
Increased cerebral perfusion in adult attention deficit hyperactivity disorder is normalised by...
6
Increased cerebral perfusion in adult attention deficit hyperactivity disorder is normalised by stimulant treatment: A non-invasive MRI pilot study Ruth L. O'Gorman, a,b,c, ⁎ Mitul A. Mehta, a Philip Asherson, d,e Fernando O. Zelaya, a Keeley J. Brookes, d,f Brian K. Toone, e David C. Alsop, g and Steven C.R. Williams a a Centre for Neuroimaging Sciences, Institute of Psychiatry, King's College London, London, UK b Department of Neuroimaging, King's College Hospital, London, UK c Department of Medical Engineering and Physics, King's College Hospital, London, UK d MRC Social, Genetic, and Developmental Psychiatry Centre, Institute of Psychiatry, London, UK e Neuropsychiatry unit, Maudsley Hospital, London, UK f Bute Medical School, University of St Andrews, Fife, UK g Department of Radiology, Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, MA, USA Received 29 November 2007; revised 28 March 2008; accepted 11 April 2008 Available online 20 April 2008 The neurobiological basis for attention deficit hyperactivity disorder (ADHD) has not yet been fully established, although there is a growing body of evidence pointing to functional and structural abnormalities involving the basal ganglia, cerebellum, and regions of frontal grey matter. The purpose of this study was to investigate regional cerebral perfusion in adults with ADHD and age-matched control subjects, and to assess the perfusion response to stimulant treatment in the ADHD group using a non-invasive magnetic resonance perfusion imaging technique. Whole-brain cerebral perfusion images were acquired from nine right-handed male patients with ADHD and eleven age-matched control subjects using a continuous arterial spin labelling (CASL) technique. The ADHD group was assessed once on their normal treatment and once after withdrawing from treatment for at least one week. An automated voxel-based analysis was used to identify regions where the cerebral perfusion differed significantly between the ADHD and control groups, and where the perfusion altered significantly with stimulant treatment. Regional cerebral perfusion was increased in the ADHD group in the left caudate nucleus, frontal and parietal regions. Psychomotor stimulant treatment acted to normalise perfusion in frontal cortex and the caudate nucleus with additional decreases in parietal and parahippocampal regions. These findings highlight the potential sensitivity of non-invasive perfusion MRI techniques like CASL in the evaluation of perfusion differences due to illness and medication treatment, and provide further evidence that persistence of ADHD symptomatology into adulthood is accompanied by abnormal- ities in frontal and striatal brain regions. © 2008 Elsevier Inc. All rights reserved. Introduction Attention deficit hyperactivity disorder (ADHD) is a developmental psychiatric disorder thought to affect approximately 4% of school-age children, of whom 30%–65% continue to exhibit symptoms into adulthood (DSM-IV, 1994; Faraone et al., 2006; Nutt et al., 2007). Over the long term those affected by ADHD tend to demonstrate reduced educational outcomes and an increased incidence of substance abuse, antisocial behaviour, anxiety, and depression (Kollins et al., 2005; Upadhyaya et al., 2005; Spencer et al., 2007). Currently ADHD is predominantly treated with stimulant medications such as methylphe- nidate or amphetamine, which primarily release and prevent the reuptake of catecholamines (dopamine and noradrenaline), increasing the activity of these neurotransmitter systems (Seeman and Madras, 1998; Arnsten, 2006). Since these stimulant medications have been demonstrated to bring about a transitory reduction in ADHD symptoms, the dopaminergic and noradrenergic pathways have been the focus of much of the existing work exploring the neurobiology of ADHD. Neuroimaging studies have provided further support for the notion that the major catecholaminergic pathways are abnormal in ADHD (for review see Castellanos and Tannock, 2002; Durston, 2003; Bush et al., 2005). Specifically, widespread reductions in frontal grey matter www.elsevier.com/locate/ynimg NeuroImage 42 (2008) 36 – 41 ⁎ Corresponding author. Neuroradiology department, King's College Hospital, Denmark Hill, London SE5 9RS, UK. E-mail address: r.o'[email protected] (R.L. O'Gorman). Available online on ScienceDirect (www.sciencedirect.com). 1053-8119/$ - see front matter © 2008 Elsevier Inc. All rights reserved. doi:10.1016/j.neuroimage.2008.04.169
-
Upload
independent -
Category
Documents
-
view
2 -
download
0
Transcript of Increased cerebral perfusion in adult attention deficit hyperactivity disorder is normalised by...
