition.
n surgical emergency in many general Is in the developing countries and it is rated with high morbidity and mortality. severity of acute peritonitis has assisted
way in decision-making and has improved the management of severely ill patients. to objectively estimate patients 2 risk for other important outcome is an important
ging severely ill patients. Empirically assessment for important clinical events extremely useful in evaluating new n monitoring resources utilization and
quality of care. Scoring systems had useful in predicting the outcome in
A patients, thus allowing application of effective use. The introduction of Injury ore by Bakers et al in 1974 and Injury Scale in 1981 successfully opened further development of severity grading y scoring systems have been designed cessfully to grade the severity of acute
peritonitis and intra-abdominal sepsis.
The most widely used index, APACHE II (Acute Physiological and Chronic ill Health Evaluation), was developed from a mixed group of medical and surgical patients. Although not specifically designed for general surgical practice it has been successfully used by many authors to assess critically ill general surgical patients. It has also been compared with other scoring systems with good results.
The aim of this study was to grade the severity of acute generalized peritonitis from typhoid Heal perforation using modified APACHE II score. This study was carried out at the Sri Krishna Medical College & Hospital, Muzaffarpur, Bihar. This study will serve as the basis for further study in the area of severity assessment of generalized peritonitis from typhoid Beal perforation.
PATIENTS AND METHODS
A prospective survey of patients with acute generalized peritonitis due to typhoid deal perforation was carried out at the Department of Surgery. Katihar Medical College & Hospital (KMCH), Katihar, Bihar.
The stud) population consisted of 80 consecutive patients who had laparotrny during a 3-year period (2012 to 2014) for acute peritonitis due to typhoid Heal perforation. All the patients with acute generalized peritonitis from typhoid ileal perforation were included; adults or children, female or male. Clinical evaluation as well as haematological and biochemical investigations were carried out. Patients were resuscitated with intravenous fluid and correction of electrolyte imbalance as indicated by the results of the electrolytes and urea. Urethral catheter was inserted to monitor hourly urinary output and naso-gastric tube inserted to decompress the stomach. Combined Amoxicillin-Clavulanic acid (Augmentin) and metronidazole or Cefuroxime (Zinace0 and metronidazole were commenced on admission in the Children Emergency Room or in the Adult Accident and Emergency unit in appropriate doses.
The following Acute Physiological parameters of APACHE II were assessed and recorded at the admission points: Temperature (degree Centigrade), Mean arterial blood pressure (mmHg), Heart rate, Respiratory rate (non-ventilated), Serum sodium (nMal), potassium (rnMo1/1), creatinine (mg/100m1),
bicarbonate (rnhitoVI venous blood): haernalocrit white blood count (total/cmm3). No patients had Arterial pH or Partial pressure of oxygen (P02) due to lack of facility. These were scored in accordance with the APACHE II chart, scoring for abnormally high or low levels. The scores ranged from 010 4 on each side of normal value. Zero score represents normal values, an increase to 4 indicating the extreme end of high or low abnormal levels. These parameters represent the Acute Physiological Scores (APS).
Included in this study as part of APS was the serum urea. This was scored using the parameter similar to that of serum creatinine as follows: Serum urea 15 mmoVI = 4, 9-14mmoVI = 3.5-8 = 2, 1.4-4 mmoVI = 0,. 1-1.39 mmoVI = 1, <1 mmoV I = 2.
Age points are as follows for adult patients: 44= 0, 45-54=2, 55-64=3, 65-74=5, 75=6 22
Age points were modified as follows for children: 15= 0, 10-14=2, 5-9=3, 1-4=5, <1=6; this followed the pattern used for adults.
Chronic ill health value were added if the patients has history of severe organ system insufficiency or is immuno-compromisecl points are assigned as follows:
(a) non-operative or emergency postoperative patients- 5
(b) elective postoperative patients- 2 points.
The Acute Physiological Scores, Age Points and Score for Chronic ill health values, is the total APACHE II SCORE.
Analysis
All these and the demographic data were entered into a personal IBM compatible Computer and analysed using Epi info version 6 (CDC, Atlanta, Georgia, USA). Frequencies, tabulation and means were determined. Groups were compared using the student Rest and proportion using the Chi-square analysis with 'fate correction or Fisher Exact lest when indicated.
RESULTS
Demography
The age ranged from 6-65 years, mean of 23.6 + 15.5 years. There were 64 male patients (80%) and 16 females (20%). Over 70% were students
1. M.B.B.S., M.S. (Gen. Surg.), Associate Professor, Department of Surgery, K.M.C.H., Katihar, Bihar.
2. M.D. (Microbiology), PG Student, K.M.C.11., Katihar, Bihar.
451(A) 109, DICAL JOURNAL I June 2015 (Annexure), Vol. 109, No. 6

while the remaining patients were distributed among the farming, trading and artisan population, Clinical parameters and operative findings
The symptoms and signs were not different from the usual symptoms and signs of acute generalized peritonitis. At operation pus with faeculent materials was drained in all the patients ranging from 100-6000 mls, mean of 11735 ± 942.4 mls. There was
single Heal perforation in 68 patients (85%), two perforations in 9 (11.3%) and three perforations in 3(3.7%) patients. The size of perforation ranged from 0.5-4 cm, mean of 1.2 + 0.7 cm. With distant from ileocaecal junction ranged from 4-60 cm, mean of 283 + 13.3 cm. All the deal perforations were located in the anti-mesenteric border of the intestine. Postoperative outcome
The postoperative complications were wound infection in 57 patients (71.3%), wound dehiscence in 22 (27.6%), residual intra-abdorninal abscess in 10 cases (12.5%), postoperative cough in 10 cases (12.5%), residual intra-abdorninal sepsis in 9 cases (11.3%), 7 (8.8%) cases of incisional hernia, enterocutaneous fistula in 3 cases (3.8%) and 14 patients (175%) died. The duration of hospital stay ranged from 1 day -75 days, mean 21 ± 14 days.
All those who suffered mortality were male accounting for 22% of mortality in male patients, whereas mortality was nil in female patients: this was found to be statistically significant (P<0.05). Also, 50% of those who died had multiple perforations and this accounts for 58.3% of the patients with multiple perforations, whereas mortality was 10.3% in patients with single intestinal perforation (P<0.05).
Mortality occurred in the first week of admission in 12 patients accounting for 87.5% of the patients who suffered mortality. The hospital stay of those who died ranged from 1-28 days, mean of 6.3 + 7.2 days, thus, spent shorter period in the hospital (P<0.05). illustrates the variables with a statistically significant influence on the postoperative outcome.
ours. These factors have been found to have a significant effect on the Irro. bidity and mortality as demonstrated in this study in accordance with the findings of previous study in Nigeria.
The objective evaluation of severity, therapeutic approach and effectiveness of treatment of acute generalized peritonitis from typhoid deal perforation is hampered by the lack of precise classification in this environment Crude morbidity and mortality data for the purpose of medical audit is often misleading. Early prognostic evaluation is desirable to be able to select high-risk patients or more aggressive treatment especially in
severe peritonitis such as seen in typhoid deal perforation.
postoperative mortality in the pati however, its ability to predict postopera could not be confirmed in this study. finding, there is a need for further sn larger number of patients with acute pi typhoid Heal perforation. It would al patients with acute peritonitis from perforation, APACHE II score would grading for the evaluation of disease s
REFERENCES 1. Adesunkanml ARK, Nao OG. Th
factors in Typhoid Ilealperforation. / study of 50 patients. J Roy Coe
Adesunkaruni ARK, Badrmts TA, At Ogunrombi AB. Acute generalized Adult African Patients: Assessment using APACHE II Score. Ann Co 2003;7:23-8.
3. Adesunkanmi ARK, Oseni SA, Ad Agbakwunr EA. Acute generalized ; Adult African Patients: Assessment using APACHE li Score. ANZ J Sum 2 9.
4. Adesunknami ARK, Badmus TA, Og Causes and determinant of cutcome obstruction in a semi-urban African Arm Coil Surg HK 8: 116-23.1- . Baker 8P O'Neff 13. Haddon W(Jr), Lor injury severity score. A method for pattern of patients with multiple in evaluating emergency cases. .1 2012;14:187-95.
6. Bion J. Outcome in intensive c, 2013;307;953-4.
7. Bohnen J. Boulanger, Mealdns JL, Mr Prognosis in generalized peritonitis: F cause and risk factors. Arch Sum 201: 90.
8. Bohnen JMA, Mustand RA. Okkohn SE 1313. APACHE II score and abdominal Prospective study. Arch Sum 2008;123:
9. Civetta JM, Hudson-Civetta JA, Na Evaluation of APACHE II for cost contain quality assurance_ Ann Sum 2010;212:5
10. Copeland GP. Jones 0, Walter M. PO scoring system for surgical audit. Br 2011;78:355-60.
11. Edwands AT, Ng K.J. Shanda AA. Price JM. Experience with APACHE II severity o scoring system in predicting outcome in intensive therapy unit. J It Coll Sur 2911;36:37-40.
12. Greenspin L. McLellan BA, Craig H. Abt Injury Scale and Injury Severity Score: A chart J Trauma 1985;25:60-4.
13. Jones OR. Copeland GP, de Cossart L Coe of POSSUM with APACHE II for predi oustcourr 199fromznal .6 surgical high-dependenny j
14. Karen wk. Drapper EA. Wegner OR Zirri JE. APACHE severity of disehse class) system. Crtt Care Med 1985;13:815.29. ;
15. Meakins JL SolomIdn JS. A/lo, MD. DMA Proposed dassification of intra-abdominal stratification of aetiology and Risk of that Trial. Arch Surg 1984;119:1372-8.
16. Panting GA. Sim AJW, Dudley HAP Conti of local and systemic of sepsis in predicting Br J Surg 1987;74:750-2. 1
modified APACHE II score ranged from 0-19, mean of 8.2 + 4, the mean APACHE II score for survivors Was 7.6 + 4, and it was 9.4 + 2 in those who died. There was no death among the patients who scored 0-4, whereas mortality was 13% in those who scored 5-9, 41.2% in those who scored 10-14, and 50% in patients who scored 15-19 (13<0.05). The modified APACHE II Score only predicted mortality (P00.05), but did not predict the incidence of other postoperative complications.
DISCUSSION
Mortality following typhoid Heal perforation ranges from 9-43%, with many survivors having to face with severe wound infection and dehiscence. Mortality of 17% was recorded in this study and morbidity from other postoperative complications was about 13.8%-71.3%. Prognosis depends on the size and number of perforations and this can further be worsened by late presentation, especially in a rural and semi-urban community like
452(A)
The present study confirmed the ability of APACHE II to predict mortality in acute peritonitis sepsis due to typhoid deal perforation. The study also showed that it could be easily applied to grade severity of acute peritonitis in centres like ours, despite inadequate facilities, with some degree of effectiveness as previously documented. There was no death among the patients that scored 0-4, whereas mortality was 13% in those who scored 5-8, 41.2% in those who scored 9-13 and 50% in patients who scored 14-18. The limitation of this study is the inability to assess all the physiological parameters in APACHE II, especially arterial pH and partial pressures of oxygen (Po2). These and other unavailable parameters were scored zero in accordance with the recommendation of Meakins et al.
CONCLUSION
In conclusion, APACHE II score predicted
APACHE II parameters have been shown to have a stronger relationship to the outcome than previous groupings such as anatomy, causes, abnormality, age and chronic ill health without consideration for systemic effect of the intra-abdominal sepsis, thus its use in this study. APACHE II score is very popular and has been used in both surgical and non- surgical patients, it has also been validated 5 using many patients over several years in many centres in the developed countries. Of the present prognostic scoring systems, APACHE II appeared to be the most widely used and had a general acceptance in assessing the critically ill patients, for its easy applicability and ability to predict outcome. Many of these studies have associated high APACHE II scores with poor outcome as previously documented and confirmed by this study, however, only able to predict mortality but not morbidity rates in this study.
INDIAN MEDICAL JOURNAL I June 2015 (Annexure), Vol 109,1

Full Member of WONCA
INDIAN MEDICAL JOUli&':Luil: ( The Official Month y Scientific Journal of All India General Practitioners' Association )
Volume 109, No. 10 ISSN No. 0091-5871 October 2015 NIC / BID / ICMR / JR 1233 dt. 14.12.2012, INDEX MEDICUS by NIC, New Delhi, Govt. of India
An Official Journal of AIGPA
Original and Clinical Research
A Study to Assess the Prevalence of Left Ventricular Dysfunction in Type 2 Diabetes Mellitus Patients Presenting with Dyspnoea with Referance to Pro-BNP Level
—Dr. Debsmita Roy, Dr. Arnab Ghosh Chaudhury, Professor Niladri Sarlcar Acute Peg in Hole Docking in the Management of Infected Non-union of Long Bones
—Dr. Binod Kumar Mehta Aetiopathological Study of Hoarseness of Voice
—Dr. Kameshwar Prasad Singh
Comparative Study of Optimal Test and Routine Microscopy of Blood in the Diagnosis of Malaria in Children
—Dr. Krishan Kumar Jha, Dr. N. P. Gupta, Dr. Shyam Bahadur Prasad Evaluation of Gastroesophageal Reflux in Children with Severe Persistent Asthma
—Dr. Krishan Kumar Jha, Dr. N. P. Gupta, Dr. Shyam Bahadur Prasad Extractability of Common Bi:e Duct Stones at Endoscopic Cholangio-Pancreatography
—Dr. Subhash Kumar
Gap Nonunion of Forearm Bones Treated by Modified Nicoll's Technique —Dr. Binod Kumar Mehta
Main Findings in Laboratory Tests Diagnosis of Acute Appendicitis —Dr. Subhash Kumar
Minimally Invasive Percutaneous Plate Osteosynthesis (MIPPO) Technique Applied in the Treatment of Humeral Shaft Distal Fractures through a Lateral Approach
—Dr. Binod Kumar Mehta
Observation of Postcholecystectomy Syndrome after Laparoscopic Cholecystectomy —Dr. Amjad Zia Mallik, Dr. M. Arif Ansari
Observation on Interstitial Cells of Leydig in Mammalian Testes —Dr. Binita Chaudhary
Prevalence of Obesity among Primary School Children in North Bihar —Dr. Krishan Kumar Jha, Dr. N. P. Gupta, Dr. Rakesh Kumar
Role of Laparoscopy in Diagnosing of Chronic Abdominal Pain and Masses —Dr. Amjad Zia Mallik, Dr. Md. Shakeb Ahmed
Selective Intraoperative Cholangiography and Single-Stage Management of Common Bile Duct Stone in Laparoscopic Cholecystectomy
—Dr. Subhash Kumar
Small Bowel Obstruction : The Eternal Dilemma of when to Intervene —Dr. Subhash Kumar
Study of Epidemiology and Clinical Profile of Acute Rheumatic Fever —Dr. Krishan Kumar Jha, Dr. N. P. Gupta, Dr. Amit Kumar
Study of Incidence of Gynecomastia in Patients taking Spironolactone —Dr. Saurabh Kumar, Dr. Remain Kumar Sinha
Surgical Treatment of Appendiceal Adenocarcinoid (Goblet Cell Carcinoid) —Dr. Subhash Kumar
Surgical Treatment of Midclavicular Fractures: A Prospective Comparison of Knowles Pinning and Plate Fixation
—Dr. Binod Kumar Mehta
9
12
13
14
16
19
21
24
26
29
30
33
34
36
37
39
40
INDIAN MEDICAL JOURNAL I October 2015, Vol. 109, No. 10 3

I
ORIGINAL & CLINICAL RESEARCH
INTRODUCTION
The abdomen has always been considered "A pandords box". The mysteries of the box has not been completely unveiled yet. Even surgeons.known for their clinical acumen and experiences are, at times, baffled by the bizzare presentation of certain - abdominal conditions, particularly abdominal masses and chronic abdominal pain. In spite of tremendous advancements in the field of radiodiagnosis including ultrasonography, endoscopy and various imaging techniques, the diagnosis of art abdominal mass and chronic abdominal pain still eludes the surgeon. In certain cases the surgeon completely fails to make an accurate preoperative diagnosis and is compelled to take the course of exploratory laparotomy just to make the diagnosis and treat accordingly. In some of such puzzling cases the surgeon is confronted with problems for which either he or the patient may not be well prepared. In moments like these every surgeon wishes that if somehow he could have made the diagnosis preoperatively he could have tackled the problem more effectively. It was in such situations that a need was felt to devise an instrument which could directly peep through the Pandora's box and make an accurate pre-operative diagnosis.
Kelling in 1901 first described the endoscopic examination of peritoneal cavity. He used a modified cystoscope for this purpose. Since then, inspite of many advances in this instrument, the endoscopic examination of the peritoneal cavity has remained the preserve of Physicians and the Gynaecologists with some exceptions of Ruddock (1937), Handly (1955), Borei (1962), Cuschieri (1975), Gaiseford 'B' Hugh et at. (1976), Gomel. V.11976), Balfour (1976), Cortesi et al. (1979). Lewis et al. (1981), Udwadia, T.E. (1986). Surgeons still tend to view peritoneoscopy with some degree of hostility or it the best, indifference (Udwadia, T.E., 1986) .Whilst peritoneoscopy is extensively performed by physicians and gynaecologists, surgeons who are better qualified often ignore it. Peritoneoscopy is as much informative as exploratory laparotomy. So, Udwadia ultimately established the usefulness of this instrument in the field of surgery. According to Udviladia, surgeons acquire a feel of tissue, normal and abnormal, after years of seeing and palpating abdominal pathology at open surgery. This feel can be translated with great advantage in the endoscopic examination of the abdomen. Since surgeons will carry out the definitive operative procedure, peritoneoscopy is of
• immense value in planning or avoiding surgery after the complete diagnosis has been established. Surgeons can take biopsy of the abdominal pathology at the same time to establish the histological diagnosis. Any complication which occurs can be dealt with by the surgeon himself immediately. All these positive points favour, the use of this instrument by the surgeons for the diagnosis of abdominal masses and chronic abdominal pain.
On the other hand, other sophisticated investigative procedures, at times, fail to provide exact diagnosis of the abdominal mass and chronic abdominal pain due to certain limitation.
Although endoscopes too provide direct visualisation, but they can only view intralurninal
• pathology of gastrointestinal tract.
Ultrasonography is a very useful non - invasive investigative procedure. But this can only differentiate between solid and cystic masses. The diagnostic accuracy is 72% as per Kawaski (1978). The diagnosis is done by indirect evidences and at the same time, there is no scope of histological diagnosis with this instrument.
Other modern investigative procedures like various imaging techniques, are not only expensive but also out of reach of common people, less than 20% of the world population has an access to these non- invasive diagnostic aids (Udwadia,1986).
In poor country like ours these sophisticated investigative procedures are only available in very selected centres in larger cities.
Conversely, laparoscopy is an inexpensive simple procedure that can be carried out even at a small medical centre where electricity is available for diagnosing the cases of abdominal masses and chronic abdominal pain, thereby preventing some unnecessarj laparotomies only for diagnosis.
Despite 111 these facts enough attention has not been given to this inexpensive and easily accessible procedure in bur country and facility for laparoscopy is still not readily available.
So the present study is proposed to be carried out in an attempt to assess the possibilities, practicabilities and effectiveness of laparoscopy as a diagnostic procedure for abdominal masses and chronic abdominal pain in general surgery.
AIMS AND OBJECTIVES
1. To evaluate the efficiency of laparoscopy in surgical practice in diagnosing abdominal masses and chronic abdominal pain vis -a-vis clinical as well as laparotomy diagnosis.
2. To compare its merits and demerits with those of diagnostic laparotomy.
MATERIAL AND METHOD
The present study was conducted in the Department of Surgery of Katihar Medical College & Hospital, Katihar, Bihar between February 2013 to Awtuct 2014.
1. M.B.B.S., M.S. (Gen. Surg.), Associate Katihar, Bihar.
2. M.B.B.S., M.S. (Gen. Sing.), Assistant Katihar, Bihar.
Role of Laparoscopy in Diagnosing of Chroni, Abdominal Pain and Masse
Dr. Amjad Zia Mallikl, Dr. Md. Shalreb ATEi
MATERIALS
(a) Patients suffering from chronic pain and or having abdominal masses different surgical wards constituted the the present study.
dal The laparoscope- This endosc included following :
(i) lOmm 300 rigid endoscope with source
(ii) Flexible fibre-optic light guide
WO Camera
(iv) Monitor
(v) Trocar with its sheaths
(vi) Veress needle for pneumo-pen
(vii) Insufflator
(c) Surgical instruments for incisi as well as draping materials.
Sterilization :_The laparoscoPe attachments was sterilized by keeping it irk designed chamber containing formald for 30 minutes.
METHODS
Screening of subjects:
(a) Clinical examination- on patients of chronic abdominal pain and/04 masses were subjected to a thor examination in order to arrive at a p diagnosis. Diagnostic investigation : corroborate and confirm clinical diagnosis investigations were carried out as per the
(b) Blood examination : Total and white cell count and erythrocytic sedi estir ration was done as evidence of acute inflammatory r rocesses.
- Serurr. creatinine and blood were done to assess the re
- Similarly serum bilirubin a function testes were carried the hepato-biliary system.
Professor, Department of Surge
Professor, Department of Surge
30
INDIAN MEDICAL JOURNAL October 2015, V
fel Radiography : Plain X-ray abdomen and pelvis to visualize urolithiasis.
- Skiagram of chest was taken to detect pulmonary focus of tuberculosis and metastatic lesion in the lung.
- Intravenous urography was done to assess structural as well as functional integrity of urinary system.
- Oral cholecystograpy was done to visualize the hepatobiliary system.
- Barium studies were carried out to find out any pathology in gastrointestinal tract.
kb Imaging : Ultrasonography and in some cases C.T. Scan were carried out as per need. After screening and elaborate clinical examination cases of following categories were selected for laparoscopic examination.
• - Those patients in whom definite diagnosis could not be arrived at.
- Those patients in whom the diagnosis was known but the extent of lesion could not be ascertained.
Preoperative preparation of patients : After routine pre-operative investigation the patients were prepared in the same way as they are prepared for laparotomy. Each patient were given single intravenous dose of cefuroxime(750mg)as a prophylaxis
All patients were asked to void urine just before putting them on operation table.
Laparoscopic procedure: (a) After induction of general anaesthesia
,antiseptic cleaning and draping was done in the usual way.
(b) A transverse incision of about 1" was given in suburnblical position.
tc) The tip of the veress needle was pushed through the incision by maintaining continuous pressure while the abdominal wall was tented by lifting the skirt with tissue forceps. The pressure on the needle was released when loss of resistance was felt as needle entered the peritoneal cavity. The confirmation was made by moving the needle in all directions and by injecting 5 ml of normal saline which could not be aspirated.
lcit Having confirmed the position of the needle, pneumoperitoneum was produced by insufflator pushing through the veress needle. About 2-3 litres of air was pushed till the area of liver dullness war obtainer,.
A continuous monitoring of oulse, B.P. and respiration was done throughout the period of pneumoperitoneum procedure.
Then the veress needle was taken out keeping it almost parallel to the anterior abdominal wall.
After this, the trocar with its sheath was introduced with the same incision in z-entry manner. The trocar was directed obliquely headwands through the sub-cutaneous tissue till the resistannce of the sheath was felt then directed obliquely footwards. The final direction of the entry was always footward,
in the midline towards the pelvis ensuring that the trocar should enter the abdominal cavity caudal to the bifur of major vessels and in the area of maximum air cushion. Then the trocar was taken out. The valve of the trocar sheath was depressed slightly to allow escape of air from the pneumoperitoneum, hearing it confirmed the proper location of the trocar sheath.
After fully depressing the piston of the trocar sheath the rigid telescope was introduced. The free passage of the telescope without any resistance confirmed that the telescope was in the peritoneal cavity. An accessory trocar and canula is then inserted under vision in the left iliac fossa. By altering the position of Table from Trendelenberg and reverse Trendelenberg to right or left lateral position different intraperitoneal structures were visualized after attaching the cold light source in it.
The abdomen was examined in a systematic and sequential manner, commencing with the falciparum ligament as the key anatomical land mark.
With patient in left lateral position, the left lobe of the liver, the diaphragm and the spleen were examined. With the patient flat, die greater curvature of the stomach anterior and inferior surface of the right lobe of liver, gall bladder and duodenum were examined. Then raising the head end of the patient and increasing and decreasing the volume of pneurnoperitoneum, the diaphragm and postero-superior surface of right lobe of liver were visualized. The mid-abdomen, omentum, transverse colon, small bowel and parietal peritoneum were then examined. The telescope was then pushed footward and small bowel, descending colon, ascending colom were examined. In female patients, by doing a steep trendelenberg position, the pelvis was •-isualized. Photographs were taken whenever required.
After the completion of the procedoe and after confirming that there was no bleeding inside, the telescope was taken out. The piston of the trocar sheath was pressed to deflate air from the peritoneal cavity and finally the trocar sheath was taken out carefully.
Then two skin sutures with silk were given in each case.
The patient was then kept on intravenous fluid for about 4-6 hours, then in the evening after assessment of the patient, light liquid diet was given.
The patients were kept on broad-spectrum antibiotics like injectable ampicillin for one day, follow by oral administration, as a prophylactic measure. Pain kiler drugs were given as per requirement of the patient.
The patients were allowed to do normal day to day work from the next day. Stitches were taken out on rh post operative day.
Laparotomy : Laparotomy was done subsequently in all cases for the purpose of confirmation of diagnosis and for curative or palliative treatment as per the needs of individual case.
RESULTS
Peritoneoscopy was carried out in 50 cases
of clinically palpable masses and/or chronic abdominal pain during the period of February 2012 to August 2013.
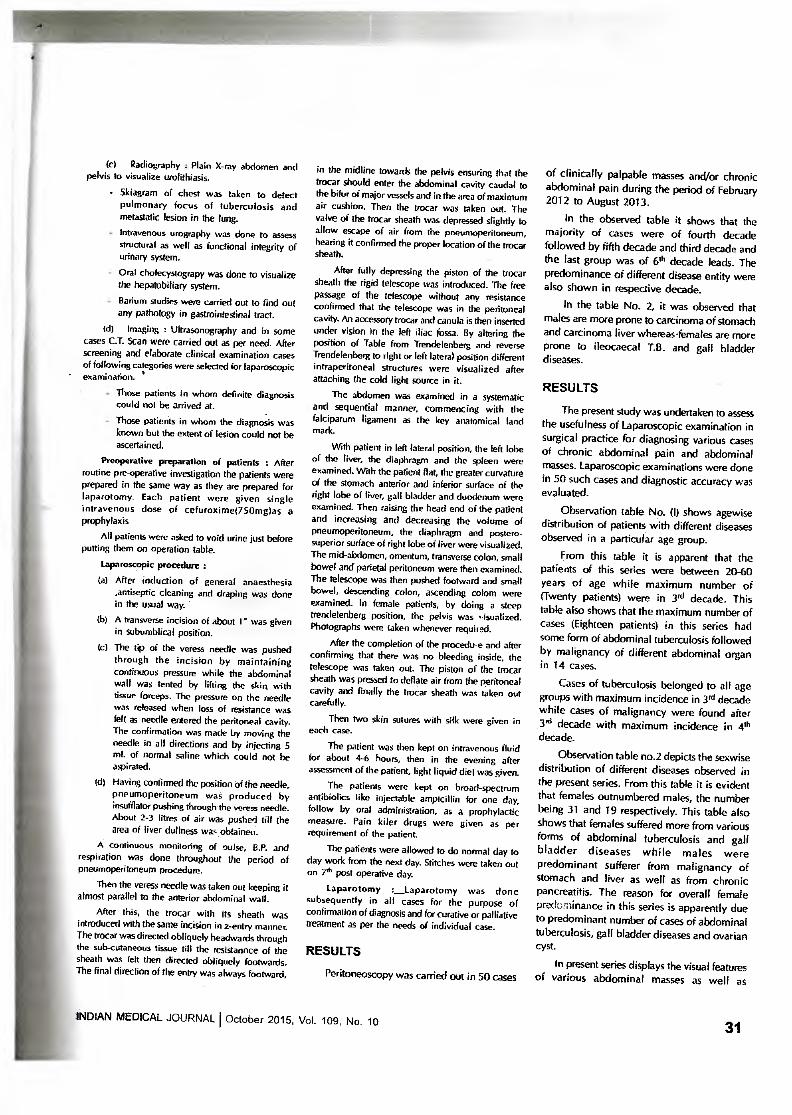
In the observed table it shows that the majority of cases were of fourth decade followed by fifth decade and third decade and the last group was of 6th decade leads. The predominance of different disease entity were also shown in respective decade.
In the table No. 2, it was observed that males are more prone to carcinoma of stomach and carcinoma liver whereas.females are more prone to ileocaecal T.B. and gall bladder diseases.
RESULTS
The present study was undertaken to assess the usefulness of Laparoscopic examination in surgical practice for diagnosing various cases of chronic abdominal pain and abdominal masses. Laparoscopic examinations were done in 50 such cases and diagnostic accuracy was evaluated.
Observation table No. (I) shows agewise distribution of patients with different diseases observed in a particular age group.
From this table it is apparent that the patients of this series were between 20-60 years of age while maximum number of (Twenty patients) were in 3rd decade. This table also shows that the maximum number of cases (Eighteen patients) in this series had some form of abdominal tuberculosis followed by malignancy of different abdominal organ in 14 cases.
Cases of tuberculosis belonged to all age groups with maximum incidence in .3rd decade while cases of malignancy were found after 3'd decade with maximum incidence in 4th decade.
Observation table no.2 depicts the sexwise distribution of different diseases observed in the present series. From this table it is evident that females outnumbered males, the number being 31 and 19 respectively. This table also shows that females suffered more from various forms of abdominal tuberculosis and gall bladder diseases while males were predominant sufferer from malignancy of stomach and liver as well as from chronic pancreatitis. The reason for overall female prtxtominance in this series is apparently due to predominant number of cases of abdominal tuberculosis, gall bladder diseases and ovarian cyst.
In present series displays the visual features of various abdominal masses as well as
INDIAN MEDICAL JOURNAL I October 2015, Vol. 109, No. 10 31
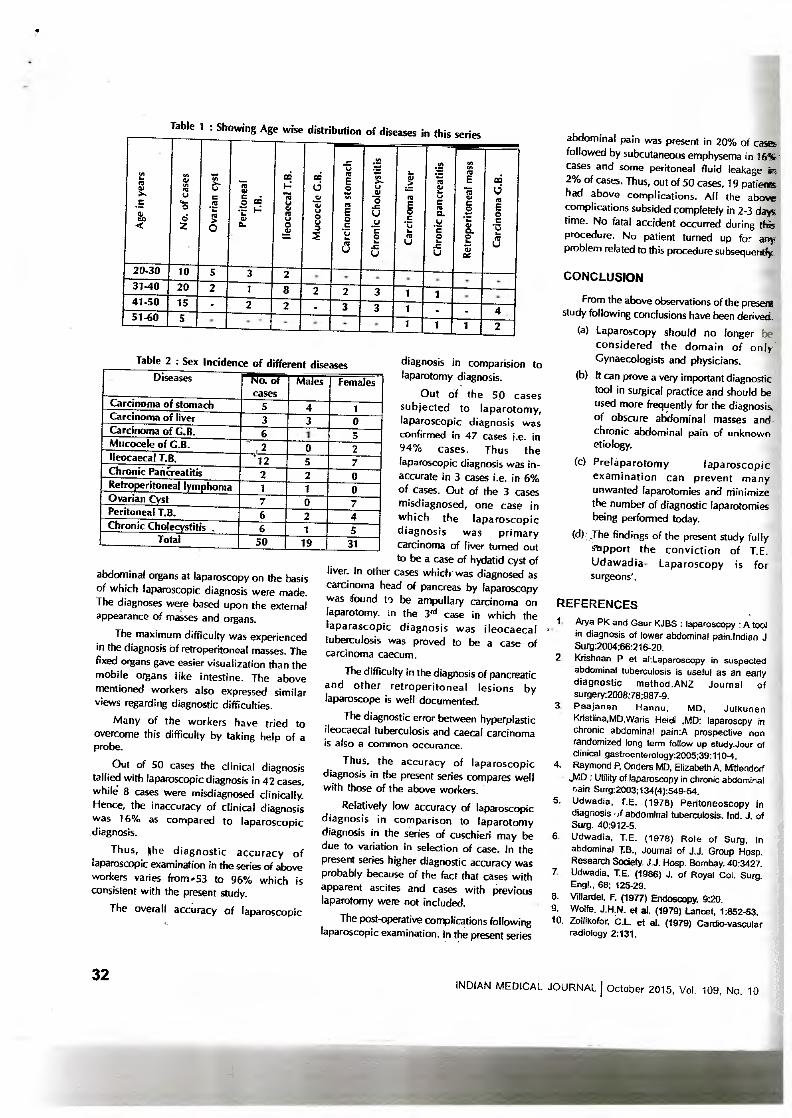
Table 1 : Showing Age wise distribution of diseases in this series
20-30 3 2 10 31-40 20 2 8 3 2 2 1 1 41-50 2 2 3 3 15 51-60 4
5 1 1 1 2
Chr
onic
Cho
lecy
stit
is
Car
c ino
ma
s tom
ach
Retr
oper
itone
a l m
ass
Chr
onic
pan
crea
titis
Car
c ino
ma
liver
I leoc
aeca
l T. B
.
Muc
oce I
e G
. B.
gel 01 co3
a-
Car
c ino
ma
C. B
.
3-)
0
Table 2 : Sex Incidence of different di Diseases No. of
cases Males Females
Carcinoma of stomach 5 4 1 Carcinoma of liver 3 3 0 Carcinoma of G.B. 6 , 1 5 Mucocele of G.B. 2 .ri 0 2 Ileocaecal T.B. 12 5 7 Chronic PanCreatitis 2 2 0 Retroperitoneal lymphoma 1 1 0 Ovarian Cyst 7 0 7 Peritoneal T.B. 6 2 4 Chronic Cholecystitis . 6 1 5
Total 50 19 31
abdominal pain was present in 20% of cases followed by subcutaneous emphysema in 16% cases and some peritoneal fluid leakage in 2% of cases. Thus, out of 50 cases, 19 patients had above complications. All the above complications subsided completely in 2-3 days time. No fatal accident occurred during this procedure. No patient turned up for any problem related to this procedure subsequently
abdominal organs at laparoscopy on the basis of which laparoscopic diagnosis were made. The diagnoses were based upon the external appearance of masses and organs.
The maximum difficulty was experienced in the diagnosis of retroperitoneal masses. The fixed organs gave easier visualization than the mobile organs like intestine. The above mentioned workers also expressed similar views regarding diagnostic difficulties.
Many of the workers have tried to overcome this difficulty by taking help of a probe.
Out of 50 cases the clinical diagnosis tallied with laparoscopic diagnosis in 42 cases, while 8 cases were misdiagnosed clinically. Hence, the inaccuracy of clinical diagnosis was 16% as compared to laparoscopic diagnosis.
Thus, he diagnostic accuracy of laparoscopic examination in the series of above workers varies from -53 to 96% which is consistent with the present study.
The overall accuracy of laparoscopic
diagnosis in comparision to laparotomy diagnosis.
Out of the 50 cases subjected to laparotomy, laparoscopic diagnosis was confirmed in 47 cases i.e. in 94% cases. Thus the laparoscopic diagnosis was in-accurate in 3 cases i.e. in 6% of cases. Out of the 3 cases misdiagnosed, one case in which the laparoscopic diagnosis was primary carcinoma of liver turned out to be a case of hydatid cyst of
liver. In other cases which was diagnosed as carcinoma head of pancreas by laparoscopy was found in be ampullary carcinoma on laparotomy. in the 3 31 case in which the laparascopic diagnosis was ileocaecal tuberculosis was proved to be a case of carcinoma caecum.
The difficulty in the diagnosis of pancreatic and other retroperitoneal lesions by laparoscope is well documented.
The diagnostic error between hyperplastic ileocaecal tuberculosis and caecal carcinoma is also a common occurance.
Thus, the accuracy of laparoscopic diagnosis in the present series compares well with those of the above workers.
Relatively low accuracy of laparoscopic diagnosis in comparison to laparotomy diagnosis in the series of cuschieri may be due to variation in selection of case. In the present series higher diagnostic accuracy was probably because of the fact that cases with apparent ascites and cases with previous laparotomy were not included.
The post-operative complications following laparoscopic examination. In the present series
CONCLUSION
From the above observations of the present study following conclusions have been derived.
(a) Laparoscopy should no longer be considered the domain of only Gynaecologists and physicians.
(b) It can prove a very important diagnostic tool in surgical practice and should be used more frequently for the diagnosis, of obscure abdominal masses and- chronic abdominal pain of unknown etiology.
(c) Pre la pa rotom y laparoscopic examination can prevent many unwanted laparotomies and Minimize the number of diagnostic laparotomies being performed today.
(d) The findings of the present study fully stipport the conviction of T.E. Udawadia- Laparoscopy is for surgeons'.
REFERENCES 1. Arya PK and Gaur KJBS laparoscopy : A tool
in diagnosis of lower abdominal pain:Indian J Surg:2004:66:216-20.
2. Krishnan P et aliaparoscopy in suspected abdominal tuberculosis is useful as an early diagnostic method.ANZ Journal of surgery:2008:28:987-9.
3. Paajanen Hannu, MD, Julkunen Kristiina,MD,Waris Heidi ,MD: laparoscpy in chronic abdominal pain:A prospective non randomized long term follow up study.Jour of clinical gastroenterology:2005;39:1104.
4. Raymond P. Onders MD, Elizabeth A, Mittendorf JvID : Utility of laparoscopy in chronic abdominal rain Surg:2003;134(4):549-54.
5. Udwadia, I.E. (1978) PeritoneOscOpy in diagnosis n abdominal tuberculosis. Ind. J. of Surg. 40:912-5.
6. Udwadia, T.E. (1978) Role of Surg. In abdominal T.B., Journal of J.J. Group Hosp. Research Society. J.J. Hosp. Bombay. 40:3427.
7. Udwadia, T.E. (1986) J. of Royal Col. Surg. Engl., 68; 125-29.
8. Villardel, F. (1977) Endosoopy. 9:20. 9. Wolfe, J.H.N. et al. (1979) Lancet, 1:852-53. 10. Zollikofor, .C.L et at. (1979) Cardio-vascular
radiology 2:131.
32 INDIAN MEDICAL JOURNAL J October 2015, Vol. 109, No. 10

INDIAN MEDICAL JOURNAL ( The Official Monthly Scientific Journal of All India General Practitioners' Association
Full Member of WONCA 110" Yr. Publication
ofAiGiv, Volume 109, No. 10 ISSN No. 0091-5871 October 2015 •
NIC / BID / ICMR / JR / 233 dt. 14.12.2012, INDEX MEDICUS by NIC, New Delhi, Govt. of India
Original and Clinical Research
A Study to Assess the Prevalence of Left Ventricular Dysfunction in Type 2 Diabetes Mellitus Patients Presenting with Dyspnoea with Referance to Pro-BNP Level
—Dr. Debsmita Roy, Dr. Amab Ghosh Chaudhuty, Professor Niladri Sarkar Acute Peg in Hole Docking in the Management of Infected Non-union of Long Bones
—Dr. Binod Kumar Mehta
Aetiopathological Study of Hoarseness of Voice —Dr. Kameshwar Prasad Singh
Comparative Study of Optimal Test and Routine Microscopy of Blood in the Diagnosis of Malaria in Children
—Dr. Krishan Kumar Jha, Dr. N. P. Gupta, Dr. Shyam Bahadur Prasad
Evaluation of Gastroesophageal Reflux in Children with Severe Persistent Asthma —Dr. Krishan Kumar Jha, Dr. N. P. Gupta, Dr. Shyam Bahadur Prasad
Extractability of Common Bie Duct Stones at Endoscopic Cholangio-Pancreatography —Dr. Subhash Kumar
Gap Nonunion of Forearm Bones Treated by Modified Nicoll's Technique —Dr. Binod Kumar Mehta
Main Findings in Laboratory Tests Diagnosis of Acute Appendicitis —Dr. Subhash Kumar
Minimally Invasive Percutaneous Plate Osteosynthesis (MIPPO) Technique Applied in the Treatment of Humeral Shaft Distal Fractures through a Lateral Approach
—Dr. Binod Kumar Mehta
Observation of Postcholecystectomy Syndrome after Laparoscopic Cholecystectomy —Dr. Amjad Zia Mallik, Dr. M. Arif Ansari
Observation on Interstitial Cells of Leydig in Mammalian Testes —Dr. Binita Chaudhary
Prevalence of Obesity among Primary School Children in North Bihar —Dr. Krishan Kumar Jha, Dr. N. P. Gupta, Dr. Rakesh Kumar
Role of Laparoscopy in Diagnosing of Chronic Abdominal Pain and Masses —Dr. Amjad Zia Mallik, Dr. Md. Shakeb Ahmed
Selective Intraoperative Cholangiography and Single-Stage Management of Common Bile Dud Stone in Laparoscopic Cholecystectomy
—Dr. Subhash Kumar
Small Bowel Obstruction : The Eternal Dilemma of when to Intervene —Dr. Subhash Kumar
Study of Epidemiology and Clinical Profile of Acute Rheumatic Fever —Dr. Krishan Kumar Jha, Dr. N. P. Gupta, Dr. Amit Kutnar
Study of Incidence of Gynecomastia in Patients taking Spironolactone —Dr. Saurabh Kumar, Dr. Hemant Kumar Sinha
Surgical Treatment of Appendiceal Adenocarcinoid (Goblet Cell Carcinoid) —Dr. Subhash Kumar
Surgical Treatment of Midclavicular Fractures: A Prospective Comparison of Knowles Pinning and Plate Fixation
—Dr. Binod Kumar Mehta
4
6
9
12
13
14
16
19
21
24
26
29
30
33
34
36
37
39
40
INDIAN MEDICAL JOURNAL I October 2015, Vol. 109, No. 10
ORIGINAL & CLINICAL RESEARCH
Observation of Postcholecystectomy Syndrome after Laparoscopic
Cholecystectomy
Dr. Amjad Zia Mallikl, Dr. M. Arif Ansari2
INTRODUCTION In
recent decades lapa roscop ic cholecystectomy has gained a status of one of the most commonly performed abdominal operations. This is due to a brisk rise in the incidence of calculus disease of the biliary tract. Also, there has been a noticeable increase in its incidence in lower age groups (<20 years). Due to the greater number of laparoscopic cholecystectomies being performed, the number of patients unimproved by the procedure has also increased Proportionately
. These unimproved .patients are said to have post-cholecystectomy syndrome. These symptoms can represent either the continuation of symptoms thought to be caused by the gallbladder or the development of new symptoms attributed to the gallbladder. PCS also includes the development of the symptoms caused b removal of the gallbladder.
As a matter of fact, the symptoms presented by such patients are not airways due to cholecystectomy but may be due to other factors related or unrelated to hepatobiliary tract disorders, thus uninfluenced by removal of gall bladder. So, the term post cholecystectomy syndrome should be precisely applied only to those post operative symptoms considered to have originated in biliary tract.
Since last two decade, laparoscopic cholecystectomy has become the preferred and more common method of treating gall bladder disease. In India also, it has became
e method of choice in advanced clinics and hospitals. The problem of PCS has decreased with laparoscopic cholecystectomy but there still remains a vast scope for attempts to decrease its incidence.
First laparoscopic cholecystectomy was done by Muhe of Germany in 1985 and Liy Mouret in Lyon in 1827. Prof. TE Udwadia, Mumbai did first laparoscopic cholecystectomy in India.
In 1947, Womack and Crider first described PCS, defining it as the presence of symptoms after cholecystectomy. These symptoms may actually represent either (1) the continuation of symptoms that had been interpreted as resulting from pathology of the '° gallbladder or (2) the developed of new 49 symptoms that might normally be attributed to yea the gallbladder. PCS is also the development of of symptoms, such as gastritis and diarrhea, f°u caused by removal of the gallbladder. 1.
Out of all laparoscopic cholecystectomies , regardless of the state of gallbladder, post 2. cholecystectomy syndrome occurs in 10-20%
24
to Fo
- gal
Professor, Department of Surgery, ICM.C.H.,
& Head, Department of Surgery, K.M.C.H.
INDIAN MEDICAL JOURNAL I October 2015, Vol. 109, No. 10
of the total cases, in 10-15% of calculus cases and in 15-40% of noncalculus cases.
According to Ernest Lack (2000), one risk factor for developing PCS includes not being certain of the diagnosis prior to gallbladder removal. Another risk factor includes having an urgent gallbladder removal. In general, the longer the symptoms lasted prior to the gallbladder removal, the greater the chance of developing PCS. If the symptoms are present less- than a year before gallbladder removal, 15.4% of patients has been shown to develop PCS. If the symptoms from 1-5 years, 21 have been shown to develop PCS. If the symptoms last from 6-10 years, 31% have been shown to develop PCS. And if the symptoms last from for more than 10 years
have . leen shown to develop PCS. If the gallbladder is removed to treat gallstone approximately 29% of patients develop PCS. If the surgery is not performed to remove allstones, anywhere from 10 to 25% of
patients develop PCS. If the common bile duct is cut open, in addition to gallbladder removal 23% of patients develop PCS. If the common bile duct is not cut open and the gallbladder is removed, 19% of patients develop PCS.
Younger patient have generally been found have an increased risk Of developing PCS. r example, people aged 20-29 that had the !bladder removed have been found to have
a 43% chance of develo in PC eas 39 year old have a 27% chance, and 40 to year olds, have a 21% chance. 50 to 59 r olds were found to have a 26% chance
developing PCS and 60-69 year olds were nd to have a 31% chance of develo 'n
M.B.B.S., M.S. (Gen. Surg.), Associate Katihar, Bihar.
M.B,B.S., M.S. (Gen. Surg.), Professor Katihar, Bihar.
PCS. Females have been found to have a greater risk of developing PCS than males. Specially, 28% of females were found to develop PCS compared to 15% of males. Another risk factor for PCS is having a psychiatric (mental health) disorder. About 50% of patients with a mental health disorder were found to develop PCS compared to patients without psychiatric disorder (of which 20% developed PCS).
MATERIALS AND METHODS
Cases after laparoscopic cholecystectomy were collected from Katihar Medical College and Hospital, Katihar, Bihar. A series of 200 cholecystectomized cases operated over a period of 5 years have studied. Followed up of cases were made by personal interview and examination either at the Hospital or at the residence, informations collected from the relatives and by correspondence. The review was made as follows :
1. Name and address of the patient 2. Registration number and date of
admission 3. Sex and age years 4. Presenting complaints — 5. Past History — other abdominal
operation performed, any other illness. 6. Fam'ty history and personal historT —
(in case of female-menstrual or menopausal history).
7. Details of previous cholecystectomy -- 8. Clinical examination —
— Pulse
- Built — Oedema - Temperature — Pallor - Lymph glands - Blood pressure
- Jaundice - Skin conditions
9. Examination of abdomen and gastrointestinal tract —
10. Examination of —
Investigations were done as following:
1. Routine examination —
a. Stool — Ova, Cyst, Occult blood, Stercobilinogen, Fat analysis.
b. Urine
c. Blood
2. Special examination
Liver function tests
Serum bilirubin, Serum protein (A:G ratio), Vanden Bergh test, Prothrombin time Serum alkaline phophatase, Serum SGPT, SGOT presence of Australia antigen.
a. Analysis of gastric secretion
b. Serum amylase estimation
3. Radiological examination
4. Electro-cardiogram
5. Laparoscopy. - This was done in cases with the views of confirming diagnosis and to institute possible surgical treatment.
6. Biopsy
Other Tests:
• In addition to the H & P and review of the old record, an ECG should be performed to screen for coronary disease.
• A stress test or Hotter monitoring may be indicated by the findings from the H & P, laboratory tests, or ECG.
• Provocation tests, such as the morphine-Prostigmin test for pain or the secretin stimulation for pancreatic-duct dilatation, have not been widely
accepted.
Diagnostic Procedures:
RESULTS AND DISCUSSION
Two hundred cholecystectomisecl cases have been observed during the period 2011-2013. All cases were examined and followed either by personal visit in surgical OPD and wards or at the residence.
Sex incidence : In the present study 150 females and 50 males were encountered. But the syndrome was seen in 40 cases in which females were 29 (58%) and males 11 (22%).
Age Incidence : In the present series majority of the cases developed symptoms between the ages of 31-60 years.
The high incidence in the present study between 31-60 years was due to the maximum number of cases of cholecystectomies performed in this age group.
AsYmotomatic period : The symptom free interval between cholecystectomy and the development of first symptom has been termed as asymptomatic period. Table III shows that the majority of the cases (40%) presented for treatment within 6 months of their cholecystectomy. The minimum and maximum symptom free interval was 0-10 years respectively with an average of two years.
In the present series (2013) of about 200 cholecystectumised patients, 40 developed PCS and their average age was 40 years. Asymptomatic period was 0-10 years with an average of two years.
Different symptoms in post laparoscopic cholecystectomy cases might take different intervals to appear. In cases of earlier arrival of symptoms, the residual pathology like hepatitis, choiangitis, left out stone in common bile duct might be responsible. In late arriv' al cases, the subsequent pathology like stricture common bile duct) reformed stone in common bile duct and flaring up of malignant conditions are considered.
Incidence of oost-cholecystectomv syndrome after laparoscopic cholecystectomy :
Total number of follow up cases have been divided into calculus and non-calculus group according to the presence of stone in their gall bladder at the cholecystectomy. The incidence of post-cholecystectomy syndrome was :we (50%) in non-calculus group than the calculus greolp (18.75%) after laparoscopic cholecystectomy.
The symptom complex referable to hepatobiliary system including pancreas have been named as "True post-cholecystectomy syndrome". Again the incidence of this true sYndrome was more (20%) in non-calculus group than calculus group (7.9%). In the present series the incidence of true syndrome, considering both of the calculus and non-calculus groups together was 8.5%.
CONCLUSION
Two hundred laparoscopic cholecystectomised cases have been following 2012-2014, out of which 150 were female and 50 male. Post-cholecystectomy syndrome was observed in 40 cases giving 20%, consisting of 29 females and 11 males.
The age group upto 30 years had minimum percentage (17.54%) of symptomatic cases whereas maximum were seen after 60 years of age.
Most of the symptomatic cases (40%) came for the treatment within 6 months of the cholecystectomy.
The complaints, details ofothe operation and the follow up observations have been recorded.
Cases were divided according to the presence of stone at their cholecystectomy into calculus and non-calculus groups. The symptomatic cases were more (50%) in non-calculus group than in the calculus group (18.75%).
Symptoms referable to hepato-biliary system including pancreas have been termed as 'True post-cholecyseectomy syndrome'. This was found in 8.5% cases.
Pain was a constant feature in almost every case and was complained before and after cholecystectomy. laundice, vomiting, nausea and fever were found in more percentage of cases after operation than before.
The causes responsible for the "True syndrome" were found to be stone in the common bile duct, stricture of common bile duct, biliary fistula, stenosis and spasm of sphincter of Oddi, biliary dvskinesia and periampullary carcinoma. Their respective incidence and relative importance have been reported and analysed.
Investigations revealed that there were several associated conditions with the biliary disease responsible for dyspeptic and other symptoms in the cases under study. They were parasitic infestations, hepatitis, cholangitis, cirrhosis, gastro-duodenal ulceration, diverticular disease of the colon and carcinoma of .the liver.
Operative treatment adopted for 18 cases (45%) offered cure or relief in 15 cases (373%). Two cases (5%) were, not benefited by surgery and one case (2.5%) died due to low condition.
Correct pre-operative diagnosis to distinguish the condition from other concomitant pathology would enable to reduce the incidence of this syndrome.
Advanced investigative techniques, correct diagnosis as far as practicable and above all mature operative judgement and meticulous surgery will certainly bring down this undesired post-cholecystectomy syndrome and finally wipe it out completely.
REFERENCES
1. Shaw, C., O'Hanlon, D.M. — Hepatogastroenterology, 2004 Jan-Feb. FenIon, H.M., McEntee, G.P.
2. Abu Farskh NA, Stietieh M & Abu Farsakh FA: J din Gastroenterol, 2009. •
3. Coakley FV, Schwartz, L.H. & Blumgari L.H — Radiology 2012 Oct; 209 (1) : 141-6(Medline ) Blumgart, L.H.
4. Corazzoari, E . — Dig Liver Dis. 2003 Jul 5. Evans, PR, Bak, Y.T., Shuter. B- Dig. Dis. Sci.
2007 Oct 6. Glenn, F. (1952) — Quoted by Schofiekl, 2006. 7. Rubini, G., Dimonte, M — Clin. Nucl. Med.,
2009. 8. Steen, W. Jensen (2002) — Medline 9. Tarik Albuzhi — Klin Khir., 2000 Oct. 10 Weir, J.F. & Snell, A.M. (1953) — Quoted by
Troppoli et at., 2012.
INDIAN MEDICAL JOURNAL 1 October 2015, Vol. 109, No. 10 25

