In pursuit of prognostic factors in children with pilocytic astrocytomas
10
ORIGINAL PAPER In pursuit of prognostic factors in children with pilocytic astrocytomas Aline Paixão Becker & Ricardo Santos de Oliveira & Fabiano Pinto Saggioro & Luciano Neder & Leila Maria Cardão Chimelli & Hélio Rubens Machado Received: 10 August 2009 / Published online: 13 October 2009 # Springer-Verlag 2009 Abstract Objective This study described a 23-year experience in the treatment of children with pilocytic astrocytomas (piloA) with the aim of identifying putative clinical, histopatholog- ical, and/or immunohistochemical features that could be related to the outcome of these patients. Methods Clinical data of 31 patients under 18 years of age with piloA were obtained from 1984 to 2006. Results The mean age at the time of surgery was 7.8± 4.2 years (1 to 17 years), and the mean follow-up was 5.7± 5.4 years (1 to 20 years). The most common site of tumor formation was the cerebellum (17), followed by brainstem (4), optic chiasmatic hypothalamic region (4), cerebral hemisphere (3), cervical spinal cord (2), and optic nerve (1). Gross total resection (GTR) was achieved in 23 (74.1%), mainly in those with tumors located in the cerebellum and cerebral hemispheres (P=0.02). The global mortality rate was 6.4%. Nine patients were reoperated. Rosenthal fibers, eosinophilic granular bodies, microvascular proliferation, and lymphocytic infiltration were observed in most cases. The mean Ki-67LI was 4.4±4.5%. In all cases, Gal-3 expression in tumor cells was observed with variable staining pattern. Conclusions Aside from GTR, no other clinical, histopath- ological, or immunohistochemical features were found to be related to the prognosis. We postulate that strict follow- up is recommended if piloA is associated with high mitotic activity/Ki67-LI, or if GTR cannot be achieved at surgery. Tumor recurrence or progression of the residual lesion should be strictly observed. In some aspects, childhood piloA remains an enigmatic tumor. Keywords Brain tumor . Pediatric neurosurgery . Pilocytic astrocytoma . Prognostic factors . Galectin-3 Introduction Pilocytic astrocytoma is the most common glioma in children that is defined as a slowly growing, relatively circumscribed grade I astrocytoma according to the WHO classification of central nervous system (CNS) tumors [1]. Pilocytic astrocytomas (piloA) account for up 6% of all gliomas, amounting to 20% of primary brain tumors in children under 15 years of age and 30% of all posterior fossa tumors in childhood [2, 3]. PiloA can be completely surgically resected, resulting in an excellent prognosis [1, 4]. The overall 5-year survival rate after complete tumor resection is 85–100% [5–7]. However, a small number of piloA recur after surgical resection and may occasionally progress to malignant transformation [8]. PiloA are most commonly located in the cerebellum, brainstem, optic chiasm, and hypothalamus, but they can also be found elsewhere in the CNS, such as in the cerebral hemispheres, ventricles, spinal cord, and even in the cerebellopontine angle [9]. A. Paixão Becker : F. P. Saggioro : L. Neder Department of Pathology, Ribeirão Preto School of Medicine, University of São Paulo, Ribeirão Preto, SP, Brazil R. S. de Oliveira (*) : H. R. Machado Division of Pediatric Neurosurgery, Department of Surgery and Anatomy, Ribeirão Preto School of Medicine, University of São Paulo, Campus Universitário, 14049-900 Ribeirão Preto, SP, Brazil e-mail: [email protected] L. M. C. Chimelli Department of Pathology, Federal University of Rio de Janeiro, Rio de Janeiro, RJ, Brazil Childs Nerv Syst (2010) 26:19–28 DOI 10.1007/s00381-009-0990-8
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of In pursuit of prognostic factors in children with pilocytic astrocytomas

ORIGINAL PAPER
In pursuit of prognostic factors in childrenwith pilocytic astrocytomas
Aline Paixão Becker & Ricardo Santos de Oliveira & Fabiano Pinto Saggioro &
Luciano Neder & Leila Maria Cardão Chimelli & Hélio Rubens Machado
Received: 10 August 2009 / Published online: 13 October 2009# Springer-Verlag 2009
AbstractObjective This study described a 23-year experience in thetreatment of children with pilocytic astrocytomas (piloA)with the aim of identifying putative clinical, histopatholog-ical, and/or immunohistochemical features that could berelated to the outcome of these patients.Methods Clinical data of 31 patients under 18 years of agewith piloA were obtained from 1984 to 2006.Results The mean age at the time of surgery was 7.8±4.2 years (1 to 17 years), and the mean follow-up was 5.7±5.4 years (1 to 20 years). The most common site of tumorformation was the cerebellum (17), followed by brainstem(4), optic chiasmatic hypothalamic region (4), cerebralhemisphere (3), cervical spinal cord (2), and optic nerve (1).Gross total resection (GTR) was achieved in 23 (74.1%),mainly in those with tumors located in the cerebellum andcerebral hemispheres (P=0.02). The global mortality ratewas 6.4%. Nine patients were reoperated. Rosenthal fibers,eosinophilic granular bodies, microvascular proliferation,and lymphocytic infiltration were observed in most cases.The mean Ki-67LI was 4.4±4.5%. In all cases, Gal-3
expression in tumor cells was observed with variablestaining pattern.Conclusions Aside from GTR, no other clinical, histopath-ological, or immunohistochemical features were found tobe related to the prognosis. We postulate that strict follow-up is recommended if piloA is associated with high mitoticactivity/Ki67-LI, or if GTR cannot be achieved at surgery.Tumor recurrence or progression of the residual lesionshould be strictly observed. In some aspects, childhoodpiloA remains an enigmatic tumor.