www.elsevier.com/locate/ynimg
NeuroImage 42 (2008) 36–41Increased cerebral perfusion in adult attention deficit hyperactivitydisorder is normalised by stimulant treatment: A non-invasiveMRI pilot study
Ruth L. O'Gorman,a,b,c,⁎ Mitul A. Mehta,a Philip Asherson,d,e Fernando O. Zelaya,a
Keeley J. Brookes,d,f Brian K. Toone,e David C. Alsop,g and Steven C.R. Williamsa
aCentre for Neuroimaging Sciences, Institute of Psychiatry, King's College London, London, UKbDepartment of Neuroimaging, King's College Hospital, London, UKcDepartment of Medical Engineering and Physics, King's College Hospital, London, UKdMRC Social, Genetic, and Developmental Psychiatry Centre, Institute of Psychiatry, London, UKeNeuropsychiatry unit, Maudsley Hospital, London, UKfBute Medical School, University of St Andrews, Fife, UKgDepartment of Radiology, Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, MA, USA
Received 29 November 2007; revised 28 March 2008; accepted 11 April 2008Available online 20 April 2008
The neurobiological basis for attention deficit hyperactivity disorder(ADHD) has not yet been fully established, although there is a growingbody of evidence pointing to functional and structural abnormalitiesinvolving the basal ganglia, cerebellum, and regions of frontal greymatter. The purpose of this study was to investigate regional cerebralperfusion in adults with ADHD and age-matched control subjects, andto assess the perfusion response to stimulant treatment in the ADHDgroup using a non-invasive magnetic resonance perfusion imagingtechnique. Whole-brain cerebral perfusion images were acquired fromnine right-handed male patients with ADHD and eleven age-matchedcontrol subjects using a continuous arterial spin labelling (CASL)technique. The ADHD group was assessed once on their normaltreatment and once after withdrawing from treatment for at least oneweek. An automated voxel-based analysis was used to identify regionswhere the cerebral perfusion differed significantly between the ADHDand control groups, and where the perfusion altered significantly withstimulant treatment. Regional cerebral perfusion was increased in theADHD group in the left caudate nucleus, frontal and parietal regions.Psychomotor stimulant treatment acted to normalise perfusion infrontal cortex and the caudate nucleus with additional decreases inparietal and parahippocampal regions. These findings highlight thepotential sensitivity of non-invasive perfusion MRI techniques likeCASL in the evaluation of perfusion differences due to illness and
⁎ Corresponding author. Neuroradiology department, King's CollegeHospital, Denmark Hill, London SE5 9RS, UK.
E-mail address: r.o'[email protected] (R.L. O'Gorman).Available online on ScienceDirect (www.sciencedirect.com).
1053-8119/$ - see front matter © 2008 Elsevier Inc. All rights reserved.doi:10.1016/j.neuroimage.2008.04.169
medication treatment, and provide further evidence that persistence ofADHD symptomatology into adulthood is accompanied by abnormal-ities in frontal and striatal brain regions.© 2008 Elsevier Inc. All rights reserved.
Introduction
Attention deficit hyperactivity disorder (ADHD) is a developmentalpsychiatric disorder thought to affect approximately 4% of school-agechildren, of whom 30%–65% continue to exhibit symptoms intoadulthood (DSM-IV, 1994; Faraone et al., 2006; Nutt et al., 2007). Overthe long term those affected by ADHD tend to demonstrate reducededucational outcomes and an increased incidence of substance abuse,antisocial behaviour, anxiety, and depression (Kollins et al., 2005;Upadhyaya et al., 2005; Spencer et al., 2007). Currently ADHD ispredominantly treated with stimulant medications such as methylphe-nidate or amphetamine, which primarily release and prevent thereuptake of catecholamines (dopamine and noradrenaline), increasingthe activity of these neurotransmitter systems (Seeman and Madras,1998; Arnsten, 2006). Since these stimulant medications have beendemonstrated to bring about a transitory reduction inADHDsymptoms,the dopaminergic and noradrenergic pathways have been the focus ofmuch of the existing work exploring the neurobiology of ADHD.
Neuroimaging studies have provided further support for the notionthat the major catecholaminergic pathways are abnormal in ADHD(for review see Castellanos and Tannock, 2002; Durston, 2003; Bushet al., 2005). Specifically, widespread reductions in frontal greymatter
37R.L. O'Gorman et al. / NeuroImage 42 (2008) 36–41
and basal ganglia volumes have been repeatedly demonstrated inchildren and adolescents with ADHD, as have reductions in ce-rebellar, and corpus callosal volumes (Castellanos et al., 1994, 1996,2001, 2002; Giedd et al., 1994; Aylward et al., 1996; Baumgardneret al., 1996; Filipek et al., 1997; Overmeyer et al., 2001; Castellanosand Tannock, 2002; Hesslinger et al., 2002), although there has beensome inconsistency with respect to the laterality of the volumechanges observed.
Evidence for functional cerebral deficits in ADHD first emergedfrom SPECT studies conducted by Lou and colleagues between1984 and 1990 (Lou et al., 1984, 1989). While these early studiessuffered from several methodological constraints (Castellanos,2002), they consistently demonstrated decreased perfusion inthe striatum relative to age-matched controls. Further SPECT stu-dies in children and adolescents with ADHD additionally demon-strated abnormal perfusion in frontal, temporal, and cerebellarregions (Amen et al., 1993; Gustafsson et al., 2000; Kim et al.,2002).