ONCA 110th Yr. Publication
INDIAN MEDICAL JOURNAL The Official Month y Scientific Journal of All India General Practitioners' Association
Volume 109, No. 8
ISSN No. 0091-5871 August 2015 (Annexure)
/ BID / ICMR / JR / 233 dt. 14.12.2012, INDEX MEDICUS by NIC, New Delhi, Govt. of India
—CME Notice 572(A)
tion News Pinaki Ghosh 582(A)
Journal PA
tice
al & I Research
A Clinical and Biochemical Study of Patients with Recent Moderate to Moderately Severe Burn with Special Reference to their Renal Function
—Dr. Athar Hussain, Dr. Sheereen Tarannum
A Clinico-Pathological Study of Persistant Diarrhoea in Infants —Dr. Kedar Nath, Dr. Manju Kumari, Dr. Keya Basu(Ghosh)
A Comparative Study of Intrathecal and Epidural Buprenorphine using Combined Spinal-epidural Technique for Caesarean Section at L2-L3 Level
—Dr. Ranjeet Kumar, Dr.Ajay Simba, Dr.Md .Alauddin Alain, Dr. Shiwangi Tiwari
A Comparative Study of Metered Dose Inhaler with Spacer and Dry Powder Inhaler for Delivery of Salbutamol in Acute Exacerbations of Asthma
—Dr. Ghulam Rasool Wani
A Prospective Duplex Sonographic Study of Intrarenal Arteries in Acute Ureteric Obstruction —Dr. Deepak Kumar, Dr. Prem Kumar
A Prospective, Randomized, Open Label Comparative Study of Efficacy and Safety of Tapentadol Versus Tramadol in Low Back Pain
—Dr. Vivek Singh, Dr. Sunita Singh A Study of Anaemia in Children
—Dr. Kedar Nath, Dr. Manju Kumari, Dr. Keya Basu(Ghosh)
A Study of Efficacy of Kangaroo Mother Care as Compared to Conventional Methods of Care on Growth in LBW Babies
—Dr. Ghulam Rasoot Wani
A Study of fall in Geriatic Patient Care —Dr. Kedar Nath, Dr. Manju Kumari
AMBLYOPIA: Out of Dark, into the Light —Dr. Bhupendra Prasad
Clinical Profile of Scrub Typhus in Pediatric Age Group in Uttrakhand — Dr. Sanjeev Kumar, Dr. Vyas Kr Rathour, Dr Anand Jain
Common Bile Duct Dilatation with Stones Indicates Requirement for Early Drainage in Patients with or without Cholangitis
—Dr. Tariq Hameed, Dr. Awadh Kumar
Comparative Evaluation of Efficacy, Safety and Acceptance of Rosuvastatin 10 mg with Atorvastatin 10 mg in Patients of Dyslipidemia
—Dr. Tanweer Ahmad
Comparison between Conventional Radiography and High Resolution Computed Tomography in Interstitial Diseases of the Lungs
—Dr. Kalaskar Ketan Arun, Dr. Rajiv Ranjan
561(A)
563(A)
564(A)
567(A)
569(A)
573(A)'
576(A)
577(A)
580(A)
581(A)
583(A)
585(A)
589(A)
592(A)
CAL JOURNAL I August 2015 (Annexure), Vol. 109, No. 8
557(A)

Oral Nifedipine for Treatment of Preterm Labour
Observation on Fetomaternal Outcome in Cases of Obstructed Labour ' Sneh Priya, Dr. Shail Kumari Sinha
—Dr. Ha Priyanka, Dr. Usha Kumari New Options for Uveitis Treatment 625(A)
—Dr. Bhupendra Prasad
Glimpse of Ovarian Tumour in Bihar 627(A)
Maternal and Perinatal Outcome following Premature Rupture of Membrane —Dr. Vidya Paul, Dr. Rakesh Kumar, Dr. Vivekanand Paul, Dr. Chandra Kiran
623(A) ' Metformin VS Myoinositol in the Management of PCOS- A Comparative Study
—Dr. Anuradha Ghosh
—Dr. Pratibha Srivastava, DE(Prof) D.N. Singh
—Dr. Vivek Singh
621(A)
632(A)
630(A)
634(A)
635(A)
637(A)
639(A)
Original & Comparison between Oral and Rectal Misoprostol to Prevent Postpartum Hemorrhage --Dr. Anuradha Ghosh Clinical Research 595(A Correlation of Hypothyroidism & Hyperprolactinemia in Women with Primary Infertility
-DE (Mrs.) Pratima Singh; Dr. Rajiva Kumar Singh; Dr. Sagar Du!al Shiba: Dr. (Prof ) S.N. Sharma 596(A Different Surgical Options and Ileostomy in Typhoid Perforation
—Dr. Anlad Zia Mallik, Dr. Md, Shami Ali
Efficacy and Tolerability of Iron Sucrose Complex Therapy in Iron Deficiency Anemia in the Pregnant women
598(A:
—Dr. Rakhi Singh, Dr. Amrita Sharan
- Electrolyte Disturbances in Diarrhea in Children 600(A) —Dr. Sanjeev'Kumar, Dr. N.P. Gupta, Dr. K.N. Mishra
Endometrial Histopatho logy in Abnormal Uterine Bleeding 602(A)
-Dr. Anuradha Ghosh
Estimation of Serum Alkaline Phosphatase and Serum Cholesterol in Cases of
603(A) Chronic Biliary Tract Diseases
—Dr. Athar Hussain, Dr. Shcen:en Tarannum
—Dr. Nidhi Jha Evaluation of Secondary Amenorrhea Cases with Special Reference to Endocrinal Disorders
604(A)
Frequency, Indications and Complications of Midline Laparotomy
606(A) —Dr. Jaikant Paswan
Eyelid Health Preservation 608(A) A —Dr. Bhupendra Prasad
Intramuscular Midazolam versus Intravenous Diazepam for Control of Seizures in Children —Dr. Ghulam Rasool Wani 611(A)
614(A)
—Dr. Anuradha Ghosh
620(A) Management of Diabetes in the Elderly with Canagliflozin : A Newer Hypoglycemic Drug on the Horizon
—Dr. Ranjeet Kumar, Dr. Ajay Simba, Dr. A4d .AlauddinAlarn, Dr. Shiwangi Tiwari 617(A) Intravaginal Misoprostol in Induction of Labour- a Randomised Controlled Study
Intraperitoneal Bupivacaine along or with Dexmedetomidine or Tramadol for Post-operative Analgesia following Laparoscopic Cholecystectomy: A Comparative Evaluation
Predictive Factors of Mortality in Burn Patients
Prevalence of Asymptomatic Bacteriuria (ASB) and UTI in Pregnancy
Pregnancy Outcome Prevalence of Lupus Anticoagulant in Pregnancy Hypertension and its Significance on
—Dr. Vidya Paul, Dr. Rakesh Kumar, Dr. Vivekanand Paul, Dr. Chandra Kiran
558(A)
INDIAN MEDICAL JOURNAL August 2015 (Annexure), Vol. 109, No. 8
—Dr. Rakhi Singh; Dr. Amrita Sharan
—DE Jaikant Paswan

Different Surgical Options and Ilpostomy in on
s Dr. Amjad Zia Nfallikl, Dr. Md. Shamim AL'
Typhoid Perforati
ORIGINAL & CLINICAL RESEARCH
ABSTRACT To find out the value of primary ileostomy as a
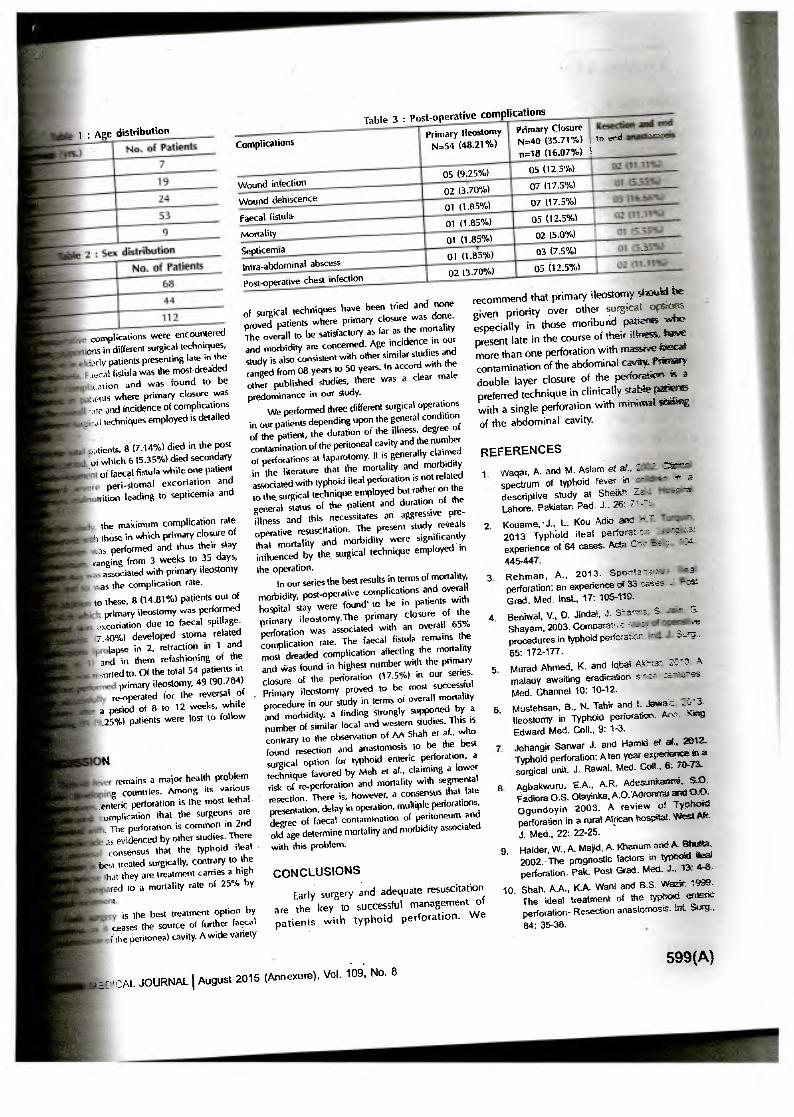
life saving procedure in patients of typhoid Heal perforation. 112 diagnosed cases were included in this study with a mean age of 18.66 years with a male to female ratio of 1.51. After diagnosis and resuscitation, all of the patients were operated within 48 h of admission. The operative procedure was determined by the general condition of the patient, number M perforations and degree of peritoneal contamination. Primary ileostomy was done in moribund patients with massive faecal contamination of peritoneal cavity, while primary double layered closure of the perforation was attempted in clinically stable patients with a single perforation and resection followed by end- to- end anastomosis was attempted in cases where-there were more than one perforations or the perforation was present too close to the ileocaecal junction. Age ranged from 8 years to 50 years and the maximum number of patients were in the age group 31-40 years, with a male dominance. On laparotomy 98 (88.5%) patients had a solitary perforation in the terminal ileum and 14 (125%) patients had more than one perforation: Primary double-layered closure was done in 40 (35:71%) patients; primary ileostomy in 54(48.21%) patients and resection followed by end-to-end anastomosis was done in remaining 18(16.07%) patients. Faecal fistula was the most dreaded and fatal complication and was found to be commonest in patients where primary closure was done (07, 17.55). Over all
mortality was (7.14%) of which 6 (5.35%) died secondary to the development of faecal fistula while one patient developed severe pen-stomal excoriation and progressive malnutrition leading to septicemia and death.
Minimum hospital stay was associated with primary ileostomy patients and so was the complication rate.
heavy faecal contamination and diffuse peritonitis.
MATERIALS AND METHODS -
One hundred and twelve patients with typhoid perforation were admitted and treated in Department of Surgery, Katihar Medical College & Hospital, Katihar, Bihar. All the admissions were carried out through the casualty department as cases of acute abdomen. All the patients were closely monitored during the post operative period in terms of post-operative complications, morbidity, mortality, total hospital stay and convalescence. All the patients were provided same management facilities. Majority (86.60%) of these patients presented with abdominal distension, tenderness and abdominal rigidity. There Was marked dehydration and toxaemia in those who presented late in the course of illness (patients were brought after 48 hours of the development of symptoms in most of the instances). Immediate resuscitative measures were taken in all the patients regardless of their age and sex. This comprised maintenance of intravenous line, catheterization, intravenous broad spectrum antibiotics and intravenous fluids. Blood transfusion was needed in 17 patients (15.17%) pre-operatively. The principle diagnostic tools in all the patients were a detailed history and examination, presence of free gas under the right dome of diaphragm and a positive widal test.
Seventy eight (78) (69.64%) patients were operated with in 24 hours of admission after preliminary investigations and resuscitation. The remaining 34 (30.35%) patients needed more aggressive resuscitation because of severe toxemia and dehydration and were therefore submitted for surgery comparatively late but with in 48 hours of admission. Laparotomy was performed by a midline incision and there was a yellow purulent material present in the abdominal cavity with patchy fibrinus coating on the bowel wall in almost all the patients. A single perforation of about 1 cm size was found on the anti- mesenteric border of terminal ileum in 98 (87.5%) patients, while more than 1 perforation was found in 14 (12.5%) patients. The abdominal cavity
INTRODUCTION
Typhoid fever is a life-threatening problem in India especially due to the emergence of multiresistant strains of salmonella typhi. Intestinal perforation is one of the most dreaded and common complication of typhoid fever, remarkably so in the developing countries where it usually leads to diffuse peritonitis. It was considered to be an almost fatal condition in
' the past and the mortality and morbidity still remains very high despite remarkable improvements in the surgical management. The current surgical options include primary double layered closure, segmental resection and end-to-end anastomosis and primary ileostomy. Studies with controversial outcome have been published and there remains a difference of opinion as to the best surgical procedure in typhoid Heal perforation. Various factors influence overall prognosis and outcome of surgical treatment such as delayed presentation, adequate pre-operative resuscitation, delay in surgery, number of perforations and degree of faecal contamination of the peritoneal cavity. The present study was conducted to compare the results of different surgical techniques employed in typhoid perforation in terms of overall morbidity and mortality and to find out the role of ileostomy as a life saving procedure especially in moribund patients presenting late in the course of illness and having
was found to be heavily contaminated in 64 157.14%a patients, while in 48 (42.85%) patients the peritone* cavity was found in a comparatively better conditiom The choice of surgical operation was determined fr* the number of perforations, general condition of the patient and the degree of faecal contamination of that peritoneal' cavity. Double layer primary closure tO the single perforations was done in 40 (35.71% patients, while primary ileostomy was performed ai
54 (48.21%) patients in which there was hew faecal contamination and the general condition the patients was not satisfactory. In 18 (16.07% patients we performed segmental resection and ea* to- end anastomosis because of multiple perforator/ and in some the perforation was very dose 4
ileocaecal valve. In all the cases, the peritoneal cavity **
thoroughly washed with copious amount of nom* saline and drains were left in pelvis. The yang* studied in the post operative period y,ere se operative complications such as wound infects" wound dehiscence, faecal fistula, mortality ao septicaemia, total hospital stay and follow up M the patients with different surgical techniqta
employed. Data collection: The data of each patient *
collected on a proforma specifically designed isr4 study and included demographic details, dew features, past medical history, interval beta of symptoms and admission, operative procedure performed, post-operative car and duration of stay in the hospital.
. Statistical analysis : The results were tie! compared and concluded on SPSS verse
RESULTS
Age ranged from 08 years to 50 the maximum number of patients si
age group 31-40 years as depicted in
The proportion of male patie significantly high (60.71%) as shov,
2.
I. M.B.B.S., M.S. (Gen. Surg.), Associate Professor, Department of Surgery,
Katihar, Bihar.
2. M.B.B.S. M.S. (Gen. Surg.), Associate Professor, Department of Surgery,
Katihar, Bihar.
598(A) INDIAN MEDICAL JOURNAL August 2015 (Annexure), Va.)
1 : Age distribution
No. of Patients
7
19
24
53
9
2 : Sex distribution
No. of Patients
68 Post-operative chest infection
112
complications were encountered ons in different surgical techniques, torly patients presenting late in the tecal fistula was the mostdreided cation and was found to be lents where primary closure was
-ate and incidence of complications :al techniques employed is detailed
:orients, 8 (7.14%) died in the post ot which 6 (5.35%) died secondary
of faecal fistula while one patient peri-stomal excoriation and
rition leading to septicemia and
to these, 8 (14,81%) patients out of , primary ileestomy was performed oxcoriation due to faecal spillage. 7.40%) developed stoma related
lapse in 2, retraction in 1 and t and in them refashioning of the - ;cried to. Of the total 54 patients in
primary ileostomy, 49 (90.784) re-operated for the reversal of
a period of a to 12 weeks, while .25%) patients were lost to follow
the maximum complication rate h those in which primary closure of as performed and thus their stay
ranging from 3 weeks to 35 days, associated with primary ileostomy as the complication rate.
remains a major health problem 'rig countries. Among its various
enteric perforation is the most lethal
44
Complications
Wound infection
Wound dehiscence
Faecal fistula
Mortality
Septicemia
Intra-abdominal abscess
of surgical techniques have been tried and none proved patients where primary closure was done. The overall to be satisfactory as far as the mortality and morbidity are concerned. Age incidence in our study is also coniistent with other similar studies and ranged from 08 years to 50 years. In accord with the other published studies, there was a clear male predominance in our study.
We performed three different surgical operations in our patients depending upon the general condition of the patient, the duration of the illness, degree of contamination of the peritoneal cavity and the number of perforations at laparotomy. It is generally claimed in the literature that the mortality and morbidity associated with typhoid ileal perforation is not related to the, surgical technique employed but rather on the general status of the patient and duration of the illness and this necessitates an aggressive pre-operative resuscitation. The present study reveals that mortality and morbidity were significantly influenced by the surgical technique employed in
the operation.
Table 3 : Post-operative complications Primary Closure N=40 (35.71%) n=18 (16.07%)
02 (3.70%)
01 (1.85%)
01(1.85%)
01 (1.85%)
01 (1.85%)
02 (3.70%1
recommend that primary ileostomy shouid be
given priority over other surgical okom especially in those moribund patients wile present late in the course of their illness, have more than one perforation with massiwe faecael contamination of the abdominal cavav. Primary
double layer closure of the perforage,n is a
preferred technique in clinically stabiepatienz with a single perforation with minimal seri&ag
of the abdominal cavity.
REFERENCES
1. \Nagar, A. and M. Astern et at.,
spectrurn of typhoid fever in _
descriptive study at Sheikh - --
Lahore. Pakistan Ped. J.. 26:
2. Kouame. •J., L. Kou Adio and 2013 Typhoid ilea! perforat : - experience of 64 cases. Ada C".' 445-447. 445-447.
05 02 5%)
07 07.5%)
07 07.5%1
05 025%)
02(5.0%)
03 (7.5%)
05 02.5%) 02 35J
resection.
In our series the best results in terms of mortality, morbidity, post-operative complications and overall hospital stay were found' to he in patients with primary ileostomy.The primary closure of the perforation was associated with an overall 65% complication rate. The faecal fistula remains the most dreaded complication affecting the mortality and Was found in highest number with the primary closure of the perforation (17.5%) in our series.
. Primary ileostomy proved to be most successful procedure in our study in terms of overall mortality and morbidity, a finding strongly supported by a number of similar local and western studies. This is contrary to the observation of AA Shah et al., who
found resection and anastornosis to be the best surgical option for typhoid enteric perforation, a
technique favored by Meh et al., claiming a lower risk of re-perforation and mortality with segmental
There is, however, a consensus that late
a
3. Rehman, A., 2013. Spoccla- s:: perforation: an experience of 33 cases _ - Grad. Med. Inst., 17: 105-110.
4. Beniwal, V., D. Jindat, J. S-a-*--?.. Shayam, 2003. Comparat..:. procedures in typhoid perfcra•-cs _
65: 172-177.
5. Murad Ahmed, K. and total kle-n- 2'7'3 A malady awaiting eradication Med. Channel 10: 10-12.
6. Mustehsan, B., N. Tahir and I. Jaitrair: 2::'-
lleostomy in Typhoid perforation. Aro.kino Edward Med. Coll., 9: 1-3.
7. Jehangir Satwar J. and Harnid at al, 2012_ Typhoid perforation: A ten year expedience in a surgical unit. J. Rawal. Med. Cod_ 6: 70-73.
8. Agbakwuru, E.A., A.R. Adesunkannit, 50.
Padiora O.S. Olayinka. A.O.Adronmu and 0,0_ Ogundoyin 2003. A review of Typhoid perforation in a rural African hospital. West Aft J. Med.. 22: 22-25.
9. Haider, W., A. Majid, A. Khanum and A_ Bhutta, 2002. The prognostic factors in typhoid ?en perforation. Pak. Post Grad. Med J.. 13: 4-8.
10. Shah, A.A., K.A. Wan) and B.S. Weak: 1999. The ideal treatment of the typhoid enteric perforation- Resection anastornosis. Int Sorg_
84: 35-38.
omplication that the surgeons are presentation, delay in operation, multiple perforations.
. The perforation is common in 2nd degree of faecal contamination of peritoneum and
as evidenced by other studies. There old age determine mortality and morbidity associated
consensus that the typhoid ileal - with this problem.
best treated surgically, contrary to the hat they are treatment carries a high red to a mortality rate of 25% by
is the best treatment option by ceases the source of further faecal
.f the peritoneal cavity. A wide variety
CONCLUSIONS
Early surgery and adequate resuscitation are the key to successful management of patients with typhoid perforation. We
. ,
CAL JOURNAL I August 2015 (Annexure), Vol. 109, No. 8
599(A)
Role of Laparoscopy in Diagnosing of Chronic Abdominal Pain and Masses
Dr. Amjad Zia MaRik', Dr. Md. Shakeb Ahmed2
1
ORIGINAL & CLINICAL RESEARCH
INTRODUCTION
The abdomen has always been considered "A pandora's box". The mysteries of the box has not been completely unveiled yet. Even surgeons.known for their clinical acumen. and experiences are, at times, baffled by the bizzare presentation of certain • abdominal conditions, particularly abdominal masses and chronic abdominal pain. In spite of tremendous advancements in the field of radiodiagnosis including ultrasonography, endoscopy and various imaging techniques, the diagnosis of an abdominal mass and chronic abdominal pain still eludes the surgeon. In certain cases the surgeon completely fails to make an accurate preoperative diagnosis and is compelled to take the course of exploratory laparotomy just to make the diagnosis and treat accordingly. In some of such puzzling cases the surgeon is confronted with problems for which either he or the patient may not be well prepared. In moments like these every surgeon wishes that if somehow he could have made the diagnosis preoperatively he could have tackled the problem more effectively. It was in such situations that a need was felt to devise an instrument which could directly peep through the Pandora's box and make an accurate pre-operative diagnosis.
Kelling in 1901 first described the endoscopic examination of peritoneal cavity. He used a modified cystoscope for this purpose. Since then, inspite of many advances in this instrument, the endoscopic examination of the peritoneal cavity has remained the preserve of Physicians and the Gynaecologists with some exceptions of Ruddock (1937), Handly (1955), Borei (1962), Cuschieri (1975), Gaiseford 'B' Hugh et al. (1976), Gomel. 14,(1976), Balfour (1976), Cortesi et al. (1979), Lewis et al. (1981), Udwadia, T.E. (1986). Surgeons still tend to view peritoneoscopy with some degree of hostility or at the best, indifference (Udwadia, I.E., 1986) .Whilst peritoneoscopy is extensively performed by physicians and gynaecologists, surgeons who are better qualified often ignore it. Peritoneoscopy is as much informative as exploratory laparotomy. So, Udwadia ultimately established the usefulness of this instrument in the field of surgery. According to Udwadia, surgeons acquire a feel of tissue, normal and abnormal, after years of seeing and palpating abdominal pathology at open surgery. This feel can be translated with great advantage in the endoscopic examination of the abdomen. Since surgeons will carry out the definitive operative procedure, peritoneoscopy is of immense value in planning or avoiding surgery after the complete diagnosis has been established. Surgeons can take biopsy of the abdominal pathology at the same time to establish the histological diagnosis. Any complication which occurs can be dealt with by the surgeon himself immediately. All these positive points favour, the use of this instrument by the surgeons for the diagnosis of abdominal masses and 'chronic abdominal pain.
On the other hand, other sophisticated investigative procedures, at times, fail to provide exact diagnosis of the abdominal mass and chronic abdominal pain due to certain limitation.
Although endoscopes too provide direct visualisation, but they can only view intralurbinal pathology of gastrbintestinal tract.
Ultrasonography is a very useful non — invasive investigative procedure. But this can only differentiate between solid and cystic masses. The diagnostic accuracy is 72% as per Kawaski (1978). The diagnosis is done by indirect evidences and at the same time, there is no scope of histological diagnosis with this instrument.
• Other modern investigative procedures like various imaging techniques, are not only expensive but also out of reach of common people, less than 20% of the world population has an access to these non- invasive diagnostic aids (Udwadia,1986).
In poor country like ours these sophisticated investigative procedures are only available in very selected centres in larger cities.
Conversely, laparoscopy is an inexpensive simple procedure that can be carried out even at a small medical centre where electricity is available for diagnosing the cases of abdominal masses and • chronic abdominal pain, thereby preventing some unnecessary laparotomies only for diagnosis.
Despite all these facts enough attention has not been given to this inexpensive and easily accessible procedure in our country and facility for laparoscopy is still not readily available.
So the present study is proposed to be carried out in an attempt to assess the possibilities, practicabilities and effectiveness of laparoscopy as a diagnostic procedure for abdominal masses and chronic abdominal pain in general surgery.
MATERIALS
(a) Patients suffering from chronic abdominal pain and or having abdominal masses admitted to different surgical wards constituted the subjects for the present study.
(b) The laparoscope- This endoscopic device included following :
(i) lOmm 30° rigid endoscope with a cold light source
(ii) Flexible fibre-optic light guide
(iii) Camera
(iv) Monitor
(v) Trocar with its sheaths
Veress needle for pneumo-peritoneum
(vii) .Insufflator
(c) Surgical instruments for incision and suture as well as draping materials.
Sterilization :__The laparoscope with its attachments was sterilized by keeping it in a specially designed chamber containing formaldehyde beads for 30 minutes.
METHODS
Screening of subjects: -(a) Clinical examination- on admission the
patients of chronic abdominal pain and/or abdominal masses were subjected to a thorough ,clinical examination in order to arrive at a probable clinical diagnosis. Diagnostic investigation : In order to corroborate and confirm clinical diagnosis all relevant investigations were carried out as per the requirement.
(b) Blood examination : Total and differential white cell count and erythrocytic sedimentation rate estimation was done as evidence of acute and chronic inflammatory r rocesses.
- Serum creatinine and blood urea estimation were done to assess the renal function.
Similarly serum bilirubin and other liver function testes were carried out to evaluate the hepato-biliary system.
1.
AIMS AND OBJECTIVES
1. To evaluate the efficiency of laparoscopy in surgical practice in diagnosing abdominal masses and chronic abdominal pain vis —a-vis clinical as well as laparotomy diagnosis.
2. To compare its merits and demerits with those of diagnostic laparotomy.
MATERIAL AND METHOD
The present study was conducted in the Department of Surgery of Katihar Medical College & Hospital, Katihar, Bihar between February 2013 to August 2014.
M.B.B.S., M.S. (Gen. Surg.), Associate Professor, Department of Surgery, K.M.C.H.,
Katihar, Bihar. 2. M.B,B.S., M.S. (Gen. Surg.), Assistant Professor, Department of Surgery, K.M.C.H.,
Katihar, Bihar.
30
INDIAN MEDICAL JOURNAL I October 2015, Vol. 109, No. 10

(c) Radiography : Plain X-ray abdomen and )elvis to visualize urolithiasis.
Skiagram of chest was taken to detect pulmonary focus of tuberculosis and metastatic lesion in the lung. Intravenous urography was done to assess structural as well as functional integrity of urinary system.
- Oral cholecystograpy was done to visualize the hepatobiliary system. Barium studies were carried out to find out any pathology in gastrointestinal tract.
(d) Imaging : Ultrasonography and in some ases C.T. Scan were carried out as per need. After creening and elaborate clinical examination cases ffollowing categories were selected for laparoscopic xamination.
- Those patients in whom definite diagnosis could not be arrived at. Those patients in whom the diagnosis was known but the extent of lesion could not be ascertained.
Preoperative preparation of patients : After )utine pre-operative investigation the patients were repared in the same way as they are prepared for iparotomy. Each patient were given single It-ravenous dose of cefuroxime(750mg)as a rophylaxis
All patients were asked to void urine just before ming them on operation table.
Laparoscopic procedure : (a) After induction of general anaesthesia
,antiseptic cleaning and draping was done in the usual way.
(a) A transverse incision of about'!" was given in subumblical position.
(c) The tip of the veress needle was pushed through the incision by maintaining continuous pressure while the abdominal wall was tented by lifting the skin with tissue forceps. The pressure on the needle was released when loss of resistance was felt as needle entered the peritoneal cavity. The confirmation was made by moving the needle in all directions and by injecting 5 ml. of normal saline which could not be aspirated.
(d) Having confirmed the position of the needle, pneumoperitoneum was produced by insufflator pushing through the veress needle. About 2-3 litres of air was pushed till the area of liver dullness wa: obtained.
A continuous monitoring of oulse, 13.P. and piration was done throughout the period of eumoperitoneum procedure.
Then the veress needle was taken out keeping it nost parallel to the anterior abdominal wall.
After this, the trocar with its sheath was roduced with the same incision in z-entry manner.
trocar was directed obliquely headwards through sub-cutaneous tissue till the resistannce of the
•ath was felt then directed obliquely footwards. ) final direction of the entry was always footward,
in the midline towards the pelvis ensuring that the trocar should enter the abdominal cavity caudal to the bifur of major vessels and in the area of maximum air cushion. Then the trocar was taken out. The valve of the trocar sheath was depressed slightly to allow escape of air from the pneumoperitoneum, hearing it confirmed the proper location of the trocar sheath.
After fully depressing the piston of the trocar sheath the rigid telescope was introduced. The free passage of the telescope without any resistance confirmed that the telescope was in the peritoneal cavity. An accessory trocar and canula is then inserted under vision in the left iliac fossa. By altering the position of Table from Trendelenberg and reverse Trendelenberg to right or left lateral position different intraperitoneal structures were visualized after attaching the cold light source in it.
The abdomen was examined in a systematic ‘. and sequential manner, commencing with the
falciparum ligament as the key anatomical land mark.
With patient in left lateral position, the left lobe of the liver, the diaphragm and the spleen were examined. With the patient flat, the greater curvature of the stomach anterior and inferior surface of the right lobe of liver, gall bladder and duodenum were examined. Then raising the head end of the patient and increasing and decreasing the volume of pneumoperitoneum, the diaphragm and postero-superior surface of right lobe of liver were visualized. The mid-abdomen, omentum, transverse colon, small bowel and parietal peritoneum were then examined. The telescope was then pushed footward and small bowel, descending colon, ascending colom were examined. In female patients, by doing a steep trendelenberg position, the pelvis was ,isualized. Photographs were taken whenever requirA.
After the completion of the procedu e and after confirming that there was no bleeding inside, the telescope was taken out. The piston of the trocar sheath was pressed to deflate air from the peritoneal cavity and finally the trocar sheath was taken out carefully.
Then Iwo skin sutures with silk were given in each case.
The patient was then kept on intravenous fluid for about 4-6 hours, then in the evening after assessment of the patient, light liquid diet was given.
The patients were kept on broad-spectrum antibiolics like injectable ampicillin for one day, follow by oral administration, as a prophylactic measure. Pain kiler drugs were given as per requirement of the patient.
The patients were allowed to do normal day to day work from the next day. Stitches were taken out on 7'h post operative day.
Laparotomy : Laparotomy was done subsequently in all cases for the purpose of confirmation of diagnosis and for curative or palliative treatment as per the needs of individual case.
RESULTS
Peritoneoscopy was carried out in 50 cases
of clinically palpable masses and/or chronic abdominal pain during the period of February 2012 to August 2013.
In the observed table it shows that the majority of cases were of fourth decade followed by fifth decade and third decade and the last group was of 6'5 decade leads. The predominance of different disease entity were also shown in respective decade.
In the table No. 2, it was observed that males are more prone to carcinoma of stomach and carcinoma liver whereas females are more prone to ileocaecal T.B. and gall bladder diseases.
RESULTS
The present study was undertaken to assess the usefulness of Laparoscopic examination in surgical practice for diagnosing various cases of chronic abdominal pain and abdominal masses. Laparoscopic examinations were done in 50 such cases and diInostic accuracy was evaluated.
Observation table No. (I) shows agewise distribution of patients with different diseases observed in a particular age group.
From this table it is apparent that the patients of this series were between 20-60 years of age while maximum number of (Twenty patients) were in 3rd decade. This table also shows that the maximum number of cases (Eighteen patients) in this series had some form of abdominal tuberculosis followed by malignancy of different abdominal organ in 14 cases.
Cases of tuberculosis belonged to all age groups with maximum incidence in 3rd decade while cases of malignancy were found after 3rd decade with maximum incidence in 4'5 decade.
Observation table no.2 depicts the sexwise distribution of different diseases observed in the present series. From this table it is evident that females outnumbered males, the number being 31 and 19 respectively. This table also shows that females suffered more from various forms of abdominal tuberculosis and gall bladder diseases while males were predominant sufferer from malignancy of stomach and liver as well as from chronic pancreatitis. The reason for overall female predominance in this series is apparently due to predominant number of cases of abdominal tuberculosis, gall bladder diseases and ovarian cyst.
In present series displays the visual features of various abdominal masses as well as
DIAN MEDICAL JOURNAL October 2015, Vol. 109, No. 10 31

Table 1 : Showing Age wise distribution of diseases in this series
fi CU >,-.
— ad ct .t
cr, cii C t)
0 • Z
C
•I',1 >" L' a r.' rz 0
76 CV C .
• — I— t,
oi I-1 7'6
f., c+ cd — M
ucoc
ele
G.B
.
Car
cino
ma
stom
ach
Chr
onic
Cho
lecy
stit
is
Car
cino
ma
liver
Chr
onic
pan
crea
titis
Retro
perit
onea
l mas
s
ICar
cino
ma
G.B
.
20-30 10 5 3 - - - - -
31-40 20 2 1 8 2 2 3 1 1 - -
41-50 15 - 2 2 - 3 3 1 - - 4
51-60 5 - - - - - - 1 1 1 2
Table 2 : Sex Incidence of different diseases
Diseases No. of cases
Males Females
Carcinoma of stomach 5 4 1 Carcinoma of liver 3 3 0
Carcinoma of G.B. 6 ., 1 5
Mucocele of G.B. i 2 —., 0 2
Ileocaecal T.B. 12 5 7
Chronic PanCreatitis 2 2 0
Retroperitoneal lymphoma 1 1 0
Ovarian Cyst 7 0 7
Peritoneal T.B. 6 2 4
Chronic Cholecystitis 6 1 5 Total 50 19 31
abdominal organs at laparoscopy on the basis of which laparoscopic diagnosis were made. The diagnoses were based upon the external appearance of masses and organs.
The maximum difficulty was experienced in the diagnosis bf retroperitoneal masses. The fixed organs gave easier visualization than the mobile organs like intestine. The above mentioned workers also expressed similar views regarding diagnostic difficulties.
Many of the workers have tried to overcome this difficulty by taking help of a probe.
Out of 50 cases the clinical diagnosis tallied with laparoscopic diagnosis in 42 cases, while 8 cases were misdiagnosed clinically. Hence, the inaccuracy of clinical diagnosis was 16% as compared to laparoscopic diagnosis.
Thus, he diagnostic accuracy of laparoscopic examination in the series of above workers varies from -53 to 96% which is consistent with the present study.
The overall accuracy of laparoscopic
diagnosis in comparision to laparotomy diagnosis.
Out of the 50 cases subjected to laparotomy, laparoscopic diagnosis was confirmed in 47 cases i.e. in 94% cases. Thus the laparoscopic diagnosis was in- , accurate in 3 cases i.e. in 6% of cases. Out of the 3 cases misdiagnosed, one case in which the laparoscopic diagnosis was primary carcinoma of liver turned out to be a case of hydatid cyst of
liver. In ot ler cases which was diagnosed as carcinoma head of pancreas by laparoscopy was found to be ampullary carcinoma on laparotomy. In the 3rd case in which the laparascopic diagnosis was ileocaecal tuberculosis was proved to be a case of carcinoma caecum.
The difficulty in the diagnosis of pancreatic and other retroperitoneal lesions by laparoscope is well documented.
The diagnostic error between hyperplastic ileocaecal tuberculosis and caecal carcinoma is also a common occurance.
Thus, the accuracy of laparoscopic diagnosis in the present series compares well with those of the above workers. "
Relatively low accuracy of laparoscopic diagnosis in comparison to laparotomy diagnosis in the series of cuschieri may be due to variation in selection of case. In the present series higher diagnostic accuracy was probably because of the fact that cases with apparent ascites and cases with previous laparotomy were not included.
The post-operative complications following laparoscopic examination. In the present series
abdominal pain was present in 20% of cases followed by subcutaneous emphysema in 16% cases and some peritoneal fluid leakage in 2% of cases. Thus, out of 50 cases, 19 patients had above complications. All the above complications subsided completely in 2-3 days time. No fatal accident occurred during this procedure. No patient turned up for any problem related to this procedure subsequently.
CONCLUSION
From the above observations of the present study following conclusions have been derived.
(a) Laparoscopy should no longer be considered the domain of only Gynaecologists and physicians.
(b) It can prove a very important diagnostic tool in surgical practice and should be used more frequently for the diagnosis, of obscure abdominal masses and, chronic•abdominal pain of unknown etiology.
(c) Prelaparotomy laparoscopic examination can prevent many unwanted laparotomies and Minimize the number of diagnostic laparotomies being performed today.
(d) The findings of the present study fully giapport the conviction of T.E. Udawadia- Laparoscopy is for surgeons'.
REFERENCES 1. Arya PK and Gaur KJBS : laparoscopy : A tool
in diagnosis of lower abdominal painindian J Surg:2004;66:216-20.
2. Krishnan P et al:Laparoscopy in suspected abdominal tuberculosis is useful as an early diagnostic method.ANZ Journal of surgery:2008;78;987-9.
3. Paajanen Hannu, MD, Julkunen Kristiina,MD,Waris Heidi ,MD: laparoscpy in chronic abdominal pain:A prospective non randomized long term follow up study.Jour of clinical gastroenterology:2005;39:110-4.
4. Raymond P, Onders MD, Elizabeth A, Mittendorf LIVID : Utility of laparoscoPY in chronic abdominal rein Surg:2003;134(4):549-54.
5. Jdwadia, I.E. (1978) PeritoneOscopY in diagnosis .;f abdominal tuberculosis. Ind. J. of Surg. 40:912-5.
6. Udwadia, T.E. (1978) Role of Surg. In abdominal T.B., Journal of J.J. Group Hosp. Research Society. J.J. Hosp. Bombay. 40:3427.
7. Udwadia, T.E. (1986) J. of Royal Col. Surg. Engl., 68; 125-29.
8. Villardel, F. (1977) Endoscopy, 9:20. 9. Wolfe, J.H.N. et al. (1979) Lancet, 1:852-53. 10. Zollikofor, C.L. et al. (1979) Cardio-vascular
radiology 2:131.
32 INDIAN MEDICAL JOURNAL I October 2015, Vol. 109, No. 10

International Surgery Journal Ahmad MS etal. Int Surg J. 2015 Nov;2(4):492-495 http://www.ijsurgery.com
Research Article
pISSN 2349-3305 I eISSN 2349-2902
DOI: http://dx.doi.org/10.18203/2349-2902.isj20150917
Causes, evaluation and surgical management of mechanical small bowel obstruction
Md. Shakeb Ahmad i , Md. Shadab l , Saif Ornar2*, Amjad Zia Md. Arif Ansari l
'Department of Surgery, Katihar Medical College, Katihar, Bihar, India 2Department of Anatomy. Katihar Medical College, Katihar. Bihar. India
Received: 22 September 2015 Accepted: 07 October 2015
*Correspondence: Dr. Saif Omar, E-mail: drsaifomar(iP,gmail.com
Copyright: © the author(s), publisher and licensee Medip Academy. This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License. which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
J
ABSTRACT
Background: Small bowel obstruction is defined as a mechanical or functional obstruction of the intestine preventing the normal transit of product of digestion. It can occur at any level distal to the duodenum and is considered to be a medical emergency. Acute intestinal obstruction has attracted wide attention and extensive research. As a consequence of experimental research, a considerable decline has been observed in the mortality of acute intestinal obstruction. The aim of this study was to observe the causes, evaluation and surgical management of small bowel obstruction among cases presenting with the same in the Department of General Surgery of Katihar Medical College. Methods: Eighty cases of small bowel obstruction were observed in this study. The cases were selected among patients visiting the outdoor clinic of General Surgery in Katihar Medical College. The selected cases belonged to different aetiology. age groups and sex. Results: Abdominal tenderness was the commonest finding during per abdomen examination. Adhesion was the commonest aetiology observed in this study followed by obstructed hernia. General trend of reporting to the hospital was observed to be on the third day of onset. Higher incidence of small bowel obstruction was observed in cases in sixth decade of life. There was predominance among the males and in cases belonging to lower socio-economic class. Conclusions: Mechanical obstruction of the small intestine due to extrinsic causes constituted a major part among the presenting cases in this study. The degree of distension has a direct relation with the duration of the symptom. Small bowel obstruction can be confirmed using a radiogram in erect posture. Mortality due to small bowel obstruction can be reduced if timely intervention is sought by the presenting cases. Early diagnosis, effective resuscitation and timely surgery are the main treatment options that should be considered.
'Keywords: Bowel, Diagnosis, Distension, Duodenum, Obstruction, Surgery
INTRODIcrioN
The small intestine consists of the duodenum, jejunum and ileum. It extends from the distal end of the pyloric canal to the ileocaecal valve. Its overall length ranges from three to seven meters in the living adult. The duodenum extends up to the duodenojejunal junction and the remaining small intestine is often referred to as the "small bowel- of which proximal two-fifths is jejunum and distal three-fifths is ileum.' Acute intestinal
obstruction occurs when there is an interruption in the forward flow of intestinal contents. This interruption can occur at any point along the length of the gastrointestinal tract, and clinical symptoms often vary based on the level of obstruction. Intestinal obstruction is most commonly caused by intraabdominal adhesions. malignancy, or intestinal herniation. The clinical presentation generally includes nausea and vomiting, colicky abdominal pain, and a failure to pass flatus or bowel movements. The classic physical examination findings of abdominal
International Surgery Journal I October-December 2015 I Vol 2 I Issue 4 Page 492

Ahmad MS et al. Int Surg J. 2015 Nov:2(4):492-195
a
distension, percussion sounds, and high-pitched bowel sounds suggest the diagnosis. Radiologic imaging can confirm the diagnosis, and can also serve as a useful investigation in less certain cases. Although radiography is often the initial study, non-contrast computed tomography is recommended if the index of suspicion is high or if suspicion persists despite negative radiography. Management of uncomplicated obstructions includes fluid resuscitation with correction of metabolic derangements, intestinal decompression, and bowel rest. Evidence of vascular compromise or perforation, or failure to resolve with adequate bowel decompression is an indication for surgical intervention. Intestinal obstruction accounts for approximately 15 percent of all emergency department visits for acute abdominal pain.2 Complications of intestinal obstruction include bowel ischemia and perforation. Morbidity and mortality associated with intestinal obstruction have declined since the advent of more sophisticated diagnostic tests, but the condition remains a challenging surgical diagnosis. Physicians who are treating patients with intestinal obstruction must weigh the risks of surgery with the consequences of inappropriate conservative management. The fundamental concerns about intestinal obstruction are its effect on whole body fluid/electrolyte balances and the mechanical effect that increased pressure has on intestinal perfusion. Proximal to the point of obstruction, the intestinal tract dilates as it fills with intestinal secretions
• and swallowed air.3 Failure of intestinal contents to pass through the intestinal tract leads to a cessation of flatus and bowel movements. Intestinal obstruction can be broadly differentiated into small bowel and large bowel obstruction. Fluid loss from emesis, bowel edema, and loss of absorptive capacity leads to dehydration. Emesis leads to loss of gastric potassium, hydrogen. and chloride ions, and significant dehydration stimulates renal proximal tubule reabsorption of bicarbonate and loss of chloride, perpetuating the metabolic alkalosis.4 In addition to derangements in fluid and electrolyte balance. intestinal stasis leads to overgrowth of intestinal flora. which may lead to the development of feculent emesis. Additionally, overgrowth of intestinal flora in the small bowel leads to bacterial translocation across the bowel wal1.5 Persistently increasing dilation of the intestine increases the luminal pressures. When the luminal pressures exceed venous pressures, loss of venous drainage causes increasing edema and hyperaemia of the bowel. This may eventually lead to compromised arterial flow to the bowel, causing ischemia. necrosis, and perforation. A closed loop obstruction, in which a section of bowel is obstructed proximally and distally. may undergo this pro-cess rapidly. with few presenting symptoms. Intestinal volvulus, the prototypical closed-loop obstruction, causes torsion of arterial inflow and venous drainage, and is a surgical emergency. The most common causes of intestinal obstruction include adhesions, neoplasms, and herniation. Adhesions resulting from prior abdominal surgery are the predominant cause of small bowel obstruction, accounting for approximately 60 percent of cases.6 Lower
abdominal surgeries, including appendectomies, colorectal surgery, gynecologic procedures, and hernia repairs. confer a greater risk of adhesive small bowel obstruction. Less common causes of obstruction include intestinal intussusceptions. volvul us. intra-abdominal abscesses, gallstones, and foreign bodies. The development of metabolic acidosis, especially in a patient with an increasing serum lactate level, may signal bowel ischem ia.
NiETIMDS •
After prior approval from the Institutional Ethics Committee (IEC). A prospective observational study of eighty cases which were admitted with small bowel obstruction was performed in the Department of General Surgery. Katihar Medical College.
RESI'LTS
All eighty cases of small bowel obstruction observed in this study presented with common symptoms of abdominal distension, absence of flatus and/or faeces. Twenty (25%) cases were in the sixth decade of life. Preponderance of males over females was observed with fifty-five (68.75%) male cases. Fifty-two (65%) cases were from lower socio-economic strata. The commonest cause was adhesion followed by hernia which were observed in thirty-three (41.25%) and twenty (25%) of the presenting cases. Thirty-eight (47.5%) cases and twenty-two (27.5%) cases reported to the hospital on the third day and second day respectively. Degree of abdominal distension was moderate in twenty-five (31.25%) cases and mild in twenty-three (28.75%) cases. High pitched or abnormal bowel sounds were heard in twenty-seven (33.75%) cases. Radiologic investigations revealed multiple fluid levels or gas shadows in fifty-five (68.75%) cases. Sonologic investigations revealed small bowel obstruction in twenty-five (31.25%) cases. Sixty (75%) cases were cured successfully without any complications.
DISCCSSION
Acute mechanical bowel obstruction is a common surgical emergency and a frequently encountered problem in abdominal surgery.' It constitutes a major cause of morbidity and financial expenditure in hospitals around the world and a significant cause of admissions to emergency surgical departments." Intestinal obstruction belongs to highly severe conditions, requiring a quick and correct diagnosis as well as immediate, rational and effective therapy.'° Surgeons are concerned about bowel obstruction cases because strangulation. causing bowel ischemia. necrosis and perforation might be involved, and it is often difficult to distinguish simple obstruction from strangulation. Accurate early recognition of intestinal strangulation in patients with mechanical bowel obstruction is important to decide on emergency surgery or to allow safe nonoperative management of carefully
International Surgery Journal I October-December 2015 I Vol 2 I Issue 4 Page 493