Keywords Brain tumor . Pediatric neurosurgery . Pilocyticastrocytoma . Prognostic factors . Galectin-3
Introduction
Pilocytic astrocytoma is the most common glioma inchildren that is defined as a slowly growing, relativelycircumscribed grade I astrocytoma according to the WHOclassification of central nervous system (CNS) tumors [1].Pilocytic astrocytomas (piloA) account for up 6% of allgliomas, amounting to 20% of primary brain tumors inchildren under 15 years of age and 30% of all posteriorfossa tumors in childhood [2, 3]. PiloA can be completelysurgically resected, resulting in an excellent prognosis[1, 4]. The overall 5-year survival rate after complete tumorresection is 85–100% [5–7]. However, a small number ofpiloA recur after surgical resection and may occasionallyprogress to malignant transformation [8]. PiloA are mostcommonly located in the cerebellum, brainstem, opticchiasm, and hypothalamus, but they can also be foundelsewhere in the CNS, such as in the cerebral hemispheres,ventricles, spinal cord, and even in the cerebellopontineangle [9].
A. Paixão Becker : F. P. Saggioro : L. NederDepartment of Pathology, Ribeirão Preto School of Medicine,University of São Paulo,Ribeirão Preto, SP, Brazil
R. S. de Oliveira (*) :H. R. MachadoDivision of Pediatric Neurosurgery,Department of Surgery and Anatomy,Ribeirão Preto School of Medicine, University of São Paulo,Campus Universitário,14049-900 Ribeirão Preto, SP, Brazile-mail: [email protected]
L. M. C. ChimelliDepartment of Pathology, Federal University of Rio de Janeiro,Rio de Janeiro, RJ, Brazil
Childs Nerv Syst (2010) 26:19–28DOI 10.1007/s00381-009-0990-8

Although the prognosis for piloA patients is usuallyfavorable, the outcome is not always predictable due tosurgical morbidity and tumor recurrence. Furthermore, theclinical behavior of piloAs is still unpredictable in somepatients, and cases of malignant transformation have beendescribed [10], usually following radiation therapy [11].There are few published studies concerning series ofexclusively childhood piloA, and the majority of themrefer to piloA admixed with pilomyxoid variants andgliomas of different subtypes and malignancy grades[4, 8, 12]. In this regard, we described the 23-yearexperience of our institution in the treatment of childrenwith piloA with the aim of identifying putative clinical,histopathological, and/or immunohistochemical featuresthat could be related to the outcome of these patients.
Clinical material and methods
We reviewed all cases of patients under 18 years of agewho were diagnosed with piloA and underwent surgery atHospital of Clinics, Ribeirão Preto Medical School,University of São Paulo from January 1984 to December2006. Ten of 41 patients with initial diagnosis of piloAwereexcluded from this series after histopathological review dueto a change in the initial diagnosis or insufficient material.Medical charts, imaging findings, operative notes, andhistopathological reports of 31 patients with piloAs(38 tissue samples) were reviewed for the purpose ofevaluating the patients’ prognosis. In each case, allhematoxylin and eosin (H&E) sections (5µm) frombuffered formalin-fixed, paraffin-embedded tissue blockswere analyzed. The slides were blinded reviewed, and thediagnosis of piloA was re-evaluated by two neuropatholo-gists (ANPPB and LN) according to the criteria of the mostrecent WHO classification of CNS tumors [1]. This studywas approved by our Internal Review Board.
Radiological studies
All neuroimaging data obtained from computerized tomog-raphy (CT) and/or magnetic resonance (MR) during thefollow-up period were reviewed. Postoperative CT scansafter surgery were reviewed in order to determine surgicalresection [13]. We observed the patients during the follow-up period so as to detect true tumor recurrence or residue.
Gross total resection (GTR) was defined as the absenceof residual tumor on postoperative CT and/or MR imaging,regardless of the surgeon’s assessment of the extent ofresection. Incomplete surgical resection (ISR; subtotal orpartial) was defined as the presence of a residual contrast-enhancing mass or nodule on the postoperative imaging
[14]. Tumor progression was defined as an increase intumor volume observed on serial scans. Spontaneousregression was defined as a reduction in tumor volume inthe absence of further surgery or adjuvant therapy.Surveillance imaging was defined as scans carried out ona routine basis for the detection of recurrent or residualdisease in the absence of new symptoms or signs.
Histopathological and immunohistochemical studies
All available histological sections were blinded reviewed.The following histopathological features were evaluated:biphasic pattern, Rosenthal fibers (RF), eosinophilicgranular bodies (EGB), microcystic changes, nuclearpleomorphism, mitotic activity (counted in ten consecu-tive high-power fields (×400)), necrosis, microvascularproliferation, lymphocytic infiltration, calcification,infiltration of adjacent parenchyma, and presence ofganglion cells.
Immunohistochemical staining was performed using theavidin–biotin–peroxidase technique on paraffin sectionsafter antigen retrieval by pressure cooking. Briefly, afterdeparaffinization and rehydration in graded alcohol, 5-µm-thick sections were incubated at room temperature for30 min in 99.7% methanol containing 0.3% hydrogenperoxide. Slides were then washed with Tris-buffered salinesolution and blocked in diluted normal goat serum. Primaryantibodies against such antigens as Ki-67 (polyclonal,Novocastra®, clone MM1, dilution 1:300), galectin-3(monoclonal, clone 9C4, dilution 1:200), CD31 (monoclo-nal, clone JC70A, Dako®, dilution 1:100), and NeuN(monoclonal, clone A60, Chemicon International®, dilution1:2000) were used according to recommendations of themanufacturer. Tissue slides were incubated with primaryantibodies overnight at room temperature, and diaminoben-zidine was used as chromogen. After washing, the slideswere immediately counterstained with Harry’s hematoxylin,dehydrated, cover slipped, and examined under a lightmicroscope (Olympus®, DX 40).