Functional abnormalities have also emerged from task-basedPositron Emission Tomography (PET) and Blood Oxygen LevelDependent (BOLD) functional MRI studies (Vaidya et al., 1998; Bushet al., 1999; Rubia et al., 1999; Schweitzer et al., 2000; Durston, 2003),which have been crucial in defining the neural correlates of task-relatedcognitive deficits in ADHD. BOLD fMRI methods offer increasedspatial and temporal resolution relative to emission tomography me-thods, but standard BOLD fMRI techniques are unable to provideinformation with regard to the baseline perfusion, known to beabnormal from the early PET and SPECT literature. The BOLD signalalso depends in a complicated way on several instrumental andbiological factors (Buxton et al., 2004), the latter of which includes therelaxation time T2* and the interaction between regional perfusion andthe metabolic rate of oxygen consumption. Since T2* and regionalperfusion are known to be altered in ADHD (Teicher et al., 2000;Anderson et al., 2002), and since these factors are not quantifiable witha typical BOLD fMRI experiment, the baseline BOLD fMRI signalcannot be easily compared between subjects or groups. The earlier
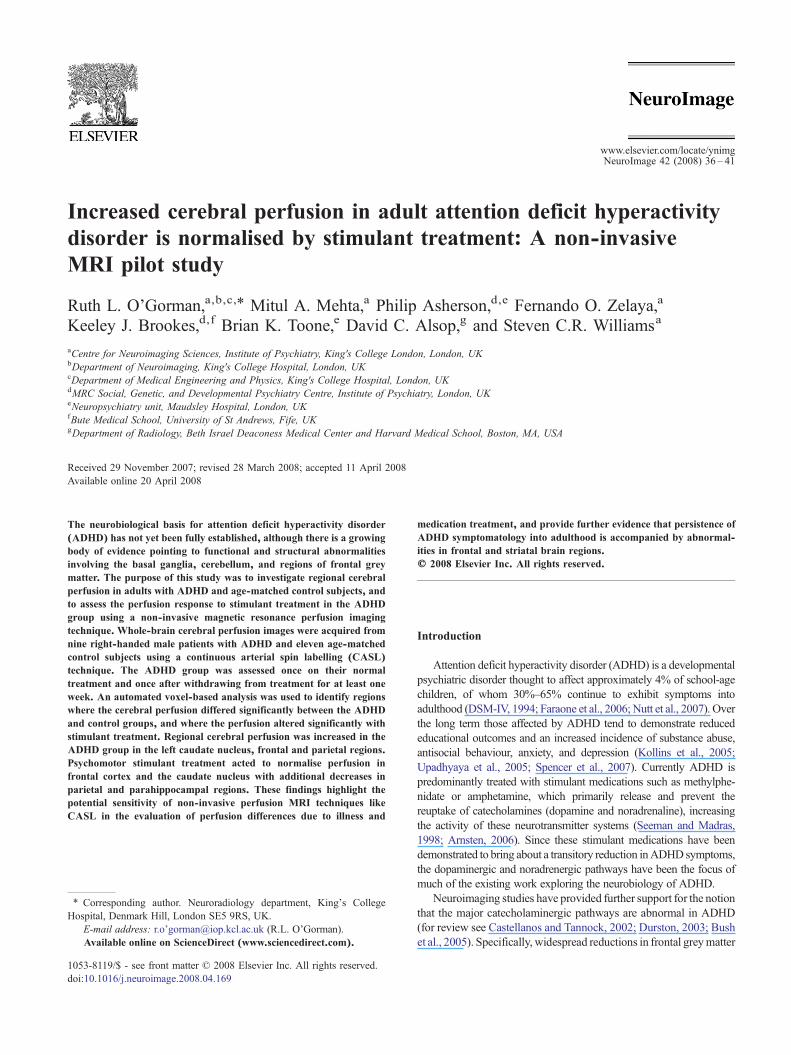
Fig. 1. Significant clusters from the group comparison between unmedicated ADHdemonstrated increased perfusion relative to controls (pb0.005, corrected). Significgyrus (CG), precuneus (pCu), medial frontal gyrus (mFG), and post-central gyrus
SPECT and PET studies have been able to identify areas of abnormalperfusion and metabolism, but many of these nuclear medicine stu-dies have been limited by the lack of a suitable control group, largelybecause of the ethical considerations associated with exposing healthyvolunteers to ionising radiation. In addition, all but one of these pre-vious neuroimaging studies have focused on children and adolescentswith ADHD, and the one previous study in adults with ADHD onlyexamined the effects of medication, without including a control group(Schweitzer et al., 2003). Given the large changes in brain structure andfunction associated with brain development and the known changes inclinical ADHD phenomenology with age (Blakemore and Choudhury,2006; Rubia et al., 2006; Shaw et al., 2006; Toga et al., 2006), acompelling argument exists for extending functional neuroimaginginvestigations of ADHD to a range of age groups. The primary purposeof this pilot study was to investigate differences in regional cerebralperfusion between adults with ADHD and controls with continuousarterial spin labelling (CASL) perfusionMRI.A secondary purposewasto assess the perfusion response to treatment with stimulant medica-tion. Although methylphenidate decreased striatal blood flow in theonly previous study in adults with ADHD, (Schweitzer et al., 2003)in consideration of the more extensive literature in children withADHD, we hypothesised that perfusion would be lower in frontal and,particularly, striatal brain regions relative to controls and that stimulanttreatment would act to normalise perfusion in these regions.