Ahmad MS et al. Int Surg J. 2015 Nov;2(4):.192-195
selected patients." Although close and careful clinical evaluation, in conjunction with laboratory and radiologic studies, is essential for the decision of proper management of patients with acute mechanical bowel obstruction, a preoperative diagnosis of bowel strangulation cannot be made or excluded reliably by any known parameter, combinations of parameters. or experienced by clinical judgement. Mechanical bowel obstruction is an old and common surgical emergency. Immediate and correct diagnosis of this condition and its etiology is essential, and appropriate treatment is of utmost importance.1113 The clinical picture, however, of these patients along with the etiology of obstruction and strangulation prevalence are variable, while appropriate management remains controversial. We, therefore, conducted this prospective study to identify and analyse the clinical presentation of patients with acute mechanical bowel obstruction in our department the etiology of obstruction as well as management and outcome of these patients. Age incidence in our study was highest in the sixth decade of life and lowest in the first decade of life respectively. However age is no bar for the acute onset of small bowel obstruction. In early age groups the common causes are congenital bands and intussusceptions whereas adhesions and obstructed hernias are more common in later age groups. Sex ratio revealed that males were more prone to the occurrence of small bowel obstructions. There is no direct relation of intestinal obstruction with sex of the person. A remarkably high incidence was observed among cases belonging to the lower socio-economic strata. The cases reported to the hospital usually on the third day after development of symptoms. It was observed that prognosis and management among cases which reported earlier was better due to minimal chances of gut injury or strangulation. Degree of abdominal distension has a direct relation with the duration and intensity of the symptom. Abdominal tenderness was observed in thirty-seven cases and eleven cases revealed visible peristalsis. Both mild and moderate distensions were observed. Confirmation of small bowel obstruction was by radiologic and sonologic investigations. Presence of peristalsis helps to differentiate small bowel obstruction from a paralytic ileus." Management of intestinal obstruction is directed at correcting physiologic derangements caused by the obstruction, bowel rest, and removing the source of obstruction.15
CONCLUSION
Abdominal distension along with absence of passage of flatus and/or faeces is the most common symptoms and physical finding of patients with acute mechanical bowel obstruction. Adhesions and hernias are the most common causes of obstruction as well as of bowel ischemia. necrosis, and perforation. A large number of these patients can be safely and effectively nonoperatively treated, particularly those with adhesive obstruction, a substantial portion requires immediate operation. Moreover, the risk of strangulation is significantly higher
in incarcerated hernias than other obstruction causes. Great caution should be taken for the treatment of patients with acute mechanical bowel obstruction since the incidence of bowel ischemia, necrosis, and perforation is significantly high. Further studies are necessary in order to determine appropriate management for treatment of these patients as well as to identify ' accurate early predictors of success of conservative or operative treatment and. particularly. of intestinal strangulation giving the greatest attention to reversible ischemia.
Funding: No funding sources Conflict of interest: None declared Ethical approval: The study was approved by the institutional ethics committee
REFERENCES
I. Standring S. Gray's Anatomy. 40th Edition: Elsevier Churchill Livingstone. Chapter 66, Small Intestine. 2008:1125.
2. Irvin TT. Abdominal pain: a surgical audit of 1190 emergency admissions. Br J Surg. 1989;76(1 I ):1121-5.
3. Wright HK, O'Brien ii. Tilson MD. Water absorption in experimental closed segment obstruction of the ileum in man. Am J Surg. 1971:121(1):96-9.
4. Wangensteen OH. Understanding the bowel obstruction problem. Am J Surg. 1978;135(2):131-49.
5. Rana SV, Bhardwaj SB. Small intestinal bacterial over-growth. Scand J Gastroenterol. 2008:43(9):1030-7.
6. Shelton BK. Intestinal obstruction. AACN Clin Issues. 1999:10(4 ):478-91.
7. Mucha P Jr. Small intestinal obstruction. Surg Clin North Am. 1987;67:597-620.
8. Miller G, Boman J. Shrier I. Gordon PH. Etiology of small bowel obstruction. Am J Surg. 2000;180:33-6.
9. Miller G. Boman J. Shrier I, Gordon PH. Natural history of patients with adhesive small bowel obstruction. Br J Surg. 2000:87:1240-7.
10. Dite P. Lata J. Novotny I. Intestinal obstruction and perforation--the role of the gastroenterologist. Dig Dis. 2003: 21:63-7.
11. Richards WO, Williams LF Jr. Obstruction of the large and small intestine. Surg Clin North Am. 1988;68:355-76.
12. Renzulli P. Krahenbuhl L. Sadowski C. al-Adili F. Maurer CA, Buehler MW. Modern diagnostic strategy in ileus. Zentralbl Chir. 1998;123:1334-9.
13. Lopez-Kostner F. Hool GR. Lavery IC. Management and causes of acute large-bowel obstruction. Surg Clin North Am. 1997;77:1265-90.
14. Frager DH. Baer JW. Distinction between postoperative ileus and mechanical small bowel obstruction: value of CT compared with clinical and
International Surgery Journal October-December 2015 I Vol 2 I Issue 4 Page 494
Ahmad MS et al. In! Surg 1 2015 Nov:2(4):492-495
other radiographic findings. AJR Am J Roentgenol. 1995;164(4):891-4.
15. Markogiannakis H. Acute mechanical bowel obstruction: Clinical presentation, etiology,
management and outcome. World .1 Gastroenterol. 2007;13(3):432-7.
Cite this article as: Ahmad MS. Shadab M, Omar S. Mallik AZ, Ansari MA. Causes, evaluation and surgical management of mechanical small bowel obstruction. Int Surg .1 2015;2:492-5.
International Surgery Journal j October-December 2015 I Vol 2 I Issue 4 Page 495

Dr Shakeb Ahmad et al JMSCR Volume 07 Issue 02 February 2019 Page 556
JMSCR Vol||07||Issue||02||Page 556-559||February 2019
Pneumatosis Intestinalis: A Rare Entity for Acute Abdomen in KMC,
Katihar
Authors
Dr Shakeb Ahmad1, Dr Ashutosh Patel
2, Dr Arif Hussain
3, Dr Md. Abdur Rahman
4,
Dr Yasir Tajdar5, Dr Saumya Sinha
6, Dr Sukesh Kumar
7
1Associate Professor, Department of General Surgery, KMC, Katihar
2,3Assistant Professor, Department of General Surgery, KMC, Katihar
4,5,6,7PGT, Department of General Surgery, KMC, Katihar
Abstract The patient who came with acute abdominal condition in the casualty of Katihar Medical College were
treated and followed up with the diagnosis of Pneumatosis intestinalis. The data of 6 patients who came in
the emergency with abdominal pain complaint between July 2016 and January 2019, followed up and
treated with the diagnosis of pneumatosis intestinalis were retrospectively evaluated. Four of the patients
were male and two of them were female. The mean age of the patients was 61.66 (52-75y). When detailed
medical histories were examined, we found that 3 patients had chronic smoking, 3 patients had the chronic
obstructive pulmonary disease, none of them had a history of surgery and known gastrointestinal system
diseases. Mean HB value was 11.25 g/dl (9.2-12.6 g/dl), white blood cell count was 8716.6/mm3 (6200-
13000/mm3). Despite the absence of acute abdominal pain, 4 out of 6 patients who were admitted to
emergency surgery due to the presence of free air in direct graphics and continuous abdominal pain
suggestive of perforation, then segmental small intestine resection and end-to-end anastomosis were
performed by open surgery, and 2 patients were followed non-operatively after regulating the medical
treatment in the hospital. Pneumatosis intestinalis is a clinical symptom. Early diagnosis can be difficult
because many systems can be associated with the disease. However, careful evaluation of clinical findings,
radiological data, secondary diseases and laboratory data will help the clinician determine the correct
diagnosis and appropriate treatment method.
Introduction
Pneumatosis intestinalis (PI) is a rare disorder
characterized by multiple gas-filled cysts in the
gastrointestinal tract, from the mouth to the anus,
often sub-serosal in the sub-mucosal part of the
intestinal wall. PI identified by Du Vernoi(3)
for
the first time in 1730 during a cadaver dissection
can be found in two forms as primary (15%) and
secondary (85%). Although the etiology is not
fully known, most of the cases can be
accompanied by gastrointestinal system diseases,
pulmonary system diseases, history of previous
abdominal surgery, trauma, connective tissue
diseases, iatrogenic injury(4)
. The development of
pneumoperitoneum as a result of rupture of cysts
without peritoneal irritation symptoms is
pathognomonic although there are not distinctive
clinical findings(5)
. In this study, the experience
www.jmscr.igmpublication.org
Index Copernicus Value: 79.54
ISSN (e)-2347-176x ISSN (p) 2455-0450
DOI: https://dx.doi.org/10.18535/jmscr/v7i2.100

Dr Shakeb Ahmad et al JMSCR Volume 07 Issue 02 February 2019 Page 557
JMSCR Vol||07||Issue||02||Page 556-559||February 2019
which was obtained from the patients who applied
to the emergency service with acute abdomen
disorder and who were treated and followed up
with the diagnosis of Pneumatosis intestinalis was
presented.
Materials and Methods
The data of 6 patients who applied to the
emergency service with abdominal pain complaint
between July 2016 and January 2019, followed up
and treated with the diagnosis of pneumatosis
intestinalis were retrospectively evaluated. The
patients' detailed medical history and treatment
during the hospitalization were noted, such as age,
gender, accompanied-disease, chronic habits and
drug use, previous operations. Laboratory values,
radiological results, and if surgical procedures
were performed, the operation, complications,
hospitalization periods, follow-up periods,
pathological examination results were also noted.
Results
Four of the patients were male and two of them
were female. Mean age was 66.66 (52-75y). All
patients were admitted to the emergency service
with sudden severe abdominal pain. In the
physical examination, there was a widespread
defense in all of them. When detailed medical
histories were examined, we found that 3 patients
had chronic smoking, 3 patients had the chronic
obstructive pulmonary disease, none of them had
a history of surgery and known gastrointestinal
system diseases. Mean HB value was 11.25 g/dl
(9.2-12.6 g/dl), white blood cell count was
8716.6/mm3(6200-13000/mm3). All patients were
evaluated X ray Erect abdomen and Computed
Tomography of whole abdomen. Although there
was no acute abdominal pain, 4 of 6 patients were
admitted to emergency surgery due to the
presence of free air in direct graphics and
continuous abdominal pain suggestive of
perforation, then segmental small intestine
resection and end-to end anastomosis were
performed by open surgery, and 2 patients were
treated conservatively by medical therapy. The
diagnosis of all patients was radiologically
confirmed by computed tomography examination.
Tomographic results showed that all of them had a
widespread free air image in the intraperitoneal
site, wall thickening of uniformed quality in the
small intestine, and intraperitoneal disseminated
free fluid in the lower quadrants of the abdomen.
The patients undergoing resection and
anastomosis had no other pathology in
intraoperative explorations that could cause these
changes in the intestinal wall. None of them
showed any evidence suggesting trauma or mass
lesions. All intestinal segments were subjected to
pathological examination. Pathological
examination of all specimens belonging to the
patients was reported as primary pneumatosis
intestinalis.
Discussion
Pneumatosis is a rare pathological condition
where multiple cysts filled with gas in the
subserosa and submucosa of intestinal wall are
seen, and its etiology has not been fully revealed
yet(6)
. It is seen most commonly in the 6th decade,
being equal to the male/female ratio(7)
. PI is often
accompanied by gastrointestinal diseases
(inflammatory intestinal diseases, pyloric stenosis,
peptic ulcer, colitis, celiac sprue, tumor etc.) or
pulmonary system diseases (chronic obstructive
pulmonary disease, chronic bronchitis, cystic
fibrosis, pulmonary fibrosis etc.), previous
abdominal surgical history (mesenteric ischemia,
transplantation, anastomosis), trauma, connective
tissue diseases (lupus variants, scleroderma),
iatrogenic injury (endoscopy, enteric tube
placement, etc.) (4)
, but three of our patients had a
continuing complaints of COPD, while the other 3
patients did not have any underlying co-morbid
disease or history of the previous operation.
Although it can be seen in the entire
gastrointestinal tract, the colon is affected by 6%
in the disease with retention of bowel loop. There
were many cysts filled with gas in jejunum
segments. The character of symptoms may be
specific or nonspecific depending on retention
Dr Shakeb Ahmad et al JMSCR Volume 07 Issue 02 February 2019 Page 558
JMSCR Vol||07||Issue||02||Page 556-559||February 2019
localization. Abdominal distension, abdominal
pain, mucous defecation, diarrhea, meteorysmus,
invagination, volvulus, mechanical obstruction,
gastrointestinal haemorrhagia may occur(8)
. All
patients had distension and epigastric sensitivity
in the abdomen. Sub-diaphragmatic free air,
dilatation of the small intestines and air-liquid
levels were present on the direct graphs of the
operated patients. These findings were confirmed
in the abdominal tomography evaluation, but no
specific sign was detected in the differential
diagnosis. Since close to half of patients have
been reported to have spontaneous remissions
during the treatment of pneumatosis intestinalis,
and recurrence of gas-filled cysts following
surgery has been reported, specific treatment is
not performed in asymptomatic cases and strict
follow-up and support are recommended(6,7)
. In
symptomatic cases, if there is no perforation,
bleeding, peritonitis, and sepsis, the nonoperative
oxygen therapy is sufficient(9)
. Complications
such as volvulus, intestinal obstruction,
intussusception, and perforation are seen only in
3% of patients(10)
. There were no significant
abdominal findings in our two patients with
underlying COPD stories, so they were first
treated by medical procedures, and they were
operated upon to dramatically reducing respond to
oxygen support therapy. However, the other six
cases were operated considering that the
perforation had developed. In patients with
intraoperative pneumatosis, internal herniation
and intestinal obstruction due to adhesions and
ligaments caused by cysts were detected.
Resection and end-to-end anastomosis were
applied to the small intestine segment with
obstruction segments and circulatory impairments.
Conclusions
It should not be forgotten that pneumatosis
intestinalis is a clinical symptom. Early diagnosis
can be difficult because many systems can be
associated with the disease. However, careful
evaluation of clinical findings, radiological data,
secondary diseases and laboratory data will help
the clinician determine the correct diagnosis and
appropriate treatment. It should also be noted that
in most cases the treatment of underlying disease
and supportive treatment are sufficient and that
emergency surgery indications may also be seen
References
1. Hwang J, Reddy SV, Sharp KW.
Penumatosiscystoides intestinalis with free
intraperitoneal air: A case report. The
American Surgeon 2003; 69:346-9
2. Yale CE, Balish E. Pneumatosiscystoides
intestinalis. Dis Colon Rectum1976;
19:107-11
3. KnechtleSJ, Davidoff AM, Rice RP.
Pneumatosis intestinalis, surgical
management and clinical outcome.
AnnSurg 1990; 212:160-65
4. Khalil PN, Huber-Wagner S, Ladurner R,
Kleespies A, Siebeck M, Mutschler
W,Hallfeldt K, Kanz KG. Natural history,
clinical pattern and surgical considerations
of penumatosis intestinalis. Eur J
MedRes (2009) 14: 231-239
5. Voboril R. Pneumatosiscystoides
intestinalis-A review. ActaMedica
(HradecKralove) 2001; 44:89-92
6. Blumberg D, Wald A. Other diseases of
the colon and rectum. In: Feldman M,
Friedman LS, Sleisenger MH, editors.
Sleisenger & Fordtran's gastrointestinal
and liver disease.7th ed. China: Saunders;
2002.p2307-9
7. Gagliardi G, Thompson IW, Hershman
MJ, Forbes A, Hawley PR, TalbotI C.
Pneumatosiscoli: a proposed pathogenesis
based on study of 25 cases and review of
the literature. Int J ColorectalDis 1996;
11:111-8
8. Oruç N, Tekin F, Çalıºkan C, Harman M,
Özütemiz Ö. Pnömatozissistoides
intestinalise bağlı gastrointestinal kanama
olgusu. Endoscopy 2009; 17:43-5

Dr Shakeb Ahmad et al JMSCR Volume 07 Issue 02 February 2019 Page 559
JMSCR Vol||07||Issue||02||Page 556-559||February 2019
9. St Peter SD, Abbas MA, Kelly KA. The
spectrum of pneumatosis intestinalis.
ArchSurg 2003; 138:68-75
10. Galandiuk S, Fazio VW.
Pneumatosiscystoides intestinalis. A
review of literature. Dis Colon Rectum
1986; 29:358-63.
Dr Shakeb Ahmad et al JMSCR Volume 07 Issue 07 July 2019 Page 408
JMSCR Vol||07||Issue||07||Page 408-410||July 2019
Incidence of wound infection post subcuticular suturing versus simple
suturing a comparative study in KMC, Katihar
Authors
Dr Shakeb Ahmad1, Dr Md. Abdur Rahman
2, Dr Yasir Tajdar
3, Dr Ankita Sharma
4,
Dr Sunil Kumar5, Dr Shashank Saurav
6, Dr Tuba Yazdani
7
1Associate Professor, Dept. of Gen. Surgery, KMC
2,3,4,5,6,7Junior Resident, Dept. of Gen. Surgery, KMC
Abstract To prevent SSI post surgery is an important aim after every surgery. There are two methods of wound
closure technique i.e. simple wound closure and subcuticular suturing which is cosmetically better
suturing technique. A prospective non-randomized study of 100 patients with surgical wound was carried
out over a period of 12 months(June 2018 to June 2019) in 50 patients (group A), wound closure was
done with simple interrupted method and in 50 patients(group B) with subcuticular method. This study
was done in Katihar medical college, Katihar. Data including age, sex, wound infection, wound type were
collected. 3% of patients in group A and 2% in group B had wound infection. Wound type of 65% of the
group A and 58% of patients in the group B were clean contaminated. 42 percent of patients in group A
and 36 % of patients in group B are located in the age of 21 to 40 years. 74% of group A and 70% of
group B were male. Surgical site of 88 %, 1%, 2% and 9% of patients in group A and 80%, 2%, 10% and
8% of patients in group B was in abdomen, thorax, head and neck and extremity, respectively. Incidence
of wound infection in patients who had surgical wounds sutured by subcuticular and simple were 8% and
4%, respectively that this difference was not statistically significant. Therefore in our study it depicts that
subcuticular suturing is having better aesthetic result. In our study, the incidence of wound infection was
lower than other studies.
Keywords: Infection, simple, subcuticular.
Introduction
The degree of bacterial contamination during an
operation is related to the risk of incisional
infections[1]
. Good suturing technique should
eliminate dead space in subcutaneous tissues,
minimize tension that causes wound separation. It
involves correct wound placement with respect to
relaxed tension lines[2]
. Simple suture, it is the
most fundamental technique of wound closure
used in cutaneous surgery. In this procedure the
needle enters one side of the wound and
penetrates well into the dermis or subcutaneous
tissue. By altering the depth or angle of the
needle, one can use this technique for wound
edges of uneven thickness. The needle is then
passed through the subcutaneous tissue to the
opposing side of the wound and exists closer to
the wound edge so that the final configuration of
the suture is flask-shaped[3,4,5]
. Another method
for suture is subcuticular stitches, the subcuticular
stitch is started by inserting a knot at one end of
the incision. A small bite is taken of the
http://jmscr.igmpublication.org/home/
ISSN (e)-2347-176x ISSN (p) 2455-0450
DOI: https://dx.doi.org/10.18535/jmscr/v7i7.76

Dr Shakeb Ahmad et al JMSCR Volume 07 Issue 07 July 2019 Page 409
JMSCR Vol||07||Issue||07||Page 408-410||July 2019
subcuticular material and the suture is pulled
through. Then on the opposite side of the wound a
similar subcuticular bite of the suturing material is
inserted and gently worked up the wound. The
subcuticular suture is used primarily to enhance
the cosmetic results[6]
. The aim of this study was
to compare the incidence of wound infection
between the two groups of patients that their
wound are sutured by subcuticular or simple
interrupted procedure.
Material and Method
A prospective non-randomized study of 100
patients with surgical wound was carried out over
a period of 12 months(June 2018 to June 2019) in
50 patients (group A), wound closure was done
with simple interrupted method and in 50 patients
(group B) with subcuticular method. The study
was conducted in Katihar Medical College,
Katihar. Data including age, sex, wound infection,
wound type was considered. The correlation
between the variables was done by IBM SPSS
statistics 18.
Result
3% of patients in group A and 2% in group B had
wound infection. All wound infections occurred in
the first weeks. Wound type of 65% of the group
A and 58% of patients in the group B were clean
contaminated. 42% of patients in group A and
36% of patients in group B were located in the age
of 21 to 40 years. 74% of group A and 70% of
group B of patients were male. 3% and 1% of
patients in group A and 4% and 2% of the group B
had diabetes and took steroids, respectively.
Surgical site of 88 %, 1%, 2% and 9% of patients
in group A and 80%, 2%, 10% and 8% of patients
in group B were in abdomen, thorax, head and
neck and extremity, respectively.
Discussion
To prevent SSI post surgery is an important aim
after every surgery. Effective skin closure is a
necessary factor in the prevention of infection[7]
.
More patients in both groups in our study were
male (group A and B). The number of patients
were maximum in the age group of 21 to 40 years
in both the groups. Subcuticular suturing provides
a better result as no skin interruption is caused by
the suturing tool, and better blood flow is
maintained[8]
. This technique is used in the areas
where better cosmetic results are required i.e. the
exposed areas most commonly demanded by the
female patients. The subcuticular suture does not
impact on deep tissues of the skin and leads to
minimal strangulation of tissue[9]
. A previous
study has reported that subcuticular method do not
increase the infection rate[10]
like in our study.
Incidence of wound infection in our patients for
which of these two techniques (subcuticular and
simple) had been used were 3% and 2%, that their
values were much lower than previous study. Chi-
square test did not show significant relationship in
the incidence of wound infection in two
techniques (simple and subcuticular) (P value
<0.05).
Conclusion
Incidence of wound infection in patients who had
surgical wounds sutured by subcuticular and
simple were 3% and 2%, respectively that this
difference was not statistically significant.
Therefore, we recommend the routine use of
subcuticular method in surgical wound closure
with better aesthetic result.
Bibliography
1. Grant SW, Hopkins J, Wilson SE;
Operative site bacteriology as an indicator
of postoperative infectious complications
in elective colorectal surgery. Am Surg.,
1995; 61(10):856-61.
2. Borges AF; Techniques of wound suture.
Elective Incisions and Scar Revision.
Boston: Little Brown., 1973;65-76.
3. Kudur MH, Pai SB, Sripathi H, Prabhu S;
Sutures and suturing techniques in skin
closure. Indian J Dermatol Venereol
Leprol., 2009;75:425-34.

Dr Shakeb Ahmad et al JMSCR Volume 07 Issue 07 July 2019 Page 410
JMSCR Vol||07||Issue||07||Page 408-410||July 2019
4. Moy RL, Waldman B, Hein DW; A review
of sutures and suturing techniques. J
Dermatol Surg Oncol., 1992;18:785-95.
5. Zachary CB; Suture techniques. In:
Zachary CB, editor. Basic Cutaneous
Surgery. New York: Churchill
Livingstone., 1991;53-75.
6. Moy RL, Lee A, Zalka A; Commonly used
suturing techniques in skin surgery.
American Family Physician., 1991;44(5):
1625–34.
7. Sakka SA, Graham K, Abdulah A; Skin
closure in hip surgery: subcuticular versus
transdermal. A prospective randomized
study. Acta Orthop Belg., 1995;61(4):331-
6.
8. Zografos GC, Martis K, Morris DL;Laser
Doppler flowmetry in evaluation of
cutaneous wound blood flow using various
suturing techniques. Ann Surg., 1992;
215(3):266-8.
9. Fiennes AG; Interrupted subcuticular
polyglactin sutures for abdominal wounds.
Ann R Coll Surg Engl., 1985;67:121.
10. Corder AP, Schache DJ, Farquharson SM,
Stephen GT; Wound infection following
high saphenous ligation. A trial comparing
two skin closure techniques: Subcuticular
polyglycolic acid and interrupted
monofilament nylon mattress sutures.
Journal of the Royal College of Surgeons
of Edinburgh., 1991;36(2):100-2.
11. Gilmore OJA., Martin TDM; Aetiology
and prevention of wound infection in
appendectomy. Br. J. Surg., 1974;
61(4):281-87.
12. Foster GE, Hardy EG, Hardcastle JD;
Subcuticular suturing after
appendicectomy. Lancet., 1977;1(8022):
1128-9.

Int J Anat Res 2015, 3(1):821-24. ISSN 2321-4287 821
Original Article
CLINICO-ANATOMICAL STUDY OF VARIATIONS IN ARTERIALSUPPLY OF ADULT HUMAN STOMACHSaif Omar *1, Md. Shakeb Ahmad 2,Nafees Fatima 3, Md. Arif Ansari 4.
ABSTRACT
Address for Correspondence: Dr. Saif Omar, Associate Professor, Department of Anatomy, KatiharMedical College, Katihar – 854105 Bihar, INDIA. Mobile No.: +919431229999E-Mail: [email protected]
Access this Article online
Quick Response code Web site:
*1 Associate Professor, Department of Anatomy, Katihar Medical College, Katihar, Bihar, India.2 Assistant Professor, Department of Surgery, Katihar Medical College, Katihar, Bihar, India.3 Senior Resident, Department of Anatomy, Indira Gandhi Institute of Medical Sciences, Patna,Bihar, India.4 Professor & Head, Department of Surgery, Katihar Medical College, Katihar, Bihar, India.
Anatomical variations in the arterial supply of adult human stomach have long baffled even the most experiencedsurgeons during surgical manipulation of the stomach. The stomach develops from the foregut hence its arterialsupply is derived from the coeliac trunk. The present study is aimed at observing the anatomical variations ofthe arteries supplying the stomach. This study has been conducted on fifty cadavers during routine dissections.The aberrant arteries observed have both embryological and clinical significance. A comprehensive knowledgeof the arteries nourishing the stomach along with their anomalies is vital for the surgeons to avoid iatrogeniccomplications during surgical manipulation involving the organ.KEYWORDS: Arterial, Foregut, Stomach, Anomalies, Complications.
INTRODUCTION
International Journal of Anatomy and Research,Int J Anat Res 2015, Vol 3(1):821-24. ISSN 2321- 4287
DOI: 10.16965/ijar.2014.499
Received: 01 Sep 2014Peer Review: 01 Sep 2014 Published (O):31 Jan 2015Accepted: 13 Jan 2015 Published (P):31 Mar 2015
International Journal of Anatomy and ResearchISSN 2321-4287
www.ijmhr.org/ijar.htm
DOI: 10.16965/ijar.2014.499
The stomach is a saclike dilatation of thealimentary canal [1]. In cadavers, the stomachis sickle shaped, the wider end being directedupwards and to the left [2]. From clinical expe-rience the arterial supply of the stomach haslong been postulated to be exceptionally rich[3]. In conventional textbooks the arterialsupply of stomach is by the coeliac trunk directlyor indirectly and the arteries reach the organalong its curvatures. The arteries are leftgastric artery branch of coeliac trunk and is theprincipal artery of the stomach; right gastricartery branch of common hepatic artery; shortgastric branches of splenic artery; left gastro-epiploic artery branch of splenic artery; right
gastroepiploic artery branch of gastroduodenalartery and posterior gastric artery occasionalbranch of splenic artery. Known to Walther [4]since 1740 and termed by Haller [5] in 1745 asthe posterior gastric branch, this artery and itssurgical importance have been at best ignoredand at worst neglected [6] in spite of severalpublications on variations of arterial supply ofthe stomach.
MATERIALS AND METHODS
Conventional cadaveric dissections for academicteaching of first year MBBS students wereperformed on 50 embalmed male cadavers agedbetween 25 to 65 years. After exposing theabdominal cavity and removing the peritonealfat, the coeliac trunk was located and each of
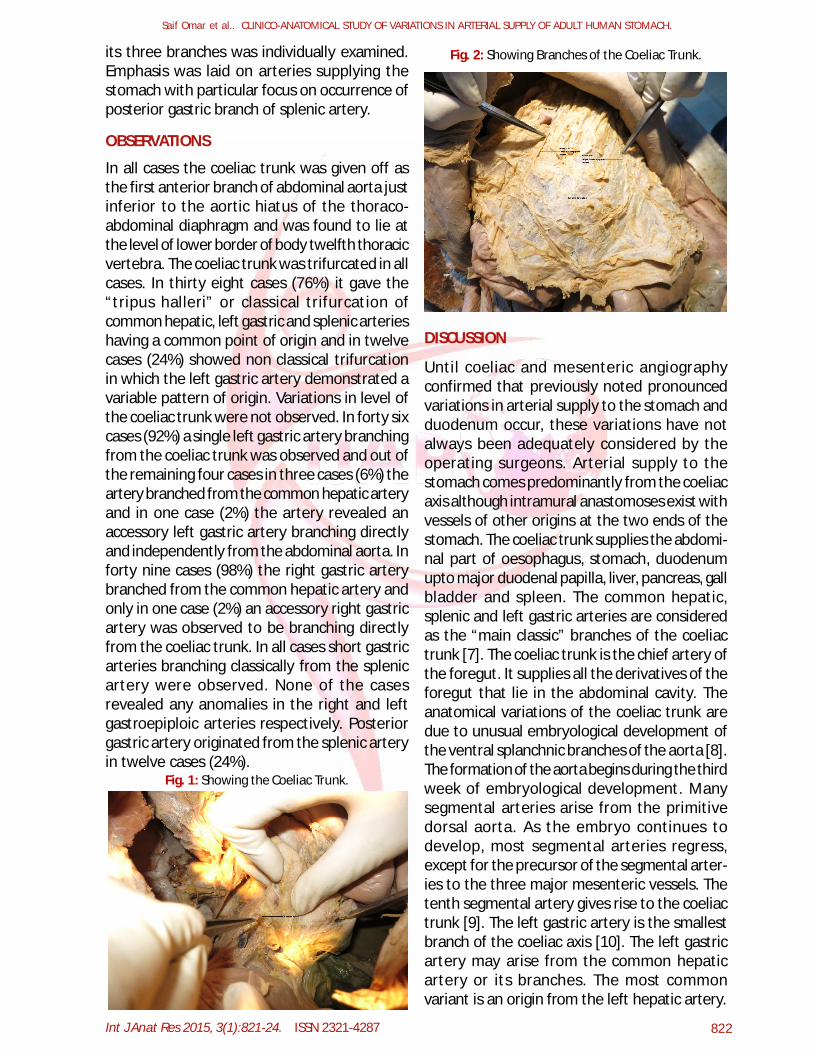
Int J Anat Res 2015, 3(1):821-24. ISSN 2321-4287 822
Saif Omar et al.. CLINICO-ANATOMICAL STUDY OF VARIATIONS IN ARTERIAL SUPPLY OF ADULT HUMAN STOMACH.
its three branches was individually examined.Emphasis was laid on arteries supplying thestomach with particular focus on occurrence ofposterior gastric branch of splenic artery.
OBSERVATIONS
In all cases the coeliac trunk was given off asthe first anterior branch of abdominal aorta justinferior to the aortic hiatus of the thoraco-abdominal diaphragm and was found to lie atthe level of lower border of body twelfth thoracicvertebra. The coeliac trunk was trifurcated in allcases. In thirty eight cases (76%) it gave the“tripus halleri” or classical trifurcation ofcommon hepatic, left gastric and splenic arterieshaving a common point of origin and in twelvecases (24%) showed non classical trifurcationin which the left gastric artery demonstrated avariable pattern of origin. Variations in level ofthe coeliac trunk were not observed. In forty sixcases (92%) a single left gastric artery branchingfrom the coeliac trunk was observed and out ofthe remaining four cases in three cases (6%) theartery branched from the common hepatic arteryand in one case (2%) the artery revealed anaccessory left gastric artery branching directlyand independently from the abdominal aorta. Inforty nine cases (98%) the right gastric arterybranched from the common hepatic artery andonly in one case (2%) an accessory right gastricartery was observed to be branching directlyfrom the coeliac trunk. In all cases short gastricarteries branching classically from the splenicartery were observed. None of the casesrevealed any anomalies in the right and leftgastroepiploic arteries respectively. Posteriorgastric artery originated from the splenic arteryin twelve cases (24%).
Fig. 1: Showing the Coeliac Trunk.
Fig. 2: Showing Branches of the Coeliac Trunk.
DISCUSSION
Until coeliac and mesenteric angiographyconfirmed that previously noted pronouncedvariations in arterial supply to the stomach andduodenum occur, these variations have notalways been adequately considered by theoperating surgeons. Arterial supply to thestomach comes predominantly from the coeliacaxis although intramural anastomoses exist withvessels of other origins at the two ends of thestomach. The coeliac trunk supplies the abdomi-nal part of oesophagus, stomach, duodenumupto major duodenal papilla, liver, pancreas, gallbladder and spleen. The common hepatic,splenic and left gastric arteries are consideredas the “main classic” branches of the coeliactrunk [7]. The coeliac trunk is the chief artery ofthe foregut. It supplies all the derivatives of theforegut that lie in the abdominal cavity. Theanatomical variations of the coeliac trunk aredue to unusual embryological development ofthe ventral splanchnic branches of the aorta [8].The formation of the aorta begins during the thirdweek of embryological development. Manysegmental arteries arise from the primitivedorsal aorta. As the embryo continues todevelop, most segmental arteries regress,except for the precursor of the segmental arter-ies to the three major mesenteric vessels. Thetenth segmental artery gives rise to the coeliactrunk [9]. The left gastric artery is the smallestbranch of the coeliac axis [10]. The left gastricartery may arise from the common hepaticartery or its branches. The most commonvariant is an origin from the left hepatic artery.
Int J Anat Res 2015, 3(1):821-24. ISSN 2321-4287 823
Saif Omar et al.. CLINICO-ANATOMICAL STUDY OF VARIATIONS IN ARTERIAL SUPPLY OF ADULT HUMAN STOMACH.
Other variants include a common origin with thecommon hepatic artery. Identification of anaberrant origin may be of importance duringsurgical mobilization of the upper stomach [10].In our study variations in origin of the leftgastric artery was observed in four cases (8%)out of which in one case an accessory leftgastric artery was also observed. Ishiqami K etal studied 118 patients with conventionalangiography for detection of an accessory leftgastric artery [11]. Result of this study revealedan accessory left gastric artery in 25 out of 118cases. According to Hollinshead W.H. [12] anaccessory left gastric artery is present in about11.5% of the population. It arises from the aortaindependently in about 4.5% of the population.The right gastric artery arises from the commonhepatic artery and its origin is often variant. Themost common alternative origins are from theleft hepatic, gastroduodenal or supraduodenalarteries [13]. An accessory right gastric arteryis present in about 1.45% of the population [7].In our study in only one case (2%) we observedthe presence of an accessory right gastric ar-tery. We did not observe any variations in rightand left gastroepiploic arteries. They were seento branch from gastroduodenal and splenicarteries respectively. The splenic artery is thelargest branch of the coeliac trunk. The splenicartery gives off five to six short gastric branchesand the left gastroepiploic artery. From themiddle part of its course the splenic artery maygive off a posterior gastric artery (PGA) to thestomach [14]. The high incidence and the widedistribution of the PGA to the stomach are insharp contrast with the absence of descriptionin most modern textbooks of anatomy. DiDio etal [15] found the PGA in 46% of their subjects.According to DiDio, the surgical importance ofthe posterior gastric arteries attributed to itsrelatively high incidence and the fact that itaugments the blood supply to the superior partof the posterior surface and to the fundus. Theartery has a deep and almost hidden origin fromthe splenic artery. Overlooking this vessel inparticular may cause postsurgical haemorrhageif this vessel is inadvertently transected duringsurgery [6]. In our study we observed PGA intwelve cases (24%) and all were observed tooriginate from the splenic artery. This artery may
be an important channel in cases where majorgastric arterial supply has been compromised.According to Loukas et al [16] the mostcommon origin of PGA was from the left gastricartery in 41.8% cases, from splenic artery in25.2% cases, double PGA in 22.4% cases andfrom coeliac trunk in 10.2% cases. Acoeliacographic study reported PGA in 55.7%cases [17]. Each artery supplying the stomachhas its own importance regarding variations. Thegastroepiploic arteries observed in our studywere least notorious.
CONCLUSION
As anatomists and surgeons we state that in ouropinion gastric arterial variations should not beoverlooked during abdominal surgeries involvingthe stomach. Many complications can beavoided with precise knowledge of theseaberrant arteries. While vascular anomalies areusually asymptomatic, they may becomeimportant in patients undergoing diagnosticangiography for gastrointestinal bleeding orcoeliac axis compression syndrome. Knowledgeof such variations can aid in the interpretationof angiographic studies.Acknowledgement: The authors wish toacknowledge the guidance and supervisionreceived from Dr. Vakil Ahmed, Professor ofAnatomy, Katihar Medical College.
[1]. Rosse C. Hollinshead’s textbook of anatomy, 5th
Edition, Lippincott – Raven, 1997, pp 553.[2]. Datta A.K. Essentials of human anatomy, 8th Edition,
Vol-1, Current Books International, pp 188.[3]. Brown R.J. Arterial supply of human stomach. AMA
Arch Surg. 1952;64(5):616-621.[4]. Walther A.F. De Vena Portae. Lipsiae, 1740.[5]. Haller A. Icones Anatomicae Quibus Praecipue
Aliquae Partes Corporis Humani DelineataeProponuntur et Arteriarum Potissimum HistoriaContinetur. Fasciculus II. Gottingae: Vandenhoeck,1745.
[6]. Suzuki K. Incidence and surgical importance of theposterior gastric artery. Ann. Surg. Feb. 1978. Vol187(2): 134-136.
[7]. Salve V.M. Multiple variation of branches ofabdominal aorta. Kathmandu Univ Med J 2011;33(1):72-76.
[8]. Chiang K. Angiographic evaluation of hepatic arteryvariations in 405 cases. Chin J Radiol 2005; 30:75-81.
Conflicts of Interests: None
REFERENCES
Int J Anat Res 2015, 3(1):821-24. ISSN 2321-4287 824
Saif Omar et al.. CLINICO-ANATOMICAL STUDY OF VARIATIONS IN ARTERIAL SUPPLY OF ADULT HUMAN STOMACH.
How to cite this article:Saif Omar, Md. Shakeb Ahmad, Nafees Fatima, Md. Arif Ansari.CLINICO-ANATOMICAL STUDY OF VARIATIONS IN ARTERIALSUPPLY OF ADULT HUMAN STOMACH. Int J Anat Res2015;3(1):821-824. DOI: 10.16965/ijar.2014.499
[9]. Lin P.H. Embryology, anatomy and surgical exposureof the great abdominal vessels. Surg. Clin. NorthAm. 2000 Feb; 80(1):417-33.
[10]. Standring S. Gray’s Anatomy, 39th Edition: ElsevierChurchil l Livingstone 2005. Stomach andabdominal oesopgahus:1146.
[11]. Ishiqami K. Accessory left gastric artery from lefthepatic artery shown on MDCT and conventionalangiography. AJR Am J Roentgenol 2006;187(4):1002-1009.
[12]. Hollinshead W.H. Anatomy for surgeons. Vol:2, 2nd
Edition, New York, Harper & Row Publisher,1961:590.
[13]. Standring S. Gray’s Anatomy, 39th Edition: ElsevierChurchil l Livingstone 2005. Stomach andabdominal oesopgahus:1148.
[14]. Sinnatamby C.S. Last’s anatomy: regional andapplied. 11th Edition. London: Churchill Livingstone2006:251.
[15]. DiDio L.J. Posterior gastric artery and itssignificance as seen on angiograms. Am J Surg 1980Mar;139(3):333-337.
[16]. Loukas M. The clinical anatomy of posterior gastricartery revisited. Surg Radiol Anat 2007Jul;29(5):361-366.
[17].Okabayashi T. Posterior gastric artery inangiograms and its surgical importance.Hepatogastroenterology 2005 Jan-Feb;52(61):298-301.
Medical Science -0EDS Calm= alginate thsss.
pbt thickness skin graft, Donor site area
11111=11111.11MMIE6 Research Paper
11, l. Sinha
The Study of Effeetiveneci,i of Calcium Alginate Dressing Over die f•.',,piit Thickness
Skin Graft Donor Site Area of Patients
MS (General Surgery). Associate Professor, Department of Surgery Katihar Medical Mazharul Hague cow, Iratikar, Bihar, India. ' Correspond-it-1F author
145 (Gemmel Surgery), Associate Professor, Department of Surgery, Darbhanga Medical Came ft ifetpital„ Darbhanga. Bihar, India_
Assaf Calming serunam dressings acre used to rire Kai eresere, :masa on the split trackness Any graft donor *earn, tar patanls. Miethavialogr Ifistary taking OrnizaZcsansinatian lavestigation. Treatment: pre opera-
a
osr operna Ye. Pcatrpierntimatinekemeed Fintopeannoginsfetornina non c.,1-erciscel specuneras afrarejaliter ulcers wereperformed Uactt. .esnUorr eke patients eare perlsolt43 mantra 5o6 months. Obscrlation- Cinserscitime leas done far a period of tat* post
igiendive days. Data s.ar analyned satutare C0102ZSZOIL: itilcium alginate dressings veer donor site ens quite easy, almostpain- im.felrEGIStal was easy a a d minim& pa6ri musrmai trauma to the rawly epithetialimd saajisceancinze alepithehzation was eery high (72%
Is) no ifith past opening? dctiK
INTRODUCTION The persons have moo. risk lir thermal hams doe to industri-alization and more .ase of electrical entimments whisib leads the increase challenge for management of burn? The modern trend of early and complete :overage of the lost skin by split thickens skin thee:oars& has nether increased the dialleages for manage-ment of recipient as o ell as oi the donor site areas of the Sian graft'
insitly was primarin befiseasedno the management of the ilkinor ate area dressings obi& was primarily managed depend
Ithr personal encores at bifrtidzatl surgeon. &MIK' of them a' ms-silk greens tiresmogt poly 12.146.11. semi permeably trans-mute& films, Ihydromilticad dressings and retention dressing etc.
Pont opentive patients may complain pain cher the donor Vitt 1,area kis die use of thew comentionaii dressings, and soatrase foam the dressings with oozing ham the donor bad is another paskillent. by applying these type of &swings heating she do-nor site alma takes a long time astai sometime it is timpredict-.Alle, reinviral of the do swigs are cif& ialt mid adtcost adherent to Me bed mad sesitionni as :uneasy and painha to tin patient?
21111inate diestangs hien age4hf lager ohm in contact with amid mound pan:id* moist emenuarient ior healing. This nil like Inter over the done site protects the eisitfachallaing maniad horn lrattima and 'limo dry-Mertes may he the season behind tar'y arid better epithiiiakzation of the donor site with alginate dressings.
Our study was to evaluated the clinical ,effectiveness of oak-mum alginale dressing over the split thickness Skin pan donor ate area .under these stages: 3 . Post operative dressing soakage. 2. Post operative pain. A. Healing time, and 4. lime of dressing ft-trouvei
A moist environment was also used to promote healing by dress-ing with calcium alginate, which possesses hemostatic, property
MAITILIAL Sr METHODS A total of St patients with varied elinidi conditions like past burn contractainsi chnloms non healing Moan. Marjohns ulcer Isle on the basis of uiciusein criteria were selected This study star done an department ,tt Surgery, Dasbbanga Medina Ceiling and Dorpitil. Darbhansa, Bihar, India between may 2005 to may 20117 Patients were carried for primary- management of ante Nue and who nomeired split thickness skin graft over the raw body Tie attendant of entire subjects signed en entormed eon-
sent approved try ethical committee of Darblaange Medical Col-lege, Dorian-safe Einar, India was sought
Methothilogy: History taking. Clinical examination Investiga-ticm. Tseatmena pre rperative and post operative, Post op-ts4sler inatiagerannt. Histopattmlogical mramanaticas of excised specimens of Maritolins dicers. Follow up the patients for a pe-Mostar; months no is months.
Psi:operative treatment Patients with olantinic non Sealing slicers and ulcers over bum war were required initial treatment with antibiotics, multhita mins Iasi antiseptic dressings till the lesions became clean and •granulating
Operative treatment: When the 7.1.5tieol seers found to be fit tie surgery on the basis of innitail examinatitin. investigation and pre anaesthetic cheek-sip then they were allmeed for surgical procedure- viz. release of nontracture.,wide excision of the margolins nicer, excisiun/scrap-ping rai the chronic non :healing ulcer followed by coverage of the raw area with split thickness skin graft.
Preoperative measures Light diet sear yrs one day before from the date of surgery. A short acting mold fodatwe like alprazolain 0.25 rag was given in night beifose mammy. Ds the day of surgery in the morrnmg proper allaying of the concerned parts of the body was done. Injection tetanus monad It ml was administered intramuscular over deltoid meanie. Hatt am hour before the surgery injection atropine or tesjection gly.copyoulatte intrarnuscularty and injection retirline 50 mg intravenously were administered. Patient was shifted to the operation theature. liner:non celtriaxone of proper dose was adminstesed intravenously at the time of induction of anaesthesia
Operative 'ones: Proper painting and ,dir ping of the donor as well as the recipi-ent sites were done Hie primary pathologies e.g. post burn con-tracture, merit/tine's after, chronic non healing Meer etc Wert dealt with first bi- EAPSW:t surgeries viz release in the contrac-ture. wide excision of okra- or scraping it the wound etsc com-plete hemostasis cif the redotent sites tiers achieved and cov-ered wail a sterile tetra. Then split thickness skin grafts were raised of a proper sizes from proper donor sites with the help of hurithey,s knife. Areas were covered with sterile tetras for the time being mai the grafts were spread over the recipient sites,
are I 1.)SE - StIOMIIMIC it£SEARCEI
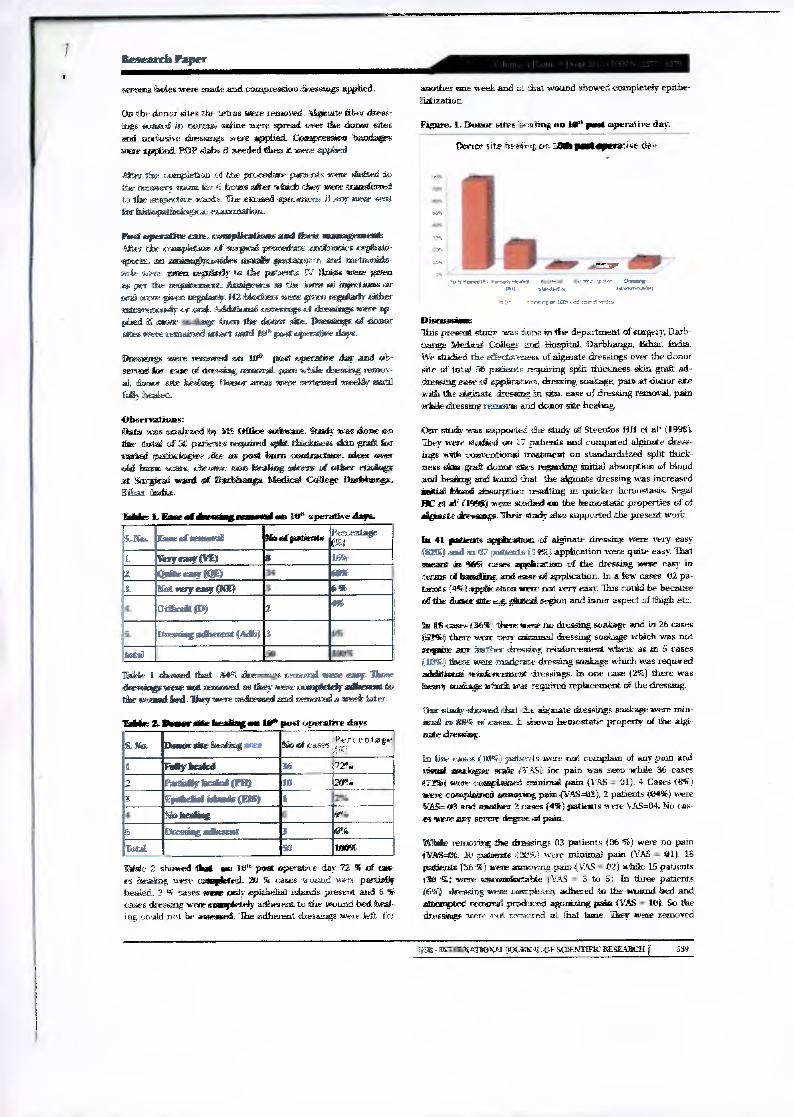
am,
ION
ever11,1 .1wrar5.c0e13
ireseateh Paper
seronaa holes were needle and compressum Mies sings applied.
On the talonor sites the tetias were nuanced 3.1spinate filer dress-ings soaked in norm:a brine were spread ever the donor sites auk( otrasive deebangs west applied. COnapression haridages were vaned. POP slabs it needed liten it were applied
Ater the ,thimpletiou st the ,prociedive pains-lots were slated to tie cenidery mow ire- 6 hours atter Whicib they were transferred a the !Respective ath.e. The excised stiondrioni id Aspl" were semi .or blinkmatiadogion examination,
Bad sapinallee care, ramiplicatitaas mad &tit management .41k£5 the seimpletion of soinporil proberbare rionlaitiths cephain-vitenti an 241111k19441111:4659e6 3,1151A* @ffetallO,Irlet arrasi metiortida wit web wren mentandy to the patients IV fatiuis were given ate gor the tespinenarse hears-saes in Ow chime rai win wive bison argatainic 02 Mechem wort gfacts wistaarly either matrannosiosityor1,104Miditisssad 2011O1110g6 Kketiiiithp were ap- plied if name - Mum the donor Fat_ Dnestings at dome 4:Atelier-ere remained intact usand Ittfa past amerattaw
Dressings west reanowid OD le pod operative ell2sy and ob-served kor: case of Mesa* removal. pain wade dinessing tesnov - al, donor site lambing amid nem area meneartal muddy matil Way healekt
Observations: flats eras acialy Office rdiforame. Dm= was done ,WO
total of 54: pe& niquired ilmeadorrs Am' gm& Lc raided pathrobgiee as pent barn contractore. Mom nem Mil buns scam drikOffldra S11013 brain= =cm of tiftem orivingi-ar dampeal ward of fi Milian= Medical Ceddier Dariebroga.
ir Gadd
TA= L Ease al flnestimg ressossi no in' onto-attic Jima
!S,.. Dia. Ease at moistralt - tie ad patient* Itierientage ty,,4 .
I. Very rosp(VIE) S IfOr
2. , ODD 03113 DWI DID .1 /DM neryretsf OSP i6 51
t 1031601111, (Di 2 433
%theasingadllierest Iarlei) 3
ientad 1
1 showed that aill% skeaeasssr remora& name carol. Mame simasings wove not reestinisil as thetcy owe enitsplekk Ahem& to
avotaitad kind liseysseire redressed and renwavel awe& latex
Talsic 2. Down site finafing ens De' poet operettas e days
S. Nia. Donor sate ismaing aunt Cper- entithe
1 Filly famintil 36 [1725,0
2 Pala* bola ONO IS 3 fpnadball(Elf) I
No letarior d''
6 Dram* adlanant 3 eqi. TotAl so
labile 2 showed DM ere 0 past operatit e day 72 % of LW sr thkoalloog were campitted. Al 5r caws wesand wen- partial* healed. 2 5 oases woe only epithelial idancis present and 6 % eases dressing were isimpletely adassent to the wound bed heal-ing could not be assersied The adherent diessings owe lett for
another one week and di that wound showed -completely epithe-lial, ation
Figure. L Donor sites beading no Waviest operative day.
Dermot site tieberitt GPO :ads postapera7iQe des
41111.,, *.R1Selif
S4,termi,..2101
5.. . . •rerrr lop,, Lrjrntrf - se-tee
Discomfit= This present baby was one in the department of surgery, Darku hangs Aficilicai Collect tub kiospital, ihriblianga %that We stitched the effectiveness of alginate dressings ,ever the donor site of inta 50 patients requiring split thickness skin graft ad-dressing ease Of appi.iimatvDra, dressing soakage, pars at tabor site with the deiniste dressing in Sit°, ease of dressing removal, pain while dressing omorni and &um site bedding.
Our study was supported the study of Steel:dos fin et ad (1998). They were Waded ,acti i7 patients and compared alginate dress-ings with nomentionail 171...Etment on standardirized split thick-ness skin grail donor sites regarding initial absorption of blood and .befailist, ZIOLI tralrod that the alginate dressing was increased initial hand absorption restating ut quicker hemostasth Segal BC et af' i1t556I were studied or the hemostatic properties of of allpinate Summates Their Moth Also supported the present work
41 panne% amilleation ,irt alginate dressier were very easy (MI and in 67 patinas .applicamin were quite easy. That meant in SW cases appacurticion of the cluissing were easy in terms of Isandling and ease of application. In a few cases 02 pa-tellas ri-rm appieenno anew oat very easy This could be because of the &mbar 4ite e,g. eeAl region and inner aspect of thigh etc.
B owes %serene-re no dressing soakage and in 26 cases i(55-lai there NOME Tell: mintarnal dressing soakage which was not simpare HUI dimElerv drt-ggittg 4x-440a:entitle:I where as an 5 cases (IteMi) there were moderate dressing soakage which was required additional reintiorrement- dressings in one ease 12%) there was hewn snairage 7101111 war required replacement of the dressing
Om bath/ dosed that the alginate dressings soakage were Milt-lamal MEK of oases. 2 shown hemostatic property of the algi-nate dressieg
irs Inie cane OW,T) patiwits INktre not complain of =I' pain and visual assalogne wade rrAS) for pain was hem while 36 cases 471a)
were transpinined minimal pain (VAS y Old, 4 Cases tit%)
were complained sonniuMg men c(VASIT), 2 patients (04%) were ft3 and annther 2 050ge6 0%) patients were VAS=04. No oas-
es's:wee anicr severe degree at pain.
Wale resuming the dressings 03 patients f96 %) were no pain till:mem lb palpates f2d5.) were minimal pain (VAS ell 18 patients (36 *) were annoying pain (VAS e tr2) while 15 patients
Si were nterninacistable i VAS = 3 to lo In three patients fib%) dressing were ouripletity adhered to the wound bed and attempted remand produced agonizing pain (VAS = RI/ So the dressings were not romered al that time. Theg were removed
ii5555 Cf ArnmAirFOLTaAg. .0F SOLATTFIC RESEARCH 539