The Ki-67 labeling index (Ki-67LI) was determined bycounting the number of tumor cells showing definitenuclear immunoreactivity among 1,000 contiguous nucleiin areas of the highest immunolabeling (“hot spots”).According to the methodology previously standardized inour institution, patients were divided into two groups: high-proliferative activity (Ki-67LI >3%) and low-proliferativeactivity (Ki-67LI <3%) [15]. Galectin-3 (Gal-3) expressionswere arbitrarily scored as diffuse (more than 50% ofpositive neoplastic cells) or focal (less than 50% ofpositivity) immunoreactivity. The Gal-3 labeling was alsodescribed at the cellular level (nucleus and/or cytoplasmicstaining). Microvascular density (MVD) was determined by
20 Childs Nerv Syst (2010) 26:19–28

counting the number of CD31-positive vessels in high-power fields (HPF, ×400). MVD evaluation was performedin the most vascularized areas, and seven microvessels perHPF was considered as reference [16]. NeuN was consid-ered positive only if staining was strong and restricted tothe nuclei of the tumor cells.
Prognostic factors
Clinical, histopathological, and immunohistochemical fea-tures were correlated with the outcome of the patients. Forclassification purpose, patients were divided into favorableoutcome (lesion-free or stable residual lesion after surgery)and adverse outcome (recurrence or regrowth of residuallesion after surgery). The clinical factors analyzed werepatient’s age at the time of surgery, tumor location, andtumor resection (GTR or ISR). The Ki-67LI (cutoff=3%),Gal-3 expression (diffuse or focal), and MVD (> or <7microvessels per HPF) were evaluated as putative prognos-tic factors.
Statistical analysis
Correlations between the various parameters werecalculated using Pearson’s and Fisher’s exact tests.The level of statistical significance was set at P<0.05.Survival and progression-free survival (PFS) curves werecalculated according to the Kaplan–Meier method. Thefollow-up period was calculated from the date of tumorresection to the date of relapse or regrowth of the residualtumor, the date of patient’s death, or the last contact withthe patient. Univariate analysis was performed using alog-rank test to evaluate association between clinicopath-ological parameters and patient’s outcome. Statisticalanalysis were performed with SPSS for Macintosh©,version 16.0.
Results
Clinical and surgical data
The patients’ mean age at diagnosis was 7.8±4.2 years(range, 1–17 years), with a female/male ratio of 1.06:1.Clinical data and tumor location are summarized in Table 1.The majority of lesions were located in the posterior fossa(67.8%), mainly in the cerebellum, in which 17 cases wereobserved (ten in the cerebellar vermis). In four cases, thetumor was located in the brainstem (two in the middlecerebellar peduncle), and in other four patients, it occurredin the optic chiasmatic hypothalamic region (OCH, 13%).
Cerebral hemispheres were affected in three patients (two inright occipital lobe).
In two patients (6.4%), the remaining lesion was locatedin the cervical spinal cord, and in one patient (case 28), itwas located in the optic nerve. This patient was known tohave neurofibromatosis type I. Neuroimaging reviewshowed that piloAs most often presented as solid enhancingmass with a cystic component (18 cases, 58%). A solidenhancing mass with no cystic component was seen in 11cases (35.4%). A large cyst with a small contrast-enhancingnodule and a heterogeneous mass was seen in two cases(cases 1 and 7, respectively).
GTR was achieved in 23 cases (74.1%), including twopatients with lesions located in the OCH, one in the brainstem,and one in the optic nerve. In eight patients whowere submittedto an incomplete surgical resection (subtotal or partial), tumorregrowth occurred between 1 and 3 years following resection.Postoperative chemotherapy for low-grade tumors was admin-istered to two patients (cases 18 and 21).
Follow-up was available for all patients. Twenty-onepatients (67.7%) showed a favorable outcome, and tenpatients (32.2%) had an adverse outcome. Residual tumorwas observed in 17 cases, but tumor progression wasobserved in seven of them. In nine patients, the residualtumor remained “silent” for a follow-up period rangingfrom 1 to 20 years (mean 6.6 years). In one patient (case14), the residual tumor regressed spontaneously after 6 yearsof surgery. Nine patients were submitted to more than onesurgical tumor resection: seven of them underwent one andtwo underwent two additional surgical procedures.
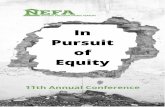
True tumor recurrence was observed in only two patients(cases 8 and 31). Figure 1 shows neuroimaging andhistopathological features of case 8. After two recurrences,the tumor spread to neuraxis via cerebrospinal fluid.Despite the fact that GTR was achieved in all the threesurgical procedures undergone by this patient, the tumorspread to the third ventricle, posterior fossa, and spinalcanal. Finally, the patient expired 2 years after the thirdsurgery. The histopathological review from the threesurgical procedures showed an ordinary cerebellar piloA,except for the brisk mitotic activity and the fact thatKi-67LI was 11.3%, 16.2%, and 10.7%, respectively.
In our series, statistical analysis showed that the adverseoutcomes were not associated with clinical factors, such asage at surgery (≤ or >5 years, P=0.22), tumor location(P=0.47), and extent of surgical resection (P=0.69). GTRwas achieved significantly when piloAs were located in thecerebellum and cerebral hemispheres (P=0.02).