Materials and methods
Participants
Nine right-handed male patients with ADHD (mean age 30 years,range 20–48) were recruited from the Maudsley adult ADHD clinic(Van Der Linden et al., 2000). All patients fulfilled DSM-IV criteria forADHD as assessed by interview with the patient and a relative or closefriend, and also fulfilled criteria as a child based on retrospectiveanalysis of school and parental reports. All patients were clinicallyresponsive to stimulant treatment and had been treated for aminimumof
D patients and controls: red regions denote clusters where ADHD patientsant clusters are in the left caudate (LC), inferior frontal gyrus (iFG), cingulate(pcG). Images are shown in radiological orientation.

Table 1Talairach coordinates (mm) for significant changes in perfusion observed in thegroup comparisons (pb0.005, corrected), derived following transformation ofthe group-specific template into Talairach space
Region Talairach coordinates [X,Y,Z] (mm)
Unmedicated ADHDNcontrolsInsula [−38, 7, −2]Superior temporal gyrus [−53, 9, −3]Caudate [−11, 15, −4]Inferior frontal gyrus [−39, 23, −7]
[−37, 33, 11][−44, 14, 32]
Cingulate gyrus [9, 34, 11][9, 4, 30]
Precuneus [37, −67, 41][−20, −47, 44]
Medial frontal gyrus [−20, 35, 26]Post-central gyrus [−30, −29, 47]
[−31, −30, 51]
Medicated ADHDNunmedicated ADHDCaudate (left) [−11, 17, −4]Caudate (right) [6, 16, −5]Inferior frontal gyrus [−41, 20, −5]
[−49, 14, 16]Parahippocampal gyrus [14, −34, 1]Post-central gyrus [−52, −14, 20]Supra-marginal gyrus [49, −41, 31]
Medicated ADHDNcontrolsPrecentral gyrus [28, −12, 42]
[30, −11, 46]Inferior frontal gyrus [−42, 13, 32]
[−36, 9, 29]Cingulate gyrus [−5, −24, 30]Inferior parietal lobule [−43, −55, 38]
38 R.L. O'Gorman et al. / NeuroImage 42 (2008) 36–41
one month prior to entry into this study. Exclusion criteria includedother current or previous psychiatric illness, neurological illness,substance abuse, WAIS IQb80, or the use of prescription drugs otherthan stimulantmedications. The control group consisted of eleven right-handed healthymale volunteers (mean age 30 years, range 22–48), withno history of psychiatric or neurological illness. All the volunteers werescreened for ADHD using the Adult Self-Report Scale (Kessler et al.,2005). Each of the ADHD patients was scanned once while ontreatment with stimulant medication (slow-release methylphenidate:n=2, fast-release methylphenidate: n=5, with one patient taking dex-troamphetamine (5/10/5 mg per day)). For the slow-release formulationthe doses prescribed were 36 mg and 54 mg (18 mg am+36 mgmidday) and for the fast-release formulation the doses prescribed were5 mg bd, 10 mg tds, 30 mg tds, 30/30/20 mg per day, and 15/15/10 mgper day. Scans were performed approximately 1 h after ingestion of thefast-release formulation or 5 h after ingestion of the slow-releaseformulation, and the order of the medicated and unmedicated scanswas counterbalanced such that five patients were first scanned offmedication and four were first scanned on medication.