Research Paper
sitiammattly ahem oise week hi our study n% of cases were taninitual eninal twin daring dressing removal.
Algoitaffir dressings Ihrita a get Ilike layer when in contact With mum wannirds e.g a id041161" sit, area This gel like layer prevents trataniar at die raw mum endings that are present at the post harvest Mann site areaf This -may explain she pain seducing el-
ad alginate doessiram
Mims j tI corahuted a study mad mindloned that M- uer rite disoussion was ntmai with denude dressings at the tame of Messing change:. They also reported that Moracculrisiate demean elimarrated the pain nyarsilly want sated herb lirie mesh maze dressings
Ender PE A A dillYS3i reported the pain milition effects of al- ginate alteasing. Avoirchog to theta Sir afiglarate dressings re- gime pain, the beg. ,ttlects wen alained elphiste dressing moistened with isupwaraine Oiplirocidardie CA" :r -Same .9thiettS
Was WOO 16.1171d ffettinger at aP (199 ret dare asoro fIrdoiollfll effects rot alginate dressings
mu present adroit 10''' post minuttine day OS patients f ithrid removal of the dressing were Atry caw trAiects Kitit%) wane mite easy 3 cases t65l. removal is sat serr; easy and 2 CAWS
(4 art-re iddficok and on anothrt three cases the iiicessing nurse reampletely adherent to the wound bed and annuipsesi menimal inoised agonizing pan, therefore redressed and fratI11203kiti of dressings were -done in alter saner week. Mine ,Otir study shooed
that ars St tr oases removal of the &essay were msy. In a few of CAW ei deeming mere onnaplete* adherents.
&Mawr 0 at al' t 19951 was conducted A iltUdIF on alginate stkimirms oar bora patients with spit thickness Slam graft and ormfroderf that alginate dressing was snore benefit-Sid over mega gauze dressings in respect at case fin cm and hemoval and it nim lammed be the mon* personal. oftur lismings ARO support-ed the findings of hatter FE et ir 1 a9a3) for ealw of removal or alighate dressings.
tbegarting die donor rate Malang when the diremings were re-monied oft4a fle gum operative day 36 cases f."72%1 wear completed iistahrig, way aDVEte was elaillatikal edam& omit( vadiereas ran twee Mffd the Orresseng were completely adlimmit to the wound bed and healing could not he mamas& This adherent Mem* was Mit tior another cox mina titYr RtVisicierte epithelia-
Mimi Thus SAW loYeke LitAtYd Ilugt aireapicW notAlieliatlazatitim OVA&
mourned
An 72% iii AVOCA OM Ca0' post aperatare slay
Wink mimed to ralrimaz airiest& diseraing :consferatmal dress- ings trikes more than fCceicrea triaci.— itpAticriAcratitin, and An
most cases at was incumnilete. Thatswhy alginate dressing was mite beneficial than comentirma I dressings
Minogbe ffit %Nati" simargrad that 91 9t cases -were athieved complete ramithelializatiors& Pt past operative day.
Hence our study was shown. that calcium alginate dressings were better tor ease of applicinon dressing soakage. pain at donor site, ease or dresimg removal in split thickness skin gofft than comentional dressings
ihnhire Research: Science is tivrarenk and there is always a scope of improvement and change an time to come ahead_ With the progressive aim to 'MOW ahead we ate to achieve highly accurate and reliable re SIMS Thus_ rimy studv "Caves hark scopes for other researcher to de suraedring mach advanced arid varied AU order to touch the itteitglit of pariertior.
This study examined 30 subjects 311 total and data collec- tion was confined to tatC11.art alginate dressings on split thick-ness Aim straft. Thus ti tire o-esearr-hers can expand the study lay including mow narnme of subjects and use of other dressing materials sa as to rum generalization of results and practice
mob experiments Sr variable Hospital setups Thus at could he applied to mat Rh sitnatim.
Relevance to pracrictm
TM remits obtained in chis study sow st that calcium alginate dressing is some beareficial than other conventional dressing. So:. these remits have 5115KAsco that teellettina alginate dressing should he rased Mr dmerangs _ices split thickness skin grids on cionar sites of patients.
Csaiclusicic
Faiditpts II present ettuPY conducted that calcium alginate dress-ings user &RUC Rtes same quite ,easy almost painless. reinoval was easy arid minimal pAnt, ankuissal trauma to the newly epi-thelia-Med surfacr anal mite deatholsahzataon was very high era 10' post Qom Mime Mix.
&CliCidOWETAIGREEECT
We wildiontedge the immense help received hom the scholars 76.1:14tSV articles are cited and riniuded in references of this manu-script. Anthers are aloe mat/4M to authorshtlitorsipublishers of all those articles. tiontals sni books from where the literature tor this article has been reviewed and discussed.
=IMP A. Bally tS.. Ivaco Nintel ytaulaue uf Stgery. 24513 t416100 4 :4. c1;44,44i 4A14,4: -ty loyantio.a.c..151 altaal. 4:1. Colytn it, tthrtet histon of trouuti heal-
tyg Ye allAng :I 11.-tittottnity SW tA 01. A fibre bye alginyie dressing an ii.inentmtnt ul kphtlindatnys abngseEN donor sites jEur, Acad.Derzynly
Yientnal. ANS taw I Y it ZI.2,tit II 5. A:opal ac 01 .1.11.-,ttieut:, ut alptafte and anal a4ItiatIrmlairdiAmVstakag w: blauld.cpagulatua. tattl playlet tyrtnyentr 3 Be Mat, Anal 199& Jun
run . 24-21Y-7, 4 t., utici.tr Ai tipia Ali tipuite tut iteritog of parent dermal wooudrP Allyeette,Ctnutda. Viefiata lamed:nal ram alari mitten:Y-3 el CalgArt. MOO 1 7. LlYa JI, et at
tEvotlitaboy ol a ectainnati ttolenites 3ydotty) alynyny And It. :ttstlizyure yotanbrnut Ck.lailVr LIO the nunageanynt tul ettne titoYin.st sym araft donor nays. Anna Masi Sag. 2001 Apr: 454 : 405 CAS Antis:, BL. tt at Bgnattrtyn nee KYllostie 5etitatlas oval alpatatire4kamt see pam..1 Mast kg 1993 rep: atty. 0-2 -2;. 1'Y Del:ugly 0.55 al.E‘aluation at calcium tagimste for dlan scan <am, Stte, Duty Case Aftbalal IVIFY lan:141%, : Dittil.i wet Dangly. lit ,ot A 1. Mac'ro of. adlaam Cooed poi...kale as dregatag and caictura Agnate on
toe held24." tft ROW ThIckney, 9kuR grab 110nar st.e.m5oultanallyetandorntattIllon11 SetyCinr Mast 111111: 421]: 14i.] i 1
540.) LNIT7KNIVIVAVAL MIESTAL ORF WIEVICIFICIRESEMUI
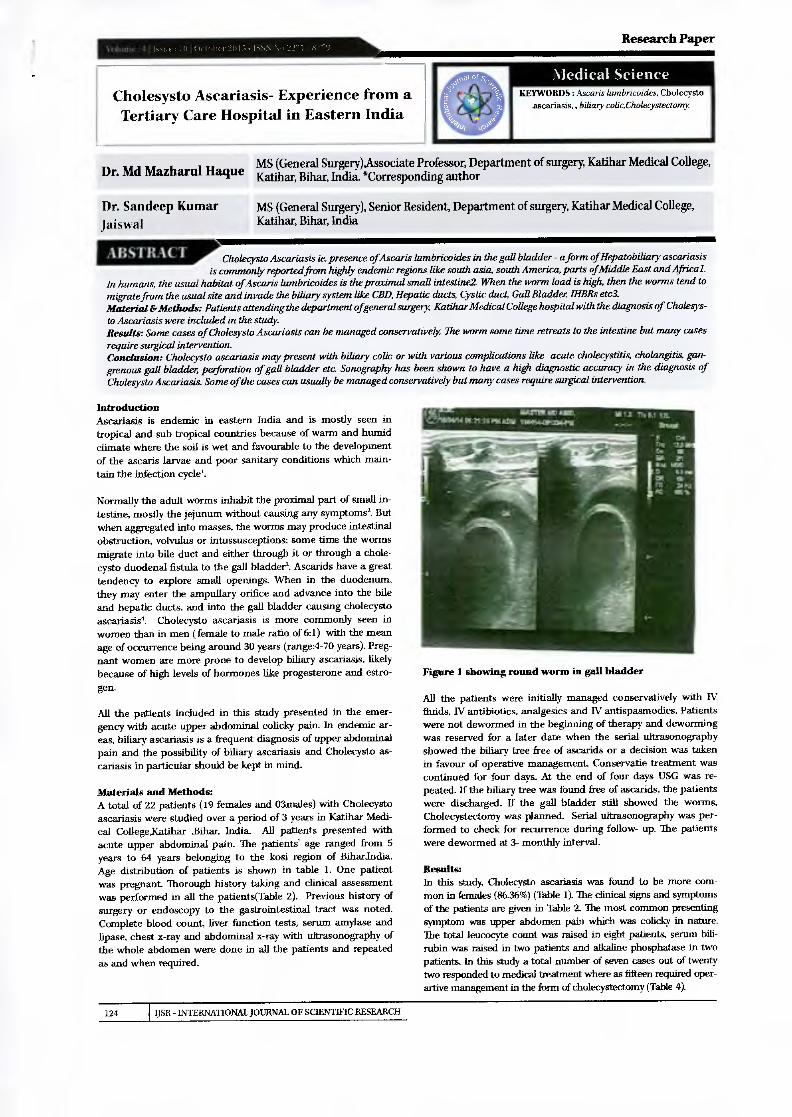
111111111=1111111111111111 Research Paper
Cholesysto Ascariasis- Experience from a Tertiary Care Hospital in Eastern India
Medical Science
KEYWORDS : Asearis lumbricoides, Cholecysto ascariasis„ biliary colic,Cholecystectomy
MS (General Surgery),Associate Professor, Department of surgery, Katihar Medical College, Dr. Md Mazhand Hague Katihar, Bihar, India. *Corresponding author
Dr. Sandeep Kumar MS (General Surgery), Senior Resident. Department of surgery, Katihar Medical College, Jaiswal Katihar, Bihar, India
Cholecysto Ascariasis ie. presence of Ascaris lumbricoides in the gall bladder - a forrn of Hepatobiliary ascariasis is commonly reported from highly endemic regions like south asia, south America, parts of Middle East and Africal.
in humans, the usual habitat of Ascaris lumbricoides is the proximal small intestine2. When the worm load is high, then the worms tend to migrate from the usual site and invade the biliary system like CBD, Hepatic ducts, Cystic duct Gall Bladder, THBRs etc3. Material &Methods: Patients attending the department ofgeneral surgery, Katihar Medical College hospital with the diagnosis of Cholesys- to Ascariasis were included in the study. Results: Some cases of Cholesysto Ascariasis can be managed conservatively The worm some time retreats to the intestine but many cases require surgical intervention. Conclusion: Cholecysto ascariasis may present with biliary colic or with various complications like acute cholecystitis, cholangitis, gan-grenous gall bladder, perforation of gall bladder etc. Sonography has been shown to have a high diagnostic accuracy in the diagnosis of Cholesysto Ascariasis. Some of the cases can usually be managed conservatively but many cases require surgical intervention.
Introduction Ascariasis is endemic in eastern India and is mostly seen in tropical and sub tropical countries because of warm and humid climate where the soil is wet and favourable to the development of the ascaris larvae and poor sanitary conditions which main-tain the infection cycle'.
Normally the adult worms inhabit the proximal part of small in-testine, mostly the jejunum without causing any symptoms'. But when aggregated into masses, the worms may produce intestinal obstruction, volvulus or intussusceptions; some time the worms migrate into bile duct and either through it or through a chole-cysto duodenal fistula to the gall bladder'. Ascarids have a great tendency to explore small openings. When in the duodenum, they may enter the ampullary orifice and advance into the bile and hepatic ducts, and into the gall bladder causing cholecysto ascariasis'. Cholecysto ascariasis is more commonly seen in women than in men ( female to male ratio of 6:1) with the mean age of occurrence being around 30 years (range:4-70 years). Preg-nant women are more prone to develop biliary ascariasis, likely because of high levels of hormones like progesterone and estro-gen.
All the patients included in this study presented in the emer-gency with acute upper abdominal colicky pain. In endemic ar-eas, biliary ascariasis is a frequent diagnosis of upper abdominal pain and the possibility of biliary ascariasis and Cholecysto as-cariasis in particular should be kept in mind.
Materials and Methods: A total of 22 patients (19 females and 03males) with Cholecysto ascariasis were studied over a period of 3 years in Katihar Medi-cal College,Katihar ,Bihar, India. All patients presented with acute upper abdominal pain. The patients age ranged from 5 years to 64 years belonging to the kosi region of BiharIndia. Age distribution of patients is shown in table 1. One patient was pregnant Thorough history taking and clinical assessment was performed in all the patients(Table 2). Previous history of surgery or endoscopy to the gastrointestinal tract was noted. Complete blood count, liver function tests, serum amylase and lipase, chest x-ray and abdominal x-ray with ultrasonography of the whole abdomen were done in all the patients and repeated as and when required.
Figure 1 showing round worm in gall bladder
All the patients were initially managed conservatively with IV W antibiotics, analgesics and IV antispasmodics. Patients
were not dewormed in the beginning of therapy and deworming was reserved for a later date when the serial ultrasonography showed the biliary tree free of ascarids or a decision was taken in favour of operative management ConservatM treatment was continued for four days. Al the end of four days USG was re-peated. If the biliary tree was found free of ascarids, the patients were discharged. If the gall bladder still showed the worms, Cholecystectomy was planned. Serial ultrasonography was per-formed to check for recurrence during follow- up. The patients were dewormed at 3- monthly interval.
Results: In this study; Cholecysto ascariasis was found to be more com-mon in females (86.36%) (Table 1). The clinical signs and symptoms of the patients are given in Table 2. The most common presenting symptom was upper abdomen pain which was colicky in nature. The total leucocyte count was raised in eight patients, serum bili-rubin was raised in two patients and alkaline phosphatase in two patients. In this study a total number of seven cases out of twenty two responded to medical treatment where as fifteen required oper-artive management in the form of cholecystectomy (Table 4).
124 USE - INTERNATIONAL JOURNAL OF SCIENTIFIC RESEARCH
Al3STRACT

Research Paper
1. Age distribution:
Age range No of male patients
No of female patients 3
Total no of patients 3 <10 0
10-20 1 2 3 21-30 0 4 4 31-40 0 4 4 41-50 1 3 4 51-60 1 2 3 61-70 0 1 1
Table 2:Clinical presentations
Symptoms/signs No ofpatients=22 Percentage
Pain right upper quadrant of abdomen 22 100
Binary colic 16 72.72
Nausea and vomiting 18 81.81
Vomiting of worms 04 18.18
Fever 13 59.09
Right upper quadrant tenderness
21 95A5
Jaundice 02 09.09
Table 3: Complications
Complications No of patients Percentage
Obstructive jaundice 02 09.09
Cholangitis 02 09.09
Acute Pancreatitis 0 00
Acute Cholecystitis 01 04.54
Discussion: In the present study, binary ascariasis was more commonly seen in the middle aged females with all presenting with acute binary symptoms. Symptoms of binary colic occur when the worm mi-grates across the papilla. If the worm remains in the bile duct and gall bladder, acute and chronic complications can occur like cholangitis, strictures, calculi, cholecystitis, perforation of gall bladder, gangrenous cholecystitis and pancreatitis etc.'. After entering the bile duct, the worms excrete various types of poly-peptides that produce allergic manifestations and cause spasm of the sphincter of Oddi by acting as chemical irritants2. The re-sultant binary stasis together with infected intestinal contents carried by the worms leads to pyogenk cholangitis, cholecysti-tis and pancreatitis' . Binary obstruction lasts only as long as a live worm remains in the binary tree; the majority of worms re-treat into the duodenum'. In contrast to the worms in the bil-iary ducts, the worms of the gall bladder do not retreat into the duodenum easily because of the anatomy of the cystic duct and the gall bladder neck. Mainstay of diagnosis is ultra sonography' which usually shows the worm in the form of Inner tube sign (round worm is seen as a thick echogenic stripe with a central anechoic tube in the gall bladder, stripe sign (thin non shadow-ing stripe without an inner tube within the gall bladder). The mobility of the worm within the gall bladder unequivocally con-firms the diagnosis. Magnetic resonance cholangio pancreatog-raphy (MRCP) may be used as another non invasive test in cases presenting with jaundice, cholangitis, pancreatitis that are not diagnosed on ultrasonography.
Approaches available for the management of cholecysto ascaria-sis are medical management and surgical intervention6. Initially the patients are managed medically for three to four days. By this time many patients become asymptomatic as the worms retreat into the duodenum. After this time period medical treat-ment is not much fruitful as complications may develop. If the patient fails to respond to medical treatment surgical interven-tion in the form of cholecystectomy is employed. In our study open cholecystectomy was done as in few cases part of the worm was in the cystic duct and in many cases pen i cholecystic adhesion was anticipated.
Table 4. Case Wise Final Treatment modality
Case No Age Sex Final Treatment Modality
05 Female Surgical Treatment
2 30 Female Medical Treatment
3 64 Female Medical Treatment
4 04 Female Surgical Treatment
5 26 Female Surgical Treatment
6 37 Female Medical Treatment
7 13 Female Surgical Treatment
8 35 Female Surgical Treatment
9 38 Female Surgical Treatment
10 28 Female Surgical Treatment
11 45 Male Medical Treatment
12 48 Female Surgical Treatment
13 29 Female Medical Treatment
14 53 Female Surgical Treatment
15 18 Female Surgical Treatment
16 42 Female Surgical Treatment
17 33 Female Medical Treatment
18 56 Male Surgical Treatment
19 08 Female Surgical Treatment
20 47 Female Medical Treatment
21 20 Male Surgical Treatment
22 55 Female Surgical Treatment
CONCLUSION Biliary ascarisis and cholecysto ascariasis in particular should be considered as a differential diagnosis of acute binary symp-toms especially in endemic areas. Ultrasonography is a useful non invasive test with a high diagnostic accuracy. Medical man-agement should be the preferred initial treatment modality and surgical treatment should be reserved for cases who do not re-spond to it.
CONSENT No special consent was taken as the treatment given was in ac-cordance with the current treatment practices in the unit.
ETHICAL APPROVAL No prior ethical approval was taken as no experimental drug or procedure was carried out in the management of this condition as highlighted in the paper
REFERENCE 1. Gonzalez Alt Regalado VC, Van den Rode J. Non-invasive management of Ascaris lumbricoides biliary tact inigrationA prospective study in 69 patients from Ecuador. Trop Med lot Health. 2001;6(2):146-50. 2. Pawlowski ZS. As,cariasis. In Warren KS, Matunoud AAP, et at editors. Tropical
and Geographical Medicine. 2nd edition. New York. McGraw- Hill. 1990;369-378. 3.Schulaman A. Lorton AJ, Hegdenrych if Abdubabaman RE Sonographic diagnosis of biliary as-cariasis. AIR Ann J Roeintgenol 1982; 139,485-459.4. Lloyd DA_ Massive hepatobiliary ascariasisin childhood_ Br J Surg 1981;68: 468-473. 5.0mar Javed Shah. Showkat Ali Zargar, Irfan Robbani. Biliary aseiniasis: a review. World J Surg 2006; 30:1500-1506. 6.Chang CC. Han CT. Biliary aseariasis in childhood. A clinical analysis of 788 cases. (lie Med J 1966; 85:167. 7.Madinunita Mukhopadhyay. Bantry ascariasis in the Indian Subcontinent a study of 42 cases. The Saudi Journal of Gastroenterology 2009:15(2): 121-124 8. Khan A. Bhowmik tiakim H, Islam M.Outcome of conservative management inbiliary ascariasis -a study of 98 ea.ses. Journal of dhaka medical college; 2010. Accessed: 17 aug, 2014
IJSR - INTERNATIONAL JOURNAL OF SCIENTIFIC RESEARCH
125

An Observation on the Significance of Prostate Specific Antigen (PSA) In Chronic Urinary
Obstruction of Prostatic Pathology
Medical Science
KEYWORDS: Prostate, Benign, Malig- nant, Prostate Specific Antigen, Adeno-
carcinoma.
PSA level 4-10 ng/ml PSA level more than 10 ng/mL According to the histopathological reports patients were divided in to two groups
Benign prostatic hypertrophy Carcinoma of prostate
190 patients out of 200 were diagnosed to have benign prostatic hypertrophy (BPH) and 10 patients with adenocarcinoma of prostate.
The data was analyzed for sensitivity, specificity, positive and negative predictive values of PSA study in prostatic disease.
Results: The patients in the study ranged from 41 years to 80 years of age with maximum patients belonging to 6th to 8th decades of life. The aim of this study was to analyze the levels of serum PSA value in prostatic pathology causing chronic urinary obstruction and to correlate this value with carcinomatous and non carcino-matous prostate. Table 1 shows the distribution of patients in re-spect to Prostate Specific Antigen (PSA )in the study group.
Group Serum PSA (ng/ml) Number of patients
1 <4 116
2 4-- 10 77
3 >10 07
Tablet-- Distribution of patients in respect to Prostate Spe-cific Antigen.
Research Paper
MS (General Surgery), Senior Resident, Department of surgery, Katihar Medical College, Katihar, Bihar, India. Sandeep Kumar Jaiswal
MS (General Surgery), Associate Professor, Department of surgery, Katihar Medical College, Katihar, Bihar, India
Md Mazharul Hague
Junior Resident, Department of surgery, Katihar Medical College, Katihar, Bihar, India. Nigar Perveen
Junior Resident, Department of surgery, Katihar Medical College, Katihar, Bihar, India. Rakhi Kumari Saw
Junior Resident, Department of surgery, Katihar Medical College, Katihar, Bihar, India. Jayesh Kumar
Chronic urinary obstruction due to prostatic pathology (Benign prostatic hypertrophy & Carcinoma of Prostate ) is a very common clinical entity. Most clinicians utilize the measurement of serum PSA as the base line screening to
differentiate between BPH &Carcinoma qfProstate in patients presenting with chronic urinary obstruction of prostatic pathology as it is a simple test to perform. In recent years, prostate specific antigen (PSA) has es-tablished itself as the most useful marker for adenocarci-noma of the prostate and has almost replaced the total acid phosphatase and prostatic acid phosphatase (PAP) for screening diagnosing and monitoring the prostate car-cinoma patients. The PSA levels also rise in benign hyper-plasia of prostate (BPH) but to a lesser extent and high values are usually diagnostic of malignant disease. The present investigation was conducted to study the relevance PSA in prostatic dis-,ease particularly in the context of hospitalized patients with retention of urine. In this study 200 cases of urinary obstruction due to prostatic pathology were studied. They were evaluated with a combination ofDRE, trans abdominal ultrasound and measurement of serum PSA and results correlated with histological findings of the operated specimens. 190 patients were diagnosed with BPH and 10 with adenocarcinoma of prostate. Serum PSA had sensitivity of 909( in detecting Ca Prostate when the level of serum PSA was greater than 4ng/ml. In the range less than 4ng/m1 it had a sensitivity of 60.52% in detection of BPH. In this study we infer that serum PSA is a good marker for diagnosis and differentiation between benign and malignant diseases of prostate.
Introduction: Benign hyperplasia of prostate (BPH) is a common disease in men above 60 years of age, whereas its malignant counterpart, carcinoma of prostate, is the leading cause of mortality amongst all the carcinoma in men. Prostate specific antigen (PSA) has been used for early screening and detection of prostate carci-noma in high risk group although its role in staging the carci-noma has been doubtful. It was first identified by Wang et al. It is a 237-amino acid monomeric serine protease, with a mo-lecular weight of 33-34 kilodaltons. It has been regarded as the best marker for prostate malignancy in recent years, although its plasma concentration also increases in BPH, but to a lesser extent. Since a majority of the prostate patients come to the hospital after urinary retention and catheterization, the levels of this marker may be falsely elevated in these patients. This study was done to see the effect of urinary retention on plasma con-centration of PSA in prostatic disease.
Materials and Methods: The present study was conducted in the department of Surgery, Katihar Medical College, Katihar. The material for the present study consisted of 200 patients of chronic urinary obstruction due to prostatic pathology, who attended the surgical outdoor and admitted in different units of the department of surgery Katihar Medical College Katihar. The criteria of inclusion were presence of features of chronic urinary obstruction with pros-tatism and aged 41 years and above. Detailed clinical history was taken. The sera samples were collected from the included patients before doing digital rectal examination. Sera samples were sent for PSA study. The biopsy or the tissue collected after transuretbral resection of prostate (TUFtP) were sent for histo-pathological examination.
ABSTRACT
According to the PSA level patients were categorized in three groups.
PSA level less than 4 ng/ml
In this study out of 200 patients 116 (58%) had PSA less than 4ng/ml, 77 (38.5% ) had PSA between 4 - 10 ng/ml and 07 (3.5% ) had PSA greater than 1 Ong/mL Table 2 (A, BSc C ) shows the serum PSA level with respect to patients having benign prostatic hypertrophy ( BPH ) and carcinoma of prostate.
IJSR - INTERNATIONAL JOURNAL OF SCIENTIFIC RESEARCH 335

Research Paper Volume :4 I Issue : 11 I November 2015 ISSN No 2277 -8179
Table 2 ( A ) : A
PSA (ng/ml) Carcinoma Total
<4 1 tis 116
4-10 4 73 77
>10 5 2 07
Table 2(B ) :
PSA (ng/ml) Carcinoma BPH Total
<4 1 ( c ) 115(4) 116
>4 9 ( a ) 75(b) 84
Sensitivity of PSA >4 ng/ml in cancer detection = a / a+c.1.00 = 9 / 9 + 1 *100 = 90%
Specificity of PSA >4 ng/ml in cancer detection = d / b+d*100 = 115 / 75+ 115*100 = 60.52%
Positive predictive value of PSA >4 ng/ml in cancer detection a/a+115100
= 9 / 9 + 75100 = 10.71 %
Negative predictive value of PSA >4 ng/ml in cancer detection = d lb + d*100
= 115/75+1151.00 = 60.52 %
Table 2 (C ) :
PSA (ng/ml) Diseased Non Diseased Total
<4 115 (a ) I ( b ) 116
>4 75(c) 9 ( d 1 84
Sensitivity of PSA <4ng/m1 in BP14 detection = a / c5100 = 115 / 115+75 = 60.52%
Specificity of PSA <4ng/m1 in BPH detection = d / b + &WO = 9 / 1+ 9*100 = 90 %
Positive predictive value of PSA <4ng/m1 in BPH detection = a / a + b5100
Discussion: With the advent of PSA in clinical practice the rate of diagnos-ing localized prostate cancer and / or prostate cancer in early stage has got a surge and at the same time incidence of regional and metastatic prostate cancer has declined. (Mettlin et al 1996 ).PSA has such a profound impact on prostate cancer screening that concern has arisen that it may detect and subsequently re-sult in the treatment of clinically insignificant tumours. ln the present study, sensitivity of PSA greater than 4 ng/ml in detec-tion of prostate cancer was 90 % and positive predictive value was 10.71 %. Positive predictive value of PSA greater than4 ng/ ml was calculated by various workers. Labrie et al (1992 ) found it to be 33 9kBrawer et al (1992 ) 31 % and Catalona et al (1994 ) 28-35 %. Brawer et al (1992 ), Catalona et al (1994 ) and Stone et al (1994 ) concluded that the approximate chance of carcino-ma prostate is one in three when PSA is between 4 - 10 ng/ml and one in two when PSA is greater than 10 ng/ml. In our study. in PSA range 4 - 10 ng/ml, 4 patients out of 77 had carcinoma prostate. In PSA greater than10 ng/ml, 5 out of 7 had carcinoma. This anomalous result may be due to less number of patients with carcinoma of prostate in this study. In PSA range 4- 10 ng/ ml, 73 out of 77had BPH whereas in the range greater than 10 ng/m1 two out of seven had BPH. In PSA range <4 ng/ml out of 116. one patient had carcinoma and 115 had BPH. In PSA range >4 ng/ml, out of 84, nine patients had carcinoma prostate and 75 had BPH. Findings of our study were broadly in conformity of the various workers from various parts of the world.
Conclusion: Chronic urinary obstruction due to prostatic pathology (Benign prostatic hypertrophy & Carcinoma of Prostate) is a very com-mon clinical entity. hi recent years, prostate specific antigen (PSA) has established itself as the most useful marker for screen-ing, diagnosing and monitoring the prostate carcinoma patients. In our study 200 patients of chronic urinary obstruction due to prostatic pathology were evaluated. The serum PSA levels were evaluated and correlated with the histopathological findings of biopsied or operated specimens of their prostates to find out the relevance of PSA study. It was found that serum PSA level cor-related well with the prostatic pathology. It had sensitivity of 90 % in detecting carcinoma of prostate when the level was greater than 4ng/ml. In the range less than 4ng/m1 it had a sensitivity of 60.52 % in detection of BPH. We conclude that serum PSA is a very good marker in detecting prostatic disease and also to dif-ferentiate between benign and malignant diseases of prostate.
= 115 /115 +rim = 99.13%
Negative predictive value of PSA <4ng/m1 in BPH detection = d / b + d5100
= 9 / 1 + 9.100 =90 96
REFERENCE lArriatage TO. Cooper EH, Newling WW at al- The value of measurement of serum PSA in patients with BPI) and untreated prostate cancer. Br J Urol 1998 ; 62: 584 I 2. Balk SP, Kom YJ, Bubley GJ- Biology of prostate specific antigen.). Cfin.Oncol. 2003; 21 (2) 383-91. I 3. 13rasver MK, Chetner
MP,Beatie J et al - Screening of prostate carcinoma with prostate specific antigen . J Urol 1992, 147 841-5.1 4. Carter H13, Pearson JD, Metter EJ.- Longitudinal evaluation of prostate specific antigen levels in men with and without prostate disease. JAMA 1992;151(4 1283-90 I 5. Catalona WI Smith D ,Ornstien D. - Prostate cancer detection in men with serum PSA concentration of 2.6 10 4.0 righail and prostate escunination.JAMA 1997:277(18): 1452-5 1 6. Ellis WI, Chetner MR Preston SD et al - Diagnosis of prostatic carcinoma The yield of serum PS& digital examination and trans rectal USG- J Um!. 1994; 152: 1520-25 1 7. Gann PH.Henuelcens CH. Stampfer MJ: A p oveitive evaluation of plasma PSA for detection of prostate cancer -AMA .1995: 272(41: 289-294 Is. Grammaticos P- Diagnostic and prognostic value of serum PSA in prostatic carcinoma -Hell J. NUel Med. 2004:7(3): 146-8 19- Mettin CJ, Murphy GP. Ho IC et al- The national cancer database report on longitudinal observation of prostate cancer. - 1996; 77 (10): 2162-661 10. Yin M. Bastcky S. ChandranU et al- Preva-lence of incidental prostate cancer in the general population: A study of healthy organ donors. J Urol 2008; 179:892 1
336 IJSR - INTERNATIONAL JOURNAL OF SCIENTIFIC RESEARCH

Volume-4, Issue-10, Oct-2015 • ISSN No 2277- 8160
Medical science
Dr. Md Mazharul Hague
MS (General Surgery),Associate Professor, Department of surgery, Katihar Medical College, Katihar, Bihar, India.*Corresponding author
Dr. Sandeep Kumar Jaiswal
MS (General Surgery), Senior Resident, Department of surgery, Katihar Medical College, Katihar, Bihar, India.
Dr Md lzhar Alam MD (Pathology), Assistant Professor, Department of Pathology, Katihar .
Medical College, Katihar, Bihar, India.
Introduction: With increased awareness among the patients and advancement in diagnostic techniques most of the diseases of gall bladder present to the clinician early and carcinoma of the gall bladder which has high mortality and very poor prognosis is usually diagnosed as an incidental finding on histopathological examination.
Methods & Materials: Patients undergoing cholecystectomy for benign diseases at a private hospital in the kosi region of Bihar, India.
Results: Out of 690 patients in whom cholecystectomy was done adenocarcinoma was detected histopathologically in 6 cases (0.87%). There was no suspicion of malignancy to any of them preoperatively.
Conclusion: In the present study the rate of incidental carcinoma of gallbladder was 0.8796. The risk factors related to gall bladder cancer are cholelithiasis, advance age etc. Upon final diagnosis of adenocarcinoma of gall bladder the patients were referred to higher centre of oncology for further treatment. All the patients whose histopathological examination showed adenocarcinoma were operated for cholelithiasis. Therefore the diagnosis of cholelithiasis is an indication for cholecystectomy.
KEYWORDS : Gallbladder, Cholelithiasis, Incidental, Carcinoma.
Research Paper
Study of Incidental carcinoma of gall bladder in benign gall bladder disease
Introduction: In the Kosi region of Bihar, India benign gall bladder disease especial-ly cholelithiasis is quite common and the occurrence of gall bladder cancer is not so uncommon. With increased awareness among the patients and advancement in diagnostic techniques most of the dis-eases of gall bladder present to the clinician early and carcinoma of the gall bladder which has high mortality and very poor prognosis is usually diagnosed as an incidental finding on histopathological exam-ination. In this present study we tried to establish the overall rate of gall bladder cancer in the patients presenting with benign gall blad-der disease based on our experience.
Methods & Materials: From August 2008 to July 2015 a total of 690 patients underwent chol-ecystectomy at a private hospital in the Kosi region of Bihar, India. We retrospectively reviewed the clinical records of all the 690 patients. There were 605 female and 85 male patients. Three patients were operated for gall bladder polyp whereas the rest 687 were operated for cholelithiasis. None of these cases had preoperative suspicion of malignancy.
Results: Out of 690 patients in whom cholecystectomy was done adenocarcino-ma was detected histopathologically in 6 cases (0.87%).There were five females (83.3%) and one male(i 6.67%) patient. Mean age of the patients was around 49 years. All the patients whose histopathological examina-tion showed adenocarcinoma were operated for cholelithiasis. Per opera-tively in one case the mucosa of the gall bladder showed a small nodule. The clinical data and follow-up are presented in Table 1.
Discussion: Gallbladder carcinoma is a highly malignant tumour and has poor prognosis. De Stall- [17711 was the first one to report gall bladder car-cinoma1. It is the fifth most common malignancy of gastrointestinal tract and the most common of the biliary tree and is usually discov-ered accidentally2. The exact etiology is unknown. The most com-mon risk factor is cholelithiasis. It is more common in females and its frequency increases with age3. The other risk factors are benign tu-mours, certain races, various carcinogens, abnormal union of pancrea-ticobiliary duct etc. Gall bladder carcinoma is diagnosed histologically in 0.3 to 1.5%4of all the cholecystectomy specimens. In our study the overall rate was 0.87%.The rate of incidentally diagnosed gall blad-der carcinoma has increased because of patient awareness, increased health facilities and advancement in diagnostic tools and techniques. Most of the cases in our study were diagnosed by histopatholgical examination. Only in one case the operated specimen had shown a suspicious small nodule on the mucosa.
Conclusion: Gall bladder carcinoma nowadays is most commonly detected inci-dentally. In the present study the rate of incidental carcinoma of gall-bladder was 0.87%. The risk factors widely related to the gallbladder cancer are advanced age and cholelithiasis. All the patients whose histopathological examination showed adenocarcinoma were oper-ated for cholelithiasis. Therefore the diagnosis of cholelithiasis is an indication for cholecystectomy.
Age (Yrs) Sex Symptoms & signs Ultrasonography Operative Finding Histopathological finding Suspicious operative finding
52 Female Pain Abdomen ' Fever cholelithiasts
h. C olelithiasis,Thickwalled GB,Adhesion at the neck
Moderately differentiated adenocarcinoma extending through serosa,Chr. Cholecystitis.
No
GJRA - GLOBAL JOURNAL FOR RESEARCH ANALYSIS e4 199
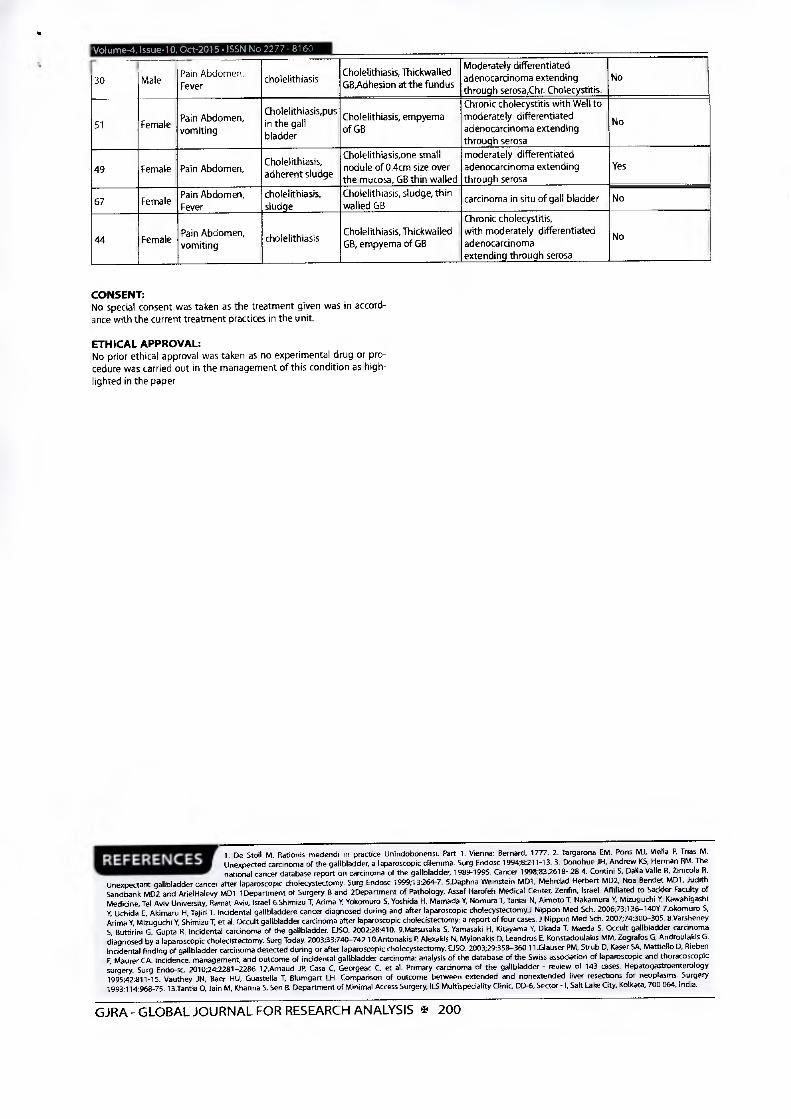
Volume-4, Issue-10, Oct-2015 .1SSN No 2277 - 8160
30 Male Pain Abdomen' Fever
cholelithiasis Cholelithiasis, Thickwalled GB,Adhesion at the fundus
Moderately differentiated adenocarcinoma extending through serosa,Chr. Cholecystitis.
No
51 Female Pain Abdomen' vomiting
Cholelithiasis pus ' in the gall bladder
Cholelithiasis, empyema of GB
Chronic cholecystitis with Well to moderately differentiated adenocarcinoma extending through serosa
No
49 Female Pain Abdomen, Cholelithiasis, adherent sludge
Cholelithiasis,one small nodule of 0.4cm size over the mucosa, GB thin walled
moderately differentiated adenocarcinoma extending through serosa
Yes
67 Female Pain Abdomen, Fever
cholelithiasis, sludge
Cholelithiasis, sludge, thin walled GB
carcinoma in situ of gall bladder No
44 Female Pain Abdomen' vomiting cholelithiasis
Cholelithiasis, Thickwalled GB, empyema of GB
Chronic cholecystitis, with moderately differentiated adenocarcinoma extending through serosa
No
CONSENT: No special consent was taken as the treatment given was in accord-ance with the current treatment practices in the unit.
ETHICAL APPROVAL: No prior ethical approval was taken as no experimental drug or pro-cedure was carried out in the management of this condition as high-lighted in the paper
1. De Stoll M. Rationis rnedendi in practice Unindobonensi. Part 1. Vienna: Bernard, 1777.2. Targarona EM, Pons Mi, Viella P. Trias M. Unexpected carcinoma of the gallbladder, a laparoscopic dilemma. Surg Endosc 1994;8213-13. 3. Donohue ill, Andrew KS, Herman RM. The national cancer database report on carcinoma of the gallbladder, 1989-1995. Cancer 19981832618- 28 4. Corrtini S. Dalla Valle R, Zinicola R.
Unexpectant gallbladder cancer after laparoscopic cholecystectomy. Sorg Endosc 1999113264-7. 5.Daphna Weinstein MD1, Mehrdad Herbert MD2, Non Bendet MD1, Judith Sandbank M02 and ArielHalevy M01 1Department of Surgery B and 2Department of Pathology, Assaf Harofeh Medical Center, Zerifin, Israel. Affiliated to Sackler Faculty of Medicine, Tel Aviv University, Ramat Aviv, Israel 6.Shimizu 7, Arima Y, Yokomuro S, Yoshida H, Mamada Y, Nomura T, Taniai N, Airnoto T, Nakamura Y. Mizuguchi Y, Kawahigashi V. Uchida E, Akimaru H, Tajiri T. Incidental gallbladdere cancer diagnosed during and after laparoscopic cholecystectomyJ Nippon Med Sch. 2006;73:136-140Y 7.okomuro 5, Arirna Y, Mizuguchi Y, Shimizu T, et al. Occult gallbladder carcinoma after laparoscopic cholecistectomy: a report of four cases. Nippon Med Sch, 2007;74:300-305. 8.Varsheney 5, Buttirini 0, Gupta R. Incidental carcinoma of the gallbladder. EEO. 2002128:410. 9.Matsusaka 5, Yamasaki H, Kitayarna V. Okada T, Maeda S. Occult gallbladder carcinoma diagnosed by a laparoscopic cholecistectomy. Sorg Today. 2003;33:740-742 10.Antonakis P. Alexakis N, Mylonakis D, Leandros E, Konstadoulakis MM, Zografos 0, Androulakis G. Incidental finding of gallbladder carcinoma detected during or after laparoscopic cholecystectomy. DSO. 200329:358-360 11.01auser PM, Strub D, Kuser SA, Mattiello D, Rieben F, Maurer CA. Incidence, management, and outcome of incidental gallbladder carcinoma: analysis of the database of the Swiss association of laparoscopic and thoracoscopic surgery. Surg Endo-sc. 2010242281-2286 12Arnaud JP, Casa C, Georgeac C, et al. Primary carcinoma of the gallbladder - review of 143 cases. Hepatogastroenterology 199542811-15. Vauthey JN, Baer HU, Guastella 7, Blumgart LH. Comparison of outcome between extended and nonextended liver resections for neoplasms. Surgery 1993;114:968-75. 13.Tantia 0, Jain M, Khanna 5, Sen B. Department of Minimal Access Surgery, ILS Multispeciality Clinic, 00-6, Sector - I, Salt Lake City, Kolkata, 700 064, India.
GJRA - GLOBAL JOURNAL FOR RESEARCH ANALYSIS E 200

124 IJSR - INTERNATIONAL JOURNAL OF SCIENTIFIC RESEARCH
Volume : 4 | Issue : 10 | October 2015 • ISSN No 2277 - 8179Research Paper
Medical Science
Dr. Md Mazharul Haque MS (General Surgery),Associate Professor, Department of surgery, Katihar Medical College, Katihar, Bihar, India. *Corresponding author
Dr. Sandeep Kumar Jaiswal
MS (General Surgery), Senior Resident, Department of surgery, Katihar Medical College, Katihar, Bihar, India
Cholesysto Ascariasis- Experience from a Tertiary Care Hospital in Eastern India
KEYWORDS : Ascaris lumbricoides, Cholecysto ascariasis, , biliary colic,Cholecystectomy.
ABSTRACT Cholecysto Ascariasis ie. presence of Ascaris lumbricoides in the gall bladder - a form of Hepatobiliary ascariasis is commonly reported from highly endemic regions like south asia, south America, parts of Middle East and Africa1.
In humans, the usual habitat of Ascaris lumbricoides is the proximal small intestine2. When the worm load is high, then the worms tend to migrate from the usual site and invade the biliary system like CBD, Hepatic ducts, Cystic duct, Gall Bladder, IHBRs etc3. Material & Methods: Patients attending the department of general surgery, Katihar Medical College hospital with the diagnosis of Cholesys-to Ascariasis were included in the study.Results: Some cases of Cholesysto Ascariasis can be managed conservatively. The worm some time retreats to the intestine but many cases require surgical intervention.Conclusion: Cholecysto ascariasis may present with biliary colic or with various complications like acute cholecystitis, cholangitis, gan-grenous gall bladder, perforation of gall bladder etc. Sonography has been shown to have a high diagnostic accuracy in the diagnosis of Cholesysto Ascariasis. Some of the cases can usually be managed conservatively but many cases require surgical intervention.
Introduction Ascariasis is endemic in eastern India and is mostly seen in tropical and sub tropical countries because of warm and humid climate where the soil is wet and favourable to the development of the ascaris larvae and poor sanitary conditions which main-tain the infection cycle1.
Normally the adult worms inhabit the proximal part of small in-testine, mostly the jejunum without causing any symptoms2. But when aggregated into masses, the worms may produce intestinal obstruction, volvulus or intussusceptions; some time the worms migrate into bile duct and either through it or through a chole-cysto duodenal fistula to the gall bladder2. Ascarids have a great tendency to explore small openings. When in the duodenum, they may enter the ampullary orifice and advance into the bile and hepatic ducts, and into the gall bladder causing cholecysto ascariasis4. Cholecysto ascariasis is more commonly seen in women than in men ( female to male ratio of 6:1) with the mean age of occurrence being around 30 years (range:4-70 years). Preg-nant women are more prone to develop biliary ascariasis, likely because of high levels of hormones like progesterone and estro-gen.
All the patients included in this study presented in the emer-gency with acute upper abdominal colicky pain. In endemic ar-eas, biliary ascariasis is a frequent diagnosis of upper abdominal pain and the possibility of biliary ascariasis and Cholecysto as-cariasis in particular should be kept in mind.
Materials and Methods: A total of 22 patients (19 females and 03males) with Cholecysto ascariasis were studied over a period of 3 years in Katihar Medi-cal College,Katihar ,Bihar, India. All patients presented with acute upper abdominal pain. The patients’ age ranged from 5 years to 64 years belonging to the kosi region of Bihar,India. Age distribution of patients is shown in table 1. One patient was pregnant. Thorough history taking and clinical assessment was performed in all the patients(Table 2). Previous history of surgery or endoscopy to the gastrointestinal tract was noted. Complete blood count, liver function tests, serum amylase and lipase, chest x-ray and abdominal x-ray with ultrasonography of the whole abdomen were done in all the patients and repeated as and when required.
Figure 1 showing round worm in gall bladder All the patients were initially managed conservatively with IV fluids, IV antibiotics, analgesics and IV antispasmodics. Patients were not dewormed in the beginning of therapy and deworming was reserved for a later date when the serial ultrasonography showed the biliary tree free of ascarids or a decision was taken in favour of operative management. Conservatie treatment was continued for four days. At the end of four days USG was re-peated. If the biliary tree was found free of ascarids, the patients were discharged. If the gall bladder still showed the worms, Cholecystectomy was planned. Serial ultrasonography was per-formed to check for recurrence during follow- up. The patients were dewormed at 3- monthly interval.
Results: In this study, Cholecysto ascariasis was found to be more com-mon in females (86.36%) (Table 1). The clinical signs and symptoms of the patients are given in Table 2. The most common presenting symptom was upper abdomen pain which was colicky in nature. The total leucocyte count was raised in eight patients, serum bili-rubin was raised in two patients and alkaline phosphatase in two patients. In this study a total number of seven cases out of twenty two responded to medical treatment where as fifteen required oper-artive management in the form of cholecystectomy (Table 4).