Pathology
Regarding the histopathological features, RF, EGB, micro-vascular proliferation, and foci of lymphocytic infiltration
Childs Nerv Syst (2010) 26:19–28 21

Tab
le1
Clin
ical
andradiolog
ical
features
ofpilocytic
astrocytom
as
Case
number
Age
(year)
andgend
erTum
orlocatio
nNeuroradiolog
ical
features
Resectio
nRecurrence
Residual
tumor
Reoperatio
nNeurological
outcom
eFollow-up
(year)
16/M
Right
cerebellu
mLarge
cystwith
contrast-enh
ancing
nodu
leGTR
No
No
No
Normal
20
212
/FCerebellarverm
isSolid
masswith
cystic
compo
nent
GTR
No
No
No
Death
inpo
stop
eratory
4days
39/M
Cerebellarverm
issolid
masswith
cystic
compo
nent
GTR
No
No
No
Normal
8
49/F
Brain
stem
(MCP)
Solid
masswith
cystic
compo
nent
Sub
total
No
Yes
(stable)
No
Normal
17
59/M
Cerebellarverm
isSolid
masswith
cystic
compo
nent
Radical
No
Yes
Yes
Mild
deficits
10
612
/FCerebellarverm
isSolid
masswith
cystic
compo
nent
Radical
No
Yes
(stable)
No
Normal
15
711/F
Right
cerebellu
mHeterog
eneous
mass
GTR
No
No
Yes
aNormal
11
818
/FLeftcerebellu
mSolid
masswith
cystic
compo
nent
GTR
Yes
No
Yes
(2tim
es)
Death
b2
913
/FCerebellarverm
isSolid
masswith
cystic
compo
nent
Radical
No
Yes
(stable)
No
Normal
12
105/M
Brain
stem
Con
trast-enhancingmass
Partial
No
Yes
(stable)
No
Normal
10
115/F
OCH
Con
trast-enhancingmass
Radical
No
Yes
(stable)
No
Mild
deficits
9
1212
/MCerebellarverm
issolid
masswith
cystic
compo
nent
Sub
total
No
Yes
Yes
Normal
8
133/F
Leftcerebellu
mSolid
masswith
cystic
compo
nent
Radical
No
Yes
Yes
Normal
7
147/M
OCH
Solid
masswith
cystic
compo
nent
Radical
No
Yes
(regressive)
No
Normal
11
158/F
Spinalcord,cervical
Con
trast-enhancingmass
Partial
No
Yes
Yes
Severescoliosis
7
1613
/MRight
occipitallobe
Con
trast-enhancingmass
GTR
No
Yes
Yes
(2tim
es)
Normal
9
173/F
Cerebellarverm
isSolid
masswith
cystic
compo
nent
GTR
No
No
No
Normal
6
181/M
Brain
stem
/spinalcord
Con
trast-enhancingmass
Partial
No
Yes
(stable)
No/chem
oScolio
sis
5
195/M
Right
cerebellu
mCon
trast-enhancingmass
GTR
No
No
No
Normal
5
203/M
Right
cerebellu
mSolid
masswith
cystic
compo
nent
GTR
No
No
No
Normal
3
215/F
OCH
Solid
masswith
cystic
compo
nent
Partial
No
Yes
Yes
chem
o(2
times)
Normal
5
221/F
Cerebellarverm
isSolid
masswith
cystic
compo
nent
GTR
No
No
No
Normal
3.5
237/M
Leftcerebellu
mSolid
masswith
cystic
compo
nent
Radical
No
Yes
(stable)
No
Normal
3
2411/M
Leftparietal
Con
trast-enhancingmass
Radical
No
Yes
Yes
Normal
3
257/M
OCH
region
Con
trast-enhancingmass
Partial
No
Yes
(stable)
No/chem
oNormal
2
262/F
Cerebellarverm
isSolid
masswith
cystic
compo
nent
GTR
No
No
No
Normal
1
2716
/MRight
occipitallobe
Con
trast-enhancingmass
GTR
No
No
No
Normal
2
2810
/FLeftop
ticnerve
Con
trast-enhancingmass
GTR
No
No
No
Normal
1.5
295/F
Brain
stem
Con
trast-enhancingmass
Partial
No
Yes
(stable)
No
Normal
1
309/F
Brain
stem
(MCP)
Solid
masswith
cystic
compo
nent
GTR
No
No
No
Normal
3
315/F
Cerebellarverm
isSolid
masswith
cystic
compo
nent
GTR
Yes
No
Yes
Normal
1
OCH
optic
chiasm
atic
region
,chem
ochem
otherapy,M
male,
Ffemale,
MCPmiddlecerebellarpedu
ncle
aSurgery
intwosteps
bDeath
afterCSFtumor
dissem
ination
22 Childs Nerv Syst (2010) 26:19–28

were observed in the majority of cases (74.2%, 74.2%,51.6%, and 61.3%, respectively). Focal degenerativenuclear atypia and foci of necrosis were seen in 25.8%and 9.7% of the cases, respectively. However, none of thesecases showed brisk mitotic activity.
The mean Ki-67 LI was 4.4±4.5% (range, 0–16.7%).The proliferative index was higher than 3% in 17 cases(54.8%). Among them, four patients had an adverseoutcome, but their KI-67 LI was not significantly differentin comparison with the whole group (P=0.617). Neverthe-less, the mean Ki-67 LI of the two patients (case 8 and 31)who showed tumor recurrence was 12.7% and 11.3%,respectively.
Nuclear and cytoplasmic immunoreactivity for Gal-3was observed in all cases. The Gal-3 immunoexpressionwas diffuse in 54.8% of the cases and focal in 45.2%(Fig. 2). Interestingly, in contrast to normal endotheliumof the adjacent brain parenchyma, the endothelial cellswithin the tumor bulk showed no Gal-3 expression(Fig. 2c).
The CD31 reaction was achieved in 27 cases, and themean value of MVD was 21.2±11.5 vessels per HPF
(range, 5.3–52.7 vessels). NeuN positivity was detected inonly two cases (cerebellar and suprasellar tumor). In 27cases, the mean MVD was 21.2±11.5 vessels per HPF(range, 5.3–52.7 vessels). Statistical analysis showed nosignificant relationships between clinical outcome andhistopathological or immunohistochemical features, asshown in Table 2.