Data acquisition
Imaging was performed with a 1.5 T GE Signa Echospeed MRIscanner (GE Medical Systems, Milwaukee, WI, USA). Cerebralperfusion images were acquired using a non-invasive multislice,continuous arterial spin labelling (CASL) sequence with an amplitudemodulated control technique (Alsop and Detre, 1998). A constant RFamplitude of 32 mG was applied with a frequency offset of 8000 Hzand a labelling gradient strength of 0.25 G/cm for adiabatic inversion,and an amplitude modulated control pulse was applied with amodulation frequency of 125Hz during the control phase. The imageswere acquiredwith a gradient-echo echo planar imaging (EPI) readoutwith a field of view (FOV) of 24 cm, a matrix of 64×64, a slicethickness of 7 mm, and a slice gap of 1 mm, resulting in a voxelresolution of 3.75×3.75×7 mm3. The repetition time (TR) andeffective echo time (TE) were 4 s and 32 ms, respectively, and a post-labelling delay of 1 s was applied in order to reduce errors from transittime effects (Alsop and Detre, 1998). In total, 90 image volumes (45control/45 label) of 15 axial slices were collected using twooverlapping acquisitions, resulting in a total scan time of 12 min.For all patients and seven of the control participants, velocity mapswere acquired at the level of the ASL inversion plane using aperipherally gated phase contrast angiography sequence, and themeasured velocity profile was used to calculate the ASL inversionefficiency, required for perfusion quantification (O'Gorman et al.,2006b). For the four control participants for whom phase contrast datawas not available, a literature value for the inversion efficiency of thissequence was assumed (Alsop and Detre, 1998). In order to confirmthe absence of any underlying pathology, high resolution structuralMR images were also acquired using a dual echo fast spin echo(TE=20/100 ms, TR=4 s, FOV=24 cm2, matrix=2562, slicethickness=3.5 mm, gap=0.5 mm) and a fast inversion-recoveryprepared spoiled gradient-echo volume (inversion time=450 ms,TR=11 ms, TE=1.9 ms, slice thickness=1.5 mm, gap=0 mm,FOV=24 cm2, matrix=2562, flip angle=90°). All scans wereperformed at the same time of day in the afternoon, and the perfusionimages were acquired after approximately 15 min of structuralscanning in order to give the participants sufficient time to acclimatiseto each session in the MR environment. The participants were notgiven an explicit task in the scanner, but simply instructed to relax andremain still during the scanning session.
Image analysis
The control images from the CASL sequence were registeredto a group-specific high resolution EPI template (Studholme et al.,1999), and the transformation matrix from this registration wasthen applied to the perfusion maps. The difference in perfusionbetween ADHD patients and controls was evaluated with Xbamm(Brain Activation and Morphological Mapping, http://www-bmu.psychiatry.cam.ac.uk), by fitting an analysis of covariance(ANCOVA) model at each intracerebral voxel, covarying for thepotentially confounding effects of age (Bullmore et al., 1999). Aninitial voxel-wise p-value of p≤0.05 was used to detect voxelspotentially demonstrating differences in perfusion betweengroups. Spatial clusters of significant voxels were then definedand the cluster mass (defined as the sum of suprathreshold voxelstatistics) was tested against a null distribution derived fromrandom permutation of the group membership, thereby testing thenull hypothesis that differences in perfusion between the groupsoccur by chance. The statistical thresholds were corrected formultiple comparisons by controlling the family-wise error rateof each cluster. Regional differences in perfusion in the ADHDgroup on and off medication were then tested with the samestatistical software and analysis method, using a paired studydesign.

Fig. 3. Distribution of perfusion values extracted from the caudate nucleuscluster showing reduced perfusion following treatment in the ADHD group.Perfusion in the same cluster for the control group is shown for comparison.The unmedicated ADHD group demonstrated a 51% increase in perfusion inthis region compared to controls; after medication these perfusion valueswere normalised (−1% relative to controls).
39R.L. O'Gorman et al. / NeuroImage 42 (2008) 36–41
Results
The results of the group comparison between the unmedicatedADHD patients and the controls are shown in Fig. 1 and Table 1.At a cluster-wise significance level of pb0.005 (corrected), theADHD patients demonstrate significantly higher perfusion in theleft caudate and regions of frontal and parietal grey and whitematter.
The results of the comparison between the ADHD group on andoff treatment are shown in Fig. 2 and Table 1. Perfusion decreasedwith medication in clusters centred in the left caudate nucleus,parahippocampal gyrus, and regions of inferior frontal and parietalgrey matter (at a cluster-wise significance level of pb0.005,corrected). Fig. 3 shows the distribution of perfusion values extractedfrom the cluster centred on the left caudate for the ADHD group onand off medication, with the perfusion values from the same region inthe control group shown for comparison. Importantly, all ADHDpatients demonstrated a decrease in perfusion in this region followingtreatment. There was no significant difference in perfusion in thisregion between the medicated ADHD patients and the control group(p=0.94). However, whole-brain analysis betweenmedicated patientsand controls (pb0.005, corrected) showed higher perfusion in theright sensorimotor and inferior frontal and parietal regions (Table 1).No significant difference in average whole-brain perfusion wasobserved between the unmedicated ADHD and control groups(p=0.41), the medicated ADHD and control groups (p=0.34), orbetween the ADHD group on and off medication (p=0.53).
Discussion
Although the neurobiological basis of ADHD has not yet beenestablished, structural and functional neuroimaging studies inchildren and adolescents have shown widespread differences infrontal, striatal, and cerebellar regions (Schweitzer et al., 2000;Teicher et al., 2000; Hesslinger et al., 2002; Durston, 2003). Theseareas are known to be involved in impulsivity and motor regula-
Fig. 2. Significant clusters from the paired comparison between ADHD patients onthe perfusion decreased with medication (offNon). Significance level: pb0.005, co(iFG), parahippocampal gyrus (pHG), post-central gyrus (pcG), and supra-margin
tion as well as the control and regulation of attention processes, andthe frontal and striatal regions are the major targets for the psy-chomotor stimulant medications used to treat some of the symp-toms of ADHD in adults and children. The increase in perfusionseen in the caudate and inferior frontal regions in ADHD grouprelative to controls (Figs. 1 and 2) therefore provides additionalevidence that these areas may be abnormally functioning in adultADHD.