IJSR - INTERNATIONAL JOURNAL OF SCIENTIFIC RESEARCH 125
Volume : 4 | Issue : 10 | October 2015 • ISSN No 2277 - 8179Research Paper
1. Age distribution:
Age range No of male patients
No of female patients
Total no of patients
<10 0 3 310- 20 1 2 321-30 0 4 431-40 0 4 441-50 1 3 451-60 1 2 361-70 0 1 1
Table 2:Clinical presentations
Symptoms/signs No ofpatients=22 PercentagePain right upper quadrant of abdomen 22 100
Biliary colic 16 72.72Nausea and vomiting 18 81.81Vomiting of worms 04 18.18Fever 13 59.09Right upper quadrant tenderness 21 95.45
Jaundice 02 09.09
Table 3: Complications
Complications No of patients Percentage
Obstructive jaundice 02 09.09
Cholangitis 02 09.09
Acute Pancreatitis 0 00
Acute Cholecystitis 01 04.54
Discussion: In the present study, biliary ascariasis was more commonly seen in the middle aged females with all presenting with acute biliary symptoms. Symptoms of biliary colic occur when the worm mi-grates across the papilla. If the worm remains in the bile duct and gall bladder, acute and chronic complications can occur like cholangitis, strictures, calculi, cholecystitis, perforation of gall bladder, gangrenous cholecystitis and pancreatitis etc7. After entering the bile duct, the worms excrete various types of poly-peptides that produce allergic manifestations and cause spasm of the sphincter of Oddi by acting as chemical irritants2. The re-sultant biliary stasis together with infected intestinal contents carried by the worms leads to pyogenic cholangitis, cholecysti-tis and pancreatitis7 . Biliary obstruction lasts only as long as a live worm remains in the biliary tree; the majority of worms re-treat into the duodenum8. In contrast to the worms in the bil-iary ducts, the worms of the gall bladder do not retreat into the duodenum easily because of the anatomy of the cystic duct and the gall bladder neck. Mainstay of diagnosis is ultra sonography3 which usually shows the worm in the form of Inner tube sign (round worm is seen as a thick echogenic stripe with a central anechoic tube in the gall bladder, stripe sign (thin non shadow-ing stripe without an inner tube within the gall bladder). The mobility of the worm within the gall bladder unequivocally con-firms the diagnosis. Magnetic resonance cholangio pancreatog-raphy (MRCP) may be used as another non invasive test in cases presenting with jaundice, cholangitis, pancreatitis that are not diagnosed on ultrasonography.
REFERENCE1. González AH, Regalado VC, Van den Ende J. Non-invasive management of Ascaris lumbricoides biliary tact migration:A prospective study in 69 patients from Ecuador. Trop Med Int Health. 2001;6(2):146-50. 2. Pawlowski ZS. Ascariasis. In Warren KS, Mahmoud AAF, et al editors. Tropical
and Geographical Medicine, 2nd edition, New York, McGraw- Hill, 1990;369-378. 3.Schulaman A, Loxton AJ, Hegdenrych JJ, Abdulrahaman KE. Sonographic diagnosis of biliary as-cariasis. AJR Am J Roentgenol 1982; 139:485-489. 4. Lloyd DA. Massive hepatobiliary ascariasisin childhood. Br J Surg 1981;68: 468-473. 5.Omar Javed Shah, Showkat Ali Zargar, Irfan Robbani. Biliary ascariasis: a review. World J Surg 2006; 30:1500-1506. 6.Chang CC, Han CT. Biliary ascariasis in childhood. A clinical analysis of 788 cases. Clin Med J 1966; 85:167. 7.Madhumita Mukhopadhyay. Biliary ascariasis in the Indian Subcontinent: a study of 42 cases. The Saudi Journal of Gastroenterology 2009;15(2): 121-124 8. Khan A, Bhowmik B, Hakim H, Islam M.Outcome of conservative management inbiliary ascariasis - a study of 98 cases. Journal of dhaka medical college; 2010. Accessed: 17 aug. 2014
Approaches available for the management of cholecysto ascaria-sis are medical management and surgical intervention6. Initially the patients are managed medically for three to four days. By this time many patients become asymptomatic as the worms retreat into the duodenum. After this time period medical treat-ment is not much fruitful as complications may develop. If the patient fails to respond to medical treatment surgical interven-tion in the form of cholecystectomy is employed. In our study open cholecystectomy was done as in few cases part of the worm was in the cystic duct and in many cases peri cholecystic adhesion was anticipated.
Table 4. Case Wise Final Treatment modality
Case No Age Sex Final Treatment Modality1 05 Female Surgical Treatment2 30 Female Medical Treatment3 64 Female Medical Treatment4 04 Female Surgical Treatment5 26 Female Surgical Treatment6 37 Female Medical Treatment7 13 Female Surgical Treatment8 35 Female Surgical Treatment9 38 Female Surgical Treatment10 28 Female Surgical Treatment11 45 Male Medical Treatment12 48 Female Surgical Treatment13 29 Female Medical Treatment14 53 Female Surgical Treatment15 18 Female Surgical Treatment16 42 Female Surgical Treatment17 33 Female Medical Treatment18 56 Male Surgical Treatment19 08 Female Surgical Treatment20 47 Female Medical Treatment21 20 Male Surgical Treatment22 55 Female Surgical Treatment
CONCLUSIONBiliary ascarisis and cholecysto ascariasis in particular should be considered as a differential diagnosis of acute biliary symp-toms especially in endemic areas. Ultrasonography is a useful non invasive test with a high diagnostic accuracy. Medical man-agement should be the preferred initial treatment modality and surgical treatment should be reserved for cases who do not re-spond to it.
CONSENTNo special consent was taken as the treatment given was in ac-cordance with the current treatment practices in the unit.
ETHICAL APPROVALNo prior ethical approval was taken as no experimental drug or procedure was carried out in the management of this condition as highlighted in the paper

IJSR - INTERNATIONAL JOURNAL OF SCIENTIFIC RESEARCH 335
Volume : 4 | Issue : 11 | November 2015 • ISSN No 2277 - 8179Research Paper
Medical Science
Sandeep Kumar Jaiswal MS (General Surgery), Senior Resident, Department of surgery, Katihar Medical College, Katihar, Bihar, India.
Md Mazharul Haque MS (General Surgery), Associate Professor, Department of surgery, Katihar Medical College, Katihar, Bihar, India.
Nigar Perveen Junior Resident, Department of surgery, Katihar Medical College, Katihar, Bihar, India.
Rakhi Kumari Saw Junior Resident, Department of surgery, Katihar Medical College, Katihar, Bihar, India.
Jayesh Kumar Junior Resident, Department of surgery, Katihar Medical College, Katihar, Bihar, India.
An Observation on the Significance of Prostate Specific Antigen (PSA) In Chronic Urinary
Obstruction of Prostatic Pathology
KEYWORDS : Prostate, Benign, Malig-nant, Prostate Specific Antigen, Adeno-
carcinoma.
ABSTRACT Chronic urinary obstruction due to prostatic pathology (Benign prostatic hypertrophy & Carcinoma of Prostate ) is a very common clinical entity. Most clinicians utilize the measurement of serum PSA as the base line screening to
differentiate between BPH &Carcinoma of Prostate in patients presenting with chronic urinary obstruction of prostatic pathology as it is a simple test to perform. In recent years, prostate specific antigen (PSA) has es¬tablished itself as the most useful marker for adenocarci¬noma of the prostate and has almost replaced the total acid phosphatase and prostatic acid phosphatase (PAP) for screening, diagnosing and monitoring the prostate car-cinoma patients. The PSA levels also rise in benign hyper¬plasia of prostate (BPH) but to a lesser extent and high values are usually diagnostic of malignant disease. The present investigation was conducted to study the relevance PSA in prostatic dis¬ease particularly in the context of hospitalized patients with retention of urine. In this study 200 cases of urinary obstruction due to prostatic pathology were studied. They were evaluated with a combination of DRE, trans abdominal ultrasound and measurement of serum PSA and results correlated with histological findings of the operated specimens. 190 patients were diagnosed with BPH and 10 with adenocarcinoma of prostate. Serum PSA had sensitivity of 90% in detecting Ca Prostate when the level of serum PSA was greater than 4ng/ml. In the range less than 4ng/ml it had a sensitivity of 60.52% in detection of BPH. In this study we infer that serum PSA is a good marker for diagnosis and differentiation between benign and malignant diseases of prostate.
Introduction:Benign hyperplasia of prostate (BPH) is a common disease in men above 60 years of age, whereas its malignant counterpart, carcinoma of prostate, is the leading cause of mortality amongst all the carcinoma in men. Prostate specific antigen (PSA) has been used for early screening and detection of prostate carci-noma in high risk group although its role in staging the carci-noma has been doubtful. It was first identified by Wang et al. It is a 237-amino acid monomeric serine protease, with a mo-lecular weight of 33-34 kilodaltons. It has been regarded as the best marker for prostate malignancy in recent years, although its plasma concentration also increases in BPH, but to a lesser extent. Since a majority of the prostate patients come to the hospital after urinary retention and catheterization, the levels of this marker may be falsely elevated in these patients. This study was done to see the effect of urinary retention on plasma con-centration of PSA in prostatic disease.
Materials and Methods:The present study was conducted in the department of Surgery, Katihar Medical College, Katihar. The material for the present study consisted of 200 patients of chronic urinary obstruction due to prostatic pathology, who attended the surgical outdoor and admitted in different units of the department of surgery, Katihar Medical College, Katihar. The criteria of inclusion were presence of features of chronic urinary obstruction with pros-tatism and aged 41 years and above. Detailed clinical history was taken. The sera samples were collected from the included patients before doing digital rectal examination. Sera samples were sent for PSA study. The biopsy or the tissue collected after transurethral resection of prostate (TURP) were sent for histo-pathological examination.
According to the PSA level patients were categorized in three groups.
PSA level less than 4 ng/ml
PSA level 4-10 ng/mlPSA level more than 10 ng/ml.According to the histopathological reports patients were divided in to two groups
Benign prostatic hypertrophyCarcinoma of prostate
190 patients out of 200 were diagnosed to have benign prostatic hypertrophy (BPH) and 10 patients with adenocarcinoma of prostate.
The data was analyzed for sensitivity, specificity, positive and negative predictive values of PSA study in prostatic disease.
Results:The patients in the study ranged from 41 years to 80 years of age with maximum patients belonging to 6th to 8th decades of life. The aim of this study was to analyze the levels of serum PSA value in prostatic pathology causing chronic urinary obstruction and to correlate this value with carcinomatous and non carcino-matous prostate. Table 1 shows the distribution of patients in re-spect to Prostate Specific Antigen (PSA )in the study group.
Group Serum PSA (ng/ml) Number of patients
1 <4 116
2 4- 10 77
3 >10 07
Table1- Distribution of patients in respect to Prostate Spe-cific Antigen. In this study out of 200 patients 116 (58%) had PSA less than 4ng/ml, 77 (38.5% ) had PSA between 4 – 10 ng/ml and 07 (3.5% ) had PSA greater than 10ng/ml. Table 2 (A, B& C ) shows the serum PSA level with respect to patients having benign prostatic hypertrophy ( BPH ) and carcinoma of prostate.

336 IJSR - INTERNATIONAL JOURNAL OF SCIENTIFIC RESEARCH
Volume : 4 | Issue : 11 | November 2015 • ISSN No 2277 - 8179Research Paper
Table 2 ( A ) : A
PSA (ng/ml ) Carcinoma BPH Total
<4 1 115 116
4-10 4 73 77
>10 5 2 07
Table 2 ( B ) : B
PSA (ng/ml ) Carcinoma BPH Total
<4 1 ( c ) 115 ( d ) 116
>4 9 ( a ) 75 ( b ) 84
Sensitivity of PSA >4 ng/ml in cancer detection = a / a+c*100 = 9 / 9 + 1 * 100 = 90 %
Specificity of PSA >4 ng/ml in cancer detection = d / b+d*100 = 115 / 75+ 115*100 = 60.52 %
Positive predictive value of PSA >4 ng/ml in cancer detection = a / a + b*100
= 9 / 9 + 75*100 = 10.71 %
Negative predictive value of PSA >4 ng/ml in cancer detection = d / b + d*100
= 115/75+115*100 = 60.52 %
Table 2 (C ) : C
PSA (ng/ml ) Diseased Non Diseased Total
<4 115 (a ) 1 ( b ) 116
>4 75 ( c ) 9 ( d ) 84
Sensitivity of PSA <4ng/ml in BPH detection = a / a + c*100 = 115 / 115+75 = 60.52 %
Specificity of PSA <4ng/ml in BPH detection = d / b + d*100 = 9 / 1+ 9*100 = 90 %
Positive predictive value of PSA <4ng/ml in BPH detection = a / a + b*100
= 115 /115 +1*100 = 99.13 %
Negative predictive value of PSA <4ng/ml in BPH detection = d / b + d*100
= 9 / 1 + 9*100 =90 %
Discussion:With the advent of PSA in clinical practice the rate of diagnos-ing localized prostate cancer and / or prostate cancer in early stage has got a surge and at the same time incidence of regional and metastatic prostate cancer has declined. (Mettlin et al 1996 ).PSA has such a profound impact on prostate cancer screening that concern has arisen that it may detect and subsequently re-sult in the treatment of clinically insignificant tumours. In the present study, sensitivity of PSA greater than 4 ng/ml in detec-tion of prostate cancer was 90 % and positive predictive value was 10.71 %. Positive predictive value of PSA greater than4 ng/ml was calculated by various workers. Labrie et al (1992 ) found it to be 33 %,Brawer et al (1992 ) 31 % and Catalona et al (1994 ) 28-35 %. Brawer et al (1992 ), Catalona et al (1994 ) and Stone et al (1994 ) concluded that the approximate chance of carcino-ma prostate is one in three when PSA is between 4 – 10 ng/ml and one in two when PSA is greater than 10 ng/ml. In our study, in PSA range 4 – 10 ng/ml, 4 patients out of 77 had carcinoma prostate. In PSA greater than10 ng/ml, 5 out of 7 had carcinoma. This anomalous result may be due to less number of patients with carcinoma of prostate in this study. In PSA range 4 – 10 ng/ml, 73 out of 77had BPH whereas in the range greater than 10 ng/ml two out of seven had BPH. In PSA range <4 ng/ml out of 116, one patient had carcinoma and 115 had BPH. In PSA range >4 ng/ml, out of 84, nine patients had carcinoma prostate and 75 had BPH. Findings of our study were broadly in conformity of the various workers from various parts of the world.
Conclusion:Chronic urinary obstruction due to prostatic pathology (Benign prostatic hypertrophy & Carcinoma of Prostate) is a very com-mon clinical entity. In recent years, prostate specific antigen (PSA) has established itself as the most useful marker for screen-ing, diagnosing and monitoring the prostate carcinoma patients. In our study 200 patients of chronic urinary obstruction due to prostatic pathology were evaluated. The serum PSA levels were evaluated and correlated with the histopathological findings of biopsied or operated specimens of their prostates to find out the relevance of PSA study. It was found that serum PSA level cor-related well with the prostatic pathology. It had sensitivity of 90 % in detecting carcinoma of prostate when the level was greater than 4ng/ml. In the range less than 4ng/ml it had a sensitivity of 60.52 % in detection of BPH. We conclude that serum PSA is a very good marker in detecting prostatic disease and also to dif-ferentiate between benign and malignant diseases of prostate.
REFERENCE1.Armitage TG, Cooper EH, Newling WW et al- The value of measurement of serum PSA in patients with BPH and untreated prostate cancer. Br J Urol 1998 ; 62: 584 | 2. Balk SP, Kom YJ, Bubley GJ- Biology of prostate specific antigen. J. Clin.Oncol. 2003; 21 (2): 383-91. | 3. Brawer MK, Chetner
MP,Beatie J et al – Screening of prostate carcinoma with prostate specific antigen . J Urol 1992, 147 841-5. | 4. Carter HB, Pearson JD, Metter EJ.- Longitudinal evaluation of prostate specific antigen levels in men with and without prostate disease. JAMA 1992;151(5): 1283-90 | 5. Catalona WJ ,Smith D ,Ornstien D. – Prostate cancer detection in men with serum PSA concentration of 2.6 to 4.0 ng/ml and prostate examination..JAMA 1997; 277(18): 1452-5 | 6. Ellis WJ, Chetner MP, Preston SD et al – Diagnosis of prostatic carcinoma : The yield of serum PSA, digital examination and trans rectal USG- J Urol 1994; 152: 1520-25 | 7. Gann PH,Hennekens CH, Stampfer MJ: A prospective evaluation of plasma PSA for detection of prostate cancer. –JAMA 1995; 272(4): 289-294 | 8. Grammaticos P- Diagnostic and prognostic value of serum PSA in prostatic carcinoma –Hell J. NUcl Med. 2004; 7(3): 146-8 | 9. Mettin CJ, Murphy GP, Ho R et al- The national cancer database report on longitudinal observation of prostate cancer. – 1996; 77 (10): 2162-66 | 10. Yin M, Bastcky S, ChandranU et al- Preva-lence of incidental prostate cancer in the general population: A study of healthy organ donors. J Urol 2008; 179: 892 |

DOI: Original Article
Intestinal Tuberculosis: Experience with Mode of Presentation and Epidemiological Profile at a Tertiary Care Centre in Eastern Bihar
Khwaja Nasim Ahnnacil, Prince Pankaj2, Deepak Pankaj3, Sweta Muni'
'Associate Professor, Department of General Surgery, Katihar Medical College, Katihar, Bihar, India, 2Ex-Junior Resident, Department of General Surgery, Katihar Medical College, Katihar, Bihar & Presently, Research Fellow, Department of Surgery &Allied Branches, Indraprastha Apollo Hospital, New Delhi, India, 3Senior Resident, Department of General Surgery, Katihar Medical College, Katihar, Bihar, India, 'Assistant Professor, Department of Microbiology, Katihar Medical College, Katihar, Bihar, India
Abstract
Introduction: Tuberculosis (TB) is a major global health problem and still considered as a social disease in India reflecting the standards of living in a community. It possesses a diagnostic and therapeutic challenge to practicing surgeon in resource-limited countries.
Aim: The aim of the present study was to study different surgical features and epidemiological profile of intestinal TB.
Materials and Methods: 100 diagnosed cases of intestinal TB were studied over a period of 3-year in the Department of General Surgery at Katihar Medical College with emphasis on mode of presentation and epidemiological profile.
Result: 64% of the cases were in the age group of 21-40 years. The sex incidence revealed a female to male ratio of 1.17:1 showing a female preponderance particularly affecting those who were engaged in household work. Persons of low socio-economic status, particularly non-vegetarians were the common victims of this disease. 50% of the cases belonged to the Muslim community. The important symptoms were abdominal pain, vomiting, loss of appetite, loss of weight, constipation, recurrent bowel upset, and distension of abdomen. The important signs were emaciated look, anemia localized, tenderness, abdominal lump, visible peristalsis, doughy feel of abdomen, distension and ascites and rigidity of the abdomen. The average duration of symptoms was 6-18 months at presentation.
Conclusion: Intestinal TB has vague presentations as shown by this study with a predominant feature of abdominal pain. Good results can be obtained by adopting a multidisciplinary approach, health education, and awareness among people as this disease is very prevalent in this region.
Keywords: Abdomen distention, Intestinal, Obstruction, Tuberculosis
INTRODUCTION
Tuberculosis (TB) is one of the most important diseases in the history of humanity and remains an extraordinary
burden on human health today. It is a chronic specific granulomatous inflammatory disease caused by an organism
Access this article online
Month of Submission : 09-2015 Month of Peer Review: 10-2015 Month of Acceptance : 11-2015 Month of Publishing :11-2015 Id"
www.surgeryijss.com
of the Mycobacterium TB complex. TB is a common and major health problem, especially in developing countries where lack of health education, ignorance, poverty, poor hygiene, overcrowding, and malnutrition are prevalent.' It is one of the most important communicable diseases worldwide and has been declared as a global emergency by World Health Organization.2 Approximately, one-third of the world's population is infected with TB, and about three million die from this disease each year.t3 In developing countries, TB remains the principal cause of death, probably due to ignorance, poverty, overcrowding, poor sanitation, malnutrition, and coexistence with emergent diseases like AIDS.' Approximately, 95% of new cases and 98% of deaths occur in developing countries:Is TB can involve any
Corresponding Author: Dr. Deepak Pankaj, Department of General Surgery, Katihar Medical College, Katihar -854 105, Bihar, India Ohnno. +e1-9421060340. E-mail: [email protected]
, 1.155 Jouinal of Surgery 1 iovemberDecem&r2015Volumell I Issue 6
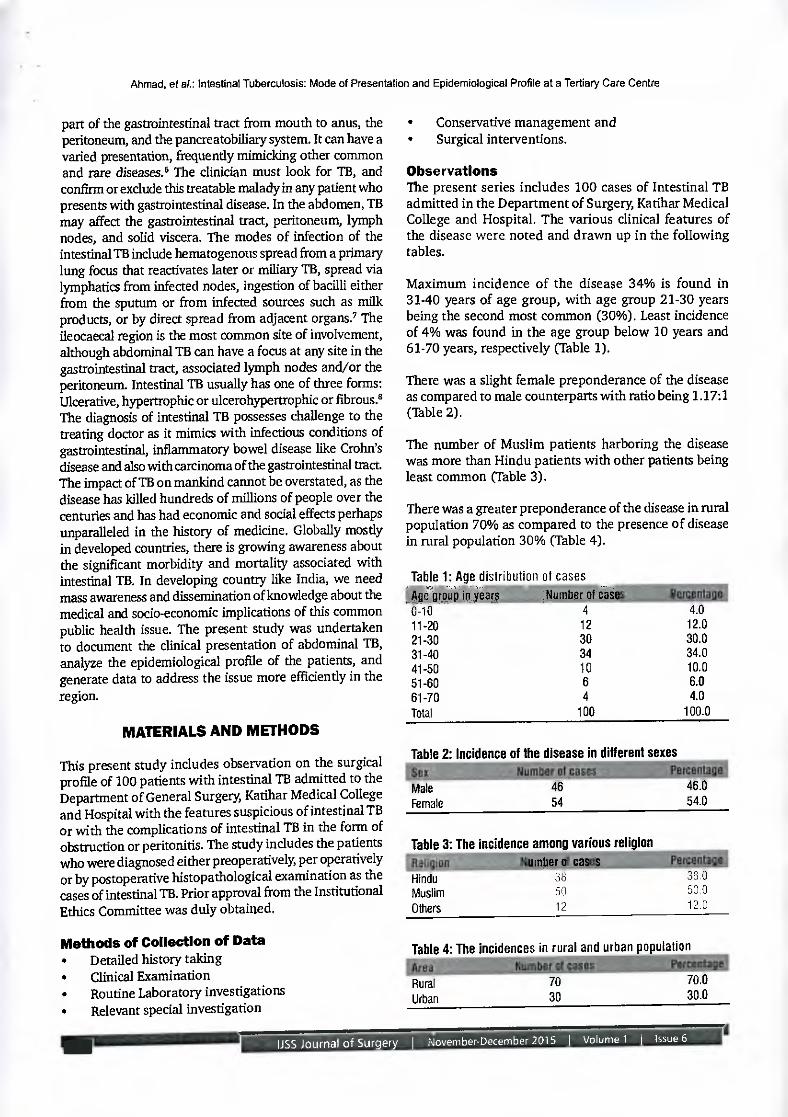
Ahmad, of at: Intestinal Tuberculosis: Mode of Presentation and Epidemiological Profile at a Tertiary Care Centre
part of the gastrointestinal tract from mouth to anus, the peritoneum, and the pancreatobiliary system. It can have a varied presentation, frequently mimicking other common and rare diseases.' The clinician must look for TB, and confirm or exclude this treatable malady in any patient who presents with gastrointestinal disease. In the abdomen, TB may affect the gastrointestinal tract, peritoneum, lymph nodes, and solid viscera. The modes of infection of the intestinal TB include hematogenous spread from a primary lung focus that reactivates later or miliary TB, spread via lymphatics from infected nodes, ingestion of bacilli either from the sputum or from infected sources such as milk products, or by direct spread from adjacent organs., The ileocaecal region is the most common site of involvement, although abdominal TB can have a focus at any site in the gastrointestinal tract, associated lymph nodes and/or the peritoneum. Intestinal TB usually has one of three forms: Ulcerative, hypertrophic or ulcerohypertrophic or fibrous.8 The diagnosis of intestinal TB possesses challenge to the treating doctor as it mimics with infectious conditions of gastrointestinal, inflammatory bowel disease like Crolufs disease and also with carcinoma of the gastrointestinal tract. The impact of TB on mankind cannot be overstated, as the disease has killed hundreds of millions of people over the centuries and has had economic and social effects perhaps unparalleled in the history of medicine. Globally mostly in developed countries, there is growing awareness about the significant morbidity and mortality associated with intestinal TB. In developing country like India, we need mass awareness and dissemination of knowledge about the medical and socio-economic implications of this common public health issue. The present study was undertaken to document the clinical presentation of abdominal TB, analyze the epidemiological profile of the patients, and generate data to address the issue more efficiently in the region.
MATERIALS AND METHODS
This present study includes observation on the surgical profile of 100 patients with intestinal TB admitted to the Department of General Surgery, Katihar Medical College and Hospital with the features suspicious of intestinal TB or with the complications of intestinal TB in the form of obstruction or peritonitis. The study includes the patients who were diagnosed either preoperatively, per operatively or by postoperative histopathological examination as the cases of intestinal TB. Prior approval from the Institutional Ethics Committee was duly obtained.
Methods of Collection of Data • Detailed history taking • Clinical Examination • Routine Laboratory investigations • Relevant special investigation
• Conservative management and • Surgical interventions.
Observations The present series includes 100 cases of Intestinal TB admitted in the Department of Surgery, Katihar Medical College and Hospital. The various clinical features of the disease were noted and drawn up in the following tables.
Maximum incidence of the disease 34% is found in 31-40 years of age group, with age group 21-30 years being the second most common (30%). Least incidence of 4% was found in the age group below 10 years and 61-70 years, respectively (Table 1).
There was a slight female preponderance of the disease as compared to male counterparts with ratio being 1.17:1 (Table 2).
The number of Muslim patients harboring the disease was more than Hindu patients with other patients being least common (Table 3).
There was a greater preponderance of the disease in rural population 70% as compared to the presence of disease in rural population 30% (Table 4).
Table 1: Age distribution of cases ._Age group in years Number of case 0-10 4 4.0 11-2o 12 12.0 21-30 30 30.0 31-40 34 34.0 41-50 10 10.0 51-60 6 6.0 61-70 4 4.0 Total 100 100.0
Table 2: Incidence of the disease in different sexes
Male 46 46.0 Female 54 54.0
Table 3: The incidence among various religion MIII.rfrrnber ill trarr Hindu 38 35.0 Muslim 50 50.0 Others 12 12.0
Table 4: The incidences in rural and urban population
Rural 70 70.0
Urban 30 30.0
IJSS Journal of Surgery I November-December 2015 I Volume 1 1 Issue 6

Ahmad, et at: Intestinal Tuberculosis: Mode of Presentation and Epidemiological Profile at a Tertiary Care Centre
Labourers are the most frequent sufferers of the disease with 50%, farmers being second 24%. Students were the least sufferers with 6% (Table 5).
The disease is more common in non-vegetarians as compared to vegetarian (Table 6).
The disease was more prevalent in poor people, i.e. a very low socio-economic group of the society with the percentage being 46%. The high socio-economic group were least sufferers of the disease with the percentage being 4% (Table 7).
A maximum number of patients reported with a duration of symptoms between 6 months and 1 V2 years. Only 4% of patients had duration of symptoms of more than 3 years (4%) (Table 8).
Among the symptoms, pain abdomen was the common symptom (96%) in our series, second being weakness and loss of weight (66%). 16% of the patients had concomitant TB of some other organ. There was a considerable overlapping of symptoms in most of the patients (Table 9).
Among the signs of Intestinal TB, anemia is present in the majority of the cases. Next common features were abdominal distension and tenderness. Tenderness was confined to right iliac fossa or umbilical region. In some acute cases, it was diffuse. Other common signs were borborygmi and doughy abdomen. Abdominal lumps were mostly due to the hyperplastic lesion, less commonly
Table 5: The incidence of disease in different occupations
Farmers 24 24.0 Labourers 50 50.0 Students 6 6.0 Others 20 20.0
Table 6: The incidence of disease in vegetarian and non-vegetarians
Vegetarian
24
24.0 Non-vegetarian
76
76.0
Table 7: The incidence of disease in relation to socio-economic status
ow-economic slalus Number Percentage of cases
Class I (high socio-economic group) 4 4.0 Class II (middle class) 16 16.0 Class III (low socio-economic group) 34 34.0 Class IV (very low socio-economic group) 46 46.0
due to enlarged mesenteric lymph nodes, or rolled up omentum (Table 10).
DISCUSSION
On the basis of the epidemiology of intestinal TB, it is obvious that the disease incidence is still higher in our country In Western developed countries, the incidence of intestinal TB in particular and TB of other organs, in general, had been decreasing, but in recent years there has been increasing the incidence of the disease due to increasing incidence of AIDS in these countries. Abdominal TB constitutes a major public health problem in developing countries and carries significant morbidity and mortality LB
Table 8: Duration of symptoms
<6 months 6 6.0 6 months-1 year 28 28.0 1-11/2 year 34 34.0 11/2-2 years 12 12.0 2-21/2 years 10 10.0 21/2-3 years 6 6.0 3 years or more 4 4.0
Table 9: Frequency of different symptoms in the patients with Intestinal tuberculosis any 'timber °Ceases Percentagel Abdominal pain JG 96.0 Weakness and loss of weight 66 66.0 Loss of appetite 60 60.0 Vomiting 62 62.0 Flatulence 24 24.0 Fever and night sweats 20 20.0 Irregular bowel habit 42 42.0 Lump 30 30.0 Constipation 40 40.0 Obstruction 34 34.0 Secondary tuberculosis 16 16.0 Scanty menstruation 4 4.0 Diarrhea 18 18.0
Table 10: The frequency of different elicited signs
Anemia 90 90.0 Abdominal distension 50 50.0 Visible peristalsis 20 20.0 Abdominal lump 30 30.0 Rigidity of abdomen 20 20.0 Tenderness of abdomen 48 48.0 Doughy feel of abdomen 10 10.0 Ascites 8 8.0 Increased frequency of bowel sound (borborygmi)
40 40.0
Crepts in the chest 6 6.0
LISS Journal of Surgery I November-December 2015 I Volume 1 I Issue 6
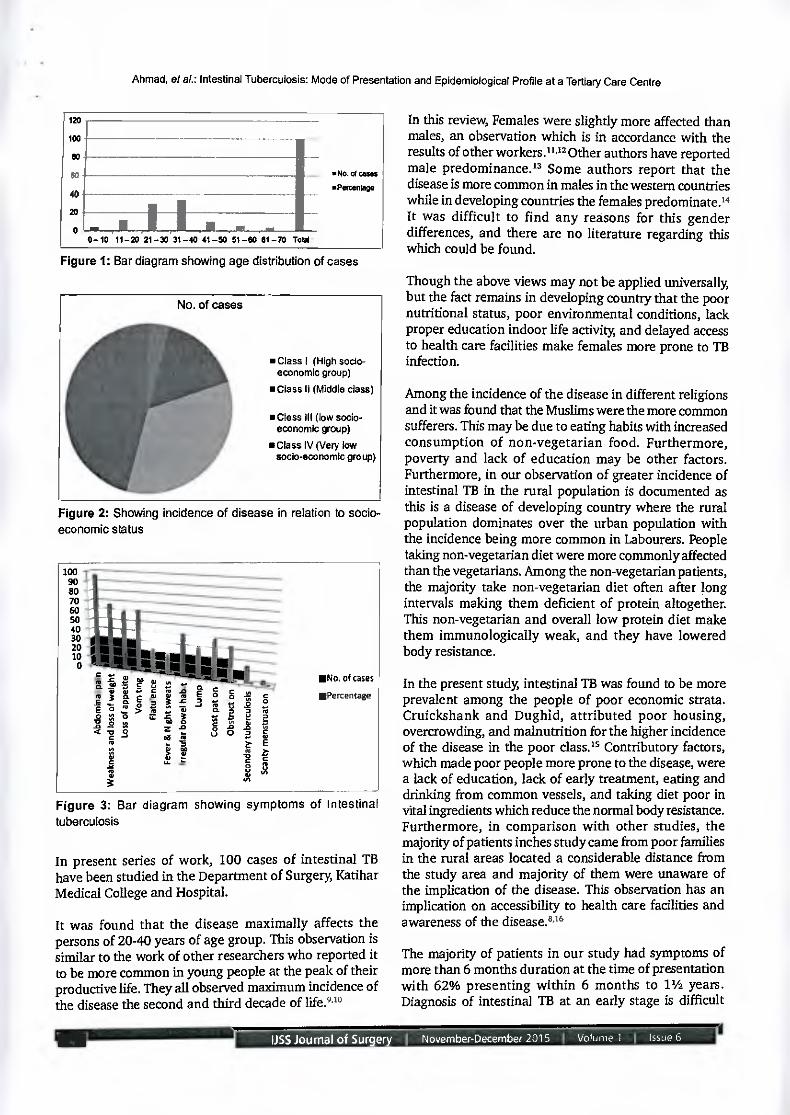
• No. of cases
aPercentage
0-10 11-20 21-30 31-40 41-50 51-00 01-70 Tots:
120
100
eo 00
40
20
100 90 80 70 60 50 40 30 20 10 0
• II III • 10 • IN •
; a
c
as !MM. ICE II/1 • • IN
g
We S
NI mi
§
mi s• •rn
1lNo. of cases
2 io EPercentage E a 2
°
9
Ahmad, et at: Intestinal Tuberculosis: Mode of Presentation and Epidemiological Profile at a Tertiary Care Centre
Figure 1: Bar diagram showing age distribution of cases
No. of cases
• Class I (High socio-economic group)
• Class II (Middle class)
• Class III (low socio-economic group)
• Class IV (Very low socioeconomic group)
Figure 2: Showing incidence of disease in relation to socio-economic status
Figure 3: Bar diagram showing symptoms of Intestine tuberculosis
In present series of work, 100 cases of intestinal TB have been studied in the Department of Surgery, Katihar Medical College and Hospital.
It was found that the disease maximally affects the persons of 20-40 years of age group. This observation is similar to the work of other researchers who reported it to be more common in young people at the peak of their productive life. They all observed maximum incidence of the disease the second and third decade of life.93°
In this review, Females were slightly more affected than males, an observation which is in accordance with the results of other workers.".° Other authors have reported male predominance.° Some authors report that the disease is more common in males in the western countries while in developing countries the females predorninate.m It was difficult to find any reasons for this gender differences, and there are no literature regarding this which could be found.
Though the above views may not be applied universally, but the fact remains in developing country that the poor nutritional status, poor environmental conditions, lath proper education indoor life activity and delayed access to health care facilities make females more prone to TB infection.
Among the incidence of the disease in different religions and it was found that the Muslims were the more common sufferers. This may be due to eating habits with increased consumption of non-vegetarian food. Furthermore, poverty and lack of education may be other factors. Furthermore, in our observation of greater incidence of intestinal TB in the rural population is documented as this is a disease of developing country where the rural population dominates over the urban population with the incidence being more common in Labourers. People taking non-vegetarian diet were more commonly affected than the vegetarians. Among the non-vegetarian patients, the majority take non-vegetarian diet often after long intervals making them deficient of protein altogether. This non-vegetarian and overall low protein diet make them immunologically weak, and they have lowered body resistance.
In the present study, intestinal TB was found to be more prevalent among the people of poor economic strata. Cruickshank and Dughid, attributed poor housing, overcrowding, and malnutrition for the higher incidence of the disease in the poor class.° Contributory factors, which made poor people more prone to the disease, were a lack of education, lack of early treatment, eating and drinking from common vessels, and taking diet poor in vital ingredients which reduce the normal body resistance. Furthermore, in comparison with other studies, the majority of patients inches study came from poor families in the rural areas located a considerable distance from the study area and majority of them were unaware of the implication of the disease. This observation has an implication on accessibility to health care facilities and awareness of the disease.8.16
The majority of patients in our study had symptoms of more than 6 months duration at the time of presentation with 62% presenting within 6 months to 11/2 years. Diagnosis of intestinal TB at an early stage is difficult
155 Journal of Surgery November-December 2015 I Volume 1 I Issue 6

Ahmad, et at: Intestinal Tuberculosis: Mode of Presentation and Epidemiological Profile at a Tertiary Care Centre
due to the vague presentation and waxing and waning of symptoms with early conservative treatment. Furthermore, lack of accessibility to health care facilities and lack of awareness may be the cause. This observation is also similar to other authors.uas
TB is notorious for the diversity of its symptoms, and the symptoms in intestinal TB are no exception to this rule. Symptoms vary with the stage of the disease, location and nature of the lesion, degree of obstruction, the extent of irritation of the nerves, the condition of the mucosa, and involvement of the peritoneum. Abdominal pain was the common symptoms and was present in 96% of the cases in this series. The pain was varied in nature ranging from the vague, dull ache in the right iliac fossa, or around the umbilicus to severe colicky pain. At the onset of the disease, the pain remained vague and generalized occurring especially after taking food. Later on the pain got localized in the right iliac fossa. In case of acute intestinal obstruction and perforation, the pain was severe and generalized. Anand in his study observed pain in all of the patients in the series while Abro et al., and Chalya et at., (93.8%) described it to be the main symptom of intestinal TB."-21
66% of the patients complained of loss of weight and loss of appetite. These symptoms were observed by Singhai et al., in 60% of the cases, Anand in 58% of cases.19,n In this series, the other common symptom was vomiting present in 62% of the cases. The cause of the vomiting among the patients with obstruction needs no explanation. However, vomiting without obstruction may be due to the protective pylorospasm or delayed emptying of the chyme due to the inflamed bowel. Abdominal distension was observed in 50% of the cases in present series Chalya etal., found distention in 36.7% of the cases. This fairly common feature and considered it to be due to collection of fluid in the peritoneal cavity or to gaseous distension in small intestine or stomach from obstruction. So, far the signs are concerned, anemia was the most common sign present in 90% of the cases. The results of the abdominal examination were not of great help in the diagnosis of the early stage of the disease. Abdominal tenderness was the other frequent sign present in 48% of the cases. Its site varied with the types and sites of the lesion. Bhansali observed tenderness in 62.5% of his series. Prakash found tenderness in 55% of patients in the right iliac fossa. Tenderness in the other region was not included in the figures given by Prakash. He attributed surrounding inflammatory reaction as a cause of tenderness.23•24 A well-defined abdominal lump was felt in 30% of cases. The lump was felt in the right iliac fossa as expected from the hyperplastic lesions in the ileocaecal region. Lumps observed in other regions were due to the involvement of greater omentum, transverse colon, retroperitoneal, or mesenteric lymph nodes. In
other studies, the lump was felt in 46% cases and 32.5%, respectively, which was similar to the present study. The mass was tender due to surrounding inflammatory reactions.23•24
In general, it is not possible to evaluate the typical symptoms and signs of an early case of gastrointestinal TB. It is only in the late stage, when symptoms of chronic and acute on chronic obstruction develop, the definitive clinical diagnosis may be possible. It has been explained by clinical findings and autopsy reports that a vast number of abdominal TB lesions do not cause significant abdominal symptoms during the life time of the patients.
CONCLUSION
Intestinal TB is a major public health problem in developing nations. Persons of low socio-economic status are the common victims of this disease with vague abdominal discomfort and varied presentation. Poverty, malnutrition, overcrowding, and HIV co-infection aid the spread of TB with a differing profile of patients around the globe. The majority of the cases are of primary intestinal variety, and a small proportion is secondary to pulmonary TB. Better nutrition and importance of early diagnosis and treatment must be emphasized to a vulnerable group of people for better survival.
REFERENCES
1. Butt 1; Karamat KA, Ahmad RN, Mahmood A. Advances in diagnosis of tuberculosis. Pak J Pathol 2001;12:1-3.
2. Lonnroth K, Raviglione M. Global epidemiology of tuberculosis: Prospects for control. Semin Respir Crit Care Med 2008;29:481-91.
3. Dolin PJ, Raviglione MC, Kochi A. Global tuberculosis incidence and mortality during 1990-2000. Bull World Health Organ 1994;72:213-20.
4. WHO. Global Tuberculosis Control. Geneva: World Health Organization; 2008.
S. Ducati AG, Ruffino-Netto A, Basso LA, Santos DS. The resumption of consumption - A review on tuberculosis. Mem hist Oswaldo Cruz 2006;101:697-714.
6. Peda Veerraju E. Abdominal tuberculosis. In: Sri SS, editor. Textbook of Pulmonary and Extra-Pulmonary Tuberculosis. 3'd ed. New Delhi: Inter Print; 1998. p. 250-2.
7. Sharma mg Bhada V Abdominal tuberculosis. Indian J Med Res 2004;120:305-15.
8. Shaikh MS, Dholia KR, Jalbani MA, Shaikh SA. Prevalence of intestinal tuberculosis in cases of acute abdomen. Pak J Surg 2007;23:52-6.
9. Khan SM, Khan KM, Than AS, Jehanzeb M, Jan WA, Than M, etal. Presentation of abdominal tuberculosis in NVVFP and its correlation with operative findings. J Postgrad Med Ina 2005;19:286-91.
10. Gondal SH, Gulshan S, Naseeb U. Intestinal tuberculosis
LISS Journal of Surgery I November-December 2015 I Volume 1 I Issue 6
Ahmad, et al.: Intestinal Tuberculosis: Mode of Presentation and Epidemiological Profile at a Tertiary Care Centre
as an abdominal emergency. Pak Postgrad Med J 2000;11:103-5.
11. Zafar A, Qureshi AM, Iqbal M. Comparison between strictureplasty and resection anastomosis in tuberculous intestinal strictures. J Coll Physicians Surg Pak 2003;13:277-9.
12. Baloch NA, Baloch MA, Baloch FA. A study of 86 cases of abdominal tuberculosis. J Sorg Pak 2008;13:30-2.
13. Rajpoot MJ, Memon AS, Rani S. Memon Al-I. Clinicopathological profile and surgical management outcomes in patients suffering from intestinal tuberculosis. J Liaqaut Univ Med Health Sci 2005;4:113-8.
14. Homan We Grafe WR, Dineen PA 44-year experience with tuberculous enterocolitis. World J Surg 1977;2:245-50.
15. Cruickshank R, Dughid J. In: Harmin BR Swain RA, editors. Microbiology 12th ed., Vol. I. Edinburgh: ELBS; 1974. p. 296.
16. Niaz K, Ashraf M. Intestinal tuberculosis. Diagnostic dilemma. Prof Med J 2010;17:532-7.
17. lqbal T, Khan A, lqbal A, Tahir F. Obstruction due to intestinal tuberculosis stricturoplasty versus resection anastomosis. Pak J Surg 2008;24:177-81.
18. Akbar M, Falchar-ul-Islam, Haider IZ, Naveed D, Akbar I, Khattak I, et al. Surgical management of tuberculous small bowel obstruction. J Ayub Med Coll Abbottabad 2010;22:171-5.
19. Anand SS. Hypertrophic ileo-caecal tuberculosis in India with a record of fifty hemicolectomies. Ann R Coil Surg Engl 1956;19:205-22.
20. Abro A, Siddiqui FG, Alchtar S, Memon AS. Spectrum of clinical presentation and surgical management of intestinal tuberculosis at tertiary care hospital. J Ayub Med Coll Abbottabad 2010;22:96-9.
21. Chalya PL, Mchembe MD, Mshana SE, Rambau PF, Jalca H, Mabula JB. Clinicopathological profile and surgical treatment of abdominal tuberculosis: A single centre experience in northwestern Tanzania. BMC Infect Dis 2013;13:270.
22. Singhai SL, Tandan PL, Hafiz MA, Singh R. Abdominal tuberculosis. Indian J Surg 1963;25:440-50.
23. Bhansali SK. Abdominal tuberculosis. Experiences with 300 cases. Am J Gastroenterol 1977;67:324-37.
24. Prakash A. International tuberculosis 18 years review. Indian Med .1 1978;40:56-64.
How to cite this article: Ahmad KN, Pankaj P, Pankaj D, Muni S. Intestinal Tuberculosis: Experience with Mode of Presentation and Epidemiological Profile at a Tertiary Care Centre in Eastern Bihar. IJSS Journal of Surgery 2015;1(6):1-6.
Source of Support: Nil, Conflict of Interest: None declared.
6
1155 Journai of Star. e November-December 2015 I Volume 1
Issue 6

IJSS Journal of Surgery | January-February 2016 | Volume 2 | Issue 16
Benign Breast Lesions in a Teaching Hospital in Rural Bihar
Shambhu Kumar Singh1, Khwaja Nasim Ahmad2, Deepak Pankaj3, Mohammad Arif Ansari4
1Assistant Professor, Department of General Surgery, Katihar Medical College, Katihar, Bihar, India, 2Associate Professor, Department of General Surgery, Katihar Medical College, Katihar, Bihar, India, 3Senior Resident, Department of General Surgery, Katihar Medical College, Katihar, Bihar, India, 4Professor and Head, Department of General Surgery, Katihar Medical College, Katihar, Bihar, India
Abstract
Background: Breast diseases has captured attention of surgeons throughout the ages with its uncertain cause. Study of a pattern of benign breast diseases (BBDs) is a challenge due to variants in occurrence and presentation in different age groups and different geographical areas. The breast is a complex structure and any unnatural change affects the body and psyche of the person.
Aim: The aim of this study was to observe age distribution, clinical signs, symptoms and pathology of benign breast lump and correlate them with pathological findings.
Materials and Methods: A total of 124 cases of benign breast lump were included in this study. These cases were selected among patients visiting the outdoor clinic of Department of General Surgery in Katihar Medical College, Katihar, Bihar, India. The selected cases belonged to different etiology, age group and sex.
Results: Maximum cases of benign breast tumors were observed in age group of 21-30 years (third decade). Fibroadenoma was the most common presentation. The majority of patients reported within 1 year of onset of disease. The painless lump was the most common mode of presentation. The right breast was involved in a more number of cases with maximum lesions noted in the upper outer quadrant.
Conclusion: BBDs are common in female patients. Clinical, sonological, mammographical, and pathological studies need to be conducted in a systemic way to find answers of complexities posed by the confusing pattern of BBDs.
Keywords: Benign breast disease, Fibroadenoma, Histopathology, Risk factors, Surgery
INTRODUCTION
Breast or mammary gland is the most important structure in the pectoral region. It is composed of
skin which consists of nipple and areola; parenchyma made up of glandular tissue and fibrofatty stroma. It is influenced by various hormones in a female during lifetime giving rise to different types of lesions. Benign tumors mostly fibroadenoma common in young women have a higher incidence as compared to inflammatory
lesions which are common in lactating women. Increasing incidence of malignancy in proliferating lesions of breast warrants for prompt diagnosis and treatment.1 Benign breast diseases (BBDs) is a group of breast diseases which is not cancer. It is the most common cause of breast problems in females, and it is a more frequent than the malignant ones.2-4 In fact, it is at least 10 times more common than breast cancer in the west.5 Up to 30% of the women who suffer from BBDs will require treatment at some point in their lifetime.6 Increasing reports of breast cancer in India has overshadowed the wide spectrum of benign breast disorders. An incidence of 1.5/1000 cases of total hospital admissions and 8.1/1000 cases of female admissions has been reported in cases of benign breast disorders.7 With regard to gender, diseases of breast are more prevalent among females and the pattern of breast diseases and their etiology varies among
Corresponding Author: Dr. Deepak Pankaj, Department of General Surgery, Katihar Medical College, Katihar - 854 105, Bihar, India.Phone: +91-9431060340. E-mail: [email protected]
Access this article online
www.surgeryijss.com
Month of Submission : 11-2015 Month of Peer Review : 12-2015 Month of Acceptance : 01-2016 Month of Publishing : 01-2016
DOI: 10.17354/SUR/2016/02
Original Article
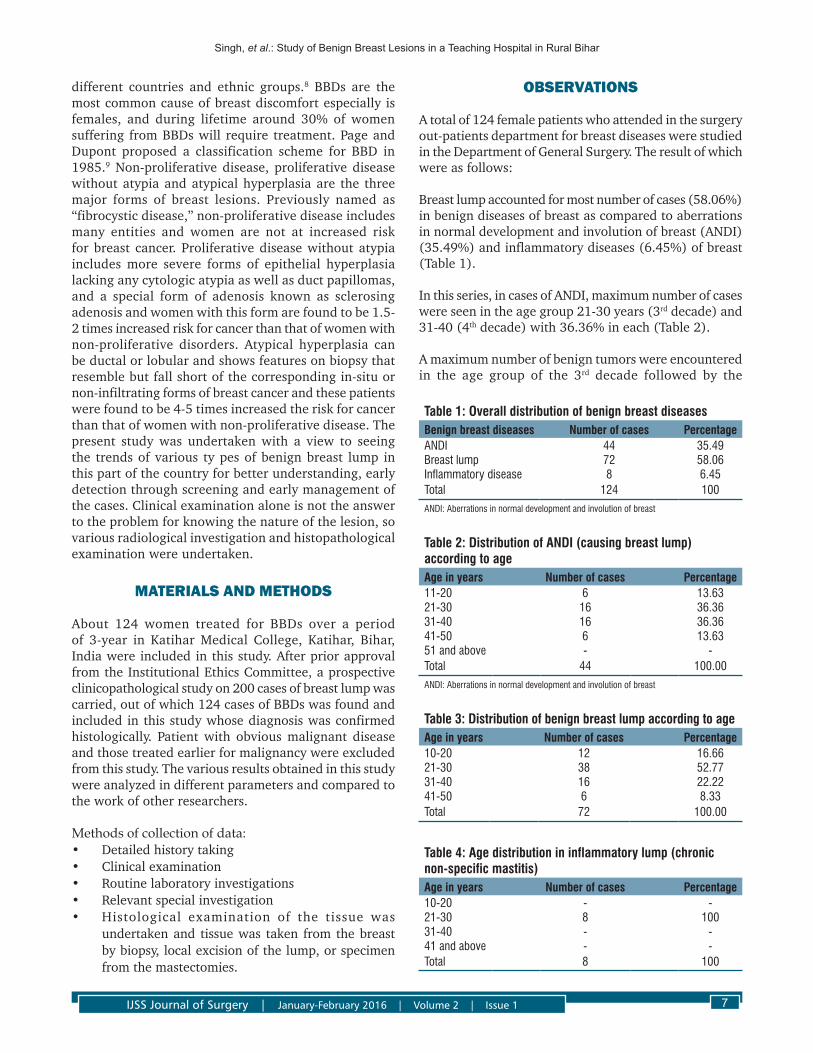
Singh, et al.: Study of Benign Breast Lesions in a Teaching Hospital in Rural Bihar
IJSS Journal of Surgery | January-February 2016 | Volume 2 | Issue 1 7
different countries and ethnic groups.8 BBDs are the most common cause of breast discomfort especially is females, and during lifetime around 30% of women suffering from BBDs will require treatment. Page and Dupont proposed a classification scheme for BBD in 1985.9 Non-proliferative disease, proliferative disease without atypia and atypical hyperplasia are the three major forms of breast lesions. Previously named as “fibrocystic disease,” non-proliferative disease includes many entities and women are not at increased risk for breast cancer. Proliferative disease without atypia includes more severe forms of epithelial hyperplasia lacking any cytologic atypia as well as duct papillomas, and a special form of adenosis known as sclerosing adenosis and women with this form are found to be 1.5-2 times increased risk for cancer than that of women with non-proliferative disorders. Atypical hyperplasia can be ductal or lobular and shows features on biopsy that resemble but fall short of the corresponding in-situ or non-infiltrating forms of breast cancer and these patients were found to be 4-5 times increased the risk for cancer than that of women with non-proliferative disease. The present study was undertaken with a view to seeing the trends of various ty pes of benign breast lump in this part of the country for better understanding, early detection through screening and early management of the cases. Clinical examination alone is not the answer to the problem for knowing the nature of the lesion, so various radiological investigation and histopathological examination were undertaken.
MATERIALS AND METHODS
About 124 women treated for BBDs over a period of 3-year in Katihar Medical College, Katihar, Bihar, India were included in this study. After prior approval from the Institutional Ethics Committee, a prospective clinicopathological study on 200 cases of breast lump was carried, out of which 124 cases of BBDs was found and included in this study whose diagnosis was confirmed histologically. Patient with obvious malignant disease and those treated earlier for malignancy were excluded from this study. The various results obtained in this study were analyzed in different parameters and compared to the work of other researchers.
Methods of collection of data:• Detailedhistorytaking• Clinicalexamination• Routinelaboratoryinvestigations• Relevantspecialinvestigation• Histological examination of the tissue was
undertaken and tissue was taken from the breast by biopsy, local excision of the lump, or specimen from the mastectomies.
OBSERVATIONS
A total of 124 female patients who attended in the surgery out-patients department for breast diseases were studied in the Department of General Surgery. The result of which were as follows:
Breast lump accounted for most number of cases (58.06%) in benign diseases of breast as compared to aberrations in normal development and involution of breast (ANDI) (35.49%) and inflammatory diseases (6.45%) of breast (Table 1).
In this series, in cases of ANDI, maximum number of cases were seen in the age group 21-30 years (3rd decade) and 31-40 (4th decade) with 36.36% in each (Table 2).
A maximum number of benign tumors were encountered in the age group of the 3rd decade followed by the
Table 1: Overall distribution of benign breast diseasesBenign breast diseases Number of cases PercentageANDI 44 35.49Breast lump 72 58.06Inflammatory disease 8 6.45Total 124 100
ANDI: Aberrations in normal development and involution of breast
Table 2: Distribution of ANDI (causing breast lump) according to ageAge in years Number of cases Percentage11‑20 6 13.6321‑30 16 36.3631‑40 16 36.3641‑50 6 13.6351 and above ‑ ‑Total 44 100.00
ANDI: Aberrations in normal development and involution of breast
Table 3: Distribution of benign breast lump according to ageAge in years Number of cases Percentage10‑20 12 16.6621‑30 38 52.7731‑40 16 22.2241‑50 6 8.33Total 72 100.00
Table 4: Age distribution in inflammatory lump (chronic non‑specific mastitis)Age in years Number of cases Percentage10‑20 ‑ ‑21‑30 8 10031‑40 ‑ ‑41 and above ‑ ‑Total 8 100