Survival
The mean follow-up was 5.7±5.4 years (range, 4 days–20 years). In this series, the overall 5-year survival ratewas 93.5%, and the 5-year PFS was 55%. When theextent of surgery was analyzed, the 5-year PFS was70% for patients who underwent GTR and 42% forpatients who were submitted to partial resection. Theextent of surgery was significant factor in determiningfavorable prognosis for patients with lesions located inthe cerebellum or cerebral hemispheres (P=0.02). Themortality rate was 6.4%: one patient (case 2) died ofpneumonia during the early postoperative period, and onepatient (case 8) expired 2 years after the initial surgery due
Fig. 1 a Patient 8 (upper left), contrast-enhanced CT scan shows amidline solid mass with cystic component. b Postoperative contrast-enhanced CT scan shows a complete resection of the lesion. cContrast-enhanced CT scan shows a true recurrence of the lesion inthe left cerebellar hemisphere. d Contrast-enhanced CT scan shows anodule in the left cerebellar hemisphere (second recurrence of thelesion). Axial T1-weighted MR after gadolinium injection shows two
ventricular lesions in the left frontal horn and third ventricle (lowerleft). Sagittal T1-weighted MR after gadolinium injection shows abasal leptomeningeal enhancement (center). There are further lepto-meningeal lesions along the falx and third ventricle. Histologicalappearance of pilocytic astrocytoma showing fusiform cells withwavy, fibrillary processes and Rosenthal fibers (lower right)
Childs Nerv Syst (2010) 26:19–28 23

to brain stem invasion and tumor spread along thecraniospinal axis.
Discussion
Since the publication of early treatises on piloAs [17],numerous studies have searched for factors that might affectthe overall patient survival [18]. Indisputably, one of themajor prognostic factors for cerebellar astrocytomas iscomplete surgical resection of the tumor [7, 19–21].However, controversy surrounds the role of other factors,such as tumor location, histopathological features, brain-stem involvement, and the presence of solid structure atneuroimaging, as well as of adjuvant therapy in selectedcases. Moreover, the dilemma of late tumor recurrenceremains constant in cases in which GTR is not achieved dueto tumor location (brain stem, OCH) and/or adverse clinicalconditions.
Clinical factors
In our series, the patient’s gender and age at surgery werenot related to the prognosis, as previously reported by someauthors [7, 22]. Similarly to the report by Strong et al.(1993) [23], preoperative CT and/or MR tumor imagingwere unreliable for predicting tumor behavior.
However, log-rank analysis indicated a straight relation-ship of piloAs located in the cerebellum and cerebralhemisphere with favorable prognoses, also corroboratingprevious studies as previously reported [7, 19, 20]. Thisfinding could be explained by the extent of surgicalresection, which is more easily attainable at those locations.It is well established that surgical resection is the standardtreatment for piloAs and that it can be curative if the tumoris completely removed [5, 7, 24, 25]. Nevertheless, theextent of surgical resection should be evaluated bypostoperative CT scans or MR, within the first 5 daysfollowing surgery, since contrast enhancement from inflam-
Fig. 2 Immunohistochemical features of pilocytic astrocytomas. a Ki-67immunolabeling shows nuclear expression in 5% of the tumor cells(×100). b Note the diffuse Galectin-3 expression occurring in the nuclei
and cytoplasm of tumor cells (×100). c Lack of Gal-3 immunoexpres-sion of endothelial cells within the tumor bulk (×100). d CD-31expression of endothelial cells within the tumor bulk (×200)
24 Childs Nerv Syst (2010) 26:19–28

Clinical status of patients (outcome) NumberHistopathological features Favorable Adverse P value
Predominant area 0.245
Microcystic 11 4
Piloid 8 3
Other 2 3
Predominant pattern 0.595
Diffuse 7 3
Loose 14 7
Calcification 0.284
Yes 3 3
No 18 7
Hemorrhage 0.173
Yes 7 1
No 14 9
Necrosis
Yes 1 2 0.237
No 20 8
Hialinized vessels 0.224
Yes 8 6
No 13 4
Angiectatic vessels 0.405
Yes 6 4
No 15 6
Rosenthal fibers 0.483
Yes 6 2
No 15 8
Eosinophilic granular bodies 0.208
Yes 17 6
No 4 4
Microcystic changes 0.152
Yes 9 7
No 12 3
Inflammation 0.384
Yes 12 7
No 9 3
Galectin-3 0.306
Strong reaction (diffuse) 13 4
Weak reaction (focal) 8 6
Ki-67 Labeling Index 0.503
>3% 12 5
≤3% 9 5
NeuN 0.452
Positive 2 0
Negative 19 10
CD31 0.872
Positive 21 10
Table 2 Clinicopathologicaland immunohistochemical fea-tures of pilocytic astrocytomas
Significant P value if≤0.05
Childs Nerv Syst (2010) 26:19–28 25

mation and neovascularization in the tumor bed can occuras early as 7 days after surgery [26, 27].
The need to perform the postoperative imaging studyarose from the observation that the surgeon’s opinion is apoor predictor of true total resection [3, 27]. In effect, theprogression of the residual tumor, often referred as “tumorrecurrence,” is more common than the actual tumorrecurrence. In analyzing 14 studies in the literature, Dirvenet al. [3] described a mean incidence of tumor recurrence of24%, ranging from 7% to 35%. However, it is unclear ifsuch recurrences represented new (de novo) tumors aftercomplete surgical resection or residual tumors incompletelyresected and showing further growth.
In the cases reported herein, no clinical factors wererelated to tumor progression or adverse patient outcome.Tumor progression after surgery was observed in 29% ofthe cases (nine patients). However, in only two of thesepatients, a “true” recurrent tumor could be defined, while inthe other seven, there was a progression of the residualtumor. It is important to stress that not every patient withresidual tumor after operation develops tumor progression.In fact, in the present series, tumor progression wasobserved in seven of 17 patients with residual tumor; andin nine patients, the residual lesion remained as a “silent”tumor for a mean follow-up period of 5.7 years (1 to20 years). Interestingly, one patient (case 14) experiencedspontaneously regression of the residual tumor after 6 yearsof surgery. The stabilization and even spontaneous regres-sion of residual piloAs many years following surgery, evenif only a small biopsy of a tumor was achieved, have beenwell described in the literature [28, 29].