The direction of the perfusion difference seen in the un-medicated adults with ADHD in this study (i.e. increased per-fusion in these regions relative to controls) is opposite to thatpreviously reported in children with ADHD, although the sameregions are involved. This result is surprising, but the level ofstatistical significance and the presence of reduced perfusion in
and off treatment with methylphenidate. Red regions denote clusters whererrected. Significant clusters are in the left caudate (LC), inferior frontal gyrusal gyrus (smG). Images are shown in radiological orientation.

40 R.L. O'Gorman et al. / NeuroImage 42 (2008) 36–41
the caudate nucleus for all patients following stimulant treat-ment are compelling. For the comparisons between patients andcontrols a potential confound arises from the fact that patients werescanned twice while controls were scanned only once, raising thepossibility that habituation effects in patients may contribute to theresults despite the fact that the order of scans was counterbalanced.However, in separate work we have shown that the coefficient ofvariation for grey matter perfusion values measured with CASLranges from 6%–10% (O'Gorman et al., 2006a, 2007), suggestingthat the pattern of results in this study (most notably the 51%increase in caudate perfusion in unmedicated patients relative tocontrols) is unlikely to be determined by habituation effects. Thebehaviour of participants was similar to that reported in previousperfusion studies in children to allow for comparisons to be made.However, it is known that the variance of imaging measures can bereduced using simple tasks (Duara et al., 1987), and the use of atask could theoretically increase power to detect changes in thisstudy. Thus, our findings may reflect differences in the ‘at rest’state of those with ADHD compared to controls and may thus alsobe represented in control conditions of cognitive tasks used infMRI studies.
Compared to perfusion changes seen in children, the apparentchange in direction of perfusion differences in adults with ADHDmay represent a long-term adaptation of the brain, but it may alsoresult partly from chronic treatment with stimulant medica-tion. Several previous studies in children and/or adolescents withADHD have noted complex changes in perfusion with methyl-phenidate, including increased perfusion in the basal ganglia anddecreased perfusion in cortical and sensorimotor areas (Lou et al.,1984), increased perfusion in frontal lobe, caudate, thalamus, andtemporal lobe (Kim et al., 2001), and reduced perfusion in leftposterior parietal regions (Szobot et al., 2003). In the present studydecreased perfusion was observed in a limited number of regions,including the left caudate nucleus and inferior frontal gyrus. Thesechanges indicate that in this group, methylphenidate may be actingto normalise the underlying difference in baseline perfusion. Theonly other study in adults (Schweitzer et al., 2003) noted a similardecrease in perfusion with medication, measured with H2
15O PET,in several regions including the left caudate nucleus and precentralgyrus, extending anteriorly, which overlap with our findings.Additionally, we have also shown the inferior frontal gyrus mayremain hyper-perfused after treatment, highlighting the regionallimitations of stimulant treatment across the brain, although itwould be necessary to consider the effects of stimulant treatment inhealthy controls in order to fully elucidate the relevance of thisfinding for ADHD.
This study represents the first application of perfusion MRIboth to the investigation of the neurobiological basis of ADHDin adults or children, and the assessment of the effects of sti-mulant medication on cerebral perfusion. Overall, we have pro-vided further evidence for a neurobiological basis for ADHD,highlighting the involvement of the fronto-striatal circuitry.This study has also established the value of non-invasive per-fusion imaging techniques such as CASL in the evaluation ofcerebral perfusion changes, raising important questions aboutpossible adaptive changes in perfusion related to developmentand treatment in ADHD. Future studies involving larger groupsand double-blind study designs will be necessary to establishthe behavioural and developmental significance of these perfu-sion changes and further clarify the persistence of ADHD intoadulthood.
References
Alsop, D.C., Detre, J.A., 1998. Multisection cerebral blood flow MRimaging with continuous arterial spin labeling. Radiology 208 (2),410–416.
Amen, D.G., Paldi, F., Thisted, R.A., 1993. Evaluating ADHD with brainSPECT imaging. J. Am. Acad. Child Adolesc. Psych. 32 (5), 1080–1081.
Anderson, C.M., Polcari, A., et al., 2002. Effects of methylphenidate onfunctional magnetic resonance relaxometry of the cerebellar vermis inboys with ADHD. Am. J. Psychiatry 159 (8), 1322–1328.
Arnsten, A.F.T., 2006. Stimulants: therapeutic actions in ADHD. Neurop-sychopharmacology 31 (11), 2376–2383.
Aylward, E.H., Reiss, A.L., et al., 1996. Basal ganglia volumes in child-ren with attention-deficit hyperactivity disorder. J. Child Neurol. 11 (2),112–115.