Singh, et al.: Study of Benign Breast Lesions in a Teaching Hospital in Rural Bihar
IJSS Journal of Surgery | January-February 2016 | Volume 2 | Issue 18
4th decade with incidence of 52.77% and 22.22% in each, respectively, in the present study (Table 3).
In the present study, all cases of chronic non-specific mastitis were seen in the age group 21-30 years (Table 4).
Maximumnumber of patientswereHindu (53.23%)followed by Muslims (46.77%) (Table 5).
In the present series, most patients (61.30%) of BBDs presented within 6 months of occurrence of the disease,
followed by patients presenting within 6-12 months of occurrence of symptoms (25.80%) (Table 6).
The most common sign and symptom of presentation in the present series was painless mass in the breast, i.e., (71.77%) followed by painful mass in the breast (28.23%) (Table 7). The nipple discharge was present in 8 cases in all cases of BBDs (6.45%).
Among the patients of BBDs, a maximum number of patients, 61.29% were having up to 3 children, followed by 30.65% having children between 3 and 6. Least number of lesions were seen in 8.06% of patients having no children (Table 8).
Among patients presenting with benign breast lump in this series, involvement of right breast (54.84%) was more than left breast (45.16%). Among the quadrants involved, upper outer quadrant (UOQ) was the most common quadrant involved with 27.42% of cases reporting with UOQ involvement in both the breast (Table 9).
Table 6: Distribution of the various lesions according to duration of illnessLesions Less than 6 months 6 months to 1 year 1‑1½ years 1½‑2 year TotalBenign tumor 40 (55.55) 20 (27.78) 4 (5.55) 8 (11.11) 72ANDI 28 (63.7) 12 (27.27) ‑ 4 (9.09) 44Chronic non‑specific mastitis 8 (100) ‑ ‑ ‑ 8Total 76 32 4 12 124% of the series 61.30 25.80 3.23 9.67 100
ANDI: Aberrations in normal development and involution of breast
Table 7: Clinical presentation of benign lesionsSign and symptoms ANDI Benign tumor Chronic non‑specific mastitis Total PercentagePainless mass in breast 29 60 89 71.77Painful mass in breast 15 12 8 35 28.23Total 44 72 8 124 100.0
ANDI: Aberrations in normal development and involution of breast
Table 8: Distribution of various breast lumps according to parityLesions No children Up to 3 children >3 up to 6 children >6 children TotalANDI 4 20 20 44Benign tumors 6 48 18 ‑ 72Chronic non‑specific mastitis ‑ 8 ‑ ‑ 8Total 10 76 38 ‑ 124Percentage 8.06 61.29 30.65 ‑ 100
ANDI: Aberrations in normal development and involution of breast
Table 9: Distribution of various breast lumps according to side and quadrantLesions Right (%) Total
(%)Left Total
(%)UOQ LOQ UIQ LIQ Central UOQ LOQ UIQ LIQ CentralANDI 12 (27.2) 4 (9.09) 4 (9.09) ‑ 4 (9.09) 24 (54.54) 12 (27.2) ‑ 4 (9.09) ‑ 4 (9.09) 20 (45.45)Benign tumors 20 (27.8) 8 (11.11) 8 (11.11) ‑ 4 (5.55) 40 (55.55) 20 (27.8) ‑ 8 (11.11) ‑ 4 (5.55) 32 (44.44)Chronic non‑specific mastitis 2 (25) 2 (25) ‑ ‑ ‑ 4 (50) 2 (25) 2 (25) ‑ ‑ ‑ 4 (50)Total 34 14 12 ‑ 8 68 34 2 12 8 56% in the series 27.42 11.29 9.68 ‑ 6.45 54.84 27.42 1.49 9.68 6.45 45.16
UOQ: Upper outer quadrant, LOQ: Lower outer quadrant, UIQ: Upper inner quadrant, LIQ: Lower inner quadrant, ANDI: Aberrations in normal development and involution of breast
Table 5: Distribution of benign breast lump according to religionReligion Number of cases PercentageHindu 66 53.23Muslim 58 46.77Others 0 0Total 124 100

Singh, et al.: Study of Benign Breast Lesions in a Teaching Hospital in Rural Bihar
IJSS Journal of Surgery | January-February 2016 | Volume 2 | Issue 1 9
Histologically in thepresentseries,allcasesofbenigntumors were fibroadenoma. Intracanalicular variety was observed in the majority of cases of benign breast lump (66.67%). Epithelial hyperplasia (adenosis) was the common picture in case of ANDI with maximum reporting in 63.64% of cases. In an inflammatory group, all cases were chronic non-specific mastitis (Table 10).
Furthermore, according to tumor size, tumors between 2.5 and 5 cm were seen in the majority of cases, followed by tumors between size 5 and 10 cm. Lymph node involvement was also seen with 12 (9.68%) cases reporting axillary lymph node involvement (Table 10).
DISCUSSION
In the present study, 124 cases of benign tumor were studied. BBDs includes a heterogeneous group of conditions which range from normal, to aberrations in the physiology, to frank disease. The patients of BBDs generally present with one or more of these complaints – breast lump, breast pain or nipple discharge.10 It has been recommended that all the patients with discrete breast lumps should undergo a triple assessment to make an early diagnosis. Breast lump which were diagnosed as fibroadenoma eventually by histology accounted for most number of cases (58.06%) among benign diseases of the breast in this study as compared to ANDI and inflammatory diseases of the breast. Most of the patients reported with benign breast lump in the third decade of life that is between 21 and 30 year of age. The finding of this study was in agreement with most of the available literature on benign breast lumps, where the frequency of fibroadenoma ranged from 46.6% to 55.6%. The peak incidence of fibroadenoma ranged from the 2nd to the 3rd decade of life, which was also consistent with the findings of other studies.11-14 According to religion, the number of HindupatientswereslightlymorethanthenumberofMuslimpatients. Other religion did not report any cases in the present study. The majority of the patients accounting for 87.1% in this study reported within 1 year of onset of symptoms of breast disease. The possible explanation for this may be that most of the patients in this study are of younger age group with increasing literacy are aware of the disease and concern about the symptoms especially in breasts affects the psyche of the patients, This leads to prompt and early reporting to the treating surgeon. This may be also due to the fact that all
patients observed were from an institutional hospital where patients report earlier with the belief that better facilities of management will be carried out than in rural practice. In the present series, all the patients with fibroadenoma presented with a lump which was painless in the majority of the cases. They were usually claimed to be discovered by the patients themselves.This result is inagreementofHaagensen,15 who reported 90% of the patients presented with painless lump and Wynder et al.16 who observed 85-90% of patients with a painless lump in their series respectively. Figures 1 and 2 shows examples of BBDs which is Fibroadenoma and Benign phylllodes tumours respectively. Among the patients of BBDs, maximum number of patients, 61.29% were having up to 3 children, followed by 30.65% having children between 3 and 6. Least number of lesions were seen in8.06%ofpatientshavingnochildren.Higherincidenceof benign lesions in multipara could be correlated with the fact that they are dependent upon hormonal, functional and physiological imbalance which has been accepted as fact nowadays. The right breast was involved in 54.84% of cases of benign breast lumps than the left breast which reveals 45.16% of cases in the present study. We could not find any literature that reveals substantial relation of the side of the breast with the development of these types of breast lesions. According to quadrants involved, these diseases were maximally observed in UOQ of both the breasts, which is in agreement with other workers.6,17 Few cases reported the involvement of axillary lymph nodes only (9.68%) as these were inflammatory in origin. This may be due to the fact that the breast drains mainly to axillary nodes, of which there are five sets.18Histologically,inthepresentseries,allcasesof benign tumors were fibroadenoma. An intracanalicular pattern was observed in 66.67% of cases while in 33.33% of cases pericanalicular pattern was observed. It is in confirmity with the results of Kern and Clark19 while contrary to the resultsofHaqueet al.17 who observed mixed pattern in majority of cases.
Epithelial hyperplasia (adenosis) was the commonest histological picture in ANDI, seen in 63.64% of the cases and rest were cystic and fibrocystic diseases in 18.18% and papillomatosis and sclerosing adenosis in 18.18%. ThisisalsoinagreementwiththefindingsofHaque0.17 These lesions have the potential to be misdiagnosed with carcinoma of the breast in a fraction of cases. The basis of false diagnosis of cancer may be abundance of fibrous tissue contributing hardness and infiltration of fat leading
Table 10: Histopathological types of various breast lumpLesions ANDI Benign InflammatoryHistological types
Cystic and fibro cystic
Epithelial, hyperplasia (adenosis and atypical lobular hyperplasia)
Papillo‑matosis (sclerosing adenosis)
Total Intracana‑ licular
Peric‑analic‑ular Total Chronic non‑specific
mastitis
Total
Number of cases 8 28 8 44 48 24 72 8 8Percentage 18.18 63.64 18.18 100 66.67 33.33 100 100 100
ANDI: Aberrations in normal development and involution of breast

Singh, et al.: Study of Benign Breast Lesions in a Teaching Hospital in Rural Bihar
IJSS Journal of Surgery | January-February 2016 | Volume 2 | Issue 110
to fixation of the tumor.
In the present series, four cases showed chronic non-specific mastitis. It was commonly a legacy of acute mastitis resulting from imperfect resolution and inadequate treatment. Most of the cases do not warrant biopsy. One case simulate carcinoma clinically but biopsy showed chronic non-specific mastitis.
CONCLUSION
BBDs are a common problem in a women’s life and has a lot of impact on the physical and mental state of the patients. A lump in the breast is the most common presentation which is mostly painless followed by painful lump and nipple discharge. Proper counselling of the patient along specific investigations with prompt diagnosis and both conservative and surgical approach as a part of surgeon’s perspective forms an essential part of treatment.
REFERENCES
1. KumarR. A clinicopathologic study of breast lumps inBhairahwa, Nepal. Asian Pac J Cancer Prev 2010;11:855-8.
2. Kelsey JL, Gammon MD. Epidemiology of breast cancer. EpidemiolRev1990;12:228-40.
3. SarnelliR,SquartiniF.Fibrocysticconditionand“atrisk”lesions in asymptomatic breasts: a morphologic study of postmenopausal women. Clin Exp Obstet Gynecol 1991;18:271-9.
4. CookMG,RohanTE.Thepatho-epidemiologyofbenignproliferative epithelial disorders of the female breast. J Pathol 1985;146:1-15.
5. Mansel RE. Benign breast disease. Practitioner1982;232:830-7.
6. Sainsbury RC. Breast. In: NormanWS, Bulstrode CJ,RonanO’ConnelP,editors.BaileyandLove’sShortPracticeof Surgery. 25th ed. London: Edward Arnold Ltd.; 2008. p. 827-48.
7. Ajitha MB, Srinivasan N, Shivaswamy BS, Abhishek V. A systemic study on fibroadenomaof the breast. IJBAR2012;3:891-5.
8. Siddiqui M, Kayani N, Gill M, Pervez S, Muzaffar S, Aziz S, et al. Breast diseases: A histopathological analysis of 3279 cases at a tertiary care center in Pakistan. J Pak Med Assoc 2003;53:94-7.
9. DupontWD, PageDL.Risk factors for breast cancer inwomen with proliferative breast disease. N Engl J Med 1985;312:146-51.
10. Sangma MB, Panda K, Dasiah S. A clinico-pathological study onbenignbreastdiseases.JClinDiagnRes2013;7:503-6.
11. AdesunkanmiAR,AgbakwuruEA.BenignbreastdiseaseatWesleyGuildHospital,Ilesha,Nigeria.WestAfrJMed2001;20:146-51.
12. Ihekwaba FN. Benign breast disease in Nigerian women: a studyof657patients.JRCollSurgEdinb1994;39:280-3.
13. Florica JV. Fibrocystic changes. Obstet Gynecol Clin N Am 1994;21:445-59.
14. GreenbergR,SkornickY,KaplanO.Managementofbreastfibroadenomas. J Gen Intern Med 1998;13:640-5.
15. HaagensenCD.Diseasesof theBreast.PhiladelphiaandLondon: W.B. Saunders; 1957.
16. Wynder EL, Bross IJ, Hirayama T. A study of theepidemiology of cancer of the breast. Cancer. 1960; 13: 559–601.
17. HaqueR,TyagiSP,KhanMH,GahlautYV.Breastlesions.A clinicopathological study of 200 cases of breast lumps. Indian J Surg 1980;42:419-25.
18. Decker GA, Plessis DJ. In: Lee McGregor’s Synopsis of Surgical Anatomy. Bristol: John Wright & Sons Ltd.; 1986. p. 161-71.
19. KernWH,ClarkRW.Retrogressionoffibroadenomasofthebreast. Am J Surg 1973;126:59-62.
Figure 1: Visible lump in upper outer quadrant of right breast
Figure 2: Benign phyllodes tumor of right breast
How to cite this article: Singh SK, Ahmad KN, Pankaj D, Ansari MA. Benign breast lesions in a teaching hospital in rural Bihar. IJSS Journal of Surgery 2016;2(1):6-10.
Source of Support: Nil, Conflict of Interest: None declared.
Dr Khwaja Nasim Ahmad et al JMSCR Volume 07 Issue 01 January 2019 Page 800
JMSCR Vol||07||Issue||01||Page 800-802||January 2019
A Study of Percutaneous Antegrade Transvesical Fulguration of Posterior
Urethral Valves in Neonates and Infants
Authors
Dr Khwaja Nasim Ahmad1, Dr Ashutosh Patel
2, Dr Md. Abdur Rahman
3,
Dr Yasir Tajdar4
1Associate Professor, Dept. of General Surgery, K.M.C. Katihar
2Assistant Professor, Dept. of General Surgery, K.M.C. Katihar
3,4PGT, Dept. of General Surgery, K.M.C. Katihar
Corresponding Author
Dr Ashutosh Patel
Assistant Professor, Dept. of General Surgery, K.M.C. Katihar, India
Abstract
Due to advancement in imaging technology especially ultrasound and routine antenatal monitoring of foetus
by ultrasound it has become easier to diagnose posterior urethral valve earliest possible, even can be
diagnosed in utero. So earliest decompression of the kidneys and fulguration of PUV with better outcome is
possible now.
Materials and Methods
This retrospective study was conducted at Katihar
Medical College, Katihar in Department of
General Surgery from 2015 to 2018. Total 25
patients were selceted who presented with – (i)
Drribbling of urine (ii) Distentded bladder (iii)
Bilateral hydronephrosis on USG (iv) Weak
urinary stream.
All the cases done under general anaesthesia with
muscle relaxant and infant feeding tube of 6 Fr
was passed per urethra after all antiseptic
precautions. Bladder was fully distended with
normal saline then the feeding tube was clamped.
With the help of large cutting needle and linen
thread the lower anterior abdominal wall and
anterior wall of urinary bladder was fixed by
taking two deep bites 2 cm apart in the midline at
the upper portion of the bladder including the
anterior abdominal wall.
Now with the help of no. 11 blade small incision
was made over anterior abdominal wall between
two sutures. Now with the help of Trocar we
puncture into the bladder. Through this rent we
passed 17 Fr cystoscope and examined interior of
the bladder and locate the per urethral feeding
tube. Using infant feeding tube as a guide, bladder
neck was located, now it was easier to enter into
posterio urethra as it was widely dilated in case of
PUV. Posterior urethral valve identified and with
the help of 4 Fr ureteric catherter and metallic
www.jmscr.igmpublication.org
Index Copernicus Value: 79.54
ISSN (e)-2347-176x ISSN (p) 2455-0450
DOI: https://dx.doi.org/10.18535/jmscr/v7i1.139

Dr Khwaja Nasim Ahmad et al JMSCR Volume 07 Issue 01 January 2019 Page 801
JMSCR Vol||07||Issue||01||Page 800-802||January 2019
stealate the posterior urethral valve was fulgurated
under vision by insulating the metallic tip ureteric
catherter between the infant feeding tube and
during fulguration we go on extending the
metallic tip laterally so it open the urethra.
The completeness of fulguration was judged on
the operating table by removing the infant feeding
tube from urethra and seeing the flow of urine by
pressing the bladder. No stitches were taken over
anterior abdominal wall or the bladder.
Foley's catheter was inserted according to the size
of urethra and remains there as needed according
to the condition of the patients.
Merits and Demerits
As most of the patients were neonates and infants
and at that moment we didn’t have such small
endoscope by which perurethral fulguration of
PUV could be possible. As it is the well
established facts mentioned all over the literature
that there is a very high percentage of urethral
stricture even >30% in children when the existing
urethroscope are used to fulguration retrogradely
(through urethra).
As there was wide dilatation of posterior urethra
in case of PUV, we took advantage of this
situation and even there was no difficulty in
entering the urethra antegradely even with 17 Fr
cystoscope and does not touches at all the wall of
urethra. So there was no question of stretching or
trauma to the urethra and valve can be easily
fulgurated and therefore there were very much
less chance of stricture of urethra in this procedure.
No sophisticated, expensive and miniature
instruments were required but the basic
instruments can be used to fulgurate the valve and
there by reducing the cost of the procedure.
Localization of the valve is very much easier in
case of PUV in antegrade method of fulguration.
Only demerit of this procedure was the abdominal
puncture of the bladder suprpubically and
sometimes extravassation of urine can be seen.
Result
Most of the patients with posterior urethral valves
improved without any complication after
Percutaneous Antegrade Transvesical Fulguration,
reoperation in 2 patients (8%) is due to under
fulguration to avoid any stricture urethra and
death in 1 patient (4%) due to pulmonary
hypoplasia and septicemia.
Discussion
PUV is a congenital disease and with the use of
different imaging modalities it can be diagnosed
early in life and even antenatally. In our study 2
patients (8%) were diagnosed antenatally. This
observation was in accordance with Casale et al.
(1990) according to him posterior urethral valve
accounts for 10% of all infants born with
significant uropathies diagnosed antenatally.
In present series 44% of patients presented in first
month of life. A.N. Gangopodhyay (2003) noted
that nearly half of the patients presented in first
three months of life. In our series it was 64%.
The incidence of posterior urethral valve in our
series was 9.3 patients per year, higher in
accordance with Bueschen et al. (1973), who
recorded 4.2 cases per year. However, this
observation was in accordance with William et al.
(1965) was noted 8 cases per year.
Voiding cystourethrography was used to
established the diagnosis of PUV which 100%
sensitive in detecting PUV and showing
vesicoureteric reflux. This study simulates with
the report of A.N. Gangapodhyay (2003) who also
used voiding cystourethrography as the role mode
of confirmatory test and to know the reflux or any
bladder abnormalities.
In our series of study we performed “Percutaneous
Antegrade Transvesical Fulguration of PUV” in
20 patients (80%) without prior diversion, rest of
5 patients having severely deranged renal
parameters and early valve ablation was not
possible, we went for urinary diversion
(vesicotomy in 4 and percutaneous ureterostomy
in 1) and delayed antegrade transvesical valve
ablation through performed tract after
improvement of renal function.
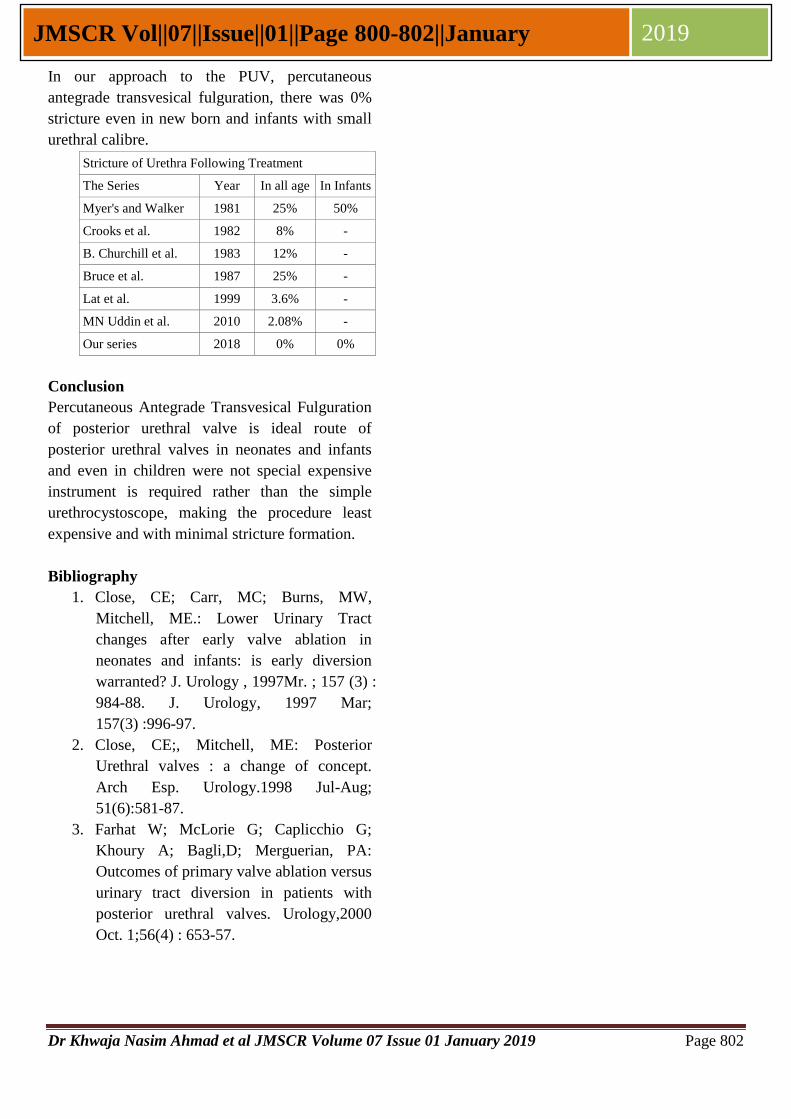
Dr Khwaja Nasim Ahmad et al JMSCR Volume 07 Issue 01 January 2019 Page 802
JMSCR Vol||07||Issue||01||Page 800-802||January 2019
In our approach to the PUV, percutaneous
antegrade transvesical fulguration, there was 0%
stricture even in new born and infants with small
urethral calibre.
Stricture of Urethra Following Treatment
The Series Year In all age In Infants
Myer's and Walker 1981 25% 50%
Crooks et al. 1982 8% -
B. Churchill et al. 1983 12% -
Bruce et al. 1987 25% -
Lat et al. 1999 3.6% -
MN Uddin et al. 2010 2.08% -
Our series 2018 0% 0%
Conclusion
Percutaneous Antegrade Transvesical Fulguration
of posterior urethral valve is ideal route of
posterior urethral valves in neonates and infants
and even in children were not special expensive
instrument is required rather than the simple
urethrocystoscope, making the procedure least
expensive and with minimal stricture formation.
Bibliography
1. Close, CE; Carr, MC; Burns, MW,
Mitchell, ME.: Lower Urinary Tract
changes after early valve ablation in
neonates and infants: is early diversion
warranted? J. Urology , 1997Mr. ; 157 (3) :
984-88. J. Urology, 1997 Mar;
157(3) :996-97.
2. Close, CE;, Mitchell, ME: Posterior
Urethral valves : a change of concept.
Arch Esp. Urology.1998 Jul-Aug;
51(6):581-87.
3. Farhat W; McLorie G; Caplicchio G;
Khoury A; Bagli,D; Merguerian, PA:
Outcomes of primary valve ablation versus
urinary tract diversion in patients with
posterior urethral valves. Urology,2000
Oct. 1;56(4) : 653-57.
Dr Khwaja Nasim Ahmad et al JMSCR Volume 05 Issue 10 October 2017 Page 29446
JMSCR Vol||05||Issue||10||Page 29446-29448||October 2017
Epidemiological Study of Urolithiasis with Special Reference to Its Chemical
Nature
Dr Khwaja Nasim Ahmad1, Dr Md. Abdur Rahman
2, Dr Md. Shadab
3,
Dr Amjad Zia Mallik4, Dr Yasir Tajdar
5, Dr Ameet Kumar
6, Dr Nadia Hasin
7
1Associate Professor, Department of Surgery, K.M.C, Katihar 2,5,6,7
Post graduate, Department of Surgery, K.M.C, Katihar 3Assistant professor, Department of Surgery, K.M.C, Katihar
4Professor, Department of Surgery, K.M.C, Katihar
Abstract
Epidemiological Study of Urolithiasis with special reference to its chemical nature. To find out the quality
of urinary stone. The collected stones were sent to the Department of Biochemistry, K.M.C.H, Katihar.
Qualitative biochemical analysis were performed to know the composition of the stones by H. Varley
method. It was a prospective study. A total of 23 patients had been studied. The study period is of 1 year
duration of which male – 14, female – 9 all were collected after intervention. Age group was from 8 years
to 70 years. 73.91% of the case studied was renal calculi. 94.11 % of all the renal calculi was unilateral.
21.73% of all the urolith was ureteric calculi and bladder stone was 8.69%.
Introduction
Urinary stones have afflicted human kind since
antiquity, with the earliest recorded example being
bladder and kidney stones detected in Egyptian
mummies dated to 4800 B.C. The incidence of
urolithiasis is increasing gradually all over the
world including Bengal region. Most accounts of
urinary stone disease, both renal and bladder,
majority were unaccompanied by observable
anatomic or metabolic disorder hence idiopathic.
Poor economic condition had been associated with
idiopathic bladder stone, composed principally of
calcium oxalate ammonium urate and uric acid
(Broek et. al. 1981, Sutor et. al. 1974). Affluent,
industrialised and developed countries were to
face predominantly the problem of idiopathic
calcium kidney stones (Letl 1934, Gherdi et. al.
1973, GU 1978). The role of socio-economic
factor in idiopathic renal stone occurrence was
mediated by dietary habit. Anderson (1972) and
Robertson et. al. 1973 noted that the men in the
higher socio-economic group were more
prevalently suffering from the disease. Power et.
al. (1989) also found that town with better socio-
economic conditions were the places with higher
incidence of renal stone.
Methods
All the patients admitted with urolithiasis in the
department of General Surgery Katihar Medical
College, Katihar were evaluated by history,
clinical examinations, routine & special
investigations, imaging techniques, stone were
collected after interventions, i.e. open operations
www.jmscr.igmpublication.org
Impact Factor 5.84
Index Copernicus Value: 71.58
ISSN (e)-2347-176x ISSN (p) 2455-0450
DOI: https://dx.doi.org/10.18535/jmscr/v5i10.165
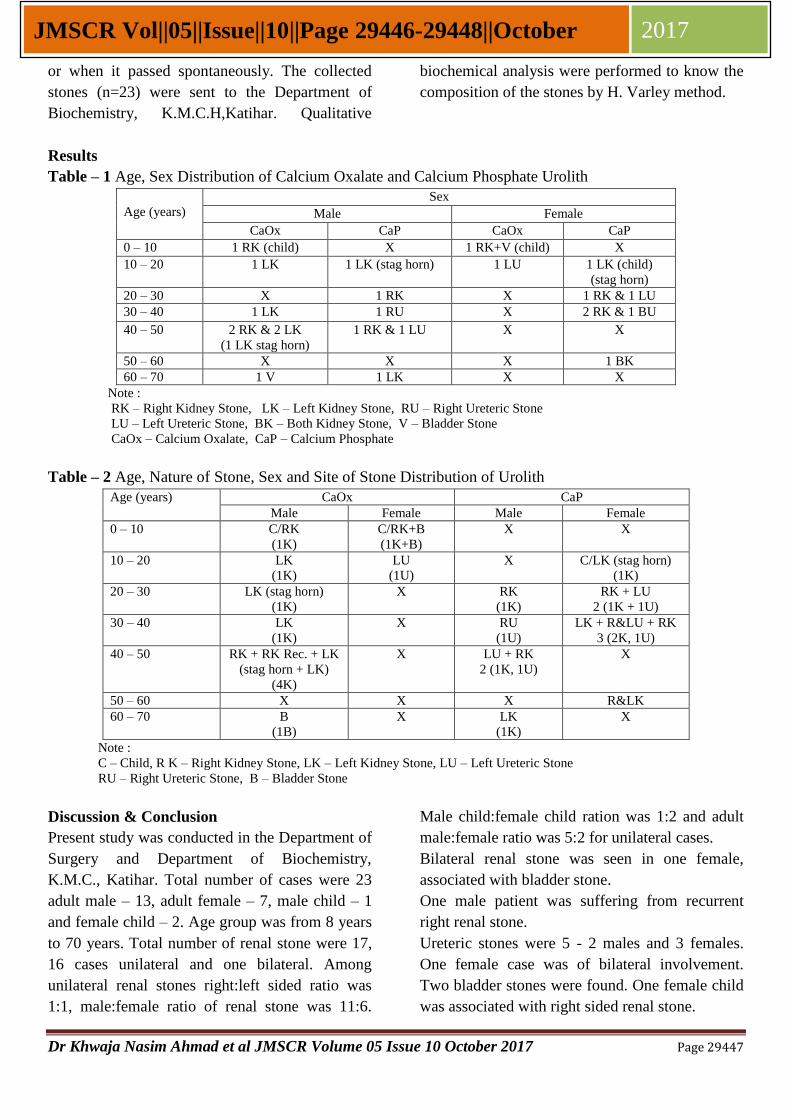
Dr Khwaja Nasim Ahmad et al JMSCR Volume 05 Issue 10 October 2017 Page 29447
JMSCR Vol||05||Issue||10||Page 29446-29448||October 2017
or when it passed spontaneously. The collected
stones (n=23) were sent to the Department of
Biochemistry, K.M.C.H,Katihar. Qualitative
biochemical analysis were performed to know the
composition of the stones by H. Varley method.
Results
Table – 1 Age, Sex Distribution of Calcium Oxalate and Calcium Phosphate Urolith
Age (years)
Sex
Male Female
CaOx CaP CaOx CaP
0 – 10 1 RK (child) X 1 RK+V (child) X
10 – 20 1 LK 1 LK (stag horn) 1 LU 1 LK (child)
(stag horn)
20 – 30 X 1 RK X 1 RK & 1 LU
30 – 40 1 LK 1 RU X 2 RK & 1 BU
40 – 50 2 RK & 2 LK
(1 LK stag horn)
1 RK & 1 LU X X
50 – 60 X X X 1 BK
60 – 70 1 V 1 LK X X
Note :
RK – Right Kidney Stone, LK – Left Kidney Stone, RU – Right Ureteric Stone
LU – Left Ureteric Stone, BK – Both Kidney Stone, V – Bladder Stone
CaOx – Calcium Oxalate, CaP – Calcium Phosphate
Table – 2 Age, Nature of Stone, Sex and Site of Stone Distribution of Urolith
Age (years) CaOx CaP
Male Female Male Female
0 – 10 C/RK
(1K)
C/RK+B
(1K+B)
X X
10 – 20 LK
(1K)
LU
(1U)
X C/LK (stag horn)
(1K)
20 – 30 LK (stag horn)
(1K)
X RK
(1K)
RK + LU
2 (1K + 1U)
30 – 40 LK
(1K)
X RU
(1U)
LK + R&LU + RK
3 (2K, 1U)
40 – 50 RK + RK Rec. + LK
(stag horn + LK)
(4K)
X LU + RK
2 (1K, 1U)
X
50 – 60 X X X R&LK
60 – 70 B
(1B)
X LK
(1K)
X
Note :
C – Child, R K – Right Kidney Stone, LK – Left Kidney Stone, LU – Left Ureteric Stone
RU – Right Ureteric Stone, B – Bladder Stone
Discussion & Conclusion
Present study was conducted in the Department of
Surgery and Department of Biochemistry,
K.M.C., Katihar. Total number of cases were 23
adult male – 13, adult female – 7, male child – 1
and female child – 2. Age group was from 8 years
to 70 years. Total number of renal stone were 17,
16 cases unilateral and one bilateral. Among
unilateral renal stones right:left sided ratio was
1:1, male:female ratio of renal stone was 11:6.
Male child:female child ration was 1:2 and adult
male:female ratio was 5:2 for unilateral cases.
Bilateral renal stone was seen in one female,
associated with bladder stone.
One male patient was suffering from recurrent
right renal stone.
Ureteric stones were 5 - 2 males and 3 females.
One female case was of bilateral involvement.
Two bladder stones were found. One female child
was associated with right sided renal stone.
Dr Khwaja Nasim Ahmad et al JMSCR Volume 05 Issue 10 October 2017 Page 29448
JMSCR Vol||05||Issue||10||Page 29446-29448||October 2017
Stones were collected after interventions
(pyelolithotomy, ureterolithotomy, cystolitho-
tomy), and retrieved stones were sent to
laboratory for chemical analysis in each case.
Calcium oxalate was found in 47.83% cases and
calcium phosphate in 52.17% cases. Among male
patients, 8 cases were found with calcium oxalate
and 5 cases with calcium phosphate In cases of
female, calcium oxalate was found in 1 case and
calcium phosphate in 6 cases. In children, one
male patient suffered from calcium oxalate stone,
1 female from calcium oxalate and other one from
calcium phosphate.
Incidence of idiopathic calcium stone disease is
increasing. Male suffers more than their female
counter part. Change in life style and food habit
probably is incriminated for rise in stone disease.
Also, genetic influences are important. It is a
multi-factorial disease, chemical nature of stones
influence the treatment procedure.
References
1. Monti E, Trinchieri A, Magri V, et. al.:
Herbal medicines for urinary stone
treatments. A systemic rerview. Arch Ital
Urol Androl. 2016: 88 (1): 38-46.
2. Scott Kreigshauser J, Naidu SG, Paden
RG, He M, Wu Q, Hara AK.Feasibility of
ultra- low radiation dose dreuctionh for
renal stone CT using model based
iterative reconstruction: Prospective pilot
study. Clin Imaghing 2015:39:99-103.
3. Huang GO, Engebretsen SR, Smith JC,
Wallner CL, Culpepper DJ, Creech JD, et
al.. Detection of uric acid stones in the
ureter using low- and concentional dose
CT. Urology 2014; 84:571-4.
4. Green W, Ratan H: Molecular Mechanism
of urolitiasis. Urology 2013; 81(4): 701-4
5. Kulkarni NM, Uppot RN, Eisner BH,
Sahni DV, Radiation Dose Reduction At
Multidetector CT with Adaptive statistical
iterative reconstruction for evaluation of
urolithiasis: How low can we go?
Radiology 2012; 265:158-66.
6. Eisner BH, McQuid JW, Hymes E,
Matlaga BR. Nephrolithiasis: What
surgeons need to know? AJR Am J
Roentgenol 2011; 196:1274-8.
7. Hsu TC, Chen J. Huang HS. Wang CJ. :
Association of changes in the pattern of
urinary calculi in Taiwanese with diet
habit change between 1956 & 1999.
Journal of the Formosan Medical
Association. 101(1):5-10 2000Jan.
8. Decoster M. Bigot JC. Carre JL. Morin
JF, Mahe JL. Tanguerel T . Cledes J, Floch
HH. : Epidemiologic study of urinary
calculi in western France. Press Medicale
31(3):113-9 2002Jan 26.
9. Sagara Y, Hara AK, Pavlicek W, Silva
AC, Paden RG, Wu Q. Abdominal CT :
Comparision of low dose CT with adaptive
statistical iterative reconstruction and
routine- dose CT with filtered back
projection in 53 patients.AJR Am J
Roentgenol 2010;195:713.
10. Safranow K: [Identification and
quantitation of purine derivatives in
urinary calculi as markers of abnormal
purine metabolism by using high-
performance liquid chromatography
11. Varley’s Practical Clinical Biochemistry
6th
edition page 758-760.
12. CAMPBELL’S UROLOGY 8th
Edition,
volume-4.

538 IJSR - INTERNATIONAL JOURNAL OF SCIENTIFIC RESEARCH
Volume : 4 | Issue : 9 | Sept 2015 • ISSN No 2277 - 8179Research Paper
Medical Science
* Md Mazharul Haque MS (General Surgery), Associate Professor, Department of Surgery, Katihar Medical College, Katihar, Bihar, India. * Corresponding author
B. K. Sinha MS (General Surgery), Associate Professor, Department of Surgery, Darbhanga Medical College & Hospital, Darbhanga, Bihar, India.
The Study of Effectiveness of Calcium Alginate Dressing Over the Split Thickness
Skin Graft Donor Site Area of Patients
KEYWORDS : Calcium alginate dressings, split thickness skin graft, Donor site area
ABSTRACT Aim: Calcuim alginate dressings were used to clinical evaluation and effectiveness on the split thickness skin graft donor site area of patients. Methodology: : History taking, Clinical examination, Investigation, Treatment: pre opera-
tive and post operative, Post operative management, Histopathological examination of excised specimens of marjolin’s ulcers were performed to the patients. Follow up the patients were a period of 3 months to 6 months. Observation: Observation was done for a period of 10th post operative days. Data was analyzed by MS Office software. Conclusion: calcium alginate dressings over donor site was quite easy, almost pain-less, removal was easy and minimal pain, minimal trauma to the newly epithelialized surface and rate of epithelialization was very high (72% patients) on 10th post operative days
INTRODUCTIONThe persons have more risk for thermal burns due to industri-alization and more use of electrical equipments which leads the increase challenge for management of burn.1 The modern trend of early and complete coverage of the lost skin by split thickens skin homograft has further increased the challenges for manage-ment of recipient as well as of the donor site areas of the skin graft. 1
Our study was primarily be focused on the management of the donor site area dressings which was primarily managed depend upon the personal choices of individual surgeon. Some of them are mesh gauze dressings, poly urethane semi permeable trans-parent films, hydrocolloid dressings and retention dressing etc.
Post operative patients may complain pain over the donor site area by the use of these conventional dressings, and soakage from the dressings with oozing from the donor bed is another problem. By applying these type of dressings healing of the do-nor site area takes a long time and sometime it is unpredict-able, removal of the dressings are difficult and almost adherent to the bed and removal is uneasy and painful to the patient.2
Alginate dressings form a gel like layer when in contact with moist wound providing moist environment for healing. This gel like layer over the donor site protects the epithelializing wound from trauma and from drying.3This may be the reason behind early and better epithelialization of the donor site with alginate dressings.
Our study was to evaluated the clinical effectiveness of calcium alginate dressing over the split thickness skin graft donor site area under these stages: 1. Post operative dressing soakage. 2. Post operative pain, 3. Healing time, and 4. Ease of dressing re-moval.
A moist environment was also used to promote healing by dress-ing with calcium alginate, which possesses hemostatic property.
MATERIAL & METHODSA total of 50 patients with varied clinical conditions like post burn contractures, chronic non healing ulcers, Marjolin’s ulcer etc on the basis of inclusion criteria were selected. This study was done in department of Surgery, Darbhanga Medical College and Hospital, Darbhanga, Bihar, India between may 2005 to may 2007 . Patients were carried for primary management of acute burn and who required split thickness skin graft over the raw body. The attendant of entire subjects signed an informed con-
sent approved by ethical committee of Darbhanga Medical Col-lege, Darbhanga, Bihar, India was sought.
Methodology: History taking, Clinical examination, Investiga-tion, Treatment: pre operative and post operative, Post op-erative management, Histopathological examination of excised specimens of Marjolin’s ulcers, Follow up the patients for a pe-riod of 3 months to 6 months.
Treatment:Preoperative treatment:Patients with chronic non healing ulcers and ulcers over burn scar were required initial treatment with antibiotics, multivita-mins and antiseptic dressings till the lesions became clean and granulating.
Operative treatment:When the patients were found to be fit for surgery on the basis of clinical examination, investigation and pre anaesthetic check-up then they were allowed for surgical procedure- viz. release of contracture, wide excision of the marjolin’s ulcer, excision/scrap-ping of the chronic non healing ulcer followed by coverage of the raw area with split thickness skin graft.
Preoperative measures:Light diet was given one day before from the date of surgery. A short acting mild sedative like alprazolam 0.25 mg was given in night before surgery. On the day of surgery in the morning proper shaving of the concerned parts of the body was done. Injection tetanus toxoid 0.5 ml was administered intramuscular over deltoid muscle. Half an hour before the surgery injection atropine or injection glycopyrolate intramuscularly and injection retidine 50 mg intravenously were administered. Patient was shifted to the operation theature. Injection ceftriaxone of proper dose was administered intravenously at the time of induction of anaesthesia.
Operative notes:Proper painting and draping of the donor as well as the recipi-ent sites were done. The primary pathologies e.g. post burn con-tracture, marjoline’s ulcer, chronic non healing ulcer etc were dealt with first by relevant surgeries viz. release of the contrac-ture, wide excision of ulcer or scraping of the wound etc. com-plete hemostasis of the recipient sites were achieved and cov-ered with a sterile tetra. Then split thickness skin grafts were raised of a proper sizes from proper donor sites with the help of humbey’s knife. Areas were covered with sterile tetras for the time being and the grafts were spread over the recipient sites,
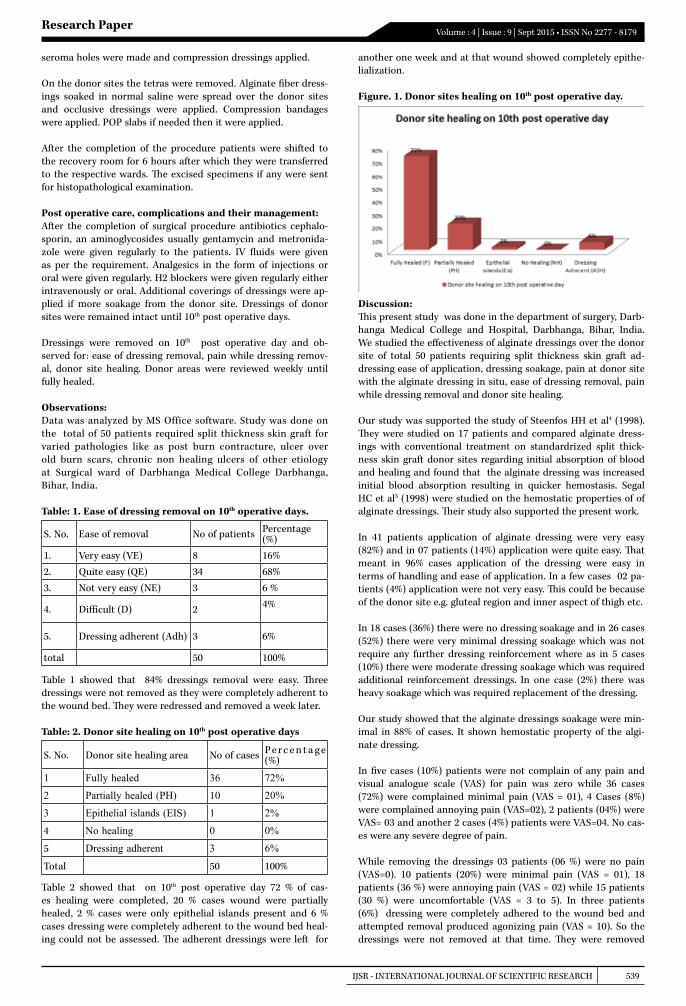
IJSR - INTERNATIONAL JOURNAL OF SCIENTIFIC RESEARCH 539
Volume : 4 | Issue : 9 | Sept 2015 • ISSN No 2277 - 8179Research Paper
seroma holes were made and compression dressings applied.
On the donor sites the tetras were removed. Alginate fiber dress-ings soaked in normal saline were spread over the donor sites and occlusive dressings were applied. Compression bandages were applied. POP slabs if needed then it were applied.
After the completion of the procedure patients were shifted to the recovery room for 6 hours after which they were transferred to the respective wards. The excised specimens if any were sent for histopathological examination.
Post operative care, complications and their management:After the completion of surgical procedure antibiotics cephalo-sporin, an aminoglycosides usually gentamycin and metronida-zole were given regularly to the patients. IV fluids were given as per the requirement. Analgesics in the form of injections or oral were given regularly. H2 blockers were given regularly either intravenously or oral. Additional coverings of dressings were ap-plied if more soakage from the donor site. Dressings of donor sites were remained intact until 10th post operative days.
Dressings were removed on 10th post operative day and ob-served for: ease of dressing removal, pain while dressing remov-al, donor site healing. Donor areas were reviewed weekly until fully healed.
Observations:Data was analyzed by MS Office software. Study was done on the total of 50 patients required split thickness skin graft for varied pathologies like as post burn contracture, ulcer over old burn scars, chronic non healing ulcers of other etiology at Surgical ward of Darbhanga Medical College Darbhanga, Bihar, India.
Table: 1. Ease of dressing removal on 10th operative days.
S. No. Ease of removal No of patients Percentage (%)
1. Very easy (VE) 8 16%
2. Quite easy (QE) 34 68%
3. Not very easy (NE) 3 6 %
4. Difficult (D) 2 4%
5. Dressing adherent (Adh) 3 6%
total 50 100%
Table 1 showed that 84% dressings removal were easy. Three dressings were not removed as they were completely adherent to the wound bed. They were redressed and removed a week later.
Table: 2. Donor site healing on 10th post operative days
S. No. Donor site healing area No of cases P e r c e n t a g e (%)
1 Fully healed 36 72%
2 Partially healed (PH) 10 20%
3 Epithelial islands (EIS) 1 2%
4 No healing 0 0%
5 Dressing adherent 3 6%
Total 50 100%
Table 2 showed that on 10th post operative day 72 % of cas-es healing were completed, 20 % cases wound were partially healed, 2 % cases were only epithelial islands present and 6 % cases dressing were completely adherent to the wound bed heal-ing could not be assessed. The adherent dressings were left for
another one week and at that wound showed completely epithe-lialization.
Figure. 1. Donor sites healing on 10th post operative day.
Discussion:This present study was done in the department of surgery, Darb-hanga Medical College and Hospital, Darbhanga, Bihar, India. We studied the effectiveness of alginate dressings over the donor site of total 50 patients requiring split thickness skin graft ad-dressing ease of application, dressing soakage, pain at donor site with the alginate dressing in situ, ease of dressing removal, pain while dressing removal and donor site healing.
Our study was supported the study of Steenfos HH et al4 (1998). They were studied on 17 patients and compared alginate dress-ings with conventional treatment on standardrized split thick-ness skin graft donor sites regarding initial absorption of blood and healing and found that the alginate dressing was increased initial blood absorption resulting in quicker hemostasis. Segal HC et al5 (1998) were studied on the hemostatic properties of of alginate dressings. Their study also supported the present work.
In 41 patients application of alginate dressing were very easy (82%) and in 07 patients (14%) application were quite easy. That meant in 96% cases application of the dressing were easy in terms of handling and ease of application. In a few cases 02 pa-tients (4%) application were not very easy. This could be because of the donor site e.g. gluteal region and inner aspect of thigh etc.
In 18 cases (36%) there were no dressing soakage and in 26 cases (52%) there were very minimal dressing soakage which was not require any further dressing reinforcement where as in 5 cases (10%) there were moderate dressing soakage which was required additional reinforcement dressings. In one case (2%) there was heavy soakage which was required replacement of the dressing.
Our study showed that the alginate dressings soakage were min-imal in 88% of cases. It shown hemostatic property of the algi-nate dressing.
In five cases (10%) patients were not complain of any pain and visual analogue scale (VAS) for pain was zero while 36 cases (72%) were complained minimal pain (VAS = 01), 4 Cases (8%) were complained annoying pain (VAS=02), 2 patients (04%) were VAS= 03 and another 2 cases (4%) patients were VAS=04. No cas-es were any severe degree of pain.
While removing the dressings 03 patients (06 %) were no pain (VAS=0). 10 patients (20%) were minimal pain (VAS = 01), 18 patients (36 %) were annoying pain (VAS = 02) while 15 patients (30 %) were uncomfortable (VAS = 3 to 5). In three patients (6%) dressing were completely adhered to the wound bed and attempted removal produced agonizing pain (VAS = 10). So the dressings were not removed at that time. They were removed

540 IJSR - INTERNATIONAL JOURNAL OF SCIENTIFIC RESEARCH
Volume : 4 | Issue : 9 | Sept 2015 • ISSN No 2277 - 8179Research Paper
REFERENCE1. Baily & Love’s Short practice of Surgery, 24th edition. | 2. Clinical guide to wound care, 5th edition. | 3. Cohen IK, Abrief history of wound heal-ing 1st edition. | 4. Steenfos HH, et al. A fibre free alginate dressing in the treatment of split thickness skin graft donoe sites. J Eur, Acad. Dermatol
Venerol. 1998 nov; 11(3): 252-6. | 5. Segal HC, et al. The effects of alginate and non alginate wound dressings on blood coagulation and platelet activation. J Bio Mater Appl, 1998 Jan; 12(3) : 249-257. | 6. Moxhan PH. Impact of alginate on healing of porcin dermal wounds. Alberta Canada; Western biomedical corp and university of Calgary, 2000. | 7. Disa JJ, et al. Evaluation of a combined calicium sodium alginate and bio occlusive membrain dressing in the management of split thickness skin graft donor sites. Anna Plast, Surg, 2001 Apr; 46(4) : 405-8. | 8. Butler PE, et al. Bupivacain and Kaltostat reduces post operative donor site pain. J. Plast Surg, 1993 sep; 46(6) : 523-24. | 9. Bettinger D, et al. Evaluation of calcium alginate for skin graft donor sites. Burn Care Rehabil 1995 Jan; 16(1) : 59-61. | 10. O’ Donoghue JM, et al. Effects of a silicon coated polyamide net dressing and calcium alginate on the healing of split thickness skin graft donor sites; a prospective randomized trial. Acta Chir Plast 2000; 42(1) : 3-6. | | |
subsequently after one week. In our study 72% of cases were minimal to mild pain during dressing removal.
Alginate dressings form a gel like layer when in contact with moist wounds e.g. a donor site area. This gel like layer prevents irritation of the raw nerve endings that are present at the post harvest donor site area.6 This may explain the pain reducing ef-fect of alginate dressings.
Disa JJ et al7 (2001) conducted a study and concluded that do-nor site discomfort was minimal with alginate dressings at the time of dressing change. They also reported that bio-occulusive dressing eliminated the pain typically associated with fine mesh gauze dressings.
Butler PE et al8 (1993) reported the pain reducing effects of al-ginate dressing. According to them alone alginate dressings re-duce pain, the best effects were obtained by alginate dressing moistened with bupivacaine hydrochloride (0.5%). Same effects was also found by Bettinger D et al9 (1995) on the pain reducing effects of alginate dressings.
In our present study on 10th post operative day 08 patients (16%) removal of the dressing were very easy, 34 patients (68%) were quite easy, 3 cases (6%) removal were not very easy and 2 cases (4%) were difficult and in another three cases the dressing were completely adherent to the wound bed and attempted removal incited agonizing pain, therefore redressed and removed of dressings were done at after one week. Hence our study showed that in 84 % cases removal of the dressing were easy. In a few of cases 6% the dressing were completely adherents.
Bettinger D et al9 (1995) was conducted a study on alginate dressings on burn patients with split thickness skin graft and concluded that alginate dressing was more beneficial over mesh gauze dressings in respect of case for care and removal and it was favored by the nursing personal. Our findings also support-ed the findings of Butler PE et al8 (1993) for ease of removal of alginate dressings.
Regarding the donor site healing when the dressings were re-moved on 10th post operative day 36 cases (72%) were completed healing, one case (2%) was epithelial islands only whereas in three cases (6%) the dressing were completely adherent to the wound bed and healing could not be assessed. This adherent dressing was left for another one week for complete epitheliali-zation. Thus we were found that complete epithelialization was occurred in 72% of cases on 10th post operative day.
With respect to calcium alginate dressing, conventional dress-ings takes more than fourteen days for epithelialization, and in
most cases it was incomplete. Thatswhy alginate dressing was more beneficial than conventional dressings.
O’ Donoghe JM (2000)10 reported that 91 % cases were achieved complete reepithelialization by 7th post operative day.
Hence our study was shown that calcium alginate dressings were better for ease of application, dressing soakage, pain at donor site, ease of dressing removal in split thickness skin graft than conventional dressings.
Future Research:Science is dynamic and there is always a scope of improvement and change in time to come ahead. With the progressive aim to move ahead we aspire to achieve highly accurate and reliable re-sults. Thus, every study leaves back scopes for other researcher to do something more advanced and varied in order to touch the height of perfection.
This study examined only 50 subjects in total and data collec-tion was confined to calcium alginate dressings on split thick-ness skin graft. Thus future researchers can expand the study by including more number of subjects and use of other dressing materials so as to make generalization of results and practice such experiments in variable Hospital setups . Thus it could be applied to real life situation.
Relevance to clinical practice:The results obtained in this study suggest that calcium alginate dressing is more beneficial than other conventional dressing. So, these results have shown that calcium alginate dressing should be used for dressings over split thickness skin graft on donor sites of patients.
Conclusion:Findings of present study concluded that calcium alginate dress-ings over donor sites were quite easy, almost painless, removal was easy and minimal pain, minimal trauma to the newly epi-thelialized surface and rate of epithelialization was very high on 10th post operative days.
ACKNOWLEDGMENTWe acknowledge the immense help received from the scholars whose articles are cited and included in references of this manu-script. Authors are also grateful to authors/editors/publishers of all those articles, journals and books from where the literature for this article has been reviewed and discussed.