A higher frequency of recurrence or progression ofpiloAs has been described in older patients [30]. In thepresent series, an adolescent (case 8) showed dissemina-tion of cerebellar piloA 2 years after GTR. The piloAspread to the third ventricle, posterior fossa, and spinalcanal. Prior to dissemination, the patient presented twolocal recurrences that were promptly extirpated. The slidereview of the three specimens showed histopathologicalfeatures similar to those seen in ordinary piloAs, exceptfor the noticeable mitotic activity and high KI-67 LI (mean of12.7%). Although infiltration of the subarachnoid space is acommon event in piloAs [8], cerebrospinal spread of anordinary piloA has been reported in few cases [6, 31, 32].
Buschmann et al. [33] described two cases of piloAsin the OCH region with leptomeningeal dissemination.According to the histological description, one of thecases (case 1) most probably represented a pilomyxoidastrocytoma, which is actually considered as an aggres-sive variant of piloAs, prone to disseminate to theleptomeninges [2]. Based on their own report andreviewing similar cases in the literature, those authorspointed out that special attention should be directed
toward patients with primary piloAs in the OCH region,since ablative surgery is difficult to be achieved, andthere is a higher incidence of subarachnoid spread inthese cases.
Histopathological features
The initial goal of this retrospective study was to identifypossible differences in the histopathological and/or immu-nohistochemical features that could better distinguishpatients with piloAs according to their outcomes. Histo-pathologically, classical features of piloAs, such as RF,EGB, biphasic pattern, and even foci of lymphocyticinfiltration, were present in our cases in similar proportionsto those found in previous studies [8, 34]; however, nuclearatypia and necrosis were seen in a higher frequency.Furthermore, in the current study, none of these featureswere related to an adverse prognosis for piloAs, similarly toother reported series [4, 7, 8, 28].
The role of Ki-67 LI in predicting prognosis for piloAsis controversial [35]. While in one study a nonsignificanttrend toward a lower/negative (absent) proliferative indexwas associated with fewer progressions of residual tumor[3], another study suggested that MIB-1 LI might identifya subset of more clinically aggressive piloAs in children[36]. The proliferative index in our study was notcorrelated with tumor location and/or patient outcome.The mean Ki-67 LI found in our series (4.4±4.5%) wassimilar to that reported by Roessler et al. (2002) [37], buthigher than that reported by other authors [36, 38, 39].More interestingly, the mean Ki-67 LI for piloAs was evenhigher than that described for grade II astrocytomas[15, 38, 40]. In reviewing the literature on Ki-67/MIB-1LI in diffuse astrocytomas of different grades of malig-nancy, Johannessen and Torp [40] described that the meanKi-67/MIB-1 LI value (±SD) of the 16 papers included inthe review was 3.0% (±2.1) for grade II. We speculate thatthe high mean Ki-67 LI for piloAs in our series may be aconsequence of the higher incidence of nuclear atypia andnecrosis. Nevertheless, differences in immunohistochem-ical and technical procedures between laboratories shouldalso be considered. Although four out of 17 patients withKi-67 LI higher than 3% had an adverse outcome,including one death (case 8), their KI-67 LI were notsignificantly different compared to the group. Despite that,the analysis of individual cases suggests that strict follow-up should be performed if piloAs is associated with highmitotic activity/Ki-67 LI or if GTR cannot be achieved atsurgery.
Regarding Gal-3 immunoexpression, we generally ob-served a diffuse nuclear and cytoplasmic tumor cellstaining. Although Gal-3 immunoexpression was notrelated to the prognosis, its expression can be used as a
26 Childs Nerv Syst (2010) 26:19–28

tool marker to differentiate piloAs from grade II diffuseastrocytomas, which do not express this lectin. Similarly,this lectin can be used to differentiate glioblastomas (Gal-3positive) from anaplastic oligodendrogliomas (Gal-3 nega-tive) [41] and anaplastic astrocytomas (Gal-3 negative)from glioblastomas [42]. The absence of immunolabelingof the endothelial cells within the tumor bulk wasanalogous to that previously reported by our group andconfirmed by other authors [41, 43]. Gordower et al. [44]reported that Gal-3 was expressed in endothelial cells ofvessels within diffuse astrocytomas, but piloAs was notincluded in such study. We speculate that the absence ofGal-3 expression in tumor vessels in piloAs can be related,in some way, to the loss of blood–brain barrier, since thesame finding is seen in glioblastomas, which also showcontrast enhancement in neuroimaging [41].
In contrast to what was described by Preusser et al. [45],NeuN immunoreactive cells were found in 3.2% of ourcases. According to our evaluation, these cells wereneurons entrapped into the neoplastic core, since they haveno morphological aspects of neoplastic cells or ganglioncells, as seen in gangliogliomas. In a series of 80 piloAs inchildren, Fernandez et al. [8] described six cases exhibitingneurons within the tumor bulk, but this finding was notconfirmed by immunohistochemistry. In fact, the role ofcells with neuronal differentiation in astrocytic tumors isstill debatable. Moreover, this matter has raised puzzlingquestions about the gold standard criteria for neuronaldifferentiation as well as about the classification ofastrocytic tumors and its prognostic value [46].
Conclusions
The main prognostic factor for patients with piloAscontinues to be the extent of surgical excision. Tumorrecurrences should be treated with additional operations,since malignant change has been rarely described forpiloAs. If a residual tumor is detected by neuroimaging, asecond surgery should be considered in case of tumorprogression. If ablative resection is unattainable, the patientshould be carefully followed up, even if lesions are stable.Despite the overall excellent prognosis, adequate postopera-tive follow-up is of the utmost importance. The favorableoutcome in patients with tumors located in the cerebellum ismost likely a consequence of the complete tumor resection.
Aside from gross tumor resection, no clinical ormicroscopic factors were significantly related to patientoutcome. Although patients at risk for an unfavorableoutcome or tumor recurrence could not be determinedherein, strict follow-up is suggested to be necessary ifpiloAs is associated with high mitotic activity/Ki-67 LI or ifGTR cannot be achieved at surgery. In some aspects,
childhood piloAs remains an enigmatic tumor. Furtherseries with molecular studies focused on genetic alterationsmay provide a better comprehension of the pathobiology ofthese tumors.