Baumgardner, T.L., Singer, H.S., et al., 1996. Corpus callosum morphologyin children with Tourette syndrome and attention deficit hyperactivitydisorder. Neurology 47 (2), 477–482.
Blakemore, S.J., Choudhury, S., 2006. Development of the adolescent brain:implications for executive function and social cognition. J. ChildPsychol. Psychiatry 47 (3–4), 296–312.
Bullmore, E.T., Suckling, J., et al., 1999. Global, voxel, and cluster tests, bytheory and permutation, for a difference between two groups of structuralMR images of the brain. IEEE Trans. Med. Imag. 18 (1), 32–42.
Bush, G., Frazier, J.A., et al., 1999. Anterior cingulate cortex dysfunction inattention-deficit/hyperactivity disorder revealed by fMRI and the count-ing stroop. Biol. Psychiatry 45 (12), 1542–1552.
Bush, G., Valera, E.M., et al., 2005. Functional neuroimaging of attention-deficit/hyperactivity disorder: a review and suggested future directions.Biol. Psychiatry 57 (11), 1273–1284.
Buxton, R.B., Uludag, K., et al., 2004. Modeling the hemodynamic responseto brain activation. NeuroImage 23, S220–S233.
Castellanos, F.X., 2002. Proceed, with caution: SPECT cerebral blood flowstudies of children and adolescents with attention deficit hyperactivitydisorder. J. Nucl. Med. 43 (12), 1630–1633.
Castellanos, F.X., Tannock, R., 2002. Neuroscience of attention-deficit/hyperactivity disorder: the search for endophenotypes. Nat. Rev. Neurosci.3 (8), 617–628.
Castellanos, F.X., Giedd, J.N., et al., 1994. Quantitative morphology of thecaudate-nucleus in attention-deficit hyperactivity disorder. Am. J. Psychiatry151 (12), 1791–1796.
Castellanos, F.X., Giedd, J.N., et al., 1996. Quantitative brain magneticresonance imaging in attention-deficit hyperactivity disorder. Arch. Gen.Psychiatry 53 (7), 607–616.
Castellanos, F.X., Giedd, J.N., et al., 2001. Quantitative brain magneticresonance imaging in girls with attention-deficit/hyperactivity disorder.Arch. Gen. Psychiatry 58 (3), 289–295.
Castellanos, F.X., Lee, P.P., et al., 2002. Developmental trajectories of brainvolume abnormalities in children and adolescents with attention-deficit/hyperactivity disorder. JAMA 288 (14), 1740–1748.
Diagnostic and StatisticalManual ofMental Disorders, 4th edition. AmericanPsychiatric Association.
Duara, R., Grossglenn, K., et al., 1987. Behavioral activation and thevariability of cerebral glucose metabolic measurements. J. Cereb. BloodFlow Metab. 7 (3), 266–271.
Durston, S., 2003. A review of the biological bases of ADHD: what have welearned from imaging studies? Ment. Retard. Dev. Disabil. Res. Rev. 9 (3),184–195.
Faraone, S.V., Biederman, J., et al., 2006. The age-dependent decline ofattention deficit hyperactivity disorder: a meta-analysis of follow-upstudies. Psychol. Med. 36 (2), 159–165.
Filipek, P.A., SemrudClikeman, M., et al., 1997. Volumetric MRI analysiscomparing subjects having attention-deficit hyperactivity disorder withnormal controls. Neurology 48 (3), 589–601.
Giedd, J.N., Castellanos, F.X., et al., 1994. Quantitative morphology of thecorpus-callosum in attention-deficit hyperactivity disorder. Am. J. Psychiatry151 (5), 665–669.

41R.L. O'Gorman et al. / NeuroImage 42 (2008) 36–41
Gustafsson, P., Thernlund, G., et al., 2000. Associations between cerebralblood-flow measured by single photon emission computed tomography(SPECT), electro-encephalogram (EEG), behaviour symptoms, cogni-tion and neurological soft signs in children with attention-deficithyperactivity disorder (ADHD). Acta Paediatr. 89 (7), 830–835.
Hesslinger, B., van Elst, L.T., et al., 2002. Frontoorbital volume reductionsin adult patients with attention deficit hyperactivity disorder. Neurosci.Lett. 328 (3), 319–321.
Kessler, R.C., Adler, L., et al., 2005. The World Health Organization adultADHD self-report scale (ASRS): a short screening scale for use in thegeneral population. Psychol. Med. 35 (2), 245–256.
Kim, B.N., Lee, J.S., et al., 2001. Methylphenidate increased regionalcerebral blood flow in subjects with attention deficit/hyperactivitydisorder. Yonsei Med. J. 42 (1), 19–29.
Kim, B.N., Lee, J.S., et al., 2002. Regional cerebral perfusion abnormalitiesin attention deficit/hyperactivity disorder — statistical parametricmapping analysis. Eur. Arch. Psychiatry Clin. Neurosci. 252 (5),219–225.