GJRA - GLOBAL JOURNAL FOR RESEARCH ANALYSIS X 199
Volume-4, Issue-10, Oct-2015 • ISSN No 2277 - 8160
Research Paper Commerce Medical science
Study of Incidental carcinoma of gall bladder in benign gall bladder disease
Dr. Md Mazharul Haque
MS (General Surgery),Associate Professor, Department of surgery, Katihar Medical College, Katihar, Bihar, India.*Corresponding author
Dr. Sandeep Kumar Jaiswal
MS (General Surgery), Senior Resident, Department of surgery, Katihar Medical College, Katihar, Bihar, India.
Dr. Md Izhar Alam MD (Pathology), Assistant Professor, Department of Pathology, Katihar Medical College, Katihar, Bihar, India.
Introduction: With increased awareness among the patients and advancement in diagnostic techniques most of the diseases of gall bladder present to the clinician early and carcinoma of the gall bladder which has high mortality and very poor prognosis is usually diagnosed as an incidental finding on histopathological examination.
Methods & Materials: Patients undergoing cholecystectomy for benign diseases at a private hospital in the kosi region of Bihar, India.
Results: Out of 690 patients in whom cholecystectomy was done adenocarcinoma was detected histopathologically in 6 cases (0.87%). There was no suspicion of malignancy to any of them preoperatively.
Conclusion: In the present study the rate of incidental carcinoma of gallbladder was 0.87%. The risk factors related to gall bladder cancer are cholelithiasis, advance age etc. Upon final diagnosis of adenocarcinoma of gall bladder the patients were referred to higher centre of oncology for further treatment. All the patients whose histopathological examination showed adenocarcinoma were operated for cholelithiasis. Therefore the diagnosis of cholelithiasis is an indication for cholecystectomy.
ABSTRACT
KEYWORDS : Gallbladder, Cholelithiasis, Incidental, Carcinoma.
Introduction: In the Kosi region of Bihar, India benign gall bladder disease especial-ly cholelithiasis is quite common and the occurrence of gall bladder cancer is not so uncommon. With increased awareness among the patients and advancement in diagnostic techniques most of the dis-eases of gall bladder present to the clinician early and carcinoma of the gall bladder which has high mortality and very poor prognosis is usually diagnosed as an incidental finding on histopathological exam-ination. In this present study we tried to establish the overall rate of gall bladder cancer in the patients presenting with benign gall blad-der disease based on our experience.
Methods & Materials: From August 2008 to July 2015 a total of 690 patients underwent chol-ecystectomy at a private hospital in the Kosi region of Bihar, India. We retrospectively reviewed the clinical records of all the 690 patients. There were 605 female and 85 male patients. Three patients were operated for gall bladder polyp whereas the rest 687 were operated for cholelithiasis. None of these cases had preoperative suspicion of malignancy.
Results: Out of 690 patients in whom cholecystectomy was done adenocarcino-ma was detected histopathologically in 6 cases (0.87%).There were five females (83.3%) and one male(16.67% ) patient. Mean age of the patients was around 49 years. All the patients whose histopathological examina-tion showed adenocarcinoma were operated for cholelithiasis. Per opera-tively in one case the mucosa of the gall bladder showed a small nodule. The clinical data and follow-up are presented in Table 1.
Discussion: Gallbladder carcinoma is a highly malignant tumour and has poor prognosis. De Stall- [1771] was the first one to report gall bladder car-cinoma1. It is the fifth most common malignancy of gastrointestinal tract and the most common of the biliary tree and is usually discov-ered accidentally2. The exact etiology is unknown. The most com-mon risk factor is cholelithiasis. It is more common in females and its frequency increases with age3. The other risk factors are benign tu-mours, certain races, various carcinogens, abnormal union of pancrea-ticobiliary duct etc. Gall bladder carcinoma is diagnosed histologically in 0.3 to 1.5%4of all the cholecystectomy specimens. In our study the overall rate was 0.87%.The rate of incidentally diagnosed gall blad-der carcinoma has increased because of patient awareness, increased health facilities and advancement in diagnostic tools and techniques. Most of the cases in our study were diagnosed by histopatholgical examination. Only in one case the operated specimen had shown a suspicious small nodule on the mucosa.
Conclusion: Gall bladder carcinoma nowadays is most commonly detected inci-dentally. In the present study the rate of incidental carcinoma of gall-bladder was 0.87%. The risk factors widely related to the gallbladder cancer are advanced age and cholelithiasis. All the patients whose histopathological examination showed adenocarcinoma were oper-ated for cholelithiasis. Therefore the diagnosis of cholelithiasis is an indication for cholecystectomy.
Table 1.Clinical data
Age (Yrs) Sex Symptoms & signs Ultrasonography Operative Finding Histopathological finding Suspicious operativefinding
52 Female Pain Abdomen, Fever cholelithiasis Cholelithiasis,Thickwalled
GB,Adhesion at the neck
Moderately differentiatedadenocarcinoma extending through serosa,Chr. Cholecystitis.
No

GJRA - GLOBAL JOURNAL FOR RESEARCH ANALYSIS X 200
Volume-4, Issue-10, Oct-2015 • ISSN No 2277 - 8160
REFERENCES 1. De Stoll M. Rationis medendi in practice Unindobonensi. Part 1. Vienna: Bernard, 1777. 2. Targarona EM, Pons MJ, Viella P, Trias M. Unexpected carcinoma of the gallbladder, a laparoscopic dilemma. Surg Endosc 1994;8:211-13. 3. Donohue JH, Andrew KS, Herman RM. The national cancer database report on carcinoma of the gallbladder, 1989-1995. Cancer 1998;83:2618- 28 4. Contini S, Dalla Valle R, Zinicola R.
Unexpectant gallbladder cancer after laparoscopic cholecystectomy. Surg Endosc 1999;13:264-7. 5.Daphna Weinstein MD1, Mehrdad Herbert MD2, Noa Bendet MD1, Judith Sandbank MD2 and ArielHalevy MD1 1Department of Surgery B and 2Department of Pathology, Assaf Harofeh Medical Center, Zerifin, Israel. Affiliated to Sackler Faculty of Medicine, Tel Aviv University, Ramat Aviv, Israel 6.Shimizu T, Arima Y, Yokomuro S, Yoshida H, Mamada Y, Nomura T, Taniai N, Aimoto T, Nakamura Y, Mizuguchi Y, Kawahigashi Y, Uchida E, Akimaru H, Tajiri T. Incidental gallbladdere cancer diagnosed during and after laparoscopic cholecystectomy.J Nippon Med Sch. 2006;73:136–140Y 7.okomuro S, Arima Y, Mizuguchi Y, Shimizu T, et al. Occult gallbladder carcinoma after laparoscopic cholecistectomy: a report of four cases. J Nippon Med Sch. 2007;74:300–305. 8.Varsheney S, Buttirini G, Gupta R. Incidental carcinoma of the gallbladder. EJSO. 2002;28:410. 9.Matsusaka S, Yamasaki H, Kitayama Y, Okada T, Maeda S. Occult gallbladder carcinoma diagnosed by a laparoscopic cholecistectomy. Surg Today. 2003;33:740–742 10.Antonakis P, Alexakis N, Mylonakis D, Leandros E, Konstadoulakis MM, Zografos G, Androulakis G. Incidental finding of gallbladder carcinoma detected during or after laparoscopic cholecystectomy. EJSO. 2003;29:358–360 11.Glauser PM, Strub D, Kaser SA, Mattiello D, Rieben F, Maurer CA. Incidence, management, and outcome of incidental gallbladder carcinoma: analysis of the database of the Swiss association of laparoscopic and thoracoscopic surgery. Surg Endo-sc. 2010;24:2281–2286 12.Arnaud JP, Casa C, Georgeac C, et al. Primary carcinoma of the gallbladder - review of 143 cases. Hepatogastroenterology 1995;42:811-15. Vauthey JN, Baer HU, Guastella T, Blumgart LH. Comparison of outcome between extended and nonextended liver resections for neoplasms. Surgery 1993;114:968-75. 13.Tantia O, Jain M, Khanna S, Sen B. Department of Minimal Access Surgery, ILS Multispeciality Clinic, DD-6, Sector - I, Salt Lake City, Kolkata, 700 064, India.
30 Male Pain Abdomen, Fever cholelithiasis Cholelithiasis, Thickwalled
GB,Adhesion at the fundus
Moderately differentiatedadenocarcinoma extending through serosa,Chr. Cholecystitis.
No
51 Female Pain Abdomen, vomiting
Cholelithiasis,pus in the gall bladder
Cholelithiasis, empyema of GB
Chronic cholecystitis with Well to moderately differentiatedadenocarcinoma extending through serosa
No
49 Female Pain Abdomen, Cholelithiasis, adherent sludge
Cholelithiasis,one small nodule of 0.4cm size over the mucosa, GB thin walled
moderately differentiatedadenocarcinoma extending through serosa
Yes
67 Female Pain Abdomen, Fever
cholelithiasis, sludge
Cholelithiasis, sludge, thin walled GB carcinoma in situ of gall bladder No
44 Female Pain Abdomen,vomiting cholelithiasis Cholelithiasis, Thickwalled
GB, empyema of GB
Chronic cholecystitis,with moderately differentiated adenocarcinomaextending through serosa
No
CONSENT:No special consent was taken as the treatment given was in accord-ance with the current treatment practices in the unit.
ETHICAL APPROVAL:No prior ethical approval was taken as no experimental drug or pro-cedure was carried out in the management of this condition as high-lighted in the paper

International Surgery Journal | January-March 2016 | Vol 3 | Issue 1 Page 32
International Surgery Journal
Singh SK et al. Int Surg J. 2016 Feb;3(1):32-36
http://www.ijsurgery.com pISSN 2349-3305 | eISSN 2349-2902
Research Article
A clinico-pathological study of malignant breast lump in a tertiary care
hospital in Kosi region of Bihar, India
Shambhu Kumar Singh1, Deepak Pankaj
1*, Rajesh Kumar
2, Rayaz Mustafa
1
INTRODUCTION
Breasts are an important feature of female anatomy and
an integral part of reproductive system. It is a glandular
organ influenced by hormones in females and composed
of various structures giving rise to different types of
lesions and lumps.1 These lesions of breast can be of
various types ranging from inflammatory to benign to
malignant with some lesions being common in young
females while other being common in elderly to older age
group. Of all the breast disorders, pain is the first
common presentation with palpable breast lump being the
second most common presentation.2 Breast cancer is one
of the commonest malignant tumours in the world and is
one of the leading causes of death due to cancer in
women.3 It is the leading cause of death in women aged
between35 to 54 years. One in eight women are
diagnosed with breast cancer during their life time.4 In
India the incidence of breast cancer is low but rising.
India is a sub – continent with wide ethnic, cultural,
ABSTRACT
Background: Breast cancer has captured attention of surgeons throughout the ages with its uncertain cause. Despite
centuries of meandering and scientific enquiry, breast cancer is still one of the most dreaded human diseases. The
breast is a complex structure and any unnatural change affects the body and psyche of the person. The aim of this
study was to observe age distribution, clinical signs and symptoms and pathology of malignant breast lump and draw
a correlation between clinical and histological diagnosis of patients presenting with breast lump.
Methods: Seventy six (76) cases of diagnosed malignant breast lump out of a total of 200 cases were included in this
study. These cases were selected among patients visiting outdoor clinic of department of General Surgery in Katihar
Medical College, Katihar. The selected cases belonged to different etiology, age group and sex.
Results: Maximum number of malignant tumours was encountered in the 5th decade of age group of patients,
followed by in 4th decade. All cases studied were females except 2 cases which were male. The commonest sign and
symptoms of presentation was painless lump in the breast followed by painful mass in the breast along with
associated features of ulceration of the skin, retraction of nipple and nipple discharge. Histologically, malignant
tumours were maximally observed as infiltrating scirrhous carcinoma, followed by medullary carcinoma & papillary
carcinoma.
Conclusions: Breast cancer is a common cancer worldwide with varied presentation. Multimodality treatment
approach is required for malignant breast lump which has shown improvement in both loco regional control and
survival.
Keywords: Breast, Histopathology, Infiltrating carcinoma of breast, Malignancy, Surgery
1Department of General Surgery, Katihar Medical College, Katihar, Bihar, India
2Department of Pathology, Katihar Medical College, Katihar, Bihar, India
Received: 09 October 2015
Revised: 17 October 2015
Accepted: 04 November 2015
*Correspondence:
Dr. Deepak Pankaj,
E-mail: [email protected]
Copyright: © the author(s), publisher and licensee Medip Academy. This is an open-access article distributed under
the terms of the Creative Commons Attribution Non-Commercial License, which permits unrestricted non-commercial
use, distribution, and reproduction in any medium, provided the original work is properly cited.
DOI: http://dx.doi.org/10.18203/2349-2902.isj20151216
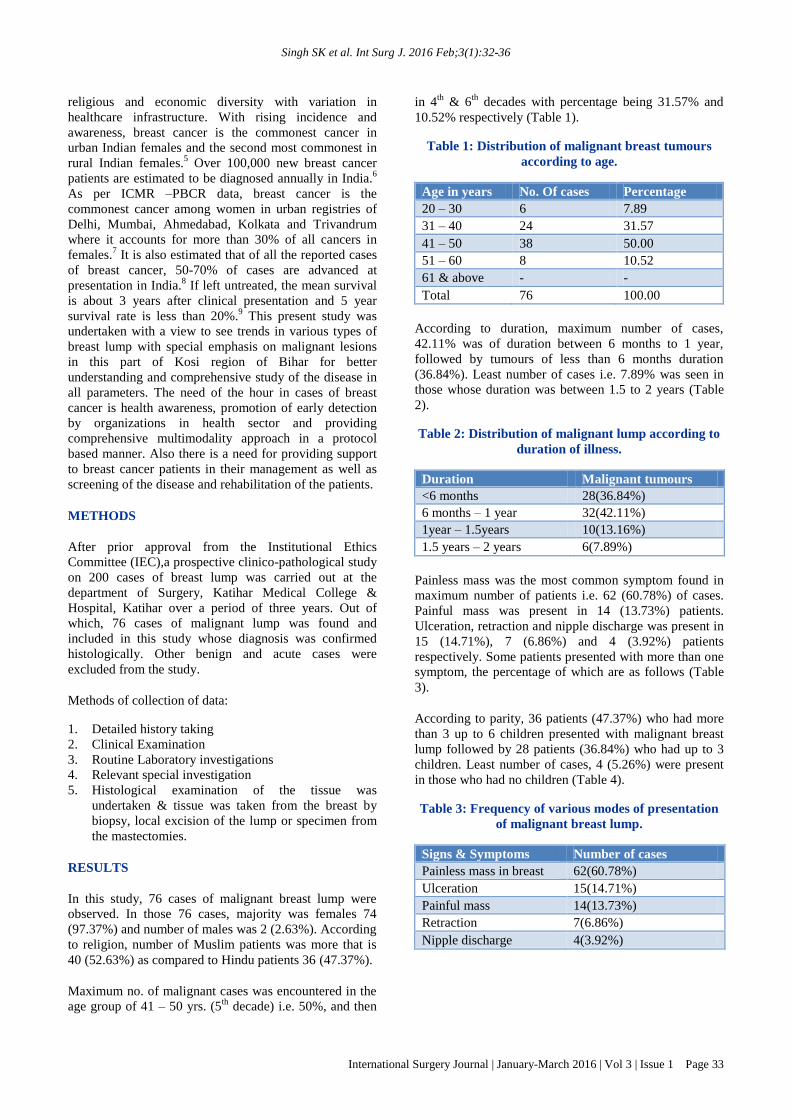
Singh SK et al. Int Surg J. 2016 Feb;3(1):32-36
International Surgery Journal | January-March 2016 | Vol 3 | Issue 1 Page 33
religious and economic diversity with variation in
healthcare infrastructure. With rising incidence and
awareness, breast cancer is the commonest cancer in
urban Indian females and the second most commonest in
rural Indian females.5 Over 100,000 new breast cancer
patients are estimated to be diagnosed annually in India.6
As per ICMR –PBCR data, breast cancer is the
commonest cancer among women in urban registries of
Delhi, Mumbai, Ahmedabad, Kolkata and Trivandrum
where it accounts for more than 30% of all cancers in
females.7 It is also estimated that of all the reported cases
of breast cancer, 50-70% of cases are advanced at
presentation in India.8 If left untreated, the mean survival
is about 3 years after clinical presentation and 5 year
survival rate is less than 20%.9 This present study was
undertaken with a view to see trends in various types of
breast lump with special emphasis on malignant lesions
in this part of Kosi region of Bihar for better
understanding and comprehensive study of the disease in
all parameters. The need of the hour in cases of breast
cancer is health awareness, promotion of early detection
by organizations in health sector and providing
comprehensive multimodality approach in a protocol
based manner. Also there is a need for providing support
to breast cancer patients in their management as well as
screening of the disease and rehabilitation of the patients.
METHODS
After prior approval from the Institutional Ethics
Committee (IEC),a prospective clinico-pathological study
on 200 cases of breast lump was carried out at the
department of Surgery, Katihar Medical College &
Hospital, Katihar over a period of three years. Out of
which, 76 cases of malignant lump was found and
included in this study whose diagnosis was confirmed
histologically. Other benign and acute cases were
excluded from the study.
Methods of collection of data:
1. Detailed history taking
2. Clinical Examination
3. Routine Laboratory investigations
4. Relevant special investigation
5. Histological examination of the tissue was
undertaken & tissue was taken from the breast by
biopsy, local excision of the lump or specimen from
the mastectomies.
RESULTS
In this study, 76 cases of malignant breast lump were
observed. In those 76 cases, majority was females 74
(97.37%) and number of males was 2 (2.63%). According
to religion, number of Muslim patients was more that is
40 (52.63%) as compared to Hindu patients 36 (47.37%).
Maximum no. of malignant cases was encountered in the
age group of 41 – 50 yrs. (5th
decade) i.e. 50%, and then
in 4th
& 6th
decades with percentage being 31.57% and
10.52% respectively (Table 1).
Table 1: Distribution of malignant breast tumours
according to age.
Age in years No. Of cases Percentage
20 – 30 6 7.89
31 – 40 24 31.57
41 – 50 38 50.00
51 – 60 8 10.52
61 & above - -
Total 76 100.00
According to duration, maximum number of cases,
42.11% was of duration between 6 months to 1 year,
followed by tumours of less than 6 months duration
(36.84%). Least number of cases i.e. 7.89% was seen in
those whose duration was between 1.5 to 2 years (Table
2).
Table 2: Distribution of malignant lump according to
duration of illness.
Duration Malignant tumours
<6 months 28(36.84%)
6 months – 1 year 32(42.11%)
1year – 1.5years 10(13.16%)
1.5 years – 2 years 6(7.89%)
Painless mass was the most common symptom found in
maximum number of patients i.e. 62 (60.78%) of cases.
Painful mass was present in 14 (13.73%) patients.
Ulceration, retraction and nipple discharge was present in
15 (14.71%), 7 (6.86%) and 4 (3.92%) patients
respectively. Some patients presented with more than one
symptom, the percentage of which are as follows (Table
3).
According to parity, 36 patients (47.37%) who had more
than 3 up to 6 children presented with malignant breast
lump followed by 28 patients (36.84%) who had up to 3
children. Least number of cases, 4 (5.26%) were present
in those who had no children (Table 4).
Table 3: Frequency of various modes of presentation
of malignant breast lump.
Signs & Symptoms Number of cases
Painless mass in breast 62(60.78%)
Ulceration 15(14.71%)
Painful mass 14(13.73%)
Retraction 7(6.86%)
Nipple discharge 4(3.92%)
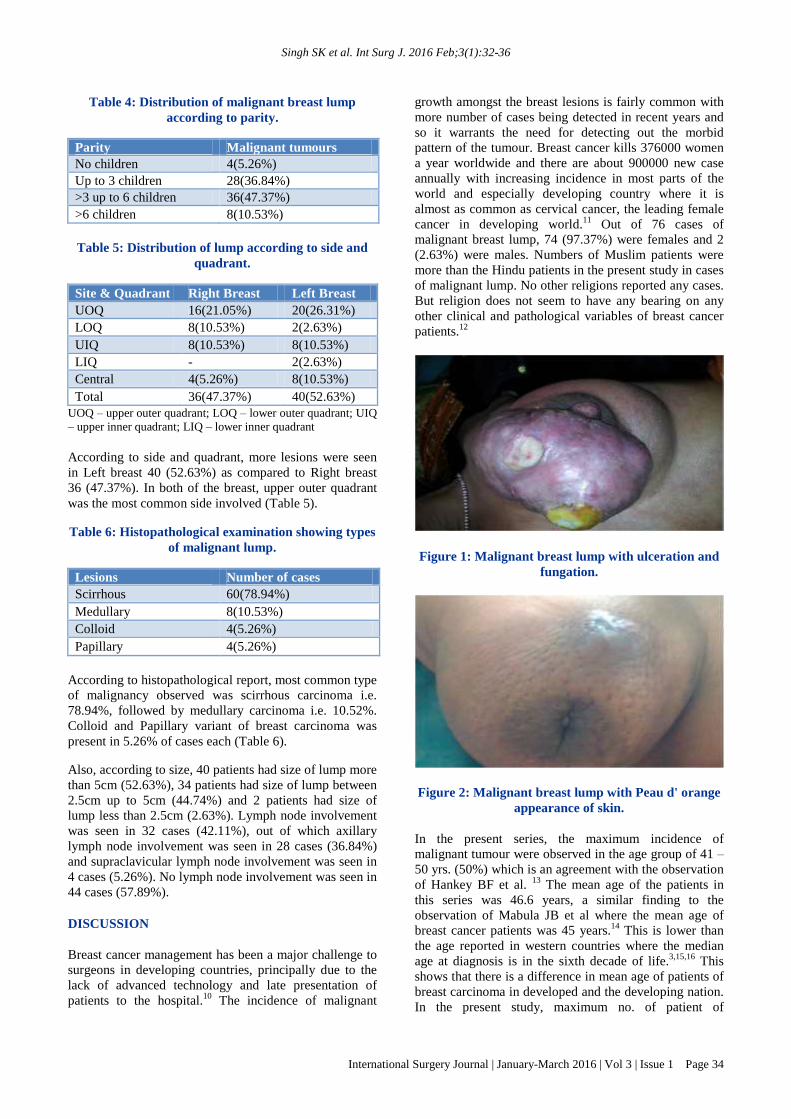
Singh SK et al. Int Surg J. 2016 Feb;3(1):32-36
International Surgery Journal | January-March 2016 | Vol 3 | Issue 1 Page 34
Table 4: Distribution of malignant breast lump
according to parity.
Parity Malignant tumours
No children 4(5.26%)
Up to 3 children 28(36.84%)
>3 up to 6 children 36(47.37%)
>6 children 8(10.53%)
Table 5: Distribution of lump according to side and
quadrant.
Site & Quadrant Right Breast Left Breast
UOQ 16(21.05%) 20(26.31%)
LOQ 8(10.53%) 2(2.63%)
UIQ 8(10.53%) 8(10.53%)
LIQ - 2(2.63%)
Central 4(5.26%) 8(10.53%)
Total 36(47.37%) 40(52.63%)
UOQ – upper outer quadrant; LOQ – lower outer quadrant; UIQ
– upper inner quadrant; LIQ – lower inner quadrant
According to side and quadrant, more lesions were seen
in Left breast 40 (52.63%) as compared to Right breast
36 (47.37%). In both of the breast, upper outer quadrant
was the most common side involved (Table 5).
Table 6: Histopathological examination showing types
of malignant lump.
Lesions Number of cases
Scirrhous 60(78.94%)
Medullary 8(10.53%)
Colloid 4(5.26%)
Papillary 4(5.26%)
According to histopathological report, most common type
of malignancy observed was scirrhous carcinoma i.e.
78.94%, followed by medullary carcinoma i.e. 10.52%.
Colloid and Papillary variant of breast carcinoma was
present in 5.26% of cases each (Table 6).
Also, according to size, 40 patients had size of lump more
than 5cm (52.63%), 34 patients had size of lump between
2.5cm up to 5cm (44.74%) and 2 patients had size of
lump less than 2.5cm (2.63%). Lymph node involvement
was seen in 32 cases (42.11%), out of which axillary
lymph node involvement was seen in 28 cases (36.84%)
and supraclavicular lymph node involvement was seen in
4 cases (5.26%). No lymph node involvement was seen in
44 cases (57.89%).
DISCUSSION
Breast cancer management has been a major challenge to
surgeons in developing countries, principally due to the
lack of advanced technology and late presentation of
patients to the hospital.10
The incidence of malignant
growth amongst the breast lesions is fairly common with
more number of cases being detected in recent years and
so it warrants the need for detecting out the morbid
pattern of the tumour. Breast cancer kills 376000 women
a year worldwide and there are about 900000 new case
annually with increasing incidence in most parts of the
world and especially developing country where it is
almost as common as cervical cancer, the leading female
cancer in developing world.11
Out of 76 cases of
malignant breast lump, 74 (97.37%) were females and 2
(2.63%) were males. Numbers of Muslim patients were
more than the Hindu patients in the present study in cases
of malignant lump. No other religions reported any cases.
But religion does not seem to have any bearing on any
other clinical and pathological variables of breast cancer
patients.12
Figure 1: Malignant breast lump with ulceration and
fungation.
Figure 2: Malignant breast lump with Peau d' orange
appearance of skin.
In the present series, the maximum incidence of
malignant tumour were observed in the age group of 41 –
50 yrs. (50%) which is an agreement with the observation
of Hankey BF et al. 13
The mean age of the patients in
this series was 46.6 years, a similar finding to the
observation of Mabula JB et al where the mean age of
breast cancer patients was 45 years.14
This is lower than
the age reported in western countries where the median
age at diagnosis is in the sixth decade of life.3,15,16
This
shows that there is a difference in mean age of patients of
breast carcinoma in developed and the developing nation.
In the present study, maximum no. of patient of

Singh SK et al. Int Surg J. 2016 Feb;3(1):32-36
International Surgery Journal | January-March 2016 | Vol 3 | Issue 1 Page 35
malignant tumour reported within a year i.e. 42.11% of
patients reported within 6 months to 1 year of onset of
symptoms followed by 36.84% of patients who presented
within 6 months from onset of symptoms. Only 7.89% of
patients presented late between 1.5 to 2 years. Even
Bloom HJG in his series of 250 patients observed that
according to duration of symptoms, maximum patients in
that series i.e. 28.8% reported within one year of onset of
symptoms followed by 26.4% within 1 to 2 years. This
early reporting in case of malignant breast lump clearly
suggests increasing awareness of patients about the
disease in the developing nation over the period of time.17
In the present study, by far the most common presenting
feature was painless mass in the breast (60.78%)
followed by painful mass (13.73%) and associated
features like ulceration of the skin, retraction of nipple
and nipple discharge.
In the present series, the brunt of the breast lump was
observed in the ladies having children between 3 to 6.
Out of 76 patients having malignant breast tumour,
maximum no. 47.37% of patients had more than 3 up to 6
children followed by up to 3 children (36.84%) and
5.26% had no children while 10.53% had more than 6
children. It has been known since longtime, that marriage
and sexual function had tremendous influence in the
development of the breast cancer. Macmohan B et al
reported higher incidence of breast cancer in nulliparous
women but an inverse correlation of breast cancer
incidence with increasing parity has been repeatedly
demonstrated.18
The most acceptable explanation for
higher incidence of breast cancer in multipara is the fact
that women of this part of country marry early & become
mother early and only a very few cases are sterile.
However, this observation warrants further study of this
nature.
Out of 76 patients of carcinoma of the breast, 40
(52.63%), patients had left breast involvement whereas
36 (47.37%) patients had right breast involvement. This
observation fully confirms to the observations of Agrawal
GP et al and Tulinius H et al who also observed increased
incidence of breast cancer on left side with the latter
reporting 13% increased incidence of carcinoma breast to
left side.19, 20
Out of 76 malignant breast tumours in
present study, 36 cases (47.36%) were seen in upper
outer quadrant followed by upper inner quadrant 16 cases
(21.06%), lower outer quadrant 10 cases (13.15%) &
central region 12 cases (10.52%), in that order. This data
is similar to the data obtained by Muqtadir et al and
Mudholkar et al who reported 53.03% and 42.05% of
involvement of upper outer quadrant of breast.21,22
Maximal involvement of upper outer quadrant as
observed in the present study was also in agreement with
the results reported by Darbre.23
The explanation for the
predilection for the cancer in the upper outer quadrant
lies in the fact that lymphatic drainage of the breast in
this region is poor because of inadequate support and
greater amount of target epithelial tissue in that region.
In the present series all cases of malignant growth were
of carcinoma of the breast. Infiltrative carcinoma with
fibrosis (scirrhous) was the commonest variety
constituting 78.94% of the malignant lesions. Usually
designated as scirrhous, it showed varying degree of
fibrosis & infiltration with cords or groups of polyhedral
or spindle cells with hyperchromatic unclei. An incidence
of more than 75% of scirrhous carcinoma had been
reported in the recent study by Muqtadir et al and
Mudholkar et al who reported 78.79% and 88% of
involvement as scirrhous carcinoma.21,22
10.53% of cases belonged to medullary carcinoma group
in which fibrous tissue was scanty & groups of round or
polyhedral cells with vesicular nuclei and abundant
cytoplasm formed the characteristic picture of the lesion.
An incidence of 8.6% of cases of medullary carcinoma
was reported by Haque et al in cases of malignant breast
lump. Also 4 cases of papillary carcinoma and colloid
carcinoma (5.26%) was seen in the present study, in
which there were papillary growths, cells showing
considerable irregularity in, size & shape of the nuclei
and hyper chromatic nuclei. Haque et al observed 1.1%
incidence of papillary carcinoma which is slightly lower
than the incidence in the present series.24
The maximum number of lymph nodes involved was the
axillary group of lymph nodes followed by two cases of
right supraclavicular lymph nodes. This is in agreement
with the observations of other workers .25,26
Axillary node
is the commonest node to be involved in cases of
malignant breast lump but involvement of supraclavicular
lymph nodes or any other contralateral lymph nodes
represents advanced nature of the disease.
CONCLUSION
Understanding the risk factors for the development of
breast carcinoma is important as it provides clues to the
pathogenesis and identifies patients likely to benefit from
reduction of risk factors. Although breast cancer can
develop in both genders, women are at greatly increased
risk and breast cancer in men is uncommon. Staging of
breast cancer is determined prior to any treatment to
categorize patient into risk categories that defines
prognosis and guides recommendations for treatment.
Breast cancer treatment in modern era involves both local
and regional control (surgery and radiation therapy) in
addition to medical therapy for systemic manifestations.
Funding: No funding sources
Conflict of interest: None declared
Ethical approval: The study was approved by the
institutional ethics committee
REFERENCES
1. Jain SB, Jain I, Srivastava J, Jain B. A
clinicopathological study of breast lumps in patients
presenting in surgery OPD in a referral hospital in
Singh SK et al. Int Surg J. 2016 Feb;3(1):32-36
International Surgery Journal | January-March 2016 | Vol 3 | Issue 1 Page 36
Madhya Pradesh, India. Int J Current Microbiol App
Sci. 2015;4(8):919-23.
2. Kumar A, Vohra LS, Bhargava K, Reddy PS.
Investigation of Breast Lump, an evaluation.
MJAPI. 1999;55:299-302.
3. Ikpatt OF, Kuopoo I, NdomaEgbe R & Collen Y.
Breast cancer in Nigeria and Finland:
epidemiological, clinical and histological
comparison. Anticancer Research. 2002;22:3005-12.
4. Jemal A, Bray F, Canter MM, Ferlay J. Global
Cancer Statistics. LA Cancer J Clin. 2011;61(2):69-
90.
5. National Cancer Registry Program. Ten years
consolidated report of the Hospital based Cancer
Registries, 1984-1993, an assessment of the burden
and care of Cancer Patients. Indian Council of
Medical Research. New Delhi, 2001.
6. Agrawal G, Pradeep PV, Agrawal V, Yip CH,
Cheung PS. Spectrum of breast cancer in Asian
women. World J Surg. 2007;31:1031-40.
7. National Cancer Registry Programme: Consolidated
report of the Hospital based Cancer Registries,
1990-1996. Indian Council of Medical Research.
New Delhi, 2001.
8. Chopra R. The Indian Scene. Journal of Clinical
Oncology. 2001;19(18 Suppl):106S-11S.
9. Baum M. Modern concept of natural history of
breast cancer: A guide to design and publication of
trials of the treatment of breast cancer. Eur J Cancer.
2013;49(1):60-4.
10. Kene TS, Odigie VI, Yusufu LMD, Shehu SM &
Kase JT. Pattern of presentation and survival of
breast cancer in a Teaching Hospital in North
Western Nigeria. Oman Medical Journal.
2010;25:104-7.
11. The State of World Health. The World Health report
1997-Conquering suffering, enriching humanity.
World Health Forum. 1997;18.
12. Paymaster TC, Gamgadharan P. Cancer in Parsi
community of Bombay. Int J Cancer. 1970;5:426-31
13. Hankey BF, Miller B, Curtis R, Kosary C. Trends in
breast cancer in younger women in contrast to older
women. J Natl Cancer Inst Monogr. 1994;(16):7-14.
14. Mabula JB, Mabula DM, Chalya PL. Stage at
diagnosis, clinicopathological and treatment patterns
of breast cancer at Bugando Medical Centre innorth-
western Tanzania. Tanzania Journal of Health
Research. 2012;14(4):1-14.
15. Fregene A, Newman LA. Breast cancer in sub-
Saharan Africa: how does it relate to a breast cancer
in African-American women Cancer.
2005;103:1540-50.
16. Awadelkarim KD, Arrizi C, Elamin EOM.
Pathological, clinical and prognostic characteristics
of breast cancer in Central Sudan versus Northern
Italy: implications for breast cancer in Africa.
Histopathology. 2008;52:445-56.
17. Bloom HJG, Richardson WW, Harries EJ. Natural
history of untreated breast cancer. Br Med J.
1962;2(5299):231-21.
18. Macmohan B, Cole P, Lin TM. Age at first birth and
breast cancer risk. Bull Wld Hlth Org. 1970;43:209-
21.
19. Aggrawal GP, Jain SP, Joshi DC. Carcinoma of
Male breast. J Ind Med Assoc. 1964;43:3-61.
20. Tulinius H, Sigvaldason H, Olafsdottir G. Left and
right sided breast cancer. Pathol Res Pract.
1990;186(1):92-4.
21. Muqtadir AMA, Shaikh JM, Anagha VS, Dawle
AV. Clinical profile and outcome of breast cancer at
tertiary care hospital in rural Maharashtra. An
observational study. Int M Jour. 2015;2(4):238-40.
22. Mudholkar VG, Kawade SB, Mashal SN.
Histopathological study of neoplastic lesions of
breast. Indian Medical Gazette. 2012:353-64.
23. Darbre PD. Recorded quadrant increase of female
breast in Great Britain suggests disproportionate
increase in upper outer quadrant of breast.
Anticancer Res. 2005;25(3c):2543-50.
24. Haque R, Tyagi SP, Khan MH, Gahlaut YVS.
Breast lesions. A clinicopathological study of 200
cases of breast lumps. Ind J Surg. 1980;42:419-25.
25. Haagensen CD. Diseases of the breast. Philadelphia
and London. WB Saunders, 1957.
26. Williams NS, Bulstrode CJK, O’Connell PR. The
Breast. In: Bailey & Love’s short practice of surgery
(25th edn.). Hodder Arnold. UK. 2008;50:827-48.
Cite this article as: Singh SK, Pankaj D, Kumar R,
Mustafa R. A clinico-pathological study of malignant
breast lump in a tertiary care hospital in Kosi region of
Bihar. Int Surg J 2016;3:32-6.

IJSS Journal of Surgery | January-February 2016 | Volume 2 | Issue 16
Benign Breast Lesions in a Teaching Hospital in Rural Bihar
Shambhu Kumar Singh1, Khwaja Nasim Ahmad2, Deepak Pankaj3, Mohammad Arif Ansari4
1Assistant Professor, Department of General Surgery, Katihar Medical College, Katihar, Bihar, India, 2Associate Professor, Department of General Surgery, Katihar Medical College, Katihar, Bihar, India, 3Senior Resident, Department of General Surgery, Katihar Medical College, Katihar, Bihar, India, 4Professor and Head, Department of General Surgery, Katihar Medical College, Katihar, Bihar, India
Abstract
Background: Breast diseases has captured attention of surgeons throughout the ages with its uncertain cause. Study of a pattern of benign breast diseases (BBDs) is a challenge due to variants in occurrence and presentation in different age groups and different geographical areas. The breast is a complex structure and any unnatural change affects the body and psyche of the person.
Aim: The aim of this study was to observe age distribution, clinical signs, symptoms and pathology of benign breast lump and correlate them with pathological findings.
Materials and Methods: A total of 124 cases of benign breast lump were included in this study. These cases were selected among patients visiting the outdoor clinic of Department of General Surgery in Katihar Medical College, Katihar, Bihar, India. The selected cases belonged to different etiology, age group and sex.
Results: Maximum cases of benign breast tumors were observed in age group of 21-30 years (third decade). Fibroadenoma was the most common presentation. The majority of patients reported within 1 year of onset of disease. The painless lump was the most common mode of presentation. The right breast was involved in a more number of cases with maximum lesions noted in the upper outer quadrant.
Conclusion: BBDs are common in female patients. Clinical, sonological, mammographical, and pathological studies need to be conducted in a systemic way to find answers of complexities posed by the confusing pattern of BBDs.
Keywords: Benign breast disease, Fibroadenoma, Histopathology, Risk factors, Surgery
INTRODUCTION
Breast or mammary gland is the most important structure in the pectoral region. It is composed of
skin which consists of nipple and areola; parenchyma made up of glandular tissue and fibrofatty stroma. It is influenced by various hormones in a female during lifetime giving rise to different types of lesions. Benign tumors mostly fibroadenoma common in young women have a higher incidence as compared to inflammatory
lesions which are common in lactating women. Increasing incidence of malignancy in proliferating lesions of breast warrants for prompt diagnosis and treatment.1 Benign breast diseases (BBDs) is a group of breast diseases which is not cancer. It is the most common cause of breast problems in females, and it is a more frequent than the malignant ones.2-4 In fact, it is at least 10 times more common than breast cancer in the west.5 Up to 30% of the women who suffer from BBDs will require treatment at some point in their lifetime.6 Increasing reports of breast cancer in India has overshadowed the wide spectrum of benign breast disorders. An incidence of 1.5/1000 cases of total hospital admissions and 8.1/1000 cases of female admissions has been reported in cases of benign breast disorders.7 With regard to gender, diseases of breast are more prevalent among females and the pattern of breast diseases and their etiology varies among
Corresponding Author: Dr. Deepak Pankaj, Department of General Surgery, Katihar Medical College, Katihar - 854 105, Bihar, India.Phone: +91-9431060340. E-mail: [email protected]
Access this article online
www.surgeryijss.com
Month of Submission : 11-2015 Month of Peer Review : 12-2015 Month of Acceptance : 01-2016 Month of Publishing : 01-2016
DOI: 10.17354/SUR/2016/02
Original Article

Singh, et al.: Study of Benign Breast Lesions in a Teaching Hospital in Rural Bihar
IJSS Journal of Surgery | January-February 2016 | Volume 2 | Issue 1 7
different countries and ethnic groups.8 BBDs are the most common cause of breast discomfort especially is females, and during lifetime around 30% of women suffering from BBDs will require treatment. Page and Dupont proposed a classification scheme for BBD in 1985.9 Non-proliferative disease, proliferative disease without atypia and atypical hyperplasia are the three major forms of breast lesions. Previously named as “fibrocystic disease,” non-proliferative disease includes many entities and women are not at increased risk for breast cancer. Proliferative disease without atypia includes more severe forms of epithelial hyperplasia lacking any cytologic atypia as well as duct papillomas, and a special form of adenosis known as sclerosing adenosis and women with this form are found to be 1.5-2 times increased risk for cancer than that of women with non-proliferative disorders. Atypical hyperplasia can be ductal or lobular and shows features on biopsy that resemble but fall short of the corresponding in-situ or non-infiltrating forms of breast cancer and these patients were found to be 4-5 times increased the risk for cancer than that of women with non-proliferative disease. The present study was undertaken with a view to seeing the trends of various ty pes of benign breast lump in this part of the country for better understanding, early detection through screening and early management of the cases. Clinical examination alone is not the answer to the problem for knowing the nature of the lesion, so various radiological investigation and histopathological examination were undertaken.
MATERIALS AND METHODS
About 124 women treated for BBDs over a period of 3-year in Katihar Medical College, Katihar, Bihar, India were included in this study. After prior approval from the Institutional Ethics Committee, a prospective clinicopathological study on 200 cases of breast lump was carried, out of which 124 cases of BBDs was found and included in this study whose diagnosis was confirmed histologically. Patient with obvious malignant disease and those treated earlier for malignancy were excluded from this study. The various results obtained in this study were analyzed in different parameters and compared to the work of other researchers.
Methods of collection of data:• Detailedhistorytaking• Clinicalexamination• Routinelaboratoryinvestigations• Relevantspecialinvestigation• Histological examination of the tissue was
undertaken and tissue was taken from the breast by biopsy, local excision of the lump, or specimen from the mastectomies.
OBSERVATIONS
A total of 124 female patients who attended in the surgery out-patients department for breast diseases were studied in the Department of General Surgery. The result of which were as follows:
Breast lump accounted for most number of cases (58.06%) in benign diseases of breast as compared to aberrations in normal development and involution of breast (ANDI) (35.49%) and inflammatory diseases (6.45%) of breast (Table 1).
In this series, in cases of ANDI, maximum number of cases were seen in the age group 21-30 years (3rd decade) and 31-40 (4th decade) with 36.36% in each (Table 2).
A maximum number of benign tumors were encountered in the age group of the 3rd decade followed by the
Table 1: Overall distribution of benign breast diseasesBenign breast diseases Number of cases PercentageANDI 44 35.49Breast lump 72 58.06Inflammatory disease 8 6.45Total 124 100
ANDI: Aberrations in normal development and involution of breast
Table 2: Distribution of ANDI (causing breast lump) according to ageAge in years Number of cases Percentage11‑20 6 13.6321‑30 16 36.3631‑40 16 36.3641‑50 6 13.6351 and above ‑ ‑Total 44 100.00
ANDI: Aberrations in normal development and involution of breast
Table 3: Distribution of benign breast lump according to ageAge in years Number of cases Percentage10‑20 12 16.6621‑30 38 52.7731‑40 16 22.2241‑50 6 8.33Total 72 100.00
Table 4: Age distribution in inflammatory lump (chronic non‑specific mastitis)Age in years Number of cases Percentage10‑20 ‑ ‑21‑30 8 10031‑40 ‑ ‑41 and above ‑ ‑Total 8 100