Acknowledgments The authors thank the CNPQ (Conselho Nacionalde Desenvolvimento Científico e Tecnológico and FAEPA (Fundaçãode Assistência de Ensino e Pesquisa) for grant support. The authors arealso grateful to Deise Simões and Ana Maria Anselmi for their experttechnical assistance.
Conflict of interest statements The authors state that there are noconflicts of interest.
References
1. Louis DN, Ohgaki H, Wiestler OD, Cavenee WK, Burger PC,Jouvet A, Scheithauer BW, Kleihues P (2007) The 2007 WHOclassification of tumours of the central nervous system. ActaNeuropathol 114:97–109
2. Ceppa EP, Bouffet E, Griebel R, Robinson C, Tihan T (2007) Thepilomyxoid astrocytoma and its relationship to pilocytic astrocy-toma: report of a case and a critical review of the entity. JNeurooncol 81:191–196
3. Dirven CM, Mooij JJ, Molenaar WM (1997) Cerebellar pilocyticastrocytoma: a treatment protocol based upon analysis of 73 casesand a review of the literature. Childs Nerv Syst 13:17–23
4. Villarejo F, de Diego JM, de la Riva AG (2008) Prognosis ofcerebellar astrocytomas in children. Childs Nerv Syst 24:203–210
5. Due-Tønnessen BJ, Helseth E, Scheie D, Skullerud K, Aamodt G,Lundar T (2002) Long-term outcome after resection of benigncerebellar astrocytomas in children and young adults (0–19 years):report of 110 consecutive cases. Pediatr Neurosurg 37:71–80
6. Mamelak AN, Prados MD, Obana WG, Cogen PH, Edwards MS(1994) Treatment options and prognosis for multicentric juvenilepilocytic astrocytoma. J Neurosurg 81:24–30
7. Pencalet P, Maixner W, Sainte-Rose C, Lellouch-Tubiana A,Cinalli G, Zerah M, Pierre-Kahn A, Hoppe-Hirsch E, BourgeoisM, Renier D (1999) Benign cerebellar astrocytomas in children. JNeurosurg 90:265–273
8. Fernandez C, Figarella-Branger D, Girard N, Bouvier-Labit C,Gouvernet J, Paz PA, Lena G (2003) Pilocytic astrocytomas inchildren: prognostic factors—a retrospective study of 80 cases.Neurosurgery 3:544–553
9. Mirone G, Schiabello L, Chibbaro S, Bouazza S, George B (2009)Pediatric primary pilocytic astrocytoma of the cerebellopontineangle: a case report. Childs Nerv Syst 25:247–251
10. Tomlinson FH, Scheithauer BW, Hayostek CJ, Patisi JE, MeyerFB, Shaw EG, Weiland TL, Katzmann JA, Jack CR (1994) Thesignificance of atypia and histologic malignancy in pilocyticastrocytoma of the cerebellum: a clinicopathologic study and flowcytometric study. J Child Neurol 9:301–310
11. Parsa CF, Givrad S (2008) Juvenile pilocytic astrocytomas do notundergo spontaneous malignant transformation. Grounds fordesignation as hamartomas. Br J Ophthalmol 92:40–46
12. Desai KI, Nadkarni TD, Muzumdar DP, Goel A (2001) Prognosticfactors for cerebellar astrocytomas in children: a study of 102cases. Pediatr Neurosurg 35:311–317
13. Schneider JH Jr, Raffel C, McComb JG (1992) Benign cerebellarastrocytomas of childhood. Neurosurgery 30:58–62 discussion62-63
Childs Nerv Syst (2010) 26:19–28 27

14. Sutton LN, Cnaan A, Klatt L, Zhao H, Zimmerman R, Needle M,Molloy P, Phillips P (1996) Postoperative surveillance imaging inchildren with cerebellar astrocytomas. J Neurosurg 84:721–725
15. Neder L, Colli BO, Machado HR, Carlotti CG Jr, Santos AC,Chimelli L (2004) MIB-1 labeling index in astrocytic tumors—aclinicopathologic study. Clin Neuropathol 23:262–270
16. Abdulrauf SI, Edvardsen K, Ho KL, Yang XY, Rock JP,Rosenblum ML (1988) Vascular endothelial growth factorexpression and vascular density as prognostic markers ofsurvival in patients with low-grade astrocytoma. J Neurosurg88:513–520
17. Cushing H (1931) Experiences with the cerebellar astrocytomas, acritical review of seventy-six cases. Surg Gynecol Obstet 52:129–204
18. Kepes JJ, Lewis RC, Vergara GG (1980) Cerebellar astrocytomainvading the musculature and soft tissues of the neck. J Neurosurg52:414–418
19. Abdollahzadeh M, Hoffman HJ, Blazer SI, Becker LE,Humphreys RP, Drake JM, Rutka JT (1994) Benign cerebellarastrocytoma in childhood: experience at the Hospital for SickChildren 1980–1992. Childs Nerv Syst 10:380–383
20. Lapras C, Patet JD, Lapras C Jr, Mottolese C (1986) Cerebellarastrocytomas in childhood. Childs Nerv Syst 2:55–59
21. Sgouros S, Fineron PW, Hockley AD (1995) Cerebellar astrocy-toma of childhood: long-term follow-up. Childs Nerv Syst 11:89–96
22. Sobel EL, Gilles FH, Leviton A, Tavaré CJ, Hedley-Whyte ET,Rorke LB, Adelman LS (1996) Survival of children withinfratentorial neuroglial tumors. The Childhood Brain TumorConsortium. Neurosurgery 39:45–54 discussion 54–56
23. Strong JA, Hatten HP Jr, Brown MT, Debatin JF, Friedman HS,Oakes WJ, Tien R (1993) Pilocytic astrocytoma: correlationbetween the initial imaging features and clinical aggressiveness.AJR Am J Roentgenol 161:369–372