Kollins, S.H., McClernon, F.J., et al., 2005. Association between smokingand attention-deficit/hyperactivity disorder symptoms in a population-based sample of young adults. Arch. Gen. Psychiatry 62 (10),1142–1147.
Lou, H.C., Henriksen, L., et al., 1984. Focal cerebral hypoperfusion inchildren with dysphasia and or attention deficit disorder. Arch. Neurol.41 (8), 825–829.
Lou, H.C., Henriksen, L., et al., 1989. Striatal dysfunction in attention deficitand hyperkinetic disorder. Arch. Neurol. 46 (1), 48–52.
Nutt, D.J., Fone, K., et al., 2007. Evidence-based guidelines for managementof attention-deficit/hyperactivity disorder in adolescents in transitionto adult services and in adults: recommendations from the BritishAssociation for Psychopharmacology. J. Psychopharmacol. 21 (1),10–41.
O'Gorman, R.L., Kumari, V., et al., 2006a. Personality factors correlate withregional cerebral perfusion. NeuroImage 31 (2), 489–495.
O'Gorman, R.L., Summers, P.E., et al., 2006b. In vivo estimation of theflow-driven adiabatic inversion efficiency for continuous arterial spinlabeling: a method using phase contrast magnetic resonance angiogra-phy. Magn. Reson. Med. 55 (6), 1291–1297.
O'Gorman, R.L., Coward, H.J., et al., 2007. Reproducibility of Pseudo-continuous ASL at 1.5T and 3T. International Society for MagneticResonance in Medicine, 15th annual meeting, Berlin, Germany.
Overmeyer, S., Bullmore, E.T., et al., 2001. Distributed grey and whitematter deficits in hyperkinetic disorder: MRI evidence for anatomi-
cal abnormality in an attentional network. Psychol. Med. 31 (8),1425–1435.
Rubia, K., Overmeyer, S., et al., 1999. Hypofrontality in attention deficithyperactivity disorder during higher-order motor control: a study withfunctional MRI. Am. J. Psychiatry 156 (6), 891–896.
Rubia, K., Smith, A.B., et al., 2006. Progressive increase of frontostriatalbrain activation from childhood to adulthood during event-related tasksof cognitive control. Hum. Brain Mapp. 27 (12), 973–993.
Schweitzer, J.B., Faber, T.L., et al., 2000. Alterations in the functionalanatomy of working memory in adult attention deficit hyperactivitydisorder. Am. J. Psychiatry 157 (2), 278–280.
Schweitzer, J.B., Lee, D.O., et al., 2003. A positron emission tomographystudy of methylphenidate in adults with ADHD: alterations in restingblood flow and predicting treatment response. Neuropsychopharmacol-ogy 28 (5), 967–973.
Seeman, P., Madras, B.K., 1998. Anti-hyperactivity medication: methyl-phenidate and amphetamine. Mol. Psychiatry 3 (5), 386–396.
Shaw, P., Greenstein, D., et al., 2006. Intellectual ability and corticaldevelopment in children and adolescents. Nature 440 (7084), 676–679.
Spencer, T.J., Biederman, J., et al., 2007. Attention-deficit/hyperactivitydisorder: diagnosis, lifespan, comorbidities, and neurobiology. J. Pediatr.Psychol. 32 (6), 631–642.
Studholme, C., Hill, D.L.G., et al., 1999. An overlap invariant entropymeasure of 3D medical image alignment. Pattern Recogn. 32 (1), 71–86.
Szobot, C.M., Ketzer, C., et al., 2003. The acute effect of methylphenidateon cerebral blood flow in boys with attention-deficit/hyperactivitydisorder. Eur. J. Nucl. Med. Mol. Imaging 30 (3), 423–426.
Teicher,M.H., Anderson, C.M., et al., 2000. Functional deficits in basal gangliaof children with attention-deficit/hyperactivity disorder shown withfunctional magnetic resonance imaging relaxometry. Nat. Med. 6 (4),470–473.
Toga, A.W., Thompson, P.M., et al., 2006. Mapping brain maturation.Trends Neurosci. 29 (3), 148–159.
Upadhyaya, H.P., Rose, K., et al., 2005. Attention-deficit/hyperactivitydisorder, medication treatment, and substance use patterns among ado-lescents and young adults. J. Child Adolesc. Psychopharmacol. 15 (5),799–809.
Vaidya, C.J., Austin, G., et al., 1998. Selective effects of methylphenidate inattention deficit hyperactivity disorder: a functional magnetic resonancestudy. Proc. Natl. Acad. Sci. U. S. A. 95 (24), 14494–14499.
Van Der Linden, G., Young, S., et al., 2000. Attention deficit hyperactivitydisorder in adults — experience of the first National Health Serviceclinic in the United Kingdom. J. Mental Health 9 (5), 527–535.




