Singh, et al.: Study of Benign Breast Lesions in a Teaching Hospital in Rural Bihar
IJSS Journal of Surgery | January-February 2016 | Volume 2 | Issue 18
4th decade with incidence of 52.77% and 22.22% in each, respectively, in the present study (Table 3).
In the present study, all cases of chronic non-specific mastitis were seen in the age group 21-30 years (Table 4).
Maximumnumber of patientswereHindu (53.23%)followed by Muslims (46.77%) (Table 5).
In the present series, most patients (61.30%) of BBDs presented within 6 months of occurrence of the disease,
followed by patients presenting within 6-12 months of occurrence of symptoms (25.80%) (Table 6).
The most common sign and symptom of presentation in the present series was painless mass in the breast, i.e., (71.77%) followed by painful mass in the breast (28.23%) (Table 7). The nipple discharge was present in 8 cases in all cases of BBDs (6.45%).
Among the patients of BBDs, a maximum number of patients, 61.29% were having up to 3 children, followed by 30.65% having children between 3 and 6. Least number of lesions were seen in 8.06% of patients having no children (Table 8).
Among patients presenting with benign breast lump in this series, involvement of right breast (54.84%) was more than left breast (45.16%). Among the quadrants involved, upper outer quadrant (UOQ) was the most common quadrant involved with 27.42% of cases reporting with UOQ involvement in both the breast (Table 9).
Table 6: Distribution of the various lesions according to duration of illnessLesions Less than 6 months 6 months to 1 year 1‑1½ years 1½‑2 year TotalBenign tumor 40 (55.55) 20 (27.78) 4 (5.55) 8 (11.11) 72ANDI 28 (63.7) 12 (27.27) ‑ 4 (9.09) 44Chronic non‑specific mastitis 8 (100) ‑ ‑ ‑ 8Total 76 32 4 12 124% of the series 61.30 25.80 3.23 9.67 100
ANDI: Aberrations in normal development and involution of breast
Table 7: Clinical presentation of benign lesionsSign and symptoms ANDI Benign tumor Chronic non‑specific mastitis Total PercentagePainless mass in breast 29 60 89 71.77Painful mass in breast 15 12 8 35 28.23Total 44 72 8 124 100.0
ANDI: Aberrations in normal development and involution of breast
Table 8: Distribution of various breast lumps according to parityLesions No children Up to 3 children >3 up to 6 children >6 children TotalANDI 4 20 20 44Benign tumors 6 48 18 ‑ 72Chronic non‑specific mastitis ‑ 8 ‑ ‑ 8Total 10 76 38 ‑ 124Percentage 8.06 61.29 30.65 ‑ 100
ANDI: Aberrations in normal development and involution of breast
Table 9: Distribution of various breast lumps according to side and quadrantLesions Right (%) Total
(%)Left Total
(%)UOQ LOQ UIQ LIQ Central UOQ LOQ UIQ LIQ CentralANDI 12 (27.2) 4 (9.09) 4 (9.09) ‑ 4 (9.09) 24 (54.54) 12 (27.2) ‑ 4 (9.09) ‑ 4 (9.09) 20 (45.45)Benign tumors 20 (27.8) 8 (11.11) 8 (11.11) ‑ 4 (5.55) 40 (55.55) 20 (27.8) ‑ 8 (11.11) ‑ 4 (5.55) 32 (44.44)Chronic non‑specific mastitis 2 (25) 2 (25) ‑ ‑ ‑ 4 (50) 2 (25) 2 (25) ‑ ‑ ‑ 4 (50)Total 34 14 12 ‑ 8 68 34 2 12 8 56% in the series 27.42 11.29 9.68 ‑ 6.45 54.84 27.42 1.49 9.68 6.45 45.16
UOQ: Upper outer quadrant, LOQ: Lower outer quadrant, UIQ: Upper inner quadrant, LIQ: Lower inner quadrant, ANDI: Aberrations in normal development and involution of breast
Table 5: Distribution of benign breast lump according to religionReligion Number of cases PercentageHindu 66 53.23Muslim 58 46.77Others 0 0Total 124 100

Singh, et al.: Study of Benign Breast Lesions in a Teaching Hospital in Rural Bihar
IJSS Journal of Surgery | January-February 2016 | Volume 2 | Issue 1 9
Histologically in thepresentseries,allcasesofbenigntumors were fibroadenoma. Intracanalicular variety was observed in the majority of cases of benign breast lump (66.67%). Epithelial hyperplasia (adenosis) was the common picture in case of ANDI with maximum reporting in 63.64% of cases. In an inflammatory group, all cases were chronic non-specific mastitis (Table 10).
Furthermore, according to tumor size, tumors between 2.5 and 5 cm were seen in the majority of cases, followed by tumors between size 5 and 10 cm. Lymph node involvement was also seen with 12 (9.68%) cases reporting axillary lymph node involvement (Table 10).
DISCUSSION
In the present study, 124 cases of benign tumor were studied. BBDs includes a heterogeneous group of conditions which range from normal, to aberrations in the physiology, to frank disease. The patients of BBDs generally present with one or more of these complaints – breast lump, breast pain or nipple discharge.10 It has been recommended that all the patients with discrete breast lumps should undergo a triple assessment to make an early diagnosis. Breast lump which were diagnosed as fibroadenoma eventually by histology accounted for most number of cases (58.06%) among benign diseases of the breast in this study as compared to ANDI and inflammatory diseases of the breast. Most of the patients reported with benign breast lump in the third decade of life that is between 21 and 30 year of age. The finding of this study was in agreement with most of the available literature on benign breast lumps, where the frequency of fibroadenoma ranged from 46.6% to 55.6%. The peak incidence of fibroadenoma ranged from the 2nd to the 3rd decade of life, which was also consistent with the findings of other studies.11-14 According to religion, the number of HindupatientswereslightlymorethanthenumberofMuslimpatients. Other religion did not report any cases in the present study. The majority of the patients accounting for 87.1% in this study reported within 1 year of onset of symptoms of breast disease. The possible explanation for this may be that most of the patients in this study are of younger age group with increasing literacy are aware of the disease and concern about the symptoms especially in breasts affects the psyche of the patients, This leads to prompt and early reporting to the treating surgeon. This may be also due to the fact that all
patients observed were from an institutional hospital where patients report earlier with the belief that better facilities of management will be carried out than in rural practice. In the present series, all the patients with fibroadenoma presented with a lump which was painless in the majority of the cases. They were usually claimed to be discovered by the patients themselves.This result is inagreementofHaagensen,15 who reported 90% of the patients presented with painless lump and Wynder et al.16 who observed 85-90% of patients with a painless lump in their series respectively. Figures 1 and 2 shows examples of BBDs which is Fibroadenoma and Benign phylllodes tumours respectively. Among the patients of BBDs, maximum number of patients, 61.29% were having up to 3 children, followed by 30.65% having children between 3 and 6. Least number of lesions were seen in8.06%ofpatientshavingnochildren.Higherincidenceof benign lesions in multipara could be correlated with the fact that they are dependent upon hormonal, functional and physiological imbalance which has been accepted as fact nowadays. The right breast was involved in 54.84% of cases of benign breast lumps than the left breast which reveals 45.16% of cases in the present study. We could not find any literature that reveals substantial relation of the side of the breast with the development of these types of breast lesions. According to quadrants involved, these diseases were maximally observed in UOQ of both the breasts, which is in agreement with other workers.6,17 Few cases reported the involvement of axillary lymph nodes only (9.68%) as these were inflammatory in origin. This may be due to the fact that the breast drains mainly to axillary nodes, of which there are five sets.18Histologically,inthepresentseries,allcasesof benign tumors were fibroadenoma. An intracanalicular pattern was observed in 66.67% of cases while in 33.33% of cases pericanalicular pattern was observed. It is in confirmity with the results of Kern and Clark19 while contrary to the resultsofHaqueet al.17 who observed mixed pattern in majority of cases.
Epithelial hyperplasia (adenosis) was the commonest histological picture in ANDI, seen in 63.64% of the cases and rest were cystic and fibrocystic diseases in 18.18% and papillomatosis and sclerosing adenosis in 18.18%. ThisisalsoinagreementwiththefindingsofHaque0.17 These lesions have the potential to be misdiagnosed with carcinoma of the breast in a fraction of cases. The basis of false diagnosis of cancer may be abundance of fibrous tissue contributing hardness and infiltration of fat leading
Table 10: Histopathological types of various breast lumpLesions ANDI Benign InflammatoryHistological types
Cystic and fibro cystic
Epithelial, hyperplasia (adenosis and atypical lobular hyperplasia)
Papillo‑matosis (sclerosing adenosis)
Total Intracana‑ licular
Peric‑analic‑ular Total Chronic non‑specific
mastitis
Total
Number of cases 8 28 8 44 48 24 72 8 8Percentage 18.18 63.64 18.18 100 66.67 33.33 100 100 100
ANDI: Aberrations in normal development and involution of breast
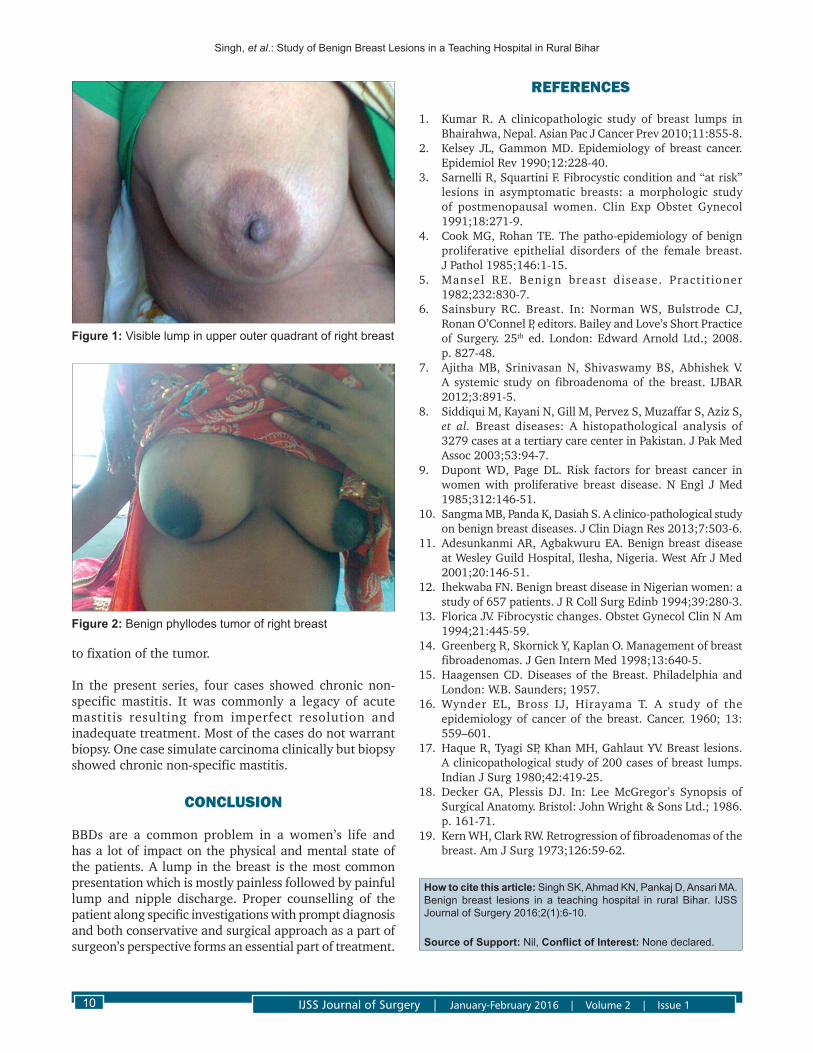
Singh, et al.: Study of Benign Breast Lesions in a Teaching Hospital in Rural Bihar
IJSS Journal of Surgery | January-February 2016 | Volume 2 | Issue 110
to fixation of the tumor.
In the present series, four cases showed chronic non-specific mastitis. It was commonly a legacy of acute mastitis resulting from imperfect resolution and inadequate treatment. Most of the cases do not warrant biopsy. One case simulate carcinoma clinically but biopsy showed chronic non-specific mastitis.
CONCLUSION
BBDs are a common problem in a women’s life and has a lot of impact on the physical and mental state of the patients. A lump in the breast is the most common presentation which is mostly painless followed by painful lump and nipple discharge. Proper counselling of the patient along specific investigations with prompt diagnosis and both conservative and surgical approach as a part of surgeon’s perspective forms an essential part of treatment.
REFERENCES
1. KumarR. A clinicopathologic study of breast lumps inBhairahwa, Nepal. Asian Pac J Cancer Prev 2010;11:855-8.
2. Kelsey JL, Gammon MD. Epidemiology of breast cancer. EpidemiolRev1990;12:228-40.
3. SarnelliR,SquartiniF.Fibrocysticconditionand“atrisk”lesions in asymptomatic breasts: a morphologic study of postmenopausal women. Clin Exp Obstet Gynecol 1991;18:271-9.
4. CookMG,RohanTE.Thepatho-epidemiologyofbenignproliferative epithelial disorders of the female breast. J Pathol 1985;146:1-15.
5. Mansel RE. Benign breast disease. Practitioner1982;232:830-7.
6. Sainsbury RC. Breast. In: NormanWS, Bulstrode CJ,RonanO’ConnelP,editors.BaileyandLove’sShortPracticeof Surgery. 25th ed. London: Edward Arnold Ltd.; 2008. p. 827-48.
7. Ajitha MB, Srinivasan N, Shivaswamy BS, Abhishek V. A systemic study on fibroadenomaof the breast. IJBAR2012;3:891-5.
8. Siddiqui M, Kayani N, Gill M, Pervez S, Muzaffar S, Aziz S, et al. Breast diseases: A histopathological analysis of 3279 cases at a tertiary care center in Pakistan. J Pak Med Assoc 2003;53:94-7.
9. DupontWD, PageDL.Risk factors for breast cancer inwomen with proliferative breast disease. N Engl J Med 1985;312:146-51.
10. Sangma MB, Panda K, Dasiah S. A clinico-pathological study onbenignbreastdiseases.JClinDiagnRes2013;7:503-6.
11. AdesunkanmiAR,AgbakwuruEA.BenignbreastdiseaseatWesleyGuildHospital,Ilesha,Nigeria.WestAfrJMed2001;20:146-51.
12. Ihekwaba FN. Benign breast disease in Nigerian women: a studyof657patients.JRCollSurgEdinb1994;39:280-3.
13. Florica JV. Fibrocystic changes. Obstet Gynecol Clin N Am 1994;21:445-59.
14. GreenbergR,SkornickY,KaplanO.Managementofbreastfibroadenomas. J Gen Intern Med 1998;13:640-5.
15. HaagensenCD.Diseasesof theBreast.PhiladelphiaandLondon: W.B. Saunders; 1957.
16. Wynder EL, Bross IJ, Hirayama T. A study of theepidemiology of cancer of the breast. Cancer. 1960; 13: 559–601.
17. HaqueR,TyagiSP,KhanMH,GahlautYV.Breastlesions.A clinicopathological study of 200 cases of breast lumps. Indian J Surg 1980;42:419-25.
18. Decker GA, Plessis DJ. In: Lee McGregor’s Synopsis of Surgical Anatomy. Bristol: John Wright & Sons Ltd.; 1986. p. 161-71.
19. KernWH,ClarkRW.Retrogressionoffibroadenomasofthebreast. Am J Surg 1973;126:59-62.
Figure 1: Visible lump in upper outer quadrant of right breast
Figure 2: Benign phyllodes tumor of right breast
How to cite this article: Singh SK, Ahmad KN, Pankaj D, Ansari MA. Benign breast lesions in a teaching hospital in rural Bihar. IJSS Journal of Surgery 2016;2(1):6-10.
Source of Support: Nil, Conflict of Interest: None declared.

AB
STR
AC
T
Acute appendicitis is the most common surgically correctable cause of abdominal pain, the diagnosis of which remains difficult in many instances. Some of the signs and symptoms can be subtle to both the clinical and the patient and may not be present in all instances. Arriving at the correct diagnosis is essential; however, a delay may allow progression to perforation and significantly increased morbidity and mortality. Incorrectly diagnosing a patient with appendicitis although not catastrophic often subjects the patients to an unnecessary operation. The diagnosis of acute appendicitis is essentially clinical; however a decision to operate based on clinical suspicion alone can lead to removal of a normal appendix in 15-30% cases. Aims and objectives of the study was to To assess the association between clinical, radiological, operative and histopathological finding and thus evaluate clinical diagnostic accuracy and radiological diagnostic accuracy,To assess the effectiveness of radiological investigation in diagnosing acute appendicitis,To assess the importance and accuracy of clinical examination in acute appendicitis,In the present study, majority of cases were in the age group of 20-40 years, The ratio of male to female was 28:22. Abdominal pain was present in 90 % of cases. Fever was present in 92 % of cases while nausea and vomiting were present in 82 % of cases. Tenderness in right iliac fossa was present in 98% of cases. 98 % of patients showed Alvarado's score of >7(s/o clinically positive). In majority of cases position of appendix was retrocaecal (62%), while pelvic position was present in 14 % of cases, and pre ileal in 10 % of cases. USG abdomen diagnosed 82 % cases of acute appendicitis and it showed negative results in 18% of cases which were clinically positive. Per operatively, in 96 % of cases appendix was diseased ( either inflammed or perforated), while only in 4 % of cases it was normal (non diseased). Histopathological examination revealed that in 96 % of cases, appendix was diseased, while in 4 % of cases it was completely normal. 96 % of cases were discharged from the hospital uneventfully. In almost all cases (98%) diagnosis is accurately made only on the basis of clinical examination, while in a significant number of cases (18 % ), radiological investigation used for diagnosis, failed to diagnose the positive cases. Acute appendicitis is a clinical diagnosis , although the radiological, biochemical and pathological evaluation in acute appendicitis is important. The history and clinical examination and Alvarado's score is more significant to treat and manage the cases of acute appendicitis which has been proved from our study and the literature. The diagnostic accuracy of clinical features is far more better than radiological investigations in the diagnosis of acute appendicitis. Therefore it is concluded that acute appendicitis is more a clinical diagnosis rather than radiological and it is better to use radiological investigation only to confirm the diagnosis of acute appendicitis rather to diagnose it.
ORIGINAL RESEARCH PAPER Surgery
A STUDY ON CLINICAL, RADIOLOGICAL AND OPERATIVE PROFILE OF ACUTE APPENDICITIS
KEY WORDS:
INTRODUCTION :-Acute appendicitis is the most common surgically correctable cause of abdominal pain, the diagnosis of which remains difficult in many instances. Some of the signs and symptoms can be subtle to both the clinical and the patient and may not be present in all instances. Arriving at the correct diagnosis is essential; however, a delay may allow progression to perforation and significantly increased morbidity and mortality. Incorrectly diagnosing a patient with appendicitis although not catastrophic often subjects the patients to an unnecessary operation. The diagnosis of acute appendicitis is essentially clinical; however a decision to operate based on clinical suspicion alone can lead to removal of a normal appendix in 15-30% cases. A number of clinical and laboratory based scoring system have been devised to assist diagnosis. The most commonly used is the Alvarado score and equally its modification, ultrasound abdomen, intraoperative and histopathological confirmation. Modified Alvarado score: This consists of three symptoms, three signs and two laboratory findings as described by Alvarado et al, later modified by Kalan et al.
Score:1-4 Appendicitis unlikely 5-6 Appendicitis possible 7-9 Appendicit is probable 9- Appendicit is definit ive. Al l patients(100%), which were positive for acute appendicitis intra-operatively and histopathologically werealso positive for the same by clinical examination, while 18% of cases were negative for the same by radiological investigations (ultrasonography).
AIMS & OBJECTIVES :-1. To assess the association between clinical, radiological,
operative and histopathological finding and thus evaluate clinical diagnostic accuracy and radiological diagnostic accuracy.
2. To assess the effectiveness of radiological investigation in diagnosing acute appendicitis.
3. To assess the importance and accuracy of clinical examination in acute appendicitis.
MATERIALS AND METHODS :-The study was conducted at Department of Surgery, Katihar Medical College & Hospital, Katihar. Fifty patients admitted to the surgery wards at , Katihar Medical College & Hospital, Katihar, with signs and symptoms of appendicitis were taken for study. This is a time bound prospective study in which patients presenting with clinical suspicion of acute appendicitis were taken into study.
Ÿ The period of study was from November 2017 to October 2018.
Ÿ 50 cases were taken up for study.
Inclusion criteriaŸ Only patients undergoing surgery were included.Ÿ All age groups and of both sex.
Exclusion criteriaPatients admitted for interval appendicectomy following recurrent appendicitis, appendicular abscess, apendicular mass previously treated conservatively. Patients were subjected to detailed history and thorough physical examination.
Ÿ Alvarado's scoring.Ÿ Patients underwent necessary investigations.Ÿ Blood counts, biochemical analysis and urine analysis, USG
abdomen / pelvis, CT abdomen(as and when required.),all diagnosed patients will be subjected to surgery.
Ÿ In all cases, operative findings and post operative diagnosis by histopathological examination were recorded.
Dr. Brish Bhan Gupta*
M.S., M.Ch., Assistant Professor, Department of Surgery, Katihar Medical College & Hospital, Katihar, Bihar *Corresponding Author
www.worldwidejournals.com 15
Dr. (Prof.) M. Arif Ansari
M.S., Professor, Department of Surgery, Katihar Medical College & Hospital, Katihar, Bihar
PARIPEX - INDIAN JOURNAL OF RESEARCH Volume-8 | Issue-4 | April-2019 | PRINT ISSN No 2250-1991
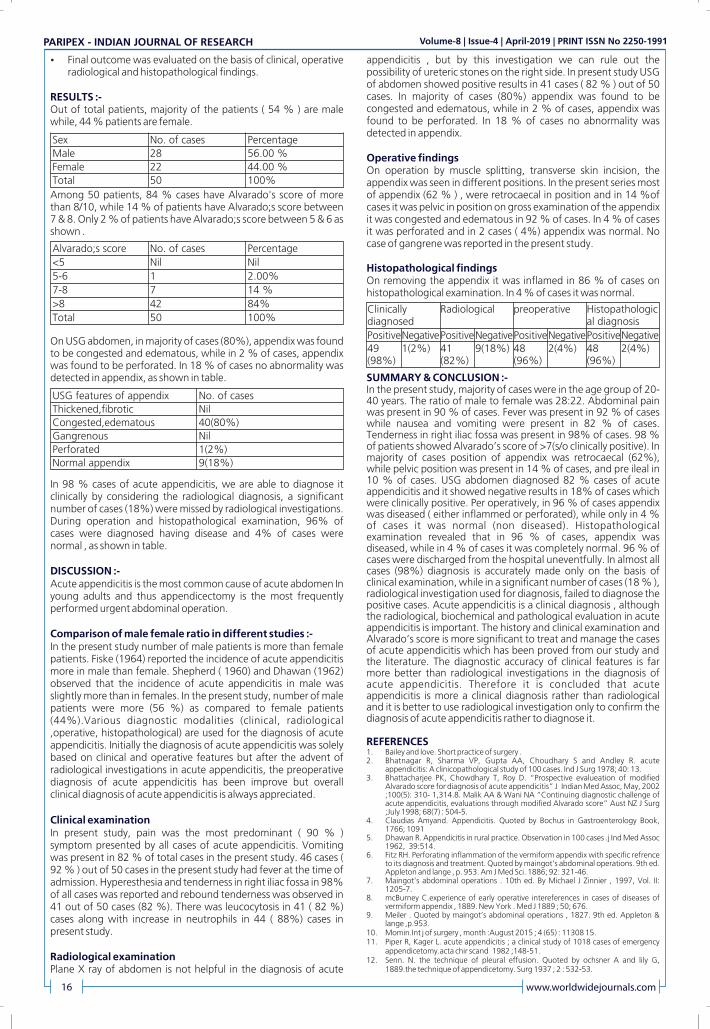
Ÿ Final outcome was evaluated on the basis of clinical, operative radiological and histopathological findings.
RESULTS :-Out of total patients, majority of the patients ( 54 % ) are male while, 44 % patients are female.
Among 50 patients, 84 % cases have Alvarado's score of more than 8/10, while 14 % of patients have Alvarado;s score between 7 & 8. Only 2 % of patients have Alvarado;s score between 5 & 6 as shown .
On USG abdomen, in majority of cases (80%), appendix was found to be congested and edematous, while in 2 % of cases, appendix was found to be perforated. In 18 % of cases no abnormality was detected in appendix, as shown in table.
In 98 % cases of acute appendicitis, we are able to diagnose it clinically by considering the radiological diagnosis, a significant number of cases (18%) were missed by radiological investigations. During operation and histopathological examination, 96% of cases were diagnosed having disease and 4% of cases were normal , as shown in table.
DISCUSSION :-Acute appendicitis is the most common cause of acute abdomen In young adults and thus appendicectomy is the most frequently performed urgent abdominal operation.
Comparison of male female ratio in different studies :- In the present study number of male patients is more than female patients. Fiske (1964) reported the incidence of acute appendicitis more in male than female. Shepherd ( 1960) and Dhawan (1962) observed that the incidence of acute appendicitis in male was slightly more than in females. In the present study, number of male patients were more (56 %) as compared to female patients (44%).Various diagnostic modalities (clinical, radiological ,operative, histopathological) are used for the diagnosis of acute appendicitis. Initially the diagnosis of acute appendicitis was solely based on clinical and operative features but after the advent of radiological investigations in acute appendicitis, the preoperative diagnosis of acute appendicitis has been improve but overall clinical diagnosis of acute appendicitis is always appreciated.
Clinical examination In present study, pain was the most predominant ( 90 % ) symptom presented by all cases of acute appendicitis. Vomiting was present in 82 % of total cases in the present study. 46 cases ( 92 % ) out of 50 cases in the present study had fever at the time of admission. Hyperesthesia and tenderness in right iliac fossa in 98% of all cases was reported and rebound tenderness was observed in 41 out of 50 cases (82 %). There was leucocytosis in 41 ( 82 %) cases along with increase in neutrophils in 44 ( 88%) cases in present study.
Radiological examinationPlane X ray of abdomen is not helpful in the diagnosis of acute
appendicitis , but by this investigation we can rule out the possibility of ureteric stones on the right side. In present study USG of abdomen showed positive results in 41 cases ( 82 % ) out of 50 cases. In majority of cases (80%) appendix was found to be congested and edematous, while in 2 % of cases, appendix was found to be perforated. In 18 % of cases no abnormality was detected in appendix.
Operative findingsOn operation by muscle splitting, transverse skin incision, the appendix was seen in different positions. In the present series most of appendix (62 % ) , were retrocaecal in position and in 14 %of cases it was pelvic in position on gross examination of the appendix it was congested and edematous in 92 % of cases. In 4 % of cases it was perforated and in 2 cases ( 4%) appendix was normal. No case of gangrene was reported in the present study.
Histopathological findingsOn removing the appendix it was inflamed in 86 % of cases on histopathological examination. In 4 % of cases it was normal.
SUMMARY & CONCLUSION :-In the present study, majority of cases were in the age group of 20-40 years. The ratio of male to female was 28:22. Abdominal pain was present in 90 % of cases. Fever was present in 92 % of cases while nausea and vomiting were present in 82 % of cases. Tenderness in right iliac fossa was present in 98% of cases. 98 % of patients showed Alvarado�s score of >7(s/o clinically positive). In majority of cases position of appendix was retrocaecal (62%), while pelvic position was present in 14 % of cases, and pre ileal in 10 % of cases. USG abdomen diagnosed 82 % cases of acute appendicitis and it showed negative results in 18% of cases which were clinically positive. Per operatively, in 96 % of cases appendix was diseased ( either inflammed or perforated), while only in 4 % of cases it was normal (non diseased). Histopathological examination revealed that in 96 % of cases, appendix was diseased, while in 4 % of cases it was completely normal. 96 % of cases were discharged from the hospital uneventfully. In almost all cases (98%) diagnosis is accurately made only on the basis of clinical examination, while in a significant number of cases (18 % ), radiological investigation used for diagnosis, failed to diagnose the positive cases. Acute appendicitis is a clinical diagnosis , although the radiological, biochemical and pathological evaluation in acute appendicitis is important. The history and clinical examination and Alvarado�s score is more significant to treat and manage the cases of acute appendicitis which has been proved from our study and the literature. The diagnostic accuracy of clinical features is far more better than radiological investigations in the diagnosis of acute appendicitis. Therefore it is concluded that acute appendicitis is more a clinical diagnosis rather than radiological and it is better to use radiological investigation only to confirm the diagnosis of acute appendicitis rather to diagnose it.
REFERENCES1. Bailey and love. Short practice of surgery .2. Bhatnagar R, Sharma VP, Gupta AA, Choudhary S and Andley R. acute
appendicitis: A clinicopathological study of 100 cases. Ind J Surg 1978; 40: 13.3. Bhattacharjee PK, Chowdhary T, Roy D. �Prospective evalueation of modified
Alvarado score for diagnosis of acute appendicitis� J Indian Med Assoc, May, 2002 ;100(5): 310- 1,314.8. Malik AA & Wani NA �Continuing diagnostic challenge of acute appendicitis, evaluations through modified Alvarado score� Aust NZ J Surg ;July 1998; 68(7) : 504-5.
4. Claudias Amyand. Appendicitis. Quoted by Bochus in Gastroenterology Book, 1766; 1091
5. Dhawan R. Appendicitis in rural practice. Observation in 100 cases .j Ind Med Assoc 1962, 39:514.
6. Fitz RH. Perforating inflammation of the vermiform appendix with specific refrence to its diagnosis and treatment. Quoted by maingot�s abdominal operations. 9th ed. Appleton and lange , p. 953. Am J Med Sci. 1886; 92: 321-46.
7. Maingot�s abdominal operations . 10th ed. By Michael J Zinnier , 1997, Vol. II: 1205-7.
8. mcBurney C.experience of early operative intereferences in cases of diseases of vermiform appendix , 1889. New York . Med J 1889 ; 50; 676.
9. Meiler . Quoted by maingot�s abdominal operations , 1827. 9th ed. Appleton & lange ,p.953.
10. Momin.Int j of surgery , month :August 2015 ; 4 (65) : 11308 15.11. Piper R, Kager L. acute appendicitis ; a clinical study of 1018 cases of emergency
appendicetomy.acta chir scand 1982 ;148-51.12. Senn. N. the technique of pleural effusion. Quoted by ochsner A and lily G,
1889.the technique of appendicetomy. Surg 1937 ; 2 : 532-53.
16 www.worldwidejournals.com
PARIPEX - INDIAN JOURNAL OF RESEARCH Volume-8 | Issue-4 | April-2019 | PRINT ISSN No 2250-1991
Sex No. of cases Percentage
Male 28 56.00 %
Female 22 44.00 %
Total 50 100%
Alvarado;s score No. of cases Percentage
<5 Nil Nil
5-6 1 2.00%
7-8 7 14 %
>8 42 84%
Total 50 100%
USG features of appendix No. of cases
Thickened,fibrotic Nil
Congested,edematous 40(80%)
Gangrenous Nil
Perforated 1(2%)
Normal appendix 9(18%)
Clinically diagnosed
Radiological preoperative Histopathological diagnosis
Positive Negative PositiveNegativePositiveNegativePositiveNegative49 (98%)
1(2%) 41 (82%)
9(18%) 48 (96%)
2(4%) 48 (96%)
2(4%)

AB
STR
AC
T
In recent decades laparoscopic cholycystectomy has gained a status of one of the most commonly performed abdominal operations. This is due to a brisk rise in the incidence of calculus disease of the biliary tract. Also there has been a noticeable increase in its incidence in lower age groups ( < 20 years). Due to the greater numbers of laparoscopic cholecystectomies being performed , the number of patients unimproved by the procedure has also increased proportionately.The study was done AT DEPARTMENT OF SURGERY, KATIHAR MEDICAL COLLEGE & HOSPITAL, KATIHAR from January 2017 to December 2018. Total 200 cases, who had undergone laparoscopic cholecystectomy were studied and followed up. Cases were studied by detailed history, thorough clinical examination and detailed investigations like routine investigations ,Imaging studies and other special investigations as and when required. Data was collected and alalysed for study. Two hundred Laparoscopic cholecystectomy cases have been followed between 2017-2018, out of which 150 were female and 50 male. Post cholecystectomy syndrome was observed in 40 cases giving 20 % , consisiting of 29 females and 11 males.The age group upto 30 years had minimum percentage ( 17.54 % ) of symptomatic cases whereas maximum were seen after 60 years of age.Most of the symptomatic cases(40 % ) came for the treatment within six months of the cholecystectomy.The complaints, details of the surgery and the follow up observations have been recorded.Cases were divided according to the presence of stone at their cholecystectomy into calculus and non calculus groups.the symptomatic cases were more ( 50 % 0 in non calculus groups than in the calculus group ( 18.75 % ).Symptoms related to hepatobiliary system including pancreas have been termed as � true post cholecystectomy syndrome.� This was found in 8.5 % cases. Advanced investigation techniques correct diagnosis as far as practicable and above all mature operative judgement and meticulous surgery will certainly bring down this undesired Post - cholecystectomy syndrome and finally wipe it out completely.
ORIGINAL RESEARCH PAPER Surgery
A STUDY ON CLINICAL PROFILE OF POST- CHOLYCYSTECTOMY SYNDROME AFTER LAPAROSCOPIC CHOLECYSTECTOMY
KEY WORDS:
INTRODUCTIONIn recent decades laparoscopic cholycystectomy has gained a status of one of the most commonly performed abdominal operations. This is due to a brisk rise in the incidence of calculus disease of the biliary tract. Also there has been a noticeable increase in its incidence in lower age groups ( < 20 years). Due to the greater numbers of laparoscopic cholecystectomies being performed , the number of patients unimproved by the procedure has also increased proportionately. These symptoms can represent either the continuation of symptoms attributed to the gall bladder. Post cholecystectomy syndrome ( PCS ) also includes the development of the symptoms caused by removal of the gall bladder.
As a matter of fact, the symptoms presented by such patients are not always due to cholecystectomy but may be due to other factors related or unrelated to hepatobiliary tract disorders , thus uninfluenced by removal of gall bladder. So the term post cholecystectomy syndrome should only be precisely applied only to those postoperative symptoms considered to have originated in biliary tract.
Since last two decades , laparoscopic cholecystectomy has become the preferred and more common method of treating gallbladder disease . In india also, it has become the method of choice in advanced clinics and hospitals. The problem of PCS has decreased with the laparoscopic cholecystectomy but there still remains a vast scope for attempts to decrease its incidence.
First laparoscopic cholecystectomy was done by Muhe of Germany in1985 . Prof. Udwadia of Mumbai did first laparoscopic cholecystectomy in India.
In 1947, Womack and Crider first described PCS, defining it as the presence of symptoms after cholecystectomy. These symptoms may actually represent either (1) the continuation of symptoms that had been interpreted as resulting from pathology of the gall bladder or (2) the development of new symptoms that might normally be attributed to the gall bladder . PCS is also the development of symptoms like gastritis or diarrhea caused by removal of the gall bladder.
Out of all laparoscopic cholecystectomies , regardless of the state of gall bladder, post cholecystectomy syndrome occurs in 10-20 % of the total cases. In 10-15 % of calculus cases and in in 15-40 % of non calculus cases.
According to Ernest lack(2000), one risk factor for PCS includes not being certain of the diagnosis prior to the gall bladder removal . In general, the longer the symptoms lasted prior to the gallbladder removal, the greater the chance of developing PCS. If the symptoms are present less than a year before gallbladder removal, 15.4% of patients has been shown to develop PCS. If the symptoms last from 6-10 years, 31% have been shown to develop PCS and if the symptoms last for more than 10 years, 34% have been shown to develop PCS. If the gallbladder is removed to treat gallstone, approximately 20 % of patients develop PCS. If the surgery is not performed to remove gallstones, anywhere from 10 to 25% of patients develop PCS. If the common bile duct is cut open, in addition to gallbladder removal 23% of patients develop PCS. If the common bile duct is cut open and the gallbladder is removed, 19% of patients develop PCS.
Younger patients have generally been found to have an increased risk of developing PCS. For example, people aged 20-29 years that had the gallbladder removed have been found to have a 43% chance of developing PCS, whereas 30-39 year old have a 27% chance, and 40-49 year olds, have a 21% of chance, 50-59 year olds were found to have a 26% chance of developing PCS and 60-69 year olds were found to have a 31% chance of developing PCS, Females were found to develop PCS more as compared to males. Another risk factor for PCS is having a psychiatric (mental health) disorder. About 50% of patients with a mental health disorder were found to develop PCS compared to patients without psychiatric disorder (of which 20% developed PCS.)
MATERIALS AND METHODSThe study was done AT DEPARTMENT OF SURGERY, KATIHAR MEDICAL COLLEGE & HOSPITAL, KATIHAR from January 2017 to December 2018. Total 200 cases, who had undergone laparoscopic cholecystectomy were studied and followed up. Cases were studied by detailed history, thorough clinical examination and detailed investigations like routine investigations
Dr. Brish Bhan Gupta*
M.S., M.Ch., Assistant Professor, Department of Surgery, Katihar Medical College & Hospital, Katihar, Bihar *Corresponding Author
Dr.(Prof.) M.Arif Ansari
M.S., Professor, Department of Surgery, Katihar Medical College & Hospital, Katihar, Bihar
PARIPEX - INDIAN JOURNAL OF RESEARCH Volume-8 | Issue-4 | April-2019 | PRINT ISSN No 2250-1991
12 www.worldwidejournals.com
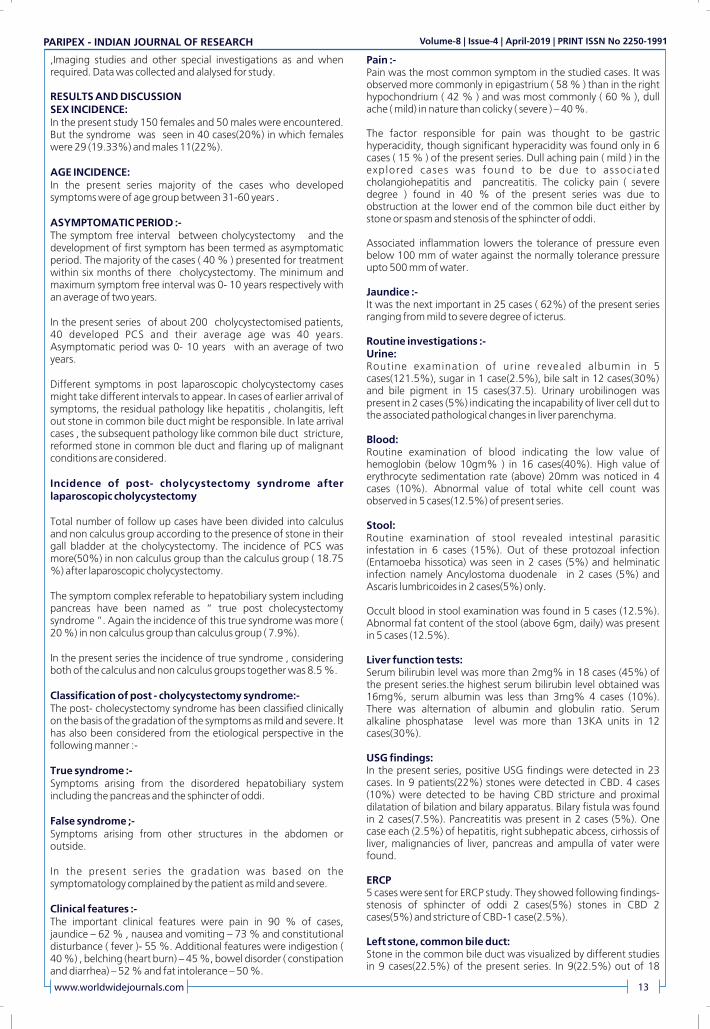
,Imaging studies and other special investigations as and when required. Data was collected and alalysed for study.
RESULTS AND DISCUSSIONSEX INCIDENCE:In the present study 150 females and 50 males were encountered. But the syndrome was seen in 40 cases(20%) in which females were 29 (19.33%) and males 11(22%).
AGE INCIDENCE:In the present series majority of the cases who developed symptoms were of age group between 31-60 years .
ASYMPTOMATIC PERIOD :-The symptom free interval between cholycystectomy and the development of first symptom has been termed as asymptomatic period. The majority of the cases ( 40 % ) presented for treatment within six months of there cholycystectomy. The minimum and maximum symptom free interval was 0- 10 years respectively with an average of two years.
In the present series of about 200 cholycystectomised patients, 40 developed PCS and their average age was 40 years. Asymptomatic period was 0- 10 years with an average of two years.
Different symptoms in post laparoscopic cholycystectomy cases might take different intervals to appear. In cases of earlier arrival of symptoms, the residual pathology like hepatitis , cholangitis, left out stone in common bile duct might be responsible. In late arrival cases , the subsequent pathology like common bile duct stricture, reformed stone in common ble duct and flaring up of malignant conditions are considered.
Incidence of post- cholycystectomy syndrome after laparoscopic cholycystectomy
Total number of follow up cases have been divided into calculus and non calculus group according to the presence of stone in their gall bladder at the cholycystectomy. The incidence of PCS was more(50%) in non calculus group than the calculus group ( 18.75 %) after laparoscopic cholycystectomy.
The symptom complex referable to hepatobiliary system including pancreas have been named as � true post cholecystectomy syndrome �. Again the incidence of this true syndrome was more ( 20 %) in non calculus group than calculus group ( 7.9%).
In the present series the incidence of true syndrome , considering both of the calculus and non calculus groups together was 8.5 %.
Classification of post - cholycystectomy syndrome:-The post- cholecystectomy syndrome has been classified clinically on the basis of the gradation of the symptoms as mild and severe. It has also been considered from the etiological perspective in the following manner :-
True syndrome :-Symptoms arising from the disordered hepatobiliary system including the pancreas and the sphincter of oddi.
False syndrome ;-Symptoms arising from other structures in the abdomen or outside.
In the present series the gradation was based on the symptomatology complained by the patient as mild and severe.
Clinical features :-The important clinical features were pain in 90 % of cases, jaundice � 62 % , nausea and vomiting � 73 % and constitutional disturbance ( fever )- 55 %. Additional features were indigestion ( 40 %) , belching (heart burn) � 45 %, bowel disorder ( constipation and diarrhea) � 52 % and fat intolerance � 50 %.
Pain :-Pain was the most common symptom in the studied cases. It was observed more commonly in epigastrium ( 58 % ) than in the right hypochondrium ( 42 % ) and was most commonly ( 60 % ), dull ache ( mild) in nature than colicky ( severe ) � 40 %.
The factor responsible for pain was thought to be gastric hyperacidity, though significant hyperacidity was found only in 6 cases ( 15 % ) of the present series. Dull aching pain ( mild ) in the explored cases was found to be due to associated cholangiohepatitis and pancreatitis. The colicky pain ( severe degree ) found in 40 % of the present series was due to obstruction at the lower end of the common bile duct either by stone or spasm and stenosis of the sphincter of oddi.
Associated inflammation lowers the tolerance of pressure even below 100 mm of water against the normally tolerance pressure upto 500 mm of water.
Jaundice :-It was the next important in 25 cases ( 62%) of the present series ranging from mild to severe degree of icterus.
Routine investigations :-Urine:Routine examination of urine revealed albumin in 5 cases(121.5%), sugar in 1 case(2.5%), bile salt in 12 cases(30%) and bile pigment in 15 cases(37.5). Urinary urobilinogen was present in 2 cases (5%) indicating the incapability of liver cell dut to the associated pathological changes in liver parenchyma.
Blood:Routine examination of blood indicating the low value of hemoglobin (below 10gm% ) in 16 cases(40%). High value of erythrocyte sedimentation rate (above) 20mm was noticed in 4 cases (10%). Abnormal value of total white cell count was observed in 5 cases(12.5%) of present series.
Stool:Routine examination of stool revealed intestinal parasitic infestation in 6 cases (15%). Out of these protozoal infection (Entamoeba hissotica) was seen in 2 cases (5%) and helminatic infection namely Ancylostoma duodenale in 2 cases (5%) and Ascaris lumbricoides in 2 cases(5%) only.
Occult blood in stool examination was found in 5 cases (12.5%). Abnormal fat content of the stool (above 6gm, daily) was present in 5 cases (12.5%).
Liver function tests:Serum bilirubin level was more than 2mg% in 18 cases (45%) of the present series.the highest serum bilirubin level obtained was 16mg%, serum albumin was less than 3mg% 4 cases (10%). There was alternation of albumin and globulin ratio. Serum alkaline phosphatase level was more than 13KA units in 12 cases(30%).
USG findings:In the present series, positive USG findings were detected in 23 cases. In 9 patients(22%) stones were detected in CBD. 4 cases (10%) were detected to be having CBD stricture and proximal dilatation of bilation and bilary apparatus. Bilary fistula was found in 2 cases(7.5%). Pancreatitis was present in 2 cases (5%). One case each (2.5%) of hepatitis, right subhepatic abcess, cirhossis of liver, malignancies of liver, pancreas and ampulla of vater were found.
ERCP5 cases were sent for ERCP study. They showed following findings-stenosis of sphincter of oddi 2 cases(5%) stones in CBD 2 cases(5%) and stricture of CBD-1 case(2.5%).
Left stone, common bile duct:Stone in the common bile duct was visualized by different studies in 9 cases(22.5%) of the present series. In 9(22.5%) out of 18
PARIPEX - INDIAN JOURNAL OF RESEARCH Volume-8 | Issue-4 | April-2019 | PRINT ISSN No 2250-1991
www.worldwidejournals.com 13

rexplored cases, choledocholithotomy was performed, constibuting to a relief in distress.
Biliary fistula:In the present series 3 cases(7.5%) had biliary fistula on the right side of the abdomen opening to the exterior through the skin, where the drainage tube was given at the end of the cholecystectomy. Those fistula started immediately after the drainage tube was removed. All of them had jaundice (plasma bilurubin above 4mg% in the post-operative system).
Stricture of common bile duct:4 cases(10%) of the present series had stricture of bile duct shown by USG & ERCP. In 1 case (2.5%) re-exploration was done and the stricture segment exercised with end to end anastomosis of the severed ends.
In the present series injury to CBD, recurrent cholangitis prior to cholecystetomy, periductal fibrosis due to extravasation of infection bile or blood after cholecystetomy are responsible for the stricture.
Stenosis of the sphincter of oddi:2 cases (5%) of the present series had stenosis of oddi which developed symptoms 1 year after the initial cholecystectomy. The patient had severe pain, fever and jaundice. Ultimately transduodinal spinchterotomy was done which was rewarded with cure.
Adhesions:Adhesion between common bile duct with surrounding structures namely duodenum, stomach, liver, colon etc. has been observed in 3 cases(7.5%) of the present series. Periductal fibrosis plays a complex role in the cholecystectomised individuals. This is probably due to leakage of bile and blood causing irritation and inflammation over the surrounding structure due to lack of care during operation by inexperienced surgeon.
Concomitant hepato - biliary disorders:The four(10%) of the present series there was involvement of liver (excluding malignant conditions) in the form of cholangitis-2 cases (5%), infective hepatitis-1(2.5%) and cirrhosis one case (2.5%). All those cases were treated with conservation measures. Except the only case of cirrhosis the rest were relieved of other symptoms.
Two cases of cholangitis of the present series had the feature of inflammation of pancreas and liver at their cholecystectomy.
In the present series it was marked that the liver disease became prominent when there was a prolonged and advanced cholecystic disease.
Gastrointestinal disorders:The cause of gastrointestinal symptoms were observed in 12 cases (30%). This consisted of chronic peptic ulcer(duodenum and stomach) -5 cases (12.5%), parasitic infestation of the intestine 5(12.5%) and 2 cases (5%) of other intestinal conditions such as diverticulitis, irritable bowel syndrome.
Hydronephrosis:Only one case 2.5% of the present series was diagnosed as mild hydronephrosis or the right kidney. The symptoms were relieved by conservative treatment.
Malignant disease:In the present series 3(7.5%) cases had malignant disease, one each of liver,pancreas and ampulla of vater. Patient with carcinoma of liver died within one year while those with carcinoma pancreas and ampullary carcinoma were in poor state two years after cholecystectomy.
The preparation and indication of cholecystectomy are the same whether it is performed by open or laparoscopy technique. Laparoscopic cholecystectomy is the procedure of choice for the majority of patients with gall bladder disease. The key in open
cholecystectomy , is identification and safe dissection of calot�s triangle.
SUMMARY AND CONCLUSIONTwo hundred Laparoscopic cholecystectomy cases have been followed between 2017-2018, out of which 150 were female and 50 male. Post cholecystectomy syndrome was observed in 40 cases giving 20 % , consisiting of 29 females and 11 males.
The age group upto 30 years had minimum percentage ( 17.54 % ) of symptomatic cases whereas maximum were seen after 60 years of age.
Most of the symptomatic cases(40 % ) came for the treatment within six months of the cholecystectomy.
The complaints, details of the surgery and the follow up observations have been recorded.
Cases were divided according to the presence of stone at their cholecystectomy into calculus and non calculus groups.the symptomatic cases were more ( 50 % 0 in non calculus groups than in the calculus group ( 18.75 % ).
Symptoms related to hepatobiliary system including pancreas have been termed as � true post cholecystectomy syndrome.� This was found in 8.5 % cases.
Pain was a constant feature in almost every case and was complained before and after cholecystectomy. Jaundice , vomiting, nausea and fever were found in more percentage of cases after operation than before.
The cause responsible for the �True syndrome� was found to be stone in the common bile duct, Stricture of common bile duct, biliary fistula, stenosis and spasm of sphincter of oddi, biliary dyskinesia and periampullary carcinoma. Their incidence and importance have been reported and analysed.
Investigations revealed that there were several associated conditions with the biliary disease responsible for dyspeptic and other symptoms in the cases under study. They were parasitic infestations, hepatitis, cholangitis, cirrhosis, gastroduodenal ulceration , diverticular disease of the colon and carcinoma of the liver.
Operative treatment adopted for 18 cases ( 45 % ) offered cure or relief in 15 cases ( 37.5 % ). Two cases were not benefited by surgery and one case 9 2.5 % ) died due to low condition.
Correct pre-operative diagnosis to distinguish the condition from other concomitant pathology would enable to reduce the incidence of this syndrome.
Advanced investigation techniques correct diagnosis as far as practicable and above all mature operative judgement and meticulous surgery will certainly bring down this undesired Post - cholecystectomy syndrome and finally wipe it out completely.
REFERENCES:1. Show, C., O Hanlon D.M. Hepatogastroenterology , 2004 Jan-Feb. Fenlon B.M.
Mc Entee,G.P.2. Abu Farsakh NA, Stietieh M & Abu Farsakh :J Clin Gastroenterol,2009.3. Coakley FV, Schwartz, L.H. & Blumgari L.H. �Radiology 2012 Oct. ; 209 (1) :141-6
(medline) Blumgart, L.H.4. Corzzoari, E. �Dig liver Dis. 2003 Jul.5. Evans, PR Bak, Y.T. Shuter B-Dig Dis.Sci. 2007 Oct.6. Glenn, F (1952) � Quoted by Schofield,20067. Rubini, G., Dimonte, M-Clin. Nucl. Med. 2009.8. Steen, W. Jensen (2002)-Medline.9. Tarik Albuzhi- Klin Khir.,2000 Oct.10. Weir. J.F. & Snell,A.m.(1953)-Quoted by Troppoli et al.,2012.
PARIPEX - INDIAN JOURNAL OF RESEARCH Volume-8 | Issue-4 | April-2019 | PRINT ISSN No 2250-1991
14 www.worldwidejournals.com




