24. Benesch M, Eder HG, Sovinz P, Raith J, Lackner H, Moser A,Urban C (2006) Residual or recurrent cerebellar low-grade gliomain children after tumor resection: is re-treatment needed? A singlecenter experience from 1983 to 2003. Pediatr Neurosurg 42:159–164
25. Fisher PG, Tihan T, Goldthwaite PT, Wharam MD, Carson BS,Weingart JD, Repka MX, Cohen KJ, Burger PC (2008) Outcomeanalysis of childhood low-grade astrocytomas. Pediatr BloodCancer 51:245–250
26. Ohki M, Sakurada K, Sonoda Y, Sato S, Saito S, Kayama T (2003)Analysis of the extent of astrocytic tumour resection evaluated bymagnetic resonance images. Neurosurg Rev 26:262–265
27. Rollins NK, Nisen P, Shapiro KN (1998) The use of earlypostoperative MR in detecting residual juvenile cerebellarpilocytic astrocytoma. AJNR Am J Neuroradiol 19:151–156
28. Austin EJ, Alvord EC Jr (1988) Recurrences of cerebellarastrocytomas: a violation of Collins’ law. J Neurosurg 68:41–47
29. Gunny RS, Hayward RD, Phipps KP, Harding BN, Saunders DE(2005) Spontaneous regression of residual low-grade cerebellarpilocytic astrocytomas in children. Pediatr Radiol 35:1086–1091
30. Stüer C, Vilz B, Majores M, Becker A, Schramm J, Simon M(2007) Frequent recurrence and progression in pilocytic astrocy-toma in adults. Cancer 110:2799–2808
31. Civitello LA, Packer RJ, Rorke LB, Siegel K, Sutton LN, Schut L(1988) Leptomeningeal dissemination of lowgrade gliomas inchildhood. Neurology 38:509–513
32. Prados MD, Edwards MSB, Rabbitt J, Lamborn K, Davis RL,Levin VA (1997) Treatment of pediatric low grade gliomas with a
nitrosourea-based multiagent chemotherapy regimen. J Neuro-oncol 32:235–241
33. Buschmann U, Gers B, Hildebrandt G (2003) Pilocytic astrocy-tomas with leptomeningeal dissemination: biological behavior,clinical course, and therapeutical options. Childs Nerv Syst19:298–304
34. Malik A, Deb P, Sharma MC, Sarkar C (2006) Neuropathologicalspectrum of pilocytic astrocytoma: an Indian series of 120 cases.Pathol Oncol Res 12:164–171
35. Faria MH, Gonçalves BP, do Patrocínio RM, de Moraes-FilhoMO, Rabenhorst SH (2006) Expression of Ki-67, topoisomeraseIIalpha and c-MYC in astrocytic tumors: correlation with thehistopathological grade and proliferative status. Neuropathology26:519–527
36. Bowers DC, Gargan L, Kapur P, Reisch JS, Mulne AF, ShapiroKN, Elterman RD, Winick NJ, Margraf LR (2003) Study of theMIB-1 labeling index as a predictor of tumor progression inpilocytic astrocytomas in children and adolescents. Clin Oncol21:2968–2973
37. Roessler K, Bertalanffy A, Jezan H, Ba-Ssalamah A, Slavc I,Czech T, Budka H (2002) Proliferative activity as measured byMIB-1 labeling index and long-term outcome of cerebellarjuvenile pilocytic astrocytomas. J Neurooncol 58:141–146
38. Giannini C, Scheithauer BW, Burger PC, Christensen MR, WollanPC, Sebo TJ, Forsyth PA, Hayostek CJ (1999) Cellular prolifer-ation in pilocytic and diffuse astrocytomas. J Neuropathol ExpNeurol 58:46–53
39. Torp SH, Alsaker M (2002) Ki-67 immunoreactivity, basicfibroblast gowth factor (bFGF) expression, and microvesseldensity as supplementary prognostic tools in low-grade astrocy-tomas. Pathol Res Pract 198:261–265
40. Johannessen AL, Torp SH (2006) The clinical value of Ki-67/MIB-1 labeling index in human astrocytomas. Pathol Oncol Res12:143–147
41. Neder L, Marie SK, Carlotti CG Jr, Gabbai AA, Rosemberg S,Malheiros SM, Siqueira RP, Oba-Shinjo SM, Uno M, AguiarPH, Miura F, Chammas R, Colli BO, Silva WA Jr, Zago MA(2004) Galectin-3 as an immunohistochemical tool to distin-guish pilocytic astrocytomas from diffuse astrocytomas, andglioblastomas from anaplastic oligodendrogliomas. Brain Pathol14:399–405
42. Camby I, Belot N, Rorive S, Lefranc F, Maurage CA, Lahm H,Kaltner H, Hadari Y, Ruchoux MM, Brotchi J, Zick Y, Salmon I,Gabius HJ, Kiss R (2001) Galectins are differentially expressed insupratentorial pilocytic astrocytomas, astrocytomas, anaplasticastrocytomas and glioblastomas, and significantly modulate tumorastrocyte migration. Brain Pathol 11:12–26
43. Park SH, Min HS, Kim B, Myung J, Paek SH (2008) Galectin-3: auseful biomarker for differential diagnosis of brain tumors.Neuropathology 28:497–506
44. Gordower L, Decaestecker C, Kacem Y, Lemmers A, Gusman J,Burchert M, Danguy A, Gabius H, Salmon I, Kiss R, Camby I(1999) Galectin-3 and galectin-3-binding site expression in humanadult astrocytic tumours and related angiogenesis. NeuropatholAppl Neurobiol 25:319–330
45. Preusser M, Laggner U, Haberler C, Heinzl H, Budka H,Hainfellner JA (2006) Comparative analysis of NeuN immunore-activity in primary brain tumours: conclusions for rational use indiagnostic histopathology. Histopathology 48:438–444
46. Rodriguez FJ, Scheithauer BW, Port JD (2006) Unusual malignantglioneuronal tumors of the cerebrum of adults: a clinicopathologicstudy of three cases. Acta Neuropathol 112:727–737
28 Childs Nerv Syst (2010) 26:19–28